Concepts, Challenges, Barriers, and Opportunities Related to Evidence-Based Practice in...
13
Rehabilitation Education, Volume 24, Numbers 3 & 4, pp. 179-190, 2010 Concepts, Challenges, Barriers, and Opportunities Related to Evidence-Based Practice in Rehabilitation Counseling Fong Chan University of Wisconsin - Madison Jill Bezyak University of Northern Colorado Maria Romero Ramirez California Sate University - Fresno Chung-Yi Chiu University of Texas Southwestern Medical Center Connie Sung Mayu Fujikawa University of Wisconsin - Madison Evidence-based practice espouses that all healthcare professionals should provide their clients with the most effective clinical services based on sound research evidence. This philosophy of practice has since permeated to an array of health care and human service disciplines, and the rehabilitation counseling profession is no exception. Although the evidence-based practice movement is not without its controversy and critics, this movement also presents a window of opportunity for the rehabilitation counseling profession to promote and support a systematic agenda for theory-driven rehabilitation counseling research. The use of scientific evidence derived from theory-driven research to inform rehabilitation counseling practices could contribute to higher employment rates and better quality of employment outcomes for people with disabilities. In this article, we provided an overview of the key concepts related to evidence-based practice, critical issues and challenges that surround the evidence-based practice movement, and the implications and opportunities of this movement for the rehabilitation counseling profession. Keywords: evidence-based practice, research utilization, rehabilitation counseling ".. .the honest clinician cannot avoid the question 'Am I doing better than I could do by flipping pennies?' " (Meehl, 1954, p. 136). The term 'evidence-based medicine' first appeared dence-Based Medicine Working Group, 1992; Guyatt, in the medical literature in the U.S. in 1991 (Evi- 1991; Montori & Guyatt, 2008). The philosophical un- Rehabilitation Education
-
Upload
michiganstate -
Category
Documents
-
view
2 -
download
0
Transcript of Concepts, Challenges, Barriers, and Opportunities Related to Evidence-Based Practice in...

Rehabilitation Education, Volume 24, Numbers 3 & 4, pp. 179-190, 2010
Concepts, Challenges, Barriers, andOpportunities Related to Evidence-Based
Practice in Rehabilitation CounselingFong Chan
University of Wisconsin - Madison
Jill BezyakUniversity of Northern Colorado
Maria Romero RamirezCalifornia Sate University - Fresno
Chung-Yi ChiuUniversity of Texas Southwestern Medical Center
Connie SungMayu Fujikawa
University of Wisconsin - Madison
Evidence-based practice espouses that all healthcare professionals should provide their clientswith the most effective clinical services based on sound research evidence. This philosophy ofpractice has since permeated to an array of health care and human service disciplines, and therehabilitation counseling profession is no exception. Although the evidence-based practicemovement is not without its controversy and critics, this movement also presents a window ofopportunity for the rehabilitation counseling profession to promote and support a systematicagenda for theory-driven rehabilitation counseling research. The use of scientific evidencederived from theory-driven research to inform rehabilitation counseling practices couldcontribute to higher employment rates and better quality of employment outcomes for peoplewith disabilities. In this article, we provided an overview of the key concepts related toevidence-based practice, critical issues and challenges that surround the evidence-basedpractice movement, and the implications and opportunities of this movement for therehabilitation counseling profession.
Keywords: evidence-based practice, research utilization, rehabilitation counseling
".. .the honest clinician cannot avoid the question 'Am I doing better thanI could do by flipping pennies?' " (Meehl, 1954, p. 136).
The term 'evidence-based medicine' first appeared dence-Based Medicine Working Group, 1992; Guyatt,in the medical literature in the U.S. in 1991 (Evi- 1991; Montori & Guyatt, 2008). The philosophical un-
Rehabilitation Education
Page 180 Chan et al.
derpinnings of evidence-based practice espouse that allhealthcare professionals should provide their clientswith the most effective clinical services based on soundresearch evidence (Chan, Tarvydas, Blalock, Strauser,& Atkins, 2009; Chronister, Chan, Cardoso, Lynch, &Rosenthal, 2008). The concept of evidence-based prac-tice has since permeated to a wide array of healthcareand human service disciplines, and the rehabilitationcounseling profession is no exception (Chan, Miller,Pmett, Lee, & Chou, 2003; Chan, Rosenthal, & Pmett,2008; Chronister et al, 2008; Pmett, Swett, Chan,Rosenthal, & Lee, 2008). However, the current state ofrehabilitation practice can still be justifiably character-ized as experience-based or habit-based (Law, 2002).To fully adopt an evidence-based approach in rehabili-tation, Dunn and Elliott (2008) proposed that we needto first embrace a comprehensive theory-driven re-search agenda; second, validate effective interventionsbased on this research agenda; and finally, facilitate theprovision of empirically supported interventions basedon the research evidence.
Clearly, intemal motivation and extemal pressuresfor rehabilitation agencies and counselors suggest us-ing an array of evidence-based assessment and plan-ning tools and interventions in practices to improve em-ployment outcomes for individuals with disabilities(Rubin, Chan, & Thomas, 2003). Specifically, thestate-federal vocational rehabilitation program wasplaced by the U.S. Government Accountability Office(GAO) on a list of high-risk programs for not keepingup with scientific advances and economic and socialchanges (GAO, 2005). Without a doubt, the current ex-pectation for healthcare and rehabilitation professionalsto use empirically supported interventions in their prac-tices will continue to sti-ongly shape the future of reha-bilitation counseling research and services. The Na-tional Institute on Disability and Rehabilitation Re-search (NIDRR) has, in recent years, underscored theneed for NIDRR-sponsored research studies to meetstandards for inclusion in evidence-based systematicreviews (Schlosser, 2006), and it also emphasizes theimportance of knowledge translation to all grantees.Similarly, the Rehabilitation Services Administrationhas begun to encourage state vocational rehabilitationagencies to integrate the best scientific evidence withclinical expertise and client perspectives (33''' Institutefor Rehabilitation Issues, 2008).
However, the evidence-based practice movement isnot without its controversy and critics. For example, so-cial and behavioral sciences researchers have raisedquestions about what constitutes "best evidence" usedto inform service delivery. The use of randomized clini-cal trials as the gold standard for scientific evidence,which works well in medicine, may be too restrictivefor other behavioral sciences because randomized clini-cal trials do not always take into account the full com-plexity of human behavior and clinical condition(̂ Wampold, 1997). Similarly, the complex nature of vo-cational rehabilitation both in the scope of services pro-vided through an array of disciplines and diverse clini-cal populations also makes process and outcome re-search challenging. Conversely, the evidence-basedpractice movement may present a window of opportu-nity for the rehabilitation counseling profession to pro-mote and support a systematic agenda for theory-drivenrehabilitation research. The use of scientific evidencederived from theory-driven research to inform rehabili-tation counseling practice could improve employmentrates and quality of employment outcomes for peoplewith significant disabilities. Without a doubt, rehabili-tation counseling professionals will increasingly beasked to integrate research evidence in their clinical de-cision-making process (Chan et al., 2003; Chwalisz &Chan, 2008; Schlosser, 2006). This article will providean overview of the key concepts related to evi-dence-based practice, critical issues and challenges thatsurround the evidence-based practice movement, andthe implications and opportunities of this movement forthe rehabilitation counseling profession.
ConceptsEvidence-based practice is a clinical decision-mak-
ing process beginning with formulating clinical ques-tions to ask, determining the best practice, and criticallyappraising the evidence for validity and applicability tothe particular situation. The best evidence must then beapplied by a clinician with expertise in considering theclient's unique values and needs. The final aspect of theprocess is evaluation of the effectiveness of care andcontinual improvement of the process (DePalma, 2000;Sackett, Rosenberg, Gray, Haynes, & Richardson,1996). From a conceptual perspective, it is clear thatevidence-based practice involves the conscientious, ex-plicit, and judicious use of current best evidence inmaking decisions about the care of individual clients(Sackett et al., 1996). The complexities occur when try-
Rehabilitation Education

Evidence-Based Practice in Rehabilitation Counseling Page 181
ing to define what constitutes 'best evidence,' as indi-cated by a growing debate in the literature regardingwhat constitutes quality research, how to best apply re-search evidence, and how to define effectiveness(Tanenbaum, 2005).
Within the field of medicine, with its positivist sci-entific methods tradition, the gold standard for scien-tific evidence has always been randomized clinical tri-als, and "best evidence" from this perspective is de-rived from a series of research results based onrandomized clinical trials that form an empirical con-sensus regarding the effectiveness of a specific treat-ment approach (Ottenbacher & Maas, 1998). However,randomized clinical trials may not be the best form ofevidence for rehabilitation and other allied health disci-plines. This type of experimental design may not takeinto account the complexities of real world clinical pop-ulations and settings associated with behavioral sci-ences (Wampold, 1997). For these reasons. Tucker andReed (2008) suggested that we should embrace eviden-tiary pluralism as a strategy for research and evi-dence-based practice in rehabilitation. Despite the de-bate regarding what constitutes "best evidence," a fivelevel hierarchical framework emphasizing the impor-tance of experimental studies offers healthcare and re-habilitation professionals a format for determining thestrength ofthe evidence based on methodological rigor(Holm, 2000; Nathan & Gorman, 1998). This hierarchyof evidence is presented in Table 1.
Evidence-based medicine also delineates a set ofskills for clinical decision making (Walker, Seay, Solo-mon, & Spring, 2006). Walker et al. (2006) suggestedthe following four specific steps: (a) formulatingwell-defined, answerable questions; (b) seeking thebest evidence available to answer the questions; (c) crit-
ically appraising the evidence; and (d) applying the evi-dence to the individual client. The steps recommendedfor evidence-based medicine can also be used by reha-bilitation counselors in their clinical decision-makingwith individuals with disabilities. A detailed descrip-tion of each step follows.
Step 1: Formulating Well-Defined,Answerable Questions
This is likely the most important step of the evi-dence-based practice process because it determineswhat evidence to look for and where to search for thebest evidence. Walker et al. (2006) provided some ex-amples of general questions the rehabilitation healthprofessional may ask. These quesfions include:• What processes/techniques make a specific rehabili-
tation intervention work?• For whom is the intervention most effective?• Are certain interventions/programs better for certain
persons?• Who should receive a specific intervention or pro-
gram? When? And for how long?In evidence-based practice, general questions or
background questions ask about a setting or context,whereas foreground questions ask about a specific casewithin that context (Walker et al., 2006). Walker et al.(2006) recommend asking foreground questions usingthe PICO format: patient group (P), intervention (I),comparison group (C), and outcome measures (O). Forexample, in the case of a 52-year old first generationChinese American with a back injury who is dissatis-fied with his transcutaneous electrical nerve stimula-tion (TENS) treatment and would like to explore acu-puncture as an altemative therapy, background ques-tions may include:
Table 1Hierarchical Levels of Evidence
Level 1: Strong evidence from at least one systematic review of multiple well-designed randomized confroUedtrials.Level 2: Strong evidence from at least one properly designed randomized controlled trials of appropriate size.Level 5: Evidence from well-designed trials without randomization, single group pre-post, cohort, time series,or matched case-controlled studies.Level 4: Evidence from well-designed nonexperimental studies from more than one center or research group.Level 5: Evidence from opinions of respected authorities, based on clinical evidence, descriptive studies, or re-ports of expert committees.
Rehabilitation Education

Page 182 Chan et al.
• What are the most effective treatments for low backpain?
• Is acupuncture an effective treatment for low backpain?
• Are there any significant risks associated with acu-puncture?The foreground PICO question may be: In mid-
dle-aged Chinese men with chronic pain (P), is thereany evidence that acupuncture (I), is superior to shamtreatment, biofeedback, relaxation training, and/orTENS (C), in reducing the frequency, intensity, and du-ration of low back pain (O)? A set of well-built back-ground and foreground questions provide direction fordetermining what evidence to look for and where tosearch for the best evidence.
Step 2: Seeking the Best Evidence Available toAnswer the Questions
After formulating the appropriate clinical hypotheses,the next step is to search for evidence-based interventionsrelated to clinical questions. The most reliable and scholarlyapproach to searching for "best evidence" is through aca-demic databases such as Academic Search Elite, CINAHLPlus with Full Text, MEDLINE, and PsycINFO. The mostuseñil websites for evidence-based mecücal, rehabilitation,and behavioral science intervention information include theCochrane Collaboration (www.cochrane.org), CampbellCollaboration (http:// www.campbellcollaboration.org).Agency for Healthcare Research and Quality (www.ahrq.gov), and American Congress of Rehabilitation Medicine(http://www.acrm.org/consumer_professional/Evidence_Based Practice.cñn).
Given the potential for a vast number of research ar-ticles with contradictory findings, the most efficientway to find best evidence is to use databases and/or spe-cific evidence-based intervention websites to search forsystematic reviews. Systematic reviews answer a spe-cific clinical question by using predetermined mies forcapturing the evidence, appraising it, and synthesizingit in a manner that is easily accessible to clinicians. Sys-tematic reviews are based on work by scholars with ex-pertise in a substantive area who review and critique theavailable data in the field (Schlosser, 2006). Strong evi-dence from at least one systematic review of multiplewell-designed randomized clinical trials is consideredthe highest level of best evidence and is frequently la-beled a meta-analytic review.
The most efficient way of searching forpsychosocial and rehabilitation treatment informationis to search the above databases and/or websites usingkey words related to the clinical problem coupled withthe terms systematic review or meta-analysis. Relatedto the example of the Chinese immigrant with backpain, entering acupuncture, low back pain, and system-atic review using Academic Search Elite, CINAHLPlus with Full Text, MEDLINE, and PsycINFO re-sulted in 12 entries. When only acupuncture was en-tered, 13,309 entries resulted; when just low back painwas entered, 14,606 entries resulted; and when acu-puncture and low back pain were entered together, 264entries resulted. As a result of this search, one of the re-views indicated that there is evidence of immediate andshort-term pain relief and functional improvement foracupuncture compared to no treatment or sham therapy.In a separate search seeking to determine the effective-ness of TENs versus acupuncture, the terms acupunc-ture and TENS were entered and six entries occurred.The lead systematic review article indicated that the ev-idence for the efficacy of TENS as an isolated interven-tion in the management of chronic low back pain issomewhat limited and inconsistent. Therefore, acu-puncture treatment may be more effective within thecontext of the dominant culture for a recent immigrantfrom China.
Step 3: Critically Appraising the EvidenceTo critically appraise evidence from a single prop-
erly designed randomized control trial requires a rela-tively strong background in research methods and aworking knowledge of concepts related to intemal andextemal validity (Schlosser, 2006). Again, rehabilita-tion counselors can save valuable time by gleaning evi-dence from systematic reviews. However, to read andunderstand systematic reviews, rehabilitation profes-sionals need to be familiar with several concepts relatedto systematic review/meta-analysis as described below:
1. Systematic review: A systematic review is athorough, comprehensive, and explicit process of col-lecting, reviewing and presenting all available evi-dence. It typically involves several steps including (a)asking an answerable clinical question (oñen the mostdifficult step), (b) identifying one or more databases tosearch, (c) developing an explicit search strategy, (d)selecting titles, abstracts, and manuscripts based on ex-plicit inclusion and exclusion criteria, (e) abstracting
Rehabilitation Education
Evidence-Based Practice in Rehabilitation Counseling Page 183
data in a standardized format, and (f) providing a sum-mary of the evidence from the primary sources(Schlosser, 2006).
2. Meta-analysis: Meta-analysis is a subtypeof systematic review. A meta-analysis reviews the re-sults of a collection of empirical studies in a specific re-search domain through statistical integration and analy-sis and synthesizes the results to determine theeffectiveness of a given clinical treatment (Durlak,1995; Schmidt & Hunter, 2003). It is a mechanism bywhich professionals can understand the effectiveness ofa practice/intervention domain in quantitative terms.
3. Randomized clinical trials: Randomizedclinical trials possess three characteristics: (a) an exper-imental group who receives the experimental interven-tion or treatment; (b) a control or comparison groupwho receive standard care or a comparison interventionthat is different from the experimental treatment; and(c) random assignment or randomization to experimen-tal and control or comparison groups (Durlak, 1995).
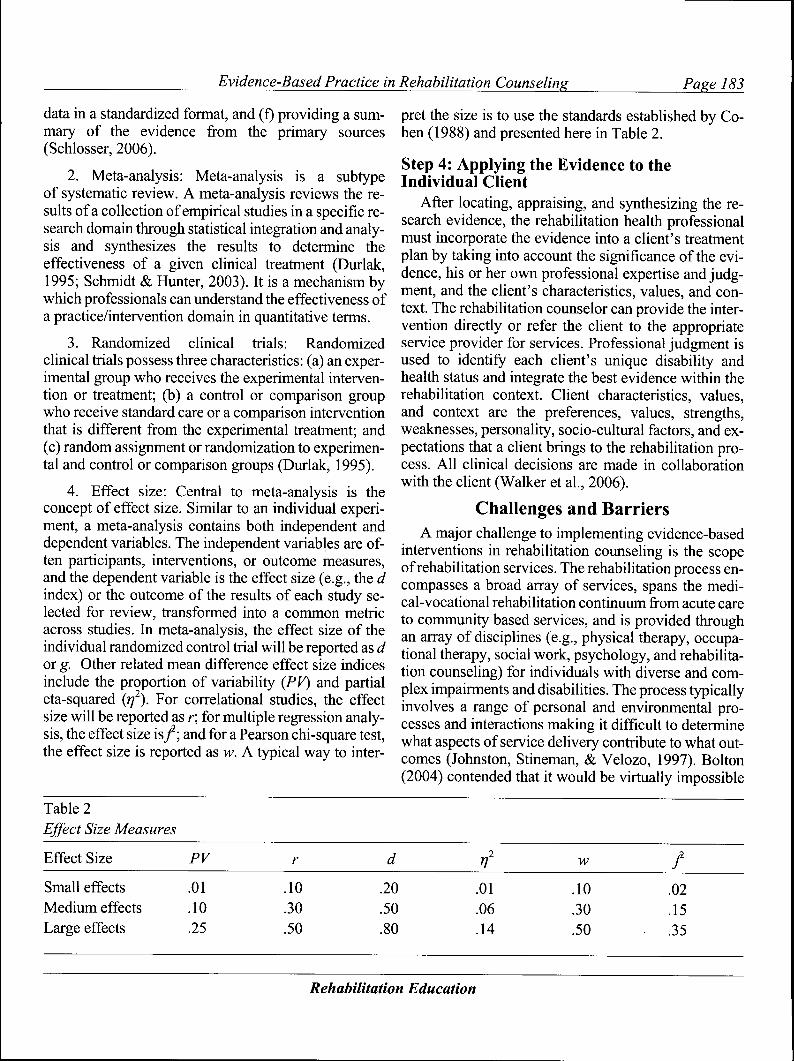
4. Effect size: Central to meta-analysis is theconcept of effect size. Similar to an individual experi-ment, a meta-analysis contains both independent anddependent variables. The independent variables are of-ten participants, interventions, or outcome measures,and the dependent variable is the effect size (e.g., the dindex) or the outcome of the results of each study se-lected for review, transformed into a common metricacross studies. In meta-analysis, the effect size of theindividual randomized control trial will be reported as dor g. Other related mean difference effect size indicesinclude the proportion of variability (PV) and partialeta-squared (rj^). For correlational studies, the effectsize will be reported as r; for multiple regression analy-sis, the effect size i s / ; and for a Pearson chi-square test,the effect size is reported as w. A typical way to inter-
pret the size is to use the standards established by Co-hen (1988) and presented here in Table 2.
Step 4: Applying the Evidence to theIndividual Client
synthesizing the re-health professional
the evidence into a client s freatmentinto account the significance of the evi-
text. The rehabilitation counselor can provide the irvention directly or refer the client to the appropriateservice provider for services. Professional judgment isused to identify each client's unique disability andhealth status and integrate the best evidence within therehabilitation context. Client characteristics, values,and context are the preferences, values, strengths,weaknesses, personality, socio-cultural factors, and ex-pectations that a client brings to the rehabilitation pro-cess. All clinical decisions are made in collaborationwith the client (Walker et al., 2006).
Challenges and BarriersA major challenge to implementing evidence-based
interventions in rehabilitation counseling is the scopeof rehabilitation services. The rehabilitation process en-compasses a broad array of services, spans the medi-cal-vocational rehabilitation continuum from acute careto community based services, and is provided through
array of disciplines (e.g., physical therapy, occupa-therapy, social work, psychology, and rehabilita-
counseling) for individuals with diverse and com-plex impairments and disabilities. The process typicallyinvolves a range of personal and environmental pro-cesses and interactions making it difficult to determinewhat aspects of service delivery contribute to what out-comes (Johnston, Stineman, & Velozo, 1997). Bolton(2004) contended that it would be virtually impossible
Table 2Effect Size Measures
Effect Size PV w
Small effectsMedium effectsLarge effects
.01
.10
.25
.10
.30
.50
.20
.50
.80
.01
.06
.14
.10
.30
.50
.02
.15
.35
Rehabilitation Education

Page 184 Chan et al.
to design and implement an experimental study to de-termine the overall effect of state vocational rehabilita-tion services because clients who are eligible for ser-vices must be served, and clients who are placed on awaiting list according to the 'order of selection' criteriaare clients with less severe disabilities and, therefore,different from clients who receive vocational rehabili-tation services immediately.
Lack of scientific rigor and sophistication is anothercommon criticism of rehabilitation counseling research(Arokiasamy, 1993). In order to effectively implementevidence-based practice, rehabilitation researchersmust provide quality evidence with a sfrong theoreticalbasis. Some professionals suggest that rehabilitation re-search is frequently non-experimental or quasi-experi-mental in nature (Bolton, 2004). As previously men-tioned, the lack of randomized confrolled trials is oftenseen as a major barrier to the successful implementationof rehabilitation counseling and psychology researchinto practice (Chwalisz & Chan, 2008). Experts outsideof the field of rehabilitation counseling suggest similarbarriers. Tannenbaum (2003) pointed out that currentevidence in the mental health field, particularly re-search of individuals with severe mental illness, maynot be satisfactory due to problems such as weak exter-nal validity and difficulty standardizing freatments.
Chan et al. (2003) suggested that the development ofcompeting models of rehabilitation counseling usingsalient and empirically supported constructs would al-low researchers to validate the effectiveness of thesemodels using a true experimental research design,which is an important indicator of research quality. Inaddition, increasing attention to the use of appropriateresearch design and statistical analysis techniques, in-cluding an emphasis on testing mediator and moderatorvariables, will further the development of model-driveninterventions for individuals with disabilities (Chwalisz& Chan, 2008). By linking model-driven interventionsto practical concems of rehabilitation counselors andthe delivery of services to people with disabilities, theapplication of evidence to practice will become increas-ingly apparent to rehabilitation practitioners and re-searchers alike.
In addition to the concem of the quality of availableevidence, rehabilitation counselors may not possess theskills necessary to evaluate and incorporate researchfindings into daily practice. According to a recent sur-vey, rehabilitation counselors agree that the application
of evidence-based practice is necessary, useful, andwill lead to improved quality of client services(Bezyak, Kubota, & Rosenthal, 2010). In addition, atti-tudes of rehabilitation counselors surveyed were posi-tive regarding interest in leaming skills needed to effec-tively incorporate evidence into rehabilitation counsel-ing practice. Despite these positive attitudes, a lack ofknowledge about evidence-based practice and insuffi-cient academic preparation has been identified by cur-rent rehabilitation counselors (Bezyak et al., 2010).
According to Bezyak et al. (2010), rehabilitationcounselors typically feel equipped to use generic searchengines in professional practice. Despite this skill,many reported receiving limited training in academicsearch strategies or strategies regarding the implemen-tation of evidence-based practice. In fact, nearly 34% ofrehabilitation counselors reported an inability to applyresearch findings to provide empirically supported in-terventions for individual clients. Survey results alsopoint to some familiarity with research-related terms,but gaps in knowledge of terminology contribute toproblems incorporating evidence into rehabilitationcounseling practice (Bezyak et al., 2010). For example,a lack of understanding of terms such as systematic re-views, randomized confrolled-trials, meta-analysis, andeffect size may easily prevent rehabilitation counselorsfrom effectively implementing empirically-based inter-ventions and techniques. Historically, it has been achallenge for educators to integrate research and prac-tice into graduate level coursework (Olson, 1996). Withan emphasis on leaming research methodology and de-scriptive and inferential statistics in graduatecoursework, students may not grasp the role of researchas clinical evidence (Foster, 2004). Clearly, to be an ef-fective evidence-based practitioner, knowledge of ba-sic concepts of research methods acquired from tradi-tional master's level rehabilitation counseling researchand statistics courses is insufficient. We must modifyour research curriculum to include a strong emphasis onevidence-based methodologies, knowledge translation,and research utilization.
Not surprisingly, insufficient time continues to bereported as a barrier to applying research evidence topractice. A recent survey of primary care physicianscited time as a major obstacle to fully implementing ev-idence-based practice (O'Donnell, 2004). Practitionersin various health professions are often required to spendat least eight hours each day providing direct service.
Rehabilitation Education

Evidence-Based Practice in Rehabilitation Counseling Page 185
and as a result, there is limited time for reviewing andleaming new evidence or implementation strategies(Corrigan, Steiner, McCracken, Blaser, & Barr, 2001).This problem extends to the field of rehabilitation coun-seling as well. An estimated 83% of respondents rankedinsufficient time as one of top three barriers to imple-menting evidence-based practice (Bezyak et al., 2010).The inability to consistently devote time to collectingnew evidence, careñilly reviewing findings, and devel-oping implementation strategies must be addressed be-fore evidence-based practice can be successfully ap-plied to all areas of rehabilitation counseling.
Winch, Henderson, and Creedy (2005) suggestedthat barriers to evidence-based practice that may also besymptoms of organizational contexts that have not beenconducive to integrate evidence into practice. A studyof occupational therapists indicated that less thanone-third of participants interviewed searched the liter-ature for research information to apply to practice(Rappolt & Tassone, 2002). The authors concluded thatany new information implemented into practice wasunsystematic and based heavily on peer consultation,rather than recent scientific eviclence. Professionals of-ten point to limited motivation and interest, poor confi-dence, negative attitudes, and limited understanding ofthe value of research as specific barriers to accessingand implementing evidence-based practice within theirorganization (Winch et al, 2005).
Other characteristics of the organizational seftingmay serve as barriers to evidence-based practice (Nel-son & Steele, 2007). For example, community mentalhealth centers may present several unique challenges tothe implementation of evidence-based practice that arenot encountered in an inpatient setting. The institutionalculture may also influence the use of evidence-basedpractice. An organization that openly acknowledgesand reviews evidence may influence practitioners to dothe same (Nelson & Steele, 2007), while a lack of atten-tion to new evidence may foster a similar trend amongcounselors. Other potentially problematic organiza-tional characteristics are a lack of knowledge to prop-erly assimilate evidence-based practice on the part ofservice providers, poor leadership, bureaucratic con-straints, and a change-averse culture (Corrigan et al,2001), as well as limited training and education of prac-titioners and limited access to evidence (Jette et al,2003; Nelson & Steele, 2007).
Difficulty evaluating current evidence in the fieldalso appears to be problematic to rehabilitation coun-selors. Although nearly all rehabilitation counselorssurveyed report reviewing academic literature, 30% ofrespondents report reviewing one or fewer articles eachmonth ft-om the professional literature, and 43% of re-habilitation counselors surveyed report using one orfewer articles in case decision making (Bezyak et al,2010). It does not appear that restricted access to re-sources is the reason for limited use of professional lit-erature. In fact, 77% of counselors indicated they hadaccess to professional joumals, and 73% of respondentsindicated access to research databases. Approximatelyhalf of all respondents reported support from their em-ploying agency in the use of evidence in daily practice(Bezyak et al, 2010). Despite this generally positive re-sponse, a large percentage of rehabilitation counselorsare not accessing and using evidence on a regular basis.The current emphasis on evidence-based practice inhealth professions including rehabilitation counselingsuggests the need for stronger support from employingagencies and higher motivation on the part of the coun-selors in order to promote the use of evidence by reha-bilitation counselors (Bruyère & Houtenville, 2006).
OpportunitiesOne of the primary goals of rehabilitation counsel-
ing is to help people with disabilities obtain and main-tain employment. However, the employment rate forindividuals with disabilities continues to be unaccept-ably low. A recent U.S. Bureau of Labor Statistics(BLS) Employment Situation report estimated the laborforce participation rate of individuals with disabilitiesto be 21.5% compared to 70.6% for people without dis-abilities (BLS, 2010). The recent recession also has adisproportionate impact on workers with disabilities,with the number of employed workers with disabilitiesdeclining at a rate more than three times that of workerswithout disabilities and the unemployment rate rising tolevels exceeding that of other workers (Kaye, 2010).These disability employment statistics also indicatedthat a large percentage of people with disabilities are nolonger looking for employment. Specifically, between1970 and 2009, the number of people receiving SocialSecurity Disability Insurance (SSDI) benefits morethan tripled, from 2.7 million to 9.7 million (Congres-sional Budget Office, 2010). Less than one percent ofindividuals on the rolls of the Disability Insurance (DI)and Supplemental Security Income (SSI) programs
Rehabilitation Education

Page 186 Chan et al.
ever resume employment (Lui et al., 2010; Roessler,2002). Without a doubt, lack of employment opportuni-ties excludes people with disabilities from full commu-nity participation, significantly affecting their qualityof life.
In order to improve the effectiveness of rehabilita-tion counseling services, Bolton and colleagues(Bolton, 1979; Bolton, Bellini, & Brookings, 2000)contend that rehabilitation outcome research needs tofocus on answering the following question: "Which ap-proach works best for whom, how, and under what con-dition?" Answering this question will provide counsel-ors with information regarding what individual charac-terisfics, environmental factors, and service provisionpattems have a high probability of predicting success-ful employment outcomes for persons with disabilities.However, little is known about what personal charac-teristics, environmental factors, and service pattemsmight contribute differentially to improve employmentrates of people with disabilities and thosesubpopulations with the lowest employment outcomes.Also, limited research has been conducted to examinethe interaction effect between individual level charac-teristics with employer practice factors on employmentoutcomes of customers (Chan, Strauser, Gervey, &Lee, 2010; Chan, Tarvydas, Blalock, Strauser, &Atkins, 2009).
Without a doubt, the consistent nature of unemploy-ment and underemployment among people with dis-abilifies cannot be reduced to only one factor (i.e., dis-ability). Vocational rehabilitation researchers andscholars have begun to recognize the need to considercontextual and environmental factors (e.g., socialstigma) in the development of efficacious and effectiveVR practice (Chan et al., 2009; Chan et al., 2010). BothNIDRR's socio-ecological model of disability (Täte &Pledger, 2003) and the World Health Organization's(WHO) Intemational Classification Functioning, Dis-ability, and Health (ICF) have underscored the impor-tance of environmental (E) factors and personal charac-teristic (P) factors and the significance ofthe P x E in-teraction effect on the full integration of individualswith disability into the community (Chan, Keegan, etal., 2009; Chan, Sasson, Ditchman, Kim, & Chiu,2009).
Recently, the ICF model has gained wide accep-tance among intemational rehabilitation health re-searchers and professionals as a framework that can be
used to support a systematic approach for understand-ing the effect of chronic illness and disability on inclu-sion and community participation across cultures, thusincreasing the available evidence for rehabilitationcounseling pracfice (Chan, Keegan, et al., 2009; Chan,Sasson, et al., 2009; Peterson & Rosenthal, 2005). TheICF is structured around three broad components: (a)body fiinctions and stmcture, (b) activities (related totasks and actions by an individual) and participation(involvement in a life situation), and (c) individual levelcharacteristics and environmental factors. Functioningand disability are viewed as a complex interaction be-tween the health condition of the individual and thecontextual factors of the environment, as well as per-sonal factors. The emphasis of the ICF is on functionrather than condition or disease and is designed to berelevant across multiple cultures as well as age, gender,and disability, making it highly appropriate for hetero-geneous populations.
Voluminous research has been generated by rehabil-itation health researchers to validate interventions thatcan be used to improve health condition, activity, andparticipation. This evidence-based practice informationis invaluable to VR counselors as they have to coordi-nate the provision of a complex web of medical, voca-tional, educational, and psychosocial services for theircustomers. Importantly, the ICF model is consistentwith the holistic philosophy of VR, and it holds signifi-cant promise as a rehabilitation model that can be usedto conceptualize VR assessment, planning, and inter-vention for improving employment outcomes and qual-ity of life of people with disabilities (Chan, Tarvydas, etal., 2009). A comprehensive taxonomy of outcomemeasures can be organized around the major constructsof the ICF to assess the effectiveness of different ser-vice providers in the rehabilitation process. The agendaof VR researchers should therefore focus on conductingsystematic research to validate relationships amongconstmcts in the ICF model and how these constructsuniquely contribute and interact with each other to af-fect full inclusion and participation of people with dis-abilities in the community as well as employment,health condition, and quality of life (Chan, Keegan, etal., 2009). This type of research agenda will signifi-cantly contribute to the availability of best evidence,which will influence rehabilitation counseling practice.Specifically, randomized controlled trials conducted tovalidate ICF-guided interventions can be used to im-
Rehabilitation Education
Evidence-Based Practice in Rehabilitation Counseling Page 187
prove flmctioning, increase activity levels, maximizeindividual strengths, modify the environment (e.g., em-ployer attitudes), encourage full participation in thecommunity, promote health and mental health well-be-ing, and increase employment opportunities for peoplewith disabilities, especially those from subpopulationswith lowest employment outcomes.
Another societal trend particularly relevant to effec-tive VR service delivery practice is the rapidly changingcomposition of the U.S. population. The Census Bureauprojects that the European American population will fallnom 81% of the population in 2000 to 52% of the popu-lation in 2050 (Shrestha, 2006). Conversely, the popula-tion of Hispanic or Latino origin will rise nom 12.6% in2000 to 24.4% in 2050. Asian Americans will also expe-rience a dramatic growth nom 3.8% in 2000 to 8% in2050. The African American population will rise nom12.7% in 2000 to 14.6% in 2050, while American In-dian, Eskimo, and Aleut will represent 1% of the popula-tion in 2050. The changing demographic makeup of theUnited States has prompted many health care researchersto question the traditional assumption that treatmentsthat work for persons of European American descentwill work for individuals from racial and ethnic minoritygroups. For the rehabilitation community, awareness ofthe effects of personal characteristics that identify a per-son as different, how one sees oneself, and how otherssee and react to this individual have long been recog-nized as central to the experience of disability and issuesthat clients bring to the rehabilitation counselor (Chan,Tarvydas, et al. 2009). Research on psychosocial aspectsof disability has also explored the powerful effects ofdisability as another aspect of human experience affect-ing psychosocial and vocational service outcomes. As aresult, researchers are becoming more interested in test-ing moderator effects in VR research, which will furtherpromote the use of evidence-based practice in the field.
Research questions involving moderators addresswhen or for whom a variable most strongly predicts orcauses an outcome variable, whereas mediators estab-lish how or why one variable predicts or causes an out-come variable (Frazier, Tix, & Barron, 2004). A media-tor provides information about the underlying mecha-nisms for change, whereas a moderator effect isbasically an interaction whereby the effect of an inde-pendent variable (e.g., treatment) differs at differentlevels of another independent variable (e.g., severity).Similar to health care research, the study of moderator
effects in VR research is important, as what works forEuropean American clients may not work for individu-als fi-om diverse racial and ethnic minority back-grounds; what works for men may not work for women;and what works for individuals with sensory impair-ments may not work for persons with psychiatric dis-abilities (Chan, Tarvydas, et al., 2009).
Similarly, moderators are extremely important inother key areas of VR research. For example, in study-ing the role of resiliency factors in adjustment to dis-ability, future research can examine whether the adjust-ment process is similar or different for persons withsudden onset versus chronic conditions. Therefore, it isvery important for VR researchers to expend more re-search efforts to test moderator effects of race, gender,disability type, health status, and immunity (e.g., socialsupport, coping skills, and resilience) and vulnerabilityfactors (e.g., stress). For theory or model building, it isequally important to study the mediator effect (i.e., theunderlying mechanisms of change) in order to betterdesign effective interventions (Hoyt, Imel, & Chan,2008). An increased emphasis on testing mediator andmoderator variables in the VR research paradigm isneeded in order to develop effective model-driven, cul-turally sensitive and evidence-based VR interventionsfor individuals with disabilities in the 21st century(Chan, Tarvydas, et al., 2009).
Incorporating research-based knowledge into VRpractice, to assure that people with disabilities receiveempirically validated assessment, intervention, andconsultation services, is particularly relevant in today'sera of accountability, research utilization, and evi-dence-based practice (Chan et al., 2008; Chronister etal., 2008; Law, 2002). As a conceptual framework orphilosophy, evidence-based practice advocates that ev-ery rehabilitation and health professional should havean interest in delivering the best possible services totheir customers, based whenever possible on the bestclinical practices available nom the strongest researchevidence. Vocational rehabilitation researchers andpractitioners must develop a strong focus on theory de-velopment, empirical evidence, and clinical applica-tion. Within the context of evidence-based practice,Dunn and Elliott (2008) argue for the primacy of theoryand its place in rehabilitation research. Advocacy forthe development of theory-driven research programsthat embrace methodological pluralism will advance
Rehabilitation Education

Page 188 Chan et al.
new theory and produce meaningful research programsthat inform practice in VR service delivery.
ReferencesArokiasamy, C. V. (1993). A theory of rehabilitation?
Rehabilitation Education, 7, 77-98.Bezyak, J. L., Kubota, C, & Rosenthal, D. (2010). Ev-
idence-based practice in rehabilitation counseling:Perceptions and practices. Rehabilitation Educa-tion, 24, 85-96.
Bolton, B. (2004). Counseling and rehabilitation out-comes. In F. Chan, N. L. Berven, & K. R. Thomas(Eds.), Counseling theories and techniques for re-habilitation professionals (pp. 444—465). NewYork: Springer.
Bolton, B. (1979). Rehabilitation counseling re-search. Baltimore, MD: University Park Press.
Bolton, B. F., Bellini, J. L., & Brookings, J. B. (2000).Predicting client employment outcomes from per-sonal history, functional limitations, and rehabilita-tion services. Rehabilitation Counseling Bulletin,44, 10-21.
Bmyere, S. M. & Houtenville, A. J. (2006). Use of sta-tistics from national data sources to inform rehabil-itation program planning, evaluation, andadvocacy. Rehabilitation Counseling Bulletin, 50,46-58.
Chan, F., Strauser, D., Gervey, R., & Lee, E. J. (2010).Introduction to demand-side factors related to em-ployment of people with chronic illness and dis-ability. Journal of Occupational Rehabilitation,20, 407-411. doi 10.1007/s 10926-010-9243-7
Chan, F., Keegan, J., Sung, C , Drout, M., Pai, C. H.,Anderson, E., & McLain, N. (2009). The WorldHealth Organization ICF model as a framework forassessing vocational rehabilitation outcomes.Journal of Rehabilitation Administration, 33,91-112.
Chan, F., Sasson, J., Ditchman, N., Kim, J. H., & Chiu,C. Y. (2009). The World Health Organization ICFmodel as a conceptual framework of disability. InF. Chan, E. Cardoso, & J. Chronister (Eds.),Psychosocial interventions for people with chronicillness and disability: A handbook for evi-dence-based rehabilitation health professionals(pp. 23-74). New York: Springer.
Chan, F., Tarvydas, V., Blalock, K., Strauser, D., &Atkins, B. J. (2009). Unifying and elevating reha-bilitation counseling through model-driven, diver-si ty-sensit ive evidence-based pract ice.Rehabilitation Counseling Bulletin, 52, 114-119.
Chan, F., Rosenthal, D. A., «fe Pmett, S. (2008). Evi-dence-based practices in the provision of rehabili-tation services. Journal of Rehabilitation, 74(2),1-5.
Chan, F., Leahy, M. J., Saunders, J. L., Tarvydas, V.M., Ferrin, J. M., & Lee, G. (2003). Training needsof certified rehabilitation counselors for contempo-rary practice. Rehabilitation Counseling Bulletin,46(2), 82-91.
Chan, F., Miller, S., Pmett, S., Lee, G., & Chou, C.(2003). Research. In D. Maki & T. Riggar (Eds.),Handbook of Rehabilitation Counseling (pp.159-170). New York: Springer.
Chronister, J. A., Chan, F., Cardoso, E., Lynch, R. T.,& Rosenthal, D. A. (2008). The evidence-basedpractice movement in healthcare: Implications forrehabilitation. Journal of Rehabilitation, 74(2),6-15.
Chwalisz, K. (2003). Evidence-based practice: Aframework for the twenty-first century scien-tist-practitioner training. The Counseling Psychol-ogist, 31, 497-528.
Chwalisz, K., & Chan, F. (2008). Methodological ad-vances and issues in rehabilitation psychology:Moving forward on the cutting edge. Rehabilita-tion Psychology, 53, 251-253.
Cohen, J. (1988). Statistical power analysis for the be-havioral sciences (2nd ed.). Hillsdale, NJ: Law-rence Erlbaum Associates.
Congressional Budget Office (2010, July). Social Se-curity Disability Insurance: Participation trendsand their fiscal implications. Economic and BudgetIssue Brief, 1-8.
Corrigan, P. W., Steiner, L., McCracken, S. G.,Blaser, B., & Barr, M. (2001). Strategies for dis-seminating evidence-based practices to staff whotreat people with serious mental illness. Psychiat-ric Services, 52, 1598-1606.
DePalma, J. A. (2002). Proposing an evidence-basedpolicy process. Nursing Administration Quarterly,26(4), 55-61.
Dunn, D. S., & Elliott, T. R. (2008). The place andpromise of theory in rehabilitation psychology. Re-habilitation Psychology, 53, 254-267.
Durlak, J. A. (1995). School-based prevention pro-grams for children and adolescents. ThousandOaks, CA: Sage.
Evidence-Based Medicine Working Group (1992).Evidence-based medicine. A new approach toteaching the practice of medicine. Journal ofAmer-
Rehabilitation Education

Evidence-Based Practice in Rehabilitation Counseling Page 189
ican Medical Association, 268, 2420-2425.doi: 10.1001/jama.268.17.2420.PMID 1404801.
Foster, R. L. (2004). Challenges in teaching evi-dence-based practice. Journal for Specialists in Pe-diatric Nursing, 9, 75-76.
Frazier, P. A., Tix, A. P., & Barron, K. E. (2004). Test-ing moderator and mediator effects in counselingpsychology research. Journal of Counseling Psy-chology, 51, 115-134.
Guyatt, G. (1991). Evidence-based medicine. ACPJournal Club, 7;4(Suppl 2), A16.
Holm, M. B. (2000). Our mandate for the new millen-nium: Evidence-based practice. American Journalof Occupational Therapy, 54, 575-585.
Hoyt, W., Imel, S. E., & Chan, F. (2008). Regressionand correlation techniques: Recent controversiesand best practices. Rehabilitation Psychology, 53,321-339.
Schmidt, F. L., & Hunter, J. E. (2003). Meta-analysis.In J. A. Schinka & W. F. Velicer (Eds.), Handbookof psychology (Vol. 2): Research methods in psy-chology (pp. 533-554). New York: John Wiley andSons.
Jette, D. U., Bacon, K., Batty, C , Carlson, M.,Ferland, A., Hemingway, R. D., . . . Volk, D.(2003). Evidence-based practice: Beliefs, attitudes,knowledge, and behaviors of physical therapists.Physical Therapy, 83, 786-805
Johnston, M. V., Stineman, M., & Velozo, C. A.(1997). Outcome research in medical rehabilita-tion. Foundations from the past and directions forthe future. In M.J. Fuhrer (Ed.). Assessing medicalrehabilitation practices. The promise of outcomesresearch. Baltimore: Paul H. Brookes.
Kaye, H. S. (March, 1998). Vocational rehabilitationin the United States. Disability Statistics Abstract,20, 1-4.
Law, M. (2002). Evidence-based rehabilitation: Aguide to practice. Thorofare, NJ: SLACK.
Lui, J., Chan, F., Fried, J., Lin, C.P., Anderson, C, &Peterson, M. (2010). Roles and ftinctions of" bene-fits counseling specialists: A multi-frait analysis.
. Journal of Vocational Rehabilitation, 32,163-173.Meehl, P. E. (1954). Clinical vs. statistical prediction.
Minneapolis: University of Minnesota Press.Montori, V.M., & Guyatt, G. H. (2008). Progress in
evidence-based medicine. X4M4, 300,1814-1816.Nathan, P. E., & Gorman, J. M. (1998). A guide to
treatments that work. New York: Oxford Univer-sity Press.
Nelson, T. D. & Steele, R. G. (2007). Predictors ofpractitioner self-reported use of evidence-basedpractices: Practitioner fraining, clinical setting, andattitudes toward research. Administration and Pol-icy in Mental Health and Mental Health ServicesResearch, 54,319-330.
O'Donnell, C. A. (2004). Attitudes and knowledge ofprimary care professionals towards evidence-basedpractice: A postal survey. Journal of Evaluation inClinical Practice, 10, 197-205.
Olson, E. A. (1996). Evidence-based practice: A newapproach to teaching the integration of researchand practice in gerontology. Educational Geron-tology, 22, 523-537.
Ottenbacher, K. J., & Maas, F. (1999). How to detecteffects: Statistical power and evidence-based prac-tice in occupational therapy research. AmericanJournal of Occupational Therapy, 40, 181-188.
Peterson, D., & Rosenthal, D. (2005). The intema-tional classification of functioning, disability, andhealth: A primer for rehabilitation educators. Reha-bilitation Education, 19, 81-94.
Pmett, S., Swett, E., Chan, F., Rosenthal, D., & Lee,G. (2008). Empirical evidence supporting the ef-fectiveness of vocational rehabilitation services.Journal of Rehabilitation, 74(2), 56-63.
Rappolt, S., & Tassone, M. (2002). How rehabilitationtherapists gather, evaluate, and implement newknowledge. Journal of Continuing Education inHealth Professions, 22, 170-180.
Roessler, R. (2002). TWWIIA initiatives and work in-centives: Retum to work implications. Journal ofRehabilitation, 68(3), 11-16.
Rubin, S. E., Chan, F., Thomas, D. (2003). Assessingchanges in life skills and quality of life resultingfrom rehabilitation services. Journal of Rehabilita-tion, 69(3), 4-9.
Sackett, D. L, Rosenberg, W. M. C, Gray, J. A. M.,Haynes, R. B., & Richardson, W. S. (1996). Evi-dence-based medicine: What it is and what it is not.British Medical Journal, 312, 71-72.
Schlosser, R. W. (2006). The role of systematic re-views in evidence-based practice, research, and de-velopment. Focus, 15, 1-4.
Shrestha, L. B. (2006). The changing demographicprofile of the United States (CRS Report RL32701). Washington, DC: Congressional R.esearchService.
Rehabilitation Education
Page 190 Chan et al.
Täte, D. G., & Pledger, C. (2003). An integrative con-ceptual framework of disability. American Psy-chologist, 58, 289-295.
Tannenbaum, S. (2003). Evidence-based practice inmental health: Practical weaknesses meet politicalstrengths. Journal of Evaluation in Clinical Prac-tice, 9,2^1-3,01.
Thirty-Third Institute on Rehabilitation Issues (2008).Evidence based practices: Improving employmentoutcomes for people with significant disabilities.Hot Springs, AK: University of Arkansas Rehabili-tation Continuing Education Center.
Tucker, J. A., & Reed, G. M. (2008). Evidentiary plu-ralism as a strategy for research and evi-dence-based practice in rehabilitation psychology.Rehabilitation Psychology, 53, 279-293.
U.S. Department of Labor Bureau of Labor Statistics(2010). The employment situation-July 2010. Re-trieved August 11, 2010, from http://www.bls.gov/news.release/pdf/empsit.pdf
U.S. Govemment Accountability Office (2005). Vo-cational Rehabilitation-Better measures and mon-itoring could improve the performance of the VRProgram (GAO-05-865). Washington, DC: Au-thor.
Walker, B. B., Seay, S. J., Solomon, A. C, & Spring,B. (2006). Treating chronic migraine headache: Anevidence-based practice approach. Journal of Clin-ical Psychology: In Session, 62, 1367-1378.
Wampold, B. E. (1997). Methodological problems inidentifying efficacious psychotherapies. Psycho-therapy Research, 7,21-43.
Winch, S., Henderson, A., & Creedy, D. (2005). Read,think, do!: A method fbr fitting research evidenceinto practice. Journal of Advanced Nursing Prac-tice, 50, 20-26.
Author NotesCorrespondence pertaining to this article should be
directed to Fong Chan, Co-Director of the Rehabilita-tion Research and Training Center on Effective Voca-tional Rehabilitation Service Delivery Practices, De-partment of Rehabilitation Psychology and Special Ed-ucation, University of Wisconsin-Madison, 403Education Building, 1000 Bascom Mall, Madison, WI53706. Email at [email protected]
The contents of this article were developed withsupport through the Rehabilitation Research andTraining Center on Effective Vocational RehabilitationService Delivery Practices (EBP-VR-RRTC) estab-
lished at both the University of Wisconsin-Madisonand the University of Wisconsin-Stout under a grantfrom the Department of Education, National Instituteon Disability and Rehabilitation Research (NIDRR)grant number PR# H133B100034. However, these con-tents do not necessarily represent the policy of the De-partment of Education, and endorsement by the FederalGovernment should not be assumed.
Rehabilitation Education

Copyright of Rehabilitation Education is the property of Elliott & Fitzpatrick, Inc. and its content may not be
copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.