
Computed tomographic cholangiography using spiral scanning and 3D image processing
6
1993, The British Journal of Radiology, 66, 762-767 Computed tomographic cholangiography using spiral scanning and 3D image processing 1 H-M KLEIN, 1 B WEIN, 2 S TRUONG, 2 F-P PFINGSTEN and 1 R W GUNTHER Departments of diagnostic Radiology and 2 Surgery, University of Technology Medical School, D-5100, Germany Abstract Volumetric computed tomography (CT) scans ("spiral CT") were performed after intravenous (i.v.) cholan- giography followed by additional 3D surface reconstructions of gallbladder and biliary ducts. 34 patients were investigated prior to cholecystectomy. No allergic adverse reactions were observed. The scan time was 24 s. Contrast enhancement in the extrahepatic bile duct and gallbladder were measured. All CT image series were reviewed independently by four experienced physicians (two radiologists, two surgeons) and compared for quality with conventional cholangiography on a three-point scale. The average rating for the demonstra- tion of the biliary tract was significantly better for spiral CT than for conventional cholangiography (p < 0.01). In all cases sufficient contrast was found in the common bile duct (mean 315 HU). 3D imaging was considered to be helpful for intraoperative orientation during laparoscopic surgery. Cholangiography prior to hepatobiliary surgery is important, particularly if minimally invasive laparo- scopic techniques are used. The most important ques- tions for the radiologist concern: (1) obstructions or calculi in the ductal system and the gallbladder; (2) the anatomy of the right hepatic duct and the cystic duct (Gotz et al, 1991). To answer these questions, intra- venous cholangiography employing conventional tomo- graphy is usually performed. The quality of the examination can be diminished by superposition of faeces or gas and small intraductal calculi may be invisible. An alternative to cholangiography for the detection of small intraductal calculi is ERCP (endoscopic retro- grade cholangiopancreatogram) which is a reliable but invasive method involving discomfort for the patient (Neuhaus et al, 1992). Single-breathhold volumetric spiral CT provides a complete registration of the upper abdomen in one 24 s scan, resulting in the acquisition of a contiguous series of CT images without respiratory artefacts (Vock et al, 1989, 1990; Kalender et al, 1990; Kalender & Polacin, 1991). The aim of this study was to assess this new method when compared with conventional cholangiography. Patients and method During a 5 month period (January-May 1992) 34 patients (age range 29-72 years, average 41 years) Received 23 October 1992 and in revised form 20 January 1993, accepted 15 March 1993. Address correspondence to Dr med. Hans-Martin Klein, Klinik fur Radiologische Diagnostik, Klinikum der RWTH Aachen, D-5100 Aachen, Germany. underwent i.v. cholangiography in the course of the pre- operative work-up for laparoscopic cholecystectomy. After an initial plain image of the right upper abdomen, 19 g iotroxindimeglumine (Schering, Germany) was infused slowly (>10min) through a cubital vein. Post-contrast images were obtained 30, 60 and 120 min after the start of the infusion (Figure la). If imaging of the biliary ducts was insufficient, conventional tomo- graphy was performed 30-60 min post-injection (13 patients). During transfer to the CT unit, the patients were placed in LAO position in order to delay emptying of the biliary ducts. For the spiral CT, we used a Somatom Plus (Siemens Medical Systems, Erlangen) allowing up to 24 con- tinuous 1 s rotations. The spiral CT was carried out 30-120 min post-injection. Table feed was 5 mm s" 1 for a 24 s scan, resulting in a total volume thickness of 11.5 cm, since the first and last images of the helical scan cannot be used for image reconstruction (Gotz et al, 1991). Slice thickness was 5 mm with an interslice incre- ment of 2 mm. Tube voltage was 137 kV at a current of 145 mA. Back-projection of the raw data was performed with standard resolution algorithm. The window width was adjusted to 512 HU and the centre at 65 HU (Figure lb). For 3D surface reconstructions, the contrast- containing areas of the biliary system and the surrounding bony structures were extracted using a threshold of 130 HU. Surface presentations were obtained in six standard views (top, bottom, front, back, left, right) and additional views oriented for the estim- ated viewing position of the surgeon. The reconstruc- tion matrix was 512 3 voxel (Figure lc). All reconstruction and rendering procedures were per- formed using the integrated 3D software of the CT system. 762 The British Journal of Radiology, September 1993
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Computed tomographic cholangiography using spiral scanning and 3D image processing

1993, The British Journal of Radiology, 66, 762-767
Computed tomographic cholangiography using spiralscanning and 3D image processing
1H-M KLEIN, 1B WEIN, 2S TRUONG, 2F-P PFINGSTEN and 1R W GUNTHER
Departments of diagnostic Radiology and 2Surgery, University of Technology Medical School, D-5100,Germany
AbstractVolumetric computed tomography (CT) scans ("spiral CT") were performed after intravenous (i.v.) cholan-giography followed by additional 3D surface reconstructions of gallbladder and biliary ducts. 34 patientswere investigated prior to cholecystectomy. No allergic adverse reactions were observed. The scan time was24 s. Contrast enhancement in the extrahepatic bile duct and gallbladder were measured. All CT image serieswere reviewed independently by four experienced physicians (two radiologists, two surgeons) and comparedfor quality with conventional cholangiography on a three-point scale. The average rating for the demonstra-tion of the biliary tract was significantly better for spiral CT than for conventional cholangiography(p < 0.01). In all cases sufficient contrast was found in the common bile duct (mean 315 HU). 3D imaging wasconsidered to be helpful for intraoperative orientation during laparoscopic surgery.
Cholangiography prior to hepatobiliary surgery isimportant, particularly if minimally invasive laparo-scopic techniques are used. The most important ques-tions for the radiologist concern: (1) obstructions orcalculi in the ductal system and the gallbladder; (2) theanatomy of the right hepatic duct and the cystic duct(Gotz et al, 1991). To answer these questions, intra-venous cholangiography employing conventional tomo-graphy is usually performed. The quality of theexamination can be diminished by superposition offaeces or gas and small intraductal calculi may beinvisible.
An alternative to cholangiography for the detectionof small intraductal calculi is ERCP (endoscopic retro-grade cholangiopancreatogram) which is a reliable butinvasive method involving discomfort for the patient(Neuhaus et al, 1992). Single-breathhold volumetricspiral CT provides a complete registration of the upperabdomen in one 24 s scan, resulting in the acquisition ofa contiguous series of CT images without respiratoryartefacts (Vock et al, 1989, 1990; Kalender et al, 1990;Kalender & Polacin, 1991).
The aim of this study was to assess this new methodwhen compared with conventional cholangiography.
Patients and methodDuring a 5 month period (January-May 1992) 34
patients (age range 29-72 years, average 41 years)
Received 23 October 1992 and in revised form 20 January1993, accepted 15 March 1993.
Address correspondence to Dr med. Hans-MartinKlein, Klinik fur Radiologische Diagnostik, Klinikumder RWTH Aachen, D-5100 Aachen, Germany.
underwent i.v. cholangiography in the course of the pre-operative work-up for laparoscopic cholecystectomy.After an initial plain image of the right upper abdomen,19 g iotroxindimeglumine (Schering, Germany) wasinfused slowly (>10min) through a cubital vein.Post-contrast images were obtained 30, 60 and 120 minafter the start of the infusion (Figure la). If imaging ofthe biliary ducts was insufficient, conventional tomo-graphy was performed 30-60 min post-injection (13patients). During transfer to the CT unit, the patientswere placed in LAO position in order to delay emptyingof the biliary ducts.
For the spiral CT, we used a Somatom Plus (SiemensMedical Systems, Erlangen) allowing up to 24 con-tinuous 1 s rotations. The spiral CT was carried out30-120 min post-injection. Table feed was 5 mm s"1 fora 24 s scan, resulting in a total volume thickness of11.5 cm, since the first and last images of the helical scancannot be used for image reconstruction (Gotz et al,1991). Slice thickness was 5 mm with an interslice incre-ment of 2 mm. Tube voltage was 137 kV at a current of145 mA. Back-projection of the raw data was performedwith standard resolution algorithm. The window widthwas adjusted to 512 HU and the centre at 65 HU(Figure lb).
For 3D surface reconstructions, the contrast-containing areas of the biliary system and thesurrounding bony structures were extracted using athreshold of 130 HU. Surface presentations wereobtained in six standard views (top, bottom, front, back,left, right) and additional views oriented for the estim-ated viewing position of the surgeon. The reconstruc-tion matrix was 5123 voxel (Figure lc). Allreconstruction and rendering procedures were per-formed using the integrated 3D software of the CTsystem.
762 The British Journal of Radiology, September 1993

CT cholangiography using spiral CT
Figure 1. (a) Conventional image of gallbladder and bile ducts, (b) The axial spiral CT scan shows the cystic duct orifice (largecurved arrow) at the dorsal circumference of the common bile duct. Small arrow = intrahepatic bile duct, (c) 3D surfacereconstruction, frontal view. Impression on the caudal gall bladder by intestinal structures (arrow).
Contrast enhancement was measured in the commonbile ducts and gallbladders. The time interval betweenthe start of the infusion and the start of CT wasrecorded. CT and conventional images of each patientwere reviewed independently by two radiologists andtwo surgeons, who assessed the intra- and extrahepaticbile ducts, the cystic duct and gallbladder. Criteria werethe completeness of visualization and the diagnosticreliability relating to intraductal pathology. Reviewerswere blinded to the patient data. A quality rating wasemployed using a three-point scale (1 — good, 3 =poor). Average quality values and standard deviation(SD) were calculated. Statistical significance for thedifference between the quality ratings of each modalitywas tested using Wilcoxon sign-rank test (p < 0.01).
Density measurements in the common bile duct werecorrelated with the delay time between infusion and CTimaging and quality of visualization of the cystic duct.
ResultsAll patients suffered from cholelithiasis. In two
patients, the cystic duct was occluded by stones(Figure 2a) and these could be seen on axial CT images.In one of these patients, the calculus was calcified andcould be seen on conventional radiographs. In one case,we found a calculus with a diameter of 4 mm in thecommon bile duct, delineated as a hypodense structurein the contrast column. This stone could also be seen inthe cholangiographic projection image. Surgery revealeda true maximum diameter of 6 mm (Figure 2b).
Vol. 66, No. 789 763

H-M Klein, B Wein, S Truong et al
Figure 2. (a) Calculus in the cystic duct. The axial CT image shows the non-calcified stone (C) in the proximal part of the cysticduct (white arrow). Conventional images only demonstrated absent opacification of the gallbladder, (b) Intraductal non-calcified stone (arrow) in the distal common bile duct.
Additional findings on CT were cortical renal cysts intwo patients and focal liver lesions in another two cases.In these patients, additional dynamic CT confirmedsmall haemangiomas between 1.5 and 2.0 cm in size.
All the examinations were completed and none of thepatients reported discomfort during the scan associatedwith the 24 s breatholding. No adverse reactions to thei.v. cholangiographic medium were observed.
Additional 3D surface reconstruction was performedin order to facilitate intraoperative orientation. 3Ddemonstration of the cystic duct orifice was consideredto be important and helpful in 54% (14/26) of cases andthe stones were shown in 73% (19/26) (Figure 3). In onecase, the retroperitoneal duodenal loop was demon-strated (Figure 4). In one case, a questionable aberrantcystic duct orifice suggested by conventional cholangio-graphy was shown to be normal by 3D reconstruction,and later confirmed at surgery (Figure 5). 3D surfacereconstruction of the biliary tree took an average addi-tional operator time of 15 min.
The quality of imaging by conventional methods andaxial CT of the intrahepatic and common bile ducts wasequal (1.1; SD 0.3). For demonstration of the cysticduct, axial CT was superior (1.6; SD 0.8) to conven-tional cholangiography (2.2; SD 0.8). The quality of thecystic duct was rated 2 or better in 80% (20/26) of CTimages and 50% (13/26) of conventional images.Evaluation of the gallbladder was considered to bebetter on axial CT (1.2; SD 0.5) than on projectionimages (1.8; SD 1.0). Overall quality was 1.4 for axialCT and 1.7 for conventional cholangiography(Figure 6). The superiority of axial CT to conventional
cholangiography in imaging selected structures wasstatistically significant (p < 0.01). For all structuresexcept the gallbladder the quality score was worst for3D reconstructed pseudo-surface images. Nevertheless,the surgeons appreciated the spatial display of thebiliary tree structures, which subjectively improved theirimpression of the anatomy.
Mean opacification of the common bile duct was315 HU (SD 101 HU) and of the gallbladder 278 HU(SD 152 HU). Optimum images were obtained between30 and 60 min after the start of infusion. Even 110 minafter infusion, a value of 300 HU could be seen in thecommon bile duct. Correlation was found betweencontrast enhancement in the common bile duct and thequality of the cystic duct visualization (r — —0.56,p<0.002) (Figure 7). If imaging was performed less than
Figure 3. Cholecystolithiasis. G = gallbladder with fillingdefects due to calculi, C = common bile duct, D = duodenum.
764 The British Journal of Radiology, September 1993

CT cholangiography using spiral CT
Figure 4. Occlusion of the cystic duct. White arrow = calculus,L = left hepatic duct, R = right hepatic duct, D = duodenemwith anatomical variation (retroperitoneal loop), S = reflux ofcontrast medium in the stomach (antrum).
30min after the commencement of contrast infusion,opacification was poor. Optimum results were achieved35-60 min after injection. If only examinations with a
Figure 5. Demonstration of normal configuration of cystic ductorifice (white arrow). Filling defects in the gallbladder due tostones (curved arrow).
Score
Intrahep.ducts Extrahep.ducU Cystic duct Gall bladder
18plr«l-CT (2D) I Cholangiography E H 8plr«l-CT (3D)
Figure 6. Qualitative results. Average quality (1 = good, 3 =poor) in demonstration of the biliary tract in conventionalcholangiography, 2D, spiral CT and 3D reconstruction.
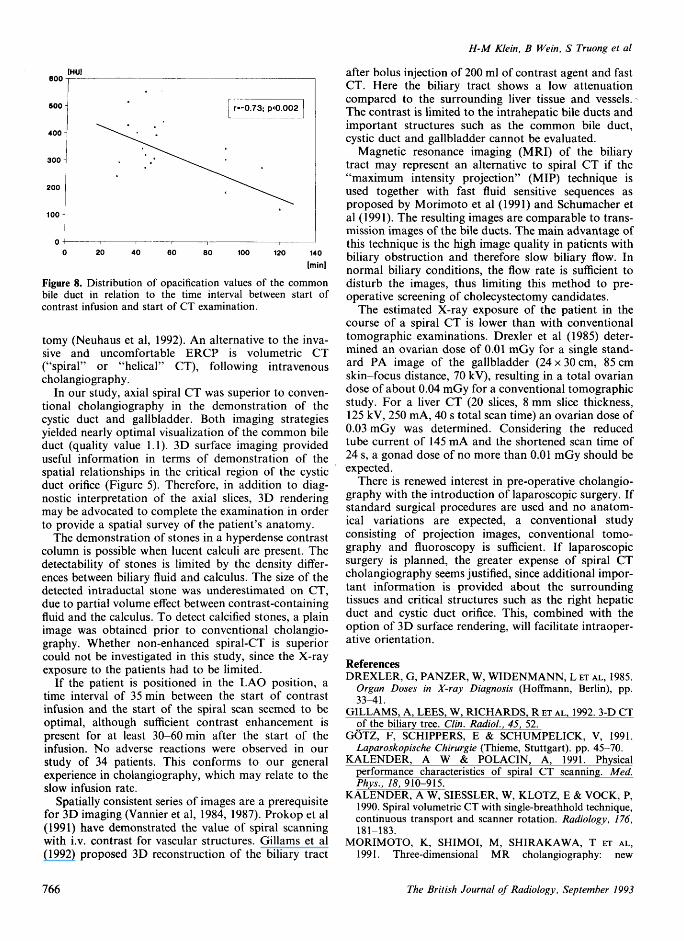
delay greater than 35 min were considered, a positivecorrelation between scan delay and opacification of thecommon bile duct was found (r = —0.73; p< 0.002)(Figure 8).
The scanning range of the spiral scan was sufficient todemonstrate the complete biliary tract from the level ofthe hepatic vein orifice to the caudal pole of the gall-bladder. The limiting parameter was the maximal scantime of 24 s.
DiscussionNew methods of laparoscopic biliary surgery require
accurate pre-operative evaluation, since the flexibilityfor intraoperative changes in the surgical strategy islimited. The decision between laparoscopic and conven-tional cholecystectomy depends on the pre-operativedetection of intraductal stones and possible associatedadditional abnormalities not only in the ductal systembut also in the adjacent upper abdominal organs (Gotzet al, 1991). Therefore preoperative ERCP has beenadvocated in candidates for laparoscopic cholecystec-
IHUl
300
r-0.56; p<0.002
1 2 3 CT score
Figure 7. Quality of visualization of the cystic duct in the axialCT images related to intensity in the common bile duct.
Vol. 66, No. 789 765
H-M Klein, B Wein, S Truong et al
[HUJ
Figure 8. Distribution of opacification values of the commonbile duct in relation to the time interval between start ofcontrast infusion and start of CT examination.
tomy (Neuhaus et al, 1992). An alternative to the inva-sive and uncomfortable ERCP is volumetric CT("spiral" or "helical" CT), following intravenouscholangiography.
In our study, axial spiral CT was superior to conven-tional cholangiography in the demonstration of thecystic duct and gallbladder. Both imaging strategiesyielded nearly optimal visualization of the common bileduct (quality value 1.1). 3D surface imaging provideduseful information in terms of demonstration of thespatial relationships in the critical region of the cysticduct orifice (Figure 5). Therefore, in addition to diag-nostic interpretation of the axial slices, 3D renderingmay be advocated to complete the examination in orderto provide a spatial survey of the patient's anatomy.
The demonstration of stones in a hyperdense contrastcolumn is possible when lucent calculi are present. Thedetectability of stones is limited by the density differ-ences between biliary fluid and calculus. The size of thedetected intraductal stone was underestimated on CT,due to partial volume effect between contrast-containingfluid and the calculus. To detect calcified stones, a plainimage was obtained prior to conventional cholangio-graphy. Whether non-enhanced spiral-CT is superiorcould not be investigated in this study, since the X-rayexposure to the patients had to be limited.
If the patient is positioned in the LAO position, atime interval of 35 min between the start of contrastinfusion and the start of the spiral scan seemed to beoptimal, although sufficient contrast enhancement ispresent for at least 30-60 min after the start of theinfusion. No adverse reactions were observed in ourstudy of 34 patients. This conforms to our generalexperience in cholangiography, which may relate to theslow infusion rate.
Spatially consistent series of images are a prerequisitefor 3D imaging (Vannier et al, 1984, 1987). Prokop et al(1991) have demonstrated the value of spiral scanningwith i.v. contrast for vascular structures. Gillams et al(1992) proposed 3D reconstruction of the biliary tract
after bolus injection of 200 ml of contrast agent and fastCT. Here the biliary tract shows a low attenuationcompared to the surrounding liver tissue and vessels.The contrast is limited to the intrahepatic bile ducts andimportant structures such as the common bile duct,cystic duct and gallbladder cannot be evaluated.
Magnetic resonance imaging (MRI) of the biliarytract may represent an alternative to spiral CT if the"maximum intensity projection" (MIP) technique isused together with fast fluid sensitive sequences asproposed by Morimoto et al (1991) and Schumacher etal (1991). The resulting images are comparable to trans-mission images of the bile ducts. The main advantage ofthis technique is the high image quality in patients withbiliary obstruction and therefore slow biliary flow. Innormal biliary conditions, the flow rate is sufficient todisturb the images, thus limiting this method to pre-operative screening of cholecystectomy candidates.
The estimated X-ray exposure of the patient in thecourse of a spiral CT is lower than with conventionaltomographic examinations. Drexler et al (1985) deter-mined an ovarian dose of 0.01 mGy for a single stand-ard PA image of the gallbladder (24 x 30 cm, 85 cmskin-focus distance, 70 kV), resulting in a total ovariandose of about 0.04 mGy for a conventional tomographicstudy. For a liver CT (20 slices, 8 mm slice thickness,125 kV, 250 mA, 40 s total scan time) an ovarian dose of0.03 mGy was determined. Considering the reducedtube current of 145 mA and the shortened scan time of24 s, a gonad dose of no more than 0.01 mGy should beexpected.
There is renewed interest in pre-operative cholangio-graphy with the introduction of laparoscopic surgery. Ifstandard surgical procedures are used and no anatom-ical variations are expected, a conventional studyconsisting of projection images, conventional tomo-graphy and fluoroscopy is sufficient. If laparoscopicsurgery is planned, the greater expense of spiral CTcholangiography seems justified, since additional impor-tant information is provided about the surroundingtissues and critical structures such as the right hepaticduct and cystic duct orifice. This, combined with theoption of 3D surface rendering, will facilitate intraoper-ative orientation.
ReferencesDREXLER, G, PANZER, W, WIDENMANN, L ET AL, 1985.
Organ Doses in X-ray Diagnosis (Hoffmann, Berlin), pp.33-41.
GILLAMS, A, LEES, W, RICHARDS, R ET AL, 1992. 3-D CTof the biliary tree. Clin. Radiol, 45, 52.
GOTZ, F, SCHIPPERS, E & SCHUMPELICK, V, 1991.Laparoskopische Chirurgie (Thieme, Stuttgart), pp. 45-70.
KALENDER, A W & POLACIN, A, 1991. Physicalperformance characteristics of spiral CT scanning. Med.Phys., 18, 910-915.
KALENDER, A W, SIESSLER, W, KLOTZ, E & VOCK, P,1990. Spiral volumetric CT with single-breathhold technique,continuous transport and scanner rotation. Radiology, 176,181-183.
MORIMOTO, K, SHIMOI, M, SHIRAKAWA, T ET AL,1991. Three-dimensional MR cholangiography: new
766 The British Journal of Radiology, September 1993

CT cholangiography using spiral CT
noninvasive technique for evaluation of biliary obstruction.Radiology, 183, 578-580.
NEUHAUS, H, UNGEHEUER, A, FEUSSNER, H ET AL,1992. Laparoscopic cholecystectomy: should ERCP be thestandard method of preoperative diagnosis? Dtsch. Med.Wochenschr., 117, 1863-1867.
PROKOP, M, SCHAEFER, C M, DOEHRING, W ET AL,1991. Spiral CT for three-dimensional imaging of complexvascular anatomy. Radiology, 181 (P), 293.
SCHUMACHER, K A, WALLNER, B, WEIDENMAIER,W & FRIEDRICH, J M, 1991. Biliary obstruction:MR-cholangiography with a rapid gradient-echo sequence(2D CE-FAST). Fortschr. Rontgenstr., 155, 332-336.
VANNIER, M W, MARSH, J L & WARREN, J O, 1984.Three-dimensional CT reconstruction images for craniofacialsurgical planning and evaluation. Radiology, 150, 179-184.
VANNIER, M W, MARSH, J L, KNAPP, R H & OFFUT,C J, 1987. Recent advantages in 3D-CT scan reconstructionfor clinical applications. Proc. CAR, pp. 657-661.
VOCK, P, JUNG, H & KALENDER, W, 1989. Singlebreathhold spiral volumetric CT of the hepato-biliarysystem. Radiology, 173(P), 7>11.
VOCK, P, JUNG, H & KALENDER, A W, 1990.Single-breathhold spiral volumetric CT of the lung.Radiology, 176, 864-867.
Vol. 66, No. 789 767




















