Comprehensive Analysis of Left Ventricular Geometry and Function by Three-Dimensional...
11
Comprehensive Analysis of Left Ventricular Geometry and Function by Three-Dimensional Echocardiography in Healthy Adults Denisa Muraru, MD, Luigi P. Badano, MD, Diletta Peluso, MD, Lucia Dal Bianco, MD, Simona Casablanca, MD, Gonenc Kocabay, MD, Giacomo Zoppellaro, MD, and Sabino Iliceto, MD, Padua, Italy Background: Recent European Association of Echocardiography and American Society of Echocardiography guidelines on three-dimensional echocardiography state that normal values of left ventricular (LV) parameters for age and body size remain to be established. Methods: In 226 consecutive healthy subjects (125 women; age range, 18–76 years), comprehensive three- dimensional echocardiographic analyses of LV parameters were performed, and values were compared with those obtained by conventional echocardiography. Results: Upper reference values (mean + 2 SDs) for three-dimensional LV end-diastolic and end-systolic volumes were 85 and 34 mL/m 2 in men and 72 and 28 mL/m 2 in women, respectively. Indexing LV volumes to body surface area did not eliminate gender differences. Lower reference values (mean 2 SDs) for ejection fraction were 54% in men and 57% in women and for stroke volume were 25 and 24 mL/m 2 , respectively. Upper reference values for LV mass were 97 g/m 2 in men and 90 g/m 2 in women and for end-diastolic sphericity index were 0.49 and 0.48, respectively. Significant age dependency of LV parameters was identified and reported across age groups. Three-dimensional echocardiographic LV volumes were larger, ejection fraction was similar, and LV stroke volume and mass were significantly smaller in comparison with the corresponding values obtained by conventional echocardiography. Conclusions: The investigators report a comprehensive analysis of LV geometry and function using three- dimensional echocardiography in a relatively large cohort of healthy Caucasian subjects with a wide age range. These may serve to establish age-specific and gender-specific reference ranges, which are crucial for the routine implementation of three-dimensional echocardiography to detect LV remodeling and dysfunc- tion in clinical practice. (J Am Soc Echocardiogr 2013;-:---.) Keywords: Echocardiography, Three-dimensional, Left ventricle, Reference values, Normal subjects The quantification of left ventricular (LV) size, geometry, and function represents the most frequent indication for an echocardiographic study and is pivotal for patient evaluation and management. Indication for cardiac surgery, suitability for device implantation, indication for med- ical treatment in systolic heart failure, and suspension of cardiotoxic agents in patients with cancer are among the most critical decisions that rely on accurate assessments of LV geometry and function. 1 Three-dimensional echocardiography (3DE) enables comprehen- sive, accurate, and reproducible LV quantitation. 2,3 The superiority of 3DE over conventional two-dimensional (2D) echocardiography (2DE) for LV volume measurement in comparison with cardiac mag- netic resonance (CMR) has been well documented. 4-6 Although there seems to be a small underestimation of LV volumes using 3DE, this modality provides LV volumes significantly closer to those measured with CMR than 2DE, and no less important, it has been proved to be more robust than 2DE when tested for intraobserver, interobserver, and test-retest reproducibility. 3 The identification of reference values for LV volumes, mass, and function is a prerequisite for the routine clinical application of quantitative 3DE. Indeed, both the European Association of Echocardiography and the American Society of Echocardiography recommend 3DE rather than 2DE for the routine clinical assessment of LV volumes. 3 However, they also acknowledge that limited norma- tive data are available, particularly because of the lack of gender-based and anthropometric analysis. These aspects have significantly contrib- uted to the limited adoption of 3DE in routine clinical practice. Accordingly, we designed this prospective, single-center, observa- tional study to (1) perform a comprehensive analysis of LV geometry and function using state-of-the-art 3D echocardiographic equipment From the Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Padua, Italy. Dr. Muraru was supported by a scientific grant awarded by the European Associ- ation of Echocardiography. Dr. Kocabay is a recipient of a research grant from the Turkish Society of Cardiology (Istanbul, Turkey). Drs. Badano and Muraru have received equipment grants and speakers’ honoraria from GE Vingmed Ultrasound AS (Horten, Norway). Dr. Badano is on the speakers’ bureau of GE Vingmed Ultrasound AS. Reprint requests: Luigi P. Badano, MD, University of Padua, Department of Cardiac, Thoracic and Vascular Sciences, Via Giustiniani 2, 35128 Padua, Italy (E-mail: [email protected]). 0894-7317/$36.00 Copyright 2013 by the American Society of Echocardiography. http://dx.doi.org/10.1016/j.echo.2013.03.014 1
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Comprehensive Analysis of Left Ventricular Geometry and Function by Three-Dimensional...

From the Dep
Padua, Padua
Dr. Muraru wa
ation of Echoc
Turkish Socie
Drs. Badano a
fromGE Vingm
bureau of GE
Reprint reque
Cardiac, Thor
(E-mail: lpbad
0894-7317/$3
Copyright 201
http://dx.doi.o
Comprehensive Analysis of Left Ventricular Geometryand Function by Three-Dimensional Echocardiography
in Healthy Adults
Denisa Muraru, MD, Luigi P. Badano, MD, Diletta Peluso, MD, Lucia Dal Bianco, MD, Simona Casablanca, MD,Gonenc Kocabay, MD, Giacomo Zoppellaro, MD, and Sabino Iliceto, MD, Padua, Italy
Background: Recent European Association of Echocardiography and American Society of Echocardiographyguidelines on three-dimensional echocardiography state that normal values of left ventricular (LV) parametersfor age and body size remain to be established.
Methods: In 226 consecutive healthy subjects (125 women; age range, 18–76 years), comprehensive three-dimensional echocardiographic analyses of LV parameters were performed, and values were comparedwith those obtained by conventional echocardiography.
Results: Upper reference values (mean + 2 SDs) for three-dimensional LV end-diastolic and end-systolicvolumes were 85 and 34 mL/m2 in men and 72 and 28 mL/m2 in women, respectively. Indexing LV volumesto body surface area did not eliminate gender differences. Lower reference values (mean� 2 SDs) for ejectionfraction were 54% in men and 57% in women and for stroke volume were 25 and 24 mL/m2, respectively.Upper reference values for LV mass were 97 g/m2 in men and 90 g/m2 in women and for end-diastolicsphericity index were 0.49 and 0.48, respectively. Significant age dependency of LV parameters was identifiedand reported across age groups. Three-dimensional echocardiographic LV volumes were larger, ejectionfraction was similar, and LV stroke volume and mass were significantly smaller in comparison with thecorresponding values obtained by conventional echocardiography.
Conclusions: The investigators report a comprehensive analysis of LV geometry and function using three-dimensional echocardiography in a relatively large cohort of healthy Caucasian subjects with a wide agerange. These may serve to establish age-specific and gender-specific reference ranges, which are crucialfor the routine implementation of three-dimensional echocardiography to detect LV remodeling and dysfunc-tion in clinical practice. (J Am Soc Echocardiogr 2013;-:---.)
Keywords: Echocardiography, Three-dimensional, Left ventricle, Reference values, Normal subjects
The quantification of left ventricular (LV) size, geometry, and functionrepresents themost frequent indication for an echocardiographic studyand is pivotal for patient evaluation and management. Indication forcardiac surgery, suitability for device implantation, indication for med-ical treatment in systolic heart failure, and suspension of cardiotoxicagents in patients with cancer are among the most critical decisionsthat rely on accurate assessments of LV geometry and function.1
artment of Cardiac, Thoracic and Vascular Sciences, University of
, Italy.
s supported by a scientific grant awarded by the European Associ-
ardiography. Dr. Kocabay is a recipient of a research grant from the
ty of Cardiology (Istanbul, Turkey).
ndMuraru have received equipment grants and speakers’ honoraria
ed Ultrasound AS (Horten, Norway). Dr. Badano is on the speakers’
Vingmed Ultrasound AS.
sts: Luigi P. Badano, MD, University of Padua, Department of
acic and Vascular Sciences, Via Giustiniani 2, 35128 Padua, Italy
6.00
3 by the American Society of Echocardiography.
rg/10.1016/j.echo.2013.03.014
Three-dimensional echocardiography (3DE) enables comprehen-sive, accurate, and reproducible LV quantitation.2,3 The superiorityof 3DE over conventional two-dimensional (2D) echocardiography(2DE) for LV volume measurement in comparison with cardiac mag-netic resonance (CMR) has been well documented.4-6 Althoughthere seems to be a small underestimation of LV volumes using3DE, this modality provides LV volumes significantly closer to thosemeasured with CMR than 2DE, and no less important, it has beenproved to be more robust than 2DE when tested for intraobserver,interobserver, and test-retest reproducibility.3
The identification of reference values for LV volumes, mass,and function is a prerequisite for the routine clinical application ofquantitative 3DE. Indeed, both the European Association ofEchocardiography and the American Society of Echocardiographyrecommend 3DE rather than 2DE for the routine clinical assessmentof LV volumes.3 However, they also acknowledge that limited norma-tive data are available, particularly because of the lack of gender-basedand anthropometric analysis. These aspects have significantly contrib-uted to the limited adoption of 3DE in routine clinical practice.
Accordingly, we designed this prospective, single-center, observa-tional study to (1) perform a comprehensive analysis of LV geometryand function using state-of-the-art 3D echocardiographic equipment
1

Abbreviations
BSA = Body surface area
BSADB = Body surface area
(Dubois and Dubois)
BSAH = Body surface area(Haycock et al.)
CMR = Cardiac magneticresonance
ICC = Intraclass correlationcoefficient
LV = Left ventricular
3D = Three-dimensional
3DE = Three-dimensionalechocardiography
2D = Two-dimensional
2DE = Two-dimensional
echocardiography
2 Muraru et al Journal of the American Society of Echocardiography- 2013
in a relatively large cohort ofhealthy subjects, (2) assess theeffects of age and gender on LV3D echocardiographic parame-ters, and (3) compare the valuesmeasured by 3DE with those ob-tained by conventional echocar-diography in the same subjects.
METHODS
Study Population
Between October 2011 andFebruary 2013, 257 healthyCaucasian volunteers were pro-spectively recruited at a singletertiary center among hospitalemployees, fellows in training,their relatives, and individualswho underwent medical visitsfor driving or working licenses
and met the inclusion criteria. The sample size of the study was deter-mined according to Altman,7 who set 200 subjects as the minimumnumber to enroll in a study aiming to assess reference values for bio-logic variables. Prospective criteria for recruitment included age > 17years, no history of cardiovascular or lung disease, no symptoms,absence of cardiovascular risk factors (i.e., systemic hypertension,smoking, diabetes, dyslipidemia), no cardioactive or vasoactive treat-ment, and normal results on electrocardiography and physical exam-ination. Exclusion criteria were athletic training, pregnancy, bodymass index > 30 kg/m2, and poor apical acoustic window, definedas more than two LV segments not adequately visualized withoutcontrast infusion.
Blood pressure was measured in all subjects immediately beforethe echocardiographic examination. Height and weight were mea-sured using a calibrated stadiometer and scale, and body surfacearea (BSA) was calculated according to the formulas of bothDubois and Dubois8 (BSADB) and Haycock et al.9 (BSAH) (modifiedby Sluysmans and Colan10).
The study was approved by the University of Padua ethics commit-tee (protocol 2380 P, approved on October 6, 2011), and writteninformed consent was obtained from all volunteers before screeningfor eligibility in the study.
Image Acquisition
Using a standardized protocol, all examinations were performed bythree cardiologists with experience in research echocardiography(L.D.B., D.M., and L.P.B.) using a commercially available Vivid E9ultrasound machine (GE Vingmed Ultrasound AS, Horten, Norway)equipped with M5S and 4V probes for 2DE and 3DE, respectively.All patients were examined in the left lateral position using grayscalesecond-harmonic 2D imaging, with the adjustment of image contrast,frequency, depth, and sector size for adequate frame rate and optimalLV border visualization. Care was taken to avoid LV foreshortening inboth apical views, and image acquisition was done during breathholding to minimize respiratory movements.
Standard transthoracic echocardiography included (1) 2D-guidedM-mode tracings of LV wall thickness and cavity diameter to calculateLV mass; (2) a zoom image of the LVoutflow tract obtained from the
parasternal 2D long-axis view; (3) spectral recordings of LV outflowtract flow sampled using a pulsed-wave Doppler sample volume po-sitioned just proximal to the aortic valve, so that the location of thevelocity recording could match the LV outflow tract measurement;and (4) apical four-chamber and two-chamber view recordings forLV volume measurements, taking care to maximize LV length andto reduce depth by excluding the left atrium to achieve the highestframe rate.11 All tracings and recordings contained at least threecardiac cycles to allow averaging of measurements.
Three-dimensional echocardiographic full-volume LV data sets ob-tained by stitching together four or six consecutive electrocardio-graphically gated subvolumes were acquired by the same examinerat the end of the standard 2D echocardiographic examination.Using multislice display of the 3D LV data set, special care was takento adequately visualize all LV segments and to exclude any stitchingartifacts between subvolumes. Data sets were stored digitally inraw-data format and exported to a separate workstation for analysis(EchoPAC BT 11; GE Vingmed Ultrasound AS).
Image Analysis
Image quality check and analysis were performed offline by two inde-pendent observers (D.M. and L.P.B.) with 3 years of experience withthe software package used in this study. LV mass was calculated usingmeasurements performed on 2DE-guidedM-mode tracings12 accord-ing to the American Society of Echocardiography’s leading-edge con-vention.13 To calculate LV stroke volume, LV outflow tract diameterwas measured in the parasternal long-axis view in midsystole, inneredge to inner edge, parallel and proximal (within 0.5 cm) to the aorticvalve plane. End-diastole and end-systole were identified from 2Dechocardiographic cine loops using frame-by-frame analysis of theapical four-chamber and two-chamber LV views as the largest andsmallest cavity during the cardiac cycle, respectively. Then, manualtracing of endocardial border was performed in both frames, payingattention to include the papillary muscles within the LV cavity. LV vol-umes were calculated using the biplane disk-summation algorithm(modified Simpson’s rule), and ejection fraction was calculated as1�end-systolic volume/end-diastolic volume. Two-dimensionalechocardiographic end-diastolic sphericity index was calculatedfrom LV end-diastolic volume and LV longitudinal axis (averagedfrom the LV longitudinal axes in four-chamber and two-chamberviews) by applying the same formula as for 3D echocardiographicsphericity index (see below).
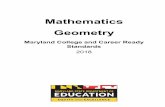
Quantification of 3D LV volumes and ejection fraction was per-formed using a commercially available software (4D AutoLVQ; GEVingmed Ultrasound AS) previously validated against CMR and ex-tensively described elsewhere14 (Figure 1). Initialization of LV endo-cardial border tracing was manually performed by the operator, byidentifying two points on the four-chamber view image at end-diastole and then at end-systole (one point in the middle of the mitralannulus and a second point at the LV apex). Manual editing of thesemiautomatically generated endocardial contours was routinely ap-plied to include the LV outflow, as well as papillary muscles and tra-beculae within the LV cavity, because this approach was found toreduce bias in comparison with CMR.14,15 Editing involved thesystematic addition of several attractor points, within a range of oneto five points for the endocardium and two to eight points for theepicardium.
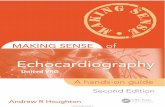
In addition, this software enabled the automatic calculation of LVsphericity index (Figure 1) and LVmass (Figure 2). LV sphericity indexis a quantitative parameter reflecting LV shape, and it is calculated

Figure 1 Measurement of LV volumes on the basis of semiautomated identification of endocardial surface by 3DE. CO, Cardiacoutput; EF, ejection fraction; EDV, end-diastolic volume; ESV, end-systolic volume; HR, heart rate; SpI, sphericity index; SV, strokevolume.
Journal of the American Society of EchocardiographyVolume - Number -
Muraru et al 3
as the ratio between the LVend-diastolic volume divided by the vol-ume of a sphere whose diameter is equal to the longitudinal LV axismeasured at end-diastole.16 For LV mass calculation (Figure 2), afterLVendocavitary volume quantitation, the software automatically de-tected also the epicardial LV contours in end-diastole and in end-systole. Both endocardial and epicardial contours were verified bythe operator and manually adjusted to fit the regional differences inLV wall thickness. Then, LV mass was automatically computed as(LV epicardial volume�LV endocardial volume) � 1.05 g/mL (thespecific weight of myocardial tissue).
Statistical Analysis
Normal distribution of variables was verified using the Kolmogorov-Smirnov test. Continuous variables are summarized as mean 6 SD,and categorical variables were reported as percentages. Variableswere compared between men and women using unpaired t tests.Three-dimensional and 2D echocardiographic measurements ob-tained from the same subject were compared using paired t testsand Bland-Altman analysis. Pearson’s correlation was used to analyzethe relationships between age and LV parameters.
Interobserver variability for 3D LV volumes andmass was analyzedin 15 random subjects by two independent observers (D.M. andL.P.B.). Intraobserver variability was analyzed in another group of15 subjects by the same observer (D.M.) repeating the measurements1 week later. For each parameter, reproducibility was reported as thecoefficient of repeatability (1.96 SDs of the differences between thetwo measurements) by Bland-Altman analysis and as the intraclasscorrelation coefficient (ICC).
All analyses were carried out using SPSS version 19.0 (SPSS, Inc.,Chicago, IL) and MedCalc version 10.0.1.0 (MedCalc Software,Mariakerke, Belgium). Differences among variables were consideredsignificant at P < .05. Upper and lower limits of normality were com-puted as mean 6 2 SDs.
RESULTS
Of the 258 healthy volunteers screened for eligibility, 32 (12%) wereexcluded for unknown cardiac pathology detected by echocardiogra-phy (n = 5), obesity (n = 5), professional athletic activity (n = 3), ele-vated blood pressure levels at enrollment (n = 5), prematureventricular contractions (n = 2), pregnancy (n = 1), and right bundlebranch block (n = 1). Another seven healthy subjects were excludedbecause of poor apical acoustic windows and three because of tech-nical inadequate 3D LV data sets identified during image analysis.Thus, the overall feasibility in our study was 88%.
Temporal resolution of 3D data sets was 346 5 volumes/sec, andfor 2D data sets, resolution was 766 7 frames/sec. The quality of 3Ddata sets for LV quantitation was judged subjectively, considering thesignal-to-noise ratio, the degree of blood-tissue contrast, and the com-pleteness of LV wall visualization; image quality was excellent in 31%,good in45%, fair in 20%, andpoor in 4%of subjects. The quality of 2DLV data sets for LV quantitation by the disk-summation method wasverified by calculating the differences in the LV longitudinal axes inthe four-chamber versus two-chamber view; <10% difference wasfound in 96% of subjects at end-diastole and in 90% at end-systole.
Table 1 summarizes the demographics and the 3D echocardio-graphic LV parameters of geometry and function in the study

Figure 2 Measurement of LV mass on the basis of semiautomated identification of endocardial and epicardial surfaces on the same3D data set used for LV volume quantitation. CO, Cardiac output; EDMass, end-diastolic mass; EDMassI, end-diastolic mass index;EDV, end-diastolic volume; EF, ejection fraction; ESV, end-systolic volume; HR, heart rate; SpI, sphericity index; SV, stroke volume.
4 Muraru et al Journal of the American Society of Echocardiography- 2013
population taken as a whole and separately by gender. Subjects’ agerange was 18 to 76 years, and 45% were men. There was no differ-ence in age or heart rate between men and women. However,women showed significantly smaller body size and lower blood pres-sure levels than men (Table 1).
LV volumes were larger in men than in women, even after normal-ization for BSADB and BSAH (Figure 3). BSADB was significantly largerthan BSAH, and using BSAH for indexing 3D echocardiographic LVvolumes and mass amplified the differences between genders(Table 1). Using BSADB for indexing, upper reference values(mean + 2 SDs) for 3D LV end-diastolic and end-systolic volumeswere 85 and 34 mL/m2 in men and 72 and 28 mL/m2 in women,respectively. Using BSAH for indexing, upper reference values(mean + 2 SDs) for 3D LV end-diastolic and end-systolic volumeswere 115 and 45 mL/m2 in men and 88 and 33 mL/m2 in women,respectively. As expected, LV end-diastolic and end-systolic volumescalculated on 2D echocardiographic images were significantly smallerthan those measured from 3D echocardiographic data sets (Table 2,Figure 4).
LVejection fractions were significantly higher in women (Table 1).However, because LV volumes in womenwere smaller, LV stroke vol-umes in women were also found to be significantly smaller than inmen, and this difference persisted after normalization for BSA(Table 1, Figure 3). Lower reference values (mean�2 SDs) for ejec-tion fraction were 54% inmen and 57% in women and for stroke vol-ume were 25 and 24 mL/m2 using BSADB, and 31 and 29 mL/m2
using BSAH, respectively. LVejection fraction was statistically smallerwith 3DE than with 2DE, but this difference was clinically irrelevant
(Table 2, Figure 4). LV stroke volume measured with 3DE was signif-icantly lower than tLV stroke volume calculated using the conven-tional 2D Doppler method (76 6 16 vs 94 6 20 mL in men and60 6 12 vs 75 6 12 mL in women, P < .0001 for both; Figure 4).
LV shape assessed in terms of sphericity index measured at end-diastole was similar between genders (Table 1). Overall, the end-diastolic LV longitudinal axis was longer by 3DE (8.4 6 0.7 cm)than its average calculated from 2D echocardiographic four-chamber and two-chamber views (8.26 0.7 cm) (P < .0001), reflect-ing LV foreshortening and accounting, at least in part, for the smallerLV volumes by 2DE. When 3D echocardiographic LV end-diastolicsphericity index was compared with the corresponding values ob-tained by 2DE, no significant differences in LV shape were identified(Table 2).
LVmass was significantly larger in men than in women, and this dif-ference persisted even after indexing to BSA (Table 1). Conversely, LVmass/volume ratios were significantly higher in women than in men.Upper limits of reference values (mean + 2 SDs) were 97 and90 g/m2 for 3D echocardiographic LV mass/BSADB, 144 and120 g/m2 for 3D echocardiographic LV mass/BSAH, and 1.60 and1.66 for 3D mass/volume ratio in men and women, respectively.LV mass measured with 3DE was significantly lower than the valuecalculated using the M-mode formula in both men (150 6 22 vs171 6 35 g) and women (124 6 16 vs 141 6 30 g) (P < .0001 forboth; Figure 5).
Table 3 summarizes the relationships of LV parameters with age.LV volumes decreased with aging in both genders (Table 4). This re-lationship was still evident after indexing to both BSADB and BSAH

Table 1 Demographics and parameters of LV geometry and function obtained by 3DE in the study population
Variable Overall (n = 226) Men (n = 101) Women (n = 125) P
Age (y) 44 6 14 43 6 14 44 6 15 .584Height (cm) 170 6 9 177 6 7 164 6 7 <.0001
Weight (kg) 68 6 11 76 6 9 61 6 8 <.0001Body mass index (kg/m2) 23 6 3 24 6 3 22 6 3 <.0001
BSADB (m2) 1.78 6 0.18 1.93 6 0.13 1.66 6 0.12 <.0001
BSAH (m2) 1.30 6 0.03 1.33 6 0.22 1.28 6 0.22 <.0001
Heart rate (beats/min) 67 6 10 67 6 11 68 6 10 .338
Systolic BP (mm Hg) 123 6 14 128 6 12 118 6 14 <.0001
Diastolic BP (mm Hg) 74 6 8 77 6 8 71 6 9 <.0001
LV EDV (mL) 106 6 25 123 6 25 93 6 16 <.0001
LV EDV/BSADB (mL/m2) 59 6 10 63 6 11 56 6 8 <.0001
LV EDV/BSAH (mL/m2) 73 6 15 83 6 16 66 6 11 <.0001
LV ESV (mL) 39 6 11 46 6 10 33 6 7 <.0001
LV ESV/BSADB (mL/m2) 22 6 5 24 6 5 20 6 4 <.0001
LV ESV/BSAH (mL/m2) 27 6 7 31 6 7 23 6 5 <.0001
LV SV (mL) 68 6 15 76 6 16 60 6 12 <.0001
LV SV/BSADB (mL/m2) 38 6 6 39 6 7 36 6 6 .001
LV SV/BSAH (mL/m2) 47 6 9 51 6 10 43 6 7 <.0001
LV ejection fraction (%) 64 6 4 62 6 4 65 6 4 <.0001
LV mass (g) 135 6 23 150 6 22 124 6 16 <.0001
LV mass/BSADB (g/m2) 76 6 9 77 6 10 74 6 8 .023
LV mass/BSAH (g/m2) 103 6 16 112 6 16 96 6 12 <.0001
LV end-diastolic sphericity index 0.35 6 0.07 0.35 6 0.07 0.34 6 0.07 .838
LV mass/EDV (g/mL) 1.30 6 0.2 1.24 6 0.18 1.30 6 0.18 <.0001
BP, Blood pressure; EDV, end-diastolic volume; ESV, end-systolic volume; SV, stroke volume.
Data are expressed as mean 6 SD.
Journal of the American Society of EchocardiographyVolume - Number -
Muraru et al 5
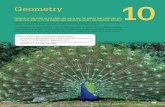
and was more evident in women than in men (Figure 3). Three-dimensional echocardiographic stroke volume and LV ejection frac-tion did not show any significant relationships with age in men, butstroke volume decreased and LV ejection fraction increased signifi-cantly with age in women. There was no correlation between ageand LV mass or LV mass indexed to BSADB in men, while LV massdecreased with age in women. The mass/volume ratio increasedwith age in both genders.
Comparisons of our findings with the 3D echocardiographic LVreference values from previous studies are reported in Table 5.
Reproducibility
Three-dimensional LV parameters showed excellent intraobserverand interobserver reproducibility (Table 6). In comparison with 3Dechocardiographic parameters, 2D LV volumes and particularly 2DLV ejection fraction showed more variability at repeated measure-ments: for 2D LV end-diastolic volume, ICCs were 0.970 and0.945; for 2D LVend-systolic volume, ICCs were 0.963 and 0.957;and for 2D LVejection fraction, ICCs were 0.741 and 0.742 for intra-observer and interobserver analyses, respectively.
DISCUSSION
The present study provides a comprehensive analysis of LV geometryand function using 3DE in a relatively large cohort of healthyCaucasian volunteers with a wide age range. The main results canbe summarized as follows: (1) reference values for LV volumes andmass by 3DE were found to be significantly different from those
obtained with conventional echocardiography, highlighting the im-portance of applying method-specific reference values for a reliableidentification of LV remodeling; (2) LV parameters measured by3DE had excellent reproducibility and were more robust than 2Dindices (particularly regarding LVejection fraction) on repeated mea-surements; and (3) most LV indices should be defined accordingto age and gender, because indexing them only for BSA does notaccount for all variations in LV geometry and function.
Method-Specific Reference Values of LV Geometry andFunction from 3DE
LV volumes, ejection fraction, and spherical shape are powerful pre-dictors of morbidity and mortality in both clinical and populationstudies. However, LV parameters derived from conventional echocar-diography (M-mode, 2DE, and Doppler) are based on a limited num-ber of actual measurements. In fact, they derive mostly fromcalculations involving several assumptions of LV geometry (i.e., LVwall thickness distribution, LV outflow tract circularity) and on theiranatomically correct imaging by 2DE, although a significant errormay result from restricted imaging capabilities inherent to a tomo-graphic technique, foreshortening errors, or insufficient experiencein image acquisition or analysis. Hence, although these LV indicesare of utmost clinical importance, traditional echocardiographicmethods are inherently flawed. This has been demonstrated in severalstudies comparing the accuracy of 2DE with CMR or cardiac com-puted tomography.17 Because CMR and cardiac computed tomogra-phy also have limitations, such as limited availability, cost, timeconsumption, use of contrast agent, and radiation exposure (for car-diac computed tomography), there is a need for a robust, noninvasive

Figure 3 Comparison of LV 3D echocardiographic parameters between genders and displayed across age groups. Indexed param-eters to BSADB
8 are shown. EF, Ejection fraction; EDV, end-diastolic volume; ESV, end-systolic volume; SV, stroke volume.
Table 2 Comparison of parameters of LV geometry and function obtained by 3DE with those derived from 2DE
Variable 3DE 2DE P Upper limit by 3DE Upper limit by 2DE
End-diastolic volume (mL) 107 6 25 97 6 25 <.0001 157 147
End-systolic volume (mL) 39 6 11 35 6 11 <.0001 61 57
Sphericity index 0.35 6 0.07 0.34 6 0.06 .35 0.49 0.46
Ejection fraction (%) 64 6 4 65 6 4 <.0001 56* 57*
Data are expressed as mean 6 SD.
*Lower limit.
6 Muraru et al Journal of the American Society of Echocardiography- 2013
imaging modality to be routinely used to quantify LV performanceand remodeling in patients with known or suspected cardiovasculardisease.
Three-dimensional echocardiographic measurements are affectedneither by cardiac chamber foreshortening nor by geometric assump-tions. Specifically, previous studies have shown that 3DE is not onlyaccurate in measuring LV volumes and mass compared with CMR5
but is also more reproducible, demonstrating low observer and test-retest variability.3,18,19 However, the lack of specific referencevalues for 3DE might have hindered, at least partially, the use of3DE in clinical and research practice. Available recommendationson LV quantification11 rely on M-mode-derived or 2DE-derived
cutoff values to define normality of LV volumes, ejection fraction,or mass, and to date, there is no clear evidence that these referencevalues can be extrapolated for 3D echocardiographic measurements.Studies comparing 3DE and 2DE with CMR in patients have foundthat LV volumes by 3DE were significantly larger than those obtainedwith 2DE,14,20 while 3D echocardiographic LV mass was larger thanthe value obtained by 2DE21 and smaller than the value calculated us-ing the cubed formula by M-mode echocardiography.22,23 Ourfindings in healthy subjects demonstrate that LV reference valuesfrom conventional echocardiography should not be usedinterchangeably with 3D LV volumes and mass, emphasizing oncemore that method-specific normality ranges should be applied for

Figure 4 Bland-Altman plots comparing LV volumes, ejection fraction, and stroke volume obtained by 3DE and 2DE. EF, Ejectionfraction; EDV, end-diastolic volume; ESV, end-systolic volume; LOA, limits of agreement; SV, stroke volume.
Figure 5 Bland-Altman plot comparing measurements of LVmass with 3DE and M-mode echocardiography. LOA, Limitsof agreement.
Table 3 Relationships between LV parameters by 3DE andage for both genders
Variable
Men (n = 101) Women (n = 125)
r P r P
EDV (mL) �0.25 .014 �0.36 <.0001
EDV/BSADB (mL/m2) �0.25 .012 �0.42 <.0001
EDV/BSAH (mL/m2) �0.22 .026 �0.35 <.0001
ESV (mL) �0.28 .005 �0.44 <.0001
ESV/BSADB (mL/m2) �0.28 .005 �0.49 <.0001
ESV/BSAH (mL/m2) �0.27 .008 �0.44 <.0001
SV (mL) �0.20 .052 �0.20 .031
SV/BSADB (mL/m2) �0.20 .053 �0.25 .005
SV/BSAH (mL/m2) �0.17 .098 �0.20 .025
Ejection fraction (%) 0.18 .067 0.28 .002
Mass (g) 0.01 .940 �0.18 .050
Mass/BSADB (g/m2) 0.03 .749 �0.20 .024
Mass/BSAH (g/m2) 0.12 .905 �0.16 .08
Sphericity index 0.16 .107 0.10 .256
Mass/EDV (g/mL) 0.32 .001 0.29 .001
Journal of the American Society of EchocardiographyVolume - Number -
Muraru et al 7
clinical decisionmaking. In addition, excellent intraobserver and inter-observer reproducibility for 3D echocardiographic parameters wasconfirmed in our study, as well as the superiority of 3DE in compar-ison with 2DE regarding LV volumes and ejection fraction measure-ment reproducibility.
Abbreviations as in Table 1.
Comparison with LV Reference Values from Other 3DEchocardiographic and CMR Studies
To our knowledge, four studies have previously reported referencevalues for LV geometry and function in healthy subjects using 3DE,and all used BSADB to index LV volumes and mass. Aune et al.24 stud-ied 166 healthy Norwegian subjects (46% men; age range, 29–80
years) and found reference values very similar to ours (differencesin upper limits of normality for end-diastolic and end-systolic LV vol-umes of 2 and 1 mL/m2, respectively). Kaku et al.25 studied the effectof aging on LV geometry and function in 280 healthy American andJapanese subjects (49%male; age range, 1–88 years). LV volumes and

Table
4LVgeometryandfunctionby3DEpresentedbyagegroupsin
menandwomen
Variable
18–3
9y
40–5
9y
$60y
Men(n
=40)
Women(n
=44)
PMen(n
=38)
Women(n
=54)
PMen(n
=24)
Women(n
=26)
P
EDV(m
L)
1286
27(182)
986
16(130)
<.0001
1196
21(161)
946
16(126)
<.0001
1166
26(168)
846
12(108)
<.0001
EDV/B
SADB(m
L/m
2)
666
11(88)
606
8(76)
.001
616
9(79)
566
8(72)
.021
626
12(86)
516
7(65)
.001
EDV/B
SAH(m
L/m
2)
866
17(110)
696
10(89)
<.0001
806
13(106)
676
11(89)
<.0001
816
17(115)
596
8(75)
<.0001
ESV(m
L)
506
11(72)
366
7(50)
<.0001
446
9(62)
336
5(43)
<.0001
446
11(66)
286
6(40)
<.0001
ESV/B
SADB(m
L/m
2)
266
5(36)
226
4(30)
<.0001
236
4(31)
206
3(26)
<.0001
236
5(33)
176
4(25)
<.0001
ESV/B
SAH(m
L/m
2)
336
7(47)
256
5(35)
<.0001
306
6(42)
236
3(29)
<.0001
306
8(46)
206
4(28)
<.0001
SV(m
L)
786
17(44*)
626
10(42*)
<.0001
756
13(49*)
606
14(32*)
<.0001
746
15(44*)
566
9(38*)
<.0001
SV/B
SADB(m
L/m
2)
416
7(27*)
376
5(27*)
.027
386
6(24*)
366
6(24*)
.261
396
7(25*)
346
5(24*)
.016
ESV/B
SAH(m
L/m
2)
536
11(31*)
436
7(29*)
<.0001
506
8(34*)
446
8(28*)
<.0001
516
10(31*)
406
6(28*)
<.0001
Ejectionfraction(%
)616
4(53*)
636
3(57*)
.016
636
3(57*)
656
4(57*)
.009
636
3(57*)
666
5(56*)
.008
Mass(g)
1496
22(193)
1246
15(154)
<.0001
1506
22(194)
1266
16(158)
<.0001
1506
23(196)
1186
19(156)
<.0001
Mass/B
SADB(g/m
2)
786
9(96)
756
8(91)
.250
766
11(98)
756
8(91)
.450
796
10(99)
726
10(92)
.027
Mass/B
SAH(g/m
2)
1126
16(144)
966
11(118)
<.0001
1136
13(139)
986
11(120)
<.0001
1136
15(143)
926
14(120)
<.0001
Mass/EDV(g/m
L)
1.196
0.16(1.51)
1.296
0.16(1.61)
.004
1.286
0.20(1.68)
1.356
0.20(1.75)
.078
1.296
0.18(1.65)
1.426
0.15(1.72)
.013
Sphericityindex
0.336
0.06(0.45)
0.346
0.07(0.48)
.827
0.356
0.08(0.51)
0.346
0.06(0.46)
.807
0.376
0.08(0.53)
0.366
0.07(0.50)
.684
Abbreviationsasin
Table
1.
Data
are
expressedasmean6
SD(upperlim
itofnorm
ality).
*Lowerlim
itofnorm
ality.
8 Muraru et al Journal of the American Society of Echocardiography- 2013
mass in their adult subgroup were very similar to those obtained inour subjects. Finally, Fukuda et al.26 recently reported referencedata for the left ventricle and left atrium obtained in 222 healthyJapanese subjects (61% men; age range, 20–69 years). Their LVend-diastolic volumes were smaller than ours (�13 mL/m2 in menand �10 mL/m2 in women; Table 5), but they studied Japanese sub-jects with smaller BSAs (1.8 m2 in men and 1.5 m2 in women). It ispossible that race or ethnicity-specific 3D echocardiographic refer-ence values for the left ventricle need to be identified as well, butonly a multicenter study specifically designed for this purpose ora meta-analysis of existing data27 could clarify for this aspect.
Recently, Chahal et al.28 reported average values of 49 6 9 and42 6 8 mL/m2 for 3D echocardiographic end-diastolic LV volumesfor men and women, respectively, in 978 healthy Europeans. Thesevolumes are significantly smaller than those from our study and pre-vious studies: 66 6 10 mL/m2 for men and 58 6 8 mL/m2 forwomen found by Aune et al.24 and 55 6 7 and 49 6 6 mL/m2, re-spectively, reported by Kaku et al.25 for the same age group.Fukuda et al.26 in their Japanese population with smaller body sizesthan Europeans also found larger end-diastolic LV volumes: 50 612 and 46 6 9 mL/m2 in men and women, respectively.Furthermore, the upper normal values (mean + 2 SDs) for 3D echo-cardiographic end-diastolic and end-systolic LV volumes reported byChahal et al. (e.g., 67 and 29 mL/m2 in men) are smaller than the 2Dechocardiographic upper normal limits reported in current guidelines(75 and 30 mL/m2, respectively11), contradicting all previous studiesreporting a large underestimation of LV volumes by 2DE in compar-ison with 3DE. Finally, European subjects were apparently in a lowflow state (average stroke volume index, 30 mL/m2 in men and26 mL/m2 in women, calculated from data in Table 1 in Chahalet al.). These data raise some concerns regarding the accuracy of the3D echocardiographic measurements performed in that study, partic-ularly because no comparison with other methods has been provided(i.e., stroke volume measured with 2DE and Doppler). One possibleexplanation for LV volume underestimation in the study by Chahalet al. may be the limited experience of the sonographers who per-formed 3D echocardiographic measurements, as acknowledged bythe authors (‘‘all underwent a 4-wk period of training in 3DE volumeacquisition and off-line analysis by the vendor representative at thebeginning of the study’’).29,30 The importance of reader experienceto the accuracy of 3D LV volume measurements has beenpreviously documented.15
Hudsmith et al.31 reported upper normal limits (mean + 2 SDs) forLVend-diastolic and end-systolic volumes by CMR in 108 apparentlyhealthy subjects (58% men): 106 mL/m2 in men and 39 mL/m2 inwomen. The upper limits for LV volumes in the study of Hudsmithet al. exceed our corresponding values for LV end-diastolic volumesby 19% in men and 34% in women, while end-systolic volumeswere very similar. An underestimation of LV volumes obtained by3DE in comparison with CMR was also documented in a meta-analysis recently performed by Dorosz et al.17 They reviewed datafrom 23 studies with 1,638 echocardiograms and found pooledbiases 6 2 SDs for 3DE of �19 6 34 mL, �10 6 30 mL, and0.6612% for LVend-diastolic and end-systolic volumes and ejectionfraction, respectively.
Mor-Avi et al.,15 in a multicenter study comparing 3DE and CMR,found that 3DE LV volumes were highly correlated with CMR mea-surements (end-diastolic volume, r = 0.91; end-systolic volume,r = 0.93) but were 26% and 29% lower, consistently across institu-tions, with a magnitude of bias inversely related to the level of ex-perience of the operators. They found that the main reason for

Table 6 Reproducibility of LV geometry and functional parameters by 3DE in 15 healthy subjects
Variable
Intraobserver Interobserver
CR ICC* 95% CI CR ICC* 95% CI
End-diastolic volume 8.5 0.998 0.968–0.996 9.3 0.990 0.971–0.997End-systolic volume 5.5 0.982 0.947–0.994 5.4 0.981 0.944–0.993
Ejection fraction 2.9 0.906 0.745–0.968 3.7 0.816 0.536–0.934
Stroke volume 6.1 0.980 0.942–0.993 8.9 0.967 0.905–0.989
Sphericity index 0.06 0.878 0.675–0.957 0.06 0.914 0.764–0.970
Mass 10.2 0.863 0.640–0.952 17.0 0.875 0.668–0.956
CI, Confidence interval; CR, coefficient of repeatability.
*P < .0001.
Table 5 Data comparison with two previous studies reporting LV parameters obtained by 3DE in healthy subjects
Variable
Present study (Vivid E9) Aune et al.24 (iE33) Fukuda et al.26 (Sonos 7500/iE33)
Men (n = 101) Women (n = 125) Men (n = 79) Women (n = 87) Men (n = 222) Women (n = 134)
EDV/BSADB (mL/m2) 63 6 11 56 6 8 66 6 10 58 6 8 50 6 12* 46 6 9*
ESV/BSADB (mL/m2) 24 6 5 20 6 4 29 6 6* 23 6 5* 19 6 5* 17 6 4*
SV/BSADB (mL/m2) 39 6 7 36 6 6 — — — —
Ejection fraction (%) 62 6 4 65 6 4 57 6 4* 61 6 6* 61 6 4† 63 6 4*
Mass (g/m2) 77 6 10 74 6 8 — — 64 6 12* 56 6 11*
Mass/EDV (g/mL) 1.24 6 0.18 1.30 6 0.18 — — 1.3 6 0.3 1.3 6 0.2
Abbreviations as in Table 1.
Data are expressed as mean 6 SD.
*P < .0001.†P < .05.
Journal of the American Society of EchocardiographyVolume - Number -
Muraru et al 9
this underestimation was the limited spatial resolution of 3DE,which cannot provide clear definition of endocardial trabeculae,which are, therefore, included in the myocardium rather beingpart of the left ventricle, as is done when tracing the endocardiumwith CMR. Greater underestimation seems to occur for LV end-diastolic volumes,6,32 and this is consistent with the fact that ourreference values for end-diastolic volume were significantly lowerthan those reported by Hudsmith et al.,31 while end-systolic volumeswere closer. The same issue of the underestimation of LV end-diastolic volumes with 3DE was reported by Aune et al.24 Thislimitation may have contributed to the underestimation of strokevolume by 3DE in comparison with the conventional 2D Dopplermethod in our study.
In their meta-analysis, Dorosz et al.17 also identified significantlylarger biases and limits of agreement for 2DE (�48 6 56 mL,�286 46 mL, and 0.1614% for LV volumes and ejection fraction)than 3DE, when both were compared with CMR. These data,together with the superior reproducibility of 3DE, warrant itsuse as the preferred method to assess LV size and function byechocardiography.
Relationships with Gender and Age
Despite their physiologic and clinical importance, the ideal methodfor indexing LV volumes and mass still remains to be defined.Sluysmans and Colan10 showed that the relationship of LV volumeswith BSA is a complex one that cannot be accounted for by adjust-ments for the square root of BSA. They demonstrated that, giventhe inverse relation of heart rate with BSA and the linear relation be-
tween cardiac output and BSA, LV volumes weremore closely relatedto BSA1.4 (BSAH). Therefore, in our report, two sets of referencevalues are provided for LV volumes, stroke volume, and mass: oneset based on gender and BSADB
8 and the other based on genderand BSAH.
10
Our findings show that reference values for most 3D echocar-diographic LV parameters should be gender-specific, because thesimple normalization of LV volumes to BSA (using either BSADB
or BSAH) does not eliminate gender differences for these parame-ters. These findings are consistent with the data reported by othersimilar studies.25,26,33 LV mass/volume ratio and ejection fractionwere also significantly higher in women than in men.Conversely, LV sphericity index was similar in men and women.These gender differences in LV geometry and function areconsistent with previous reports in which both 3DE and CMRwere used.25,31
It is widely accepted that age-related changes in cardiovascularstructure and function occur in healthy subjects. In our study popula-tion, LV size decreased with age, whereas LV mass and shape did notchange. As a result, the LV mass/volume ratio increased with age.These age-related changes evolving as concentric LV remodeling andinterpreted as a ‘‘physiologic’’ response to increased arterial pressureand afterload with age,34,35 were particularly evident in women. LVvolume reductions are compensated by an increase in LV ejectionfraction (which was statistically significant in women in our study) tomaintain cardiac output. Our findings are consistent with thosereported by others who used either echocardiography25 orCMR20,34 to assess age-related changes in LV morphology andfunction.

10 Muraru et al Journal of the American Society of Echocardiography- 2013
Study Limitations
Three-dimensional echocardiographic data set acquisitions and quan-tifications were performed using a single vendor platform and its pro-prietary analysis algorithm, which may have implications for theapplicability of these reference values to volumetric data sets that areacquired or analyzed with other vendor-specific platforms. However,to the best of our knowledge, no significant intervendor variabilityhas been reported for 3D echocardiographic volumes, in contrast tothe recent evidence regarding myocardial deformation measure-ments.36,37 In fact, we previously reported excellent agreementbetween 3D echocardiographic LV volumes obtained with the samevendor equipment used in this study and those measured usingvendor-independent software, when both were compared in a rela-tively large number of patients with a wide range of LV volumes.14
This study did not include validation of 3D echocardiographic LVvolumes and mass against CMR. Limited availability and costs ofCMR, as well as ethical reasons, prevented its use for studying healthysubjects with no clinical indications for CMR. In addition, we previ-ously validated the 3D echocardiographic software used in this studyagainst CMR.14
The samples of men and womenwere not equal, particularly in themiddle age group, raising the possibility that some gender differencesmay have been amplified or not adequately detected. In addition, thenumber of subjects aged > 60 years was limited. However, in ourstudy, we prioritized the quality over the quantity of data by adoptinga rather strict protocol to enroll a priori healthy subjects, not patientsreferred to the echocardiography lab for clinical reasons and inciden-tally found to have ‘‘normal’’ echocardiographic results. With our strictinclusion criteria, the enrollment of truly healthy volunteers, particu-larly those aged > 50 years, is rather challenging, and only a multicen-ter study could allow the enrollment of such a large number of normalsubjects. On the other hand, a multicenter study would have to facethe challenge of quality control on the fulfillment of enrollment crite-ria and of standardization of 3D echocardiographic acquisition and/oranalysis across centers. The European Association of CardiovascularImaging has undertaken such an initiative.38
Our study population was composed of Caucasian subjects only,which may limit the applicability of our reference values to otherracial groups.
Finally, although subjects fulfilled all the inclusion criteria as healthyadults, we cannot exclude the possibility of subclinical coronary arterydisease, particularly in older subjects.
CONCLUSIONS
Our study provides a comprehensive analysis of LV geometry andfunction obtained by 3DE in a relatively large population of healthyadult subjects. Because age and gender significantly influenced LVmorphology and function, reference values have been provided ac-cording to gender for each age group. The availability of referencevalues and age-specific and gender-specific cutoff values should facil-itate the implementation of 3DE to identify LV remodeling and dys-function in both clinical routine and research.
REFERENCES
1. Kirkpatrick JN, Vannan M, Narula J, Lang RM. Echocardiography in heartfailure. Applications, utility, and new horizons. J AmColl Cardiol 2007;50:381-96.
2. Lang RM, Mor-Avi V, Sugeng L, Nieman PS, Sahn DJ. Three-dimensionalechocardiography: the benefits of the additional dimension. J Am CollCardiol 2006;48:2053-69.
3. Lang RM, Badano LP, TsangW, AdamsDH, Agricola E, Buck T, et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. Eur Heart J Cardiovasc Imaging 2012;13:1-46.
4. Shimada YJ, Shiota T. A meta-analysis and investigation for the source ofbias of left ventricular volumes and function by three-dimensional echo-cardiography in comparison with magnetic resonance imaging. Am J Car-diol 2011;107:126-38.
5. Badano LP, Boccalini F, Muraru D, Dal Bianco L, Peluso D, Bellu R, et al.Current clinical applications of transthoracic three-dimensional echocardi-ography. J Cardiovasc Ultrasound 2012;20:1-22.
6. Shimada YJ, Shiota T. Meta-analysis of accuracy of left ventricular massmeasurement by three-dimensional echocardiography. Am J Cardiol2012;110:445-52.
7. Altman DG. Practical statistics for medical research. London: Chapman &Hall; 1991. 419-426.
8. Dubois D, Dubois EF. Clinical calorimetry. A formula to estimate the ap-proximate surface area if height andweight be known. Arch Int Med 1916;17:863-71.
9. Haycock GB, Schwartz GJ, Wisotsky DH. Geometric method for measur-ing body surface area: height-weight formula validated in infants, children,and adults. J Pediatr 1978;93:62-6.
10. Sluysmans T, Colan SD. Theoretical and empirical derivation of cardiovas-cular allometric relationships in children. J Appl Physiol 2005;99:445-57.
11. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA,et al. Recommendations for chamber quantification: a report from theAmerican Society of Echocardiography’s Guidelines and StandardsCommittee and the Chamber Quantification Writing Group, developedin conjunction with the European Association of Echocardiography,a branch of the European Society of Cardiology. J Am Soc Echocardiogr2005;18:1440-63.
12. Ilercil A, O’Grady MJ, Roman MJ, Paranicas M, Lee ET, Welty TK, et al.Reference values for echocardiographic measurements in urban and ruralpopulations of differing ethnicity: the Strong Heart Study. J Am Soc Echo-cardiogr 2001;14:601-11.
13. SahnDJ, DeMariaA,Kisslo J,WeymanA. TheCommittee onM-Mode Stan-dardizationof theAmericanSocietyofEchocardiography: recommendationsregarding quantitation in M-mode echocardiography: results of a survey ofechocardiographic measurements. Circulation 1978;58:1072-83.
14. Muraru D, Badano LP, Piccoli G, Gianfagna P, Del Mestre L,Ermacora D, et al. Validation of a novel automated border-detection al-gorithm for rapid and accurate quantitation of left ventricular volumesbased on three-dimensional echocardiography. Eur J Echocardiogr2010;11:359-68.
15. Mor-Avi V, Jenkins C, Kuhl HP, Nesser HJ, Marwick T, Franke A, et al.Real-time 3-dimensional echocardiographic quantification of left ventricu-lar volumes: multicenter study for validation with magnetic resonance im-aging and investigation of sources of error. JACC Cardiovasc Imaging2008;1:413-23.
16. Mannaerts HF, van der Heide JA, Kamp O, Stoel MG, Twisk J, Visser CA.Early identification of left ventricular remodelling after myocardial infarc-tion, assessed by transthoracic echocardiography. Eur Heart J 2004;25:680-7.
17. Dorosz JL, Lezotte DC, Weitzenkamp DA, Allen LA, Salcedo EE. Perfor-mance of 3-dimensional echocardiography in measuring left ventricularvolumes and ejection fraction: a systematic review and meta-analysis.J Am Coll Cardiol 2012;59:1799-808.
18. Jenkins C, Bricknell K, Hanekom L, Marwick TH. Reproducibility and ac-curacy of echocardiographic measurements of left ventricular parametersusing real-time three-dimensional echocardiography. J Am Coll Cardiol2004;44:878-86.
19. Pouleur AC, le Polain de Waroux JB, Pasquet A, Gerber BL, Gerard O,Allain P, et al. Assessment of left ventricular mass and volumes by three-dimensional echocardiography in patients with or without wall motion

Journal of the American Society of EchocardiographyVolume - Number -
Muraru et al 11
abnormalities: comparison against cine magnetic resonance imaging.Heart 2008;94:1050-7.
20. Nikitin NP, Loh PH, de Silva R, Witte KK, Lukaschuk EI, Parker A, et al.Left ventricular morphology, global and longitudinal function in normalolder individuals: a cardiac magnetic resonance study. Int J Cardiol2006;108:76-83.
21. Mor-Avi V, Sugeng L, Weinert L, MacEneaney P, Caiani EG, Koch R, et al.Fast measurement of left ventricular mass with real-time three-dimen-sional echocardiography: comparison with magnetic resonance imaging.Circulation 2004;110:1814-8.
22. Missouris CG, Forbat SM, Singer DR, Markandu ND, Underwood R,MacGregor GA. Echocardiography overestimates left ventricular mass:a comparative study with magnetic resonance imaging in patients with hy-pertension. J Hypertens 1996;14:1005-10.
23. Kuhl HP, Hanrath P, Franke A. M-mode echocardiography overestimatesleft ventricular mass in patients with normal left ventricular shape: a com-parative study using three-dimensional echocardiography. Eur J Echocar-diogr 2003;4:312-9.
24. Aune E, BaekkevarM, RodevandO,Otterstad JE. Reference values for leftventricular volumes with real-time 3-dimensional echocardiography.Scand Cardiovasc J 2010;44:24-30.
25. KakuK, TakeuchiM,Otani K, Sugeng L, Nakai H, Haruki N, et al. Age- andgender-dependency of left ventricular geometry assessed with real-timethree-dimensional transthoracic echocardiography. J Am Soc Echocar-diogr 2011;24:541-7.
26. Fukuda S, Watanabe H, Daimon M, Abe Y, Hirashiki A, Hirata K, et al.Normal values of real-time 3-dimensional echocardiographic parametersin a healthy Japanese population: the JAMP-3D Study. Circ J 2012;76:1177-81.
27. Poppe KK, Doughthy RN,Whalley G. Redefining normal reference rangesfor echocardiography: a major new individual person data meta-analysis.Eur Heart J Cardiovasc Imaging 2013;14:347-8.
28. Chahal NS, Lim TK, Jain P, Chambers JC, Kooner JS, Senior R.Population-based reference values for 3D echocardiographic LV vol-umes and ejection fraction. JACC Cardiovasc Imaging 2012;5:1191-7.
29. Badano LP. Defining normative values for 3D left ventricular volumes: thedevil is in the details. JACC Cardiovasc Imaging 2013;6:530.
30. Marwick TH. Application of 3D echocardiography to everyday practice:development of normal range is step 1. JACC Cardiovasc Imaging2012;5:1198-200.
31. Hudsmith LE, Petersen SE, Francis JM, Robson MD, Neubauer S. Normalhuman left and right ventricular and left atrial dimensions using steadystate free precession magnetic resonance imaging. J Cardiovasc MagnReson 2005;7:775-82.
32. Chang SA, Lee SC, Kim EY, Hahm SH, Jang SY, Park SJ, et al. Feasibility ofsingle-beat full-volume capture real-time three-dimensional echocardiog-raphy and auto-contouring algorithm for quantification of left ventricularvolume: validation with cardiac magnetic resonance imaging. J Am SocEchocardiogr 2011;24:853-9.
33. Abo K, Hozumi T, Fukuda S, Matsumura Y, Matsui M, Fujioka K, et al.Usefulness of transthoracic freehand three-dimensional echocardiographyfor the evaluation of mitral valve prolapse [article in Japanese]. J Cardiol2004;43:17-22.
34. Cheng S, Fernandes VR, Bluemke DA, McClelland RL, Kronmal RA,Lima JA. Age-related left ventricular remodelling and associated risk forcardiovascular outcomes: the Multi-Ethnic study of atherosclerosis. CircCardiovasc Imaging 2009;2:191-8.
35. Lakatta EG. Cardiovascular regulatory mechanisms in advanced age.Physiol Rev 1993;73:413-67.
36. Badano LP, Cucchini U, Muraru D, Al Nono O, Sarais C, Iliceto S. Use ofthree-dimensional speckle tracking to assess left ventricular myocardialmechanics: inter-vendor consistency and reproducibility of strain mea-surements. Eur Heart J Cardiovasc Imaging 2013;14:285-93.
37. Gayat E, Ahmad H, Weinert L, Lang RM, Mor-Avi V. Reproducibility andinter-vendor variability of left ventricular deformation measurements bythree-dimensional speckle-tracking echocardiography. J Am Soc Echocar-diogr 2011;24:878-85.
38. Lancellotti P, Badano LP, Lang RM, Akhaladze N, Athanassopoulos GD,Barone D, et al. Normal Reference Ranges for Echocardiography: ratio-nale, study design, and methodology (NORRE study). Eur Heart J Cardi-ovasc Imaging 2013;14:303-8.