COMPARISON OF TRIAGE REVISED TRAUMA SCORE AND ...
91
COMPARISON OF TRIAGE REVISED TRAUMA SCORE AND CRAMS SCALE AS PREDICTORS OF OUTCOME FOR ADULT TRAUMA PATIENT IN EMERGENCY DEPARTMENT, HOSPITAL UNIVERSITI SAINS MALAYSIA DR NOOR HAFIZA BINTI CHE ANI Dissertation Submitted In Partial Fulfillment Of The Requirements For The Degree Of Master Of Medicine (EMERGENCY MEDICINE) UNIVERSITI SAINS MALAYSIA 2017
-
Upload
khangminh22 -
Category
Documents
-
view
7 -
download
0
Transcript of COMPARISON OF TRIAGE REVISED TRAUMA SCORE AND ...
COMPARISON OF TRIAGE REVISED TRAUMA SCORE AND
CRAMS SCALE AS PREDICTORS OF OUTCOME FOR ADULT
TRAUMA PATIENT IN EMERGENCY DEPARTMENT, HOSPITAL
UNIVERSITI SAINS MALAYSIA
DR NOOR HAFIZA BINTI CHE ANI
Dissertation Submitted In Partial Fulfillment Of The
Requirements For The Degree Of Master Of Medicine
(EMERGENCY MEDICINE)
UNIVERSITI SAINS MALAYSIA
2017

ii
ACKNOWLEDGEMENT
First of all, I am grateful to Allah the Almighty for establishing me to complete this
dissertation.
I wish to express my sincere thanks to my supervisor, Dr Tuan Hairulnizam Tuan
Kamauzaman, Lecturer and Emergency physician HUSM for all the knowledge, valuable
guidance, constant encouragement and necessary facilities throughout the process of
producing this study. All the deeds only Allah SWT can be repay.
I also thanks to Dr Najib Wajdi, lecturer of Biostatistic Department, School of Medical
Sciences, USM and Mr Aiman, Statistician, Clinical Research Center, Hospital Sultanah
Bahiyah. I am grateful for their expert and guidance in the process of this study.
I would like to take this opportunity to record my sincere thankful to all the lecturers of
Emergency Department, School of Medical Sciences, Universiti Sains Malaysia for all the
knowledge that I obtained through out this master programme. I also thanks to my colleagues,
and all the staff of Emergency department for all the joy and difficulties that we had been
through together.
I also like to expressed my gratitude to anybody that involved in my study; direct or indirectly
and gave help in this study.
And last but not least to my family, especially Mak and Ayah for unceasing encouragement,
love, support and tolerance throughout my life.

iii
TABLE OF CONTENTS
PAGE
TITLE i
ACKNOWLEDGEMENT ii
TABLE OF CONTENTS iii
ABSTRAK vi
ABSTRACT viii
CHAPTER 1: INTRODUCTION
1.1 Introduction 1
CHAPTER 2: OBJECTIVES
2.1 General Objectives 4
2.2 Specific Objectives 4
CHAPTER 3: MANUSCRIPT
3.1 Title Page 5
3.2 Abstract 6
iv
3.3 Introduction 8
3.4 Methodology 11
3.5 Results 13
3.6 Discussion 15
3.7 Conclusion 17
3.8 References 18
3.9 Tables 21
3.10 Guidelines/Instruction to Authors Of Selected Journal 25
Chapter 4: Study Protocol
4.1 Study Protocol Submitted For Ethical Approval 28
4.2 Patient Information and Consent Form 54
4.3 Ethical Approval Letter 68
Chapter 5: Appendices
5.1 Additional Tables/Graph 73
5.2 Assessment Form 78

v
5.3 Additional Literature Review 80
5.4 Additional References 81
5.5 Raw Data On SPSS Soft Copy 82
vi
ABSTRAK (BAHASA MELAYU)
PENGENALAN: Trauma merupakan masalah kesihatan yang penting dan penyebab
kematian utama dikalangan remaja dan belia. Mengenalpasti tahap kecederaan pesakit
terutamanya yang mengalami kecederaan parah di peringkat awal membantu dalam
perawatan pesakit. Sistem pemarkahan ‘triage’ yang baik dapat meramal tahap kecederaan
pesakit dan dapat membantu pesakit untuk medapat rawatan segera di pusat rawatan trauma.
OBJEKTIF: Membandingkan keberkesanan penggunaan ‘Triage Revised Trauma Score (T-
RTS)’ dan ‘CRAMS Scale’ dalam meramal keadaan pesakit trauma di Jabatan Kecemasan,
Hospital Universiti Sains Malaysia (HUSM)
METODOLOGI: Satu kajian ‘prospective cohort’ yang telah dijalankan selama tiga bulan
bermula dari Disember 2015 sehingga Februari 2016. Penilaian pesakit trauma dewasa telah
dinilai di ‘triage’ dan juga ketika pesakit dipindahkan dari Jabatan Kecemasan, HUSM.
KEPUTUSAN: Seramai 91 pesakit terlibat dalam kajian ini. Keputusan penggunaan T-RTS
menunjukkan seramai 12 orang pesakit (13.2%) telah dikategorikan sebagai major dan 79
orang pesakit (86.8%) telah dikategorikan sebagai minor (median=12, IQR=0). Keputusan
penggunaan ‘CRAMS scale’ pula menunjukkan, seramai 10 orang (11.0%) telah
dikategorikan sebagai major, dan 91 orang pesakit (89.0%) telah dikategorikan sebagai minor
(median-=10, IQR=1). Sensitiviti T-RTS ialah 71.4% manakala sensitiviti ‘CRAMS scale’
ialah 72.4 %. Spesifisiti CRAMS Scale lebih tinggi iaitu 94.0% jika dibandingkan spesifisiti
vii
T-RTS iaitu 91.7%. kedua-dua sistem pemarkahan mempunyai ‘negative predictive value’
yang tinggi iaitu, 97.5% . CRAMS Scale mempunyai nilai ‘positive predictor value’ lebih
tinggi berbanding T-RTS (50.0% dan 41.7%)
KESIMPULAN: Kajian ini menunjukkan bahawa pengunaan CRAMS Scale dapat meramal
keadaan pesakit ketika dipindahkan daripada jabatan kecemasan dengan lebih tepat
berbanding T-RTS. Kajian lanjutan dengan jumlah subjek yang lebih besar dan julat masa
yang lebih lama perlu untuk memastikan kajian seperti ini boleh diaplikasikan
penggunaannya.
viii
ABSTRACT
INTRODUCTION: Trauma is an important health problem and a leading cause of death
among young adults. Early recognition of injury severity could aid in managing trauma
patient. Triage scores that capable to predict outcome would give better assessment of patient
urgency to get proper treatment at trauma center.
OBJECTIVE: To compare the utility of Triage Revised Trauma Score (T-RTS) with
CRAMS Scale in determining outcome of adult trauma patient in Emergency Department
(ED), Hospital Universiti Sains Malaysia (HUSM).
METHODS: A Prospective cohort study that was conducted within three months study
period from December 2015 until February 2016 by assessing adult trauma patients at triage
and their disposition from ED.
RESULT: 91 patients were recruited. For T-RTS, 12 patients (13.2%) were score as major,
and 79 patients (86.8%) were scored as minor (median=12, IQR=0). For CRAMS, 10 patients
(11.0%) were scored as major, and 81 patients (89.0%) were scored as minor (median-=10,
IQR=1). T-RTS sensitivity is 71.4% while CRAMS Scale sensitivity is 72.4 %. CRAMS
score have higher specificity 94.0% compare to T-RTS specificity 91.7%. Both scoring
system have high negative predictive value, 97.5%. CRAMS Scale had higher positive
predictive value compared to T-RTS (50.0% and 41.7% respectively).

ix
CONCLUSION: Our study showed CRAMS Scale was better than T-RTS in predicting
patient outcome from ED. Further study needed to be done with larger sample size and longer
duration in order to improve the reliability of the study.
1
1.1 Introduction
Trauma remains the leading cause of morbidity and mortality in adolescent and young adults
in Malaysia. Malaysia Ministry of Health 2013 report showed that trauma is the third
principal causes of hospital admission and the fifth leading cause of death.1 It is neglected
cause of morbidity and mortality despite many campaigns regarding injury and road traffic
accident prevention had been addressed to public. Most of trauma patients were within their
productive age and disability as result from trauma will reduce patient’s productivity.2
Differences of trauma patients’ mortality and morbidity rates in between countries reflected
the countries health care quality and standard.2
Triage systems are method of systematically prioritizing patient base on patients’ condition
and severity. Its goal is to identify the right patient, bring them to the right place and to get
treatment at the right time.3 Trauma patients will be effectively distributed and will be
managed accordingly at the designated trauma centre.4 A good scoring system with high
accuracy, reliability and specificity enable to predict patients’ outcome.4 It is also will be a
useful tool for prehospital and emergency care triage personnel in managing trauma. Certain
prehospital triage scores able to predict severity of injury, prolonged Intensive Care Unit stay
and massive haemorrhage.5
There are multiple types of trauma triage scoring systems that assessed either patients’
physiological, anatomical or combination of both. Triage score that assessed physiological
component can be done at prehospital or emergency department triage as it used simple
measurement tool such as standard vital sign monitoring devices and also rapid bedside
clinical assessment. Physiological assessment reflects patient’s acute dynamic change post
2
trauma.6 Triage score that used anatomical assessment need more complicated diagnostic
tool especially radiological investigation and only reflects patient injury at one point of time;
thus it is not suitable to be done at prehospital or emergency triage level. Triage Revised
Trauma Score (T-RTS) and CRAMS Scale are the example of trauma scores used
physiological indices, Abbreviated Injury Scale (AIS), Injury Severity Score (ISS) and
Anatomic Profile (AP) are the example of trauma scores that used anatomical indices and
Trauma Score- Injury Severity Score (TRISS) is the example of trauma score that used both
anatomical and physiological indices.7
T-RTS and CRAMS scale were chosen as both scoring system used physiology severity
assessment. Both of this scoring systems could be done at prehospital level and also primary
triage at any hospital. Both scoring systems can be used by inexperienced triage personnel in
identifying severely injured. 7,8 However, comparison of both scoring systems in Malaysia
was not known as no comparison study has been conducted before.
Revision of Trauma Score (TS) consists of Triage Revised Trauma Score (T-RTS) and
Revised Trauma Score (RTS).7,9 Certain parameters of TS are found difficult to be assessed
at field especially capillary refilling time and respiratory expansion. The usage of TS as a
triage tool is replaced by T-RTS; while RTS is used for quality assurance and outcome
prediction.10 The RTS is measured in coded form which GCS is weighted heavily in RTS as
RTS emphasizes the significant impact of traumatic brain injury outcome.9,11
T-RTS is a physiologic injury severity score that numerically summarize assessment of
circulation, respiration and central nervous system function.11 The component of T-RTS
consisted of respiratory rate that were calculated as breath per minute, systolic blood pressure
in mmHg, and Glasgow Coma Scale (GCS). Each component had maximum score of 4
3
(normal value of component being assessed) and minimum score of 0(abnormal value of
component being assessed). Total maximum score is 12 and total minimum score is 0. Score
equal or less than 11 consider major trauma9 with sensitivity of 59% and specificity 82%.11
CRAMS scale is a 10 points scoring system that develop for the purposed of determining
which patient should be sent in trauma centre.12 It consists of 5 component; circulation,
respiration, abdomen/thorax, motor and speech. For each component of CRAMS scale,
normal value is scored as 2, mildly abnormal value is scored as 1 and severely abnormal is
scored as 0. CRAMS scale provides effective in identifying major trauma while ensuring that
minor trauma was not necessarily sent to trauma centre. CRAMS Scale defined major trauma
if score equal of less than 8 and minor trauma with score of 9 and above.12 Patients’ CRAMS
scale score were compared with the final disposition from emergency department.11 The
outcome of CRAMS Scale is considered major if patient died in emergency department, or
went to operating theatre or intensive care unit while outcome is considered minor if patient
was allowed discharge from emergency department.6 CRAMS Scale have high sensitivity,
92 percent, high specificity 98 percent12 and can discriminate well between minor and major
trauma.6,12
The purpose of this study is to compare the utility of T-RTS with CRAMS scale in
determining outcome of adult trauma patient in Hospital Universiti Sains Malaysia (HUSM).
4
2.1 General Objective
To compare the utility of Triage Revised Trauma Score with CRAMS Scale in determining
outcome of adult trauma patient in emergency department HUSM.
2.2 Specific Objectives
1. To determine mean score of Triage Revised Trauma Score and CRAMS Scale of adult
trauma patient who visit emergency department HUSM.
2. To determine the association between patient outcome (major injury/minor injury) with
Triage Revised Trauma Score and CRAMS Scale.
3. To compare sensitivity and specificity of Triage Revised Trauma Score and CRAMS
Scale in determining outcome of adult trauma patient in emergency department HUSM.
5
3.1 Title Page
Comparison of Triage Revised Trauma Score (T-RTS) and CRAMS Scale as Predictors of
Outcome for Adult Trauma Patient in Emergency Department, Hospital Universiti Sains
Malaysia.
Author:
Dr Noor Hafiza binti Che Ani
Emergency Department,
School of Medical Sciences, Universiti Sains Malaysia
16150, Kubang Kerian, Kelantan
Corresponding Author:
Dr Noor Hafiza binti Che Ani
Emergency Department, School of Medical Sciences, Universiti Sains Malaysia
16150, Kubang Kerian, Kelantan, MALAYSIA
Email : [email protected]
Tel. number: +6097676721
Fax. number: +6097673219
6
3.2 Abstract
INTRODUCTION: Trauma is an important health problem and a leading cause of death
among young adults. Early recognition of injury severity could aid in managing trauma
patient. Triage scores that capable to predict outcome would give better assessment of patient
urgency to get proper treatment at trauma center.
OBJECTIVE: To compare the utility of Triage Revised Trauma Score (T-RTS) with
CRAMS Scale in determining outcome of adult trauma patient in Emergency Department,
Hospital Universiti Sains Malaysia.
METHODS: A Prospective cohort study was conducted within three months study period
from December 2015 until February 2016 by assessing adult trauma patients at triage and
their disposition from ED.
RESULT: 91 patients were recruited. For T-RTS, 12 patients (13.2%) were score as major,
and 79 patients (86.8%) were scored as minor (median=12, IQR=0). For CRAMS, 10 patients
(11.0%) were scored as major, and 81 patients (89.0%) were scored as minor (median-=10,
IQR=1). T-RTS sensitivity is 71.4% while CRAMS Scale sensitivity is 72.4 %. CRAMS
score have higher specificity 94.0% compare to T-RTS specificity 91.7%. Both scoring

7
system have high negative predictive value, 97.5%. CRAMS Scale had higher positive
predictive value compared to T-RTS (50.0% and 41.7% respectively).
CONCLUSION: Our study showed CRAMS Scale was better than T-RTS in predicting
patient outcome from ED. Further study needed to be done with larger sample and longer
duration in order to improve the reliability of the study.
Keywords: trauma, injury, triage, Triage Revised Trauma Score, CRAMS Scale

8
3.3 Introduction
Trauma remains the leading cause of morbidity and mortality in adolescent and young adults
in Malaysia. Malaysia Ministry of Health 2013 report showed that trauma is the third
principal causes of hospital admission and the fifth leading cause of death.1 It is neglected
cause of morbidity and mortality despite many campaigns regarding injury and road traffic
accident prevention had been addressed to public. Most of trauma patients were within their
productive age and disability as result from trauma will reduce patient’s productivity.2
Differences of trauma patients’ mortality and morbidity rates in between countries reflected
the countries health care quality and standard.2
Triage systems are method of systematically prioritizing patient base on patients’ condition
and severity. Its goal is to identify the right patient, bring them to the right place and to get
treatment at the right time.3 Trauma patients will be effectively distributed and will be
managed accordingly at the designated trauma centre.4 A good scoring system with high
accuracy, reliability and specificity enable to predict patients’ outcome.4 It is also will be a
useful tool for prehospital and emergency care triage personnel in managing trauma. Certain
prehospital triage scores able to predict severity of injury, prolonged Intensive Care Unit stay
and massive haemorrhage.5
There are multiple types of trauma triage scoring systems that assessed either patients’
physiological, anatomical or combination of both. Triage score that assessed physiological
component can be done at prehospital or emergency department triage as it used simple
measurement tool such as standard vital sign monitoring devices and also rapid bedside
9
clinical assessment. Physiological assessment reflects patient’s acute dynamic change post
trauma.6 Triage score that used anatomical assessment need more complicated diagnostic
tool especially radiological investigation and only reflects patient injury at one point of time;
thus it is not suitable to be done at prehospital or emergency triage level. Triage Revised
Trauma Score (T-RTS) and CRAMS Scale are the example of trauma scores used
physiological indices, Abbreviated Injury Scale (AIS), Injury Severity Score (ISS) and
Anatomic Profile (AP) are the example of trauma scores that used anatomical indices and
Trauma Score- Injury Severity Score (TRISS) is the example of trauma score that used both
anatomical and physiological indices.7
T-RTS and CRAMS scale were chosen as both scoring system used physiology severity
assessment. Both of this scoring systems could be done at prehospital level and also primary
triage at any hospital. Both scoring systems can be used by inexperienced triage personnel in
identifying severely injured. 7,8 However, comparison of both scoring systems in Malaysia
was not known as no comparison study has been conducted before.
Revision of Trauma Score (TS) consists of Triage Revised Trauma Score (T-RTS) and coded
Revised Trauma Score (RTSc).7,9 Certain parameters of TS are found difficult to be assessed
at field especially capillary refilling time and respiratory expansion. The usage of TS as a
triage tool is replaced by T-RTS; while RTSc is used for quality assurance and outcome
prediction.10 The RTSc is measured in coded form which GCS is weighted heavily in RTSc
as RTSc emphasizes the significant impact of traumatic brain injury outcome.9,11
T-RTS is a physiologic injury severity score that numerically summarize assessment of
circulation, respiration and central nervous system function.11 The component of T-RTS
consisted of respiratory rate that were calculated as breath per minute, systolic blood pressure
10
in mmHg, and Glasgow Coma Scale (GCS). Each component had maximum score of 4
(normal value of component being assessed) and minimum score of 0(abnormal value of
component being assessed). Total maximum score is 12 and total minimum score is 0. Score
equal or less than 11 consider major trauma9 with sensitivity of 59% and specificity 82%.11
CRAMS scale is a 10 points scoring system that develop for the purposed of determining
which patient should be sent in trauma centre.12 It consists of 5 component; circulation,
respiration, abdomen/thorax, motor and speech. For each component of CRAMS scale,
normal value is scored as 2, mildly abnormal value is scored as 1 and severely abnormal is
scored as 0. CRAMS scale provides effective in identifying major trauma while ensuring that
minor trauma was not necessarily sent to trauma centre. CRAMS Scale defined major trauma
if score equal of less than 8 and minor trauma with score of 9 and above.12 Patients’ CRAMS
scale score were compared with the final disposition from emergency department.11 The
outcome of CRAMS Scale is considered major if patient died in emergency department, or
went to operating theatre or intensive care unit while outcome is considered minor if patient
was allowed discharge from emergency department.6 CRAMS Scale have high sensitivity,
92 percent, high specificity 98 percent12 and can discriminate well between minor and major
trauma.6,12
The purpose of this study is to compare the utility of T-RTS with CRAMS scale in
determining outcome of adult trauma patient in Hospital Universiti Sains Malaysia (HUSM).
11
3.4 Methodology
This was a prospective cohort study conducted in Emergency Department(ED), HUSM,
Kubang Kerian, Kelantan from December 2015 until February 2016. All trauma patients age
18 years old and above chosen via convenience sampling were included in this study.
Referred trauma patients from other hospital were excluded.
Adult trauma patients were identify and selected at triage upon visited to ED. Patient
demographic data such as age, gender, race and type of trauma were recorded. Vital signs
such as blood pressure, respiratory rate, Glasgow coma Scale (GCS) and examination
findings of the thorax and abdomen were obtained to calculate score for T-RTS and CRAMS
scale. For T-RTS, parameters needed were respiratory rate per minute, systolic blood
pressure in mmHg and GCS. Each parameter had been divided into range of value and the
highest score of each parameters was 4 and the lowest was 0. The summation of each
parameter score were calculated and noted in assessment form (total score maximum was 12,
minimum total score was 0). Score of 12 was categorized as minor injury while score 11 and
below were categorized as major injury.12
Parameter that needed for CRAMS Scale were circulation, respiration, abdomen and thorax,
motor and speech. Each parameter highest score was 2 and lowest score was 0. For
circulation, patients were evaluated based on capillary refilling time or systolic blood
pressure and for respiration was based on breathing pattern. Abdomen and thorax were
evaluated based on present of tender part or patient having rigid abdomen or flail chest. Motor
functions assessment was evaluated based on respond or posture while speech was evaluated
based on vocalization respond. Score from each parameter were sum up (maximum total

12
score was 10, minimum total score was 0). Score of 9 and above were categorized as minor
injury while score 8 and below were categorized as major injury.13
Endpoint of this study was patients’ outcome from emergency department. Patients’
disposition from ED were followed up. The parameter for outcome was either patient was
discharged, admitted to general ward, admitted to intensive care unit or directly to operation
theatre or death in emergency department. Patients’ outcome were categorized into two
categories; major injury or minor injury. They were considered have major injury outcome
if patient died in the emergency department or admission to intensive care unit or directly to
operation theatre.13 Patients who were discharged or admitted to general ward were
considered to have minor injury outcome.11,12
Data management and statistical analysis were done using software IBM SPSS version 22.0.
Descriptive statistic were used for demographic data. The continuous variable was described
in mean and standard deviation while categorical variables such were described in frequency
and percentage. Both scoring systems, T-RTS and CRAMS were divided into major (T-RTS
score <12, CRAMS score < 9) and minor (RTS score 12, CRAMS score >8) injury describe
in frequency, percentage and interquartile range.
Independent T -test was used for association of patients’ age and outcome while Fisher Exact
test was used to analyse association of both scoring systems and categorical variables with
patient’s outcome. Sensitivity and specificity of T-RTS and CRAMS scale were evaluated
using crosstabs. Negative Predictive Value (NPV) and Positive Predictive Value (PPV) were
estimated for both T-RTS and CRAMS Scale. Kappa statistic test were used to obtained
accuracy and agreement for both scoring.
13
This study had obtained ethical approval from Human research Ethics Committee, Universiti
Sains Malaysia (USM/JEPeM/15030102).
3.5 Results
A total number of 91 adult trauma patients who visited ED between December 2015 and
February 2016 were included in this study. The mean age of all adult trauma patient was
38.5±19.29 years old. The majority of the respondents were male (n=68, 74.7%). Most of
patients were Malay (n=86, 94.5%), followed by Chinese (n=3, 3.3%), Indian (n=1, 1.1%)
and others (n=1, 1.1%). Majority of patients involved in road traffic accident (n=54, 59.3%).
All patients were scored on both T-RTS and CRAMS Scale. The median score for T-RTS
was 12 (IQR=0). Twelve patients (13.2%) were classified as major injury, while the rest
(n=79, 86.8%) were classified as minor injury. By CRAMS Scale, the median score was 10
(IQR=1). Ten patients (11.0%) were classified as major injury, while the rest (n=81, 89.0%)
were classified as minor injury. All patients were followed up for their outcome. Our study
showed that 84 patients (92.3%) had minor injury outcome which was either discharged
home after emergency visit or been admitted to general ward. Seven patients (7.7%) had
major injury outcome which was either admitted to ICU, sent directly to operation theatre or
died in ED (Table 1).
The mean age for major injury outcome was 27±7.42 years old while the mean age for minor
injury outcome was 39±19.68 years old. There was a significant association of patient age
with patients’ outcome (p=0.003). Among trauma patients who had involved in road traffic
14
accident, 42 patients (87.0%) had minor injury outcome while another 7 patients (13.0%) had
major injury outcome. All patients who had not involved in road traffic accident had minor
injury outcome (n=37, 100%). Type of trauma had a significant association with patients’
outcome (p=0.039).
For male patients, 61 patients (89.7%) outcome were minor injury while another 7 patients
(10.3%) outcome were major injury. All female patients had minor injury outcome. However,
there was no significant association of patients’ gender with their outcome (p=0.185). Our
results also showed that there was no significant association of patients’ race with their
outcome post trauma (p=1.000). Among the Malays, outcome of 79 patients (89.7%) were
minor injury and outcome for another 7 patients (8.1%) were major injury.
Among the twelve patients who were classified by T-RTS as major injury, 7 patients (58.3%)
had major outcome and 5 patients (41.7%) had minor outcome. Among the 79 minor injury
patients as classified by T-RTS, 77 patients (97.5%) had minor outcome while other 2
patients (2.5%) had major outcome. Ten patients had been classified by CRAMS Scale as
major injury of which five patients (50%) had major outcome while another five patients
(50%) had minor outcome. For 81 patients with CRAMS Scale classified as minor injury, 79
patients (97.5%) had minor outcome while another 2 patients (2.5%) had major outcome.
There was a significant association for both patients’ T-RTS and CRAMS Scale scores with
patients’ outcome (p<0.001). (Table 2)
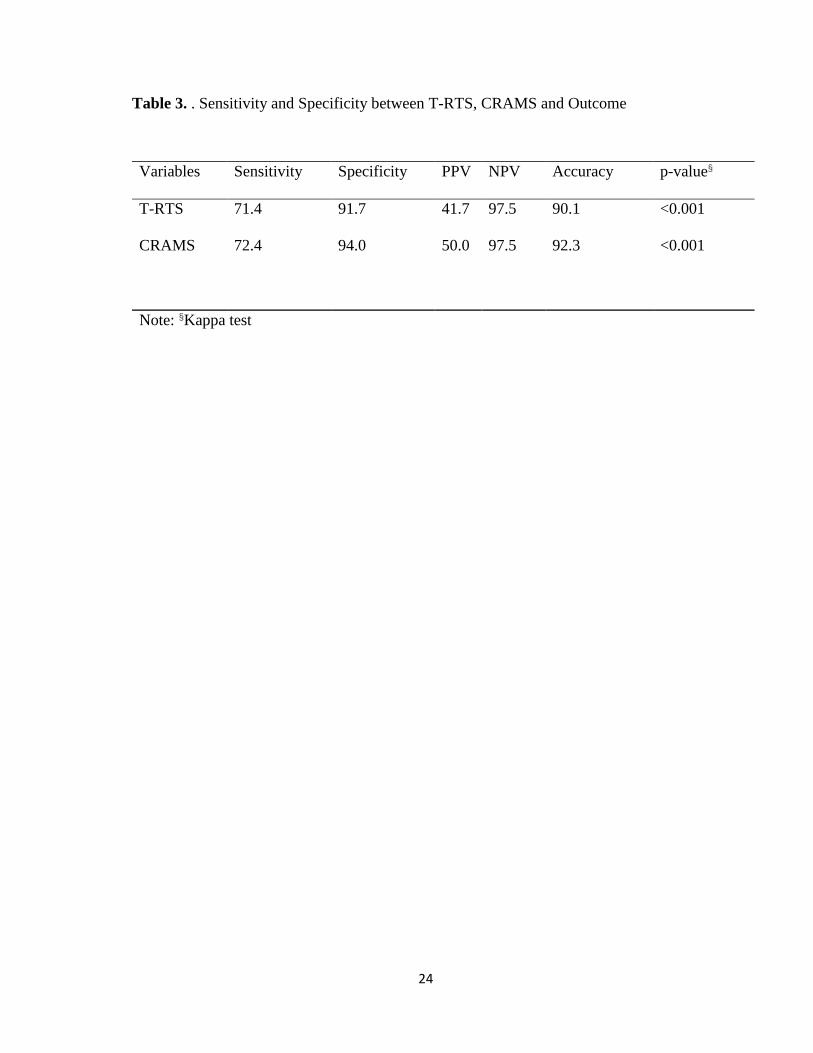
With crosstabs analysis, T-RTS had a sensitivity of 71.4% while CRAMS Scale had
sensitivity of 72.4% of predicting patient outcome in ED. CRAMS Scale had higher
specificity (94.0% as compared to T-RTS (91.7%). T-RTS and CRAMS Scale have high
NPV (97.5%) with high accuracy (90.1% and 92.3% respectively). Both scoring systems

15
however had low PPV (T-RTS 41.7% and CRAMS 50.0%). Comparison of both scoring
systems using Kappa test analysis showed moderate agreement with Kappa=0.54 (p<0.001).
(Table 3)
3.6 Discussion
Trauma among adults were more common in younger age group especially between 21 to 40
years old.14-15 Majority of trauma patients were Malay. There was different findings with
other center in Malaysia in view of high Malay population in study area, Kelantan (92.3%)
in 2015 compared to Malaysia population (50.78%).16 Road traffic accident was major type
of trauma encountered by patients. However the percentage was lower in these study
population compared with other centers.14-15 The differences were due to only adult trauma
patients who visited to emergency department in HUSM were chosen to be involved in this
study and referral cases were excluded.
Most of trauma patients were categorized as minor for both T-RTS and CRAMS Scale. The
figure showed similar result with other study.17 The percentage of trauma patients scored
major were very minimal due to multiple factor. Few factors were identified such as
investigator had difficulty in getting consent as the surrogate relatives were not available and
referral case from other hospitals were excluded. Actual comparison with other study was
not feasible with limited references in view of most study involving T-RTS and CRAMS
were done retrospectively rather than prospectively. The outcome of trauma patients that had
been followed up also showed major injury comprised only small number of patient
16
compared to minor injury. The percentage of major injury also differed from other study due
to similar factor stated before prior to data collection.12
Age factor did correlates with severity of injury. Majority of patients who had major injury
were within young age group and the figure similar to Malaysia’s figure with 54.3% of major
injury occur in patients within 15 to 34 years old.14 This situation was not bizarre in view of
urbanization and economic status with vehicle ownership at younger age and involvement in
high risk behavior such as disobedience to the road traffic laws, non-adherences to the
personal protective equipment such as helmets and safety belt and also illegal racing.18
Types of trauma did correlate with severity of injury. Among major injury victims, majority
were due to road traffic accident and it was similar to Malaysia’s figure.14 Majority of road
traffic accidents involved high impact mechanism especially the vehicular speed prior to
incidents and these caused severe injuries especially to the head, neck, limb and abdomen.
T-RTS and CRAMS Scale had low sensitivity (71.4% for T-RTS and 72.4% for CRAMS).
Sensitivity from this study was low compared to similar study that had been done in United
Kingdom (UK).17 However this study and study that had been done in UK showed the
sensitivity of CRAMS Scale were low compared to actual CRAMS Scale study (92.0%) and
also it validation study (100%).5,12-13 For T-RTS, it showed different result. In this study
sensitivity was 71.4% compared to study had been done in UK (61.0%).18 Actual T-RTS
study showed lower sensitivity (59%). Despite of lower T-RTS sensitivity compared to
CRAMS Scale, it is widely used and being studied in multiple trauma center in the world due
to feasibility of assessment that involved only three physiological parameter.

17
Our study shows that T-RTS and CRAMS Scale had high specificity (T-RTS for 91.7% and
94.0% for CRAMS Scale). The findings varies if compared to actual study. For T-RTS, actual
T-RTS study showed lower specificity (82%). However, result showed higher specificity
(90%) in a study done in UK.11,18 CRAMS Scale had high specificity (94%). However, actual
CRAMS Scale showed higher specificity (98%). A study done in UK showed different result
as CRAMS Scale specificity was only 75%. Our study and a study done in UK showed
similar findings; both studies had high negative predictive values with low positive predictive
values.
Presence of results variability and also limited number of comparison studies that had been
conducted using these two scoring system made it difficult to determine which scoring
systems could be used for adult trauma patient in prehospital or triage in ED.
Limited number of study used CRAMS Scale as prehospital triage tool even though it has
higher sensitivity and specificity if compare to T-RTS. Few studies had been conducted
against the usage of T-RTS in view of poor prognostic value. Study done Switzerland showed
that high incidence of major injuries to chest, abdomen and extremities among patients with
T-RTS maximum score 12.19 The T-RTS also was noted inaccurately triage patients with
major injuries. Some patients were scored as minor injury using T-RTS however were noted
to have major injuries during treatment.20

18
3.7 Conclusion
Our study showed CRAMS Scale was better than T-RTS in predicting patients’ outcome
from ED. Further study needed to be done with larger sample size and longer duration in
order to improve the reliability of the study.
Acknowledgement
Special thanks to Dr Tuan Hairulnizam Tuan Kamauzaman, Supervisor and Senior Lecturer,
Emergency Department, School of Medical Sciences, Universiti Sains Malaysia (USM), Dr
Najib Wajdi, Statistician, Biostatic Unit, School of Medical Sciences, USM and En. Aiman,
Statistician, Clinical Research Center, Hospital Sultanah Bahiyah, Alor Setar for their expert
advice and guidance along the process for completion of this study.
3.8 References
1. Planning Division HIC. Health Facts 2014. In: Ministry of Health M, editor. 2014.
2. Arokiasamy JT, Krishnan R. Some epidemiological aspects and economic costs of
in Malaysia. Asia-Pacific Journal of Public Health. 1994;7(1):16-20.
3. Batchelor J. Adult prehospital scoring systems: a critical review. Trauma. 2000;2(4):253-
60.
4. Chawda M, Hildebrand F, Pape HC, Giannoudis PV. Predicting outcome after multiple
19
trauma: which scoring system? Injury. 2004;35(4):347-58.
5. Raux M, Sartorius D, Le Manach Y, David J-S, Riou B, Vivien B. What do prehospital
trauma scores predict besides mortality? Journal of Trauma and Acute Care Surgery.
2011;71(3):754-9.
6. Champion H. Trauma scoring. Scandinavian Journal of Surgery. 2002;91(1):12-22.
7. Gilpin D, Nelson P. Revised trauma score: a triage tool in the accident and emergency
department. Injury. 1991;22(1):35-7
8. Chew KS, Chan HC. Prehospital care in Malaysia: issues and challenges. International
Paramedic Practice. 2011;1(2):47-51.
9. Rehn M, Perel P, Blackhall K, Lossius HM. Prognostic models for the early care of
trauma patients: a systematic review. Scandinavian journal of trauma, resuscitation and
emergency medicine. 2011;19(1):17.
10. Nickson C. Trauma Scoring Systems lifeinthefastlane.com; 2014 [cited 2017].
11. Champion HR, Sacco WJ, COPES WS, GANN DS, Gennarelli TA, Flanagan ME. A
revision of the Trauma Score. Journal of Trauma and Acute Care Surgery.
1989;29(5):6239
12. Gormican SP. CRAMS scale: field triage of trauma victims. Annals of emergency
medicine. 1982;11(3):132-5.Champion H. Trauma scoring. Scandinavian Journal of
Surgery. 2002;91(1):12-22.
13. Lidal IB, Holte HH, Vist GE. Triage systems for pre-hospital emergency medical
services-a systematic review. Scandinavian journal of trauma, resuscitation and
emergency medicine. 2013;21(1):1-6.
20
14. Sabariah Faizah Jamaluddin MAW, Fatahul Laham Mohamed,, IsmailMohd Saiboon
MIZ, Mohd Yusof Abdul Wahab. National Trauma Database January 2008 to December
2008 – Third Report. National Trauma Database
15. Andrew Gunn RIA, Yuzaidi Mohamad, Azuddin Mohd Khairy, Norazlin Md Noh,
Izzianie Ibrahim, Mohamad Faizul Sanusi. Trauma Registry Report 2011-2012. Ministry
of Health, Malaysia. 2012
16. Jabatan Perangkaan Malaysia. Penduduk Malaysia Mengikut Negeri dan Kumpulan
Etnik, 2015 http://pmr.penerangan.gov.my/:
17. Gray A, Goyder E, Goodacre S, Johnson G. Trauma triage: a comparison of CRAMS and
TRTS in a UK population. Injury. 1997;28(2):97-101.
18. Rehman H, Zulkifli N, Subramaniam K, editors. Car occupants accidents and injuries
among adolescents in a state in Malaysia. Proceedings of the Eastern Asia Society for
Transportation Studies; 2005
19. Giannakopoulos GF, Saltzherr TP, Lubbers WD, Christiaans HM, van Exter P, de Lange–
de Klerk ES, et al. Is a maximum Revised Trauma Score a safe triage tool for Helicopter
Emergency Medical Services cancellations? European Journal of Emergency Medicine.
2011;18(4):197-201.
20. Sturms LM, Hoogeveen JM, Le Cessie S, Schenck PE, Pahlplatz PV, Hogervorst M, et
al. Prehospital triage and survival of major trauma patients in a Dutch regional trauma
system: relevance of trauma registry. Langenbeck's Archives of Surgery.
2006;391(4):343-9.

21
3.9 Tables
Table 1. Sociodemographic Characteristics and Clinical Variables of the Samples
Variables n (%) Mean (SD) Median (IQR)
Age
38.5(19.29)
Gender
Male 68(74.7)
Female 23(25.3)
Race
Malay 86(94.5)
Chinese 3(3.3)
Indian 1(1.1)
Others 1(1.1)
Type of Trauma
RTA 54(59.3)
non RTA 37(40.7)
T-RTS
12(0)
Major 12(13.2)
Minor 79(86.8)
CRAMS
10(1)
Major 10(11.0)
Minor 81(89.0)
Outcome

22
Discharge 49(53.8)
Admit 35(38.5)
ICU/Operation Theatre 4(4.4)
Death 3(3.3)
notes: SD = Standard Deviation, IQR= Interquartile Range
23
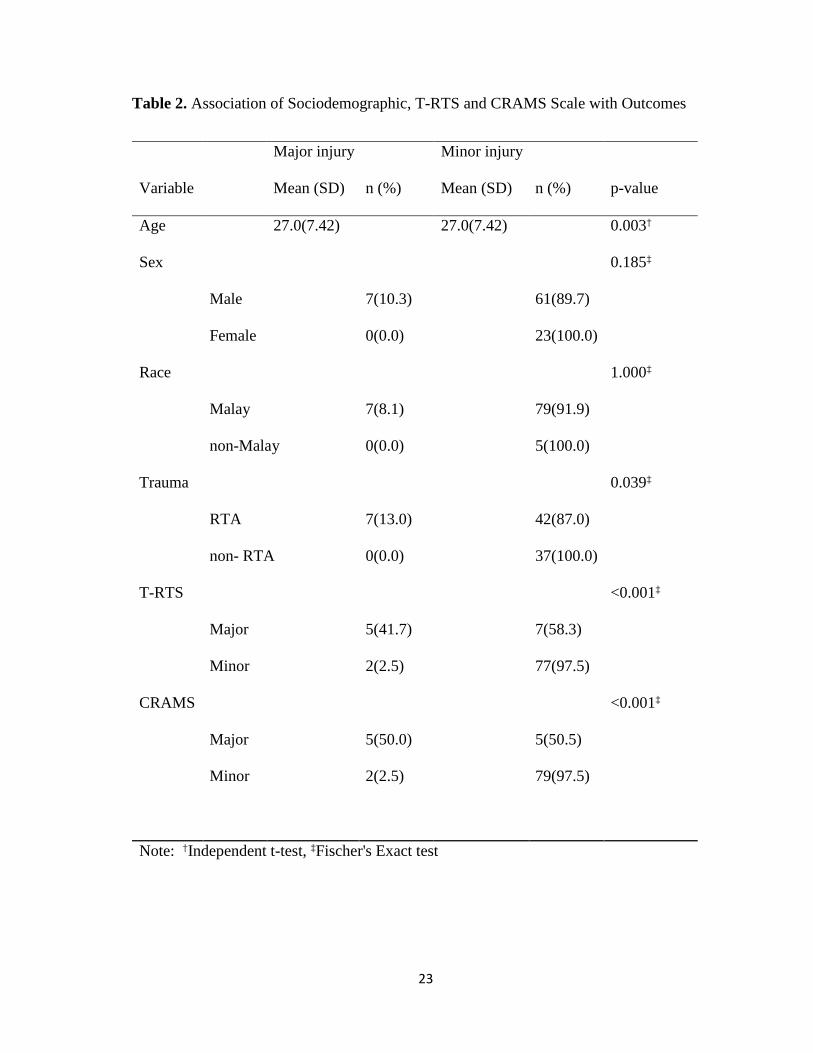
Table 2. Association of Sociodemographic, T-RTS and CRAMS Scale with Outcomes
Major injury Minor injury
Variable Mean (SD) n (%) Mean (SD) n (%) p-value
Age
27.0(7.42) 27.0(7.42) 0.003†
Sex
0.185‡
Male
7(10.3)
61(89.7)
Female
0(0.0)
23(100.0)
Race
1.000‡
Malay
7(8.1)
79(91.9)
non-Malay 0(0.0)
5(100.0)
Trauma
0.039‡
RTA
7(13.0)
42(87.0)
non- RTA 0(0.0)
37(100.0)
T-RTS
<0.001‡
Major
5(41.7)
7(58.3)
Minor
2(2.5)
77(97.5)
CRAMS
<0.001‡
Major
5(50.0)
5(50.5)
Minor
2(2.5)
79(97.5)
Note: †Independent t-test, ‡Fischer's Exact test
24
Table 3. . Sensitivity and Specificity between T-RTS, CRAMS and Outcome
Variables Sensitivity Specificity PPV NPV Accuracy p-value§
T-RTS 71.4 91.7 41.7 97.5 90.1 <0.001
CRAMS 72.4 94.0 50.0 97.5 92.3 <0.001
Note: §Kappa test

25
3.10 Guidelines/Instruction to Authors of Selected Journal
Hong Kong journal of Emergency Medicine
GlUU! II ~IIHU
Instruction to Authors
I
Tha Hong Kong Journal of Emergency Medicine is a peerrevieY.ed bi-monthly biomodical pl.tllication of the Hong KorQ Colege of
Emergency Medicine and Tha Hong KorQ Society for Emergency Mecicine and Surgery. Tha Journal pttishes origonal research atticiBs,
review articles, case reports. and arucational inlorrretion relsled lo alespec1s of clnical practice and emergency medicine research in the hospital and prehospital sailings. Tha Journal is indexed in EMBASE!Excerpta Medica, Science Citation Index Expended (SCIE) and
Scopus.
Copyright
AI manuscripts subrrltted 1o the Hong KorQ JOt.rnal of Ernotgency Medici'la roost be original WD<1<s that haw nol been previously publshed. Folowing acceptance, the Hong KorQ Journal of Emergency Medicine reserws c:opyriglt of al published materials and such materials may
not be reproduced In any form wilhout the witten pemission of the Journal
Uablllty and ethlca AI statements in er1ides are the rosponsibility of the authors. Tha Editorial Board, the Hong Kong Colege of Emergency Medicine and Tha Hong Kong Society for Emergency Medicine and Surgery accept no responsibiity or lability for materials comined herein. Authors
are expected to COI11liY with the provisions of the Declaretion of Helsinki. Patient confodereiaity and anonyrrity shotAd ~ys be preserved.
Style and ravl- procau AI rn&roJScripts should be witten In Englsh. Speling shotAd ~ lha Concise Oxford Dictionary. Maoosetipts shotAd folow the style of lha Vancouver agreement detailed In the International Cornnittee of Medical Jo<Xnal Editors' "Uriform Requlremants for Maoosetipts Submitted
1o BlomeQcal Journals: Writing and Editing for Biomedical Pldcation".
AI rnaroscripts wil be subjected lo edlorial review. Those that do not COI11liY with lha instructions lo authors, or those that are of insufficiert
lnteres~ wil be returned. Retained rneruscripts wil be sent for peer review. Re~ and authors wil be blnded to e ach other. Tha final decision of acceptance rests with lha Editorial Boanl. Rejected manuscripts wil be destroyed ll'lless requesled by lha author, in advance, to
be returned.
1he Editorial BoarO reserves lha right 1o edt al ar1ides for lha PlXJX>S9 of style. lonna! and clarity. Authors may be requored 1o revise their
maoosetipts for reasons of style and content Manuscripts with excessive typograptical errors may be returned 10 authors for retyping.
Compliance by authors to requesled revisions does not autorneticaly bind lha Journallo publsh the articles. SIIJrritled maoosetipts for one category may be publshed LWlder another category, suqect 10 the decision of the Editorial Board llustrelions wil generaly be published In blacll and ..ole. Special request from authors for reproduciag colour figures wil be enlertained fri.J if they pay lha ...nota cost in advance.
Manuacript aubmiaaion Manuscripts can only be subrrltted electronicaly tlvotql the email.
Manuscripts shotAd be sent to: E<ilor..Jn..Chief, Hong KorQ Jou:nel of Emergency Medicine
Hong Kong Colege of Emergency Medicine
Room 809. HK Academy of Medicine Jockey Cklb Building
99 Wong Chuk Hang Roed, Aberdeen Hong Korg. Chine
let (852) 28718877 Fax: (852) 2554 2913
ErnaR: hkjem@hi<am.org.hk
N.....,.,. al pages in the folowing sequence, begirdlg with
the title page as 1, as: •
t . Title pege;
2. Abstract; 3. Text;
26
4 . Ackoo-.Aedgements;
5. References;
6. Tables and legends;
7. Agu-es and legends; and
8 . Appendix.
Type al metler on A4 size paper (212 x 297 nm), dol.tllespaced and on one side only. Leave 25 nm rnal'jjns on al sides of the page. The
right hand mel'jjn of the text sho"*l not be )Jstified.
Conventional menuiiUipts
The manuscripts should be arranged as folows, wilh each seetion beginning on a separate page: -
The covering lettBr
Manusaipls should be 8CCOf11l8l1ied by a cowring letter sig'oed by al co-au1hors. l1is should include: a. Information on prior pU:icalion or submission eisa>lhere of any part of the ...,ri<; b. A statement lhal the n.ruscript has been read and approved by al authors;
c. Disclosure of al fonancial support and potential conficts of irmrests; and
d. ArTy ad<ilional information lhal may be he\>lul to the Echlrial Board.
Tttlepage The title page should lncJude, in the toilo'Mng Older: -
1. The title of the article (do nol use abbreviations);
2. A short n.rnng title of nol more lhan 50 characters (inc:Uing spaces);
3. Ful names of authors (Uflderine farrily names and prollide Chinese names, if available);
4. A maximum of th,.... quallllcatlona for each author;
5. Position of authors and nan.s of departments and institutions to ...tich they are attached, incWng COf1lllele postal addressas; and 6. Name, address, email address, telephone and fax r'UI"bers of the author for correspondence.
Abstmct
A surrrnary of the paper rrust be In the form of a structured abstract (maxirn.mof 250 ..,.,.-<~s for original articles and reviews, and 150 ...,rds for case reports) using the folowing format lnlroduction, Methods, Results and ConcaJsKlns.
KIJywords
Select up to a mexirn.m of five keY""'fds lhat do not ~te words in the title, in alphabetical order. Key..,.,.-ds should be taken from the US
National Ubrary of Medicine's Subject Headings (MeSH) browser tisL If suitable MeSH terms aro not yet available for recently introduced terms, present terms rrey be used. Do not abbrwate Key..,.,.-ds.
Mamtext
Original articles should norrrely nol exceed 15 typewltl8n pages Including tables, ilustrations and references unless absolJ!ety necessary.
It should be divided Into the folowing sections: Introduction. Methods, Results, and Discussion. Cite In numerical order every reference,
f~e and table. The order of mention in the text determnes the number given to each.
SlaliSiical methods
ArTy statistical method used should be detailed in the methodology section of the paper and any nol ln comnon use should be described in
detail and supported by reference. Urits of measurement System lntemational (SI) urits should be used for measurements.
Drug names In general, generic names should be used. Brand names may be Inserted in parenthesis.
Abbroviations Abbrwalions may be used and should be defoned In the Ab5tract and on first mention in the texL In general, a term should not be
abbreviated unless 11 IS used repeatedy. Avoid abbreVIBbOns in the title.
Acknowledgement As a footnote to the text, one or more statements co"*l specify:
a. Persons 1M1o have mede gerUn& conlrlbutions and 1M1o endorse the data and concl.lslon6;
b. Grants, olher financial or rreterlal support; andlor c. Tedrical he_,.
R&f&rences
Provide a ist ol references after the main text. Place ir'd1IOJal reference I1Uil'bers lnme<iately alter lhe text In Arable numerals in
27
superscript. Nl.<liler the references in the oroer of which they are mentioned in teld in Vancouver style. References cited od/f in tables or
in legends to f~gLn~s should be nl.<lilered in aceotdance ¥lith a sequence estabished by the first ldentifocation in the teld of the particular
table or ilkJstration. Cite ~shed data and personal COITilUlications in the teld only. In the reference is1, abbreviate the titles of journals
according to MEDLIN E.
If the pumal is not indexed, the tille should be v.ritten in ful. Ust the first six authors of each reference, folo....OO by et alv.t.en there ere more
than six. Cite also the issue nl.<liler, if available.
Tables Tables should be included on a separate page, nl.<lilered \lith Arabic numerals and IICCOII'4l'lnied by short tilles at the top. Each table must
be referred to in the teld in consecutl\19 order. Data presented should, in general, not be dupicated in the teld or ~s. Explanatory
matter should be placed in foolnotes below the table and not included in the title. AI non-standard abbreviations should also be explained in lhe footnotes. Footnotes should be indicated by·. t, :t. §.Vertical rules and horizontal rules between entries should be orritted.
Figure legends
AI ilkJstrations are classified as figlxes and should be nl.<1ilered \lith Arabic runerals in the oroer in \V1ich they are referred to in the text.
When syrrbols, arrows and ~s or letters are used to identify parts of ilkJstrations. each one should be identified and explained in the
legend.
Figures
Une dra>Mngs and ga~ should be professionaly dra'MI. AI lettering should be done professionaly end should be of edaquate size 1o
retain clarity after reduction. Photographs must be sherp, glossy black and v.tite prints. Photomicrographs should have internal scale
markers. For radiogaphs, n subrrission of photographic prints is not possible, please enclose one copy of each of the radioga~. Please
note that original materiai-MI not be reh.med to the author lriess a specific request is made in the covering letter. Indicate the top end by
use of an arrow at the back of the print. Patients shown in photogra~ shoukl have their identity concealed (cropped sufficiently or eye bar
used) or should have given 'Mitten consent for pubicetion.
The size of photog-aphs end chv.ings should not exceed 280 mn x 400 nm. Identify and nurrber in Arabic ftgUres in the oroer of v.tich they
are mentioned In the text. Toties and detailed eJqllanations should be confined to legends and not Included in the ilkJstrations.
Alternatively, the Illustrations may be subrritted in highresOOtion electronic files.
Permission Wholesale reproduction of al previously pubished tables, cherts, ftgUres and photog-a~ v.il require written permission from the pubisher or author concerned. The source must be given in lui. Reproduction of modified data \Iii require at least a reference citing.
Proofs Authors ¥lith their article in production v.ill be provided v.ith page-proofs to proofread for typesetting errors. Proofs must be returned by the
specified date; olherv.ise the articles may be signed off by the E<itor-irH:hief or held over to the next issue.
67001 reads
28
4.1 Study Protocol Submitted For Ethical Approval
COMPARISON OF TRIAGE REVISED TRAUMA SCORE AND CRAMS SCALE
AS PREDICTORS OF OUTCOME FOR ADULT TRAUMA PATIENT IN
EMERGENCY DEPARTMENT HUSM
Introduction
Trauma is important health problem and leading cause of death in adolescent and young
adults. In Malaysia, mortality from trauma, especially road traffic accident is the fifth leading
causes of death in 2008 (Jabatan perangkaan Malaysia:statistic cause of death 2008) and
the number is forecast to be elevated (Rohayu et al, 2012).Is a neglected causes of morbidity
and mortality despite multiple campaigns have been addressed and advocated to public
regarding trauma and road traffic accident prevention.
Presence variability of mortality and morbidity of trauma patient in between centres and
countries reflects the differences in quality of management (Chawda et al, 2004). It is vital a
study to be conduct in order to make sure the population comparable with the prognostic
variable used. Presence of satisfactory scoring system that fulfil certain requirement is
needed. A good scoring system able to predict the outcome, give good comparison of
therapeutic methods and a useful tool for pre-hospital and emergency care triage if it provides
good accuracy, reliability and specificity (Chawda et al, 2004).

29
Goal of triage is to identify trauma patients that will need a high level of trauma care. It will
bring patient the center that will be most capable of managing patient and efficiently
distribute patients from multiple casualty events. In a study, 56 % of all trauma patient and
36 % of major trauma patient failed to receive care at designated trauma facilities. Triage
system are method for systematic prioritizing system of patient for urgency of treatment and
care. However, there is lack scientific documentation evaluating whether or not pre-hospital
triage system are effective (Lidal et al, 2013).
Literature Review
Triage Revised Trauma Score
Revised trauma score (RTS) is develop in 1989 (Champion et al, 1989). It is revision of
Trauma Score (TS) consists of Triage Revised Trauma Score (T-RTS) and coded Revised
Trauma Score (RTSc). The usage of TS as a triage tool is replaced by T-RTS; while RTS is
used for quality assurance and outcome prediction. The RTS is measured in coded form
which GCS is weighted heavily in RTSc as RTSc emphasizes the significant impact of
traumatic brain injury outcome.
T-RTS it is a physiologic injury severity score that numerically summarize assessment of
circulation, respiration and central nervous system function. It is develop as noted difficulty
in previous Trauma Score that was develop in 1981(Champion et al, 1981) in assessing
certain parameter at field especially capillary filling time and respiratory expansion. T-RTS
can be used in pre-hospital and emergency care setting. (Champion et al, 1989).
30
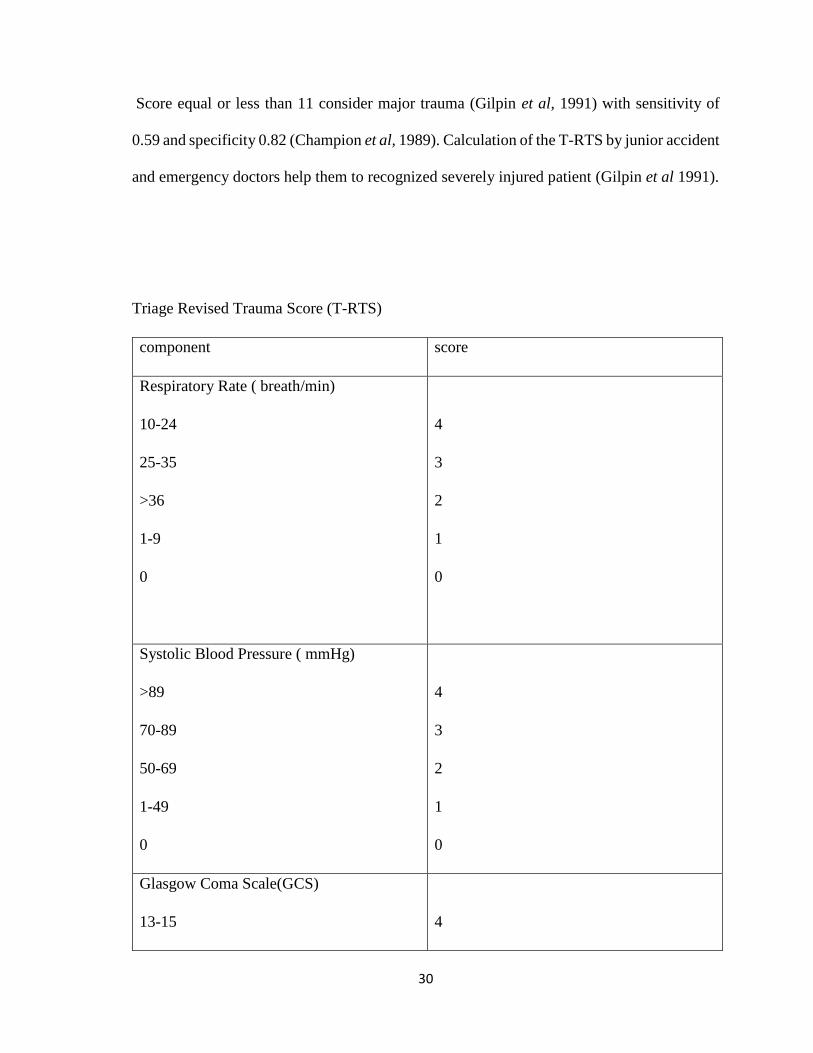
Score equal or less than 11 consider major trauma (Gilpin et al, 1991) with sensitivity of
0.59 and specificity 0.82 (Champion et al, 1989). Calculation of the T-RTS by junior accident
and emergency doctors help them to recognized severely injured patient (Gilpin et al 1991).
Triage Revised Trauma Score (T-RTS)
component score
Respiratory Rate ( breath/min)
10-24
25-35
>36
1-9
0
4
3
2
1
0
Systolic Blood Pressure ( mmHg)
>89
70-89
50-69
1-49
0
4
3
2
1
0
Glasgow Coma Scale(GCS)
13-15
4
31
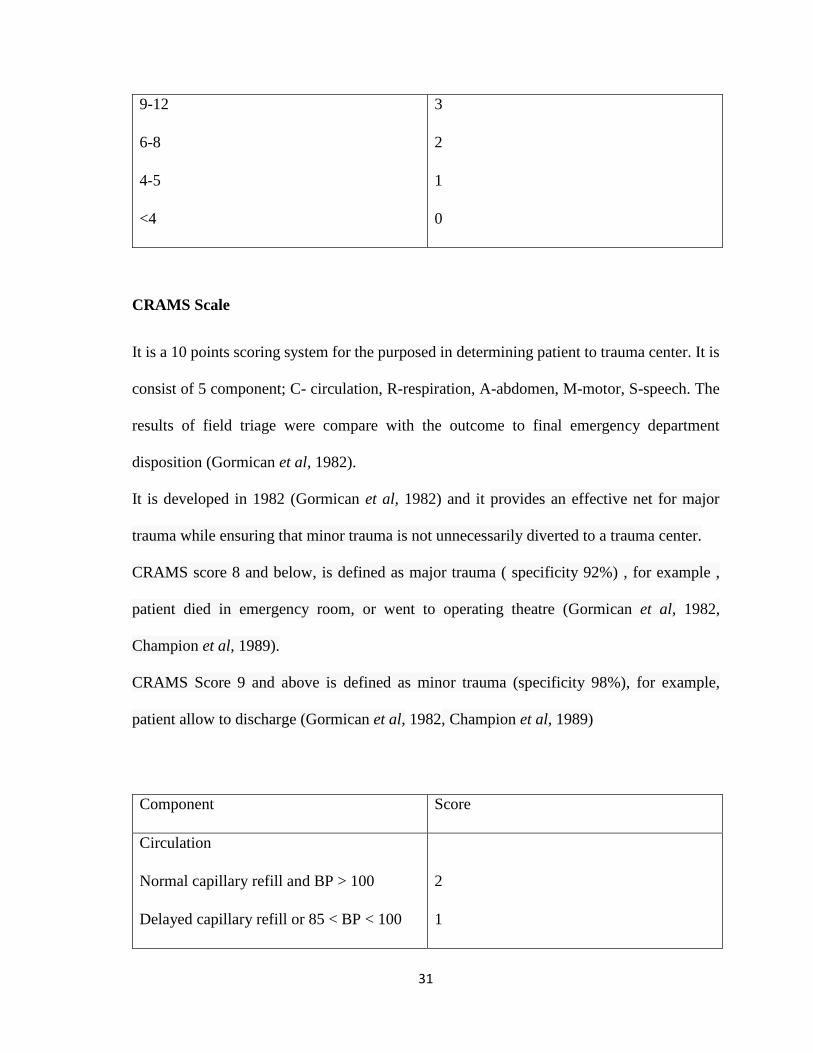
9-12
6-8
4-5
<4
3
2
1
0
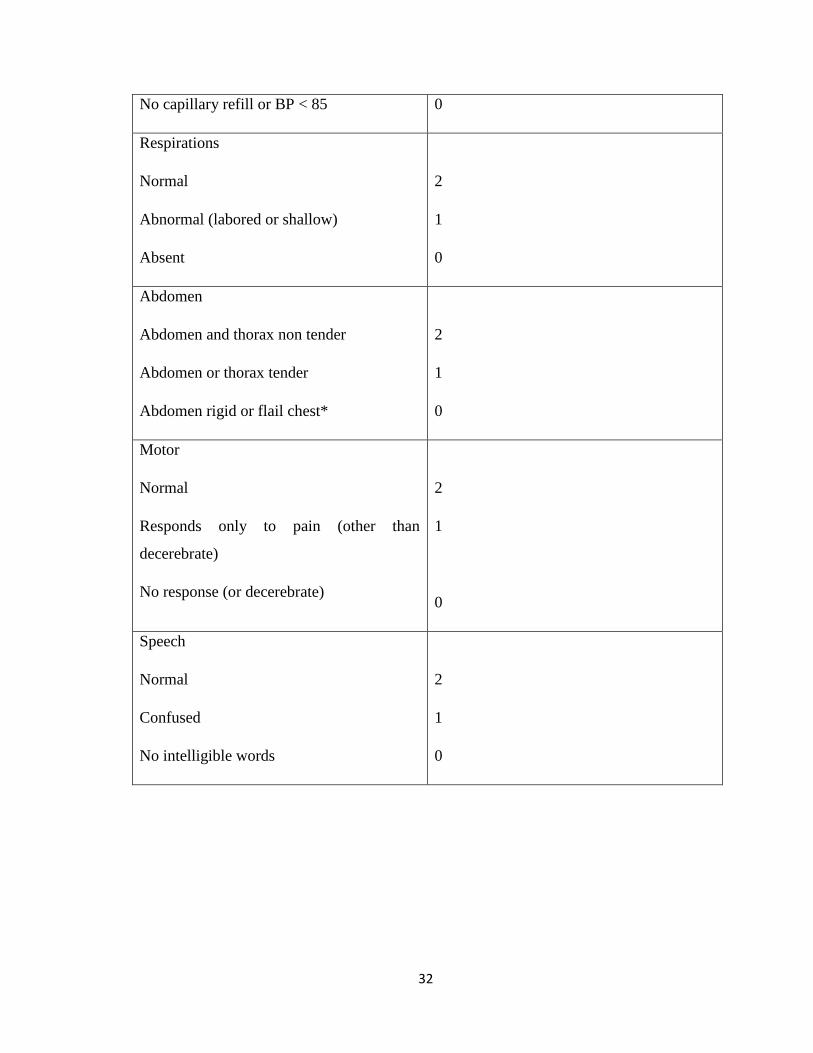
CRAMS Scale
It is a 10 points scoring system for the purposed in determining patient to trauma center. It is
consist of 5 component; C- circulation, R-respiration, A-abdomen, M-motor, S-speech. The
results of field triage were compare with the outcome to final emergency department
disposition (Gormican et al, 1982).
It is developed in 1982 (Gormican et al, 1982) and it provides an effective net for major
trauma while ensuring that minor trauma is not unnecessarily diverted to a trauma center.
CRAMS score 8 and below, is defined as major trauma ( specificity 92%) , for example ,
patient died in emergency room, or went to operating theatre (Gormican et al, 1982,
Champion et al, 1989).
CRAMS Score 9 and above is defined as minor trauma (specificity 98%), for example,
patient allow to discharge (Gormican et al, 1982, Champion et al, 1989)
Component Score
Circulation
Normal capillary refill and BP > 100
Delayed capillary refill or 85 < BP < 100
2
1
32
No capillary refill or BP < 85 0
Respirations
Normal
Abnormal (labored or shallow)
Absent
2
1
0
Abdomen
Abdomen and thorax non tender
Abdomen or thorax tender
Abdomen rigid or flail chest*
2
1
0
Motor
Normal
Responds only to pain (other than
decerebrate)
No response (or decerebrate)
2
1
0
Speech
Normal
Confused
No intelligible words
2
1
0

33
Problem Statement
Triage systems are method for systematic prioritizing system of patient for urgency of
treatment and care. However, there is lack scientific documentation evaluating whether or
not emergency triage system are effective (Lidal et al, 2013).
Justification to Conduct Study
Emergency care triage important for early recognition of severely injured patient. However,
there is lack scientific evidence about the effects of using emergency care triage system but
does not mean such systems are ineffective (Lidal et al, 2013).
Emergency care triage systems have served some useful purposes and have proved popular
over time, but it now seems that there is no ideal scoring system available. Therefore caution
should be exercised when using any of the existing scoring systems until an ideal one
becomes available (Chawda et al, 2004).
Benefits of the Study
To identify the reliable scoring system for emergency triage in aided for emergency medical
responder to prioritize trauma patient that need urgent care. It helps clinician to speak
common language in quality assurance and quality control program (Chawda et al, 2004).
34
Objectives
General Objective
To compare the utility of Triage Revised Trauma Score with CRAMS Scale in determining
outcome of adult trauma patient in emergency department HUSM.
Specific Objectives
1. To determine mean score of Triage Revised Trauma Score and CRAMS Scale of adult
trauma patient who visit emergency department HUSM.
2. To determine the association between patient outcome (major injury/minor injury) with
Triage Revised Trauma Score and CRAMS Scale.
3. To compare sensitivity and specificity of Triage Revised Trauma Score and CRAMS Scale
in determining outcome of adult trauma patient in emergency department HUSM.
35
Hypothesis
Hypothesis 1
Ho- The mean score of trauma patient using Triage Revised Trauma Score is not different
with the mean score of CRAMS Scale.
HA- The mean score of trauma patient using Triage Revised Trauma Score is different with
the mean score of CRAMS Scale.
Hypothesis 2
HO - The outcome of trauma patient in emergency HUSM (major injury/minor injury) is not
associated with the Triage Revised Trauma score and CRAMS Scale.
HA - The outcome of trauma patient in emergency HUSM (major injury/minor injury) is
associated with the Triage Revised Trauma score and CRAMS Scale.
Hypothesis 3
HO- The sensitivity and specificity of Triage Revised Trauma Score had no difference with
CRAMS Scale in determining outcome of adult trauma patient in emergency department
HUSM.
36
HA- The sensitivity and specificity of Triage Revised Trauma Score had no difference with
CRAMS Scale in determining outcome of adult trauma patient in emergency department
HUSM.
Methodology
Study Design: Prospective cohort study
Study Period: Study will be conducted from December 2015 till February 2016
Study Location: Emergency Department, Hospital Universiti Sains Malaysia, Kubang
Kerian Kelantan
Reference Population: Adult trauma patient visited to emergency department HUSM
Source Population: Adult trauma patients who come to emergency department HUSM
who visit on December 2015 until February 2016.
Study Participants: Adult trauma patient who come to emergency department HUSM and
agree to be involved in study.
Inclusion and Exclusion Criteria
Inclusion Criteria
Involved in physical trauma

37
Age 18 years old and above
Exclusion Criteria
trauma patient who refuses to be involved in study
referral case from other hospital
Sample Size Determination
Sample Size Calculated Using Formula for Single Proportion
p value - prevalence of major trauma - 0.46
q value - 1 - p value- 0.54
Z alpha- value from normal distribution 1.96
D- value- precision estimate - 10% (0.1)
n - sample size
n = (Z alpha/D)² (p) (q)
= (1.96/0.10)² (0.46)(0.54)
= 95.42
38
Calculation Base on Probability
Using formula
n = P1(1-P1) + P2(1-P2) (Zα+Zβ)²
(P1-P2)²
n = sample size
Zα= critical value for α = 1.96
Zβ= critical value for 1-β = 0.84
P1 = estimate probability of exposure in major trauma
P2= estimate probability of exposure in minor trauma
m= ratio minor trauma to major trauma
For Triage Revised Trauma Score
P1 = 6%
P2= 94%
m = 15
n = 1
n (major trauma) =1
39
n ( minor trauma) = 15
Total = 16
For CRAMS Scale
P1=4%
P2= 96 %
m= 26
n = 1
n (major trauma) =1
n ( minor trauma) =26
n total= 27
Calculation of Sample Size Base on Specificity and Specificity
Sample Size Based On Sensitivity
n = (Zα/2)²SN (1-SN)
L²P
SN = sensitivity

40
L= absolute precision - taken 10%
P= prevalence
Zα/2= 1.96
For Triage Revised Trauma score:
SN = 59%
L= absolute precision - taken 10%
P= 46%
Zα/2= 1.96
n for sensitivity=90
For CRAMS Scale:
SN = 92%
L= absolute precision - taken 10%
P= 46%
Zα/2= 1.96
n for sensitivity=14
41
Sample Size Based On Specificity
n = (Zα/2)²SP(1-SP)
L²( 1-P)
L= absolute precision - taken 10%
P= prevalence
Zα/2= 1.96
For Triage Revised Trauma score:
SN = 59%
SP= 82%
P= 46%
n for specificity= 4
For CRAMS Scale:
SN=92%
SP= 98%
P= 46%
42
n for sensitivity= 7
n for specificity=28
Based on above calculations, largest size calculated is 95.
Number of sample size is 106(including 10% drop out rate) is taken for this study.
Sampling Method
Convenience sampling is chosen in view unfeasible of other method. This is because visit
time of trauma patient to emergency department in unpredictable and number of trauma
patient visit to emergency department varies from day by day.
Research Tools
All adult trauma patient who visited emergency department Hospital Universiti Sains
Malaysia during period time of study will be taken. It includes patient who visit emergency
HUSM by walk in, brought by relative, health clinic and ambulance call. Patient who fulfil
the inclusion criteria will be included in the study while patient who fulfil exclusion criteria
will be excluded.

43
Data Collection
Adult trauma patient who visit emergency department HUSM will be identify at triage
counter. Each patient that fulfil inclusion criteria will be selected. Consent will be obtained
by investigator after informed consent to trauma patient if patient is alert, conscious,
understood and agree to be involved in study. For trauma patient who is not fully conscious
and GCS less than 15, informed consent will be given to patient legal representative (spouse,
biological children, biological siblings and biological parents). Consent will be obtained from
legal representative if they understood and agree for patient to be involved in study. If patient
is not fully conscious and GCS level less than 15 and no legal representative present during
study, he will not be included in study.
After consent taken, patient personal data, date and time and type of trauma will be recorded
in assessment form. Patient will be seen by triage officer as usual (routinely be done to every
patient at emergency department HUSM following department standard operating
procedure). Vital sign such as blood pressure, respiratory rate, conscious level (using
Glasgow coma Scale) and focused examination will be taken and done by triage officer.
Investigator will not interfere triage officer in duty during parameter taken and bedside
examination done at triage. Parameters and examination taken at triage will be scored base
on Triage Revised Trauma Score and CRAMS Scale and will be recorded in assessment form
provided. Patient will be triage accordingly by triage officer and will be managed
accordingly by emergency team. Patient disposition from emergency department will be
followed up and will be recorded again on same assessment form.
44
Study Variables
Demographic Variable
Age
Sex
Race
Type of trauma
Independent Variable
Severity of injury
Patient disposition from emergency department
Dependent Variable
Respiratory rate per minute
Blood pressure
GCS score
Time of capillary refill/ blood pressure value
Abnormality of breathing
Tenderness of abdomen/ thorax
Motor function
Speech abnormality
45
Data Entry
Data will be enter and analyze by using SPSS version 22.0.
Validity and Reliability of the Measurement Tools
Revised Trauma Scoret
The reliability of T-RTS were tested against two large databases (Champion et al, 1989). The
Washington Hospital Center database (the database of the principal author) containing 2,166
patients and the Major Trauma Outcome Study (MTOS) database (as developed by the
American College of Surgeons Committee on Trauma) containing 26,000 patients were
evaluated by T-RTS. Results showed that an T-RTS<11 accurately identified 97.2% of the
fatally injured and most of the severely injured as determined by regression analysis
(Senkowski et al, 1999).
CRAMS Scale
The derivation study included consecutive paramedic runs involving trauma and collected
predictors both in the pre-hospital and early in-hospital phase, and internally it remains
unclear how it was validated (Rehn et al, 2011).
It is validated external in 2 studies. Baxt et al (1989) evaluated 2434 patients with ROC
curves presented. Emerman et al (1992) evaluated 1027 patients with outcome of major
injury (CRAMS < 9) with sensitivity of 100%; specificity 83% (Rehn et al, 2011).
46
Definition of Operational Terms
Major Injury
Patient is consider having major injury if patient died during the injury or admission to
intensive care unit ( Champion et al, 1989) or directly to operation theatre ( Gormicon et al,
1982).
Minor Injury
Patient is consider as minor injury if discharge for emergency department, or admitted to
general ward ( Gormicon et al, 1982).
Conflict of Interest
This study is a self fund by principal investigator and have no affiliations with or involvement
in any organization or entity with any financial or nonfinancial interest in the subject matter
discuss in this study. Participant confidentiality is our priority and participant safety will not
jeopardized. If any information regarding participant that is life threatening that obtained
during this study, participants and his legal representative will be informed regarding his
current condition and emergency personnel that involved in managing this participant also
will be informed for participant own benefit.
47
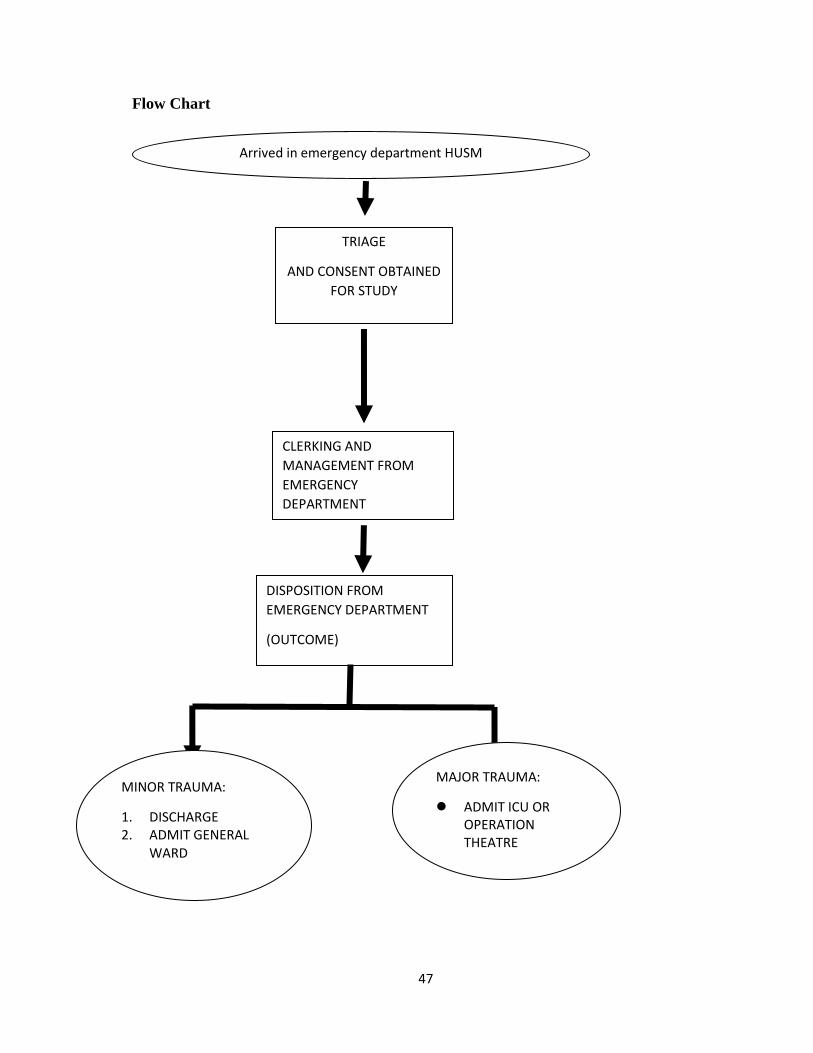
Flow Chart
Arrived in emergency department HUSM
TRIAGE
AND CONSENT OBTAINED
FOR STUDY
DISPOSITION FROM
EMERGENCY DEPARTMENT
(OUTCOME)
MINOR TRAUMA:
1. DISCHARGE 2. ADMIT GENERAL
WARD
MAJOR TRAUMA:
ADMIT ICU OR OPERATION THEATRE
DEATH
CLERKING AND
MANAGEMENT FROM
EMERGENCY
DEPARTMENT

48
Intended Statistical Analysis
For demographic data, the continuous variables will be described either in mean and standard
deviation. The categorical variables will be described in frequency and percentage.
Expected result (dummy table):
Variables Numerical mean (SD) Categorical frequency (%)
Age
Sex
Race
Type of trauma
For hypothesis 1, intended statistical statistic is parametric test, using independent t-test
to determine mean distribution of both Triage Revised Trauma Score and CRAMS Scale.
group Mean Standard deviation(SD)
T-RTS
CRAMS
49
For hypothesis 2, intended statistical analysis is using the Pearson Chi-square test for
association of both scoring system (Triage Revised Trauma Score and CRAMS Scale)
with patients’ outcome.
T-RTS SCORE INJURY x ²(df) p-value
MAJOR
INJURY
MINOR
INJURY
0-11
12
CRAMS
SCALE
INJURY x² (df) p-value
MAJOR
INJURY
MINOR
INJURY
0-8
9-10
For hypothesis 3, by comparing specificity and sensitivity of Triage Revised Trauma
Score and CRAMS Scale
50
Triage Revised Trauma Score
T-RTS estimate 95% CI
sensitivity
specificity
PPV
NPV
LR+
LR+
CRAMS Scale
CRAMS estimate 95% CI
sensitivity
specificity
PPV
NPV
LR+
LR+
51
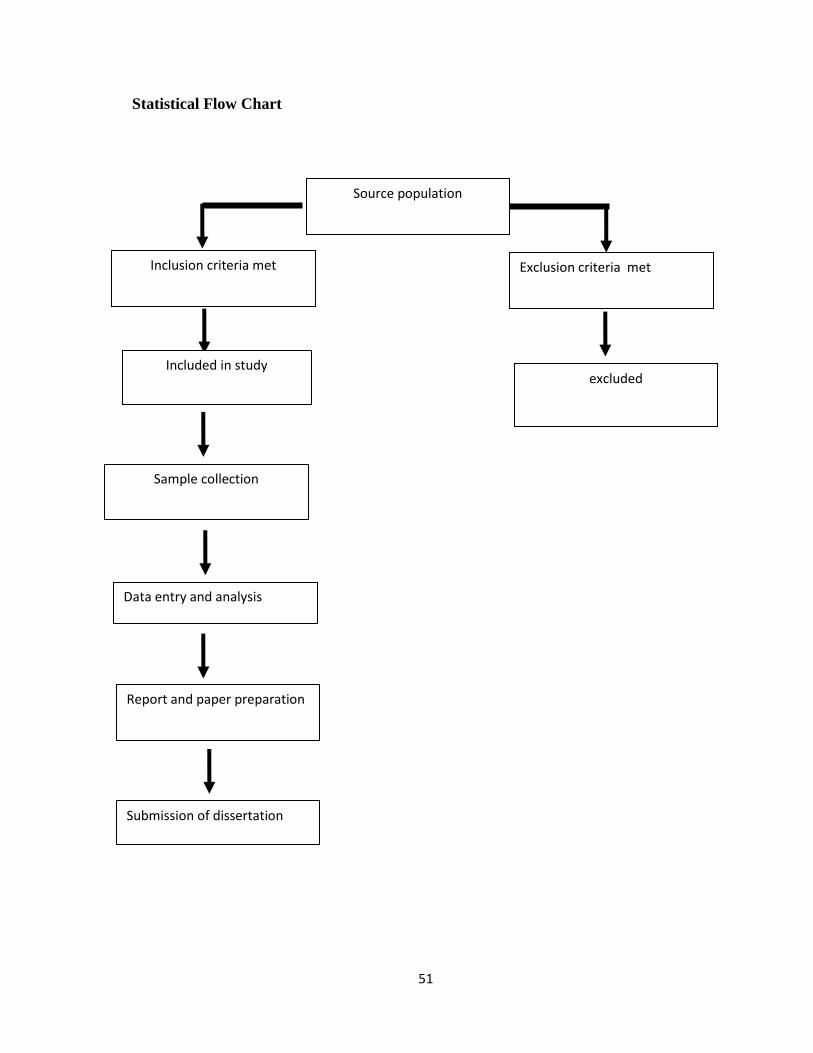
Statistical Flow Chart
Source population
Exclusion criteria met
Submission of dissertation
Report and paper preparation
Data entry and analysis
Sample collection
Inclusion criteria met
excluded Included in study
52
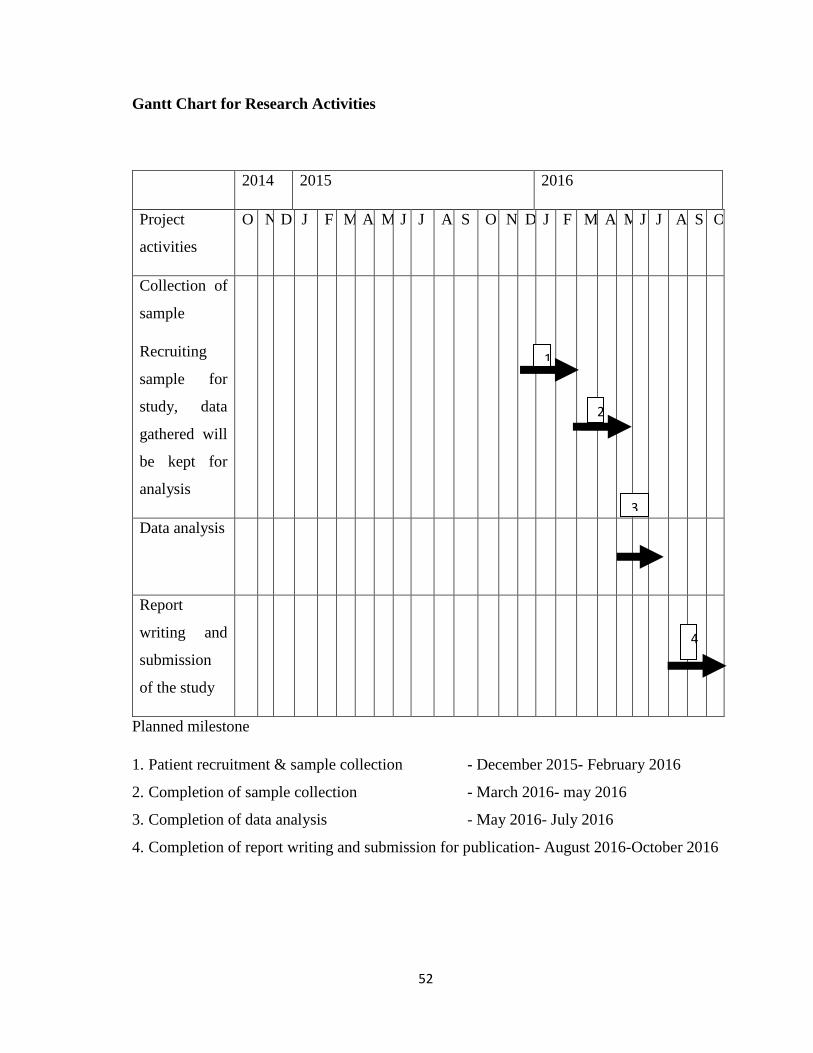
Gantt Chart for Research Activities
2014 2015 2016
Project
activities
O N D J F M A M J J A S O N D J F M A M J J A S O
Collection of
sample
Recruiting
sample for
study, data
gathered will
be kept for
analysis
Data analysis
Report
writing and
submission
of the study
Planned milestone
1. Patient recruitment & sample collection - December 2015- February 2016
2. Completion of sample collection - March 2016- may 2016
3. Completion of data analysis - May 2016- July 2016
4. Completion of report writing and submission for publication- August 2016-October 2016
1
2
3
4
53
References
1. Champion HR, Sacco WJ, COPES WS, GANN DS, Gennarelli TA, Flanagan ME. A
revision of the Trauma Score. Journal of Trauma and Acute Care Surgery.
1989;29(5):623-9.
2. Gray A, Goyder E, Goodacre S, Johnson G. Trauma triage: a comparison of CRAMS
and TRTS in a UK population. Injury. 1997;28(2):97-101.
3. Chawda M, Hildebrand F, Pape HC, Giannoudis PV. Predicting outcome after
multiple trauma: which scoring system? Injury. 2004;35(4):347-58.
4. Gilpin D, Nelson P. Revised trauma score: a triage tool in the accident and emergency
department. Injury. 1991;22(1):35-7.
5. Lefering R. Trauma score systems for quality assessment. European Journal of
Trauma. 2002;28(2):52-63.
6. Ma M, MacKenzie EJ, Alcorta R, Kelen GD. Compliance with prehospital triage
protocols for major trauma patients. The Journal of trauma. 1999;46(1):168-75.
7. Rohayu S, Sharifah Allyana S, Jamilah M, Wong S. Predicting Malaysian road
fatalities for year 2020. 2012.
8. Lidal IB, Holte HH, Vist GE. Triage systems for pre-hospital emergency medical
services-a systematic review. Scandinavian journal of trauma, resuscitation and
emergency medicine. 2013;21(1):1-6.
9. Senkowski CK, McKenney MG. Trauma scoring systems: a review 1 2. Journal of
the American College of Surgeons. 1999;189(5):491-503.
10. Rehn M, Perel P, Blackhall K. Prognostic models for the early care of trauma patients:
a systematic review. Scand J Trauma Resusc Emerg Med. 2011;19:17.

54
4.2 Patient Information and Consent Form
JAWATANKUASA ETIKA PENYELIDIKAN (MANUSIA) -
JEPeM
RESEARCH ETHICS COMMITTEE (HUMAN)
_______________________________________________________________________________
BORANG MAKLUMAT DAN KEIZINAN PESAKIT/ SUBJEK
PATIENT INFORMATION AND CONSENT FORM
(PROJEK PENYELIDIKAN)
(RESEARCH PROJECT)
Borang Maklumat dan Keizinan Pesakit/Subjek yang digunakan dalam Projek Penyelidikan
mestilah mengikuti format maklumat berikut:
The Patient Infomation and Consent Form used in the Research Project must be according to
these information formats:
Tajuk Kajian / Topic of the Research
Pengenalan / Introduction
Tujuan Kajian / Purpose of the Study
Kelayakan Penyertaan / Qualification to Participate
Prosedur-prosedur Kajian / Study Procedures
Risiko / Risks
Melaporkan Pengalaman Kesihatan / Reporting Health Experiences
Penyertaan dalam Kajian / Participation in the Study
Manafaat yang Mungkin Diperolehi / Possible Benefits
Soalan / Questions
Kerahsiaan / Confidentiality
Tandatangan / Signatures
Sebagai CONTOH, sila rujuk Borang Maklumat dan Keizinan Pesakit yang dilampirkan.
As an EXAMPLE, please refer to the attached Patient Infomation and Consent Form.
(Versi Bahasa Malaysia) / (Bahasa Malaysia Version)
1. LAMPIRAN A
<TAJUK KAJIAN>
2. LAMPIRAN S (Borang Keizinan Pesakit)
3. LAMPIRAN G (Borang Keizinan Pesakit – Sampel Genetik)
BORANG ETIKA - 02
55
4. LAMPIRAN P (Borang Keizinan Penerbitan Bahan yang Berkaitan dengan Subjek)
(Versi Bahasa Inggeris) / (English Version) N
1. ATTACHMENT B
<RESEARCH TITLE>
2. ATTACHMENT S (Patient Information and Consent Form)
3. ATTACHMENT G (Patient Information and Consent Form – Genetic Sample)
4. ATTACHMENT P (Subject’s Material Publication Consent Form)
JEPeM/EthicalForm02/Ver.4.0 – 2011
Updated
: 13/02/2011

56
Consent Form (English)
ATTACHMENT B
RESEARCH INFORMATION
Research Title: COMPARISON OF REVISED TRAUMA SCORE VERSUS CRAMS
SCALE AS A PREDICTOR OF OUTCOME FOR ADULT TRAUMA
PATIENT IN EMERGENCY DEPARTMENT HUSM
Researcher’s Name: DR NOOR HAFIZA BINTI CHE ANI
MMC Registration No. : MPM 48502
INTRODUCTION
You or your legal representative are invited to take part voluntarily in a research study. This study
involve evaluation of injury when participants arrives at triage in emergency department HUSM using
Revised Trauma Score and CRAMS Scale and comparison of participant outcome from Emergency
Department HUSM. Before agreeing to participate in this research study, it is important that you or
your legal representative read and understand this form. If you or your legal representative
participate, you or your legal representative will receive a copy of this form to keep for your records.
Participation in this study is expected to last up to 1 day. Up to 280 participants will be expected to
participate in this study.
PURPOSE OF THE STUDY
Purpose of this study to compare the effectiveness of Revised Trauma Score and CRAMS Scale in
predicting adult trauma patient outcome from Emergency Department HUSM. There is probability of
the collected information from this study will be analyzed by other researcher in the future in order to
evaluate the effectiveness of scoring system that have been used.
QUALIFICATION TO PARTICIPATE
The doctor in charge of this study or has discussed with you or your legal representative the
requirements for participation in this study. It is important that you or your legal representative are
57
completely truthful with the doctor and about participant health history. Participants should not
participate in this study if participant do not meet all qualifications.
Some of the requirements to be in this study are:
Involved in physical trauma Age above 18 years old
You cannot participate in this study if:
referral from other hospital Refused to be involved in this study
STUDY PROCEDURES
Participant injury will be evaluated at triage counter and will be scored following prepared scoring
system. Summation of score will be recorded. Total score that gain based on scoring system will be
compare with participant outcome during disposition from emergency department HUSM. These are
the scoring systems that will be used in this study
Revised Trauma Score (RTS) - This scoring system will evaluate participant severity of injury based on physiological finding by scoring blood pressure, rate of breathing and patient mental status during arrival to emergency HUSM.
CRAMS Scale (CRAMS)- This scoring system will evaluate participants severity of injury based on blood pressure and circulation, breathing pattern, injury to abdomen or chest, mental status and speech.
RISKS
Estimated there will be risk of underestimated or overestimated assessment that will interfere
participant further management in emergency department. If any important new information is found
during this study that may affect you or your legal representative wanting to continue to be part of
this study, you will be told about it right away.
REPORTING HEALTH EXPERIENCES.
If you have any injury, bad effect, or any other unusual health experience during this study, make
sure that you immediately tell the nurse or Dr. Noor Hafiza Binti Che Ani [MMC Registration No.:
58
MPM 48502] at 09-7673226 or 016-4115904. You can call at anytime, day or night, to report such
health experiences.
PARTICIPATION IN THE STUDY
Your taking part in this study is entirely voluntary. You may refuse to take part in the study or you
may stop participation in the study at anytime, without a penalty or loss of benefits to which you are
otherwise entitled. Your participation also may be stopped by the study doctor or sponsor without
your consent.
POSSIBLE BENEFITS [Benefit to Individual, Community, University]
Study procedures will be provided at no cost to you. You may receive information about your health
from any physical examination to be done in this study. We hope that the outcome and information
regarding this research will beneficial to future patients.
QUESTIONS
If you have any question about this study or your rights, please contact;
Dr Noor Hafiza Che Ani, MPM 48502
Jabatan kecemasan
Pusat Pengajian Sains Perubatan
USM Kampus Kesihatan
No tel : 09 -7673226/016-4115904
Email: [email protected]
If you have any questions regarding the Ethical Approval or any issue / problem related to this
study, please contact;
En. Mohd Bazlan Hafidz Mukrim
Setiausaha Jawatankuasa Etika Penyelidikan (Manusia) USM
Pusat Inisiatif Penyelidikan -Sains Klinikal & Kesihatan
USM Kampus Kesihatan.
No. Tel: 09-767 2354 / 09-767 2362
59
Email: [email protected]/[email protected]
CONFIDENTIALITY
Your medical information will be kept confidential by the study doctor and staff and will not be made
publicly available unless disclosure is required by law.
Data obtained from this study that does not identify you individually will be published for knowledge
purposes.
Your original medical records may be reviewed by the researcher, the Ethical Review Board for this
study, and regulatory authorities for the purpose of verifying clinical trial procedures and/or data. Your
medical information may be held and processed on a computer.
By signing this consent form, you or your legal representative authorize the record review, information
storage and data transfer described above.
SIGNATURES
To be entered into the study, you or a legal representative must sign and data the signature page
[ATTACHMENT S and ATTACHMENT P]
60
ATTACHMENT S
Patient/Subject Information and Consent Form
(Signature Page)
Research Title: COMPARISON OF REVISED TRAUMA SCORE VERSUS CRAMS SCALE AS A PREDICTOR OF OUTCOM FOR ADULT TRAUMA PATIENT IN EMERGENCY DEPARTMENT HUSM
Researcher’s Name: DR NOOR HAFIZA BINTI CHE ANI
MMC Registration No. : MPM 48502
To become a part this study, you or your legal representative must sign this page. By
signing this page, I am confirming the following:
I have read a l l o f the in format ion in th is Pat ient In format ion and Consent Form inc lud ing an y in form at ion regard ing the r isk in th i s s tudy and I have had t ime to th ink about i t .
Al l o f my quest ions have been answered to my sat isfact ion. I vo luntar i ly agree to be part o f th is research study, to fo l low the
study procedures, and to prov ide necessary in format ion to the doctor , nurses, o r o ther staf f members, as requested.
I may f reely choose to stop being a part o f th is study at anyt ime. I have received a copy of th is Pat ient In format ion and Consent
Form to keep fo r mysel f .
Patient Name (Print or type) Patient Initials and Regisistration Number
Patient I.C No. (New) Patient I.C No. (Old)
Signature of Patient or Legal Representative Date (dd/MM/yy)
Name of Individual Conducting Consent Discussion (Print or Type)
Signature of Individual Conducting Consent Discussion Date (dd/MM/yy)
Name & Signature of Witness Date (dd/MM/yy)
Note: i) All subject/patients who are involved in this study will not be covered by insurance.

61
ATTACHMENT P
Patient’s Material Publication Consent Form
Signature Page
Research Title: COMPARISON OF REVISED TRAUMA SCORE VERSUS CRAMS SCALE AS A PREDICTOR OF OUTCOME FOR ADULT TRAUMA PATIENT IN EMERGENCY DEPARTMENT HUSM
Researcher’s Name: DR NOOR HAFIZA BINTI CHE ANI
MMC Registration No. : MPM 48502
To become a part this study, you or your legal representative must sign this page.
By signing this page, I am confirming the following:
I unders tood tha t m y nam e wi l l no t appear on the m ater ia ls pub l i shed and there has been e f fo r ts to m ake sure tha t the pr i vac y o f m y nam e is kept conf ident ia l a l though the conf ident ia l i t y is no t com ple te l y guaranteed due to unexpec ted c i rcumstances .
I have read the materials or general description of what the material contains and reviewed all photographs and figures in which I am included that could be published.
I have been offered the opportunity to read the manuscript and to see all materials in which I am included, but have waived my right to do so.
A l l the pub l ished m ater ia ls w i l l be shared am ong the m edica l p rac t i t i oners , sc ien t is ts and journa l is t wor ld wide.
The m ater ia ls w i l l a lso be used in loca l pub l ica t ions , book pub l ica t ions and accessed by m any loca l and in ternat iona l doc to rs wor ld w ide.
I hereb y agree and a l low the m ater ia ls to be used in o ther pub l ica t ions requ i red by o ther pub l ishers w i th these cond i t ions :
The m ater ia ls w i l l no t be used as a dver t isem ent purposes nor as packag ing m ater ia ls .
The m ater ia ls w i l l no t be used out o f contex – i .e . : Sam ple p ic tu res w i l l no t be used in an ar t ic le wh ich is unre la ted sub jec t to t he p ic tu re .
Patient Name Patient Initials or Number
Patient I.C No. Patient’s Signature or legal representative Date(dd/MM/yy)
Name and Signature of Individual Conducting Consent Discussion Date(dd/MM/yy)
Note: i) All subject/patients who are involved in this study will not be covered by insurance.
62
Consent Form (Bahasa Melayu)
LAMPIRAN A
MAKLUMAT KAJIAN
Tajuk Kajian: PERBANDINGAN DI ANTARA 'REVISED TRAUMA SCORE' DAN 'CRAMS
SCALE' SEBAGAI PANDUAN UNTUK MERAMAL TAHAP KECEDERAAN
PESAKIT TRAUMA DEWASA DI JABATAN KECEMASAN HUSM
Nama Penyelidik: DR NOOR HAFIZA BINTI CHE ANI
No. Pendaftaran MMC: MPM 48502
PENGENALAN
Anda atau wakil sah anda dipelawa untuk menyertai satu kajian penyelidikan secara sukarela. Kajian
ini melibatkan penilaian tahap kecederaan pesakit ketika tiba di kaunter 'triage', Jabatan Kecemasan,
Hospital Universiti Sains Malaysia (HUSM) menggunakan format pemarkahan 'Revised Trauma
Score' dan 'CRAMS Scale dan mencatatkan keadaan pesakit ketika dipindahkan dari jabatan ini .
Sebelum anda atau wakil sah anda bersetuju untuk menyertai kajian penyelidikan ini, adalah penting
anda atau waris anda membaca dan memahami borang ini. Sekiranya anda atau wakil sah anda
menyertai kajian ini, anda atau wakil sah anda akan menerima satu salinan borang ini untuk disimpan
sebagai rekod anda atau wakil sah anda.
Penyertaan pesakit di dalam kajian ini dijangka mengambil masa selama sehari. Seramai 280 pesakit
akan menyertai kajian ini.
TUJUAN KAJIAN
Kajian ini bertujuan adalah untuk menentukan sama ada skema pemarkahan tahap kecederaan yang
dinilai dapat meramal tahap kecederaan yang di alami pesakit semasa berada di Jabatan Kecemasan
HUSM.
Terdapat kemungkinan maklumat yang dikumpulkan semasa kajian ini akan dianalisa oleh pihak
penyelidik pada masa depan untuk menilai keberkesanan skema pemarkahan tahap kecederaan
yang di nilai.

63
KELAYAKAN PENYERTAAN
Doktor yang bertanggungjawab dalam kajian ini akan membincangkan kelayakan untuk menyertai
kajian ini dengan anda atau wakil sah anda. Adalah penting untuk anda berterus terang dengan
doktor tersebut tentang kecederaan pesakit. Pesakit tidak seharusnya menyertai kajian ini sekiranya
pesakit tidak memenuhi semua syarat kelayakan.
Beberapa keperluan untuk menyertai kajian ini adalah
.
Anda terlibat dengan kemalangan fizikal
Berumur 18 tahun dan ke atas
Anda tidak boleh menyertai kajian ini sekiranya
Di rujuk dari hospital lain
Tidak bersetuju menyertai kajian ini
PROSEDUR-PROSEDUR KAJIAN
Kecederaan yand dialami pesakit akan di nilai mengikut format pemarkahan yang disediakan ketika
di kaunter " triage" Jabatan Kecemasan HUSM. Jumlah markah pesakit akan di rekodkan. Jumlah
markah yang di dapati akan di bandingkan dengan keadaan anda semasa dipindahkan dari
Jabatan Kecemasan HUSM.
Berikut adalah format pemarkahan yang dinilai:
Revised Trauma Score( RTS) - Format permakahan RTS ini menilai tahap kecederaan mangsa dari segi keadaan keupayaan fizikal pesakit seperti tekanan darah, bilangan pernafasan dan keadan fungsi otak pesakit ketika tiba di jabatan kecemasan HUSM
CRAMS Scale (CRAMS)- Format pemarkahan CRAMS ini menilai tahap kecederaan anda dengan memberi markah berpandukan tekanan dan peredaran darah, pernafasan, kecederaan di bahagian abdomen atau dada, fungsi pergerakan fizikal dan pertuturan .
RISIKO
Risiko yang boleh dihadapi adalah kesilapan dalam penilaian yang mungkin akan mempengaruhi
rawatan peserta. Jika apa-apa maklumat penting yang baru dijumpai semasa kajian ini yang mungkin
mengubah persetujuan anda atau wakil sah anda untuk meneruskan penyertaan pesakit dalam kajian
ini, anda atau wakil sah anda akan dimaklumkan secepat mungkin.
64
MELAPORKAN PENGALAMAN KESIHATAN
Jika pesakit mengalami kesan buruk, atau apa-apa pengalaman kesihatan yang luar biasa semasa
kajian ini, pastikan anda memberitahu jururawat atau Dr. Noor Hafiza binti Che Ani [No.
Pendaftaran Penuh Majlis Perubatan Malaysia: 48502] di talian 09-7673226 atau 016-4115904
secepat mungkin. Anda atau wakil sah anda boleh membuat panggilan pada bila-bila masa, siang
atau malam, untuk melaporkan pengalaman sedemikian.
PENYERTAAN DALAM KAJIAN
Penyertaan anda atau wakil sah anda dalam kajian ini adalah secara sukarela. Anda atau wakil sah
anda berhak menolak untuk menyertai kajian ini atau anda atau wakil sah anda boleh menamatkan
penyertaan anda pada bila-bila masa, tanpa sebarang hukuman atau kehilangan manfaat yang
sepatutnya anda atau wakil sah anda perolehi.
Penyertaan anda atau wakil sah anda juga mungkin boleh diberhentikan oleh doktor yang terlibat
dalam kajian ini tanpa persetujuan anda atau wakil sah anda. Sekiranya anda atau wakil sah anda
berhenti menyertai kajian ini, doktor yang terlibat di dalam kajian ini atau salah seorang kakitangan
akan berbincang dengan anda atau wakil sah anda mengenai apa-apa isu perubatan berkenaan
dengan pemberhentian penyertaan anda atau waris anda.
MANFAAT YANG MUNGKIN [Manfaat terhadap Individu, Masyarakat, Universiti]
Prosedur kajian ini akan diberikan kepada anda atau wakil sah anda tanpa kos. Anda atau wakil sah
anda mungkin menerima maklumat tentang kesihatan anda daripada pemeriksaan fizikal yang
dilakukan dalam kajian ini. Hasil atau maklumat kajian ini diharapkan, dapat memberi manfaat kepada
pesakit-pesakit pada masa hadapan. Anda atau wakil sah anda tidak akan menerima sebarang
pampasan kerana menyertai kajian ini. Namun sebarang keperluan perjalanan berkaitan dengan
penyertaan ini akan diberi.
PERSOALAN
Sekiranya anda atau wakil sah anda mempunyai sebarang soalan mengenai prosedur kajian ini atau
hak-hak anda, sila hubungi;
Dr Noor Hafiza Che Ani, MPM 48502
Jabatan kecemasan
Pusat Pengajian Sains Perubatan
USM Kampus Kesihatan
No tel : 09 -7673226/016-4115904

65
Email: [email protected]
Sekiranya anda atau wakil sah anda mempunyai sebarang soalan berkaitan kelulusan Etika atau
sebarang pertanyaan dan masalah berkaitan kajian ini, sila hubungi;
En. Mohd Bazlan Hafidz Mukrim
Setiausaha Jawatankuasa Etika Penyelidikan (Manusia) USM
Pusat Inisiatif Penyelidikan -Sains Klinikal & Kesihatan
USM Kampus Kesihatan.
No. Tel: 09-767 2354 / 09-767 2362
Email : [email protected]/[email protected]
KERAHSIAAN
Maklumat perubatan anda akan dirahsiakan oleh doktor dan kakitangan kajian. Ianya tidak akan
didedahkan secara umum melainkan jika ia dikehendaki oleh undang-undang.
Data yang diperolehi dari kajian yang tidak mengenalpasti anda secara perseorangan mungkin akan
diterbitkan untuk tujuan memberi pengetahuan baru.
Rekod perubatan anda yang asal mungkin akan dilihat oleh pihak penyelidik, Lembaga Etika kajian
ini dan pihak berkuasa regulatori untuk tujuan mengesahkan prosedur dan/atau data kajian klinikal.
Maklumat perubatan anda mungkin akan disimpan dalam komputer dan diproses dengannya.Dengan
menandatangani borang persetujuan ini, anda atau wakil sah anda membenarkan penelitian rekod,
penyimpanan maklumat dan pemindahan data seperti yang dihuraikan di atas.
TANDATANGAN
Untuk dimasukkan ke dalam kajian ini, anda atau wakil sah anda mesti menandatangani serta
mencatatkan tarikh dihalaman tandatangan [ LAMPIRAN S dan LAMPIRAN P]
66
LAMPIRAN S
Borang Keizinan Pesakit/ Subjek
(Halaman Tandatangan)
Tajuk Kajian: PERBANDINGAN DI ANTARA 'TRIAGE REVISED TRAUMA
SCORE' DAN 'CRAMS SCALE’ SEBAGAI PANDUAN UNTUK
MERAMAL TAHAP KECEDERAAN PESAKIT TRAUMA
DEWASA DI JABATAN KECEMASAN HUSM
Nama Penyelidik: DR NOOR HAFIZA BINTI CHE ANI , No. Pendaftaran MPM : MPM 48502 Untuk menyertai kajian ini, anda atau wakil sah anda mesti menandatangani mukasurat ini. Dengan
menandatangani mukasurat ini, saya mengesahkan yang berikut:
Sa ya te lah m em baca sem ua m ak l um at da lam Borang Mak lum at dan Ke iz inan Pesak i t in i t e rm asuk apa-apa m ak lum at berka i tan r is iko yang ada da lam ka j ian dan saya te lah pun d iber i m asa yang m encukup i un tuk m em per t im bangkan m ak lum at te rsebu t .
Sem ua soa lan -soa lan saya te lah d i jawab dengan m em ua skan. Sa ya, secara sukare la , berse tu ju m enyer ta i ka j ian pen ye l id ikan in i ,
m em atuh i sega la prosedur ka j ian dan m em ber i m ak lum at yang d iper lukan kepada dok tor , para ju rurawa t dan juga kak i tangan la in yang berka i tan apab i la d im in ta .
Sa ya bo leh m enam atkan penyer taan sa ya da lam kaj ian in i pada b i la -b i l a m asa.
Sa ya te lah pun m ener im a satu sa l inan Borang Mak lum at dan Ke iz inan Pesak i t un tuk s im panan per ibad i saya .
Nama Pesakit (Dicetak atau Ditaip) Nama Singkatan & No. Pesakit
No. Kad Pengenalan Pesakit (Baru) No. K/P (Lama)
Tandatangan Pesakit atau Wakil Sah Tarikh (dd/MM/yy)
Nama & Tandatangan Individu yang Mengendalikan Tarikh (dd/MM/yy)
Perbincangan Keizinan
Nama Saksi dan Tandatangan Tarikh (dd/MM/yy)
Nota: i) Semua subjek/pesakit yang mengambil bahagian dalam projek penyelidikan ini tidak dilindungi insuran.

67
LAMPIRAN P
Borang Keizinan bagi Penerbitan Bahan yang berkaitan dengan Pesakit/ Subjek
(Halaman Tandatangan)
Tajuk Kajian: PERBANDINGAN DI ANTARA 'TRIAGE REVISED TRAUMA SCORE' DAN 'CRAMS SCALE' SEBAGAI PANDUAN UNTUK MERAMAL TAHAP KECEDERAAN PESAKIT TRAUMA DEWASA DI JABATAN KECEMASAN HUSM
Nama Penyelidik: DR NOOR HAFIZA BINTI CHE ANI No. Pendaftaran MPM : MPM 48502 Untuk menyertai kajian ini, anda atau wakil sah anda mesti menandatangani mukasurat ini.
Dengan menandatangani mukasurat ini, saya memahami yang berikut:
Bahan yang akan d i t e rb i tkan tanpa d i lampi rkan dengan nam a saya dan se t iap percubaan yang akan d ibuat un tuk mem ast ikan ke tanpanam aan saya. Sa ya m em aham i , wa laubaga im anapun, ke tanpanam aan yang sempurna t idak dapa t d i j am in . Kem ungk inan ses iapa yang m enjaga saya d i hosp i ta l a tau saudara dapat m engena l i sa ya.
Bahan yang akan d i te rb i tkan da lam penerb i tan m ingguan/bu lanan/dw ibu lanan/suku tahunan/dwi t ahunan m erupakan sa tu pen yebaran yang luas dan te rsebar ke se luruh dun ia . Keban yakan penerb i tan in i akan te rsebar kepada dok tor -dok tor dan juga bukan dok tor te rm asuk ah l i sa ins dan ah l i j u rna l .
Bahan te rsebut j uga akan d i lam pi rkan pada lam an web ju rna l d i se lu ruh dun ia . Sesetengah lam an web in i bebas d ikun jung i o leh sem ua orang.
Bahan te rsebut j uga akan d igunakan sebaga i penerb i tan t em patan dan d isam paikan o leh ramai dok tor dan ah l i sa ins d i se luruh dun ia .
Bahan te rsebut j uga akan d igunakan sebaga i penerb i tan buku o leh penerb i t j u rna l .
Bahan te rsebut t idak akan d igunakan untuk peng ik lanan a taupun bahan untuk m em bungkus .
Sa ya juga m em ber i ke iz inan bahawa bahan te rsebu t bo leh d igunakan sebaga i penerb i tan la in yang d im in ta o leh penerb i t dengan k r i te r ia ber iku t :
Bahan te rsebut t i dak akan d igunakan untuk peng ik lanan a tau bahan un tuk m em bungkus .
Bahan te rsebut t i dak akan d igunakan d i luar k onteks – contohnya : Gam bar t idak akan d igunakan untuk m enggam barkan sesuatu ar t ike l yang t idak berka i tan dengan sub jek da lam fo to te rsebut .
Nama Pesakit (Dicetak atau Ditaip) Nama Singkatan atau No. Pesakit
No. Kad Pengenalan Pesakit T/tangan Pesakit Tarikh (dd/MM/yy)
Nama & Tandatangan Individu yang Mengendalikan Tarikh (dd/MM/yy)
Perbincangan Keizinan (Dicetak atau Ditaip)
Nota: i) Semua subjek/pesakit yang mengambil bahagian dalam projek
68
4.3 Ethical Approval Letter
1\ IIHMI ~V: J awatankuasa Etika Penyelidikan Manusia USM (JEPcM) !I uman Research Ethics Committee USM (II REC)
2l'h May 2015
Dr Noor Hafiza Chc Ani Jabatan Kecemasan Pusat Pengajian Sa ins Perubatan USM Kampus Kcsihatau
JEPeM-USM Code: USMJJEPEMJ IS030102
Universili Sains Malaysia Kampus Kcsihutan, 16150 Kubang Kerian, Kelantan. Malaysia. T · GOO· 767 SOOO .lllmb. ~S5 .. h !UJ"'!! f , G09 • 76HS51 E.: [email protected]$Jn.IIIY wwwjepcm.kk.usm.my
Protocol Title: Comparison of Revised Trauma Score and Crams Scoring System as Predictors of Outcome for Adult Trauma Patient in Emergency Department HUSM
Dear Dr:
We wish to inform you that the Jawatankuasa Etika Penyelidikan (Manusia) JEPeM -USM has reviewed your submission received on 261h March 2015 . Upon review by the primary reviewers, we found issues requiring your clarifications.
ln this regard, our primary reviewer' s requests for a clarificatory interview with you during the next deliberated review meeting on 281h Mav 2015 from 9.00 am till 2 .00 pm at the Meeting Room, Centre for Research Initiatives, USM llealth Campus. Your session will be star t at 11.45 am.
Should you have any questions or clarifications regarding the abovementioned matters, please contact tbe undersigned through the JEPeM-USM Secretariat at 09-7672362/097672354 or jepem@ usm.my.
The JEPeM-USM looks forward to your immediate response and action.
Thank you.
"ENSURING A SUSTAINABLE TOMORROW"
Very truly yours,
&1. MOHD BAZLAN HA.I<"IDZ M UKRlM Secretary Jawatankuasa Etika Penyelidikan (Manusia) JEPeM Universiti Sains Malaysia
Clarificatory Interview< D1· Noor Hafi'za >USM/JEPeM/15030102

69
/ Jawatankuasa Etika Penyelidikan Manusia USM (JEPeM) Human Research Ethi cs Committee USM (HREC')
18th June 2015
Dr. Noor Hafiza Che Ani,
Department of Emergency Medicine,
School of Medical Sciences,
USM Health Campus.
JEPeM Code : USM/JEPeM/15030102
Universiti Sains Malaysia Kounpus Kesihatom, ltiiJo Kubang Kerian, Ktlantan. Malaysia. T: 6<.V - 767 !SOOO mmb. ~.:J.; "1~36'.! F: 609 • 7(;7 ~3,; 1 E: j~::pem(fyusm.my www jepem.kk.usm.my
Protocol Title : Comparison of Revised Trauma Score Versus Crams Scoring System as a Predictor of Outcome for Adult Trauma Patient in Emergency Department HUSM.
Dear Dr,
We wish to inform you that the Jawatankuasa Etika Penyelidikan Manusia, Universiti Sains Malaysia (JEPeM-USM ) reviewed your proposed ethical application during its regular meet ing on 28th May 2015
(Meeting No.309). Your study has been assigned study protocol code USM/JEPeM/15030102 which should be used for all communication to the JEPeM related to this study.
As a result of the review, the decision of the committee is APPROVED WITH CORRECTION.
Recommended revisions and/or clarifications are summarized in the 'conclusion and recommendations' part in the provided attachment.
Please note that revisions requested by the JEPeM-USM should:
1. Be integrated into a revised STUDY PROTOCOL and related documents in one printed copy
2. Be SUMMARIZED in a cover letter indicating in which page of the revised study protocol the respective revision may be found;
3. Modified part should be underlined and bold.
Please note that the cut-off date for submission of revised study protocol is on 2 August 2015. Also,
please note that resubmissions can only be accepted w ithin 30 working days from the date of this letter. Failure to respond within 30 working days from the date of this letter will inactivate the
application and study protocol will be archived. Subsequent submissions will be processed as initial review. Should you have any quest ions or clarifications regarding the abovementioned recommendations, please contact the undersigned through the JEPeM Secretariat at 09 7672352/2354
The JEPeM-USM looks forward to your immediate response and action.
"ENSURING A SUSTAINABLE TOMORROW"
Very truly yours,
ctj Secretary On behalf of Chairperson Jawatankuasa Etika Penyelidikan (Manusia)
Universit i Sa ins Malaysia
<USM/ IEPeM/15030102> Dr. Noor Hafiw Che Ani Page 1
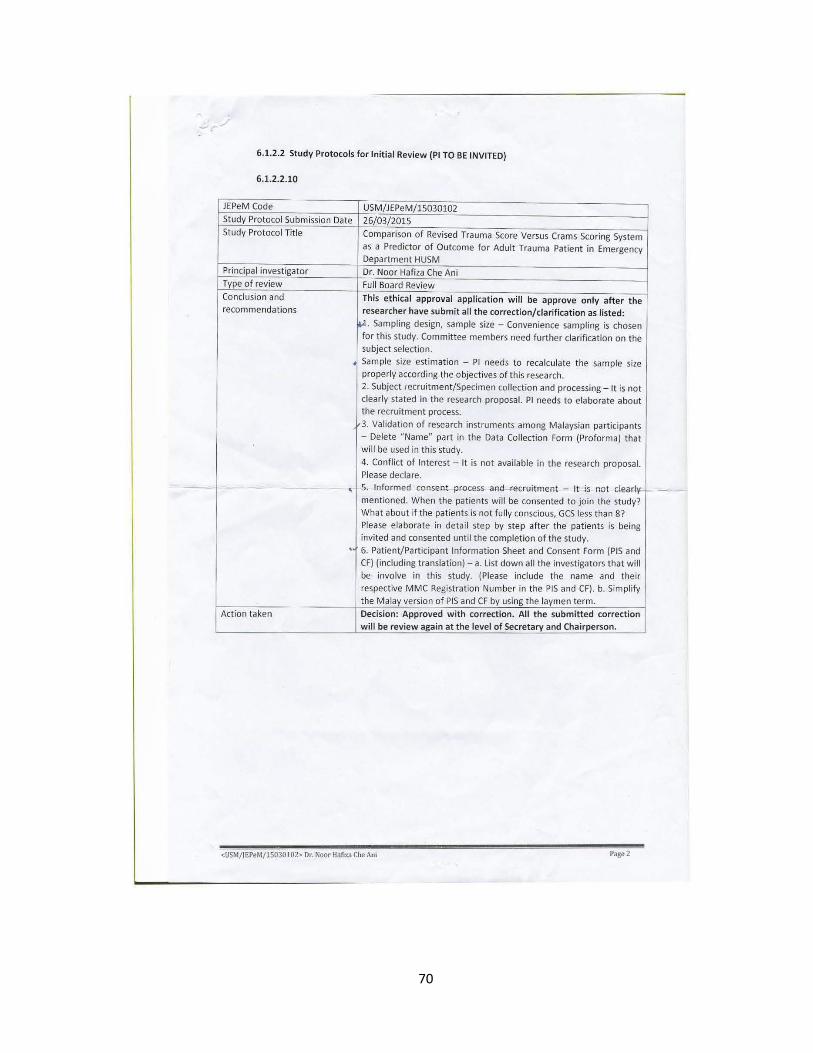
70
-' .-./
6.1.2.2 Study Protocols for Initial Review (PI TO BE INVITED)
6.1.2.2.10
JEPeM Code USM/JEPeM/15030102 Study Protocol Submission Date 26/03/2015 Study Protocol Title Comparison of Revised Trauma Score Versus Crams Scoring System
as a Predictor of Outcome for Adult Trauma Patient in Emergency Department HUSM
Principal investigator Dr. Noor Hafiza Che Ani Type of review Full Board Review Conclusion and This ethical approval application will be approve only after the recommendations researcher have submit all the correction/clarification as listed:
~· Sampling design, sample size - Convenience sampling is chosen for this study. Committee members need further clarification on the subject selection.
Sample size estimation - PI needs to recalculate the sample size properly according the objectives of this research. 2. Subject fecruitment/Specimen collection and processing- It is not clearly stated in the research proposal. PI needs to elaborate about the recruitment process.
3. Validation of research instruments among Malaysian participants - Delete "Name" part in the Data Collection Form (Proforma) that will be used in this study.
4. Conflict of Interest- It is not available in the research proposal. Please declare.
- - ' 5. lnfcrme.d consent "Process and recruitment - It is not clearl't r mentioned. When the patients will be consented to join the study? What about if the patients is not fully conscious, GCS less than 8? Please elaborate in detail step by step after the patients is being invited and consented until the completion of the study. . 6. Patient/Participant Information Sheet and Consent Form (PIS and CF) (including translation)- a. List down all the investigators that will be involve in this study. (Please include the name and their respective MMC Registration Number in the PIS and CF). b. Simplify the Malay version of PIS and CF by using the laymen term.
Action taken Decision: Approved with correction. All the submitted correction will be review again at the level of Secretary and Chairperson.
<USM/ IEPeM/15030102> Dr. Noor Hofiza Che Am
71

72

73
5.1 Additional Tables/Graph
5.1.1 Triage Revised Trauma Score
component score
respiratory rate (breath/min)
10 to 24 4
25 to 36 3
>36 2
1 to 9 1
0 0
systolic blood pressure (mmHg)
>89 4
70 to 89 3
50 to 69 2
1 to 49 1
0 0
Glasgow Coma Scale
13 to 15 4
9 to 12 3
6 to 8 2
4 to 5 1
3 0

74
5.1.2 CRAMS Scale
component score
Circulation
Normal capillary refill and BP > 100
2
Delayed capillary refill or 85 < BP <
100
1
No capillary refill or BP < 85
0
Respiration
Normal
2
Abnormal (labored or shallow)
1
Absent
0
Abdomen/thorax
Abdomen and thorax non tender
2
Abdomen or thorax tender
1
Abdomen rigid or flail chest*
0
Motor
Normal
2
Responds only to pain (other than decerebrate) 1
No response (or decerebrate)
0
Speech
Normal
2
Confused
1
No intelligible words
0
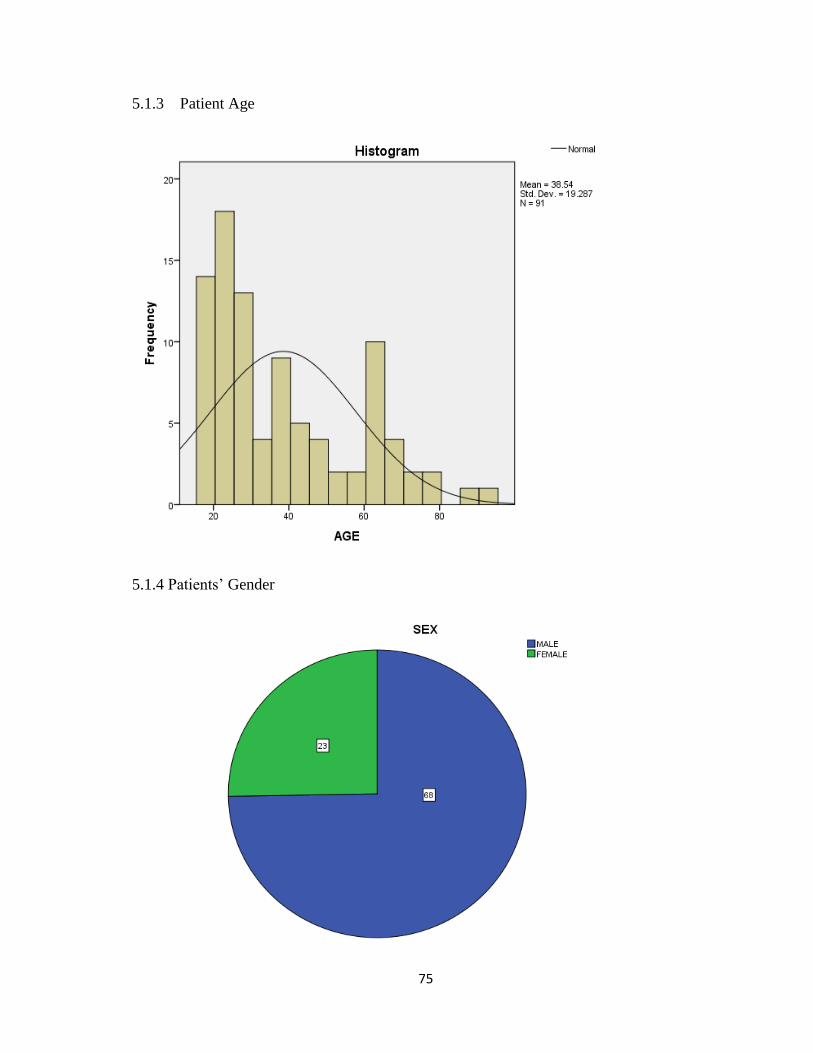
75
5.1.3 Patient Age
5.1.4 Patients’ Gender
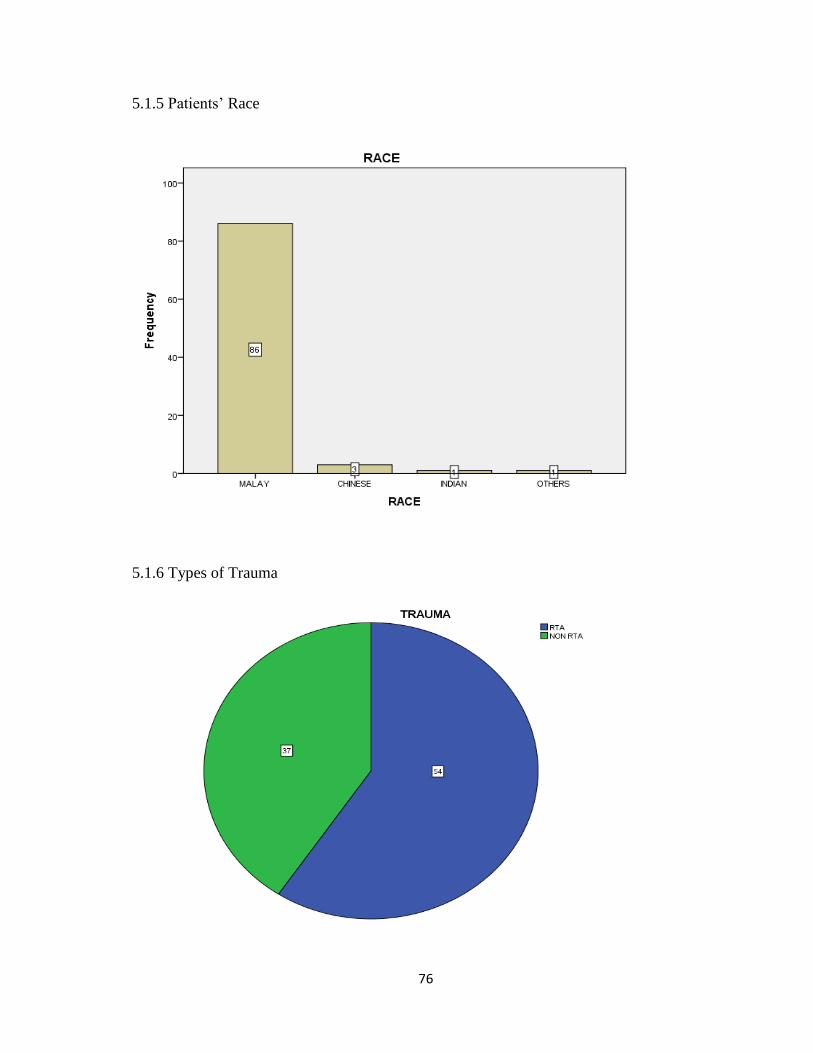
76
5.1.5 Patients’ Race
5.1.6 Types of Trauma

77
5.1.7 Patients’ Outcome/Disposition from Emergency Department

78
5.2 Assessment Form
COMPARISON OF REVISED TRAUMA SCORE VERSUS CRAMS SCALE AS A
PREDICTOR OF OUTCOME FOR ADULT TRAUMA PATIENT IN
EMERGENCY DEPARTMENT HUSM
ASSESSMENT FORM
AGE
SEX FEMALE
MALE
RACE MALAY / CHINESE / INDIAN / OTHERS
TYPE OF
INJURY
ROAD TRAFFIC ACCIDENT
NON ROAD TRAFFIC ACCIDENT
REVISED TRAUMA SCORE CRAMS SCALE
COMPONENT VALUE SCO
RE
COMPONEN
T
VALUE SCO
RE
RESPIRATOR
Y RATE
(BREATH/MIN
)
10-24 4 CIRCULATIO
N
(CAPILLARY
REFILL/ SBP)
NORMAL/ SBP>100 2
25-35 3 DELAYED/ SBP 85-
100 1
>36 2 NO CRT/ SBP< 85 0
1-9 1 REPIRATION NORMAL 2
0 0 ABNORMAL 1
SYSTOLIC
BLOOD
PRESSURE
(SBP mmHg)
>89 4 ABSENT 0
70-89 3 ABDOMEN/
THORAX
NON TENDER 2
50-69 2 TENDER 1
1-49 1 RIGID
ABDOMEN/FLAIL
CHEST
0
0 0 MOTOR NORMAL 2
13-15 4 RESPOND TO PAIN 1

79
GLASGOW
COMA SCALE
9-12 3 NO
RESPOND/DECEBRA
TE
0
6-8 2 SPEECH NORMAL 2
4-5 1 CONFUSED 1
<4 0 NO INTELIGIBLE
WORDS 0
TOTAL TOTAL
OUTCOME ( DISPOSITION FROM EMERGENCY DEPARTMENT)
DISCHARGE INTENSIVE CARE UNIT/
OPERATION THEATRE
ADMIT GENERAL WARD DEATH
ASSESSED BY :
NAME : _______________________________________
MPM : _______________________________________
DATE :________________________________________
80
5.3 Additional Literature Review
1. The reliability of both T-RTS and CRAMS Scale already tested and validated. Patients
were considered major injury if T-RTS was score 11 and below. Champion et al (1989) tested
the reliability of RTS against two large databases. The Washington Hospital Center database
(the database of the principal author) containing 2,166 patients and the Major Trauma
Outcome Study (MTOS) database (as developed by the American College of Surgeons
Committee on Trauma) containing 26,000 patients were evaluated by T-RTS. Results
showed that an T-RTS<11 accurately identified 97.2% of the fatally injured and most of the
severely injured as determined by regression analysis.1
2. For CRAMS Scale, patients were considered to have major injury if scored 8 and below.
It was validated external in two studies. Baxt et al (1989) evaluated 2434 patients with ROC
curves presented.2 Emerman et al evaluated 1027 patients with outcome of major injury
(CRAMS < 9) with Sensitivity of 100%; Specificity 83%.3-4
81
5.4 Additional References
1. Senkowski CK, McKenney MG. Trauma scoring systems: a review 1 2. Journal of the
American College of Surgeons. 1999;189(5):491-503.
2. Baxt WG, Berry CC, Epperson MD, Scalzitti V. The failure of prehospital trauma
prediction rules to classify trauma patients accurately. Annals of emergency medicine.
1989;18(1):1-8.
3. Emerman CL, Shade B, Kubincanek J. A comparison of EMT judgment and prehospital
trauma triage instruments. Journal of Trauma and Acute Care Surgery. 1991;31(10):1369-
75.
4. Rehn M, Perel P, Blackhall K, Lossius HM. Prognostic models for the early care of trauma
patients: a systematic review. Scand J Trauma Resusc Emerg Med. 2011;19:17.
82
5.5 Raw Data on SPSS (Soft Copy)
COMPARISON OF TRIAGE REVISED
TRAUMA SCORE AND CRAMS SCALE
AS PREDICTORS OF OUTCOME IN
EMERGENCY DEPARTMENT,
HOSPITAL UNIVERSITI SAINS
MALAYSIA
BY : DR NOOR HAFIZA BINTI CHE ANI
SPSS RAW DATA