Comparison of three commercially available ektacytometers with different shearing geometries
14
Biorheology 46 (2009) 251–264 251 DOI 10.3233/BIR-2009-0536 IOS Press Technical report Comparison of three commercially available ektacytometers with different shearing geometries Oguz K. Baskurt a,∗ , M.R. Hardeman b , Mehmet Uyuklu a , Pinar Ulker a , Melike Cengiz a , Norbert Nemeth c , Sehyun Shin d , Tamas Alexy e and Herbert J. Meiselman e a Department of Physiology, Akdeniz University, Faculty of Medicine, Antalya, Turkey b Department of Physiology, Academic Medical Center, Amsterdam, The Netherlands c Institute of Surgery, Department of Operative Techniques and Surgical Research, Medical and Health Science Center, University of Debrecen, Hungary d Department of Mechanical Engineering, Korea University, Seoul, Korea e Department of Physiology and Biophysics, University of Southern California, Keck School of Medicine, Los Angeles, CA, USA Received 23 February 2009 Accepted in revised form 3 April 2009 Abstract. In December 2008, the International Society for Clinical Hemorheology organized a workshop to evaluate and com- pare three ektacytometer instruments for measuring deformability of red blood cells (RBC): LORCA (Laser-assisted Optical Rotational Cell Analyzer, RR Mechatronics, Hoorn, The Netherlands), Rheodyn SSD (Myrenne GmbH, Roetgen, Germany) and RheoScan-D (RheoMeditech, Seoul, Korea). Intra-assay reproducibility and biological variation were determined using normal RBC, and cells with reduced deformability (i.e., 0.001–0.02% glutaradehyde (GA), 48 ◦ C heat treatment) were em- ployed as either the only RBC present or as a sub-population. Standardized difference values were used as measure of the power to detect differences between normal and treated cells. Salient results include: (1) All instruments had intra-assay vari- ations below 5% for shear stress (SS) > 1 Pa but a sharp increase was found for Rheodyn SSD and RheoScan-D at lower SS; (2) Biological variation was similar and markedly increased for SS < 3–5 Pa; (3) All instruments detected GA-treated RBC with maximal power at 1–3 Pa, the presence of 10% or 40% GA-modified cells, and the effects of heat treatment. It is concluded that the LORCA, Rheodyn SSD and RheoScan-D all have acceptable precision and power for detecting reduced RBC deformability due to GA treatment or heat treatment, and that the SS range selected for the measurement of deformability is an important determinant of an instrument’s power. Keywords: Erythrocyte deformability, ektacytometry * Address for correspondence: Dr. Oguz K. Baskurt, Department of Physiology, Akdeniz University, Faculty of Medicine, Antalya, Turkey. Tel.: +90 242 310 1560; Fax: +90 242 310 1561; E-mail: [email protected]. 0006-355X/09/$17.00 © 2009 – IOS Press and the authors. All rights reserved
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Comparison of three commercially available ektacytometers with different shearing geometries

Biorheology 46 (2009) 251–264 251DOI 10.3233/BIR-2009-0536IOS Press
Technical report
Comparison of three commercially availableektacytometers with different shearinggeometries
Oguz K. Baskurt a,∗, M.R. Hardeman b, Mehmet Uyuklu a, Pinar Ulker a, Melike Cengiz a,Norbert Nemeth c, Sehyun Shin d, Tamas Alexy e and Herbert J. Meiselman e
a Department of Physiology, Akdeniz University, Faculty of Medicine, Antalya, Turkeyb Department of Physiology, Academic Medical Center, Amsterdam, The Netherlandsc Institute of Surgery, Department of Operative Techniques and Surgical Research, Medical and HealthScience Center, University of Debrecen, Hungaryd Department of Mechanical Engineering, Korea University, Seoul, Koreae Department of Physiology and Biophysics, University of Southern California, Keck School ofMedicine, Los Angeles, CA, USA
Received 23 February 2009Accepted in revised form 3 April 2009
Abstract. In December 2008, the International Society for Clinical Hemorheology organized a workshop to evaluate and com-pare three ektacytometer instruments for measuring deformability of red blood cells (RBC): LORCA (Laser-assisted OpticalRotational Cell Analyzer, RR Mechatronics, Hoorn, The Netherlands), Rheodyn SSD (Myrenne GmbH, Roetgen, Germany)and RheoScan-D (RheoMeditech, Seoul, Korea). Intra-assay reproducibility and biological variation were determined usingnormal RBC, and cells with reduced deformability (i.e., 0.001–0.02% glutaradehyde (GA), 48◦C heat treatment) were em-ployed as either the only RBC present or as a sub-population. Standardized difference values were used as measure of thepower to detect differences between normal and treated cells. Salient results include: (1) All instruments had intra-assay vari-ations below 5% for shear stress (SS) > 1 Pa but a sharp increase was found for Rheodyn SSD and RheoScan-D at lowerSS; (2) Biological variation was similar and markedly increased for SS < 3–5 Pa; (3) All instruments detected GA-treatedRBC with maximal power at 1–3 Pa, the presence of 10% or 40% GA-modified cells, and the effects of heat treatment. It isconcluded that the LORCA, Rheodyn SSD and RheoScan-D all have acceptable precision and power for detecting reducedRBC deformability due to GA treatment or heat treatment, and that the SS range selected for the measurement of deformabilityis an important determinant of an instrument’s power.
Keywords: Erythrocyte deformability, ektacytometry
*Address for correspondence: Dr. Oguz K. Baskurt, Department of Physiology, Akdeniz University, Faculty of Medicine,Antalya, Turkey. Tel.: +90 242 310 1560; Fax: +90 242 310 1561; E-mail: [email protected].
0006-355X/09/$17.00 © 2009 – IOS Press and the authors. All rights reserved

252 O.K. Baskurt et al. / Comparison of three commercially available ektacytometers
1. Introduction
Deformability of red blood cells (RBC) is an important parameter frequently used for hemorheolog-ical evaluations in experimental and clinical studies. A variety of methods have been used to quantitateRBC deformability, including filtration techniques, micropipette aspiration and ektacytometry [9]. Ek-tacytometry is a technique using diffraction patterns produced by laser light traversing a sheared lowhematocrit RBC suspension; the geometry of the diffraction pattern reflects the deformed cell shapeand is usually expressed as a dimensionless elongation index (EI). This technique has become the mostutilized method in the field to test for RBC deformability, mainly due to its precision, sensitivity andconvenience. Currently, there are several commercially available ektacytometers, all using the samelaser-diffraction principle [10] but different shearing geometries (e.g., Couette, plate–plate, microchan-nel). All commercially-available instruments report EI measured over a range of shear stresses (SS), andin some devices this SS range is user selectable.
Obviously, the value of an instrument used for research or clinical purposes is determined by itsprecision and sensitivity to alterations of RBC deformability. However, there are no generally-acceptedstandards for calibration or evaluation of hemorheological instruments, including devices to measureRBC deformability and aggregation. Therefore, a workshop was organized under the auspices of theInternational Society of Clinical Hemorheology to compare and evaluate three commercially-availableektacytometers. This report presents results from this workshop held in Antalya, Turkey, December 8–13, 2008.
2. Materials and methods
2.1. Blood samples
Venous blood samples were obtained from 10 healthy male volunteers, aged between 25 and 52 years.A tourniquet was applied to locate the antecubital vein prior to venipuncture and kept in place duringthe blood sampling. Thirty ml of blood was obtained from each donor using commercial vacuum tubescontaining ethylenediamine-tetraacetic acid (EDTA, 1.5 mg/ml). All blood sampling was completedwithin two minutes after the application of the tourniquet. A five ml aliquot of each sample was savedfor control measurements. The remaining 25 ml of each sample was centrifuged at 1400 × g for sixminutes, the plasma aspirated and saved, and the buffy coat discarded. RBC were then washed twicewith isotonic phosphate-buffered saline (0.01 M phosphate, PBS, pH = 7.4).
2.2. Glutaraldehyde treatment of RBC
A portion of the washed RBC were re-suspended in PBS at 0.05 l/l hematocrit and divided into fouraliquots. Glutaraldehyde (GA, Sigma Chemical Company, St. Louis, MO, USA) was added to achievefinal concentrations of 0.001, 0.003, 0.005 and 0.02% and the suspensions incubated at room temperature(22◦C) for 30 minutes. Following incubation with GA the RBC were washed three times with PBS.
The washed RBC previously incubated with 0.001, 0.003 and 0.005% GA were re-suspended in au-tologous plasma at 0.4 l/l hematocrit. Additionally, mixtures of normal (untreated) and GA-treated RBCwere prepared as follows: (1) 10% GA-treated (at 0.005%) RBC + 90% normal RBC; (2) 40% GA-treated (at 0.005%) RBC + 60% normal RBC; (3) 10% GA-treated (at 0.02%) RBC + 90% normalRBC; (4) 40% GA-treated (at 0.02%) RBC + 60% normal RBC. These RBC mixtures were also sus-pended in autologous plasma at 0.4 l/l hematocrit.

O.K. Baskurt et al. / Comparison of three commercially available ektacytometers 253
2.3. Heat treatment of RBC
Washed RBC were re-suspended in PBS at 0.1 l/l hematocrit and 20 ml of the suspension was trans-ferred to a 50 ml Erlenmeyer flask. The flask was immersed in a water bath at 48◦C for 9 min with gentlemixing, following which the flask was immediately cooled in a water bath at room temperature and theRBC used for deformability measurements.
2.4. RBC deformability measurements
All measurements were carried out using RBC suspended at low hematocrit in an isotonic, viscouspolymer solution: 40 µl of blood or RBC suspension added to 8 ml of a 6% polyvinylpyrrolidone solution(PVP, 360 kDa, Sigma, 30 mPa s at 37◦C). Two types of RBC suspensions were used for deformabilitymeasurements: (1) to evaluate reproducibility a whole blood sample from one donor was used to de-termine intra-assay variation for each device; for this purpose, 10 separate aliquots of the dilute RBCsuspension were measured; (2) to evaluate the ability of each device to detect altered RBC rigidity, nor-mal samples, GA-treated and heat-treated RBC, and mixtures of normal and treated cells were employedusing blood from each of the 10 individual donors.
2.5. Evaluated ektacytometers
Three commercially-available ektacytometers having different shearing geometries were evaluated.
2.5.1. LORCA – Laser-assisted Optical Rotational Cell AnalyzerThe details of the LORCA (RR Mechatronics, Hoorn, The Netherlands) have been described else-
where [7]. The dilute RBC suspension is sheared in a Couette system composed of a glass cup and aprecisely fitting bob, with a gap of 0.3 mm between the cylinders. A laser beam is directed through thesheared sample and the diffraction pattern produced by the deformed cells is captured by a CCD cameraand analyzed by a microcomputer. Based upon the geometry of the ellipsoidal diffraction pattern, anelongation index is calculated as: EI = (L − W )/(L + W ), where L and W are the length and widthof the diffraction pattern. An increased EI at a given SS indicates greater cell deformation and hencegreater RBC deformability. EI values were measured for nine SS at 0.3–75 Pa. All measurements werecarried out at 37◦C.
2.5.2. Rheodyn SSDThe Rheodyn SSD (Myrenne GmbH, Roetgen, Germany) utilizes two parallel, transparent circular
discs separated by a 0.5 mm gap as the shearing system [11]. The bottom disc is stationary and the upperone rotates at eight different pre-determined speeds to generate eight levels of shear rate. A polarizedlaser beam is directed through the sample perpendicular to the discs, and the geometry of the diffractionpattern on the opposite side sensed using four light-sensing diodes arranged in a square pattern. Themean length and width of the diffraction pattern is determined from the light intensities recorded by thediode array using a calibration factor, and the elongation index calculated as described above. The pre-determined rotational speeds of the upper disc yielded a SS range of 0.3–75 Pa with the 30 mPa s PVPsolution used in this study. The instrument is not temperature controlled, but was placed in a temperaturecontrolled box throughout the measurements with the temperature maintained at 37◦C.

254 O.K. Baskurt et al. / Comparison of three commercially available ektacytometers
2.5.3. RheoScan-D slit-flow ektacytometerThe RheoScan-D (RheoMeditech, Seoul, Korea) consists of a disposable element, a laser, a CCD-
camera, a screen, a pressure sensor and a vacuum-generating mechanism [12]. The disposable element,which is made of transparent plastic, consists of a microchannel and reservoirs at each end; the dimen-sions of the microchannel are 0.2 mm high × 4.0 mm wide × 40 mm long. The dilute RBC suspensionis sheared in the microchannel under continuously decreasing pressure-differentials. A laser beam is di-rected through the sheared sample and the diffraction pattern produced by the deformed cells is capturedby a CCD camera and analyzed by a computer. Based upon the captured elliptical diffraction patterns,an elongation index is determined as described above. EI values are given for sixteen SS levels at 0.5–20 Pa, with SS calculated using an average shear rate (i.e., one-half wall shear rate, assuming a parabolicvelocity profile); SS values utilized herein were selected to be comparable to those from the other twoinstruments.
The RheoScan-D instrument is not temperature controlled, but in the present study the plastic dis-posable elements were placed in a 37◦C temperature controlled box prior to use. Due to the short testtime (i.e., ∼30 s) and the use of pre-warmed suspensions, the sample temperature was assumed to bemaintained at 37◦C during the measurement period.
2.6. Other methods
Mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH) and mean corpuscularhemoglobin concentration (MCHC) values were determined using a hematology analyzer (Cell-Dyn3500R, Abbott Diagnostic Division, IL, USA). RBC shape was examined in dilute wet-mount, unstainedpreparations under light microscopy. The viscosity of the PVP solution was measured at 37◦C using aWells–Brookfield cone–plate viscometer (DV II + Pro, Brookfield Engineering Labs, Middleboro, MA,USA; shear rate = 750 s−1).
2.7. Calculations and statistics
Intra-assay variation was calculated as the coefficient of variation (CV) of 10 repeated measurementson the same sample. Biological variation was expressed as the CV of the data obtained using the bloodsamples from 10 donors.
The results for RBC suspensions with reduced deformability (i.e., GA or heat-treated) are expressedas mean ± standard error (SE); statistical comparisons were done using a two-way ANOVA for EIdata measured at various SS followed by appropriate statistical post-tests. Additionally, standardizeddifferences from control values were calculated by dividing the mean difference of EI between normaland the treated RBC at a given SS by the “pooled standard deviation” of the normal plus treated data.That is
[mean normal (10 donors) − mean treated (10 donors)]/pooled standard deviation.
The pooled standard deviation is calculated as the square root of the mean of squared standard deviationsof the two groups being compared [5]. The standardized difference has been accepted as a measure ofthe power of each measurement condition to detect a difference between two groups [14].

O.K. Baskurt et al. / Comparison of three commercially available ektacytometers 255
3. Results
3.1. Hematological parameters and red blood cell shape
MCV, MCH and MCHC values were 84.7 ± 1.2 fl, 31.8 ± 0.5 pg and 37.3 ± 0.1 g/dl respectively. RBCshape was observed to be normal in normal and treated samples, except for heat-treated RBC wheresome stomatocyte formation and fragmentation were noted.
3.2. Intra-assay variation
The CV values of the 10 repeated EI measurements on the same sample were below 5% at all SS forthe LORCA (Fig. 1). CV results exceeded 5% only at lowest SS for the Rheodyn SSD and RheoScan-D,being markedly increased for the Rheodyn SSD at 0.38 Pa.
3.3. Biological variability
Biological variability for normal samples from the 10 donors were similar and SS dependent, beingless than 10% for all three instruments if the SS was above 0.5 Pa (Fig. 2).
3.4. Deformability measurements for glutaraldehyde-treated RBC
Figure 3 presents EI versus shear stress data for RBC treated with GA at 0.001%, 0.003% and 0.005%concentrations. Inspection of these results indicates: (1) Data obtained for the three instruments haveessentially similar shapes over comparable SS ranges; (2) The concentration-dependent effect of GA wasobserved with all three instruments, with EI progressively decreased with increased GA concentrationsat most SS. Treatment of RBC with 0.001% GA resulted in a very slight decrease of deformability, withthe differences statistically significant over SS ranges of 1.2–4.8 Pa for the LORCA, 1.5–3.8 Pa for theRheodyn SSD and 0.5–15 Pa for the RheoScan-D. Differences between normal and GA-treated RBCwere significant (p < 0.001) over a wider range of SS for RBC treated with 0.003% and 0.005% GA:(1) LORCA at all SS except the lowest (0.3 Pa) for both concentrations; (2) Rheodyn SSD at SS between1.5 and 15 Pa for 0.003% and at all SS except the lowest (0.4 Pa) for 0.005% GA; (3) RheoScan-D at allSS over its range of 0.5–20 for both 0.003 and 0.005% GA.
Fig. 1. Coefficients of variation (CV) of 10 repeated measurements using the same blood sample.

256 O.K. Baskurt et al. / Comparison of three commercially available ektacytometers
Fig. 2. Coefficients of variation (CV) of the measurements on normal samples from the 10 donors (i.e., biological variability).Note the similar dependence on shear stress with the three instruments.
Fig. 3. Elongation indexes of RBC treated with 0.001, 0.003 and 0.005% glutaradehyde. Data are presented as mean ± standarderror, n = 10. Standard error lines remain inside the symbol for most data points. See Section 3.4 for statistical comparisons.

O.K. Baskurt et al. / Comparison of three commercially available ektacytometers 257
Fig. 4. Standardized differences calculated using the data presented in Fig. 3. Each graph corresponds to RBC treated with GAconcentrations of 0.001% (A), 0.003% (B) and 0.005% (C).
Figure 4 presents standardized differences for GA-treated RBC, where it is obvious that they increasewith GA concentration and hence with increasing cell rigidity (Fig. 3). It is also obvious from Fig. 4 thatthe level of SS is also a determinant of standardized difference, with peak values at about 0.5–1.5 Paand significantly lower levels at higher SS. Standardized differences for all three instruments in theirlower SS range were similar for RBC treated with GA at the two lower concentrations (i.e., 0.001 and0.003%). At 0.005% GA, the RheoScan-D had the highest standardized differences over the SS range forthis device (0.5–20 Pa). Standardized differences for all GA concentrations were lowest for the RheodynSSD at SS > 10 Pa.
3.5. Mixtures of GA-treated and normal RBC
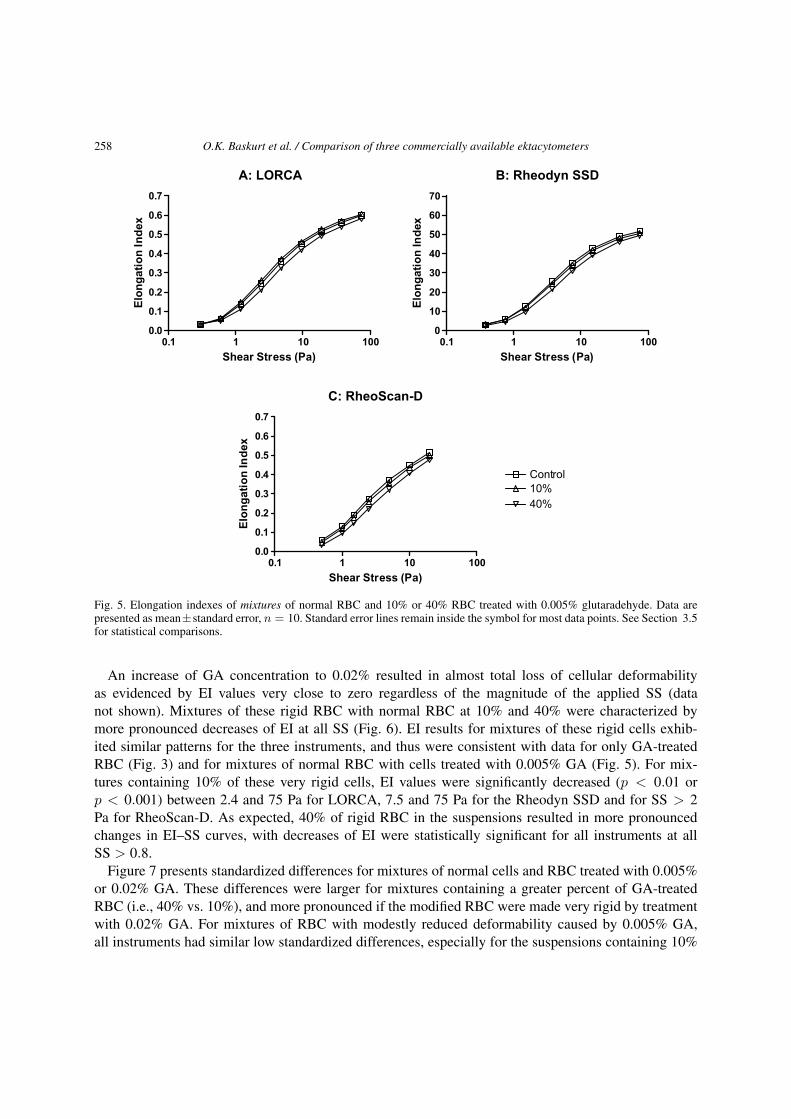
EI–SS data for mixtures of normal RBC and RBC treated with 0.005% GA are presented in Fig. 5. In-clusion of 10% GA-treated RBC resulted in a very slight decrease of EI, with the LORCA and RheodynSSD not detecting significant differences and the RheoScan-D yielding significant alterations (p < 0.05only at 15 and 17 Pa). All three devices were more sensitive to the presence of 40% of GA-treated cells(Fig. 5): LORCA EI values were significantly decreased at SS > 1.2 Pa; Rheodyn SSD results weresignificantly decreased between 1.5 and 75 Pa (p < 0.001 between 3.8 and 15 Pa), and RheoScan-Dindicated significant EI decreases over its entire SS range (p < 0.001).
258 O.K. Baskurt et al. / Comparison of three commercially available ektacytometers
Fig. 5. Elongation indexes of mixtures of normal RBC and 10% or 40% RBC treated with 0.005% glutaradehyde. Data arepresented as mean ± standard error, n = 10. Standard error lines remain inside the symbol for most data points. See Section 3.5for statistical comparisons.
An increase of GA concentration to 0.02% resulted in almost total loss of cellular deformabilityas evidenced by EI values very close to zero regardless of the magnitude of the applied SS (datanot shown). Mixtures of these rigid RBC with normal RBC at 10% and 40% were characterized bymore pronounced decreases of EI at all SS (Fig. 6). EI results for mixtures of these rigid cells exhib-ited similar patterns for the three instruments, and thus were consistent with data for only GA-treatedRBC (Fig. 3) and for mixtures of normal RBC with cells treated with 0.005% GA (Fig. 5). For mix-tures containing 10% of these very rigid cells, EI values were significantly decreased (p < 0.01 orp < 0.001) between 2.4 and 75 Pa for LORCA, 7.5 and 75 Pa for the Rheodyn SSD and for SS > 2Pa for RheoScan-D. As expected, 40% of rigid RBC in the suspensions resulted in more pronouncedchanges in EI–SS curves, with decreases of EI were statistically significant for all instruments at allSS > 0.8.
Figure 7 presents standardized differences for mixtures of normal cells and RBC treated with 0.005%or 0.02% GA. These differences were larger for mixtures containing a greater percent of GA-treatedRBC (i.e., 40% vs. 10%), and more pronounced if the modified RBC were made very rigid by treatmentwith 0.02% GA. For mixtures of RBC with modestly reduced deformability caused by 0.005% GA,all instruments had similar low standardized differences, especially for the suspensions containing 10%

O.K. Baskurt et al. / Comparison of three commercially available ektacytometers 259
Fig. 6. Elongation indexes of mixtures containing 10 or 40% RBC treated with 0.02% glutaraldehyde. Data are presented asmean ± standard error, n = 10. Standard error lines remain inside the symbol for most data points. See Section 3.5 for statisticalcomparisons.
GA-treated RBC (Fig. 7A). Standardized differences for suspensions containing 40% of these cells wereslightly increased with a rank order of RheoScan-D > LORCA > Rheodyn SSD (Fig. 7B). The patternfor standardized difference versus SS for mixtures containing 10% of RBC treated with 0.02% GAcontinued to increase with SS for each instrument (Fig. 7C). However, for suspensions containing 40%of RBC treated with 0.02% GA, maximum values were reached at 1–2 Pa followed by decreases athigher SS (Fig. 7D).
3.6. Heat-treated RBC
Heating RBC at 48◦C for 9 minutes resulted in a marked decrease of deformability, with this changedetected similarly by all three instruments (Fig. 8). Differences between heat-treated and normal RBCwere statistically significant at all SS (p < 0.001), with the exception of the lowest levels (0.3–0.8 Pa)for the LORCA and Rheodyn SSD. Standardized differences for heat-treated RBC (Fig. 9) demonstrateda pattern similar to that for RBC treated with 0.005% GA (Fig. 7B): The LORCA and Rheodyn SSDhad a maximum at around 1 Pa that gradually declined at higher SS, with the RheoScan-D exhibiting alower degree of dependence on SS.

260 O.K. Baskurt et al. / Comparison of three commercially available ektacytometers
Fig. 7. Standardized differences calculated using the data presented in Figs 5 and 6 for mixtures of normal and GA-treated cells.Panels A and B are for 10 or 40% RBC treated with 0.005% GA, and panels C and D are for 10 or 40% RBC treated with0.02% GA.
4. Discussion
The three ektacytometers evaluated in this study were characterized by a very low intra-assay variation(i.e., CV for repeated measurements of the same sample), with intra-assay variations below 5% forSS > 1 Pa. However, for the RheoScan-D and Rheodyn SSD instruments, there were sharp increases ofintra-assay variation at SS < 1 Pa; CV values were approximately 10% at 0.5 Pa and reached ∼40% at0.38 Pa (Fig. 1). This low reproducibility may thus limit the value of these two devices for measurementsat less than 1 Pa. The dependence of intra-assay variation on SS observed herein for the LORCA isconsistent with previous reports indicating a CV of about 4% at 0.5 Pa and 0.4% at 50 Pa [7]. Wang etal. report that for 6 repeated measures on the same normal blood sample, the reproducibility for both theLORCA and Rheodyn SSD was less than 5% but unfortunately do not indicate the shear stress range forthese results [15].
The biological variation of EI for 10 normal donors (Fig. 2) also reflects a dependence on SS, in thatall instruments indicated a markedly increased variation at SS less than about 3–5 Pa. Wang et al. alsoindicate a SS-dependence of biological variability for the LORCA and Rheodyn SSD: 28–33% CV at0.5 Pa and 3–10% at 30 Pa. Note, however, that their studies used a 30 mPa s PVP solution for theLORCA and a 25%, 24 mPa s solution of 40 kDa dextran for the Rheodyn SSD. In addition, unequal

O.K. Baskurt et al. / Comparison of three commercially available ektacytometers 261
Fig. 8. Elongation indexes of RBC heated at 48◦C for 9 minutes. Data are presented as mean ± standard error, n = 10. Standarderror lines remain inside the symbol for most data points. See Section 3.6 for statistical comparisons.
Fig. 9. Standardized differences calculated using the data presented in Fig. 8.
temperatures were employed (22◦C for Rheodyn SSD, 37◦C for LORCA) and thus direct comparisonsare inappropriate.
In addition to determining reproducibility as an index to the merit of a hemorheological device, theuse of standardized differences provides a parameter that allows comparison of instruments. Note thatthis parameter is determined by both the sensitivity of the instrument to a given change in deformability

262 O.K. Baskurt et al. / Comparison of three commercially available ektacytometers
from normal and the variation within the two groups being compared [14] and is thus similar to a poweranalysis of a method [5].
Two separate approaches were utilized to compare the power (i.e., standardized difference) of eachinstrument for detecting differences between two RBC populations: (1) Comparisons between untreatedRBC and RBC treated with 0.001, 0.003 or 0.005% GA in which all cells being tested had been exposedto this agent. GA at these low concentrations results in very slight and gradual alterations of deforma-bility [1,14]; (2) Comparisons between untreated RBC and mixtures of untreated and GA-treated RBCusing mixtures containing either 10% or 40% cells with slightly reduced deformability (0.005% GA)or with very rigid RBC (0.02% GA). The second approach was designed to model samples that maybe obtained from patients where only a sub-population of RBC have impaired deformability [13,14].Both approaches have been previously used to evaluate ektacytometers and alterations of EI, with con-centrations of GA and percentages of rigid cells similar to those utilized herein [1,8,15]. GA treatmentrigidifies RBC by cross-linking membrane proteins. It should be noted that this approach may not berepresentative for all clinically relevant mechanisms of deformability alterations (e.g., change in surfacearea/volume ration, change in cytoplasmic viscosity).
In samples where all cells were treated with GA, the three instruments detected alterations induced byGA even at the lowest concentration (0.001%) and showed dose-dependent depression of SS–EI curves(Fig. 3). These measurements were all characterized by low coefficients of variation, with standard errorbars being within the symbols used in Fig. 3. The CV values for these suspensions varied with SS (e.g.,for the LORCA, 1.3–57% for the highest and lowest SS levels) and were similar to biological variabilityresults for untreated, normal cells (Fig. 2); they also tended to increase with GA concentration and hencewith increased differences between untreated and normal samples.
Although the three instruments demonstrated very similar standardized differences between the un-treated and GA-treated RBC at 0.001 and 0.003% concentrations, the RheoScan-D had a higher power(i.e., higher standardized difference) for 0.005% GA-treated RBC (Fig. 4C). It is also clear from Fig. 4that standardized differences reached a maximum at about 1–2 Pa SS then gradually decreased withincreased SS. This decreasing standardized difference with increasing SS is due to smaller differencesbetween treated and untreated RBC at high stress levels, and not to poorer performance; the CV levelsfor these modified cell suspensions were smaller at higher SS than at lower SS.
The instruments evaluated in this study also yielded similar results for samples with GA-treated RBCsub-populations. However, the changes caused by the presence of 10% of 0.005% GA-treated RBCcould only be detected by the RheoScan-D at high SS (15–17 Pa, Fig. 7A); this instrument exhibitedsomewhat greater power for detecting the presence of 40% of 0.005% GA-treated RBC (Fig. 7B). Allthree instruments had similar power in detecting the presence of 10% or 40% RBC treated with 0.02%GA. EI–SS relations were remarkably similar for heat-treated RBC (Fig. 8) and are consistent with theknown increased rigidity of such cells [3,8,15]. Standardized differences were also very similar, althoughthe LORCA values were slightly higher (Fig. 9).
It follows from the above discussion that the LORCA, Rheodyn SSD and RheoScan-D all had accept-able precision and power for detecting the various degrees of alterations induced by GA treatment andheat treatment. It is also obvious that the SS range selected for the measurement of EI is an importantdeterminant of the power. Measurements at low SS are characterized by higher variation which may sig-nificantly decrease the power of the measurement. Further, differences between normal and altered RBCbecome smaller at higher SS, especially if the alteration of deformability is relatively small (Fig. 4).However, this is not true for RBC suspensions containing non-deformable RBC. Rather, in the presence

O.K. Baskurt et al. / Comparison of three commercially available ektacytometers 263
of rigid RBC subpopulations, differences at higher SS became larger, thereby increasing the standard-ized differences (Fig. 7C and D). It is thus essential that each of these ektacytometers be operated ina shear stress range that optimizes their performance and ability to detect differences; it is especiallyimportant to avoid very low stress levels where instrument reproducibility is low (Fig. 1).
While similar in performance, there are important differences between the three instruments:
1. The RheoScan-D operates over a smaller SS range (0.5–20 Pa) than the LORCA or RheodynSSD (0.35–75 Pa). However, this difference in measurement range does not impair the value ofRheoScan-D since the highest sensitivity, and hence the most useful SS region for detecting differ-ences, is available with all three instruments;
2. While all three devices were operated at 37◦C, both the RheoScan-D and the Rheodyn SSD re-quired the use of a temperature controlled box since neither presently have built-in temperatureregulation. Since measurement temperature does affect sensitivity to changes of deformability [2]as well as the viscosity of the suspending medium, temperature control for all devices is warranted;
3. In the disc–disc Rheodyn SSD system, shear rate is uniform across the gap and is determined bythe rotational speed of one disc and by the radial position of the laser beam. The LORCA usesa bob-in-cup Couette geometry in which variation of shear rate across the gap is proportional tothe ratio of each radii squared. The nominal variation is approximately 5% and an average valueis used. The RheoScan-D uses a parallel plate flow system having a parabolic flow velocity acrossthe gap, and hence the shear is maximum at the walls and zero in the center. An average value ofshear rate is also used in this instrument;
4. Both the LORCA and RheoScan-D use a computer-controlled video system to capture and ana-lyze the diffraction image, with the LORCA obtaining repeated images at each shear rate and theRheoScan-D continuously recording images as the shear rate decreases. The Rheodyn SSD usesa set of diodes arranged parallel and perpendicular to the long axis of the diffraction pattern andobtains light intensity data at each of several shear rates.
Given the above differences it is remarkable that each instrument provides very similar results fornormal and modified RBC. In particular, it is curious that systems with small variations of shear ratethroughout the sample (i.e., LORCA, Rheodyn-D) are in agreement with a device in which shear ratevaries from maximum to zero across the suspension being measured. The resolution of this apparentdilemma must lie in an optical averaging process in which all cells in the path of the laser beam contributeto the resulting diffraction pattern, and an average shear rate is appropriate for computing shear stress[4]. It would thus be of potential value to incorporate an optical and image system in which individualRBC deformation is measured and a population distribution of RBC deformability determined. Such anapproach has been utilized for counter-rotating rheoscopes in which the cells are deformed but remainstationery in the flow field [6]. If such an approach was automated and applied to the shear fields used inthese ektacytometers, it would be possible to detect sub-populations of rigid cells and thus should supplyadditional information useful for research studies and hopefully improved patient care.
In conclusion, the results of the current study indicates that all three evaluated instruments have ac-ceptable sensitivity to alterations in deformability induced by GA treatment. Although GA treatment ofRBC is a widely used model of deformability alterations, it should be noted that this approach may notbe representative for all clinically relevant mechanisms of deformability alterations.

264 O.K. Baskurt et al. / Comparison of three commercially available ektacytometers
Acknowledgements
The workshop that provided data for this report was sponsored and financially supported by the In-ternational Society for Clinical Hemorheology. This study was also supported by NIH Research GrantsHL15722, HL 70595 and HL 090511, by the Akdeniz University Research Projects Unit, and by ajoint project supported by the Turkish Scientific and Technical Research Council (SBAG-MACAR-6;106S251) and the National Office for Research and Technology of Hungary (BILAT TR-03/2006).
References
[1] O.K. Baskurt, T.C. Fisher and H.J. Meiselman, Sensitivity of the cell transit analyzer (CTA) to alterations of red bloodcell deformability: role of cell size-pore size ratio and sample preparation, Clin. Hemorheol. 16 (1996), 753–765.
[2] O.K. Baskurt and F. Mat, Importance of measurement temperature in detecting the alterations of red blood cell aggregationand deformability studied by ektacytometry: a study on experimental sepsis in rats, Clin. Hemorheol. Microcirc. 23 (2000),43–49.
[3] O.K. Baskurt and H.J. Meiselman, Cellular determinants of low-shear blood viscosity, Biorheology 34 (1997), 235–247.[4] C.F. Bohren and D.R. Huffman, Absorption and Scattering of Light by Small Particles, Wiley, New York, 1983.[5] J. Cohen, Statistical Power Analysis for the Behavioral Sciences, Lawrance Earlbaum Associates, Hillsdale, NJ, 1988.[6] J.G.G. Dobbe, M.R. Hardeman, G.J. Steekstra and C.A. Grimbergen, Validation and application of an automated rheo-
scope for measuring red blood cell deformability distributions in different species, Biorheology 41 (2004), 65–77.[7] M.R. Hardeman, P.T. Goedhart, J.G.G. Dobbe and K.P. Lettinga, Laser-assisted optical rotational cell analyzer (LORCA).
I. A new instrument for measurement of various structural hemorheological parameters, Clin. Hemorheol. 14 (1994),605–618.
[8] M.R. Hardeman, P.T. Goedhart and N.H. Schut, Laser-assisted optical rotational cell analyzer (LORCA). II. Red bloodcell deformability: elongation index versus cell transit time, Clin. Hemorheol. 14 (1994), 619–630.
[9] M.R. Hardeman, P.T. Goedhart and S. Shin, Methods in hemorheology, in: Handbook Hemorheology and Hemodynamics,O.K. Baskurt, M.R. Hardeman, M.W. Rampling and H.J. Meiselman, eds, IOS Press, Amsterdam, 2007, pp. 242–266.
[10] R.M. Johnson, Ektacytometry of red blood cells, Methods Enzymol. 173 (1989), 35–54.[11] H. Schmid-Schönbein, P. Ruef and O. Linderkamp, The shear stress diffractometer Rheodyne SSD for determination of
erythrocyte deformability. I. Principles of operation and reproducibility, Clin. Hemorheol. 16 (1996), 745–748.[12] S. Shin, Y.H. Ku, M.S. Park and J.S. Suh, Laser diffraction in a slit rheometer, Cytometry 65B (2005), 6–13.[13] J. Stuart, A.J. Keidan, P.C.W. Stone and M.C. Sowter, Rheological study of erythrocyte sub-populations prepared by
density-gradient fractionation, Clin. Hemorheol. 8 (1988), 467–475.[14] J. Stuart, P.C.W. Stone, G. Freyburger, M.R. Boisseau and D.G. Altman, Instrument precision and biological variability
determine the number of patients required for rheological studies, Clin. Hemorheol. 9 (1989), 181–197.[15] X. Wang, H. Zhao, F.Y. Zhuang and J.F. Stoltz, Measurement of erythrocyte deformability by two laser diffraction meth-
ods, Clin. Hemorheol. Microcirc. 21 (1999), 291–295.