
Plasmodium vivax antigen discovery based on alpha-helical coiled coil protein motif
Upload
independentCategory
view
0download
0
COMPARISON OF IgG REACTIVITIES TO PLASMODIUM VIVAX MEROZOITEINVASION ANTIGENS IN A BRAZILIAN AMAZON POPULATION
TUAN M. TRAN, JOSELI OLIVEIRA-FERREIRA, ALBERTO MORENO, FATIMA SANTOS, SYED S. YAZDANI,CHETAN E. CHITNIS, JOHN D. ALTMAN, ESMERALDA V-S. MEYER, JOHN W. BARNWELL, AND MARY R. GALINSKI*
Emory Vaccine Center & Yerkes National Primate Research Center, Emory University, Atlanta, Georgia; Department ofImmunology, Institute Oswaldo Cruz, Oswaldo Cruz Foundation, Rio de Janeiro, Brazil; Fundação Nacional de Saúde, Ministry of
Health, Rondônia, Brazil; Malaria Research Group, International Centre for Genetic Engineering and Biotechnology (ICGEB), NewDelhi, India; Malaria Branch, Division of Parasitic Diseases, National Center for Infectious Diseases, Centers for Disease Controland Prevention, Atlanta, Georgia; Department of Medicine, Division of Infectious Diseases, Emory University, Atlanta, Georgia
Abstract. Naturally acquired antibody reactivity to two major Plasmodium vivax vaccine candidates was investigatedin 294 donors from three malaria-endemic communities of Rondônia state, Brazil. Antibody recognition of recombi-nantly expressed antigens covering five different regions of P. vivax reticulocyte binding protein 1 (PvRBP1) and regionII of P. vivax Duffy binding protein (PvDBP-RII) were compared. Positive IgG responses to these antigens weresignificantly related to the level of malaria exposure in terms of past infections and years of residence in the endemic areawhen corrected for age. The highest prevalence of anti-PvRBP1 total IgG antibodies corresponded to the amino acidregions denoted PvRBP1431-748 (41%) and PvRBP1733-1407 (47%). Approximately one-fifth of positively responding serahad titers of at least 1:1,600. Total IgG responses to PvDBP-RII were more prevalent (67%), of greater magnitude, andacquired more rapidly than those to individual PvRBP1 antigens. Responses to both PvRBP1 and PvDBP-RII werebiased toward the cytophilic subclasses IgG1 and IgG3. These data provide the first insights on acquired antibodyresponses to PvRBP1 and a comparative view with PvDBP-RII that may prove valuable for understanding protectiveimmune responses to these two vaccine candidates as they are evaluated as components of multitarget blood-stagevaccines.
INTRODUCTION
Plasmodium vivax accounts for an estimated 80 millioncases occurring throughout most of Asia, Oceania, southeast-ern Europe, Central and South America, and parts of Africa.1
Despite its wide geographic distribution, P. vivax has longbeen overshadowed by the burden caused by Plasmodiumfalciparum, which causes more than 1 million deaths per yearin sub-Saharan Africa alone.2 The disproportionate morbidityand mortality figures are a major reason why research on P.vivax has lagged far behind that of P. falciparum. As of now,more than 23 different P. falciparum vaccines are currentlyundergoing clinical trials compared with only two P. vivaxvaccine trials.3,4 However, the phylogenetic and antigenic dis-parity between the two species implies that effective falci-parum vaccines will not be cross-protective against vivax in-fections. In light of rising drug resistance in P. vivax and itsincreasing prevalence, it is imperative to advance the devel-opment of more P. vivax antigens as vaccine candidates.5
Malaria blood-stage vaccines aim to disrupt interactionsbetween receptors on Plasmodium merozoites and theirerythrocytic ligands by eliciting inhibitory antibodies that tar-get the parasitic receptors. One such target unique to P. vivaxis the Duffy binding protein (PvDBP),6,7 a Type I integralmembrane protein whose homologues in Plasmodiumknowlesi and P. falciparum have been localized by immuno-electron microscopy to the micronemes of merozoites.8,9
PvDBP mediates the invasion of erythrocytes via interactionswith its erythrocytic ligand, the Duffy antigen receptor forchemokines (DARC).6 Invasion of human erythrocytes by P.vivax requires this interaction, as individuals deficient in
DARC are not susceptible to infection.10 The PvDBP eryth-rocyte binding domain, designated region II (PvDBP-RII),has been mapped to an ∼350 amino acid cysteine-rich regionnear the amino-terminus.11 Region II has significantly higherdiversity than the rest of the PvDBP and appears to be understrong selective pressure.12 In addition, naturally occurringantibodies from humans exposed to malaria have been dem-onstrated to inhibit the in vitro binding of erythrocytes toregion II, suggesting an antiparasitic role of the naturally ac-quired immune response.13 The functional and immunologicsignificance of PvDBP-RII has supported its candidacy as avaccine.
Two other P. vivax candidate antigens are the reticulocytebinding proteins (PvRBP1 and PvRBP2), which were identi-fied based on their ability to preferentially adhere to reticu-locyte-enriched populations of erythrocytes.14,15 Evidencesuggests that the two PvRBPs form a complex at the apicalpole of the merozoite and confer the reticulocyte-specificityof P. vivax blood-stage infections.14,16 PvRBP1 and PvRBP2are both Type I integral membrane proteins of approximately330 kDa, each consisting of a large extracellular domain, asingle transmembrane domain, and a short cytoplasmic tail.Homologues with similar structures have subsequently beenidentified and characterized in P. falciparum.17–19 Global di-versity analysis of these genes has revealed a cluster of non-synonymous polymorphisms within the first 750 amino acidsof the PvRBP1 extracellular domain,20 suggesting that thisregion may be the target of immune selection. Despite evi-dence that the PvRBPs play an important role during the P.vivax invasion of reticulocytes, the immunogenicity of theseproteins has yet to be studied. Furthermore, evidence fornaturally occurring antibodies reactive against PvRBPs hasnot been demonstrated in a malaria-exposed population.Given the large size of PvRBP1, the identification of func-tional subdomains and protective B-cell epitopes would provevaluable in the development of a PvRBP1 subunit vaccine.
Toward these goals, we have screened plasma samples from
* Address correspondence to Mary R. Galinski, Emory Vaccine Cen-ter, Yerkes National Primate Research Center, Emory University,954 Gatewood Rd., Atlanta, Georgia 30329. E-mail: [email protected]
Am. J. Trop. Med. Hyg., 73(2), 2005, pp. 244–255Copyright © 2005 by The American Society of Tropical Medicine and Hygiene
244

a cross section of three epidemiologically distinct communi-ties in the Brazilian Amazon state of Rondônia for the pres-ence of IgG antibodies against five recombinant fragmentsspanning the length of the PvRBP1 extracellular domain. Forcomparative purposes, we also tested the same plasmasamples for antibodies against a recombinant, refoldedPvDBP-RII.21 We used malaria infection and exposure his-tories obtained from individual donors to assess the relation-ship between exposure and naturally acquired antibody re-sponses to PvRBP1 and PvDBP-RII. Previous seroepidemio-logical studies in hyperendemic areas of Africa have showncytophilic antibody subclasses IgG1 and IgG3 to be associatedwith acquired protection to falciparum malaria.22 Further-more, in vitro studies have demonstrated that cytophilic an-tibodies mediate their antiparasitic effect by engaging withFc� receptors on monocytes.23,24 We therefore evaluated theIgG subclass reactivities in positive responders and deter-mined the subclass distribution for both PvRBP1 and PvDBP-RII. This study provides the first insights into immune re-sponses made against these two blood-stage vaccine candi-dates upon natural exposure to P. vivax.
MATERIALS AND METHODS
Study site and subjects. Cohort studies were conducted inpopulations living in three communities in the malaria en-demic region of Rondônia state, Brazil, where vivax malariaaccounts for more than 70% of all malaria cases in the past 3years (Brazilian Ministry of Health, 2004, unpublished data).Samples and survey data were collected during the drymonths of June and July of 2001, coinciding with the period ofincreased malaria transmission. The two communities ofColina and Ribeirinha have been described previously.25–27
Briefly, Colina consists primarily of transmigrants from non-endemic areas of Brazil who have lived in the region for 10years or more. They reside in rural settlements alongside un-paved roads that traverse the transnational highway BR-364
approximately 50–100 km southeast of the capital, PortoVelho. Ribeirinha encompasses riverine communities alongthe banks of the Madeira River and its tributaries approxi-mately 30–60 km northeast of the capital. Families in Ribeir-inha have lived in the malaria-endemic region for more than25 years, and many are native to the region. The third grouplives in Buritis, a newly developed municipality situated ap-proximately 300 km due south of the capital. Most individualsfrom this group consist of transmigrants who have resided inthe endemic region for less than 10 years. The study popula-tion consisted of 87 donors from Colina, 177 donors fromRibeirinha, and 30 donors from Buritis. Age ranged from 9years to 85 years, but most donors were between 20 to 40years of age. Written informed consent was obtained from alladult donors or from parents of donors in the case of minors.The study was reviewed and approved by the Fundação Os-waldo Cruz Ethical Committee.
Epidemiologic survey. Donors giving informed consent an-swered questions from an epidemiologic survey. Questions onthe survey related to demographics, time of residence in theendemic area, personal and family histories of malaria, use ofmalaria prophylaxis, presence of malaria symptoms, and per-sonal knowledge of malaria. Survey data was entered into adatabase created with Epi Info 2002 (Centers for DiseaseControl and Prevention, Atlanta, GA). Demographic andepidemiologic data are summarized in Table 1.
Collection of human blood samples and malaria diagno-sis. Intravenous blood was collected in sodium heparin Vacu-tainer tubes (Becton Dickinson, Franklin Lakes, NJ). Cellularcomponents were separated from plasma by centrifugation,and aliquots of plasma were frozen and stored at −20°C untiluse for antibody analysis. Thin and thick blood smears of alldonors were examined for malaria parasites. The numbers ofdonors positive for P. vivax and P. falciparum at the time ofphlebotomy are listed in Table 1. Parasitemia for smear-positive donors was determined by counting the number ofparasites against a predetermined number of white blood cells
TABLE 1Characteristics of three communities in Rondonia, Brazil
Characteristics
Study population (N)
Statistical analysis¶ PBuritis (30) Colina (87) Ribeirinha (177)
Gender, male (%) 12 (41.4) 60 (68.2) 96 (54.2) �2 � 8.57 0.014Median age in years (range) 24 (9–62) 35 (11–75) 32 (10–85) KW � 3.7 NSTransmigrants* (%) 27 (90%) 64 (74%) 20 (11%) �2 � 135 < 0.0001Median number of years residing in endemic area 7.0 21.0 28.0 KW � 51.3 < 0.0001
Males 7.0 20.0 29.0 KW � 26.0 < 0.0001Females 8.0 24.5 28.0 KW � 27.6 < 0.0001
Median number of previous malaria episodes 3.5 8.0 4.0 KW � 11.9 0.003Males 4.0 10.0 4.0 KW � 7.1 0.029Females 3.0 5.0 4.5 KW � 3.6 NS
Months since previous malaria episode† 1.6–5.6 10.6–24.2 11.2–19.7 F � 9.4‡ 0.0001Males 0.8–8.2 10.6–27.2 13.0–27.6 F � 5.4‡ 0.005Females 1.2–6.8 5.4–33.6 7.4–17.4 F � 3.5‡ 0.035
Patent malaria infection by blood smear (%) 11 (37%) 7 (8.0%) 19 (10.7%) �2 � 18.0 0.0001Plasmodium vivax 9 (30%) 5 (5.7%) 13 (7.3%) �2 � 17.5 < 0.001
Asymptomatic§ 4 (44%) 5 (100%) 12 (92%) �2 � 8.8 0.012Plasmodium falciparum 2 (6.7%) 2 (2.3%) 6 (3.4%) �2 � 1.30 NS
Asymptomatic§ 1 (50%) 2 (100%) 4 (67%) �2 � 1.27 NS* Transmigrants are defined as individuals who migrated into the endemic area from a nonendemic state of Brazil.† Back-transformed 95% confidence intervals of transformed data shown. Only donors with a positive history for malaria were included.‡ Raw data was transformed using the function log (x + 1) to produce a normal distribution before one-way analysis of variance.§ Asymptomatic individuals were defined as blood smear positive donors who did not report malaria-like symptoms at the time of collection and during their next day follow-up.¶ KW, Kruskal-Wallis statistic; F, F statistic; NS, not statistically significant. Statistical significance was set as P � 0.05.
ANTIBODY RESPONSES TO VIVAX INFECTIONS 245

in thick blood smears, and, from this, the number of parasitesper �l of blood was calculated.28 Infected donors who wereasymptomatic at the time of phlebotomy were followed upthe next day to confirm absence of malaria symptoms. Allsmear-positive donors were subsequently treated for P. vivaxor P. falciparum per the regimen recommended by the Bra-zilian Ministry of Health.
Protein expression and purification. Five overlapping frag-ments spanning the PvRBP1 extracellular domain andPvDBP-RII were expressed as recombinant proteins in Es-cherichia coli and subsequently purified as described below.The expression and purification of recombinant, refoldedPvDBP-RII have been described previously.21 In addition,thioredoxin, used as a control for nonspecific IgG reactivity,was expressed and purified from Escherichia coli BL21(DE3)(Novagen, Madison, WI) containing the plasmid pET32b(Novagen) using standard procedures suggested by the manu-facturer. Recombinant proteins were used to detect theprevalence of antibodies in plasma samples by enzyme-linkedimmunosorbant assays (ELISA).
Five overlapping regions of Pvrbp1 spanning nucleotides 67to 7832 of the coding sequence were amplified from P. vivaxBelem strain genomic DNA using the Expand High Fidelitypolymerase chain reaction (PCR) system (Roche, Indianapo-lis, IN). The regions (shown in Figure 1) were selected basedon global diversity data20 and protein stability index as deter-mined by ExPASy ProtParam program.29 The primers, clon-ing sites, and expression vectors used for each construct arelisted in Table 2. The PCR product PvRBP123-458 was clonedinto pDONOR2.1 (Invitrogen, Carlsbad, CA) before sub-cloning into the expression vector pDEST17, yielding the re-combinant plasmid PvRBP123-458/pDEST17. Escherichia coliBL21(SI) (Invitrogen) was transformed with plasmidPvRBP123-458/pDEST17. The PCR product PvRBP1431-748
was digested with EcoR I and cloned into the expressionvector pET32b to yield plasmid PvRBP1431-748/pET32b. The
PCR products PvRBP1733-1407 and PvRBP11392-2076 were di-gested with Kpn I and cloned into the expression vectorpET32b to yield plasmids PvRBP1733-1407/pET32b andPvRBP11392-2076/pET32b, respectively. The PCR productPvRBP12038-2611 was cloned into the Kpn I site of expressionvector pET29b (Novagen) to yield PvRBP12038-2611/pET29bplasmid. Each plasmid was transformed into E. coliBL21(DE3). All cloned constructs were verified for properorientation, reading frame, and fidelity to the template.
PvRBP123-458 was expressed as an N-terminal hexa-histidine(6-His) fusion protein; PvRBP1431-748, PvRBP1733-1407, andPvRBP11392-2076 as N-terminal thioredoxin/6-His double fu-sion proteins; and PvRBP12038-2611 as a C-terminal 6-His fu-sion protein. For PvRBP1431-748, PvRBP1733-1407, andPvRBP11392-2076, Luria-Bertania media containing 100 �g/mLampicillin (LB-amp) was inoculated and cultured at 37°C un-til the optical density at 600 nm (OD600) reached 0.6-0.8. Cellswere induced to produce protein with 1 mM isopropyl-1-thio-�-galactopyranoside (IPTG) for 3 hours at 37°C. The soluble6-His recombinant proteins were purified with Ni-NTA aga-rose (Qiagen, Valencia, CA) per the manufacturer’s instruc-tions before gel filtration chromatography. Protein sampleswere loaded on a Sephacryl S-300 (Amersham PharmaciaBiotech, Piscataway, NJ) gel filtration column equilibratedwith 20 mM Tris-HCl, pH 8.0, and eluted with 20 mM Tris-HCl buffer, pH 8.0, containing 500 mM NaCl. Fractions fromthe major peak based on absorbance280 were pooled, dialyzedovernight against phosphate-buffered saline, pH 7.4 (PBS;Cellgro, Herndon, VA), concentrated by ultrafiltration, andstored at −80°C.
The insoluble recombinant proteins PvRBP123-458 andPvRBP12038-2611 were isolated as inclusion bodies, reconsti-tuted by step dialysis, and purified by gel filtration chroma-tography. Escherichia coli BL21(SI) containing plasmidPvRBP123-458/pDEST17 was cultured in salt-free LB-amp at37°C until an OD600 of 0.8–1.0, and protein expression was
FIGURE 1. Expression of the extracellular domain of Plasmodium vivax reticulocyte binding protein 1 (PvRBP1) as overlapping recombinantfragments in Escherichia coli. The five antigens span residues 23 through 2611 of the Belem strain nascent polypeptide sequence. For details onthe expression and purification of the proteins, see “Materials and Methods.” N � amino terminus, C � carboxyl terminus, trx � thioredoxin.
TRAN AND OTHERS246

induced with 0.3 M NaCl for 4 hours. For PvRBP12038-2611,LB containing 50 �g/mL kanamycin (LB-kan) was inoculatedand grown at 37°C to an OD600 of 0.8–1.0, and protein ex-pression was induced with 1 mM IPTG for 4 hours. Bacteriapellets were harvested and resuspended in 50 mM Tris-HCl,pH 8.0 containing 25% (w/v) sucrose, 1 mM ethylenediamine-tetraacetic acid (EDTA), and 10 mM dithiothreitol (DTT)before freezing at −80°C. The resuspension was thawed, and1 mg/mL lysozyme, 5 mM MgCl2, 2 mg/mL DNase, 1% Tri-ton-X 100, and 10 mM DTT were added. Cells were lysed bysonication and pelleted by centrifugation before resuspensionin 50 mM Tris-HCl, pH 8.0, containing 0.5% Triton X-100,100 mM NaCl, 1 mM EDTA, 0.1% azide, and 1 mM DTT.Sonication, centrifugation, and resuspension steps were re-peated four more times, with Triton X-100 excluded in thelast wash. The washed pellets were dissolved in 25 mM 2-[N-morpholino] ethane sulfonic acid, pH 6.0, containing 8 Murea, 10 mM EDTA, 0.1 mM DTT, and these inclusion bodieswere stored at −80°C. PvRBP123-458 and PvRBP12038-2611 in-clusion bodies were reconstituted by 1:2 dilution with 50 mMglycine, pH 8.0 containing 10% w/v sucrose, 1 mM EDTA, 1mM reduced gluthathione, 0.1 mM oxidized glutathione, and4 M urea and dialyzed for 24 hours at 4°C against a 50×volume of the same buffer. The dialysis buffer was exchangedwith a 50x volume of 20 mM Tris-HCl, pH 8.0, containing10% w/v sucrose, 1 mM EDTA, 0.1 mM reduced glutathione,0.01 mM oxidized glutathione and dialyzed for 24 hours at4°C. Samples were concentrated to an appropriate volumeand further purified by gel filtration chromatography as de-scribed above. Purity and stability of all recombinant proteinswere verified by SDS-PAGE (Figure 2) and Western blotanalysis using an anti-penta-His monoclonal antibody (mAb;Qiagen; supplemental Figure 1).
Measurement of antibody levels. Plasma samples fromstudy participants were screened for total IgG reactivityagainst the five PvRBP1 constructs, PvDBP-RII, and purifiedthioredoxin using ELISA for total IgG antibodies. Maxisorp96-well plates (Nunc, Rochester, NY) were coated with 200ng of antigen overnight at 4°C in PBS, pH 7.4. Plates werewashed four times with PBS-0.05% Tween 20 (PBS-T) andblocked with blocking buffer (PBS-T containing 5% skimmilk) for 2 hours at 37°C. Plates were washed once and in-cubated for 1 hour at 22°C with plasma diluted 1:100 in block-ing buffer. After washing four times, the plates were incu-bated for 1 hour at 22°C with peroxidase-conjugated goatanti-human IgG (� chain specific) (KPL, Gaithersburg, MD)
diluted 1:3000 in blocking buffer. Plates were washed fourtimes and incubated for 30 minutes at 22°C with 2, 2’-azino-di(3-ethylbenzthiazoline-6-sulfonate) substrate (ABTS, KPL)per the manufacturer’s instructions. The ODs were measuredat 405 nm, and the threshold for positivity was an OD valueset at 3 SD above the mean OD of 30 residents of either theUnited States or Brazil who have never been exposed to ma-laria transmission. For the three thioredoxin fusion proteins,background antibody reactivity to thioredoxin was subtractedfrom raw ODs before further analysis. Average cutoffs were0.607 (PvRBP123-458), 0.723 (PvRBP1431-748), 0.289(PvRBP17 3 3 - 1 4 0 7) , 0 .272 (PvRBP11 3 9 2 - 2 0 7 6) , 0 .616(PvRBP12038-2611), and 0.388 (PvRII). All samples weretested in duplicate. All plates included the same positive ref-erence plasma and PvRBP1431-748 to standardize develop-ment time. For positive responders, end-point titers were de-termined using 1:2 serial dilutions starting at 1:100. The endpoints were determined as the highest titers in which the ODwas greater than the threshold for positivity at a control
TABLE 2Primers used to amplify PvRBP1 polymerase chain reaction products for cloning into expression vectors*
Construct Forward primer Reverse primer Cloning site Expression vector
PvRBP123–458 5�GGGGACAAGTTTGTACAAAAAAGCAGGCTCCGAAAATGCAGAAGAAGACATAAG 3�
5�GGGGACCACTTTGTACAAGAAAGCTGGGTCCTATTTTCCTAACGTGTCTATAATGG 3�
att recombination pDEST17
PvRBP1431–748 5�TCCGAATTCGAACGAACCAATTAAGAAAGCATAT 3�
5�CCACGAATTCTTCTATAATTTAGCAAAAGTTTCTTTGGC 3�
EcoRI pET32b
PvRBP1733–1407 5�GGGGGTACCGAAATGGAAGAGAAGCTACAGGAT 3�
5�AGGGGTACCTTAGGCACTTGCGTTTTTCTCTTC 3�
Kpn I pET32b
PvRBP11392–2076 5�GAGGGTACCGGGGAATTTACAAAGGCTGAAGGT 3�
5�GGGGGTACCCTAATAGGTGTTCATTTCGTTCTCCATTTC 3�
Kpn I pET32b
PvRBP12038–2611 5�CACGGTACCCTAGACAATACAGAGGAGCTTGAAAA 3�
5�GAGGGTACCCTGTACTAGTTGGCCTATTTCTCG 3�
Kpn I pET29b
* PvRBP1, Plasmodium vivax reticulocyte binding protein 1. Cloning sites on primer sequences indicated by italics and underscoring.
FIGURE 2. Polyacrylamide gel of recombinant Plamodium vivaxreticulocyte binding protein 1 (PvRBP1) and P. vivax Duffy bindingprotein region II (PvDBP-RII) proteins. Approximately 5 �g of eachprotein were electrophoresed on a 10% polyacrylamide gel andstained with Coomassie R-250 to visualize the bands. The minorbands below PvRBP1733-1407, PvRBP11392-2076, PvRBP12038-2611 repre-sent degradation products. See “Materials and Methods” for detailson expression and purification of proteins. Molecular weights in ki-lodaltons (kDa) are indicated. Refer to supplemental Figure 1 forWestern blot analysis of these recombinant proteins.
ANTIBODY RESPONSES TO VIVAX INFECTIONS 247

plasma dilution of 1:100. An ELISA to detect the IgG sub-classes of the anti-DBP and anti-RBP antibodies was alsoperformed for positive responders. Plates were coated withantigen, blocked, and incubated with plasma diluted 1:100 asin the ELISA for total IgG. After washing, plates were incu-bated for 1 hour at 22°C with mouse mAbs to human IgGsubclasses diluted in blocking buffer according to the manu-facturer’s specifications. The mAbs were from clones HP-6001 for IgG1, HP-6002 for IgG2, HP-6050 for IgG3, andHP-6023 for IgG4 (Sigma, St. Louis, MO) and have been usedpreviously to characterize IgG subclass reactivity in theRibeirinha population. After incubation, plates were washedand incubated for 1 hour at 22°C with peroxidase-labeled goatanti-mouse antibody (KPL) diluted 1:1,000 in blocking buffer.Plates were washed, incubated with ABTS, and the OD mea-sured as described above. Subclass-specific prevalence foreach antigen was determined from OD values using 3 SDabove the appropriate mean OD of 24 nonexposed controls asthe cutoff for positivity (Table 3). In addition, standard curves
were prepared to enable conversion of OD values to concen-tration (�g/mL) values, thus allowing for the comparison ofdifferent subclasses. Purified human IgG kappa myelomaproteins from each of the four subclasses (The Binding Site,San Diego, CA) were coated overnight at 4°C in PBS at 100�L per well onto 96-well plates in 1:2 serial dilutions from 24
�g/mL to 2−11 �g/mL. After washing four times, plates wereincubated with the appropriate human IgG subclass-specificmAb, washed four times, incubated with peroxidase-labeledgoat anti-mouse antibody, washed a final four times, devel-oped with ABTS, and measured as described above for sub-class-specific ELISA. Subclass-specific OD values were con-verted to concentration values (�g/mL) using sigmoidalcurve-fit equations derived from subclass-specific standardcurves (supplemental Figure 2).
Statistical analysis. Differences in medians for the studypopulation data were tested by non-parametric Kruskal-Wallis test where appropriate. Normalizing transformationswere performed on raw data before testing by one-way analy-sis of variance where appropriate. Differences in proportionswere evaluated by �2 test. Relationships between years ofresidence in the endemic area and number of past malariainfections or months since last known malaria episode wereassessed with Spearman’s rank correlation. Multivariate lo-gistic regression was used to assess the relationship betweenantigen-specific total IgG responses and the independentvariables of gender, age, years of residence in the endemicarea, number of past malaria episodes, and months since lastknown malaria infection. For comparison of IgG subclass-specific antibody responses, �2 test was used to evaluate dif-ferences in prevalence. Normalizing transformations wereperformed on subclass concentrations before one-way analy-sis of variance (for evaluating differences in subclass distri-
FIGURE 3. Seroprevalence of IgG antibodies against Plasmodium vivax reticulocyte binding protein 1 (PvRBP1) recombinant antigens and P.vivax Duffy binding protein region II (PvDBP-RII) for Buritis, Colina, and Ribeirinha communities as determined by enxyme-linked immuno-sorbent assay. Total IgG seroprevalence refers to the frequency of IgG positive responders to an antigen in a population. A positive responsewas defined as a response having an optical density405 that was greater than three standard deviations above the mean of nonexposed controls.The solid black bars represent seroprevalence for all three communities combined. �2 analyses were performed to determine if a statisti-cally significant difference existed between the seroprevalence of the three populations for each antigen. The level of significance is indicated by*(P < 0.05), **(P < 0.01), and ***(P < 0.001).
TABLE 3Optical density cutoffs for IgG subclass-specific positivity
Antigen
Subclass
IgG1 IgG2 IgG2 IgG4
PvRBP123–458 0.114 0.255 0.093 0.117PvRBP1431–748 0.119 0.542 0.214 0.151PvRBP1733–1407 0.061 0.123 0.057 0.089PvRBP11392–2076 0.077 0.227 0.043 0.054PvRBP12038–2611 0.122 0.560 0.089 0.113PvDBP-RII 0.180 0.525 0.110 0.156
PvRBP1, Plasmodium vivax reticulocyte binding protein 1; PvDBP-RII, P. vivax Duffybinding protein region II. Cutoff values represent the mean + 3 SD of subclass-specificoptical densities for 24 nonexposed controls.
TRAN AND OTHERS248

bution within responders or within controls for each antigen)or Student’s t test (for evaluating subclass-specific differencesbetween responders and controls for each antigen). Spear-man’s rank correlation coefficients were calculated to deter-mine the relationships between IgG subclass levels andmonths since last known malaria episode. Analyses weredone using Epi Info 2002 and Prism 3.0 (GraphPad Software,San Diego, CA).
RESULTS
Characteristics of Buritis, Colina, and Ribeirinha. Table 1shows the characteristics of the three communities studied.Among our sample set, the communities differ significantly ingender ratio, with Colina donors being disproportionatelymale. Median age is similar between the three communities.The proportion of transmigrants is highest in Buritis (90%)and lowest in Ribeirinha (11%). The communities differ sig-nificantly in years of residence in the endemic area, number ofpast malaria episodes, months since last malaria episode, and
proportion of patent malaria infections as listed. Data wasstratified by gender to account for male bias among Colinaresidents.
Relationship between years of residence in the endemicarea and malaria history. For this study, we used years ofresidence in the endemic area and number of past malariaepisodes as reported by donors as indices of malaria expo-sure. Absence of recent symptomatic malaria infection, mea-sured as the number of months since a donor’s last knownmalaria episode, was used as a crude approximation of pro-tection. The number of past malaria episodes did not corre-late significantly with years of residence in the endemic area(Spearman r � 0.086, P � 0.14, N � 294). Among donorswith a positive history of malaria, years of residence in theendemic area correlated positively with the number ofmonths since a donor’s last malaria episode (Spearman r �0.29, P < 0.0001, N � 258).
Anti-PvRBP1 and anti-PvDBP-RII seroprevalence inthree communities of Rondônia. Naturally acquired antibodyresponses to PvDBP-RII have been shown to have high
FIGURE 4. Seroprevalence of IgG antibodies against Plasmodium vivax reticulocyte binding protein 1 (PvRBP1) and P. vivax Duffy bindingprotein region II (PvDBP-RII) in 294 residents of Rondônia, Brazil. Donors were grouped by (A) years of residence in the endemic area and (B)past number of malaria episodes. Servoprevalence is the proportion of donors responding to the different antigens among the total for each group.Responses to the five PvRBP1 antigens are shown as filled shapes. Anti-PvDBP-RII responses are shown as open squares.
ANTIBODY RESPONSES TO VIVAX INFECTIONS 249

prevalence in regions of vivax endemicity.13,30–32 Thus, anti-PvDBP-RII IgG reactivity was used in this study to estimatethe rate of exposure to P. vivax. Anti-PvDBP-RII seropreva-lence was 67% among all 294 donors and 43%, 70%, and 70%for Buritis, Colina, and Ribeirinha communities, respectively.In comparison, seroprevalence for any of the five PvRBP1fragments was 66% among all donors and 57%, 58%, and72% for Buritis, Colina, and Ribeirinha, respectively. Ofthese five PvRBP1 fragments, the highest frequencies of posi-tive responses among all donors were for PvRBP1431-748
(41%) and PvRBP1733-1407 (47%). Total IgG reactivity toPvRBP123-458 and PvRBP1431-748 differed significantly amongthe three communities (�2 � 10.08, P � 0.0065 and �2 �17.20, P � 0.0002, respectively), with increased prevalence toboth in Colina and Ribeirinha. The results are summarized inFigure 3. Although there was a trend for anti-PvRBP1 IgGantibodies to be more prevalent in males than females, thisdifference was not statistically significant.
Magnitude of IgG responses. To compare the relativemagnitude of antibody responses, we determined IgGend-point titers for positive responders to each antigen. Thegeometric means of IgG titers for each antigen were 196.0for PvRBP123-458, 371.1 for PvRBP1431-748, 455.8 forPvRBP1733-1407, 394.4 for PvRBP11392-2076, 243.1 forPvRBP12038-2611, and 488.8 for PvDBP-RII. Positive respond-ers to each antigen were subdivided by their total IgG anti-body titers into low responders (titers < 1,600) and high re-sponders (titers � 1,600). High responders were frequentlyobserved for PvDBP-RII (27% of all PvDBP-RII positiveresponders), PvRBP11392-2076 (24%), PvRBP1733-1407 (22%),and PvRBP1431-748 (20%), while PvRBP123-458 andPvRBP12038-2611 had a lower proportion of high responders(4.4% and 8.7%, respectively). The maximum total IgGtiter achieved for each antigen was 6,400 for PvRBP123-458
(N � 1), 12,800 for PvRBP1431-748 (N � 1), 25,600 forPvRBP1733-1407 (N � 1), 12,800 for PvRBP11392-2076 (N � 2),3,200 for PvRBP12038-2611 (N � 2), and 51,200 for PvDBP-RII (N � 2). Maximum titers were obtained in donors fromeither Ribeirinha or Colina but never from Buritis.
Multivariate logistic regression analysis of total IgG anti-body reactivity according to gender, age, and indices of ma-laria exposure. The contributions of five independent vari-ables related to malaria exposure to total IgG antibody re-sponses against each of the six vivax recombinant proteinswere determined using stepwise, multivariate logistic regres-sion. The variables initially tested were gender, age, years ofresidence in the malaria endemic area, number of past ma-laria episodes, and months since last known malaria episode.The initial analysis showed that gender did not affect IgGantibody responses to any of the recombinant antigens andwas subsequently removed from the final regression analysis(Table 4). The analysis demonstrated that IgG responsesto the recombinant antigens were generally age independentbut exposure dependent, except for responses againstPvRBP123-458, which appeared independent of both age andexposure. Individuals living in the malaria-endemic area formore than 30 years were 3.3 to 4.6 times more likely to reactto PvRBP1431-748, PvRBP2038-20611, and PvDBP-RII than themost recently migrated individuals. Donors who reportedhaving greater than 15 malaria infections were 4.4 to 7 timesmore likely to respond to PvRBP1431-748, PvRBP1733-1407,PvRBP11392-2076, PvRBP12038-2611, and PvDBP-RII than self-
reported malaria-naïve individuals. Donors who have had arecent malaria infection (within two months preceding samplecollection) were significantly more likely to respond toPvRBP12038-2611 and PvDBP-RII than those who have beenmalaria-free within this same period.
Seroprevalence and malaria exposure. All 294 donors fromRondônia were stratified according to years of residence inthe endemic area (< 11, 11–20, 21–30, and > 30 years) andnumber of past malaria episodes (0, 1–5, 6–15, and > 15 ma-laria infections). The prevalence of total IgG antibodiesagainst each antigen was plotted for each group (Figure 4).Seroprevalence generally increased with years of residence inthe endemic area and number of past malaria episodes for allantigens. This trend of rising seroprevalence was similaramong the five PvRBP1 antigens. However, the prevalence ofanti-PvRBP1 antibody responses was shown to increase at aslower rate than that of anti-PvDBP-RII antibody responses.Many donors who reported never having malaria respondedto PvDBP-RII (11 of 31), PvRBP1 (16 of 31), or either anti-gen (21 of 31).
IgG subclass distribution of anti-PvDBP-RII and anti-PvRBP1 antibodies. We assessed the overall subclass distri-bution of the IgG antibody responses to each antigen usingtwo different comparative analyses. Firstly, we determinedsubclass-specific prevalence of total IgG positive respondersfor each antigen using background-subtracted OD values andOD cutoffs determined from ODs of controls. Secondly, an-tigen-specific IgG1, IgG2, IgG3, and IgG4 concentrations fortotal IgG positive responders were determined from OD val-ues using subclass-specific standard curves and the resultscompared with the concentrations of controls using paramet-ric statistics. Both analyses are summarized in Table 5. Withthe exception of PvRBP1392-2076 responses, the results of bothanalyses were comparable. Using prevalence as the basis ofcomparison, the predominant responses to PvRBP123-458,PvRBP12038-2611, and PvDBP-RII were IgG3, while IgG1 pre-dominated in responses to PvRBP1431-748, PvRBp1733-1407,and PvRBP11392-2076. When concentrations were compared,positive responses to PvRBP1431-748 and PvRBP1733-1407
showed increases in IgG1 levels relative to nonexposed con-trols, while positive responses to PvRBP123-458 andPvRBP12038-2611 showed statistically significant increases forall IgG subclasses. Positive responses to PvDBP-RII showedincreased IgG1, IgG3, and IgG4 levels relative to controls. Incontrast, responses to PvRBP11392-2076 showed increasedIgG2 and IgG4 but decreased IgG3 relative to controls.
IgG subclass levels and months since last known malariaepisode. Time (in months) since a donor’s last known malariaepisode was used as a crude approximation of the donor’slevel of protection from malaria. To assess if IgG subclasslevels correlated with this approximation, we calculatedSpearman’s correlation coefficients between IgG subclassconcentrations and months since last known malaria episodefor each antigen. Only donors who were identified as positiveresponders to a particular antigen were included in the analy-ses for that antigen. Donors who either had detectable levelsof parasitemia or reported themselves as malaria-naïve wereexcluded from analyses. Months since last known malaria epi-sode positively correlated with IgG3 concentration forPvRBP1733-1407 (r � 0.20, P < 0.05, N � 110) and with IgG2concentration for PvRBP1733-1407 (r � 0.22, P < 0.02, N �110) and PvRBP11392-2076 (r � 0.34, P < 0.002, N � 82).
TRAN AND OTHERS250

TA
BL
E4
Mul
tiva
riat
elo
gist
icre
gres
sion
ofP
vRB
P1
and
PvD
BP
-RII
IgG
anti
body
resp
onse
s*
Inde
pend
ent
vari
able
sN
Dep
ende
ntva
riab
le(a
ntig
enre
spon
se)
PvR
BP
1 23–
458
PvR
BP
1 431
–748
PvR
BP
1 733
–140
7P
vRB
P1 1
392–
2076
PvR
BP
1 203
8–26
11P
vDB
P-R
II
Odd
sra
tio
(95%
CI)
PO
dds
rati
o(9
5%C
I)P
Odd
sra
tio
(95%
CI)
PO
dds
rati
o(9
5%C
I)P
Odd
sra
tio
(95%
CI)
PO
dds
rati
o(9
5%C
I)P
Age
(in
year
s)9–
1965
Ref
eren
ceR
efer
ence
Ref
eren
ceR
efer
ence
Ref
eren
ceR
efer
ence
20–3
598
1.05
(0.2
9–3.
83)
0.94
70.
66(0
.24–
1.80
)0.
418
0.76
(0.3
1–1.
90)
0.56
10.
57(0
.20–
1.63
)0.
299
1.05
(0.3
6–3.
10)
0.93
00.
69(0
.27–
1.80
)0.
451
36–5
066
0.94
(0.2
4–3.
66)
0.92
30.
60(0
.20–
1.75
)0.
346
1.23
(0.4
7–3.
23)
0.68
00.
84(0
.28–
2.48
)0.
749
0.92
(0.2
9–2.
92)
0.88
40.
49(0
.18–
1.34
)0.
165
51–8
565
3.25
(0.8
7–12
.20)
0.08
10.
83(0
.28–
2.46
)0.
743
1.64
(0.6
1–4.
46)
0.33
01.
29(0
.43–
3.87
)0.
651
3.79
(1.2
1–11
.89)
0.02
30.
88(0
.30–
2.57
)0.
821
Yea
rsof
resi
denc
ein
ende
mic
area
0–10
29R
efer
ence
Ref
eren
ceR
efer
ence
Ref
eren
ceR
efer
ence
Ref
eren
ce11
–20
850.
73(0
.18–
2.92
)0.
659
1.02
(0.3
3–3.
16)
0.97
40.
70(0
.26–
1.87
)0.
477
0.45
(0.1
6–1.
29)
0.13
71.
00(0
.30–
3.32
)0.
994
1.21
(0.4
4–3.
33)
0.70
821
–30
740.
94(0
.24–
3.65
)0.
927
3.49
(1.0
9–11
.21)
0.03
61.
31(0
.48–
3.61
)0.
602
1.82
(0.6
3–5.
26)
0.26
82.
24(0
.67–
7.44
)0.
189
2.25
(0.7
9–6.
43)
0.12
9>
3010
62.
65(0
.72–
9.73
)0.
141
4.64
(1.4
5–14
.86)
0.01
01.
61(0
.59–
4.36
)0.
350
1.12
(0.3
9–3.
20)
0.83
13.
36(1
.03–
10.9
5}0.
044
3.30
(1.1
7–9.
35)
0.02
5N
umbe
rof
past
mal
aria
epis
odes
031
Ref
eren
ceR
efer
ence
Ref
eren
ceR
efer
ence
Ref
eren
ceR
efer
ence
1–5
143
2.20
(0.6
1–7.
90)
0.22
70.
84(0
.32–
2.22
)0.
732
1.06
(0.4
1–2.
78)
0.90
11.
74(0
.59–
5.10
)0.
311
3.20
(0.9
1–11
.28)
0.07
02.
27(0
.88–
5.91
)0.
092
6–15
943.
47(0
.89–
13.6
)0.
074
1.61
(0.5
6–4.
62)
0.37
11.
85(0
.65–
5.25
)0.
245
2.06
(0.6
5–6.
55)
0.21
94.
11(1
.10–
15.4
6)0.
036
5.37
(1.8
3–15
.79)
0.00
2>
1526
3.83
(0.8
4–17
.5)
0.08
33.
83(1
.09–
13.4
8)0.
037
4.40
(1.2
3–15
.67)
0.02
24.
40(1
.19–
16.2
5)0.
026
5.30
(1.2
1–23
.24)
0.02
76.
98(1
.79–
27.1
7)0.
005
Mon
ths
sinc
ela
stm
alar
iaep
isod
e0–
164
Ref
eren
ceR
efer
ence
Ref
eren
ceR
efer
ence
Ref
eren
ceR
efer
ence
2–18
710.
63(0
.26–
1.54
)0.
308
0.50
(0.2
3–1.
06)
0.07
20.
74(0
.36–
1.51
)0.
402
0.69
(0.3
3–1.
47)
0.33
90.
37(0
.17–
0.81
)0.
013
0.31
(0.1
3–0.
73)
0.00
719
–60
640.
63(0
.25–
1.55
)0.
311
0.81
(0.3
8–1.
73)
0.58
70.
79(0
.38–
1.67
)0.
536
0.79
(0.3
7–1.
71)
0.55
50.
36(0
.16–
0.80
)0.
013
0.30
(0.1
2–0.
73)
0.00
8>
60or
neve
rin
fect
ed89
0.95
(0.3
9–2.
33)
0.91
00.
59(0
.27–
1.30
)0.
189
0.57
(0.2
6–1.
34)
0.15
80.
74(0
.33–
1.65
)0.
460
0.36
(0.1
6–0.
83)
0.01
70.
28(0
.11–
0.69
)0.
006
*P
vRB
P1,
Pla
smod
ium
viva
xre
ticu
locy
tebi
ndin
gpr
otei
n1;
PvD
BP
-RII
,P.v
ivax
Duf
fybi
ndin
gpr
otei
nre
gion
II.D
onor
sw
ere
grou
ped
asin
dica
ted
acco
rdin
gto
the
inde
pend
ent
vari
able
sof
age
(in
year
s),y
ears
ofre
side
nce
inen
dem
icar
ea,n
umbe
rof
past
mal
aria
epis
odes
,and
mon
ths
sinc
ela
stm
alar
iaep
isod
e.M
ulti
vari
ate
logi
stic
regr
essi
onw
aspe
rfor
med
com
pari
ngth
elik
elih
ood
ofpo
siti
vere
spon
ses
inea
chgr
oup
toth
ere
fere
nce
grou
pfo
rea
chan
tige
n.L
ikel
ihoo
dis
mea
sure
das
odds
rati
osan
d95
%co
nfid
ence
inte
rval
s(C
I).S
tati
stic
alsi
gnif
ican
cew
asse
tat
P�
0.05
.
ANTIBODY RESPONSES TO VIVAX INFECTIONS 251

DISCUSSION
Naturally acquired antibody responses against PvRBP1,one of the proteins implicated in conferring reticulocytespecificity of P. vivax invasion of red blood cells, have notbeen studied to date. This study attempts to characterize theacquired antibody response to PvRBP1 and PvDBP in ma-laria-endemic populations of Rondônia state in the BrazilianAmazon. Malaria transmission in this area is low but continu-ous throughout the year, with sharp increases in malaria in-cidence during the dry months of June, July, and August.33,34
Distinct rural communities of Rondônia represent the varioustemporal cohorts of transmigrants who have settled inthe region during the past 40 years as a result ofgovernment social programs.35 The seroepidemiology of ma-laria infection in these communities has been studied exten-sively for P. falciparum; however, studies on antibody re-sponses to specific P. vivax antigens have been limited tosmall fragments of the long-standing vaccine candidatesmerozoite surface protein 1 (PvMSP1) and the circumsporo-zoite protein (PvCSP).25–27,36–42
We investigated three communities that have comparablemedian age but are clearly epidemiologically distinct, differ-ing in time of residence in the endemic area, number of past
malaria episodes, and number of patent vivax malaria infec-tions (Table 1). Male bias in the Colina community may be aconfounding variable, especially in regard to analyses withnumber of past malaria episodes. The effect of gender biasmust be considered when interpreting comparative analysesbetween the communities since men in these communitiestypically engage in outdoor activities (farming, fishing, log-ging, etc.) during peak transmission hours and thus havegreater overall exposure than women. The communities listedin order of increasing time of residence in the malaria en-demic area are 1) Buritis, 2) Colina, and 3) Ribeirinha. Cu-riously, residents of Ribeirinha reported having the leastnumber of past malaria episodes, despite being natives of theendemic area. This finding is probably a limitation of donor-reported data. Most likely, natives underestimate past malariahistories because they do not recall childhood infections.Comparable times since last malaria episode between Colinaand Ribeirinha (Table 1) not only argues against alternativeexplanations such as lower malaria transmission or enhancedacquired clinical immunity in the Ribeirinha community, buteven suggests that the transmigrant Colina population is ac-quiring a level of clinical immunity similar to that of the na-tive Ribeirinha population. This is not surprising given thatthe median number of years of residence in the endemic re-
TABLE 5Prevalence (% positive) and 95% confidence intervals (�g/mL) of IgG subclass-specific responses to PvRBP1 and PvDBP-RII in responders
positive for total IgG*
Antigen N
Antibody subclass†
P‡IgG1 IgG2 IgG3 IgG4
PvRBP123–458
Prevalence 54.4% 39.7% 64.7% 44.1% 0.02Responders 68 5.556–6.485 1.781–2.196 7.893–9.091 0.456–0.546 < 0.0001Controls 23 4.769–5.110 1.301–1.542 6.317–6.631 0.354–0.411 < 0.0001P† < 0.0001 < 0.0001 < 0.0001 < 0.0001
PvRBP1431–748Prevalence 42.5% 12.5% 20.0% 18.3% < 0.0001Responders 120 4.677–8.375 1.194–1.702 4.529–6.124 0.244–0.356 < 0.0001Controls 24 1.968–3.221 0.885–1.567 3.828–5.623 0.193–0.297 < 0.0001P† < 0.0001 NS NS NS
PvRBP1733–1407Prevalence 34.1% 27.5% 28.3% 15.2% 0.004Responders 138 2.301–3.540 0.804–1.104 2.904–3.963 0.109–0.159 < 0.0001Controls 24 1.268–2.009 0.548–0.940 2.218–3.443 0.062–0.154 < 0.0001P† 0.0004 NS NS NS
PvRBP11392–2076Prevalence 23.2% 4.0% 18.2% 12.1% < 0.001Responders 99 1.936–2.944 1.954–2.812 1.245–1.888 1.306–1.811 < 0.001Controls 24 1.816–2.642 0.615–1.096 1.977–2.999 0.094–0.156 < 0.0001P† NS < 0.0001 0.002 < 0.0001
PvRBP12038–2611Prevalence 73.8% 36.9% 83.5% 66.0% < 0.0001Responders 103 7.722–9.074 2.108–2.609 8.850–9.814 0.603–0.707 < 0.0001Controls 24 4.960–5.330 1.527–1.965 6.333–6.596 0.390–0.425 < 0.0001P† < 0.0001 0.0007 < 0.0001 < 0.0001
PvDBP-RIIPrevalence 55.3% 31.5% 72.1% 55.8% < 0.0001Responders 187 6.680–7.770 1.559–1.785 7.564–8.432 0.952–1.122 < 0.0001Controls 24 5.447–6.184 1.504–1.960 6.297–6.716 0.381–0.4394 < 0.0001P† < 0.0001 NS < 0.0001 < 0.0001
* PvRBP1, Plasmodium vivax reticulocyte binding protein 1; PvDBP-RII, P. vivax Duffy binding protein region II. Prevalence refers to the percentage of responders determined as positivefor a particular subclass based on optical densities (OD) from subclass-specific enzyme-linked immunosorbent assays. Responders are donors previously determined as having a positive totalimmunoglobulin G (IgG) response to the indicated antigen. Controls are non-malaria-exposed donors. OD values were converted to �g/mL using standard curves for each IgG subclass (see“Materials and Methods” for details). Log or reciprocal transformations were performed as appropriate to normalize the distribution of data points before parametric statistical analyses.Back-transformed 95% confidence intervals of means in �g/ml are shown.
† Student’s t test was used to compare differences between responders and controls within each IgG subclass for a single antigen. Bold typeface indicates the statistically greater of the twogroups.
‡ For each antigen, differences in proportions of subclass-specific positive responders (subclass-specific seroprevalence) were compared by �2 test. One-way analysis of variance was used tocompare differences between IgG subclass levels within responders or within controls for each antigen. Statistical significance was set at P � 0.05. NS, not statistically significant.
TRAN AND OTHERS252

gion for the Colina population approaches that of Ribeirinha.The community of recent transmigrants (Buritis) has the low-est seroprevalence of antibodies against all of the antigenstested when compared with the established communities ofColina and Ribeirinha. Although no significant relationshipswere found between infection status and seropositivity forany of the antigens (data not shown), the higher frequency ofpatent P. vivax infections, relative absence of asymptomaticinfections, and lowered P. vivax antibody responses observedin the Buritis residents may be indicative of their nonimmunestatus.
It has long been known that acquired clinical immunity tofalciparum malaria depends on repeated exposure to theparasite, a conclusion based on the observation that effectivenatural immunity to P. falciparum is restricted to areas of highlevel transmission.43 The presence of asymptomatic cases inAmazonian communities with long-term malaria exposure re-ported here and elsewhere suggests that a parallel phenom-enon occurs in areas of low P. vivax transmission.44,45 This isfurther supported by our finding that the time that has passedsince a donor’s last malaria episode positively correlates withthe time the donor has resided in the endemic area. Thebiological basis for such clinical immunity has yet to be elu-cidated, but it is likely that the effect is partially mediated byantibodies against P. vivax blood stage antigens. We demon-strate that IgG antibody responses to PvDBP and PvRBP1are dependent on indices of malaria exposure such as time ofresidence in the endemic area and number of past malariaepisodes. Our results coincide with other studies investigatingthe antibody responses to malaria antigens in areas of lowtransmission, supporting the view that natural immunologicboosting occurs even with less frequent transmission pat-terns.25,30,46 Studies on nonimmune transmigrants to hyper-endemic areas of Indonesia suggest that immunity to falci-parum malaria is age-dependent and that adults acquire pro-tective immunity to chronic infection more rapidly thanchildren.47 We were not able to investigate whether the clini-cal immunity we observed was age-dependent as our studywas limited primarily to adults. However, incidental cross-reactivity of malaria-naïve plasma with Plasmodium antigens,a major component of the age-dependent hypothesis, is sug-gested in our study by 1) high OD values among a few non-exposed North American and Brazilian controls for several ofthe antigens tested, resulting in unexpectedly high OD cutoffsand 2) the high frequency of seropositivity (67%) among ex-posed donors who reported themselves as malaria-naïve. Analternative explanation for seropositivity in this latter groupmay be unrecalled or subclinical P. vivax infections, as men-tioned previously.
Studies on IgG responses against P. falciparum antigenshave consistently shown that cytophilic subclasses IgG1 andIgG3 play an important role in a protective antibody responsein humans.22,48–51 The proposed mechanism involves parasiticinhibition effected by engagement of Plasmodium-specific cy-tophilic Ig antibodies to Fc� receptors on the surface ofmonocytes.23,24,52 To date, however, only a small number ofstudies have investigated cytophilic antibody responsesagainst P. vivax.53,54 In this study, we have demonstrated thatpositive IgG responses to both PvRBP1 and PvDBP-RIIshow increased levels of the cytophilic subclasses relative tononexposed controls. Specifically, positive responses toPvRBP1431-748 and PvRBP733-1407 were predominantly IgG1,
while positive responses to PvRBP123-458, PvRBP12038-2611,and PvDBP-RII demonstrated increases in IgG3. Curiously,positive responses to PvRBP11392-2076 demonstrated discor-dant subclass distributions between our two analyses, withone analysis suggesting a predominance of non-cytophilic an-tibodies.
Although we demonstrate a general predominance of cy-tophilic IgG antibodies, the correlation to clinical immunity israther tenuous. The cross-sectional design of this study lim-ited our investigation to retrospective malaria histories, andthe best approximation of an individual’s protection was theestimated amount of time that had passed since their lastmalaria episode, a measurement that may be confounded bylow or absent exposure to the parasite. We were only able toobserve modest, positive correlations between subclass reac-tivities against the PvRBP1733-1407 and PvRBP11392-2076 anti-gens and the amount of time since the last infection, only oneof which involved a cytophilic subclass. Prospective studies onhumoral immune responses or biologic studies addressing theability of P. vivax antibodies to inhibit merozoite invasion ordevelopment will provide more direct evidence with regardsto their protective efficacy.
This study attempts to determine the target of antibodyresponses to PvRBP1 by screening for IgG antibodies to re-combinant fragments spanning the extracellular region of theprotein. The prevalence of IgG responses to individualPvRBP1 antigens and PvDBP-RII approached 50% and 70%,respectively, comparable to levels previously observed for thePvCSP repeat region and the N-terminal region ofPvMSP1.36,39 Our results highlight PvRBP1431-748 andPvRBP1733-1407 as targets of a natural antibody response, asthese regions demonstrate both broad and high-titer re-sponses. Although responses to PvRBP1733-1407 were moreprevalent than those to PvRBP1431-748, the latter antigenspans only 318 amino acids of the 2749 residues comprisingthe PvRBP1 extracellular domain (compared with 675 aminoacids for PvRBP1733-1407). Furthermore, of the 25 total poly-morphic residues in PvRBP1, 12 (48%) reside in the regionspanned by PvRBP1431-748.20 These data taken together sug-gest that PvRBP1431-748 may be under immunologic selectionpressure. Finer mapping studies are needed to further definethe B cell epitopes contained within this region.
The leading strategy for malaria vaccine design calls for amultiple target approach against several blood-stage anti-gens.55 Direct comparisons of the natural antibody responseto these antigens provide valuable insight as to how such avaccine might work. We have compared the antibody re-sponses for two promising P. vivax blood-stage targets,PvRBP1 and PvDBP. In addition to the differences in sub-class distribution, we show that their IgG responses differ intwo important characteristics. First, anti-PvDBP-RII IgG re-sponses appear more prevalent and of higher magnitude thananti-PvRBP1 responses. Second, the rate of IgG antibody ac-quisition differs between the two antigens. Individuals seemto require less exposure to build up detectable levels of anti-bodies to PvDBP-RII compared with PvRBP1, implying im-munodominance of PvDBP-RII over PvRBP1; the lone ex-ception is the response against PvRBP12038-2611, which showsa rate of increase similar to that of the anti-PvDBP-RII re-sponse, albeit at lower prevalence and magnitude. We quan-tified the rapid acquisition of anti-PvDBP-RII antibodies bylogistic regression, showing that donors with more than five
ANTIBODY RESPONSES TO VIVAX INFECTIONS 253

malaria episodes were more than five times as likely to re-spond to this antigen compared with malaria-naïve individu-als (Table 4). However, the regression also suggests that theanti-PvDBP-RII response may be short-lived. Donors whohave not had a recent malaria infection (within two monthspreceding sample collection) were significantly less likely torespond to PvDBP-RII than their recently infected counter-parts. In contrast, with the exception of PvRBP12038-2611, theprevalence of responses to PvRBP1 antigens was independentof time since the last known malaria episode. The evidenceimplies that although anti-PvRBP1 IgG responses may beslowly acquired relative to anti-PvDBP-RII responses, thelongevity of such responses may be greater in the absence ofclinical malaria episodes.
In conclusion, we have characterized the IgG antibody re-sponses to five distinct regions spanning the extracellular do-main of PvRBP1. We show that both PvRBP1 with PvDBP-RII elicit predominantly cytophilic IgG responses but theseresponses differ in magnitude, breadth, and rate of acquisi-tion, with PvDBP-RII eliciting the more robust and rapidantibody response in three communities of the BrazilianAmazon. These data provide information on the characteris-tics of acquired humoral immunity to two key vivax antigensin populations exposed to malaria transmission that could bebeneficial in the development of a multitarget, blood-stagevaccine for P. vivax. Prospective studies are needed to deter-mine whether synergistic, additive, or antagonistic interac-tions exist between IgG antibody responses to PvDBP-RIIand PvRBP1 as well as their roles in clinical immunity.
Received October 7, 2004. Accepted for publication March 18, 2005.
Note: Supplemental figures 1 and 2 appear online at www.ajtmh.org.
Acknowledgments: The authors thank the Fundação Nacional deSaude (Brazilian Ministry of Health) and the Secretary of Health ofRondônia for providing fieldwork support and K.B. Anderson forhelp with statistical analyses. We are grateful to all donors who par-ticipated in this study.
Financial support: This research is supported by the National Insti-tute of Allergy and Infectious Diseases, National Institutes of Health,grant no. R01AI247-18. Tuan M. Tran was also a recipient of anAmerican Society of Tropical Medicine and Hygiene Benjamin H.Kean Fellowship in Tropical Medicine. Chetan E. Chitnis is aWellcome Trust International Senior Research Fellow and HowardHughes International Research Scholar.
Authors’ addresses: Tuan M. Tran, Alberto Moreno, John D. Alt-man, Esmeralda V-S. Meyer, and Mary R. Galinski, Emory VaccineCenter, Yerkes National Primate Research Center, Emory Univer-sity, 954 Gatewood Rd., Atlanta GA 30329. Joseli Oliveira-Ferreira,Laboratorio de Pesquisas em Malaria, Fundação Oswaldo Cruz –FIOCRUZ, Av. Brasil, 4365 – Manguinhos, Rio de Janeiro, RJ, Bra-zil. Fatima Santos, Fundação Nacional de Saúde, Av George TeixeiraS/N, Porto Velho, Rondônia, Brazil. Syed S. Yazdani and Chetan E.Chitnis, Malaria Research Group, International Centre for GeneticEngineering and Biotechnology (ICGEB), Aruna Asaf Ali Marg, NewDelhi 110067, India. John W. Barnwell, Malaria Branch, Division ofParasitic Diseases, National Center for Infectious Diseases, Centers forDisease Control and Prevention, MS F-36, Atlanta, GA 30341.
Reprint requests: Mary R. Galinski, Emory Vaccine Center atYerkes, Emory University, 954 Gatewood Rd., Atlanta, GA 30329,Telephone: 404-727-7214, Fax: 404-727-8199, E-mail: [email protected].
REFERENCES1. Mendis K, Sina BJ, Marchesini P, Carter R, 2001. The neglected
burden of Plasmodium vivax malaria. Am J Trop Med Hyg 64:97–106.
2. Breman JG, 2001. The ears of the hippopotamus: manifestations,determinants, and estimates of the malaria burden. Am J TropMed Hyg 64: 1–11.
3. Moorthy VS, Good MF, Hill AV, 2004. Malaria vaccine devel-opments. Lancet 363: 150–156.
4. Ballou WR, Arevalo-Herrera M, Carucci D, Richie TL, CorradinG, Diggs C, Druilhe P, Giersing BK, Saul A, Heppner DG,Kester KE, Lanar DE, Lyon J, Hill AV, Pan W, Cohen JD,2004. Update on the clinical development of candidate malariavaccines. Am J Trop Med Hyg 71: 239–247.
5. Sina B, 2002. Focus on Plasmodium vivax. Trends Parasitol 18:287–289.
6. Wertheimer SP, Barnwell JW, 1989. Plasmodium vivax interac-tion with the human Duffy blood group glycoprotein: identifi-cation of a parasite receptor-like protein. Exp Parasitol 69:340–350.
7. Fang XD, Kaslow DC, Adams JH, Miller LH, 1991. Cloning ofthe Plasmodium vivax Duffy receptor. Mol Biochem Parasitol44: 125–132.
8. Adams JH, Hudson DE, Torii M, Ward GE, Wellems TE,Aikawa M, Miller LH, 1990. The Duffy receptor family ofPlasmodium knowlesi is located within the micronemes of in-vasive malaria merozoites. Cell 63: 141–153.
9. Sim BK, Toyoshima T, Haynes JD, Aikawa M, 1992. Localizationof the 175-kilodalton erythrocyte binding antigen in micron-emes of Plasmodium falciparum merozoites. Mol BiochemParasitol 51: 157–159.
10. Miller LH, Mason SJ, Clyde DF, McGinniss MH, 1976. The re-sistance factor to Plasmodium vivax in blacks. The Duffy-blood-group genotype, FyFy. N Engl J Med 295: 302–304.
11. Chitnis CE, Miller LH, 1994. Identification of the erythrocytebinding domains of Plasmodium vivax and Plasmodiumknowlesi proteins involved in erythrocyte invasion. J Exp Med180: 497–506.
12. Cole-Tobian J, King CL, 2003. Diversity and natural selection inPlasmodium vivax Duffy binding protein gene. Mol BiochemParasitol 127: 121–132.
13. Michon P, Fraser T, Adams JH, 2000. Naturally acquired andvaccine-elicited antibodies block erythrocyte cytoadherence ofthe Plasmodium vivax Duffy binding protein. Infect Immun 68:3164–3171.
14. Galinski MR, Medina CC, Ingravallo P, Barnwell JW, 1992. Areticulocyte-binding protein complex of Plasmodium vivaxmerozoites. Cell 69: 1213–1226.
15. Galinski MR, Xu M, Barnwell JW, 2000. Plasmodium vivaxreticulocyte binding protein-2 (PvRBP-2) shares structural fea-tures with PvRBP-1 and the Plasmodium yoelii 235 kDa rhop-try protein family. Mol Biochem Parasitol 108: 257–262.
16. Galinski MR, Barnwell JW, 1996. Plasmodium vivax: merozoites,invasion of reticulocytes and considerations for vaccine devel-opment. Parasitol Today 12: 20–29.
17. Rayner JC, Galinski MR, Ingravallo P, Barnwell JW, 2000. TwoPlasmodium falciparum genes express merozoite proteins thatare related to Plasmodium vivax and Plasmodium yoelii adhe-sive proteins involved in host cell selection and invasion. ProcNatl Acad Sci U S A 97: 9648–9653.
18. Rayner JC, Vargas-Serrato E, Huber CS, Galinski MR, BarnwellJW, 2001. A Plasmodium falciparum homologue of Plasmo-dium vivax reticulocyte binding protein (PvRBP1) defines atrypsin-resistant erythrocyte invasion pathway. J Exp Med 194:1571–1581.
19. Triglia T, Thompson J, Caruana SR, Delorenzi M, Speed T, Cow-man AF, 2001. Identification of proteins from Plasmodiumfalciparum that are homologous to reticulocyte binding pro-teins in Plasmodium vivax. Infect Immun 69: 1084–1092.
20. Rayner JC, Tran TM, Corredor V, Huber CS, Barnwell JW, Ga-linski MR, 2005. Dramatic difference in diversity betweenPlasmodium falciparum and Plasmodium vivax reticulocytebinding-like genes. Am J Trop Med Hyg 72: 666–674.
21. Singh S, Pandey K, Chattopadhayay R, Yazdani SS, Lynn A,
TRAN AND OTHERS254
Bharadwaj A, Ranjan A, Chitnis C, 2001. Biochemical, bio-physical, and functional characterization of bacterially ex-pressed and refolded receptor binding domain of Plasmodiumvivax duffy-binding protein. J Biol Chem 276: 17111–17116.
22. Bouharoun-Tayoun H, Druilhe P, 1992. Plasmodium falciparummalaria: evidence for an isotype imbalance which may be re-sponsible for delayed acquisition of protective immunity. InfectImmun 60: 1473–1481.
23. Bouharoun-Tayoun H, Attanath P, Sabchareon A, Chong-suphajaisiddhi T, Druilhe P, 1990. Antibodies that protect hu-mans against Plasmodium falciparum blood stages do not ontheir own inhibit parasite growth and invasion in vitro, but actin cooperation with monocytes. J Exp Med 172: 1633–1641.
24. Bouharoun-Tayoun H, Oeuvray C, Lunel F, Druilhe P, 1995.Mechanisms underlying the monocyte-mediated antibody-dependent killing of Plasmodium falciparum asexual bloodstages. J Exp Med 182: 409–418.
25. Banic DM, de Oliveira-Ferreira J, Pratt-Riccio LR, Conseil V,Goncalves D, Fialho RR, Gras-Masse H, Daniel-Ribeiro CT,Camus D, 1998. Immune response and lack of immune re-sponse to Plasmodium falciparum P126 antigen and its amino-terminal repeat in malaria-infected humans. Am J Trop MedHyg 58: 768–774.
26. Jacobson KC, Thurman J, Schmidt CM, Rickel E, Oliviera deFerreira J, Ferreira-da-Cruz MF, Daniel-Ribeiro CT, HowardRF, 1998. A study of antibody and T cell recognition of rhop-try-associated protein-1 (RAP-1) and RAP-2 recombinantproteins and peptides of Plasmodium falciparum in migrantsand residents of the state of Rondonia, Brazil. Am J Trop MedHyg 59: 208–216.
27. Banic DM, Goldberg AC, Pratt-Riccio LR, De Oliveira-FerreiraJ, Santos F, Gras-Masse H, Camus D, Kalil J, Daniel-RibeiroCT, 2002. Human leukocyte antigen class II control of theimmune response to p126-derived amino terminal peptidefrom Plasmodium falciparum. Am J Trop Med Hyg 66: 509–515.
28. Shute GT, 1988. The microscopic diagnosis of malaria. Werns-dorfer WH, McGregor SI, eds. Malaria: Principles and Practiceof Malariology. New York: Churchill Livingstone, 781–814.
29. Guruprasad K, Reddy BV, Pandit MW, 1990. Correlation be-tween stability of a protein and its dipeptide composition: anovel approach for predicting in vivo stability of a protein fromits primary sequence. Protein Eng 4: 155–161.
30. Michon PA, Arevalo-Herrera M, Fraser T, Herrera S, Adams JH,1998. Serologic responses to recombinant Plasmodium vivaxDuffy binding protein in a Colombian village. Am J Trop MedHyg 59: 597–599.
31. Fraser T, Michon P, Barnwell JW, Noe AR, Al-Yaman F, KaslowDC, Adams JH, 1997. Expression and serologic activity of asoluble recombinant Plasmodium vivax Duffy binding protein.Infect Immun 65: 2772–2777.
32. Xainli J, Cole-Tobian JL, Baisor M, Kastens W, Bockarie M,Yazdani SS, Chitnis CE, Adams JH, King CL, 2003. Epitope-specific humoral immunity to Plasmodium vivax Duffy bindingprotein. Infect Immun 71: 2508–2515.
33. Camargo LM, Noronha E, Salcedo JM, Dutra AP, Krieger H,Pereira da Silva LH, Camargo EP, 1999. The epidemiology ofmalaria in Rondonia (Western Amazon region, Brazil): studyof a riverine population. Acta Trop 72: 1–11.
34. Salcedo JM, Camargo EP, Krieger H, Silva LH, Camargo LM,2000. Malaria control in an agro-industrial settlement of Ron-donia (Western Amazon region, Brazil). Mem Inst OswaldoCruz 95: 139–145.
35. Singer BH, de Castro MC, 2001. Agricultural colonization and ma-laria on the Amazon frontier. Ann N Y Acad Sci 954: 184–222.
36. Oliveira-Ferreira J, Nakaie CR, Daniel-Ribeiro C, 1992. Lowfrequency of anti- Plasmodium falciparum circumsporozoiterepeat antibodies and rate of high malaria transmission in en-demic areas of Rondonia State in northwestern Brazil. Am JTrop Med Hyg 46: 720–726.
37. Mertens F, Levitus G, Camargo LM, Ferreira MU, Dutra AP,Del Portillo HA, 1993. Longitudinal study of naturally ac-quired humoral immune responses against the merozoite sur-face protein 1 of Plasmodium vivax in patients from Rondonia,Brazil. Am J Trop Med Hyg 49: 383–392.
38. Ferreira MU, Kimura ES, Camargo LM, Alexandre CO, da SilvaLH, Katzin AM, 1994. Antibody response against Plasmodiumfalciparum exoantigens and somatic antigens: a longitudinalsurvey in a rural community in Rondonia, western BrazilianAmazon. Acta Trop 57: 35–46.
39. Levitus G, Mertens F, Speranca MA, Camargo LM, Ferreira MU,del Portillo HA, 1994. Characterization of naturally acquiredhuman IgG responses against the N-terminal region of themerozoite surface protein 1 of Plasmodium vivax. Am J TropMed Hyg 51: 68–76.
40. Balthazar-Guedes HC, Ferreira-Da-Cruz MF, Montenegro-James S, Daniel-Ribeiro CT, 1995. Malaria diagnosis: identifi-cation of an anti-40-kDa polypeptide antibody response asso-ciated with active or recent infection and study of the IgG/IgMratio of antibodies to blood-stage Plasmodium falciparum an-tigens. Parasitol Res 81: 305–309.
41. Ferreira-da-Cruz MF, Deslandes DC, Oliveira-Ferreira J, Mon-tenegro-James S, Tartar A, Druilhe P, Daniel-Ribeiro CT,1995. Antibody responses to Plasmodium falciparum sporozo-ite-, liver- and blood-stage synthetic peptides in migrant andautochthonous populations in malaria endemic areas. Parasite2: 23–29.
42. Oliveira-Ferreira J, Pratt-Riccio LR, Arruda M, Santos F, DanielRibeiro CT, Carla Golberg A, Banic DM, 2004. HLA class IIand antibody responses to circumsporozoite protein repeats ofP. vivax (VK210, VK247 and P. vivax-like) in individuals natu-rally exposed to malaria. Acta Trop 92: 63–69.
43. Riley E, 1994. Malaria. Kierszenbaum F, ed. Parasitic Infectionsand the Immune System. San Diego: Academic Press, xii, 254.
44. Camargo EP, Alves F, Pereira da Silva LH, 1999. SymptomlessPlasmodium vivax infections in native Amazonians. Lancet353: 1415–1416.
45. Alves FP, Durlacher RR, Menezes MJ, Krieger H, Silva LH,Camargo EP, 2002. High prevalence of asymptomatic Plasmo-dium vivax and Plasmodium falciparum infections in nativeAmazonian populations. Am J Trop Med Hyg 66: 641–648.
46. Braga EM, Barros RM, Reis TA, Fontes CJ, Morais CG, MartinsMS, Krettli AU, 2002. Association of the IgG response toPlasmodium falciparum merozoite protein (C-terminal 19 kD)with clinical immunity to malaria in the Brazilian Amazonregion. Am J Trop Med Hyg 66: 461–466.
47. Baird JK, 1998. Age-dependent characteristics of protection v.susceptibility to Plasmodium falciparum. Ann Trop Med Para-sitol 92: 367–390.
48. Druilhe P, Khusmith S, 1987. Epidemiological correlation be-tween levels of antibodies promoting merozoite phagocytosisof Plasmodium falciparum and malaria-immune status. InfectImmun 55: 888–891.
49. Oeuvray C, Bouharoun-Tayoun H, Gras-Masse H, Bottius E,Kaidoh T, Aikawa M, Filgueira MC, Tartar A, Druilhe P, 1994.Merozoite surface protein-3: a malaria protein inducing anti-bodies that promote Plasmodium falciparum killing by coop-eration with blood monocytes. Blood 84: 1594–1602.
50. Nguer CM, Diallo TO, Diouf A, Tall A, Dieye A, Perraut R,Garraud O, 1997. Plasmodium falciparum- and merozoite sur-face protein 1-specific antibody isotype balance in immuneSenegalese adults. Infect Immun 65: 4873–4876.
51. Taylor RR, Allen SJ, Greenwood BM, Riley EM, 1998. IgG3antibodies to Plasmodium falciparum merozoite surface pro-tein 2 (MSP2): increasing prevalence with age and associationwith clinical immunity to malaria. Am J Trop Med Hyg 58:406–413.
52. Druilhe P, Bouharoun-Tayoun H, 2002. Antibody-dependent cel-lular inhibition assay. Methods Mol Med 72: 529–534.
53. Kirchgatter K, del Portillo HA, 1998. Molecular analysis of Plas-modium vivax relapses using the MSP1 molecule as a geneticmarker. J Infect Dis 177: 511–515.
54. Soares IS, da Cunha MG, Silva MN, Souza JM, Del Portillo HA,Rodrigues MM, 1999. Longevity of naturally acquired anti-body responses to the N- and C-terminal regions of Plasmo-dium vivax merozoite surface protein 1. Am J Trop Med Hyg60: 357–363.
55. Good MF, 2001. Towards a blood-stage vaccine for malaria: arewe following all the leads? Nat Rev Immunol 1: 117–125.
ANTIBODY RESPONSES TO VIVAX INFECTIONS 255
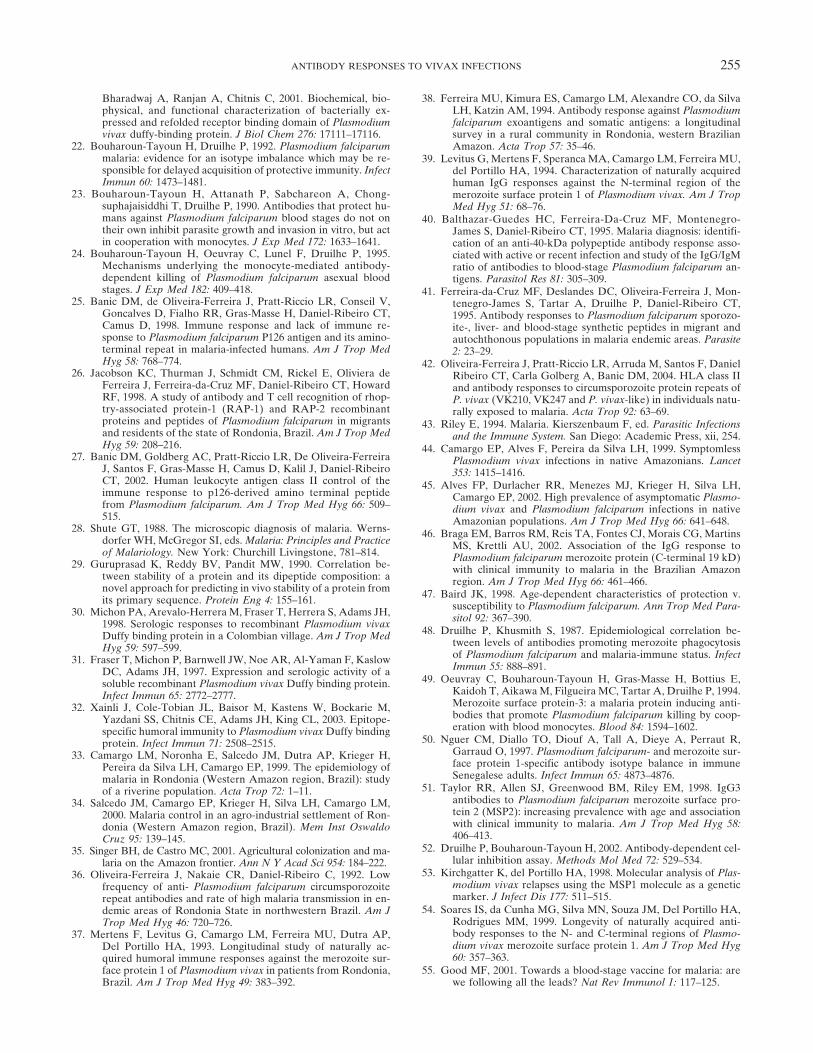
SUPPLEMENTAL FIGURE 1. Anti-penta-His Western blot of recom-binant Plasmodium vivax reticulocyte binding protein 1 (PvRBP1)and P. vivax Duffy binding protein region II (PvDBP-RII) proteins.Approximately 2 �g of each protein were run on a 10% polyacryl-amide gel and transferred to a nitrocellulose membrane. Western blotwas performed using an anti-penta-His monoclonal antibody(Qiagen, Valencia, CA) according to the manufacturer’s specifica-tions. See “Materials and Methods” for details on expression andpurification of proteins. Molecular weights in kilodaltons (kDa) areindicated.
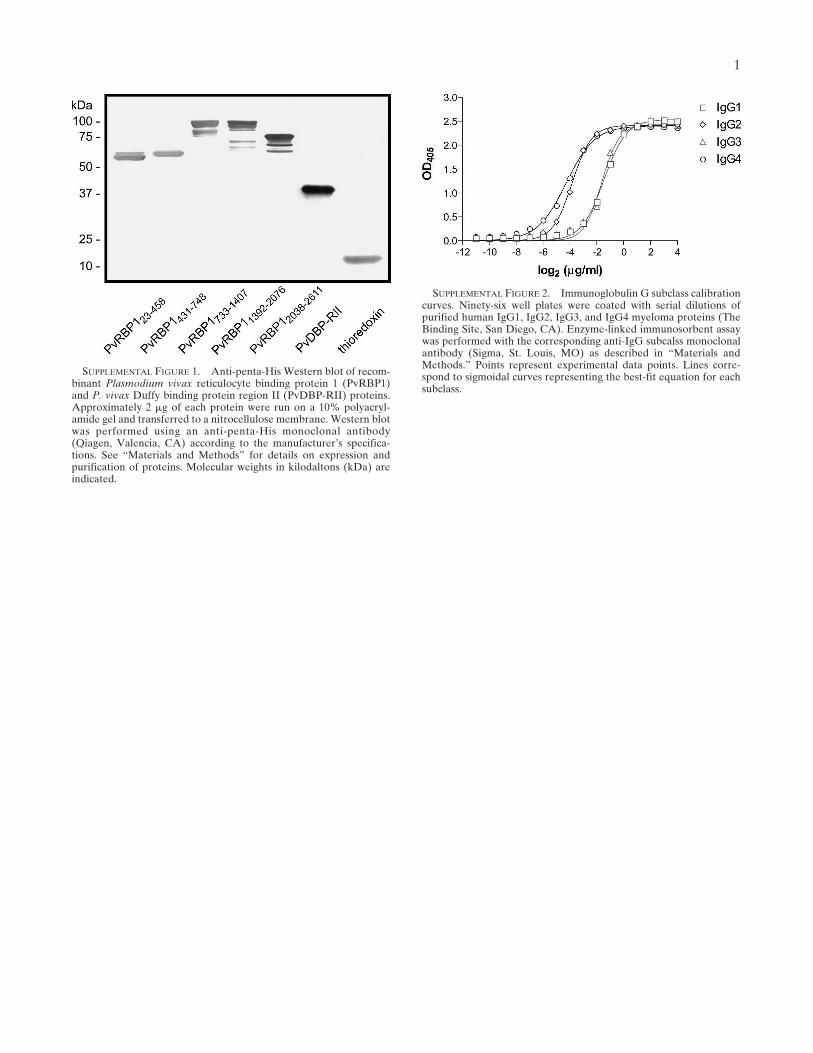
SUPPLEMENTAL FIGURE 2. Immunoglobulin G subclass calibrationcurves. Ninety-six well plates were coated with serial dilutions ofpurified human IgG1, IgG2, IgG3, and IgG4 myeloma proteins (TheBinding Site, San Diego, CA). Enzyme-linked immunosorbent assaywas performed with the corresponding anti-IgG subcalss monoclonalantibody (Sigma, St. Louis, MO) as described in “Materials andMethods.” Points represent experimental data points. Lines corre-spond to sigmoidal curves representing the best-fit equation for eachsubclass.
1
Copyright © 2022 FDOKUMEN




















