Communication within Families at-risk for Type 2 Diabetes
51
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Communication within Families at-risk for Type 2 Diabetes

i
Communication within Families at-risk for Type 2 Diabetes
A thesis submitted to the
Graduate School
of the University of Cincinnati
in partial fulfillment of the
requirements for the degree of
Master of Science
In the Department of Pediatrics
Of the College of Medicine
April 2013
by
Jennifer Hopper
M.S. Valdosta State University, 2008
Committee Chair: Melanie F. Myers, PhD, MS, CGC1, 2
Committee Members: Laura M. Koehly, PhD3, Robert Smith, MD1, Carrie Atzinger, MS, CGC1, 2
1 University of Cincinnati, Cincinnati, OH, USA 2 Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA
3 Social and Behavioral Research Branch, National Human Genome Research Institute, Bethesda, MD, USA
ii
Abstract
Purpose: 1) To identify characteristics within families at-risk for Type 2 diabetes (T2D),
based on a family history of T2D, which either facilitate or hinder risk communication and 2) To
gather participants’ perspectives on ways to increase risk communication about T2D within at-
risk families and ways to reduce the risk of developing T2D among at-risk family members.
Methods: Semi-structured qualitative interviews were conducted with adults diagnosed
with T2D, who were recruited through a pharmacogenetic database used in a previous research
study at the University of Cincinnati. Themes were developed using deductive codes based on
pre-determined interview questions and inductive codes based on interviewee responses, and
then coded by two coders.
Results: Themes were grouped and discussed under four major categories: 1)
Characteristics facilitating and impeding communication 2) Familial communication patterns 3)
Role of family and the role of society in communication about T2D risk and 4) Perceived causes
of T2D.
Conclusions: Communication within at-risk T2D families informs genetic counseling
practice as well as public health practice. Genetic counselors can help families facilitate
discussion about T2D based on familial characteristics. Public health interventions should be
developed based on relationships between individuals within at-risk families, potential barriers
to communication, individuals’ family and social environments, and perceived cause of T2D.

iii
iv
Acknowledgements
I would like to thank my research advisory committee for their valuable input on this project.
Also I would like to thank Brandon Smith, BS, for his help with data collection and Sara
Fernandes, BS for her help with data collection and coding. Finally, this project was funded by a
grant from the National Institute of Health and a K-award, both awarded to Melanie Myers,
PhD, for her work in T2D research.
v
Table of Contents
Introduction………………………………………………………………………………………………………………………………7
Methods………………………………………………………………….………………………………………………………………10
Results……………………………………..………………………………………………………………………………………………14
Discussion………………………..………………………………………………………………………………………………………27
References….……………………………………………………………………………………………………………………………34
Appendices, Tables, Figures.…………………………………………………………………………………………………….36

vi
Appendices, Tables, Figures
Appendix A: Qualitative interview guide…………………………………………………………………………………36
Appendix B: Codebook…………………………………………………………………………………………………………….37
Table 1: Inter-rater reliability for each theme…………………………………………………………………………47
Table 2: Participant characteristics…………………………………………………………………………………………49
Figure 1: Types and flow of communication……………………………………………………………………………50

7
Introduction
Diabetes is the seventh leading cause of death in the United States and affects 25.8
million people or 8.3% of the U.S. population. An estimated 90-95 % of individuals diagnosed
with diabetes have type 2 diabetes (T2D). Another 79 million Americans are estimated to have
“pre-diabetes,” where their blood glucose levels are higher than normal but not high enough to
be placed in the diabetic category [1]. In 2007 the estimated total direct and indirect costs to
society associated with diabetes, including medical costs, disability, work loss and premature
mortality, were $174 billion [1]. Multiple studies report that physical activity and a low calorie
and low fat diet can help prevent T2D or at least delay the onset of the condition [2, 3].
However, the current prevalence of T2D is significantly high at 16 million Americans [1] and if
current trends continue, the Centers for Disease Control and Prevention estimates 1 in 3 U.S.
adults could have T2D by 2050 [4].
Based on an analysis of the 6-year National Health and Nutrition Examination Survey
(NHANES), the prevalence of diabetes in high risk families, which are those families with at least
two first-degree relatives or one first-degree relative and at least two second-degree relatives
with diabetes from the same lineage, is 30%. Individuals in these high-risk families are 5.5 times
more likely to develop T2D than individuals in average risk families, which are families with no
history of diabetes, or at most, one second-degree relative with diabetes [5]. Family health
history (FHH) has been identified as an important indicator of risk and a catalyst for
communication of risks of common and chronic diseases [6-10].
Patients who are informed of their risks for developing T2D by their physicians are more
likely to engage in risk reducing behaviors, such as making lifestyle changes, than patients who
8
are not informed of their risks [11]. Studies have posited that people with knowledge of their
risk for T2D based on their family history are also more likely to engage in risk-reducing
behaviors [11, 12]. If individuals at an increased risk of T2D, based on FHH, are identified early
by communication about FHH then these individuals can be educated about the potential risk
of developing T2D, as well as the risk-reducing actions they can take to help prevent T2D.
Explanations of risk that are generated to target a general audience are difficult to
connect to on a personal level, and appear to be insufficient for motivating behavior change
[13] ;as a result, individuals may not recognize the importance of changing their lifestyles to
reduce disease risk. Royak-Schaler, et al., conducted focus groups with 25 African-American and
17 Hispanic females, ages 40-60, with no personal history of breast or colorectal cancer [13].
Participants answered open-ended questions about their understanding of cancer risk factors,
their perceptions of personal cancer risk, strategies for reducing risk, and risk communication.
Results indicated that participants had limited knowledge about general cancer risks and they
wanted to receive more information about risks, but preferred that the risk information be
conveyed at an individualized level, and include personal risk factors such as family history [13].
Family communication about T2D risk among families impacted by T2D is an approach to risk
communication that allows family members to act as ambassadors in providing risk information
at a more individualized level that is tailored to their personal risk factors [8, 13].
Whitford, et al., examined how receptive first-degree relatives of a family member with
T2D were to risk communication by their T2D affected relative [14]. Survey questionnaires were
mailed to a random sample of 703 patients with T2D who attended an urban hospital diabetes
clinic, and the patients were instructed to pass along the survey to at least one first-degree
9
relative. Relatives from 257 families completed and returned the survey and answered
questions, among others, on perceived susceptibility to T2D, knowledge of risk factors for T2D
and desire to be spoken to about the possibility of reducing their risk of diabetes. Results
showed that first-degree relatives of patients with T2D who had been informed about their risk
of developing T2D by their affected relatives had increased perceived susceptibility to T2D,
increased knowledge of risk factors and an increased sense of the seriousness of T2D compared
to those first-degree relatives who had not been informed of their risk for developing T2D.
Additionally, T2D patients and their relatives had similar attitudes, knowledge and anxiety
about the risk of developing T2D within their families. Therefore, it was suggested that
encouraging individuals who are affected with T2D to communicate with their unaffected
family members about the risk of developing T2D and potential risk-reducing behaviors would
lead to an increase in knowledge about risk for disease; hopefully communication would then
lead to a change in lifestyle behaviors that could help reduce the risk for developing T2D [14].
Family dynamics are complex and tend to be unique to every family. In order to increase
communication about disease risk within at-risk families, it is important to understand the role
that family communication plays in the flow of T2D risk information. In a study looking at the
family role of melanoma risk communication [6], 313 first degree relatives of melanoma
patients completed multiple surveys assessing family coping type, family adaptation, family
cohesion and family health beliefs. Results illustrated those families who engaged in active
coping, and reported to be adaptable and cohesive had an open style of risk communication
and an increased frequency of communication compared to those families who did not engage
in active coping, and did not report to be adaptable or cohesive. [6].
10
Another study by McCann, et al., on family communication of information about
colorectal cancer risk, also identified family variables related to risk communication [9]. Thirty
people from 17 families with a FHH of colorectal cancer participated in qualitative interviews,
and results indicated that communication within families about risk can be affected by family
members’ feelings of duty to listen to relatives affected with cancer and responsibility to inform
children who may become affected in the future of their risks. Risk communication among the
families was inhibited in cases of a recent diagnosis of colorectal cancer or bereavement from a
recent death, due to the sensitive nature of these occurrences, and was also inhibited where
there was less frequency of contact between relatives [9].
Identifying factors that impact risk communication in at-risk families can provide insight
on the best approach to utilizing FHH as a way to promote the adoption of healthy behaviors
that could lead to a decreased risk of disease. The purpose of this study is to identify themes
within families at-risk for T2D, based on a family history of T2D, which either facilitate or hinder
risk communication. Additionally the study aims to gather participants’ perspectives on ways to
increase risk communication about T2D within at-risk families and ways to reduce the risk of
developing T2D among at-risk family members.
Methods
Study Type
Semi-structured qualitative interviews were conducted with adults diagnosed with T2D
to identify perceived factors that affect T2D risk communication within respective families. A
phenomenological approach guided the qualitative research to understand the participants’
11
lived experiences from their own perspectives [15]. Institutional Review Board (IRB) approval
was obtained from the University of Cincinnati.
Interview Guide
Questions from a previous qualitative study that looked at explanations of risk in
families with a history of colorectal cancer [16] guided the development of questions for the
current study. These questions were piloted on three colleagues to assess face validity and
comprehension of questions. Based on feedback, that some questions did not have good face
validity and additional topics should be addressed, the survey was revised by deleting a few
questions and adding questions to encompass the additional topics. Questions added covered
the topics of how participants felt about diabetes, challenges to talking with family members
about T2D, ways to increase communication about T2D and ways to reduce the risk of T2D. The
final questions asked about participants’ experience with T2D, their feelings about T2D, who in
their family had been diagnosed with T2D, who in the family participants talked to or did not
talk to about T2D, whether participants thought any family members were at risk of T2D, and
thoughts on how to increase T2D-related communication as well as reduce the risks of T2D (see
Appendix A).
Study Subjects
Participants were randomly selected from a database of patients with T2D who
previously participated in a preliminary pharmacogenetic (PGx) study. The participants from the
PGx database were labeled as the index participants. As part of the PGx study, clinical data was
collected from T2D patients from multiple family practice sites in the Greater Cincinnati area.
12
The aim of the PGx study was to examine the effect of common genetic variants in the PPARG
gene on patients’ responses to thiazolidinediones, a class of medications used to treat T2D.
There are 247 participants with T2D in the PGx database who range in age from 30-96.
We invited proportionally random samples of individuals up to age 85 who self-identified in the
PGx study as African American, Appalachian or Caucasian, non-Appalachian to participate in the
family communication study to better reflect the diversity of individuals impacted by T2D.
Participants were sorted in the database according to their racial/ethnic identification, and then
their unique identification numbers were entered into an online number randomizer tool,
through which 10 individuals from each race/ethnic group were selected. Thirty individuals (10
from each group) comprised each wave of participants, and a total of 4 waves of participants
were invited to participate in the study. Individuals unable to provide verbal consent were
excluded. All interviews were conducted in English.
Data Collection
Potential index participants who met the inclusion criteria were sent a recruitment
letter, asking them to participate in 2 phone interviews (the qualitative interview and a
quantitative survey to identify familial characteristics that are related to the dissemination of
T2D risk information in at-risk families), as well as an initial phone contact to confirm eligibility.
Invited participants were asked to either check a box indicating whether they did or did not
wish to participate. Individuals agreeing to participate were asked to provide preferred days,
times and phone numbers when they could be contacted by phone. All invited participants
were asked to mail their response back to the researchers in a postage-paid envelope. If a
response was not received within two weeks, the invitation letter was mailed again. If there

13
was no response within four weeks of the initial mailing, potential participants were contacted
by phone to ask if they would like to participate in the study.
During the initial telephone contact, participants were asked to provide demographic
information, to list additional individuals in their families who might also be willing to
participate in the study and to indicate a convenient time for a follow-up phone call. During a
second phone call, the qualitative interview was conducted. Contact information for
participants’ family members and permission to contact these family members was also
obtained, and a time for the quantitative phone interview was scheduled. Both index cases and
unaffected relatives participated in qualitative interviews, however, only results from the
qualitative interviews with individuals who had been diagnosed with T2D are reported here.
Each participant received a $25 gift card to a popular retail store after completing the
qualitative assessment. Participation was voluntary and individuals were informed that they
could discontinue participation at any time.
Coding
Themes were developed using deductive codes based on pre-determined interview
questions and inductive codes based on interviewee responses. For example, themes that
emerged when participants were asked about reasons for not talking with family members
about T2D included not feeling close to their family members (“no close bond”) or that their
relatives lived too far away to have discussions (“distance”). [17]. Data organization and coding
was performed with the use of the qualitative software analysis program NVIVO. After training,
two coders analyzed three transcripts together to standardize application of codes. The primary

14
coder then coded all transcripts and the secondary coder coded 40% (8) of randomly selected
transcripts.
Cohen’s Kappa was used to calculate agreement and κ-values above 0.60 were
considered to be in agreement [18]. After the transcripts coded by both the primary and
secondary coder were evaluated, any themes not reaching a κ-value of greater than 0.60 were
discussed between the coders. The coders reached consensus on the best code to apply, and
the remaining transcripts were reanalyzed to ensure proper application of codes across all
documents. All themes had a κ-value of greater than 0.60 (see Table 1). Emergent themes were
grouped into 14 different categories (see Appendix B). In this paper, themes are discussed
under the following topics: characteristics facilitating and impeding communication, types and
flow of familial communication, role of family and the role of society in communication about
T2D risk, and perceived cause of T2D.
Results
Participant characteristics
Overall, 105 invitation letters to participate in the qualitative survey were mailed to
individuals from the PGx database. From those letters, 25 individuals agreed to participate, 20
individuals actually participated, 67 were unreachable or declined to participate, and 13 letters
were undeliverable. Fifteen of the participants were female and 5 were male. Based on self-
reports in this study, 6 identified as Appalachian, 7 as African American and 6 as Caucasian,
non-Appalachian. The majority of participants were married (n = 12), 3 were never married, 3
were widowed, 1 was separated and 1 was divorced. When asked about education, 8 reported
that they received a four year college education or higher, 7 participants reported having an
15
associate’s degree and 5 had a high school diploma or GED. Based on the definitions of at-risk
families used in the NHANES survey [5], 11 participants had a high risk family, 7 had a moderate
risk family, and 2 had an average risk family (see Table 2 for additional participant
characteristics).
Characteristics facilitating and impeding communication
Some individuals reported that they most often spoke to family members with whom
they shared a close bond about T2D (n = 4). Conversely, other participants (n = 6) reported that
they did not discuss T2D related information with family members with whom they did not
share a close bond. For example, one participant explained that she did not talk with her
relatives about T2D because they were no longer close: “Over the last year we’ve just become
somewhat estranged, after my mom died. You know, and they just don’t want to hear from me.
I go by and try to talk to them anyway but they really don’t want to talk to me, really.” (3, F,
African American)
Those with T2D often preferred to talk with family members and friends who were also
affected with T2D because they felt there would be common shared experiences among them
(n = 9). Participants who indicated that they preferred to talk to a family member or friend
because that person was also T2D affected, had an associate’s degree or less education. One
participant explained that she chose to talk to a close friend about T2D because this friend was
also affected by T2D, “She and I, we’re the same age, we’ve known each other our whole lives
and we both have Type II diabetes, and we found out about the same time.” (10, F, Caucasian)
Three participants chose not to communicate with their family members about T2D because
their family members did not have T2D. The affected participants felt that their unaffected
16
family members would not be able to relate or take T2D seriously because they weren’t
affected by it. One participant explained, “I don’t really talk to my sisters and brothers about it. I
mean it’s kind of hard. I guess I would talk to them but if you never, if you’re not a type 2
diabetic then they can’t relate until they actually walk through your shoes.” (8, F, African
American)
Four participants thought that the family members who might benefit most from
communication about T2D and its risks were too young to understand the information. One
participant expressed that she was concerned about her grandchildren’s risk for getting
diabetes, but when questioned if she had discussed her concerns with him she stated, “No, I
haven’t. They’re not really at the age that I would do that.” (5, F, Caucasian) Others felt some
of their family members would listen to information about T2D and risks, but would not actively
engage in the conversation or give feedback. These participants wanted to engage in
communication about risk with their unaffected family members, but felt that these individuals
would not successfully receive the risk information. One participant explained, “It’s like you talk
to somebody and they don’t really hear you…I can see the wheels turning, she’s [sister] busy,
dialing up a conversation and getting ready to tell me everything she’s been through.” (2, F,
Caucasian)
A few participants stated that communicating about T2D wasn’t a priority with some
family members because these individuals live too far away (n = 3). When the participants get
together with these relatives who live far away, T2D was not a topic that took priority in the
communication process. One participant explained, “But as far as my siblings go, there again,
because of the distance, it’s just – when we talk to each other on the phone, it’s not something
17
that we talk about.” (1, M, Appalachian) Other participants reported that their family members
are too busy with other things going on in their lives to discuss T2D (n = 4). Others reported that
family members were too wrapped up in careers and family or personal issues. One participant
discussed how she chooses not to talk to a cousin because she is dealing with her own sickness:
“People just don’t wanna hear about a whole lot of sickness. It’s not that they don’t care,
they have problems of their own and sometimes some of their problems are so bad, or so
much more than mine, you know you don’t mention that to them. When you got a
cousin that’s dying of cancer you really don’t wanna talk about it, you know?” (20, F,
African American)
Types and flow of familial communication
Communication resulted from affected T2D participants discussing T2D with both
affected and unaffected family members and friends. Often, the type of communication
differed between affected participants and their family members and friends due to maturity
(e.g. developmental stage of unaffected family member) and disease status (e.g. affected or
unaffected with T2D) (See Table 3). Of note, supportive communication between affected
participants and both their affected and unaffected relatives was only reported in Appalachian
and African American populations. Finally, there were some communication themes that
applied to all family members and friends, regardless of disease status and maturity.
Communication between affected participants and younger children:
Some affected participants shared examples of how younger, unaffected children in
their families made sure that the participants were adhering to lifestyle “rules” for T2D. A
participant described how her nephew kept his grandfather, who was affected with T2D, in line
18
with eating habits, “My nephew was 2 or 3 at the time and if he’d catch my dad eating
something he shouldn’t be eating you’d hear his little bare feet come patting through the house
and he’d be like ‘grammy, paw’s eating shugnar’.” (19, F, Appalachian)
Participants often felt that sharing their knowledge about and personal experiences
with T2D would help with risk reduction efforts in their children and grandchildren. A
participant shared that having knowledge about the risks for T2D and then sharing and
reinforcing that knowledge with her children and grandchildren could help reduce their risks of
getting T2D:
“Sister and I, she’ll probably get diabetes too but we might be able to prevent my
daughter and my granddaughter-grandchildren from getting it. If we can teach them,
reinforce with them, show them. Showing is a big deal. You know, then hopefully the
next generation won’t get it until late if they get it at all.” (7, F, Caucasian)
Communication between affected participants and other affected individuals:
Affected participants often commiserated with one another over their experiences with
T2D. One participant indicated that she and her T2D affected sister served as a support system
for one another, “My sister has to keep me with my head up cause like I said she has type II
diabetes too. We just talk to each other and keep each other from being depressed all the time.”
(12, F, African American) Another participant explained how he and his sister, who is also
affected by T2D, encourage each other about diabetes management: “But you know I try to
encourage my sister anyways, we’re probably the closest out of my family. *** and I, you know
we try to encourage each other about eating sweets and kinda watching your diet and uh
making sure we’re taking the medications.” (4, M, Appalachian)
19
Affected individuals would share their personal experiences of living with T2D with one
another, sometimes with the intention of learning new or better ways to manage their T2D.
One participant explained the conversations that she had with a T2D affected coworker about
T2D:
“Well, there’s this girl at work. We speak about it because she’s got diabetes; she’s not
managing hers very well. I discuss with her and I guess I’m telling her about my journey
and how she can try to do things and make things better for herself. So I discuss that
with her.” (14, F, African American)
T2D affected individuals also created support networks with other T2D affected
individuals. One participant talked about how she and several of her coworkers supported each
other through their diabetic journey:
“We jokingly called it our diabetic support group, even though we jokingly called it that I
think it was good for all of us, because on days when you just felt like you were pounding
your head against the wall no matter what you did, you just couldn’t control your
numbers, you had someone there who understood.” (19, F, Appalachian)
Supportive communication between affected participants and unaffected adult relatives:
T2D affected individuals reported that they received both tangible and verbal support
from their unaffected family members. Often unaffected family members encouraged their T2D
affected family members to make good lifestyle choices. A participant shared,
“Well we eat dinner every week and my dad has gone from regular hot dogs to fat free.
And my mom tries to make the side dishes with me in mind. She makes tea, and makes

20
unsweetened tea for me and then everybody else has the sweet tea.” (15, F,
Appalachian)
Unaffected family members also provided support to their affected relatives by showing
concern about their affected relatives’ health and well-being. One participant talked about how
her son always checks in with her about her T2D, “He’s (son) always asking me ‘Momma are
you taking your medicine? Is there anything I can do?’” (6, F, African American)
Risk communication between affected participants and unaffected adult relatives:
About half of the affected participants (n = 12) reported that they communicate with
unaffected family members about T2D because they want to help reduce the risk of T2D from
occurring in these family members. Some participants felt that simply sharing what they knew
about T2D and how they manage their T2D would be helpful information for unaffected family
members. One participant explained,
“Well if I need to mention it (T2D) to them (unaffected family members) or it comes up in
conversation or something, then I’ll tell them what I know. I will do what I can to give
them guidance or help…I don’t know everything about it, but I know what kind of sort of
works for me.” (11, M, Caucasian)
A few participants specified that they thought using scare tactics were the best way to
bring about a change in behaviors that could lead to risk reduction in unaffected family
members. One of these participants shared, “I do mention to them (daughters), ‘Ok, get that
weight off of you. You know I’m diabetic, it runs through the family.’ You know, I try to scare
them up, my two daughters.” (14, F, African American)
Barriers to communication between affected participants and unaffected adult relatives:
21
Affected participants also reported that there were several barriers to communicating
with their unaffected relatives. Some participants (n = 4) reported that unaffected family
members tended to avoid having discussions about T2D with them because these relatives did
not want to discuss scary or negative topics. One affected participant explained that his kids
tried to avoid potentially negative topics:
“My wife and I have wanted to discuss funeral plans with them down the road and they
don’t even want to discuss that. I guess they operate under the philosophy that no news
is good news. They don’t really want to discuss that. So if I sit down with them and
discuss diabetes, I’d be beatin’ my head against the wall.” (18, M, Caucasian)
Two participants talked about how some of their unaffected family members just did
not engage in communication about T2D, for unknown reasons. One woman tried to talk to her
unaffected son, but was not successful, “He really don’t say much about it. He just don’t, I don’t
know. He don’t really feel here nor there about it…He just don’t talk about it.” (12, F, African
American)
One participant shared that she believes her children are not open to discussing T2D
because they don’t think it could happen to them: “I just think they think it couldn’t affect them
like it’s affected me. Just because mommy got it or big grandma got it, that ain’t gonna happen
to me.” (6, F, African American) Another participant stated that her kids felt like it was
“personal attack against them” if she tried to discuss their risk for T2D. When discussing her
daughter’s weight, the daughter became defensive:
“I said, ‘But you know you could really afford to lose some weight because you don’t
want to become diabetic.’ And she immediately was like, she took offense to it, she was
22
like ‘Well you just-the older you get, you just become more rude, I just can’t believe that
you’re so rude to tell me about losing weight.’” (3, F, African American)
One participant also shared that she did try to talk to her daughter about T2D, but her
daughter did not think she was at risk, so the participant does not try to talk to her daughter
anymore about T2D: “I brought it up once before and she told me that she’s not worried about
these type 2 diabetes and that’s why I don’t talk to her anymore.” (12, F, African American)
Communication between affected participants and all family members and friends:
Some affected participants reported that emergency preparation was discussed with all
family members and friends. Four participants shared that they wanted their relatives to be
prepared in the event that they a bad complication of T2D occurred. For example, one person
explained:
“I mean, because I almost died last year, we’ve already talked about the end of life
decisions, you know, so I’ve got a living will and I’ve already told the kids that because of
the diabetes…’Well we may have to do that and thank you but I don’t really want to.’ So
I talked to my sister, my kids, my grandkids.” (7, F, Caucasian)
In a few instances affected participants had a difficult time discussing T2D with all family
members and friends, regardless of maturity and disease status. A fatalistic attitude was
described in one family due to the amount of family members already affected by T2D. The
participant from this family explained:
“We all saw how it affected other family members and uh that’s probably another
reason why we don’t talk about it so much because we’ve been through it so much, so
23
many times, with so many other family members that we all kinda shrug our shoulders
and go that’s diabetes, that’s life. We just have to deal with it.” (19, F, Appalachian)
A few participants (n= 3) suggested a threshold of severity related to their T2D had to be
reached before family members placed importance on discussing T2D. These participants felt
like once this threshold was met, T2D would become a priority, and families would therefore
have to be faced with the saliency of T2D and engage in communication about T2D as a result.
For example, when asked why T2D was not discussed with her unaffected sister one participant
stated, “Unless I was in the hospital facing something imminent, she (sister) wouldn’t want to
hear about it, she wouldn’t want to talk about it.” (19, F, Appalachian) Two participants
reported that their families only discussed T2D right after they were diagnosed. T2D was not
discussed again after the diagnosis, because there was nothing new to discuss: “I mean when I
was first diagnosed (we talked about T2D), but not anymore after that. It’s not like ‘Hey, how’s
that going?’ Nobody questions and I don’t really have to talk to them about it.” (13, F, African
American)
Role of family and the role of society in communication about T2D risk
All participants were asked how they thought communication about T2D and risks could
be increased within at-risk families. Participants reported several ways that at-risk families
could take an active role in increasing communication and reducing risks in their own families.
They also provided many suggestions on how society could potentially take an active role in
increasing communication and reducing risks in at-risk families.
Many participants (n = 9) thought that if unaffected family members looked at
educational materials about T2D, these materials would help create an awareness or reality
24
about the risks for developing T2D and the complications associated with T2D. Participants
thought this awareness could help increase communication about T2D and its risks among
family members. One participant suggested that reading something that paints a realistic
picture of the negative side of T2D might be helpful for his unaffected relatives, “Is there
literature that they could read to say they were a threat? Maybe if they got somethin’ like that,
they’d read it and it might shake ‘em up a little bit or show them the results of diabetes.” (9, M,
Caucasian) Also, one participant cited improved knowledge as a way to bring about risk-
reducing behaviors: “I think if my parents had the knowledge that I have now about diabetes,
they could have or they would have…have taken better choices, made better choices.” (17, F,
Appalachian)
Some participants (n = 3) suggested using family gatherings as way to increase
communication about T2D. One participant said that when families get together they need to
discuss family health history: “I think when you start talking about family history, you know
when you sit down with your children or your brothers or sisters, they need to talk about the
family history and the things that are going on in the family. My children know their family
health history.” (20, F, African American) Another participant said that she thought creating a
genealogical health chart to send to family members would be a good way to increase
communication, “And I did suggest to them that we do a health, uh a genealogical health chart,
you know…and send that to each of the family members.” (3, F, African American)
When asked about ways to increase communication in her family, another participant
thought that she would need to overcome T2D in order to get her family members talking:
“(Increase communication) within my family? Probably that I would be able to overcome where I
25
am now. I think they would be inspired and see what good eating and exercise does.” (15, F,
Appalachian)
When asked about ways to reduce the risk of developing T2D in their families, the
majority of participants (n = 15) responded that changing lifestyle factors would be the best
way to reduce risk, including watching diet and increasing activity. A participant shared:
“Try to get them involved in healthier lifestyles. If you’re big on going out and walking up
and down the street or in the park or whatever, try to get them to go with you. Try to
encourage them to eat the right kind of foods…you just have to eat in moderation or
very limited quantities.” (11, M, Caucasian)
Some participants suggested that reducing risks were the responsibility of those with
T2D. One woman said; “You can do something about it if you want to. But you have to have the
wanting. Just like any other disease, it can be treated if it’s caught in time.” (17, F, Appalachian)
Another woman, who takes T2D medications and has made better lifestyle choices in terms of
diet and exercise, displayed anger that her sibling who also had T2D had not made more of an
effort to control the disease: “She’s (participant’s sister) not here anymore because she chose
not to be. She chose to accept the fact that she was gonna die anyways….but had you sought
more treatment or not refused your treatment, then maybe you’d still be here.” (6, F, African
American)
There was also mention of societal interventions that could help increase
communication about and reduce risks for T2D among at-risk families. Two African American
participants said that if T2D was discussed at church, then families would take the disease more
seriously and increase their communication about it. For example, one participant said, “If the

26
church took on as much emphasis of lifestyles as they do the teachings of God, then maybe we’d
know that if we don’t take care of our bodies, they’re not going to take care of us.” (8, F,
African American)
Several participants (n = 4) felt strongly that actions to reduce risk should start early in
the schools. One participant suggested: “Show them (kids in school) what happens, you
know…why their body needs, you know, those sugars for energy and what are good and what
are bad and what can happen. It might stick with them.” (2, F, Caucasian)
One participant suggested that there is a negative stereotype attached to individuals
who have T2D, and getting rid of this negative stereotype would help increase communication.
“I think there’s a stigma on the disease that it attacks people who are overweight and
therefore people think they’re lazy and they brought it on themselves type thing. It’s not
cancer that just hits anybody and everybody. I think there’s a stigma attached to it…I
think if people didn’t judge others by thinking like that, you have this disease so
therefore I judge you as being fat or lazy or whatever, if they just said, ‘Yeah that’s what
you have. Ok, how do you deal with it? What do you do?’ it would be different.” (5, F,
Caucasian)
Perceived cause of T2D
Many of the participants (n = 15) indicated that the cause of T2D in their families was
due to factors over which they had no control, such as genetics and ethnicity, whereas about
half of the participants (n = 11) listed lifestyle factors as the cause of T2D in their families. The
two individuals who reported their race/ethnicity as a risk factor were African American
females. Only 7 individuals recognized that the T2D in their families could be caused by a
27
combination of lifestyle and uncontrollable factors. For example, when asked about the cause
of diabetes in her family one participant said, “I think some of it is inherited and some of it is
just poor choices that you make.” (17, F, Appalachian)
There seemed to be disagreement between perceived cause of T2D in families and
perceived reasons why unaffected family members were at-risk for T2D. Despite many
participants reporting the perceived cause of T2D in their families as genetics, many individuals
identified lifestyle factors as playing a role in risk for family members. For example, one of the
participants who originally reported genetics as the perceived cause of the diabetes in her
family, “what I know is that it’s genetic based…just the fact that one person had it, it can trickle
down, we just don’t know when and how,” identified lifestyle factors as the reason for her
perceived risk for her grandson, “*** is 13 and he’s borderline obese. And if he’s borderline
obese, that means he has the potential to be diabetic.” (6, F, African American) When looking
at differences in responses across themes based on family risk category, those individuals who
reported genetics as the cause of T2D in their families were from either a high risk or moderate
risk family.
Discussion
Patenaude, et al., suggested that as the need for preventive programs for individuals at
increased genetic risk of disease grows, the need for research related to how people
understand risk, how they communicate risk information and health concerns within their
families, and how awareness of risk affected self-management of health will grow as well [19].
To our knowledge, our study was the first to examine the different characteristics within
families at-risk for T2D that facilitate or impede communication about the risks for developing
28
T2D, as well as the types and flow of communication in at-risk T2D families. Results indicate
future directions and efforts for genetic counseling practice and health education.
In genetic counseling practice, common, chronic diseases are noted frequently when
taking a family history from a patient. Therefore, a genetic counseling session is an ideal
platform for discussing risks for T2D based on FHH. A previous study looked at the effectiveness
of genetic counseling techniques focused on communicating T2D risk in at-risk families [20].
Participants in this study reported favorable perceived control of and satisfaction with a genetic
counseling session that incorporated clinical recommendations and lifestyle changes to address
T2D risk. The current study demonstrates that family dynamics can facilitate or impede
communication about T2D, and that the types and flow of communication vary based on
maturity and disease status of family members. Genetic counselors can assess family dynamics,
disease status, and development stage to more effectively develop strategies for disseminating
T2D risk information amongst family members.
Furthermore, patients could benefit from having conversations with genetic counselors about
how to facilitate discussion with their family members about T2D disease risk.
This study also reported many findings about communication in T2D at-risk families that
can inform health education practices. One element to think about for health education is the
audience, specifically the characteristics of the audience that could potentially change the
effectiveness of interventions. This study found that T2D affected individuals have different
types of relationships amongst family members (affected vs. unaffected), and that
communication about T2D changes based on these relationships. Affected T2D participants
demonstrated homophily in their preference to discuss T2D with other affected family
29
members or friends, as opposed to unaffected relatives and friends. The participants suggested
that an unaffected relative would not be able to relate to the participants’ experience with the
disease. Other studies have also noted homophily as a variable in risk communication [8, 21].
Participants also chose to discuss T2D with individuals with whom they shared a close bond,
and chose not to discuss T2D with certain relatives because they did not share a close bond.
Understanding the structure of close ties in the family might identify pathways of information
exchange in at-risk T2D families. These pathways of communication can be then targeted for
interventions that aim to deliver information about risks and risk reducing behaviors to at-risk
families.
Our study also found that affected individuals from Appalachian and African American
populations more often engaged in supportive communication with relatives than Caucasian
families; this finding speaks to the possibility of higher family cohesion in Appalachian and
African American families. Support, encouragement and sharing experiences could serve as
methods to teach unaffected relatives about risks and complications associated with T2D in
families with high cohesion. If an unaffected relative is providing support and/or
encouragement to their affected family member, the unaffected relative may also learn about
lifestyle modifications that are used in the management of T2D. Future studies could look at
how supportive relationships that exist between affected and unaffected relatives teach
unaffected relatives risk reducing strategies.
Another finding from this study relates to communication about T2D between older and
younger individuals in at-risk families. Affected individuals had a strong desire for risk reduction
in children and grandchildren, indicating a sense of duty to these younger generations [9]. One
30
explanation may be that some affected individuals who are older may be entrenched in their
bad behaviors related to T2D and decide to focus on younger individuals who are not set in
their ways. Starting risk reduction efforts early may be critical to obtaining the most successful
adoption of risk reducing behaviors that could help in the prevention of T2D.
When looking to implement health interventions, the potential barriers are a second
element to take into consideration. There were many familial characteristics reported that act
as barriers to communication about T2D between affected participants and unaffected adult
relatives. Many participants stated that their unaffected relatives tried to avoid potentially
negative or scary conversations about disease and some seemed to be generally uninterested
in the topic of T2D. Saliency of T2D also seems to impede communication in at-risk families
[22]. Some participants reported that their unaffected relatives didn’t think that T2D could
affect them and that they would not be willing to discuss T2D unless a significant health event
occurred. Future research should aim to investigate what would make T2D more salient for
unaffected individuals in families at-risk for T2D, in the absence of a significant health event.
One participant explained how fatalism was a variable that was present in her at-risk family.
This participant discussed her family’s acceptance of T2D as fate, and cited this belief as the
reason her family did not discuss the risks of developing T2D. The participant was self-reported
Appalachian, which may play a role, as fatalistic attitudes have been cited previously in
Appalachian populations [23]. Geographic location of a relative was another variable that
hindered communication; this variable has also been identified as a barrier in other familial
communication studies [8, 9, 21]. Because geographic location is consistently cited as a barrier

31
to communication, efforts to understand how and why distance seems to create gaps in
relationships would be important.
A third element of health education to think about is tailoring interventions based on a
person’s familial and social environments. An article on adolescent obesity proposed
implementing multiple interventions simultaneously to target family and social influence [24].
The interventions focused on 3 settings: the household and the child’s family outside the
household, the neighborhood and community, and the school.
When asked about ways to increase communication about and reduce the risk of T2D in
at-risk families, participants in this study suggested a few different strategies, including ones
that involve families taking action. Many of the individuals suggested that awareness about T2D
could be increased by family members reading educational materials about T2D, and that this
awareness could then lead to a change in lifestyle in unaffected relatives. Using FHH to facilitate
discussion about risks for disease has also been suggested to increase communication about
T2D risks [6-10]. Some participants agreed with the utility of FHH as a method to increase
communication, and said that talking to their families about their family’s history of T2D is
important; discussions about FHH can help encourage unaffected relatives to take steps to
improve health and reduce the risks of developing T2D. Finally, respondents felt that
unaffected relatives could make lifestyle and behavior changes to help reduce risk. Other
studies have also noted the success of making lifestyle and behavior changes for risk reduction
[2, 3].
Participants also suggested ways that society could help increase communication about
T2D, including discussion in schools to generate T2D awareness and communication. Two
32
African American participants suggested that talking about T2D in churches may help
encourage unaffected individuals who are at-risk to start talking about T2D within their
families. Targeting churches within African American communities may be a good starting point
for developing interventions to increase T2D communication.
Another suggestion that emerged from this study is that there is a negative stigma
associated with individuals who have T2D, and this stigma hinders affected T2D individuals from
wanting to disclose their diagnosis with T2D or talk about T2D with others. This participant
postulated that if society were more informed and took a less judgmental stand on their views
of individuals with T2D, then more affected individuals would be willing to talk about their
experiences with T2D. Future studies could target individuals affected with T2D and focus on
finding out whom in society, specifically, creates this negative environment for the affected
individuals (i.e. healthcare providers, family members, or the general public). This knowledge
could provide direction of who would be best to target with efforts to increase awareness and
sensitivity towards individuals with T2D.
A final consideration for health education is to understand how an individual’s
perception of the cause of T2D can influence how they communicate about T2D within their
families. We found discordance in the perceived cause and perceived risk of T2D. While many
respondents felt that the cause of T2D in their family was due to uncontrollable factors such as
genetics and ethnicity, they also perceived their unaffected relatives to be at-risk for T2D due to
lifestyle factors. Future research could include quantitative studies that look at these reported
differences between perceived cause and perceived risk of T2D in at-risk families, because
these differences could potentially be affecting communication about risk in families.

33
Limitations
Our study also aimed to identify racial/cultural differences in communication patterns
within at-risk families; however the only trend noted to have differences across populations
was support. For future studies, there is a need for larger samples to address racial/cultural
trends. A smaller sample size is expected with a qualitative design; however, this limits external
generalization of the findings. Also, qualitative studies cannot establish causality, so it cannot
be concluded that the variables developed in this study affect communication. There were
multiple interviewers, which could result in interviewer bias. Attempts to limit this bias were
made by training all interviewers in qualitative interviewing techniques, and having them
conduct practice interviews before collecting data.
This study had a majority of female participants, who tend to be more often involved in
communication over males. Future qualitative studies could investigate whether
communication variables change with a predominantly male population of affected T2D
participants. All families reported some level of communication about T2D, so families who are
not actively engaging in communication about T2D were not examined. Future studies could
target at-risk families who are not communicating about T2D to identify additional variables
that may be associated with a lack of communication. Finally, this study only presents the
perspectives of individuals affected with T2D. Future studies could examine similar themes
from the perspectives of unaffected individuals in families at-risk for T2D.
34
References
1. Prevention, C.f.D.C.a., National Diabetes Fact Sheet: General Information and National Estimates on Diabetes in the United States 2011, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA.
2. Knowler, W.C., et al., Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med, 2002. 346(6): p. 393-403.
3. Tuomilehto, J., et al., Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med, 2001. 344(18): p. 1343-50.
4. Boyle, J.P., et al., Projection of the year 2050 burden of diabetes in the US adult population: dynamic modeling of incidence, mortality, and prediabetes prevalence. Popul Health Metr, 2010. 8: p. 29.
5. Valdez, R., et al., Family history and prevalence of diabetes in the US population: 6-year results from the National Health and Nutrition Examination Survey (NHANES, 1999 2004). Diabetes, 2007.
6. Harris, J.N., et al., Using a family systems approach to investigate cancer risk communication within melanoma families. Psychooncology, 2010. 19(10): p. 1102-11.
7. Harrison, T.A., et al., Family history of diabetes as a potential public health tool. Am J Prev Med, 2003. 24(2): p. 152-9.
8. Loescher, L.J., J.D. Crist, and L.A. Siaki, Perceived intrafamily melanoma risk communication. Cancer Nurs, 2009. 32(3): p. 203-10.
9. McCann, S., et al., Family communication, genetic testing and colonoscopy screening in hereditary non-polyposis colon cancer: a qualitative study. Psychooncology, 2009. 18(11): p. 1208-15.
10. Yoon, P.W., et al., Can family history be used as a tool for public health and preventive medicine? Genet Med, 2002. 4(4): p. 304-10.
11. Qureshi, N. and J. Kai, Informing patients of familial diabetes mellitus risk: How do they respond? A cross-sectional survey. BMC Health Services Research, 2008. 8(37).
12. Pijl, M., et al., Impact of communication familial risk of diabetes on illness perceptions and self-reported behavioral outcomes. Diabetes Care, 2009. 32(4): p. 3.
13. Royak-Schaler, R., et al., Breast and colorectal cancer risk communication approaches with low-income African-American and Hispanic women: implications for healthcare providers. J Natl Med Assoc, 2004. 96(5): p. 598-608.
14. Whitford, D.L., H. McGee, and B. O'Sullivan, Reducing health risk in family members of patients with type 2 diabetes: views of first degree relatives. BMC Public Health, 2009. 9(455).
15. Patton, M.Q., Qualitative Evaluation and Research Methods. 2 ed1990, Newbury Park, CA: Sage Publications.
16. Ersig, A.L., et al., Explanations of Risk in Families Without Identified Mutations for Hereditary Nonpolyposis Colorectal Cancer. Journal of Nursing Scholarship, 2010. 42(2): p. 8.
17. Ayres, L., K. Kavanaugh, and K.A. Knafl, Within-Case and Across Case Approaches to Qualitative Data Analysis. Qualitative Health Research, 2003. 13(6): p. 13.
18. Landis, J.R. and G.G. Koch, The measurement of observer agreement for categorical data. Biometrics, 1977. 33(1): p. 159-74.
19. Patenaude, A.F., A.E. Guttmacher, and F.S. Collins, Genetic testing and psychology. New roles, new responsibilities. Am Psychol, 2002. 57(4): p. 271-82.
20. Waxler, J.L., et al., Genetic Counseling as a Tool for Type 2 Diabetes Prevention: A Genetic Counseling Framework for Common Polygenetic Disorders. J Genet Couns, 2012.
35
21. Ashida, S., et al., Family Health History Communication Networks of Older Adults: Importance of Social Relationships and Disease Perceptions. Health Educ Behav, 2013.
22. Walter, F.M., et al., Lay understanding of familial risk of common chronic diseases: a systematic review and synthesis of qualitative research. Ann Fam Med, 2004. 2(6): p. 583-94.
23. Cree, R.A., et al., Decisions to seek healthcare based on family health history among urban Appalachian women. J Genet Couns, 2009. 18(6): p. 534-50.
24. Koehly, L. and A. Loscalzo, Adolescent Obesity and Social Networks. Preventing Chronic Disease: Public Health Research, Practice and Policy, 2009. 6(3).
36
Appendix A
Qualitative Interview Guide
For this portion of the study, I have some questions for you about Type II Diabetes. These questions are meant to be discussion-based: please be open and honest and feel free to share as much detail as you feel comfortable. There are no right or wrong answers, we just want to hear your perspective about diabetes, how it has impacted your life and who you talk to about diabetes. Just to remind you, the information that you provide will not be shared with your family members. In order for me to better remember what we discussed, the interview will be audio recorded. Do you give consent to participate in a recorded interview? 1. Can you start by telling me about your experiences with diabetes?
2. Tell me more about how diabetes has impacted your life?
3. How do you feel about diabetes?
4. Who in your family has diabetes?
a. What do you think causes diabetes in your family?
5. Who do you talk to about diabetes? a. If family members aren’t mentioned – Do you talk to any of your family members about
diabetes? b. What do you talk about related to diabetes? c. Are there family members who you don’t talk to about diabetes? Why? d. What are the challenges to talking with your family members about diabetes?
6. Do you think any of your family members are at risk of developing diabetes?
a. Why do you think they are at risk? b. If participant NOT diagnosed with diabetes – Do you think that you are at risk for developing
diabetes? Why?
7. What do you think could be done to help increase communication about diabetes within your family?
a. What do you think would work for another family?
8. What do you think could be done to help reduce the risk of developing diabetes (in family members)?
a. What do you think would work for another family?
9. Thank you for answering these questions. Is there anything else you think it is important for me to know about diabetes and your family?
37
Appendix B
Codebook
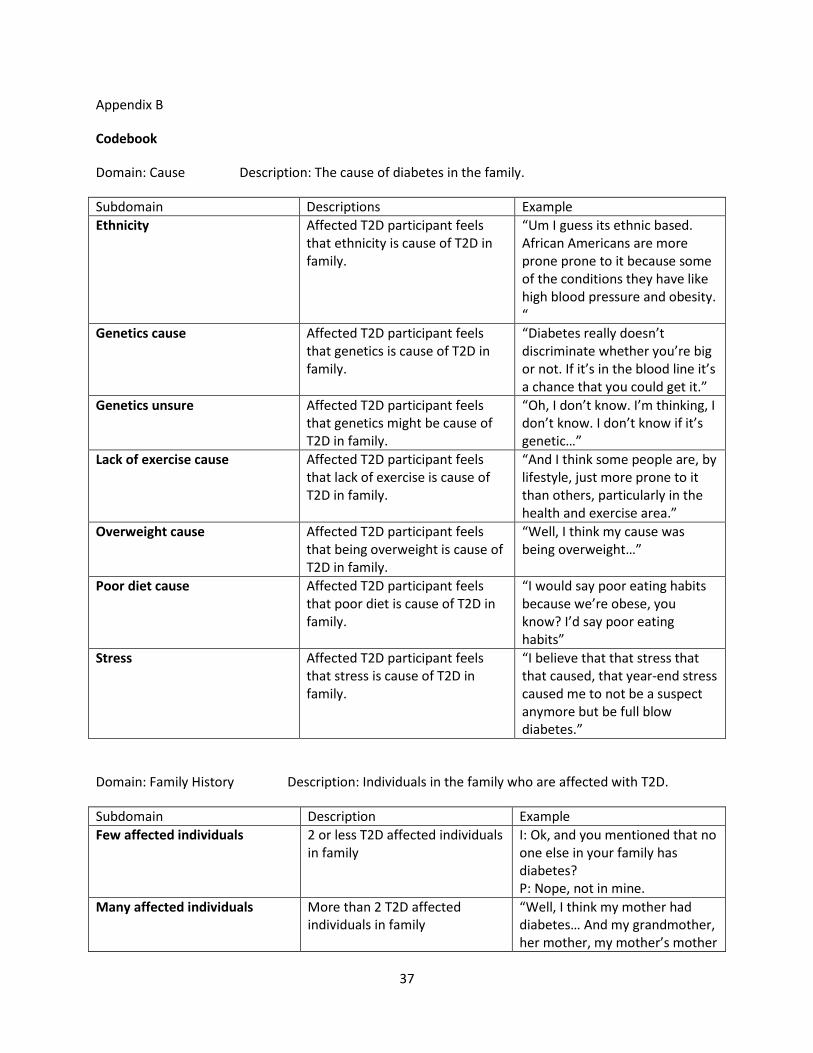
Domain: Cause Description: The cause of diabetes in the family.
Subdomain Descriptions Example
Ethnicity Affected T2D participant feels that ethnicity is cause of T2D in family.
“Um I guess its ethnic based. African Americans are more prone prone to it because some of the conditions they have like high blood pressure and obesity. “
Genetics cause Affected T2D participant feels that genetics is cause of T2D in family.
“Diabetes really doesn’t discriminate whether you’re big or not. If it’s in the blood line it’s a chance that you could get it.”
Genetics unsure Affected T2D participant feels that genetics might be cause of T2D in family.
“Oh, I don’t know. I’m thinking, I don’t know. I don’t know if it’s genetic…”
Lack of exercise cause Affected T2D participant feels that lack of exercise is cause of T2D in family.
“And I think some people are, by lifestyle, just more prone to it than others, particularly in the health and exercise area.”
Overweight cause Affected T2D participant feels that being overweight is cause of T2D in family.
“Well, I think my cause was being overweight…”
Poor diet cause Affected T2D participant feels that poor diet is cause of T2D in family.
“I would say poor eating habits because we’re obese, you know? I’d say poor eating habits”
Stress Affected T2D participant feels that stress is cause of T2D in family.
“I believe that that stress that that caused, that year-end stress caused me to not be a suspect anymore but be full blow diabetes.”
Domain: Family History Description: Individuals in the family who are affected with T2D.
Subdomain Description Example
Few affected individuals 2 or less T2D affected individuals in family
I: Ok, and you mentioned that no one else in your family has diabetes? P: Nope, not in mine.
Many affected individuals More than 2 T2D affected individuals in family
“Well, I think my mother had diabetes… And my grandmother, her mother, my mother’s mother
38
had diabetes. My nephew actually has diabetes…”
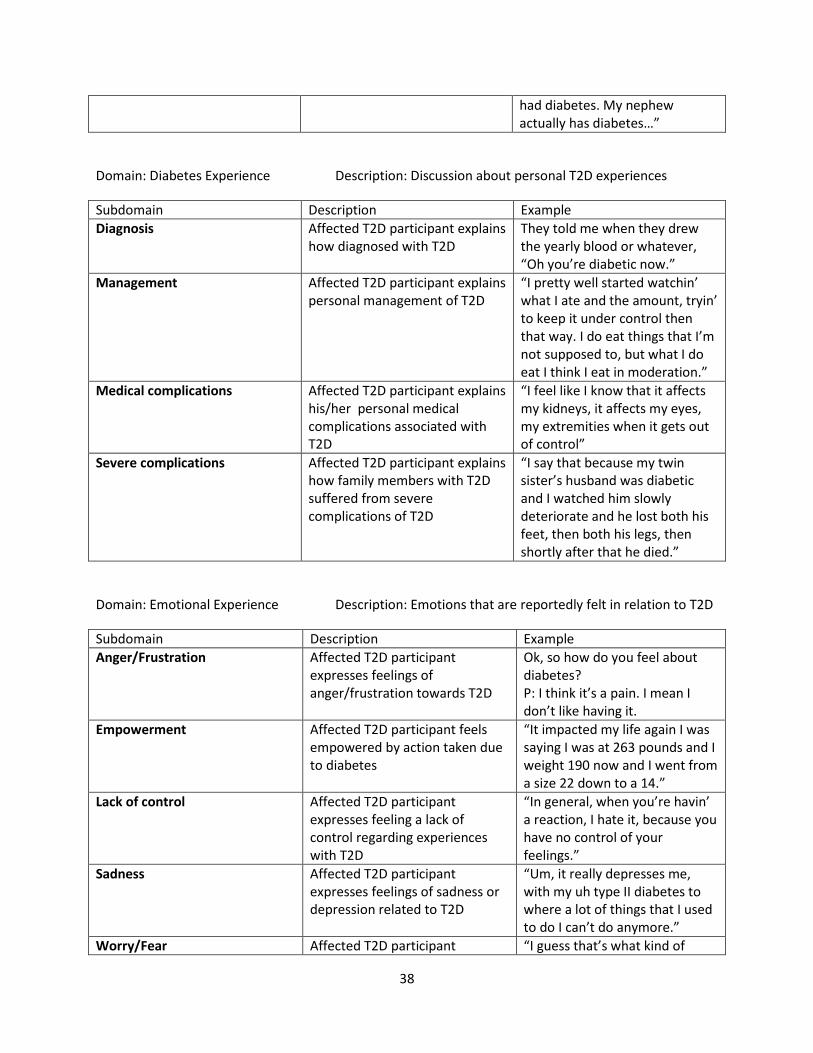
Domain: Diabetes Experience Description: Discussion about personal T2D experiences
Subdomain Description Example
Diagnosis Affected T2D participant explains how diagnosed with T2D
They told me when they drew the yearly blood or whatever, “Oh you’re diabetic now.”
Management Affected T2D participant explains personal management of T2D
“I pretty well started watchin’ what I ate and the amount, tryin’ to keep it under control then that way. I do eat things that I’m not supposed to, but what I do eat I think I eat in moderation.”
Medical complications Affected T2D participant explains his/her personal medical complications associated with T2D
“I feel like I know that it affects my kidneys, it affects my eyes, my extremities when it gets out of control”
Severe complications Affected T2D participant explains how family members with T2D suffered from severe complications of T2D
“I say that because my twin sister’s husband was diabetic and I watched him slowly deteriorate and he lost both his feet, then both his legs, then shortly after that he died.”
Domain: Emotional Experience Description: Emotions that are reportedly felt in relation to T2D
Subdomain Description Example
Anger/Frustration Affected T2D participant expresses feelings of anger/frustration towards T2D
Ok, so how do you feel about diabetes? P: I think it’s a pain. I mean I don’t like having it.
Empowerment Affected T2D participant feels empowered by action taken due to diabetes
“It impacted my life again I was saying I was at 263 pounds and I weight 190 now and I went from a size 22 down to a 14.”
Lack of control Affected T2D participant expresses feeling a lack of control regarding experiences with T2D
“In general, when you’re havin’ a reaction, I hate it, because you have no control of your feelings.”
Sadness Affected T2D participant expresses feelings of sadness or depression related to T2D
“Um, it really depresses me, with my uh type II diabetes to where a lot of things that I used to do I can’t do anymore.”
Worry/Fear Affected T2D participant “I guess that’s what kind of
39
expresses feelings of worry or fear related to T2D
scared me when I found out I had it, because my father was just out of control.”
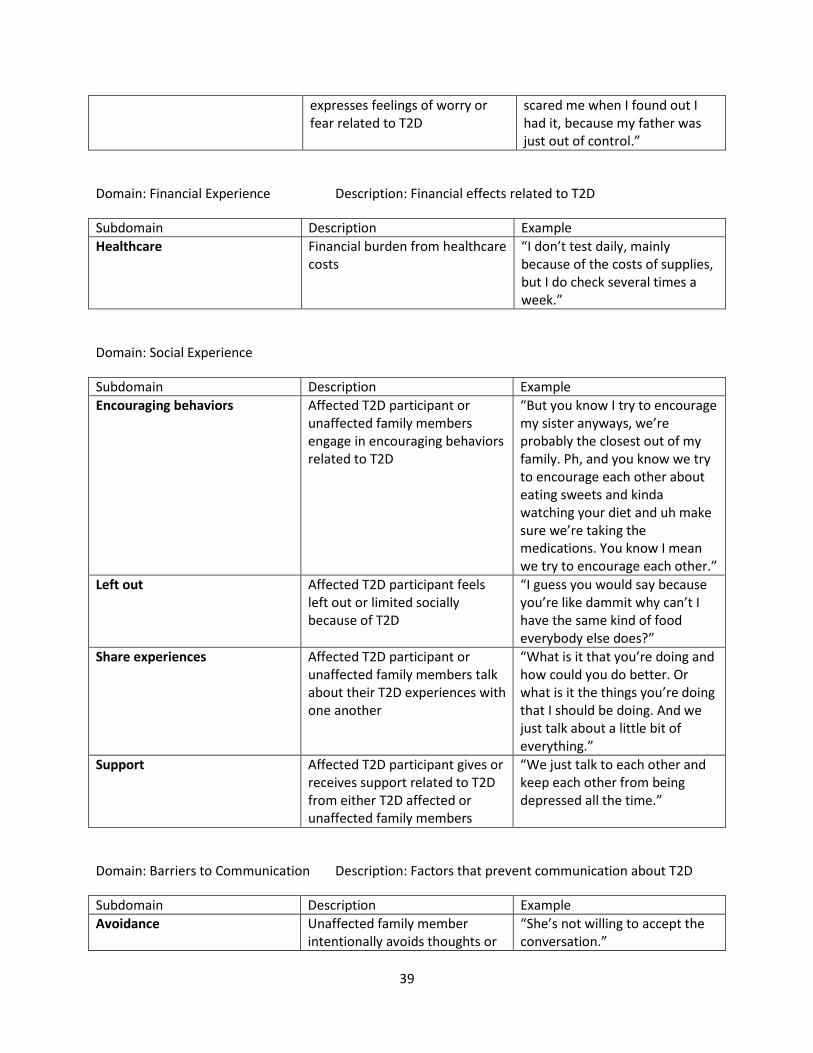
Domain: Financial Experience Description: Financial effects related to T2D
Subdomain Description Example
Healthcare Financial burden from healthcare costs
“I don’t test daily, mainly because of the costs of supplies, but I do check several times a week.”
Domain: Social Experience
Subdomain Description Example
Encouraging behaviors Affected T2D participant or unaffected family members engage in encouraging behaviors related to T2D
“But you know I try to encourage my sister anyways, we’re probably the closest out of my family. Ph, and you know we try to encourage each other about eating sweets and kinda watching your diet and uh make sure we’re taking the medications. You know I mean we try to encourage each other.”
Left out Affected T2D participant feels left out or limited socially because of T2D
“I guess you would say because you’re like dammit why can’t I have the same kind of food everybody else does?”
Share experiences Affected T2D participant or unaffected family members talk about their T2D experiences with one another
“What is it that you’re doing and how could you do better. Or what is it the things you’re doing that I should be doing. And we just talk about a little bit of everything.”
Support Affected T2D participant gives or receives support related to T2D from either T2D affected or unaffected family members
“We just talk to each other and keep each other from being depressed all the time.”
Domain: Barriers to Communication Description: Factors that prevent communication about T2D
Subdomain Description Example
Avoidance Unaffected family member intentionally avoids thoughts or
“She’s not willing to accept the conversation.”

40
conversations about T2D
Can’t happen to me barrier Unaffected family member feels that diabetes can’t happen to them
“I just think they don’t think it could affect them like it’s affected me. Just because mommy got it or big grandma got it, that ain’t gonna happen to me.”
Distance Lack of communication between affected T2D participant and unaffected family member due to distance
“My family, I have a sister in Boston, Massachusetts. I have a brother in Charleston, Indiana and one in Louisville and one in Lexington. So it’s not like we’re centrally located where we can get together and talk.”
Lack of engagement Attempted discussion with unaffected family member, but the person doesn't give feedback or seem to listen
“My sister, though, I don’t talk a whole lot to her, she’s a somewhat introverted and basically she doesn’t really- it’s more of a one-sided conversation with her.”
Lack of salience Unaffected family member unwilling or unable to grasp seriousness of diabetes because he/she has no firsthand experience with the disease
“I guess they don’t take it as serious because they’re not a diabetic.”
Lack of understanding Unaffected family member would not understand due to age or mental capacity
I: Do you ever talk to her about t2d? P: No because I basically manages everything that goes on around her because she’s mentally handicapped. And some of the things she wouldn’t understand.
Lecturing Unaffected family member feels like he/she is being talked down to or preached to
“Yeah. They consider things when I say you need to stop smoking or you need to stop drinking, they feel like I’m preaching to them. And I’m not. “
No close bond No communication between affected T2D participant and unaffected family member because there is not a close bond between the individuals
“If it wasn’t somethin’ within the confines of the family, I don’t think it’s a subject that you approach, that people talk about.”
No perceived risk Don't talk with unaffected family member because that person
“I brought it up once before and she told me that she’s not
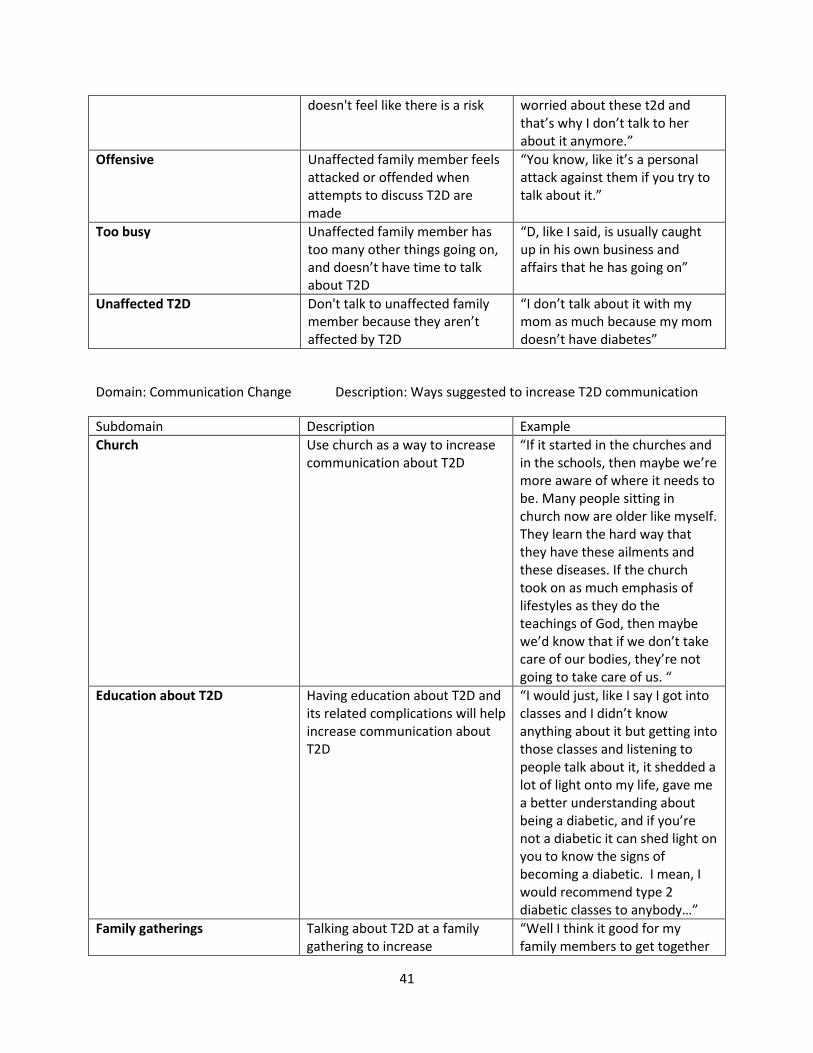
41
doesn't feel like there is a risk worried about these t2d and that’s why I don’t talk to her about it anymore.”
Offensive Unaffected family member feels attacked or offended when attempts to discuss T2D are made
“You know, like it’s a personal attack against them if you try to talk about it.”
Too busy Unaffected family member has too many other things going on, and doesn’t have time to talk about T2D
“D, like I said, is usually caught up in his own business and affairs that he has going on”
Unaffected T2D Don't talk to unaffected family member because they aren’t affected by T2D
“I don’t talk about it with my mom as much because my mom doesn’t have diabetes”
Domain: Communication Change Description: Ways suggested to increase T2D communication
Subdomain Description Example
Church Use church as a way to increase communication about T2D
“If it started in the churches and in the schools, then maybe we’re more aware of where it needs to be. Many people sitting in church now are older like myself. They learn the hard way that they have these ailments and these diseases. If the church took on as much emphasis of lifestyles as they do the teachings of God, then maybe we’d know that if we don’t take care of our bodies, they’re not going to take care of us. “
Education about T2D Having education about T2D and its related complications will help increase communication about T2D
“I would just, like I say I got into classes and I didn’t know anything about it but getting into those classes and listening to people talk about it, it shedded a lot of light onto my life, gave me a better understanding about being a diabetic, and if you’re not a diabetic it can shed light on you to know the signs of becoming a diabetic. I mean, I would recommend type 2 diabetic classes to anybody…”
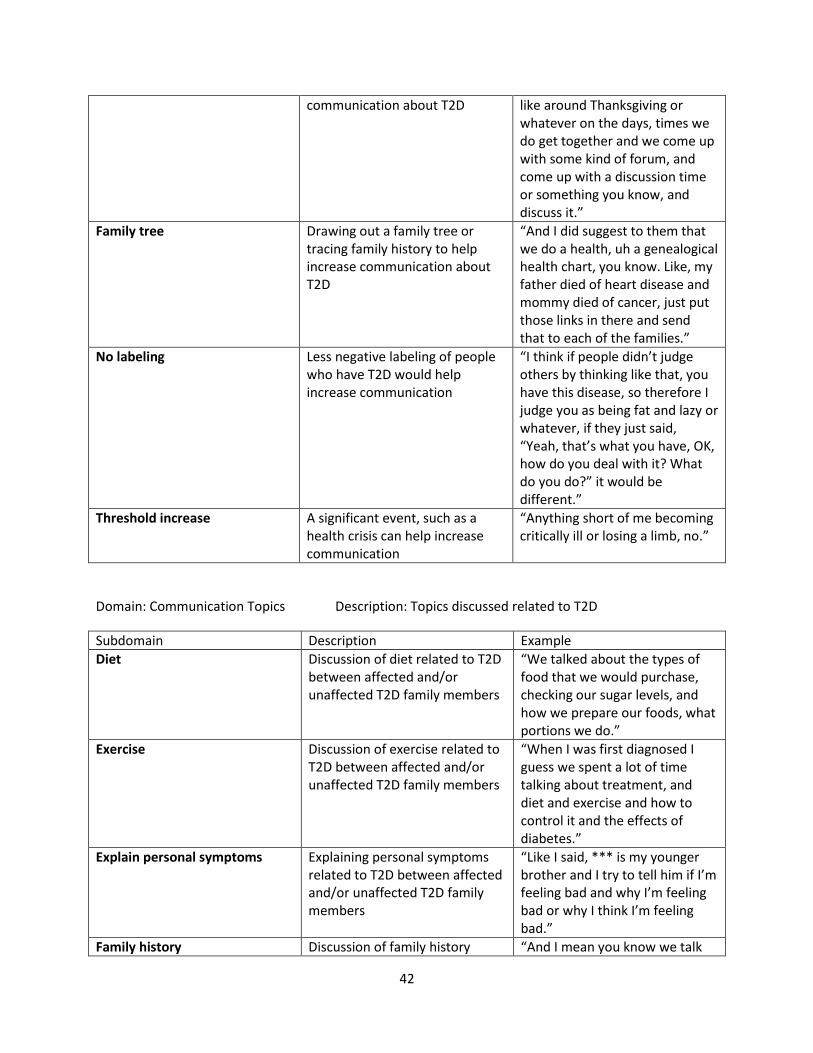
Family gatherings Talking about T2D at a family gathering to increase
“Well I think it good for my family members to get together
42
communication about T2D like around Thanksgiving or whatever on the days, times we do get together and we come up with some kind of forum, and come up with a discussion time or something you know, and discuss it.”
Family tree Drawing out a family tree or tracing family history to help increase communication about T2D
“And I did suggest to them that we do a health, uh a genealogical health chart, you know. Like, my father died of heart disease and mommy died of cancer, just put those links in there and send that to each of the families.”
No labeling Less negative labeling of people who have T2D would help increase communication
“I think if people didn’t judge others by thinking like that, you have this disease, so therefore I judge you as being fat and lazy or whatever, if they just said, “Yeah, that’s what you have, OK, how do you deal with it? What do you do?” it would be different.”
Threshold increase A significant event, such as a health crisis can help increase communication
“Anything short of me becoming critically ill or losing a limb, no.”
Domain: Communication Topics Description: Topics discussed related to T2D
Subdomain Description Example
Diet Discussion of diet related to T2D between affected and/or unaffected T2D family members
“We talked about the types of food that we would purchase, checking our sugar levels, and how we prepare our foods, what portions we do.”
Exercise Discussion of exercise related to T2D between affected and/or unaffected T2D family members
“When I was first diagnosed I guess we spent a lot of time talking about treatment, and diet and exercise and how to control it and the effects of diabetes.”
Explain personal symptoms Explaining personal symptoms related to T2D between affected and/or unaffected T2D family members
“Like I said, *** is my younger brother and I try to tell him if I’m feeling bad and why I’m feeling bad or why I think I’m feeling bad.”
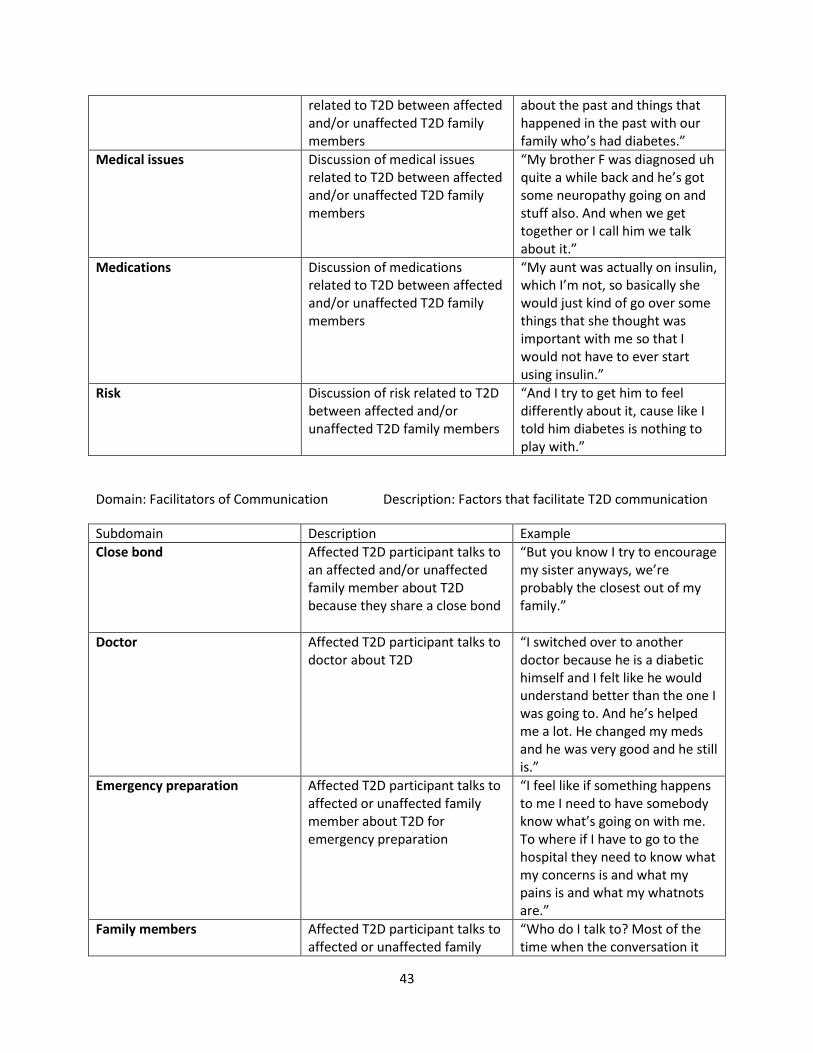
Family history Discussion of family history “And I mean you know we talk
43
related to T2D between affected and/or unaffected T2D family members
about the past and things that happened in the past with our family who’s had diabetes.”
Medical issues Discussion of medical issues related to T2D between affected and/or unaffected T2D family members
“My brother F was diagnosed uh quite a while back and he’s got some neuropathy going on and stuff also. And when we get together or I call him we talk about it.”
Medications Discussion of medications related to T2D between affected and/or unaffected T2D family members
“My aunt was actually on insulin, which I’m not, so basically she would just kind of go over some things that she thought was important with me so that I would not have to ever start using insulin.”
Risk Discussion of risk related to T2D between affected and/or unaffected T2D family members
“And I try to get him to feel differently about it, cause like I told him diabetes is nothing to play with.”
Domain: Facilitators of Communication Description: Factors that facilitate T2D communication
Subdomain Description Example
Close bond Affected T2D participant talks to an affected and/or unaffected family member about T2D because they share a close bond
“But you know I try to encourage my sister anyways, we’re probably the closest out of my family.”
Doctor Affected T2D participant talks to doctor about T2D
“I switched over to another doctor because he is a diabetic himself and I felt like he would understand better than the one I was going to. And he’s helped me a lot. He changed my meds and he was very good and he still is.”
Emergency preparation Affected T2D participant talks to affected or unaffected family member about T2D for emergency preparation
“I feel like if something happens to me I need to have somebody know what’s going on with me. To where if I have to go to the hospital they need to know what my concerns is and what my pains is and what my whatnots are.”
Family members Affected T2D participant talks to affected or unaffected family
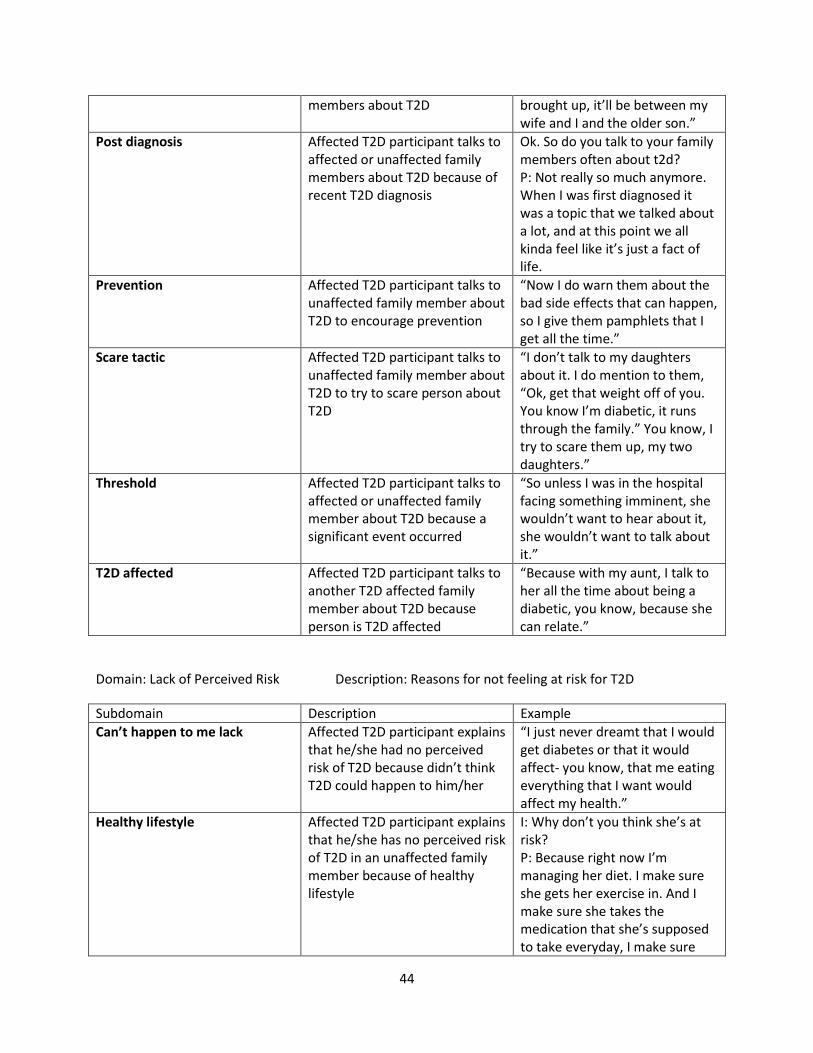
“Who do I talk to? Most of the time when the conversation it
44
members about T2D brought up, it’ll be between my wife and I and the older son.”
Post diagnosis Affected T2D participant talks to affected or unaffected family members about T2D because of recent T2D diagnosis
Ok. So do you talk to your family members often about t2d? P: Not really so much anymore. When I was first diagnosed it was a topic that we talked about a lot, and at this point we all kinda feel like it’s just a fact of life.
Prevention Affected T2D participant talks to unaffected family member about T2D to encourage prevention
“Now I do warn them about the bad side effects that can happen, so I give them pamphlets that I get all the time.”
Scare tactic Affected T2D participant talks to unaffected family member about T2D to try to scare person about T2D
“I don’t talk to my daughters about it. I do mention to them, “Ok, get that weight off of you. You know I’m diabetic, it runs through the family.” You know, I try to scare them up, my two daughters.”
Threshold Affected T2D participant talks to affected or unaffected family member about T2D because a significant event occurred
“So unless I was in the hospital facing something imminent, she wouldn’t want to hear about it, she wouldn’t want to talk about it.”
T2D affected Affected T2D participant talks to another T2D affected family member about T2D because person is T2D affected
“Because with my aunt, I talk to her all the time about being a diabetic, you know, because she can relate.”
Domain: Lack of Perceived Risk Description: Reasons for not feeling at risk for T2D
Subdomain Description Example
Can’t happen to me lack Affected T2D participant explains that he/she had no perceived risk of T2D because didn’t think T2D could happen to him/her
“I just never dreamt that I would get diabetes or that it would affect- you know, that me eating everything that I want would affect my health.”
Healthy lifestyle Affected T2D participant explains that he/she has no perceived risk of T2D in an unaffected family member because of healthy lifestyle
I: Why don’t you think she’s at risk? P: Because right now I’m managing her diet. I make sure she gets her exercise in. And I make sure she takes the medication that she’s supposed to take everyday, I make sure

45
she takes it every day.
No genetics Affected T2D participant had no perceived risk of T2D because genetics was not thought of as cause
“Maybe I just didn’t know that it was hereditary, I mean that it was a possibility that somebody else in the family could have it because she had it.”
Domain: Risk Perception Family Description: Persons in family suspected to be at risk for T2D
Subdomain Description Example
FDR FDR at risk for T2D “Right, and she said to me, she says, “Well the doctor said I don’t have diabetes.” And I said, “No, you could be pre-diabetic.”
SDR SDR at risk for T2D “I think her feeding habits of her grandkids has led to the fact that now her grandson is being tested for diabetes.”
Domain: Risk Perception Why Description: Why family members are thought to be at risk for T2D
Subdomain Description Example
Alcohol risk Affected T2D participant perceives unaffected family member to be at risk for T2D because of alcohol
“Why do I think she’s at risk? She’s overweight, she doesn’t exercise, she doesn’t eat right and she drinks a lot. A lot.”
Genetics risk Affected T2D participant perceives unaffected family member to be at risk for T2D because of genetics
“Why do you think they’re at risk of developing diabetes? P: My daughter eats very very healthy. I think a lot of it is the genetics.”
Lack of exercise risk Affected T2D participant perceives unaffected family member to be at risk for T2D because of no exercise
“They don’t exercise, you know, they just- all the lifestyle choices of what they eat is just adding more weight to them, I guess.”
Overweight risk Affected T2D participant perceives unaffected family member to be at risk for T2D because overweight
“*** is 13 and he’s borderline obese. And if he’s borderline obese, that means he has the potential to be diabetic.”
Symptoms suggest diabetes Affected T2D participant perceives unaffected family member to be at risk for T2D because various physical manifestations
I: What kind of concerns do you have? P: Well I know he’s always saying that he’s tired. And I know he sweats a lot and be clammy in the hands. So I tells him you need to go to the doctor and
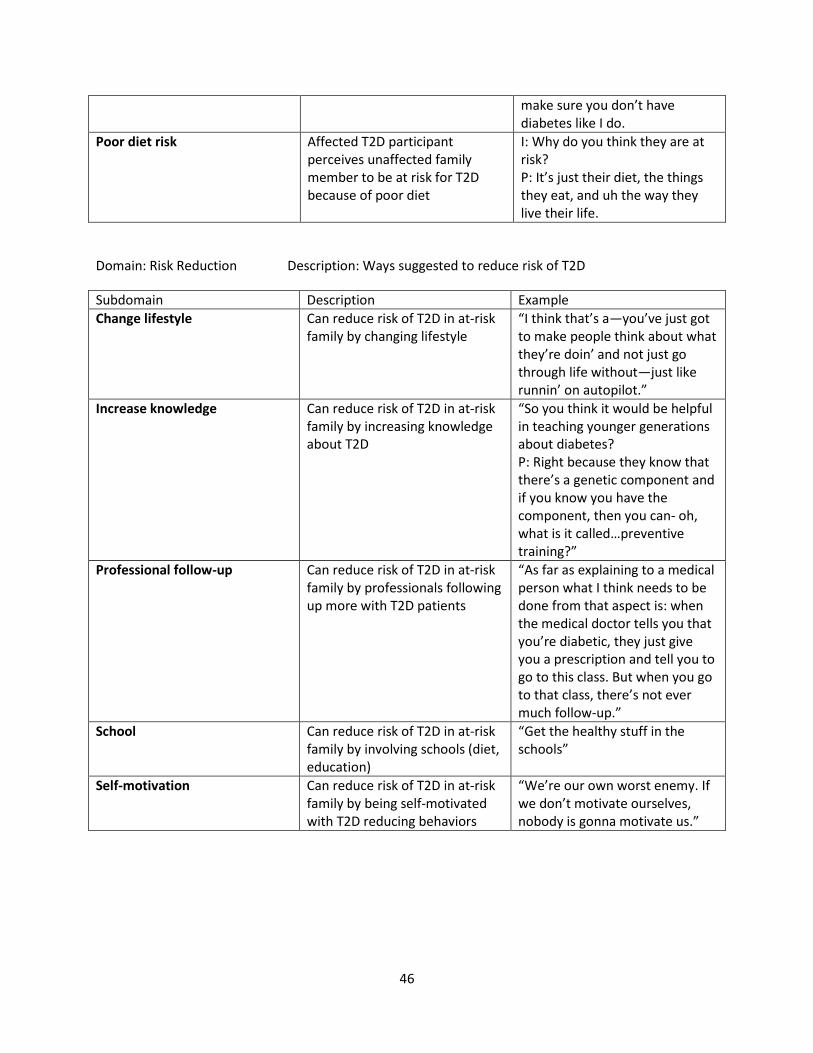
46
make sure you don’t have diabetes like I do.
Poor diet risk Affected T2D participant perceives unaffected family member to be at risk for T2D because of poor diet
I: Why do you think they are at risk? P: It’s just their diet, the things they eat, and uh the way they live their life.
Domain: Risk Reduction Description: Ways suggested to reduce risk of T2D
Subdomain Description Example
Change lifestyle Can reduce risk of T2D in at-risk family by changing lifestyle
“I think that’s a—you’ve just got to make people think about what they’re doin’ and not just go through life without—just like runnin’ on autopilot.”
Increase knowledge Can reduce risk of T2D in at-risk family by increasing knowledge about T2D
“So you think it would be helpful in teaching younger generations about diabetes? P: Right because they know that there’s a genetic component and if you know you have the component, then you can- oh, what is it called…preventive training?”
Professional follow-up Can reduce risk of T2D in at-risk family by professionals following up more with T2D patients
“As far as explaining to a medical person what I think needs to be done from that aspect is: when the medical doctor tells you that you’re diabetic, they just give you a prescription and tell you to go to this class. But when you go to that class, there’s not ever much follow-up.”
School Can reduce risk of T2D in at-risk family by involving schools (diet, education)
“Get the healthy stuff in the schools”
Self-motivation Can reduce risk of T2D in at-risk family by being self-motivated with T2D reducing behaviors
“We’re our own worst enemy. If we don’t motivate ourselves, nobody is gonna motivate us.”
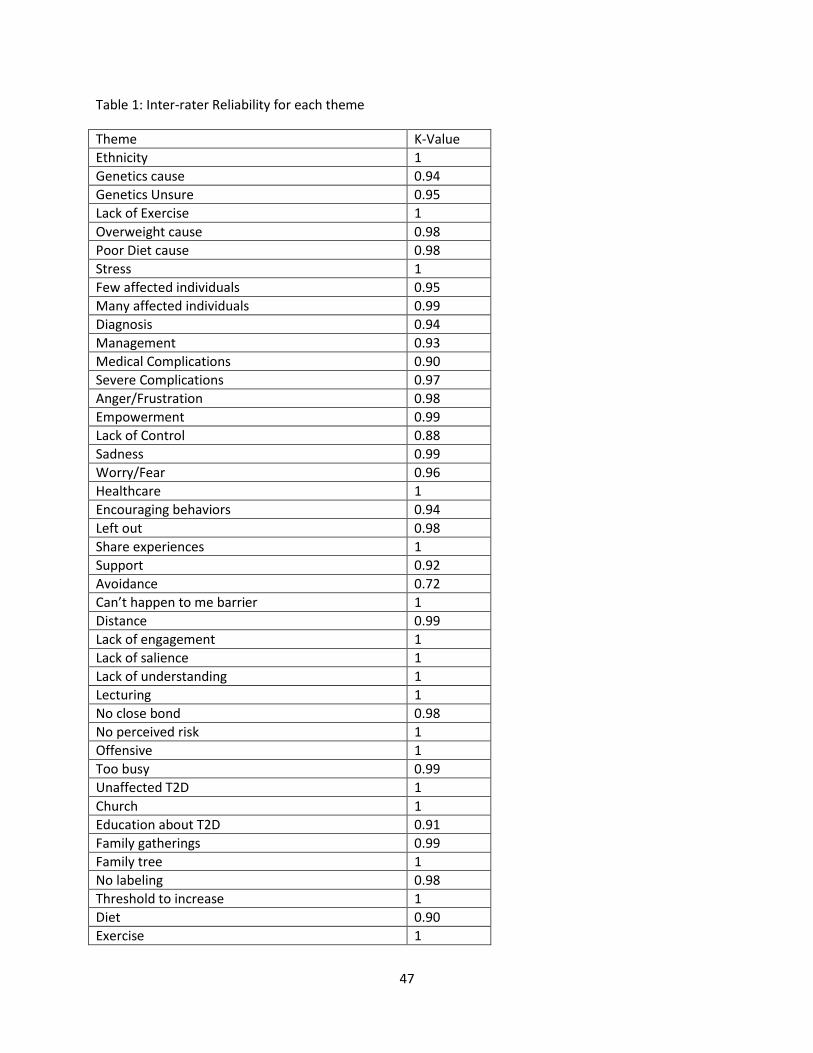
47
Table 1: Inter-rater Reliability for each theme
Theme K-Value
Ethnicity 1
Genetics cause 0.94
Genetics Unsure 0.95
Lack of Exercise 1
Overweight cause 0.98
Poor Diet cause 0.98
Stress 1
Few affected individuals 0.95
Many affected individuals 0.99
Diagnosis 0.94
Management 0.93
Medical Complications 0.90
Severe Complications 0.97
Anger/Frustration 0.98
Empowerment 0.99
Lack of Control 0.88
Sadness 0.99
Worry/Fear 0.96
Healthcare 1
Encouraging behaviors 0.94
Left out 0.98
Share experiences 1
Support 0.92
Avoidance 0.72
Can’t happen to me barrier 1
Distance 0.99
Lack of engagement 1
Lack of salience 1
Lack of understanding 1
Lecturing 1
No close bond 0.98
No perceived risk 1
Offensive 1
Too busy 0.99
Unaffected T2D 1
Church 1
Education about T2D 0.91
Family gatherings 0.99
Family tree 1
No labeling 0.98
Threshold to increase 1
Diet 0.90
Exercise 1
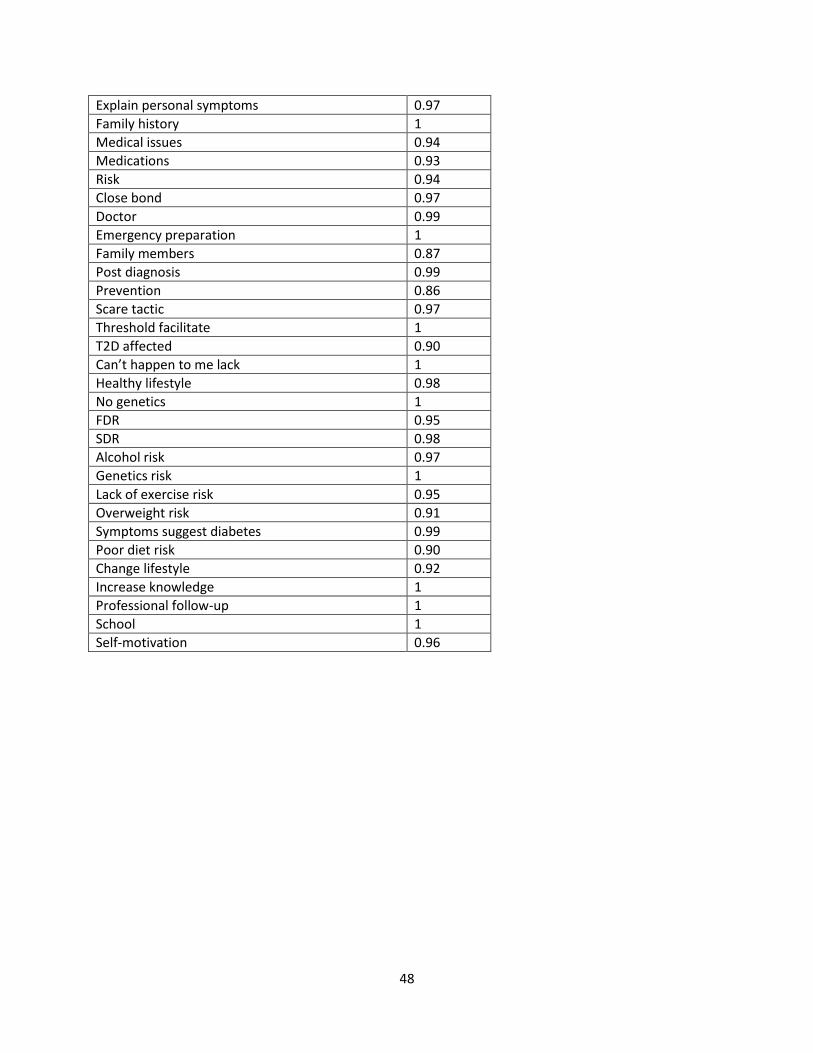
48
Explain personal symptoms 0.97
Family history 1
Medical issues 0.94
Medications 0.93
Risk 0.94
Close bond 0.97
Doctor 0.99
Emergency preparation 1
Family members 0.87
Post diagnosis 0.99
Prevention 0.86
Scare tactic 0.97
Threshold facilitate 1
T2D affected 0.90
Can’t happen to me lack 1
Healthy lifestyle 0.98
No genetics 1
FDR 0.95
SDR 0.98
Alcohol risk 0.97
Genetics risk 1
Lack of exercise risk 0.95
Overweight risk 0.91
Symptoms suggest diabetes 0.99
Poor diet risk 0.90
Change lifestyle 0.92
Increase knowledge 1
Professional follow-up 1
School 1
Self-motivation 0.96
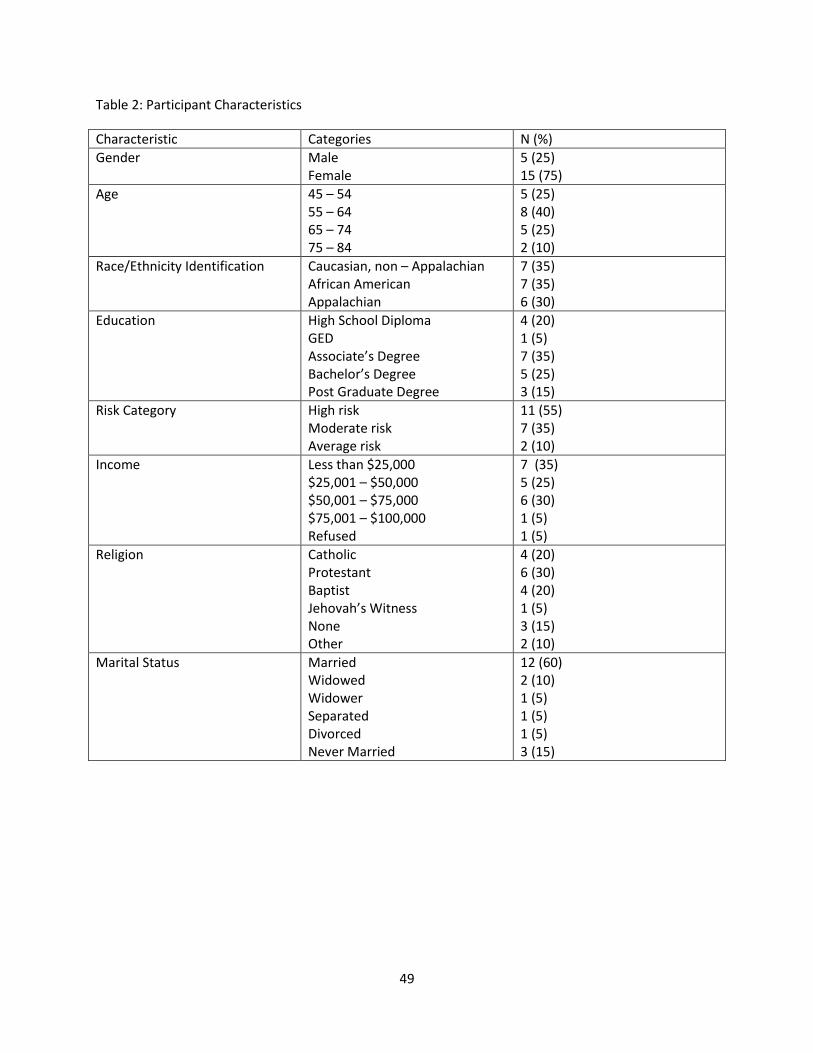
49
Table 2: Participant Characteristics
Characteristic Categories N (%)
Gender Male Female
5 (25) 15 (75)
Age 45 – 54 55 – 64 65 – 74 75 – 84
5 (25) 8 (40) 5 (25) 2 (10)
Race/Ethnicity Identification Caucasian, non – Appalachian African American Appalachian
7 (35) 7 (35) 6 (30)
Education High School Diploma GED Associate’s Degree Bachelor’s Degree Post Graduate Degree
4 (20) 1 (5) 7 (35) 5 (25) 3 (15)
Risk Category High risk Moderate risk Average risk
11 (55) 7 (35) 2 (10)
Income Less than $25,000 $25,001 – $50,000 $50,001 – $75,000 $75,001 – $100,000 Refused
7 (35) 5 (25) 6 (30) 1 (5) 1 (5)
Religion Catholic Protestant Baptist Jehovah’s Witness None Other
4 (20) 6 (30) 4 (20) 1 (5) 3 (15) 2 (10)
Marital Status Married Widowed Widower Separated Divorced Never Married
12 (60) 2 (10) 1 (5) 1 (5) 1 (5) 3 (15)
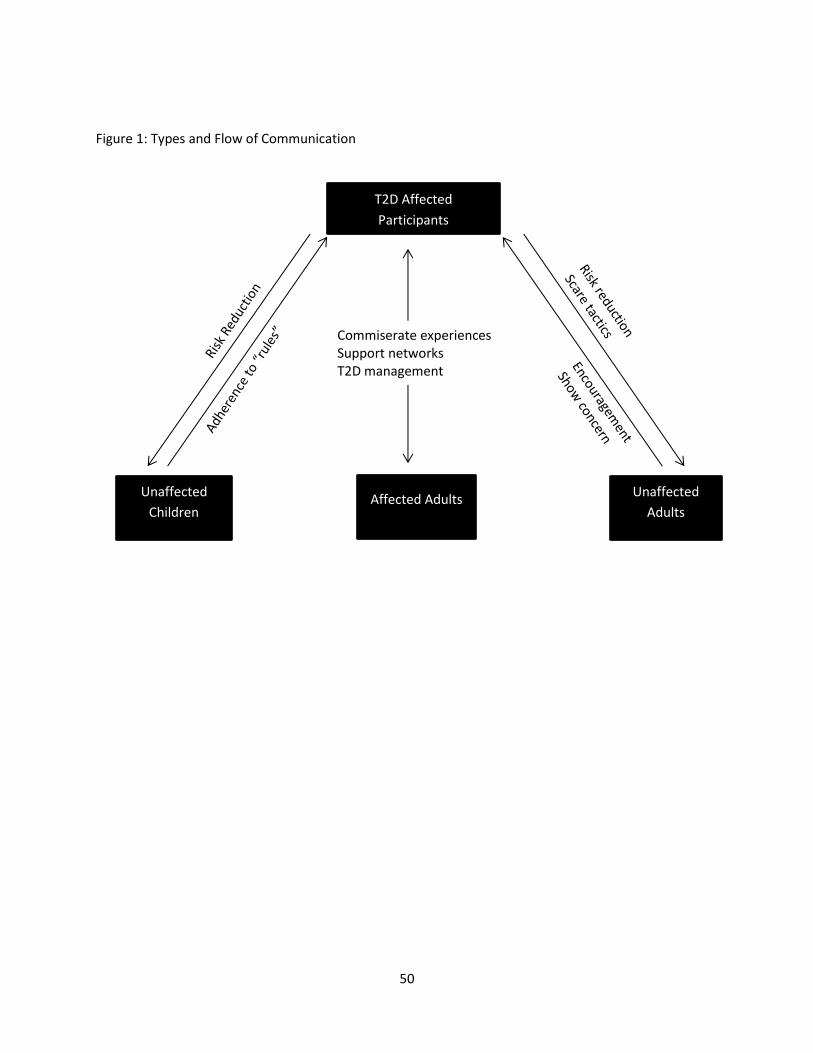
50
Figure 1: Types and Flow of Communication
T2D Affected
Participants
Unaffected
Children Affected Adults
Unaffected
Adults
Commiserate experiences Support networks T2D management