
Coccidioidomycosis in Latin America - Oxford Academic
10
Medical Mycology, 2019, 57, S46–S55 doi: 10.1093/mmy/myy037 Review Article Review Article Coccidioidomycosis in Latin America Rafael Laniado-Labor´ ın 1, ∗ , Eduardo G. Arathoon 2 , Cristina Canteros 3 , Raquel Mu ˜ niz-Salazar 4 and Adri ´ an Rendon 5 1 Facultad de Medicina y Psicolog´ ıa, Universidad Aut ´ onoma de Baja California, 2 Asociaci ´ on de Salud Integral, Hospital General San Juan de Dios, Guatemala, 3 Servicio Micosis Profundas, Departamento Micolog´ ıa, INEI-ANLIS “Dr Carlos G. Malbr ´ an,” Rep ´ ublica Argentina, 4 Escuela de Ciencias de la Salud, Universidad Aut ´ onoma de Baja California and 5 CIPTIR, Hospital Universitario de Monterrey UANL, Mexico ∗ To whom correspondence should be addressed. Rafael Laniado-Labor´ ın MD, MPH, Tel: +52 +664 686–5626; E-mail: [email protected] Received 18 November 2017; Revised 24 April 2018; Accepted 15 May 2018; Editorial Decision 6 May 2018 Abstract Coccidioidomycosis is a highly prevalent systemic mycosis in Latin America and has been reported (human and zoonotic cases) in M ´ exico, Guatemala, Honduras, Colombia, Venezuela, Brazil, Paraguay, Bolivia, and Argentina. The incidence of coccidioidomycosis in Latin America is unknown due to lack of clinical awareness and limited access to laboratory diagnosis. Coccidioidomycosis is as prevalent in Mexico as in the endemic regions of the United States. The number of cases reported in Brazil and Argentina has progressively increased during the last decade, including areas that were not considered as endemic. Genetic studies have shown that the prevalent species in Latin America is Coccidioides posadasii. Coccidioides immitis has been reported sporadically in indigenous cases from Mexico and Colombia. Coccidioidomycosis and tuberculosis share some risk factors such as immunosuppression and residing in areas endemic for these conditions, so their coexistence in the same patient is not uncommon in Latin America. In most regions, clinical diagnosis of coccidioidomycosis is based on direct sputum examination and histopathology results from biopsies or autopsies. This would explain why primary coccidioidomycosis is rarely diagnosed, and most cases published are about chronic pulmonary or disseminated disease. Key words: coccidioidomycosis, Latin America, epidemiology, tuberculosis. Introduction The enormous geographic and climatic diversity of Latin Amer- ica provides a great diversity of ecosystems that allow the de- velopment of different microorganisms, including pathogenic fungi. Coccidioidomycosis is a systemic mycosis that has been reported in many Latin American countries. The re- gion has a high proportion of rural population dedicated to agricultural work, exposed to diverse habitats for fungi, be- ing therefore exposed to inhalation (or transcutaneous in- oculation) of Coccidioides arthroconidia. Coccidioidomycosis has an important impact on public health; however, despite the reporting of clinical cases in several countries of the re- gion, clinical and epidemiological information is scarce and fragmentary. Coccidioidomycosis in Mexico Coccidioidomycosis (CM) is the most prevalent of the systemic mycosis in Mexico. CM was first diagnosed in Mexico by Dr. Gast ´ on Madrid, who reported a case in 1945. 1 The patient was referred due to the possible diagnosis of tuberculosis (TB) to the 80-bed TB sanatorium in Hermosillo, the capital of Sonora, a state that shares the United States (U.S.)–Mexico border with Arizona. Bacteriology for TB in this patient was negative despite the clinical and radiological features suggestive of TB. A fungal culture was ordered and Coccidioides spp. was isolated from the sputum. Three years later, Madrid reported a series of coccid- ioidomycosis cases diagnosed in the region. 2 A few years later 3 Coccidioides spp. was isolated for the first time in Mexico, in the soil from a snake burrow in the outskirts of Hermosillo. In S46 C The Author(s) 2019. Published by Oxford University Press on behalf of The International Society for Human and Animal Mycology. All rights reserved. For permissions, please e-mail:[email protected] Downloaded from https://academic.oup.com/mmy/article/57/Supplement_1/S46/5300138 by guest on 22 August 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Coccidioidomycosis in Latin America - Oxford Academic

Medical Mycology, 2019, 57, S46–S55doi: 10.1093/mmy/myy037
Review Article
Review Article
Coccidioidomycosis in Latin America
Rafael Laniado-Laborın1,∗, Eduardo G. Arathoon2, Cristina Canteros3,
Raquel Muniz-Salazar4 and Adrian Rendon5
1Facultad de Medicina y Psicologıa, Universidad Autonoma de Baja California, 2Asociacion de Salud Integral,Hospital General San Juan de Dios, Guatemala, 3Servicio Micosis Profundas, Departamento Micologıa, INEI-ANLIS“Dr Carlos G. Malbran,” Republica Argentina, 4Escuela de Ciencias de la Salud, Universidad Autonoma de BajaCalifornia and 5CIPTIR, Hospital Universitario de Monterrey UANL, Mexico∗To whom correspondence should be addressed. Rafael Laniado-Laborın MD, MPH, Tel: +52 +664 686–5626;E-mail: [email protected]
Received 18 November 2017; Revised 24 April 2018; Accepted 15 May 2018; Editorial Decision 6 May 2018
Abstract
Coccidioidomycosis is a highly prevalent systemic mycosis in Latin America and has been reported (humanand zoonotic cases) in Mexico, Guatemala, Honduras, Colombia, Venezuela, Brazil, Paraguay, Bolivia, andArgentina. The incidence of coccidioidomycosis in Latin America is unknown due to lack of clinical awarenessand limited access to laboratory diagnosis. Coccidioidomycosis is as prevalent in Mexico as in the endemicregions of the United States. The number of cases reported in Brazil and Argentina has progressivelyincreased during the last decade, including areas that were not considered as endemic. Genetic studieshave shown that the prevalent species in Latin America is Coccidioides posadasii. Coccidioides immitishas been reported sporadically in indigenous cases from Mexico and Colombia. Coccidioidomycosis andtuberculosis share some risk factors such as immunosuppression and residing in areas endemic for theseconditions, so their coexistence in the same patient is not uncommon in Latin America. In most regions,clinical diagnosis of coccidioidomycosis is based on direct sputum examination and histopathology resultsfrom biopsies or autopsies. This would explain why primary coccidioidomycosis is rarely diagnosed, andmost cases published are about chronic pulmonary or disseminated disease.
Key words: coccidioidomycosis, Latin America, epidemiology, tuberculosis.
Introduction
The enormous geographic and climatic diversity of Latin Amer-ica provides a great diversity of ecosystems that allow the de-velopment of different microorganisms, including pathogenicfungi. Coccidioidomycosis is a systemic mycosis that hasbeen reported in many Latin American countries. The re-gion has a high proportion of rural population dedicated toagricultural work, exposed to diverse habitats for fungi, be-ing therefore exposed to inhalation (or transcutaneous in-oculation) of Coccidioides arthroconidia. Coccidioidomycosishas an important impact on public health; however, despitethe reporting of clinical cases in several countries of the re-gion, clinical and epidemiological information is scarce andfragmentary.
Coccidioidomycosis in Mexico
Coccidioidomycosis (CM) is the most prevalent of the systemicmycosis in Mexico. CM was first diagnosed in Mexico by Dr.Gaston Madrid, who reported a case in 1945.1 The patient wasreferred due to the possible diagnosis of tuberculosis (TB) to the80-bed TB sanatorium in Hermosillo, the capital of Sonora, astate that shares the United States (U.S.)–Mexico border withArizona. Bacteriology for TB in this patient was negative despitethe clinical and radiological features suggestive of TB. A fungalculture was ordered and Coccidioides spp. was isolated from thesputum. Three years later, Madrid reported a series of coccid-ioidomycosis cases diagnosed in the region.2 A few years later3
Coccidioides spp. was isolated for the first time in Mexico, inthe soil from a snake burrow in the outskirts of Hermosillo. In
S46 C© The Author(s) 2019. Published by Oxford University Press on behalf of The International Society for Human and AnimalMycology. All rights reserved. For permissions, please e-mail:[email protected]
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022

Laniado-Laborın et al. S47
1974, Madrid publishes the book Coccidioidomycosis, the onlymonograph on CM published to date in Mexico.4
Infection by Coccidioides sp. is as prevalent in Mexico as inthe endemic regions of the United States.5 The first skin sur-veys with coccidioidin were carried out in Sonora from the late1940s to the early 1970s, at different sites in the state. Rates ofinfection were high all over the state and ranged from 64% to90% in adults; in children, the rate was reported at 16%.5 In1966 Gonzalez-Ochoa reported the first national survey on coc-cidioidomycosis infection; rates were significantly higher in thenorthwestern states (Baja California, Sonora, Sinaloa, and Chi-huahua) of the country with rates that ranged from 30% to morethan 50%.6 These high rates of infection have been corroboratedin later surveys with coccidioidin and spherulin.7,8
The endemic regions in Mexico are characterized by a dryclimate, alkaline soil, summers with very high temperatures (upto 50◦C), and annual precipitation indexes as low as 10 cm; thiscombination of environmental factors facilitates the spread ofCoccidioides spores in the air. The high prevalence of infectionin the semi-arid northwestern region of Mexico correlates wellwith the evidence from the United States, where the highest ratesof disease are found also in California and Arizona, states withlarge desert regions that are likely to serve as ecological nichesfor Coccidioides.9
The prevalent species in Mexico is Coccidioides posadasii;10
the only isolates of Coccidioides immitis have been found inBaja California, a state located in the most northwestern re-gion of the country; no geographical overlap of the species hasbeen reported.11 The clinical burden of disease in Mexico is cur-rently unknown.12 CM was a reportable disease in Mexico upto 1994, with an average of 1500 cases reported per year; since1995 there are no data on the clinical burden of CM, when thedisease was eliminated from the national epidemiological reg-istry for reportable diseases. From 1988 through 1994 the meanincidence of CM in Mexico was 0.8 per 10.5 The states (all ofthem northern states, located in the U.S.–Mexico border) withthe highest rates of clinical cases were Nuevo Leon, Tamaulipas,Chihuahua, Baja California, and Sonora.9
An important barrier for the clinical diagnosis in Mexico isthe lack of access to laboratory mycological diagnosis. There arejust a few centers in the country (some of them dedicated to basicresearch more than to clinical diagnosis) with the capability andbiosafety standards for culture and identification of Coccidioidesand/or serological diagnosis. In most regions, clinical diagnosis isbased on direct sputum examination and histopathology resultsfrom biopsies or autopsies. This would explain why primarycoccidioidomycosis is rarely diagnosed, and most cases publishedare about chronic pulmonary or disseminated CM.
The literature on the interrelationship of diabetes mellitus andcoccidioidomycosis suggest that these patients may experiencesevere, progressive, and complicated coccidioidal infections.13
Diabetes is one of the main causes of death in Mexico; the
prevalence of diabetes in the country, according to the latest na-tional survey is 9.4%;14 severe forms of CM have been reportedin diabetics in Mexico for more than 30 years.15 Tuberculosisand CM share the same risks factors and its coexistence is alsoa common clinical finding in Mexico.16 The coexistence of CMand human immunodeficiency virus (HIV) has also been re-ported in Mexico,17 although not with the frequency that shouldbe expected based on the prevalence of HIV in the country.
Travelers from nonendemic areas should be aware of the po-tential risk of infection when visiting endemic areas in Mexico.An example of this risk would be an outbreak that included 21serologically confirmed CM cases (17% attack rate) among achurch group from Washington State in the United States. Thegroup had just stayed for 6 days at an orphanage in Tecate, Mex-ico, a town in the Sonoran Desert adjacent to the U.S.–Mexicoborder to build a church.18
A group of clinicians and microbiologist from Baja Califor-nia, Sonora, and Nuevo Leon have founded the Mexican Coc-cidioidomycosis Study Group in 2014. The first objective of thegroup was to develop the Mexican Guidelines for the Diagno-sis and Treatment of Coccidioidomycosis; they were published inthe journal of the National Infectious Diseases Society in 2015.19
Funding has been an issue for the regular meeting of the group.
Coccidioidomycosis Research in Mexico
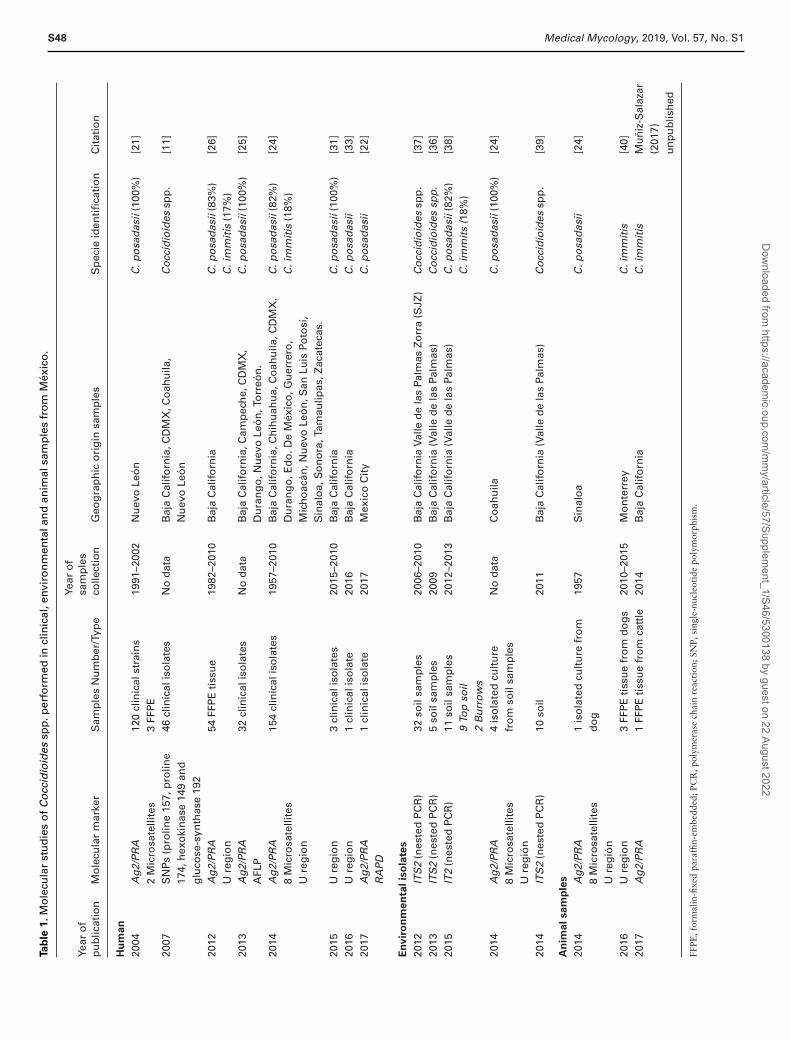
Coccidioidomycosis in humans (Table 1)
The first molecular study on CM in Mexico was reported in2004; it dealt with the development of a conventional nestedand a real-time polymerase chain reaction (PCR) assay specificfor the identification of C. posadasii DNA by targeting a genecoding for the antigen 2/proline-rich antigen (Ag2/PRA). Thestudy included 120 clinical strains isolated from 114 patientsand three formalin-fixed paraffin embedded specimens during a10-year period (1991–2002) in Monterrey, Mexico. The sampleswere amplified using two microsatellite loci (GAC and 621);20 allstrains were correctly identified as C. posadasii, whereas DNAfrom related members of the family Onygenaceae tested nega-tive. Also, specific DNA was amplified by conventional nestedPCR from three microscopically spherule-positive formalin-fixedtissue samples and identified as C. posadasii, whereas 20 humantissue samples tested positive for other dimorphic fungi testednegative.21 This assay is used directly in clinical samples,22,23 aswell in clinical isolates and formalin-fixed tissues.24–28
In 2007, Castanon-Olivares analyzed 56 clinical isolates ofCoccidioides spp. from Mexican patients by real-time PCR usingTaqMan probes to amplify single nucleotide polymorphisms(SNPs) in four target sequences loci (proline 157, proline 174,hexokinase 149, and glucose-synthase 192). In total, 54 isolatesidentified as C. posadasii and two as C. immitis. Only proline157, proline 174, and glucose-synthase 192 gave consistentresults on SNP differentiation between the two species, while
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022
S48 Medical Mycology, 2019, Vol. 57, No. S1Ta
ble
1.M
ole
cula
rst
ud
ies
of
Co
ccid
ioid
essp
p.p
erfo
rmed
incl
inic
al,e
nvir
on
men
tala
nd
anim
alsa
mp
les
fro
mM
exic
o.
Year
of
pu
blic
atio
nM
ole
cula
rm
arke
rS
amp
les
Nu
mb
er/T
ype
Year
of
sam
ple
sco
llect
ion
Geo
gra
ph
ico
rig
insa
mp
les
Sp
ecie
iden
tifi
cati
on
Cit
atio
n
Hu
man
2004
Ag
2/P
RA
120
clin
ical
stra
ins
1991
–200
2N
uev
oLe
on
C.p
osa
das
ii(1
00%
)[2
1]2
Mic
rosa
telli
tes
3FF
PE
2007
SN
Ps
(pro
line
157,
pro
line
174,
hex
oki
nas
e14
9an
dg
luco
se-s
ynth
ase
192
46cl
inic
alis
ola
tes
No
dat
aB
aja
Cal
ifo
rnia
,CD
MX
,Co
ahu
ila,
Nu
evo
Leo
nC
occ
idio
ides
spp
.[1
1]
2012
Ag
2/P
RA
Ure
gio
n54
FFP
Eti
ssu
e19
82–2
010
Baj
aC
alif
orn
iaC
.po
sad
asii
(83%
)C
.im
mit
is(1
7%)
[26]
2013
Ag
2/P
RA
AFL
P32
clin
ical
iso
late
sN
od
ata
Baj
aC
alif
orn
ia,C
amp
ech
e,C
DM
X,
Du
ran
go
,Nu
evo
Leo
n,T
orr
eon
.C
.po
sad
asii
(100
%)
[25]
2014
Ag
2/P
RA
8M
icro
sate
llite
sU
reg
ion
154
clin
ical
iso
late
s19
57–2
010
Baj
aC
alif
orn
ia,C
hih
uah
ua,
Co
ahu
ila,C
DM
X,
Du
ran
go
,Ed
o.D
eM
exic
o,G
uer
rero
,M
ich
oac
an,N
uev
oLe
on
,San
Luis
Poto
sı,
Sin
alo
a,S
on
ora
,Tam
aulip
as,Z
acat
ecas
.
C.p
osa
das
ii(8
2%)
C.i
mm
itis
(18%
)[2
4]
2015
Ure
gio
n3
clin
ical
iso
late
s20
15–2
010
Baj
aC
alif
orn
iaC
.po
sad
asii
(100
%)
[31]
2016
Ure
gio
n1
clin
ical
iso
late
2016
Baj
aC
alif
orn
iaC
.po
sad
asii
[33]
2017
Ag
2/P
RA
1cl
inic
alis
ola
te20
17M
exic
oC
ity
C.p
osa
das
ii[2
2]R
AP
D
En
vir
on
men
tal
iso
late
s
2012
ITS
2(n
este
dP
CR
)32
soil
sam
ple
s20
06–2
010
Baj
aC
alif
orn
iaVa
lled
ela
sPa
lmas
Zo
rra
(SJZ
)C
occ
idio
ides
spp
.[3
7]20
13IT
S2
(nes
ted
PC
R)
5so
ilsa
mp
les
2009
Baj
aC
alif
orn
ia(V
alle
de
las
Palm
as)
Co
ccid
ioid
essp
p.
[36]
2015
IT2
(nes
ted
PC
R)
11so
ilsa
mp
les
2012
–201
3B
aja
Cal
ifo
rnia
(Val
led
ela
sPa
lmas
)C
.po
sad
asii
(82%
)[3
8]9
Top
soil
C.i
mm
its
(18%
)2
Bu
rro
ws
2014
Ag
2/P
RA
8M
icro
sate
llite
sU
reg
ion
4is
ola
ted
cult
ure
fro
mso
ilsa
mp
les
No
dat
aC
oah
uila
C.p
osa
das
ii(1
00%
)[2
4]
2014
ITS
2(n
este
dP
CR
)10
soil
2011
Baj
aC
alif
orn
ia(V
alle
de
las
Palm
as)
Co
ccid
ioid
essp
p.
[39]
An
imal
sam
ple
s
2014
Ag
2/P
RA
8M
icro
sate
llite
sU
reg
ion
1is
ola
ted
cult
ure
fro
md
og
1957
Sin
alo
aC
.po
sad
asii
[24]
2016
Ure
gio
n3
FFP
Eti
ssu
efr
om
do
gs
2010
–201
5M
on
terr
eyC
.im
mit
is[4
0]20
17A
g2/
PR
A1
FFP
Eti
ssu
efr
om
catt
le20
14B
aja
Cal
ifo
rnia
C.i
mm
itis
Mu
niz
-Sal
azar
(201
7)u
np
ub
lish
ed
FFPE
,for
mal
in-fi
xed
para
ffin-
embe
dded
;PC
R,p
olym
eras
ech
ain
reac
tion
;SN
P,si
ngle
-nuc
leot
ide
poly
mor
phis
m.
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022

Laniado-Laborın et al. S49
hexokinase 149 gave negative results in 34 samples. Clinicalisolates were from sputum, cerebrospinal fluid, bronchoalveolarlavage, pus or tissues, and the tip of a ventriculoperitoneal shuntcatheter and patients clinically diagnosed with coccidioidomyco-sis in Baja California, Coahuila, Nuevo Leon, and Mexico City.
Gonzalez-Becuar in 2012,26 analyzed a total of 129 formalin-fixed tissue samples with histopathology diagnosis of CM. Thesamples were obtained from the collection of the pathology lab-oratory from the Tijuana General Hospital from 1982 through2010. In total, 54 (83%) samples identified as C. posadasii, and11 (17%) as C. immitis, which distributed in five haplotypes forC. posadasii and three for C. immitis.
In 2013, Duarte-Escalante25 analyzed 32 clinical isolatesfrom Mexico (Mexico City, Durango, Torreon, Baja California,Nuevo Leon, and Campeche) and Argentina. All isolates wereidentified as C. posadasii. Also, the study reported a high geneticvariability in the isolates from Mexico (0.5011 ± 0.0382) andArgentina (0.3951 ± 0.0503). A small but significant geneticdifferentiation between countries (P = .0001) was detected, sug-gesting that there is a single genetic population in Latin Amer-ica. This is the first study in Mexico, which explores the geneticstructure of Coccidioides using the molecular marker amplifiedfragment length polymorphism (AFLP).
In 2014, Luna-Isaac et al.24 used nine-microsatellites,Ag2/PRA and Umeyama region to establish the predominantCoccidioides species in Mexico, to delineate the current geo-graphical locations of both species, and to identify a possiblecorrelation between clinical symptoms and a specific genotype.One hundred sixty isolates (155 clinical, four environmental,and one animal) recovered from culture collections of differentinstitutions in Mexico stored from 1957 and 2010. The pre-dominant species was C. posadasii (82%). Among 28 C. immitisstrains, 14 unique multilocus genotypes and six clones were ob-served. While 126 C. posadasii strains showed 29 unique multi-locus genotypes and 16 clones. Finally, based solely on the sizescores of microsatellite locus 621, which was the most commonlyused to discriminate between species, 28 samples identified as C.immitis (416–426 bp) and 126 as C. posadasii (399 bp). Inter-estingly, samples 5233, 5234, M60 09, M61 09, and TJ3835showed sequences and fragment sizes that corresponded to C.posadasii using U region that identified as C. immitis based onthe Ag2/PRA and 621 loci. This situation has been observed byTintelnot et al.29 who identified one strain of Coccidioides as onespecies using restriction fragment length polymorphism (RFLP)and as another using U region. That strain was previously iden-tified as C. immitis and postulated to be a hybrid genotype ofboth species. Neafsey et al.30 suggest that sexual reproductionbetween the two species could occur, causing the hybridizationand introgression of genomic fragments from one species intothe genome of another. On the other hand, Luna-Isaac et al.24
reported the correlation between genotype and clinical presenta-tion was not significant (P > .05). However, 83% of C. immitis
isolates were associated with cutaneous dissemination, suggest-ing this species exhibits a higher tendency to disseminate to theskin, while C. posadasii was related to all forms of clinical pre-sentation. It is important to highlight that this is the only studyon the genetic structure of Coccidioides in Mexico.
Recently, clinical cases have used molecular markers toidentify species of Coccidioides. In 2015, Moreno-Coutino31
reported six Mexican male cases, residents of Tijuana BajaCalifornia—three of them with primary pulmonary infection andfurther cutaneous dissemination, and three cases of primary cu-taneous coccidioidomycosis. Half of the cases were identified asC. posadasii using U region.32 In 2016, Arce et al.33 reported aprimary cutaneous coccidioidomycosis caused by C. posadasii ina male patient 41 years of age, a native and resident of Tijuana,Baja California, who for 27 years worked as a surveyor in thisregion. Recently, Fernandez22 reported the case of a MexicanHIV+ patient with a probable endogenous reactivation of coc-cidioidomycosis. A direct microscopic examination using potas-sium hydroxide (KOH) on a sample taken from the cheek nodulerevealed the presence of spherules. The fungus was isolated, andits identity was confirmed by phenotypic and molecular methods(Ag2/PRA).
Coccidioidomycosis in environmentalsamples (Table 1)
The screening of environmental samples has had low effective-ness, mainly because of the weak characterization of Coccid-ioides ecological niche. Coccidioides spp. has been identifiedfrom airborne and soil samples by culture and molecular assays.The first environmental report of Coccidioides was by Laniado-Laborin et al.34 who isolated Coccidioides from one air samplein Tijuana. The most studied site in Mexico is Valle de Las Pal-mas in Baja California. The interest to study this site is because aCM outbreak occurred in 1996 when a Washington State churchgroup traveled to VDP to build an orphanage.35 As mentioned,after they returned to the United States, 17% (21/126) serologi-cal cases of coccidioidomycosis were confirmed.
A total of 108 soil samples from Baja California has been ana-lyzed, mainly from Valle de las Palmas (101 samples); 54% of theisolated strains are identified as Coccidioides spp. amplifying theinternal transcribed spacer (ITS) region. Most of the soil sampleswere from heteromyid latrines, and in a lower frequency fromtopsoil, heteromyids’ active burrows and large mammal dens.No Coccidioides spp. has been found in soils collected in Ense-nada, Baja California. Luna-Isaac24 reported the molecular iden-tification of four soil isolates as C. posadasii (M47–06, M49–06,M50–06, and M51–06), sheltered in the culture collection of theUniversidad Nacional Autonoma de Mexico (UNAM), but thecollection date is unknown.
Romero-Olivares36 constructed a Dikarya-specific gene li-brary for the ITS region of nuclear ribosomal DNA in order
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022

S50 Medical Mycology, 2019, Vol. 57, No. S1
to determine the diversity of the mycobiota in Baja California.Although this assay was able to identify species like Penicilliumdipodomyicola, Coprinellus radians, Alternaria spp., among oth-ers, it was not able to identify Coccidiodes. Thus, a nested PCRwas used to determine this species.37 The most recent work ana-lyzes the ITS region by a metagenomic approach in a 454 Rochepyrosequencer.38 The objective was to identify environmentalfactors determining fungal community structure in two differ-ent microhabitats, burrows (influenced by rodent activity), andtopsoil and were compared in winter and summer. Differencesin composition between microhabitats were mainly correlated tosignificant differences in environmental factors, such as moistureand clay content in topsoil samples, and temperature and electri-cal conductivity in burrow samples. Overall, the fungal commu-nity structure (dominated by Ascomycota and Basidiomycota)was less variable between seasons in burrow than in topsoil sam-ples. Similarly, 13 Coccidioides spp. went undetected by pyrose-quencing. However, a nested PCR approach revealed its higherprevalence in burrows.
The last study reported until now in Valle de las Palmas wasperformed during 2010–2011by Catalan-Dibene.39 DNA wasextracted directly from 24 soil samples to amplify the ITS2 re-gion of rDNA.37 A 170 bp amplicon was recovered from 15out of 24 samples; however, just 10 samples were confirmedas Coccidioides spp. The rest of the sequences correspondedto members of the genus Aphanoascus (A. Canadensis and A.pinarensis) and Penicillium.
Coccidioides in animals (Table 1)
The available published studies on animal CM in Mexico arescarce; heteromyids, prairie dogs, dogs, and cattle are the onlyspecies reported. Consequently, the actual prevalence of CMinfection in domestic and wild mammals in Mexico is unknown.
In 2014, Catalan-Dibene39 detected antibodies against Coc-cidioides in two species of heteromyids (Peromyscus maniculatusand Neotoma lepida) sampled in Valle de las Palmas, Baja Cali-fornia.
Ramirez-Romero40 analyzed 765 dog biopsies with a pre-sumptive diagnosis of neoplasm between April 1, 2010, andMarch 31, 2015, from Monterrey, Nuevo Leon. In total, threecases of CM were found (3/765 = 0.39%). The presumptivediagnoses in these cases were osteosarcoma, lymphoma, andneurofibroma, respectively. Molecular analysis of formalin-fixedparaffin-embedded (FFPE) positive samples amplifying the U re-gion32 showed C. posadasii in one of these cases.
Sera from urban dogs and wild rodents (prairie dogs) weretested employing the Ouchterlony double immunodiffusion tech-nique, with coccidioidin produced at UNAM as an antigen.One hundred domestic dog sera were tested, and three (3%)tested positive for anti-Coccidioides antibodies; of 158 sera fromprairie dogs, 113 (71.5%) tested positive.
Only a few studies of CM in cattle have been reported in Mex-ico. Six cases of CM in beef (3) and dairy (3) cattle slaughteredand inspected in 1995 and 1996 were reported in Mexicali, BajaCalifornia. The identification was performed just by histopatho-logical analysis. After that, there are no reports in this area until2017, when a post-mortem examination in 1 out of 319 cattleslaughtered at Mexicali, using histopathological and molecular(Ag2/PRA) testing identified C. immitis (Muniz-Salazar unpub-lished data).
Coccidioidomycosis and tuberculosis:
Differential diagnosis
CM and tuberculosis (TB) share very similar pathogenic mech-anisms: they usually start with a primary lung infection thatmay lead to a chronic condition in which they may present thesame symptoms and radiologic manifestations.41–45 In endemicregions for both diseases, the clinicians may face quite a chal-lenge when considering these two infections in the differentialdiagnosis. Support from specialized TB and mycology labora-tories is needed but, even when this is available, confirmationof either (or both) infection can be difficult. In the followingsection, we present a clinical approach for the differential diag-nosis of tuberculosis and/or coccidioidomycosis in Monterrey,Mexico.
Diagnostic work-up for TB and CM
Monterrey is located close to the United States–Mexican bor-der, an endemic region for coccidioidomycosis;43 also it is oneof the cities with the highest incidence of TB in Mexico.46 Clin-ical guidelines and recommendations to diagnose CM47,48 orTB44,49 are readily available; in individual cases, the diagnosisof either disease can be straightforward in some cases but inothers, it can be extremely complicated. Due to this difficulty,a number of diagnostic modalities may be needed. Cultures arestill considered as the gold standard tests for both infections, buttheir sensitivity is far from perfect, creating the need for com-plementary methods to support the diagnosis.44,47 Diagnosis ofTB is based on the initial finding of acid-fast bacilli (AFB) ei-ther in sputum or bronchoalveolar lavage (BAL) stains and theposterior isolation of Mycobacterium tuberculosis in culture; inthe past decade, molecular methods have improved the rapiddiagnosis of TB, and nowadays they are widely used and rec-ommended as the preferred initial tests.44 On the other hand,diagnosis of CM based on sputum microscopy and culture ismuch less sensitive. BAL stains and culture also lack sensitiv-ity but bronchoscopy is usually indicated in severe cases whena specific diagnosis is urgently needed.47 Serodiagnosis is notrecommended for TB44 but can be very useful for the diagnosisof CM.47,49 Several tests are commercially available for clinicallaboratories but others need to be sent to reference laborato-ries. Serology is probably the most commonly ordered diagnostic
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022

Laniado-Laborın et al. S51
test, but their results must be interpreted judiciously since mis-interpretation can lead to false positive or negative diagnosis; apositive serology test by itself does not make the CM diagnosisand a negative one does not rule out the disease, mainly in themost seriously ill patients.47 Skin testing, when available, canalso be used to detect either infection, but they are not usefulfor the diagnosis of the disease.44,47 Interferon-gamma releaseassays (IGRAs) for the detection of TB infection, are basicallyinterpreted in a similar way than the tuberculin test but with ahigher sensitivity and specificity.44 However, as mentioned, skintests and IGRA tests do not distinguish active disease from latentinfection.
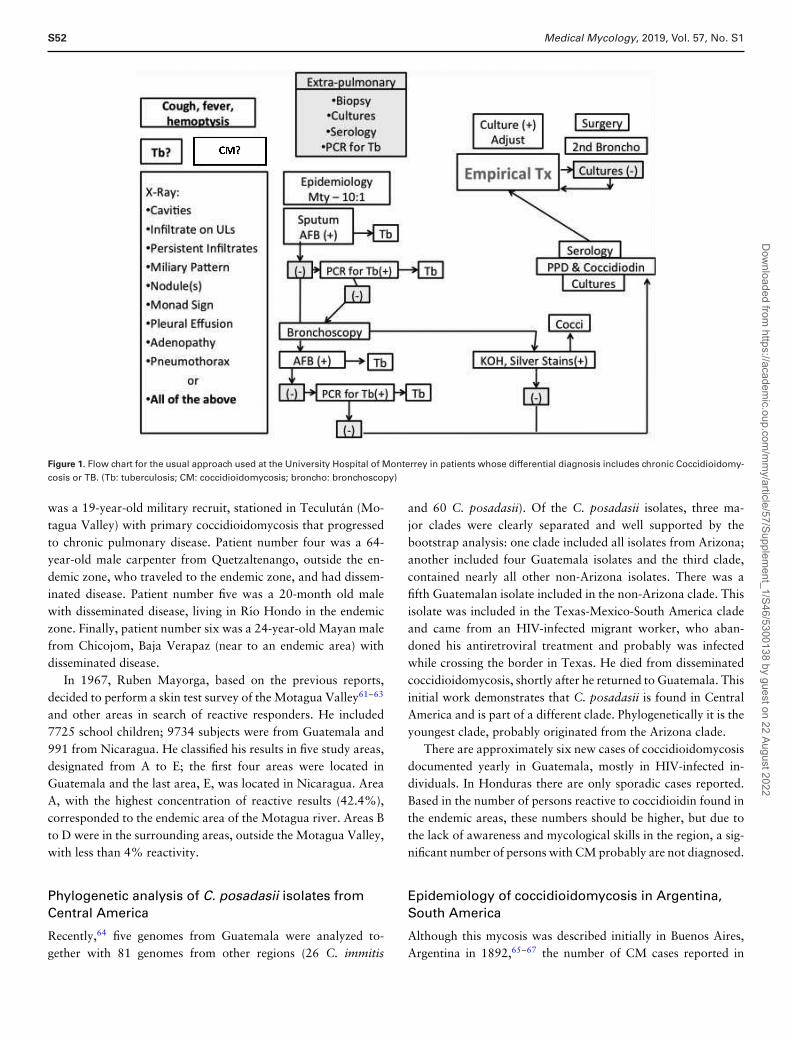
Frequently, a combination of clinical data, radiologic presen-tation, and results of diagnostic tests should be used in order tomake a specific diagnosis.44,47 Guideline algorithms for the diag-nosis of TB or CM are designed to search for a specific diagnosis,either TB or CM, but they do not consider into their algorithmsthe possibility of the other infection.44, 47–49 Complicating mat-ters even more, the two infections may and do coexist.50 Eventhough we try to be aligned with international recommenda-tions, we must adapt them to our local needs and resources.A modified algorithm for the differential diagnosis when fac-ing a patient in whom TB or cocci are possible is shown inFigure 1.
The approach suggests to first rule out TB since this infec-tion is more common and is contagious. We begin the diagnosticwork-up with the sputum smear for AFB. If AFB is positive, westart treatment for TB, while we wait for the diagnosis to be con-firmed by the cultures. If AFB is negative, a molecular test is per-formed: if positive, TB is diagnosed, if negative, a bronchoscopyis performed. TheBAL is simultaneously tested for TB and cocciwith stains, cultures, and molecular TB tests. Any positive test isconsidered a definite diagnosis. Transbronchial biopsies are per-formed mainly on those with interstitial infiltrates or on thosewith no cavities. For those with stains and negative moleculartests, we order skin test for both diseases. Negative results mayhelp to rule out any of the two infections. Positive results arecarefully considered since they do not confirm active disease. Insome cases, Cocci serology is also sent to a reference laboratory.For patients in which results are all negative and cultures are stillbeing processed, we may prescribe empirical therapy if the clin-ical conditions deserve it. Empirical therapy is chosen analyzingall the available data for each case on an individual basis. Inmost cases, the empirical treatment prescribed is for presumedTB. According to the clinical response and the cultures results,treatment is further adjusted. For those patients with HIV infec-tion, diabetes or on any kind of immunosuppressive therapy, anearlier more aggressive diagnostic approach is used including in-vasive procedures to obtain tissues for histopathology study andcultures. Thereare no data to support if our approach is better orworse compared to the one used in other centers with differentepidemiology and different resources.
Coccidioidomycosis in Central America
Coccidioidomycosis is an endemic fungal infection found in cer-tain arid and semi-arid regions of Central America.51 Reportsof its presence in the region are scarce, and documented reportsof autochthonous human CM are found in only two countries,Guatemala and Honduras.
Two early attempts to investigate the presence of disease inCentral America using coccidioidin skin test surveys exist. Thefirst one by Andrade in 1945,52 included 1200 persons, children,and adults in Guatemala City. A second study in 1950 included500 persons in the Canal Zone of Panama.53 The reactivity tothe coccidioidin in both studies was less than 1% of the subjectstested.
A few years later in 1951, the first human case of CM in Cen-tral America,54 was documented, by two pathologists from CostaRica who received lymph node tissue belonging to a 53-year-oldtruck driver born in Nacaome, Honduras, and who lived andworked for the last 24 years in the Comayagua Valley. In 1946,he developed a cough, chest pain, hemoptysis, night sweats, andweight loss. In 1950 he traveled to Costa Rica, developing at thattime bilateral supraclavicular lymphadenopathy, with a bloodypurulent discharge. Spherules were documented in the purulentsecretion and in sputum. A chest X-ray suggested mediastinallymphadenopathy. Tuberculin test and CM skin tests were re-active. He received intramuscular colloidal copper, with littleimprovement.
It should be mentioned that in 1959, a dog from Nicaraguawas diagnosed with coccidioidomycosis in Norway, after itsarrival,55 raising the possibility of human coccidioidomycosisthere.
Nine years after the first human case from Honduras wasfound, two veterinarians reported several infected animals withcoccidioidomycosis in Guatemala. Two bulls56 and seven dogs,57
none of them came from the endemic areas documented later.Also, during the same year (1960), the first human case inGuatemala was documented by Eduardo Perez-Guisasola,58 andthe clinical findings were described by Garcıa Valdes.59
The patient was a 16-year-old black male, who lived inGualan Zacapa, part of the Motagua Valley. His chest X-rayshowed pulmonary infiltrates and skin and bone dissemination.Perez-Guisasola, during the next 6 years, found and documentedsix more persons with the disease.60 Based on the climatic char-acteristics of Guatemala, and the region where the patients lived,Perez-Guisasola proposed the Motagua Valley, an arid region inthe western part of the country, as the potential endemic area. Hecarefully described the clinical, microbiologic and epidemiologicorigin of the infected persons. Patient number one, was 34-year-old 9-month pregnant female, from Guatemala City (outsidethe endemic zone), with disseminated disease. Patient numbertwo was a 64-year-old diabetic female from Salama (near to anendemic zone) with disseminated disease. Patient number three
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022
S52 Medical Mycology, 2019, Vol. 57, No. S1
Figure 1. Flow chart for the usual approach used at the University Hospital of Monterrey in patients whose differential diagnosis includes chronic Coccidioidomy-cosis or TB. (Tb: tuberculosis; CM: coccidioidomycosis; broncho: bronchoscopy)
was a 19-year-old military recruit, stationed in Teculutan (Mo-tagua Valley) with primary coccidioidomycosis that progressedto chronic pulmonary disease. Patient number four was a 64-year-old male carpenter from Quetzaltenango, outside the en-demic zone, who traveled to the endemic zone, and had dissem-inated disease. Patient number five was a 20-month old malewith disseminated disease, living in Rıo Hondo in the endemiczone. Finally, patient number six was a 24-year-old Mayan malefrom Chicojom, Baja Verapaz (near to an endemic area) withdisseminated disease.
In 1967, Ruben Mayorga, based on the previous reports,decided to perform a skin test survey of the Motagua Valley61–63
and other areas in search of reactive responders. He included7725 school children; 9734 subjects were from Guatemala and991 from Nicaragua. He classified his results in five study areas,designated from A to E; the first four areas were located inGuatemala and the last area, E, was located in Nicaragua. AreaA, with the highest concentration of reactive results (42.4%),corresponded to the endemic area of the Motagua river. Areas Bto D were in the surrounding areas, outside the Motagua Valley,with less than 4% reactivity.
Phylogenetic analysis of C. posadasii isolates fromCentral America
Recently,64 five genomes from Guatemala were analyzed to-gether with 81 genomes from other regions (26 C. immitis
and 60 C. posadasii). Of the C. posadasii isolates, three ma-jor clades were clearly separated and well supported by thebootstrap analysis: one clade included all isolates from Arizona;another included four Guatemala isolates and the third clade,contained nearly all other non-Arizona isolates. There was afifth Guatemalan isolate included in the non-Arizona clade. Thisisolate was included in the Texas-Mexico-South America cladeand came from an HIV-infected migrant worker, who aban-doned his antiretroviral treatment and probably was infectedwhile crossing the border in Texas. He died from disseminatedcoccidioidomycosis, shortly after he returned to Guatemala. Thisinitial work demonstrates that C. posadasii is found in CentralAmerica and is part of a different clade. Phylogenetically it is theyoungest clade, probably originated from the Arizona clade.
There are approximately six new cases of coccidioidomycosisdocumented yearly in Guatemala, mostly in HIV-infected in-dividuals. In Honduras there are only sporadic cases reported.Based in the number of persons reactive to coccidioidin found inthe endemic areas, these numbers should be higher, but due tothe lack of awareness and mycological skills in the region, a sig-nificant number of persons with CM probably are not diagnosed.
Epidemiology of coccidioidomycosis in Argentina,South America
Although this mycosis was described initially in Buenos Aires,Argentina in 1892,65–67 the number of CM cases reported in
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022

Laniado-Laborın et al. S53
Table 2. Epidemiological studies in Coccidioidomycosis performed
in South America.
Country Period Cases reported (n) Infection rate∗ (%)
Colombia 1958–2015 5 3–13Venezuela 1948–2014 114 11–46Brazil 1978–2015 829 26Paraguay 1950–1967 3 15–44Bolivia 1948 1 . . .Argentina 1892–2015 2–40
∗Infection rate in each country varies according to the geographical area of thecountry.
South America is much lower than those diagnosed in NorthAmerica, and the real incidence is unknown perhaps because itis not a reportable disease, because it may be misdiagnosed astuberculosis, which is very endemic, and also because there isa high percentage of subclinical cases. However, available datasuggest that its prevalence is increasing in some areas of SouthAmerica.68–70
As in North America, the geographical endemic areas forCM in South America are characterized by arid and semi-aridareas with sandy, alkaline soils and extreme temperatures inColombia, Venezuela, Brazil, Paraguay, Bolivia, and Argentina.
In Colombia, five cases were reported from 1958 to 2015 andlow infection rate was detected using coccidioidin skin tests (3–13%).71 Venezuela reported 114 cases from 1948 to 2004 andan infection rate of about 50% in major endemic areas of thiscountry.72
The area that has most recently been described as endemic forCM is the northeast of Brazil, where the first autochthonous casewas reported in 1978 in a patient from Bahia.73 Epidemiologicalstudies show autochthonous cases in Ceara, Bahia, Piauı, andMaranhao.70 In 2016 the Brazilian Ministry of Health reported829 hospitalizations due to CM (incidence 7.12/1000 hospitaladmissions).69 In the state of Ceara in Brazil, a coccidioidin skinsurvey showed a prevalence of infection of 26.4%.74
In the southernmost areas of South America coccidioidomy-cosis is endemic in the west of Paraguay, southeast of Bolivia,and in the arid geographic areas from the province of Jujuy tothe province of Rıo Negro in Argentina.68,75,76
Both Paraguay and Bolivia report only occasional cases; how-ever in the northwest of Paraguay, the infection rate has beenreported as high as 44% in aboriginal population and oil com-pany employees.75 Table 2 summarizes the epidemiological stud-ies performed in South America using the coccidioidin skin test.
In Argentina, epidemiological studies revealed highest infec-tion rates in Catamarca province, with values about 40% ofreactors. Other areas with high infection rates were describedin the northwest of Cordoba (34%); the west of Santiago delEstero (19.8%); and La Rioja (19.13%); all of these provincesare adjacent to Catamarca.
Only a small number of CM cases had been reported inArgentina before the year 2000, despite the large extent of theendemic area. In 2009 the first retrospective review of all CMcases reported in the country documented 128 cases from theoriginal case reported by Posadas in 1892 to the year 2009.From 1892 through 1939 only six cases were registered; between1940 and 1999, 59 more cases were reported, and finally, theremaining 63 cases (49% of total cases) were reported from2000 to 2009, with the Catamarca province having the highestnumber of cases.68 The National Mycology Network reported48 new CM human cases from 2010 through 2015. Almost50% of these cases occurred in patients who lived or visited ageographic region in the Central Valley of Catamarca. Annualdisease incidence rates in this province increased from historicalvalues below 0.5/100 000 to 2/100 000 inhabitants from 2000to 2009;68 incidence from 2010 to 2015 is reported between 1and 2 cases/100 000 inhabitants.
Probably the dramatic changes in the ecosystem that occurredbetween the years of 1973 and 2007 in the central valley ofCatamarca (an increase of 4 times the urbanized areas and 38times the cultivated areas) was a factor in the increase of CMin the region.77 Coccidioides has been isolated from the soil inArgentina (Province of Cordoba).78
In addition, increased diagnosis capability could be a factorin this incidence increase because the Reference National My-cology Laboratory of Argentina has provided reagents for CMimmunodiffusion tests to the laboratories of the laboratory net-work since the year 2000.79
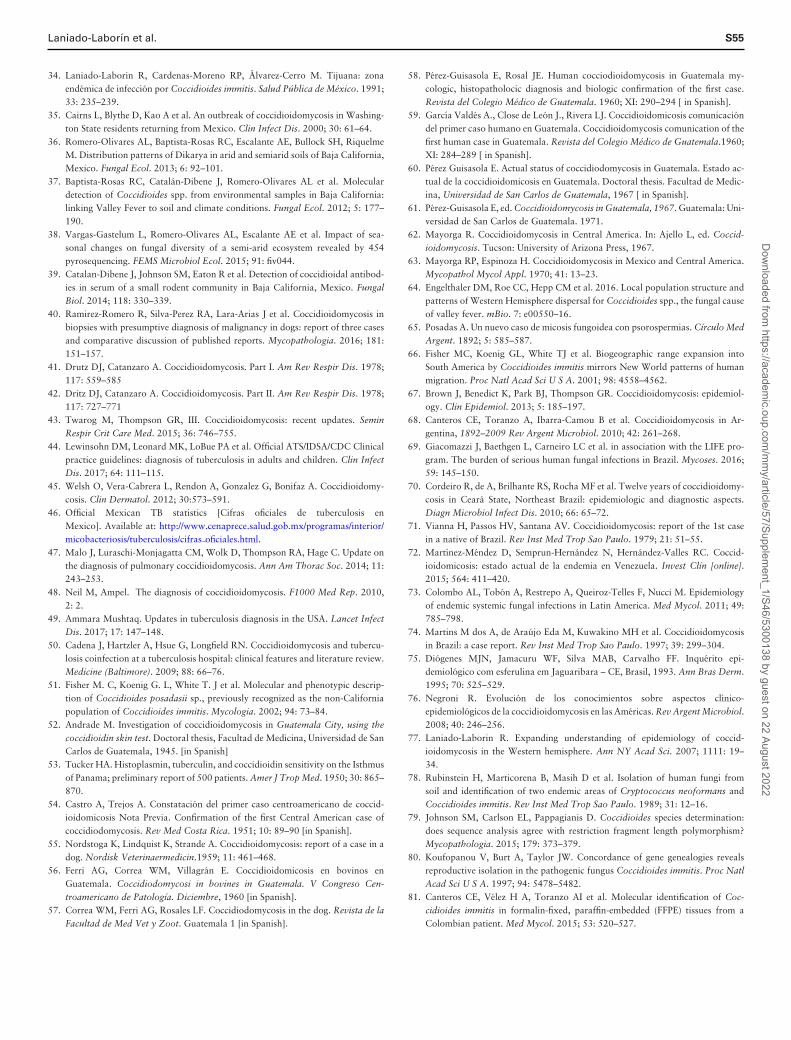
With respect to zoonotic CM, data collected by the Refer-ence National Mycology laboratory registered only three casesbefore to 2005 in dogs from Catamarca. In 2005, an increase inthe number of CM cases in dogs was reported in this province.Animals showed fever, cough, and lameness and osteomyelitislesions. Up to 2014, the total number of canine CM cases inCatamarca Province was 86. All cases were confirmed by detect-ing anti-Coccidioides antibodies by immunodiffusion test withtiter >1:4 plus clinical and radiological findings. Figure 2 showsthe evolution of reported dog and human cases by year from1997 to 2014 in Catamarca Province.
Coccidioides posadasii is the most prevalent etiological agentof CM in South America68,70; there have been two reportsof C. immitis cases in South American patients, one fromVenezuela80 and the other by Argentina,81 but in these cases,it was impossible to exclude travel by the patients to regionswhere C. immitis is prevalent. In 2015, Coccidioides immitisDNA has been detected in a specimen from a patient fromPinto, Colombia (the patient never traveled abroad). Althoughthis species is primarily found in California, it has been re-ported in other geographical areas as shown by this case fromColombia; there is the possibility that C. immitis endemic ar-eas may be extending from the formerly proposed geographicalborders.71
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022

S54 Medical Mycology, 2019, Vol. 57, No. S1
0
2
4
6
8
10
12
14
16
18
20N
umbe
r of r
epor
ted
case
s
year
dog human
Figure 2. Evolution of reported dog and human cases from 1997 to 2014 inCatamarca Province, Argentina∗. (*Data obtained from the Reference NationalLaboratory for Mycology of Argentina.)
Coccidioidomycosis is a highly prevalent systemic mycosis inLatin America and has been reported in Mexico, Guatemala,Honduras, Colombia, Venezuela, Brazil, Paraguay, Bolivia, andArgentina. However, despite the reporting of clinical cases inseveral countries of the region, clinical and epidemiological in-formation is scarce and fragmentary. The incidence of CM in theregion is unknown, mainly due to lack of clinical awareness andlimited access to a laboratory. Clinical training in this conditionand the strengthening of the network of mycology laboratoriesin the region is necessary to adequately characterize this mycosisin the region.
Declaration of interest
The authors report no conflicts of interest. The authors alone areresponsible for the content and writing of this paper.
References
1. Madrid GS. Coccidioidomicosis. Prensa Medica. 1946; 6: 1033–1035.2. Madrid GS. Las micosis pulmonares. 1a parte. Rev Mex Tuber Ap Resp. 1948;
9: 32–55.3. Sotomayor C, Madrid GS, Torres EA. Aislamiento de Coccidioides immitis del
suelo de Hermosillo, Sonora Mexico. Rev Latinoamericana Microbiol. 1960; 3:237–238.
4. Madrid GS. Coccidioidomicosis. Talleres de Impresion y Editorial. Hermosillo,Mexico. Primera Edicion, 1974.
5. Ajello L. Comparative ecology of respiratory mycotic disease agents. BacteriolRev. 1967; 31: 6–24.
6. Gonzalez-Ochoa A. La coccidioidomicosis en Mexico. Rev Invest Salud Publica(Mex). 1966; 26: 245–262.
7. Fredrich BE. A skin test survey of valley fever in Tijuana, Mexico. Soc Sci Med.1989; 29: 121–127.
8. Padua A, Martinez-Ordaz VA, Velasco-Rodriguez VM, Lazo-Saenz JG, CiceroR. Prevalence of skin reactivity to coccidioidin and associated risk factors insubjects living in a northern city of Mexico. Arch Med Res. 1999; 30: 388–392.
9. Baptista Rosas RC, Riquelme M. Epidemiologıa de la coccidioidomicosis enMexico. Rev Iberoam Micol. 2007; 24: 100–105.
10. Bialek B, Kern J, Hermann T et al. PCR assays for identification of Coccidioidesposadasii based on the nucleotide sequence of the antigen 2/proline-rich antigen.J Clin Microbiol. 2004; 42: 778–783.
11. Castanon-Olivares LR, Guerena-Elizalde D, Gonzalez-Martınez MR, Licea-Navarro AF, Gonzalez-Gonzalez GM, Aroch-Calderon A. Molecular identifi-cacion of Coccidioides isolates from Mexican patients. Ann NY Acad Sci. 2007;1111: 326–335.
12. Castanon-Olivares LR, Aroch-Calderon A, Bazan-Mora E, Cordova-MartınezE. Coccidioidomicosis y su escaso conocimiento en nuestro paıs. Rev FacultadMed UNAM. 2004; 47: 4.
13. Santelli AC, Blair JE, Roust LR. Coccidioidomycosis in patients with diabetesmellitus. Am J Med. 2006; 119: 964–969.
14. Encuesta Nacional de Salud y Nutricion de Medio Camino 2016, Secretarıa deSalud, Mexico, 2016.
15. Forsbach-Sanchez GB, Fuentes-Pensamiento R. Coccidioidomicosis pulmonarcronica progresiva en una paciente con diabetes mellitus II. Rev Inv Clin. 1985;37: 49–51.
16. Castaneda-Godoy R, Laniado-Laborın R. Coexistencia de tuberculosis y coccid-ioidomicosis: presentacion de dos casos clınicos. Rev Inst Nal Enf Resp Mex.2002; 15: 98–101.
17. Laniado-Laborın R. Coccidioidomicosis. Mas que una enfermedad regional. RevInst Nal Enf Resp Mex. 2006; 19: 301–330.
18. Gabe LM, Malo J, Knox KS. Diagnosis and management of coccidioidomycosis.Clin Chest Med. 2017; 38: 417–433.
19. Mendoza-Mendoza A, Acuna-Kaldman M, Alvarez-Hernandez G et al. Guıa delGrupo Mexicano de Diagnostico y Tratamiento de la coccidioidomicosis. EnfInf Microbiol. 2015; 35: 18–31.
20. Fisher MC, White TJ, Taylor JW. Primers for genotyping single nucleotide poly-morphisms and microsatellites in the pathogenic fungus Coccidioides immitis.Mol Ecol. 1999; 8: 1082–1084.
21. Bialek R, Kern J, Herrman T et al. PCR assays for identification of Coccidioidesposadasii based on the nucleotide sequence of the antigen 2/proline-rich antigen.J Clin Microbiol. 2004; 42: 778–783.
22. Fernandez R, Arenas R, Duarte-Escalante E et al. Diagnosis of coccidioidomy-cosis in a non-endemic area: inference of the probable geographic area of aninfection. Rev Iberoamericana Micol. 2017; 34: 237–240.
23. Brilhante RSN, Cordeiro RA, Rocha MFG et al. Coccidioidal pericarditis: arapid presumptive diagnosis by an in-house antigen confirmed by mycologicaland molecular methods. J Med Microbiol. 2008; 57: 1288–1292.
24. Luna-Isaac J, Muniz-Salazar R, Baptista-Rosas R et al. Genetic analysis of theendemic fungal pathogens Coccidioides posadasii and C. immitis in Mexico. MedMycol. 2014; 52: 156–166.
25. Duarte-Escalante E, Zuniga G, Frias-De-Leon MG et al. AFLP analysis revealshigh genetic diversity but low population structure in Coccidioides posadasiiisolates from Mexico and Argentina. BMC Infect Dis. 2013; 13: 411.
26. Gonzalez-Becuar CG. Identificacion de Coccidioides spp. en muestras de tejidosparafinizados utilizando tres tipos de marcadores moleculares. Ensenada, BajaCalifornia, Mexico: Universidad Autonoma de Baja California; 2012 (Thesis).
27. Canteros C, Toranzo A, Suarez-Alvarez R et al. Genetic characterization of thefungus involved in the first case of coccidioidomycosis described by AlejandroPosadas in 1892. Medicina (Buenos Aires). 2009; 69: 215–220.
28. Canteros CE, Velez H A, Toranzo AI et al. Molecular identification of Coc-cidioides immitis in formalin-fixed, paraffin-embedded (FFPE) tissues from aColombian patient. Med Mycol. 2015; 53: 520–527.
29. Tintelnot K, De Hoog GS Antweiler E et al. Taxonomic and diagnostic mark-ers for identification of Coccidioides immitis and Coccidioides posadasii. MedMycol. 2007; 45: 385–393.
30. Neafsey DE, Barker BM, Sharpton TJ et al. Population genomic sequencing ofCoccidioides fungi reveals recent hybridization and transposon control. GenomeRes. 2010; 20: 938–946.
31. Moreno-Coutino G, Arce-Ramırez M, Medina A et al. Coccidioidomicosiscutanea: Comunicacion de seis casos mexicanos. Rev Chil Infect. 2015; 32:339–343.
32. Umeyama T, Sano A, Kamei K et al. Novel approach to designing primers foridentification and distinction of the human pathogenic fungi Coccidioides immitisand Coccidioides posadasii by PCR amplification. J Clin Microbiol. 2006; 44:1859–1862.
33. Arce M, Ramırez V, Castaneda R, Castanon-Olivares L. Primary cutaneouscoccidioidomycosis due to Coccidioides posadasii. Dermatol Rev Mex. 2016;60: 520–525.
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022
Laniado-Laborın et al. S55
34. Laniado-Laborin R, Cardenas-Moreno RP, Alvarez-Cerro M. Tijuana: zonaendemica de infeccion por Coccidioides immitis. Salud Publica de Mexico. 1991;33: 235–239.
35. Cairns L, Blythe D, Kao A et al. An outbreak of coccidioidomycosis in Washing-ton State residents returning from Mexico. Clin Infect Dis. 2000; 30: 61–64.
36. Romero-Olivares AL, Baptista-Rosas RC, Escalante AE, Bullock SH, RiquelmeM. Distribution patterns of Dikarya in arid and semiarid soils of Baja California,Mexico. Fungal Ecol. 2013; 6: 92–101.
37. Baptista-Rosas RC, Catalan-Dibene J, Romero-Olivares AL et al. Moleculardetection of Coccidioides spp. from environmental samples in Baja California:linking Valley Fever to soil and climate conditions. Fungal Ecol. 2012; 5: 177–190.
38. Vargas-Gastelum L, Romero-Olivares AL, Escalante AE et al. Impact of sea-sonal changes on fungal diversity of a semi-arid ecosystem revealed by 454pyrosequencing. FEMS Microbiol Ecol. 2015; 91: fiv044.
39. Catalan-Dibene J, Johnson SM, Eaton R et al. Detection of coccidioidal antibod-ies in serum of a small rodent community in Baja California, Mexico. FungalBiol. 2014; 118: 330–339.
40. Ramirez-Romero R, Silva-Perez RA, Lara-Arias J et al. Coccidioidomycosis inbiopsies with presumptive diagnosis of malignancy in dogs: report of three casesand comparative discussion of published reports. Mycopathologia. 2016; 181:151–157.
41. Drutz DJ, Catanzaro A. Coccidioidomycosis. Part I. Am Rev Respir Dis. 1978;117: 559–585
42. Dritz DJ, Catanzaro A. Coccidioidomycosis. Part II. Am Rev Respir Dis. 1978;117: 727–771
43. Twarog M, Thompson GR, III. Coccidioidomycosis: recent updates. SeminRespir Crit Care Med. 2015; 36: 746–755.
44. Lewinsohn DM, Leonard MK, LoBue PA et al. Official ATS/IDSA/CDC Clinicalpractice guidelines: diagnosis of tuberculosis in adults and children. Clin InfectDis. 2017; 64: 111–115.
45. Welsh O, Vera-Cabrera L, Rendon A, Gonzalez G, Bonifaz A. Coccidioidomy-cosis. Clin Dermatol. 2012; 30:573–591.
46. Official Mexican TB statistics [Cifras oficiales de tuberculosis enMexico]. Available at: http://www.cenaprece.salud.gob.mx/programas/interior/micobacteriosis/tuberculosis/cifras oficiales.html.
47. Malo J, Luraschi-Monjagatta CM, Wolk D, Thompson RA, Hage C. Update onthe diagnosis of pulmonary coccidioidomycosis. Ann Am Thorac Soc. 2014; 11:243–253.
48. Neil M, Ampel. The diagnosis of coccidioidomycosis. F1000 Med Rep. 2010,2: 2.
49. Ammara Mushtaq. Updates in tuberculosis diagnosis in the USA. Lancet InfectDis. 2017; 17: 147–148.
50. Cadena J, Hartzler A, Hsue G, Longfield RN. Coccidioidomycosis and tubercu-losis coinfection at a tuberculosis hospital: clinical features and literature review.Medicine (Baltimore). 2009; 88: 66–76.
51. Fisher M. C, Koenig G. L, White T. J et al. Molecular and phenotypic descrip-tion of Coccidioides posadasii sp., previously recognized as the non-Californiapopulation of Coccidioides immitis. Mycologia. 2002; 94: 73–84.
52. Andrade M. Investigation of coccidioidomycosis in Guatemala City, using thecoccidioidin skin test. Doctoral thesis, Facultad de Medicina, Universidad de SanCarlos de Guatemala, 1945. [in Spanish]
53. Tucker HA. Histoplasmin, tuberculin, and coccidioidin sensitivity on the Isthmusof Panama; preliminary report of 500 patients. Amer J Trop Med. 1950; 30: 865–870.
54. Castro A, Trejos A. Constatacion del primer caso centroamericano de coccid-ioidomicosis Nota Previa. Confirmation of the first Central American case ofcoccidiodomycosis. Rev Med Costa Rica. 1951; 10: 89–90 [in Spanish].
55. Nordstoga K, Lindquist K, Strande A. Coccidioidomycosis: report of a case in adog. Nordisk Veterinaermedicin.1959; 11: 461–468.
56. Ferri AG, Correa WM, Villagran E. Coccidioidomicosis en bovinos enGuatemala. Coccidiodomycosi in bovines in Guatemala. V Congreso Cen-troamericano de Patologıa. Diciembre, 1960 [in Spanish].
57. Correa WM, Ferri AG, Rosales LF. Coccidiodomycosis in the dog. Revista de laFacultad de Med Vet y Zoot. Guatemala 1 [in Spanish].
58. Perez-Guisasola E, Rosal JE. Human cocciodioidomycosis in Guatemala my-cologic, histopatholocic diagnosis and biologic confirmation of the first case.Revista del Colegio Medico de Guatemala. 1960; XI: 290–294 [ in Spanish].
59. Garcıa Valdes A., Close de Leon J., Rivera LJ. Coccidioidomicosis comunicaciondel primer caso humano en Guatemala. Coccidioidomycosis comunication of thefirst human case in Guatemala. Revista del Colegio Medico de Guatemala.1960;XI: 284–289 [ in Spanish].
60. Perez Guisasola E. Actual status of coccidiodomycosis in Guatemala. Estado ac-tual de la coccidioidomicosis en Guatemala. Doctoral thesis. Facultad de Medic-ina, Universidad de San Carlos de Guatemala, 1967 [ in Spanish].
61. Perez-Guisasola E, ed. Coccidioidomycosis in Guatemala, 1967. Guatemala: Uni-versidad de San Carlos de Guatemala. 1971.
62. Mayorga R. Coccidioidomycosis in Central America. In: Ajello L, ed. Coccid-ioidomycosis. Tucson: University of Arizona Press, 1967.
63. Mayorga RP, Espinoza H. Coccidioidomycosis in Mexico and Central America.Mycopathol Mycol Appl. 1970; 41: 13–23.
64. Engelthaler DM, Roe CC, Hepp CM et al. 2016. Local population structure andpatterns of Western Hemisphere dispersal for Coccidioides spp., the fungal causeof valley fever. mBio. 7: e00550–16.
65. Posadas A. Un nuevo caso de micosis fungoidea con psorospermias. Cırculo MedArgent. 1892; 5: 585–587.
66. Fisher MC, Koenig GL, White TJ et al. Biogeographic range expansion intoSouth America by Coccidioides immitis mirrors New World patterns of humanmigration. Proc Natl Acad Sci U S A. 2001; 98: 4558–4562.
67. Brown J, Benedict K, Park BJ, Thompson GR. Coccidioidomycosis: epidemiol-ogy. Clin Epidemiol. 2013; 5: 185–197.
68. Canteros CE, Toranzo A, Ibarra-Camou B et al. Coccidioidomycosis in Ar-gentina, 1892–2009 Rev Argent Microbiol. 2010; 42: 261–268.
69. Giacomazzi J, Baethgen L, Carneiro LC et al. in association with the LIFE pro-gram. The burden of serious human fungal infections in Brazil. Mycoses. 2016;59: 145–150.
70. Cordeiro R, de A, Brilhante RS, Rocha MF et al. Twelve years of coccidioidomy-cosis in Ceara State, Northeast Brazil: epidemiologic and diagnostic aspects.Diagn Microbiol Infect Dis. 2010; 66: 65–72.
71. Vianna H, Passos HV, Santana AV. Coccidioidomycosis: report of the 1st casein a native of Brazil. Rev Inst Med Trop Sao Paulo. 1979; 21: 51–55.
72. Martınez-Mendez D, Semprun-Hernandez N, Hernandez-Valles RC. Coccid-ioidomicosis: estado actual de la endemia en Venezuela. Invest Clın [online].2015; 564: 411–420.
73. Colombo AL, Tobon A, Restrepo A, Queiroz-Telles F, Nucci M. Epidemiologyof endemic systemic fungal infections in Latin America. Med Mycol. 2011; 49:785–798.
74. Martins M dos A, de Araujo Eda M, Kuwakino MH et al. Coccidioidomycosisin Brazil: a case report. Rev Inst Med Trop Sao Paulo. 1997; 39: 299–304.
75. Diogenes MJN, Jamacuru WF, Silva MAB, Carvalho FF. Inquerito epi-demiologico com esferulina em Jaguaribara – CE, Brasil, 1993. Ann Bras Derm.1995; 70: 525–529.
76. Negroni R. Evolucion de los conocimientos sobre aspectos clınico-epidemiologicos de la coccidioidomycosis en las Americas. Rev Argent Microbiol.2008; 40: 246–256.
77. Laniado-Laborin R. Expanding understanding of epidemiology of coccid-ioidomycosis in the Western hemisphere. Ann NY Acad Sci. 2007; 1111: 19–34.
78. Rubinstein H, Marticorena B, Masih D et al. Isolation of human fungi fromsoil and identification of two endemic areas of Cryptococcus neoformans andCoccidioides immitis. Rev Inst Med Trop Sao Paulo. 1989; 31: 12–16.
79. Johnson SM, Carlson EL, Pappagianis D. Coccidioides species determination:does sequence analysis agree with restriction fragment length polymorphism?Mycopathologia. 2015; 179: 373–379.
80. Koufopanou V, Burt A, Taylor JW. Concordance of gene genealogies revealsreproductive isolation in the pathogenic fungus Coccidioides immitis. Proc NatlAcad Sci U S A. 1997; 94: 5478–5482.
81. Canteros CE, Velez H A, Toranzo AI et al. Molecular identification of Coc-cidioides immitis in formalin-fixed, paraffin-embedded (FFPE) tissues from aColombian patient. Med Mycol. 2015; 53: 520–527.
Dow
nloaded from https://academ
ic.oup.com/m
my/article/57/Supplem
ent_1/S46/5300138 by guest on 22 August 2022




















