CNS Erdheim–Chester Disease: A Challenge to Diagnose
11
REVIEW ARTICLE CNS Erdheim–Chester Disease: A Challenge to Diagnose Zenggang Pan, MD, PhD and Bette K. Kleinschmidt-DeMasters, MD Abstract Erdheim–Chester disease (ECD) is a rare nonLangerhans cell his- tiocytosis. Although approximately 50% of cases eventually involve the central nervous system (CNS), the CNS has seldom been reported as the initial biopsy site. The diagnosis of CNS ECD can be challenging due to morphologic overlap with reactive histiocytic proliferation, Langerhans cell histiocytosis (LCH), and extranodal Rosai–Dorfman disease (RDD). We present 3 cases from our files that illustrate the protean manifestations of ECD. Case 1 was a 47- year-old man with ataxia, dysarthria, and intermittent ophthalmople- gia whose cerebellar biopsy had shown only profuse, nonspecific Rosenthal fiber-rich piloid gliosis; ECD was diagnosed only at au- topsy. The gliosis and marked variations in histiocyte morphology in different anatomical sites added to the diagnostic challenge. Case 2 was a 67-year-old female with chronic progressive symptoms and a pontine lesion that had been considered to be CLIPPERS by neuro- imaging. Identification of a BRAFV600E mutation allowed an ECD diagnosis and treatment with the specific BRAFV600E inhibitor vemurafenib, which resulted in a marked sustained clinical response. Case 3 was diagnosed as ECD after positive bone biopsy with typi- cal foamy histiocytes. Six years later, there was massive dural in- volvement that showed RDD-like, BRAF-mutation-negative histiocytosis. These cases highlight the clinical and histologic over- lap that can occur among these disorders. Key Words: Central nervous system, Erdheim–Chester disease, Langerhans cell histiocytosis, NonLangerhans cell histiocytosis, Rosai–Dorfman disease. INTRODUCTION Erdheim–Chester disease (ECD) is a rare nonLanger- hans cell histiocytosis characterized by xanthomatous or xan- thogranulomatous infiltrates in tissues (1). The number of cases has increased recently due to more recognition of this entity, improved diagnostic criteria, and reliable molecular studies. In the 2016 World Health Organization Classification, ECD has been reclassified as a distinct entity and separated from disseminated juvenile xanthogranuloma (2). The clinical course of ECD is mainly dependent on the disease extent and distribution, ranging from asymptomatic bone involvement to systemic life-threatening disease with poor prognosis, particu- larly in the cases with central nervous system (CNS) or cardio- vascular involvement (3). The diagnosis of ECD is typically based on the charac- teristic radiologic findings and pathologic features in the ap- propriate clinical context. However, recognition of CNS ECD can be challenging due to variable clinical courses, often lim- ited tissue biopsies and mimicries with other reactive and neo- plastic histiocytic lesions; this is particularly problematic in localized CNS ECD cases without stereotypic radiographic changes elsewhere. Here, we review the major clinicopatho- logic characteristics of CNS ECD with emphasis on the diagnostic workups and differential diagnosis through several illustrative case presentations. Case 1. ECD Diagnosed at Autopsy After Inconclusive Cerebellar Biopsy With Profuse Piloid Gliosis The decedent was a 47-year-old Hispanic man with a history of a left cerebellar lesion since 2006. Symptoms con- sisted of ataxia, dysarthria, and intermittent ophthalmoplegia. The patient had no other chronic medical problems but had been hospitalized in the spring of 2009 for pneumonia. In May 2009, he developed decreasing mental status and was taken to the emergency department in the southern part of Colorado where computerized tomography imaging revealed obstruc- tive hydrocephalus. Magnetic resonance imaging (MRI) showed a combination of bilateral cerebellar lesions epicen- tered on the dentate nuclei with enhancement (Fig. 1A), upper cervical cord lesions (Fig. 1B), and, in retrospect, enhance- ment in the pituitary stalk (Fig. 1C). An external ventricular drain was placed and the patient was transferred to the Univer- sity of Colorado Hospital Neuro ICU soon thereafter. He was suspected to have neurosarcoidosis and respiratory failure. Biopsy of the cerebellar mass revealed no foamy macro- phages or granuloma formation. The most conspicuous feature was profuse Rosenthal fiber-rich piloid gliosis (Fig. 2A), with modest collections of cytologically bland, CD68-positive his- tiocytes without granuloma formation (Fig. 2B). The findings were not diagnostic for a specific disease process. The patient’s respiratory status remained poor and he was placed From the Department of Pathology (ZP, BKK-D); Department of Neurology (BKK-D); and Department of Neurosurgery, University of Colorado Denver, Aurora, Colorado (BKK-D) Send correspondence to: Bette K. Kleinschmidt-DeMasters, MD, Department of Pathology, University of Colorado School of Medicine, Mailstop F768, 12605 East 16th Avenue, Aurora, CO 80045; E-mail: [email protected] The authors declare no specific funding. The authors have no duality or conflicts of interest to declare. 986 V C 2017 American Association of Neuropathologists, Inc. All rights reserved. J Neuropathol Exp Neurol Vol. 76, No. 12, December 2017, pp. 986–996 doi: 10.1093/jnen/nlx095 Downloaded from https://academic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of CNS Erdheim–Chester Disease: A Challenge to Diagnose

REVIEW ARTICLE
CNS Erdheim–Chester Disease: A Challenge to Diagnose
Zenggang Pan, MD, PhD and Bette K. Kleinschmidt-DeMasters, MD
AbstractErdheim–Chester disease (ECD) is a rare nonLangerhans cell his-
tiocytosis. Although approximately 50% of cases eventually involve
the central nervous system (CNS), the CNS has seldom been
reported as the initial biopsy site. The diagnosis of CNS ECD can be
challenging due to morphologic overlap with reactive histiocytic
proliferation, Langerhans cell histiocytosis (LCH), and extranodal
Rosai–Dorfman disease (RDD). We present 3 cases from our files
that illustrate the protean manifestations of ECD. Case 1 was a 47-
year-old man with ataxia, dysarthria, and intermittent ophthalmople-
gia whose cerebellar biopsy had shown only profuse, nonspecific
Rosenthal fiber-rich piloid gliosis; ECD was diagnosed only at au-
topsy. The gliosis and marked variations in histiocyte morphology in
different anatomical sites added to the diagnostic challenge. Case 2
was a 67-year-old female with chronic progressive symptoms and a
pontine lesion that had been considered to be CLIPPERS by neuro-
imaging. Identification of a BRAFV600E mutation allowed an ECD
diagnosis and treatment with the specific BRAFV600E inhibitor
vemurafenib, which resulted in a marked sustained clinical response.
Case 3 was diagnosed as ECD after positive bone biopsy with typi-
cal foamy histiocytes. Six years later, there was massive dural in-
volvement that showed RDD-like, BRAF-mutation-negative
histiocytosis. These cases highlight the clinical and histologic over-
lap that can occur among these disorders.
Key Words: Central nervous system, Erdheim–Chester disease,
Langerhans cell histiocytosis, NonLangerhans cell histiocytosis,
Rosai–Dorfman disease.
INTRODUCTIONErdheim–Chester disease (ECD) is a rare nonLanger-
hans cell histiocytosis characterized by xanthomatous or xan-thogranulomatous infiltrates in tissues (1). The number ofcases has increased recently due to more recognition of thisentity, improved diagnostic criteria, and reliable molecularstudies. In the 2016 World Health Organization Classification,
ECD has been reclassified as a distinct entity and separatedfrom disseminated juvenile xanthogranuloma (2). The clinicalcourse of ECD is mainly dependent on the disease extent anddistribution, ranging from asymptomatic bone involvement tosystemic life-threatening disease with poor prognosis, particu-larly in the cases with central nervous system (CNS) or cardio-vascular involvement (3).
The diagnosis of ECD is typically based on the charac-teristic radiologic findings and pathologic features in the ap-propriate clinical context. However, recognition of CNS ECDcan be challenging due to variable clinical courses, often lim-ited tissue biopsies and mimicries with other reactive and neo-plastic histiocytic lesions; this is particularly problematic inlocalized CNS ECD cases without stereotypic radiographicchanges elsewhere. Here, we review the major clinicopatho-logic characteristics of CNS ECD with emphasis on thediagnostic workups and differential diagnosis through severalillustrative case presentations.
Case 1. ECD Diagnosed at Autopsy AfterInconclusive Cerebellar Biopsy WithProfuse Piloid Gliosis
The decedent was a 47-year-old Hispanic man with ahistory of a left cerebellar lesion since 2006. Symptoms con-sisted of ataxia, dysarthria, and intermittent ophthalmoplegia.The patient had no other chronic medical problems but hadbeen hospitalized in the spring of 2009 for pneumonia. In May2009, he developed decreasing mental status and was taken tothe emergency department in the southern part of Coloradowhere computerized tomography imaging revealed obstruc-tive hydrocephalus. Magnetic resonance imaging (MRI)showed a combination of bilateral cerebellar lesions epicen-tered on the dentate nuclei with enhancement (Fig. 1A), uppercervical cord lesions (Fig. 1B), and, in retrospect, enhance-ment in the pituitary stalk (Fig. 1C). An external ventriculardrain was placed and the patient was transferred to the Univer-sity of Colorado Hospital Neuro ICU soon thereafter. He wassuspected to have neurosarcoidosis and respiratory failure.
Biopsy of the cerebellar mass revealed no foamy macro-phages or granuloma formation. The most conspicuous featurewas profuse Rosenthal fiber-rich piloid gliosis (Fig. 2A), withmodest collections of cytologically bland, CD68-positive his-tiocytes without granuloma formation (Fig. 2B). The findingswere not diagnostic for a specific disease process. Thepatient’s respiratory status remained poor and he was placed
From the Department of Pathology (ZP, BKK-D); Department of Neurology(BKK-D); and Department of Neurosurgery, University of ColoradoDenver, Aurora, Colorado (BKK-D)
Send correspondence to: Bette K. Kleinschmidt-DeMasters, MD, Departmentof Pathology, University of Colorado School of Medicine, MailstopF768, 12605 East 16th Avenue, Aurora, CO 80045; E-mail:[email protected]
The authors declare no specific funding.The authors have no duality or conflicts of interest to declare.
986 VC 2017 American Association of Neuropathologists, Inc. All rights reserved.
J Neuropathol Exp NeurolVol. 76, No. 12, December 2017, pp. 986–996doi: 10.1093/jnen/nlx095
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

on comfort care measures before dying 10 days later. Permis-sion was given for a full autopsy.
At autopsy, there was bilateral pneumonia and atrophyof the testes. Although numerous systemic organs microscopi-cally contained small, amorphously grouped, nongranuloma-tous collections of histiocytes, these small collections hadbeen overlooked by the general autopsy pathologist. Indeed,only after neuropathological examination of the brain yieldeda postmortem diagnosis of ECD did rereview confirm the find-ings of ECD in the lung, testis, parathyroid capsule, bone, ad-ventitia of coronary arteries, and very focally in the kidney,the latter with a rare Touton giant cell (Fig. 3A–F). As is typi-cal of ECD, the histiocytes showed cytologically bland nuclei,inconspicuous nucleoli, and quite varying degrees of foamy
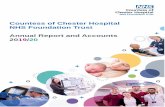
FIGURE 1. Case 1. (A) T1-weighted coronal magneticresonance imaging (MRI) with gadolinium illustrates thebilateral enhancing cerebellar lesions with epicenters nearthe dentate nuclei. (B) T1-weighted sagittal MRI withgadolinium of the spine shows patchy, somewhat linearenhancement in the upper cervical cord, without cord
FIGURE 1. Continuedexpansion. (C) T1-weighted sagittal MRI with gadoliniumreveals increased signal in the infundibular stalk and posteriorpituitary gland, which can be seen in patients with ECD even ifdiabetes insipidus is not clinically evident. Posterior fossalesions in this patient are also seen well on this sagittal image.
FIGURE 2. Case 1. (A, B) The nondiagnostic biopsy showedprominent piloid gliosis with profuse numbers of Rosenthal fibers(arrows, A) not accompanied by neoplastic piloid tumor cells.Small collections of cytologically bland, CD68-immunopositivehistiocytes are less conspicuous (B).
J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017 Diagnosis of CNS Erdheim–Chester Disease
987
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

(Fig. 3C) versus eosinophilic cytoplasm (Fig. 3D). Admixedlymphocytes and plasma cells were also variable in number,but in some sites, they were more pronounced than the histio-cytes (Fig. 3E).
The most striking macroscopic finding was in the brain.The cerebellum manifested bright yellow lesions measuring1.0 cm in greatest diameter, involving the dentate nuclei of thecerebellum bilaterally (Fig. 4). Although Rosenthal fiberswere still prominent, microscopic examination of the brainand spinal cord at autopsy demonstrated massive lipogranu-lomatous disease. Maximally affected areas included thecentral portion of the cerebellar white matter near the dentatenucleus bilaterally (Fig. 5A–D), hypothalamus (Fig. 5E), spi-
nal cord (Fig. 5F), and portions of the brainstem. These areascontained cohesive collections of lipid-laden histiocytes bothwithin parenchyma and around blood vessels that werehighlighted by periodic acid Schiff stain (Fig. 5A) and CD68immunohistochemistry (IHC) (Fig. 5D). They were composedof epithelioid histiocytes with small, round, eccentricallyplaced nuclei and abundant eosinophilic to focally foamy cyto-plasm (Fig. 5B, E). In a few areas, diffuse microglial activationwas even more prominent than the perivascular CD68 IHC-positive histiocytic collections (Fig. 5F). There was no evi-dence in the brain of an infectious process or tight small granu-lomas. No necrosis, multinucleated giant cells or Touton giantcells were found in the CNS, unlike the rare example of the
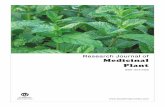
FIGURE 3. Case 1. (A–F) The diagnosis of ECD was made only at autopsy, based on the much more striking brain findings thanin the biopsy. Interestingly, histiocytic collections in systemic organs had been overlooked by the general pathologist but onretrospective review, non-CNS organs were clearly affected by ECD, yielding small multifocal nodular histiocytic collections inthe lung (A), histiocytes with eosinophilic cytoplasm in the testis (B), and foamy histiocytes in the parathyroid (C). Bonemarrow was focally involved, even if not clinically apparent (D); and in a few locations, the numbers of other types ofmononuclear inflammatory cells exceeded that of the histiocytes, as in the kidney (E). Touton giant cells (arrow), a characteristicfinding in ECD when present, were quite rare; this one was identified in the kidney, however (F).
Pan and Kleinschmidt-DeMasters J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017
988
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

latter in systemic organs (Fig. 5F), although the latter is not es-sential for the diagnosis of ECD. No cholesterol clefts wereidentified anywhere in the brain or systemic organs, excludingdiagnostic consideration of cerebrotendinous xanthomatosis.IHC for BRAF VE1, performed in retrospect, was positive.
Case 2. ECD Diagnosed at BiopsyA 67-year-old female was found to have an enhancing
pontine lesion of unclear etiology, which had been stable for3 years. She initially experienced diplopia, which was im-proved with prism glasses; later she developed worseningataxia, balance deficits, and intermittent dysarthria. Onworkup, lumbar puncture pressure and cerebrospinal fluidanalysis were normal. MRI studies detected a heterogeneousmultifocal lesion centered in the pons (Fig. 6A). This case oc-curred soon after the seminal report on chronic lymphocyticinflammation with pontine perivascular enhancement respon-sive to steroids (CLIPPERS), and after we had encountered acase of CLIPPERS at our institution seen by the same clinicalservice (4). The current patient’s condition was, therefore, ini-tially clinically felt to be CLIPPERS. No enhancing lesionswere noted elsewhere in the brain.
The patient underwent biopsies of the pontine lesion.Histologically, there was a prominent histiocytic infiltrate in abackground of reactive lymphocytes and plasma cells(Fig. 6C). The large histiocytes showed round to ovoid nucleiwith fine chromatin, occasional small nucleoli, and abundantpale cytoplasm (Fig. 6D). No microorganisms, hemophagocy-tosis, or emperipolesis was seen. Histiocytes revealed no sig-nificant cytologic atypia, increased mitotic rate, or areas ofgranuloma formation or necrosis. Histiocytes were immuno-positive for CD68 (Fig. 6E), but negative for S100 and CD1a.Notably, the lesional cells had a diffuse cytoplasmic stainingfor BRAF VE1 (Fig. 6F), an antibody reactive to the mutantprotein, BRAFV600E. Molecular assays with polymerasechain reaction and subsequent sequencing detectedBRAFV600E mutation in this case. Although BRAF mutation
is not essential for diagnosis (see below), when identified inconjunction with the correct clinicopathological features as inthe case, the diagnosis of ECD is solidified.
The patient was further evaluated with positron emis-sion tomography–computed tomography and was found tohave no evidence of systemic disease, including perirenal softtissues or suspicious bone involvement. She was treated withvemurafenib and had a marked response 1 month later withdramatic decrease of the lesion in the pons (Fig. 6B, placedimmediately adjacent to the initial pretreatment scan). She hasremained disease free on the drug for 3 years.
Case 3. Patient With Clinical Features of ECDIncluding Bone Involvement but HistologicalFeatures in Dura of RDD
A 46-year-old female experienced the onset of head-aches associated with facial tingling on the left cheek in 2009.Headaches were progressive, with gradual loss of sensation oftaste on the left side of her tongue and mouth. MRI scan of thebrain showed an enhancing mass in the left middle cranialfossa, left cerebellopontine angle, and hyperostosis of the pe-trous apex. Further and systemic studies then revealed axillaryand right inguinal lymph nodes, and soft tissue nodules in thelow anterior pelvis, concerning for metastases.
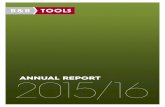
Excisional biopsies of the left trigeminal nerve and massin 2009 demonstrated massive expansion and distortion of theganglion by a mixed inflammatory infiltrate in which reactivelymphocytes and plasma cells were just as numerous as foamyhistiocytes. Multinucleated or Touton giant cells were notfound, nor were there tight granulomas. There was no molecu-lar evidence for a monoclonal T or B cell neoplasm (i.e. noneurolymphomatosis) and the diagnosis was descriptive only.A bone biopsy was performed soon thereafter in 2009 and thisdemonstrated small collections of foamy histiocytes. A bonescan was performed in 2010 (Fig. 7A); ECD was suspectedgiven the histiocytic features in the bone biopsy combined withpositive bone scans, particularly the increased bilateral uptakein the distal femur, proximal tibia, and humeral head (Fig. 7A).
The patient initially had a clinical response to Gleevec,but then showed persistent and progressive disease. She then de-veloped left eye fullness, vision changes and diplopia, and imag-ing in 2014 demonstrated a left intraconal mass, 13 � 15 �15 cm. That displaced the lateral rectus muscle and optic nervesheath complex, without definite signal abnormalities or en-hancement in the optic nerve (Fig. 7B). This mass was notapproached surgically.
In 2015, she developed more neurological symptoms,resulting in imaging studies performed at an outside hospitalthat showed a new, massive dural lesion over the convexity(Fig. 7C). An excision of this dural mass was performed at theoutside local hospital 7 years after the initial presentation. Theresection specimen was referred to our institution for consulta-tive diagnosis.
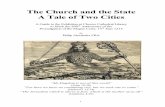
Previous bone and trigeminal biopsies were retrievedfor comparison and showed a range of morphological features(Fig. 8A–D). The bone biopsy contained very small nests offoamy histiocytes with nuclei showing indistinct nucleoli(Fig. 8A), whereas the left trigeminal nerve and ganglion
FIGURE 4. Case 1. The most striking gross finding at autopsywas multifocal bright yellow histiocytic deposits in bilateralcerebellar hemispheres, encompassing the dentate nuclei.Compare with premortem neuroimaging in Figure 1A, C.
J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017 Diagnosis of CNS Erdheim–Chester Disease
989
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

biopsy showed fewer histiocytes, albeit also with relatively in-distinct nucleoli and no emperipolesis; lymphocytes andplasma cells were more conspicuous (Fig. 8B). Morphologi-cally, the new meningeal lesion manifested placode-like tobulbous expansion of dura and contained sheets of histiocyteswith slightly different cytological features than previous biop-sies. Notably, there were sheets of abnormal histiocytes thathad enlarged nuclei with fine chromatin and frequent large nu-cleoli. The cytoplasm was abundant and often dense pale orpink staining with frequent viable intracytoplasmic lympho-cytes and plasma cells, so called “emperipolesis” (Fig. 8C).
A subset of histiocytes also showed foamy cytoplasm. The his-tiocytes were diffusely immunopositive for CD68 and S100(Fig. 8D) on both trigeminal and dural biopsies but were nega-tive for CD1a and BRAF VE1. Molecular studies on the duralmass detected no significant gene mutations, including BRAF,NRAS, MAP2K1, and PIK3CA. Overall, the CNS disease hadoverlapping clinicopathologic features of RDD and ECD, al-though the presence of cells with large nucleoli was thought tobe archetypal for the former.
The patient is still alive with slowly enlarging brainlesions in multiple sites on recent MRI imaging. Recent
FIGURE 5. Case 1. (A–F) Cerebellum at autopsy demonstrated numerous Rosenthal fibers in surrounding gliotic brain tissue butthere were more prominent perivascular histiocytic collections (A, B), as well as diffuse parenchymal histiocytic infiltrates (B). Arange of morphological features was seen within a single aggregate of the ECD histiocytes, with some showing mild foamycytoplasmic features and others showing completely eosinophilic cytoplasm (C). The rounded cytoplasmic profiles distinguishedthese from stellate, reactive gemistocytic astrocytes, as did CD68 immunoreactivity (D). Histiocytic collections were identified inthe hypothalamus, another frequently involved anatomical CNS site in ECD (E). Although lesions had been identified onpremortem imaging in the spinal cord (see Fig. 1B), even at autopsy many areas of involvement were subtle, as seen with anti-CD68 immunohistochemistry (F). As in the premortem biopsy, such areas were clearly abnormal but not fully and specificallydiagnostic for ECD without corroborating the lesion with findings in other areas in the same brain (A–E).
Pan and Kleinschmidt-DeMasters J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017
990
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

clinical laboratory studies showed normal serum interleukin-6and IgG4 levels.
DISCUSSIONBased on the presence of BRAFV600E and other related
mutations, ECD, along with LCH, is recognized today to be a
true neoplastic, rather than inflammatory disorder (5).Haroche et al have long reported the overlapping clinical fea-tures seen in some patients. This is an interesting observation,given the fact that ECD and LCH, but not RDD, share similargenetic underpinnings. Case 3 in this series underscores theclinical and even histologic overlap between ECD and RDDthat can occur. The most frequent overlap, however, is
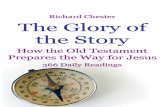
FIGURE 6. Case 2. (A, B) Axial MRI, T-weighted, with contrast scan(s) detected a heterogeneous expansile lesion in the pons ofthe patient (A). After vemurafenib treatment there has been a sustained, near-total regression of the pontine lesion, as seen onthis MRI scan taken 1 month after start of therapy following diagnosis of ECD made on biopsy (B). (C–F) Biopsy of the pontinelesion revealed a prominent histiocytic infiltration with scattered lymphocytes and plasma cells (C). Histiocytes had no overtcytologic atypia and abundant pale, nonfoamy cytoplasm (D), CD68 immunoreactivity (E), and diffuse cytoplasmic positivity toanti-BRAF VE1 antibody (F).
J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017 Diagnosis of CNS Erdheim–Chester Disease
991
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

between ECD and LCH, with some cases initially showingLCH and eventuating in ECD (6). LCH is predominantly a dis-order of childhood whereas most ECD patients are middle-aged to elderly, ranging from 40 to 80 years with a mean ageof 55 years. ECD shows a strong male predilection, with amale to female ratio of 3:1 (3).
Like other histiocytoses, ECD can virtually affect ev-ery organ system. The resultant variable clinical presenta-tions depend upon the extent and distribution of the disease.Skeletal involvement is nearly always present and eventu-ally develops in approximately 96% of ECD cases with
characteristic bilateral osteosclerotic lesions of long bonesin the lower extremities. Generally, the clinical features arechronic, and sometimes of sufficiently long duration thatECD is not in the differential considerations. The majorextraskeletal manifestations include neurological symptoms,diabetes insipidus, cardiovascular involvement with circum-ferential thickening of the aorta (“coated aorta”), and retro-peritoneal fibrosis (“hairy kidney”). It is when patientspresent with prominent neurological symptoms that over-shadow or predate the systemic signs and symptoms thatdiagnostic confusion often arises.
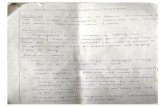
FIGURE 7. Case 3. (A) One year after presentation, the patient underwent nuclear medicine bone scans that showed bilateralincreased uptake in the distal femur, proximal tibia, and humeral head. (B) Five years later, she developed eye fullness and visualchanges that prompted an MRI scan (sagittal, T-weighted, with contrast), which demonstrated a left intraconal mass intimatelyassociated with the ocular musculature. (C) Six years later, new neurological symptoms prompted another MRI scan thatshowed an enhancing convexity dural mass.
Pan and Kleinschmidt-DeMasters J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017
992
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

CNS involvement is present in up to 50% of ECD casesand less than one third of ECD cases initially present with neu-rological symptoms (7–9). The major CNS manifestations arecerebellar and pyramidal syndromes, with central diabetes in-sipidus as the most common CNS manifestation, reported inapproximately 25% of patients. Other symptoms include seiz-ures, headaches, neuropsychiatric manifestations, cognitiveimpairment, sensory disturbances, and cranial nerve paralysis.The CNS symptoms may last for several years before the diag-nosis, as noted in our Cases 1 and 2. In the French series, overa decade of unexplained diabetes insipidus was present insome patients before other symptoms developed that led toECD diagnosis (10). CNS involvement is an independent, ad-verse prognostic factor of ECD (3). Due to the high prevalenceof CNS involvement, all new ECD patients should be system-atically examined on the brain with imaging studies, even ifthey are asymptomatic.
CNS ECD may occur throughout the neuraxis, with bothintraaxial and extraaxial infiltrations. Pachymeninges-basedlesions can be expansile and gadolinium-enhancing along thecerebral hemispheres or in the cerebellar tentorium, which canmimic meningioma, granulomatous disease, meningeal RDD,and LCH (11, 12). Intraaxially, ECD most commonly involvesthe cerebellar dentate nuclei and the pons (12), causing cere-bellar symptoms (i.e. ataxia and dysarthria) and brainstem
symptoms, which may resemble metastatic tumor, demyelin-ating disease, and/or inflammatory processes. Unilateral or bi-lateral infiltration of the orbits occurs in approximately 25% ofpatients (13) and typically shows bilateral intraconal masses(Fig. 7B), a hypointense signal on both T1- and T2-weightedimages, and intense enhancement on gadolinium-enhancedT1-weighted images. Patients can clinically present with ex-ophthalmos, retro-orbital pain, oculomotor palsies, or blind-ness, resembling Graves’ disease, lymphoma, IgG4-relatedsclerosing disease, and granulomatous disease.
Radiographic StudiesBone involvement is present in almost all ECD patients
and represents the most common clinical feature. Plain radio-graph shows bilateral, symmetric cortical osteosclerosis of thediaphyseal and/or metaphyseal regions of the distal ends oflower extremities, which can be highlighted by the sensitivebone scintigraphy using technetium Tc 99 m with symmetricuptakes in the long bones (Fig. 7A).
In the brain, the hypothalamic-pituitary axis is most fre-quently involved, and the high signal intensity of the posteriorpituitary lobe is normally seen on T1-weighted MR images(Fig. 1C) (9). Meningeal involvement occurs in 23% ofpatients, presenting as single or multiple dural masses or
FIGURE 8. Case 3. (A–C) Over the course of her disease, 3 anatomical sites have had biopsy/excisional material: bone (A), lefttrigeminal nerve and ganglion (B), and dura (C). Side-by-side comparison of the histiocytic features from these 3 sites shows anECD to RDD spectrum. The bone (A) and the left trigeminal nerve and ganglion (B) contained foamy histiocytes but had noapparent emperipolesis, consistent with ECD; histiocytes were similar in the trigeminal biopsy but accompanying nonneoplasticlymphocytes and plasma cells were more conspicuous (B). In contrast, the dural mass showed histiocytes with frequentemperipolesis (C, arrows) and histiocytes manifested more open chromatin pattern, larger nuclei and more distinct nucleoli (C).The histiocytes were diffusely positive for S100 both on the trigeminal biopsy (D) and the dural mass, with negativeimmunostaining for CD1a and BRAF VE1 on the latter.
J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017 Diagnosis of CNS Erdheim–Chester Disease
993
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

diffuse pachymeningeal thickening. The intraaxial involve-ment shows one or multiple mass lesions in the supratentorialor infratentorial area (Fig. 1A). These meningeal or intraaxiallesions typically reveal an iso- or hypointense signal on T2-weighted images, and intense homogeneous enhancement ongadolinium-enhanced T1-weighted images. ECD in the den-tate nucleus demonstrates bilateral symmetric high signal in-tensity areas on T2-weighted MR images and correspondinglow signal intensity on T1-weighted images.
Clinical FeaturesClinical features have been reviewed by Parisi et al (14),
with symptoms referable to this posterior fossa/cerebellar pre-dilection, including central diabetes insipidus, cerebellar syn-dromes, orbital lesions, and extraaxial masses involving thedura. When only the brainstem is involved, the differential di-agnosis may be broader, as illustrated by Case 2.
Histomorphologic FeaturesThe diagnosis of ECD is made based upon the appropri-
ate clinical and radiologic context, characteristic morphologicfeatures, and necessary immunohistochemical and molecularstudies (1). Lesional tissue typically contains foamy or lipid-laden macrophages with mixed fibrosis and frequent plasmacells in the background. The histiocytes are often organizedinto polymorphic xanthogranulomatous nests; and they haveround nuclei and abundant foamy cytoplasm with no apparentcytologic atypia or increase in mitosis or apoptosis. Touton gi-ant cells are often, but not invariably, present (e.g. Fig. 3F). Asillustrated by our Case 1, the variability of foamy versus paleeosinophilic cytoplasm and presence of Touton giant cells isbest appreciated on cases that come to autopsy. Difficulty withdiagnosis on small biopsy or suboptimally targeted biopsies isalso underscored by Case 1.
By immunohistochemical staining, ECD histiocytes arepositive for CD68, CD163, and factor XIIIa, whereas immu-nostains for CD1a, S100, and Langerin (CD207) are negative.Immunohistochemical staining on paraffin sections with theBRAFV600E mutant-specific antibody (VE1) can be used toassist in the diagnosis of ECD, although it must be emphasizedthat absence of mutation does not exclude ECD.
Molecular StudiesBRAFV600E mutation is detected in about 55%–60% of
ECD cases (15–20). BRAF is a serine/threonine protein kinase,with a crucial role in the regulation of cell proliferation andsurvival, as it contributes to the RAS/RAF-MEK-ERK proteinkinase pathway. The mutation causes the amino acid substitu-tion of glutamic acid for valine at position 600 of the BRAFprotein (V600E). Recently, it has been shown that ECDpatients treated with vemurafenib, a selective BRAFV600E in-hibitor, had dramatic clinical and radiographic improvement(21, 22), as observed in our Case 2. In ECD patients with wildtype BRAF, 10.9% and 3.7% of patients have mutations inPIK3CA and NRAS, respectively. PIK3CA and NRAS are bothimplicated in MAPK activation pathway which further
highlights the importance of MAPK signaling to ECDpathogenesis (23, 24).
Differential DiagnosisCNS ECD must be distinguished from reactive and neo-
plastic processes with a histiocytic component, particularlyextranodal RDD and LCH (Table). Like CNS ECD, CNSRDD usually contains histiocytic infiltration, prominent fibro-sis, and abundant plasma cells in the tissue (Fig. 6C, D). How-ever, the histiocytes in RDD are usually larger and have alarge nucleus with a prominent nucleolus and mild cytologicatypia (Fig. 8C). The cytoplasm is typically homogeneouspale or pink staining with characteristic emperipolesis, thepresence of viable intracytoplasmic lymphocytes, plasmacells, and/or neutrophils, although it may not be as obvious asthe nodal disease. Immunostaining for S100 is positive inRDD but not ECD.
CNS LCH has similar distribution and radiographicappearances to CNS ECD, although ECD is often expansile inmeninges, and spinal cord is often spared in LCH. Both lesionsmay share the features of diabetes insipidus. Morphologically,LCH cells are epithelioid with obvious cytologic atypia andfrequent nuclear grooves. Abundant background eosinophils,increased mitoses and apoptotic bodies, and areas of necrosisare commonly seen in LCH. LCH cells express CD1a, S100and Langerin. Despite these differences mentioned above,both ECD and LCH commonly have a BRAFV600E mutation;and 12%–19% of ECD cases have concurrent LCH, suggestingthat they are clonally related in some cases (6, 25).
IgG4-related sclerosing disease may involve the CNSand mostly manifests as hypertrophic pachymeningitis andhypophysitis with infrequent direct parenchymal brain in-volvement (26). Histologically, IgG4-related disease containsprominent fibrosis and lymphoplasmacytic infiltration, whichis like ECD, whereas features of foamy histiocytes and xan-thogranuloma are generally absent in IgG4-related disease.However, immunostaining for IgG4 may be considered in theinitial workup if no apparent etiology is uncovered.
Prominent histiocytic and/or granulomatous reaction isfrequently seen in the brain following infection and necrosisdue to infarction or hemorrhage, which may resemble ECD;therefore, essential clinical examinations, careful morphologicevaluation, and necessary ancillary studies are required for acorrect diagnosis.
Finally, sellar region histiocytic/xanthomatous lesionssecondary to ruptured Rathke cleft cyst, leakage of adamanti-nomatous craniopharyngioma cyst contents, or uncertaincauses must be distinguished from histiocytic disorders thataffect the sellar region/pituitary stalk (27).
Management and TherapyMany different therapeutic approaches for ECD have
been explored so far; these include steroids, cytotoxic drugs,and autologous hematopoietic stem cell transplant, but theclinical efficacy is limited. Interferon-a (IFN-a) became thefirst-line drug in the management of symptomatic ECD, andthe therapeutic modality with the largest amount of supporting
Pan and Kleinschmidt-DeMasters J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017
994
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

evidence in ECD is IFN-a and pegylated IFN-a (28). Treat-ment with the recombinant interleukin 1-receptor antagonistanakinra has been attempted and found effective in somepatients (29). The discovery of BRAFV600E mutation in ECDhas led to the very promising treatment with vemurafenib, aninhibitor of the BRAFV600E mutation, with dramatic and un-precedented clinical and radiographic responses (21, 30). Al-though anecdotal, the response seen in Case 2 in this seriesunderscores that unlike targeted therapies for some conditions,the response appears to be better sustained in BRAF-mutatedECD patients treated with targeted drug (21, 22, 31–33).
ConclusionIn summary, for a brain lesion with prominent histio-
cytic proliferation, an initial workup is necessary to rule outreactive processes based on the clinical presentations and mor-phologic features. For persistent and progressive lesions, spe-cial considerations include ECD, LCH, and RDD, and furtherimmunohistochemical stains can be utilized to separate theseentities. Additional radiologic examinations and molecularstudies may be required to confirm the diagnosis of CNS ECDand open the possibility of targeted therapy treatments. Takehome messages include the fact that the neoplastic histiocytesmay be quite variable in number and cytoplasmic content, andthat the hypothalamic/pituitary and posterior fossa are epicen-ters of involvement in the CNS, although certainly disease canextend beyond these sites. Diabetes insipidus may antedateother symptoms by years and although ECD presenting withneurological, not systemic organ clinical manifestations, is the
most challenging to diagnose, initial CNS presentation iscertainly not rare and must be recognized. Overlap betweenECD and especially LCH has been better appreciated by clini-cian experts in histiocytic disorders than by pathologists, butoccasional morphological overlap also occurs.
ACKNOWLEDGMENTSThe authors thank Ms. Lisa Litzenberger for photo-
graphic expertise and Mrs. Diane Hutchinson for manuscriptpreparation.
REFERENCES1. Diamond EL, Dagna L, Hyman DM, et al. Consensus guidelines for the
diagnosis and clinical management of Erdheim–Chester disease. Blood
2014; 124:483–922. Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World
Health Organization classification of lymphoid neoplasms. Blood 2016;
127:2375–903. Arnaud L, Hervier B, Neel A, et al. CNS involvement and treatment with
interferon-alpha are independent prognostic factors in Erdheim–Chester
disease: a multicenter survival analysis of 53 patients. Blood 2011; 117:
2778–824. Kleinschmidt-DeMasters BK, West M. CLIPPERS with chronic small
vessel damage: more overlap with small vessel vasculitis? J Neuropathol
Exp Neurol 2014; 73:262–75. Haroche J, Papo M, Cohen-Aubart F, et al. Erdheim–Chester disease
(ECD), an inflammatory myeloid neoplasia. Presse Med 2017; 46:
96–1066. Hervier B, Haroche J, Arnaud L, et al. Association of both Langerhans
cell histiocytosis and Erdheim–Chester disease linked to the
BRAFV600E mutation. Blood 2014;124:1119–26.7. Cuello-Oderiz C, Pigretti S, Patrucco L. Neurological onset of Erdheim–
Chester disease. Rev Neurol 2014; 59:572–4
TABLE. Differential Diagnosis of Erdheim–Chester Disease with Langerhans Cell Histiocytosis and Rosai–Dorfman Disease
Erdheim–Chester Disease Langerhans Cell Histiocytosis Rosai–Dorfman Disease
Locations in CNS Cerebellum, pons, dura,
brain parenchyma
Cerebellum, pons, dura, brain parenchyma Dura
Morphology
Nucleus Round Epithelioid, frequent grooves Often enlarged with mild atypia
Nucleolus Small Variable Variable. May be prominent
Cytoplasm Abundant, foamy, or lipid-laden Moderate, pink Abundant, dense pale or pink,
frequent emperipolesis
Mitosis/necrosis None May be present None
Other features Touton cells Occasional osteoclast-like giant cells
Background Fibrosis, plasma cells Abundant eosinophils Fibrosis and plasma cells
Immunophenotype
CD1a � þ �CD68 þ þ þCD207 (langerin) � þ �Factor XIIIa þ � �S100 � þ �VE1 þ* þ* �
BRAF V600E 55%–60% �64% �Other Mutations MAP2K1
PIK3CA 10.9%NRAS 3.7%
MAP2K1 12%–27.5%(mutually exclusive to BRAF V600E)
KRAS 19%MAP2K1 14% (mutually exclusive)
*Positive in the cases with BRAF V600E mutation.
J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017 Diagnosis of CNS Erdheim–Chester Disease
995
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022

8. Perez A, Crahes M, Laquerriere A, et al. Neurological form of Erdheim–Chester disease: Case report and review of the literature. Neurochirurgie2014; 60:316–20
9. Drier A, Haroche J, Savatovsky J, et al. Cerebral, facial, and orbital in-volvement in Erdheim–Chester disease: CT and MR imaging findings.Radiology 2010; 255:586–94
10. Courtillot C, Laugier Robiolle S, Cohen Aubart F, et al. Endocrine mani-festations in monocentric cohort of 64 patients with Erdheim–Chesterdisease. J Clin Endocrinol Metab 2016; 101:305–13
11. Wilejto M, Abla O. Langerhans cell histiocytosis and Erdheim–Chesterdisease. Curr Opin Rheumatol 2012; 24:90–6
12. Haroche J, Arnaud L, Amoura Z. Erdheim–Chester disease. Curr OpinRheumatol 2012; 24:53–9
13. Haroche J, Arnaud L, Cohen-Aubart F, et al. Erdheim–Chester disease.Rheum Dis Clin North Am 2013; 39:299–311
14. Wright RA, Hermann RC, Parisi JE. Neurological manifestations ofErdheim–Chester disease. J Neurol Neurosurg Psychiatry 1999; 66:72–5
15. Haroche J, Charlotte F, Arnaud L, et al. High prevalence of BRAF V600Emutations in Erdheim–Chester disease but not in other non-Langerhanscell histiocytoses. Blood 2012;120:2700–3
16. Cangi MG, Biavasco R, Cavalli G, et al. BRAFV600E-mutation is invari-ably present and associated to oncogene-induced senescence inErdheim–Chester disease. Ann Rheum Dis 2015; 74:1596–602
17. Blombery P, Wong SQ, Lade S, et al. Erdheim–Chester disease harboringthe BRAFV600E mutation. J Clin Oncol 2012;30:e331–2
18. Cohen Aubart F, Emile JF, Maksud P, et al. Efficacy of the MEK inhibi-tor cobimetinib for wild-type BRAF Erdheim–Chester disease. Br J Hae-matol 2016; doi: 10.1111/bjh.14284.
19. Emile JF, Charlotte F, Amoura Z, et al. BRAF mutations in Erdheim–Chester disease. J Clin Oncol 2013;31:398.
20. Nordmann TM, Juengling FD, Recher M, et al. Trametinib after diseasereactivation under dabrafenib in Erdheim–Chester disease with bothBRAF and KRAS mutations. Blood 2017;129:879–82
21. Haroche J, Cohen-Aubart F, Emile JF, et al. Reproducible and sustainedefficacy of targeted therapy with vemurafenib in patients withBRAF(V600E)-mutated Erdheim–Chester disease. J Clin Oncol 2015;33:411–8
22. Haroche J, Cohen-Aubart F, Emile JF, et al. Dramatic efficacy of vemur-afenib in both multisystemic and refractory Erdheim–Chester disease
and Langerhans cell histiocytosis harboring the BRAF V600E mutation.Blood 2013;121:1495–500
23. Emile JF, Diamond EL, Helias-Rodzewicz Z, et al. Recurrent RAS andPIK3CA mutations in Erdheim–Chester disease. Blood 2014; 124:
3016–924. Diamond EL, Abdel-Wahab O, Pentsova E, et al. Detection of an NRAS
mutation in Erdheim–Chester disease. Blood 2013; 122:1089–9125. Liersch J, Carlson JA, Schaller J. Histopathological and clinical findings
in cutaneous manifestation of Erdheim–Chester disease and Langerhanscell histiocytosis overlap syndrome associated with the BRAFV600E
Mutation. Am J Dermatopathol 2017; 39:493–50326. Regev K, Nussbaum T, Cagnano E, et al. Central nervous system mani-
festation of IgG4-related disease. JAMA Neurol 2014; 71:767–7027. Kleinschmidt-DeMasters BK, Lillehei KO, Hankinson TC. Review of
xanthomatous lesions of the sella. Brain Pathol 2017; 27:377–9528. Hervier B, Arnaud L, Charlotte F, et al. Treatment of Erdheim–Chester
disease with long-term high-dose interferon-alpha. Sem Arthritis Rheum2012; 41:907–13
29. Aouba A, Georgin-Lavialle S, Pagnoux C, et al. Rationale and efficacyof interleukin-1 targeting in Erdheim–Chester disease. Blood 2010; 116:
4070–630. Haroche J, Abla O. Uncommon histiocytic disorders: Rosai–Dorfman,
juvenile xanthogranuloma, and Erdheim–Chester disease. HematologyAm Soc Hematol Educ Program 2015; 2015:571–8
31. Gupta A, Yeganeh A, Rootman D, et al. Vemurafenib (BRAF inhibitor)therapy for orbital Erdheim–Chester disease. Ophthal Plast Reconstr
Surg 2017; doi: 10.1097/IOP.0000000000000866.32. Janku F, Vibat CR, Kosco K, et al. BRAFV600E mutations in urine and
plasma cell-free DNA from patients with Erdheim–Chester disease.Oncotarget 2014;5:3607–10
33. Varadi Z, Banusz R, Csomor J, et al. Effective BRAF inhibitor vemurafe-nib therapy in a 2-year-old patient with sequentially diagnosed Langer-
hans cell histiocytosis and Erdheim–Chester disease. Onco Targets Ther2017; 10:521–6
Pan and Kleinschmidt-DeMasters J Neuropathol Exp Neurol • Volume 76, Number 12, December 2017
996
Dow
nloaded from https://academ
ic.oup.com/jnen/article/76/12/986/4583594 by guest on 23 August 2022