Self-Efficacy, Outcome Expectation and Health-Promotion Practice among Nigerian Physiotherapists
Upload
khangminh22Category
view
1download
0
Clinical Practice Guidelines
for Physiotherapists working with persons with
Bleeding Disorders
2021
Companion document for
CPHC Standards of Physiotherapy Care
for Persons with Bleeding Disorders

Page 1 of 61
Canadian Physiotherapists in Hemophilia Care Clinical Practice Guidelines
Revised January 11, 2021
Contents:
Introduction
1. The Physiotherapist as a core team member page 4
2. Physiotherapy assessment of acute bleeds page 7
3. Physiotherapy treatment after acute bleeds page 15
4. The annual assessment page 19
5. Physiotherapy treatment of MSK complications of bleeding disorders page 27
6. Physiotherapy before and after MSK surgery page 36
A. Prior to MSK surgery page 36
B. Following MSK surgery page 41
C. Special Considerations regarding Total Knee Arthroplasty page 42
7. Consultation with other care providers page 47
8. Encouraging a healthy lifestyle page 50
9. Continuing competence page 51
Appendix 1: Incidence and clinical symptoms of Rare Bleeding Disorders page 54
Appendix 2: Levels of evidence page 56
Appendix 3: Grades of recommendation page 57
Appendix 4: Summary of Practice Statements page 58

Page 2 of 61
Introduction:
CPHC Clinical Practice Guidelines were originally developed in 2018 as a companion
document to the CPHC Standards of Physiotherapy Care for Persons with Bleeding
Disorders.
Revisions to this 2021 version include:
• Updated references, and inclusion of Levels of Evidence for all references
• Revised section on Physiotherapy before and after musculoskeletal surgery
• Conversion of the guidelines into Practice Statements
• Inclusion of “Grade of recommendation” for each Practice Statement
Additional modifications were made to align these guidelines with the 2020 Canadian
Hemophilia Society Canadian Integrated and Comprehensive Care Standards for
Inherited Bleeding Disorders.
https://www.hemophilia.ca/integrated-and-comprehensive-care-standards/
Key changes to the integrated and comprehensive standards include:
• The standards apply to “the entire family of inherited bleeding disorders”,
not only to hemophilia
• The standards apply to all Persons with a Bleeding Disorder (PWBD)
regardless of gender at birth
• The term Hemophilia Treatment Center (HTC) has been replaced with
Treatment Center (TC)
Finally, in light of the new products coming available we have changed “factor
replacement/coverage” to Hemostasis Management, which could also include non-
infused products like DDAVP, and non-factor products such as Emicizumab.
2020 Working group members: Kathy Mulder, Winnipeg JoAnn Nilson, Saskatoon Erin McCabe, Edmonton
Contributors to Section 6: Physiotherapy before and after MSK surgery:
Greig Blamey, Winnipeg Laurence Boma-Fischer, Toronto
Stacey Cave, Vancouver Pamela Hilliard, Toronto
Sandra Squire, Vancouver Karen Strike, Hamilton
Marie-Eve Toussaint, Montreal

Page 3 of 61
Thanks to the 2018 working group:
Julia Brooks, Edmonton
Anne Ducharme, Montreal
Elia Fong, Edmonton
Pamela Hilliard, Toronto
Erin McCabe, Edmonton
Kathy Mulder, Winnipeg
Sandra Squire, Vancouver
Marie-Eve Toussaint, Montreal

Page 4 of 61
Standard 1: Each Canadian integrated and comprehensive bleeding
disorders care team includes a physiotherapist.
Practice Statement 1.1
The TC physiotherapist should meet the PWBD /family soon after diagnosis*, and will
provide assessment, treatment and education throughout the person’s lifespan.
Grade of recommendation: Theoretical
*Bleeding disorders that are associated with Musculoskeletal (MSK) bleeding include:
Frequent Common Less Common
Hemophilia A (FVIII deficiency)
Prothrombin deficiency Factor V deficiency
Hemophilia B (FIX deficiency)
Factor X deficiency Factor VII deficiency
Type 3 von Willebrand disease
Factor XIII deficiency
See Appendix A: Incidence and Clinical symptoms of Rare Bleeding Disorders
For individuals diagnosed with these conditions:
• The TC physiotherapist performs baseline and longitudinal assessments, and
participates in the assessment of suspected MSK bleeds. [See also Assessment of
acute bleeds (S-2), Annual Assessment (S-4), and Pre-and post-operative
assessments (S-6)]
• The TC physiotherapist arranges rehabilitation after acute bleeds, and for the
sequelae of bleeding. [See Treatment after Acute Bleeds (S-3) and Treatment of
MSK Complications (S-5)]
• The TC physiotherapist will educate PWBD and their families regarding prevention,
identification and management of bleeds and the potential MSK complications of
bleeding disorders.
Rationale:
The WHO Chronic Care Model states that patients and families need to be informed
about their chronic condition, including the expected course, potential complications,
and effective strategies to prevent complications and manage symptoms.
PWBD need to be prepared with sufficient knowledge and skills to manage their
condition at home. In addition to education about preventing and managing MSK bleeds
and their sequelae, the physiotherapist will promote a healthy active lifestyle.

Page 5 of 61
References:
de Moerloose P, Fischer K, Lambert T, et al. Recommendations for assessment,
monitoring and follow-up of patients with haemophilia. Haemophilia. 2012;18(3):319-
325. doi:10.1111/j.1365-2516.2011.02671.x
Level of evidence: V- expert opinion
Canadian Integrated and Comprehensive Care Standards for Inherited Bleeding
Disorders 2020. https://www.hemophilia.ca/integrated-and-comprehensive-care-
standards/ Accessed December 14, 2020
Level of evidence: V- expert opinion
Haemophilia Chartered Physiotherapists Association (HCPA). Service Provision of
Physiotherapy for Adults with Haemophilia & other Inherited Bleeding Disorders 2020.
http://www.ukhcdo.org/haemophilia-associations/physiotherapy-information/
Accessed December 14, 2020.
Level of evidence: V- expert opinion
Lillicrap D, James P. Von Willebrand disease: An introduction for the primary care
physician. World Federation of Hemophilia. 2009. Treatment of Hemophilia No. 47.
https://elearning.wfh.org/find-a-resource/ Accessed January 15, 2021
Level of evidence: Review
Palla R, Peyvandi F, Shapiro AD. Rare bleeding disorders: diagnosis and treatment. Blood
2015; 125 (13): 2052–2061. doi.org/10.1182/blood-2014-08-532820
Level of evidence: Review.
Srivastava, A, Santagostino, E, Dougall, A, et al. WFH Guidelines for the Management of
Hemophilia, 3rd edition. Haemophilia. 2020: 26(Suppl 6): 1‐ 158.
doi.org/10.1111/hae.14046
Level of evidence: V- expert opinion
World Health Organization. Innovative Care for Chronic Conditions: Building Blocks for
Action- Chapter 3. https://www.who.int/chp/knowledge/publications/icccreport/en/
Accessed December 14, 2020
Level of evidence: V- expert opinion

Page 6 of 61
Practice Statement 1.2
The physiotherapist should consider using telerehabilitation, including online video
conferencing platforms, for assessment, treatment and/or education of PWBD.
Grade of recommendation: Theoretical
Rationale:
The use of communications technology, if available and permitted by the TC/institution,
can enhance self-management and decrease patient burden, such as lost time from
school/work.
References:
Flannery T, Bladen M, Hopper D, Jones S, McLaughlin P, Penn A, Sayers F, Wells A,
Stephensen D. Physiotherapy after COVID-19—"Zoom or room". Haemophilia. 2020;
doi: 10.1111/hae.14166
Level of evidence: V-expert opinion
O'Donovan M, Buckley C, Benson J, et al. Telehealth for delivery of haemophilia
comprehensive care during the COVID-19 pandemic. Haemophilia. 2020;26(6):984-990.
doi:10.1111/hae.14156
Level of evidence: III - Case controlled study

Page 7 of 61
Standard 2: The physiotherapist participates in the assessment of acute
musculoskeletal bleeds.
Practice Statement 2.1
Physiotherapy assessment of acute bleeds should include a detailed history of the
present condition.
Grade of recommendation: Theoretical
Rationale/Discussion:
The earliest symptom of a musculoskeletal bleed is pain, BUT not all pain is due to
bleeding.
History of present condition includes:
• details of bleed onset and progression of symptoms
• mechanism of injury
• hemostasis management used to date and response to treatment
• other treatment (first aid) used and response to treatment
• pain qualities, location, intensity, aggravating/alleviating factors
• pain with movement
By taking a detailed history, the physiotherapist might be able to recognize mechanisms
of injury that correspond with the symptoms and subsequent physical exam findings.
References:
Blamey G, Forsyth A, Zourikian N, et al. Comprehensive elements of a physiotherapy
exercise programme in haemophilia--a global perspective. Haemophilia. 2010;16 Suppl
5:136-145. doi:10.1111/j.1365-2516.2010.02312.x
Key point: “the cause of the injury must be known, and the potential impact on the
involved structures as well as their role in overall function must be recognized.”
Level of evidence: V- expert opinion
Flood E, Pocoski J, Michaels LA, McCoy A, Beusterien K, Sasanè R. Patient-reported
experience of bleeding events in haemophilia. Eur J Haematol. 2014;93 Suppl 75:19-28.
doi:10.1111/ejh.12329
Key point: reports the words PWBD use to describe their sensation of bleeding in joints
and muscles
Level of evidence: Cross-sectional study/Qualitative
Sørensen B, Benson GM, Bladen M, et al. Management of muscle hematomas in

Page 8 of 61
patients with severe hemophilia in an evidence-poor world. Hemophilia.
2012;18(4):598-606. doi:10.1111/j.1365-2516.2011.02720.x
Key point: “Cause of bleed should be determined by explicit questioning, especially in
children”
Level of evidence: V- expert opinion
Timmer MA, Pisters MF, de Kleijn P, et al. How do patients and professionals
differentiate between intra-articular joint bleeds and acute flare-ups of arthropathy in
patients with haemophilia? Haemophilia. 2016;22(3):368-373. doi:10.1111/hae.12858
Key point: Focus groups generated a list of items that patients and professionals use to
differentiate between a joint bleed and a flare-up of Hemophilic Arthropathy.
Level of evidence: Other/Qualitative
Witkop M, Lambing A, Divine G, Kachalsky E, Rushlow D, Dinnen J. A national study of
pain in the bleeding disorders community: a description of haemophilia pain.
Haemophilia. 2012;18(3):e115-e119. doi:10.1111/j.1365-2516.2011.02709.x
Key point: describes the language used by patients to describe and differentiate acute
and persistent pain
Level of evidence: Other/Qualitative
Practice Statement 2.2
Physiotherapy assessment of acute bleeds should include past medical history.
Grade of recommendation: Theoretical
Rationale:
Past medical history includes:
• recent joint or muscle bleeds
• reasons for those bleeds
• previous target joints: location and number
• usual activities
• usual hemostasis management regime
o (factor or non-factor products)
• usual response to treatment for bleeds
Repeated episodes of bleeding at the same site may indicate incomplete recovery of
previous episodes, or shed light on a particular recurrent activity that contributes to re-
injury.

Page 9 of 61
References:
de Moerloose P, Fischer K, Lambert T et al. Recommendations for assessment,
monitoring and follow-up of patients with haemophilia. Haemophilia. 2012;18(3):319-
325. doi:10.1111/j.1365-2516.2011.02671.x
Key point: changes in bleeding frequency or severity should be thoroughly investigated
and treatment modified as necessary
Level of evidence: V- expert opinion
Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and
hematomas. J Blood Med. 2014; 5:207-218. Published 2014 Oct 17.
doi:10.2147/JBM.S50644
Key point: “subacute hemarthroses arise after repeated episodes…in the same joint.
Joint becomes a ‘target joint’ due to incomplete recovery.”
Level of evidence: V- expert opinion
Sørensen B, Benson GM, et al. Management of muscle hematomas in patients with
severe hemophilia in an evidence-poor world. Haemophilia. 2012;18(4):598-606.
doi:10.1111/j.1365-2516.2011.02720.x
Key point: “good history taking … will allow planning of subsequent treatment and
rehabilitation and enable an accurate prognosis.”
Level of evidence: V- expert opinion
Practice Statement 2.3
Physiotherapy assessment of acute bleeds should include a physical examination.
Grade of recommendation: Theoretical
Rationale/Discussion:
Physical exam should include:
• Observation/inspection:
o posture/resting position
o bruising** (see Notes)
o swelling
o redness
• Active Movement:
o compare to contralateral limb or, in the case of chronic arthropathy,
baseline measurements on file

Page 10 of 61
o pain with movement
• Palpation:
o warmth
o swelling
o tenderness
o spasm
• Testing:
o Joint end feel (within limits of pain)
o Muscle length, especially two-joint muscles
o Muscle strength, noting pain and/or weakness with active contraction
o Sensation, especially if nerve compression is suspected
Physiotherapists routinely perform a physical exam to determine a clinical diagnosis and
develop a treatment plan.
In PWBD, it is important to differentiate MSK bleeding from other sources of pain.
Presentation of joint bleeds may include the following:
• Warmth
• Swelling
• Joint held in a position of comfort (open pack position)
• Tender when joint is touched or moved
• Reduced range of motion
• Altered gait or inability to bear weight
Presentation of muscle bleeds may include the following:
• Pain if the muscle contracts or is stretched
• Muscle tightness and limited arc of motion
Superficial muscle bleeds will feel warm and tender to touch, and be accompanied by a
palpable swelling/hematoma.
Deep muscle bleeds may be difficult to palpate, but have potential for compartment
syndrome, with paresthesia and distal pallor or pulselessness.
**NOTES:
**Bruising:
• May be an indication of a superficial soft tissue bleed.
• Bruising is NOT a feature of joint bleeds

Page 11 of 61
• Bruising MAY be a late feature of a muscle bleed, but is not always present.
Accurate muscle testing will differentiate superficial soft tissue bleeds from
muscles bleeds.
** Presentation of an iliopsoas bleed may mimic that of appendicitis, or be confused
with a hip bleed.
Signs of an iliopsoas bleed can include:
• Pain in groin, thigh, hip, OR lower back
• Hip flexed, sometimes externally rotated
• Abdominal tenderness
• Tingling or numbness in distribution of femoral nerve
• Weakness of quadriceps and/or decreased patellar reflex
• Unable to stand straight: hyperlordosis, knee flexed, and unable to place foot flat
on floor
• Unable to lie flat
[Also note that psoas bleeds can be associated with sexual activity. Inquiry regarding
recent sexual activity should be included in ‘history of present condition’.]
References:
Blamey G, Forsyth A, Zourikian N, et al. Comprehensive elements of a physiotherapy
exercise programme in haemophilia--a global perspective. Haemophilia. 2010;16 Suppl
5:136-145. doi:10.1111/j.1365-2516.2010.02312.x
Key point: “Thorough assessment must follow any acute injury to ensure that
comprehensive and complete rehabilitation is being pursued”
Level of evidence: V- expert opinion
Blanchette VS, Key NS, Ljung LR, et al. Definitions in hemophilia: communication from
the SSC of the ISTH. J Thromb Haemost. 2014;12(11):1935-1939. doi:10.1111/jth.12672
Key Point: International group of Hematologists developed definitions of Joint Bleed,
Target Joint, Muscle Bleeds based on presenting symptoms, in order to facilitate
uniform documentation of outcomes in clinical studies.
Level of evidence: V- expert opinion
Flood E, Pocoski J, Michaels LA, McCoy A, Beusterien K, Sasanè R. Patient-reported
experience of bleeding events in haemophilia. Eur J Haematol. 2014;93 Suppl 75:19-28.
doi:10.1111/ejh.12329
Key point: reports the words PWBD use to describe their sensation of bleeding in joints
and muscles
Level of evidence: Cross-sectional study /Qualitative

Page 12 of 61
MASAC Recommendations Regarding Physical Therapy Guidelines in Patients with
Bleeding Disorders: Iliopsoas.
https://www.hemophilia.org/sites/default/files/document/files/238ptiliopsoas.pdf
Accessed January 10, 2021
Key Point: describes presenting signs and symptoms, and differential diagnosis
Level of evidence: V-expert opinion
Sørensen B, Benson GM, et al. Management of muscle hematomas in patients with
severe hemophilia in an evidence-poor world. Haemophilia. 2012;18(4):598-606.
doi:10.1111/j.1365-2516.2011.02720.x
Key point: describes common symptoms of muscle bleeds, including iliopsoas
Level of evidence: V- expert opinion
Srivastava A, Santagostino E, Dougall A, et al. WFH Guidelines for the Management of
Hemophilia, 3rd edition. Haemophilia. 2020;26 Suppl 6:1-158. doi:10.1111/hae.14046
Key points: Physical examination for joint changes (e.g., in joint circumference, muscle
strength, joint effusion, joint angle, pain according to a visual analogue scale) should be
conducted at all routine follow-ups. (Chapter 10: Musculoskeletal Complications)
Level of evidence: V- expert opinion
Timmer MA, Pisters MF, de Kleijn P, de Bie RA, Fischer K, Schutgens RE. Differentiating
between signs of intra-articular joint bleeding and chronic arthropathy in haemophilia: a
narrative review of the literature. Haemophilia. 2015;21(3):289-296.
doi:10.1111/hae.12667
Key Points: symptoms of hemarthrosis partly overlap with symptoms of flare-ups of
Hemophilic Arthropathy. “Differentiating based on imaging techniques or biomarkers
causes practical difficulties. Clinical assessment still seems the most convenient and
practical solution.”
Level of evidence: V- expert opinion
Timmer MA, Pisters MF, de Kleijn P, et al. How do patients and professionals
differentiate between intra-articular joint bleeds and acute flare-ups of arthropathy in
patients with haemophilia?. Haemophilia. 2016;22(3):368-373. doi:10.1111/hae.12858
Key point: Focus groups generated a list of items patients and professionals use to
differentiate between a joint bleed and a flare-up of Hemophilic Arthropathy
Level of evidence: Other/Qualitative

Page 13 of 61
Practice Statement 2.4
Physiotherapists who have received appropriate training may use point of care
ultrasound (POCUS), if available, to confirm diagnosis and monitor resolution.
Grade of recommendation: Moderate
Rationale:
There is considerable overlap between signs and symptoms of acute bleeding and
arthritis, which can make accurate diagnosis of joint bleeds challenging.
Deep muscle bleeds may not be easy to palpate or measure.
POCUS may be used as an adjunct to clinical assessment to confirm diagnosis, guide the
treatment plan, and confirm whether hematoma/synovitis is resolved.
References:
Ceponis A, Wong-Sefidan I, Glass CS, Von Drygalski A. Rapid musculoskeletal ultrasound
for painful episodes in adult haemophilia patients. Haemophilia. 2013;19(5):790-798.
doi:10.1111/hae.12175
Key points: MSK-US is a valuable point-of-care imaging tool to distinguish whether acute
joint and/or musculoskeletal pain episodes in adult PWH are due to bleeding or not.
Only approximately 1/3rd of the painful musculoskeletal episodes were judged
correctly, either by the patient or physician, and arthritis was being incorrectly treated
with factor.
Level of evidence: IV-Case series
Stephensen D, Bladen M, McLaughlin P. Recent advances in musculoskeletal
physiotherapy for haemophilia. Ther Adv Hematol. 2018;9(8):227-237. Published 2018
Jul 2. doi:10.1177/2040620718784834
Key point: Point-of-care ultrasound (POCUS) has potential value in acute hemarthrosis
to objectively identify presence of blood in joints, measure size, pinpoint location, assess
evolution and confirm complete disappearance.
Level of evidence: V- expert opinion
Stephensen, D, Classey, S, Harbidge, H, Patel, V, Taylor, S, Wells, A. Physiotherapist
inter‐rater reliability of the Haemophilia Early Arthropathy Detection with Ultrasound
protocol. Haemophilia. 2018;24(3):471-476. doi:10.1111/hae.13440
Key point: US imaging complements the physical examination when screening and
monitoring joint health of people with haemophilia at the point of care; inter-rater
reliability between physiotherapists was good.
Level of evidence: I

Page 14 of 61
Practice Statement 2.5
The physiotherapist should communicate assessment findings and treatment plans to
the relevant other team members.
Grade of recommendation: Theoretical
Rationale:
Communication with the other core team members is essential, to confirm clinical
diagnosis and to ensure adequate follow-up until full resolution and return to full
activity.
In some situations, hemostatic management may need to be adjusted to provide
optimum hemostasis during rehabilitation and/or during return to full activity.
References:
Canadian Alliance of Physiotherapy Regulators Core Standards of Practice – Updated
December 2019
https://www.alliancept.org/announcement/core-standards-practice-physiotherapists-
canada-now-available/
Accessed January 22, 2021
Key Points: Shares information with clients, team members, and other stakeholders
about the roles and responsibilities of physiotherapists in client-centred care.
Sørensen B, Benson GM, et al. Management of muscle hematomas in patients with
severe hemophilia in an evidence-poor world. Hemophilia 2012.18:598-606
Key point: need to ensure adequate hemostatic management especially for people with
inhibitors.
Level of evidence: V- expert opinion

Page 15 of 61
Standard 3: The physiotherapist will become involved as soon as possible
after acute bleeds to assist the individual to regain pre-bleed status while
preventing new injury or re-bleeding.
Practice Statement 3.1
Early management of acute MSK injuries may include:
• Monitoring and education
• Hemostatic management, as prescribed by the hematologist
• Protection of the injury with splints, slings
• Complete rest of the injured area, including:
o no weight bearing for joint or muscle bleeds
o no ambulation for psoas bleeds
• Ice for pain relief
• Compression
• Elevation
Grade of recommendation: Theoretical
Rationale/Discussion:
The primary goal of Physiotherapy treatment following any acute musculoskeletal injury
is to regain pre- injury status as soon as possible.
Physiotherapy management of acute MSK bleeding in PWBD has been informed largely
by the literature pertaining to other populations, such as sports injuries.
In PWBD, attention must also be paid to ensuring that bleeding has stopped, and to
preventing new bleeding during the rehabilitation period. The physiotherapist must be
familiar with contraindications and safety precautions applicable to treating PWBD.
References:
Hanley J, McKernan A, Creagh MD, et al. Guidelines for the management of acute joint
bleeds and chronic synovitis in haemophilia: A United Kingdom Haemophilia Centre
Doctors' Organisation (UKHCDO) guideline. Haemophilia. 2017;23(4):511-520.
doi:10.1111/hae.13201
Key point: Review by a physiotherapist is recommended as soon as a patient presents
with or reports a joint bleed, to advise and educate on the anticipated timeline for
rehabilitation.
Level of evidence: V- expert opinion
Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and
hematomas. J Blood Med. 2014; 5:207-218. Published 2014 Oct 17.

Page 16 of 61
doi:10.2147/JBM.S50644
Key point: contains detailed description of early management, with rationale and
precautions.
Level of evidence: V- expert opinion
Simpson ML, Valentino LA. Management of joint bleeding in hemophilia. Expert Rev
Hematol. 2012;5(4):459-468. doi:10.1586/ehm.12.27
Key point: “Rest, ice, compression and elevation are generally recommended as an
adjunct to factor replacement therapy during acute hemarthrosis…… evidence
supporting the use of ancillary therapies (in addition to factor replacement) is lacking.”
Level of evidence: V- expert opinion
Sørensen B, Benson GM. Management of muscle hematomas in patients with severe
hemophilia in an evidence-poor world. Haemophilia. 2012;18(4):598-606.
doi:10.1111/j.1365-2516.2011.02720.x
Key point: Protection, rest, ice, compression and elevation (PRICE) should be
implemented in the initial acute stage. An exception is young children, in whom
compression is not advocated.
Level of evidence: V- expert opinion
Practice Statement 3.2
After bleeding has stopped, the physiotherapist should introduce exercise to restore:
• Joint motion
• Muscle length (may also require serial splinting)
• Muscle strength
• Proprioception (upper limb as well as lower limb)
• Balance
• Gait
• Function (including ADL and sports)
Grade of recommendation: Theoretical
Rationale/Discussion:
Prior to modern clotting factor products, treatment of acute bleeds involved lengthy
periods of immobilization and/or inactivity which resulted in muscle weakness and loss
of sensorimotor skills.

Page 17 of 61
It is now recognized that an exercise program is essential for return to full function and
to minimize the risk of recurrent bleeding.
The most effective post-bleeding exercise parameters for PWBD are unknown: exercise
prescription guidelines for the general population should be followed, however, to
decrease the risk of injury, exercise should commence in limited range, at low velocity
and submaximal load, and within patient tolerance, while closely monitoring for signs of
new bleeding.
References:
Blamey G, Forsyth A, Zourikian N, et al. Comprehensive elements of a physiotherapy
exercise programme in haemophilia--a global perspective. Haemophilia. 2010;16 Suppl
5:136-145. doi:10.1111/j.1365-2516.2010.02312.x
Key points: Describes rationale for exercise for Flexibility, Strength, Proprioception,
Balance and Function within the context of hemophilia.
Level of evidence: V- expert opinion
Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and
hematomas. J Blood Med. 2014; 5:207-218. Published 2014 Oct 17.
doi:10.2147/JBM.S50644
Key point: An appropriate balance should be established between rest, early
mobilization, and weight-bearing so as to prevent unwanted complications associated
with immobilization
Level of evidence: V- expert opinion
Mulder K. Exercises for People with Hemophilia. World Federation of Hemophilia 2006.
http://www1.wfh.org/publications/files/pdf-1302.pdf Accessed November 3, 2020
Key point: Includes “Dos and Don’ts” for therapists who have limited experience with
PWBD.
Level of evidence: V- expert opinion
Sørensen B, Benson GM, Bladen M, et al. Management of muscle haematomas in
patients with severe haemophilia in an evidence-poor world. Haemophilia.
2012;18(4):598-606. doi:10.1111/j.1365-2516.2011.02720.x
Key point: Current literature divides physiotherapy and rehabilitation for muscle bleeds
in athletes into four phases: (i) control of haemorrhage, (ii) restoration of ROM and
strength, (iii) functional rehabilitation, and (iv) and return to normal living.

Page 18 of 61
Practice Statement 3.3
The physiotherapist may consider using electrophysical modalities to enhance
hematoma resolution.
Grade of recommendation: Research
Rationale:
Some authors have reported using Pulsed Ultrasound and/or Pulsed Short-Wave
Diathermy to assist tissue healing and/or hematoma resolution in PWBD. There are no
known references that specify parameters for treating acute bleeds in PWBD.
It is the opinion of the working group that any heat-generating modalities should be
applied with caution.
Deep heating is not advisable, and pulsed settings should always be used.
References:
Ravanbod R, Torkaman G and Esteki A. Comparison between pulsed ultrasound and low
level laser therapy on experimental haemarthrosis. Haemophilia. 2013;19(3):420-425.
doi:10.1111/hae.12061
Key point: in the lab, pulsed Ultrasound seems more effective than LLLT.
Level of evidence: Experimental- Animal study
Sørensen B, Benson GM, Bladen M. Management of muscle hematomas in patients with
severe hemophilia in an evidence-poor world. Haemophilia. 2012;18(4):598-606.
doi:10.1111/j.1365-2516.2011.02720.x
Key point: summarizes relevant studies on US and PSWD in athletes.
Level of evidence: V- expert opinion
Tiktinsky R, Chen L and Narayan P. Electrotherapy: yesterday, today and tomorrow.
Haemophilia. 2010;16 Suppl 5:126-131. doi:10.1111/j.1365-2516.2010.02310.x
Key point: a review of how modalities could be used in PWBD: hypothetically speaking
Level of evidence: V- expert opinion
Watson T. Current concepts in electrotherapy. Haemophilia. 2002;8(3):413-418.
doi:10.1046/j.1365-2516.2002.00613.x
Key Point: Expert review of theories and applications of electrotherapy intervention,
with separate section on using modalities for PWBD.
Level of evidence: V-review, expert opinion

Page 19 of 61
Standard 4: The physiotherapist will perform a complete musculoskeletal
assessment annually on each patient*, regardless of severity of the
bleeding disorder.
(*each PWBD with a potential for MSK bleeding- see intro)
World Federation of Hemophilia recommends a multidisciplinary check-up including
hematologic, musculoskeletal, and quality-of-life assessments by the core
comprehensive care team members at least yearly and every six months for children.
(This applies to all bleeding disorders.)
Individuals with no bleeds, no recent treatment changes and no musculoskeletal or
psychosocial concerns may be reviewed in person less frequently as deemed to be
appropriate by the comprehensive care team.
Reference: Canadian Integrated and Comprehensive Care Standards for Inherited
Bleeding Disorders 2020, Appendix 5. https://www.hemophilia.ca/integrated-and-
comprehensive-care-standards/ Accessed December 14, 2020
Practice Statement 4.1
The physiotherapist should review the individual’s bleeding history.
Grade of recommendation: Theoretical
Rationale:
Regular review of the history of bleeding episodes will identify sites of repeated
bleeding, so-called ‘target joints’, and perhaps incomplete rehabilitation of some
injuries. It may also help the individual correlate specific activities with their bleeds, and
indicate if changes to hematologic management regime are needed.
Reference:
de Moerloose P, Fischer K, Lambert T et al. Recommendations for assessment,
monitoring and follow-up of patients with haemophilia. Haemophilia. 2012;18(3):319-
325. doi:10.1111/j.1365-2516.2011.02671.x
Key point: European consensus exercise regarding components and frequency of
assessments.
Level of evidence: V expert opinion
Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and
hematomas. J Blood Med. 2014; 5:207-218. Published 2014 Oct 17.

Page 20 of 61
doi:10.2147/JBM.S50644
Key point: “any patient with severe hemophilia should be followed-up by a hemophilia
specialist, with one or two visits conducted per year. For patients with moderate or
minor deficit, annual follow-ups are also essential. The evaluation of joint status, along
with its evolution and the impact on QoL, represent an integral part of the hemophilia
consultation”.
Level of evidence: V-expert opinion
Practice Statement 4.2
The physiotherapist should perform a detailed musculoskeletal examination.
Grade of recommendation: Theoretical
Rationale:
Assessment of Body Structures and Function should include, at a minimum:
• range of joint motion of all peripheral joints* (See note)
• joint swelling
• crepitus with movement
• muscle wasting
• functional muscle strength
• gait
Assessment of joint end feel, balance and proprioception is also recommended.
The Hemophilia Joint Health Score (HJHS) is a reliable, validated disease-specific
assessment tool that was developed to assess early arthropathy in children. The use of
HJHS for teens and adults, as well as for individuals with chronic arthropathy, is being
investigated.
An instruction manual and video are available at https://www.ipsg.ca/portal/terms-and-
conditions
*Note: the HJHS does NOT include hips or shoulders.
References:
Compendium of assessment tools. World Federation of Hemophilia.
https://elearning.wfh.org/resource/compendium-of-assessment-tools/
Accessed December 14,2020

Page 21 of 61
Key point: Describes the psychometric properties of disease specific tools, including
HJHS
Level of evidence: V expert opinion
David JA, Feldman BM. Assessing activities, participation, and quality of life in
hemophilia: relevance, current limitations, and possible options. Semin Thromb Hemost.
2015;41(8):894-900. doi:10.1055/s-0035-1552564
Key point: Discusses use of ICF, including relevant “impairment measures”.
Level of evidence: V-expert opinion
Fischer, K. and de Kleijn, P. Using the Haemophilia Joint Health Score for assessment of
teenagers and young adults: exploring reliability and validity. Haemophilia.
2013;19(6):944-950. doi:10.1111/hae.12197
Key point: Interobserver reliability of the HJHS1.0 in teenagers and young adults with
limited joint damage is excellent. Preliminary data on validity were similar or better than
those in children.
Level of evidence: I
Practice Statement 4.3
The physiotherapist should assess pain.
Grade of recommendation: Weak
Rationale/discussion:
Pain is a prominent feature in persons with bleeding disorders, and can be due to
diverse factors including acute bleeding, venous access, and chronic joint disease.
PWBD may experience pain that is acute, chronic or acute ON chronic. A large number
of adults with bleeding disorders experience pain on a daily basis, which impacts their
daily activities, quality of life and mental health.
Pain is a complex biopsychosocial phenomenon. A ‘static’ pain measurement such as
the VAS, which was designed to measure intensity of acute pain, may not be adequate
for assessing the complex pain experienced by PWBD.
Different tools will be necessary for children and adults.
Hemophilia-specific tools are available.
References:

Page 22 of 61
Birnie KA, Hundert AS, Lalloo C, Nguyen, Stinson JN. Recommendations for selection of
self-report pain intensity measures in children and adolescents: a systematic review and
quality assessment of measurement properties. Pain. 2019 Jan; 160(1):5-18. doi:
10.1097/j.pain.0000000000001377.
Key points: Analysis of psychometric properties of 8 pediatric pain scales. Weak
recommendations at best could be made across all measures for chronic pain.
Measures were not recommended for children younger than 6 years, and sometimes up
to 8 years old.
Level of evidence: I - Systematic review
Forsyth AL, Witkop M, Lambing A, et al. Associations of quality of life, pain, and self-
reported arthritis with age, employment, bleed rate, and utilization of haemophilia
treatment center and health care provider services: results in adults with haemophilia in
the HERO study. Patient Prefer Adherence. 2015;9: 1549-1560. Published 2015 Oct 29.
doi:10.2147/PPA.S87659
Key points: Increased disability and pain were associated with increased age, lower
employment, higher reported bleed frequency, and lower HRQoL.
Level of evidence: III- case controlled study
Tupper SM, Nilson JA, King J, Downe P, Hodgson N, Schlosser T, Brose K. Development
and clinical feasibility testing of the Pain Treatment Planning Questionnaire. J Haem
Pract. 2020; 7(1): 12–[12-24]. doi.org/10.17225/jhp00155
Key point: a patient-reported outcome tool, designed in Canada, to be used with adults
attending outpatient bleeding disorder clinics. Objective: to facilitate discussions about
pain management options as a means of promoting self-efficacy.
Level of evidence: III
Witkop M, Lambing A, Divine G, Kachalsky E, Rushlow D, Dinnen J. A national study of
pain in the bleeding disorders community: a description of haemophilia pain.
Haemophilia. 2012;18(3):e115-e119. doi:10.1111/j.1365-2516.2011.02709.x
Key point: how PWBD (hemophilia) describe their pain, as well as what they do (or don’t
do) to manage it.
Level of evidence: Prospective survey (other)
Young G, Tachdjian R, Baumann K, Panopoulos G. Comprehensive management of
chronic pain in haemophilia. Haemophilia. 2014;20(2):e113-e120.
doi:10.1111/hae.12349

Page 23 of 61
Key point: Although the title says “management’, includes a good description of chronic
pain in people with hemophilia.
Level of evidence: V- review
Practice Statement 4.4
The physiotherapist should will assess the individual’s activities and participation
throughout the lifespan, including:
• gross motor development
• school/work
• physical activity/sports
• leisure/social activities
• self-care
Grade of Recommendation: Theoretical
Rationale:
The presence of a bleeding disorder will have different impacts on Activities and
Participation at different life stages, and a combination of objective and self-reported
instruments is necessary to give a complete picture of the impact of the condition on
the individual.
Bleeds, or fear of bleeding, particularly in young children may result in some
parents/caregivers restricting activities that promote normal development. Gross motor
delays have been identified in children with hemophilia (Hernandez). Physiotherapists
should monitor overall development, and ensure that children with BD are able to
participate with their peers in school and leisure activities.
During the lifespan, musculoskeletal bleeding may alter movement patterns and cause
pain, which begin to limit activities and participation in normal social roles.
As PWBD live longer, issues often associated with “normal aging” may appear- such as
decreased activity levels, decline in muscle strength, issues related to balance. These
may be amplified or accelerated by the bleeding disorder.
Therefore, regular review of activities and participation, using age-appropriate patient-
reported measures, should be done to identify issues that are important to the
individual, and assist with goal-setting and treatment planning.
References:

Page 24 of 61
Canadian Integrated and Comprehensive Care Standards for Inherited Bleeding
Disorders 2020 https://www.hemophilia.ca/integrated-and-comprehensive-care-
standards/ Accessed December 14-2020
Key point: See Appendix 4: outcomes to be measured. Level- V-expert working group
David JA, Feldman BM. Assessing activities, participation, and quality of life in
hemophilia: relevance, current limitations, and possible options. Semin Thromb Hemost.
2015;41(8):894-900. doi:10.1055/s-0035-1552564
Key point: Emphasizes need to assess activities/participation as well as impairments.
Level of evidence: V- expert opinion
de Moerloose P, Fischer K, Lambert T et al. Recommendations for assessment,
monitoring and follow-up of patients with haemophilia. Haemophilia. 2012;18(3):319-
325. doi:10.1111/j.1365-2516.2011.02671.x
Key Point: recommends using Hemophilia Activities List once a year
Level of evidence: V- expert opinion
Fischer K, Nijdam A, Holmström M, Petrini P, Ljung R, van der Schouw YT, and Berntorp
E. Evaluating outcome of prophylaxis in haemophilia: objective and self-reported
instruments should be combined. Haemophilia. 2016;22(2):e80-e86.
doi:10.1111/hae.12901
Key point: objective and self-reported instruments should be combined.
Level of evidence: V-expert opinion
Hernandez G, Kunicki M. Prevalence of gross motor delays in boys with hemophilia ages
4-14: single site study.
https://www.postersessiononline.eu/173580348_eu/congresos/WFH2016/aula/-PP-
T_152_WFH2016.pdf Accessed December 14, 2020
Key point: more than 50% of the boys tested had gross motor delays. The percentage of
boys showing deficits increased and persisted after age 7.
Level of evidence: III case-controlled study
Timmer MA, Gouw SC, Feldman BM, et al. Measuring activities and participation in
persons with haemophilia: A systematic review of commonly used instruments.
Haemophilia. 2018;24(2):e33-e49. doi:10.1111/hae.
Key points: Supports use of HAL, FISH, and PedHAL, with some caveats
Level of evidence: I - Systematic review

Page 25 of 61
Practice Statement 4.5
Physiotherapists should use standardized and validated assessment tools, including
patient-reported outcomes, to evaluate changes in condition, identify areas of concern,
and assist with goal-setting.
Grade of Recommendation: Theoretical
Rationale:
Disease specific tools have been developed, including:
• Hemophilia Joint Health Score
• Hemophilia Activities List (HAL and PedHAL)
• Functional Independence Scale for Hemophilia (FISH)
• Pain Treatment Planning Questionnaire
Generic tools, or tools developed for other populations (e.g., osteoarthritis), may also be
useful, and allow comparison between PWBD and other groups. Some examples of
these are:
• Alberta Infant Motor Scale
• Peabody Developmental Gross Motor Scale
• SF-36
• Community Balance and Mobility Scale
• Timed Up and Go
• 6-minute Walk test
Work is being done to develop a Core Set of assessment tools specifically for
Hemophilia, based on the ICF.
Different tools will be needed for pediatric and adult populations.
Selection of tools should be guided by reason for use (clinical vs research tools).
References:
Birnie KA, Hundert AS, Lalloo C, Nguyen, Stinson JN. Recommendations for selection of
self-report pain intensity measures in children and adolescents: a systematic review and
quality assessment of measurement properties. Pain. 2019 Jan; 160(1):5-18. doi:
10.1097/j.pain.0000000000001377.
Key point: There are presently no pain scales suitable for children under 6.
Level of evidence: I- systematic review

Page 26 of 61
Compendium of assessment tools. World Federation of Hemophilia.
https://elearning.wfh.org/resource/compendium-of-assessment-tools/ Accessed
December 14-2020
Key point: Describes the psychometric properties of disease specific tools, including
HJHS
Level of evidence: V –expert opinion
Fischer K, Nijdam A, Holmström M, et al. Evaluating outcome of prophylaxis in
haemophilia: objective and self-reported instruments should be combined.
Haemophilia. 2016;22(2):e80-e86. doi:10.1111/hae.12901
Key point: multiple domains must be assessed; tools are available
Level of evidence: V-expert opinion
Stephensen D, Bladen M, McLaughlin P. Recent advances in musculoskeletal
physiotherapy for haemophilia. Ther Adv Hematol. 2018;9(8):227-237. Published 2018
Jul 2. doi:10.1177/2040620718784834
Key point: highlights advances and limitations in current research, and calls for
development of a core set of outcome measures that will enable future meta-analyses.
Level of evidence: V-expert opinion
Tupper SM, Nilson JA, King J, Downe P, Hodgson N, Schlosser T, Brose K. Development
and clinical feasibility testing of the Pain Treatment Planning Questionnaire. The Journal
of Haemophilia Practice. 2020; 7(1):12-24. doi.org/10.17225/jhp00155
Key point: A new disease-specific tool for adults.
Level of evidence: III

Page 27 of 61
Standard 5: The TC physiotherapist will arrange for the provision of
Physiotherapy treatment (in-house or elsewhere) to address the MSK
complications associated with bleeding disorders.
Practice Statement 5.1
Physiotherapists should use therapeutic exercise to address hemophilic arthropathy.
Grade of recommendation: Strong
Rationale:
Features of hemophilic arthropathy include joint swelling, pain and stiffness,
contracture and deformity, muscle imbalance and atrophy, as well as alterations in the
individual’s ability to function and participate normally.
Exercises that have been studied in PWBD (particularly Hemophilia A and Hemophilia B)
include:
• exercise in water (hydrotherapy)
• active, isometric, and resisted exercise
• aerobic exercise
• functional (closed chain) exercise
• treadmill walking
• supervised exercise for groups or individuals
• Tai Chi
• Nordic walking
• home exercise programs
In randomized controlled studies, exercise for PWBD has been shown to improve range
of motion, strength, walking tolerance, gait, balance, and quality of life (Calatayud,
Runkel, Strike), in addition to decreasing pain and anxiety (Firoozabadi).
Exercise combined with education sessions also reduced illness behaviour (Cuesta-
Barriuso 2017).
The findings are consistent with the many non-controlled reports in the literature, as
well as the experience of the working group: exercise is safe and effective for people
with bleeding disorders.
References:
Calatayud J, Pérez-Alenda S, Carrasco JJ, et al. Safety and Effectiveness of Progressive
Moderate-to-Vigorous Intensity Elastic Resistance Training on Physical Function and

Page 28 of 61
Pain in People With Hemophilia. Phys Ther. 2020;100(9):1632-1644.
doi:10.1093/ptj/pzaa106
Level of evidence: I- RCT
Cuesta-Barriuso R, Torres-Ortuño A, Nieto-Munuera J, López-Pina JA. Effectiveness of an
Educational Physiotherapy and Therapeutic Exercise Program in Adult Patients With
Hemophilia: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2017;98(5):841-
848. doi:10.1016/j.apmr.2016.10.014
Level of evidence: I- RCT
Danusantoso H, Heijnen L. Tai Chi Chuan for people with haemophilia. Haemophilia.
2001;7(4):437-439. doi:10.1046/j.1365-2516.2001.0538b.x
Level of evidence: V- expert opinion
Firoozabadi MD, Mahdavinejad R, Ghias M, Rouzbehani R. The Effects of an Exercise
Therapy Program on Joint Range of Motion, Aerobic Fitness and Anxiety of Hemophilia A
Patients. J Isfahan Medical School. 2012. 30(177):1-9
Level of evidence: II
McLaughlin P, Hurley M, Chowdary P, Khair K. Physiotherapy interventions for pain
management in haemophilia: A systematic review. Haemophilia. 2020;26(4):667-684.
doi:10.1111/hae.14030
Level of evidence: I – systematic review
Runkel B, Czepa D, Hilberg T. RCT of a 6-month programmed sports therapy (PST) in
patients with haemophilia- Improvement of physical fitness. Haemophilia.
2016;22(5):765-771. doi:10.1111/hae.12957
Level of evidence: I-RCT
Runkel B, Von Mackensen S, Hilberg T. RCT - subjective physical performance and quality
of life after a 6-month programmed sports therapy (PST) in patients with haemophilia.
Haemophilia. 2017;23(1):144-151. doi:10.1111/hae.13079
Level of evidence: I-RCT
Salim M, Brodin E, Spaals-Abrahamsson Y, Berntorp E, Zetterberg E. The effect of Nordic
Walking on joint status, quality of life, physical ability, exercise capacity and pain in adult
persons with haemophilia. Blood Coagul Fibrinolysis. 2016;27(4):467-472.
doi:10.1097/MBC.0000000000000554

Page 29 of 61
Level of evidence: II- small study
Strike K, Mulder K, Michael R. Exercise for haemophilia. Cochrane Database Syst Rev.
2016;12(12):CD011180. Published 2016 Dec 19. doi:10.1002/14651858.CD011180.pub2
Level of evidence: I - Systematic review
Practice Statement 5.2
Physiotherapists may recommend orthotics for PWBD
Grade of recommendation: Theoretical
Rationale:
Orthoses and footwear modifications can be used in PWBD to control or prevent joint
movement, stabilize a specific joint or relieve joint stress or loading.
References:
de la Corte-Rodriguez H and Rodriguez-Merchan EC. The current role of orthoses in
treating haemophilic arthropathy. Haemophilia. 2015;21(6):723-730.
doi:10.1111/hae.12779
Key point: a very good review article: Includes pertinent studies, discusses shoe
modifications/inserts, and orthotics for ankles, knees, AND elbows
Level of evidence: V- review article
Srivastava A, Santagostino E, Dougall A, et al. WFH Guidelines for the Management of
Hemophilia, 3rd edition. Haemophilia. 2020;26 Suppl 6:1-158. doi:10.1111/hae.14046
Level of evidence: V- expert opinion
Practice Statement 5.3
Physiotherapists may use low load prolonged passive stretching and serial splinting to
address flexion contractures.
Grade of recommendation: Theoretical
Rationale:
Flexion contractures can develop in PWBD if prevention and management of bleeding
are not optimal.

Page 30 of 61
Repeated bleeding leads to progressive fibrosis of the synovium with development of
fibrous intraarticular bands. Pain, spasm and shortening in the surrounding muscles, and
eventually fibrosis of the joint capsule, will follow if not addressed.
In the early stages (contractures < 30 degrees), slow stretching and serial splinting can
be used to improve extension. To maintain the improvement, this should always be
accompanied by strengthening exercises for the extensor muscles.
References:
Heijnen L, De Kleijn P. Physiotherapy for the treatment of articular contractures in
haemophilia. Haemophilia. 1999;5 Suppl 1:16-19. doi:10.1046/j.1365-
2516.1999.0050s1016.x
Key point: Describes uses of manual traction, joint mobilization techniques, muscle
stretching.
Level of evidence: IV- case series
Solimeno L, Goddard N, Pasta G, et al. Management of arthrofibrosis in haemophilic
arthropathy. Haemophilia. 2010;16 Suppl 5:115-120. doi:10.1111/j.1365-
2516.2010.02308.x
Key point: Quick review of conservative measures, and a precaution: Vigorous attempts
to restore motion through manipulation or excessive force with serial casting should be
avoided as it can result in avulsion of articular surfaces at sites of attachment of fibrous
bands.
Level of evidence: V- review, expert opinion
Sørensen B, Benson GM, Bladen M, Classey S, Keeling DM, McLaughlin P, Yee, TT, Makris
M. Management of muscle hematomas in patients with severe hemophilia in an
evidence-poor world. Haemophilia. 2012;18(4):598-606. doi:10.1111/j.1365-
2516.2011.02720.x
Key point: “Stretching techniques in phase 2 of treatment should be progressive, of very
light intensity and within the limits of pain”
Level of evidence: V-review, expert opinion
Practice Statement 5.4
Physiotherapists may use manual techniques.
Grade of recommendation: Strong
Page 31 of 61
Rationale:
Manual techniques that have been studied include joint traction, joint gliding
techniques, fascial therapy and manual stretching.
These techniques were found to be safe (no new bleeding) and effective in decreasing
pain.
One group suggests that bleeding frequency may also be reduced (Donoso-Úbeda).
However, this was self-reported bleeding: as people with arthropathy sometimes have
difficulty distinguishing bleed pain from arthritic pain, and vice versa, this finding should
be interpreted with caution.
References:
Cuesta-Barriuso R, Gómez-Conesa A, López-Pina JA. Manual and educational therapy in
the treatment of hemophilic arthropathy of the elbow: a randomized pilot study.
Orphanet J Rare Dis. 2018;13(1):151. Published 2018 Sep 3. doi:10.1186/s13023-018-
0884-5
Manual therapy: joint traction, passive muscles stretching.
Level of evidence: I RCT
Donoso-Úbeda E, Meroño-Gallut J, López-Pina JA, Cuesta-Barriuso R. Effect of manual
therapy in patients with hemophilia and ankle arthropathy: a randomized clinical trial.
(Clin Rehabil. 2019 Sep 27) Published correction appears in Clin Rehabil. 2020;34(1):111-
119. doi:10.1177/0269215519879212
Manual therapy: fascial therapy.
Level of evidence: I RCT
Heijnen L, De Kleijn P. Physiotherapy for the treatment of articular contractures in
haemophilia. Haemophilia. 1999;5 Suppl 1:16-19. doi:10.1046/j.1365-
2516.1999.0050s1016.x
Manual therapy: manual traction, joint mobilization techniques, muscle stretching.
Level of evidence: IV case series
Practice Statement 5.5
Physiotherapists may use electrotherapy, following the usual clinical indications and
precautions.
Grade of recommendation: Theoretical

Page 32 of 61
Rationale:
Applications of energy, including Short-Wave Diathermy, Ultrasound, LASER, magnetic
therapy, TENS, IFC and NMES have been proposed for pain management,
neuromuscular reeducation (and to promote tissue healing and hematoma resolution in
acute phases).
It is the opinion of the authors of these guidelines that such modalities may be used for
PWBD according to the usual clinical indications and precautions in the general
population, but should be considered as ADJUNCTS to exercise, education and other
self-management techniques.
References:
McLaughlin P, Hurley M, Chowdary P, Khair K. Physiotherapy interventions for pain
management in haemophilia: A systematic review. Haemophilia. 2020;26(4):667-684.
doi:10.1111/hae.14030
Key point: LASER with exercise and hydrotherapy/land-based exercise appears to have
some positive effect on knee pain in PWBD (Hemophilia).
Level of evidence: I -Systematic review
Tiktinsky R, Chen L and Narayan P. Electrotherapy: yesterday, today and tomorrow.
Haemophilia. 2010;16 Suppl 5:126-131. doi:10.1111/j.1365-2516.2010.02310.x
Key points: a review of theory and possible applications; some clinical experience with
EMG with PWBD
Level of evidence: V- Theoretical, review
Practice Statement 5.6
Physiotherapists who have the necessary training may use acupuncture.
Grade of recommendation: Theoretical
Rationale:
There is some evidence that acupuncture can be effective in decreasing chronic arthritic
pain in PWBD. Some patients received factor prior to acupuncture, some did not, but no
adverse effects or bleeding was reported in these studies.
Having a bleeding disorder may pose a small increased risk of bruising and mild bleeding
with acupuncture treatment, but should not be a contraindication.

Page 33 of 61
The working group suggests that acupuncture can be used with caution in PWBD;
hematological management should be discussed with the team.
References:
Lambing A, Kohn-Converse B, Hanagavadi S, Varma V. (2012), Use of acupuncture in the
management of chronic haemophilia pain. Haemophilia. 2012;18(4):613-617.
doi:10.1111/j.1365-2516.2012.02766.x
Key point: Small study in 2 centers: Local and distal points were used; no bleeding and
50% of patients reported pain relief.
Level of evidence: IV case series
Wallny TA, Brackmann HH, Gunia G, Wilbertz P, Oldenburg J, Kraft CN. Successful pain
treatment in arthropathic lower extremities by acupuncture in haemophilia patients.
Haemophilia. 2006;12(5):500-502. doi:10.1111/j.1365-2516.2006.01308.x
Key points: Small study: used a single skull point; decreased pain in lower extremities;
no adverse effects.
Level of evidence: Level II- cohort study
Practice Statement 5.7
Physiotherapists should provide education to PWBD.
Grade of recommendation: Theoretical
Rationale:
WFH endorses ongoing education of PWBD and their families to enable self-
management. Education from the physiotherapist should include prevention,
identification and management of MSK bleeding and its sequelae. Education should be
specific to the age and situation of the individual, although group education can also be
useful (opinion of the working group).
There is some preliminary evidence that education can be effective in improving the
health of PWBD, as well as decreasing parental stress. The education sessions in the
research included anatomy, biomechanics, pathophysiology and treatment of bleeds,
proprioception, and activity selection.
References:
Cuesta-Barriuso R, Torres-Ortuño A, Nieto-Munuera J, López-Pina JA. Effectiveness of an
Educational Physiotherapy and Therapeutic Exercise Program in Adult Patients With

Page 34 of 61
Hemophilia: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2017;98(5):841-
848. doi:10.1016/j.apmr.2016.10.014
Level of evidence: I- RCT
Cuesta-Barriuso R, Gómez-Conesa A, López-Pina JA. Manual and educational therapy in
the treatment of hemophilic arthropathy of the elbow: a randomized pilot study.
Orphanet J Rare Dis. 2018;13(1):151. Published 2018 Sep 3. doi:10.1186/s13023-018-
0884-5
Level of evidence: I -RCT
Cuesta-Barriuso R, Torres-Ortuño A, López-García M, Nieto-Munuera J. Effectiveness of
an educational intervention of physiotherapy in parents of children with haemophilia.
Haemophilia. 2014;20(6):866-872. DOI: 10.1111/hae.12447.
Level of evidence: IV
Practice Statement 5.8
The physiotherapist may recommend environmental adaptation and mobility aids.
Grade of recommendation: Theoretical
Rationale:
PWBD with advancing arthropathy and/or with inhibitors may need assistance such as
mobility aids to enhance functional activities and participation. Modifications to the
home and/or workplace may also be needed to ensure safety and optimal function.
This may require consultation with a community-based physiotherapist and/or
occupational therapist.
Reference:
Srivastava A, Santagostino E, Dougall A, et al. WFH Guidelines for the Management of
Hemophilia, 3rd edition. Haemophilia. 2020;26 Suppl 6:1-158. doi:10.1111/hae.14046
Level of evidence: V expert opinion
Practice Statement 5.9
The physiotherapist should arrange for referral of clients to other health professionals
when indicated.
Grade of recommendation: Theoretical

Page 35 of 61
Rationale:
Many PWBD have complex needs, and might require services of health professionals
who are outside of the TC care team. These could include other Physiotherapists,
Occupational Therapists, Pain Management Specialists, Orthotists, or other multi-
disciplinary programs (e.g., pain program)
[See also S 7: Consultation with other care providers]
References:
Canadian Integrated and Comprehensive Care Standards for Inherited Bleeding
Disorders 2020 https://www.hemophilia.ca/integrated-and-comprehensive-care-
standards/ Accessed December 14-2020
Key point: See Appendix 2: Core team and extended team members. Level of Evidence: V- Expert opinion
Srivastava A, Santagostino E, Dougall A, et al. WFH Guidelines for the Management of
Hemophilia, 3rd edition. Haemophilia. 2020:00: -158.
https://doi.org/10.1111/hae.14046
Key point: Describes Core team and “others”
Level of evidence: V expert opinion

Page 36 of 61
Standard 6: The TC physiotherapist must participate in discussions with
the core team, the surgical team and the PWBD about optimal timing,
pre-operative planning and post-operative rehabilitation for all MSK
procedures.
This paper, by an international multidisciplinary panel of experts, outlines the roles and
responsibilities of all team members, including the PWBD, during the pre-operative,
intra-operative, and post-operative phases. It is relevant to all the practice statements
related to Standard 6.
Escobar MA, Brewer A, Caviglia H, et al. Recommendations on multidisciplinary
management of elective surgery in people with haemophilia. Haemophilia.
2018;24:693–702. https://doi.org/10.1111/hae.13549
Level of evidence: V- expert opinion
A. Prior to MSK Surgery:
Practice Statement 6.1
The physiotherapist should ensure that the individual has had access to appropriate
rehabilitation prior to recommending surgical intervention.
Grade of Recommendation: Theoretical
Rationale:
Surgical options may range from simple (intraarticular injection, radioactive
synovectomy) to complex (arthroscopy, osteotomy, debridement, arthrodesis, or
arthroplasty).
In some situations, it will be the TC physiotherapist who suggests to the team that it is
time to consider surgery. In other situations, the request for surgical opinion might
come from the PWBD or another team member.
In all cases, conservative therapy, including exercise, orthotic support, and
environmental modification should be explored prior to considering surgery. (See
Section 5: Physiotherapy Treatment of MSK Complications)
References: (in addition to Escobar)

Page 37 of 61
Solimeno L, Goddard N, Pasta G, et al. Management of arthrofibrosis in haemophilic
arthropathy. Haemophilia. 2010;16 Suppl 5:115-120. doi:10.1111/j.1365-
2516.2010.02308.x
Key point: International panel of surgical experts; summary of types of surgeries.
Level of evidence: V – expert opinion
Practice Statement 6.2
The bleeding disorders team, the surgical team and the PWBD should discuss goals
and expectations for elective orthopedic surgery, including post-operative
requirements.
Grade of Recommendation: Theoretical
Rationale:
The usual goals for surgical intervention are to decrease bleeding, reduce pain and/or
optimize function.
Improved range of motion is not always expected and can be difficult to achieve, and
the PWBD must understand this.
The PWBD must also understand that a lengthy period of out-patient rehabilitation may
be required.
Pre-operative planning and coordination among all parties is imperative. The teams
must discuss potential post-operative requirements such as:
• hemostatic management
• pain management
• anticipated length of hospital stay
• possible need for ICU (patients with inhibitors, complex surgeries with high risk
of bleeding)
• anticipated time for restriction of usual activities, such as lifting, driving,
work/school, or sports
• logistics regarding post-op rehab (e.g., location, frequency, transportation if the
PWBD is unable to drive)
References:
Escobar MA, Brewer A, Caviglia H, et al. Recommendations on multidisciplinary
management of elective surgery in people with haemophilia. Haemophilia.
2018;24:693–702. https://doi.org/10.1111/hae.13549
Level of evidence: V-expert opinion

Page 38 of 61
Practice Statement 6.3
After the decision is made to proceed with surgery, the physiotherapist should assess
for indications for pre-operative physiotherapy.
Grade of Recommendation: Theoretical
Rationale:
PWBD often have multiple joint arthropathy which can limit their ability to maintain
post-op weight-bearing restrictions. Consideration of upper extremity joint status
should be made for weight-bearing status and use of mobility aids.
Depending on the procedure, pre-operative physiotherapy (“pre-hab”) could include:
• preparation of other joints that may be subjected to increased stress post-
operatively, by improving strength, ROM, or stability.
• preparing the operative joint, to optimize the recuperation and maximize the
effects of the surgery
o As long as the joint is not too painful, the physiotherapist should help the
PWBD optimize range of motion and strength. For example, quads function
may be poor due to prolonged pain, patellar adhesions and altered
mechanics, making it difficult to achieve active knee extension.
o It has been demonstrated that for Total Knee Arthroplasty, post-operative
ROM correlates closely with pre-operative ROM (Moore 2016).
o The working group feels that pre-operative preparation will optimize
results of arthroplasty for other joints as well.
• ensuring that mobility aids, adaptive equipment, and environmental adaptations
are in place to allow safe functioning after discharge
“Pre-hab” can also prepare the PWBD for the types of exercise he/she will need to do
post-op.
References: (in addition to Escobar)
De Kleijn P, Blamey G, Zourikian N, Dalzell R, Lobet S. Physiotherapy following elective
orthopedic procedures. Haemophilia. 2006;12 Suppl 3:108-112. doi:10.1111/j.1365-
2516.2006.01266.x
Key point: international panel of physiotherapy experts.
Level of evidence: V-expert opinion

Page 39 of 61
Lobet S, Pendeville E, Dalzell R, Defalque A, Lambert C, Pothen D and Hermans C. The
role of physiotherapy after total knee arthroplasty in patients with haemophilia.
Haemophilia. 2008;14(5):989-998. doi:10.1111/j.1365-2516.2008.01748.x
Key point: Notwithstanding the title, they do address importance and suggest content of
a “pre-hab” program.
Level of evidence: V expert opinion
Moore MF, Tobase P, Allen DD. Meta-analysis: outcomes of total knee arthroplasty in
the haemophilia population. Haemophilia. Haemophilia. 2016;22(4):e275-e285.
doi:10.1111/hae.12885
Key point: Pre-op range and strength influences post-op results.
Level of evidence: II
Practice Statement 6.4
The physiotherapist from the TC should establish and maintain regular communication
with other physiotherapists who may need to be involved post-operatively.
Grade of Recommendation: Theoretical
Rationale:
There will be situations where TC physiotherapist will not be supervising the post-op
therapy: e.g.,
• the surgery and immediate post-op rehab may take place in a facility different
from where the TC is located
• out-patient post-op rehab may take place a local clinic closer to the individual’s
home.
The TC physiotherapist should be available to consult with the treating
physiotherapist(s) who will plan and carry out appropriate therapy. Communication
should emphasize the need to prevent new bleeding during mobilization and rehab.
Discussion could also include factors specific to the individual (e.g., status of other
joints, environmental considerations for discharge, individual’s pain tolerance) that
might impact post-op management.
All physiotherapists must be aware that:

Page 40 of 61
• longer than normal hospital admission and rehabilitation time should be
expected
• post-op bleeding may delay or interrupt mobilization, and make it difficult to
optimize range of motion
• joint stiffness is more likely to occur in PWBD due to slower progression and the
pre-existing state of the peri-articular structures
• PWBD are more likely to develop complications such as delayed wound healing
and infection
• pain management may be complicated because the individual
o may interpret post-operative pain as pain due to new bleeding
o may already be using high levels of analgesics, including narcotics or
cannabis, to manage chronic complex pain
o may have developed other protective behaviours, such as avoiding
activity, to manage persistent pain
o may have strong and specific expectations about their complex pain and
how it should be managed
(See also: Special Considerations for TKA)
Reference: (in addition to Escobar)
Haemophilia Chartered Physiotherapists Association (HCPA). Service Provision of
Physiotherapy for Adults with Haemophilia & other Inherited Bleeding Disorders. 2020.
http://www.ukhcdo.org/haemophilia-associations/physiotherapy-information/
Accessed December 14, 2020.
Key point: the TC physiotherapist ‘oversees’ the program.
Level of evidence: V
Lobet S, Pendeville E, Dalzell R, et al. The role of physiotherapy after total knee
arthroplasty in patients with haemophilia. Haemophilia. 2008;14(5):989-998.
doi:10.1111/j.1365-2516.2008.01748.x
Key point: need to develop partnership with local physiotherapist who may be
supervising the long-term rehabilitation.
Level of evidence: V-expert opinion
Solimeno L, Luck J, Fondanesche C, et al. Knee arthropathy: When things go wrong.
Haemophilia. 2012 Jul;18(SUPPL.4):105-111. https://doi.org/10.1111/j.1365-
2516.2012.02834.x

Page 41 of 61
Key points: International surgeons and physiotherapists emphasize the need for long-
term rehabilitation after several different procedures.
Level of evidence: V-expert opinion
B. Following MSK surgery:
Practice Statement 6.5
Before beginning post-operative physiotherapy, the treating physiotherapist must be
aware of:
• the type of bleeding disorder and its severity
• the hematological management plan
• the detailed procedure of the surgery including
o the condition of the joint and surrounding muscles observed during the
surgery
o the range of motion obtained during surgery (if appropriate to the
procedure)
Grade of Recommendation: Theoretical
Rationale:
All possible steps must be taken to prevent new bleeding while optimizing post-
operative function. Therapy sessions should be coordinated with optimum hemostasis,
analgesics, and other pain management strategies (e.g., relaxation).
The physiotherapist should discuss intra-operative findings directly with the surgeon.
Sometimes surgery in PWBD may become more complex than was anticipated pre-
operatively, e.g., need for wider field synovial resection, additional soft tissue or
capsular releases, patellectomy.
References: (in addition to Escobar)
Solimeno L, Luck J, Fondanesche C, et al. Knee arthropathy: When things go wrong.
Haemophilia. 2012 Jul;18(SUPPL.4):105-111. https://doi.org/10.1111/j.1365-
2516.2012.02834.x
Key point: “Patients going to surgery with very limited flexion may require
quadricepsplasty, which is often associated with an extensor lag for six months or
longer”.
Level of evidence: V- expert opinion

Page 42 of 61
C. Special Considerations regarding Total Knee Arthroplasty:
Practice Statement 6.6
The treating physiotherapist should be aware that PWBD may present challenges that
are not seen in other populations undergoing TKA.
Grade of Recommendation: Theoretical
Rationale:
Since the knee joint is a common site for hemarthrosis in PWBD, many PWBD require
TKA due to degenerative changes.
There are several differences in the characteristics of PWBD, compared to other
populations, that may require special consideration during the post-operative period,
including (but not limited to):
• PWBD undergoing TKA are often younger
• PWBD may have significant arthropathy of several joints, and may undergo
multiple procedures during one admission
• PWBD may be undergoing revision of a previous TKA
• PWBD have been conditioned to interpret pain as a sign of bleeding
• PWBD may already be using high levels of narcotic analgesics due to severe
arthropathy
• Complication rates, including bleeding and infection, may be higher than in other
populations
• PWBD may achieve good post-op range of motion initially, but have difficulty
maintaining it
• PWBD may benefit from ‘pre-hab’, and extended post-operative rehabilitation
including hydrotherapy even though these may not be used routinely with other
populations undergoing TKA.
References: (in addition to Escobar)
Lobet S, Pendeville E, Dalzell R, et al. The role of physiotherapy after total knee
arthroplasty in patients with haemophilia. Haemophilia. 2008;14(5):989-998.
doi:10.1111/j.1365-2516.2008.01748.x
Key Point: Description of components of In-patient and on-going out-patient
rehabilitation programs.
Level of evidence: V-expert opinion

Page 43 of 61
MASAC Recommendations Regarding Physical Therapy Guidelines in Patients with
Bleeding Disorders: Total Knee Replacement 2015
https://www.hemophilia.org/sites/default/files/document/files/238pttotalkneereplace
ment.pdf Accessed January 10, 2021
Key points: From USA; describes Physiotherapy treatment, challenges and long-term
expectations.
Level of evidence-V-expert opinion
Solimeno L, Luck J, Fondanesche C, et al. Knee arthropathy: When things go wrong.
Haemophilia. 2012 Jul;18(SUPPL.4):105-111. https://doi.org/10.1111/j.1365-
2516.2012.02834.x
Key point: “progressive postoperative loss of motion can occur in the most cooperative
patients”.
Level of evidence: V- expert opinion
Practice Statement 6.7
The treating physiotherapist must actively and regularly watch for any signs of
bleeding or infection.
Grade of Recommendation: Weak
Rationale:
Post-operative bleeding is not unusual, especially during the first week. Active bleeding
will delay rehabilitation.
If bleeding occurs, the physiotherapist should stop the rehabilitation program, allow the
limb to rest, and discuss with the hematologist and the surgeon.
References: (in addition to Escobar)
De Kleijn P, Fischer K, Vogely HC, Hendriks C, Lindeman E. In-hospital rehabilitation after
multiple joint procedures of the lower extremities in haemophilia patients: clinical
guidelines for physical therapists. Haemophilia. 2011;17(6):971-978. doi:10.1111/j.1365-
2516.2011.02527.x
Key points: Fairly high rate of post-op bleeding and infections; difficulty achieving good
knee extension
Level of evidence: IV

Page 44 of 61
MASAC Recommendations Regarding Physical Therapy Guidelines in Patients with
Bleeding Disorders: Total Knee Replacement 2015
https://www.hemophilia.org/sites/default/files/document/files/238pttotalkneereplace
ment.pdf
Accessed January 10, 2021
Key points: From USA; describes signs of infection after TKA
Level of evidence: V -expert opinion
Moore MF, Tobase P, Allen DD. Meta-analysis: outcomes of total knee arthroplasty in
the haemophilia population. Haemophilia. 2016;22(4):e275-e285.
doi:10.1111/hae.12885
Key point: higher rate of bleeding and infection than in PWOBD
Level of evidence: II
Practice Statement 6.8
The physiotherapist should consider use of hydrotherapy after hip or knee
arthroplasty.
Grade of Recommendation: Weak
Rationale:
Several authors recommend the use of exercise in water during the post-operative
period.
Advantages:
• Buoyancy can be used to assist or resist movement, and provide support and
tactile stimulation.
• Warmth of the water assists with relaxation.
• Weight bearing can be progressed by varying depths of water as strength and
confidence improve.
Prior to starting hydrotherapy, the wound must be completely healed, with no signs of
infection.
References: (in addition to Escobar)
De Kleijn P, Fischer K, Vogely HC, Hendriks C and Lindeman E. In -hospital rehabilitation
after multiple joint procedures of the lower extremities in haemophilia patients: clinical

Page 45 of 61
guidelines for physical therapists. Haemophilia. 2011;17(6):971-978.
doi:10.1111/j.1365-2516.2011.02527.x
Level of evidence: IV Case series and expert opinion
Lobet S, Pendeville E, Dalzell R, et al. The role of physiotherapy after total knee
arthroplasty in patients with haemophilia. Haemophilia. 2008;14(5):989-998.
doi:10.1111/j.1365-2516.2008.01748.x
Level of evidence: V-expert opinion
Passeri EV, Martinelli M, Gatteri V, et al. Standard and water rehabilitation: An analysis
of over 14 years' experience in patients with haemophilia or other clotting factor
disorders after orthopaedic surgery. Haemophilia. 2019;25:699-707.
doi.org/10.1111/hae.13748
Level of evidence: IV Case series
Practice Statement 6.9
The TC physiotherapist should ensure that on-going out-patient rehabilitation has
been arranged.
Grade of recommendation: Theoretical
Rationale:
Although it may not be common practice in other populations, an extended program of
supervised progressive rehabilitation may be useful for PWBD to help regain range of
motion and strength, and re-educate posture and gait.
PWBD often have more difficulty regaining knee extension after TKA, which will affect
their gait and overall function.
Referral for out-patient rehab should be organized by the in-patient physiotherapist OR
the TC physiotherapist, depending on local practice. During the rehab program regular
communication between the TC physiotherapist and the treating physiotherapist is
recommended for optimal care.
(See also Practice Statements 6.4 and 7.1)
References:
Key point: all recommend extended course of post-op rehab
De Kleijn P, Fischer K, Vogely HCh, Hendriks C, Lindeman E. In-hospital rehabilitation

Page 46 of 61
after multiple joint procedures of the lower extremities in haemophilia patients: clinical
guidelines for physical therapists. Haemophilia. 2011;17(6):971-978. doi:10.1111/j.1365-
2516.2011.02527.x
Level of evidence: IV Case series and expert opinion
Escobar MA, Brewer A, Caviglia H, et al. Recommendations on multidisciplinary
management of elective surgery in people with haemophilia. Haemophilia.
2018;24(5):693-702. doi:10.1111/hae.13549
Level of evidence: V- expert opinion
Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and
hematomas. J Blood Med. 2014; 5:207-218. Published 2014 Oct 17.
doi:10.2147/JBM.S50644
Level of evidence: V-expert opinion
MASAC Recommendations Regarding Physical Therapy Guidelines in Patients with
Bleeding Disorders: Total Knee Replacement. 2015.
https://www.hemophilia.org/sites/default/files/document/files/238pttotalkneereplace
ment.pdf Accessed January 10, 2021
Solimeno L, Luck J, Fondanesche C, et al. Knee arthropathy: When things go wrong.
Haemophilia. 2012 Jul;18(SUPPL.4):105-111. https://doi.org/10.1111/j.1365-
2516.2012.02834.x
Level: V - expert opinion

Page 47 of 61
Standard 7: The TC physiotherapist will be available for consultation with
other care providers.
Practice Statement 7.1
The TC physiotherapist should be available for consultation with physiotherapists
outside the TC who may be seeing PWBD.
Grade of recommendation: Theoretical
Rationale:
There are many circumstances where PWBD may receive physiotherapy assessment and
treatment from physiotherapists who are not affiliated with a comprehensive treatment
center (TC).
Reasons include, but are not limited to:
• The protected time allocation of the TC physiotherapist is not sufficient to meet
all the needs of the PWBDs within the program
• the PWBD requires therapy outside the skill set of the TC physiotherapist
• the PWBD undergoes surgery in a facility that is different from the TC
• The PWBD lives far away from the TC, and is receiving treatment from a
physiotherapist closer to home.
In these situations, the TC physiotherapist will ensure that the treating physiotherapist:
• is familiar with contraindications and precautions to be observed when treating
ANY PWBD
• is aware of known chronic impairments and limitations specific to the PWBD
being treated that may not be amenable to treatment
• is aware of the hemostasis management plan recommended by the TC team
• is aware of signs and symptoms of new bleeding
• is aware of whom to contact in the event of new bleeding
References:
Canadian Integrated and Comprehensive Care Standards for Inherited Bleeding
Disorders 2020 https://www.hemophilia.ca/integrated-and-comprehensive-care-
standards/ Accessed December 14-2020
Key point: “provide education and treatment recommendations to other community
professionals who provide services to PWBD (e.g., surgery, dentistry).”
Level of evidence: V Expert working group

Page 48 of 61
Haemophilia Chartered Physiotherapists Association (HCPA). Service Provision of
Physiotherapy for Adults with Haemophilia & other Inherited Bleeding Disorders. 2020.
http://www.ukhcdo.org/haemophilia-associations/physiotherapy-information/
Accessed December 14, 2020.
Key point: “The overall responsibility of physiotherapy management should remain with
the specialist physiotherapist with effective communication between professionals”
Level of evidence: V -Expert working group
Canadian Alliance of Physiotherapy Regulators Core Standards of Practice – Updated
December 2019
https://www.alliancept.org/announcement/core-standards-practice-physiotherapists-
canada-now-available/
Accessed January 22, 2021
Key points: “Consults with/refers to the appropriate team member when aspects of
clients’ goals are best addressed by another provider.”
“Takes appropriate actions (e.g., referral to another physiotherapist or health care
provider, courses, mentorship) in situations where he/she does not have the required
competence to deliver quality client-centred care.”
Practice Statement 7.2
The physiotherapist should be available for consultation with coaches, teachers.
Grade of recommendation: Theoretical
Rationale:
All people who are responsible for a child’s safety, such as babysitters, teachers,
coaches etc. need to have sufficient information to minimize risk of bleeding and
respond appropriately to suspected bleeds.
The physiotherapist can provide information about
• prevention of bleeding, including activity selection and modification (See S-8:
Health promotion)
• identification of acute bleeding
• first aid management of bleeding
• return to activity following a bleed
There are several suitable educational resources at www.hemophilia.ca that can assist
with this.

Page 49 of 61
References:
Srivastava A, Santagostino E, Dougall A, et al. WFH Guidelines for the Management of
Hemophilia, 3rd edition. Haemophilia. 2020;26 Suppl 6:1-158. doi:10.1111/hae.14046
Level of evidence: V Expert opinion
Practice Statement 7.3
The physiotherapist should be available to consult with other team members
regarding identification and management of musculoskeletal complications of
bleeding disorders
Grade of recommendation: Best Practice
Rationale:
Physiotherapists have specific training in identifying subtle changes in MSK health, and
management of acute and chronic MSK conditions.
As the MSK expert on the team, the physiotherapist will assist other team members,
other physiotherapists, and students to develop the skills they need to work with PWBD.
References: Opinion of the working group

Page 50 of 61
Standard 8: Physiotherapists will encourage PWBD of all ages to lead
active, healthy lifestyles.
Practice Statement 8.1
The Physiotherapist should encourage all PWBD to participate regularly in physical
activities that are enjoyable to the individual, and discuss ways to minimize injury.
Grade of Recommendation: Theoretical
Rationale:
An active healthy lifestyle promotes cardiovascular fitness, healthy body weight,
psychological well-being, and ability to maintain independence.
References:
Negrier C, Seuser A, Forsyth A, et al. The benefits of exercise for patients with
haemophilia and recommendations for safe and effective physical activity. Haemophilia.
2013; 19(4):487–498.
Key point: Comprehensive review of relevant literature.
Level of evidence: II
Practice Statement 8.2
The physiotherapist should work with the individual and the TC team to develop a
personalized activity plan which includes a plan for injury management.
Grade of recommendation: Theoretical
Rationale:
Personalized activity plans should take into account each person’s bleeding tendency,
physical capabilities and interests. The prophylactic hemostasis management plan and a
plan for management of injuries must be discussed with the whole team.
A tool has been developed by CPHC to assist this process: In the Driver’s Seat: A
Workbook is designed to guide personalized decision-making about physical activities.
https://www.hemophilia.ca/files/In%20the%20Drivers%20Seat%20-%20EN_LR.pdf
accessed Jan 14, 2021
References:

Page 51 of 61
Stephensen D, Bladen M, McLaughlin P. Recent advances in musculoskeletal
physiotherapy for haemophilia. Ther Adv Hematol. 2018;9(8):227-237. Published 2018
Jul 2. doi:10.1177/2040620718784834
Key point: “Studies have reported between 50% and 80% of PWH avoid exercise and
activity due to pain and arthropathy, but there is reasonable evidence emerging that
exercise via its effect on pain, joint ROM, strength and mobility can have a positive
impact on maximizing mobility and function as well as quality of life in PWH”.
Level of evidence: V
Wittmeier K, Mulder K. Enhancing lifestyle for individuals with haemophilia through
physical activity and exercise: the role of physiotherapy. Haemophilia. 2007;13 Suppl
2:31-37. doi:10.1111/j.1365-2516.2007.01504.x

Page 52 of 61
Standard 9: Continuing Competence: The TC Physiotherapist will
maintain clinical competence
Practice Statement 9.1
The TC Physiotherapist should participate in learning activities specific to bleeding
disorders, and be familiar with current relevant literature.
Grade of recommendation: Best Practice
Rationale:
Bleeding disorders are rare, and recently there have been recent rapid changes in
assessment and management options.
The TC Physiotherapists should take an active role in maintaining their knowledge and
competence to treat PWBD.
Examples of resources include:
Journals:
• Haemophilia: The Official Journal of the World Federation of Hemophilia.
• The Journal of Haemophilia Practice
Websites:
• World Federation of Hemophilia: www.wfh.org.
• Canadian Hemophilia Society www.hemophilia.ca.
• National Hemophilia Foundation (USA) https://www.hemophilia.org/Bleeding-
Disorders
• Hemophilia Foundation of Australia http://www.haemophilia.org.au
• Haemophilia Chartered Physiotherapists Association (HCPA)-UK
http://www.ukhcdo.org/haemophilia-associations/physiotherapy-information/
Congresses and Meetings:
• CHS New team member workshops: designed for Treatment Center team
members with 3 years or less of experience
• CPHC education days and annual meetings
• World Federation of Hemophilia:
o Congress
o Musculoskeletal Congress
o Global Forum

Page 53 of 61
• Congress of the European Association for Haemophilia and Allied Disorders.
http://eahad.org/

Page 54 of 61
Appendix 1: Rare Bleeding Disorders: Incidence and clinical symptoms
Modified from:
• Palla R, Peyvandi F, Shapiro AD. Rare bleeding disorders: diagnosis and treatment. Blood
2015; 125 (13): 2052–2061. doi: https://doi.org/10.1182/blood-2014-08-532820
• WFH elearning Introduction to Hemophilia https://elearning.wfh.org/elearning-
centres/introduction-to-hemophilia/#hemophilia_faq
Deficiency Incidence
Factor VIII (Hemophilia A) 1/10,000 Factor IX (Hemophilia B) 1/50,000
Von Willebrand Type 3 1 in 1 million
Fibrinogen 1 in 1 million
Prothrombin 1 in 2 million Factor V 1 in 1 million
Combined FV and FVIII 1 in 1 million
Factor VII deficiency 1 in 500,000
Factor X deficiency 1 in 1 million Factor XI 1 in 1 million
Factor XIII 1 in 2 million
Vitamin K-dependent factors deficiency
< 50 families

Page 55 of 61

Page 56 of 61
Appendix 2: Levels of Evidence
Levels of evidence were assigned using this system:
Source: Kaplan SL, Coulter C, Fetters L. Physical therapy management of congenital
muscular torticollis: an evidence-based clinical practice guideline: from the Section on
Pediatrics of the American Physical Therapy Association. Pediatr Phys Ther.
2013;25(4):348-394. doi:10.1097/PEP.0b013e3182a778d2
An expanded version of this table, based on Oxford Centre for Evidence-Based
Medicine—Levels of Evidence, can be found in
APTA Clinical Practice Guideline Process Manual. Alexandria, VA: American Physical
Therapy
Association; 2018. Page 29.
For these guidelines, Qualitative studies and animal studies were classified as “Other”.
Additional tools, such as AGREE and AMSTAR 2 were also used when necessary to
further refine the classification.

Page 57 of 61
Appendix 3: Grading the Action Statements
Source: Kaplan SL, Coulter C, Fetters L. Physical therapy management of congenital
muscular torticollis: an evidence-based clinical practice guideline: from the Section on
Pediatrics of the American Physical Therapy Association. Pediatr Phys Ther.
2013;25(4):348-394. doi:10.1097/PEP.0b013e3182a778d2
And APTA Clinical Practice Guideline Process Manual. Alexandria, VA: American
Physical Therapy Association; 2018. Page 31.
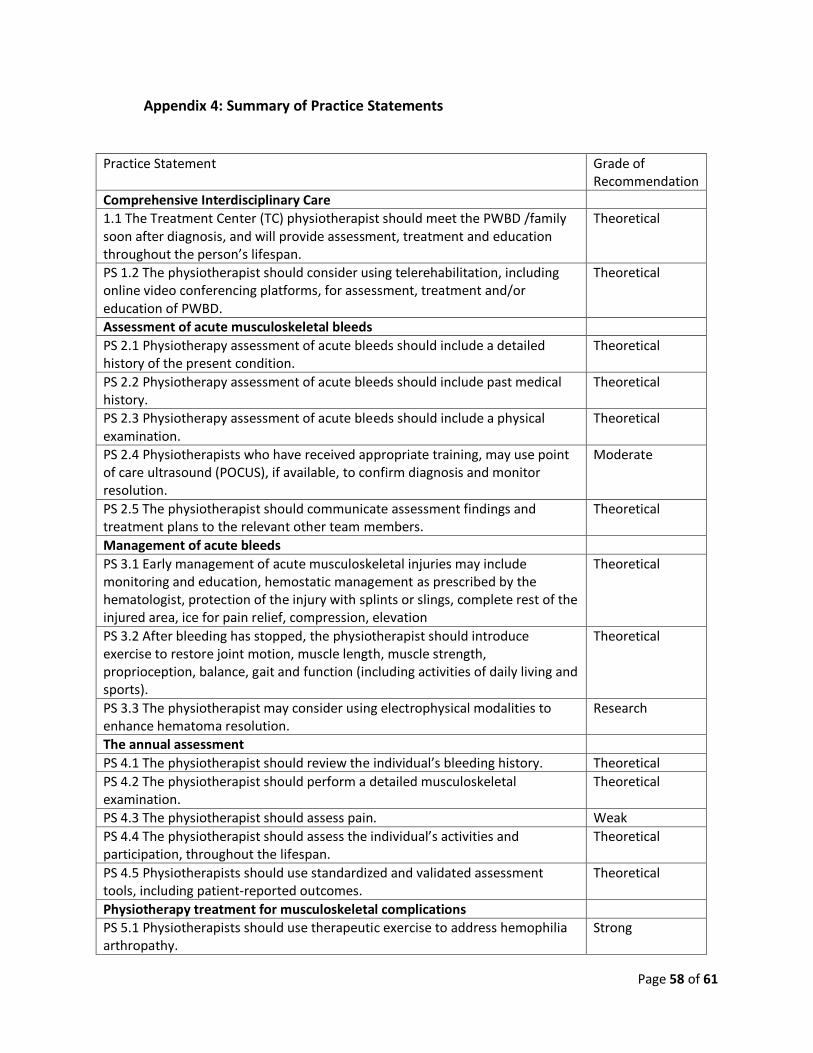
Page 58 of 61
Appendix 4: Summary of Practice Statements
Practice Statement Grade of Recommendation
Comprehensive Interdisciplinary Care
1.1 The Treatment Center (TC) physiotherapist should meet the PWBD /family soon after diagnosis, and will provide assessment, treatment and education throughout the person’s lifespan.
Theoretical
PS 1.2 The physiotherapist should consider using telerehabilitation, including online video conferencing platforms, for assessment, treatment and/or education of PWBD.
Theoretical
Assessment of acute musculoskeletal bleeds
PS 2.1 Physiotherapy assessment of acute bleeds should include a detailed history of the present condition.
Theoretical
PS 2.2 Physiotherapy assessment of acute bleeds should include past medical history.
Theoretical
PS 2.3 Physiotherapy assessment of acute bleeds should include a physical examination.
Theoretical
PS 2.4 Physiotherapists who have received appropriate training, may use point of care ultrasound (POCUS), if available, to confirm diagnosis and monitor resolution.
Moderate
PS 2.5 The physiotherapist should communicate assessment findings and treatment plans to the relevant other team members.
Theoretical
Management of acute bleeds
PS 3.1 Early management of acute musculoskeletal injuries may include monitoring and education, hemostatic management as prescribed by the hematologist, protection of the injury with splints or slings, complete rest of the injured area, ice for pain relief, compression, elevation
Theoretical
PS 3.2 After bleeding has stopped, the physiotherapist should introduce exercise to restore joint motion, muscle length, muscle strength, proprioception, balance, gait and function (including activities of daily living and sports).
Theoretical
PS 3.3 The physiotherapist may consider using electrophysical modalities to enhance hematoma resolution.
Research
The annual assessment
PS 4.1 The physiotherapist should review the individual’s bleeding history. Theoretical
PS 4.2 The physiotherapist should perform a detailed musculoskeletal examination.
Theoretical
PS 4.3 The physiotherapist should assess pain. Weak
PS 4.4 The physiotherapist should assess the individual’s activities and participation, throughout the lifespan.
Theoretical
PS 4.5 Physiotherapists should use standardized and validated assessment tools, including patient-reported outcomes.
Theoretical
Physiotherapy treatment for musculoskeletal complications
PS 5.1 Physiotherapists should use therapeutic exercise to address hemophilia arthropathy.
Strong

Page 59 of 61
PS 5.2 Physiotherapists may recommend orthotics for PWBD Theoretical
PS 5.3 Physiotherapists may use low load prolonged passive stretching, and serial splinting to address flexion contractures.
Theoretical
PS 5.4 Physiotherapists may use manual techniques, including traction, joint gliding, fascial therapy and manual stretching.
Strong
PS 5.5 Physiotherapists may use electrotherapy. Theoretical
PS 5.6 Physiotherapists who have the necessary training may use acupuncture. Theoretical
PS 5.7 Physiotherapists should provide education to PWBD Theoretical
PS 5.8 The physiotherapist may recommend environmental adaptation and mobility aids.
Theoretical
PS 5.9 The physiotherapist should arrange for referral of clients to other health professionals when indicated.
Theoretical
Physiotherapy management before and after musculoskeletal surgery
PS 6.1 The physiotherapist should ensure that the individual has had access to appropriate rehabilitation prior to recommending surgical intervention.
Theoretical
PS 6.2 The bleeding disorders team, the surgical team and the PWBD should discuss goals and expectations for elective orthopedic surgery, including post-operative requirements.
Theoretical
PS 6.3 After the decision is made to proceed with surgery, the physiotherapist should assess for indications for pre-operative physiotherapy.
Theoretical
PS 6.4 The Physiotherapist from the TC should establish and maintain regular communication with other physiotherapists who may need to be involved post-operatively.
Theoretical
PS 6.5 Before beginning post-operative physiotherapy, the treating physiotherapist must be aware of the type and severity of the bleeding disorder, the hematological management plan, the detailed procedure of the surgery including the condition of the tissues observed during the surgery and the range of motion obtained during surgery (if appropriate to the procedure).
Theoretical
PS 6.6 The treating physiotherapist should be aware that PWBD may present challenges that are not seen in other populations undergoing similar procedures. For example, PWBD may be younger, may have arthropathy at multiple joints, have been conditioned to interpret pain as a sign of bleeding, may be accustomed to using high levels of narcotic analgesia, and may have higher post-op complication rates.
Theoretical
PS 6.7 The treating therapist must actively and regularly watch for any signs of bleeding or infection
Weak
PS 6.8 The physiotherapist should consider use of hydrotherapy after hip or knee arthroplasty.
Weak
PS 6.9 The TC physiotherapist should ensure that on-going out-patient rehabilitation has been arranged.
Theoretical
Consultation with other care providers
PS 7.1 The TC physiotherapist should be available for consultation with physiotherapists outside the TC who may be seeing PWBD.
Theoretical
PS 7.2 The physiotherapist should be available for consultation with coaches, school teachers (etc.) regarding activity modification, bleed prevention and injury management.
Theoretical

Page 60 of 61
PS 7.3 The physiotherapist should be available to consult with other team members regarding identification and management of musculoskeletal complications of bleeding disorders.
Best Practice
Encouraging a healthy lifestyle
PS 8.1 The physiotherapist should encourage all PWBD to participate regularly in physical activities that are enjoyable to the individual, and discuss ways to minimize injury.
Theoretical
PS 8.2 The physiotherapist should work with the individual and the TC team to develop a personalized activity plan which includes a plan for injury management.
Theoretical
Continuing Competence
PS 9.1 The TC physiotherapist should participate in learning activities specific to bleeding disorders, and be familiar with current relevant literature.
Best Practice
Copyright © 2022 FDOKUMEN