
Hodgkin's lymphoma: Diagnostic difficulties in fine-needle aspiration cytology
Upload
independentCategory
view
3download
0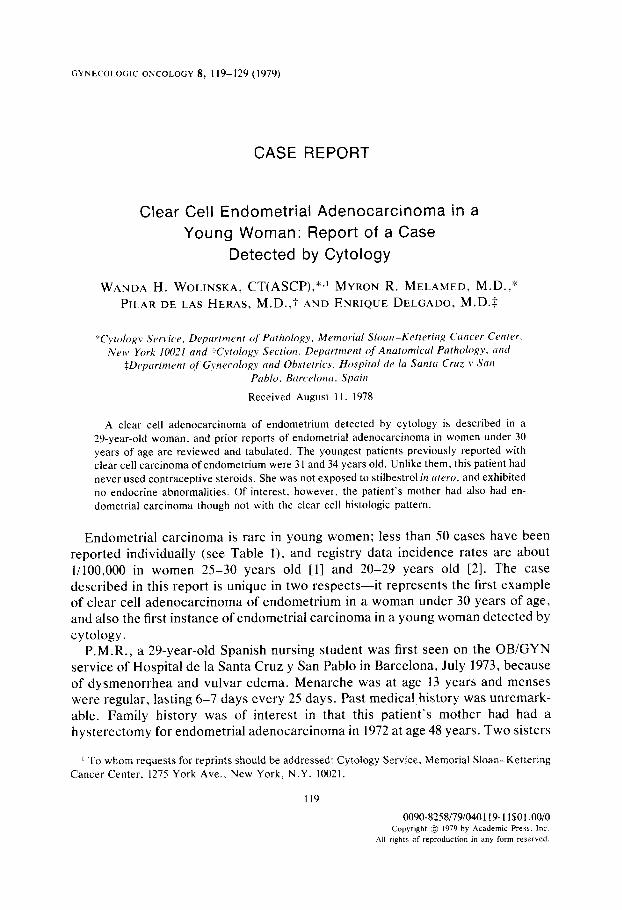
GYNECOLOGIC ONCOLOGY 8, 119-129 (1979)
CASE REPORT
Clear Cell Endometrial Adenocarcinoma in a Young Woman: Report of a Case
Detected by Cytology
WANDA H. WOLINSKA, CT(ASCP),*,’ MYRON R. MELAMED, M.D.,* PILAR DE LAS HERAS, M.D.,? AND ENRIQUE DELGADO, M.D.S
“Cytology SerLticr, Department of Pathology, Memoriul Slow-Kettering Cancer Centrr.
Near, York 10021 and tC.vtology Section. Depurfment of Anatomical Pathology, and $Departmrnt of Gynecology and Obstetrics, Hospital de la Santa Cruz y Sun
Pablo. Barcc4ona. Spuin
Received August 1 I. 1978
A clear cell adenocarcinoma of endometrium detected by cytology is described in a 29-year-old woman, and prior reports of endometrial adenocarcinoma in women under 30 years of age are reviewed and tabulated. The youngest patients previously reported with clear cell carcinoma of endometrium were 31 and 34 years old. Unlike them, this patient had never used contraceptive steroids. She was not exposed to stilbestrol in utero, and exhibited no endocrine abnormalities. Of interest, however, the patient’s mother had also had en- dometrial carcinoma though not with the clear cell histologic pattern.
Endometrial carcinoma is rare in young women; less than 50 cases have been reported individually (see Table l), and registry data incidence rates are about 11100,000 in women 25-30 years old [I] and 20-29 years old [2]. The case described in this report is unique in two respects-it represents the first example of clear cell adenocarcinoma of endometrium in a woman under 30 years of age, and also the first instance of endometrial carcinoma in a young woman detected by cytology.
P.M.R., a 29-year-old Spanish nursing student was first seen on the OBiGYN service of Hospital de la Santa Cruz y San Pablo in Barcelona, July 1973, because of dysmenorrhea and vulvar edema. Menarche was at age 13 years and menses were regular, lasting 6-7 days every 25 days. Past medical history was unremark- able. Family history was of interest in that this patient’s mother had had a hysterectomy for endometrial adenocarcinoma in 1972 at age 48 years. Two sisters
r To whom requests for reprints should be addressed: Cytology Service, Memorial Sloan-Kettering Cancer Center. 1275 York Ave., New York, N.Y. 10021.
119
0090-8258/79/040119- 1 1 $0 1.0010 Copyright @ 1979 by Academic Press. Inc.
All rlght% of reproduction m any form reserved.

TABL
E I
REPO
RTED
CA
SES
OF
ENDO
MET
RIAL
AD
ENOC
ARCI
NOM
A IN
W
OMEN
UN
DER
30
YEAR
S OF
AG
E
Year
Au
thor
Tota
l No
. of
ca
ses
Belo
w st
udie
d 30
Ty
pe”
Ovary
1924
Hi
rst
I I
1949
Sp
eert
255
2 19
49
Som
mer
s et
(2
1.
30
8
1951
19
60
1694
4
1 1
I963
1
1 Ad
enoc
a Cy
stic
1967
19
67
1968
I 1
Aden
oca
650
2 Ad
enoc
a 22
2
Aden
oca
1970
19
71
244
3 Ad
enoc
a 70
7 3
Aden
oca
1972
Dock
erty
et
rrl.
Andr
ews
and
Andr
es
DeVe
re
and
Dem
pste
r Ca
irns
et al
. Pe
ters
on
Kem
pson
an
d Po
korn
y Ng
an
d Re
agan
Ch
risto
pher
son
et
121.
Cu
tler
et al
. 2
1973
19
74
Frick
et
al
. Fe
chne
rand
Ka
ufm
an
Silve
rber
g an
d M
akow
ski
Kelle
y et
al.
Lyon
an
d Fr
ich
Mem
orial
Ho
spita
l
348
2 4
2
1975
21
7
1976
19
76
1967
- 19
73
3
534
1 1 3
Aden
oca
Aden
oca
5-Ad
enoc
a,
2-Ad
enos
q,
I-Und
iff Ad
enoc
a Ad
enoc
a
Aden
osq
Aden
oca
Aden
oca
Aden
oca
Aden
oca
Cyst
ic 4-
Fibr
osis
Cyst
ic Po
lycys
tic
Polyc
ystic
l-C
ystic
Gon
adal
dysg
enes
is
2-Po
lycys
tic
Som
e po
lycys
tic
Aden
oca,
in
sit
u I-A
deno
ca
I-Cys
tic
Blee
ding
Re
mar
ks
Refe
renc
e
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Irreg
ular
Horm
onal
imba
lanc
e,
stou
t
Two
obes
e
Obes
e 12
21
Stein
-Lev
enth
al sy
ndro
me
WI
Stein
-Lev
enth
al sy
ndro
me
WI
Obe
se,
Stein
-Lev
enth
al sy
ndro
me
Obes
e [7
1 [I3
1 12
41
Stilb
estro
l Rx
11
71
Stein
-Lev
enth
al sy
ndro
me
WI
PI
Oral
cont
race
ptive
12
91
Oral
cont
race
ptive
[3
01
Cont
race
ptive
[3
11
1 Ob
ese
Unpu
blish
ed
1191
PO1
P]l
WI
WI
a Ad
enoc
a,
aden
ocar
cinom
a;
Aden
osq,
ad
enos
quam
ous;
Undi
ff,
undi
ffere
ntia
ted.
b FI
G.
I La
rge
singl
e ce
lls
with
irr
egula
r co
arse
ly gr
anula
r nu
cleus
an
d pr
omine
nt
mac
ronu
cleol
us.
The
cells
ar
e ro
unde
d,
with
we
ll-def
ined
m
argi
ns
and
abun
dant
cy
topl
asm
th
at
varie
s fro
m
opaq
ue
(a)
to
finel
y va
cuola
ted
(c).
Note
th
e cy
topl
asm
of
on
e ce
ll (b
) wh
ich
appe
ars
rath
er
dens
e an
d gr
anula
r ce
ntra
lly,
and
beco
mes
cle
ar
at
the
perip
hery
. Th
is
type
of
cell
sugg
ests
a
clear
ce
ll ca
rcin
oma,
wh
ich
we
have
pr
eviou
sly
asso
ciate
d wi
th
clear
ce
ll ad
enoc
arcin
oma
of
cerv
ix an
d kid
ney.
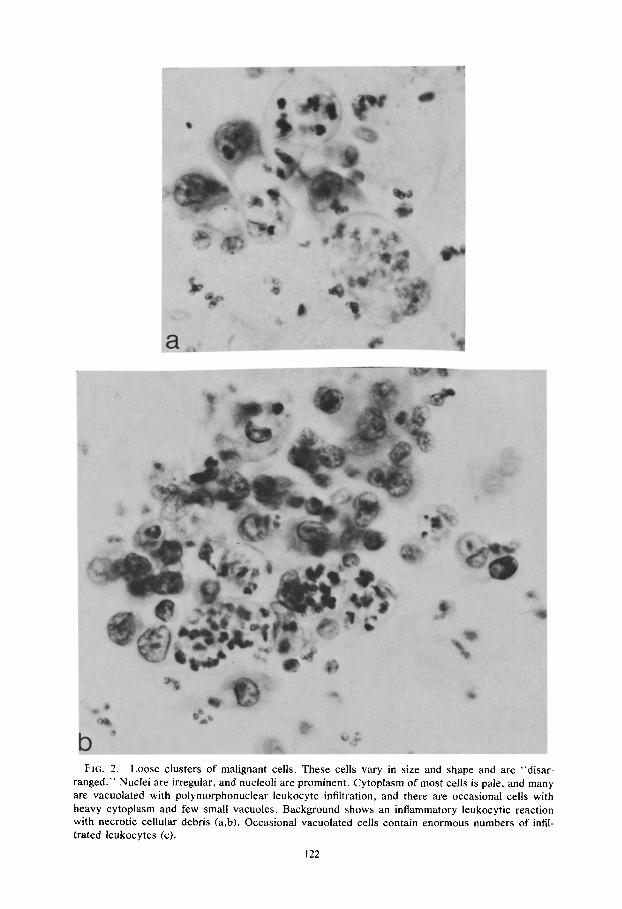
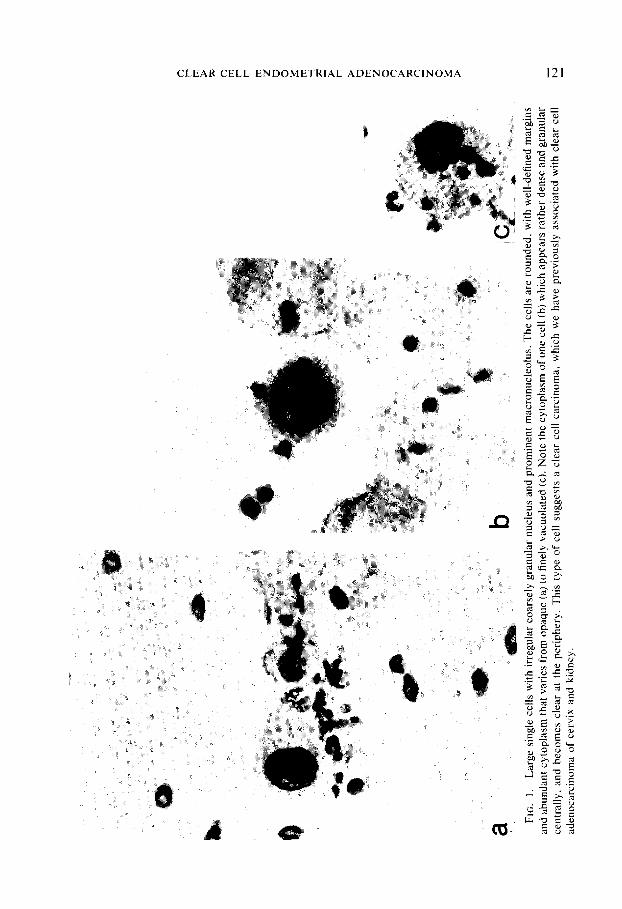
FIG. 2. Loose clusters of malignant cells. These cells vary in size and shape and are “disar- ranged.” Nuclei are irregular, and nucleoli are prominent. Cytoplasm of most cells is pale, and many are vacuolated with polymorphonuclear leukocyte infiltration, and there are occasional cells with heavy cytoplasm and few small vacuoles. Background shows an inflammatory leukocytic reaction with necrotic cellular debris (a,b). Occasional vacuolated cells contain enormous numbers of infil- trated leukocytes (c).
122
CLEAR CELL ENDOMETRIAL ADENOCARCINOMA 123
were in good health. No abnormalities were found on general physical examina- tion. Pelvic examination revealed a virginal introitus, normal external genitalia, and normal manual examination. The cervix was not visualized. Cytology smears were taken from the vaginal pool and were normal.
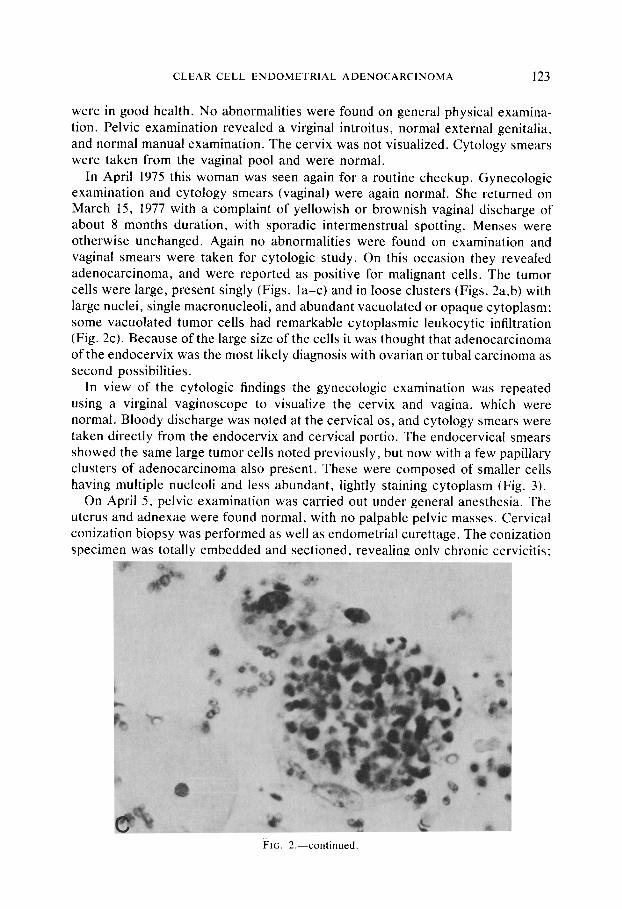
In April 1975 this woman was seen again for a routine checkup. Gynecologic examination and cytology smears (vaginal) were again normal. She returned on March 15, 1977 with a complaint of yellowish or brownish vagina1 discharge of about 8 months duration, with sporadic intermenstrual spotting. Menses were otherwise unchanged. Again no abnormalities were found on examination and vaginal smears were taken for cytologic study. On this occasion they revealed adenocarcinoma, and were reported as positive for malignant cells. The tumor cells were large, present singly (Figs. la-c) and in loose clusters (Figs. 2a,b) with large nuclei, single macronucleoli, and abundant vacuolated or opaque cytoplasm; some vacuolated tumor cells had remarkable cytoplasmic leukocytic infiltration (Fig. 2~). Because of the large size of the cells it was thought that adenocarcinoma of the endocervix was the most likely diagnosis with ovarian or tubal carcinoma as second possibilities.
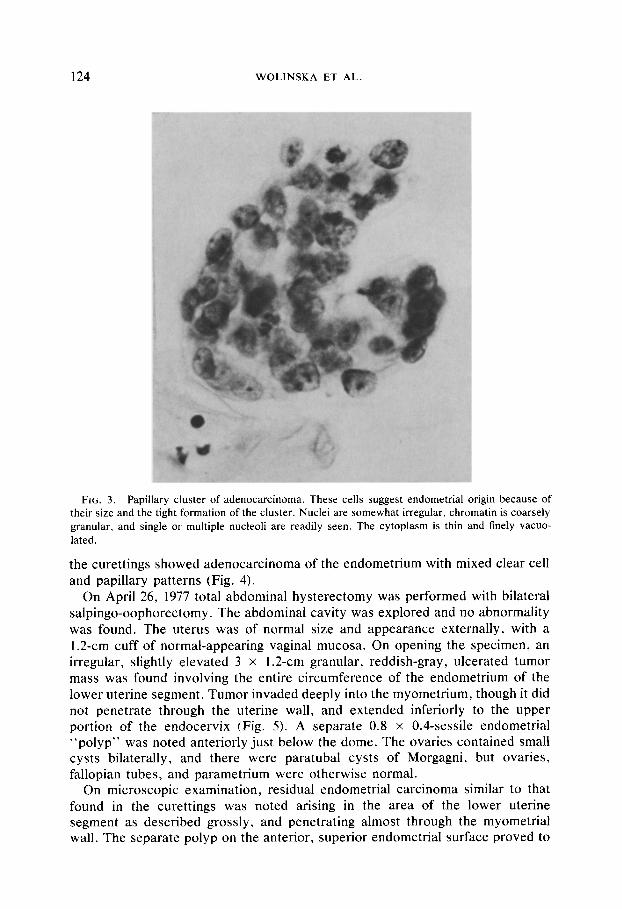
In view of the cytologic findings the gynecologic examination was repeated using a virginal vaginoscope to visualize the cervix and vagina, which were normal. Bloody discharge was noted at the cervical OS, and cytology smears were taken directly from the endocervix and cervical portio. The endocervical smears showed the same large tumor cells noted previously, but now with a few papillary clusters of adenocarcinoma also present. These were composed of smaller cells having multiple nucleoli and less abundant, lightly staining cytoplasm (Fig. 3).
On April 5, pelvic examination was carried out under genera1 anesthesia. The uterus and adnexae were found normal, with no palpable pelvic masses. Cervical conization biopsy was performed as well as endometrial curettage. The conization specimen was totally embedded and sectioned, revealing only chronic cervicitis;
FIG. 2.-continued
124 WOLINSKA ET AL.
FIG. 3. Papillary cluster of adenocarcinoma. These cells suggest endometrial origin because of their size and the tight formation of the cluster. Nuclei are somewhat irregular, chromatin is coarsely granular, and single or multiple nucleoli are readily seen. The cytoplasm is thin and finely vacuo- lated.
the curettings showed adenocarcinoma of the endometrium with mixed clear cell and papillary patterns (Fig. 4).
On April 26, 1977 total abdominal hysterectomy was performed with bilateral salpingo-oophorectomy. The abdominal cavity was explored and no abnormality was found. The uterus was of normal size and appearance externally, with a 1.2-cm cuff of normal-appearing vaginal mucosa. On opening the specimen, an irregular, slightly elevated 3 x 1.2-cm granular, reddish-gray, ulcerated tumor mass was found involving the entire circumference of the endometrium of the lower uterine segment. Tumor invaded deeply into the myometrium, though it did not penetrate through the uterine wall, and extended inferiorly to the upper portion of the endocervix (Fig. 5). A separate 0.8 x 0.4-sessile endometrial “polyp” was noted anteriorly just below the dome. The ovaries contained small cysts bilaterally, and there were paratubal cysts of Morgagni, but ovaries, fallopian tubes, and parametrium were otherwise normal.
On microscopic examination, residual endometrial carcinoma similar to that found in the curettings was noted arising in the area of the lower uterine segment as described grossly, and penetrating almost through the myometrial wall. The separate polyp on the anterior, superior endometrial surface proved to

CLEAR CELL ENDOMETRIAL ADENOCARCINOMA 125
FIG. 4. Clear cell endometrial adenocarcinoma present in the curettage specimen.
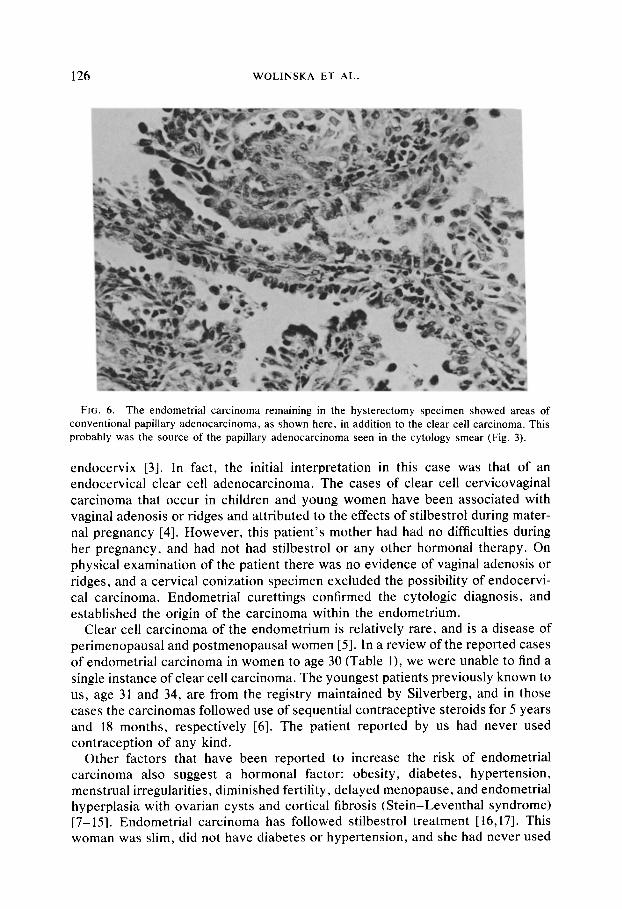
be a small, noninvasive papillary endometrial carcinoma. In addition to the clear cell pattern noted in the curettings, there were areas of more conventional papil- lary adenocarcinoma as well (Fig. 6).
The postoperative course was normal and the patient was discharged within 7 days. She received a course of external irradiation, 4,000 rad, and 8 months following surgery is making plans for marriage.
DlSCUSSlON
The cytologic presentation of clear cell adenocarcinoma in the cervico-vaginal smears of this patient was quite similar to that seen in miillerian carcinomas of the
FIG. 5. Gross photograph of the uterus showing lower uterine segment and cervix. The car- cinoma involves the entire circumference of the endometrial cavity in the lower uterine segment, and extends to the upper portion of the endocervix. Tumor invades almost completely through the muscularis. The cervix is postconization.
126 WOLINSKA ET AL.
FIG. 6. The endometrial carcinoma remaining in the hysterectomy specimen showed areas of conventional papillary adenocarcinoma, as shown here, in addition to the clear cell carcinoma. This probably was the source of the papillary adenocarcinoma seen in the cytology smear (Fig. 3).
endocervix [3]. In fact, the initial interpretation in this case was that of an endocervical clear cell adenocarcinoma. The cases of clear cell cervicovaginal carcinoma that occur in children and young women have been associated with vaginal adenosis or ridges and attributed to the effects of stilbestrol during mater- nal pregnancy [4]. However, this patient’s mother had had no difficulties during her pregnancy, and had not had stilbestrol or any other hormonal therapy. On physical examination of the patient there was no evidence of vaginal adenosis or ridges, and a cervical conization specimen excluded the possibility of endocervi- cal carcinoma. Endometrial curettings confirmed the cytologic diagnosis, and established the origin of the carcinoma within the endometrium.
Clear cell carcinoma of the endometrium is relatively rare, and is a disease of perimenopausal and postmenopausal women [5]. In a review of the reported cases of endometrial carcinoma in women to age 30 (Table l), we were unable to find a single instance of clear cell carcinoma. The youngest patients previously known to us, age 31 and 34, are from the registry maintained by Silverberg, and in those cases the carcinomas followed use of sequential contraceptive steroids for 5 years and 18 months, respectively [6]. The patient reported by us had never used contraception of any kind.
Other factors that have been reported to increase the risk of endometrial carcinoma also suggest a hormonal factor: obesity, diabetes, hypertension, menstrual irregularities, diminished fertility, delayed menopause, and endometrial hyperplasia with ovarian cysts and cortical fibrosis (Stein-Leventhal syndrome) [7- 151. Endometrial carcinoma has followed stilbestrol treatment [ 16,171. This woman was slim, did not have diabetes or hypertension, and she had never used

CLEAR CELL ENDOMETRIAL ADENOCARCINOMA 127
any contraceptives or received stilbestrol or any other hormone. She did have minimal menstrual irregularities and a brownish discharge that led to a gynecologic examination, but that appeared most likely a symptom of her en- dometrial carcinoma rather than an indication of hormonal imbalance. In all other respects she considered herself well and was planning marriage when the car- cinoma was discovered.
A family history of endometrial carcinoma increases risk of this disease, though one must be wary of reports particularly in the older literature that fail to distin- guish cervical from endometrial carcinoma in families that have several members with uterine cancer [18]. In a recent epidemiologic study of 154 patients with endometrial carcinoma, Lynch found that 26 (16%) had first degree relatives with endometrial carcinoma including 16 mother-daughter combinations [ 1 I]. He also reported on a group of families at high risk [ 121.
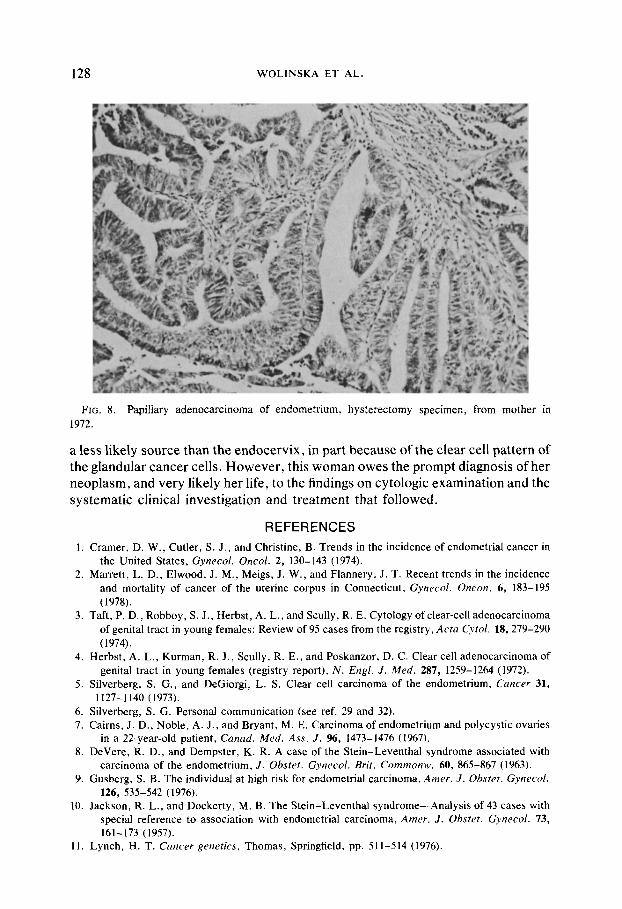
Because of the unique clear cell histology of the endometrial carcinoma in our patient, and her young age, the family history of endometrial carcinoma in the mother seems worthy of emphasis. We had the opportunity to review histologic sections of the mother’s surgically resected uterus, ovaries, and fallopian tubes, and were able to obtain a photograph of the gross specimen (Fig. 7). The histologic pattern was that of a conventional papillary adenocarcinoma of endometrium which did not have clear cell or secretory features (Fig. 8). Nevertheless, the maternal carcinoma must be considered a predisposing factor in this patient who had no apparent hormonal imbalance and no exposure to exogenous steroids.
Because of her young age, the menstrual irregularities that brought this woman to her physician were initially considered to be functional. Even after adenocar- cinema was identified by cytologic examination the endometrium was considered
FIG. 7. Gross photograph of the mother’s uterus showing endometrial adenocarcinoma which, interestingly, arises in the lower uterine segment resembling the carcinoma in the daughter.
128 WOLINSKA ET AL.
FIG. 8. Papillary adenocarcinoma of endometrium, hysterectomy specimen, from mother in 1972.
a less likely source than the endocervix, in part because of the clear cell pattern of the glandular cancer cells. However, this woman owes the prompt diagnosis of her neoplasm, and very likely her life, to the findings on cytologic examination and the systematic clinical investigation and treatment that followed.
REFERENCES
1. Cramer. D. W., Cutler, S. J., and Christine, B. Trends in the incidence of endometrial cancer in the United States, Gynecol. Oncol. 2, 130-143 (1974).
2. Marrett, L. D., Elwood, J. M., Meigs, J. W., and Flannery, J. T. Recent trends in the incidence and mortality of cancer of the uterine corpus in Connecticut, Gynecol. Oncon. 6, 183-195 (1978).
3. Taft, P. D., Robboy, S. J., Herbst, A. L., and Scully, R. E. Cytology of clear-cell adenocarcinoma of genital tract in young females: Review of 95 cases from the registry, Acta Cyfol. 18, 279-290 (1974).
4. Herbst, A. L., Kurman, R. J., Scully, R. E., and Poskanzor, D. C. Clear cell adenocarcinoma of genital tract in young females (registry report), N. EngI. J. Med. 287, 1259-1264 (1972).
5. Silverberg, S. G., and DeGiorgi, L. S. Clear cell carcinoma of the endometrium, Cancer 31, 1127-l 140 (1973).
6. Silverberg, S. G. Personal communication (see ref. 29 and 32). 7. Cairns, J. D., Noble, A. J., and Bryant, M. E. Carcinoma of endometrium and polycystic ovaries
in a 22-year-old patient, Canad. Med. Ass. J. %, 1473-1476 (1967). 8. DeVere, R. D., and Dempster, K. R. A case of the Stein-Leventhal syndrome associated with
carcinoma of the endometrium, J. O&ret. Gynecol. Bn’t. Commons. 60, 865-867 (1963). 9. Gusberg, S. B. The individual at high risk for endometrial carcinoma, Amer. J. Obsret. Gynecol.
126, 535-542 (1976). 10. Jackson, R. L., and Dockerty, M. B. The Stein-Leventhal syndrome-Analysis of 43 cases with
special reference to association with endometrial carcinoma, Amer. J. Obsret. Gynecol. 73, 161-173 (1957).
11. Lynch, H. T. Cancer generics, Thomas, Springfield, pp. 511-514 (1976).
CLEAR CELL ENDOMETRIAL ADENOCARCINOMA 129
12. Lynch, H. T., Harris, R. E., Lynch, P. M., Guirgis, H. A.. Lynch. J. F., and Bardawil. W. A. Role of heredity in multiple primary cancer, C~/tcer 40, 1849-1854 (1977).
13. Peterson, E. P. Endometrial carcinoma in young women, Obsref. Gynrcol. 31, 702-707 (1968).
14. Scully, R. E. Estrogens and endometrial carcinoma, Ifron. Purhol. 8, 481-485 (1977). 15. Wynder, E. L., Escher, G. C., and Mantel, N. An epidemiological investigation of cancer of the
endometrium, Concrr 19, 489-520 (1966). 16. Bromberg, Y. M., Liban, E., and Laufer, A. Early endometrial carcinoma following prolonged
estrogen administration in an ovariectomized woman, Ohsre~. G~tzrc~ol. 14, 221-226 (1959). 17. Cutler, B. S., Forbes. A. P.. Ingersoll, F. M.. and Scully, R. E. Endometrial carcinoma after
stilbestrol therapy in gonadal dysgenesis, N. ERR/. .I. Mrd. 287, 628-631 (1972). 18. Savage, D. A family history of uterine and gastro-intestinal cancer, Brir. Med. .I. 2, 341-343 (1956). 19. Hirst, B. C. Malignant growths of the uterus in young girls. Amer. J. Oh.sfc~r. Gynrcol. 18,
104-105, 150-151 (1929). 20. Speert, H. Carcinoma of the endometrium in young women, Surf. G~nrcol. Ohstrr. 88, 332-336
(1949). 21. Sommers, S. C., Hertig, A. T., and Bengloff. H. Genesis ofendometrial carcinoma. II. Cases I9 to
35 years old, Gamer 2, 957-963 (1949). 22. Dockerty, M. B., Lovelady. S. B., and Foust. G. T. Carcinoma of the corpus uteri in young
women, Amer. J. Ohsret. G~~nrw~/. 61, 966-981 (1951). 23. Andrews, W. C., and Andres, M. C. Stein-Leventhal syndrome with associated adenocarcinoma
of the endometrium-report of a case in a 22 year old woman, Amer. J. Ohwr. G~rwcd. 80, 632-636 (1960).
24. Kempson. R. L., and Pokorny, G. E. Adenocarcinoma of the endometrium in women aged forty and younger. Cancer 21, 650-662 (1968).
25. Ng, A. B. P.. and Reagan, J. W. Incidence and prognosis of endometrial carcinoma by histologic grade and extent. Obstet. Gyned. 35, 437-443 (1970).
26. Christopherson, W. M., Mendez, W. M., Parker, J. E., Lundin, F. E., and Ahuja, E. M. Carcinoma of the endometrium: A study of changing rates over a 15-year period, Carlcrr- 27, 1005-1008 (1971).
27. Frick, H. C., Munnell. E. W., Richart, R. M., Berger, A.. and Lawry, M. F. Carcinoma of the endometrium. Amer. J. Obsrcv. Gyww~l. 115, 663-676 (1973).
28. Fechner. R. E., and Kaufman, R. H. Endometrial adenocarcinoma in Stein-Leventhal syndrome, Cancer 34, 444-452 (1974).
29. Silverberg, S. G., and Makowski, E. L. Endometrial carcinoma in young women taking oral contraceptive agents, Obstrr. Gywcd. 46, 503-506 (1975).
30. Kelley, H. W., Miles, P. A., Buster, J. E.. and Scragg. W. H. Adenocarcinoma of the endome- trium of women taking sequential oral contraceptives, Ohsr~~r. Gynrcoi. 47, 200-202 (1976).
31. Lyon, F. A., and Frisch, M. J. Endometrial abnormalities occurring in young women on long-term sequential oral contraception, Obstrt. Gyrvxo/. 47, 636-643 (1976).
32. Silverberg, S. G., Makowski, E. L., and Roche, W. D. Endometrial carcinoma in women under 40 years of age, Cunccr 39, 592-598 (1977).
Copyright © 2022 FDOKUMEN




















