Childhood injuries: a population-based study of emergency room visits in Jerusalem
15
Paediatric and Perinatal Epidemiology 1989, 3, 174-188 Childhood injuries: a population-based study of emergency room visits in Jerusalem Rosa Gofin, Hava Palti, Bella Adler and Edet Edet Department of Social Medicine, Hadassah Medical Organisation and the Hebrew University-Hadassah School of Public Health and Community Medicine, lerusalem, lsrael Summary. A study of childhood injuries of 0-17-year-old Jewish children based on emergency room records of the four major hospitals and the first aid stations was conducted in Jerusalem during 1986. The incidence of visits was 99.7/1000 child-years with 95% confidence intervals (C1)--98.0-101.5. The rate was 97.2/1000 child-years (CI- 94.4-100.0) among the 0-5-year-olds, 114.6/1000 child-years (CI- 111.3-118.0) in the 6-12 age group, and was 93.6/1000 child-years (CI-90.1-97.1) among 13-17-year-olds. The male to female rate ratio was 1.7 for the 0-5-year-olds, 2.1 for the 6-12-year-olds and 2.3 for the 13-17-year-olds. The most frequent causes of injuries were falls, 38.5/1000 child-years (CI-37.4-39.6), being struck or caught, 21.1/1000 child-years (CI-20.3-21.9), and road accidents, 5.4/1000 child-years (CI-5.0-5.8). Only bums among children aged 6 years and over and poisoning among 13-1 7-year-olds showed a higher incidence among females than among males. The head was the most frequently injured part of the body (45.2/1000 child-years, CIz44.0-46.4). Head injuries decreased as age increased, while injuries to the extremities and trunk increased with increasing age. Two per cent of the injured children were admitted to hospital. Introduction Only in the late 1940s was it recognised that injuries are an ecological problem and that they should be studied by epidemiological methods.'. Better understand- ing of the natural history of injuries, their incidence and definition of risk groups can assist policy makers in deciding priorities, planning interventions and furthering investigation^.^-^ Address for correspondence: Dr R. Gofin, Department of Social Medicine, Faculty of Medicine of the Hebrew University and Hadassah School of Public Health and Community Medicine, POB 1172, Jerusalem 91010, Israel. 174
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Childhood injuries: a population-based study of emergency room visits in Jerusalem

Paediatric and Perinatal Epidemiology 1989, 3, 174-188
Childhood injuries: a population-based study of emergency room visits in Jerusalem
Rosa Gofin, Hava Palti, Bella Adler and Edet Edet Department of Social Medicine, Hadassah Medical Organisation and the Hebrew University-Hadassah School of Public Health and Community Medicine, lerusalem, lsrael
Summary. A study of childhood injuries of 0-17-year-old Jewish children based on emergency room records of the four major hospitals and the first aid stations was conducted in Jerusalem during 1986. The incidence of visits was 99.7/1000 child-years with 95% confidence intervals (C1)--98.0-101.5. The rate was 97.2/1000 child-years (CI- 94.4-100.0) among the 0-5-year-olds, 114.6/1000 child-years (CI- 111.3-118.0) in the 6-12 age group, and was 93.6/1000 child-years (CI-90.1-97.1) among 13-17-year-olds. The male to female rate ratio was 1.7 for the 0-5-year-olds, 2.1 for the 6-12-year-olds and 2.3 for the 13-17-year-olds. The most frequent causes of injuries were falls, 38.5/1000 child-years (CI-37.4-39.6), being struck or caught, 21.1/1000 child-years (CI-20.3-21.9), and road accidents, 5.4/1000 child-years (CI-5.0-5.8). Only bums among children aged 6 years and over and poisoning among 13-1 7-year-olds showed a higher incidence among females than among males. The head was the most frequently injured part of the body (45.2/1000 child-years, CIz44.0-46.4). Head injuries decreased as age increased, while injuries to the extremities and trunk increased with increasing age. Two per cent of the injured children were admitted to hospital.
Introduction
Only in the late 1940s was it recognised that injuries are an ecological problem and that they should be studied by epidemiological methods.'. Better understand- ing of the natural history of injuries, their incidence and definition of risk groups can assist policy makers in deciding priorities, planning interventions and furthering investigation^.^-^
Address for correspondence: Dr R. Gofin, Department of Social Medicine, Faculty of Medicine of the Hebrew University and Hadassah School of Public Health and Community Medicine, POB 1172, Jerusalem 91010, Israel.
174

Childhood injuries 175 In the developed world, accidental injuries rank as the main cause of death in
child and adolescent populations and are becoming increasingly important in the developing world as a cause of morbidity and While mortality statistics of injuries are available for most countries, they represent only the ‘tip of the iceberg’. Data on non-fatal occurrences are not available due to lack of compulsory reporting. There are few comprehensive epidemiological studies dealing with the whole range of accidental injuries in a total population.*-”
The present study investigates injuries to Jewish children and adolescents which occurred during 1 year in the city of Jerusalem and required attention at an emergency room. The city has four major hospitals with emergency rooms providing care for the population. It is an appropriate framework in which to study and estimate the incidence of accidental injuries, their cause, nature and outcome. Up till now, there are no data available on non-fatal childhood injuries dealing with all types of injuries in a defined population in Israel.
Data from this study will allow identification of ‘high risk’ groups and will serve as a basis for planning interventions to reduce morbidity and mortality.
Population and methods The study is based on the Jewish population of children aged 0-17 years born between 1 January 1969 and 31 December 1986 who are residents of Jerusalem (n= 123 630). They are a heterogeneous population regarding ethnic and sociocultural background. The hospitals and the first aid station ‘Magen David Adom‘ (MDA) are accessible and available to all members of the population, more than 954b of whom are insured by sick funds’* and the rest by social welfare insurance. The maximum travel distance to any facility is 15 km. The hospital emergency facilities accept all patients on specific days of the month on a rotating basis.
The study refers to the period between 1 January 1986 and 31 December 1986. A 2546 sample of the attendances at the above facilities was randomly selected, 91 days for each hospital and MDA. For one of the hospitals only a 12.5% sample could be obtained. The weight of each one of the sampling fractions was considered when rates or proportions were calculated. On the selected days in each facility, the records of every child who met the criteria for inclusion in the study were reviewed and extracted on standard forms. A small proportion of the records (1.6%) could not be located.
’Accident‘ was defined as an unintentional unexpected violent event affecting the child with or without detectable injury and subsequently leading to medical attention in an emergency room. Repeat accidents for the same child were also included. Data were collected on sex, year of birth, place of residence, time of

176 R. Gofin et al. arrival and departure to the facility, place of accident, type, nature and location of injury and its outcome (whether released with or without follow-up or hospitalised). Cause and nature were grouped according to categories defined in terms of ICD codes” as will be shown in Tables 3 and 4.
To enhance reliability of coding, a sample of the records was coded by all four recorders and the project director, and discrepancies were discussed. Linkage between records of the patients attending more than one institution was not possible due to lack of a common identification system. This lack of identification was important for cases referred from the first aid station (MDA) to the hospitals’ emergency rooms. The total number of injury visits to the emergency rooms and MDA was 16 140. Fifty-one per cent of the injuries attending the MDA services were subsequently referred to the emergency room of the hospital on duty. These 3760 cases were counted only once as hospital emergency room cases, leaving 12380 visits. The rates.presented in this study are considered a conservative estimate since we assumed that all children referred from MDA actually paid a visit to the emergency room of one of the hospitals whereas from checking on a sample of the referrals, only 73% of them arrived at the emergency room.
Proportions for cause, nature and location of injury were calculated based on number of visits in each age group. Since each child could have been injured by more than one cause, and would have more than one kind of injury which could affect more than one part of the body, the sum of the injuries in each age category exceeded the total number of visits. Rates of injury are expressed per 1000 child- years with 9546 confidence intervals (CI) calculated using a binomial distribu- tion.14 Denominator information is based on publications of the Central Bureau of Statistics by sex and age groups (0-4,5-14,15-19). To obtain a regrouping for the purpose of this analysis it was necessary to estimate the number in single years of age. The estimates were based on number of live births per year in Jerusalem from 1969 to 1986.15 In order to correct for deaths and out-migration during the period studied, the ratio between the population estimate for Jerusalem by broad age groups (0-4, 5-14, 15-19)16 and the number of live births for that age group was calculated. An additional method was used to check for the possibility of bias. In this calculation, the Central Bureau of Statistics population estimates for the whole country by calendar year15 were multiplied by the percentage of Jerusalemites of the specific age category. The results of this calculation were similar to the previous one. The final population estimates are shown in Table 1.
The percentage of missing information for cause of injury was 19.596, for nature of injury 9.570, and for the location of injury 3%. Missing information for other variables ranged from 0.1% to 0.890. Cases with missing information are excluded from the relevant tables. In most cases, there was no indication of the place of injury.
The numbers of accidental events in the sample were 880 and 684 at the two big university hospitals, 558 at the third hospital and only 44 at the hospital where

Childhood injuries 177
Table 1. injury incidence rates per thousand child-years by age and sex. Emergency rooms. Jerusalem, 1986
~~
Males Females Total
~~~
0-5 24880 121.7 23 230 70.9 48 110 97.2
6-12 23470 143.8 22 000 66.7 45 470 106.5
13-17 15650 128.1 14 400 56.1 30 050 93.6
(117.4-126.1) (67.5-74.4) (94.4-100.0)
(139.0-148.8) (63.3-70.2) (103.5-109.6)
(122.5-133.8) (52.3-60.1) (90.1-97.1) -~
Total 64000 131.4 59 630 65.8 123 630 99.7 (128.6-134.2) (63.7-67.9) (98.0-101.5)
CI =confidence intervals.
Age ( y r )
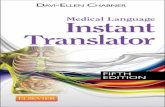
Figure 1. Injury incidence rates and 95% confidence intervals by age and sex. Emergency rooms. Jerusalem, 1986. O=males; 0 -females.
a 12.50/0 sample was obtained. This hospital is a small one and does not have orthopaedic or neurosurgery departments. There were 1825 visits to the MDA Service. Data were analysed using the SPSSX program.”
Results
Incidence rates are shown in Table 1. The male to female rate ratio (M:F) was 2.0 for children 0-17 years old. It increased from 1.7 among the 0-5-year-olds to 2.1

178 R. Gofin et al. among the 6-12-year-olds and 2.3 among the 13-17-year-olds. Rates by single years of age are shown in Figure 1. The rates were low for the first year of life. A marked increase in the rate of accidents occurred for both sexes during the second year of life. Thereafter, the rate remained high, with a decrease for girls older than 5 years of age and boys older than 6 years of age. Girls show a peak in incidence rate at 13 years of age with a subsequent decline as opposed to adolescent boys who show an increase in incidence after 15 years of age. The M: F ratio increased to 3.5 at 17 years of age.
The peak number of visits took place during July and October (Table 2). There were somewhat more visits during the weekend (Friday and Saturday) and on Wednesdays. The frequency of attendance was highest during afternoon hours.
Table 2. Attendance at emergency rooms by month, day of the week and time of arrival (n-12380)
Yo 96
Month January February March April May June July August September October November December
7.1 5.9 8.6 6.9 8.1 8.3
11.0 9.2 9.2
12.4 7.2 5.9
Day Sunday 14.4 Monday 10.8 Tuesday 13.1 Wednesday 17.0 Thursday 14.3 Friday 15.7 Saturday 14.7
Time of arrival (h) 0-7 2.7 8-12 18.4
13-15 20.4 16-19 33.0 20-24 25.4
Cause of injury The most common injuries were falls (Table 3) followed by 'being struck/caught'. Within this category there were 48% struck/caught by a blunt object, 4246 by a sharp object and 1046 by a person. Of the 668 road accidents, 43% occurred while travelling in cars, 25% were pedestrians, 2146 cyclists, 6% motorcyclists and 4% were 'other' or undetermined. The rates of road accidents by specific cause are shown in Table 4. Poisonings, bums, sports injuries and bites/stings had low incidence rates. There were only 4 cases of drowning.
A marked decline in the rates of falls was noted with age, while being struck/caught, road injuries, sports injuries and bites/stings increased with age.

Childhood injuries 179
Table 3. Cause of injury by age and sex*
Age f Y 4
Cause of injury 0-5 6-12 13-17 Total
Falls 880-888
Struck/caught 9 16-920
Road accidents 810-829
Foreign body 9 14-915
Bums 890-899, 924
sports
Bites/stings 905-906
Poisonings 850-869
No. Rate CI 90
M:F
No. Rate CI YO
M:F
No. Rate CI 90
M:F
No. Rate CI %
M:F
No. Rate CI %
M:F
No. Rate CI YO
M:F
No. Rate CI 96
M:F
No. Rate CI 46
M:F
2272 47.2
45.3-49.2 57.8
1.7
860 17.9
16.7-1 9.1 21.9 2.1
164 3.4
2.9-4.0 4.2 2.0
256 5.3
4.7-6.0 6.5 1.0
280 5.8
5.2-6.5 7.1 1.8
76 1.6
1.3-2.0 1.9 2.0
68 1.4
1.1-1.8 0.3 1.7
108 2.2
1.8-2.7 2.7 4.1
1832 40.3
50.7 2.4
1048 23.0
21.7-24.5 29.0 2.8
260 5.7
5 .O-6.5 7.2 1.3
156 3.4
2.9-4.0 4.3 1.7
100 2.2
1.8-2.7 2.8 0.7
204 4.5
3.9-5.1 5.6 3.9
180 3.9
3.4-4.6 5.0 3.7
4 0.1
0.0-0.2 0.1
38.5-42.2
-
660 22.0
20.3-23.7 33.7 2.2
696 23.2
35.6 3.2
244 8.1
7.1-9.2 12.5 3.1
96 3.2
2.6-3.9 4.9 1.1
68 2.3
1.7-2.9 3.5 0.8
156 5.2
4.4-6.1 8.0 5.0
88 2.9
2.3-3.6 4.5 1.3
28 0.9
0.6-1.3 1.4 0.7
21.5-24.9
4764 38.6
37.5-39.7 50.1
2.0
., 2604 21.1
20.3-21.9 27.5 2.6
668 5.4
5.0-5.8 7.0 2.0
508 4.1
3.8-4.5 5.4 1.2
448 3.6
3.3-4.0 4.7 1.3
436 3.5
3.2-3.9 4.6 3.7
336 2.7
2.4-3 .O 3.5 2.3
140 1.1
0.9-1.3 1.5 2.7

180 R. Gofin et al. Table 3.-continued
Cause of injury 0-5 6-12 13-17 Total
Others No. 24 16 36 76 Rate 0.5 0.3 1.3 0.7 CI 0.3-0.7 0.2-0.6 0.9-1.9 0.5-0.8 96 0.6 0.4 1.8 0.8
M : F 0.5 0.5 0.1 0.3 ~~ ~ ~
Total number of visits 3932 3616 1956 9504 Total number of injuries 4108 3800 2072 9980
* Rates are expressed by 1000 child-years; CI-confidence interval; % are of total number of visits in each’age group. A child may have suffered more than one injury; M:F-male to female rate ratio; -indicates all male cases. E codes (ICD-9-CM) are given for each cause of injury when applicable.
Bums and poisonings decrease after age five, the lowest rates being among the 6-12 age group.
The findings indicated a predominance among males except for the following: bums from water and steam among the 6-12-year-olds (M:F=0.7) and among the 13-1 7-year-olds (M : F= 0.9), and for bums from fire among the O-5-year-olds (M:F=0.9) and poisonings among adolescent girls aged 13 to 17 (M:F-0.7).
Nature of injuty
Puncture/laceration wounds were the most frequent followed by contusions and haematomas, dislocation and tearing of joints/muscles and fractures (Table 5). Dislocations and tearing of joints and muscles, contusions and haematomas increased with age. Puncture/laceration wounds were lower among the 13-1 7- year-olds than among other age groups. The majority of fractures (61.5%) occurred among the 6-12-year-olds, 25.9% among the 13-1 7-year-olds and only 12.6% among the O-5-year-olds.
Eighty per cent of the fractures were caused by falls, 1046 by sports accidents and 8.7% by road accidents.
The result of being caught/struck was mainly puncture and/or laceration wounds (73%), and contusions and haematomas occurred in 174b.
Six per cent of the children attending for accidents did not have any evident injury at the time of the emergency room visit. Boys aged 13-17 attended the emergency room 2.6 times more often than girls of the same age, with no evident injury.

Childhood injuries 181
Table 4. Road accidents by age and sex*
Age (yr)
Road accidents 0-5 6-12 13-17 Total
Travelling in cars No. Rate CI
M:F
Pedestrians No. Rate CI
M:F
Cyclists No. . Rate
CI M:F
Motorcycle No. Rate CI
M:F
Other and No. undetermined Rate
CI M:F
92 1.9
1.5
32 0.7
2.8
36 0.7
0.5-1.0 3.3
0
1.5-2.3
0.5-0.9
4 0.1
0.0-0.2 (-)
96 100 2.1 3.3
1.7-2.6 2.7-4.0 1.6 2.3
84 52 1.8 1.7
1.5 1.5
60 48 1.3 1.6
1.0-1.7 1.2-2.1 0.6 -
0 40 1.3
4.0
20 4 0.4 0.2
0.3-0.7 0.0-0.4 3.5 (-1
1.5-2.3 1.3-2.3
0.9-1.8
288 2.3
1.7
168 1.3
1.7
144 1.2
1 .O-1.4 2.1
40 0.3
5.0
28 0.2
0.1-0.3 4.0
2.1-2.6
1.2-1.6
0.2-0.4
Total No. Rate CI
M:F
164 260 244 668 3.4 5.7 8.1 5.4
2.9-4.0 5.0-6.5 7.1-9.2 5.0-5.8 2.0 1.3 3.1 2.0
~~~~~ ~
* Rates are expressed by 1000 child-years; CI-confidence interval; M:F male to female rate ratio, -indicates all male cases. Among cyclists, (-) indicates too few cases to calculate M : F.
Location of injury The most frequent part of the body injured was the head (Table 6) , followed by the upper and lower extremities. Head injuries decreased with increasing age while injuries of the upper and lower extremities increased with age.
Falls caused injury to the head in 67.1% of the cases, to the upper extremities in 19.90’0, and to the lower extremities in 13.6%. Injuries caused by being struck/caught were evenly distributed between the head and the upper extremities, 42.5% and 40.246, respectively, 16.4% were injured in the lower extremities and 1.9% in the trunk. Among children injured while travelling in cars, 55.790 suffered head injuries, 31.1% injuries to the lower extremities, 13.2%

182 R. Gofin et al. Table 5. Nature of injury by age and sex*
Nature of injury 0-5 6-12 13-17 Total
Puncture/lacera tion 870-884,890494 910-919
Contusions, haematomas 920, 924
Dislocation and tearing of joints and muscles 830-848
Fractures 800-829
Foreign body 930-939
Bums 940-949
Poisonings 960-989
Other
No. Rate CI YO
M:F No. Rate CI YO
M:F
No. Rate CI 46
M:F
No. Rate CI 46
M:F No. Rate CI %
M:F No. Rate CI 70 M:F No. Rate CI %
M:F NO. Rate CI %
M:F
2352 48.9
46.9-50.9 50.7 2.2 864
18.0
18.6 1.3 344 7.1
6.4-7.9 7.4 1.2 72
1.5
1.9 4.8 268 5.6
4.9-6.3 5.8 1.1 264 5.5
4.9-6.2 5.7 1.9 116 2.4
2.0-2.9 2.5 4.5 32
0.7
0.7 5.0
16.8-19.2
1.2-1.9
0.5-0.9
2476 54.5
52.3-56.6 51.7 2.5
1144 25.1
23.7-26.7 23.9 2.1 508
11.2 10.2-12.2
10.6 1.3 352 7.7
6.9-8.6 7.3 2.0 160 3.5
3.0-4.1 3.3 1.7 108 2.4
2.3 0.7 24
0.5 0.3-0.8
0.5 4.7 16
0.3
0.3 2.5
1.9-2.9
0.2-0.6
1044 34.7
32.7-3 6.9 37.5
2.9 864
28.7 26.9-30.7
31.0 2.1 528
17.6 16.1-19.1
19.0 - 2.0 148 4.9
4.2-5.8 5.3 2.2 96
3.2 2.6-3.9
3.4 1.5 68
2.3 1.7-2.9
2.4 1.0 32
1.1 0.7-1.5
1.1 0.9 28
0.9 0.6-1.3
1 .o 0.6
5872 47.5
46.3-48.7 48.1
2.4 2872 23.2
23.5 1.8
1380 11.2
10.6-1 1.8 11.3 1.5 5 72 4.6
4.3-5.0 4.7 2.9 524 4.2
3.9-4.6 4.3 1.3 440 3.6
3.6 1.3 172 1.4
1.4 3.1
0.6
0.6 1.4
22.4-24.1
3.2-3.9
1.2-1.6
76
0.5-0.8

Childhood injuries 183
Table 5.-continued
Age (yr)
Nature of injury 0-5 6-12 13-17 Total
No evident injury No. 436 200 124 760 Rate 9.1 4.4 4.1 6.1
% 9.4 4.2 4.5 6.2 M:F 1.2 1.8 2.6 1.5
CI 8.2-9.9 3.8-5.1 3.4-4.9 5.7-6.6
Total number of visits 4640 4784 2784 12 208 Total number of injuries 4748 4988 2932 12 668
* Rates are expressed by 1000 child years; CI=confidence intervals; % are of total number of visits in each group; M:F=male to female rate ratio; corresponding ICD-9-CM codes are given for nature of injury.
to the trunk and 9.8% to the upper extremities. Nintey per cent of motorcycle riders had lesions in the lower extremities, 4090 in the upper extremities, 20% in the trunk and 10% in the head. Among the pedestrians injured, there were 41.2% with head injuries, 47.1% were injured in the lower extremities, 35.3% in the upper extremities and 8.7% had trunk injuries. Cyclists suffered mostly head injuries (57.10/0), but 32% of the cases suffered injuries to the lower extremities and 26% to the upper extremities. Forty-eight per cent of bites/stings were in the upper extremities and 32.0% in the lower extremities. Bums caused injuries in the upper extremities in 41.9% of the cases and in the lower extremities in 35.2% of the cases with a lower proportion in the head (18.1%) and the trunk (l6.29b). (Some children suffered lesions in more than one location.)
Outcome of injury Twelve per cent of the injuries did not require treatment; 22.3% were treated and did not require follow-up; 63.5% were treated and referred for follow-up and 246 were hospitalised. There was one death in the emergency room in the sample, so the estimated number of such deaths will be four per year. Of the children who suffered injuries due to falls, only 1.84b were hospitalised; 6.6Yo of the road accident victims required hospitalisation; 20’30 of the poisoning victims and 6.296 of the children who suffered bums were hospitalised.
Figure 2 indicates that children who were involved in falls and road accidents account for most of the hospitalisations. Poisonings and bums, with lower incidence than other causes, accounted for a relatively higher proportion of hospitalisations.

184 R. Gofin et al. Table 6. Location of injury by age and sex*
Age (yr)
Location of injury 0-5 6-12 13-17 Total
Head and neck No. Rate CI Yo
M:F
Upper extremities No. Rate CI YO
Lower extremities No. Rate CI %
M:F
No. Rate CI %
M:F
, M:F
Trunk
2820 58.6
67.3 1.9
976 20.3
23.3 1.5
428 8.9
8.1-9.8 10.2 1.4
120 2.5
2.1-3.0 2.9 2.3
56.5-60.8
19.0-21.6
2096 46.1
44.1-48.1 44.9
2.5
1612 35.5
33.7-3 7.2 34.5
1.7
1004 22.1
20.7-23.5 21.5
2.1
140 3.1
3.0 1.9
2.6-3.6
668 22.2
20.6-24.0 24.7
3.2
1192 39.7
37.4-42.0 44.1
2.8
888 29.5
32.8 1.7
132 4.4
3.7-5.2 4.9 1.4
27.6-31.6
5584 45.2
44.0-46.4 48.3
2.2
3780 30.6
29.7-31.6 32.7
1.9
2320 18.8
18.0-19.5 20.1
1.8
392 3.2
2.9-3.5 3.4 1.8
Total number of visits 4188 4668 2704 11 560 Total number of injuries 4344 4852 2880 12 076
~~ ~ ~
* Rates are expressed by 1000 child-years; CI-confidence intervals; YO are of total number of visits in each age group; M:F-male to female rate ratio.
Discussion This study provides information on occurrence of injuries in the city of Jerusalem among its Jewish population of 0-17-year-olds during a whole year. The study is based on injuries leading to emergency room consultations. The injury rates presented do not represent all injuries which required medical attention. We did not include injuries treated by primary health care clinics of the sick funds, or private physicians, or school injuries that were treated by the school nurse at the place of occurrence.
Comparisons with incidence rates obtained by other studies is problematic due to differences in study methods, definition, source of data, denominator information, classification and presentation of data. Nevertheless comparisons of injuries between studies are useful in particular for assessing trends by age and sex.

Childhood injuries 185
Figure 2. Hospitalisation by cause of injury. Jerusalem, 1986.
A decline in the frequency of injuries with age among school age children has been shown in some European ~tudies,~J ' but not in several American studies;8J0 our study showed a decline similar to the European studies (see Figure 1). This may indicate an actual decrease in injuries with age or a decreased use of emergency room facilities. In the public school system in Israel, the presence of a school nurse for several days of the week may reduce the attendance at the emergency room either by providing first aid at the school site, or by referring mild injuries to the neighbourhood primary health care clinics.
The predominance of injuries among boys has been previously described.18 In our population the male : fem'ale ratio is even greater than that described by others and is evident also for both the school and preschool aged g r o ~ p s , ~ J ~ - ~ ~ appearing as early as 2 years of age. It seems that despite the different socio-cultural background of the various ethnic groups and different child-rearing practices, the male child has more injuries. He probably is involved in more adventurous behaviour than the female. This is particularly striking in our population at age 17, where there is an increase in incidence among males and a decrease in females, thus widening the gap between the sexes. It may well be that boys of this age are involved in more risk taking behaviour to 'prove themselves'.
It is interesting to note that there is a sex difference for children attending the emergency rooms for accidents without objective signs of injury. This is particularly striking for the 13-17-year-olds. Nearly three times more boys than girls attended the emergency room without evident injury following an accident. It is possible that the parents express more concern toward a male than toward a female child or that the adolescent male himself is more concerned with the physical consequences of an accident. Male preference in child rearing practices such as better feeding, more hospitalisations and lower prevalence of malnutrition is known from various studies.*'

186 R. Gofin et al.
There were two groups in which there was a female predominance of injuries: girls in the preschool years who suffered more from bums from flames and 6-12- year-olds and 13-17-year-old girls who suffered bums from water or steam, The sex difference is probably due to increased exposure to fire and boiling water by girls who are more involved in play and chores around the kitchen than boys. Special attention should be given to the predominance of poisoning among adolescent girls. Although there was no indication of purposely ingesting medicines or toxic agents, this possibility should be investigated. This finding shows a different direction than the national statistics of mortality which indicate that the suicide rate among adolescent girls aged 15-19 for the years 1974-1980 in Israel was 3.3 times lower than for boys from the same age groupeZ2
The higher rate of head injuries among the 0-5-year-olds is explained by the high head to body ratio for this age group. This is especially important in car accidents where children are propelled head first and crushed against the hard surfaces of the car or against other passengers. In Israel, there is no compulsory use of car restraints for children except for those up to the age of 14 sitting in the front seat of a car, Only 8Yo of the 0-14 age group were observed to use car restraint^.^^ The low rate of head injuries among motorcycle riders is probably due to the use of helmets which is compulsory.
During the summer months of July and August with longer and warmer days, there was a higher proportion of accidents, probably due to more intensive outdoor activities. The higher frequency of injuries in October was probably due to the traditional holidays, lasting 10 days, when picnics and travelling are a custom and there is a school break.
The increased frequency during the weekends may also indicate increased exposure to potentially dangerous activities. The peak number of visits at the emergency rooms in the afternoon is probably due to leisure time activities after school hours and lack of primary health care services which close down at 18.00. On Wednesday afternoon, particularly, there is a peak number of visits at the emergency room due to complete lack of primary care services from 12.00. The increased frequency in the afternoon hours when children are not attending school or in day care facilities has been, described by other^.^
Only 2% of the children visiting the emergency rooms were hospitalised, a much lower proportion than the 13% in the Yvelines study in France" and the 8% in Goteborg9 but closer to the 3.4% found in Massachusetts.20 This may indicate that the emergency rooms are utilised as a primary health care facility, throughout the day and particularly after closure time of the neighbourhood clinics of the sick funds.
The similarity of findings in different c o u n t r i e ~ ~ ~ ~ ~ J ~ * ~ ~ for cause, nature and location of injuries indicates that in spite of the different ecology, children are exposed to the same hazards resulting in similar injuries.
The present study indicates that the 'high risk' groups are toddlers and

Childhood injuries 187
adolescent boys. The most severe injuries leading to a high proportion of hospitalisations are road accidents, burns and poisonings.
There is a need for health education programmes and other preventive measures in order to reduce the incidence of injuries. There is also a need for education of parents, caretakers and children towards more rational utilisation of the health service in order to reduce the load on the emergency rooms and promote self-help and self-care.
It is advisable to introduce an ongoing surveillance system of injuries on a national basis. Such information should include not only the available data as presented here, but also information on place and circumstance of the accident and the products involved in it. A standardised procedure of data collection specifying the cause of injury will allow for analysis by cause and thereby enable the development of specific preventive programmes to modify the high risk environment and increase the safety of specific products. It is also important to try to score the seventy of the injury. The above-mentioned monitoring would provide better understanding of the epidemiology of injuries and would form a basis for planning intervention and evaluation of preventive and promotive programmes.
Acknowledgements
We are grateful to Professor I. Michel, Director of Hadassah Mount Scopus Hospital, Dr Z. Stern, Director of Hadassah Ein Karem Hospital, Dr Y. Adler, Director of Emergency Room Services at Shaarei Zedek Hospital, Professor S. Stern, Director of Bikur Holim Hospital, Mr H. Vigolic, Director of Magen David Adom and to the staff of the archives of the above institutions for allowing access to the data of the emergency room services.
References
1
2 Public Health Reports 1980; 95411-421. 3 Medicine Clinics of North America 1984; 2:701-715. 4 Pediatric Clinics of North America 1985; 325-15. 5 Society Meeting. The Journal of Trauma 1987; 27343-348. 6 Statistics Quarterly 1986; 39232-256. 7
Gordon, J.E. The epidemiology of accidents. American Journal of Public Health 1949;
Haddon, W. Jr. Advances in the epidemiology of injuries as a basis for public policy.
Withers, B.F., Baker, S.P. Epidemiology and prevention of injuries. Emergency
Guyer, B., Gallagher, S.S. An approach to the epidemiology of childhood injuries.
Baker, S.P. Injuries: the neglected epidemic: Stone Lecture, 1985. American Trauma
Taket, A. Accident mortality in children, adolescents and young adults. World Health
Wintemute, G.J. The Size of the Problem. Proceedings of an international course
39504-5 15.

188 R. Gofin et al. organised by the Johns Hopkins University School of Hygiene and Public Health and The World Health Organisation. Baltimore, June 1983. World Health Organisation, 1985. 8 Gallagher, S.S., Guyer, B., Kotelchuck, M. et al. A strategy for the reduction of childhood injuries in Massachusetts: SCIPP. New England Journal of Medicine 1985;
9 Westfelt, J.A.R.N. Environmental factors in childhood accidents. A prospective study in Goteborg, Sweden. Acta Paediatrica Scandinmica 1982; Suppl. 2 9 6-75. 10 Baranick, J.I., Chattejee, B.F., Greene, Y.C. et al. Northeastern Ohio Trauma Study. I. Magnitude of the problem. American Journal of Public Health 1983; 73:746-751. 11 Tursz, A., Crost, M., Guyot, M.M., et'al. Childhood accidents. A registration in public and private medical facilities of a French Health Care Area. Public Health; London 1985;
12 Central Bureau of Statistics. Use of Health Services Survey 1981. Special Series No. 717. Jerusalem: Central Bureau of Statistics, 1983. 13 International Classification of Diseases, 9th Revision (ICD-9-CM). Geneva: World Health Organisation, 1978. 14 Abramson, J.H., Peritz, E. Calculation Programs for the Health SerPices. New York: Oxford University Press, 1983; pp. 62-64. 15 Central Bureau of Statistics. Statistical Abstract of Israel. Years 1970-1987. Jerusalem: Central Bureau of Statistics. 16 Central Bureau of Statistics. Unpublished data. 17 SPSS Inc. Statistical Package for the Social Sciences fSPSSXJ. User's Guide. New York: McGraw Hill, 1983. 18 Rivara, F., Bergman, A.B., LoGerfo, J,P. et al. Epidemiology of childhood injuries. 11. Sex differences in injury rates. American Journal of Diseases of Children 1982; 136502-506. 19 Fife, D., Baranick, J.I., Chatterjee, B.F. North-eastern Ohio Trauma Study. 11. Injury rates by age, sex and cause. American Journal of Public Health 1984; 74473-478. 20 Gallagher, S.S., Finison, K., Guyer, 8. et al. The incidence of injuries among 87,000 Massachusetts children and adolescents: results of the 1980-81 Statewide Childhood Injury Prevention Program Surveillance System. American Journal of Public Health 1984;
21 Williams, C., Baumshlay, D., Jeliffe, D.B. Mother and Child Health. London: Oxford Medical Publications, 1985; pp. 21, 53, 127, 140. 22 Marshlkovitz, I. Patterns of adolescent mortality in Israel 1974-1980. MD thesis. Jerusalem: The Hebrew University and Hadassah Medical School, 1983. 23 Levi, E. The use of safety restraint for children in motor vehicles in Jerusalem. January 1985, MPH thesis. Jerusalem: The Hebrew university and Hadassah Medical School, 1985.
3W1015-1019.
99: 1 56-1 64.
74340-347.