
Research Article Personality Profiles Identify Depressive ...
Upload
independentCategory
view
4download
0
www.elsevier.com/locate/jadJournal of Affective Disorders 82 (2004) 9–20
Research report
Child and adolescent clinical features as forerunners of
adult-onset major depressive disorder: retrospective evidence
from an epidemiological sample
Holly C. Wilcoxa,b,*, James C. Anthonyb
aDepartment of Psychiatry and Behavioral Sciences, Center for Family Research, George Washington University, Washington, DC 20037, USAbDepartment of Mental Health, Bloomberg School of Public Health, Johns Hopkins University, 624 N. Broadway, Room 888, Baltimore,
MD 21205, USA
Received 24 September 2002; accepted 17 October 2003
Abstract
Background: Adult-onset cases of DSM-III-R major depressive disorder (MDD) often have had a history of mood
disturbances and allied clinical features during childhood or adolescence. This study seeks to illuminate these early-life
disturbances, as recalled and reported by adult-onset MDD cases (i.e. those whose first episode of MDD occurred after age 18)
and non-cases. Methods: Our research group has re-assessed survivors in the Baltimore Epidemiologic Catchment Area (ECA)
community sample roughly 13.5 years after first diagnostic assessments in 1981. Of the 1920 participants, 150 were found to
have a history of adult-onset MDD; 1755 were sub-threshold with respect to DSM criteria or reported few or no depression-
related problems. Survival analysis was used to plot and study the cumulative occurrence of each clinical feature of depression
from age 6 through 18 years for cases of adult-onset MDD versus non-cases. Results: The earliest and most frequently occurring
forerunners of adult-onset MDD were persistent depressed mood, anhedonia, feelings of worthlessness, and thoughts of death or
suicide, with persistent anhedonia and worthlessness having a special prognostic value. One-third of adult-onset cases of MDD
reported at least one clinical feature before age 19 versus only 7.3% of non-cases. Limitations: The study’s estimates are based
on retrospective recall, although a life chart methodology sought to reduce recall inaccuracies. Conclusions: The ECA follow-
up sample data, though based on retrospection, provide new details about early forerunners of adult-onset depression from a
sample of survivors. When they appear in children or adolescents, persistent anhedonia and persistent feelings of worthlessness
merit special attention. These two clinical features, in particular, may help predict later risk of adult-onset major depression.
D 2003 Elsevier B.V. All rights reserved.
Keywords: Major depression; Epidemiologic studies; Survival analysis; Natural history; Adolescent; Children
0165-0327/$ - see front matter D 2003 Elsevier B.V. All rights reserved.
doi:10.1016/j.jad.2003.10.007
* Corresponding author. Department of Mental Health, Bloom-
berg School of Public Health, Johns Hopkins University, 624 N.
Broadway, Room 888, Baltimore, MD 21205, USA. Tel.: +1-410-
614-2852; fax: +1-410-955-9088.
E-mail address: [email protected] (H.C. Wilcox).
1. Introduction
Our aim in this study is to use epidemiological and
field survey diagnostic methods in order to identify
specific early markers or precursors that may help
clinicians identify young people at excess risk for
developing adult-onset major depressive disorder

H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–2010
(MDD). A specific focus is upon persistent anhedonia
and persistent feelings of worthlessness, two clinical
features recently identified by Pine et al. (1999) and
Murphy et al. (2002) as having special prognostic
significance.
Three features differentiate this study from virtu-
ally all previous work of this type. First, we use
survival analysis and generalized estimating equation
(GEE) methods to reconstruct the emergence of dis-
turbed mental life during the years of childhood and
adolescence. This statistical approach, sometimes re-
ferred to as, ‘multivariate response profile analysis’,
takes the interdependencies of other clinical features
into account while estimating risk of adult-onset
MDD for each clinical feature and adjusting for
possible confounding by age, sex, and race-ethnic
minority status. Second, while other studies of this
type have recruited from clinical samples, this re-
search is based upon an epidemiological sample.
More than one-half of the community cases of major
depression in this sample had never received treat-
ment for their depression. Third, we compared char-
acteristics of 1755 young people who did not develop
MDD to 150 individuals who did develop MDD. All
cases and non-cases were drawn from the same
community sample.
Dryman and Eaton (1991), in an analysis of 1-
year follow-up data from ECA samples assessed in
the early 1980s, found that adult-onset MDD was
most strongly associated with prior feelings of
worthlessness, trouble concentrating, diminished sex
drive, and either sleep disturbance (women) or
fatigue (men). More recently, Pine et al. (1999)
extended this line of inquiry by studying a longitu-
dinal community sample of young adults in New
York State, first observed in childhood or adoles-
cence during two waves and then followed to a
mean age of 22 years (range 17–26). In this re-
search, the experience of anhedonia and thoughts of
death during childhood or adolescence helped pre-
dict which individuals subsequently developed MDD
by age 22. However, since the peak risk for adult-
onset major depression is after age 22 years, it is
very likely that most cases of adult-onset MDD were
not identified by these investigators (Eaton et al.,
1989).
The finding on early-life anhedonia was somewhat
of a surprise because prior clinical and epidemiolog-
ical studies of MDD had not suggested that anhedonia
was a common forerunner of adult-onset MDD. An-
hedonia has been found to increase with age, but has
been one of the less common clinical features of MDD
in clinical sample research on childhood and adoles-
cent patients with MDD (e.g. see Roberts et al., 1995).
The experience of general anhedonia was not a
prominent characteristic of MDD cases identified by
Dryman and Eaton (1991) nor by Weissman et al.
(1991) in the prior ECA studies of adults, although
Dryman and Eaton identified ‘‘loss of interest in sex’’
as a noteworthy predictive feature.
In the present study, we use the terms ‘forerunner’
and ‘antecedent’ in order to convey our uncertainty
about the associations linking the earlier clinical
features that emerge before adulthood with the later
major depressive episodes that occur in adulthood. If
the strength of association is large, many youngsters
who report the forerunner or antecedent will become
MDD cases as adults. From an epidemiological stand-
point, we might assert that the positive predictive
value (PPV) of each clinical feature approaches
100%. If so, the clinical feature might be part of the
MDD prodrome (e.g. see Eaton et al., 1995). Due to
recently published evidence, we give special attention
to the clinical features of persistent anhedonia (see
Pine et al., 1999) and persistent feelings of worthless-
ness (see Murphy et al., 2002), which may have
special prognostic significance as forerunners or ante-
cedents of adult-onset major depression, or as part of
the MDD prodrome.
2. Methods
2.1. Sample
This study makes use of data from the longitudi-
nal follow-up of the Baltimore sample of the Epide-
miologic Catchment Area Survey (ECA). More
detailed reports of the Baltimore ECA follow-up
methodology have appeared elsewhere (Eaton et
al.,; Badawi et al., 1999; 1997; Neumark et al.,
2000; Rosenberg and Anthony, 2001). The ECA
program began with five epidemiological surveys
carried out by independent research teams in collab-
oration with National Institute of Mental Health
(NIMH) staff; the ECA sites were Los Angeles,
H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–20 11
New Haven, St. Louis, the Raleigh-Durham Pied-
mont area and Baltimore City. The ECA program
was designed to assess occurrence of psychiatric
disorders and the use of mental health services
(Eaton et al., 1981). The methods of the ECA
program are described in more detail elsewhere
(Eaton and Kessler, 1985; Robins and Regier, 1991).
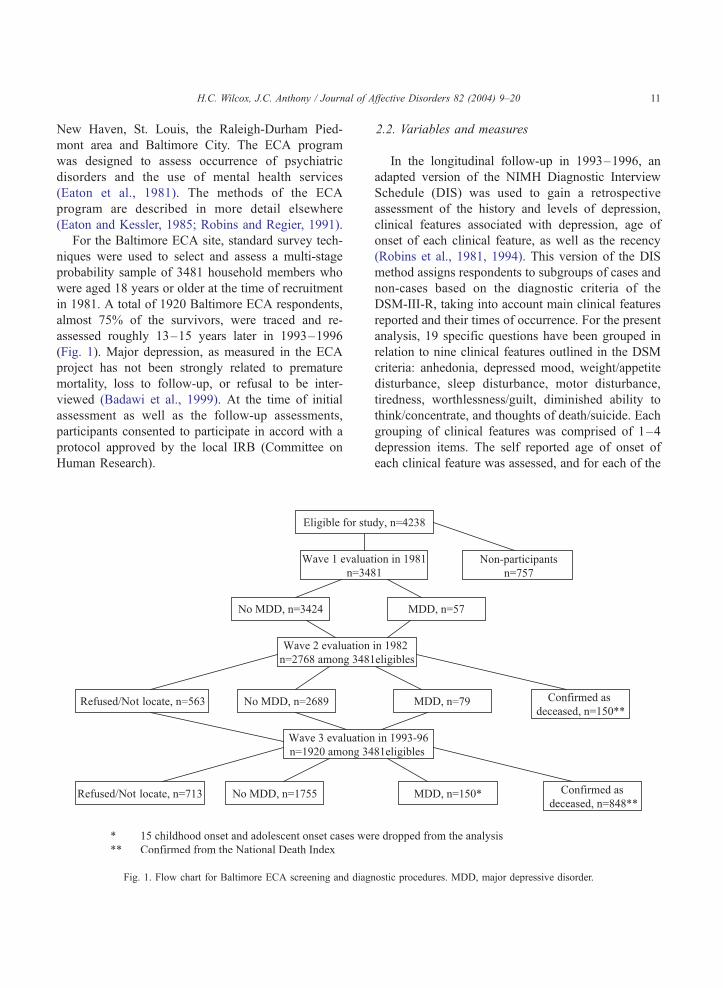
For the Baltimore ECA site, standard survey tech-
niques were used to select and assess a multi-stage
probability sample of 3481 household members who
were aged 18 years or older at the time of recruitment
in 1981. A total of 1920 Baltimore ECA respondents,
almost 75% of the survivors, were traced and re-
assessed roughly 13–15 years later in 1993–1996
(Fig. 1). Major depression, as measured in the ECA
project has not been strongly related to premature
mortality, loss to follow-up, or refusal to be inter-
viewed (Badawi et al., 1999). At the time of initial
assessment as well as the follow-up assessments,
participants consented to participate in accord with a
protocol approved by the local IRB (Committee on
Human Research).
Fig. 1. Flow chart for Baltimore ECA screening and diagn
2.2. Variables and measures
In the longitudinal follow-up in 1993–1996, an
adapted version of the NIMH Diagnostic Interview
Schedule (DIS) was used to gain a retrospective
assessment of the history and levels of depression,
clinical features associated with depression, age of
onset of each clinical feature, as well as the recency
(Robins et al., 1981, 1994). This version of the DIS
method assigns respondents to subgroups of cases and
non-cases based on the diagnostic criteria of the
DSM-III-R, taking into account main clinical features
reported and their times of occurrence. For the present
analysis, 19 specific questions have been grouped in
relation to nine clinical features outlined in the DSM
criteria: anhedonia, depressed mood, weight/appetite
disturbance, sleep disturbance, motor disturbance,
tiredness, worthlessness/guilt, diminished ability to
think/concentrate, and thoughts of death/suicide. Each
grouping of clinical features was comprised of 1–4
depression items. The self reported age of onset of
each clinical feature was assessed, and for each of the
ostic procedures. MDD, major depressive disorder.

H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–2012
groups, the earliest reported age of onset for the 1–4
items was considered the age of onset for the clinical
features grouping. Clinical features groups were stud-
ied individually, not in combination.
A note about the persistence or prominence of
clinical features is in order, which will help clarify
the distinctions between the ‘clinical features’ under
study here versus the ‘symptoms of MDD’ that count
toward DSM criteria. In general, the DSM criteria for
MDD require a disturbance of mental life or behavior
that is either persistent or impairing. Most typically, the
DSM criteria require the presence of a full 2 weeks of a
disturbance of mental life or behavior, but an exception
is a single suicide attempt, which is sufficient to satisfy
DSM criteria. Hereinafter, when we refer to ‘‘feelings
of worthlessness’’ or other clinical features with the
exception of suicide attempt, the respondent has
reported clinical features pertinent to mood disturban-
ces that have persisted for 2 weeks or more.
However, suppose an MDD case (or a non-case)
has experienced 2 weeks of feeling worthless, but
never has suffered impairment as a result, and neither
told a doctor nor sought help for this particular clinical
feature. In this instance, the experience of the clinical
feature would not meet the impairment or help-seek-
ing standards that are imposed if a clinical feature is to
be counted toward the MDD diagnosis (e.g. see
Narrow et al., 2002). However, the DIS age of onset
question is asked anyway, which has allowed us to
plot the experience of each clinical feature in relation
to the age of the case (or non-case). As such, this is
research on ‘clinical features’, some of which do not
qualify formally as ‘symptoms’ of an underlying
MDD and do not count toward fulfillment of DSM
diagnostic criteria.
We also note that the DIS assessment of age of onset
of each clinical feature is not specific with respect to
issues of presumed etiology. That is, if the clinical
feature is to be counted toward DSM criteria, it must
occur without attribution to known etiological factors
such as the use of alcohol and other drugs, or to general
medical conditions such as pregnancy or malignancies.
This issue of etiological specificity has been found to
account for some of the observed mismatch between
DIS diagnoses of major depression and standardized
clinical examination diagnoses made by board-eligible
psychiatrists. For this reason, some observers prefer to
eschew DIS diagnoses in favor of standardized assess-
ments by clinicians (e.g. see Anthony et al., 1985).
Moreover, the DIS questions about age of onset of
MDD clinical features do not require the degree of
etiological specificity that might be achieved in a
thorough clinical examination. In the balance, howev-
er, a reliance on DIS diagnoses frees the research from a
diagnostic work-up bias that might be created when
clinicians conduct diagnostic assessments for research
purposes. Namely, unless special precautions are taken
to constrain ordinary diagnostic practices, clinicians
might probe more deeply for MDD when a respondent
reports an early suicide ideation or attempt. This form
of potential work-up bias is constrained when lay
interviewers use the DIS method because they are not
permitted to probe and cross-examine in a work-up
process that is one of the real strengths of a psychia-
trist’s diagnostic examination (e.g. see Anthony et al.,
1985).
As described in detail by Lyketsos et al. (1994), the
follow-up methodology sought to address the problem
of deterioration of recall by means of a standardized
procedure called the Life Chart Interview. At the start
of every interview, the Life Chart Interview method
generates age and calendar linked personal memory
cues for the respondent by means of an interactive
visually oriented life calendar that focuses the respon-
dent’s attention on designated time periods during the
follow-up.
At the time of the follow-up assessment for DSM-
III-R major depression during 1993–1996, a total of
150 Baltimore ECA respondents had ever qualified
for adult-onset MDD (i.e. met DSM-III-R criteria as
evaluated by the adapted DIS, and reported first
episode as having occurred after age 18). A total of
1755 people had few or no depression-related prob-
lems, and had not developed MDD by the time of the
follow-up, when the median age and minimum age of
ECA interviewees were 50 and 27 years, respectively.
To sharpen this study’s focus on the early-life expe-
riences of adult-onset MDD, we have excluded the 15
cases whose experience of the onset of the first
episode of MDD occurred before age 19.
2.3. Statistical analyses
Kaplan–Meier survival analyses were used to plot
and estimate the cumulative occurrence of each clin-
ical feature from age 6 through 18 years, contrasting

Table 1
Sociodemographic characteristics of adults with and without adult-
onset MDD, data from the Baltimore ECA follow-up sample,
1981–1993/1996
No past history of
MDD* (n= 1755)
MDD case, both recent
and past (n= 150)*
Sex
Female 1093 (62%) 110 (73%)
Male 662 (38%) 40 (27%)
Age at 1993–1996 assessment
27–39 412 (23%) 44 (29%)
40–49 436 (24%) 59 (39%)
50–59 232 (13%) 28 (19%)
60–69 213 (12%) 8 (5%)
70 + 472 (27%) 11 (7%)
Race
White,
non-Hispanic
1100 (63%) 103 (69%)
Other** 655 (37%) 47 (31%)
*As explained in accompanying text and footnote to Fig. 1,
there were 15 MDD cases with child or adolescent onset MDD.
These early-onset cases were excluded from this study of predictors
for adult-onset MDD.
**Mainly African–American.
H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–20 13
the 150 adult-onset MDD cases and the non-cases.
Making use of information about each respondent’s
age at assessment and the reported age of onset of
each clinical feature, this actuarial approach estimates
annual occurrence by calculating the years at risk for
individuals as they pass through ages 6–18 years.
This approach provides a graphical display of infor-
mation about the retrospectively recalled experiences
of adult-onset cases and non-cases of MDD, as these
experiences emerged during childhood and adoles-
cence. In this way, it has been possible to reconstruct
the progression of features of depression over time,
displaying features that appear most rapidly and at an
increased occurrence.
For these analyses, clinical features with first onset
at ages 1–5 were recoded to age 6.5, which we
designated as the start of the observation interval of
primary interest to us. Twenty-eight individuals met
criteria for childhood or adolescent dysthymic disor-
der that preceded adult-onset MDD; these cases were
retained in the analyses because their exclusion might
have distorted our findings on anhedonia. Dysthmia
was not studied with MDD because the evolution and
clinical course is distinct from MDD (Akiskal, 1994).
Overall results (based on all male and female cases)
and female results are presented to explore potential
differences in the frequency and onset of clinical
features. Results specific for males are not presented
because there were too few cases for precise estimates
(n = 40 male adult-onset cases). Consistent with stan-
dard survival analysis conventions (Lawless, 1982),
the time of occurrence of clinical features was spec-
ified in relation to the midpoint through the age-year
reported by the respondent as the ‘age of onset’ (i.e. at
age 16.5 for someone who reported onset at 16 years
of age).
Multivariate response modeling (GLM/GEE), with
application of the general linear model and the gener-
alized estimating equations, was used to estimate the
association that links each early clinical feature to
occurrence of adult-onset MDD, based on methods
described by Liang et al. (1992) and as illustrated in
Andrade et al. (1994), Chen and Anthony (2003), and
others. This statisticalmethod, sometimes referred to as,
‘GEE multivariate response profile analysis’, takes the
interdependencies of the binary responses into account,
with statistical adjustments for covariates (here, birth
cohort, sex, and race-ethnicminority status). The result-
ing estimates are in the form of the familiar odds ratio
(i.e. the covariate-adjusted odds of reporting a given
clinical feature for cases with adult-onset MDD vs. the
corresponding odds for adults without MDD). To aid in
interpretation, 95% confidence intervals (CI) and P-
values are presented, with variance estimators based
upon a GEE exchangeable working correlation struc-
ture and robust specification for variance estimation.
3. Results
3.1. Description of study sample
In general, as described previously (Eaton et al.,
1997; Chen et al., 2000), major depression was more
prevalent among females, younger people, and Cau-
casians as compared to other race-ethnicity subgroups
in the Baltimore ECA follow-up sample (Table 1). Of
the 150 adult-onset cases of MDD, 110 are females
and 40 are males. It is important to note that, at the
time of follow-up, the youngest person in the sample
was 27 years old, and when the study began in 1981
all the respondents were 18 years of age or older. This

H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–2014
community sample had generally received little for-
mal clinical intervention for depression. When evalu-
ated in 1993–1996, a total of 47% of cases of MDD
had ever spoken with a doctor or mental health
professional about depression; fewer had been in
treatment for depression.
3.2. Survival analysis
Within the Baltimore ECA sample, there were
1755 adults who had not developed DSM-III-R major
depression by the time of follow-up in the 1990s.
Among the 1755 MDD non-cases, a total of 128 (7–
8%) reported at least one clinical feature of depression
before age 19. In comparison, among the 150 adults
who had developed MDD by the time of follow-up, a
total of 50 (i.e. one-third) had experienced at least one
clinical feature of depression by age 19.
Survival analysis curves for adult-onset MDD
cases and non-cases depict estimated cumulative oc-
currence of clinical features, with separate curves used
to display male– female differences (Fig. 2a–d).
Kaplan–Meier life-table estimates were derived, and
curves were plotted, in order to depict the cumulative
incidence of each clinical feature by two groups
defined in terms of adult-onset MDD status. This
method produced a cumulative age-specific estimate
of the probability of each clinical feature among those
with and without adult-onset MDD at each age under
study. Persistent anhedonia was reported by 5–6% of
female cases before age 19 years (vs. 0.2% for female
non-cases), and by 2–3% of male cases (vs. 0.5% for
male non-cases; Fig. 2a). (An inset figure was placed
in Fig. 2a to show more refined details about early
anhedonia while maintaining the same scale of the
main figure for direct comparison to other clinical
features.)
Before age 19 years, suicidal thoughts or behav-
iors were reported by 20% of female cases (vs. 2–
3% of female non-cases) and by 15% of male cases
(vs. 1–2% of male non-cases as depicted in Fig.
2b). Persistent depressed mood was reported by 21–
22% female cases (vs. almost 3% of non-cases) and
by 10% of male cases (vs. 2–3% of male non-
cases; as depicted in Fig. 2c). When we considered
all clinical features in the same analyses, a total of
36–37% of female MDD cases had experienced at
least one clinical feature of depression before age
19; for male adult-onset cases, this value was 25%.
Corresponding values for female and male non-cases
were in the 6–8% range (Fig. 2d). For most adult-
onset cases of MDD, the first disturbances occurred
after age 12 years, and occurred more frequently
among female cases than male cases.
3.3. Multivariate response modeling (GLM/GEE)
The next analysis in our series is one that expresses
the occurrence of a multivariate profile of child–
adolescent disturbances as a function of membership
in the adult-onset MDD case group versus the non-
case group, first with females and males combined,
followed by separate GEE profile analyses for
females. As explained in our Section 2, this multivar-
iate response analysis is important because it takes the
interdependencies of these reported disturbances into
account and provides an analogue to multivariate
analysis of covariance, with an allowance for statisti-
cal adjustments (i.e. for birth cohort, sex, race-ethnic-
ity). Results are presented in order of strength of
association. Table 2a provides evidence that confirms
the earlier report of Pine et al. (1999) with respect to
persistent anhedonia. Here, within the context of the
multivariate analysis, persistent anhedonia in child-
hood and adolescence is observed some 17 times
more often among adult-onset MDD cases than
among non-cases (P < 0.001), and there is no more
than modest attenuation of this association with sta-
tistical adjustment for birth cohort, sex, and race-
ethnicity (estimated relative risk (RR) = 14.1; 95%
CI = 4.5, 44.8; P < 0.001).
Table 2a also shows the overall results for other
clinical features strongly associated with MDD, such
as persistent feelings of worthlessness (RR = 19.8;
95% CI = 7.5, 51.8; P < 0.001) and diminished ability
to think or concentrate (RR = 13.8; 95% CI = 5.8,
33.1; P < 0.001). The associations with occurrence
of adult-onset MDD were not appreciably altered with
statistical adjustment for cohort, sex and race
(RR = 11.4; 95% CI = 4.8, 27.5; P < 0.001, respective-
ly). Weight/appetite disturbance in adolescence was
the clinical feature group least associated with devel-
oping adult-onset MDD after adjusting for demo-
graphic variables. Adolescents reporting weight or
appetite problems were about three to four times more
likely to develop MDD as adults than adolescents not

Fig. 2. (a) Estimated cumulative occurrence of anhedonia during the child and adolescent years, cross-classified to show the different
experiences of adult-onset MDD cases and non-cases, males and females. Data from Baltimore ECA sample, 1993–1996.* Inset figure is a plot
of the same data, but with a rescaled y-axis. (b) Estimated cumulative occurrence of thoughts of death/suicide and/or suicide attempt during the
child and adolescent years, cross-classified to show the different experiences of adult-onset MDD cases and non-cases, males and females. Data
from Baltimore ECA sample, 1993–1996. (c) Estimated cumulative occurrence of depressed mood during the child and adolescent years, cross-
classified to show the different experiences of adult-onset MDD cases and non-cases, males and females. Data from Baltimore ECA sample,
1993–1996 *. (d) Estimated cumulative occurrence of any clinical feature during the child and adolescent years, cross-classified to show the
different experiences of adult-onset MDD cases and non-cases, males and females. Data from Baltimore ECA sample, 1993–1996 *.
H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–20 15

Fig. 2 (continued).
H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–2016
reporting these clinical features (RR = 4.3; 95%
CI = 2.3, 8.1; P < 0.001).
Table 2b provides separate estimates for females.
Based on these exploratory sex-specific analyses, the
association linking earlier anhedonia to later onset of
MDD is quite pronounced for females, who were about
31 times more likely to develop MDD as adults than
their female peers who did not suffer from anhedonia
(RR = 31.5; P < 0.001). Even after adjusting for demo-
graphic variables, women who had experienced per-

Table 2
Estimated association between the occurrence of each observed clinical feature before age 19 and the development of adult-onset MDD
Clinical features Unadjusted Adjusted for cohort, sex and race
RR P-value 95% CI RR P-value 95%CI
(a) Both sexes combined
Worthlessness 19.8 < 0.001 7.5–51.8 16.4 < 0.001 6.2–43.2
Anhedonia 17.1 < 0.001 5.4–54.6 14.1 < 0.001 4.5–44.8
Think/concentrate 13.8 < 0.001 5.8–33.1 11.4 < 0.001 4.8–27.5
Sleep disturbance 11.2 < 0.001 5.3–23.4 9.3 < 0.001 4.4–19.8
Death/suicide 10.1 < 0.001 6.0–17.0 8.5 < 0.001 5.1–14.3
Tiredness 7.9 < 0.001 3.4–18.7 6.6 < 0.001 2.8–15.4
Depressed mood 7.6 < 0.001 4.7–12.6 6.5 < 0.001 3.9–10.8
Motor disturbance 6.7 0.001 2.2–20.2 5.5 0.003 1.8–16.6
Weight/appetite 4.3 < 0.001 2.3–8.1 3.6 0.001 1.9–6.9
Any feature 6.4 < 0.001 4.3–9.3 5.5 < 0.001 3.7–8.2
Clinical features Unadjusted Adjusted for cohort and race
RR P-value 95% CI RR P-value 95% CI
(b) For females
Anhedonia 31.5 < 0.001 6.3–158.0 27.0 < 0.001 5.4–134.7
Worthlessness 21.4 < 0.001 6.3–72.2 18.3 < 0.001 5.4–62.5
Think/concentrate 15.5 < 0.001 5.8–41.7 13.3 < 0.001 5.0–35.7
Death/suicide 9.9 < 0.001 5.4–18.1 8.6 < 0.001 4.7–15.6
Sleep disturbance 9.0 < 0.001 3.8–21.4 7.7 < 0.001 3.2–18.6
Depressed mood 9.0 < 0.001 5.1–15.9 7.8 < 0.001 4.3–14.0
Motor disturbance 7.6 0.008 1.7–34.6 6.5 0.015 1.4–29.3
Tiredness 6.7 < 0.001 2.5–17.6 5.7 < 0.001 2.2–15.2
Weight/appetite 5.2 < 0.001 2.5–10.7 4.5 < 0.001 2.1–9.5
Any feature 6.8 < 0.001 4.3–10.6 6.0 < 0.001 3.8–9.6
H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–20 17
sistent anhedonia were 27 times more likely to develop
MDD as adults (RR= 27.0; P < 0.001). Other obser-
vations of possible note with respect to females in-
volve persistent feelings of worthlessness during
childhood or adolescence (RR= 21.4; 95% CI = 6.3,
72.2; P < 0.001) and periods of diminished ability to
think or concentrate during childhood or adolescence,
which were also highly associated with increased risk
of developing MDD as adults (RR = 15.5; 95%
CI = 5.8, 41.7; P < 0.001) (see Table 2b). There was
no appreciable shift in the summary estimates when
terms were added to include statistical adjustment for
cohort and race (RR = 18.3; 95% CI = 5.4, 62.5;
P < 0.001; RR= 13.3; 95% CI = 5.0, 35.7; P < 0.001,
respectively).
3.4. Positive predictive value (PPV)
Sample-based PPVs were calculated as an indica-
tion of how often the early-life appearance of each
clinical feature was followed by adult-onset MDD.
Estimates of PPVs for each clinical feature were
calculated for the total sample and for females. Over-
all, the PPV estimate for persistent anhedonia was
58%, which means that 58% of adolescents reporting
anhedonia had developed MDD as adults. In the case
of female adolescents, the PPV was notably higher
(75%). For persistent feelings of worthlessness, the
estimated PPV was 61% overall and 67% for females.
The estimated PPV for persistent problems with
concentration was the next highest with 52% overall
and 59% for females. The lowest PPV was for
persistent weight/appetite disturbances, 25% overall
and 32% for females.
4. Discussion
There are four main findings: first, an estimated
33% of adult-onset cases of MDD reported early-life

H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–2018
clinical features before age 19, whereas only 7% of
non-cases reported clinical features. Females were
more likely than males to report disturbances in mood
and allied clinical features before age 19 years; 36%
of female cases and 25% of male cases reported at
least one clinical feature. Second, an estimated 75% of
females with child–adolescent anhedonia were found
to have developed adult-onset MDD, and for males
and females combined, the PPV estimate was about
60%. Third, persistent anhedonia in childhood and
adolescence is observed some 17 times more often
among adult-onset MDD cases than among non-cases,
and some 31–32 times more often for females.
Fourth, in the multivariate response profile analysis,
persistent feelings of worthlessness were most strong-
ly associated with MDD. Almost 70% of females with
childhood–adolescent persistent feelings of worth-
lessness later developed MDD in adulthood, whereas
the PPV for both sexes combined was about 60%.
Before detailed discussion of these results, several
limitations merit attention. First, because the range of
ages in the ECA sample did not include adolescents,
this study’s estimates are based upon an adult’s
retrospective recall of the age of onset of individual
clinical features, and are subject to errors of recall and
accuracy in reporting, although the life chart method-
ology was used to address the problem of deteriora-
tion of recall. The ECA has a prospective design, but
the age of onset questions were not administered for
each clinical feature until the ECA follow-up in
1993–1996.
A second limitation is the modest number of MDD
cases, especially male cases, which places a limit on
what can be learned from the Baltimore ECA sample,
despite its large sample, with coverage of many adult
years of life. A third limitation involves diagnostic
criteria and methods of assessment (e.g. orientation to
DSM-III-R as opposed to DSM-IV, and reliance on
the DIS, as mentioned in our Section 2). It is possible
that different results might be obtained with the DSM-
IV or ICD-10 diagnostic criteria, or with standardized
clinical examinations by psychiatrists. We must also
acknowledge a possibility that some of our adult-onset
MDD cases actually were adolescent-onset cases, with
our assessment of age-of-onset subject to a distortion
in the measurement process. Finally, we will mention
the distinction we have drawn between the ‘clinical
feature’ age of onset information that is elicited by our
survey questions versus the ‘symptom’ age of onset.
As noted in our description of methods, age of onset
questions about ‘clinical features’ are less specific
than age of onset questions about ‘symptoms’, and
not all of the experiences tallied in our Kaplan–Meier
analyses and survival plots would qualify as a ‘symp-
tom of MDD’ if an experienced psychiatrist were to
have conducted a careful examination. Some readers
may prefer to see a study focused more specifically on
‘symptoms’ of MDD, which might well lead to even
greater separation of survival curves and subgroup
differences to the extent that ‘MDD symptoms’ are
defined as observable self-report manifestations of the
underlying pathology of MDD.
Despite limitations such as these, several features of
the study’s evidence merit attention. The results of this
new study help to strengthen and confirm the thesis
advanced by Pine et al. (1999) with respect to the
prognostic significance of persistent anhedonia when it
appears before young adulthood. These new results
also help to strengthen and confirm the thesis ad-
vanced by Murphy et al. (2002) with respect to
appearance of feelings of worthlessness in children
or adolescents. Results are generally consistent with
studies of a rather insidious or slow MDD onset. These
results are also consistent with the literature on MDD
clinical features as predictors of onset among adults
(Dryman and Eaton, 1991; Horwath et al., 1992).
As to the meaning or potential clinical utility of
these findings, we note that the results provide some
support for clinical observation that early depression-
like clinical features in childhood and adolescence
have a prognostic significance with respect to later
adult-onset MDD, and it might be useful to pose
questions about distinguishing these clinical features
from variations in ‘‘normal’’ development. As such,
these early features may be a manifestation of sus-
ceptibility for later adult-onset psychiatric disturban-
ces (Pine et al., 1999; Orvaschel et al., 1995; Aronen
and Soininen, 2000). This study may also stimulate
interest in dimensional conceptualizations of depres-
sive disorder as characterized by a dynamic fluctuat-
ing course with a common disease process whereby
clinical features of depression are neither normal nor
non-specific variations of normal mood, but rather are
clinical markers of significance (e.g. see Judd and
Akiskal, 2000). From a public health standpoint,
identifying specific early clinical features of MDD

H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–20 19
might make it possible to provide anticipatory guid-
ance or other early interventions that might prevent or
reduce the impact of the disorder.
Working along these lines, Costello (1992) as well
as Eaton et al. (1995) have discussed the importance
of studying the earliest clinical features in the screen-
ing and prevention of mental disorders. However,
definitive evidence on potentially distinctive child
and adolescent elements of an MDD prodrome may
require periodic follow-up assessments of a large
epidemiological sample from the childhood years
through the full period of risk for MDD. What is
needed is a longitudinal community study, similar to
the work by Pine et al. (1999) but with more frequent
assessments and with follow-up into and through the
periods of peak MDD risk in adulthood.
A word of caution may be necessary about the
current public health applications of this study’s find-
ings. The prospective study by Pine et al. (1999) and
our own retrospective study both highlight persistent
anhedonia (and other clinical features) as forerunner
experiences of adult-onset major depression. Grimes
and Schulz (2002) recently outlined a rationale to be
cautious about launching mass screening initiatives on
the basis of early epidemiological evidence of this type.
Until there is more evidentiary support, these findings
merit attention in new investigations, but not premature
application in the context of public health work. Ulti-
mately, the clinical and public health significance of
these findings will be demonstrated if early interven-
tion before or during the prodromal interval is effective
and leads to reduced risk, severity, duration, or disabil-
ity associated with adult-onset major depression.
5. Uncited references
Eaton, 1995; Lewinsohn et al., 1994.
Acknowledgements
We thank Dr. Li-Shiun Chen and Dr. William W.
Eaton for their assistance. This work was funded by
research training grants T32 DA07292 and F31
DA14454 from the National Institute on Drug Abuse
and research grant R01 MH47447 from the National
Institute of Mental Health.
References
Akiskal, H.S., 1994. Dysthymia: clinical and external validity. Acta
Psychiatr. Scand. 89 (Suppl. 383), 19–23.
Andrade, L., Eaton, W.W., Chilcoat, H., 1994. Lifetime comorbid-
ity of panic attacks and major depression in a population-based
study: symptom profiles. Br. J. Psychiatry 165, 363–369.
Anthony, J.C., Folstein, M., Romanoski, A.J., Von Korff, M.R.,
Nestadt, G.R., Chahal, R., Merchant, A., Brown, C.H., Sha-
piro, S., Kramer, M., Gruenberg, E.M., 1985. Comparison of
the lay Diagnostic Interview Schedule and a standardized psy-
chiatric diagnosis. Experience in eastern Baltimore. Arch. Gen.
Psychiatry 42 (7), 667–675.
Aronen, E.T., Soininen, M., 2000. Childhood depressive symptoms
predict psychiatric problems in young adults. Can. J. Psychiatry
45, 465–470.
Badawi, M., Eaton, W.W., Myllyluoma, J., Weimer, L.G., Gallo, J.,
1999. Psychopathology and attrition in the Baltimore ECA 15-
year follow-up 1981–1996. Soc. Psychiatry Psychiatr. Epide-
miol. 34, 91–98.
Chen, C.Y., Anthony, J.C., 2003. Possible age-associated bias in
reporting of clinical features of drug dependence: epidemiolo-
gical evidence on adolescent-onset marijuana use. Addiction 98
(1), 71–82.
Chen, L., Eaton, W.W., Gallo, J.J., Nestadt, G., 2000. Understan-
ding the heterogeneity of depression through the triad of symp-
toms, course and risk factors: a longitudinal, population-based
study. J. Affect. Disord. 59, 1–11.
Costello, C.G., 1992. Research on symptoms versus research on
syndromes: arguments in favour of allocating more research
time to the study of symptoms. Br. J. Psychiatry 160, 304–308.
Dryman, A., Eaton, W.W., 1991. Affective symptoms associated
with the onset of major depression in the community: findings
from the US National Institute of Mental Health Epidemiologic
Catchment Area Program. Acta Psychiatr. Scand. 84, 1–5.
Eaton, W.W., 1995. Studying the natural history of psychopatho-
logy. In: Tsuang, M., Tohen, M., Zahner, G. (Eds.), Textbook
in Psychiatric Epidemiology. Wiley-Liss Inc, New York, NY,
pp. 157–177.
Eaton, W.W., Kessler, L.G. (Eds.), 1985. Epidemiological Field
Methods in Psychiatry: The NIMH Epidemiological Catchment
Area Program. Academic Press, Orlando, FL.
Eaton, W.W., Regier, D.A., Locke, B.Z., Taube, C.A., 1981. The
Epidemiologic Catchment Area Program of the National Insti-
tute of Mental Health. Public Health Rep. 96, 319–325.
Eaton, W.W., Kramer, M., Anthony, J.C., Dryman, A., Shapiro, S.,
Locke, B.Z., 1989. The incidence of specific DIS/DSM-III men-
tal disorders: data from the NIMH Epidemiologic Catchment
Area Program. Acta Psychiatr. Scand. 79 (2), 163–178.
Eaton, W.W., Badawi, M., Melton, B., 1995. Prodromes and pre-
cursors: epidemiologic data for primary prevention of disorders
with slow onset. Am. J. Psychiatry 152, 967–972.
Eaton, W.W., Anthony, J.C., Gallo, J., Cai, G., Tien, A., Romanos-
ki, A., Lyketsos, C., Chen, L.S., 1997. Natural history of Diag-
nostic Interview Schedule/DSM-IV major depression. The
Baltimore Epidemiologic Catchment Area follow-up. Arch.
Gen. Psychiatry 54, 993–999.

H.C. Wilcox, J.C. Anthony / Journal of Affective Disorders 82 (2004) 9–2020
Grimes, D.A., Schulz, K.F., 2002. Uses and abuses of screening
tests. Lancet 359, 881–884.
Horwath, E., Johnson, J., Klerman, K., Weissman, M., 1992.
Depressive symptoms as relative and attributable factors for
first onset depression. Arch. Gen. Psychiatry 49, 817–823.
Judd, L.L., Akiskal, H.S., 2000. Delineating the longitudinal struc-
ture of depressive illness: beyond clinical subtypes and duration
thresholds. Pharmacopsychiatry 33, 3–7.
Lawless, J.F., 1982. Statistical Models and Methods for Lifetime
Data. Wiley, New York, NY.
Lewinsohn, P.M., Clarke, G., Seeley, J.R., Rohde, P., 1994. Major
depression in community adolescents: age at onset, episode
duration, and time to recurrence. J. Am. Acad. Child Adolesc.
Psychiatry 33, 809–818.
Liang, K.Y., Zeger, S.L., Qaqish, B., 1992. Multivariate regression
analyses for categorical data. J. R. Stat. Soc. Ser. B—Methodo-
logical 54, 3–40.
Lyketsos, C.G., Heithoff, K., Nesdadt, G., Cwi, J., Eaton, W.W.,
1994. The life-chart interview: a standardized method to describe
the course of psychopathology. Int. J. Methods Psychiatr. Res. 4,
143–155.
Murphy, J.M., Nierenberg, A.A., Monson, R.R., Laird, N.M.,
Sobol, A.M., Leighton, A.H., 2002. Self-disparagement as
feature and forerunner of depression: findings from the Stirling
County Study. Compr. Psychiatry 43 (1), 13–21.
Narrow, W.E., Rae, D.S., Robins, L.N., Regier, D.A., 2002. Revised
prevalence estimates of mental disorders in the United States:
using a clinical significance criterion to reconcile 2 surveys’
estimates. Arch. Gen. Psychiatry 59 (2), 115–123.
Neumark, Y.D., Van Etten, M.L., Anthony, J.C., 2000. Drug de-
pendence and death: survival analysis of the Baltimore ECA
sample from 1981–1995. Substance Use Misuse 35, 313–327.
Orvaschel, H., Lewinsohn, P.M., Seeley, J.R., 1995. Continuity of
psychopathology in a community sample of adolescents. J. Am.
Acad. Child Adolesc. Psychiatry 34, 1525–1535.
Pine, D.S., Cohen, E., Cohen, P., Brook, J., 1999. Adolescent
depression symptoms as predictors of adult depression: moodi-
ness or mood disorder? Am. J. Psychiatry 156, 133–135.
Roberts, R.E., Lewinsohn, P.M., Seeley, J.R., 1995. Symptoms of
DSM-III-R major depression in adolescence: evidence from an
epidemiological survey. J. Am. Acad. Child Adolesc. Psychiatry
34, 1608–1617.
Robins, L.N., Regier, D.A., 1991. Psychiatric Disorders in Amer-
ica. Free Press, New York.
Robins, L.N., Helzer, J.E., Croughan, J., Ratcliff, K.S., 1981.
National Institute on Mental Health Diagnostic Interview
Schedule: its history, characteristics, and validity. Arch. Gen.
Psychiatry 38, 381–389.
Robins, L.N., Helzer, J.E., Croughan, J., Ratcliff, K.S., 1994. Na-
tional Institute on Mental Health Diagnostic Interview Schedule.
In: Mezzich, J.E., Jorge, M.R., Salloum, I.M. (Eds.), Psychiatric
Epidemiology: Assessment, Concepts and Methods. The Johns
Hopkins University Press, Baltimore, MD.
Rosenberg, M.F., Anthony, J.C., 2001. Early clinical manifestations
of cannabis dependence in a community sample. Drug Alcohol
Depend. 64, 123–131.
Weissman, M.M., Bruce, M.L., Leaf, P.J., Florio, L.P., Holzer III, C.
1991. Affective disorders. In: Robins, L.N., Regier, D.A. (Eds.),
Psychiatric Disorders in America. The Free Press, New York,
NY, pp. 53–80.
Copyright © 2022 FDOKUMEN




















