
Accuracy of bacterial DNA testing for central venous catheter ...
Upload
independentCategory
view
0download
0
1222
Recent studies have demonstrated the importance of cathe-ter–tissue contact force (CF) during radiofrequency abla-
tion (RFA).1,2 A novel CF-sensing ablation catheter that allows real-time assessment of CF between an open irrigated cath-eter tip and target tissue interface has been shown to provide additionally useful information during endocardial catheter ablation procedures to treat atrial flutter and atrial fibrillation (AF).3 CF seems to have a relationship with the force–time integral, lesion size formation, acute procedural success, and recurrence rates.1,4,5
Editorial see p 1053 Clinical Perspective on p 1228
There remains a paucity of literature on the impact of CF dur-ing epicardial ablation procedures. It can be problematic when using traditional epicardial ablation techniques to determine ablation catheter–tissue contact. Furthermore, the impact of applied CF during RF application at sites over or adjacent to
epicardial fat, coronary vessels, or the phrenic nerve (PN) has not been systematically described.6–8 Therefore, CF-sensing ablation catheters could potentially improve epicardial RFA efficacy.
The aims of this study were to evaluate and characterize the effect of CF-sensing technology on RF epicardial lesion size in an ovine beating heart model, and the effect of RF appli-cation with increasing CF over or adjacent to epicardial fat, coronary arteries, and the PN.
MethodsThis study was approved by the Faculty of Veterinary Science Animal Research Ethics Committee of the University of Melbourne.
ProcedureOvine Model Preparation—General AnesthesiaTwelve female crossbred sheep weighing 34±5.7 (range 30–40) kg were studied. Each animal underwent induction of gen-eral anesthesia (mean anesthetic time, 153±18.4 minutes) with
© 2013 American Heart Association, Inc.
Circ Arrhythm Electrophysiol is available at http://circep.ahajournals.org DOI: 10.1161/CIRCEP.113.000184
Original Article
Background—Contact force (CF) during radiofrequency ablation (RFA) is an important determinant of endocardial lesion size with limited data on epicardial RFA and CF. We evaluated CF characteristics using irrigated RFA on the epicardium in an ovine model.
Methods and Results—In 12 sheep, a 7-F irrigated RFA catheter with CF sensor was introduced via a pericardial incision onto/in parallel with ventricular epicardium. RFA (30 W per 30 second duration) was applied at 5g, 10g, 20g, 40g, and 70g: (1) over left and right ventricular myocardium with or without fat, (2) either directly over or adjacent to a coronary artery, or directly over the phrenic nerve. Force–time integral, lesion dimensions, and coronary artery/phrenic nerve injury were recorded. Lesion size, volume, and force–time integral progressively increased with higher CF (P<0.05). Steam pops occurred with high CF. Epicardial fat had an attenuating effect on RF penetration into myocardium (P<0.05); however, myocardial RF lesions could be created at sites with >3.5 mm epicardial fat. At sites with epicardial fat, each 10g increment in CF led to a 0.6 mm increase in lesion depth, whereas each 1 mm of fat reduced lesion depth into underlying myocardium by 0.7 mm. Extent of acute coronary injury with direct and indirect RFA and phrenic nerve palsy occurrence was proportional to CF.
Conclusions—CF is a determinant of epicardial RF lesion size, steam pops, acute coronary artery injury, and phrenic nerve injury. Although epicardial fat limits lesion size, RFA with high CF can produce small myocardial RF lesions at sites of thick epicardial fat. (Circ Arrhythm Electrophysiol. 2013;6:1222-1228.)
Key Words: catheter ablation ◼ models, animal
Received January 15, 2013; accepted September 30, 2013.From the Department of Cardiology, The Royal Melbourne Hospital, Melbourne, Australia (M.C.G.W., S.J.S., J.M.K., S.K., J.B.M.); Department of
Medicine, University of Melbourne, Parkville, Australia (M.C.G.W., J.M.K., S.K., J.B.M.); Department of Veterinary Science, University of Melbourne, Werribee, Australia (G.E.); and Department of Cardiology, Western Hospital, Melbourne, Australia (S.A.J.).
The online-only Data Supplement is available at http://circep.ahajournals.org/lookup/suppl/doi:10.1161/CIRCEP.113.000184/-/DC1.Correspondence to Joseph Morton, MBBS, PhD, Department of Cardiology, Royal Melbourne Hospital, Melbourne 3050, Australia. E-mail
Characterization of Catheter–Tissue Contact Force During Epicardial Radiofrequency Ablation in an Ovine Model
Michael C.G. Wong, MBBS; Glenn Edwards, BVetSc; Steven J. Spence, GradDipSc (Cardiac EP); Jonathan M. Kalman, MBBS, PhD;
Saurabh Kumar, BSc (Med)/MBBS, PhD; Stephen A. Joseph, MBBS, PhD; Joseph B. Morton, MBBS, PhD
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

Wong et al Contact Force During Epicardial RF Ablation 1223
thiopentone sodium 20 mg/kg and buprenorphine 0.01 mg/kg fol-lowed by a continuous infusion of fentanyl. Sheep were intubated and mechanically ventilated with oxygen and nitrous oxide. An intravenous bolus of lignocaine 40 mg was administered at the start of each case followed by a continuous infusion throughout the procedure as prophylaxis against ventricular arrhythmias.
Access to Pericardial CavityA left open thoracotomy was performed. The left and right ventricular (LV/RV) aspects of the beating heart were exposed and a 1-cm incision into the parietal pericardium was per-formed under direct vision. Prewarmed (37°C) normal saline was introduced into the pericardial space to allow for zero calibration of CF when there was no electrode–tissue contact (ie, catheter floating) as visualized by the operator. The CF-sensing catheter was then inserted via the pericardial incision into the pericardial space.
CF RFA ProtocolA novel CF-sensing 7-F quadripolar ablation catheter (Tac-tiCath; Endosense SA, Geneva, Switzerland; distributed by Biotronik, Germany) with 3.5 mm open irrigation tip electrode (total catheter length, 115 cm) was used. The interelectrode distance was 2-5-2 mm with a thermocouple positioned at the tip. The CF-sensing catheter contains a triaxial sensor located between the second and third electrode, which measures the force (amplitude and direction) of contact between tissue and catheter tip electrode.2,4 The sensor measures the lateral and axial force every 100 ms and displays this on a viewing station that is integrated into the electrophysiology laboratory.
An 8.5-F steerable long sheath (Agilis NxT; St Jude Medical, St Paul, MN) was used to improve catheter tip sta-bility and facilitate optimal transmission of CF to the target epicardial structures during each RFA application. A Stockert Radiofrequency Power Generator (Biosense-Webster Inc, Diamond Bar, CA) was used for radiofrequency energy delivery. Power, temperature, and impedance were continu-ously monitored throughout each RFA application and stored on a computer-based digital amplifier/recorder system (Bard LabSystem Pro; Lowell, MA) for offline data analysis. The catheter was positioned parallel to the epicardial surface structures under the overlying pericardium. The operator ensured that the point of contact was against the epicar-dial surface and not against overlying lung or pericardium. Catheter–tissue CF was applied at the following predeter-mined sites: LV myocardium at a site without epicardial fat; RV myocardium at a site without epicardial fat; LV myocar-dium at a site with visible overlying epicardial fat; RV myo-cardium at a site with visible overlying epicardial fat; directly overlying a coronary artery (usually the left anterior descend-ing artery); directly adjacent to, but not in immediate contact with, a coronary artery (usually the left circumflex artery); and directly onto the left PN.
Predefined constant CF was applied at 5g, 10g, 20g, 40g, and 70g at each of the above sites as measured by the cath-eter contact sensor. Each RFA application was delivered at 30 W for 30 seconds (17 mL/min irrigation) at a temperature limit of 48ºC unless an impedance rise occurred first. The RF
application was not terminated prematurely in the event of a steam pop occurring without impedance rise, and the total number of steam pops was recorded for each application.
It was observed in preparing the model that basal epicardial fat was thicker and became progressively thinner toward the apex. Therefore, when performing RF over fat, the highest CF was applied at the most basal site and CF reduced over each subsequent more apical location.
Direct application of RF energy over the PN was com-menced at the most cranially accessible site that ensured con-sistent stability of applied CF. Diaphragmatic stimulation was observed with PN pacing during each RF application over the PN with loss of diaphragmatic contraction indicative of sig-nificant PN injury. Each subsequent RF application over the PN was applied in a more caudal site to the previous applica-tion to evaluate intact PN function.
Postprocedure Preparation of Ovine HeartAt the end of ablation procedure, the aorta was cannulated and 20 mL of 1% 2,3,5-triphenyl-tetrazolium chloride (TTC) solu-tion was administered via the coronary arteries. The animal was euthanized and its heart harvested, immediately immersed in TTC solution for 20 to 30 minutes at room temperature to ensure adequate staining of the epicardium, and subsequently transferred to 10% formalin solution for fixation before subse-quent macroscopic and microscopic histopathologic analysis.
CF Sensing DataData consisting of force characteristics (amplitude and direction) from catheter tip electrode and target tissue were recorded by Endosense software and exported for offline anal-ysis. Visual display of tip-to-tissue orientation of the catheter was available to the operator to ensure that adequate catheter–tissue contact was maintained during each RF application.
Pathological AnalysisLesions made over the myocardium and epicardial fat were measured macroscopically with a surgical ruler to determine diameter and depth. Baseline myocardial and epicardial fat thickness was measured immediately adjacent to each lesion. Lesion dimensions and lesion volume were measured and determined using a previously published formula.9 Lesion volume at sites where RF was applied over fat could not be accurately assessed with this formula. At sites of epicardial fat, the lesion size was determined from the amount of ablated myocardium directly underlying the fat. For example, if the epicardial fat was 5 mm thick and the lesion 7 mm deep, the depth of lesion was recorded as 2 mm to account only for the extent of myocardial ablation.
Sections from lesions made over or adjacent to coronary arteries and over the PN and adjacent to the left circumflex artery were taken and fixed in 10% neutrally buffered forma-lin. The tissue was dehydrated, embedded in paraffin, sec-tioned at 2 mm thickness, and stained with hematoxylin and eosin. Coronary lesions were analyzed by assessing for evi-dence of vacuolation within the tunica media and disruption of the tunica intima (internal elastic lamina and endothelium), perivascular edema, and fat necrosis.
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

1224 Circ Arrhythm Electrophysiol December 2013
Specimens were examined under light microscopy with microscopic measurements performed using the ScanScope XT system and analyzed with proprietary software.
Statistical AnalysisData analysis was performed using the statistical package SPSS (release 17.0; IBM). Continuous variables were expressed as mean±SD. Means of lesion depth with versus without fat were compared at each CF using an independent samples t-test. A Mann–Whitney U-test was used when the normal distribu-tion assumption was questionable. A linear mixed model was fitted across the entire data to determine the relationship between lesion depth into myocardium (response), fat thick-ness (covariate), and CF (continuous covariate). In addition to the above fixed effects, sheep was fitted as a random effect in the mixed model, with lesions nested within sheep. A 2-tailed P value <0.05 was considered statistically significant.
ResultsA total of 420 lesions were analyzed. Twenty applications were excluded because of impedence rise prematurely termi-nating the RFA application, occurrence of ventricular fibrilla-tion, or inconsistent CF during RFA application.
Baseline Tissue CharacteristicsOf the areas targeted by ablation, the baseline LV wall thick-ness was 15±3.2 (range 11–22) mm and RV wall thickness was 5.6±0.9 (range 3–6.5) mm. For sites of ablation, the mean thickness (depth) of the fat layer overlying myocardium was 3.7±2.2 mm over the LV (range 0.5–8 mm) and 4.5±2.7 mm over the RV (range 1–7 mm). LV myocardium was up to 3 times thicker compared with RV myocardium. As expected, there was variability in the thickness of epicardial fat over dif-ferent ventricular sites (Table 1).
Effect of RF Over Epicardial Sites Without FatThere was a progressive increase in lesion size according to the delivered CF (Table 2; Figures 1 and 2). The smallest lesion depth (LV, 2.2±0.6 mm; RV, 1.8±0.5 mm) and width (LV, 2.8±0.9 mm; RV, 1.8±0.8 mm) occurred with the lowest CF of 5g, which significantly increased with higher CFs up to 70g (depth: LV, 7.3±1.4 mm; RV, 6.4±1.0 mm; width: LV, 10.3±1.6 mm; RV, 9.9±1.9 mm). This resulted in an approxi-mate doubling of lesion volume for each step-up in CF from 5g to 40g. Between 40g and 70g, lesion volume increased by 1 to 1.5 times. In the LV, even the largest lesions were not transmural because of the significant baseline wall thickness.
However, transmural lesions were frequently seen at 70g applications over the RV and occasionally at 40g applications (Figure 3A).
Steam pops were observed rarely at 5g or 10g CF, but fre-quently at 40g (12%) and 70g (33%). In no cases was there myocardial perforation with any steam pop. However, tissue cavitation or cratering was evident at RF lesion points that correlated with steam pop occurrence (Figure 3B).
Effect of RF Lesions Applied at Sites Covered by Epicardial Fat Lesions were substantially smaller in depth of penetration into myocardium underlying areas of fat; however, even with a mean fat thickness 5.1±2.6 mm overlying the LV, 70g of CF during RF did produce a mean 1.4±2.0 mm deep myocardial lesion under the fat. Comparing myocardial lesion depth at LV or RV sites with and without epicardial fat (Figures 1 and 2), there was a highly significant difference. There was a strong relationship between both applied CF and lesion depth at sites with and without fat. There was a statistically significant relationship between fat thickness and lesion depth across all CFs (P<0.05). The mixed model using CF and fat thickness as covariates for all lesions (at all forces and fat thickness) resulted in estimated coefficient of 0.064 for force and –0.670 for fat thickness. This showed that, on average, for each addi-tional 10g of force there was a 0.6 mm increase in lesion depth; however, for each additional 1 mm of fat, there was a 0.7 mm reduction in lesion depth. See Figure 4 and Table I (online-only Data Supplement) for details.
Effects of RF Delivered Over PN and Coronary ArteriesPN paralysis was seen for almost all applied lesions with applied force of ≥20g (Table 2) but in no case at 5g CF and 2 of 12 cases using 10g CF.
Direct RF application over the left anterior descending cor-onary artery at forces from 5g to 70g did not result in vascular occlusion. However, marked acute coronary vessel injury was observed on histopathology at 70g CF and moderate injury at 40g CF (Table II in the online-only Data Supplement).
At the highest forces (Figure 4D), transmural vacuolation of the tunica media and disruption of the internal elastic lamina and endothelium were clearly observed in 9 cases. Even when RF was applied adjacent to but not directly over the coronary artery, there was evidence of vessel injury (Table III in the online-only Data Supplement). Fat necrosis around the vessels, perivascular edema, and perivascular
Table 1. Baseline Characteristics
Contact Force P Value5g 10g 20g 40g 70g
Mean LV wall thickness, mm 15.8±4.4 14.8±2.8 14.3±2.5 15.4±2.7 17.0±3.1 0.30
Mean RV wall thickness, mm 5.4±0.6 5.7±1.1 5.5±1.0 5.9±0.8 6.1±1.4 0.59
Mean LV fat layer, mm 2.7±2.1 2.9±1.8 3.3±1.4 4.0±2.0 5.1±2.6 <0.05
Mean RV fat layer, mm 2.6±1.1 3.5±1.3 4.5±1.7 6.0±3.4 6.2±3.8 <0.05
Values are expressed as mean±SD. LV indicates left ventricular; and RV, right ventricular.
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

Wong et al Contact Force During Epicardial RF Ablation 1225
hemorrhage into the epicardial fat layer were frequently observed. Although not systematically assessed, the pres-ence of an overlying (as opposed to adjacent) coronary vein did seem to reduce the degree of arterial injury in 5 cases.
DiscussionThis study of epicardial RF application in an ovine model using a novel CF-sensing catheter provided the following main findings:
1. Epicardial lesion volume is related to increasing CF when this CF is applied directly over the myocardium with the catheter tip lying parallel to the surface as would usually be the case in clinical epicardial VT abla-tion in humans.
2. For each doubling of tissue contact between 5g and 40g of applied CF, there was a corresponding doubling in the absolute lesion volume.
3. At sites of thinner myocardium (in this model, RV with mean wall thickness 5.6±0.9 mm), transmural lesions can be created with epicardial RF applications.
4. Epicardial fat attenuates the effect of RF penetration into underlying myocardium, but myocardial ablation does still occur and is proportional to the applied CF and thickness of the fat layer.
5. PN injury occurs with increasing directly applied CF. At CF of ≥20g, this injury was virtually universal.
6. Acute coronary artery injury was also related to the deliv-ered CF. Even at sites where RF was applied adjacent to the coronary artery, lesions with higher CF produced ves-sel wall injury as evidenced by vacuolation of the tunica media. When RF was directly applied over a coronary vessel at high CF, these changes were frequently trans-mural and extended to the tunica intima (endothelium).
Epicardial Lesion Volume and Applied CFPrevious experimental studies have demonstrated the influ-ence that CF has on lesion size formation during RF appli-cations.1,2 In clinical studies, sites of low applied CF have been shown to correlate with sites of less effective ablation and sites more likely to demonstrate tissue recovery with recovery of functional conduction properties.3,10 Similarly, in this study CF has a significant effect on lesion size. In sheep, the RV wall is thinner than the LV wall and transmu-ral lesions were produced here when using higher CF. The application of strong CF on the epicardium was also more likely to produce steam pops and cavitation. It has been shown previously that impedance-controlled ablation was associated with a low risk of popping regardless of catheter–tissue contact when compared with fixed power ablation.11 However, given the importance of catheter contact for ade-quate lesion formation through tissue heating, CF represents another indicator of steam pop risk. We demonstrated that at
Figure 1. Left ventricular myocardial lesion depth with/without epicardial fat.
Figure 2. Right ventricular myocardial lesion depth with/without epicardial fat.
Table 2. Radiofrequency Application Over Sites Not Covered With Epicardial Fat
Contact Force P Value5g 10g 20g 40g 70g
Lesion depth in LV, mm 2.2±0.6 2.9±0.8 4.1±1.4 5.5±1.8 7.3±1.4 <0.05
Lesion width in LV, mm 2.8±0.9 4.1±1.5 6.0±2.2 7.9±2.0 10.3±1.6 <0.05
Mean LV lesion volume, mm3 4.3±2.5 11.4±10.8 22.3±17.4 47.0±0.1 73.0±23.1 <0.05
RV lesion depth, mm 1.8±0.5 3.0±0.9 4.1±0.8 5.0±0.6 6.4±1.0 <0.05
RV lesion width, mm 1.8±0.8 4.1±1.0 6.4±1.5 7.9±2.3 9.9±1.9 <0.05
Mean RV lesion volume, mm3 3.1±2.0 8.4±4.9 19.0±10.6 35.7±23.6 62.7±33.1 <0.05
Steam pop LV/RV (n lesions) 0 (84) 1 (84) 9 (84) 10 (84) 28 (84) <0.05
PN paralysis (n sheep) 0 (12) 2 (12) 11 (12) 12 (12) 12 (12) <0.05
Vessel injury present (n sheep) 0 (12) 3 (12) 5 (12) 11 (12) 12 (12) <0.05
Values are expressed as mean±SD. LV indicates left ventricle; PN, phrenic nerve; and RV, right ventricle.
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

1226 Circ Arrhythm Electrophysiol December 2013
lower CFs the chance of steam pops occurring is small but this risk increased significantly with higher CFs (ie, >20g).
Sacher et al12 recently demonstrated larger epicardial than endocardial lesion formation in an ovine model with 60 sec-onds of irrigated RF at 30 W (mean total epicardial CF of 21g). The present study does not point to the optimal CF when performing ablation with 30 W irrigated RF (30-second dura-tion), but even at 10g and 20g, significant lesions were created.
Influence of Epicardial FatPrevious studies have reported on the protective role epicar-dial fat may have during RF ablation,6,13 and this may limit
the use of epicardial RF. This can be particularly challenging in patients with nonischemic cardiomyopathy where there may be a predominance of low bipolar voltage correlating with scar substrate in the perivalvular regions that have exten-sive fat distribution epicardially.14,15 Moreover in humans, fat volumes around the heart have been found to correlate with advancing age and are larger in men compared with women.16
The low electric and thermal conductivity properties of fat reduce the penetrating effect of RF current and heat to the underlying myocardium, thereby creating shallower lesions compared with epicardial areas without fat. It has been found that irrigated tip RFA was unable to produce epicardial lesions
Figure 3. A, Five-centimeter-deep transmural lesion at 40g contact force (CF) over right ventricle (no overlying fat). Lesion volume is cal-culated using the formula volume=(1/6)×π×(a×b2+c×d2/2) where a=maximum depth of lesion, b=maximum diameter of lesion, c=depth of maximum diameter, and d=surface diameter of lesion. B, Steam pop occurrence with extensive right ventricular wall cavitation at 70g CF.
Figure 4. Hematoxylin and eosin–stained epicardial lesions. A, Layer of overlying thin fat with significant lesion formation into underlying myocardium at 70g contact force (CF). B, Medium fat with moderate myocardial lesion formation at 70g CF. C, Thick fat with reduced but still significant lesion penetration into underlying myocardium at 70g CF. D, Radiofrequency lesion directly over coronary artery at 70g CF showing extensive tunica media injury with transmural vacuolation and fat necrosis.
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

Wong et al Contact Force During Epicardial RF Ablation 1227
through fat thicker than 3.5 mm, but this is dependent on power/temperature settings and does not take into account the amount of CF involved.13
The present study has shown that RF lesions using high CF can produce small myocardial lesions of mean depth 1 to 2 mm at sites of even the thickest fat (>5 mm). Whether these small lesions produce clinically relevant effects on epicardial circuits is unknown. The ANOVA model demonstrated that, on aver-age, for each 10g of force there was a 0.6 mm increase in lesion depth; however, for each 1 mm of fat, there was a 0.7 mm reduc-tion in lesion depth. Therefore, at 40g applied force over 4 mm of fat, there would be no lesion (2.4 mm calculated depth atten-uated by 2.8 mm reduction in lesion penetration). However, at 3.5 mm of fat thickness (2.45 mm lesion depth attenuation), a 50g CF lesion (3.0 mm predicted lesion depth below fat) would produce a 0.5 mm lesion. In other words, a high CF would be required to create a meaningful lesion below 3.5 mm of fat.
Neurovascular Injury and Epicardial AblationCoronary vessel injury has been reported in rare cases of epi-cardial ablation.17,18 A large clinical case series reported acute coronary injury in 2 of 131 epicardial ablation procedures with both involving small branch vessel occlusion.17 Several studies have demonstrated that acute vascular wall changes, including endothelial disruption, neointimal thickening, and intravascular thrombosis, occur when delivering RFA in the vicinity of a coronary artery with risk of chronic vascular damage inversely proportional to vessel size.19,20 Moreover, more significant changes were noted to only occur in vessels of small calibre with the suggestion that larger vessels are pro-tected from such changes due to greater blood flow.13
RF application over or immediately adjacent to a coronary artery is best avoided, and based on our data, coronary injury is greater when CF is high.
PN injury is an uncommon complication of epicardial abla-tion. Our study showed that PN injury appeared unlikely at 5g or 10g of CF but that it was consistently injured at forces >20g. Importantly in our model, RF was directly applied over the PN, whereas clinically, the PN sits on the external surface of the fibrous pericardium. It is not known what CF can be applied/transmitted to the PN during clinical epicardial abla-tion procedures.
Study LimitationsThe use of an open left thoracotomy approach with saline-filled pericardium was chosen as our model of epicardial ablation, but this may be limiting the clinical relevance of our results. The model was chosen to (1) ensure optimal and consistent positioning of the CF catheter tip, (2) permit reliable applica-tion of RFA across all levels of CF, and (3) facilitate repro-ducible lesion formation over fat/coronaries and PN. Different results might have been achieved if perpendicular or angled catheter orientation had been attempted; however, applying the catheter tip parallel to the tissue surface in this study did reflect the usual epicardial ablation technique in humans.
ConclusionsCF is a major determinant of epicardial RF lesion size, occur-rence of steam pops, coronary artery injury, and PN injury.
The epicardial fat layer has an important role in limiting the penetrating depth of ablation into the underlying myocardium. At sites of thickest epicardial fat, applying RF with the highest CF can produce small myocardial RF lesions.
Acknowledgments We thank Carol Bradley and Gail Squires for their assistance with this project, and Graham Hepworth for statistical data analysis.
Sources of Funding This study was made possible by a research grant from Biotronik.
Disclosures Dr Wong is the recipient of the Keith Goldsbury Postgraduate Research Scholarship Award (ID PC11M 6218) from the National Heart Foundation of Australia. Dr Kumar is the recipient of a post-graduate research scholarship cofunded by the National Health and Medical Research Council and the National Heart Foundation of Australia (ID 628996).
References 1. Yokoyama K, Nakagawa H, Shah DC, Lambert H, Leo G, Aeby N, Ikeda
A, Pitha JV, Sharma T, Lazzara R, Jackman WM. Novel contact force sensor incorporated in irrigated radiofrequency ablation catheter predicts lesion size and incidence of steam pop and thrombus. Circ Arrhythm Electrophysiol. 2008;1:354–362.
2. Thiagalingam A, D’Avila A, Foley L, Guerrero JL, Lambert H, Leo G, Ruskin JN, Reddy VY. Importance of catheter contact force during irri-gated radiofrequency ablation: evaluation in a porcine ex vivo model using a force-sensing catheter. J Cardiovasc Electrophysiol. 2010;21:806–811.
3. Kumar S, Morton JB, Halloran K, Spence SJ, Lee G, Wong MC, Kistler PM, Kalman JM. Effect of respiration on catheter-tissue contact force dur-ing ablation of atrial arrhythmias. Heart Rhythm. 2012;9:1041–1047.e1.
4. Kuck KH, Reddy VY, Schmidt B, Natale A, Neuzil P, Saoudi N, Kautzner J, Herrera C, Hindricks G, Jaïs P, Nakagawa H, Lambert H, Shah DC. A novel radiofrequency ablation catheter using contact force sensing: Toccata study. Heart Rhythm. 2012;9:18–23.
5. Shah DC, Lambert H, Nakagawa H, Langenkamp A, Aeby N, Leo G. Area under the real-time contact force curve (force-time integral) predicts ra-diofrequency lesion size in an in vitro contractile model. J Cardiovasc Electrophysiol. 2010;21:1038–1043.
6. Desjardins B, Morady F, Bogun F. Effect of epicardial fat on electroana-tomical mapping and epicardial catheter ablation. J Am Coll Cardiol. 2010;56:1320–1327.
7. Dixit S, Narula N, Callans DJ, Marchlinski FE. Electroanatomic mapping of human heart: epicardial fat can mimic scar. J Cardiovasc Electrophysiol. 2003;14:1128.
8. Tung R, Nakahara S, Ramirez R, Lai C, Fishbein MC, Shivkumar K. Distinguishing epicardial fat from scar: analysis of electrograms using high-density electroanatomic mapping in a novel porcine infarct model. Heart Rhythm. 2010;7:389–395.
9. Wittkampf FH, Nakagawa H, Foresti S, Aoyama H, Jackman WM. Saline-irrigated radiofrequency ablation electrode with external cooling. J Cardiovasc Electrophysiol. 2005;16:323–328.
10. Reddy VY, Shah D, Kautzner J, Schmidt B, Saoudi N, Herrera C, Jaïs P, Hindricks G, Peichl P, Yulzari A, Lambert H, Neuzil P, Natale A, Kuck KH. The relationship between contact force and clinical outcome during radiofrequency catheter ablation of atrial fibrillation in the TOCCATA study. Heart Rhythm. 2012;9:1789–1795.
11. Thiagalingam A, D’Avila A, McPherson C, Malchano Z, Ruskin J, Reddy VY. Impedance and temperature monitoring improve the safety of closed-loop irrigated-tip radiofrequency ablation. J Cardiovasc Electrophysiol. 2007;18:318–325.
12. Sacher F, Wright M, Derval N, Denis A, Ramoul K, Roten L, Pascale P, Bordachar P, Ritter P, Hocini M, Dos Santos P, Haissaguerre M, Jais P. Endocardial versus epicardial ventricular radiofrequency ablation: util-ity of in vivo contact force assessment. Circ Arrhythm Electrophysiol. 2013;6:144–150.
13. d’Avila A, Houghtaling C, Gutierrez P, Vragovic O, Ruskin JN, Josephson ME, Reddy VY. Catheter ablation of ventricular epicardial tissue: a
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

1228 Circ Arrhythm Electrophysiol December 2013
comparison of standard and cooled-tip radiofrequency energy. Circulation. 2004;109:2363–2369.
14. Hsia HH, Callans DJ, Marchlinski FE. Characterization of endocar-dial electrophysiological substrate in patients with nonischemic car-diomyopathy and monomorphic ventricular tachycardia. Circulation. 2003;108:704–710.
15. Soejima K, Stevenson WG, Sapp JL, Selwyn AP, Couper G, Epstein LM. Endocardial and epicardial radiofrequency ablation of ventricular tachy-cardia associated with dilated cardiomyopathy: the importance of low-voltage scars. J Am Coll Cardiol. 2004;43:1834–1842.
16. Alexopoulos N, McLean DS, Janik M, Arepalli CD, Stillman AE, Raggi P. Epicardial adipose tissue and coronary artery plaque characteristics. Atherosclerosis. 2010;210:150–154.
17. Roberts-Thomson KC, Steven D, Seiler J, Inada K, Koplan BA, Tedrow UB, Epstein LM, Stevenson WG. Coronary artery injury due
to catheter ablation in adults: presentations and outcomes. Circulation. 2009;120:1465–1473.
18. Sacher F, Roberts-Thomson K, Maury P, Tedrow U, Nault I, Steven D, Hocini M, Koplan B, Leroux L, Derval N, Seiler J, Wright MJ, Epstein L, Haissaguerre M, Jais P, Stevenson WG. Epicardial ventricu-lar tachycardia ablation a multicenter safety study. J Am Coll Cardiol. 2010;55:2366–2372.
19. D’Avila A, Gutierrez P, Scanavacca M, Reddy V, Lustgarten DL, Sosa E, Ramires JA. Effects of radiofrequency pulses delivered in the vicin-ity of the coronary arteries: implications for nonsurgical transthoracic epicardial catheter ablation to treat ventricular tachycardia. Pacing Clin Electrophysiol. 2002;25:1488–1495.
20. Viles-Gonzalez JF, de Castro Miranda R, Scanavacca M, Sosa E, d’Avila A. Acute and chronic effects of epicardial radiofrequency applications delivered on epicardial coronary arteries. Circ Arrhythm Electrophysiol. 2011;4:526–531.
CLINICAL PERSPECTIVEContact force (CF) has been established as an important determinant of endocardial lesion formation during radiofrequency ablation (RFA). This study demonstrates the use of novel CF catheter technology during epicardial RFA in an ovine open beating heart model and how it can influence lesion size and geometry over areas with or without epicardial fat as well as potential injury to critical vascular/neural structures. The presence of thick epicardial fat is shown to attenuate the effect of RF penetration into underlying myocardium, but contrary to previous suggestion that myocardial lesion formation does not occur under areas with >3.5 mm overlying fat, we have shown that higher levels of CF can overcome this issue. Our data further quantify the incremental effect of every 10g CF and 1 mm of fat thickness on lesion depth penetration, although it is important to remember that our model differs from the typical percutaneous approach of clinical epicardial RFA. Although higher CF can lead to effective lesion formation, potential pitfalls that remain include higher incidence of steam pops and greater extent of acute coronary and phrenic nerve injury, both of which have been reported to occur rarely but remain impor-tant considerations during clinical epicardial VT ablation. CF, therefore, can play an important role in reducing complica-tions and improving epicardial RFA efficacy.
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

Stephen A. Joseph and Joseph B. MortonMichael C.G. Wong, Glenn Edwards, Steven J. Spence, Jonathan M. Kalman, Saurabh Kumar,
Ablation in an Ovine ModelTissue Contact Force During Epicardial Radiofrequency−Characterization of Catheter
Print ISSN: 1941-3149. Online ISSN: 1941-3084 Copyright © 2013 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleCirculation: Arrhythmia and Electrophysiology
doi: 10.1161/CIRCEP.113.0001842013;6:1222-1228; originally published online October 17, 2013;Circ Arrhythm Electrophysiol.
http://circep.ahajournals.org/content/6/6/1222World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org/content/suppl/2013/10/17/CIRCEP.113.000184.DC1.htmlData Supplement (unedited) at:
http://circep.ahajournals.org//subscriptions/
is online at: Circulation: Arrhythmia and Electrophysiology Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Answer
Permissions and Rights Question andunder Services. Further information about this process is available in thepermission is being requested is located, click Request Permissions in the middle column of the Web pageClearance Center, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the CopyrightCirculation: Arrhythmia and Electrophysiologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

CIRCAE/2013/000184 Page R1 of R4
SUPPLEMENTAL MATERIAL
Supplemental Table 1 - RF application over sites covered with epicardial fat
Contact force (grams) 5g 10g 20g 40g 70g LV myocardium lesion
depth (mm) 2.2 ± 0.6 2.9 ± 0.8 4.1 ± 1.4 5.5 ± 1.8 7.3 ± 1.4
Myocardial lesion depth under LV fat (mm) 0 ± 0 0.1 ± 1.4 0.6 ± 1.5 1.0 ± 2.1 1.4 ± 2.0
P value <0.05 <0.05 <0.05 <0.05 <0.05
RV myocardium lesion depth (mm) 1.8 ± 0.5 3.0 ± 0.9 4.1 ± 0.8 5.0 ± 0.6 6.4 ± 1.0
Myocardial lesion depth under RV fat (mm) 0 ± 0 0 ± 0 0 ± 0 0 ± 0 0.3 ± 2.9
P value <0.05 <0.05 <0.05 <0.05 <0.05 Values are expressed as mean ± SD. LV indicates left ventricle; RV, right ventricle.
Supplemental Table 2 - Histopathology of RF application directly over coronary vessel
Sheep Vacuolation Internal Elastic Lamina intact?
Haemorrhage - in adventitia
Haemorrhage - in perivascular fat
5g N Y N N
10g N or mild Y N Y
20g N or mild Y N Y
40g mild or mod Y N Y
70g mod or sev Y/N Y Y N indicates no; Y, yes; mod, moderate; sev, severe.

CIRCAE/2013/000184 Page R2 of R4
Supplemental Table 3 – Histopathology of RF application adjacent to coronary vessel
Sheep Vacuolation Internal Elastic Lamina intact?
Haemorrhage - in adventitia
Haemorrhage - in perivascular fat
5g N Y N N 10g N Y N N 20g N Y N Y 40g N or mild Y N Y 70g mild or mod Y/N N Y
N indicates no; Y, yes; mod, moderate; sev, severe.
Supplemental Table 4 – Actual real time contact force applied at various epicardial sites
Contact Force Level
(grams) LV LV fat RV RV fat Adjacent
to vessel Directly
over vessel
5g 6.1±1.8 5.1±0.5 5.5±0.9 5.9±0.8 5.2±1.0 6.0±0.8
10g 11.1±1.1 12.5±5.2 11.2±1.5 10.4±1.0 9.6±3.1 10.5±2.3
20g 20.2±2.7 20.2±1.5 21.1±2.2 21.0±2.5 21.2±4.0 21.3±4.4
40g 40.7±2.2 39.8±3.5 41.1±0.8 40.2±1.2 40.2±1.2 39.6±9.6
70g 71.3±2.1 70.1±1.9 72.2±2.1 70.8±2.9 71.2±3.5 74.4±2.9
Values are expressed as mean ± SD. LV indicates left ventricle; RV, right ventricle.

CIRCAE/2013/000184 Page R3 of R4
Supplemental Figure 1 – Sample CF tracing of epicardial RF application at CF 20g
CIRCAE/2013/000184 Page R4 of R4
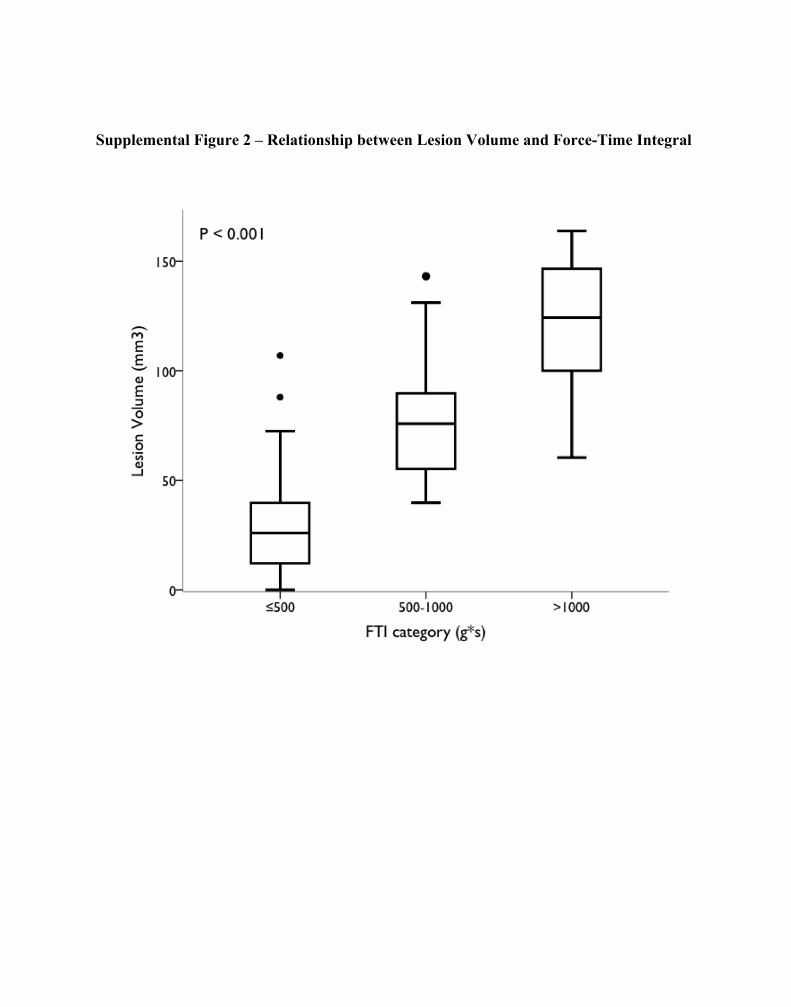
Supplemental Figure 2 – Relationship between Lesion Volume and Force-Time Integral
Copyright © 2022 FDOKUMEN




















