A Framework To Create A Virtual Organization Breeding Environment In The Mould And Die Sector

3
Historical Vignette on Radiation Cross-Fire: Paris 1905 to Stanford University 1994
CHA P T E R
1John R. Adler Jr
Richard F. Mould
Abstract
Cross-firing of radium gamma ray or X-ray beams has been an integral feature of therapeutic radiation practice for more than a century. The concept origi-nated in 905 in Paris with locally applied radium sources (surface brachytherapy) for the treatment of sciatic neuralgia. Its application then rapidly devel-oped for use with radium needle implants (interstitial brachytherapy) and X-rays (external beam radio-therapy) and eventually radium bomb machines (radium teletherapy). The latter were the forerunners of post-World War II kilocurie tele60Cobalt machines. Cross-firing techniques are relevant not only for fixed field treatments but also for rotational therapy. The milestones in radiation cross-fire are summarized, starting in Paris in 905 and continuing via the Gamma Knife to the CyberKnife® in 994 at Stanford University.
Introduction
The CyberKnife radiosurgical system was initially described in principle in 99 by Guthrie and Adler .1
It incorporates several distinctive features, including those of image-guided target localization, robotically administered radiation, a small X-band linear accel-erator, dynamic compensation for respiratory motion, and finally the potential use of up to ,200 intersect-ing beams of therapeutic radiation. This last feature, cross-fired photon beams, was first proposed in 905 .2 Thus, in 994, when the first CyberKnife was installed at Stanford, cross-fired beams had been in routine use for 90 years.
Origins of the CyberKnife
The modern lineage of the CyberKnife begins with Lars Leksell’s concept of radiosurgery. More than anyone, Leksell and his Karolinska team in Stockholm demonstrated over several decades that the combina-tion of precise target localization and large numbers of cross-fired beams could enable an entire new class of neurosurgical techniques. It was during a one-year neurosurgical fellowship in 985 at the Karolinska Institute that Adler came to fully compre-hend Lars Leksell’s enormous accomplishment in the
3rd Page Proofs*DDAdD

4 PA RT I : History
development of the Gamma Knife, which had made possible a near-magical procedure for ablating tissue in the brain.3–6 However, Adler quickly realized that the same radiophysical principles of cross-fire should be clinically applicable to targets in the spine, chest or abdomen with comparable success. It was also soon obvious to him that the concept of frame-based targeting embodied by the Gamma Knife could not practically be extrapolated to this potentially new therapeutic universe. This critical understanding proved to be the genesis of the CyberKnife.
Dawn of Therapeutic Cross-Fire Irradiation: Paris 1905
X-rays were discovered in November 895, 7, 8 radioac-tivity in March 896 9 and radium in December 898.10 Within five years, radium therapy was finding its first clinical applications, primarily for surface lesions. However, it was not long before radium was utilized for intracavitary techniques, such as for cancers of the cervix, rectum and nasopharynx. It was also soon used for interstitial treatments where radium needles were inserted into the tumor, Figure .
In 90 Pierre Curie and Henri Becquerel con-ducted self-exposure experiments with radium .11 Pierre Curie then loaned a radium source to Henri Danlos of Hôpital St. Louis, Paris, who used it for the very first clinical application.12 The Hôpital St. Louis would remain the leading hospital for radium brachytherapy in Paris until Marie Curie founded the Institut du Radium in 93.
At the beginning, surface brachytherapy with radium used only a single flat or curved applicator containing the sources. This design restricted treat-ments to superficial conditions such as lupus vulgaris, naevi, hypertrichosis acne vulgaris, and skin cancers.
The case history for the first cross-fire treated patient was described in Wickham & Degrais’ report
Therapeutic Results,2 in the section entitled Sciatic Neuralgia:
“Two patients suffering from sciatic neuralgia, treated in 905, were considerably relieved by radium. One of these cases deserves special notice, for the tech-nique adopted served as the basis for our invention of the “cross-fire” system. It was that of a workman who could only come three times a week to undergo treat-ment. He came from a great distance, partly on foot, and partly by omnibus, and was much fatigued by the journey. The conditions under which the treatment was carried out were therefore quite unfavourable, and yet decided improvement was obtained. The patient, who at the time of his first visits was hardly able to walk, certainly had much better freedom of movement after
Figure . An interstitial technique for the treatment of an inoperable malignant tumor in the neck region described by pioneer French radium therapists Louis Wickham & Paul Degrais. The goose quills allowed introduction of radium tubes deep into the tissues at the four opposite points of the tumor. The two flat, screened varnish radium applicators taped to the skin provided additional cross-fired irradiation of the underlying tissues.14

CHAPTER 1: Historical Vignette on Radiation Cross-Fire: Paris 905 to Stanford University 994 5
twelve applications. Feeling better, he gave up coming on account of the loss of time. The neuralgia had con-tinued for two years, and was aggravated by standing or walking. The difficulty was therefore to obtain deep action with sufficiently numerous and penetrating rays, without irritating the skin.”
This particular patient was treated by “. . . the simultaneous application of three instruments” (i.e., three radium applicators). The specific method here is much akin to the Gamma Knife concept of concur-rent irradiation.
With other patients, Wickham & Degrais “. . . repeated the applications over an entire series of neighbouring points in succession, with the object of making the rays converge toward the deep-seated painful parts.” Each exposure was required to be less than that “. . . required to produce a slight erythema.” With this alternative procedure, Wickham & Degrais’ treatment parallels the step and shoot concept that underlies CyberKnife cross-firing. Despite the primi-tive technology of the time, the principle initially described by these medical pioneers continues to be valid into the 2st century.
Arrival of Mechanical Cross-Fire: 1915
The first radiation therapy machine to include mechanical rotation was designed and built in 95 at the Royal Cancer Hospital, London. It was used successfully in the clinic for more than a decade .13
Because treatment with multiple fixed-field 200 kV X-ray beams was inadequate for many deep-seated tumors, such as those of the esophagus and bronchus, this new device was developed specifically to deliver large doses of radiation to smaller and deeper seated target volumes. During the rotational treatment, the external beam apparatus rotates at a constant speed around the stationary patient and continuously irra-diates over one or two planned prescribed arcs.
The earliest calculations of the total dose of radia-tion were represented by the sum of what would otherwise be a series of small, discrete beams admin-istered throughout a treatment arc. For example, the dose for a 300-degree arc around a fixed center of rotation was calculated to be equivalent to fixed fields delivered every 0 degrees. Although all modern linear accelerators and tele60Cobalt machines have the ability to treat using rotation therapy, in practice most cancer patients are treated using a fixed field technique.
Emergence of Treatment Planning: 1919
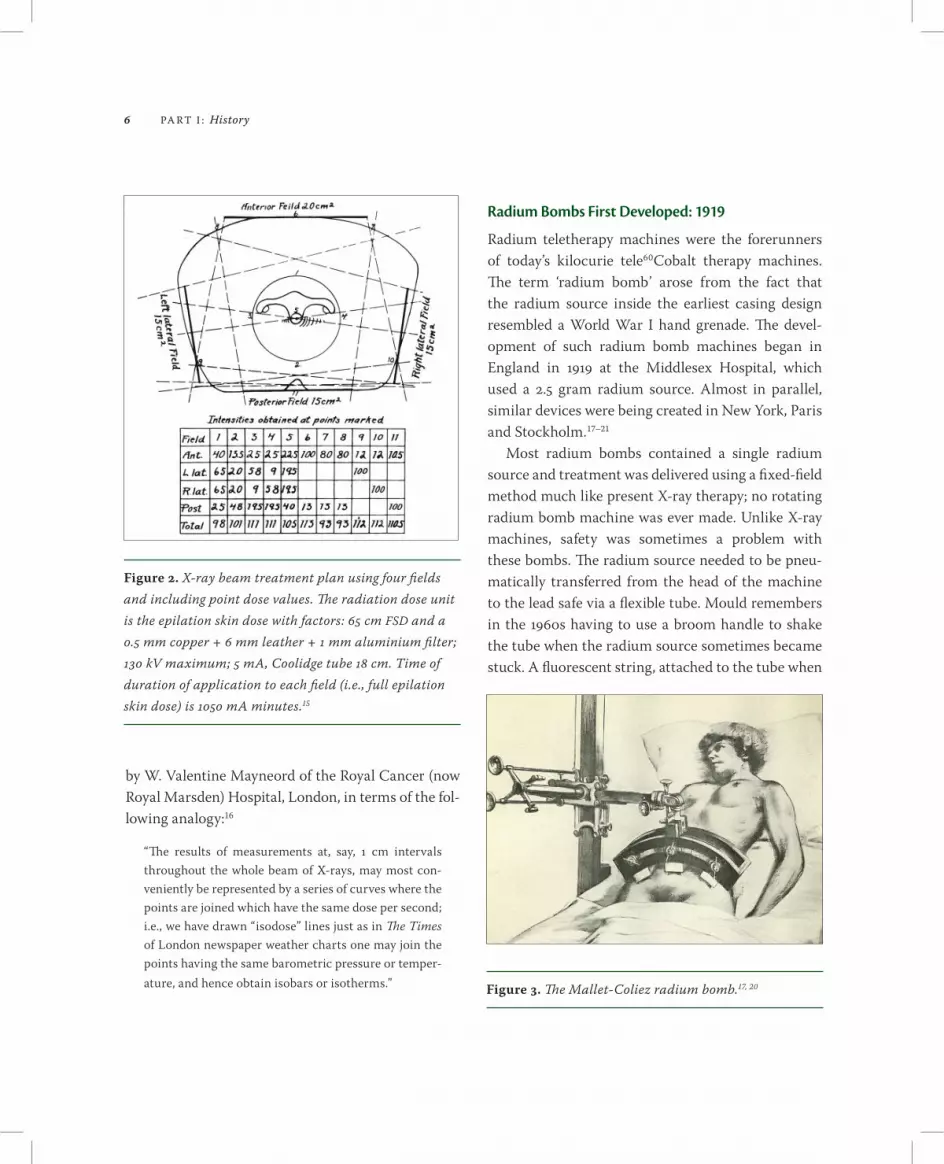
The quantity of radiation administered to a patient was first depicted as a series of point doses of which Figure 2 is probably the earliest example in any American or European radiological journal. 15 Although published in 922, this figure was made in Chicago in 99. The pelvic tumor volume is depicted by the central circle with intensity dose points , 2, 3 and 4 on its periphery and dose point 5 at its center. The primary clinical objective was to achieve a homo-geneous radiation intensity throughout this volume: 98–0%. However, it can also be seen that regions outside the targeted region received a similar thera-peutic dose of radiation.
Isodose curves, which have formed the basis for presentation of dose distributions for more than 70 years, were first proposed in 920 by Otto Glasser when he was working in Freiburg, Germany. Later he would immigrate to the USA and become the Director of the Radiation Research Department of the Cleveland Clinic Foundation.
With the acuity of hindsight, it now seems a simple idea to join points of equal intensity, but it cannot always have been so obvious when only low energy X-rays were available for therapy. Nevertheless, the concept soon found widespread adoption, and in 929, the intuitive nature of isodose curves was explained
6 PA RT I : History
by W. Valentine Mayneord of the Royal Cancer (now Royal Marsden) Hospital, London, in terms of the fol-lowing analogy:16
“The results of measurements at, say, cm intervals throughout the whole beam of X-rays, may most con-veniently be represented by a series of curves where the points are joined which have the same dose per second; i.e., we have drawn “isodose” lines just as in The Times of London newspaper weather charts one may join the points having the same barometric pressure or temper-ature, and hence obtain isobars or isotherms.”
Radium Bombs First Developed: 1919
Radium teletherapy machines were the forerunners of today’s kilocurie tele60Cobalt therapy machines. The term ‘radium bomb’ arose from the fact that the radium source inside the earliest casing design resembled a World War I hand grenade. The devel-opment of such radium bomb machines began in England in 99 at the Middlesex Hospital, which used a 2.5 gram radium source. Almost in parallel, similar devices were being created in New York, Paris and Stockholm. 17–21
Most radium bombs contained a single radium source and treatment was delivered using a fixed-field method much like present X-ray therapy; no rotating radium bomb machine was ever made. Unlike X-ray machines, safety was sometimes a problem with these bombs. The radium source needed to be pneu-matically transferred from the head of the machine to the lead safe via a flexible tube. Mould remembers in the 960s having to use a broom handle to shake the tube when the radium source sometimes became stuck. A fluorescent string, attached to the tube when
Figure 2. X-ray beam treatment plan using four fields and including point dose values. The radiation dose unit is the epilation skin dose with factors: 65 cm FSD and a 0.5 mm copper + 6 mm leather + mm aluminium filter; 30 kV maximum; 5 mA, Coolidge tube 8 cm. Time of duration of application to each field (i.e., full epilation skin dose) is 050 mA minutes.15
Figure 3. The Mallet-Coliez radium bomb.17, 20

CHAPTER 1: Historical Vignette on Radiation Cross-Fire: Paris 905 to Stanford University 994 7
the source transfer took place, would often look like a moving glow-worm or firefly!
The machine in Figure 3 is a French design for cross-fire using three radium sources—not one. Each of the three applicators held a number of 0 mg radium tubes and for “continued and prolonged irradiation” 00–200 mg was recommended per applicator. The apparatus weighed 33 kg and was sup-ported by a tube stand of the kind ordinarily used in radiology.20 In 930 the design was modified to carry 8 radium applicators. 17 This represented the maxi-mum available number of cross-fire positions until the development of the Gamma Knife.
Analog Computing Begins for Cross-Fire Planning: 1922
Portal Selector
The device known as a portal selector was almost certainly the first example of an analog computing device for X-ray cross-fire beams: 22
“In an attempt to increase the accuracy and the safety of cross-firing and portal plotting, a graphic method has been devised called a portal selector device. It consists of a box illuminated with electric bulbs from beneath. Over it is placed a translucent plate of glass upon which are printed certain geometrical figures, squares, trian-gles, points and circles, which are used as signals. They are printed in one color with the different symbols in percentages of strength of color, the circles being darker than the points, the points darker than the squares and the triangles showing the lightest.
A drawing is made with a wax pencil upon a glass plate representing a cross-section of the body and showing the location of the organs and the location of the growth. This is now placed over the illuminated plate on which the symbols are printed. There are a series of celluloid dummies representing the beam of X-rays produced at different voltages and through dif-ferent values of filters at different distances from the
body and of different dimensions of field, on which are shown the percentage depth dose at varying depths by decreasing intensity of color starting with 00% at the surface. They are calculated at depth dose percentages of 5%, 20%, 25%, 30%, etc., each percentage depth dose having a number of dummies.
They are stained with the same color as the symbols printed upon the plate, and when two or more of these dummies are laid upon the diagram in such as way as to cover the lesion, one observes whether the different symbols are visible or whether they have become invis-ible, when viewed through the superimposed celluloid films. The triangles disappear when 30–40% of the standard skin dose is reached in the color values of the dummies. The quadrangles disappear at 60–70% of the standard skin dose and the points at 05–5%, and all the figures are invisible at 35%.
The danger signals which are represented by the dots should at all times be visible. When they are no longer visible, then the dose has exceeded 35% of the standard skin dose and represents an amount of radia-tion which will cause a burn.” 23
Light Boxes
Analog computers using light boxes were standard dose computation equipment until digital computers became generally available in hospital physics depart-ments in the late 960s. The individual beams usually were represented by isodose curves from 0–00% in intervals of 0%, with the curves drawn in different colors. For a three-field technique, the first two beams would be added together and the next stage would be to add the third beam to the composite formed by the first two.24
The initial Holfelder idea of symbols for the portal selector 23 was discarded by 925 , but the basic con-cept of the light box continued for more than 50 years. In the 2st century "light box planning" is obso-lete, except for teaching purposes. This device can be useful in teaching students of therapeutic radiation that treatment planning computations are more than
8 PA RT I : History
just pressing a button and activating sophisticated computer software whose underlying background they do not fully understand.
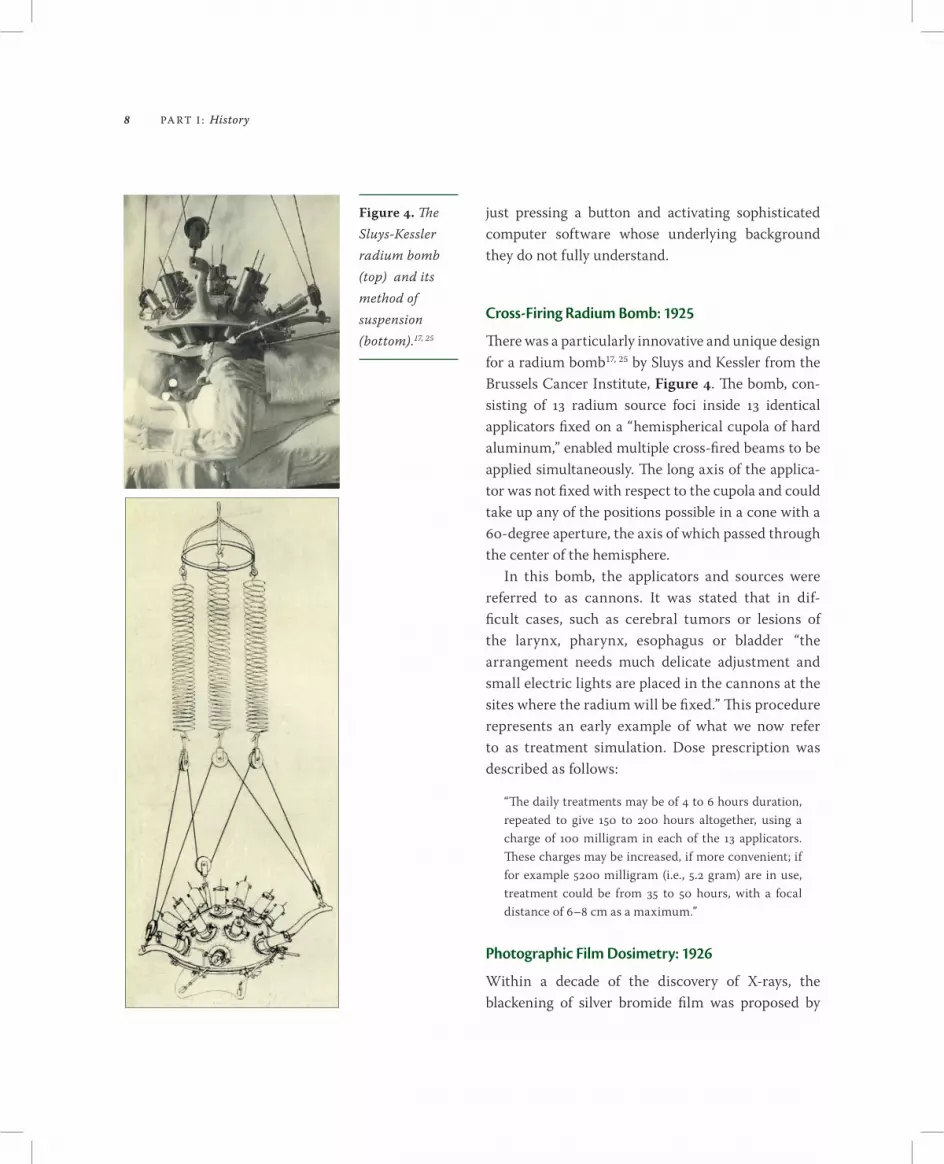
Cross-Firing Radium Bomb: 1925
There was a particularly innovative and unique design for a radium bomb 17, 25 by Sluys and Kessler from the Brussels Cancer Institute, Figure 4. The bomb, con-sisting of 3 radium source foci inside 3 identical applicators fixed on a “hemispherical cupola of hard aluminum,” enabled multiple cross-fired beams to be applied simultaneously. The long axis of the applica-tor was not fixed with respect to the cupola and could take up any of the positions possible in a cone with a 60-degree aperture, the axis of which passed through the center of the hemisphere.
In this bomb, the applicators and sources were referred to as cannons. It was stated that in dif-ficult cases, such as cerebral tumors or lesions of the larynx, pharynx, esophagus or bladder “the arrangement needs much delicate adjustment and small electric lights are placed in the cannons at the sites where the radium will be fixed.” This procedure represents an early example of what we now refer to as treatment simulation. Dose prescription was described as follows:
“The daily treatments may be of 4 to 6 hours duration, repeated to give 50 to 200 hours altogether, using a charge of 00 milligram in each of the 3 applicators. These charges may be increased, if more convenient; if for example 5200 milligram (i.e., 5.2 gram) are in use, treatment could be from 35 to 50 hours, with a focal distance of 6–8 cm as a maximum.”
Photographic Film Dosimetry: 1926
Within a decade of the discovery of X-rays, the blackening of silver bromide film was proposed by
Figure 4. The Sluys-Kessler radium bomb (top) and its method of suspension (bottom).17, 25

CHAPTER 1: Historical Vignette on Radiation Cross-Fire: Paris 905 to Stanford University 994 9
Robert Kienböck of Vienna as the basis for a unit of measurement for X-ray dosage. The density of the radiation- exposed film was compared to an arbitrary scale of blackening and the measurement recorded in X units. The small pieces of film, ‘Kienböck strips,’ were placed on the patient’s skin. 26
Photographic film blackening was later used for radium bomb dosimetry, and Figure 5 shows a “pho-tograph of three converging beams produced by the Mallet-Coliez apparatus,” 17 which is in Figure 3. The film density is white fading to grey; it is clearly seen that the maximum dose for the combined three beam cross-fire technique occurs at the surface and not at the depth at which the three beams cross.
Radium Cross-Fire for Cerebral Tumors: 1931
An example of cross-fire treatment of a cerebral tumor using several radium sources is shown in Figure 6 and was a typical treatment of the 930s. It was described as follows: 17
“Radium therapy gives good results in certain cerebral tumors. Gliomata are specially sensitive to irradia-tion, but the use of radium must always be preceded by decompression. Radium is indicated if operative removal has been incomplete, or in cases where, after decompression, the growth has been found difficult to access. A moulded apparatus should be used, either by cross-fire, or by an apparatus in the shape of a crown or helmet. Dosage may be pushed to the limits of radio-dermatitis.”
Radiation Therapy: 1940s–1980s
By the latter part of the 940s, treatment plans had become relatively standardized for orthovoltage (also termed deep X-ray) therapy. Although a few machines operated as high as 400 kV, the prevail-ing X-ray energy at that time was 200–250 kV using 50 cm FSD applicator-defined or light field-defined beams. Multiple field irradiation was often utilized,
Figure 5. Photographic film dosimetry for the radium bomb in Figure 3. 17
Figure 6. Surface applicator for treatment of a cerebral tumor using multiple radium sources for cross-firing.17

0 PA RT I : History
but seldom exceeded four beams. The exception was for esophageal cancer, where six fields could be used. With the emergence of such X-ray machines, radium bombs with an SSD of only 8–0 cm were largely rel-egated to the treatment of head and neck tumors.
By the 960s, radium had been replaced by large kilocurie sources of 60Cobalt in teletherapy devices, and in doing so the SSD was increased to 70 cm, 80 cm or even 00 cm. However, not long afterward, the introduction of linear accelerators would change the entire scope of modern radiation oncology—that is, everywhere but in Stockholm, where Leksell’s surgi-cal instrument for cross-fired 60Co irradiation was
just getting started. 3–6, 27, 28 After initial tests of his "radiosurgical" method using a narrow proton beam in the Physics Department of Uppsala University, the first apparatus for clinical use was designed and built for the Karolinska Institute,29, 30 Figure 7.
Recycling the Past: Stanford 1994
Our historical vignette ends with the clinical introduc-tion of the first CyberKnife at Stanford in 994 .1, 31–36 The contemporary world of radiation delivery has been shaped by dozens of technical developments, such as the arrival of higher energy X-ray sources, modern computerized imaging and treatment plan-ning, sophisticated algorithms for dose calculation, etc. Despite all this technical ferment, there has been virtually no more recurrent and enduring theme in therapeutic irradiation than the principle of cross-fire. 2 The invention of the CyberKnife builds on this legacy.
In an increasingly more powerful world of com-puters and robotics, the CyberKnife promises to take the cross-fire concept to an ever-greater level of sophistication. Instead of today’s starting point of 200 cross-firing beams, it is well within the realm of the future CyberKnife to bring physicians unlimited numbers of beams. By recognizing this potential, ever-greater dose conformality will become an everyday reality. As embodied by the CyberKnife, continued technical progress has meant that the clinical scope of radiation delivery is also rapidly outgrowing its core application of cancer radiotherapy. In fact, Wickham & Degrais’ early 20th century description of using cross-fired radium gamma-ray beams to treat sciatic neuralgia may soon in the 2st century appear prescient. The CyberKnife must be considered an important contemporary development in medicine. The following chapters will demonstrate the signifi-cant impact this advance is now having on surgery and radiation medicine.
Figure 7. Sketch of the prototype for the Leksell Gamma Knife. () Protective housing. (2) In all, 279 60Cobalt sources, mm diameter, distributed over a spherical sector. (3) Primary collimators. (4) Secondary collimators (exchangeable) mounted on treatment table. (5) Sliding treatment table with stereotactical adjustment of patient position. (6) Folding protection barrier. Courtesy: Rune Walstam.30

CHAPTER 1: Historical Vignette on Radiation Cross-Fire: Paris 905 to Stanford University 994
References
. Guthrie BL, Adler JR. Computer-assisted pre-operative planning, interactive surgery, and frameless stereo-taxy. In: Selman W, ed. Clinical Neurosurgery, Vol. 38, Baltimore: Williams & Wilkins, 99, 2–3.
2. Wickham L, Degrais P. Radiumtherapy. English trans. Dore SE. London: Cassell, 90.
3. Leksell L. A stereotaxic apparatus for intracranial sur-gery. Acta Chir Scand 949;99:229–233.
4. Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand 95;02:36–39.
5. Leksell D. Lars Leksell—an historical vignette. In: Steiner L, ed. Radiosurgery: Baseline and Trends. New York: Raven Press, 992, 257–26.
6. Leksell L. Brain fragments [Hjärn fragment, Stockholm: Norstedts, trans. from Swedish, Steiner M]. In: Steiner L, ed. Radiosurgery: Baseline and Trends. New York: Raven Press, 992, 264–292.
7. Röntgen WC. Ueber eine neue Art von Strahlen [Vorläufige Mittheilung]. Sitzungsberichte der Physikal-ische-medizinischen Gessellschaft zu Würzburg 895;9:32–4. [Reprinted in English: On a new kind of rays: preliminary communication. See Mould RF. Röntgen and the discovery of X-rays. Br J Radiol 995;68:45–76.]
8. Röntgen WC. Ueber eine neue Art von Strahlen [2. Mittheilung]. Sitzungsberichte der Physikalische-medi-zinischen Gessellschaft zu Würzburg 896;2:–7.
9. Becquerel H. Sur les radiations invisibles émises par les corps phosphorescents. Comptes Rendus de l’Académie des Sciences, Paris 896;22:50–503.
0. Curie P, Curie M, Bémont G. Sur une nouvelle substance fortement radio-active contenue dans la pechblende. Comptes Rendus de l’Académie des Sciences, Paris 898;27:25–28. [See also Mould RF. The discovery of radium in 898 by Maria Sklodowska-Curie (867–934) and Pierre Curie (859–906) with a commentary on their life and times. Br J Radiol 898;7:229–254.]
. Becquerel H, Curie P. L’action physiologique des rayons du radium. Comptes Rendus de l’Académie des Sciences, Paris 90;32:289–29.
2. Danlos H, Bloch E. Note sur le traitement du lupus erythemateux par des applications du radium. Ann Dermatol et Syphilog 90;2:986–988.
3. Knox R, Caulfield A. A new therapeutic X-ray localiser. Archives of Radiol & Electrotherapy [Archives of the Roentgen Ray] 95–6;20:76–83.
4. Wickham L, Degrais P. Radium–As Employed in the Treatment of Cancer, Angiomata, Kloids, Local Tuberculosis and Other Affectations. New York: Paul B Hoeber, 93.
5. Schmitz H. Technique and statistics in the treatment of carcinoma of the uterus and contiguous organs with the combined use of radium and X-rays. Am J Roentgenol 922;9:662–670.
6. Mayneord WV. The Physics of X-ray Therapy. London: J & A Churchill, 929, 3.
7. Union Minière du Haut Katanga [Radium Department]. Radium: Production, General Properties, Its Applications in Therapeutics, Apparatus. Brussels: Union Minière du Haut Katanga, 93.
8. Medical Research Council. Medical Uses of Radium. MRC Special report series 62. London: MRC, 922.
9. Lysholm E. Apparatus for the production of a narrow beam of gamma-rays in treatment by radium at a dis-tance. Acta Radiol 923;2:56.
20. Mallet L, Coliez R. Techniques de curiethérapie pro-fonde. Br J Radiol [BIR Section] 926;3:393.
2. Laborde S. La Technique de la Curiethérapie. Paris: Gauthier-Villars, 933.
22. Holfelder HG. Deep radiotherapy in malignant tumors and tuberculosis. Strahlenther 922;3 (2).
23. Holzknecht G. Dosage formula and dosage table. In: Hirsch S. The Principles and Practice of Roentgen Therapy. New York: American X-ray Publishing Company, 925.

2 PA RT I : History
24. Mould RF. Radiotherapy Treatment Planning. Medical physics handbook 7. Bristol: Adam Hilger, 98.
25. Sluys F, Kessler E. Gammathérapie. Le Cancer 925; 2:88–07 and 50–76.
26. Kienböck R. Ueber Dosimeter und das quantrimetrische Verfahren. Fortschr Geb Röntgenstrahlen 905;9:276.
27. Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chirurg Scand 95;02:36–39.
28. Leksell L. Stereotaxis and Radiosurgery. Springfield: Charles C Thomas, 97.
29. Larsson B, Lidén K, Sarby B. Irradiation of small structures through the intact skull. Acta Radiol Ther 974;3:52–534.
30. Walstam R. A historical review on radiotherapeu-tic applications. In: Bernier J. 895–995 Radiation Oncology: A Century of Progress and Achievement.Leuven: European Society for Therapeutic Radiology & Oncology (ESTRO), 995, 9–46.
3. Adler JR. Frameless radiosurgery. In: Goetsch SJ, De Salles AA, eds. Stereotactic Surgery and Radiosurgery. Madison: Medical Physics Publishing, 993, 237–248.
32. Adler JR, Schweikard A, Tombropoulos R et al. Modeling and planning for sensor based intelligent robot systems. In: Selman W, ed. Image-Guided Robotic Radiosurgery. Baltimore: World Scientific Publishing Company, 995, 460–470.
33. Adler JR, Cox RS. Preliminary experience with the CyberKnife: image-guided stereotactic Radiosurgery. In: Alexander E, Kondziolka D, Loeffler JS, eds. Radiosurgery. Basel: S Karger, 996, 2–3.
34. Adler JR, Chang SD, Murphy MJ et al. The CyberKnife: a frameless robotic system for radiosurgery. Stereotact Func Neurosurg 997;69:24–28.
35. Adler JR, Schweikard A, Murphy M et al. Image-guided stereotactic radiosurgery: the CyberKnife. In: Barnett G, Roberts D, Macunias R, eds. Image-Guided Neurosurgery: Clinical Applications of Interactive Surgical Navigation. St Louis: Quality Medical Publishing Inc, 998, 93–204.
36. Adler JR, Murphy MJ, Chang SD et al. Image-guided robotic radiosurgery. Neurosurg 999;44:299–307.
37. Souttar HS. Radium and Its Surgical Applications. London: Heinemann, 929.
Angioma of meninges treated using radium needles in 929.37
Copyright © 2022 FDOKUMEN