
Capecitabine and Oxaliplatin for Advanced Esophagogastric Cancer
Upload
uni-heidelbergCategory
view
0download
0
CLINICAL INVESTIGATION Rectum
CETUXIMAB IN COMBINATION WITH CAPECITABINE, IRINOTECAN, ANDRADIOTHERAPY FOR PATIENTS WITH LOCALLY ADVANCED RECTAL CANCER:
RESULTS OF A PHASE II MARGIT TRIAL
KAROLINE HORISBERGER, M.D.,* ANNE TRESCHL, M.D.,y SABINE MAI, M.D.,z
MANUEL BARRETO-MIRANDA, M.D.,y PETER KIENLE, M.D.,* PHILIPP STROBEL, M.D.,x
PHILIPP ERBEN, M.D.,y CHRISTOPH WOERNLE, M.D.,* DIETMAR DINTER, M.D.,{ GEORG KAHLER, M.D.,k
ANDREAS HOCHHAUS, M.D.,y STEFAN POST, M.D.,* FRANK WILLEKE, M.D.,*** FREDERIK WENZ, M.D.,z
AND RALF-DIETER HOFHEINZ, M.D.,y ON BEHALF OF THE MARGIT (MANNHEIMER ARBEITSGRUPPE FUR
GASTROINTESTINALE TUMOREN)
*Chirurgische Klinik und Poliklinik, yOnkologisches Zentrum, III. Medizinische Klinik, zKlinik fur Strahlentherapie undRadioonkologie, x Institut fur Pathologie, { Institut fur Radiologie und Nuklearmedizin, kSektion fur Chirurgische Endoskopie,
Medizinische Fakultat Mannheim der Universitat Heidelberg, Germany; and **Chirurgische Klinik, Marienhospital Siegen, Germany
Purpose: To evaluate the safety and efficacy of preoperative radiotherapy (RT) in combination with cetuximab,capecitabine, and irinotecan in patients with locally advanced rectal cancer.Methods and Materials: Patients with rectal cancer (clinical stage T3/4 or N+) were scheduled to receive cetuximab(400 mg/m2 Day 1, 250 mg/m2 Days 8, 15, 22, 29) in combination with weekly irinotecan 40 mg/m2 and capecitabine500 mg/m2 twice daily (Days 1–38). RT was given to a dose of 50.4 Gy (45 + 5.4 Gy). Primary endpoint was toxicity,and antitumor activity as assessed by the pathologic complete remission (pCR) rate was a secondary endpoint.Results: Fifty patients were enrolled; 88% showed T3 or T4 and 76% nodal-positive tumors with a median distancefrom the anal verge of 7.5 cm. The actual dose intensity was as follows (median/mean, %): cetuximab 100/92, iri-notecan 100/91, capecitabine 100/89). Main adverse events Grades 2/3/4 were (National Cancer Institute commontoxicity criteria version 3.0, %): leukocytopenia 6/2/2, nausea/vomiting 4/2/0, diarrhea 34/30/0, proctitis 26/2/0,elevation of liver transaminases 8/10/0, and acnelike skin rash 46/6/0. All patients underwent surgery, and no post-operative deaths occurred. Eighty-four percent underwent low-anterior resection, and 68% of the specimenexhibited moderate or good tumor regression, but only 4 patients had a pCR.Conclusion: Preoperative chemoradiation with cetuximab-CapIri-RT has manageable toxicity, with diarrheabeing the most commonly observed adverse event. Nevertheless, the efficacy of this regimen with a pCR rate ofonly 8% was significantly lower than that observed in a previous Phase I trial. � 2009 Elsevier Inc.
Capecitabine, Cetuximab, Chemoradiotherapy, Irinotecan, Rectal cancer.
Int. J. Radiation Oncology Biol. Phys., Vol. 74, No. 5, pp. 1487–1493, 2009Copyright � 2009 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/09/$–see front matter
doi:10.1016/j.ijrobp.2008.10.014
INTRODUCTION
Advances in surgery have significantly improved the progno-
sis of rectal cancer. Despite optimized resection techniques
including total mesorectal excision (TME), preoperative
radiotherapy (RT) further reduces local recurrence rates with-
out improving overall survival (1). On the basis of the results
of 3 randomized trials neoadjuvant 5-fluorouracil-(5-FU)-
based chemoradiotherapy is regarded as a standard of care
for locally advanced rectal tumors (2–4). In these trials the
rates of local recurrences in patients undergoing 5-FU-based
preoperative treatment ranged between 6% and 8%, but
Reprint requests to: Ralf-Dieter Hofheinz, M.D., OnkologischesZentrum, III. Medizinische Klinik, Universitatsklinikum Mannheimder Universitat Heidelberg, Theodor-Kutzer-Ufer 1-3, D-68135Mannheim, Germany. Tel: (+49) 621-3832854; Fax: (+49) 621-832488; E-mail: [email protected]
14
distant metastases represented the most common site of
treatment failure in approximately 35%–40% of the patients
(2–4).
Thus far, the biomodulation of 5-FU (5), the combination
of 5-FU with older cytostatics (e.g., semustine) (6), and the
prolongation of chemotherapy (7) have not improved dis-
ease-free or overall survival. Newer drugs such as irinotecan
or oxaliplatin are expected to improve treatment results. For
instance, the safety of irinotecan in combination with 5-FU or
its pro-drug capecitabine during chemoradiotherapy has been
investigated in several Phase II trials (8–15). Summarizing
Anne Treschl and Karoline Horisberger contributed equally tothis study.
Conflict of interest: none.Received Aug 13, 2008, and in revised form Sept 10, 2008.
Accepted for publication Oct 1, 2008.
87

1488 I. J. Radiation Oncology d Biology d Physics Volume 74, Number 5, 2009
the data from these trials, the rate of pathologic complete re-
missions (pCR) using irinotecan/5-FU-based combinations
appears to be at least twice as high as in 5-FU-based regimens
(approximately 8% in trials with quality-controlled pathol-
ogy) (8–15).
The pCR rate has been identified as a prognostic factor for
patients undergoing neoadjuvant chemoradiation for rectal
cancer (16, 17), and the long-term outcome of patients exhib-
iting pCR is favorable (local relapse rate 1.6%, 5-year cancer-
specific survival 94%) (18). Two-drug regimens were shown
to be associated with higher pCR rates in an analysis of sev-
eral trials including a total of 3,157 patients (19). Therefore
increasing pCR rates is of major interest because it may
also improve long-term results.
Biological factors and molecular targeted agents have
a growing role in the treatment of colorectal cancer. Cetuxi-
mab, an antibody targeting the epidermal growth factor
receptor (EGFR), was initially used as treatment for chemo-
therapy-refractory colorectal cancer (20) and is now also
considered first-line treatment for patients with metastatic
colorectal cancer in combination with chemotherapy (21).
Overexpression of EGFR is a negative prognostic factor
and is associated with resistance to radiotherapy (22, 23).
Therefore, EGFR has emerged as a promising target in radio-
oncology. In head and neck cancer, the addition of cetuximab
to RT resulted in superior outcomes with respect to locore-
gional failure and survival (24). In retrospective analyses, pa-
tients with EGFR expressing rectal cancer undergoing
neoadjuvant RT had a significantly lower disease-free sur-
vival and a lower chance of pCR (25). Thus, there is a clear
rationale to combine cetuximab with radiochemotherapy for
rectal cancer.
We have previously established a dosing regimen for ce-
tuximab in combination with capecitabine and irinotecan-
based chemoradiotherapy (cetuximab-CapIri-RT) (26). The
preliminary efficacy in 20 patients included in this Phase I
trial was promising with 5 patients exhibiting pCR. The ob-
jective of the present Phase II trial was to assess the tolerabil-
ity (primary endpoint) and efficacy (secondary endpoint) of
the cetuximab-CapIri-RT regimen in a larger cohort of
patients.
METHODS AND MATERIALS
The protocol was reviewed and approved by the institutional
review board, and the study was performed according to the
Declaration of Helsinki. All patients provided written informed
consent.
Patients eligibility criteriaPatients with histologically confirmed, locally advanced nonme-
tastatic rectal adenocarcinoma (cT3/4, or cN+ [nodal positivity as
determined by transrectal ultrasonography]; 0–16 cm distance
from anal verge as measured by rigid rectoscopy) were eligible.
We classified every visible lymph node in the transrectal ultrasound
as positive. Cases in which the probe could not pass the tumor com-
pletely were regarded as uTx uNx. In these patients, the cT cN stag-
ing was determined by magnetic resonance imaging (MRI).
Otherwise, we continued the transrectal ultrasound examination
up to the aortic bifurcation to visualize the iliac and mesorectal
lymph nodes as well. Positive EGFR staining was not required. Fur-
ther inclusion criteria were as follows: Eastern Cooperative Oncol-
ogy Group (ECOG) performance status #2; age $18 years;
adequate bone marrow (leukocyte count >3,000/mL, platelet count
>100,000/mL), renal (serum creatinine #1.4 mg/dL or creatinine
clearance >60 mL/min), and hepatic function (bilirubin #2 mg/
dL). Patients with a history of Gilbert-Meulengracht’s disease
were excluded. Patients of childbearing potential were required to
be using contraception. Patients were excluded if they suffered
from other cancers or had known hypersensitivity to 5-FU, irinote-
can, or cetuximab.
Pretreatment evaluationAll patients underwent a complete history, physical examination,
digital rectal examination, rigid rectoscopy with biopsy, transrectal
ultrasonography, pelvic and abdominal computed tomographic (CT)
scans, MRI, colonoscopy, and chest X-rays. A full blood count with
differential and serum chemistry (including blood electrolytes, cre-
atinine, urea, uric acid, liver transaminases, alkaline phosphatase, to-
tal bilirubin, and lactic dehydrogenase) was obtained before the start
of treatment. Weekly blood counts and serum chemistry every 3
weeks were scheduled during chemoradiotherapy or whenever clin-
ically indicated.
RadiotherapyRT was delivered with a linear accelerator using 18–23 MeV
photons and a three-field box technique consisting of a poste-
rior-anterior and 2 lateral fields. A total dose of 50.4 Gy was given
in daily fractions of 1.8–Gy, 5 days a week. The clinical target
volume (CTV) included the sacrum, the presacral space, and the
posterior wall of the bladder and prostate or vagina. The common
iliac lymph nodes were included in the CTV. The upper border of
the CTV was at the L5–S1 interspace for cN0 and at L4–L5 for
cN+ patients. The lower field border was 5 cm below the macro-
scopic tumor. After a dose of 45 Gy, an additional dose of 5.4 Gy
was given to the boost volume using a shrinking field technique.
To keep the boost volume as large as possible, it was defined as
the initial CTV minus the small bowel as identified on the treat-
ment planning CT or on simulation films after oral contrast admin-
istration in prone position using a belly board. The maximal dose
to small bowel was limited to 46 Gy, accepting potential under-
dosages to small parts of the gross tumor volume in tumors of
the upper third.
Preoperative chemo- and antibody therapy (cetuximab-CapIri regimen)
Starting at Day 1 of RT, patients received weekly cetuximab (400
mg/m2 Day 1 and 250 mg/m2 Days 8, 15, 22, 29; 2 hours before ir-
radiation), weekly irinotecan (40 mg/m2 Days 1, 8, 15, 22, 29;
1 hour before irradiation), and capecitabine orally twice daily (500
mg/m2 twice daily Days 1–38). All patients received standard anti-
emetic prophylaxis using 5-HT3 antagonists and dexamethasone.
If a patient experienced one of the following adverse events
according to National Cancer Institute common toxicity criteria
(version 3.0) at the day of planned irinotecan application, chemo-
therapy was interrupted until adverse events had resolved to Grade
0 or 1: leukocytopenia Grade $2, thrombocytopenia Grade $2,
diarrhea Grade $2, mucositis/stomatitis Grade $2, skin toxicity
Grade $2, other adverse events Grade >2. Treatment was resumed
with a dose reduction of 25% for either drug. Cetuximab dosing

Phase II study with cetuximab and CapIri-RT in rectal cancer d K. HORISBERGER et al. 1489
remained identical. In case of adverse events Grade $2 in the inter-
val between irinotecan applications, we suggested interruption of
chemotherapy and dose reduction of both drugs of 25%. On the sec-
ond occurrence of adverse events Grade $2, the chemotherapy dose
was reduced by 50%.
Every effort was made to continue RT without interruption. The
RT schedule was not modified unless an adverse event Grade $2
was clearly related to radiation. In these cases, RT was withheld
until adverse events resolved to Grades 0 or 1.
Surgery and histopathologySurgical resection with TME was scheduled 4–6 weeks after com-
pletion of chemoradiotherapy. Pathological examination of the
specimen involved opening the specimen, identification of the for-
mer tumor-bearing area, and macroscopic description followed by
fixation in 10% neutral buffered formalin for 24 h. After fixation,
specimens were processed according to standard protocols (27).
For obvious residual tumor, at least 4 paraffin blocks were pro-
cessed. If no obvious residual tumor was present, the former tu-
mor-bearing area was sliced and embedded. The completion of
TME, circumferential resection margins, proximal and distal tu-
mor-free margins, tumor mass, fibrotic changes, and irradiation vas-
culopathy were evaluated. Grades of histopathologic regression
were described as defined by the Japanese Society for Cancer of
the Colon and Rectum (JSCCR) (28). Tumors were classified as
good responders when assigned tumor regression Grades 2 or 3
(TRG 2 or TRG 3) and as bad responders in regression Grades
0 or 1 (TRG 0 or TRG 1).
Study design, definitions, and endpointsThe main focus of this Phase II study was to assess the toxicity
(primary endpoint) and efficacy (tumor regression using the JSCCR
grading; secondary endpoint) of the cetuximab-CapIri-RT regimen.
The statistical calculation was made on toxicity issues and was
based on the dose-limiting toxicities (DLT). DLT was defined by
the occurrence of one of the following adverse events: Grade 4 leu-
kocytopenia/neutropenia or thrombocytopenia, symptomatic throm-
bocytopenia, Grade 3/4 febrile neutropenia, diarrhea Grade 3 lasting
for $72 hours despite adequate treatment, or any other Grade $3
nonhematological adverse events except renal adverse events
(Grade $2), nausea/vomiting, and acnelike skin rash. We deter-
mined that the rate of DLTs during this Phase II trial should have
been lower than 17% (i.e., approximately one in six patients).
With a total of 47 patients, a rate of at least 83% of patients experi-
encing no DLTs during radiochemotherapy can be assumed with
a power of 80% and an alpha value of 0.2 if fewer than 8 of 47
patients experienced DLTs.
RESULTS
Fifty patients entered this single-center trial between
March 2006 and February 2008. Patient characteristics are
listed in Table 1. The median age of the patients was 57 years
(range, 33–80 years). All but one patient with a local relapse
had newly diagnosed rectal adenocarcinoma. The median
distance from the lower border of the primary to the anal
verge was 7.5 cm.
Safety and dose intensityAll patients were evaluable for toxicity analysis. No treat-
ment-related deaths occurred, and only 1 patient developed
a Grade 4 toxicity according to National Cancer Institute
common toxicity criteria (leukocytopenia). Adverse events
observed during chemoradiation are listed in Table 2. Diar-
rhea was the most commonly observed toxicity with 15 pa-
tients (30%) developing Grade 3 diarrhea. The median time
to onset of Grade 3 diarrhea was 22 days calculated from
the start of chemoradiation (range, 12–33 days). In 7 patients,
diarrhea Grade 3 lasted <72 hours, but eight patients had di-
arrhea Grade 3 lasting $72 hours despite adequate treatment
using loperamide and oral fluid intake. These patients were
hospitalized for safety reasons and rehydrated. The median
hospital stay of these patients was 7.5 days (range, 5–11
days). No patient developed renal failure as a consequence
of diarrhea. Acnelike skin rash Grades 2 or 3 was seen in
approximately half of the patients.
Hematologic toxicity was mild with only 5 patients
developing Grade 2–4 leukocytopenia. No episode of neutro-
penic fever was reported, and no patient received prophylac-
tic or therapeutic granulocyte colony-stimulating factors
during chemoradiotherapy. The median decrease of the he-
moglobin level was 1.4 g/dL (range, 0–5.6 g/dL), but Grade
4 anemia or major bleeding was not observed. No prophylac-
tic recombinant human erythropoetin was given and no blood
transfusions were required during chemoradiation.
In all, 8 patients (16%) had DLTs. All DLTs (diarrhea $72 h,
n = 8; elevation of liver transaminases, n = 5; elevation of
bilirubin, n = 1; abdominal pain, n = 1; proctitis, n = 1; leuko-
cytopenia, n = 1) were observed in these 8 patients.
Table 1. Patient and tumor characteristics (n = 50)
Age (years)Median 57Range 33–80
SexMale 33 (66)Female 17 (34)
ECOG performance status0 34 (68)1 16 (32)
CEAMedian (mg/L) 2.4Range 0.4–50.3
CA 19-9 (kU/L)Median 10Range 1–298
Clinical stage*cT2 5 (10)cT3 42 (84)cT4 2 (4)Local relapse 1 (2)cN0 13 (26)cN+ 37 (74)
Lower tumor margin to anal verge distance (cm)Median 7.5Range 1–13
Abbreviations: CA = cancer antigen; CEA = carcinoembryonicantigen. ECOG = Eastern Cooperative Oncology Group.
Data presented as number of patients, with percentage in paren-theses, unless otherwise noted.
* As determined by transrectal ultrasonography and magnetic res-onance imaging.
1490 I. J. Radiation Oncology d Biology d Physics Volume 74, Number 5, 2009
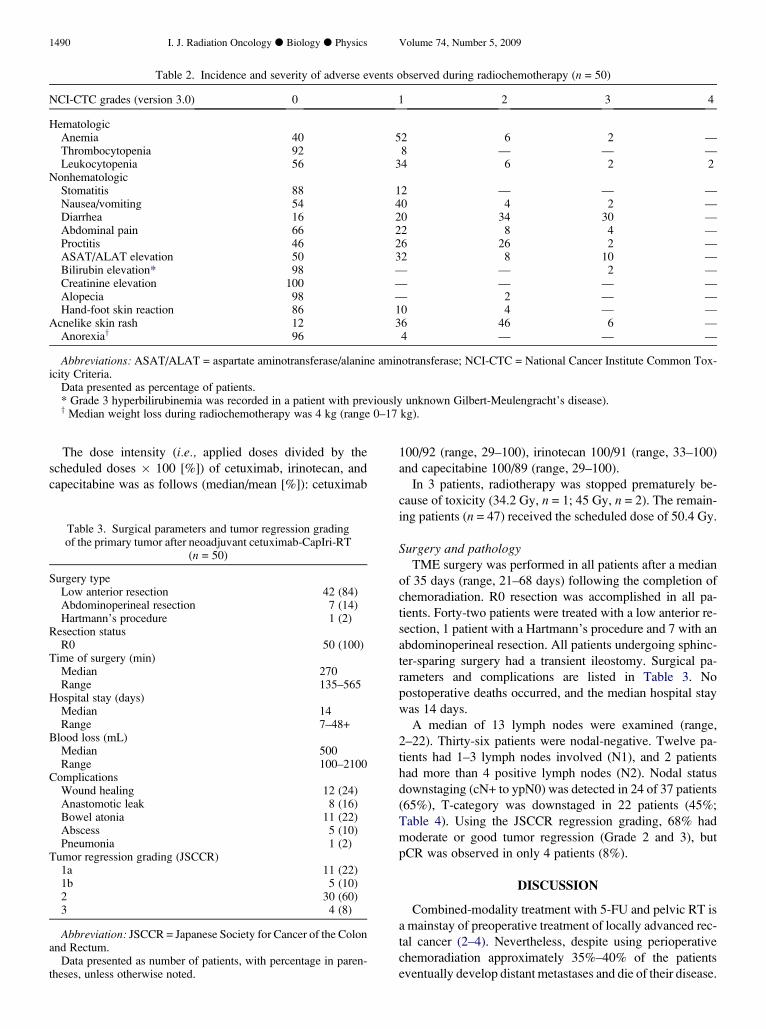
Table 2. Incidence and severity of adverse events observed during radiochemotherapy (n = 50)
NCI-CTC grades (version 3.0) 0 1 2 3 4
HematologicAnemia 40 52 6 2 —Thrombocytopenia 92 8 — — —Leukocytopenia 56 34 6 2 2
NonhematologicStomatitis 88 12 — — —Nausea/vomiting 54 40 4 2 —Diarrhea 16 20 34 30 —Abdominal pain 66 22 8 4 —Proctitis 46 26 26 2 —ASAT/ALAT elevation 50 32 8 10 —Bilirubin elevation* 98 — — 2 —Creatinine elevation 100 — — — —Alopecia 98 — 2 — —Hand-foot skin reaction 86 10 4 — —
Acnelike skin rash 12 36 46 6 —Anorexiay 96 4 — — —
Abbreviations: ASAT/ALAT = aspartate aminotransferase/alanine aminotransferase; NCI-CTC = National Cancer Institute Common Tox-icity Criteria.
Data presented as percentage of patients.* Grade 3 hyperbilirubinemia was recorded in a patient with previously unknown Gilbert-Meulengracht’s disease).y Median weight loss during radiochemotherapy was 4 kg (range 0–17 kg).
The dose intensity (i.e., applied doses divided by the
scheduled doses � 100 [%]) of cetuximab, irinotecan, and
capecitabine was as follows (median/mean [%]): cetuximab
Table 3. Surgical parameters and tumor regression gradingof the primary tumor after neoadjuvant cetuximab-CapIri-RT
(n = 50)
Surgery typeLow anterior resection 42 (84)Abdominoperineal resection 7 (14)Hartmann’s procedure 1 (2)
Resection statusR0 50 (100)
Time of surgery (min)Median 270Range 135–565
Hospital stay (days)Median 14Range 7–48+
Blood loss (mL)Median 500Range 100–2100
ComplicationsWound healing 12 (24)Anastomotic leak 8 (16)Bowel atonia 11 (22)Abscess 5 (10)Pneumonia 1 (2)
Tumor regression grading (JSCCR)1a 11 (22)1b 5 (10)2 30 (60)3 4 (8)
Abbreviation: JSCCR = Japanese Society for Cancer of the Colonand Rectum.
Data presented as number of patients, with percentage in paren-theses, unless otherwise noted.
100/92 (range, 29–100), irinotecan 100/91 (range, 33–100)
and capecitabine 100/89 (range, 29–100).
In 3 patients, radiotherapy was stopped prematurely be-
cause of toxicity (34.2 Gy, n = 1; 45 Gy, n = 2). The remain-
ing patients (n = 47) received the scheduled dose of 50.4 Gy.
Surgery and pathologyTME surgery was performed in all patients after a median
of 35 days (range, 21–68 days) following the completion of
chemoradiation. R0 resection was accomplished in all pa-
tients. Forty-two patients were treated with a low anterior re-
section, 1 patient with a Hartmann’s procedure and 7 with an
abdominoperineal resection. All patients undergoing sphinc-
ter-sparing surgery had a transient ileostomy. Surgical pa-
rameters and complications are listed in Table 3. No
postoperative deaths occurred, and the median hospital stay
was 14 days.
A median of 13 lymph nodes were examined (range,
2–22). Thirty-six patients were nodal-negative. Twelve pa-
tients had 1–3 lymph nodes involved (N1), and 2 patients
had more than 4 positive lymph nodes (N2). Nodal status
downstaging (cN+ to ypN0) was detected in 24 of 37 patients
(65%), T-category was downstaged in 22 patients (45%;
Table 4). Using the JSCCR regression grading, 68% had
moderate or good tumor regression (Grade 2 and 3), but
pCR was observed in only 4 patients (8%).
DISCUSSION
Combined-modality treatment with 5-FU and pelvic RT is
a mainstay of preoperative treatment of locally advanced rec-
tal cancer (2–4). Nevertheless, despite using perioperative
chemoradiation approximately 35%–40% of the patients
eventually develop distant metastases and die of their disease.
Phase II study with cetuximab and CapIri-RT in rectal cancer d K. HORISBERGER et al. 1491
This highlights the need for more effective perioperative sys-
temic treatment. Two main strategies are currently pursued:
(1) treatment intensification with newer chemotherapeutic
agents such as irinotecan or oxaliplatin and (2) the use of mo-
lecular targeted therapies, for example, cetuximab, a mono-
clonal EGFR antibody. The rate of pCR is regarded as
a potential early marker to estimate the efficacy of radioche-
motherapy regimens involving newer agents in view of its
prognostic value and the outstanding prognosis of patients
achieving pCR.
In this study, we conjointly investigated both strategies
adding cetuximab and irinotecan to capecitabine-based
chemoradiotherapy (cetuximab-CapIri-RT). This regimen
showed promising results in a previous Phase I study in
20 patients. In this Phase II trial, we sought to expand
the safety data before investigating this regimen in a ran-
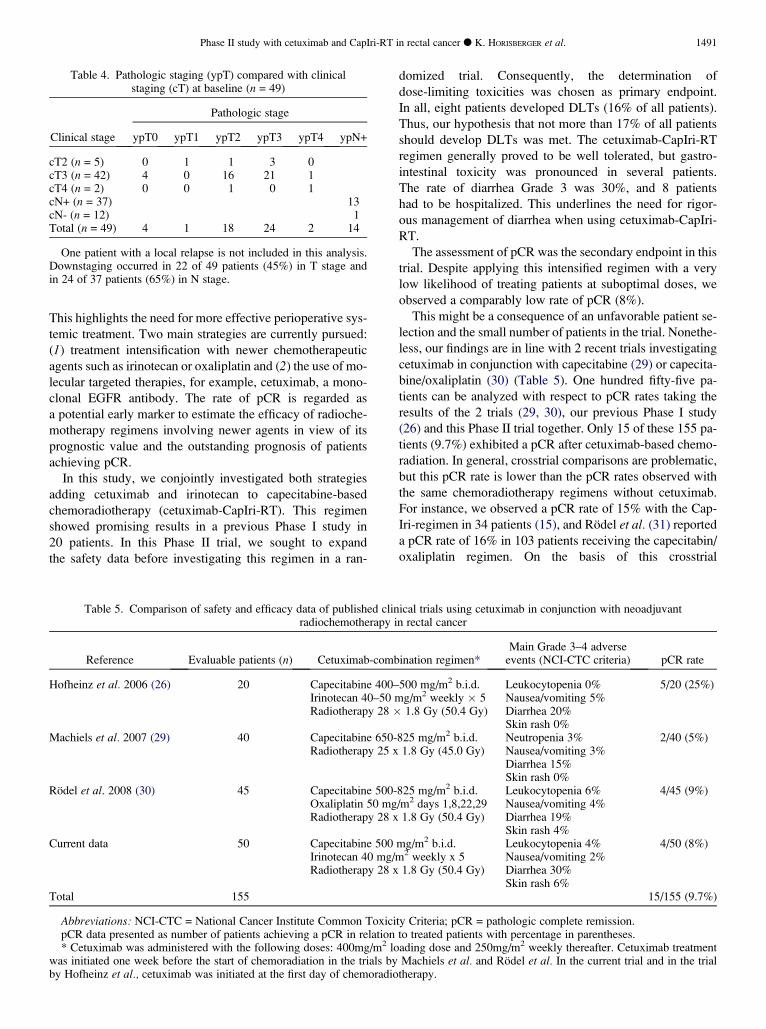
Table 4. Pathologic staging (ypT) compared with clinicalstaging (cT) at baseline (n = 49)
Pathologic stage
Clinical stage ypT0 ypT1 ypT2 ypT3 ypT4 ypN+
cT2 (n = 5) 0 1 1 3 0cT3 (n = 42) 4 0 16 21 1cT4 (n = 2) 0 0 1 0 1cN+ (n = 37) 13cN- (n = 12) 1Total (n = 49) 4 1 18 24 2 14
One patient with a local relapse is not included in this analysis.Downstaging occurred in 22 of 49 patients (45%) in T stage andin 24 of 37 patients (65%) in N stage.
domized trial. Consequently, the determination of
dose-limiting toxicities was chosen as primary endpoint.
In all, eight patients developed DLTs (16% of all patients).
Thus, our hypothesis that not more than 17% of all patients
should develop DLTs was met. The cetuximab-CapIri-RT
regimen generally proved to be well tolerated, but gastro-
intestinal toxicity was pronounced in several patients.
The rate of diarrhea Grade 3 was 30%, and 8 patients
had to be hospitalized. This underlines the need for rigor-
ous management of diarrhea when using cetuximab-CapIri-
RT.
The assessment of pCR was the secondary endpoint in this
trial. Despite applying this intensified regimen with a very
low likelihood of treating patients at suboptimal doses, we
observed a comparably low rate of pCR (8%).
This might be a consequence of an unfavorable patient se-
lection and the small number of patients in the trial. Nonethe-
less, our findings are in line with 2 recent trials investigating
cetuximab in conjunction with capecitabine (29) or capecita-
bine/oxaliplatin (30) (Table 5). One hundred fifty-five pa-
tients can be analyzed with respect to pCR rates taking the
results of the 2 trials (29, 30), our previous Phase I study
(26) and this Phase II trial together. Only 15 of these 155 pa-
tients (9.7%) exhibited a pCR after cetuximab-based chemo-
radiation. In general, crosstrial comparisons are problematic,
but this pCR rate is lower than the pCR rates observed with
the same chemoradiotherapy regimens without cetuximab.
For instance, we observed a pCR rate of 15% with the Cap-
Iri-regimen in 34 patients (15), and Rodel et al. (31) reported
a pCR rate of 16% in 103 patients receiving the capecitabin/
oxaliplatin regimen. On the basis of this crosstrial
Table 5. Comparison of safety and efficacy data of published clinical trials using cetuximab in conjunction with neoadjuvantradiochemotherapy in rectal cancer
Reference Evaluable patients (n) Cetuximab-combination regimen*Main Grade 3–4 adverse
events (NCI-CTC criteria) pCR rate
Hofheinz et al. 2006 (26) 20 Capecitabine 400–500 mg/m2 b.i.d. Leukocytopenia 0% 5/20 (25%)Irinotecan 40–50 mg/m2 weekly � 5 Nausea/vomiting 5%Radiotherapy 28 � 1.8 Gy (50.4 Gy) Diarrhea 20%
Skin rash 0%Machiels et al. 2007 (29) 40 Capecitabine 650-825 mg/m2 b.i.d. Neutropenia 3% 2/40 (5%)
Radiotherapy 25 x 1.8 Gy (45.0 Gy) Nausea/vomiting 3%Diarrhea 15%Skin rash 0%
Rodel et al. 2008 (30) 45 Capecitabine 500-825 mg/m2 b.i.d. Leukocytopenia 6% 4/45 (9%)Oxaliplatin 50 mg/m2 days 1,8,22,29 Nausea/vomiting 4%Radiotherapy 28 x 1.8 Gy (50.4 Gy) Diarrhea 19%
Skin rash 4%Current data 50 Capecitabine 500 mg/m2 b.i.d. Leukocytopenia 4% 4/50 (8%)
Irinotecan 40 mg/m2 weekly x 5 Nausea/vomiting 2%Radiotherapy 28 x 1.8 Gy (50.4 Gy) Diarrhea 30%
Skin rash 6%Total 155 15/155 (9.7%)
Abbreviations: NCI-CTC = National Cancer Institute Common Toxicity Criteria; pCR = pathologic complete remission.pCR data presented as number of patients achieving a pCR in relation to treated patients with percentage in parentheses.* Cetuximab was administered with the following doses: 400mg/m2 loading dose and 250mg/m2 weekly thereafter. Cetuximab treatment
was initiated one week before the start of chemoradiation in the trials by Machiels et al. and Rodel et al. In the current trial and in the trialby Hofheinz et al., cetuximab was initiated at the first day of chemoradiotherapy.

1492 I. J. Radiation Oncology d Biology d Physics Volume 74, Number 5, 2009
comparison, an additional benefit for the addition of cetuxi-
mab appears unlikely. Nevertheless, the rate of gastrointesti-
nal toxicity (i.e., diarrhea) is clearly augmented by the
addition of cetuximab, an effect that has also been observed
in randomized clinical trials in patients with metastatic colo-
rectal cancer (21).
There are several possible reasons for the low pCR rate,
as well as various conclusions to be drawn from these ob-
servations. First, a possible explanation, as suggested by
Rodel et al. (30), for the low efficacy is the G1 cell-cycle
arrest caused by the addition of cetuximab which impairs
the efficacy of 5-FU-derivatives, oxaliplatin, or irinotecan,
all of which exert their main cytotoxic or radiosensitizing
mode of action mainly in the S/G2/M phases. Second, for
patients with metastastic colorectal cancer, the negative im-
pact of KRAS mutations on the efficacy of EGFR anti-
bodies was recently demonstrated (32). Moreover, the
addition of cetuximab to standard chemotherapy (capecita-
bin/oxaliplatin/bevacizumab) in patients with KRAS muta-
tions not only had no additional effect but was harmful
for these patients, resulting in a significantly shorter time
to tumor progression (33). However, the KRAS mutational
status has not been investigated thus far in either of the rec-
tal cancer trials using cetuximab. Third, although the results
of cetuximab-based chemoradiation obtained in several
Phase I/II trials indicate no benefit for the addition of the
EGFR antibody, from a methodological point of view, it
should be noted that the small sample size is susceptible
to biased statistical results. Only randomized, adequately
powered trials are required to answer the question satisfac-
torily. Fourth and finally, pCR is an early surrogate end-
point that is far from being universally accepted (34).
Clearly, patients exhibiting pCR after conventional chemo-
radiation have an excellent long-term prognosis (18).
Whether this also holds true for regimens including mono-
clonal antibodies remains to be shown.
The data on chemoradiation including EGFR tyrosine-ki-
nase inhibitors are contradictory. A trial investigating capeci-
tabine/gefitinib-based chemoradiotherapy was closed early
because of toxicity issues (35), and a recent trial using
5-FU instead of capecitabine reported acceptable gastrointes-
tinal toxicity and a pCR rate of 30% in 41 patients (36).
In conclusion, this study shows that the cetuximab-CapIri
regimen has pronounced albeit manageable toxicity. Never-
theless, the pCR rate was only 8%. This adds to a growing
body of evidence suggesting that the combination of anti-
EGFR antibodies with conventional chemoradiotherapy pro-
vides no additional antitumor activity. We do not recommend
using this regimen outside of clinical trials. Nevertheless, the
combination of anti-EGFR molecular drugs with radiother-
apy should be investigated further, ideally within randomized
trials. These trials should also focus on correlative tumor tis-
sue and biomarker analysis to gain more information on
potential benefits of such combinations.
REFERENCES
1. Peeters E, Marijnen CA, Nagtegaal ID, et al. The TME trial after
a median follow-up of 6 years: increased local control but no
survival benefit in irradiated patients with resectable rectal car-
cinoma. Ann Surg 2007;246:693–701.2. Sauer R, Becker H, Hohenberger W, et al. Preoperative versus
postoperative chemoradiotherapy for rectal cancer. N Engl JMed 2004;351:1731–1740.
3. Bosset JF, Collette L, Calais G, et al. Chemotherapy with pre-
operative radiotherapy in rectal cancer. N Engl J Med 2006;
355:1114–1123.4. Gerard JP, Conroy T, Bonnetain F, et al. Preoperative radiother-
apy with or without concurrent fluorouracil and leucovorin in
T3-4 rectal cancers: Results of FFCD 9203. J Clin Oncol2006;24:4620–4625.
5. Tepper JE, O’Connell M, Niedzwiecki D, et al. Adjuvant ther-
apy in rectal cancer: Analysis of stage, sex, and local control-fi-
nal report of intergroup 0114. J Clin Oncol 2002;20:
1744–1750.6. O’Connell MJ, Martenson JA, Weiand HS, et al. Improving ad-
juvant therapy by combining protracted infusion fluorouracil
with radiation therapy after curative surgery. N Engl J Med1994;331:502–507.
7. Queißer W, Hartung G, Kopp-Schneider A, et al. for the study
group Colon and Rectum Carcinoma, Mannheim. Adjuvant Ra-
dio-Chemotherapy with 5-Fluorouracil and Folinic Acid in
Stage II and III Rectal Cancer: 12 vs. 6 months of therapy.
Onkologie 2000;23:334–339.8. Mohiuddin M, Winter K, Mitchell E, et al. Randomized Phase II
study of neoadjuvant combined-modality chemoradiation for
distal rectal cancer: Radiation Therapy Oncology Group Trial
0012. J Clin Oncol 2006;24:650–655.
9. Mehta VK, Cho C, Ford JM, et al. Phase II trial of preoperative
3D conformal radiotherapy, protracted venous infusion 5-fluo-
rouracil, and weekly CPT-11, followed by surgery for ultra-
sound-staged T3 rectal cancer. Int J Radiat Oncol Biol Phys2003;55:132–137.
10. Iles S, Gollins S, Susnerwala S, et al. Irinotecan+5-fluorouracil
with concomitant pre-operative radiotherapy in locally ad-
vanced non-resectable rectal cancer: A Phase I/II study. Br JCancer 2008;98:1210–1216.
11. Klautke G, Kirchner R, Hopt U, et al. Continuous infusion of
5-FU and weekly irinotecan with concurrent radiotherapy as
neoadjuvant treatment for locally advanced or recurrent rectal
cancer. Br J Cancer 2005;92:1215–1220.12. Klautke G, Kuchenmeister U, Foitzik T, et al. Concurrent che-
moradiation with capecitabine and weekly irinotecan as preop-
erative treatment for rectal cancer: Results from a phase I/II
study. Br J Cancer 2006;94:976–981.13. Gollins S, Myint S, Levine E, et al. Phase I study of capeci-
tabine plus weekly irinotecan (CAPIRI) plus radiotherapy as
preoperative downstaging treatment for locally advanced rec-
tal cancer (LARC) [abstract]. Proc Am Soc Clin Oncol 2005;
23:3565.14. Hofheinz RD, von Gerstenberg-Helldorf B, Wenz F, et al.
Phase I trial of capecitabine and weekly irinotecan in combina-
tion with radiotherapy for neoadjuvant therapy of rectal cancer.
J Clin Oncol 2005;23:1350–1357.15. Willeke F, Horisberger K, Kraus-Tiefenbacher U, et al. A phase
II study of capecitabine and irinotecan in combination with con-
current pelvic radiotherapy (CapIri-RT) as neoadjuvant treat-
ment of locally advanced rectal cancer. Br J Cancer 2007;96:
912–917.
Phase II study with cetuximab and CapIri-RT in rectal cancer d K. HORISBERGER et al. 1493
16. Rodel C, Martus P, Papadoupolos T, et al. Prognostic signifi-cance of tumor regression after preoperative chemoradiotherapyfor rectal cancer. J Clin Oncol 2005;23:8688–8696.
17. Roh MS, Colangelo L, Wieand S, et al. Response to preopera-tive multimodality therapy predicts survival in patients with car-cinoma of the rectum [abstract]. Proc Am Soc Clin Oncol 2004;22:3505.
18. Capirci C, Valentini V, Cionini L, et al. Prognostic value ofpathologic complete response after neoadjuvant therapy in lo-cally advanced rectal cancer: Long-term analysis of 566ypCR patients. Int J Radiat Oncol Biol Phys 2008;72:99–107.
19. Hartley A, Ho KF, McConkey C, et al. Pathological completeresponse following pre-operative chemoradiotherapy in rectalcancer: Analysis of Phase II/III trials. Br J Radiol 2005;78:934–938.
20. Cunningham D, Humblet Y, Siena S, et al. Cetuximab mono-therapy and cetuximab plus irinotecan in irinotecan-refractorymetastatic colorectal cancer. N Engl J Med 2004;351:337–345.
21. van Cutsem E, Lang I, D’haens G, et al. KRAS status and effi-cacy in the first-line treatment of patients with metastatic colo-rectal cancer (mCRC) treated with FOLFIRI with or withoutcetuximab: The CRYSTAL experience. J Clin Oncol 2008;26(suppl):abstract 2.
22. Krause M, Ostermann G, Petersen C, et al. Decreased repopu-lation as well as increased reoxygenation contribute to the im-provement in local control after targeting of EGFR by C225during fractionated irradiation. Radiother Oncol 2005;76:162–167.
23. Huang SM, Bock JM, Harari PM. Epidermal growth factor re-ceptor blockade with C225 modulates proliferation, apoptosis,and radiosensitivity in squamous cell carcinomas of the headand neck. Cancer Res 1999;59:1935–1940.
24. Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetux-imab for squamous cell carcinoma of the head and neck. N EnglJ Med 2006;354:567–578.
25. Giralt J, de las Heras M, Cerezo L, et al. The expression of epi-dermal growth factor receptor results in a worse prognosis forpatients with rectal cancer treated with preoperative radiother-apy: A multicenter, retrospective analysis. Radiother Oncol2005;74:101–108.
26. Hofheinz RD, Horisberger K, Woernle C, et al. Phase I trial ofcetuximab in combination with capecitabine, weekly irinotecan,and radiothrapy as neoadjuvant therapy for rectal cancer. Int JRadiat Oncol Biol Phys 2006;66:1384–1390.
27. Compton CC for the members of the Cancer Committee, Col-lege of American Pathologists. Updated protocol for the exam-ination of specimens from patients with carcinomas of the colonand rectum, excluding carcinoid tumors, lymphomas, sarcomas,and tumors of the vermiform appendix. A basis for checklists.Arch Pathol Lab Med 2000;124:1016–1025.
28. Japanese Society for Cancer of the Colon and Rectum (JSCCR).Japanese classification of colorectal carcinoma, 1st English ed.Tokyo: Kanehara; 1997.
29. Machiels JP, Sempoux C, Scalliet P, et al. Phase I/II study ofpreoperative cetuximab, capecitabine, and external beam radio-therapy in patients with rectal cancer. Ann Oncol 2007;18:738–744.
30. Rodel C, Arnold D, Hipp M, et al. Phase I–II trial of cetuximab,capecitabine, oxaliplatin, and radiotherapy as preoperativetreatment in rectal cancer. Int J Radiat Oncol Biol Phys 2008;70:1081–1086.
31. Rodel C, Liersch T, Hermann RM, et al. Multicenter Phase IItrial of chemoradiation with oxaliplatin for rectal cancer.J Clin Oncol 2007;25:110–117.
32. van Cutsem E, Nowacki M, Lang I, et al. Randomized Phase IIIstudy of irinotecan and 5-FU/FA with or without cetuximab inthe first-line treatment of patients with metastatic colorectalcancer (mCRC): The CRYSTAL trial. J Clin Oncol 2007;25(suppl):abstract 4000.
33. Punt CJ, Tol J, Rodenburg CJ, et al. Randomized Phase IIIstudy of capecitabine, oxaliplatin, and bevacizumab with orwithout cetuximab in advanced colorectal cancer (ACC), theCAIRO2 study of the Dutch Colorectal Cancer Group(DCCG). J Clin Oncol 2008;26(suppl):abstr LBA4011.
34. Glynne-Joes R, Anyamene N. Just how useful an endpoint iscomplete pathological response after neoadjuvant chemoradia-tion in rectal cancer? Int J Radiat Oncol Biol Phys 2006;66:319–320.
35. Czito BG, Willett CG, Bendell JC, et al. Increased toxicity withgefitinib, capecitabine, and radiation therapy in pancreatic andrectal cancer: Phase I trial results. J Clin Oncol 2006;24:656–662.
36. Valentini V, De Paoli A, Gambacorta MA, et al. Infusional5-fluorouracil and ZD1839 (gefitinib-Iressa) in combinationwith preoperative radiotherapy in patients with locally ad-vanced rectal cancer: A Phase I and II trial (1839IL/0092).Int J Radiat Oncol Biol Phys 2008 (April 3), Epub ahead ofprint.
Copyright © 2022 FDOKUMEN




















