
Cell populations and membrane attack complex in glomeruli of patients with post-streptococcal...
9
Cell Populations and Membrane Attack Complex in Glomeruli of Patients with Post-streptococcal Glomerulonephritis: Identification Using Monoclonal Antibodies by Indirect Immunofluorescence GLJSTAVO PARKA,'JEFFKEY L. PLAT~,~ RONALD J. FALL BERNARDORODRIGUEZ-ITURBE." AND ALFRED F. MICHAEL Depurtments of Pediutrics and Laboratory Medicine urrtl Pathology, UGivt-.sity of Minnrsotri Medicul School. Minnrapolis, Minnesota 55455, and *Rem11 Scr~ic~e. Department of Medicine Hospital Universiturio and Universidad de1 Zulitr. Muruwiho, Vcne:uelo Poststreptococcal glomerulonephritis (PSGN) had been thought to arise from renal deposition of immune complexes and as such is analogous to acute serum sickness. Recent studies of acute serum sickness in animals and PSGN in humans, however, have suggested a pathogenetic role for cellular immunity. To enlarge on these observation?. cellular components of glomeruli were characterized by indirect immunofluorescence in Ii tissues from individuals with PSGN using monoclonal antibodies. These studies dem- onstrate infiltration of glomeruli by monocytes, granulocytes. and lymphoid cells. Focal accumulations of T lymphocytes were also observed adjacent to Bowman’s capsule. Analysis of glomerular T-cell subpopulations revealed a predominance of cells reactive with OKT4 early and with OKT8 later in the course of disease. Proliferation of parietal and visceral epithelial cells was associated with increased binding of BA-I and J.5, re- spectively. The presence of the membrane attack complex of complement was demon- strated by glomerular reactivity with a monoclonal antibody (poly-CY MA) which rec- ognizes a neoantigen present in poly-C9. Fluorescence was present along the glomerular basement membrane early and within the mesangium late in the course of disease. a distribution similar to that observed for C3 and C5. These observations suggest that immune cells as well as terminal components of complement either provoke or mark tissue injury in PSGN. Cl 1984 Academtc Prec\. Ini- INTRODUCTION Poststreptococcal glomerulonephritis (PSGN) is thought to be triggered by for- mation of soluble immune complexes in serum and deposition of these complexes in glomeruli (1). Immunofluorescence studies reveal granular patterns of reac- tivity for immunoglobulin and complement components early and late in the course of the disease and focal deposits of C3 have been observed in some in- stances as late as 10 years after the acute episode (2). The pathogenesis of PSGN is thought to be similar to that of acute serum sickness, since both diseases are characterized by a latent period between exposure to the atigen and development of disease: formation of immune complexes in the circulation; similar patterns of ’ Under the tenure of a Fundaciti Grant. ’ Supported by a Clinician Scientist Award from the American Heart Association 324 0090-1229/84 $1.50 Copyright ‘0 1984 by Academic Press. Inc.
-
Upload
udistrital -
Category
Documents
-
view
3 -
download
0
Transcript of Cell populations and membrane attack complex in glomeruli of patients with post-streptococcal...

Cell Populations and Membrane Attack Complex in Glomeruli of Patients with Post-streptococcal Glomerulonephritis:
Identification Using Monoclonal Antibodies by Indirect Immunofluorescence
GLJSTAVO PARKA,'JEFFKEY L. PLAT~,~ RONALD J. FALL BERNARDORODRIGUEZ-ITURBE." AND ALFRED F. MICHAEL
Depurtments of Pediutrics and Laboratory Medicine urrtl Pathology, UGivt-.sity of Minnrsotri Medicul School. Minnrapolis, Minnesota 55455, and *Rem11 Scr~ic~e. Department of Medicine
Hospital Universiturio and Universidad de1 Zulitr. Muruwiho, Vcne:uelo
Poststreptococcal glomerulonephritis (PSGN) had been thought to arise from renal deposition of immune complexes and as such is analogous to acute serum sickness. Recent studies of acute serum sickness in animals and PSGN in humans, however, have suggested a pathogenetic role for cellular immunity. To enlarge on these observation?. cellular components of glomeruli were characterized by indirect immunofluorescence in Ii tissues from individuals with PSGN using monoclonal antibodies. These studies dem- onstrate infiltration of glomeruli by monocytes, granulocytes. and lymphoid cells. Focal accumulations of T lymphocytes were also observed adjacent to Bowman’s capsule. Analysis of glomerular T-cell subpopulations revealed a predominance of cells reactive with OKT4 early and with OKT8 later in the course of disease. Proliferation of parietal and visceral epithelial cells was associated with increased binding of BA-I and J.5, re- spectively. The presence of the membrane attack complex of complement was demon- strated by glomerular reactivity with a monoclonal antibody (poly-CY MA) which rec- ognizes a neoantigen present in poly-C9. Fluorescence was present along the glomerular basement membrane early and within the mesangium late in the course of disease. a distribution similar to that observed for C3 and C5. These observations suggest that immune cells as well as terminal components of complement either provoke or mark tissue injury in PSGN. Cl 1984 Academtc Prec\. Ini-
INTRODUCTION
Poststreptococcal glomerulonephritis (PSGN) is thought to be triggered by for- mation of soluble immune complexes in serum and deposition of these complexes in glomeruli (1). Immunofluorescence studies reveal granular patterns of reac- tivity for immunoglobulin and complement components early and late in the course of the disease and focal deposits of C3 have been observed in some in- stances as late as 10 years after the acute episode (2). The pathogenesis of PSGN is thought to be similar to that of acute serum sickness, since both diseases are characterized by a latent period between exposure to the atigen and development of disease: formation of immune complexes in the circulation; similar patterns of
’ Under the tenure of a Fundaciti Grant. ’ Supported by a Clinician Scientist Award from the American Heart Association
324 0090-1229/84 $1.50 Copyright ‘0 1984 by Academic Press. Inc.

CELLPOPULATIONS IN ACUTEGLOMERULONEPHRITIS 325
immunoglobulin and complement deposition; and depression of serum comple- ment levels (1).
In addition to evidence of humoral immunity light microscopic analysis of the kidney in PSGN and acute serum sickness reveals glomerular hypercellularity reflecting proliferation of mesangial and endothelial cells (3) and infiltration of polymorphonuclear cells (PMN) and monocytes (4). The relative pathogenic roles of the proliferative and infiltrative elements, however, is uncertain. Recent in- vestigations have demonstrated that monocytes may evoke endothelial and mes- angial damage (5-7). Although lymphocytes have not been observed in situ in PSGN (8), a role for these cells is suggested by lymphocyte transfer studies of experimental anti-glomerular basement membrane (GBM) and immune complex glomerulonephritis (9, 10).
We have studied renal tissues of 11 patients with PSGN using monoclonal antibodies directed against renal, lymphoid, and myeloid cells to identify and characterize proliferative and infiltrative cells. Our findings demonstrate that lym- phocytes as well phagocytes are present in glomeruli of patients with PSGN. Additionally, a monoclonal antibody directed against a neoantigen on C9 of the membrane attack complex of complement (MAC) documented the presence of MAC in early and late stages of disease.
MATERIALS AND METHODS
Source of tissues. Renal tissues were obtained for diagnostic purposes from 11 patients (5 males, 6 females, ages 5 to 14 years) with acute PSGN and from 6 normal controls (kidney donors at the time of transplantation). The diagnosis of acute PSGN was based upon clinical evidence of nephritis associated with se- rological or bacteriologic evidence of recent streptococcal infection [positive throat or skin lesion culture, elevated titers of antistreptolysin 0 (ASO), anti- DNase B, or streptozyme] (11, 12). The time between the onset of clinical disease and biopsy ranged from 14 to 120 days.
Eight renal tissues obtained at the Hospital Universitario de Maracaibo were each divided into two fragments, one of which was snap-frozen in dry ice and acetone and stored at -70°C until used and the other fixed in Formalin. Three tissues obtained at the University of Minnesota Hospitals were likewise each divided into portions some of which were immersed in isopentane precooled in liquid nitrogen and stored at -70°C until used and some fixed in Zenker’s.
Patients with PSGN were divided arbitrarily into two groups: Group I consisted of five patients in whom clinical onset occurred less than 4 weeks (14, 16, 23, 24, 25 days) prior to percutaneous renal biopsy, while group II contained six patients with an onset of 4-17 weeks (28, 31, 35, 39, 43, 120 days) prior to biopsy.
Light microscopy revealed diffuse hypercellularity, as previously reported (2), more prominent in group I than in group II. Crescents were observed in biopsies obtained 14 and 120 days following the onset of the clinical disease. Routine immunofluorescence studies revealed granular deposits of immunoglobulin and C3 as previously reported (2).
Monoclonal and polyclonal antibodies. Mouse IgG subclass and specificity of monoclonal antibodies used are indicated in Table 1. OKT3, OKT4, OKT8, and
326 PARRA ET AL.
TABLE I MONOCLONAL ANTIBODIES
- -~ ---- - .- --.-. ~--. ...~_ -~
Antibody Subclass Specificity Reference
Tll w, T lymphocytes (E receptor) (19) OKT3 lgGza T lymphocytes IT!% OKT4 k% Helper T lymphocytes (30) OKT8 ML1 Cytotoxicisuppressor T lymphocytes (311 Anti-Tat w2, Interleukin ‘2 receptor !i!i OKMl ks2R Monocytes/null cells/PMN (CR31 (37) MN41 w, Monocytesinull cells/PMN tCR3) (13) B-l W,, B lymphocytes (331 BA-1 W B lymphocytes, PMN, renal epithelium t35: J.5 kG!% Leukemia antigen renal epithelium (19) Poly-C9 MA W, Membrane attack complex of complement / I41
----- __- -~-_ ..~_._. .-~..-~-
OKMl were obtained from Ortho Pharmaceutical Corporation (Raritan. N.J.); Tll, anti-B-l, and J5 were from Coulter, Inc. (Hialeah, Fla.); BA-I was from Tucker W. LeBien, University of Minnesota; anti-Tat was from Thomas Wald- mann, National Institutes of Health; MN41 (anti-CR3) (13) and poly-C9 MA. which has specificity for a neoantigen of C9 present on the MAC but absent from monomeric C9, were made at the University of Minnesota (14).
Fluorescein isothiocyanate (FlTC)-conjugated monspecific goat anti-human C3 was prepared as previously described (2), and monospecific goat anti-human C5 obtained from Miles Laboratories, Inc. (Elkart, lnd.) was absorbed with human (X-deficient sera (14). FITC-conjugated rabbit anti-human lactoferrin (Cappel Laboratories, West Chester, Pa.) was used to identify PMN in tissue sections.
Preparation and stuining of tisslre sections. Four-micrometer-thick frozen sec- tions were prepared as previously described (1.5). Frozen sections of each tissue were sequentially reacted with a monoclonal antibody, FITC-labeled F(ab’), rabbit anti-mouse IgG (heavy and light chains) (Cappel), FITC-labeled F(ab), goat anti-rabbit IgG (heavy and light chains) (Cappel), ethidium bromide to stain the nuclei, and p-phenylenediamine to retard fluorescence fading (16, 17). All fluo- rochromes were affinity isolated and human plasma absorbed. Frozen tissue sec- tions were also reacted with poly-C9 MA, and then with human plasma-absorbed FITC-goat anti-mouse lg (Cappel); goat anti-human CS, and FITC-F(ab’)? rabbit anti-goat IgG (Cappel) (14); and finally with FITC-goat anti-human C3. Frozen sections prepared from selected biopsies were reacted with OKMl followed by the double fluorochrome layer as described above: and adjacent sections were reacted with FITC-labeled anti-human lactoferrin.
Standurdization of reugents and controls. Tl I, OKT3, OKT4, OKT8, anti-Bl. OKMl, anti-Tat, BA-1, and J5 were standardized by analysis of reactivity with appropriate human lymphoid, renal and skin tissues as previously described ( 15, 18). Monoclonal antibody MN41 was shown to react with CR3 of monocytes and null cells (13). FITC-anti-human lactoferrin was standardized by immunofluores- cence using smears of peripheral blood cells obtained from normal donors and kidney biopsy tissues from patients with PSGN known to have substantial PMN infiltration. Control sections for each tissue were reacted with the single and

CELL POPULATIONS IN ACUTE GLOMERULONEPHRITIS 327
double flurochrome layers described above without prior application of unlabeled monoclonal or polyclonal antisera.
Analysis oftissues. Tissues were examined using a Zeiss Universal microscope equipped for epifluorescence with appropriate filters and dichroic mirrors through a x 63 plan apochromatic oil immersion objective and 10 x oculars fitted with a lo-mm indexing grid. Cells with orange fluorescent nuclei (ethidium bromide) surrounded by apple green fluorescent plasma membrane were considered reac- tive. Cells without nuclei were excluded.
For each section the following were enumerated: (i) reactive intraglomerular cells (excluding cells associated with Bowman’s capsule), (ii) total intraglomerular cells, (iii) reactive cells in contact with Bowman’s capsule, (iv) reactive cells in glomerular crescents. These data were then expressed as reactive cells per 100 intraglomerular cells, reactive Bowman’s capsule cells per glomerulus, and reac- tive cells per crescent. Because of variation in the number of glomeruli present in tissues from group I (3- 1.5), from group II (2- 17), and from controls (2-8) the weighted mean percentage of glomerular cells reactive with each of the mono- clonal antibodies was calculated as previously described (19).
In four tissues, monocytes and PMN could not be easily distinguished on the basis of nuclear morphology. Therefore, the difference between the proportion of cells reactive with OKMl (which binds to both PMN and monocytes) and the proportion reactive with anti-human lactoferrin (which identifies PMN) in serial sections was used to define the intraglomerular monocyte population.
RESULTS
immune cell populations The proportions of glomerular cells reactive with monoclonal antibodies directed against lymphoid cells, monocytes, and PMN are presented in Fig. 1. The proportions of cells recognized by OKT4 was similar in both groups. Cells reactive with OKT8, however, were less frequently observed in group I than in group II. Because of focal and segmental distribution of reactive cells and variation in the numbers of glomeruli in tissues studied, a weighted mean percentage of glomerular cells reactive with each antibody was also deter- mined for each group (Table 2). These data demonstrated T-lymphocyte and phagocyte infiltration of glomeruli in both groups.
T-Lymphocyte infiltration was also observed along the external aspect of Bow- man’s capsule in 8 of 11 tissues (Fig. 2A). Cells in this locus were more frequently reactive with OKT8 than with OKT4. These periglomerular foci were most prom- inent in tissues containing crescents.
Anti-B1 reactive cells were not observed in glomeruli or crescents. Some in- terstitial cells however reacted with this antibody. Evidence of T-lymphocyte activation was sought by the use of anti-Tat antibody to identify cells bearing interleukin 2 receptors but reactive cells were seen in the interstitium of only two tissues and intraglomerular anti-Tat-reactive cells were not observed.
Renal cell populations. In normal human kidney tissue monoclonal antibody BA-1 reacts with parietal epithelial cells of Bowman’s capsule and with distal tubule (18). In PSGN tissues this antibody was a sensitive indicator of prolifer- ation of cells along Bowman’s capsule (Fig. 2C). Cells associated with active

PARRA ET AI..
OKTB Tll OKT4
Fm. 1. Proportion of glomerular cells reactive with monoclonal antibodies which identify lymphoid and phagocytic cells in glomeruli of 11 patients with PSGN. Results expressed a\ positive cells per 100 glomerular cells are displayed on log scale.
crescent formation in the 14-day tissue reacted with BA- I, whereas fibrotic cres- cents in a 120-day tissue were unreactive.
Another monoclonal antibody, J5 reacts with visceral epithelium of the glo- merulus and proximal tubular epithelium in normal kidney tissues, reflecting the
TABLE 2 WIXHTED MEAN PERCENTAGE” OF LELKOCYTES REACI IVI: WII-H MONOC‘I.ONAI. A~TIBODI~-.~ 13
GLOMEKUI OF PATIENTS WITH PSGN .%ND NORMAL CONTROL.S
Positive cells per 100 glomerular cells
PSGN
14-X days ‘X- I?0 days after onset after onset
(II = 5) 01 = 6)
T11 0.48 0.28 0. I2 OKT4 0.25 0 I9 0 OKT8 0.07 0.19 o.oti PMNh 4.94 2.6 Il. I Monocytes’ 3.35 I .06 !i OKT410KT8 3.57 0.4x
” The weighted mean percentage equals the sum of all cells reactive with a given antibody m all sections of all tissues in a particular group divided by the sum of all glomerular cells in all sections reacted with that antibody x 100.
b Identified using FITC-anti-human lactoferrin. ’ Proportion of glomerular cells reactive with OKMl minus PMN.

CELL POPULATIONS IN ACUTE GLOMERULONEPHRITIS 329
FIG. 2. Immunofluorescence of glomeruli in PSGN reacted with monoclonal antibodies which iden- tify immune cells (A,B) and renal epithelium (C,D) in tissues obtained 120 days (A), 14 days (B,C), and 16 days after onset (D). (A) Glomerular lymphoid cells are reactive with OKT8 (arrows). Auto- fluorescent cells (arrowheads) are also observed. (B) Numerous glomerular cells are reactive with OKMI (arrows). (C) Proliferation of Bowman’s capsule epithelium (arrow) is detected with BA-1. (D) Reactivity of visceral glomerular epithelium with J5 reveals focal segmental lobular expansion (*) and proliferation (arrow).
presence of the common acute lymphoblastic leukemia antigen (CALLA) (18, 20). In PSGN tissues it reacted with intact visceral epithelium and identified focal proliferation (Fig. 2D). However, sclerotic and crescentic lesions were not reac- tive.
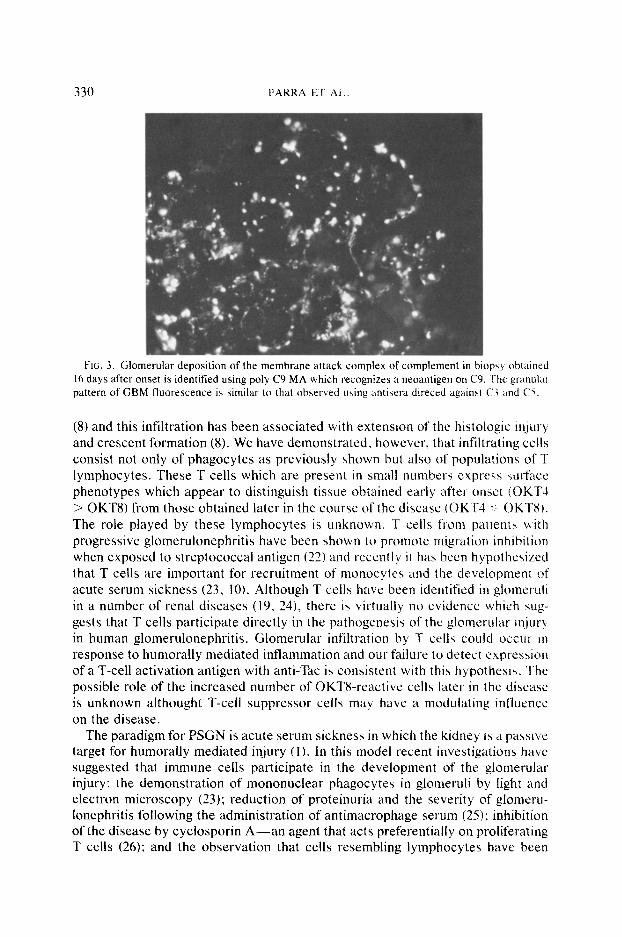
Membrane attack complex of complement. Poly-C9 MA, a monoclonal anti- body directed against a neoantigen of the polymerized 9th component of com- plement, reacted with granular deposits along the GBM and mesangium in six of seven tissues studied. Tissues obtained 14 and 16 days after onset of glomeru- lonephritis revealed primarily GBM-oriented deposits (Fig. 3) whereas those ob- tained at 25, 28, and 35 days revealed increasing mesangial deposits. C3 and CS were present in a similar distribution. Poly-C9 MA did not react with a tissue obtained 120 days after onset of disease.
DISCUSSION
PSGN is thought to be caused by circulating immune complexes. In glomeruli of patients with PSGN monocytes but not lymphoid cells have been recognized by ultrastructural techniques (21) and more recently by monoclonal antibodies
330 PARKA ET Al
FIG. 3. Glomerular deposition of the membrane attack complex of complement in biopsy obtained 16 days after onset is identified using poly C9 MA which recognizes a neoantigen on C9. The granular pattern of GBM fluorescence is similar to that observed using antisera direccd against (1’1 and (‘5.
(8) and this infiltration has been associated with extension of the histologic injury and crescent formation (8). We have demonstrated, however, that infiltrating cells consist not only of phagocytes as previously shown but also of populations of T lymphocytes. These T cells which are present in small numbers express surface phenotypes which appear to distinguish tissue obtained early after onset fOK1’4 > OKT8) from those obtained later in the course of the disease (OKT4 -;I OKTI!). The role played by these lymphocytes is unknown, T cells from patlen with progressive glomerulonephritis have been shown to promote migration inhibition when exposed to streptococcal antigen (22) and recently4 it has been hypothesized that T cells are important for recruitment of monocytes and the developmenr of acute serum sickness (23. 10). Although T cells have been identified in glomeruli in a number of renal diseases (19, 24), there is virtually no evidence which xup- gests that T cells participate directly in the pathogenesis of the glomerular injury in human glomerulonephritis. Glomerular infiltration by T cells could occur in response to humorally mediated inflammation and our failure to detect expression of a T-cell activation antigen with anti-Tat is consistent with this hypothesis. The possible role of the increased number of OKT8-reactive cells later in the disease is unknown althought T-cell suppressor cells may have a modulating influence on the disease.
The paradigm for PSGN is acute serum sickness in which the kidney 13 a passive target for humorally mediated injury (I ). In this model recent investigations have suggested that immune cells participate in the development of the glomerular injury: the demonstration of mononuclear phagocytes in glomeruli by light and electron microscopy (23); reduction of proteinuria and the severity of glomcru- lonephritis following the administration of antimacrophage serum (25); inhibition of the disease by cyclosporin A-an agent that acts preferentially on proliferating T cells (26): and the observation that cells resembling lymphocytes have been

CELL POPULATIONS IN ACUTE GLOMERULONEPHRITIS 331
recognized adjacent to monocytes in the glomerular lesion (23). In addition, cell transfer experiments have shown that sensitized lymphocytes can interact with heterologous antigen bound to GBM (9) or located within immune complexes, resulting in an increase in the number of infiltrating mononuclear cells and seg- mental glomerular hypercellularity (10).
A monoclonal antibody which recognizes a neoantigen on the C9 portion of the membrane attack complex of complement was used to seek evidence of in- volvement of terminal complement components in the PSGN lesion. MAC, which is present in a variety of other glomerular lesions (14, 27) and in chronic serum sickness in rabbits (28), was observed in all PSGN tissues except one obtained late in the course of disease. The pattern of poly-C9 MA binding was homologous to that of C3 and C5. The importance of MAC in the pathogenesis of PSGN, however, remains uncertain, although it has been postulated to induce plasma membrane damage of endothelial and epithelial cells with impairment in the syn- thesis and repair of GBM (28).
ACKNOWLEDGMENTS
This study was supported by grants from the National Institutes of Health (AI10704, AM25518. AM26149), the American Health Association, Minnesota Affiliate, and the Viking Children’s Fund. The authors thank Mr. Marshall Hoff and Ms. Kathy Divine for technical assistance and Ms. Jan Aplin for preparaing the manuscript.
REFERENCES
1. Michael, A. F., and Kim, Y., In “Streptococcal Disease and Immune Response” (S. E. Reap and J. Zabriskie, Eds.), pp. 53-77. Academic Press. New York, 1980.
2. Michael, A. F., Drummond, K., Good, R. A., and Vernier, R, L.. J. C/in. Invest. 45, 237, 1966. 3. Lewy, E. J., Madrigal-Salinas. L.. Herdson, P. B., Pirani, C. L.. and Metcoff, J.. Medicine 50,
453, 1971. 4. Monga, G.. Mazzucco, G., di Belgiojoso, G. B., and Busnach, G., Lab. Invest. 44, 4, 381. 5. MacCarthy, E. P., Ooi, Y. M., Hsu, A., and Ooi. B. S., In “16th Annual Meeting of American
Society of Nephrology (Abstracts).” p. 78A, 1983. 6. Lovett, D., Sterzel. B.. and Ryan. J. In “16th Annual Meeting of American Society ofNephrology
(Abstracts).” p. 77A, 1983. 7. Polverini, P., Cotran, R. S., and Shelley, M.. J. Immunol. 118, 2, 529. 1977. 8. Atkins, R. C.. Holdswoth, S. R., Hancock. W. W,, Thomson, N. M., and Glasgow, E. F.,
Springer Semin. Immunopathol. 5, 269, 1982. 9. Bhan. A. K., Schneeberger, E.. Colin, A. B., and McCluskey, R. T., J. Exp. Med. 148, 246,
1978. IO. Bhan. A. K.. Colin. A. B.. Schneeberger. E., and McCluskey, R. T., /. Exp. Med. 150, 1410,
1979. 11. Rodriguez-Iturbe, B., Garcia, R.. Rubio, L., Treser, G., and Lange, K., C/in. Nephrol. 5, 197.
1976. 12. McIntosh, R., Garcia, R., Rubio, L., Rabideau, D., Allen, J., Carr. R., and Rodriguez-Iturbe.
B., Kidney Int. 14, 501, 1978. 13. Eddy, A.. Newman, S. L., Cosio, F.. LeBien, T., and Michael, A. F., C/in. Immunol. Immuno-
pathol. 31, 371, 1984. 14. Falk. R. J.. Dalmasso, A. P., Kim, Y,, Tsai. C. H.. Scheinman. J. I., Gewurz, H.. and Michael,
A. F., J. Clin. Invest. 72, 560, 1983. IS. Platt, J. L., LeBien, T. W., and Michael, A. F., J. Exp. Med. 155, 17, 1982. 16. Franklin, W. A., and Locker, J. D., J. Histochem. Cytochem. 29, 572, 1981. 17. Platt, J. L., and Michael, A. F., J. Histochem. Cytochem. 31, #6. 840. 1983.

332 PARRA ET‘ AL,.
IS. Platt, J. L.. LeBien, T., and Michael. A. F., J. &. Med. 157. 155. 1983. 19. Nagata, K., Platt. J. L.. and Michael. A. F. Kidrq Itzt. 25, 88. 1984. 20. Ritz, J.. Pesando, J. M.. Notis-McConarty. J. Lazarus, H.. and Schlossman. S. F.. ;Vu/urc,
(London) 283, 583, 1980. 21. Shigematsu, H.. Shishido, H., Kuhara. K.. Tsuchiada. H.. Suzuki. H., Hirose. K.. and ‘Iojo. 5..
Virchm*s Arch. B. 12, 367. 1973. 22. Zabriskie. J. B.. Lewishenia, R.. Moller, G., Wehle. B.. and Falk. K. J.. .\c,i<,r~t o ( Wushirrg:(o~,
D.C.) 168, 1105, 1970. 23. Hunsicker, L. G., Shearer, T. P.. Plattner. S. B., and Weisenburger. D.. ./. Ilfp. Med. 1.50, 413.
1979. 24. Stachura, I., Si, L., Madan E., and Whiteside T.. C‘lirl. Irn~nrrnol. Itnr,7ltnoptrtilo/.. 30, 362. IYXJ, 25. Holdsworth, S. R., Neale. T. J., and Curtis, C. B.. .f. Clir~. Inise.rt. 68, 686. 19X1. 26. Neild, G. H.. Ivory, K., Hiramatsu, M.. and Willimas, D. G.. C/in. ,Urp. I~nrnnrzol. 52, 586. 1983. 27. Biesecker, G.. Lab. Itwest. 49, 237, 1983. 28. Groggel. G.. Adler, S., Helmut. R., Couser, W.. and Salant. I>.. J. C‘lirl. lt~~~rvt. 72. 194X. iYK3. 29. Kung, P. C.. Goldstein, G., Reinherz. E. L., and Schlossman. S. F.. Sc~iewc.c~ (Washington. D.C’.)
206, 347. 1979. 30. Reinherz, E. L.. Kung, I?. C.. Goldstein. G.. and Schloasman. S. F., f’roc-. ,Vcltl. A(,cicl. <S(,,. C!SA
76, 4061. 1979. 31. Reinherz, E. L., Kung, P. C., Goldstein, G.. Levey. K. H., and Schlossman. S. E. I+~~~ ,Vliti.
Acud. Sci. USA 77, 1588, 1980. 32. Uchiyama, T., Broder, S.. and Waldmann, T., J. f~rrnr~tol. 126, 13Y3. 1981. 33. Breard, J., Reinherz, E. L.. Kung. P. C., and Schlossman. S. F., J. I~nmunol. 124, 1943, lY80. 34. Stashenko. P. L., Nadler, L. M., Hardy, R.. and Schlossman. S. E. J. Itnmunt)/. 125. 1678, 1980. 35. Abramson. C. S.. Kersey, J. H., and LeBien. T. W.. 1. Ir?rrn~no/. 126. 83. 1981.
Received April 4, 1984: accepted with revisions June 28. lY84.




















