
Case Report - Oxford Academic
12
Treatment for a 14-Year-Old Girl With Lyme Disease Using Therapeutic Exercise and Gait Training Myriam M.C. Moser Background and Purpose. Lyme disease is well documented in the literature; however, specific physical therapy interventions for the pediatric population with residual effects of Lyme disease have not been addressed. The purposes of this retrospective case report are: (1) to present an example of a therapeutic intervention for a pediatric patient in the late stages of Lyme disease with related musculoskeletal dysfunction and severely impaired quality of life, (2) to report the patient’s functional outcomes from treatment, and (3) to discuss implications for treatment of patients with musculoskeletal dysfunction in the late stages of Lyme disease. Case Description. The patient was a 14-year old girl who had contracted Lyme disease 1 year prior to initiation of physical therapy. She was unable to participate with her peers in school, church, and sporting events due to significant impairments in strength (force-generating capacity), endurance, and gait; fatigue; pain; and total body tremor. Therapeutic exercise and gait training were used for treatment. The patient actively participated in managing her care by providing feedback during interventions and setting goals. Outcomes. After 18 weeks of treatment, the patient achieved 96.7% of her predicted distance on the Six-Minute Walk Test with normal gait mechanics and returned to playing high school sports. She had a manual muscle test grade of 4/5 or greater in major extremity muscle groups. She returned to school and church participation with minimal total body tremor when fatigued and daily pain rated 0 to 3/10. Discussion. Therapeutic exercise and gait training may facilitate return to func- tion in an adolescent patient with late effects of Lyme disease. Further investigation is advised to establish treatment effects in a broader population. M.M.C. Moser, PT, DPT, New England Rehabilitation Hospital, 2 Rehabilitation Way, Woburn, MA 01801 (USA). Address all corre- spondence to Dr Moser at: [email protected]. [Moser MMC. Treatment for a 14-year-old girl with Lyme disease using therapeutic exercise and gait training. Phys Ther. 2011; 91:1412–1423.] © 2011 American Physical Therapy Association Published Ahead of Print: July 7, 2011 Accepted: May 16, 2011 Submitted: January 25, 2011 Case Report Post a Rapid Response to this article at: ptjournal.apta.org 1412 f Physical Therapy Volume 91 Number 9 September 2011 Downloaded from https://academic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Case Report - Oxford Academic

Treatment for a 14-Year-Old Girl WithLyme Disease Using TherapeuticExercise and Gait TrainingMyriam M.C. Moser
Background and Purpose. Lyme disease is well documented in the literature;however, specific physical therapy interventions for the pediatric population withresidual effects of Lyme disease have not been addressed. The purposes of thisretrospective case report are: (1) to present an example of a therapeutic interventionfor a pediatric patient in the late stages of Lyme disease with related musculoskeletaldysfunction and severely impaired quality of life, (2) to report the patient’s functionaloutcomes from treatment, and (3) to discuss implications for treatment of patientswith musculoskeletal dysfunction in the late stages of Lyme disease.
Case Description. The patient was a 14-year old girl who had contracted Lymedisease 1 year prior to initiation of physical therapy. She was unable to participatewith her peers in school, church, and sporting events due to significant impairmentsin strength (force-generating capacity), endurance, and gait; fatigue; pain; and totalbody tremor. Therapeutic exercise and gait training were used for treatment. Thepatient actively participated in managing her care by providing feedback duringinterventions and setting goals.
Outcomes. After 18 weeks of treatment, the patient achieved 96.7% of herpredicted distance on the Six-Minute Walk Test with normal gait mechanics andreturned to playing high school sports. She had a manual muscle test grade of 4/5 orgreater in major extremity muscle groups. She returned to school and churchparticipation with minimal total body tremor when fatigued and daily pain rated 0 to3/10.
Discussion. Therapeutic exercise and gait training may facilitate return to func-tion in an adolescent patient with late effects of Lyme disease. Further investigationis advised to establish treatment effects in a broader population.
M.M.C. Moser, PT, DPT, NewEngland Rehabilitation Hospital, 2Rehabilitation Way, Woburn, MA01801 (USA). Address all corre-spondence to Dr Moser at:[email protected].
[Moser MMC. Treatment for a14-year-old girl with Lyme diseaseusing therapeutic exercise andgait training. Phys Ther. 2011;91:1412–1423.]
© 2011 American Physical TherapyAssociation
Published Ahead of Print: July 7,2011
Accepted: May 16, 2011Submitted: January 25, 2011
Case Report
Post a Rapid Response tothis article at:ptjournal.apta.org
1412 f Physical Therapy Volume 91 Number 9 September 2011
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

Lyme disease is the most commontick-borne disease in the UnitedStates and occurs through infec-
tion by the spirochete bacteria Bor-relia burgdorferi.1,2 Lyme disease isa “multisystem disorder with diversecutaneous, arthritic, neurologic,[and] cardiac” manifestations, whichmay occur within days or weeks fol-lowing infection, but may notbecome apparent until months oryears after the initial infection.3 Thetypical disease course begins whenan infected tick bites and remains onthe host for at least 48 hours. Thiscontact with the tick is followed bythe characteristic bull’s-eye rash (ery-thema migrans), which occurs in70% to 80% of people who areinfected.4 Flu-like symptoms, myal-gia, and large-joint inflammation mayresult.4–6 The incidence among chil-dren aged 5 to 10 years (23 per100,000) is twice that among adoles-cents and adults aged 20 to 35 years(8–12 per 100,000). The incidencepeaks in the adult populationbetween 60 and 70 years of age(19 per 100,000). The cases ofreported Lyme disease occur with ahigher frequency in densely woodedareas—especially of New Englandstates.2,7 In 2009, 95% of reportedcases occurred in 12 northeastern USstates alone.4
Typically, 60% of those diagnosedwith Lyme disease develop Lymearthritis, especially in the knees, dur-ing early dissemination of the dis-ease.4,8 In the late stages of the dis-ease, patients may developcontinuing or relapsing generalizedsymptoms such as fatigue and mus-culoskeletal pain.8 Cases have beendocumented where patients exhib-ited fibromyalgia-like symptoms orgeneral self-limiting, nonspecificsymptoms persisting longer than 6months after the original infection,but their incidence has not beenestablished.5,6,9 Some authors havereported pain occurring in largejoints, which may or may not be
polyarticular, and that may appearpost–Lyme infection.5,10 Theseauthors recommended physical ther-apy interventions, although they didnot specify any particular methodsof intervention.
Lyme disease has been classified as arheumatic disease. Several authorshave reported incorporating physi-cal therapy in the treatment of peo-ple with general rheumatic diseas-es.10–13 Physical therapy for latestages of Lyme disease has been men-tioned by a few authors as an adjuncttherapy for persistent musculo-skeletal dysfunction.5,14–16 The pub-lication by Ellenbogen14 is not anexperimental study but rather a com-mentary, and Sigal5 mentioned phys-ical therapy for patellofemoral painthat might occur due to quadricepsmuscle weakness from joint painafter Lyme infection. Although notspecifically addressing physical ther-apy interventions, Klempner et al6
performed a double-blind, placebo-controlled study of the effects ofantibiotics on adult patients withseropositivity to B. burgdorferi andpatients with seronegativity and adocumented incident of erythemamigrans. Patients included in thisstudy had onset of chronic symp-toms within 6 months of the initialtick bite that interfered with theirfunctioning such as “widespreadmusculoskeletal pain, cognitiveimpairment, radicular pain, paresthe-sias, or dysesthesias.”6(p85) Theyfound that patients with the chroniceffects of Lyme disease persistingafter unsuccessful antibiotic treat-ment were considerably impaired intheir health-related quality of life.Most notably, according to the Med-ical Outcomes Study 36-Item Short-Form Health Survey questionnaire(SF-36) scores they recorded, thesepatients were as impaired as otherpatient populations with congestiveheart failure or osteoarthritis.
Rheumatoid arthritis (RA) also is clas-sified as rheumatic disease.13 A num-ber of studies of varying quality haveinvestigated the effects of physicaltherapy interventions and therapeu-tic exercises for adult patients withRA.18–20 The general consensus isthat therapeutic exercise appears tobe a beneficial intervention foradults with RA. In the pediatric pop-ulation, numerous authors have con-cluded that physical therapy wasbeneficial for patients with juvenilerheumatoid arthritis (JRA). Interven-tions ranged from splinting, rest, andpalliative modalities (ie, ice, heat,and ultrasound) to therapeutic exer-cise and aquatic therapy, with thera-peutic exercise promoted as a viableapproach to restoring function inpatients with JRA.11,21–23
In light of these findings for the treat-ment of rheumatic diseases, thera-peutic exercise was postulated toproduce similar outcomes in apatient affected by the late stages ofLyme disease. Of note, neither thestudies on general rheumatic diseasenor the articles specifically mention-ing physical therapy for musculo-skeletal dysfunction as a result ofLyme disease addressed specificphysical therapy interventions orguidelines for treating the general orpediatric population with adversefunctional sequelae associated withthe late stages of Lyme disease.
The purposes of this retrospectivecase report are: (1) to present anexample therapeutic interventionfor a pediatric patient in the latestages of Lyme disease with relatedmusculoskeletal dysfunction andseverely impaired quality of life,
Available WithThis Article atptjournal.apta.org
• Video recorded during the gaittraining program.
Therapeutic Exercise and Gait Training in Lyme Disease
September 2011 Volume 91 Number 9 Physical Therapy f 1413
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

(2) to report the patient’s functionaloutcomes from treatment, and (3) todiscuss implications for treatmentof patients with musculoskeletal dys-function in the late stages of Lymedisease.
Patient History and Reviewof SystemsThe patient was a very thin, 170-cm(5.58-ft)-tall, 14-year-old girl diag-nosed with Lyme disease after receiv-ing a tick bite while playing outdoorson a warm winter day in February inNew England. She reported findingand removing the tick. The site ofthe bite became sore and developedthe characteristic erythema migransrash. Two days after finding the tick,the patient was seen by a nurse prac-titioner at her primary care physi-cian’s office. The nurse practitionerrecognized the rash, ordered bloodwork, and prescribed 1 month ofdoxycycline. The initial test returneda negative result, and the antibioticswere discontinued.
Over the next few weeks, the patientbegan to report increased fatigueand joint pain radiating from her jawto her knees initially, then to herelbows, back, and ankles, with herknees and ankles being the worst.The primary care physicianre-ordered blood work 1 month afterthe initial episode. The patient testedpositive for Lyme disease andreceived another course of doxycy-line for 1 month, with continuedworsening of symptoms. Sevenmonths after the initial bite, thepatient was withdrawn from schooland referred to another physicianwho prescribed a cocktail of medica-tions, including doxycycline, amoxi-cillin, clarithromycin, probenecid,and Mepron* (atovaquone). Fourmonths later, the patient had diffi-culty ambulating and had constanttotal body tremors, as reported by
the patient’s mother. One year afterthe original tick bite, the patient con-tinued to experience total body pain,fatigue, and constant tremor. Shewas referred to a pediatric rheuma-tologist and specialist in Lyme dis-ease, who discontinued the antibiot-ics and ordered physical therapy. Atthe time of the patient’s referral, shewas not receiving outside medicalcare, and she was taking only over-the-counter Aleve† (naproxen) asneeded for pain relief.
At the initial assessment, the patientand her mother reported that sincethe infection she had not beenattending school, participating in herchurch youth group, playing sports,or doing light chores. She also hadepisodes of falling down stairs dueto her knees buckling. She statedthat falling episodes had diminishedat the time of her physical therapyevaluation. Prior to the Lyme infec-tion, her past medical history wasunremarkable. The patient’s goalsfor physical therapy were “to run,participate in sports, pick up thingswithout hurting, and go to the[church] youth group.”
Clinical ImpressionThe patient reported impaired func-tional mobility in activities of dailyliving (ADL) and instrumental activi-ties of daily living (IADL) due to totalbody pain, fatigue, and constanttremor resulting from the originalLyme infection. She was unable toparticipate with her peers in school,church, and sporting events. Theevaluating physical therapist deter-mined the patient needed a thor-ough strength (force-generatingcapacity) and range-of-motion(ROM) examination, gait analysis,balance testing, pain and fatigueassessment, and a brief neurologicworkup to rule out any possible cen-tral nervous system dysfunction. The
patient’s unusual history and signifi-cant limitations afforded a uniqueopportunity to research and presentinterventions for a patient affectedby Lyme disease.
Informed consent was obtained fromthe patient and her mother to useher case for this article. In accor-dance with HIPAA regulations andhospital policies, permission wasobtained from the hospital privacyofficer to use the medical recordsin this case. The records werede-identified for confidentialitypurposes.
Physical ExaminationThe patient exhibited a total bodyresting tremor greatest in all 4extremities when sitting. The tremordisappeared with joint approxima-tion such as in quadruped stance.Tremors have not been documentedas a common primary or secondarysymptom of Lyme disease. Thetremor the patient exhibited mayhave been a visible manifestation ofphysiological tremor due to an emo-tional component,24 such as anxietyfrom the pain related to the Lymedisease and inability to interact withher peers or due to physical exhaus-tion resulting from the fatigue that iscommonly associated with Lyme dis-ease.3,4 The tremor also may havebeen an adverse side effect of theprescribed medications. Her reflexeswere normal. The patient wasscreened for central nervous systemdysfunction using rapid dorsiflexionof the ankles for abnormal tone(velocity-dependent resistance tostretch), and she tested negative forankle clonus bilaterally. No otherspecific neurologic tests were per-formed because the patient’s sponta-neous movements did not appeardysmetric or uncoordinated. Whenstanding, she assumed a forwardhead posture with flexed hips andknees. The Wong-Baker Faces PainRating Scale25 was used to assess herself-reported pain (Tab. 1, Fig. 1). A
* GlaxoSmithKline, 5 Moore Dr, Research Tri-angle Park, NC 27709.
† Bayer Health Care LLC, 36 Columbia Rd, POBox 1910, Morristown, NJ 07962-1910.
Therapeutic Exercise and Gait Training in Lyme Disease
1414 f Physical Therapy Volume 91 Number 9 September 2011
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

scale with faces was chosen becausethis type of scale has been well doc-umented and validated in the litera-ture for pediatric populations.26,27
Once the patient learned the scale,she used numbers in subsequent ses-sions to report her pain.
Gait assessment was performedusing observational gait analysis asdescribed by Levangie and Norkin.28
During gait on level surfaces, thepatient continued her forward flexedtrunk posture with flexion at thehips and knees, decreased right
Wong-Baker FACES Pain Rating Scale
0 2 4 6 8 10HurtsWorst
HurtsEven More
HurtsLittle Bit
NoHurt
Hurts LittleMore
HurtsWhole Lot
Figure 1.Pain scale used to determine the patient’s subjective pain report. Copyright 1983,Wong-Baker FACES Foundation. Used with permission.
Table 1.Measurements Taken Periodically Throughout Treatmenta
Measure
Baseline Week 8 Week 10 Week 12 Week 18
Right Left Right Left Right Left Right Left Right Left
Passive range of motion Glenohumeral flexion 158° 150° 180° 180° N/T
Straight leg raise 70° 70° N/T
All other joints WNL WNL
Manual muscle test Anterior deltoid muscles 3�/5 3�/5 4/5 4/5
Upper trapezius muscles 4/5 4/5 N/T
Biceps muscles 4/5 4�/5 N/T
Triceps muscles 4/5 4�/5 N/T
Hip flexion 3�/5 3�/5 4/5 4/5
Hip extension 3�/5 3�/5 4/5 4/5
Hip abduction 4�/5 4�/5 N/T
Hip adduction 4�/5 4�/5 N/T
Knee extension 4�/5 3�/5 4/5 4/5
Plantar flexionb 4/5 4/5 5/5 5/5 N/T
Dorsiflexion 3�/5 4�/5 4/5 4/5
Eversion 3�/5 4/5 4/5 4/5
Inversion 4�/5 4�/5 4�/5 4/5
Upper abdominals 4�/5 4�/5 N/T
Lower abdominals 4/5 4/5 N/T
Subjective pain rating scale 4/10–9/10 3/10–4/10 3.5/10 0–4/10 0–3/10
Unilateral stance �30 s �30 s N/T
Dynamic stancec Bilateral WNL WNL
Single-leg stability 1.0 1.5
Six-Minute Walk Test 277.37 m(910 ft)
564.49 m(1,852 ft)
643.74 m(2,112 ft)
a WNL�within normal limits, as defined by Norkin and White40; N/T�not tested further, as no further testing was indicated based on overall function.b Nonstandardized testing position used initially for evaluation. All other manual muscle tests refer to Reese.33 To differentiate muscle strength of 3�/5 from4�/5, 2-finger resistance was applied. If the patient’s extremity could be moved with 2 fingers, muscle strength was considered 3�/5. If the patient couldresist 2 fingers but could not maintain muscle contraction for longer than 1 second against the whole hand, muscle strength was considered 4�/5. Toreceive a muscle strength grade of 5/5, she had to resist maximally for 5 seconds.c Tested on the Biodex Balance System force platform.
Therapeutic Exercise and Gait Training in Lyme Disease
September 2011 Volume 91 Number 9 Physical Therapy f 1415
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

lower-extremity (LE) terminal stancetime, decreased trunk rotation, andno upper-extremity (UE) swing. Toestablish baseline gait speed andendurance, a Six-Minute Walk Test(6MWT) was performed similar tothe procedure described by Li et al,29
except due to space constraints dur-ing the initial evaluation, it was per-formed on a continuous looping cir-cuit rather than in a long hallway. Allsubsequent 6MWT trials were per-formed in a straight 45.72-m (150-ft)hallway. The 6MWT has been welldocumented in the literature,30,31
and 2 recent studies have describednorms in children who werehealthy.29,32 Although the 6MWT hasnot yet been validated in children, itwas chosen for this patient becauseit was conducive to setting measure-able goals and to indicating a likelyteenage level of ambulatory gaitspeed and endurance.
Manual muscle testing (MMT) wasperformed (in the positions describedby Reese33) on major muscle groupsto design individualized interventionsaddressing the patient’s strength def-icits (Tab. 1). The grading scale usedwas adapted from Kendall et al.34
Manual muscle testing has beendescribed as having variable sensitiv-ity but is considered reliable andmoderately to strongly correlatedwith handheld dynamometry.35,36 Ithas been validated for use in myositisand has good reliability and validityin neuromusculoskeletal dysfunc-tion,37,38 but it particularly lacks sen-sitivity and precision when assessingmuscle grades of 4/5 and higher.35,39
In this case, the patient had globalstrength deficits bilaterally aboveand below 4/5. Since a handhelddynamometer was not available inthis clinic, a general MMT screen ofmajor muscle groups was deemedadequate to determine strengthimpairments and their relationshipto the patient’s function.
The patient had normal or functionalROM in all joints except the gleno-humeral joints bilaterally (Tab. 1).Joint ROM was assessed as describedby Norkin and White40 unless other-wise noted. Joint goniometry hasbeen validated radiographically forthe knee (intraclass correlation coef-ficient [ICC]�.98)41 and found tohave high intratester reliability in theshoulder (ICC�.87–.99),42 knee,43
and elbow.43
Balance was assessed first by unilat-eral stance in quiet standing witheyes open on a stable surface(Tab. 1). Eight weeks into treatmentbalance was further assessed usingan athlete single-leg stability (SLS)test (Tab. 1) on the Biodex BalanceSystem‡ in preparation for progres-sion of interventions to include plyo-metrics and higher-speed agility lad-der work. The Biodex BalanceSystem consists of a circular multi-axial force platform connected to acomputer output screen. The athleteSLS test is performed for each LE andconsists of three 20-second tests on aplatform with a setting of 4 (1�leaststable, 12�most stable), with10-second rests between tests. Theplatform measures medial-lateral andanterior-posterior postural stability.Similar balance testing on dynamicplatforms has been outlined for usein adolescents.44 Normative datahave been generated using the ath-lete SLS test in 20- to 28-year-oldadults who were healthy but not inchildren.45 Paterno et al46 demon-strated good between-session reli-ability (ICC�.72) using the level 4athlete SLS test in femaleadolescents.
Clinical ImpressionThe evaluating physical therapistdetermined that the patient wouldbenefit from skilled physical therapyto address her primary impairments
of decreased strength, decreasedROM, abnormal gait, fatigue, andpain. Interventions were targetedtoward these deficits to improve herability to perform ADL and IADLtasks and return to all previous age-appropriate social activities. Physicaltherapy was scheduled for 2 timesper week for 8 weeks. The patientwas re-evaluated at 8 weeks, atwhich point goals were revised andprogressed for another 4 weeks ofcontinued treatment. She wasre-evaluated at 12 weeks, and goalswere again progressed over 6 weeksuntil the patient’s discharge fromtherapy. Frequency of treatment wascontinued after the first 8 weeks buttapered over the remaining 10weeks to once a week. This taperingof treatment was done to accommo-date the patient’s insurance limita-tions and to optimize her ability toachieve her goals as she regainedfunction and learned to self-manageher symptoms.
InterventionThe patient and her mother wereactively involved in setting her initialgoals and revising them at weeks 8and 12 (Tab. 2). Interventions weredesigned with these goals in mindand based on active feedback fromboth the patient and her mother. A6MWT goal chart (Fig. 2) wasassigned for the patient to track herprogress and was periodicallyreviewed throughout treatment.There were no contraindications toproceeding with physical therapy.All interventions were performed bythe evaluating therapist except forone land treatment where the pri-mary therapist was off site, and theaquatic session in the clinic was per-formed with the aquatic therapistwith input from the primarytherapist.
A combination of therapeutic exer-cise and a home exercise program(HEP) was designed to address thepatient’s strength and ROM deficits.
‡ Biodex Medical Systems, 20 Ramsay Rd, Shir-ley, NY 11967-4704.
Therapeutic Exercise and Gait Training in Lyme Disease
1416 f Physical Therapy Volume 91 Number 9 September 2011
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022
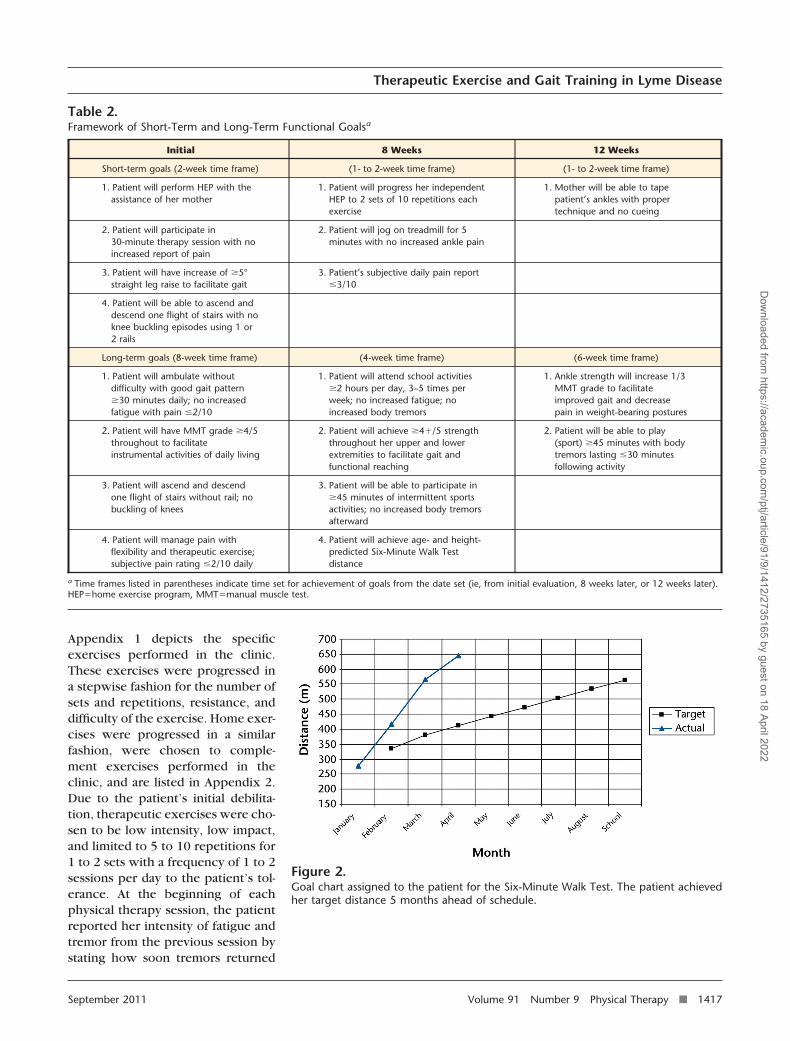
Appendix 1 depicts the specificexercises performed in the clinic.These exercises were progressed ina stepwise fashion for the number ofsets and repetitions, resistance, anddifficulty of the exercise. Home exer-cises were progressed in a similarfashion, were chosen to comple-ment exercises performed in theclinic, and are listed in Appendix 2.Due to the patient’s initial debilita-tion, therapeutic exercises were cho-sen to be low intensity, low impact,and limited to 5 to 10 repetitions for1 to 2 sets with a frequency of 1 to 2sessions per day to the patient’s tol-erance. At the beginning of eachphysical therapy session, the patientreported her intensity of fatigue andtremor from the previous session bystating how soon tremors returned
Figure 2.Goal chart assigned to the patient for the Six-Minute Walk Test. The patient achievedher target distance 5 months ahead of schedule.
Table 2.Framework of Short-Term and Long-Term Functional Goalsa
Initial 8 Weeks 12 Weeks
Short-term goals (2-week time frame) (1- to 2-week time frame) (1- to 2-week time frame)
1. Patient will perform HEP with theassistance of her mother
1. Patient will progress her independentHEP to 2 sets of 10 repetitions eachexercise
1. Mother will be able to tapepatient’s ankles with propertechnique and no cueing
2. Patient will participate in30-minute therapy session with noincreased report of pain
2. Patient will jog on treadmill for 5minutes with no increased ankle pain
3. Patient will have increase of �5°straight leg raise to facilitate gait
3. Patient’s subjective daily pain report�3/10
4. Patient will be able to ascend anddescend one flight of stairs with noknee buckling episodes using 1 or2 rails
Long-term goals (8-week time frame) (4-week time frame) (6-week time frame)
1. Patient will ambulate withoutdifficulty with good gait pattern�30 minutes daily; no increasedfatigue with pain �2/10
1. Patient will attend school activities�2 hours per day, 3–5 times perweek; no increased fatigue; noincreased body tremors
1. Ankle strength will increase 1/3MMT grade to facilitateimproved gait and decreasepain in weight-bearing postures
2. Patient will have MMT grade �4/5throughout to facilitateinstrumental activities of daily living
2. Patient will achieve �4�/5 strengththroughout her upper and lowerextremities to facilitate gait andfunctional reaching
2. Patient will be able to play(sport) �45 minutes with bodytremors lasting �30 minutesfollowing activity
3. Patient will ascend and descendone flight of stairs without rail; nobuckling of knees
3. Patient will be able to participate in�45 minutes of intermittent sportsactivities; no increased body tremorsafterward
4. Patient will manage pain withflexibility and therapeutic exercise;subjective pain rating �2/10 daily
4. Patient will achieve age- and height-predicted Six-Minute Walk Testdistance
a Time frames listed in parentheses indicate time set for achievement of goals from the date set (ie, from initial evaluation, 8 weeks later, or 12 weeks later).HEP�home exercise program, MMT�manual muscle test.
Therapeutic Exercise and Gait Training in Lyme Disease
September 2011 Volume 91 Number 9 Physical Therapy f 1417
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

after treatment, how long theylasted, and how long she had to restbefore she could resume her regularactivities without tremor. Exerciseswere progressed or regressed at thebeginning of each session basedon her tremor, fatigue, and painresponse from the previous session(Appendix 1). When she could per-form 2 to 3 sets of each exerciseeasily without cues for techniqueand no increased body tremors aftershe finished her exercises, the exer-cises were progressed either inintensity, with resistance providedby Thera-Band,§ or in repetitions.If exercises were progressed withresistance, the number of sets andrepetitions were decreased for thatday. If exercises were progressed inintensity (ie, from walking speed torunning speed on the agility ladderor from low impact to high impact),the patient was given longer restsor performed fewer repetitions foreach set. Using this graded approachto resistive exercise with ongoingassessment of the patient’s bodyresponses, the physical therapistcould readily progress or regress theexercises.
For generalized pain and myalgia,some authors have advocated theuse of warm water to alleviate pain-ful joints and stiffness in childrenand adolescents.11,21 Aquatic therapywas initiated in water at a tempera-ture of 94°F. Prior to initiating theaquatherapy, the primary land thera-pist discussed with the aquatic ther-apist the patient’s current limita-tions, fatigue, and pain levels and theplan of care. The patient reporteddecreased joint and muscle painwith the warmth of the water butreported increased lumbar pain andtotal body tremor after the first ses-sion. The patient tried 2 additionalindependent sessions with similarresults. Aquatic therapy was discon-
tinued at this time because of theincreased pain and tremors, andinterventions were continued onland only. Given the patient’s age,exercises were chosen to be fun yetfunctional and challenging. Sheassisted in directing her care bychoosing between certain exercisesoffered by the therapist. For exam-ple, the patient would choosebetween trunk exercises such asprone planks on elbows versus hook-lying abdominal crunches or, for run-ning tasks, hopping on the trampo-line versus performing agility ladderdrills. In weeks 14 and 15, thepatient did not participate in thera-peutic exercises in the clinic. Theseclinical sessions were spent educat-ing the patient’s mother on ankletaping techniques to alleviate anklepain as the patient returned to play-ing soccer (Appendix 1).
The patient participated in gait train-ing to normalize cadence, to increasespeed and fluidity of movements,and to increase aerobic endurance(Appendix 1). Cues were given toincrease hip and knee extension dur-ing walking speeds on level ground.As she improved at level walkingspeeds, she was progressed to jog-ging. The phases of running werebroken down into parts, including:(1) active ankle plantar flexion anddorsiflexion while maintaining hipand knee extension and a stabletrunk position; (2) active ankle plan-tar flexion with hip and knee exten-sion and contralateral limb ankle dor-siflexion with hip and knee flexion;and (3) progression of the entiremovement into cyclical ankle dorsi-flexion with hip and knee flexion,hip flexion with knee extension, andreturning to hip and knee extensionwith ankle plantar flexion (see videorecorded during the gait trainingprogram available at ptjournal.apta.org). King47 outlined a similar pro-gression for optimizing speed andcoordination in an athlete. When thepatient had mastered these basics,
she was progressed to walking andjogging drills with an agility ladderand then to sprinting with quickdirectional changes (Appendix 1).
The patient also learned to monitorher heart rate. She used her heartrate in conjunction with her HEPand a simple flow chart for self-monitoring of intensity and deter-mining appropriate work rates formanaging postexercise tremors. Shereceived guidelines on the range ofheart rates that would place herbetween 60% to 80% of her pre-dicted maximal heart rate (calcu-lated as: 220�age).48 Although thereis substantial inter- and intra-variability between children and ado-lescents for predicted and measuredmaximal heart rate, the general equa-tion was used to provide a startingpoint to assign intensity of workouts.The patient then reported on herfatigue and tremor response follow-ing high-intensity exercise. If herfatigue and tremor were worse,intensity was decreased; if fatigueand tremor were the same or better,intensity (as measured by heart rateresponse) and duration of intenseexercise were gradually increased.
OutcomeUpon discharge after 18 weeks oftreatment, the patient achieved hergoal to play high-intensity sports(soccer) for up to 2 hours with trem-ors lasting between 30 to 45 minutesafterward. Initially, tremors wereconstant throughout the day. Threeweeks into treatment, the patientreported tremors lasting 2 to 3 hoursafter treatment and then diminish-ing. Although the patient could notattend school because it was the endof the school year, she was attendingmorning chapel exercises, selectedclasses 3 times per week, and all ofher usual church activities.
By week 12, the patient manifestedno remarkable deviations in her gaitpattern at walking, running, and
§ The Hygienic Corporation, 1245 Home Ave,Akron, OH 44310.
Therapeutic Exercise and Gait Training in Lyme Disease
1418 f Physical Therapy Volume 91 Number 9 September 2011
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

sprinting speeds. She achieved96.7% (643.7 m) of her height-predicted 6MWT distance—2.32times her initial distance (Tab. 1)—using the prediction equationderived by Li et al based on heightand change in heart rate. In theirstudy, the overall mean (�SD) dis-tance for children who were healthyand between the ages of 7 and 16years was 664�65.3 m (2,178.5�214.2 ft). The patient’s outcomeplaced her around the 40th percen-tile of the female cohort.29 Accord-ing to the study by Geiger et al,32
the patient’s final distance fell wellwithin the predicted mean (�SD) of663�50.8 m (2,174.6�166.6 ft).
By week 8, the patient had achievedfull glenohumeral motion (Tab. 1).She had achieved at least a 4/5strength rating in both lower extrem-ities (initially, 50% of motions testedscored below 4/5; Tab. 1). The samephysical therapist performed initialand follow-up measurements andwas the treating therapist. In bothjoint goniometry and MMT, studiessuggest a higher intratester reliabil-ity.38,42 As this is a retrospective casereport, the evaluating physical ther-apist was not blinded to the treat-ment and expected outcomes.
The patient self-monitored her heartrate and activity levels to manage hertremors and related fatigue, and shereported performing her home exer-cises twice daily. Her back, knee,and UE pain had resolved. Thepatient reported only some anklepain (3/10) but was able to managethe pain with taping and ankle exer-cises using Thera-Band as part of herregular HEP.
The patient demonstrated excellentbalance at baseline, so no interven-tions were specifically designed forbalance training. She had no loss ofbalance with unilateral stance on astatic surface. On the Biodex BalanceSystem platform, the patient demon-
strated an overall stability for each LE(right LE: 1.0, left LE, 1.5; Tab. 1) thatwas excellent and showed far loweranterior-posterior and medial-lateralstability indices compared with agroup of females who were healthyand 13 to 17 years of age.46
DiscussionNumerous authors have observedthat the late effects of Lyme diseasecan severely limit a patient’s func-tion, but few have provided non-pharmacological solutions to restorefunction. This case report presentsphysical therapy interventions aimedat restoring function, which wereadministered to a 14-year-old girlwith the late effects of Lyme disease.At the end of treatment, the patienthad achieved her personal goals andresumed her prior level of function.A summary of interventions used toaddress impairments has been pre-sented in the “Intervention” sectionand in Appendixes 1 and 2. It isimpossible in a single-case report todemonstrate a causal relationshipbetween the interventions providedand the patient outcomes. A positiveassociation can be seen between theinterventions and outcomes; how-ever, the patient may have alreadybegun healing at the time of referralto physical therapy. Other factorsmay have influenced her return tofunction. The patient was highlymotivated with very supportive par-ents, was healthy prior to this epi-sode, and reported high adherenceto her HEP—performing it twicedaily. Her school was very support-ive in allowing her to resume activi-ties on a limited basis without beingfully enrolled for the year.
It is not clear whether the aquatictherapy had any influence on painresolution. As the aquatic therapywas performed for only 1 supervisedsession and 2 independent sessionsand generally made the patient feelworse (increased pain and tremors),it is unlikely that it had a significant
influence on the patient’s recovery.As no other analgesic modalitieswere used throughout treatment, theimprovement seen in subjective painreport may have resulted from ben-eficial effects of regular exercisesuch as increased oxygenation to tis-sues, improved mood, and decreasedpain,23,49–50 or the improvement ingait mechanics, endurance, and mus-cle strength may have relievedundue stress on joint and muscle tis-sue. Burrascano16 noted that B. burg-dorferi is sensitive to both oxygenand temperature changes and theo-rized that regular, vigorous exercisemay assist in eradicating any remain-ing effects caused by B. burgdorferiin patients with chronic effects fromLyme disease, but this theory has notbeen substantiated by formal studies.
The 6MWT was used to provide aquantitative measure to track gainsin gait distance and endurance onlevel surfaces. The distance gainedappeared to be related to theobserved return to function, and thepatient’s final distance placed herwell within the means for adoles-cents who were healthy observed byLi et al29 and Geiger et al.32 A rela-tionship may exist between improve-ments in the 6MWT scores and mus-cle strength, but it is not possibleto establish this relationship in asingle-case report. As MMT scoresimproved, 6MWT distances increased,and posture while walking, jogging,and sprinting began to normalize.The weakness and fatigue the patientdemonstrated on the initial evalua-tion may have been a result ofreduced mobility from the pain andillness of the initial Lyme infectionfollowed by the persistent musculo-skeletal pain. Thus, muscle strengthmay have improved because thepatient was encouraged to be moremobile and to walk more frequentlyand farther, thereby increasingstrength through regular use. Con-versely, the patient may havebecome more mobile and able to
Therapeutic Exercise and Gait Training in Lyme Disease
September 2011 Volume 91 Number 9 Physical Therapy f 1419
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

walk farther because of strengthimprovements gained from specifictherapeutic exercise interventions.The 6MWT and MMT outcomes pre-sented measurable improvements inthe clinic setting. Combined withachievement of the patient’s func-tional goals, they suggest a probablepath to restoration of functionthrough physical therapy. However,they lack the ability to measureactual changes in function as relatedto quality of life. The patient’s chiefcomplaints related to limitations inactivity participation. A global mea-sure of function such as the PediatricQuality of Life Inventory (Peds-QL)51
or the KIDSCREEN-5252 might haveprovided a better quantified measureof the impact of the patient’s impair-ments on her daily function.
Throughout this case, the patient’sfeedback was sought on exerciseprogression, fatigue, pain, andtremor intensity. Slade et al53 dis-cussed the importance patientsplace on negotiation between thecaregiver and the recipient todevelop a plan incorporating thepatient’s personal values, prefer-ences, and lifestyle. Their findingssuggest that patients with chroniclow back pain prefer active involve-ment in their care. Slujis et al54 foundthat adherence to home exercise reg-imens was significantly (P�.001)influenced by positive feedbackfrom the therapist. Furthermore,they suggested that when therapistsfrequently cued patients to beinvolved in stating demands and tobe motivated to exercise at home,the patients demonstrated increasedadherence. Throughout treatment,the patient’s and her mother’s activeinvolvement in providing feedbackand choosing her course of care mayhave promoted the positive out-comes demonstrated. Successfulapplication of the interventions toother similar cases would necessitatefrequent communication between
the clinician and the patient to pur-sue patient-driven outcomes.
Klempner et al noted that patientsmay be diagnosed with Lyme diseaseand receive antibiotic therapy duringthe acute stages, yet months laterreport “persistent musculoskeletalpain, neurocognitive symptoms, ordysesthesia, often associated withfatigue.”6(p85) The patient describedin this case report had similar symp-toms despite 3 courses of antibiotictherapy. Some authors have postu-lated that lingering symptoms aredue to: (1) the initial Lyme infectionnot being completely eradicated,55
(2) a co-infection by another tick-borne pathogen,1 or (3) the initialinfection triggering a fibromyalgia-like response that may last formonths or even years.5,6,8,9 Patientswith persistent symptoms have sig-nificant limitations in daily functionand may respond to physical therapyinterventions as described in thisreport.
The use of therapeutic exercise andgait training elicited a positiveresponse and nonpharmacologicalrestoration of function for thepatient with late effects of Lyme dis-ease in this case report. The studiesdiscussing RA and JRA highlight ageneral trend that therapeutic exer-cise is beneficial in the treatment ofpatients with functional impairmentsresulting from these diseases in boththe adult and pediatric populations.Recommendations for the use oftherapeutic exercise for RA11,21,22
support the present case report’smode of intervention if Lyme diseaseis classified as being a subcategory ofthe rheumatic diseases. The inter-ventions in this report may be cau-tiously applied to patients with sim-ilar presentations. Careful attentionshould be paid to consistently reas-sess patients’ post-exercise response,and interventions should be adjustedaccordingly. In order to apply thefindings of this case report to a
broader population, future researchfocusing on addressing nonpharma-cological interventions for patientswith persistent musculoskeletal def-icits more than 6 months after initialLyme infection is advised. Such stud-ies could include a design wherepatients received antibiotic therapyas suggested by Stricker,55 antibiot-ics with concurrent physical ther-apy, and physical therapy interven-tions alone.
The author thanks the patient and thepatient’s parents for their diligence, for all theytaught her as a therapist, and for consenting tohave her case presented professionally. Theauthor also thanks Sean Collins, PT, ScD, SusanB. O’Sullivan, PT, EdD, and Deirdre Murphy,PT, DPT, MHA, of the University of Massachu-setts at Lowell, who provided critical analysisand feedback on content and presentation;Keith Poulin, PT, MSPT, and StacyMcDonough, PT, MSPT, of New EnglandRehabilitation Hospital for their valuable feed-back and support; and Peter Moser who con-tributed to the design of the tables and appen-dices. The author gives thanks to God for thedaily privilege to serve patients’ needs.
DOI: 10.2522/ptj.20110020
References1 Owen DC. Is Lyme disease always poly
microbial?—The jigsaw hypothesis. MedHypotheses. 2006;67:860–864.
2 Shapiro ED, Gerber MA. Lyme disease.Clin Infect Dis. 2000;31:533–542.
3 Stafford KC III. The Tick ManagementHandbook. New Haven, CT: The Connect-icut Agricultural Experimentation Station;2007. Available at: http://www.cdc.gov/ncidod/dvbid/lyme/resources/handbook.pdf. Accessed March 9, 2011.
4 Centers for Disease Control and Preven-tion. Lyme disease symptoms. Availableat: http://www.cdc.gov/lyme. AccessedMarch 26, 2010.
5 Sigal LH. Management of Lyme arthritis.Compr Ther. 1999;25:228–238.
6 Klempner MS, Hu LT, Evans J, et al. Twocontrolled trials of antibiotic treatment inpatients with persistent symptoms and ahistory of Lyme disease. N Engl J Med.2001;345:85–92.
7 Centers for Disease Control and Preven-tion. Lyme disease incidence rates by state,2004–2008. Available at: http://www.cdc.gov/ncidod/dvbid/lyme/resources/ld_stateIncidence2004_2008.pdf. Accessed March26, 2010.
Therapeutic Exercise and Gait Training in Lyme Disease
1420 f Physical Therapy Volume 91 Number 9 September 2011
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

8 Meletis CD, Zabriskie N, Rountree R. Iden-tifying and treating Lyme disease. Alterna-tive and Complementary Therapies.2009;15:17–23.
9 Sigal LH. Toward a more complete appre-ciation of the clinical spectrum of Borreliaburgdorferi infection: early Lyme diseasewithout erythema migrans. Am J Med.2003;114:74–75.
10 Dressler F, Girschick H, Huppertz H, Lah-denne P. Pediatric Rheumatology Euro-pean Society clinical guidelines: Lymearthritis. Pediatric Rheumatology OnlineJournal. Available at: http://www.pedrheumonlinejournal.org/july-august/PDF/guidelines%20lyme.pdf. AccessedJune 22, 2010.
11 Kimura Y, Walco GA. Pain in children withrheumatic diseases. Curr Rheumatol Rep.2006;8:480–488.
12 Ross JJ, Hu LT. Bacterial and Lyme arthri-tis. Curr Infect Dis Rep. 2004;6:380–387.
13 Sangha O. Epidemiology of rheumatic dis-eases. Rheumatology (Oxford). 2000;39(suppl 2):3–12.
14 Ellenbogen C. Lyme disease: shift the par-adigm! Arch Fam Med. 1997;6:191–195.
15 Schwartz B. Lyme disease. The Johns-Hopkins Arthritis Center. Available at:http://www.hopkins-arthritis.org/arthritis-info/lyme-disease/lyme.html. AccessedMarch 18, 2011.
16 Burrascano JJ. Advanced topics in Lymedisease diagnostic hints and treatment:guidelines for Lyme and other tick borneillnesses. 16th ed. 2008. Available at: http://www.lymenet.org/BurrGuide200810.pdf.Accessed April 4, 2011.
17 Ware JE Jr. SF-36 Health Survey: Manualand Interpretation Guide. Boston, MA:Health Institute, New England MedicalCenter; 1993.
18 Ottawa Panel Evidence-Based ClinicalPractice Guidelines for Therapeutic Exer-cises in the Management of RheumatoidArthritis in Adults. Phys Ther. 2004;84:934–972.
19 Christie A, Jamtvedt G, Dahm KT, et al.Effectiveness of nonpharmacological andnonsurgical interventions for rheumatoidarthritis: an overview of systematicreviews. Phys Ther. 2007;87:1697–1715.
20 Bell MJ, Lineker SC, Wilkins AL, et al. Arandomized controlled trial to evaluate theefficacy of community based physical ther-apy in the treatment of people with rheu-matoid arthritis. J Rheumatol. 1998;25:231–237.
21 Cakmak A, Bolukbas N. Juvenile rheuma-toid arthritis: physical therapy and rehabil-itation. South Med J. 2005;98:212–216.
22 Rhodes VJ. Physical therapy managementof patients with juvenile rheumatoidarthritis. Phys Ther. 1991;71:910–919.
23 Klepper S. Exercise and fitness in childrenwith arthritis: evidence of benefits forexercise and physical activity. ArthritisRheum. 2003;49:435–443.
24 National Institute of Neurological Disor-ders and Stroke. Tremor fact sheet. Avail-able at: http://www.ninds.nih.gov/disorders/tremor/detail_tremor.htm. PublishedJune 2006. Accessed March 26, 2011.
25 Wong-Baker FACES pain rating scale. Avail-able at: http://www.wongbakerfaces.org/wp-content/uploads/2010/12/FACES_English1.pdf. Accessed January 19, 2011.
26 Freeman K, Smyth C, Dallam L, Jackson B.Pain measurement scale: a comparison ofthe visual analogue and faces rating scalesin measuring pressure ulcer pain. JWound Ostomy Continence Nurs. 2001;28:290–296.
27 Garra G, Singer AJ, Taira BR, et al. Validationof the Wong-Baker FACES Pain Rating Scalein pediatric emergency department patients.Acad Emerg Med. 2010;17:50–54.
28 Levangie PK, Norkin CC. Joint Structureand Function: A Comprehensive Analysis.4th ed. Philadelphia, PA: FA Davis Co; 2005.
29 Li AM, Yin J, Au JT, et al. Standard refer-ence for the six-minute-walk test inhealthy children aged 7 to 16 years. Am JRespir Crit Care Med. 2007;176:174–180.
30 Enright PL, Sherrill DL. Reference equa-tions for the six-minute walk in healthyadults. Am J Respir Crit Care Med. 1998;158(pt 1):1384–1387.
31 Gibbons WJ, Fruchter N, Sloan S, Levy RD.Reference values for a multiple repetition6-minute walk test in healthy adults olderthan 20 years. J Cardiopulm Rehabil.2001;21:87–93.
32 Geiger R, Strasak A, Tremul B, et al. Six-minute walk test in children and adoles-cents. J Pediatr. 2007;150:395–399, e1–e2.
33 Reese NB. Muscle and Sensory Testing.2nd ed. St Louis, MO: Elsevier Inc; 2005.
34 Kendall FP, McCreary EK, Provance PG.Muscles: Testing and Function, With Pos-ture and Pain. 5th ed. Baltimore, MD:Lippincott, Williams & Wilkins; 2005.
35 Bohannon RW, Corrigan D. A broad rangeof forces is encompassed by the maximummanual muscle test grade of five. PerceptMot Skills. 2000;90(3 pt 1):747–750.
36 Bohannon RW. Manual muscle testing:does it meet the standards of an adequatescreening test? Clin Rehabil. 2005;19:662–667.
37 Rider LG, Koziol D, Giannini EH, et al. Val-idation of manual muscle testing and a sub-set of eight muscles for adult and juvenileidiopathic inflammatory myopathies.Arthritis Care Res (Hoboken). 2010;62:465–472.
38 Cuthbert SC, Goodheart GJ Jr. On the reli-ability and validity of manual muscle test-ing: a literature review. Chiropr Osteopat.2007;15:4.
39 Dvir Z. Grade 4 in manual muscle testing:the problem with submaximal strengthassessment. Clin Rehabil. 1997;11:36–41.
40 Norkin CC, White DJ. Measurement ofJoint Motion: A Guide to Goniometry.Philadelphia, PA: FA Davis Co; 2003.
41 Gogia PP, Braatz JH, Rose SJ, Norton BJ.Reliability and validity of goniometric mea-surements at the knee. Phys Ther. 1987;67:192–195.
42 Riddle DL, Rothstein JM, Lamb RL. Gonio-metric reliability in a clinical setting:shoulder measurements. Phys Ther. 1987;67:668–673.
43 Rothstein JM, Miller PJ, Roettger RF. Gon-iometric reliability in a clinical setting:elbow and knee measurements. PhysTher. 1983;63:1611–1615.
44 Emery CA, Cassidy JD, Klassen TP, et al.Development of a clinical static anddynamic standing balance measurementtool appropriate for use in adolescents.Phys Ther. 2005;85:502–514.
45 Arnold BL, Schmitz RJ. Examination of bal-ance measures produced by the biodexstability System. J Athl Train. 1998;33:323–327.
46 Paterno MV, Myer GD, Ford KR, HewettTE. Neuromuscular training improvessingle-limb stability in young female ath-letes. J Orthop Sports Phys Ther. 2004;34:305–316.
47 King I. MC Project Parts 1 and 2 [video-tape]. Reno, NV: King Sports Internation-al; 2002.
48 American Heart Association. Target heartrates. Available at: http://www.americanheart.org/presenter.jhtml?identifier�4736. Updated October 18, 2010. Ac-cessed October 18, 2010.
49 Oberg E. Physical activity prescription:our best medicine. Integrative Medicine.2007;6:18–22.
50 Fletcher GF, Balady G, Blair SN, et al. State-ment on exercise, benefits and recommen-dations for physical activity programs forall Americans: a statement for health pro-fessionals by the Committee on Exerciseand Cardiac Rehabilitation of the Councilon Clinical Cardiology, American HeartAssociation. Circulation. 1996;94:857–862.
51 Varni JW. Peds QL: Measurement Modelfor the Pediatric Quality of Life Inventory.Mapi Research Institute, 27 rue de la Vil-lette, 69003 Lyon, France, 1998–2011.Available at: http://www.pedsql.org.Accessed January 19, 2011.
52 Ravens-Sieberer U, Gosch A, Rajmil L, et al.KIDSCREEN-52 quality-of-life measure forchildren and adolescents. Expert RevPharmacoecon Outcomes Res. 2005;5:353–364.
53 Slade SC, Molloy E, Keating JL. “Listen tome, tell me”: a qualitative study of partner-ship in care for people with non-specificchronic low back pain. Clin Rehabil.2009;23:270–280.
54 Sluijs EM, Kok GJ, van der Zee J. Correlatesof exercise compliance in physical ther-apy. Phys Ther. 1993;73:771–786.
55 Stricker RB. Counterpoint: long-term anti-biotic therapy improves persistent symp-toms associated with Lyme disease. ClinInfect Dis. 2007;45:149–157.
Therapeutic Exercise and Gait Training in Lyme Disease
September 2011 Volume 91 Number 9 Physical Therapy f 1421
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

Ap
pen
dix
1.Pr
ogre
ssio
nof
Phys
ical
Ther
apy
Sess
ion-
to-S
essi
onIn
terv
entio
nsa
Inte
rven
tio
n
Wee
k
12
34
56
78
910
11
12
13
14
15
16
17
18
HEP
Hom
eEx
erci
sePr
ogra
m
Stab
ilit
yB
all
BLE
onba
ll:hi
pex
tens
ion,
low
ertr
unk
rota
tion,
abdo
min
alcu
rls
Qua
drup
edov
erba
ll:hi
pex
tens
ion,
GH
flexi
on,
and
alte
rnat
ing
hip
exte
nsio
nw
ithG
Hfle
xion
Neu
tral
brid
gew
ithth
orac
icsp
ine
onba
ll,w
ithdu
mbe
llp
ress
,w
ithG
Hfle
xon
Pron
eel
bow
son
ball
roll
outs
Tru
nk
Stab
ilit
yQ
uadr
uped
:hi
pex
tens
ion
with
GH
flexi
on
Hoo
k-ly
ing:
GH
flexi
on,
trun
kco
unte
rrot
atio
n,p
rogr
esse
dto
abdo
min
alcr
unch
varia
tions
Hoo
k-ly
ing
onfo
amro
ller:
alte
rnat
ing
LEm
arch
Pron
e:p
lank
onel
bow
sw
ithhi
ps/
knee
sof
fgr
ound
Pron
e:al
tern
atin
gG
Hfle
xion
with
hip
exte
nsio
n
Sup
ine:
BLE
flexi
on/e
xten
sion
Late
ralp
lank
Low
erEx
trem
ity
Wal
lsq
uat:
varia
tions
with
rubb
erba
nds
and
balls
;p
rogr
esse
dto
squa
ts,
now
allo
rw
eigh
ts
Seat
edkn
eeex
tens
ion
pro
gres
sed
tose
ated
onba
ll
Seat
edha
mst
ring
mus
cle
curls
pro
gres
sed
tost
oolp
ulls
and
brid
geon
ball
with
ham
strin
gm
uscl
ecu
rl
Stan
ding
:hi
pex
tens
ion,
hip
abdu
ctio
n
Late
rals
qua
tw
alk
pro
gres
sed
tosq
uat
wal
kw
ithru
bber
band
resi
stan
ce
15.2
cm(6
in)
late
rals
tep
-dow
nta
ps
pro
gres
sed
to20
.32
cm(8
in)
Ligh
tp
lyom
etric
s:1
and
2LE
jum
pin
gat
low
heig
hts,
low
rep
etiti
ons,
mul
tidire
ctio
nal,
freq
uent
rest
s
Cal
fra
ises
pro
gres
sed
toca
lfra
ises
onst
ep
Sup
ine:
BLE
onba
ll,os
cilla
ting
hip
exte
nsio
nfo
llow
edby
brid
gew
ithha
mst
ring
mus
cle
curls
and
ankl
eD
F/PF
Ank
le:
resi
sted
3-w
ay(in
vers
ion,
ever
sion
,an
ddo
rsifl
exio
n)
Mul
tidire
ctio
nall
unge
sp
rogr
esse
dto
varia
tions
with
med
icin
eba
ll
Late
rall
unge
jum
ps
pro
gres
sed
toov
er15
.2-c
m(6
-in)
box
Dep
thhu
mp
s:8
in-
floor
-6-
inbo
x
Up
per
Extr
emit
yW
allp
ush-
ups
Mod
ified
floor
pus
h-up
s
Full
pus
h-up
s
Gai
tT
rain
ing
Leve
lsur
face
s:m
ultid
irect
iona
l,br
aidi
ng,
late
ral,
brie
fbo
uts
ofjo
ggin
g,w
ithba
ll,ob
stac
les
Wal
king
sprin
tsw
ithba
ll
Hee
lwal
k,to
ew
alk,
skip
,m
arch
with
ankl
eD
F
Kick
ing
ball
for
socc
er
Agi
lity
ladd
er:
wal
king
spee
dp
rogr
esse
dto
jogg
ing
and
runn
ing
spee
ds
Trea
dmill
:2.
0m
ph
pro
gres
sed
to5.
0m
ph
Mod
ified
pus
h-up
into
sprin
t;ac
cele
ratio
nsin
tofu
llsp
rint
Jog
with
emp
hasi
son
ankl
eD
F/PF
Dyn
amic
Bal
ance
Ball
toss
:BL
Eon
bala
nce
beam
,on
air-
fille
ddi
sks,
with
late
rals
huffl
ing
Uni
late
rals
tanc
eva
riatio
ns:
com
plia
ntsu
rfac
es,
dyna
mic
forc
ep
latf
orm
,ai
r-fil
led
disk
Tram
pol
ine:
bila
tera
lhop
s,la
tera
lhop
s
aEx
erci
ses
liste
dfo
rea
chw
eek
wer
ep
erfo
rmed
2tim
esp
erw
eek,
then
tap
ered
toon
cea
wee
k,as
indi
cate
din
the
pla
nof
care
.H
EP�
hom
eex
erci
sep
rogr
am,
BLE�
bila
tera
llow
erex
trem
ities
,G
H�
glen
ohum
eral
,LE
�lo
wer
extr
emity
,D
F�do
rsifl
exio
n,PF
�p
lant
arfle
xion
.
Therapeutic Exercise and Gait Training in Lyme Disease
1422 f Physical Therapy Volume 91 Number 9 September 2011
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022

Appendix 2.Progression of Home Exercise Program
Week Exercises
1 1. Prayer stretch with lateral trunk flexion2. Hamstring muscle stretch3. Straight leg raise, side-lying hip abduction, standing mini-squats4. Seated on stability ball: gentle bouncing, pelvic circles, long-arc quadriceps knee extension5. Gait: walk 5–7 minutes, 2–3 times a day, setting number 1 on home treadmillAll exercises were performed for 5 repetitions, 1 set, 2 times a day; stretches were held for 5–15 seconds,2 times per set, 1–2 times a day.
3 1. Patient given chart to log Six-Minute Walk Test distances and goals to return to school2. Week 1 exercises continued3. Treadmill time: 6 minutes � 2 sets, setting number 2, once a day
4 1. Exercises as in week 1 but increased to 8 repetitions per exercise2. Heart rate monitoring3. Postexercise tremor used as gauge for exercise intensity and duration
6 1. Treadmill time: 8–9 minutes � 2 sets, setting number 2, once a day2. Week 1 exercises discontinued3. Standing: hip abduction, adduction, extension, and flexion; squats4. Stretches: half-kneeling psoas muscle stretch, hamstring muscle stretch, prayer stretch5. Stability ball: prone over ball, bilateral glenohumeral flexion with trunk extension, upper trunk
rotation with glenohumeral horizontal abduction; seated on ball, proprioceptive neuromuscularfacilitation diagonal 1 and 2 flexion and extension with trunk flexion and extension; seated on ballglenohumeral flexion and abduction
All exercises were performed for 8 repetitions, 2 sets, 1–2 times a day; stretches were held for 10–20seconds, 2 sets, 1–2 times a day
9 1. Treadmill time: 10–12 minutes each set2. Week 6 exercises continued3. Increased exercise repetitions to 10 � 2 sets, 1–2 times a day
11 1. Treadmill time: 15 minutes each set2. Light soccer practice with frequent rests and heart rate monitoring
12 1. Flow chart assigned to self-assess intensity of exercise and how to adjust exercises independently2. Ankle exercises: dorsiflexion, inversion, and eversion with Thera-Band
13 1. Under the guidance of the physical therapist, the patient self-designed collection of exercises topick out of hat each week; exercises were grouped into low and high intensity with aid of therapistso the patient could self-progress her exercises using her flow chart assigned in week 12
14 1. Ankle taping with mother: preparation, stirrups, heel-lock
Therapeutic Exercise and Gait Training in Lyme Disease
September 2011 Volume 91 Number 9 Physical Therapy f 1423
Dow
nloaded from https://academ
ic.oup.com/ptj/article/91/9/1412/2735165 by guest on 18 April 2022




















