Case Conference
74
Case Conference Reporter : 許珮寧 Instructor :蔡宗伯醫師 Date: 2013/09/14 1. Basic Information Name :詹吳x妹 Chart No. : 2765225 Gender : female Birth : 1926/05/17 Occupation : nil Patient identification -
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of Case Conference
Case Conference
Reporter : 許珮寧 Instructor :蔡宗伯醫師
Date: 2013/09/14
1. Basic Information
Name :詹吳x妹
Chart No. : 2765225
Gender : female
Birth : 1926/05/17
Occupation : nil
Patient identification -

This 85 years-old female came to our dental OPD for full mouth dental check and treatment
2. Chief Complaint
I want to restore my upper missing teeth with removable denture
3. PMH Hypertension D.M. Peptic ulcer Drug allergy: Pyrine
4. PDH FPDs made at LDC
admin
矩形

Extraction (O.S. department)
Scaling at LDC
PERSONAL HABITS ØSmoking (-)
ØBetal-nut chewing (-)
ØDrinking (-)
ØBruxism (-)
5.present Illness
This 85 years old female came to our OPD on 99.06.11 for full mouth prosthesis fabrication. She have never worn any removable denture. Her remnant teeth were #12, #13, #14, #15 and #32, #33, #34, #35. Teeth of #14 #15 #33 #34 #35 have been restored with metal splinted crowns without antagonists for several years. Upper and lower edentulous ridge were severe resorbed. (#12,#13,#32) Dental caries, poor oral hygiene and gingival inflammation were noted .
6.Extraoral Examination
Frontal view -- facial asymmetry(-)
•Lateral view -- convex profile

•No gummy smile
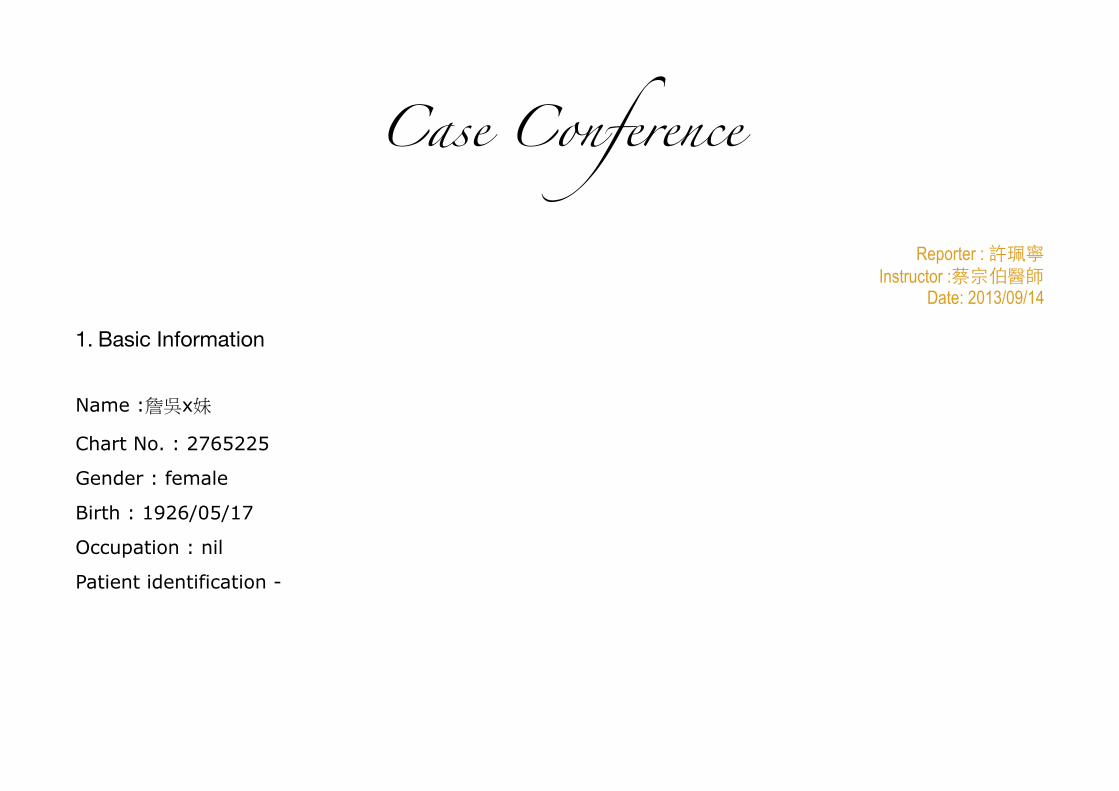
7. Intraoral Examination
Present dentition: 5 4 3 2 2 3 4 5
•FPDs:#14#15,#33#34#35
•Dental caries:12,13,32
admin
矩形
admin
矩形
admin
矩形
14,15 metal crowns
12,Atrophy edentulous ridge 33,34,35 metal crowns
8.Radiographic examination

13,15,33,34,35 incomplete endo. Tx teeth 33,34 apical lesion 14,15,33,34,35 metal crowns 32 moderate bone destruction
9.Probing Data
#15 #14 #13 #12 #32 #33 #34 #35PD-B 212 413 213 423 223 322 996 222
PD-L 422 443 334 422 233 322 1098 322
10.Diagnosis and Problem List
DENTAL PROBLEM LIST ØFull mouth plaque deposition

ØChronic periodontitis
ØMissing:
7 6 1 1 2 3 4 5 6 7
7 6 5 4 3 2 1 1 6 7
ØDental caries :12,13,32
TREATMENT SEQUENCE ØEmergency care
ØPre-prosthetic corrective care
ØHygienic and maintenance care
ØRehabilitative care
ØMaintenance and supportive care
TREATMENT OBJECTIVES ØRemove ill-fitted prostheses (99.07.23) ØRemove hopeless teeth (99.08.03) ØEndodontic treatment ( 99.08.10~99.10.27) ØPeriodontal treatment (99.07.23~) ØFull mouth prostheses fabrication

- provisional restoration (99.07.23~99.09.17) - definitive restoration (100.10.27~101.01.03)
11.Diagnostic Wax-up
Tentative Treatment
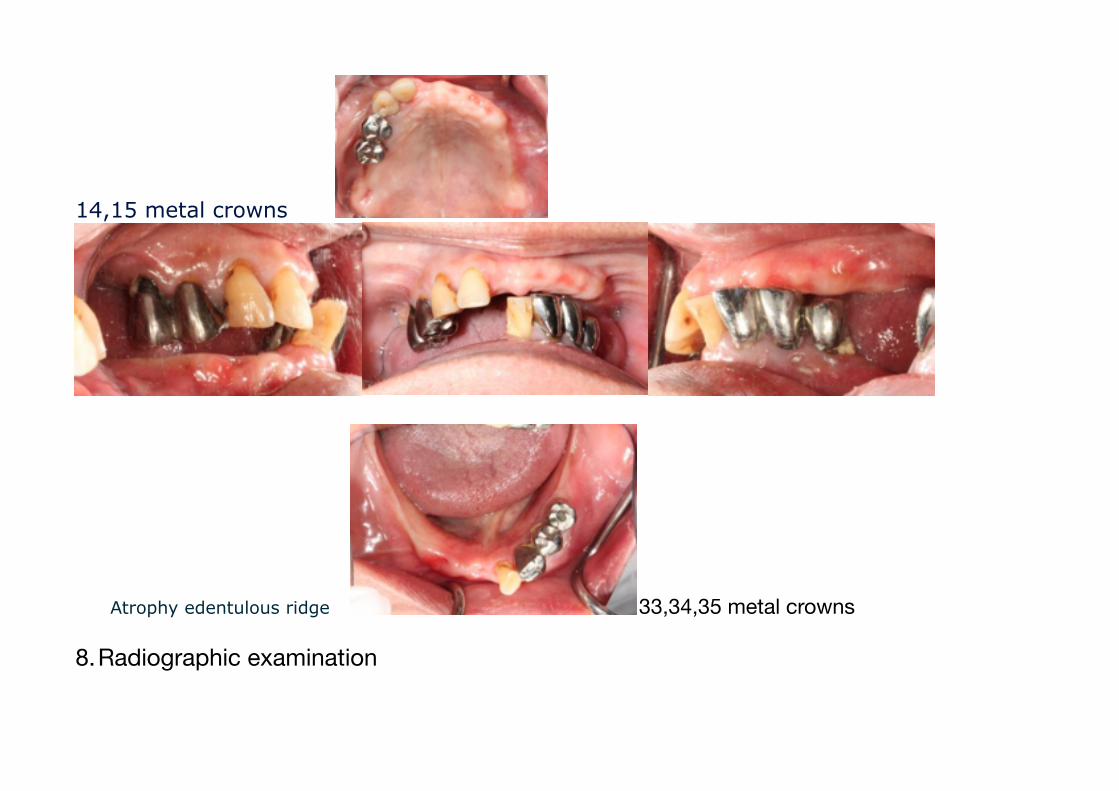
34 extraction
•13,15,33,35 endo. Tx
•Present dentition : 5 4 3 2 2 3 5 •13,14,15,33x35 provisional FPDs
• Upper and lower interim removable partial denture
12.Provisionals and Interim Dentures- Intraoral
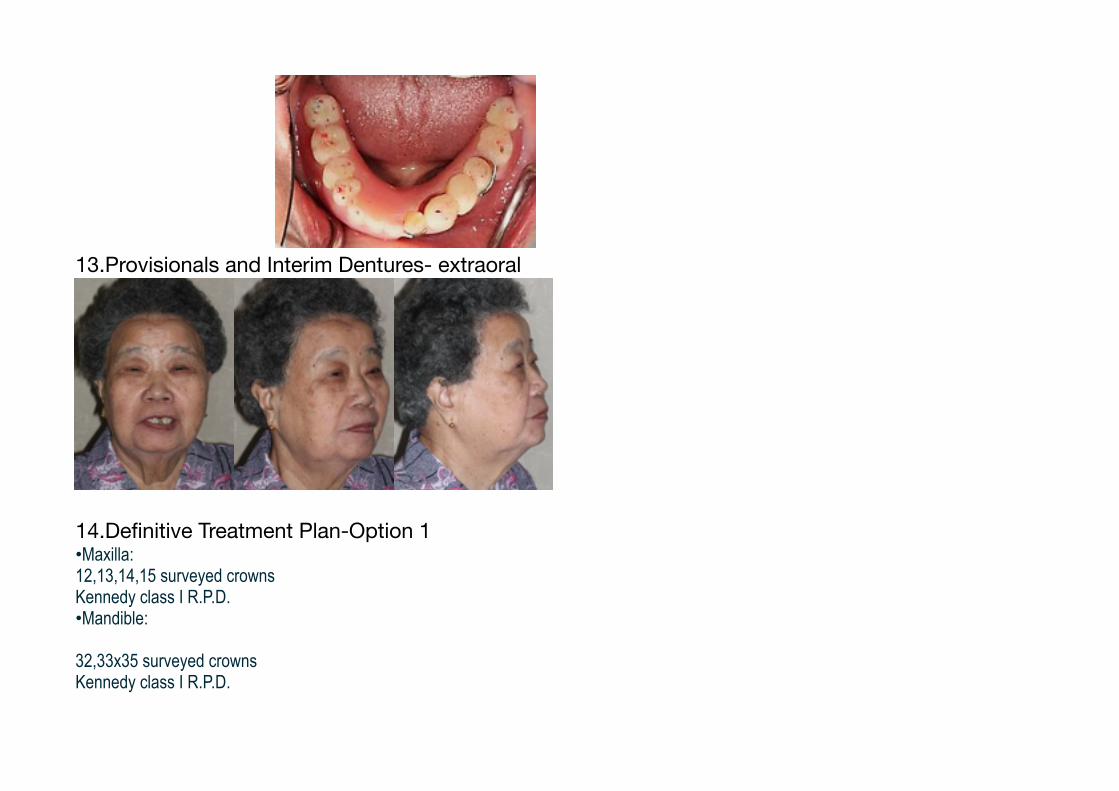
13.Provisionals and Interim Dentures- extraoral
14.Definitive Treatment Plan-Option 1•Maxilla: 12,13,14,15 surveyed crowns Kennedy class I R.P.D. •Mandible:
32,33x35 surveyed crowns Kennedy class I R.P.D.
admin
矩形
admin
矩形
admin
矩形

15.Definitive Treatment Plan-Option2
Maxilla: 13,14,15 surveyed crowns Kennedy class I R.P.D. •Mandible:
33x35 surveyed crowns Kennedy class I R.P.D.
16.Definitive Treatment Plan-Option3
Maxilla: 12,13,14,15 surveyed crowns implants assisted Kennedy class I R.P.D. •Mandible:
32,33x35 surveyed crowns implants assisted Kennedy class I R.P.D. 17.Definitive Treatment CourseSurveyed Crowns



18.RPD design and framework

19.Altered cast and wax up


20.Denture Delivery
MIP protrusion
Excentric movement21.Months Follow-up22.Q&A病例討論會Q&AQ1:請問你所取的咬合紀錄是C.O.還是C.R. bite?怎麼取?A1:CR;利用bilateral manipula8on of the mandible的方式:使用此法時每隻手的四根手指放在病患下顎的下緣,拇指放置於靠近顎部隆突處。當

病患下顎可自由地旋轉時,以手指施予一結實向上的壓力,拇指則施予一往上和往後的壓力。這些動作將引導一往後旋轉的下顎運動(hinge movement)。Q2:有考慮swing-‐lock的設計嗎?為何最後沒有做此設計?A2:一開始有考慮swing-‐lock的設計,但因為病患年紀較大,手的靈巧度比較不 好,所以後來就沒有作此設計。Q3:如何決定咬合平面?A3:利用上頷的recording base與occlual rim,incisal plane平行interpupillary line而側方平行Camper’s line而決定。Q4:作surveyed crown時bite時如何取的?A4:印製有裝戴上下provisional restora8on的study cast,取咬合紀錄及facebow transfer,及印製上下surveyed crown的master cast,分別取下顎及上頷study cast 對master cast的咬合紀錄,作cross mount將製作surveyed crown的上下master cast轉移至半調節咬合器上。 Q5:請問這患者在假牙製作後,在病人卸下活動假牙時,有什麼方式可以保護他 的無牙嵴?A5:可以製作occlusal splint去保護無牙嵴或如果病患口腔衛生照顧許可的話,可在睡覺時只裝其中一頷的活動假牙。Q6:在這類有牙對上無牙的患者,就mechanical方面在咬合上請問有什麼考量或 想法嗎?A6:希望減少自然牙對咬側無牙嵴的受力,所以occlusal scheme設計成group func8on以分擔咬合力量,減緩其吸收速度。

Case Conference
Reporter : 魏敏佳醫師 Instructor: 徐光蔚醫師
Date: 2013/09/14
1. General informa8onName :李x英 Gender : Female
Age : 69 y/o
Marriage: married
Occupa8on: re8red
AXtude : philosophic, live in Chiayi and Taoyuan
2.Chief complaint : My teeth are loosening

Referred from periodontal department for prosthe8c treatment
3. Past History•Past Medical History -‐ Denied of major systemic disease -‐ Denied any drug allergy •Past Dental History
-‐ OD, Endo, Ext, FPD
-‐ Examina8on and treatment at LDC 4. Personal habit
Smoking (-‐)
Betal-‐nut chewing (-‐)
Drinking (-‐)
Bruxism (-‐)
TMD symptom/sign : denied

5. Pre-‐treatment X-‐ray
6. Extra-‐oral examina8on:

Frontal view -‐ facial asymmetry (-‐) Ovoid outline form Low smile line Lateral view -‐ convex profile (class III profile)
Nasolabial angle: nearly 90°
7. Intra-‐oral examina8on 2012.02.21:
admin
矩形
admin
矩形
admin
矩形

#13-12-11-xx-23 ext Arch form: upper & lower -- taper
#18-28,38-33,44-48 missing #32,31,41 residual roots #42 advanced periodontitis with mobility Gr II #43 periodontitis with caries
FM chronic periodontitis lower anterior teeth and bone protrude to buccal side Edentulous area with moderate to severe alveolar bone resorption
8. Diagnosis & problem listdiagnosis:
#18-‐28,38-‐33,44-‐48 missing
FM chronic periodon88s
Ø #42 advanced periodon88s
Ø #43 caries and apical periodon88s
#32,31,41 residual roots
Lower anterior teeth and bone protrude to buccal side
Edentulous area with moderate to severe alveolar bone resorp8on
Problem list:
#18-‐28,38-‐33,44-‐48 missing
Lower anterior teeth and bone protrude to buccal side
Edentulous area with moderate to severe alveolar bone resorp8on
Unesthe8c profile
Poor chewing func8on
9. Tenta8ve treatment plan
Op8on 1. -‐ #32,31,41,42 extrac8on -‐ #33 endodon8c treatment -‐ upper and lower interim denture Op8on 2.
-‐ Extract all teeth -‐ Upper and lower interim denture -‐-‐ preprosthe8c correc8ve phase: -‐
2012/02/21: #13-‐12-‐11-‐xx-‐23 extrac8on
2012/02/24: #32,31,41,42,43 extrac8on -‐10. Interim denture fabrica8on

Lower anterior teeth lingual tilting 11. interim denture photosintraoral
extraoral
admin
矩形

12. Treatment sequence
Preprosthe8c correc8on and interim prosthesis phase 2012/02/24:primary impression and #32,31,41,42,43 extrac8on 2012/03/02:bite registra8on, facebow transfer 2012/03/09:wax denture try-‐in 2012/03/19:interim denture delivery 2012/04/25:alveoloplasty 2012/06/29:interim denture adjustment for teeth re-‐arrangement
Defini8ve prosthesis treatment phase 2012/08/01:CT taken 2012/10/12:#33,43 implanta8on
admin
矩形
admin
矩形
admin
矩形
admin
矩形

2013/02/19:primary impression 2013/03/26:maxilla final impression 2013/03/26:locator abutment selec8on 2013/03/29:locator abutment delivery and mandible final impression 2013/04/12:bite registra8on with base plate and wax rim, facebow transfer 2013/04/17:metal framework fabrica8on 2013/04/26:wax denture try-‐in 2013/05/09:denture delivery and pick up locator aiachment 2013/06/18:replace locator aiachment
13.Plan for alveoloplasty
1 month after lower teeth extraction prominent alveolar height & width (to buccal side) between #33-45

Fitchecker + PVS light body (Imprint II)

OSSEOUS FINDING: incomplete healed sockets with granulation tissue invaded, sharp edge
before after

OSSEOUS CORRECTION: osteoplasty to reduce the height & buccal prominence, approximately 3mm in height & 2mm in width, using rotary instrument & bone file
SOFT TISSUE CORRECTION: B & L flaps were apically posi8oned
14.Aker alveoloplastya. relief denture and cover with sok liner(12/05/02)b. repair resin(12/05/29)c. 34-‐43 re-‐arrange teeth

15.Prepare for implanta8on
admin
矩形
admin
矩形
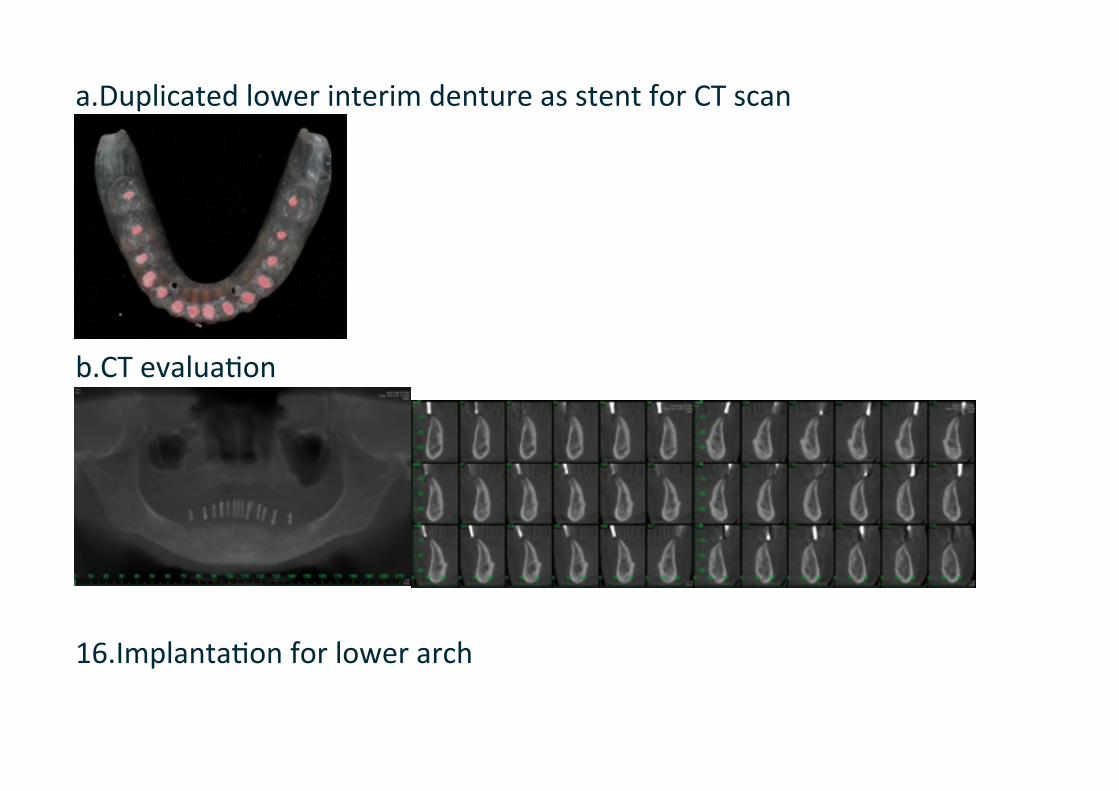
a.Duplicated lower interim denture as stent for CT scan
b.CT evalua8on
16.Implanta8on for lower arch

SURGERY: #33,43 implant installa8on
SOCKET: complete healed
SOFT TISSUE: TH: B=2mm; W: B=7,7; L=4,4
BONE QUALITY: type II
BONE QUANTITY: sufficient OSSEOUS: 4mm reduc8on of ridge height

IMPLANT: Straumann @4.1x12mm SP RNI at #33 & 43
BC-‐SHOULDER: #33=1.5, 2, 1, 1; #43= 1.5, 2, 1.5, 1.5
BONE TH: #33=1, 1.5; #43=1, 1.5mm
ISQ: #33=75,75; #43=76,75
HEALING ABUTMENT: 1.5mm
STAGE: non-‐submerged
SOFT TISSUE: B-‐flap spliced & apically posi8oned

17.Aker surgerya. Not to wear denture for 2 weeks

b. aker 2 wks, reline with Soklinerc. one month later, reline with Sokliner Tough18.Defini8ve Prosthesesa. Primary impression

b. Final impression/Maxilla
c. Final impression/Mandible

19.Bite registra8on with wax rim, and facebow transfer
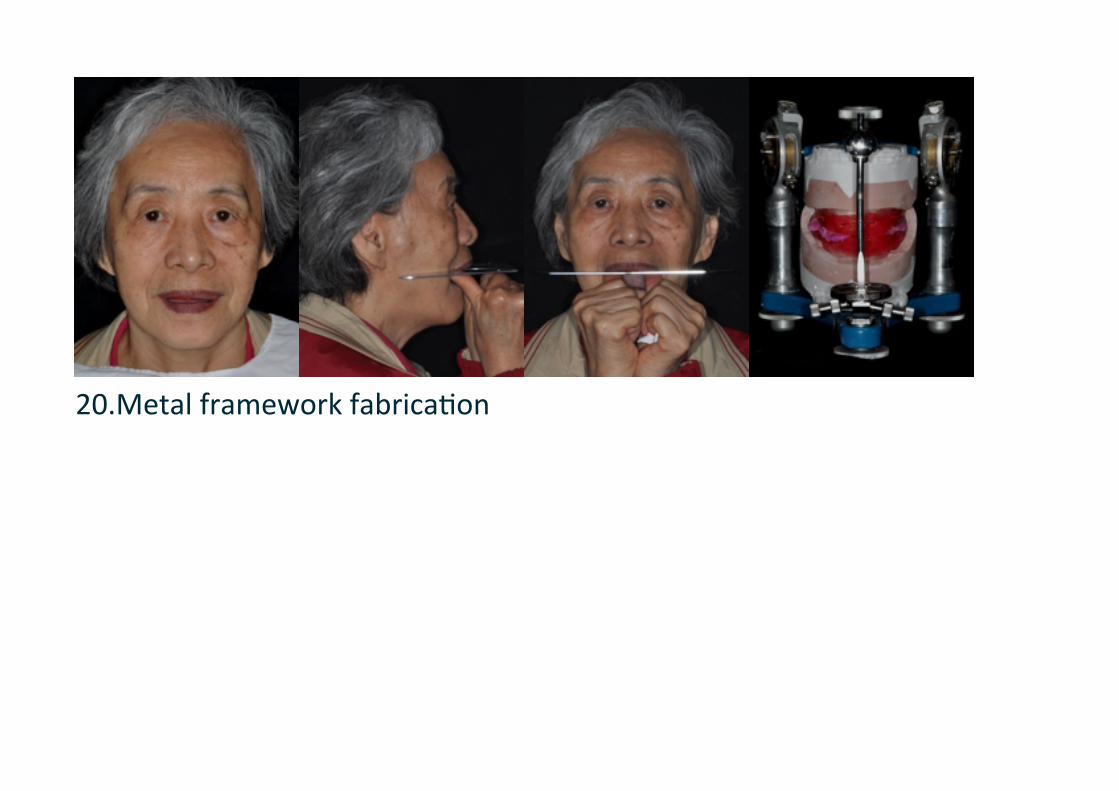
20.Metal framework fabrica8on
admin
矩形
admin
矩形
admin
矩形
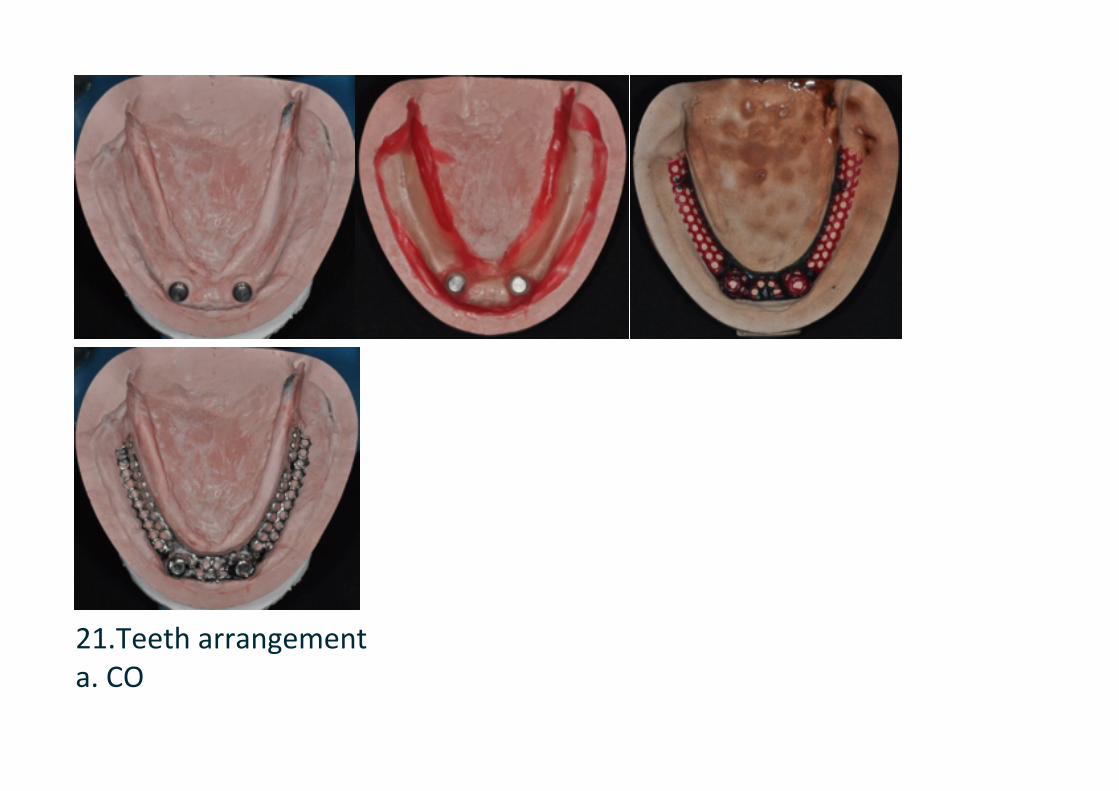
21.Teeth arrangementa. CO

b. Rt working
c. Lt working
d. protrusion


e. intraoral view
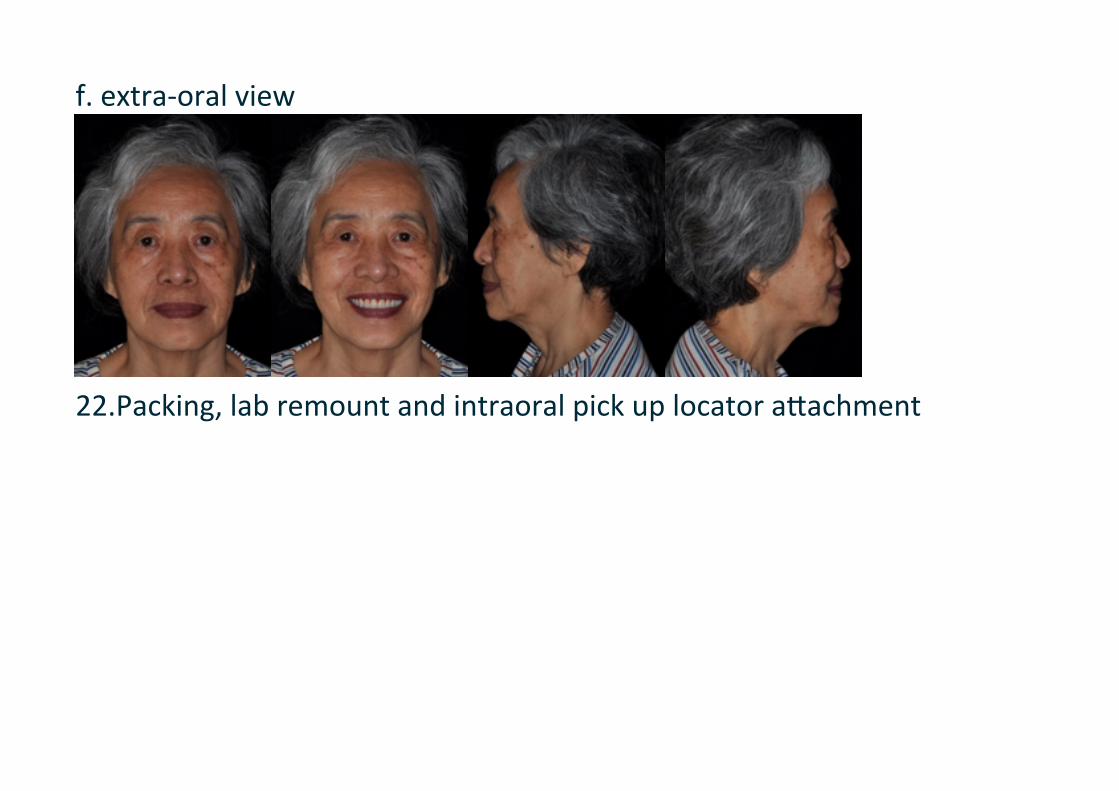
f. extra-‐oral view
22.Packing, lab remount and intraoral pick up locator aiachment
admin
矩形
admin
矩形
admin
矩形
admin
矩形
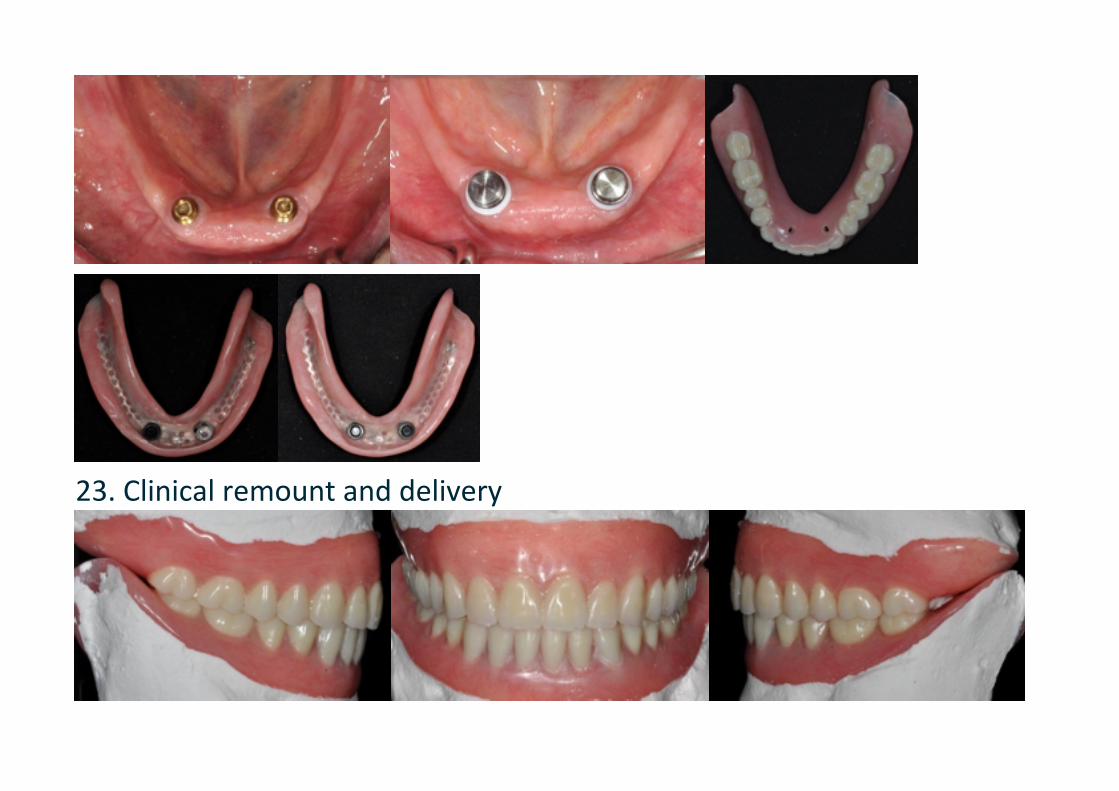
23. Clinical remount and delivery


24.Before and aker
admin
矩形
admin
矩形
admin
矩形
admin
矩形
Q & A (by魏敏佳)Q1. 為何不在拔牙的同時做alveoloplasty?A1: 確實可以在拔牙的同時做alveoloplasty或是針對比較sharp的bone做修整,但當時是只有單純做拔牙並沒有翻開flap去做alveoloplasty,是等bone經過一段時間自行remodeling後覺得bone仍然偏向buccal side protrusion才決定進行alveoloplasty,或許若預先知道resorp8on後的bone型態仍會不如預期,應該可以在拔牙就同時翻開flap做alveoloplasty。
Q2. 選擇在chair-‐side pick up aiachment的時機應該在denture delivery當次或是應讓病患戴denture一段時間後再pick up?A2: 理論上應先讓denture戴一段時間,讓sok 8ssue適當seiling,確保sok 8ssue與implant能同時均勻受力之後再pick up aiachment會更好,但研究上沒有確切數據指出應該要戴denture多長的時間才能達到效果,且此患者在deliver new denture之前已經有一副interim denture,sok 8ssue已經過一段時間的受力,而new denture在pick up aiachment之前的reten8on效果與interim denture也差不多,因此這個case是在deliver當次就直接pick up aiachment。
admin
矩形
admin
矩形
admin
矩形
admin
矩形

Q3. 為什麼沒有在pick up aiachment之後立刻換藍色male part?A3: 在此case是隔了一段時間才換藍色male part,原先是想讓病患先適應denture reten8on增加的感覺,follow up就換藍色,只是病患後來回南部一段時間才回來換,這段期間病患表示denture沒有不舒服的狀況。
Q4. Aiachment在lab processing過程直接完成與臨床上chair-‐side pick up有何差異?A4: 在locator操作說明是寫可以lab processing直接完成,但由於臨床操作經驗覺得由lab直接完成的aiachment位置常有誤差,需要整個挖掉重新pick up,因此在此case是選擇最後再進行chair-‐side pick up。
Q5. 此case是否考慮過增加implant數量或使用其他aiachment方式?A5: 以2 implants overdenture而言locator是簡易又方便的aiachment方式。曾與病患討論過是否增加到4 implants,但病患表示費用上考量,選擇2 implants贋復方式,若增加到4 implants,implant種植位置、aiachcment方式或是否配合使用bar,則需要再另外分析討論。
Q6. 在chair-‐side pick up aiachment時應請病患輕咬或是咬緊?A6: 依照locator的操作說明是請病患輕咬到MICP的位置來做pick up,但要讓sok 8ssue達到一定的沉降量似乎又應該請病患咬緊,而目前沒有針對咬力大小對於aiachment pick up精準度的相關研究。因為locator aiachment本身有resilient,因此臨床上大多數醫師還是選擇請病患輕咬到MICP做chair-‐side pick up。

Case Conference
Reporter : 簡君倩 醫師 Instructor : 徐光蔚 醫師
Date : 2013/09/14
1. General informationName :李 X 風
pGender : male
pBirth : 1960.07.10
pOccupation : 南亞成品課
pFirst visit :2010/10/05
pAttitude: philosophic
pPast medical history :
ØDM (-)
ØHTN (-)

ØDenied other systemic disease
ØDenied any drug allergy
ØTMD (-)
pPast dental history :
ØOD at LDC
ØExtraction at LDC
ØRoot canal treatment at LDC
ØFPDs were made at LDC
2. Chief complaintI had toothache at upper right side for almost a month, and the local dentist suggested me to receive FM periodontal treatment.
3. Personal habit
Cigarette (+,1 ppd/day for 20yrs)
ØBetel-nut chewing (-)
ØDrinking (+,高粱 1-2 cup/week)
ØBruxism(-)
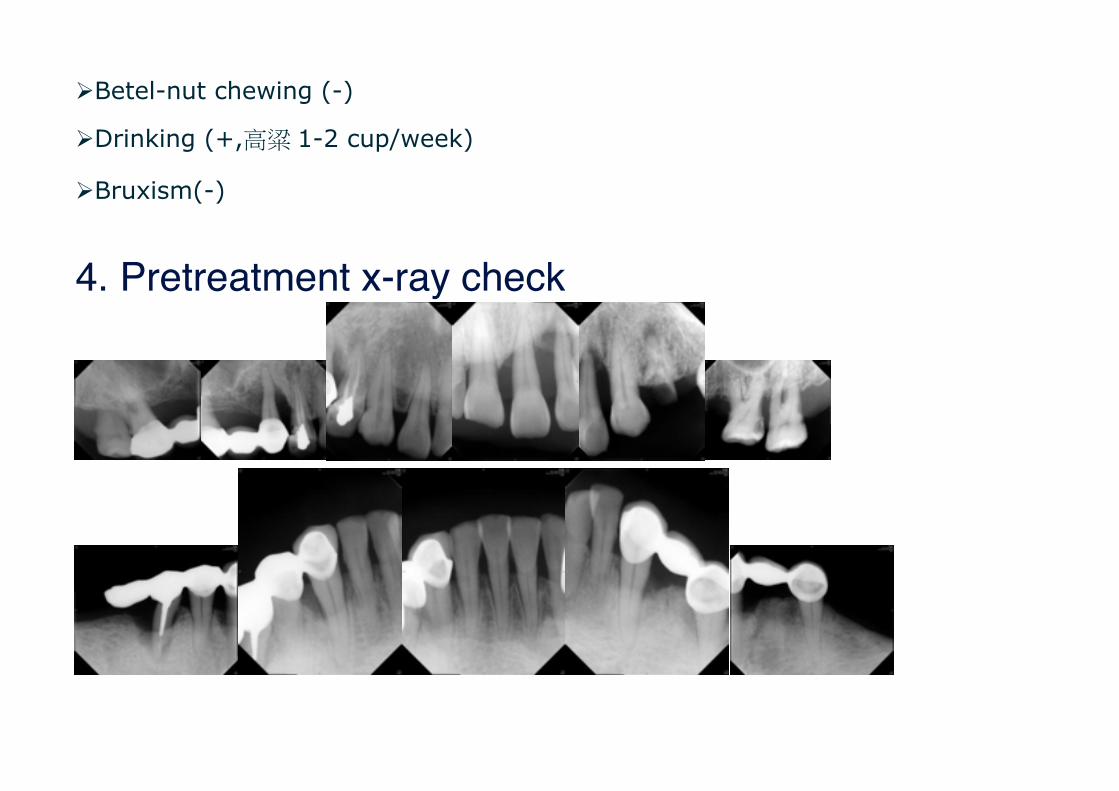
4. Pretreatment x-ray check
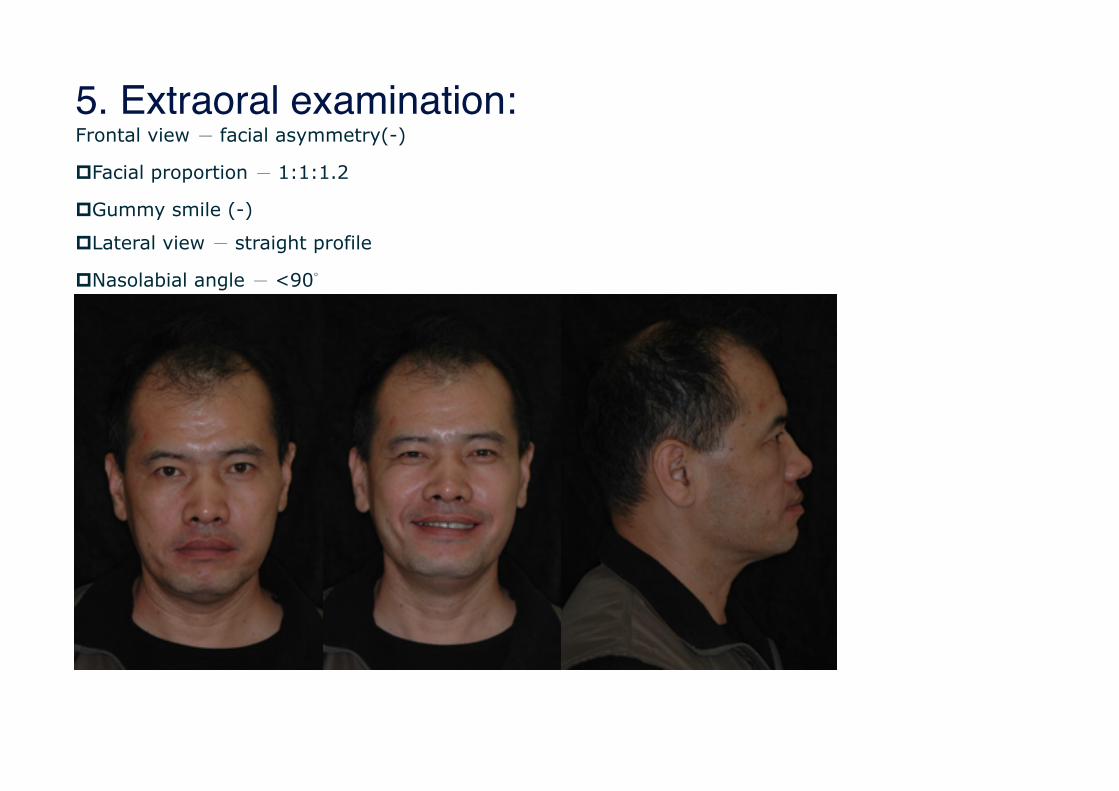
5. Extraoral examination:Frontal view - facial asymmetry(-)
pFacial proportion - 1:1:1.2
pGummy smile (-)
pLateral view - straight profile
pNasolabial angle - <90°
admin
矩形
admin
矩形
admin
矩形
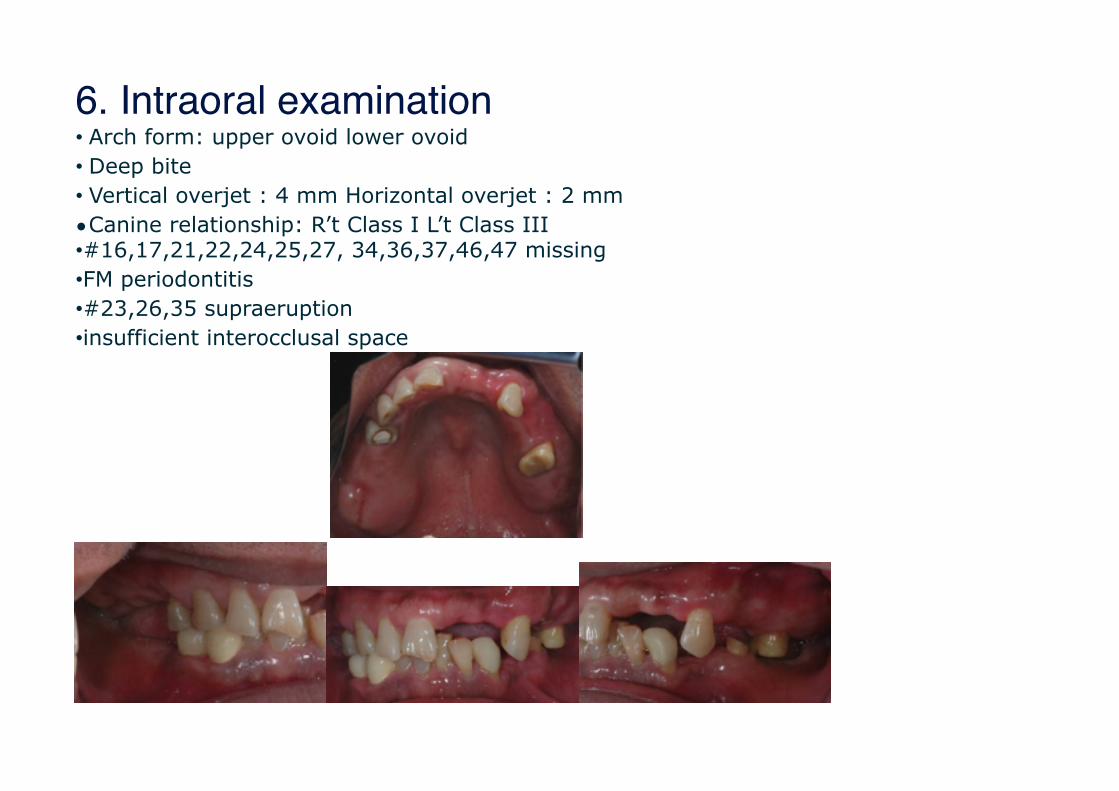
6. Intraoral examination• Arch form: upper ovoid lower ovoid • Deep bite • Vertical overjet : 4 mm Horizontal overjet : 2 mm •Canine relationship: R’t Class I L’t Class III •#16,17,21,22,24,25,27, 34,36,37,46,47 missing •FM periodontitis •#23,26,35 supraeruption •insufficient interocclusal space

7. Diagnosisp#18,17,15,21,22,24,27,45 extraction
p#33x35, #43-44-45x FPDs removal then abutment reevaluation
pFM periodontal treatment
p#14 endodontic retreatment
pInterim denture
Problem list

pInsufficient interocclusal space for prostheses
p#23,26,35 supra-eruption
pChronic periodontitis
8. Periodontal probing data
Tooth
18 17 16 15 14 13 12 11
PD(B) 665866637 535525 426 636 PD(B)
665 PD(B)
665 866 637
PD(P) 10 86
67 10
10 12 8
445535 436 635 PD(P)
10 86
PD(P)
10 86
67 10
10 12 8
M III II III I - II I M III M III II III

7. Treatment planning
Option 1) maintain VD
n#35 CLP and LL residual ridge alveoloplasty
nUR and UL tuberosity alveoloplasty
n#23,26,35 occlusal adjustment
n#14,26,33,35,43,44 FPDs
nmaxillary and mandibular RPDs

Option 2) maintain VD
n#35 extraction
nUR and UL tuberosity alveoloplasty
n#23,26 occlusal adjustment
n#14,26,33,43,44 FPDs
nmaxillary and mandibular RPD

Option 3) maintain VD
n#35 extraction
nLL alveoloplasty
n#23,26 occlusal adjustment
n#14,26,33,43,44 FPDs
n#34x36,45x47 implant-supported FPDs
nmaxillary RPD
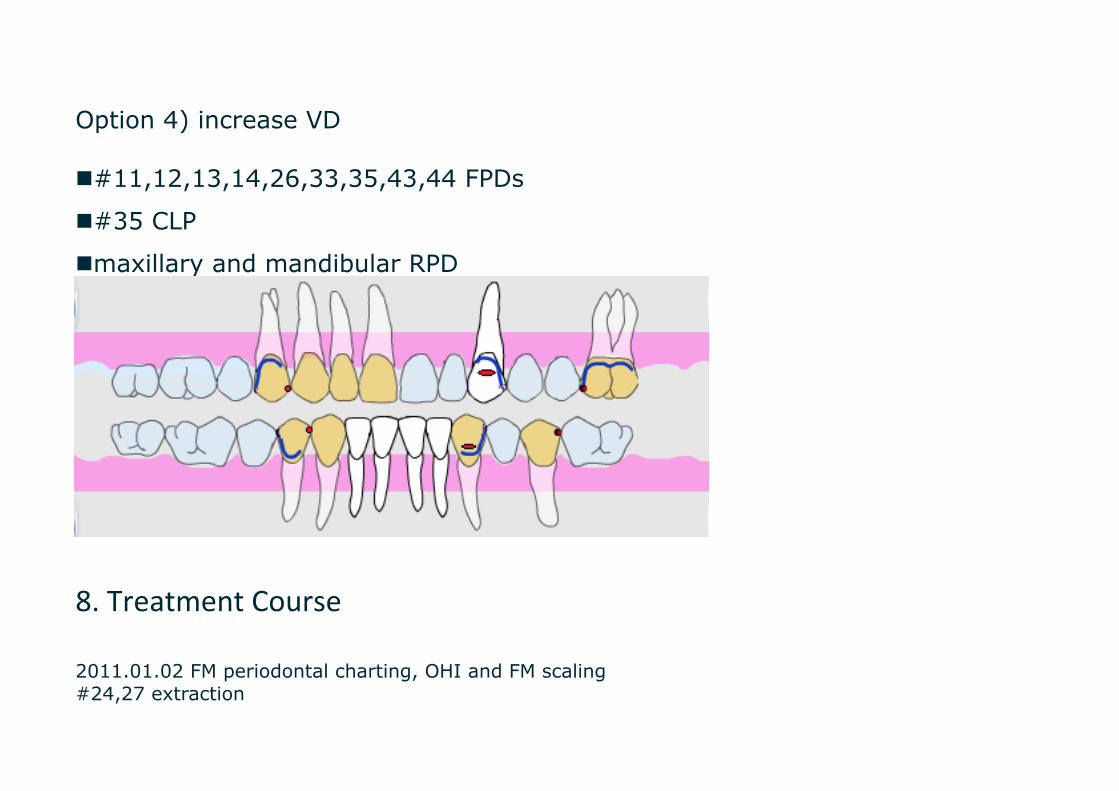
Option 4) increase VD
n#11,12,13,14,26,33,35,43,44 FPDs
n#35 CLP
nmaxillary and mandibular RPD
8. Treatment Course
2011.01.02 FM periodontal charting, OHI and FM scaling #24,27 extraction
p2011.03.07 UR and LR subgingival root planing p2011.03.18 #26 emergency open chamber and occlusal reduction p2011.03.25 #33x35 ill-fitted FPDs removal
#26 occlusal reduction impression for upper interim denture fabrication section at #44 distal side and #45 extraction p2011.04.04 LL subgingival root planing
#18,17,15 extraction p2011.04.11 #21,22 extraction p2011.04.12 upper interim denture delivery
p2011.04.13 #35 root canal treatment p2011.05.15 #14 root canal treatment p2011.05.16 FM periodontal charting(reevaluation) p2011.05.17 #26 local periodontal flap operation p2011.05.31 #33,35,43,44 local periodontal flap operation p2012.06.11 #26 root canal treatment p2012.08.10 #43-44 FPDs removal p2012.08.12~2012.08.25 #43 root canal treatment
9. Defini8ve treatment
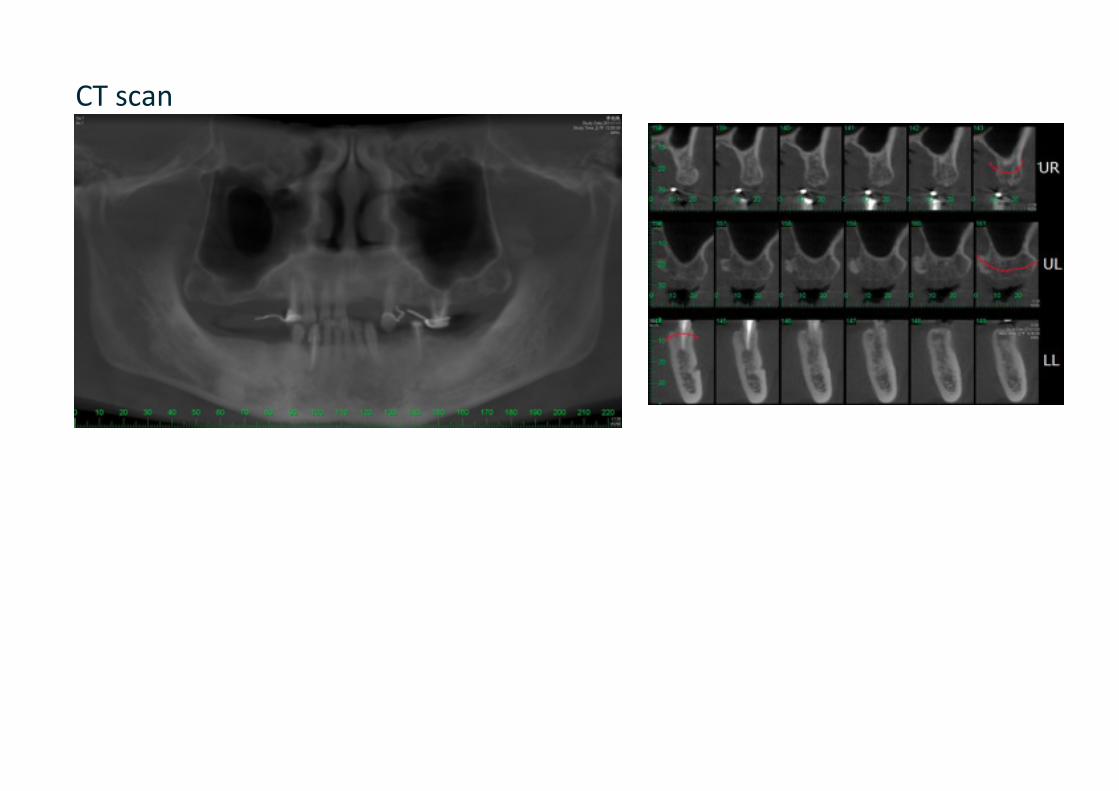
CT scan

UR and UL alveoloplasty 2012.06.05
p#35 CLP and LL alveoloplasty 2012.08.01
Aker surgery, the final ver8cal height

#11→#41: 14 mm #13→#43: 16 mm
Diagnostic wax up

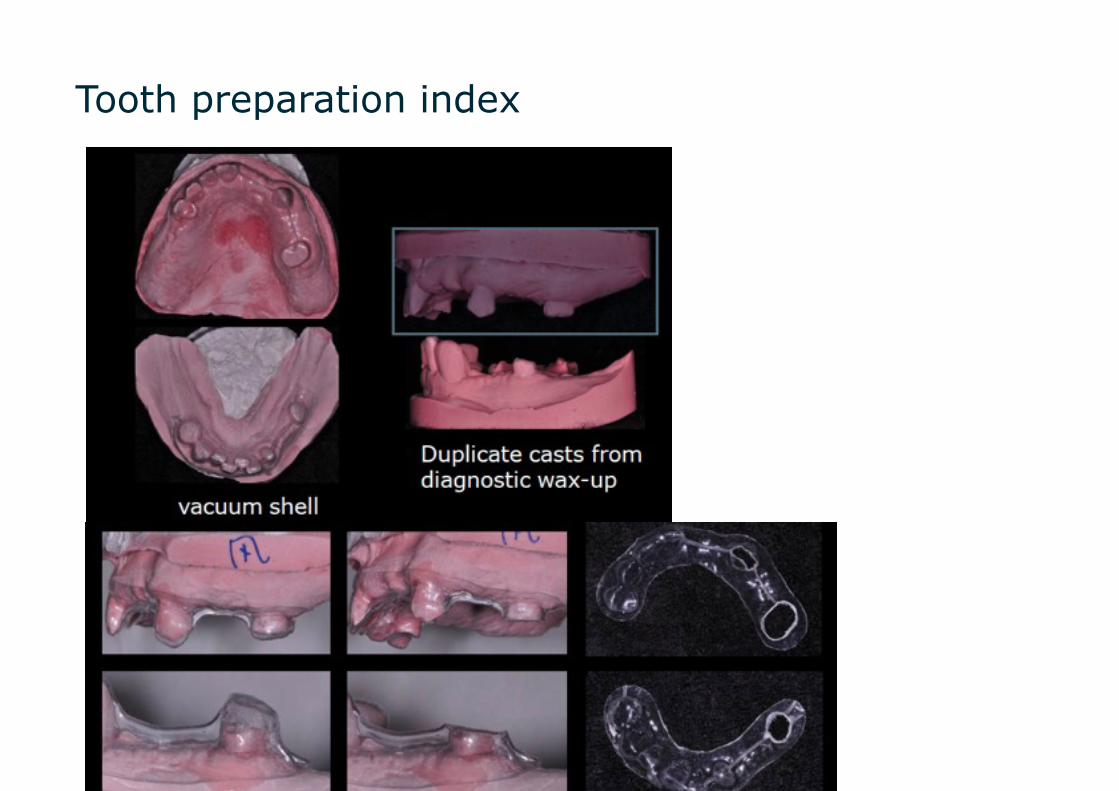
Tooth preparation index

surveyed crown impression and take bite

Fully wax up and surveyed

Take RPD impression

wax denture try in
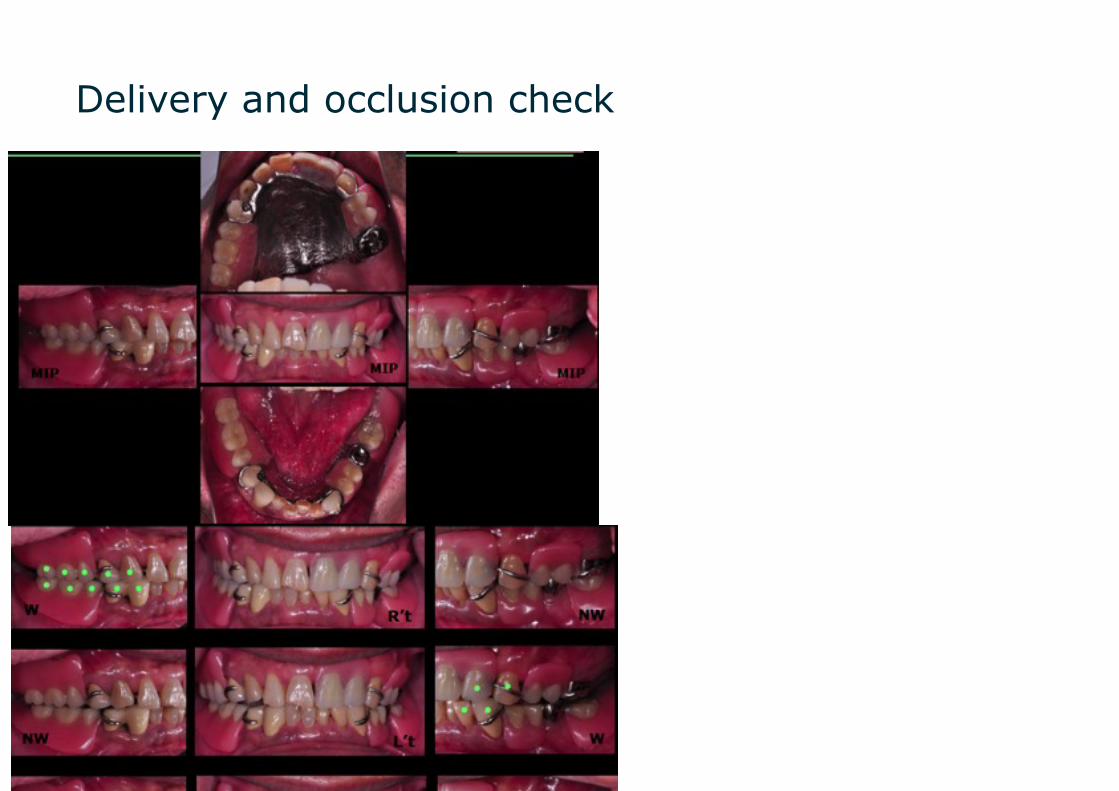
Delivery and occlusion check

admin
矩形
admin
矩形
admin
矩形
admin
矩形

Q:6個Txplan中,哪一個是最理想的?A: op8on 3能夠維持原本的ver8cal dimension來進行贗復,而不需要面對增加VD的風險,而上顎因為8ssue support較足夠以及deep bite的顧慮,所以維持RPD的設計;而lower den88on是以#34x36和#45x47 implant-‐supported FPDs來restore,這樣的優點是能夠增加occluding pair,左側也可建立 ver8cal stop,但缺點是要犧牲#35,並且implant 的費用也較高,所以仍然需要與病人完整的溝通。
Q: 若lower den88on以implant-‐supported FPDs來贗復,則#45x47 進行implant的意義為何?A: lower den88on以#34x36和#45x47 implant-‐supported FPDs來restore,是希望lower den88on能夠全部做為fixed prostheses,而不考慮做implant-‐assisted RPD。
Q: 若不做alveoloplasty,有其他的治療計畫嗎?A: 可以選擇單純以RPD來提高ver8cal dimension,讓病人不戴RPD的時候是咬在自己的牙齒上,而戴上RPD時,是在提高VD的狀態下,咬在RPD的framework上。
Q: 若上顎前牙做成#12-‐#23 FPDs,是否更為理想?A: 因為病人沒有意願再多prepare牙齒,所以上顎最後只有做#14,26兩顆surveyed crowns,此外考慮病人為deep bite,且#21,22缺牙的space較大,所以在前牙prostheses的製作上會比較保守。
Q: 預計#35的prognosis與後續追蹤的情況?A: #35 的crown-‐root ra8o 約為5:9,也沒有明顯的mobility,surveyed crown的設計為short guiding plane,再加上病人經過OHI後,oral hygiene維持得還不錯,所以prognosis還算理想;但之後仍然須維持 regular follow up,評估RPD與abutments的狀況,若#35的情況變差需要拔除,也已跟病人告知RPD repair的處理方式。














![[ CONFERENCE TENTATIVE ]](https://static.fdokumen.com/doc/165x107/6332727f3108fad7760ea090/-conference-tentative-.jpg)


