Cardiovascular dysfunction in symptomatic primary hyperparathyroidism and its reversal after...
11
Cardiovascular dysfunction in symptomatic primary hyperparathyroidism and its reversal after curative parathyroidectomy: Results of a prospective case control study Gaurav Agarwal, MS, FACS, a Gitika Nanda, MS, a Aditya Kapoor, MD, DM (Cardiol), b Kul Ranjan Singh, MS, a Gyan Chand, MS, a Anjali Mishra, MS, PDC (EndocrSurg), a Amit Agarwal, MS, a Ashok K. Verma, MS, FACS, a Saroj K. Mishra, MS, FACS, a and Sanjeev K. Syal, MD, DM (Cardiol), b Lucknow, India Background. Cardiovascular mortality in primary hyperparathyroidism (PHPT) is attributed to myocardial and endothelial dysfunction. In this prospective, case-control study we assessed cardiovascular dysfunction in patients with symptomatic PHPT and its reversal after successful parathyroidectomy. Methods. Fifty-six patients with symptomatic PHPT underwent two-dimensional echocardiography, tissue Doppler (diastolic function assessment), serum N-terminal pro-brain natriuretic peptide (s-NTproBNP, a myocardial damage marker), and endothelial- and smooth muscle dependent vasodilatory response (vascular dysfunction) studies before, 3, and 6 months after parathyroidectomy; 25 age-matched controls were studied similarly. Results. Patients had greater left ventricular mass (192 ± 70 vs 149 ± 44 g; P = .006), interventricular septal thickness (10.8 ± 2.5 vs 9.0 ± 1.6 mm; P = .001), posterior wall thickness (9.9 ± 2.0 vs 8.6 ± 2.2 mm; P = .004), and diastolic dysfunction (lower E/A trans-mitral flow velocity ratio [1.0 ± 0.4 vs 1.3 ± 0.4; P = .01). Patients had greater s-NTproBNP (4,625 ± 1,130 vs 58 ± 49 pg/mL; P = .002) and lower endothelial-mediated vasodilation (9.3 ± 8.6 vs 11.7 ± 6.3%; P = .03) and smooth mu- scle mediated vasodilation (20.1 ± 17.9 vs 23.8 ± 11.2%; P = .01). Improvements in left ventricular mass, systolic and diastolic function, and smooth muscle mediated vasodilation were noted from 3 to 6 months after parathyroidectomy. Endothelial-mediated vasodilation did not improve significantly. S- NTproBNP levels mirrored echocardiographic changes with a substantial, sustained decrease. Results were similar in hypertensive and normotensive patients. Conclusion. Symptomatic PHPT patients have substantial cardiac and vascular dysfunction, which improve by 6 months after parathyroidectomy. Objective cardiovascular evaluation may improve outcomes in symptomatic PHPT patients. (Surgery 2013;j:j-j.) From the Departments of Endocrine & Breast Surgery, a and Cardiology, b Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India THE CARDIOVASCULAR (CV) effects of parathyroid hor- mone (PTH) have been studied extensively. 1 The risk of mortality due to CV disorders is considered greater in patients with primary hyperparathyroid- ism (PHPT), 2,3 although this belief is contested by some. 4 In a population-based study, Wermers et al reported mortality to be correlated with greater levels of serum calcium. 4 CV deaths in patients with PHPT decreased steadily between 1965 and 1992, as PHPT evolved into an asymptomatic disor- der with modest hypercalcemia. 1 Because of con- flicting reports, whether parathyroidectomy (PTx) Supported by SGPGI Intramural research grant no. PGI/DIR/ 1270/2010 to GA. Institutional ethics committee clearance vide IEC Code: A-22:PGI/IMP/IEC/53/18.02.2011. G.A. and G.N. contributed equally and should be considered joint first authors. Accepted for publication June 26, 2013. Reprint requests: Prof Gaurav Agarwal, MS, FACS, Department of Endocrine & Breast Surgery, SGPGIMS, Raebareli Road, Lucknow 226014, India. E-mail: [email protected]. 0039-6060/$ - see front matter Ó 2013 Mosby, Inc. All rights reserved. http://dx.doi.org/10.1016/j.surg.2013.06.047 SURGERY 1 ARTICLE IN PRESS
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Cardiovascular dysfunction in symptomatic primary hyperparathyroidism and its reversal after...

ARTICLE IN PRESS
Support1270/20vide IEC
G.A. anjoint fir
Accepte
Reprintof EndoLuckno
0039-60
� 2013
http://d
Cardiovascular dysfunctionin symptomatic primaryhyperparathyroidism and its reversalafter curative parathyroidectomy:Results of a prospective case controlstudyGaurav Agarwal, MS, FACS,a Gitika Nanda, MS,a Aditya Kapoor, MD, DM (Cardiol),b
Kul Ranjan Singh, MS,a Gyan Chand, MS,a Anjali Mishra, MS, PDC (EndocrSurg),a
Amit Agarwal, MS,a Ashok K. Verma, MS, FACS,a Saroj K. Mishra, MS, FACS,a andSanjeev K. Syal, MD, DM (Cardiol),b Lucknow, India
Background. Cardiovascular mortality in primary hyperparathyroidism (PHPT) is attributed tomyocardial and endothelial dysfunction. In this prospective, case-control study we assessed cardiovasculardysfunction in patients with symptomatic PHPTand its reversal after successful parathyroidectomy.Methods. Fifty-six patients with symptomatic PHPT underwent two-dimensional echocardiography,tissue Doppler (diastolic function assessment), serum N-terminal pro-brain natriuretic peptide(s-NTproBNP, a myocardial damage marker), and endothelial- and smooth muscle�dependentvasodilatory response (vascular dysfunction) studies before, 3, and 6 months after parathyroidectomy;25 age-matched controls were studied similarly.Results. Patients had greater left ventricular mass (192 ± 70 vs 149 ± 44 g; P = .006), interventricularseptal thickness (10.8 ± 2.5 vs 9.0 ± 1.6 mm; P = .001), posterior wall thickness (9.9 ± 2.0 vs 8.6 ± 2.2mm; P = .004), and diastolic dysfunction (lower E/A trans-mitral flow velocity ratio [1.0 ± 0.4 vs 1.3 ±0.4; P = .01). Patients had greater s-NTproBNP (4,625 ± 1,130 vs 58 ± 49 pg/mL; P = .002) andlower endothelial-mediated vasodilation (9.3 ± 8.6 vs 11.7 ± 6.3%; P = .03) and smooth mu-scle�mediated vasodilation (20.1 ± 17.9 vs 23.8 ± 11.2%; P = .01). Improvements in left ventricularmass, systolic and diastolic function, and smooth muscle�mediated vasodilation were noted from 3 to 6months after parathyroidectomy. Endothelial-mediated vasodilation did not improve significantly. S-NTproBNP levels mirrored echocardiographic changes with a substantial, sustained decrease. Resultswere similar in hypertensive and normotensive patients.Conclusion. Symptomatic PHPT patients have substantial cardiac and vascular dysfunction, whichimprove by 6 months after parathyroidectomy. Objective cardiovascular evaluation may improveoutcomes in symptomatic PHPT patients. (Surgery 2013;j:j-j.)
From the Departments of Endocrine & Breast Surgery,a and Cardiology,b Sanjay Gandhi PostgraduateInstitute of Medical Sciences, Lucknow, India
ed by SGPGI Intramural research grant no. PGI/DIR/10 to GA. Institutional ethics committee clearanceCode: A-22:PGI/IMP/IEC/53/18.02.2011.
d G.N. contributed equally and should be consideredst authors.
d for publication June 26, 2013.
requests: Prof Gaurav Agarwal, MS, FACS, Departmentcrine & Breast Surgery, SGPGIMS, Raebareli Road,w 226014, India. E-mail: [email protected].
60/$ - see front matter
Mosby, Inc. All rights reserved.
x.doi.org/10.1016/j.surg.2013.06.047
THE CARDIOVASCULAR (CV) effects of parathyroid hor-mone (PTH) have been studied extensively.1 Therisk of mortality due to CV disorders is consideredgreater in patients with primary hyperparathyroid-ism (PHPT),2,3 although this belief is contested bysome.4 In a population-based study, Wermers et alreported mortality to be correlated with greaterlevels of serum calcium.4 CV deaths in patientswith PHPT decreased steadily between 1965 and1992, as PHPT evolved into an asymptomatic disor-der with modest hypercalcemia.1 Because of con-flicting reports, whether parathyroidectomy (PTx)
SURGERY 1

ARTICLE IN PRESSSurgeryj 2013
2 Agarwal et al
reduces the risk ofCVdeath inpatients with PHPT isunclear.5 Usual cardiac derangements in PHPT arecardiac hypertrophy with preserved systolic andimpaired diastolic functions,6 although recentstudies on asymptomatic patients with PHPT donot report these abnormalities.7 Serum N-terminalpro brain natriuretic peptide (NT-proBNP), a cleav-age product of BNP secreted by ventricular cardio-myocytes in response to stretch, is a sensitivemarker of chronic cardiac dysfunction, and fewstudies have used it to objectively assess myocardialdamage in PHPT.8
Experimental studies have documented PTH-mediated structural and functional cardiovascularchanges.9 Various mechanisms of myocardial dam-age in PHPT have been proposed, including PTH-mediated endothelial dysfunction, and tunicamedia sclerosis leading to impaired coronary vaso-dilatation. Endothelial dysfunction in the periph-eral and coronary vessels is closely correlated;however, the association of PHPT with endothelialand/ or vascular smooth muscle dysfunction re-mains unestablished.10 There are no comprehen-sive, prospective, case-control studies reportingCV dysfunction in PHPT that use objectivemethods. The few studies that exist in the litera-ture have almost exclusively reported such changesin mild, asymptomatic PHPT. No studies have beenconducted on overtly symptomatic PHPT patientsin recent years. The aim of our study was to inves-tigate the nature and prevalence of cardiac andvascular damage in symptomatic PHPT patientsby using objective evaluation tools and to docu-ment their reversal, if any, after successful PTx.
METHODS
This prospective, case-control study was conduct-ed at SGPGIMS Lucknow, a tertiary-care referralteachinghospital innorth India, with approval of theinstitutional ethics committee. Consecutive consent-ing PHPT patients who underwent successful PTxduring October 2010 to September 2012 wereincluded. One patient with a pre-existing structuralcardiac defect was excluded, as were three patientsfor whom follow-up evaluation was incomplete, andone who had persistent PHPT after excision of amediastinal parathyroid adenoma. The study groupcomprised 56 patients (22 males, 34 females), withmean age of 46.5 ± 13.6 years (range, 14–73). Thecontrol group consisted of 25 healthy, normotensiveand normocalcemic subjects (6 males, 19 females)with mean age of 44 ± 11.2 years (range, 14–62).
Patients with PHPTunderwent biochemical eval-uation, including serum lipids profile, radiologicevaluation and parathyroid imaging, and were
treated as per standard protocols.11,12 Patients un-derwent the appropriate PTxprocedure---minimallyinvasive PTx (n = 36), bilateral neck exploration (n =18), or mediastinal PTx (n = 2)–and were followed-up. In addition, the patients underwent a detailedCV evaluation with 2D-echocardiography (2DEcho), tissue Doppler imaging (TDI), serum NT-proBNP estimation, and flow-mediated vasodilatorystudies by Doppler ultrasonography of the brachialartery to assess the endothelial-dependent (hyper-emia induced, using a blood pressure cuff, FMD)and smooth muscle–dependent (nitroglycerin-induced, NMD) vasodilatory responses. All thesestudies were performed as baseline before opera-tion and at 3 and 6 months after PTx. The controlswere evaluated similarly, but only once.
2D Echo was conducted by a single experiencedcardiologist, who used a GE Vivid 7 ECHOmachine(GE Healthcare, Waukesha, WI), with a multifre-quency transducer. Various 2D Echo and Dopplerindices, as described previoulsy,13 were docu-mented, including the following:
(1) systolic function indices (left ventricular [LV]mass [LVM], LV dimensions and volumes, and LVejection fraction [LVEF]). LVM was calculatedfrom the parasternal M-mode projection by the De-vereux formula.14 LV hypertrophy (LVH) wasconsidered present if the LVM exceeded 162 g inwomen and 224 g in men.
(2) Diastolic or relaxation indices: trans-mitraldiastolic flow by pulsed-wave Doppler and myocar-dial velocity by TDI were obtained from an apicalfour-chamber view with the use of standardizedtechniques, and the following parameters weredetermined: peak velocities of the early (E wave)and late (A wave) phase of the mitral inflowpattern and their ratio (E/A); deceleration timeof E wave; iso-volumic relaxation time (IVRT); andpeak early (Ea) diastolic velocity of the lateralmitral annulus. The presence of calcification wasassessed in the mitral and aortic annulus, myocar-dium, and pericardium.
(3) Vascular function indices: Endothelium-dependent FMD and endothelium-independentNMD were assessed as described previously.15 Base-line diameter of the brachial artery was measured 3cm above the ante-cubital fossa with a high–resolu-tion,10-MHz linear array transducer (GE VingmedUltrasound AS, N-3191, Horten, Norway). A stan-dard blood pressure cuff was placed on the fore-arm distal to the ante-cubital fossa, inflated 50mmHg above systolic blood pressure for 5 minutes,and then released to induce reactive hyperemia. Arepeat measurement of brachial artery diameterwas obtained 30 seconds after cuff deflation.FMD

Table I. Symptoms and end-organ damage inPHPT patients (n = 56)
Symptoms %
Bone pain 42 75Bone swelling/deformity 11 19.6Fractures 10 17.8Osteoporosis (t score < �2.5) 33 58.9Muscle weakness 23 41.1Nephrocalcinosis/Nephrolithiasis 25 44.6Behavioral problems 14 25Acute or chronic pancreatitis 9 16.1Acid peptic disease 28 50
PHPT, Primary hyperparathyroidism.
ARTICLE IN PRESSSurgeryVolume j, Number j
Agarwal et al 3
was calculated with the following formula: FMD(%) = 100 3 [(brachial artery diameter at peak hy-peremia- diameter at rest)/diameter at rest].
NMD was measured after sublingual administra-tion of 5 mg of isosorbide di-nitrate given 15minutes after deflation of the blood pressurecuff. Scans of brachial artery were taken at thesame site. Diameter measurements were takenfrom one media-intima interface to the other atbaseline and 30 seconds after reactive hyperemia/after the administration of isosorbide di-nitrate.Impaired FMD was defined as values <4.5%.16
Serum NT-proBNP estimation was performed onvenous blood sample collected in an EDTA vial us-ing a fluorescence immunoassay (Triage; RocheDiagnostics) using murine and sheep monoclonalantibodies against NT-proBNP labeled with fluo-rescent dye and immobilized on the solid phase.
Statistical analyses were performed using aSPSS-16 software package (SPSS, Inc, Chicago,IL). All data are expressed as mean ± SD. Para-metric tests were used: the v2 test for categoricalvariables, and paired t-test for normally distributeddata. Nonparametric (Mann-Whitney) test wasused for skewed data. Pearson’s product momentcorrelation was used to measure the strength of as-sociation between biochemical data and LVM asdependent variable. Logistic regression analysiswas used to determine the strongest predictors ofLVM among serum calcium, PTH, 25-hydroxyvitamin D, NT-proBNP, and hypertension.
RESULTS
The mean age of patients with PHPT (47 ± 14years) was comparable (P = .407) with that ofthe control subjects (44 ± 11 years). All patientshad symptomatic PHPT, with 54 (96%) havingend-organ damage or complications, includingnephrolithiasis, bone disease- fragility fracture(s),brown tumor(s) or osteoporosis, and muscle weak-ness (Table I). The serum PTH levels in patientsranged from 56 to 1,723 pg/mL, with a mean of338.3 ± 311 (reference range, 9–55 pg/mL).Mean serum creatinine levels were 1.2 ± 0.07mg/dL (range, 0.5–3.3). Seven patients had mildlyelevated serum creatinine levels due to obstructiveuropathy, but none of them required hemodialy-sis. Mean serum 25-hydroxy vitamin D levels were20 ± 2.5 ng/mL (range 1–94, normal levels 9–47).
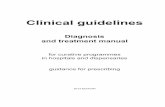
Table II provides a comparative summary of thebiochemical, 2D Echo, TDI, and FMD findings inPHPT patients and control groups. At the baseline,patients with PHPT had a greater LVM (P = .006)with a mean value of 192 ± 70 g and greater inter-ventricular septal (IVS, mean 10.8 ± 2.5 mm) and
posterior wall (PW, mean 9.9 ± 2 mm) thicknesscompared with the control subjects. The LV end-diastolic dimension (LVEDD), LV end-systolicdimension (LVESD), LV end-diastolic volume(LVEDV), LV end-systolic volume (LVESV), andLV ejection fraction (LVEF) were not significantlydifferent among patients and controls. Patientsalso had greater impairment of LV diastolic func-tion as evidenced by lesser trans-mitral E/A veloc-ity ratio (1.1 ± 0.5, P = .017) and peak early (E)diastolic velocity of the lateral mitral annulus(0.11m/sec, p = 0.02). Thirty of the 56 patientshad an abnormal trans-mitral E/A ratio at diag-nosis, with 26 (46.4%) having grade I, and 4(7.1%) having grade III diastolic dysfunction.
Dispersed myocardial, pericardial, valvularannulus (mitral and aortic being commonest), orIVS calcifications were seen in 28% patients. Calci-fications also were seen in two controls in the IVS.The mean serum NT-proBNP in PHPT patients wasgreater compared with the control group (P = .002).SerumNT-proBNP levels>120 pg/mL were seen in15 (27%), and were extremely high (>300 pg/mL)in 12 (21%)patients with PHPT. The FMDwas lesserin PHPT patients with a mean of 9.3 ± 8.6 %, asagainst 11.7 ± 6.3% in the controls (P = .03). Fifteen(27%) patients with PHPT had an abnormal abso-lute FMD (<4.5%). The NMD was also less in pa-tients with a value of 20.1 ± 17.9 % vs 23.8 ± 11.7%in controls (P = .01).
Twenty-one patients (37.5%) had history ofhypertension and were on treatment with anti-hypertensive medications. Secondary hypertensionwas ruled out with appropriate tests in all thesepatients. Table III provides a comparison ofvarious indices between normotensive and hyper-tensive PHPT patients versus controls, all ofwhom were normotensive. The mean LVM ofnormotensive PHPT patients (180 ± 68 g) wasgreater (P = .042) compared with controls (149 ±44). They also had diastolic dysfunction, with
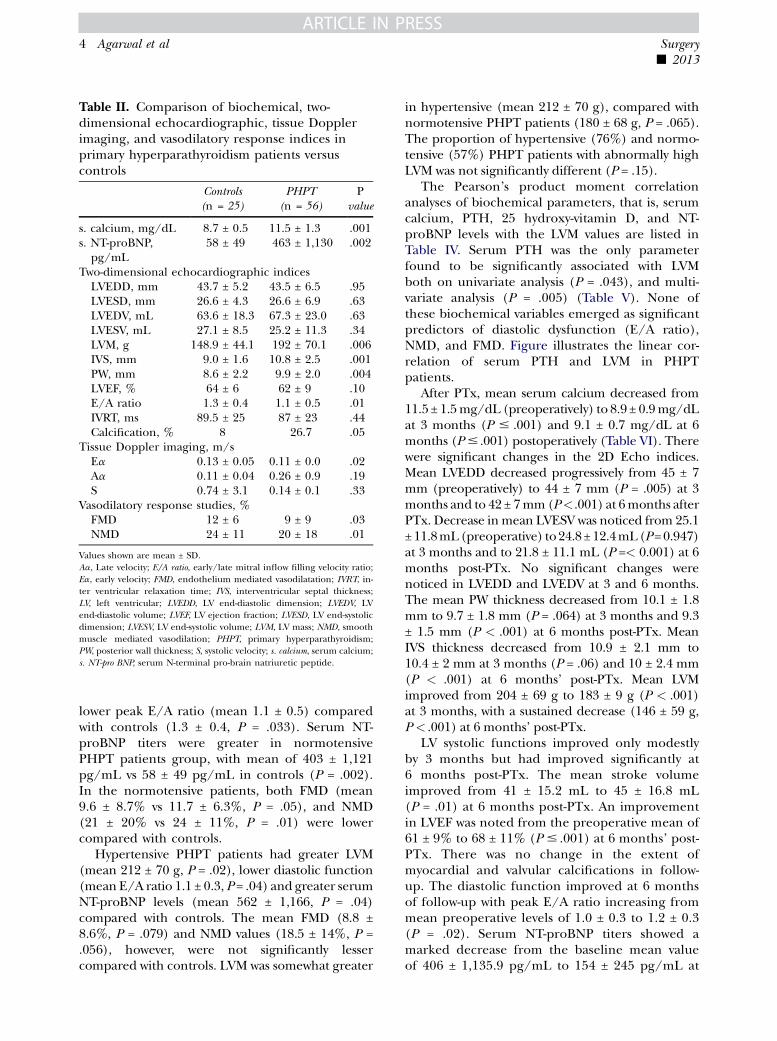
Table II. Comparison of biochemical, two-dimensional echocardiographic, tissue Dopplerimaging, and vasodilatory response indices inprimary hyperparathyroidism patients versuscontrols
Controls(n = 25)
PHPT(n = 56)
Pvalue
s. calcium, mg/dL 8.7 ± 0.5 11.5 ± 1.3 .001s. NT-proBNP,
pg/mL58 ± 49 463 ± 1,130 .002
Two-dimensional echocardiographic indicesLVEDD, mm 43.7 ± 5.2 43.5 ± 6.5 .95LVESD, mm 26.6 ± 4.3 26.6 ± 6.9 .63LVEDV, mL 63.6 ± 18.3 67.3 ± 23.0 .63LVESV, mL 27.1 ± 8.5 25.2 ± 11.3 .34LVM, g 148.9 ± 44.1 192 ± 70.1 .006IVS, mm 9.0 ± 1.6 10.8 ± 2.5 .001PW, mm 8.6 ± 2.2 9.9 ± 2.0 .004LVEF, % 64 ± 6 62 ± 9 .10E/A ratio 1.3 ± 0.4 1.1 ± 0.5 .01IVRT, ms 89.5 ± 25 87 ± 23 .44Calcification, % 8 26.7 .05
Tissue Doppler imaging, m/sEa 0.13 ± 0.05 0.11 ± 0.0 .02Aa 0.11 ± 0.04 0.26 ± 0.9 .19S 0.74 ± 3.1 0.14 ± 0.1 .33
Vasodilatory response studies, %FMD 12 ± 6 9 ± 9 .03NMD 24 ± 11 20 ± 18 .01
Values shown are mean ± SD.Aa, Late velocity; E/A ratio, early/late mitral inflow filling velocity ratio;Ea, early velocity; FMD, endothelium mediated vasodilatation; IVRT, in-ter ventricular relaxation time; IVS, interventricular septal thickness;LV, left ventricular; LVEDD, LV end-diastolic dimension; LVEDV, LVend-diastolic volume; LVEF, LV ejection fraction; LVESD, LV end-systolicdimension; LVESV, LV end-systolic volume; LVM, LV mass; NMD, smoothmuscle�mediated vasodilation; PHPT, primary hyperparathyroidism;PW, posterior wall thickness; S, systolic velocity; s. calcium, serum calcium;s. NT-pro BNP, serum N-terminal pro-brain natriuretic peptide.
ARTICLE IN PRESSSurgeryj 2013
4 Agarwal et al
lower peak E/A ratio (mean 1.1 ± 0.5) comparedwith controls (1.3 ± 0.4, P = .033). Serum NT-proBNP titers were greater in normotensivePHPT patients group, with mean of 403 ± 1,121pg/mL vs 58 ± 49 pg/mL in controls (P = .002).In the normotensive patients, both FMD (mean9.6 ± 8.7% vs 11.7 ± 6.3%, P = .05), and NMD(21 ± 20% vs 24 ± 11%, P = .01) were lowercompared with controls.
Hypertensive PHPT patients had greater LVM(mean 212 ± 70 g, P = .02), lower diastolic function(mean E/A ratio 1.1 ± 0.3, P = .04) and greater serumNT-proBNP levels (mean 562 ± 1,166, P = .04)compared with controls. The mean FMD (8.8 ±8.6%, P = .079) and NMD values (18.5 ± 14%, P =.056), however, were not significantly lessercompared with controls. LVM was somewhat greater
in hypertensive (mean 212 ± 70 g), compared withnormotensive PHPT patients (180 ± 68 g, P = .065).The proportion of hypertensive (76%) and normo-tensive (57%) PHPT patients with abnormally highLVM was not significantly different (P = .15).
The Pearson’s product moment correlationanalyses of biochemical parameters, that is, serumcalcium, PTH, 25 hydroxy-vitamin D, and NT-proBNP levels with the LVM values are listed inTable IV. Serum PTH was the only parameterfound to be significantly associated with LVMboth on univariate analysis (P = .043), and multi-variate analysis (P = .005) (Table V). None ofthese biochemical variables emerged as significantpredictors of diastolic dysfunction (E/A ratio),NMD, and FMD. Figure illustrates the linear cor-relation of serum PTH and LVM in PHPTpatients.
After PTx, mean serum calcium decreased from11.5 ± 1.5mg/dL (preoperatively) to 8.9 ± 0.9mg/dLat 3 months (P # .001) and 9.1 ± 0.7 mg/dL at 6months (P# .001) postoperatively (Table VI). Therewere significant changes in the 2D Echo indices.Mean LVEDD decreased progressively from 45 ± 7mm (preoperatively) to 44 ± 7 mm (P = .005) at 3months and to 42 ± 7mm(P<.001) at 6months afterPTx. Decrease inmean LVESV was noticed from 25.1± 11.8mL(preoperative) to24.8± 12.4mL(P=0.947)at 3 months and to 21.8 ± 11.1 mL (P =< 0.001) at 6months post-PTx. No significant changes werenoticed in LVEDD and LVEDV at 3 and 6 months.The mean PW thickness decreased from 10.1 ± 1.8mm to 9.7 ± 1.8 mm (P = .064) at 3 months and 9.3± 1.5 mm (P < .001) at 6 months post-PTx. MeanIVS thickness decreased from 10.9 ± 2.1 mm to10.4 ± 2 mm at 3 months (P = .06) and 10 ± 2.4 mm(P < .001) at 6 months’ post-PTx. Mean LVMimproved from 204 ± 69 g to 183 ± 9 g (P < .001)at 3 months, with a sustained decrease (146 ± 59 g,P < .001) at 6 months’ post-PTx.
LV systolic functions improved only modestlyby 3 months but had improved significantly at6 months post-PTx. The mean stroke volumeimproved from 41 ± 15.2 mL to 45 ± 16.8 mL(P = .01) at 6 months post-PTx. An improvementin LVEF was noted from the preoperative mean of61 ± 9% to 68 ± 11% (P # .001) at 6 months’ post-PTx. There was no change in the extent ofmyocardial and valvular calcifications in follow-up. The diastolic function improved at 6 monthsof follow-up with peak E/A ratio increasing frommean preoperative levels of 1.0 ± 0.3 to 1.2 ± 0.3(P = .02). Serum NT-proBNP titers showed amarked decrease from the baseline mean valueof 406 ± 1,135.9 pg/mL to 154 ± 245 pg/mL at
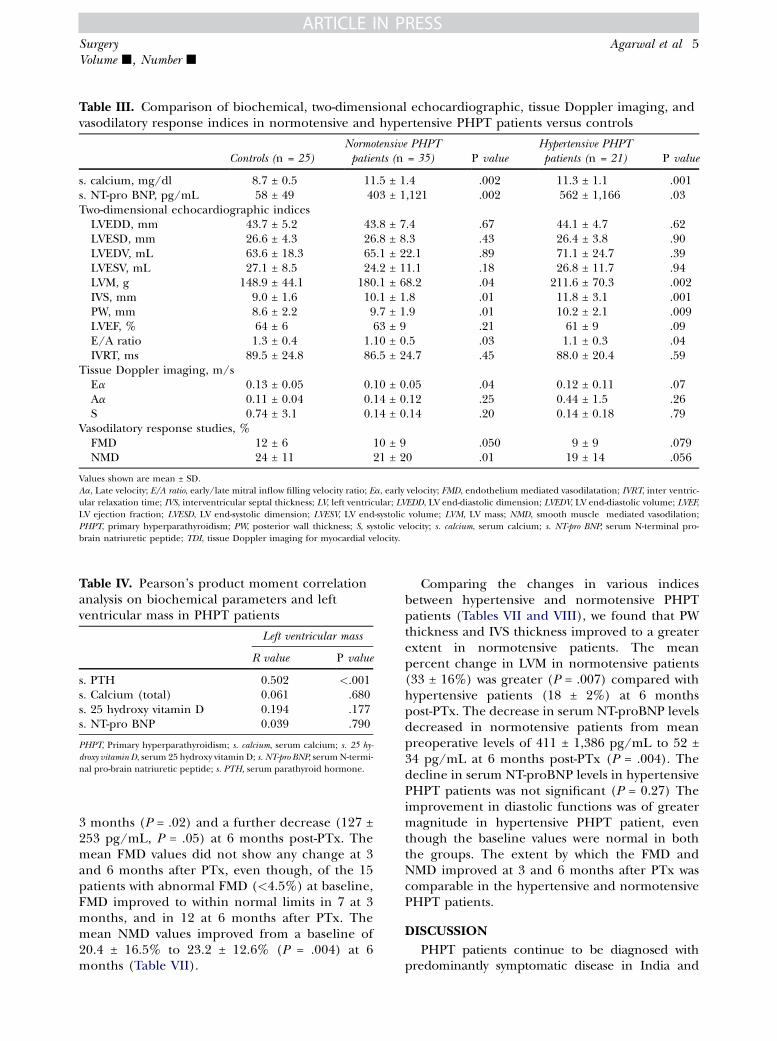
Table III. Comparison of biochemical, two-dimensional echocardiographic, tissue Doppler imaging, andvasodilatory response indices in normotensive and hypertensive PHPT patients versus controls
Controls (n = 25)Normotensive PHPTpatients (n = 35) P value
Hypertensive PHPTpatients (n = 21) P value
s. calcium, mg/dl 8.7 ± 0.5 11.5 ± 1.4 .002 11.3 ± 1.1 .001s. NT-pro BNP, pg/mL 58 ± 49 403 ± 1,121 .002 562 ± 1,166 .03Two-dimensional echocardiographic indices
LVEDD, mm 43.7 ± 5.2 43.8 ± 7.4 .67 44.1 ± 4.7 .62LVESD, mm 26.6 ± 4.3 26.8 ± 8.3 .43 26.4 ± 3.8 .90LVEDV, mL 63.6 ± 18.3 65.1 ± 22.1 .89 71.1 ± 24.7 .39LVESV, mL 27.1 ± 8.5 24.2 ± 11.1 .18 26.8 ± 11.7 .94LVM, g 148.9 ± 44.1 180.1 ± 68.2 .04 211.6 ± 70.3 .002IVS, mm 9.0 ± 1.6 10.1 ± 1.8 .01 11.8 ± 3.1 .001PW, mm 8.6 ± 2.2 9.7 ± 1.9 .01 10.2 ± 2.1 .009LVEF, % 64 ± 6 63 ± 9 .21 61 ± 9 .09E/A ratio 1.3 ± 0.4 1.10 ± 0.5 .03 1.1 ± 0.3 .04IVRT, ms 89.5 ± 24.8 86.5 ± 24.7 .45 88.0 ± 20.4 .59
Tissue Doppler imaging, m/sEa 0.13 ± 0.05 0.10 ± 0.05 .04 0.12 ± 0.11 .07Aa 0.11 ± 0.04 0.14 ± 0.12 .25 0.44 ± 1.5 .26S 0.74 ± 3.1 0.14 ± 0.14 .20 0.14 ± 0.18 .79
Vasodilatory response studies, %FMD 12 ± 6 10 ± 9 .050 9 ± 9 .079NMD 24 ± 11 21 ± 20 .01 19 ± 14 .056
Values shown are mean ± SD.Aa, Late velocity; E/A ratio, early/late mitral inflow filling velocity ratio; Ea, early velocity; FMD, endothelium mediated vasodilatation; IVRT, inter ventric-ular relaxation time; IVS, interventricular septal thickness; LV, left ventricular; LVEDD, LV end-diastolic dimension; LVEDV, LV end-diastolic volume; LVEF,LV ejection fraction; LVESD, LV end-systolic dimension; LVESV, LV end-systolic volume; LVM, LV mass; NMD, smooth muscle�mediated vasodilation;PHPT, primary hyperparathyroidism; PW, posterior wall thickness; S, systolic velocity; s. calcium, serum calcium; s. NT-pro BNP, serum N-terminal pro-brain natriuretic peptide; TDI, tissue Doppler imaging for myocardial velocity.
Table IV. Pearson’s product moment correlationanalysis on biochemical parameters and leftventricular mass in PHPT patients
Left ventricular mass
R value P value
s. PTH 0.502 <.001s. Calcium (total) 0.061 .680s. 25 hydroxy vitamin D �0.194 .177s. NT-pro BNP 0.039 .790
PHPT, Primary hyperparathyroidism; s. calcium, serum calcium; s. 25 hy-
droxy vitamin D, serum 25 hydroxy vitamin D; s. NT-pro BNP, serumN-termi-nal pro-brain natriuretic peptide; s. PTH, serum parathyroid hormone.
ARTICLE IN PRESSSurgeryVolume j, Number j
Agarwal et al 5
3 months (P = .02) and a further decrease (127 ±253 pg/mL, P = .05) at 6 months post-PTx. Themean FMD values did not show any change at 3and 6 months after PTx, even though, of the 15patients with abnormal FMD (<4.5%) at baseline,FMD improved to within normal limits in 7 at 3months, and in 12 at 6 months after PTx. Themean NMD values improved from a baseline of20.4 ± 16.5% to 23.2 ± 12.6% (P = .004) at 6months (Table VII).
Comparing the changes in various indicesbetween hypertensive and normotensive PHPTpatients (Tables VII and VIII), we found that PWthickness and IVS thickness improved to a greaterextent in normotensive patients. The meanpercent change in LVM in normotensive patients(33 ± 16%) was greater (P = .007) compared withhypertensive patients (18 ± 2%) at 6 monthspost-PTx. The decrease in serum NT-proBNP levelsdecreased in normotensive patients from meanpreoperative levels of 411 ± 1,386 pg/mL to 52 ±34 pg/mL at 6 months post-PTx (P = .004). Thedecline in serum NT-proBNP levels in hypertensivePHPT patients was not significant (P = 0.27) Theimprovement in diastolic functions was of greatermagnitude in hypertensive PHPT patient, eventhough the baseline values were normal in boththe groups. The extent by which the FMD andNMD improved at 3 and 6 months after PTx wascomparable in the hypertensive and normotensivePHPT patients.
DISCUSSION
PHPT patients continue to be diagnosed withpredominantly symptomatic disease in India and

Table V. Univariate and multivariate analysis of correlation between biochemical parameters and leftventricular mass
Variable
Left ventricular mass
Univariate analysis Multivariate analysis
OR 95% CI P value OR 95% CI P value
s. calcium (total) 1.051 0.70–1.57 .809s. PTH 0.994 0.988–1.000 .043* 0.987 0.979–0.996 .005*s. 25 hydroxy vitamin D 1.008 0.976–1.041 .628Hypertension
(yes/no)0.417 0.125–1.393 .155
s. NT-proBNP 1.000 1.000–1.001 .869
*Statistically significant (P < .05) correlation.Binary logistic regression analysis, forward linear regression analysis.95% CI, 95% Confidence interval; OR, odds ratio; s. calcium, serum calcium; s. 25 hydroxy vitamin D, serum 25 hydroxy vitamin D; s. NT-pro BNP, serumN-terminal pro-brain natriuretic peptide; s. PTH, serum parathyroid hormone.
Figure. Correlation between serum PTH levels and LVMin patients with PHPT. R2 = 0.188; P < .001 (afterexcluding the outliers).
ARTICLE IN PRESSSurgeryj 2013
6 Agarwal et al
often have a long duration of illness, with high serumcalcium and PTH levels, at a relatively youngerage.11,12 Patients with extremely high serum PTHlevels and severe hypercalcemia over long durationare likely to have more extensive target organ dam-age, including CV dysfunction. CV changes in mildasymptomatic PHPT are subtle, but patients with se-vere PHPT have greater CVmortality.4,17 The degreeofhypercalcemiaby itself is an independentpredictorof CV mortality.4 North American studies on asymp-tomatic and mildly hypercalcemic PHPT patientsfound no excess CV mortality,5 unlike the Europeanstudies between 1965 and 1992, which correlatedgreater CV mortality with serum calcium levels.4
Numerous studies have evaluated CV functions inasymptomatic PHPT patients with mild-to-moderatehypercalcemia and hyperparathyroidism,7,8 some ofwhich used rather subjective methods for assessmentofCVfunction.7 In thisprospective case-control study,weused contemporary objectivemethods and tools toassess systolic, diastolic, myocardial, and vascularfunctions in consecutive symptomatic PHPTpatients,most of whom had end-organ damage in form of
osteitis fibrosa cystica and nephrocalcinosis/nephro-lithiasis. We also studied linear changes in their CVindices after curative PTx.
The patients with PHPT in our study had LVHas evidenced by greater dimensions of IVS, PWthicknesses, LV dimensions, and LVM, withoutevident systolic dysfunction, all of which weregreater compared with the controls. Thirty-eightof 56 (68%) patients had LVH; both hypertensive(16 of 21, 76%) as well as normotensive (20 of 35,57%) had high LVM. They had poorer diastolicfunctions compared with controls though meanabsolute values were in low normal range. Theseresults are in agreement with most6,18,19 but notall6 previous studies. LVM is considered a strongindicator of CV morbidity and mortality.6,18 Thepresence of LVH was found to be independentof hypertension because it was found in normo-tensive PHPT patients as well. This finding is inagreement with other studies.1,6 In vitro studiessuggest that LVH is due to action of PTH onPTHrP receptors, which leads to calcium influxand activation of protein kinase C, thus promot-ing hypertrophic effects.1,6 Various studies haveshown LVH to be correlated with serum levels ofPTH19 or vitamin D,20 rather than calcium orblood pressure.6 We found LVM positively core-lated to serum PTH levels, but not to serumcalcium, 25-hydroxy vitamin D titers, andhypertension.
Myocardial, IVS, and valvular (aortic, mitral)calcifications were found in 28% of our patients.Previous studies report the incidence of suchcalcification in up to 70%patients.6,19 In our experi-ence, the lesser incidence of cardiac calcification inour patients mirrors overall relatively lesser rate ofectopic calcification, which is perhaps a reflection

Table VI. Linear changes in biochemical, two-dimensional echocardiographic, tissue Doppler imaging, andvasodilatory response indices in primary hyperparathyroidism patients after parathyroidectomy
Baseline value 3 month after PTx P value 6 month after PTx P value
s. calcium, mg/dL 11.5 ± 1.5 8.9 ± 0.9 <.001 9.1 ± 0.7 <.001s. NT-proBNP, pg/mL 406 ± 1,135 154 ± 245 .002 127 ± 253 .005Two-dimensional echocardiographic indices
LVEDD, mm 45.4 ± 7.0 43.6 ± 7.3 .005 41.6 ± 7 <.001LVEDS, mm 27.2 ± 7.3 26.3 ± 4.9 .601 26.6 ± 5.3 .676LVEDV, mL 65.7 ± 24.7 65.9 ± 21.7 .991 66.7 ± 24.3 .533LVESV, mL 25.1 ± 11.8 24.8 ± 12.4 .947 21.8 ± 11.1 <.001IVS, mm 10.9 ± 2.1 10.4 ± 2.0 .064 10.1 ± 2.4 <.001PW, mm 10.1 ± 1.78 9.7 ± 1.8 .094 9.3 ± 1.5 <.001LVEF, % 61 ± 9 64 ± 11 .102 68 ± 11 <.001Stroke volume, mL 41.0 ± 15.2 41.2 ± 16.5 .923 45.0 ± 16.8 .01LVM, g 204.2 ± 68.6 182.6 ± 68.7 <.001 146.1 ± 59.1 <.001E/A ratio 1.0 ± 0.3 1.1 ± 0.4 .530 1.2 ± 0.3 .02IVRT, ms 88.1 ± 21.4 88.7 ± 16.9 .893 84.9 ± 17.4 .04
Tissue Doppler imaging, m/sEa 0.10 ± 0.05 0.13 ± 0.11 .14 0.12 ± 0.03 .004Aa 0.31 ± 1.16 0.10 ± 0.03 .01 0.10 ± 0.03 .005S 0.13 ± 0.14 0.11 ± 0.05 .65 0.13 ± 0.13 .334
Vasodilatory response studies, %FMD 10 ± 9 11 ± 9 .55 13 ± 17 .44NMD 20 ± 17 18 ± 13 .68 23 ± 13 .004
Values shown are mean ± SD.Aa, Late velocity; E/A ratio, early/late mitral inflow filling velocity ratio; Ea, early velocity; FMD, endothelium mediated vasodilatation; IVRT, inter ventric-ular relaxation time; IVS, interventricular septal thickness; LV, left ventricular; LVEDD, LV end-diastolic dimension; LVEDV, LV end-diastolic volume; LVEF,LV ejection fraction; LVESD, LV end-systolic dimension; LVESV, LV end-systolic volume; LVM, LV mass; NMD, smooth muscle�mediated vasodilation;PHPT, primary hyperparathyroidism; PTx, parathyroidectomy; PW, posterior wall thickness; S, systolic velocity; s. calcium, serum calcium; s. NT-pro BNP,serum N-terminal pro-brain natriuretic peptide.
ARTICLE IN PRESSSurgeryVolume j, Number j
Agarwal et al 7
of vitaminD�deficient status of ourpatients and thelow calcium-phosphorus product, consequent to di-etary calcium and phosphorus deficiency.11,12 Dia-stolic dysfunction has been reported even inpatients with mild-to-moderate PHPT18 and isconsidered a predictor of CV death.21
We used TDI, a contemporary objectivemethod for assessing peak early (Ea) diastolicvelocity of the lateral mitral annulus, and otherdiastolic indices. These studies revealed mildlyimpaired diastolic functions in PHPT patients,which were less compared with controls. SerumNT-pro BNP estimation is a sensitive marker ofmyocardial dysfunction, both in the presence andabsence of systolic dysfunction. It has emerged asa useful tool for the identification and manage-ment of cardiac dysfunction irrespective of un-derlying pathology.13 We reported the value ofthis marker in the evaluation and managementof CV dysfunction in patients with pheochromocy-toma.13 Serum NT-proBNP titers were high (>120pg/mL) in 48% of PHPT patients in our study,with very high values (>300 pg/mL) in 21% pa-tients. Mean serum NT-proBNP levels weregreater in patients compared with controls. Very
few published studies have reported serumNT-pro BNP evaluation in PHPT patients, withsomewhat inconsistent results.8
Endothelial dysfunction of coronary arteries isan important antecedent event in the develop-ment of coronary atherosclerosis and coronaryartery disease and correlates closely with brachialartery FMD.22 Hypercalcemia leads to stiffening inthe peripheral as well as in the coronary arteriesdue to intimal and medial calcification. Brachialartery ultrasonography for measuring FMD, ameasure of arterial wall compliance, is impairedin asymptomatic subjects with hypercholesterole-mia, healthy smokers, and patients with coronaryartery disease. FMD impairment has been corre-lated to vitamin D deficiency in patients withcoronary artery disease.16 The results of FMD inPHPT are not consistent, with some studiesreporting impaired23 and other reporting normalFMD.24 We found impaired FMD in PHPT pa-tients compared with controls. Impaired FMD inPHPT is attributed to an early preclinicalphase of atherogenesis and to parathyroid hor-mone or hypercalcemia�mediated endothelialdysfunction.24

Table VII. Linear changes in biochemical, two-dimensional echocardiographic, tissue Doppler imaging,and vasodilatory response indices in hypertensive primary hyperparathyroidism patients afterparathyroidectomy
Baseline value 3 month after PTx P value 6 month after PTx P value
s. calcium, mg/dL 11.5 ± 1.2 9.1 ± 1.1 <.001 9.1 ± 0.7 <.001s. NT-proBNP, pg/mL 399 ± 695 236 ± 363 0.211 231 ± 372 .272Two-dimensional echocardiographic indices
LVEDD, mm 45.2 ± 4.5 43.6 ± 7.3 .020 42.1 ± 3.9 .001LVEDS, mm 27.2 ± 3.7 27.7 ± 3.9 .605 27.0 ± 4.1 .872LVEDV, mL 67.5 ± 25.4 65.3 ± 22.6 .551 68.9 ± 25.6 .626LVESV, mL 25.3 ± 11.5 25.5 ± 15.4 .944 21.6 ± 11.4 .037IVS, mm 11.8 ± 2.3 11.6 ± 2.0 .454 11.3 ± 2.9 .189PW, mm 10.2 ± 1.6 10.3 ± 1.7 .806 9.7 ± 1.6 .150LVEF, % 60 ± 9 65 ± 12 .117 68 ± 14 .011Stroke volume, mL 42.0 ± 17.1 38.7 ± 18.9 .535 47.3 ± 19.6 .071LVM, g 215.0 ± 59.9 202.7 ± 61.3 .059 171.3 ± 63.6 .014E/A ratio 1.1 ± 0.4 1.1 ± 0.4 .043 1.2 ± 0.4 .001IVRT, ms 88.3 ± 23.1 89.7 ± 18.2 .778 91.1 ± 15.9 .471
Tissue Doppler imaging, m/sEa 0.098 ± 0.04 0.11 ± 0.04 .034 0.12 ± 0.02 .003Aa 0.58 ± 1.7 0.10 ± 0.02 .31 0.10 ± 0.02 .02S 0.17 ± 0.21 0.10 ± 0.03 .26 0.11 ± 0.04 .09
Vasodilatory response studies, &FMD 10 ± 10 12 ± 8 .28 11 ± 6 .77NMD 21 ± 16.5 21 ± 16 .56 26 ± 17 .036
Values shown are mean ± SD.Aa, Late velocity; E/A ratio, early/late mitral inflow filling velocity ratio; Ea, early velocity; FMD, endothelium mediated vasodilatation; IVRT, inter ventric-ular relaxation time; IVS, interventricular septal thickness; LV, left ventricular; LVEDD, LV end-diastolic dimension; LVEDV, LV end-diastolic volume; LVEF,LV ejection fraction; LVESD, LV end-systolic dimension; LVESV, LV end-systolic volume; LVM, LV mass; NMD, smooth muscle�mediated vasodilation;PHPT, primary hyperparathyroidism; PTx, parathyroidectomy; PW, posterior wall thickness; S, systolic velocity; s. calcium, serum calcium; s. NT-pro BNP,serum N-terminal pro-brain natriuretic peptide.
ARTICLE IN PRESSSurgeryj 2013
8 Agarwal et al
Although the short-term administration of PTHcauses a dose-dependent transient vasodilation,long-term PTH infusion results in vasoconstric-tion.1,6 Endothelial independent vasodilatation-NMD primarily reflects smoothmuscle dysfunction,and is impaired even before calcification in theintima and media of artery can be detected. NMDimpairment suggests that hypercalcemia predomi-nantly causes altered smooth muscle reactivity,although it is not related to PTH and calcium levelsindependently.24 In our study, NMD was foundimpaired in PHPT patients, which is in agreementwith the only other study which reported NMDimpairment in PHPT.24
All PHPT patients in our study had successfulPTx with predictable and substantial decrease inserum calcium levels at 3 and 6 months after PTx.The reversal of CV changes and hypertension afterPTx in PHPT patients is a contentious issue, withcontradictory results reported in the litera-ture.7,18,19 Reduction in LVM after PTx by 50–60% has been reported.1,6 In our study, LVMdecreased 3 months postoperatively, and had sus-tained progressive reduction at 6 months after
PTx. Improvements were seen in LVEDD andLVESV, with improvement in stroke volume andLVEF from 3 to 6 months after PTx. The diastolicfunction also improved progressively between 3 to6 months. The decrease in LVM itself leads to bet-ter diastolic relaxation of myocardium, which inturn brings about optimal systolic contraction(Starling law), leading to a decrease in LVEDDand improvement in LVESV. Previous studies,almost all conducted in mild PHPT, have not re-ported similar marked improvements in systolicand diastolic functions after PTx. To the contrary,our patients, with greater baseline levels of PTHand calcium levels, more severe disease, and pro-longed duration of illness11,12 and hence worseCV indices at baseline, had more marked improve-ment in systolic and diastolic functions, as hasbeen postulated by others.25 The myocardial andvalvular calcifications did not regress during the6 months’ follow-up, which is in agreement withother studies.6
The extent of regression of LVM after PTx inour study was greater in normotensive PHPTpatients compared with their hypertensive

Table VIII. Linear changes in biochemical, two-dimensional echocardiographic, tissue Doppler imaging,and vasodilatory response indices in normotensive primary hyperparathyroidism patients afterparathyroidectomy
Baseline value 3 month after PTx P value 6 month after PTx P value
s. calcium, mg/dL 11.4 ± 1.7 8.8 ± 0.7 <.001 9.1 ± 0.8 .001s. NT-proBNP, pg/mL 410 ± 1,385 81 ± 61 .007 52 ± 34 .004Two-dimensional echocardiographic indices
LVEDD, mm 45.5 ± 8.5 44.2 ± 9.1 .021 41.4 ± 8.7 <.001LVEDS, mm 27.2 ± 9.1 25.8 ± 5.3 .478 26.4 ± 6.1 .705LVEDV, mL 64.5 ± 24.8 66.0 ± 23.1 .506 65.2 ± 23.9 .714LVESV, mL 24.8 ± 12.2 24.4 ± 11.3 .629 21.9 ± 11.1 .002IVS, mm 10.3 ± 1.8 9.9 ± 1.8 .130 9.3 ± 1.6 <.001PW, mm 9.9 ± 1.9 9.5 ± 1.8 .058 8.9 ± 1.5 <.001LVEF, % 60 ± 10 65 ± 12 .452 68 ± 14 .012Stroke volume, mL 40.2 ± 13.9 41.6 ± 15.1 .513 43.3 ± 14.7 .109LVM, g 196.4 ± 74.7 178.7 ± 72.4 .001 128.2 ± 49.7 <.001E/A ratio 1.0 ± 0.6 1.1 ± 0.3 .757 1.2 ± 0.3 .260IVRT, ms 88.1 ± 20.6 87.9 ± 17.2 .967 80.7 ± 17.6 .050
Tissue Doppler imaging, m/sEa 0.11 ± 0.05 0.10 ± 0.03 .76 0.12 ± 0.03 .19Aa 0.12 ± 0.05 0.09 ± 0.04 .02 0.10 ± 0.03 .07S 0.11 ± 0.37 0.12 ± 0.06 .65 0.15 ± 0.17 .81
Vasodilatory response studies, %FMD 10 ± 9 10 ± 9 .84 15 ± 22 .45NMD 21 ± 18 16 ± 10 .39 22 ± 9 .054
Values shown are mean ± SD.Aa, Late velocity; E/A ratio, early/late mitral inflow filling velocity ratio; Ea, early velocity; FMD, endothelium mediated vasodilatation; IVRT, inter ventric-ular relaxation time; IVS, interventricular septal thickness; LV, left ventricular; LVEDD, LV end-diastolic dimension; LVEDV, LV end-diastolic volume; LVEF,LV ejection fraction; LVESD, LV end-systolic dimension; LVESV, LV end-systolic volume; LVM, LV mass; NMD, smooth muscle�mediated vasodilation;PHPT, primary hyperparathyroidism; PTx, parathyroidectomy; PW, posterior wall thickness; S, systolic velocity; s. calcium, serum calcium; s. NT-pro BNP,serum N-terminal pro-brain natriuretic peptide.
ARTICLE IN PRESSSurgeryVolume j, Number j
Agarwal et al 9
counterparts, again similar to previous reports.19
Our normotensive PHPT patients, who had noother condition that could possibly have influ-enced the LVM, exhibited a decrease in LV thick-ness of 7.3% (IVS thickness) and 6.7% (PWthickness). The regression of LV thicknesscontinued up to 6 months after PTx. These obser-vations are indicative of the fact that hyperparathy-roidism and hypercalcemia themselves, and nothypertension, resulted in reversible LVH. Thechanges in serum NT-pro BNP titers mirrored thechanges in LVM indicating myocardial dysfunctionand improved at 3 and 6 month after PTx. The NT-proBNP titers did not revert to within the normalrange until 6 months after PTx, indicating residualpersistent myocardial damage.
Unlike most cardiac function indices, thevascular dysfunction, as evidenced by impairedFMD, did not exhibit improvement within 6months after PTx, similar to observations madein previous studies.10 NMD, a marker of smoothmuscle (endothelium-independent) vasculardysfunction is an early change, while FMD,endothelium-dependent gets impaired later. The
temporal sequence of improvement of these fol-lows the same sequence, leading to earlierimprovement in NMD as observed in our study,as compared to improvement in FMD. The rela-tively moderate improvement in vascular compli-ance is probably due to calcium deposits in themyocytes of the vessel wall, which occurs in symp-tomatic patients, and does not reverse after PTx,akin to persistence of the valvular and myocardialcalcifications after PTx.
In conclusion, symptomatic Indian patients withPHPT have substantial CV manifestations in formof systolic and diastolic dysfunction, and increasedlevels of serum NT-proBNP, which improve aftersuccessful PTx. These patients also have impairedarterial wall compliance, the extent of improve-ment of which after successful PTx is rathermodest. Improvement in NT-pro BNP mirrorsimprovement in cardiac functions. Cardiovascularevaluation should be performed in symptomaticPHPT patients to detect subclinical cardiac andvascular dysfunction so that their recovery can bemonitored, and the cardiovascular outcomes ofsuch patients be improved.

ARTICLE IN PRESSSurgeryj 2013
10 Agarwal et al
REFERENCES
1. Fitzpatrick LA, Bilezikian JP, Silverberg SJ. Parathyroid hor-mone and the cardiovascular system. Curr Osteoporos Rep2008;6:77-83.
2. Palm�er M, Adami HO, Bergstr€om R, Akerstr€om G, Ljun-ghall S. Mortality after surgery for primary hyperparathy-roidism: a follow-up of 441 patients operated on from1956 to 1979. Surgery 1987;102:1-7.
3. Hedb€ack G, Tisell LE, Bengtsson BA, Hedman I, Oden A.Premature death in patients operated on for primary hy-perparathyroidism. World J Surg 1990;14:829-35; discus-sion 836.
4. Wermers RA, Khosla S, Atkinson EJ, Grant CS, Hodgson SF,O’Fallon WM, et al. Survival after the diagnosis of hyper-parathyroidism: a population-based study. Am J Med 1998;104:115-22.
5. S€oreide JA, van Heerden JA, Grant CS, Yau Lo C, Schleck C,Ilstrup DM. Survival after surgical treatment for primaryhyperparathyroidism. Surgery 1997;122:1117-23.
6. Andersson P, Rydberg E, Willenheimer R. Primary hyper-parathyroidism and heart disease---a review. Eur Heart J2004;25:1776-87.
7. Luigi P, Chiara FM, Laura Z, Cristiano M, Giuseppina C, Lu-ciano C, et al. Arterial hypertension, metabolic syndromeand subclinical cardiovascular organ damage in patientswith asymptomatic primary hyperparathyroidism beforeand after parathyroidectomy: preliminary results. Int JEndocrinol 2012;2012:408295.
8. Almqvist EG, Becker C, Bondeson AG, Bondeson L, Svens-son J, Svensson SE. Increased plasma concentrations ofN-terminal pro-B-type natriuretic peptide in patients withmild primary hyperparathyroidism. Clin Endocrinol (Oxf)2006;65:760-6.
9. Rashid G, Bernheim J, Green J, Benchetrit S. Parathyroidhormone stimulates the endothelial nitric oxide synthasethrough protein kinase A and C pathways. Nephrol DialTransplant 2007;22:2831-7.
10. Neunteufl T, Heher S, Prager G, Katzenschlager R, Abela C,Niederle B, et al. Effects of successful parathyroidectomy onaltered arterial reactivity in patients with hypercalcaemia:results of a 3-year follow-up study. Clin Endocrinol (Oxf)2000;53:229-33.
11. Agarwal G, Mishra SK, Kar DK, Singh AK, Arya V, Gupta SK,et al. Recovery pattern of patients with osteitis fibrosa cysticain primary hyperparathyroidism after successful parathy-roidectomy. Surgery 2002;132:1075-85.
12. Agarwal G, Prasad KK, Kar DK, Krishnani N, Pandey R, Mis-hra SK. Indian primary hyperparathyroidism patients withparathyroid carcinoma do not differ in clinicoinvestigativecharacteristics from those with benign parathyroid pathol-ogy. World J Surg 2006;30:732-42.
13. Agarwal G, Sadacharan D, Kapoor A, Batra A, Dabadghao P,Chand G, et al. Cardiovascular dysfunction and catechol-amine cardiomyopathy in pheochromocytoma patientsand their reversal following surgical cure: results of a pro-spective case-control study. Surgery 2011;150:1202-11.
14. Devereux RB, Reichek N. Echocardiographic determina-tion of left ventricular mass in man. Anatomic validationof the method. Circulation 1977;55:613-8.
15. Celermajer DS, Sorensen KE, Gooch VM, Spiegelhalter DJ,Miller OI, Sullivan ID, et al. Non-invasive detection of endo-thelial dysfunction in children and adults at risk of athero-sclerosis. Lancet 1992;340:1111-5.
16. Syal SK, Kapoor A, Bhatia E, Sinha A, Kumar S, Tewari S,et al. Vitamin D deficiency, coronary artery disease, and
endothelial dysfunction: observations from a coronaryangiographic study in Indian patients. J Invasive Cardiol2012;24:385-9.
17. Barletta G, De Feo ML, Del Bene R, Lazzeri C, VecchiarinoS, La Villa G, et al. Cardiovascular effects of parathyroid hor-mone: a study in healthy subjects and normotensive patientswith mild primary hyperparathyroidism. J Clin EndocrinolMetab 2000;85:1815-21.
18. Almqvist EG, Bondeson AG, Bondeson L, Nissborg A,Smedg�ardP, SvenssonSE.Cardiacdysfunction inmildprimaryhyperparathyroidism assessed by radionuclide angiographyand echocardiography before and after parathyroidectomy.Surgery 2002;132:1126-32.
19. Stefenelli T, Abela C, Frank H, Koller-Strametz J, Globits S,Bergler-Klein J, et al. Cardiac abnormalities in patients withprimary hyperparathyroidism: implications for follow-up.J Clin Endocrinol Metab 1997;82:106-12.
20. Walker MD, Fleischer JB, Di Tullio MR, Homma S, RundekT, Stein EM, et al. Cardiac structure and diastolic functionin mild primary hyperparathyroidism. J Clin EndocrinolMetab 2010;95:2172-9.
21. Mogelvang R, Sogaard P, Pedersen SA, Olsen NT, Marott JL,Schnohr P, et al. Cardiac dysfunction assessed by echocar-diographic tissue Doppler imaging is an independent pre-dictor of mortality in the general population. Circulation2009;119:2679-85.
22. Neunteufl T, Katzenschlager R, Hassan A, Klaar U, Schwar-zacher S, Glogar D, et al. Systemic endothelial dysfunctionis related to the extent and severity of coronary artery dis-ease. Atherosclerosis 1997;129:111-8.
23. Carrelli AL, Walker MD, Di Tullio MR, Homma S, Zhang C,McMahon DJ, et al. Endothelial function in mild primaryhyperparathyroidism. Clin Endocrinol (Oxf) 2013;78:204-9.
24. Neunteufl T, Katzenschlager R, Abela C, Kostner K, Nie-derle B, Weidinger F, et al. Impairment of endothelium-independent vasodilation in patients with hypercalcemia.Cardiovasc Res 1998;40:396-401.
25. Dalberg K, Brodin LA, Juhlin-Dannfelt A, Farnebo LO. Car-diac function in primary hyperparathyroidism before andafter operation. An echocardiographic study. Eur J Surg1996;162:171-6.
DISCUSSION
Dr Collin J. Weber (Atlanta, GA): Why does it take solong to get better? The reason I ask you that is that wehave evidence in release of a variety of cytokines fromparathyroid tumors, primarily, interleukin (IL)-6, IL-8,tumor necrosis factor alpha (TNFa), interferon-gamma, and even some IL-1 beta. What they’re doingthere, we have no idea, but they are noxious and createa proinflammatory stress-related situation. The BNP, forexample, is quite an interesting observation that may berelated to that. But all of these factors are reduced in mi-nutes to an hour. Why does it take 6 months to see thebeneficial effects of this procedure?
Dr Gaurav Agarwal: We studied two different sets ofthings: the structural cardiovascular changes and func-tional cardiovascular changes in patients with PHPT.And, as you’ve rightly said, the functional changesand the humoral changes can very well be expectedto reverse within minutes to days. The structuralchanges would, however, definitely take longer to bereversed.

ARTICLE IN PRESSSurgeryVolume j, Number j
Agarwal et al 11
Unfortunately, given the design of our study, wherewe reevaluated our patients only at 3 months afterparathyroidectomy, we did not carry out an earlyevaluation. It’s quite possible that in at least some ofthe patients, the serum NT-proBNP levels and otherfunctional indices might have improved earlier, but,unfortunately, we have not documented that.
Dr Nancy D. Perrier (Houston, TX): Can you give usa recommendation on how these symptoms preopera-tively can be objectively assessed to have this consideredfor falling into the category of symptomatic hyperpara-thyroidism? We use that term asymptomatic, which, truly,as data like yours show, these patients may not be asymp-tomatic. But what can we use these as objective criteria?Do you have any suggestions for us?
Dr Gaurav Agarwal: Based on some of our previouswork, we have tried to segregate patients into categories.We do not have any truly asymptomatic patients, only afew mildly symptomatic, but most are overtly symptom-atic, and quite a few have complicated disease. Roughly40% of patients that we treat have fragility fractures,nephrocalcinosis, brown tumors, and these are what weconsidered as falling in the complicated disease group.But then, a whole lot of others, almost all of the others,have overt bone pains, muscular weakness, symptomaticrenal calculus disease, whom we consider as havingovertly symptomatic disease.
Even the few who are left, after a careful history-taking, are found to have subtle symptoms, includingsome degree of behavioral changes or muscular weak-ness and bone pains. There are other ways of looking atthis whole issue, including categorizing patients on thebasis of their bone mineral densitometry. If a patient hasovert osteoporosis, then of course you can very wellimagine that patient is indeed symptomatic.
Dr Nancy D. Perrier (Houston, TX): We’re talkingabout that group that you mentioned all the way to theleft, that small group. Is there any way that we can objec-tively quantify the cardiovascular issues and to knowwhat we could expect in those that we could objectivelyquantitate that would improve?
Dr Gaurav Agarwal: None of our patients had any car-diovascular symptoms. In terms of their overall symptom-atology and quality of life, our group is at this momentinvolved with another study, where we are trying to
objectively study the quality of life based on a question-naire. We know from works of Dr Pasieka and othersthat there are various ways of looking at quality of lifeand symptomatology in these mildly symptomaticpatients.
Dr Nancy D. Perrier (Houston, TX): Could any ofyour parameters be used that aren’t so subjective, butsomething that could be measured?
Dr Gaurav Agarwal: Yes. In terms of cardiovascularmanifestations, we can use serum NT-proBNP titer,which is a fairly straightforward blood investigation.There is a correlation between the LV mass and PTH ti-ters, as we have documented in this study. These areperhaps few objective things that we can use for assess-ment of cardiovascular changes.
Dr Saif S. Al Sobhi (Riyadh, Saudi Arabia): We havealmost-similar population, like in India, advanced calci-fied soft tissue. And some of these patients, you have tomanage their cardiac situation before parathyroidectomy.What’s your contraindication for parathyroidectomy forthese patients and how they do after their cardiac surgery?
Dr Gaurav Agarwal: For the purpose of this study, oneof the exclusion criteria we used was presence of any pre-existing structural cardiac defect, including atrial septaldefect, myocardial ischemia and other things. So we didnot have any patients who would have required cardiacsurgery before or after parathyroidectomy in this subsetof patients. But, to answer your question, yes, there arefortunately very few patients with cardiac conditions whoneed to be managed. And because the patients that wetreat are by and large young patients, they do not requirea cardiac intervention before or after parathyroid surgery.
Dr James Lee (New York, NY): You’ve matched forage and sex. Did you give consideration to matchingfor things like vitamin D, which is an independent riskfactor for cardiovascular disease, as well as lipid profile?
Dr Gaurav Agarwal: We didn’t assess the vitamin Dstatus for all the controls, and that is why we had to leaveout these data. Initially, we had 20 controls to begin with,and we had data on vitamin D and BMD for them. Andthey matched the study patients fairly well for thevitamin D status. I believe, that is a reflection of overallvitamin D deficiency in our population, which hasbeen amply documented in various studies by our groupand others.




















