Campbell Collaboration-handout
10
1 New Trend in Actualizing Evidence- Based Practice in Social Work Setting Daniel TL Shek, PhD, FHKPS, BBS, JP Chair Professor of Applied Social Sciences Department of Applied Social Sciences The Hong Kong Polytechnic University 2 Knowledge Claims - Believe It Or Not? • “The cranes send the babies to town. When there were more cranes in the town last winter, the number of babies in the next year will increase.” • “Acid in the stomach is the major cause of stomach ulcer.” • “After the Big Bang, the universe has expanded at a slower rate.” • “Chinese fathers are stricter and less kind than Chinese mothers” ("yan fu ci mu”) . • Adventure-based counseling is an effective intervention approach in changing the behavior of delinquents. • After school care service is helpful to students. 3 The Counting Horse - Believe It Or Not? • A horse (Clever Hans) was claimed by its owner that it could count and do simple addition and subtraction (including fractions). • Hans gave his answers by tapping his forefoot or by pointing his nose at different answers displayed to him. 4 What is Evidence-Based Practice? How much do you know about EBP? EBP is “the integration of best research evidence with clinical experience and client values.” (Sackett et al., 2000, p.1) Sackett, D.L., Straus, S.E., Richardson, W.C., Rosenberg, W., & Haynes, R.M. (2000). Evidence-based medicine: How to practice and teach EBM. New York: Churchill Livingstone. “Use of best current knowledge as a basis for decisions about groups of patients or populations.” (Gray, 2001, p.20) Gray, J.A.M. (2001). Evidence-based medicine for professionals. In A. Edwars & G. Elwyn (Eds.), Evidence- based patient choice: Inevitable or impossible? (pp. 19-33). New York: Oxford University Press. 5 5 Steps of EBP 1. Converting information needs related to practice decisions into well-structured answerable questions. 2. Tracking down, with maximum efficiency, the best evidence with which to answer them. 3. Critically appraising that evidence for its validity, impact (size of effect), and applicability (usefulness in practice). 4. Applying the results of this appraisal to practice and policy decisions (decisions on generalizability of findings). 5. Evaluating effectiveness and efficiency in carrying out. Steps 1 to 4 and seeking ways to improve them in the future. (Sackett et al., 2000, pp. 3-4) 6 An Updated Model for Evidence-Based Decisions: Gambrill, E. (2006). Evidence-based practice and policy: Choice ahead. Research on Social Work Practice, 16, 338-357. Clinical Characteristics and Circumstances Clinical Expertise Client Preferences and Actions Research Evidence
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Campbell Collaboration-handout
1
New Trend in Actualizing Evidence-Based Practice in Social Work Setting
Daniel TL Shek, PhD, FHKPS, BBS, JPChair Professor of Applied Social Sciences
Department of Applied Social SciencesThe Hong Kong Polytechnic University
2
Knowledge Claims - Believe It Or Not?• “The cranes send the babies to town. When there
were more cranes in the town last winter, the number of babies in the next year will increase.”
• “Acid in the stomach is the major cause of stomach ulcer.”
• “After the Big Bang, the universe has expanded at a slower rate.”
• “Chinese fathers are stricter and less kind than Chinese mothers” ("yan fu ci mu”) .
• Adventure-based counseling is an effective intervention approach in changing the behavior of delinquents.
• After school care service is helpful to students.
3
The Counting Horse - Believe It Or Not?• A horse (Clever Hans) was claimed by its
owner that it could count and do simple addition and subtraction (including fractions).
• Hans gave his answers by tapping his forefoot or by pointing his nose at different answers displayed to him.
4
What is Evidence-Based Practice?How much do you know about EBP?
EBP is “the integration of best research evidence with clinical experience and client values.” (Sackett et al., 2000, p.1)Sackett, D.L., Straus, S.E., Richardson, W.C., Rosenberg, W., & Haynes, R.M. (2000). Evidence-based medicine: How to practice and teach EBM. New York: Churchill Livingstone.
“Use of best current knowledge as a basis for decisions about groups of patients or populations.” (Gray, 2001, p.20)Gray, J.A.M. (2001). Evidence-based medicine for professionals. In A. Edwars & G. Elwyn (Eds.), Evidence-based patient choice: Inevitable or impossible? (pp. 19-33).New York: Oxford University Press.
5
5 Steps of EBP1. Converting information needs related to practice
decisions into well-structured answerable questions.2. Tracking down, with maximum efficiency, the best
evidence with which to answer them.3. Critically appraising that evidence for its validity, impact
(size of effect), and applicability (usefulness in practice).4. Applying the results of this appraisal to practice and
policy decisions (decisions on generalizability of findings).
5. Evaluating effectiveness and efficiency in carrying out. Steps 1 to 4 and seeking ways to improve them in the future.
(Sackett et al., 2000, pp. 3-4)6
An Updated Model for Evidence-Based Decisions:Gambrill, E. (2006). Evidence-based practice and policy: Choice ahead. Research on Social Work Practice, 16, 338-357.
Clinical Characteristics and Circumstances
Clinical Expertise
Client Preferences and Actions Research Evidence
7
Rubin, A., & Parrish, D. (2007). Challenges to the future of evidence-based practice in social work education. Journal of social Work Education, 43, 405-428.
• Evidence-based practice as an empowerment process
• Attempts to maximize the likelihood that the clients will receive the most effective intervention
• Associated with a higher probability of treatment success, but not a guarantee (program with higher probability of adolescent drug prevention – carnival; singing concert; curricular-based intervention?)
8
Gambrill (2006): Critical Thinking Values as the Foundation of EBP
ValuesCourage Curiosity Intellectual Empathy Humility Integrity Persistence
Honor Ethical ObligationsTransparencyAvoiding harmInformed consentMaximizing autonomySelf determinationEmpowerment
9
Rubin and Parrish (2007):Common Myths Against EBP
• Myth 1: Ignores clinical expertise and client values
• Myth 2: Inconsistent with client empowerment• Myth 3: Inadequate studies on various
populations• Myth 4: Lag time in demonstrating
effectiveness• Myth 5: Evidence-based practice is the
concern of academics only• Your myths and understanding about EBP?
10
Choices in EBP (Gambrill, 2006)How systemic to be (educators, researchers, practitioners)?Who will select the practice?What outcome and indicators will be focused on?What style of EBP will be used (e.g. knowledge manager)?How transparent regarding the evidentiary status of services?How and in what ways to involve the clients?Whether to implement needed organization change?How rigorous to be in reviewing the evidentiary status of services?How transparent to be regarding the evidentiary status of services?
11
How to Get the Best Available Evidence?• How often do you read social work journals?• Professional and academic journals – A MUST• Journal: Evidence-based Social Work• Journal: Research on Social Work Practice• Database: Social Work Abstracts (Social Work and allied
disciplines)• PsycINFO (Psychology, social work and allied disciplines)• Medline (Medicine and allied disciplines)• Sociological Abstracts (Sociology and allied disciplines)• ERIC (Education and allied disciplines)• CINAHL Plus (Clinical professions and allied disciplines)• Government databases: SAMHSA and NREPP• Campbell Collaboration 12
The Campbell Collaboration (C2)• helps people make well-informed decisions by preparing,
maintaining and disseminating systematic reviews in education, crime and justice, and social welfare
• an international research network that produces systematic reviews of the effects of social interventions
• voluntary cooperation among researchers of a variety of backgrounds
• Campbell currently has five Coordinating Groups: Social Welfare, Crime and Justice, Education, Methods, and the Users group
• The Coordinating Groups are responsible for the production, scientific merit, and relevance of our systematic reviews
• Campbell's International Secretariat is now located in Oslo and hosted by the Norwegian Knowledge Centre for the Health Services

13
10 Key Principles• Collaboration: internally and externally fostering good
communications• Building on the enthusiasm of individuals• Avoiding duplication, by good management and co-
ordination to ensure economy of effort.• Minimizing bias, through a variety of approaches such as
scientific rigor• Keeping up to date: incorporation of new evidence. • Striving for relevance, by promoting the assessment of
policies and practices using outcomes that matter to people. • Promoting access: wide dissemination of the outputs• Ensuring quality, by being open and responsive to criticism,
applying advances in methodology• Continuity: key functions is maintained and renewed. • Enabling wide participation by reducing barriers to
contributing and by encouraging diversity. 14
• The Campbell Collaboration (C2) grew out of a meeting in London in 1999
• 80 people from four countries attended the meeting, many from our sibling organization The Cochrane Collaboration (C1).
• Cochrane had been producing systematic reviews in healthcare, since 1994. Many of its members saw the need for an organization that would produce systematic reviews of research evidence on the effectiveness of social interventions.
• Creation of The Campbell Collaboration in 2000: inaugural meeting in Philadelphia, USA attracting 85 participants from 13 countries
• With partnerships developing in a number of countries, Campbell has held eight Annual Colloquia to date
• A Nordic Campbell Centre was added to the Collaboration in 2001, supported by the Danish Government and the Nordic Council of Ministers.
15 16
17 18
19 20
21 22
23 24
25
Oversea Experiences of Evidence-Based Practice• Numerous examples! Do you know them?• Campbell Collaboration Library• Mental health, substance abuse, suicide abuse prevention
programs• Durlak, J. A., & Wells, A. M. (1997). Primary prevention
mental health programs for children and adolescents: A meta-analytic review. American Journal of Community Psychology, 25, 115-152.
• Catalano, R. F., Berglund, M. L., Ryan, J. A. M., Lonczak, H. S., & Hawkins, J.D. (2002, June 24). Positive youth development in the United States: Research findings on evaluations of positive youth development programs. Prevention & Treatment, 5, Article 15. Retrieved November 17, 2004, from http://www.journals.apa.org/prevention/volume5/pre0050015a.html
26
• Zwi K, Woolfenden S, Wheeler D, O'Brien T, Tait P, Williams K. School-based education programmes for the prevention of child sexual abuse. Campbell Systematic Reviews 2007:5 DOI: 10.4073/csr.2007.5
• Studies evaluated in this review report significant improvements in knowledge measures and protective behaviours. Several studies reported harms, suggesting a need to monitor the impact of similar interventions. Retention of knowledge should be measured beyond School-based education programmes for the prevention of child sexual abuse3-12 months. Further investigation of the best forms of presentation and optimal age of programme delivery is required.
27
• Fisher H, Montgomery P, Gardner F. Opportunities provision for preventing youth gang involvement for children and young people (7-16). Campbell Systematic Reviews 2008:8 DOI: 10.4073/csr.2008.8
• No evidence from randomised controlled trials or quasi-randomised controlled trials currently exists regarding the effectiveness of opportunities provision for gang prevention. Only two studies addressed opportunities provision as a gang prevention strategy, a case study and a qualitative study, both of which had such substantial methodological limitations that even speculative conclusions as to the impact of opportunities provision were impossible. Rigorous primary evaluations of gang prevention strategies are crucial to develop this research field, justify funding of existing interventions, and guide future gang prevention programmes and policies. 28
• Smedslund G, Hagen KB, Steiro A, Johme T, Dalsbø TK, Rud MG. Work programmes for welfare recipients. Campbell Systematic Reviews 2006:9 DOI: 10.4073/csr.2006.9
• Welfare-to-work programmes in the USA have shown small, but consistent effects in moving welfare recipients into work, increasing earnings, and lowering welfare payments. The results are not clear for reducing the proportion of recipients receiving welfare. Little is known about the impacts of welfare-to-work programmes outside of the USA.
29
Question for Reflection and Discussion:
It is commonly believed that organizing visits for high-risk youths will lower juvenile crime rates. Based on such a belief, many District Fight Crime Committees, Correctional Services Department and NGOs in Hong Kong organize visits for high risk young people. Do you think such programs are really effective in reducing juvenile crime rates?
3030
Rosenbaum, D.P., & Hanson, G.S. (1998). Assessing the effects of school-based drug education: A six-year multi-level analysis of Project D.A.R.E. Journal of Research in Crime and Delinquency, 35(4), 381-412.• Drug Abuse Resistance Education Program
(DARE) – reaching 25 million students in the US, adopted in 44 foreign countries.
• 18 pairs of elementary schools in urban, suburban and rural areas of Illinos
• Matched for school characteristics, random assignment
• Pretest and posttest measurement (6 years), with data collected from students and teachers

3131
• Outcome measures – drug use behavior; onset of alcohol use; general attitudes toward drugs; Attitudes toward the use of specific drugs; perceived benefits and costs of using drugs; self-esteem; attitude towards police; peer resistance skills, school performance, delinquent and violent behavior
• Multi-level analyses with seven waves of posttreatment data showed that D.A.R.E. had no long term effect on a wide range of drug use measures
32
33
Cost-Benefit Analysis Via an Longitudinal Experimental Study
• Wortman, P.D. (1995). An Exemplary Evaluation of a Program that Worked: The High/Scope Perry Preschool Project. Evaluation Practice, 16(3), 257-265.
• Is there a high-quality, randomized evaluative study that shows that preschool education provides these benefits or prevents these negative social consequences?
• What is the real solution to poverty?33 34
• The program consisted of a 2.5 hour morning session on weekdays and one 1.5 hour “home visit” session per week with the mother and child
• The program’s teaching curriculum followed the principles of the developmental psychologist Jean Piaget and used “active learning” where the children plan and carry out learning activities (what did Piaget say?)
34
35
• The goal was to provide a successful initial educational experience that would continue into the regular (K-12) school years
• Hypothesis: In the long run, such students would do better
• Hypothesis: They would have fewer placements in special education programs, fewer would be retained in grade (or “held back”), fewer would commit crimes, and more would graduate from high school 35 36
• How much will the program cost and how much does the American public benefit?
• The first cost-benefit analysis, reported by Gramlich (1986), a professor of economics at The University of Michigan, concluded that “the program is a winner.”.
• Equally “remarkable”, according to Gramlich, nearly 80 percent of the benefits went to the American public, with the program participants getting the remaining 20 percent 36
37
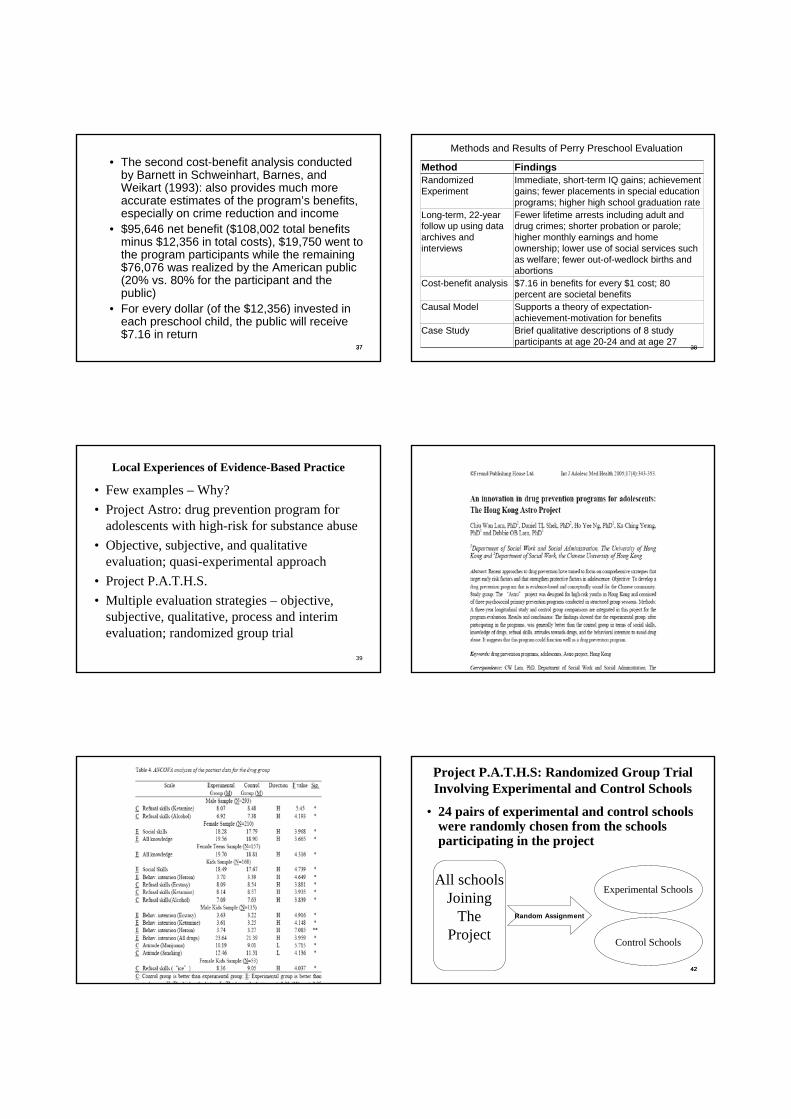
• The second cost-benefit analysis conducted by Barnett in Schweinhart, Barnes, and Weikart (1993): also provides much more accurate estimates of the program’s benefits, especially on crime reduction and income
• $95,646 net benefit ($108,002 total benefits minus $12,356 in total costs), $19,750 went to the program participants while the remaining $76,076 was realized by the American public (20% vs. 80% for the participant and the public)
• For every dollar (of the $12,356) invested in each preschool child, the public will receive $7.16 in return
37 38
Methods and Results of Perry Preschool Evaluation
Method FindingsRandomized Experiment
Immediate, short-term IQ gains; achievement gains; fewer placements in special education programs; higher high school graduation rate
Long-term, 22-year follow up using data archives and interviews
Fewer lifetime arrests including adult and drug crimes; shorter probation or parole; higher monthly earnings and home ownership; lower use of social services such as welfare; fewer out-of-wedlock births and abortions
Cost-benefit analysis $7.16 in benefits for every $1 cost; 80 percent are societal benefits
Causal Model Supports a theory of expectation-achievement-motivation for benefits
Case Study Brief qualitative descriptions of 8 study participants at age 20-24 and at age 27
38
39
Local Experiences of Evidence-Based Practice
• Few examples – Why?• Project Astro: drug prevention program for
adolescents with high-risk for substance abuse• Objective, subjective, and qualitative
evaluation; quasi-experimental approach• Project P.A.T.H.S.• Multiple evaluation strategies – objective,
subjective, qualitative, process and interim evaluation; randomized group trial
40
41 4242
Project P.A.T.H.S: Randomized Group Trial Involving Experimental and Control Schools
• 24 pairs of experimental and control schools were randomly chosen from the schools participating in the project
All schoolsJoining
TheProject
Random Assignment
Experimental Schools
Control Schools
4343
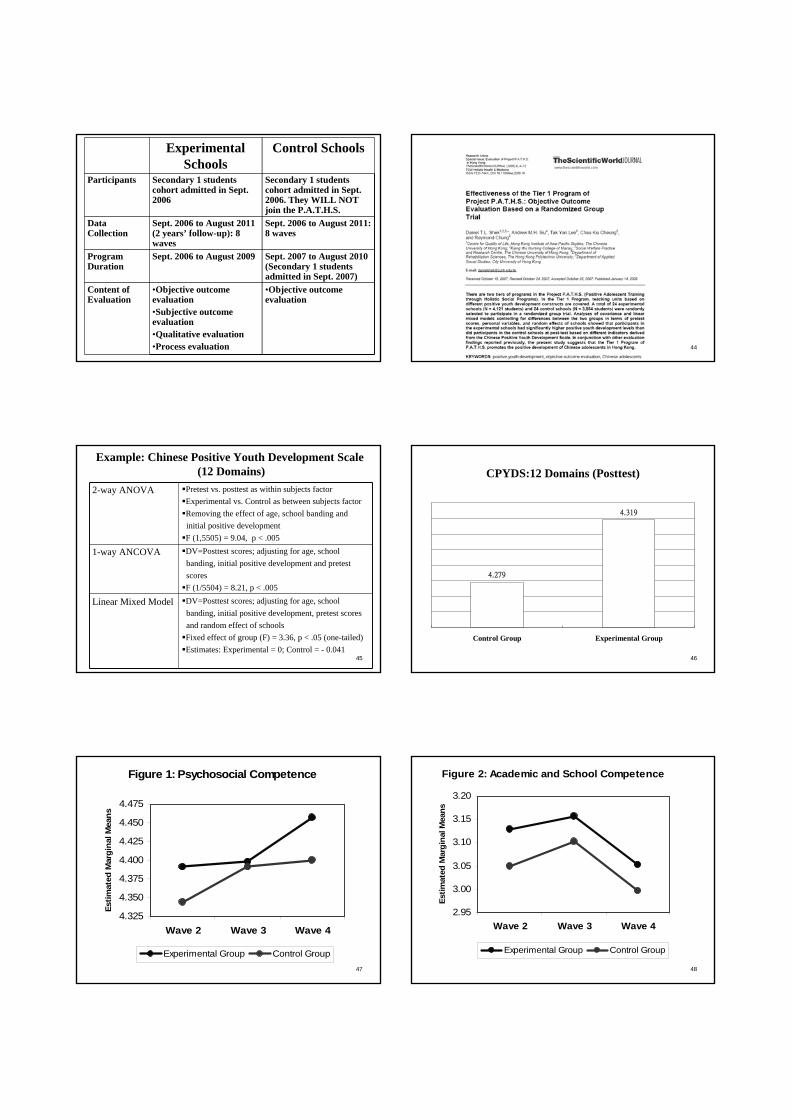
Experimental Schools
Control Schools
Participants Secondary 1 students cohort admitted in Sept. 2006
Secondary 1 students cohort admitted in Sept. 2006. They WILL NOT join the P.A.T.H.S.
Data Collection
Sept. 2006 to August 2011 (2 years’ follow-up): 8 waves
Sept. 2006 to August 2011: 8 waves
Program Duration
Sept. 2006 to August 2009 Sept. 2007 to August 2010 (Secondary 1 students admitted in Sept. 2007)
Content of Evaluation
•Objective outcome evaluation•Subjective outcome evaluation•Qualitative evaluation•Process evaluation
•Objective outcome evaluation
44
45
Example: Chinese Positive Youth Development Scale(12 Domains)
2-way ANOVA Pretest vs. posttest as within subjects factorExperimental vs. Control as between subjects factorRemoving the effect of age, school banding andinitial positive developmentF (1,5505) = 9.04, p < .005
1-way ANCOVA DV=Posttest scores; adjusting for age, schoolbanding, initial positive development and pretest scoresF (1/5504) = 8.21, p < .005
Linear Mixed Model DV=Posttest scores; adjusting for age, school banding, initial positive development, pretest scores and random effect of schoolsFixed effect of group (F) = 3.36, p < .05 (one-tailed)Estimates: Experimental = 0; Control = - 0.041
46
CPYDS:12 Domains (Posttest)
4.319
4.279
Control Group Experimental Group
47
Figure 1: Psychosocial Competence
4.325
4.350
4.375
4.400
4.425
4.450
4.475
Wave 2 Wave 3 Wave 4
Estim
ated
Mar
gina
l Mea
ns
Experimental Group Control Group48
2.95
3.00
3.05
3.10
3.15
3.20
Wave 2 Wave 3 Wave 4
Estim
ated
Mar
gina
l Mea
ns
Experimental Group Control Group
Figure 2: Academic and School Competence
49
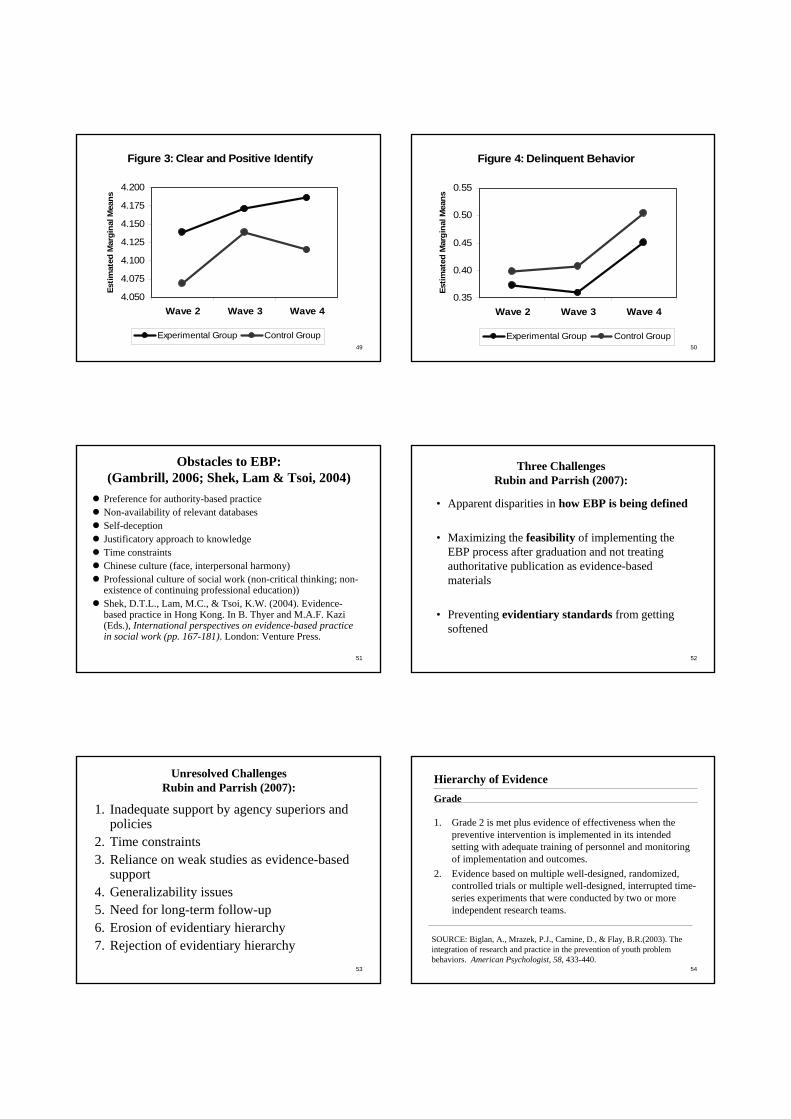
Figure 3: Clear and Positive Identify
4.050
4.075
4.100
4.125
4.150
4.175
4.200
Wave 2 Wave 3 Wave 4
Estim
ated
Mar
gina
l Mea
ns
Experimental Group Control Group50
Figure 4: Delinquent Behavior
0.35
0.40
0.45
0.50
0.55
Wave 2 Wave 3 Wave 4
Estim
ated
Mar
gina
l Mea
ns
Experimental Group Control Group
51
Obstacles to EBP:(Gambrill, 2006; Shek, Lam & Tsoi, 2004)
Preference for authority-based practiceNon-availability of relevant databasesSelf-deception Justificatory approach to knowledgeTime constraintsChinese culture (face, interpersonal harmony) Professional culture of social work (non-critical thinking; non-existence of continuing professional education))Shek, D.T.L., Lam, M.C., & Tsoi, K.W. (2004). Evidence-based practice in Hong Kong. In B. Thyer and M.A.F. Kazi (Eds.), International perspectives on evidence-based practice in social work (pp. 167-181). London: Venture Press.
52
Three ChallengesRubin and Parrish (2007):
• Apparent disparities in how EBP is being defined
• Maximizing the feasibility of implementing the EBP process after graduation and not treating authoritative publication as evidence-based materials
• Preventing evidentiary standards from getting softened
53
Unresolved ChallengesRubin and Parrish (2007):
1. Inadequate support by agency superiors and policies
2. Time constraints3. Reliance on weak studies as evidence-based
support4. Generalizability issues5. Need for long-term follow-up6. Erosion of evidentiary hierarchy7. Rejection of evidentiary hierarchy
54
Hierarchy of EvidenceGrade
1. Grade 2 is met plus evidence of effectiveness when the preventive intervention is implemented in its intended setting with adequate training of personnel and monitoring of implementation and outcomes.
2. Evidence based on multiple well-designed, randomized, controlled trials or multiple well-designed, interrupted time-series experiments that were conducted by two or more independent research teams.
SOURCE: Biglan, A., Mrazek, P.J., Carnine, D., & Flay, B.R.(2003). The integration of research and practice in the prevention of youth problem behaviors. American Psychologist, 58, 433-440.
55
Hierarchy of EvidenceGrade
3. Evidence based on multiple well-designed, randomized, controlled trials or multiple well-designed, interrupted time-series experiments that were conducted by a single research team.
4. Evidence based on at least one well-designed, randomized, controlled trial or an interrupted time-series design that was replicated across three cases.
56
Hierarchy of EvidenceGrade
5. Evidence based on non-equivalent group design(i.e., comparisons between groups that were not effectively randomized to conditions).
6. Evidence based on pre-post evaluation with no comparison group or multiple posttests (i.e., pre-experimental design).
7. Evidence based on clinical experience by respected authorities (researchers and practitioners), descriptions of programs, and case reports.
57
Rubin and Parrish (2007):Recommendations
• Social Work education: defining and strengthening the related EBP components
• Removing obstacles in EBP• Improve colleagues’ understanding of EBP• Avoid softening of evidentiary evidence• Critical appraisal of research studies• Guidelines for describing conclusions of
research studies
58
The Quest for Effective Social Work Intervention Program
6 possible types of programs:
1. Ineffective or harmful intervention2. Intervention unlikely to be beneficial3. Intervention with unknown effectiveness4. Intervention with both benefits and adverse effects5. Intervention likely to be beneficial6. Intervention is effective reflected by clear evidence
Shek, D.T.L. (2008) Enthusiasm-based or evidence-based charities: personal reflections based on the Project P.A.T.H.S. in Hong Kong. TheScientificWorldJOURNAL: 8, 802–810.