BY STRAIGHT LEG RAISE (SLR) AND - Best Physiotherapy ...
39
Volume 5 • Number 1 • September 2016 A STUDY TO KNOW THE EFFECT OF HOLD RELAX STRETCHING ON FLEXIBILITY OF HAMSTRINGS WHEN PERFORMED: BY STRAIGHT LEG RAISE (SLR) AND PASSIVE KNEE EXTENSION (PKE) Ram Babu, Meenakshi Arora, Gagandeep Kaur COMPARISON BETWEEN TWO ACTIVE ASSISTED SLUMP TEST TECHNIQUES: SENSORY RESPONSES IN ASYMPTOMATIC SUBJECTS Dr. Shefali kapoor, Dr. Vinay Jagga, Dr. Megha Gakhar EFFICACY OF SOFT TISSUE MANIPULATION ON CHRONIC NECK PAIN IN COMPUTER PROFESSIONALS IN RELIEVING PAIN AND IMPROVING FUNCTIONAL OUTCOME Kirti Chawla, Shagun Agarwal SENSORY-MOTOR SKILLS IN SCHOOL CHILDREN BORN BY CAESAREAN SECTION DELIVERY AND NORMAL VAGINAL DELIVERY AT TERM: A COMPARATIVE STUDY Rajnish Kumar, Reena Kumari, Sukriti Gupta
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of BY STRAIGHT LEG RAISE (SLR) AND - Best Physiotherapy ...
Volume 5 • Number 1 • September 2016
A STUDY TO KNOW THE EFFECT OF HOLD RELAX STRETCHING ON FLEXIBILITY OF HAMSTRINGS WHEN PERFORMED: BY STRAIGHT LEG RAISE (SLR) AND PASSIVE KNEE EXTENSION (PKE)
Ram Babu, Meenakshi Arora, Gagandeep Kaur
COMPARISON BETWEEN TWO ACTIVE ASSISTED SLUMP TEST TECHNIQUES:
SENSORY RESPONSES IN ASYMPTOMATIC SUBJECTS
Dr. Shefali kapoor, Dr. Vinay Jagga, Dr. Megha Gakhar
EFFICACY OF SOFT TISSUE MANIPULATION ON CHRONIC NECK PAIN IN COMPUTER PROFESSIONALS IN RELIEVING PAIN AND IMPROVING FUNCTIONAL OUTCOME
Kirti Chawla, Shagun Agarwal
SENSORY-MOTOR SKILLS IN SCHOOL CHILDREN BORN BY CAESAREAN SECTION DELIVERY AND NORMAL VAGINAL DELIVERY AT TERM:
A COMPARATIVE STUDY
Rajnish Kumar, Reena Kumari, Sukriti Gupta

Dr. Poonam Singh, Dr. Vaishali Chaudhary, Dr. Monika Sharma, Dr. Shivani Tickoo
Dr. Ali Irani (PT) HOD, Physiotherapy and Sports MedicineDr. Balabhai Nanavati Hospital, Mumbai
Dr. Dharampani PandeyHOD, BL KApur Hospital,New Delhi
Dr. Harpreet SinghSenior Physiotherapist, AIIMS
Dr. Jasmine HOD, Sir Ganga Ram Hospital, Delhi
Dr. K GanesanDirector, Movment SolutionsChennai
Dr. Maneesh Arora Principal, SBSPGI Dehradun
Dr. Neelima PatelSr. Lecturer, College of Physiotherapy, S S G Hospital, Baroda
Dr. Nikita JoshiPrincipal, Dept of PhysiotherapySikkim Manipal University, Gangtok.Dr. Shabnam AggarwalDirector, Dept. of Physiotherapy,Nopany Group of Institutions, Kolkata
Dr. S.K.S MaryaVice Chairman, Max Health Care, Saket, New Delhi Chairman- Max Institute of Orthopaedics & Joint Replacement Surgery.
Dr. Tejbir singhDirector, Kamal Hospital
Dr. Sarvanan SivanithiPaediatric Therapy Associates, Chennai.
Dr. Narkeesh ArumugamHOD, Punjab University, Patiala
Prof. Umashankar MohantyPresident, Manual Therapy Foundation of India.


A STUDY TO KNOW THE EFFECT OF HOLD RELAX STRETCHING ON FLEXIBILITY OF 1-9HAMSTRINGS WHEN PERFORMED: BY STRAIGHT LEG RAISE (SLR) AND PASSIVE KNEE EXTENSION (PKE)Ram Babu, Meenakshi Arora, Gagandeep Kaur
COMPARISON BETWEEN TWO ACTIVE ASSISTED SLUMP TEST TECHNIQUES: 10-12SENSORY RESPONSES IN ASYMPTOMATIC SUBJECTSDr. Shefali kapoor, Dr. Vinay Jagga, Dr. Megha Gakhar
EFFICACY OF SOFT TISSUE MANIPULATION ON CHRONIC NECK PAIN IN COMPUTER 13-21PROFESSIONALS IN RELIEVING PAIN AND IMPROVING FUNCTIONAL OUTCOMEKirti Chawla, Shagun Agarwal
SENSORY-MOTOR SKILLS IN SCHOOL CHILDREN BORN BY CAESAREAN SECTION 22-30DELIVERY AND NORMAL VAGINAL DELIVERY AT TERM: A COMPARATIVE STUDYRajnish Kumar, Reena Kumari, Sukriti Gupta
Volume 5 • Number 1 • September 2016


1
A STUDY TO KNOW THE EFFECT OF HOLD RELAX STRETCHING ON FLEXIBILITY OF HAMSTRINGS
A STUDY TO KNOW THE EFFECT OF HOLD RELAXSTRETCHING ON FLEXIBILITY OF HAMSTRINGS WHEN
PERFORMED: BY STRAIGHT LEG RAISE (SLR) AND PASSIVEKNEE EXTENSION (PKE)
Ram Babu* , Meenakshi Arora** , Gagandeep Kaur**
* Assistant Professor, DAV Institute of Physiotherapy & Rehabilitation, GT Road, Jalandhar, Punjab, India.** Students, DAV Institute of Physiotherapy & Rehabilitation, GT Road, Jalandhar, Punjab, India.
INTRODUCTIONFlexibility: “the available range of motion of a joint ora series of joints that are influenced by ligaments,bones and bony structure”1 is an importantcomponent of physical fitness helps in reducingthe potential for injury and also for improvingperformance during physical activity and sport6.Flexibility can be altered by stretching andacitivities.”Stretching is a general term used todescribe any therapeutic maneuver designed to lengthen(elongate) pathologically shortened soft tissue structuresand there by incresing the range of motion of a jointor a series of joints.”4,5,28
The most commonly used stretching techniques forincreasing flexibility of hamstrings are static
Objectives: The purpose of this Study was to compare the effectiveness of Straight Leg Raise (SLR) and PassiveKnee Extension (PKE) stretching procedures using Hold-Relax as a stretching technique for the hamstringsmuscles.
Background: Stretching of hamstrings muscles can be performed by keeping hip joint in full flexion and movingknee Passively into extension (Passive Knee Extension) and also by keeping knee joint in full extension movinghip into flexion (Straight leg raise). Both variation of stretching are used in past to compare the differentstretching techniques, different protocols and different parameters.
Methodology: Fifty-four asymptomatic healthy Physiotherapy students, aged between 17- 23 years, withhamstrings tightness, were recruited for this study. The subjects were allocated into three groups - CG, SLR andPKE respectively using convenient sampling. They underwent assigned stretching procedure for hamstrings,group SLR was on hold relax stretching by straight leg raise (SLR), group PKE was on hold relax stretching bypassive knee extension (PKE), for five times per week for four weeks and group CG serve as control and nostretching were given. Length of the hamstrings was measured prior and after four weeks of stretching, usingAKE test.
Result: Upon analysis of data using one-way ANOVA significant values were found, F Ratio Equals to 37.249,P<0.000. Scheffe multiple range test significant differences were found in between PKE and SLR at P<0.01(F=14.829) with the SLR group benefiting more than PKE.Conclusion: Stretching of hamstrings is more effective in increasing the length if performed by SLR, if choice oftechnique is Hold Relax.
Keywords: Hamstrings, Stretching, Straight Leg Raise, Passive Knee extension, Hold Relax, PNF
stretching (SS), PNF stretching such as hold-relax(HR) and contract-relax (CR)9,31,24,21,20,14
Static Stretching of hamstrings muscles can beperformed by stabilizing hip joint in full flexionand moving knee Passively into extension (PKE)20
or by keeping knee joint in full extension andmoving hip into flexion (SLR)17,29,16,31,25,3,8,12,19,24. Bothvariation of stretching were used in past tocompare the different stretching techniques,different protocols and different parameters.
Hamstrings group of muscles are biarticular, theycross hip anteriorly and knee posteriorly, at kneethey act as flexor of knee joint and at hip theyhelps in extension. Their work effectiveness at
2
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 1-9
hip and at knee depends upon the relativeposition of these two joints. When knee joint is infull extension they work efficiently and effectivelyat hip as an extensor and when hip is in fullflexion they work efficiently and effectively at kneeas a flexor13. Kapandji (1970) documented, whenhamstrings are lengthen by hip flexion theirefficiency as knee flexors increases: thus duringstair climbing one lower limb moves forward;flexion of hip increases the efficiency of the kneeflexors. Conversely knee extension promotes theextensor action of these muscles on the hip: thisoccurs as one tries to straighten the trunk when itis bent forward. So in both situations hamstringefficiency at knee or hip is going to vary. In thisstudy we used hold relax technique to comparetwo variations, so that the active involvement ofthe muscles can be utilized to generate theeffective tension caused by isometric contractionand most of the literature supports the view thatPNF stretching, which involves a pre-stretchisometric muscle contraction 14, are better thanstatic stretching.21,20,9,8,22,7 In figure 2 when subjectspush the therapist shoulder hamstrings producedmore efficient contraction or tension as hipextensors. In figure 3 when hip is fully flexed andsubjects were instructed to bend the knee,hamstrings are more efficient as knee flexors.
Aim of this study was to measure right kneeextension range of motion pre test and post-testusing AKE in control and experiment group, andanalysis of recorded data for any significantdifference.
METHODOLOGYSubject: - healthy students of DAV Institute ofPhysiotherapy and Rehabilitation, Jalandharranging in the age from 17-23 yrs, male andfemale participated in this study. They wereexplained about the procedure prior in hand andverbal consent was taken. Sixty-nine subjects whowere not having any history of orthopedic andneurological disorder were considered forscreening. After screening fifty four subjects wereselected whose right knee flexion angle was lessthan 300 or reciprocating angle not more than 1500
the upper limit for knee flexion angle was notrecorded.
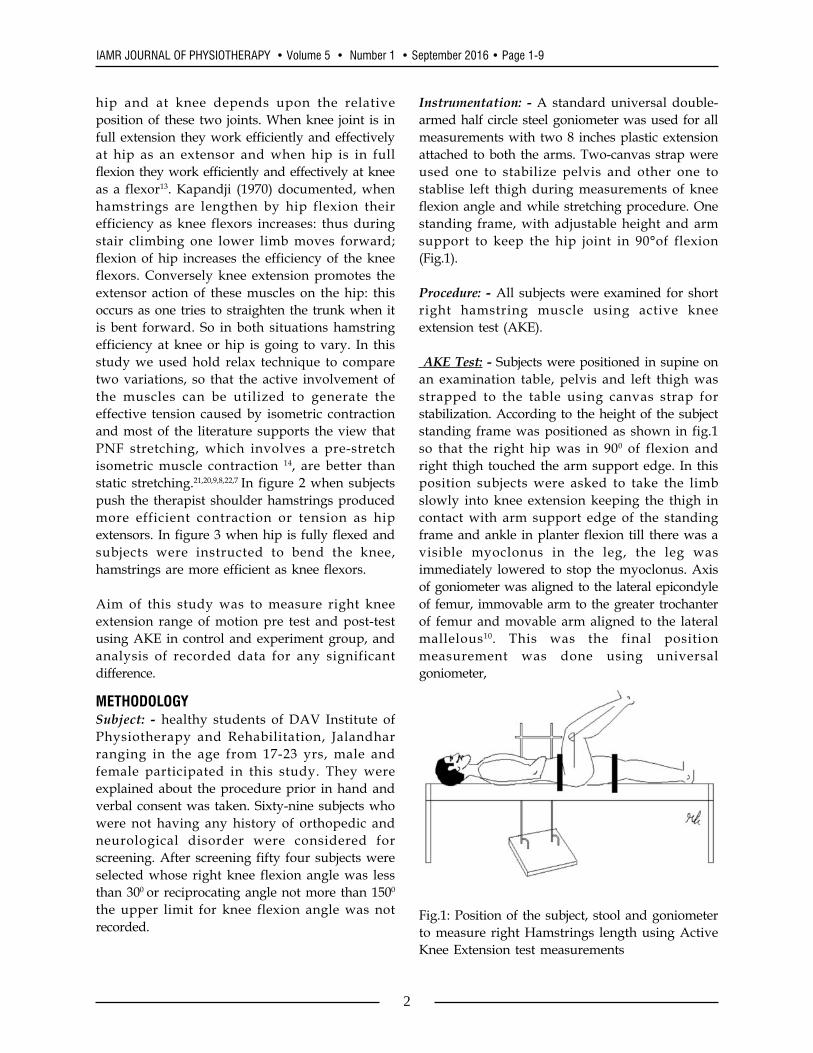
Instrumentation: - A standard universal double-armed half circle steel goniometer was used for allmeasurements with two 8 inches plastic extensionattached to both the arms. Two-canvas strap wereused one to stabilize pelvis and other one tostablise left thigh during measurements of kneeflexion angle and while stretching procedure. Onestanding frame, with adjustable height and armsupport to keep the hip joint in 90°of flexion(Fig.1).
Procedure: - All subjects were examined for shortright hamstring muscle using active kneeextension test (AKE).
AKE Test: - Subjects were positioned in supine onan examination table, pelvis and left thigh wasstrapped to the table using canvas strap forstabilization. According to the height of the subjectstanding frame was positioned as shown in fig.1so that the right hip was in 900 of flexion andright thigh touched the arm support edge. In thisposition subjects were asked to take the limbslowly into knee extension keeping the thigh incontact with arm support edge of the standingframe and ankle in planter flexion till there was avisible myoclonus in the leg, the leg wasimmediately lowered to stop the myoclonus. Axisof goniometer was aligned to the lateral epicondyleof femur, immovable arm to the greater trochanterof femur and movable arm aligned to the lateralmallelous10. This was the final positionmeasurement was done using universalgoniometer,
Fig.1: Position of the subject, stool and goniometerto measure right Hamstrings length using ActiveKnee Extension test measurements
3
A STUDY TO KNOW THE EFFECT OF HOLD RELAX STRETCHING ON FLEXIBILITY OF HAMSTRINGS
In this study we measured the opposite angle tothe knee flexion angle, as our aim was to measurethe changes in range of motion that did not affectour study, for the convenience such 3 readingswere taken with a time interval of 2 mins. and themean was recorded as pre test AKE reading.
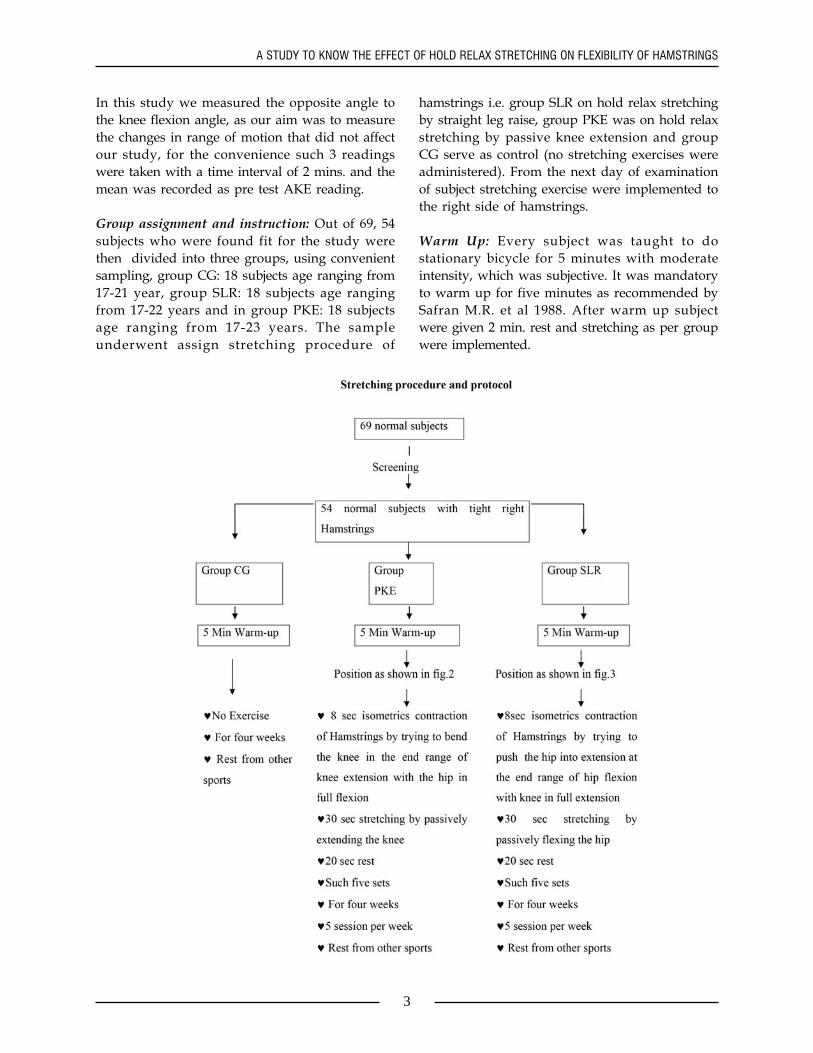
Group assignment and instruction: Out of 69, 54subjects who were found fit for the study werethen divided into three groups, using convenientsampling, group CG: 18 subjects age ranging from17-21 year, group SLR: 18 subjects age rangingfrom 17-22 years and in group PKE: 18 subjectsage ranging from 17-23 years. The sampleunderwent assign stretching procedure of
hamstrings i.e. group SLR on hold relax stretchingby straight leg raise, group PKE was on hold relaxstretching by passive knee extension and groupCG serve as control (no stretching exercises wereadministered). From the next day of examinationof subject stretching exercise were implemented tothe right side of hamstrings.
Warm Up: Every subject was taught to dostationary bicycle for 5 minutes with moderateintensity, which was subjective. It was mandatoryto warm up for five minutes as recommended bySafran M.R. et al 1988. After warm up subjectwere given 2 min. rest and stretching as per groupwere implemented.
4
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 1-9
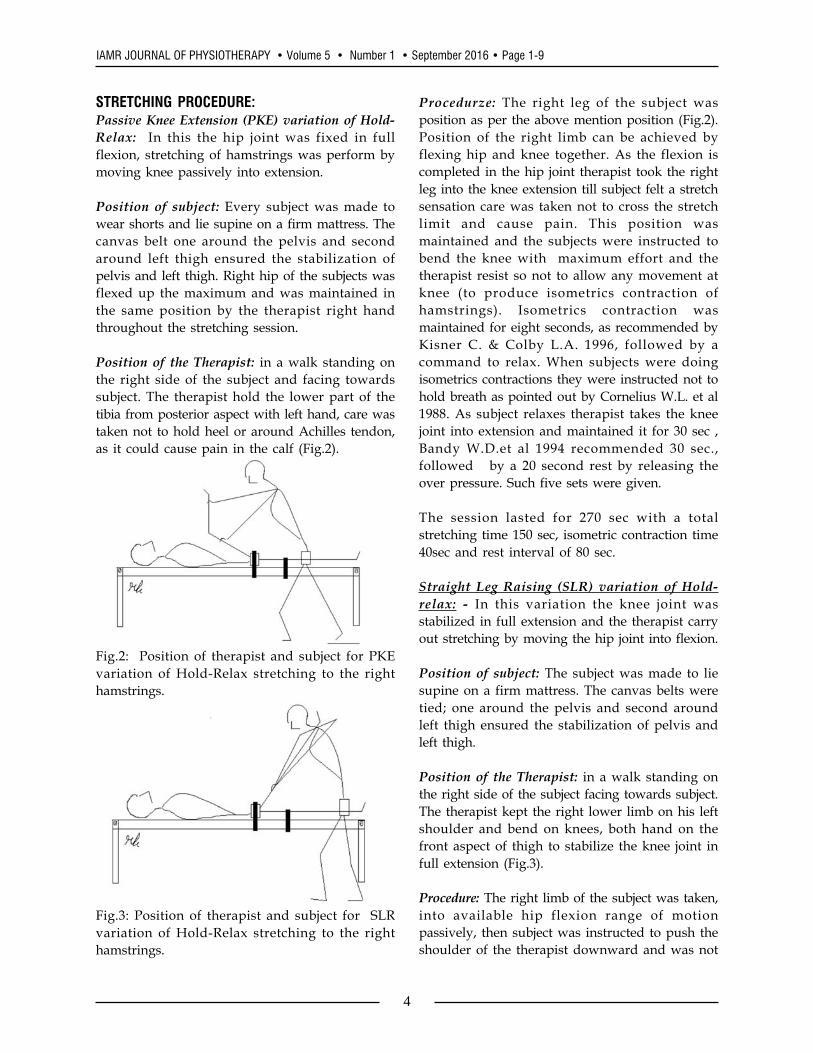
STRETCHING PROCEDURE:Passive Knee Extension (PKE) variation of Hold-Relax: In this the hip joint was fixed in fullflexion, stretching of hamstrings was perform bymoving knee passively into extension.
Position of subject: Every subject was made towear shorts and lie supine on a firm mattress. Thecanvas belt one around the pelvis and secondaround left thigh ensured the stabilization ofpelvis and left thigh. Right hip of the subjects wasflexed up the maximum and was maintained inthe same position by the therapist right handthroughout the stretching session.
Position of the Therapist: in a walk standing onthe right side of the subject and facing towardssubject. The therapist hold the lower part of thetibia from posterior aspect with left hand, care wastaken not to hold heel or around Achilles tendon,as it could cause pain in the calf (Fig.2).
Fig.2: Position of therapist and subject for PKEvariation of Hold-Relax stretching to the righthamstrings.
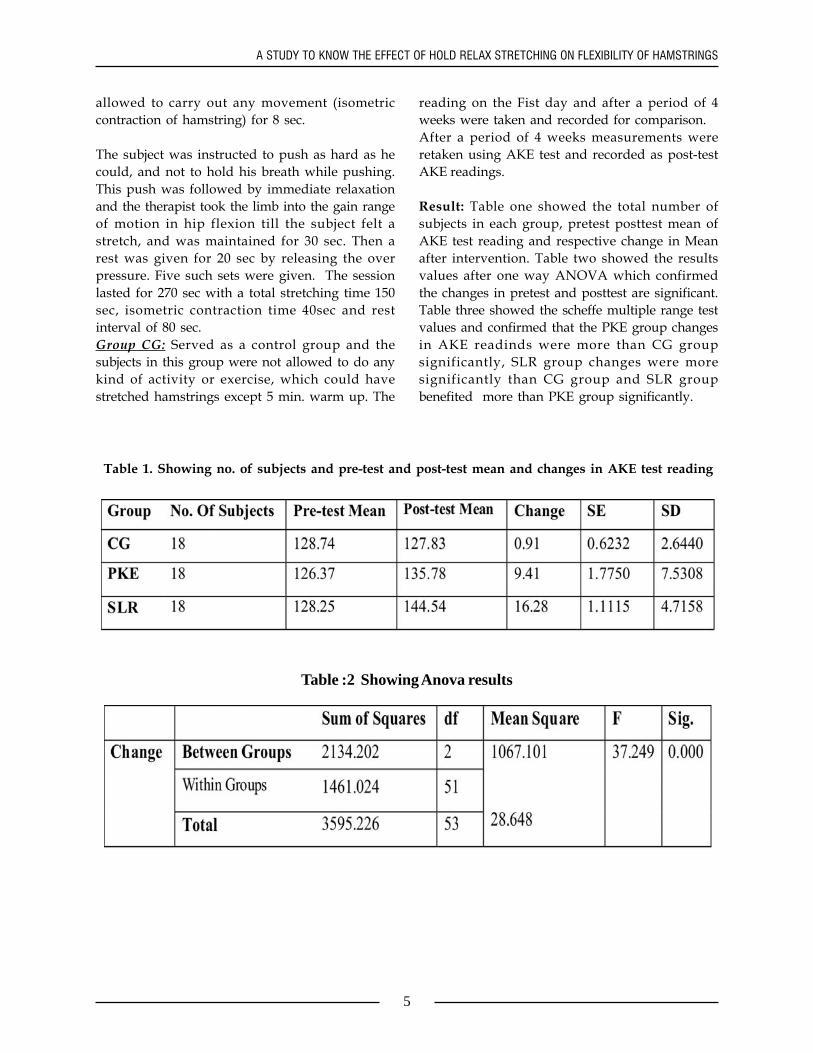
Fig.3: Position of therapist and subject for SLRvariation of Hold-Relax stretching to the righthamstrings.
Procedurze: The right leg of the subject wasposition as per the above mention position (Fig.2).Position of the right limb can be achieved byflexing hip and knee together. As the flexion iscompleted in the hip joint therapist took the rightleg into the knee extension till subject felt a stretchsensation care was taken not to cross the stretchlimit and cause pain. This position wasmaintained and the subjects were instructed tobend the knee with maximum effort and thetherapist resist so not to allow any movement atknee (to produce isometrics contraction ofhamstrings). Isometrics contraction wasmaintained for eight seconds, as recommended byKisner C. & Colby L.A. 1996, followed by acommand to relax. When subjects were doingisometrics contractions they were instructed not tohold breath as pointed out by Cornelius W.L. et al1988. As subject relaxes therapist takes the kneejoint into extension and maintained it for 30 sec ,Bandy W.D.et al 1994 recommended 30 sec.,followed by a 20 second rest by releasing theover pressure. Such five sets were given.
The session lasted for 270 sec with a totalstretching time 150 sec, isometric contraction time40sec and rest interval of 80 sec.
Straight Leg Raising (SLR) variation of Hold-relax: - In this variation the knee joint wasstabilized in full extension and the therapist carryout stretching by moving the hip joint into flexion.
Position of subject: The subject was made to liesupine on a firm mattress. The canvas belts weretied; one around the pelvis and second aroundleft thigh ensured the stabilization of pelvis andleft thigh.
Position of the Therapist: in a walk standing onthe right side of the subject facing towards subject.The therapist kept the right lower limb on his leftshoulder and bend on knees, both hand on thefront aspect of thigh to stabilize the knee joint infull extension (Fig.3).
Procedure: The right limb of the subject was taken,into available hip flexion range of motionpassively, then subject was instructed to push theshoulder of the therapist downward and was not
5
A STUDY TO KNOW THE EFFECT OF HOLD RELAX STRETCHING ON FLEXIBILITY OF HAMSTRINGS
allowed to carry out any movement (isometriccontraction of hamstring) for 8 sec.
The subject was instructed to push as hard as hecould, and not to hold his breath while pushing.This push was followed by immediate relaxationand the therapist took the limb into the gain rangeof motion in hip flexion till the subject felt astretch, and was maintained for 30 sec. Then arest was given for 20 sec by releasing the overpressure. Five such sets were given. The sessionlasted for 270 sec with a total stretching time 150sec, isometric contraction time 40sec and restinterval of 80 sec.Group CG: Served as a control group and thesubjects in this group were not allowed to do anykind of activity or exercise, which could havestretched hamstrings except 5 min. warm up. The
reading on the Fist day and after a period of 4weeks were taken and recorded for comparison.After a period of 4 weeks measurements wereretaken using AKE test and recorded as post-testAKE readings.
Result: Table one showed the total number ofsubjects in each group, pretest posttest mean ofAKE test reading and respective change in Meanafter intervention. Table two showed the resultsvalues after one way ANOVA which confirmedthe changes in pretest and posttest are significant.Table three showed the scheffe multiple range testvalues and confirmed that the PKE group changesin AKE readinds were more than CG groupsignificantly, SLR group changes were moresignificantly than CG group and SLR groupbenefited more than PKE group significantly.
Table 1. Showing no. of subjects and pre-test and post-test mean and changes in AKE test reading
Table :2 Showing Anova results

6
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 1-9
Table:3 Showing scheffe Multiple range test
Graph 1 : percentage change in AKE reading ofright Knee
Graph one showed the percentage of changes inMean AKE pre and post test readings in whichmaximum percentage cnage was in PKE groupfollowed by PKE group and in cg group changesof 0.71% was also reported.
DISCUSSION:Among the comparative hamstrings flexibilitystudies, which includes at least one PNF method,changes were reported as a result of variousstretching techniques. The objective of this studywas to compare the response of short hamstringsmuscles to hold relax technique by two variationsPKE (stretching by moving knee) and SLR(stretching by moving hip). The results of thisstudy reveals that the way of performing
stretching technique was more important thanstretching technique for increasing hamstringsflexibility when hold –relax is the choice oftechnique to stretch hamstrings.
In this study both the groups weresignificantly befitted when compare with thecontrol group. Both the variation of PNFstretching technique were significantly effective inincreasing hamstring length with a mean gain inROM of 9.41 degress with PKE stretching and16.28 degrees with SLR variation of PNFstretching. This finding of our study was inaccordance with the finding reported by OsterningL.R.et al.1987 they reported a gain in kneeextension range of motion when hamstrings werestretched using contract relax technique usingpassive knee extension consist of five trials ofthree stretch and three contraction phases.Cornelius W.L. et al 1988 also concluded that thehold relax stretching technique using SLR variationincreased hamstrings length significantly frombaseline, he used three trial of static stretching asbaseline and after a rest executed hold relax threerepetitions. Moller m et al 1985 also reported aincrease in hamstring flexibility using Hold relaxstretching technique he used five repetitions of 4-6 sec maximum isometric contraction, 2sec restand 8 sec of stretch.

7
A STUDY TO KNOW THE EFFECT OF HOLD RELAX STRETCHING ON FLEXIBILITY OF HAMSTRINGS
The improved range of motion gains demonstratedby both stretching may be because of stressrelaxation26,18 , lengthening changes 11,27,30, autogenicinhibition2 , increase in stretch tolerance12 and byenhanced autogenic inhibition21. Taylor D.C.et al.(1990) did a study to know the effect of staticstretching on rabbit in vivo and reportedmusculotendinous unit elongation due to Stress-relaxation, stimulated by static stretching andduring isometric contraction during PNFtechniques might have caused contribution inlengthening in our both stretching techniques. McHug M.P. et al. 1992 provide further support forviscoelastic stress relaxation using a human staticstretching model by SLR, which increases thehamstrings flexibility. Gajdosik R.L. (1991)reported an increased hamstrings length andresistance to passive stretching following 3 weeksof daily static stretching. Avela (1999) did a studyon triceps surae and proposed when a repeatedstretch is given it induces relaxation of the samemuscle by Autogenic inhibition and there is also adecrease in a motor pool activity, in our studystretch was maintained so this inhibition of motorpool could have played role in both the groups torelax muscles and so gain in range of motion. Allthe above-proposed mechanisms could havecontributed in increasing the resting length of amuscle by passive stretching. In hold-relax,because of pre-stretch isometric contraction thatinduces relaxation all the benefits of stretching areenhanced to increase muscle length.
In this study the PKE variation changed the Activeknee extension test values 9.41° which is inagreement with Webright W.G.et al (1997), theyreported a 10.2° increment after a six-week of staticstretching in neural slump position (stretchinghamstring by extending knee joint). This result ofour study was in agreement with Osterning L.R.etal.(1987) they reported a 4% gain in kneeextension range of motion when hamstrings werestretched using contract relax technique usingpassive knee extension consist of five trials ofthree stretch and three contraction phases thetechnique CR, was same as used in this studywith different stretching protocols in terms of time,repetition and session. Later 1989 they reported a4.86%, 9.74% and3.19% increment in kneeextension range of motion, in endurance, high
intensity athletes and normal subjects respectively.Magnussion S. Peter in 1996 reported decrease instiffness after five consecutive stretches. They putthe subjects on KinKom and stretch hamstrings bypassive knee extension and reported that in thisposition tension was placed primarily on themuscle and tendon without involvement of theposterior capsular constraints about the knee.
By SLR way of stretching we found 16.28°changein the knee extension range of motion. This resultof our study was in accordance with CornelusWilliams et al 1988 did a study to know the acuteeffect of PNF stretching on ABP and reported 16.2°increase in hip flexion range of motion from thebase line after one session of PNF stretching bySLR. Wiemann K. and Hahn K. (1997) alsoreported 7.8° gain in SLR after implementing staticstretching of hamstrings by Passive SLR. MollerMargareta in 1985 reported about 6° increase inhip flexion range of motion after one session ofhold relaxstretching using hip movement forstretching of hamstrings and hip extension forisometric contraction as in our study but theyperformed the procedure in standing position. In1994 Bandy William D et al. study the effect oftime on static stretching with passive SLR andreported a 3.78°gain in knee extension with 15 sec.12.50° with 30 sec. & 10.83° with 60 sec stretchingafter six week, six time per week and concludedthat there is no benefit of increasing the staticstretching duration from 30 sec. to 60 seconds inour study also stretch position was maintained for30 seconds and hamstring length were found to beincreased. In 1996 Halbertsma Jan P.K. et al.reported an 8.9° increase in hip flexion range ofmotion after 5min static stretching session bybending forward which is same maneuver tostretch hamstrings by moving hips as in SLRvariation.
In our study we reported a change in AKEreadings was more with SLR variation (16.27)than PKE variation (9.41) and the results werehighly significant. This may be because in PKEvariation the neural tissue behind the knee jointare fully taut and the subjects were not able toreach the actual end range and so not elongatedtheir hamstrings beyond their resting length asdiscussed by Webright W.G..et at 1997. There may

8
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 1-9
be more effective stretching of hamstrings when westretch them by hold relax, involving isometriccontraction, as also suggested by Kapandji (1987)that if the hamstrings are stretched by moving hipand keeping the knee joint in full extension, morethe hip is flexed the greater the degree of relativeshortening of these muscles and the more stretchedthey become.
CONCLUSION AND SUGGESTIONSIf we summarize the results we come to thefollowing conclusions. Both the techniques werefound to be effective in increasing the length ofshort hamstring muscle in healthy individuals. Byusing two variations of the Hold Relax we cansay the way of stretching is more important whenHold-Relax is the choice of technique. Stretching ofhamstrings is more effective in increasing thelength if performed by SLR, if choice of techniqueis Hold Relax. This is the first study of this typeof comparing these two variation and only usingHold –Relax stretching: therefore conclusioncannot be generalized further study can be carryout to compare these two variations using otherstretching technique. The conclusion cannot begeneralized to the symptomatic individuals havingneural tissue involvement.
REFERENCES1) Anderson B, Burke ER, Scientific, medical
and practical aspects of stretching. Clin.Sports Med. 1991;10:63-86.
2) Avela J, Kynolainen H, Komi PV. AlteredReflex sensitivity after repeated andprolonged passive muscle stretching. J.Appl. Phyisol. 1999; 86:1283-91.
3) Bandy WD, Irion JM. The effect of time onstatic stretch on flexibility of thehamstring muscles. Phys.Ther.1994;74:845-50.
4) Basmajian JV. Manipulation, traction andMassage (3rd edition) Williams andWilkins, Baltimore, pp. 157, (1985).
5) Beaulieu J. Developing a stretchingprogram. Physician and Sports Med.1981;9: 59-65.
6) Corbin CB, Noble L. Flexibility: a majorcomponent of physical fitness. J. PhysicalEdu. 1981;51:23-60.
7) Cornelius WL, Jackson AW. The effect of
cryotherapy and PNF on hip extensionflexibility. Athletic Training. 1984;19: 183-4.
8) Cornelius WL, Hamm K.C. Proprioceptiveneuromuscular facilitation flexibilitytechnique: Acute effects on arterial bloodpressure. The Phys. and Sport med.1988;16: 152-61.
9) Etnyre RB, Lee EJ. Chronic and acuteflexibility of men and women using threedifferent stretching techniques. Resc. Quar.for Ex. and Sports. 1988; 59: 222-28.
10) Gajdosik RL, Lusin G. Hamstring muscletightness: reliability of an active kneeextension test. Phys. Ther. 1983;63:1085-9.
11) Gajdosik RL. Effect of static stretching onthe maximal length and resistance topassive stretch of short hamstring muscles.J. Orthop. Sports. Phys. Ther. 1991;14: 250-5.
12) Halbertsma JPK, Balhuis ALV, GoekenLNH. Sport stretching effect on the passivemuscle stiffness of short hamstring. Arch.Phys. Med. Rehabil. 1996;77:688-92.
13) Kapandji IA. The Physiology of the joints.Volume –II, 5th edition. churchilllivingstone new york. 1987.
14) Knott M, Voss D. Proprioceptiveneuromuscular facilitation : patterns andtechniques. Harper and Row, New York.1968.
15) Kisner C, Colby L. Therapeutic Exercise :Foundations and techniques. 3rd edition.F.A. Davis Co. Philadelphia. pp.143-182.1996.
16) Li Yerchin, Mc Clure PW, Pratt N. Theeffect of hamstring muscle stretching onstanding posture and on lumbar and hipmotion during forward bending . PhysicalTherapy. 1996;75:836-50.
17) Magnunsson SP, Simonsen EB, Aagaard P,Kjaer M. Biomechanical response torepeated stretches in human hamstringmuscle in vivo. The American J. of sportsmedicine. 1996;24: 622-8.
18) Mchugh MP, Magnasson SP, Glein GW,Nicholas JA. Viscoelastic stress relaxationin human skeletal muscles. Med. Sci.Sports Exer. 1992;12: 1375-82.
9
A STUDY TO KNOW THE EFFECT OF HOLD RELAX STRETCHING ON FLEXIBILITY OF HAMSTRINGS
19) Moller M, Ekstrund J, Oberg B, Gillguist J.Duration of static stretching effect onrange of motion in lower extremities. Arch.Phys. Med. Rehabil. 1985;44:171-3.
20) Osternig LR, Robertson R, Troxel R,Hansen P. Muscle activation during PNFstretching techniques. Am. J. PhysicalMed. 1987;66:298-307.
21) Prentice WE. A comparison of staticstretching and PNF stretching forimproving hip joint flexibility. AthleticTrain. J. 1983;18:56-59.
22) Rosenberg BS, Cornelius WL, Jackson AW.The effects of cryotherapy and PNFstretching techniques on hip extensionflexibility in elderly females. J of PhysicalEdu. And Sports Sciences. 1990;2:31-36.
23) Safron MR, Garret WE, Seaber AV, GlissonRR, Ribbeck BM. The role of warm-up inmuscle injury prevention. Am. J. Sport.Med. 1988;16:123-9.
24) Sullivan MK, Dejulia JJ, Worrell TW. Effectof pelvic position and stretching methodon hamstring muscle flexibility. Med. Sci.Sports. Exerc. 1992;24:1383-9.
25) Starring DT, Gouman MR, Nicholson GG,Lemons J. Comparison of cyclic andsustained passive stretching using amechanical device to increase restinglength of hamstring muscles. Phys. Ther.1988;68:314-20.
26) Taylor DC, Dalton JD, Seaber AV, GarrettWE. Viscoelastic properties of muscletendon units:The biomechanical effects ofstretching. The American journal of sportsmedicine. 1990;18:300-8.
27) Tobary JC, Tabary C, Tardieu C,Tardieu G,Goldspink G. Physiological and structuralchanges in the cat’s soleus muscle due toimmobilizationat different length byplanter casts. J Physiology. 1972;224:231-44.
28) Trombly CA.: Occupational therapy forphysical dysfunction (2nd edition).Williams and Wilkinson, Baltimore (1983).
29) Webright WG, Radalph BJ, Perrin DH.Comparison of non ballistic active kneeextension in neural slump position andstatic stretch technique on hamstringflexibility. J. Orthop. Sports. Phys. Ther.1997;25:7-13.
30) Williams PE, Goldspink G. Change insarcomere length and physiologicalproperties in immobilized muscle. JAnatomy. 1978;127:459–68.
31) Worrell TW, Smith TL, Winegardner J.Effect of hamstring stretching onhamstring muscle performance. J. Orthop.Sports. Phys. Ther. 1994;20:154-9.

10
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 10-12
Comparison Between Two Active Assisted Slump TestTechniques: Sensory Responses In
Asymptomatic Subjects.
Dr. Shefali kapoor*, Dr. Vinay Jagga **, Dr. Megha Gakhar***
* Asst. Professor, Prem Physiotherapy and Rehabilitation College, Panipat, Haryana.** Principal / Professor, Prem Physiotherapy and Rehabilitation College, Panipat, Haryana.*** Asst. Professor, College of Physiotherapy, Pt. B.D.Sharma Uni. of Health Sciences, Rohtak.
INTRODUCTIONSlump test is used as fast, low cost diagnostic toolin the evaluation of leg & back pain disorder. It isa physical examination procedure used forevaluating patient with spinal and lower extremitycomplaints. The test seeks to rule out or identifytension in the neuromeringeal tract. Theperformance of test places traction on theneuromenigeal tract from head to foot & slumptest consist of a series of passive movementsdesigned to assess the mechanics & physiology ofneural tissue.Throughout the procedure pain orany other sensation, available rage of movementand muscle response are monitored 1,2.Anatomical studies confirm that components of theslump test do place extra stress on neuralstructures, for example full flexion of cervical,thoracic and lumbar region of the spine lengthenthe vertebral canal and are associated with the
Introduction: Slump test is used as fast, low cost diagnostic tool in the evaluation of leg & back pain disorder.It is a physical examination procedure used for evaluating patient with spinal and lower extremity complaints
The purpose of this study: Was to compare the normative sensory response with two different active slump testtechnique in asymptomatic subjects
Method: 120 asymptomatic subjects volunteered for the study. Subject meeting any of the following exclusioncriteria were excluded from the study: (1) Any history of leg or back problem from last 6 months to 1 year (2)Any pathophysiological limitation to performing slump test (3) Any history of trauma of upper limb and spinefrom past 6 months to 1 year (4) Any history of general medical condition. Main outcome measures: VAS forintensity of response and body chart for location of response
Results: There was significant difference between two active assisted techniques i.e. long sitting & high sitting ofSLUMP test.
Conclusion: we conclude that SLUMP long sitting technique is more effective in producing sensory responses inasymptomatic subjects and this is an effective mass screening test to predict the progressing muscle tightness andneural tension.
Key words: SLUMP test; sensory response; intensity
stretching of the spinal dura mater and lumbarsacral nerve roots 3. Special variation of slump testexists. The principle difference between variationsis only the order of the test. One variation uses thedorsiflexion of foot prior to the knee extension,another uses cervical flexion after knee extensionand foot dorsiflexion. A test is begins with thepatient in a seated position on the examiner tablewith the lower extremity is extended along thetable. If symptoms of slump test can be changedby adding or subtracting a distal maneuver ofslump test, the test response is interpreted to berelated to the pathological changes affecting themechanics of neural system. The pathologicalchanges or sources of symptoms may be neuralsystem itself or adjacent interfacing tissue. 2,4

11
Comparison Between Two Active Assisted Slump Test Techniques :
There are many active assisted slump testtechnique. So in this study we are comparing 2techniques as there is lack of evidence regardingwhich active assisted slump test technique isbetter for assessing the sensory response inasymptomatic subjects. In some studies it has beenobserved that slump test is also positive inasymptomatic subjects.
MATRIAL & METHODA convenient sample was taken from PremPhysiotherapy and Rehabilitation College Panipatand Central Parks at model town and Sadarbazaar kernal. 120 subjects were taken which wereequally dividing into 3 groups with 20 males and20 females in each group. The subjects wereexplained about the procedure and then group Aperformed slump long sitting, group B performedslump high sitting and group C performing bothlong sitting & high sitting after fulfillment ofinclusion criteria Volunteers of 18-25 yrs. of age,both male & female, able to understand simpleEnglish words & never visited to a doctor due toleg or back pain from last 6 month to 1 year areincluded in this study.
PROCEDUREAll subjects will be equally divided into 3 groupsA.B & C in which subject in Group A performslump long sitting & Group B perform slump highsitting with ankle dorsiflexion & Group C performboth high sitting & long sitting. Standardizedverbal instructions will be given by the examinerto explain the test to each subject. Any Sensationor response will be recorded in the startingposition and at the four stages of slump test[slump sitting/thoracolumbar and cervical flexion(SS), knee extension (KE), ankle dorsiflexion (AD)and cervical extension (CE)] & again when subjectreturned to comfortable sitting position. At eachstage of test, nature, location and intensity of anysensory response will be recorded.
To determine location of response subject will beshown a body diagram with eight regions clearlyoutlined. At each stage of test, subject will beasked to identify the location of each responseaccording to body diagram. To determine intensity,subject will be asked to rate the intensity ofresponse on a verbal descriptor scale of 0 to 10.
RESULT & DISCUSSIONThe results demonstrate that SLUMP long sittingtechnique is more effective in producing sensoryresponses in asymptomatic subjects. All the valuesof intensities in group A, group B, group C areexpressed in terms of mean + S.D for males &females respectively. By applying “unpaired t-test”significant different between the intensities ofgroup A and group B, group A and group C,group B and C are noted. A significant differencewas observed between group A and group B,group A and group C, group B and C for males &females at 5% level of significance. In this studygroup A showed 45% of sensory response duringthe slump sitting (SS) stage while 52.5% subjectexperience during cervical extension (CE) andankle dorsiflexion (AD) stage of slump test. Whilein group B, 15% of subjects experience sensoryresponse in SS where as 85% experience sensoryresponse in CE and 100% subjects experiencesensory response in DF. In group C out of 40patients, 27.5% of subjects performing long sittinghave sensory response in SS where as 65% ofsubject have sensory response in CE while 2.5% ofsubjects have no response in DF . Where as inhigh sitting 17.5% of subjects have response in SS,70% have response in KLS and 40% have responsein DF where as 12.5% of patients experience nosensory response in KE.
Table 1: Showing the mean value of intensity between group A andgroup B for males and females
Table 2 : Showing the mean value of intensity between group Cfor males and females
The result in my studies reveals that the meanintensity of the response of slump test is higher inmales than females. This variation in the averageintensities may be due to the physiologicalvariation in males & females. After performingslump test it has been found that the mostly

12
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 10-12
recorded sensory response is stretch, tightness &pain. Stretch as a response is due to the course ofsciatic nerve mainly and pain is due tooverstretching of Dura at axilla of intervertebralforamen. It implies that symptom arising from thestructure within the canal is due to the Duramater exclusively. 5
In this study greater number of responses arelocated at the calf region which in may be due tothe stretching of common peroneal nerve which isa branch of sciatic nerve. 6
During this study is has been reported that rangeof knee extension is increased after cervicalextension. This may be due to the fact thatcervical spine flexion produces tension in thespinal cord and dura which is transmittedcaudally, pulling the nerve root of caudal equinacranially. This stretching and cephaleddisplacement of the lumbosacral nerve roots andsacral plexus reduces the available caudal mobilityof sciatic nerve. As a result subsequent lowerextremity motion which exert a caudal pull onlumbosacral trunk and nerve root may berestricted . 7,8
Following the slump test it is noted that there issubsequently increase in intensity after thedorsiflexion stage of slump test. This may be dueto the fact that ankle dorsiflexion is a sensitizingmaneuver and is known to increase tensionprimarily along the tibial tract. 9
CONCLUSIONThe study was on comparison between two activeassisted slump test techniques to see sensoryresponses in asymptomatic subjects and the resultof our study conclude that slump long sittingtechnique is more effective in producing sensoryresponse in asymptomatic subjects and this test isan effective mass screening test to predict theprogressing muscle tightness and neural tension.
REFRENCES
1. Jeremy Walsh, Kathleen Bennett and NiallJohnstons(2007).’Slump test:SensoryResponses in Asymptomatic subject’, JMan Manip Ther, 15 (4), 231-238.
2. K. Jeffrey Miller.(1998)’The slump test:clinical application and interpretation’,Chiropactic Orthopardist, November.
3. Steven Z. George.(2002) ‘Characteristic ofpatient with lower extremity symptomstreated with slump stretching: A caseseries’, J orthop sports phys Ther, 32 ,391-398.
4. Sterling M, Treleaven J, Jull G.(2003)‘Response to a clinical test of mechanicalprovocation of nerve tissue in whiplashassociate disorder’, Man Ther. Feb, 8 (1)52-53
5. Butler DA.(1991): Mobilization of thenervous system Melbourne, AustralianChurchill Livingstone.
6. Chaurusia’s BD.(2004): Human Anatomy7. Kathleen Philip, Paul Lew, Thomas A
Matyas. ‘The inter therapist reliability ofslump test’, The Australian journal ofphysiotherapy, 35 (2)
8. Evan K. Johson, Cynthia MChiarello.(1997) ‘The Slump test: the effectof head & lower extremity position onknee extension’ JOSPT, Dec, 26(6)Pahor S, Toppenberg R.(1996) ‘Aninvestigation of neural tissue involvementin ankle invrsion sprain’, ManTher,Sep,1(4,192-197).
13
EFFICACY OF SOFT TISSUE MANIPULATION ON CHRONIC NECK PAIN
EFFICACY OF SOFT TISSUE MANIPULATION ONCHRONIC NECK PAIN IN COMPUTER PROFESSIONALS
IN RELIEVING PAIN AND IMPROVINGFUNCTIONAL OUTCOME
Kirti Chawla*, Shagun Agarwal**
* Research Scholar, Department of Physiotherapy, Institute of Applied Medicines & Research, Gzb** Head of Department, Department of Physiotherapy, Institute of Applied Medicines & Research Gzb
INTRODUCTIONChronic neck pain is a common problem amongadults in developed countries and contributesimportantly to the demand for medical servicesand the economic burden of absence from workdue to sickness. Work related neck disorders arecommon problems in the office workers, especiallyamong those who are intensive computer users.(1)
Neck pain is complicated by many factors. Someof these factors are intrinsic to the patient (ie,concurrent medical or psychosocial factors), andsome are environmental (ie, occupational,ergonomic,or medicolegal issues).(2)Psychosocialfactors are known to be important predictors ofoutcome for neck pain.(3)It has been estimated thatabout 70% of adults are afflicted by neck pain at
Introduction: Chronic neck pain is a common problem among adults in developed countries and contributes importantlyto the demand for medical services and the economic burden of absence from work due to sickness. Work related neckdisorders are common problems in the office workers, especially among those who are intensive computer users. (1)
Aim of the study: To find the efficacy of soft tissue manipulation compared with conventional physical therapytreatment in management of non-specific chronic neck pain in computer professionals.
Methodology: Total of 30 subjects, having neck pain for more than 6 months, aged between 20 - 35 years was takenin the study. The patients in the study were taken from the IT companies who are working on computer for more than6 hours daily. A sample of convenience of 30 subjects, who fitted the inclusion and exclusion criteria were taken in thestudy. The individuals were then divided into two groups of 15 individuals each in experimental group (Group A) andcontrol group (Group B), by random allocation.
Results: Thirty subjects (N = 30) were taken which were divided into two groups ie. Group A (n = 15) and Group B(n = 15). A treatment protocol of three weeks was administered to both the groups and the two groups were evaluatedat week 0 and week 3 on the basis of two different scales these are: Visual analogue scale (VAS): Mean for VAS at week0 = 6.3 and at week 3 = 2.5.Neck disability index (NDI): Mean for NDI at week 0 = 20.6 and at week 3 = 4.6.
Conclusion: This study found that soft tissue manipulation techniques were more effective than conventional physicaltherapy treatment but both the treatments showed significant improvement in the management of chronic neck pain. Alloutcome measures improved significantly in both the treating groups but the experimental group receiving soft tissuemanipulation showed significant improvement over the group receiving conventional physical therapy treatment.
Keywords: Non Specific Neck Pain, NDI, VAS, Soft tissue manipulation
some time in their lives, 10 to 40% of adults arebothered by neck pain each year, 10 to 15% ofadults report neck pain that has persisted morethan 6 months in the past year, and 5% of adultsare currently experiencing disabling neck pain.(4)
Neck pain is responsible for huge personal andsocietal costs, and is major cause of workdisability. Contrary to traditional thinking, neckpain is not a problem that always resolves itself.Recurrences are usual and their course isvariable.(5-8)
The management of neck pain presents a commonclinical problem. The high frequency of neck painand its impact on functioning, including workperformance, make this an important problem for

14
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 13-21
the patient, industry, and society.(2)
All treatment of neck pain is empiric, because theprecise pathology of the pain and the tissue that isgenerating it is not certain in most cases.(2)
There are many treatment options available forneck pain and these options are muscle relaxants,steroid injections, manual therapy, soft tissuemanipulation massage therapy, physical therapy,behavioural therapy, acupuncture, traction andelectromagnetic therapy.(9) Physical therapyconsists of electrotherapy like ultrasound, IFT,TENS, etc. and various exercises to combat pain.Various surgical options are also availabledepending upon the patient’s condition.
Soft Tissue Manipulation, commonly known asMassage therapy aims at imparting mechanicalenergy to the soft tissue of body through the skinwithout producing any change in the position ofjoint, in order to elicit certain physiological orpsychological effect which can be utilized fortherapeutic, restorative or preventive purposeseither on sick or a healthy individual.Thisscientific manipulation manoeuvers of the softtissues of body can be done either with the palmaraspect of hand(s) and or fingers.(10)
Application of touch and pressure in variousmanners constitute the maneuvers of massage. Theeffects produced by a technique entirely dependupon the type of tissue approached during aparticular technique and the character of thetechnique governs this. Any given technique canbe analysed and compared with other techniquesof massage in terms of
• Magnitude of force• Direction of force• Duration of force• Means of application of force
So, the characters of technique could be one of thebases of classification. Massage can also beclassified on the basis of depth of tissueapproached during a technique. The region ofbody, to which massage is given, has also beenused to classify massage. Massage maneuvers canbe done either by hands of the therapist or by
various mechanical devices. This can be anotherbasis of classifying massage.(10)
Basis of classification of massage:
On the Basis of Character of Techniques
1. Stroking manipulation: Superficial strokingand Deep stroking or effleurage
2. Pressure manipulation: Kneading (Palmarkneading, Digital kneading and Ironing),Petrissage (Picking up, Wringing and Skinrolling) and Friction (Circular friction andTransverse friction)
3. Percussion manipulations: Clapping, Hacking,Tapping, Beating, Pounding,Tenting andContact heel percussion(10)
4. Vibratory manipulations: Vibration andShaking
On the Basis of Depth of Tissue Approached
Light massage and deep massage techniques.(10)
On the Basis of Region Massaged
General massage and local massage.(10)
On the Basis of Means of Administration ofTechnique
Manual massage and mechanical massage.(10)
Techniques used for intervention in this study areeffleurage, kneading, picking up, muscle rolling,scapula rolling and hacking and clapping.Evaluation of the patients was done on the basisof VAS scores for pain and NDI scores forfunctional outcome or disability.
METHODS:
NUMBER AND SOURCE:Total of 30 subjects, having neck pain for morethan 6 months, aged between 20 - 35 years weretaken in the study. The patients in the study weretaken from the IT companies who are working oncomputer for more than 6 hours daily.

15
EFFICACY OF SOFT TISSUE MANIPULATION ON CHRONIC NECK PAIN
INCLUSION CRITERIA:• Age 20-35 years• Computer professional(>5-6 working hours)• Neck pain lasing more than 6 months• Pain on VAS = 5
EXCLUSION CRITERIA:• Systemic diseases• Cervical spondylosis• Pain more than 8 on VAS• Vertigo• Dizziness• Headache• Cervical radiculopathy• VBI
SAMPLINGA sample of convenience of 30 subjects, who fittedthe inclusion and exclusion criteria were taken inthe study. The individuals were then divided intotwo groups of 15 individuals each inexperimental group (Group A) and control group(Group B), by random allocation.
INSTRUMENTS AND TOOLS USEDINSTRUMENTS:StepperPlinthPillowsTowelsUltrasound (Serial no.: 1067 and Company name:ATS)Interferential therapy unit (Model no.: IF-9 andCompany name: ATS)
TOOLS:Visual Analogue Scale (VAS)Neck Disability Index (NDI)
PROCEDURE
DESIGN OF STUDYExperimental comparative study.
METHODOLOGYTotal 30 subjects, having neck pain for more than6 months, were selected in the study on the basisof the inclusion criteria and divided into twogroups of 15 individuals in each.
Group A- Soft tissue manipulation techniques
Group B- Conventional physical therapy treatment
After taking the consent from each individual thepatients were randomly assigned into two groups-Group A and Group B, of 15 patients in each. Thepatients were then explained about the fullprocedure in detail to be administered.
Protocol for Group A- The patients of group weregiven moist heat for 10 minutes in supine lyingposition before starting with soft tissuemanipulation before each session.
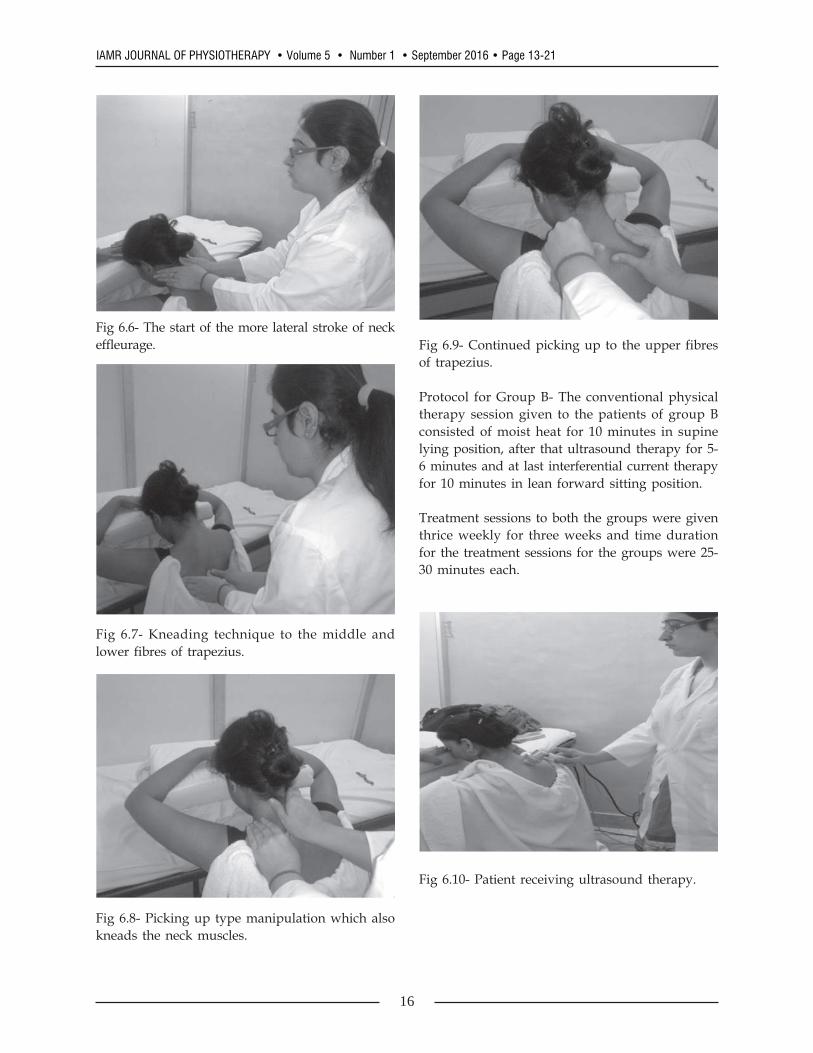
The hands-on manipulation techniques whichwere administered are effleurage, kneading,picking up, muscle rolling, and hacking andclapping. Each soft tissue manipulation sessionwas for 15-20 minutes with patient in leanforward sitting position.
Fig 6.5- Lean forward sitting position of the modelfor neck massage.
16
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 13-21
Fig 6.6- The start of the more lateral stroke of neckeffleurage.
Fig 6.7- Kneading technique to the middle andlower fibres of trapezius.
Fig 6.8- Picking up type manipulation which alsokneads the neck muscles.
Fig 6.9- Continued picking up to the upper fibresof trapezius.
Protocol for Group B- The conventional physicaltherapy session given to the patients of group Bconsisted of moist heat for 10 minutes in supinelying position, after that ultrasound therapy for 5-6 minutes and at last interferential current therapyfor 10 minutes in lean forward sitting position.
Treatment sessions to both the groups were giventhrice weekly for three weeks and time durationfor the treatment sessions for the groups were 25-30 minutes each.
Fig 6.10- Patient receiving ultrasound therapy.

17
EFFICACY OF SOFT TISSUE MANIPULATION ON CHRONIC NECK PAIN
Fig 6.11- Patient receiving IFT.
DATA COLLECTIONTo find out the effectiveness of the therapyevaluation was done on the basis of the scoresobtained in the following scales:• Visual Analogue Scale (VAS)• Neck Disability Index (NDI)
This evaluation was performed on week 0 andweek 3 in the 3 weeks study and the data wascollected on the basis of the tests given above.
RESULTSThirty subjects (N = 30) were taken which weredivided into two groups ie. Group A (n = 15) andGroup B (n = 15). A treatment protocol of threeweeks was administered to both the groups andthe two groups were evaluated at week 0 andweek 3 on the basis of two different scales theseare:Visual analogue scale (VAS)Neck disability index (NDI)
GROUP A
VASMean for VAS at week 0 = 6.3 and at week 3 =2.5. Variance for VAS at week 0 = 0.6 and at week3 = 0.3. P value for group A = 4.5641E-12 whichis a significant value (as the level of significanceis 0.05).(Table 8.1 and graph 8.1).
NDIMean for NDI at week 0 = 20.6 and at week 3 =4.6. Variance for NDI at week 0 = 5.5 and at week
3 = 0.9. P value for group B = 8.00691E-15 whichis a significant value (as the level of significanceis 0.05).(Table 8.2 and graph 8.2)
GROUP BVASMean for VAS at week 0 = 6.3 and at week 3 =3.4. Variance for VAS at week 0 = 1.1 and at week3 = 0.8. P value for group B = 2.68714E-10 whichis a significant value (as the level of significanceis 0.05).(Table 8.3 and graph 8.3).
NDIMean for NDI at week 0 = 20.1 and at week 3 =6.8. Variance for NDI at week 0 = 5.9 and at week3 = 1.4. P value for group B = 2.0393E-14 which isa significant value (as the level of significance is0.05).(Table 8.4 and graph 8.4).
GROUP ABVASMean for group A = 2.57 and mean for group B =.47. Variance for group A = 0.32 and variance forgroup B = 0.84. Since P value for one tailed t-testi.e. 0.0018 for VAS scores is less than the level ofsignificance i.e. .05, therefore, null hypothesis isrejected and experimental hypothesis isaccepted.(Table 8.5 and graph 8.5 and 8.6).
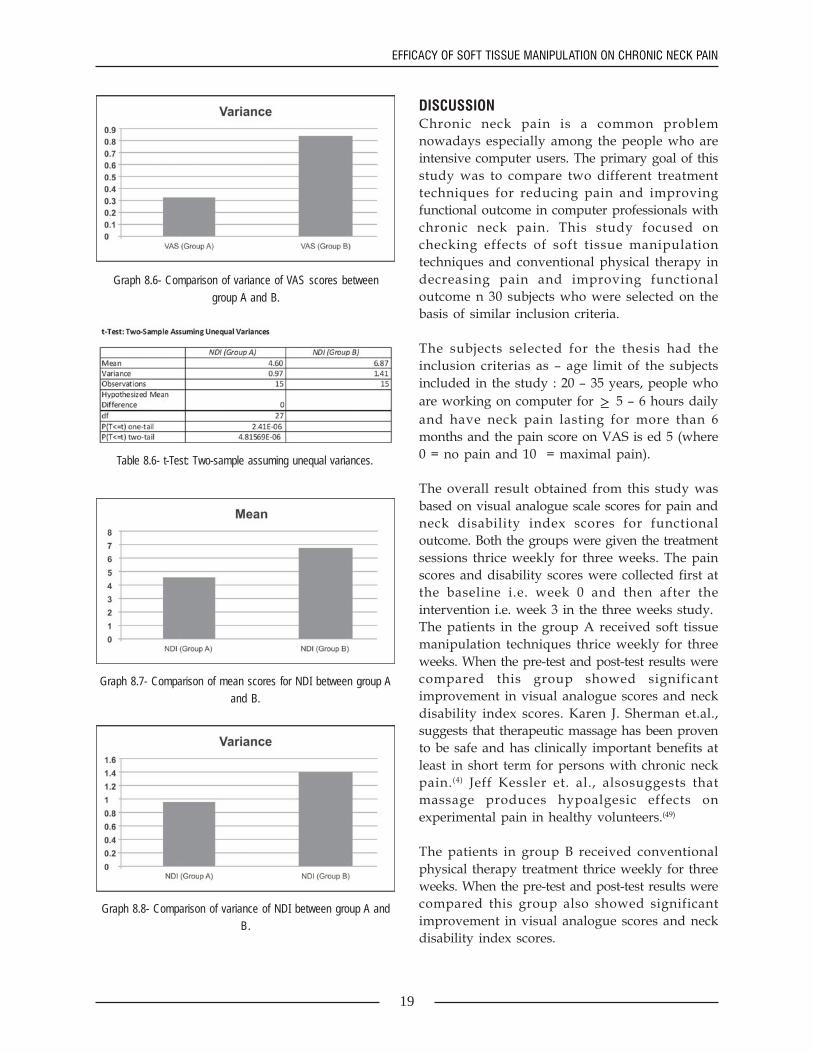
NDIMean for group A = 4.60 and mean for group B =6.87. Variance for group A = 0.97 and variance forgroup B = 1.41. Since P value for one tailed t-testi.e. 2.41E-06 for NDI scores is less than the level ofsignificance i.e. .05, therefore, null hypothesis isrejected and experimental hypothesis isaccepted.(Table 8.6 and graph 8.7 and 8.8).
Table 8.1- t-Test: Paired Two Sample for Means for Group A(VAS Scores)

18
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 13-21
Graph 8.1- Comparison of mean VAS scores for Group A.
Table 8.2- t-Test: Paired Two Sample for Means for Group A(NDI Scores)
Graph 8.2- Comparison for mean scores for NDI for Group A.
Table 8.3- t-Test: Paired Two Sample for Means for Group B(VAS Scores)
Graph 8.3- Comparison of mean scores for VAS for group B.
Table 8.4- t-Test: Paired Two Sample for Means for Group B(NDI Scores)
Graph 8.4- Comparison of mean scores for NDI for group B.
Table 8.5- t-Test: Two-sample assuming unequal variances.
Graph 8.5- Comparison of mean scores of VAS between group Aand B.
19
EFFICACY OF SOFT TISSUE MANIPULATION ON CHRONIC NECK PAIN
Graph 8.6- Comparison of variance of VAS scores betweengroup A and B.
Table 8.6- t-Test: Two-sample assuming unequal variances.
Graph 8.7- Comparison of mean scores for NDI between group Aand B.
Graph 8.8- Comparison of variance of NDI between group A andB.
DISCUSSIONChronic neck pain is a common problemnowadays especially among the people who areintensive computer users. The primary goal of thisstudy was to compare two different treatmenttechniques for reducing pain and improvingfunctional outcome in computer professionals withchronic neck pain. This study focused onchecking effects of soft tissue manipulationtechniques and conventional physical therapy indecreasing pain and improving functionaloutcome n 30 subjects who were selected on thebasis of similar inclusion criteria.
The subjects selected for the thesis had theinclusion criterias as – age limit of the subjectsincluded in the study : 20 – 35 years, people whoare working on computer for ≥ 5 – 6 hours dailyand have neck pain lasting for more than 6months and the pain score on VAS is ed 5 (where0 = no pain and 10 = maximal pain).
The overall result obtained from this study wasbased on visual analogue scale scores for pain andneck disability index scores for functionaloutcome. Both the groups were given the treatmentsessions thrice weekly for three weeks. The painscores and disability scores were collected first atthe baseline i.e. week 0 and then after theintervention i.e. week 3 in the three weeks study.The patients in the group A received soft tissuemanipulation techniques thrice weekly for threeweeks. When the pre-test and post-test results werecompared this group showed significantimprovement in visual analogue scores and neckdisability index scores. Karen J. Sherman et.al.,suggests that therapeutic massage has been provento be safe and has clinically important benefits atleast in short term for persons with chronic neckpain.(4) Jeff Kessler et. al., alsosuggests thatmassage produces hypoalgesic effects onexperimental pain in healthy volunteers.(49)
The patients in group B received conventionalphysical therapy treatment thrice weekly for threeweeks. When the pre-test and post-test results werecompared this group also showed significantimprovement in visual analogue scores and neckdisability index scores.

20
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 13-21
When the results of both the groups werecompared it showed that both groups showedsignificant improvement but the group A whichreceived soft tissue manipulation as thetherapeutic intervention showed better improvedscores than group B which received conventionalphysical therapy. Soft tissue manipulation wasfound to be quiet more effective than conventionalphysical therapy. Both the treatments aimed atdecreasing pain and improving functionaloutcome but therapeutic massage proved to bemore effective because it further leads to re-orientation of the muscle fibres which yield betterresults.
Harald Walach et.Al, suggests that massage canbe atleast effective as standard medical care inchronic pain syndromes. Because of political andorganizational problems, only 29 patients wererandomized, 19 to receive massage, 10 to standardmedical care (SMC). Pain improved significantly inboth groups, but only in the massage group was itstill significantly improved at follow-up.Depression and anxiety were improvedsignificantly by both treatments, yet only in themassage group maintained at follow-up. While theamount of change is comparable in both groupsin nearly all parameters at post-treatment, it isonly the massage-treated group that tends tomaintain its improvement in nearly all variablesthat were sensitive to change. This is apparent,apart from pain, in depression, anxiety, andtiredness. This study quantified this by calculatingeffect sizes for the most important parameters:pain, depression, and anxiety.
Therefore, it seems safe to conclude that this studyprovides initial evidence for the fact that massageis at least as effective as SMC for the treatment ofvarious pain syndromes. While SMC is alsoeffective in reducing pain on the short term, theeffects are more short lived and do not generalizeas readily into psychologic domains as depression,anxiety, or mood. It showed that massage is apromising intervention, at least as effective asSMC, and that it needs to be studied moreclosely.(50)
Thus, the results from this study will contribute toevidence based recommendations for the
usefulness of soft tissue manipulation techniquesin the management of chronic neck pain.
Future research:-In this study both the treatments i.e., soft tissuemanipulation and conventional physical therapyshowed significant improvement but soft tissuemanipulation techniques were more effective thanconventional physical therapy treatment. Therewere 30 subjects taken for the study. In each groupnumbers of subjects were 15 and they were givenintervention for three weeks on alternate days. Thesample size was small and follow-up treatmentwas not recorded. So, for future research longersample size should be taken and follow-uptreatment should be recorded for stronger evidenceof the study.
Relevance to clinical practice:-For effective management of chronic neck pain,this study recommends clinicians to use soft tissuemanipulation techniques as a major tool ofintervention. But, before this more trials are neededto validate its clinical significance overconventional physical therapy treatment incomputer professionals with chronic neck pain.
CONCLUSIONThis study found that soft tissue manipulationtechniques were more effective than conventionalphysical therapy treatment but both the treatmentsshowed significant improvement in themanagement of chronic neck pain. All outcomemeasures improved significantly in both thetreating groups but the experimental groupreceiving soft tissue manipulation showedsignificant improvement over the group receivingconventional physical therapy treatment.
Thus, for early and effective management ofchronic neck pain, this study recommendsclinicians to consider soft tissue manipulationtechniques as a major tool for the intervention. Butbefore that more trials are needed to validate itsclinical significance in general population.

21
EFFICACY OF SOFT TISSUE MANIPULATION ON CHRONIC NECK PAIN
LIMITATIONSFollowing are the limitations of this study:-
• Sample size was small.• Follow-up was not included, therefore, it is not
known whether the improvement in neck painwas maintained or not when treatment wasstopped after 3 weeks.
• Study was not for the generalized population.• Time duration was less.• More variables should be studied.• No work restriction was there.
REFERENCES
1. B. Cagnie., L Danneels, D.Van Tiggelen.,et. al., Individual and work related riskfactors for neck pain among officeworkers: a cross sectional study. Eur SpineJ (2007) 16:679-686.
2. Rand S. Swenson, DC, MD, PhD,Therapeutic modalities in the managementof nonspecific neck pain, Phys MedRehabil Clin N Am 14 (2003) 605-627.
3. Erdinc Civelek Aykut Karasu et. al.,Surgical anatomy of the cervicalsympathetic trunk during anterolateralapproach to cervical spine, Journal list EurSpine J v.17(8); Aug (2008)
4. Karen J. Sherman, Phd, MPH, et. al.,Randomized trial of therapeutic massagefor chronic neck pain, Clin J Pain. 2009;25(3): 233-238.
5. J. Moffett and S. Mclean, The role ofphysiotherapy in the management of non-specific back pain and neck pain,Rheumatology 2006;45:371-378.
6. SBU. Back pain and neck pain: anevidence based review. Stockholm:Swedish Council on TechnologyAssessment in Health Care, 2000.
7. Nachemson A, Vingard E.Assessment ofpatients with neck and back pain: a bestevidence synthesis. In: Nachemson A,Jonsson E, eds. Neck and back pain: thescientific evidence of causes. Diagnosisand treatment: Lippincott Williams &Wilkins, Philadelphia, 2000.
8. Carter J, Birrell L. Occupational healthguidelines for the management of lowback pain at work-principalrecommendations. London: Faculty ofOccupational Medicine, 2000.
9. Alf L. Nachemson, M.D., PH.D., EgonJonsson, PH.D.: Neck and Back Pain:Lippincott Williams & Wilkins,2000,p349-352.
10. Akhoury Gourang Sinha: Principles andPractices of Therapeutic Massage: JaypeeBrothers, 2006, p2.

22
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 22-30
Sensory-Motor Skills in School Children born by CaesareanSection Delivery and Normal Vaginal Delivery at Term:
A Comparative Study
Rajnish Kumar*, Reena Kumari**, Sukriti Gupta***
* Post graduate student of Physiotherapy, SBSPGI, Balawala, Dehradun.** Associate professor,, Department of Physiotherapy, SBSPGI, Balawala, Dehradun.*** Assistant professor Department of Physiotherapy, SBSPGI, Balawala, Dehradun.
INTRODUCTIONIn recent years, caesarean section has become afrequently performed surgical procedure with 18%of Indian mothers giving birth by caesareansection .. The WHO recommends no more than a15% cesarean rate. The increase in the rates of CSis a global phenomenon that has got theprofession, the public and those who care forwomen’s health worried, because the rise has notcontributed to an improved pregnancy outcome 1.A study by the Indian Council of MedicalResearch (ICMR) in 33 tertiary care institutionsnoted that the average CS rate increased from 21.8per cent in 1993-1994 to 25.4 per cent in 1998-19992. A study in Jaipur showed that CS rates in aleading hospitals raised from 5% in 1972 to 10%in the late 1970s and to 19.7% between 1980- 85.The rates were as high as 23% in 1989. InpChennai, the CS rate was reported to be 45% ofall live births, based on reporting by mothers of210 children aged 12-36 months3. In Mumbai, theCS rate has increased over the last four decadesupto 16% since the early 1990s4. A rising trends inCS rates, from 11.9% in 1987 to 21.4% in 1996,has also been reported from Kerala, the state withthe best demographic characteristics and access to
Abstract: As there is an increased prevalence of cognitive and other neuro-development disability, there is need forearly identification of children with sensory and motor performance deficit. But data still lack regarding prevalence ofthese problems in children born by caesarean section at full term. Therefore this study aimed at assessing andcomparing the sensory-motor skills of term children born by caesarean section and those born with normal vaginaldelivery. In this study 35 caesarean delivery and 35 normal vaginal delivery children of both male and female wereselected from different schools of Dehradun. The sensory skills were assessed by Short Sensory Profile and motorskills were assessed by BOTMP-sf. It was concluded that caesarean section delivered children are on weaker side insensory skills but no effect was found in motor skills. Physiological basis for the results need to be further studied.
Key words: Caesarean section, Full term, Sensory-Motor skills, Normal vaginal delivery, BOTMP-SF, SSP.
healthcare within Indian. CS delivery rates inKerala has indicated that they are more likely tooccur in private healthcare institutions 5. Surveyshave confirmed the rates of CS are higher inprivate hospitals6
Several studies have documented the highincidence of respiratory morbidity and NICUadmissions in infants born by cesarean delivery. Accurate data about the occurrence of respiratoryfailure and long-term outcomes in term and near-term infants are hard to obtain because of the lackof large databases such as those available forpreterm infants; however, it is estimated that asignificant number of term infants delivered by CSare admitted to neonatal intensive care units eachyear in the US7 with the diagnosis of transienttachypnea of the newborn (TTN), respiratorydistress syndrome (RDS) and severe persistentpulmonary hypertension of the newborn. Ininfants who develop respiratory distress after CS,the need for mechanical ventilation wasdramatically higher. It was believed that at leastsome of the respiratory morbidity in newbornsdelivered by ECS was secondary to iatrogenic

23
Sensory-Motor Skills in School Children born by Caesarean Section Delivery
prematurity. Indeed, studies evaluating large seriesof patients have shown a higher rate ofprematurity and surfactant deficiency in thesepatients 8Chances of serious respiratory morbidityare higher among 37, 38 and 39 weeks gestationinfants delivered by ECS when compared to thosedelivered vaginally9 Changes in the pulmonaryvasculature, such as slowing of smooth muscle cellreplication and involution at birth, increase in thesmall pulmonary blood vessels (up to 40 times) inthe 3rd trimester, and changes in the epithelialsodium channels with increased ability to clearfetal lung fluid at term and with labor, all play animportant role. Further, it is clear that, in additionto prematurity and RDS, infants delivered by CSare at higher risk for developing transienttachypnea of the newborn and persistentpulmonary hypertension unrelated to theirgestational age at the time of delivery10. Theincidence of persistent pulmonary hypertension ofthe newborn was approximately 0.37% amongneonates delivered by elective cesarean that wasalmost fivefold higher than those deliveredvaginally11
Cesarean section seems to be a major barrier tobreastfeeding initiation12 The most critical periodof breastfeeding initiation is the first 0.5 to 2 hrsafter. The first milk, colostrum, containsimmunologic and nutritious properties not only toprotect the newborn from infections but also tospeed up their normal intestinalfunctions14.Furthermore, early touch of the nippleand areola within 30 minutes influences thematernal/infant relationship positively13 . Earlyskin to skin contact and opportunity to sucklewithin the first hour or so after birth are bothimportant15 . It has an important bearing onsurvival and development of babies. The infantwho is in close contact with its mother can sucklewhen it shows signs of readiness, such assuckling movements, which are often presentduring the first hour of birth. The effect of skin-to-skin and suckling contact immediately after birthincreases the median duration of breastfeeding by2½ months to 1 year16 ). It has been observed thatthe suckling reflex of the newborn is at its heighttwenty to thirty minutes after birth. If the infants isnot fed then the reflex diminishes rapidly only toreappear adequately forty hours later. Oxytocin is
known to play a role in bonding and it has beendemonstrated that oxytocin level increases duringfirst 45 minutes and return to normal levels in 60minutes17 .
Study also suggests that respiratory complicationsat the time of birth also lead to damage of braincells and finally children suffers from neurologicconditions. Because of an increased prevalence ofcognitive and other neuro-development disability,there is need for early identification of childrenwith sensory and motor performance deficit. Butdata still lack regarding prevalence of theseproblems in children born by caesarean section atfull term. Therefore this study aims at assessingand comparing the sensory-motor skills of termchildren born by caesarean section and those bornwith normal vaginal delivery at full term.
METHODSStudy performed on 70 school going children (35caesarean section delivered and 35 normal vaginaldelivered) of either gender taken from the localschools of Dehradun under the age group of 4½-7½ years. They were divided into two groups- A(Normal vaginal delivery children) and B(Caesarean section delivery children). This was anexperimental study, which was performed in thelocal schools of Dehradun. Study was performedin accordance with ethical considerations of theinstitute and consent from the parents/caregiver ofthe children was taken prior to the study.
Testing equipment and procedureShort sensory profile: The Short Sensory Profile18is a standardized, abbreviated version of thesensory profile designed so that clinicians canquickly identify if a child is experiencing sensorymodulation difficulties. It is a 38-item, judgmentbased questionnaire using a 5-point Likert scalethat the primary caregiver completes. A PhysicalTherapist or health professional trained in sensoryprocessing scores the sensory profile. Scores thatfall within one standard deviation of the mean foreach category represent “Typical Performance” oneto two standard deviations below the mean“Probable Difference”, and scores below twostandard deviations below the mean “DefiniteDifference”. Scores that result in a probable ordefinite difference indicate that further assessment
24
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 22-30
and possible therapeutic intervention may bewarranted. Because the Short Sensory Profile canbe completed by the caregiver in 10 minutes andscored by the examiner in 10 minutes, it is widelyused in clinics and school based settings.According to author, internal consistency of thesections within the scale ranges from 0.70 to 0.90.Internal validity correlations for the sectionsranged from 0.25 to 0.76.
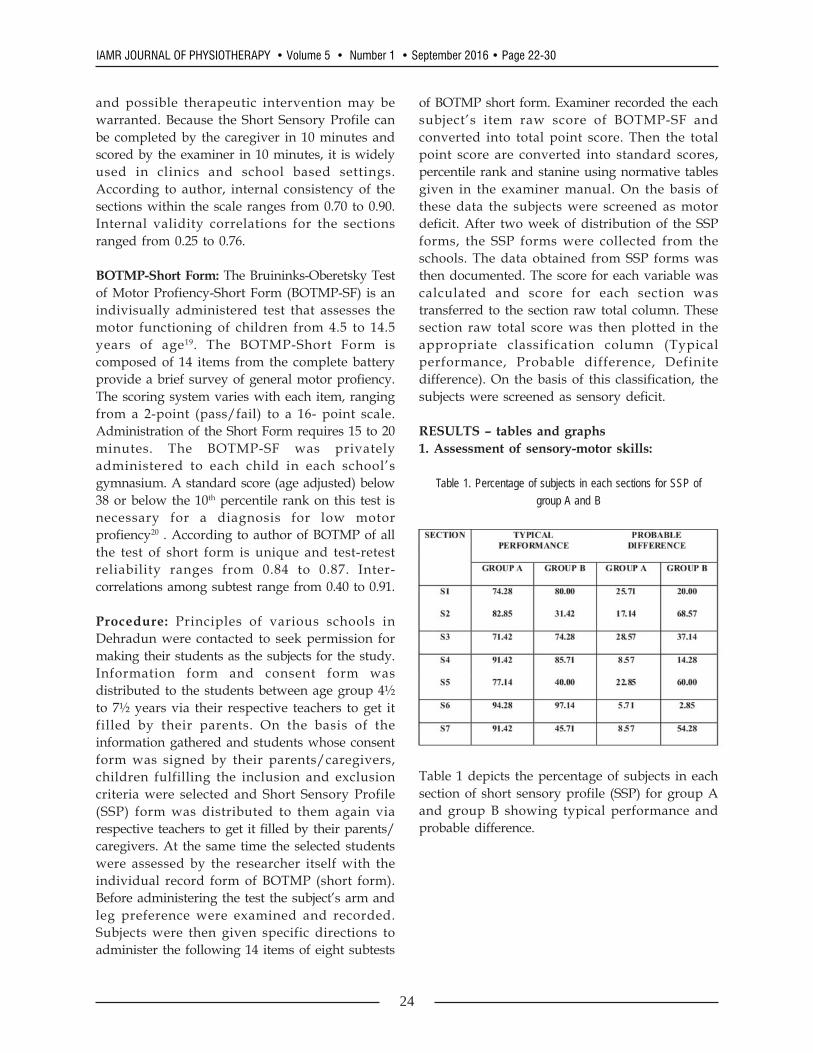
BOTMP-Short Form: The Bruininks-Oberetsky Testof Motor Profiency-Short Form (BOTMP-SF) is anindivisually administered test that assesses themotor functioning of children from 4.5 to 14.5years of age19. The BOTMP-Short Form iscomposed of 14 items from the complete batteryprovide a brief survey of general motor profiency.The scoring system varies with each item, rangingfrom a 2-point (pass/fail) to a 16- point scale.Administration of the Short Form requires 15 to 20minutes. The BOTMP-SF was privatelyadministered to each child in each school’sgymnasium. A standard score (age adjusted) below38 or below the 10th percentile rank on this test isnecessary for a diagnosis for low motorprofiency20 . According to author of BOTMP of allthe test of short form is unique and test-retestreliability ranges from 0.84 to 0.87. Inter-correlations among subtest range from 0.40 to 0.91.
Procedure: Principles of various schools inDehradun were contacted to seek permission formaking their students as the subjects for the study.Information form and consent form wasdistributed to the students between age group 4½to 7½ years via their respective teachers to get itfilled by their parents. On the basis of theinformation gathered and students whose consentform was signed by their parents/caregivers,children fulfilling the inclusion and exclusioncriteria were selected and Short Sensory Profile(SSP) form was distributed to them again viarespective teachers to get it filled by their parents/caregivers. At the same time the selected studentswere assessed by the researcher itself with theindividual record form of BOTMP (short form).Before administering the test the subject’s arm andleg preference were examined and recorded.Subjects were then given specific directions toadminister the following 14 items of eight subtests
of BOTMP short form. Examiner recorded the eachsubject’s item raw score of BOTMP-SF andconverted into total point score. Then the totalpoint score are converted into standard scores,percentile rank and stanine using normative tablesgiven in the examiner manual. On the basis ofthese data the subjects were screened as motordeficit. After two week of distribution of the SSPforms, the SSP forms were collected from theschools. The data obtained from SSP forms wasthen documented. The score for each variable wascalculated and score for each section wastransferred to the section raw total column. Thesesection raw total score was then plotted in theappropriate classification column (Typicalperformance, Probable difference, Definitedifference). On the basis of this classification, thesubjects were screened as sensory deficit.
RESULTS – tables and graphs1. Assessment of sensory-motor skills:
Table 1. Percentage of subjects in each sections for SSP ofgroup A and B
Table 1 depicts the percentage of subjects in eachsection of short sensory profile (SSP) for group Aand group B showing typical performance andprobable difference.
25
Sensory-Motor Skills in School Children born by Caesarean Section Delivery
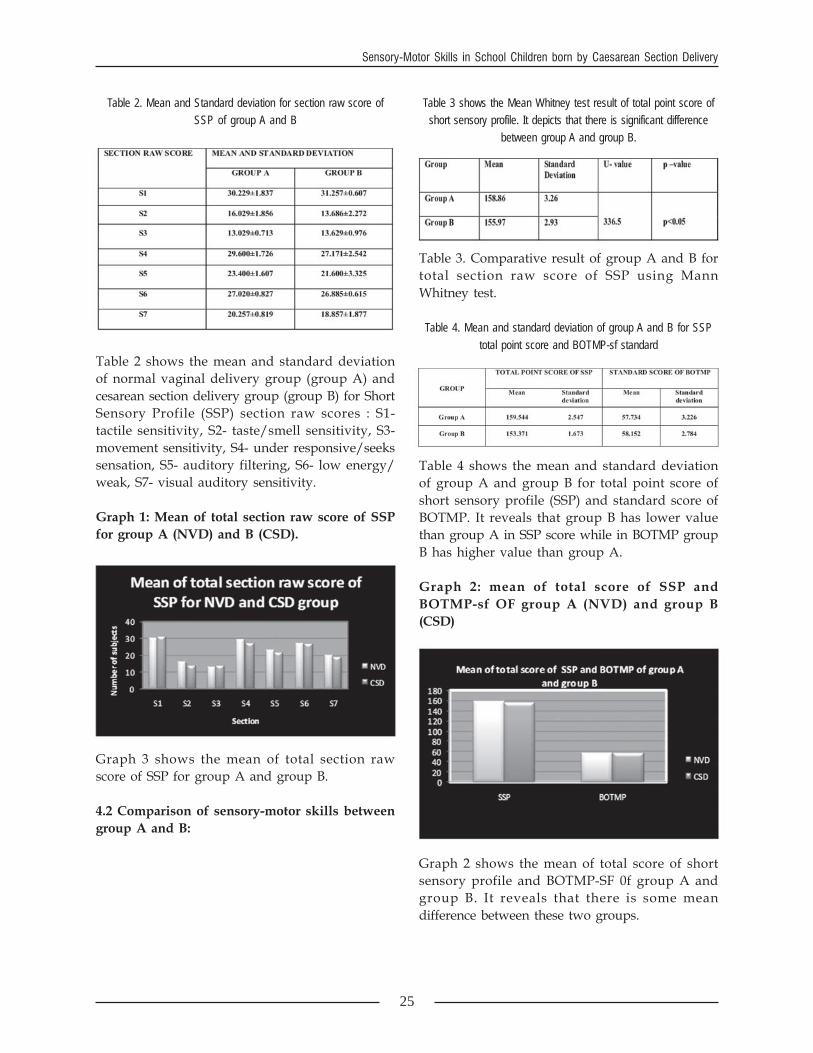
Table 2. Mean and Standard deviation for section raw score ofSSP of group A and B
Table 2 shows the mean and standard deviationof normal vaginal delivery group (group A) andcesarean section delivery group (group B) for ShortSensory Profile (SSP) section raw scores : S1-tactile sensitivity, S2- taste/smell sensitivity, S3-movement sensitivity, S4- under responsive/seekssensation, S5- auditory filtering, S6- low energy/weak, S7- visual auditory sensitivity.
Graph 1: Mean of total section raw score of SSPfor group A (NVD) and B (CSD).
Graph 3 shows the mean of total section rawscore of SSP for group A and group B.
4.2 Comparison of sensory-motor skills betweengroup A and B:
Table 3 shows the Mean Whitney test result of total point score ofshort sensory profile. It depicts that there is significant difference
between group A and group B.
Table 3. Comparative result of group A and B fortotal section raw score of SSP using MannWhitney test.
Table 4. Mean and standard deviation of group A and B for SSPtotal point score and BOTMP-sf standard
Table 4 shows the mean and standard deviationof group A and group B for total point score ofshort sensory profile (SSP) and standard score ofBOTMP. It reveals that group B has lower valuethan group A in SSP score while in BOTMP groupB has higher value than group A.
Graph 2: mean of total score of SSP andBOTMP-sf OF group A (NVD) and group B(CSD)
Graph 2 shows the mean of total score of shortsensory profile and BOTMP-SF 0f group A andgroup B. It reveals that there is some meandifference between these two groups.

26
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 22-30
Table 5. Comparative result of group A and B of BOTMP-SF meanscore using independent t-test
Table 5 shows the independent t test value ofBOTMP-short form for three age group 5 (4 ½ to 5½ years), age group 6 (5 ½ to 6 ½ years) and agegroup 6 (6 ½ to 7 ½ years). This reveals that thereis no significant difference of BOTMP-SF betweengroup A and group B although some meandifference is there.
DISCUSSIONMounting evidence suggests that the children bornby cesarean section at full term has increased riskfor respiratory complications and late initiation ofbreastfeeding. Many of the follow up studies tilldate have focused on C-section at pre-term or post-term or breech presentation rather than full term.The present study was designed to assess andcompare the sensory-motor skills of children bornby cesarean delivery and those born by normalvaginal delivery at full term in between 4½ to 7½years of age group. Sensory perception skill wasexamined in children using Short Sensory Profileand motor skill was assessed with the use ofBruininks-Oberetsky Test Motor Performance- shortform. Assessment of sensory-motor skills: Theprimary aim of this study was to assess thesensory- motor skills. For sensory perception skillour results depicts that out of 35 childrendelivered by caesarean section, 12 children wasgrouped in probable difference and 23 children intypical performance. None of the children foundas having definite difference. Thus 34.28%children were suffering from mild sensoryperception disorders. In sub sections, 68.57%children in taste/smell sensitivity, 60% childrenin auditory filtering and 54.28% children invisual/auditory sensitivity showed poorperformance. For motor assessment the childrenwere divided into three age groups. Childrenbetween aged 54 months to 66 months weregrouped in age group 5, children between aged 67months to 78 months were in age group 6 and
children between aged 79 months to 90 monthswere grouped in age group 7. After the analysis ofdata of BOTMP-short form all children performedas average or good performance. Mean score of thedata was 57.73(±) for normal vaginal group and58.15(±) for caesarean section group. The highervalue found in caesarean section group may bedue to small sample size. Mean score of bothgroup was in sixth stanine (Table 27 in theBOTMP manual). It showed that maximumchildren were average or good in performance.None of the children were found below average orlow motor performance. Comparison of sensoryperception skill: For comparison of the databetween normal vaginal delivery group andcaesarean section group, the data were analyzed itwas found that cesarean section group performedpoorer than normal vaginal delivery group in threesection of Short Sensory Profile, that is, in taste/smell sensitivity, auditory filtering and visual/auditory sensitivity. There was large difference inmean of total point score found between normalvaginal delivery group and caesarean sectiongroup. Mann Whitney test was used betweengroup A and B to compare the data obtained bySSP. It showed that there was significantdifference for total point score of Short SensoryProfile (p<0.05) between these two groups. Variousfactors seemed to affect sensory perception skills asshown by many studies. The relationship betweencesarean section delivery and sensory perceptionskills is complex. Birth asphyxia and low apgarscore are established risk factors for a broad rangeof developmental disabilities. Birth asphyxia is theresult of an adequate exchange of oxygen andcarbon dioxide due to respiratory complicationsduring pregnancy and at the time of delivery. Theimpact of an episode of asphyxia causes hypoxicischemic encephalopathy (HIE) which is the mostcommon cause of neurologic defects by perinatalevents. Study have found that lesions associatedwith HIE include selective neuronal damageincluding basal ganglia and brainstem,parasagittal cerebral injury21. Mercury et al (1997)in his study found that basal ganglia wasresponsible for the visual development in thechildren. Any lesion in the basal ganglia due toHIE or birth asphyxia may disrupt the visualpathway.22 Olusanya et al (2009) in his studyexamined the sensorineural hearing loss and

27
Sensory-Motor Skills in School Children born by Caesarean Section Delivery
found that infants delivered by caesarean sectionwere likely to be at a greater risk than thosedelivered by vaginal delivery.23 Ehrenestein et al(2009) in their study found that low apgar scoreis responsible for neurological disorders in earlyadulthood24. Various studies has been conductedto evaluate the relationship between low apgarscore and caesarean section delivery. Thus it maybe one of the factors associated with the results ofthis study. Other studies have also found thatcesarean section is associated with adverse longterm health of survivors through reduced rates ofbreastfeeding25. Delayed breast feeding may be thecause for such abnormalities. They relate to theabnormalities in nutrition of infants, metabolicfunctioning and environmental stress. They maydisrupt the normal brain development even thechild does not suffer major insult. Comparison ofmotor skills: For comparison of data obtained byBOTMP-sf (standard score), children were dividedinto three age groups- age group 5 (54-66 months),age group 6 (67-78 months), age group 7 (79-90months). Independent t-test was used to comparethe mean score of different age group. After theanalysis of the data of subtests of BOTMP shortform it was found that there was no significant(p>0.05) difference between the children born bycesarean delivery and normal vaginal delivery atfull term may be due to small sample size. Thisresult showed that there may be no effect of minorasphyxia or delayed breastfeeding in newborn onmotor deficits later in childhood. Handley-Derryet al (1997) found that the term newborn infantsexposed to mild intrapartum fetal asphyxia do nothave minor motor deficits later in childhood.Although there are many factors which maycontribute to sensory-motor and cognitiveneurodevelopment variability in childhood likematernal intelligence, maternal intelligence,maternal education, socioeconomic status, homeenvironment, and attendance at school, from theresults of our study, it can be hypothesized thatlow scores in short sensory profile in cesareansection delivery child at term could have due torespiratory complications at the time of birth ordelayed initiation of breastfeeding26 . Thoughfurther physiologic evidences are required insupport and reasoning for the results of the study.
Limitations of the studyLarger sample size would have brought in moresignificant results in all the scores.Information regarding birth history was obtainedfrom the parents/caregivers of children anddocumented birth records could not be obtained foreach and every child.
Type of cesarean section delivery was notmentioned in this work.
I.Q. level of children could not be assessed.Social and environmental factors were notcontrolled.
Attention and concentration of the child could notbe very much considered.
Future scope of the studyStudy can be carried out on larger sample size.Other scales that assess sensory-motor skills canbe used.
The research may be conducted in different area.Study can be conducted on other aspects likecognitions and learning.
CONCLUSIONOur study results indicate that there exists adifference between the three sections of shortsensory profile that is taste/smell sensitivity,auditory filtering and visual/auditory sensitivity ofcesarean section delivery and normal vaginaldelivery term child in between 4 ½ to 7 ½ years ofage group. The motor assessment done byBOTMP-sf has no significant difference betweenchildren born by cesarean section and normalvaginal delivery at full term. Thus it can beconcluded that caesarean section deliveredchildren are on weaker side in sensory perceptionskills. Physiological basis for the results need tobe further studied. And thus by identifying theseproblems at an early age, age specificinterventions can be made to stimulatedevelopment of various aspects of sensoryperception

28
IAMR JOURNAL OF PHYSIOTHERAPY • Volume 5 • Number 1 • September 2016 • Page 22-30
REFERENCES
1) Asha O. (2006). “Rising Rates ofCaesarean Section: The Way Ahead”.Indian Journal of Medical Research, vol.124, no. 8, pp 119-122
2) Kambo I., Bedi N., Dhillon B.S., SaxenaN.C. (2002). “A Critical Appraisal ofCaesarean Section Rates at TeachingHospitals in India”. International Journalof Gynaecology and Obstetrics, vol. 79, no.2, pp 151-158
3) Pai M. Sundaram P, Radhakrishnan KK,Mullyll JP (1999). “A High Rates ofCaesarean Section in an AffluentSection of Chennai: Is it Cause forConcern?” National Medical Journal ofIndia, vol. 12, no. 4, pp 156-58
4) Mehta A., Apers L., Verstraelen H.,Temmerman M. (2001). “Trends inCaesarean Section Rates at a MaternityHospital in Mumbai, India”. Journal ofHealth Population and Nutrition, vol. 19.no. 4, pp 306-312
5) Padmadas S.S., Kumar S., Nair S.B.,Kumari A. (2000). “Caesarean SectionDelivery in Kerala, India: Evidence from aNational Family Health Survey”. SocialScience Med, vol. 51, no. 4, pp 511-21
6) Mishra U.S. and Ramanathan M. (2002).“Delivery Related Complications andDeterminants of Caesarean Rates inIndia”. Health Policy Planning, vol. 17,no. 1, pp 90-98.
7) Angus D.C., Linde-Zwirble W.T.,Clermont G., Griffin M.F., Clark R.H.(2001). “Epidemiology of NeonatalRespiratory Failure in the United States:Projections from California and NewYork”. American Journal of RespiratoryCritical Care Medicine, vol. 164, no. 7, pp1154-60
8) Roth-kleiner M., Wagner B.P., BachmannD., Pfenninger F. (2003). “RespiratoryDistress Syndrome in Near Term Babiesafter Caesarean Section”. Swiss MedicalWeekly, vol. 133, pp 283-88.
9) Hansen A.K., Wisborg K., Uldbjerg N.,Henriksen T.B. (2008). “Risk of
Respiratory Morbidity in Term InfantsDelivered by Elective Cesarean Section: ACohort Study”. BMJ, vol. 336, pp 85-7
10) Derbent A., Tatli M.M., Duran M., TonbulA., Kafali H., Akyol M., Turhan N.O.(2010). “Transient Tachypnea of theNewborn: Effects of Labor and DeliveryType in Term and Preterm Pregnancies”.Archive of Gynecology & Obstetrics, vol.30.
11) Levine E.M., Ghai V., Barton J.J., StromC.M. (2001). “Mode ofDelivery and Risk of Respiratory Diseasesin Newborns”. Obstetrics and Gynecology,vol. 97, no. 3, pp 439-42
12) Rowe-Murray H.J. and Fisher J.R. (2002).“Baby Friendly Hospital Practices:Caesarean Section is a Persistent Barrier toEarly Initiation of Breastfeeding”. Birth,vol. 29, no. 2, pp 124-31
13) Widstrom A.M. and Paulsson T.J. (1993).“The Positions of the Tongue duringRooting Reflexes elicited in NewbornInfants before the First Suckle”. ActaPaediatr, vol. 82, no. 3, pp 281-83
14) Gartner L.M., Eidelman A.I., Morton J.,Lawrence R.A., Naylor A.J., O’Harre D.,Schanler R.J. (2005). “Breastfeeding andUse of Human Milk”. Pediatrics, vol. 115,no. 2, pp 496-506
15) Taylar P.M., Maloni J.A., Brown D.R.(1986). “Early Suckling and ProlongedBreastfeeding”. American Journal of DisChild, vol. 140, no. 2, pp 151-154
16) Bystrova K., Ivanova V., Edhborg M.,Matthiesen A.S., Widstrom A.M. (2009).“Early Contact versus Separation Effectson Mother-Infant Interaction One YearLater”. Birth, vol. 36, no. 2, pp 97-109
17) Nissen E., Lilja G., Widstrom A.M., Uvnas-Moberg K. (1995). “Evaluation of OxytocinLevels Early Post Partum in Women”. ActaObstet Gynecol Scand, vol. 74, no. 7, pp530-33.
18) Dunn W. (1999). “The Short SensoryProfile: User’s Manual”. San Antonio, TX:Psychological Corporation
19) Bruininks R.H. (1978). “Bruininks-Oseretsky test of Motor Profiency:
29
Sensory-Motor Skills in School Children born by Caesarean Section Delivery
Examiner’s Manual”. Circle Pines, M.N.:American Guidance Services.
20) Cairney J., Hay J., Faught B, Corna L.M.,Flouris A.D. (2006). “DevelopmentalCoordination Disorder, Age, and Play: ATest of the Divergence in Activity-Deficitwith Age Hypothesis. Adapted PhysicalActivity Quaterly, vol. 23, pp 261-276.
21) Tecklin JS (1999). “Pediatric PhysicalTherapy”. 3rd edition, Philadelphia:Lippincot Williams & Wilkins. pp 75-78.
22) Mercury E., Atkinson J., Braddick O.,Anker S., Cowan F., Rutherford M.,Pennock J., Dubowitz L. (1997). “BasalGanglia Damage and Impaired VisualFunction in the Newborn Infant”. ArchDis Childhood, vol. 77, F111-1 14
23) Olusanya B.O. and Solanke O.A. (2009).“Maternal and neonatal factors associatedwith mode of delivery under a universalnewborn hearing screening programme inNigeria”. BMC Pregnancy and Childbirth,vol. 9, p 41
24) Ehrenstein V., Pederson L., Grijota M.,Neilsen G.L., Rothman K.J., SorensenH.T. (2009). “Association of Apgar scoreat five minutes with long term NeurologicDisability and Cognitive Function in aPrevalence study of Danish conscripts”.BMC Pregnancy and Childbirth 2009, vol.9, no. 14.1, pp 124-26
25) Evans K.C., Evans R.G., Royal R.,Esterman A.J., James S.L. (2003). “Effect ofCaesarean Section on Breast Milk Transferto the Normal Term Newborn over theFirst Week of Life”. Arch Dis Child FetalNeonatal, vol. 88, pp F380-82
26) Handley-Derry M., Low J.A., Burke S.O.,Waurick M., Killen H., Derrick E.J. (1997).“Intrapartum Fetal Asphyxia and theOccurrence of Minor Motor Deficits in 4 to8 year old Children”. DevelopmentalMedical Child Neurology, vol. 39, no. 8,pp 508-514