Brief and Precarious Lives: infant mortality in contrasting sites from medieval and post-medieval...
13
Brief and Precarious Lives: Infant Mortality in Contrasting Sites from Medieval and Post-Medieval England (AD 850–1859) Mary E. Lewis 1 * and Rebecca Gowland 2 1 School of Human and Environmental Studies, Department of Archaeology, University of Reading, Reading, Berkshire RG6 6AB, UK 2 Department of Archaeology, University of Durham, South Road, Durham DH1 3LE, UK KEY WORDS post-neonatal deaths; neonatal deaths; medieval England; Bays’ theorem; regression equations ABSTRACT This study compares the infant mortal- ity profiles of 128 infants from two urban and two rural cemetery sites in medieval England. The aim of this paper is to assess the impact of urbanization and industrializa- tion in terms of endogenous or exogenous causes of death. In order to undertake this analysis, two different methods of estimating gestational age from long bone lengths were used: a traditional regression method and a Bayesian method. The regression method tended to produce more marked peaks at 38 weeks, while the Bayesian method pro- duced a broader range of ages and were more comparable with the expected ‘‘natural’’ mortality profiles. At all the sites, neonatal mortality (28–40 weeks) out- weighed post-neonatal mortality (41–48 weeks) with ru- ral Raunds Furnells in Northamptonshire, showing the highest number of neonatal deaths and post-medieval Spitalfields, London, showing a greater proportion of deaths due to exogenous or environmental factors. Of the four sites under study, Wharram Percy in Yorkshire showed the most convincing ‘‘natural’’ infant mortality profile, suggesting the inclusion of all births at the site (i.e., stillbirths and unbaptised infants). Am J Phys Anthropol 000:000–000, 2007. V V C 2007 Wiley-Liss, Inc. This study compares the infant mortality profiles of 128 infants from two urban (Christ Church Spitalfields, St. Helen-on-the-Walls) and two rural (Raunds Furnells, Wharram Percy) cemetery sites in medieval England with the aim of interpreting the differences observed in terms of endogenous or exogenous causes of death. Infant mor- tality has a profound effect upon the crude death rate of a population and, consequently, is considered a sensitive indicator of overall population ‘‘fitness’’ (Adler and Ostrove, 1999; Saunders and Barrans, 1999; Murray and Frenk, 2002). This study follows earlier work that exam- ined the health of children from contrasting medieval environments in an attempt to assess whether urbaniza- tion and industrialization had a detrimental effect on the health of the inhabitants (Lewis, 2002). This previous study demonstrated a decline in child health and an increase in child mortality due to the detrimental envi- ronmental effects of industrial London. In the current analysis, it is hypothesized that failure in the population’s ability to adapt to these environments will be evident in higher rates of infant mortality, with deaths related to external factors (post-neonatal mortality) exceeding those relating to internal causes (neonatal mortality) in the industrial sample of post-medieval London. Infant mortality is calculated as the number of infant deaths in one calendar year, per 1000 live births (Stock- well, 1993). Infant survivability has been found to be largely dependent on the physical environment into which the child is born, in particular, the level of sanita- tion and availability of health care facilities. It is the improvement in these factors that is largely believed to have resulted in the rapid decline in infant mortality in England and Wales during the eighteenth and early nineteenth centuries, contributing to the ‘‘demographic transition’’ (Williams and Galley, 1995). Estimated infant mortality figures from modern preindustrial populations have been found to vary widely, up to approximately 200 per 1000 live births (Hobbs and Kigguridu, 1992). Infant mortality rates for many past populations are uncertain; however, in sixteenth century England, it was estimated that around 27% of children died before the age of 1 year (Orme, 2001). Graunt (1962) claimed that in London during nonplague years, 36% of children died under the age of 6 years, and that urban deaths exceeded rural ones. However, given the inconsistency with which stillbirths and neonatal deaths were reported in the past, historical documents such as the London Bills of Mortality, which recorded deaths in London from the sixteenth century, are likely to reflect a minimum number only (Robertson, 1996). The absence of infant mortality records in England prior to the late 1550s means that skeletal remains from cemetery excavations are the primary source of evidence for infant death. This archaeological evidence does, of course, have many limitations, which have been ad- dressed at length in the literature (e.g., Sundick, 1978; *Correspondence to: Mary Lewis, School of Human and Environ- mental Studies, Department of Archaeology, University of Reading, Reading, Berkshire RG6 6AB, UK. E-mail: [email protected] Received 29 June 2006; accepted 26 March 2007 DOI 10.1002/ajpa.20643 Published online in Wiley InterScience (www.interscience.wiley.com). V V C 2007 WILEY-LISS, INC. AMERICAN JOURNAL OF PHYSICAL ANTHROPOLOGY 000:000–000 (2007)
Transcript of Brief and Precarious Lives: infant mortality in contrasting sites from medieval and post-medieval...

Brief and Precarious Lives: Infant Mortality inContrasting Sites from Medieval and Post-MedievalEngland (AD 850–1859)
Mary E. Lewis1* and Rebecca Gowland2
1School of Human and Environmental Studies, Department of Archaeology, University of Reading, Reading,Berkshire RG6 6AB, UK2Department of Archaeology, University of Durham, South Road, Durham DH1 3LE, UK
KEY WORDS post-neonatal deaths; neonatal deaths; medieval England; Bays’ theorem; regressionequations
ABSTRACT This study compares the infant mortal-ity profiles of 128 infants from two urban and two ruralcemetery sites in medieval England. The aim of this paperis to assess the impact of urbanization and industrializa-tion in terms of endogenous or exogenous causes of death.In order to undertake this analysis, two different methodsof estimating gestational age from long bone lengths wereused: a traditional regression method and a Bayesianmethod. The regression method tended to produce moremarked peaks at 38 weeks, while the Bayesian method pro-duced a broader range of ages and were more comparablewith the expected ‘‘natural’’ mortality profiles.
At all the sites, neonatal mortality (28–40 weeks) out-weighed post-neonatal mortality (41–48 weeks) with ru-ral Raunds Furnells in Northamptonshire, showing thehighest number of neonatal deaths and post-medievalSpitalfields, London, showing a greater proportion ofdeaths due to exogenous or environmental factors. Ofthe four sites under study, Wharram Percy in Yorkshireshowed the most convincing ‘‘natural’’ infant mortalityprofile, suggesting the inclusion of all births at the site(i.e., stillbirths and unbaptised infants). Am J PhysAnthropol 000:000–000, 2007. VVC 2007 Wiley-Liss, Inc.
This study compares the infant mortality profiles of128 infants from two urban (Christ Church Spitalfields,St. Helen-on-the-Walls) and two rural (Raunds Furnells,Wharram Percy) cemetery sites in medieval England withthe aim of interpreting the differences observed in termsof endogenous or exogenous causes of death. Infant mor-tality has a profound effect upon the crude death rate ofa population and, consequently, is considered a sensitiveindicator of overall population ‘‘fitness’’ (Adler andOstrove, 1999; Saunders and Barrans, 1999; Murray andFrenk, 2002). This study follows earlier work that exam-ined the health of children from contrasting medievalenvironments in an attempt to assess whether urbaniza-tion and industrialization had a detrimental effect on thehealth of the inhabitants (Lewis, 2002). This previousstudy demonstrated a decline in child health and anincrease in child mortality due to the detrimental envi-ronmental effects of industrial London. In the currentanalysis, it is hypothesized that failure in the population’sability to adapt to these environments will be evident inhigher rates of infant mortality, with deaths related toexternal factors (post-neonatal mortality) exceeding thoserelating to internal causes (neonatal mortality) in theindustrial sample of post-medieval London.
Infant mortality is calculated as the number of infantdeaths in one calendar year, per 1000 live births (Stock-well, 1993). Infant survivability has been found to belargely dependent on the physical environment intowhich the child is born, in particular, the level of sanita-tion and availability of health care facilities. It is theimprovement in these factors that is largely believed tohave resulted in the rapid decline in infant mortality inEngland and Wales during the eighteenth and early
nineteenth centuries, contributing to the ‘‘demographictransition’’ (Williams and Galley, 1995). Estimated infantmortality figures from modern preindustrial populationshave been found to vary widely, up to approximately 200per 1000 live births (Hobbs and Kigguridu, 1992). Infantmortality rates for many past populations are uncertain;however, in sixteenth century England, it was estimatedthat around 27% of children died before the age of1 year (Orme, 2001). Graunt (1962) claimed that inLondon during nonplague years, 36% of children diedunder the age of 6 years, and that urban deathsexceeded rural ones. However, given the inconsistencywith which stillbirths and neonatal deaths were reportedin the past, historical documents such as the LondonBills of Mortality, which recorded deaths in London fromthe sixteenth century, are likely to reflect a minimumnumber only (Robertson, 1996).
The absence of infant mortality records in Englandprior to the late 1550s means that skeletal remains fromcemetery excavations are the primary source of evidencefor infant death. This archaeological evidence does, ofcourse, have many limitations, which have been ad-dressed at length in the literature (e.g., Sundick, 1978;
*Correspondence to: Mary Lewis, School of Human and Environ-mental Studies, Department of Archaeology, University of Reading,Reading, Berkshire RG6 6AB, UK. E-mail: [email protected]
Received 29 June 2006; accepted 26 March 2007
DOI 10.1002/ajpa.20643Published online in Wiley InterScience
(www.interscience.wiley.com).
VVC 2007 WILEY-LISS, INC.
AMERICAN JOURNAL OF PHYSICAL ANTHROPOLOGY 000:000–000 (2007)

Gordon and Buikstra, 1981; Johnston and Zimmer, 1989;Goode et al., 1993). Differential burial practices, togetherwith preservation and recovery biases can limit theextent to which infants excavated from cemetery popula-tions represent the true proportion of those dying withina particular society at any one time (Saunders, 2000).Furthermore, anthropologists are unable to calculateactual mortality ‘‘rates’’ from this type of informationbecause data concerning the total population at risk (i.e.,the number of live births) is not available. It is also fre-quently impossible to narrow the dates of archaeologicalsamples into yearly, or even decadal, increments.
In the 1980s, palaeodemographers began to recognizethe influence fertility had on age at death distributions,and hence the mortality profiles derived from archaeo-logical samples (Sattenspiel and Harpending, 1983;Buikstra et al., 1986; Milner et al., 1989; Paine and Har-pending, 1996). Average age at death within a skeletalpopulation was demonstrated to be more a reflection ofits birth rate and fertility, rather than a measure of mor-tality or life expectancy (Sattenspiel and Harpending,1983). Thus, a large number of infants within a cemeterysample would reflect the greater number of infantsentering the population, rather than a population strug-gling to adapt to their environment (Larsen, 1997, p.339). However, determining fertility in past populationsis problematic and in 1986, Buikstra and coworkersintroduced a method to examine nonadult mortalitystructure by comparing the proportion of children dyingbetween 1 and 5 years (weaning age deaths) with thosewho died between 1 and 10 years. Populations with ahigh mortality would have a greater proportion of deathsbetween 1 and 5 years. However, it does not follow thata population with large numbers of infants in its mortu-ary sample is successful; it could also mean that thehigh mortality rate of infants within the communitycaused shorter birth intervals and a greater number ofpregnancies. The ability of the population to keep thesechildren alive into adulthood is the true measure of theirsuccess.
We argue that examining mortality in archaeologicalsamples still has value and explore the age structure ofthe infants that died in medieval England as a means ofelucidating the cultural and environmental factors thatled to their death. That is not to say that we are notaware of taphonomic limitations and/or cultural biases isburial practice. Although some authors have argued thatthe generally low numbers of infant remains in ourarchaeological populations may actually reflect true mor-tality rates (Brothwell, 1986–1987; Panhuysen, 1999),cemetery samples, such as St. Andrew Fishergate, yield-ing only 11 infants over a 500 year period, suggest sig-nificant under-representation exists (Stroud and Kemp,1993). In the rare cases where burial records from anexcavated sample survive, the proportion of infantsreported to have died, and those excavated, are at odds.For example, the low number of infants from the Voegtlycemetery in Pittsburgh, where 311 infants were reportedto have died but only 200 children under 5 years wererecovered, was suggested by Jones and Ubelaker (2001)to demonstrate taphonomic bias in preservation. Con-versely, Herring et al. (1994) found a greater number ofinfants in the skeletal sample from Belleville, Ontario,than were listed in the burial record. These studies dem-onstrate both the cultural and taphonomic problems in-herent in interpreting infant mortality from both burialregisters and cemetery samples.
Despite these shortcomings, Saunders (2000) andSaunders and Barrans (1999) have convincingly arguedthe necessity and advantages of studying infant mortal-ity rates from archaeological cemetery evidence. It isunfortunate that in many studies of infant burials it isissues of infanticide (Smith and Kahila, 1992; Mays,1993, 2003; Gowland and Chamberlain, 2002) and prob-lems of under-representation in palaeodemography thatare the main focus of attention, and in some cases, theyoungest children are excluded from studies altogether(Bocquet-Appel, 2002; Paine, 2000; Ribot and Roberts,1996). One of the key aspects of infant mortality studiesin bioarchaeology is that they provide information on thepopulation’s ability to adapt to their environment, theircultural practices, fertility rates, demography, maternalhealth, disease epidemics, birthing practices, and socialattitudes towards children.
ENDOGENOUS VERSUS EXOGENOUSINFANT MORTALITY
Infant mortality rates are traditionally subdivided intothose who die before birth (late fetal or stillbirths), thosedying at birth or within the first 27 days of extrauterinelife (neonatal mortality), and those who die between 28days and 1 year (post-neonatal mortality). It is an unfor-tunate drawback of archaeological studies of perinatalmortality that we are unable to determine whether achild was premature, stillborn, or survived for the firstfew days of life (Saunders and Barrans, 1999). It is gen-erally accepted that, in the past, children under the ageof 28 weeks, or 7 months from conception, were lesslikely to survive the extrauterine environment due tothe immaturity of their vital internal structures. In for-ensic and archaeological science, the presence or absenceof the neonatal line has been used to assess whether achild was stillborn, or was possibly the victim of infanti-cide (Smith and Avishai, 2005). Visible as a microscopichypoplastic defect on the deciduous teeth, the neonatalline is thought to represent a period of enamel stasis af-ter the stress of birth. Research on the survivability,location, and visualization of the neonatal line has raisedquestions about the reliability of this feature (Sarnatand Schour, 1941; Whittaker and MacDonald, 1989);however, it continues to be a useful marker in recon-structing the life history of the infant (Humphrey et al.,2005). Nevertheless, it is not always possible to carryout destructive analysis on collections held in Nationalmuseums or Universities, hindering such investigationson a large scale.
Clinically, the majority of neonatal deaths are consid-ered to reflect the endogenous state of the infant as theresult of genetic and maternal influences (e.g., congeni-tal anomalies, prematurity, low birth weight, birthtrauma), and post-neonatal mortality is seen more as aconsequence of the child’s external environment or exoge-nous factors (infectious diseases, poor nutrition, poison-ings, accidents) (Scott and Duncan, 1999). This ‘‘biomet-ric model’’ developed by Bourgeois-Pichat (1951) workson the premise that all endogenous deaths occur withinthe first month, and that exogenous mortality is propor-tional to the number of days, after the first month, theinfant survives. The ability of a given population to pro-vide the biocultural means for a child’s survival once itis born provides an insight into their adaptive success.Today in industrialized countries, sanitation measuresensure that the vast majority of infant deaths are due to
2 M.E. LEWIS AND R. GOWLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa

endogenous factors (Stockwell, 1993), but the reversewas true in urban centers of the past (Vogele, 1994). Thebiometric model has been used by historical demogra-phers to identify, among other things, breastfeeding pat-terns. Knodel and Kinter (1977) demonstrated that inareas where breastfeeding was common practice, exoge-nous mortality remained low until weaning, and wherebreastfeeding was uncommon, mortality was high in theearlier months of life. However, both exogenous and en-dogenous mortality are affected by the nutritional statusof the mother and baby (Scott and Duncan, 1999).
Historical evidence suggests that neonatal deathswere higher in rural areas than in urban communities,where environmental factors have a greater effect onchild mortality, producing higher post-neonatal deaths(Vogele, 1994). Examining the archaeological evidence,Saunders et al. (1995) estimated the proportions of neo-natal to post-neonatal deaths in infants from Belleville,Ontario. They found that 74% of infant skeletons werepost-neonates and 26% neonates, reflecting the strongerexogenous influence of infant death in this industrializedCanadian sample. However, historical infant mortalitydata from preindustrial England (1550–1649) has shownneonatal mortality (excluding unregistered stillbirths) tooutweigh post-neonatal mortality samples (Hart, 1998).In a study of birth and death records from Penrith,Cumbria (1557–1806), Scott and Duncan (1998) foundthat both neonatal and post-neonatal mortality fluctu-ated in accordance with the rise and fall of wheat prices.However, neonatal mortality lagged behind by 1 year,suggesting that early mortality was indirectly related tothe nutritional status of the mother during pregnancy,whereas post-neonatal mortality was directly related tolactation and weaning during the first year of life.
Previous research has indicated that in later medievalEngland, urban and rural differences in health were lim-ited, and that the greatest strain on the children inthese societies occurred during the post-medieval indus-trial period, where environmental factors resulted inhigher rates of infectious and metabolic disease, andincreased child mortality (Lewis, 2002). This study willfocus on the infant remains from four sites in medievaland post-medieval England to explore whether infantmortality patterns can provide more detail about thecontrasting environmental conditions during these peri-ods, and whether inferences about birth practices andmaternal health can also be made from the data.
MATERIALS
The four sites were originally selected for their geo-graphical location, large nonadult sample sizes, and con-trasting settlement character (Table 1, Fig. 1). RaundsFurnells, the earliest of the settlements, dates betweenthe ninth to twelfth centuries (Boddington, 1996) andthus, predates the industrial developments that occurredin England during the thirteenth century. The skeletons
from St. Helen-on-the-Walls (St. Helens), Aldwark (AD950–1550) in later medieval York represent infants froman urban sample. Medieval York was at its height interms of wealth and influence between the eleventh andfifteenth centuries and was the focus of social, political,and religious activities for the North of England(Andrews, 1984). However, Aldwark was documented tohave been one of the poorest parishes in York (Palliser,1980), and during the fourteenth century experienced ashift in its demography from mostly craftsmen tofemales, some of whom are suspected to have been work-ing as prostitutes (Hall et al., 1988). Wharram Percy(AD 950–1550), a rural settlement in the YorkshireWolds, was contemporaneous with St. Helens and situ-ated eight miles from the city of York (Bell and Beres-ford, 1987). Because of trading practices and its location,individuals from Wharram Percy would probably havebeen exposed to similar environmental pathogens astheir urban counterparts in York (Hall et al., 1988;Milne and Richards, 1992). Finally, infants excavatedfrom the London crypt of Christ Church, Spitalfields,dating from AD 1729 to 1859, were selected to representthe industrial sample. The church is located in east Lon-don, and parish records reveal that the individualsinterred in the crypt were the middle to upper classmembers of the congregation (Cox, 1996). Georgian soci-ety did not have the sophisticated sewage, water supply,and disposal systems of the Victorian Age, but the peopleof Spitalfields did benefit from the Lighting and Cleans-ing Act of 1759 and the Paving Act of 1778. In the1700s, the population of London was estimated to be
Fig. 1. Map of England showing the location of the studysites.
TABLE 1. Site information and number of infants included in the study
Site Period (AD) ContextTotal
nonadultsTotal infants(% nonadults)
%Nonadults
Raunds Furnells 850–1100 Rural (early medieval) 142 40 28.1St. Helen-on-the-Walls 950–1550 Urban (later medieval) 200 12 6.0Wharram Percy 950–1500 Rural (later medieval) 303 64 21.1Christ Church, Spitalfields 1729–1859 Industrial (post-medieval) 186 47 25.2Total 831 163 19.6
3INFANT MORTALITY IN MEDIEVAL ENGLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa

20,000 and, whatever their status, the residents of Spi-talfields would have experienced the effects of over-crowding, air pollution, and inadequate sewage disposal(Cox, 1996).
METHODS
Estimating age-at-death
Dental development is generally considered the mostaccurate method of estimating age-at-death of nonadults.However, the developing tooth crowns of perinates areextremely fragile and this, together with the fact thatthey are situated within relatively large crypt spaces inthe mandible and maxilla, means that they are fre-quently lost. Age estimates of perinatal skeletons are,therefore, usually based on approximations from longbone diaphyseal lengths (Clement and Kosa, 1992).Errors in the relationship between diaphyseal lengthsand gestational age are well known, but difficult to con-trol for in archaeological populations. In addition to fac-tors pertaining directly to the mother, such as ethnicgroup, age, height, and parity, external factors such asseason, social class, and pollutants have all been shownto affect the size and weight of the infant at birth (Adair,2004; Hauspie et al., 1994). It has also been proposedthat female fetuses mature earlier than do males interms of both leg length and weight (Lampl and Jeanty,2003), potentially resulting in longer diaphyseal lengths,and hence, older age estimates in female dominatedsamples.
Despite these problems, long bone growth is still con-sidered to be a useful index to estimate the age of peri-natal skeletons because of the rapidity of growth duringthis period (Jeanty and Romaro, 1984). Several well-known standards have been produced for use on perina-tal skeletal samples (e.g., Fazekas and Kosa, 1978; Sche-uer et al., 1980). Similar studies have been made of longbone diaphyseal length based on in utero ultrasoundmeasurement of long bones (e.g., Jeanty et al., 1981,1982; Jeanty and Romaro, 1984). All of these methodshave a common element in their construction; they useregression equations to derive age from long bone length.A number of authors have demonstrated that ageingtechniques based on regression equations are statisti-cally biased towards producing an age structure akin tothat of their reference population (Bocquet-Appel andMasset, 1982, 1996; Konigsberg and Frankenberg, 1992;Lucy et al., 1996; Aykroyd et al., 1997, 1999; Konigsberget al., 1997). Recent work in paleodemography hasemphasized the utility of Bayesian inference in age-at-death estimation of skeletal populations (Hoppa andVaupel, 2002, p. 2). Bayesian data analysis allows us tomake inferences from data using probability models forobservable quantities (known age data) and for quanti-ties that are unknown (archaeological data), but that wewish to learn about (Gelman et al., 1995). Consequently,this study of neonatal and post-neonatal mortality inmedieval England has employed two methods of age esti-mation. The first is the regression method produced byScheuer et al. (1980)—the most commonly used methodfor ageing perinatal skeletons in the UK—and the sec-ond, a Bayesian method for ageing perinatal skeletonsproduced by Gowland and Chamberlain (2002). Whilesome consensus on appropriate methods for estimatingage-at-death is being attained, debates continue (seeHoppa and Vaupel, 2002; Chamberlain, 2006; Samworthand Gowland, 2006). Consequently, we have included the
raw long bone data from each of the sites in an appendixso that it is available for further study using othermethods.
Neonatal and post-neonatal mortality
In historical demographic studies, cumulative exoge-nous mortality is proportional to the log 3 (n+1) where nis the age in days within the first year of life. This cu-mulative death rate is then plotted on a graph, with thevertical axis representing the number of deaths, and thehorizontal axis the days in a year, spaced according tothe above formula. The points representing the cumula-tive total of deaths will lie on a straight line or veryclose to it. Projecting a horizontal line to the left until itcuts the vertical axis, enables exogenous and endogenousdeaths to be separated (Wrigley, 1977). For archaeologi-cal populations, as we do not know the number of infantdeaths per year, in the long time span of our cemeteries,or can we age our skeletons to as accurately as days,such statistics cannot be applied. However, a crude esti-mate of exogenous and endogenous deaths can be estab-lished by looking at the numbers of individuals dyingbetween the ages of 28–40 weeks of gestation comparedwith 41–48 weeks. Hence, the percentage of neonataldeaths, including possible stillbirths (28–40 weeks) andpost-neonatal deaths (41–48 weeks), aged by both meth-ods, were compared between rural and urban samples tosee if different patterns of infant mortality could be dis-cerned.
RESULTS
Regression statistics
Of a total of 163 infant skeletons (under 48 weeks),128 (78.5%) were aged using the available diaphyseallengths (humerus, radius, ulna, femur, tibia) for eachindividual (Tables 2 and 3). In 1929, the Infant LifePreservation Act set 28 weeks gestation as the period atwhich a child was developed enough to be viable outsidethe mother’s womb, although with modern medical inter-vention this period has been reduced to 24 weeks(Knight, 1996). In the past, it is logical that the later achild was born the more likely it was to survive. Tradi-tionally, a full-term fetus is aged between 38 and 40weeks gestation (Saunders, 2000) and for the purpose ofour study 40 weeks was taken as the time of birth. Anyindividuals below this age were considered to have beenpremature, with a reduced chance of survival, spontane-ously aborted, or stillborn. This method would clearlyplace any small-for-gestational-age (SGA) babies withina younger, or premature, age category as methods toidentify these children are limited (Lewis, 2007).
The age at death of the infants based on regressionequations is presented in Figures 2–5. It is clear thatthere is a stark under-representation of infants in theSt. Helens sample, and this has been a matter of debatein the literature before. Only 12 (6%) infants were recov-ered from this site in a period spanning 500 years, withone child found within the pelvis of an adult female(Grauer, 1991; Lewis, 2002). The peak at 38 weeks usingregression equations, may suggests that children weredying at birth, and has prompted speculation that theseinfants were being killed by their impoverished mothers.Documentary evidence from St. Helens has indicatedthat many of the female tenants were involved in prosti-tution (Palliser, 1980), and it is possible that the high
4 M.E. LEWIS AND R. GOWLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa
number of neonatal deaths represent their disposal bywomen who needed to remain unburdened by babies tocontinue in their trade. However, this pattern may alsoreflect the burial practices of the medieval period, whereunbaptised infants were either disposed of away fromconsecrated ground, or buried in a specific, unexcavatedarea of the cemetery. Unfortunately, detailed plans of the
excavation are not available and it is not possible toidentify where within the cemetery the recovered infantswere located. What is clear is that the tiniest of babies(under 38 weeks) are not in the sample and it is possiblethat these bones were overlooked at the time of excava-tion. While the under-enumeration provides interestinginformation in itself regarding attitudes towards infant
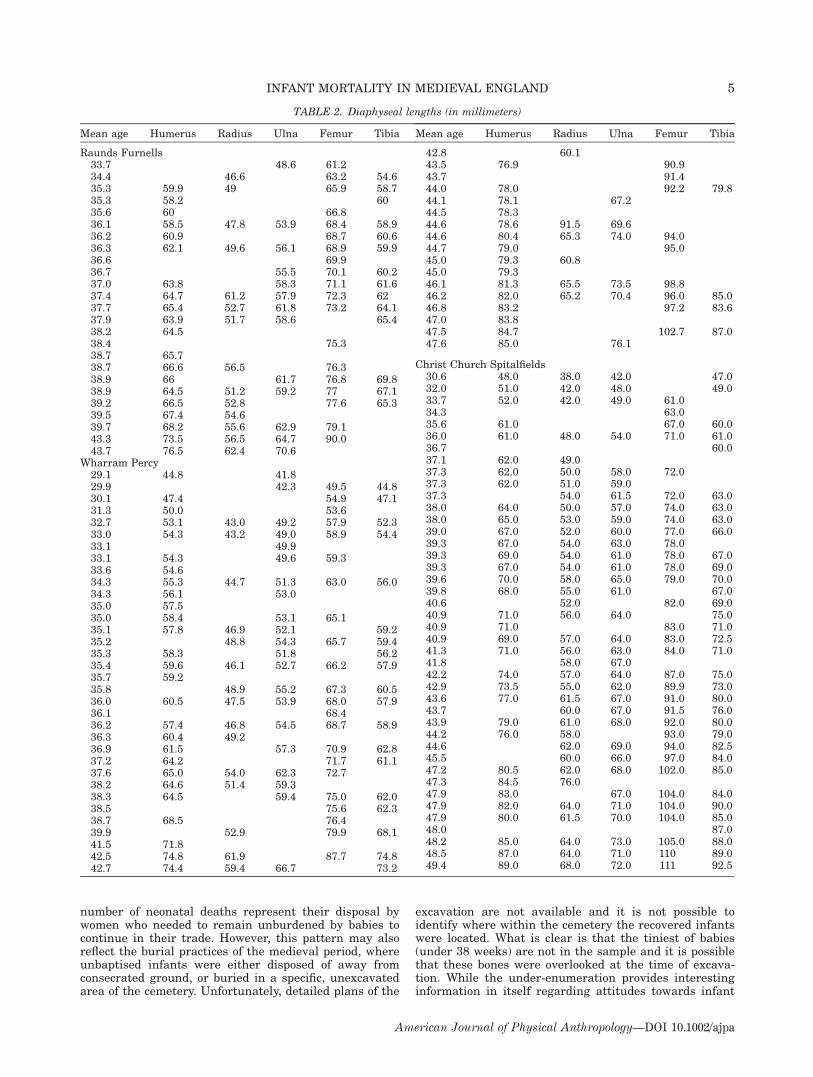
TABLE 2. Diaphyseal lengths (in millimeters)
Mean age Humerus Radius Ulna Femur Tibia
Raunds Furnells33.7 48.6 61.234.4 46.6 63.2 54.635.3 59.9 49 65.9 58.735.3 58.2 6035.6 60 66.836.1 58.5 47.8 53.9 68.4 58.936.2 60.9 68.7 60.636.3 62.1 49.6 56.1 68.9 59.936.6 69.936.7 55.5 70.1 60.237.0 63.8 58.3 71.1 61.637.4 64.7 61.2 57.9 72.3 6237.7 65.4 52.7 61.8 73.2 64.137.9 63.9 51.7 58.6 65.438.2 64.538.4 75.338.7 65.738.7 66.6 56.5 76.338.9 66 61.7 76.8 69.838.9 64.5 51.2 59.2 77 67.139.2 66.5 52.8 77.6 65.339.5 67.4 54.639.7 68.2 55.6 62.9 79.143.3 73.5 56.5 64.7 90.043.7 76.5 62.4 70.6
Wharram Percy29.1 44.8 41.829.9 42.3 49.5 44.830.1 47.4 54.9 47.131.3 50.0 53.632.7 53.1 43.0 49.2 57.9 52.333.0 54.3 43.2 49.0 58.9 54.433.1 49.933.1 54.3 49.6 59.333.6 54.634.3 55.3 44.7 51.3 63.0 56.034.3 56.1 53.035.0 57.535.0 58.4 53.1 65.135.1 57.8 46.9 52.1 59.235.2 48.8 54.3 65.7 59.435.3 58.3 51.8 56.235.4 59.6 46.1 52.7 66.2 57.935.7 59.235.8 48.9 55.2 67.3 60.536.0 60.5 47.5 53.9 68.0 57.936.1 68.436.2 57.4 46.8 54.5 68.7 58.936.3 60.4 49.236.9 61.5 57.3 70.9 62.837.2 64.2 71.7 61.137.6 65.0 54.0 62.3 72.738.2 64.6 51.4 59.338.3 64.5 59.4 75.0 62.038.5 75.6 62.338.7 68.5 76.439.9 52.9 79.9 68.141.5 71.842.5 74.8 61.9 87.7 74.842.7 74.4 59.4 66.7 73.2
Mean age Humerus Radius Ulna Femur Tibia
42.8 60.143.5 76.9 90.943.7 91.444.0 78.0 92.2 79.844.1 78.1 67.244.5 78.344.6 78.6 91.5 69.644.6 80.4 65.3 74.0 94.044.7 79.0 95.045.0 79.3 60.845.0 79.346.1 81.3 65.5 73.5 98.846.2 82.0 65.2 70.4 96.0 85.046.8 83.2 97.2 83.647.0 83.847.5 84.7 102.7 87.047.6 85.0 76.1
Christ Church Spitalfields30.6 48.0 38.0 42.0 47.032.0 51.0 42.0 48.0 49.033.7 52.0 42.0 49.0 61.034.3 63.035.6 61.0 67.0 60.036.0 61.0 48.0 54.0 71.0 61.036.7 60.037.1 62.0 49.037.3 62.0 50.0 58.0 72.037.3 62.0 51.0 59.037.3 54.0 61.5 72.0 63.038.0 64.0 50.0 57.0 74.0 63.038.0 65.0 53.0 59.0 74.0 63.039.0 67.0 52.0 60.0 77.0 66.039.3 67.0 54.0 63.0 78.039.3 69.0 54.0 61.0 78.0 67.039.3 67.0 54.0 61.0 78.0 69.039.6 70.0 58.0 65.0 79.0 70.039.8 68.0 55.0 61.0 67.040.6 52.0 82.0 69.040.9 71.0 56.0 64.0 75.040.9 71.0 83.0 71.040.9 69.0 57.0 64.0 83.0 72.541.3 71.0 56.0 63.0 84.0 71.041.8 58.0 67.042.2 74.0 57.0 64.0 87.0 75.042.9 73.5 55.0 62.0 89.9 73.043.6 77.0 61.5 67.0 91.0 80.043.7 60.0 67.0 91.5 76.043.9 79.0 61.0 68.0 92.0 80.044.2 76.0 58.0 93.0 79.044.6 62.0 69.0 94.0 82.545.5 60.0 66.0 97.0 84.047.2 80.5 62.0 68.0 102.0 85.047.3 84.5 76.047.9 83.0 67.0 104.0 84.047.9 82.0 64.0 71.0 104.0 90.047.9 80.0 61.5 70.0 104.0 85.048.0 87.048.2 85.0 64.0 73.0 105.0 88.048.5 87.0 64.0 71.0 110 89.049.4 89.0 68.0 72.0 111 92.5
5INFANT MORTALITY IN MEDIEVAL ENGLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa
deaths, the impossibly small sample size meant thatdata from this site was not examined further.
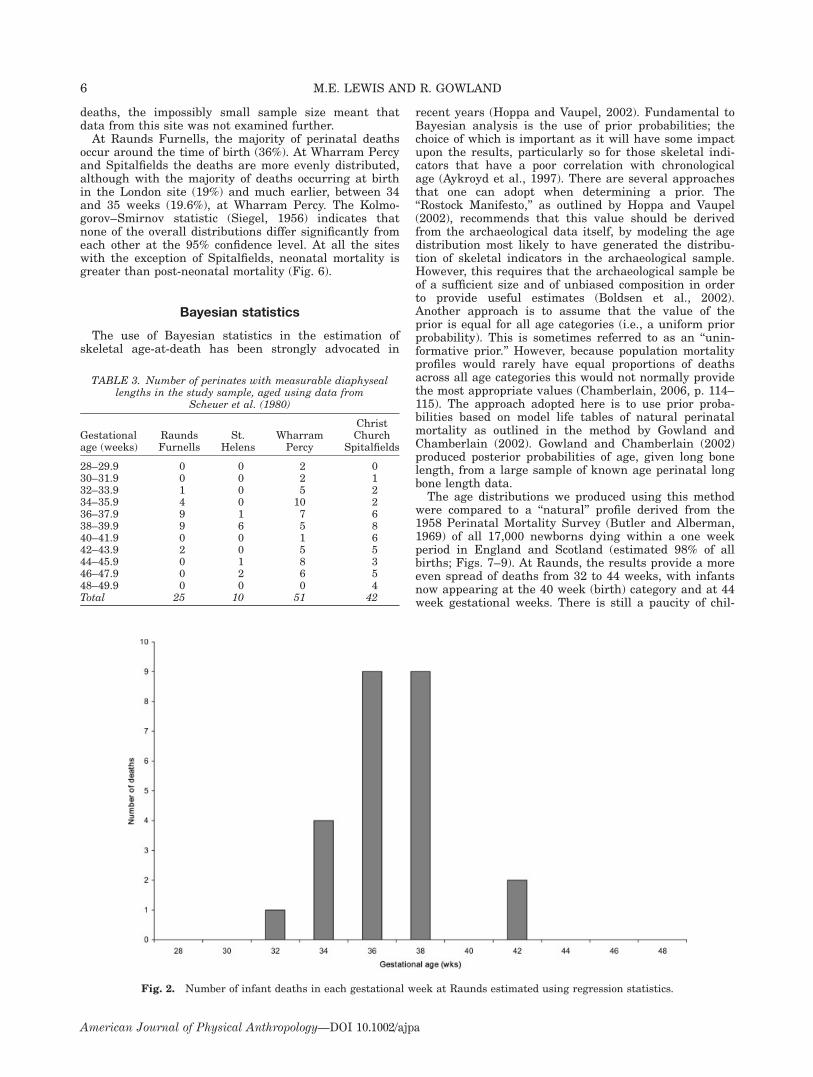
At Raunds Furnells, the majority of perinatal deathsoccur around the time of birth (36%). At Wharram Percyand Spitalfields the deaths are more evenly distributed,although with the majority of deaths occurring at birthin the London site (19%) and much earlier, between 34and 35 weeks (19.6%), at Wharram Percy. The Kolmo-gorov–Smirnov statistic (Siegel, 1956) indicates thatnone of the overall distributions differ significantly fromeach other at the 95% confidence level. At all the siteswith the exception of Spitalfields, neonatal mortality isgreater than post-neonatal mortality (Fig. 6).
Bayesian statistics
The use of Bayesian statistics in the estimation ofskeletal age-at-death has been strongly advocated in
recent years (Hoppa and Vaupel, 2002). Fundamental toBayesian analysis is the use of prior probabilities; thechoice of which is important as it will have some impactupon the results, particularly so for those skeletal indi-cators that have a poor correlation with chronologicalage (Aykroyd et al., 1997). There are several approachesthat one can adopt when determining a prior. The‘‘Rostock Manifesto,’’ as outlined by Hoppa and Vaupel(2002), recommends that this value should be derivedfrom the archaeological data itself, by modeling the agedistribution most likely to have generated the distribu-tion of skeletal indicators in the archaeological sample.However, this requires that the archaeological sample beof a sufficient size and of unbiased composition in orderto provide useful estimates (Boldsen et al., 2002).Another approach is to assume that the value of theprior is equal for all age categories (i.e., a uniform priorprobability). This is sometimes referred to as an ‘‘unin-formative prior.’’ However, because population mortalityprofiles would rarely have equal proportions of deathsacross all age categories this would not normally providethe most appropriate values (Chamberlain, 2006, p. 114–115). The approach adopted here is to use prior proba-bilities based on model life tables of natural perinatalmortality as outlined in the method by Gowland andChamberlain (2002). Gowland and Chamberlain (2002)produced posterior probabilities of age, given long bonelength, from a large sample of known age perinatal longbone length data.
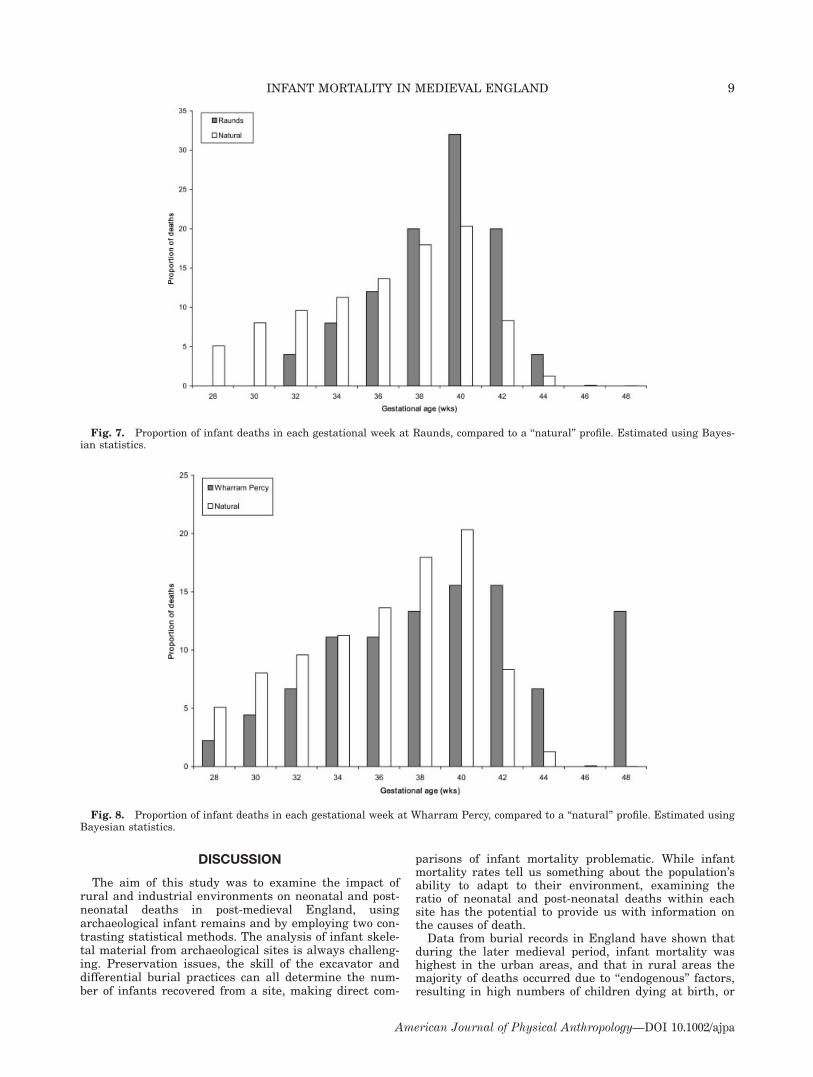
The age distributions we produced using this methodwere compared to a ‘‘natural’’ profile derived from the1958 Perinatal Mortality Survey (Butler and Alberman,1969) of all 17,000 newborns dying within a one weekperiod in England and Scotland (estimated 98% of allbirths; Figs. 7–9). At Raunds, the results provide a moreeven spread of deaths from 32 to 44 weeks, with infantsnow appearing at the 40 week (birth) category and at 44week gestational weeks. There is still a paucity of chil-
TABLE 3. Number of perinates with measurable diaphyseallengths in the study sample, aged using data from
Scheuer et al. (1980)
Gestationalage (weeks)
RaundsFurnells
St.Helens
WharramPercy
ChristChurch
Spitalfields
28–29.9 0 0 2 030–31.9 0 0 2 132–33.9 1 0 5 234–35.9 4 0 10 236–37.9 9 1 7 638–39.9 9 6 5 840–41.9 0 0 1 642–43.9 2 0 5 544–45.9 0 1 8 346–47.9 0 2 6 548–49.9 0 0 0 4Total 25 10 51 42
Fig. 2. Number of infant deaths in each gestational week at Raunds estimated using regression statistics.
6 M.E. LEWIS AND R. GOWLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa

dren aged from 28 to 30 weeks compared to the‘‘natural’’ mortality profile, but it follows it much moreclosely than with the regression statistics. One mightexpect this because the prior probability is based on nat-ural perinatal mortality, though that is not to say thatthe prior absolutely determines the outcome as evi-denced by the different mortality curves produced. AtWharram Percy, the profile changed from two peaks at34 and 44 weeks, to a much more gradual peak of infantdeaths between 40 and 42 weeks, with many of the
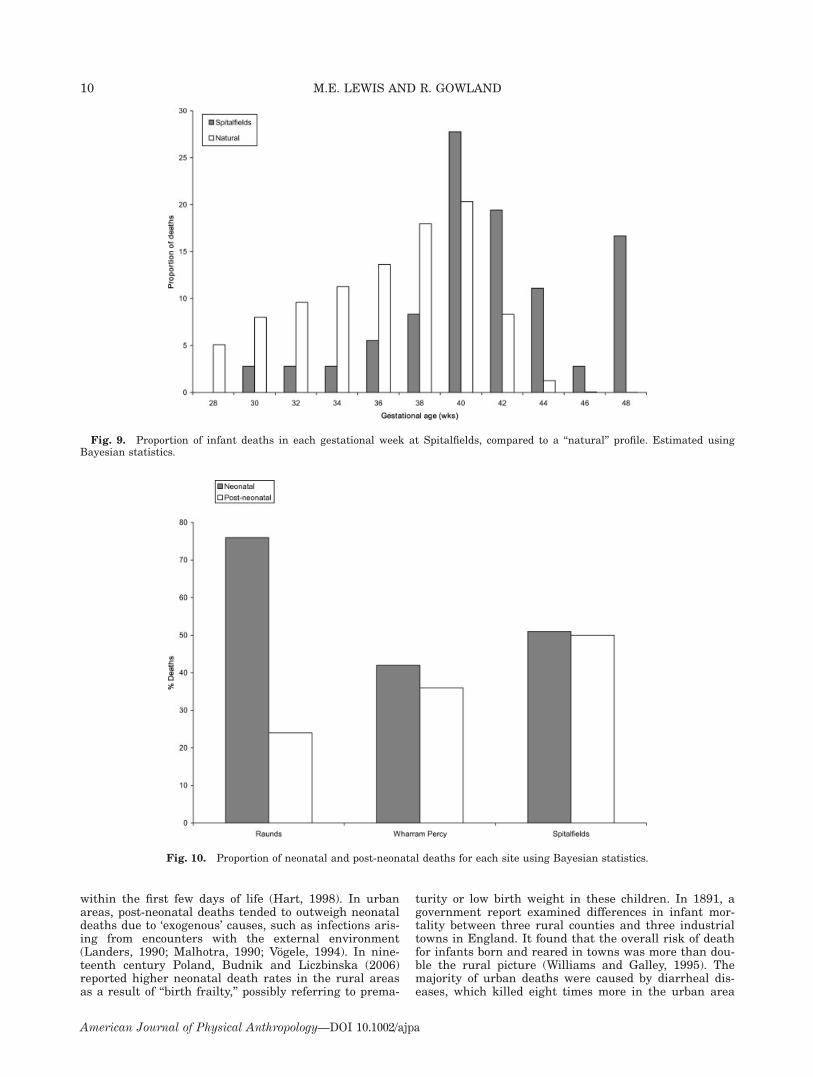
infants shifting to the 40 weeks age category, againreflecting the ‘‘natural’’ profile. The previous two peakshave disappeared, but there are a number of deathsoccurring at 48 weeks, out of step with the ‘‘natural’’ pro-file. Finally, Spitalfields still shows an even spread ofinfant deaths from 30 to 48 weeks, but the peak hasshifted from 36–38 to 40 weeks gestation, and the largenumber of deaths in the 46 week category has disap-peared. As with Wharram Percy, there is an increase inthe number of deaths at 48 weeks.
Fig. 3. Number of infant deaths in each gestational week at St. Helens estimated using regression statistics.
Fig. 4. Number of infant deaths in each gestational week at Wharram Percy estimated using regression statistics.
7INFANT MORTALITY IN MEDIEVAL ENGLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa

The analysis of neonatal and post-neonatal mortalityhas also altered with more children dying in the post-neonatal period at all of the sites (Fig. 10). At Raunds,however, neonatal deaths remain high (76%), and atWharram Percy they outweighed post-neonatal deaths.The results from both of these rural sites are in tune
with documentary evidence for the medieval periodwhere deaths due to endogenous factors exceed those asthe result of exogenous causes. At Spitalfields, neonataland post-neonatal deaths are almost equal suggestingthat environmental factors were beginning to influencethe pattern of infant death in this industrial sample.
Fig. 5. Number of infant deaths in each gestational week at Spitalfields estimated using regression statistics.
Fig. 6. Percentage of neonatal and post-neonatal deaths for each site using regression statistics.
8 M.E. LEWIS AND R. GOWLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa
DISCUSSION
The aim of this study was to examine the impact ofrural and industrial environments on neonatal and post-neonatal deaths in post-medieval England, usingarchaeological infant remains and by employing two con-trasting statistical methods. The analysis of infant skele-tal material from archaeological sites is always challeng-ing. Preservation issues, the skill of the excavator anddifferential burial practices can all determine the num-ber of infants recovered from a site, making direct com-
parisons of infant mortality problematic. While infantmortality rates tell us something about the population’sability to adapt to their environment, examining theratio of neonatal and post-neonatal deaths within eachsite has the potential to provide us with information onthe causes of death.
Data from burial records in England have shown thatduring the later medieval period, infant mortality washighest in the urban areas, and that in rural areas themajority of deaths occurred due to ‘‘endogenous’’ factors,resulting in high numbers of children dying at birth, or
Fig. 7. Proportion of infant deaths in each gestational week at Raunds, compared to a ‘‘natural’’ profile. Estimated using Bayes-ian statistics.
Fig. 8. Proportion of infant deaths in each gestational week at Wharram Percy, compared to a ‘‘natural’’ profile. Estimated usingBayesian statistics.
9INFANT MORTALITY IN MEDIEVAL ENGLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa
within the first few days of life (Hart, 1998). In urbanareas, post-neonatal deaths tended to outweigh neonataldeaths due to ‘exogenous’ causes, such as infections aris-ing from encounters with the external environment(Landers, 1990; Malhotra, 1990; Vogele, 1994). In nine-teenth century Poland, Budnik and Liczbinska (2006)reported higher neonatal death rates in the rural areasas a result of ‘‘birth frailty,’’ possibly referring to prema-
turity or low birth weight in these children. In 1891, agovernment report examined differences in infant mor-tality between three rural counties and three industrialtowns in England. It found that the overall risk of deathfor infants born and reared in towns was more than dou-ble the rural picture (Williams and Galley, 1995). Themajority of urban deaths were caused by diarrheal dis-eases, which killed eight times more in the urban area
Fig. 9. Proportion of infant deaths in each gestational week at Spitalfields, compared to a ‘‘natural’’ profile. Estimated usingBayesian statistics.
Fig. 10. Proportion of neonatal and post-neonatal deaths for each site using Bayesian statistics.
10 M.E. LEWIS AND R. GOWLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa

(40%) than in the rural (5%), and crowd diseases such asmeasles and scarlet fever were three times more preva-lent, with tuberculosis double that of the rural areas.
While we know stillborn and unbaptised babies wereofficially excluded from burial in the latter part of themedieval period (Gilchrist and Slone, 2005), we have noinformation on parental or cultural attitudes towardsthe children who survived for a few days after birth(neonates), as opposed to children who lived for weeks ormonths before their death, and who may have made adeeper emotional connection with their parents. If neo-nates were buried in a different location or manner topost-neonates, this would affect the proportions of thesechildren recovered. At Raunds Furnells, whatever statis-tic is used, neonatal deaths exceed post-neonatal deaths,indicating no such discrimination existed, and that en-dogenous factors such as congenital defects have moreinfluence on the death rate than environmental ones.Infants make up 28% of the nonadult sample at this site,but the very young infants (28–30 weeks) and olderinfants (44–48 weeks) are few in number. At WharramPercy, the age distribution was similar to that expectedfrom a normal mortality profile when both stillborn andneonatal deaths are accorded similar burials. The agedistribution for this site, however, is flatter thanexpected, with a slight peak at 34–35 weeks, indicatingthat a greater number of premature births were includedat this site. This suggests that there may have been agreater tradition within rural areas of burying stillbornor unbaptised infants within the main cemetery. The sit-uation at Spitalfields may have been different. From doc-umentary evidence we know that urban infants whodied while being wet-nursed in the countryside wouldnot have been returned home for burial and this mayhave had some affect on the age profile of the infants inthe crypt. However, Molleson and Cox (1993, p. 132)refer to the burial of at least one stillborn child, suggest-ing that midwives were performing baptisms in utero.The spread of infant deaths is again similar to the‘‘natural’’ mortality profile, indicating that the majorityof babies were buried within the crypt, with childrenaged between 30 and 48 weeks all represented, andinfants making up a quarter (25%) of the nonadultsample.
Overall, a much greater spread of gestational ages wasobtained at each site when the infants were aged usingthe Bayesian method as opposed to the regressionmethod. This is what one would expect, as the Bayesiantechnique does not assign all individuals with the samelong bone length to the same gestational age (as theregression technique does), instead it takes into accountthe fact that individuals with the same long bone lengthmay fall within a range of gestational ages (Gowlandand Chamberlain, 2002). It does this by incorporating aprobability distribution of gestational age given the longbone length based on observations of a large sample ofknown age data. Therefore, while this technique doesnot provide ages for individuals, it does generate a prob-ability distribution of gestational ages from the observedlong bone lengths, and as such would seem to be bettersuited to the analytical purposes of this study. In addi-tion to the broader range of gestational ages observedusing the Bayesian method, the peaks in ages at deathtend to be less pronounced and occur at 40 weeks asopposed to 38 weeks when using the regression method(see Gowland and Chamberlain, 2002 for a discussion ofthe methodological reasons for this). Using the Bayesian
data, all sites with the exception of Raunds, show anincrease in infant deaths at the 48 week cut-off point.This pattern is likely to have occurred because theBayesian method does not provide probabilities for thoseinfants dying over the age of 48 weeks. Hence, the upperlimit of this method is effectively truncated, and some ofthe infants falling within this 48 week age category mayin fact have died at the slightly older ages of 50, 51, or52 weeks.
At all sites, the regression and Bayesian results showneonatal deaths outweighing post-neonatal deaths. How-ever, the Bayesian results increase the number of chil-dren dying after 41 weeks, and at Spitalfields, the per-centage of neonatal and post-neonatal deaths is almostequal (see Figures 6 and 10). The London Bills of Mor-tality for the period of the Spitalfields crypt use, showthat infant mortality rates were high and fluctuatedbetween 341 per 1000 live births (1725–1749) to 151(1825–1829), above the national rate, and greater thanthe rural areas with rates of 191 and 144 respectively(Galley and Shelton, 2001, p. 69). The greater number ofchildren surviving birth at Spitalfields may be explainedby the apparent wealth of the Spitalfields mothers whowere mostly skilled silk-weavers, and medical advances,such as the introduction of the forceps and man-mid-wives in the early eighteenth century (Loudon, 1992;Wear, 1992). The age of enamel hypoplasia formationand cribra orbitalia in the Spitalfields sample, comparedto the other sites, suggest that weaning may haveoccurred by around 7 months (Lewis, 2002), increasingthe child’s risk of exposure to contaminated food, diar-rhea, and malnutrition, and contributing to the greaterpost-neonatal mortality rates.
CONCLUSIONS
This study has analyzed and compared the mortalitypatterns of infants excavated from both urban and ruralmedieval sites in England, with the aim of interpretingthe differences observed in terms of endogenous or exog-enous causes. In order to undertake this analysis, twodifferent methods of estimating gestational age fromlong bone lengths were used: a traditional regressionmethod and a Bayesian method. The regression methodtended to produce more marked peaks at 38 weeks,while the Bayesian method produced a broader range ofages, although the differences in age distributions didnot affect the interpretation of the results significantly.Of the three sites, it is Wharram Percy that provides themost convincing evidence for a total infant sample, withall infants represented and the expected peak between38 and 42 weeks, indicating that both stillborn and neo-natal deaths were accorded burial within the main ceme-tery. Raunds also showed a ‘‘natural’’ mortality pattern,although fewer infants of younger gestational ages wereburied than at Wharram Percy. At Spitalfields a greaterproportion of infants were of post-neonatal age withfewer very young, possibly stillborn, infants. It is likelythat there was a more strict observance of the exclusionof unbaptised infants within this urban crypt than atthe rural burial sites of Wharram Percy and Raunds.This pattern may also indicate the success of medicaladvances during childbirth, coupled with the greaterimpact of exogenous causes on infant death within thisurban setting, as the result of poor sanitation and earlyweaning ages.
11INFANT MORTALITY IN MEDIEVAL ENGLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa
ACKNOWLEDGMENTS
Part of this research was funded by a University ofBradford Studentship. Thanks are also due to the peopleand institutions that allowed ML access to the skeletalmaterial. Firstly, to the Yorkshire Museum and YorkArchaeological Trust, for making the St. Helen-on-the-Walls material available, to Northants County Councilfor access to the Raunds Furnells collection via BradfordUniversity and, to Simon Mays (English Heritage) foraccess to the Wharram Percy skeletons. ML is alsograteful to Louise Humphrey (Natural History Museum)for access to the Spitalfields collection. We thank thereviewers and Clark Spenser Larsen, whose useful com-ments helped to improve this paper.
LITERATURE CITED
Adair L. 2004. Fetal adaptations to maternal nutritional statusduring pregnancy. Am J Phys Anthropol 38:50.
Adler NE Ostrove JM. 1999. Socioeconomic status and health:what we know and what we don’t. Ann New York Acad Sci896:3–15.
Andrews G. 1984. Archaeology in York: an assessment. In:Addyman PV, Black VE, editors. Archaeological papers fromYork: Presented to M.W. Barley. York: York ArchaeologicalTrust. p 173–187.
Aykroyd R, Lucy D, Pollard A, Roberts C. 1999. Nasty, brutish,but not necessarily short: a reconsideration of the statisticalmethods used to calculate age at death from adult humanskeletal and dental age indicators. Am Antiquity 64:55–70.
Aykroyd R, Lucy D, Pollard A, Solheim T. 1997. Technical note:regression analysis in adult age estimation. Am J PhysAnthropol 104:259–265.
Bell RD, Beresford M. 1987. Wharram Percy: the Church of St.Martin. London: Society for Medieval Archaeology.
Bocquet-Appel JP. 2002. Paleoanthropological traces of a neo-lithic demographic transition. Curr Anthropol 43:637–650.
Bocquet-Appel JP, Masset C. 1982. Farewell to paleodemogra-phy. J Hum Evol 11:321–333.
Bocquet-Appel JP, Masset C. 1996. Paleodemography: expect-ancy and false hope. Am J Phys Anthropol 99:571–583.
Boddington A. 1996. Raunds Furnells. The Anglo-Saxon churchand churchyard. London: English Heritage.
Boldsen JL, Milner GL, Konigsberg LW, Wood JW. 2002. Transi-tion analysis: a new method for estimating age from skele-tons. In: Hoppa RD, Vaupel JW, editors. Paleodemography:age distributions from skeletal samples. WP: Cambridge:Cambridge University Press. p 73–106.
Bourgeois-Pichat J. 1951. La measure de la mortalite infantile:I. Principes et methodes. Population 6:233–48.
Brothwell DR. 1986–7. The problem of the interpretation ofchild mortality in earlier populations. Anthropol Port 4–5:135–143.
Budnik A, Liczbinska G. 2006. Urban and rural differences inmortality and causes of death in historic Poland. Am J PhysAnthropol 129:294–304.
Buikstra J, Konigsberg L, Bullington J. 1986. Fertility and thedevelopment of agriculture in the prehistoric midwest. AmAntiquity 51:191–204.
Butler NR, Alberman ED. 1969. Perinatal problems: the secondreport of the 1958 perinatal mortality survey. Edinburgh: Liv-ingstone.
Chamberlain A. 2006. Demography in archaeology. Cambridge:Cambridge University Press.
Clement J, Kosa F. 1992. The fetal skeleton. In: Clark D, editor.Practical forensic odontology. London: Butterworth-Heinemann,p 43–52.
Cox M. 1996. Life and death in Spitalfields 1700 to 1850. York:Council for British Archaeology.
Fazekas IG, Kosa F. 1978. Forensic fetal osteology. Budapest:Academic Press.
Galley C, Shelton N. 2001. Bridging the gap: determining long-term changes in infant mortality in pre-registration Englandand Wales. Popul Studies 55:65–77.
Gelman A, Carlin J, Stern H, Rubin D. 1995 Bayesian dataanalysis. London: Chapman & Hall.
Gilchrist R, Slone B. 2005. Requiem: the monastic cemeteries inBritain. London: Museum of London.
Goode H, Waldron T, Rogers J. 1993. Bone growth in juveniles:a methodological note. Int J Osteoarch 3:321–323.
Gordon CC, Buikstra J. 1981. Soil pH, bone preservation,and sampling bias at mortuary sites. Am Antiquity 48:566–571.
Gowland R, Chamberlain A. 2002. A Bayesian approach to age-ing perinatal skeletal material from archaeological sites:implications for the evidence for infanticide in Roman-Britain.J Arch Sci 29:677–685.
Grauer AL. 1991. Life patterns of women from medieval York.In: Walde D, Willows ND, editors. Proceedings of the 22ndAnnual Chacmool Conference. University of Calgary, Chac-mool: The Archaeological Association of the University of Cal-gary. p 407–413.
Graunt J. 1662. Natural and political observations. London:Thomas Roycroft.
Hall RA, MacGregor H, Stockwell M. 1988. Medieval tenementsin Aldwark, and other sites. London: Council for BritishArchaeology.
Hart N. 1998. Beyond infant mortality: gender and stillbirth inreproductive mortality before the twentieth century. PopulStudies 52:215–229.
Hauspie R, Chrzastek-Spruch H, Verleyen G, Kozlowska M,Suzsanne C. 1994. Determinates of growth in body lengthfrom birth to 6 years of age: a longitudinal study of Dublinchildren. Int J Anthropol 9:202.
Herring D, Saunders S, Boyce G. 1994. Bones and the burialregisters: infant mortality in a 19th century cemetery fromUpper Canada. C Northeast Hist Arch J 20:54–70.
Hobbs C, Kigguridu M. 1992. A global analysis of life expect-ancy and infant mortality. Canada: Carleton UniversityPress.
Hoppa R, Vaupel J. 2002. The Rostock manifesto for paleode-mography: the way from age to stage. In: Hoppa R, Vaupel J,editors. Paleodemography: age distributions from skeletalsamples. Cambridge: Cambridge University Press. p 1–8.
Humphrey L, Dean M, Jeffries T. 2005. Identification of the neo-natal line using LA-ICP-MS. Am J Phys Anthropol Suppl.40:119–120.
Jeanty P, Dramaix-Wilmet D, van Kerkem J, Schwers J. 1982.Ultrasonic evaluation of fetal limb growth. Part I. Radiology143:751–754.
Jeanty P, Kirkpatrick C, Dramaix-Wilmet D, Struyven J. 1981.Ultrasonic evaluation of fetal limb growth: Part II. Radiology140:165–168.
Jeanty P, Romaro R. 1984. Obstetrical ultrasound. London:McGraw Hill.
Johnston FE, Zimmer LO. 1989. Assessment of growth and agein the immature skeleton. In: Iscan MY, Kennedy KAR, edi-tors: Reconstruction of life from the skeleton. New York: AlanR. Liss. p 11–21.
Jones E, Ubelaker D. 2001. Demographic analysis of the Voegtlycemetery sample, Pittsburgh, Pennsylvania. Am J PhysAnthropol 32:86.
Knight B. 1996. Forensic pathology, 2nd ed. London: Arnold.Knodel J, Kintner H. 1977. The impact of breast feeding pat-
terns on the biometric analysis of infant mortality. Demogra-phy 14:391–409.
Konigsberg L, Frankenberg S, Walker R. 1997. Regress what onwhat? Palaeodemographic age estimation as a calibrationproblem. In: Paine RR, editor. Integrating archaeologicaldemography: Multidisciplinary approaches to prehistoric pop-ulations. Carbondale: Center from Archaeological Investiga-tions, Southern Illinois University. p 64–88.
Konigsberg LW, Frankenberg SR. 1992. Estimation of age struc-ture in anthropological demography. Am J Phys Anthropol89:235–256.
12 M.E. LEWIS AND R. GOWLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa

Lampl M, Jeanty P. 2003. Timing is everything: a reconsidera-tion of fetal growth velocity patterns identifies the importanceof individual and sex differences. Am J Hum Bio 15:667–680.
Landers J. 1990. Age patterns of mortality in London duringthe ‘long eighteenth century’: a test of the ‘high potential’model of metropolitan mortality. Soc Hist Med 3:27–60.
Larsen CS. 1997. Bioarcheology: Interpreting behavior from thehuman skeleton. Cambridge: Cambridge University Press.
Lewis M. 2002. The impact of industrialisation: comparativestudy of child health in four sites from medieval and post-me-dieval England (850–1859 AD). Am J Phys Anthropol 119:211–223.
Lewis M. 2007. The bioarchaeology of children. Perspectivesfrom biological and forensic anthropology. Cambridge: Cam-bridge University Press.
Loudon I. 1992. Death in childbirth: An international study ofmaternal care and maternal mortality 1800–1950. Oxford:Clarendon Press.
Lucy D, Aykroyd R, Pollard A, Solheim T. 1996. A Bayesianapproach to adult human age estimation from dental observa-tions by Johansson’s age changes. J For Sci 41:189–194.
Malhotra KC. 1990. Changing patterns of disease in India withspecial reference to childhood mortality. In: Swedlund AC,Armelagos GJ, editors. Disease in populations in transition:Anthropological and epidemiological perspectives. New York:Bergin and Garvey.
Mays S. 1993. Infanticide in Roman Britain. Antiquity 67:883–888.
Mays S. 2003. Comment on ‘‘A Bayesian approach to aging peri-natal skeletal material from archaeological sites: implicationsfor the evidence for infanticide in Roman Britain’’ by GowlandRL, Chamberlain AT. J Arch Sci 30:1695–1700.
Milne G, Richards J. 1992. Two Anglo-Saxon buildings and asso-ciated finds. York: York University Archaeological Publica-tions 9.
Milner G, Humpf D, Harpending H. 1989. Pattern matching ofage-at-death distributions in paleodemographic analysis. AmJ Phys Anthropol 80:49–58.
Molleson T, Cox M. 1993. The Spitalfields Project, volume II–The Middling Sort. York: Council for British Archaeology,Research Report 86.
Murray C, Frenk J. 2002. Summary measures of populationhealth in the context of the WHO framework for health sys-tem performance assessment. In: Murray CJ, Salomon JA,Mathers CD, Lopex AD, editors. Summary measures of popu-lation health. Concepts, ethics, measurement and application.Geneva: World Health Organization, p 1–12.
Orme N. 2001. Medieval children. New Haven: Yale UniversityPress.
Paine R. 2000. If a population crashes in prehistory, and thereis no palaeodemographer there to hear it, does it make asound? Am J Phys Anthropol 112:181–190.
Paine R, Harpending H. 1996. Assessing the reliability of paleo-demographic fertility estimators in stimulated skeletal distri-butions. Am J Phys Anthropol 101:151–159.
Palliser DM. 1980. Location and history. In: Magilton J, editor.The archaeology of York: The medieval walled city north-eastof the Ouse. London: Council for British Archaeology. p 2–14.
Panhuysen R. 1999. Child mortality in early medieval Maas-tricht: missing children? J Paleopathol 11:94.
Ribot I, Roberts CA. 1996. A study of non-specific stress indica-tors and skeletal growth in two mediaeval subadult popula-tions. J Arch Sci 23:67–79.
Robertson J. 1996. Reckoning with London: interpreting thebills of mortality before John Graunt. Urban Hist 23:325–350.
Samworth RJ, and Gowland RL. 2006. Estimation of adult skel-etal age-at-death: statistical assumptions and applications.Int J Osteoarch 16:1–15.
Sarnat B, and Schour I. 1941. Enamel hypoplasia (chronologicalenamel aplasia) in relation to systemic disease: a chronologic,morphologic and etiologic classification. J Am Dent Ass28:1989–2000.
Sattenspiel L, Harpending H. 1983. Stable populations and skel-etal age. Am Antiquity 48:489–498.
Saunders SR. 2000. Subadult skeletons and growth-relatedstudies. In: Katzenberg M, Saunders S, editors. Biologicalanthropology of the human skeleton. New York: Wiley-Liss.p 1–20.
Saunders SR, Barrans L. 1999. What can be done about theinfant category in skeletal samples? In: Hoppa RD, FitzgeraldCM, editors. Human growth in the past: studies from bonesand teeth. Cambridge: Cambridge University Press. p 183–209.
Saunders SR, Herring DA, Boyce G. 1995. Can skeletal samplesaccurately represent the living populations they come from?The St. Thomas’ cemetery site, Belleville, Ontario. In: GrauerAL, editor. Bodies of evidence: reconstructing history throughskeletal analysis. New York: Wiley-Liss. p 69–89.
Scheuer JL, Musgrave JH, Evans SP. 1980. The estimation oflate fetal and perinatal age from limb bone length by linearand logarithmic regression. Ann Human Biol 7:257–265.
Scott S, Duncan C. 1998. Human demography and disease.Cambridge: Cambridge University Press.
Scott S, Duncan CJ. 1999. Malnutrition, pregnancy and infantmortality: a biometric model. J Interdis Hist 30:37–60.
Siegel S. 1956. Nonparametric statistics for the behavioral sci-ences. London: McGraw-Hill.
Smith P, Avishai G. 2005. The use of dental criteria for estimat-ing postnatal survival in skeletal remains of infants. J ArchSci 32:83–89.
Smith P, Kahila G. 1992. Identification of infanticide in archaeo-logical sites: a case study from the Late Roman-Early Byzan-tine Periods at Ashkelon, Israel. J Arch Sci 19:667–675.
Stockwell E. 1993. Infant mortality. In: Kiple K, editor. TheCambridge world history of human disease. Cambridge: Cam-bridge University Press. p 224–229.
Stroud G, Kemp RL, editors. 1993. Cemeteries of the Churchand Priory of St Andrew, Fishergate. The archaeology of York,Vol. 12: The medieval cemeteries. York: Current BritishArchaeology.
Sundick RI. 1978. Human skeletal growth and age determina-tion. Homo 29:228–249.
Vogele JP. 1994. Urban infant mortality in Imperial Germany.Soc Hist Med 7:401–426.
Wear A. 1992. Making sense of health and the environment inearly modern England. In: Andrew W, editor. Medicine in so-ciety. Cambridge: Cambridge University Press. p 119–147.
Whittaker D, MacDonald D. 1989. A colour atlas of forensic den-tistry. London: Wolfe.
Williams N, Galley C. 1995. Urban-rural differentials in infantmortality in Victorian England. Popul Studies 49:401–420.
Wrigley E. 1977. Births and baptisms: the use of Anglican bap-tism registers as a source of information about numbers ofbirths in England before the beginning of civil registration.Popul Studies 31:281–312.
13INFANT MORTALITY IN MEDIEVAL ENGLAND
American Journal of Physical Anthropology—DOI 10.1002/ajpa