Brain mass estimation by head circumference and body mass methods in neonatal glycaemic modelling...
8
Please cite this article in press as: C.A. Gunn, et al., Brain mass estimation by head circumference and body mass methods in neonatal glycaemic modelling and control, Comput. Methods Programs Biomed. (2014), http://dx.doi.org/10.1016/j.cmpb.2014.03.006 ARTICLE IN PRESS COMM-3781; No. of Pages 8 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e x x x ( 2 0 1 4 ) xxx–xxx jo ur nal ho me p ag e: www.intl.elsevierhealt h.com/journals/cmpb Brain mass estimation by head circumference and body mass methods in neonatal glycaemic modelling and control Cameron Allan Gunn ∗ , Jennifer L. Dickson, Christopher G. Pretty, Jane M. Alsweiler, Adrienne Lynn, Geoffrey M. Shaw, J. Geoffrey Chase Department of Mechanical Engineering, University of Canterbury, Private Bag, Christchurch, Canterbury 8140, New Zealand a r t i c l e i n f o Article history: Received 23 August 2013 Received in revised form 5 March 2014 Accepted 17 March 2014 Keywords: Central nervous system Brain mass Preterm infants Glycaemic control Insulin therapy Physiological modelling a b s t r a c t Introduction: Hyperglycaemia is a common complication of stress and prematurity in extremely low-birth-weight infants. Model-based insulin therapy protocols have the abil- ity to safely improve glycaemic control for this group. Estimating non-insulin-mediated brain glucose uptake by the central nervous system in these models is typically done using population-based body weight models, which may not be ideal. Method: A head circumference-based model that separately treats small-for-gestational-age (SGA) and appropriate-for-gestational-age (AGA) infants is compared to a body weight model in a retrospective analysis of 48 patients with a median birth weight of 750 g and median gestational age of 25 weeks. Estimated brain mass, model-based insulin sensitivity (S I ) pro- files, and projected glycaemic control outcomes are investigated. SGA infants (5) are also analyzed as a separate cohort. Results: Across the entire cohort, estimated brain mass deviated by a median 10% between models, with a per-patient median difference in S I of 3.5%. For the SGA group, brain mass deviation was 42%, and per-patient S I deviation 13.7%. In virtual trials, 87–93% of rec- ommended insulin rates were equal or slightly reduced ( < 0.16 mU/h) under the head circumference method, while glycaemic control outcomes showed little change. Conclusion: The results suggest that body weight methods are not as accurate as head cir- cumference methods. Head circumference-based estimates may offer improved modelling accuracy and a small reduction in insulin administration, particularly for SGA infants. © 2014 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Hyperglycaemia, the elevation of blood glucose (BG) concen- tration, is common in extremely preterm infants, typically ∗ Corresponding author. Tel.: +64 3 364 2571. E-mail addresses: [email protected], [email protected] (C.A. Gunn). of 27 weeks gestation or less and is closely correlated with morbidity and mortality [1–3]. Hyperglycaemia in neonates is frequently treated with insulin to lower BG concentra- tions [4]. However, reported insulin protocols have increased the risk of hypoglycaemia in this cohort [5,6], which is http://dx.doi.org/10.1016/j.cmpb.2014.03.006 0169-2607/© 2014 Elsevier Ireland Ltd. All rights reserved.
Transcript of Brain mass estimation by head circumference and body mass methods in neonatal glycaemic modelling...

C
Bbm
CJDZ
a
A
R
R
5
A
K
C
B
P
G
I
P
1
Ht
h0
ARTICLE IN PRESSOMM-3781; No. of Pages 8
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e x x x ( 2 0 1 4 ) xxx–xxx
jo ur nal ho me p ag e: www.int l .e lsev ierhea l t h.com/ journa ls /cmpb
rain mass estimation by head circumference andody mass methods in neonatal glycaemicodelling and control
ameron Allan Gunn ∗, Jennifer L. Dickson, Christopher G. Pretty,ane M. Alsweiler, Adrienne Lynn, Geoffrey M. Shaw, J. Geoffrey Chaseepartment of Mechanical Engineering, University of Canterbury, Private Bag, Christchurch, Canterbury 8140, Newealand
r t i c l e i n f o
rticle history:
eceived 23 August 2013
eceived in revised form
March 2014
ccepted 17 March 2014
eywords:
entral nervous system
rain mass
reterm infants
lycaemic control
nsulin therapy
hysiological modelling
a b s t r a c t
Introduction: Hyperglycaemia is a common complication of stress and prematurity in
extremely low-birth-weight infants. Model-based insulin therapy protocols have the abil-
ity to safely improve glycaemic control for this group. Estimating non-insulin-mediated
brain glucose uptake by the central nervous system in these models is typically done using
population-based body weight models, which may not be ideal.
Method: A head circumference-based model that separately treats small-for-gestational-age
(SGA) and appropriate-for-gestational-age (AGA) infants is compared to a body weight model
in a retrospective analysis of 48 patients with a median birth weight of 750 g and median
gestational age of 25 weeks. Estimated brain mass, model-based insulin sensitivity (SI) pro-
files, and projected glycaemic control outcomes are investigated. SGA infants (5) are also
analyzed as a separate cohort.
Results: Across the entire cohort, estimated brain mass deviated by a median 10% between
models, with a per-patient median difference in SI of 3.5%. For the SGA group, brain mass
deviation was 42%, and per-patient SI deviation 13.7%. In virtual trials, 87–93% of rec-
ommended insulin rates were equal or slightly reduced (� < 0.16 mU/h) under the head
circumference method, while glycaemic control outcomes showed little change.
Conclusion: The results suggest that body weight methods are not as accurate as head cir-
cumference methods. Head circumference-based estimates may offer improved modelling
accuracy and a small reduction in insulin administration, particularly for SGA infants.
© 2014 Elsevier Ireland Ltd. All rights reserved.
morbidity and mortality [1–3]. Hyperglycaemia in neonates
. IntroductionPlease cite this article in press as: C.A. Gunn, et al., Brain mass estimation bmodelling and control, Comput. Methods Programs Biomed. (2014), http://
yperglycaemia, the elevation of blood glucose (BG) concen-ration, is common in extremely preterm infants, typically
∗ Corresponding author. Tel.: +64 3 364 2571.E-mail addresses: [email protected], cameron.gunn@can
ttp://dx.doi.org/10.1016/j.cmpb.2014.03.006169-2607/© 2014 Elsevier Ireland Ltd. All rights reserved.
of 27 weeks gestation or less and is closely correlated with
y head circumference and body mass methods in neonatal glycaemicdx.doi.org/10.1016/j.cmpb.2014.03.006
terbury.ac.nz (C.A. Gunn).
is frequently treated with insulin to lower BG concentra-tions [4]. However, reported insulin protocols have increasedthe risk of hypoglycaemia in this cohort [5,6], which is

ARTICLE IN PRESSCOMM-3781; No. of Pages 8
s i n
2 c o m p u t e r m e t h o d s a n d p r o g r a massociated with neurological complications [7]. Hypogly-caemia is overrepresented in preterm infants, most severelyin small-for-gestational-age (SGA) infants [8]. STAR (StochasticTARgeted) is a model-based glycaemic control framework forcritically ill patients [9,10]. In the neonatal intensive care unit(NICU) setting, STAR has delivered tight glycaemic control andreduced hypoglycaemia [11]. Its main attribute is a stochasticforecast of possible BG outcomes enabling a quantified levelof risk of hypoglycaemia [12]. Hence, it directly mitigates therisk of inter- and intra-patient variability when using insulin.
STAR utilizes the NICING model [13] to simulate insulintherapy. The NICING model is a pharmacokinetic descriptionof insulin–glucose dynamics in the preterm infant that usesthe same fundamental dynamics as a clinically well-validatedadult model of acute care hyperglcaemia [14–16]. This modelis similar in fundamental dynamics to well-known type-1diabetes models [17,18]. Patients are fit to this model to cre-ate treatment-independent insulin sensitivity profiles, whichserve as the basis for describing patient condition. The glucosecompartment of this model, with parameters given in Table 1,is defined:
G = −pGG(t) − SIG(t)Q(t)
1 + ˛GQ(t)
+ P(t) + EGP × mbody − CNS × mbrain
Vg,frac(t) × mbody(1)
Non-insulin-mediated glucose uptake by the central ner-vous system (CNS) is the rate at which glucose is removed fromthe blood for use in the brain. This rate is relatively constant[19], irrespective of the body’s plasma insulin concentrations[20]. CNS uptake is a required parameter in the NICING model,as [13] notes that in contrast to the adult case, the brain rep-resents a major source of glucose uptake in infants, due totheir larger brain-to-body weight ratio. Hence, given signif-icant variability between preterm infants and no clinicallypractical ability to measure it directly, this parameter shouldbe modelled as accurately as feasibly possible.
In Eq. (1), CNS is weighted by a patient-specific brain massmbrain. Currently, mbrain is calculated as 14% of body mass mbody
[13]:
mbrain = 0.14mbody (2)
This calculation assumes that brain mass is directly pro-portional to body mass (mbody). Eq. (2) is clinically convenient,as it requires only mbody data, which is easily available. How-ever, it may not be accurate. Dobbing and Sands [21] showeda trend between mbody and brain mass, but with notable vari-ance. A more precise measure for estimating brain mass maybe head circumference (HC) [22].
Improving the estimation of the patient-specific CNS termin the NICING model is projected to have three potential ben-efits for patients and clinicians:
Please cite this article in press as: C.A. Gunn, et al., Brain mass estimation bmodelling and control, Comput. Methods Programs Biomed. (2014), http://
(1) It may improve glycaemic control and outcomes ofpatients;
(2) It will improve the physiological accuracy of the model;and
b i o m e d i c i n e x x x ( 2 0 1 4 ) xxx–xxx
(3) It will provide a method of brain mass estimation that isbetter justified by the existing literature.
Thus, this work serves as a feasibility study as to whethergrowth metrics, such as head circumference [22], which arealso readily measured in infants, should be used in model-based glycaemic control methods to better account for andmanage the inter-patient variability that can make control dif-ficult for preterm infants [11,23]. Ultimately, improvements inglycaemic control that may come by this investigation couldreduce the incidence of hyper- and hypo-glycaemia in thisfragile cohort.
This work attempts to mitigate a limitation of STAR’smodel-based stochastic forecasting technique by improvingphysiological parameter estimation. Methods are not onlylimited by parameter estimation and modelling constraints,but also on the quality of the stochastic forecasting. A keycomponent of improving stochastic models is understandinginter-patient variability [24]. Accounting for head circumfer-ence in the physiological model can reduce variability instochastic modelling and forecasting.
2. Methods
2.1. Values for brain mass
Eq. (2) is estimated using data from Ho et al. [25]. This paperreports the mean and standard deviation body and brain massfor a range of preterm infants, divided into sub-cohorts by sexand ethnicity. Ethnicity was defined by ‘black’ or ‘white’, withno further detail provided.
The ratio of these group means was taken for blackfemale and black male cohorts, which had the lowest meangestational ages (mean GA = 27.3 weeks and 28.4 weeks,respectively), and then averaged to give mbrain = 0.140mbody.White cohorts were neglected due to the larger mean bodymass (1367 g for the white cohort versus 1058 g for the blackcohort) and greater gestational age (30.0 weeks versus 27.9weeks), which do not reflect the weight of infants who typi-cally require glycaemic control [5,11]. If the same method wasapplied to the white cohort, it would give mbrain = 0.131mbody,and if the entire cohort was used, then mbrain = 0.136mbody. Thecalculated ratio for each cohort is summarized in Table 2.
While Eq. (2) captures a ratio that may be applicable to apatient around the median mass of 1055 g, it assumes a linearrelationship with no offset between mbrain and mbody, whichis not realistic far from this value. Because the cohort thismethod will be applied to is typically much smaller than 1055 g[11], the errors from this assumption will be amplified. Finally,the apparent choice of ethnic cohort may not best reflect thepopulation of patients in New Zealand, where patients are pre-dominantly of New Zealand European, Maori, Pacific Island,and Asian descent.
2.2. Head circumference and brain mass
y head circumference and body mass methods in neonatal glycaemicdx.doi.org/10.1016/j.cmpb.2014.03.006
A model relating HC to brain mass from Cooke et al. [22] iscompared to the original NICING assumption that brain massis 14% of mbody, based on Ho et al. [25] and in Eq. (2).

ARTICLE IN PRESSCOMM-3781; No. of Pages 8
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e x x x ( 2 0 1 4 ) xxx–xxx 3
Table 1 – Parameters and variables in Eq. (1) of the NICING model.
Variable Description Value
G(t) BG concentration mg/dLpG Non-insulin-mediated endogenous glucose clearance 0.0030/minSI Insulin sensitivity L/mU/minQ(t) Interstitial insulin concentration mU/L˛G Saturation parameter for insulin mediated glucose removal 0 L/mUP(t) Total glucose appearance in plasma from enteral and parenteral sources mg/minEGP Endogenous glucose production 5.112 mg/minmbody Body mass kgCNS Central nervous system glucose uptake 15.84 mg/minmbrain Brain mass kgVg,frac Plasma glucose distribution volume 0.5961 L/kg
Table 2 – Mean statistics on body and brain mass from Ho et al. [25].
Cohort Gestational age (weeks) mbody (g) mbrain (g) mbrain/mbody (g/g)
Black female 27.3 958 139 0.145
biSufSgam
m
wia
auttsamcarwppo
patients [29] using the NICING model. Finally, glycaemic con-trol outcomes were simulated in clinically validated virtualtrials [29], to assess the effect on glycaemia and interventions.
Black male 28.4
White female 29.2
White male 30.4
Cooke et al. [22] provide a relationship between HC andrain mass following a post-mortem study of 485 premature
nfants with gestational ages (GA) between 18 and 43 weeks.mall-for-gestational-age (SGA) infants are accounted forsing a different parameter set to those that were appropriate-
or-gestational-age (AGA). This separation was the result ofGA infants having a statistically higher brain mass for theirestational age than AGA infants [22]. Such a distinction maylso be necessary in the relationship between mbody and brainass, which has not been investigated using the mbody model.The HC model from Cooke et al. [22] is defined:
brain = Cb × k (3)
here C is the head circumference in centimetres and mbrain
s the brain mass in grams. The remaining parameters givenre in Table 3.
Head circumference and weight data for this feasibilitynalysis are taken from the HINT trial of 88 preterm infantsndergoing tight glycaemic control, for which the popula-ion is described in [6]. Of this cohort, patients were includedhat had episodes of insulin therapy with five or more con-ecutive BG measurements that were recorded less than 8 hpart. Inclusion also required a head circumference measure-ent during, or 24 h before the start of the episode. These
riteria were necessary to fit patients to the NICING model,nd to compare brain mass estimates. Multiple episodes wereecorded per patient where applicable. A total of 48 patientsere selected, totalling 82 episodes. None of the mothers of
Please cite this article in press as: C.A. Gunn, et al., Brain mass estimation bmodelling and control, Comput. Methods Programs Biomed. (2014), http://
atients in the study experienced maternal diabetes. 17 of 48atients experienced intraventricular haemorrhage (IVH), allf whom were AGA infants. IVH was rated on a scale of 1–5
Table 3 – Parameters in HC model [22].
Cohort b k
Appropriate-for-gestational-age 3.001 0.0093Small-for-gestational-age 3.225 0.0048
1151 157 0.1361258 165 0.1311434 190 0.132
in order of increasing severity; the 17 patients had a median[IQR] IVH score of 2 [1–3.5]. Table 4 has demographic data fromthe overall cohort with further details in [6].
The SGA cohort is investigated in greater detail in eachanalysis to discern the effect of separating this group in esti-mation, and whether they may be more at-risk. Of the entirecohort, 5 of 48 patients were SGA, corresponding to 7 of 82patient episodes. SGA infants were defined as patients at orbelow the 10th percentile of weight for their GA using growthcharts from New South Wales, Australia [26] that have beenused in New Zealand hospitals. 4 of the 5 SGA patients wereasymmetric SGA, as determined by the Ponderal index [27].Due to the small SGA cohort, asymmetric and symmetricpatients are not analyzed separately.
2.3. Analyses
First, changes in the estimated value of mbrain were inves-tigated. For each head circumference measurement, patientbrain mass is estimated using both models of Eqs. (2) and (3).
Next, changes in glycaemic control were analyzed usingclinically validated virtual patients [11,28]. In particular, bothmodels for estimating brain mass were compared by fittingdata to create virtual patients. Patients were fit for treatment-independent insulin sensitivity profiles (SI) to create virtual
y head circumference and body mass methods in neonatal glycaemicdx.doi.org/10.1016/j.cmpb.2014.03.006
Table 4 – Median [IQR] cohort demographics.
Birth weight (g) 750 [678–894]GA at birth (weeks) 25.0 [24.0–26.5]Age at start of trial (days) 4 [2–7]Ethnicity (%)
NZ European 28Maori 35Pacific Islander 6Asian 10

ARTICLE IN PRESSCOMM-3781; No. of Pages 8
4 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e x x x ( 2 0 1 4 ) xxx–xxx
Table 5 – Combinations of assumed model and controller-perceived model used in virtual trials.
SI profile in control
HC-fit control mbody-fit control
SI profile insimulation
HC-fit virtual profile A.Assume HC gives the bestestimate, and control with it.
B.Assume HC gives the bestestimate, but control with mbody.
mbod
e, bu
mbody-fit virtual profile C.Assumeestimat
Because it is not known which of the two brain massestimation methods is most accurate or useful in control, SI
profiles from both are used to create virtual patients. Bothmodels are also tested within the model-based control. Hence,four combinations are tested, shown in Table 5. Cases B and Cin Table 5 give estimates of the worst-case effects of estimationwhere model-based control and physiology are mismatched,in relation to A and D respectively.
Control simulations used the STAR controller defined in[30], with four-hourly insulin interventions. Insulin infusionsare given through an IV pump, with a minimum rate of0.1 mL/h and step size of 0.01 U/kg/h.
Nonparametric statistics were used in this analysis. Dis-tributed data are compared using the Wilcoxon rank-sum(Mann–Whitney U test). Values of p < 0.05 are considered sta-tistically significant.
3. Results
3.1. Model comparison
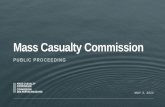
Estimations of brain mass from the mbody model, f(mbody), basedon body weight, and the HC model, f(HC), based on head cir-cumference are compared in a Bland–Altman plot in Fig. 1.The figure shows a bias towards the mbody model estimating
Please cite this article in press as: C.A. Gunn, et al., Brain mass estimation bmodelling and control, Comput. Methods Programs Biomed. (2014), http://
a significantly lower value for mbrain (p < 0.005). The mediandifference (f(mbody) − f(HC)) was −11.4 g, with an inter-quartilerange (IQR) of (−22.3, 0.8) g. The median brain mass estimatedfor the mbody model was 110 g, and was 121 g for the HC model.
80 10 0 12 0 1 -100
-50
0
50
Average br
m(f( ecnereffiD
niar
b)g( ssa
m niarb ni ))C
H(f – )
Compa ring brain mass es
Fig. 1 – Comparison of mbody and HC estimation
y gives the bestt control with HC.
D.Assume mbody gives the bestestimate, and control with it.
Hence, the HC model predicts a median increase in the brainmass of approximately 10%.
SGA infants are discriminated in Fig. 1. These patientsare clearly biased, with a median difference of −40 g (42%),and inter-quartile range of (−49, −33) g (p � 0.001). This resultshows that the distinction between AGA and SGA infants thatCooke et al. [22] required for their HC model may also be nec-essary when using a body mass estimate, this highlightingdifficulty with Eq. (2).
Two infants in Fig. 1 with average estimated brain massgreater than 150 g had a bias of over 80 g. This result sug-gests a further, nonlinear deviation between the two models atgreater brain mass. However, the scarcity of data in this regionis a reflection of the typical cohort and, as such, only a verysmall minority of patients undergoing insulin therapy mightbe expected to exist in this region.
Fig. 2 classifies the points in Fig. 1 by the GA percentilebands. In general, infants in the lower GA percentiles, who arethus low weight for their GA, were underestimated by the mbody
model, and those with higher percentiles were overestimated.This result indicates that the body weight and head circum-ference methods represent significantly different measures ofbrain mass.
3.2. Effect on model-based insulin sensitivity
y head circumference and body mass methods in neonatal glycaemicdx.doi.org/10.1016/j.cmpb.2014.03.006
Patients are fit to the NICING model to generate SI profiles forvirtual patients using both methods of brain estimation. Theresulting SI profiles identified are summarized in Table 6.
40 16 0 18 0 20 0
ain mass (g)
timation (Bland– Altman plot)
SGA
AGA
s for brain mass, highlighting SGA infants.

ARTICLE IN PRESSCOMM-3781; No. of Pages 8
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e x x x ( 2 0 1 4 ) xxx–xxx 5
80 10 0 12 0 14 0 16 0 18 0 20 0-100
-50
0
50
Average brain mass (g)
m(f( ecnereff iD
yd
ob
)g ( ssam niar b ni ) )
CH(f –
Compa ring brain mass estimation (Bland– Altman plot)
<5th
5th--10 th10th--25th
25th--50th
50th--75th
75th--90th90th-95th
>95th
Fig. 2 – Comparison of mbody and HC estimations for brain m
Table 6 – Deviations in SI profiles under different models.
Entire cohort SGA only
SI with mbody model (Med[IQR]) (mL/mU/min)
1.09 [0.70–1.49] 0.82 [0.66–1.35]
SI with HC model (Med 1.08 [0.68–1.43] 0.75 [0.59–1.22]
w[(bm
[[wrtbId
caf[g
all simulations, indicating another underlying reason for dif-
[IQR]) (mL/mU/min)Per-patient % �SI (Med) 3.5 13.7
The median [IQR] SI for the cohort fit by the mbody modelas 1.09 [0.70–1.49] mL/mU/min, and for the HC model, 1.08
0.68–1.43] mL/mU/min. Per patient, the median change in SI
f(mbody) − f(HC)) was 3.5% (p = 0.0048). This result shows a smallut significant reduction in model-based SI under the Cookeodel using HC.For the SGA group, mbody-fit SI was 0.82
0.66–1.35] mL/mU/min while HC-fit SI was 0.750.59–1.22] mL/mU/min. Per-patient median change in SI
as much greater for this group at 13.7% (p = 0.0015). Theesults for this cohort are much more significant than forhe wider cohort, indicating that this particular group maye particularly poorly modelled by the current mbody model.n particular, significantly different SI may yield significantlyifferent insulin interventions in model-based control.
Despite changes in the absolute values of SI, both the fullohort and the SGA subgroup displayed relatively similar IQRscross the two models. Variability is a much more important
Please cite this article in press as: C.A. Gunn, et al., Brain mass estimation bmodelling and control, Comput. Methods Programs Biomed. (2014), http://
actor in glycaemic control and forecasting than absolute SI
12,23,31], particularly for safety from hypoglycaemia. Hence,lycaemic control outcomes for SGA patients may not be
Table 7 – Control interventions and outcomes from virtual trials
Whole cohort statistics A.Simulate HCControl HC
SimCon
Median insulin rate [IQR] (U/kg/h) 0.042[0.030–0.061]
0[
% BG within 4.0–8.0 mmol/L 68.92 6% BG > 10 mmol/L 7.89 8% BG < 4.0 mmol/L 1.50 1% BG < 2.6 mmol/L 0.17 0
ass at different expected weight percentile bands [26].
compromised by this discrepancy if, despite differing valuesof median SI, profiles are only shifted, rather than alteredwith changed variability.
3.3. Effect on control
Results for virtual trials across the entire cohort are shownin Table 7. The 82 episodes simulated constituted 7032 h ofcare, with 1881 BG measurements (mean 3.7 h/intervention).Electing to use HC in control instead of body mass could poten-tially decrease insulin interventions by as much as a medianof 0.03 U/kg/h or 7.1% (compare A–B or C–D in Table 7). BG out-comes are not significantly altered, with a negligible changeto the time in band (% of BG measurements 4.0–8.0 mmol/L)and hypoglycaemia (% of BG measurements < 2.6 mmol/L). Forboth simulation SI profiles, controlling with HC gave a smalldecrease in excessive hyperglycaemia (% BG > 10 mmol/L).
Control is also assessed for patients for the SGA cohort only.Results from just these virtual trials are shown in Table 8. Timein band is marginally improved by controlling using the HCmodel. This simulation of 7 patient episodes was 622 h, with166 BG measurements (9% of total hours).
The same trend for insulin interventions and glycaemicoutcomes are seen in the SGA cohort simulation. However,the time in band for this group is significantly lower across
y head circumference and body mass methods in neonatal glycaemicdx.doi.org/10.1016/j.cmpb.2014.03.006
ficulty in control. It is worth noting that SGA infant data (N = 7),contributing only 9% of total hours, is reasonably sparse andhighly influenced by outlying patients.
for entire cohort.
B.ulate HCtrol mbody
C.Simulate mbody
Control HC
D.Simulate mbodyControl mbody
.0450.032–0.062]
0.040[0.030–0.061]
0.042[0.030–0.061]
8.41 69.58 68.92.49 6.94 7.72.48 1.66 1.52.17 0.18 0.16

ARTICLE IN PRESSCOMM-3781; No. of Pages 8
6 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e x x x ( 2 0 1 4 ) xxx–xxx
Table 8 – Control interventions and outcomes from virtual trials for SGA infants.
Whole cohort statistics A.Simulate HC
Control HC
B.Simulate HCControl mbody
C.Simulate mbody
Control HC
D.Simulate mbodyControl mbody
Median insulin rate [IQR] (U/kg/h) 0.046[0.036–0.075]
0.051[0.039–0.085]
0.041[0.033–0.064]
0.046[0.037–0.073]
% BG within 4.0–8.0 mmol/L 62.96 61.84 64.07 62.80202.0.
% BG > 10 mmol/L 17.97
% BG < 4.0 mmol/L 2.70
% BG < 2.6 mmol/L 0.16
The matched difference in insulin interventions betweenCases A–B and A–D are shown in Fig. 3 and summarized inTable 9. Comparing A–B shows the difference between dosesfor either controller method, assuming that the HC model isa true in simulation, while using HC (Case A) or mbody (CaseB) in model-based control. Comparing A–D shows the differ-ence between best-case model selections, with no mismatch
Please cite this article in press as: C.A. Gunn, et al., Brain mass estimation bmodelling and control, Comput. Methods Programs Biomed. (2014), http://
between virtual patient and controller model. For both com-parisons, Case A is most likely to give the equal or slightly lessinsulin (87–93% of doses across comparisons and sub-cohorts).
0 0.5 1 1.5 0
0.5
1
1.5
2
2.5
3
3.5
Case A: Sim H
m lortnoC ,
CH
miS :
B esaC
yd
ob
Insuli n intervention comparison betwe
0 0.5 1 1.5 0
0.5
1
1.5
2
2.5
3
3.5
Case A: Sim H
m mi
S :D esa
Cy
do
b m lortno
C ,y
do
b
Insuli n intervention comparison betwe
Fig. 3 – Changes in insulin interventions be
.19 13.35 17.6538 3.18 2.7016 0.32 0.16
This result shows that changes in interventions are small, andthat the majority of these changes reduce insulin and there-fore associated risk. Less than 1% of interventions would beincreased by more than 0.16 U/h, the standard step increasein insulin between STAR interventions.
y head circumference and body mass methods in neonatal glycaemicdx.doi.org/10.1016/j.cmpb.2014.03.006
4. Discussion
Across the entire cohort, parameter changes in SI were negligi-ble. However, for SGA infants, mbrain fit under the HC model was
2 2.5 3 3.5C, Control HC
en mbrain
estimates (Cases A–B)
2 2.5 3 3.5C, Control HC
en mbrain
estimates (Cases A–D)
AGASGA
AGASGA
tween Cases A–B (top) and Cases A–D.

ARTICLE IN PRESSCOMM-3781; No. of Pages 8
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e x x x ( 2 0 1 4 ) xxx–xxx 7
Table 9 – Changes in insulin dosing comparing Cases A–B and A–D.
Cohort Percent change in insulin rates by using Case A (%)
Largedecrease
(by > 0.16 U/h)
Decreasewithin
0.00–0.16 U/h
Equal Increasewithin
0.00–0.16 U/h
Largeincrease
(by > 0.16 U/h)
A–B AGA 3.4 37.0 50.8 7.9 0.9SGA 7.5 64.2 24.9 2.9 0.6
16.134.7
nTotmawu
mwHswo
hfdSccuaeoi
rgmHriia
mtmopaa
itwa
A–D AGA 1.7
SGA 0.0
otably larger, and the resulting SI profiles fit were reduced.his indicates that insulin has less effect in BG changesbserved, assuming this model. Hence, there is an indicationhat any discrepancies in between the two methods of esti-
ation are exacerbated in SGA infants. This result may bettributed to the median mass of 1055 g of the cohort fromhich Eq. (2) was derived [25], versus the median mass of 750 gsed here and 760 g in Le Compte et al. [11].
Control performance negligibly improved by using the HCodel for control decisions. This result was independent ofhich model was used in simulation. However, the using theC model resulted in less insulin being recommended for theame glycaemic outcomes. Such a result indicates that insulinas used more effectively, and potentially improves the safetyf care by reducing the risks associated with insulin intake.
It is worth noting that the data acquired from the HINT trialas some longer periods between interventions than those
or which NICING was designed. This difference may haveegraded some of the virtual trials by reducing some potential
I variability [12]. However, in each case, these virtual trials areomparing the patients and cohort as their own control. Headircumference data has not yet been analyzed for patientsndergoing STAR at Christchurch Women’s Hospital NICU, orny other cohort with more frequent BG measurement, whichliminated other sources of clinical data. Other than frequencyf measurement, data from the HINT trial contains sufficient
nformation that is of practical use in glycaemic modelling.The introduction of the Cooke method using HC would
equire an additional input for clinical staff when startinglycaemic control. Additional complexity to clinical protocolsay increase clinical burden and potential for error [32,33].owever, HC is routinely measured, and thus should not
equire any additional effort at the point of care. Furthermore,f for computer-based protocols this input was left as optionaln a graphical user interface (e.g. “Head circumference (if avail-ble):”), it would minimize clinical burden when inconvenient.
As the comparative accuracy of both the HC and body massodels is not known it would be beneficial to have an objec-
ive study compare the two models against a more accurateethod. For example, both could be compared to PET scans
f patients, using approaches such as in [34], which wouldrovide a significantly better estimate, although is impracticalt the bedside. HC and body mass methods could be comparedgainst this baseline metric.
The discrepancies observed between SGA and AGA infants
Please cite this article in press as: C.A. Gunn, et al., Brain mass estimation bmodelling and control, Comput. Methods Programs Biomed. (2014), http://
s of interest, however, more data on SGA infants is necessaryo claim robust conclusions. In particular, this investigationas not able to distinguish differences in symmetric and
symmetric SGA infants due to lack of data. As SGA infants are
74.1 7.1 0.9 57.8 7.5 0.0
the most affected by model choice, this distinction may be ofclinical use. Future research should investigate these cohortsin greater detail. Additionally, further variables of interestcould be investigated. These variables could include placen-tal insufficiency, maternal anti-hyperintensive therapy, andenteral/parenteral, protein, calorie and lipid intake. Finally,as noted in Section 1, this feasibility study indicates that thevariables studied can improve the model accuracy and thuscontrol quality, and the study of these further variables basedon this outcome is therefore more strongly supported by theoutcomes presented here.
Although the HC model is much more likely to be physio-logically accurate both due to the nature of the measurement[21] and because the method is derived from a cohort of thesame demographics it will be used on, it may not neces-sarily affect clinical outcomes. However, the authors suggestthat it should be used in preference to body mass-basedestimates for neonatal glycaemic modelling, particularly forSGA infants. The similarity in glycaemic control outcomesdemonstrates the robustness of the model-based stochasticforecasting approach for glycaemic control that STAR utilizes.
5. Conclusions
An alternative model for estimating brain mass using headcircumference in preterm infants has been investigated. Thismodel is likely to have greater physiological accuracy thanprevious and better reflects the demographics of the cohortof patients that typically require glycaemic control. Cohort-wide, changes in brain mass were significant, but changes inresulting insulin sensitivity profiles were negligible. The SGAsubgroup was estimated to have a median brain mass dif-ference of 40 g, reducing median insulin sensitivity by 13.7%.These results were statistically significant. Simulated gly-caemic control under the STAR protocol suggested that 87–93%of insulin interventions would be the same or slightly reduced(within 0.16 U/h), for similar glycaemic outcomes. Further,prospective research with larger cohorts is necessary to fullyunderstand the implications of the discussed modelling differ-ences. Due to the improved physiological accuracy and mildlyreduced insulin intake, there are preliminary indications thathead circumference-based models for glycaemic modellingand model-based control may be preferable, particularly forSGA infants.
y head circumference and body mass methods in neonatal glycaemicdx.doi.org/10.1016/j.cmpb.2014.03.006
Conflicts of interest
The authors have no conflicts of interest to declare.

ARTICLE IN PRESSCOMM-3781; No. of Pages 8
s i n
r
8 c o m p u t e r m e t h o d s a n d p r o g r a m
e f e r e n c e s
[1] D.I. Alaedeen, M.C. Walsh, W.J. Chwals, Total parenteralnutrition-associated hyperglycemia correlates withprolonged mechanical ventilation and hospital stay in septicinfants, J. Pediatr. Surg. 41 (1) (2006) 239–244 (discussion239-44).
[2] K. Beardsall, et al., Prevalence and determinants ofhyperglycemia in very low birth weight infants: cohortanalyses of the NIRTURE study, J. Pediatr. 157 (5) (2010)715–719, e1–e3.
[3] S. Hays, E. Smith, A. Sunehag, Hyperglycemia is a risk factorfor early death and morbidity in extremely low birth-weightinfants, Pediatrics 118 (5) (2006) 1811–1818.
[4] J.M. Alsweiler, C.A. Kuschel, F.H. Bloomfield, Survey of themanagement of neonatal hyperglycaemia in Australasia, J.Paediatr. Child Health 43 (9) (2007) 632–635.
[5] K. Beardsall, et al., Early insulin therapy invery-low-birth-weight infants, N. Engl. J. Med. 359 (18) (2008)1873–1884.
[6] J.M. Alsweiler, J.E. Harding, F.H. Bloomfield, Tight glycemiccontrol with insulin in hyperglycemic preterm babies: arandomized controlled trial, Pediatrics 129 (4) (2012) 639–647.
[7] A. Lucas, R. Morley, T.J. Cole, Adverse neurodevelopmentaloutcome of moderate neonatal hypoglycaemia, Br. Med. J.297 (6659) (1988) 1304–1308.
[8] L.O. Lubchenco, H. Bard, Incidence of hypoglycemia innewborn infants classified by birth weight and gestationalage, Pediatrics 47 (5) (1971) 831–838.
[9] L. Fisk, et al., STAR development and protocol comparison,IEEE Trans. Biomed. Eng. PP (99) (2012) 1.
[10] A. Evans, et al., Pilot proof of concept clinical trials ofStochastic Targeted (STAR) glycemic control, Ann. IntensiveCare 1 (1) (2011) 38.
[11] A.J. Le Compte, et al., Pilot study of a model-based approachto blood glucose control in very-low-birthweight neonates,BMC Pediatr. 12 (1) (2012) 117.
[12] A.J. Le Compte, et al., Blood glucose prediction usingstochastic modeling in neonatal intensive care, IEEE Trans.Biomed. Eng. 57 (3) (2010) 509–518.
[13] A. Le Compte, et al., Modeling the glucose regulatory systemin extreme preterm infants, Comput. Methods ProgramsBiomed. 102 (3) (2011) 253–266.
[14] A.J. Le Compte, et al., Impact of variation in patient responseon model-based control of glycaemia in critically ill patients,Comput. Methods Programs Biomed. 109 (2) (2013) 211–219.
[15] S. Penning, et al., First pilot trial of the STAR-Liege protocolfor tight glycemic control in critically ill patients, Comput.Methods Programs Biomed. 108 (2) (2012) 844–859.
[16] C. Pretty, et al., Impact of sensor and measurement timingerrors on model-based insulin sensitivity, Comput. Methods
Please cite this article in press as: C.A. Gunn, et al., Brain mass estimation bmodelling and control, Comput. Methods Programs Biomed. (2014), http://
Programs Biomed. (2013),http://dx.doi.org/10.1016/j.cmpb.2013.08.007 (in press).
[17] P. Colmegna, R. Sánchez Pena, Analysis of three T1DMsimulation models for evaluating robust closed-loop
b i o m e d i c i n e x x x ( 2 0 1 4 ) xxx–xxx
controllers, Comput. Methods Programs Biomed. 113 (1)(2014) 371–382.
[18] Z. Wu, et al., Glucose–insulin regulation model withsubcutaneous insulin injection and evaluation usingdiabetic inpatients data, Comput. Methods ProgramsBiomed. 111 (2) (2013) 347–356.
[19] R. Gruetter, K. Ugurbil, E.R. Seaquist, Steady-state cerebralglucose concentrations and transport in the human brain, J.Neurochem. 70 (1) (1998) 397–408.
[20] R.M. Cowett, H.M. Farrag, Selected principles ofperinatal-neonatal glucose metabolism, Semin. Neonatol. 9(1) (2004) 37–47.
[21] J. Dobbing, J. Sands, Quantitative growth and developmentof human brain, Arch. Dis. Child. 48 (10) (1973) 757–767.
[22] R. Cooke, et al., Head circumference as an index of brainweight in the fetus and newborn, Early Hum. Dev. 1 (2) (1977)145–149.
[23] J.G. Chase, et al., Tight glycemic control in critical care – theleading role of insulin sensitivity and patient variability: areview and model-based analysis, Comput. MethodsPrograms Biomed. 102 (2) (2011) 156–171.
[24] R.P. Floyd, et al., External validation and sub-cohort analysisof stochastic forecasting models in NICU cohorts, 2012.
[25] K.C. Ho, et al., Newborn brain weight in relation to maturity:sex, and race, Ann. Neurol. 10 (3) (1981)243–246.
[26] P.J. Beeby, T. Bhutap, L.K. Taylor, New South Walespopulation-based birthweight percentile charts, J. Paediatr.Child Health 32 (6) (1996) 512–518.
[27] T. Vik, et al., Prenatal growth in symmetric and asymmetricsmall-for-gestational-age infants, Early Hum. Dev. 48 (1-2)(1997) 167–176.
[28] A.J. Le Compte, et al., Development of blood glucose controlfor extremely premature infants, Comput. MethodsPrograms Biomed. 102 (2) (2011) 181–191.
[29] J.G. Chase, et al., Validation of a model-based virtual trialsmethod for tight glycemic control in intensive care, Biomed.Eng. 9 (2010) 84.
[30] J.L. Dickson, et al., Development and optimisation ofstochastic targeted (STAR) glycaemic control for pre-terminfants in neonatal intensive care, Biomed. Signal Process.Control 8 (2) (2013) 215–221.
[31] J.L. Dickson, et al., External validation and sub-cohortanalysis of stochastic forecasting models in NICU cohorts,Biomed. Signal Process. Control (2013).
[32] J.G. Chase, et al., Impact of human factors on clinicalprotocol performance: a proposed assessment frameworkand case examples, J. Diabetes Sci. Technol. 2 (3) (2008)409–416.
[33] D. Aragon, Evaluation of nursing work effort and perceptionsabout blood glucose testing in tight glycemic control, Am. J.Crit. Care 15 (4) (2006) 370–377.
[34] Z. Rausova, et al., System approach to modeling of liver
y head circumference and body mass methods in neonatal glycaemicdx.doi.org/10.1016/j.cmpb.2014.03.006
glucose metabolism with physiologically interpreted modelparameters outgoing from [18F] FDG concentrationsmeasured by PET, Comput. Methods Programs Biomed. 107(2) (2012) 347–356.