
Brachial plexus blocks: a review of approaches and techniques
13
662 CANADIAN JOURNAL OF ANESTHESIA CAN J ANESTH 54: 8 www.cja-jca.org August, 2007 Purpose: The purpose of this narrative review is to summarize the evidence derived from randomized controlled trials (RCTs) regarding established approaches and techniques for brachial plexus anesthesia. Source: Using the MEDLINE (January 1966 to November 2006) and EMBASE (January 1980 to November 2006) databas- es, key words “brachial plexus”, “nerve blocks”, “interscalene”, “cervical paravertebral”, “suprascapular”, “supraclavicular”, “infraclavicular”, “axillary”, “brachial canal” and “humeral canal” were searched for full text articles pertaining to the evaluation of recognized approaches and techniques for brachial plexus anesthesia. The search was limited to RCTs involving human subjects and published in the English language. Seventy-six RCTs were identified. Principal findings: Many of the published studies were under- powered and contained various methodological limitations. We found that, for shoulder and proximal humeral surgery, interscalene and cervical paravertebral approaches to the brachial plexus appear to provide equally effective surgical anesthesia. Intersternocleidomastoid supraclavicular blocks are not associated with improved postoperative analgesia despite eliciting more complete anesthesia of the brachial plexus. For surgery at or below the elbow, an infraclavicular block may result in decreased performance time and block-related pain while providing similar efficacy compared to (multiple-stimula- tion) axillary and brachial canal approaches. With respect to technique, it is unclear if nerve stimulation provides a more effective interscalene block than elicitation of paresthesiae. For supraclavicular blocks, nerve stimulation with a minimal thresh- old of 0.9 mA is recommended, whereas a double-stimulation technique is optimal for infraclavicular blocks. For the axillary approach, a triple-stimulation technique, involving injections of the musculocutaneous, median and radial nerves, is the most effective option. Conclusions: Published reports of RCTs provide evidence to formulate limited recommendations regarding optimal approaches and techniques for brachial plexus anesthesia. Further well-designed and meticulously executed RCTs are warranted, particularly in light of new techniques involving ultrasound or combining neurostimulation and echoguidance. CAN J ANESTH 2007 / 54: 8 / pp 662–674 Objectif : L’objectif de ce compte-rendu narratif est de résumer les données probantes dérivées des études randomisées con- trôlées (RCT) quant aux approches et techniques reconnues pour l’anesthésie du plexus brachial. Source : A l’aide des bases de données MEDLINE (janvier 1966 à novembre 2006) et EMBASE (janvier 1980 à novembre 2006), les mots clés « brachial plexus », « nerve blocks », « interscalene », « cervical paravertebral », « suprascapular », « supraclavicular », « infraclavicular », « axillary », « brachial canal » et « humeral canal » ont été utilisés pour sélectionner les articles intégraux dont le sujet était l’évaluation des approches et techniques reconnues pour le bloc du plexus brachial. La recherche a été limitée aux RCT portant sur des sujets humains et publiées en anglais. Soixante- seize RCT ont été identifiées. Constatations principales : Nombre d’études publiées man- quaient de puissance et comportaient diverses limitations méthodologiques. Nous avons découvert que dans les cas de chirurgies de l’épaule et de l’humérus proximal, les approches interscalénique et cervicale paravertébrale au plexus brachial semblent offrir une anesthésie chirurgicale d’efficacité semblable. Les blocs supra-claviculaires intersternocléidomastoïdiens ne sont pas associés à une meilleure analgésie postopératoire malgré le fait qu’ils permettent une anesthésie plus complète du plexus 662 CAN J ANESTH 54: 8 www.cja-jca.org August, 2007 Review Articles/Brief Reviews Brachial plexus blocks: a review of approaches and techniques [Les blocs du plexus brachial : compte-rendu des approches et techniques] Quang Hieu De Tran MD FRCPC, Antonio Clemente MD, Julian Doan MD, Roderick J. Finlayson MD FRCPC From the Department of Anesthesia, Montreal General Hospital, McGill University, Montreal, Quebec, Canada. Address correspondence to: Dr. De QH Tran, Montreal General Hospital, Department of Anesthesia, 1650 Ave Cedar, D10-144, Montreal, Quebec H3G 1A4, Canada. Phone: 514-934-1934, ext. 43261; Fax: 514-934-4289; E-mail: [email protected] Competing interests: There were no direct funding sources associated with the preparation of this manuscript. Accepted for publication March 23, 2007. Revision accepted April 19, 2007. Final revision accepted May 8, 2007.
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Brachial plexus blocks: a review of approaches and techniques
662 CANADIAN JOURNAL OF ANESTHESIA
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
Purpose: The purpose of this narrative review is to summarize the evidence derived from randomized controlled trials (RCTs) regarding established approaches and techniques for brachial plexus anesthesia.
Source: Using the MEDLINE (January 1966 to November 2006) and EMBASE (January 1980 to November 2006) databas-es, key words “brachial plexus”, “nerve blocks”, “interscalene”, “cervical paravertebral”, “suprascapular”, “supraclavicular”, “infraclavicular”, “axillary”, “brachial canal” and “humeral canal” were searched for full text articles pertaining to the evaluation of recognized approaches and techniques for brachial plexus anesthesia. The search was limited to RCTs involving human subjects and published in the English language. Seventy-six RCTs were identified.
Principal findings: Many of the published studies were under-powered and contained various methodological limitations. We found that, for shoulder and proximal humeral surgery, interscalene and cervical paravertebral approaches to the brachial plexus appear to provide equally effective surgical anesthesia. Intersternocleidomastoid supraclavicular blocks are not associated with improved postoperative analgesia despite eliciting more complete anesthesia of the brachial plexus. For surgery at or below the elbow, an infraclavicular block may result in decreased performance time and block-related pain while providing similar efficacy compared to (multiple-stimula-tion) axillary and brachial canal approaches. With respect to technique, it is unclear if nerve stimulation provides a more effective interscalene block than elicitation of paresthesiae. For supraclavicular blocks, nerve stimulation with a minimal thresh-old of 0.9 mA is recommended, whereas a double-stimulation technique is optimal for infraclavicular blocks. For the axillary approach, a triple-stimulation technique, involving injections of the musculocutaneous, median and radial nerves, is the most effective option.
Conclusions: Published reports of RCTs provide evidence to formulate limited recommendations regarding optimal approaches and techniques for brachial plexus anesthesia. Further well-designed and meticulously executed RCTs are warranted, particularly in light of new techniques involving ultrasound or combining neurostimulation and echoguidance.
CAN J ANESTH 2007 / 54: 8 / pp 662–674
Objectif : L’objectif de ce compte-rendu narratif est de résumer les données probantes dérivées des études randomisées con-trôlées (RCT) quant aux approches et techniques reconnues pour l’anesthésie du plexus brachial.
Source : A l’aide des bases de données MEDLINE (janvier 1966 à novembre 2006) et EMBASE (janvier 1980 à novembre 2006), les mots clés « brachial plexus », « nerve blocks », « interscalene », « cervical paravertebral », « suprascapular », « supraclavicular », « infraclavicular », « axillary », « brachial canal » et « humeral canal » ont été utilisés pour sélectionner les articles intégraux dont le sujet était l’évaluation des approches et techniques reconnues pour le bloc du plexus brachial. La recherche a été limitée aux RCT portant sur des sujets humains et publiées en anglais. Soixante-seize RCT ont été identifiées.
Constatations principales : Nombre d’études publiées man-quaient de puissance et comportaient diverses limitations méthodologiques. Nous avons découvert que dans les cas de chirurgies de l’épaule et de l’humérus proximal, les approches interscalénique et cervicale paravertébrale au plexus brachial semblent offrir une anesthésie chirurgicale d’efficacité semblable. Les blocs supra-claviculaires intersternocléidomastoïdiens ne sont pas associés à une meilleure analgésie postopératoire malgré le fait qu’ils permettent une anesthésie plus complète du plexus
662
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
Review Articles/Brief Reviews
Brachial plexus blocks: a review of approaches and techniques [Les blocs du plexus brachial : compte-rendu des approches et techniques]Quang Hieu De Tran MD FRCPC, Antonio Clemente MD, Julian Doan MD, Roderick J. Finlayson MD FRCPC
From the Department of Anesthesia, Montreal General Hospital, McGill University, Montreal, Quebec, Canada.Address correspondence to: Dr. De QH Tran, Montreal General Hospital, Department of Anesthesia, 1650 Ave Cedar, D10-144,
Montreal, Quebec H3G 1A4, Canada. Phone: 514-934-1934, ext. 43261; Fax: 514-934-4289; E-mail: [email protected] interests: There were no direct funding sources associated with the preparation of this manuscript.
Accepted for publication March 23, 2007.Revision accepted April 19, 2007.Final revision accepted May 8, 2007.

Tran et al.: APPROACHES AND TECHNIQUES FOR BRACHIAL PLEXUS BLOCKS 663
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
brachial. Pour les chirurgies du coude ou inférieures au coude, un bloc infra-claviculaire peut avoir comme résultat une réduction de la durée de performance et une douleur associée au bloc, bien qu’il fournisse une efficacité comparable à des approches axillaires ou du canal brachial (à stimulation multiple). En ce qui concerne la technique employée, nous n’avons pu déterminer si la stimulation nerveuse permettait d’obtenir un bloc interscalénique plus efficace que l’élicitation de paresthésies. Dans le cas des blocs supra-cla-viculaires, la stimulation nerveuse avec un seuil minimal de 0,9 mA est recommandée, alors qu’une technique de stimulation double est optimale pour les blocs infra-claviculaires. Lors d’une approche axillaire, une technique de stimulation triple, qui consiste en des injections au niveau des nerfs musculocutanés, médians et radiaux, est l’option la plus efficace.
Conclusions : Les comptes-rendus publiés de RCT fournissent des données probantes qui ne permettent que de formuler des recom-mandations limitées quant aux approches et techniques optimales pour les blocs du plexus brachial. D’autres RCT bien conçues et exécutées avec soin sont justifiées, plus particulièrement pour les nouvelles techniques impliquant l'échographie ou combinant cette dernière à la neurostimulation.
FOR over a century, brachial plexus anesthesia has been an indispensable tool in the anes-thesiologist’s armamentarium.1 By providing surgical anesthesia and postoperative analge-
sia to the entire upper limb, brachial plexus anesthesia has been intimately linked with advances in ambula-tory orthopedic and plastic surgery. Furthermore, with the recent surge in popularity of echoguided regional techniques, there has been a renewed interest amongst anesthesiologists to perform brachial plexus blocks.2 However, despite this enthusiasm, there are many variances in clinical methods of brachial plexus anesthesia. Accordingly, a literature search of random-ized clinical trials was undertaken to determine the best available approaches and techniques for regional anesthesia of the upper limb. For the purposes of this narrative review, the term “approach” refers to the site where the brachial plexus is accessed (interscalene, cervical paravertebral, supraclavicular, infraclavicular, axillary, humeral canal). The term “technique” refers to the modality (loss of resistance, fascial clicks, trans-arterial injection, paresthesia, neurostimulation, ultra-sound) or endpoints (type of neurostimulation, single or multiple injections) needed to identify and anesthe-tize the brachial plexus for any given approach.
MethodsSearch strategy and selection criteriaThe literature search for this review was conducted in November 2006, using the MEDLINE (January 1966 to November 2006) and EMBASE (January 1980 to November 2006) databases. Key words “brachial plexus” and “nerve blocks” were searched and com-bined with the term “and”. Key words “interscalene”, “cervical paravertebral”, “suprascapular”, “supracla-vicular”, “infraclavicular”, “axillary”, “brachial canal”, “humeral canal” were also queried for additional full text articles. Furthermore, the results were limited to peer-reviewed reports of human studies published in the English language. From this initial search, only randomized controlled trials (RCTs) (level I evidence) comparing different approaches or techniques of brachial plexus block were retained. After selecting the initial articles, the latter’s reference lists, as well as the authors’ personal files, were also checked for additional sources. Seventy-six RCTs were thus identi-fied. All studies containing an appropriately identified randomization process and active control groups were retained. Non-randomized studies, observational case reports and cohort studies were excluded to avoid potential biases introduced by institutional practices. Furthermore, only articles pertaining to approaches and techniques related to brachial plexus anesthesia were retained. Studies dealing with local anesthetic manipulation (thermoalteration, alkalinization, addi-tion of adjuncts, mixing, dose fractionation) and patient-related factors (body or limb position, muscu-lar exercise) exceeded the scope of this review.
ResultsOf the 76 RCTs surveyed (average sample size = 76 subjects), approximately half provided sample size justification and blinded assessment (43 and 57% respectively). Only one study provided data about allocation concealment. Primary endpoints varied greatly: definitions of block success included surgical anesthesia, sensory analgesia (patient cannot feel cold or pinprick), sensory anesthesia (patient cannot feel touch) and motor blockade. Furthermore, the nerve distributions tested were also variable: while some RCTs examined blockade of all brachial plexus end branches, others considered only those directly impli-cated in the surgical site.
THE APPROACHES
Interscalene block (ISB) vs cervical paravertebral block (CPVB) and supraclavicular block (SCB)Although often labelled “posterior interscalene”, the CPVB is very different from the classic ISB: in fact it
Tran et al.: APPROACHES AND TECHNIQUES FOR BRACHIAL PLEXUS BLOCKS 663

664 CANADIAN JOURNAL OF ANESTHESIA
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
is more radicular or paravertebral in nature.3 In one RCT allocating 21 patients to ISB or CPVB, the lat-ter was found to produce a better block of the medial arm, forearm and hand.3 Another RCT, reporting on 80 patients undergoing upper humeral and shoulder surgery, found that both approaches yielded similar surgical success rates (93–95%). The extent, onset and offset of the block were also equivalent. However, compared to CPVB, ISB required a slightly longer performance time (6.2 vs 8.4 min respectively; P < 0.001).4 In 77 patients undergoing shoulder or upper extremity surgery above the elbow, Dewees et al.5 compared ISB to (intersternocleidomastoid) SCB. The latter approach was associated with a higher inci-dence of complete sensorimotor blockade of the radi-al, median, ulnar and musculocutaneous nerves (92 vs 74% respectively; P = 0.038) and a shorter block per-formance time (7.1 ± 2.9 vs 9.6 ± 5.3 minutes respec-tively; P = 0.039). Moreover, there was a decreased incidence of side effects: Horner’s syndrome (16 vs 50% of patients; P = 0.01), recurrent laryngeal nerve paralysis (5 vs 21% of patients; P = 0.049), symptom-atic diaphragmatic paralysis (5 vs 15% of patients; P = 0.05) in the ISB vs SCB groups, respectively. However block duration, patient satisfaction, postoperative pain scores and analgesic requirements were similar with both approaches.
INTERPRETATION
Based on the limited evidence, for shoulder and upper humeral surgery, ISB and CPVB are associated with similar onset and offset times as well as block success rates. The (intersternocleidomastoid) SCB, despite eliciting a better block of the median, radial, ulnar and musculocutaneous nerves, does not alter post-operative pain scores; nonetheless, compared to ISB, SCB may be associated with fewer side effects and a decreased block performance time.
Supraclavicular block vs infraclavicular block (ICB) and axillary block (AXB)Using echoguidance combined with nerve stimula-tion, Arcand et al.6 compared SCB and ICB: in a RCT of 80 patients undergoing surgery of the distal arm, forearm and hand, they found a similar rate of surgi-cal anesthesia without supplementation (80–87%). However the radial nerve needed more frequent supplementation with the ICB (18 vs 0% of patients respectively; P = 0.006). Despite shorter image acqui-sition time with ICB (12 vs 28 sec; P < 0.0001), mean performance times were similar in both groups (4–4.7 min). No differences were noted in terms of tech-nique-related pain and sedation requirements.
Two RCTs have compared SCB and AXB in patients undergoing forearm and hand surgery. In one study (n = 40) comparing paresthesia-guided or transarterial AXB to SCB using nerve stimulation, the proportion of patients not requiring supplementation was not statistically different (80 vs 65% of patients respectively).7 In a second RCT (n = 40), Kapral et al.8 compared echoguided SCB and AXB approaches: they found an identical rate of surgical anesthesia (95%). However the musculocutaneous nerve was adequately blocked for surgery in only 75% of patients with AXB (compared to 100% of patients in the SCB group).
INTERPRETATION
Based on the limited available evidence, SCB produces a similarly successful brachial plexus block compared to ICB or AXB.
Infraclavicular block vs axillary and humeral canal blocks (HCB)Eight RCTs comparing ICB to AXB were identified. Despite differences in infraclavicular surface landmarks and varying definitions of success rate, the findings were remarkably consistent.
In three RCTs (100 adults and 40 children), a single-stimulation ICB reliably produced a higher success rate than a single-stimulation AXB (97–100 vs 80–85%; P ≤ 0.05) possibly due to better blockade of the axillary, radial and musculocutaneous nerves. However both approaches yielded a similar onset and block duration.9–11 In an effort to improve the success rate of the AXB, Heid et al.12 inserted a stimulating catheter in the axillary brachial plexus sheath and directed it cephalad. Compared to a single-stimulation ICB, despite a similar rate of surgical anesthesia, this method still resulted in inferior anesthesia at 30 min in three nerve territories (axillary, radial and musculo-cutaneous).
When compared to a triple- or quadruple-stimula-tion AXB, two RCTs (total n = 180) reported that a single-stimulation ICB was associated with a similar success rate (85–92%).13,14 However, because of the reduced number of needle passes, ICB resulted in a shorter block performance time,13,14 decreased pain and fewer side effects (paresthesiae, vascular punc-ture).13 However, in one RCT of 59 patients, a qua-druple-stimulation AXB resulted in a higher success rate (83 vs 53% of patients; P = 0.03), a decrease in block performance time (17 vs 30 min; P < 0.05) and anesthesia-related time (29 vs 41 min; P < 0.05) as well as less pain during the block (visual analogue score = 0.6 vs 1.4 cm; P < 0.05).15 Finally one RCT, allocat-
664 CANADIAN JOURNAL OF ANESTHESIA

Tran et al.: APPROACHES AND TECHNIQUES FOR BRACHIAL PLEXUS BLOCKS 665
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
ing 30 patients to (non-stimulating) infraclavicular and axillary catheters, reported similar success rates, performance times and block durations. However the axillary catheters resulted in more vascular puncture (30 vs 0%; P < 0.05).16
In two RCTs (combined n = 224), Minville et al.17,18 compared HCB to a double-stimulation ICB: both approaches yielded similar success rates (90–95%). Although requiring a shorter performance time, ICB resulted in a longer latency time; thus the total anesthesia-related time was not different. One of the two RCTs however reported that ICB produced less pain related to skin puncture and nerve stimula-tion (visual analogue score = 19 ± 18 vs 35 ± 27 mm; P = 0.011).18
INTERPRETATION
Most studies suggest that ICB is more reliable than a single-stimulation AXB. When compared to a mul-tiple-stimulation AXB or HCB, ICB provides similar efficacy. However it may be associated with a shorter performance time and less procedure-related pain for the patient.
Axillary vs HCBIn the peer-reviewed literature, five RCTs have com-pared AXB and HCB in patients undergoing surgery at the elbow or below. In 60 patients, Bouaziz et al.19 reported that HCB yielded a higher success rate than a double-stimulation AXB (88 vs 54%; P < 0.01). However this finding was not reproduced by Fuzier et al.20 who observed a similar effectiveness (80–91%) despite a better musculocutaneous block with HCB (98 vs 80%; P < 0.05). Furthermore, these authors found the axillary approach more efficient because of decreased performance (8 ± 3 vs 13 ± 5 min; P < 0.01) and anesthesia-related (22 ± 6 vs 27 ± 9 min; P < 0.01) times. Moreover AXB was better tolerated by patients. A triple-stimulation AXB was compared to HBC in 96 patients by March et al.21 The axillary method resulted in a higher success rate (94 vs 79%; P < 0.05) as well as decreases in performance (8 ± 4 vs 11 ± 4 min; P < 0.01), onset (16 ± 8 vs 21 ± 9 min; P < 0.05) and total anesthesia-related (24 ± 8 vs 33 ± 10 min; P < 0.0001) times. However it also caused more vascular puncture (22 vs 8%; P < 0.05). Finally two RCTs (total n = 173) have compared quadruple-stimulation AXB to HBC: there was no difference in success rate and performance times.22,23 The axillary approach however resulted in less procedure-related pain (visual analogue score = 16 ± 9 vs 22 ± 12 mm; P < 0.005) in one study22 and quicker readiness for surgery (26 ± 8 vs 30 ± 6 minutes; P = 0.04) in the other.23
INTERPRETATION
Humeral canal blocks and multiple-stimulation AXB produce similar block efficacy. However AXB may be associated with decreases in time related to block performance and onset.
THE TECHNIQUES
Interscalene blockIdentification of the brachial plexus in the interscalene groove can be achieved with elicitation of paresthesiae, nerve stimulation or ultrasonography. In two RCTs totalling 257 patients, the first two modalities pro-duced similar onsets,24 success rates (94–96%),24 ease of performance,25 patient satisfaction24,25 and transient postoperative neurologic symptoms (9.3–10.1%).24 In contrast, Boezaart et al.26 found nerve stimulation superior to a paresthesia-seeking technique. They allocated 120 patients to receive a 20-mL bolus of bupivacaine 0.5% through a needle positioned in the groove by paresthesia, nerve stimulation or through a stimulating catheter: higher failure rates (10 vs 0%; P < 0.05) and postoperative pain scores were recorded in the paresthesia group. Additionally, the incidence of complete phrenic blockade was also increased (85 vs 20–35%; P < 0.05). Compared to a blind, purely landmarked-based technique, ultrasonography improved the quality of the block.27 However no RCT has compared echoguidance to the more commonly used techniques of nerve stimulation and elicitation of paresthesiae.
Urmey et al.28,29 have shown that ISB (with 35–50 mL of mepivacaine 1.5%) resulted in a 100% inci-dence of hemidiaphragmatic paresis as well as a 27% decrease in forced vital capacity and forced expiratory volume at one second. Moreover, the peak expira-tory flow rate was lowered by 15%.29 In one RCT (n = 20), decreasing the local anesthetic volume from 45 to 20 mL was not found to alter the impairment in diaphragmatic excursion, forced vital capacity and forced expiratory volume at one second.30 Digital pressure above the injection site did not decrease dia-phragmatic paresis.31,32 In one RCT combining both low volume of local anesthetics (20 mL mepivacaine 1.5%) and digital pressure, Sala-Blanch et al.33 again found no reduction in phrenic paralysis. However, in 11 healthy volunteers, ISB with 10 mL of bupivacaine 0.25% was not associated with significant changes in diaphragmatic excursion, FVC and FEV1.34
Cervical paravertebral blockThe optimal technique for CPVB has not been inves-tigated with RCTs.

666 CANADIAN JOURNAL OF ANESTHESIA
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
Suprascapular block (SSB)Because of the combined risks of hemidiaphragmatic paralysis and protracted postoperative mechanical ventilation, patients with severe lung compromise undergoing shoulder surgery can be problematic. To avoid the need for general anesthesia and ISB or SCB, some authors have favoured a combined ICB and SSB to provide analgesia to the anterior and posterior shoulder joint respectively.35 However the efficacy of SSB in shoulder surgery is controversial. In a RCT involving 50 patients undergoing ambulatory arthroscopic shoulder surgery, Ritchie et al.36 report-ed that, in contrast to the placebo group, the study group experienced less pain (P < 0.05), consumed 31% less opioids (P ≤ 0.05) and experienced 5.5 times less nausea (P < 0.05) in the immediate postoperative period; furthermore discharge occurred, on average, 64 min sooner (P < 0.05). These changes persisted at 24 hr. In another RCT involving 120 patients under-going ambulatory acromioplasty, when compared to placebo or intraarticular local anesthetic infiltration, SSB resulted in improved analgesia but did not affect postoperative opioid consumption or side effects.37 This is in keeping with the results of Neal et al.,38 who showed that, in non-arthroscopic shoulder surgery, when added to an ISB, SSB delayed the request to first analgesia by 3.6 hr but did not influence postoperative recovery, pain scores, analgesic use or quality of life outcomes (activity level, sleep quality).
INTERPRETATION
Based on the available evidence, it is unclear if nerve stimulation provides a better technique for ISB than elicitation of paresthesiae. Because of the high inci-dence of associated phrenic nerve block, ISB is prob-lematic in patients with limited pulmonary reserve. To date, the only maneuver proven to spare diaphragmat-ic function is the use of 10 mL of bupivacaine 0.25%. However the efficacy of such a small dose for surgi-cal anesthesia of the shoulder has not been studied. Furthermore SSB, although possessing a debatable role in postoperative analgesia, has not been shown to reliably provide (alone or in conjunction with ICB) adequate intraoperative conditions.
Supraclavicular blockAlthough many different surface landmarks have been advocated for SCB, only one RCT has addressed the issue. In 120 children, Dalens et al.39 compared the classic Kulenkampff to new parascalene landmarks (puncture site at the junction of the lower third and upper two thirds of a line joining mid clavicle and Chassaignac’s tubercle).40 The latter method yielded a
higher first pass success rate (88 vs 77%; P < 0.05) as well as a decreased incidence of vascular puncture (2 vs 10%) and Horner’s syndrome (3 vs 70%).
In regards to adjunctive nerve stimulation, Franco et al.41 conducted a RCT (n = 60) comparing 0.9 mA to 0.5 mA as minimal stimulatory currents to obtain a motor response (finger flexion or extension) prior to injection of local anesthetics. A 100% success rate was obtained in both groups. Furthermore no differences were noted in terms of onset or duration of anesthe-sia as well as patient satisfaction. In 1990, Hickey et al.42 proposed a new technique involving transarterial injection anterior or posterior to the subclavian artery. After recruiting 18 patients, the authors discontinued enrolment because 60–63% of patients required block supplementation. The incidence of side effects (hema-toma, Horner’s syndrome, recurrent laryngeal nerve paralysis) approached 20–25%.
Ultrasonography has also proven to be a valuable adjunct. In one RCT allocating 80 patients receiving SCB to nerve stimulation alone or nerve stimulation with ultrasound, Williams et al.43 found that, in the latter group, the time required to perform the proce-dure was significantly reduced (5.0 ± 2.4 vs 9.8 ± 7.5 min; P = 0.0001).
INTERPRETATION
Nerve stimulation guidance with a minimal threshold of 0.9 mA seems to provide a dependable SCB. One study suggests that echoguidance in combination with nerve stimulation can shorten the performance time of SCB.
Infraclavicular blockAlthough many different surface landmarks have been advocated for ICB, no RCT has proven the superiority of one over another. With ultrasonography, in a RCT of 196 patients, a medial approach at the apex of the delto-pectoral groove (with the patient’s arm exter-nally rotated and abducted 110º as well as the elbow flexed 90º) provided better visualization, a quicker performance time (9 ± 5 vs 13 ± 4 min; P < 0.05) and more effective block of tourniquet pain (97 vs 83% of patients; P < 0.01) than a lateral infracoracaoid tech-nique performed with the patient’s arm adducted to the side.44
For single-stimulation ICB, one RCT compared success rates with median and musculocutaneous nerve responses: in 121 patients, at 20 min, Rodriguez et al.45 found that a median response resulted in better sensory and motor blockade of the radial/ ulnar and radial/ ulnar/ median nerves respectively. However the incidence of complete paralysis and complete

Tran et al.: APPROACHES AND TECHNIQUES FOR BRACHIAL PLEXUS BLOCKS 667
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
anesthesia of the upper limb was similarly low in both groups (≤ 40%). Although two large series (total of 864 patients) have reported good success with pos-terior cord stimulation (90–94%), this finding still requires validation with RCTs.46,47
The low success rate associated with single-stimula-tion ICB has led many authors to advocate a dual- or triple-injection technique. In three RCTs (totalling 215 patients), a multiple-stimulation technique con-sistently produced better sensory and motor blockade at 20 min in the musculocutaneous, ulnar and radial territories.48–50 This was associated with increased patient satisfaction (9.3 ± 1.1 vs 7.5 ± 3.3 on a ten-point scale; P = 0.007) and an overall success rate of 72.5% (compared to 40% for a single-injection technique; P < 0.0001).48 Furthermore, multiple injections may allow a 25% decrease in the volume of local anesthetics (from 40 to 30 mL) without affecting the quality of the block.51 No differences were found between a double- and a triple-injection technique.50 While a dual- or triple-injection technique significantly increased the success rate of ICB, the time needed for its performance was slightly greater (9 ± 3 vs 7.5 ± 6 min; P = 0.04) or no different from the one required by its single-injection counterpart.48,51 In addition it is a simple technique to learn: in one RCT enroll-ing 220 patients, dual-injection blocks performed by staff anesthesiologists and residents resulted in similar onsets, adverse events and success rates.52
In a RCT involving 40 children undergoing fore-arm and hand surgery, when compared to a single-neurostimulation technique, ICB, using 0.5 mL·kg–1 of ropivacaine 0.5% and relying solely on echoguid-ance, resulted in less procedure-related pain (3 vs 3.75; P = 0.03) as well as a faster onset (9 vs 15 min; P < 0.001) and a longer duration (384 vs 310 min; P < 0.001) of sensory blocks. However after 30 min, the quality of the block was similar in the two groups.53
INTERPRETATION
Current evidence points to a double-stimulation technique as the optimal choice for ICB. The best combination of cords to stimulate has not been stud-ied using RCTs. In children, echoguidance offers a reliable and potentially superior alternative to nerve stimulation.
Axillary blockIdentification of the brachial plexus in the axilla can be achieved with different methods: loss of resistance, fascial clicks (snaps), transarterial injection, elicitation of paresthesiae, nerve stimulation and ultrasonogra-phy.
A) LOSS OF RESISTANCE
In a RCT allocating 60 patients to a paresthesia-seeking technique or loss of resistance, the latter was observed to provide an increased success rate (73 vs 43%; P < 0.05), better block of the axillary, muscu-locutaneous and radial nerves, as well as a decreased incidence of vascular puncture (7 vs 33%).54
B) FASCIAL CLICKS
In a RCT allocating 100 patients to an AXB by paresthesia, nerve stimulation or through a catheter inserted with the fascial click method, Baranowski et al.55 showed that the latter technique blocked the median and ulnar nerves less frequently (85 vs 100% and 75 vs 100% respectively; P < 0.01). In another RCT of 60 patients, when compared to nerve stimula-tion, fascial clicks yielded a higher failure rate (13 vs 0%) and a decreased incidence of complete blockade (60 vs 73%) but these findings did not achieve statisti-cal significance.56
In an effort to refine the technique, Rodriguez et al.57 combined fascial clicks with cold-induced par-esthesiae. A RCT of 46 patients showed that, when compared to normothermic saline, cold saline (8–11ºC) consistently elicited one or more paresthesiae, thus making fascial snaps more brachial plexus sheath-specific. In turn, this led to an increased success rate of (100 vs 75%; P < 0.02). In a follow-up study, the same authors compared cold-induced paresthesiae to nerve stimulation (one motor response below the elbow) as adjuncts for fascial clicks: both methods yielded a positive response in 85–95% of cases and a success rate of 95%.58
C) TRANSARTERIAL INJECTION
Due in part to different definitions, the success rate of transarterial axillary block ranges from 62 to 90%.59,60 However most RCTs report success rates of 70 to 82%.61–63
With the transarterial technique, local anesthetics can be injected anterior or posterior to the artery. Alternately, half of the bolus may be deposited pos-teriorly and half anteriorly. Of the three variants, a single injection behind the artery yielded a slower onset and a decreased incidence of sensory blockade in the median nerve territory. In the same RCT of 49 patients, no differences were noted between the pre-arterial and half-half methods.64
Two RCTs compared the transarterial to the snap/ paresthesia-seeking technique and found no differ-ence. However combining both methods increased the block’s duration and success rate (94 vs 78–82%; P = 0.04).59,61 The transarterial technique has also been

668 CANADIAN JOURNAL OF ANESTHESIA
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
shown to be equivalent to a single-nerve stimulation technique.62 One study reported that a transarterial technique is superior to a double-nerve stimulation technique (success rate of 66 vs 47%; P < 0.05).65 However, in two RCTs (total n = 200), a quadruple-nerve stimulation technique yielded a higher success rate (88–94 vs 62–64%; P < 0.001) and, despite a longer performance time (10–11 vs 7–8 min; P < 0.001), resulted in a decreased anesthesia-related time (23–30 vs 37–38 min; P < 0.001) because of a shorter latency and a decreased need for supplementation.60,63 Similar findings were reported in one RCT that compared a quadruple-stimulation to a transarterial (or paresthesia-seeking) technique: again the former produced a higher success rate (87 vs 54%; P < 0.001) and, despite a longer performance time (11 vs 7 min; P < 0.05), the total anesthetic time was reduced (32 vs 39 min; P < 0.05).66 Finally, one RCT of 59 patients, comparing transarterial, paresthesia-seeking and (uni)neurostimulatory techniques, concluded that all three methods were equivalent.67
D) ELICITATION OF PARESTHESIAE
Because of differences in definition, the success rate of AXB with a paresthesia-seeking technique ranges from 40 to 90%.59,68 However most RCTs report rates of 76 to 82%.56,61,67,69
While many authors have elicited only a single paresthesia before local anesthetic injection, in a RCT comparing fascial click, elicitation of paresthesiae and nerve stimulation, Baranowski et al.55 observed a positive correlation between the number of paresthe-siae sought and block success rate (60, 82 and 100% for one, two and three paresthesiae respectively). However these results must be interpreted cautiously as subjects in the paresthesia group were not randomly assigned to one, two or three paresthesiae.
Using a two-paresthesiae technique, Rucci et al.70 reported that, compared to a tangential angle, inser-tion of the needle perpendicularly to the axillary artery provided a better block of the median, ulnar, radial and musculocutaneous nerves, as well as a higher overall success rate (84 vs 42%; P < 0.00001). Moreover the same authors have demonstrated that a slow (30 sec) injection of local anesthetics after elicitation of paresthesiae yielded better results than a rapid (ten seconds) injection (success rate = 70 vs 40% respectively; P < 0.05).68
As stated in the previous section, three RCTs (com-bined n = 186) have reported no differences between single-paresthesia and transarterial techniques.59,61,67
Three RCTs compared (one, two or three) pares-thesiae-seeking and (single, double or triple) nerve
stimulation techniques. In two RCTs, no differences were observed (success rate of 70–82%).55,67 A recent RCT compared a triple-paresthesiae technique aug-mented by coracobrachialis infiltration to a quadruple-nerve stimulation technique. In 96 patients, the latter method yielded a higher success rate (91 vs 76%; P < 0.05) coupled with a reduced anesthesia-related time (25 ± 8 vs 35 ± 9 min; P < 0.001) due to decreased performance and latency times. Moreover the inci-dence of venous puncture was also lower (4 vs 12 instances of puncture; P < 0.05).69
E) NERVE STIMULATION
For single-stimulation AXB, the ideal response is radial nerve stimulation: Rodriguez et al.71 have shown that, compared to median stimulation, it produced similar blockade of the median nerve and better blockade of the radial and ulnar nerves. Furthermore, contrary to popular belief, digital pressure on the neurovascular sheath (distal to the injection site) does not promote proximal spread of local anesthetics. In a RCT of 98 patients, digital pressure did not increase the success rate of single-stimulation AXB.72
In adults, despite differences in the definition of success and in the number of stimulations (two, three or four), a multiple-stimulation technique was consis-tently found to be superior to its single stimulatory counterpart. In four RCTs (total n = 285), the former resulted in a higher success rate (90–93% vs 43–63%; P < 0.05).71,73–75 Furthermore, despite a longer per-formance time (8–9.5 ± 2.2-5 vs 3.3–5.5 ± 0.9–2.5 min; P < 0.005), the multiple-stimulation technique resulted in decreased latency and anesthesia-related times (25 ± 6 vs 38.5 ± 6 min; P < 0.001).71,74 In children, despite a quicker onset time (25 ± 7 vs 29 ± 4 min; P < 0.001), a double-stimulation technique did not result in more complete blocks. The authors attributed this phenomenon to a better circumferen-tial diffusion of local anesthetics in the pediatric bra-chial plexus sheath.76
For double-stimulation AXB, one RCT of 60 patients showed that the combination of muscu-locutaneous and radial stimulations yielded better sensorimotor blockade of the radial nerve than the combination of musculocutaneous and ulnar stimula-tions. However this had no impact on block success rate.77
In the literature, four RCTs compared double- to triple- and quadruple-stimulation AXB with mixed results. In one study, double- and quadruple-injection techniques resulted in similar success rates (93%).73 In another RCT of 100 patients, compared to a double-stimulation technique, three stimulations produced a

Tran et al.: APPROACHES AND TECHNIQUES FOR BRACHIAL PLEXUS BLOCKS 669
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
better block of the musculocutaneous nerve but did not improve the success rate.78 Finally two RCTs have concluded that a triple-stimulation technique yielded a higher success rate (93–97 vs 53–77%; P < 0.05)71,79 attributable to better blockade of the median71 and radial nerves.79
In 2001, Sia et al.80 compared a triple- (musculo-cutaneous, median and radial stimulations) to quadru-ple-injection AXB. In 81 patients randomly allocated to either technique, they reported a similar frequency of complete block (90–92%). Despite a shorter per-formance time for the triple-injection technique (5 ± 2 vs 8 ± 3 min; P < 0.01), the latency (17–19 min) and anesthesia-related times (25 min) were not differ-ent. However the triple-stimulation AXB caused less procedure-related pain (visual analogue score = 8 ± 2 vs 13 ± 2 mm; P < 0.01). In two follow-up RCTs, the same authors refined the triple-stimulation AXB: com-pared to the stimulatory pattern of musculocutaneous-median-ulnar, despite a longer performance time (7.8 ± 1.8 vs 6.5 ± 1.7 min; P < 0.01), the combination of musculocutaneous-median-radial produced a higher success rate (91 vs 73%; P< 0.05).81 Furthermore, dur-ing radial nerve stimulation, compared to a proximal response (forearm extension), a distal motor response (supination, wrist or finger extension) has been shown to produce a decreased onset time (9.9 ± 6 vs 15.4 ± 7 min; P < 0.01) and better sensory blockade (95 vs 81%; P < 0.05) of the distal radial branches, which innervate the dorsum of the hand. However, location of a distal response required more time (8.4 ± 1.9 vs 7 ± 1.7 min; P < 0.01).82
F) ULTRASONOGRAPHY
Two RCTs have compared echoguided to transarte-rial and anatomically-placed AXBs. Adjunctive ultra-sonography was shown to decrease the performance time (7.9 ± 3.9 vs 11.1 ± 5.7 min; P < 0.05) and failure rate (0 vs 29%; P = 0.01) when compared to a transarterial technique.83 Furthermore it provided a better sensorimotor block, a shorter onset time and a lower incidence of paresthesiae than a technique relying on blind placement of the needle superior or inferior to the artery.27 No RCT has compared ultra-sonography to the more successful multiple-stimula-tion technique.
INTERPRETATION
With AXB, fascial clicks, transarterial injection, elicita-tion of paresthesiae and single-nerve stimulation result in a similar efficacy. A triple-stimulation technique, with injections on the musculocutaneous, median and radial nerves, constitutes the best AXB technique.
When stimulating the radial nerve, a distal motor response should be preferentially sought.
Humeral canal blockIn one RCT allocating 60 patients to radial before ulnar or ulnar before radial blockade, Guntz et al.84 found that, with the former sequence, while looking for the radial nerve, an ulnar (motor) response was recorded in 50% of cases. With the latter sequence, while searching for the ulnar nerve, a radial response was found 10% of the time. Thus radial blockade should precede ulnar blockade to minimize the risk of ulnar injury during radial nerve localization. The sequence for median and musculocutaneous neural blockade has not been established with RCTs.
Limitations For practical reasons, a decision was taken to limit this review to RCTs published in the English language. Although such a restriction may constitute a method-ological limitation, we believe that its impact on the paper’s conclusions is small: expansion of our search criteria (using the same databases and time periods) to languages other than English only yielded an addi-tional eight RCTs.85–92 Furthermore, no attempt was made to produce a meta-analysis. In our view, given the wide array of approaches and techniques com-monly used for brachial plexus anesthesia, patient enrolment would have been insufficient for many approaches and techniques to support a systematic pooling of data. The heterogeneous definitions of endpoints such as block success would also make this task very difficult. The only area that would be amena-ble to such an analysis would be the optimal number of stimulations in AXB (single vs multiple): this has already been analyzed in a previous review.93 Finally, all RCTs published in English were retained for the analysis: no studies were excluded based on factors such as sample size justification, statistical power, blinding, definition of intervention allocation or pri-mary and secondary outcomes. This may represent a limitation to our review as it may serve to overempha-size evidence derived from “weaker” RCTs.
ConclusionsFor shoulder and proximal humeral surgery, inter-scalene and cervical paravertebral approaches pro-vide similar rates of successful surgical anesthesia. Intersternocleidomastoid supraclavicular blockade, despite eliciting a more complete block of the median, radial, ulnar and musculocutaneous nerves, does not improve postoperative analgesia; nonetheless it may result in fewer side effects. For surgery at the elbow
670 CANADIAN JOURNAL OF ANESTHESIA
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
or below, infraclavicular blockade, while providing a similar efficacy to (multiple-stimulation) axillary and brachial canal approaches, may result in decreased patient discomfort and performance time.
In terms of technique, based on the available evi-dence, it is unclear if nerve stimulation provides a bet-ter interscalene block than elicitation of paresthesiae. For supraclavicular blockade, nerve stimulation with a minimal threshold of 0.9 mA can offer a dependable block. Current evidence points to a double-stimu-lation as the best technique for the infraclavicular approach. For axillary blockade, a triple-stimulation technique, with injections on the musculocutaneous, median and radial nerves, represents the best tech-nique. Furthermore, when stimulating the radial nerve, a distal motor response should be preferentially sought.
A critical survey of the available RCTs can pro-vide an effective tool to establish the most effective approaches and techniques for brachial plexus anes-thesia. Despite current best evidence, many technical issues regarding single-shot brachial plexus blocks remain unresolved and require further elucidation through well designed and meticulously conducted RCTs (Table). The best approaches and techniques to brachial plexus perineural catheterization for different types of surgical procedures require further investiga-tion. Finally, the roles of adjunctive ultrasonography and combined electrical stimulation/ echoguidance need to be better and systematically defined for bra-chial plexus anesthesia.
References 1 Neal JM, Hebl JR, Gerancher JC, Hogan QH. Brachial
plexus anesthesia: essentials of our current understand-ing. Reg Anesth Pain Med 2002; 27: 402–28.
2 Perlas A, Chan VW, Simons M. Brachial plexus exami-nation and localization using ultrasound and electrical stimulation: a volunteer study. Anesthesiology 2003; 99: 429–35.
3 Rucci FS, Pippa P, Barbagli R, Doni L. How many interscalenic blocks are there? A comparison between the lateral and posterior approach. Eur J Anaesthesiol 1993; 10: 303–7.
4 Rettig HC, Gielen MJ, Jack NT, Boersma E, Klein J. A comparison of the lateral and posterior approach for brachial plexus block. Reg Anesth Pain Med 2006; 31: 119–26.
5 Dewees JL, Schultz CT, Wilkerson FK, Kelly JA, Biegner AR, Pellegrini JE. Comparison of two approaches to brachial plexus anesthesia for proximal upper extrem-ity surgery: interscalene and intersternocleidomastoid. AANA J 2006; 74: 201–6.
6 Arcand G, Williams SR, Chouinard P, et al. Ultrasound-guided infraclavicular versus supraclavicular block. Anesth Analg 2005; 101: 886–90.
7 Fleck JW, Moorthy SS, Daniel J, Dierdorf SF. Brachial plexus block. A comparison of the supraclavicular lat-eral paravascular and axillary approaches. Reg Anesth 1994; 19: 14–7.
8 Kapral S, Kraft P, Eibenberger K, Fitzgerald R, Gosch M, Weinstabl C. Ultrasound-guided supraclavicular approach for regional anesthesia of the brachial plexus. Anesth Analg 1994; 78: 507–13.
9 Kapral S, Jandrasits O, Schabernig C, et al. Lateral infraclavicular plexus block vs. axillary block for hand and forearm surgery. Acta Anaesthesiol Scand 1999; 43: 1047–52.
10 Fleischmann E, Marhofer P, Greher M, Waltl B, Sitzwohl C, Kapral S. Brachial plexus anesthesia in children: lateral infraclavivular vs axillary approach. Paediatr Anaesth 2003; 13: 103–8.
11 Rettig HC, Gielen JM, Boerma E, Klein J. A compari-son of the vertical infraclavivular and axillary approach-es for brachial plexus anaesthesia. Acta Anaesthesiol Scand 2005; 49: 1501–8.
12 Heid FM, Jage J, Guth M, Bauwe N, Brambrink AM. Efficacy of vertical infraclavicular plexus block vs. mod-ified axillary plexus block: a prospective, randomized, observer-blinded study. Acta Anaesthesiol Scand 2005; 49: 677–82.
13 Deleuze A, Gentili ME, Marret E, Lamonerie L, Bonnet F. A comparison of a single-stimulation lateral infra-clavicular plexus block with a triple-stimulation axillary block. Reg Anesth Pain Med 2003; 28: 89–94.
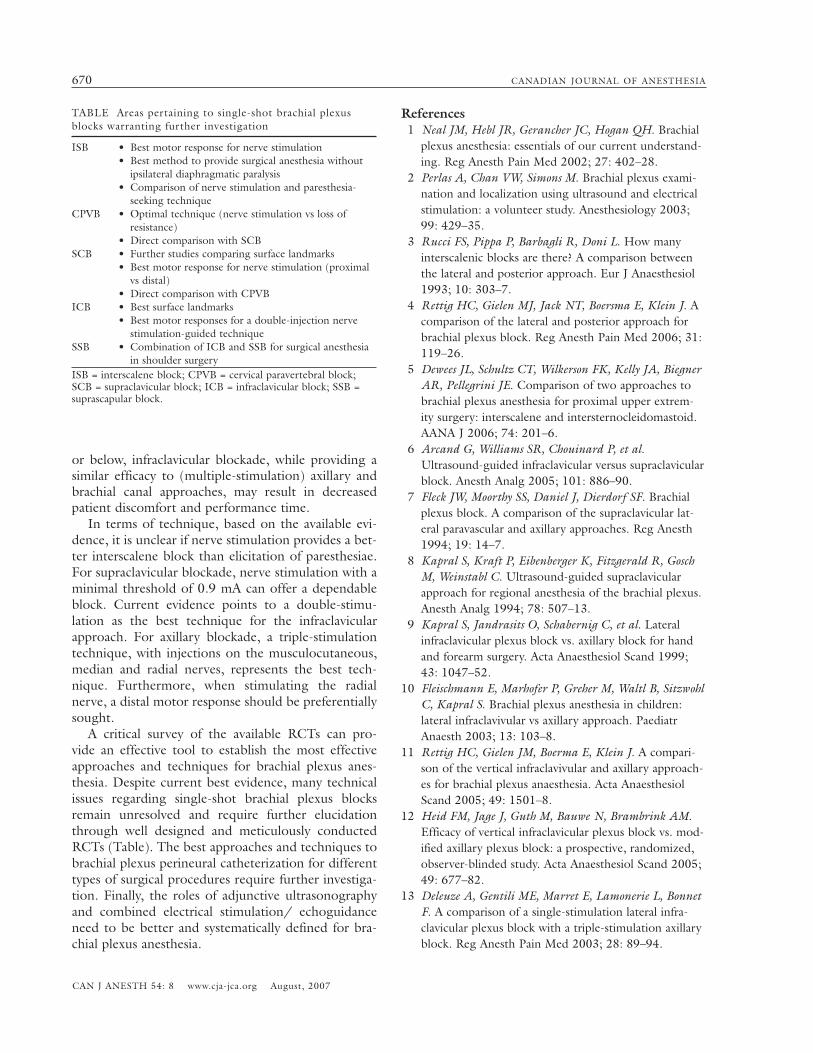
TABLE Areas pertaining to single-shot brachial plexus blocks warranting further investigation
ISB • Best motor response for nerve stimulation • Best method to provide surgical anesthesia without ipsilateral diaphragmatic paralysis • Comparison of nerve stimulation and paresthesia- seeking techniqueCPVB • Optimal technique (nerve stimulation vs loss of resistance) • Direct comparison with SCBSCB • Further studies comparing surface landmarks • Best motor response for nerve stimulation (proximal vs distal) • Direct comparison with CPVBICB • Best surface landmarks • Best motor responses for a double-injection nerve stimulation-guided techniqueSSB • Combination of ICB and SSB for surgical anesthesia in shoulder surgeryISB = interscalene block; CPVB = cervical paravertebral block; SCB = supraclavicular block; ICB = infraclavicular block; SSB = suprascapular block.

Tran et al.: APPROACHES AND TECHNIQUES FOR BRACHIAL PLEXUS BLOCKS 671
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
14 Koscielniak-Nielsen ZJ, Rasmussen H, Hesselbjerg L, Nielsen TP, Gurkan Y. Infraclavicular block causes less discomfort than axillary block in ambulatory patients. Acta Anaesthesiol Scand 2005; 49: 1030–4.
15 Koscieniak-Nielsen ZJ, Rotboll Nielsen P, Risby Mortensen C. A comparison of coracoid and axillary approaches to the brachial plexus. Acta Anaesthesiol Scand 2000; 44: 274–9.
16 Ertug Z, Yegin A, Ertem S, et al. Comparison of two different techniques for brachial plexus block: infra-clavicular versus axillary technique. Acta Anaesthesiol Scand 2005; 49: 1035–9.
17 Minville V, Amathieu R, Luc N, et al. Infraclavicular brachial plexus block versus humeral approach: com-parison of anesthetic time and efficacy. Anesth Analg 2005; 101: 1198–201.
18 Minville V, Fourcade O, Idabouk L, et al. Infraclavicular brachial plexus block versus humeral block in trauma patients: a comparison of patient comfort. Anesth Analg 2006; 102: 912–5.
19 Bouaziz H, Narchi P, Mercier FJ, et al. Comparison between conventional axillary block and a new approach at the midhumeral level. Anesth Analg 1997; 84: 1058–62.
20 Fuzier R, Fourcade O, Pianezza A, Gilbert ML, Bounes V, Olivier M. A comparison between double-injection axillary brachial plexus block and midhumeral block for emergency upper limb surgery. Anesth Analg 2006; 102: 1856–8.
21 March X, Pardina B, Torres-Bahi S, Navarro M, del Mar Garcia M, Villalonga A. A comparison of a triple-injection axillary brachial plexus block with the humer-al approach. Reg Anesth Pain Med 2003; 28: 504–8.
22 Sia S, Lepri A, Campolo MC, Fiaschi R. Four-injection brachial plexus block using peripheral nerve stimulator: a comparison between axillary and humeral approaches. Anesth Analg 2002; 95: 1075–9.
23 Koscielniak-Nielsen ZJ, Rasmussen H, Nielsen PT. Patients’ perception of pain during axillary and humer-al blocks using multiple nerve stimulations. Reg Anesth Pain Med 2004; 29: 328–32.
24 Liguori GA, Zayas VM, YaDeau JT, et al. Nerve local-ization techniques for interscalene brachial plexus blockade: a prospective, randomized comparison of mechanical paresthesia versus electrical stimulation. Anesth Analg 2006; 103: 761–7.
25 Smith BL. Efficacy of a nerve stimulator in regional anesthesia; experience in a resident training pro-gramme. Anaesthesia 1976; 31: 778–82.
26 Boezaart AP, de Beer JF, du Toit C, van Rooyen K. A new technique of continuous interscalene nerve block. Can J Anesth 1999; 46: 275–81.
27 Soeding PE, Sha S, Royse CE, Marks P, Hoy G, Royse
AG. A randomized trial of ultrasound-guided brachial plexus anaesthesia in upper limb surgery. Anaesth Intensive Care 2005; 33: 719–25.
28 Urmey WF, Talts KH, Sharrock NE. One hundred percent incidence of hemidiaphragmatic paresis asso-ciated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg 1991; 72: 498–503.
29 Urmey WF, McDonald M. Hemidiaphragmatic paresis during interscalene brachial plexus block: effects on pulmonary function and chest wall mechanics. Anesth Analg 1992; 74: 352–7.
30 Urmey WF, Gloeggler PJ. Pulmonary function changes during interscalene brachial plexus block: effects of decreasing local anesthetic injection volume. Reg Anesth 1993; 18: 244–9.
31 Urmey WF, Grossi P, Sharrock N, Stanton J, Gloeggler PJ. Digital pressure during interscalene block is clini-cally ineffective in preventing anesthetic spread to the cervical plexus. Anesth Analg 1996; 83: 366–70.
32 Bennani SE, Vandenabele-Teneur F, Nyarwaya JB, Delecroix M, Krivosic-Horber R. An attempt to prevent spread of local anaesthetic to the phrenic nerve by compression above the injection site during the inter-scalene brachial plexus block. Eur J Anaesthesiol 1998; 15: 453–6.
33 Sala-Blanch X, Lazaro JR, Correa J, Gomez-Fernandez M. Phrenic nerve block caused by interscalene brachial plexus block: effects of digital pressure and a low vol-ume of local anesthetic. Reg Anesth Pain Med 1999; 24: 231–5.
34 al-Kaisy AA, Chan VW, Perlas A. Respiratory effects of low-dose bupivacaine interscalene block. Br J Anaesth 1999; 82: 217–20.
35 Martinez J, Sala-Blanch X, Ramos I, Gomar C. Combined infraclavicular plexus block with supra-scapular nerve block for humeral head surgery in a patient with respiratory failure: an alternative approach. Anesthesiology 2003; 98: 784–5.
36 Ritchie ED, Tong D, Chung F, Norris A, Miniaci A, Vairavanathan SD. Suprascapular nerve block for post-operative pain relief in arthroscopic shoulder surgery: a new modality? Anesth Analg 1997; 84: 1306–12.
37 Singelyn FJ, Lhotel L, Fabre B. Pain relief after arthroscopic shoulder surgery: a comparison of intraar-ticular analgesia, suprascapular nerve block, and inter-scalene brachial plexus block. Anesth Analg 2004; 99: 589–92.
38 Neal JM, McDonald SB, Larkin KL, Polissar NL. Suprascapular nerve block prolongs analgesia after non-arthroscopic shoulder surgery but does not improve outcome. Anesth Analg 2003; 96: 982–6.
39 Dalens B, Vanneuville G, Tanguy A. A new parascalene
672 CANADIAN JOURNAL OF ANESTHESIA
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
approach to the brachial plexus in children: comparison with the supraclavicular approach. Anesth Analg 1987; 66: 1264–71.
40 Kulenkampff D, Persy MA. Brachial plexus anesthesia: its indications, technique and dangers. Ann Surg 1928; 87: 883–91.
41 Franco CD, Domashevich V, Voronov G, Rafizad AB, Jelev TJ. The supraclavicular block with a nerve stimu-lator: to decrease or not to decrease, that is the ques-tion. Anesth Analg 2004; 98: 1167–71.
42 Hickey R, Hoffman J, Ramamurthy S. Transarterial techniques are not effective for subclavian perivascular block. Reg Anesth 1990; 15: 245–9.
43 Williams SR, Chouinard P, Arcand G, et al. Ultrasound guidance speeds the execution and improves the qual-ity of supraclavicular block. Anesth Analg 2003; 97: 1518–23.
44 Bigeleisen P, Wilson M. A comparison of two tech-niques for ultrasound guided infraclavicular block. Br J Anaesth 2006; 96: 502–7.
45 Rodriguez J, Taboada-Muniz M, Barcena M, Alvarez J. Median versus musculocutaneous nerve response with single-injection infraclavicular coracoid block. Reg Anesth Pain Med 2004; 29: 534–8.
46 Lecamwasam H, Mayfield J, Rosow L, Chang Y, Carter C, Rosow C. Stimulation of the posterior cord predicts successful infraclavicular block. Anesth Analg 2006; 102: 1564–8.
47 Bloc S, Garnier T, Komly B, et al. Single-stimulation, low-volume infraclavicular plexus block: influence of the evoked distal motor response on success rate. Reg Anesth Pain Med 2006; 31: 433–7.
48 Gaertner E, Estebe JP, Zamfir A, Cuby C, Macaire P. Infraclavicular plexus block: multiple injection versus single injection. Reg Anesth Pain Med 2002; 27: 590–4.
49 Rodriguez J, Barcena M, Lagunilla J, Alvarez J. Increased success rate with infraclavicular brachial plexus block using a dual-injection technique. J Clin Anesth 2004; 16: 251–6.
50 Rodriguez J, Barcena M, Taboada-Muniz M, Lagunilla J, Alvarez J. A comparison of single versus multiple injections on the extent of anesthesia with coracoid infraclavicular brachial plexus block. Anesth Analg 2004; 99: 1225–30.
51 Fuzier R, Fourcade O, Fuzier V, Albert N, Samii K, Olivier M. Double- vs. single-injection infraclavicular plexus block in the emergency setting: higher suc-cess rate with lower volume of local anaesthetic. Eur J Anaesthesiol 2006; 23: 271–5.
52 Minville V, Asehoune K, Chassery C, et al. Resident versus staff anesthesiologist performance: coracoid approach to infraclavicular brachial plexus blocks using
a double-stimulation technique. Reg Anesth Pain Med 2005; 30: 233–7.
53 Marhofer P, Sitzwohl C, Greher M, Kapral S. Ultrasound guidance for infraclavicular brachial plexus anaesthesia in children. Anaesthesia 2004; 59: 642–6.
54 Hill DA, Campbell WI. Two approaches to the axillary brachial plexus. Loss of resistance to saline or paraes-thesia? Anaesthesia 1992; 47: 207–9.
55 Baranowski AP, Pither CE. A comparison of three methods of axillary brachial plexus anaesthesia. Anaesthesia 1990; 45: 362–5.
56 Tuominen MK, Pitkanen MT, Numminen MK, Rosenberg PH. Quality of axillary brachial plexus block. Comparison of success rate using perivascular and nerve stimulator techniques. Anaesthesia 1987; 42: 20–2.
57 Rodriguez J, Carceller J, Barcena M, Pedraza I, Calvo B, Alvarez J. Cold saline is more effective than room temperature saline in inducing paresthesia during axil-lary block. Anesth Analg 1995; 81: 329–31.
58 Rodriguez J, Barcena M, Alvarez J. Axillary brachial plexus anesthesia: electrical versus cold saline stimula-tion. Anesth Analg 1996; 83: 752–4.
59 Youssef MS, Desgrand DA. Comparison of two methods of axillary brachial plexus anaesthesia. Br J Anaesth 1988; 60: 841–4.
60 Koscielniak-Nielsen ZJ, Hesselbjerg L, Fejlberg V. Comparison of transarterial and multiple nerve stimu-lation techniques for an initial axillary block by 45 mL of mepivacaine 1% with adrenaline. Acta Anaesthesiol Scand 1998; 42: 570–5.
61 Turkan H, Baykal B, Ozisik T. Axillary brachial plexus blockade: an evaluation of three techniques. Mil Med 2002; 167: 723–5.
62 Pere P, Pitkanen M, Tuominen M, Edgren J, Rosenberg PH. Clinical and radiological comparison of perivas-cular and transarterial techniques of axillary brachial plexus block. Br J Anaesth 1993; 70: 276–9.
63 Koscielniak-Nielsen ZJ, Nielsen PR, Nielsen SL, Gardi T, Hermann C. Comparison of transarterial and mul-tiple nerve stimulation techniques for axillary block using a high dose of mepivacaine with adrenaline. Acta Anaesthesiol Scand 1999; 43: 398–404.
64 Hickey R, Hoffman J, Tingle LJ, Rogers JN, Ramamurthy SJ. Comparison of the clinical efficacy of three perivascular techniques for axillary brachial plexus block. Reg Anesth 1993; 18: 335–8.
65 Jones TS. Comparison of axillary block techniques: is there a difference in success rates? AANA J 1997; 65: 257–9.
66 Koscielniak-Nielsen ZJ, Rotboll Nielsen P, Sorensen T, Stenor M. Low dose axillary block by targeted injec-tions of the terminal nerves. Can J Anesth 1999; 46:
Tran et al.: APPROACHES AND TECHNIQUES FOR BRACHIAL PLEXUS BLOCKS 673
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
658–64. 67 Goldberg ME, Gregg C, Larijani GE, Norris MC, Marr
AT, Seltzer JL. A comparison of three methods of axillary approach to brachial plexus blockade for upper extremity surgery. Anesthesiology 1987; 66: 814–6.
68 Rucci FS, Pippa P, Boccaccini A, Barbagli R. Effect of injection speed on anaesthetic spread during axillary block using the orthogonal two-needle technique. Eur J Anaesthesiol 1995; 12: 505–11.
69 Sia S, Bartoli M, Lepri A, Marchini O, Ponsecchi P. Multiple-injection axillary brachial plexus block: a comparison of two methods of nerve localization-nerve stimulation versus paresthesia. Anesth Analg 2000; 91: 647–51.
70 Rucci FS, Boccaccini A, Doni L, Pippa P. The ortho-gonal two-needle technique: a new axillary approach to the brachial plexus. Eur J Anaesthesiol 1995; 12: 333–9.
71 Rodriguez J, Taboada M, Del Rio S, Barcena M, Alvarez J. A comparison of four stimulation patterns in axillary block. Reg Anesth Pain Med 2005; 30: 324–8.
72 Koschielniak-Nielsen ZJ, Christensen LQ, Pedersen HL, Brusho J. Effect of digital pressure on the neurovascular sheath during perivascular axillary block. Br J Anaesth 1995; 75: 702–6.
73 Lavoie J, Martin R, Tetrault JP, Cote DJ, Colas MJ. Axillary plexus block using a peripheral nerve stimula-tor: single or multiple injections. Can J Anaesth 1992; 39: 583–6.
74 Koscielniak-Nielsen ZJ, Stens-Pedersen HL, Lippert FK. Readiness for surgery after axillary block: single or multiple injection techniques. Eur J Anaesthesiol 1997; 14: 164–71.
75 Inberg P, Annila I, Annila P. Double-injection method using peripheral nerve stimulator is superior to single injection in axillary plexus block. Reg Anesth Pain Med 1999; 24: 509–13.
76 Carre P, Joly A, Cluzel Field B, Wodey E, Lucas MM, Ecoffey C. Axillary block in children: single or multiple injection? Paediatr Anaesth 2000; 10: 35–9.
77 Rodriguez J, Taboada M, Valino C, Barcena M, Alvarez J. A comparison of stimulation patterns in axillary block: part 2. Reg Anesth Pain Med 2006; 31: 202–5.
78 Sia S, Lepri A, Ponzecchi P. Axillary brachial plexus block using peripheral nerve stimulator: a comparison between double- and triple-injection techniques. Reg Anesth Pain Med 2001; 26: 499–503.
79 Coventry DM, Barker KF, Thomson M. Comparison of two neurostimulation techniques for axillary brachial plexus blockade. Br J Anaesth 2001; 86: 80–3.
80 Sia S, Bartoli M. Selective ulnar nerve localization is not essential for axillary brachial plexus block using a multiple nerve stimulation technique. Reg Anesth Pain
Med 2001; 26: 12–6. 81 Sia S. A comparison of injection at the ulnar and the
radial nerve in axillary block using triple stimulation. Reg Anesth Pain Med 2006; 31: 514–8.
82 Sia S, Lepri A, Magherini M, Doni L, Di Marco P, Gritti G. A comparison of proximal and distal radial nerve motor responses in axillary block using triple sti-mulation. Reg Anesth Pain Med 2005; 30: 458–63.
83 Sites BD, Beach ML, Spence BC, et al. Ultrasound guidance improves the success rate of a perivascular axillary plexus block. Acta Anaesthesiol Scand 2006; 50: 678–84.
84 Guntz E, Herman P, Delbos A, Sonowski M. The radial nerve should be blocked before the ulnar nerve during a brachial plexus block at the humeral canal. Can J Anesth 2004; 51: 354–7.
85 Ortells-Polo MA, Garcia-Guiral M, Garcia-Amigueti FJ, Carral-Olondris JN, Garcia-Godino T, Aguiar-Mojarro JA. Brachial plexus anesthesia: results of a modified perivascular supraclavicular technique (Spanish). Rev Esp Anestesiol Reanim 1996; 43: 94–8.
86 Nitta K, Yamamoto K, Itoh H, Ohmura S, Kobayashi T. Comparison of transarterial technique and paresthesia technique of axillary brachial plexus block (Japanese). Masui 1998; 47: 156–60.
87 Neuburger M, Kaiser H, Rembold-Schuster I, Landes H. Vertical infraclavicular brachial-plexus blockade. A clini-cal study of reliability of a new method for plexus anes-thesia of the upper extremity (German). Anaesthesist 1998; 47: 595–9.
88 Desbordes J, Mille FX, Adnet P, Boittiaux P, Forget AP. Brachial plexus anesthesia via an axillary route for emergency surgery: comparison of three approach methods (French). Ann Fr Anesth Reanim 1998; 17: 674–80.
89 Caputo F, Ventura R. Brachial plexus block. Effect of low interscalenic approach on phrenic nerve paresis (Italian). Minerva Anestesiol 2000; 66: 195–9.
90 Liu FC, Liou JT, Tsai YF, Li AH, Day YY, Hui YL, Lui PW. Efficacy of ultrasound-guided axillary brachial plexus block: a comparative study with nerve stimula-tor-guided method (Chinese). Chang Gung Med J 2005; 28: 396–402.
91 Sarradell Catalan AS, Moncho Rodriguez JM, Santos Carnes JA, Herrero Carbo R, Villanueva Ferrer JA, Masdeu Castellvi J. Axillary brachial plexus anesthesia. how many nerve stimulation responses do we look for? (Spanish). Rev Esp Anestesiol Reanim 2001; 48: 356–63.
92 Che XH, Liang WM, Chen JY. Triple-injection axillary brachial plexus block: a comparison of two nerve-local-ization techniques, nerve stimulation versus paresthesia (Chinese). Acta Acad Med Shanghai 2005; 32: 529–35.
674 CANADIAN JOURNAL OF ANESTHESIA
CAN J ANESTH 54: 8 www.cja-jca.org August, 2007
93 Handoll HH, Koscielniak-Nielsen ZJ. Single, double or multiple injection techniques for axillary brachial plexus block for hand, wrist or forearm surgery. Cochrane Database Syst Rev 2006; 1: CD003842.
Prague - Czech Republic




















