Body mass, tobacco and alcohol and risk of esophageal, gastric cardia, and gastric non-cardia...
10
Body mass, tobacco and alcohol and risk of esophageal, gastric cardia, and gastric non-cardia adenocarcinoma among men and women in a nested case-control study q Mats Lindblad 1, *, Luis A. Garcı´a Rodrı´guez 2 & Jesper Lagergren 1,3 1 Department of Surgical Sciences, Karolinska University Hospital, Karolinska Institutet, Stockholm, Sweden; 2 Centro Espan ˜ol de Investigacio ´n Farmacoepidemiolo ´gica, Madrid, Spain; 3 Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden Received 24 June 2004; accepted in revised form 20 September 2004 Key words: esophageal adenocarcinoma, cardia adenocarcinoma, gastric cancer, body mass, smoking. Abstract Objectives: To prospectively assess the influence of body mass index (BMI), tobacco, and alcohol on the occurrence of esophageal, gastric cardia, and non-cardia gastric adenocarcinoma, and to detect any sex differences that could explain the male predominance of these tumors. Methods: A case-control study nested in the General Practitioner Research Database in the United Kingdom, 1994– 2001. Odds ratios (ORs) were calculated with 95% confidence intervals (CI), including multivariate analysis. Results: During follow-up of 4,340,207 person-years, we identified 287 esophageal adenocarcinomas, 195 gastric cardia adenocarcinomas, 327 gastric non-cardia adenocarcinomas, and 10,000 controls. A positive association was found between overweight (BMI > 25 kg/m 2 ) and esophageal adenocarcinoma (OR 1.67, 95% CI 1.22–2.30), and gastric cardia adenocarcinoma (OR 1.46, 95% CI 0.98–2.18), but not non-cardia gastric adenocarcinoma. The association between BMI and esophageal and gastric cardia adenocarcinoma were dose-dependent and seemingly independent of reflux. No strong sex differences were identified. Smokers, particularly females, were at increased risk of all studied adenocarcinomas, while no association with alcohol was found. Conclusions: Overweight increases risk of esophageal and gastric cardia adenocarcinoma, while tobacco smoking increases risk of esophageal, gastric cardia, and non-cardia gastric adenocarcinoma. The male predominance is not explained by sex differences in risk factor profiles of the studied exposures. Abbreviations: BMI–body mass index; CI–confidence interval; GP–general practitioner; GPRD–general practitio- ners research database; OR–odds ratio Introduction Major changes of the incidence rates of esophageal and gastric adenocarcinoma have taken place in the western world during the last decades. Recent reports reveal steeply rising incidence rates of esophageal adenocarci- noma and moderately increasing rates of gastric cardia adenocarcinoma, while the incidence of more distally located gastric cancer is gradually decreasing [1–10]. The increase in incidence of adenocarcinoma of the esoph- agus and gastric cardia in the United Kingdom is more rapid than that reported of any other country worldwide [7]. Another striking feature is the strong (7:1) male predominance among patients with esophageal and cardia adenocarcinoma [5, 11]. The reasons for these variations of incidence have not been identified, under- lining the need for further risk factor detection and evaluation. The incidence of esophageal squamous-cell carcinoma is more stable, the main risk factors in western societies are well established, i.e. tobacco and q Grant support: AstraZeneca R&D and the Swedish Cancer Society. *Address correspondence to: Mats Lindblad, Department of Sur- gical Sciences P9:03, Karolinska University Hospital, Solna, SE-171 76 Stockholm, Sweden. Ph.: +46-8-517 728 01; Fax: +46-8-33 15 87; E-mail: [email protected] Cancer Causes and Control (2005) 16:285–294 Ó Springer 2005 DOI 10.1007/s10552-004-3485-7
-
Upload
psmvalencia -
Category
Documents
-
view
0 -
download
0
Transcript of Body mass, tobacco and alcohol and risk of esophageal, gastric cardia, and gastric non-cardia...

Body mass, tobacco and alcohol and risk of esophageal, gastric cardia, and gastric
non-cardia adenocarcinoma among men and women in a nested case-control studyq
Mats Lindblad1,*, Luis A. Garcıa Rodrıguez2 & Jesper Lagergren1,31Department of Surgical Sciences, Karolinska University Hospital, Karolinska Institutet, Stockholm, Sweden; 2CentroEspanol de Investigacion Farmacoepidemiologica, Madrid, Spain; 3Department of Medical Epidemiology andBiostatistics, Karolinska Institutet, Stockholm, Sweden
Received 24 June 2004; accepted in revised form 20 September 2004
Key words: esophageal adenocarcinoma, cardia adenocarcinoma, gastric cancer, body mass, smoking.
Abstract
Objectives: To prospectively assess the influence of body mass index (BMI), tobacco, and alcohol on the occurrenceof esophageal, gastric cardia, and non-cardia gastric adenocarcinoma, and to detect any sex differences that couldexplain the male predominance of these tumors.Methods: A case-control study nested in the General Practitioner Research Database in the United Kingdom, 1994–2001. Odds ratios (ORs) were calculated with 95% confidence intervals (CI), including multivariate analysis.Results: During follow-up of 4,340,207 person-years, we identified 287 esophageal adenocarcinomas, 195 gastriccardia adenocarcinomas, 327 gastric non-cardia adenocarcinomas, and 10,000 controls. A positive association wasfound between overweight (BMI > 25 kg/m2) and esophageal adenocarcinoma (OR 1.67, 95% CI 1.22–2.30), andgastric cardia adenocarcinoma (OR 1.46, 95% CI 0.98–2.18), but not non-cardia gastric adenocarcinoma. Theassociation between BMI and esophageal and gastric cardia adenocarcinoma were dose-dependent and seeminglyindependent of reflux. No strong sex differences were identified. Smokers, particularly females, were at increasedrisk of all studied adenocarcinomas, while no association with alcohol was found.Conclusions: Overweight increases risk of esophageal and gastric cardia adenocarcinoma, while tobacco smokingincreases risk of esophageal, gastric cardia, and non-cardia gastric adenocarcinoma. The male predominance is notexplained by sex differences in risk factor profiles of the studied exposures.
Abbreviations: BMI–body mass index; CI–confidence interval; GP–general practitioner; GPRD–general practitio-ners research database; OR–odds ratio
Introduction
Major changes of the incidence rates of esophageal andgastric adenocarcinoma have taken place in the westernworld during the last decades. Recent reports revealsteeply rising incidence rates of esophageal adenocarci-noma and moderately increasing rates of gastric cardia
adenocarcinoma, while the incidence of more distallylocated gastric cancer is gradually decreasing [1–10]. Theincrease in incidence of adenocarcinoma of the esoph-agus and gastric cardia in the United Kingdom is morerapid than that reported of any other country worldwide[7]. Another striking feature is the strong (7:1) malepredominance among patients with esophageal andcardia adenocarcinoma [5, 11]. The reasons for thesevariations of incidence have not been identified, under-lining the need for further risk factor detection andevaluation. The incidence of esophageal squamous-cellcarcinoma is more stable, the main risk factors inwestern societies are well established, i.e. tobacco and
qGrant support: AstraZeneca R&D and the Swedish Cancer
Society.
*Address correspondence to: Mats Lindblad, Department of Sur-
gical Sciences P9:03, Karolinska University Hospital, Solna, SE-171 76
Stockholm, Sweden. Ph.: +46-8-517 728 01; Fax: +46-8-33 15 87;
E-mail: [email protected]
Cancer Causes and Control (2005) 16:285–294 � Springer 2005DOI 10.1007/s10552-004-3485-7

alcohol use, but not obesity, and the moderate (3:1)male predominance is explained by baseline differencesin the prevalence of risk factors [11, 12].Obesity has been found to be a strong risk factor for
esophageal adenocarcinoma in some previous studies[13–18], but not in all [19, 20]. However, its role as anindependent risk factor, free from the influence ofgastroesophageal reflux, has been questioned [21]. Whiletobacco smoking seems to be a potential weak riskfactor for gastric adenocarcinoma [18, 22–26], theresults on the association with esophageal adenocarci-noma are contradictory [18, 22, 27]. Excessive use ofalcohol is not known to be associated with raised risk ofesophageal or gastric adenocarcinomas [18, 22, 27–29].A problem shared by all previous studies that evaluatedthe role of body mass, and most that address the roles oftobacco and alcohol use in the etiology of these tumors,is the retrospective exposure assessment. The risk ofboth non-random misclassification, i.e. recall bias,which would distort the findings, and random misclas-sification of the exposure, which would dilute anyassociations, is considerable. There is a need forepidemiological studies with prospective data collectionto firmly establish and define the strength of thesepotential associations. Another limitation of the previ-ous literature is the limited number of female patientswith esophageal adenocarcinoma in each individualstudy, which has prevented valid estimates of riskfactors specifically among women.Therefore, the aims of the present study were to
prospectively assess the influence of body mass, tobaccosmoking, and alcohol consumption on the developmentof esophageal, cardia, and gastric adenocarcinoma, andto detect potential differences in risk factor profilesbetween sexes that could contribute to explaining themale predominance among patients with esophageal andcardia adenocarcinoma in a geographical area with ahigh incidence of these tumors, i.e. the United Kingdom.
Materials and methods
Design
We conducted a prospective nested case-control studywithin the General Practitioners Research Database(GPRD) in the United Kingdom during the study periodJanuary 1, 1994 through December 31, 2001. Therelation between exposure to obesity, tobacco smoking,and alcohol consumption and risk of esophageal, cardia,and gastric adenocarcinomas was explored. For com-parison, we also included patients with squamous-cellcarcinoma of the esophagus. They represent a group
with a well established relation to all exposuresaddressed in this investigation, and can therefore beused to evaluate the internal validity of the study.
General practitioners research database (GPRD)
The GPRD has been described in more detail elsewhere[30]. In brief, it is one of the largest computerizeddatabases of longitudinal patient records in the world,containing more than 35 million patient-years of Britishprimary care data. The GPRD contains prospectivelyrecorded information routinely recorded by GPs duringtheir standard medical care, including patients’ demo-graphics, medical disorders, diagnoses from hospitalreferrals and drug prescriptions. This database has beenused in numerous pharmacoepidemiological and clinicalepidemiological studies, and is continuously validatedand proven to be of high quality for research purposes[31–34].
Study cohort and follow-up
All patients aged between 40 and 84 years during thestudy period became members of the study cohort whenthey had been enrolled in the GPRD for at leasttwo years. Patients with any cancer recorded in theGPRD before the start of the study period were noteligible for the study cohort. The members of the studycohort were followed up until the earliest occurrence ofany of the following endpoints: (1) detection of anesophageal or gastric cancer, (2) detection of any othercancer, (3) age of 85 years, (4) death, or (5) end of studyperiod (December 31, 2001).
Selection of study participants
During follow-up of the study cohort 2128 patients witha diagnosis code indicating esophageal or gastric cancerwere found. The computerized profiles of all thesepatients were reviewed by one investigator (ML), whowas kept blinded to the exposure information during thereview process. Patients were excluded as cases if: (1) thetumor was benign, (2) the site of the primary cancer wasunknown, (3) the tumor was a metastasis, (4) the patienthad another, concurrent cancer, (5) the cancer was firstdiagnosed before the start date in the study cohort, or(6) the histological diagnosis was of another type thanadenocarcinoma or squamous-cell carcinoma. For asample of 1280 (60%) consecutively computer-detectedcase patients, the general practitioners (GPs) were askedto provide additional information on the site andhistology of the tumor and to send all available paper-based information related to the diagnosis. This
286 M. Lindblad et al.

information was evaluated on 993 (78%) patients,resulted in the additional exclusion of a mere 2.7% ofthe computer-detected cases. Therefore, we did notrequest such complementary information for theremaining computer-detected case patients. Index dateamong the case patients was set as the date when thetumor was first recorded or when the review revealed anearlier date of diagnosis.The control subjects and their index date were
randomly selected. A date within the study period wasgenerated at random for each of the members of theentire study cohort. If this random date was included inthe eligible person-time for that cohort member, we usedthis date as the index date and marked that person as aneligible control subject. Thereafter, a total of 10,000controls, free of cancer, were randomly selected andfrequency-matched by sex, age (within one year) andsame calendar year from the pool of eligible controlsubjects. We decided to select 10,000 controls, since itapproached the ratio of five controls per case, a ratioconsidered to bring close to as much information as anyother ratio greater than it.
Exposure information
For the evaluated exposures, only information recordedat least two years before the index date was considered.We used this two-year lag time to reduce the influence ofreversed causality due to the possibility that the level ofexposure was influenced by early symptoms of a yetundetected cancer. Recordings of body length andweight were collected from the database, and bodymass index (BMI) was calculated as body weight inkilograms divided by the square of body height inmeters (kg/m2). Exposure to tobacco smoking in theGPRD was recorded as smoking status, i.e. non-smoker,current smoker, ex-smoker, or unknown. Recordings ofalcohol consumption were reported as units of alcoholper day. In the United Kingdom, one unit of analcoholic beverage equals 10 ml (7.9 g) of pure ethanol.
Statistical analyses
The main analyses were performed in unconditionallogistic regression, calculating odds ratios (ORs) with95% confidence intervals (CIs). In the multivariateanalyses, all estimates of risk were adjusted for thefollowing potential confounding factors: age (in ten-yearcategories), sex, calendar year, and a history of gastro-esophageal reflux (yes or no), i.e. any recordings ofheartburn, reflux or esophagitis in the database. Thecut-off points for BMI were pre-determined and basedon the World Health Organization classification of
overweight and obesity [35], where a BMI value between25 and 29.9 is defined as overweight, and a BMI of 30and above represents obesity. Moreover, a BMI of 35and above is often referred to as severe obesity. Weconsidered a BMI value between 20 and 24.9 as normaland used this interval as the reference value, while BMIbelow 20 was regarded as sub-normal, i.e. underweight.Additionally, BMI was also grouped into sex-specificquartiles by using cut-off points among the controls.The lowest quartile was considered as reference.
Ethics
The study was approved by the Scientific and EthicalAdvisory Group (SEAG) in the United Kingdom.
Results
Study participants
In total, the study cohort comprised 4,340,207 person-years at risk. From this cohort, we identified 2128patients with a computer code of esophageal or gastriccancer, and 10,000 control subjects. The manual reviewof the computer-selected cases, including computer filesand the additional information provided by the GPs,revealed that 178 computer-selected patients fulfilled atleast one of the pre-determined exclusion criteria.Furthermore, the review process rendered a change oftumor site from esophageal to gastric in 74 (8%)patients and from gastric to esophageal in 14 (2%)patients. Thereafter, 1950 case patients remained in thestudy, 1315 males and 635 females, and among thecontrols there were 6713 male and 3287 female partic-ipants. The tumors were classified into 909 esophagealcancers, 1023 gastric cancers, and 18 where it was notpossible to discern whether the tumor site was esoph-ageal or gastric. The patients with a cancer located in theesophagus were further divided histologically into 287adenocarcinomas, 140 squamous-cell carcinomas, and482 without a specified recorded histology. The patientswith a gastric cancer were classified according to sitewithin the stomach: 195 cancers were located in thegastric cardia, 327 more distally in the stomach, (i.e.gastric non-cardia), and in 501 patients the specific sitewithin the stomach was not possible to determine duringthe review of the records.
Body mass index (BMI)
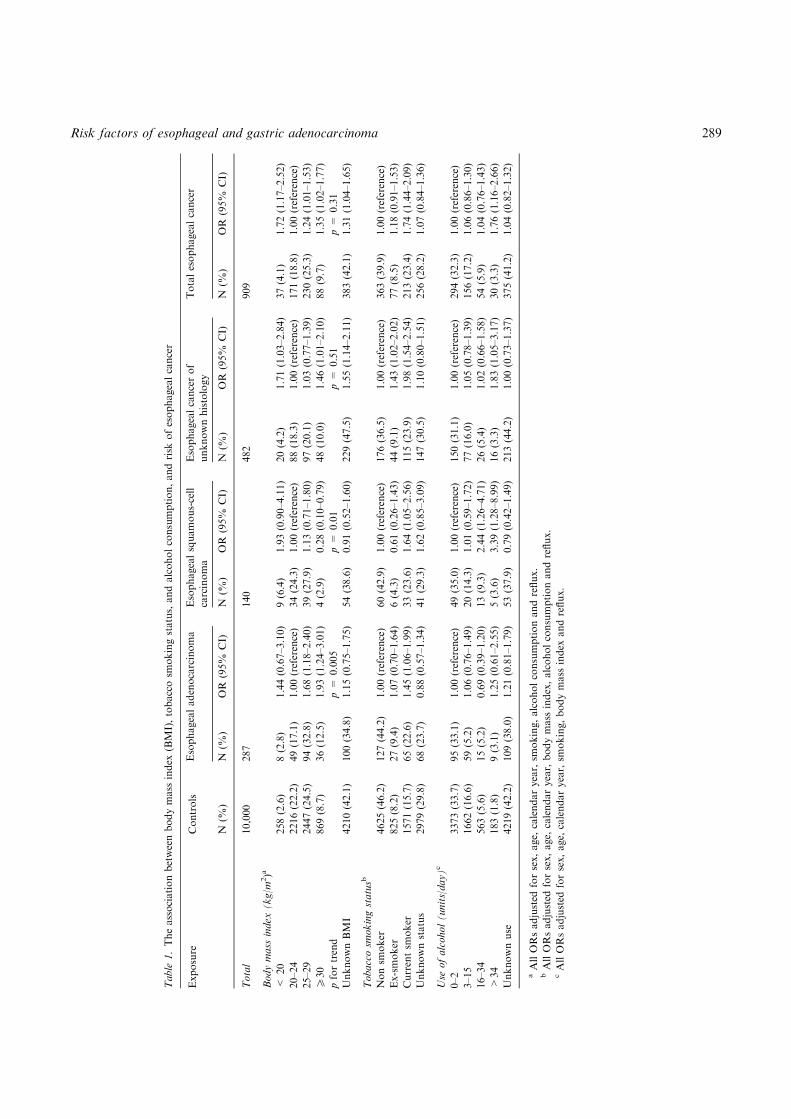
Overweight or obese individuals, i.e. all persons with aBMI of 25 kg/m2 or higher, were at a nearly 70% raised
Risk factors of esophageal and gastric adenocarcinoma 287

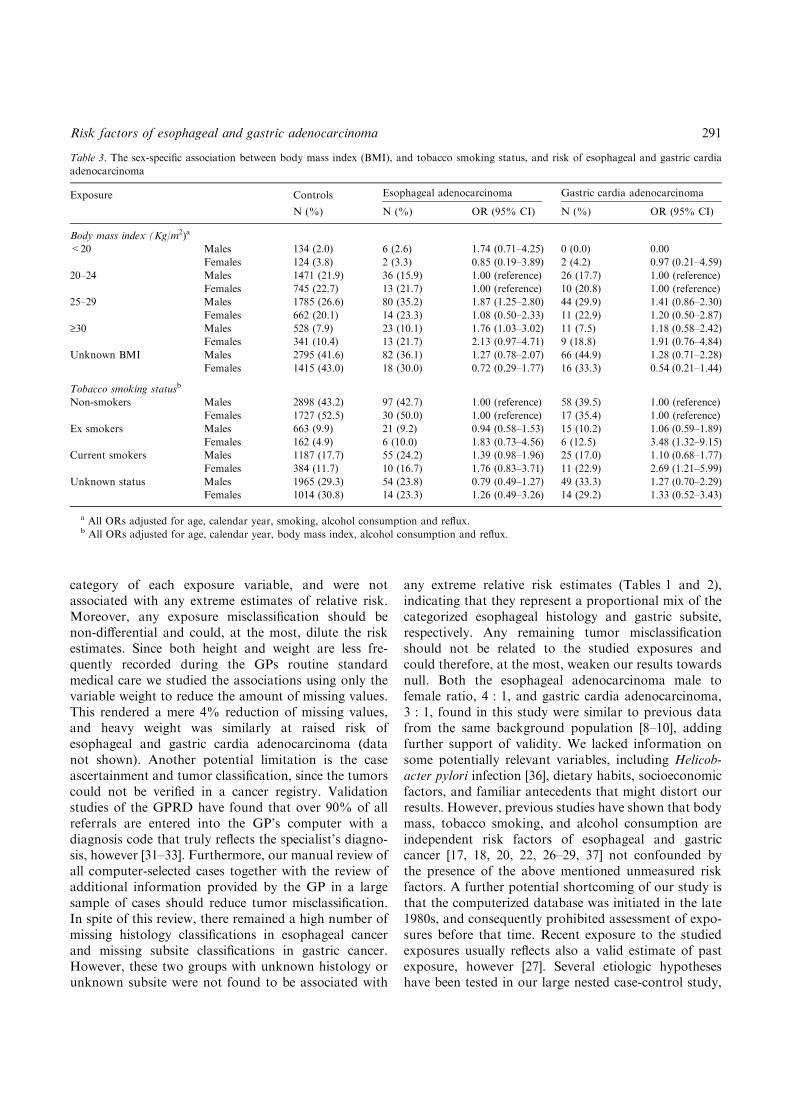
risk of esophageal adenocarcinoma (OR 1.67, 95% CI1.22–2.30), and a nearly 50% increased risk of gastriccardia adenocarcinoma (OR 1.46, 95% CI 0.98–2.18).There was an indication of an inverse association withesophageal squamous-cell carcinoma (OR 0.79, 95% CI0.52–1.22), while no association was found with gastricnon-cardia adenocarcinoma (OR 0.97, 95% CI 0.73–1.30). The analyses of sex-specific BMI-quartiles asdefined by the BMI values among control subjects aswell as the pre-defined BMI categories, revealed astatistically significant positive dose-response relationbetween BMI and risk of esophageal adenocarcinoma(Table 1). A similar dose-response association wassuggested for gastric cardia adenocarcinoma (Table 2),while a statistically significant negative dose-responseassociation was found for esophageal squamous-cellcarcinoma (Table 1). Among persons with severe obes-ity, i.e. BMI of at least 35 kg/m2, the OR was 3.68 (95%CI 1.81–7.51) for esophageal adenocarcinoma, and 1.47(95% CI 0.44–4.88) for gastric cardia adenocarcinoma,indicating a stronger association with the former type ofcancer. The raised risks of esophageal and gastric cardiaadenocarcinoma among women seemed mainly re-stricted to the obese persons, i.e. women in the highestBMI quartile or with a BMI of at least 30 kg/m2, whilethe increased risks among men were found also at amore modest excess body mass (Table 3). Body massappeared to be a risk factor acting independently ofreflux, since the risk estimates were not reduced inanalyses restricted to persons without reflux or hiatushernia (Table 4) or after adjustment for reflux in thelogistic regression model. The other potential confound-ing variables did not materially change the risk esti-mates.
Tobacco smoking
Current smoking status, as defined two years prior toindex date, was associated with a moderately increasedrisk of both esophageal (Table 1) and gastric cancer(Table 2). Current smokers were at an increased risk ofesophageal adenocarcinoma (OR 1.45, 95% CI 1.06–1.99), gastric cardia adenocarcinoma (OR 1.38, 95% CI0.92–2.09), gastric non-cardia adenocarcinoma (OR1.70, 95% CI 1.26–2.29), as well as esophageal squa-mous-cell carcinoma (OR 1.64, 95% CI 1.05–2.56).With regard to risk of esophageal and cardia adenocar-cinoma, female smokers were at a seemingly higher riskcompared to men (Table 3). This pattern was found alsofor gastric non-cardia adenocarcinoma among women(OR 2.37, 95% CI 1.44–3.88) compared to men (OR1.41, 95% CI 0.97–2.05). Among ex-smokers, the resultsindicated an increased risk of gastric cardia adenocar-
cinoma (OR 1.40, 95% CI 0.85–2.30), but not of gastricnon-cardia adenocarcinoma, esophageal adenocarci-noma, or esophageal squamous-cell carcinoma(Tables 1 and 2).
Alcohol consumption
Excessive use of alcohol was not associated with risk ofadenocarcinoma of the esophagus, cardia, or non-cardiastomach (Tables 1 and 2). Consumers of more than34 units of alcohol per day were at a more than three-fold increased risk of esophageal squamous-cell carci-noma (OR 3.39, 95% CI 1.28–8.99). The raised risks ofesophageal squamous-cell carcinoma among alcoholconsumers were evenly distributed between the sexes(data not shown).
Discussion
This study adds prospective evidence that BMI is adose-dependent risk factor for both esophageal adeno-carcinoma and, to a more moderate extent, gastriccardia adenocarcinoma, seemingly independent of theoccurrence of gastroesophageal reflux. Our resultsfurther indicate that tobacco smoking increases the riskof adenocarcinoma of the esophagus, cardia andnon-cardia stomach, particularly among females, whilealcohol consumption does not increase the risk of thesetumors.Strengths of our study include the prospectively
collected exposure data and the large sample size.Prospective recording of exposure data ensures thatthe information is not affected by the occurrence of anycancer, and is equally good for cases and controls. Thisprovides exposure information free of recall bias, amajor concern in case-control studies using retrospectiveexposure data collected by personal interviews orpatient-administered questionnaires after the cancerdiagnosis has been confirmed. Other advantages includethe large sample size in the country with the highestknown incidence of esophageal and cardia adenocarci-noma, the United Kingdom. A large sample size reducesthe risk of bias and chance errors, and providesopportunities to study subgroups of interest.A limitation of the study is the relatively large
proportion of missing values among the studied expo-sures. This should not influence our main findings,however, since the extent of missing data was equallydistributed between cases and controls, and not per seassociated with raised risk of esophageal or gastriccancer (data not shown). Furthermore, the missingvalues were included in all analyses as a separate
288 M. Lindblad et al.
Table
1.Theassociationbetweenbodymass
index
(BMI),tobaccosm
okingstatus,andalcoholconsumption,andrisk
ofesophagealcancer
Exposure
Controls
Esophagealadenocarcinoma
Esophagealsquamous-cell
carcinoma
Esophagealcancerof
unknownhistology
Totalesophagealcancer
N(%
)N
(%)
OR
(95%
CI)
N(%
)OR
(95%
CI)
N(%
)OR
(95%
CI)
N(%
)OR
(95%
CI)
Total
10,000
287
140
482
909
Bodymass
index
(kg/m
2)a
<20
258(2.6)
8(2.8)
1.44(0.67–3.10)
9(6.4)
1.93(0.90–4.11)
20(4.2)
1.71(1.03–2.84)
37(4.1)
1.72(1.17–2.52)
20–24
2216(22.2)
49(17.1)
1.00(reference)
34(24.3)
1.00(reference)
88(18.3)
1.00(reference)
171(18.8)
1.00(reference)
25–29
2447(24.5)
94(32.8)
1.68(1.18–2.40)
39(27.9)
1.13(0.71–1.80)
97(20.1)
1.03(0.77–1.39)
230(25.3)
1.24(1.01–1.53)
P30
869(8.7)
36(12.5)
1.93(1.24–3.01)
4(2.9)
0.28(0.10–0.79)
48(10.0)
1.46(1.01–2.10)
88(9.7)
1.35(1.02–1.77)
pfortrend
p=
0.005
p=
0.01
p=
0.51
p=
0.31
UnknownBMI
4210(42.1)
100(34.8)
1.15(0.75–1.75)
54(38.6)
0.91(0.52–1.60)
229(47.5)
1.55(1.14–2.11)
383(42.1)
1.31(1.04–1.65)
Tobaccosm
okingstatusb
Nonsm
oker
4625(46.2)
127(44.2)
1.00(reference)
60(42.9)
1.00(reference)
176(36.5)
1.00(reference)
363(39.9)
1.00(reference)
Ex-smoker
825(8.2)
27(9.4)
1.07(0.70–1.64)
6(4.3)
0.61(0.26–1.43)
44(9.1)
1.43(1.02–2.02)
77(8.5)
1.18(0.91–1.53)
Currentsm
oker
1571(15.7)
65(22.6)
1.45(1.06–1.99)
33(23.6)
1.64(1.05–2.56)
115(23.9)
1.98(1.54–2.54)
213(23.4)
1.74(1.44–2.09)
Unknownstatus
2979(29.8)
68(23.7)
0.88(0.57–1.34)
41(29.3)
1.62(0.85–3.09)
147(30.5)
1.10(0.80–1.51)
256(28.2)
1.07(0.84–1.36)
Use
ofalcohol(units/day)c
0–2
3373(33.7)
95(33.1)
1.00(reference)
49(35.0)
1.00(reference)
150(31.1)
1.00(reference)
294(32.3)
1.00(reference)
3–15
1662(16.6)
59(5.2)
1.06(0.76–1.49)
20(14.3)
1.01(0.59–1.72)
77(16.0)
1.05(0.78–1.39)
156(17.2)
1.06(0.86–1.30)
16–34
563(5.6)
15(5.2)
0.69(0.39–1.20)
13(9.3)
2.44(1.26–4.71)
26(5.4)
1.02(0.66–1.58)
54(5.9)
1.04(0.76–1.43)
>34
183(1.8)
9(3.1)
1.25(0.61–2.55)
5(3.6)
3.39(1.28–8.99)
16(3.3)
1.83(1.05–3.17)
30(3.3)
1.76(1.16–2.66)
Unknownuse
4219(42.2)
109(38.0)
1.21(0.81–1.79)
53(37.9)
0.79(0.42–1.49)
213(44.2)
1.00(0.73–1.37)
375(41.2)
1.04(0.82–1.32)
aAllORsadjusted
forsex,age,
calendaryear,sm
oking,alcoholconsumptionandreflux.
bAllORsadjusted
forsex,age,
calendaryear,bodymass
index,alcoholconsumptionandreflux.
cAllORsadjusted
forsex,age,
calendaryear,sm
oking,bodymass
index
andreflux.
Risk factors of esophageal and gastric adenocarcinoma 289

Table
2.Theassociationbetweenbodymass
index
(BMI),tobaccosm
okingstatus,andalcoholconsumption,andrisk
ofgastricadenocarcinoma
Exposure
Controls
Gastriccardia
adenocarcinoma
Non-cardia
gastric
adenocarcinoma
Unknownsubsite
of
gastricadenocarcinoma
Totalgastric
adenocarcinoma
N(%
)N
(%)
OR
(95%
CI)
N(%
)OR
(95%
CI)
N(%
)OR
(95%
CI)
N(%
)OR
(95%
CI)
Total
10,000
195
327
501
1023
Bodymass
index
(kg/m
2)a
<20
258(2.6)
2(1.03)
0.50(0.12–2.10)
16(4.9)
1.75(1.00–3.08)
11(2.2)
0.77(0.40–1.45)
29(2.8)
1.05(0.69–1.58)
20–24
2216(22.2)
36(18.5)
1.00(reference)
70(21.4)
1.00(reference)
111(22.2)
1.00(reference)
217(21.2)
1.00(reference)
25–29
2447(24.5)
55(28.2)
1.37(0.89–2.10)
83(25.4)
1.11(0.80–1.54)
116(23.2)
0.97(0.74–1.28)
254(24.8)
1.09(0.90–1.32)
‡30
869(8.7)
20(10.3)
1.46(0.84–2.54)
23(7.0)
0.87(0.54–1.41)
55(11.0)
1.34(0.96–1.87)
98(9.6)
1.21(0.94–1.56)
pfortrend
p=
0.04
p=
0.18
p=
0.11
p=
0.21
UnknownBMI
4210(42.1)
82(42.0)
1.01(0.61–1.66)
135(41.3)1.25(0.87–1.81)
208(41.5)
0.90(0.67–1.21)
425(41.5)
1.02(0.82–1.26)
Tobaccosm
okingstatusb
Nonsm
oker
4625(46.2)
75(38.5)
1.00(reference)
134(41.0)1.00(reference)
196(39.1)
1.00(reference)
405(39.6)
1.00(reference)
Ex-smoker
825(8.2)
21(10.8)
1.40(0.85–2.30)
25(7.6)
1.10(0.71–1.70)
48(9.6)
1.39(1.00–1.93)
94(9.2)
1.30(1.02–1.65)
Currentsm
oker
1571(15.7)
36(18.5)
1.38(0.92–2.09)
75(22.9)
1.70(1.26–2.29)
111(22.2)
1.81(1.42–2.32)
222(21.7)
1.70(1.42–2.03)
Unknownstatus
2979(29.8)
63(32.3)
1.26(0.76–2.07)
93(28.4)
1.48(0.97–2.26)
146(29.1)
1.05(0.77–1.43)
302(29.5)
1.19(0.94–1.50)
Use
ofalcohol(units/day)c
0–2
3373(33.7)
55(28.2)
1.00(reference)
124(37.9)1.00(reference)
172(34.3)
1.00(reference)
351(34.3)
1.00(reference)
3–15
1662(16.6)
33(16.9)
1.08(0.70–1.69)
61(18.6)
0.99(0.72–1.36)
72(14.4)
0.82(0.61–1.09)
166(16.2)
0.92(0.75–1.12)
16–34
563(5.6)
14(7.2)
1.22(0.67–2.24)
19(5.8)
0.91(0.55–1.51)
25(5.0)
0.79(0.51–1.22)
58(5.7)
0.91(0.67–1.22)
>34
183(1.8)
4(2.0)
1.04(0.37–2.93)
2(0.6)
0.29(0.07–1.18)
10(2.0)
0.96(0.49–1.87)
16(1.6)
0.75(0.44–1.27)
Unknownuse
4219(42.2)
89(45.6)
1.38(0.84–2.26)
121(37.0)0.57(0.38–0.87)
222(44.3)
1.20(0.89–1.62)
432(42.2)
0.99(0.80–1.24)
aAllORsadjusted
forsex,age,
calendaryear,sm
oking,alcoholconsumptionandreflux.
bAllORsadjusted
forsex,age,
calendaryear,bodymass
index,alcoholconsumptionandreflux.
cAllORsadjusted
forsex,age,
calendaryear,sm
oking,bodymass
index
andreflux.
290 M. Lindblad et al.
category of each exposure variable, and were notassociated with any extreme estimates of relative risk.Moreover, any exposure misclassification should benon-differential and could, at the most, dilute the riskestimates. Since both height and weight are less fre-quently recorded during the GPs routine standardmedical care we studied the associations using only thevariable weight to reduce the amount of missing values.This rendered a mere 4% reduction of missing values,and heavy weight was similarly at raised risk ofesophageal and gastric cardia adenocarcinoma (datanot shown). Another potential limitation is the caseascertainment and tumor classification, since the tumorscould not be verified in a cancer registry. Validationstudies of the GPRD have found that over 90% of allreferrals are entered into the GP’s computer with adiagnosis code that truly reflects the specialist’s diagno-sis, however [31–33]. Furthermore, our manual review ofall computer-selected cases together with the review ofadditional information provided by the GP in a largesample of cases should reduce tumor misclassification.In spite of this review, there remained a high number ofmissing histology classifications in esophageal cancerand missing subsite classifications in gastric cancer.However, these two groups with unknown histology orunknown subsite were not found to be associated with
any extreme relative risk estimates (Tables 1 and 2),indicating that they represent a proportional mix of thecategorized esophageal histology and gastric subsite,respectively. Any remaining tumor misclassificationshould not be related to the studied exposures andcould therefore, at the most, weaken our results towardsnull. Both the esophageal adenocarcinoma male tofemale ratio, 4 : 1, and gastric cardia adenocarcinoma,3 : 1, found in this study were similar to previous datafrom the same background population [8–10], addingfurther support of validity. We lacked information onsome potentially relevant variables, including Helicob-acter pylori infection [36], dietary habits, socioeconomicfactors, and familiar antecedents that might distort ourresults. However, previous studies have shown that bodymass, tobacco smoking, and alcohol consumption areindependent risk factors of esophageal and gastriccancer [17, 18, 20, 22, 26–29, 37] not confounded bythe presence of the above mentioned unmeasured riskfactors. A further potential shortcoming of our study isthat the computerized database was initiated in the late1980s, and consequently prohibited assessment of expo-sures before that time. Recent exposure to the studiedexposures usually reflects also a valid estimate of pastexposure, however [27]. Several etiologic hypotheseshave been tested in our large nested case-control study,
Table 3. The sex-specific association between body mass index (BMI), and tobacco smoking status, and risk of esophageal and gastric cardia
adenocarcinoma
Exposure Controls Esophageal adenocarcinoma Gastric cardia adenocarcinoma
N (%) N (%) OR (95% CI) N (%) OR (95% CI)
Body mass index (Kg/m2)a
<20 Males 134 (2.0) 6 (2.6) 1.74 (0.71–4.25) 0 (0.0) 0.00
Females 124 (3.8) 2 (3.3) 0.85 (0.19–3.89) 2 (4.2) 0.97 (0.21–4.59)
20–24 Males 1471 (21.9) 36 (15.9) 1.00 (reference) 26 (17.7) 1.00 (reference)
Females 745 (22.7) 13 (21.7) 1.00 (reference) 10 (20.8) 1.00 (reference)
25–29 Males 1785 (26.6) 80 (35.2) 1.87 (1.25–2.80) 44 (29.9) 1.41 (0.86–2.30)
Females 662 (20.1) 14 (23.3) 1.08 (0.50–2.33) 11 (22.9) 1.20 (0.50–2.87)
‡30 Males 528 (7.9) 23 (10.1) 1.76 (1.03–3.02) 11 (7.5) 1.18 (0.58–2.42)
Females 341 (10.4) 13 (21.7) 2.13 (0.97–4.71) 9 (18.8) 1.91 (0.76–4.84)
Unknown BMI Males 2795 (41.6) 82 (36.1) 1.27 (0.78–2.07) 66 (44.9) 1.28 (0.71–2.28)
Females 1415 (43.0) 18 (30.0) 0.72 (0.29–1.77) 16 (33.3) 0.54 (0.21–1.44)
Tobacco smoking statusb
Non-smokers Males 2898 (43.2) 97 (42.7) 1.00 (reference) 58 (39.5) 1.00 (reference)
Females 1727 (52.5) 30 (50.0) 1.00 (reference) 17 (35.4) 1.00 (reference)
Ex smokers Males 663 (9.9) 21 (9.2) 0.94 (0.58–1.53) 15 (10.2) 1.06 (0.59–1.89)
Females 162 (4.9) 6 (10.0) 1.83 (0.73–4.56) 6 (12.5) 3.48 (1.32–9.15)
Current smokers Males 1187 (17.7) 55 (24.2) 1.39 (0.98–1.96) 25 (17.0) 1.10 (0.68–1.77)
Females 384 (11.7) 10 (16.7) 1.76 (0.83–3.71) 11 (22.9) 2.69 (1.21–5.99)
Unknown status Males 1965 (29.3) 54 (23.8) 0.79 (0.49–1.27) 49 (33.3) 1.27 (0.70–2.29)
Females 1014 (30.8) 14 (23.3) 1.26 (0.49–3.26) 14 (29.2) 1.33 (0.52–3.43)
a All ORs adjusted for age, calendar year, smoking, alcohol consumption and reflux.b All ORs adjusted for age, calendar year, body mass index, alcohol consumption and reflux.
Risk factors of esophageal and gastric adenocarcinoma 291

apart from those considered in this report. This multipletesting raises the risk of chance findings, i.e. type I error.Yet, we rest in assurance in that our hypotheses werepre-determined and well grounded on previous findings.Finally, our results with regard to squamous-cell carci-noma of the esophagus are well in line with the previouswell established results, indicating good overall internalvalidity of our study.To our knowledge, this is the first study that uses
prospective BMI data in the evaluation of the associa-tion with esophageal and gastric cancer. Our results
support the conclusion of six previous case-controlstudies that reported a positive association between BMIand risk of esophageal or gastric cardia adenocarcinoma[13–18]. A lack of association was indicated in two case-control studies, however [19, 20]. In one of thesenegative studies BMI values were assessed relativelyclose to the cancer diagnosis [20], which might haveintroduced reversed causality, i.e. the cancer reducedbody mass. The present study suggests that the raisedrisk of esophageal and gastric cardia adenocarcinomaamong overweight women was mainly restricted to
Table 4. Association between body mass index (BMI) and risk of esophageal and gastric cardia adenocarcinoma in stratified analyses by history
of reflux only and by history of reflux or hiatus herniaa
Variable Odds ratio (95% CI)b
Quartile 1c Quartile 2d Quartile 3e Quartile 4f Unknown BMI
Esophageal adenocarcinoma
Reflux No 1.0 (reference) 0.81 (0.47–1.40) 1.63 (1.02–2.60) 1.79 (1.13–2.81) 1.09 (0.67–1.78)
(Number of
cases/number
of controls)
(31/1317) (24/1324) (47/1319) (54/1312) (93/3954)
Yes 1.0 (reference) 1.24 (0.39–3.96) 0.78 (0.24–2.58) 1.44 (0.48–4.31) 0.65 (0.18–2.35)
(Number of
cases/number
of controls)
(6/130) (8/113) (7/141) (10/134) (7/256)
Reflux or
hiatus hernia
No 1.0 (reference) 0.78 (0.44–1.36) 1.60 (0.99–2.57) 1.70 (1.07–2.72) 1.07 (0.65–1.77)
(Number of
cases/number
of controls)
(30/1276) (22/1281) (44/1276) (49/1255) (87/3819)
Yes 1.0 (reference) 1.16 (0.41–3.28) 1.02 (0.36–2.83) 1.56 (0.61–4.04) 0.71 (0.24–2.09)
(Number of
cases/number
of controls)
(7/171) (10/156) (10/184) (15/191) (13/391)
Gastric Cardia adenocarcinoma
Reflux No 1.0 (reference) 0.71 (0.36–1.39) 1.44 (0.82–2.55) 1.54 (0.88–2.70) 0.94 (0.52–1.70)
(Number of
cases/number
of controls)
(21/1317) (15/1324) (30/1319) (32/1312) (73/3954)
Yes 1.0 (reference) 1.30 (0.30–5.76) 1.03 (0.23–4.55) 0.97 (0.20–4.71) 1.20 (0.28–5.14)
(Number of
cases/number
of controls)
(4/130) (4/113) (4/141) (3/134) (9/256)
Reflux or
hiatus hernia
No 1.0 (reference) 0.64 (0.31–1.33) 1.62 (1.90–2.90) 1.69 (0.94–3.02) 0.98 (0.53–1.81)
(Number of
cases/number
of controls)
(19/1276) (12/1281) (30/1276) (31/1255) (70/3819)
Yes 1.0 (reference) 1.39 (0.44–4.40) 0.59 (0.16–2.18) 0.61 (0.16–2.25) 0.97 (0.29–3.17)
(Number of
cases/number
of controls)
(6/171) (7/156) (4/184) (4/191) (12/391)
a Reflux includes any recordings of gastroesophageal reflux, esophagitis or heartburn.b Lowest BMI quartile, for men <23.6 and for women <22.9.c Lower-middle BMI quartile, for men 23.6–25.8 and for women 22.9–25.4.d Higher-middle BMI quartile, for men 25.9–28.1 and for women 25.5–28.7.e Highest BMI quartile, for men >28.1 and for women >28.7.f All ORs adjusted for sex, age, calendar year, smoking and alcohol consumption.
292 M. Lindblad et al.

individuals belonging to the highest BMI category (nonlinear response), whereas men were at a raised risk at alllevels of overweight. This could imply a differencebetween the sexes with regard to the association betweenBMI and these cancers, a hypothesis that is supported inthree previous studies [15, 17, 18], but not in a fourth[16]. The number of observations was small in all studieshowever, which advocates a cautious interpretation. Thebiological mechanism behind the association betweenbody mass and esophageal and gastric cardia adenocar-cinoma is unclear. One often suggested pathway is that ahigher BMI increases gastroesophageal reflux [21, 38,39], possibly due to higher abdominal pressure [40]. Thecurrent study, in line with previous findings [16], did notreveal any support for this hypothesis, however. More-over, our raised relative risk estimates among personswith a high BMI remained equally elevated when werestricted the analysis to persons without a recordedhistory of reflux symptoms or presence of a hiatal hernia(Table 4). Therefore, the mechanism behind the relationbetween BMI and these tumors is probably not reflux,and needs to be addressed in further research. Thefinding of an inverse association between higher BMIand esophageal squamous-cell carcinoma in our studyhas been reported previously [19, 41], and is most likelybecause persons at increased risk of this type ofesophageal cancer, i.e. persons using high combinedlevels of tobacco and alcohol, are often malnourished[13].There has been controversy regarding the role of
tobacco smoking as a risk factor of esophageal adeno-carcinoma. Two out of three large population-basedcase-control studies, designed to identify risk factors ofesophageal adenocarcinoma, found an increased riskamong smokers [18, 22], while the third – from ourgroup – did not [27]. The present study adds evidence toa true, but moderate positive association betweencurrent smoking and esophageal adenocarcinoma. Cur-rent female smokers were at a seemingly higher risk ofboth esophageal and gastric cardia adenocarcinomathan men, but the confidence intervals were overlapping.Ex-smokers were not at an elevated risk, indicatingbenefit of stopping smoking. These data must beinterpreted with caution, however, since former smokingis not recorded with high validity in the GPRD [34]. Thecausal mechanism by which tobacco smoking acts onupper gastrointestinal carcinogenesis is uncertain, but asuggestion has been that tobacco-specific N-nitrosoam-ines and other carcinogens contained in tobacco smokeare ingested and brought in direct contact with theupper gastrointestinal mucosa [42].Our lack of association between alcohol consumption
and risk of adenocarcinomas of the esophagus, gastric
cardia and non-cardia stomach is well in agreement withrecent well designed population-based case-controlstudies in the United States and in Sweden that haveaddressed the role of alcohol in the etiology of esoph-ageal and gastric cancers [18, 22, 27–29]. Therefore, incombination with existing data it seems reasonable tostate that no association exists.Our study included more female patients with esoph-
ageal and gastric cardia adenocarcinoma than any of thethree large-scale population-based case-control studiesaddressing the etiology of these tumors that have beencompleted [16–18]. The risk factors that we addresseddid not seem to explain any of the striking malepredominance among patients with esophageal or gas-tric cardia adenocarcinoma, however. Thus, the hypoth-esis that sex differences in risk factor profiles with regardto body mass, tobacco, or alcohol contribute to thisunexplained feature was not confirmed by our findings.In conclusion, our large prospective nested case-
control study supports that a higher body mass isassociated with an increased risk of esophageal andgastric cardia adenocarcinoma. Furthermore, tobaccosmoking is a moderately strong risk factor for esoph-ageal, gastric cardia and non-cardia gastric adenocarci-noma, while alcohol is not. Moreover, there were nostrong differences between the sexes in risk factorprofiles of the studied exposures that could contributeto explaining the strong male predominance amongpatients with esophageal or gastric cardia adenocarci-noma.
Acknowledgements
We wish to thank all participants and collaborators inthe GPRD for making this study possible. We are indebt to Weimin Ye at Karolinska Institutet for valuablestatistical and epidemiological input.
References
1. Howson CP, Hiyama T, Wynder EL (1986) The decline in gastric
cancer: epidemiology of an unplanned triumph. Epidemiol Rev 8:
1–27.
2. Sipponen P, Jarvi O, Kekki M, Siurala M (1987) Decreased
incidences of intestinal and diffuse types of gastric carcinoma in
Finland during a 20-year period. Scand J Gastroenterol 22: 865–
871.
3. Blot WJ, Devesa SS, Kneller RW, Fraumeni JF Jr (1991) Rising
incidence of adenocarcinoma of the esophagus and gastric cardia.
JAMA 265: 1287–1289.
4. Hansson LE, Sparen P, Nyren O (1993) Increasing incidence of
both major histological types of esophageal carcinomas among
men in Sweden. Int J Cancer 54: 402–407.
Risk factors of esophageal and gastric adenocarcinoma 293
5. Devesa SS, Blot WJ, Fraumeni JF Jr (1998) Changing patterns in
the incidence of esophageal and gastric carcinoma in the United
States. Cancer 83: 2049–2053.
6. Ekstrom AM, Hansson LE, Signorello LB, Lindgren A, Bergstrom
R, Nyren O (2000) Decreasing incidence of both major histologic
subtypes of gastric adenocarcinoma – a population-based study in
Sweden. Br J Cancer 83: 391–396.
7. Bollschweiler E, Wolfgarten E, Gutschow C, Holscher AH (2001)
Demographic variations in the rising incidence of esophageal
adenocarcinoma in white males. Cancer 92: 549–555.
8. Wayman J, Forman D, Griffin SM (2001) Monitoring the
changing pattern of esophago-gastric cancer: data from a UK
regional cancer registry. Cancer Causes Control 12: 943–949.
9. Powell J, McConkey CC, Gillison EW, Spychal RT (2002)
Continuing rising trend in oesophageal adenocarcinoma. Int J
Cancer 102: 422–427.
10. Newnham A, Quinn MJ, Babb P, Kang JY, Majeed A (2003)
Trends in the subsite and morphology of oesophageal and gastric
cancer in England and Wales 1971–1998. Aliment Pharmacol Ther
17: 665–676.
11. Parkin DM (2001) Global cancer statistics in the year 2000. Lancet
Oncol 2: 533–543.
12. Enzinger PC, Mayer RJ (2003) Esophageal cancer. N Engl J Med
349: 2241–2252.
13. Brown LM, Swanson CA, Gridley G, et al. (1995) Adenocarci-
noma of the esophagus: role of obesity and diet. J Natl Cancer Inst
87: 104–109.
14. Vaughan TL, Davis S, Kristal A, Thomas DB (1995) Obesity,
alcohol, and tobacco as risk factors for cancers of the esophagus
and gastric cardia: adenocarcinoma versus squamous cell carci-
noma. Cancer Epidemiol Biomarkers Prev 4: 85–92.
15. Ji BT, Chow WH, Yang G, et al. (1997) Body mass index and the
risk of cancers of the gastric cardia and distal stomach in
Shanghai, China. Cancer Epidemiol Biomarkers Prev 6: 481–485.
16. Chow WH, Blot WJ, Vaughan TL, et al. (1998) Body mass index
and risk of adenocarcinomas of the esophagus and gastric cardia.
J Natl Cancer Inst 90: 150–155.
17. Lagergren J, Bergstrom R, Nyren O (1999) Association between
body mass and adenocarcinoma of the esophagus and gastric
cardia. Ann Intern Med 130: 883–890.
18. Wu AH, Wan P, Bernstein L (2001) A multiethnic population-
based study of smoking, alcohol and body size and risk of
adenocarcinomas of the stomach and esophagus (United States).
Cancer Causes Control 12: 721–732.
19. Kabat GC, Ng SK, Wynder EL (1993) Tobacco, alcohol intake,
and diet in relation to adenocarcinoma of the esophagus and
gastric cardia. Cancer Causes Control 4: 123–132.
20. Zhang ZF, Kurtz RC, Sun M, et al. (1996) Adenocarcinomas of
the esophagus and gastric cardia: medical conditions, tobacco,
alcohol, and socioeconomic factors. Cancer Epidemiol Biomarkers
Prev 5: 761–768.
21. Romero Y, Cameron AJ, Locke GRIII, et al. (1997) Familial
aggregation of gastroesophageal reflux in patients with Barrett’s
esophagus and esophageal adenocarcinoma. Gastroenterology 113:
1449–1456.
22. Gammon MD, Schoenberg JB, Ahsan H, et al. (1997) Tobacco,
alcohol, and socioeconomic status and adenocarcinomas of the
esophagus and gastric cardia. J Natl Cancer Inst 89: 1277–1284.
23. Chao A, Thun MJ, Henley SJ, Jacobs EJ, McCullough ML, Calle
EE (2002) Cigarette smoking, use of other tobacco products and
stomach cancer mortality in US adults: the Cancer Prevention
Study II. Int J Cancer 101: 380–389.
24. Sasazuki S, Sasaki S, Tsugane S (2002) Cigarette smoking, alcohol
consumption and subsequent gastric cancer risk by subsite and
histologic type. Int J Cancer 101: 560–566.
25. Gonzalez CA, Pera G, Agudo A, et al. (2003) Smoking and the
risk of gastric cancer in the European Prospective Investigation
Into Cancer and Nutrition (EPIC). Int J Cancer 107: 629–634.
26. Machida-Montani A, Sasazuki S, Inoue M, et al. (2004) Associ-
ation of Helicobacter pylori infection and environmental factors in
non-cardia gastric cancer in Japan. Gastric Cancer 7: 46–53.
27. Lagergren J, Bergstrom R, Lindgren A, Nyren O (2000) The role
of tobacco, snuff and alcohol use in the aetiology of cancer of the
oesophagus and gastric cardia. Int J Cancer 85: 340–346.
28. Hansson LE, Baron J, Nyren O, Bergstrom R, Wolk A, Adami HO
(1994) Tobacco, alcohol and the risk of gastric cancer. A popula-
tion-based case-control study in Sweden. Int J Cancer 57: 26–31.
29. Ye W, Ekstrom AM, Hansson LE, Bergstrom R, Nyren O (1999)
Tobacco, alcohol and the risk of gastric cancer by sub-site and
histologic type. Int J Cancer 83: 223–229.
30. Garcıa Rodrıguez LA, Perez Gutthann S (1998) Use of the UK
General Practice Research Database for pharmacoepidemiology.
Br J Clin Pharmacol 45: 419–425.
31. Jick H, Jick SS, Derby LE (1991) Validation of information
recorded on general practitioner based computerised data resource
in the United Kingdom. BMJ 302: 766–768.
32. Jick H, Jick S, Derby LE, Vasilakis C, Myers MW, Meier CR
(1997) Calcium-channel blockers and risk of cancer. Lancet 349:
525–528.
33. Jick SS, Kaye JA, Vasilakis-Scaramozza C, et al. (2003) Validity of
the general practice research database. Pharmacotherapy 23: 686–
689.
34. Lewis JD, Brensinger C (2004) Agreement between GPRD
smoking data: a survey of general practitioners and a popula-
tion-based survey. Pharmacoepidemiol Drug Saf 13: 437–441.
35. Joint FAO/WHO/UNU Expert Consultation (1985) Energy and
Protein requirements. World Health Organization Technical Report
Series No. 724; 1–67. Geneva: World Health Organization,
pp. 1–67.
36. IARC International Agency for Research on Cancer, World
Health Organization (1994) Infection with Helicobacter pylori. In:
Shistosomes, Liver Flukes and Helicobacter pylori. Lyon: IARC.
37. Lagergren J, Ye W, Lindgren A, Nyren O (2000) Heredity and risk
of cancer of the esophagus and gastric cardia. Cancer Epidemiol
Biomarkers Prev 9: 757–760.
38. Nilsson M, Johnsen R, Ye W, Hveem K, Lagergren J (2003)
Obesity and estrogen as risk factors for gastroesophageal reflux
symptoms. JAMA 290: 66–72.
39. Wu AH, Tseng CC, Bernstein L (2003) Hiatal hernia, reflux
symptoms, body size, and risk of esophageal and gastric adeno-
carcinoma. Cancer 98: 940–948.
40. La Vecchia C, Negri E, Lagiou P, Trichopoulos D (2002)
Oesophageal adenocarcinoma: a paradigm of mechanical carcino-
genesis? Int J Cancer 102: 269–270.
41. Brown LM, Blot WJ, Schuman SH, et al. (1988) Environmental
factors and high risk of esophageal cancer among men in coastal
South Carolina. J Natl Cancer Inst 80: 1620–1625.
42. De Stefani E, Barrios E, Fierro L (1993) Black (air-cured) and
blond (flue-cured) tobacco and cancer risk. III: Oesophageal
cancer. Eur J Cancer 29A: 763–766.
294 M. Lindblad et al.