board-main-papers-31119.pdf - Hertfordshire Community ...
125
1 Hertfordshire Community NHS Trust Board Meeting in Public Thursday 31 January 2019 1.30 to 3.30 Mill Green Golf Club Gypsy Lane Welwyn Garden City AL7 4TY For map and directions please see: https://millgreengolf.co.uk Parking: Parking available at the venue AGENDA Lead For Att. Allocated Time Approx. Timing (A) Patient / Service Story 15 mins 13.30 –13.45 AP/SH Patient Story ( Community Paediatrics) To note (B) HealthWatch 5 mins 13.45 –13.50 A verbal report from Maryrose Brennan, HealthWatch observer, on HealthWatch news and issues pertinent to the Trust. To note for assurance (verbal) 5 mins (C) Opening administration 5 mins 13.55 –14.00 DO’F 1. Welcomes, Introductions and Apologies for Absence To note DO’F 2. Chair’s Announcements / Notice of Urgent Business (to include confirmation of Board appointments and leavers): To note DO’F 3. Declarations of Interest (Members to declare any interests material to items on the agenda) To note Board 4. Ratification of items of Chair’s and Chief Executive’s Action taken since the last meeting under Standing Order 5.2 To ratify DO’F 5. To approve the Minutes of the meeting held on 29 November 2018 To approve (C1)
-
Upload
khangminh22 -
Category
Documents
-
view
14 -
download
0
Transcript of board-main-papers-31119.pdf - Hertfordshire Community ...

1
Hertfordshire Community NHS Trust Board Meeting in Public
Thursday 31 January 2019
1.30 to 3.30
Mill Green Golf Club Gypsy Lane
Welwyn Garden City AL7 4TY
For map and directions please see: https://millgreengolf.co.uk
Parking: Parking available at the venue
AGENDA
Lead For Att. Allocated Time
Approx. Timing
(A) Patient / Service Story 15 mins 13.30 –13.45
AP/SH Patient Story ( Community Paediatrics) To note
(B) HealthWatch 5 mins 13.45 –13.50
A verbal report from Maryrose Brennan, HealthWatch observer, on HealthWatch news and issues pertinent to the Trust.
To note for assurance (verbal) 5 mins
(C) Opening administration 5 mins 13.55 –14.00
DO’F 1. Welcomes, Introductions and Apologies for Absence To note
DO’F
2. Chair’s Announcements / Notice of Urgent
Business (to include confirmation of Board appointments and leavers):
To note
DO’F
3. Declarations of Interest (Members to declare any interests material to items on the agenda) To note
Board
4. Ratification of items of Chair’s and Chief
Executive’s Action taken since the last meeting under Standing Order 5.2
To ratify
DO’F 5. To approve the Minutes of the meeting held on 29 November 2018 To approve (C1)

2
Lead For Att. Allocated Time
Approx. Timing
(C) Opening administration 5 mins 14.00 –14.05
DO’F 6. Matters arising from the Minutes of the
meeting held on 29th November 2018 (Tracker).
To note (C2)
(D) Strategy, Resources and Engagement 30 mins 14.05 –14.35
CEO 1. Chief Executive’s Report To note (D1)
DB 2. Finance Report (Month 9) To note (D2)
(E) Clinical Services and Healthcare Governance 20 mins 14.35 –14.55
HP 1. Clinical Quality and Medical Directorate Report To note (E1)
TW 3. Community Hospital Safe Staffing Report Oct/Nov
To note for assurance (E2)
HP 2. Learning from Death (Qtr 3 2018/19) (previously Mortality Report
To note for assurance (E3)
AM 3. Chair of Healthcare Governance Committee’s
Assurance Report for the meeting held on 22 January 2019
To note for assurance (E4)
(F) Performance and Operations 5 mins 14.55 –15.00
DB 1. Summary Integrated Board Performance Report
To note for assurance (F1) 5 mins
(G) Board Governance and Leadership 5 mins 15.00 –15.05
RB 1. Update on Remuneration Committee Meeting To note (G1)
JP 2. Audit Committee Chair’s Assurance report
and minutes from the meeting held on 11 December 2018
To note (G2)
(H) Urgent Business 5 mins 15.05- 15.10
(As notified under Item (B) 2 above)

3
Lead For Att. Allocated Time
Approx. Timing
(J) Risks Arising / Observations 5 mins 15.10 –15.15
TW 1. Summary of High Level Risk Register To review (J1)
TW 2. Board Assurance Framework To review (J2)
MD 3. EPRR Core Standards Compliance To note letter from NHSE dated 18.12.18 To note (J3)
DO’F 4. Summary of Risks Arising To discuss (verbal)
(K) Supporting Papers / Items for Receipt and Noting Only 5 mins 15.15 –15.20
D1 i. NHS Long Term Plan – NHS Providers (K1)
D2 ii. Finance Report (Month 9) (K2)
E4 iii. Minutes of the Healthcare Governance Committee held on 20th November 2018 (K3)
F1 iv. Integrated Board Performance Report (K4)
G2 v. Minutes from the Audit Committee meeting held on 11 December 2018 (K5)
(L) Date, Time & Venue of Next Meeting(s) 2 mins 15.20-15.22
DO’F 13.30 pm to 15.30pm 28th March 2019 venue tbc
(M) Questions from the Public 5 mins 15.22 –15.27
DO’F
The Chair will take questions from members of the public. Questions which cannot be addressed at the meeting or in the time allocated will be noted. Replies will be communicated to questioners following the meeting and reported to the next Board meeting in public.
(M) Informal Review of Meeting 5 mins 15.27 –15.30
Please note that Board papers and Trust papers referenced in Reports are available on the Trust’s Website at:
https://www.hct.nhs.uk/about-us/our-board/meeting-papers/
Hard copies or copies in large size font or in translation can be provided on application to:
The Assistant Board Secretary Hertfordshire Community NHS Trust Unit 1A Howard Court, 14 Tewin Road, Welwyn Garden City, Hertfordshire, AL7 1BW

Board 31st January 2019 Attachment C1
Page 1 of 19
HERTFORDSHIRE COMMUNITY NHS TRUST
Minutes of the Hertfordshire Community NHS Trust Board Meeting Held in Public on 29P
thP November 2018
Christchurch (Peartree) Baptist,
20 Tewin Road, Welwyn Garden City Herts AL& 1BW
Key Points from the meeting for the Board to note: The following were approved / ratified
(i) The Board ratified the Chair’s action taken on 25th October 2018 to sign off the Herts Valley Clinical Commissioning Groups Adult Community Service tender prior to submission.
(ii) The Corporate Trustees delegated authority to the Audit Committee on the 11 December to sign off the Charitable Funds Annual Accounts and Annual report 2017/18
The following were noted: (i) The Board noted the content of the Chief Executive’s Report. (ii) The Board noted the content of the Finance Report (Month 7) (iii) The Board noted the content of the Clinical Quality and Medical Director Update (iv) The Board noted the content of the Quality Report Quarter 2 (v) The Board noted the content of the Community Hospital Safe Staffing Report Q2. (vi) The Board noted the Mortality Reviews Q1 and Q2 (vii) The Board noted the Healthcare Governance Committee verbal Chair’s report for the meeting
held on 20P
thP November 2018
(viii) The Board noted the content of the Integrated Board Performance Report (ix) The Board noted the remuneration committee update (x) The Board noted the Freedom to Speak Up (FTSU) update. (xi) The Board noted the Board Governance Update (xii) The Board noted changes to the HLRR during September/ October and progress and
assurance on the management of risks (xiii) The Board noted that the full Board Assurance Framework was reviewed and discussed in the
Trust Board meeting held in Private on 29 P
thP November due to commercially sensitive
information.
PRESENT (* Voting Member of the Board) Declan O’Farrell (DOF) Chair* Anne McPherson (AM) Non-Executive Director* Alan Russell (AR) Non-Executive Director (Vice Chair)* Dr Linda Sheridan (LS) Non-Executive Director* Brenda Griffiths (BG) Non-Executive Director (Designate) Clare Hawkins (CH) Chief Executive Officer* Dr Hari Pathmanathan (HP) Medical Director and Acting Deputy Chief Executive* David Bacon (DB) Director of Finance (Interim)*
Marion Dunstone (MD) Director of Operations
Julie Hoare (JH) Director of Partnerships and Service Development
Antonia Robson (ARo) Director of Business Services

Board 31st January 2019 Attachment C1
Page 2 of 19
IN ATTENDANCE Alison Ryder (ARy) Deputy Director of HR and OD Tracey Westley (TW) Assistant Director Risk & Quality Assurance Meg Carter (MC) HealthWatch Observer Lorraine (L) Early Support Discharge Team (ESDT) Patient Kate Crossland (KC) Early Support Discharge Team (ESDT) Occupational Therapist Hana Bond (HB) Early Support Discharge Team (ESDT) Physiotherapist Anthony Power (AP) Head of Patient Experience Mark Graver (MG) Head of Communications and Engagement Marina Sweatman (MS) Assistant Board Secretary (minutes)
APOLOGIES Jeff Phillips (JP) Non-Executive Director* Tricia Wren (TW) Director of Quality and Nursing (Acting)*
Raj Bhamber (RB) Director of Human Resources and Organisational Development (Interim)
Andy Nuckcheddee (AN) Deputy Director of Quality & Nursing Deputy Director of Quality & Governance and Deputy Chief Nurse
(A)
150/18 Patient Story
Today’s patient story provided an overview of the 6 weeks intensive, home-based therapy provided for stroke patients on their discharge from hospital by the West Hertfordshire Early Supported Discharge (ESD) team. The team, which was set up in 2015, receive the majority of their referrals from the Acute Stroke unit from Watford General Hospital. The care and therapy provided is patient centred and involves an extensive multidisciplinary team (MDT). The team set clear Goal Attainment Scaling (GAS) in rehabilitation goals which are closely monitored over the 6 week treatment period. The team are audited on accessibility and outcomes which include meeting key performance indicators, GAS goal outcomes and therapy specific improvement outcomes. Patients are given the opportunity to give feedback at the end of their treatment plan and more recently through patient stories. Lorraine, a mother of two young children, who worked as a professional at senior level in a fast paced role with a large team prior to her illness explained very clearly, confidently and enthusiastically about her involvement with the ESD team and their contribution to her rehabilitation. She gave a clear insight into the impact that her condition had had on her physical, mental and psychological ability and confidence to undertake the basic tasks in everyday family life. Lorraine explained in detail how the ESD team had personalised their rehabilitation approach to maximise the relevance of the treatment to make a difference to her world and family. The team supported and educated her about fatigue, limitations and pace. They always made her feel important and never rushed their treatments. The MDT working

Board 31st January 2019 Attachment C1
Page 3 of 19
enabled the treatment to progress at her pace and not to a service schedule and their method of teaching both visual and practical, enabled her to build her confidence and to plan and carry out family tasks and outings. Lorraine expressed that she had very good family support and the team included the family, providing support and guidance throughout and she felt this was an example of excellent partnership working. Lorraine thanked the ESD team and HCT for the incredible personalised service and advised that following her six month review she is planning a phased return to work in January 2019.
150/18 Observations and response to Patient Story
a) JH expressed that it was really interesting to understand the involvement with the service from both sides and pleasing to hear that the service worked in partnership with the family to provide support and guidance.
b) MD asked if Lorraine had had any involvement with voluntary stroke services. Lorraine advised that she had been signposted to a number of voluntary services and they are available should she want to access ongoing community support. KC advised that all patients on the stroke pathway are contacted by the Stroke Association and they are involved in a large proportion of the six month reviews.
c) MC expressed how inspirational Lorraine’s account was and
observed that the team approach to personalised care is one that continues to have a powerful effect on patients and has become a generic approach for the Trust. Lorraine expressed that this is an example of a personal health budget in a notional way and a shining example of MDT working.
d) AM expressed that this story shows remarkable courage and
determination both physically and psychologically and asked if there was anything that she had experienced that could be passed onto other patients in the future. Lorraine advised that she had had good family support; this can be difficult for patients if they don’t have this support and motivation is difficult when fatigued. Lorraine recognised that peer to peer support is important.
HB explained about the programme “Living well with stroke” which is offered after the treatment has concluded. One patient has developed a social support group. The team are thinking of other ways of supporting patients and encouraging patients to become engaged in peer support. KC advised that currently there are two “living well with stroke” groups on each side of the county but this is being reduced to one each side next year, this will have an impact on the waiting list which currently stands at three years.
e) KC expressed that she feels incredibly fortunate to have worked in
this team from the start, working with exceptional staff and very engaged and involved patients. She “loves” her job.

Board 31st January 2019 Attachment C1
Page 4 of 19
f) ARo asked if Lorraine had any advice on how to convey the benefits
of this service to the commissioner. Lorraine advised that today’s presentations and sharing quality information with commissioners could help and seek out others involved to demonstrate this to them. Lorraine volunteered to help in this journey.
Decision(s), Outcome(s) and Action(s)
1. DOF thanked Lorraine for sharing her story and wished her the best
for the future. KC, HB and AP were thanked for their involvement and making this story possible.
(B) 151/18 HealthWatch Action
MC apologised for not attending the last meeting, apologies were sent but not received. MC confirmed that this is her last meeting with HCT as the HealthWatch Hertfordshire (HWH) observer as she is moving to West Herts Hospitals NHS Trust. MC will be focus on supporting and engaging with West Hertfordshire Hospitals Trust in respect of the Hospital development programme. Mary Rose Brennan will take over as the HCT HWH observer from January 2019. Q. TW asked how HWH fits with the National HealthWatch agenda and
contract development as a whole. R MC advised that HWH is aligned with the national group and the
communication between the two is very good. The focus for both is facilitating meaningful engagement with family members, users and services. HWH are negotiating with NHS England for funding to support this. HWH is independent but their role is to ensure that the voice of patients is heard, especially as how linked to service delivery.
(C) Opening administration 152/18 Welcome, Introductions and apologies
The Chair welcomed members of the Board and those in attendance to the meeting. Apologies were received from TWr, JP, RB, AN.
153/18 Chair’s Announcements / Notice of Urgent Business (to include confirmation of Board appointments and leavers)
The chair announced that: i) This is MC’s last meeting with HCT as HWH Observer. Thanks were
extended to her for her input and involvement during her term as representative.
ii) Mary Rose Brennan will commence as the new HWH observer in January 2019.

Board 31st January 2019 Attachment C1
Page 5 of 19
iii) Paul Burstow has been appointed as the Independent Chair to the Herts & West Essex Sustainability and Transformation Partnership (STP).
iv) Clare Hawkins has recently been appointed as HCT’s Chief Executive Officer. CH was welcomed into her new substantive role.
v) Tricia Wren will be retiring from her post as Director of Nursing and Quality (Acting) in December. Thanks were extended to Tricia for all her involvement and hard work and she will be missed.
vi) Sarah Browne has been appointed to the role of Director of Nursing and Quality and is expected to be in post early in 2019.
154/18 Declarations of Interest (Members to declare any interests material to items on the agenda)
No items declared
155/18 Ratification of items of Chair’s and Chief Executive’s Action taken since the last meeting under Standing Order 5.2
The Board was asked to ratify the Chair’s action taken on 25P
thP October
2018 to sign off the Herts Valleys Clinical Commissioning Group’s (HVCCG) Adult Community Service tender prior to submission.
Decision(s), Outcome(s) and Action(s)
1. Herts Valleys Clinical Commissioning Groups Adult Community
Service tender sign off was ratified.
156/18 Minutes of the meeting held in Public on 27 September 2018
The minutes of the meeting in Public held on 27P
PSeptember 2018 were
agreed as a correct record.
157/18 Matters arising from the Minutes of the meeting held on 27P
thP
September 2018 (Tracker) Action
137/18 Community Hospitals Safe Staffing
MD reported there are two elements to this item, firstly Discharge Home to Assess (DH2A) has now been extended to the east of the county including the Princess Alexandra Hospital and secondly the Winter plan may lead to HCT opening extra escalation beds. Staffing safety will be considered before these are implemented. The winter plan update and any staffing issues will be scrutinised in the Board committees. Action: Board action to be shown as complete.
114/18 Workforce Race Equality Standard (WRES) Report
This work will be incorporated into the Equality Delivery Scheme 2 which will be considered at the March Board. A revised date March 2019 was approved.

Board 31st January 2019 Attachment C1
Page 6 of 19
CH advised that one of the CEO’s objectives is to provide leadership in Equality and Diversity for the organisation. A small exploratory group has been formed to discuss and develop a proposal on the roles and proactive approach to be taken by the leaders of the organisation. This will be discussed with staff and shared with the Board in the Equality Delivery Scheme. Action: A brief update to be included in the January meeting.
CH/RB
146/18 Freedom to Speak Up (FTSU)
It was noted that the Freedom to Speak Up Q2 report is an agenda item for this meeting. The Board had agreed that this would in the future be reported six monthly to protect the confidentiality of individuals as there are small numbers reported.
(D) Strategy, Resources and Engagement 158/18 Chief Executive’s Report
CH asked the Board to note a number of areas referred to in the Chief Executive’s Report, some of the subject areas were discussed in detail in the Board meeting in Private. An update of items not covered by the report included: i) The Trust has agreed to support the Hertfordshire County Council
Public Health Team (PHT) in their application as a trailblazer for Childhood Obesity. Hertfordshire Community NHS Trust (HCT) will partner with PHT and has committed to introducing Childhood Obesity into the Sustainability Transformation Partnership (STP) as a key area of focus for the whole of the system.
ii) Thanks were given to Andy Nuckcheddee for his contribution not
only undertaking the Deputy Director of Nursing role but also covering a large proportion of the Chief Nurse portfolio during TWr’s absence, along with being instrumental in supporting the Care Quality Commission (CQC) inspection.
Recently Andy has supported the team that work at HMP the Mount through an extensive Coroner’s inquest and is currently preparing for another one due shortly. The Mount healthcare team previously reported they did not feel well supported in this area, The feedback from staff on this occasion confirmed that they felt much more supported. It was noted that the outcome of the inquest stated that there was no criticism of any person of organisation or specific factors which contributed to the prisoner’s death. The Board extended their condolences to Mr Nichols family who were present throughout the inquest.
Chief Executive Report 3.0 The National/Regional updates
The National and Regional update included:

Board 31st January 2019 Attachment C1
Page 7 of 19
• Investment into Social Care to support the NHS over winter • NHS England (NHSE) and NHS Improvement (NHSI) Regional
Urgent & Emergency Care Reporting • NHS Violence Reduction Strategy • Draft Brexit Agreement and Outline UK’s future relationship with
the EU • “Prevention is better than cure”- The government’s vision for
helping people to live well for longer • Health Service Journal (HSJ) Award 2018- System Led Support
for Carers • Announcement of funding for community services under the long
term plan by Matt Hancock, Secretary of State for Health & Social Care
Chief Executive Report 4.0 Matters Internal and local to the Trust
The matters internal and local to the Trust included:
• Clare Hawkins appointment as Chief Executive of the Trust • Director of Nursing and Quality/ Chief Nurse update • Annual General Meeting and Annual Leader Conference feedback • Care Quality Commission Inspection – Quality update • Ofsted inspection of Children’s Social Care Services outcomes • Herts Valleys Adult Community Services tender • Coroner’s Inquest update, outcome and condolences to the family.
Chief Executive Report 5.0 Human Resources and Organisational Development
The Human Resources and Organisational Development updates included:
• Temporary Staffing and Agency cost controls • Annual staff survey • Apprenticeship programme • Mandatory training – My learning zone update • Reimbursement of EU staff applying to settle in the UK
Chief Executive Report 5.2 Vacancy Rates
HCT overall vacancy rate across the Trust has reduced to 10.5 % for the month of October, down from 12.4% in September. This is due to a combination of successful recruitment activity, coupled with a reduction in the budgeted establishments in E&N Herts Adult Community Services and Children’s Public Health Nursing as a result of commissioning changes. Recruitment and retention remains a focus for the organisation.
Chief Executive Report 5.4 Influenza Vaccination Campaign for Healthcare staff
This year’s campaign to meet the 75% staff flu vaccination target is well advanced, with the Occupational Health drop-in clinics now complete and

Board 31st January 2019 Attachment C1
Page 8 of 19
further clinics being run by internal champions. Currently 55% of frontline staff have received their vaccination which is behind uptake at this time in the 2017 campaign. Every staff member that has not yet taken up the vaccination has been contacted, it is hoped that this will result in further uptake. In line with the letter from NHSE and NHSI on 7 September 2018, the best practice management checklist, including a self-assessment against these measures, is included for information in the supporting papers.
Chief Executive Report 6.0 Update from Operational Services
The Operational Services update included:
• East and North Herts Integrated Care Teams (ICTs) update • Discharge Home to Assess – Herts Valley • Discharge Home to Asses – East and North Herts • Community Paediatrics Service • Public Health Nursing Service • Children’s and Young People Specialist Partnership Event
Chief Executive Report 6.1 Patient Flow
NHSE and NHSI wrote to all Trusts in respect of Winter Planning, reminding them of the ambition to reduce the number of beds occupied by long stay patients by 25% to thereby free up 4,000 beds as compared to 2017, supporting patients to move out of the acute setting and ensuring patients receive the appropriate level of care in the community and in their own homes. HCT has noted significant improvement in patient flow following the introduction of new clinical pathways which has reduced average length of stay (ALoS) by 6 days during October. This will need to be sustained during the winter period.
Chief Executive Report 6.2 Winter Planning
Work is continuing with system partners in both Herts Valleys and E&N Herts to plan and prepare for winter with escalation plans being tested both internally and across the system. Additional community capacity (Discharge Home to Assess and Virtual Beds) are being commissioned and additional bed based capacity will be available when required in line with the system Operational Pressures Escalation Levels (OPEL) status.
Chief Executive Report 6.7 Nascot Lawn
Nascot Lawn was decommissioned from 22 November 2018 by Herts Valleys CCG. HCT was able to continue to deliver a service at Nascot Lawn until October 2018 despite significant staffing challenges.

Board 31st January 2019 Attachment C1
Page 9 of 19
All staff have now successfully been redeployed and the children have safely been transitioned to their new respite provision. Thanks were extended to all staff and management at Nascot Lawn who remained dedicated and committed to supporting the children, young people and their families through the transition process in spite of the extended period of uncertainty.
Chief Executive Report 7.0 Finance, Estates and Information Governance
Other areas in the Finance, Estates and Information Governance update included:
• Performance and benchmarking, HCT’s attendance at the National conference
• Adult Frailty working with ENCCG in the development of ICT (Frailty) and associated key performance indicators (KPI)
• Herts- wide analytics • Clinical Support Systems • Project Management Office – Portfolio Assurance Group
DB provided an update on the Harpenden Memorial Hospital Outline Business Case (OBC). The OBC was presented to Herts Valleys CCG for sign off; HVCCG asked for additional information which was supplied, they has been a subsequent request for further information which is currently being provided. It was noted that the additional information requested would usually be provided in the Full Business Case. HCT awaits receipt of HVCCG support in order to progress the planning application. CH advised that the CEO of HVCCG has advised that The HVCCG Board intend to support this application in their January Board meeting.
Chief Executive Report 7.3 Daily Downloads
The national programme of converting historical organisation identifiers has had some impacts on the Trust’s daily reporting. The Trust is currently working with Bluefish and TPP to implement a solution that minimises the impact in future phases.
Chief Executive Report 7.4 Information Management & Technology (IM&T) Update
i) Network upgrades for increased network performance and video conferencing have continued. One priority 1 site remains, this will be completed before the end of 2018 and the priority 2 sites will commence in 2019.
ii) Deployment of new phone systems for various Customer Service
Transformation (CST) sites is underway. The first wave of 300 Smartphones has been deployed in Watford and Hertsmere. The deployment of the remainder (approx. 2000+) continues.

Board 31st January 2019 Attachment C1
Page 10 of 19
Chief Executive Report 8.00 Estates Update
Other areas in the Estates update not mentioned below included:
• Capital Developments for 2018/19 – schemes are progressing
Chief Executive Report 8.1 Strategy
The Estates update included:
• The development of a joint HCT/Hertfordshire Partnership University Foundation Trust (HPFT) Integrated Estates Strategy is underway; this will be in draft form by January 2019. STP wave 5 bids are expected to be submitted in April 2019 to potentially allow the Trust to utilise some of these funds to deliver schemes in the strategy.
Chief Executive Report 8.3 Operational Estates
The new staff structure for the joint HCT/HPFT Estates and Facilities Department was launched on 1 October 2018. The staffing of this structure is almost complete.
Observations (O) Questions (Q) and Response (R) to Chief Executive’s Report
Q. MC asked for clarification on the term “virtual bed” and what this involves.
R MD advised that Early Support Discharge (ESD) or virtual beds can be described as the patient bed in the patient’s home or care home with a care team providing the care within the home that would otherwise be provided in an inpatient unit. This approach is proven to be more effective for patients by remaining in their own home environment.
O The Board proposed to write to thank all Nascot Lawn staff and
management for their commitment, dedication and contribution supporting the patients and families during the closure process of Nascot Lawn
O AM asked for clarification around the location of St Paul’s as
mentioned in the estates report. R. It was advised this is a temporary base for HCT staff Slippers Hill,
Hemel Hempstead.
Q LS asked what impact is the further delay on the Harpenden Memorial Hospital OBC having on the Trust’s capital plan?
R DB advised that this year’s plan is not significantly affected as it is still in the planning and application stage but future years will factor in larger sums of investment. HVCCG have been asked to support the scheme to take this forward to a planning application.
159/18 Decision(s), Outcome(s) and Action(s)
i. The Board noted the content of the Chief Executive’s Report.

Board 31st January 2019 Attachment C1
Page 11 of 19
ii. Letter to be sent to staff and management of Nascot Lawn on behalf
of the Board expressing gratitude for their commitment, dedication and professionalism during the transition of respite services.
CH
160/18 Finance Report (Month 7)
The highlights were discussed:
• Trust performance against the control total is on plan in month 7 and ahead of plan year to date.
• The Trust's single oversight risk rating is still maintained at a 1. • The Trust is forecasting to achieve the control total of £2,077K as
per the 2018/2019 Operating Plan Submission. • Agency Expenditure is £621K against the target of £541k. This
has shown improvement against previous months. • The Trust Cost Improvement Programme delivered £460K against
a target of £460K and year to date £2,797K against a target of £2,797K.
• Capital expenditure was £1,565K delivered against a target of £2,380K. Options are being developed to ensure that the target will be met in year. This could potentially involve bringing forward some programmes.
• The Cash Plan for month 7 is £24,991K which is above the target of £17,304K
Observations (O) Questions (Q) and Response (R) to Finance Report (Month 5)
Q. BG asked that if there has been significant recruitment of staff why is this not reflected in the agency expenditure?
R. ARy advised that the agency expenditure is reducing but it is not directly correlated to vacancies, as covering vacancies is only one of the uses of agency staff.
O DOF acknowledged the improved performance and that the challenges are being managed.
Decision(s), Outcome(s) and Action(s)
i. The Board noted the content of the Finance Report (Month 7)
(E) Clinical Services and Healthcare Governance
161/18 Clinical Quality and Medical Director Update
Dr Hari Pathmanathan provided highlights on current work streams. Other areas in the Clinical Quality and Medical Director Update not mentioned below included:
• Frailty Programme update • Learning from Deaths • Medical Job Planning • Clinical Effectiveness group • Medical Revalidation • Infection Prevention and Control- Healthcare Associated Infections
(HCAI) – Outbreaks and appeals

Board 31st January 2019 Attachment C1
Page 12 of 19
• Safeguarding Children o CQC Well Led Inspection o Ofsted Inspection o Safeguarding Training update
• Safeguarding Adults Review update o Policy update
• Safe Staffing o NHS Improvement’s Retention Direct Support Programme o New NMC Standards of Education & Training o NMC Quality Assurance Framework
• CQUIN update
Clinical Quality and Medical Director Update 3.1 Do Not Attempt Cardiopulmonary Resuscitation (DNACPR)
In response to queries raised by CQC inspectors regarding DNACPR forms and mental capacity assessments a number of actions have been taken. These include the production of a DNACPR audit form and updating the DNACPR policy to reflect the remedial and sustained actions. Additional training for medical and nursing staff is being planned
Clinical Quality and Medical Director Update 3.4 Sepsis Management
Sepsis has been identified as a quality improvement for 2019/20. A new group has been established, chaired by Dr Elizabeth Kendrick, Deputy Medical Director, to undertake a baseline assessment and formulate a robust strategy on sepsis prevention and management.
Clinical Quality and Medical Director Update 5.1 Medicines Management and Safety
The CQC inspection reviewed Medicines Management in the inpatient units and the inspector reported a series of findings. These show that there are some gaps in Medicines Management across our Community inpatients units. In order to address the issues the Chief Pharmacist is developing a proposal to strengthen the pharmacy provision across HCT.
Observations (O) Questions (Q) and Response (R) to Clinical Quality and Medical Director Update Action
Q. DOF advised that it is really pleasing to see that there are plans underway to strengthen the Pharmacy service, however as this is funded by a block contract what are the plans to fund this additional service as it is not commissioned?
R. HP confirmed that this was the historic approach, however in light of the changing workforce, an increase in nurse prescribing and with community services taking on more of the GP work load; he agreed that this will need to be addressed via a contract review with the commissioners.

Board 31st January 2019 Attachment C1
Page 13 of 19
Decision(s), Outcome(s) and Action(s)
i. The Board noted the content of the Clinical Quality and Medical
Director’s Update
162/18 Quality Report Quarter One
TW provided the detail of the quality achievements and challenges during Quarter Two, 2018/19. The full report was supplied in the supporting papers. An additional challenge not noted in the report related to the achievement of the Influenza CQUIN which requires an uptake of 75%. This currently stands at 55%. A variety of actions are being taken. However the non achievement of the CQUIN remains a risk. Clarification and assurance was given on the two areas on the dash board which appear to have deteriorated. This is not an accurate reflection as the Safeguarding training figures were affected by a technical issue with the new training system data flow and the Friends and Families Test scope has been widened which has impacted on the scoring.
Achievements
• CQC report following inspection at HMP The Mount identified best practice for the management of blue light incidents.
• Infection Prevention & Control report: No outbreaks and cases of MRSA bacteraemia maintained at zero.
• There has been improved achievement of CQUIN targets in Q2. • Quality Assurance Visits demonstrate general improvements in
areas visited with remedial actions continuing where relevant. • Freedom to Speak Up has been actively promoted during Q2. • 15 Step Challenge has been completed in all community inpatient
units noting positive patient feedback and ideas for improvements are being taken forward..
Challenges
• The Quality Priority for patient experience response rates identified that negative Friends and Families Test (FFT) responses within the School Nursing survey, primarily around survey design, impacted on FFT scores in the quarter. The survey has been amended taking on board comments and suggestions received.
• The Quality Priority relating to Patient Reported Outcome Measures (PROMs) has been partially achieved with resource support under current review.
• Changes in alignment and data validation for safeguarding training are being monitored whilst the new Learning Management System is embedded. There are no concerns in safeguarding training compliance.
• Items identified for improvement following Quality Assurance Visits are being actioned and monitored.
Observations (O) Questions (Q) and Response (R) to Quality Report Quarter One

Board 31st January 2019 Attachment C1
Page 14 of 19
Q. AM asked for future clarification on the challenge which involved improvements following Quality Assurance visits.
R. TW advised that the challenge relates to ensuring that actions that have been taken to achieve improvements are sustained and embedded and changes in practice achieved. All Quality Improvements are being reviewed to ensure improvements are sustained. This will be reworded to clarify.
Q. DOF acknowledged the continuous effort involved to achieve the Influenza CQUIN, and asked if there are any examples of good practice elsewhere that could help HCT focus this approach and achieve the target?
R. HP advised that at the Medical Director Forum only 4 or 5 Trusts have reached 70% compliance but there is no ideal solution or approach.
R CH advised that a considerable number of actions are been employed and considerable effort is being made despite the resulting figures. The Executive Team are receiving regular updates and approving targeted approaches. This is being addressed at the Operational Senior Management Team. Learning will be taken forward to support future years target achievement.
Decision(s), Outcome(s) and Action(s)
i. The Board noted the content of the Quality Report Quarter Two.
ii. To review any scheduled staff development events up to Christmas that the Flu Champions could attend to increase staff CQUIN target compliance.
ARy
163/18 Community Hospital Safe Staffing Report Q2 Action
• The average safe staffing levels for all wards remained above the NHS England threshold of 80% throughout Q2 for registered nurses.
• Vacancy levels were above the Trust’s target of 10% in the majority of bed based units throughout Q2. The areas with the high vacancy rates and with the greatest challenge are noted on the high level risk register.
• All Inpatient Units continued to provide care for high numbers of patients with complex needs with 525 patients requiring additional support throughout Quarter 2.
Decision(s), Outcome(s) and Action(s)
i. The Board noted the content of the Community Hospital Safe Staffing Report Q2
164/18 Mortality Review Quarter One and Quarter Two
HP presented the Mortality Review for quarter one and two. In quarter one 18 deaths and in quarter two 11 death were reviewed. All deaths reviewed were assessed as being unavoidable and no patterns have emerged to date. HP advised that the processes and outcomes are currently being considered and reviewed along with the method of cascading learning to clinicians. A bi monthly training programme is being rolled out to provide

Board 31st January 2019 Attachment C1
Page 15 of 19
updates on learning going forward.
Observations (O) Questions (Q) and Response (R) to Mortality Review Quarter One and Quarter Two
Q. CH remarked that recent feedback from Doctors in the In-patient units identified that they feel disengaged with the organisation and it is acknowledged that there are plans in place to address this. However what assurances are there that the Doctors are receiving and acting upon the learning?
R. HP advised that there is limited assurance that the Doctors are receiving and acting upon the learning. To address these bi monthly education events will be held for the Doctors, Advanced Nurse Practitioners, Ward staff and out of hours Doctors to ensure that learning is embedded.
O. AM advised that this is reviewed at Healthcare Governance
Committee and the changes and improvements being taken forward are most welcome.
164/18 Chair of Healthcare Governance Committee’s Assurance Report of meeting held on 20 November 2018
AM provided a verbal update on the Healthcare Governance Committee (HGC) meeting held on 20P
thP of November 2018.
i) The CQC action plan was presented and discussed following the
core service and well led inspections. It was confirmed that the improvement work will need to demonstrate to CQC that actions were taken and embedded. There was good assurance that the action taken following the verbal and written report had been rigorously addressed. Work will continue to ensure that this is sustained. The action plan will be ongoing. It provided good evidence and will become part of the Quality Improvement Programme Risk Rating Amber/ Red
ii) HGC was informed of the findings from the Ministry of Justice CQC Inspection undertaken in April – May 2018 at HMP the Mount. The introduction to the report states that Health services were good overall. There was good assurance that the actions raised were completed within 14 days. The actions mainly related to the mental health support provided by HPFT to the Prison Healthcare team which included: o Support to provide clinical supervision for HCT staff delivering
primary mental health care. o Single prison health record for men receiving both healthcare
and mental health care. A quality improvement plan is being developed in conjunction with the Commissioners and the Ministry of Justice. Risk Rating: Amber/Green Both these reports will provide the Board with ongoing assurance via the HGC.

Board 31st January 2019 Attachment C1
Page 16 of 19
Decision(s), Outcome(s) and Action(s)
i. The Board noted the content of the Chair’s verbal assurance report for
the Healthcare Governance Committee meeting held on 20 November 2018
(F) Performance and Operations
165/18 Summary of Integrated Board Performance Report
DB asked the Board to note the key messages set out in the IBPR for October 2018 that included four performance highlights and six areas for Board review. It was noted the detailed report is in the supporting papers. DB highlighted that three of the six areas for Board review e.g. Delayed Transfers of Care (DToC), Non Stroke length of stay and underlying staff turnover are all showing improvement and are over the threshold. The improvement was noted and the teams are to be thanked for their contribution.
Observations (O) Questions (Q) and Response (R) to Summary of Integrated Board Performance Report
O. LS remarked that it is disappointing that two cases of c.difficile have
been recorded as this related to one patient who had a reoccurrence 29 days later. This highlights an issue with targets and measurements.
O. TW advised that two of the c.difficile total cases are being successfully
challenged; the outcome is likely to be successful and will be reported in due course.
Decision(s), Outcome(s) and Action(s)
i. The Board noted the content of the Summary of Integrated Board Performance Report
(G)) Board Governance and Leadership 166/18 Remuneration Committee update
The Board received the minutes of the Remuneration Committee meeting held on 23 October 2018. O It was confirmed that the Fit and Proper Person (FPP) process was
reviewed at this committee in order to provide a speedy resolution to a CQC query. Assurance was provided that all CQC actions are captured on the CQC action plan and there will be ongoing assurance to the Board. It was agreed that any future changes to FPP process to be reported to the Board.
Decision(s), Outcome(s) and Action(s)
The Board noted receipt of the minutes of the Remuneration Committee meeting held on 23 October 2018.

Board 31st January 2019 Attachment C1
Page 17 of 19
167/18 Update on Freedom to Speak Up (FTSU)
The Board received the Freedom to Speak up Q2 report.
Decision(s), Outcome(s) and Action(s)
i. The Board noted the FTSU update.
168/18 Board Governance Update
The Board received and noted the revised Board Governance structure
(H) Charitable Funds
169/18
The Corporate Trustees delegated authority to the Audit Committee to sign off the Charitable Funds Annual Report and Accounts 2017/18 on 11 December 2018. The audited accounts must be submitted to the Charities Commission no later than 31 January 2019
(I) Urgent Business
170/18 No urgent business declared.
(J) Risks Arising / Observations Action
171/18 Summary of High Level Risk Register (HLRR)
TW introduced a paper that reported the status of risks associated with activity and business across all of the Trust’s Business Units as at the end of October. Clarification was given on adjustment/ amendments to be made:
• Risk Ref 622: The narrative will be amended to clarify data referred to Length of Stay and Delayed Transfers of Care (DToC) and not clinical patient records.
• Ref 577 will be removed now that the services at Nascot Lawn have been decommissioned and the service is closed. This service has been de registered with CQC
The Trust Executive Team and the Healthcare Governance Committee reviewed these risks. The Risk Team continues to work with Operational and Corporate services to deliver timeliness of reviews and improved understanding of managing risk registers which includes a review of the effectiveness of the controls and the actions
Decision(s), Outcome(s) and Action(s)

Board 31st January 2019 Attachment C1
Page 18 of 19
i. The Board noted changes to the HLRR during October and progress
and assurance on the management of risks.
172/18 Summary of Board Assurance Framework (BAF)
The Executive Team and the Healthcare Governance Committee have reviewed the BAF risks during October 2018; this will be submitted to the Audit Committee in December. • One new risk added to the BAF; • The changes in the BAF (highlighted blue) relate to September and
October reviews; • The revised format & layout of the BAF captures recommendations
from the Trust’s internal auditors • The Trust annual risk appetite review is scheduled for February 2019.
Observations (O) Questions (Q) and Response (R) to Summary of the Board Assurance Framework
O In the future the BAF supplied to this meeting should to be a
summary version; only as this level of detail is not required.
Decision(s), Outcome(s) and Action(s)
i. The Board noted the full Board Assurance Framework was reviewed
and discussed in the Trust Board meeting held in Private on 29 November due to commercially sensitive information.
173/18 Summary of Risks Arising Decision(s), Outcome(s) and Action(s)
i) The risk in respect of Social care provision needs to be reviewed and a decision made on how this is to be recorded and what mitigations are required.
ii) The Living with Stroke programme curtailment as mentioned in the
patient story is an issue. Changes in commissioning maybe responsible for this in the future, however creative options to fund/ deliver this service to be investigated.
(K) Supporting Papers / Items for Receipt and Noting Only
Members of the Board noted
• Finance Report (Month 7), • Quality Report Q2, • Minutes of the Healthcare Governance Committee 18 September
2018 • Integrated Board Performance Report
(L) Date, time and Venue of the Next Meeting Action
The next Trust Board meeting in Public would be held on Thursday 31 January at 13.30 pm to 15.30 pm. A change of venue noted due to construction noise.

Board 31st January 2019 Attachment C1
Page 19 of 19
(K) Questions from the Public
No questions notified.
Meeting closed at 16.15 pm

Trust Board in Public 31 January 2019 Attachment C2
1
HERTFORDSHIRE COMMUNITY NHS TRUST BOARD TRACKER
RAG Traffic Light Key:
To be considered at current meeting
(i.e. action deadline reached)
No Action Required
Action Deferred
Action not yet initiated but within target
Action not yet initiated and likely
to miss target
Action In Progress but not on target or target has expired
Action in progress and on target
Action Completed
Minute Ref No.
Meeting Date Item / Action Required Board
Lead Target /
Finish Date Progress R/A/G
Board Tracker From 29 November 2018
162/18 29.11.18
Influenza Campaign To review any scheduled staff development events up to Christmas that the Flu Champions could attend to increase staff CQUIN target compliance.
ARy Dec 2018 Action taken Action Complete
159/18 29.11.18
Nascot lawn Letter to be sent to staff and management of Nascot Lawn on behalf of the Board expressing gratitude for their commitment, dedication and professionalism during the transition of respite services.
CH Nov 2018 Letter of thanks sent Action Complete
Board Tracker From 27 September 2018
137/18 27.09.18 Community Hospital Safe Staffing report Q1 Noted the need to develop a collective plan for the interface with West Essex Princess Alexandra Hospital NHS Trust. MD 29.11.2018
Discharge Home to Assess service for PAH patients commenced and increasing capacity. Winter planning including approach to escalation beds.
Action Complete

Trust Board in Public 31 January 2019 Attachment C2
2
Minute Ref No.
Meeting Date Item / Action Required Board
Lead Target /
Finish Date Progress R/A/G
144/18 27.09.18 Workforce Race Equality Standard (WRES) Report The Board noted it should receive a further update on action in relation to the WRES report in November 2018 or January 2019 at the latest.
RB 28.3.19
Incorprated into the Equality Delivery Scheme 2 which will be considered at March Board
Action in progress and
on target
28.11.19 Brief update to be given at January 19 meeting
Action in progress and
on target 146/18 27.09.18 Update on Freedom to Speak Up (FTSU)
The Board noted the results of the FTSU self-review tool would be reported to Board on 29 November 2018.This report would include key themes and an action plan
RB 29.11.2018 Quarter 2 FTSUG report on agenda, key themes included
Action Complete

Board 31st January 2019 Attachment D1
Page | 1
Chief Executive’s Report
1.0 Executive Summary
1.1 This report provides the Board with an overview of matters of current interest at a national and local level together with an update on the work of the Executive Team since December’s Board meeting that are not covered elsewhere on the agenda for this meeting.
2.0 Recommendations
2.1 The Board members are asked to note the content of this report.
3.0 Matters pertaining to national/regional updates
• NHS Long Term Plan
3.1 The much awaited and welcomed NHS Long Term Plan was published on 7 January 2019 and comprises a practical and realistic set of changes that should bring about important improvements in the quality of care and outcomes, while also tackling the pressures in the sector. The publication of the plan is one important milestone. We now need to work together to deliver these improvements and make the Long Term Plan a reality; this is what will make a difference for patients and staff. The plan includes a commitment to increasing investment in primary and community health services, recognizing the contribution that these services make to patient care. Investing in these services will enable us to provide more care in people’s homes and the community, supporting them to stay at home wherever possible and avoiding them getting to the point where they have to be admitted to an acute hospital.
We are committed to integrated multi-disciplinary working with primary care and neighborhood teams comprising GPs, pharmacists, community staff, social workers and the voluntary sector.
We also welcome the Long Term Plan intentions around children’s mental
health and are looking forward to working with commissioners on how we translate this into delivery across our Step2 and PALMS services, and for children with neuro developmental issues (i.e. ASD, ADHD).

Board 31st January 2019 Attachment D1
Page | 2
The recognition in the plan of the issues associated with tendering in the NHS in terms of cost and fragmented provision is helpful, as is the commitment to an increasing focus on integration and collaboration over competition; with the stated intention to press for legislative change where necessary to avoid unnecessary procurements
The NHS Providers briefing on the NHS Long Term Plan forms can be found in the supporting papers (K1)
• NHS Annual Planning Guidance 2019/20
3.2 Following the publication of the NHS Long term plan, NHSE published the Annual planning guidance 2019/10 and are developing our Operational Plan for next year to the required timelines. The first draft is to be submitted on 12 February and final plan on 4 April, as well as inputting to the aggregate STP system plan. The guidance sets a deadline for NHS 2019/20 contract signature of 21 March and HCT is progressing its contract negotiations.
• NHS England and NHS Improvement joint senior leadership team – NHS
Executive-Group
3.3 NHS England and NHS Improvement announced a joint senior leadership team – the NHS Executive Group on 11 December 2018, as part of closer working arrangements between the two organisations, NHS England and NHS Improvement will share the new combined management group chaired by the two Chief Executives. Appointments to the new group are as follows:
NHS Chief Financial Officer – Julian Kelly National Medical Director – Professor Stephen Howis Chief Nursing Officer – Ruth May Deputy Chief Executive NHS England – Matthew Swindells National Director for Emergency & Elective Care – Pauline Phillip National Director for Strategy & Innovation – Ian Dodge National Director for Transformation & Corporate Development – Emily Lawson South West Regional Director – Elizabeth O’Mahony South East Regional Director – Anne Eden Midland Regional Director – Dale Bywater East of England Regional Director - Anne Radmore North West Regional Director – Bill McCarthy North East & Yorkshire Regional Director – Richard Barker London Regional Director– Sir David Sloman

Board 31st January 2019 Attachment D1
Page | 3
The NHS Executive Group is set to hold its first meeting this month with the new national and regional directors expected to formally lead their integrated directorates by April 2019.
• Quality Accounts 2018/19 Requirements
3.4 All providers are required to publish a quality account by 30 June each year.
The requirements for 2018/19 include new considerations for disclosures on seven day hospital services and arrangements for staff who speak up. • Quality reports arrangements for 2018/19
3.5 NHS foundation trusts are required to include a quality report in their annual report each year, and obtain assurance from their auditors on aspects of it. The requirements for 2018/19 have been published, including guidance for NHS trusts like ours that may also choose to adopt the same principles.
4.0 Matters Internal and Local to the Trust
• Appointment of Substantive Director of Nursing & Quality
4.1 Following my appointment in October 2018 and a statutory recruitment and selection process, I was delighted to announce the appointment of Sarah Browne as our new Director of Nursing and Quality, in November 2018. The role attracted a strong field of applicants and Sarah was the unanimous decision of the interview and stakeholder panels.
Sarah will formally join us on 25 February 2019 and is currently Deputy Director of Nursing and Director of Infection Prevention and Control at Essex Partnership NHS Foundation Trust (EPUT) - a combined mental health and community trust with services in Essex and Bedfordshire. Before this she was Acting Executive Nurse at South Essex Partnership University NHS Foundation Trust and she has worked at a senior level in the former Bedfordshire Community Health Services Trust.
Sarah lives in Hertfordshire and will bring a breadth and depth of experience to the role. She has extensive experience of integrated community and mental health services, nursing and clinical leadership and workforce transformation across complex systems. She has worked at local, regional and national levels.
• Appointment of Substantive Director of Finance
4.2 In December 2018, I was also delighted to announce the appointment of David Bacon as our substantive Director of Finance following a national advertisement and statutory recruitment and selection process. David formally

Board 31st January 2019 Attachment D1
Page | 4
joined us in July 2018. He qualified as a Chartered Accountant in 1986 and joined the NHS in 1990 becoming Deputy Director of Finance of Leicestershire Health Authority in 1995. Between 2001 and 2010 David held Director of Finance and Turnaround Director Posts in both the East Midlands and the East of England. Since 2010, David has been providing senior financial expertise to NHS organisations on an interim basis, working in a variety of senior roles in both commissioning and NHS trusts across England in line management and project roles. David holds an MBA and has completed the Strategic Financial Leadership Programme at Cass Business School.
David is an active member of the Healthcare Financial Management Association (HFMA), He chairs the National Accounting and Standards Committee, the HFMA’s annual pre-accounts planning conferences and the HFMA’s Finance Team of the Year Award judging panel. He is also the Chief Assessor for the HFMA Academy. His work for the HFMA was recognised in April 2011 when he received an HFMA inaugural Key Contributor award.
• Appointment of Substantive Deputy Chief Executive
4.3 Following the Remuneration Committee meeting in December 2018, I am also delighted to confirm the appointment of Dr Hari Pathmanathan as our substantive Deputy Chief Executive. Hari has been a GP in Hertfordshire for twenty years and been involved with NHS management and Clinical Leadership for fifteen years. He has held board level positions as Director and Non-Executive Director in Welwyn and Hatfield PCT; NHS Hertfordshire PCT; and East & North Hertfordshire CCG. Between 2014-2018 he was Chairman of East & North Hertfordshire CCG.
Hari brings a wealth of experience to the board and continues to work two days a week as a Partner at Bridge Cottage Surgery in Old Welwyn.
• Quality Update - Care Quality Commission Inspection
4.4 The Trust welcomes the Care quality commission report following the inspection September 2018. Services have once again been rated ‘Good’ and highlights our staff are compassionate and involve patients in their care enabling effective pain management and seeking to minimise emotional distress. This is a testament to the hard work of staff since 2016. A comprehensive improvement programme with particular focus on medicines management, patient records and safety is underway to address areas which require improvement as part of our overall journey from being rated ‘good’ to ‘outstanding’.
• Safeguarding adult reporting

Board 31st January 2019 Attachment D1
Page | 5
4.5 Safeguarding adult reporting is increasing across the county and the Trust continues to work with partner colleagues to ensure safety of vulnerable adults in our community.
• C Difficile
4.6 The total cases of C Difficile at the end of January year to date is 5, however 2 have been appealed with 1 appeal approved to date.
• Screening for Flu
4.7 Due to the expected increase in respiratory symptoms the Trust is observing an increase in screening for flu – no cases to date.
5.0 Our people
• HCT Superstars and Celebration Events 5.1 We are introducing new regular staff recognition arrangements to complement
the annual Leading Lights Awards. These will involve monthly Superstar awards, with quarterly recognition events where Superstar winners can be congratulated and meet members of the senior team. These events will also provide the opportunity to recognise retirees and colleagues reaching long service milestones in a timely way.
• Annual Staff Survey
5.2 The fieldwork for the 2018 National Annual Staff Survey closed on the 30th
November, with 55% of staff responding (slightly down on last year’s response rate of 58%). The official publication date for the survey outcome is expected to be 26th February 2019.
• Influenza Vaccination Campaign for healthcare staff
5.3 The Trust is required by NHS England to use its public board papers to report details of its staff flu vaccination uptake as follows:
The current Trust uptake (as at 17th January 2019) is 66.7%. This means that the Trust has met the 65% threshold which attracts three-quarters off the related CQUIN funding, but the 75% target remains at risk.
The Trust has identified the Respiratory Service and Children’s Community Nursing as ‘higher-risk’ services in relation to patients with immune-supressed conditions and the uptake in these areas is currently 100% and 81% respectively.
To date, 281 staff have actively opted out of the vaccination using the Trust’s reporting process. The final analysis of reasons for declining will be provided on request to NHS England at the end of the campaign.

Board 31st January 2019 Attachment D1
Page | 6
The Trust has successfully met national uptake targets in previous years using a well-established action plan, incorporating occupational health service run clinics, staff peer vaccinators and a comprehensive communication campaign using all Trust channels. As part of the commitment to achieving maximum uptake again this year, individual conversations are being held with staff to encourage them to be vaccinated and these will continue throughout January and February.
• Temporary Staffing and Agency Cost Reductions
5.4 The work that has been done to introduce the Bank Network (shared staff bank), review bank pay rates, move senior interims onto fixed term contracts and encourage the migration of agency workers onto the bank is now paying off with reductions in agency use and corresponding increases in bank use across all staff groups. In particular, agency fill for non-nursing unqualified shifts (mostly Administrative and Clerical) has fallen from 69.7% in April 2018 to 41.1% in December 2018. • Learning Management System
5.5 A staff survey has been undertaken to identify the impact of the new Learning
Management System on staff time, with around 120 staff participating. The outcome was positive, with 56% identifying that using the system means it takes less time or a lot less time to complete training activities. A case study is being created with the supplier to share with other Trusts on the benefits of the system.
• Administrative Conference
5.6 A further Conference for Administration staff will take place in March 2019 and will include strategic updates, a session on building confidence and Glimpses of Brilliance highlighting the career achievements of our staff.
• Mandatory Training- My Learning Zone
5.7 Mandatory training was 94.2% at the end of December which is the highest recorded figure since an overall compliance figure was introduced in April 2015. Appraisal compliance is steady at 91.1%.
• Making a Difference Programme
5.8 The latest cohort of staff completing Making a Difference Foundations in Leadership and Management completed their programme in January – 5 staff have achieved promotion during the programme. The next programme will start in April 2018.

Board 31st January 2019 Attachment D1
Page | 7
24 staff members have completed the 2018 Making a Difference Programme and recruitment will start soon for the next programme which will start in April 2019. 5 staff have already secured promotion during the course.
6. Update from Operational Services
• Patient Flow
6.1 Patient flow in community bedded units through Dec 2018 and into Jan 2019
across both sides of the County has been good with availability of beds averaging an OPEL 2 score daily. The new enhanced community bedded pathways started in East and North on 17th Dec 2018. Further workshops have been agreed with the CCG and ENHT to embed these. The progress in Herts Valley bed bases have remained very positive with length of stay for the rehabilitation pathway in Dec 2018 being 23 days and overall length of stay in Dec 2018 being 26.6 days. The provision of daily patient information from SystmOne has improved and is supporting the operational team. The KPIs for the new pathways will now be reflected in the Herts Valley contract monitoring moving forward
• Winter Planning
6.2 Internal escalation calls have been held through Jan 2019 to manage
escalation and co-ordination of resources with all senior Adults managers. This has enabled a much improved co-ordination of service delivery and positive feedback from both CCGs and other local partners. The escalation plan has been further updated and has been tested during this period. 9 winter escalation beds have been used in Jan 2019 in Herts Valleys at St Peters, Simpson and Potters Bar Community Hospital. In East and North 2 winter escalation beds have been opened at Herts and Essex Hospital for West Essex CCG patients. Discharge to Assess in East and North has a caseload increase to 60 in Nov 2018 to include patients discharged from Princess Alexandra Hospital. This caseload through Dec and Jan period has not reached capacity due to

Board 31st January 2019 Attachment D1
Page | 8
availability of care provision. Discharge home to assess in Herts Valleys has a caseload of 40 and has been almost at capacity during this period. In addition, the Virtual beds currently have a commissioned capacity of 13; usage was slow to increase initially but is now at capacity.
Adults and Children’s Services
• East and North Integrated Care Teams
6.3 The EN ICT rollout continues to be positively received with acknowledgement of improvement in the referral hub and positive assurance with staffing and workforce. The North Herts ICT team will undergo a Quality Improvement (QI) approach to understand the delivery of the model and its outcomes. This will then be taken into each team over coming months. • Skin Health
6.4 The service remains an escalated service.
A further review was commissioned by an external expert and this has initially provided positive assurance on the service. We are working with WHHT who have been positive in their response to working with us to provide medical leadership to strengthen the governance.
The service challenge currently is managing the demand due to staff shortages, action have been agreed to increase capacity in Jan/Feb 2019. • Community Paediatric Service
6.5 The community paediatric service continues to breach the 18 week referral to treatment target, including a significant number of children and young people waiting for ASD assessments. The service has undertaken a detailed data diagnostic exercise from which we have identified key actions to take as part of a service transformation plan. A number of these actions have been implemented including updated referral forms and review and update of all triage and waiting list processes. Other interventions underway are the introduction of multi-disciplinary teams (skill mix) and job planning to more closely match demand capacity to changing service demand. The impact of the actions taken to address the waiting lists

Board 31st January 2019 Attachment D1
Page | 9
will be closely monitored and reported as appropriate to commissioners. The transformation work is being overseen by our Medical Director. • Children’s and Young People Specialist Services Transformation
6.6 We have initiated work to transform our children’s and young people’s specialist services. Our vision is that by October 2019 children and young people will experience an integrated Specialist Children and Young People’s Health Service in Herts Valleys. The transformation will deliver embedded integrated care pathways and enhanced care co-ordination and will be delivered in hubs locally. An important part of it will be to ensure that the services provide outcomes that are personalised to children, young people and their families. We are co-designing our transformation with Parents / carers, commissioners and provider partners and we will be holding a partnership meeting on 12 February, building on the previous event held in November. • Public Health Nursing Service
6.7 The Public Health Nurse Service continues to work in partnership with our
Family Support Services colleagues towards full service delivery together from April 2019. There are a series of events forming part of a Welcome Week for the new Family Centre Services in January. The event hosted at Highfield Community Centre in Hemel Hempstead was attended by Cllrs Teresa Heritage and Tim Hutchings as well as Jim McManus - Director of Public Health and HCT board members. • Nascot Lawn
6.8 Nascot Lawn has been decommissioned from 22 November 2018 and demobilisation is underway. Over the course of the last 11 months, the team have worked as part of a system-wide operational group to secure the safe transition of children and young people to new provision or secure alternative arrangements. The Nascot Lawn staff have worked hard to continue to offer the service and support the children and young people alongside the transition process.

Board 31st January 2019 Attachment D1
Page | 10
7.0 Finance, Performance & Information 7.1 Business planning for 2019/20 is underway linking in closely with services
and contract team to provide activity plans. The first cut of the plan was shared with ENHCCG on 14th January 2019.
7.2 Business Intelligence
Development of a solution to enable single unit downloads into HCT data warehouse has been successfully completed. This means that single units can be downloaded from SystmOne without having to do a full bulk of every unit. This greatly reduces the processing time of any unit changes (unit merges and/or unit ID changes). Successful processing of a single unit with RY4 changes for 2 units has now taken place.
Improved online appraisal forms for use by all staff have been developed. Development of updated Minimum Data Sets (MDS) for HVCCG due to
changes in reporting for Diabetes service. 7.3 Information Management & Technology (IM&T)
Patient and Guest Wi-Fi is now available in all HCT sites Guest printing on MFDs is now available PHN CST sites live on 2/1/19 Migration to smartphones continues Capital plans for 2019/20 being developed Trail new HP mobile working devices with windows 10 Further network upgrades Further CST deployments
7.4 Clinical Systems Support
Jo Goulden (former Head of Clinical systems) has returned 2 days a week as a Clinical Systems Specialist, working on configuration of SystmOne Publishing unit.
EMIS Interoperability Pilot successful. Plan now for this to be rolled out across all HV GP’s. Expect national roll out of functionality in early 2019.
ERS (Electronic Referral Service) roll out to begin in February. Bid for funding from STP provisionally approved for additional £39k.
7.5 Project Management Office The current list of improvement initiatives far exceeds the Trust’s capacity to
deliver. The PMO estimates that there are around 49 ‘active’ programmes and projects within the Trust portfolio, an increase of around 15 projects compared with this time last year. This is in addition to other improvement initiatives, priorities and objectives. The Portfolio Assurance Group will be reviewing

Board 31st January 2019 Attachment D1
Page | 11
the prioritisation of existing projects and during Q4 we aim to release resource by delaying or stopping lower priority projects.
The Director of People & OD formally launched the Transformation of Corporate Services programme on 24th January 2019.
8.0 Estates Update 8.1 Estate Strategy Development The HCT/HPFT Integrated Estates Strategy will be drafted by the end of
January 2019 for comment and approval. The strategy will be an overarching document which details the key principles, aims and objectives etc. of both organisations and will form a joint document. There will be a delivery plan which will detail the alignment, configuration and will reflect the national and local direction as well as identify the programme of investment and disinvestment. The delivery plan will include a backlog maintenance/lifecycle cost and program together with the 5 year capital plan – this will be complete by May 2019.
8.2 STP The Strategic Estates and Delivery Plan will contain proposals to develop STP
capital bids which will be due for wave 5 approval in December 2019 the bids however will be completed by July 2019 to meet various internal approval processes. Cheshunt Health and Wellbeing Centre is likely to be one of the bids developed
8.3 Capital Program - St Albans Civic Centre Development
St Albans Civic Centre development has experienced delays as the costs advised by Kier Construction through the SCAPE form of contract proved to be too high. An alternative contractor (ASHE) using the same form of contact has been approached and costs have significantly reduced enabling the Trust to proceed with the development. Completion July 2019.
8.4 Capital Program 2018/19 Whilst the majority of the 2018/19 capital program is complete a new bid to
address environmental and issues identified within the PLACE inspections has been approved. Work on this will commence imminently and is due for completion on 31st March 2019.

Board 31st January 2019 Attachment D1
Page | 12
8.5 STF Funding
The STF funding program will be detailed following a Survey Monkey staff survey as well as advice from various service including estates – details of this program will be contained within the March estates report.
End of Report

1
TRUST BOARD
Title: Month 9 2018/19 Finance Report
Meeting Date: 31 January 2019
Executive Lead: David Bacon, Director of Finance
Author(s): Finance Department
For: Note / Discussion
Risk rating: Green /Amber
1.0 Purpose & Recommendations
1.1 To advise the committee regarding the Month 9 2018/19 financial position.
1.2 To ask the committee to: (1) Note the M9 position (2) Raise any issues / concerns.
2.0 Executive Summary
2.1 a. Income and Expenditure position:
The Trust performance against the control total is as per plan in month 9 and £29K ahead of plan year to date. In achieving plan, funds from reserves have been utilised to offset non-pay over spend and under performance of the CIP. Notable over spends include IT costs for Microsoft licences, Drug costs and Clinical supplies in the bed units. The Trust's single oversight risk rating is still maintained at a 1, despite continued pressure around agency usage.
The Trust is forecasting to achieve the control total of £2,077K as per the 18/19 Operating Plan Submission, however significant monitoring and control is required over the spend for the rest of the financial year.
b. Agency Expenditure: Month 9: £543K actual, target £547K Year to date £6,247K actual, target £4,923K
c. Cost Improvement Programme: Month 9: £460K delivered, target £460K Year to date: £3,717K delivered, target £3,717K
Board 31st January 2019 Attachment D2

2
Continued achievement through contribution of £1,146 of non-recurrent schemes and savings
d. Capital Expenditure: Year to date: £2,377K delivered, target £2,380K
e. Cash Plan:
Month 9: £24,900K delivered, target £18,078K 3.0 Relevant Strategic Objective(s) / Strategies
3.1 Trust Strategic Objectives
4 We will use resources efficiently to enhance our ability to improve
services.
4.0 References, Appendices & Attachments Appendices & Attachments
None
Author(s) of paper: Director of Finance – David Bacon Date: January 2019

3
Sign Off: To be completed as part of papers to Executive Team, Board Committees and Board Committee Consideration This Report has previously been considered by the following committees: Committee: Date (Month / Year): Strategy & Resources Committee January 2019
Data Quality Statement By way of assurance to the Board, and in order to inform discussion / decision, the accountable executive director confirms that to the best of their knowledge, and subject to any exceptions identified, data contained in this report is: Data Quality Domain
Description Comments / Exceptions √ / x
Complete Information is as comprehensive as possible to inform the board and no significant known facts or statistics which may influence a decision are omitted.
√
Accurate As far as can be reasonable ascertained or validated, information in the report is accurate.
√
Relevant Information contained in the report is relevant to the matters considered in the report.
√
Up To Date
Information in the report is as up to date as reasonably possible in the context of the time at which the paper is written
√
Valid Information is presented in a format which complies with internal or national models or standards
√
Clearly Defined
The meaning of any data in the report is clearly explained
√
Executive Director Sign-Off
This paper has been approved by the accountable executive director who is satisfied that (i) the implications for risks, (ii) quality/service/regulatory impacts and (iii) resource implications, have been considered.
David Bacon, Director of Finance
√
Company Secretary Sign-Off (Board papers only) This paper has been quality control checked and approved by the Company Secretary √ / x

Board 31st January 2019 Attachment E1
1
Clinical Quality and Medical Directors Report 1.0 Medical Directorate 1.1 The medical directorate has been involved in providing clinical leadership
within the organisation and externally. Since the last report, the directorate has been supporting preparation; assessment; and implementation of recommendations from our recent CQC inspection.
1.2 I have taken on Executive Lead for the CYP Transformation. After chairing a
very successful Children’s Transformation Board, our case for change will be made to HV CCG at the end of this month.
1.3 As Executive Lead for the Dermatology transformation, a new staffing model
is soon to be implemented which will augment the STP Dermatology model. 1.4 Aside from the business as usual functions of the directorate, work has been
ongoing in our role of providing system leadership and delivering the organisation’s strategy. Regular meetings have been had with clinical leaders in the HWE STP.
1.5 Work is also underway to work more collaboratively with General Practice, for
example: Evaluation of a collaborative approach to provide community
phlebotomy with GP federations. Hosting of GP fellows within our services for HV CCG. Joint work with Herts & Beds. Local Medical Council (LMC) to potentially
support vulnerable practices. 2.0 Learning from Deaths 2.1 There is work ongoing to put into place the improvements we agreed at the
Learning from Deaths workshop in Q3. There is a new draft policy with amended scope and we are piloting new administrative processes to try to reduce duplication. We plan to improve timeliness of reviews and more systematically evidence the learning from each patient, linking to evidence of change which follows. Our biggest challenge is embedding and evidencing the Trust’s learning. As an interim measure the panel will send required actions directly to individual lead clinicians, while new Trust quality

Board 31st January 2019 Attachment E1
2
improvement processes are developed. We are also exploring the use of existing Datix software to support the review process, reducing administration time and holding the action plans.
2.2 Dr Carol Scholes, Deputy Medical Director and Responsible Officer attended
the Hertfordshire LeDeR (Learning Disability Mortality Review Programme) meeting to develop links and ensure our own policy and processes link as well as possible to achieve the overall goals of the national Learning from Deaths programme in Hertfordshire. We plan to pilot one of their administrative processes to evidence improvements required from each mortality review.
2.3 Christine Stock, Head of Patient Safety and Dr Carol Scholes met the two
leads for Learning from Deaths in HPFT. We shared current processes, challenges and desired improvements, and they have both accepted the invitation to join HCT Structured Judgement Review training in February.
2.3 There are differences in the number and nature of the patients and national
requirements for review, but both parties seem committed to working together where possible. We will also have Non-Executive Director oversight with Brenda Griffiths attending panel meetings.
3.0 Clinical Effectiveness 3.1 A subgroup of Clinical Effectiveness Group met in December to review the
terms of reference and the current working of the group. Improved processes were agreed to focus the annual work plan and meeting agenda, ensuring members can be well prepared to make the decisions required to meet the existing terms of reference.
3.2 This has enabled more time for clinical discussion and improved decision
making and feedback from members is very positive. 3.3 Outcome Based Healthcare leaders visited the executive team again in
January, and the Medical Directorate will be supporting the delivery of this programme to measure and report on clinical outcomes.
4.0 Medical Revalidation 4.1 The medical revalidation officer has left their post and there is agreement that
the function will be expanded to include medical job planning, and will now sit within the operational business units under the HR business partners.
4.2 With help from the Trust Lead Medical Appraiser, Dr Thakur, we have
selected new appraisal software which principally will improve appraisee

Board 31st January 2019 Attachment E1
3
experience and save them time. All Doctors will be offered training and will use this system from April 2019. The system also eliminates manual entry of required data returns regarding medical appraisal, and may soon be able to support quality assurance using the tool currently used by the Responsible Officer. We are uploading existing appraisals within this revalidation cycle for every Doctor onto the new system.
4.3 One Consultant has recently been revalidated, with six more due in 2019.
There are no concerns about Doctors working for the Trust which have been escalated to the Responsible Officer.
4.4 Following the audit of pre-recruitment checks of medical staff there are still a
few Doctors where the required information is missing. This is being followed up by the recruitment team in HR.
5.0 Skin health 5.1 A commissioned report on the service has been received from an external
Consultant Dermatologist / University Lecturer. It describes a well-supported community service which provides an important service for people with skin conditions living in Hertfordshire. It includes an options appraisal for future prescribing of isotretinoin for acne within the service. A Consultant dermatologist is expected to support the service soon.
6.0 Job planning 6.1 Further amendments to the job planning policy are proposed to strengthen the
input of operational management in every job planning meeting, and the policy will be discussed at the next Joint Local Negotiating Committee (JLNC). The Paediatrics business unit is exploring ways of resourcing the administrative support required to help the Trust job planning lead, Dr Rudran, implement e-job planning tool Trust-wide. The Trust’s annual job planning cycle is February / March, meaning that all the medical e-job plans should be completed and signed off within that window. This is the first of these cycles so some exceptions to this deadline are expected. For the four community hospital specialty Doctors and the locum prison GP this will be their first job planning process. It will also be the first time that operational management have been so closely engaged, so the training morning in Q4 included both Doctors and managers. We will review early in 2019-20 and seek improvements for the next round.

Board 31st January 2019 Attachment E1
4
7.0 Frailty update 7.1 A frailty task and finish group has been formed within the Trust and we have
developed our approach to frailty. This is now going to be made into a frailty programme, with governance via the clinical operations group.
7.2 Comprehensive geriatric assessment was developed in SystmOne for use in
frailty clinics and being reviewed by community staff to see if fit for community. 7.3 We have started pilot frailty clinics in North Hertfordshire and are due to start
frailty clinics in Hertsmere and Watford localities in January. 8.0 Sepsis 8.1 Sepsis has been identified as a key topic to focus on going forward and
possible quality priority. 8.2 We have started a new sepsis group within the Trust chaired by Dr Elizabeth
Kendrick to establish where the Trust is, what it needs to do to become outstanding on sepsis care and build a strategy going forward
8.3 We will be looking at ways to introduce NEWS2 across the Trust and feel that
this will be ground breaking work in a community setting. 9.0 Medical Cover for Bed bases 9.1 We are trying to move away from ad hoc cover by locums to a more
sustainable approach and to ensure that units are buddied with other units and leave is coordinated. Medical training to commence in March for all ward based doctors and for band 7 and above staff – this will be a bi-monthly programme.
10.0 Personalisation 10.1 Dr Elizabeth Kendrick attended the Sustainability and Transformation
Partnership (STP) personalisation group regarding “My Plan” (STP personalised patient held care plan). The Plan is due for sign off at the STP workstream on the 18th January and then signed off by the Chief Executive.
10.2 The likely cohorts will be frail patients, end of life patients and frequent ED
attenders where HCT is likely to be an early adopter.

Board 31st January 2019 Attachment E1
5
10.3 There is a Queens Nursing Institute (QNI) submission for £5,000 being drawn up around patient experience for frailty clinics, a PFS roll out for nurses and use of “My Plan” in clinics.
11.0 Leadership opportunities 11.1 Dr Kendrick applied for and was offered a place on the Nye Bevan leadership
programme commencing in February 2019 and finishing in September 2019. 12.0 Hyperkalaemia 12.1 The Hyperkaleamia guidelines have been written in response to Central
Alerting System (CAS) alert for Trust. 13.0 Patient Group Directives for antibiotics for ECPs and non-prescribers 13.1 The guidelines have been written for North Hertfordshire. HomeFirst has been
reviewed and updated. These will then be discussed at MMF for next steps. 14.0 At Risk Feeding Pathway 14.1 We have agreed for this to become an STP wide workstream led by Ruth Bird
from HCT. 15.0 Medicines Management & Safety 15.1 The CQC’s confidential Draft Report has confirmed that in their inspection of
our Community Health In-patient services, within the “safe” Key Line of Enquiry, found that Medicines Management requires improvement. As such, we have been given a Requirements notice under Regulation 12 HSCA (RA) Regulations 2014 Safe care, for the activity of “Treatment of disease, disorder or injury”.
15.2 There are two “must dos”, which are: a) ensure it follows its medicines management policy in relation to the safe
handling of medicine including, supply, storage, administration, supply, handling and recording and
b) prescribe for patients the right drugs, by the right route in the right
dosage at the right time.

Board 31st January 2019 Attachment E1
6
15.2 In response, the Chief Pharmacist has created a 10-point plan to tackle Issue a) and a 14-point plan to tackle Issue b). The approach is a multidisciplinary one and its success requires the cooperation of colleagues from Pharmacy, Nursing, Medical, Operations and Learning & Development. Buy-in has been strong from all the disciplines. Each plan is multi-staged with immediate, short, medium and long term actions. The time frames for the actions range from 2 weeks to 9 months and some of the longer-term actions will require additional Pharmacy resources to be invested.
15.3 The objective is that we will achieve a “good” rating for Medicines
Management at the end of the programme. 15.4 Work is underway to review the Medicines Management team resources and
team structure. 15.5 We have included senior clinical pharmacist role in our service model
proposal for the Herts Valleys CCG Pilot Community Specialist Frailty Service. Following the successful outcome of the bid, we will now be recruiting to a pharmacist role for a 9 to 12-month period. This post will out to advert by mid-quarter 4 of 2018/19.
15.6 Insulin medication incidents have been a concern for the Trust during the first
half of 2018/19, with rising numbers. Following the work and initiatives of the Pharmacy, Nursing and Operations Teams, insulin incidents have fallen by 40% quarter on quarter. The Chief Pharmacist continues to lead work to reduce insulin and other medication errors in the Trust.
January 2019 Dr Hari Pathmanathan End of Report

Board 31st January 2019 Attachment E2
1
TRUST BOARD Title: Safe Staffing Levels in Community Hospitals (Inpatients) Meeting Date: 31 January 2019 Executive Lead: Andy Nuckcheddee, Director of Nursing & Quality (Acting) Author(s): Charlotte Reynolds, Service Manager for Community Inpatient Units. For: Noting and Assurance Risk Rating: Amber/ Green 1.0 Purpose & Recommendations
1.1 The purpose of the report is to provide the Board with a progress report on Safe Staffing levels within HCT’s Inpatient Units during October and November 2018).
1.2 The Board members are asked to:
a) Note the Safe Staffing levels for this period 2.0 Key Points
2.1 During October and November 2018, safe staffing data demonstrates that the average safe staffing levels for all wards remained above the NHS England threshold of 80% for registered nurses.
2.2 Staff vacancy rate and sickness levels rate are high. HR are working with
teams proactively to fill vacancies. There is a Facebook and Twitter campaign currently running to improve recruitment and a ‘Golden Hello’ initiative has been introduced into Potters Bar, Herts & Essex and Langley House. The Trust Sickness Policy continues to be implemented with support from HR colleagues where necessary.
2.3 All Inpatient Units continue to provide care for high numbers of patients with
complex needs (risk of falls, DOLs, patients requiring enhanced care). 3.0 Relevant Strategic Objective(s) / Strategies
3.1 This report links to the following Trust Strategic Objectives:
SO 2: We will improve clinical outcomes and enhance patient safety. SO 4: We will use resources efficiently to enhance our ability to improve
services. SO 5: We will develop the organisational capacity to deliver our vision and
objectives.

Board 31st January 2019 Attachment E2
2
4.0 Appendices & Supporting Information
Safe Staffing In-Patient units Author(s) of paper: Charlotte Reynolds, Service Manager for Community Inpatient Units January 2018

Board 31st January 2019 Attachment E2
3
To be completed as part of paper Committee Consideration This Report has previously been considered by the following committees: Committee: BUPR data Date (Month / Year): Dec 2018 Healthcare Governance Committee January 2019
Data Quality Statement By way of assurance to the Board, and in order to inform discussion / decision, the accountable executive director confirms that to the best of their knowledge, and subject to any exceptions identified, data contained in this report is: Data Quality Domain
Description Comments / Exceptions √ / x
Complete Information is as comprehensive as possible to inform the board / committee and no significant known facts or statistics which may influence a decision are omitted.
√
Accurate As far as can be reasonable ascertained or validated, information in the report is accurate.
√
Relevant Information contained in the report is relevant to the matters considered in the report.
√
Up To Date
Information in the report is as up to date as reasonably possible in the context of the time at which the paper is written
√
Valid Information is presented in a format which complies with internal or national models or standards
√
Clearly Defined
The meaning of any data in the report is clearly explained
√
Executive Director Sign-Off
This paper has been approved by the accountable executive director who is satisfied that (i) the implications for risks, (ii) quality/service/regulatory impacts and (iii) resource implications, have been considered.
T Westley AD Risk & Quality Assurance on behalf A Nuckcheddee Director of Nursing & Quality (Acting)
√ / x
Company Secretary Sign-Off (Board papers only) This paper has been quality control checked and approved by the Company Secretary N/A

Board 31st January 2019 Attachment E2
4
Safe Staffing Levels in Community Inpatient Units Update Report
October and November 2018 1.0 Introduction
This report provides the Healthcare Governance Committee and the Board with an overview of the safe staffing levels within our Community Inpatient Units for October and November 2018. There is no nationally agreed RAG rating to determine safe staffing thresholds for nursing care; however, NHS England has applied a threshold where organisations declaring less than 80% fill rates for Registered Nurses (RN) will be subject to additional scrutiny as this level of nursing staff would be determined as unsafe. 2.0 Executive Summary Throughout October and November, safe staffing data demonstrates that the average safe staffing levels for all wards remained above the NHS England threshold of 80% for registered nurses. All Community Inpatient Units continue to care for high numbers of patients with complex needs. Vacancy levels were above the Trust’s target of 10% on all units in October and November, apart from QVM in October (4.91%) November(7.29%). The Inpatient Unit vacancy rate was 17.49% in October and 16.70% in November, which is slightly less than the 19% vacancy rates reported across Q2. Vacancy levels on the Inpatient Units are gradually decreasing (17.49% in October, reduced to 16.70% in November) with active recruitment ongoing. A ‘Golden Hello’ initiative is now in place for the units who have been having the most difficulty recruiting, Potters Bar, Langley and Herts and Essex. This has been successful across all units, particularly Langley, where the vacancy rate has gone from 23% in October to 16% in November. The Facebook and Twitter campaign is ongoing. Bank and agency use has remained high throughout October and November. The use on most units was associated with additional HCAs required to support patients requiring one to one care. The units with the highest Bank and Agency use across October and November are listed below, along with the number of specials required on the units: Unit B&A Use % No of additional
‘special’ shifts Oct
No of additional ‘special’ shifts
Nov Oct Nov St Peters 33% 28% 99 80 Holywell 32% 30% 103 43 Langley 30% 28% 82 75 HEH 30 30% 46 53

Board 31st January 2019 Attachment E2
5
Bank & Agency use at Langley and HEH was also associated with their high vacancy factor (8 x WTE RN vacancies on each unit). There is a considerable amount of work being undertaken to convert long term agency HCA and RNs. So far we have 7/11 converted to fixed term contracts or substantive positions. This work is ongoing. Sickness absence rates continue to fluctuate on all units throughout October and November, with the highest rates being approx. 11% in Langley, HEH and Simpson during October. This had decreased to approx. 6% on all units except Langley by November. The Trust absence policy continues to be enacted to manage sickness with support from HR, where necessary.
Papers Appendix 1 - Safe staffing dashboard October 2018
Appendix 2 - Safe staffing dashboard November 2018
Appendix 3 – Number of Patients on Units with Additional Needs.
3.0 Staffing Levels Safe staffing data met the required staffing levels for wards and remained above the NHS England threshold of 80% throughout October and November. Three of the Inpatients Units (Danesbury, Herts & Essex and Holywell) had staffing levels just above 90% during October. This level increased slightly during November to approx. 92%. Langley staffing was particularly low at 83% in October, but this has increased significantly to 94% in November, with the introduction of the ‘Golden Hello’ and the target recruitment. It is important to note that these figures relate to RN staffing levels for day shifts. All wards were staffed above 95% for RN’s for night shifts for October and November. The majority of units were also staffed above 100% for unregistered staff. Detailed information is shown in the staffing dashboards in Appendices 1 and 2. 4.0 Risks Patients with additional needs During October and November, across all of our units, there were 25 patients with Deprivation of Liberty Safeguards (DOLS) in place. Patients required 44 staff escorts off site. 679 additional HCA shifts were required to care for patients with complex needs across all of our units.

Board 31st January 2019 Attachment E2
6
282 patients were assessed as being at high risk of falls. This is a considerably higher number than in previous reports. The reason for this is that HCT have updated and implemented our new HCT Inpatient Falls Prevention Policy to reflect changes to the NICE guidelines. All patients admitted to hospital who are 65+ are considered to be at risk of falls and therefore need to have individualised risk assessments and intervention plans. Previously, we were using a MORSE score to predict the level of risk around a patient falling, and this is no longer recommended, since all patients 65+ who have been admitted to hospital are now considered at risk. This change in risk assessment will change the way we are reporting falls risk and the majority of our patients should be considered as at risk. A breakdown by Unit of shifts for additional needs is provided in Appendix 3. Vacancy Levels Vacancy levels were above the Trust’s target of 10% on all units in October and November, apart from QVM in October (4.91%), November (7.29%). The Inpatient Unit vacancy rate was 17.49% in October and 16.70% in November, which is slightly less than the 19% vacancy rates reported across Q2. Vacancy levels on the Inpatient Units are gradually decreasing (17.49% in October, reduced to 16.70% in November) with active recruitment ongoing. A ‘Golden Hello’ initiative is now in place for the units who have been having the most difficulty recruiting, Potters Bar, Langley and Herts and Essex. This has been successful across all units, particularly Langley, where the vacancy rate has gone from 23% in October to 16% in November. The Facebook and Twitter campaign is ongoing. 5.0 Quality Indicators
Falls
One fall was reported in October in Danesbury which resulted in ‘moderate’ harm to a patient. No falls resulting in ‘moderate/severe’ harm reported in November.
Pressure Ulcers There were no avoidable pressure ulcers reported in the units during October or November. Serious Incidents One Serious Incident was declared in October for Simpson Ward. This was a Safeguarding concern, which was raised via Hertfordshire County Council regarding a patient’s discharge from Simpson Ward, which resulted in a readmission to the Acute Hospital. This is being investigated by the Lead Nurse for Neuro and a report will be provided in due course.

Board 31st January 2019 Attachment E2
7
Healthcare Associated Infections (HCAIs) There were two cases of C-diff reported on the Units during October. One case was reported in Langley House and one case in Potters Bar. No HCAIs were reported on the units during November. Complaints No complaints were received for the Inpatient Units during October. Five complaints were received for the Inpatient Units during November. Of these 5 complaints, 3 were for QVM, 1 for Potters Bar and 1 for Simpson. Two of the complaints for QVM related to poor communication and discharge planning. Both of these complaints were resolved locally and the lessons learnt from these complaints were shared with the team. The third complaint for QVM related to poor care and poor communication. The complaint was investigated by the Service Manager and a written response provided to the family in January. The family were offered meeting, but declined this offer. The complaint is now closed. The complaint related to Simpson Ward was related to EOL care and poor discharge planning. A local resolution meeting is being held between the family and the Service Manager to discuss the issues. The Potters Bar complaint related to poor discharge planning. This complaint was investigated by the Service Manager and a written response was send to the family. This complaint is now closed. 6.0 Monitoring The Trust has a robust system in place which monitors staffing levels of RN and care staff on all units each day. This is supported via the Safe Staffing Reporting and Escalation Standard Operating Procedure, confirming minimum staffing levels and escalation procedures. Ward staff are required to report daily on their agreed staffing levels and actual level of staff on duty. Unresolved risks are escalated to the Director of Operations Monday to Friday and the Tier 1 Director/General Manager at weekends. In addition, episodes of low staffing levels requiring mitigating action are reported via a Datix incident report to ensure accurate monitoring. End of Report

Board 31st January 2019 Attachment E2
8
Appendix 1: October 2018 Safe Staffing Dashboard

Board 31st January 2019 Attachment E2
9

Board 31st January 2019 Attachment E2
10
Appendix 2: November 2018 Safe Staffing Dashboard

Board 31st January 2019 Attachment E2
11
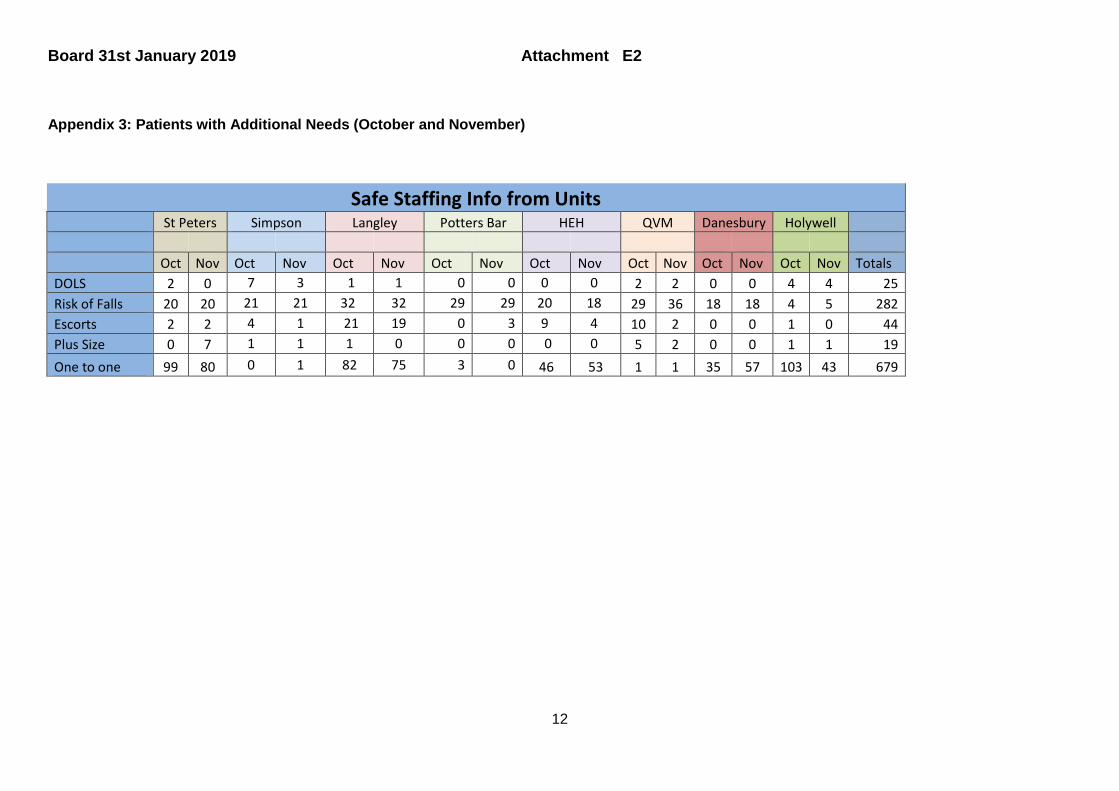
Board 31st January 2019 Attachment E2
12
Appendix 3: Patients with Additional Needs (October and November)
Safe Staffing Info from Units St Peters Simpson Langley Potters Bar HEH QVM Danesbury Holywell Oct Nov Oct Nov Oct Nov Oct Nov Oct Nov Oct Nov Oct Nov Oct Nov Totals DOLS 2 0 7 3 1 1 0 0 0 0 2 2 0 0 4 4 25 Risk of Falls 20 20 21 21 32 32 29 29 20 18 29 36 18 18 4 5 282 Escorts 2 2 4 1 21 19 0 3 9 4 10 2 0 0 1 0 44 Plus Size 0 7 1 1 1 0 0 0 0 0 5 2 0 0 1 1 19 One to one 99 80 0 1 82 75 3 0 46 53 1 1 35 57 103 43 679

Board 31st January 2019 Attachment E3
1
TRUST BOARD Title: LEARNING FROM DEATHS REPORT Q3 2018/19 (previously named ‘Mortality Review’) Meeting Date: 31 January 2019 Executive Lead: Hari Pathmanathan, Medical Director Author(s): Christine Stock, Head of Patient Safety For: Assurance and noting Risk Rating: Amber/Green 1.0 Purpose and Recommendations The Q3 assurance report provides:
1. An overview of deaths occurring; 2. Learning identified; 3. Conclusions and next steps.
2.0 Executive Summary
2.1 5 deaths were reviewed at Panel during Q3 (community and inpatients). All deaths were assessed as not being due to problems in care and were judged to be unavoidable.
2.2 Incidental learning identified at Panel will be disseminated to all staff during
January and will include the importance of: − Holding early end of life conversations with patient/family; − Maintaining fluid balance charts; − Completing DNACPR forms − Undertaking mental capacity assessments
2.3 The workshop held in November identified a number of key actions including
that the policy should be reviewed and re-written to more closely align with the ‘National Guidance on Learning from Deaths’ and its implementation supported
by clear procedural guidance. A revised policy will be circulated for consultation and approval during Q4.
3.0 Relevant Strategic Objective(s) / Strategies
The Statement impacts on all strategic objectives and links to all Trust strategies.
4.0 Appendices and Attachments
(1) None

Board 31st January 2019 Attachment E3
2
Author(s) of paper: Name Christine Stock, Head of Patient Safety Date: January 2019 To be completed as part of paper Committee Consideration This Report has previously been considered by the following committees: Committee: Date (Month / Year): Healthcare Governance Committee January 2019
Data Quality Statement By way of assurance to the Board, and in order to inform discussion / decision, the accountable executive director confirms that to the best of their knowledge, and subject to any exceptions identified, data contained in this report is: Data Quality Domain
Description Comments / Exceptions √ / x
Complete Information is as comprehensive as possible to inform the board / committee and no significant known facts or statistics which may influence a decision are omitted.
√
Accurate As far as can be reasonable ascertained or validated, information in the report is accurate.
√
Relevant Information contained in the report is relevant to the matters considered in the report.
√
Up To Date
Information in the report is as up to date as reasonably possible in the context of the time at which the paper is written
√
Valid Information is presented in a format which complies with internal or national models or standards
√
Clearly Defined
The meaning of any data in the report is clearly explained
√
Executive Director Sign-Off
This paper has been approved by the accountable executive director who is satisfied that (i) the implications for risks, (ii) quality/service/regulatory impacts and (iii) resource implications, have been considered.
Hari Pathmanathan Medical Director
√ / x
Company Secretary Sign-Off (Board papers only) This paper has been quality control checked and approved by the Company Secretary N/A

Board 31st January 2019 Attachment E3
3
LEARNING FROM DEATHS (previously named ‘Mortality Review’) REPORT
2018/19 Quarter 3
Background The mortality policy and procedure has been in place since September 2017. In November 2018 the Deputy Medical Director, who chairs the Mortality Review panel, led an annual review of the existing policy and procedure and a number of changes were agreed, two of which are:
− To review and rewrite the policy, incorporating procedural changes agreed at the workshop; − To re-name both the policy and the panel as the Learning from Death policy and the Learning from Deaths panel.
Quarterly assurance reports for 2018/19 will continue to provide information and the learning from review of deaths and will follow the same format with information being added to provide a 2018/19 cumulative overview. This Q3 assurance report provides:
1. An overview of deaths occurring meeting the criteria for completing case note review; 2. An overview of mortality reviews undertaken; 3. Learning identified; 4. Conclusions and next steps.
1. Overview of deaths occurring (within scope for review) The following tables provide an overview of deaths occurring in Q3 meeting the scope for mortality reviews. Information is provided by quarter and place of death. Inpatient unit deaths 2017/18
End of year total 2018/19
Q1 Q2 Q3 Q4 Total Danesbury Neurology Service 0 0

Board 31st January 2019 Attachment E3
4
Herts & Essex Hospital 2 1 1 2 Holywell Neurology Service 0 0 Langley House 0 0 Potters Bar Community Hospital 5 2 1 1 4 Queen Victoria Memorial Hospital 2 0 St Peters Ward HHGH 5 1 1 2 Simpson Ward HHGH 11 (part year) 3 4 3 10
Total 25 6 7 5 18 To note - each quarter the previous quarter’s data will be reviewed and updated to ensure all data is complete and accurate. This is to ensure that all deaths in scope are captured, including those where notification falls outside the reporting period. • 5 inpatient deaths were reported in Q3; numbers are in line with previous quarters and no exceptional patterns are emerging. • All inpatient unit deaths were expected. • Nascot Lawn (Children) closed during Q3. No deaths occurred at Nascot Lawn during 2017/18 or 2018/19 therefore reference to Nascot Lawn has
been removed from in this report. A profile of inpatients who died during Q3, including ages and known causes of death, is included below:
Age No. of patients 75 - 79 1 80 -84 1 85-89 1 90+ 2
Known causes of death - 1a on death certificate (number of patients) − Advanced dementia (1) − Frailty of old age (1) − Metastatic ovarian cancer (1) − Pulmonary embolus (1) − Cause of death for one patient will be confirmed when case note review is completed
Community deaths 2017/18
End of year total 2018/19
Q1 Q2 Q3 Q4 Total

Board 31st January 2019 Attachment E3
5
Specialist Palliative Care 2 0 Dacorum CAHS 1 2 2 Hertsmere CAHS 2 2 2 Lower Lea Valley 1 0 North Herts ICT 1 2 2 St Albans CAHS 1 1 1 2 WelHat ICT 1 1 2 3
Total 9 6 2 3 11 To note - each quarter the previous quarter’s data will be reviewed and updated to ensure it is complete and accurate. This is to make sure that all deaths within scope for review are captured, including those where notification falls outside the reporting period. • 3 community patient deaths were reported in Q3 meeting the criteria for undertaking case record review. • Community deaths fell within scope for review because the deaths were unexpected and the patient had had contact with a member of HCT staff
within the preceding seven days. A profile of community patients who died during Q3, including ages and known causes of death, is included below:
Age No. of patients 65 – 69 1 70 – 74 1 80-84 1
Known causes of death - 1a on death certificate (number of patients)
− Ischaemic heart disease (1) − The Coroner’s Office has been asked to confirm the cause of death for two community patients.
Deaths of children and people with learning disability No deaths of children have been reported requiring review. In December, HCT reported the death of an adult with learning disability to the Learning Disabilities Mortality Review (LeDeR) programme. The person was living in an assisted living facility in the community and died at home. Reporting all deaths of people with learning disability aged four years and over to the LeDeR programme is in line with expectations. The review of this death will be coordinated as part of the national programme using

Board 31st January 2019 Attachment E3
6
specific LeDeR methodology and the findings will be feedback to the Hertfordshire LeDeR Steering Group, which has HCT representation. The HCT representative will ensure that learning from the review is considered by the Learning from Deaths panel. 2. Overview of mortality reviews undertaken The following dashboard has been developed taking into consideration:
− The ‘assessment of avoidability’ scoring used by NHSI and which HCT has adopted; − Patients with learning disability will be identified separately as this supports the Learning Disability Mortality Review (LeDeR) programme; − The number of deaths occurring each quarter may be different to the number of deaths where (case-note) reviews are completed each quarter; − The mandated reporting requirements within the annual Quality Account, i.e. number of deaths occurring each quarter is to be reported
separately to the number of case reviews undertaken each quarter.
INPATIENT UNIT DEATHS 2018-2019
Deaths
occurring in quarter (not LD)
Mortality reviews
completed in quarter (not LD)
Panel assessment of avoidability LD deaths
occurring in quarter
LD Mortality reviews
completed in quarter
Definitely avoidable
Strong evidence of avoidability
Probably avoidable (more than 50:50)
Probably avoidable but not
very likely Slight evidence of avoidability
Definitely not avoidable
1 2 3 4 5 6 Q1 6 8 7 0 n/a
Q2 7 6 1 6 0 n/a
Q3 5 4 4 0 n/a
Q4
COMMUNITY PATIENT DEATHS 2018-2019
Deaths
occurring in quarter (not LD)
Mortality reviews
completed in quarter (not LD)
Panel assessment of avoidability LD deaths
occurring in quarter
LD Mortality reviews
completed in quarter
Definitely avoidable
Strong evidence of avoidability
Probably avoidable (more than 50:50)
Probably avoidable but not
very likely Slight evidence of avoidability
Definitely not avoidable
1 2 3 4 5 6 Q1 6 10 11 0 n/a

Board 31st January 2019 Attachment E3
7
Q2 2 4 5 0 n/a
Q3 3 2 1 1 0
Q4
Deaths occurring in quarter No. of deaths recorded as occurring during the quarter within scope for undertaking a review Reviews completed/returned in quarter No. of structured judgment reviews completed (may include reviews for deaths occurring in the preceding quarter) Panel assessment of avoidability Assessment of avoidability made by the Learning from Deaths Panel (may include deaths occurring in preceding quarter) • During Q3 5 deaths were reviewed at panel (1 community and 4 inpatient) who assessed that the deaths were not due to problems in care and
judged the deaths to be ‘definitely not avoidable’, score 6.
• One death of a learning disabled adult was reported to LeDeR during Q3. Once LeDeR review is completed the findings will be shared with HCT Learning from Deaths panel.
• Review of all 2018-2019 information has identified an error within the previous Q2 report; the error has been corrected in this report. − The error concerns one inpatient death that had been reviewed at panel during Q2, but where the panel’s assessment had not been included
within the above ‘Inpatient Overview’ table; this has now been added to the table. − The inpatient death had been judged at panel as ‘slight evidence of avoidability’, score 5. The patient was 90 years old and had died within
four days of admission; cause of death is recorded as pneumonia. The case note review failed to evidence that sepsis had been considered. Whilst it was recognised that in the frail and elderly it can be difficult to recognise sepsis, and that active treatment may not have made a difference to the outcome, the panel considered it reasonable to expect evidence that sepsis had been considered, especially as the urgent blood test that the ward had ordered suggested infection.
− The findings of this review provided further support for a trust-wide sepsis group with medical and senior nurse leadership to be established. This group was convened during Q2 and is chaired by a Deputy Medical Director.
3. Learning identified Learning is gathered through review and discussion at the Mortality Panel when the Structured Judgement Reviews are considered by senior doctors, nurses, AHPs and managers. Learning is summarised and communicated to all staff via Sharing Lessons in Practice (all-staff trust communication) and the next Sharing Lessons in Practice will be developed at the end of January.

Board 31st January 2019 Attachment E3
8
Specific learning is directed to the relevant service managers and by way of example, one death reviewed during Q3 is detailed below, including how the learning has been shared: An elderly patient was on an inpatient in one of the trust’s units for one month; they died on the unit. Cause of death has been confirmed as ‘Advanced Dementia’. Whilst the panel judged that problems in care did not contribute to the death, areas of poor care were identified and included:
− No fluid balance chart − No mental capacity assessments during admission − DNACPR incomplete − No End of Life conversations
Following discussion at panel, the Chair shared the completed review and requested that the ward consultant and ward manager facilitate a meeting with their ward team to discuss the findings and consider what actions they will take to improve the areas of poor care and prevent these occurring again - ‘If this patient was on the ward now, what would they do differently?’ The senior operational management have been requested to gather feedback from the consultant and ward manager who are to report the changes in practice that are made back. Feedback is to be to the panel, with any necessary assurance. 4. Conclusions and next steps Next steps agreed at the November workshop include:
a) The policy will be re-written to more closely align with the ‘National Guidance on Learning from Deaths’ and will provide clearer procedural guidance;
b) All inpatient deaths will continue to be reviewed and the scope for community deaths will be revised; c) The Deputy Medical Director has completed tier one Structured Judgement Review training and will lead a training event during Q4 with a
focus on training up a smaller group of reviewers and supporting an improvement in the quality of case reviews. Christine Stock, Head of Patient Safety, January 2019

Board 31st January 2019 Attachment E4
1
Board Committee Chair’s Assurance Report
Healthcare Governance Committee Date of Board Meeting: 31th January 2019 Committee Chair: Anne McPherson Date of Committee Meeting: 22 January 2019 Date of Report: Dates of Committee Meetings Held Since Last Board Meeting: None Date of Next meeting: 19 March 2019
Item Ref
Subject Director’s Risk
Assessment (H/M/L) (R/A/G)
Committee Assurance
Assessment (R/AR/AG/G)
Committee Chair’s Observations
Risks Arising From Minutes / Tracker Updates: Tr1
Assurance: 4.1 CQC Update
verbal
Amber/ Green
Review carried out by CQC Relationship Manager prior to attending HGC. No concerns. Current SMT action plan to be developed into an HCT Quality Improvement Plan to achieve the behavioural changes needed to embed improvement in HCT services. Will be subject to regular review by HGC.
4.2 • East & North Herts ICT QIA
Amber/ Green
Amber/ Green
Reasonable assurance that the short-term, moderate risk to patient safety, experience and clinical effectiveness as staff move base and adopt new models of working with new skills following the planned equalisation of resource in East & North Herts has not

Board 31st January 2019 Attachment E4
2
had a negative impact. HGC will continue to overview for assurance by reviewing the performance and service specific KPI’s in March 2019.
4.3 Skin Health Independent Review
Amber/ Green
Amber/ Green
External report by Dr Julia Schofield MBE Consultant Dermatologist & Principal Lecturer, Post Graduate Medical School, University of Hertfordshire provides evidence of sound clinical governance & professional support systems are in place. Arrangements to provide Consultant input to the service is close to being finalised to enable the safe prescribing of Isotretinoin for the treatment of Acne by the Skin Health Service.
4.4 Community paediatrics Harm Review
Amber/Red
Amber/ Green
Administrative data cleanse of systm1 caseloads in the Community Paediatric service completed. Plus a review of all clinical records requiring Harm Review carried out by the Consultant Paediatricians. 10 cases of low harm identified relating to follow up appointments with immediate mitigation action taken. Risk rating reduced.
4.5i Complaints report Q3
Amber /Green
Amber /Green
36 complaints in quarter 3 5280 compliments. In Q3 29 Prison Healthcare complaints all managed at stage 1. The details of all prison complaints (92) 86 stage 1 & 6 stage 2 since the beginning of the year reviewed. Both HCT and Prison Service complaint numbers relatively stable within 30-38 range on average. 1 PHSO referral in Q3. No lapses of care found in PHSO review of a Q1 complaint referred 2018.

Board 31st January 2019 Attachment E4
3
4.5ii Serious Incident Report (bi monthly)
Green Amber /Green
Two SI reported in the last 2 months. 6 SI’s this year to date of which 4 are categorised as sub optimal care. Assurance that changes are made and embedded in practice via evidence presented to the SI Assurance Panel. HGC down-graded the RAG rating because the two new SI’s are being investigated but the outcome is not known at this time to provide assurance.
4.5iii Safe staffing Community Hospitals (Oct/ Nov)
Amber /Green
Amber /Green
October/November outturn with 80% staffing levels achieved by the use of temporary staff. HEH on the HLRR. Vacancies continue to be high but gradually reducing as various recruitment initiatives begin to have effect. Quality Indicators including training and appraisal rates maintained.
4.5iv Safe staffing ICT Teams (Oct/Nov)
Amber /Green
Amber /Green
Reduced allocation in North Herts locality from the E&N Herts new workforce model & Equalisation Agenda is having an adverse impact on staffing. Deep dive underway. Watford ICT continues be successful in recruitment and is now approaching a good level with the potential to achieve a nearly full establishment. Agency staff are actively being encouraged to become substantive or join NHSP. Training and Appraisal rates are good.
4.6 High Level Risk Register (January 2019)
N/A N/A
Two risks require to be re-assessed since the level of clinical risk has reduced. . These are 567 Skin Health and 458 Watford ICT.

Board 31st January 2019 Attachment E4
4
4.7 Board Assurance Framwork
N/A N/A BAF reviewed. Quality & Regulatory 01 CQC Compliance requires updating once the CQC Report on the September 2018 Inspection is in the public domain.
4.8 Freedom to Speak Up Policy to approve
N/A
N/A
Approved by the Healthcare Governance Committee. Pictorial depiction of the policy on a page highly commended.
5 Patient Safety & Patient Experience
5.1 Patient Safety& Experience Group, Chair’s Assurance report and minutes 13th December 2018
N/A N/A HGC noted the escalation of by the Medical Devices Advisory Forum regarding the lack of capacity within the team. This has resulted in a delay in the servicing and maintenance of medical devices and audit of DEC training folders, leading to a lack of assurance that clinical staff are competent to manage medical devices locally. PSEG RED negative assurance. Assurance given that this is being addressed and will be reported back to HGC via the normal governance route.
5.2 Duty Of Candour Q3
Green Green Fully compliant with good assurance that the duty of candour is being met. No longer required to provide a quarterly assurance to HGC but will be reported through the IBPR.

Board 31st January 2019 Attachment E4
5
6 Clinical Effectiveness
6.1 Learning from Deaths Q3
Amber/Green Amber/ Green
Revised policy to be presented in Q4. Work to improve the working of the Panel and the processes involved in Learning from Deaths ongoing. Numbers of unavoidable deaths remain similar to previous Quarters.
6.2 Clinical Reference Group minutes from the meeting on 13 December 2018
N/A N/A Clinical Reference Group Minutes noted
6.3 Clinical Effectiveness Group Chair’s assurance and minutes from 7 November 2018
N/A N/A Action to turn around the negative assurance on the CPR & Blood Transfusion Policy reviews to be completed within 1 week. Assurance to be provided to HGC that this has been done as requested.
7.00 Key Items for Noting
8.00 Key Items for Escalation
Supporting Papers for information
FI1 Clinical Quality Review minutes from 30th November 2018

Board 31st January 2019 Attachment E4
6
Summary of Committee governance issues and any other points for the Board’s Attention
• The Self- Assessment for Committees Questionnaire approved by the Audit Committee in December 2018 has been completed by the Chair of HGC. It has been circulated to committee members for comment before being formally reviewed for agreement and sign off in March.
• Appropriateness of items on the tracker reviewed. A number have been reverted either to the Business Cycle or to come through the normal governance route as business/reports from the sub groups and forums reporting to HGC.
Definitions and Key: Green Amber/ Green Amber/ Red Red (A) Executive Director’s Risk Assessment High (Red) Risks associated with this issue: (1) Include high scoring risks (15+) which have been recorded on the appropriate
risk register (ie HLRR (Operational) or BAF (strategic)) or (2) Will be recorded on the appropriate risk register following committee / Board /
Executive Team deliberation. Medium to High (Amber / Red) Risks associated with this issue: (1) Include Medium scoring risks which have been recorded on the appropriate
risk register (ie Business Unit (Operational) or BAF (strategic)) or (2) Will be recorded on the appropriate risk register following committee / Board /
Executive Team deliberation. Medium to Low (Amber / Green) Risks associated with this issue:

Board 31st January 2019 Attachment E4
7
(1) Do not require recording on the relevant risk register but continued monitoring for any risks emerging required or
(2) Associated risks have been recorded on the relevant risk register but
circumstances are now such whereby de-escalation is proposed. Low (Green) (1) No risks or insignificant (low scoring: risks) not necessary to record on risk
registers. (B) Committee Chair’s Assurance: Red (Negative Assurances): The Committee considers that there are currently significant gaps / weaknesses in actions to manage risks, controls or assurances which are of sufficient concern to the Committee to require escalation to the Board for consideration and agreement on actions required Amber / Red (Limited Assurances): The Committee considers that there are some gaps / weaknesses in actions to manage risks, controls or assurance which are of sufficient concern to require escalation to the Board for information at this stage Amber / Green (Reasonable Assurances): The Committee has received reasonable assurance on behalf of the Board as to actions to manage risks, controls and assurances. Green (Significant Assurances): The Committee has received significant assurance on behalf of the Board as to actions, to manage risks, controls and assurances.

Board 31st January 2019 Attachment F1
1
TRUST BOARD Title: SUMMARY OF INTEGRATED BOARD PERFORMANCE
REPORT (December 2018) Meeting Date: 31 January 2019
Executive Lead(s): ROSHAN JHOREE – Assistant Director of Performance & Information (Acting) Author(s): INFORMATION For: NOTING Risk Rating: Not Applicable 1.0 Purpose & Recommendations
1.1 This paper provides the Trust scorecard and headlines from the Integrated Board Performance Report for December 2018. The full report is included in Supporting Papers.
1.2 The Board is requested to note the Trust scorecard and headlines of the
Integrated Business Performance Report.
2.0 Performance Highlights & Areas for Board Review December 2018 Key Messages Performance highlights • Zero C.Diff cases reported for second consecutive month. • Friends & Family test on target at 95% in December. • Stroke LoS within rehab pathway thresholds. • Non-stroke (Rehab pathway) LOS below 21 day threshold in December. • 93.5% of patients waiting within 18 weeks for their initial appointment. • 77% of End of life care patients have been offered, completed or refused an
advanced care plan. • Staff Mandatory training figures above target with 94.2% in December • Safeguarding Children supervision now above target • Information Governance training at 94.9%. Areas for Board review • 11 avoidable category 3-4 Pressure ulcers reported in December. • DTOC rate above the 5% threshold with 6.9% health delays recorded in
December. • Underlying Staff turnover over threshold with 14.4% recorded in December.

Board 31st January 2019 Attachment F1
2
• Absence rate above threshold for December. 3.0 Relevant Strategic Objective(s) / Strategies
This report impacts on all strategic objectives and links to all Trust strategies.
4.0 Appendices and Attachments Summary Trust Scorecard (December 2019) K4 Integrated Board Performance Report (December 2019) Author(s) of paper: Roshan Jhoree Assistant Director of Performance & Information (Acting) January 2019

Board 31st January 2019 Attachment F1
3
Committee Consideration This Report has previously been considered by the following committees: Committee: Date (Month / Year):
Strategy & Resource Committee January 2019 Data Quality Statement By way of assurance to the Board, and in order to inform discussion / decision, the accountable executive director confirms that to the best of their knowledge, and subject to any exceptions identified, data contained in this report is: Data Quality Domain
Description Comments / Exceptions √ / x
Complete Information is as comprehensive as possible to inform the board and no significant known facts or statistics which may influence a decision are omitted.
√
Accurate As far as can be reasonable ascertained or validated, information in the report is accurate.
√
Relevant Information contained in the report is relevant to the matters considered in the report.
√
Up To Date
Information in the report is as up to date as reasonably possible in the context of the time at which the paper is written
√
Valid Information is presented in a format which complies with internal or national models or standards
√
Clearly Defined
The meaning of any data in the report is clearly explained
√
Executive Director Sign-Off This paper has been approved by the accountable executive director who is satisfied that (i) the implications for risks, (ii) quality/service/regulatory impacts and (iii) resource implications, have been considered.
David Bacon Director of Finance (Interim)
√
Company Secretary Sign-Off (Board papers only) This paper has been quality control checked and approved by the Company Secretary √

December 2018 Attachment F1
Indicator
2018/19
Target /
Threshold
Current period
performance18-19 YTD
Current
Period
RAG
YTD RAG
Trend from
previous
month
Trend over
time
HCT
Benchmarking
Rank
Trusts
Participating
97.4% 98.0%
11.6% A A � 11
A A �
�
� 5 14
Work
forc
e &
Fin
ance
% of staff who have received an appraisal in the last 12 months 90% 91.1% G G
15
(Overall
Turnover)
Absence Rate <=3.6% 4.70% R
13
15
(Overall Turnover)
Underlying Staff turnover (Voluntary resignations excluding retirements, redundancy and the end of
FTCs)
% posts vacant
(vacant WTE/budgeted WTE).10%
12% 14.4%
2 14
94.9%
14.4%
4.70%
91.4%
11.6%
% of staff completing Information Governance training (Rolling Year) 95% 94.9% A A �
�% of staff who have undertaken level 1 / 2 safeguarding adults training every 3 years 95% 97.3% G G
% of all clinical and medical relevant staff (all clinical staff including staff in supervisory roles
requiring a clinical registration) will undertake
Level 2 safeguarding adults�95% 97.3% G G
�% of eligible staff trained at appropriated level of safeguarding children in accordance with IC
document Level 1, Level 2, Level 395% 95.0% G G
L &
D
% staff who have undertaken mandatory training 90.0% 94.2% G G � 10 15
Patient waiting list (including Consultant & Non-consultant led services) 92.0% 93.5% G G �
5%
for health
delays
Community Hospitals - Average length of stay in HCT community hospital - Non Stroke (Rehab
Pathway)19 days 14.9 G R �
Total 15.7%
(Health 6.9%
HCS 8.7%
Both 0.1%)
Total 16.4%
(Health 9.6%
HCS 6.6%
Both 0.2%)
Perf
orm
ance
Community Hospitals - Average length of stay in HCT community hospital - ALL Stroke (Rehab
Pathway)42 Days 29.1 G G
All data entered on S1 within 24 hours of contact >=90% 89.7% R R
Community Hospitals - % of NHS (health) bed days lost due to delayed transfers of care
�
0 G R
Friends and Family test 95% 95% G G
No of avoidable category 2 pressure ulcers acquired in HCT care (Reported one month in arrears) 0
C.difficile cases occurring post 3 days following admission into HCT bed based facilities (i.e.
acquired in our facility)
Full Year 5
monthly
trajectory
0 - Nov
0 G
% of patients receiving harm free care (Safety Themometer data - New Harms only) 5 13Compliant
TRUST SCORECARD 18/19
Quality
�
� 5 15
� 14 15
�
R
G G �
Number of complaints received in monthFor
information12
R
R R �
�
5
111
95%
25
32.7
21.3
88.5%
94.4%
94.2%
95.0%
97.3%
97.3%

December 2018 Attachment F1
December 2018 Key Messages
Performance highlights
• Zero C.Diff cases reported for second consecutive month.
• Friends & Family test on target at 95% in December.
• Stroke LoS within rehab pathway thresholds.
• Non-stroke (Rehab pathway) LOS below 21 day threshold in December.
• 93.5% of patients waiting within 18 weeks for their initial appointment.
• 77% of End of life care patients have been offered, completed or refused an advanced care plan.
• Staff Mandatory training figures above target with 94.2% in December
• Safeguarding Children supervision now above target
• Information Governance training at 94.9%.
Areas for Board review
• 11 avoidable category 3-4 Pressure ulcers reported in December.
• DTOC rate above the 5% threshold with 6.9% health delays recorded in December.
• Underlying Staff turnover over threshold with 14.4% recorded in December.
• Absence rate above threshold for December.

December 2018 Attachment F1 HCT SCORECARD EXCEPTION REPORT ( 18 KPIs RAG RATED)
4 6 8
ACTION NHS Health Delayed Transfer of Care (DTOC) HCT were over the 5% threshold after recording 6.9% health delays in December. This is the lowest figure since May 2018 and an improvement of 1.3% on previous month. The main delay reasons for December were Funding (B), Patient/Family choice (G) and Community Equipment (F). The combined number of bed days delayed for these reasons were 291 which equates to 84% of total delays.
Actions Focused work continues in the Community Inpatient Units to ensure that they are used for patients requiring an appropriate pathway of care, working closely with partners in the acute hospitals and social care to ensure that the patient’s journey is optimised from admission.
All data entered on S1 within 24 hours of contact HCT are below the 90% target in December with 89.7% of contacts recorded within 24hrs. The percentage increases to 93% within 48hrs. This will be monitored and where certain services are below the target this will be escalated to Service managers during business unit reviews.
% of staff completing Information Governance training (Rolling Year) Compliance is 94.9% for December. HCT is confident the target will be achieved by end of financial year.
% Posts Vacant The Trust vacancy rate increased to 11.6% in December 2018, up from the 10.5% low in October and November. This is due to a combination of a reduction in staff in-post (more leavers than starters) and some increases in budgeted establishments, particularly with the setting up of the new cost centres for the admin hubs in the Childrens Business Unit.
Underlying Staff turnover The Trust-wide underlying turnover rate for December 2018 was 14.4% which remains relatively stable (it was 14.3% this time last year). However, whereas in December 2017, Adult Services turnover was highest at 16.46% (with Corporate at 10.08%), now Corporate turnover is higher than either of the operational business units at 15.2% (with the Adult Business Unit down to 14.5%).
Absence Rate The Trust sickness absence rate was up to 4.7% in December, well above the 3.6% target. The sickness rate for the Childrens Business unit has reduced down below target this month (at 3.5%); however the rate in the Adult Business Unit has increased to 5.7%. This is mainly due to very high absence rates in the Community Inpatients Units at 8.8% (6.5% long term). Corporate sickness absence remains low at 1.6%.

Board 31st January 2019 Attachment G1
Remuneration Committee
18 December 2018 08.30 – 09. 05hrs
Main Items of Discussion
Present: Anne McPherson (AMcP) Chair of Remuneration Committee Declan O’Farrell (DO’F) Board Chair Jeff Phillips (JP) Chair of Audit Committee
In attendance: Raj Bhamber (RB) Interim Director of People & OD
Clare Hawkins (CH) CEO
1. Introductions & apologies The Chair of the Remuneration Committee welcomed everyone to the meeting.
2. Notes of meeting held on 23 October 2018 were approved, subject to a correction of the initials, which should have been RB rather DE for Raj Bhamber, Interim Director of Human Resources & OD who was in attendance at the meeting.
3. Matters Arising There were no matters arising that were not already agenda items for the meeting.
4. Proposal (supplemented by independent report) The committee considered an independent report relating to a former employee and approved the proposal.
5. Appointment of the Director of Nursing & Quality The committee were delighted to note the appointment ( and associated terms and conditions of employment) of Sarah Browne as the new substantive Director of Nursing & Quality who will be joining the Trust formally on the 25th February 2019 with attendance at key events beforehand where possible. Members also reflected on the leadership provided by Andy Nuckcheddee as the Acting Director of Nursing & Quality and recorded their gratitude for his sterling stewardship of the remit and achievements.
6. Appointment of the Director of Finance The committee was pleased to note the appointment (and associated terms and conditions of employment) of David Bacon as the substantive Director of Finance following a national advertisement and a statutory recruitment and selection process involving internal and external stakeholders and assessors. The Chief Executive informed the committee that the all of the formal appointment processes had been completed and that the appointment had been well received.
7. Interim Director of People & OD ( the Interim Director of HR & OD left the meeting for this item) The committee noted the agreement to extend the arrangements for Raj Bhamber as the Interim Director of People & OD.

Board 31st January 2019 Attachment G1
8. Deputy Chief Executive and Medical Director The committee approved the substantive appointment of the Deputy Chief Executive and Medical Director. It also welcomed the review and future executive structure and portfolios.
9. Executive Salary Review The committee considered the analysis of executive salaries at HCT for the last two financial years, external benchmarks for community Trusts and proposed changes
10. Any Other Business There was no other business.
11.
Date of next meeting: 26 March 2019 at noon, after the SRC at Howard Court unless required sooner.

Board 31st January 2019 Attachment G2
1
Board Committee Chair’s Assurance Report
Audit Committee Date of Board Meeting: 31 January 2019 Committee Chair: Jeff Phillips Date of Committee Meeting: 11 December 2018 Date of Report: 23.1.19 Dates of Committee Meetings Held Since Last Board Meeting: None Date of Next meeting: 12 March 2019
Item Ref Subject
Director’s Risk
Assessment (H/M/L) (R/A/G)
Committee Assurance Assessment (R/AR/AG/G)
Committee Chair’s Observations
Risks Arising From Minutes / Tracker Updates:
51/18
Consistent reporting of ALOS
Remains dependent on CCG engagement
Assurance:
Internal Audit
B1 Internal Audit progress report and action tracker
Green Slippage to timeframes has now been rectified, and the planned audits will all be completed by end of March. Two management actions remain, a substantial improvement on the 20+ reported at the last Audit Committee.

Board 31st January 2019 Attachment G2
2
B2
Internal Audit Final Report: 3.18/19 General Data Protection Regulations
Amber/ Green
The audit opinion contained one low and five medium actions. However, gaps remain:- 1. Completion of data flow
mapping and information asset registers
2. Identification of a Data Protection Officer
3. Development of robust processes for incident and data breaches.
These will be in place by March 2019
4.18/19 STP Governance & Assurance
N/A HCT have been proactive in managing issues that need to be delivered, but gaps exist:- 1. Information retained re implementation of work streams. 2.Limited STP assurance to manage STP risks 3.HCT strategic objectives need to play into the wider STP 4.The STP is not subject to internal audit as yet
5.18/19 Business Unit Quality & Governance
N/A Rigour and clarity around managing identified risks needs improvement, and the timing of Exec challenge needs to be done before submission to the Board sub-committees.
6.18/19 Estates
N/A Three gaps identified:- 1.Lack of an agreed MOU with HFPT 2. Consistency in policies and procedures across both organisations.

Board 31st January 2019 Attachment G2
3
3.Clear lines of responsibility and accountability Significant progress on these was reported, and a draft joint estate strategy is out for comment, with a target implementation of March 2019 There will be a follow-up audit in late 2019/2020
B3 1./18/19 E Rostering update report
N/A HCT have been cited as following good practice in a follow up Carter Review case study. However, practice across the Trust is still patchy, but the E-Roster team are actively supporting business units in achieving that consistency in approach, shared learning and practical use of the system. IA are happy with progress, but a cost benefit analysis is needed to prove the benefits gained, and the ER team’s resource requirement need to be agreed by the Exec.
External Audit C1 External Audit
Progress Report
N/A
Early testing is underway and the programme plan will be presented at the March meeting. Two issues of concern for the audit are the impact of Brexit and the outcome of the HVACS bid as they affect the going concern and value for money opinions
Quality, Clinical Governance and Risk& Assurance D1 High Level Risk
Register
N/A 11 risks on the Register, 3 corporate and 8 operational. One of the corporate risks relates to HCT’s ability to maintain current CQC regulatory standards. However, it is worth noting

Board 31st January 2019 Attachment G2
4
that that there has been noticeable improvement in the engagement of operational leads in respect of articulating risks and related controls. Training programme now in place for front-line staff
D2 Board Assurance Framework
N/A The alignment of the BAF with risk registers and controls remains work in progress, and IA are advising on the format for the public document/ Governance processes aligning the BAF remain a key element of this work Worth noting that many NHS organisations do not publish the BAF or the HLRR
D3 Clinical Audit Programme (half yearly update)
N/A Clinical effectiveness has been reviewed, but in future will be more outcome focussed. HCT has participated in 100% of the national and local audits, but the articulation of the full outcomes achieved needs to be improved, particularly as regards lessons learned. Worth noting that CQC were impressed by how well embedded clinical audits were across HCT
Financial & Procurement E1 Charitable Funds
Accounts (For Approval)
N/A The audited accounts were approved on behalf of the Corporate Trustee following the external audit by Ernst &Young
E2 Charitable Funds Annual Report (For Approval)
N/A The annual report was approved on behalf of the Corporate Trustee following the external audit by Ernst &Young

Board 31st January 2019 Attachment G2
5
E3 Letter of Representation
N/A A joint letter of representation from the Chair of the Charitable Funds Committee and Director of Finance has been drafted
E4 Review of Tender Waivers
N/A To date there are 8 tender waivers in 2018/9 totalling £264k and there were no SFI breaches in the year
E5 IFRS 9, 15 And 16 Adoption Update
N/A IFRS 9 and 15 will not impact the 18/19 accounts, and IFRS 16 covering accounting for leases has been deferred by HM Treasury until 20/21. The primary impact of IFRS 16 is to bring ALL leases agreements on to the Statement of Financial Position. HCT has made progress in assessing the impact of this standard, and an update will be provided for the next Audit meeting
Counter Fraud F1 Local Counter Fraud
Progress Report
N/A eLearning programme is underway, and the second phase will start in the New Year. Information has been circulated on gambling awareness and phishing telephone scamming. 2 referrals of false representation re working elsewhere whilst on sick leave. One of these is being pursued and a prosecution file is being prepared. A Trust wide communication on this case will be actioned once the outcome is established. No action required on the other case

Board 31st January 2019 Attachment G2
6
Audit Committee Governance G1 Review annual
Business Cycle
N/A The updated business cycle report was agreed
G2 Board Committee effectiveness self-assessment
N/A The revised self-assessment document was accepted, subject to some minor amendments and a pilot was agreed to be signed off by the next meeting
H1 Circulated for information
For information: Governance return supplied to Herts Valleys CCG Any Other Urgent Business None
Summary of Committee Governance issues and any other points for the Board’s Attention
See individual items reported above

Board 31st January 2019 Attachment G2
7
Definitions and Key: Green Amber/ Green Amber/ Red Red (A) Executive Director’s Risk Assessment High (Red) Risks associated with this issue: (1) Include high scoring risks (15+) which have been recorded on the appropriate risk register (ie
HLRR (Operational) or BAF (strategic)) or (2) Will be recorded on the appropriate risk register following committee / Board / Executive Team
deliberation. Medium to High (Amber / Red) Risks associated with this issue: (1) Include Medium scoring risks which have been recorded on the appropriate risk register (ie
Business Unit (Operational) or BAF (strategic)) or (2) Will be recorded on the appropriate risk register following committee / Board / Executive Team
deliberation. Medium to Low (Amber / Green) Risks associated with this issue: (1) Do not require recording on the relevant risk register but continued monitoring for any risks
emerging required or (2) Associated risks have been recorded on the relevant risk register but circumstances are now
such whereby de-escalation is proposed. Low (Green) (1) No risks or insignificant (low scoring: risks) not necessary to record on risk registers. (B) Committee Chair’s Assurance: Red (Negative Assurances): The Committee considers that there are currently significant gaps / weaknesses in actions to manage risks, controls or assurances which are of sufficient concern to the Committee to require escalation to the Board for consideration and agreement on actions required Amber / Red (Limited Assurances): The Committee considers that there are some gaps / weaknesses in actions to manage risks, controls or assurance which are of sufficient concern to require escalation to the Board for information at this stage Amber / Green (Reasonable Assurances): The Committee has received reasonable assurance on behalf of the Board as to actions to manage risks, controls and assurances.

Board 31st January 2019 Attachment G2
8
Green (Significant Assurances): The Committee has received significant assurance on behalf of the Board as to actions, to manage risks, controls and assurances.

Board 31st January 2019 Attachment J1
1
TRUST BOARD
Title: High-Level Risk Register Meeting Date: 31st January 2019 Executive Lead: Andy Nuckcheddee: Acting Director of Nursing & Quality & Chief
Nurse/Governance Lead Author(s): Nico Kamera: Head of Risk & Clinical Effectiveness Gerry Phee: Risk & Assurance Manager For: Assurance 1.0 Purpose and Recommendations
1.1 To inform Trust Board of the current status of Risks associated with activity and business across all Hertfordshire Community NHS Trust (HCT) Business Units as of 23rd January 2019. 1.2 To provide assurance that the High-Level Risk Register (HLRR) reflects the Trust’s current ‘high level’ risks. The Risk Team continues to work with our Operational and Corporate services to deliver timeliness of reviews and improved understanding of managing risk registers.
2.0 Executive Summary
The number of high-level risks is currently 8 (eight) compared with 9 (nine) in December. Two of the high-level risks are corporate and six are operational.
This paper outlines changes to the HLRR during December 2018 and January
2019 and provides progress and assurance on the management of these risks. All risk scores have been reviewed in collaboration with the risk leads and updated accordingly. The scores are defined as consequences of risk multiplied by the likelihood of risk materialising. The risk Model 5x5 Matrix has been attached as an appendix to provide rationalisation as to how risks are scored, noting consequence x likelihood = score.
The top five risks on the HLRR scoring 16 or above are:
1. Ref 526 Workforce (HR) - Insufficient supply of workforce with the right skills may lead to difficulties in meeting current and future service needs impacting on the ability to transform services, provide quality of care and financial sustainability. (Risk score: 4x4=16)
2. Ref 605 Community In-Patient Units Herts Valleys - There are a high number of patients whose onward destination from a community hospital bed is delayed (DTOC) and who do not meet the intermediate care service

Board 31st January 2019 Attachment J1
2
specification criteria, leading to high numbers of patients waiting for admission into, or remaining in a community hospital bed within the Herts Valley locality for longer than the commissioned target. This is resulting in patients waiting in an acute and a community bed for longer than they should, and HCT not meeting its commissioned targets for overall average length of stay and rehabilitation length of stay. (Risk score: 4x4=16)
3. Ref 634 Community Paediatrics – Increasing demand for consultant community paediatric assessment, review and treatment for Autism Spectrum Disorder and a lack of clarity for referral and access between providers has led to referral to treatment breaches, increased follow-up waiting lists resulting in an increase in first to follow up appointments and support for families, increased scrutiny within the Trust and from commissioners with potential increase in reputational risk and increase of stress within the team. (Risk score 4x4=16)
4. Ref 670 Herts & Essex Inpatient Unit - High Nursing vacancy rates, sickness
absence and reliance on use of bank and Agency staff may lead to an inability to maintain safe staffing levels for nursing resulting in potential for reduced quality and continuity of care, increase in patient harm, poor patient experience, reduced staff morale, reputational damage and increased scrutiny by commissioners and regulators. (Risk score: 4x4=16)
5. Ref 600 Public Health Nursing (This risk was escalated in December 2018)
- Successful Public Health Nursing bid within Family Centre Service (FSC) provision commissioned by HCC, leading to the need to mobilise the new service model as described in HCT's bid; and align and integrate with Family Support Services to form FSC. Potentially resulting in an inability to deliver the services as expected and within agreed timescales, possible quality impact on children, young people (CYP) and families, possible negative impact on staffing, loss of reputation and financial penalties. (Risk score: 4x4=16)
2.1.1 De-escalated Risks:
1. Ref 458 Watford CAHS - Ongoing shortage of staff as difficulty in recruiting leading to unfilled vacancies, recruitment of bank and agency staff, increase in resignations, long term sickness, resulting in risk to continuity of care, patients safety and patient experience. The risk was reviewed at January 2019 Healthcare Governance Committee and de-escalated as the staffing levels have improved. The risk score has been re-assessed and consequently de-escalated from the HLRR. (Risk score: 4x3=12)
2. Ref 685 Care Quality Commission - Inability to maintain the current CQC
standards or achieve a higher CQC compliance following a formal inspection may adversely impact on the Trust’s reputation in delivering safe and quality services, loss in confidence by key stakeholders such as

Board 31st January 2019 Attachment J1
3
commissioners, local population and partner organisations and also, impacting on staff morale. The risk was reviewed at January 2019 Healthcare Governance Committee and de-escalated in light of the positive CQC report. The risk has reduced, subsequently this risk score has reduced and the risk has been de-escalated from the High Level Risk Register. (Risk score: 4x3=12)
2.2 The diagrams (below) illustrate the number of risks on the risk register for the past four months and their current risk status.
3.0 Monitoring of HLRR
Risks are reviewed monthly at Operational Senior Management Team (OSMT) and with The Head of Risk and Clinical Effectiveness. Regular face-to-face meetings continue between the Risk Team and Senior Managers to improve communication, support for staff and embed a culture of risk management and the delivery of safe care.
4.0 Controls & Assurance
Evaluation of controls and assurances are monitored through the use of associated Key Performance Indicators and other metrics to evidence their robustness and effectiveness to address gaps and mitigate risks and are included within the Datix Risk Management System. These are reviewed at monthly BUPRs and by the Executive team. This provides assurance of the effectiveness of controls to mitigate and manage the risk to the desired outcome and supports the risk rating score reported within this summary paper.
1 1
0 0 0 0 0
1
0 0 0
2
1
0
2
0 0
1
2
3
October November December January
Risks by Status New
Escalated
De-escalated
Closed
2 3 3 2
8 8 6 6
10 11 9 8
0
5
10
15
October November December January
Risks by Type
Risks in HLRR Corp
Risks in HLRR Ops
Risks in HLRR Total

Board 31st January 2019 Attachment J1
4
Current risks for January 2019 ID Service Executive Lead Cause (X) Rating 567 Skin Health Service Director of
Operations Failure to address the current increase in service demand and to commission a fully integrated pathway for Dermatology across East and North Hertfordshire, may lead to loss of income and reputation for HCT.
15
622 Community In-patient Units
Director of Operations
Poor quality data inputting into the Ward Dashboards may result in loss of confidence within and outside the organisation and impacting on contractual performance issues with commissioners.
15
526 Workforce Director of HR Insufficient availability of workforce with the skills to fill Trust vacancies and meet future requirements, may lead to difficulties in delivering current services.
16
589 Corporate Director of Service Development and Partnerships
Failure of HCT to succeed in the tendering of services will lead to a reduction in financial income leading to the Trust’s in ability to financially sustain the delivery of some services, reputational loss, loss in confidence by key stakeholders as well as partner organisations, impacting on staff morale, recruitment and retention.
15
605 Community In-Patient Units Herts Valleys
Director of Operations
There are a high number of patients whose onward destination from a community hospital bed is delayed (DTOC) and who do not meet the intermediate care service specification criteria, leading to high numbers of patients waiting for admission into, or remaining in a community hospital bed within the Herts Valley locality for longer than the commissioned target. This is resulting in patients waiting in an acute and a community bed for longer than they should, and HCT not meeting its commissioned targets for overall average length of stay and rehabilitation length of stay.
16
634 Community Paediatrics
Director of Operations
Increasing demand for consultant community paediatric assessment, review and treatment for Autism Spectrum Disorder and a lack of clarity for referral and access between providers has led to referral to treatment breaches, increased follow-up waiting lists resulting in an increase in first to follow up appointments and support for families, increased scrutiny within the Trust and from commissioners with potential increase
16

Board 31st January 2019 Attachment J1
5
in reputational risk and increase of stress within the team
670 Herts & Essex Inpatient Unit
Director of Operations
High Nursing vacancy rates, sickness absence and reliance on use of bank and Agency staff may lead to an inability to maintain safe staffing levels for nursing resulting in potential for reduced quality and continuity of care, increase in patient harm, poor patient experience, reduced staff morale, reputational damage and increased scrutiny by commissioners and regulators.
16
600 Public Health Nursing Director of Operations
Successful Public Health Nursing bid within Family Centre Service (FSC) provision commissioned by HCC, leading to the need to mobilise the new service model as described in HCT's bid; and align and integrate with Family Support Services to form FSC. Potentially resulting in an inability to deliver the services as expected and within agreed timescales, possible quality impact on children, young people (CYP) and families, possible negative impact on staffing, loss of reputation and financial penalties.
16
De-escalated Risks for January 2019 458 Community Nursing &
Integrated Teams West
Director of Operations
Ongoing shortage of staff as difficulty in recruiting leading to unfilled vacancies, recruitment of bank and agency staff, increase in resignations, long term sickness, resulting in risk to continuity of care, patients safety and patient experience.
12
685 Corporate Director of Quality & Governance
Inability to maintain the current CQC standards or achieve a higher CQC compliance following a formal inspection may adversely impact on the Trust’s reputation in delivering safe and quality services, loss in confidence by key stakeholders such as commissioners, local population and partner organisations and also, impacting on staff morale.
12
Author: Gerry Phee Risk & Assurance Manager Nico Kamera Head of Risk & Clinical Effectiveness (Interim) 23rd January 2019

Board 31st January 2019 Attachment J1
6
Committee Consideration This Report has previously been considered by the following committees: Committee: OSMT/Executive/Healthcare Governance Committee
Date (Month / Year): 01/2019
Data Quality Statement By way of assurance to the Board, and in order to inform discussion / decision, the accountable executive director confirms that to the best of their knowledge, and subject to any exceptions identified, data contained in this report is: Data Quality Domain
Description Comments / Exceptions √
Complete Information is as comprehensive as possible to inform the board / committee and no significant known facts or statistics which may influence a decision are omitted.
√
Accurate As far as can be reasonable ascertained or validated, information in the report is accurate.
√
Relevant Information contained in the report is relevant to the matters considered in the report.
√
Up To Date
Information in the report is as up to date as reasonably possible in the context of the time at which the paper is written.
√
Valid Information is presented in a format which complies with internal or national models or standards.
√
Clearly Defined
The meaning of any data in the report is clearly explained.
√
Executive Director Sign-Off
This paper has been approved by the accountable executive director who is satisfied that (i) the implications for risks, (ii) quality/service/regulatory impacts and (iii) resource implications, have been considered.
Tracey Westley, Assistant Director Risk & Quality Assurance on Acting Director of Nursing & Quality & Chief Nurse/Governance Lead
√
Company Secretary Sign-Off (Board papers only) This paper has been quality control checked and approved by the Company Secretary. √

Board 31st January 2019 Attachment J2
1
TRUST BOARD Title: Board Assurance Framework Report Date: 31st January 2019 Executive Lead: Andy Nuckcheddee, Acting Director of Nursing & Quality & Chief
Nurse/Governance Lead Author(s): Tracey Westley, Associate Director of Quality and Risk Assurance
Nico Kamera, Interim Head of Risk and Clinical Effectiveness For: Discussion & Assurance 1.0 Purpose & Recommendations 1.1 To inform the Trust Board of the current status of Board Assurance Framework (BAF). 1.2 To provide assurance that the BAF reflects the Trust’s current principal risks that may
compromise the achievement of HCT’s Strategic Objectives and that the risks are robustly and timely managed.
1.3 The Risk Team continues to work with the Executive members who are BAF risk leads
to deliver timeliness of reviews and improved understanding of managing BAF risk registers. Note Executive Team may provide further update in their individual reports and this will be reflected in future BAF reports.
2.0 Executive Summary
2.1 The BAF currently has eight (9) risks, the same risks presented to Board in November 2018, of these two (2) risks feature on the HLRR and they are:
• Corporate risk-01(HLRR-526); a risk relating to staffing, and • Corporate risk-06 (HLRR-589); a risk relating to failure of HCT to succeed in
Tenders. 2.2 The BAF incorporates recommendations from Trust internal Auditors and its
scoring is aligned with the HLRR in accordance with the (5x5) Risk Matrix. 3.0 Criteria defining Board Assurance Framework Risks
3.1 A risk featuring on the BAF has the potential to severely impact on the Trust achieving its Strategic Objectives irrespective of the likelihood of occurrence. A risk on the BAF may also compromise the Trust from achieving more than one or all of its Strategic Objectives. Therefore, BAF risks have been mapped and aligned to the most appropriate Strategic Objective in order that there is clear accountability at Executive Level in both ownership and management of risks which facilitates the achievement of the Strategic Objectives.

Board 31st January 2019 Attachment J2
2
3.2 The impact determines whether or not the risk is critical and therefore, has
severe consequences for the Trust in terms of level of harm (severe/fatality), patient safety, financial sustainability, reputational damage, shut down of a particular service impacting on service delivery and patient outcomes, breach of contractual obligations and severe non-compliance with regulatory framework.
The (5x5) Risk Matrix is attached as a point reference to facilitate the
discussion. 4.0 Risks on Board Assurance Framework 4.1 There are nine (9) risks on the Board Assurance Framework and they are as follows:
1. Financial-01: Increased demand and financial pressures as a result of real terms cuts in financial resources available to the Trust which could lead to Trust’s inability to transform and implement productivity improvement at sufficient scale or pace to mitigate financial pressures leading to pressure to deliver financial targets set by NHSE.
2. Corporate-01(HLRR-526): Insufficient supply of workforce with the right skills may lead to difficulties in meeting current and future service needs impacting on the ability to transform services provide quality of care and financial sustainability.
3. Corporate-02: There is a risk that the current climate of external and internal
pressure will have a negative impact on staff satisfaction, wellness and turnover.
4. Quality & Regulatory-01: Inability to maintain the current CQC standards or achieve a higher CQC compliance following a formal inspection may adversely impact on the Trust’s reputation, for delivering safe, effective, well led care resulting in a potential loss of confidence by key stakeholders including the local population, commissioners and partner organisations and a potential reduction in staff morale.
5. Corporate-03: Insufficient consistent reporting of clinical measure intervention and
outcomes may lead to difficulties in demonstrating evidence based clinical interventions potentially leading queries about clinical effectiveness.
6. Corporate-04: Misalignment or changing delivery priorities for those with whom the Trust partners may potentially lead to HCT being unable to deliver its services within its defined timelines potentially impacting on; patient’s experience, performance monitoring , HCT’s reputation and patient flow through HCT services.
7. Corporate-05: Underdeveloped / ineffective use of technology and Cyber Security Risks may result in having outdated, or vulnerable technical systems and /or working practices thereby (1) hindering delivery of modern, effective healthcare and (ii) presenting barriers to (a) efficiency or (b) operational viability / vulnerability or (c) market competitive advantages leading to Trust’s information being at risk and Trust’s services’ functions being compromised and impact healthcare delivery.
8. Corporate-06(HLRR-589): Failure of HCT to succeed in the tendering of services will
led to a reduction in financial income leading to the Trust’s in ability to financially sustain the delivery of some services, reputational loss, loss in confidence by key stakeholders as well as partner organisations, impacting on staff morale, recruitment and retention.

Board 31st January 2019 Attachment J2
3
9. Corporate Risk 07: Inadequate strategy for downside mitigation and contingency planning may compromise service delivery thereby impacting on Trust meeting its contractual obligations.
5.0 Monitoring of risks on Board Assurance Framework
5.1 Evaluation of controls, actions and assurances are monitored through the use of associated Key Performance Indicators and other metrics to evidence their robustness, including internal and external management reports and effectiveness to address gaps and mitigate risks and are included within the Datix Risk Management System. These are reviewed by the Executive Team and the respective Committees. The role of the Audit Committee is to challenge the rationale and decision making of the Executive and the responsible Committees in the mitigation of all risks including those featuring on the BAF.
5.2 The Audit Committee will provide assurance of the effectiveness of controls and
actions to mitigate and manage the risk to the desired outcome and supports the risk rating score reported within this summary paper. Note for this month Healthcare Care Governance Committee who includes the chair of the Audit Committee has provided interim oversight to enable Board comment. This paper will be received by Audit Committee in due course.
5.3 In addition Executive and Risk Management team will seek to review additional
external or internal reports that also demonstrate controls are effective. If the risk score and output of the controls and additional assurance reports therefore identifies the score is within the expected risk appetite the controls will be seen as effective. This will therefore, provide the required level of assurance to the Board. Should the converse be presented as part of either KPIs or assurance management reports the controls should be reviewed as actions and controls are not providing adequate assurance and therefore, indicate that there are gaps in the system of internal controls which require constant review and oversight.
Appendix A – Risk Matrix End of Report

Board 31st January 2019 Attachment J2
4
Sign Off: To be completed as part of papers to Executive Team, Board Committees and Board, Committee Consideration This report has approved by the following committee: Healthcare Governance Committee January 2019
Data Quality Statement By way of assurance to the Board, and in order to inform discussion / decision, the accountable executive director confirms that to the best of their knowledge, and subject to any exceptions identified, data contained in this report is: Data Quality Domain
Description Comments / Exceptions √ / x
Complete Information is as comprehensive as possible to inform the board and no significant known facts or statistics which may influence a decision are omitted.
√
Accurate As far as can be reasonable ascertained or validated, information in the report is accurate.
√
Relevant Information contained in the report is relevant to the matters considered in the report.
√
Up To Date
Information in the report is as up to date as reasonably possible in the context of the time at which the paper is written
√
Valid Information is presented in a format which complies with internal or national models or standards
√
Clearly Defined
The meaning of any data in the report is clearly explained
√
Executive Director Sign-Off
This paper has been approved by the accountable executive director who is satisfied that (i) the implications for risks, (ii) quality/service/regulatory impacts and (iii) resource implications, have been considered.
Tracey Westley, Assistant Director Risk & Quality Assurance on Acting Director of Nursing & Quality & Chief Nurse/Governance Lead
√
Company Secretary Sign-Off (Board papers only) This paper has been quality control checked and approved by the Company Secretary

1
Board Assurance Framework. The board assurance framework is a structured means of identifying and mapping the principal risks that may compromise the achievement of HCT’s Strategic Objectives. It provides the board with key assurances that there are adequate systems in place to monitor the effectiveness of controls and actions in the mitigation of principal risks.

2
Trust’s Strategic Objectives
3.We will support the substantial expansion of community services through the delivery of excellent core services for adults and children and the development of ambulatory services. 4.We will use resources efficiently to enhance our ability to improve services. 5.We will develop the organisational capacity to deliver our vision and objectives.
Risk description: Financial-01
Increased demand and financial pressures as a result of real terms cuts in financial resources available to the Trust could lead to Trust’s inability to transform and implement productivity improvement at sufficient scale or pace to mitigate financial pressures leading to pressure to deliver financial targets set by NHSI.
Director Lead: D Bacon, Director of Finance. Responsible Committee: Strategy Resource Committee (SRC) Executive Management Committee (EMC) Date Last Reviewed: Executive Management Committee-21-Nov-18 Healthcare Governance Committee (HGC) -18-Sept -18 Board-29-Nov-18. Name/ Date last reviewed by Author: David Bacon, Director of Finance, 11-Jan-19.
Risk Rating: (consequence x likelihood)
Risk History: Date of entry: March 2016
Rationale for Score: (Explain any impact new control(s) have on current risk score, any change in risk score between iterations) Financial plan to achieve surplus in place for 2018/19.
Initial Risk Before Mitigation: 4 x 4=16
Comment on Current Risk: Risk currently stable. Current risk score: 4x4=12
Tolerance: Risk related to wider financial operating environment, no update for December. Target date: N/A

3
Main Controls in place: (New controls highlighted). 1. Standing Financial Instructions and Delegation of Powers provide a financial control structure that budget holders operate within.
2. HCT has Transformation programmes which are:
• Reviewing Patient Pathways • Reviewing flow of patients • Relocating services to more strategic locations.
3. Trust’s Cost Improvement Programmes and Wider engagement across the STP 4. Delivering services as per Service Level Agreement. 5. Local negotiations with commissioners with regards to level of funding values through demonstrating sufficient increase in demand.
Internal assurances/ management reports received / frequency: (How do we know if the things we are doing are having an impact?) December 2018 update: Key Financial Controls. 5th March 2018 / RSM – Internal Auditors. External Assurances/ management reports received/ frequency: (How do we know if the things we are doing are having an impact?) December 2018 update:
Annual Audit Letter 2017/18. June 2018 / Grant Thornton –External Auditors.
Gaps in Assurances and Controls: (Re-assess, leading to removal, or amendment in next iteration) None
Actions to address Gaps in Assurances and Controls: December 2018 update. No gaps in Assurance and Controls.
Additional comments: (With these actions taken, how serious is the problem?)
None Changes in Actions and Controls: (Closed actions that have been reflected in new controls; narrative to explain delay in actions or closed actions not leading to new control, including cause and how risk is being managed) None

4
Trust’s Strategic Objectives
5. We will develop the organisational capacity to deliver our vision and objectives.
Risk Description: Corporate-01 Insufficient supply of workforce with the right skills and culture may lead to difficulties in meeting current and future service needs impacting on the ability to deliver our vision and objectives.
Director Lead: Raj Bhamber, Director of HR & OD
Responsible Committee:
Strategy Resource Committee (SRC). Date last reviewed : Executive Management Committee- 21- Nov-18 HGC-18 Sept- 18 Board- 29-Nov-18 Name/ Date last reviewed by risk owner: Raj Bhamber , Director of HR & OD and Alison Ryder Deputy Director of HR and OD: 09-Jan-19.
Risk Rating: (consequence x likelihood)
Risk History: Date of entry: November 2018
Rationale for current score: (Explain any impact new controls(s) have on current risk score, any change in risk score between iterations) Controls in place effective in controlling vacancy rates
Initial risk before mitigation: 4 x 4=16
Comment on direction of Risk: Currently stable
Current: 4 x 4 =16 Tolerance rating: 4 x 3 =12 Target Date: 31/03/2019

5
Main Controls in place: (What are we currently doing about the risk?) (New controls highlighted)
1. Resourcing Plan in place and progress monitored
2. E-recruitment system/reporting
3. Resourcing Group to drive activities
4. IBPR and BUPR KPI Reporting
5. Safer staffing processes
6. Competency frameworks for range of bands/roles
7. Apprenticeship scheme and levy plans in place
8. Extended roles for HCAs piloted
9. STP meeting structure in place
10. Plans for pilot integrated workforce development process.
Internal assurances/ management reports received / frequency: (How do we know if the things we are doing are having an impact?) December 2018 update: Hertfordshire Community Trust’s workforce strategy delivery plan Bimonthly- Recruitment and Retention Monitoring Report Hertfordshire Community Trust’s monthly workforce KPI Dashboard. External Assurances/ management reports received/frequency: (How do we know if the things we are doing are having an impact?) •National and STP Benchmark Reports.
Gaps in Assurances and Controls: (Re-assess, leading to removal, or amendment in next iteration) Uncertainties in direction of national labour market, e.g., impact of Brexit, University bursaries etc
Actions to address Gaps in Assurances and Controls:
Implement Trust Resourcing and Retention Plan. Additional comments: (With these actions taken, how serious is the problem?) None Changes in Actions and Controls: (Closed actions that have been reflected in new controls; narrative to explain delay in actions or closed actions not leading to new control, including cause and how risk is being managed) None.

6
Trust’s Strategic Objectives.
5. We will develop the organisational capacity to deliver our vision and objectives.
Risk description Corporate-02 There is a risk that the current climate of external and internal pressure will have a negative impact on staff satisfaction, wellness and turnover.
Director Lead: Raj Bhamber, Director of HR & OD
Responsible Committee:
Strategy Resource Committee (SRC). Date last reviewed: Executive Management Committee-21 Nov-18 HCT Board- 29-Nov-18. Name/ Date last reviewed by Risk owner: Raj Bhamber , Director of HR & OD and Alison Ryder Deputy Director of HR and OD: 09- Jan -19.
Risk Rating: (consequence x likelihood)
Risk History Date of entry: November 2018
Rationale for current score: (Explain any impact new controls(s) have on current risk score, any change in risk score between iterations) Turnover rates improving and above target. Annual staff survey and pulse survey results plateauing.
Initial risk before mitigation: 3x4=12
Comment on direction of Risk: Current: 3 x4 =12

7
Tolerance rating: 3 x2=6 Target tolerance date: 31/03/2020
Stable.
Main controls in place: (New controls highlighted) 1.Trust retention plan activities 2. Engaging, consulting and involving colleagues in change programmes.
Internal assurances/ management reports received: (How do we know if the things we are doing are having an impact?) •Hertfordshire Community Trust’s workforce strategy delivery plan. •Bimonthly- Recruitment and Retention Monitoring Report •Hertfordshire Community Trust’s monthly workforce KPI Dashboard. External Assurances/ management reports received: (How do we know if the things we are doing are having an impact?) •National NHS Staff Survey •National and STP Benchmark Reports.
Gaps in Assurances and Controls: (Re-assess, leading to removal, or amendment in next iteration) •Externally driven service change reduce the control of HCT, e.g. demographic increases in demand.
Actions to address Gaps in Assurances and Controls: (What more should we do?) December 2018 update: • Implement Workforce Strategy Delivery Plan
Additional comments: (With these actions taken, how serious is the problem?) None Changes in Actions and Controls: (Closed actions that have been reflected in new controls; narrative to explain delay in actions or closed actions not leading to new control, including cause and how risk is being managed) None

8
Trust’s Strategic Objectives.
1.We will support the people we serve to manage their own health and wellbeing
2.We will improve clinical outcomes and enhance patient safety
3.We will support the substantial expansion of community services through the delivery of excellent core services for adults and children and the development of ambulatory services
5. We will develop the organisational capacity to deliver our vision and objectives.
Risk Description: Quality & Regulatory-01 Inability to maintain the current CQC regulatory standards or achieve a higher CQC compliance following a formal inspection may adversely impact on the Trusts reputation for delivering safe, effective, well led care resulting in a potential loss of confidence by key stakeholders including the local population, commissioners and partner organisations and a potential reduction in staff morale.
Director Lead: Andy Nuckcheddee, Director of Nursing & Quality/Chief Nurse (Acting) Responsible Committee(s): Executive Management Team (EMT). Healthcare Governance Committee (HGC) Date last reviewed: Executive Management Committee- 21- Nov-18 HGC-18-Sept- 18 Board- 29-Nov-18 Name/ Date last reviewed by risk owner: Tracey Westley , Assistant Deputy Director Risk and Clinical Quality Assurance, 09-Jan-2019
Risk Rating: (consequence x likelihood)
Risk History: Date of entry: January 2018. Period in months:12
Rationale for current score: (Explain any impact new controls(s) have on current risk score, any change in risk score between iterations)

9
Controls in place are effective to control the risk.
Initial risk before mitigation:(5x3) = 15 Current:( 4x3=12) Tolerance rating: 2 x 3=6 Target Date: Revised Dec 2019 Must do to be confirmed
Comment on direction of Risk: Trust has undergone a formal inspection; the risk scores have been reviewed in line with CQC formal report.
Main controls in place: (What are we currently doing about the risk?) (New controls highlighted) Controls/Mitigation 1.Current CQC rating is good since last formal inspection in April 2016 2.A senior manager has been designated to lead on CQC preparation, PIR submission and subsequent inspection by working across all business units 3.An internal Trust-wide CQC assurance Team is in place 4.Regular/quarterly CQC/ Quality Assurance visits are undertaken by the Trust Board members and Quality Directorate which includes Infection Prevention and Control Team 5.Unannounced Quality Assurance visits based on the CQC’s KLOEs are undertaken by the commissioners 6.PLACE visits take place on an annual basis 7. Maintenance via Quality Improvement programme, including quality wheel review overseen by Executive team and reported to Board.
Internal assurances/ management reports received / Type and frequency: (How do we know if the things we are doing are having an impact?) December 2018 update: •Trust’s Business Unit Performance (BUPR) reports and Integrated Business Unit Performance Reports (IBUPR). External Assurances/ management reports received: (How do we know if the things we are doing are having an impact?) December 2018 update: •Quality Assurance Visits by commissioners •Quarterly Quality Review Meetings with CCGs •Monthly Contract Review Meetings with CCGs •Regular meetings with CQC Compliance Inspector.

10
Gaps in Assurances and Controls: (Re-assess, leading to removal, or amendment in next iteration) 1. Inadequate local monitoring and checks- Quality Checklist 2. Inadequate implementation of clinical policies such as DNACPR/MCAs.
Actions to address Gaps in Assurances and Controls: (What more should we do?) December 2018 update: 1.CQC Remedial Action Plan has been put in place following initial feedback from inspectors 2.Quality Assurance visits to all the ICTs and Inpatient Units have been increased to provide support to staff 3. Quality Improvement programme revised.
Additional comments: (With these actions taken, how serious is the problem?) None Changes in Actions and Controls: (Closed actions that have been reflected in new controls; narrative to explain delay in actions or closed actions not leading to new control, including cause and how risk is being managed) None

11
Trust’s Strategic Objectives
2. We will improve clinical outcomes and enhance patient safety 3.We will support the substantial expansion of community services through the delivery of excellent core services for adults and children and the development of ambulatory services 4.We will use resources efficiently to enhance our ability to improve services
Risk description: Corporate-03 Insufficient consistent reporting of clinical measure intervention and outcomes may lead to difficulties in demonstrating evidence based clinical interventions potentially leading queries about clinical effectiveness.
Director Lead: Dr H Pathmanathan, Medical Director. Responsible Committee: Healthcare Governance Committee (HGC). Executive Management Team (EMT). Date last reviewed: Executive Management Team- 21- Nov-18 HCGC 18 Sept- 18 Board- 29-Nov-18 Name/ Date last reviewed by risk owner: Dr Hari Pathmanathan, Medical Director, 19 Nov-18
Risk Rating: (consequence x likelihood)
Risk History: Date of entry: July 2016. Period in months:28
Rationale for current score: (Explain any impact new controls(s) have on current risk score, any change in risk score between iterations) Clinical outcome measures not in use in all in HCT services.
Initial risk before mitigation: 4x4=16
Comment on direction of Risk: Current: 4x4=16

12
Tolerance rating: 4 x 2 = 8 Target Date: October 2019.
Starting to reduce.
Main controls in place: (What are we currently doing about the risk?) (New controls highlighted) 1. A project in place to review the use and implement use of patient reported outcome measures and clinical outcome measures 2. Clinical outcome measures are currently in use in various teams in the Trust however their use and outcomes are not currently reported to Trust committees.
Internal assurances/ management reports received/ frequency: (How do we know if the things we are doing are having an impact?)
Clinical Effectiveness Group- held Bi- Monthly. External Assurances/ management reports received/ frequency (How do we know if the things we are doing are having an impact?) Health Care Governance Committee Report- Held Bi Monthly.
Gaps in Assurances and Controls: (Re-assess, leading to removal, or amendment in next iteration) • Clinical outcome measures not currently reported to Trust comities and plans in place for these to be formally reported. • Outcomes measures to be reported formally as part of the BUPR and through Clinical Effectiveness Group which both feed into the Health Care Governance Committee
Further actions required/ Actions to address gaps: (What more should we do?) December 2018 update: Implementation of the Outcomes based Healthcare Work Programme.
Additional comments: (With these actions taken, how serious is the problem?) None Changes in Actions and Controls: (Closed actions that have been reflected in new controls; narrative to explain delay in actions or closed actions not leading to new control, including cause and how risk is being managed) None

13
Trust’s Strategic Objectives.
1.We will support the people we serve to manage their own health and wellbeing 2.We will improve clinical outcomes and enhance patient safety 3.We will support the substantial expansion of community services through the delivery of excellent core services for adults and children and the development of ambulatory services 4.We will use resources efficiently to enhance our ability to improve services 5.We will develop the organisational capacity to deliver our vision and objectives.
Risk description:Corporate-04 Misalignment or changing delivery priorities for those with whom the Trust partners may potentially lead to HCT being unable to deliver its services within its defined timelines potentially impacting on; patient’s experience , performance monitoring, HCT’s reputation and patient flow through HCT services.
Director Lead: J Hoare , Director of Service Development and Partnerships Responsible Committee: Strategy Resource Committee (SRC). Executive Management Committee (EMC). Date last reviewed: Executive Management Committee: 21-Nov-18 HCGC-18-Sept-18 HCT Board-29/11/2018 Name/Date last reviewed by Risk owner: Julie Hoare, Director of Service Development and Partnerships , 14-Jan-19
Risk Rating: (consequence x likelihood)
Risk History: Date of entry: March 2016. Period in months: 31
Rationale for current score: (Explain any impact new controls(s) have on

14
current risk score, any change in risk score between iterations) Competing priorities and resource constraints impact on the performance of the system which in turn impacts on the effectiveness of HCT to deliver its commissioned services.
Initial risk before mitigation: 5 x 3 = 15
Comment on direction of Risk: Risk currently stable
Current: 4 x 3 = 12 Tolerance rating: 4 x 2 =8 Target Date: To be reviewed in line with new NHS Plan. Main controls in place: (What are we currently doing about the risk?) (New controls highlighted)
1. HCT engages in Partnership forum discussions to strategically and operationally optimize co-delivery and mitigate risks e.g. A&E delivery board, System Resilience Group
2. Trust performance monitored through Business Unit Performance Reports and discussions where emerging issues are identified early and assurance on actions taken reported to executive team monthly and strategy and resources committee
3. Recovery Action Plan (RAP) in place for HCT actions to improve patient flow through services reported to Strategy Resource Committee
4. System RAP in place to improve patient flow through wider services across the system
5. HCT effective contract management including oversight of performance of sub contracted system partners 6. Linked to mitigating actions of the High Level Risk Register ID number 605 management of patient flow in
the system 7. The Trust is a key partner and actively engaged in the Hertfordshire & West Essex Sustainability Transformation
Partnership (STP).
Internal assurances/ management reports received/frequency: (How do we know if the things we are doing are having an impact?) December 2019 update: HCT Business Unit Monthly Performance Report: BUPR assurance to executive team and to strategy and resources committee. External Assurances/ management reports received/frequency: (How do we know if the things we are doing are having an impact?) STP Monthly programme report.

15
Gaps in Assurances and Controls: (Re-assess, leading to removal, or amendment in next iteration)
• Updating STP clinical strategy and financial plan. • Reviewing System performance in Herts valley for delays in patient flow.
Actions to address Gaps in Assurances and Controls : (What more should we do?) December 2019 update: Risk reduction through effective joint working on the management of patient flow across the system with social care and CCG. Resulting in changes to commissioned service capacity.
Additional comments: (With these actions taken, how serious is the problem?) None Changes in Actions and Controls: (Closed actions that have been reflected in new controls; narrative to explain delay in actions or closed actions not leading to new control, including cause and how risk is being managed) None

16
Trust’s Strategic Objectives.
1. We will support the people we serve to manage their own health and wellbeing
2. We will improve clinical outcomes and enhance patient safety
3. We will support the substantial expansion of community services through the delivery of excellent core services for adults and children and the development of ambulatory services
4. We will use resources efficiently to enhance our ability to improve services
5. We will develop the organizational capacity to deliver our vision and objectives.
Risk description: Corporate-05 Underdeveloped / ineffective use of technology and Cyber Security Risks may result in having outdated, or vulnerable technical systems and /or working practices thereby
(i) hindering delivery of modern, effective healthcare and (ii) presenting barriers to
(a) efficiency or (b) operational viability / vulnerability or (c) market competitive advantages
leading to Trust’s information being at risk and Trust’s services’ functions being compromised and impact healthcare delivery.
Director Lead: D Bacon, Director of Finance
Responsible Committee:
Strategy Resource Committee (SRC). Date last reviewed : Executive Mgt Committee- 21-Nov-18 HGC-18 Sept- 18 Board- 29-Nov-18 Name/ Date last reviewed by risk owner: David Bacon, Director of Finance, 11th Jan-19
Risk Rating: (consequence x likelihood)
Risk History: Date of entry: March 2016 .Period in months: 32
Rationale for current score: (Explain any impact new controls(s) have on current risk score, any change in risk score between iterations) Risks currently stable as current strategy effective.
Initial risk before mitigation: 5 x 4= 20
Comment on direction of Risk: Risk rating stable. Current: 5 x 3 =15
Tolerance rating: 5x2=10

17
Target Date: March 2020 Main controls in place : (What are we currently doing about the risk?) (New controls highlighted) Controls for Effective use of technology: 1.Robust system availability through HBL Infrastructure agreements and planned (minimal) downtime 2.Licensing agreements with clinical system suppliers maintained 3.Development of WiFi coverage including completion of the NHS Digital ‘NHS Wi-Fi Secondary Care Implementation’ project to increase coverage and mobile working accessibility 4.Rollout of Smartphones to front line staff Controls for Cyber Security: 1. The risk is on Hertfordshire Bedfordshire and Luton (HBL) ICT shared Services High
Level Risk Registers ref; ICT 231:Loss of Environment due to Cyber Attack – caused by Tech due to Cyber Attack – caused by Tech)
2. The risk is on Hertfordshire Bedfordshire and Luton (HBL) ICT shared Services High Level Risk Registers ref: ICT 015: Risk of Inadequate Disaster Recovery capability of IT services leading to lack of critical services to partners.
3. The risk is on Hertfordshire Bedfordshire and Luton (HBL) ICT shared Services High Level Risk Registers ref: ICT-198: Unplanned cost for additional Licensing for Primary Care.
4. Disaster Recovery plan in place: • Backups in place for key systems • Automatic failover between DataCentres • System checks carried 24x7 with alerting in place • Note all services used by HBL ICT do automatically failover • Antivirus on all end points and Intercept X in place across end points
Internal assurances/ management reports received/ frequency: (How do we know if the things we are doing are having an impact?) December 2018 update: 1. Cyber Security Update report to SRC July 2018. 2. Yearly external cyber security review (penetration ‘pen’ testin).. External Assurances/ management reports received/ frequency: (How do we know if the things we are doing are having an impact?) Information Management and Information Technology Maturity Review completed November 2018
Gaps in Assurances and Controls: (Re-assess, leading to removal, or amendment in next iteration)
Actions to address Gaps in Assurances and Controls: (What more should we do?)

18
Effective Technology use: The Information Management and Information Technology Maturity Review identifies areas where user uptake of the technology available could be strengthened and improved (Nov 2018). Cyber Security: Trust is now compliant with DHSC Cyber security standards (the 2017/18 Data security protection requirements). Cyber security will be further strengthened by moving with HBLICT towards the Cyber Essential Plus security standard (scheduled to be achieved by 2020)
Appropriate policies are in place but the Trust remains reliant on end users fully complying with Trust and HBL advice and guidance on managing/responding to cyber security threats.
December 2018 update: Effective Technology use: Action plan in place and being implemented across HCT. Cyber Security: Cyber security risks are environmental risks. The Trust is continuing to work with its partners to strengthen its cyber security defences to mitigate this risk.
Additional comments: (With these actions taken, how serious is the problem?) None Changes in Actions and Controls: (Closed actions that have been reflected in new controls; narrative to explain delay in actions or closed actions not leading to new control, including cause and how risk is being managed) None

19
Trust’s Strategic Objectives
1. We will support the people we serve to manage their own health and wellbeing 2. We will improve clinical outcomes and enhance patient safety 3. We will support the substantial expansion of community services through the delivery of excellent core services for
Adults and children and the development of ambulatory services 4. We will use resources efficiently to enhance our ability to improve services 5. We will develop the organizational capacity to deliver our vision and objectives.
Risk Description: Corporate-06
Failure of HCT to succeed in the tendering of services will lead to a reduction in financial income leading to the Trust’s in ability to financially sustain the delivery of some services, reputational loss, and loss in confidence by key stakeholders as well as partner organizations, impacting on staff morale, recruitment and retention.
Director Lead: J Hoare, Director of Service Development and Partnerships. Responsible Committee: Strategy Resource Committee (SRC). Date last reviewed: HCT Board: 29-Nov-18 HCGC-18-Sept-18 Executive Management Team-21-Nov-18 Name/ Date last reviewed by Author/risk owner: Julie Hoare, Director of Service Development and Partnerships, 14-Jan-2018.
Risk Rating: (consequence x likelihood)
Risk History: Date of entry: December 2017. Period in months: 13
Rationale for current score: (Explain any impact new controls(s) have on current risk score, any change in risk score between iterations) Current controls effective.
Initial risk before mitigation: 5 x 4 =20
Comment on direction of Risk: Risk stable
Current: 5 x 3 =15

20
Tolerance rating: N/A
Target Date: N/A.
Main controls in place: (What are we currently doing about the risk?) (New controls highlighted)
1. Identified Executive Owner to lead work required to succeed in the tenders 2. Programme management and team in place 3. High-Level programme plan in place 4. Liaison with key stakeholders and partners 5. Assurance reporting from steering group to executive team 6. Regular reporting to strategy and resources committee
7.Two weekly assurance reporting from steering group to executive team 8.Monthly reporting to strategy and resources committee 9. Annual planning programme will include mitigation for potential reduction in financial income and service contracts.
Internal assurances/ management reports received/frequency: (How do we know if the things we are doing are having an impact?) December 2018 update Assurances remain in place - Full Business Case signed off. External Assurances/ management reports received/frequency: (How do we know if the things we are doing are having an impact?) None.
Gaps in Assurances and Controls: (Re-assess, leading to removal, or amendment in next iteration)
1. Revision of downside mitigation plan for the Organization.
Actions to address Gaps in Assurances and Controls: (What more should we do?) 1. To refresh down side mitigation plan.
Additional comments: (With these actions taken, how serious is the problem?) None
Changes in Actions and Controls: (Closed actions that have been reflected in new controls; narrative to explain delay in actions or closed actions not leading to new control, including cause and how risk is being managed)
None.
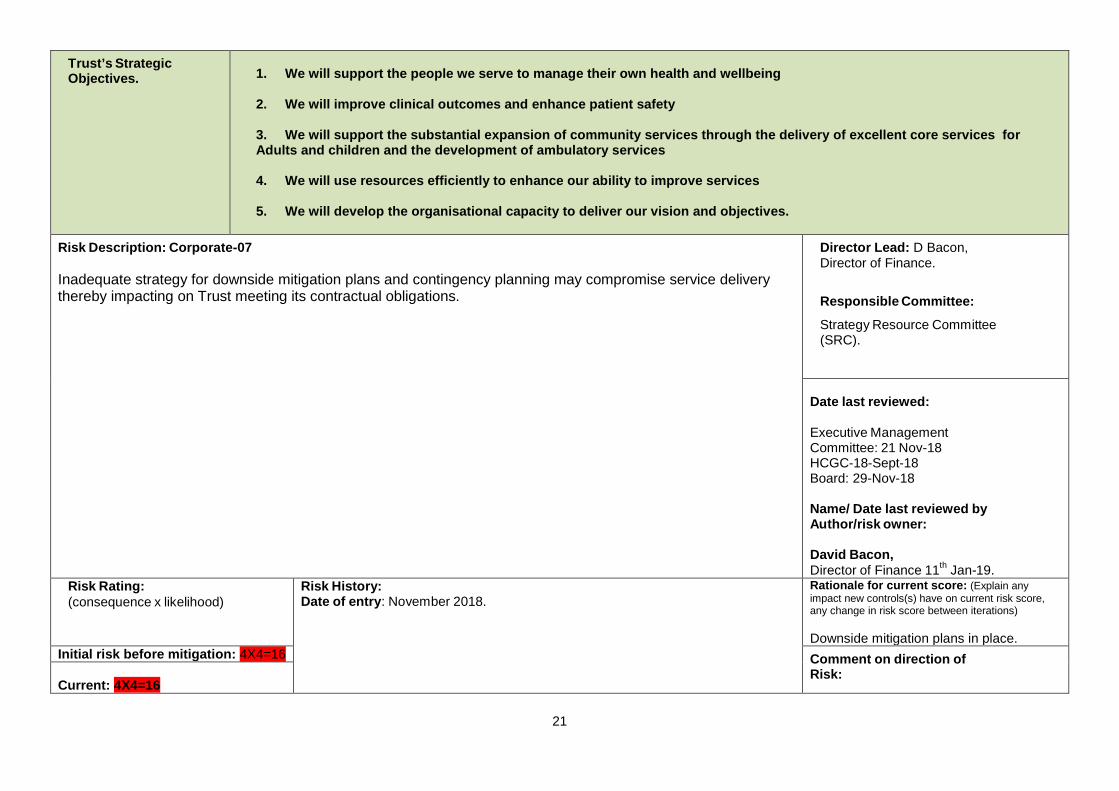
21
Trust’s Strategic Objectives.
1. We will support the people we serve to manage their own health and wellbeing 2. We will improve clinical outcomes and enhance patient safety 3. We will support the substantial expansion of community services through the delivery of excellent core services for Adults and children and the development of ambulatory services 4. We will use resources efficiently to enhance our ability to improve services 5. We will develop the organisational capacity to deliver our vision and objectives.
Risk Description: Corporate-07 Inadequate strategy for downside mitigation plans and contingency planning may compromise service delivery thereby impacting on Trust meeting its contractual obligations.
Director Lead: D Bacon, Director of Finance.
Responsible Committee:
Strategy Resource Committee (SRC).
Date last reviewed:
Executive Management Committee: 21 Nov-18 HCGC-18-Sept-18 Board: 29-Nov-18
Name/ Date last reviewed by Author/risk owner: David Bacon, Director of Finance 11th Jan-19.
Risk Rating: (consequence x likelihood)
Risk History: Date of entry: November 2018.
Rationale for current score: (Explain any impact new controls(s) have on current risk score, any change in risk score between iterations) Downside mitigation plans in place.
Initial risk before mitigation: 4X4=16 Comment on direction of Risk:
Current: 4X4=16

22
End of BAF
Tolerance rating: 4X2=8 Target Date: Feb-2019.
Risk reducing.
Main controls in place: (What are we currently doing about the risk?) (New controls highlighted) HCT’s 2018/19 Financial plan.
Internal assurances/ management reports received/frequency: (How do we know if the things we are doing are having an impact?) December 2018 update:
• Review and updating of current Business continuity strategy underway.
External Assurances/ management reports received/frequency (How do we know if the things we are doing are having an impact?)
None.
Gaps in Assurances and Controls: (Re-assess, leading to removal, or amendment in next iteration) Review and updating the downside mitigation plans.
Actions to address Gaps in Assurances and Controls: (What more should we do?) December 2018 update: Review downside mitigation plans.
Additional comments: (With these actions taken, how serious is the problem?)
None Changes in Actions and Controls: (Closed actions that have been reflected in new controls; narrative to explain delay in actions or closed actions not leading to new control, including cause and how risk is being managed)
None.

Board 31st January 2019 Attachment J2 Risk Model matrix
The scoring of risk at HCT is based on the adapted Australian/New Zealand risk management standard AS/NZS 4360:2004. Table 1 - Consequence score (C)
1. Choose the most appropriate domain for the identified risk from the left hand side of the table. 2. Then work along the columns in same row to assess the severity of the risk on the grade scale of 1 to 5 to determine the consequence score, which is the number given at the top of the column. 3. If a risk impacts falls into more than one domain, select the domain with the most significant score as the basis for grading the risk (e.g. if the risk would score a 3 for Patient care but a 4 for Financial, it should be scored as a 4).
Domain Grade 1 Grade 2 Grade 3 Grade 4 Grade 5 Insignificant Minor Moderate Major Catastrophic
Patient Experience / Complaints / Claims (Quality)
Informal complaint resolved within ward/department
Complaint peripheral to clinical care
Complaint involving lack of appropriate care. Claim £10,000 - £99,999
Multiple complaints. Claim £100,000 to £999,999
Multiple claims or single major claim - £1M+
Compliance (Statutory breaches)
Any assessment, inspection or audit that highlights minor non compliances
Any assessment, inspection or audit recommendation that indicates partial compliance or insufficient assurance with an element of a CQC registration standard
Any assessment, inspection or audit that indicates reduced rating. Report with challenging recommendations. Partial compliance or insufficient assurance for more than one element of CQC registration standard
Any assessment, inspection or audit that indicates enforcement action. Critical report with multiple challenging recommendations. Partial compliance or insufficient assurance for more than one CQC registration standard
Any assessment with a Zero rating. Significant lapse or non-compliance with statutory requirements (e.g. Major non-compliance with CQC registration standard). Severely critical reports. Risk of prosecution
Confidentiality Minor breach of confidentiality. Only a single individual involved.
Potentially serious breach. Less than 20 people affected or risk assessed as low, e.g. files were encrypted.
Serious breach of confidentiality & risk assessed as high, e.g. unencrypted clinical records. Up to 100 people affected.
Serious breach with either particular sensitivity, e.g. sexual health details or up to 1000 people affected.
Serious breach with potential for ID theft or over 1000 people affected
Injury/Harm
Minor injury not requiring first aid or treatment
Minor injury or illness. First aid or short-term medical treatment needed.
Injuries reportable to external agencies / statutory bodies (e.g. RIDDOR (7 day injury), MHRA etc.)
Major injuries or long term incapacity / disability (fracture or dislocation of major limb e.g. leg / arm, amputation)
Death or major permanent incapacity. “Never event”
Financial (insured/uninsured loss)
Less than £1,000 £1,000 to £9,999 £10,000 - £99,999 £100,000 to £999,999 £1M+
Objectives and projects
Barely noticeable reduction in scope or quality. Less than £1,000 cost increase / schedule slippage.
Minor reduction in quality/scope. £1,000 to £9,999 budget / schedule slippage.
Reduction in scope or quality requiring client approval. £10,000 - £99,999 budget / schedule slippage.
Does not meet secondary objective(s). £100,000 to £999,999 budget / schedule slippage.
Does not meet primary objectives. £1M+ budget / schedule slippage.
Patient Care Unsatisfactory patient experience - readily resolvable
Unsatisfactory patient experience – not readily resolvable
Mismanagement of patient care / minor breach of working practices
Serious mismanagement of patient care / significant breach of working practices
Totally unsatisfactory patient care / serious breach of working practices
Reputation No significant reflection on any individual or body. Media interest very unlikely
Damage to individual reputation. Possible local media interest.
Minor effect on staff morale. Damage to team/service reputation. Local media interest likely to go public.
Significant effect on staff morale. Damage to organisation reputation. Adverse local /national media coverage lasting up to 3 days. Local MP concern.
Damage to NHS reputation. Adverse National Media coverage lasting more than 3 days. MP concern. DOH concern.
Service Loss/interruption of service or business of less
Loss/interruption of service or business greater
Loss/interruption of service or business greater than 8 hours
Loss/interruption of service or business greater than 24 hours
Loss/interruption of service or business greater

Board 31st January 2019 Attachment J2
than 1 hour than 1 hour and less than 8 hours
and less than 24 hours and less than 1 week than 1 week
Staffing Short term low staffing level temporarily reduces service quality (less than 1 day)
Ongoing low staffing level minimal impact on service quality
Late delivery of key objective/service due to lack of staff (recruitment, retention or sickness). Minor error due to insufficient training. Ongoing unsafe staffing level(s)
Uncertain delivery of key objective/service due to lack of staff (recruitment, retention or sickness). Serious error due to insufficient staff training
Non delivery of key objective/service due to lack of staff. Very high turnover. Critical error due to insufficient staff training.
Stress Stress symptoms (work related) are mild or temporary. Staff quickly recover
Stress symptoms can be self-managed and are one off response to unexpected stressful situation.
Stress symptoms are more frequent and show a pattern. Can be dealt with by workplace adjustments
Stress symptoms are frequently apparent and in danger of becoming chronic. Increasing staff sickness
Staff on long term sick leave with stress (work related) or physical illness associated with chronic stress. Suicide risk
Table 2 - Likelihood score (L)
What is the likelihood of the consequence occurring?
The frequency-based score is appropriate in most circumstances and is easier to identify. It should be used whenever it is possible to identify a frequency based on the controls currently in place:
Likelihood score 1 2 3 4 5 Descriptor Rare Unlikely Possible Likely Almost certain Frequency How often might it/does it happen
This will probably never happen/recur
Do not expect it to happen/recur but it is possible it may do so
Might happen or recur occasionally
Will probably happen/recur but it is not a persisting issue
Will undoubtedly happen/recur, possibly frequently
Table 3 - Risk scoring = Consequence x Likelihood (C x L)
Likelihood score
1 2 3 4 5
Consequence score Rare Unlikely Possible Likely Almost certain
5 Catastrophic 5 10 15 20 25
4 Major 4 8 12 16 20
3 Moderate 3 6 9 12 15
2 Minor 2 4 6 8 10
1 Negligible 1 2 3 4 5
For grading a risk the scores obtained from the risk matrix are assigned grades as follows: 1-3 Negligible Risk 4-6 Low Risk 8-12 Moderate (Medium) Risk 15-25 High Risk Instructions for use
1. Define the risk(s) explicitly in terms of the adverse consequence(s) that might arise from the risk.

Board 31st January 2019 Attachment J2 2. Use table 1 to determine the consequence score(s) (C) for the potential adverse outcome(s)
relevant to the risk being evaluated.
3. Use table 2 (to determine the likelihood score(s) (L) for those adverse outcomes. If possible, score the likelihood by assigning a predicted frequency of occurrence of the adverse outcome. If this is not possible, assign a probability to the adverse outcome occurring within a given time frame, such as the lifetime of a project or a patient care episode.

Page 1 of 2
Dear Marion,
RE: Emergency Preparedness Resilience and Response (“EPRR”) Core Standards
Assurance Meeting 2018
Thank you for participating in the NHS Core Standards for EPRR Assurance meeting held
on 19th October 2018. The purpose of the assurance meeting was to discuss your Core
Standards submission in an open and facilitative forum, seeking assurance that you are
compliant with each of the core standards; that you are meeting your emergency planning
duties both contractually and under the Civil Contingencies Act (2004); and to set priorities
moving forward. The Core Standards Panel will then make recommendations to the Local
Health Resilience Partnership (LHRP) and in turn, the Local Resilience Forum (LRF) in
response to your submission.
Governance
NHS England accepts that the Trust has achieved 75% attendance at the LHRP and is
therefore compliant for 2017/2018. If an appropriate director level representative is unable to
attend on an occasion then an appropriate deputy must in order to maintain attendance.
The panel also noted your change of Emergency Planning Manager in place, Mandy Shoben
who holds extensive experience in this field would prove beneficial to the Trust.
We discussed the challenges and risks for the trust. You considered winter as your current
risk including workforce to be a challenge and recognised that change across many services
meant Partnership working would be vital. You were working on your Electronic Staff
Records (ESR) to ensure staff competencies are added to their profiles and for the purpose
of identifying which staff members are available to support locally and out of hours. A staff
list has been compiled to identify availability out of hours.
Health Protection
Flu clinics had been set up to cover the County which provided a positive uptake. You
advised the Trust has a Flu Champion in place to support with the administering the
vaccination.
Business Continuity
Your main focus for improvement is regarding Business Continuity. You advised the Trust
had recently commenced a new pilot regarding the communication of your Business
Private and Confidential
Marion Dunstone
Accountable Emergency Officer
Hertfordshire Community NHS Trust
Central Midlands (South Locality)
Charter House
Parkway
Welwyn Garden City
Hertfordshire
AL8 6JL
Email: [email protected]
Tel: 0113 8248831
18 December 2018
Board 31st January 2019 Attachment J3

Page 2 of 2
Continuity Plans ensuring ease of access for key contacts to all organisations.
You also advised that the Trust is trialling a new way of testing its Business Continuity Plans
by looking into the ISO Standards and Business Continuity Best Practice Guidance.
The Trust also reports multi-agency collaboration with Fire and Police Services around
media training and is inputting the health specific perspective into this training that they
deliver in order to build a joint approach.
Brexit
It is welcoming to hear that the Trust are considering the implications should a Brexit ‘no
deal’ occur. In specific, the Trust identified the need for a formal report to go to the Trust
Board however, after assessing the risk and potential mitigations, the Trust considered the
risk to be low based on low numbers of European Union (EU) staff employed. You also
confirmed, the Trust do not stockpile large quantities of pharmaceutical supplies.
Heatwave
To manage through the recent heatwave, the Trust increased their communication
messages to staff and patients regarding the importance of keeping hydrated. You
encountered challenges with patients with specific medical conditions such as UTI etc. A
particular issue is communication to older patients in their own homes about managing
dehydration. This highlighted the need for the Trust to broaden communications.
Lessons from Incidents
Due to the number of real incidents/opportunities this year, the Trust has had opportunities
to test its resilience and plans. Some of which include flooding at Danesbury. You advised
that the Trust will continue testing throughout winter. Avian Flu testing also provided
opportunities for learning. You also reported the Trust had planned IT upgrades which will
be used as a test.
Deep Dive: Command and Control
The Trust is fully compliant with the deep dive questions.
Summary
In your EPRR Core Standards self-assessment, you have rated your overall level of
compliance as Fully Compliant. Following the assurance meeting and review of your
submission, we agree with your EPRR Core Standards Assurance rating of: FULLY
COMPLIANT.
Yours sincerely,
Georgie Brown Prof Jim McManus
LHRP Co-Chair LHRP Co-Chair
Locality Director (South) Director of Public Health
Midlands and East (Central Midlands) Hertfordshire County Council
Cc: Mandy Shoben, Emergency planning and resilience manager, HCT