BMJ Open is committed to open peer review. As part of this ...
96
BMJ Open is committed to open peer review. As part of this commitment we make the peer review history of every article we publish publicly available. When an article is published we post the peer reviewers’ comments and the authors’ responses online. We also post the versions of the paper that were used during peer review. These are the versions that the peer review comments apply to. The versions of the paper that follow are the versions that were submitted during the peer review process. They are not the versions of record or the final published versions. They should not be cited or distributed as the published version of this manuscript. BMJ Open is an open access journal and the full, final, typeset and author-corrected version of record of the manuscript is available on our site with no access controls, subscription charges or pay-per-view fees (http://bmjopen.bmj.com ). If you have any questions on BMJ Open’s open peer review process please email [email protected] on February 2, 2022 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of BMJ Open is committed to open peer review. As part of this ...

BMJ Open is committed to open peer review. As part of this commitment we make the peer review history of every article we publish publicly available. When an article is published we post the peer reviewers’ comments and the authors’ responses online. We also post the versions of the paper that were used during peer review. These are the versions that the peer review comments apply to. The versions of the paper that follow are the versions that were submitted during the peer review process. They are not the versions of record or the final published versions. They should not be cited or distributed as the published version of this manuscript. BMJ Open is an open access journal and the full, final, typeset and author-corrected version of record of the manuscript is available on our site with no access controls, subscription charges or pay-per-view fees (http://bmjopen.bmj.com). If you have any questions on BMJ Open’s open peer review process please email
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review onlyHealth-related outcomes among female informal workers in debt: Retrospective quasi-experimental study on the impact
of microfinance health interventions in Pakistan
Journal: BMJ Open
Manuscript ID bmjopen-2020-043544
Article Type: Original research
Date Submitted by the Author: 09-Aug-2020
Complete List of Authors: Jafree, Sara; Forman Christian CollegeZakar, Rubeena; The University of LahoreAhsan, Humna; Forman Christian CollegeMustafa, Mudasir; Utah State UniversityFischer, Florian; Charité Universitätsmedizin Berlin, Institute of Public Health; University of Applied Sciences Ravensburg-Weingarten, Doggenriedstraße
Keywords: Health policy < HEALTH SERVICES ADMINISTRATION & MANAGEMENT, PUBLIC HEALTH, EPIDEMIOLOGY
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on F
ebruary 2, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-043544 on 5 January 2021. Dow
nloaded from

For peer review onlyI, the Submitting Author has the right to grant and does grant on behalf of all authors of the Work (as defined in the below author licence), an exclusive licence and/or a non-exclusive licence for contributions from authors who are: i) UK Crown employees; ii) where BMJ has agreed a CC-BY licence shall apply, and/or iii) in accordance with the terms applicable for US Federal Government officers or employees acting as part of their official duties; on a worldwide, perpetual, irrevocable, royalty-free basis to BMJ Publishing Group Ltd (“BMJ”) its licensees and where the relevant Journal is co-owned by BMJ to the co-owners of the Journal, to publish the Work in this journal and any other BMJ products and to exploit all rights, as set out in our licence.
The Submitting Author accepts and understands that any supply made under these terms is made by BMJ to the Submitting Author unless you are acting as an employee on behalf of your employer or a postgraduate student of an affiliated institution which is paying any applicable article publishing charge (“APC”) for Open Access articles. Where the Submitting Author wishes to make the Work available on an Open Access basis (and intends to pay the relevant APC), the terms of reuse of such Open Access shall be governed by a Creative Commons licence – details of these licences and which Creative Commons licence will apply to this Work are set out in our licence referred to above.
Other than as permitted in any relevant BMJ Author’s Self Archiving Policies, I confirm this Work has not been accepted for publication elsewhere, is not being considered for publication elsewhere and does not duplicate material already published. I confirm all authors consent to publication of this Work and authorise the granting of this licence.
Page 1 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 1 -
Health-related outcomes among female informal workers in debt:
Retrospective quasi-experimental study on the impact of microfinance health
interventions in Pakistan
Sara Rizvi Jafree, Rubeena Zakar, Humna Ahsan, Mudasir Mustafa, Florian Fischer
Dr. Sara Rizvi JafreeDepartment of Sociology, Forman Christian College University, Lahore, Pakistan; [email protected]
Prof. Dr. Rubeena ZakarInstitute of Social and Cultural Studies, University of the Punjab, Lahore, Pakistan; [email protected]
Dr. Humna AhsanDepartment of Economics, Forman Christian College University, Lahore, Pakistan; [email protected]
Mudasir MustafaDepartment of Sociology, Social Work, and Anthropology, Utah State University, Logan, United States of America; [email protected]
Dr. Florian Fischer 1) Institute of Public Health, Charité – Universitätsmedizin Berlin, Germany; [email protected] 2) Institute of Gerontological Health Services and Nursing Research, Ravensburg-Weingarten University of Applied Sciences, Germany; [email protected]
Corresponding author:Dr. Florian FischerCharité – Universitätsmedizin BerlinInstitute of Public HealthCharitéplatz 1 10117 BerlinE-Mail: [email protected]
Word count: 4,259
Page 2 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 2 -
1 Abstract
2 In countries where dependable public health service structure and universal financial protection
3 for health coverage is missing, particularly impoverished families are at risk. In the past years,
4 different kinds of microfinance health interventions were established to promote health among
5 disadvantaged population groups. The purpose of this study is to assess the impact of microfinance
6 health interventions (health insurance and health awareness programs) on health-related outcomes
7 of female informal workers in Pakistan. We conducted a retrospective quasi-experimental study
8 among a total of 447 female borrowers from seven microfinance providers (MFPs) in 2018. A
9 standardized tool was used for data collection. Probit regression has been used to identify the
10 probability of female borrowers gaining improvement in health outcomes based on their socio-
11 demographic characteristics. Propensity score matching (PSM) has been used to assess the overall
12 impact of health interventions. Results show that women receiving health insurance and health
13 awareness programs had greater probability of better health outcomes when they were from
14 Punjab, borrow in groups, and attend monthly meetings at MFPs. The results of the PSM show
15 significant improvements in overall perceived health status when women received health insurance
16 and improvement in the purchase of prescribed medicine when women received a health awareness
17 program. Health and social policies are vital to secure health and wellbeing of poor women
18 working in the informal sector of the economy. Targeting improved equity across female
19 population groups for health intervention will in the long run improve women’s health, capacity
20 expansion and income-earning abilities.
21
22 Keywords: borrow, informal sector, health insurance, health awareness, microfinance
23
Page 3 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 3 -
24 Strengths and limitations of the study
25 This study is part of a larger mixed-methods study on the well-being of female
26 microfinance borrowers.
27 Potentially the first study which focuses on female microfinance borrowers in Pakistan to
28 assess the impact of health interventions on health-related outcomes of poor women.
29 Although a quasi-experimental analysis framework has been used, the two-group cross-
30 sectional designs suffers from the limitations related to a single measurement for all
31 subjects.
32 Future studies need to consider additional burdens of loan repayment and small business
33 investment.
34
Page 4 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 4 -
35 Introduction
36 More than half (57%) of the female population in Pakistan is illiterate. Less than a quarter (23%)
37 of women is employed, with a majority working in the informal sector [1]. There are several
38 problems to consider with regard to the health of female informal workers in Pakistan, including
39 high rates of poverty and low health literacy, as well as inadequate access to public health services
40 [2], reinforced by low government health budget allocation for this population group [3]. In
41 addition to the overall absence of universal health coverage, there are limited coverage for public
42 health emergencies like pandemics [4] and greater risks for acquiring infectious diseases in female
43 informal workers due to mostly unsanitary living conditions in disadvantaged communities [5].
44 Pakistan has one of the largest out-of-pocket healthcare expenditures globally, with an
45 overwhelming proportion of 90% [6]. Although health insurance can become an important support
46 system for buffering the poor in out-of-pocket payments, it covers only 1% of health expenditure
47 in the country yet [2]. This is because health insurances are mainly used by richer and urban
48 populations.
49 The efficacy and limitations of private providers for health interventions in Pakistan are not clear.
50 One of the few private providers offering health interventions to women employed in the informal
51 sector are microfinance providers (including banks, institutes and non-governmental organizations
52 [NGOs]) [7]. Microfinance providers (MFPs) are mainly operational in under-developed
53 communities providing loans to the poorest women for small business development [8]. There are
54 50 MFPs operating in Pakistan, with nearly 40 reporting some form of health intervention for
55 clients, including health insurance and health awareness programs [9]. The MFPs are regulated
56 either by the State Bank of Pakistan or the Securities Exchange Commission Pakistan. An inherent
57 function of the original model of microfinance was to catalyze wider social development for
Page 5 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 5 -
58 women, including improved health behavior and, therefore, better health-related outcomes [10]. It
59 is in the interest of MFPs to couple health interventions with loan services as healthy clients are
60 more likely to return loans and run successful businesses [11].
61 The role of microfinance health interventions is even more critical for countries like Pakistan,
62 where poverty is high and out-of-pocket payments are not possible for impoverished families.
63 Additionally, the public sector did not have a dependable service structure for complete or quality
64 healthcare and universal financial protection for health coverage is absent [4]. More than 2 million
65 poor women are loan-takers of microfinance in the country [12]. As poor populations do not have
66 the money to take traditional health insurance, microfinancing for health insurance becomes the
67 only option for them. However, small health insurance schemes have been severely criticized for
68 their minimal impact on clients lives due to minimal coverage and large burden of disease faced
69 by poor populations [13]. Evidence also suggests that poor populations receiving minimal health
70 insurance, in the event of sustaining large health costs, may resort to damaging practices such as
71 reducing household nutrition, removing children from school, and taking more loans [14]. In the
72 most recent times of the corona pandemic, debt-ridden poor women attempting to repay loans are
73 facing even more challenges in generating income from small businesses due to social isolation
74 and lockdown [15]. Therefore, health security is a major concern in women borrowers and there
75 is a need to improve research and policy to financially protect poor women and also improve their
76 health literacy [16].
77 To the best of our knowledge, there are no studies which have used female microfinance borrowers
78 as a sample to assess the impact of health interventions on health-related outcomes of poor women
79 [17]. Using a sample of female microfinance borrowers who are availing health insurance from a
80 private provider will help to identify suited policies for disease prevention and health promotion
Page 6 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 6 -
81 in Pakistan. The following research questions are addressed in this study include: 1) Do female
82 borrowers of microfinance who are provided with health interventions show improved health-
83 related outcomes?, and 2) What are the socio-demographic, household, and loan portfolio
84 characteristics of female borrowers of microfinance that are associated with improved health-
85 related outcomes?
86
87 Methods
88 This study is part of a larger mixed-methods study on the wellbeing of female microfinance
89 borrowers. The qualitative part has already been published [18]. The results presented here are
90 based on a cross-sectional survey, in which females who have been borrowers of microfinance for
91 more than one year were interviewed with a structured quantitative questionnaire. We used the
92 framework of a quasi-experimental study to estimate the impact of microfinance health
93 interventions.
94
95 Sampling
96 First, seven MFPs were sampled randomly through a list available on Pakistan Microfinance
97 Network. All MFPs were asked for permission to interview their clients. Afterwards, 500 women
98 borrowing money from these MFPs were contacted to participate in the study. The sampling took
99 place in all four provinces of Pakistan (Punjab, Sindh, Balochistan, and Khyber Pakhtunkhwa
100 [KPK]), not considering the two autonomous territories and the federal territory of Islamabad. The
101 sampling frame at the level of individual women took the population weightage of the provinces
102 into account. A total of 442 women were willing to participate in the study and provided informed
103 written consent, which is a response rate of 88.4%. These women were sampled from seven cities
Page 7 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 7 -
104 within the four provinces (Punjab: n=252 [cities: Gujranwala, Lahore, Khanewal, Sheikhapura];
105 Sindh: n=100 [city: Matiari]; Balochistan: n=50 [city: Lasbela]; KPK: n=40 [city: Abbottabad].
106 Study participants received financial support from the following types of MFPs: four microfinance
107 banks (n=340), one microfinance institute (n=41), one government microfinance scheme (n=50),
108 and one Islamic microfinance organization (n=11),
109
110 Data collection
111 Data collection took place between February and November 2018. Each city had one research team
112 leader and two assistants in the data collection team, comprising a total of 21 persons for data
113 collection. The assistants were all MPhil graduates who had experience in field research and were
114 hired through the assistance of universities in each city. Training of the data collection team took
115 place over a two-week period and was done either in person or through video calls. The structured
116 surveys were completed on behalf of the female respondents with the assistance of the trained
117 research team, as most of the women were illiterate or semi-literate. Data collection took place in
118 face-to-face-interviews in a private space at the MFP premises, in order to preserve the privacy of
119 women in lieu of the personal questions.
120
121 Measures
122 A structured interview schedule was used for data collection (see Supplementary Appendix).
123 Questions in this tool were taken from instruments used in various studies, such as Women’s
124 Healthcare Experiences Survey [19], Baseline Nutrition and Food Security Survey by UNICEF
125 [20], WHO Multi-country Study on Women’s Health and Domestic Violence against Women [21],
126 and WHO Survey on Workplace Violence [22].
Page 8 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 8 -
127 This study assesses the association of health interventions offered by MFPs on four dependent
128 health-related variables: 1) women perceive health to be good overall, 2) women visit a general
129 practitioner in the last year, 3) women have the ability to purchase prescribed medicine in the last
130 year, and 4) women’s intake of multivitamins has improved in the last year. The four dependent
131 variables have been categorized as binominal and coded as either “Yes” (1) or “No” (0).
132 Several socio-demographic variables such as age (0=less than 30 years; 1=30 years and older),
133 religion (0=Muslim; 1=Other than Muslim), literacy of the female borrower (0=Illiterate;
134 1=Literate), literacy of the spouse (0=Illiterate; 1=Literate), house ownership (0=Yes; 1=No), and
135 number of depending children living in the house (0=None; 1=One or more) have been assessed
136 as confounding variables. It is necessary to control for these variables as they have an impact on
137 each of the dependent variables mentioned above. Province is also controlled as the region is a
138 proxy for socio-cultural norms which would impact how women perceive their health and whether
139 they are able to visit a general practitioner or to purchase medicine (0=Other than Punjab [Sindh,
140 Balochistan, or KPK]; 1=Punjab).
141 The other set of variables related to microfinance provider services such as loan amount
142 (0=10,000–20,000 PKR; 1=21,000 PKR and more), monthly meetings (0=No; 1=Yes), interest
143 rate, which is the amount charged on top of the principal by a lender to a borrower (0=2.5–10%;
144 1=11% and more), group loan, meaning that a group of customers are willing to guarantee each
145 other for the repayment of loan (0=No; 1=Yes), and debt age (0=1–2 years; 1=3 or more years)
146 have been included as they assess the impact of the provision of non-financial services on each of
147 the dependent variables.
148
Page 9 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 9 -
149 Intervention
150 Using a quasi-experimental framework, the study estimates the impact of getting access to health
151 interventions against the counterfactual of those women who are receiving the loan for small
152 business mobilization in the absence of health interventions. The control group ( consists 𝑇 = 0)
153 of women who have been provided the loan but lack the provision of health intervention and the
154 treatment group ( includes women who will have provision of both, the loan as well as 𝑇 = 1)
155 health intervention.
156 The three independent variables for microfinance health intervention are: 1) receiving health
157 insurance, 2) attended at least one health workshop, and 3) received health-related talks by loan
158 officers. The last two independent variables of health workshop and health-related talks by loan
159 officers were compounded to make one variable indicating whether the women received a health
160 awareness program (0=No; 1=Yes).
161
162 Data analysis
163 Data were analyzed using SPSS and STATA. The impact of health insurance and health awareness
164 programs provided by the MFP on the four dependent health-related variables will first be
165 estimated using a Probit estimation for the following linear regression equation:
166 𝑌𝑖 = 𝛽0 + 𝛽1𝑇 + 𝛽2𝑋𝑖 + 𝛽3𝑍𝑖 + 𝛽4𝐿𝑖 + 𝜀𝑖
167 where is the dependent variable measuring the four health-related outcomes. T is the treatment 𝑌𝑖
168 variable (1 if “yes”, and 0 otherwise) measuring the three microfinance health interventions. is 𝑋𝑖
169 a set of socio-demographic characteristics including age, religion, province, and literacy; is a 𝑍𝑖
170 set of household characteristic including house ownership and number of dependent children living
Page 10 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 10 -
171 in the house; is a set of loan portfolio characteristics including debt age, group loan, loan amount, 𝐿𝑖
172 interest rate, and monthly meetings; and is the error term. 𝜀𝑖
173 Following Rosenbaum and Rubin, we used Propensity Score Matching (PSM) to estimate the
174 unobserved counterfactuals and make an impact analysis of health interventions. PSM is a non-
175 parametric statistical method which matches the treated (those receiving health intervention) and
176 the controlled on the basis of conditional probability of participation, given observable
177 characteristics [23]. As we only have cross-sectional data, we can compare the dependent variables
178 related to women’s health and wellbeing in terms of those who have access to non-financial health-
179 related services provided by the microfinance provider (in this study called “health awareness
180 program”) and those who do not, as long as these services are randomly distributed and there is no
181 selection bias. The estimation of instrumental variables is one technique that is frequently used
182 within PSM. However, these results are only robust if a valid instrument is being used. As it not
183 easy to find a valid instrument in our study, we used statistical matching which has been widely
184 used before as well [24-26].
185 Our study satisfies the main conditions of PSM, which are 1) using a rich set of control variables,
186 which are observable characteristics, 2) using the same survey for treated and control groups, and
187 3) having the same community belonging to treated and control group [27]. The PSM model
188 constructs a statistical comparison group based on the probability of participating in the treatment
189 T, conditional on observed characteristics, X or the propensity score,
190 𝑝(𝑋) = 𝑃𝑟(𝑇 = 1│𝑋).
191 where T = {0, 1} is the indicator of exposure to treatment and X is the multidimensional vector of
192 pre-treatment characteristics. Following the estimation for the propensity score, the region for
193 common support is defined where distributions of the propensity score for the treatment and
Page 11 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from
For peer review only
- 11 -
194 comparison group overlap. Observations within the control and treatment group that lie outside
195 the common support are eliminated [28]. As PSM is intended to help in identifying the impact of
196 the health intervention, we used the computation of ‘average treatment effect on the treated’
197 (ATT). We used two matching criteria (Nearest Neighbor Matching [NNM] and Kernel Matching
198 [KM]), to assess statistical significance from different perspectives and to test the robustness of
199 the results [24]. NNM is used to evaluate absolute differences between propensity scores and KM
200 is used to compare each treated unit to a weighted average of the outcomes of all untreated units.
201
202 Patient and Public Involvement
203 This research was conducted without involvement of public or patients. However, the view of
204 females was already included in the qualitative part of this mixed-methods approach, which has
205 already been published elsewhere [18].
206
207 Results
208 Sample characteristics
209 All women in our sample earned less than $4.82 per day and belonged to the poorest strata of
210 society. They were taking loans for small business mobilization to improve their life opportunities.
211 The majority of women were Muslim, from Punjab, and illiterate. About three quarters had been
212 borrowers for more than 3 years, were attending monthly meetings with loan officers, and were
213 paying interest rates less than 10%. Out of the 442 women borrowers in the sample, 64.2% (n=284)
214 were taking health insurance and 71.0% (n=314) have participated in a health awareness program
215 by attending a health workshop or receiving health talks by loan officers (Table 1).
216
217
Page 12 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 12 -
218 Table 1: Descriptive statistics of women borrowers receiving health interventions (n=442)
Variable
Receiving health insurance
n (%)(N=284)
Chi-square test1
Receiving health awareness program
n (%)(N=314)
Chi-square test1
Age <29 years ≥30 years
165 (58.1%)119 (41.9%)
0.557 177 (56.4%)137 (43.6%)
0.077
Religion Muslim Other
254 (89.4%)30 (10.6%)
0.740 276 (87.9%)38 (12.1%)
0.337
Province Punjab Other
197 (69.4%)87 (30.6%)
37.977*** 203 (64.6%)111 (35.4%)
16.372***
Literacy Illiterate Literate
195 (68.7%)89 (31.3%)
3.770* 219 (69.7%)95 (30.3%)
9.109**
Spouse literacy Illiterate Literate
191 (67.3%)93 (32.7%)
7.135** 199 (63.4%)115 (36.6%)
0.231
House ownership Other Owned
225 (79.2%)59 (20.8%)
9.583** 233 (74.2%)81 (25.8%)
0.030
Children None One or more
116 (40.8%)168 (59.2%)
1.907 121 (38.5%)193 (61.5%)
0.002
Debt age 1–2 years ≥3 years
75 (26.4%)209 (73.6%)
15.755*** 83 (26.4%)231 (73.6%)
21.342***
Group loan No Yes
168 (59.2%)116 (40.8%)
0.102 173 (55.1%)141 (44.9%)
5.480**
Loan amount (in PKR) 10,000–20,000 ≥21,000
123 (43.3%)161 (56.7%)
25.096*** 121 (38.5%)193 (61.5%)
6.515**
Interest rate 2.5–10% ≥11%
202 (71.7%)82 (28.9%)
1.044 237 (75.5%)77 (24.5%)
18.527***
Monthly meeting No Yes
70 (24.6%)214 (75.4%)
0.091 73 (23.2%)241 (76.8%)
2.005
Overall perceived good health No Yes
185 (65.1%)99 (34.9%)
5.545** 216 (68.8%)98 (31.2%)
0.023
Improved ability to visit general practitioner No Yes
124 (43.7%)160 (56.3%)
0.065 127 (40.4%)187 (59.6%)
3.383*
Improved ability to purchase prescribed medicine No Yes
152 (53.5%)132 (46.5%)
19.127*** 175 (55.7%)139 (44.3%)
13.073***
Improved intake of multivitamins No Yes
182 (64.1%)102 (35.9%)
6.6040** 214 (68.2%)100 (31.8%)
0.015
219 1 *** Significant at 1% level, ** Significant at 5% level, * Significant at 10% level
Page 13 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 13 -
220
221 Women taking loans from the Government Scheme or Islamic Finance Provider were not receiving
222 health insurance interventions. However, both the Government Scheme and Islamic Finance
223 Provider were giving health awareness interventions. The Government Providers offered the
224 women a separate government health insurance scheme, called Sehat Sahulat Program, but none
225 of the study participants was availing this scheme. The Islamic Finance provider was supporting
226 Lahore-based women clients with a free medical camp for diabetes and heart disease (Table 2).
227
228 Table 2: Health insurance schemes of microfinance providers sampled in this study
Microfinance Bank(n=340)
Microfinance Institute(n=41)
Government Scheme(n=50)
Islamic Finance(n=11)
Coverage Female borrower + any family member
Female borrower + spouse
- -
Term One year One year - -Premium PKR 490–990 per
family memberPKR 1,200 (if unmarried);PKR 1,850 (married)
- -
Insurance Only hospitalizationPKR 2,000–4,000 daily
Only hospitalizationPKR 30,000
- -
Limit Between 10–30 days One-off payment - -Life insurance PKR 25,000–50,000
in event of death- - -
Other Option to take government Sehat Sahulat Program.
Health clinic in Lahore only; treating patients with diabetes and heart disease
229 Information in this table is based on data from microfinance provider loan officers
230
231 Women borrowing from the banks can take insurance for themselves and any family member.
232 They have to pay a premium ranging from PKR 490–990 per person and are insured only in the
233 event of hospital admission. However, the insurance does not cover hospital costs and instead pays
234 the client the amount of daily wages lost, ranging from PKR 2,000–4,000 daily. The scheme also
235 covers a one-off payment in the event of death ranging from PKR 25,000–50,000. Female
Page 14 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 14 -
236 borrowers from the microfinance institute are only covered for themselves and spouse. They have
237 to pay a premium of PKR 1,200 if unmarried or PKR 1,850 if married. Clients are provided with
238 a one-off payment of PKR 30,000 in the event of hospitalization.
239
240 Determinants of health-related outcomes after health insurance intervention
241 Table 3 presents the determinants of health-related outcomes for recipients of a health insurance.
242 Overall perceived good health was significantly associated with group borrowers, small loan
243 amount, and smaller interest rate. Improved ability to visit a general practitioner shows a positive
244 correlation with women borrowers from Punjab province, attending monthly meetings, group loan,
245 and smaller loan amount. Women had a significantly improved ability to purchase prescribed
246 medicine when they were from Punjab, took smaller loans, owned a house. The uptake of
247 multivitamins was increased in women with smaller loans, owning a house, being borrowers since
248 no longer than two years, and attending monthly meetings. Therefore, only a small loan amount
249 was a significant determinant in all four health-related outcomes among recipients of a health
250 insurance.
Page 15 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 15 -
251 Table 3: Probit analysis on determinants of health-related outcomes among recipients of health insurance
Overall perceivedgood health
Improved ability to visit general practitioner
Improved ability to purchase prescribed
medicine
Improvedmultivitamin
uptake
Coeff. Z-Score Coeff. Z-
Score Coeff. Z-Score Coeff. Z-
ScoreAge -0.2588 -1.43 0.2754 1.39 -0.2915 -1.51 0.0703 0.36Religion 0.4079 1.37 -0.2711 -0.97 0.4165 1.46 -0.0102 -0.03Province -0.2676 -1.04 0.9990*** 4.05 1.043*** 4.21 0.0315 0.12Literacy -0.0999 -0.49 0.2018 0.96 0.0828 0.42 0.1994 0.98Spouse literacy 0.2410 1.18 0.1779 0.85 0.2424 1.20 0.1323 0.64House ownership 0.1550 0.69 -0.3397 -1.45 -0.6825** -2.65 -0.5699** -2.17Children 0.2094 1.15 0.2213 1.20 0.1530 0.85 0.2829 1.54Debt age -0.4130 -0.16 0.1650 0.63 0.3807 1.50 -0.6088** -2.41Group loan 0.8582*** 3.76 0.4813** 2.25 0.1567 0.73 -0.3705* -1.69Loan amount -0.7765*** -3.27 -0.8863** -3.50 -1.2028*** -5.05 -1.9933*** -4.13Interest rate 0.7250** 2.94 0.2777 1.12 -0.0691 -0.28 0.2345 0.98Monthly meetings 0.1370 0.61 0.7753*** 3.58 0.0166 0.08 -0.4233* -1.84No. of observationsWald Chi2
Prob> Chi2
Log likelihood
28442.740.0001
-158.6116
28476.930.0000
-146.0385
28464.570.0000
-157.5241
28453.150.0000
-153.7125252 *** Significant at 1% level, ** Significant at 5% level, * Significant at 10% level
253
254 Determinants of health-related outcomes after health awareness intervention
255 In Table 4, the determinants for all four health-related outcomes among recipients of a health
256 awareness program are presented. Women with the following characteristics have a greater
257 probability of overall perceived good health: group borrowers, smaller loans, smaller interest rates,
258 younger women, and those with literate spouses. The ability of visiting the general practitioner for
259 regular checkups in the last year was higher in women from Punjab province, with smaller loans,
260 attending monthly meetings, above 29 years of age, and non-Muslim women. Similarly, women
261 from Punjab province, having smaller loans, owning their house, and younger women had a higher
262 probability of improved ability to purchase prescribed medicine. The probability of increased
263 uptake of multivitamins was greater in women who took smaller loans, had not been in debt for
264 more than 2 years, were group borrowers, and who attended monthly meetings. As for health
265 insurance, the only variable significantly associated with all health-related outcomes among
266 recipients of a health awareness program was the small loan amount.
Page 16 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 16 -
267
268 Table 4: Probit analysis on determinants of health-related outcomes among recipients of health awareness 269 programs
Overall perceivedgood health
Improved ability to visit general practitioner
Improved ability to purchase prescribed
medicine
Improvedmultivitamin
uptake
Coeff. Z-Score Coeff. Z-
Score Coeff. Z-Score Coeff. Z-
ScoreAge -0.3747* -1.70 0.3781* 1.70 -0.4329* -2.02 0.1058 0.48Religion 0.5185 1.59 -0.5503* -1.76 0.3880 1.24 0.1904 0.56Province -0.3898 -1.24 1.3048*** 4.39 1.029*** 3.83 0.1983 0.65Literacy -0.1537 -0.65 0.2229 0.91 0.1405 0.61 0.3411 1.43Spouse literacy 0.4163* 1.80 0.2546 1.09 0.0860 0.38 0.2310 1.00House ownership 0.3495 1.42 -0.2453 -0.96 -0.6360** -2.48 -0.4271 -1.54Children 0.3209 1.55 0.2765 1.33 0.2424 1.21 0.2833 1.36Debt age -0.0066 -0.02 0.4529 1.49 0.3817 1.36 -0.7164** -2.51Group loan 0.8817*** 3.33 0.3640 1.51 0.1030 0.43 -0.6352** -2.55Loan amount -0.7199** -2.65 -0.6511** -2.28 -1.9361*** -3.52 -0.9170*** -3.35Interest rate 0.6739** 2.23 0.3860 1.28 0.2428 0.83 0.3726 1.26Monthly meetings 0.2357 0.88 0.7689** 3.08 -0.0556 -0.22 -0.5816** -2.10No. of observationsWald Chi2
Prob> Chi2
Log likelihood
31435.680.0004
-126.4054
31464.570.0000
-116.6811
31453.250.0000
-128.2105
31448.790.0000
-121.2616270 *** Significant at 1% level, ** Significant at 5% level, * Significant at 10% level
271
272 Impact of interventions on health-related outcomes
273 The results from the PSM model (Table 5) show that women receiving health insurance had a
274 significantly greater chance of overall perceived good health. According to NNM, 17.4% of
275 women with health insurance had greater likelihood for overall perceived good health; the results
276 for KM showed a greater likelihood in 11.8%. Female borrowers receiving a health awareness
277 program from the MFP in the form of health workshop or health talk by loan officer show
278 significant improvement in their ability to purchase prescribed medicine (NNM=10.1%; KM
279 =11.7%). For the two other outcomes, neither of the interventions showed a significant effect.
280
Page 17 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 17 -
281 Table 5: Impact of interventions on health-related outcomes based on propensity score matching
Overallperceived
good health
Improved ability to visit general practitioner
Improved ability to purchase prescribed
medicine
Improved multivitamin
uptake
Coeff. Z-Score Coeff. Z-
Score Coeff. Z-Score Coeff. Z-
ScoreNearest Neighbor MatchingHealth insurance 0.1740*** 3.45 0.0038 0.04 0.1271 1.46 0.0343 0.38Health awareness program 0.0599 0.97 0.0141 0.23 0.1016* 1.70 0.0291 0.42
Kernel MatchingHealth insurance 0.1175* 1.67 -0.0256 -0.32 0.1062 1.21 0.0775 1.09Health awareness program 0.0240 0.42 0.0292 0.41 0.1167** 2.08 0.0703 1.15
282 *** Significant at 1% level, ** Significant at 5% level, * Significant at 10% level
283
284 Discussion
285 In the absence of universal health coverage and compulsory educational enrollment, poor and
286 predominantly illiterate female informal workers and borrowers of microfinance are dependent on
287 MFP for receiving health coverage and promoting health. This study has measured four health-
288 related outcomes in female borrowers. The results show that there is inequity in uptake of health
289 insurance and health-related outcomes.
290 Women from Punjab have better health-related outcomes compared to women from Sindh,
291 Balochistan and KPK. National health surveys of Pakistan also report that Punjab has better health-
292 related outcomes compared to other provinces, as the provincial government of Punjab has greater
293 budget allocation for running health awareness campaigns [29]. The fact that our results show that
294 older women and non-Muslim women have higher likelihood of improved ability to visit general
295 practitioner after receiving health awareness intervention indicates that younger Muslim women
296 face barriers to health access due to regressive norms [30]. Muslim families are known to prevent
297 fertile women from accessing healthcare in an attempt to control their reproductive choices and
298 health options. Our results align with other research which suggests that Muslims suffer from
299 health disparities due to religious fallacies [31].
Page 18 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 18 -
300 Conversely, younger women show better overall perceived health and ability to purchase
301 prescribed medicine This may be because at a younger age less health issues occur and also
302 because of greater state and NGO efforts for maternal healthcare [32]. Our results confirm that
303 women under the age of 29 years receive privileged support in a patriarchal society during prime
304 childbearing years to consume maternal health related medication [33]. Women with literate
305 spouses are also showing improvement in overall general health after receiving health insurance.
306 This may be because spouse literacy has a direct effect on women’s improved health behavior and
307 mental health [34].
308 Women who borrow the loan in groups show better health-related outcomes compared to women
309 who are single borrowers. Our results suggest that women in groups share their health knowledge
310 and encourage each other toward improved health behavior [35]. Similarly, women who attend
311 monthly meetings with loan officers have better health-related outcomes. The results suggest that
312 caring loan officers are fulfilling an important responsibility in supporting women borrowers in
313 improved health behavior and health-related outcomes. Given the conservative culture of Pakistan
314 and the disadvantaged background of the female borrowers, loan-taking women might not be able
315 to utilize health services due to issues of permission or ignorance.
316 Women who receive smaller microfinance loans and do not have a long debt age show improved
317 health-related outcomes. This finding suggests that women with debt burden over a longer period
318 of time may be suffering from debt fatigue converting to declined health-related outcomes [36].
319 Women and their families who live in owned houses also have better health-related outcomes,
320 specifically related to the ability to visit general practitioners and improved uptake of
321 multivitamins. The results imply that provision of health insurance and not having to pay
322 household rents on a monthly basis translates to better health-related outcomes. Impoverished
Page 19 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from
For peer review only
- 19 -
323 families that have to pay high rents for accommodation are usually employed in multiple jobs and
324 have little time for health and wellbeing [37].
325 The impact of microfinance is only visible on two health-related variables. Although there are no
326 effects on general practitioner visitation and uptake of multivitamins, we found that a microfinance
327 health insurance has an impact on an improved perception of general health. This shows that being
328 insured is an emotional support and wellbeing facilitator for poor women. The emotional buttress
329 provided by health insurance can go a long way in improving perceived wellbeing, which can
330 translate to greater commitment to self, family, and business development in poor women from
331 disadvantaged backgrounds [38]. In addition, microfinance health awareness interventions have
332 an impact on improved purchase of prescribed medicine. Many poor women in Pakistan do not
333 take prescribed medicine unless it is freely available due to the greater need to prioritize purchase
334 of basic necessities and household consumption [39]. The impact of microfinance interventions is
335 comparable to previous research. A review highlighted that most interventions combined
336 microfinance with health education. However, positive effects were mainly found for health
337 knowledge and behavior, but not health status [40]. A meta-analysis indicated the potential for
338 females, as microfinance may lead to changes in the use of contraceptives, strengthen female
339 empowerment and improve children’s nutrition [41].
340 However, for female borrowers of microfinance, there might be additional burdens of loan
341 repayment and small business investment. Our results suggest that illiterate and poor women of
342 the country are benefiting from health awareness in recognizing that if they do not consume
343 prescribed medicine for chronic ailments (heart disease, cholesterol, or diabetes) it can have
344 serious consequences for their own life and the future livelihood of their families. There needs to
345 be urgent recognition that a triadic health insurance safety net is necessary, instead of dependency
Page 20 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 20 -
346 on private providers to protect informal working women in Pakistan. Employers and the
347 government must join forces to ensure universal health insurance and – particularly in times of the
348 corona pandemic – infectious disease outbreak insurances for health emergencies. State financing
349 of healthcare is essential through increased allocations of gross domestic product (GDP),
350 government-run business profits, and increasing income and corporate tax base from the elite.
351 With regard to women microfinance borrowers, we recommend microfinance regulatory bodies to
352 urgently legislate the following reforms: (i) coverage of children and other dependents, maternity
353 costs, and non-hospitalization costs, (ii) expand coverage for religious and ethnic minorities, (iii)
354 reduce interest rates for those paying high house rents and introduce house ownership loans, (iv)
355 introduce mandatory group borrowing and monthly meetings with loan officers, and (iv) alter
356 repayment timelines and interest rate packages for women taking bigger loans.
357 We recommend the following urgent social policy improvements, which would adjoin in helping
358 health policy efforts: (i) development of public primary healthcare services for women in the
359 communities with mandatory quarterly General Practitioner meeting, (ii) upgrading of poverty
360 alleviation programs for support of poor women, (iii) capping for housing rents and improvement
361 of neighborhood sanitation to curb infection, (iv) advancement of home-based business
362 opportunities for informal women workers for income maintenance, including digitalization and
363 internet access in the homes, and (v) income supplementation and cash transfers for multivitamin
364 and food nutrition intake for immunity and health overall [42].
365
366 Limitations
367 This study has some limitations, most important the cross-sectional design. Although we were able
368 to compare the effects of an intervention because of the quasi-experimental analysis framework,
Page 21 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 21 -
369 two-group cross-sectional designs are suffering from the limitations related to a single
370 measurement for all subjects. Therefore, within-person changes over time are not observable.
371 Without repeated measures in a two-group design, causality cannot be identified, because temporal
372 sequencing on the intervention and outcomes cannot be established. For that reason, we
373 recommend longitudinal data collection in future studies. Furthermore, the results need to be
374 interpreted with caution, because the four health-related outcomes are non-homogenous and
375 dependent on socio-environmental factors specific to the region and community where the
376 interventions are taking place. Despite the limitations, we feel this study is significant for the
377 development of microfinance health services in Pakistan and the role of state and interest-free
378 microfinance health interventions.
379
380 Conclusion
381 It is critical to assess the health needs of women employed in the informal sector. As primary
382 caregivers at home as well as primary contributors for household income, the health of women
383 assumes a salience that would place both structures of the family and the economy at risk. Health
384 policy must consider several social policies for protecting disadvantaged women, who are poverty-
385 ridden, illiterate or semi-literate, and loan takers. Health insurance schemes and health promotion
386 at the workplace must be made mandatory by employers, microfinance providers, and the
387 government, given the cultural barriers of uptake for women. Targeting improved equity across
388 female population groups for health intervention will in the long run improve women’s health,
389 capacity expansion and income-earning abilities.
390 Designing and implementing a health and social policy protection net for female informal workers
391 requires empirical evidence regarding health interventions and socio-demographic characteristics
392 impacting on health outcomes. Since public sector health sector shortages and inefficiencies are a
Page 22 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 22 -
393 concern in Pakistan, the ‘health card’ must be accepted in both the private and public sector,
394 whichever is able to serve the poor first. As Pakistan is struggling with low GDP and tax collection
395 base, we recommend more research into options for social franchising, and partnership with
396 independent health insurance companies to serve disadvantaged women.
397
398 Acknowledgements
399 We thank the female borrowers who consented and gave their time to participate in the study. We
400 are grateful to our research team members in charge of logistical planning and coordination for
401 data collection across Pakistan including Rizwan Haider and Amir Naseem. Individual data
402 collection heads for each city are thanked for their efforts, especially for resolving gate keeping
403 issues, including Nida Abbas (Lahore), Zainab Asif (Abbotabad), Hina Bukhari (Gujranwala),
404 Sadia BiBi (Khanewal), Ansari Abbass (Sheikhapura), Azra Shakeel and Shumaila Sadique
405 (Matari), and Javaria Imran (Lasbela). The research assistant Bilal Asghar is also thanked for
406 entering all data.
407 We acknowledge support from the German Research Foundation (DFG) and the Open Access
408 Publication Fund of Charité – Universitätsmedizin Berlin.
409
410 Competing interests
411 The authors declare that no competing interests exist.
412
413 Funding
414 This study received funding by the Office of Research, Innovation and Commercialization at
415 Forman Christian College.
416
417 Data sharing
418 Data is available upon reasonable request from the corresponding author.
419
Page 23 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 23 -
420 Ethical considerations
421 Ethical approval for this study was taken from the Institutional Review Board of the Forman
422 Christian College University. Study participants were informed about the aims of the study and
423 provided informed consent either in written form or through thumb impression.
424
425 Author’s contributions
426 SRJ designed the study and was responsible for the research project, including data collection and
427 analysis; FF supervised this process. HA and MM supported in data collection. RZ and FF
428 contributed to the interpretation of the data. SRJ drafted the manuscript; all authors revised it
429 critically for important intellectual content. All authors approved the final version of this
430 manuscript.
431
432 References
433
434 1. United Nations Pakistan. One United Nations Programme III 2018-2022. United Nations
435 Sustainable Development Framework for Pakistan; 2018.
436 2. Malik MA. Universal health coverage assessment Pakistan. Karachi: Aga Khan University;
437 2015.
438 3. Nishtar S. Choked pipes: reforming Pakistan’s mixed health system: Oxford University
439 Press Karachi; 2010.
440 4. Nishtar S, Bhutta ZA, Jafar TH, et al. Health reform in Pakistan: a call to action. Lancet
441 2013;381(9885):2291–7.
442 5. Nishtar S, Boerma T, Amjad S, et al. Pakistan’s health system: performance and prospects
443 after the 18th Constitutional Amendment. Lancet 2013;381(9884):2193–206.
444 6. Pakistan Bureau of Statistics. Pakistan National Health Accounts 2013-14. Islamabad:
445 Pakistan Bureau of Statistics; 2014.
446 7. Garikipati S, Johnson S, Guérin I, Szafarz A. Microfinance and gender: Issues, challenges
447 and the road ahead. The Journal of Development Studies 2017;53(5):641–8.
448 8. Salim MM. Revealed objective functions of microfinance institutions: evidence from
449 Bangladesh. Journal of Development Economics 2013;104:34–55.
Page 24 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 24 -
450 9. Saba A, Saquiba A. Conceptualizing Health and Microfinance Nexus in Pakistan; 2017.
451 URL: http://www.pmn.org.pk/assets/articles/69106cec5d4f0132b45673990ab4622d.pdf
452 (accessed August 1, 2020).
453 10. Al-Shami SSA, Majid IBA, Rashid NA, Hamid MSRBA. Conceptual framework: The role
454 of microfinance on the wellbeing of poor people cases studies from Malaysia and Yemen.
455 Asian Social Science 2014;10(1):230.
456 11. Leatherman S, Dunford C. Linking health to microfinance to reduce poverty. Bull World
457 Health Organ 2010;88(6):470-1.
458 12. Zulfiqar G. Does microfinance enhance gender equity in access to finance? Evidence from
459 Pakistan. Feminist Economics 2017;23(1):160–85.
460 13. Escobar M-L, Griffin CC, Shaw RP. The impact of health insurance in low-and middle-
461 income countries. Brookings Institution Press; 2011.
462 14. Heltberg R, del Ninno C, Dorosh P, et al. Social protection in Pakistan: Managing
463 household risks and vulnerability. Washington, DC: Human Development Unit, South Asia
464 Region, World Bank; 2007.
465 15. Malik K, Meki M, Morduch J, Ogden T, Quinn S, Said F. COVID-19 and the Future of
466 Microfinance: Evidence and Insights from Pakistan. Oxford Review of Economic Policy;
467 2020
468 16. Mersland R, Strøm RØ. Microfinance: Costs, lending rates, and profitability. In: Caprio G,
469 Arner DW, Beck T, et al., eds. Handbook of key global financial markets, institutions, and
470 infrastructure. London: Academic Press 2016:489–99.
471 17. O’Malley T, Burke J. A systematic review of microfinance and women’s health literature:
472 Directions for future research. Global Pub Health 2017;12(11):1433–60.
473 18. Jafree SR, Mustafa M. The triple burden of disease, destitution, and debt: Small business-
474 women’s voices about health challenges after becoming debt-ridden. Health Care Women
475 Int Published Online First: 30 January 2020. doi: 10.1080/07399332.2020.1716236.
476 19. Women’s and Children’s Health Policy Center. Women’s Health Care Experiences Survey.
477 Baltimore: Hopkins University Bloomberg School of Public Health; 2000.
478 20. Quinn VJ, Kennedy E. Food security and nutrition monitoring systems in Africa: A review
479 of country experiences and lessons learned. Food Policy 1994;19(3):234–54.
Page 25 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 25 -
480 21. World Health Organization. WHO multi-country study on women's health and domestic
481 violence against women: summary report of initial results on prevalence, health outcomes
482 and women's responses. Geneva: World Health Organization; 2005.
483 22. Di Martino V. Relationship between work stress and workplace violence in the health
484 sector. Geneva: World Health Organization; 2003.
485 23. Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies
486 for causal effects. Biometrika 1983;70(1):41–55.
487 24. Becker SO, Ichino A. Estimation of average treatment effects based on propensity scores.
488 The Stata Journal 2002;2(4):358–77.
489 25. Dehejia R. Practical propensity score matching: a reply to Smith and Todd. Journal of
490 Econometrics 2005;125(1-2):355–64.
491 26. Dehejia RH, Wahba S. Propensity score-matching methods for nonexperimental causal
492 studies. Review of Economics and Statistics 2002;84(1):151–61.
493 27. Abadie A, Imbens GW. Matching on the estimated propensity score. Econometrica
494 2016;84(2):781–807.
495 28. Caliendo M, Kopeinig S. Some practical guidance for the implementation of propensity
496 score matching. Journal of Economic Surveys 2008;22(1):31–72.
497 29. Akram M, Khan FJ. Health care services and government spending in Pakistan. PIDE-
498 Working Papers 32. Pakistan Institute of Development Economics.
499 30. Mumtaz Z, Salway S. ‘I never go anywhere’: extricating the links between women's
500 mobility and uptake of reproductive health services in Pakistan. Soc Sci Med
501 2005;60(8):1751–65.
502 31. Padela AI, Zaidi D. The Islamic tradition and health inequities: A preliminary conceptual
503 model based on a systematic literature review of Muslim health-care disparities. Avicenna
504 J Med 2018;8(1):1–13.
505 32. Bhutta ZA, Hafeez A, Rizvi A, et al. Reproductive, maternal, newborn, and child health in
506 Pakistan: challenges and opportunities. Lancet 2013;381(9884):2207–18.
507 33. Hafeez A, Mohamud BK, Shiekh MR, Shah SAI, Jooma R. Lady health workers
508 programme in Pakistan: challenges, achievements and the way forward. Journal of the
509 Pakistan Medical Association 2011;61(3):210.
Page 26 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 26 -
510 34. Hamid SA, Roberts J, Mosley P. Evaluating the health effects of micro health insurance
511 placement: Evidence from Bangladesh. World Development 2011;39(3):399–411.
512 35. Prost A, Colbourn T, Seward N, et al. Women’s groups practising participatory learning
513 and action to improve maternal and newborn health in low-resource settings: a systematic
514 review and meta-analysis. Lancet 2013;381(9879):1736–46.
515 36. Jacoby MB. Does indebtedness influence health? A preliminary inquiry. The Journal of
516 Law, Medicine & Ethics 2002;30(4):560–71.
517 37. Taylor L. Housing and Health: An Overview Of The Literature. Health Affairs Health
518 Policy Brief. 7 June 2019. doi: 10.1377/hpb20180313.396577.
519 38. Bauhoff S, Hotchkiss DR, Smith O. The impact of medical insurance for the poor in
520 Georgia: a regression discontinuity approach. Health Economics 2011;20(11):1362–78.
521 39. Zaidi S, Bigdeli M, Aleem N, Rashidian A. Access to essential medicines in Pakistan:
522 policy and health systems research concerns. PloS One 2013;8(5):e63515.
523 40. Lorenzetti LMJ. Evaluating the effect of integrated microfinance and health interventions:
524 an updated review of the evidence. Health Policy Plan 2017;32(5):732–56.
525 41. Gichuru W, Ojha S, Smith S, Smyth AR, Szatkowski L. Is microfinance associated with
526 changes in women's well-being and children's nutrition? A systematic review and meta-
527 analysis. BMJ Open 2019;9(1):e023658.
528 42. Saha S. Provision of health services for microfinance clients: Analysis of evidence from
529 India. International Journal of Medicine and Public Health 2011;1(1):1–5.
Page 27 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Relationship between Microfinance, Social Development and Women’s Health
Cover Letter for Participants Questionnaire Information for Women Microfinance Borrowers Researcher: Dr. Sara Rizvi Jafree, e-mail: [email protected]; 0300 400 5740
Thank you for your valuable time! Your name is not required and all research analysis will be undertaken with confidentiality and complete anonymity. At any point during the interview you may leave, if you wish to do so. (Translation in Roman Urdu: Apka Bohat Shukirya apke eemtay waat ke liye! Apke Nam Ka Bharna Zaruri Nahi Hai Aur Yeh Tehkeek Ko Khoofiya Rakha Jaye Ga. Interview ke doran ap kabhi bhi uth ke jaana chahey to apko puri ijazat hai.) The questionnaire has been designed to collect information about your loan portfolio and your self-rated health. Our aim is to understand your needs and challenges, and ultimately try to improve your loan portfolio and health access and services. ((Translation in Roman Urdu: Is questionnaire Ka Masad Hai ke apse chand sawal loan aur sehat ke bare mein puchna. Humara masad ye hai ke apke arze ki sahuliyat aur sehat dono ko behtar kiya jaye.) Your honest and reliable answers will be appreciated, so that we can recommend the best solutions with regard to optimal loan portfolios and health satisfaction. ((Translation in Roman Urdu: Apke Sache Aur Ba Aitibar Jawab Ke Shukarguzar Honge, Thake loan aur sehat ke hawale se hum apke mushkilay ya rukawaton ko Samajh Sake.) In the event that you feel disturbed or upset after answering questions or recalling memories related to health problems or experiences of violence/ harassment, you may call or text the researcher for free consultation services from trained female psychologists. ((Translation in Roman Urdu: Agar apko in sawal aur jawab ki wajeh se koi preshani ho ya koi aisa waiya yad a jaye jo apki zehni pareshani mein izafa kare, tho ap upar diye gaye number par call ya text kar ke rabta kar le. Hum apki muft mein madat zanana mahir-e-nafsiyat se karwayenge.)
Page 28 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Instrument The questionnaire will be read out and completed by the researcher, on behalf of the participant. Province/City: ____________________________ Microfinance Provider:________________________ Area/locality: Participant Code:
SECTION A: SOCIO-DEMOGRAPHIC CHARACHTERISTICS
Code Entry
Q1.Age Umar?
1.20-29 2.30-39 3.40-49 4.50+
Q2.Religion Mazhab
1.Muslim 2.Christian 3.Hindu 4.Other
Q3.Province Sooba?
1.Punjabi 2.Sindhi 3.Baluchi 4.KPK
Q4.City Shehr?
1.Lahore 2.Islamabad
3.Karachi 4.Hyderabad
1.Quetta 1.Peshawar
Q5.City-Area Q6.Language spoken at home with family Madri zubaan?
Q7.Race (β) Zaat
Q8.Marital Status Kya ap shadi shuda hain?
1.Married 2.Single 3.Divorced 4.Seperated
Q9.Literacy Taleem-i-qabiliyat
1.None 2.Primary 3.Secondary 4.Graduate
Q10.Occupation Pesha
Q10.Spouse literacy Aapkay khaawand ki taleemi qabiliyat kya hai?
1.None 2.Primary 3.Secondary 4.Graduate
Q12.Spouse Occupation Apkay khawand ka pesha kya hai?
Q13.Your earning in last month Pichlay mahinay aap ki kamai kitni thi?
1.Less than 5k 2.>5k-10k 2.>10k-20k 4.Other
Q14.Your earning in last year Pichlay saal apki kitni kamai thi?
1.Less than 50k 2.>50k-70k 2.>70k-90k 4.Other
Q15.Combined household income in a month (on average) Tamaam ghar ki amdani kitni hai?
1.Less than 10k 2.>10k-15k 2.>15k-20k 4.Other
Q16.House Ownership Ghar ka malik kaun hai?
1.Owned 2.Rented 3.Living with someone
4.Other
Q17.Number of children Apkay kitnay bachay hain?
1. None 2. 1-2 3. 3-5 4. >6
Q18.Age of last child Akhri bachay ki umar?
Q19.Number of people living in house Ghar mai kitnay afraad rehte hain?
1. 1-2 2. 3-5 3. 6-9 4. >10
Sign or Thumb Impression for Written Consent
Page 29 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q20.Number of rooms in house Ghar mai kitnay kamray hain?
1. 1 2. 2-3 3. 4-5 4. >6
Q21.Are you currently taking care of a disabled/ dependent family member Kya apkay ghar mai koi mazoor/jiska ap par inhasaar ho, shakhs hai?
1.No 2.Yes If Yes, who:
Q22.Source of drinking water Pani penay ka kya zarya hai?
1.Plain Tap 2.Filtered 3.Local Pump
4.Other
Q23.Type of energy used for cooking in house Ghar mai khana pakanay ke liye kis chiz ka istemaal kartay hain? (gas, coal, electric etc.)
1.Gas 2.Wood 3.Electricity 4.Other
Q24.Do you have toilet facility in house Apkay ghar mai bait-ul-khala hai?
1.Yes 2.No If No, what do you use
Q25.How many toilets in the house Ghar mai kitnay bait-ul-khala hain?
1. None 2. 1-2 3. 3-5 4. >6
Q26.Does the toilet have a flush Bait-ul-khala mai flush hai?
1.Yes 2.No If No, what do you use
Q27.Is the drainage and gutter system of your house satisfactory Ganday pani ke ikhraj ka nizaam darust hai?
1.Yes 2.No
Q28.How do you dispose of the garbage Ghar ki gandagi kahan phenkhtay hain?
1.Throw it on street/ far away
from home
2.Garbage collectors come to house
3.Set Fire 4.Other
Q29.Are you taking any health insurance (not provided by the microfinance provider)? (If so, from where, how much installment) Sehat ke liye insurance le rae hain?
1.Yes 2.No If Yes, who
SECTION B: MICROFINANCE LOAN CHARACHTERISTICS
Q30.Why are you taking loan (describe your work type, hours of work, working conditions in detail) Aap karz kyun le rahe hain? (kis tarah ka kaam hai, kitnay ghantay kaam kartay hain, jahan kaam kartay hain uskay halaat)
Q31.What type of loan are you currently taking/ duration Kis tarah ka karz le rahay hain/kitnay arsay se?
Q32.How long have you been a microfinance borrower for Kitne arsay se karz le rahay hain?
1. 1-2 years 2. 3-5 years 3. 6-9 years 4. >10 years
Q33.Is it a group loan Kya ap ne kisi ke sath mil ke karz liya hai?
1.Yes 2.No If Yes, who
Q34.How much is the loan for Kitna karz liya hai?
Q35.What is the installment rate per month Karz ko ada karnay ki mahana kist kya hai?
Q36.Do you attend monthly meetings with loan officers Karz denay walay officer se kya apki mahwar mulakaat hoti hai?
1.Yes 2.No
Q37.Do you attend weekly meetings with loan officers Karz dene walay officer se kya apki haftawar mulkaat hoti hai?
1.Yes 2.No
Q38.Who helps you in loan repayment Karz ada karnay mai kya koi apki madad karta hai?
1.No one 2.Husband 3.Parents 4.Other
Q39.What exactly has the loan been used for Ap karz kis liye istemal karti hain?
1.Business 2.Household expenditure
3.Old Loans
4.Health Costs
4.Other
Page 30 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q40.How much of the loan taken has been invested in business Karz ka kitna hissa karobar mai kharch kiya hai?
1.All 2.Half 3.Quarter 4.Other
Q41.Are you satisfied with loan amount Kya aap karz ki rakam se mutmaeen hai?
1.Yes 2.No
Q42.Are you satisfied with loan repayment rate Kya ap karz ki adaigi ki kist se mutmaeen hai?
1.Yes 2.No
Q43.Will you be renewing loan Kya aap karz dobara lena chahain gae?
1.Yes 2.No
Q44.Have you received any skill development training Kya apki silahiyaton ko barhanay ki koi tarbiyat mili hai?
1.Yes 2.No
Q45.Have you participated in any health workshop/awareness campaign/talk… Kya sehat se mutalik ap kisi agahi mohim ka hissa banay hai?
1.Yes 2.No
Q46.Has your loan officer or center ever talked to you about health awareness or access Kya karz denay walay officer ne ap se sehat ke mutalik koi agahi di hai?
1.Yes 2.No
Q47.Have you been offered saving insurance by your MFP Kya idaray ne apko bachat insurance ki peshkash ki hai?
1.Yes 2.No
Q48.Are you taking saving insurance with your MFP Kya idara ap ko bachat insurance de raha hai?
1.Yes 2.No
Q49.Have you been offered health insurance by your MFP Kya idara aap ko sehat insurance deta hai?
1.Yes 2.No
Q50.Are you taking health insurance with your MFP Kya ap idaray se sehat insurance le rahay hain?
1.Yes 2.No
Q51.Has the loan so far satisfied your business needs Kya karz ki rakam ne apki karobari zaroriyat ko pura kiya hai?
1.Yes 2.No
Q52.Has your loan taking from MF enabled you to visit a trained private general practitioner, if needed in last 12 months Karzay k baad pichlay 12 maheenay mein kya app private doctor ko dekhanay gaye hain?
1.Yes 2.No
Q53.Has your employment from MF loan enabled you to visit a trained private specialist practitioner, if needed in last 12 months Karzay k baad pichlay 12 maheenay mein kya app baday doctor ko dekhanay gaye hain?
1.Yes 2.No
Q54.How is your ability to purchase prescribed medicines (in case recommended by doctor) since loan-taking? Kya karz lene ke bad dawayan khareednay ki istata’at mai koi tabdeeli ai hai?
1.Very Good 2.Good 3.Fair 4.Poor
SECTION C WOMEN’S HEALTH CARE EXPERIENCES SURVEY
Q55. How would you rate your health in general? Apki sehat kis mayar ki hai?
1.Very Good 2.Good 3.Fair 4.Poor
Q56.Compared to other women your age, how would you rate your health Apni hum umar auraton ki nisbat aap apni sehat ka kya mayaar samjhtay hain?
1.Very Good 2.Good 3.Fair 4.Poor
Q57. Do you feel your health could be better than 1.Yes 2.No If yes, could you say why/ how:
Page 31 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
it is presently? Kya apki sehat ke mayaar mai koi behtari lai ja sakti hai?
Q58.Does your husband/ male relative/in-laws decide/ give approval when you or your children need consultation from a medical practitioner Kya apka khawand/susral apko doctor pe janay ki ijazat deta hai? Kya ye faisla bhi apka susral/khawand krta hai?
1.Yes 2. I decide myself independently
If yes, can you specify which relatives:
Q59.Does your husband/ male relative/in-laws decide/ give approval when you or your children need to visit a clinic/ hospital Kya apka khawand/susral apko hospital janay ki ijazat deta hai or kya ye faisla kaun leta hai?
1.Yes 2. I decide myself independently
If yes, can you specify which relatives:
Please indicate if you have experienced any of the following health issues in the last 12 months?
1.Yes 2.No
Q60.Minor illness like the flu or an infection Pichlay 12 mahinay mai apko nazla ya infection hua hai?
Q61.Had to go for a checkup or routine physical exam Jismani muaaenay ke liye gae hain?
Q62.Were you pregnant? Kya app hamla theen?
Q63.Did you need family planning or preconceptional services? Kya apko munsoba bandi ki zaroorat thee?
Q64.Did you have an injury that you have not already mentioned? Kya apko koi chot lagi hai?
Q65.Did you need care for a chronic health problem, (that is one that goes on for a long time)? Kya apko kisi taweel bemari ke liye hospital jana para hai?
Q66.Did you need surgery for a condition not already mentioned? Kya apko operation keranay ki zaroorat parhi?
If yes, what?
Q67.Were you feeling depressed, anxious, or highly stressed? Kya iski waja se apko kisi kisam ka zehni dabao ya bechaini mehsoos hui hai?
Could you pinpoint why?
Have you had one of the following tests in the last 12 months?
1.Yes 2.No
Q68.Colon cancer screening, such as a check for blood in your stool, sigmoidoscopy, or colonoscopy
Q69.Test for glaucoma or pressure in the eye Q70.Blood cholesterol test Q71.Check for high blood pressure Q72.Test for diabetes Q73.Breast exam by a doctor or nurse Q74.Mammogram Q75.Pap test Q76.Bone density test (for osteoporosis) Q77.Genetic screening test Q78.Screening for HIV/AIDS
Page 32 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q79.Screening for other sexually transmitted diseases
Q80.Dental exam Q81.Shot for flu or pneumonia Q82.Pregnancy test Q83.Family planning services or contraception Q84.Tests for infertility Q85.Abortion information or services Q86.Alcohol or drug abuse counseling or treatment
In the past 12 months, did any of your health care providers or microfinance loan managers talk with you or give you information about? (pichlay 12 mahino mai kya apkay doctor/nurse ya apkay karz dene walay officer ne aap se in chizon ke baray mai maloomat di hain?)
1.Yes 2.No If yes, can you specify who gave you this information:
Q87.Smoking, second-hand smoke, or quitting smoking Tambako noshi, kisi aisay shaks k saath bethtna/rehna jo tambako noshi mein mulawis ho, ya tambako noshi chorna
Q88.Nutrition or diet (Khuraak)
Q89.Alcohol or drug use Shraab ya adviyaat?
Q90.Physical fitness or exercise Jismani sehat ya warzish?
Q91.Menopause or hormone replacement therapy San – e - yaas ya hormone tabdeeli therapy?
Q92.Violence in the home or workplace Kya ghar ya kaam pe kisi tashadud ka shikar hue hain?
Q93.Work or financial problems Kaam ya muaashi mushkilaat ka samna hua hai?
Q94.Family or relationship problems Ghar walon ya rishtadaron ke masa’il?
Q95.Importance of child health and nutrition Bachon ki sehat or khuraak ki ehmiyat?
Q96.Stress management Zehani dabao ko kum karna
Q97.Preventing unintended pregnancies & birth spacing Bachon ke darmiya wakfa?
Q98.Using alternative therapies, such as herbs or acupuncture
Q99.Preventing osteoporosis Hadion ke dard se bachao
Are there any dietary supplements that you have used in the last 12 months?
1.Yes 2.No
Q100.Vitamin C Q101.Vitamin D Q102.Vitamin E Q103.B Complex Q104.Calcium Q105.Pregnancy Vitamin Q106.Lactation Vitamin
Page 33 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q107.General Multi-vitamin What is your personal preference for health services? Tibbi saholiyat se mutalik apki zaati tarjihaat kya hain?
1.Yes 2.No 3.Indfferent
Q108.Family (e.g. mother/ mother-in-law/ aunt) Ghar walay?
If Yes, describe who:
Q109.A women’s health center where you can get most of your basic health care, including gynecological care, in one place Khawateen ki sehat markaz?
Q110.Trusted community member Baradari?
Q111.A nurse or LHW (Not a physician/ surgeon/ medical consultant)
Q112.PublicHospital Q113.Local female healer Q114.Private Clinic Q115.In general, how difficult have you found it to talk to health care providers about your personal health concerns? doctor/nurse se baat krna apko kitna mushkil lagta hai?
1.Very difficult 2.Somewhat difficult
2.Not too difficult
3.Not difficult at all
Please rate the health practitioner services as you have experienced them?
1.Excellent 2.Good 3.Fair 4.Poor
Q116.Listening to what you have to say Kya apki baat ghor se suntay hain?
Q117.Talking to you in a respectful and caring manner
Kya ap se izzat se baat kartay hai?
Q118.Speaking to you in the language/ dialect you understand better
Kya apse apki madri zubaan mai baat krtay hai
Q119.Answering your questions clearly Ap ke sawalon ka sahi se jawaab detay hai?
Q120.Giving you the opportunity to ask all of your questions Apko sawaal puchnay ka wakt detay hai?
Q121.Helping you to feel comfortable talking about your personal or sensitive health concerns Kya ap asaani se unhe apnay masaael ke baray mai bata deti hain?
Q122.Giving you complete health information Kya sehat se mutalik tamaam jankari detay hain?
Q123.Discussing alternative therapies, diet and lifestyle Kya ap se mutabadil therapy ya khuraq ya roz mara ki zindagi guzarnay kay tareekay pe tabadal e khayal kya hai?
Q124.Giving you complete information about any tests or services Test ke baray mai mukamal jaankari detay hain?
Q125.Giving you the results of your tests Test ke nataij batatay hain?
Page 34 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q126.Giving you complete information about all your options for treatments Kya ilaaj ke mutalik apko mukamal jaankari detay hai?
Q127.Giving you the opportunity to make important decisions about your health care Kya sehat se mutalik tamam faislay apko karnay detay hai?
Q128.Giving you written or printed information when you need it Malumaat likh kr dete hai?
Q129.Spending enough time with you during your visits Apko tasali bakhsh wakt detay hai?
Q130.Treating you like a partner in your health care Apka sathi bun kr apki sehat ka khayal rakhtay hai?
Which are the primary/ most important sources you depend on for making health decisions? Sehat se mutalik faislon ke liye ap kis se mashwara leti hai?
Tick relevant options
Q131.Husband Q132.Mother in law Q133.Other in-laws (list please) Q134.Blood family (parents, siblings, children…) Q135.Newspapers / magazines Q136.Heath newsletter Q137.TV Q138.Radio Q139.Microfinance provider Q140.Internet Q141.Mobile services Q142.Family/ friends Q143.Community Q144.Medical Practitioner Q145.Local Healer Q146.Local Imam/ religious leader Q147.Other (Please list) Current Health Risks Q148.Do you currently smoke? Kya app tambako noshi mein mulawis hain?
1.Yes
2.No
Q149.How many in a day? Din ke kitnay ?
Q150.Does anyone else smoke in the house when you/ children are in same room? Kya koi aur tambako noshi mein mulawis hain
1.Yes 2.No If yes, who is this:
Q151.Do you feel anxious, stressed, depressed, suicidal? Kya app kabhi bechain hotay hain ya zehni dabao ka shakar ya khud kushi ka khayal aya hai?
1.Yes 2.No
Indicate which:
Q152.Do you take any drugs (to relieve yourselves of stress or an ailment? Kya app in ke liye koi dawa laitay hain?
1.Yes
2.No
If yes, which ones:
Page 35 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
In the past 5 years, has a doctor ever told you that you have any of the following conditions Kya pichlay paanch salon mai doctor ne aapko bataya ke apko ye bemari hai?
Tick relevant options
Q153.Hypertension/ BP High blood pressure
Q154.Heart disease Dil ki bemari
Q155.High cholesterol Q156.Diabetes (sugar)
Q157.Depression Zehni dabao
Q158.Anxiety Bechaini
Q159.Migraine headaches (sar dard)
Q160.Arthritis Joro ki dard
Q161.Osteoporosis Q162.Obesity/ Over-weight problems (mutapa)
Q163.Urinary incontinence (pishaap ki takleef)
Q164.Cancer Q165.Eating disorder like bulimia/ anorexia Khanay k hawaly se koi mushkil, jaisay bhook na lagna ya kha k ulti kerna
Q166.Thyroid problems Q167.Malaria/ Dengue Are you facing any disability which? Kya aap kisi mazoori ka shikaar hain?
1.Yes
2.No
Q168.Keeps you from participating fully in your ability to take care of your family Jiski waja se ap apnay ghar walon ka khayal na rakh sakain
If yes, please describe this disability:
Q169.Keeps you from participating fully in your ability to continue with your business Apnay karobaar mai sahi se kaam na kr sakain
If yes, please describe this disability:
SECTION D BASELINE NUTRITION AND FOOD SECURITY SURVEY UNICEF
Q170.In the past 6 months did you find it too expensive to purchase the foods you needed to feed your family? Pichlay 6 maah mai kya apko khaandan ko palnay ke liye khana lenay mai mushkilaat hoti hai?
1.Yes
2.No
Q171.Did you find it too expensive to purchase fruit? Kya phal khareedna bohat mehnga hai?
1.Yes
2.No
Q172.Did you find it too expensive to purchase 1.Yes
2.No
Page 36 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
vegetables? Kya sabzi khareedna bohat mehnga hai?
Q173.Did you find it too expensive to purchase meat? Kya gosht khareedna bohat mehnga hai?
1.Yes
2.No
Q174.Did you find it too expensive to purchase eggs? Kya anday khareedna bohat mehnga hai?
1.Yes
2.No
Q175.Did you find it too expensive to purchase milk? Kya doodh khareedna bohat mehnga hai?
1.Yes
2.No
Q176.Did you find it too expensive to purchase wheat, for roti? Kya roti khareedna bohat mehnga hai?
1.Yes
2.No
Q177.In the last 3 months were you worried about running out of food because of high costs? Pichlay 3 maah mai mehngai ki waja se khana na khareed panay ka dart ha?
1.Yes
2.No
Q178.In the last 3 months did you run out of food because of expense? Pichlay 3 maah mai kya mehngai ki waja se kabhi ghar mai khana khatam ho gaya ho?
1.Yes
2.No
Q179.In the last 3 months did you or any other adult in the house skip meals because there was not enough food? Pichlay 3 maah mai aap ya kisi or ghar walay se khana kum honay ki waja se khana na khaya ho?
1.Yes
2.No
Q180.In the last 3 months did you ever think your children are still hungry because of not being fed enough food? Pichlay 3 maah mai apko kabhi laga ke apkay bachay bhookay hai kyunkay khana pura nai tha?
1.Yes
2.No
Q181.In the last 3 months did any of your children go to bed hungry? Pichlay 3 maah mai kya apkay bachay kabhi bhookay soe houn?
1.Yes
2.No
SECTION E WHO MULTI-COUNTRY STUDY ON WOMEN’S HEALTH AND DOMESTIC VIOLENCE AGAINST WOMEN Psychological violence experienced at home 1.Yes 2.No If yes, who were these
household members?
Q182.Has someone in your home insulted you or made you feel bad about yourself? Kya ghar mai kisi ne apki bezati ki hai?
Q183.Has someone in your home belittled or humiliated you in front of other people? Kya ghar mai kisi ne apko dosron ke samnay hakeer dikhaya hai?
Q184.Has someone in your home done things to scare or intimidate you on purpose? Kya ghar mai kisi ne apko daraya hai?
Q185.Has someone in your home threatened to hurt you or someone you care about? Kisi ne apko damkhaya hai?
Physical violence experienced at home 1.Yes 2.No If yes, who were these
Page 37 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from
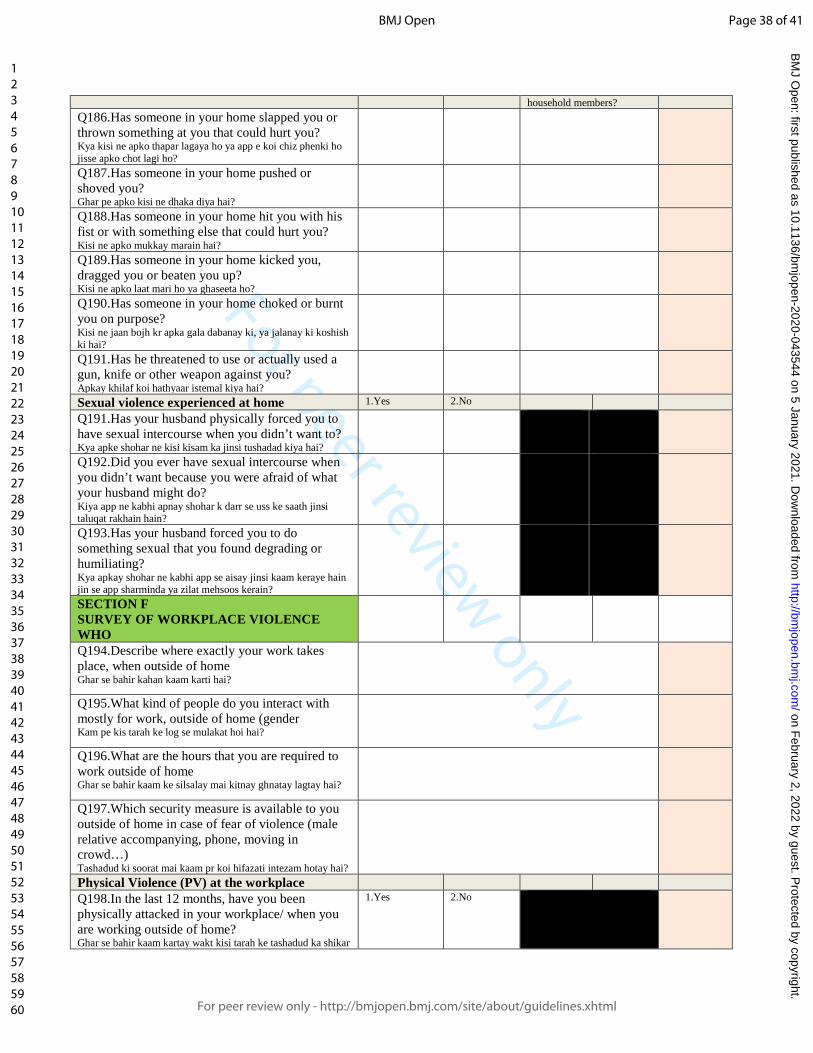
For peer review only
household members? Q186.Has someone in your home slapped you or thrown something at you that could hurt you? Kya kisi ne apko thapar lagaya ho ya app e koi chiz phenki ho jisse apko chot lagi ho?
Q187.Has someone in your home pushed or shoved you? Ghar pe apko kisi ne dhaka diya hai?
Q188.Has someone in your home hit you with his fist or with something else that could hurt you? Kisi ne apko mukkay marain hai?
Q189.Has someone in your home kicked you, dragged you or beaten you up? Kisi ne apko laat mari ho ya ghaseeta ho?
Q190.Has someone in your home choked or burnt you on purpose? Kisi ne jaan bojh kr apka gala dabanay ki, ya jalanay ki koshish ki hai?
Q191.Has he threatened to use or actually used a gun, knife or other weapon against you? Apkay khilaf koi hathyaar istemal kiya hai?
Sexual violence experienced at home 1.Yes 2.No
Q191.Has your husband physically forced you to have sexual intercourse when you didn’t want to? Kya apke shohar ne kisi kisam ka jinsi tushadad kiya hai?
Q192.Did you ever have sexual intercourse when you didn’t want because you were afraid of what your husband might do? Kiya app ne kabhi apnay shohar k darr se uss ke saath jinsi taluqat rakhain hain?
Q193.Has your husband forced you to do something sexual that you found degrading or humiliating? Kya apkay shohar ne kabhi app se aisay jinsi kaam keraye hain jin se app sharminda ya zilat mehsoos kerain?
SECTION F SURVEY OF WORKPLACE VIOLENCE WHO
Q194.Describe where exactly your work takes place, when outside of home Ghar se bahir kahan kaam karti hai?
Q195.What kind of people do you interact with mostly for work, outside of home (gender Kam pe kis tarah ke log se mulakat hoi hai?
Q196.What are the hours that you are required to work outside of home Ghar se bahir kaam ke silsalay mai kitnay ghnatay lagtay hai?
Q197.Which security measure is available to you outside of home in case of fear of violence (male relative accompanying, phone, moving in crowd…) Tashadud ki soorat mai kaam pr koi hifazati intezam hotay hai?
Physical Violence (PV) at the workplace Q198.In the last 12 months, have you been physically attacked in your workplace/ when you are working outside of home? Ghar se bahir kaam kartay wakt kisi tarah ke tashadud ka shikar
1.Yes 2.No
Page 38 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
hui hain? Q199.Was this PV with a weapon? (If yes, what kind) Kya is tashadud ke liye koi aslaah istemal kiya gaya tha?
Q200.Is this a typical incident at your workplace/ when you are working outside of home? Kya is tarah ka tashadud kaam pr mamool ki baat hai?
1.Yes 2.No
Q201.Who attacked you? Kis ne app r tashadud kiya?
Q202.Where exactly did it take place? Tashadud kis jaga hua?
Q203.What time was it? Kis wakt hua?
Q204.Do you think it could be prevented? Kya is tashadud roka ja sakta tha?
1.Yes 2.No
Q205.Were you injured? Kya apko kisi kisam ki chot ai thi?
1.Yes 2.No
Q206.Did you require treatment for the injury? Kya is chot/zakham ke liye apko kisi ilaj ki zarorat hui?
1.Yes 2.No If yes, can you describe this treatment:
Q207.How did you respond to the incident? Tashadud ke natijay mai ap ne kya kiya?
Did you suffer any of the following due to PV: Q208.Repeated, disturbing memories, thoughts, or images of the attack? Tashadud ke bad kya apko iske baray mai aksar khayalat atay the?
1.Yes 2.No
Q209.Avoiding thinking about or talking about the attack or avoiding having feelings related to it? Kya is tashadud ke baray mai baat karne se ap ghabrati thi?
1.Yes 2.No
Q210.Being "super-alert" or watchful and on guard? Tashadud ke bad dar ke rehne lagi?
1.Yes 2.No
Q211.Feeling like everything you did was an effort? Har kaam mushkil ho gaya?
1.Yes 2.No
Verbal Violence (VV) at the workplace Q212.In the last 12 months, have you been verbally assaulted in your workplace/ when you are working outside of home? Kya pichlay 12 mah mai kaam pr kisi ne ap pr zabani tashadud kiya hai?
1.Yes 2.No
Q213.How often has this happened in the last 12 months? Kitni dafa?
1.Daily 2.About once in a week
3.About once in a month
4.Other
Q214.Is this a typical incident at your workplace/ when you are working outside of home? Kya ye kaam pr mamool ki baat hai?
1.Yes 2.No
Q215.Who abused you? Kis ne aap per zabani tashadud kiya?
Q216.Where exactly did it take place? Kahan kiya?
Q217.What time was it? Kis wakt kiya?
Page 39 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q218.Do you think it could be prevented? Kya isse roka ja sakta tha?
1.Yes 2.No
Q219.How did you respond to the incident? Iske natijay mai aap ne kya kiya?
Did you suffer any of the following due to VV: Q220.Repeated, disturbing memories, thoughts, or images of the attack? Tashadud ke bad kya apko iske baray mai aksar khayalat atay the?
1.Yes 2.No
Q221.Avoiding thinking about or talking about the attack or avoiding having feelings related to it? Kya is tashadud ke baray mai baat karne se ap ghabrati thi?
1.Yes 2.No
Q222.Being "super-alert" or watchful and on guard? Tashadud ke bad dar ke rehne lagi?
1.Yes 2.No
Q223.Feeling like everything you did was an effort? Har kaam mushkil ho gaya?
1.Yes 2.No
Sexual Harassment (SH) at the workplace Q224.In the last 12 months, have you been sexually harassed in your workplace/ when you are working outside of home? Kya pichlay 12 maheenay mein ap ko kisi kisam k jinsi harasaan ka samna kerna parha hai?
1.Yes 2.No
Q225.How often have you been sexually harassed in the last 12 months? Pichlay 12 maheenay mein yeh kitni dafa hua?
1.Daily 2.About once in a week
3.About once in a month
4.Other
Q226.Is this a typical incident at your workplace/ when you are working outside of home? Kya yeh kaam kernay wali jaga pe amoman hota hai?
1.Yes 2.No
Q227.Who attacked you? Hamla awar kaun tha?
Q228.Where exactly did it take place? Yeh kis jaga pe hua?
Q229.What time was it? Waqt kya tha?
Q230.Do you think it could be prevented? Kya app isko rok sakti theen?
1.Yes 2.No
Q231.How did you respond to the incident? Apnay iska samna kaisay kiya?
Did you suffer any of the following due to SH: Q232.Repeated, disturbing memories, thoughts, or images of the attack? Kya apko iss hadsay k baad baar baar buray khaylat ya yaadain pareshan kerti hain?
1.Yes 2.No
Q233.Avoiding thinking about or talking about the attack or avoiding having feelings related to it? Kya app iss hadsay ko bhulanay ki koshih ya iskay baray mein baat kernay se guraiz kertay hain?
1.Yes 2.No
Q234.Being "super-alert" or watchful and on guard?
1.Yes 2.No
Page 40 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Kya app chak o chawbund rehtay hain? Q235.Feeling like everything you did was an effort? Kya apko zehni dabao mehsoos hota hai?
1.Yes 2.No
Racial Harassment (RH) at the workplace Q236.In the last 12 months, have you been racially harassed in your workplace/ when you are working outside of home? Pichlay 12 maah mai apki zaat ki waja se kisi ne apko harasaan kiya hai?
1.Yes 2.No
Q237.How often have you been racially harassed in the last 12 months? Kitni dafa?
1.Daily 2.About once in a week
3.About once in a month
4.Other
Q238.Is this a typical incident at your workplace/ when you are working outside of home? Ghar se bahir kaam pe kya ye aam ma’mool ki baat hai?
1.Yes 2.No
Q239.Who attacked you? Kis ne harasaan kiya?
Q240.Where exactly did it take place? Kahan
Q241.What time was it? Kis wakt?
Q242.Do you think it could be prevented? Kya issay roka ja sakta tha?
1.Yes 2.No
Q243.How did you respond to the incident? Iske natijay mai aap ne kya kiya?
Did you suffer any of the following due to RH: Q244.Repeated, disturbing memories, thoughts, or images of the attack? Tashadud ke bad kya apko iske baray mai aksar khayalat atay the?
1.Yes 2.No
Q245.Avoiding thinking about or talking about the attack or avoiding having feelings related to it? Kya is tashadud ke baray mai baat karne se ap ghabrati thi?
1.Yes 2.No
Q246.Being "super-alert" or watchful and on guard? Tashadud ke bad dar ke rehne lagi?
1.Yes 2.No
Q247.Feeling like everything you did was an effort? Har kaam mushkil ho gaya?
1.Yes 2.No
SECTION F OPEN-ENDED QUESTIONS
Q248.What are the main health challenges you face in the last 12 months? Pichlay sal mein kaunsi sehat ki takleef thi apko? Behtareen tibbi saholiyat ke wasool mai sub se eham 3 rukawatain?
Q249.What are the top 3 barriers preventing you from access to health services? Kaunsi theen chezay apko sehat ki sahulat laney mein rukawat hai
Page 41 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q250. What are the main problems which prevent you from being satisfied with your health since taking loan? Kaunsi sehat ke mutalik cheezay apko ----- ?
β- Punjabis (1), Pashtuns (2), Sindhis (3), Siddis (4), Saraikis (5), Muhajirs (6), Balochis (7), Hindkowans (8), Chitralis (9), Gujarati (10), Kashmiris (11), Kalash (12), Burusho (13), Brahui (14), Khowar (15), Hazara (16), Shina (17), Kalyu (18), Balti (19), Afghan refugees (20), Other (21). *- Doctors clinic (private/primary-secondary) (1), Hospital Clinic (tertiary) (2), LHW (3), BHU (4), Local Hakim (5), Homeopath (6), Other (7). +- No money (1), not serious/ took care it of it myself (2), too busy (3), no childcare (4), no transport (5), too embarrassed (6), don’t have permission (7), prescription/ paperwork/ referral got lost (8), didn’t know where to get care (9), provider too far away (10), don’t like the local provider (11), couldn’t find specific specialist (12), other (13). # Physical violence refers to the use of physical force against another person or group, that results in physical harm, sexual or psychological harm. It can include beating, kicking, slapping, stabbing, shooting, pushing, biting, and/or pinching, among others. Psychological violence is defined as: Intentional use of power, including threat of physical force, against another person or group, that can result in harm to physical, mental, spiritual, moral or social development. Psychological violence includes verbal abuse, bullying/mobbing, harassment, and threats. Sexual Harassment refers to any unwanted, unreciprocated and unwelcome behavior of a sexual nature that is offensive to the person involved, and causes that person to be threatened, humiliated or embarrassed. Racial Harassment refers to any threatening conduct that is based on race, color, language, national origin, religion, association with a minority, birth or other status that is unreciprocated or unwanted and which affects the dignity of women and men at work. @ took no action (1), tried to pretend it never happened (1), told the person to stop (1), tried to defend myself (1), told friends/family (1), sought counseling (1), told a colleague (1), reported it to a colleague (1), discussed/ complained to MF loan officer (1), sought help from MFP (1), sought help from the union/community (1), pursued prosecution (1), other (1)
Page 42 of 41
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review onlyImpact of microfinance health interventions on health-
related outcomes among female informal workers in Pakistan: A retrospective quasi-experimental study
Journal: BMJ Open
Manuscript ID bmjopen-2020-043544.R1
Article Type: Original research
Date Submitted by the Author: 02-Nov-2020
Complete List of Authors: Jafree, Sara; Forman Christian CollegeZakar, Rubeena; The University of LahoreAhsan, Humna; Forman Christian CollegeMustafa, Mudasir; Utah State UniversityFischer, Florian; Charité Universitätsmedizin Berlin, Institute of Public Health; University of Applied Sciences Ravensburg-Weingarten, Doggenriedstraße
<b>Primary Subject Heading</b>: Public health
Secondary Subject Heading: Epidemiology, Evidence based practice, Global health
Keywords: Health policy < HEALTH SERVICES ADMINISTRATION & MANAGEMENT, PUBLIC HEALTH, EPIDEMIOLOGY
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on F
ebruary 2, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-043544 on 5 January 2021. Dow
nloaded from

For peer review onlyI, the Submitting Author has the right to grant and does grant on behalf of all authors of the Work (as defined in the below author licence), an exclusive licence and/or a non-exclusive licence for contributions from authors who are: i) UK Crown employees; ii) where BMJ has agreed a CC-BY licence shall apply, and/or iii) in accordance with the terms applicable for US Federal Government officers or employees acting as part of their official duties; on a worldwide, perpetual, irrevocable, royalty-free basis to BMJ Publishing Group Ltd (“BMJ”) its licensees and where the relevant Journal is co-owned by BMJ to the co-owners of the Journal, to publish the Work in this journal and any other BMJ products and to exploit all rights, as set out in our licence.
The Submitting Author accepts and understands that any supply made under these terms is made by BMJ to the Submitting Author unless you are acting as an employee on behalf of your employer or a postgraduate student of an affiliated institution which is paying any applicable article publishing charge (“APC”) for Open Access articles. Where the Submitting Author wishes to make the Work available on an Open Access basis (and intends to pay the relevant APC), the terms of reuse of such Open Access shall be governed by a Creative Commons licence – details of these licences and which Creative Commons licence will apply to this Work are set out in our licence referred to above.
Other than as permitted in any relevant BMJ Author’s Self Archiving Policies, I confirm this Work has not been accepted for publication elsewhere, is not being considered for publication elsewhere and does not duplicate material already published. I confirm all authors consent to publication of this Work and authorise the granting of this licence.
Page 1 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 1 -
Impact of microfinance health interventions on health-related outcomes
among female informal workers in Pakistan: A retrospective quasi-
experimental study
Sara Rizvi Jafree, Rubeena Zakar, Humna Ahsan, Mudasir Mustafa, Florian Fischer
Dr. Sara Rizvi JafreeDepartment of Sociology, Forman Christian College University, Lahore, Pakistan; [email protected]
Prof. Dr. Rubeena ZakarInstitute of Social and Cultural Studies, University of the Punjab, Lahore, Pakistan; [email protected]
Dr. Humna AhsanDepartment of Economics, Forman Christian College University, Lahore, Pakistan; [email protected]
Mudasir MustafaDepartment of Sociology, Social Work, and Anthropology, Utah State University, Logan, United States of America; [email protected]
Dr. Florian Fischer 1) Institute of Public Health, Charité – Universitätsmedizin Berlin, Germany; [email protected] 2) Institute of Gerontological Health Services and Nursing Research, Ravensburg-Weingarten University of Applied Sciences, Germany; [email protected]
Corresponding author:Dr. Florian FischerCharité – Universitätsmedizin BerlinInstitute of Public HealthCharitéplatz 1 10117 BerlinE-Mail: [email protected]
Word count: 4,941
Page 2 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 2 -
1 Abstract
2 Objective: The purpose of this study is to assess the impact of microfinance health interventions
3 (health insurance and health-awareness programmes) on health-related outcomes among female
4 informal workers in Pakistan.
5 Design: We conducted a retrospective, quasi-experimental study among a total of 442 female
6 borrowers from seven microfinance providers (MFPs) across four provinces of Pakistan in 2018.
7 A standardised tool was used for data collection. Probit regression was used to identify the
8 probability of female borrowers gaining improvements in health outcomes based on their socio-
9 demographic characteristics. Propensity score matching (PSM) was used to assess the overall
10 impact of health interventions.
11 Primary outcome measures: Four health-related outcomes reported by the women were used:
12 perception of good health overall, ability to visit a general practitioner, ability to purchase
13 prescribed medicine, and intake of multivitamins.
14 Results: We found that women receiving health interventions had a greater probability of better
15 health outcomes when they were from Punjab province, borrowing in groups, and attending
16 monthly meetings at MFPs. Even with a small loan amount, all four health-related outcomes were
17 significantly associated with receiving health insurance and health-awareness programmes. PSM
18 results show a greater likelihood of overall perceived good health (NNM=17.4%; KM=11.8%)
19 when health insurance is provided and a significant improvement in the ability to purchase
20 prescribed medicine when a health-awareness programme is provided (NNM=10.1%; KM
21 =11.7%).
22 Conclusion: Health and social policies are vital to secure health and wellbeing among poor women
23 working in the informal sector. Targeting improved equity across female population groups for
Page 3 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 3 -
24 health interventions will in the long run improve poor women’s health, income-earning abilities,
25 and capacity expansion for small businesses.
26 Keywords: borrow, informal sector, health insurance, health awareness, microfinance
27
28 Strengths and limitations of the study
29 This study uses a nationally representative sample of 442 female borrowers of
30 microfinance from four provinces in Pakistan.
31 It is the first study which focuses on female microfinance borrowers in Pakistan to assess
32 the impact of health interventions on health-related outcomes among poor women.
33 We were able to identify health improvements when women received health insurance and
34 health-awareness programmes.
35 Due to the cross-sectional study design and quasi-experimental analysis framework, the
36 results must be interpreted with caution.
37 Future studies need to consider additional burdens of loan repayment and small-business
38 investment.
39
Page 4 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 4 -
40 Introduction
41 More than half (57%) of the female population of Pakistan is illiterate. Less than a quarter (23%)
42 of women are employed, with a majority working in the informal sector [1]. Informal workers in
43 Pakistan are usually self-employed or involved in small-scale work. They are not protected by the
44 country’s labour laws and regulations. Therefore, they do not receive employment benefits like a
45 permanent contract, minimum wage, medical allowances, a pension or provident fund. There are
46 several problems to consider with regard to the health of female informal workers in Pakistan,
47 including high rates of poverty and low health literacy, as well as inadequate access to public
48 health services [2], reinforced by low government health budget allocations for this population
49 group [3]. In addition to the overall absence of universal health coverage, there is limited coverage
50 for public health emergencies like pandemics [4] and greater risks of acquiring infectious diseases
51 among female informal workers due to mostly unsanitary living conditions in disadvantaged
52 communities [5]. Pakistan has one of the largest out-of-pocket healthcare expenditures globally,
53 at an overwhelming proportion of 90% [6]. Although health insurance can become an important
54 support system for buffering the poor against out-of-pocket payments, so far it covers only 1% of
55 health expenditure in the country [2]. This is because health insurance is mainly used by richer and
56 urban populations.
57 The efficacy and limitations of private providers of health interventions in Pakistan are not clear.
58 One of the few private providers offering health interventions to women employed in the informal
59 sector are microfinance providers (including banks, institutes and non-governmental organisations
60 [NGOs]) [7]. Microfinance providers (MFPs) are mainly operational in under-developed
61 communities, providing loans to the poorest women for small-business development [8]. There are
62 50 MFPs operating in Pakistan, with nearly 40 reporting some form of health intervention for
Page 5 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 5 -
63 clients, including health insurance and health-awareness programmes [9]. The MFPs are regulated
64 either by the State Bank of Pakistan or the Securities Exchange Commission of Pakistan. An
65 inherent function of the original model of microfinance was to catalyse wider social development
66 for women, including improved health behaviour and, therefore, better health-related outcomes
67 [10]. It is in the interests of MFPs to couple health interventions with loan services because healthy
68 clients are more likely to repay loans and run successful businesses [11].
69 The role of microfinance health interventions is critical in countries like Pakistan, where poverty
70 is high and out-of-pocket payments are not possible for impoverished families. Additionally, the
71 public sector does not have a dependable service structure for complete or quality healthcare and
72 universal financial protection for health coverage is absent [4]. More than two million poor women
73 are loan-takers of microfinance in the country [12]. As poor populations do not have the money to
74 take out traditional health insurance, microfinancing for health insurance becomes the only option
75 for them. However, small health insurance schemes have been severely criticised for their minimal
76 impact on clients’ lives due to their minimal coverage and the large burden of disease faced by
77 poor populations [13]. Evidence also suggests that poor populations holding minimal health
78 insurance, in the event of sustaining large healthcare costs, may resort to damaging practices such
79 as reducing household nutrition, removing children from school, and taking out more loans [14].
80 During the most recent times of the coronavirus pandemic, debt-ridden poor women attempting to
81 repay loans are facing even more challenges in generating income from small businesses due to
82 social isolation and lockdown [15]. Therefore, health security is a major concern among female
83 borrowers and there is a need to improve research and policy in order to financially protect poor
84 women and improve their health literacy [16].
85
Page 6 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 6 -
86 Aims of the study
87 To the best of our knowledge, there are no studies that have used female microfinance borrowers
88 as a sample to assess the impact of health interventions on health-related outcomes among poor
89 women [17]. Our objective for this study was to use a sample of female microfinance borrowers,
90 who are availing themselves of health insurance from a private provider, to help identify suitable
91 policies for disease prevention and health promotion in Pakistan. The following research questions
92 are addressed in this study: 1) Do female borrowers of microfinance who are provided with health
93 interventions show improved health-related outcomes? 2) What are the socio-demographic,
94 household, and loan portfolio characteristics of female borrowers of microfinance that are
95 associated with improved health-related outcomes?
96
97 Methods
98 This study is part of a larger, mixed-methods study on the wellbeing of female microfinance
99 borrowers. The qualitative part has already been published [18]. The results presented here are
100 based on a cross-sectional survey, in which women who had been borrowers of microfinance for
101 more than one year were interviewed using a structured, quantitative questionnaire. We used the
102 framework of a quasi-experimental study to estimate the impact of microfinance health
103 interventions. The data was analysed using SPSS and STATA.
104
105 Sampling
106 We used a list available on the Pakistan Microfinance Network to contact the 20 MFPs across
107 Pakistan. Seven MFPs agreed to provide permission to interview their clients. The sampling took
108 place in all four provinces of Pakistan (Punjab, Sindh, Balochistan, and Khyber Pakhtunkhwa
Page 7 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 7 -
109 [KPK]), but not in the two autonomous territories or the federal territory of Islamabad. The
110 sampling frame at the level of individual women took the population weightage of the provinces
111 into account. We were able to contact 500 women randomly, as they visited the MFP offices to
112 make their monthly loan repayment. A final total of 442 women were willing to participate and
113 provided informed written consent, which is a response rate of 88.4%. These women were sampled
114 from seven cities within the four provinces, based on MFP permission and access (Punjab: n=252
115 [cities: Gujranwala, Lahore, Khanewal, Sheikhapura]; Sindh: n=100 [city: Matiari]; Balochistan:
116 n=50 [city: Lasbela]; KPK: n=40 [city: Abbottabad]. Study participants received financial support
117 from the following types of MFPs: four microfinance banks (n=340), one microfinance institute
118 (n=41), one government microfinance scheme (n=50), and one Islamic microfinance organisation
119 (n=11).
120 Information related to the services provided by the sampled MFPs in this study is presented in
121 Table 1. None of the MFPs provide mandatory health insurance schemes. Neither the government
122 scheme nor the Islamic finance provider were offering health insurance, but they were providing
123 health awareness interventions. The government scheme offered a separate health insurance
124 scheme (called the Sehat Sahulat Programme), but none of the study participants was enrolled in
125 this scheme. Women borrowing from banks have the option to take out health insurance for
126 themselves and any family members. They have to pay a premium ranging from PKR 490–990
127 (USD 3.00–6.08)1 per person and are insured only in the event of hospital admission. However,
128 the insurance does not cover hospital costs but instead pays the client the amount of daily wages
129 lost, ranging from PKR 2,000–4,000 (USD 12.28–24.56) daily. The scheme also covers a one-off
130 payment in the event of death, ranging from PKR 25,000–50,000 (USD 153.55–307.10). Female
1 All PKR to USD conversions in this study have made done at the rate of 1 USD = 162.805 PKR.
Page 8 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from
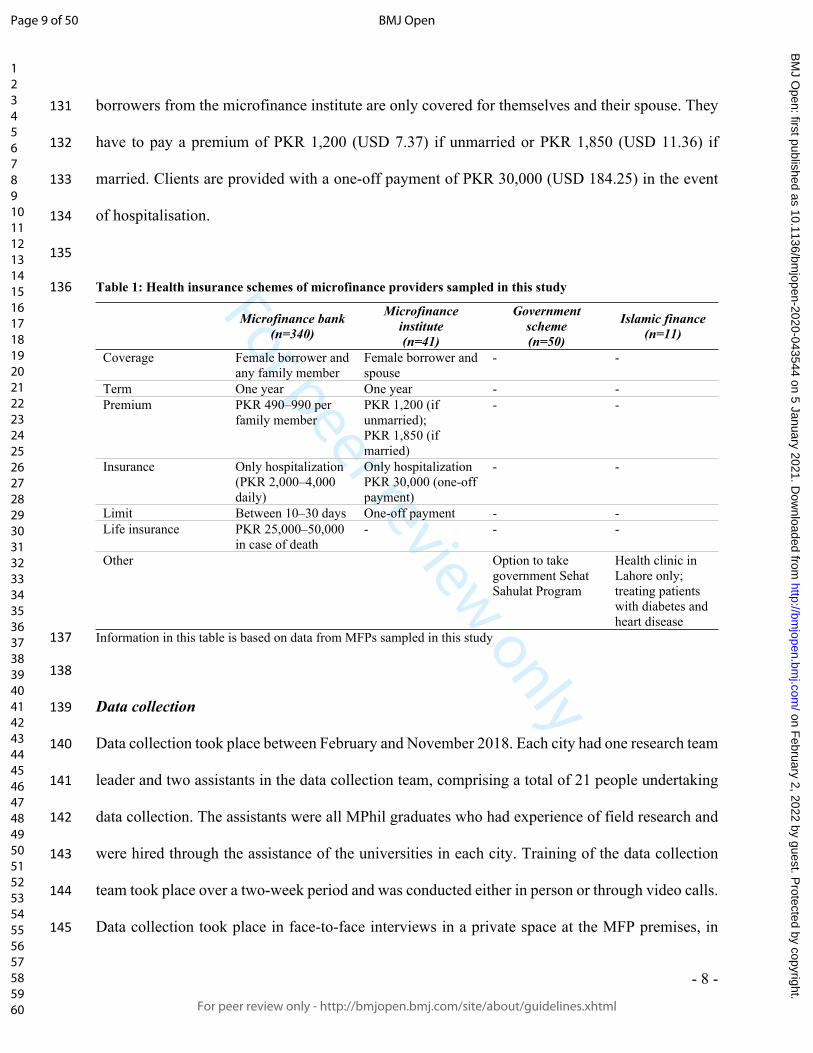
For peer review only
- 8 -
131 borrowers from the microfinance institute are only covered for themselves and their spouse. They
132 have to pay a premium of PKR 1,200 (USD 7.37) if unmarried or PKR 1,850 (USD 11.36) if
133 married. Clients are provided with a one-off payment of PKR 30,000 (USD 184.25) in the event
134 of hospitalisation.
135
136 Table 1: Health insurance schemes of microfinance providers sampled in this study
Microfinance bank(n=340)
Microfinance institute(n=41)
Government scheme(n=50)
Islamic finance(n=11)
Coverage Female borrower and any family member
Female borrower and spouse
- -
Term One year One year - -Premium PKR 490–990 per
family memberPKR 1,200 (if unmarried);PKR 1,850 (if married)
- -
Insurance Only hospitalization(PKR 2,000–4,000 daily)
Only hospitalizationPKR 30,000 (one-off payment)
- -
Limit Between 10–30 days One-off payment - -Life insurance PKR 25,000–50,000
in case of death- - -
Other Option to take government Sehat Sahulat Program
Health clinic in Lahore only; treating patients with diabetes and heart disease
137 Information in this table is based on data from MFPs sampled in this study
138
139 Data collection
140 Data collection took place between February and November 2018. Each city had one research team
141 leader and two assistants in the data collection team, comprising a total of 21 people undertaking
142 data collection. The assistants were all MPhil graduates who had experience of field research and
143 were hired through the assistance of the universities in each city. Training of the data collection
144 team took place over a two-week period and was conducted either in person or through video calls.
145 Data collection took place in face-to-face interviews in a private space at the MFP premises, in
Page 9 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 9 -
146 order to preserve the women’s privacy due to the personal nature of the questions. The structured
147 surveys were completed on behalf of the female respondents with the assistance of the trained
148 research team. During pilot-testing, we utilised both a self-administered and researcher-
149 administered approach, and found that the latter showed lower rates of non-response. This could
150 be due to the length of the questionnaire and the low literacy rate among the interviewed women.
151 Although the questionnaire was translated into Urdu, women having less than eight years of
152 schooling required assistance to read and fill in the questionnaire.
153
154 Measures
155 A structured interview schedule was used for data collection (Supplementary File 1). Questions in
156 this tool were taken from instruments used in various studies, such as the Women’s Healthcare
157 Experiences Survey [19], the Baseline Nutrition and Food Security Survey developed by UNICEF
158 [20], the WHO Multi-Country Study on Women’s Health and Domestic Violence against Women
159 [21], and the WHO Survey on Workplace Violence [22].
160
161 Dependent variables: Health outcomes
162 This study assesses the association of health interventions offered by MFPs with four dependent
163 health-related outcome variables: 1) women perceive health to be good overall, 2) women visited
164 a general practitioner in the last year, 3) women had the ability to purchase prescribed medicine in
165 the last year, and 4) women’s intake of multivitamins has improved in the last year. The four
166 dependent variables were categorised as binominal and coded as either “Yes” (1) or “No” (0).
167
Page 10 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 10 -
168 Independent variables: Socio-demographic and loan characteristics
169 Several socio-demographic variables, such as age (0=less than 30 years; 1=30 years and older),
170 religion (0=Muslim; 1=Other than Muslim), literacy of the female borrower (0=Illiterate;
171 1=Literate), literacy of the spouse (0=Illiterate; 1=Literate), house ownership (0=Yes; 1=No), and
172 number of dependent children living in the house (0=None; 1=One or more) were assessed as
173 confounding variables. It is necessary to control for these variables because they have an impact
174 on each of the dependent variables mentioned above. Province is also controlled because the region
175 is a proxy for socio-cultural norms that would impact upon how women perceive their health and
176 whether they are able to visit a general practitioner or purchase medicine (0=Other than Punjab
177 [Sindh, Balochistan, or KPK]; 1=Punjab).
178 The other set of variables is related to microfinance provider services, such as: loan amount
179 (0=10,000–20,000 PKR; 1=21,000 PKR or more), monthly meetings (0=No; 1=Yes), interest rate,
180 which is the amount charged on top of the principal by a lender to a borrower (0=2.5–10%; 1=11%
181 or more), group loan, meaning that a group of customers are willing to guarantee each other for
182 the repayment of the loan (0=No; 1=Yes), and debt age (0=1–2 years; 1=3 or more years). These
183 have been included because they assess the impact of the provision of non-financial services on
184 each of the dependent variables.
185
186 Independent variables: Health intervention
187 The three independent variables for microfinance health intervention are: 1) receiving health
188 insurance, 2) attended at least one health workshop, and 3) received health-related talks by loan
189 officers. The two independent variables of health workshop and health-related talks by loan
190 officers were compounded to make one variable indicating whether the women had attended a
Page 11 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 11 -
191 health-awareness programme (0=No; 1=Yes). In this way, the control group for the study (T=0)
192 consists of female borrowers who lack the provision of a health intervention, and the treatment
193 group (T=1) includes female borrowers who are receiving a health intervention.
194
195 Comparison group
196 Using a quasi-experimental framework, the study estimates the impact of gaining access to health
197 interventions (health insurance and health-awareness programmes) against the counterfactual of
198 those women who are receiving a loan for small business mobilisation in the absence of health
199 interventions.
200
201 Probit analysis
202 The impacts of health insurance and health-awareness programmes provided by the MFP on the
203 four dependent, health-related variables have first been estimated using a probit estimation for the
204 following linear regression equation:
205 𝑌𝑖 = 𝛽0 + 𝛽1𝑇 + 𝛽2𝑋𝑖 + 𝛽3𝑍𝑖 + 𝛽4𝐿𝑖 + 𝜀𝑖
206 where is the dependent variable measuring the four health-related outcomes. T is the treatment 𝑌𝑖
207 variable (1 if “yes”, and 0 otherwise) measuring the three microfinance health interventions. is 𝑋𝑖
208 a set of socio-demographic characteristics including age, religion, province, and literacy; is a 𝑍𝑖
209 set of household characteristics, including house ownership and number of dependent children
210 living in the house; is a set of loan portfolio characteristics including debt age, group loan, loan 𝐿𝑖
211 amount, interest rate, and monthly meetings; and is the error term. 𝜀𝑖
212
Page 12 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 12 -
213 Propensity score matching
214 We used Propensity Score Matching (PSM) to estimate the unobserved counterfactuals and make
215 an impact analysis of health interventions. PSM is a non-parametric statistical method which
216 matches the treated (those receiving the health intervention) and the controlled on the basis of
217 conditional probability of participation, given the observable characteristics [23]. As we only have
218 cross-sectional data, we can compare the dependent variables related to women’s health in terms
219 of those who have access to non-financial, health-related services provided by the microfinance
220 provider (in this study called the “health-awareness programme”) and those who do not, as long
221 as these services are randomly distributed and there is no selection bias. The estimation of
222 instrumental variables is one technique that is frequently used within PSM. However, these results
223 are only robust if a valid instrument is being used. As it was not easy to find a valid instrument for
224 our study, we used statistical matching, which has also been widely used before [24-26].
225 The study will be using the following functional form:
226 𝑌𝑖 = 𝛽0 + 𝛽1𝑇 + 𝛽1𝑋𝑖 + 𝜀𝑖
227 where is the dependent variable measuring the four health-related outcomes. T is the treatment 𝑌𝑖
228 variable (1 if “yes”, and 0 otherwise) measuring the microfinance health interventions. are the 𝑋𝑖
229 covariates used for matching the data, including age, religion, literacy, spouse’s literacy, house
230 ownership, access to drinking water, access to gutter drainage, access to toilet facility, children,
231 debt age, group loan, loan amount, interest rate, and monthly meetings, and is the error term. 𝜀𝑖
232 These control variables have been used in a large and growing volume of studies [27].
233 Our study satisfies the main conditions of PSM, which are: 1) using a rich set of control variables,
234 which are observable characteristics, 2) using the same survey for treated and control groups, and
235 3) having the same community belonging to the treated and control groups [28]. The PSM model
Page 13 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 13 -
236 constructs a statistical comparison group based on the probability of participating in the treatment
237 T, conditional on observed characteristics, X, or the propensity score:
238 𝑝(𝑋) = 𝑃𝑟(𝑇 = 1│𝑋).
239 where T = {0, 1} is the indicator of exposure to treatment and X is the multidimensional vector of
240 pre-treatment characteristics. Following the estimation of the propensity score, the region for
241 common support is defined as being where distributions of the propensity score for the treatment
242 and comparison group overlap. Observations within the control and treatment group that lie outside
243 the region for common support are eliminated [29]. As PSM is intended to help in identifying the
244 impact of the health intervention, we used the computation of “average treatment effect on the
245 treated” (ATT). We used two matching criteria (Nearest Neighbour Matching [NNM] and Kernel
246 Matching [KM]), to assess statistical significance from different perspectives and to test the
247 robustness of the results [24]. NNM is used to evaluate absolute differences between propensity
248 scores, and KM is used to compare each treated unit to a weighted average of the outcomes of all
249 untreated units.
250
251 Patient and public involvement
252 This research was conducted without the involvement of the public or patients. However, the views
253 of women from this study have been published elsewhere [18].
254
255 Results
256 Sample characteristics
257 All the women in our sample earned less than $4.82 per day and belonged to the poorest stratum
258 of society. They were taking out loans for small business mobilisation in order to improve their
Page 14 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 14 -
259 life opportunities. The majority of the women were Muslim, from Punjab, and illiterate. About
260 three-quarters had been borrowers for more than three years, were attending monthly meetings
261 with loan officers, and were paying interest rates of less than 10%. Out of the 442 female borrowers
262 in the sample, 64.2% (n=284) had taken out health insurance (Table 2) and 71.0% (n=314) had
263 participated in a health-awareness programme by attending a health workshop or receiving health
264 talks by loan officers (Table 3).
265
266 Table 2: Descriptive statistics of women borrowers with regard to health insurance
Variable
Not receiving health insurance
n (%) (n=158)
Receiving health insurance
n (%)(n=284)
Chi-square test1
Age <29 years ≥30 years
86 (54.4%)72 (45.6%)
165 (58.1%)119 (41.9%)
0.557
Religion Muslim Other
137 (86.7%) 21 (13.3%)
254 (89.4%)30 (10.6%)
0.740
Province Punjab Other
62 (39.2%)96 (60.8%)
197 (69.4%)87 (30.6%)
37.977***
Literacy Illiterate Literate
94 (59.5%)64 (40.5%)
195 (68.7%)89 (31.3%)
3.770*
Spouse literacy Illiterate Literate
86 (54.4%)72 (45.6%)
191 (67.3%)93 (32.7%)
7.135**
House ownership Other Owned
104 (65.8%) 54 (34.2%)
225 (79.2%)59 (20.8%)
9.583**
Children None One or more
54 (34.2%)104 (65.8%)
116 (40.8%)168 (59.2%)
1.907
Debt age 1–2 years ≥3 years
71 (44.9%)87 (55.1%)
75 (26.4%)209 (73.6%)
15.755***
Group loan No Yes
91 (57.6%)67 (42.4%)
168 (59.2%)116 (40.8%)
0.102
Loan amount PKR 10,000–20,000 (USD 61.42-122.84) PKR 21,000–100,000 (USD 129.45-616.41)
31 (19.6%)127 (80.4%)
123 (43.3%)161 (56.7%)
25.096***
Interest rate 2.5–10% ≥11%
105 (66.5%)53 (33.5%)
202 (71.7%)82 (28.9%)
1.044
Page 15 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 15 -
Monthly meeting No Yes
41 (25.9%)117 (74.1%)
70 (24.6%)214 (75.4%)
0.091
Overall perceived good health No Yes
120 (75.9%)38 (24.1%)
185 (65.1%)99 (34.9%)
5.545**
Improved ability to visit general practitioner No Yes
67 (42.4%)91 (57.6%)
124 (43.7%)160 (56.3%)
0.065
Improved ability to purchase prescribed medicine No Yes
118 (74.7%)40 (25.3%)
152 (53.5%)132 (46.5%)
19.127***
Improved intake of multivitamins No Yes
120 (75.9%)38 (24.1%)
182 (64.1%)102 (35.9%)
6.6040**
267 1 *** Significant at 1% level, ** Significant at 5% level, * Significant at 10% level268269 Table 3: Descriptive statistics of women borrowers with regard to health awareness
Variable
Not receiving health awareness
n (%)(n=128)
Receiving health awareness
n (%)(n=314)
Chi-square test1
Age <29 years ≥30 years
74 (57.8%)54 (42.2%)
177 (56.4%)137 (43.6%)
0.077
Religion Muslim Other
115 (89.8%)13 (10.2%)
276 (87.9%)38 (12.1%)
0.337
Province Punjab Other
56 (43.8%)72 (56.3%)
203 (64.6%)111 (35.4%)
16.372***
Literacy Illiterate Literate
70 (54.7%)58 (45.3%)
219 (69.7%)95 (30.3%)
9.109**
Spouse literacy Illiterate Literate
78 (60.9%)50 (39.1%)
199 (63.4%)115 (36.6%)
0.231
House ownership Other Owned
96 (75.0%)32 (25.0%)
233 (74.2%)81 (25.8%)
0.030
Children None One or more
49 (38.3%)79 (61.7%)
121 (38.5%)193 (61.5%)
0.002
Debt age 1–2 years ≥3 years
63 (49.2%)65 (50.8%)
83 (26.4%)231 (73.6%)
21.342***
Group loan No Yes
86 (67.2%)42 (32.8%)
173 (55.1%)141 (44.9%)
5.480**
Loan amount PKR 10,000–20,000 (USD 61.42-122.84) PKR 21,000–100,000 (USD 129.45-616.41)
33 (25.8%)95 (74.2%)
121 (38.5%)193 (61.5%)
6.515**
Interest rate 2.5–10% 70 (54.7%) 237 (75.5%) 18.527***
Page 16 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 16 -
≥11% 58 (45.3%) 77 (24.5%)Monthly meeting No Yes
38 (29.7%)90 (70.3%)
73 (23.2%)241 (76.8%)
2.005
Overall perceived good health No Yes
89 (69.5%)39 (30.5%)
216 (68.8%)98 (31.2%)
0.023
Improved ability to visit general practitioner No Yes
64 (50.0%)64 (50.0%)
127 (40.4%)187 (59.6%)
3.383*
Improved ability to purchase prescribed medicine No Yes
95 (74.2%)33 (25.8%)
175 (55.7%)139 (44.3%)
13.073***
Improved intake of multivitamins No Yes
88 (68.8%)40 (31.3%)
214 (68.2%)100 (31.8%)
0.015
270
271 Determinants of health-related outcomes after the health insurance intervention
272 Table 4 presents the determinants of health-related outcomes for recipients of health insurance.
273 Overall, perceived good health was significantly associated with group borrowers, small loan
274 amounts, and lower interest rates. Improved ability to visit a general practitioner shows a positive
275 correlation with female borrowers from Punjab province, who attending monthly meetings, had a
276 group loan, and a smaller loan amount. Women had a significantly improved ability to purchase
277 prescribed medicine when they were from Punjab, took out smaller loans, and owned a house. The
278 uptake of multivitamins was increased among women with smaller loans, who owned a house, had
279 been borrowers for no longer than two years, and were attending monthly meetings. Therefore,
280 only a small loan amount was a significant determinant in all four health-related outcomes among
281 recipients of health insurance.
282
Page 17 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 17 -
283 Table 4: Probit analysis on determinants of health-related outcomes among recipients of health insurance
Overall perceivedgood health
Improved ability to visit general practitioner
Improved ability to purchase prescribed
medicine
Improvedmultivitamin
uptake
Coeff. Z-Score Coeff. Z-
Score Coeff. Z-Score Coeff. Z-
ScoreAge -0.2588 -1.43 0.2754 1.39 -0.2915 -1.51 0.0703 0.36Religion 0.4079 1.37 -0.2711 -0.97 0.4165 1.46 -0.0102 -0.03Province -0.2676 -1.04 0.9990*** 4.05 1.043*** 4.21 0.0315 0.12Literacy -0.0999 -0.49 0.2018 0.96 0.0828 0.42 0.1994 0.98Spouse literacy 0.2410 1.18 0.1779 0.85 0.2424 1.20 0.1323 0.64House ownership 0.1550 0.69 -0.3397 -1.45 -0.6825** -2.65 -0.5699** -2.17Children 0.2094 1.15 0.2213 1.20 0.1530 0.85 0.2829 1.54Debt age -0.4130 -0.16 0.1650 0.63 0.3807 1.50 -0.6088** -2.41Group loan 0.8582*** 3.76 0.4813** 2.25 0.1567 0.73 -0.3705* -1.69Loan amount -0.7765*** -3.27 -0.8863** -3.50 -1.2028*** -5.05 -1.9933*** -4.13Interest rate 0.7250** 2.94 0.2777 1.12 -0.0691 -0.28 0.2345 0.98Monthly meetings 0.1370 0.61 0.7753*** 3.58 0.0166 0.08 -0.4233* -1.84No. of observationsWald Chi2
Prob> Chi2
Log likelihood
28442.740.0001
-158.6116
28476.930.0000
-146.0385
28464.570.0000
-157.5241
28453.150.0000
-153.7125284 *** Significant at 1% level, ** Significant at 5% level, * Significant at 10% level
285
286 Determinants of health-related outcomes after the health-awareness intervention
287 In Table 5, the determinants for all four health-related outcomes among recipients of a health-
288 awareness programme are presented. Women with the following characteristics have a greater
289 probability of overall perceived good health: group borrowers, smaller loans, lower interest rates,
290 younger women, and those with literate spouses. The ability to visit a general practitioner for
291 regular check-ups during the previous year was higher among women from Punjab province, with
292 smaller loans, attending monthly meetings, above 29 years of age, and who were non-Muslim.
293 Similarly, women from Punjab province, having smaller loans, owning their house, and younger
294 women had a higher probability of improved ability to purchase prescribed medicine. The
295 probability of increased uptake of multivitamins was greater in women who took out smaller loans,
296 had not been in debt for more than two years, were group borrowers, and who attended monthly
Page 18 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 18 -
297 meetings. The only variable that was significantly associated with all four health-related outcomes
298 among recipients of a health-awareness programme was the small loan amount.
299
300 Table 5: Probit analysis on determinants of health-related outcomes among recipients of health awareness 301 programs
Overall perceivedgood health
Improved ability to visit general practitioner
Improved ability to purchase prescribed
medicine
Improvedmultivitamin
uptake
Coeff. Z-Score Coeff. Z-
Score Coeff. Z-Score Coeff. Z-
ScoreAge -0.3747* -1.70 0.3781* 1.70 -0.4329* -2.02 0.1058 0.48Religion 0.5185 1.59 -0.5503* -1.76 0.3880 1.24 0.1904 0.56Province -0.3898 -1.24 1.3048*** 4.39 1.029*** 3.83 0.1983 0.65Literacy -0.1537 -0.65 0.2229 0.91 0.1405 0.61 0.3411 1.43Spouse literacy 0.4163* 1.80 0.2546 1.09 0.0860 0.38 0.2310 1.00House ownership 0.3495 1.42 -0.2453 -0.96 -0.6360** -2.48 -0.4271 -1.54Children 0.3209 1.55 0.2765 1.33 0.2424 1.21 0.2833 1.36Debt age -0.0066 -0.02 0.4529 1.49 0.3817 1.36 -0.7164** -2.51Group loan 0.8817*** 3.33 0.3640 1.51 0.1030 0.43 -0.6352** -2.55Loan amount -0.7199** -2.65 -0.6511** -2.28 -1.9361*** -3.52 -0.9170*** -3.35Interest rate 0.6739** 2.23 0.3860 1.28 0.2428 0.83 0.3726 1.26Monthly meetings 0.2357 0.88 0.7689** 3.08 -0.0556 -0.22 -0.5816** -2.10No. of observationsWald Chi2
Prob> Chi2
Log likelihood
31435.680.0004
-126.4054
31464.570.0000
-116.6811
31453.250.0000
-128.2105
31448.790.0000
-121.2616302 *** Significant at 1% level, ** Significant at 5% level, * Significant at 10% level303
304 Balancing covariates and common support diagnostics
305 Figure 1(a) exhibits the Kernel Density graphs for the propensity score of treated and control
306 groups before matching, while Figure 1(b) exhibits it after matching. It can be clearly seen that the
307 kernel densities are significantly overlapping in the latter, indicating that the treatment and control
308 groups have a comparable propensity score as estimated using the covariates. A similar
309 comparison of treatment and control groups can be observed in Figures 2(a) and 2(b) using
310 histograms.
Page 19 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 19 -
311 Figures 3(a) and 3(b) exhibit the common support between the control and treatment groups. While
312 in Figure 3(a) we can see that certain observations in the treated group are not matched, in Figure
313 3(b) all the observations in the treated and control groups are successfully matched.
314 The balancing of covariates can also be observed using standardised mean difference and ratio of
315 variances. Table 6 gives the standardised mean difference and ratio of variances for the control
316 and treatment groups before and after matching. It can be observed that the standardised mean
317 difference in the matched sample is much improved and close to zero for all covariates. The ratio
318 of variances is approximately equal to one in the matched sample for all covariates except monthly
319 meetings. Using these diagnostics, we can infer that the sample has matched well using propensity
320 score matching.
321
322 Table 6:Balancing of covariates using standardized mean difference and ratio of variances
Standardized differences Variance ratioRaw Matched Raw Matched
Age -0.1320698 -0.1058939 0.9619896 0.9611875Religion 0.1586396 -0.0071039 1.451878 0.9828996Literacy -0.3073917 -0.1159204 0.7931779 0.9171598Spouse literacy -0.0719588 0.027969 0.9641836 1.014213Earning month -0.0491266 0.0305069 1.129418 0.9202911House ownership 0.2189877 0.1585524 0.7669609 0.8061959Drinking water 0.2226595 0.0116275 0.6952835 0.9813404Toilet Facility 0.0445714 0.1247478 0.9471727 0.8276644Gutter drainage -0.0290293 0.0423519 1.035531 0.9496166Group loan 0.0250079 0.0549512 1.01166 1.017812Loan amount -0.6030964 -0.1454947 1.331749 1.081931Interest rate -0.0851667 0.0594108 1.075376 0.9483068Monthly meetings 0.5404452 0.337374 0.4480249 0.6085328
323
324 Impact of the interventions on health-related outcomes
325 The descriptive statistics for comparison between control and treatment group for health insurance
326 (Supplementary Table 1) and the health-awareness programme (Supplementary Table 2), before
Page 20 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from
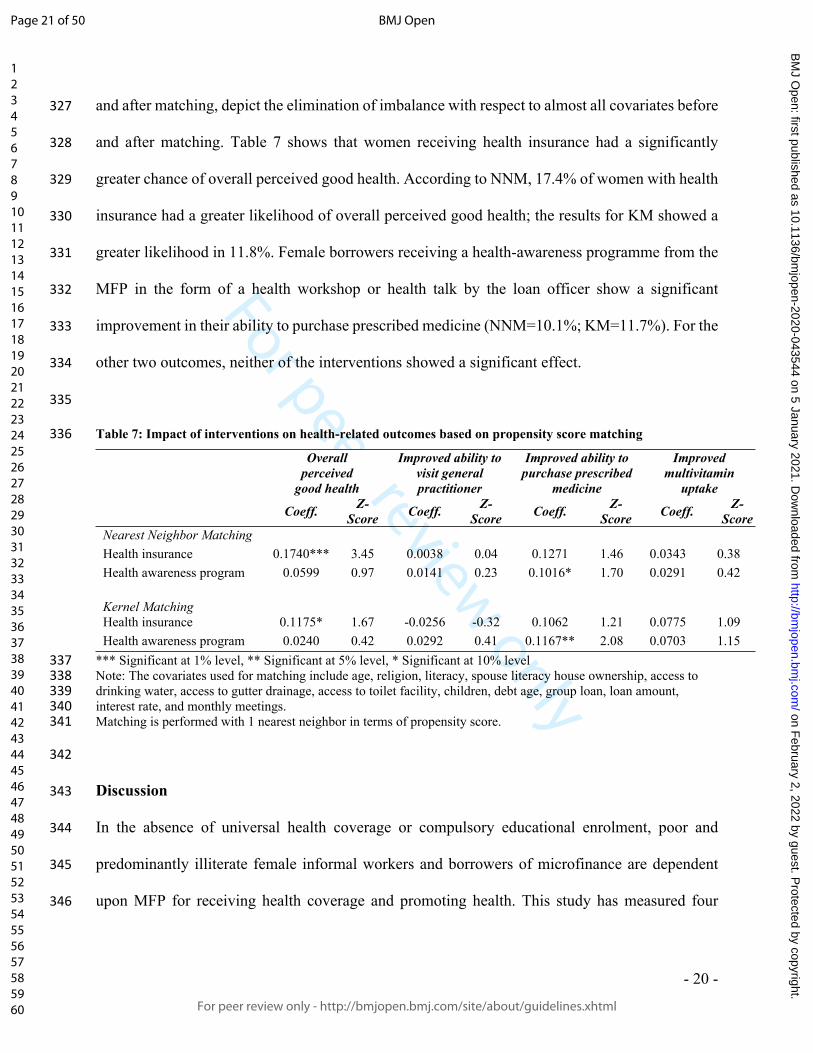
For peer review only
- 20 -
327 and after matching, depict the elimination of imbalance with respect to almost all covariates before
328 and after matching. Table 7 shows that women receiving health insurance had a significantly
329 greater chance of overall perceived good health. According to NNM, 17.4% of women with health
330 insurance had a greater likelihood of overall perceived good health; the results for KM showed a
331 greater likelihood in 11.8%. Female borrowers receiving a health-awareness programme from the
332 MFP in the form of a health workshop or health talk by the loan officer show a significant
333 improvement in their ability to purchase prescribed medicine (NNM=10.1%; KM=11.7%). For the
334 other two outcomes, neither of the interventions showed a significant effect.
335
336 Table 7: Impact of interventions on health-related outcomes based on propensity score matching
Overallperceived
good health
Improved ability to visit general practitioner
Improved ability to purchase prescribed
medicine
Improved multivitamin
uptake
Coeff. Z-Score Coeff. Z-
Score Coeff. Z-Score Coeff. Z-
ScoreNearest Neighbor MatchingHealth insurance 0.1740*** 3.45 0.0038 0.04 0.1271 1.46 0.0343 0.38Health awareness program 0.0599 0.97 0.0141 0.23 0.1016* 1.70 0.0291 0.42
Kernel MatchingHealth insurance 0.1175* 1.67 -0.0256 -0.32 0.1062 1.21 0.0775 1.09Health awareness program 0.0240 0.42 0.0292 0.41 0.1167** 2.08 0.0703 1.15
337 *** Significant at 1% level, ** Significant at 5% level, * Significant at 10% level338 Note: The covariates used for matching include age, religion, literacy, spouse literacy house ownership, access to 339 drinking water, access to gutter drainage, access to toilet facility, children, debt age, group loan, loan amount, 340 interest rate, and monthly meetings. 341 Matching is performed with 1 nearest neighbor in terms of propensity score.
342
343 Discussion
344 In the absence of universal health coverage or compulsory educational enrolment, poor and
345 predominantly illiterate female informal workers and borrowers of microfinance are dependent
346 upon MFP for receiving health coverage and promoting health. This study has measured four
Page 21 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 21 -
347 health-related outcomes in female borrowers. The results show that there is inequity in the uptake
348 of health insurance and health-related outcomes.
349 Women from Punjab have better health-related outcomes compared to women from Sindh,
350 Balochistan and KPK. National health surveys of Pakistan also report that Punjab has better health-
351 related outcomes compared to other provinces, because the provincial government of Punjab has
352 a greater budget allocation for running health-awareness campaigns [30]. The fact that our results
353 show that older women and non-Muslim women have a greater likelihood of improved ability to
354 visit a general practitioner after receiving a health-awareness intervention indicates that younger
355 Muslim women face barriers to healthcare access due to regressive norms [31]. Muslim families
356 are known to prevent fertile women from accessing healthcare in an attempt to control their
357 reproductive choices and health options. Our results align with other research, which suggests that
358 Muslims suffer from health disparities due to religious fallacies [32].
359 Conversely, younger women show better overall perceived health and ability to purchase
360 prescribed medicine. This may be because at a younger age fewer health issues occur, and also
361 because of greater state and NGO efforts directed towards maternal healthcare [33]. Our results
362 confirm that women under the age of 29 years receive privileged support in a patriarchal society
363 during their prime childbearing years to consume maternal-health-related medication [34]. Women
364 with literate spouses also show improvements in overall general health after receiving health
365 insurance. This may be because spouse literacy has a direct effect on women’s improved healthcare
366 behaviour and mental health [35].
367 Women who take out their loan in groups show better health-related outcomes compared to women
368 who are single borrowers. Our results suggest that women in groups share their healthcare
369 knowledge and encourage each other towards improved healthcare behaviour [36]. Similarly,
Page 22 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 22 -
370 women who attend monthly meetings with loan officers have better health-related outcomes. The
371 results suggest that caring loan officers are fulfilling an important responsibility in supporting
372 female borrowers to engage in improved health behaviour and health-related outcomes. Given the
373 conservative culture of Pakistan and the disadvantaged backgrounds of these female borrowers,
374 loan-taking women might not be able to utilise healthcare services due to issues of permission or
375 ignorance.
376 Women who receive smaller microfinance loans and do not have a long debt age show improved
377 health-related outcomes. The finding that only women who receive smaller loans show
378 significantly better health-related outcomes may be seen as an endogenous result (i.e., because
379 individuals who need only a small loan may be better off to start with in terms of health), and
380 difficult to interpret in terms of causality, given the cross-sectional nature of the data. However,
381 we have only sampled women from the poorest stratum, and they have taken out small loans
382 because they are not eligible for bigger loans. Therefore, one can expect that there is no association
383 between health condition at the time of loan-taking and the loan amount.
384 Furthermore, the finding related to debt age suggests that women with a debt burden over a longer
385 period of time may be suffering from debt fatigue, which is converting to declining health-related
386 outcomes [37]. Women and their families who own their houses also have better health-related
387 outcomes, specifically related to the ability to visit general practitioners and improved uptake of
388 multivitamins. The results imply that the provision of health insurance and not having to pay
389 household rents on a monthly basis translates into better health-related outcomes. Impoverished
390 families who have to pay high rents for accommodation are usually employed in multiple jobs and
391 have little time for health and wellbeing [38].
Page 23 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from
For peer review only
- 23 -
392 The impact of microfinance is only visible on two health-related variables. Although there are no
393 effects on general practitioner visits or uptake of multivitamins, we found that microfinance health
394 insurance has an impact by creating an improved perception of general health. This shows that
395 being insured is an emotional support and wellbeing facilitator for poor women. The emotional
396 buttress provided by health insurance can go a long way towards improving perceived wellbeing,
397 which can translate into a greater commitment to self, family, and business development among
398 poor women from disadvantaged backgrounds [39]. In addition, microfinance health-awareness
399 interventions have an impact by improving the purchase of prescribed medicine. Many poor
400 women in Pakistan do not take prescribed medicine unless it is freely available due to the greater
401 need to prioritise the purchase of basic necessities and household consumption [40]. The impact
402 of microfinance interventions is comparable to previous research. A review highlighted that most
403 interventions combined microfinance with health education. However, positive effects were
404 mainly found for health knowledge and behaviour, but not health status [41]. A meta-analysis
405 indicated the potential for women and girls, because microfinance may lead to changes in the use
406 of contraceptives, strengthen female empowerment and improve children’s nutrition [42].
407 However, for female borrowers of microfinance, there might be additional burdens in the form of
408 loan repayments and small-business investment. Our results suggest that illiterate and poor women
409 in the country are benefiting from health awareness by recognising that if they do not consume
410 prescribed medicine for chronic ailments (heart disease, cholesterol, or diabetes) it can have
411 serious consequences for their own lives and the future livelihood of their families. There needs to
412 be an urgent recognition that a triadic health insurance safety net is necessary, instead of
413 dependency on private providers to protect informal working women in Pakistan. Employers and
414 the government must join forces to ensure universal health insurance and – particularly in these
Page 24 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 24 -
415 times of the coronavirus pandemic – infectious disease outbreak insurance for health emergencies.
416 State financing of healthcare is essential through an increased allocation of gross domestic product
417 (GDP), government-run business profits, and increasing the income and corporate tax base from
418 the elite.
419 With regard to female microfinance borrowers, we recommend microfinance regulatory bodies to
420 urgently legislate the following reforms: (i) coverage for children and other dependents, maternity
421 costs, and non-hospitalisation costs, (ii) expand coverage for religious and ethnic minorities, (iii)
422 reduce interest rates for those paying high housing rents and introduce home ownership loans, (iv)
423 introduce mandatory group borrowing and monthly meetings with loan officers, and (iv) alter
424 repayment timelines and interest-rate packages for women taking out bigger loans.
425 We recommend the following urgent social policy improvements, which would join in helping
426 health policy efforts: (i) the development of public primary healthcare services for women in the
427 communities, with a mandatory quarterly general practitioner meeting, (ii) the upgrading of
428 poverty alleviation programmes to support poor women, (iii) the capping of housing rents and
429 improvements in neighbourhood sanitation to curb infection, (iv) the advancement of home-based
430 business opportunities for informal female workers to assist in maintaining incomes, including
431 digitalisation and internet access in their homes, and (v) income supplementation and cash
432 transfers for multivitamins and food nutritional intake to improve overall immunity and health
433 [43].
434
435 Limitations
436 This study has some limitations, most importantly the cross-sectional design. Although we were
437 able to compare the effects of an intervention because of the quasi-experimental analysis
Page 25 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 25 -
438 framework, two-group cross-sectional designs suffer from the limitations related to a single
439 measurement for all subjects. Therefore, within-person changes over time are not observable.
440 Without repeated measures in a two-group design, causality cannot be identified, because temporal
441 sequencing on the intervention and outcomes cannot be established. For that reason, we
442 recommend longitudinal data collection in future studies. This study focused on comparatively
443 small loans. Therefore, the impact of larger loans (> PKR 100,000) on health is not known.
444 Furthermore, the results need to be interpreted with caution, because the four health-related
445 outcomes are non-homogeneous and dependent on socio-environmental factors that are specific to
446 the region and community where the interventions are taking place. In addition, outcome data are
447 based on self-reporting, which can lead to potential measurement errors. Despite these limitations,
448 we feel that this study is significant for the development of microfinance health services in Pakistan
449 and the role of state and interest-free microfinance health interventions.
450
451 Conclusion
452 It is critical to assess the health needs of women employed in the informal sector. As primary
453 caregivers at home as well as primary contributors to household income, women’s health assumes
454 a salience that could place the structures of both the family and the economy at risk. Health policy
455 must consider several social policies for protecting disadvantaged women, who are poverty-ridden,
456 illiterate or semi-literate, and loan takers. Health insurance schemes and health promotion in the
457 workplace must be made mandatory for employers, microfinance providers, and the government,
458 given the cultural barriers to uptake for women. Targeting improved equity across female
459 population groups for health interventions will in the long run improve women’s health, capacity
460 expansion and income-earning abilities.
Page 26 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 26 -
461 Designing and implementing a health and social policy protection net for female informal workers
462 requires empirical evidence regarding which health interventions and socio-demographic
463 characteristics impact upon health outcomes. Since public-sector and health-sector shortages and
464 inefficiencies are a concern in Pakistan, the ‘health card’ must be accepted in both the private and
465 public sector, whichever is able to serve the poor first. As Pakistan is struggling with a low GDP
466 and tax collection base, we recommend more research into options for social franchising, and
467 partnerships with independent health insurance companies to serve disadvantaged women.
468
469 Acknowledgements
470 We thank the female borrowers who consented and gave their time to participate in the study. We
471 are grateful to our research team members in charge of logistical planning and coordination for
472 data collection across Pakistan including Rizwan Haider and Amir Naseem. Individual data
473 collection heads for each city are thanked for their efforts, especially for resolving gate keeping
474 issues, including Nida Abbas (Lahore), Zainab Asif (Abbotabad), Hina Bukhari (Gujranwala),
475 Sadia BiBi (Khanewal), Ansari Abbass (Sheikhapura), Azra Shakeel and Shumaila Sadique
476 (Matari), and Javaria Imran (Lasbela). The research assistant Bilal Asghar is also thanked for
477 entering all data.
478 We acknowledge support from the German Research Foundation (DFG) and the Open Access
479 Publication Fund of Charité – Universitätsmedizin Berlin.
480
481 Competing interests
482 The authors declare that no competing interests exist.
483
484 Funding
485 This study received funding by the Office of Research, Innovation and Commercialization at
486 Forman Christian College. The grant number is IRB-180/04-2017. The funding body was not
487 involved in data collection, data analysis, or data interpretation and presentation.
488
Page 27 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 27 -
489 Data sharing
490 Data is available upon reasonable request from the corresponding author.
491
492 Ethical considerations
493 Ethical approval for this study was taken from the Institutional Review Board of the Forman
494 Christian College University. Study participants were informed about the aims of the study and
495 provided informed consent either in written form or through thumb impression.
496
497 Author’s contributions
498 SRJ designed the study and was responsible for the research project, including data collection and
499 analysis; FF supervised this process. HA and MM supported in data collection. RZ and FF
500 contributed to the interpretation of the data. SRJ drafted the manuscript; all authors revised it
501 critically for important intellectual content. All authors approved the final version of this
502 manuscript.
503
504 References
505
506 1. United Nations Pakistan. One United Nations Programme III 2018-2022. United Nations
507 Sustainable Development Framework for Pakistan; 2018.
508 2. Malik MA. Universal health coverage assessment Pakistan. Karachi: Aga Khan University;
509 2015.
510 3. Nishtar S. Choked pipes: reforming Pakistan’s mixed health system: Oxford University
511 Press Karachi; 2010.
512 4. Nishtar S, Bhutta ZA, Jafar TH, et al. Health reform in Pakistan: a call to action. Lancet
513 2013;381(9885):2291–7.
514 5. Nishtar S, Boerma T, Amjad S, et al. Pakistan’s health system: performance and prospects
515 after the 18th Constitutional Amendment. Lancet 2013;381(9884):2193–206.
516 6. Pakistan Bureau of Statistics. Pakistan National Health Accounts 2013-14. Islamabad:
517 Pakistan Bureau of Statistics; 2014.
518 7. Garikipati S, Johnson S, Guérin I, Szafarz A. Microfinance and gender: Issues, challenges
519 and the road ahead. The Journal of Development Studies 2017;53(5):641–8.
Page 28 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 28 -
520 8. Salim MM. Revealed objective functions of microfinance institutions: evidence from
521 Bangladesh. Journal of Development Economics 2013;104:34–55.
522 9. Saba A, Saquiba A. Conceptualizing Health and Microfinance Nexus in Pakistan; 2017.
523 URL: http://www.pmn.org.pk/assets/articles/69106cec5d4f0132b45673990ab4622d.pdf
524 (accessed August 1, 2020).
525 10. Al-Shami SSA, Majid IBA, Rashid NA, Hamid MSRBA. Conceptual framework: The role
526 of microfinance on the wellbeing of poor people cases studies from Malaysia and Yemen.
527 Asian Social Science 2014;10(1):230.
528 11. Leatherman S, Dunford C. Linking health to microfinance to reduce poverty. Bull World
529 Health Organ 2010;88(6):470-1.
530 12. Zulfiqar G. Does microfinance enhance gender equity in access to finance? Evidence from
531 Pakistan. Feminist Economics 2017;23(1):160–85.
532 13. Escobar M-L, Griffin CC, Shaw RP. The impact of health insurance in low-and middle-
533 income countries. Brookings Institution Press; 2011.
534 14. Heltberg R, del Ninno C, Dorosh P, et al. Social protection in Pakistan: Managing
535 household risks and vulnerability. Washington, DC: Human Development Unit, South Asia
536 Region, World Bank; 2007.
537 15. Malik K, Meki M, Morduch J, Ogden T, Quinn S, Said F. COVID-19 and the Future of
538 Microfinance: Evidence and Insights from Pakistan. Oxford Review of Economic Policy;
539 2020
540 16. Mersland R, Strøm RØ. Microfinance: Costs, lending rates, and profitability. In: Caprio G,
541 Arner DW, Beck T, et al., eds. Handbook of key global financial markets, institutions, and
542 infrastructure. London: Academic Press 2016:489–99.
543 17. O’Malley T, Burke J. A systematic review of microfinance and women’s health literature:
544 Directions for future research. Global Pub Health 2017;12(11):1433–60.
545 18. Jafree SR, Mustafa M. The triple burden of disease, destitution, and debt: Small business-
546 women’s voices about health challenges after becoming debt-ridden. Health Care Women
547 Int Published Online First: 30 January 2020. doi: 10.1080/07399332.2020.1716236.
548 19. Women’s and Children’s Health Policy Center. Women’s Health Care Experiences Survey.
549 Baltimore: Hopkins University Bloomberg School of Public Health; 2000.
Page 29 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 29 -
550 20. Quinn VJ, Kennedy E. Food security and nutrition monitoring systems in Africa: A review
551 of country experiences and lessons learned. Food Policy 1994;19(3):234–54.
552 21. World Health Organization. WHO multi-country study on women's health and domestic
553 violence against women: summary report of initial results on prevalence, health outcomes
554 and women's responses. Geneva: World Health Organization; 2005.
555 22. Di Martino V. Relationship between work stress and workplace violence in the health
556 sector. Geneva: World Health Organization; 2003.
557 23. Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies
558 for causal effects. Biometrika 1983;70(1):41–55.
559 24. Becker SO, Ichino A. Estimation of average treatment effects based on propensity scores.
560 The Stata Journal 2002;2(4):358–77.
561 25. Dehejia R. Practical propensity score matching: a reply to Smith and Todd. Journal of
562 Econometrics 2005;125(1-2):355–64.
563 26. Dehejia RH, Wahba S. Propensity score-matching methods for nonexperimental causal
564 studies. Review of Economics and Statistics 2002;84(1):151–61.
565 27. Thuong NTT. Impact of health insurance on healthcare utilisation patterns in Vietnam: a
566 survey-based analysis with propensity score matching method. BMJ Open
567 2020;10:e040062.
568 28. Abadie A, Imbens GW. Matching on the estimated propensity score. Econometrica
569 2016;84(2):781–807.
570 29. Caliendo M, Kopeinig S. Some practical guidance for the implementation of propensity
571 score matching. Journal of Economic Surveys 2008;22(1):31–72.
572 30. Akram M, Khan FJ. Health care services and government spending in Pakistan. PIDE-
573 Working Papers 32. Pakistan Institute of Development Economics.
574 31. Mumtaz Z, Salway S. ‘I never go anywhere’: extricating the links between women's
575 mobility and uptake of reproductive health services in Pakistan. Soc Sci Med
576 2005;60(8):1751–65.
577 32. Padela AI, Zaidi D. The Islamic tradition and health inequities: A preliminary conceptual
578 model based on a systematic literature review of Muslim health-care disparities. Avicenna
579 J Med 2018;8(1):1–13.
Page 30 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
- 30 -
580 33. Bhutta ZA, Hafeez A, Rizvi A, et al. Reproductive, maternal, newborn, and child health in
581 Pakistan: challenges and opportunities. Lancet 2013;381(9884):2207–18.
582 34. Hafeez A, Mohamud BK, Shiekh MR, Shah SAI, Jooma R. Lady health workers
583 programme in Pakistan: challenges, achievements and the way forward. Journal of the
584 Pakistan Medical Association 2011;61(3):210.
585 35. Hamid SA, Roberts J, Mosley P. Evaluating the health effects of micro health insurance
586 placement: Evidence from Bangladesh. World Development 2011;39(3):399–411.
587 36. Prost A, Colbourn T, Seward N, et al. Women’s groups practising participatory learning
588 and action to improve maternal and newborn health in low-resource settings: a systematic
589 review and meta-analysis. Lancet 2013;381(9879):1736–46.
590 37. Jacoby MB. Does indebtedness influence health? A preliminary inquiry. The Journal of
591 Law, Medicine & Ethics 2002;30(4):560–71.
592 38. Taylor L. Housing and Health: An Overview Of The Literature. Health Affairs Health
593 Policy Brief. 7 June 2019. doi: 10.1377/hpb20180313.396577.
594 39. Bauhoff S, Hotchkiss DR, Smith O. The impact of medical insurance for the poor in
595 Georgia: a regression discontinuity approach. Health Economics 2011;20(11):1362–78.
596 40. Zaidi S, Bigdeli M, Aleem N, Rashidian A. Access to essential medicines in Pakistan:
597 policy and health systems research concerns. PloS One 2013;8(5):e63515.
598 41. Lorenzetti LMJ. Evaluating the effect of integrated microfinance and health interventions:
599 an updated review of the evidence. Health Policy Plan 2017;32(5):732–56.
600 42. Gichuru W, Ojha S, Smith S, Smyth AR, Szatkowski L. Is microfinance associated with
601 changes in women's well-being and children's nutrition? A systematic review and meta-
602 analysis. BMJ Open 2019;9(1):e023658.
603 43. Saha S. Provision of health services for microfinance clients: Analysis of evidence from
604 India. International Journal of Medicine and Public Health 2011;1(1):1–5.
Page 31 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Figure 1: Kernel Density balancing plot (a) before and (b) after matching
255x104mm (144 x 144 DPI)
Page 32 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Figure 2: Density balancing plot (a) before and (b) after matching
256x106mm (144 x 144 DPI)
Page 33 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Figure 3: Common support graph of propensity scores (a) before and (b) after matching
256x104mm (144 x 144 DPI)
Page 34 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Relationship between Microfinance, Social Development and Women’s Health
Cover Letter for Participants Questionnaire Information for Women Microfinance Borrowers Researcher: Dr. Sara Rizvi Jafree, e-mail: [email protected]; 0300 400 5740
Thank you for your valuable time! Your name is not required and all research analysis will be undertaken with confidentiality and complete anonymity. At any point during the interview you may leave, if you wish to do so. (Translation in Roman Urdu: Apka Bohat Shukirya apke eemtay waat ke liye! Apke Nam Ka Bharna Zaruri Nahi Hai Aur Yeh Tehkeek Ko Khoofiya Rakha Jaye Ga. Interview ke doran ap kabhi bhi uth ke jaana chahey to apko puri ijazat hai.) The questionnaire has been designed to collect information about your loan portfolio and your self-rated health. Our aim is to understand your needs and challenges, and ultimately try to improve your loan portfolio and health access and services. ((Translation in Roman Urdu: Is questionnaire Ka Masad Hai ke apse chand sawal loan aur sehat ke bare mein puchna. Humara masad ye hai ke apke arze ki sahuliyat aur sehat dono ko behtar kiya jaye.) Your honest and reliable answers will be appreciated, so that we can recommend the best solutions with regard to optimal loan portfolios and health satisfaction. ((Translation in Roman Urdu: Apke Sache Aur Ba Aitibar Jawab Ke Shukarguzar Honge, Thake loan aur sehat ke hawale se hum apke mushkilay ya rukawaton ko Samajh Sake.) In the event that you feel disturbed or upset after answering questions or recalling memories related to health problems or experiences of violence/ harassment, you may call or text the researcher for free consultation services from trained female psychologists. ((Translation in Roman Urdu: Agar apko in sawal aur jawab ki wajeh se koi preshani ho ya koi aisa waiya yad a jaye jo apki zehni pareshani mein izafa kare, tho ap upar diye gaye number par call ya text kar ke rabta kar le. Hum apki muft mein madat zanana mahir-e-nafsiyat se karwayenge.)
Page 35 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Instrument The questionnaire will be read out and completed by the researcher, on behalf of the participant. Province/City: ____________________________ Microfinance Provider:________________________ Area/locality: Participant Code:
SECTION A: SOCIO-DEMOGRAPHIC CHARACHTERISTICS
Code Entry
Q1.Age Umar?
1.20-29 2.30-39 3.40-49 4.50+
Q2.Religion Mazhab
1.Muslim 2.Christian 3.Hindu 4.Other
Q3.Province Sooba?
1.Punjabi 2.Sindhi 3.Baluchi 4.KPK
Q4.City Shehr?
1.Lahore 2.Islamabad
3.Karachi 4.Hyderabad
1.Quetta 1.Peshawar
Q5.City-Area Q6.Language spoken at home with family Madri zubaan?
Q7.Race (β) Zaat
Q8.Marital Status Kya ap shadi shuda hain?
1.Married 2.Single 3.Divorced 4.Seperated
Q9.Literacy Taleem-i-qabiliyat
1.None 2.Primary 3.Secondary 4.Graduate
Q10.Occupation Pesha
Q10.Spouse literacy Aapkay khaawand ki taleemi qabiliyat kya hai?
1.None 2.Primary 3.Secondary 4.Graduate
Q12.Spouse Occupation Apkay khawand ka pesha kya hai?
Q13.Your earning in last month Pichlay mahinay aap ki kamai kitni thi?
1.Less than 5k 2.>5k-10k 2.>10k-20k 4.Other
Q14.Your earning in last year Pichlay saal apki kitni kamai thi?
1.Less than 50k 2.>50k-70k 2.>70k-90k 4.Other
Q15.Combined household income in a month (on average) Tamaam ghar ki amdani kitni hai?
1.Less than 10k 2.>10k-15k 2.>15k-20k 4.Other
Q16.House Ownership Ghar ka malik kaun hai?
1.Owned 2.Rented 3.Living with someone
4.Other
Q17.Number of children Apkay kitnay bachay hain?
1. None 2. 1-2 3. 3-5 4. >6
Q18.Age of last child Akhri bachay ki umar?
Q19.Number of people living in house Ghar mai kitnay afraad rehte hain?
1. 1-2 2. 3-5 3. 6-9 4. >10
Sign or Thumb Impression for Written Consent
Page 36 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q20.Number of rooms in house Ghar mai kitnay kamray hain?
1. 1 2. 2-3 3. 4-5 4. >6
Q21.Are you currently taking care of a disabled/ dependent family member Kya apkay ghar mai koi mazoor/jiska ap par inhasaar ho, shakhs hai?
1.No 2.Yes If Yes, who:
Q22.Source of drinking water Pani penay ka kya zarya hai?
1.Plain Tap 2.Filtered 3.Local Pump
4.Other
Q23.Type of energy used for cooking in house Ghar mai khana pakanay ke liye kis chiz ka istemaal kartay hain? (gas, coal, electric etc.)
1.Gas 2.Wood 3.Electricity 4.Other
Q24.Do you have toilet facility in house Apkay ghar mai bait-ul-khala hai?
1.Yes 2.No If No, what do you use
Q25.How many toilets in the house Ghar mai kitnay bait-ul-khala hain?
1. None 2. 1-2 3. 3-5 4. >6
Q26.Does the toilet have a flush Bait-ul-khala mai flush hai?
1.Yes 2.No If No, what do you use
Q27.Is the drainage and gutter system of your house satisfactory Ganday pani ke ikhraj ka nizaam darust hai?
1.Yes 2.No
Q28.How do you dispose of the garbage Ghar ki gandagi kahan phenkhtay hain?
1.Throw it on street/ far away
from home
2.Garbage collectors come to house
3.Set Fire 4.Other
Q29.Are you taking any health insurance (not provided by the microfinance provider)? (If so, from where, how much installment) Sehat ke liye insurance le rae hain?
1.Yes 2.No If Yes, who
SECTION B: MICROFINANCE LOAN CHARACHTERISTICS
Q30.Why are you taking loan (describe your work type, hours of work, working conditions in detail) Aap karz kyun le rahe hain? (kis tarah ka kaam hai, kitnay ghantay kaam kartay hain, jahan kaam kartay hain uskay halaat)
Q31.What type of loan are you currently taking/ duration Kis tarah ka karz le rahay hain/kitnay arsay se?
Q32.How long have you been a microfinance borrower for Kitne arsay se karz le rahay hain?
1. 1-2 years 2. 3-5 years 3. 6-9 years 4. >10 years
Q33.Is it a group loan Kya ap ne kisi ke sath mil ke karz liya hai?
1.Yes 2.No If Yes, who
Q34.How much is the loan for Kitna karz liya hai?
Q35.What is the installment rate per month Karz ko ada karnay ki mahana kist kya hai?
Q36.Do you attend monthly meetings with loan officers Karz denay walay officer se kya apki mahwar mulakaat hoti hai?
1.Yes 2.No
Q37.Do you attend weekly meetings with loan officers Karz dene walay officer se kya apki haftawar mulkaat hoti hai?
1.Yes 2.No
Q38.Who helps you in loan repayment Karz ada karnay mai kya koi apki madad karta hai?
1.No one 2.Husband 3.Parents 4.Other
Q39.What exactly has the loan been used for Ap karz kis liye istemal karti hain?
1.Business 2.Household expenditure
3.Old Loans
4.Health Costs
4.Other
Page 37 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q40.How much of the loan taken has been invested in business Karz ka kitna hissa karobar mai kharch kiya hai?
1.All 2.Half 3.Quarter 4.Other
Q41.Are you satisfied with loan amount Kya aap karz ki rakam se mutmaeen hai?
1.Yes 2.No
Q42.Are you satisfied with loan repayment rate Kya ap karz ki adaigi ki kist se mutmaeen hai?
1.Yes 2.No
Q43.Will you be renewing loan Kya aap karz dobara lena chahain gae?
1.Yes 2.No
Q44.Have you received any skill development training Kya apki silahiyaton ko barhanay ki koi tarbiyat mili hai?
1.Yes 2.No
Q45.Have you participated in any health workshop/awareness campaign/talk… Kya sehat se mutalik ap kisi agahi mohim ka hissa banay hai?
1.Yes 2.No
Q46.Has your loan officer or center ever talked to you about health awareness or access Kya karz denay walay officer ne ap se sehat ke mutalik koi agahi di hai?
1.Yes 2.No
Q47.Have you been offered saving insurance by your MFP Kya idaray ne apko bachat insurance ki peshkash ki hai?
1.Yes 2.No
Q48.Are you taking saving insurance with your MFP Kya idara ap ko bachat insurance de raha hai?
1.Yes 2.No
Q49.Have you been offered health insurance by your MFP Kya idara aap ko sehat insurance deta hai?
1.Yes 2.No
Q50.Are you taking health insurance with your MFP Kya ap idaray se sehat insurance le rahay hain?
1.Yes 2.No
Q51.Has the loan so far satisfied your business needs Kya karz ki rakam ne apki karobari zaroriyat ko pura kiya hai?
1.Yes 2.No
Q52.Has your loan taking from MF enabled you to visit a trained private general practitioner, if needed in last 12 months Karzay k baad pichlay 12 maheenay mein kya app private doctor ko dekhanay gaye hain?
1.Yes 2.No
Q53.Has your employment from MF loan enabled you to visit a trained private specialist practitioner, if needed in last 12 months Karzay k baad pichlay 12 maheenay mein kya app baday doctor ko dekhanay gaye hain?
1.Yes 2.No
Q54.How is your ability to purchase prescribed medicines (in case recommended by doctor) since loan-taking? Kya karz lene ke bad dawayan khareednay ki istata’at mai koi tabdeeli ai hai?
1.Very Good 2.Good 3.Fair 4.Poor
SECTION C WOMEN’S HEALTH CARE EXPERIENCES SURVEY
Q55. How would you rate your health in general? Apki sehat kis mayar ki hai?
1.Very Good 2.Good 3.Fair 4.Poor
Q56.Compared to other women your age, how would you rate your health Apni hum umar auraton ki nisbat aap apni sehat ka kya mayaar samjhtay hain?
1.Very Good 2.Good 3.Fair 4.Poor
Q57. Do you feel your health could be better than 1.Yes 2.No If yes, could you say why/ how:
Page 38 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
it is presently? Kya apki sehat ke mayaar mai koi behtari lai ja sakti hai?
Q58.Does your husband/ male relative/in-laws decide/ give approval when you or your children need consultation from a medical practitioner Kya apka khawand/susral apko doctor pe janay ki ijazat deta hai? Kya ye faisla bhi apka susral/khawand krta hai?
1.Yes 2. I decide myself independently
If yes, can you specify which relatives:
Q59.Does your husband/ male relative/in-laws decide/ give approval when you or your children need to visit a clinic/ hospital Kya apka khawand/susral apko hospital janay ki ijazat deta hai or kya ye faisla kaun leta hai?
1.Yes 2. I decide myself independently
If yes, can you specify which relatives:
Please indicate if you have experienced any of the following health issues in the last 12 months?
1.Yes 2.No
Q60.Minor illness like the flu or an infection Pichlay 12 mahinay mai apko nazla ya infection hua hai?
Q61.Had to go for a checkup or routine physical exam Jismani muaaenay ke liye gae hain?
Q62.Were you pregnant? Kya app hamla theen?
Q63.Did you need family planning or preconceptional services? Kya apko munsoba bandi ki zaroorat thee?
Q64.Did you have an injury that you have not already mentioned? Kya apko koi chot lagi hai?
Q65.Did you need care for a chronic health problem, (that is one that goes on for a long time)? Kya apko kisi taweel bemari ke liye hospital jana para hai?
Q66.Did you need surgery for a condition not already mentioned? Kya apko operation keranay ki zaroorat parhi?
If yes, what?
Q67.Were you feeling depressed, anxious, or highly stressed? Kya iski waja se apko kisi kisam ka zehni dabao ya bechaini mehsoos hui hai?
Could you pinpoint why?
Have you had one of the following tests in the last 12 months?
1.Yes 2.No
Q68.Colon cancer screening, such as a check for blood in your stool, sigmoidoscopy, or colonoscopy
Q69.Test for glaucoma or pressure in the eye Q70.Blood cholesterol test Q71.Check for high blood pressure Q72.Test for diabetes Q73.Breast exam by a doctor or nurse Q74.Mammogram Q75.Pap test Q76.Bone density test (for osteoporosis) Q77.Genetic screening test Q78.Screening for HIV/AIDS
Page 39 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q79.Screening for other sexually transmitted diseases
Q80.Dental exam Q81.Shot for flu or pneumonia Q82.Pregnancy test Q83.Family planning services or contraception Q84.Tests for infertility Q85.Abortion information or services Q86.Alcohol or drug abuse counseling or treatment
In the past 12 months, did any of your health care providers or microfinance loan managers talk with you or give you information about? (pichlay 12 mahino mai kya apkay doctor/nurse ya apkay karz dene walay officer ne aap se in chizon ke baray mai maloomat di hain?)
1.Yes 2.No If yes, can you specify who gave you this information:
Q87.Smoking, second-hand smoke, or quitting smoking Tambako noshi, kisi aisay shaks k saath bethtna/rehna jo tambako noshi mein mulawis ho, ya tambako noshi chorna
Q88.Nutrition or diet (Khuraak)
Q89.Alcohol or drug use Shraab ya adviyaat?
Q90.Physical fitness or exercise Jismani sehat ya warzish?
Q91.Menopause or hormone replacement therapy San – e - yaas ya hormone tabdeeli therapy?
Q92.Violence in the home or workplace Kya ghar ya kaam pe kisi tashadud ka shikar hue hain?
Q93.Work or financial problems Kaam ya muaashi mushkilaat ka samna hua hai?
Q94.Family or relationship problems Ghar walon ya rishtadaron ke masa’il?
Q95.Importance of child health and nutrition Bachon ki sehat or khuraak ki ehmiyat?
Q96.Stress management Zehani dabao ko kum karna
Q97.Preventing unintended pregnancies & birth spacing Bachon ke darmiya wakfa?
Q98.Using alternative therapies, such as herbs or acupuncture
Q99.Preventing osteoporosis Hadion ke dard se bachao
Are there any dietary supplements that you have used in the last 12 months?
1.Yes 2.No
Q100.Vitamin C Q101.Vitamin D Q102.Vitamin E Q103.B Complex Q104.Calcium Q105.Pregnancy Vitamin Q106.Lactation Vitamin
Page 40 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q107.General Multi-vitamin What is your personal preference for health services? Tibbi saholiyat se mutalik apki zaati tarjihaat kya hain?
1.Yes 2.No 3.Indfferent
Q108.Family (e.g. mother/ mother-in-law/ aunt) Ghar walay?
If Yes, describe who:
Q109.A women’s health center where you can get most of your basic health care, including gynecological care, in one place Khawateen ki sehat markaz?
Q110.Trusted community member Baradari?
Q111.A nurse or LHW (Not a physician/ surgeon/ medical consultant)
Q112.PublicHospital Q113.Local female healer Q114.Private Clinic Q115.In general, how difficult have you found it to talk to health care providers about your personal health concerns? doctor/nurse se baat krna apko kitna mushkil lagta hai?
1.Very difficult 2.Somewhat difficult
2.Not too difficult
3.Not difficult at all
Please rate the health practitioner services as you have experienced them?
1.Excellent 2.Good 3.Fair 4.Poor
Q116.Listening to what you have to say Kya apki baat ghor se suntay hain?
Q117.Talking to you in a respectful and caring manner
Kya ap se izzat se baat kartay hai?
Q118.Speaking to you in the language/ dialect you understand better
Kya apse apki madri zubaan mai baat krtay hai
Q119.Answering your questions clearly Ap ke sawalon ka sahi se jawaab detay hai?
Q120.Giving you the opportunity to ask all of your questions Apko sawaal puchnay ka wakt detay hai?
Q121.Helping you to feel comfortable talking about your personal or sensitive health concerns Kya ap asaani se unhe apnay masaael ke baray mai bata deti hain?
Q122.Giving you complete health information Kya sehat se mutalik tamaam jankari detay hain?
Q123.Discussing alternative therapies, diet and lifestyle Kya ap se mutabadil therapy ya khuraq ya roz mara ki zindagi guzarnay kay tareekay pe tabadal e khayal kya hai?
Q124.Giving you complete information about any tests or services Test ke baray mai mukamal jaankari detay hain?
Q125.Giving you the results of your tests Test ke nataij batatay hain?
Page 41 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q126.Giving you complete information about all your options for treatments Kya ilaaj ke mutalik apko mukamal jaankari detay hai?
Q127.Giving you the opportunity to make important decisions about your health care Kya sehat se mutalik tamam faislay apko karnay detay hai?
Q128.Giving you written or printed information when you need it Malumaat likh kr dete hai?
Q129.Spending enough time with you during your visits Apko tasali bakhsh wakt detay hai?
Q130.Treating you like a partner in your health care Apka sathi bun kr apki sehat ka khayal rakhtay hai?
Which are the primary/ most important sources you depend on for making health decisions? Sehat se mutalik faislon ke liye ap kis se mashwara leti hai?
Tick relevant options
Q131.Husband Q132.Mother in law Q133.Other in-laws (list please) Q134.Blood family (parents, siblings, children…) Q135.Newspapers / magazines Q136.Heath newsletter Q137.TV Q138.Radio Q139.Microfinance provider Q140.Internet Q141.Mobile services Q142.Family/ friends Q143.Community Q144.Medical Practitioner Q145.Local Healer Q146.Local Imam/ religious leader Q147.Other (Please list) Current Health Risks Q148.Do you currently smoke? Kya app tambako noshi mein mulawis hain?
1.Yes
2.No
Q149.How many in a day? Din ke kitnay ?
Q150.Does anyone else smoke in the house when you/ children are in same room? Kya koi aur tambako noshi mein mulawis hain
1.Yes 2.No If yes, who is this:
Q151.Do you feel anxious, stressed, depressed, suicidal? Kya app kabhi bechain hotay hain ya zehni dabao ka shakar ya khud kushi ka khayal aya hai?
1.Yes 2.No
Indicate which:
Q152.Do you take any drugs (to relieve yourselves of stress or an ailment? Kya app in ke liye koi dawa laitay hain?
1.Yes
2.No
If yes, which ones:
Page 42 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from
For peer review only
In the past 5 years, has a doctor ever told you that you have any of the following conditions Kya pichlay paanch salon mai doctor ne aapko bataya ke apko ye bemari hai?
Tick relevant options
Q153.Hypertension/ BP High blood pressure
Q154.Heart disease Dil ki bemari
Q155.High cholesterol Q156.Diabetes (sugar)
Q157.Depression Zehni dabao
Q158.Anxiety Bechaini
Q159.Migraine headaches (sar dard)
Q160.Arthritis Joro ki dard
Q161.Osteoporosis Q162.Obesity/ Over-weight problems (mutapa)
Q163.Urinary incontinence (pishaap ki takleef)
Q164.Cancer Q165.Eating disorder like bulimia/ anorexia Khanay k hawaly se koi mushkil, jaisay bhook na lagna ya kha k ulti kerna
Q166.Thyroid problems Q167.Malaria/ Dengue Are you facing any disability which? Kya aap kisi mazoori ka shikaar hain?
1.Yes
2.No
Q168.Keeps you from participating fully in your ability to take care of your family Jiski waja se ap apnay ghar walon ka khayal na rakh sakain
If yes, please describe this disability:
Q169.Keeps you from participating fully in your ability to continue with your business Apnay karobaar mai sahi se kaam na kr sakain
If yes, please describe this disability:
SECTION D BASELINE NUTRITION AND FOOD SECURITY SURVEY UNICEF
Q170.In the past 6 months did you find it too expensive to purchase the foods you needed to feed your family? Pichlay 6 maah mai kya apko khaandan ko palnay ke liye khana lenay mai mushkilaat hoti hai?
1.Yes
2.No
Q171.Did you find it too expensive to purchase fruit? Kya phal khareedna bohat mehnga hai?
1.Yes
2.No
Q172.Did you find it too expensive to purchase 1.Yes
2.No
Page 43 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
vegetables? Kya sabzi khareedna bohat mehnga hai?
Q173.Did you find it too expensive to purchase meat? Kya gosht khareedna bohat mehnga hai?
1.Yes
2.No
Q174.Did you find it too expensive to purchase eggs? Kya anday khareedna bohat mehnga hai?
1.Yes
2.No
Q175.Did you find it too expensive to purchase milk? Kya doodh khareedna bohat mehnga hai?
1.Yes
2.No
Q176.Did you find it too expensive to purchase wheat, for roti? Kya roti khareedna bohat mehnga hai?
1.Yes
2.No
Q177.In the last 3 months were you worried about running out of food because of high costs? Pichlay 3 maah mai mehngai ki waja se khana na khareed panay ka dart ha?
1.Yes
2.No
Q178.In the last 3 months did you run out of food because of expense? Pichlay 3 maah mai kya mehngai ki waja se kabhi ghar mai khana khatam ho gaya ho?
1.Yes
2.No
Q179.In the last 3 months did you or any other adult in the house skip meals because there was not enough food? Pichlay 3 maah mai aap ya kisi or ghar walay se khana kum honay ki waja se khana na khaya ho?
1.Yes
2.No
Q180.In the last 3 months did you ever think your children are still hungry because of not being fed enough food? Pichlay 3 maah mai apko kabhi laga ke apkay bachay bhookay hai kyunkay khana pura nai tha?
1.Yes
2.No
Q181.In the last 3 months did any of your children go to bed hungry? Pichlay 3 maah mai kya apkay bachay kabhi bhookay soe houn?
1.Yes
2.No
SECTION E WHO MULTI-COUNTRY STUDY ON WOMEN’S HEALTH AND DOMESTIC VIOLENCE AGAINST WOMEN Psychological violence experienced at home 1.Yes 2.No If yes, who were these
household members?
Q182.Has someone in your home insulted you or made you feel bad about yourself? Kya ghar mai kisi ne apki bezati ki hai?
Q183.Has someone in your home belittled or humiliated you in front of other people? Kya ghar mai kisi ne apko dosron ke samnay hakeer dikhaya hai?
Q184.Has someone in your home done things to scare or intimidate you on purpose? Kya ghar mai kisi ne apko daraya hai?
Q185.Has someone in your home threatened to hurt you or someone you care about? Kisi ne apko damkhaya hai?
Physical violence experienced at home 1.Yes 2.No If yes, who were these
Page 44 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
household members? Q186.Has someone in your home slapped you or thrown something at you that could hurt you? Kya kisi ne apko thapar lagaya ho ya app e koi chiz phenki ho jisse apko chot lagi ho?
Q187.Has someone in your home pushed or shoved you? Ghar pe apko kisi ne dhaka diya hai?
Q188.Has someone in your home hit you with his fist or with something else that could hurt you? Kisi ne apko mukkay marain hai?
Q189.Has someone in your home kicked you, dragged you or beaten you up? Kisi ne apko laat mari ho ya ghaseeta ho?
Q190.Has someone in your home choked or burnt you on purpose? Kisi ne jaan bojh kr apka gala dabanay ki, ya jalanay ki koshish ki hai?
Q191.Has he threatened to use or actually used a gun, knife or other weapon against you? Apkay khilaf koi hathyaar istemal kiya hai?
Sexual violence experienced at home 1.Yes 2.No
Q191.Has your husband physically forced you to have sexual intercourse when you didn’t want to? Kya apke shohar ne kisi kisam ka jinsi tushadad kiya hai?
Q192.Did you ever have sexual intercourse when you didn’t want because you were afraid of what your husband might do? Kiya app ne kabhi apnay shohar k darr se uss ke saath jinsi taluqat rakhain hain?
Q193.Has your husband forced you to do something sexual that you found degrading or humiliating? Kya apkay shohar ne kabhi app se aisay jinsi kaam keraye hain jin se app sharminda ya zilat mehsoos kerain?
SECTION F SURVEY OF WORKPLACE VIOLENCE WHO
Q194.Describe where exactly your work takes place, when outside of home Ghar se bahir kahan kaam karti hai?
Q195.What kind of people do you interact with mostly for work, outside of home (gender Kam pe kis tarah ke log se mulakat hoi hai?
Q196.What are the hours that you are required to work outside of home Ghar se bahir kaam ke silsalay mai kitnay ghnatay lagtay hai?
Q197.Which security measure is available to you outside of home in case of fear of violence (male relative accompanying, phone, moving in crowd…) Tashadud ki soorat mai kaam pr koi hifazati intezam hotay hai?
Physical Violence (PV) at the workplace Q198.In the last 12 months, have you been physically attacked in your workplace/ when you are working outside of home? Ghar se bahir kaam kartay wakt kisi tarah ke tashadud ka shikar
1.Yes 2.No
Page 45 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
hui hain? Q199.Was this PV with a weapon? (If yes, what kind) Kya is tashadud ke liye koi aslaah istemal kiya gaya tha?
Q200.Is this a typical incident at your workplace/ when you are working outside of home? Kya is tarah ka tashadud kaam pr mamool ki baat hai?
1.Yes 2.No
Q201.Who attacked you? Kis ne app r tashadud kiya?
Q202.Where exactly did it take place? Tashadud kis jaga hua?
Q203.What time was it? Kis wakt hua?
Q204.Do you think it could be prevented? Kya is tashadud roka ja sakta tha?
1.Yes 2.No
Q205.Were you injured? Kya apko kisi kisam ki chot ai thi?
1.Yes 2.No
Q206.Did you require treatment for the injury? Kya is chot/zakham ke liye apko kisi ilaj ki zarorat hui?
1.Yes 2.No If yes, can you describe this treatment:
Q207.How did you respond to the incident? Tashadud ke natijay mai ap ne kya kiya?
Did you suffer any of the following due to PV: Q208.Repeated, disturbing memories, thoughts, or images of the attack? Tashadud ke bad kya apko iske baray mai aksar khayalat atay the?
1.Yes 2.No
Q209.Avoiding thinking about or talking about the attack or avoiding having feelings related to it? Kya is tashadud ke baray mai baat karne se ap ghabrati thi?
1.Yes 2.No
Q210.Being "super-alert" or watchful and on guard? Tashadud ke bad dar ke rehne lagi?
1.Yes 2.No
Q211.Feeling like everything you did was an effort? Har kaam mushkil ho gaya?
1.Yes 2.No
Verbal Violence (VV) at the workplace Q212.In the last 12 months, have you been verbally assaulted in your workplace/ when you are working outside of home? Kya pichlay 12 mah mai kaam pr kisi ne ap pr zabani tashadud kiya hai?
1.Yes 2.No
Q213.How often has this happened in the last 12 months? Kitni dafa?
1.Daily 2.About once in a week
3.About once in a month
4.Other
Q214.Is this a typical incident at your workplace/ when you are working outside of home? Kya ye kaam pr mamool ki baat hai?
1.Yes 2.No
Q215.Who abused you? Kis ne aap per zabani tashadud kiya?
Q216.Where exactly did it take place? Kahan kiya?
Q217.What time was it? Kis wakt kiya?
Page 46 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q218.Do you think it could be prevented? Kya isse roka ja sakta tha?
1.Yes 2.No
Q219.How did you respond to the incident? Iske natijay mai aap ne kya kiya?
Did you suffer any of the following due to VV: Q220.Repeated, disturbing memories, thoughts, or images of the attack? Tashadud ke bad kya apko iske baray mai aksar khayalat atay the?
1.Yes 2.No
Q221.Avoiding thinking about or talking about the attack or avoiding having feelings related to it? Kya is tashadud ke baray mai baat karne se ap ghabrati thi?
1.Yes 2.No
Q222.Being "super-alert" or watchful and on guard? Tashadud ke bad dar ke rehne lagi?
1.Yes 2.No
Q223.Feeling like everything you did was an effort? Har kaam mushkil ho gaya?
1.Yes 2.No
Sexual Harassment (SH) at the workplace Q224.In the last 12 months, have you been sexually harassed in your workplace/ when you are working outside of home? Kya pichlay 12 maheenay mein ap ko kisi kisam k jinsi harasaan ka samna kerna parha hai?
1.Yes 2.No
Q225.How often have you been sexually harassed in the last 12 months? Pichlay 12 maheenay mein yeh kitni dafa hua?
1.Daily 2.About once in a week
3.About once in a month
4.Other
Q226.Is this a typical incident at your workplace/ when you are working outside of home? Kya yeh kaam kernay wali jaga pe amoman hota hai?
1.Yes 2.No
Q227.Who attacked you? Hamla awar kaun tha?
Q228.Where exactly did it take place? Yeh kis jaga pe hua?
Q229.What time was it? Waqt kya tha?
Q230.Do you think it could be prevented? Kya app isko rok sakti theen?
1.Yes 2.No
Q231.How did you respond to the incident? Apnay iska samna kaisay kiya?
Did you suffer any of the following due to SH: Q232.Repeated, disturbing memories, thoughts, or images of the attack? Kya apko iss hadsay k baad baar baar buray khaylat ya yaadain pareshan kerti hain?
1.Yes 2.No
Q233.Avoiding thinking about or talking about the attack or avoiding having feelings related to it? Kya app iss hadsay ko bhulanay ki koshih ya iskay baray mein baat kernay se guraiz kertay hain?
1.Yes 2.No
Q234.Being "super-alert" or watchful and on guard?
1.Yes 2.No
Page 47 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Kya app chak o chawbund rehtay hain? Q235.Feeling like everything you did was an effort? Kya apko zehni dabao mehsoos hota hai?
1.Yes 2.No
Racial Harassment (RH) at the workplace Q236.In the last 12 months, have you been racially harassed in your workplace/ when you are working outside of home? Pichlay 12 maah mai apki zaat ki waja se kisi ne apko harasaan kiya hai?
1.Yes 2.No
Q237.How often have you been racially harassed in the last 12 months? Kitni dafa?
1.Daily 2.About once in a week
3.About once in a month
4.Other
Q238.Is this a typical incident at your workplace/ when you are working outside of home? Ghar se bahir kaam pe kya ye aam ma’mool ki baat hai?
1.Yes 2.No
Q239.Who attacked you? Kis ne harasaan kiya?
Q240.Where exactly did it take place? Kahan
Q241.What time was it? Kis wakt?
Q242.Do you think it could be prevented? Kya issay roka ja sakta tha?
1.Yes 2.No
Q243.How did you respond to the incident? Iske natijay mai aap ne kya kiya?
Did you suffer any of the following due to RH: Q244.Repeated, disturbing memories, thoughts, or images of the attack? Tashadud ke bad kya apko iske baray mai aksar khayalat atay the?
1.Yes 2.No
Q245.Avoiding thinking about or talking about the attack or avoiding having feelings related to it? Kya is tashadud ke baray mai baat karne se ap ghabrati thi?
1.Yes 2.No
Q246.Being "super-alert" or watchful and on guard? Tashadud ke bad dar ke rehne lagi?
1.Yes 2.No
Q247.Feeling like everything you did was an effort? Har kaam mushkil ho gaya?
1.Yes 2.No
SECTION F OPEN-ENDED QUESTIONS
Q248.What are the main health challenges you face in the last 12 months? Pichlay sal mein kaunsi sehat ki takleef thi apko? Behtareen tibbi saholiyat ke wasool mai sub se eham 3 rukawatain?
Q249.What are the top 3 barriers preventing you from access to health services? Kaunsi theen chezay apko sehat ki sahulat laney mein rukawat hai
Page 48 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Q250. What are the main problems which prevent you from being satisfied with your health since taking loan? Kaunsi sehat ke mutalik cheezay apko ----- ?
β- Punjabis (1), Pashtuns (2), Sindhis (3), Siddis (4), Saraikis (5), Muhajirs (6), Balochis (7), Hindkowans (8), Chitralis (9), Gujarati (10), Kashmiris (11), Kalash (12), Burusho (13), Brahui (14), Khowar (15), Hazara (16), Shina (17), Kalyu (18), Balti (19), Afghan refugees (20), Other (21). *- Doctors clinic (private/primary-secondary) (1), Hospital Clinic (tertiary) (2), LHW (3), BHU (4), Local Hakim (5), Homeopath (6), Other (7). +- No money (1), not serious/ took care it of it myself (2), too busy (3), no childcare (4), no transport (5), too embarrassed (6), don’t have permission (7), prescription/ paperwork/ referral got lost (8), didn’t know where to get care (9), provider too far away (10), don’t like the local provider (11), couldn’t find specific specialist (12), other (13). # Physical violence refers to the use of physical force against another person or group, that results in physical harm, sexual or psychological harm. It can include beating, kicking, slapping, stabbing, shooting, pushing, biting, and/or pinching, among others. Psychological violence is defined as: Intentional use of power, including threat of physical force, against another person or group, that can result in harm to physical, mental, spiritual, moral or social development. Psychological violence includes verbal abuse, bullying/mobbing, harassment, and threats. Sexual Harassment refers to any unwanted, unreciprocated and unwelcome behavior of a sexual nature that is offensive to the person involved, and causes that person to be threatened, humiliated or embarrassed. Racial Harassment refers to any threatening conduct that is based on race, color, language, national origin, religion, association with a minority, birth or other status that is unreciprocated or unwanted and which affects the dignity of women and men at work. @ took no action (1), tried to pretend it never happened (1), told the person to stop (1), tried to defend myself (1), told friends/family (1), sought counseling (1), told a colleague (1), reported it to a colleague (1), discussed/ complained to MF loan officer (1), sought help from MFP (1), sought help from the union/community (1), pursued prosecution (1), other (1)
Page 49 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Supplementary Table 1a: Descriptive statistics before matching for health insurance (T=0 and T=1)
Variable No health insurance (T=0)
Health insurance (T=1)
Mean SD Mean SD Difference p-value Age 0.455 0.499 0.390 0.489 0.065 0.188 Religion 0.097 0.297 0.150 0.358 -0.052 0.103 Literacy 0.396 0.490 0.253 0.436 0.142 0.003 Spouse Literacy 0.385 0.488 0.351 0.479 0.035 0.473 House ownership 0.712 0.454 0.805 0.397 -0.093 0.032 Children 0.563 0.497 0.714 0.453 -0.152 0.002 Drinking water 0.771 0.421 0.857 0.351 -0.086 0.034 Toilet facility 0.760 0.428 0.779 0.416 -0.019 0.657 Gutter drainage 0.747 0.436 0.733 0.443 0.013 0.771 Debt age 0.670 0.471 0.669 0.472 0.001 0.978 Group loan 0.410 0.493 0.422 0.496 -0.012 0.802 Loan amount 0.750 0.433 0.468 0.501 0.283 <0.001 Interest rate 0.708 0.455 0.669 0.472 0.040 0.391 Monthly meetings 0.674 0.470 0.890 0.314 -0.216 <0.001
Supplementary Table 1b: Descriptive statistics after matching for health insurance (T=0 and T=1)
Variable No health insurance (T=0)
Health insurance (T=1)
Mean SD Mean SD Difference p-value Age 0.450 0.500 0.433 0.498 0.017 0.796 Religion 0.125 0.332 0.150 0.359 -0.025 0.576 Literacy 0.308 0.464 0.308 0.464 0 1.000 Spouse literacy 0.425 0.496 0.375 0.486 0.050 0.431 House ownership 0.825 0.382 0.792 0.408 0.033 0.514 Children 0.650 0.479 0.642 0.482 0.008 0.893 Drinking water 0.833 0.374 0.817 0.389 0.017 0.735 Toilet facility 0.842 0.367 0.792 0.408 0.050 0.319 Gutter drainage 0.725 0.448 0.750 0.435 -0.025 0.662 Debt age 0.658 0.476 0.683 0.467 -0.025 0.682 Group loan 0.467 0.501 0.400 0.492 0.067 0.299 Loan amount 0.475 0.501 0.483 0.502 -0.008 0.898 Interest rate 0.667 0.473 0.625 0.486 0.042 0.502 Monthly meetings 0.892 0.312 0.858 0.350 0.333 0.437
Page 50 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from

For peer review only
Supplementary Table 2a: Descriptive statistics before matching for health awareness programme (T=0 and T=1)
Variable No health awareness programme
(T=0)
Health awareness programme
(T=1)
Mean SD Mean SD Difference p-value Age 0.476 0.501 0.394 0.490 0.082 0.084 Religion 0.087 0.283 0.140 0.348 -0.05 0.086 Literacy 0.383 0.487 0.314 0.465 0.070 0.124 Spouse literacy 0.379 0.486 0.369 0.483 0.010 0.829 House ownership 0.762 0.427 0.729 0.446 0.033 0.424 Children 0.573 0.496 0.653 0.477 -0.080 0.086 Drinking water 0.820 0.385 0.784 0.412 0.037 0.034 Toilet facility 0.728 0.446 0.801 0.400 -0.727 0.072 Gutter drainage 0.699 0.460 0.780 0.415 -0.081 0.053 Debt age 0.636 0.482 0.699 0.460 -0.063 0.159 Group loan 0.442 0.498 0.390 0.489 0.052 0.270 Loan amount 0.767 0.424 0.551 0.498 0.216 0.000 Interest rate 0.660 0.475 0.725 0.448 -0.064 0.143 Monthly meetings 0.626 0.485 0.856 0.352 -0.230 <0.001
Supplementary Table 2b: Descriptive statistics after matching for health awareness programme (T=0 and T=1)
Variable No health awareness programme
(T=0)
Health awareness programme
(T=1)
Mean SD Mean SD Difference p-value Age 0.469 0.502 0.424 0.496 0.045 0.923 Religion 0.135 0.343 0.139 0.347 -0.003 0.940 Literacy 0.344 0.477 0.285 0.453 0.059 0.334 Spouse literacy 0.375 0.487 0.417 0.495 -0.042 0.521 House ownership 0.833 0.375 0.792 0.408 0.042 0.424 Children 0.604 0.491 0.674 0.471 -0.069 0.272 Drinking water 0.813 0.392 0.833 0.374 -0.021 0.679 Toilet facility 0.781 0.416 0.840 0.368 -0.059 0.249 Gutter drainage 0.677 0.477 0.778 0.417 -0.101 0.083 Debt age 0.667 0.474 0.674 0.470 -0.007 0.911 Group loan 0.448 0.500 0.424 0.496 0.024 0.711 Loan amount 0.573 0.497 0.417 0.495 0.156 0.018 Interest rate 0.667 0.474 0.632 0.484 0.035 0.584 Monthly meetings 0.854 0.355 0.889 0.315 -0.035 0.428
Page 51 of 50
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 2, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2020-043544 on 5 January 2021. D
ownloaded from