
BIOLOGICAL OPTIMIZATION IN VOLUMETRIC MODULATED ARC RADIOTHERAPY FOR PROSTATE CARCINOMA
7
PHYSICS CONTRIBUTION BIOLOGICAL OPTIMIZATION IN VOLUMETRIC MODULATED ARC RADIOTHERAPY FOR PROSTATE CARCINOMA IVAYLO B. MIHAYLOV,PH.D.,* y MIREK FATYGA,PH.D., z KARL BZDUSEK, B.S., x KENNETH GARDNER, M.D., y AND EDUARDO G. MOROS,PH.D. y *Department of Radiation Oncology, Rhode Island Hospital/Brown Medical Center, Providence, RI; y Department of Radiation Oncology, University of Arkansas for Medical Sciences, Little Rock, AK; z Department of Radiation Oncology, Virginia Commonwealth University, Richmond, VA 23298; and x Philips Radiation Oncology Systems, Fitchburg, WI Purpose: To investigate the potential benefits achievable with biological optimization for modulated volumetric arc (VMAT) treatments of prostate carcinoma. Methods and Materials: Fifteen prostate patient plans were studied retrospectively. For each case, planning target volume, rectum, and bladder were considered. Three optimization schemes were used: dose–volume histogram (DVH) based, generalized equivalent uniform dose (gEUD) based, and mixed DVH/gEUD based. For each scheme, a single or dual 6-MV, 356 VMAT arc was used. The plans were optimized with Pinnacle 3 (v. 9.0 beta) treatment planning system. For each patient, the optimized dose distributions were normalized to deliver the same prescrip- tion dose. The quality of the plans was evaluated by dose indices (DIs) and gEUDs for rectum and bladder. The tallied DIs were D 1% ,D 15% ,D 25% , and D 40% , and the tallied gEUDs were for a values of 1 and 6. Statistical tests were used to quantify the magnitude and the significance of the observed differences. Monitor units and treatment times for each optimization scheme were also assessed. Results: All optimization schemes generated clinically acceptable plans. The statistical tests indicated that biolog- ical optimization yielded increased organs-at-risk sparing, ranging from 1% to more than 27% depending on the tallied DI, gEUD, and anatomical structure. The increased sparing was at the expense of longer treatment times and increased number of monitor units. Conclusions: Biological optimization can significantly increase the organs-at-risk sparing in VMAT optimization for prostate carcinoma. In some particular cases, however, the DVH-based optimization resulted in superior treat- ment plans. Ó 2012 Elsevier Inc. VMAT, Volumetric, Arc, Optimization, Dose, Prostate cancer. INTRODUCTION Intensity-modulated radiation therapy (IMRT) is rapidly be- coming a standard of care. The primary reason is that it offers great flexibility in delivering highly conformal dose distribu- tions to complex targets while sparing the surrounding healthy tissue and anatomical structures. IMRT treatments can be delivered either with a fixed gantry angle technique or with a recently commercially available volumetric modulated arc (VMAT) technique. VMAT evolved from intensity-modulated arc therapy (1), allowing for simulta- neous variation of dose rate, gantry speed, and multileaf col- limator (MLC) segments. The technique promises some dosimetric benefits (2), together with reduced treatment times (1, 3–6), which in turn can have significant radiobiological impact (7–9). IMRT inverse plan optimization is routinely performed by dose–volume histogram (DVH) optimization objectives. In DVH optimization, the planner specifies dose level(s) to dif- ferent partial or total volumes of the anatomical organs and targets of interest. The widespread use of DVH-based optimi- zation stems from the wealth of clinical information, as well as clinicians’ experience (10), relating organ volumes and dose levels resulting in complications to the surrounding or- gans at risk (OARs). DVH-based objective functions how- ever do not adequately represent (11, 12) the nonlinear response of tumors or OARs to dose—in particular, for highly heterogeneous dose distributions, which are common in IMRT. Therefore, the use of biological information in the IMRT optimization holds tremendous promise for improving local control or reduction of normal tissue toxicity. The biological information can be supplied Reprint requests to: Ivaylo B. Mihaylov, Ph.D., Department of Radiation Oncology, Warren Alpert Medical School of Brown Uni- versity, Rhode Island Hospital, 593 Eddy St., Providence, RI 02903. Tel: (401) 444-8546; Fax: (401) 444-2149; E-mail: imihaylov@ Lifespan.org This work was supported in part by Central Arkansas Radiation Therapy Institute (CARTI). Conflict of interest: Karl Bzdusek is an employee of Philips Ra- diation Oncology Systems. Received Oct 9, 2009, and in revised form June 3, 2010. Accepted for publication June 9, 2010. 1292 Int. J. Radiation Oncology Biol. Phys., Vol. 82, No. 3, pp. 1292–1298, 2012 Copyright Ó 2012 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ - see front matter doi:10.1016/j.ijrobp.2010.06.020
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of BIOLOGICAL OPTIMIZATION IN VOLUMETRIC MODULATED ARC RADIOTHERAPY FOR PROSTATE CARCINOMA

Int. J. Radiation Oncology Biol. Phys., Vol. 82, No. 3, pp. 1292–1298, 2012Copyright � 2012 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/$ - see front matter
jrobp.2010.06.020
doi:10.1016/j.iPHYSICS CONTRIBUTION
BIOLOGICAL OPTIMIZATION IN VOLUMETRIC MODULATED ARCRADIOTHERAPY FOR PROSTATE CARCINOMA
IVAYLO B. MIHAYLOV, PH.D.,*y MIREK FATYGA, PH.D.,z KARL BZDUSEK, B.S.,x
KENNETH GARDNER, M.D.,y AND EDUARDO G. MOROS, PH.D.y
*Department of Radiation Oncology, Rhode Island Hospital/Brown Medical Center, Providence, RI; yDepartment of RadiationOncology, University of Arkansas for Medical Sciences, Little Rock, AK; zDepartment of Radiation Oncology, Virginia Commonwealth
University, Richmond, VA 23298; and xPhilips Radiation Oncology Systems, Fitchburg, WI
ReprinRadiationversity, RTel: (401Lifespan.
Purpose: To investigate the potential benefits achievable with biological optimization for modulated volumetric arc(VMAT) treatments of prostate carcinoma.Methods and Materials: Fifteen prostate patient plans were studied retrospectively. For each case, planning targetvolume, rectum, and bladder were considered. Three optimization schemes were used: dose–volume histogram(DVH) based, generalized equivalent uniform dose (gEUD) based, and mixed DVH/gEUD based. For each scheme,a single or dual 6-MV, 356� VMAT arc was used. The plans were optimized with Pinnacle3 (v. 9.0 beta) treatmentplanning system. For each patient, the optimized dose distributions were normalized to deliver the same prescrip-tion dose. The quality of the plans was evaluated by dose indices (DIs) and gEUDs for rectum and bladder. Thetallied DIs were D1%, D15%, D25%, and D40%, and the tallied gEUDs were for a values of 1 and 6. Statistical testswere used to quantify the magnitude and the significance of the observed differences. Monitor units and treatmenttimes for each optimization scheme were also assessed.Results: All optimization schemes generated clinically acceptable plans. The statistical tests indicated that biolog-ical optimization yielded increased organs-at-risk sparing, ranging from �1% to more than �27% depending onthe tallied DI, gEUD, and anatomical structure. The increased sparing was at the expense of longer treatment timesand increased number of monitor units.Conclusions: Biological optimization can significantly increase the organs-at-risk sparing in VMAT optimizationfor prostate carcinoma. In some particular cases, however, the DVH-based optimization resulted in superior treat-ment plans. � 2012 Elsevier Inc.
VMAT, Volumetric, Arc, Optimization, Dose, Prostate cancer.
INTRODUCTION
Intensity-modulated radiation therapy (IMRT) is rapidly be-
coming a standard of care. The primary reason is that it offers
great flexibility in delivering highly conformal dose distribu-
tions to complex targets while sparing the surrounding
healthy tissue and anatomical structures. IMRT treatments
can be delivered either with a fixed gantry angle technique
or with a recently commercially available volumetric
modulated arc (VMAT) technique. VMAT evolved from
intensity-modulated arc therapy (1), allowing for simulta-
neous variation of dose rate, gantry speed, and multileaf col-
limator (MLC) segments. The technique promises some
dosimetric benefits (2), together with reduced treatment times
(1, 3–6), which in turn can have significant radiobiological
impact (7–9).
t requests to: Ivaylo B. Mihaylov, Ph.D., Department ofOncology, Warren Alpert Medical School of Brown Uni-
hode Island Hospital, 593 Eddy St., Providence, RI 02903.) 444-8546; Fax: (401) 444-2149; E-mail: imihaylov@org
1292
IMRT inverse plan optimization is routinely performed by
dose–volume histogram (DVH) optimization objectives. In
DVH optimization, the planner specifies dose level(s) to dif-
ferent partial or total volumes of the anatomical organs and
targets of interest. The widespread use of DVH-based optimi-
zation stems from the wealth of clinical information, as well
as clinicians’ experience (10), relating organ volumes and
dose levels resulting in complications to the surrounding or-
gans at risk (OARs). DVH-based objective functions how-
ever do not adequately represent (11, 12) the nonlinear
response of tumors or OARs to dose—in particular, for
highly heterogeneous dose distributions, which are
common in IMRT. Therefore, the use of biological
information in the IMRT optimization holds tremendous
promise for improving local control or reduction of normal
tissue toxicity. The biological information can be supplied
This work was supported in part by Central Arkansas RadiationTherapy Institute (CARTI).
Conflict of interest: Karl Bzdusek is an employee of Philips Ra-diation Oncology Systems.
Received Oct 9, 2009, and in revised form June 3, 2010. Acceptedfor publication June 9, 2010.

Biological optimization in VMAT therapy for prostate carcinoma d I. B. MIHAYLOV et al. 1293
in terms of normal tissue complication probability models
(13, 14) or generalized equivalent uniform doses (gEUDs)
(15, 16).
Generally, in DVH optimization several (2–4) DVH
objectives must be specified for any target or OAR. In
contrast, in gEUD or combination of DVH and gEUD
(hybrid) optimizations fewer (no more than 2) objectives
per anatomical structures are enough for adequate IMRT
optimization. It has been shown that biological
optimization is superior to DVH-based optimization in
OAR sparing (with satisfactory target coverage) for multiple
fixed gantry angle IMRT (11, 17–23).
The purpose of this study is to compare the results and
evaluate the achievable dosimetric benefits, as well as the
possible pitfalls, of DVH- (ArcDVH), gEUD- (ArcgEUD),
and hybrid-based (ArcHybrid) optimization for VMAT tech-
nique in prostate carcinoma
METHODS AND MATERIALS
PatientsThe data set for this work consisted of 15 prostate IMRT treat-
ment plans, derived from patients treated at the Department of Radi-
ation Oncology at University of Arkansas for Medical Sciences. For
each patient, clinical target volume (CTV) and planning target vol-
ume (PTV) were contoured by the attending physician. The PTV
was obtained from the CTV by a uniform expansion of approxi-
mately 1 cm. In addition, rectum and bladder were outlined as
OARs and used in the IMRT optimization as critical anatomical
structures limiting the PTV dose escalation.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 1564006600680070007200740076007800640066006800700072007400760078008000
ArcDVHArcHybrid
PTV
D95
%[c
Gy]
Patient Number
ArcDVH ArcgEUD
PTV
D95
%[c
Gy]
Fig. 1. Comparison among planning target volume (PTV) D95%
dose indices achieved with the three different optimization schemes.In addition, dose standard deviations (two s) across the PTV are pre-sented as error bars. ArcDVH = dose–volume histogram–based arctherapy; ArcgEUD = generalized equivalent uniform doses–basedarc therapy; ArcHybrid = combination of ArcDVH and ArcgEUD.
Treatment planningThe treatment planning was performed with Pinnacle3 (beta v.
9.0, Philips Radiation Oncology Systems, Fitchburg, WI) treatment
planning system. The patient plans were optimized for a VMAT
treatment (3) on a Varian 21EX (Varian Medical Systems, Palo
Alto, CA) linear accelerator equipped with a 120-leaf Millennium
MLC. Each plan used either a single or a dual volumetric modulated
arc covering 356�, from 2� to 358� (Varian convention). All plans
were optimized for a single photon energy of 6 MV. Control points
were set 4� apart across the arcs for the machine parameter optimi-
zation. The dose calculations were performed with Pinnace3 col-
lapsed cone convolution superposition (24, 25) dose calculation
algorithm.
The ArcDVH optimization was performed with the Pinnacle3
IMRT optimization algorithm, whereas the ArcgEUD and ArcHy-
brid optimizations used the Pinnacle3 gEUD-based biological opti-
mization algorithm. The details of the VMAT arc generation and
optimization have been described elsewhere (3).
The ArcDVH optimization was performed first. The prescription
doses to 95% of the PTV ranged from 6,600 to 7,800 cGy, depend-
ing on the patient anatomy. The prescription doses were varied on
a case-by-case bases, subject to the following OAR constraints.
Doses to 15%, 25%, and 40% of the rectum were limited to
7,500, 7,000, and 6,000 cGy, respectively. Similar constraints
were used for bladder, although in some cases, slightly higher doses
were accepted as clinically viable because the bladder has somewhat
higher tolerances (26) than the rectum. In addition, the prescription
dose to 95% of the PTV was subject (affected) to the requirement
that the standard deviation of the dose over the PTV was within
3% (27). The IMRT objectives for the ArcDVH optimization used
minimum, maximum, and uniform dose for PTV, as well as the
above-mentioned three constraints of 6,000, 7,000, and 7,500 cGy
for rectum and bladder. The relative weights of the PTV were set be-
tween 10 and 20, and the relative weights fro the OARs were slightly
lower, ranging between 5 and 20. The doses to 15%, 25%, and 40%
of rectum and bladder volumes were reduced as much as possible
given that therapeutic prescription dose with small standard devia-
tion was achieved. Usually four to six manual interventions in the
optimization process were adequate for a clinically acceptable
plan. The same parameters, such as arc length, number of optimiza-
tion iterations, and convergence criteria, were used for the ArcgEUD
optimization. The PTV objectives for minimum and maximum
gEUDs with ‘‘a values’’ of –10 and +10 (11) were used in the Arc-
gEUD optimization. Similarly, two maximum EUD parameters
were used for either rectum and bladder, with a values of 6 (11)
and 1 (average dose), respectively. In the gEUD formalism, ‘‘a’’
is an organ-specific parameter describing dose–volume effects. If
a = N, the gEUD represents the maximum dose, whereas if a =
–N, the gEUD represents the minimum dose. For a = 1, the
gEUD is the mean dose. The a value can be determined empirically
by fitting published dose response data (26). This parameter usually
has large negative value for tumors, large positive values for serial
structures such as the spinal cord, and small (�1) positive value
for structures that exhibit large volume effect, such as lungs or pa-
rotid glands. The gEUD-based optimization in the Pinnacle3 treat-
ment planning system is realized by incorporating gEUDs (20),
rather than a sum of doses on a voxel-by-voxel basis, in a quadratic
objective function, which is subsequently minimized by the IMRT
optimization algorithm. In the ArcgEUD optimization, PTV relative
weights were set in the range of 80 to 100, and the OAR relative
weights were similar to the weights used in the ArcDVH optimiza-
tion. The maximum gEUDs for rectum and bladder for a value of 6
were set between 5,000 and 6,500 cGy, whereas for a value of 1,
they were set between 3,000 and 5,500 cGy on a case-by-case basis.
Through several trial-and-error steps, the objectives were lowered as
much as possible without compromising the prescription dose and

1294 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 3, 2012
PTV dose uniformity. The number of required manual interventions
was similar to that used in ArcDVH optimization.
The ArcHybrid optimization utilized the same objectives for the
PTV as the ArcDVH optimization, i.e., minimum, maximum, and
uniform dose, while using the gEUD constraints for the OARs in
the ArcgEUD-based optimization with the same a values. The clin-
ical viability of the ArcgEUD and ArcHybrid plans was based on the
same criteria used for ArcDVH results. In the ArcHybrid optimiza-
tion, PTV relative weights were set in the range of 20 to 100,
whereas the OAR relative weights were similar to the weights
used in the ArcgEUD optimization. The maximum gEUDs for rec-
tum and bladder, as well as the manual intervention frequency in the
optimization process, were the same as in ArcgEUD optimization.
AnalysesThe dose distributions computed with ArcDVH optimization
were used as a reference to which the dose distributions computed
with the ArcgEUD and ArcHybrid optimizations were compared.
The metric used in the comparison was based on dose indices
(DI) and generalized equivalent uniform doses. The evaluated
dose indices were PTV D95% (dose covering 95% of the PTV vol-
ume), and rectum and bladder D1%, D15%, D25%, and D40%. They
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
0.40.50.60.70.80.91.00.5
0.6
0.7
0.8
0.9
1.0
1.10.75
0.80
0.85
0.90
0.95
1.00
1.05
1.10
D40%ArcgEUD D40% ArcHybrid
Patient Number
D25% ArcgEUD D25% ArcHybrid
Nor
mal
ized
dos
e in
dice
s D
com
pare
d/Dre
fere
ncefo
r rec
tum
D15% ArcgEUD D15% ArcHybrid
Fig. 2. Comparison of normalized dose indices for rectum. The nor-malization was performed with respect to the dose indices derivedfrom ArcDVH optimization scheme. Open symbols denote the re-sults for ArcgEUD optimization, and the filled symbols denote theresults for ArcHybrid optimization. The top, middle, and bottompanels denote the comparisons for rectum D15%, D25%, and D40%,respectively. The ‘‘one’’ level is denoted in each panel by a dashedline. It indicates where the compared dose indices equal each other.ArcDVH = dose–volume histogram–based arc therapy; ArcgEUD =generalized equivalent uniform doses–based arc therapy; ArcHybrid= combination of ArcDVH and ArcgEUD.
were the same as the DIs used in establishing the IMRT DVH-
based optimization objectives (except D1%) in ArcDVH optimiza-
tion. The evaluated gEUDs were for PTV, rectum, and bladder.
The a value for the PTV was –10, whereas for rectum and bladder,
it was 6. In addition, the average doses for the OARs were also eval-
uated. The evaluated gEUDs were essentially the same as the
gEUDs used in the ArcgEUD and ArcHybrid optimizations as opti-
mization objectives. In the comparison between the DIs and gEUDs
derived from the various optimization schemes, the difference of 3%
was used as a threshold for clinical significance (28–30).
Statistical significance tests were used to determine the magnitude
of the differences between the tallied DIs and gEUDs derived from
the various optimization schemes. The details and the implementa-
tion of the tests have been presented elsewhere (31, 32). Briefly, the
statistical tests comprised two one-tailed paired t tests (33), where
statistical significance was determined by p value (34) <5% (0.05).
RESULTS
The plans optimized with the various optimization
schemes for each patient were normalized such that 95% of
the PTV received the same dose. In addition, the standard de-
viation of the dose across the PTV was within 3% (27) for
each plan. The target coverage and the dose uniformity result-
ing from the different optimization schemes were essentially
the same, as can be observed in Fig. 1.
Dose index comparisonsThe results for the rectum DIs, D15%, D25%, D40%, are
presented in the top, middle, and bottom panels of Fig. 2 re-
spectively. ArcgEUD and ArcHybrid evaluation metrics
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
0.30.40.50.60.70.80.91.01.10.5
0.6
0.7
0.8
0.9
1.0
1.10.75
0.80
0.85
0.90
0.95
1.00
1.05
1.10
D40%ArcgEUD D40% ArcHybrid
Patient Number
D25% ArcgEUD D25% ArcHybrid
Nor
mal
ized
dos
e in
dice
s D
com
pare
d/Dre
fere
ncefo
r bla
dder
D15% ArcgEUD D15% ArcHybrid
Fig. 3. The same comparisons as in Fig. 2 but for bladder.

0.85
0.90
0.95
1.00
0.90
0.92
0.94
0.96
0.98
1.00
1.02
a = 6 ArcgEUDa = 6 ArcHybrid
gEU
Ds
gEU
Dco
mpa
red/g
EUD
refe
renc
efo
r bla
dder
Biological optimization in VMAT therapy for prostate carcinoma d I. B. MIHAYLOV et al. 1295
were expressed as fractions of the corresponding ArcDVH
metrics. Consequently, the dose indices derived from Arc-
gEUD and ArcHybrid optimization were normalized to the
dose indices derived from ArcDVH optimization. This nor-
malization eases the comparison, especially when different
patients have different prescription doses (32) and different
OAR objectives. In majority of the cases, the normalized
DIs are less than unity, indicating increased rectum sparing
for ArcgEUD and ArcHybrid optimization schemes. Similar
results are evident on Fig. 3, where bladder normalized DIs
are presented. For some patient plans, the normalized DIs
are slightly greater than unity, indicating that no improve-
ment is achievable with the gEUD or the hybrid optimization.
However, in the majority of the cases, the normalized DIs are
less than unity, demonstrating the potential of biological op-
timization methods for increased OAR sparing.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
0.65
0.70
0.75
0.80
Patient Number
a = 1 ArcgEUDa = 1 ArcHybrid
Nor
mal
ized
gEUD comparisonsThe results from the gEUD comparisons for rectum and
bladder are presented in Figs. 4 and 5, respectively. The
ArcgEUD and ArcHybrid gEUDs (a value of 6) and
average doses (a value of 1) have been normalized with
respect to the gEUDs and the average doses derived from
1 2 3 4 5 6 7 8 9 10 11 12 13 14 150.65
0.70
0.75
0.80
0.85
0.90
0.95
1.00
0.88
0.90
0.92
0.94
0.96
0.98
1.00
1.02
Patient Number
a = 1 ArcgEUDa = 1 ArcHybrid
a = 6 ArcgEUDa = 6 ArcHybrid
Nor
mal
ized
gEU
Ds
gEU
Dco
mpa
red/g
EUD
refe
renc
efo
r rec
tum
Fig. 4. Comparison of normalized gEUDs for rectum. The top andbottom panels represent the average doses (a value of 1) and thegEUDs for a value of 6, respectively. The open symbols are forthe ArcgEUD comparison, and the filled symbols are for the ArcH-ybrid comparison. The ‘‘one’’ level is denoted in each panel bya dashed line. It indicates where the compared gEUDs equal eachother. ArcgEUD = generalized equivalent uniform doses–basedarc therapy; ArcHybrid = combination of dose–volume histo-gram–based arc therapy and ArcgEUD.
Fig. 5. The same comparisons as in Fig. 4 but for bladder.
the ArcDVH optimization in the same fashion as the DIs.
The results are qualitatively similar to the results for the
DIs. In majority of the cases, the ArcgEUD and ArcHybrid
optimization schemes resulted in an increased sparing of
the OARs.
Statistical analysisTable 1 contains the average values of the tallied DIs for
rectum, the statistically different dose interval, and the per-
cent change in the dose index necessary to establish statistical
equivalence for the results derived from ArcDVH, Arc-
gEUD, and ArcHybrid optimization schemes. It is evident
from the table that as the tallied DI corresponds to a bigger
and bigger OAR volume, the statistically significant differ-
ence increases from �1% to almost 28%. This indicates
that there is an increased OAR sparing with volumes above
decreasing dose limits. The gEUD statistical analyses among
the three optimization schemes are presented in Table 2.
Those results also indicate a statistically significant increase
in the sparing of rectum and bladder with increasing OAR
volume because higher values of a correspond to increased
importance of higher doses (10), which in turn are the doses
to smaller volumes of the OARs.
DISCUSSION
The plans generated by ArcgEUD optimization yielded
slightly higher dose heterogeneity within the PTV22. The
ArcHybrid scheme generated slightly better dose homogene-
ity than ArcgEUD scheme. However, this optimization re-
sulted in somewhat smaller OAR sparing. Statistical
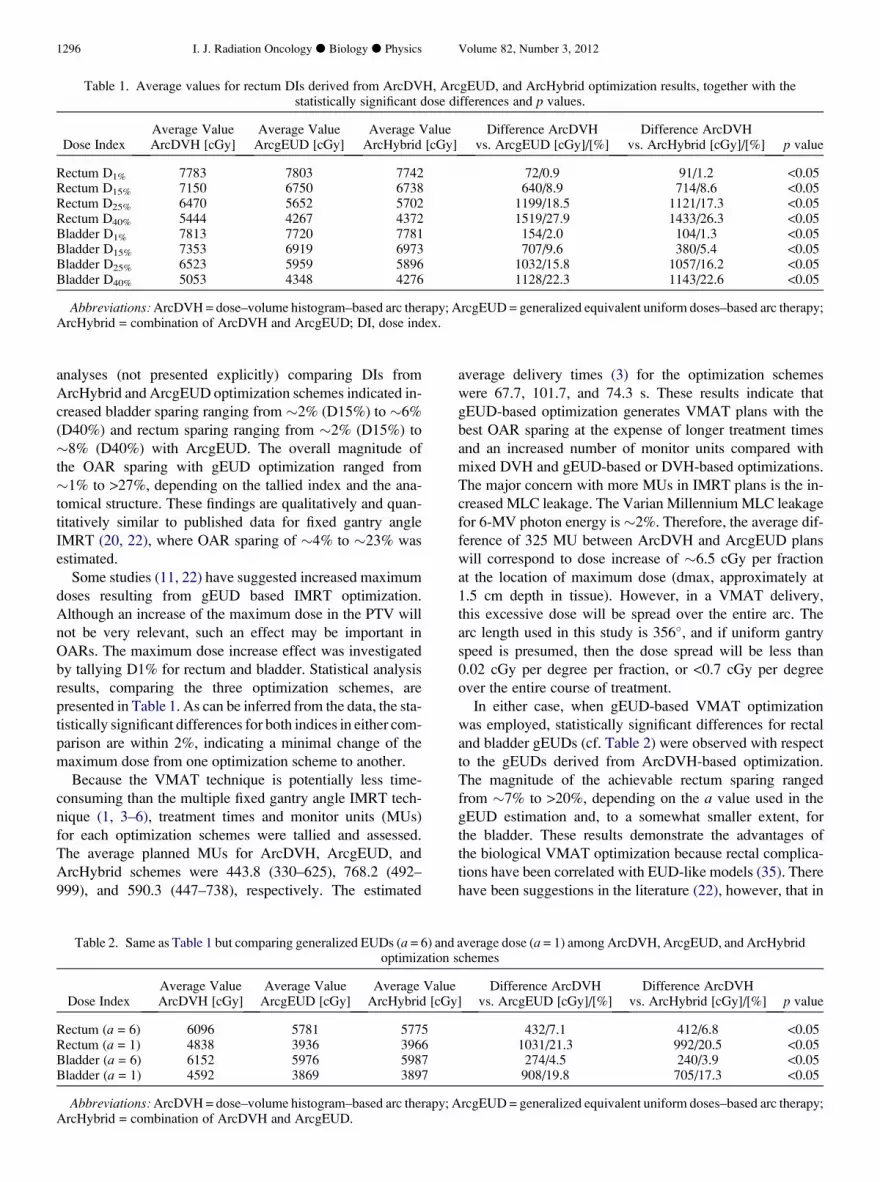
Table 1. Average values for rectum DIs derived from ArcDVH, ArcgEUD, and ArcHybrid optimization results, together with thestatistically significant dose differences and p values.
Dose IndexAverage ValueArcDVH [cGy]
Average ValueArcgEUD [cGy]
Average ValueArcHybrid [cGy]
Difference ArcDVHvs. ArcgEUD [cGy]/[%]
Difference ArcDVHvs. ArcHybrid [cGy]/[%] p value
Rectum D1% 7783 7803 7742 72/0.9 91/1.2 <0.05Rectum D15% 7150 6750 6738 640/8.9 714/8.6 <0.05Rectum D25% 6470 5652 5702 1199/18.5 1121/17.3 <0.05Rectum D40% 5444 4267 4372 1519/27.9 1433/26.3 <0.05Bladder D1% 7813 7720 7781 154/2.0 104/1.3 <0.05Bladder D15% 7353 6919 6973 707/9.6 380/5.4 <0.05Bladder D25% 6523 5959 5896 1032/15.8 1057/16.2 <0.05Bladder D40% 5053 4348 4276 1128/22.3 1143/22.6 <0.05
Abbreviations: ArcDVH = dose–volume histogram–based arc therapy; ArcgEUD = generalized equivalent uniform doses–based arc therapy;ArcHybrid = combination of ArcDVH and ArcgEUD; DI, dose index.
1296 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 3, 2012
analyses (not presented explicitly) comparing DIs from
ArcHybrid and ArcgEUD optimization schemes indicated in-
creased bladder sparing ranging from �2% (D15%) to �6%
(D40%) and rectum sparing ranging from �2% (D15%) to
�8% (D40%) with ArcgEUD. The overall magnitude of
the OAR sparing with gEUD optimization ranged from
�1% to >27%, depending on the tallied index and the ana-
tomical structure. These findings are qualitatively and quan-
titatively similar to published data for fixed gantry angle
IMRT (20, 22), where OAR sparing of �4% to �23% was
estimated.
Some studies (11, 22) have suggested increased maximum
doses resulting from gEUD based IMRT optimization.
Although an increase of the maximum dose in the PTV will
not be very relevant, such an effect may be important in
OARs. The maximum dose increase effect was investigated
by tallying D1% for rectum and bladder. Statistical analysis
results, comparing the three optimization schemes, are
presented in Table 1. As can be inferred from the data, the sta-
tistically significant differences for both indices in either com-
parison are within 2%, indicating a minimal change of the
maximum dose from one optimization scheme to another.
Because the VMAT technique is potentially less time-
consuming than the multiple fixed gantry angle IMRT tech-
nique (1, 3–6), treatment times and monitor units (MUs)
for each optimization schemes were tallied and assessed.
The average planned MUs for ArcDVH, ArcgEUD, and
ArcHybrid schemes were 443.8 (330–625), 768.2 (492–
999), and 590.3 (447–738), respectively. The estimated
Table 2. Same as Table 1 but comparing generalized EUDs (a = 6) andoptimization s
Dose IndexAverage ValueArcDVH [cGy]
Average ValueArcgEUD [cGy]
Average ValueArcHybrid [cGy
Rectum (a = 6) 6096 5781 5775Rectum (a = 1) 4838 3936 3966Bladder (a = 6) 6152 5976 5987Bladder (a = 1) 4592 3869 3897
Abbreviations: ArcDVH = dose–volume histogram–based arc therapy; AArcHybrid = combination of ArcDVH and ArcgEUD.
average delivery times (3) for the optimization schemes
were 67.7, 101.7, and 74.3 s. These results indicate that
gEUD-based optimization generates VMAT plans with the
best OAR sparing at the expense of longer treatment times
and an increased number of monitor units compared with
mixed DVH and gEUD-based or DVH-based optimizations.
The major concern with more MUs in IMRT plans is the in-
creased MLC leakage. The Varian Millennium MLC leakage
for 6-MV photon energy is �2%. Therefore, the average dif-
ference of 325 MU between ArcDVH and ArcgEUD plans
will correspond to dose increase of �6.5 cGy per fraction
at the location of maximum dose (dmax, approximately at
1.5 cm depth in tissue). However, in a VMAT delivery,
this excessive dose will be spread over the entire arc. The
arc length used in this study is 356�, and if uniform gantry
speed is presumed, then the dose spread will be less than
0.02 cGy per degree per fraction, or <0.7 cGy per degree
over the entire course of treatment.
In either case, when gEUD-based VMAT optimization
was employed, statistically significant differences for rectal
and bladder gEUDs (cf. Table 2) were observed with respect
to the gEUDs derived from ArcDVH-based optimization.
The magnitude of the achievable rectum sparing ranged
from �7% to >20%, depending on the a value used in the
gEUD estimation and, to a somewhat smaller extent, for
the bladder. These results demonstrate the advantages of
the biological VMAT optimization because rectal complica-
tions have been correlated with EUD-like models (35). There
have been suggestions in the literature (22), however, that in
average dose (a = 1) among ArcDVH, ArcgEUD, and ArcHybridchemes
]Difference ArcDVH
vs. ArcgEUD [cGy]/[%]Difference ArcDVH
vs. ArcHybrid [cGy]/[%] p value
432/7.1 412/6.8 <0.051031/21.3 992/20.5 <0.05
274/4.5 240/3.9 <0.05908/19.8 705/17.3 <0.05
rcgEUD = generalized equivalent uniform doses–based arc therapy;

Biological optimization in VMAT therapy for prostate carcinoma d I. B. MIHAYLOV et al. 1297
principle, it is possible to achieve similar plan quality with
DVH- and gEUD-based optimization schemes. The major
difference between the two types of optimization implied in
that study is the overall time required to achieve the optimal
solution. It requires more planning experience as well as
more trial-and-error steps with DVH-based compared with
gEUD-based optimization for comparable plans. To asses
each optimization scheme fairly, the same approach should
be applied in all cases. An initial educated guess, derived
from the planner experience, should be followed by consec-
utive manual interventions aimed at delivering a uniform tar-
get dose while sparing OARs as much as possible.
DVH-based objectives are simplified surrogates of biolog-
ical outcomes from a radiotherapy treatment. Arguably (11),
there is a multitude of DVHs that can lead to a similar dose
response for a particular anatomical structure. The high de-
generacy of the DVHs makes a large space of biologically
equivalent dose distributions for each organ equally accept-
able. Therefore, biologically based optimization achieves
better OAR sparing, at the expense of a minimal increase
in maximum target doses, for a preset number of human in-
terventions in the treatment planning process.
CONCLUSIONS
The findings presented here indicate that biological opti-
mization has a significant potential to improve the treatment
plans for VMAT delivery. The results demonstrate that
a combination of DVH and gEUD objectives delivers accept-
able dose uniformity across the targets, increased sparing of
the surrounding critical structures, and a reasonable compro-
mise for treatment time and delivered monitor units com-
pared with the routinely used DVH optimization. Readers
should be cautioned that our conclusions are based on statis-
tical inferences, and, in some cases, DVH-based optimization
may yield better VMAT plans.
REFERENCES
1. Yu CX. Intensity-modulated arc therapy with dynamic multileafcollimation: An alternative to tomotherapy. Phys Med Biol1995;40:1435–1449.
2. Bortfeld T, Webb S. Single-Arc IMRT? Phys Med Biol 2009;54:N9–20.
3. Bzdusek K, Friberger H, Eriksson K, et al. Development andevaluation of an efficient approach to volumetric arc therapyplanning. Med Phys 2009;36:2328–2339.
4. Earl MA, Shepard DM, Naqvi S, et al. Inverse planning forintensity-modulated arc therapy using direct aperture optimiza-tion. Phys Med Biol 2003;48:1075–1089.
5. Otto K. Volumetric modulated arc therapy: IMRT in a singlegantry arc. Med Phys 2008;35:310–317.
6. Shepard DM, Cao D, Afghan MK, et al. An arc-sequencing al-gorithm for intensity modulated arc therapy. Med Phys 2007;34:464–470.
7. Moiseenko V, Duzenli C, Durand RE. In vitro study of cell sur-vival following dynamic MLC intensity-modulated radiationtherapy dose delivery. Med Phys 2007;34:1514–1520.
8. Mu X, Lofroth PO, Karlsson M, et al. The effect of fraction timein intensity modulated radiotherapy: Theoretical and experi-mental evaluation of an optimisation problem. Radiother Oncol2003;68:181–187.
9. Wang JZ, Li XA, D’Souza WD, et al. Impact of prolonged frac-tion delivery times on tumor control: A note of caution forintensity-modulated radiation therapy (IMRT). Int J Radiat On-col Biol Phys 2003;57:543–552.
10. Das SK. A role for biological optimization within the cur-rent treatment planning paradigm. Med Phys 2009;36:4672–4682.
11. Wu Q, Mohan R, Niemierko A, et al. Optimization of intensity-modulated radiotherapy plans based on the equivalent uniformdose. Int J Radiat Oncol Biol Phys 2002;52:224–235.
12. Ling CC, Li XA. Over the next decade the success of radiationtreatment planning will be judged by the immediate biologicalresponse of tumor cells rather than by surrogate measuressuch as dose maximization and uniformity. Med Phys 2005;32:2189–2192.
13. Kallman P, Agren A, Brahme A. Tumour and normal tissue re-sponses to fractionated non-uniform dose delivery. Int J RadiatBiol 1992;62:249–262.
14. Lyman JT. Complication probability as assessed from dose-volume histograms. Radiat Res Suppl 1985;8:S13–19.
15. Niemierko A. Reporting and analyzing dose distributions: Aconcept of equivalent uniform dose. Med Phys 1997;24:103–110.
16. Niemierko A. A generalized concept of equivalent uniform dose(EUD). Med Phys 1999;26:1100.
17. Choi B, Deasy JO. The generalized equivalent uniform dosefunction as a basis for intensity-modulated treatment planning.Phys Med Biol 2002;47:3579–3589.
18. Thieke C, Bortfeld T, Niemierko A, et al. From physical doseconstraints to equivalent uniform dose constraints in inverse ra-diotherapy planning. Med Phys 2003;30:2332–2339.
19. Thomas E, Chapet O, Kessler ML, et al. Benefit of using bio-logic parameters (EUD and NTCP) in IMRT optimization fortreatment of intrahepatic tumors. Int J Radiat Oncol Biol Phys2005;62:571–578.
20. Widesott L, Strigari L, Pressello MC, et al. Role of the param-eters involved in the plan optimization based on the generalizedequivalent uniform dose and radiobiological implications. PhysMed Biol 2008;53:1665–1675.
21. Penagaricano JA, Papanikolaou N, Wu C, et al. An assessmentof biologically-based optimization (BORT) in the IMRT era.Med Dosim 2005;30:12–19.
22. Qi XS, Semenenko VA, Li XA. Improved critical structuresparing with biologically based IMRT optimization. MedPhys 2009;36:1790–1799.
23. Semenenko VA, Reitz B, Day E, et al. Evaluation of a commer-cial biologically based IMRT treatment planning system. MedPhys 2008;35:5851–5860.
24. Ahnesjo A, Andreo P, Brahme A. Calculation and applicationof point spread functions for treatment planning with high en-ergy photon beams. Acta Oncol 1987;26:49–56.
25. Mackie TR, Scrimger JW, Battista JJ. A convolution method ofcalculating dose for 15-MV x rays. Med Phys 1985;12:188–196.
26. Emami B, Lyman J, Brown A, et al. Tolerance of normal tissueto therapeutic irradiation. Int J Radiat Oncol Biol Phys 1991;21:109–122.
27. Aaltonen P, Brahme A, Lax I, et al. Specification of dose deliv-ery in radiation therapy. Recommendation by the Nordic Asso-ciation of Clinical Physics (NACP). Acta Oncol 1997;36(Suppl10):1–32.
28. Bentzen SM. High-tech in radiation oncology: Should there bea ceiling? Int J Radiat Oncol Biol Phys 2004;58:320–330.

1298 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 3, 2012
29. Dutreix A. When and how can we improve precision in radio-therapy? Radiother Oncol 1984;2:275–292.
30. Dutreix J, Tubiana M, Dutreix A. An approach to the interpre-tation of clinical data on the tumour control probability-dose re-lationship. Radiother Oncol 1988;11:239–248.
31. Mihaylov IB, Penagaricano J, Moros EG. Quantification of theskin sparing effect achievable with high-energy photon beamswhen carbon fiber tables are used. Radiother Oncol 2009;93:147–152.
32. Mihaylov IB, Siebers JV. Evaluation of dose prediction errorsand optimization convergence errors of deliverable-based
head-and-neck IMRT plans computed with a superposition/con-volution dose algorithm. Med Phys 2008;35:3722–3727.
33. Rosner B. Fundamentals of biostatistics. Boston: DuxberryPress; 1986. 54–58.
34. Bevington PR, Robinson KD. Data reduction and error analysis.3rd ed. New York: McGraw-Hill; 2003.
35. Sohn M, Yan D, Liang J, et al. Incidence of late rectal bleedingin high-dose conformal radiotherapy of prostate cancer usingequivalent uniform dose-based and dose-volume-based normaltissue complication probability models. Int J Radiat Oncol BiolPhys 2007;67:1066–1073.





![[- 200 [ PROVIDING MODULATED COMMUNICATION SIGNALS ]](https://static.fdokumen.com/doc/165x107/6328adc85c2c3bbfa804c60f/-200-providing-modulated-communication-signals-.jpg)













