Bevacizumab in older patients with advanced colorectal or breast cancer
14
Critical Reviews in Oncology/Hematology 87 (2013) 41–54 Bevacizumab in older patients with advanced colorectal or breast cancer Giuseppe Aprile a,∗,1 , Laura Ferrari a,1 , Caterina Fontanella a,1 , Fabio Puglisi a,b,1 a Department of Medical Oncology, University of Udine, Italy b Department of Medical and Biological Science, University of Udine, Italy Accepted 20 November 2012 Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42 2. Mechanism of action of bevacizumab . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42 3. Major bevacizumab-related toxicities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42 3.1. Hypertension . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42 3.2. Proteinuria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43 3.3. Thromboembolic events . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43 3.3.1. Arterial thromboembolic events (ATEs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43 3.3.2. Venous thromboembolic events (VTEs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43 3.4. Bleeding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43 3.5. Congestive heart failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44 3.6. Gastrointestinal perforation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44 3.7. Wound-healing complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44 4. Bevacizumab in the treatment of older patients: the quest for fine tuning to maximize efficacy and minimize toxicity . . . . . . . . . . . . 44 4.1. Colorectal cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44 4.2. Breast cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48 5. Recommendations for the selection of older patients to be offered anti-angiogenic treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 6. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 Biographies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54 Abstract The incidence of colorectal and breast cancer is growing among the 550 million living people aged 65 or older. Bevacizumab was the first anti-angiogenic agent approved for the treatment of the advanced phase of these cancers. Although older chronological age still hampers the use of modern treatments, there is a widespread awareness that chronological and physiological (i.e. functional) ages may largely differ, and that seniority itself should not be a stringent limit for the introduction of anti-angiogenics. However, the use of bevacizumab in the general older population is questionable. There is limited evidence of a favorable risk-to-benefit ratio, with efficacy data deriving from clinical trials that selected only elderly patients in rather good health. While summarizing the recent advances, this review highlights specific clinical features characterizing those older patients who may benefit the most from receiving bevacizumab. © 2012 Elsevier Ireland Ltd. All rights reserved. Keywords: Bevacizumab; Elderly; Colorectal cancer; Breast cancer ∗ Corresponding author at: Department of Medical Oncology, Piazzale Santa Maria della Misericordia, University Hospital Santa Maria della Misericordia, 33100 Udine, Italy. Tel.: +39 0432559308; fax: +390 432559305; mobile: +39 3470048600. E-mail address: [email protected] (G. Aprile). 1 All authors have equally contributed to the writing, and they all have read and approved the final manuscript. 1040-8428/$ – see front matter © 2012 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.critrevonc.2012.11.006
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Bevacizumab in older patients with advanced colorectal or breast cancer

C
123
4
56
A
autpsc©
K
3
1h
Critical Reviews in Oncology/Hematology 87 (2013) 41–54
Bevacizumab in older patients with advanced colorectal or breast cancer
Giuseppe Aprile a,∗,1, Laura Ferrari a,1, Caterina Fontanella a,1, Fabio Puglisi a,b,1
a Department of Medical Oncology, University of Udine, Italyb Department of Medical and Biological Science, University of Udine, Italy
Accepted 20 November 2012
ontents
. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
. Mechanism of action of bevacizumab . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
. Major bevacizumab-related toxicities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 423.1. Hypertension . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 423.2. Proteinuria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 433.3. Thromboembolic events . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
3.3.1. Arterial thromboembolic events (ATEs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 433.3.2. Venous thromboembolic events (VTEs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
3.4. Bleeding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 433.5. Congestive heart failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 443.6. Gastrointestinal perforation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 443.7. Wound-healing complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
. Bevacizumab in the treatment of older patients: the quest for fine tuning to maximize efficacy and minimize toxicity . . . . . . . . . . . . 444.1. Colorectal cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 444.2. Breast cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
. Recommendations for the selection of older patients to be offered anti-angiogenic treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
. Conclusions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50Biographies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
bstract
The incidence of colorectal and breast cancer is growing among the 550nti-angiogenic agent approved for the treatment of the advanced phase ofse of modern treatments, there is a widespread awareness that chronologhat seniority itself should not be a stringent limit for the introduction of antiopulation is questionable. There is limited evidence of a favorable risk-telected only elderly patients in rather good health. While summarizing thharacterizing those older patients who may benefit the most from receivi
2012 Elsevier Ireland Ltd. All rights reserved.
eywords: Bevacizumab; Elderly; Colorectal cancer; Breast cancer
∗ Corresponding author at: Department of Medical Oncology, Piazzale Santa Ma3100 Udine, Italy. Tel.: +39 0432559308; fax: +390 432559305; mobile: +39 347
E-mail address: [email protected] (G. Aprile).1 All authors have equally contributed to the writing, and they all have read and a
040-8428/$ – see front matter © 2012 Elsevier Ireland Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.critrevonc.2012.11.006
million living people aged 65 or older. Bevacizumab was the first these cancers. Although older chronological age still hampers theical and physiological (i.e. functional) ages may largely differ, and-angiogenics. However, the use of bevacizumab in the general oldero-benefit ratio, with efficacy data deriving from clinical trials thate recent advances, this review highlights specific clinical features
ng bevacizumab.
ria della Misericordia, University Hospital Santa Maria della Misericordia,0048600.
pproved the final manuscript.

4 n Oncol
1
acpstmceimp[tmmifabsoia[
eachfiaratpnaetacofba
2
tnh
[t[etaHsecfgs
bp(siFpeas1wb
3
3
soiiu[w[tfiaftrbph
2 G. Aprile et al. / Critical Reviews i
. Introduction
In developed countries, cancer incidence and prevalencere rising among older generations [1]: over 60% of all can-ers are diagnosed in people over 65 years of age [2], androjections seem to confirm this trend [3]. As a result, theoaring demand for care of older people with cancer is likelyo increase further. Chronic medical disorders also are com-on in the elderly. Most older patients with cancer have
oncurrent morbidities requiring medical treatment [4], butven if they were otherwise healthy they may present dimin-shed organ functions, impairment of daily vital activities, orinor cognitive deficits. Nevertheless, the majority of those
atients will receive systemic chemotherapy and/or biologics5]. Age is an important risk factor for breast cancer, withhe average age at diagnosis being 61 years. According to theost recent Surveillance Epidemiology and End Results data,ore than 35% of new invasive breast cancers are diagnosed
n women aged over 65 [6]. It is worthy of note that in the lastew decades the rate of breast cancer-related death decreasedt least 2% per year in patients younger than 75 years old,ut only 1.1% per year in older patients [7]. Among the pos-ible reasons for reduced survival improvement observed inlder patients, under-treatment is likely to have a significantmpact [8]. Nearly 75% of all colorectal cancer patients areged ≥65 years, with a median age at diagnosis of 70 years9].
Bevacizumab, a humanized antibody against vascularndothelial growth factor (VEGF), is the first anti-angiogenicgent approved for clinical use. When added to systemichemotherapy, it has demonstrated superior outcomes andas gained market approval – regardless of patients’ age – inrst line of treatment for metastatic breast cancer (MBC) [10]nd in first or subsequent lines of therapy for metastatic colo-ectal carcinoma (CRC) [11,12]. Historically, chronologicalge has been a major barrier to clinicians offering standardreatments to older populations. However, chronological andhysiological ages may largely differ, and age itself shouldot be used as a stringent limit for the introduction of targetedgents. Different types and grades of comorbidities make thelderly highly heterogeneous in health status, but it is difficulto tailor treatment decisions on the basis of factors other thange. Moreover, older patients are under-represented in clini-al trials, and the few included are highly selected. The aimf this review is to critically analyze the available literatureocusing on the use of bevacizumab in older patients withreast or colorectal cancers, specifically addressing safetynd efficacy results.
. Mechanism of action of bevacizumab
Tumor cells can induce their own blood supply fromhe pre-existing vasculature with a mimetic process calledeo-angiogenesis, a recognized hallmark of cancer [13] thatas triggered significant research during the last decade
btiu
ogy/Hematology 87 (2013) 41–54
14–16]. The best-characterized angiogenic factors belong tohe VEGF family or to their related tyrosine kinases receptors17]. Since tumors are unable to grow beyond 2 mm in diam-ter without oxygen and blood supply [18], hypoxia itselfriggers the “angiogenic switch”, a biological process thatlters the balance between pro- and anti-angiogenic factors.ypoxia-inducible factor-1 (HIF-1) stimulates VEGF tran-
cription and VEGF causes enlarged vessel permeability withndothelial cell migration and proliferation [19]. Since can-er cells proliferate aberrantly, tumor neovasculature differsrom normal blood vasculature by being irregular and hetero-eneous, with similarly disorganized arteriolar and venulartructures [20].
Bevacizumab is a recombinant, humanized, function-locking monoclonal antibody that binds to VEGF-A andrevents its association with the endothelial receptor-2VEGFR-2) [21], inducing regression of existing microves-els, normalization of surviving mature vasculature, andnhibition of vessel growth and neovascularization [22–24].urthermore, maintaining the VEGF ligand inhibition mayrevent tumor growth and cause tumor shrinkage [25]. How-ver, the mechanism of action of bevacizumab is still unclear,nd specific predictive biomarkers are still lacking. A recenttudy suggests that a genetic locus in the VEGF receptor-
(VEGFR-1) tyrosine-kinase domain could be associatedith increased VEGFR1 expression and poor outcome ofevacizumab treatment [26].
. Major bevacizumab-related toxicities
.1. Hypertension
Bevacizumab-induced hypertension, the most frequentide effect of systemic inhibition of VEGF signaling, mayccur at any time during therapy [27], but its pathogenesiss not thoroughly understood. In preclinical studies, VEGFnhibition results in glomerulopathy associated with protein-ria, endotheliosis, and hyaline deposits in renal capillaries28]; furthermore, the silencing of the VEGF-mediated path-ays may reduce the endothelial production of nitric oxide
29]. An exploratory meta-analysis of randomized controlledrials showed that bevacizumab was associated with a four-old higher risk for hypertension (RR, 4.30; 95% confidencenterval [CI], 2.97–6.21) [30]. In addition, a weighted aver-ge of a 4.5% increase in the incidence of hypertensionor women with MBC exposed to bevacizumab comparedo those receiving placebo was reported [31]. Notably, ret-ospective studies suggest that hypertension may predictevacizumab efficacy [32,33], while specific VEGF geneticolymorphisms forecast both the development of severeypertension and prolonged survival [34]. Management of
evacizumab-induced hypertension usually requires standardreatments such as angiotensin-converting enzyme (ACE)nhibitors [35]. Despite the lack of randomized trials, thepfront use of ACE inhibitors is reasonable because of
n Oncol
tgiase
ir2aohr
3
wd(dtarctmfpd
3
octc
3
aowac0oetaitt
6y
3
6tct(estidaf
3
hbgwno(awr(rdmsm
arsatAi1taa
s
G. Aprile et al. / Critical Reviews i
heir ability to counteract bevacizumab-induced plasmino-en activator inhibitor-1 [36]. Add-on second-line therapiesnclude non-dihydropyridine calcium channel blockers orldosterone receptor antagonists [27]. However, the optimaltrategy for the management of this toxicity has not yet beenstablished.
Among risk factors for the development of bevacizumab-nduced hypertension, older age is to be considered. Aetrospective review found an incidence of hypertension of9% in MCRC patients aged >75 years versus 11% in thoseged 65–75 [37]. It should be noted that community-dwellinglder patients may have more comorbidities compared withighly selected trial patients and may therefore be at increasedisk of developing this side effect.
.2. Proteinuria
The overall incidence of proteinuria in cancer patientsho received bevacizumab ranged from 21% to 63%, with aose-dependent relative risk of 1.4 for low-dose exposure5 mg/kg/week) rising to 2.2 for patients receiving higheroses (10–15 mg/kg/week) [38]. Mainly asymptomatic pro-einuria spontaneously resolves as soon as treatment ends,nd only in 1–2% of cases does it cause serious impairment ofenal function [28,38,39]. To some degree, hypertension itselfontributes to facilitate the genesis of proteinuria. However,he frequent co-occurrence of hypertension and proteinuria
ay also reflect the importance of VEGF in normal renalunction. ACE inhibitors may decrease urine protein loss inatients with diabetic-induced nephropathy or other kidneyiseases [40].
.3. Thromboembolic events
Thromboembolic events are one of the leading causesf morbidity and mortality in patients with advanced can-er; their occurrence is related to cancer type and burden,reatment type and duration, underlying comorbidities, andoncomitant medications [41,42].
.3.1. Arterial thromboembolic events (ATEs)Among MCRC patients receiving bevacizumab, arterial
dverse events are more frequently observed in subjectslder than 75 years [43]. The overall incidence of ATEsas 3.8% in advanced cancer patients receiving bevacizumab
nd chemotherapy, compared to 1.7% in those receivinghemotherapy alone. Event-related death was low, being.62% in the bevacizumab-treated patients and 0.26% in thethers [44]. While the overall increase in the risk was mod-st, it appeared to be significant in patients with previoushromboembolic history (HR 2.17, 95%CI 1.17–4) or those
ged over 65 (HR 3.65, 95%CI 1.92–6.92) [44]. Moreover,n a separate evaluation of 1953 elderly patients with MCRCreated with bevacizumab [45], there was 4.3% of ATEs inhose older than 80 years versus 1.5% in those younger thanhtOo
ogy/Hematology 87 (2013) 41–54 43
5. In the light of these data, patients who are older than 65ears should be always considered at a higher risk.
.3.2. Venous thromboembolic events (VTEs)A pooled analysis of ten randomized trials enrolling over
000 patients showed no statistically significant increase inhe incidence of all-grade VTEs for bevacizumab versusontrols [42]. The unadjusted incidence in the bevacizumab-reated group was 10.9% versus 9.8% in the control groupOR 1.14; 95%CI, 0.96–1.35), with similar figures for severevents in both groups [39]. After bevacizumab exposure, theimultaneous risk for both thrombosis and bleeding reflectshe multiplicity of actions of VEGF on the vascular walls andts interference with the coagulation cascade [46]. However,ata suggest that the interaction of bevacizumab with plateletggregation should not be considered a major contributingactor to either thrombotic events or bleeding [47].
.4. Bleeding
The initial serious concern that a severe or fatalemorrhage might occur much more frequently in theevacizumab-treated than in non-exposed patients was trig-ered by the premarketing analysis of 1132 cancer patients,here the incidence of severe bleeding events was 4%. Whileot fully dismissed, the concern has at least been temperedver time thanks to reassuring available data. In the BRITEBevacizumab Regimens: Investigation of Treatment Effectsnd safety) study, a large cohort of 1953 MCRC patientsho were treated with first-line bevacizumab and concur-
ent chemotherapy, the incidence of serious bleeding eventsSBEs) was 2.6%, with 6 months as the median time to occur-ence [48]. Patients with rectal cancer as the primary site hadouble the rate of SBEs compared to patients with the pri-ary tumor located in the colon (4% versus 2%; P = 0.012),
uggesting that primary cancer site may be a risk factor forajor bleeding.It is unclear whether patients on anticoagulant or
ntiplatelet therapy can be safely treated. Notably, patientseceiving full-dose anticoagulants share a limited risk ofevere bleeding (<1%) that does not seem to be affected bynti-angiogenic exposure [42]. Moreover, MCRC patientsreated with bevacizumab while receiving prophylaxis forTEs with low-dose acetylsalicylic acid experienced sim-
lar rates of bleeding compared to the others (11% versus4%, P = 0.13) [49]. Nonetheless, because of the retrospec-ive nature of the data, caution should be used in patients whore candidates for bevacizumab and are receiving full-dosenticoagulation or full-dose antiplatelet therapy.
In MBC patients enrolled in five clinical trials [50],erious hemorrhagic events were uncommon (<1.7%), and
igher than 5% only in the taxane–bevacizumab arm ofhe RIBBON-1 (Regimens In Bevacizumab for BreastNcology-1). It should be noted that trials allowed the usef aspirin or anticoagulants.
4 n Oncol
nVgmecHacbs
(a(etasrwrcp
3
wdef
hwipsmltt–h
btpMis[ac
tc
3
iicFpnpa1tdra
3
tcaarowo
4tm
otord
4
W5ops
4 G. Aprile et al. / Critical Reviews i
SBEs associated with bevacizumab use include centralervous system (CNS) hemorrhage. Higher expression ofEGF mRNA in tumor cells directly correlated with therowth of brain metastasis, suggesting that VEGF expressionay play a role in the development of brain lesions [51]. Nev-
rtheless, patients with brain metastases were excluded fromlinical trials because of the worry of CNS hemorrhages [52].owever, subsequent case series, retrospective exploratory
nalysis, and phase-II/III trials show that the addition of beva-izumab to different chemotherapy agents in patients withrain metastases treated with whole-brain radiotherapy seemsafe, producing a low incidence of CNS hemorrhage [53–56].
In SAiL (Safety of Avastin in Lung) [57] and ATHENAAvastin THErapy for advaNced breAst cancer) [58] tri-ls only three cases of cerebral hemorrhage in 321 patients0.9%) with occult CNS metastases were reported. In anxploratory analysis of the AVADO (AVastin And DOce-axel) trial, no major CNS bleeding events were reportedmong women who developed brain metastases while on thetudy [46]. Although reports indicate no clear increase in theisk of cerebral hemorrhage in bevacizumab-treated patientsith brain metastases, patient selection may be a potential
eason for the lower rates of cerebral hemorrhage. Extremeaution should be exercised when treating common canceropulations with symptomatic CNS metastases.
.5. Congestive heart failure
The benefits and risks of using bevacizumab in patientsith a significant cardiovascular history, including myocar-ial infarction or cerebral vascular accidents, have not beenstablished, mainly because these patients were excludedrom clinical studies [59].
A significant five-fold increase in the risk of congestiveeart failure (CHF) in bevacizumab-treated MBC patientsas recently reported, with a cumulative incidence of 1.6%
n the exposed patients compared to 0.4% in the unexposedatients [60]. Despite the large sample size, the analysisuffers from several limitations: (1) individual patient infor-ation was unavailable, and data were retrieved from the
iterature; (2) the definition of CHF was blurred; (3) risk fac-ors for the development of CHF – including prior exposureo cardiotoxic agents or potentially contributing conditions
were not considered; (4) death, significant disability fromigh-grade CHF, and timing of CHF were not captured.
Although the greater risk of CHF in patients exposed toevacizumab may have been related to hypertension or ATEs,he role of the drug in the genesis of cardiotoxicity will remainartially unclear until more in-depth analyses are conducted.oreover, since the advent of the use of tyrosine kinase
nhibitors (TKIs), anti-angiogenic agents (i.e. sorafenib and
unitinib) may sometimes result in increased rates of CHF61,62], and cardiovascular toxicity could be considered asclass side effect rather than a specific bevacizumab-relatedonsequence. Nonetheless, whenever bevacizumab is given
rist
ogy/Hematology 87 (2013) 41–54
o patients with known cardiac risk factors, strict cardiovas-ular monitoring is strongly recommended.
.6. Gastrointestinal perforation
Gastrointestinal (GI) perforations were initially observedn the pivotal phase-III trial for bevacizumab in MCRC [11],n which six events occurred in the bevacizumab group (1.5%)ompared with no events in the control group. Afterwards, theirst BEATrial (First Bevacizumab Expanded Access Trial)rovided new data on bevacizumab safety in a large commu-ity population [63]. Among 223 patients with unresectedrimary tumor, 3.6% had GI perforation. On the other hand,mong 1373 patients with resected primary tumors, only.2% had GI perforation, suggesting that an intact primaryumor may be an important risk factor. In addition, the inci-ence of GI perforation seemed to be higher in patients withecent history of sigmoidoscopy or colonoscopy, or previousdjuvant radiotherapy [64].
.7. Wound-healing complications
Since wound healing depends on angiogenesis [65], theiming of bevacizumab initiation and cessation warrantsareful consideration. Considering the pharmacokineticsnd half-life of bevacizumab, a 6-week interval betweennti-angiogenic exposure and major surgery is consideredeasonably safe [66,67]. Moreover, a retrospective reviewn 195 patients confirmed that having received bevacizumabithin 10 days of port placement caused a higher incidencef wound dehiscence [68].
. Bevacizumab in the treatment of older patients:he quest for fine tuning to maximize efficacy and
inimize toxicity
Data regarding the use of bevacizumab for older MCRCr MBC patients are limited and derive from (a) subpopula-ion analyses of large phase-III randomized controlled trialsf bevacizumab-containing therapies, (b) non-randomizedegistries of community-based studies, or (c) specificallyesigned small phase-II trials.
.1. Colorectal cancer
Median age at diagnosis usually exceeds 70 years inestern countries [9]. Generally, older people treated with
-fluorouracil alone [69] or combined with irinotecan [70]r oxaliplatin [71] derive the same advantage as youngeratients in terms of response rate (RR), progression-freeurvival (PFS), and overall survival (OS). After the first
eport merging data from 439 patient aged >65 enrolledn the AVF2107/AVF2192 studies [72], a broader retro-pective exploratory pooled analysis of four randomizedrials suggested that when bevacizumab is combined with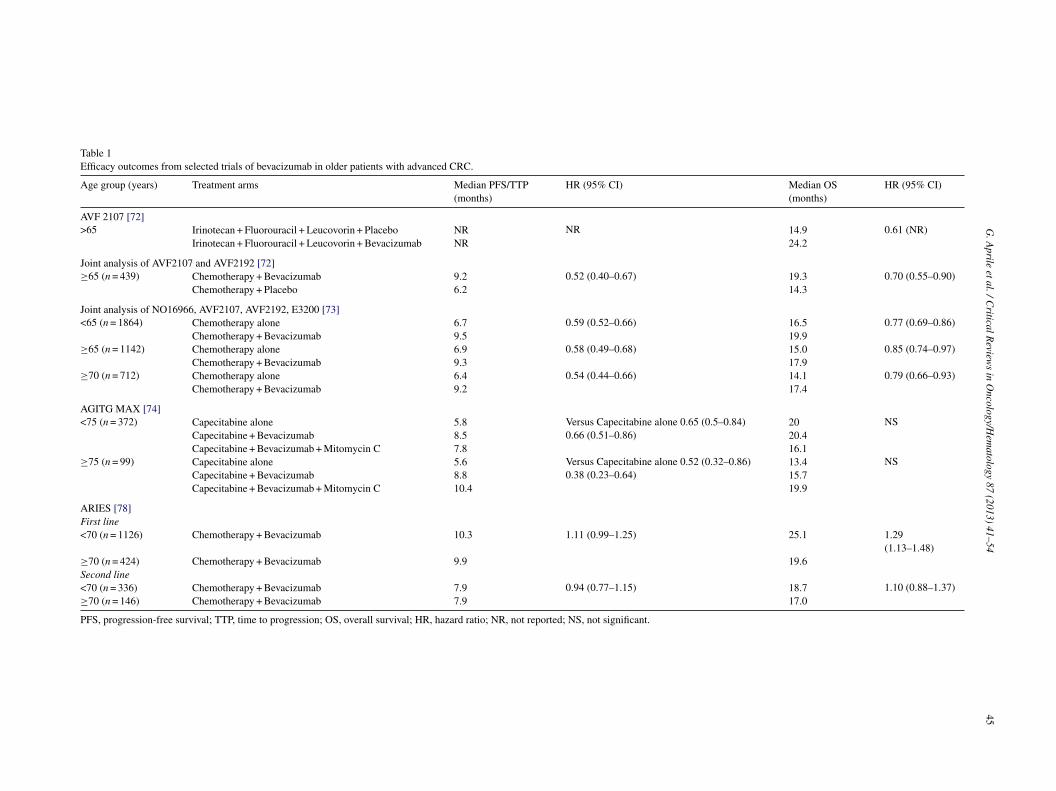
G.
Aprile
et al.
/ C
ritical R
eviews
in O
ncology/Hem
atology 87
(2013) 41–54
45
Table 1Efficacy outcomes from selected trials of bevacizumab in older patients with advanced CRC.
Age group (years) Treatment arms Median PFS/TTP(months)
HR (95% CI) Median OS(months)
HR (95% CI)
AVF 2107 [72]>65 Irinotecan + Fluorouracil + Leucovorin + Placebo NR NR 14.9 0.61 (NR)
Irinotecan + Fluorouracil + Leucovorin + Bevacizumab NR 24.2
Joint analysis of AVF2107 and AVF2192 [72]≥65 (n = 439) Chemotherapy + Bevacizumab 9.2 0.52 (0.40–0.67) 19.3 0.70 (0.55–0.90)
Chemotherapy + Placebo 6.2 14.3
Joint analysis of NO16966, AVF2107, AVF2192, E3200 [73]<65 (n = 1864) Chemotherapy alone 6.7 0.59 (0.52–0.66) 16.5 0.77 (0.69–0.86)
Chemotherapy + Bevacizumab 9.5 19.9≥65 (n = 1142) Chemotherapy alone 6.9 0.58 (0.49–0.68) 15.0 0.85 (0.74–0.97)
Chemotherapy + Bevacizumab 9.3 17.9≥70 (n = 712) Chemotherapy alone 6.4 0.54 (0.44–0.66) 14.1 0.79 (0.66–0.93)
Chemotherapy + Bevacizumab 9.2 17.4
AGITG MAX [74]<75 (n = 372) Capecitabine alone 5.8 Versus Capecitabine alone 0.65 (0.5–0.84)
0.66 (0.51–0.86)20 NS
Capecitabine + Bevacizumab 8.5 20.4Capecitabine + Bevacizumab + Mitomycin C 7.8 16.1
≥75 (n = 99) Capecitabine alone 5.6 Versus Capecitabine alone 0.52 (0.32–0.86)0.38 (0.23–0.64)
13.4 NSCapecitabine + Bevacizumab 8.8 15.7Capecitabine + Bevacizumab + Mitomycin C 10.4 19.9
ARIES [78]First line<70 (n = 1126) Chemotherapy + Bevacizumab 10.3 1.11 (0.99–1.25) 25.1 1.29
(1.13–1.48)≥70 (n = 424) Chemotherapy + Bevacizumab 9.9 19.6Second line<70 (n = 336) Chemotherapy + Bevacizumab 7.9 0.94 (0.77–1.15) 18.7 1.10 (0.88–1.37)≥70 (n = 146) Chemotherapy + Bevacizumab 7.9 17.0
PFS, progression-free survival; TTP, time to progression; OS, overall survival; HR, hazard ratio; NR, not reported; NS, not significant.

4 n Oncol
ceSpcopaa(
t(aCm(((fs
mlbd≥fdn7tarwaoaos
ti(v([
tPPCscet
dv
SOalsfvf(a
79dwsPlwacaEaocvratpt
Caiwotpicbaocdei
6 G. Aprile et al. / Critical Reviews i
hemotherapy both tolerance and outcome are not influ-nced by age, at least in medically fit older patients [73].pecifically, compared to the PFS benefit that the youngeratients derived from the addition of bevacizumab to standardhemotherapy (HR 0.59, 95%CI 0.52–0.66), the magnitudef PFS benefit for the use of bevacizumab was similar amongatients aged over 70 (HR 0.54, 95%CI 0.44–0.66). The samedvantage was maintained for the benefit in OS, with anlmost identical risk reduction for death (23% versus 21%)Table 1).
In the subgroup analysis of the Australasian Gastroin-estinal Study Group (AGITG) Mitomycine–Avastin–XelodaMAX) trial, restricted to 99 patients older than 75 [74], olderge did not significantly impact on the outcome (Table 1).hemotherapy dose intensity was also maintained, with noajor differences in toxicity patterns between age cohorts
Table 2). Of note, baseline comorbidities such as diabetes15%), hypertension (56%), previous ischemic heart disease15%) or cerebrovascular accidents (10%) were similar inrequency to those reported in the general population of theame age.
A subgroup analysis from BRITE (Bevacizumab Regi-ens investigation of Treatment Effects and Safety), the
argest observational registry of CRC patients exposed toevacizumab, included 896 patients aged ≥65 years that wereivided into three age cohorts (65–74 n = 533; 75–80 n 202;80 n = 161) [75]. Compared to the median PFS reported
or the 1057 patients aged <65 (9.8 months), no significantifferences in median PFS among older age cohorts wereoted (9.6 months in those aged 65–74; 10 months in those5–80; 8.6 in those ≥80). Nevertheless, median OS tendedo decrease with age, shrinking from 24.6 months in thoseged <65–16.8 months in those >80. Rates of bevacizumab-elated AEs appeared to be similar across age subgroups,ith no differences in proteinuria, bleeding, or hypertension
mong age cohorts. However, increased rates of ATEs in thelder age cohorts were reported (4.8% in patients between 75nd 80 years, 4% in those over 80 years versus 1.4% in thether two categories), although 60-day mortality rates wereimilar (Table 2).
The subgroup analysis of 1559 CRC patients enrolled inhe Czech observational registry showed a slight increasen the rate of bevacizumab-related AEs in those aged >65n = 280) compared to that in the younger patients (11.3%ersus 9.2%), with no significant differences in median PFS11 versus 12.6 months) or OS (27 months versus not reached)76].
ETNA is a French cohort study including over 400 patientsreated with upfront chemotherapy and bevacizumab [77].atients aged <75 years (n = 360) had a slightly longer medianFS (10.9 versus 9.9 months) compared to those >75 (n = 51).ompared to the younger cohort, those aged >75 years had
imilar exposure to irinotecan, similar duration of beva-izumab treatment, and comparable incidences of adversevents (any grade) (43.1% versus 41.7%). The scope ofoxicity was also similar between age groups, with minor
8p
t
ogy/Hematology 87 (2013) 41–54
ifferences in the incidence of hypertension, proteinuria, orascular events.
ARIES (Avastin Registry: Investigation of Efficacy andafety), a US observational cohort study, reported PFS andS of elderly patients (>70 years) receiving bevacizumab
nd chemotherapy in first- or second-line treatment. First-ine efficacy results paralleled those of other registries, againhowing similar PFSs and slightly reduced median survivalor elderly MCRC patients. Interestingly, neither PFS (7.9ersus 7.9 months) nor OS (18.7 versus 17.2 months) dif-ered in second-line treatment between the two age categoriesTable 1). The incidences of bevacizumab-specific AEs werelso similar, regardless of age and previous treatments [78].
In a Spanish phase-II trial, 59 CRC patients aged at least0 were treated up front with capecitabine 1250 mg/m2 (or50 mg/m2 if creatinine clearance of 30–50 ml/min) twiceaily on days 1–14 and bevacizumab 7.5 mg/kg every 3eeks obtaining an overall RR of 34%. [79]. Hyperten-
ion was reported in 36 patients (60%) at baseline. MedianFS and OS were 10.8 and 18 months, respectively, in
ine with expected values. The toxicity profile, however,as significant. Although most AEs were mild or moder-
te (74%), 32 patients reported severe side effects, the mostommon being HFS (19%), diarrhea (9%) and VTEs (7%),nd four of them died because of treatment-related toxicities.leven patients reported mild to moderate hypertension,nd one patient had grade 3. Indeed, a higher frequencyf bevacizumab-unrelated severe AEs was noted in thoseycles in which creatinine clearance was <50 ml/min (23ersus 13%; P < 0.05), but whether the patients included wereeally unselected is not clear. Notwithstanding the unsuit-bility for receiving oxaliplatin or irinotecan-based doubletshat had been specified among the inclusion criteria, someatients received combination chemotherapy as second-linereatment.
In a Croatian phase-II study, 41 patients with advancedRC (median age 75) were treated up front with bevacizumabnd capecitabine at standard doses. The ORR was 65%,ncluding 13% of complete responses. Median PFS and OSere 11.5 and 21.2 months, respectively. Rates and patternsf toxicity were similar to those expected [80]. Two similarrials by the same Italian group were reported, both enrollingatients aged over 70. In the first study 42 patients receivedrinotecan (180 mg/mq), bevacizumab (7.5 mg/kg q21) andapecitabine assumed continuously at a fixed dose of 1000 mg.i.d. Median PFS was 12.3 months, median OS 22 months,nd no life-threatening toxicities were reported [81]. The sec-nd study evaluated the efficacy and safety of the metronomicombination of oxaliplatin (65 mg/m2), capecitabine (fixedose of 1000 mg b.i.d.) and bevacizumab (7.5 mg/kg) in 76lderly CRC patients. No patient experienced grade 4 toxic-ty. Median PFS was 12.3 months with a 6-month PFS rate of
2%. Median OS was 23.5 months with a 12-month survivalrobability of nearly 80% [82].Data derived from the large German registry confirmedhat bevacizumab-based treatment combinations can be
G.
Aprile
et al.
/ C
ritical R
eviews
in O
ncology/Hem
atology 87
(2013) 41–54
47
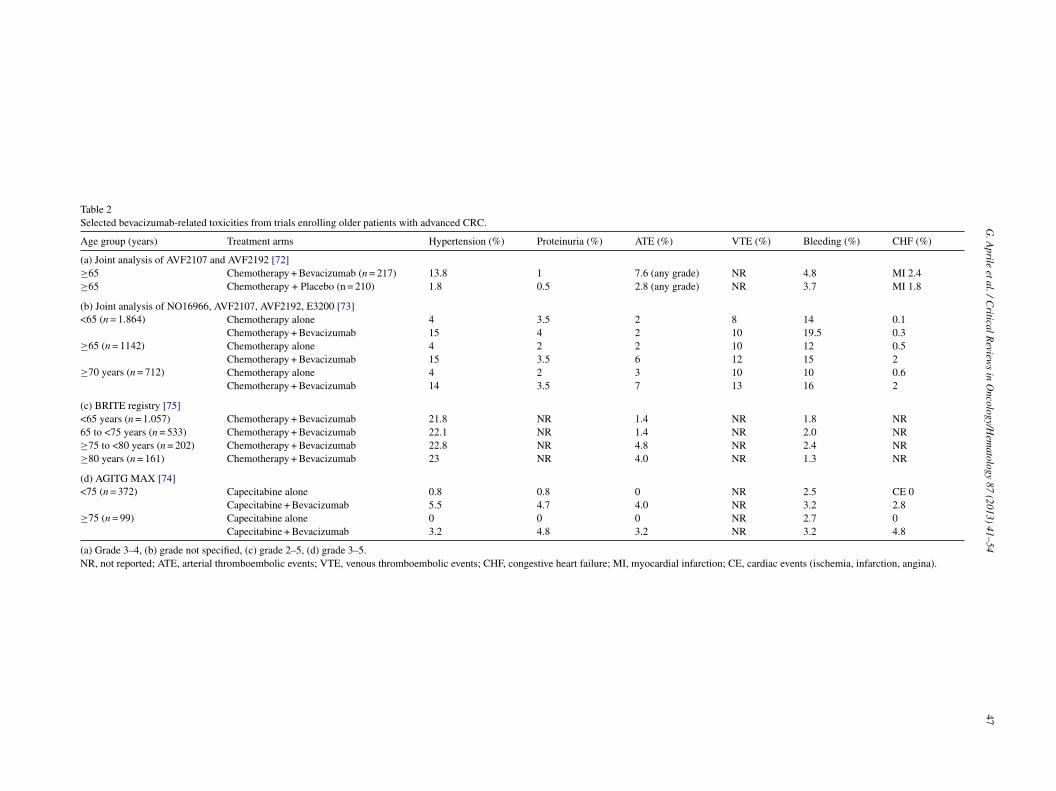
Table 2Selected bevacizumab-related toxicities from trials enrolling older patients with advanced CRC.
Age group (years) Treatment arms Hypertension (%) Proteinuria (%) ATE (%) VTE (%) Bleeding (%) CHF (%)
(a) Joint analysis of AVF2107 and AVF2192 [72]≥65 Chemotherapy + Bevacizumab (n = 217) 13.8 1 7.6 (any grade) NR 4.8 MI 2.4≥65 Chemotherapy + Placebo (n = 210) 1.8 0.5 2.8 (any grade) NR 3.7 MI 1.8
(b) Joint analysis of NO16966, AVF2107, AVF2192, E3200 [73]<65 (n = 1.864) Chemotherapy alone 4 3.5 2 8 14 0.1
Chemotherapy + Bevacizumab 15 4 2 10 19.5 0.3≥65 (n = 1142) Chemotherapy alone 4 2 2 10 12 0.5
Chemotherapy + Bevacizumab 15 3.5 6 12 15 2≥70 years (n = 712) Chemotherapy alone 4 2 3 10 10 0.6
Chemotherapy + Bevacizumab 14 3.5 7 13 16 2
(c) BRITE registry [75]<65 years (n = 1.057) Chemotherapy + Bevacizumab 21.8 NR 1.4 NR 1.8 NR65 to <75 years (n = 533) Chemotherapy + Bevacizumab 22.1 NR 1.4 NR 2.0 NR≥75 to <80 years (n = 202) Chemotherapy + Bevacizumab 22.8 NR 4.8 NR 2.4 NR≥80 years (n = 161) Chemotherapy + Bevacizumab 23 NR 4.0 NR 1.3 NR
(d) AGITG MAX [74]<75 (n = 372) Capecitabine alone 0.8 0.8 0 NR 2.5 CE 0
Capecitabine + Bevacizumab 5.5 4.7 4.0 NR 3.2 2.8≥75 (n = 99) Capecitabine alone 0 0 0 NR 2.7 0
Capecitabine + Bevacizumab 3.2 4.8 3.2 NR 3.2 4.8
(a) Grade 3–4, (b) grade not specified, (c) grade 2–5, (d) grade 3–5.NR, not reported; ATE, arterial thromboembolic events; VTE, venous thromboembolic events; CHF, congestive heart failure; MI, myocardial infarction; CE, cardiac events (ischemia, infarction, angina).

4 n Oncol
sPmbi
afidwPPv
4
iiMidfktrsd[ed
wtlp
wtbt
itoI(cwEasoit
aarptNecsAbirwcsc6
tctmtcmps
Ade2Ia1aMictwweeSsdrrit
8 G. Aprile et al. / Critical Reviews i
uccessfully used in patients aged ≥75 years. However, bothFS (8.9 versus 10.5 months) and OS (20.8 versus 25.8onths) were significantly shorter in older patients, probably
ecause of greater comorbidity and possibly because of lessntensive second-line treatment in the older subgroup [83].
In clinical practice, advanced CRC Medicare beneficiariesged at least 65 derived survival advantage when treated upront with chemotherapy and bevacizumab, particularly whenrinotecan-based chemotherapy was chosen as the companionoublet [84]. The addition of bevacizumab, even associatedith a modestly increased risk of stroke (4.9% versus 2.5%;
< 0.01) and gastrointestinal perforation (2.3% versus 1.0%; < 0.01), was not linked with increased cardiac events orenous thrombosis.
.2. Breast cancer
Since the incidence of breast cancer increases with age,t is not surprising that over 50% of new cases are detectedn women older than 65 [85]. Generally, older patients with
BC are expected to derive benefits from chemotherapy sim-lar to those of younger patients, but toxicity and quality of lifeeterioration may be greater [86]. As a result, life expectancy,unctional status, comorbidities and potential toxicities are alley elements to consider when choosing the most appropriatereatment strategy [8]. For example, in the case of diabetes-elated peripheral neuropathy, a taxane-containing regimenhould be avoided [87], while the presence of coronary arteryisease should suggest caution in prescribing anthracyclines83]. The multidimensional geriatric assessment and the pres-nce of suitable care-givers are also critical in the treatmentecision [88]
Although few phase-II trials have been conducted in olderomen [89,90], oral chemotherapies [91,92] appear attrac-
ive because of excellent tolerance and the possibility ofimiting hospitalizations while preserving functional inde-endence [93].
Data regarding the use of bevacizumab in older patientsith MBC have been recently updated. Overall, subpopula-
ion analysis of randomized clinical trials have suggested PFSenefits for bevacizumab exposure in older patients similaro those in younger patients [94–98].
No differences in OS were observed among different armsn trials comparing bevacizumab-containing regimens versushe corresponding single-agent therapy. These results werebtained either in the entire population or in the older patients.t is important to note that the Food and Drugs AdministrationFDA) originally granted accelerated approval for beva-izumab for use in combination with paclitaxel in patientsith MBC, based on the advantage in PFS observed in the2100 trial [10]. It is important to point out that there was
warning in the registration document, based on that trial,
tating that higher toxicity and mortality were observed inlder patients [99]. Recently, the license for bevacizumabn MBC has been revoked in the US because of addi-ional results from other studies that failed to demonstrateibn
ogy/Hematology 87 (2013) 41–54
significant improvement in OS or a clinically relevant ther-peutic benefit. Nonetheless, debate about the benefit/riskatio of bevacizumab in MBC continues, and the combinationaclitaxel–bevacizumab is still considered a valid therapeu-ic option by the Breast Cancer Guideline Committee of theCCN and by the European Medicines Agency (EMA). In
ffect, similar to the large majority of trials in breast can-er [100], several factors may explain the lack of overallurvival differences between experimental and control arms.mong other reasons, the fact that OS may be influencedy therapies used after discontinuation of treatment receivedn a given trial, including crossover, seems to be extremelyelevant [101]. In RIBBON-1 [102], median PFS in olderomen who received bevacizumab combined with anthracy-
lines or taxanes was 10.1 months versus 9.1 in the youngerubgroup. Moreover, median PFS in the bevacizumab-plus-apecitabine cohort was 8.6 months in patients younger than5 years versus 9.1 months in the older subgroup (Table 3).
The RIBBON-2 trial [103] was designed to evaluatehe efficacy and safety of combining bevacizumab withommonly used second-line regimens. Adding bevacizumabo chemotherapy resulted in a 2.2-month improvement inedian PFS and a statistically significant 22% reduction in
he risk of events (HR 0.78; P = 0.0072). This benefit wasonfirmed in patients older than 65 years with an improve-ent in PFS from 4.5 to 7.4 months (Table 3). The safety
rofile was in line with that reported in previous phase-IIItudies.
In the sub-analysis of elderly patients included in theVADO trial [97], the combination of bevacizumab andocetaxel improved PFS compared to docetaxel alone in thelderly intention-to-treat (ITT) population, paralleling the-month increase reported for the overall ITT population.ndeed, the median PFS of 7.7 months in the docetaxel-alonerm was incremented to 9.0 months (HR 0.83; P = 0.48) or0.3 months (HR 0.68; P = 0.095) for elderly patients wholso received bevacizumab at 7.5 or 15 mg/kg (Table 3).edian PFS values were 7.6 months in the placebo arm, 9.0
n the bevacizumab 7.5 mg/kg arm, and 10.3 in the beva-izumab 15 mg/kg arm. As in the overall ITT population, inhe elderly the extent of benefit versus placebo was greaterith bevacizumab at 15 mg/kg (HR = 0.63; P = 0.07) thanith the 7.5 mg/kg dose (HR = 0.76; P = 0.35). Within the
lderly cohort, 43% presented at baseline with mild or mod-rate hypertension. In older MBC patients the incidence ofAEs was slightly higher than in the overall population,pecifically for those exposed to the higher bevacizumabose, where a 6.3% incidence of grade ≥3 hypertension waseported (Table 4). Compared to the others, elderly patientseporting baseline hypertension had an 80% higher probabil-ty of worsening hypertension during high-dose bevacizumabreatment.
Among elderly patients, the rates of grade 3–5 bleed-ng were 2.7% in the placebo arm, 2.4% in the low-doseevacizumab, and 4.2% in the high-dose bevacizumab, sig-ificantly higher than the corresponding figures reported in

G. Aprile et al. / Critical Reviews in Oncology/Hematology 87 (2013) 41–54 49
Table 3Efficacy outcomes in randomized phase III and phase IV trials of bevacizumab in MBC.
Median PFS/TTP months HR (CI)
AVADO [97]Docetaxel + Placebo (n = 241) 8.2 Placebo versus Bevacizumab7,5 mg/kg 0.86 (0.72–1.04)Docetaxel + Bevacizumab 7.5 mg/kg (n = 248) 9.0 Placebo versus Bevacizumab15mg/kg 0.77 (0.64–0.93)Docetaxel + Bevacizumab 15 mg/kg (n = 247) 10.1Docetaxel + Placebo (n = 38 ≥65 years) 7.7 Placebo versus Bevacizumab7,5 mg/kg 0.83 (0.52–1.13)Docetaxel + Bevacizumab 7.5 mg/kg (n = 41 ≥65 years) 9.0 Placebo versus Bevacizumab15mg/kg 0.68 (0.43–1.08)Docetaxel + Bevacizumab 15 mg/kg (n = 48 ≥65 years) 10.3
RIBBON-1 [102]CAPECITABINE <65 years (n = 462)Capecitabine + Placebo 4.7 0.67 (0.53–0.84)Capecitabine + Bevacizumab 8.6CAPECITABINE ≥65 years (n = 153)Capecitabine + Placebo 6.2 0.69 (0.47–1.02)Capecitabine + Bevacizumab 9.1ANTHRACYCLINES/TAXANE <65 years (n = 498)Anthracyclines/Taxanes + Placebo 7.9 0.63 (0.50–0.78)Anthracyclines/Taxanes + Bevacizumab 9.1ANTHRACYCLINES/TAXANE ≥65 years (n = 124)Anthracyclines/Taxanes + Placebo 8.5 0.83 (0.52–1.34)Anthracyclines/Taxanes + Bevacizumab 10.1
RIBBON-2 [103]Chemotherapy + Placebo 5.2 0.82 (0.66–1.00)Chemotherapy + Bevacizumab 7.0Chemotherapy + Placebo (≥65 years) 4.5 0.58 (0.38–0.88)Chemotherapy + Bevacizumab (≥65 years) 7.4
ATHENA [98]Chemotherapy + Bevacizumab (n = 2251) 9.5 NRChemotherapy + Bevacizumab (n = 176 ≥70 years) 10.4 NR
P NR, no
ttVwriap
tMmp
TS
ADDDDDD
ACC
ACC
A
FS, progression-free survival; TTP, time to progression; HR, hazard ratio;
he overall population. Similarly, the rates of grade ≥3 pro-einuria (4.2% versus 2.0%), ATEs (2.1% versus 0.8%) orTEs (6.3% versus 1.2%) in the bevacizumab 15 mg/kg armere also increased in the elderly cohort compared to those
eported in the overall safety population (Table 4). Interest-
ngly, no difference was seen in severe cardiovascular events,nd the only congestive heart failure reported occurred in aatient enrolled in the low-dose bevacizumab arm.p
[
able 4afety in randomized phase III trials of bevacizumab in MBC (adverse events grad
Hypertension (%)
VADO [97]ocetaxel + Placebo (n = 231) 1.3
ocetaxel + Placebo (n = 38 ≥65 years) 2.7
ocetaxel + Bevacizumab 7.5 mg/kg (n = 252) 0.8
ocetaxel + Bevacizumab 7.5 mg/kg (n = 41 ≥65 years) 0
ocetaxel + Bevacizumab 15 mg/kg (n = 247) 4.5
ocetaxel + Bevacizumab 15 mg/kg (n = 48 ≥65 years) 6.3
THENA (on treatment) [98]hemotherapy + Bevacizumab (n = 2076 <70 years) 3.2
hemotherapy + Bevacizumab (n = 176 ≥70 years) 5.1
THENA (entire study period = during treatment and up to 6 months after) [98]hemotherapy + Bevacizumab (n = 2076 <70 years) 4.2
hemotherapy + Bevacizumab (n = 176 ≥70 years) 6.9
TE/VTE, arterial thromboembolic events/venous thromboembolic events; CHF, c
t reported.
The AVEREL trial [104] showed that adding bevacizumabo trastuzumab and docetaxel in women with HER2-positive
BC resulted in a statistically significant 3-month improve-ent in median PFS. This benefit was confirmed in the 77
atients older than 65 years, with an HR of 0.40. The safety
rofile is currently not available.In the age subgroup analysis of the ATHENA trial98] median time to progression was 10.4 months (95%CI
e 3–5).
Proteinuria (%) ATE/VTE (%) Bleeding (%) CHF (%)
0 0/3.0 0.9 00 2.7/8.1 2.7 00.8 0/1.6 1.2 1.22.4 0/2.4 2.4 2.42.0 0.8/1.2 0.8 04.2 2.1/6.3 4.2 0
1.0 1.2 0.3 0.12.3 0.6 1.1 0
1.5 3.3 1.4 0.44.0 2.9 1.1 0.6
ongestive heart failure.

5 n Oncol
87cab
mtmSlhg
uoiaporo
talsbemt
5p
pibHipg
tfishtrC(ai
HntptiaabupaeuotpasoMMt
6
coIottrcamgAas
C
Aoi
0 G. Aprile et al. / Critical Reviews i
.8–11.8) (Table 3), overall RR was 42% in patients aged0 years or older, and 60% of grade 3–5 AE were reportedompared to 54% in those aged <70. Death rate was 5.1%,lthough none of the events was considered to be related toevacizumab.
Data on bevacizumab-related AEs were collected for 6onths after completion of therapy. Hypertension and pro-
einuria were the only bevacizumab-related SEAs reportedore frequently in older than in younger patients (Table 4).till, the relationship between presence or severity of base-
ine hypertension and the severity of bevacizumab-inducedypertension is uncertain. Notably, there was no excess ofrade ≥3 ATE/VTE, in contrast with previous findings [44].
Interestingly, in ATHENA bevacizumab was discontin-ed because of ATE/VTE in 2.9% of patients ≥70 years, yetccurred at grade 3–5 in only 0.6% during treatment, suggest-ng that bevacizumab was often withheld for minor toxicities,nd that the discontinuation rate for ATE/VTE may reflect thehysician’s cautiousness rather than an increased incidencef the side-effect during bevacizumab therapy. Severe hemor-hage during the treatment period occurred in 1.1% of patientsver 69 years versus 1.4% in younger patients (Table 4).
A recent overview of five randomized placebo-controlledrials enrolling MBC patients exposed to chemother-py ± bevacizumab [50] showed that the higher risk for AEseading to treatment discontinuation was not paralleled by aimilar increased risk of AEs leading to death. Notably, whenevacizumab was given together with capecitabine, no differ-nces in AEs leading to discontinuation or death were found,aking this combination particularly appealing regardless of
he line of treatment.
. Recommendations for the selection of olderatients to be offered anti-angiogenic treatment
Prospectively validated specific scores to select olderatients who are suitable for anti-angiogenic therapy are lack-ng. In clinical practice, the choice is often individual andased on the physicians’ personal judgment and experience.owever, as mentioned above, older patients enrolled in clin-
cal trials are usually in very good health or at least do notresent any important morbidity, and may not represent theeneral older population.
Hence, to merely transfer results from clinical trials tohe general older population may prove to be hazardous. Inact, older patients are more likely to present with functionalmpairment, malnutrition, cognitive dysfunction, or depres-ion. A number of tools help physicians to define the overallealth status of elderly patients. Historically, the Cumula-ive Illness Rating Scale (CIRS) has provided quantitativeatings of chronic illness burden [105]. More recently, the
hemotherapy Risk Assessment Scale for High-age patientsCRASH) [106], the first score integrating both chemother-py type and clinical risk for older patients, stratifies patientsn four different toxicity risk categories.
R
ogy/Hematology 87 (2013) 41–54
Frail elderly patients, according to the Cardiovascularealth Study (CHS), were defined by weight loss, weak-ess, exhaustion, slowness, and low activity [107]. Overall,he use of five or more medications can be defined asolypharmacy exposure, and it is associated with worse func-ional abilities [108]. Therefore, the decision-making processn the older population is complex and requires a holisticpproach, considering not only tumor features (i.e. biologynd sites of disease, previous and current cancer treatments)ut also age, comorbidities, and polypharmacy. In partic-lar, the presence of severe comorbidities or the need forolypharmacy to maintain a delicate steady state of health,voiding cardiovascular or renal flaws, should be consid-red a contraindication for bevacizumab prescription. These of bevacizumab should be judged with extreme caution inlder patients with peritoneal carcinomatosis or CNS metas-ases. However, in order to decide appropriately for theseatients, an approach involving a comprehensive geriatricssessment (CGA) is advocated. The systematic CGA con-ists of various validated tests and questionnaires focusingn somatic, psychological, functional and social domains.oreover, the addition of bevacizumab to chemotherapy inCRC and MBC provides a borderline clinical benefit in
erms of QALYs gained [109].
. Conclusions
Since elderly patients are still under-represented in clini-al trials, clinicians are less confident in extrapolating resultsn new therapeutic agents to this specific patient population.n an effort to obtain more information on safety and efficacyf bevacizumab in elderly patients with advanced colorec-al or breast cancer, we collected the evidence from clinicalrials and retrospective series. Overall, age per se does notepresent an absolute contraindication for the use of beva-izumab. Indeed, specific characteristics of the patients thatre often age-related (i.e. comorbidities and polypharmacy)ay influence the clinical decision-making process by sug-
esting caution in the use of bevacizumab in older patients. careful benefit-to-risk evaluation is therefore mandatory
nd strict monitoring for possible side-effects is stronglyuggested.
onflict of interest statement
No funding source was used for this review. Dr Giuseppeprile and Dr Fabio Puglisi have received consulting feesr honoraria from Roche. All authors declare no conflict ofnterest.
eferences
[1] Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA: ACancer Journal for Clinicians 2012;62(1):10–29.
n Oncol
G. Aprile et al. / Critical Reviews i[2] Yancik R. Cancer burden in the aged: an epidemiologic and demo-graphic overview. Cancer 1997;80(October (7)):1273–83.
[3] Smith BD, Smith GL, Hurria A, Hortobagyi GN, Buchholz TA.Future of cancer incidence in the United States: burdens upon anaging, changing nation. Journal of Clinical Oncology 2009;27(June(17)):2758–65.
[4] Cashman J, Wright J, Ring A. The treatment of co-morbidities inolder patients with metastatic cancer. Supportive Care in Cancer2010;18(May (5)):651–5.
[5] Muss HB. Older age – not a barrier to cancer treatment. New EnglandJournal of Medicine 2001;345(October (15)):1127–8.
[6] Howlader N, Noone AM, Krapcho M, et al. SEER CancerStatistics Review, 1975–2009 (Vintage 2009 Popula-tions). Bethesda, MD: National Cancer Institute; 2012http://seer.cancer.gov/csr/1975 2009 pops09/ (based on November2011 SEER data submission, posted to the SEER web site, April).
[7] Smith BD, Jiang J, McLaughlin SS, et al. Improvement in breastcancer outcomes over time: are older women missing out? Journal ofClinical Oncology 2011;29(35):4647–53.
[8] Muss HB, Busby-Whitehead J. Older women with breast cancer:slow progress, great opportunity, now is the time. Journal of ClinicalOncology 2011;29(35):4608–10.
[9] Köhne CH, Folprecht G, Goldberg RM, Mitry E, Rougier P.Chemotherapy in elderly patients with colorectal cancer. Oncologist2008 Apr;13(4):390–402.
[10] Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab versuspaclitaxel alone for metastatic breast cancer. New England Journal ofMedicine 2007;357(December (26)):2666–76.
[11] Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plusirinotecan, fluorouracil, and leucovorin for metastatic colorectalcancer. New England Journal of Medicine 2004;350(June (23)):2335–42.
[12] Giantonio BJ, Catalano PJ, Meropol NJ, et al. Eastern CooperativeOncology Group Study E3200. Bevacizumab in combination withoxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previouslytreated metastatic colorectal cancer: results from the Eastern Coop-erative Oncology Group Study E3200. Journal of Clinical Oncology2007;25(April (12)):1539–44.
[13] Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation.Cell 2011;144(March (5)):646–74.
[14] Baffert F, Thurston G, Rochon-Duck M, Le T, Brekken R,McDonald DM. Age-related changes in vascular endothelialgrowth factor dependency and angiopoietin-1-induced plasticityof adult blood vessels. Circulation Research 2004;94(April (7)):984–92.
[15] Kamba T, Tam BY, Hashizume H, et al. VEGF-dependent plastic-ity of fenestrated capillaries in the normal adult microvasculature.American Journal of Physiology-Heart and Circulatory Physiology2006;290(February (2)):H560–76.
[16] de Castro Junior G, Puglisi F, de Azambuja E, El Saghir NS, Awada A.Angiogenesis and cancer: a cross-talk between basic science and clin-ical trials (the “do ut des” paradigm). Critical Reviews in OncologyHematology 2006;59(July (1)):40–50.
[17] Jain RK. Molecular regulation of vessel maturation. Nature Medicine2003;9(June (6)):685–93.
[18] Carmeliet P. Mechanisms of angiogenesis and arteriogenesis. NatureMedicine 2000;6(April (4)):389–95.
[19] Forsythe JA, Jiang BH, Iyer NV, et al. Activation of vascularendothelial growth factor gene transcription by hypoxia-induciblefactor 1. Molecular and Cellular Biology 1996;16(September (9)):4604–13.
[20] Papetti M, Herman IM. Mechanisms of normal and tumor-derivedangiogenesis. American Journal of Physiology-Cell Physiology
2002;282(May (5)):C947–70.ogy/Hematology 87 (2013) 41–54 51
[21] Genentech, Inc., United States Securities and Exchange Commission.http://www.sec.gov/Archives/edgar/data/318771/000031877109000003/form10-k 2008.htm [accessed 04.05.12].
[22] Jain RK. Normalizing tumor vasculature with anti-angiogenic ther-apy: a new paradigm for combination therapy. Nature Medicine2001;7(September (9)):987–9.
[23] Wang Y, Fei D, Vanderlaan M, Song A. Biological activity of beva-cizumab, a humanized anti-VEGF antibody in vitro. Angiogenesis2004;7(4):335–45.
[24] Augustin HG. Translating angiogenesis research into the clinic: thechallenges ahead. British Journal of Radiology 2003;76. Spec No 1,S3–S10.
[25] Homsi J, Daud AI. Spectrum of activity and mechanism of action ofVEGF/PDGF inhibitors. Cancer Control Journal of the Moffitt CancerCenter 2007;14(July (3)):285–94.
[26] Lambrechts D, Claes B, Delmar P, et al. VEGF pathway geneticvariants as biomarkers of treatment outcome with bevacizumab: ananalysis of data from the AViTA and AVOREN randomised trials.Lancet Oncology 2012;13(July (7)):724–33.
[27] Gressett SM, Shah SR. Intricacies of bevacizumab-induced toxicitiesand their management. Annals of Pharmacotherapy 2009;43(March(3)):490–501.
[28] Kincaid-Smith P. The renal lesion of preeclampsia revisited. Ameri-can Journal of Kidney Diseases 1991;17(February (2)):144–8.
[29] Horowitz JR, Rivard A, van der Zee R, et al. Vascular endothelialgrowth factor/vascular permeability factor produces nitric oxide-dependent hypotension. Evidence for a maintenance role in quiescentadult endothelium. Arteriosclerosis Thrombosis and Vascular Biology1997;17(November (11)):2793–800.
[30] Geiger-Gritsch S, Stollenwerk B, Miksad R, Guba B, Wild C,Siebert U. Safety of bevacizumab in patients with advanced can-cer: a meta-analysis of randomized controlled trials. Oncologist2010;15(11):1179–91.
[31] Cuppone F, Bria E, Vaccaro V, et al. Magnitude of risks and benefitsof the addition of bevacizumab to chemotherapy for advanced breastcancer patients: meta-regression analysis of randomized trials. Journalof Experimental & Clinical Cancer Research 2011;30(May):54.
[32] Mir O, Coriat R, Cabanes L, et al. An observational study ofbevacizumab-induced hypertension as a clinical biomarker of anti-tumor activity. Oncologist 2011;16(9):1325–32.
[33] Scartozzi M, Galizia E, Chiorrini S, et al. Arterial hypertension cor-relates with clinical outcome in colorectal cancer patients treatedwith first-line bevacizumab. Annals of Oncology 2009;20(February(2)):227–30.
[34] Schneider BP, Wang M, Radovich M, et al. ECOG 2100.Association of vascular endothelial growth factor and vascu-lar endothelial growth factor receptor-2 genetic polymorphismswith outcome in a trial of paclitaxel compared with pacli-taxel plus bevacizumab in advanced breast cancer: ECOG2100. Journal of Clinical Oncology 2008;26(October (28)):4672–8.
[35] Escalante CP, Zalpour A. Vascular endothelial growth factor inhibitor-induced hypertension: basics for primary care providers. CardiologyResearch and Practice 2011;2011:816897.
[36] Dincer M, Altundag K. Angiotensin-converting enzyme inhibitorsfor bevacizumab-induced hypertension. Annals of Pharmacotherapy2006;40(December (12)):2278–9.
[37] Raman AK, Lombardo JC, Chandrasekhar R, Fakih MG. Beva-cizumab related adverse events among various age groups of elderlypatients with advanced colorectal cancer (abstract). Journal of ClinicalOncology 2007;25(18S):14546. ASCO Annual Meeting ProceedingsPart I [June 20 Supplement].
[38] Zhu X, Wu S, Dahut WL, Parikh CR. Risks of proteinuria
and hypertension with bevacizumab, an antibody against vascu-lar endothelial growth factor: systematic review and meta-analysis.
5 n Oncol
2 G. Aprile et al. / Critical Reviews iAmerican Journal of Kidney Diseases 2007;49(February (2)):186–93.
[39] Eremina V, Jefferson JA, Kowalewska J, et al. VEGF inhibition andrenal thrombotic microangiopathy. New England Journal of Medicine2008;358(March (11)):1129–36.
[40] KDOQI. Clinical practice guidelines and clinical practice recommen-dations for diabetes and chronic kidney disease. American Journal ofKidney Diseases 2007;49(February (2 Suppl. 2)):S12–54.
[41] Lyman GH, Khorana AA, Falanga A, Clarke-Pearson D, Flowers C,Jahanzeb MW, et al. American Society of Clinical Oncology guide-line: recommendations for venous thromboembolism prophylaxisand treatment in patients with cancer. Journal of Clinical Oncology2007;25(December (34)):5490–505.
[42] Hurwitz HI, Saltz LB, Van Cutsem E, et al. Venous thromboembolicevents with chemotherapy plus bevacizumab: a pooled analysis ofpatients in randomized phase II and III studies. Journal of ClinicalOncology 2011;29(May (13)):1757–64.
[43] Francois E, Guérin O, Follana P, Evesque L, Mari V, Aparicio T. Useof bevacizumab in elderly patients with metastatic colorectal cancer:Review. Journal of Geriatric Oncology 2011;2(January (1)):64–71.
[44] Scappaticci FA, Skillings JR, Holden SN, et al. Arterial throm-boembolic events in patients with metastatic carcinoma treated withchemotherapy and bevacizumab. Journal of the National Cancer Insti-tute 2007;99(August (16)):1232–9.
[45] Kozloff M, Sugrue M, Berlin J, et al. Safety and effectiveness ofbevacizumab and chemotherapy in elderly patients with metastaticcolorectal cancer: results from the BRITE prospective cohort study(abstract). Journal of Clinical Oncology 2008;May (Suppl.). Abstr.4026.
[46] Kilickap S, Abali H, Celik I. Bevacizumab, bleeding, thrombo-sis, and warfarin. Journal of Clinical Oncology 2003;21(September(18)):3543 [3542; author reply].
[47] Fehr M, Catschegn S, Reinhart WH, et al. The influence of beva-cizumab on platelet function. Swiss Medical Weekly 2011;141(July),http://dx.doi.org/10.4414/smw.2011.13243w13243.
[48] Flynn PJ, Sugrue MM, Feng S, et al. Incidence of serious bleed-ing events in patients with metastatic colorectal cancer receivingbevacizumab as part of a first-line regimen: results from theBRITE observation cohort study (abstract). Journal of ClinicalOncology 2008;26(May (15S Suppl.)):4104 [ASCO annual meetingproceedings (post-meeting edition)].
[49] Hambleton J, Skillings J, Kabbinavar F, et al. Safety of low-doseaspirin (ASA) in a pooled analysis of 3 randomized, controlled trials ofbevacizumab with chemotherapy in patients with metastatic colorectalcancer (abstract). Journal of Clinical Oncology 2005;23(June (16SSuppl.)):3554 [ASCO Annual Meeting Proceedings].
[50] Hamilton EP, Blackwell KL. Safety of bevacizumab inpatients with metastatic breast cancer. Oncology 2011;80(5–6):314–25.
[51] Yano S, Shinohara H, Herbst RS, et al. Expression of vascularendothelial growth factor is necessary but not sufficient for productionand growth of brain metastasis. Cancer Research 2000;60(September(17)):4959–67.
[52] Gordon MS, Margolin K, Talpaz M, et al. safety and pharmacoki-netic study of recombinant human anti-vascular endothelial growthfactor in patients with advanced cancer. Journal of Clinical Oncology2001;19(February (3)):843–50.
[53] Labidi SI, Bachelot T, Ray-Coquard I, et al. Bevacizumab andpaclitaxel for breast cancer patients with central nervous sys-tem metastases: a case series. Clinical Breast Cancer 2009;9(May(2)):118–21.
[54] Socinski MA, Langer CJ, Huang JE, et al. Safety of bevacizumab inpatients with non-small-cell lung cancer and brain metastases. Journal
of Clinical Oncology 2009;27(November (31)):5255–61.ogy/Hematology 87 (2013) 41–54
[55] Besse B, Lasserre SF, Compton P, Huang J, Augustus S, Rohr UP.Bevacizumab safety in patients with central nervous system metas-tases. Clinical Cancer Research 2010;16(January (1)):269–78.
[56] De Braganca KC, Janjigian YY, Azzoli CG, et al. Efficacy and safetyof bevacizumab in active brain metastases from non-small cell lungcancer. Journal of Neurooncology 2010;100(December (3)):443–7.
[57] Crinò L, Dansin E, Garrido P, et al. Safety and efficacy offirst-line bevacizumab-based therapy in advanced non-squamousnon-small-cell lung cancer (SAiL, MO19390): a phase 4 study. LancetOncology 2010;11(August (8)):733–40.
[58] Smith IE, Pierga JY, Biganzoli L, et al., ATHENA Study Group.First-line bevacizumab plus taxane-based chemotherapy for locallyrecurrent or metastatic breast cancer: safety and efficacy in an open-label study in 2,251 patients. Annals of Oncology 2011;22(March(3)):595–602.
[59] Verma N, Swain SM. Bevacizumab and heart failure risk in patientswith breast cancer: a thorn in the side? Journal of Clinical Oncology2011;29(February (6)):603–6.
[60] Choueiri TK, Mayer EL, Je Y, et al. Congestive heart failure riskin patients with breast cancer treated with bevacizumab. Journal ofClinical Oncology 2011;29(February (6)):632–8.
[61] Richards CJ, Je Y, Schutz FA, et al. Incidence and risk of conges-tive heart failure in patients with renal and nonrenal cell carcinomatreated with sunitinib. Journal of Clinical Oncology 2011 Sep1;29(25):3450–6.
[62] Pantaleo MA, Mandrioli A, Saponara M, et al. Development of coro-nary artery stenosis in a patient with metastatic renal cell carcinomatreated with sorafenib. BMC Cancer 2012;12(June (1)):231.
[63] Kretzschmar A, Cunningham D, Berry S, et al. First BEAT Inves-tigators. Incidence of gastrointestinal perforations and bleeding inpatients starting bevacizumab treatment in first-line mCRC withoutprimary tumour resection: preliminary results from the First BEATrial(abstract 248). In: Paper presented at American Society of ClinicalOncology Gastrointestinal Symposium. 2006.
[64] Sugrue M, Kozloff M, Hainsworth J, et al. Risk factors for gas-trointestinal perforations in patients with metastatic colorectal cancerreceiving bevacizumab plus chemotherapy (abstract 3535). Journal ofClinical Oncology 2006;24(June (18S Suppl.)):3535 [ASCO AnnualMeeting Proceedings Part I].
[65] Gaur P, Bose D, Samuel S, Ellis LM. Targeting tumor angiogenesis.Seminars in Oncology 2009;36(April (2 Suppl. 1)):S12–9.
[66] Ellis LM, Curley SA, Grothey A. Surgical resection after downsizingof colorectal liver metastasis in the era of bevacizumab. Journal ofClinical Oncology 2005;23(August (22)):4853–5.
[67] Eng C. Toxic effects and their management: daily clinical challengesin the treatment of colorectal cancer. Nature Reviews Clinical Oncol-ogy 2009;6(April (4)):207–18.
[68] Zawacki WJ, Walker TG, DeVasher E, et al. Wound dehiscence orfailure to heal following venous access port placement in patientsreceiving bevacizumab therapy. Journal of Vascular and InterventionalRadiology 2009;20(May (5)):624–7 [quiz 571].
[69] Folprecht G, Cunningham D, Ross P, et al. Efficacy of 5-fluorouracil-based chemotherapy in elderly patients with metastatic colorectalcancer: a pooled analysis of clinical trials. Annals of Oncology2004;15(September (9)):1330–8.
[70] Folprecht G, Seymour MT, Saltz L, et al. Irinotecan/fluorouracilcombination in first-line therapy of older and younger patientswith metastatic colorectal cancer: combined analysis of 2,691patients in randomized controlled trials. Journal of Clinical Oncology2008;26(March (9)):1443–51.
[71] Goldberg RM, Tabah-Fisch I, Bleiberg H, et al. Pooled analysis ofsafety and efficacy of oxaliplatin plus fluorouracil/leucovorin admin-istered bimonthly in elderly patients with colorectal cancer. Journal
of Clinical Oncology 2006;24(September (25)):4085–91.[72] Kabbinavar FF, Hurwitz HI, Yi J, Sarkar S, Rosen O. Addition ofbevacizumab to fluorouracil-based first-line treatment of metastaticcolorectal cancer: pooled analysis of cohorts of older patients

n Oncol
G. Aprile et al. / Critical Reviews ifrom two randomized clinical trials. Journal of Clinical Oncology2009;27(January (2)):199–205.
[73] Cassidy J, Saltz LB, Giantonio BJ, Kabbinavar FF, Hurwitz HI, RohrUP. Effect of bevacizumab in older patients with metastatic colorectalcancer: pooled analysis of four randomized studies. Journal of CancerResearch and Clinical Oncology 2010;136(May (5)):737–43.
[74] Price TJ, Zannino D, Wilson K, et al. Bevacizumab is equally effec-tive and no more toxic in elderly patients with advanced colorectalcancer: a subgroup analysis from the AGITG MAX trial: an interna-tional randomised controlled trial of Capecitabine, Bevacizumab andMitomycin C. Annals of Oncology 2012;23(6):1531–6.
[75] Kozloff MF, Berlin J, Flynn PJ, et al. Clinical outcomes in elderlypatients with metastatic colorectal cancer receiving bevacizumab andchemotherapy: results from the BRiTE observational cohort study.Oncology 2010;78(5–6):329–39.
[76] Kubala E, Bartos J, Petruzelka LB, et al. Safety and effectiveness ofbevacizumab in combination with chemotherapy in elderly patientswith metastatic colorectal cancer: results from a large Czech obser-vational registry. In: Gastrointestinal Cancers Symposium. 2010. p.467.
[77] Smith D, Rouyer M, Noize P, et al., ETNA Study Group. Effective-ness and safety in very elderly patients treated by bevacizumab pluschemotherapy in first-line therapy of metastatic colorectal cancer:results of ETNA, a French cohort study. Journal of Clinical Oncology2011;29(February (1 Suppl.)):555.
[78] Kozloff M, Bekaii-Saab TS, Bendell JC, et al. Effectiveness of first- orsecond-line bevacizumab (BV) treatment (tx) in elderly patients (pts)with metastatic colorectal cancer (mCRC) in ARIES, an observationalcohort study (OCS). Journal of Clinical Oncology 2011;29(May (20Suppl.)):3625.
[79] Feliu J, Safont MJ, Salud A, et al. Capecitabine and bevacizumabas first-line treatment in elderly patients with metastatic colorectalcancer. British Journal of Cancer 2010;102(May (10)):1468–73.
[80] Vrdoljak E, Omrcen T, Boban M, Hrabar A. Phase II study of beva-cizumab in combination with capecitabine as first-line treatment inelderly patients with metastatic colorectal cancer. Anticancer Drugs2011;22(February (2)):191–7.
[81] Carreca IU, Bellomo F, Burgio SL, Pernice G, Piazza D, Balducci L.Metronomic therapy irinotecan (IRI) capecitabine (CAP) plus beva-cizumab (BEV) in treatment of advanced colorectal cancer (ACRC)in very elderly people. Journal of Clinical Oncology 2010;28(May(20 Suppl.)):3552.
[82] Carreca IU, Bellomo F, Pernice G, Antista M, Amelio R, Bal-ducci L. Metronomic (M), capecitabine (C), and oxaliplatin (O)plus bevacizumab (B) as treatment of advanced colorectal can-cer (ACRC) in very elderly people (M-COB): Efficacy and safety(E&S) evaluation—a 2-year monitoring. Journal of Clinical Oncology2011;29(Suppl.). Abstr. e14086.
[83] Hofheinz R, Grothe W, Tummes D, et al. Bevacizumab in the first-linetreatment of elderly patients with metastatic colorectal cancer: Matureresults from a large community-based observational study. Journal ofClinical Oncology 2012;30(Suppl. 4). Abstr. 566.
[84] Meyerhardt JA, Li L, Sanoff HK, Carpenter 4th W, Schrag D. Effec-tiveness of bevacizumab with first-line combination chemotherapy formedicare patients with stage IV colorectal cancer. Journal of ClinicalOncology 2012;30(February (6)):608–15.
[85] Siegel R, Naishadham D, Jemal A. Cancer statistics. CA: ACancer Journal for Clinicians 2012;62(January–February):10–29,http://dx.doi.org/10.3322/caac.20138.
[86] Wildiers H, Kunkler I, Biganzoli L, et al. International Society of Geri-atric Oncology. Management of breast cancer in elderly individuals:recommendations of the International Society of Geriatric Oncology.Lancet Oncology 2007;8(December (12)):1101–15.
[87] Jaggi AS, Singh N. Mechanisms in cancer-chemotherapeuticdrugs-induced peripheral neuropathy. Toxicology 2012;291(January(1–3)):1–9.
ogy/Hematology 87 (2013) 41–54 53
[88] Viale PH, Yamamoto DS. Cardiotoxicities of breast cancer treatment.Oncology (Williston Park) 2009;23(April (4 Suppl.)):19–24 [nurseEd].
[89] Extermann M, Meyer J, McGinnis M, et al. A comprehensive geri-atric intervention detects multiple problems in older breast cancerpatients. Critical Reviews in Oncology Hematology 2004;49(January(1)):69–75.
[90] Hamberg P, Verweij J, Seynaeve C. Cytotoxic therapy forthe elderly with metastatic breast cancer: a review on safety,pharmacokinetics and efficacy. European Journal of Cancer2007;43(July (10)):1514–28.
[91] Brunello A, Roma A, Falci C, Basso U. Chemotherapy and targetedagents for elderly women with advanced breast cancer. Recent Patentson Anticancer Drug Discovery 2008;3(November (3)):187–201.
[92] Bajetta E, Procopio G, Celio L, et al. Safety and efficacy of twodifferent doses of capecitabine in the treatment of advanced breastcancer in older women. Journal of Clinical Oncology 2005;23(April(10)):2155–61.
[93] Colleoni M, Rocca A, Sandri MT, et al. Low-dose oral methotrexateand cyclophosphamide in metastatic breast cancer: antitumor activityand correlation with vascular endothelial growth factor levels. Annalsof Oncology 2002;13(January (1)):73–80.
[94] Aapro M, Monfardini S, Jirillo A, Basso U. Management of primaryand advanced breast cancer in older unfit patients (medical treatment).Cancer Treatment Reviews 2009;35(October (6)):503–8.
[95] Glaspy J, Dieras V, Brufsky A, Miles DW, Phan SC, O’ShaughnessyJ. Bevacizumab in combination with chemotherapy in the treatmentof HER2- metastatic breast cancer: PFS subgroup results from twophase III studies. European Journal of Cancer 2010;8(Suppl.):202.
[96] Dieras V, Glaspy J, Brufsky A, et al. Efficacy in patient subgroups inRIBBON-1, a randomized, double-blind, phase III trial of chemother-apy with or without bevacizumab (B) for first-line treatment ofHER2-negative locally recurrent or metastatic breast cancer (MBC)[meeting abstracts]. European Journal of Cancer 2009;7(Suppl.):265.Abstr. 5016.
[97] Pivot X, Schneeweiss A, Verma S, et al. Efficacy and safetyof bevacizumab in combination with docetaxel for the first-line treatment of elderly patients with locally recurrentor metastatic breast cancer: results from AVADO. Euro-pean Journal of Cancer 2011;47(November (16)):2387–95,http://dx.doi.org/10.1016/j.ejca.2011.06.018.
[98] Biganzoli L, Di Vincenzo E, Jiang Z, et al. First-line bevacizumab-containing therapy for breast cancer: results in patients aged ≥70 yearstreated in the ATHENA study. Annals of Oncology 2012;23(January(1)):111–8.
[99] www.fda.gov/ohrms/dockets/ac/07/briefing/2007-4332b1-03-Genentech.pdf
[100] Verma S, McLeod D, Batist G, Robidoux A, Martins IR, MackeyJR. In the end what matters most? A review of clinical endpoints inadvanced breast cancer. Oncologist 2011;16(1):25–35.
[101] Broglio KR, Berry DA, Detecting an overall survival benefit that isderived from progression-free survival. Journal of the National CancerInstitute 2009;101(23):1642–9.
[102] Robert NJ, Diéras V, Glaspy J, et al. RIBBON-1: randomized,double-blind, placebo-controlled, phase III trial of chemotherapywith or without bevacizumab for first-line treatment of humanepidermal growth factor receptor 2-negative, locally recurrent ormetastatic breast cancer. Journal of Clinical Oncology 2011;29(April(10)):1252–60.
[103] Brufsky AM, Hurvitz S, Perez E, et al. RIBBON-2: a randomized,double-blind, placebo-controlled, phase III trial evaluating the effi-cacy and safety of bevacizumab in combination with chemotherapyfor second-line treatment of human epidermal growth factor recep-
tor 2-negative metastatic breast cancer. Journal of Clinical Oncology2011;29(November (32)):4286–93.[104] Gianni L, Romieu G, Lichinitser M, et al.AVEREL, arandomized phase III trial to evaluate bevacizumab in com-

5 n Oncol
B
oBBtU
iah
UOi
iaI
lhUniversity of Udine, Italy. Dr. Puglisi is author of severalpapers in peer-reviewed journals, focusing on breast cancerand prognostic/predictive factors.
4 G. Aprile et al. / Critical Reviews i
bination with trastuzumab + docetaxel as first-line therapyfor HER2-positive locally recurrent/metastatic breast cancer.2011.
[105] Linn BS, Linn MW, Gurel L. Cumulative illness rating scale. Journalof the American Geriatrics Society 1968;16(May (5)):622–6.
[106] Extermann M, Boler I, Reich RR, et al. Predicting the risk ofchemotherapy toxicity in older patients: the chemotherapy riskassessment scale for high-age patients (CRASH) score. Cancer2012;118(July (13)):3377–86, http://dx.doi.org/10.1002/cncr.26646.
[107] Fried LP, Tangen CM, Walston J, et al. Cardiovascular Health StudyCollaborative Research Group. Frailty in older adults: evidence fora phenotype. Journals of Gerontology Series A-Biological Sciencesand Medical Sciences 2001;56(March (3)):M146–56.
[108] Gnjidic D, Hilmer SN, Blyth FM, et al. Polypharmacy cutoff andoutcomes: five or more medicines were used to identify community-dwelling older men at risk of different adverse outcomes. Journal ofClinical Epidemiology 2012;June.
[109] Gonsalves W, Ganti AK. Targeted anti-cancer therapy in theelderly. Critical Reviews in Oncology Hematology 2011;78(June(3)):227–42.
iographies
Giuseppe Aprile, has been a Specialist in Medical Oncol-gy since October 2001. He was a Research Fellow atrigham and Women’s Hospital-Harvard Medical School,
oston, MA, US in 2006, and currently leads the Gas-rointestinal Unit at the Department of Medical Oncology,niversity Hospital, Udine, Italy. He has been principal
ogy/Hematology 87 (2013) 41–54
nvestigator or co-investigator of more than 40 clinical trialsnd co-author of 50 full papers. Gastrointestinal oncology isis main clinical and research interest.
Laura Ferrari received her MD degree in 2008 from theniversity of Siena, Italy. She is currently training in Medicalncology at the University of Udine, Italy. Her main clinical
nterest is gastrointestinal oncology.
Caterina Fontanella (MD) completed her medical trainingn 2010 at the Univeristy of Trieste, Italy. Currently, she is
resident in Medical Oncology at the University of Udine,taly. Her clinical and research interests include breast cancer.
Fabio Puglisi (MD, PhD) gained his medical degree (cumaude) in 1993 from University of Palermo, Italy. Currently,e is researcher and professor of Medical Oncology at the