
Behavioral and Cognitive Therapies in Psychiatric ... - Penn Lab
61
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/348395904 Behavioral and Cognitive Therapies in Psychiatric Rehabilitation for the Schizophrenia Spectrum: Finding the Forgotten Stepchild Article · January 2021 CITATIONS 0 READS 120 4 authors, including: Some of the authors of this publication are also working on these related projects: Comparing the CASI-4R and the PGBI-10M for Differentiating Bipolar Spectrum Disorders from Other Outpatient Diagnoses in Youth View project Tate Halverson Durham VA Medical Center 25 PUBLICATIONS 113 CITATIONS SEE PROFILE All content following this page was uploaded by Tate Halverson on 12 January 2021. The user has requested enhancement of the downloaded file.
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Behavioral and Cognitive Therapies in Psychiatric ... - Penn Lab

See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/348395904
Behavioral and Cognitive Therapies in Psychiatric Rehabilitation for the
Schizophrenia Spectrum: Finding the Forgotten Stepchild
Article · January 2021
CITATIONS
0READS
120
4 authors, including:
Some of the authors of this publication are also working on these related projects:
Comparing the CASI-4R and the PGBI-10M for Differentiating Bipolar Spectrum Disorders from Other Outpatient Diagnoses in Youth View project
Tate Halverson
Durham VA Medical Center
25 PUBLICATIONS 113 CITATIONS
SEE PROFILE
All content following this page was uploaded by Tate Halverson on 12 January 2021.
The user has requested enhancement of the downloaded file.

the Behavior TherapistI S S N 0 2 7 8 - 8 4 0 3
VOLUME 44, NO. 1 • JANUARY 2021
[continued on p. 3]
ABCT
s
association forbehavioral andcognitive therapies
Contents
January • 2021 1
President’s MessageDavid F. Tolinengaging our stakeholders • 1
At ABCTMary Jane EimerFrom Your executive Director: what Your leadership and staffare working on to serve You Better • 4
Original ResearchJessica L. Schleider, Jenna Y. Sung, Amanda Bianco, Adam Gonzalez,Dina Vivian, Michael C. Mullarkeyopen Pilot trial of a single-session consultation service for clientson Psychotherapy wait-lists • 8
Literature ReviewTate F. Halverson, Charlie A. Davidson, William Spaulding, David L. PennBehavioral and cognitive therapies in Psychiatric rehabilitation forthe schizophrenia spectrum: Finding the Forgotten stepchild • 15
Clinical Practice ForumAlana J. McVey, Hillary K. Schiltz, Henry Boeha call for compassion: evidence-Based strategies for workingwith autistic clients without co-occuring intellectual Disabilityin therapy • 23
Jessica L. Hawks, Clio Pitula, Jamie Shoopa transdiagnostic approach to the treatment of autonomic Dysfunctionassociated with orthostatic intolerance in Pediatric Patients • 32
NewsShannon M. Blakeya summary of Dr. martin antony’s aBct Presidential address • 38
Amy Sewart and Karla Lopeza synopsis of Dr. Philip c. Kendall’s lifetime achievement awardaddress: “managing anxiety in Youth: more action than talk” • 40
Dana Strauss and Jade Gallosummary of Dr. luana marques’s invited address: “leveragingimplementation science and community-Based Partnerships to Bridgethe science-Practice Gap among Diverse Populations” • 41
Arthur R. Andrews, IIIinvited address: Dr. allison harvey and looking to the next Phaseof transdiagnostic interventions • 43
[Contents continued on p. 2]
PRESIDENT’S MESSAGE
Engaging OurStakeholdersDavid F. Tolin, The Institute
of Living
as i write this column, the54th aBct annual conven-tion has just wrapped up, andour pivot to a virtual meetingseems to have gone extremelywell. i’d like to express mydeepest gratitude to the
aBct central office staff who made it happen,with a special thanks to stephen crane, ourconvention manager, for his exceptional work.we had 2,334 attendees; i’m particularly happythat of those, 225 were nondoctoral clinical pro-fessionals attending their first aBct conven-tion, suggesting that our efforts to expand ourtent are working. although i have not yet beenable to review all of the attendees’ commentsabout the convention, the anecdotal informa-tion i’ve received thus far suggests that ourattendees were particularly appreciative of theincreased emphasis on diversity in our offer-ings. here i want to acknowledge the tremen-dous efforts of the 2020 Program chair, shan-non wiltsey stirman, and the associateProgram chair, Daniel cheron. Know that2021 Program chair Gregory chasson, associ-ate Program chair elizabeth Katz, and i haveevery intention of continuing, and evenexpanding on, their work and vision for a con-vention that embraces diversity in all its mani-festations.
i’d also like to thank our immediate Past-President, martin antony, for his steady lead-

2
the Behavior TherapistPublished by the Association for
Behavioral and Cognitive Therapies305 seventh avenue - 16th Floor
new York, nY 10001 | www.abct.org(212) 647-1890 | Fax: (212) 647-1865
Editor: richard leBeau
Editorial Assistant: resham Gellatly
Associate Editorsraeann andersontrey andrewsshannon Blakeylily Brownamanda chuenajwa culverBrian FeinsteinDavid hansenangela morelandsamantha moshieramy murrellalayna ParkJae PuckettJennifer reganamy sewarttony wellsmonnica williamsKatherine Young
ABCT President: David F. TolinExecutive Director: Mary Jane EimerDirector of Communications & Deputy
Executive Director: David TeislerConvention Manager: Stephen CraneManaging Editor: Stephanie SchwartzMembership Services Manager:
Dakota McPherson
copyright © 2021 by the association for Behavioraland cognitive therapies. all rights reserved. no partof this publication may be reproduced or transmittedin any form, or by any means, electronic or mechan-ical, including photocopy, recording, or any infor-mation storage and retrieval system, without permis-sion in writing from the copyright owner.
Subscription information: tBT is published in 8issues per year. it is provided free to aBct members.nonmember subscriptions are available at $40.00 peryear (+$32.00 airmail postage outside northamerica). Change of address: 6 to 8 weeks arerequired for address changes. send both old and newaddresses to the aBct office.
aBct is committed to a policy of equal opportu-nity in all of its activities, including employment.aBct does not discriminate on the basis of race,color, creed, religion, national or ethnic origin, sex,sexual orientation, gender identity or expression,age, disability, or veteran status.
all items published in the Behavior Therapist,including advertisements, are for the information ofour readers, and publication does not imply endorse-ment by the association.
the association for Behavioral and cog-nitive therapies publishes the BehaviorTherapist as a service to its membership.eight issues are published annually. thepurpose is to provide a vehicle for therapid dissemination of news, recentadvances, and innovative applications inbehavior therapy.
Feature articles that are approxi-mately 16 double-spaced manuscriptpages may be submitted.
Brief articles, approximately 6 to 12double-spaced manuscript pages, arepreferred.
Feature articles and brief articlesshould be accompanied by a 75- to100-word abstract.
letters to the editor may be used torespond to articles published in theBehavior Therapist or to voice a profes-sional opinion. letters should be lim-ited to approximately 3 double-spacedmanuscript pages.
Submissions must be accompanied by aCopyright Transfer Form (which can bedownloaded on our website: http://www.abct.org/Journals/?m=mJournal&fa=tBt): submissions will not be reviewed with-out a copyright transfer form. Prior topublication authors will be asked tosubmit a final electronic version of theirmanuscript. authors submitting materi-als to tBT do so with the understandingthat the copyright of the published mate-rials shall be assigned exclusively toaBct. electronic submissions are pre-ferred and should be directed to theeditor, richard leBeau, Ph.D., [email protected]. Please include thephrase tBT submission and the author’slast name (e.g., tBT Submission - Smith etal.) in the subject line of your e-mail.include the corresponding author’s e-mail address on the cover page of themanuscript attachment. Please alsoinclude, as an attachment, the completedcopyright transfer document.
INSTRUCTIONS Ñçê AUTHORS
[Contents continued]
News (continued)
Joel Lopezsummary of eric Youngstrom’s invited address: “helping Give awayPsychological science: Bringing the Best of our work to the People whowould Benefit” • 44
Samantha Moshiersummary of Dr. Zindel segal’s invited address: “strange Bedfellows sharemutual Dreams: increasing access to mindfulness-Based interventions formood and anxiety Disorders” • 45
Angela Morelandsummary of invited Panel “Promoting Better, equitable access to evidence-Basedmental health services in a community Behavioral health system” • 47
Amy Sewart and Amanda Brashearsummary of invited Panel “Personalizing treatment to improve cBtoutcomes” • 49
ABCT Launches Inaugural Briefing Books Initiative • 50Preparing to Submit an Abstract • 51Call for Ticketed Sessions—55th Annual Convention • 52Call for Papers—55th Annual Convention • 53Understanding the ABCT Convention • 54ABCT and Continuing Education • 55Call for Award Nominations • 58
convention2021

p r e s i d e n t ’ s m e s s a g e
January • 2021 3
ership during a turbulent year. the year2020 brought us coViD-19, an increasedfocus on systemic racism, and a disputedelection. throughout the year, Dr. antonymanaged to keep aBct on track, address-ing timely topics in his presidentialcolumns and guiding us toward a moreconscientious and inclusive future. he hasleft some very big shoes to fill.
as you may have read in a previousissue of the Behavior Therapist, 2020 alsobrought a strategic retreat, which occursevery 3 years (antony, 2020). Facilitated byconsultant Jeff De cagna, this meetingincluded the Board of Directors, coordina-tors, and senior staff. among the manytopics of discussion was a challenge tothink of who our stakeholders are, and howto best engage with those stakeholders.Britannica defines a stakeholder as anyindividual, social group, or actor who pos-sesses an interest, a legal obligation, a moralright, or other concern in the decisions oroutcomes of an organization. thus, foraBct, our stakeholders are any individu-als or organizations who have a vestedinterest in what our organization does andthe decisions we make.
For us to engage with a stakeholder doesnot necessarily mean that the stakeholdermust become a member of aBct. that isone way to engage—and i am broadly infavor of expanding our membership—butit is not the only way. rather, the aim ofstakeholder engagement is to build somekind of mutually beneficial relationship.central to the process, therefore, is starting(or continuing) conversations with variousgroups in order to explore how aBct canbest meet their needs. in this column, i willdiscuss several (though certainly not all) ofour prospective stakeholder groups. i donot claim to have the solution for how bestto engage all of these stakeholder groups;rather, my hope is to start a discussion onthe topic.
our members are, of course, our pri-mary stakeholders. at present, there are2,938 of us. that number is down fromprior years, likely due to diminished atten-dance at the virtual convention. this linkbetween membership and conventionattendance highlights the fact that ourmain way of engaging members has histor-ically been through the annual conven-tion, but that is certainly not the only way.indeed, during the strategic retreat, theidea that “aBct is primarily the aBctconvention” was identified as an orthodoxbelief that potentially holds us back from aricher relationship with our members. sohow else can we build a mutually beneficial
relationship with our members—both fullmembers and students? one ready avenueis our 41 special interest Groups (siGs),which can provide a smaller and more top-ically focused group with which our mem-bers can interact. to join a siG, visit the“For members” section at www.abct.org. inaddition, members wishing to work onbehalf of the organization can join one of anumber of committees, including (but notlimited to) the continuing educationcommittee; academic training & educa-tional standards committee; researchFacilitation committee; awards & recog-nition committee; self-help Book recom-mendation committee; Dissemination,implementation, & stakeholder engage-ment committee; Public education &media Dissemination committee; mem-bership committee; and social network-ing media committee. if you’re interestedin learning more about, or joining, a com-mittee, email our executive Director, maryJane eimer ([email protected]). Further-more, we are in need of members whowould like to review 2021 convention sub-missions; for more information, [email protected].
aBct is also working to increaseengagement with our members from tradi-tionally marginalized groups. our mem-bers who represent ethnic, racial, sexual, orgender minorities should know that theyhave a welcoming and inclusive profes-sional home in aBct, and those of us inleadership should continuously strive tomake it so. recently, the task Force to Pro-mote equity, inclusion, and access,chaired by Drs. sandra Pimentel, shireenrizvi, and laura seligman, recommendedspecific steps for aBct to consider inorder to better engage with, and meet theneeds of, our members and prospectivemembers from these groups. the Board ofDirectors is currently discussing their sug-gestions, and a report on their work isforthcoming in a future issue of thisnewsletter.
the list of stakeholders, however, doesnot end with the membership. Practicingclinicians in the community constituteanother important group that has an inter-est in, and can contribute meaningfully to,aBct’s activities, with or without aBctmembership. although our full membersmostly (91%) have doctoral degrees, weshould be mindful of the fact that the aPacommission on accreditation is nowworking towards accrediting master’sdegree programs in health service psychol-ogy (hsP), comprised of clinical, counsel-ing, and school psychology programs
(commission on accreditation, 2020). wewould be well served to enhance our rela-tionship with these master-level clinicians.our journal Cognitive and Behavioral Prac-tice provides a unique potential for a two-way communication, in which we can bothprovide information to, and solicit infor-mation from, these stakeholders. there is aunique opportunity here for us not only todisseminate information about evidence-based cBt, but also to hear back fromthese clinicians about how our treatmentsare working in their practices, and whatmight improve uptake and efficacy of thetreatments. this strategy of two-way com-munication is consistent with prior recom-mendations for the dissemination of evi-dence-based practices (e.g., Goldfried et al.,2014). one area of our work that i’d partic-ularly like to highlight is our continuingeducation program, which i hope to prior-itize during my term as President. aBct iswell poised to provide educational work-shops that appeal to practicing clinicians,regardless of whether they are aBct mem-bers. and again, because dissemination isbest conceptualized as a dialogue, ratherthan a lecture, aBct should solicit inputfrom these stakeholders about their train-ing needs. we should further exploreengaging these clinicians as presenters, notjust as consumers, as i am sure there ismuch that they can teach us while stillmaintaining a strong aBct “brand.”
we should also consider how best toengage training programs. this includesnot only our strong existing relationshipwith clinical psychology Ph.D. programs,but also counseling psychology programs,Psy.D. programs, msw programs, andmaster’s-level hsP programs. Given ourincreasing emphasis on diversity and inclu-sion, we may wish to reach out in particularto programs housed in historically Blackuniversities, universities with largely his-panic/latinx students, and organizationsof underrepresented students. conversa-tions with directors of clinical training atthese institutions would help us under-stand how to create a mutually beneficialrelationship.
another stakeholder group thatdeserves our attention—companies andother organizations with a vested interestin the work of aBct—includes healthinsurance companies, administrators oflarge mental health systems, schools, thejudicial system, and our colleagues in pub-lishing. Funding agencies such as thenational institute of mental health(nimh) and the substance abuse andmental health services administration

4 the Behavior Therapist
(samhsa) are also important stakehold-ers, and ongoing dialogue with these agen-cies is critical.
Finally, a list of aBct stakeholderswould not be complete without individualswith lived experience of behavioral healthproblems. certainly they stand to benefitfrom the work that aBct does, and ourresources such as the fact sheets (which arenow expanding to Youtube videos) andFind a cBt therapist search engine on ourwebsite are a great start. however, wewould likely benefit from increased dia-logue with, and input from, those withlived experience.
as we think about engaging stakehold-ers, we need to consider how we articulateto those stakeholders what our organiza-tion is about. our current mission state-ment was carefully crafted and provides athorough description of our aims. how-ever, at 101 words long, it may not be theoptimal message for rapid communicationwith certain stakeholders, especially when
“bandwidth” is limited. as the leadershipdiscusses how aBct can interact with var-ious stakeholders and the relationships wecould build, we are considering a statementof simplified purpose that is not intendedto replace the mission statement, but ratherwill serve as a shorthand way to communi-cate to prospective stakeholders aBct’sreason for being that reflects its mostimportant work:
ABCT promotes the use of scienceto understand and treat humanproblems.
the Board is continuing to address thissimplified purpose, along with guidingprinciples and critical outcomes. in futurecolumns i will describe additional propos-als from the strategic meeting. in the mean-time, i welcome your comments and ques-tions. Please feel free to email me [email protected].
Referencesantony, m. m. (2020). Planning for
aBct's future. the Behavior Therapist,43(7), 229-231.
commission on accreditation. (2020,march). Master’s level accreditation: Astatus update from the Master’s Accredi-tation Work Group. retrieved november21, 2020, from https://www.apa.org/ed/accreditation/newsletter/2020/03/masters-accreditation
Goldfried, m. r., newman, m. G., cas-tonguay, l. G., Fuertes, J. n., magnavita,J. J., sobell, l., & wolf, a. w. (2014). onthe dissemination of clinical experiencesin using empirically supported treat-ments. Behavior Therapy, 45(1), 3-6.
. . .
no conflicts of interest or funding todisclose.Address correspondence to David F.tolin, Ph.D., 200 retreat avenue, hartford,ct 06106; [email protected]
we DiD it! aBctoffered its first virtualconvention, and themajority of our atten-dees were satisfied,according to evaluationsand feedback. thankyou shannon wiltsey
stirman, Program chair; Daniel cheron,associate Program chair; and all of ourmembers for accommodating the extraeffort required by the cadmium system,the additional time required to prerecordor record “live!,” and being flexible. staffare coming down the home stretch inreviewing and editing the 40 Zoom-basedwebinars.
thank you, President antony, for pro-ducing an opening ceremony and shakingthings up by presenting your Presidentialaddress wednesday evening. and thankyou to Katharina Kircanski, our conven-
tion and education issues coordinator,who presented an orientation session forour virtual format and worked closely withour committee chairs: Brian Baucom,amass; samantha Farris, institutes;courtney Benjamin wolk, master clini-cian seminars; cole hooley, research andProfessional Development seminars; andchristina Boisseau, workshops (mini and3-hour ticketed). special thanks to abbyadler, our local arrangements chair, whohelped staff in identifying appropriateaudiences for our virtual format andhelped organize our first virtual saturday-night party. and thank you to an outstand-ing Program committee who reviewed thesubmissions. it does take many dedicatedand generous members to develop the con-tent for our annual conventions. Yourservice to aBct is greatly appreciated.
i also want to acknowledge our amazingstaff, who took on added responsibilities,
learned new systems, white-knuckled ouropening sessions, and faithfully came to theoffice each day to monitor sessions, answerthe constant ringing phones to help mem-bers and nonmembers renew, join, register,gain their access code, and manage thisyear’s process to earn continuing educationcredits. Kudos and a sincere thank you tomy colleagues: stephen crane, conventionmanager, for learning how to put on a vir-tual convention and stay on top of cad-mium complex program; Dakota mcPher-son, membership and marketing manager,and Veronica Bowen, membership ser-vices assistant, for applying their technicalskills in helping sort out a few glitches;David teisler, Director of communica-tions, and amanda marmol, administra-tive secretary, for monitoring a livestreamchannel and staffing the phones; stephanieschwartz, managing editor, for hergraphic design skills that grace the plat-form and our website; Kelli long, Book-keeper, for nurturing the staff even whileshe keeps our books in GaaP-approvedorder; and, of course, tonya childers, ourconvention registrar, who was never offthe phone and was totally focused onanswering questions and solving numer-ous problems to get our attendees in ses-sions as quickly as possible. Yours trulyalso handled several Zoom webinars andmonitored a live stream. we also hired 3temps to help monitor the concurrent ses-sions. clearly, it was a team effort.
AT ABCT
From Your Executive Director:What Your Leadership and StaffAre Working on to Serve You BetterMary Jane Eimer, Executive Director
e i m e r

January • 2021 5
Earn 5 CE credits forreading books in theAdvances in Psychotherapybook seriesPsychologists and other healthcare providers may earn fivecontinuing education credits for reading the books in theAdvances in Psychotherapy series and taking a multiplechoice exam. This continuing education program is apartnership of Hogrefe Publishing and the National Registerof Health Service Psychologists.
The National Register of Health Service Psychologistsis approved by the American Psychological Associationto sponsor continuing education for psychologists. TheNational Register maintains responsibility for this programand its content.
Readers who are not members of National Register canpurchase each exam for US $25.00 or access to the entireseries of exams for US $200.00. National Register memberscan take the exams free of charge. Exams are available for30 topics / books, with new titles being continually added.
Learn more at hogrefe.com/us/cenatreg
Vol. 42, 2019, viii + 94 pp.US $29.80ISBN 978-0-88937-415-7
Vol. 41, 2019, iv + 86 pp.US $29.80ISBN 978-0-88937-501-7
Vol. 40, 2019, viii + 76 pp.US $29.80ISBN 978-0-88937-407-2
Vol. 43, 2019, vi + 106 pp.US $29.80ISBN 978-0-88937-505-5
www.hogrefe.com

6 the Behavior Therapist
e i m e r
and then . . . we were hitting our stridewith membership renewals, donations toour awards programs, and convention reg-istrations, when bam! — a hacker compro-mised our online store, making fraudulentcharges on some members’ credit cards.we apologize for the inconvenience andthank our members and convention atten-dees for their good will and understandingas we sorted out and addressed the prob-lems. we contacted the FBi, Ftc, and ussecret service, the latter of which has juris-diction over cyber-crimes. Both the FBiand Ftc recommended that those whosecards were used to make reports to the Ftcand to give and get information from anyof the three major credit bureaus. amongthose compromised credit cards we weremade aware of, the individual cardholdershave been contacted by our Director ofcommunications, David teisler. he hasgiven formal statements to the FBi andFtc and has spoken with an agent at usss.we are well aware we are not the first orga-nization they have heard from and it is along line of organizations ahead of us forfurther follow-up.
this was an insidious hack—it left notrace. in the past, our systems show ananomaly, but not this time. we are alsoaware that our firewalls are fighting dailyagainst brute-force attack. we shut downour e-store and had our consultants andstaff work to find the problem and deter-mine the solution(s). we understand theneed for our membership and profession-als to trust our system. so we upgraded sys-tems, added security, and reopened thestore, monitoring transactions there andon our merchant portal. as you know frompast columns, we are migrating to a newplatform in april. there is an awareness ofoptics and the cost; but we wanted you tohave a fully functioning system in the inter-vening 4 months. we all know that hackinghas increased world-wide during the pan-demic. all of us are monitoring our credit
card usage and bank accounts with a closereye. staff continues to come to the office,but we are back to a staggered scheduleddue to the increased number of coViDcases in nYc, so calling us with your infor-mation is still an option in addition to mail-ing in a check. we’re here to facilitatethings for you.
now is the time to look forward. workis already under way in planning for thenovember 18-21, 2021, convention in neworleans’ hyatt, a new venue for us. theportal to submit ticketed sessions opensJanuary 4 followed closely by the generalcall for papers on February 8. Programchair chasson is working with leadershipand staff on what an aBct hybrid meetingwould offer.
President tolin has laid out the broadtopics the aBct leadership intends toaddress over the coming year. each stand-ing committee and think tank has a staffliaison to ensure clear communication thatruns both vertically and horizontally. timespent is a precious commodity and we wantall of our volunteers to feel their time hasbeen spent in meaningful ways during theirservice at aBct. as President tolin men-tioned in his column, many of our commit-tees appreciate more participation fromour members. You can contact the chairdirectly or you can write to me with yourinterest and skill sets and i can help youidentify a committee or two that wouldbenefit from your participation. Feel free towrite to me at [email protected].
a top priority for staff over the past yearthat is continuing in the new year is transi-tioning to a more robust database systemthat is fully integrated with a more user-friendly website. our goal is to have moreindividual transaction history (capturingthe conventions and ce credits), indicatingthe special interest Groups joined, addressand email changes updated in real timeacross various directories available on theweb, the ability for staff to update the
annual election records directly rather thansending to a third party, and capturingmore demographic and biographic infor-mation to help aBct be mindful of ourgoals for equity, inclusion, and access. inaddition to our web editors regine Galanti,succeeded by laura Payne, and associateweb editors shelley avny, nicholascrimarco, courtney Deangelis, andmiriam Korbman, many of our membershave been tapped into service to help us.we have focused on the rather long list ofspecialties and exploring how professionalsand the public use our site and what theymight want in the future. we also areexpanding our cyber security coverage.
it is no secret that these are turbulenttimes for you, our members. thank you forthose who have already renewed yourmembership. For those that have not, i dohope you will do that now. aBct is amember-driven organization with over 20standing committees, three journals, twothink tanks, and over 40 special interestGroups. we are expanding our webinarprogram to provide quality and diversepresentations and the ability to earn con-tinuing education credits from our live andrecorded offerings. we are here for your24/7—and we are more than our annualconvention. Don’t make this your lastissue of tBT, dropped from our list serve oryour favorite siG, cut loose from your pro-fessional home.
and as mentioned earlier, let us hearfrom you. a new year brings new goals,aspirations, and hope. i wish you and yoursa very happy and healthy new year withcoViD-19, one hopes, rapidly becoming adistant memory.
. . .
Correspondence to mary Jane eimer, cae,executive Director, aBct, 305 seventhave., suite 1601, new York, nY 10001;[email protected]
A B C T P I O N E E R S S E R I E S
Russell BarkleyDavid BarlowDavid BurnsAndrew ChristensenPhil KendallJudith BeckEsther DeblingerSteven C. HayesSteve Hollon
Alan KazdinArt NezuChristine Maguth NezuPatricia ResickTom OllendickSteven SafrenGail SteketeeGreg Siegle
ExploreABCT’s growing CBT Pioneers series:Interviews with CBT’s influential thinkers,researchers, and practitioners—
www.abct.org ABCT > FOR MEMBERS > CBT PIONEERS

January • 2021 7
1-800-748-6273 | newharbinger.com
newharbingerpub l i ca t i ons
Learn more about evidence-based continuing education and training with praxiscet.com
Download a FREE e-book of our most popular tips: newharbinger.com/quicktips
Essential Resources for Your Practice
ISBN: 978-1684034321 | US $24.95
ISBN: 978-1684035120 | US $25.95ISBN: 978-1684034550 | US $54.95ISBN 978 1684034550 | US $54 95
ISBN: 978-1684035489 | US $25.95
NEWEDITION
ISBN: 978-1684035915 | US $17.95ISBN 978 1684035915 | US $17 95
CARDDECK
ISBN: 978-1684035151 | US $64.95
NEWEDITION
NEWEDITION
NEWEDITION

8 the Behavior Therapist
the DemanD For mental health ser-vices dramatically exceeds the number ofavailable providers, rendering months-long waits for therapy the rule, rather thanthe exception, facing treatment-seekingindividuals. in the united states, wait-times for outpatient psychotherapy oftenspan weeks to several months (Blech et al.,2017; steinman et al., 2015), and waitingfor care can itself may cause harm. longerwait-times are linked to worsening mentalhealth symptoms (steinert et al., 2017),even when compared to “no treatment”conditions (where individuals do notexpect to receive future care (Furukawa etal., 2014), along with smaller symptomimprovements and greater odds of prema-ture dropout once treatment is accessed(reitzel et al., 2006; swift et al., 2012). thus,there is a need for efficient, sustainable ser-vice-delivery models that enable quickaccess to treatment for as many patients aspossible. offering interim, low-intensitysupports to treatment seekers may helpmitigate adverse effects of waiting forlonger-term care. to explore this possibil-ity, we tested the acceptability, feasibility,and short-term effects of a solution-focused single-session consultation service,offered to individuals waiting for therapy attwo outpatient clinics with mean wait-times of 2 to 6 months.
What Are Single-Session Interven-tions and Why Deliver Them?
single-session interventions (ssis) aredefined as “specific, structured programsthat intentionally involve just one visit orencounter with a clinic, provider, or pro-gram” (schleider et al., 2020). ssis mayserve as stand-alone programs (e.g., whereno other treatment is accessible, as is truefor many individuals with mental healthneeds; Kazdin, 2019) or as adjunctive sup-ports within existing care systems (seehoyt et al., 2018, for examples of bothapplication types). evidence supports both
applications. ssis have reduced anxiety,depression, self-harm, and interpersonalchallenges, among other psychosocial con-cerns (cartwright-hatton et al., 2018;Davis et al., 2012; hymmen et al., 2013;ranney et al., 2017; schleider et al., 2019).a meta-analysis of 50 randomized trialsfound a significant, positive effect of ssison mental health problems, versus controlconditions, at post-intervention (g = .32;schleider & weisz, 2017)—an effect com-parable to that observed for longer-termtherapies lasting 16 weeks on average (g =.46; weisz et al.). ssis may also improvetreatment expectancies, which predict sub-sequent engagement and response (swift etal., 2012; thiruchselvam et al., 2019; wu etal., 2020). For instance, relative to a placebocontrol, a 15-minute, online ssi teachingthat emotions are malleable strengthenedadults’ beliefs that therapy could be effec-tive (schleider & weisz, 2018).
Because ssis may improve both symp-toms and treatment expectancies, deliver-ing an ssi when individuals initially seektherapy might augment expectancies forchange, capitalize on motivation, and pre-vent symptom increases while waiting forlonger-term care. hoyt and colleagues(2018) note that ssis may confer at leastthree structural benefits if integrated intotraditional outpatient clinics: (a) ssisincrease access to immediate support, pro-viding patients with meaningful therapeu-tic interactions at just the right moment(when they are first compelled to seek sup-port); (b) ssis may reduce risks of delayedtreatment (or prevent overtreatment, as anssi may be sufficient to address certainpatients’ needs); and (c) ssi services couldprovide a valuable clinical training oppor-tunity to trainees, given that weekly ther-apy is infeasible in many clinical settings(e.g., inpatient clinics, schools, primarycare). as such, it is important to identifyssis best-suited for flexible, broad useacross diverse clinical settings—especially
ssis that are easy to implement, requiringminimal training to deliver.
SSIs for Individuals Waiting forTherapy: A Solution-Focused
Approachalthough many existing ssis might be
usefully integrated into existing clinical set-tings, we opted to test a novel “single-ses-sion consultation” service (schleider, 2020;full intervention protocol accessible atosf.io/xnz2t/ and draws heavily from prin-ciples of solution-Focused Brief therapy;sFBt; Bannink, 2007; De shazer, 1985).sFBt is focused on identifying and mobi-lizing a patient’s present goals, hopes, andstrengths (i.e., a strengths-based, patient-centered approach as opposed to a deficits-focused, therapist-driven approach). inter-ventions based on sFBt have guidedsingle-session clinical services internation-ally, though few such services exist in theunited states (several exist in canada, newZealand, and australia; see hoyt et al, 2018,for case examples). Given its emphasis onpresent hopes, patient strengths, and con-crete strategies, sFBt fits naturally into asingle-session format. therapists helppatients identify the tools and capacitiesthey already possess to solve a problem athand, and to take steps, however small,toward a future in which that problem isless influential. sFBt asserts that all peoplepossess inner resources to solve life’s chal-lenges; that one does not need to knowwhat caused a problem (e.g., via compre-hensive clinical assessment) to begin solv-ing it; and that the client is expert in theirlife and best positioned to address theirproblems (de shazer, 1985).
we designed the single-session con-sultation (ssc) as a flexible, sBFt-basedprogram for use with adolescents andadults, regardless of problem type or sever-ity. using the ssc, therapists help clientsidentify (1) a specific, modifiable problem(and associated “hope” for their ssc ses-sion); (2) the “smallest-possible step” theycan take toward overcoming their problem;and (3) a personalized action Plan, draw-ing on their inner abilities and externalresources to help them enact this smallest-possible step. this process aims toempower the client, helping them realizeand mobilize their existing resources tocope more effectively. notably, the ssc isdesigned to be delivered by therapists withany level of clinical training, from traineesto seasoned professionals, and training isapproximately 90 minutes in length(schleider, 2020). thus, the ssc is designed
ORIGINAL RESEARCH
Open Pilot Trial of a Single-SessionConsultation Service for Clients onPsychotherapy Wait-ListsJessica L. Schleider, Jenna Y. Sung, Amanda Bianco, Adam Gonzalez,
Dina Vivian, and Michael C. Mullarkey, Stony Brook University

January • 2021 9
for immediate scalability across diverse set-tings.
Present Studythis open pilot trial examined the feasi-
bility, perceived acceptability, and short-term effects of the ssc service, which wasoffered to clients on waiting-lists at two out-patient clinics at stony Brook universityacross a 6-month period. at both of theseclinics, wait-times for psychotherapy aver-age 2 to 6 months. Preregistered hypotheseswere as follows (see https://clinicaltrials.gov/ct2/show/nct04069832):
1. clinically relevant constructs of hope-lessness and perceived agency (primaryoutcomes) will significantly improvefrom pre-ssc to immediately post-ssc.
2. ssc participants will view the programas acceptable and useful in addressingtheir clinical needs, indexed by meanratings of at least 3.5 out of 5 across thefive items (each rated on 1–5 likertscales) on the “consultation FeedbackForm” developed for this study (avail-able at osf.io/zwphv).
3. the ssc will show feasibility as a serviceprovision model based on patient atten-dance (i.e., >50% of patients offered thessc service will elect to receive it, and>75% of clients who schedule an sscwill attend, which would reflect a sub-stantially lower “no-show” rate thanaverage for community-based mentalhealth clinics, where 40-60% of sched-uled sessions are attended (lefforge etal., 2007; oldham et al., 2012).
4. clients' overall psychological distresswill significantly decrease from baselineto 2 weeks after their ssc.
last, to explore whether ssc might pro-vide sufficient clinical care for some subsetof clients, we documented patients’ choicesabout whether to remain on (or removethemselves from) clinic wait lists 2 weeksafter their ssc.
MethodProcedure
all clients 13 years or older whoinquired about outpatient therapy servicesat two outpatient clinics (described below)from september 2019 to February 2020
were offered an ssc. Prospective clientscompleted a brief phone screen to collectcontact information, a brief summary oftheir primary reason for seeking services,and an abbreviated risk assessment todetermine appropriateness for outpatienttherapy (versus emergency services ifimminent risk is present). if emergencyservices are not required, clients wereplaced on clinic wait-lists (estimated at 2–6months). clients were then informed of thessc service and invited to take part in aone-time, face-to-face consultation with atrained clinician while waiting for treat-ment. clients expressing interest in the sscwere scheduled for a session within 2 weeksof this invitation, choosing among 6 to 8preexisting ssc appointment times (1–2session options per weekday). clientsreceived confirmation emails shortly afterscheduling and 24 hours before their ses-sion. Prior to scheduling, clients wereinformed that the cost of an ssc is identicalto the cost for a single session of psy-chotherapy (between $20 and $65, per theclinics’ sliding fee schedules).
Participants were asked to arrive 30minutes prior to their ssc to complete
Celebrat ing Our 49th Year
Steven T. Fishman, Ph.D., ABPP | Barry S. Lubetkin, Ph.D., ABPPDirectors and Founders
Since 1971, our professional staff has treated over 30,000 patients with compassionate, empirically-based CBT.Our specialty programs include: OCD, Social Anxiety Disorder, Panic Disorder, Depression, Phobias, PersonalityDisorders, and ADHD-Linked Disorders, and Child/Adolescent/Parenting Problems.
Our externs, interns, postdoctoral fellows and staff are from many of the area’s most prestigious universitiesspecializing in CBT, including: Columbia, Fordham, Hofstra, Rutgers, Stony Brook, St. John’s, and YeshivaUniversities.
Conveniently located in the heart of Manhattan just one block from Rockefeller Center. Fees are affordable,and a range of fees are offered.
For the safety and welfare of our patients and our mental health colleagues, the Institute is offering virtualindividual therapy sessions, as well as virtual supervisory sessions by our senior staff members.
New York CityINSTITUTE for BEHAVIOR THERAPY
For referrals and/or information, please call: (212) 692-928820 East 49th St., Second Floor, New York, NY 10017e-mail: [email protected] | web: www.ifbt.com
s i n g l e - s e s s i o n c o n s u l t a t i o n s e r v i c e

10 the Behavior Therapist
s c h l e i d e r e t a l .
baseline questionnaires. upon arrival, afterproviding informed consent to take part inthe ssc trial, participants self-reportedoverall psychological distress, levels ofhopelessness, and levels of perceivedagency at baseline. Participants then tookpart in their 1-hour ssc with a trained clin-ician. immediately after the ssc, partici-pants again self-reported levels of hopeless-ness and perceived agency, along withfeedback on the session’s acceptability. Par-ticipants were then contacted via phone fora two-week follow-up assessment, whereinthey again self-reported overall psycholog-ical distress and received the option ofremaining on or removing themselves fromthe clinic waitlist for therapy. clinic staffattempted to contact ssc recipients up to 3times for their follow-up call. if noresponse was received, clients were consid-ered unresponsive and were automaticallyremoved from the clinic waitlist, per bothclinics’ standard policies.
Clinical Settingsthis trial took place at two mental
health clinics affiliated with stony Brookuniversity, the leonard Krasner Psycho-logical center (KPc) and the mind-Bodyclinical research center (mBcrc). theKPc is the training facility for students instony Brook university’s clinical psychol-ogy doctoral program. student cliniciansprovide a variety of evidence-based assess-ments and therapies, including outpatientservices for children, adolescents, andadults under the supervision of licensedpsychologists. the mBcrc, housed in theDepartment of Psychiatry at stony Brookhospital, provides evidence-based adultoutpatient mental health services and isstaffed by predoctoral and postdoctoraltrainees, social workers, and clinical psy-chologists.1
Inclusion Criteriaall english-speaking adolescents (age
13+) and adults on waitlists for outpatienttherapy services at the KPc and mBcrcreceived invitations to take part in thisstudy. child clients < age 13 were not eligi-ble to take part in this study, as the ssc wasdesigned for use with adolescents andadults. Due to unusually low rates of ser-vice inquiries from prospective adolescent
clients during the recruitment period, allparticipants in this study were adults (> 18years). informed consent was obtainedprior to study initiation with each partici-pant.
Therapist Training, Supervision, andFidelity
six advanced doctoral student cliniciansfrom the KPc and three postdoctoral clin-icians from the mBcrc attended a 90-minute ssc training, led by the first author(Jls). this training provided backgroundinformation on single-session and solu-tion-focused therapeutic techniques; astep-by-step walkthrough of the ssc pro-gram protocol; an overview of potentialchallenges (and recommended solutions)faced by ssc providers; and guidelines foraddressing imminent risk during an sscsession. clinicians in this study wereadvised to utilize standard clinic proce-dures to assess risk in participants report-ing non-zero suicidal ideation at pre-inter-vention. if risk to the client was deemedimminent, clinicians were instructed toprioritize risk management and triage overssc completion. although several partici-pants in this study (26.67%) reported pas-sive suicidal ideation at pre-intervention,risk was assessed and deemed imminent innone of these cases, and all of these clientsengaged successfully in the ssc.
to promote clinician fidelity, therapistsreceived a step-by-step guide to deliveringthe ssc in its intended format (availablehere: https://osf.io/r5gk3/) and an “actionPlan” worksheet to be completed jointlywith clients during the ssc (available here:https://osf.io/7jt6m/). the action Plan isdesigned to impose a uniform, linear struc-ture onto each ssc while generating a per-sonal coping plan for each client. actionplans were successfully (at least 80%) com-pleted for all ssc sessions in this study,suggesting fidelity to the intended format.additionally, all ssc sessions delivered atthe KPc (23 of 30 in this study) were video-recorded for supervision purposes andviewed in full by the first author (Jls).consistent with the successfully completedaction Plans, recordings suggested thera-pists’ fidelity to the ssc structure.
Single-Session Consultation Overviewthe ssc is designed to last approxi-
mately 1 hour, although a session may last30–90 minutes, depending on clinical set-ting, client needs, and therapist availability.Below we summarize the key tasks withinan ssc. a more comprehensive descrip-tion of the ssc and its delivery, includingexample responses to client concerns,strategies for incorporating strengths-based language throughout the interven-tion, and solutions to common problems,is available in the open-access ssc manual:https://osf.io/tua4h/.
after briefly assessing readiness toengage in the ssc (i.e., assessing imminentrisk, which takes precedence over the ssc ifpresent), the ssc therapist briefly intro-duces the purpose and parameters of thessc; sets client expectations (i.e., this ses-sion will not become a long-term therapeu-tic relationship; it is simply a means of pro-viding short-term support while you arewaiting for services); praises the client fortaking initiative to engage in the ssc; andintroduces the action Plan, which willguide the session’s structure and will becompleted jointly over the upcoming hour.next, the client is asked to identify their topproblem in the present moment (which ledthem to seek services), along with their tophope for today’s session (framed as a dis-crete, tangible step they would like to taketowards a future where their top problem ismore manageable). if needed, the therapistredirects the client to identify a top prob-lem and commensurate top hope that ismodifiable—i.e., changeable via personaleffort. examples for ways to reframe“external” top problems to relatively “inter-nal” alternatives are noted in the sscmanual.
next, the clinician poses the “miraclequestion,” a common sFBt technique:Imagine that a miracle occurs overnight;while you are sleeping, your reason for seek-ing services has completely disappeared.When you wake up, how will you know thatthere has been a miracle? What will you do,think, or feel differently? the therapist sup-ports their client in crafting as vivid adescription as possible of their “miracleday” wherein their top problem is absent.next, the therapist asks the client to rate, ona 1-to-10 scale, “how close they are to[their] miracle day” at the present moment,with “10” representing their problemhaving disappeared entirely, and “1” repre-senting their problem being at its worst(completely incapacitating). the remain-der of the session is dedicated to crafting apersonalized action Plan, geared towards
1there were no significant differences across clinics in uptake of the ssc when offered, buta larger number of clients at the KPc (versus the ssc) were offered the ssc, as there weremore staff members available at the KPc to assist with recruitment calls for this study. wewere unable to examine differences in outcome by clinic, as only 7 individuals completedthe ssc at the mBcrc; thus, results of statistical tests would have been uninterpretable.

January • 2021 11
s i n g l e - s e s s i o n c o n s u l t a t i o n s e r v i c e
helping the client “move up by just onepoint on your miracle Day scale”—forinstance, if a client rates themselves at a “4out of 10” in terms of closeness to theirmiracle day, their plan is geared towardssupporting them in reaching a “5 out of10.” the action Plan includes up to threeconcrete things that the client can do(including where and when they will dothose things) to increase their miracle dayscale rating by a single point. therapistsencourage the client to choose action Planstrategies reflecting small steps they havetaken before (e.g., based on times whentheir miracle day scale rating was slightlyhigher than today’s rating), drawing on theclient’s existing strengths, habits, connec-tions, and coping skills as heavily as possi-ble. clients are also guided to identify twopeople or community resources that canhelp them implement their plan. once theaction Plan is constructed, the client isasked to identify an inner obstacle that maykeep them from following through withtheir plan: a “thought, feeling, or bad habitthat could get in the way” of carrying outthe action Plan as intended. upon identi-fying an inner obstacle, the client is askedto generate a “phrase, thought, or action tohelp them overcome their inner obstacle.”the therapist works with the client to helpthem generate an inner obstacle that feelspersonally important, and to craft a way toovercome it that “rings true” to them.
upon ending the ssc, the therapisttakes a few moments to write a personal-ized note to their client at the bottom of theaction Plan worksheet. this note is writtenin the second person (using “you” pro-nouns) and identifies two specific reasonswhy the clinician personally believes thatthe client is capable of following-throughon their action plan, based on their ownobservations during the ssc. the clientreceives a copy of their action plan, includ-ing the note from their clinician, at thessc’s conclusion. clients are also providedwith a list of referrals to local emergencyservices and crisis hotlines and textlines,should they require immediate supportbefore beginning psychotherapy.
MeasuresState Hope Scale(SHS; Snyder et al., 1996)the shs is a 6-item self-report measure
of agentic, goal-directed thinking. respon-dents rate 6 items on a likert scale from 1(definitely false) to 8 (definitely true).higher mean scores reflect a greater senseof personal agency (i.e., personal capacityto pursue and sense of having attained
goals). scores range from 1–8, with higherscores reflecting greater perceived agency.the shs was administered at pre-ssc andimmediately post-ssc. internal consis-tency was α= 0.86 and 0.92 at pre-and post-ssc, respectively.
Beck Hopelessness Scale-4(Perczel Forintos et al., 2013)the brief, 4-item Bhs asks respondents
to report agreement with 4 items on a 0–3scale. higher scores reflect greater hope-lessness; scores range from 0–12. the Bhs-4 was administered at pre- and immedi-ately post-ssc. internal consistency was α=0.87 at both pre- and post-ssc.
Brief Symptom Inventory-18(BSI-18; Derogatis, 2001)the Bsi-18 assesses self-reported psy-
chopathology and distress. it was selectedas the primary outcome measure for thisstudy because it is brief, normed on anational u.s. sample of adults, and inclu-sive of multiple domains of psychopathol-ogy (depressive symptoms, anxiety symp-toms, somatic symptoms). respondentsrate endorsement of 18 physical and emo-tional complaints on a 0–4 likert scale. thetotal sum score yields an additional totaldistress score (range: 0–72). higher scoresindicate higher levels of overall psycholog-ical distress. the Bsi-18 was administeredpre-ssc and at 2-week follow up. internalconsistency was α= 0.85 and 0.90 at pre-and post-ssc, respectively.
Consultation Feedback Formthe consultation feedback form,
designed for this trial and administered atpost-ssc, contains 5 items rated on a 1(Not at all) to 5 (Very much) likert scale,reflecting endorsement of a series of state-ments about the ssc (e.g., "Did you findthe consultation helpful in addressing yourconcerns?" and "how hopeful are you thatthe action plan will be useful?" higherscores indicate greater perceived usefulnessof the ssc. internal consistency was α=0.86.
Sample Size Justificationwe were interested in obtaining precise
estimates of feasibility and acceptabilityoutcomes; client satisfaction ratings; andchanges in proximal intervention out-comes to aid in the planning of a larger-scale efficacy trial. a sample of 30 partici-pants was sufficient for these objectives, perguidelines for pilot study-planning pro-posed by Joulius (2005) and whitehead etal (2016).
Analytic PlanPer preregistered analyses, we ran two
2-tailed paired samples t-tests to assesswhether participants’ hopelessness andperceived agency significantly improvedfrom pre- to post-ssc. a pre-post differ-ence with p < .05 indexed a significantchange, in either case. we next examinedconsultation Feedback Form scores; meanscores of >3.5/5 on each item indicated that
CAREER OPPORTUNITY
Licensed ClinicianMountain Valley, a residential
treatment program for adolescentssuffering from debilitating anxiety
and OCD, is hiring.Rewarding experience with
opportunities for developmentand advancement.
Contact Dr. Tim DiGiacomo, Clinical Director, [email protected],
or 203-913-3744.
Located in New Hampshire’sDartmouth College region.
As featured in the New York Times Magazineand People Magazine
s c h l e i d e r e t a l .
12 the Behavior Therapist
participants found the ssc more thansomewhat acceptable along all dimensionsexamined. to gauge service model feasibil-ity, we first divided the number of wait-listed individuals who accepted the sscinvitation by the number of people whoreceived ssc invitations; we then dividedthe number of people who attended theirscheduled ssc by the total number of whoscheduled an ssc. an “accepted ssc invi-tation” rate of >50% and an “attendedscheduled ssc” rate of >75% suggested thessc’s feasibility as a service delivery modelin these clinics. last, we ran a 2-tailedpaired samples t-test to test whether partic-ipants’ psychological distress (Bsi-18scores) significantly (p < .05) reduced frompre-ssc to follow-up.
For paired-samples t-tests, the false dis-covery rate (FDr) was applied to identifypotential false-positive results. Q-valueswere computed for p-values from t testsusing an online calculator applying Ben-jamini and hochberg’s (1995) approach(www.sdmproject.com/utilities/?show=FDr).
results were considered significant if FDrcorrected q < 0.05.
Resultsanonymized data and code for all
analyses are available here: https://osf.io/xnz2t/
Descriptives and Feasibilityof the 90 treatment-seeking individuals
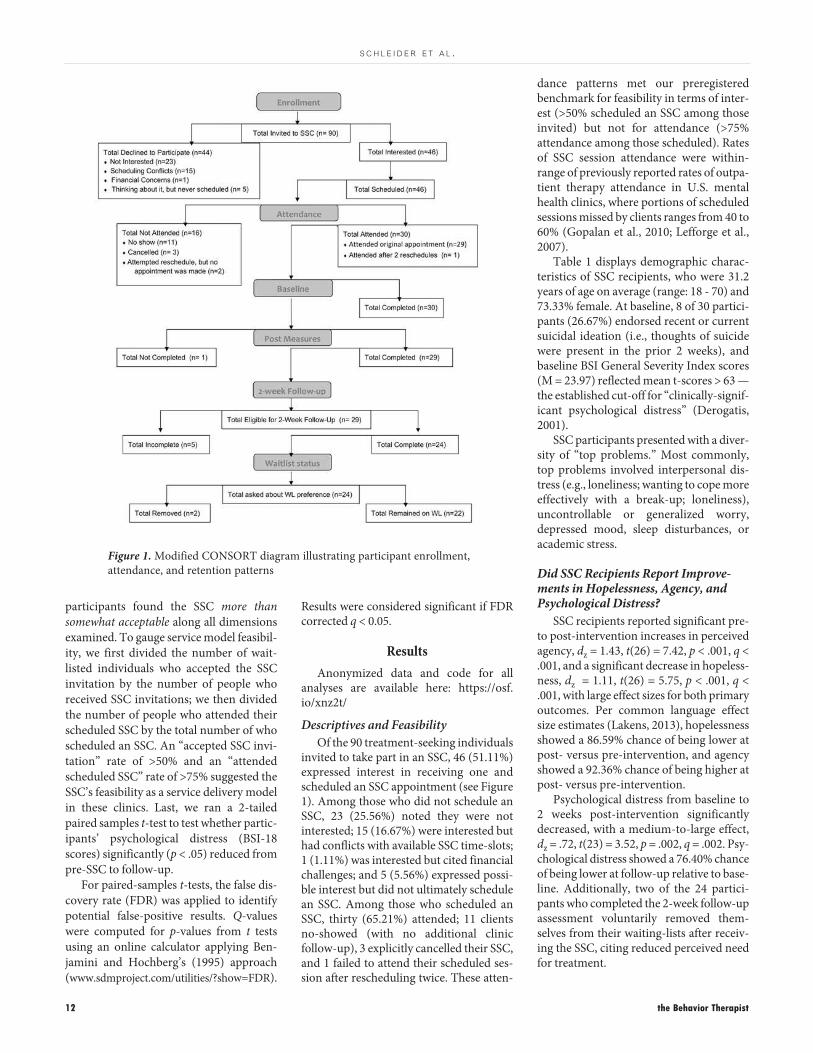
invited to take part in an ssc, 46 (51.11%)expressed interest in receiving one andscheduled an ssc appointment (see Figure1). among those who did not schedule anssc, 23 (25.56%) noted they were notinterested; 15 (16.67%) were interested buthad conflicts with available ssc time-slots;1 (1.11%) was interested but cited financialchallenges; and 5 (5.56%) expressed possi-ble interest but did not ultimately schedulean ssc. among those who scheduled anssc, thirty (65.21%) attended; 11 clientsno-showed (with no additional clinicfollow-up), 3 explicitly cancelled their ssc,and 1 failed to attend their scheduled ses-sion after rescheduling twice. these atten-
dance patterns met our preregisteredbenchmark for feasibility in terms of inter-est (>50% scheduled an ssc among thoseinvited) but not for attendance (>75%attendance among those scheduled). ratesof ssc session attendance were within-range of previously reported rates of outpa-tient therapy attendance in u.s. mentalhealth clinics, where portions of scheduledsessions missed by clients ranges from 40 to60% (Gopalan et al., 2010; lefforge et al.,2007).
table 1 displays demographic charac-teristics of ssc recipients, who were 31.2years of age on average (range: 18 - 70) and73.33% female. at baseline, 8 of 30 partici-pants (26.67%) endorsed recent or currentsuicidal ideation (i.e., thoughts of suicidewere present in the prior 2 weeks), andbaseline Bsi General severity index scores(m = 23.97) reflected mean t-scores > 63 —the established cut-off for “clinically-signif-icant psychological distress” (Derogatis,2001).
ssc participants presented with a diver-sity of “top problems.” most commonly,top problems involved interpersonal dis-tress (e.g., loneliness; wanting to cope moreeffectively with a break-up; loneliness),uncontrollable or generalized worry,depressed mood, sleep disturbances, oracademic stress.
Did SSC Recipients Report Improve-ments in Hopelessness, Agency, andPsychological Distress?
ssc recipients reported significant pre-to post-intervention increases in perceivedagency, dz = 1.43, t(26) = 7.42, p < .001, q <.001, and a significant decrease in hopeless-ness, dz = 1.11, t(26) = 5.75, p < .001, q <.001, with large effect sizes for both primaryoutcomes. Per common language effectsize estimates (lakens, 2013), hopelessnessshowed a 86.59% chance of being lower atpost- versus pre-intervention, and agencyshowed a 92.36% chance of being higher atpost- versus pre-intervention.
Psychological distress from baseline to2 weeks post-intervention significantlydecreased, with a medium-to-large effect,dz = .72, t(23) = 3.52, p = .002, q = .002. Psy-chological distress showed a 76.40% chanceof being lower at follow-up relative to base-line. additionally, two of the 24 partici-pants who completed the 2-week follow-upassessment voluntarily removed them-selves from their waiting-lists after receiv-ing the ssc, citing reduced perceived needfor treatment.
Figure 1. modified consort diagram illustrating participant enrollment,attendance, and retention patterns

s i n g l e - s e s s i o n c o n s u l t a t i o n s e r v i c e
Did SSC Recipients Find It Acceptable?Participants perceived their ssc ses-
sions as highly acceptable. on a scale from1 (not at all) to 5 (very much), participantsrated their sessions as “helpful in address-ing their concerns,” M(SD) = 4.31(0.76)and as having “helped them develop anaction plan to address their concerns,”M(SD) = 4.55 (0.78). Participants generallyrated themselves as “hopeful that the actionplan will be useful,” M(SD) = 4.07 (0.80),and “motivated to use their action plan,”M(SD) = 4.24 (0.79). all but one of the par-ticipants (96.67%) reported that theywould “mostly” or “very much” recom-mend the consultation service to others,M(SD) = 4.72(0.52). additionally, severalssc recipients provided positive writtenfeedback about their experience. as exam-ples: “i didn't expect to feel this differentlyafter a single consultation. it's a big relief";“Great communication, the consultationdidn't feel rushed. everything was patientand led to a new revelation/idea/goal thatwas set”; “i feel very positive about my planand i am excited to begin trying it out.thank you.” other study participants pro-vided either neutral written feedback (e.g.,“thank you”) or no written feedback. noparticipants provided negative writtenfeedback on their ssc.
Discussionthis open pilot trial tested the feasibil-
ity, perceived acceptability, and short-termeffects of the single-session consultation,a 1-hour solution-focused intervention foradults on waiting-lists for outpatient psy-chotherapy. clients who completed thessc reported significant pre- to post-inter-vention reductions in hopelessness (dz =1.43) and perceived agency (dz = 1.11),along with significant reductions in psy-chological distress from pre-interventionto 2-week follow-up (dz = 0.73). ssc recip-ients viewed the intervention as highlyacceptable, per preregistered benchmarks.regarding feasibility, attendance patternsmet our preregistered benchmark withrespect to client interest (51% of thoseoffered an ssc elected to receive one, aboveour 50% benchmark) but not attendance(65% of those who scheduled an sscattended one, below our 75% benchmark).overall, results suggest the ssc’s potentialutility among high-symptom, treatment-seeking individuals.
our study, though preliminary, sug-gests that a novel ssi may help fill gaps inexisting services. Given the shortages ofmental health providers and needs to
expand service access across numerous set-tings, the ssc might prove helpful withinand beyond outpatient mental health clin-ics. Providers in hospital and primary caresettings, where time with patients is lim-ited, may find the ssc’s self-containedstructure useful. therapists in this studyincluded both pre- and postdoctoral clini-cians, suggesting the ssc’s ease of deliveryafter a 90-minute training. of course, thesepossibilities require further study in diversecontexts and populations. we have thusmade ssc materials freely available,including ssc training slides, the interven-tion protocol, the action Plan, and theconsultation Feedback Form used in thisstudy (https://osf.io/xnz2t/), which wehope spur further tests of the program’spotential.
some aspects of our results warrant fur-ther consideration. For instance, due tologistical constraints, we were able to offerclients only a handful of time-slot optionsfor ssc appointments, and those appoint-ments were available in-person only. walk-in clinics, teletherapy options, and otherapproaches conferring more flexible sched-uling capacity could yield broader sscinterest and improved attendance.although the ssc attendance rate in thistrial (65%) compares favorably with ses-sion attendance rates in outpatient mentalhealth clinics nationally (40–60%), alterna-tive delivery models could further boost thessc’s accessibility and uptake—and inturn, its feasibility for clinics to provide.
separately, most clients in this studychose to remain on their respective therapywaiting lists after completing an ssc.notably, we do not view this as evidencethat the ssc was ineffective. this samplewas composed of treatment-seeking adults
with no prior knowledge of the ssc, whocontacted clinics specifically in pursuit ofweekly therapy; thus, their continued inter-est in this type of treatment is unsurprising.indeed, the fact that two participants per-ceived no need for therapy after their sscssuggests its potential utility, for some, as astand-alone intervention. as is discussedelsewhere (schleider et al., 2020), most ssismay operate as either stand-alone oradjunctive supports, depending on context,setting, and clinical need. this prospectshould be explored in future, larger-scaletrials of the ssc as a stand-alone supportand as a means of enhancing client motiva-tion and engagement once therapy begins.
this study has important limitations.results of any nonrandomized pilot trialare preliminary. Further, this pilot trial hada relatively brief follow-up period com-pared the average waiting time for psy-chotherapy at the participating clinics, and
nagesex
maleFemale
3031.2 (14.9)
8 ( 26.7%)22 (73.3%)
2326.3 (11.2)
7 (30.4%)16 (69.6%)
747.0 (15.1)
1 (14.3%)6 (85.7%)
Full sampleM (SD) or (%)
Note. KPc (Krasner Psychological center); mBcrc (mind Body clinicalresearch center). Due to the KPc’s and mBcrc’s transitions to tele-mental health services in april 2020, data on participants’ race/ethnicity(stored on paper documents in both clinics) were inaccessible to theresearchers at the time of data analysis for this manuscript.
Table 1. Demographics, individuals attending an ssc session
KPc sampleM (SD) or (%)
mBcrc sampleM (SD) or (%)
agencyPre-sscPost-sscdz [95% ci]
hopelessnessPre-sscPost-sscdz [95% ci]
PsychologicalDistress
Pre-ssc2-weeks
dz [95% ci]
26.30 (8.73)19.48 (8.04)1.43 [0.88, 1.96]
5.37 (3.59)2.78 (2.50)1.11 [0.62, 1.58]
25.83 (11.24)18.00 (11.83)0.72 [0.26, 1.16]
M (SD)
Table 2. means, standard Deviations,and effect sizes
January • 2021 13

14 the Behavior Therapist
s c h l e i d e r e t a l .
a subset of participants were lost to attri-tion (though no differences emerged inbaseline psychological distress levelsbetween participants who did versus didnot complete the follow-up assessment).nonetheless, it is notable that treatment-seeking individuals often report stable orworsening symptoms while waiting fortherapy, yet participants in this trialreported symptom reductions 2 weekspost-ssc. Future randomized trials areneeded to determine the longevity androbustness of effects observed in this study.separately, due to the ssc’s brief format(and its omission of a formal assessment,which might have lasted longer than theintervention itself), data on participants’diagnostic profiles were unavailable. wethus cannot comment on the ssc’s utilityas a function of problem type. anecdotally,study authors (upon viewing video-recorded ssc sessions) and ssc therapistsobserved that some conditions renderedthe program more challenging to deliver.examples included traumatic brain injury(resulting in memory impairment) and aneating disorder (resulting in medical prob-lems)—both noted spontaneously by sscrecipients during sessions (these twoclients were referred to specialty servicesfollowing their sscs). at the same time,several clients reporting clinically elevatedpsychological distress and suicidal ideationengaged successfully in the ssc; thus, clin-ical severity alone does not appear to pre-clude acceptability, but formal investiga-tion is needed as to whether the ssc’sutility varies by clinical profile.
overall, results support the single-ses-sion consultation’s acceptability in a high-symptom, treatment-seeking adult sample.ssc recipients reported improvements inhopelessness, perceived agency, and psy-chological distress while waiting forlonger-term treatment. Both pre- and post-doctoral therapists successfully deliveredthe ssc following a brief, 90-minute train-ing. Future studies will help gauge thessc’s best-fit applications and potentialcontraindications.
ReferencesBannink, F. (2007). solution-Focused Brief
therapy. Journal of Contemporary Psy-chotherapy, 2, 87–94.
Benjamini, Y., & hochberg, Y. (1995).controlling the false discovery rate: apractical and powerful approach to mul-tiple testing. Journal of the Royal Statisti-cal Society: Series B, 57, 289–300.
Blech, B., west, J. c., Yang, Z., Barber, K.D., wang, P., & coyle, c. (2017). avail-
ability of network Psychiatrists amongthe largest health insurance carriers inwashington, Dc. Psychiatric Services,68(9), 962–965.
cartwright-hatton, s., ewing, D., Dash, s.,hughes, Z., thompson, e. J., hazell, c.m., Field, a. P., & startup, h. (2018).Preventing family transmission of anxi-ety: Feasibility rct of a brief interven-tion for parents. British Journal of Clini-cal Psychology, 57(3), 351–366.
Davis, t. e., iii, ollendick, t. h., & Öst,l.-G. (2012). Intensive One-SessionTreatment of Specific Phobias. springerscience & Business media.
Derogatis, l. r. (2001). Brief SymptomInventory 18: Administration, Scoringand Procedures Manual.
De shazer, s. (1985). Keys to Solution inBrief Therapy. w w norton.
Furukawa, t. a., noma, h., caldwell, D.m., honyashiki, m., shinohara, K., imai,h., chen, P., hunot, V., & churchill, r.(2014). waiting list may be a nocebocondition in psychotherapy trials: a con-tribution from network meta-analysis.Acta Psychiatrica Scandinavica, 130(3),181–192.
hoyt, m. F., Bobele, m., slive, a., Young,J., & talmon, m. (2018). Single-session/one-at-a-time walk-in therapy.routledge.
hoyt, m. F., & talmon, m. e. (2014). Cap-turing the Moment: Single Session Ther-apy and Walk-In Services. crown housePublishing limited.
hymmen, P., stalker, c. a., & cait, c.-a.(2013). the case for single-session ther-apy: Does the empirical evidence supportthe increased prevalence of this servicedelivery model? Journal of MentalHealth, 22, 60–71.
Kazdin, a. e. (2019). annual researchreview: expanding mental health ser-vices through novel models of interven-tion delivery. Journal of Child Psychologyand Psychiatry, 60(4), 455-472.
lakens, D. (2013). calculating and report-ing effect sizes to facilitate cumulativescience: a practical primer for t-tests andanoVas. Frontiers in Psychology, 4, 863.
lefforge, n. l., Donohue, B., & strada, m.J. (2007). improving session attendancein mental health and substance abuse set-tings: a review of controlled studies.Behavior Therapy, 38(1), 1–22.
oldham, m., Kellett, s., miles, e., &sheeran, P. (2012). interventions toincrease attendance at psychotherapy: ameta-analysis of randomized controlledtrials. Journal of Consulting and ClinicalPsychology, 80(5), 928–939.
Perczel Forintos, D., rózsa, s., Pilling, J., &Kopp, m. (2013). Proposal for a shortversion of the Beck hopelessness scale
based on a national representative surveyin hungary. Community Mental HealthJournal, 49(6), 822–830.
ranney, m. l., Goldstick, J., eisman, a.,carter, P. m., walton, m., & cunning-ham, r. m. (2017). effects of a brief eD-based alcohol and violence interventionon depressive symptoms. General Hospi-tal Psychiatry, 46, 44–48. https://doi.org/10.1016/j.genhosppsych.2017.01.008
reitzel, l. r., stellrecht, n. e., Gordon, K.h., lima, e. n., wingate, l. r., Brown, J.s. … Joiner, t. e. (2006). Does timebetween application and case assignmentpredict therapy attendance or prematuretermination in outpatients? PsychologicalServices, 3, 51–60.
schleider, J., l. (2020) single-session con-sultation for emotional and Behavioralhealth. https://doi.org/10.17605/osF.io/XnZ2t
schleider, J. l., Burnette, J. l., widman, l.,hoyt, c., & Prinstein, m. J. (2019, inpress). randomized trial of a single-ses-sion Growth mind-set intervention forrural adolescents’ internalizing andexternalizing Problems. Journal of clini-cal child and adolescent Psychology.
schleider, J. l., Dobias, m. l., sung, J. Y., &mullarkey, m. c. (2020). Future Direc-tions in single-session Youth mentalhealth interventions. Journal of ClinicalChild and Adolescent Psychology, 49(2),264–278.
schleider, J. l., & weisz, J. r. (2017). littletreatments, Promising effects? meta-analysis of single-session interventionsfor Youth Psychiatric Problems. Journalof the American Academy of Child &Adolescent Psychiatry, 56, 107–115.https://doi.org/10.1016/j.jaac.2016.11.007
schleider, J. l., & weisz, J. r. (2018).Parent expectancies and Preferences formental health treatment: the roles ofemotion mind-sets and Views of Failure.Journal of Clinical Child and AdolescentPsychology, 47, s480–s496.
slive, a., mcelheran, n., & lawson, a.(2008). how Brief Does it Get? walk-insingle session therapy. Journal of Sys-temic Therapies, 27, 5–22.https://doi.org/10.1521/jsyt.2008.27.4.5
snyder, c. r., sympson, s., Ybasco, F.,Borders, t., Babyak, m., & higgins, r. l.(1996). Development and validation ofthe state hope scale. Journal of Personal-ity and Social Psychology, 70(2), 321–335.
steinert, c., stadter, K., stark, r., & leich-senring, F. (2017). the effects of waitingfor treatment: a meta-analysis of wait-list control Groups in randomized con-trolled trials for social anxiety Disorder.Clinical Psychology & Psychotherapy,24(3), 649–660.
steinman, K. J., shoben, a. B., Dembe, a.e., & Kelleher, K. J. (2015). how long Do

January • 2021 15
adolescents wait for Psychiatryappointments? Community MentalHealth Journal, 51(7), 782–789.
swift, J. K., whipple, J. l., & sandberg, P.(2012). a prediction of initial appoint-ment attendance and initial outcomeexpectations. Psychotherapy , 49(4), 549–556.
thiruchselvam, t., Dozois, D. J. a.,Bagby, r. m., lobo, D. s. s., ravindran,l. n., & Quilty, l. c. (2019). the role ofoutcome expectancy in therapeuticchange across psychotherapy versuspharmacotherapy for depression. Jour-nal of Affective Disorders, 251, 121–129.
weisz, J. r., Kuppens, s., ng, m. Y., eck-shtain, D., ugueto, a. m., … Fordwood,s. r. (2017). what five decades ofresearch tells us about the effects ofyouth psychological therapy: a multi-level meta-analysis and implications forscience and practice. American Psycholo-gist, 72(2), 79–117.
wu, m. s., caporino, n. e., Peris, t. s.,Pérez, J., thamrin, h., … Piacentini, J.(2020). the impact of treatment expec-tations on exposure Process and treat-ment outcome in childhood anxietyDisorders. Journal of Abnormal ChildPsychology, 48(1), 79–89.
. . .
Jls receives grant and research supportfrom the national institutes of health(DP5oD28123), the Klingenstein thirdGeneration Foundation, the american Psy-chological Foundation, and limbix, inc. JYsreceives research funding from the Psi chihonor society. Jls and mcm are undercontract with new harbinger Publicationsto co-author a therapeutic workbook foradolescents. Jls is under contract withoxford university Press to co-edit a bookon low-intensity youth mental health inter-ventions. the authors report no other finan-cial conflicts.Correspondence to Jessica l. schleider,Ph.D., stony Brook university, stonyBrook, nY, 11794- 2500; [email protected]
alan BellacK famously characterizedschizophrenia as cognitive behavioral ther-apy’s “forgotten stepchild” in his 1985association for advancement of Behaviortherapy (later renamed the association forBehavioral and cognitive therapies) pres-idential address, a characterization thatlargely rings true today (see snyder et al.,2016). at aBct’s 52nd annual conven-tion in 2019, the president of the aBctPsychosis and schizophrenia spectrumspecial interest Group (Pass-siG), Dr.Jerome Yoman, co-organized a panel dis-cussion, including senior serious mentalillness (smi) expert panelists (i.e., Drs.shirley Glynn, Kim mueser, David Penn,steven silverstein, and will spaulding),and moderated by one of the authors ofthis article (Dr. charlie Davidson). thispanel commemorated 50 years of behav-ioral and cognitive therapies for schizo-phrenia spectrum disorders (ssDs). it wasa lively panel discussion regarding the stateof smi/ssD treatment research (emphasiz-ing effective ssD interventions) and con-cerns that mental health practitioners andtrainees unfamiliar with smi view ssD astoo severe, too distinct, or even too risky totreat (see combs et al., 2006, for anoverview of smi misconceptions and rec-ommendations).
we pause here to address stigma andrelated factors that too often preclude anindividual with ssD from receiving anytype of care (corrigan, 2004; corrigan etal., 2014). rates of institutionalization haverapidly declined since the 1950s, but ratesof criminalization of mental illness andaccompanying incarceration have in-creased (e.g., individuals with a mental ill-ness are 50% more likely to receive a jail
sentence for a misdemeanor conviction), asare rates of homelessness, and lack ofinsurance coverage in ssD (Davis et al.,2012; hall et al., 2019). individuals withssD also experience stigma at alarmingrates from the general population (Ger-linger et al., 2013) and from primary andmental health care providers (e.g.,increased social distancing, stereotyping,and attribution of mental illness; mittal etal., 2014). however, as our health care sys-tems are increasingly pushed towards moreefficient integrated care, clinicians andresearchers are more likely than ever toencounter individuals with ssD, a historyof psychosis, or psychosis secondary toanother condition. a move towards inclu-sive care for individuals with ssD candecrease barriers to treatment, increaseaccess to medications and effective psy-chosocial treatments, and combat stigmathrough increased interactions and visibil-ity of recovery (i.e., if individuals haveaccess to better treatment, providers seemore individuals with ssD doing well andmodify misconceptions that perpetuatestigma). the present article is a call for clin-icians and researchers to reevaluate whatthey may have learned about ssD. Giventhe low prevalence rates of ssD, these mis-conceptions are perhaps not surprising andare likely the result of unfamiliarity ratherthan ill intentions. to this end, the presentreview provides a brief background onssD, an overview of effective behavioraland cognitive treatments, and summarizesintegrated services needed to provide trulyintegrated care for individuals with ssD.
LITERATURE REVIEW
Behavioral and Cognitive Therapies inPsychiatric Rehabilitation for the SchizophreniaSpectrum: Finding the Forgotten StepchildTate F. Halverson, University of North Carolina at Chapel Hill
Charlie A. Davidson, Emory University and Mercer University Collegeof Health Professions
William Spaulding, University of Nebraska–Lincoln
David L. Penn, University of North Carolina at Chapel Hilland Australian Catholic University

16 the Behavior Therapist
h a l v e r s o n e t a l .
BackgroundBefore proceeding further, we offer a
couple of simple definitions. the term“schizophrenia spectrum disorders”encompasses a range of diagnoses includ-ing schizophrenia, schizoaffective disorder,and psychosis not otherwise specified,which are diagnosed by the presence of atleast one of the following: delusions, hallu-cinations, disorganized thinking, disorga-nized or abnormal motor behavior, andnegative symptoms (e.g., diminished emo-tion expression and avolition; americanPsychiatric association, 2013). the term“psychosis” is used to describe conditionsthat affect the mind where there has beensome loss of contact with consensus realityand typically includes symptoms from theaforementioned domains (national insti-tute of mental health, 2019). For this arti-cle, we will focus on schizophrenia spec-trum disorders (hereafter referred tosimply as “ssD”) to focus our review ofpublications and treatment guidelines. Psy-chotic symptoms exist on a spectrum andare observed across diagnoses with varyingseverity (e.g., positive symptoms in schizo-phrenia, grandiosity in bipolar disorders,superstitious beliefs in obsessive compul-sive disorder, nihilistic delusions in severedepression, and concern for constantwatch by others in social anxiety disorder;see Guloksuz & van os, 2018). anotherterm used throughout this review, seriousmental illness (smi), is a term typicallyassociated with mental health policy. it wasoriginally used in federal policy discourseto denote people with ssD and other com-parably disabling conditions. For presentpurposes, “smi services” refers to peoplewith ssD.
Prevalence and Costs of SSDPrevalence rates of ssD are relatively
low, around 0.5% to 0.75% (moreno-Küst-ner et al., 2018; wu et al., 2006). Yet, ssDremains one of the most impairing andcostly diseases, consistently ranked as the15th leading global cause of years lost todisability (the third leading mental illnessdiagnosis) since 1990 behind major depres-sion and anxiety disorders, which haveprevalence rates at least 10 times greaterthan ssD (Global health metrics, 2017;Greenberg et al., 2015; remes et al., 2016).an individual diagnosed with ssD willhave a life expectancy, on average, 14.5years shorter than their cohort members,and premature mortality rates exceed triplethat of the general population (hjorthøj etal., 2019; olfson et al., 2019). one of the
misconceptions of premature mortality inssD is that these deaths are due to suicide,when, in fact, the majority (more than85%) of these premature deaths are due tonatural causes such as cardiovascular dis-eases (most common), cancer, diabetes,influenza, and pneumonia (olfson et al.).actual causes of death in this populationseem to reflect a sedentary low-socioeco-nomic lifestyle and social disadvantageoften related to disability rather than vio-lence or substance use. only one in sevendeaths in ssD is related to unnatural causesand suicide makes up only 25% of thosedeaths with a global prevalence rate of 8.9%in ssD populations (Global health met-rics, 2017; walker et al., 2015). in short,suicide and substance use are serious risksfor people with ssD, as with other mentalillnesses, but they do not account for themuch lower life expectancy and substantialimpairments observed.
equally striking are the substantial eco-nomic costs associated with ssD. while theprevalence of ssD is less than 1%, annualnational economic costs related to directhealth care, nondirect health care, andindirect costs (e.g., unemployment, care-giver costs) total around $155 billion(cloutier et al., 2016). compared withdepressive disorders, with a prevalence ratemore than 20 times higher (20.6% preva-lence, $210.5 billion estimated economiccosts), and anxiety disorders, with a preva-lence almost 30 times higher (28.8% preva-lence, $46.6 billion estimated economiccosts), the economic costs of ssD are stag-gering (Devane et al., 2005; Greenberg etal., 2015). From both a human life and eco-nomic perspective, improving treatmentand outcomes for individuals with ssDremains one of our toughest and mostpressing challenges as mental healthproviders and clinical researchers.
Risk of Violence in SSD:Stigma and Misperceptions
similar to misconceptions regardingssD and mortality, misconceptions alsoexist around ssD and risk of violence toothers. Despite widespread media atten-tion, reviews of epidemiological datarobustly demonstrate that most individualswith ssD are never violent towards others(swanson et al., 2015). Globally, individu-als with ssD were shown to have a 9.9%risk for engaging in violence comparedwith 1.6% in the general population; how-ever, the meta-analysis presenting thisfinding cautioned against significant het-erogeneity in reports and emphasized theneed to examine predictors of violence
comorbid with ssD rather than ssD as astand-alone risk factor (Fazel et al., 2009).For example, this meta-analysis found thatelevated rates of engaging in violent behav-ior may be better explained by substanceuse. rates of violence were higher amongpeople with substance use disorder but notssD (seven times higher than the generalpopulation) than among people withcomorbid substance use and ssD (fivetimes higher than the general population).
a large prospective study also shed lighton the misconceptions surrounding therelationship between ssD and rates of vio-lence (sariaslan et al., 2016). this studyfound that it may be more prudent for clin-icians to screen for high-risk characteristicsmore broadly (e.g., recent stressful lifeevents, injury-related events such as self-harm and traumatic brain injury, sub-stance use) rather than screening out indi-viduals with ssD and denying them accessto care and research opportunities (sari-aslan et al.).
considering recent large-scale findings,clinicians and researchers alike are encour-aged to rethink excluding individuals fromclinical care or research based solely on adiagnosis of ssD. instead, we advocate for ashift towards more accurate and inclusion-ary practices such as screening for violencerisk factors more broadly (e.g., head injury,PtsD, homelessness, and substance use;elbogen et al., 2008) and emphasizing indi-vidual protective factors (e.g., engagementin treatment, social support) when decid-ing if a person is an appropriate fit for therisk and liability capabilities of a treatmentor research setting. For example, studiesmay consider excluding individuals basedon the level of specific symptoms that mayprohibit safe or effective engagement in theintervention (e.g., high scores on hostility,mania, suicidality; see himle et al., 2019,for an example) rather than an ssD diag-nosis.
we pause briefly to reiterate that whilethere is some evidence for slightly elevatedrisk of violence in ssD, individuals withssD and smi are far more likely (2.3 to140.4 times higher than the general popu-lation) to be victims of criminalization,highlighting that victimization seems to bea greater public health concern among ssDpopulations than perpetration (choe et al.,2008; maniglio, 2009). these rates of vic-timization are associated with substanceuse, homelessness, and more severe symp-tomatology—factors that can be addressedand alleviated if individuals have access toeffective treatments and social supports.

January • 2021 17
s c h i z o p h r e n i a s p e c t r u m
Psychosocial Treatmentsfor People With SSD
For organizing research, policy, andpractice, behavioral and cognitive therapiesare often categorized as psychosocial treat-ment, in contradistinction to pharmaco-logical (drug) treatment. there have beensystematic efforts to identify best practicesin the psychosocial treatment domain forssD, including behavioral and cognitivetherapies, e.g., the Patient outcomesresearch team (Port; Dixon et al., 2009),mueser et al. (2013), and the nationalinstitute for health and care excellence inthe united Kingdom (nice; Kuipers et al.,2014). these efforts are comparable tobroader efforts to identify and disseminateevidence-based practices in health caremore generally and are meant to addresspersistent difficulties in dissemination ofnew treatments for ssD (spaulding & sul-livan, 2016). the following section brieflysummarizes these efforts, leading to a cur-rent agenda for developing and dissemi-nating practices of known effectiveness.this review is a primer and by no meansmeant as an exhaustive review of evi-denced-based treatment recommendationsfor ssD. the following sections review psy-chosocial treatments with consensus acrosswidely disseminated practice guidelinesand a focus on services psychologists areuniquely trained to provide (i.e., Dixon etal.; Kuipers et al.; mueser et al.). Psychoso-cial treatments summarizes approaches tospecifically target symptoms and function-ing related to ssD on an individual level(e.g., cBt), while integrated care reviewsapproaches that target concerns related toor comorbid with ssD symptoms, often ina broader context (e.g., trauma, substanceuse, family therapy, and supportedemployment).
Before we begin, it is important to rec-ognize that different psychosocial treat-ments for ssD target different dimensionsof the disorder. historically, there is a focuson targeting hallucinations and delusions.this focus can ignore impairments in func-tioning, particularly interpersonal andbroader social functioning, which tend tobe more disabling and more subjectivelydistressing to individuals with ssD (e.g.,halverson et al., 2019, Van rooijen et al.,2019). the rise of the recovery movement,a consumer movement that favors abroader concept of functional recovery(treichler & spaulding, 2017), parallels thefocus of modern behavioral and cognitivetherapies and other psychosocial treat-ments that address a much broader scope
of treatment targets (e.g., symptom man-agement, interpersonal problem-solving,occupational functioning, family rela-tions).
antipsychotic medications are effectivefirst-line treatments to resolve acute psy-chotic episodes in the short term and maysuppress persistent psychotic symptoms inthe longer term. however, effects are het-erogeneous across individuals (citrome &stroup, 2006), with estimates that half ofindividuals demonstrate “minimal im-provement,” indicated by a 20% reductionin symptoms, while less than a quarter ofindividuals demonstrate “good improve-ment,” indicated by a 50% reduction insymptoms (haddad & correll, 2018).rarely are antipsychotic medications aloneenough to fully restore premorbid func-tioning. additionally, medication benefitstarget positive symptoms (e.g., hallucina-tions, delusions, acute behavioral disorga-nization) with limited effects for negativesymptoms (e.g., anhedonia, amotivation)and impairments in interpersonal andsocial functioning (haddad & correll). thelatter are significant predictors of func-tional outcomes in ssD (Fusar-Poli et al.,2015; nielsen et al., 2015; sergi et al., 2007).the relative limitations of psychopharma-cological treatment for ssD have been animportant impetus for development ofbehavioral and cognitive therapies.
Social Skills Trainingsocial skills training is a behavioral
approach utilizing role-modeling,rehearsal, and corrective feedback toimprove skills related to everyday func-tioning and social interactions and can beadministered in individual or group for-mats. For example, a therapist and clientmay take turns role-playing how to social-ize at an upcoming family event. the ther-apist may recommend and model differentstrategies and then switch and have theclient try preferred actions while receivingfeedback during and after the role-play(e.g., recommending increased eye contactduring a greeting to seem more engaged).this approximates methods used forclients with other diagnoses who havesocial skill deficits but less severe disability.contemporary social skills training canalso target deficits in social perception,social cognitive processes and social anxi-ety (e.g., mueser et al., 2013), as well asovert behavior, and is designed to facilitategeneralization of new skills to diverse set-tings and context, and to promote develop-ment of a social support network. a recentmeta-analysis on skills training supports
the Port (2009) and mueser and col-leagues recommendations, with findingsdemonstrating improvements in negativesymptoms, general psychopathology, andsocial outcome measures with improve-ments maintained during follow-up peri-ods (turner et al., 2018).
Cognitive Behavioral TherapycBt treatment research in ssD has
been prolific albeit somewhat fragmentedand divergent. one direction has focusedon positive symptom reduction, usingtechniques collectively identified as cogni-tive behavioral therapy for psychosis(cBtp), with demonstrated efficacy reduc-ing positive symptoms (e.g., turner et al.,2020). another direction is based on theattribution-focused techniques associatedwith the work of aaron Beck and is typi-cally described as recovery-oriented cogni-tive therapy (e.g., Grant et al., 2014). moredirect attention to the cognitive processingdeficits of ssDs are also incorporated inconventional group and dyadic cBtmodalities, such as social skills training andcognitive process interventions (e.g., orderet al., 2010; Granholm et al., 2016). cBtmodalities that directly address motiva-tion, such as motivational interviewing(mi) and acceptance and commitmenttherapy (act), are especially applicable toindividuals with ssD, and have an evi-dence-base for that purpose (e.g., Fiszdonet al., 2016). therefore, a “cBt” treatmentdesignation in ssD may range widelyacross studies.
outcome analyses of cBt for ssD havenot always kept up with the diversificationof purposes, techniques, and treatment tar-gets. Bighelli and colleagues (2018), in ameta-analysis of over 50 studies, found thatcBt for ssD is associated with reductionsin positive and negative symptoms andimprovements in functioning and qualityof life. however, a recent cochrane reviewof 36 randomized controlled trials foundno added benefits of cBt to standard care(e.g., antipsychotic medication regimen)compared with other psychosocial treat-ments, often requiring less resources (e.g.,social skills training groups; Jones et al.,2019). this conclusion was based on arange of outcomes including symptomreduction, rates of rehospitalization, andemphasized average endpoint scores forfunctional outcomes rather than individualdomains of functioning (e.g., interpersonalfunctioning, daily living skills). it is alsoimportant to note that Jones and colleaguesrated most studies as “low” in quality. reli-able meta-analytic studies require inclu-

18 the Behavior Therapist
h a l v e r s o n e t a l .
sion of more rigorous treatment studiesand greater sensitivity to the heterogeneityof cBt as applied to the heterogeneoustreatment targets associated with ssD.
one final note regarding cBt and ssD.cBt is recommended as an “add-on” treat-ment for ssD by the national institute ofmental health (nimh) and the nationalinstitute for health and care excellence(nice; Jones et al., 2019). this is an unfor-tunate terminological relic of a past era inwhich symptom reduction was consideredthe most important outcome (rather thanfunctional recovery). the term “add-on”also ignores the importance of improvedsymptom management in individuals withsymptoms refractory to drug treatment(i.e., symptom reduction does not meet aclinically defined “good response” butsymptoms are stable and overall function-ing is improved).
First-Episode Psychosisa clinical practice guideline for treating
schizophrenia perhaps less known to prac-titioners outside of smi specialty care is theneed for distinct and comprehensive coor-dinated care programs specifically for indi-viduals experiencing first-episode psy-chosis (FeP). typically, the designation of“FeP” is used to refer to individuals withssD experiencing illness onset within thepast three to five years. individuals in theearly stage of ssD present with uniquetreatments needs (e.g., emphasis on low-dose psychopharmacological treatments tominimize side effects and decrease nonad-herence, delivery of services in a group set-ting with other young persons, familyinvolvement, emphasis on school and workfunctioning; for a brief review see mueser& cook, 2014), and interventions address-ing these unique treatment needs showimproved outcomes and reduced symp-toms (Kane et al., 2016).
FeP programs today trace back to thework of Dr. Patrick mcGorry and his groupin australia and their work with the earlyPsychosis Prevention and interventioncentre (ePPic; mcGorry et al., 1996).ePPic was the first comprehensive pro-gram targeting early detection and inten-sive treatment of psychosis with noveltreatment components including familytherapy, vocational rehabilitation, and peersupport. the success of ePPic in australiaprompted a roll-out of programs in theunited states emulating the ePPic model(Breitborde & moe, 2016). two of the mostwell-known FeP studies in the unitedstates include the large-scale randomizedcontrolled trial, recovery after an initial
schizophrenia episode (raise) initiative(Kane et al., 2015) and the large-scaleimplementation study ontracknY (Belloet al., 2018). the raise study imple-mented a treatment recovery program ofcoordinated specialty care called naVi-Gate, which comprises medication man-agement, individual and family therapy,and supported employment and education.the naViGate model emphasizesshared decision-making, resiliency, psy-choeducation, and cBt methods. theraise study randomized 34 clinicsaround the country to deliver naViGateor traditional community care from 2010–2014. results demonstrated the naVi-Gate model improved quality of life,decreased symptoms, improved involve-ment in work and school and increasedtreatment retention (Kane et al., 2016).this model of coordinated specialty care isalso cost-effective and efficacious, demon-strating improved outcomes comparedwith treatment as usual (correll et al., 2017;rosenheck et al., 2016). since the inceptionof raise, clinics around the country haveadopted this model of recovery, and theavailability of FeP clinics is rapidly grow-ing (azrin et al., 2016). it should be notedthat the dissemination of raise was spear-headed by Dr. robert heinssen at nimh,who founded the siG in 1990 and was itschair until 1996; his advocacy and policywork with congress resulted in the consol-idated appropriations act of 2014 thatprovided funding to support the imple-mentation of evidence-based programs forindividuals with ssD.
these psychosocial treatments arebased on recommendations from consis-tent findings of large-scale studies (eitherlarge sample sizes or a large combinedsample of smaller studies). therefore, aquick note is warranted that this is by nomeans an exhaustive list of efficacious psy-chosocial treatments for ssD (other effec-tive psychosocial treatments that may be ofinterest to readers include therapies target-ing neurocognition, social cognition, andmetacognition). as researchers and clini-cians continue to develop and disseminatenew treatments, more information is con-tinually made available on which to basemore definitive clinical practice recom-mendations. readers are also cautionedthat ssD is a heterogeneous diagnosis andtherefore a “one size fits all” approach riskspolicy reforms advantageous to a majorityat the expense of a significant minority(spaulding et al., 2010). new treatmentswill invariably create subsets of individualswith refractory forms of ssD that do not
respond to these new treatments, whichcan lead to further stigmatization (spauld-ing et al.). treatment recommendationsimpact administrative decisions and “toooften, administrators perceive mentalhealth services to be like commodities likepork bellies and iron ore—generic andinvariant in quality and cost-effectiveness”(spaulding et al., p. 5). therefore, cliniciansand researchers are advised to carefullyconsider the effects of advocating for noveland “tried and true” interventions alike.
Integrated CarePsychiatric Rehabilitation
Psychiatric rehabilitation was arguablythe first integrated approach to treatmentin ssD and still serves as a paradigm forsystematic integrated care. it is notable thatmost or all empirically supported treat-ments integrate easily within a larger psy-chiatric rehabilitation program. it isbroader than a “treatment” modality. thisapproach derives from the same roots asmodern behavioral therapies, including itsconceptual basis in social learning theory,individualized functional assessment, useof evidence-based interventions for specificpurposes, emphasis on patient perspectiveand values, and objective evaluation ofprogress toward operationalized outcomes(spaulding et al., 2003). Psychiatric reha-bilitation emphasizes the importance of amultimodal approach to assessment andtreatment and balances pharmaceuticallevels of intervention with behavioral, cog-nitive, and socio-environmental levels aswell as conceptualization of ssD as a dis-ability to be overcome rather than anincurable disease. central to the approachof psychiatric rehabilitation is the idea thata diagnosis of ssD reflects impairmentacross multiple domains. Prior to the dein-stitutionalization of ssD in the 1950s, psy-chiatric rehabilitation involved integrated,interdisciplinary teams, able to targetimpairment on multiple levels. however,this integrated approach became more dif-ficult after deinstitutionalization. whilelarge-scale health care systems still imple-ment integrated programs of care with suc-cess (e.g., Veterans health administration;Goldberg & resnick, 2010) communitycare has become increasingly specializedand compartmentalized so that today thereis a need to restore the integration factor tocommunity-based care.
specialized packages of evidence-basedintegrated services, such as raise, can beconceptualized as contemporary models ofpsychiatric rehabilitation for first-episode

January • 2021 19
s c h i z o p h r e n i a s p e c t r u m
psychosis (FeP). and, while the effective-ness of the integrated raise model waspreviously discussed in the context of FeP,there is also strong support for the efficacyand sustained durability of integrated carefor more chronic ssD compared withtreatment-as-usual (e.g., malm et al., 2003;schöttle et al., 2013).
Family Therapyrecommendations from both Port
and the raise initiative highlight theimportance of family support interventionsto improve outcomes for individuals withssD in both early and chronic stages of ill-ness (Dixon et al., 2009; Dixon et al., 2018).ssD is marked by a change in functioning(e.g., loss of job, withdrawal from school)and family members become integralsources of support, ranging from assistancewith daily activities to active participationin treatment. Family therapy can rangefrom a modest amount of education forfamily members about the nature of ssDsand the requirements for recovery to thebehavioral interventions that comprisebehavioral family therapy (BFt). in addi-tion to information about the disorder,BFt involves functional analysis of partic-ular behaviors that cause family stress andconflict, identification and change ofbeliefs and attitudes that drive reactions,strengthening collective problem-solvingand communication skills, and negotiatingnormal developmental transitions compli-cated by the onset of psychosis (e.g.,mueser & Glynn, 1999). Family therapy isshown to decrease frequency of relapse,increase treatment adherence, decreasesocial impairment, and improve familymember outcomes such as perceivedburden of caregiving and well-being (clax-ton et al., 2017; Pharoah et al., 2010; weis-man de mamani et al., 2014).
Traumathe role of trauma in ssD is also worthy
of mention here. roughly 30–60% of indi-viduals with ssD endorse a history oftrauma and/or meet diagnostic criteria forPtsD (mauritz et al., 2013). theoreticalmodels propose that PtsD worsens theseverity and course of ssD through directeffects (e.g., overarousal, reexperiencingtrauma) as well as indirect effects (e.g., sub-stance abuse, retraumatization, poor work-ing alliance with care providers), and PtsDin ssD is linked with more severe depres-sion, higher rates of stigma, and treatmentunderutilization in both early and chronicssD highlighting the importance of inter-ventions targeting trauma (Detore et al.,
2019; mueser et al., 2002; mueser et al.,2004). while many smi clinicians arefamiliar with evidence-based trauma inter-ventions, these treatments (e.g., cognitiveprocessing therapy, prolonged exposure)require specialized training and structuredsessions, which may not be feasible oraccessible during regular group or individ-ual sessions. individuals with ssD may beunderrepresented participants in expo-sure-based therapies due to perceived riskbased on stigmatized misperceptions; how-ever, evidence-based trauma interventionssuch as prolonged exposure have beenshown to be safe, effective, and feasiblewith individuals with ssD (De Bont et al.,2016; Van Den Berg et al., 2015). thesefindings suggest individuals may benefitfrom work with both their primary smiprovider and participation in time-limited(e.g., often 8 to 12 sessions) trauma inter-ventions with clinicians trained in evi-dence-based treatments.
Substance UseBoth Port and raise recommenda-
tions highlight the need for psychosocialtreatments addressing co-occurring sub-stance use, and a comprehensive review ofthe literature suggests around 42% of indi-viduals (22% in women) with ssD have aco-occurring substance use disorder (huntet al., 2018). this problem exploded in thewake of deinstitutionalization. similar toPtsD, many smi clinicians have experi-ence assessing and treating substance use,but there is an urgent need for providerswith expertise in substance use and misuseto deliver this treatment to ssD popula-tions. the feasibility and efficacy of inte-grating treatments targeting substance usein ssD is well-established (e.g., Drake et al.,2004; lubman et al., 2010). however, moreresearch is needed to recommend specificinterventions. current evidence suggestsoptimal outcomes are achieved with effec-tive antipsychotic medication regimensand addiction-based psychosocial inter-ventions; however, the definition of “addic-tion-based psychosocial interventions” isbroad (crockford & addington, 2017).currently, best-practice recommendationsemphasize an integration of substance usetreatment with mental health services, alow-stress and harm-reduction approach,enhancing motivation, cBt to improveinterpersonal and coping skills, supportingfunctional recovery (e.g., improving qual-ity of relationships and supported employ-ment), and engagement of an individual’ssocial network (mueser & Gingerich,2013). as with smi treatment generally,
integrated treatment appears crucial whensubstance use is co-occurring.
Supported Employment Servicesthe unemployment rate in ssD is
alarming, with some estimates as high as58% (cloutier et al., 2016) despite consis-tent support across decades of researchdemonstrating that individuals diagnosedwith ssD want to work (crowther et al.,2001). this statistic is also troubling con-sidering meta-analytic evidence illustratingthe success of employment interventionswith competitive job placement and retain-ment (carmona et al., 2017). today, rec-ommendations for vocational rehabilita-tion focus on supported employment andare based on the individual Placement andsupport model, which emphasizes collabo-rative job searches for competitive jobsinformed by client preferences (Khare etal., 2016). recommendations for successfulsupported employment also highlight theneed to integrate cognitive remediation toimprove cognitive abilities necessary forsuccessful job performance (lystad et al.,2017; mcGurk et al., 2017). Despiteimproved outcomes (e.g., schennach et al.,2012), access and awareness of theseimportant services remain limited. theimportance of supported education andemployment in smi treatment also high-lights the general importance of multidis-ciplinary teams in integrated care; occupa-tional therapists, social workers, and otherprofessions are often crucial to an individ-ual’s recovery (e.g., Kuipers et al., 2014).
Concluding Remarksthis review is a primer and by no means
meant as an exhaustive review of ssD gen-erally, evidenced-based treatment recom-mendations, or efficacious integrated ser-vices for people with ssD. although thepresent review focuses on services psychol-ogists are uniquely trained to provide, sev-eral other modalities are often critical ele-ments of effective and integrated treatment(e.g., assertive community treatment,cognitive remediation). contrary topublic perceptions that ssDs are perma-nent and only amenable to medications,evidence of recovery and the foundationsof these psychosocial approaches have beenaround for half a century (allyon & azrin,1968). our hope in presenting this primeris to increase awareness, combat stigma,provide exposure to helpful literature andresources, and perhaps encourage clini-cians to participate in care of individualsdiagnosed with ssD, thereby increasing

20 the Behavior Therapist
accessibility to treatment. individuals withssD are underserved in our communitiesbut there is vast potential for improve-ments in quality of life, meaningful rela-tionships, and competitive occupationalpursuits. moreover, in our personal andprofessional experience, working withthese individuals and their families isimmensely rewarding, as we perform ourroles as mental health providers and clini-cal researchers.
Referencesayllon, t., & azrin, n. h. (1968). rein-
forcer sampling: a technique for increas-ing the behavior of mental patients. Jour-nal of Applied Behavior Analysis, 1,13-20. https://doi.org/10.1901/jaba.1968.1-13
american Psychiatric association (2013).Diagnostic and statistical manual ofmental disorders (5th ed.). washington,Dc: author.
azrin, s. t., Goldstein, a. B., & heinssen,r. K. (2016). expansion of coordinatedspecialty care for first-episode psychosisin the us. Focal Point: Youth, YoungAdults and Mental Health, 30, 9–11.
Bello, i., lee, r., malinovsky, i., watkins,l., nossel, i., smith, t., ... radigan, m.(2017). ontracknY: the development ofa coordinated specialty care program forindividuals experiencing early psychosis.Psychiatric Services, 68, 318-320.https://doi.org/10.1176/appi.ps.201600512
Bighelli, i., salanti, G., huhn, m., schnei-der-thoma, J., Krause, m., reitmeir, c.,… leucht, s. (2018). Psychological inter-ventions to reduce positive symptoms inschizophrenia: systematic review andnetwork meta-analysis. World Psychiatry,17, 316–329. https://doi.org/10.1002/wps.20577
Breitborde, n. J. K., & moe, a. m. (2016).early intervention in psychosis in theunited states: From science to policyreform. Early Intervention, 4, 79–87.https://doi:10.1177/2372732216683965
carmona, V. r., Gómez-Benito, J., huedo-medina, t. B., & rojo, J. e. (2017).employment outcomes for people withschizophrenia spectrum disorder: ameta-analysis of randomized controlledtrials. International Journal of Occupa-tional Medicine and EnvironmentalHealth, 30, 345. https://doi.org/10.13075/ijomeh.1896.01074
choe, J., teplin, l. a., & abram, K. m.(2008). Perpetration of violence, violentvictimization, and severe mental illness:Balancing public health concerns. Psychi-atric Services, 59, 153–164.https://doi.org/10.1176/appi.ps.59.2.153
citrome, l., & stroup, t.s. (2006). schizo-phrenia, clinical antipsychotic trials ofintervention effectiveness (catie) andnumber needed to treat: how can catieinform clinicians? International Journalof Clinical Practice, 60, 933-940.https://doi.org/10.1111/j.1742-1241.2006.01044.x
claxton, m., onwumere, J., & Fornells-ambrojo, m. (2017). Do family interven-tions improve outcomes in early psy-chosis? a systematic review andmeta-analysis. Frontiers in Psychology, 8,1-17. https://doi.org/10.3389/fpsyg.2017.00371
cloutier, m., aigbogun, m. s., Guerin, a.,nitulescu, r., ramanakumar, a. V,Kamat, s. a., … wu, e. (2016). the eco-nomic burden of schizophrenia in theunited states in 2013. Journal of ClinicalPsychiatry, 77, 764–771. https://doi.org/10.4088/JcP.15m10278
combs, D.r., Penn, D.l., spaulding, w.D.,adams, s.D., roberts, D.l., & iyer, s.n.(2006). Graduate training in cognitive-behavioral therapy for psychosis: theapproaches of three generations of clini-cal researchers. the Behavior Therapist,29, 12-16.
correll, c. u., solmi, m., Veronese, n.,Bortolato, B., rosson, s., santonastaso,P., … Kohler, c. (2017). Prevalence, inci-dence and mortality from cardiovasculardisease in patients with pooled and spe-cific severe mental illness: a large-scalemeta-analysis of 3,211,768 patients and113,383,368 controls. World Psychiatry,16, 163–180. https://doi.org/10.1002/wps.20420
corrigan, P. w. (2004). how stigma inter-feres with mental health care. AmericanPsychologist, 59, 614-625.https://doi.org/10.1037/0003-066X.59.7.614
corrigan, P.w., Druss, B.G., & Perlick,D.a. (2014). the impact of mental illnessstigma on seeking and participating inmental health care. Psychological Sciencein the Public Interest, 15, 37-70.https://doi.org/10.1177/1529100614531398
crockford, D., & addington, D. (2017).canadian schizophrenia guidelines:schizophrenia and other psychotic disor-ders with coexisting substance use disor-ders. Canadian Journal of Psychiatry, 62,624–634. https://doi.org/10.1177/0706743717720196
Davis, l., Fulginiti, a., Kriegel, l., &Brekke, J. s. (2012). Deinstitutionaliza-tion? where have all the people gone?Current Psychiatry Reports, 14, 259–269.https://doi.org/10.1007/s11920-012-0271-1
De Bont, P. a. J. m., Van Den Berg, D. P.G., Van Der Vleugel, B. m., De roos, c.,
De Jongh, a., Van Der Gaag, m., & Vanminnen, a. m. (2016). Prolonged expo-sure and emDr for PtsD v. a PtsDwaiting-list condition: effects on symp-toms of psychosis, depression and socialfunctioning in patients with chronic psy-chotic disorders. Psychological Medicine,46, 2411–2421. https://doi.org/10.1017/s0033291716001094
Detore, n. r., Gottlieb, J. D., & mueser,K. t. (2019). Prevalence and correlates ofPtsD in first episode psychosis: Findingsfrom the raise-etP study. PsychologicalServices. advance online publication.https://doi.org/10.1037/ser0000380
Devane, c. l., chiao, e., Franklin, m., &Kruep, e. J. (2005). anxiety disorders inthe 21st century: status, challenges,opportunities, and comorbidity withdepression. American Journal of Man-aged Care, 11, s344-53.
Dixon, l. B., Dickerson, F., Bellack, a. s.,Bennett, m., Dickinson, D., Goldberg, r.w., … Kreyenbuhl, J. (2009). the 2009schizophrenia Port psychosocial treat-ment recommendations and summarystatements. Schizophrenia Bulletin, 36,48–70. https://doi.org/10.1093/schbul/sbp115
Dixon, l. B, Goldman, h. h., srihari, V.h., & Kane, J. m. (2018). transformingthe treatment of schizophrenia in theunited states: the raise initiative.Annual Review of Clinical Psychology, 14,237–258. https://doi.org/10.1146/annurev-clinpsy-050817-084934
Drake, r. e., mueser, K. t., Brunette, m.F., & mchugo, G. J. (2004). a review oftreatments for people with severe mentalillnesses and co-occurring substance usedisorders. Psychiatric RehabilitationJournal, 27, 360 - 374. https://doi.org/10.2975/27.2004.360.374
elbogen, e. B., Beckham, J. c., Butterfield,m. i., swartz, m., & swanson, J. (2008).assessing risk of violent behavior amongveterans with severe mental illness. Jour-nal of Traumatic Stress, 21, 113–117.https://doi.org/10.1002/jts
Fazel, s., Gulati, G., linsell, l., Geddes, J.r., & Grann, m. (2009). schizophreniaand violence: systematic review andmeta-analysis. PLoS Medicine, 6, 1-15.https://doi.org/10.1371/journal.pmed.1000120
Fiszdon, J. m., Kurtz, m. m., choi, J., Bell,m. D., & martino, s. (2016). motiva-tional interviewing to increase cognitiverehabilitation adherence in schizophre-nia. Schizophrenia Bulletin, 42, 327-334.https://doi.org/10.1093/schbul/sbv143
Fusar-Poli, P., Papanastasiou, e., stahl, D.,rocchetti, m., carpenter, w., shergill, s.,& mcGuire, P. (2015). treatments ofnegative symptoms in schizophrenia:meta-analysis of 168 randomized
h a l v e r s o n e t a l .

s c h i z o p h r e n i a s p e c t r u m
January • 2021 21
placebo-controlled trials. SchizophreniaBulletin, 41, 892–899. https://doi.org/10.1093/schbul/sbu170
Gerlinger, G., hauser, m., De hert, m.,lacluyse, K., wampers, m., & correll, c.u. (2013). Personal stigma in schizophre-nia spectrum disorders: a systematicreview of prevalence rates, correlates,impact and interventions. World Psychi-atry, 12, 155–164. https://doi.org/10.1002/wps.20040
Global health metrics. (2017). Global,regional, and national incidence, preva-lence, and years lived with disability for328 diseases and injuries for 195 coun-tries, 1990-2016: a systematic analysisfor the Global Burden of Disease study2016. Lancet, 390, 1211–1259.https://doi.org/10.1016/s0140-6736(17)32154-2
Goldberg, r. w., & resnick, s. G. (2010).us Department of Veterans affairs (Va)efforts to promote psychosocial rehabili-tation and recovery. Psychiatric Rehabili-tation Journal, 33, 255 – 258.https://doi.org/10.2975/33.4.2010.255.258
Granholm, e. l., mcQuaid, J. r., &holden, J. l. (2016). Cognitive-behavioralsocial skills training for schizophrenia: Apractical treatment guide. Guilford Publi-cations.
Grant, P. m., reisweber, J., luther, l.,Brinen, a. P., & Beck, a. t. (2014). suc-cessfully breaking a 20-year cycle of hos-pitalizations with recovery-oriented cog-nitive therapy for schizophrenia.Psychological Services, 11, 125 - 133.https://doi.org/10.1037/a0033912
Greenberg, P. e., Fournier, a. a., sisitsky,t., Pike, c. t., & Kessler, r. c. (2015).the economic burden of adults withmajor depressive disorder in the unitedstates (2005 and 2010). Journal of Clini-cal Psychiatry, 76, 155–162.https://doi.org/10.4088/JcP.14m09298
Guloksuz s., van os J. (2018). the slowdeath of the concept of schizophreniaand the painful birth of the psychosisspectrum. Psychological Medicine, 48,229‐244.doi:10.1017/s0033291717001775
haddad, P. m., & correll, c. u. (2018).the acute efficacy of antipsychotics inschizophrenia: a review of recent meta-analyses. Therapeutic Advances in Psy-chopharmacology, 8, 303-318.https://doi.org/10.1177/2045125318781475
halverson, t. F., orleans-Pobee, m., mer-ritt, c., sheeran, P., Fett, a. K., & Penn,D. l. (2019). Pathways to functional out-comes in schizophrenia spectrum disor-ders: meta-analysis of social cognitiveand neurocognitive predictors. Neuro-science & Biobehavioral Reviews, 105,
212-219. https://doi.org/10.1016/j.neu-biorev.2019.07.020
hall, D., lee, l. w., manseau, m. w.,Pope, l., watson, a. c., & compton, m.t. (2019). major mental illness as a riskfactor for incarceration. Psychiatric Ser-vices, 70, 1088-1093. https://doi.org/10.1176/appi.ps.201800425
himle, J. a., leBeau, r. t., weaver, a.,Brydon, D. m., Bybee, D., Kilbourne, a.m., ... smith, F. n. (2019). study proto-col: a multisite trial of work-related cog-nitive behavioral therapy for unem-ployed persons with social anxiety.Contemporary Clinical Trials Communi-cations, 16, 100464. https://doi.org/10.1016/j.conctc.2019.100464
hjorthøj, c., stürup, a. e., mcgrath, J. J.,& nordentoft, m. (2019). Years of poten-tial life lost and life expectancy in schizo-phrenia: a systematic review and meta-analysis. The Lancet Psychiatry, 4,295–301. https://doi.org/10.1016/s2215-0366(17)30078-0
hunt, G. e., large, m. m., cleary, m., lai,h. m. X., & saunders, J. B. (2018). Preva-lence of comorbid substance use in schiz-ophrenia spectrum disorders in commu-nity and clinical settings, 1990–2017:systematic review and meta-analysis.Drug and Alcohol Dependence, 191, 234–258. https://doi.org/10.1016/j.drugal-cdep.2018.07.011
Jones, c., hacker, D., cormac, i., meaden,a., irving, c. B., Xia, J., … chen, J.(2019). cognitive behavioral therapy plusstandard care versus standard care plusother psychosocial treatments for peoplewith schizophrenia. Schizophrenia Bul-letin, 45, 284–286. https://doi.org/10.1093/schbul/sby188
Kane, J. m., robinson, D. G., schooler, n.r., mueser, K. t., Penn, D. l., rosen-heck, r. a., … heinssen, r. K. (2016).comprehensive versus usual communitycare for first-episode psychosis: 2-yearoutcomes from the nimh raise earlytreatment program. American Journal ofPsychiatry, 173, 362–372. https://doi.org/10.1176/appi.ajp.2015.15050632
Kane, J. m., schooler, n. r., marcy, P.,correll, c. u., estroff, s. e., robinson, J.,… robinson, D. G. (2015). the raiseearly treatment program for first-episodepsychosis: Background, rationale, andstudy design. Journal of Clinical Psychia-try, 76, 240–246. https://doi.org/10.4088/JcP.14m09289
Khare, c., mueser, K. t., & mcGurk, s. r.(2016). Vocational rehabilitation forindividuals with schizophrenia. CurrentTreatment Options in Psychiatry, 3, 99-110. https://doi.org/10.1007/s40501-016-0082-9
Kuipers, e., Yesufu-udechuku, a., taylor,c., & Kendall, t. (2014). management of
psychosis and schizophrenia in adults:summary of updated nice guidance.BMJ, 348, g1173. https://doi.org/10.1136/bmj.g1173
lubman, D. i., King, J. a., & castle, D. J.(2010). treating comorbid substance usedisorders in schizophrenia. InternationalReview of Psychiatry, 22, 191-201.https://doi.org/10.3109/09540261003689958
lystad, J. u., Falkum, e., haaland, V. Ø.,Bull, h., evensen, s., mcGurk, s. r., &ueland, t. (2017). cognitive remediationand occupational outcome in schizo-phrenia spectrum disorders: a 2 yearfollow-up study. Schizophrenia Research,185, 122-129. https://doi.org/10.1016/j.schres.2016.12.020
malm, u., ivarsson, B., allebeck, P., & Fal-loon, i. r. h. (2003). integrated care inschizophrenia: a 2-year randomizedcontrolled study of two community-based treatment programs. Acta Psychi-atrica Scandinavica, 107, 415-423.https://doi.org/10.1034/j.1600-0447.2003.00085.x
maniglio, r. (2009). severe mental illnessand criminal victimization: a systematicreview. Acta Psychiatrica Scandinavica,119, 180–191. https://doi.org/10.1111/j.1600-0447.2008.01300.x
mauritz, m. w., Goossens, P. J. J., Draijer,n., & van achterberg, t. (2013). Preva-lence of interpersonal trauma exposureand trauma-related disorders in severemental illness. European Journal of Psy-chotraumatology, 4, 1-15.https://doi.org/10.3402/ejpt.v4i0.19985
mcGorry, P. D., edwards, J., mihalopou-los, c., harrigan, s. m., & Jackson, h. J.(1996). ePPic: an evolving system ofearly detection and optimal manage-ment. Schizophrenia Bulletin, 22, 305–326. https://doi.org/10.1093/schbul/22.2.305
mcGurk, s. r., mueser, K. t., watkins, m.a., Dalton, c. m., & Deutsch, h. (2017).the feasibility of implementing cognitiveremediation for work in communitybased psychiatric rehabilitation pro-grams. Psychiatric Rehabilitation Journal,40, 79-86. https://doi.org/10.1037/prj0000257
mittal, D., corrigan, P., sherman, m. D.,morris, s., & sullivan, G. (2014). health-care providers’ attitudes toward personswith schizophrenia. Psychiatric Rehabili-tation Journal, 37, 297–303.https://doi.org/10.1037/prj0000095.supp
moreno-Küstner, B., martín, c., & Pastor,l. (2018). Prevalence of psychotic disor-ders and its association with method-ological issues. a systematic review andmeta-analyses. PLoS One, 13, 1-25.https://doi.org/10.1371/journal.pone.0195687

h a l v e r s o n e t a l .
22 the Behavior Therapist
mueser, K. t., & cook, J. a. (2014). edito-rial: rising to the challenge of firstepisode psychosis: the nimh recoveryafter initial schizophrenia episode(raise) initiative. Psychiatric Rehabilita-tion Journal, 37, 267–269.https://doi.org/10.1037/prj0000108
mueser, K. t., Deavers, F., Penn, D. l., &cassisi, J. e. (2013). Psychosocial treat-ments for schizophrenia. Annual Reviewof Clinical Psychology, 9, 465-497.https://doi.org/10.1146/annurev-clinpsy-050212-185620
mueser, K. t., & Gingerich, s. (2013).treatment of co-occurring psychotic andsubstance use disorders. Social Work inPublic Health, 28, 424-439. https://doi.org/10.1080/19371918.2013.774676
mueser, K.t., & Glynn, s. m. (1999).Behavioral family therapy for psychiatricdisorders (2nd ed.). new harbinger Pub-lications.
mueser, K. t., rosenberg, s. D., Good-man, l. a., & trumbetta, s. l. (2002).trauma, PtsD, and the course of severemental illness: an interactive model.Schizophrenia Research, 53, 123–143.https://doi.org/10.1016/s0920-9964(01)00173-6
mueser, K. t., salyers, m. P., rosenberg, s.D., Goodman, l. a., essock, s. m., osher,F. c., … Butterfield, m. i. (2004). inter-personal trauma and posttraumatic stressdisorder in patients with severe mentalillness: Demographic, clinical, and healthcorrelates. Schizophrenia Bulletin, 30, 45–57. https://doi.org/10.1093/oxfordjour-nals.schbul.a007067
national institute of mental health(2019). What is psychosis. Mental HealthInformation. https://www.nimh.nih.gov/health/topics/schizophrenia/raise/what-is-psychosis.shtml
nielsen, r. e., levander, s., Kjaersdamtelléus, G., Jensen, s. o. w., Østergaardchristensen, t., & leucht, s. (2015).second-generation antipsychotic effecton cognition in patients with schizophre-nia: a meta-analysis of randomized clini-cal trials. Acta Psychiatrica Scandinavica,131, 185–196. https://doi.org/10.1111/acps.12374
olfson, m., Gerhard, t., huang, c., crys-tal, s., & stroup, t. s. (2019). Prematuremortality among adults with schizophre-nia in the united states. JAMA Psychia-try, 72, 1172–1181. https://doi.org/10.1001/jamapsychiatry.2015.1737
Pharoah, F., mari, J., rathbone, J., &wong, w. (2010). Family interventionfor schizophrenia. Cochrane Databse ofSystematic Reviews, 12, 1-109.https://doi.org/10.1002/14651858.cD000088.pub3
remes, o., Brayne, c., van der linde, r., &lafortune, l. (2016). a systematic review
of reviews on the prevalence of anxietydisorders in adult populations. Brain andBehavior, 6, 1-33. https://doi.org/10.1002/brb3.497
roder, V., müller, D. r., Brenner, h. D., &spaulding, w. D. (2010). Integrated psy-chological therapy (IPT): For the treat-ment of neurocognition, social cognition,and social competency in schizophreniapatients. hogrefe Publishing.
rosenheck, r., leslie, D., sint, K., lin, h.,robinson, D. G., schooler, n. r., …Kane, J. m. (2016). cost-effectiveness ofcomprehensive, integrated care for firstepisode psychosis in the nimh raiseearly treatment program. SchizophreniaBulletin, 42, 896–906. https://doi.org/10.1093/schbul/sbv224
sariaslan, a., lichtenstein, P., larsson, h.,& Fazel, s. (2016). triggers for violentcriminality in patients with psychoticdisorders. JAMA Psychiatry, 73, 796–803.https://doi.org/10.1001/jamapsychia-try.2016.1349
schennach, r., musil, r., möller, h. J., &riedel, m. (2012). Functional outcomesin schizophrenia: employment status as ametric of treatment outcome. CurrentPsychiatry Reports, 14, 229-236.https://doi.org/10.1007/s11920-012-0261-3
schöttle, D., Karow, a., schimmelmann,B. G., & lambert, m. (2013). integratedcare in patients with schizophrenia:results of trials published between 2011and 2013 focusing on effectiveness andefficiency. Current Opinion in Psychiatry,26, 384-408. https://doi.org/10.1097/Yco.0b013e328361ec3b
sergi, m. J., Green, m. F., widmark, c.,reist, c., erhart, s., Braff, D. l., … mintz,J. (2007). social cognition and neurocog-nition: effects of risperidone, olanzapine,and haloperidol. American Journal ofPsychiatry, 164, 1585–1592.https://doi.org/10.1176/appi.ajp.2007.06091515
snyder, J., spaulding, w., & sullivan, m.(2016). schizophrenia and other seriousmental illnesses siG: after 30 years, stillthe forgotten stepchild. the BehaviorTherapist, 39, 291-292.
spaulding, w. D., & sullivan, m. e. (2016).treatment of cognition in the schizo-phrenia spectrum: the context of psychi-atric rehabilitation. Schizophrenia Bul-letin, 42, s53-s61. https://doi.org/10.1093/schbul/sbv163
spaulding, w. D., sullivan, m. e., &Poland, J. s. (2003). Treatment and reha-bilitation of severe mental illness. Guil-ford Press.
spaulding, w., sullivan, m., Poland, J., &ritchie, a.J. (2010). state pscyhiatricinstitutions and the left-behinds ofmental health reform. American Journal
of Orthopsychiatry, 80, 327-333.https://doi.org/10.1111/j.1939-0025.2009.01036.x
swanson, J. w., mcGinty, e. e., Fazel, s., &mays, V. m. (2015). mental illness andreduction of gun violence and suicide:Bringing epidemiologic research topolicy. Annals of Epidemiology, 25, 366-376. https://doi.org/10.1016/j.annepi-dem.2014.03.004
treichler, e. B., & spaulding, w. D.(2017). Beyond shared decision-making:collaboration in the age of recovery fromserious mental illness. American Journalof Orthopsychiatry, 87, 567-574.https://doi.org/10.1037/ort0000256
turner, D. t., Burger, s., smit, F., Valmag-gia, l. r., & van der Gaag, m. (2020).what constitutes sufficient evidence forcase formulation–driven cBt for psy-chosis? cumulative meta-analysis of theeffect on hallucinations and delusions.Schizophrenia Bulletin [advance onlinepublication]. https://doi.org/10.1093/schbul/sbaa045
turner, D. t., mcGlanaghy, e., cuijpers,P., Van Der Gaag, m., Karyotaki, e., &macBeth, a. (2018). a meta-analysis ofsocial skills training and related interven-tions for psychosis. Schizophrenia Bul-letin, 44, 475–491. https://doi.org/10.1093/schbul/sbx146
Van Den Berg, D. P. G., De Bont, P. a. J.m., Van Der Vleugel, B. m., De roos, c.,De Jongh, a., Van minnen, a., & VanDer Gaag, m. (2015). Prolonged expo-sure vs eye movement desensitizationand reprocessing vs waiting list for post-traumatic stress disorder in patients witha psychotic disorder: a randomized clini-cal trial. JAMA Psychiatry, 72, 259–267.https://doi.org/10.1001/jamapsychia-try.2014.2637
van rooijen, G., van rooijen, m., maat, a.,Vermeulen, J. m., meijer, c. J., ruhé, h.G., ... Bruggeman, r. (2019). longitudi-nal evidence for a relation betweendepressive symptoms and quality of lifein schizophrenia using structural equa-tion modeling. Schizophrenia Research,208, 82-89. https://doi.org/10.1016/j.schres.2019.04.011
walker, e. r., mcGee, r. e., & Druss, B. G.(2015). mortality in mental disorders andglobal disease burden implications: asystematic review and meta-analysis.JAMA Psychiatry, 72, 334–341.https://doi.org/10.1001/jamapsychia-try.2014.2502
weisman de mamani, a., weintraub, m.J., Gurak, K., & maura, J. (2014). a ran-domized clinical trial to test the efficacyof a family-focused, culturally informedtherapy for schizophrenia. Journal ofFamily Psychology, 28, 800-810.https://doi:10.1037/fam0000021
January • 2021 23
s t r a t e g i e s f o r w o r k i n g w i t h a u t i s t i c c l i e n t s
wu, e. Q., shi, l., Birnbaum, h., hudson,t., & Kessler, r. (2006). annual preva-lence of diagnosed schizophrenia in theusa: a claims data analysis approach.Psychological Medicine, 36, 1535–1540.https://doi.org/10.1017/s0033291706008191.
. . .
no conflicts of interest or fundingto disclose.Correspondence to tate F. halverson, uni-versity of north carolina at chapel hill,Dept. of Psychology and neuroscience (cB3270), 235 e cameron ave., chapel hill,nc 27599-3270; [email protected]
autism sPectrum DisorDer is a lifelongneurodevelopmental condition that affectsapproximately 1 in 54 eight-year-old chil-dren in the united states (maenner, 2020)and is characterized by distinct social andcommunication challenges in tandem withrestricted interests and/or repetitive behav-iors (american Psychiatric association,2013). the last decade of clinical researchhas illuminated that mental health con-cerns are highly prevalent and may presentdifferently in autistic people comparedwith the general population (e.g., hollockset al., 2019). Few providers, however,receive training in working with autisticclients (maddox, crabbe, Beidas, et al.,2019; maddox, crabbe, Fishman, et al.,2019). as such, there is a need for trainingin working effectively with autistic peopleamong mental health providers. it isimportant for providers to have a founda-tional knowledge of and comfort in work-ing with autistic people. this article is
intended to provide concepts relevant tothe aforementioned knowledge and com-fort.
while mental health providers are oftentaught to view autism through the lens ofthe medical model—as a disorder to be pre-vented or cured—the social model pro-vides another perspective. the socialmodel of disability identifies that chal-lenges arise from the person-environmentfit (Goering, 2015). the neurodiversity, orautism rights, movement, driven by autisticself-advocates, seeks to highlight thestrengths and talents of autistic people andto celebrate autism as natural biologicalvariation (Jaarsma & welin, 2012; Kapp etal., 2013). congruent with this, labels of“high” and “low” functioning do not accu-rately reflect unique strengths and differ-ences of autistic people. this, along withthe incongruence between functional abil-ities and intelligence in autism, has led toautistic self-advocates and researchers alike
to recommend that we stop using theseterms (alvares et al., 2019; Kapp, 2018). inaddition, many autistic self-advocates havevoiced their preference for identity-first, asopposed to person-first, language, high-lighting that autism is a core component oftheir identity (Kapp et al., 2013). in thispaper, we use identity-first language (i.e.,“autistic client”) to respect this stated pref-erence. in the therapy setting, we recom-mend that providers explore each client’spreference.
Competence in Working WithAutistic Clients in Therapy
the high rates of mental health con-cerns among autistic people (hollocks etal., 2019; van steensel et al., 2011), coupledwith mental health providers’ reports oflimited knowledge, experience, compe-tence, and confidence in working effec-tively with this population (maddox,crabbe, Beidas, et al., 2019; maddox,crabbe, Fishman, et al., 2019), leave manyautistic people without access to adequatemental health care (crane et al., 2019). infact, autistic people may be turned away byprofessionals who feel they lack expertise inworking with this population (lipinski etal., 2019). commensurate with this, a lackof training in neurodevelopmental disor-ders was recently identified as a concernamong health providers generally (morriset al., 2019), and autistic adults feel asthough mental health providers are notwell-trained in working with autisticpeople (camm-crosbie et al., 2018). Forinstance, one autistic adult stated:
the biggest difficulty in getting thesupport i need is the lack of under-standing of autism. even after
CLINICAL PRACTICE FORUM
A Call for Compassion: Evidence-BasedStrategies for Working With Autistic ClientsWithout Co-occurring Intellectual Disabilityin TherapyAlana J. McVey, The University of British Columbia and MarquetteUniversity
Hillary K. Schiltz, Marquette University
Henry Boeh, Center for Behavioral Medicine, Brookfield, WI
• COVID-19• Resources for Anxiety• Coping in the Real World• Telehealth Resources
ABCT Has Links to Incredible ResourcesPertaining to COVID-19 and Telehealth
https://www.abct.org/Information/?m=mInformation&fa=COVID19

m c v e y e t a l .
24 the Behavior Therapist
decades of research, many institu-tions still don’t have the first clue indealing with such a condition . . .(camm-crosbie et al., p. 5)
the lack of competence in autism andresulting dearth of mental health servicesfor autistic people presents an immediateand urgent need for mental healthproviders to receive adequate training todevelop competence in working with autis-tic people and to implement treatmentseffectively for this population.
in this paper, we provide a briefoverview of the literature on the preva-lence, assessment, and treatment of themost commonly identified co-occurringmental health concerns in autism to pro-vide context and operational definitions forthe reader. thereafter, we provide a set ofstrategies, guided by the treatment litera-ture for this population, that mental healthproviders may draw upon in their workwith autistic clients. the focus here is onpsychotherapy; however, the strategiesbelow will likely prove helpful to psychia-trists and primary care physicians as well aspsychologists, counselors, social workers,and other mental health providers.
Co-occurring Mental HealthConcerns in Autism
as described above, autistic peoplecommonly experience co-occurringmental health concerns. historically, diag-nostic overshadowing—when the salienceof one disorder limits consideration orrecognition of another disorder (matson &williams, 2013)—resulted in these co-occurring symptoms going undetected. infact, prior to the current diagnostic manual(Dsm-5), autism and attention-deficit/hyperactivity disorder (aDhD) could notbe diagnosed together (american Psychi-atric association, 2013). recently, there hasbeen more widespread recognition of theseco-occurring mental health concerns inautism. the areas with the most establishedlines of evidence are co-occurring aDhDand anxiety, in particular among youth.recently, more attention has been paid toco-occurring depression and suicidality,and a new area of focus is co-occurringposttraumatic stress disorder (PtsD). thisresearch on etiology, mechanisms, andmeasurement has led to improved identifi-cation of mental health concerns amongautistic people and prompted a burgeoningline of research on treatment strategies forthese clinical presentations. of note, inassessing co-occurring mental health con-
cerns, we encourage clinicians to utilizemeasures that have been created for or val-idated with this population, when possible,as the literature suggests these tools mayfunction differently among autistic people(cassidy et al., 2018a, 2018b; hoover, 2015;magiati et al., 2017; schiltz et al., 2019;Yerys et al., 2017).
Co-occurring ADHDthe combined prevalence of aDhD
and autism is strikingly high. estimatesrange from 12–86% of autistic youth meet-ing criteria for aDhD, depending on thesubtype examined (Gadow et al., 2005; lee& ousley, 2006; mattila et al., 2010). in thegeneral population, the estimated preva-lence of aDhD is 5% of children and 2.5%of adults (american Psychiatric associa-tion, 2013; Polanczyk et al., 2007). as neu-rodevelopmental disorders, the functionalpresentation of aDhD and autism may beclosely intertwined, and thus, core symp-toms must be considered carefully. in par-ticular, attention to a person’s behaviorswithin the social context is crucial, asendorsement of a symptom may be relatedto social difficulties inherent to autismversus inattention or impulsivity pertain-ing to aDhD (Yerys et al., 2017).
in addition to psychopharmacology,treatments for aDhD rely heavily onbehavioral strategies for parents of children(e.g., chronis et al., 2004), and cognitive-behavioral approaches for adults (Goode etal., 2018). while few studies have evaluatednonpharmacological treatments specifi-cally designed for children with combinedautism and aDhD (antshel & russo,2019), parent training programs have beentested among parents of autistic youth anddisruptive behaviors, demonstrating pre-liminary evidence for symptom improve-ment (e.g., Bearss et al., 2013; lecavalier etal., 2017). unstuck and on target is anintervention designed to improve execu-tive functions among autistic children—which are additively compromised amongchildren with combined autism andaDhD (antshel & russo, 2019). unstuckand on target has been shown to improvehigher-order executive functions, includ-ing problem-solving and organizationamong autistic children (cannon et al.,2011; Kenworthy et al., 2014).
Co-occurring Anxietythe estimated rate of co-occurring anx-
iety among autistic youth is approximately40% (van steensel et al., 2011). this is incontrast with just 7.1% in the general pop-ulation (Ghandour et al., 2019). less is
known about rates of anxiety among autis-tic adults, but estimates are approximately33–50% (hollocks et al., 2019; uljarević etal., 2019; white et al., 2018). importantly,anxiety symptoms may be difficult to teaseapart from autism symptoms and/or maypresent differently in autistic people com-pared with the general population (Kernset al., 2014). thus, careful assessment iscrucial due to the intricacies of disentan-gling the two syndromes (american Psy-chiatric association, 2013; Kerns, rump, etal., 2016; spain et al., 2018).
researchers have developed severalinterventions to address co-occurring anx-iety, and studies have demonstrated theirefficacy, mostly among autistic youth.these interventions include: Facing YourFears (FYF; reaven et al., 2012), Behavioralinterventions for anxiety in children withautism (Biaca; storch et al., 2013; woodet al., 2009, 2015), and the multimodalanxiety and social skills intervention(massi; white et al., 2009, 2013). Deliveryof these interventions varies from group-based (FYF), individual (Biaca), or acombination (massi). although treat-ment programs differ in delivery modalityand session content, common componentsare evident. in particular, these treatmentsare based in cognitive-behavioral theoryand employ techniques commonly used totreat anxiety in the general population (i.e.,relaxation, exposure with response preven-tion, cognitive restructuring). a recent ran-domized clinical trial examining copingcat (Kendall, 2006)—an interventiondesigned to treat anxiety disorders inyouth—and Biaca found that both inter-ventions were efficacious at reducing clini-cally elevated anxiety, compared to treat-ment as usual, although Biaca showedsome additional benefits (wood et al.,2019). manuals for Facing Your Fears andcoping cat are available for purchase, andtraining in Biaca is publicly availableonline.
Co-occurring Depressionand Suicidality
co-occurring depression occurs at ratesof approximately 22–72% among autisticyouth, depending upon age and iQ (mayeset al., 2011), compared to only 3.2% in thegeneral population (Ghandour et al., 2019).among autistic adults, estimates indicate acurrent and lifetime prevalence of 23% and37%, respectively (hollocks et al., 2019).Depression may be linked with social chal-lenges common among autistic youth andadults, including perceived group affilia-tion, loneliness, and social support (hedley

January • 2021 25
s t r a t e g i e s f o r w o r k i n g w i t h a u t i s t i c c l i e n t s
et al., 2017, 2019; hedley, uljarević, Foley,et al., 2018; hedley, uljarević, wilmot, etal., 2018; hedley & Young, 2006; uljarevićet al., 2019). within the past few years, sui-cidality has been identified as a highlyprevalent concern among autistic adults(cassidy, Bradley, shaw, et al., 2018; cas-sidy et al., 2014; hedley et al., 2017; hedley,uljarević, Foley, et al., 2018; hirvikoski etal., 2019; Kirby et al., 2019), and qualitativeresearch has concerningly identified theseadults receive little support for suicidalideation and self-harm (camm-crosbie etal., 2018). as yet, few tools have demon-strated strong psychometric properties incapturing co-occurring depression or sui-cidality (cassidy, Bradley, Bowen, et al.,2018a, 2018b), and careful assessment ismerited given that some symptoms ofdepression can be conflated with autism(e.g., temper tantrums in children, socialinterest versus anhedonia among youth oradults; american Psychiatric association,2013).
Despite the high co-occurrence ofdepression and links with self-harm(hedley, uljarević, wilmot, et al., 2018)and suicidal ideation (hedley et al., 2017),there is considerably less empirical evi-dence on the treatment of co-occurringdepression compared to anxiety (white etal., 2018), with much of it focused on autis-tic adolescents and young adults. evidenceindicates that group-based cognitive-behavioral therapy (cBt) (mcGillivray &evert, 2014; santomauro et al., 2016) andmindfulness-based therapy (sizoo &Kuiper, 2017; spek et al., 2013) showmodest and comparable improvement indepressive symptoms among autistic ado-lescents and young adults (sizoo & Kuiper,2017). it has been theorized that a mindful-ness-based approach might offer treatmentgains similar to a traditional cBt approachwhen addressing depression in autism(white et al., 2018). unfortunately for ourautistic clients currently suffering with thispresentation, much remains to be learnedabout efficacious treatment for co-occur-ring depression and suicidality across thelifespan.
Co-occurring PTSDautistic people are more likely to expe-
rience traumatic events (Brenner et al.,2018; Kerns, newschaffer, et al., 2015;mandell et al., 2005) and adverse childhoodexperiences (aces) than the general popu-lation (Berg et al., 2016; hoover & Kauf-man, 2018; rigles, 2016), placing them atan elevated risk for developing co-occur-ring PtsD (roberts et al., 2015). assessing
PtsD among autistic youth and adults maybe challenging, as recent literature suggeststhat PtsD symptoms may present differ-ently among autistic people than in thegeneral population (haruvi-lamdan et al.,2018; hoover, 2015; Kerns, newschaffer, etal., 2015). adding to this challenge, there isa lack of validated PtsD measures in thispopulation (hoover, 2015), however, arecently developed interactive trauma-scale (hoover & romero, 2019) showspromise, boasting satisfaction amongautistic youth and good psychometricproperties (internal consistency and valid-ity). more research is needed to clarify thepresentation of co-occurring PtsD symp-toms in autism for accurate diagnosticassessment.
in terms of treatment for co-occurringPtsD, much of the research is in its earlystages and, while promising, it is too soonto identify which treatments are effica-cious. single case and case series designstudies have pointed to preliminary evi-dence for the effect of cBt in this popula-tion (carrigan & allez, 2017; weiss &lunsky, 2010). researchers have also putforth recommendations for modifying thetreatment of co-occurring PtsD (Petersonet al., 2019; stack & lucyshyn, 2019); theseinclude cognitive, behavioral, and affectregulation strategies shown to be effica-cious for autistic people.
Implications for Providersco-occurring mental health concerns
are highly prevalent and often challengingto accurately assess among autistic people,yet there is burgeoning evidence for suc-cessful treatment of these concerns viainterventions designed or modified for this
population. common elements in thetreatments described above are well withinreach for mental health providers. recog-nizing and employing these strategies canhelp to close a critical gap in the mentalhealth care of autistic youth and adults.
Recommended Strategies forCompetence in Working With
Autistic Clientsconsidering empirical evidence from
the field, including the studies of adaptedintervention described above, we providebelow a set of recommended strategies forworking effectively and compassionatelywith autistic clients without intellectualdisability in therapy. Cognitive-BehavioralTherapy for Adults With Autism SpectrumDisorder (Gaus, 2019) is an excellentresource, and we encourage readers toreview this text as well. here, we hope toprovide broad recommendations that maybe utilized in conjunction with treatmentmodalities including, but not limited to,cBt with autistic people across much ofthe lifespan. Please note that some of thesetechniques remain largely theoretical formuch of the autism population—as statedabove, much work has focused on the treat-ment of anxiety among autistic youth. Forclarity, strategies that have not been explic-itly tested in treatment studies, to ourknowledge, are marked with an asterisk.Please note that the recommendationsbelow assume the provider is non-autistic.Figure 1 lists the strategies described below.
Focus on Strengths*when a client initially presents for
treatment, we as mental health providers
Figure 1. strategies for working with autistic clients without co-occurringintellectual Disability in therapy

26 the Behavior Therapist
m c v e y e t a l .
identify the client’s goals and begin to clar-ify their strengths (i.e., existing tools formanaging their presenting concerns) aswell as areas for growth (i.e., ways to inter-vene). this is especially crucial for autisticclients as they may have been viewed onlyfrom the vantage point of their “deficits”their entire lives. when working withautistic clients, providers may inadver-tently overfocus on a client’s weaknessesand areas for growth. instead, we want toempower our autistic clients and highlighttheir natural abilities and the effective waysin which they navigate the world. in thisway, we seek to normalize their symptomsand instill hope (Kerns, roux, et al., 2016).narratives that “flip the script” aboutautism may be helpful for providers look-ing to capitalize on their autistic clients’strengths (e.g., Kaufman, 2019; tesfaye etal., 2019). For instance, recognizing thatautistic people may use different modes ofcommunication but nonetheless demon-strate ability and desire to communicate(tesfaye et al.), and that strong attention todetail, as commonly seen in autism, may beviewed as a strength (Kaufman).
Employ Concrete Strategies andStructured Sessions
similarly, providers benefit from utiliz-ing tangible strategies in sessions with ourautistic clients, that is, making abstractconcepts into concrete tasks or activities(Kerns, roux, et al., 2016). in particular,the use of visual materials such as videos,images, drawing, and writing, as well ashands-on activities and worksheets, havebeen found to be efficacious in treating co-occurring anxiety and are recommended(chalfant et al., 2007; reaven et al., 2012;white et al., 2013). Depending on the goalsof treatment, providers may find modelingskills and in vivo or videotaped practice ofskills especially helpful (reaven et al.;white et al.). we also encourage the use ofimmediate, direct, and specific feedback forskills acquisition (white et al.). autisticadults have identified written communica-tion, clearly structured and more slowlypaced sessions, and clear expectations to behelpful (lipinski et al., 2019; maddox,crabbe, Beidas, et al., 2019).
Use Literal Language and ExplainNonliteral Language
autistic people often communicate dif-ferently than neurotypical people, both interms of expressive and receptive language(Kwok et al., 2015). as providers, we mayneed to be flexible and patient to commu-nicate most effectively with our autistic
clients (Kerns, roux, et al., 2016). on onehand, we may choose to rely on literal, con-crete, and direct language (maddox,crabbe, Beidas, et al., 2019; mcnallyKeehn, et al., 2013) while limiting the useof metaphors, sarcasm, and idioms (Kalan-dadze et al., 2018). on the other hand,because these communication styles arewidely used, as rapport is built, we maywant to integrate them into treatment.when we do this compassionately, check-ing in with our clients to ensure we arecommunicating well (e.g., explaining themeanings of idioms, discussing our inten-tions when using sarcasm), we provide nat-ural opportunities for bolstering socialcommunication.
Capitalize on Your Client’s InterestsBecause many autistic people have
restricted or circumscribed interests—aninterest or intensity of interest that is con-sidered unusual to nonautistic people—and find them especially motivating, incor-porating them into therapy can have manybenefits (Kerns, roux, et al., 2016; maddox,crabbe, Beidas, et al., 2019; mcnally Keehnet al., 2013; wood et al., 2009, 2015). inter-ests can be knit into therapeutic materialsor activities in sessions, often leading toimproved rapport and motivation toengage in activities. interests may also beused as reinforcement in therapy. that is,clients may earn time engaging in a desiredactivity or talking about a subject of interestafter participating in a therapeutic task.with autistic youth, parents may helpemploy reinforcement schedules withinterests as rewards for desired behavior athome, to aid in generalization of therapeu-tic work.
Foster Your Own Creativityworking in mental health requires cre-
ativity, and, for providers working withautistic clients, we should feel inspired tofoster our creativity to best meet our clientswhere they are (Kerns, roux, et al., 2016).the creator of coping cat and colleagueshave written about the crucial importanceof “flexibility within fidelity” (e.g., Beidas etal., 2010; chu & Kendall, 2009; Kendall etal., 2008), that is, delivering interventionsauthentically and using strategies that pro-mote engagement in treatment. this maymean augmenting tools used within ourpractice so that they are more accessibleand/or motivating to our autistic clientsand relying more heavily on written strate-gies (lipinski et al., 2019), images, videos,or cartoons to facilitate therapeutic growth.we also encourage providers to involve
your autistic clients in this process—askwhat they would find most helpful!
Meet Your Client Where They Are*when working with autistic clients, we
should not immediately assume that theyneed or want to work on changing theirautism symptoms, such as social skills(maddox & Gaus, 2018). through the lensof the medical model, this assumption mayoccur automatically for providers, and weneed to be careful. it is crucial that we curi-ously and collaboratively develop a treat-ment plan based on where the client is andwhat they want to change in their life(Kerns, roux, et al., 2016). after all, thetreatment is the client’s, not the provider’s,and we must align our intervention withour client’s goals, not our own.
Open the Door for Social andEmotional Competence
social inclusion and acceptance areclosely tied to mental health and quality oflife for autistic adults (Kapp, 2018).research has highlighted the intercon-nected nature of social engagement and co-occurring mental health concerns, includ-ing aDhD (Yerys et al., 2017), anxiety(Kerns, Kendall, et al., 2015; locke et al.,2010), depression (hedley, uljarević,wilmot, et al., 2018), and trauma (hoover,2015). therefore, promoting social under-standing and positive social experiencesmay emerge as treatment targets whenworking with autistic clients (Kerns, roux,et al., 2016). in fact, tailored treatments forco-occurring anxiety (i.e., massi, FYF,and Biaca) include social skills compo-nents that involve didactic instruction andin-session practice. Furthermore, socialskills interventions may, in and of them-selves, result in secondary improvementsin social anxiety (mcVey et al., 2016;schohl et al., 2014), depression, and suici-dality (schiltz et al., 2017). as stated above,not all autistic clients will want social skillsintervention. skills for managing peer vic-timization, perhaps including advocacyfrom the provider, parents, teachers, orother important adults or peers, may behelpful, as the social environment—i.e.,how others treat autistic people—is linkedwith mental health for autistic people(Kapp, 2018). mental health providers mayalso wish to use their position to help pro-mote inclusion of autistic people in society(see Bölte, 2019).
Emotional competence is a broad termencompassing skills pertaining to the expe-rience of emotions (saarni, 1999). autisticpeople may or may not struggle with skills

s t r a t e g i e s f o r w o r k i n g w i t h a u t i s t i c c l i e n t s
January • 2021 27
such as emotion recognition and regula-tion (harms et al., 2010; mazefsky et al.,2013; nuske et al., 2013); in fact, symptomsof alexithymia may be more likely to pre-dict these difficulties in autism (cook et al.,2013). our autistic clients may present withchallenges with emotional competence,and these may or may not be areas ofdesired treatment. Because emotion regu-latory processes have been linked with co-occurring mental health concerns—namely, anxiety (mazefsky & white,2014)—focusing on these skills may dove-tail nicely with treatment.
Assume Intelligence*Just as binary categories can prime our
brains to ignore varied and unique forms ofintelligence among autistic clients, so canimplicit biases lead us to unfairly denigratecertain behaviors associated with autism.our autistic clients may demonstratebehaviors such as repetitive motor move-ments (“stimming”), echolalia, and/orcommunication challenges that can mis-leadingly give the impression of cognitivelimitations, when the function or source ofthese behaviors may or may not be linkedwith intelligence (Bishop et al., 2006). thisimplicit assumption can hinder providershaving reasonable expectations of clients,pushing clients toward change, viewingclients as unique people, and respectingclients’ skillsets and views of the world. it iscritical for us to assume intelligence in ourautistic clients. For instance, a client’s diffi-culty expressing cognitive experiences ver-bally does not necessarily indicate lack of arich inner life (e.g., Jones, 2017). autisticclients may have insights akin to or exceed-ing nonautistic clients, though they maystruggle to convey these to providers. itwould be harmful for a provider to imme-diately assume, because signs of insight arenot clear through verbal language, that theydo not exist.
Be Aware of Your Assumptionsand Biases*
mental health providers are encouragedto consider autism as similar to a minorityculture (maddox & Gaus, 2018; mcVey etal., 2017), and, as with any minority cul-ture, providers may have preexisting biasesagainst autistic people that can uninten-tionally hurt the therapeutic alliance. asproviders, we must be aware of these biasesin order to effectively challenge them andprevent them from impacting our treat-ment delivery. some examples of biasestowards the autistic population includebeliefs that all autistic people have signifi-
cant cognitive limitations (maddox,crabbe, Beidas, et al., 2019), are savants,are incapable of social lives—includingfriendships and romantic relationships—cannot feel and/or understand emotionsand cannot experience empathy. suchbeliefs beget clinical assumptions and deci-sions that are not based in the reality of theautistic client and, in turn, decrease thechances that effective psychotherapy cantake place.
Be Compassionate and Curious*curiosity paired with compassion can
solve many clinical conundrums, regard-less of a mental health provider’s level oftraining or expertise in autism. Given theheterogeneity in the expression and expe-rience of autism (masi et al., 2017), ourclients are often our best teachers when wewant to understand their lived experienceand determine how to help them meet theirtreatment goals. as symptoms of autismbecome apparent in therapy, we can bemost effective by asking the client for theirexperience of that symptom. For example,if an autistic client mentions confusion sur-rounding social cues, ask them about theirexperience of social interactions. ask abouttheir thoughts, emotions, behaviors,assumptions, fears, frustrations, and goals.Do not assume that they will give a text-book answer; be prepared to trust theiranswers and adapt your clinical conceptu-alization and treatment plan appropriately.
Seek to Understand the Functionof Behaviors*
in most forms of therapy, proper assess-ment of behaviors is crucial to developempathy for and understanding of a client.this is equally important when trying tohelp a client change their behavior. whentherapists rely too heavily on interpreta-tions, assumptions, or past experiences,they may incorrectly identify the functionof a behavior and risk both invalidatingtheir client and delivering an ineffectiveintervention. asking clients why they thinkthey engage in certain behaviors, or howthey experience those behaviors, can leadto more accurate understanding. addition-ally, closely observing behaviors as theyoccur in session can help to illuminate thepossible antecedents and consequences ofthose behaviors, leading to an understand-ing of their function. it is crucial to recog-nize that many behaviors common toautism are not an indication of pathologyand may instead reflect a person or a soci-ety’s discomfort with diversity (Kapp et al.,2019). For instance, repetitive motor
movements (or “stimming”) are com-monly used for emotion regulation byautistic adults (Kapp et al., 2019), and maytherefore be a coping strategy to capitalizeupon in treatment rather than a behavior toextinguish.
Ask Your Client About TheirExperience of Autism*
autistic people often experience theworld differently than neurotypicals, and itis important to explore this in therapy(Kerns, roux, et al., 2016). they may haveemotional or behavioral reactions to stim-uli that would elicit a much differentresponse from a nonautistic person. ther-apists who step into the minds of theirclients with curiosity and attempt to expe-rience the world through their client’s eyesstand a better chance of expressing empa-thy in therapy. the more curious we are ofour clients’ experiences, and the moreempathic and clinically driven questionswe ask them, the better we will be able tounderstand their emotional and behavioralexperiences. this should be balanced witha respect that our autistic clients are not tobe expected to teach us about autism(camm-crosbie et al., 2018) and we mustengage in our own education. empathizingand understanding can result in flexiblyadapting therapy to best suit each client.
Assume a Nonjudgmental StanceFinally, and perhaps most important,
work to foster a nonjudgmental stance inyour practice. it is human nature to experi-ence automatic judgments when weencounter new behaviors, cognitions, andemotional expressions, or if an autisticclient is struggling with something that anonautistic therapist believes should beeasy. the goal is not to erase our brain’scapacity for judging, but to gently acknowl-edge our judgments and return to a non-judgmental, empathy-based stance. indoing this, we are being kind to ourselvesand ensuring that we can provide the bestcare for our clients.
Conclusionour autistic clients deserve access to
high-quality mental health care. theydeserve to work with mental healthproviders who have an understanding ofand openness toward neurodiversity, tonot be turned away from treatment, nor tobe expected to teach their providers aboutautism. as such, developing competence inworking with autistic clients is a necessary

28 the Behavior Therapist
m c v e y e t a l .
component of a mental health provider'straining.
the recommendations provided hereare based on the current evidence and rep-resent merely a starting point for a mentalhealth provider’s training in working withautistic clients. as this area of clinicalresearch continues to develop, and we learnmore about the most effective ways toassess and treat co-occurring mental healthconcerns among autistic people, these rec-ommendations will inevitably change. aswith all areas of competence, providers areencouraged to continue to develop theirunderstanding of autistic clients throughcontinuing education, self-study, and com-passion in their practice. Fortunately,mental health providers already possess thecore skills needed for this important work.
Referencesalvares, G. a., Bebbington, K., cleary, D.,
evans, K., Glasson, e. J., maybery, m. t.,Pillar, s., uljarević, m., Varcin, K., wray,J., & whitehouse, a. J. (2019). the mis-nomer of “high functioning autism”:intelligence is an imprecise predictor offunctional abilities at diagnosis. autism:International Journal of Research andPractice, 1362361319852831.https://doi.org/10.1177/1362361319852831
american Psychiatric association. (2013).Diagnostic and statistical manual ofmental disorders (5th ed). author.
antshel, K. m., & russo, n. (2019).autism spectrum disorders and aDhD:overlapping phenomenology, diagnosticissues, and treatment considerations.Current Psychiatry Reports, 21(5), 34.
Bearss, K., lecavalier, l., minshawi, n.,Johnson, c., smith, t., handen, B.,sukhodolsky, D., aman, m., swiezy, n.,& Butter, e. (2013). toward anexportable parent training program fordisruptive behaviors in autism spectrumdisorders. Neuropsychiatry, 3(2), 169.
Beidas, r. s., Benjamin, c. l., Puleo, c. m.,edmunds, J. m., & Kendall, P. c. (2010).Flexible applications of the coping catprogram for anxious youth. Cognitiveand Behavioral Practice, 17(2), 142–153.
Berg, K. l., shiu, c.-s., acharya, K., stol-bach, B. c., & msall, m. e. (2016). Dis-parities in adversity among children withautism spectrum disorder: a population-based study. Developmental Medicine &Child Neurology, 58(11), 1124–1131.https://doi.org/10.1111/dmcn.13161
Bishop, s. l., richler, J., & lord, c. (2006).association Between restricted andrepetitive Behaviors and nonverbal iQin children with autism spectrum Dis-orders. Child Neuropsychology, 12(4–5),
247–267. https://doi.org/10.1080/09297040600630288
Bölte, s. (2019). hey autism researcher,what’s on your mind today about inclu-sion? Autism, 1362361319870994.https://doi.org/10.1177/1362361319870994
Brenner, J., Pan, Z., mazefsky, c., smith,K. a., & Gabriels, r. (2018). Behavioralsymptoms of reported abuse in childrenand adolescents with autism spectrumdisorder in inpatient settings. Journal ofAutism and Developmental Disorders,48(11), 3727–3735.
camm-crosbie, l., Bradley, l., shaw, r.,Baron-cohen, s., & cassidy, s. (2018).‘People like me don’t get support’: autis-tic adults’ experiences of support andtreatment for mental health difficulties,self-injury and suicidality. Autism,1362361318816053. https://doi.org/10.1177/1362361318816053
cannon, l., Kenworthy, l., alexander, K.c., werner, m. a., & anthony, l. (2011).unstuck and on target! an executivefunction curriculum to improve flexibil-ity for children with autism spectrumdisorders. ERIC.
carrigan, n., & allez, K. (2017). cognitiveBehaviour therapy for Post-traumaticstress Disorder in a person with anautism spectrum condition and intel-lectual Disability: a case study. Journalof Applied Research in Intellectual Dis-abilities, 30(2), 326–335.
cassidy, s., Bradley, l., Bowen, e.,wigham, s., & rodgers, J. (2018a). mea-surement properties of tools used toassess depression in adults with andwithout autism spectrum conditions: asystematic review. Autism Research,11(5), 738–754.
cassidy, s., Bradley, l., Bowen, e.,wigham, s., & rodgers, J. (2018b). mea-surement properties of tools used toassess suicidality in autistic and generalpopulation adults: a systematic review.Clinical Psychology Review, 62, 56–70.
cassidy, s., Bradley, l., shaw, r., & Baron-cohen, s. (2018). risk markers for suici-dality in autistic adults. MolecularAutism, 9(1), 42.
cassidy, s., Bradley, P., robinson, J., alli-son, c., mchugh, m., & Baron-cohen, s.(2014). suicidal ideation and suicideplans or attempts in adults withasperger’s syndrome attending a special-ist diagnostic clinic: a clinical cohortstudy. The Lancet Psychiatry, 1(2), 142–147.
chalfant, a. m., rapee, r., & carroll, l.(2007). treating anxiety disorders inchildren with high functioning autismspectrum disorders: a controlled trial.Journal of Autism and DevelopmentalDisorders, 37(10), 1842–1857.
chronis, a. m., chacko, a., Fabiano, G.a., wymbs, B. t., & Pelham, w. e.(2004). enhancements to the BehavioralParent training Paradigm for Families ofchildren with aDhD: review andFuture Directions. Clinical Child andFamily Psychology Review, 7(1), 1–27.https://doi.org/10.1023/B:ccFP.0000020190.60808.a4
chu, B. c., & Kendall, P. c. (2009). thera-pist responsiveness to child engagement:Flexibility within manual-based cBt foranxious youth. Journal of Clinical Psy-chology, 65(7), 736–754.
cook, r., Brewer, r., shah, P., & Bird, G.(2013). alexithymia, not autism, Pre-dicts Poor recognition of emotionalFacial expressions. Psychological Science,24(5), 723–732. https://doi.org/10.1177/0956797612463582
crane, l., adams, F., harper, G., welch, J.,& Pellicano, e. (2019). ‘something needsto change’: mental health experiences ofyoung autistic adults in england. Autism,23(2), 477–493.
Gadow, K. D., Devincent, c. J., Pomeroy,J., & azizian, a. (2005). comparison ofDsm-iV symptoms in elementaryschool-age children with PDD versusclinic and community samples. Autism,9(4), 392–415.
Gaus, V. l. (2019). Cognitive-BehavioralTherapy for Adults with Autism SpectrumDisorder (2nd ed.). Guilford Press.https://www.guilford.com/books/cogni-tive-Behavioral-therapy-adults-autism-spectrum-Disorder/Valerie-Gaus/9781462537686
Ghandour, r. m., sherman, l. J., Vladutiu,c. J., ali, m. m., lynch, s. e., Bitsko, r.h., & Blumberg, s. J. (2019). Prevalenceand treatment of Depression, anxiety,and conduct Problems in us children.Journal of Pediatrics, 206, 256-267.e3.https://doi.org/10.1016/j.jpeds.2018.09.021
Goering, s. (2015). rethinking disability:the social model of disability andchronic disease. current reviews in Mus-culoskeletal Medicine, 8(2), 134–138.https://doi.org/10.1007/s12178-015-9273-z
Goode, a. P., coeytaux, r. r., maslow, G.r., Davis, n., hill, s., namdari, B.,laPointe, n. m. a., Befus, D., lallinger,K. r., & Bowen, s. e. (2018). nonphar-macologic treatments for attention-deficit/hyperactivity disorder: a system-atic review. Pediatrics, 141(6),e20180094.
harms, m. B., martin, a., & wallace, G. l.(2010). Facial emotion recognition inautism spectrum disorders: a review ofbehavioral and neuroimaging studies.Neuropsychology Review, 20(3), 290–322.https://doi.org/10.1007/s11065-010-9138-6

January • 2021 29
s t r a t e g i e s f o r w o r k i n g w i t h a u t i s t i c c l i e n t s
haruvi-lamdan, n., horesh, D., & Golan,o. (2018). PtsD and autism spectrumdisorder: co-morbidity, gaps in research,and potential shared mechanisms. Psy-chological Trauma: Theory, Research,Practice, and Policy, 10(3), 290.
hedley, D., uljarević, m., Bury, s. m., &Dissanayake, c. (2019). Predictors ofmental health and well-being inemployed adults with autism spectrumdisorder at 12-month follow-up. AutismResearch, 12(3), 482–494.https://doi.org/10.1002/aur.2064
hedley, D., uljarević, m., Foley, K.-r.,richdale, a., & trollor, J. (2018). riskand protective factors underlying depres-sion and suicidal ideation in autismspectrum Disorder. Depression and Anx-iety, 35(7), 648–657. https://doi.org/10.1002/da.22759
hedley, D., uljarević, m., wilmot, m.,richdale, a., & Dissanayake, c. (2017).Brief report: social support, depressionand suicidal ideation in adults withautism spectrum disorder. Journal ofAutism and Developmental Disorders,47(11), 3669–3677.
hedley, D., uljarević, m., wilmot, m.,richdale, a., & Dissanayake, c. (2018).understanding depression and thoughtsof self-harm in autism: a potential mech-anism involving loneliness. Research inAutism Spectrum Disorders, 46, 1–7.https://doi.org/10.1016/j.rasd.2017.11.003
hedley, D., & Young, r. (2006). socialcomparison processes and depressivesymptoms in children and adolescentswith asperger syndrome. Autism, 10(2),139–153.
hirvikoski, t., Boman, m., chen, Q.,D’onofrio, B. m., mittendorfer-rutz, e.,lichtenstein, P., Bölte, s., & larsson, h.(2019). individual risk and familial liabil-ity for suicide attempt and suicide inautism: a population-based study. Psy-chological medicine, 1–12. https://doi.org/10.1017/s0033291719001405
hollocks, m. J., lerh, J. w., magiati, i.,meiser-stedman, r., & Brugha, t. s.(2019). anxiety and depression in adultswith autism spectrum disorder: a sys-tematic review and meta-analysis. Psy-chological Medicine, 49(4), 559–572.
hoover, D. w. (2015). the effects of psy-chological trauma on children withautism spectrum disorders: a researchreview. Review Journal of Autism andDevelopmental Disorders, 2, 287-299.
hoover, D. w., & Kaufman, J. (2018).adverse childhood experiences in chil-dren with autism spectrum disorder.Current Opinion in Psychiatry, 31(2),128–132. https://doi.org/10.1097/Yco.0000000000000390
hoover, D. w., & romero, e. m. G.(2019). the interactive trauma scale: a
web-Based measure for children withautism. Journal of Autism and Develop-mental Disorders, 49(4), 1686–1692.https://doi.org/10.1007/s10803-018-03864-3
Jaarsma, P., & welin, s. (2012). autism asa natural human variation: reflectionson the claims of the neurodiversitymovement. Health Care Analysis, 20(1),20–30.
Jones, J. (Director). (2017). Spectrum: AStory of the Mind [Film].
Kalandadze, t., norbury, c., nærland, t.,& næss, K.-a. B. (2018). Figurative lan-guage comprehension in individuals withautism spectrum disorder: a meta-ana-lytic review. Autism, 22(2), 99–117.
Kapp, s. K. (2018). social support, well-being, and quality of life among individu-als on the autism spectrum. Pediatrics,141(supplement 4), s362–s368.https://doi.org/10.1542/peds.2016-4300n
Kapp, s. K., Gillespie-lynch, K., sherman,l. e., & hutman, t. (2013). Deficit, dif-ference, or both? autism and neurodi-versity. Developmental Psychology, 49(1),59.
Kapp, s. K., steward, r., crane, l., elliott,D., elphick, c., Pellicano, e., & russell,G. (2019). ‘People should be allowed todo what they like’: autistic adults’ viewsand experiences of stimming. Autism,1362361319829628. https://doi.org/10.1177/1362361319829628
Kaufman, s. B. (2019). Autism: More ThanMeets the Eye. scientific american Blognetwork. https://blogs.scientificameri-can.com/beautiful-minds/autism-more-than-meets-the-eye/
Kendall, P. c. (2006). Coping cat work-book. workbook Pub.
Kendall, P. c., Gosch, e., Furr, J. m., &sood, e. (2008). Flexibility within fidelity.Journal of the American Academy ofChild & Adolescent Psychiatry, 47(9),987-993.
Kenworthy, l., anthony, l. G., naiman,D. Q., cannon, l., wills, m. c.,luong‐tran, c., werner, m. a., alexan-der, K. c., strang, J., Bal, e., sokoloff, J.l., & wallace, G. l. (2014). randomizedcontrolled effectiveness trial of executivefunction intervention for children on theautism spectrum. Journal of Child Psy-chology and Psychiatry, 55(4), 374–383.https://doi.org/10.1111/jcpp.12161
Kerns, c. m., Kendall, P. c., Berry, l.,souders, m. c., Franklin, m. e., schultz,r. t., miller, J., & herrington, J. (2014).traditional and atypical presentations ofanxiety in youth with autism spectrumdisorder. Journal of Autism and Develop-mental Disorders, 44(11), 2851–2861.https://doi.org/10.1007/s10803-014-2141-7
Kerns, c. m., Kendall, P. c., Zickgraf, h.,Franklin, m. e., miller, J., & herrington,J. (2015). not to Be overshadowed oroverlooked: Functional impairmentsassociated with comorbid anxiety Dis-orders in Youth with asD. BehaviorTherapy, 46(1), 29–39. https://doi.org/10.1016/j.beth.2014.03.005
Kerns, c. m., newschaffer, c. J., &Berkowitz, s. J. (2015). traumatic child-hood events and autism spectrum disor-der. Journal of Autism and Developmen-tal Disorders, 45(11), 3475–3486.
Kerns, c. m., roux, a. m., connell, J. e., &shattuck, P. t. (2016). adapting cogni-tive behavioral techniques to addressanxiety and depression in cognitivelyable emerging adults on the autism spec-trum. Cognitive and Behavioral Practice,23(3), 329–340. https://doi.org/10.1016/j.cbpra.2016.06.002
Kerns, c. m., rump, K., worley, J., Kratz,h., mcVey, a., herrington, J., & miller, J.(2016). the differential diagnosis of anxi-ety disorders in cognitively-able youthwith autism. Cognitive and BehavioralPractice, 23(4), 530–547. https://doi.org/10.1016/j.cbpra.2015.11.004
Kirby, a. V., Bakian, a. V., Zhang, Y.,Bilder, D. a., Keeshin, B. r., & coon, h.(2019). a 20-year study of suicide deathin a statewide autism population. AutismResearch, 12(4), 658–666.
Kwok, e. Y., Brown, h. m., smyth, r. e., &cardy, J. o. (2015). meta-analysis ofreceptive and expressive language skillsin autism spectrum disorder. Research inAutism Spectrum Disorders, 9, 202–222.
lecavalier, l., smith, t., Johnson, c.,Bearss, K., swiezy, n., aman, m. G.,sukhodolsky, D. G., Deng, Y., Dziura, J.,& scahill, l. (2017). moderators ofparent training for disruptive behaviorsin young children with autism spectrumdisorder. Journal of Abnormal Child Psy-chology, 45(6), 1235–1245.
lee, D. o., & ousley, o. Y. (2006). atten-tion-deficit hyperactivity disorder symp-toms in a clinic sample of children andadolescents with pervasive developmen-tal disorders. Journal of Child & Adoles-cent Psychopharmacology, 16(6), 737–746.
lipinski, s., Blanke, e. s., suenkel, u., &Dziobek, i. (2019). outpatient Psy-chotherapy for adults with high-Func-tioning autism spectrum condition:utilization, treatment satisfaction, andPreferred modifications. Journal ofAutism and Developmental Disorders,49(3), 1154–1168. https://doi.org/10.1007/s10803-018-3797-1
locke, J., ishijima, e. h., Kasari, c., &london, n. (2010). loneliness, friend-ship quality and the social networks ofadolescents with high-functioning

30 the Behavior Therapist
autism in an inclusive school setting.Journal of Research in Special Educa-tional Needs, 10(2), 74–81.https://doi.org/10.1111/j.1471-3802.2010.01148.x
maddox, B. B., crabbe, s., Beidas, r. s.,Brookman-Frazee, l., cannuscio, c. c.,miller, J. s., nicolaidis, c., & mandell, D.s. (2019). “i wouldn’t know where tostart”: Perspectives from clinicians,agency leaders, and autistic adults onimproving community mental health ser-vices for autistic adults. Autism,1362361319882227. https://doi.org/10.1177/1362361319882227
maddox, B. B., crabbe, s. r., Fishman, J.m., Beidas, r. s., Brookman-Frazee, l.,miller, J. s., nicolaidis, c., & mandell, D.s. (2019). Factors influencing the use ofcognitive–Behavioral therapy withautistic adults: a survey of communitymental health clinicians. Journal ofAutism and Developmental Disorders, 1–8.
maddox, B. B., & Gaus, V. l. (2018). com-munity mental health services for autis-tic adults: Good news and Bad news.Autism in Adulthood, 1(1), 15–19.https://doi.org/10.1089/aut.2018.0006
maenner, m. J. (2020). Prevalence ofautism spectrum Disorder among chil-dren aged 8 Years—autism and Devel-opmental Disabilities monitoring net-work, 11 sites, united states, 2016.mmwr. surveillance summaries, 69.https://doi.org/10.15585/mmwr.ss6904a1
magiati, i., lerh, J. w., hollocks, m. J.,uljarevic, m., rodgers, J., mcconachie,h., ozsivadjian, a., south, m., Vanhecke, a., hardan, a., libove, r.,leekam, s., & simonoff, e. (2017). themeasurement properties of the spencechildren’s anxiety scale-parent version ina large international pooled sample ofyoung people with autism spectrum dis-order. Autism Research, 10, 1629–1652.https://doi.org/10.1002/aur.1809
mandell, D. s., walrath, c. m., manteuffel,B., sgro, G., & Pinto-martin, J. a. (2005).the prevalence and correlates of abuseamong children with autism served incomprehensive community-basedmental health settings. Child Abuse &Neglect, 29(12), 1359–1372.
masi, a., Demayo, m. m., Glozier, n., &Guastella, a. J. (2017). an overview ofautism spectrum disorder, heterogeneityand treatment options. Neuroscience Bul-letin, 33(2), 183–193.
matson, J. l., & williams, l. w. (2013).Differential diagnosis and comorbidity:Distinguishing autism from other mentalhealth issues. Neuropsychiatry, 3(2), 233.
mattila, m.-l., hurtig, t., haapsamo, h.,Jussila, K., Kuusikko-Gauffin, s., Kieli-nen, m., linna, s.-l., ebeling, h., Bloigu,r., Joskitt, l., Pauls, D., & moilanen, i.
(2010). comorbid psychiatric disordersassociated with aspergersyndrome/high-functioning autism: acommunity- and clinic-based study.[references]. Journal of Autism andDevelopmental Disorders, 40(9), 1080–1093. http://dx.doi.org/10.1007/s10803-010-0958-2
mayes, s. D., calhoun, s. l., murray, m. J.,& Zahid, J. (2011). Variables associatedwith anxiety and depression in childrenwith autism. Journal of Developmentaland Physical Disabilities, 23(4), 325–337.
mazefsky, c. a., herrington, J., siegel, m.,scarpa, a., maddox, B. B., scahill, l., &white, s. w. (2013). the role of emo-tion regulation in autism spectrum Dis-order. Journal of the American Academyof Child & Adolescent Psychiatry.http://www.sciencedirect.com/science/article/pii/s0890856713003080
mazefsky, c. a., & white, s. w. (2014).emotion regulation: concepts & Prac-tice in autism spectrum Disorder. Childand Adolescent Psychiatric Clinics ofNorth America, 23(1).https://doi.org/10.1016/j.chc.2013.07.002
mcGillivray, J. a., & evert, h. t. (2014).Group cognitive behavioural therapyprogram shows potential in reducingsymptoms of depression and stressamong young people with asD. Journalof Autism and Developmental Disorders,44(8), 2041–2051.
mcnally Keehn, r. h., lincoln, a. J.,Brown, m. Z., & chavira, D. a. (2013).the coping cat program for childrenwith anxiety and autism spectrum disor-der: a pilot randomized controlled trial.Journal of Autism and DevelopmentalDisorders, 43(1), 57–67. https://doi.org/10.1007/s10803-012-1541-9
mcVey, a. J., Dolan, B. K., willar, K. s.,Pleiss, s., Karst, J. s., casnar, c. l.,caiozzo, c., Vogt, e. m., Gordon, n. s.,& Van hecke, a. V. (2016). a replica-tion and extension of the Peers® forYoung adults social skills intervention:examining effects on social skills andsocial anxiety in Young adults withautism spectrum Disorder. Journal ofAutism and Developmental Disorders.https://doi.org/10.1007/s10803-016-2911-5
mcVey, a. J., schiltz, h. K., & Van hecke,a. V. (2017). How do we study autism asneurodiversity? A review of theoreticalperspectives, empirical findings, andimplications for future research. interna-tional meeting for autism research(imFar), san Francisco, ca.
morris, r., Greenblatt, a., & saini, m.(2019). healthcare Providers’ experi-ences with autism: a scoping review.Journal of Autism and DevelopmentalDisorders, 49(6), 2374–2388.
https://doi.org/10.1007/s10803-019-03912-6
nuske, h. J., Vivanti, G., & Dissanayake,c. (2013). are emotion impairmentsunique to, universal, or specific in autismspectrum disorder? a comprehensivereview. Cognition and Emotion, 27(6),1042–1061. https://doi.org/10.1080/02699931.2012.762900
Peterson, J. l., earl, r. K., Fox, e. a., ma,r., haidar, G., Pepper, m., Berliner, l.,wallace, a. s., & Bernier, r. a. (2019).trauma and autism spectrum Disorder:review, Proposed treatment adapta-tions and Future Directions. Journal ofChild & Adolescent Trauma.https://doi.org/10.1007/s40653-019-00253-5
Polanczyk, G., de lima, m. s., horta, B. l.,Biederman, J., & rohde, l. a. (2007). theworldwide prevalence of aDhD: a sys-tematic review and metaregressionanalysis. American Journal of Psychiatry,164(6), 942–948.
reaven, J., Blakeley-smith, a., leuthe, e.,moody, e., & hepburn, s. (2012). Facingyour fears in adolescence: cognitive-behavioral therapy for high-functioningautism spectrum disorders and anxiety.Autism Research and Treatment.http://www.hindawi.com/journals/aurt/2012/423905/abs/
rigles, B. (2016). the relationshipBetween adverse childhood events,resiliency and health among childrenwith autism. Journal of Autism andDevelopmental Disorders, 47(1), 187–202.https://doi.org/10.1007/s10803-016-2905-3
roberts, a. l., Koenen, K. c., lyall, K.,robinson, e. B., & weisskopf, m. G.(2015). association of autistic traits inadulthood with childhood abuse, inter-personal victimization, and posttrau-matic stress. Child Abuse & Neglect, 45,135–142.
saarni, c. (1999). The development of emo-tional competence. Guilford Press.
santomauro, D., sheffield, J., & sofronoff,K. (2016). Depression in adolescents withasD: a pilot rct of a group interven-tion. Journal of Autism and Developmen-tal Disorders, 46(2), 572–588.
schiltz, h. K., magnus, B. e., mcVey, a. J.,haendel, a. D., Dolan, B. K., stanley, r.e., willar, K. a., Pleiss, s. J., carson, a.m., carlson, m., murphy, c., Vogt, e. m.,Yund, B. D., & Van hecke, a. V. (2019).a Psychometric analysis of the socialanxiety scale for adolescents amongYouth with autism spectrum Disorder:caregiver–adolescent agreement,Factor structure, and Validity. Assess-ment, 1073191119851563. https://doi.org/10.1177/1073191119851563
m c v e y e t a l .

January • 2021 31
s t r a t e g i e s f o r w o r k i n g w i t h a u t i s t i c c l i e n t s
schiltz, h. K., mcVey, a. J., Dolan, B. K.,willar, K. s., Pleiss, s., Karst, J. s.,carson, a. m., caiozzo, c., Vogt, e. m.,& Yund, B. D. (2017). changes inDepressive symptoms among adoles-cents with asD completing the Peers®social skills intervention. Journal ofAutism and Developmental Disorders, 1–10.
schohl, K. a., Van hecke, a. V., carson,a. m., Dolan, B., Karst, J., & stevens, s.(2014). a replication and extension of thePeers intervention: examining effectson social skills and social anxiety in ado-lescents with autism spectrum disorders.Journal of Autism and DevelopmentalDisorders, 44(3), 532–545.https://doi.org/10.1007/s10803-013-1900-1
sizoo, B. B., & Kuiper, e. (2017). cognitivebehavioural therapy and mindfulnessbased stress reduction may be equallyeffective in reducing anxiety and depres-sion in adults with autism spectrum dis-orders. Research in Developmental Dis-abilities, 64, 47–55.
spain, D., sin, J., linder, K. B., mcmahon,J., & happé, F. (2018). social anxiety inautism spectrum disorder: a systematicreview. Research in Autism Spectrum Dis-orders, 52, 51–68.
spek, a. a., Van ham, n. c., & nyklíček,i. (2013). mindfulness-based therapy inadults with an autism spectrum disorder:a randomized controlled trial. Researchin Developmental Disabilities, 34(1), 246–253.
stack, a., & lucyshyn, J. (2019). autismspectrum Disorder and the experience oftraumatic events: review of the currentliterature to inform modifications to atreatment model for children withautism. Journal of Autism and Develop-mental Disorders, 49(4), 1613–1625.https://doi.org/10.1007/s10803-018-3854-9
storch, e. a., arnold, e. B., lewin, a. B.,nadeau, J. m., Jones, a. m., De nadai, a.s., mutch, P. J., selles, r. r., ung, D., &murphy, t. K. (2013). the effect of cog-nitive-behavioral therapy versus treat-ment as usual for anxiety in children withautism spectrum disorders: a random-ized, controlled trial. Journal of theAmerican Academy of Child & AdolescentPsychiatry, 52(2), 132–142.
tesfaye, r., courchesne, V., Yusuf, a.,savion-lemieux, t., singh, i., shikako-thomas, K., mirenda, P., waddell, c.,smith, i. m., nicholas, D., szatmari, P.,Bennett, t., Duku, e., Georgiades, s.,Kerns, c. m., Vaillancourt, t., Zaidman-Zait, a., Zwaigenbaum, l., & elsabbagh,m. (2019). assuming ability of youthwith autism: synthesis of methods cap-turing the first-person perspectives of
children and youth with disabilities.Autism, 1362361319831487. https://doi.org/10.1177/1362361319831487
uljarević, m., hedley, D., rose-Foley, K.,magiati, i., cai, r. Y., Dissanayake, c.,richdale, a., & trollor, J. (2019). anxietyand Depression from adolescence to oldage in autism spectrum Disorder. Jour-nal of Autism and Developmental Disor-ders. https://doi.org/10.1007/s10803-019-04084-z
van steensel, F. J., Bögels, s. m., & Perrin,s. (2011). anxiety disorders in childrenand adolescents with autistic spectrumdisorders: a meta-analysis. Clinical Childand Family Psychology Review, 14, 302–317.
weiss, J. a., & lunsky, Y. (2010). Groupcognitive behaviour therapy for adultswith asperger syndrome and anxiety ormood disorder: a case series. ClinicalPsychology & Psychotherapy, 17(5), 438–446.
white, s. w., ollendick, t., albano, a. m.,oswald, D., Johnson, c., southam-Gerow, m. a., Kim, i., & scahill, l.(2013). randomized controlled trial:multimodal anxiety and social skill inter-vention for adolescents with autism spec-trum disorder. Journal of Autism andDevelopmental Disorders, 43(2), 382–394.
white, s. w., ollendick, t., scahill, l.,oswald, D., & albano, a. m. (2009). Pre-liminary efficacy of a cognitive-behav-ioral treatment program for anxiousyouth with autism spectrum disorders.Journal of Autism and DevelopmentalDisorders, 39(12), 1652–1662.
white, s. w., simmons, G. l., Gotham, K.o., conner, c. m., smith, i. c., Beck, K.B., & mazefsky, c. a. (2018). Psychoso-cial treatments targeting anxiety andDepression in adolescents and adults onthe autism spectrum: review of thelatest research and recommendedFuture Directions. Current PsychiatryReports, 20(10), 82.https://doi.org/10.1007/s11920-018-0949-0
wood, J. J., Drahota, a., sze, K., har, K.,chiu, a., & langer, D. a. (2009). cogni-tive behavioral therapy for anxiety inchildren with autism spectrum disorders:a randomized, controlled trial. Journal ofChild Psychology and Psychiatry, 50(3),224–234.
wood, J. J., ehrenreich-may, J., alessan-dri, m., Fujii, c., renno, P., laugeson, e.,Piacentini, J. c., De nadai, a. s., arnold,e., lewin, a. B., murphy, t. K., & storch,e. a. (2015). cognitive behavioral ther-apy for early adolescents with autismspectrum disorders and clinical anxiety:a randomized, controlled trial. BehaviorTherapy, 46(1), 7–19. https://doi.org/10.1016/j.beth.2014.01.002
wood, J. J., Kendall, P. c., wood, K. s.,Kerns, c. m., seltzer, m., small, B. J.,lewin, a. B., & storch, e. a. (2019). cog-nitive Behavioral treatments for anxietyin children with autism spectrum Dis-order: a randomized clinical trial.JAMA Psychiatry. https://doi.org/10.1001/jamapsychiatry.2019.4160
Yerys, B. e., nissley-tsiopinis, J., demarchena, a., watkins, m. w.,antezana, l., Power, t. J., & schultz, r.t. (2017). evaluation of the aDhDrating scale in Youth with autism. Jour-nal of Autism and Developmental Disor-ders, 47(1), 90–100.
. . .
this research did not receive any specificgrants from funding agencies in the public,commercial, or not-for-profit sectors. thefirst and second authors would each like toacknowledge that portions of this researchwere carried out while they were richard w.Jobling Distinguished research assistants(am: 2018–2019, hs: 2019–2020) at mar-quette university.
the authors wish to acknowledge theautistic clients with whom they have workedin therapy for the willingness and wisdomthey have shared. the authors presentedportions of this paper as a clinical workshopat the wisconsin Psychological association2019 annual meeting under the title, “cur-rent Best Practices for working with autis-tic clients in therapy.” the authors wouldlike to extend their gratitude to Brennamaddox, Ph.D., for her support and insight-ful comments on a draft of this manuscript.
the authors declare that they have noconflict of interest.Correspondence to alana J. mcVey, Ph.D.,the university of British columbia, 2136west mall, Vancouver, Bc V6t 1Z4,canada; [email protected]

32 the Behavior Therapist
DisorDers oF autonomic dysfunction(aD) associated with orthostatic intoler-ance (oi), such as Postural orthostatictachycardia syndrome (Pots), arechronic health conditions characterized bysymptoms such as dizziness, lightheaded-ness, nausea, fatigue, and difficulties focus-ing (i.e., “brain fog”), as well as sympatheticoveractivation such as shakiness, palpita-tions, excessive perspiration, and pain (Jar-jour, 2013). these physiological symptomsare commonly associated with functionalimpairment in major life domains includ-ing academics, sleep, physical activity,interpersonal relationships, and activitiesof daily living (Junghans-rutelonis et al.,2019). Pots and/or disorders of oi havebeen associated with significant negativeoutcomes including psychological distress,academic failure, social isolation, and func-tional disability (Kizilbash et al., 2014).Functional disability in pediatric patientsranges from mild limitations of activity tosevere impairment, with research indicat-ing patients presenting for treatment in atertiary care setting have moderate tosevere functional disability (Kritzberger etal., 2011).
although Pots has become increas-ingly recognized and diagnosed by themedical community, additional research isnecessary to understand how to effectivelytreat this condition. it is estimated that 1 to3 million americans have Pots (mirandaet al., 2018). individuals with Pots typi-cally experience the onset of symptoms inadolescence (median age of 13.1 years),oftentimes after an identifiable trigger, typ-ically a viral illness or injury (Johnson et al.,2010). additionally, most individuals withPots are female (5:1) and caucasian(Boris & Bernadzikowski, 2018). interest-ingly, most adolescents with Pots are alsocharacterized as being “high achievers,”typically receiving excellent grades andbeing highly successful in multipleextracurricular activities. although no spe-cific biochemical pattern has been identi-
fied in those with Pots and/or disordersof oi, it is hypothesized that the hyper-stimulated nervous system of a highachiever may increase the risk of develop-ing neurotransmitter abnormalities (Kizil-bash et al., 2018).
POTS and Mental Healththe possible presence of psychiatric dif-
ficulties in a pediatric Pots patient isoftentimes a source of contention betweenthe patient and their medical team. unfor-tunately, it is not uncommon for providersto convey (purposefully or otherwise) tothese patients that their physical symptomsare psychogenic in nature (Junghans-rutelonis et al., 2019), which can result inpatients feeling stigmatized and more resis-tant to participating in psychological treat-ment. the relationship between mentalhealth concerns and Pots is complicatedby the fact that psychiatric symptoms over-lap with aD symptoms associated with oi,particularly those involving sympatheticoveractivation. For example, physiologicalsymptoms such as shakiness, palpitations,increased heartrate, excessive perspiration,and lightheadedness can all be symptomsof both Pots and/or disorders of oi andanxiety/panic.
within adult populations, someresearch suggests that disorders of aDassociated with oi are associated withhigher rates of anxiety and depression(anderson et al., 2014), while other workhas not revealed a higher prevalence of psy-chiatric comorbidities in this population(raj et al., 2009). Prior research consis-tently shows youth with somatic com-plaints, such as chronic pain, demonstrateheightened levels of anxiety and depression(for a review, see Vinall et al., 2016). Giventhat over half of individuals with Potsreport chronic pain, there is reason tobelieve the high rates of comorbid mentalhealth concerns seen within chronic painpopulations may be mirrored among indi-
viduals with Pots (ojha et al., 2011).there is now preliminary evidence thatPots is associated with mental health dif-ficulties in children and adolescents. Forexample, several studies have documentedthe strong association between psychologi-cal distress, namely anxiety and depression,and Pots for pediatric patients treated inintensive outpatient programs (Bruce et al.,2016; mctate & weiss, 2016). althoughcausal conclusions cannot be drawn fromthese studies, it does make clear that symp-toms of Pots, anxiety, and depressioncluster together (Kizilbash et al., 2014).
Psychosocial Factors AssociatedWith POTS
research has identified several psy-chosocial factors common to youth withdisorders of aD associated with oi thatsupport the notion that psychologicallyinformed treatment for this patient popu-lation may be useful. For example, there issome evidence youth with Pots and/ordisorders of oi may suffer from “somatichypervigilance,” or a tendency to experi-ence mild sensory experiences in an intenseor distressing manner (Junghans-rutelonix et al., 2019). Furthermore,regardless of whether a patient has premor-bid anxiety, a common experience ofpatients with Pots, as well as their parents,is a tendency to experience anticipatoryanxiety about engaging in any activitiesthey fear might exacerbate their symptoms,such as attending school, exercising, orgoing out with friends. these anxieties canbe associated with “pain catastrophizing,”which involves a tendency to magnify thethreat value of pain stimuli, to feel helplessin the context of pain, and be unable toinhibit pain-related thoughts in anticipa-tion of, during, or following a painfulencounter (Kizilbash et al., 2018). inresponse to these fears, youth with Potsmay reduce their engagement in dailyactivities, which is oftentimes supported byparents who frequently engage in accom-modating and protective behaviors withchildren with Pots. this cycle of avoid-ance can perpetuate and exacerbate symp-toms of anxiety, contribute to furtherdeconditioning, and lead to a worsening infunctional disability. those who experi-ence significant functional disability are, inturn, at increased risk of also experiencingsymptoms of depression (Kritzberger et al.,2011).
CLINICAL PRACTICE FORUM
A Transdiagnostic Approach to the Treatmentof Autonomic Dysfunction Associated WithOrthostatic Intolerance in Pediatric PatientsJessica L. Hawks and Clio Pitula, University of Colorado
Jamie Shoop, Children’s Hospital of Pittsburgh

January • 2021 33
t r a n s d i a g n o s t i c a p p r o a c h t o a u t o n o m i c d y s f u n c t i o n
Traditional Treatment of POTSthe american autonomic society has
published evidence-based guidelinesemphasizing the use of nonpharmacologicinterventions as first-line therapy for disor-ders of aD associated with oi, contendingthat these interventions are most impor-tant to long-term outcomes (stewart et al.,2018). to this end, the mayo clinic (2009)has developed a framework (i.e., stePs)for discussing these interventions withPots patients. specific interventions focuson increasing sodium intake (s), taking inextra fluids (t), increasing exercise (e),taking medications as prescribed (P), andpromoting engagement in a variety of well-ness behaviors (i.e., sleep, school reengage-ment, setting priorities/goals, and access-ing a support system; s).
together with these nonpharmacologicrecommendations, researchers have high-lighted the benefits of including psycholog-ical interventions when working with thispatient population (Johnson et al., 2010).interventions have typically aligned withthe treatment for chronic pain, as theseinterventions have been widely studied(eccleston et al., 2014), and there are manysimilarities in the clinical needs of patientswith Pots and those with chronic pain(Bruce et al., 2016; Kizilbash et al., 2014).effective psychological interventions forchronic pain have included psychoeduca-tion and behavioral strategies that modifylifestyle factors (e.g., sleep, exercise; lynch-Jordan et al., 2015; Palermo, 2012), cogni-tive behavioral therapy (cBt; e.g., cogni-tive modification techniques, behavioralactivation, relaxation training, positivepatient coping, and activity pacing; eccle-ston et al., 2014; lynch-Jordan et al., 2015;Palermo, 2012), and acceptance and com-mitment therapy (act; e.g., limits of con-trol, focus on experience, values, cognitivedefusion, mindfulness, and committedaction; wetherell et al., 2011).
literature published on effective inter-ventions for pediatric Pots have focusedon treating acute patients in intensive mul-tidisciplinary settings (armstrong et al.,2017; Bruce et al., 2016). while these stud-ies have demonstrated the positive impactof behavioral health supports on psychi-atric symptoms and functional disability,these findings are limited by a high dropoutrate and an inability to generalize findingsto less intensive intervention settings.
Transdiagnostic Treatment of POTSto date, most interventions for pedi-
atric disorders of aD associated with oi
have focused on patients that are signifi-cantly disabled and in need of intensiveintervention, while less attention has beengiven to providing services to these patientsin an ambulatory setting, particularlywithin a group-based format. there aremany advantages to using a group therapyformat with this patient population. First,it is an equally efficacious alternative toindividual therapy (Federoff & taylor,2001), while also maximizing treatmentaccessibility in terms of time- and cost-effectiveness (Bastien et al., 2004). a groupformat also provides increased opportuni-ties for social connections and support forpatients and families, which has beenreported as particularly valuable forpatients with Pots. in fact, there is accru-ing evidence of the critical role of reducingsocial isolation and perceived hopelessnessfor positive health outcomes in patientswith chronic medical conditions (Freeden-berg et al., 2017). many teens with Pots,as well as their parents, disclose havingnegative interpersonal interactions withpeers, family, and providers that leave themfeeling ostracized and with the impressionthat others think they are “faking” their ill-ness (teen) or enabling them (parent). agroup-based therapeutic approach canhelp to address these concerns by facilitat-ing increased access to others who under-stand their symptoms and associated diffi-culties, reduce social isolation, andcontribute to increased feelings of hopeful-ness.
historically, youth with chronic med-ical conditions have been grouped andtreated by diagnosis and symptom clusters.more recently, there has been increasedappreciation for the commonalities in theneeds of patients with chronic medicalconditions and their families (Kieckhefer etal., 2014). this closely aligns with recentefforts from the national institute ofmental health to develop a transdiagnosticapproach to the assessment and treatmentof pediatric behavioral health concerns(rohde, 2012). this innovative approachaims to develop treatment protocols thatfocus on targeting underlying mechanismsof concern, rather than categorical diag-noses/symptoms (twohy et al., 2017). thisis particularly relevant to pediatric disor-ders of aD associated with oi, as the symp-tom presentation, level of functional dis-ability, and presence of secondarysymptoms/diagnoses is heterogeneous,although many of the underlying mecha-nisms responsible for these factors areshared across patients (Johnson et al.,2010). consequently, a unified treatment
targeting shared mechanisms could effec-tively treat these patients with diverse clin-ical presentations. Furthermore, develop-ing programs that are informed by atransdiagnostic framework results in a des-tigmatized approach to mental health(rohde, 2012), which is particularly impor-tant when working with this patient popu-lation.
thus, we developed a 10-week group-based transdiagnostic intervention forteens with disorders of aD associated withoi, most notably Pots (the restore Pro-gram). this intervention targets severalcandidate transdiagnostic mechanismscommonly implicated in teens with Pots,regardless of the clinical presentation: (1)emotion regulation, (2) information pro-cessing, (3) experiential avoidance, (4) par-enting behaviors, (5) sleep disturbances,and (6) peer relationships. these mecha-nisms were chosen based on a review of theliterature related to shared mechanismsacross emotional disorders and chronichealth conditions, such as Pots andchronic pain (twohy et al., 2017; ojha etal., 2011). the current study aimed toexamine the feasibility and acceptability ofthis intervention when implementedwithin an ambulatory care setting.
MethodProcedure
Prior to conducting this pilot study, wereceived approval from the university’sinstitutional review Board. Patients wereprimarily recruited through referrals frommental health providers in an outpatientpsychiatry clinic and by medical providersin various medical clinics (e.g., neurology,cardiology, and gastroenterology) in a largeteaching hospital. all participants receivedan initial health and behavior assessmentand were enrolled in the study if they metall inclusion criteria. Patients were eligibleto participate in the study if they were: (a)between the ages of 13–18; (b) had beendiagnosed with aD associated with oi orPots; and (c) had moderate functionalimpairment and/or were experiencingsymptoms of anxiety and/or depression.
ParticipantsParticipants included 25 youth-parent
dyads, with teens ranging in age from 13 to18 (M = 15.8). the majority of participantsidentified as female (n = 24; 96%) and werecaucasian (n = 24; 96%). while this reflectsa highly homogenous sample, these demo-graphic characteristics align with researchreflecting who is most likely to be diag-

34 the Behavior Therapist
h a w k s e t a l .
nosed with pediatric disorders of aD asso-ciated with oi (Boris & Bernadzikowski,2018). the most common primary medicaldiagnosis included Pots (n = 20; 80%) anddysautonomia associated with oi (n = 4;16%).
Interventionthe intervention used in this study was
a 10-session, 90-minute, group-basedtransdiagnostic psychological treatmentdeveloped for teens with disorders of aDassociated with oi, such as Pots. Groupswere facilitated by a psychologist, a psy-chology fellow, and a psychology intern.Both teens and parents attended all weeklysessions, meeting separately for the major-ity of the group, and coming together for aparent-teen exercise at the end of each ses-sion for approximately 20 minutes. thejoint portion of the group session focusedon practicing a skill discussed in bothgroups (e.g., progressive muscle relaxation)or facilitated collaboration of the teen-parent dyad in discussing effective applica-tion of a learned skill into the home/com-munity environment. see table 1 for adetailed description of each session’s focus.
Teen Curriculumthe initial sessions of the teen curricu-
lum focus on promoting treatment engage-ment and eliciting behavior changethrough application of motivational inter-viewing and act (i.e., values) techniques,providing psychoeducation about Pots,and reviewing healthy lifestyle behaviorsthat are critical to the effective manage-ment of Pots based on the stePsacronym (mayo clinic, 2009). we modi-fied this acronym to emphasize the impor-tance of pacing and shaping (P and s), asthese principles are of paramount impor-tance when discussing how to promotebehavior change and appropriately addressfunctional disability. an entire session isdevoted to sleep difficulties, as this is ahighly common complaint among patientswith Pots. a review of sleep hygiene prin-ciples is included, as is a description of astimulus control intervention commonlyused to support patients with sleep difficul-ties. treatment then shifts to a focus onusing relaxation techniques, such as pro-gressive muscle relaxation and visualimagery, to address the hyperarousal of thesympathetic nervous system. the remain-der of the curriculum is focused on high-lighting the differences between active andpassive coping with Pots and promotingthe use of a variety of active coping tech-niques such as mindfulness, cognitive flex-ibility, and opposite action. teens are sup-
ported in applying these strategies duringstructured exposures during a final session,as well as problem solving ways to ensuretreatment gains are maintained followingthe ending of the group. throughout allsessions of the group, group leaders use acombination of providing psychoeduca-tion, facilitating group discussion, andengaging teens in experiential exercises inorder to promote understanding of thematerial. the importance of teens havingopportunities to socially connect with oneanother during group sessions was alsofound to be highly beneficial.
Parent Curriculummuch of the content and structure
described in the teen curriculum was paral-leled in the parent curriculum, includinginitial discussion of values (focused on par-enting), psychoeducation about Pots, andreview of healthy lifestyle habits critical toeffective management of Pots (i.e., stePsand sleep strategies). throughout thesediscussions, an emphasis was placed onhow parents can effectively promote treat-ment adherence and functional improve-ments in their teen, despite their symp-toms, through application of principlessuch as shaping and pacing. Parents wereempowered to establish expectations oftheir teen and use contingency manage-ment (e.g., privilege loss, earning rewards)to provide extrinsic motivation for teens toengage in health promoting behaviors. Par-ents were also taught relaxation strategies,active coping techniques (e.g., cognitiveflexibility, mindfulness, acceptance, etc.),and how to support their teens in engagingin exposures. For example, if a teen’s expo-sure was focused on attending a socialevent they would typically avoid due tofears of worsening their symptoms, par-ents might provide extrinsic motivationsthrough use of contingency managementprinciples, engage their teen in a discussionfocused on promotion of cognitive flexibil-ity, and provide support in using pacingprinciples in order to successfully partici-pate in the activity. similar to the teensgroup, group leaders used a combination ofpsychoeducation, group discussion, andexperiential exercises. the value of parentsproviding emotional support, encourage-ment, and ideas to one another cannot beoverstated.
Treatment Feasibility and AcceptabilityFeasibility and acceptability of the inter-
vention were measured by evaluating themean number of sessions attended and thepercentage of patients considered “treat-ment completers.” additionally, teens and
their parents completed an 8-item self-report measure assessing satisfaction andperceived benefits of their participation inthe group. items were rated on a 4-pointlikert scale, with response descriptorsvarying.
ResultsTreatment Feasibilityof the 25 youth-parent dyads that
enrolled in the study, 9 dropped out of thegroup prematurely (i.e., after 0–4 sessions),resulting in an overall completion rate of64%. Dropout varied across the three sepa-rate groups comprising the study sample,ranging from 1 to 6 per group, andincluded factors related to cost, level ofimpairment (i.e., too low to need group ortoo high to attend), transportation, and dif-ficulty relating to other group members.this completion rate is relatively promis-ing given the difficulty this patient popula-tion has with maintaining functioningdespite their symptoms. importantly, par-ticipants who completed the group hadexcellent attendance, missing a mean of 1.3sessions (range 0–3), providing support forthe overall feasibility of this treatmentapproach.
Treatment Acceptabilityresponses from the satisfaction survey
suggested that adolescents and parentsfound the acceptability of this interventionto be quite high. aggregating across all 8items, adolescents’ overall satisfaction wasrated, on average, as 3.3 out of 4, where 4 =most satisfied, and parents’ average scorewas even higher, i.e., 3.6 out of 4. examina-tion of individual items revealed that, onaverage, adolescents were satisfied overallwith the help they received (i.e., 3.4 out of 4,where 4 = very satisfied), and they felt thegroup helped them learn ways to moreeffectively cope with their aD (i.e., 3.2 outof 4, where 4 = yes, definitely).
Free-response items provide furtherinformation about adolescents’ percep-tions at post-intervention: “i’ve gottenbetter at keeping up with my goals. i’velearned more coping skills and made morefriends.” “i found many new ways to helpwith my illnesses and made some goodfriends.” Parents’ satisfaction scoresdemonstrated that they found the interven-tion helpful and enjoyable. Parentsreported that overall, they were very satis-fied (3.8 out of 4, where 4 = very satisfied),and the group had helped them learn waysto more effectively support their child incoping with their aD (i.e., 3.6 out of 4,where 4 = yes, definitely). in expanding ontheir ratings, parents described, “[the

January • 2021 35
t r a n s d i a g n o s t i c a p p r o a c h t o a u t o n o m i c d y s f u n c t i o n
1
2
3
4
5
6
7
8
9
10
treatmentstructure/rationale;goals & values
healthy lifestylebehaviors
sleep strategies
relaxation
coping with achronic illness
emotional awareness
cognitive flexibility
cognitive flexibility
opposite action
relapse prevention
Psychoeducationabout Pots; treat-ment goal setting;identify values
stePs
sleep hygiene; stimu-lus control sleepingintervention
Diaphragmaticbreathing; visualimagery
Passive vs activecoping; experientialavoidance vs mindful-ness; acceptance
cBt model ofemotions
cognitiverestructuring
cognitive defusion
exposure hierarchy;complete exposures
review all strategies;problem solve possi-ble future barriers
treatmentstructure/rationale;psychoeducationabout Pots; goals &values
Parenting strategiesto promote teen’swellbeing
Parenting strategiesto promote teen’ssleep; parent self-care
reducing conflictwith teens; mindfulparenting
coping with a teenwith a chronic illness
emotional awarenessand opposite actionparenting
cognitive flexibility
cognitive flexibility
opposite action
relapse prevention
Psychoeducationabout Pots; treat-ment goal setting;identify parentingvalues
stePs; contingencymanagement
sleep hygiene;shaping & pacing;diaphragmaticbreathing
empathy; mindful-ness
experiential avoid-ance vs mindfulness;acceptance
cBt model of emo-tions; double before-during-after (BDa)framework
cognitiverestructuring
cognitive defusion
complete teenexposure
review all strategies;accommodating vsencouraging func-tioning; shaping andpacing
everyone shares 1personal value andgoal
teens identify 1stePs goal. Parentsidentify how they’llsupport teens.
teens identify 1sleep-related goal.Parents identify howthey’ll support teens.
Progressive musclerelaxation exercise
mindfulness exercise
complete thought logexample
Discuss how to col-laborate on cognitiverestructuring duringupcoming week
Discuss how parentscan support teens inachieving weeklygoals
Debrief exposures
teens identify anongoing goal andparents identify howthey’ll support teen
Table 1. outline of treatment Protocol
session teen Goals session content Parent Goals session content teen-Parent combined

36 the Behavior Therapist
h a w k s e t a l .
intervention] was very empowering.helped me to help my teen better. helpedher to help herself better.” “as a parent, itwas incredibly reassuring, comforting, andempowering to meet other parents of teenswith Pots. i am much calmer and happierand so is my teen.” “learning how to helpher pace herself and build up slowly is veryhelpful. i feel much more equipped toparent my child with dysautonomia.”
Conclusionthe treatment of disorders of pediatric
aD associated with oi, such as Pots, con-tinues to be in its infancy, but several con-sistent themes have begun to emerge: (a)the clinical presentation of this patientpopulation is heterogeneous, while severalcommon mechanisms are shared acrosspatients, and oftentimes is associated withsignificant functional impairment; (b)symptoms of Pots, anxiety, and depres-sion frequently cluster together; (c) treat-ment adherence can be problematic for thispatient population; and (d) psychologicalinterventions can be helpful in improvingfunctional disability, addressing psychi-atric symptoms, and learning ways to effec-tively manage symptoms of Pots and/oraD associated with oi. unfortunately, it isnot uncommon for patients to report that amedical provider has conveyed to themthat their symptoms are “all in their head,”which makes the patient much more resis-tant to the prospect of participating intreatments involving psychological inter-ventions. Furthermore, empirical evalua-tion of psychological interventions devel-oped for this patient population havetypically focused on intensive settings, withlittle attention having been given to theutility of providing treatment in an ambu-latory setting.
the restore Program was developed inan effort to fill this treatment gap by pro-viding a group-based intervention to teenswith aD associated with oi in an ambula-tory setting. Development of this treatmentprotocol was purposefully constructedwithin a transdiagnostic framework tobetter account for the heterogeneous pre-sentation of this population, as well as tofacilitate reduced mental health stigma byfocusing on treatment of underlying mech-anisms, rather than psychological symp-toms. a group-based format was chosen tocapitalize on the therapeutic power ofsocial connection. Qualitative data col-lected from satisfaction surveys during thepilot study revealed that the opportunity toconnect with other teens with Pots was a
critical element of treatment that likelypositively contributed to treatment out-comes and acceptability of the treatment.Data collected from the pilot study alsorevealed this treatment approach was bothfeasible and acceptable to patients and fam-ilies that participated.
Given the profound negative impactpoorly managed Pots can have on a teen’slife, it is imperative that effective treat-ments be available at every level of care.availability of psychological supports atthe ambulatory level of care will assist withintervening earlier on in a patient’s clinicalcourse, and hopefully, help to alter the pro-gression of symptoms away from signifi-cant distress and impairment. recentefforts have also been made to integratepsychological supports into ambulatorymedical teams treating Pots and/or aDassociated with oi, which should continueto assist with reducing mental healthstigma and improving access to this criticalcomponent of treatment. Future researchshould be conducted to determine whetherthe restore Program is sufficient as astand-alone intervention in an ambulatorysetting, as well as evaluate the feasibilityand value added of integrating additionalinterdisciplinary approaches, consistentwith what has been observed in moreintensive treatment settings. evaluation ofhow this group-based curriculum impactskey treatment targets (e.g., parenting prac-tices, treatment adherence) should also beconducted. Finally, it is recommended thatalternative delivery methods, such as tele-health, be considered as another way ofimproving access to effective treatmentsfor this patient population.
Referencesanderson, J. w., lambert, e. a. sari, c. i.,
Dawood, t., esler, m. D., Vaddadi, G., &lambert, G. w. (2014). cognitive func-tion, health-related quality of life, andsymptoms of depression and anxiety sen-sitivity are impaired in patients with pos-tural orthostatic tachycardia syndrome(Pots). Frontiers in Physiology, 5, 1-9.doi:10.3389/fphys.2014.00230
armstrong, K. r., De souza, a. m., sned-don, P. l., Potts, J. e., claydon, V. e., &sanatani, s. (2017). exercise and the mul-tidisciplinary holistic approach to adoles-cent dysautonomia. Acta Paediatrica,106, 612-618. doi:10.1111/apa.13750
Bastien, c. h., morin, c. m., ouellet, m.c., Blais, F. c., & Bouchard, s. (2004).cognitive behavioral therapy for insom-nia: comparison of individual therapy,group therapy, and telephone consulta-tions. Journal of Consulting and Clinical
Psychology, 72(4), 653. doi:10.1037/0022-006X.72.4.653
Boris, J.r., & Bernadzikowski, t. (2018).Demographics of a large paediatric Pos-tural orthostatic tachycardia syndromeprogram. Cardiology in the Young, 28(5),668-674.doi:10.1017/s1047951117002888
Bruce, B. K., harrison, t. e., Bee, s. m., etal. (2016). improvement in functioningand psychological distress in adolescentswith postural orthostatic tachycardiasyndrome following interdisciplinarytreatment. Clinical Pediatrics, 55, 1300-1304. doi:10.1177/0009922816638663
eccleston, c., Palermo, t.m., williams,a.c., lewandowski, h.a., morley, s.,Fisher, e. & law, e. (2014). Psychologicaltherapies for the management of chronicand recurrent pain in children and ado-lescents. Cochrane Database of SystemicReviews, 5, no.: cD003968.doi:10.1002/14651858.cD003968.pub4
Fedoroff i.c., taylor s. (2001). Psychologi-cal and pharmacological treatments ofsocial phobia: a meta-analysis. Journal ofClinical Psychopharmacology 21, 311–324. doi:10.1097/00004714-200106000-00011
Freedenberg, V. a., hinds, P. s., & Fried-mann, e. (2017). mindfulness-basedstress reduction and group supportdecrease stress in adolescents with car-diac diagnoses: a randomized two-groupstudy. Pediatric Cardiology, 38(7), 1415-1425. doi:10.1007/s00246-017-1679-5
Jarjour, i.t. (2013). Postural tachycardiasyndrome in children and adolescents.Seminars in Pediatric Neurology, 20(1),18-26. doi:10.1016/j.spen.2013.01.001
Johnson, J.n., mack, K.J., Kuntz, n.l.,Brands, c.K., Porter, c.J., & Fischer, P.r.(2010). Postural orthostatic tachycardiasyndrome: a clinical review. PediatricNeurology, 42(2), 77-85.doi:10.1016/j.pediatrneurol.2009.07.002
Junghauns-rutelonis, a.n., Postier, a.,warmuth, a., schwantes, s., & weiss,K.e. (2019). Pain management in pedi-atric patients with postural orthostatictachycardia syndrome: current insights.Journal of Pain Research, 12, 2969-2980.doi:10.2147/JPr.s194391
Kieckhefer, G.m., trahms, c.m.,churchill, s.s., Kratz, l., uding, n., &Villareale, n. (2014). a randomized clin-ical trial of the Building on Familystrengths Program: an education pro-gram for parents of children with chronichealth conditions. Maternal and ChildHealth Journal, 18(3), 563-574.doi:10.1007/s10995-013-1273-2
Kizilbash, s.J., ahrens, s.P., Bruce, B.K.,chelimsky, G., Driscoll, s.w., harbeck-weber, c., lloyd, r.m., mack, K.J.,nelson, D.e., ninis, n., Pianosi, P.t.,

t r a n s d i a g n o s t i c a p p r o a c h t o a u t o n o m i c d y s f u n c t i o n
stewart, J.m., weiss, K.e., & Fischer, P.r.(2014). adolescent fatigue, Pots, andrecovery: a guide for clinicians. currentProblems in Pediatric and AdolescentHealth Care, 44(5), 108-133.doi:10.1016/j.cppeds.2013.12.014
Kritzberger, c.J., antiel, r.m., wallace,D.P., Zacharias, J.D., Brands, c.K., Fis-cher, P.r., & harbeck-weber, c. (2011).Functional disability in adolescents withorthostatic intolerance and chronic pain.Journal of Child Neurology, 26(5), 593-598. doi:10.1177/0883073810390366
lynch-Jordan, a. m., sil, s., cunningham,n. r., Joffe, n., slater, s. K., tran, s. t., &crosby, l. e. (2015). measuring treat-ment response in an outpatient pediatricpain program. Clinical Practice in Pedi-atric Psychology, 3, 1-11.doi:10.1037/cpp0000081
mayo clinic. (2009). Teens and AutonomicDysfunction [Patient education Booklet].https://www.ehlers-danlos.org/wp-con-tent/uploads/2017/07/maYo_clinic_teens_Dysautonomia_copy.pdf
mctate, e., a. & weiss, K. e. (2016). Psy-chosocial dimensions and functioning inyouth with Postural orthostatic tachy-cardia syndrome. Clinical Pediatrics,55(10), 979-982.
miranda, n.a., Boris, J.r., Kouvel, K.m., &stiles, l. (2018). activity and exerciseintolerance after concussion: identifica-tion and management of Postural ortho-static tachycardia syndrome. Journal ofNeurologic Physical Therapy, 42(3), 163-171. doi:10.1097/nPt.0000000000000231
ojha, a., chelimsky, t. c., & chelimsky,G. (2011). comorbidities in pediatricpatients with postural orthostatic tachy-cardia syndrome. Journal of Pediatrics,158, 20-23. doi:10.1016/j.jpeds.2010.07.005
Palermo, t. m. (2012). Cognitive-behav-ioral therapy for chronic pain in childrenand adolescents. oxford universityPress.
raj, V, haman, K. l., raj, s. r., Byrne, D.,Blakely, r.D., Biaggioni, i., robertson,D., & shelton, r.c. (2009). Psychiatricprofile and attention deficits in posturaltachycardia syndrome. Journal of Neurol-ogy, Neurosurgery, and Psychiatry, 80,339-344. doi:10.1136/jnnp.2008.144360
rohde, P. (2012). applying transdiagnos-tic approaches to treatments with chil-dren and adolescents: innovative modelsthat are ready for more systematic evalu-ation. Cognitive and Behavioral Practice,19, 83-86. doi:10.1016/j.cbpra.2011.06.006
stewart, J.m., Boris, J.r., chelimsky, G.,Fischer, P.r., Fortunato, J.e., Grubb,B.P., heyer, G.l., Jarjour, i.t., medow,m.s., numan, m.t., Pianosi, P.t., singer,w., tarbell, s., chelimsky, t.c., & the
Pediatric writing Group of the ameri-can autonomic society. (2018). Pediatricdisorders of orthostatic intolerance. Pedi-atrics, 141(1), e20171673.doi:10.1542/peds.2017-1673
twohy, e., malmberg, J., & williams, J.(2017). a comprehensive transdiagnosticapproach to pediatric behavioral health.Colorado Journal of Psychiatry & Psy-chology, 2, 43-57.doi:10.25677/10968/4320
Vinall, J., Pavlova, m., asmundson, G. J.G., rasic, n. & noel, m. (2016). mentalhealth comorbidities in pediatric chronicpain: a narrative review of epidemiology,models, neurobiological mechanismsand treatment. Children, 40, 1-31.doi:10.3390/children3040040
wetherell, J. l., afari, n., rutledge, t.,sorrell, J. t., stoddard, J. a., Petkus, a. J.,solomon, B.c., lehman, D.h., liu, l. &atkinson, J. h. (2011). a randomized,controlled trial of acceptance and com-mitment therapy and cognitive-behav-ioral therapy for chronic pain. Pain, 152,2098-2107.doi:10.1016/j.pain.2011.05.016
. . .
the authors wish to thank sally tarbell,Ph.D., for providing us with her expertknowledge on the topic of pediatric dysau-tonomia and significantly contributing tothe conceptualization and development ofthe restore Program.
the authors whose names are listedimmediately below certify that they have noaffiliations with or involvement in any orga-nization or entity with any financial interest(such as honoraria; educational grants; par-ticipation in speakers’ bureaus; membership,employment, consultancies, stock owner-ship, or other equity interest; and expert tes-timony or patent-licensing arrangements),or non-financial interest (such as personalor professional relationships, affiliations,knowledge or beliefs) in the subject matteror materials discussed in this manuscript.
no conflicts of interest or fundingto disclose.Correspondence to Jessica l. hawks, Ph.D.,Department of Psychiatry, university ofcolorado, 13123 east 16th avenue, B130,aurora, co 80045; [email protected]
Find a CBT Therapist
ABCT’s Find a CBT Therapistdirectory is a compilation of prac‐
titioners schooled in cognitive and
behavioral techniques. In addition
to standard search capabilities
(name, location, and area of exper‐
tise), ABCT’s Find a CBT Therapist
offers a range of advanced search
capabilities, enabling the user to
take a Symptom Checklist, review
specialties, link to self‐help books,
and search for therapists based on
insurance accepted.
We urge you to sign up for the
Expanded Find a CBT Therapist(an extra $50 per year). With this
addition, potential clients will see
what insurance you accept, your
practice philosophy, your website,
and other practice particulars.
To sign up for the Expanded Find
a CBT Therapist, click mEmBEr
logIn on the upper left‐hand of the
home page and proceed to the
ABCT online store, where you will
click on “Find CBT Therapist.”
For further questions, call the
ABCT central office at 212‐647‐
1890.
January • 2021 37

38 the Behavior Therapist
aBct’s 2020 convention differed from pre-vious conventions in ways big and small.the 54th annual meeting was held virtuallyfor the first time, of course, but the multi-day meeting also began with what usuallyoccurs late saturday: the presidentialaddress. Prerecorded a week prior to theaBct 2020 Virtual convention, Dr.martin (marty) antony delivered anengaging presentation, titled “cBt in theera of coViD-19.”
after a friendly introduction from theaBct President-elect (Dr. David tolin),current aBct President Dr. marty antonyopened his presidential address by dis-cussing the convention theme, “Betteraccess, Better outcomes: enhancing theimpact of Behavioral and cognitive thera-pies.” he also acknowledged several aBctmembers and staff who were critical to thedevelopment and execution of aBct’sfirst-ever virtual convention on relativelyshort notice: Dr. shannon wiltsey stirman,Dr. Daniel cheron, Dr. Katharina Kircan-ski, stephen crane, and the rest of theaBct staff who all helped to make thisyear’s convention a success (mary Janeeimer, David teisler, Dakota mcPherson,tonya childers, Veronica Bowen, amandamarmol, Kelli long, and stephanieschwartz).
though the 2020 convention theme wasdecided prior to the coViD-19 initial out-break and subsequent global pandemic, afocus on “access and outcomes” remainscritically important during the ongoingcoViD-19 pandemic. specifically, there isa critical need to increase access to evi-dence-based mental health treatments forpeople who cannot easily access them intraditional settings, and there is still roomto enhance outcomes for mental healthtreatments that have existed for decades. ina mere 65 minutes, Dr. antony skillfullycontextualized the convention’s themewithin the professional challenges andopportunities associated with the coViD-19 pandemic.
Dr. antony first discussed the psychol-ogy of pandemics, drawing largely from the
work of Dr. steven taylor, whose timelybook on the psychology of pandemics(taylor, 2020) can help us understand sev-eral intra- and interpersonal phenomenasalient to many of us today. For example,pandemics are associated with experiencessuch as uncertainty, confusion, urgency,and unpredictability; disruption in dailyroutines and the ability to satisfy basicneeds; economic, financial, housing, andfood instability; social isolation and loneli-ness; and the death of loved ones. extremebehaviors such as agoraphobic avoidance,excessive checking, reassurance-seeking,and cleaning rituals typically associatedwith psychopathology are common amongthe general public. Dr. antony highlightedhow pandemics strain health care systemsand disproportionately affect the poor dueto systemic and income-associated envi-ronmental variables. he also commentedon how pandemics are generally associatedwith a seeming rise of conspiracy theories,scientific misinformation, anti-sciencefalsehoods, and pseudoscientific claimsand “cures”—as well as how certain cogni-tive-behavioral and motivational inter-viewing strategies can be used to combatthem.
coViD-19 was not the only key eventin 2020, however: north america and theworld experienced tense political elections,natural disasters (e.g., wildfires, hurri-canes) tied to climate change, and murderhornets! another critical focus of 2020 cen-tered on race-related killings and race-based violence, leading to international dis-cussion around how to address systemicracism. aBct and several other high-pro-file organizations (e.g., american Psycho-logical association, american Psychiatricassociation, national association of socialworkers) released public statements, cre-ated task forces and workgroups, and havefocused resources toward ending the “pan-demic of racism.” Dr. antony acknowl-edged the interaction between coViD-19and systemic racism before reviewingresearch showing how coViD-19 dispro-portionately affects people from different
racial and ethnic backgrounds. Dr. antonycited research indicating hospitalizationrates differ across racial/ethnic groups(u.s. centers for Disease control and Pre-vention) as well as other studies showingthat although non-english speakers are lesslikely to receive coViD-19 tests than eng-lish speakers, non-english speakers aremore likely to test positive when they aretested (e.g., Kim et al., 2020). he also dis-cussed how ethnic and racial minorities areunderrepresented in coViD-related clini-cal trials, which poses serious limitationsand problems for equitably addressing thepandemic (chastain et al., 2020).
Dr. antony also addressed several chal-lenges and opportunities related to theenhancement of health and well-being byadvancing the scientific understanding,assessment, prevention, and treatment ofhuman problems through the global appli-cation of behavioral, cognitive, and biolog-ical evidence-based principles (that’s theaBct mission statement, in case youdidn’t know!). the coViD-19 pandemicand associated disruption in daily livinghas brought with it psychological, medical,social, vocational, and economic tolls,which could perhaps be exacerbated bysocial distancing and quarantine mandates.moreover, people may be engaging withsocial media and news outlets more oftenthan normal, which could potentially posedeleterious effects on mental health. manyprofessionals have also encounteredcoViD-related distress: the experiences ofanxiety, xenophobia, and traumatic stresssymptoms, which can be distressing andimpairing for many (asmundson &taylor, 2020; taylor et al., 2020). someinvestigators argue that coViD-19 and itsassociated consequences create “a perfectstorm” for suicide, although there ispresently insufficient evidence that suicidalideation and/or behavior has changed as aresult of the pandemic. Furthermore,although certain mental health conditionsseem especially likely to exacerbate due tothe pandemic (e.g., obsessive-compulsivedisorder [ocD] or depression), not allpeople with clinical disorders report moresevere mental health symptoms or func-tioning (e.g., Benatti et al., 2020). thus, asDr. antony reminded viewers, it is impor-tant not to make overly broad assumptionsin our professional roles as clinicians, edu-cators, and investigators.
next, Dr. antony discussed to the roleof cBt in the era and wake of coViD-19.he began by acknowledging the impressiveresponsiveness of mental health profes-sionals (including many aBct members)
NEWS
A Summary of Dr. Martin Antony’s ABCTPresidential AddressShannon M. Blakey, Durham VA Health Care System and VA Mid-Atlantic Mental Illness Research, Education and Clinical Center

January • 2021 39
a n t o n y ’ s p r e s i d e n t i a l a d d r e s s
in generating and disseminating psycho-educational and coping resources for thegeneral public, clinical materials and toolsto practitioners, and assessment scales foruse in coViD-related research. Dr.antony pointed to cBt interventionsdesigned to address the needs of front-lineworkers, including dissemination andimplementation efforts to train cliniciansand first responders in cBt for coViD-related distress. cognitive-behavioral andrelated techniques that might be particu-larly useful for addressing coViD-relateddistress include adopting flexible and bal-anced thinking (i.e., cognitive restructur-ing), confronting safe-yet-anxiety-provok-ing situations (i.e., exposure), engaging inpleasant and important activities (i.e.,behavioral activation), problem-solving,mindfulness and acceptance-based strate-gies, relaxation-based strategies, and com-munication training.
Dr. antony also acknowledged how thepandemic has pressed clinicians (as well aseducators and investigators) to be creativein translating and adapting “usual practice”in light of the real-world constraints onbehaviors and situations we may have pre-viously taken for granted (e.g., mcKay etal., 2020). other clinical challenges includediscriminating between an adaptive copingbehavior and an excessive “safety behavior”(e.g., thwaites & Freeston, 2005), whichcan vary over time as public health agenciesrevise health-related guidelines and recom-mendations. Beyond simply deliveringexisting treatments via teletherapy, notableadaptations of cBt referenced by Dr.antony include cBt for psychosis(Kopelovich & turkington, 2020), compli-cated grief (Boelen et al., 2020), social anx-iety (warnock-Parkes et al., 2020), post-traumatic stress disorder (PtsD; wells etal. 2020; wild et al., 2020), eating disorders(murphy et al., 2020), and ocD (Jassi et al.,2020; Krompinger et al., 2020). addition-ally, consultation with fellow aBct mem-bers and other professional colleagues canbe another helpful strategy for ensuringpatients receive the safest, yet also mostefficacious, care during this time.
Finally, Dr. antony turned to what hesaw as some potentially positive lastingconsequences, as well as general futuredirections. First, he discussed the ontariostructured Psychotherapy Program, whichfocuses on implementing a canadianprovince-wide, publicly funded, stepped-care cBt program for depression and anx-iety-related disorders (including PtsD andocD). informed by the improving accessto Psychological therapies (iaPt) pro-
gram in the united Kingdom, the ontariostructured Psychotherapy Program drawson teletherapy to increase access to cBt forcommon mental health problems, and willhopefully contribute valuable scientificknowledge about the utility and therapeu-tic effects of stepped cBt delivered overvirtual platforms. Dr. antony alsoexpressed what he hoped would be contin-ued research and policy efforts aimed ataddressing discrimination and systemicracism.
the year 2020 has certainly been ademanding and unprecedented year innumerous ways, several of which Dr.antony spoke to in his aBct presidentialaddress. Dr. antony—as well as othermembers of aBct’s Board of Directors,coordinators, committees, and full-timestaff—have all worked tirelessly for thisorganization and its members. if you havenot viewed Dr. antony’s presidentialaddress already, you can find it on demandalong with hundreds of other aBctrecorded offerings. You can also findcoViD-related aBct content athttps://www.abct.org/information/?m=minformation&fa=coViD19 and on theaBct Youtube channel (https://www.youtube.com/channel/ucue6712YKqw-pnf8uwfGp1kQ).
Referencesasmundson, G. J. G., & taylor, s. (2020).
coronaphobia revisited: a state-of-the-art on pandemic-related fear, anxiety,and stress. Journal of Anxiety Disorders,76. doi:10.1016/j.janxdis.2020.102326
Benatti, B., albert, u., maina, G., Fiorillo,a., celebre, l., Girone, n., Fineberg, n.,Bramante, s., rigardetto, s., & Dell'osso,B. (2020). what happened to patientswith obsessive compulsive disorderduring the coViD-19 pandemic? a mul-ticentre report from tertiary clinics innorthern italy. Frontiers in Psychiatry,11, 720. doi:10.3389/fpsyt.2020.00720
Boelen, P. a., eisma, m. c., smid, G. e., deKeijser, J., & lenferink, l. i. m. (2020).remotely delivered cognitive behaviortherapy for disturbed grief during thecoViD-19 crisis: challenges and oppor-tunities. Journal of Loss and Trauma.doi:10.1080/15325024.2020.1793547
chastain, D. B., osae, s. P., henao-martínez, a. F., Franco-Paredes, c.,chastain, J. s., & Young, h. n. (2020).racial disproportionality in covid clini-cal trials. New England Journal of Medi-cine, 383, e59.doi:10.1056/neJmp2021971
Jassi, a., shahriyarmolki, K., taylor, t.,Peile, l., challacombe, F., clark, B., &
Veale, D. (2020). ocD and coViD-19:a new frontier. Cognitive BehaviourTherapist, 13, e27.doi:10.1017/s1754470X20000318
Kim, l., Garg, s., o’halloran, a.,whitaker, m., Pham, h., … langley, G.e. (2020). risk factors for intensive careunit admission and in-hospital mortalityamong hospitalized adults identifiedthrough the us coronavirus Disease2019 (coViD-19)-associated hospital-ization surveillance network (coViD-net). Clinical Infections Diseases.doi:10.1093/cid/ciaa1012
Kopelovich, s. l., & turkington, D.(2020). remote cBt for psychosisduring the coViD-19 pandemic: chal-lenges and opportunities. CommunityMental Health Journal.doi:10.1007/s10597-020-00718-0
Krompinger, J. w., Kuckertz, J. m.,schreck, m., nota, J. a., Van Kirk, n., &Falkenstein, m. J. (2020). adapting expo-sure and response prevention in the ageof coViD-19. the Behavior Therapist, 43,166-171. retrieved from https://www.abct.org/docs/Pastissue/43n5.pdf
mcKay, D., minaya, c., & storch, e. a.(2020). conducting exposure andresponse prevention treatment for conta-mination fears during coViD-19: thebehavioral immune system impact onclinician approaches to treatment. Jour-nal of Anxiety Disorders, 74.doi:10.1016/j.janxdis.2020.102270
murphy, r., calugi, s., cooper, Z., & DalleGrave, r. (2020). challenges and oppor-tunities for enhanced cognitive behav-iour therapy (cBt-e) in light of coViD-19. Cognitive Behaviour Therapist, 13,e14. doi:10.1017/s1754470X20000161
reger, m. a., stanley, i. h., & Joiner, t. e.(2020). suicide mortality and coron-avirus Disease 2019: a Perfect storm?Jama Psychiatry. doi:10.1001/jamapsychiatry.2020.1060
taylor, s. (2020). The psychology of pan-demics: Preparing for the next global out-break of infectious disease. cambridgescholars Publishing.
taylor, s., landry, c. a., Paluszek, m. m.,Fergus, t. a., mcKay, D., & asmundson,G. J. G. (2020). Development and initialvalidation of the coViD stress scales.Journal of Anxiety Disorders, 72.doi:10.1016/j.janxdis.2020.102232
thwaites, r., & Freeston, m. h. (2005).safety-seeking behaviours: Fact or func-tion? how can we clinically differentiatebetween safety behaviours and adaptivecoping strategies across anxiety disor-ders? Behavioural and Cognitive Psy-chotherapy, 33, 177-188.doi:10.1017/s1352465804001985
u.s. centers for Disease control and Pre-vention (2020). Demographic trends of

40 the Behavior Therapist
coViD-19 cases and deaths in the usreported to cDc. covid.cdc.gov.retrieved from https://covid.cdc.gov/covid-data-tracker/#demographics
warnock-Parkes, e., wild, J., thew, G. r.,Kerr, a., Grey, n., stott, r., ehlers, a., &clark, D. m. (2020). treating social anxi-ety disorder remotely with cognitivetherapy. Cognitive Behaviour Therapist,13, e30.doi:10.1017/s1754470X2000032X
wells, s. Y., morland, l. a., wilhite, e. r.,Grubbs, K. m., rauch, s. a. m., acierno,r., & mclean, c. P. (2020). DeliveringProlonged exposure therapy via video-conferencing during the coViD-19pandemic: an overview of the researchand special considerations for providers.Journal of Traumatic Stress.doi:10.1002/jts.22573
wild, J., warnock-Parkes, e., murray, h.,Kerr, a., thew, G., Grey, n., clark, D.m., & ehlers, a. (2020). treating post-traumatic stress disorder remotely withcognitive therapy for PtsD. europeanJournal of Psychotraumatology, 11.doi:10.1080/20008198.2020.1785818
. . .
Dr. Blakey was supported by the Depart-ment of Veterans affairs office of academicaffiliations advanced Fellowship in mentalillness research and treatment. the viewsexpressed in this article are those of theauthor and do not necessarily reflect theposition or policy of the united states Gov-ernment or Department of Veterans affairs.
Correspondence to shannon m. Blakey,Ph.D., 3022 croasdaile rd., suite 300 (Visn6 mirecc), Durham, nc 27705;[email protected]
at last Year’s aBct convention inatlanta, Dr. Philip c. Kendall was awardedaBct’s career/lifetime achievementaward, recognizing his undeniablygroundbreaking contributions to the fieldof cognitive behavioral therapy, specificallyin the treatment of child and adolescentanxiety. as a Distinguished Professor attemple university, Dr. Kendall currentlyserves as the Director of the child andadolescent anxiety Disorders clinic,which has served thousands of childrenover the years and fostered generations ofpioneering youth mental healthresearchers. it would not be hyperbolic tosay that perhaps all of us within aBct arefamiliar with his work, whether this bethrough his influential papers (oftenrequired reading in graduate programs),through the use of coping cat with ourchild clients, or—for the most fortunateamong us—through direct collaboration.Dr. Kendall has been an integral figure inaBct for several decades, serving as PastPresident and as editor of the BehaviorTherapist.
in his lifetime achievement address,Dr. Kendall provided an overview of hisresearch on youth anxiety, first posing thequestion, “Do we want to tackle anxiety inyouth?” the answer here is an overwhelm-ing yes—research unequivocally showsthat failure to treat internalizing problemsin youth leads to a host of adult issues,including adult anxiety, depression, sub-stance use, and suicidality. “Do we want toremove all anxiety in youth?” no—rather,we should focus our efforts on giving chil-dren the necessary skills to cope with andadaptively manage anxiety. Dr. Kendallhighlighted that this requires considerationof how common behaviors that both par-ents and educators engage in contribute tothe maintenance and/or amplification ofyouth anxiety. these behaviors include (a)an intrusive and controlling style (e.g., “imust know what my child is doing at alltimes”), (b) the immediate involvement of
a mental health professional at the first signof anxiety (e.g., “my child is anxious abouther upcoming spelling test, it’s time to see aprofessional”), (c) efforts to avoid andescape the experience of anxiety-provokingsituations and associated negative emo-tions (e.g., “my child gets anxious whilespeaking to strangers, so i just speak forthem”), (d) prevention of limited risk-taking (e.g., “my students love soccer, but idon’t let them play during recess. theymay seriously injure themselves!”), (e)unpredictable and punitive caretakerbehaviors (e.g., inconsistently giving time-out or week-long grounding for similarmisdeeds), (f) modeling maladaptive anx-ious responding, and accommodating (e.g.,“oh my god, a spider!”). these behaviorsseverely jeopardize the child’s perceivedcapability to cope with distressing situa-tions and emotions and remove criticallearning experiences necessary for thedevelopment of adaptive responding.
next, Dr. Kendall highlighted the essen-tial elements to emphasize during the treat-ment of youth anxiety, (a) including astrong, collaborative therapist-child rela-tionship; (b) addressing anxious self-talk;(c) ensuring strengthening and generaliza-tion of in-session learning through home-work, which may be reinforced throughrewards; (d) problem solving; (e) psychoe-ducation regarding emotions; and, criti-cally (f) exposure tasks. Dr. Kendall notedthat community-based treatment provid-ers frequently ask, “wouldn’t exposure todistressing stimuli compromise the thera-peutic alliance, an essential element neces-sary for treatment engagement?” no,research demonstrates that exposure doesnot rupture alliance.
also highlighted was Dr. Kendall’sresearch demonstrating that early, effectivetreatment of youth anxiety reduces the riskof chronic depressive symptoms and suici-dal ideation. no doubt, many of us withinaBct now consider the points mentionedabove common knowledge; this under-
NEWS
A Synopsis of Dr. Philip C. Kendall’s LifetimeAchievement Award Address: “ManagingAnxiety in Youth: More Action Than Talk”Amy Sewart and Karla Lopez, California State University,Dominguez Hills

January • 2021 41
m a r q u e s ’ s i n v i t e d a d d r e s s
scores the importance and foundationalnature of Dr. Kendall’s research. theimportance of flexibility within fidelity, oradherence to scientifically supported inter-vention strategies while being flexible intheir application, was emphasized as criti-cal. Dr. Kendall’s address concluded withoutlining necessary future directions inchild anxiety research, including researchon optimal treatment approaches for non-responders, improved methods for dissem-inating evidence-based treatments, in-creased awareness and destigmatization of
child anxiety, early identification efforts,and a more dimensional understanding ofchildhood psychopathology aligning withthe research Domain criteria (rDoc).the address concluded with sincere appre-ciation for his colleagues and students, cur-rent and former, and acknowledgment oftheir critical role in the research above. Dr.Kendall ended his talk by saying, “i’m notdone yet.” we certainly look forward tonew research by Dr. Kendall and col-leagues.
. . .
no conflicts of interest or fundingto disclose.Correspondence to amy sewart, Ph.D.,california state university, Dominguezhills, 1000 east Victoria street, carson, ca90747; [email protected]
Dr. luana marQues and her lab at themassachusetts General hospital (mGh)community Psychiatry Program forresearch in implementation and Dissemi-nation of evidence-Based treatments(PriDe) strive to bridge the gap betweenscience and practice in diverse communi-ties using implementation science. Dr.luana marques started as a clinical psy-chology intern at mGh in Boston, ma,where she learned from and worked withindividuals who developed and tested evi-dence-based protocols across disorders.this work furthered her interest in servingdiverse communities, leading her to beginher current research at a satellite mGhlocated in chelsea, a primarily latinx area.mGh chelsea is home to many commu-nity-led initiatives to combat the high levelsof poverty and violence that afflict the area.
Why Is the Science-PracticeGap Important?
after years of working in the ivorytower in psychiatry at mGh, Dr. marquesexperienced, firsthand, the gap betweenscience and practice. For example, themajority of the population at mGhchelsea had acute trauma and a long
trauma history. though the mental healthproviders were determined to treat theirpatients, they did not have adequate train-ing in evidence-based protocols fortrauma. in fact, she later learned that ittakes 17 years for scientific findings toreach practice, and of these, only 14% endup reaching practice (Boren & Balas, 2000;institute of medicine, 2006). this meantthat it was unlikely that clinicians at mGhwere using the most current and well-vali-dated approaches.
Dr. marques noted that what was hap-pening at mGh chelsea was not an anom-aly, but part of a broader pattern of mentalhealth disparities in which communities ofcolor, particularly latinx and Black com-munities, do not have access to high-qual-ity mental health care, and as a result, theirmental health needs are not met (wells etal., 2001). a recent study highlighting dis-parities in the provision of mental healthservices showed that in massachusettsduring coViD-19, non-hispanic whitesused mental health services far more oftenthan Black and latinx communities despitethe disproportionate impact of coViD-19on racialized and marginalized communi-ties (Yang et al., 2020). Dr. marques’ lab,community Psychiatry PriDe, believes
that everyone deserves access to high qual-ity mental health care, and they activelywork towards this goal.
How to Bridge the Gapimplementation science, in combina-
tion with community-based participatoryresearch, can help bridge the gap betweenscience and practice. implementation sci-ence is the development of frameworks andguidelines that allow practitioners to tailormental health research to specific commu-nities. in community-based participatoryresearch, theory meets lived experience asresearchers work as equals with commu-nity partners to find community-specificsolutions to inaccessibility and poor qual-ity of care. to ensure the resulting treat-ments are respectful, accessible, and rele-vant, Dr. marques emphasized that diverseperspectives must be engaged at every level,from community members to staff andfrom organizations to communities.researchers need to think about how theycan give back to the communities theystudy, and develop reciprocity and rela-tionships. Dr. marques often asks her com-munity partners, “how can i be of service?”
What the Lab Has Done to Bridgethe Gap: Three Studies With Diverse
Populations
Study 1: Implementation ScienceApplied to Diverse Populations
though many of the patients at mGhchelsea were hispanic and most had histo-ries of chronic traumatic experiences, therewas limited use of evidence-based treat-ments (eBt) for PtsD among mentalhealth providers, contributing to the exist-ing gap between science and practice. mis-guided fears and perceptions surroundingeBt can contribute to therapists’ reluc-tance to learn eBt (marques, 2020). Dr.marques and her lab conducted a study
NEWS
Summary of Dr. Luana Marques’s InvitedAddress: “Leveraging Implementation Scienceand Community-Based Partnerships to Bridgethe Science-Practice Gap Among DiversePopulations”Dana Strauss, University of Ottawa
Jade Gallo, University of Connecticut

42 the Behavior Therapist
s t r a u s s & g a l l o
where cognitive Processing therapy(cPt) was analyzed to refine the trainingmanual to be more feasible for clinicians.their study used the replicating effectivePrograms (reP) Framework with threemain phases: (1) “Pre-conditions”(addressing barriers and facilitators of cPtat the provider level), (2) “Pre-implemen-tation” (adjusting the protocol for differentcultures; e.g., latino patients), and (3)“implementation” (determining theimpact of provider modification on patientoutcome). they found that provider mod-ifications that demonstrated greater fidelityto the treatment protocol were associatedwith larger reductions in PtsD symptoms.this research produced a cPt communitymanual that is culturally appropriate, feasi-ble, effective, and sustainable (Valentine etal., 2017).
Study 2: Developing a CBT Curriculumfor Justice-Involved Youth
the community Psychiatry PriDe labpartnered with roca in chelsea, a non-profit that works with young men at highrisk for a number of adverse psychosocialoutcomes (e.g., incarceration). roca wasusing an intervention model to help pro-vide positive outcomes for these youngmen; however, they were missing a mentalhealth component. they established an evi-dence-based manual to address this issue,thinking for a change (national instituteof corrections, & united states of america,2001), but this model failed to engage theparticipants. after the partnership, a needsassessment found that cBt was perceivedas too long, complex, and formal to addressthe issues facing the young men (e.g.,trauma, grief, substance use, anxiety,depression, and emotion dysregulation).Dr. marques and her team then designed asimple way to deliver and teach cBt skillsin small doses that would be engaging andimpactful for the men in roca. this led tocBt being practiced through formal andinformal deliveries, as frequently as possi-ble, with paraprofessionals possessing lowspecialization in mental health, who them-selves were like the men they were trying tohelp. they found that practicing at leastone cBt skill resulted in lower risk ofunenrolling from the roca program andincreased chances of maintaining a job.this research resulted in an integrated cur-riculum that provides training and supportfor staff, can be delivered by paraprofes-sionals, and fully addresses the needs of theparticipants while also being sustainable(marques, 2020).
one roca participant commented onthe skills he learned in the program: “if i’msad, instead of doing a bunch of drugs, ithink it’s, like, skill 2 or 3, feel your feelings,ride the wave. i just deal with my feelingswithout fogging my mind up with any-thing.” roca assistant Director, emily,said, “the cBt can kind of just give us thismore concrete way of talking about thingsthat we’ve already talked with youngpeople about many times, but it gives us,like, a format.” Xavier, another roca par-ticipant, reflected, “they teach you how tothink in other ways. they teach you how toact in line with your values, and not act onyour emotions. if i value being a model cit-izen and i value being free and not in jail,i’m not going to beat this person up and goto jail tonight.” though the staff had notexpected the youth to embrace the cBt-based curriculum, they greatly valued theskills they learned and were able to applythem to their everyday lives.
Study 3: Skills to Support Resilience:A Summer Internship for Chelsea Teens
while less than 1% of the u.s. popula-tion and the massachusetts populationcontracted coViD-19 during the pan-demic, it was contracted by 11% of chelsearesidents. in response to the increasedthreat of coViD-19 to chelsea residents,Dr. marques and her lab developed thePride summer scholars Program, a cBtprogram adapted for inner-city studentyouth (marques, 2020). the Pride summerscholars program ran for 4 weeks plus anadditional 5th week in which the studentscompleted a final project. it included 150youths ranging in age from 14 to 18+, andit was taught through virtual learning dueto the coViD-19 pandemic. the primarygoal of the program was to teach cBt asskills rather than therapy. the youths in theprogram reimagined cBt as thoughts,emotions and Behaviors (teB), and theylearned a new skill each week. they firstlearned the science of stress and observingthe teB cycle, then, charging up, facingtheir fears, exploring their thoughts, andthey completed a final project.
results showed that although studentsexpressed differences in the skills theyfound to be most helpful, most of the stu-dents that participated in the programfound all the skills helpful, and the majorityfound the skills helpful to apply to theirlives. one student described teB as allow-ing students to “learn to control their emo-tions, not overreact in school, not overre-act with their teachers, and as a way forthem to become better people in general.”
the students also believe these skills shouldbe integrated into school curricula to helpregulate emotions and generate positiveoutcomes. through this study, Dr. mar-ques and her lab were able to anchor fivenecessary skills: observe the teB cycle andcreate a “pause button”; explore thoughts(i.e., cognitive restructuring); problemsolve; charge up (i.e., behavioral activa-tion); and face fears (i.e., exposure ther-apy). this study demonstrated that theseskills can be taught through virtual learn-ing grounded in cBt. in order to bridgethe gap between science and practice, cBtmust be delivered in such a way that indi-viduals in diverse communities, in this caseinner-city latinx youth, can learn andapply basic cBt to their lives.
Conclusionimplementation science is a solid foun-
dation on which researchers can conceptu-alize, develop, and grow their research. itallows researchers to think about the chal-lenges that face diverse communities andask the questions that are relevant to thosecommunities. implementation sciencemust be done through equitable partner-ships in order to effectively bridge the gapbetween science and practice and increaseaccessibility and quality of care.
mental health care is still largely inac-cessible: 20% of adult americans strugglewith mental health (u.s. Department ofhealth and human services, 2016), andmental health professionals make up lessthan 1% of the u.s. population (andrilla etal., 2018). therefore, there is a critical needto train paraprofessionals, particularly indiverse communities, to increase accessthrough innovation.
Dr. marques’s lab at mGh chelsea,community Psychiatry Pride, haslaunched a training institute that providesa basic life skills curriculum, evidence-based training, customized coaching, andaccess to data anywhere. the goal is to trainas many paraprofessionals as possible tomake evidence-based mental health carewidely accessible and to breach thatsupply-and-demand gap in mental healthcare. You can learn more about Dr. mar-ques’s work at her website: drluana.com
Referencesandrilla, c. h. a., Patterson, D. G., Gar-
berson, l. a., coulthard, c., & larson, e.h. (2018). Geographic variation in thesupply of selected behavioral healthproviders. American Journal of Preven-tive Medicine, 54(6), s199-s207.

January • 2021 43
Balas, e. a., & Boren, s. a. (2000). Manag-ing clinical knowledge for health careimprovement. center for health careQuality, university of missouri.
institute of medicine (us) committee oncrossing the Quality chasm, adaptationto mental health, & addictive Disorders.(2006). Improving the Quality of HealthCare for Mental and Substance-Use Con-ditions: Quality Chasm Series. nationalacademy Press.
marques, l. (2020, november 18). Lever-aging implementation science and com-munity-based partnerships to bridge thescience-practice gap among diverse popu-lations. invited address live streamed atthe aBct 2020 54th annual convention[virtual conference].
national institute of corrections, &united states of america. (2001). Think-ing for a Change: Integrated CognitiveBehavior Change Program (lessonPlans). revised [ed.].
us Department of health and humanservices. (2016). National projections ofsupply and demand for selected behav-ioral health practitioners: 2013–2025.rockville, maryland. https://bhw.hrsa.gov/sites/default/files/bhw/healthwork-force-analysis/research/projections/behavioral-health2013-2025. pdf.
Valentine, s. e., Borba, c. P., Dixon, l.,Vaewsorn, a. s., Guajardo, J. G., resick,P. a., stirman, s. w., & marques, l.(2017). cognitive Processing therapy forspanish‐speaking latinos: a formativestudy of a model‐driven cultural adapta-tion of the manual to enhance imple-mentation in a usual care setting. Journalof Clinical Psychology, 73(3), 239-256.
wells, K., Klap, r., Koike, a., & sher-bourne, c. (2001). ethnic disparities inunmet need for alcoholism, drug abuse,and mental health care. American Jour-nal of Psychiatry, 158(12), 2027-2032.
Yang, J., landrum, m. B., Zhou, l., &Busch, a. B. (2020). Disparities in outpa-tient visits for mental health and/or sub-stance use disorders during the coViDsurge and partial reopening in massa-chusetts. General Hospital Psychiatry, 67,100-106.
. . .
the authors would like to thank Dr.monnica williams for mentorship, input,and guidance on this article.no conflicts of interest or fundingto disclose.Correspondence to Dana strauss, univer-sity of ottawa, 136 Jean-Jacques lussierPvt., ottawa, on, K1n [email protected]
it seems as thouGh each year at aBct’sannual convention we see great examplesof the potential for broad spectrum inter-ventions that move beyond diagnostic clas-sifications. these approaches fit neatlywithin the cognitive behavioral frameworkand mindset as the diagnostic taxons werenever rooted in the general principles wesee within cBt. setting aside the debateregarding diagnostic classification systems,Dr. allison harvey, a professor of psychol-ogy at the university of california, Berke-ley, provided another example of the effec-tive and broadly applicable approaches thatextend beyond a single diagnostic categoryand adds to the growing transdiagnosticmovement. the target this time? sleep dis-ruptions.
in her invited address, Dr. harvey pro-vided the empirically driven and scientifi-cally rigorous rationale for the use of trans-diagnostic approaches generally and asapplied to sleep more specifically. mostnotably, sleep disruptions occur within andexacerbate a host of problem types (e.g.,sarsour et al., 2010). Dr. harvey centeredmuch of this discussion on her and others’work within bipolar disorder. to thepoint, sleep disruptions lead to and forecastonset of manic and depressive episodes(Gruber et al., 2011). Further, addressingsleep-related problems improved out-comes for individuals with bipolar disorder(harvey et al., 2015). combining this withdata regarding the multiple mechanismsfor sleep disruption and the mechanismsthat maintain appropriate sleep function,she provided an overview of the develop-ment of transdiagnostic intervention forsleep and circadian Dysfunction (trans-c). trans-c follows the groundbreakingmodularized format chorpita and weiszdeveloped for treating emotional andbehavioral issues in children and adoles-cents (chorpita & weisz, 2009). Dr.harvey presented data that at least throughinitial clinical trials, trans-c appears effec-tive across a variety of sleep domains,though perhaps less with adolescents.
importantly, her data suggested thattrans-c reduces symptoms of other seri-ous mental illnesses in addition to improv-ing sleep. Dr. harvey ended her address bynoting the importance of translatingtrans-c into community-based settingsand testing the most crucial aspect of trans-diagnostic approaches more generally:expediting uptake of effective mentalhealth interventions and improving stan-dard of care.
Dr. harvey recounted her path to con-cluding that transdiagnostic researchneeded to prioritize implementation. herstory likely felt familiar to many of us ataBct. she came to realize that her clinicwhere she tested these wonderful innova-tions did not represent the broader com-munity. it is now almost cliché to acknowl-edge that clinical innovations do not reachthose who would be most likely to benefitfrom them and access to such innovationperpetuates the same inequality that wehave seen for decades. Dr. harvey is nowmoving forward to implement this inter-vention within community-based settingsto test the mechanism that makes transdi-agnostic approaches appealing, which isthat therapists have to learn fewer treat-ments to treat a greater number of clients.this has the potential to expand thenumber of people who can receive evi-dence-based interventions and at a com-munity-level improves the effectiveness ofour interventions. it ties directly to acommon public health formula that theoverall impact of an intervention operatesas a function of its effectiveness, its reachand the fidelity to the intervention when itis translated to a community setting.
i, personally, was relieved to see Dr.harvey’s move toward approaches thatconsider the overall impact of the interven-tion and seek to deliver on its promise toexpand access to quality mental health. Fortoo long our field has focused on improv-ing interventions without considering whohas access to them and how could wedesign them so that we are producing
NEWS
Invited Address: Dr. Allison Harvey andLooking to the Next Phase of TransdiagnosticInterventionsArthur R. Andrews III, University of Nebraska-Lincoln

44 the Behavior Therapist
equity rather than enriching the resourcesof those who already have access. movingtoward community-based implementationof transdiagnostic interventions for such across-cutting problem as sleep is a highlywelcome next step. at aBct, we shouldbe striving to move further down this path.if we are committed to inclusion andantiracism, we must continuously ask forwhom and by whom are our interventionsdesigned. without this, we will always fallshort in the full potential of cBt and sci-ence-based interventions.
Referenceschorpita, B. F., & weisz, J. r. (2009).
Modular approach to therapy for childrenwith anxiety, depression, trauma, or con-duct problems (match-aDtc).
Gruber, J., miklowitz, D. J., harvey, a. G.,Frank, e., Kupfer, D., thase, m. e.,sachs, G. s., & Ketter, t. a. (2011). sleepmatters: sleep functioning and course ofillness in bipolar disorder. Journal ofAffective Disorders, 134(1–3), 416–420.https://doi.org/10.1016/j.jad.2011.05.016
harvey, a. G., soehner, a. m., Kaplan, K.a., hein, K., lee, J., Kanady, J., li, D.,rabe-hesketh, s., Ketter, t. a., neylan,t. c., & Buysse, D. J. (2015). treatinginsomnia improves mood state, sleep,and functioning in bipolar disorder: apilot randomized controlled trial. Jour-nal of Consulting and Clinical Psychol-ogy, 83(3), 564–577.https://doi.org/10.1037/a0038655
sarsour, K., morin, c. m., Foley, K.,Kalsekar, a., & walsh, J. K. (2010). asso-ciation of insomnia severity and comor-bid medical and psychiatric disorders ina health plan-based sample: insomniaseverity and comorbidities. Sleep Medi-cine, 11(1), 69–74. https://doi.org/10.1016/j.sleep.2009.02.008
. . .
no conflicts of interest or fundingto disclose.Correspondence to arthur r. andrewsiii, Ph.D., 317 Burnett hall, university ofnebraska-lincoln, lincoln, ne [email protected]
PsYcholoGists anD researchers alikededicate much of their lives to improvingthe impact of psychological science, whichwe see in the implementation of new mea-sures, treatments, and frameworks. itbecame apparent to Dr. eric Youngstromthat the work of psychologists andresearchers often leaks through the currentpipeline, never making it to widespreadaudiences that need the information andresources most. this pipeline Youngstromspeaks of more specifically describes theprocess from the initial breakthrough inpsychological science to the intended ben-efit to the individual. the leaks in thispipeline Youngstrom speaks of includecost, language, and accessibility barriersthat are found around the world. throughdiscussion of the pitfalls within this processand his proposed open-source methods tolimit the information lost along the way,Dr. Youngstrom’s presentation fallsdirectly in line with the theme of aBct’s54th annual convention: “Better access,Better outcomes.”
Dr. Youngstrom envisions a world inwhich the public has immediate access tomaterials used by professionals within cen-tralized locations, thereby maximizingpotential benefit. a service thatYoungstrom sees as foundational for theimplementation of this open-access frame-work is wikipedia, the world’s largestonline encyclopedia and 13th most popu-lar website on the internet (alexa internet,2020; wikipedia, 2020). Youngstrom illus-trates his point by comparing the amountof views a “top 5% Journal Paper” wouldreceive (~3,000 views) to a “mediocre”wikipedia page, which garners approxi-mately 30,000 views. more specifically,wikipedia articles on psychological topicsgenerally garner approximately 100,000–1,000,000 views. the sheer amount ofmaterial that has come from wikipediaand subsequent audiences for such mater-ial is astounding, as is found within themetrics available on the platform. this
underscores the advantage of usingwikipedia alone as a location for profes-sionals and researchers to distribute theirwork, not to mention other services thatare available. while the information andwriting found on wikipedia may not meetthe quality standards or rigor expected ofacademic writing, wikiversity, a subserviceof wikipedia used by researchers and pro-fessionals alike, consists of information ofhigher quality (Youngstrom, 2018).Youngstrom highlighted that while most ofthese topics are consistently trafficked onboth platforms by humans who can correctmisinformation, wikipedia algorithmsdetermine that the information within psy-chological science pages tends to be of lowquality or infrequently updated.
a solution to this issue comes in theform of a function of wikipedia that actu-ally allows authors to submit their writtenwork directly to wikipedia for peer review,allowing the preliminary material to bepreviewed while undergoing the peer-review process. additionally, academicmaterial could be co-published throughwikipedia and scientific journals as well,further enhancing the reach that an articlecould have. another solution to this issueis that Youngstrom and Dr. mian-li ongdeveloped an organization called helpingGive away Psychological science(hGaPs). hGaPs originated as an orga-nization that aimed to keep various psy-chology-related wikipedia pages as up-to-date as possible with peer-reviewedcontent. hGaPs has since evolved into anorganization that explores various issuesand creatively answers the broader ques-tion of how to give away psychological sci-ence (Youngstrom & cotuna, 2020). otherprojects developed by hGaPs include theassessment center, a self-assessment andtriage service that utilizes assessment mea-sures found online for free to collectresponses and score responses (hGaPs,2020). this service allows individuals toundergo self-assessments for various psy-
NEWS
Summary of Eric Youngstrom’s Invited Address“Helping Give Away Psychological Science:Bringing the Best of Our Work to the PeopleWho Would Benefit”Joel Lopez, University of Connecticut

January • 2021 45
s e g a l ’ s i n v i t e d a d d r e s s
chological disorders to be used as an indi-cator for follow-on care. the assessmentcenter offers a service for clinicians as well,allowing for a patient’s responses to bescored and confidentially shared with theprovider online (hGaPs, 2020). theassessment center faces challenges in theirefforts to effectively accomplish their goalof giving away psychological science; forexample, language barriers, translations ofmeasures, and resources are required toacquire highest quality and most up-to-date measures.
another topic that Youngstrom dis-cussed at length is the idea of creativecommons. as people develop programsand processes to disseminate the informa-tion that has been created, there is animpasse surrounding ownership and right-ful compensation for the material that wascarefully curated. traditional ways to dis-tribute a publisher's information came inthe form of requesting permission andoften providing compensation for the pub-lished material. information that comesfrom open access journals is, as the namesuggests, open to the public for use and dis-tribution. Youngstrom discusses the vari-ous creative commons classifications andhighlights “cc-BY.” cc-BY means “cre-ative commons by…”, as in who the workis attributed to. this classification requiresonly kudos to the author, thereby negatingthe fees that are often associated with dis-tributing an author's work. as literaturebecomes older, it is a simple process to
change the distribution classification onthe work to cc-BY. this designationwould allow organizations to discuss anddisseminate the author’s work, andYoungstrom takes the audience through anexample on how to do this for their ownwork.
in summary, Dr. Youngstrom fulfilledthe intention set forth by aBct for their54th annual convention with his invitedaddress, and he embodies this with hisrelentless efforts to streamline the processof bringing psychological science to thepublic. Youngstrom’s high energy andengaging invited address was a highlight tothe scheduled presenters in their inauguralall-virtual convention. with the rapidadvancement of technology and increasedability for lay-people to access information,Youngstrom believes that the dissemina-tion process should come with ease as thereis a more explicit effort to effectively sharethis information in a mutually beneficialprocess. Youngstrom is leading the way fordeveloping creative and inexpensive waysto distribute their contributions to psycho-logical science, and urges professional andacademic research communities alike tofollow suit.
Referencesalexa. (2020). The top 500 sites on the web.
alexa internet.
helping Give away Psychological science.(hGaPs). (2020). Assessment Center.hGaPs.org/assessment-center.html
helping Give away Psychological science(hGaPs) (2020). Assessment Center forClinicians. hGaPs.org/for-clinicians.html
wikipedia. (2020). Largest encyclopedia.wikipedia.
Youngstrom, e. (2018). Students learnscience communication throughWikiversity. https://www.psychologi-calscience.org/observer/students-learn-science-communica tion-through-wikiversity.
Youngstrom, e., & cotuna, a. (2020).helping give away psychological science:Putting information and resources wherethe public and professionals can find anduse them. North Carolina Medical Jour-nal, 81(2), 117-119.
…
the author reports no conflicts of interestor funding to disclose.the author would like to thank Dr. monnicawilliams for mentorship, input, and guid-ance on this article.Correspondence to Joel lopez, universityof connecticut, Department of Psychologi-cal sciences, 406 Babbidge road, unit 1020,storrs, ct 06269-1020;[email protected]
one oF the inViteD aDDresses at thisyear’s aBct convention was delivered byDr. Zindel segal, a Distinguished Professorof Psychology in mood Disorders at theuniversity of toronto scarborough and asenior scientist in the campbell Familymental health research institute at thecentre for addiction and mental health.
a pioneer in the area of mindfulness med-itation interventions, he is one of thefounders of mindfulness Based cognitivetherapy (mBct) and has developed avariety of books, online tools, and otherresources for patients and therapists alike.
Dr. segal opened his address by high-lighting an unusual commercial that aired
on national tV during the election cover-age this month: 30 seconds of rain fallingon leaves. the ad was sponsored by calm,a digital application for meditation prac-tice. Dr. segal described the strong poten-tial for public health intervention arisingfrom this unique advertisement: a messageof mindfulness, with direct access (in theform of an app), viewed by tens of millionsof viewers. simultaneously, he noted, con-cerns come to mind: is calm evidence-based? if not, might such advertisementsdisrupt efforts within our field to dissemi-nate empirically supported mindfulnesstreatments?
Dr. segal’s address focused on a majorgap that exists in the current status ofmindfulness-based interventions: limitedpublic reach. For instance, in a review ofmindfulness intervention research he co-authored with Dr. sona Dimidjian (Dimid-jian & segal, 2015), approximately 98% ofresearch was dedicated to basic research,
NEWS
A Summary of Dr. Zindel Segal’s InvitedAddress “Strange Bedfellows Share MutualDreams: Increasing Access to Mindfulness-Based Interventions for Mood and AnxietyDisorders”Samantha Moshier, Emmanuel College

46 the Behavior Therapist
m o s h i e r
intervention development, and efficacystudies conducted in research clinics.Because meta-analyses (e.g., Goldberg etal., 2018) already provide support for theefficacy of mindfulness-based interventionfor anxiety and depression, Dr. segalargued that focusing on efficacy is likelynot the most productive avenue for futureresearch. instead, he said, the questionshould be asked: “how can we get clinicallyrobust treatments in the hands of morepeople?”
Dr. segal described this as the “chal-lenge of our field” in the coming years andpresented three examples of innovativework being done to address this problem.First, with a $100,000 grant for advertisingusing Google adwords, Dr. ricardomunoz and colleagues (2016) have imple-mented and evaluated a massive onlineopen intervention for smoking cessationtreatment. the intervention website wasviewed by hundreds of thousands of indi-viduals and the study enrolled over 7,000participants, a vast increase in sample sizecompared to that of the typical randomizedclinical trial for a face-to-face treatment.second, Dr. andrea Graham and col-leagues (2020) have partnered with pri-mary care networks to deliver digitaldepression and anxiety interventionsthrough a mobile platform, showing howdigital tools can be more easily rolled outwhen relying on patients’ existing relation-ships. Finally, the government of ontariohas responded to the coViD-19 pandemicby offering free mental health resources,including an online cBt program calledBeacon health, an effort that Dr. segalnoted will go far in reducing barriers tocare and normalizing the need for mentalhealth treatment.
acknowledging that these examples aresnapshots at the end of a longer journey,Dr. segal discussed his own experience inmaking mBct accessible to a wider audi-ence. he described that in the process ofdeveloping mBct, he had done everythingthat his graduate training had suggestedwas required for successful disseminationof a treatment: developing an efficacioustherapy, creating a treatment manual and apatient workbook, and publishing in top-tier journals. Yet these accomplishmentsdid not increase the adoption rate ofmBct into public spaces. in order toaddress this, he and Dr. Dimidjian havedeveloped, evaluated, and implemented adigital mBct intervention called mindfulmood Balance (mmB). their experienceof translating an evidence-based face-to-face treatment into a digital intervention
offers important lessons for aBct mem-bers with similar goals.
Dr. segal described that the essentialfirst step of digitizing a treatment is to iden-tify the core elements of intervention thatmust be captured in order to maintainfidelity. he gave several examples of howhe and his team “safeguarded” the corecomponents of mBct. First, mmB wasdeveloped to teach mindfulness in a scaf-folded manner similar to in-person mBct,focusing first on mindfulness of tangiblestimuli (activities or physical sensations),and moving on to intangible stimuli (emo-tions and thoughts). second, mmB re-cre-ated the tripartite learning consisting ofexperiential practice, didactic learning, andvicarious learning that takes place duringan in-person mBct group. For instance,participants might first complete a 30-minute breath meditation and would thenbe asked to reflect on their experiencethrough a series of written prompts. then,they could view a video of an in-persongroup discussing the same meditationpractice that they have just completed,allowing for consolidation of learning. Dr.segal also described how the online formatof mmB allowed for several new ways ofteaching the core skills and information:for instance, to encourage a metacognitiverelationship to thoughts, mmB contains anexercise in which patients can populate andrearrange a “playlist” of their most frequentautomatic thoughts.
Dr. segal next reported on the recentlypublished results of his randomized trialutilizing mmB to treat residual depressivesymptoms (segal et al., 2020). exemplify-ing his earlier point about the need toexpand mindfulness intervention researchbeyond the traditional efficacy study, thetrial was conducted among patients receiv-ing usual depression care within the KaiserPermanente health care system. Patientswere 460 individuals with residual symp-toms of depression and were randomlyassigned to receive either eight sessions ofmmB + usual depression care or usualdepression care alone. mmB was highlycost-effective and resulted in significantlygreater reductions in depressive symptoms,anxiety, and mental functioning relative tousual care alone. importantly, 60% ofpatients completed the minimum thera-peutic dose of four or more sessions,despite receiving only minimal supportfrom a coach by phone or email.
Dr. segal concluded his address by dis-cussing how we in the aBct communitycan best utilize our skills to help evidence-based treatments reach a broader audience.
he emphasized that we have a uniqueskillset: we are able to conceive of, develop,structure, and evaluate psychological treat-ments. however, we must step out of ourcomfort zone to ensure that these treat-ments don’t just “sit on a shelf.” to thisend, Dr. segal made two specific sugges-tions. First, we need to consider partneringwith those we may not usually collaboratewith. whether we find ourselves workingwith computer programmers or e-learn-ing experts, pursuing collaborations out-side of our academic spheres will increasethe reach of our treatments. Dr. segalemphasized that our biggest “zone of influ-ence” in these collaborations is ensuringtreatment fidelity. second, we need toacknowledge the role of commercializa-tion; money must be a part of the conversa-tion because it is required to develop andmaintain any digitally based therapy thatcan reach large numbers of individuals.relatedly, Dr. segal noted that outside thetraditional academic world, we may needto embrace alternative value sets; forinstance, satisfaction survey data may beweighed more heavily than efficacy data formany of our collaborators.
the development of the digital versionof mBct and its subsequent evaluationoutside the traditional research clinic is avaluable case study in making evidence-based care more widely available to thepublic. as calm’s election-day advertisingdemonstrates, myriad programs havebegun to fill the gaps that exist worldwidein access to mental health treatment. Dr.segal timely message encourages each of usto forge new paths and partnerships inorder to ensure that the options reachingthe public represent the best that our fieldhas to offer.
ReferencesDimidjian, s., & segal, Z. V. (2015).
Prospects for a clinical science of mind-fulness-based intervention. AmericanPsychologist, 70(7), 593-620.
Goldberg, s. B., tucker, r. P., Greene, P.a., Davidson, r. J., wampold, B. e.,Kearney, D. J., & simpson, t. l. (2018).mindfulness-based interventions for psy-chiatric disorders: a systematic reviewand meta-analysis. Clinical PsychologyReview, 59, 52-60.
Graham, a. K., Greene, c. J., Kwasny, m.J., Kaiser, s. m., lieponis, P., Powell, t.,& mohr, D. c. (2020). coached mobileapp platform for the treatment ofdepression and anxiety among primarycare patients: a randomized clinicaltrial. JAMA Psychiatry, 77(9), 906-914.

January • 2021 47
i n v i t e d p a n e l
muñoz, r. F., Bunge, e. l., chen, K.,schueller, s. m., Bravin, J. i., shaugh-nessy, e. a., & Pérez-stable, e. J. (2016).massive open online interventions: anovel model for delivering behavioral-health services worldwide. Clinical Psy-chological Science, 4(2), 194-205.
segal, Z. V., Dimidjian, s., Beck, a., Boggs,J. m., Vanderkruik, r., metcalf, c. a.,Gallob, r., Felder, J. n., & levy, J. (2020).outcomes of online mindfulness-basedcognitive therapy for patients with resid-ual depressive symptoms: a randomizedclinical trial. JAMA Psychiatry, 77(6),563-573.
. . .
no conflicts of interest or fundingto disclose.Correspondence to samantha moshier,Ph.D., emmanuel college, 400 the Fenway,Boston, ma 02115 [email protected]
the coViD-19 PanDemic has taken thelives of over 300,000 americans over thepast year, with minority groups showingdisproportional rates of death at more than2.7 to 3.3 times that of white americans(aPm research lab, 2020). Placingminorities at an even greater disadvantagethan nonminority individuals sufferingfrom coViD-19, minority populationshave historically experienced greater diffi-culties accessing both medical and mentalhealth care.
recent attention has been brought tothis significant gap in the experience ofcoViD-19 among minority versus non-minority populations, which has oftenbeen additionally discussed due to conver-sations surrounding racial injustice andsystemic racism that plague our country.as mental health professionals, there is acritical need to bring these conversationsinto our clinical care and to discuss waysthat both coViD-19 and systemic racismimpact the clients that we serve, and poten-tially more importantly, how we respond asclinicians. led by Dr. torrey creed, aninvited panel discussion at the 54th aBctconvention not only brought together bril-liant leaders in our field to discuss ways topromote better, equitable access to evi-dence-based mental health services in ourcountry, but also shared their own experi-ences and knowledge about essential nextsteps in clinical care, systems, and policy toaddress current issues in health disparitiesto care.
the panel opened with Dr. creed intro-ducing each of the panelists, whichincluded Dr. sosunmolu shoyinka from
the Department of Behavioral health andintellectual disability services; hectorayala from the hispanic communitycounseling services; Dr. amber callowayfrom the university of Pennsylvania; toddinman from the mental heaven show andFounder of aristocrat tV; and Dr. Karriemsalaam from Drexel university college ofmedicine. the panel had a special focus onPhiladelphia, which was the intended siteof the aBct convention before the pan-demic forced it to transition to being a vir-tual experience. the panelists initiallydescribed that Philadelphia has a long his-tory of innovating behavioral health treat-ments within a recovery-oriented, person-centered system to drive evidence-BasedPractices (eBPs), which helped agencies inPhiladelphia to quickly adapt and increaseaccess to necessary mental health servicesfor individuals and families at the begin-ning of the coViD-19 pandemic. the pan-elists shared some of their personal experi-ences during the pandemic, which has beena challenging period for all, but has beenespecially challenging for minority individ-uals and families. the panelists then high-lighted some of the barriers and solutionsthat were seen in Philadelphia when thecoViD-19 pandemic initially began andhow these barriers and solutions havechanged over the past year.
all four of the panelists described thelast 9 months as both transformative andchallenging. while Philadelphia is a“vibrant city full of diversity,” it is also oneof the largest and poorest cities in theunited states. all of the individuals on thepanel spoke passionately about work being
conducted in Philadelphia and their com-mitment to broad access of eBP among allindividuals and families. Dr. callowaydescribed that getting access to high-qual-ity eBPs into the system in a routine way ischallenging in “regular situations,” but thatchallenge was heightened exponentiallyduring the coViD-19 pandemic. Panelmembers discussed several immediatechanges that were incorporated inPhiladelphia to improve access to mentalhealth treatment, which included the citysuspending the need for prior authoriza-tions for providers, ability to set up alterna-tive payment methods, the sudden move totelehealth services for mental health, push-ing out materials through websites andother platforms, and agencies offeringguidance on unique ways to access care.
when stay-at-home orders were ini-tially placed and businesses were forced toclose their doors, many agencies began thetransition to serving clients solely throughtelehealth, although this transition was notswift or easy and worked better for someagencies compared to others. specifically,many agencies did not have the infrastruc-ture in place to quickly adopt telehealth orthe policies that accompany the shift to aremote platform. Disparities in the mentalhealth workforce additionally impacted theability to deliver telehealth during the pan-demic, as many clinicians had difficultyaccessing the typical needs for successfulwork and contacting clients, such as email,computer access, or stable internet connec-tion. Because of this, clinicians had tospend extra time in each work day todevelop strategies to conduct everydaywork activities.
while effort was being made to improveaccess to mental health services and careduring the pandemic, many logistical bar-riers impeded successful implementationof telehealth. First, many clients did nothave access to computers or stable internetconnections, forcing a significant amountof time in session being spent providing itsupport, which cut into time for delivery ofmental health treatment. Panelistsdescribed that these barriers have changedover the past year, but that they are consis-tent and continue to impact equitable
NEWS
Summary of Invited Panel: “Promoting Better,Equitable Access to Evidence-Based MentalHealth Services in a Community BehavioralHealth System”Angela Moreland, Medical University of South Carolina

48 the Behavior Therapist
m o r e l a n d
access to evidence-based mental health ser-vices. in addition, many clients were sud-denly faced with multiple additional rolesin the household, including working fromhome, assisting children with remote edu-cation, and household responsibilities.Because of these competing roles, manyclients had difficulty scheduling sessionsduring typical business hours or wereunable to schedule at all. many cliniciansmet this barrier by meeting the client wherethey were and agreeing to hold the sessionlate at night after the children went to bed,or over the weekend when additional assis-tance with childcare or other responsibili-ties was available.
while these methods were helpful,providers in community agencies werecoping with many of the same barriers thatclients faced, including childcare concerns,furlough from jobs, and loss of incomeamong other stressors. Privacy and spacealso served as a barrier for both clients andclinicians, as many sessions were con-ducted from cars, bathroom floors, or clos-ets in attempt to establish privacy on eitherthe clients end or the clinicians end withother family members also working orattending school from home.
offering a different perspective, Dr.salaam discussed his experiences as aprovider within an inpatient setting duringthe pandemic. he described that the typi-cal flow of patients did not change with thepandemic under way, as people continuedto have the same mental health problemsthat require inpatient hospitalization, butthat the manner in which care was deliv-ered changed in a significant way. Dr.salaam explained that the way providersdressed, the protective measures taken(PPe gear, face masks), and the cancelingof in-person sessions brought on addi-tional stress and often created distancebetween patients and clinicians. Further, allvisitation was suspended during parts ofthe pandemic, which impacted the criticalfamily and social support that clients need,especially during a time when more stressand anxiety are inherently present. whilethe impact on patients is clearly seen, stressand anxiety of clinicians was also height-ened given the constant worry about get-ting sick and the additional bandwidth nec-essary to keep themselves and their familiessafe. clinicians work very hard on a dailybasis to help patients decrease emotionalpain, but it becomes more difficult to pro-vide the needed support when the clinicianis constantly thinking about maintaininghis/her safety as well.
to provide some insight and next steps,Dr. creed asked the panel what they feelpeople have learned from the first 9months of the pandemic that has beenhelpful during this new surge. the pan-elists highlighted that people are dealingwith a great deal of change and are notalways prepared for it, coupled with the factthat the parameters of the pandemic areconsistently changing and can be over-whelming for individuals and families.People are dealing with a great deal of loss,including loss of jobs, loss of income, andisolation, which raises concern for mal-adaptive coping mechanisms. a mainlesson learned provided by the panelincluded the need for flexibility to addressthis constant change in parameters andnumbers, as well as openness to changes instructure, routine, rules, and everyday life.additionally, many panel membersstressed the importance of support systemsand finding unique ways to connect withother people, as well as the emphasis onself-care. while significant suffering andstress have surrounded the coViD-19pandemic, the silver lining is the enormousimprovement in access to care due to lever-aging technology and other unique ways toreach individuals and families. as this pan-demic continues, it is imperative that wecontinue to leverage the unique ways wehave connected with others while alsofocusing on the people and populationsthat are not being reached through tradi-tional mental health services.
Dr. creed thanked the panel membersfor their insightful thoughts and experi-ences, then transitioned to the topic of sys-temic racism and broadened awareness,posing the critical question of what strate-gies have been employed to address theseissues and what are the important stepsmoving forward. Dr. calloway opened thediscussing by noting that it is essential thatwe move beyond the notion that cognitivebehavioral therapy and mental health dis-orders are equal among all individuals, byacknowledging that they do not persist orexist in the same way across people fromdifferent identities and cultures. cliniciansacross the united states are increasinglyhaving conversations about how to incor-porate these differences into care and prac-tice. this power that clinicians hold has thebenefit of influencing outcomes and can bevery useful for clients, but power with thelack of insight into privilege and differ-ences across cultures can be harmful toclients and the field as a whole. thus, it iscrucial that clinicians increase their knowl-edge of the lived experience of their clients
and not assume that racism is a new con-cept, although broad awareness might be.Given health disparities in mental healthcare, minorities often experience myriadadditional stressors when compared tononminority individuals, and cliniciansneed to understand how these stressors canlead to negative mental health outcomes.Because of this, it is critical to build cultur-ally responsive techniques into every aspectof mental health services, and particularlycognitive behavioral therapy, to ensure thatwe are considering cultural backgroundand experiences of clients in assessment,case conceptualization, treatment plan-ning, ongoing treatment, and termination.
Given the enormous impact that cul-tural identification has on all treatmentcomponents, it is the clinician’s responsi-bility to invite conversations about culturalbackground, systemic racism, and experi-ences, and to critically and carefully exam-ine how they impact treatment. the pan-elists discussed that successful mentalhealth treatment is built upon rapport withthe client, which cannot be built withoutunderstand the client’s background andexperiences.
this invited panel discussion concludedwith Dr. creed asking about next steps andwhat the panelists would like to see in ourfield moving forward. the panelists pro-vided several suggestions with the themerevolving around agencies and systemsbuilding an infrastructure to specificallyfocus on systemic racism and making aneeded shift within and among clinics tosustain implementation of culturallyresponsive therapies. this could includeadaptation of eBPs to create connectionwith patients and incorporate culturalexperiences and background, but the panelmembers felt that it was essential to con-sider the factors discussed in that panelwhen connecting with clients and deliver-ing evidence-based interventions.
. . .
no conflicts of interest or fundingto report.Correspondence to angela D. moreland,Ph.D., national crime Victims research andtreatment center, medical university ofsouth carolina, 67 President street, 2 south,charleston, sc [email protected]

January • 2021 49
DesPite General imProVements in theefficacy of empirically supported treat-ments for psychological disorders, bothclinicians and researchers continue to befaced with an ever-present problem as oldas the field of psychotherapy itself. a sig-nificant proportion of patients either con-tinue to experience treatment nonresponseor experience a relapse of symptoms post-treatment. methods to enhance precisionand individualization of evidence-basedtreatments are critical to the improvementof treatment outcomes. to discuss currentapproaches aimed at creating more tar-geted and effective interventions, aBct2020 hosted an invited panel entitled “Per-sonalizing treatment to improve cBtoutcomes,” moderated by Dr. michellecraske, a past president of aBct and aDistinguished Professor of Psychology atthe university of california, los angeles.
First, Dr. Jacqueline Persons (oaklandcBt center) provided her case-formula-tion-driven approach as a means toenhance treatment response (Persons,2006). taking a hypothesis-testingapproach to each case, selected interven-tions are guided by evidence-based theory,ongoing assessment (i.e., measurement-based care), and process monitoring (i.e.,homework compliance, working alliance).current findings suggest that individual-ized (i.e., “modularized”) applications ofempirically supported treatment elementsguided by case-formulation-driven princi-ples are comparable to (Persons et al.,2006) or outperform (lewis et al., 2019;weisz et al., 2012) standard, manualizedtreatment protocols. Dr. rob Derubeis(university of Pennsylvania) completedthis approach in the second presentation,which discussed the use of multivariatemodels, such as the employment of “prog-nostic indices”—composite variables ofmultiple pre-treatment characteristics (i.e.,moderators)—as a promising tool for indi-vidualized matching to an appropriate levelof care (lorenzo-luaces et al., 2017). thiseffort addresses the lack of replicability forsingle moderators across randomized con-
trolled trials, limitations to multiple mod-erator analyses with shared underlyingconstructs, and, hypothetically, dropoutthrough better-matched care.
next, Dr. aaron Fisher (university ofcalifornia, Berkeley) discussed the use ofindividual-level behavioral data to person-alize psychotherapy, wherein individualcharacteristics inform (a) personalizedcontent and sequencing of modularized,evidence-based treatments and (b) “just-in-time” adaptive interventions. critically,Dr. Fisher highlighted that nomothetic sta-tistical approaches traditionally used intherapy outcome research, which assessbetween-group differences, fail to captureintraindividual experiences and outcomesthat are essential to treatment personaliza-tion (Fisher et al., 2018). with lack ofgroup-to-individual generalizability, Dr.Fisher emphasized the need to create gen-eralizable processes for model derivationand construction that facilitate the reliablecreation of personalized models.
Finally, Dr. Greg siegle (university ofPittsburgh) presented ways in which neu-roscience can be harnessed to personalizecognitive behavior therapies to enhanceoutcomes. Dr. siegle highlighted thatneural predictors of nonresponse (e.g.,decreased executive control) are not neces-sarily targeted directly within cognitivebehavior therapies, and methods to inter-vene upon these predictors through afford-able adjunctive training (e.g., cognitivecontrol; siegle et al., 2014) and “emotionprosthetics” (e.g., a vibrating wrist strap toassist with emotion regulation through anincrease in parasympathetic tone) haveshown promise in optimizing treatmentresponse.
During the Q&a, important considera-tions in the implementation of treatmentpersonalization methods were discussed.the panel noted that improving treatmentresponse requires that we also focus effortson reducing demoralization during ther-apy and subsequent dropout, and toachieve this requires that we listen to andrespect patient treatment preferences—
even when this preference is perhaps con-traindicated by research indicating whowill and will not respond, or what treat-ment module best maps onto one’s pri-mary presenting problems. the benefits ofpersonalized treatment using a modular-ized or component-based approach tar-geted at identified deficits were discussedfurther, including potential cost-cuttingthrough briefer interventions and per-ceived translatability and acceptabilityamong real-world settings. at this time, asDr. siegle noted, insurance companies donot reimburse for assessments that informindividualized treatment and a shift inwhat insurance covers as part of psy-chotherapy is necessary. Furthermore, dis-semination of aforementioned technolo-gies is a notoriously long process. Dr. siegleurged collaboration with industry toincrease the rate at which these technolo-gies can be tested within real-world set-tings. Finally, Dr. Fisher noted that we needto be able to effectively communicate thepurpose of assessment methods to patientsto reduce perceived burdensomeness andenhance acceptability. in sum, this panelhighlighted various promising methods topersonalize cognitive behavioral therapiesinformed by data ranging from self-reportto neuroimaging, and through the applica-tion of advanced statistical and conceptualmodels. efforts presented by these panelistsare promising and bring us one step closerto cracking the code of treatment nonre-sponse and symptom relapse, and, mostimportant, to having the ability to provideevery individual psychotherapy that worksbest for each individual.
ReferencesFisher, a. J., medaglia, J. D., & Jeronimus,
B. F. (2018). lack of group-to-individualgeneralizability is a threat to human sub-jects research. Proceedings of the NationalAcademy of Sciences, 115(27), e6106–e6115.
lewis, c. c., Boyd, m., Puspitasari, a.,navarro, e., howard, J., Kassab, h.,hoffman, m., scott, K., lyon, a., & Dou-glas, s. (2019). implementing measure-ment-based care in behavioral health: areview. JAMA Psychiatry, 76(3), 324–335.
lorenzo-luaces, l., Derubeis, r. J., vanstraten, a., & tiemens, B. (2017). aprognostic index (Pi) as a moderator ofoutcomes in the treatment of depression:a proof of concept combining multiplevariables to inform risk-stratified steppedcare models. Journal of Affective Disor-ders, 213, 78–85.
NEWS
Summary of Invited Panel “PersonalizingTreatment to Improve CBT Outcomes”Amy Sewart and Amanda Brashear, California State University,Dominguez Hills

50 the Behavior Therapist
s e w a r t
Persons, J. B. (2006). case formulation–driven psychotherapy. Clinical Psychol-ogy: Science and Practice, 13(2), 167–170.
Persons, J. B., roberts, n. a., Zalecki, c.a., & Brechwald, w. a. G. (2006). natu-ralistic outcome of case formulation-driven cognitive-behavior therapy foranxious depressed outpatients. BehaviourResearch and Therapy, 44(7), 1041–1051.
siegle, G. J., Price, r. B., Jones, n. P., Ghi-nassi, F., Painter, t., & thase, m. e.(2014). You gotta work at it: Pupillaryindices of task focus are prognostic for
response to a neurocognitive interven-tion for rumination in depression. Clini-cal Psychological Science, 2(4), 455–471.
weisz, J. r., chorpita, B. F., Palinkas, l. a.,schoenwald, s. K., miranda, J., Bearman,s. K., Daleiden, e. l., ugueto, a. m., ho,a., martin, J., Gray, J., alleyne, a.,langer, D. a., southam-Gerow, m. a.,Gibbons, r. D., & research network onYouth mental health, and the. (2012).testing standard and modular designsfor psychotherapy treating depression,anxiety, and conduct problems in youth:a randomized effectiveness trial.
Archives of General Psychiatry, 69(3),274–282. https://doi.org/10.1001/archgenpsychiatry.2011.147
. . .
no conflicts of interest or fundingto disclose.Correspondence to amy sewart, Ph.D.,california state university, Dominguezhills, 1000 east Victoria street, carson, ca90747; [email protected]
To coincide with the its 54th AnnualConvention, ABCT launched its inau-gural Briefing Books project. The ini-tiative is the brainchild of Emily L.Bilek, Ph.D., ABPP, of the PublicEducation and Media Dissemination(PEMD) Committee, and DavidTeisler, CAE, Director of Communi-cations/Deputy Director. PEMD coor-dinates projects with the Publica-
tions Committee and handles press relations for ABCT. Thedriving force behind the Briefing Books was the desire to pro-vide resources for media and the public who want quickaccess to materials that explain evidence-based treatmentsfor mental health. In January the committee put out a call tomembers asking for volunteers to spearhead the project andmanage a small team to produce these resources. Fast trackto November and the first Briefing Book is available to down-load on the ABCT website.
The first Briefing Book is entitled Suicide Across theLifespan, with 160-plus pages covering the prevalence ofdeath by suicide in youth (5 to 24 years), adulthood andmidlife, and seniors. In addition, death by suicide within sexu-al and gender minorities and veterans is included, as well asthe contributing role of nonsuicidal self-injury, trauma, anddisease.
The book’s editor and contributing author of the Seniors &Veterans section of the Briefing Book’s project, Rita Hitching,MSc., explains the reasoning behind the decision to cover sui-cide in the first edition: “Our first issue is being released at atime when society is experiencing an unprecedented level ofstress. Emotionally demanding circumstances, persistentstress, and depression are strong risk factors for suicide, and
when someone ends their own life, the impact is felt by theentire community, and often, long after the event. The globalcoronavirus pandemic has led to a substantial increase in thenumber of people experiencing anxiety and depression, and2020 has highlighted many social injustices and inequities.We felt that by providing evidence-based information that wasaccessible to all on death by suicide would be very timely.”
By design, and with the needs of the reader in mind, flexi-bility has been built in by providing the option to download theentire book or individual sections. The book, or its sections,can provide useful background information for the busy jour-nalist, as well as supplement the available expertise offeredvia phone or Zoom conversation by volunteer ABCT subjectmatter experts through the ABCT office.
Each of the six Briefing Book sections can stand alone,and covers the risk and protective factors, assessment, andtreatment of suicidal behavior. Sections are co-authored byABCT members and leading experts in their field, includingPeggy Andover, Ph.D., who contributed to the Non-SuicidalSelf-Injury section; Emily Bilek, Ph.D., who wrote the Adults &Mid-Life section; Lily Brown, Ph.D., who wrote the Trauma &Disease section; Mitch Prinstein, Ph.D., and his teamBenjamin W. Nelson, Ph.D., Maya Massing-Schaffer, M.A.,who penned the Youth section; and Iliana Seager van Dyk,Ph.D., who contributed the section on Sexual & GenderMinorities. The Briefing Books team hope, in future, to writeabout other topics such as PTSD, stress, gun violence, schoolshootings, grief, and survivor's guilt, to name a few.
ABCT Launches Inaugural Briefing Books Initiative

the aBct convention is designed for scientists, practitioners, students, and scholars whocome from a broad range of disciplines. the central goal is to provide educational experi-ences related to behavioral and cognitive therapies that meet the needs of attendees acrossexperience levels, interest areas, and behavioral and cognitive theoretical orientations. somepresentations offer the chance to learn what is new and exciting in behavioral and cognitiveassessment and treatment. other presentations address the clinical-scientific issues of howwe develop empirical support for our work. the convention also provides opportunities forprofessional networking. the aBct convention consists of General sessions, targeted andspecial Programming, and ticketed events.
aBct uses the cadmium scorecard system for the submission of general session events.the step-by-step instructions are easily accessed from the abstract submission Portal, andthe aBct home page. attendees are limited to speaking (e.g., presenter, panelist, discus-sant) during no more than Four events. as you prepare your submission, please keep inmind:
• Presentation type: For descriptions of the various presentation types, please visithttp://www.abct.org/conventions/?fa=understanding_the_aBct_convention• Number of presenters/papers: For symposia please have a minimum of four presenters,including one or two chairs, only one discussant, and 3 to 5 papers. the total number ofspeakers may not exceed 6. symposia are either 60 or 90 minutes in length. the chair maypresent a paper, but the discussant may not. symposia are presentations of data, usuallyinvestigating the efficacy, effectiveness, dissemination or implementation of treatmentprotocols. For Panel Discussions and clinical round tables, please have one moderator andbetween three to five panelists.• Title: Be succinct.• Authors/Presenters: Be sure to indicate the appropriate order. Please ask all authorswhether they prefer their middle initial used or not. Please ask all authors their degree,aBct category (if they are aBct members), and their email address. (Possibilities for“aBct category” are current member; lapsed member or nonmember; postbaccalaureate;student member; student nonmember; new professional; emeritus.)• Institutions: the system requires that you enter institutions before entering authors. thisallows you to enter an affiliation one time for multiple authors. Do not list DePart-ments. in the following step you will be asked to attach affiliations with appropriateauthors.• Key Words: Please read carefully through the pull-down menu of defined keywords anduse one of the keywords on the list. Keywords help aBct have adequate programmingrepresentation across all topic areas.• Objectives: For symposia, Panel Discussions, and clinical round tables, write three state-ments of no more than 125 characters each, describing the objectives of the event. samplestatements are: “Described a variety of dissemination strategies pertaining to the treatmentof insomnia”; “explained data on novel direction in the dissemination of mindfulness-basedclinical interventions.”• Overall: ask a colleague to proof your abstract for inconsistencies or typos.
For an in-depth explanation of aBct’s convention program, including the differencesamong ticketed, general, and special programming, visit us at:
www.abct.org > Conventions & CE > Understanding the ABCT Convention
Questions? FaQs are at http://www.abct.org/conventions/ > abstract submission FaQs
Thinking about submitting anabstract for the ABCT 55thAnnual Convention in NewOrleans? the submission portal willbe opened from February 8–march 8.look for more information in the com-ing weeks to assist you with submittingabstracts for the aBct 55th annualconvention. the deadline for submis-sions will be 3:00 a.m. (est), Feb. 8-march 8.
Preparingto Submit
an Abstract
ABCT’s 55th Annual ConventionNovember 18–21, 2021 • New Orleans
January • 2021 51
52 the Behavior Therapist
call 55th Annual ConventionNovember 18–21, 2021 | New Orleans
ticketedsessions
for Ticketed Sessions
Workshops & Mini WorkshopsWorkshops cover concerns of the practitioner/ educator/researcher. Workshopsare 3 hours long, are generally limited to 60 attendees, and are scheduled forFriday and Saturday. Please limit to no more than 4 presenters. Mini Workshopsaddress direct clinical care or training at a broad introductory level. They are 90minutes long and are scheduled throughout the convention. Please limit to nomore than 4 presenters. When submitting for Workshops or Mini Workshop,please indicate whether you would like to be considered for the other format aswell.
For more information or to answer any questions before you submit yourabstract, email Christina Boisseau, Workshop Committee Chair, [email protected]
InstitutesInst itutes, designed for clinical practitioners, are 5 hours or 7 hours long, aregenerally limited to 40 attendees, and are scheduled for Thursday. Please limit tono more than 4 presenters.
For more information or to answer any questions before you submit yourabstract, email Samantha G. Farris, Institutes Committee Chair, [email protected]
Master Clinician SeminarsMaster Clinician Seminars are opportunities to hear the most skilled cliniciansexplain their methods and show taped demonstrations of client sessions. Theyare 2 hours long, are limited to 40 attendees, and are scheduled Friday throughSunday. Please limit to no more than 2 presenters.
For more information or to answer any questions before you submit yourabstract, email Tejal Jakatdar, Master Clinician Seminars Committee Chair,[email protected]
Research and Professional DevelopmentPresentations focus on “how to” develop one’s own career and/or conductresearch, rather than on broad-based research issues (e.g., a methodological ordesign issue, grantsmanship, manuscript review) and/or professional develop-ment topics (e.g., evidence-based supervision approaches, establishing a privatepractice, academic productivity, publishing for the general public). Submissionswill be of specific preferred length (60, 90, or 120 minutes) and format (panel dis-cussion or more hands-on participation by the audience). Please limit to no morethan 4 presenters, and be sure to indicate preferred presentation length and for-mat.
For more information or to answer any questions before you submit yourabstract, email Cole Hooley, Research and Professional Development Committee Chair,[email protected]
Information about the con-vention and how to submit
abstracts will be on ABCT'swebsite, www.abct.org,after January 1, 2021.
Submission deadline: February 8, 2021, 3:00 A.M. ESTPortal Opens: Monday, Jan. 4
Conference Theme:
“Championing CBT:Promoting Cognitive
and BehavioralPractice and Science
in the Context ofPublic Health,Social Justice,
Policy, Research,Practice, and
Training”

January • 2021 53
ABCT is proud to announce the 2021 convention theme of Championing CBT:Promoting Cognitive and Behavioral Practice and Science in the Context of PublicHealth, Social Justice, Policy, Research, Practice, and Training.
Sometimes it can feel like swimming against a strong current when advocating forcognitive and behavioral science and practice (i.e., henceforth, "CBT") outside of ourclose professional circles. The international landscape of mental health prevention,intervention, and training is replete with alternative theories, practices, and inter-ests. The 2021 Annual Convention will place a spotlight on success stories, trials,and lessons learned related to promoting CBT and differentiating it from the othermental health worldviews. In doing so, the ABCT community will come together for arich discussion that facilitates a core component of the organization's mission tofacilitate "the global application of behavioral, cognitive, and biological evidence-based principles." Examples of topics consistent with this theme include, but are notlimited to, the following (in no particular order):
• Advocating for the value of CBT in the priorities of major funding agencies andorganizations (e.g., importance of promoting cognitive and behavioral sciencewithin the NIMH RDoC framework).
• Providing a platform for CBT in the context of social justice (e.g., using cognitiveand behavioral science and practice to affect change in prejudice and stigma).
• Encouraging CBT with policymakers to enhance public health through scienceand practice (e.g., adopting cognitive and behavioral science and practice toreduce unhealthy behaviors, like smoking).
• Promoting CBT priorities in the training of the mental health researchers andpractitioners of tomorrow (e.g., encouraging CBT principles as part of establish-ing training competencies and standards).
• Educating the public about CBT on social media and other public-facing plat-forms (e.g., impacting public perception of CBT via #CBTWorks).
• Supporting dissemination and implementation of CBT (e.g., integrating CBTprinciples in a population-level health initiative or system).
Submissions may be in the form of symposia, clinical round tables, panel discus-sions, and posters. Information about the convention and how to submit abstractswill be on ABCT's website, www.abct.org, after January 1, 2021. The online submis-sion portal for general submission will open on February 8, 2021.
DDeeaadldliinene for subfor submismissions:sions: Monday, March 8, 2021
••• P RO G R A M C H A I R : Gregory Chasson •••••• A S S O C I AT E P RO G R A M C H A I R : Elizabeth Katz •••
generalsessions
CALL for PAPERS
*

54 the Behavior Therapist
Understanding the ABCT ConventionGENERAL SESSIONS
there are between 150 and 200 generalsessions each year competing for yourattention. an individual must limit to6 the number of general session submis-sions in which he or she is a sPeaKer(including symposia, panel discussions,clinical round tables, and research spot-lights). the term sPeaKer includes rolesof chair, moderator, presenter, panelist,and discussant. acceptances for any givenspeaker will be limited to 4. all generalsessions are included with the registrationfee. these events are all submittedthrough the aBct submission system.the deadline for these submissions is 3:00a.m. et, monday, march 8, 2021.General session types include:
Symposia. In responding to conventionfeedback requesting that senior research-ers/faculty present papers at symposia,while also recognizing the importance ofopportunities for early career, student, andpostdoctoral fellows to present their work,we strongly encourage symposia submis-sions that include a mix of senior and earlycareer presenters. Presentations of data,usually investigating the efficacy, effective-ness, dissemination or implementation oftreatment protocols. symposia are either60 or 90 minutes in length. they have oneor two chairs, one discussant, and betweenthree and five papers. the total number ofspeakers may not exceed 6.
Clinical Round Tables. Discussions (ordebates) by informed individuals on acurrent important topic directly related topatient care, treatment, and/or the appli-cation/implementation of a treatment.examples of topics for clinical roundtables include (but are not limited to)challenges/suggestions for treating a cer-tain disorder or group of patients, appli-cation of a treatment protocol or type oftreatment to a novel population, consid-erations in applying cBts to marginal-ized communities and/or minoritygroups. some topics may be appropriatefor either clinical round tables or PanelDiscussions, and authors are invited touse their judgment in making this deci-sion. clinical round tables are organizedby a moderator and include between three
and six panelists with a range of experi-ences and attitudes. the total number ofspeakers may not exceed 7.
Panel Discussions. Discussions (ordebates) by informed individuals on acurrent important topic that are concep-tual in nature, rather than pertainingdirectly to clinical care. examples of top-ics for panel discussions include (but arenot limited to) supervision/trainingissues, ethical considerations in treatmentor training, the use of technology in treat-ment, and cultural considerations in theapplication of cBts. some topics may beappropriate for either clinical roundtables or Panel Discussions, and authorsare invited to use their judgment in mak-ing this decision. these are organized by amoderator and include between three andfive panelists with a range of experiencesand attitudes. the total number of speak-ers may not exceed 7.
Spotlight Research Presentations. thisformat provides a forum to debut newfindings considered to be groundbreakingor innovative for the field. a limited num-ber of extended-format sessions consist-ing of a 45-minute research presentationand a 15-minute question-and-answerperiod allows for more in-depth presenta-tion than is permitted by symposia orother formats.
Poster Sessions. one-on-one discussionsbetween researchers, who display graphicrepresentations of the results of theirstudies and interested attendees. Becauseof the variety of interests and researchareas of the aBct attendees, between1,200 and 1,500 posters are presentedeach year.
TARGETED and SPECIALPROGRAMMING
targeted and special programming eventsare also included with the registration fee.these events are designed to address arange of scientific, clinical, and profes-sional development topics. they also pro-vide unique opportunities for networking.invited addresses/Panels. speakers well-established in their field, or who holdpositions of particular importance, share
their unique insights and knowledge.
Mini Workshops. Designed to addressdirect clinical care or training at a broadintroductory level and are 90 minuteslong.
Clinical Grand Rounds. clinical expertsengage in simulated live demonstrationsof therapy with clients, who are generallyportrayed by graduate students studyingwith the presenter.
Membership Panel Discussion. organ-ized by representatives of the member-ship committees, these events generallyemphasize training or career develop-ment.
Research Facilitation Sessions. organ-ized by members of the researchFacilitation committee, these events aimto highlight research resources for thosewho study or practice behavioral and cog-nitive principles.
Special Sessions. these events aredesigned to provide useful informationregarding professional rather than scien-tific issues. For more than 20 years, theinternship and Postdoctoral overviewshave helped attendees find their educa-tional path. other special sessions ofteninclude expert panels on getting intograduate school, career development,information on grant applications, and ameeting of the Directors of clinicaltraining.
Special Interest Group (SIG) Meetings.more than 40 siGs meet each year toaccomplish business (such as electing offi-cers), renew relationships, and often offerpresentations. siG talks are not peer-reviewed by the association.
Research and Professional Development.Provides opportunities for attendees tolearn from experts about the developmentof a range of research and professionalskills, such as grant writing, reviewingmanuscripts, and professional practice.

January • 2021 55
TICKETED EVENTSticketed events offer educational oppor-tunities to enhance knowledge and skills.these events are targeted for attendeeswith a particular level of expertise (e.g.,basic, moderate, and/or advanced).ticketed sessions require an additionalpayment. the deadline for these submis-sions is 3:00 am et, monday, February8, 2021.
Clinical Intervention Training. one-and two-day events emphasizing the"how-to" of clinical interventions. theextended length allows for exceptionalinteraction.
Institutes. leaders and topics forinstitutes are selected from previousaBct workshop presentations. institutesare offered as a 5- or 7-hour session onthursday and are generally limited to 40attendees.
Workshops. covering concerns of thepractitioner/educator/researcher, theseremain an anchor of the convention.workshops are offered on Friday andsaturday, are 3 hours long, and are gener-ally limited to 60 attendees.
Master Clinician Seminars. the mostskilled clinicians explain their methodsand show videos of sessions. these 2-hour sessions are offered throughout theconvention and are generally limited to40 to 45 attendees.
Advanced Methodology and StatisticsSeminars. Designed to enhanceresearchers' abilities, they are 4 hourslong and limited to 40 attendees.
Thinking about submitting an abstract forthe ABCT 55th Annual Convention inNew Orleans? The submission portal willbe opened until 3 AM EST March 8. Lookfor more information in the coming weeksto assist you with submitting abstracts forthe ABCT 55th Annual Convention.
Deadline for submissions: 3:00 A.M.(EST), Monday, March 8, 2021
at the aBct annual convention, thereare ticketed events (meaning you usuallyhave to buy a ticket for one of thesebeyond the general registration fee) andGeneral sessions (meaning you can usual-ly get in by paying the general registrationfee), the vast majority of which qualify force credit. see the end of this documentfor a list of organizations that haveapproved aBct as a ce sponsor. notethat we do not offer cmes. attendance ateach continuing education session in itsentirety is required to receive ce credit.no partial credit is awarded; late arrival orearly departure will preclude awarding ofce credit. General session attendees mustcheck in and out and answer evaluationquestions regarding each session attend-ed. For those who have met all require-ments according to the organizationswhich have approved aBct as a cesponsor, certificates will be available elec-tronically.
TICKETED EVENTS Eligible for CEall ticketed events offer ce in addition toeducational opportunities to enhanceknowledge and skills. these events aretargeted for attendees with a particularlevel of expertise (e.g., basic, moderate,and/or advanced). ticketed sessionsrequire an additional payment beyond thegeneral registration fee. For ticketedevents, attendees must complete an indi-vidual evaluation form. it remains theresponsibility of the attendee to check inat the beginning of the session and out atthe end of the session. ce will not beawarded unless the attendees checks inand out.
Clinical Intervention Trainingone- and two-day events emphasizing the"how-to" of clinical interventions. theextended length allows for exceptionalinteraction. Participants attending a full-day session can earn 7 continuing educa-tion credits, and 14 continuing educationcredits for the two-day session.
Institutesleaders and topics for institutes areselected from previous aBct workshoppresentations. institutes are offered as a 5-or 7-hour session on thursday and are
generally limited to 40 attendees.Participants in the full-day institute canearn 7 continuing education credits, andin the half-day institutes can earn 5 con-tinuing education credits.
Workshopscovering concerns of the practitioner/educator/researcher, these remain ananchor of the convention. workshopsare offered on Friday and saturday, are 3hours long, and are generally limited to 60attendees. Participants in these work-shops can earn 3 continuing educationcredits per workshop.
Master Clinician Seminars (MCS)the most skilled clinicians explain theirmethods and show videos of sessions.these 2-hour sessions are offeredthroughout the convention and are gen-erally limited to 40 to 45 attendees.Participants in these seminars can earn 2continuing education credits per seminar.
Advanced Methodology and StatisticsSeminars (AMASS)Designed to enhance researchers' abilities,there are generally two seminars offeredon thursday. they are 4 hours long andlimited to 40 attendees. Participants inthese courses can earn 4 continuing edu-cation credits per seminar.
GENERAL SESSIONS Eligible for CEthere are more than 200 general sessionseach year competing for your attention.all general sessions are included with theregistration fee. most of the sessions areeligible for ce, with the exception of theposter sessions, some membership PanelDiscussions, the special interest Groupmeetings (siG), and a few special ses-sions. You are eligible to earn 1 ce creditper hour of attendance.
General session attendees must checkin and out and answer evaluation ques-tions regarding each session attended.
General session types that are eligiblefor ce include the following:
ABCT & Continuing EducationUnderstanding the ABCTConvention, continued

56 the Behavior Therapist
Clinical Grand Roundsclinical experts engage in simulated livedemonstrations of therapy with clients,who are generally portrayed by graduatestudents studying with the presenter.
Invited Panels and Addressesspeakers well-established in their field, orwho hold positions of particular impor-tance, share their unique insights andknowledge on a broad topic of interest.
Mini-WorkshopsDesigned to address direct clinical care ortraining at a broad introductory level andare 90 minutes long. mini-workshops areoffered on Friday and saturday and aregenerally limited to 80 attendees.Participants can earn 1.5 continuing edu-cation credits.
Panel DiscussionDiscussions (or debates) by informedindividuals on a current important topicthat are conceptual in nature, rather thanpertaining directly to clinical care.examples of topics for panel discussionsinclude (but are not limited to) supervi-sion/training issues, ethical considera-tions in treatment or training, the use oftechnology in treatment, and culturalconsiderations in the application of cBts.some topics may be appropriate for eitherclinical round tables or PanelDiscussions, and authors are invited touse their judgment in making this deci-sion. these are organized by a moderatorand include between three and five pan-elists with a range of experiences and atti-tudes. the total number of speakers maynot exceed 7.
Clinical Round TablesDiscussions (or debates) by informedindividuals on a current important topicdirectly related to patient care, treatment,and/or the application/implementation ofa treatment. examples of topics forclinical round tables include (but are notlimited to) challenges/suggestions fortreating a certain disorder or group ofpatients, application of a treatment proto-col or type of treatment to a novel popula-tion, considerations in applying cBts tomarginalized communities and/or minor-ity groups. some topics may be appropri-
ate for either clinical round tables orPanel Discussions, and authors are invitedto use their judgment in making this deci-sion. clinical round tables are organizedby a moderator and include between threeand six panelists with a range of experi-ences and attitudes. the total number ofspeakers may not exceed 7.
Spotlight Research Presentationsthis format provides a forum to debutnew findings considered to be ground-breaking or innovative for the field. alimited number of extended-format ses-sions consisting of a 45-minute researchpresentation and a 15-minute question-and-answer period allows for more in-depth presentation than is permitted bysymposia or other formats.
SymposiaPresentations of data, usually investigat-ing the efficacy, effectiveness, dissemina-tion or implementation of treatment pro-tocols. symposia are either 60 or 90 min-utes in length. they have one or twochairs, one discussant, and between threeand five papers. the total number ofspeakers may not exceed 6.
GENERAL SESSIONS NOTELIGIBLE for CE
Membership Panel Discussionorganized by representatives of themembership committee and studentmembership committees, these eventsgenerally emphasize training or careerdevelopment.
Poster Sessionsone-on-one discussions betweenresearchers, who display graphic repre-sentations of the results of their studiesand interested attendees. Because of thevariety of interests and research areas ofthe aBct attendees, between 1,100 and1,500 posters are presented each year.
Special Interest Group (SIG) Meetingsmore than 40 siGs meet each year toaccomplish business (such as electing offi-cers), renew relationships, and often offerpresentations. siG talks are not peer-reviewed by the association.
Special Sessionsthese events are designed to provide use-ful information regarding professionalrather than scientific issues. For morethan 20 years the internship andPostdoctoral overviews have helpedattendees find their educational path.other special sessions often includeexpert panels on getting into graduateschool, career development, informationon grant applications, and a meeting ofthe Directors of clinical training. thesesessions are not eligible for continuingeducation credit.
Other Sessionsother sessions not eligible for ce arenoted as such on the itinerary planner, inthe PDF program book and on the con-vention app.
How Do I Get CEat the ABCT Convention?
the continuing education fee must bepaid (see registration form) for a person-alized continuing education credit letterto be distributed. those who have includ-ed ce in their pre-registration will gainaccess to the ce module. others can stillpurchase access at the registration areaduring the convention.
Which Organizations HaveApproved ABCT as a CE Sponsor?
PsychologyaBct is approved by the americanPsychological association to sponsorcontinuing education for psychologists.aBct maintains responsibility for thisprogram and its content. attendance ateach continuing education session in itsentirety is required to receive ce credit.no partial credit is awarded; late arrival orearly departure will preclude awarding ofce credit.
For ticketed events attendees mustcheck in and check out and complete anindividual evaluation form. For generalsessions attendees must check in andcheck out and answer questions regardingeach session attended. it remains theresponsibility of the attendee to check inat the beginning of the session and out atthe end of the session.
ABCT & Continuing Education (continued)

January • 2021 57
Social WorkaBct program is approved by thenational association of social workers(approval # 886427222). note: theapproval number and unique identifiernumber along with the social work cate-gory will be provided on your approvalletter.
CounselingaBct is approved by the national Boardof certified counselors (nBcc)approved continuing educationProvider, aceP no. 5797 and may offernBcc-approved clock hours for eventsthat meet nBcc requirements. Programsthat do not qualify for nBcc credit areclearly identified. aBct is solely respon-sible for all aspects of the program.
Licensed ProfessionalsaBct’s approval is pending by thecalifornia association of marriage andFamily therapists (camFt) to sponsorcontinuing education for counselors andmFt’s, lmFts, lcsws, lPccs, and/orlePs as required by the california Boardof Behavioral sciences. aBct maintainsresponsibility for this program/courseand its contents.
Continuing Education (CE)Grievance Procedure
aBct is fully committed to conductingall activities in strict conformance withthe american Psychological association'sethical Principles of Psychologists. aBctwill comply with all legal and ethicalresponsibilities to be non-discriminatoryin promotional activities, program con-tent and in the treatment of program par-ticipants. the monitoring and assessmentof compliance with these standards will bethe responsibility of the coordinator ofconvention and education issues in con-junction with the convention manager.
although aBct goes to great lengthsto assure fair treatment for all participantsand attempts to anticipate problems,there will be occasional issues which cometo the attention of the convention staffwhich require intervention and/or actionon the part of the convention staff or anofficer of aBct. this procedural descrip-tion serves as a guideline for handlingsuch grievances.all grievances must be filed in writing toensure a clear explanation of the problem.if the grievance concerns satisfaction witha ce session the convention managershall determine whether a full or partial
refund (either in money or credit for afuture ce event) is warranted. if the com-plainant is not satisfied, their materialswill be forwarded to the coordinator ofconvention and continuing educationissues for a final decision.
if the grievance concerns a speakerand particular materials presented, theconvention manager shall bring the issueto the coordinator of convention andeducation issues who may consult withthe members of the continuing educationissues committees. the coordinator willformulate a response to the complaintand recommend action if necessary,which will be conveyed directly to thecomplainant. For example, a grievanceconcerning a speaker may be conveyed tothat speaker and also to those planningfuture educational programs.
records of all grievances, the processof resolving the grievance and the out-come will be kept in the files of theconvention manager.
a copy of this Grievance Procedurewill be available upon request.
if you have a complaint, please contactstephen r. crane, convention manager,at [email protected] or (212) 646-1890 forassistance.
Webinarwww.abct.org/Conventions/?m=mConvention&fa=Webinars
RegisterNow!
Cultural Psychotherapy: Concepts, Interventionsand Telepsychiatry— Martin La Roche, Ph.D.
MODERATOR: Janie Hong, Ph.D.11 am – 12:30 pm Eastern | 10 am – 11:30 pm Central9 am – 10:30 am Mountain | 8 am – 9:30 am Pacific
During 2020, the twin pandemics of COVID-19 and social unrestexposed significant socioeconomic and racial/ethnic disparities withinthe United States. Unfortunately, psychotherapy has often reflectedthese disparities. If psychotherapy is to remain meaningful and credi-ble it needs to be inclusive of the needs and characteristics of all, notjust of a privileged few. Cultural Psychotherapy addresses this issue byunderscoring how our interventions/relationships and who we are isembedded within socio-economic cultural contexts that confine ourrelationships and meanings. In this presentation CulturalPsychotherapy’s integrative and systematic model is underscoreddescribing its specific applications.
MARCH 12
$20 for ABCT members$30 for nonmembers
CE Credit: 1.5

58 the Behavior Therapist
Career/Lifetime Achievementeligible candidates for this award should be members of aBct in good standing who have made significant contributions over a number ofyears to cognitive and/or behavior therapy. recent recipients of this award include thomas h. ollendick, lauren B. alloy, lyn abramson,David m. clark, marsha linehan, Dianne l. chambless, linda carter sobell and mark B. sobell, and Philip c. Kendall. applications shouldinclude a nomination form (available at www.abct.org/awards), three letters of support, and the nominee’s curriculum vitae. Please e-mail thenomination materials as one pdf document to [email protected]. include “career/lifetime achievement” in the subject line.Nomination deadline: march 1, 2021.
Outstanding Training Programthis award will be given to a training program that has made a significant contribution to training behavior therapists and/or promotingbehavior therapy. training programs can include graduate (doctoral or master's), predoctoral internship, postdoctoral programs, institutes,or continuing education initiatives. recent recipients of this award include the Doctoral Program in clinical Psychology at sunY albany,massachusetts General hospital/harvard medical school Predoctoral internship in clinical Psychology, the university of nebraska-lincolnclinical Psychology training Program, the charleston consortium Psychology internship training Program, clinical science Ph.D. Programat Virginia Polytechnic institute & state university, and Florida state university’s clinical Psychology Ph.D. program. Please complete theon-line nomination form at www.abct.org/awards. then e-mail the completed form and associated materials as one pdf document [email protected]. include “outstanding training Program” in your subject heading. Nomination deadline: march 1, 2021.
Outstanding Contribution by an Individual for Research Activitieseligible candidates for this award should be members of aBct in good standing who have provided significant contributions to the literatureadvancing our knowledge of behavior therapy. recent recipients of this award include alan e. Kazdin, David h. Barlow, terence m. Keane,thomas Borkovec, steven D. hollon, michelle craske, and Jennifer P. read. applications should include a nomination form (available atwww.abct.org/awards), three letters of support, and the nominee’s curriculum vitae. Please e-mail the nomination materials as one pdf docu-ment to [email protected]. include “outstanding researcher” in the subject line.Nomination deadline: march 1, 2021.
The Francis C. Sumner Excellence Awardthe Francis cecil sumner excellence award is named in honor of Dr. sumner, the first african american to receive a Ph.D. in psychology in1920. commonly referred to as the “Father of Black Psychology,” he is recognized as an american leader in education reform. this awardcan be given on an annual basis, awarded in even years to a graduate student and in odd years to an early career professional within the first10 years of terminal degree. candidate must be a current member of aBct at the time of the awards ceremony and priority will be given tostudents and professional members of aBct at the time of the nomination. the award is intended to acknowledge and promote the excel-lence in research, clinical work, teaching, or service by an aBct member who is a doctoral student or early career professional within 10years of award of the PhD/PsyD/edD/scD/mD who identifies as Black or indigenous. the award is given to recognize that Black andindigenous practitioners and scholars are underrepresented in clinical psychology, despite making important contributions to our field. theFrancis c. sumner excellence award is meant to reflect the overarching goal of aBct supporting its members of color. the recipient willreceive $1,000 and a certificate. Please complete the online nomination materials at www.abct.org/awards. then email the nomination mate-rials as one PDF document to [email protected]. include “Francis c. sumner award” in the subject line. Nomination deadline: march1, 2021.
Anne Marie Albano Early Career Award for Excellence in the Integration of Science and PracticeDr. anne marie albano is recognized as an outstanding clinician, scientist, and teacher dedicated to aBct’s mission. she is known for hercontagious enthusiasm for the advancement of cognitive and behavioral science and practice. the purpose of this award is to recognize earlycareer professionals who share Dr. albano’s core commitments. this award includes a cash prize of $1,000 to support travel to the aBctannual convention and to sponsor participation in a clinical treatment workshop. eligibility requirements are as follows: (1) candidatesmust be active members of aBct, (2) new/early career Professionals within the first 10 years of receiving his or her doctoral degree (PhD,PsyD, edD). Preference will be given to applicants with a demonstrated interest in and commitment to child and adolescent mental healthcare. applicants should submit: nominating cover letter, cV, personal statement up to three pages (statements exceeding 3 pages will not bereviewed), and 2 to 3 supporting letters. application materials should be emailed as one pdf document to [email protected]. includecandidate's last name and “albano award” in the subject line. Nomination deadline: march 1, 2021.
Call for Award Nominations2021����������������
t o b e p r e s e n t e d a t t h e 5 5 t h A n n u a l C o n v e n t i o n i n n e w o r l e a n s
The ABCT Awards and Recognition Committee, chaired by Sara R. Elkins, Ph.D., of University of HoustonClear Lake is pleased to announce the 2021 awards program. Nominations are requested in all categories listedbelow. Given the number of submissions received for these awards, the committee is unable to consider addi-tional letters of support or supplemental materials beyond those specified in the instructions below. Please notethat award nominations may not be submitted by current members of the ABCT Board of Directors.

January • 2021 59
a w a r d s & r e c o g n i t i o n
Michael J. Kozak Critical Inquiry and Analytical Thinking Award“clarity of writing reflects clarity of thinking.” this statement reflects the overarching goal that michael J. Kozak sought to achieve himselfand that he vigorously encouraged others to reach as well. his penchant for critical inquiry cut across contexts: whether in providing cogni-tive-behavioral treatment itself, offering supervision of treatment, in scientific inquiry and writing, or in advising investigators about how toput their grant applications in the best possible position for success. Dr. Kozak was always in search of clarity. accordingly, recipients of themichael J. Kozak critical inquiry and analytical thinking award from aBct should embody this same spirit in their own work. michaelwas able to achieve this high standard and promote its achievement in others with great skill and kindness, so recipients should also conductthemselves in such a way in their professional lives. this award will be given in alternate years. the recipient will receive $1,500 and a plaque.Please complete the online nomination materials at www.abct.org/awards. then email the nomination materials as one PDF document [email protected]. include “michael J. Kozak award” in the subject line. Nomination deadline: march 1, 2021.
Student Dissertation Awards• Virginia a. roswell student Dissertation award ($1,000)• leonard Krasner student Dissertation award ($1,000)• John r. Z. abela student Dissertation award ($500)each award will be given to one student based on his/her doctoral dissertation proposal. accompanying this honor will be a monetary award(see above) to be used in support of research (e.g., to pay participants, to purchase testing equipment) and/or to facilitate travel to the aBctconvention. eligibility requirements for these awards are as follows: 1) candidates must be student members of aBct, 2) topic area of dis-sertation research must be of direct relevance to cognitive-behavioral therapy, broadly defined, 3) the dissertation must have been success-fully proposed, and 4) the dissertation must not have been defended prior to november 2020. Proposals with preliminary results includedare preferred. to be considered for the abela award, research should be relevant to the development, maintenance, and/or treatment ofdepression in children and/or adolescents (i.e., under age 18). self-nominations are accepted, or a student's dissertation mentor may com-plete the nomination. the nomination must include a letter of recommendation from the dissertation advisor. Please complete the nomina-tion form found online at www.abct.org/awards/. then e-mail the nomination materials (including letter of recommendation) as one pdfdocument to [email protected]. include candidate’s last name and “student Dissertation award” in the subject line.Nomination deadline: march 1, 2021
President’s New Researcher AwardaBct's 2020-21 President, David F. tolin, Ph.D., invites submissions for the 43rd annual President's new researcher award. the winnerwill receive a certificate and a cash prize of $500. the award will be based upon an early program of research that reflects factors such as: con-sistency with the mission of aBct; independent work published in high-impact journals; and promise of developing theoretical or practicalapplications that represent clear advances to the field. requirements: must have had terminal degree (Ph.D., m.D., etc.) for at least 1 year butno longer than 5 years (i.e., completed during or after 2015); must submit an article for which they are the first author (in press, or publishedduring or after 2018); 2 letters of recommendation must be included; self-nominations are accepted; the author's cV, letters of support, andpaper must be submitted in electronic form. applicants from traditionally underrepresented backgrounds, or whose work advances ourunderstanding of behavioral health disparities, are particularly encouraged to apply. e-mail the nomination materials (including letter of rec-ommendation) as one pdf document to [email protected]. include candidate's last name and "President's new researcher" in the subjectline. Nomination deadline: march 1, 2021.
Graduate Student Research Grantthe aBct research Facilitation committee is sponsoring a grant of up to $1000 to support graduate student research. the grant will beawarded based on a combination of merit and need. eligible candidates are graduate student members of aBct seeking funding for anunfunded (including internal sources of funding) thesis or dissertation project that has been approved by either the faculty advisor or the stu-dent's full committee. applications should include all of the materials listed in GsrG application Guidelines(https://www.abct.org/resources/index.cfm?m=mresources&fa=GraduatestudentGrant) and one letter of support from a faculty advisor.Please email the application, excluding the advisor letter, in a single pdf to the chair of the research Facilitation committee, shannon sauer-Zavala, PhD, at [email protected]. include "Graduate student research Grant" in your subject heading.Please ask your faculty advisor to e-mail a letter of support separately.Application deadline: march 1, 2021
Nominations for the following award are solicited from members of the ABCT governance:
Outstanding Service to ABCTPlease complete the nomination form found online at www.abct.org/awards/. then e-mail the completed form and associated materials asone pdf document to [email protected]. include “outstanding service” in the subject line.Nomination deadline: march 1, 2021.
For details on all ABCT Awards,visit our website at www.abct.org

PRSRT STDU.S. POSTAGE
PAIDHanover, PAPermit No. 4
the Behavior TherapistAssociation for Behavioraland Cognitive Therapies305 seventh avenue, 16th floornew York, nY 10001-6008212-647-1890 | www.abct.org
ADDRESS SERV ICE REQUESTED
This may be your LAST issue.
There is one way to remedy
this unexpected plight:
renew your membership!
Visit www.abct.org & click
RENEW
View publication statsView publication stats




















