
Laccase Immobilization on Enzymatically Functionalized Polyamide 6, 6 Fibres
Upload
independentCategory
view
4download
0
The Journal of Emergency Medicine, Vol 14. No 3. pp 193-298. 1996 Copyright 0 1996 Elsaier Science Inc. Printed in the USA. All rights reserved
0'36.4679/M S15.W A- IH)
ELSEVIER PII SO736-4679( %)00034-O
BACKBOARD VERSUS MA’l-flXSS SPLINT #3VW#ON: A COMPARtSON OF SYMPTOMS Gl%%ZRATED
Dennis Chan, MD, Richard M. Goldberg, MD, Jennifer Mason, MS, and Linda Chan, r=hD
Department of Emergency Medicine, Los Angeles County and University of Southern California Medical Center, Los Angeles, California Reprint Address: Richard M. Goldberg, MD, Department of Emergency Medicine, Los Angeles County and University of Southern
California Medical Center, 1200 No. State Street, Room GH-1011, Los Angeles, CA 90033-i 084
q Abstract-The study objective was to compare spinal hnmohilization techniques to a vacuum mattress-splint (VMS) with respect to the incidence of symptoms gener- ated by the immobllization process. We used a prospec- tive, cross-over study in a university hospital setting. Par- ticipants consisted of 37 healthy volunteers without his- tory of back pain or spinal disease.
Interventions consisted of two phases. In Phase I, sub- jects were randomly assigned to be immobilized on either a wooden backboard or a mattress-splint for 30 min. The incidence and severity of any symptoms generated by the immoblIization process were recorded. In Phase II, the two groups were again tested after a 2-week washout period, with the method of immobilization being re- versed. Symptoms and severity were again recorded.
Pain symptoms were conflned to four anatomic sites: Occipital prominence, lumbosacral spine, scapulae, and cervical spine. After adjusting for the effect of order of exposure, subjects were 3.08 times more likely to have symptoms when immobilized on a backboard than when immobilized on the VMS. They were 7.88 times more likely to complain of occipital pain and 4.27 times more likely to complain of lumbosacral pain. Severity of occipi- tal and hunbosacral pain was also significantly greater during backboard immobilization.
We conclude that, when compared to a VMS, stan- dard backboard immobilization appears to be associated with an increased incidence of symptoms ln general and an increased incidence and severity of occipital and lum- bosacral pain in particular.
0 Keywords-emergency medical services; immobiliza- tion; orthopedic equipment; spinal injuries
INTRODUCTION
Standard spinal immobilization (hard backboard, rigid cervical collar, sandbags, and tape or straps) is well- accepted and widely used in the prehospital and emer- gency department care of trauma victims in the United States. The results of a recent study indicate that cur- rent immobilization techniques may cause significant pain at certain points of bony contact, particularly the occipital prominence and lumbosacral spine ( 1) . These observations suggest that the standard process of im- mobilization may complicate the evaluation of the trauma victim by generating additional symptoms. Such symptoms may lead to unnecessary laboratory tests and X-ray studies, time of immobilization, and ultimately, health care costs. Additionally, standard backboard immobilization has been associated with the development of pressure necrosis along points of bony contact (23).
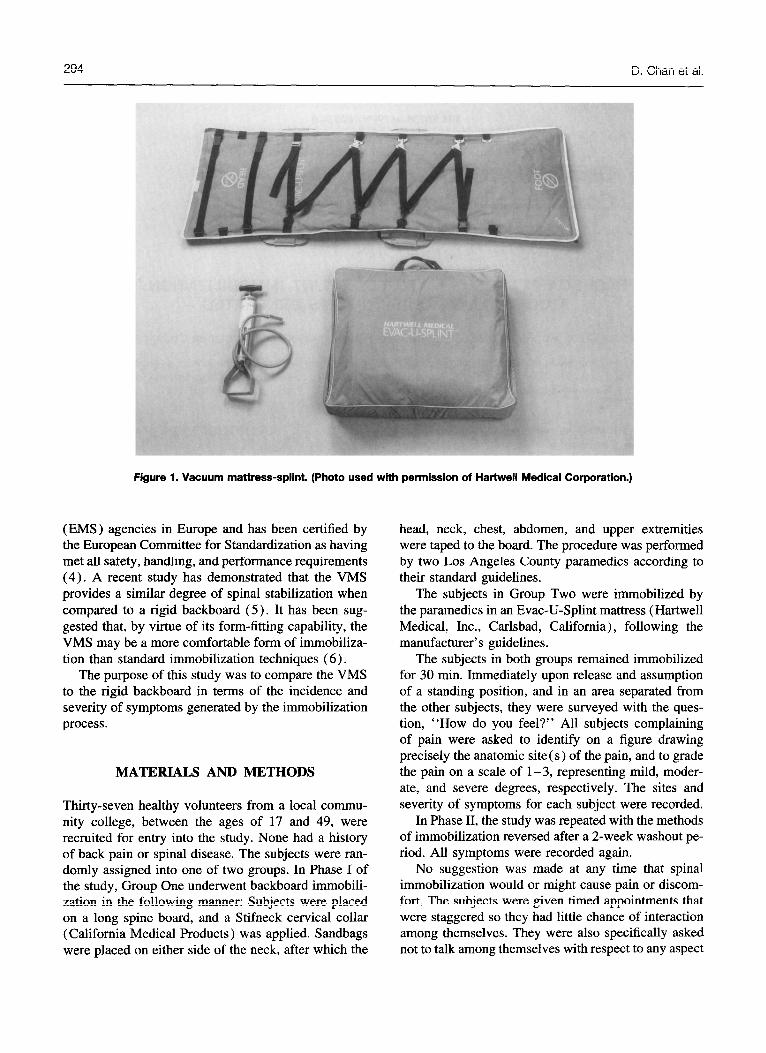
A recent innovation in the area of spinal immobili- zation is the vacuum mattress-splint (VMS) (Figs. 1 and 2). This device consists essentially of a large poly- ester bag (mattress) filled with thousands of tiny poly- ester foam spheres and fitted with an evacuation tube and valve. The patient is placed on the mattress, and a vacuum pump evacuates the interior causing the mat- tress to conform rigidly to the contours of the patient’s body. The mattress thus provides support as well as constraint for the patient at all points of contact. It has been used extensively by Emergency Medical Service
RECEIVED: 7 July 1995; FINALSUBMISSIONRECEIVED: 17 November 1995; ACCEPTED: 1 December 1995
293
D. Chan et al.
Figure 1. Vacuum mattress-splint. (Photo used with permission of Hartwell Medical Corporation.)
(EMS ) agencies in Europe and has been certified by the European Committee for Standardization as having met all safety, handling, and performance requirements (4). A recent study has demonstrated that the VMS provides a similar degree of spinal stabilization when compared to a rigid backboard (5 ) . It has been sug- gested that, by virtue of its form-fitting capability, the VMS may be a more comfortable form of immobiliza- tion than standard immobilization techniques (6).
The purpose of this study was to compare the VMS to the rigid backboard in terms of the incidence and severity of symptoms generated by the immobilization process.
MATERIALS AND METHODS
Thirty-seven healthy volunteers from a local commu- nity college, between the ages of 17 and 49, were recruited for entry into the study. None had a history of back pain or spinal disease. The subjects were ran- domly assigned into one of two groups. In Phase I of the study, Group One underwent backboard immobili- zation in the following manner: Subjects were placed on a long spine board, and a Stifneck cervical collar (California Medical Products) was applied. Sandbags were placed on either side of the neck, after which the
head, neck, chest, abdomen, and upper extremities were taped to the board. The procedure was performed by two Los Angeles County paramedics according to their standard guidelines.
The subjects in Group Two were immobilized by the paramedics in an Evac-U-Splint mattress (Hartwell Medical, Inc., Carlsbad, California), following the manufacturer’s guidelines.
The subjects in both groups remained immobilized for 30 min. Immediately upon release and assumption of a standing position, and in an area separated from the other subjects, they were surveyed with the ques- tion, “How do you feel?” All subjects complaining of pain were asked to identify on a figure drawing precisely the anatomic site(s) of the pain, and to grade the pain on a scale of l-3, representing mild, moder- ate, and severe degrees, respectively. The sites and severity of symptoms for each subject were recorded.
In Phase II, the study was repeated with the methods of immobilization reversed after a 2-week washout pe- riod. All symptoms were recorded again.
No suggestion was made at any time that spinal immobilization would or might cause pain or discom- fort. The subjects were given timed appointments that were staggered so they had little chance of interaction among themselves. They were also specifically asked not to talk among themselves with respect to any aspect
Spinal Immobilization
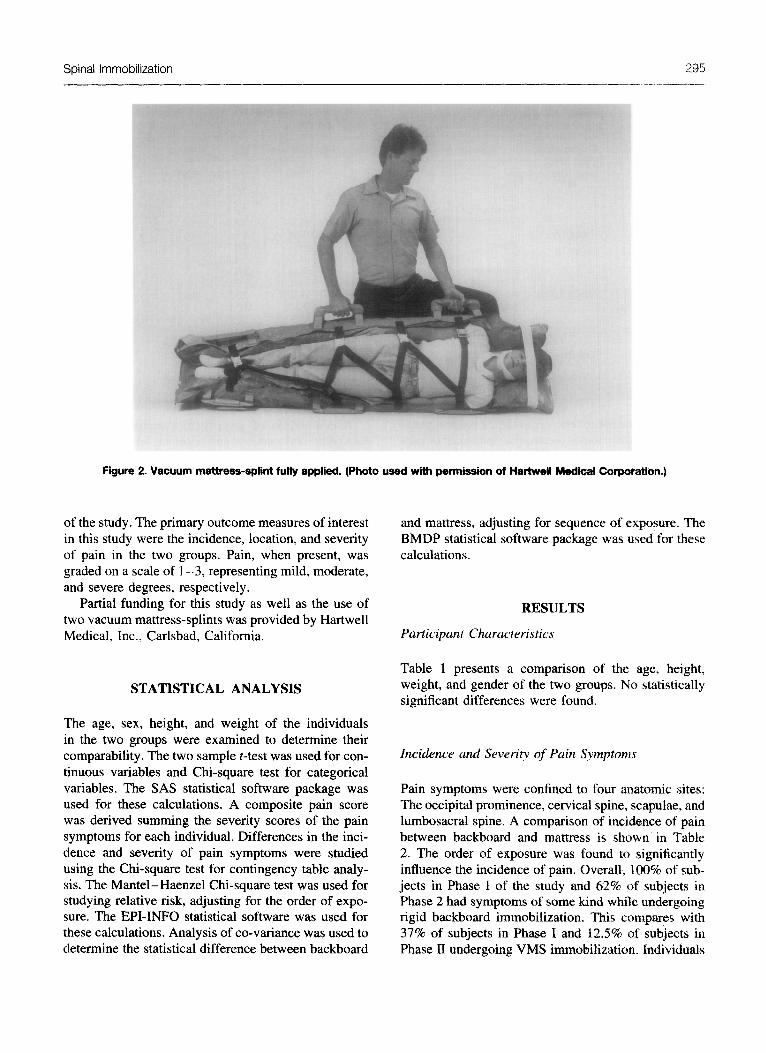
Figure 2. Vacuum mattress-splint fully applied. (Photo used with permission of Hartwell Medical Corporation.)
of the study. The primary outcome measures of interest in this study were the incidence, location, and severity of pain in the two groups. Pain, when present, was graded on a scale of l-3, representing mild, moderate, and severe degrees, respectively.
Partial funding for this study as well as the use of two vacuum mattress-splints was provided by Hartwell Medical, Inc., Carlsbad, California.
STATISTICAL ANALYSIS
The age, sex, height, and weight of the individuals in the two groups were examined to determine their comparability. The two sample t-test was used for con- tinuous variables and Chi-square test for categorical variables. The SAS statistical software package was used for these calculations. A composite pain score was derived summing the severity scores of the pain symptoms for each individual. Differences in the inci- dence and severity of pain symptoms were studied using the Chi-square test for contingency table analy- sis. The Mantel-Haenzel Chi-square test was used for studying relative risk, adjusting for the order of expo- sure. The EPI-INFO statistical software was used for these calculations. Analysis of co-variance was used to determine the statistical difference between backboard
and mattress, adjusting for sequence of exposure. The BMDP statistical software package was used for these calculations.
RESULTS
Participant Characteristics
Table 1 presents a comparison of the age, height, weight, and gender of the two groups. No statistically significant differences were found.
Incidence and Severity of Pain Symptoms
Pain symptoms were confined to four anatomic sites: The occipital prominence, cervical spine, scapulae, and lumbosacral spine. A comparison of incidence of pain between backboard and mattress is shown in Table 2. The order of exposure was found to significantly influence the incidence of pain. Overall, 100% of sub- jects in Phase I of the study and 62% of subjects in Phase 2 had symptoms of some kind while undergoing rigid backboard immobilization. This compares with 37% of subjects in Phase I and 12.5% of subjects in Phase II undergoing VMS immobilization. Individuals
D. Chan et al.
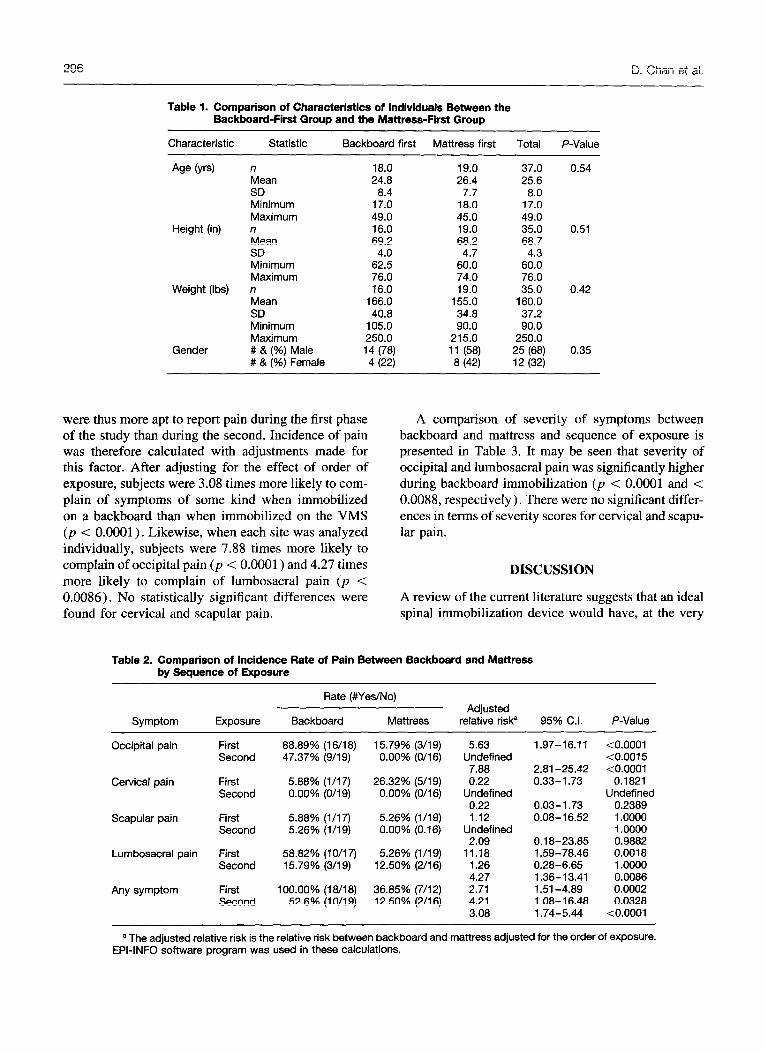
Table 1. Comparison of Characteristics of Individuals Between the Backboard-First Group and the Mattress-First Group
Characteristic Statistic Backboard first Mattress first Total P-Value
Age b-4 n 18.0 19.0 37.0 0.54 Mean 24.8 26.4 25.6 SD 8.4 7.7 8.0 Minimum 17.0 18.0 17.0 Maximum 49.0 45.0 49.0
Height (in) n 16.0 19.0 35.0 0.51 Mean 69.2 68.2 68.7 SD 4.0 4.7 4.3 Minimum 62.5 60.0 60.0 Maximum 76.0 74.0 76.0
Weight (Ibs) n 16.0 19.0 35.0 0.42 Mean 166.0 155.0 160.0 SD 40.8 34.8 37.2 Minimum 105.0 90.0 90.0 Maximum 250.0 215.0 250.0
Gender # & (%) Male 14 (78) 11 (58) 25 (68) 0.35 # & (%) Female 4 (22) 8 (42) 12 (32)
were thus more apt to report pain during the first phase of the study than during the second. Incidence of pain was therefore calculated with adjustments made for this factor. After adjusting for the effect of order of exposure, subjects were 3.08 times more likely to com- plain of symptoms of some kind when immobilized on a backboard than when immobilized on the VMS (p < 0.0001). Likewise, when each site was analyzed individually, subjects were 7.88 times more likely to complain of occipital pain (p < 0.0001) and 4.27 times more likely to complain of lumbosacral pain (p < 0.0086). No statistically significant differences were found for cervical and scapular pain.
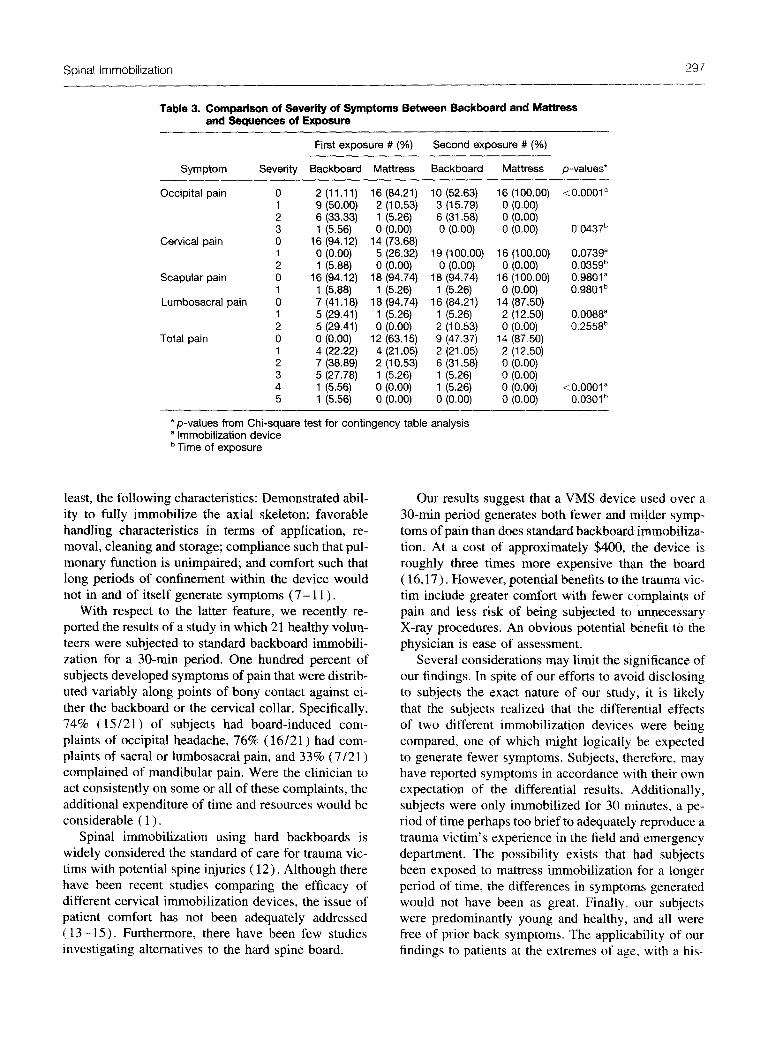
A comparison of severity of symptoms between backboard and mattress and sequence of exposure is presented in Table 3. It may be seen that severity of occipital and lumbosacral pain was significantly higher during backboard immobilization (p < 0.0001 and < 0.0088, respectively). There were no significant differ- ences in terms of severity scores for cervical and scapu- lar pain.
DISCUSSION
A review of the current literature suggests that an ideal spinal immobilization device would have, at the very
Table 2. Comparison of Incidence Rate of Pain Between Backboard and Mattress by Sequence of Exposure
Symptom Exposure
Rate (#Yes/No)
Backboard Mattress Adjusted
relative risk= 95% Cl. P-Value
Occipital pain First 88.89% (16/l 8) 15.79% (3/l 9) 5.63 1.97-16.11 <0.0001 Second 47.37% (9/19) 0.00% (O/16) Undefined <0.0015
7.88 2.81-25.42 <0.0001 Cervical pain First 5.88% (l/17) 26.32% (5/l 9) 0.22 0.33-l .73 0.1821
Second 0.00% (O/l 9) 0.00% (O/l 6) Undefined Undefined 0.22 0.03-l .73 0.2389
Scapular pain First 5.88% (l/l 7) 5.26% (l/19) 1.12 0.08-16.52 I .oooo Second 5.26% (l/19) 0.00% (0.16) Undefined 1 .oooo
2.09 0.18-23.85 0.9882 Lumbosacral pain First 58.82% (1 O/l 7) 5.26% (l/l 9) 11.18 1.59-78.46 0.0018
Second 15.79% (3/l 9) 12.50% (2/l 6) 1.26 0.28-6.65 1 .oooo 4.27 1.36-13.41 0.0086
Any symptom First 100.00% (18/i 8) 36.85% (7/12) 2.71 1.51-4.89 0.0002 Second 52.6% (10/19) 12.50% (2/16) 4.21 1.08-l 6.48 0.0328
3.08 1.74-5.44 <0.0001
a The adjusted relative risk is the relative risk between backboard and mattress adjusted for the order of exposure. EPI-INFO software program was used in these calculations.
Spinal Immobilization 297 -.--..- ____..--
Table 3. Comparison of Severity of Symptoms Between Backboard and Mattress and Sequences of Exposure -
First exposure # (%) Second exposure # 1%)
Symptom Severity Backboard Mattress Backboard Mattress p-values*
Occipital pain 0 2 (11 .ll) 16 (84.21) 10 (52.63) 16 (100.00) <O.OOOl a 1 9 (50.00) 2 (10.53) 3 (15.79) 0 (0.00) 2 6 (33.33) 1 (5.26) 6 (31.58) 0 (0.00) 3 1 (5.56) 0 (0.00) 0 (0.00) 0 (0.00) 0.0437”
Cervical pain 0 16 (94.12) 14 (73.68) 1 0 (0.00) 5 (26.32) 19 (100.00) 16 (100.00) 0.0739” 2 1 (5.88) 0 (0.00) 0 (0.00) 0 (0.00) 0.035gb
Scapular pain 0 16 (94.12) 18 (94.74) 18 (94.74) 16 (100.00) 0.9801” 1 1 (5.88) 1 (5.26) 1 (5.26) 0 (0.00) 0.9801 b
Lumbosacral pain 0 7 (41.18) 18 (94.74) 16 (84.21) 14 (87.50) 1 5 (29.41) 1 (5.26) 1 (5.26) 2 (12.50) 0.0088a 2 5 (29.41) 0 (0.00) 2 (10.53) 0 (0.00) 0.2558b
Total pain 0 0 (0.00) 12 (63.15) 9 (47.37) 14 (87.50) 1 4 (22.22) 4 (21.05) 2 (21.05) 2 (12.50) 2 7 (38.89) 2 (10.53) 6 (31.58) 0 (0.00) 3 5 (27.78) 1 (5.26) 1 (5.26) 0 (0.00) 4 1 (5.56) 0 (0.00) 1 (5.26) 0 (0.00) <0.0001 B 5 1 (5.56) 0 (0.00) 0 (0.00) 0 (0.00) 0.0301b
_-
*p-values from Chi-square test for contingency table analysis a immobilization device b Time of exposure
least, the following characteristics: Demonstrated abil- ity to fully immobilize the axial skeleton; favorable handling characteristics in terms of application, re- moval, cleaning and storage; compliance such that pul- monary function is unimpaired; and comfort such that long periods of confinement within the device would not in and of itself generate symptoms (7- 11) .
With respect to the latter feature, we recently re- ported the results of a study in which 21 healthy volun- teers were subjected to standard backboard immobili- zation for a 30-min period. One hundred percent of subjects developed symptoms of pain that were distrib- uted variably along points of bony contact against ei- ther the backboard or the cervical collar. Specifically, 74% ( 15/21) of subjects had board-induced com- plaints of occipital headache, 76% ( 16/21) had com- plaints of sacral or lumbosacral pain, and 33% (7/21) complained of mandibular pain. Were the clinician to act consistently on some or all of these complaints, the additional expenditure of time and resources would be considerable ( 1) ,
Spinal immobilization using hard backboards is widely considered the standard of care for trauma vic- tims with potential spine injuries ( 12). Although there have been recent studies comparing the efficacy of different cervical immobilization devices, the issue of patient comfort has not been adequately addressed ( 13 - 15). Furthermore, there have been few studies investigating alternatives to the hard spine board.
Our results suggest that a VMS device used over a 30-min period generates both fewer and milder symp- toms of pain than does standard backboard immobiliza- tion. At a cost of approximately $400, the device is roughly three times more expensive than the board ( 16,17). However, potential benefits to the trauma vic- tim include greater comfort with fewer complaints of pain and less risk of being subjected to unnecessary X-ray procedures. An obvious potential benefit to the physician is ease of assessment.
Several considerations may limit the significance of our findings. In spite of our efforts to avoid disclosing to subjects the exact nature of our study, it is likely that the subjects realized that the differential effects of two different immobilization devices were being compared, one of which might logically be expected to generate fewer symptoms. Subjects, therefore, may have reported symptoms in accordance with their own expectation of the differential results. Additionally, subjects were only immobilized for 30 minutes, a pe- riod of time perhaps too brief to adequately reproduce a trauma victim’s experience in the field and emergency department. The possibility exists that had subjects been exposed to mattress immobilization for a longer period of time, the differences in symptoms generated would not have been as great. Finally, our subjects were predominantly young and healthy. and all were free of prior back symptoms. The applicability of our findings to patients at the extremes of‘ age, with a his-

298 D. Chan et al.
tory of a variety of back disorders, or with significant injuries as a source of pain is indeterminate.
Future studies of the mattress-like device are recom- mended to document the adequacy of immobilization, effects (if any) on pulmonary function, and extent of induced flexion and extension of the cervical spine in pediatric patients.
variably at four anatomic sites: Occipital prominence, lumbosacral spine, scapulae, and cervical spine. When compared to the mattress-splint, standard backboard immobilization appears to be associated with an in- creased incidence of complaints of back and occipital pain and increased severity of pain at all of the above anatomic sites.
CONCLUSION
Healthy subjects undergoing spinal immobilization for Acknowledgment-Funded in part by Hartwell Medical, Inc., a period of 30 min appear disposed to develop pain Carlsbad, California.
REFERENCES
1. Chan D, Goldberg R, Tascone A, et al. The effect of spinal immobilization on healthy volunteers. Ann Emerg Med. 1994; 23~48-51.
2. Linares HA, Mawson AR, Suarez E. Association between pres- sure sores and immobilization in the immediate post-injury pe- riod. Orthopedics 1987; 10571-3.
3. Mawson AR, Biundo JJ, Neville P. Risk factors for early oc- curring pressure ulcers following spinal cord injury. Am J Phys Med Rehab. 1988;67:123-7.
4. European Standard: Medical Vehicles and Their Equipment. European Committee for Standardization. Central Secretariat: rue de Stassart 36, B-1050. Brussels. February, 1994.
5. Johnson DR, Hauswald M, Stockhoff C. Comparison of a vac- uum splint device to a rigid backboard for spinal immobilization. Am J Emerg Med. in press.
6. McCarty LH. Polyester spheres immobilize accident victims: Vacuum causes particles to rigidly conform to body contours. Design News. 1991:89-90.
7. Herzenberg JE, Hensinger RN, Dedrick DK, et al. Emergency transport and positioning of young children who have an injury of the cervical spine. J Bone and Joint Surg. 1989;7-A:15-22.
8. Schriger DL, Larmon B, LeGarrick T, et al. Spinal immobiliza- tion on a flat backboard: Does it result in neutral position of the cervical spine? AM Emerg Med. 1991;20:878-81.
9. Schafermeyer RW, Ribbeck BM, Gaskins J, et al. Respiratory effects of spinal immobilization in children. Ann Emerg Med. 1991;20:1017-9.
10. Bauer D, Kowalski R. Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man. Ann Emerg Med.-1988; 17:915-8.
11. Barney RN, Cordell WH, Miller E. Pain associated with immo- bilization on rigid spine boards (Abstract). Ann Emerg Med. 1989; 18:918.
12. American College of Surgeons. Advanced trauma life support student manual. Chicano: ACS 1992: DD. 193. 201. 215.
13. Podolsky S, Baraff Uy Simon RR, et’& Efficacy of cervical spine immobilization methods. J Trauma. 1983;23(6):461-5.
14. Huerta C, Griffity R, Joyce SM. Cervical spine stabilization in pediatric patients: evaluation of current techniques. Ann Emerg Med. 1987;16:1121-6.
15. Chandler DR, Nemejc C, Adkins RH, et al. Emergency cervical spine immobilization. AM Emerg Med. 1992;21:1185-8.
16. Rosen PB, McSwain NE, Arata M, et al. Comparison of two new immobilization collars. Ann Emerg Med. 1992;21:1189- 95.
17. Personal communication: Steve Bodalatto, Hartwell Medical, Inc., Carlsbad, California.
18. Dyna Med Sales, Catalog No. 1032. Summer, 1995. Page 30.
Copyright © 2022 FDOKUMEN



















