
Automated multidetector computed tomography evaluation of subacutely infarcted myocardium

Circulation Journal Vol.72, August 2008
linical observational studies have demonstrated thatboth angiotensin-converting enzyme inhibitors andangiotensin type I receptor blockades can attenuate
left ventricular (LV) enlargement in association with re-duced mortality after myocardial infarction (MI).1–3 How-ever, despite the application of pharmacotherapeutics1–3 ormechanical intervention,4 dead cardiomyocytes followingMI cannot be regenerated.
Growing experimental evidence indicates that bone mar-row-derived mesenchymal stem cells (BMDMSCs) appearto be highly advantageous for cell therapy.5–7 Experimentaland clinical studies have recently demonstrated that autolo-gous BMDMSC transplantation improved ischemic-inducedor infarct-related cardiac dysfunction.5–7 Thus, autologousBMDMSC transplantation has been proposed as a promis-
ing novel therapeutic strategy for ameliorating ischemia-induced myocardial dysfunction and restoring heart func-tion following acute MI (AMI).5–11 Although short-term andintermediate-term results5–8,12 are attractive and promising,the mechanisms underlying improvement of cardiac functionfollowing BMDMSC therapy remain poorly defined.7,10,13
Experimental studies have demonstrated that damage to injured and remote viable myocardium from AMI isfrequently progressive.14,15 Additionally, living cells arechallenged by myriad acute and chronic stresses,16–18 andprogrammed cell death, or “apoptosis,” has been shown toincrease following various cardiac insults, such as ischemia-reperfusion injury and cardiac failure.19 Moreover, gapjunctions, which are composed of connexin (Cx) subunits,play a key role in electrical coupling between cardiomyo-cytes.20,21 Changes in Cx expression patterns, which areassociated with a variety of cardiac pathologies, contributeto the development of cardiac arrhythmia.22–24 Neverthe-less, the impact of AMI on remote (non-infarct area) viablemyocardium, which undoubtedly plays an essential role inmaintaining heart function following infarction, remainsuncertain. This study tested the hypothesis that AMI in-duced apoptotic body formation and suppressed Cx43 gapjunction expression in viable myocardium, and examinedthe effects of autologous transplantation of bone marrow-derived mononuclear cells (BMDMNCs) on preserving LVfunction and preventing molecular and cellular pertur-bations in a rat MI model. Additionally, this study alsomeasured the impact of BMDMNC therapy on mRNA
Circ J 2008; 72: 1336–1345
(Received January 29, 2008; revised manuscript received March 10,2008; accepted April 10, 2008)Division of Cardiology, *Department of Cardiovascular Surgery,**Department of Hematology, †Department of General Surgery,Chang Gung Memorial Hospital-Kaohsiung Medical Center, ChangGung University College of Medicine, Kaohsiung, ††Basic Science,Nursing Department, Meiho Institute of Technology, Pingtung,Taiwan, R.O.C and ‡Cardiology Department, Suez Canal UniversityHospital, Ismailia, EgyptMailing address: Cheuk-Kwan Sun, MD, PhD, Division of Cardiolo-gy, Department of Internal Medicine, Chang Gung Memorial Hospital,123 Ta Pei Road, Niao Sung Hsiang, Kaohsiung Hsien, 83301, Taiwan.E-mail: tangadm.cgmh.org.twAll rights are reserved to the Japanese Circulation Society. For per-missions, please e-mail: [email protected]
Autologous Bone Marrow-Derived Mononuclear Cell Therapy Prevents the Damage of Viable Myocardium
and Improves Rat Heart Function Following Acute Anterior Myocardial Infarction
Hon-Kan Yip, MD; Li-Teh Chang, PhD††; Chiung-Jen Wu, MD; Jiunn-Jye Sheu, MD*; Ali A.Youssef, MD‡; Sung-Nan Pei, MD**;
Fan-Yen Lee, MD*; Cheuk-Kwan Sun, MD, PhD†
Background We examined the effects of bone marrow-derived mononuclear cells (BMDMNCs) on prevent-ing viable myocardium damage from myocardial infarction (MI) in a rat MI model.Methods and Results Saline (group 1) or BMDMNCs (group 2) were implanted into the infarct area (IA) of 1-week-old anterior wall MI Sprague –Dawley (SD) rats. Twenty SD rats without MI served as the controls(group 3). The results demonstrated that in remote viable myocardium, the integrated area (μm2) of connexin43spots was lower, whereas the number of apoptotic nuclei were higher in group 1 than in groups 2 and 3 on day 90following BMDMNC implantation (all p<0.001). Additionally, the number of vessels and survival myocardiumin the IA was lower in group 1 than in groups 2 and 3 (all p<0.005). Furthermore, the mRNA expressions of nitricoxide synthase, interleukin-8/Gro-α, interleukin-10 and matrix metalloproteinase-9 were higher in group 2 thanin groups 1 and 3 in peri-IA (all p<0.05). On days 42 and 90, the left ventricular (LV) function was lower ingroup 1 than in groups 2 and 3 (p<0.001).Conclusions Autologous BMDMNC therapy improves LV function, and mitigates molecular and cellularperturbation following MI. (Circ J 2008; 72: 1336–1345)
Key Words: Bone marrow-derived mononuclear cell therapy; Left ventricular function; Molecular and cellularperturbation; Myocardium infarction
C
EXPERIMENTAL INVESTIGATIONS

1337Bone Marrow Cells Therapy on MI
Circulation Journal Vol.72, August 2008
expressions of endothelial nitric oxide synthase (eNOS),interleukin (IL)-8/Gro-αCXC chemokine family, IL-10 andmatrix metalloproteinase (MMP)-9, which were identifiedto regulate the myocardial homing and neovascularizationfrom bone marrow to damaged myocardium.25
MethodsAnimals, Protocol and Procedure
Pathogen-free, adult male Sprague–Dawley (SD) rats,weighing 250–300g (Charles River Technology, BioLASCOTaiwan Co, Ltd, Taipei, Taiwan) were anesthetized by chlo-ral hydrate (35mg/kg, ip) and placed in a supine positionon a warming pad at 37°C, followed by endotracheal intu-bation with positive-pressure ventilation (180ml/min) withroom air using a Small Animal Ventilator (SAR-830/A,CWE, Inc, Ardomore, PA, USA). Under sterile conditions,the heart was exposed via a left thoracotomy.
AMI was induced in 40 SD rats by left coronary arteryligation (LCAL) just below the left atrium in the atrioven-tricular groove with 7-0 prolene sutures. These rats wereassigned to a saline-treated group (group 1, n=20) and aBMDMNC-treated group (group 2, n=20). Rats (n=20)receiving thoracotomy without LCAL served as over shamcontrol (group 3).
Preparation of BMDMNCs for Autologous TransplantationThe group 2 rats were anesthetized by chloral hydrate
(35mg/kg, ip) on day 3 following LCAL and placed on awarming pad at 37°C. After carefully separating the liga-ment from the patella, an electric rotablator with a diameterof 0.2mm was used to screw straight into the femoral bone.A sterile 22-gauge needle syringe was then used to aspiratethe bone marrow.
Bone marrow cells from each rat were buffered in 10mlRPMI1640 medium (Gibco) and then digested for 40minwith 0.01% collagenase B and DNase1, and filtered througha 30μmol/L nylon mesh. The BMDMNCs were then isolatedby Ficoll-paque (Amersham) density-gradient centrifuga-tion. Finally, the interphase of BMDMNCs was collected.These cells were washed twice with PBS and finally cen-trifuged at 400 g for 5 min. Approximately 1.2–2.0×106
BMDMNCs were obtained from each rat (both femoralbones) via this method and then cultured in a 60mm diame-ter dish using 10ml DMEM culture medium containing 10%5,637 cell-culture supernatant. The 5-azacytidin (Sigma)100μmol/L was added to the culture medium on day 3 fol-lowing BMDMNC culture for 24 h stimulation beforeimplantation. By day 7, 30min before BMDMNCs wereimplanted, 4’,6-diamidino-2-phenylindole (DAPI) (Sigma)(50μg/ml) was added into the culture medium for identi-fication of these cells in an infarct area. Cell viability bytrypan blue exclusion was >95% in all experiments.
Approximately 1.2×106 BMDMNCs in 750μl culturemedium IMDM were implanted in the 1-week-old infarctedarea in group 2 rats and 750μl saline was implanted into the1-week-old infarcted area using a-30 gauge syringe ingroup 1 rats.
Functional Assessment by EchocardiographyTransthoracic echocardiography was performed preopera-
tively as described26 using a commercially available echo-cardiographic system (UF-750XT) equipped with an 8-MHzlinear-array transducer for animals (FUKUDA Denshi Co,Tokyo, Japan), on days 21, 42, and 90 after BMDMNC im-
plantation under anesthesia. LV internal dimensions–[end-systolic diameter (ESD) and end-diastolic diameter (EDD)]–were measured according to the American Society of Echo-cardiography leading-edge method using at least 3 consecu-tives cardiac cycles.27
Immunolabeling of Cx43 and Quantitative Image Data Analysis
Calculation of the integrated area (μm2) of Cx43 spots inthe slides was achieved using Image Tool 3 image analysissoftware (University of Texas, Health Science Center, SanAntonio, UTHSCSA; Image Tool for Windows, Version 3.0,Arlington, TX, USA). Three selected slides for each animalwere quantified. Three randomly selected high-power fields(HPFs) (400×) were analyzed in each slide. The number ofpixels in each Cx43 spot per HPF was first determined, fol-lowed by summation of the pixels number obtained fromthe 3 HPFs in each slide. The mean pixels number per HPFfor each animal was then determined by summation of allpixel numbers divided by 9. The mean Cx43 area per HPFwas obtained by adopting a conversion factor of 19.24 (1μm2 represented 19.24 pixels).
Histological and Immunohistochemical StudiesImmunolabeling of troponin-I-positive, CD31-positive,
andα-smooth muscle actin (α-SMA)-positive stained cellsfor assessment of engrafted cells were examined in the in-farct area. Primary antibodies including anti-troponin I(Sigma), anti-CD31 (JC/70A, Dako) and anti-α-SM actin(Sigma) and secondary antibody, anti-mouse polyvalent-PE conjugate (Sigma), were incubated for 30mins at roomtemperature. Irrelevant antibodies were used as a control.
Immunocytochemical StainingBMDMNCs were also obtained from 4 other rats. These
BMDMNCs (1.2×106 cells/each rat) were then cultured in10ml DMEM culture medium containing 10% 5,637 cell-culture supernatant for 21 days to examine the presence oftroponin-I-positive, CD31-positive, andα-SMA-positivecells. The 5-azacytidin was added into the culture mediumon day 3 following culturing for 24h stimulation.
Western Blot Analysis for Cx43To investigate the impact of BMDMNC therapy on pre-
venting down-regulation of Cx43, protein aliquots (30mg)of LV myocardium were Western blotted for Cx43 accord-ing to manufacturer instructions. The membranes were incu-bated with the indicated primary antibody (Cx43: 1:1,000,Chemicon) for 1h at room temperature. Horseradish peroxi-dase (HPF)-conjugated anti-mouse immunoglobulin IgG(1:2,000, Amersham Biosciences) was used as a secondaryantibody for 1h at room temperature. Immunoreactive bandswere visualized by enhanced chemiluminescence (ECL;Amersham Biosciences) and exposed to Biomax L film(Kodak). Protein bands were quantified using a Labworksoftware (UVP) densitometer.
Real-Time (RT) Quantitative Polymerase Chain Reaction (PCR) Analysis for IL-8/Gro-α, IL-10, MMP-9 and eNOS
A RT-PCR was conducted using a LighCycler TaqManMaster (Roche, Mannheim, Germany) in a single capillarytube according to the manufacturer’s guidelines for individu-al component concentrations.
1338 YIP HK et al.
Circulation Journal Vol.72, August 2008
Vessel Density in Infarct AreaImmunohistochemical stain of blood vessels was per-
formed withα-SMA (1:400) as a primary antibody at roomtemperature for 1h, followed by washing with PBS thrice.The anti-mouse-HRP conjugated secondary antibody wasthen added for 10 min, followed by washing with PBSthrice. The 3,3’ diaminobenzidine (0.7gm/tablet) (Sigma)was added for 1min, followed by washing with PBS thrice.Finally, hematosylin was added for 1min as a counter stainfor nuclei, followed by washing twice. For quantification, 3 sections of the infarct area were chosen for each rat and 3 randomly selected HPFs (×100) were analyzed in eachslide. The mean number per HPF for each animal was thendetermined by summation of all numbers divided by 9.
TUNEL Assay for Apoptotic NucleiFor each rat, 6 sections (3 longitudinal and 3 transverse
sections of LV myocardium) were analyzed by an in situCell Death Detection Kit, AP (Roche), according to themanufacture’s guidelines. The TUNEL-positive cells wereexamined in 3 randomly chosen HPFs (×400) and normal-ized to the total number of cells divided by 18.
Statistical AnalysisData are expressed as mean values (mean±SD). The sig-
nificance of differences between groups was evaluated witha t-test. Continuous variables among 4 groups were com-pared using the Kruskal-Wallis test, followed by a multiplecomparison procedure with the Wilcoxon’s rank sum testand Bonferroni’s correction. SAS statistical software for
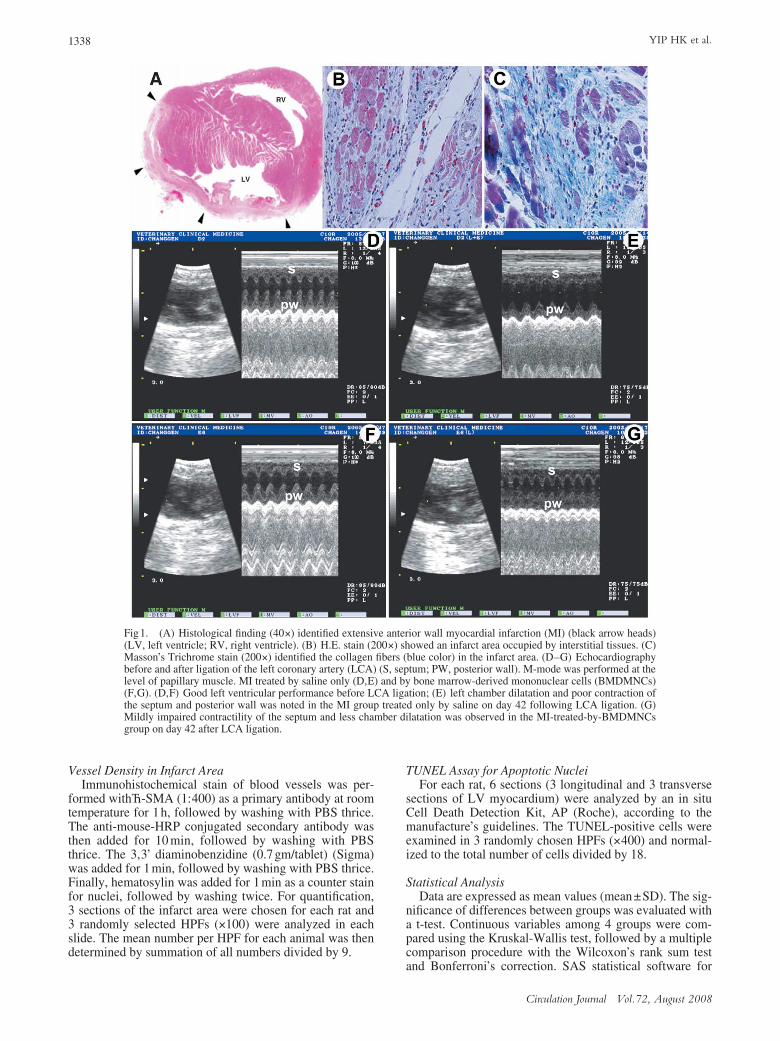
Fig1. (A) Histological finding (40×) identified extensive anterior wall myocardial infarction (MI) (black arrow heads)(LV, left ventricle; RV, right ventricle). (B) H.E. stain (200×) showed an infarct area occupied by interstitial tissues. (C)Masson’s Trichrome stain (200×) identified the collagen fibers (blue color) in the infarct area. (D–G) Echocardiographybefore and after ligation of the left coronary artery (LCA) (S, septum; PW, posterior wall). M-mode was performed at thelevel of papillary muscle. MI treated by saline only (D,E) and by bone marrow-derived mononuclear cells (BMDMNCs)(F,G). (D,F) Good left ventricular performance before LCA ligation; (E) left chamber dilatation and poor contraction ofthe septum and posterior wall was noted in the MI group treated only by saline on day 42 following LCA ligation. (G)Mildly impaired contractility of the septum and less chamber dilatation was observed in the MI-treated-by-BMDMNCsgroup on day 42 after LCA ligation.
1339Bone Marrow Cells Therapy on MI
Circulation Journal Vol.72, August 2008
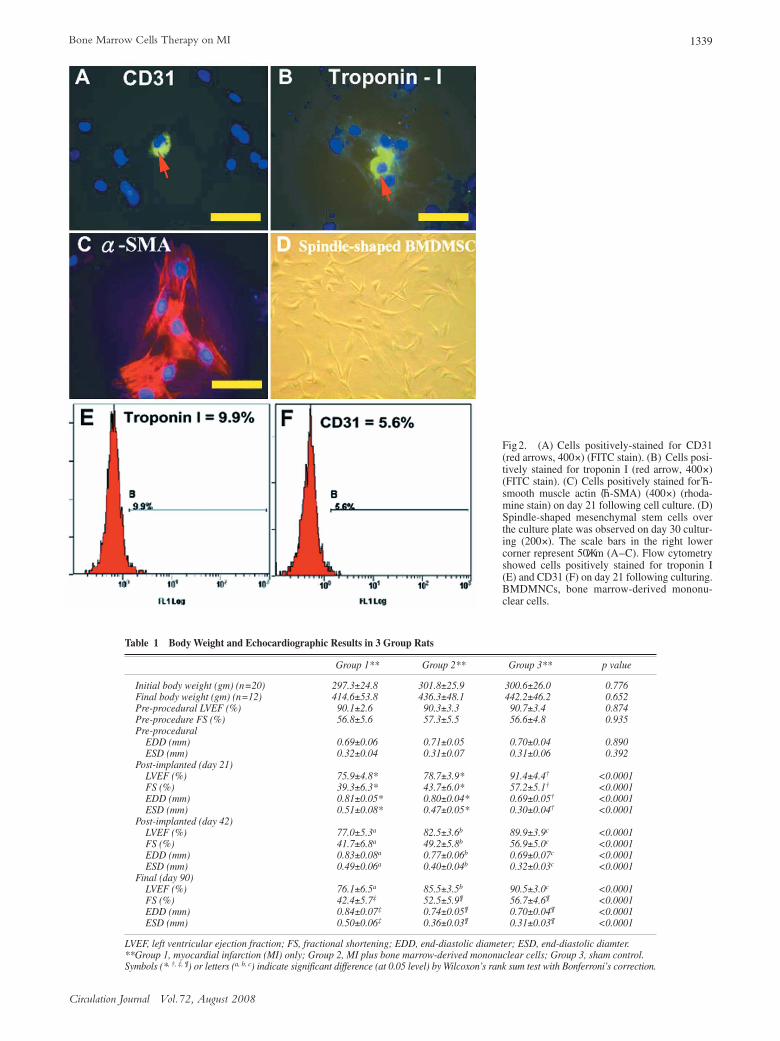
Fig 2. (A) Cells positively-stained for CD31(red arrows, 400×) (FITC stain). (B) Cells posi-tively stained for troponin I (red arrow, 400×)(FITC stain). (C) Cells positively stained forα-smooth muscle actin (α-SMA) (400×) (rhoda-mine stain) on day 21 following cell culture. (D)Spindle-shaped mesenchymal stem cells overthe culture plate was observed on day 30 cultur-ing (200×). The scale bars in the right lowercorner represent 50μm (A–C). Flow cytometryshowed cells positively stained for troponin I(E) and CD31 (F) on day 21 following culturing.BMDMNCs, bone marrow-derived mononu-clear cells.
Table 1 Body Weight and Echocardiographic Results in 3 Group Rats
Group 1** Group 2** Group 3** p value
Initial body weight (gm) (n=20) 297.3±24.8 301.8±25.9 300.6±26.0 0.776Final body weight (gm) (n=12) 414.6±53.8 436.3±48.1 442.2±46.2 0.652Pre-procedural LVEF (%) 90.1±2.6 90.3±3.3 90.7±3.4 0.874Pre-procedure FS (%) 56.8±5.6 57.3±5.5 56.6±4.8 0.935Pre-procedural EDD (mm) 0.69±0.06 0.71±0.05 0.70±0.04 0.890 ESD (mm) 0.32±0.04 0.31±0.07 0.31±0.06 0.392Post-implanted (day 21) LVEF (%) 75.9±4.8* 78.7±3.9* 91.4±4.4† <0.0001 FS (%) 39.3±6.3* 43.7±6.0* 57.2±5.1† <0.0001 EDD (mm) 0.81±0.05* 0.80±0.04* 0.69±0.05† <0.0001 ESD (mm) 0.51±0.08* 0.47±0.05* 0.30±0.04† <0.0001 Post-implanted (day 42) LVEF (%) 77.0±5.3a 82.5±3.6b 89.9±3.9c <0.0001 FS (%) 41.7±6.8a 49.2±5.8b 56.9±5.0c <0.0001 EDD (mm) 0.83±0.08a 0.77±0.06b 0.69±0.07c <0.0001 ESD (mm) 0.49±0.06a 0.40±0.04b 0.32±0.03c <0.0001 Final (day 90) LVEF (%) 76.1±6.5a 85.5±3.5b 90.5±3.0c <0.0001 FS (%) 42.4±5.7‡ 52.5±5.9¶ 56.7±4.6¶ <0.0001 EDD (mm) 0.84±0.07‡ 0.74±0.05¶ 0.70±0.04¶ <0.0001 ESD (mm) 0.50±0.06‡ 0.36±0.03¶ 0.31±0.03¶ <0.0001
LVEF, left ventricular ejection fraction; FS, fractional shortening; EDD, end-diastolic diameter; ESD, end-diastolic diamter.**Group 1, myocardial infarction (MI) only; Group 2, MI plus bone marrow-derived mononuclear cells; Group 3, sham control.Symbols (*, †, ‡, ¶) or letters (a, b, c) indicate significant difference (at 0.05 level) by Wilcoxon’s rank sum test with Bonferroni’s correction.
1340 YIP HK et al.
Circulation Journal Vol.72, August 2008
Windows version 8.2 (SAS institute, Cary, NC, USA) wasused. A probability value <0.05 was considered statisticallysignificant.
ResultsMortality in Each Group
No mortality was observed within group 3 in the studyperiod. However, 5 rats in group 1 and 6 rats in group 2were dead within 7 days after the procedure. Therefore, intotal, 25 rats in group 1 and 26 rats in group 2, respectively,were originally used in the present study.
Histological Findings Indicating LV Anterior Wall Infarction (Fig1: Upper Panel)
Extensive LV MI was identified grossly (Fig1A) and fur-
ther confirmed histopathologically using H.E. (Fig1B) andMasson Trichrome (Fig1C) stains.
Immunoflourescence and Flow Cytometry Findings of Cultured BMDMNCs (Fig2)
By immunofluorescence staining, the cells positive forCD31, a marker of an endothelial phenotype, and cellspositive for troponin I, a cardiomyocyte specific marker,and those positive forα-SMA were observed on day 21 fol-lowing culturing (Figs 2A–C). Plentiful spindle-shapedBMDMSCs were also noted on day 30 of culture (Fig2D).Furthermore, flow cytometric measurement also identifiedthe presence of troponin-I (Fig2E) and CD31 positivelystained cells (Fig2F) following 21-day culture.
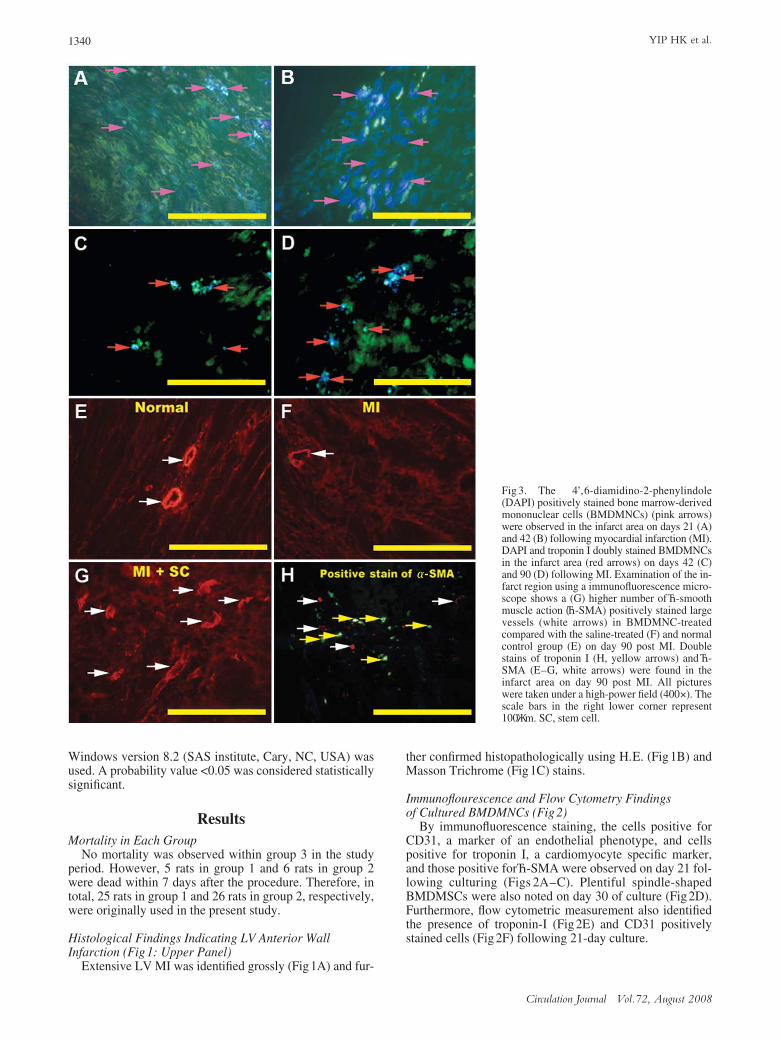
Fig 3. The 4’,6-diamidino-2-phenylindole(DAPI) positively stained bone marrow-derivedmononuclear cells (BMDMNCs) (pink arrows)were observed in the infarct area on days 21 (A)and 42 (B) following myocardial infarction (MI).DAPI and troponin I doubly stained BMDMNCsin the infarct area (red arrows) on days 42 (C)and 90 (D) following MI. Examination of the in-farct region using a immunofluorescence micro-scope shows a (G) higher number ofα-smoothmuscle action (α-SMA) positively stained largevessels (white arrows) in BMDMNC-treatedcompared with the saline-treated (F) and normalcontrol group (E) on day 90 post MI. Doublestains of troponin I (H, yellow arrows) andα-SMA (E–G, white arrows) were found in theinfarct area on day 90 post MI. All pictureswere taken under a high-power field (400×). Thescale bars in the right lower corner represent100μm. SC, stem cell.
1341Bone Marrow Cells Therapy on MI
Circulation Journal Vol.72, August 2008
Initial and Final Body Weight and Serial EchocardiographicFindings (Table1)
Initial and final body weight did not differ between the 3groups. There were no significant differences in initial LVejection fraction (LVEF), fractional shortening (FS),LVEDD, and LVESD between the 3 groups. The LVEF,FS, LVEDD, and LVESD did not differ between groups 1and 2 on day 21 following BMDMNC implantation. How-ever, LVEF and FS on day 21 were significantly lower,whereas LVEDD and LVESD were markedly higher ingroups 1 and 2 than in group 3. Both LVEF and FS on days
42 and 90 (Figs 1D–G) following BMDMNC implantationwere significantly lower in group 1 than in groups 2 and 3.Additionally, LVEDD and LVESD were significantlyhigher in group 1 than in groups 2 and 3. The LVEF and FSwere significantly lower, whereas LVED and LVESD weresignificantly higher in group 2 than in group 3 on day 42following BMDMNC implantation. Moreover, LVEF wassignificantly lower in group 2 than in group 3 on day 90 fol-lowing BMDMNC implantation. However, FS, LVEDD,and LVESD did not differ between groups 2 and 3 on day90 following BMDMNC implantation.
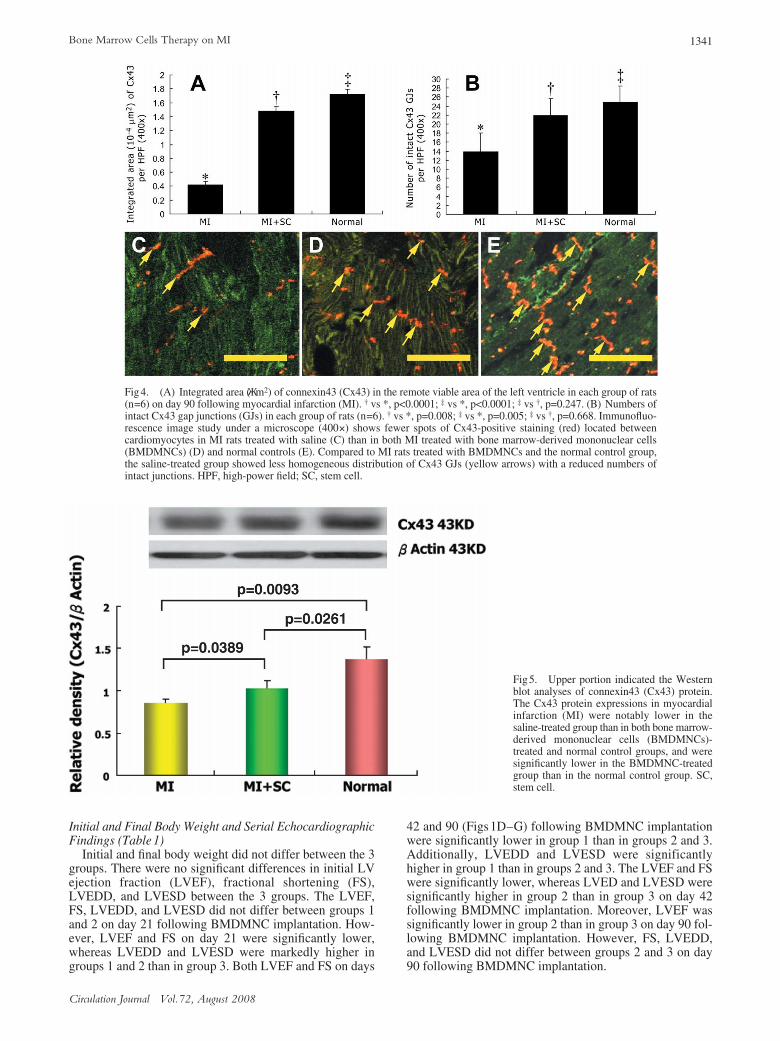
Fig4. (A) Integrated area (μm2) of connexin43 (Cx43) in the remote viable area of the left ventricle in each group of rats(n=6) on day 90 following myocardial infarction (MI). † vs *, p<0.0001; ‡ vs *, p<0.0001; ‡ vs †, p=0.247. (B) Numbers ofintact Cx43 gap junctions (GJs) in each group of rats (n=6). † vs *, p=0.008; ‡ vs *, p=0.005; ‡ vs †, p=0.668. Immunofluo-rescence image study under a microscope (400×) shows fewer spots of Cx43-positive staining (red) located betweencardiomyocytes in MI rats treated with saline (C) than in both MI treated with bone marrow-derived mononuclear cells(BMDMNCs) (D) and normal controls (E). Compared to MI rats treated with BMDMNCs and the normal control group,the saline-treated group showed less homogeneous distribution of Cx43 GJs (yellow arrows) with a reduced numbers ofintact junctions. HPF, high-power field; SC, stem cell.
Fig5. Upper portion indicated the Westernblot analyses of connexin43 (Cx43) protein.The Cx43 protein expressions in myocardialinfarction (MI) were notably lower in thesaline-treated group than in both bone marrow-derived mononuclear cells (BMDMNCs)-treated and normal control groups, and weresignificantly lower in the BMDMNC-treatedgroup than in the normal control group. SC,stem cell.
1342 YIP HK et al.
Circulation Journal Vol.72, August 2008
Identification of Implanted BMDMNCs in the Infarct AreaBy days 21 and 42 following transplantation, numerous
DAPI-stained undifferentiated BMDMNCs were engraftedinto the infarct area (Figs3A,B). By days 42 and 90, someDAPI-stained engrafted cells presenting as muscle-like cellswere stained positively for troponin I in the infarct area(Figs 3C,D). Additionally, DAPI-stained engrafted cells,which were stained positively forα-SMA, were also clearlyidentified (Lower panel of Fig3H). Moreover, the numberof vessels stained positively forα-SMA was notably higherin group 2 than in group 1 rats [group 2 (5.67±1.07) vs group3 (2.0±0.89) vs group 1 (0.83±0.75), p=0.0012] (Lowerpanel of Figs3E–G).
Cx43 Expression in the LV Remote AreaFig4A shows the results of quantification of an integrated
area (μm2) of clustered Cx43 spots in each group of LVmyocardium on day 90 following BMDMNC therapy. Thesummation area of Cx43 did not differ between group 2 andgroup 3. However, the summation area of Cx43 spots was
substantially lower in group 1 than in groups 2 and 3.Figs 4B–E shows the results of numbers of intact Cx43
gap junctions in each group of rats. The number did not dif-fer between groups 2 and 3. However, it was significantlylower in group 1 than in groups 2 and 3.
Western Blot Analysis of Cx43 in an LV Remote Area (Fig5)
The Cx43 protein expression of an LV remote area wassubstantially lower in group 1 than in groups 2 and 3 onday 90 following BMDMNC treatment. Additionally,Cx43 protein expression in an LV remote area was signifi-cantly lower in group 2 than in group 3.
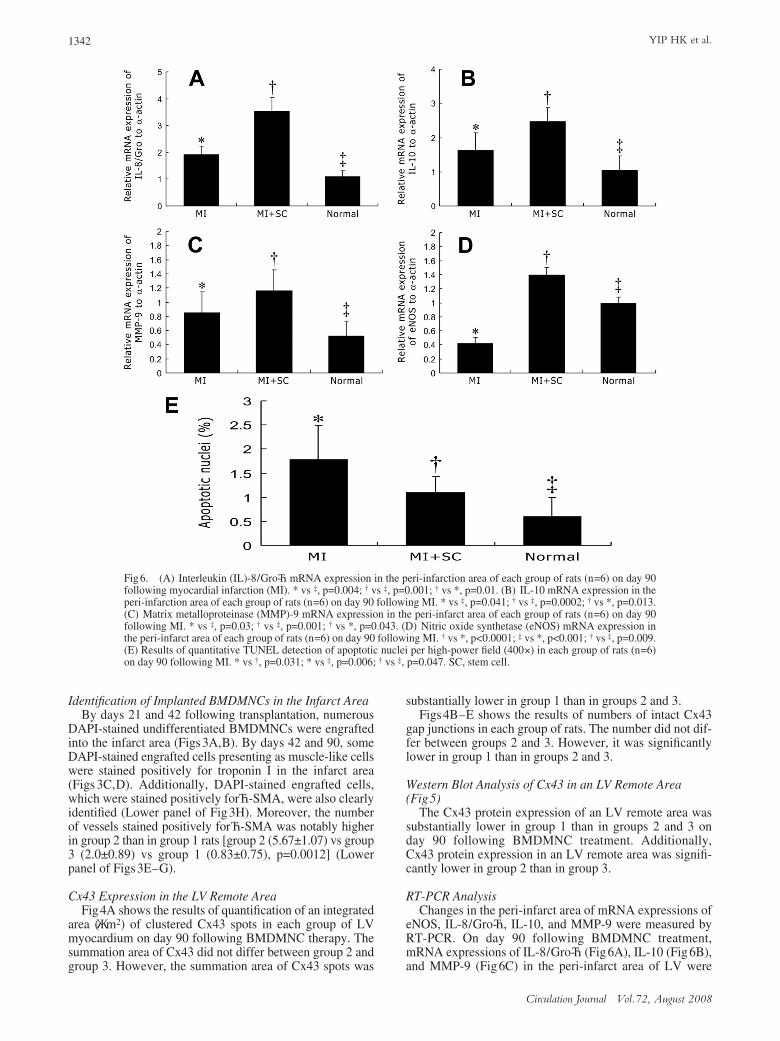
RT-PCR AnalysisChanges in the peri-infarct area of mRNA expressions of
eNOS, IL-8/Gro-α, IL-10, and MMP-9 were measured byRT-PCR. On day 90 following BMDMNC treatment,mRNA expressions of IL-8/Gro-α(Fig6A), IL-10 (Fig6B),and MMP-9 (Fig6C) in the peri-infarct area of LV were
Fig6. (A) Interleukin (IL)-8/Gro-αmRNA expression in the peri-infarction area of each group of rats (n=6) on day 90following myocardial infarction (MI). * vs ‡, p=0.004; † vs ‡, p=0.001; † vs *, p=0.01. (B) IL-10 mRNA expression in theperi-infarction area of each group of rats (n=6) on day 90 following MI. * vs ‡, p=0.041; † vs ‡, p=0.0002; † vs *, p=0.013.(C) Matrix metalloproteinase (MMP)-9 mRNA expression in the peri-infarct area of each group of rats (n=6) on day 90following MI. * vs ‡, p=0.03; † vs ‡, p=0.001; † vs *, p=0.043. (D) Nitric oxide synthetase (eNOS) mRNA expression inthe peri-infarct area of each group of rats (n=6) on day 90 following MI. † vs *, p<0.0001; ‡ vs *, p<0.001; † vs ‡, p=0.009.(E) Results of quantitative TUNEL detection of apoptotic nuclei per high-power field (400×) in each group of rats (n=6)on day 90 following MI. * vs †, p=0.031; * vs ‡, p=0.006; † vs ‡, p=0.047. SC, stem cell.
1343Bone Marrow Cells Therapy on MI
Circulation Journal Vol.72, August 2008
significantly higher in groups 1 and 2 than in group 3, andsignificantly higher in group 2 than in group 1. Conversely,eNOS mRNA expression (Fig6D) in the peri-infarct areawas significantly lower in group 1 than in groups 2 and 3and significantly higher in group 2 than in group 3.
Apoptotic Nuclei Formation in Remote Viable Myocardium
Fig6E shows the results of quantitative TUNEL detectionof apoptotic nuclei. Experimental results showed that thenumber of apoptotic nuclei was significantly increased ingroup 1 than in groups 2 and 3, and in group 2 than in group3.
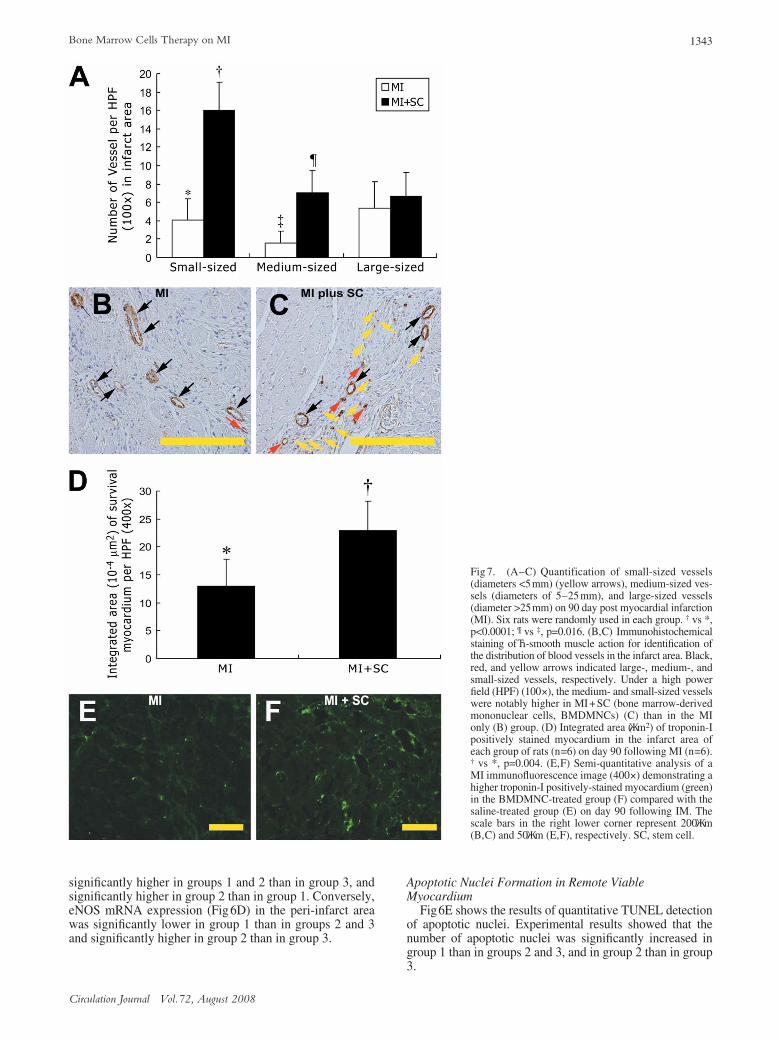
Fig 7. (A–C) Quantification of small-sized vessels(diameters <5mm) (yellow arrows), medium-sized ves-sels (diameters of 5–25 mm), and large-sized vessels(diameter >25mm) on 90 day post myocardial infarction(MI). Six rats were randomly used in each group. † vs *,p<0.0001; ¶ vs ‡, p=0.016. (B,C) Immunohistochemicalstaining ofα-smooth muscle action for identification ofthe distribution of blood vessels in the infarct area. Black,red, and yellow arrows indicated large-, medium-, andsmall-sized vessels, respectively. Under a high powerfield (HPF) (100×), the medium- and small-sized vesselswere notably higher in MI+SC (bone marrow-derivedmononuclear cells, BMDMNCs) (C) than in the MIonly (B) group. (D) Integrated area (μm2) of troponin-Ipositively stained myocardium in the infarct area ofeach group of rats (n=6) on day 90 following MI (n=6).† vs *, p=0.004. (E,F) Semi-quantitative analysis of aMI immunofluorescence image (400×) demonstrating ahigher troponin-I positively-stained myocardium (green)in the BMDMNC-treated group (F) compared with thesaline-treated group (E) on day 90 following IM. Thescale bars in the right lower corner represent 200μm(B,C) and 50μm (E,F), respectively. SC, stem cell.

1344 YIP HK et al.
Circulation Journal Vol.72, August 2008
Vascular Density and Quantitative Survival Myocardium in an Infarct Area
The number of large-sized vessels in an infarct area didnot differ between groups 1 and 2. However, the number ofsmall-sized and medium-sized vessels in the infarct areawas significantly higher in group 2 than in group 1 on day90 after BMDMNC implantation (Figs7A–C). Additional-ly, the integrated area of survival myocardium was signifi-cantly higher in group 2 than in group 1 on day 90 afterimplantation (Figs7D–F).
DiscussionExperimental evidence has suggested that BMDMSCs
are highly advantageous for cell therapy.5–7 Increasing datahas also shown that BMDMSCs can be successfully im-planted into ischemic or infarct myocardium by differentmethods.5–11,13 Additionally, these engrafted BMDMSCscan differentiate into myogenic cells and cells with CD31endothelial phenotype in the infarct area.5,8,13 In the presentstudy, we observed that BMDMNCs were successfullyimplanted into an infarct myocardium and survived in theinfarct area as long as 3 months. Additionally, differentia-tion of these engrafted BMDMNCs into myogenic cellsandα-SMA-positive cells were clearly identified in theinfarct area. Thus, our results are consistent with those ob-tained from recent experimental studies5,8,9,13 and furthersupport findings acquired by in vitro study.28
In this study, although the engrafted BMDMNCs differ-entiated into troponin I-positive cells in the infarct myocar-dium, a rather large number of these engrafted BMDMNCswere found to present either as undifferentiated orα-SMA-positive phenotype. The mechanism by which mesenchymalstem cells develop into cardiac myocyte-like cells remainsunclear.9 Furthermore, poor cell viability associated withtransplantation and difficulty obtaining clinically meaningfulnumbers of transplanted BMDMSCs that have differentiatedinto myocyte-like cells have been suggested as limitationsin the reparative capacity for replacing lost myocardiumthrough these cells.9,29 A recent study13 also demonstratedthat implanted allogenic mesenchymal stem cells in post-infarcted rat myocardium did not fully evolve into adultcardiomyocytes. Accordingly, our findings further supportthe observations9,12,29 that the number of myogenic-like cellsin the infarct area having differentiated from BMDMSCs istypically insufficient for restoring MI.
Interestingly, serial echocardiographic measurementsshowed that LV function was significantly improved andLV chamber size was notably reduced in the BMDMNCtherapy group compared with those in the saline-treated MIgroups on post-transplant days 42 and 90 in this study. Thefindings of an inadequate number of BMDMNCs differenti-ating into myogenic-like cells and the distinctive improve-ment in LV remodeling and post-transplantation LV func-tion in this study suggest that other unidentified confoundersexist. In fact, proposed mechanisms, including angiogene-sis,5,7 myogenesis,5,9 cytokine effects,7 effect of paracrinemediators,8,9 or a myocardial homing by BMDMSCs to themyocardium for reparation and angiogenesis,30,31 underlyingimproved cardiac function following BMDMSC therapy inischemic or infarcted myocardium have been extensivelydebated. However, the exact mechanism remains poorlydefined.7,10,13 Collectively, we suggest that the significanceof any single mechanism acting alone is unlikely. Further-more, because it appeared that the site of BMDMSC injec-
tion is irrelevant, the BMDMSC-derived paracrine media-tors might be the key elements in improving LV functionand remodeling.
The effects of cytokines on myocardial homing of bonemarrow angioblasts and neovascularization have beendemonstrated in a recent experimental study.25 Importantly,RT-PCR identified that mRNA expressions of IL-8/Gro-α,IL-10, and MMP-9 in a peri-infarct area were significantlyhigher in the BMDMNC therapy group than that in thesaline-treated MI group in the present study. Moreover,eNOS gene expression in the peri-infarct area and thenumber of vessels in the infarct area were both markedlyhigher in the BMDMNC therapy group than in the saline-treated MI group. Therefore, our findings, together withthose from other studies,25 might explain the substantiallyhigher summation area of survival myocardium in the in-farct zone after BMDMNC treatment compared to thesaline-treated MI group in this study. More importantly, ourfindings suggest that the new vessel formation is the resultof angiogenesis and vasculogenesis and the effects of cyto-kines following BMDMNC transplantation. Interestingly,in vitro studies32,33 have recently demonstrated that eithercytokine or shock wave therapy applied to BMDMNC canenhance angiogenesis, expression of vascular endothelialgrowth factor, and positive CD31 cellular staining. Otherrecent investigations5–7,34,35 have also shown that autologousbone marrow cell transplantation elicits angiogenesis,which in turn improves ischemia-induced organ dysfunc-tion. Accordingly, the current findings could also, at least inpart, explain the improved cardiac function after BMDMNCtransplantation.
Damage to injured and remote viable myocardium fromAMI is often progressive,14,15 as in post-infarcted LV re-modeling. Most previous experimental studies focused onexamining the differentiation of implanted mesenchymalstem cells into myogenic-like cells or endothelial cells in aninfarcted area rather than the additional beneficial effects ofthese implanted cells on remote viable myocardium. Theprincipal finding in this study was that the total area of Cx43and the number of intact Cx43 gap junctions were signifi-cantly higher, whereas cellular apoptosis was significantlylower in the remote myocardium in the BMDMNC therapygroup compared with the saline-treated group. Studies havepreviously demonstrated that Cx43 gap junctions are clustersof cell membrane aqueous channels linked to cytoplasmiccompartments of adjacent cells, thereby providing path-ways with minimal resistance for electrical coupling, directintercellular ion exchanges, secondary messengers, andsmall signaling molecules.20–24,36,37 Programmed cell death,or “apoptosis”, which has been shown to increase followinga variety of cardiac insults, such as ischemia-reperfusioninjury and cardiac failure,19 would be initiated following aloss of cell-to-cell communication mediated by gap junc-tions. The decreased number of apoptotic nuclei in theremote area of LV in this study, therefore, might explainthe reduction in LVESD and LVEDD on post-transplanta-tion days 42 and 90 in the BMDMNC therapy comparedwith the saline-treated group.
In conclusion, autologous BMDMNC implantation intothe infarct myocardium can elicit more than 1 harmonicallybiological effect– reducing LV remodeling, improving LVfunction, and reversing the adverse effects of AMI onmolecular and cellular perturbation in the remote viablemyocardium.
1345Bone Marrow Cells Therapy on MI
Circulation Journal Vol.72, August 2008
AcknowledgementThis study is supported by a program grant from the National Science
Council, Taiwan, R.O.C (Grant no. NSC-95-2745-B-182A-001).
References1. St John Sutton M, Pfeffer MA, Plappert T, Rouleau JL, Moye LA,
Dagenais GR, et al. Quantitative two-dimentional echocardiographicmeasurements are major predictors of adverse cardial events afteracute myocardial infarction: The protective effects of captopril.Circulation 1994; 89: 68–75.
2. The Acute Infarction Ramipril Efficacy (AIRE) Study Investigators.Effect of ramipril on morality and morbidity of survivors of acutemyocardial infarction with clinical evidence of heart failure. Lancet1993; 342: 812–828.
3. Pfeffer MA, McMurray JJ, Velazquez EJ, Rouleau JL, Køber L,Maggioni AP. Valsartan, captopril, or both in myocardial infarctioncomplicated by heart failure, left ventricular dysfunction, or both. NEngl J Med 2003; 349: 1893–1906.
4. Stone GW, Webb J, Cox DA, Brodie BR, Qureshi M, Kalynych A, etal. Distal microcirculatory protection during percutaneous coronaryintervention in acute ST-segment elevation myocardial infarction: Arandomized controlled trial. JAMA 2005; 293: 1063–1072.
5. Tomita S, Ki RK, Weisel RD, Mickle DAG, Kim EJ, Sakai T, et al.Autologous transplantation of bone marrow cells improves damagedheart function. Circulation 1999; 100(Suppl): II-247– II-256.
6. Strauer BE, Brehm M, Zeus T, Kostering M, Hernandez A, Sorg RV,et al. Repair of infarcted myocardium by autologous intracoronarymononuclear bone cell transplantation in humans. Circulation 2002;106: 1913–1918.
7. Tse HF, Kwong YL, Chan JK, Lo G, Ho CL, Lau CP. Angiogenesisin ischemic myocardium by intramyocardial autologous bone marrowmononuclear cell implantation. Lancet 2003; 4: 47–49.
8. Davani S, Marandin A, Merisin N, Royer B, Kantelip B, Herve P, etal. Mesenchymal progenitor cells differentiate into an endothelialphenotype, enhance vascular density, and improve heart function in arat cellular cardiomyoplasty model. Circulation 2003; 108(Suppl):II-253 – II-258.
9. Mangi AA, Noiseux N, Kong D, He H, Rezvani M, Ingwall JS, et al.Mesenchymal stem cells modified with Akt prevent remodeling andrestore performance of infracted hearts. Nat Med 2003; 9: 1195–1201.
10. Makino S, Fukuda K, Miyoshi S, Konishi F, Kodama H, Pan J, et al.Cardiomyocytes can be generated from marrow stromal cell in vitro.J Clin Invest 1999; 103: 697–705.
11. Wang JS, Shum-Tim D, Chedrawy E, Chiu RC. The coronary deliv-ery of marrow stromal cells for myocardial regeneration: Pathophysi-ologic and therapeutic implications. J Thorac Cardiovasc Surg 2001;122: 699–705.
12. Nagaya N, Kangawa K, Itoh T, Iwase T, Murakami S, Miyahara Y,et al. Transplantation of mesenchymal stem cells improves cardiacfunction in a rat model of dilated cardiomyopathy. Circulation 2005;112: 1128–1135.
13. Dai W, Hale SL, Martin BJ, Kuang IQ, Dow JS, Wold LE, et al. Al-logeneic mesenchymal stem cell transplantation in postinfarcted ratmyocardium: Short- and long-term effects. Circulation 2005; 112:214–223.
14. Chen KR. Stress pathways and heart failure. Cell 1999; 98: 555–558.
15. Bloom NV, Leor J, Ohad DG, Hasin Y, Amar M, Fixler R, et al.Cytotoxic T lymphocytes are activated following myocardial infarc-tion and can recognize and kill healthy myocytes in vitro. J Mol CellCardiol 2000; 32: 2141–2149.
16. Oppenheim RW. Cell death during development of the nervoussystem. Annu Rev Neurosci 1991; 14: 453–459.
17. Raff MC, Barres BA, Burne JF, Coles HS, Ishizaki Y, Jacobson MD.Programmed cell death and the control of cell survival: Lessons from
the nervous system. Science 1993; 262: 695–700.18. Shacter E, Beecham EJ, Covey JM, Kohn KW, Potter M. Activated
neutrophil induced prolonged DNA damage in neighboring cells.Carcinogenesis 1998; 9: 2297–2304.
19. Scarabelli TM, Knight R, Stephanou A, Townsend P, Chen-ScarabelliC, Lawrence K, et al. Clinical implications of apoptosis in ischemicmyocardium. Curr Probl Cardiol 2006; 31: 181–264.
20. Jalife J, Morley GE, Vaidya D. Connexins and impulse propagationin the mouse heart. J Cardiovasc Electrophysiol 1999; 10: 1649–1663.
21. Vozzi C, Dupont E, Coppen SR, Yeh HI, Severs NJ. Chamber-re-lated differences in connexin expression in human heart. J Mol CellCardiol 1999; 31: 991–1003.
22. Severs NJ, Rothery S, Dupont E, Coppen SR, Yeh HI, Ko YS, et al.Immunocytochemical analysis of connexin expression in healthy anddiseased cardiovascular system. Microsc Res Tech 2001; 52: 301–322.
23. Kirchhoff S, Nelles E, Hagendorff A, Krüger O, Traub O, Willecke K.Reduced cardiac conduction velocity and predisposition to arrhyth-mias in connexin40-deficient mice. Curr Biol 1998; 8: 299–302.
24. Lerner DL, Yamada KA, Schuessler RB, Saffitz JE. Acceleratedonset and increased incidence of ventricular arrhythmias induced byischemia in Cx43-deficient mice. Circulation 2000; 101: 547–552.
25. Kocher AA, Schuster MD, Bonaros N, Lietz K, Xiang G, MartensTP, et al. Myocardial homing and neovascularization by human bonemarrow angioblasts is regulated by IL-8/Gro CXC chemokines. J MolCell Cardiol 2006; 40: 455–464.
26. Litwin SE, Katz SE, Morgan JP, Douglas PS. Serial echocardiogra-phic assessment of left ventricular geometry and function after largemyocardial infarction in the rat. Circulation 1994; 89: 345–354.
27. Jiang Y, Jahagirdar BN, Reinhardt RL, Schwartz RE, Keene CD,Ortiz-Gonzalez XR. Recommendations of regarding quantification inM-mode echocardiography: Results of a survey of echocardiographicmeasurements. Circulation 1978; 58: 1072–1083.
28. Jiang Y, Jahagirdar BN, Reinhardt RL, Schwartz RE, Keene CD,Ortiz-Gonzalez XR, et al. Pluripotency of mesenchymal stem cellsderived from adult marrow. Nature 2002; 418: 41–49.
29. Jackson KA, Majka SM, Wang H, Pocius J, Hartley CJ, MajeskyMW. Human mesenchymal stem cells differentiate to a cardiomyo-cyte phenotype in the adult marine heart. Circulation 2002; 105: 93–98.
30. Jackson KA, Majka SM, Wang H, Pocius J, Hartley CJ, MajeskyMW, et al. Regeneration of ischemic cardiac muscle and vascularendothelium by adult stem cells. J Clin Invest 2001; 107: 1395–1402.
31. Quaini F, Urbanek K, Beltrami AP. Chimerism of the transplantedheart. N Engl J Med 2002; 346: 5–15.
32. Qin SL, Li TS, Takahashi M, Hamano K. In vitro assessment of theeffect of interleukin-1 beta on angiogenic potential of bone marrowcells. Circ J 2006; 70: 1195–1199.
33. Yip HK, Chang LT, Sun CK, Youssef AA, Sheu JJ, Wang CJ. Shockwave therapy applied to rat bone marrow-derived mononuclear cellsenhances formation of cells stained positive for CD31 and vascularendothelial growth factor. Circ J 2008; 72: 150–156.
34. Umemura T, Kishioka K, Igarashi A, Kato Y, Ochi M, Chayama K, etal. Autologous bone marrow mononuclear cell implantation inducesangiogenesis and bone regeneration in a patient with compartmentsyndrome. Circ J 2006; 70: 1362–1364.
35. Kajiguchi M, Kondo T, Izawa H, Kobayashi M, Yamamoto K,Shintani S, et al. Safety and efficacy of autologous progenitor celltransplantation for therapeutic angiogenesis in patients with criticallimb ischemia. Circ J 2007; 71: 196–201.
36. Yeh HI, Lupu F, Dupont E, Severs NJ. Upregulation of connexin43gap junctions between smooth muscle cells after balloon catheterinjury in the rat carotid artery. Aterioscler Thromb Vasc Biol 1997;17: 3174–3184.
37. Kumar NM, Gilula NB. The gap junction communication channel.Cell 1996; 84: 381–388.
Copyright © 2022 FDOKUMEN




















