
Neuropsychological, neurological, and neuroanatomical profile of Williams syndrome
Upload
univ-paris5Category
view
1download
0
Autobiographical memory after temporal loberesection: neuropsychological and MRIvolumetric findingsM. Noulhiane,1,2 P. Piolino,3,4 D. Hasboun,1,5 S. Clemenceau,6,7,8 M. Baulac7,8 and S. Samson2,7
1Laboratoire de Neurosciences Cognitives et d’Imagerie Ce¤ re¤ brale, LENA CNRS UPR 640, Universite¤ Pierre et MarieCurie-Paris 6, CHU Pitie¤ Salpe“ trie' re, Paris, 2Neuropsychologie et Cognition Auditive, JE 2497, Universite¤ Charles deGaulle-Lille 3,Villeneuve d’Ascq, 3Laboratoire de Psychologie et Neurosciences Cognitives, CNRS FRE 2987, Universite¤ Paris-Descartes, Boulogne-Billancourt, 4INSERM ^ EPHE ^ Universite¤ de Caen Basse-Normandie,Unite¤ E0218,GIP Cyceron,CHUCo“ te de Nacre, Caen, 5Service de Neuroradiologie, CHU Pitie¤ Salpe“ trie' re, Paris, 6Service de Neurochirurgie, CHU Pitie¤Salpe“ trie' re, Paris, 7Unite¤ d’Epileptologie, CHU Pitie¤ Salpe“ trie' re, Paris and 8INSERM U739, Cortex et Epilepsie, Universite¤Pierre et Marie-Paris 6, CHU Pitie¤ Salpe“ trie' re, Paris, France
Correspondence to: Marion Noulhiane, LPNCog CNRS FRE 2987, e¤ quipe de recherche: ‘Me¤ moire et Apprentissage’ 71, aveEdouard Vaillant F-92774 Boulogne-Billancourt Cedex, FranceE-mail: [email protected]
This study examined the contribution of medial temporal lobe (MTL) structures in autobiographical memory.While some investigators have reported a temporal gradient in memory performance, characterized byretrieval difficulties limited to recent periods of life [Squire and Alvarez (Retrograde amnesia and memoryconsolidation: a neurobiological perspective. Curr Opin Neurobiol 1995; 5: 169^77)], others have suggested thatthis impairment involves all life-time periods [Nadel and Moscovitch (Memory consolidation, retrograde amne-sia and the hippocampal complex.Curr Opin Neurobiol 1997; 7: 217^27)]. In this study, autobiographicalmemorywas assessed in 22 patients who had undergone a left (n=12) or a right (n=10) MTL resection for the relief ofepileptic seizures and in 22 normal control participants. For this purpose, we used an autobiographicalmemorytask (TEMPau, Piolino et al., 2003) across four time periods covering the subjects’ entire lifespan. For eachperiod, an overall autobiographical memory score (AM score) was obtained, from which a strictly episodicscore (SE score), characterized by specificity and richness of details, was computed. For all events recalled,Remember responses justified by specificity of factual, spatial and temporal contents (jR responses) weremeasured using the Remember/Know paradigm.MRI volumetric analyses performed on the medial (i.e. hippo-campus, temporopolar, entorhinal, perirhinal and parahippocampal cortices) and lateral temporal (i.e. superior,middle and inferior temporal gyri) lobe structures stated that the resection mainly included MTL structures.AM and SE scores were impaired in patients with right and left MTL resections as compared to normal controlsacross all time periods, reflecting the patients’ particular difficulty in producing specific and detailed memoriesacross all periods. This impairment was associated with poor autonoetic consciousness, revealed by the smallnumber of jR responses across all periods. Results of correlation analysis between MRI volume measuresof temporal lobe structures and autobiographical memory scores suggest that the right MTL structures areparticularly responsive in reliving the encoding context regardless of remoteness.Our results support the bilat-eral MTL contribution to episodic autobiographical memory covering the entire lifespan, which is consistentwith the multiple trace theory of MTL function [Moscovitch et al. (Functional neuroanatomy of remote epi-sodic, semantic and spatialmemory: a unified account based onmultiple trace theory. J Anat 2005; 207: 35^66.)].
Keywords: autobiographical memory; autonoetic consciousness; temporal lobe epilepsy surgery; MRI volumetric analysis
Abbreviations: MTL=medial temporal lobe; TLE=temporal lobe epilepsy; TPC=temporopolar cortex; PRC=perirhinalcortex; EC=entorhinal cortex; PHC=Parahippocampal cortex
Received April 17, 2007. Revised September 24, 2007. Accepted October 1, 2007. Advance Access publication November 6, 2007
doi:10.1093/brain/awm258 Brain (2007), 130, 3184^3199
� The Author (2007). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: [email protected]
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

IntroductionIt is generally accepted that damage to the hippocampusand related medial temporal lobe (MTL) structures leads tosevere anterograde memory deficits. This finding has beenwell documented in patients who have undergone MTLresection for the relief of intractable epilepsy (e.g. Milneret al., 1968; Milner, 1975; Smith and Milner, 1981; Saykinet al., 1989; Hermann et al., 1992; Helmstaedter and Elger,1996; Berenbaum et al., 1997). However, relatively fewstudies have examined retrograde memory impairments andin particular, episodic autobiographical memory in thesesame patients. Autobiographical memory refers to a multi-faceted concept encompassing different kinds of knowledge,from general knowledge about oneself (semantic compo-nent) to very specific personal events related to the self(episodic component) (Tulving et al., 1988; Kopelmanet al., 1989; Conway and Pleydell-Pearce, 2000). Thismemory ability appears to be necessary to construct a senseof identity and continuity. More specifically, episodicautobiographical memory refers to personally relevantevents acquired in a specific spatio-temporal context andcharacterized by an autonoetic state of consciousness(Tulving, 1985). This latter component enables consciousrecollection of a personal event in its original encodingcontext and implies a kind of mental time travel involvinga personal subjective experience of remembering. Hence,episodic autobiographical memory contains specific‘sensory-perceptual-cognitive-affective details’ (Conway,2001; Conway and Holmes, 2004) that elicit the autonoeticexperience of mentally reliving a past event. In contrast,semantic autobiographical memory is characterized bya noetic state of consciousness allowing one to retrievegeneral facts about an event without re-experiencing it.In neuropsychology, several investigations involving
single-case or group studies have examined autobiographi-cal memory in epileptic patients tested before or aftertemporal lobe resection. However, their results are stillcontroversial regarding the impact of unilateral lesions onthe extent of retrograde autobiographical memory deficit.The differences between the methods used to assessautobiographical memory, the severity of the epilepsy orthe extent of the resection may be responsible for suchdiscrepancies. In 1957, Scoville and Milner reported thecase of HM who had undergone a bilateral MTL removalto control intractable epilepsy (Scoville and Milner, 1957).The initial evaluation of HM’s retrograde memory, basedon post-operative interviews, indicated an autobiographicalretrograde amnesia for a period of 3 years prior to hissurgery. Further evaluations of HM’s autobiographicalretrograde memory using more detailed testing methodsrevealed impairments extending 11 years back (Corkin,1984) or even longer (Corkin, 2002). By applying a string-ent new scoring method proposed by Levine et al. (2002),Steinvorth et al. (2005) showed that HM presented retro-grade amnesia for episodic components of autobiographical
events throughout his entire life without a temporal grad-ient, whereas personal semantic and generic memories werespared. This finding emphasized the permanent involve-ment of MTL structures in retrograde memory. Barr et al.(1990) further explored this issue in a group of patientswho had undergone unilateral temporal lobectomy using anextensive battery of remote memory tests tapping intoepisodic and semantic personal memories. They found thatonly patients with left temporal lobectomy showed remoteautobiographical memory impairments. Using a standardtest of autobiographical memory (AMI, Kopelman et al.,1989), Viskontas et al. (2000) found that patients witheither right or left MTL damage had a poorer memory forautobiographical events than normals, even for those datingfrom early childhood, suggesting that both left and righttemporal lobe lesions affect autobiographical memory.These deficits, which were also present in patients withlate-onset seizures, were noted in pre- and post-surgicalcases. Conversely, personal semantic memory was notimpaired. By using an autobiographical fluency taskdeveloped by Dritschel et al. (1992), Lah et al. (2004)assessed retrieval of names of personal acquaintances(i.e. personal semantic memory) or of personal events(i.e. episodic memory) in patients who had undergoneunilateral temporal lobectomy. These authors found thatpatients generated significantly fewer names than controlsbut there was no group difference for personal eventfluency. More recently, Lah et al. (2006), using the sametask in patients with right and left temporal lobe epilepsy(TLE), reported that the two patient groups were impairedin the subtest of fluency names. In the personal eventfluency, however, they found that patients with right TLEwere more impaired than patients with left TLE.Voltzenlogel et al. (2006) also showed that patients withboth right and left temporal lobe epilepsy produced deficitsin memory for autobiographical episodes assessed bythe AMI and the Modified Crovitz Test (Crovitz andSchiffman, 1974; Graham and Hodges, 1997) across all timeperiods. In addition, an effect of laterality was noted, withright TLE patients obtaining significantly better scores thanleft TLE patients. In contrast, personal semantic memorywas spared in both groups. Except in the study of Lah et al.(2006) which found that young age at onset (younger than14 years) was associated with greater difficulties in recallof famous events, all these studies agreed that the durationof epilepsy and the age of seizure onset did not influenceperformance on remote memory measures. In brief, therecent neuropsychological findings in epileptic patientsobtained before or after MTL resection attested to thepreservation of personal semantic memory but generallyshowed deficits of episodic autobiographical memory.The issue of the impact of unilateral lesions is still amatter for debate.
The temporally graded or un-graded episodic retrogradememory impairments found in epileptic patients withtemporal lobe resection can be explained by two competing
Autobiographical memory afterTLE surgery Brain (2007), 130, 3184^3199 3185
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

neurobiological models of long-term episodic memory.According to the standard model (McClelland et al., 1995;Squire and Alvarez, 1995; Murre, 1996; Bayley et al., 2005),MTL structures are not only involved in encoding but theymay also contribute to storage and retrieval of declarativememory (either episodic or semantic) for a limited periodof time (i.e. few years). The MTL would serve as a tempo-rary index for retrieval, whereas the neocortex wouldprovide permanent long-term memory repositories. After acouple of years (Graham and Hodges, 1997; Schmidtke andVollmer, 1997) or approximately 10 years (Rempel-Cloweret al., 1996; Reed and Squire, 1998), the links between theMTL and the neocortex vanish. This model thereforepredicts a temporally graded retrograde memory deficitof episodic information in patients with MTL resection.An alternative model, the multiple trace model, suggeststhat the hippocampus and related MTL structures arepermanently involved in the recollection of episodicmemories (Nadel and Moscovitch, 1997, 2001; Nadel andHardt, 2004; Moscovitch et al., 2005). As time passes, newlinks are created within the MTL so that remote episodicmemories are stored even more deeply in multiple traces,i.e. represented by multiple hippocampal–neocortical traces.This theory gives a comprehensive account of episodicretrograde memory deficits observed in patients withMTL lesions (see Fujii et al., 1999; Cipolotti et al., 2001;Rosenbaum et al., 2001; Moscovitch et al., 2005). The MTLis therefore necessary to re-experience detailed episodicmemories no matter how old they are. This model suggeststhat the MTL may permanently contribute to the differ-ent aspects of episodic autobiographical memory but itprovides no indication about the specific involvement ofeach MTL structure in such memory abilities (Moscovitchet al., 2005). In this current debate on the role of MTLstructures in episodic autobiographical memory, anatomicaldata describing the extent damage within the temporal lobeconstitute precious findings.The aim of the present study was therefore to investigate the
role of various MTL regions in episodic autobiographicalmemory in patients who had undergone unilateral MTLresection for the relief of intractable epilepsy. For this purpose,we used an autobiographical memory task (TEMPau task,Piolino et al., 2003) that allows one to obtain a stringent scoreof episodicity and to differentiate Remember from Knowresponses (Tulving, 1985; Gardiner, 2001) by asking factual,spatial and temporal details associated with specific personalevents. A ‘Remember’ response corresponds to the retrieval ofan event based on the recollection of details about the sourceof acquisition. A ‘Know’ response corresponds to a feelingof familiarity without any precise recollection. This task haspreviously been used to specify features of episodic auto-biographical memory deficits in ageing, neurodegenerativediseases and traumatic brain injury as well as psychiatricdiseases (e.g. Piolino et al., 2003, 2004, 2006, 2007), but not yetin patients with unilateral MTL resection. We quantified theremaining temporal lobe tissue after the resection by means
of MRI volumetric measures of MTL structures (i.e. thetemporopolar, perirhinal, entorhinal and parahippocampalcortices and the hippocampus). To ensure that the resectionmainly concerned the MTL structures, we also performedMRI volumetric analysis of the lateral temporal lobe struc-tures (i.e. the superior, middle and inferior temporal gyri).We used a correlative approach between episodic autobio-graphical memory measures across different time periods(recent and remote periods) and MRI volumetric measures(see Kopelman et al., 2003; Gilboa et al., 2005) of medial andlateral temporal lobe structures. According to the standardmodel, we predicted correlations between remaining volumesof the MTL and episodic memory deficits for recent but notremote periods. Conversely, if the multiple trace model isvalid, correlations between remaining volumes of the MTLand episodic memory deficits regardless of the time periodwould be expected.
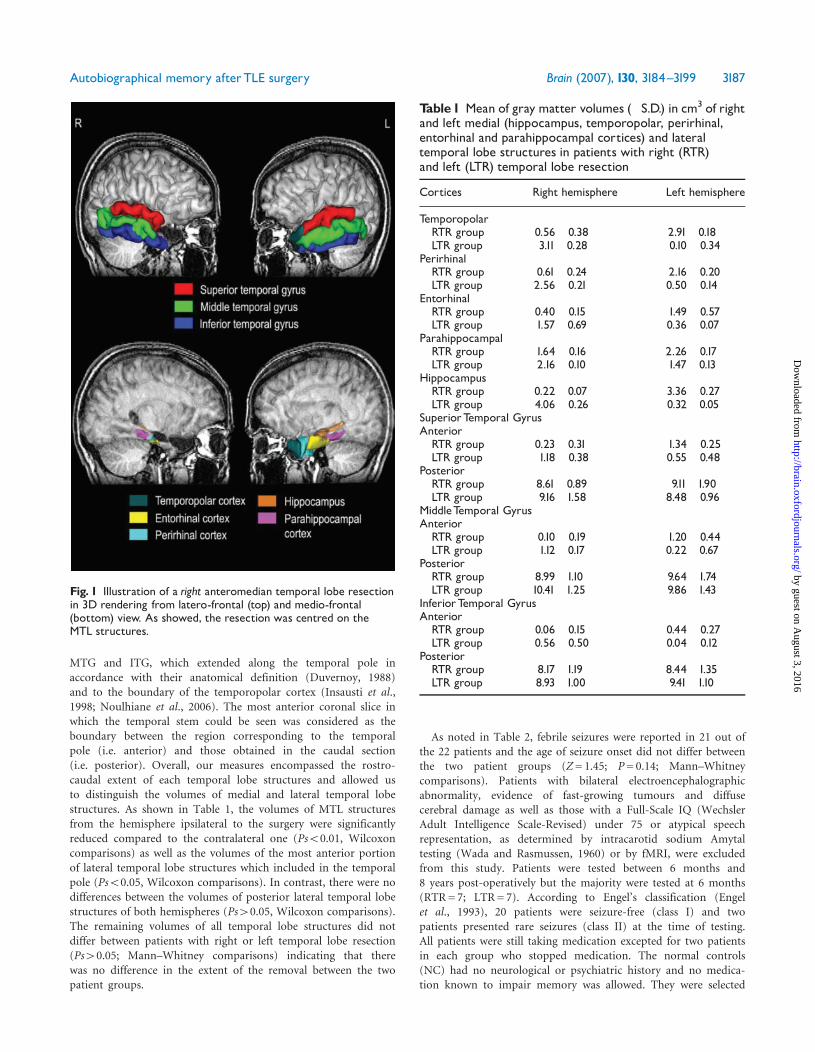
MethodsParticipantsTwenty-two patients who had undergone a left (LTR, n= 12)or right (n=10) MTL resection for the relief of medicallyintractable epilepsy associated with hippocampal sclerosis (diag-nosed by pre-operative MRI) and 22 normal controls participatedin this study. The patients were operated at La Salpetriere Hospital(Paris). Patients underwent a temporal lobe resection by using thetranscortical approach across the superior temporal gyrus (Fig. 1).The resections, performed microsurgically under operative micro-scope by the same neurosurgeon (SC), included the removal of themajor portion of the amygdala (with respect of its most medialand superior parts), the uncus, the hippocampus, various amountsof the surrounding cortices (entorhinal, perirhinal and para-hippocampal cortex) and the anterior portion of the superiortemporal gyri caudally to the temporal pole. The temporal polewas resected in all patients except for two RTR patients andone LTR patient for whom the surgery consisted of a selectiveamygdalo-hippocampectomy. Besides the temporal pole, thelateral and basal temporal lobe cortices, except the most anteriorpart of the superior temporal gyrus, were preserved in all patients.The patients underwent imaging with a 1.5-T MRI scanner
using a standard head coil and tilted coronal 3D magnetization-prepared rapid acquisition gradient-echo sequence with thefollowing parameters: 14.3/6.3/1 (repetition time/echo time/excitation). This resulted in 124 contiguous T1-weighted parti-tions with a 1.5-mm section thickness. High-resolution MRIvolumetric measurements of the gray-matter of MTL structuresincluding the temporopolar cortex (TPC), perirhinal cortex(PRC), entorhinal cortex (EC), parahippocampal cortex (PHC)and hippocampus (H), were carried out using a protocoldeveloped by Noulhiane et al. (2006). We also measured graymatter volumes of the lateral temporal lobe structures, namely thesuperior temporal gyrus (STG), the middle temporal gyrus (MTG)and the inferior temporal gyrus (ITG) in reference to the protocolof Onitsuka et al. (2004). T1-weighted images were used in anautomatic segmentation program to classify brain tissue into grayand white matter (Brainvisa environment, Cointepas et al., 2001).In this protocol, the most anterior part of the STG, MTG andITG, as it could be considered as the temporal pole (Broadmann’sarea 38), was not included. We added the measure of the STG,
3186 Brain (2007), 130, 3184^3199 M. Noulhiane et al.
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from
MTG and ITG, which extended along the temporal pole inaccordance with their anatomical definition (Duvernoy, 1988)and to the boundary of the temporopolar cortex (Insausti et al.,1998; Noulhiane et al., 2006). The most anterior coronal slice inwhich the temporal stem could be seen was considered as theboundary between the region corresponding to the temporalpole (i.e. anterior) and those obtained in the caudal section(i.e. posterior). Overall, our measures encompassed the rostro-caudal extent of each temporal lobe structures and allowed usto distinguish the volumes of medial and lateral temporal lobestructures. As shown in Table 1, the volumes of MTL structuresfrom the hemisphere ipsilateral to the surgery were significantlyreduced compared to the contralateral one (Ps50.01, Wilcoxoncomparisons) as well as the volumes of the most anterior portionof lateral temporal lobe structures which included in the temporalpole (Ps50.05, Wilcoxon comparisons). In contrast, there were nodifferences between the volumes of posterior lateral temporal lobestructures of both hemispheres (Ps40.05, Wilcoxon comparisons).The remaining volumes of all temporal lobe structures did notdiffer between patients with right or left temporal lobe resection(Ps40.05; Mann–Whitney comparisons) indicating that therewas no difference in the extent of the removal between the twopatient groups.
As noted in Table 2, febrile seizures were reported in 21 out ofthe 22 patients and the age of seizure onset did not differ betweenthe two patient groups (Z= 1.45; P= 0.14; Mann–Whitneycomparisons). Patients with bilateral electroencephalographicabnormality, evidence of fast-growing tumours and diffusecerebral damage as well as those with a Full-Scale IQ (WechslerAdult Intelligence Scale-Revised) under 75 or atypical speechrepresentation, as determined by intracarotid sodium Amytaltesting (Wada and Rasmussen, 1960) or by fMRI, were excludedfrom this study. Patients were tested between 6 months and8 years post-operatively but the majority were tested at 6 months(RTR= 7; LTR= 7). According to Engel’s classification (Engelet al., 1993), 20 patients were seizure-free (class I) and twopatients presented rare seizures (class II) at the time of testing.All patients were still taking medication excepted for two patientsin each group who stopped medication. The normal controls(NC) had no neurological or psychiatric history and no medica-tion known to impair memory was allowed. They were selected
Fig. 1 Illustration of a right anteromedian temporal lobe resectionin 3D rendering from latero-frontal (top) and medio-frontal(bottom) view. As showed, the resection was centred on theMTL structures.
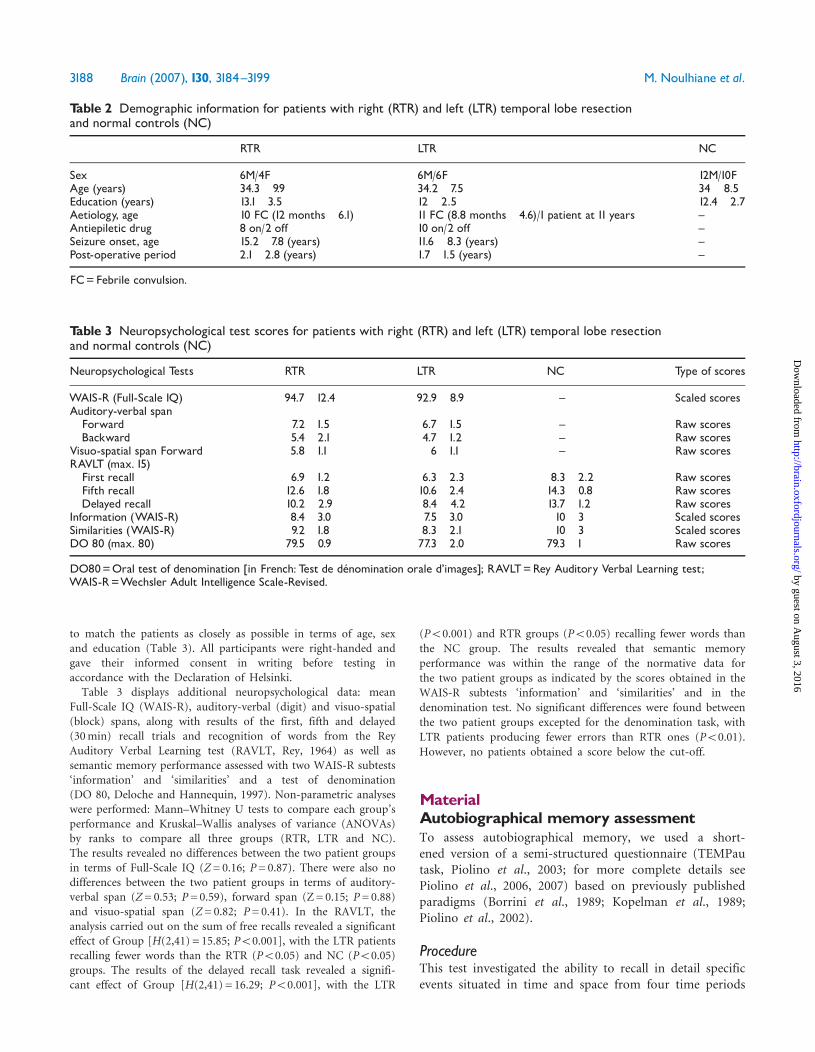
Table1 Mean of gray matter volumes (�S.D.) in cm3 of rightand left medial (hippocampus, temporopolar, perirhinal,entorhinal and parahippocampal cortices) and lateraltemporal lobe structures in patients with right (RTR)and left (LTR) temporal lobe resection
Cortices Right hemisphere Left hemisphere
TemporopolarRTR group 0.56� 0.38 2.91�0.18LTR group 3.11�0.28 0.10� 0.34
PerirhinalRTR group 0.61�0.24 2.16� 0.20LTR group 2.56� 0.21 0.50� 0.14
EntorhinalRTR group 0.40� 0.15 1.49� 0.57LTR group 1.57�0.69 0.36� 0.07
ParahippocampalRTR group 1.64� 0.16 2.26� 0.17LTR group 2.16� 0.10 1.47�0.13
HippocampusRTR group 0.22� 0.07 3.36� 0.27LTR group 4.06� 0.26 0.32� 0.05
SuperiorTemporal GyrusAnteriorRTR group 0.23� 0.31 1.34� 0.25LTR group 1.18� 0.38 0.55� 0.48
PosteriorRTR group 8.61�0.89 9.11�1.90LTR group 9.16�1.58 8.48� 0.96
MiddleTemporal GyrusAnteriorRTR group 0.10� 0.19 1.20� 0.44LTR group 1.12� 0.17 0.22� 0.67
PosteriorRTR group 8.99�1.10 9.64�1.74LTR group 10.41�1.25 9.86�1.43
InferiorTemporal GyrusAnteriorRTR group 0.06� 0.15 0.44� 0.27LTR group 0.56� 0.50 0.04� 0.12
PosteriorRTR group 8.17�1.19 8.44�1.35LTR group 8.93�1.00 9.41�1.10
Autobiographical memory afterTLE surgery Brain (2007), 130, 3184^3199 3187
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from
to match the patients as closely as possible in terms of age, sexand education (Table 3). All participants were right-handed andgave their informed consent in writing before testing inaccordance with the Declaration of Helsinki.Table 3 displays additional neuropsychological data: mean
Full-Scale IQ (WAIS-R), auditory-verbal (digit) and visuo-spatial(block) spans, along with results of the first, fifth and delayed(30min) recall trials and recognition of words from the ReyAuditory Verbal Learning test (RAVLT, Rey, 1964) as well assemantic memory performance assessed with two WAIS-R subtests‘information’ and ‘similarities’ and a test of denomination(DO 80, Deloche and Hannequin, 1997). Non-parametric analyseswere performed: Mann–Whitney U tests to compare each group’sperformance and Kruskal–Wallis analyses of variance (ANOVAs)by ranks to compare all three groups (RTR, LTR and NC).The results revealed no differences between the two patient groupsin terms of Full-Scale IQ (Z= 0.16; P= 0.87). There were also nodifferences between the two patient groups in terms of auditory-verbal span (Z= 0.53; P=0.59), forward span (Z= 0.15; P= 0.88)and visuo-spatial span (Z= 0.82; P= 0.41). In the RAVLT, theanalysis carried out on the sum of free recalls revealed a significanteffect of Group [H(2,41) = 15.85; P50.001], with the LTR patientsrecalling fewer words than the RTR (P50.05) and NC (P50.05)groups. The results of the delayed recall task revealed a signifi-cant effect of Group [H(2,41) = 16.29; P50.001], with the LTR
(P50.001) and RTR groups (P50.05) recalling fewer words than
the NC group. The results revealed that semantic memory
performance was within the range of the normative data for
the two patient groups as indicated by the scores obtained in theWAIS-R subtests ‘information’ and ‘similarities’ and in the
denomination test. No significant differences were found between
the two patient groups excepted for the denomination task, with
LTR patients producing fewer errors than RTR ones (P50.01).
However, no patients obtained a score below the cut-off.
MaterialAutobiographical memory assessmentTo assess autobiographical memory, we used a short-ened version of a semi-structured questionnaire (TEMPautask, Piolino et al., 2003; for more complete details seePiolino et al., 2006, 2007) based on previously publishedparadigms (Borrini et al., 1989; Kopelman et al., 1989;Piolino et al., 2002).
ProcedureThis test investigated the ability to recall in detail specificevents situated in time and space from four time periods
Table 2 Demographic information for patients with right (RTR) and left (LTR) temporal lobe resectionand normal controls (NC)
RTR LTR NC
Sex 6M/4F 6M/6F 12M/10FAge (years) 34.3� 9.9 34.2� 7.5 34� 8.5Education (years) 13.1�3.5 12� 2.5 12.4� 2.7Aetiology, age 10 FC (12 months� 6.1) 11 FC (8.8 months� 4.6)/1 patient at 11 years ^Antiepiletic drug 8 on/2 off 10 on/2 off ^Seizure onset, age 15.2� 7.8 (years) 11.6� 8.3 (years) ^Post-operative period 2.1�2.8 (years) 1.7�1.5 (years) ^
FC=Febrile convulsion.
Table 3 Neuropsychological test scores for patients with right (RTR) and left (LTR) temporal lobe resectionand normal controls (NC)
Neuropsychological Tests RTR LTR NC Type of scores
WAIS-R (Full-Scale IQ) 94.7�12.4 92.9� 8.9 ^ Scaled scoresAuditory-verbal spanForward 7.2�1.5 6.7�1.5 ^ Raw scoresBackward 5.4� 2.1 4.7�1.2 ^ Raw scores
Visuo-spatial span Forward 5.8�1.1 6�1.1 ^ Raw scoresRAVLT (max. 15)First recall 6.9�1.2 6.3�2.3 8.3�2.2 Raw scoresFifth recall 12.6�1.8 10.6�2.4 14.3� 0.8 Raw scoresDelayed recall 10.2� 2.9 8.4� 4.2 13.7�1.2 Raw scores
Information (WAIS-R) 8.4�3.0 7.5�3.0 10�3 Scaled scoresSimilarities (WAIS-R) 9.2�1.8 8.3�2.1 10�3 Scaled scoresDO 80 (max. 80) 79.5� 0.9 77.3�2.0 79.3�1 Raw scores
DO80=Oral test of denomination [in French: Test de de¤ nomination orale d’images]; RAVLT=Rey Auditory Verbal Learning test;WAIS-R=Wechsler Adult Intelligence Scale-Revised.
3188 Brain (2007), 130, 3184^3199 M. Noulhiane et al.
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

[P1: 0–17 years old, P2: 18–30 years old, P3: the last 5 years(except the last 12 months) and P4: the last 12 months]as well as the subjective states of conscious awarenessassociated with such memories (Tulving, 1985, 2002). Sincethe average age of the participants was 34 years, this proce-dure covered their whole life. Very precise instructions,emphasizing the notions of specificity (i.e. unique eventlasting less than a day, with spatial and temporal location)and the reliving of affective-sensory-perceptual details weregiven to the participants.The ability to recall memories from each time period,
except the last one (the most recent lifetime period), wasassessed using four topics (a meeting or an event linked toa person, a school or professional event, a trip or journey,a family event). For the most recent lifetime period, eightquestions were asked in order to conduct a chronologicalstudy of the recent past (last summer, last Christmas orlast New Year’s Eve, last month, last weekend, 2 days ago,yesterday, today).Immediately after each recall, the participants were asked
to indicate the subjective states of conscious awarenessassociated separately with the recall of what happened (thefactual content), where (the place) and when (the time),always in this order. They were instructed to givea Remember, Know or Guess response (Mantyla, 1993)according to whether each aspect of the recalled event wasassociated with conscious recollection, simply knowingor guessing, respectively. A Remember response was definedas the ability to mentally relive specific aspects such asperceptions, thoughts or feelings that occurred or wereexperienced at the time of the event. The participants wereasked to give details aloud to ensure that they were usingRemember responses properly. An example of a consistentlyrecollected memory refers to a meeting (the participantrecollected very specific details of the scene, his/her feelingsand thoughts) that took place in a particular environment(the participant relived the specific atmosphere, his/herposition in the scene) 2 years ago (the participant recollec-ted the thoughts he had with regard to the fact that themeeting took place exactly 5 years after his school gradua-tion, the time of day). A Know response was describedas simply knowing what happened, where and when, butwithout this knowledge being accompanied by anyconscious recollection (in an example like the one above,the participant simply knew he/she had attended thismeeting). A Guess response corresponded to aspects of theevent that were neither consciously recollected nor simplyknown, but guessed (the participant guessed the meetinghe/she attended took place 2 years ago).
ScoringEach event was scored on a 5-point scale as proposed byBaddeley and Wilson (1986). This scale took into accountthe specificity of the content (single or repeated event),its spatio-temporal situation and the presence of details
(perceptions, thoughts, feelings). A specific event withoutany details but situated in time and space scored 3 points.A repeated or extended event scored 2 points or 1 pointaccording to whether or not it was situated in time andspace. The absence of any recollection, or only generalinformation about the topic, was scored 0. Two differenttotal scores were calculated for each period: (i) an overallautobiographical score (AM), which included all scoresregardless of their nature (max. 4� 4 = 16), and corre-sponded to the classic episodic memory score used in thewell-known AMI (Kopelman et al., 1989); (ii) a strictlyepisodic score (SE), which used a stringent criterion,including only the most episodic memories, i.e. memoriesscoring 4 (max. 4� 4 = 16).
For the purpose of this study, we focussed our intereston the proportion of Remember (R) responses rather thanKnow and Guess responses. We also used a procedureto check the R responses for specificity. In this way,we considered R responses as justified when they corre-sponded to specific memories scoring 4 or 3. Thus, justifiedR (jR) was expressed as a percentage per period (numberof the justified R responses divided by the number ofmemories recalled�100) for each content (what, where,when) or globally with the overall content. For example, the‘where jR’ score corresponded to the ratio of R responsesper period given for the spatial features of the recalledevents when they corresponded to a memory scored 4 or 3.The mean jR responses obtained for ‘what’, ‘where’ and‘when’ was used to compute the percentage of total jRresponses (% total jR responses) per period. For each score,we recorded the results for the period corresponding tothe last 12 months, which had eight items instead of four.
We conducted a retest 15� 2 days after the initial taskto check each memory by using a cued recall task whichinvolved asking the subjects to recall in random order thecontent and spatio-temporal situation of each memory.Two independent experts (MN and PP) rated each memoryuntil a consensus was reached.
Data analysis
Autobiographical memory retrieval tasksBecause of the small patient groups and the variabilityof the data, non-parametric statistics were used throughoutthe analysis of the autobiographical memory test, expressedin terms of a total score per period. Kruskal–Wallis analyseswere carried out to examine the influence of group (RTR,LTR and NC) as a between-subject factor on memoryscores and Mann–Whitney U tests were then conductedto determine group differences across each time period.To test the effect of period within each group, Friedmananalyses were performed. For Remember responses, theseanalyses included the content (what, where, when) aswithin-subject factor. Wilcoxon tests were then processedindividually for each group to determine differences
Autobiographical memory afterTLE surgery Brain (2007), 130, 3184^3199 3189
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

between each period (P1: 0–17 years old; P2: 18–30 yearsold; P3: last 5 years; P4: last 12 months).
Relationships between autobiographical memory scoresand volumetry of temporal lobe structuresSpearman’s rank–order correlations were performedbetween volumetric measurements, taking into accountthe lateralization of the resection, and autobiographicalmemory scores. The latter corresponded to the AM, SEand total jR scores for the recent (combining P3 and P4)and the remote (combining P1 and P2) periods. To betterdelineate what best characterized episodicity, we conductedstepwise regression analyses to predict the autobiographicalmemory measures, either for the recent past or the remotepast, using the volumetric values as predictors. Stepwiseregression analyses are a special case of forward selectionof predictive independent variables: in addition to the stepsperformed in the forward selection algorithm, all variableswere tested if their contribution was significant after anew variable had been added. This led to the eliminationof an already selected variable, if this variable had becomesuperfluous because of its relationship to the othervariables. The stepwise method employs a combination ofthe procedures used in the forward entry and backwardremoval methods. Then, we carried out a multiple regres-sion on the significant predictive variables selected by thestepwise regression, including tables to show the regressioncoefficient and associated significance probability of eachvariable. Considering the small number of patients pergroup, these regression analyses were exploratory. A statis-tical threshold of P50.05 was considered as significant.
Analyses of epilepsy variablesRelationships between every autobiographical memorymeasure for each period and epilepsy variables (age ofseizure onset and post-operative delay) were calculatedusing Spearman’s rank–order correlation in both patientgroups considering the lateralization of the resection.
ResultsUnlike control subjects, who responded to all autobiogra-phical questions, the RTR group responded to 91% andthe LTR to 90.4% of the questions (Fisher’s exact test,P50.001), but no significant difference was found betweenthe two patient groups. In all three groups of participants,all the memories that were given at the test were also givenat the retest.
Autobiographical memory retrieval tasksOverall autobiographical memory scoreFigure 2 displays the results of statistical analyses for theAM score for the three groups of participants as a functionof time period. The group comparisons for each timeperiod revealed significant differences. The two patient
groups were impaired across all periods in comparison tothe NC group (from Ps50.001 to Ps50.05). Moreover,no significant difference was found between the RTR andLTR groups. Otherwise, the comparisons of the perfor-mance at different time periods showed a ‘recency effect’ inthe NC group (P44P1, P50.01; P44P2, P50.05; P44P3,P50.01) but not in the RTR and LTR groups. However,a tendency (P= 0.07) was observed in the LTR group, withperformance for P2 being better than for P3 and P4 (fordetails, see Table 4 and Fig. 2 for planned comparisons).
Strictly episodic autobiographical memory scoreFigure 3 displays the results for the strictly episodicautobiographical memory score (SE) for the three groupsof participants as a function of time period. The groupcomparisons for each time period revealed that both patientgroups were impaired in comparison to the NC groupacross all time periods. No significant differences werefound between the two patient groups although a tendencywas observed in P2, where the LTR group performed betterthan the RTR group (P= 0.06). Otherwise, comparisons ofperformance for different time periods within each groupshowed that performance tend to decrease with remotenessin the NC (P= 0.07), but not in the LTR or RTR groups(for details, see Table 4)
To sum up, the results showed impairments in boththe RTR and the LTR groups in the AM or SE scores.The data emphasized that patients found it difficult toretrieve single events, located in time and in space, withphenomenological details (perceptions, thoughts, feelings)related the source of acquisition. The LTR group,however, had a tendency to report more memories forthe 18–30 period (the so-called autobiographical memory
Fig. 2 Autobiographical memory score (AM) according to timeperiod in patients with left (LTR, n=12) or right (RTR, n=10)MTL resection and normal control participants (NC, n=22).Planned comparisons to illustrate the Group effect for eachperiod as indicated in the figure. P=Period, P1=0^17 years old,P2=18^30 years old, P3= last 5 years; P4= last 12 months,�P_0.05; ��P_0.01, ���P_0.001. (Bars indicate the standarderrors of the mean.)
3190 Brain (2007), 130, 3184^3199 M. Noulhiane et al.
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from
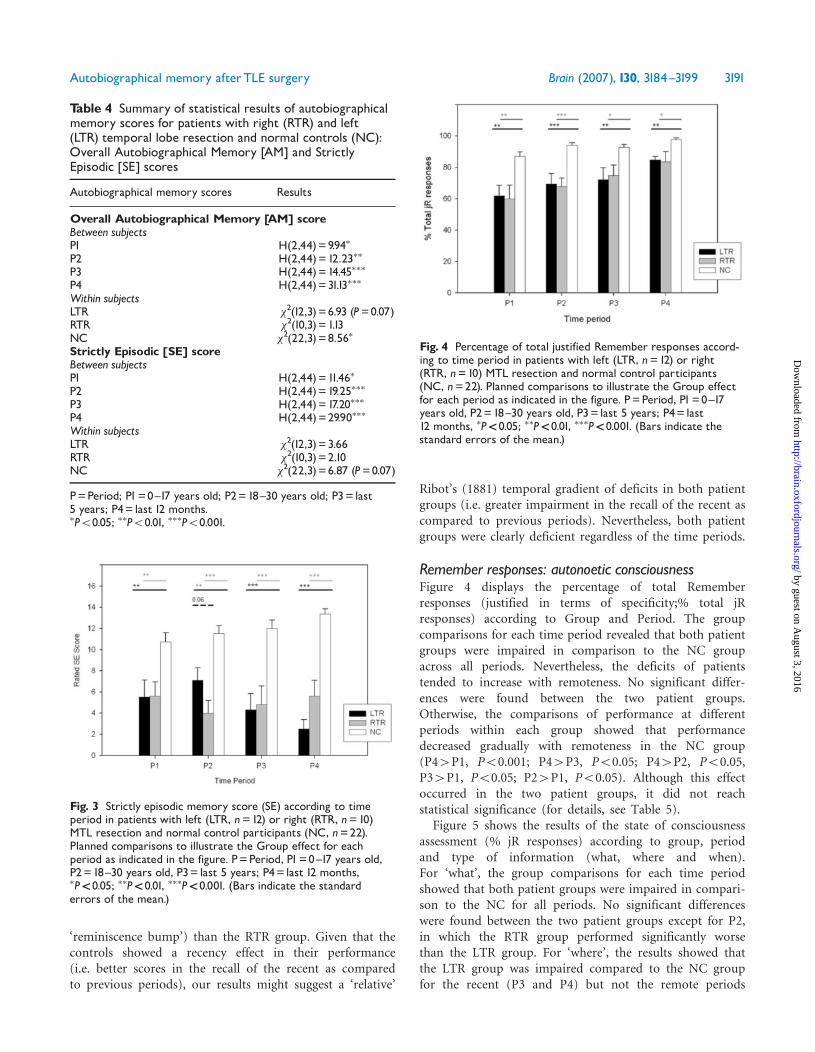
‘reminiscence bump’) than the RTR group. Given that thecontrols showed a recency effect in their performance(i.e. better scores in the recall of the recent as comparedto previous periods), our results might suggest a ‘relative’
Ribot’s (1881) temporal gradient of deficits in both patientgroups (i.e. greater impairment in the recall of the recent ascompared to previous periods). Nevertheless, both patientgroups were clearly deficient regardless of the time periods.
Remember responses: autonoetic consciousnessFigure 4 displays the percentage of total Rememberresponses (justified in terms of specificity;% total jRresponses) according to Group and Period. The groupcomparisons for each time period revealed that both patientgroups were impaired in comparison to the NC groupacross all periods. Nevertheless, the deficits of patientstended to increase with remoteness. No significant differ-ences were found between the two patient groups.Otherwise, the comparisons of performance at differentperiods within each group showed that performancedecreased gradually with remoteness in the NC group(P44P1, P50.001; P44P3, P50.05; P44P2, P50.05,P34P1, P50.05; P24P1, P50.05). Although this effectoccurred in the two patient groups, it did not reachstatistical significance (for details, see Table 5).
Figure 5 shows the results of the state of consciousnessassessment (% jR responses) according to group, periodand type of information (what, where and when).For ‘what’, the group comparisons for each time periodshowed that both patient groups were impaired in compari-son to the NC for all periods. No significant differenceswere found between the two patient groups except for P2,in which the RTR group performed significantly worsethan the LTR group. For ‘where’, the results showed thatthe LTR group was impaired compared to the NC groupfor the recent (P3 and P4) but not the remote periods
Table 4 Summary of statistical results of autobiographicalmemory scores for patients with right (RTR) and left(LTR) temporal lobe resection and normal controls (NC):Overall Autobiographical Memory [AM] and StrictlyEpisodic [SE] scores
Autobiographical memory scores Results
Overall Autobiographical Memory [AM] scoreBetween subjectsP1 H(2,44)=9.94�
P2 H(2,44)=12.23��
P3 H(2,44)=14.45���
P4 H(2,44)=31.13���
Within subjectsLTR �2(12,3)=6.93 (P=0.07)RTR �2(10,3)=1.13NC �2(22,3)=8.56�
Strictly Episodic [SE] scoreBetween subjectsP1 H(2,44)=11.46�
P2 H(2,44)=19.25���
P3 H(2,44)=17.20���
P4 H(2,44)=29.90���
Within subjectsLTR �2(12,3)=3.66RTR �2(10,3)=2.10NC �2(22,3)=6.87 (P=0.07)
P=Period; P1=0^17 years old; P2=18^30 years old; P3= last5 years; P4= last 12 months.�P50.05; ��P50.01, ���P50.001.
Fig. 3 Strictly episodic memory score (SE) according to timeperiod in patients with left (LTR, n=12) or right (RTR, n=10)MTL resection and normal control participants (NC, n=22).Planned comparisons to illustrate the Group effect for eachperiod as indicated in the figure. P=Period, P1=0^17 years old,P2=18^30 years old, P3= last 5 years; P4= last 12 months,�P_0.05; ��P_0.01, ���P_0.001. (Bars indicate the standarderrors of the mean.)
Fig. 4 Percentage of total justified Remember responses accord-ing to time period in patients with left (LTR, n=12) or right(RTR, n=10) MTL resection and normal control participants(NC, n=22). Planned comparisons to illustrate the Group effectfor each period as indicated in the figure. P=Period, P1=0^17years old, P2=18^30 years old, P3= last 5 years; P4= last12 months, �P_0.05; ��P_0.01, ���P_0.001. (Bars indicate thestandard errors of the mean.)
Autobiographical memory afterTLE surgery Brain (2007), 130, 3184^3199 3191
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

(P1 and P2); conversely, the RTR group was impairedfor the remote (P1 and P2) but not for the recent periods(P3 and P4). No significant difference was found betweenthe two patient groups. For ‘when’, the results revealed thatboth patient groups were impaired compared to the NCgroup in the remote period (P1 and P2) and the LTR groupwas also impaired in P4. The comparisons of performanceat different time periods within each group were carried outregarding the type of information. Overall, the resultsrevealed that performance decreased with remoteness in theNC group for ‘what’ (P44P1, P50.05; P34P1, P50.05)and ‘when’ (P44P3, P50.01; P44P2, P50.05; P44P1,
Table 5 Summary of statistical results of autonoeticconsciousness for patients with right (RTR) and left (LTR)temporal lobe resection and normal controls (NC):justified Remember [jR] score
Autobiographical memory scores Results
% total jRBetween subjectsP1 H(2,44)=15.02���
P2 H(2,44)=20.60���
P3 H(2,44)=11.51���
P4 H(2,44)=15.47���
Within subjectsLTR �2(12,3)=6.33RTR �2(10,3)=6.97NC �2(22,3)=18.83��
% what jRBetween subjectsP1 H(2,44)=14.51���
P2 H(2,44)=15.87���
P3 H(2,44)=12.49���
P4 H(2,44)=19.42���
Within subjectsLTR �2(12,3)=8.34�
RTR �2(10,3)=3.55NC �2(22,3)=8.15�
% where jRBetween subjectsP1 H(2,44)=7.01�
P2 H(2,44)=9.84�
P3 H(2,44)=8.89�
P4 H(2,44)=8.46�
Within subjectsLTR �2(12,3)=3.16RTR �2(10,3)=0.94NC �2(22,3)=1.56% when jRBetween subjectsP1 H(2,44)=13.15��
P2 H(2,44)=18.74���
P3 H(2,44)=1.31P4 H(2,44)=8.51�
Within subjectsLTR �2(12,3)=15.44�
RTR �2(10,3)=12.54�
NC �2(22,3)=19.76���
P=Period; P1=0^17 years old; P2=18^30 years old; P3= last5 years; P4= last 12 months.�P_0.05; ��P_0.01, ���P_0.001.
Fig. 5 Percentage of justified Remember responses for (A) ‘what’,(B) ‘where’, (C) ‘when’ according to time period in patients withleft (LTR, n=12) or right (RTR, n=10) MTL resection and normalcontrol participants (NC, n=22). Planned comparisons toillustrate the Group effect for each period as indicated in thefigure. P=Period; P1=0^17 years old, P2=18^30 years old,P3= last 5 years; P4= last 12 months, �P50.05; ��P50.01,���P50.001. (Bars indicate the standard errors of the mean.)
3192 Brain (2007), 130, 3184^3199 M. Noulhiane et al.
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from
P50.001; P24P1, P50.01) but not for ‘where’. This effectwas significant in the LTR group for ‘what’ (P24P1,P50.05; P24P4, P50.05) and ‘when’ (P44P1, P50.01;P44P2, P50.05; P34P1, P50.05; P24P1, P50.05) andin the RTR group only for ‘when’ (P44P3, P50.01;P44P2, P50.01; P44P1, P50.01; P34P2, P50.05;P34P1, P50.05) (Table 5).
Relationships between autobiographicalmemory scores and volumetry oftemporal lobe structures
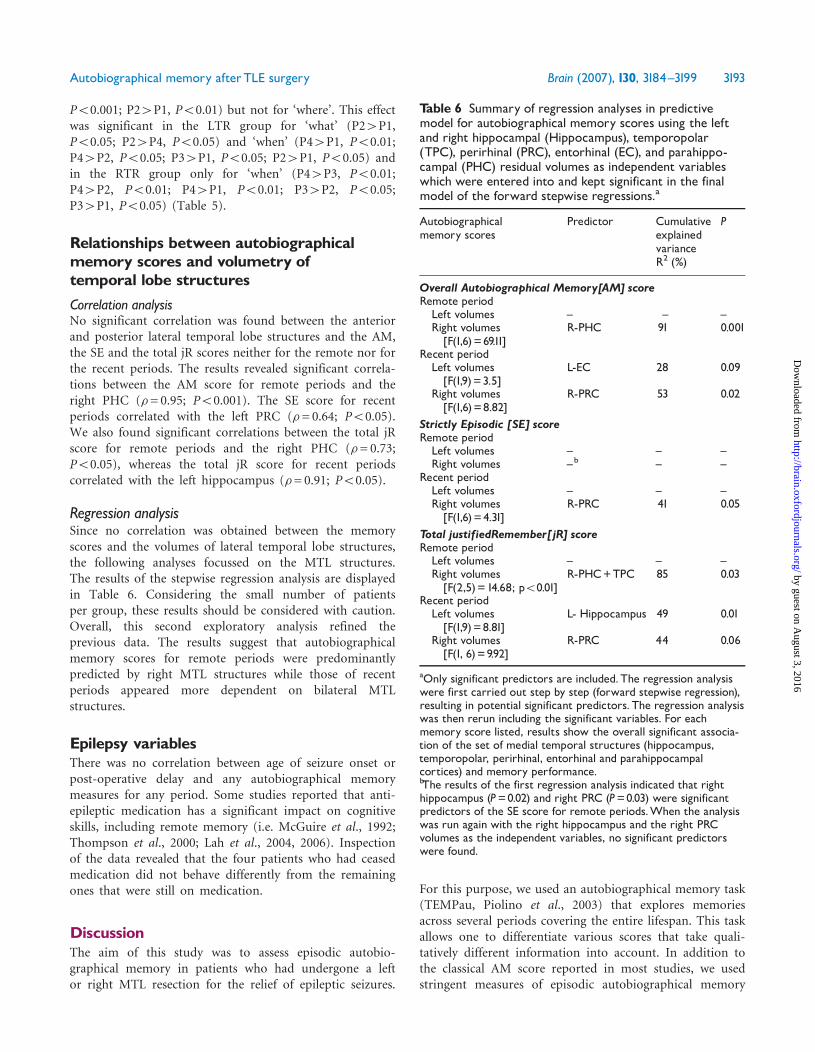
Correlation analysisNo significant correlation was found between the anteriorand posterior lateral temporal lobe structures and the AM,the SE and the total jR scores neither for the remote nor forthe recent periods. The results revealed significant correla-tions between the AM score for remote periods and theright PHC (�= 0.95; P50.001). The SE score for recentperiods correlated with the left PRC (�= 0.64; P50.05).We also found significant correlations between the total jRscore for remote periods and the right PHC (�= 0.73;P50.05), whereas the total jR score for recent periodscorrelated with the left hippocampus (�= 0.91; P50.05).
Regression analysisSince no correlation was obtained between the memoryscores and the volumes of lateral temporal lobe structures,the following analyses focussed on the MTL structures.The results of the stepwise regression analysis are displayedin Table 6. Considering the small number of patientsper group, these results should be considered with caution.Overall, this second exploratory analysis refined theprevious data. The results suggest that autobiographicalmemory scores for remote periods were predominantlypredicted by right MTL structures while those of recentperiods appeared more dependent on bilateral MTLstructures.
Epilepsy variablesThere was no correlation between age of seizure onset orpost-operative delay and any autobiographical memorymeasures for any period. Some studies reported that anti-epileptic medication has a significant impact on cognitiveskills, including remote memory (i.e. McGuire et al., 1992;Thompson et al., 2000; Lah et al., 2004, 2006). Inspectionof the data revealed that the four patients who had ceasedmedication did not behave differently from the remainingones that were still on medication.
DiscussionThe aim of this study was to assess episodic autobio-graphical memory in patients who had undergone a leftor right MTL resection for the relief of epileptic seizures.
For this purpose, we used an autobiographical memory task(TEMPau, Piolino et al., 2003) that explores memoriesacross several periods covering the entire lifespan. This taskallows one to differentiate various scores that take quali-tatively different information into account. In addition tothe classical AM score reported in most studies, we usedstringent measures of episodic autobiographical memory
Table 6 Summary of regression analyses in predictivemodel for autobiographical memory scores using the leftand right hippocampal (Hippocampus), temporopolar(TPC), perirhinal (PRC), entorhinal (EC), and parahippo-campal (PHC) residual volumes as independent variableswhich were entered into and kept significant in the finalmodel of the forward stepwise regressions.a
Autobiographicalmemory scores
Predictor CumulativeexplainedvarianceR2 (%)
P
Overall Autobiographical Memory[AM] scoreRemote periodLeft volumes ^ ^ ^Right volumes[F(1,6)=69.11]
R-PHC 91 0.001
Recent periodLeft volumes[F(1,9)=3.5]
L-EC 28 0.09
Right volumes[F(1,6)=8.82]
R-PRC 53 0.02
Strictly Episodic [SE] scoreRemote periodLeft volumes ^ ^ ^Right volumes ^b ^ ^
Recent periodLeft volumes ^ ^ ^Right volumes[F(1,6)=4.31]
R-PRC 41 0.05
Total justifiedRemember[jR] scoreRemote periodLeft volumes ^ ^ ^Right volumes[F(2,5)=14.68; p50.01]
R-PHC+TPC 85 0.03
Recent periodLeft volumes[F(1,9)=8.81]
L- Hippocampus 49 0.01
Right volumes[F(1, 6)=9.92]
R-PRC 44 0.06
aOnly significant predictors are included.The regression analysiswere first carried out step by step (forward stepwise regression),resulting in potential significant predictors. The regression analysiswas then rerun including the significant variables. For eachmemory score listed, results show the overall significant associa-tion of the set of medial temporal structures (hippocampus,temporopolar, perirhinal, entorhinal and parahippocampalcortices) and memory performance.bThe results of the first regression analysis indicated that righthippocampus (P=0.02) and right PRC (P=0.03) were significantpredictors of the SE score for remote periods.When the analysiswas run again with the right hippocampus and the right PRCvolumes as the independent variables, no significant predictorswere found.
Autobiographical memory afterTLE surgery Brain (2007), 130, 3184^3199 3193
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

by taking into account the number of specific and detailedmemories associated with phenomenological details andautonoetic consciousness (Tulving, 1985, 2002). To the bestof our knowledge, this is the first study to assess thespecificity of details combined with autonoetic conscious-ness in patients who had undergone a unilateral MTLresection for the relief of epileptic seizures. In addition, anoriginal feature of this study was the use of a correlativeapproach between autobiographical memory measuresacross remote and recent periods and MRI volumetricmeasures of medial (i.e. the temporopolar, perirhinal,entorhinal and parahippocampal cortices and the hippo-campus) and lateral (i.e. the superior, middle, inferior gyri)temporal lobe structures. This approach allowed us toensure that the resection mainly included the MTLstructures as well as the temporal pole, and to clarify theinvolvement of these structures in episodic autobiographicalmemory.
Overall autobiographical memory scoreOur study revealed that patients who had undergone aleft or right MTL resection displayed difficulties in retriev-ing autobiographical memories across all time periods.The contribution of bilateral MTL structures to autobio-graphical memory confirmed findings previously obtainedby Viskontas et al. (2000) and Voltzenlogel et al. (2006)with another autobiographical memory task (Autobio-graphical Memory Interview-AMI, Kopelman et al., 1989).This result is not surprising since the AM score measuredby the TEMPau is very similar to the episodic autobio-graphical score assessed by the AMI. All these studiesrevealed that patients with either right or left MTL lesionsexhibited profound episodic autobiographical memorydeficits extending to the most remote periods of earlychildhood. Unlike our study, Voltzenlogel et al. (2006) alsoshowed that patients with left MTL lesions performedworse than patients with right MTL lesions on the AMI orthe modified version of the Crovitz Test (Graham andHodges, 1997), regardless of the remoteness of the period.As proposed by the authors, this episodic autobiographicalmemory deficit characterizing patients with left temporallobe epilepsy can be attributed, at least in part, to addi-tional anterograde memory dysfunction affecting encodingability, but this interpretation needs further investigation.Neither our results nor those of Viskontas et al. replicatethe findings obtained in Barr et al.’s (1990) study of post-operative patients, which used an extensive survey assessingautobiographical memory without a stringent criterionfor episodicity. In this latter study, only patients who hadundergone left temporal lobe resection were found to beimpaired in both episodic and semantic autobiographicalmemory. The authors examined only a small number ofpatients (six in each group), and thus it seems plausiblethat they were not able to demonstrate a deficit after a righttemporal lobe lesion.
Overall, the results of these studies emphasize thebilateral contribution of the MTL in retrieving autobio-graphical memories across all time periods. However, ourinvestigation also provides new information by differentiat-ing the overall autobiographical memory score (i.e. AMscore, as previously discussed) from the strictly episodicscore (SE score) and by assessing autonoetic consciousness.
Strictly episodic score and autonoeticconsciousnessUsing a strict assessment criterion (i.e. SE score character-ized by specificity and richness of details), our datahighlighted the fact that the patients were severely impaired,as compared to the normal controls, in recalling memoriesfrom across the entire lifespan. They presented a flattemporal distribution of their performance compared to thenormal controls who presented the classic ‘recency effect’(i.e. superiority in specific and detailed recent memories)that has already been described in the literature on youngadults (Rubin and Schulkind, 1997; Piolino et al., 2002,2006, 2007). Given this recency effect in controls, bothpatient groups appear to be more specifically impairedfor the most recent time period. It is worth noting thatthe SE score was clearly lower than the overall autobio-graphical memory score in both patient groups, reflectingthe patients’ particular difficulty in producing specific anddetailed memories across all periods. According to thenormal performance observed in semantic memory, thisdifference between the two scores makes it clear that bothpatient groups retrieved generic memories (i.e. semanticizedones) more easily than strictly episodic memories. This isin keeping with the view that personal semantic memory isrelatively spared after unilateral temporal lobe resection(Viskontas et al., 2000). Our data therefore emphasize theimportance of considering the presence of details associatedwith specific memories in order to reliably identify residualepisodic memories (Moscovitch and Nadel, 1999; Piolinoet al., 2003). Moreover, our methodology also documentedthe autonoetic consciousness associated with each memoryby using a Remember/Know paradigm (Tulving, 1985;Gardiner, 1988; Mantyla, 1993; Gardiner, 2001; Tulving,2002). In this study, we showed that the percentage ofRemember responses justified by specificity was significantlylower in RTR and LTR patients than in normal controlsacross all time periods, suggesting that the MTL contributesbilaterally to autonoetic consciousness. Interestingly, ourresults are consistent with neuroimaging data showingmore bilateral MTL activation in healthy subjects duringconscious re-experiencing (remembering) than duringfeelings of familiarity (knowing) (Eldridge et al., 2000;Wheeler and Buckner, 2004). In the normal control partici-pants, autonoetic consciousness decreased as a functionof the remoteness of events, confirming previous findings(Piolino et al., 2006, 2007). However, this effect was notobserved in patient groups. Our results emphasize that
3194 Brain (2007), 130, 3184^3199 M. Noulhiane et al.
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from
patients with unilateral MTL lesions have a deficit inre-experiencing or reliving the past and mentally travellingback in subjective time. More specifically, the TEMPau task,which allows one to investigate the consistency of consciousrecollection by considering the sense of rememberingseparately for factual, spatial and temporal information(what, where and when, respectively), provides qualitativeinformation about the autonoetic features of autobiogra-phical memories in those patients. Globally, the normalcontrol participants’ results showed that these three types ofinformation are retrieved to a similar extent except for the‘when’ responses, which were less accessible for remote thanfor recent periods, in keeping with previous results obtainedin young adults (Piolino et al., 2006, 2007). The data fromthe two patient groups demonstrated less consistentconscious recollection, regardless of the type of informa-tion. Our results point to the bilateral involvement of theMTL in re-experiencing either phenomenological or spatio-temporal features of single autobiographical events, evenmore with remoteness. Accordingly, some neuroimagingstudies have detected bilateral MTL activation whensubjects are engaged in the retrieval of specific autobio-graphical memories that are highly rated in terms ofspecificity, mental imagery, richness of details, emotionality,re-experiencing or personal significance (Ryan et al., 2001;Piefke et al., 2003; Piolino et al., 2004; Greenberg et al.,2005; Steinvorth et al., 2006; Viard et al., 2007). The resultsfor ‘what’ responses revealed that the justified senseof reliving perceptive and affective details of events wasimpaired in both patient groups, except for the 18–30-yearperiod in the LTR patients. Interestingly, this may reflectthe reminiscence ‘memory bump’ generally reported inelderly subjects. The memory bump corresponds to thesuperior recollection of vivid events that occurred betweenthe ages of 18 and 30 years as compared to recent or moreremote epochs of our life (Rubin and Schulkind, 1997;Berntsen and Rubin, 2002). Indeed, the visual imagery,emotion and spatial details are particularly vivid for remotememories corresponding to this encoding period (Rubinand Wetzler, 1986; Conway and Rubin, 1993; Fitzgerald,1996; Rubin and Schulkind, 1997; Piolino et al., 2002,2006). Since visual imagery, spatial details and emotionalprocessing in autobiographical memory have been pre-dominantly associated with right-hemisphere functionincluding the temporal lobe structures (Fink et al., 1996;Conway, 2001; Piolino et al., 2004), we can suggest thatpatients with left temporal lobe lesions but relatively sparedright temporal lobe structures were able to use these cuesto retrieve specific phenomenologically detailed events.For ‘where’ responses, the results revealed that the RTRgroup was impaired in recalling the most remote periods(P1 and P2), whereas the LTR group was impaired inrecalling the most recent ones (P3 and P4). Again, thesefindings supported the importance of the right MTLstructures in the evocation of the episodic spatial contextof memories that consist of detailed perceptual–spatial
representations of experienced environments (Moscovitchet al., 2005). The left MTL appears important in the evoca-tion of more mundane memories, like those generallyretrieved for recent periods (Viard et al., 2007). The ‘when’responses revealed that both RTR and LTR patientsproduced fewer responses than normal control participantsfor the remote periods (P1 and P2), whereas there wasno difference for the recent ones (P3 and P4). The roleof MTL structures has been emphasized in memory forsequences of events (Fortin et al., 2002). In addition, theintegrity of those structures seems to be important in timeestimation, as indicated by several reports revealing a severedistortion of temporal processing in amnesic patients withbilateral MTL damage (Richards, 1973; Williams et al.,1989). A recent study has also reported that patientswith either right or left unilateral MTL lesions wereimpaired when estimating duration in the range of minutes(Noulhiane et al., 2007). In agreement with these studies,our results suggest that MTL structures are bilaterallyinvolved in processing of temporal attributes of events(e.g. the date, the moment in the day or the duration ofthe event). We found that the two patient groups wereimpaired in remote periods although the LTR patients werealso affected in the most recent period (P4). Nevertheless,given the lack of data in this domain, further studies willbe necessary to clarify the role of MTL structures in thetemporal attributes of episodic autobiographical memory.
Interestingly, the mixed findings obtained for thetemporal gradient question its operationalization in thecontext of the two competing neurobiological models oflong-term episodic memory. Results of strictly episodicautobiographical memories (SE) revealed that the controlgroup showed a recency effect, while the patients seemed toshow a ‘relative’ temporal gradient (i.e. greater impairmentin the recall of the recent as compared to previous periods),although they performed below the control group regardlessof the time period. This result appears to be consistentwith the consolidation theory, which proposes differentialsparing of remote and recent memories (Squire andAlvarez, 1995). However, the global impairment of patientsin all the time periods is compatible with the multi tracetheory (MTT) model (Nadel and Moscovitch, 1997, 2001;Nadel and Hardt, 2004; Moscovitch et al., 2005) andsuggests that MTL structures are permanently involved inthe recall of episodic events. This latter interpretationis further supported by the results observed with the (total)remember responses given that the deficits of patientstended to increase with remoteness. All these resultssuggest that different cognitive processes are requiredfor memory of autobiographical events. The SE score isbased on the specific properties of narrative reports ofmemories (uniqueness, spatiotemporal context and details),whereas the remember responses focused on the subjectivefeeling of remembering and the capacity to justify thisfeeling. Therefore, the temporal gradient obtained withthe remember responses indicates that the judgments
Autobiographical memory afterTLE surgery Brain (2007), 130, 3184^3199 3195
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

of patients on their sense of remembering were morereliable for the recent as compared to remote memories.While our findings underline the complexity of relationsbetween the passage of time and the recall, they suggest thatour data may be more compatible with the MTT modelthan the consolidation theory.Concerning the issue of specific mechanisms (i.e. antero-
grade versus retrograde) involved in autobiographicalmemory deficits, the results revealed that the patientswith left or right MTL resections were impaired in episodicautobiographical memory as well as in autonoetic con-sciousness even for the early childhood period. Although itis difficult to disentangle the anterograde and retrogrademechanisms of deficits, it is plausible that some additionalanterograde deficits may have supplemented retrogradeones in these patients. Indeed, the long-standing epilepticdisease associated with hippocampal sclerosis might havedisrupted the acquisition and consolidation of memoriesacquired before the surgery, as the data reported by Kapurand Prevett (2003) suggest. Such impairments would resultin a limited stock of accumulated knowledge about personalevents from childhood or adolescence. In our study,however, as in most studies reported in the literature, wewere not able to demonstrate a relation between seizureonset and different autobiographical memory scores. Thislack of correlation is consistent with previous findings(Bergin et al., 2000; Viskontas et al., 2000; Lah et al., 2004;Voltzenlogel et al., 2006). Viskontas and his colleagues forexample did not find significant differences in memoryscores when they compared early and late seizure onsets.According to these authors, the absence of poorer perfor-mance in the early onset group weakens this conclusion,although the possibility of defective encoding in bothgroups cannot be discounted. The age of onset of ongoingseizure disorders did not reflect the beginning of thehippocampal sclerosis. The damage to MTL tissue probablyoccurs during the latent period before experiencingrecurrent seizures. For instance, some studies have reportedthat febrile seizures were preceded by changes in hippo-campal morphology (Cavazos et al., 1994; Grunewald et al.,2001). Lah et al. (2006) suggested that seizures themselvesmay not only interfere with encoding and consolidation ofinformation, but also corrupt already established memorystores. These authors also reported that young age of onset(younger than 14 years) of temporal lobe epilepsy wasassociated with greater difficulties in the subtest of recall offamous events from ‘The Australian Remote MemoryBattery’. Nevertheless, this result was not observed inthe other subtests with the same patient groups (e.g. the‘Autobiographical Fluency Test’). In our study, manypatients were younger than 14 years old at epilepsy onset.Thus, it seems possible that an early encoding andconsolidation impairment could be partially responsiblefor retrograde memory deficits in childhood andadolescence.
Relationships between autobiographicalmemory scores and volumetry oftemporal lobe structuresThe correlation results suggest that unlike the lateraltemporal structures, MTL areas are involved in autobio-graphical memory, regardless of remoteness. They revealedthat for the most remote periods, the AM and total jRscores involved the right parahippocampal cortex, whichis well known for its contribution to visual imagery andspatial processing (Bohbot et al., 1998; O’Craven andKanwisher, 2000; Burgess et al., 2002; Ganis et al., 2004).As suggested earlier, mental visual imagery and emotionwere particularly important in the retrieval of remotememories (Rubin and Wetzler, 1986; Conway and Rubin,1993; Fitzgerald, 1996; Rubin and Schulkind, 1997; Piolinoet al., 2002, 2007). Moreover, the most remote periodsincluded in the total jR score were also correlated with thevolume of the right temporopolar cortex; this mightbe explained by its involvement in emotional processes(Piefke et al., 2003) and retrieval of remote episodicmemories (Markowitsch, 1995; Conway, 2001). Moregenerally, these results may be considered to be in linewith neuroimaging data suggesting that right-sided MTLactivations are obtained during the retrieval of emotionalproperties of autobiographical memories (Fink et al., 1996)or of spatial details operating on the visual mental imagery,which are especially relevant for remote autobiographicalmemory ecphory (Mayes et al., 2000; Piolino et al., 2004).
For the most recent periods, the AM, SE and total jRscores were correlated with the volume of the rightperirhinal cortex and the left hippocampus. The contribu-tion of the right perirhinal cortex to recall of the mostrecent periods could be related to the novelty of thestimulus (Brown and Aggleton, 2001; Nyberg, 2005), whilethose of the left hippocampus suggest its involvement inassociative novelty (Nyberg, 2005). Moreover, the findingof left-sided involvement for recent periods may be in linewith the fact that memories from the most recent periods(relative to more remote periods) are partly composedof non-emotional events that had happened very recently(a few days, weeks or months ago). Although such recentmemories are episodic in nature, they are unlikely to bestored for the long term, unless they are highly goal-specificand rehearsed (Conway, 2001). Our correlational andregression results also support the multiple trace theorymodel, which suggests that various MTL regions perma-nently contribute to the different aspects of either recentor remote episodic autobiographical memory (Moscovitchet al., 2005).
Overall, this study highlights the role of bilateral MTLin episodic autobiographical memory independently ofremoteness, and suggests that the right MTL structuresare particularly responsive to the sense of reliving theencoding context. Our findings are in keeping with neuro-imaging studies detecting bilateral or preferential right MTL
3196 Brain (2007), 130, 3184^3199 M. Noulhiane et al.
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

activation when subjects are engaged in the retrieval ofspecific autobiographical memories rated high for mentalimagery, richness of detail, emotionality, re-experiencing orpersonal significance (Mayes et al., 2000; Ryan et al., 2001;Graham et al., 2003; Piefke et al., 2003; Piolino et al., 2004;Greenberg et al., 2005; Steinvorth et al., 2006; Viard et al.,2007). Our results also confirm recent data indicating thatthe qualities of retrieved memories influence the MTLengagement independently of factors such as remoteness(Graham et al., 2003; Addis et al., 2004; Gilboa et al., 2004;Piolino et al., 2004; Viard et al., 2007). Moreover, they arein accordance with Gilboa et al.’ s (2005) finding that thereis a significant correlation between remote autobiographicalmemory in patients with brain lesions and the amount ofremaining tissue in bilateral MTL, which is stronger on theright than the left. In our study, the major role of the rightMTL may be due to the fact that we specifically sought theautonoetic qualities of autobiographical memories, such asmental ‘time travel’ through subjective time, from thepresent to the past, and re-experiencing, through self-awareness, one’s own previous experiences (Tulving, 2001).Therefore, our results suggest that the right MTLcontributes to the successful retrieval of episodic memories(e.g. from the reminiscence bump) that are greatlydependent upon the richness of spatio-temporal detailsand more specifically of phenomenal ones.In conclusion, our results substantiate that patients with
left or right temporal lobe resections have impairedepisodic autobiographical memories. This impairmentconcerns the entire lifespan including the early childhoodperiod and also affects autonoetic consciousness. Ouradditional findings, based on correlation analysis, indicatedthat this impairment was related to the medial rather thanthe lateral temporal lobe structures. Our results suggestthat the right-hemisphere MTL structures are particularlyresponsive to the sense of reliving the encoding context.In agreement with the multi trace theory model, we foundthat various MTL regions are permanently involved inthe different aspects of episodic autobiographical memory(Moscovitch et al., 2005) in patients with unilateraltemporal lobe resection.
AcknowledgementsThis work was supported by the French League AgainstEpilepsy (Novartis to M.N.) and the Regional Councilof Nord Pas de Calais Picardie (Ph.D. fellowship to M.N.).We thank Marie Chupin and Amee Baird for her helpfultechnical assistance, Dr Gilles Huberfeld and Dr JohanPallud for their clinical expertise, Marisa Denos for theneuropsychological assessment.
ReferencesAddis DR, Moscovitch M, Crawley AP, McAndrews MP. Recollective
qualities modulate hippocampal activation during autobiographical
memory retrieval. Hippocampus 2004; 14: 752–62.
Baddeley AD, Wilson B. Amnesia, autobiographical memory and
confabulation. In: Rubin DC, editor. Autobiographical memory.
Cambridge, England: Cambridge University Press; 1986. p. 225–52.
Barr WB, Goldberg E, Wasserstein J, Novelly RA. Retrograde amnesia
following unilateral temporal lobectomy. Neuropsychologia 1990; 28:
243–55.
Bayley PJ, Gold JJ, Hopkins RO, Squire LR. The neuroanatomy of remote
memory. Neuron 2005; 46: 799–810.
Berenbaum SA, Baxter L, Seidenberg M, Hermann B. Role of the
hippocampus in sex differences in verbal memory: memory outcome
following left anterior temporal lobectomy. Neuropsychology 1997; 11:
585–91.
Bergin PS, Thompson PJ, Baxendale SA, Fish DR, Shorvon SD. Remote
memory in epilepsy. Epilepsia 2000; 41: 231–9.
Berntsen D, Rubin DC. Emotionally charged autobiographical memories
across the life span: the recall of happy, sad, traumatic, and involuntary
memories. Psychol Aging 2002; 17: 636–52.
Bohbot VD, Kalina M, Stepankova K, Spackova N, Petrides M, Nadel L.
Spatial memory deficits in patients with lesions to the right hippo-
campus and to the right parahippocampal cortex. Neuropsychologia
1998; 36: 1217–38.
Borrini G, Dall’Ora P, Della Sala S, Marinelli L, Spinnler H. Auto-
biographical memory. Sensitivity to age and education of a standardized
enquiry. Psychol Med 1989; 19: 215–24.
Brown MW, Aggleton JP. Recognition memory: what are the roles of the
perirhinal cortex and hippocampus? Nat Rev Neurosci 2001; 2: 51–61.
Burgess N, Maguire EA, O’Keefe J. The human hippocampus and spatial
and episodic memory. Neuron 2002; 35: 625–41.
Cavazos JE, Das I, Sutula TP. Neuronal loss induced in limbic pathways by
kindling: evidence for induction of hippocampal sclerosis by repeated
brief seizures. J Neurosci 1994; 14: 3106–21.
Cipolotti L, Shallice T, Chan D, Fox N, Scahill R, Harrison G, et al.
Long-term retrograde amnesia . . . the crucial role of the hippocampus.
Neuropsychologia 2001; 39: 151–72.
Cointepas Y, Mangin JF, Garnero L, Poline JB, Benali H. BrainVISA:
software platform for visualization and analysis of multimodality brain
data. Seventh Human Brain Mapping. NeuroImage 2001; 13: S98.
Conway MA. Sensory-perceptual episodic memory and its context:
autobiographical memory. Philos Trans R Soc Lond B Biol Sci 2001;
356: 1375–84.
Conway MA, Holmes A. Psychosocial stages and the accessibility of
autobiographical memories across the life cycle. J Pers 2004; 72: 461–80.
Conway MA, Pleydell-Pearce CW. The construction of autobiographical
memories in the self-memory system. Psychol Rev 2000; 107: 261–88.
Conway MA, Rubin DC. The structure of autobiographical memory. In:
Collins AE, Gathercole SE, Conway MA, Morris PEM, editors. Theories
of memory. Hove, UK: Erlbaum; 1993. p. 103–37.
Corkin S. Lasting consequences of bilateral medial lobectomy: clinical
course and experimental findings in H.M. Seminars in Neurology 1984;
41: 249–59.
Corkin S. What’s new with the amnesic patient H.M.? Nat Rev Neurosci
2002; 3: 153–60.
Crovitz H, Schiffman H. Frequency of episodic memories as a function of
their age. Bull Psychol Soc 1974; 4: 517–8.
Deloche G, Hannequin D. Test de Denomination orale d’images (DO 80).
Paris: Centre de Psychologie Appliquee; 1997.
Dritschel BH, Williams JM, Baddeley AD, Nimmo-Smith I. Autobiogra-
phical fluency: a method for the study of personal memory.
Mem Cognit 1992; 20: 133–40.
Duvernoy HM. The human brain: surface, three-dimensional sectional
anatomy and MRI. Wien: Springer; 1988.
Eldridge LL, Knowlton BJ, Furmanski CS, Bookheimer SY, Engel SA.
Remembering episodes: a selective role for the hippocampus during
retrieval. Nat Neurosci 2000; 3: 1149–52.
Engel J, Van Ness PC, Rasmussen TB, et al. Outcome with respect to
epileptic seizures. In: Engel J, editor. Surgical treatment of the epilepsies.
2nd edn., New York: Raven Press; 1993. p. 609–21.
Autobiographical memory afterTLE surgery Brain (2007), 130, 3184^3199 3197
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

Fink GR, Markowitsch HJ, Reinkemeier M, Bruckbauer T, Kessler J,
Heiss WD. Cerebral representation of one’s own past: neural networks
involved in autobiographical memory. J Neurosci 1996; 16: 4275–82.
Fitzgerald J. Intersecting meanings of reminiscence in adult development
and aging. In: Rubin DC, editor. Remembering our past: studies in
autobiographical memory. Cambridge: Cambridge University Press;
1996. p. 360–83.
Fortin NJ, Agster KL, Eichenbaum HB. Critical role of the hippocampus in
memory for sequences of events. Nat Neurosci 2002; 5: 458–62.
Fujii T, Yamadori A, Endo K, Suzuki K, Fukatsu R. Disproportionate
retrograde amnesia in a patient with herpes simplex encephalitis. Cortex
1999; 35: 599–614.
Ganis G, Thompson WL, Kosslyn SM. Brain areas underlying visual
mental imagery and visual perception: an fMRI study. Brain Res Cogn
Brain Res 2004; 20: 226–41.
Gardiner JM. Functional aspects of recollective experience. Mem Cognit
1988; 16: 309–13.
Gardiner JM. Episodic memory and autonoetic consciousness: a first-
person approach. Philos Trans R Soc Lond B Biol Sci 2001; 356:
1351–61.
Gilboa A, Ramirez J, Kohler S, Westmacott R, Black SE, Moscovitch M.
Retrieval of autobiographical memory in Alzheimer’s disease: relation to
volumes of medial temporal lobe and other structures. Hippocampus
2005; 15: 535–50.
Gilboa A, Winocur G, Grady CL, Hevenor SJ, Moscovitch M.
Remembering our past: functional neuroanatomy of recollection of
recent and very remote personal events. Cereb Cortex 2004; 14:
1214–25.
Graham K, Hodges J. Differentiating the role of the hippocampus complex
and neocortex in long-term memory storage: evidence from the study of
semantic dementia and Alzheimer disease. Neuropsychology 1997; 3:
13–36.
Graham KS, Lee AC, Brett M, Patterson K. The neural basis of
autobiographical and semantic memory: new evidence from three PET
studies. Cogn Affect Behav Neurosci 2003; 3: 234–54.
Greenberg DL, Rice HJ, Cooper JJ, Cabeza R, Rubin DC, Labar KS.
Co-activation of the amygdala, hippocampus and inferior frontal gyrus
during autobiographical memory retrieval. Neuropsychologia 2005; 43:
659–74.
Grunewald RA, Farrow T, Vaughan P, Rittey CD, Mundy J. A magnetic
resonance study of complicated early childhood convulsion. J Neurol
Neurosurg Psychiatry 2001; 71: 638–42.
Helmstaedter C, Elger CE. Cognitive consequences of two-thirds anterior
temporal lobectomy on verbal memory in 144 patients: a three-month
follow-up study. Epilepsia 1996; 37: 171–80.
Hermann BP, Wyler AR, Bush AJ, Tabatabai FR. Differential effects of left
and right anterior temporal lobectomy on verbal learning and memory
performance. Epilepsia 1992; 33: 289–97.
Insausti R, Juottonen K, Soininen H, Insausti AM, Partanen K, Vainio P,
Laakso MP, Pitkanen A. MR volumetric analysis of the human
entorhinal, perirhinal, and temporopolar cortices. AJNR Am J
Neuroradiol. 1998; 19: 659–71.
Kapur N, Prevett M. Unexpected amnesia: are there lessons to be learned
from cases of amnesia following unilateral temporal lobe surgery? Brain
2003; 126: 2573–85.
Kopelman MD, Lasserson D, Kingsley DR, Bello F, Rush C, Stanhope N,
et al. Retrograde amnesia and the volume of critical brain structures.
Hippocampus 2003; 13: 879–91.
Kopelman MD, Wilson BA, Baddeley AD. The autobiographical
memory interview: a new assessment of autobiographical and personal
semantic memory in amnesic patients. J Clin Exp Neuropsychol 1989;
11: 724–44.
Lah S, Grayson S, Lee T, Miller L. Memory for the past after temporal
lobectomy: impact of epilepsy and cognitive variables. Neuropsychologia
2004; 42: 1666–79.
Lah S, Lee T, Grayson S, Miller L. Effects of temporal lobe epilepsy on
retrograde memory. Epilepsia 2006; 47: 615–25.
Levine B, Svoboda E, Hay JF, Winocur G, Moscovitch M. Aging and
autobiographical memory: dissociating episodic from semantic retrieval.
Psychol Aging 2002; 17: 677–89.
Mantyla T. Knowing but not remembering: adult age differences in
recollective experience. Mem Cognit 1993; 21: 379–88.
Markowitsch HJ. Which brain regions are critically involved in the
retrieval of old episodic memory? Brain Res Brain Res Rev 1995; 21:
117–27.
Mayes AR, Mackay CE, Montaldi D, Downest JJ, Singh KD, Norberst N.
Does retrieving decades-old spatial memories activate the medial
temporal lobes less than retrieving recently acquired spatial memories?
NeuroImage 2000; 11: S421.
McClelland JL, McNaughton BL, O’Reilly RC. Why there are comple-
mentary learning systems in the hippocampus and neocortex: insights
from the successes and failures of connectionist models of learning and
memory. Psychol Rev 1995; 102: 419–57.
McGuire AM, Duncan JS, Trimble MR. Effects of vigabatrin on cognitive
function and mood when used as add-on therapy in patients with
intractable epilepsy. Epilepsia 1992; 33: 128–34.
Milner B. Psychological aspects of focal epilepsy and its neurosurgical
management. Adv Neurol 1975; 8: 299–321.
Milner B, Corkin S, Teuber HL. Further analysis of the hippocampal
amnesic syndrome: 14-year follow-up of H.M. Neuropsychologia 1968;
6: 215–34.
Moscovitch M, Nadel L. Multiple-trace theory and semantic dementia:
response to K.S. Graham (1999). Trends Cogn Sci 1999; 3: 87–9.
Moscovitch M, Rosenbaum RS, Gilboa A, Addis DR, Westmacott R,
Grady C, et al. Functional neuroanatomy of remote episodic, semantic
and spatial memory: a unified account based on multiple trace theory.
J Anat 2005; 207: 35–66.
Murre JM. TraceLink: a model of amnesia and consolidation of memory.
Hippocampus 1996; 6: 675–84.
Nadel L, Hardt O. The spatial brain. Neuropsychology 2004; 18: 473–6.
Nadel L, Moscovitch M. Memory consolidation, retrograde
amnesia and the hippocampal complex. Curr Opin Neurobiol 1997; 7:
217–27.
Nadel L, Moscovitch M. The hippocampal complex and long-term
memory revisited. Trends Cogn Sci 2001; 5: 228–30.
Noulhiane M, Pouthas V, Hasboun D, Baulac M, Samson S. Role of the
medial temporal lobe in time estimation in the range of minutes.
Neuroreport 2007; 18: 1035–8.
Noulhiane M, Samson S, Clemenceau S, Dormont D, Baulac M,
Hasboun D. A volumetric MRI study of the hippocampus and the
parahippocampal region after unilateral medial temporal lobe resection.
J Neurosci Methods 2006; 156: 293–304.
Nyberg L. Any novelty in hippocampal formation and memory? Curr Opin
Neurol 2005; 18: 424–8.
O’Craven KM, Kanwisher N. Mental imagery of faces and places activates
corresponding stiimulus-specific brain regions. J Cogn Neurosci 2000;
12: 1013–23.
Onitsuka T, Shenton ME, Salisburry DF, Dickey CC, Toner SK, Frumin M,
et al. Middle and inferior temporal gyrus gray matter volume abnorma-
lities in chronic schizophrenia: an MRI study. Am J Psychiatry 2004;
161: 1603–11.
Piefke M, Weiss PH, Zilles K, Markowitsch HJ, Fink GR. Differential
remoteness and emotional tone modulate the neural correlates of
autobiographical memory. Brain 2003; 126: 650–68.
Piolino P, Desgranges B, Belliard S, Matuszewski V, Lalevee C, De la
Sayette V, et al. Autobiographical memory and autonoetic conscious-
ness: triple dissociation in neurodegenerative diseases. Brain 2003; 126:
2203–19.
Piolino P, Desgranges B, Benali K, Eustache F. Episodic and
semantic remote autobiographical memory in ageing. Memory 2002;
10: 239–57.
Piolino P, Desgranges B, Clarys D, Guillery-Girard B, Taconnat L,
Isingrini M, et al. Autobiographical memory, autonoetic consciousness,
and self-perspective in aging. Psychol Aging 2006; 21: 510–25.
3198 Brain (2007), 130, 3184^3199 M. Noulhiane et al.
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from

Piolino P, Desgranges B, Manning L, North P, Jokic C, Eustache F.
Autobiographical memory, the sense of recollection and executive
functions after severe traumatic brain injury. Cortex 2007; 43: 176–95.
Piolino P, Giffard-Quillon G, Desgranges B, Chetelat G, Baron JC,
Eustache F. Re-experiencing old memories via hippocampus: a PET
study of autobiographical memory. Neuroimage 2004; 22: 1371–83.
Reed JM, Squire LR. Retrograde amnesia for facts and events: findings
from four new cases. J Neurosci 1998; 18: 3943–54.
Rempel-Clower NL, Zola SM, Squire LR, Amaral DG. Three cases of
enduring memory impairment after bilateral damage limited to the
hippocampal formation. J Neurosci 1996; 16: 5233–55.
Rey A. L’examen clinique en Psychologie. Paris; 1964.
Richards W. Time reproductions by H.M. Acta Psychol 1973; 37: 279–82.
Rosenbaum RS, Winocur G, Moscovitch M. New views on old memories:
re-evaluating the role of the hippocampal complex. Behav Brain Res
2001; 127: 183–97.
Rubin DC, Schulkind MD. The distribution of autobiographical memories
across the lifespan. Mem Cognit 1997; 25: 859–66.
Rubin DC, Wetzler SE. Autobiographical memory across life span. In:
Rubin DC, editor. Autobiographical memory. Cambridge: Cambridge
University Press; 1986. p. 202–21.
Ryan L, Nadel L, Keil K, Putnam K, Schnyer D, Trouard T, et al.
Hippocampal complex and retrieval of recent and very remote
autobiographical memories: evidence from functional magnetic
resonance imaging in neurologically intact people. Hippocampus 2001;
11: 707–14.
Saykin AJ, Gur RC, Sussman NM, O’Connor MJ, Gur RE. Memory deficits
before and after temporal lobectomy: effect of laterality and age of onset.
Brain Cogn 1989; 9: 191–200.
Schmidtke K, Vollmer H. Retrograde amnesia: a study of its relation to
anterograde amnesia and semantic memory deficits. Neuropsychologia
1997; 35: 505–18.
Scoville WB, Milner B. Loss of recent memory after bilateral hippocampal
lesions. J Neurol Neurosurg Psychiatry 1957; 20: 11–21.
Smith ML, Milner B. The role of the right hippocampus in the recall of
spatial location. Neuropsychologia 1981; 19: 781–93.
Squire LR, Alvarez P. Retrograde amnesia and memory consolidation: a
neurobiological perspective. Curr Opin Neurobiol 1995; 5: 169–77.
Steinvorth S, Corkin S, Halgren E. Ecphory of autobiographical memories:
an fMRI study of recent and remote memory retrieval. Neuroimage
2006; 30: 285–98.
Steinvorth S, Levine B, Corkin S. Medial temporal lobe structures are
needed to re-experience remote autobiographical memories: evidence
from H.M. and W.R. Neuropsychologia 2005; 43: 479–96.
Thompson PJ, Baxendale SA, Duncan JS, Sander JW. Effects of
topiramate on cognitive function. J Neurol Neurosurg Psychiatry
2000; 69: 636–41.
Tulving E. How many memory systems are there ? Am Psychol 1985; 40:
385–98.
Tulving E. Episodic memory and common sense: how far apart? Philos
Trans R Soc Lond B Biol Sci 2001; 356: 1505–15.
Tulving E. Episodic memory: from mind to brain. Annu Rev Psychol 2002;
53: 1–25.
Tulving E, Schacter DL, McLachlan DR, Moscovitch M. Priming of
semantic autobiographical knowledge: a case study of retrograde
amnesia. Brain Cogn 1988; 8: 3–20.
Viard A, Piolino P, Desgranges B, Chetelat G, Lebreton K, Landeau B,
et al. Hippocampal activation for autobiographical memories over the
entire lifetime in healthy aged subjects: an fMRI study. Cereb Cortex
2007; 17: 2453–67.
Viskontas IV, McAndrews MP, Moscovitch M. Remote episodic memory
deficits in patients with unilateral temporal lobe epilepsy and excisions.
J Neurosci 2000; 20: 5853–7.
Voltzenlogel V, Despres O, Vignal JP, Steinhoff BJ, Kehrli P, et al. Remote
memory in temporal lobe epilepsy. Epilepsia 2006; 47: 1329–36.
Wada J, Rasmussen T. Intracarotid injection of sodium amytal for the
lateralization of cerebral speech dominance: experimental and clinical
observations. J Neurosurg 1960; 17: 266–82.
Wheeler ME, Buckner RL. Functional-anatomic correlates of remembering
and knowing. Neuroimage 2004; 21: 1337–49.
Williams JM, Medwedeff CH, Haban G. Memory disorder and subjective
time estimation. J Clin Exp Neuropsychol 1989; 11: 713–23.
Autobiographical memory afterTLE surgery Brain (2007), 130, 3184^3199 3199
by guest on August 3, 2016
http://brain.oxfordjournals.org/D
ownloaded from
Copyright © 2022 FDOKUMEN




















