
Attitudes and practices towards micronutrient supplementation among pregnant women in rural Tibet
12
This article was downloaded by: [University of Rochester], [Timothy Dye] On: 05 September 2014, At: 06:50 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Global Public Health: An International Journal for Research, Policy and Practice Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/rgph20 Attitudes and practices towards micronutrient supplementation among pregnant women in rural Tibet Timothy De Ver Dye a , Gretel Pelto b , Sibylle Kristensen c , Arlene Samen c & Ann Dozier d a Department of Obstetrics and Gynecology, School of Medicine and Dentistry, University of Rochester, Rochester, NY, USA b Division of Nutritional Sciences, College of Human Ecology, Cornell University, Ithaca, NY, USA c OneHEART Worldwide, San Francisco, CA, USA d Division of Social and Behavioral Health, Department of Community and Preventive Medicine, University of Rochester, Rochester, NY, USA Published online: 03 Sep 2014. To cite this article: Timothy De Ver Dye, Gretel Pelto, Sibylle Kristensen, Arlene Samen & Ann Dozier (2014): Attitudes and practices towards micronutrient supplementation among pregnant women in rural Tibet, Global Public Health: An International Journal for Research, Policy and Practice, DOI: 10.1080/17441692.2014.944551 To link to this article: http://dx.doi.org/10.1080/17441692.2014.944551 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or
Transcript of Attitudes and practices towards micronutrient supplementation among pregnant women in rural Tibet
This article was downloaded by: [University of Rochester], [Timothy Dye]On: 05 September 2014, At: 06:50Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Global Public Health: An InternationalJournal for Research, Policy andPracticePublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/rgph20
Attitudes and practices towardsmicronutrient supplementation amongpregnant women in rural TibetTimothy De Ver Dyea, Gretel Peltob, Sibylle Kristensenc, ArleneSamenc & Ann Dozierd
a Department of Obstetrics and Gynecology, School of Medicineand Dentistry, University of Rochester, Rochester, NY, USAb Division of Nutritional Sciences, College of Human Ecology,Cornell University, Ithaca, NY, USAc OneHEART Worldwide, San Francisco, CA, USAd Division of Social and Behavioral Health, Department ofCommunity and Preventive Medicine, University of Rochester,Rochester, NY, USAPublished online: 03 Sep 2014.
To cite this article: Timothy De Ver Dye, Gretel Pelto, Sibylle Kristensen, Arlene Samen & AnnDozier (2014): Attitudes and practices towards micronutrient supplementation among pregnantwomen in rural Tibet, Global Public Health: An International Journal for Research, Policy andPractice, DOI: 10.1080/17441692.2014.944551
To link to this article: http://dx.doi.org/10.1080/17441692.2014.944551
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or
howsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4

Attitudes and practices towards micronutrient supplementationamong pregnant women in rural Tibet
Timothy De Ver Dyea*, Gretel Peltob, Sibylle Kristensenc, Arlene Samenc andAnn Dozierd
aDepartment of Obstetrics and Gynecology, School of Medicine and Dentistry, University ofRochester, Rochester, NY, USA; bDivision of Nutritional Sciences, College of Human Ecology,Cornell University, Ithaca, NY, USA; cOneHEART Worldwide, San Francisco, CA, USA; dDivisionof Social and Behavioral Health, Department of Community and Preventive Medicine, University ofRochester, Rochester, NY, USA
(Received 22 October 2013; accepted 21 May 2014)
The objective of this study was to identify trends and change in micronutrientsupplementation (MNS) knowledge across pregnancy and post-partum and to assessthe impact of MNS knowledge (MNS-k) on practice in pregnancy in rural Tibet, anarea with endemic micronutrient deficiency. A prospective cohort with repeatedmeasures at early, late and after pregnancy in a rural area in the Tibetan AutonomousRegion included women receiving care by community workers. Key messages aboutMNS-k and optimal MNS practice were communicated through health workerencounters with pregnant women. Outcomes included MNS consumption practice,knowledge and attitudes. The proportion of women in the highest MNS-k categoryincreased by 35% from early to late pregnancy (37.5–50.7%, respectively; p < .005).MNS-k was associated with MNS consumption in a dose–response manner overpregnancy (trend X 2 p-value < .0001), with increasing knowledge associated withincreased MNS consumption. By late pregnancy, 32.5% of women had neverconsumed an MNS in this pregnancy, and 51.5% had not consumed an MNS on theassessed day or the day before. Sustained knowledge of MNS improved in pregnancyand post-partum. Best practice around MNS consumption increased though remainedsub-optimal.
Keywords: micronutrient; supplementation; Tibet; pregnancy; maternal health
Introduction
Micronutrients provided in pharmaceutically prepared supplements are common inter-ventions in pregnancy aimed at reducing micronutrient deficiency and its subsequentmorbidity and mortality (Institute of Medicine Committee on Micronutrient Deficiencies,1998). Micronutrient supplementation (MNS) in pregnancy has been recommended as acomponent of standard prenatal care in low- and middle-income countries (Fawzi et al.,2007), especially in areas with low to very low food security (World Health Organization,World Food Program, & UNICEF, 2006). Unfortunately, interventions aimed at providingantenatal micronutrient supplements to populations at nutritional risk often fail due todifferential and incomplete coverage (Schultink, 1996), inconsistent pill consumption
*Corresponding author. Email: [email protected]
Global Public Health, 2014http://dx.doi.org/10.1080/17441692.2014.944551
© 2014 Taylor & Francis
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4

practices by pregnant women (Sloan, 1998) and confusing or unclear regimens andschedules for consumption (Pena-Rosas & Viteri, 2006).
Micronutrient deficiencies are commonly found in Tibetan communities (Harris et al.,2001; Moreno-Reyes et al., 1998), which also observe some of the highest maternal andinfant mortality rates in the region (United Nations Health Partners Group, 2005). Mostrural Tibetan communities are remote, in high-altitude environments, with low fooddiversity that lack micronutrient variation in diet (Goldstein & Beall, 1990). Studies fromhigh-altitude Himalayan communities in this region of the world have helped demonstratethat MNS in pregnancy improves foetal growth (Osrin et al., 2005) and helps reduce earlyneonatal mortality (Zeng et al., 2008). Evidence around the impact of iron supplementa-tion in pregnancy is more elusive but suggests positive benefits on birthweight (Haideret al., 2013). Community, participatory approaches to design and implementation ofprogrammes and interventions can help regions make progress towards nutritional goals(Underwood, 2003).
In the present study, community health workers in a rural Tibetan county who provideongoing maternal and child health care, including prenatal multivitamin and ironsupplementation, received enhanced training and support (including in-service training,on-site mentoring and written health education materials) to improve the effectiveness oftheir supplementation work. Community health workers prior to this enhanced supportoften remarked that women did not use supplements appropriately, either saving them,giving them to their animals, family or friends, or consuming the supplements sporadically.Further, as a tea-based society (tea consumption could complicate micronutrient absorption,Zijp, Korver, & Tijburg, 2000, and butter tea and black tea are consumed regularly as part ofthe Tibetan diet), promotion of optimal pill ingestion practice is an important component ofimproving the effectiveness of antenatal MNS overall. The purpose of this study is toidentify trends and change in MNS knowledge (MNS-k) across pregnancy and post-partum;we hypothesise that MNS-k impacts MNS practice in pregnancy in a remote, ruralpopulation in Tibet.
MethodsStudy design
This project represents a quasi-experimental, non-random prospective evaluation designof a public health nutrition education intervention that used Skilled Birth Attendants(SBAs) and community-based paraprofessionals to provide a range of prenatal services topregnant women residing in a rural area of Tibet (Medrogongkar County). The projectrepresents a community-based participatory approach to collaborating with communityorganisations and a large non-governmental organisation (OneHEART, Health Educationand Research in Tibet) that managed several maternal and child health programmes in thearea. OneHEART provided training, supplies and logistical support to communityworkers who provide care to pregnant women residing in Medrogongkar; the careprovided by community workers includes prenatal health education, micronutrientsupplement distribution, birth education and linkage to SBAs (if the community workeris not a midwife). This present project – termed the TSAMPA project (Tibet Supplementsand Micronutrients in Pregnancy Assessment) – aimed to provide training to thesecommunity workers on micronutrient deficiency and to collaboratively develop strategiesto improve it through supplementation and dietary diversity for the pregnant women theyvisit.
2 T.D.V. Dye et al.
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4

Study site
Medrogongkar is a rural county located east of the city of Lhasa and contains eighttownships that sustain an approximate population of 40,000 in more than 200 villages(Phuoc, Jones-Le, Bell, & Miller, 2009). Medrogongkar County is one of the poorest inTibet (Goldstein, Jiao, Beall, & Tsering, 2003), and much of the county is at an altitudethat exceeds 4000 metres (12,000 feet). Approximately 20% of Medrogongkar’s villagesare nomadic, while the remaining villages sustain farming communities. Groups ofcommunity workers were trained on the tracking procedures that comprised this project inaddition to receiving enhanced training on micronutrients in pregnancy to help thembetter provide prenatal nutritional educational services.
Sample
Community health workers sequentially enrolled pregnant women in the project as theymade visits to women estimated to be in their first trimester. In total, 344 pregnant womenwere enrolled at baseline (early pregnancy), 204 (59.3%) of whom were followed up atlate pregnancy and 322 (93.6%) of whom were followed up post-partum. The latepregnancy follow-up sample was significantly less likely (p < .01) to reside in the remote,nomadic areas of the sample (Tsashue and Memba) than the overall sample. Thisdifference can be attributed to the logistical and practical difficulties in reaching womenin highly remote areas before delivery. The late pregnancy follow-up sample and the post-partum sample did not differ from the overall intake sample with respect to the MNS-kscore, the main variable of interest. Self-reported median weeks pregnant (based on eitherself-reported gestational age or due date) was 19 weeks at intake (25th–75th percentilerange: 12–24 weeks), 32 weeks at late pregnancy (25th–75th percentile range: 28–37weeks) and 4 weeks post-partum (25th–75th percentile range: 0–13 weeks post-partum).
Interviews
The data collection instrument was developed based on the project’s objectives, fromreviewing the existing literature on micronutrients in pregnancy and from qualitativeinterviews conducted with stakeholders. The linguistic and conceptual frame for theproject was influenced by ethnographic research conducted by the authors and with othersaffiliated with the same maternal and child health programme (e.g., see Craig, 2009). Theinstrument was further drawn from the experience of Sloan, Jordan, and Winikoff (2002),Kuhnlein and Pelto (1997) and Swindale and Ohri-Vachaspati (1999). The finalinstrument contained 39 questions covering a range of demographic characteristics,dietary and micronutrient knowledge, attitudes and practices and was translated intoTibetan for administration. Interviews lasted a median of 40 minutes overall, longer atintake (median = 46 minutes) than at late pregnancy (median = 43 minutes) or post-partum (median = 32 minutes).
MNS-k index
MNS-k items assessed included perceptions of influence of supplements on pregnantwomen, perceptions of influence of supplements on the foetus, knowledge ofrecommended consumption practices, MNS as a source of nutrition and practices toavoid MNS side effects (Figure 1). An MNS-k index was constructed by taking allknowledge questions correlated (using Spearman’s r) with at least half of all knowledge
Global Public Health 3
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4
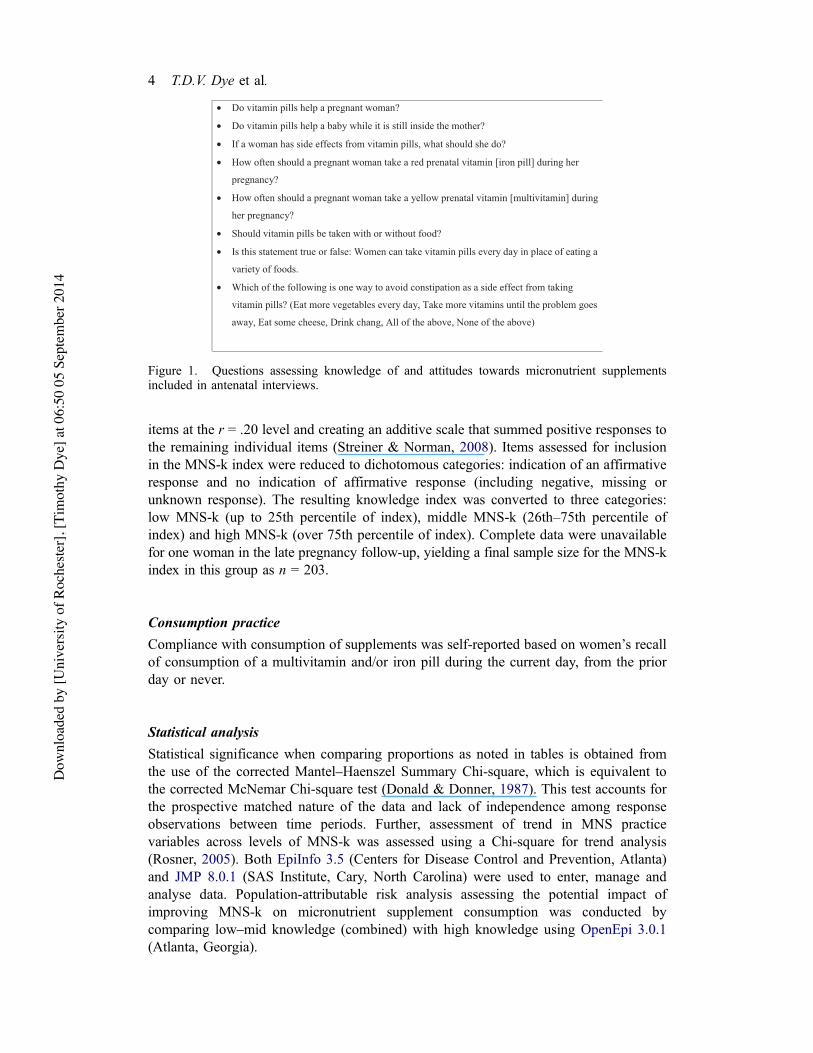
items at the r = .20 level and creating an additive scale that summed positive responses tothe remaining individual items (Streiner & Norman, 2008). Items assessed for inclusionin the MNS-k index were reduced to dichotomous categories: indication of an affirmativeresponse and no indication of affirmative response (including negative, missing orunknown response). The resulting knowledge index was converted to three categories:low MNS-k (up to 25th percentile of index), middle MNS-k (26th–75th percentile ofindex) and high MNS-k (over 75th percentile of index). Complete data were unavailablefor one woman in the late pregnancy follow-up, yielding a final sample size for the MNS-kindex in this group as n = 203.
Consumption practice
Compliance with consumption of supplements was self-reported based on women’s recallof consumption of a multivitamin and/or iron pill during the current day, from the priorday or never.
Statistical analysis
Statistical significance when comparing proportions as noted in tables is obtained fromthe use of the corrected Mantel–Haenszel Summary Chi-square, which is equivalent tothe corrected McNemar Chi-square test (Donald & Donner, 1987). This test accounts forthe prospective matched nature of the data and lack of independence among responseobservations between time periods. Further, assessment of trend in MNS practicevariables across levels of MNS-k was assessed using a Chi-square for trend analysis(Rosner, 2005). Both EpiInfo 3.5 (Centers for Disease Control and Prevention, Atlanta)and JMP 8.0.1 (SAS Institute, Cary, North Carolina) were used to enter, manage andanalyse data. Population-attributable risk analysis assessing the potential impact ofimproving MNS-k on micronutrient supplement consumption was conducted bycomparing low–mid knowledge (combined) with high knowledge using OpenEpi 3.0.1(Atlanta, Georgia).
• Do vitamin pills help a pregnant woman?
• Do vitamin pills help a baby while it is still inside the mother?
• If a woman has side effects from vitamin pills, what should she do?
• How often should a pregnant woman take a red prenatal vitamin [iron pill] during her
pregnancy?
• How often should a pregnant woman take a yellow prenatal vitamin [multivitamin] during her pregnancy?
• Should vitamin pills be taken with or without food?
• Is this statement true or false: Women can take vitamin pills every day in place of eating a
variety of foods.
• Which of the following is one way to avoid constipation as a side effect from taking
vitamin pills? (Eat more vegetables every day, Take more vitamins until the problem goes
away, Eat some cheese, Drink chang, All of the above, None of the above)
Figure 1. Questions assessing knowledge of and attitudes towards micronutrient supplementsincluded in antenatal interviews.
4 T.D.V. Dye et al.
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4

Ethical considerations
This project was reviewed and approved by the University of Rochester ResearchSubjects Review Board and the Tibetan Autonomous Region Tibetan Medicine ClinicalResearch Institute Institutional Review Board.
ResultsAttitudes towards and knowledge of micronutrient supplements
As shown in Table 1, there was a statistically significant increase (p < .01) in theproportion of women indicating that ‘vitamin pills can help pregnant women’ and/or ‘canhelp foetuses’ between the baseline antenatal and post-partum periods. The proportion ofwomen indicating ‘vitamin pills can help pregnant women’ increased by 22% from earlyantenatal to post-partum, and the proportion of women indicating vitamins ‘can helpfoetuses’ increased by 19%.
At both baseline (i.e., early antenatal) and post-partum, women were significantlymore likely to report that they thought supplements helped the foetus than they were toreport that supplements helped the pregnant woman (p < .05 at baseline and p < .01 atpost-partum). The most common reasons indicated for benefits of supplements for bothwomen and foetuses include ‘increase nutrition’, ‘increase the blood’, ‘grow well’, ‘goodsleep’, ‘baby becomes fat and grows well’ and ‘become strong and healthy’.
Table 1. Knowledge and attitudes towards prenatal micronutrient supplements among pregnantwomen in a rural Tibetan county.
Earlyantepartum(n = 344),% (n)
Lateantepartum(n = 204),% (n)
Post-partum(n = 322),% (n)
Vitamin pills help a pregnant woman(‘Yes’ response)
53.8 (185) 68.6 (140)** 65.8 (212)**
Vitamin pills help a baby while stillinside the mother (‘Yes’ response)
63.4 (218) 74.0 (151) 75.5 (243)**
Vitamin pills should be taken withfood (‘Yes’ response)
50.3 (173) 68.6 (140)*** 59.9 (193)
Women can take vitamin pills everyday in place of eating a variety of foods (‘True’response)
18.0 (62) 14.7 (30) 7.8 (25)***
Should take yellow pill (multivitamin) daily(‘Yes’ response)
48.0 (165) 63.7 (130)*** 74.8 (241)***
Should take red pill (iron) daily (‘Yes’ response) 58.1 (200) 75.9 (153)*** 73.9 (238)***Ways to avoid constipation as a side effect of taking vitamin pillsEat more vegetables 56.1 (193) 60.8 (124) 59.3 (191)Take more vitamins 14.8 (51) 15.7 (32) 17.1 (55)Eat cheese 18.0 (62) 18.1 (37) 22.4 (72)Drink changa 16.9 (58) 18.6 (38) 19.3 (62)All of the above 20.1 (69) 22.5 (46) 21.1 (68)None of the above 9.9 (34) 10.3 (21) 10.2 (33)
Note: Statistical significance: **p < .01; ***p < .001 (not noted = not statistically significant), compared tobaseline (early antepartum).achang is a commonly consumed fermented beverage made from barley.
Global Public Health 5
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4
Knowledge of basic MNS consumption practice changed over pregnancy as well. Aspresented in Table 1, the proportion of women indicating that ‘vitamins should be takenwith food’ significantly increased (p < .001) across pregnancy, as did the proportion ofwomen indicating that supplements should be ‘taken every day’ (p < .001). No significantdifference over pregnancy was observed in how women should treat constipation, acommonly reported side effect of micronutrient supplement consumption.
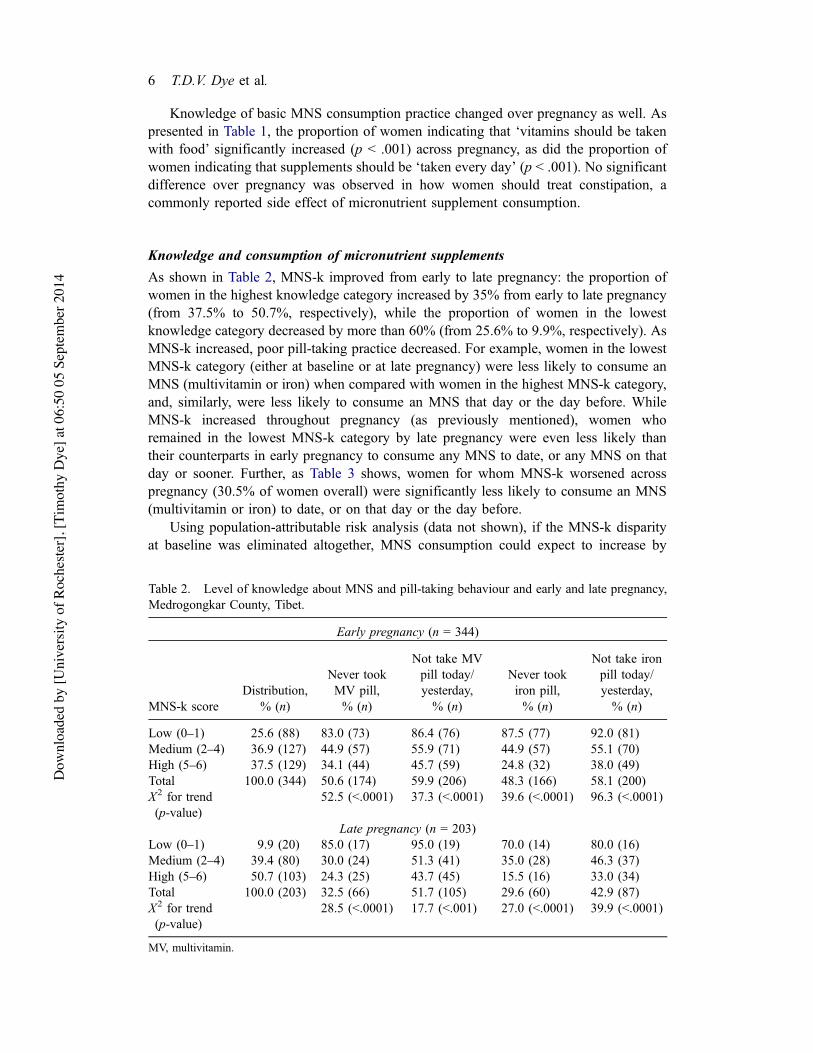
Knowledge and consumption of micronutrient supplements
As shown in Table 2, MNS-k improved from early to late pregnancy: the proportion ofwomen in the highest knowledge category increased by 35% from early to late pregnancy(from 37.5% to 50.7%, respectively), while the proportion of women in the lowestknowledge category decreased by more than 60% (from 25.6% to 9.9%, respectively). AsMNS-k increased, poor pill-taking practice decreased. For example, women in the lowestMNS-k category (either at baseline or at late pregnancy) were less likely to consume anMNS (multivitamin or iron) when compared with women in the highest MNS-k category,and, similarly, were less likely to consume an MNS that day or the day before. WhileMNS-k increased throughout pregnancy (as previously mentioned), women whoremained in the lowest MNS-k category by late pregnancy were even less likely thantheir counterparts in early pregnancy to consume any MNS to date, or any MNS on thatday or sooner. Further, as Table 3 shows, women for whom MNS-k worsened acrosspregnancy (30.5% of women overall) were significantly less likely to consume an MNS(multivitamin or iron) to date, or on that day or the day before.
Using population-attributable risk analysis (data not shown), if the MNS-k disparityat baseline was eliminated altogether, MNS consumption could expect to increase by
Table 2. Level of knowledge about MNS and pill-taking behaviour and early and late pregnancy,Medrogongkar County, Tibet.
Early pregnancy (n = 344)
MNS-k scoreDistribution,
% (n)
Never tookMV pill,% (n)
Not take MVpill today/yesterday,% (n)
Never tookiron pill,% (n)
Not take ironpill today/yesterday,% (n)
Low (0–1) 25.6 (88) 83.0 (73) 86.4 (76) 87.5 (77) 92.0 (81)Medium (2–4) 36.9 (127) 44.9 (57) 55.9 (71) 44.9 (57) 55.1 (70)High (5–6) 37.5 (129) 34.1 (44) 45.7 (59) 24.8 (32) 38.0 (49)Total 100.0 (344) 50.6 (174) 59.9 (206) 48.3 (166) 58.1 (200)X2 for trend(p-value)
52.5 (<.0001) 37.3 (<.0001) 39.6 (<.0001) 96.3 (<.0001)
Late pregnancy (n = 203)Low (0–1) 9.9 (20) 85.0 (17) 95.0 (19) 70.0 (14) 80.0 (16)Medium (2–4) 39.4 (80) 30.0 (24) 51.3 (41) 35.0 (28) 46.3 (37)High (5–6) 50.7 (103) 24.3 (25) 43.7 (45) 15.5 (16) 33.0 (34)Total 100.0 (203) 32.5 (66) 51.7 (105) 29.6 (60) 42.9 (87)X2 for trend(p-value)
28.5 (<.0001) 17.7 (<.001) 27.0 (<.0001) 39.9 (<.0001)
MV, multivitamin.
6 T.D.V. Dye et al.
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4
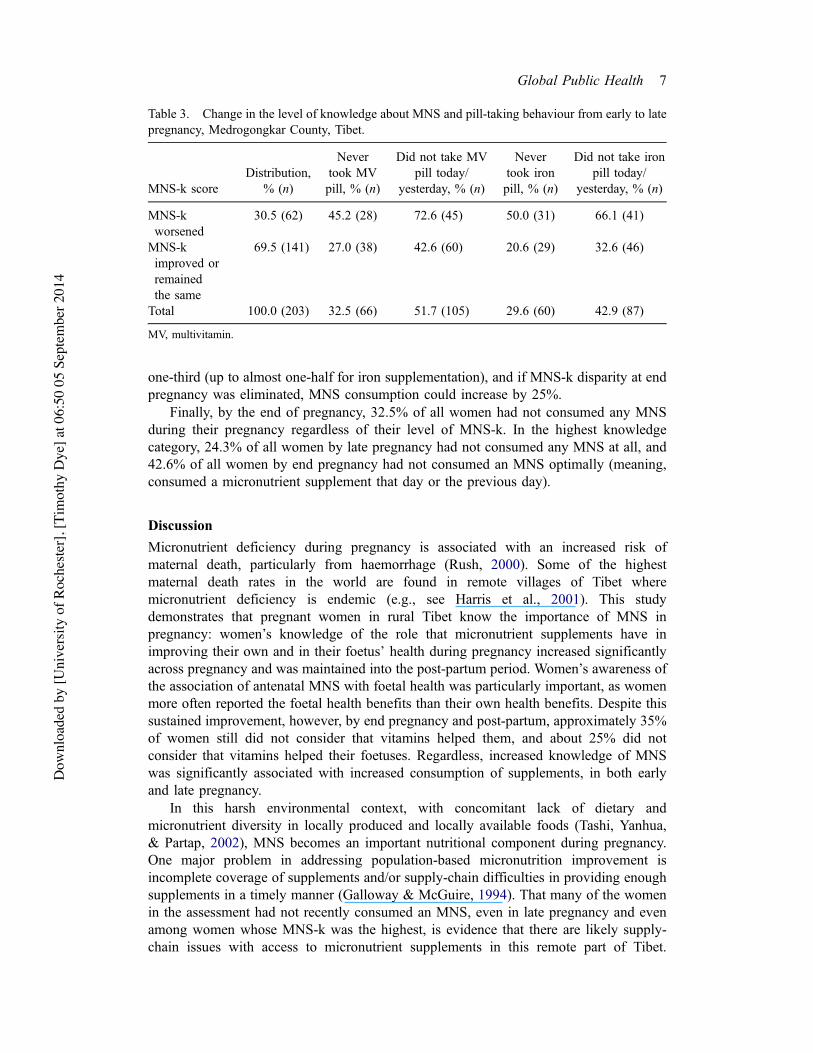
one-third (up to almost one-half for iron supplementation), and if MNS-k disparity at endpregnancy was eliminated, MNS consumption could increase by 25%.
Finally, by the end of pregnancy, 32.5% of all women had not consumed any MNSduring their pregnancy regardless of their level of MNS-k. In the highest knowledgecategory, 24.3% of all women by late pregnancy had not consumed any MNS at all, and42.6% of all women by end pregnancy had not consumed an MNS optimally (meaning,consumed a micronutrient supplement that day or the previous day).
Discussion
Micronutrient deficiency during pregnancy is associated with an increased risk ofmaternal death, particularly from haemorrhage (Rush, 2000). Some of the highestmaternal death rates in the world are found in remote villages of Tibet wheremicronutrient deficiency is endemic (e.g., see Harris et al., 2001). This studydemonstrates that pregnant women in rural Tibet know the importance of MNS inpregnancy: women’s knowledge of the role that micronutrient supplements have inimproving their own and in their foetus’ health during pregnancy increased significantlyacross pregnancy and was maintained into the post-partum period. Women’s awareness ofthe association of antenatal MNS with foetal health was particularly important, as womenmore often reported the foetal health benefits than their own health benefits. Despite thissustained improvement, however, by end pregnancy and post-partum, approximately 35%of women still did not consider that vitamins helped them, and about 25% did notconsider that vitamins helped their foetuses. Regardless, increased knowledge of MNSwas significantly associated with increased consumption of supplements, in both earlyand late pregnancy.
In this harsh environmental context, with concomitant lack of dietary andmicronutrient diversity in locally produced and locally available foods (Tashi, Yanhua,& Partap, 2002), MNS becomes an important nutritional component during pregnancy.One major problem in addressing population-based micronutrition improvement isincomplete coverage of supplements and/or supply-chain difficulties in providing enoughsupplements in a timely manner (Galloway & McGuire, 1994). That many of the womenin the assessment had not recently consumed an MNS, even in late pregnancy and evenamong women whose MNS-k was the highest, is evidence that there are likely supply-chain issues with access to micronutrient supplements in this remote part of Tibet.
Table 3. Change in the level of knowledge about MNS and pill-taking behaviour from early to latepregnancy, Medrogongkar County, Tibet.
MNS-k scoreDistribution,
% (n)
Nevertook MVpill, % (n)
Did not take MVpill today/
yesterday, % (n)
Nevertook ironpill, % (n)
Did not take ironpill today/
yesterday, % (n)
MNS-kworsened
30.5 (62) 45.2 (28) 72.6 (45) 50.0 (31) 66.1 (41)
MNS-kimproved orremainedthe same
69.5 (141) 27.0 (38) 42.6 (60) 20.6 (29) 32.6 (46)
Total 100.0 (203) 32.5 (66) 51.7 (105) 29.6 (60) 42.9 (87)
MV, multivitamin.
Global Public Health 7
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4
Inconsistent availability of supplements leads to insufficient bioavailable micronutrientsof a magnitude to impact maternal or foetal health (Sloan et al., 2002). Especially inremote or isolated communities, such as rural Tibet, ensuring a consistent supply ofsupplements to adequately cover a population’s nutritional needs is challenging, at best(Galloway et al., 2002). In addition, some studies show that adherence with consumptionof micronutrient supplements varies and that pill-taking behaviour varies with culturaland personal priorities, oftentimes in a manner that disadvantages optimal release ofmicronutrients in a nutritionally beneficial manner (Galloway & McGuire, 1994). Forexample, Milman (2006) has shown that some commonly consumed foods such as teaand some dairy products can interfere with iron absorption, and it should be noted thatthese foods comprise an important component of the Tibetan diet (see Dickersonet al., 2008).
In this population of pregnant women, both micronutrient knowledge and consump-tion increased throughout pregnancy, in a related manner. Importantly, as MNS-kincreased, consumption increased, with those women remaining in the lowest knowledgecategory least likely to consume a micronutrient supplement at any point in theirpregnancy. Further, women whose knowledge of MNS decreased over pregnancy werenearly twice as likely as other women to not consume an MNS.
Regardless of the association between knowledge and consumption, a considerableproportion of women (about one-quarter) did not consume a multivitamin or ironsupplement at any point in pregnancy, and about half of all women did not consume asupplement on the day of the assessment or the day before. Even among women in thehighest knowledge category, nearly half did not consume a supplement on the day of theinterview or the day before (rising to nearly 95% for women in the lowest knowledgecategory). Particularly in the context of increasing knowledge in pregnancy of theimportance and proper practice for consuming micronutrient supplements daily, this gapsuggests a supply difficulty where perhaps women ran out of supplements, for somereason did not take them as instructed or simply did not have access to a supply ofsupplements.
This study did have some limitations. Adherence measurement was limited to self-reported consumption during the index or prior day, without lab confirmation or pillcount. Given logistical challenges and practice standards, the project had no control groupto assess micronutrient supplement consumption among other pregnant women. Follow-up at late pregnancy (though not post-partum) was challenging and differed from intake,largely due to the nomadic nature of much of the population, unclear due dates andinclement weather or other accessibility challenges. Regardless, no statistically significantdifferences were identified in the population at intake, follow-up at late pregnancy orfollow-up post-partum when assessing the following variables: residing in nomadictownship, month of year interviewed, weeks pregnant at intake, age and education statusat intake, interview time, consumption of multivitamin supplement and consumption ofiron supplement. Further, the distribution of study participants for all three study timeperiods reflected the distribution of pregnancies by township, with the exception that oneof the remote townships (Memba) is slightly but statistically significantly over-represented at the second interview (end pregnancy), likely due to enhanced vigilancein interviewing women at end pregnancy that was emphasised in training and particularlyimplemented in Memba by the community workers. Additionally, information womenprovided in the study is self-reported, which could possibly reflect information and/orrecall bias in some cases. Finally, while community health worker interviewers attended
8 T.D.V. Dye et al.
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4

trainings, had their completed interviews reviewed and participated actively in the project,bias introduced by interviewers cannot be ruled out.
Since the conclusion of this project, a new integrated micronutrient product thatcontains both the prenatal vitamin formulation plus iron has replaced the multiple pillsrequired daily that was available during this study. Logistically, this single-pillformulation should improve the simplicity and dosing of MNS consumption in thisregion. However, the aforementioned challenges of supply-chain difficulties, improvingregular daily consumption, eliminating sharing the supplements with others, improvingconsumption practice and maintaining sustained high levels of knowledge about theimportance of MNS remain. Micronutrient deficiency and low dietary diversity continueto impact this region of the world that faces considerable health risk; improving theeffectiveness of MNS through practices and policies informed by women’s beliefs andbehaviours is an important component overall in concomitantly improving maternal andchild health in Tibetan communities.
AcknowledgementsThis project was funded through US Centers for Disease Control and Prevention – Association ofTeachers of Preventive Medicine (CDC-ATPM) Cooperative Agreement to the University ofRochester, Community-based Micronutrient Consumption in Tibet, TD Dye, Principal Investigator,Award # TS1252. The authors are very grateful to the women who participated in this project and toour many Tibetan colleagues who assisted with this work.
ReferencesCraig, S. R. (2009). Pregnancy and childbirth in Tibet: Knowledge, perspectives, and practices. InH. Selin & P. K. Stone (Eds.), Childbirth across cultures: Ideas and practices of pregnancy,childbirth and the postpartum (pp. 145–160). New York, NY: Springer.
Dickerson, T., Fernandez, D., Topgyal, Samen, A., Gelek, Nyima, … Dye, T. (2008). From buttertea to Pepsi®: A rapid appraisal of food preferences and procurement strategies in a contemporaryTibetan township. Ecology of Food and Nutrition, 47, 229–253. doi:10.1080/03670240701781861
Donald, A., & Donner, A. (1987). Adjustments to the Mantel–Haenszel chi-square statistic andodds ratio variance estimater when the data are clustered. Statistics in Medicine, 6, 491–499.doi:10.1002/sim.4780060408
EpiInfo (Version 3.5) [Computer Software]. Atlanta, GA: Centers for Disease Control andPrevention.
Fawzi, W. W., Msamanga, G. I., Urassa, W., Hertzmark, E., Petraro, P., Willett, W. C., &Spiegelman, D. (2007). Vitamins and perinatal outcomes among HIV-negative women inTanzania. New England Journal of Medicine, 356, 1423–1431. doi:10.1056/NEJMoa064868
Galloway, R., Dusch, E., Elder, L., Achadi, E., Grajeda, R., Hurtado, E., … Stephen, C. (2002).Women’s perceptions of iron deficiency and anemia prevention and control in eight developingcountries. Social Science & Medicine, 55, 529–544. doi:10.1016/S0277-9536(01)00185-X
Galloway, R., & McGuire, J. (1994). Determinants of compliance with iron supplementation:Supplies, side effects, or psychology? Social Science & Medicine, 39, 381–390. doi:10.1016/0277-9536(94)90135-X
Goldstein, M. C., & Beall, C. M. (1990). Nomads of western Tibet: The survival of a way of life.Berkeley: University of California Press.
Goldstein, M. C., Jiao, B., Beall, C., & Tsering, P. (2003). Development and change in rural Tibet:Problems and adaptations. Asian Survey, 43, 758–779. doi:10.1525/as.2003.43.5.758
Haider, B. A., Olofin, I., Wang, M., Spiegelman, D., Ezzati, M., & Fawzi, W. W. (2013). Anaemia,prenatal iron use, and risk of adverse pregnancy outcomes: Systematic review and meta-analysis.BMJ: British Medical Journal, 346, f3443. doi:10.1136/bmj.f3443
Harris, N. S., Crawford, P. B., Yangzom, Y., Pinzo, L., Gyaltsen, P., & Hudes, M. (2001).Nutritional and health status of Tibetan children living at high altitudes. New England Journal ofMedicine, 344, 341–347. doi:10.1056/NEJM200102013440504
Global Public Health 9
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4

Institute of Medicine Committee on Micronutrient Deficiencies. (1998). Prevention of micronutrientdeficiencies: Tools for policy makers and public health workers. Washington, DC: NationalAcademy Press.
JMP (Version 8.0.1) [Computer Software]. Cary, NC: SAS Institute.Kuhnlein, H. V., & Pelto, G. H. (Eds.). (1997). Culture, environment, and food to prevent vitamin Adeficiency. Ottawa: International Nutrition Foundation for Developing Countries & InternationalDevelopment Research Centre.
Milman, N. (2006). Iron and pregnancy: A delicate balance. Annals of Hematology, 85, 559–565.doi:10.1007/s00277-006-0108-2
Moreno-Reyes, R., Suetens, C., Mathieu, F., Begaux, F., Zhu, D., Rivera, M. T., … Vanderpas, J.(1998). Kashin-Beck osteoarthropathy in rural Tibet in relation to selenium and iodine status.New England Journal of Medicine, 339, 1112–1120. doi:10.1056/NEJM199810153391604
OpenEpi (Version 3.0.1) [Computer Software]. Atlanta, GA: Centers for Disease Control andPrevention.
Osrin, D., Vaidya, A., Shrestha, Y., Baniya, R., Manandhar, D., Adhikari, R., … Costello, A.(2005). Effects of antenatal multiple micronutrient supplementation on birthweight andgestational duration in Nepal: Double-blind, randomized, controlled trial. The Lancet, 365,955–962. doi:10.1016/S0140-6736(05)71084-9
Pena-Rosas, J. P., & Viteri, F. E. (2006). Effects of routine oral iron supplementation with orwithout folic acid for women during pregnancy (Review). Cochrane Database of SystematicReviews, 3, CD004736.
Phuoc, V. L., Jones-Le, E., Bell, C., & Miller, S. (2009). Preferences for perinatal healthcommunication of women in rural Tibet. Journal of Obstetric, Gynecologic, and NeonatalNursing, 38(1), 108–117. doi:10.1111/j.1552-6909.2008.00312.x
Rosner, B. (2005). Fundamentals of biostatistics (6th ed.). Florence, KY: Cengage Learning.Rush, D. (2000). Nutrition and maternal mortality in the developing world. The American Journalof Clinical Nutrition, 72(Suppl. 1), 212s–240s.
Schultink, W. (1996). Iron-supplementation programmes: Compliance of target groups andfrequency of tablet intake. Food and Nutrition Bulletin, 17(1), 22–26.
Sloan, N. (1998). Pill taking behavior: Implications for micronutrient supplementation for SafeMotherhood. Population Council #03851. New York, NY: Population Council.
Sloan, N. L., Jordan, E., & Winikoff, B. (2002). Effects of iron supplementation on maternalhematologic status in pregnancy. American Journal of Public Health, 92, 288–293. doi:10.2105/AJPH.92.2.288
Streiner, D., & Norman, G. (2008). Health measurement scales: A practical guide to theirdevelopment and use (4th ed.). Oxford: Oxford University Press.
Swindale, A., & Ohri-Vachaspati, P. (1999). Measuring household food consumption: A technicalguide. Washington, DC: Food and Nutrition Technical Assistance Project (FANTA).
Tashi, N., Yanhua, L., & Partap, T. (2002). Making Tibet food secure: Assessment of scenarios.Kathmandu: International Centre for Integrated Mountain Development.
Underwood, B. A. (2003). Scientific research: Essential, but is it enough to combat world foodinsecurities? The Journal of Nutrition, 133(5 Suppl. 1), 1434S–1437S.
United Nations Health Partners Group. (2005). A health situation assessment of the People’sRepublic of China. Beijing: United Nations Health Partners Group in China.
World Health Organization, World Food Program, & UNICEF. (2006). Preventing and controllingmicronutrient deficiencies in populations affected by an emergency. Joint Statement. Retrieved fromhttp://www.who.int/nutrition/publications/micronutrients/WHO_WFP_UNICEFstatement.pdf
Zeng, L., Cheng, Y., Dang, S., Yan, H., Dibley, M. J., Chang, S., & Kong, L. (2008). Impact ofmicronutrient supplementation during pregnancy on birthweight, duration of gestation, andperinatal mortality in rural western China: Double blind cluster randomized controlled trial. BMJ:British Medical Journal, 337, a2001–a2012. doi:10.1136/bmj.a2001
Zijp, I. M., Korver, O., & Tijburg, L. B. (2000). Effect of tea and other dietary factors on ironabsorption. Critical Reviews in Food Science and Nutrition, 40, 371–398. doi:10.1080/10408690091189194
10 T.D.V. Dye et al.
Dow
nloa
ded
by [U
nive
rsity
of R
oche
ster],
[Tim
othy
Dye
] at 0
6:50
05
Sept
embe
r 201
4




















