Association B etween T elomerase A ctivity a nd O utcome i n Patients W ith N onmetastatic E wing F...
8
Association Between Telomerase Activity and Outcome in Patients With Nonmetastatic Ewing Family of Tumors By A. Ohali, S. Avigad, I.J. Cohen, I. Meller, Y. Kollender, J. Issakov, I. Gelernter, Y. Goshen, I. Yaniv, and R. Zaizov Purpose: Telomerase is considered a molecular marker for malignancy. The aim of this study was to determine telomer- ase activity (TA) as a prognostic factor at diagnosis and as a marker for minimal residual disease during therapy and fol- low-up in nonmetastatic Ewing family of tumors (EFT). Patients and Methods: Primary tumor specimens and 97 peripheral blood (PBL) samples from 31 EFT patients were analyzed for TA by the Telomeric Repeat Amplification Pro- tocol (TRAP assay). The telomerase catalytic subunit (human telomerase reverse transcriptase [hTERT]) gene expression was evaluated by quantitative reverse transcriptase poly- merase chain reaction (RT-PCR) and telomere length was determined by Southern blotting. The presence of the EFT chimeric transcripts was analyzed by RT-PCR. Correlations with progression-free survival were evaluated. Results: At diagnosis, TA in primary tumors did not cor- relate with outcome. During therapy and follow-up, highly significant correlation was observed between high TA in PBL samples and adverse prognosis (P < .0001). None of the patients harboring low TA progressed, with a long fol- low-up (median, 60 months) and a progression-free sur- vival (PFS) of 100%. In nine patients, high TA actually could predict relapse, long before overt clinical relapse. The group of patients with high TA and positive RT-PCR had the most adverse outcome; PFS of 20% (P .0025). TA was found to be a better prognostic factor than RT-PCR and histopatho- logic response at surgery. Conclusion: The results suggest that TA is a significant prognostic variable, superior to the established clinical prognostic parameters during therapy and tumor surveil- lance. It could be used in combination with RT-PCR for a new risk classification. J Clin Oncol 21:3836-3843. © 2003 by American Society of Clinical Oncology. E WING’S SARCOMA (ES) is the second most common primary malignant bone tumor in children and adolescents, and it belongs to a group of neuroectodermal tumors known as the ES family of tumors (EFT). 1 All EFT share one of the following specific translocations: t(11;22), t(21;22), t(7;22), t(17;22), and t(2;22). 2-7 These translocations result in the fusion of the EWS gene on 22q12 with different ETS oncogene superfamily-related genes, FLI-1 (85% to 90%), ERG (5% to 10%), ETV-1, E1AF (1%), and rarely, FEV. The various EWS rearrangements seem to be pivotal events in EFT tumorigenesis and these genetic alterations are considered distinct diagnostic features of these tumors. 3 At diagnosis, approximately 25% of patients have detectable metastatic disease, but the majority of patients may have micrometastases, undetectable by conven- tional methods, as evidenced by a very low cure rate with local therapy. The standard care includes combination of aggressive chemotherapy, radiotherapy, and surgery. Initial response to therapy, assessed by histologic analysis of surgical specimens as the degree of tumor necrosis, has become an accepted valid prognostic factor, especially in localized tumors of the extrem- ities. Despite advances in therapy, more than 50% eventually relapse, even after 5 years. 8 Several groups have used reverse transcriptase polymerase chain reaction (RT-PCR) for the accurate diagnosis and for determining the presence of occult micrometastases in bone marrow (BM) or peripheral blood (PBL) at diagnosis and during therapy. 9,10 Some studies have shown an association between outcome and the presence or absence of tumor cells in BM at diagnosis and in PBL during therapy, 11,12 and recently in both at diagnosis. 13 Telomeres are specialized structures at the ends of eukaryotic chromosomes, consisting of hundreds of repeated hexanucleotides (TTAGGG) n . 14 Telomeres protect the chromosomes from DNA degradation, end-to-end fusions, rearrangements, and chromosome loss. 15,16 Due to the inability of DNA polymerase to replicate the ends of double-stranded DNA, known as the “end replication problem,” telomeres are progressively shortened with each round of cell division, leading to cellular senescence. 17 A reduction in telomere lengths has been described in a wide range of human cancers, 18-22 and progressive telomere shortening has been shown to contribute to genomic instability. 23 Telomerase expression is a characteristic feature of permanent cell lines and a vast majority of human malignant tumors, whereas most normal somatic tissues do not express telomer- ase. 24 Recent findings support the concept that activation of From the Department of Molecular Oncology, Felsenstein Medical Re- search Center, and the Department of Pediatric Hematology/Oncology, Schneider Children’s Medical Center of Israel, Petah Tikva; and Sourasky Medical Center, Sackler Faculty of Medicine, and Statistical Laboratory, School of Mathematics, Tel Aviv University, Tel Aviv, Israel. Submitted May 7, 2002; accepted July 28, 2003. This work was supported by the Josefina Maus and Gabriela Cesarman Maus Chair for Pediatric Hematology Oncology (R.Z.). This work was performed in partial fulfillment of the requirements for the PhD degree of Anat Ohali, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel. Authors’ disclosures of potential conflicts of interest are found at the end of this article. Address reprint requests to Smadar Avigad, PhD, Molecular Oncology, Felsenstein Medical Research Center, Rabin Medical Campus, Petah Tikva 49100, Israel; e-mail: [email protected]. © 2003 by American Society of Clinical Oncology. 0732-183X/03/2120-3836/$20.00 3836 Journal of Clinical Oncology, Vol 21, No 20 (October 15), 2003: pp 3836-3843 DOI: 10.1200/JCO.2003.05.059 Downloaded from jco.ascopubs.org on June 13, 2013. For personal use only. No other uses without permission. Copyright © 2003 American Society of Clinical Oncology. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Association B etween T elomerase A ctivity a nd O utcome i n Patients W ith N onmetastatic E wing F...

Associat ion Between Telomerase Act i v i t y and Outcome inPat ients With Nonmetastat ic Ewing Family of Tumors
By A. Ohali, S. Avigad, I.J. Cohen, I. Meller, Y. Kollender, J. Issakov, I. Gelernter, Y. Goshen, I. Yaniv, and R. Zaizov
Purpose: Telomerase is considered a molecular marker formalignancy. The aim of this study was to determine telomer-ase activity (TA) as a prognostic factor at diagnosis and as amarker for minimal residual disease during therapy and fol-low-up in nonmetastatic Ewing family of tumors (EFT).
Patients and Methods: Primary tumor specimens and 97peripheral blood (PBL) samples from 31 EFT patients wereanalyzed for TA by the Telomeric Repeat Amplification Pro-tocol (TRAP assay). The telomerase catalytic subunit (humantelomerase reverse transcriptase [hTERT]) gene expressionwas evaluated by quantitative reverse transcriptase poly-merase chain reaction (RT-PCR) and telomere length wasdetermined by Southern blotting. The presence of the EFTchimeric transcripts was analyzed by RT-PCR. Correlationswith progression-free survival were evaluated.
Results: At diagnosis, TA in primary tumors did not cor-relate with outcome. During therapy and follow-up, highly
significant correlation was observed between high TA in PBLsamples and adverse prognosis (P < .0001). None of thepatients harboring low TA progressed, with a long fol-low-up (median, 60 months) and a progression-free sur-vival (PFS) of 100%. In nine patients, high TA actually couldpredict relapse, long before overt clinical relapse. The groupof patients with high TA and positive RT-PCR had the mostadverse outcome; PFS of 20% (P � .0025). TA was found tobe a better prognostic factor than RT-PCR and histopatho-logic response at surgery.
Conclusion: The results suggest that TA is a significantprognostic variable, superior to the established clinicalprognostic parameters during therapy and tumor surveil-lance. It could be used in combination with RT-PCR for a newrisk classification.
J Clin Oncol 21:3836-3843. © 2003 by AmericanSociety of Clinical Oncology.
EWING’S SARCOMA (ES) is the second most commonprimary malignant bone tumor in children and adolescents,
and it belongs to a group of neuroectodermal tumors known asthe ES family of tumors (EFT).1 All EFT share one of thefollowing specific translocations: t(11;22), t(21;22), t(7;22),t(17;22), and t(2;22).2-7 These translocations result in the fusionof the EWS gene on 22q12 with differentETS oncogenesuperfamily-related genes,FLI-1 (85% to 90%),ERG (5% to10%), ETV-1,E1AF (1%), and rarely,FEV. The variousEWSrearrangements seem to be pivotal events inEFT tumorigenesisand these genetic alterations are considered distinct diagnosticfeatures of these tumors.3 At diagnosis, approximately 25% ofpatients have detectable metastatic disease, but the majority of
patients may have micrometastases, undetectable by conven-tional methods, as evidenced by a very low cure rate with localtherapy. The standard care includes combination of aggressivechemotherapy, radiotherapy, and surgery. Initial response totherapy, assessed by histologic analysis of surgical specimens asthe degree of tumor necrosis, has become an accepted validprognostic factor, especially in localized tumors of the extrem-ities. Despite advances in therapy, more than 50% eventuallyrelapse, even after 5 years.8
Several groups have used reverse transcriptase polymerase chainreaction (RT-PCR) for the accurate diagnosis and for determiningthe presence of occult micrometastases in bone marrow (BM) orperipheral blood (PBL) at diagnosis and during therapy.9,10 Somestudies have shown an association between outcome and thepresence or absence of tumor cells in BM at diagnosis and in PBLduring therapy,11,12and recently in both at diagnosis.13
Telomeres are specialized structures at the ends of eukaryoticchromosomes, consisting of hundreds of repeated hexanucleotides(TTAGGG)n.
14 Telomeres protect the chromosomes from DNAdegradation, end-to-end fusions, rearrangements, and chromosomeloss.15,16 Due to the inability of DNA polymerase to replicate theends of double-stranded DNA, known as the “end replicationproblem,” telomeres are progressively shortened with each round ofcell division, leading to cellular senescence.17 A reduction intelomere lengths has been described in a wide range of humancancers,18-22and progressive telomere shortening has been shown tocontribute to genomic instability.23
Telomerase expression is a characteristic feature of permanentcell lines and a vast majority of human malignant tumors,whereas most normal somatic tissues do not express telomer-ase.24 Recent findings support the concept that activation of
From the Department of Molecular Oncology, Felsenstein Medical Re-search Center, and the Department of Pediatric Hematology/Oncology,Schneider Children’s Medical Center of Israel, Petah Tikva; and SouraskyMedical Center, Sackler Faculty of Medicine, and Statistical Laboratory,School of Mathematics, Tel Aviv University, Tel Aviv, Israel.
Submitted May 7, 2002; accepted July 28, 2003.This work was supported by the Josefina Maus and Gabriela Cesarman
Maus Chair for Pediatric Hematology Oncology (R.Z.).This work was performed in partial fulfillment of the requirements for the
PhD degree of Anat Ohali, Sackler School of Medicine, Tel Aviv University,Tel Aviv, Israel.
Authors’ disclosures of potential conflicts of interest are found at the endof this article.
Address reprint requests to Smadar Avigad, PhD, Molecular Oncology,Felsenstein Medical Research Center, Rabin Medical Campus, Petah Tikva49100, Israel; e-mail: [email protected].
© 2003 by American Society of Clinical Oncology.0732-183X/03/2120-3836/$20.00
3836 Journal of Clinical Oncology, Vol 21, No 20 (October 15), 2003: pp 3836-3843DOI: 10.1200/JCO.2003.05.059
Downloaded from jco.ascopubs.org on June 13, 2013. For personal use only. No other uses without permission.Copyright © 2003 American Society of Clinical Oncology. All rights reserved.

telomerase may be a critical, if not obligatory step in thedevelopment of cancer.25 Telomerase, a multisubunit ribonucle-oprotein, is capable of adding telomeric DNA to the ends oflinear chromosomes using its RNA template.26 Previous studieshave found telomerase activity (TA) to be a useful diagnosticand prognostic marker in various neoplasms.27-30 High levels ofTA have been found in a variety of malignancies in adults,particularly in gastric, prostate, colon, ovarian cancer, and braintumors.21,31-34 Among pediatric solid tumors, the most studiedone is neuroblastoma, where TA has been found as an indepen-dent prognostic factor.35,36 Recently, the telomerase catalyticsubunit (human telomerase reverse transcriptase [hTERT]) wascloned, and its expression revealed a strong correlation withTA.37-39 Early detection and treatment of relapse may prevent ordelay tumor progression. The search for new molecular markersfor assessing the individual patient’s prognosis is of vitalimportance. We postulated that telomerase might be a goodcandidate for these goals.
In our study, 31 EFT patients were analyzed for TA, hTERTexpression and telomere length in primary tumors, and in PBL atdiagnosis, during therapy and during surveillance; the resultswere correlated with clinical parameters and outcome.
PATIENTS AND METHODS
Patients
Twenty-five primary tumor specimens, 97 PBL samples, and two BMsamples were obtained from 31 EFT patients with nonmetastatic disease whowere admitted to the Pediatric Hematology/Oncology Department at Schnei-der Children’s Medical Center (Petah Tikva, Israel). Informed consent wasobtained from the patients or their guardians, and the local and nationalethics committees approved the research project. All patients were treatedaccording to the protocol for EFT, including a combination of aggressivechemotherapy, radiotherapy, and surgery. Median age at diagnosis was 14years (range, 0.3 to 27 years). Twelve patients were females, and 19 weremales. Primary sites were: nine pelvis, three sacrum, 14 limbs, and fiveothers. Response to therapy was defined by histopathologic response andassessed by percentage of tumor necrosis at the time of surgery (limb salvageprocedure) following neoadjuvant chemotherapy and radiotherapy. Nineteenpatients were good responders (� 90% tumor necrosis at the time ofresection), nine were poor responders (� 90% of tumor necrosis) and threehad an inoperable tumor (primary site: cranium, chest sacrum). Nine patients(29%) progressed, four locally, three in the lung, and two in distal bone.Median follow-up was 60 months (range, 7 to 153 months). All tissuesamples were snap-frozen in liquid nitrogen immediately after surgery, andall samples were stored at �80°C until use. All patients were clinically wellwith no evidence of disease at the time before relapse. In addition, PBLsamples from 20 age-matched healthy individuals were included as controls.
TA
Tissue and PBL samples were analyzed for semiquantitative TA using theTRAPeze telomerase detection kit (Intergene Company, Purchase, NY),according to manufacturer’s instructions. The protein concentration in cellextracts was determined by the Bradford assay (Bio-Rad; Hercules, CA), and0.6 �g protein was used for each reaction. After 30 minutes incubation at30°C for telomerase-mediated extension of the TS primer (-5�-AATCCGTC-GAGCAGAGTT-3�), the reaction mixture was subjected to 35 polymerasechain reaction (PCR) cycles of 94°C for 30 seconds, 58°C for 30 seconds,and 72°C for 45 seconds. The PCR products were then electrophoresed in10% polyacrylamide gels and silver stained. Each analysis included a heatinactivation control (sample incubated at 85°C for 20 minutes before
reaction), a negative control (buffer lysis only) and a TSR8 positivequantitative control. TSR8 is an oligonucleotide that serves as a standard forestimating the amount of primers with telomeric repeats extended bytelomerase in a given extract. Telomerase-positive cells derived from a cellline, provided in the kit, were also used as a positive control. TA wasmeasured by a densitometer using Quantity One software (PDI, HuntingtonStation, NY). Based on statistical analysis of the values’ range, we defined �
80% of mean optical density (OD) values of TSR8 as high TA. The low TAgroup was comprised of negative samples and samples exhibiting less than80% of the positive quantitative control. An extract was considered negativefor TA when the 36-bp band (the internal assay control) was present and nodetectable ladder pattern was found. All analyses were conducted induplicates and results were reproducible.
Telomere Length Determination
Six microgram aliquots of genomic DNA was digested with HinfI andseparated on 0.8% agarose gels. Fractionated DNA fragments were blottedonto nylon membranes (Qiagen GmbH, Hilden, Germany) and hybridizedwith the telomeric probe (TTAGGG)3 that had been labeled with [�-33p]ATPat the 5� end by using T4 polynucleotide kinase (New England Biolabs Inc,Beverly, MA). The intensity of the hybridization was evaluated by densito-metric analysis with Quantity One software and terminal restriction frag-ments (TRF), an indicator of mean telomere length of a sample, wasestimated at the peak position of the hybridization signal over the range of 2to 23 kb. Telomere shortening or elongation were defined as less than 80%or greater than 120% of the median length (9.0 Kb) of the correspondingnormal PBL, respectively.40
Telomerase Catalytic Subunit (hTERT) Expression Analysis
Total RNA was isolated from tumor and PBL samples using Tri Reagent(Molecular Research Center Inc, Cincinnati, OH) according to manufacturer’sprotocol. Gene expression of hTERT was evaluated by quantitative RT-PCRperformed on the LightCycler (Roche Diagnostics GmbH, Mannheim, Germa-ny), using the LightCycler TeloTAGGG hTERT quantification kit followingsupplier’s instructions. Gene expression of the housekeeping gene porphobilino-gen deaminase (PBGD) was used as a control. Quantitative analysis wasperformed using the LightCycler software. The copy numbers of startingtemplates was calculated by comparing the relative fluorescence signals of thesamples with external hTERT mRNA standards. The RNA standards used were
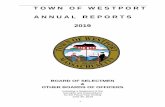
Fig 1. Telomeric repeat amplification protocol assay in Ewing family of tumors.Positive telomerase activity is detected in samples 2,4, and 7. In each sample, theadjacent lane is a heat inactivation control; negative control in lane 9 and positivequantitative control (TSR8) in lane 10. M, DNA marker; ITAS, an internaltelomerase assay standard.
3837TELOMERASE AS A PROGNOSTIC FACTOR IN ES
Downloaded from jco.ascopubs.org on June 13, 2013. For personal use only. No other uses without permission.Copyright © 2003 American Society of Clinical Oncology. All rights reserved.

10-fold dilutions starting from 106 copies/reaction, to 102 copies resulting instandard curves. High expression of hTERT was defined as equal or more than100 copies, while less than that was considered low expression.
RT-PCR Analysis
Twenty-five samples of PBL were analyzed by RT-PCR for the chimerictranscript which was identified in the primary tumor of these patients atdiagnosis. All samples harbored only the EWS-FLI1 transcript. Total RNAwas isolated as mentioned above. RT-PCR was performed with the AccessRT-PCR System (Promega, Madison, WI) according to instructions with 1�g total RNA, 2.5 �mol/L magnesium, random hexamers, and previouslydescribed primers.3,9,41
Statistical Analysis
TA was assessed for potential association with a number of clinical andmolecular parameters, including patients’ age, sex, primary site, tumornecrosis, hTERT expression, and presence or absence of chimeric transctriptsby RT-PCR. The associations were evaluated using the Fisher’s exact testand P � .05 was considered to be statistically significant. Distributions ofprogression-free survival (PFS) were estimated by the Kaplan-Meier analysis(using log-rank). Results were considered significant for P � .05. Univariateand multivariate analysis were performed using Cox regression study.
RESULTS
At Diagnosis
TA. TA was tested on 25 EFT primary tumors and nine PBLsamples available at diagnosis. TA was detected in 84% (21 of25) and in 67% (six of nine) of the tumor and PBL samples
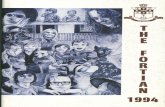
Fig 2. Quantitative reverse transcriptase polymerase chain reaction of human telomerase reverse transcriptase expression (hTERT). (A) Standard dilution series andpositive controls curves are marked by asterisks, and the other curves are patients’ samples with various degrees of expression. (B) Linear regression of standard dilutionseries indicates accuracy and reproducibility of the analysis.
Table 1. Telomerase Activity in Primary Tumors Compared With ClinicalParameters
Parameter
Telomerase Activity
P
High Low
No. of Patients % No. of Patients %
Age� 12 years 4 67 2 33 .5� 12 years 11 58 8 42
Site of primary tumorPelvis and sacrum 8 73 3 27 .2Limbs and others 7 50 7 50
SexMale 9 56 7 44 .5Female 6 67 3 33
Percent of tumor necrosis� 90 7 50 7 50 .09� 90 7 88 1 12
hTERT� 100 copies 3 33 6 67 .038� 100 copies 9 82 2 18
Abbreviation: hTERT, human telomerase reverse transcriptase gene.
3838 OHALI ET AL
Downloaded from jco.ascopubs.org on June 13, 2013. For personal use only. No other uses without permission.Copyright © 2003 American Society of Clinical Oncology. All rights reserved.

respectively. The telomerase positive tissue extracts produced acharacteristic 6-bp ladder as shown in Figure 1.
High TA (HTA) was observed in 71% (15 of 21) of thetumors. Of these patients, eight relapsed (53%), while in the 10low-TA patients, four (40%) relapsed. Evaluation of progres-sion-free survival (PFS) analysis did not reach a significantdifference between high and low TA groups.
Among the PBL samples, 56% (five of nine) showed high TA; ofthese patients, 40% (two of five) relapsed and as in the primarytumors, had no significant correlation with clinical outcome.
By Fisher’s exact test, TA was correlated to known clinicalparameters such as age at diagnosis, primary site of tumor, sex,and response to therapy (Table 1). No significant correlation wasfound between any of these clinical parameters and TA.
hTERT expression. Twenty tumor samples were tested forexpression of hTERT mRNA (Fig 2). High expression of hTERT(� 100 copies) was identified in 55% (11 of 20), and itsignificantly correlated with high TA as nine of the 11 samplesoverexpressing hTERT mRNA, also presented high TA (P �.038, Table 1).
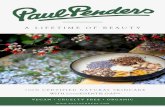
Telomere length. Twelve tumor DNA samples were ana-lyzed using Southern blot for telomere length (Fig 3). Eight of 12tumors exhibited changes in telomere lengths: five shorter andthree longer than the median benign samples. Alteration intelomere length was associated with high TA in five (71%) ofseven tumors. No significant correlation was found betweentelomere length and TA.
During Therapy and Follow-Up
TA. A retrospective analysis of TA was performed in 88PBL and two BM samples from 26 patients at different timepoints during a long follow-up ranging from 7 to 153 months(median, 60 months). One to 10 samples were analyzed perpatient (mean, five samples per patient). For the PFS and theprediction of relapse, the last available sample per patient wasevaluated (24 PBL and two BM samples).
TA from the last sample analyzed was correlated with thesame clinical parameters, as at diagnosis (Table 2). A significantcorrelation was found between high TA and age below 12 years(P � .003). No association was found with sex, site of theprimary tumor, or response to therapy.
High TA was observed in 11 patients (42%). Nine (82%) of11 patients with high TA relapsed, while none of the 15patients with low TA did. Highly significant correlation was
Fig 3. Telomere length determined by Southern blot in three patients. Eachtumor sample (T) was compared with normal tissue (NT) from the same patient.Telomere shortening is observed in the first two tumors (from the right), and one isunchanged.
Fig 4. Kaplan-Meier survival curves by telomerase activity (TA) during follow-up.
Table 2. Telomerase Activity in Peripheral Blood and Bone Marrow Samples(last analyzed) During Follow-Up Compared With Clinical Parameters
Parameter
Telomerase Activity
P
High Low
No. of Patients % No. of Patients %
Age� 12 years 7 88 1 12 .003� 12 years 4 22 14 78
Site of primary tumorPelvis and sacrum 4 44 5 56 .6Limbs and others 7 41 10 59
SexMale 7 44 9 56 .6Female 4 40 6 60
Percent of tumor necrosis� 90 7 37 12 63 .2� 90 3 75 1 25
hTERT� 100 copies 3 20 12 80 .0136� 100 copies 5 71 2 29
Abbreviation: hTERT, human telomerase reverse transcriptase gene.
3839TELOMERASE AS A PROGNOSTIC FACTOR IN ES
Downloaded from jco.ascopubs.org on June 13, 2013. For personal use only. No other uses without permission.Copyright © 2003 American Society of Clinical Oncology. All rights reserved.

observed between TA in PBL samples and PFS. Low TApatients had 100% PFS, while high-TA patients had 18% PFS(P � .0001; Fig 4).
Since we analyzed many samples during a long follow-up, itwas possible to observe the kinetics of TA. Low TA in allsamples analyzed from the same patient was detected in sevenpatients (27%); high TA was detected in all samples from sevenpatients (27%). Samples from eight patients (31%) turned fromhigh to low TA. In four patients, low TA turned to high TA. Allseven patients that consistently exhibited high TA relapsed. Ofthe four patients who had a shift to high TA, two relapsed. Noneof the patients who consistently harbored low TA or turned tolow TA relapsed.
In nine patients, high TA could predict relapse before overtclinical relapse (Table 3). In six of these patients, earlier samples
were studied, and four of the samples harbored high TA. In twopatients, samples turned from low to high TA.
Twenty-five samples of PBL were analyzed for both TA andthe presence of the chimeric transcript EWS-FLI1 by RT-PCR(Table 4). Nineteen (76%) of 25 samples were in concordance,meaning they were RT-PCR positive with high TA, or RT-PCRnegative with low TA. Of the six samples that were not inconcordance, three were RT-PCR positive with low TA, ofwhich no patient has progressed, and three were RT-PCRnegative with high TA, of which one patient progressed. Of the19 concordant results, nine relapsed, all with high TA andpositive RT-PCR. A significant correlation between TA andRT-PCR was observed (P � .030), and their predictive value ofrelapse was similar.
Age older than 12 years at diagnosis (P � .01, data notshown), and a greater than 90% tumor necrosis at the time oftumor resection (P � .0001; Fig 5) were favorable prognosticfactors for predicting PFS. We attempted to identify whichindependent factor had a significant influence on survival. It wasnot mathematically possible to establish the Cox multivariatestudy including TA, because one subset of events was empty (nocases of relapse within the group of low telomerase samples).
Fig 5. Kaplan-Meier survival curves by percentage of tumor necrosis at thetime of tumor resection.
Table 3. Prediction of Relapse by High Telomerase Activity in the Last Sample Analyzed
Patient No.
1 5 6 7 10 14 15 19 20
High TA, months from diagnosis 41 25 26 51 12 15 35 23 7Time to relapse, months from diagnosis 51 29 41 61 15 17 37 31 12Site of relapse Lung Local
(cranium)Arm Lung Lung Local
(chest)Local
(pelvis)Pelvis Local
(abdomen)Prediction, months from last TA
analysis10 4 15 10 3 2 2 8 5
Abbreviation: TA, telomerase activity.
Table 4. Correlation Between RT-PCR of the Chimeric Transcript and TA DuringFollow-Up
Patient No. TART-PCR ofEWS/FLI-1 Relapse
1 High � Yes2 Low � No3 High � No5 High � Yes6 High � Yes7 High � Yes8 Low � No9 Low � No
10 High � Yes11 Low � No12 High � No13 Low � No14 High � Yes15 High � Yes16 Low � No17 Low � No18 High � No19 High � Yes20 High � Yes21 High � No22 Low � No24 High � No25 Low � No26 Low � No31 High � Yes
Abbreviations: RT-PCR, reverse transcriptase polymerase chain reaction; TA,telomerase activity; �, positive; �, negative.
3840 OHALI ET AL
Downloaded from jco.ascopubs.org on June 13, 2013. For personal use only. No other uses without permission.Copyright © 2003 American Society of Clinical Oncology. All rights reserved.

Therefore, we performed Kaplan-Meier analysis of PFS with TAin the favorable group of patients who had more than 90% oftumor necrosis (Fig 6), and with both TA and positive/negativeRT-PCR in this group (Fig 7).
Our data show that for patients with greater than 90% tumornecrosis, low TA was a significant favorable parameter and highTA was an adverse prognostic parameter regardless of theirinitial good histopathologic response (P � .0006), and therefore,TA is a better prognostic indicator. The same results wereachieved when both TA and RT-PCR were analyzed. Norelapses occurred in patients with low TA and negative or
positive RT-PCR, with 100% PFS at a median follow-up of 60months. High TA and negative RT-PCR determined an interme-diate-risk group with 50% of 5-years PFS. The most adverse-riskgroup was high TA and positive RT-PCR with only 20% PFS(P � .0025). Thus, the combination of TA and RT-PCR resultscould identify three risk groups: good-, intermediate-, andhigh-risk. When we performed a multivariate analysis with highTA cases only, tumor necrosis was a significant protectiveparameter (P � .04) while RT-PCR lost its significance (P � .1;data not shown). According to our data, TA turned to be asignificant prognostic factor in EFT patients during follow-up.
hTERT expression. The expression of hTERT was tested in22 PBL samples of EFT patients during follow-up. The samplesof seven patients expressed high hTERT (�100 copies), four ofthem relapsed (57%), while of the 15 patients whose samplesexpressed low hTERT (�100 copies), only two relapsed (13%).PFS comparing patients with high and low hTERT expressionwas statistically significant (P � .038; Fig 8). All these samplesthat were tested for hTERT were also analyzed for TA andcorrelated significantly (P � .0136, Table 2).
Normal cohort. All 20 normal PBL samples studied showedno detectable TA by TRAP assay.
DISCUSSION
The present study is, to the best of our knowledge, the firstreport on TA and its possible prognostic significance in patientswith EFT over a long period of follow-up (7 to 153 months;median, 60 months). Moreover, this is the first extensive studythat attempted to evaluate TA in PBL as a marker for minimal
Fig 6. Kaplan-Meier survival curves by telomerase activity (TA) during fol-low-up in the group of patients with more than 90% necrosis.
Fig 7. Kaplan-Meier survival curves by both telomerase activity (TA) andreal-time polymerase chain reaction (RT-PCR) analyses in patients with more than90% tumor necrosis.
Fig 8. Kaplan-Meier survival curves by human transcriptase reverse telomer-ase (hTERT) expression during follow-up. hTERT�, low expression (<100 copies);hTERT�, high expression (> 100 copies).
3841TELOMERASE AS A PROGNOSTIC FACTOR IN ES
Downloaded from jco.ascopubs.org on June 13, 2013. For personal use only. No other uses without permission.Copyright © 2003 American Society of Clinical Oncology. All rights reserved.

residual disease (MRD). Many studies in various other malig-nancies showed that high TA in primary tumors at diagnosis wasassociated with unfavorable clinical features, and some of themrevealed a significant correlation between TA and survival incancer patients.21,22,27-36 In some of these studies, hTERTexpression also correlated with TA.
In contrast to these reports, we did not find in EFT primarytumors any correlation between TA and clinical outcome atdiagnosis. Even so, there was a significant correlation betweenTA and hTERT expression in these tumors (P � .038).
Numerous studies have shown that changes in telomerelengths are associated with unfavorable outcome. A reduction intelomere length has been reported in several malignancies:colorectal carcinoma, renal cell carcinoma, and childhood leu-kemia.18,19,42 A correlation between shortened telomeres and TAwas also established for ovarian and gastric cancer.21,31 How-ever, telomeres can be stabilized at virtually any length. Indeedsome cancers, such as basal cell carcinomas, may have un-changed or elongated TRFs, whereas liposarcomas show acharacteristically large variation in telomeric length, shortenedor elongated in comparison with normal tissues.43,44 This couldexplain why, in contrast to enzyme activity, relatively fewstudies regard TRF measurements as a useful prognostic factor.TRFs in EFT revealed a heterogeneous pattern. In our smallcohort study, we found changes in TRF in 69%; six hadshortened TRFs, three had elongated ones, and the rest wereunchanged. Seventy-five percent of the tumor samples withchanges in TRF also expressed high TA. The three patientswhose tumors showed elongated TRFs are well with no evidenceof disease, while three of the six patients whose tumors exhibitedshortened TRFs had relapsed. However, of the four patients withunchanged TRFs, three relapsed. Our preliminary data suggestthat elongated TRFs may be associated with a more favorableoutcome in EFT patients, but the study should be extended to amuch larger cohort.
In order to evaluate the potential use of TA as a marker forMRD, we analyzed PBL samples from 20 healthy donors by theTRAP assay and no TA could be detected in any of them,suggesting that TA determination could be used in PBL samples.Eighty-eight PBL and two BM samples were analyzed for TAduring follow-up, many of which were also tested for hTERTexpression. In the present study, a highly significant correlationbetween high TA and poor outcome was observed (P � .0001),and TA could distinguish between patients with a high- orlow-risk of relapse. While 82% of the patients with high TArelapsed, none of the low TA group did. In nine patients, highTA actually could predict relapse long before overt clinicalrelapse (2 to 15 months). Tumor necrosis, which is considered astrong clinical prognostic factor, was also highly correlated with
outcome. Five patients who were good responders still relapsed,and all of them harbored high TA. This suggests that high TAduring follow-up significantly correlates with clinical outcome.The data that high TA in the PBL could be used as a reliableprognostic marker has additional added value for monitoringresidual disease, particularly in children.
Based on the presence of unique chimeric transcripts in EFTcells, the feasibility of RT-PCR for follow-up of MRD in EFTpatients has been demonstrated recently by several groups9-11
including ours (manuscript submitted for publication). In 25patients, both TA and RT-PCR analysis of the chimeric tran-scripts were performed. A significant correlation between TAand RT-PCR was observed (P � .030). In the group of patientswith over 90% tumor necrosis at surgery, TA turned to be amuch stronger indicator when comparing the value of TA andRT-PCR in predicting the risk to relapse, as shown in Figure 7.Patients with high TA and positive RT-PCR had the mostadverse prognosis (5-year PFS of 20%), but the crucial param-eter was TA, as patients with low TA and negative or positiveRT-PCR had 100% PFS. Patients with high TA and negativeRT-PCR had an intermediate prognosis; PFS of 50%. Thus, thecombination of TA and RT-PCR results may form a new riskclassification with clinical relevance: low-, intermediate-, andhigh-risk of relapse.
Qualitative RT-PCR is known to be a very sensitive methodwhich can detect as little as one tumor cell in 106 normal cells,45
therefore, positive RT-PCR samples may represent residual tumorcells which do not yet indicate evidence for early relapse. Thesensitivity of detection TA by the TRAP assay is 1:104.24 Therefore,a sample harboring high TA may imply a higher number of tumorcells which by now already indicate relapse. This may explain thediscrepancy between RT-PCR and TA results.
A significant correlation between expression of hTERT andTA was observed during follow-up, and it was associated withadverse prognosis (P � .038).
High TA during follow-up was a significant prognostic factorfor PFS and was more predictive than the known clinicalprognostic parameters. Low TA during follow-up may indicate afavorable localized group with low-risk of relapse.
Although the number of patients in our study is small, ourresults suggest that TA could be used as a marker for monitoringEFT patients during follow-up. This study should be extended toa larger cohort of patients to further validate our observations.TA analysis, performed at precise time points, could be used forstratification of patients at risk of relapse.
AUTHORS’ DISCLOSURES OF POTENTIALCONFLICTS OF INTEREST
The authors indicated no potential conflicts of interest.
REFERENCES
1. Ginsberg JP, Woo SY, Johnson ME, et al: Ewing sarcoma family oftumors: Ewing’s sarcoma of bone and soft tissue and the peripheral primitiveneuroectodermal tumors, in Pizzo PA and Poplack DG (eds): Principles andPractice of Pediatric Oncology (ed 4), Philadelphia, PA, Lippincott-RavenPublishers, 2002, pp 973-1016
2. Dehner LP: Primitive neuroectodermal tumor and Ewing’s sarcoma.Am J Surg Pathol 17:1-13, 1993
3. Delattre O, Zucman J, Melot T, et al: The Ewing family of tumors: Asubgroup of small-round-cell tumors defined by specific chimeric transcripts.N Engl J Med 331:294-299, 1994
3842 OHALI ET AL
Downloaded from jco.ascopubs.org on June 13, 2013. For personal use only. No other uses without permission.Copyright © 2003 American Society of Clinical Oncology. All rights reserved.

4. Sorensen PH, Lessnick SL, Lopez-Terrada D, et al: A second Ewing’ssarcoma translocation, t(21; 22), fuses the EWS gene to another ETS-familytranscription factor, ERG. Nat Genet 6:146-151, 1994
5. Jeon IS, Davis JN, Braun BS, et al: A variant Ewing’s sarcomatranslocation (7:22) fuses the EWS gene to the ETS gene ETV1. Oncogene10:1229-1234, 1995
6. Urano F, Umezawa A, Hong W, et al: A novel chimera gene betweenEWS and E1A-F, encoding the adenovirus E1A enhancer-binding protein, inextraosseous Ewing’s sarcoma. Biochem Biophys Res Commun 219:608-612, 1996
7. Peter M, Couturier J, Paquement H, et al: A new member of the ETSfamily fused to EWS in Ewing tumors. Oncogene 14:1159-1164, 1997
8. Terrier P, Llombart-Bosch A, Contess G: Small round blue cell tumorsin bone: Prognostic factors correlated to Ewing’s sarcoma and neuroecto-dermal tumors. Semin Diagn Pathol 13:250-257, 1996
9. Peter M, Magdelenat H, Michon J, et al: Sensitive detection of occultEwing’s cells by the reverse transcriptase-polymerase chain reaction. Br JCancer 72:96-100, 1995
10. Pfleiderer C, Zoubek A, Gruber B, et al: Detection of tumor cells inperipheral blood and bone marrow from Ewing tumor patients by RT-PCR.Int J Cancer 64:135-139, 1995
11. Zoubek A, Ladenstein R, Windhager R, et al: Predictive potential oftesting for bone marrow involvement in Ewing tumor patients by RT-PCR:A preliminary evaluation. Int J Cancer 79:56-60, 1998
12. De Alava E, Lozano MD, Patino A, et al: Ewing family tumors:Potential prognostic value of reverse-transcriptase polymerase chain reactiondetection of minimal residual disease in peripheral blood samples. DiagnMol Pathol 6:152-157, 1998
13. Schleiermacher G, Peter M, Oberlin O, et al: Increased risk ofsystemic relapses associated with bone marrow micrometastasis and circu-lating tumor cells in localized Ewing Tumor. J Clin Oncol 21:85-91, 2003
14. Moyzis RK, Buckingham JM, Cram S, et al: A highly conservedrepetitive DNA sequence (TTAGGG)n present at the telomere of humanchromosomes. Proc Natl Acad Sci USA 85:6622-6626, 1988
15. Blackburn EH: Structure and function of telomere. Nature 350:569-573, 1991
16. Zakian VA: Telomeres: Beginning to understand the end. Science270:1601-1607, 1995
17. Allsopp RC, Vaziri H, Patterson C, et al: Telomere length predictsreplicative capacity of human fibroblasts. Proc Natl Acad Sci USA 89:10114-10118, 1992
18. Hastie ND, Dempster M, Dunlop MG, et al: Telomere reduction inhuman colorectal carcinoma and with aging. Nature 346:866-871, 1990
19. Adamson DJA, King DJ, Haits NE: Significant telomere shortening inchildhood leukemia. Cancer Genet Cytogenet 61:204-205, 1992
20. Hiyama E, Yokohama K, Yokohama T, et al: Length of telomericrepeats in neuroblastoma: Correlation with prognosis and other biologicalcharacteristics. Jpn J Cancer Res 83:159-164, 1992
21. Counter CM, Hirte HW, Baccetti S, et al: Telomerase activity inhuman ovarian carcinoma. Proc Natl Acad Sci U S A 91:2900-2904, 1994
22. Counter CM, Gupta J, Harley CB, et al: Telomerase activity in normalleukocytes and in hematologic malignancies. Blood 85:2315-2320, 1995
23. Ducray C, Pommier JP, Martins L, et al: Telomere dynamics, end toend fusions and telomerase activation during the human fibroblast immor-talization process. Oncogene 18:4211-4223, 1999
24. Kim NW, Piatyszek MA, Prowse KR, et al: Specific association ofhuman telomerase activity with immortal cells and cancer. Science 266:2011-2015, 1994
25. Shay JW, Gazdar AF: Telomerase in the early detection of cancer.J Clin Pathol 50:106-109, 1997
26. Nugent CI, Lundblad B: The telomerase reverse transcriptase: Com-ponents and regulation. Genes Dev 12:1073-1085, 1998
27. Yoshida TK, Sugino T, Tahara H, et al: Telomerase activity in bladdercarcinoma and its implication for noninvasive diagnosis by detection ofexfoliated cancer cells in urine. Cancer 79:362-369, 1997
28. Umbricht H, Saji M, Westra WH, et al: Telomerase activity: A markerto distinguish follicular thyroid adenoma from carcinoma. Cancer Res57:2144-2147, 1997
29. Hiyama E, Kodama T, Shinbara K, et al: Telomerase activity isdetected in pancreatic cancer but not in benign tumors. Cancer Res57:326-331, 1997
30. Rohde V, Sattler HP, Oehlenschlager B, et al: Genetic changes andtelomerase activity in human renal cell carcinoma. Clin Cancer Res 4:197-202, 1998
31. Hiyama E, Yokoyama T, Tatsumoto N, et al: Telomerase activity ingastric cancer. Cancer Res 55:3258-3262, 1995
32. Sommerfeld HJ, Meeker AK, Piatyszek MA, et al: Telomeraseactivity: A prevalent marker of malignant human prostate tissue. Cancer Res56:218-222, 1996
33. Chadeneau C, Hay K, Hirte HW, et al: Telomerase activity associatedwith acquisition of malignancy in human corolectal cancer. Cancer Res55:2533-2536, 1995
34. Langford LA, Piatyszek MA, Ruishu XU, et al: Telomerase activity inordinary meningiomas predicts poor outcome. Hum Pathol 28:416-420, 1997
35. Hiyama E, Hiyama K, Yokoyama T, et al: Correlating telomeraseactivity with neuroblastoma outcomes. Nat Med 1:249-255, 1995
36. Poremba C, Willenbring H, Hero B, et al: Telomerase activitydistinguishes between neuroblastomas with good and poor prognosis. AnnOncol 10:715-721, 1999
37. Takakura M, Kyo S, Kanaya T, et al: Cloning of human telomerasecatalytic subunit (hTERT) gene promoter and identification of proximal corepromoter sequences essential for transcriptional activation in immortalizedand cancer cells. Cancer Res 59:551-557, 1999
38. Ramakrishnan S, Eppenberger U, Mueller H, et al: Expression profileof the putative catalytic subunit of the telomerase gene. Cancer Res58:622-625, 1998
39. Meyerson M, Counter CM, Eaton EN, et al: hEST2, the putativehuman telomerase catalytic subunit gene, is up-regulated in tumor cells andduring immortalization. Cell 90:785-795, 1997
40. Takagi S, Kinouchi Y, Hiwatashi N, et al: Telomere shortening andthe clinicopathologic characteristics of human colorectal carcinomas. Cancer86:1431-1436, 1999
41. Zucman J, Melot T, Desmaze C, et al: Combinatorial generation ofvariable fusion proteins in the Ewing family of tumors. EMBO J 12:4481-4487, 1993
42. Dahase R, Fidler F, Ernst G, et al: Changes in telomere lengths inrenal cell carcinomas. Cell Mol Biol 42:477-485, 1996
43. Wainwright J, Middleton PG, Rees JL: Changes in mean telomerelength in basal cell carcinomas of the skin. Genes Chromosomes Cancer12:45-49, 1995
44. Schneider-Stock R, Epplen JT, Walter H, et al: Telomeric lengths andtelomerase activity in liposarcomas. Mol Carcinog 24:144-151, 1999
45. Downing JR, Head DR, Parham DM, et al: Detection of the (11;22)(q24;q12) translocation of Ewing’s sarcoma and peripheral neuroectoder-mal tumor by reverse transcription polymerase chain reaction. Am J Pathol143:1294-1300, 1993
3843TELOMERASE AS A PROGNOSTIC FACTOR IN ES
Downloaded from jco.ascopubs.org on June 13, 2013. For personal use only. No other uses without permission.Copyright © 2003 American Society of Clinical Oncology. All rights reserved.








![t] x| f} + of] hgf -cf=j](https://static.fdokumen.com/doc/165x107/631922cab41f9c8c6e099861/t-x-f-of-hgf-cfj.jpg)