
Substance Use among a Sample of Healthcare Workers in Kenya: A ...
Upload
independentCategory
view
3download
0
G
J
1
Avav
1
2
3
4
PQ1
HC
5
6
7
aQ28b9c10
11
a12
13
A14
R15
R2
16
17
A18
A
19
K20
I21
V22
H23
P24
S25
126
27
(28
a29
o30
a31
I32
c33
t34
v35
36
p37
p38
i39
0d
ARTICLE IN PRESSModel
VAC 11407 1–6
Vaccine xxx (2011) xxx–xxx
Contents lists available at ScienceDirect
Vaccine
journa l homepage: www.e lsev ier .com/ locate /vacc ine
re Kenyan healthcare workers willing to receive the pandemic influenzaaccine? Results from a cross-sectional survey of healthcare workers in Kenyabout knowledge, attitudes and practices concerning infection with andaccination against 2009 pandemic influenza A (H1N1), 2010
risca A. Oriaa,∗ , Wycliffe Matinib , Ian Nelligana , Gideon Emukulea , Martha Scherzerc , Beryl Oyiera ,ezron N. Ochienga, Laura Hoopera, Anne Kanyugab, Phillip Muthokab, Kathleen F. Moralesa,harles Nziokab, Robert F. Breimana, Mark A. Katza,c
Kenya Medical Research Institute/Centers for Disease Control and Prevention-Kenya (KEMRI/CDC-Kenya), Nairobi, KenyaMinistry of Public Health and Sanitation (MoPHS), KenyaCenters for Disease Control and Prevention (CDC) – Atlanta, GA, USA
r t i c l e i n f o
rticle history:eceived 29 September 2010eceived in revised form8 December 2010ccepted 21 January 2011vailable online xxx
a b s t r a c t
Over 1200 cases of 2009 pandemic influenza A H1N1 (pH1N1) have been identified in Kenya since thefirst case in June 2009. In April 2010 the Kenyan government launched a program to immunize high-riskgroups and healthcare workers (HCWs) with pH1N1 vaccines donated by the World Health Organization.To characterize HCWs’ knowledge, attitudes and practices regarding pH1N1 vaccination, we conducteda quantitative and qualitative survey in 20 healthcare facilities across Kenya between January 11 and 26,2010. Of 659 HCWs interviewed, 55% thought there was a vaccine against pH1N1, and 89% indicated that
eywords:nfluenzaaccinationealthcare workersandemicurvey
they would receive pH1N1 vaccine if it became available. In focus group discussions, many HCWs said thatpH1N1 virus infection did not cause severe disease in Kenyans and questioned the need for vaccination.However, most were willing to accept vaccination if they had adequate information on safety and efficacy.In order for the influenza vaccination campaign to be successful, HCWs must understand that pH1N1 cancause severe disease in Kenyans, that pH1N1 vaccination can prevent HCWs from transmitting influenzato their patients, and that the vaccine has been widely used globally with few recognized adverse events.
40
41
42
43
44
45
46
47
48
49
50
. Introduction
The first confirmed cases of 2009 pandemic A (H1N1) influenzapH1N1) were reported in two children in Southern California [1],nd the World Health Organization (WHO) declared the presencef a pandemic on June 11, 2009 [2]. pH1N1 vaccine first becamevailable in October 2009 in North America, Europe, and Australia.nitially, limited doses were available. WHO recommended that allountries prioritize immunization of healthcare workers (HCWs)o protect vital health infrastructure and to limit transmission toulnerable patients [3].
Please cite this article in press as: Oria PA, et al. Are Kenyan healthcare wora cross-sectional survey of healthcare workers in Kenya about knowledgeagainst 2009 pandemic influenza A (H1N1), 2010. Vaccine (2011), doi:10.1
Transmission of seasonal and pandemic influenza within hos-itals and nursing homes, including transmission from staff toatients, has been widely documented [4–11]. Transmission of
nfluenza among medical staff causes absenteeism and consid-
∗ Corresponding author. Tel.: +254 723824047.E-mail addresses: [email protected], [email protected] (P.A. Oria).
51
52
53
264-410X/$ – see front matter © 2011 Elsevier Ltd. All rights reserved.oi:10.1016/j.vaccine.2011.01.063
© 2011 Elsevier Ltd. All rights reserved.
erable disruption of health care services [12–14]. Nosocomialoutbreaks have typically been associated with low vaccination ratesamong healthcare workers [15], highlighting the need for contin-ued efforts to develop efficient influenza immunization programsfor hospital staff [12].
While influenza has been recognized as an important cause ofacute respiratory infections (ARI) in many developed countries, lit-tle is known about influenza in tropical countries in the Africa, andinfluenza vaccine is rarely used in this part of the world [16,17].Influenza vaccination is an effective way to prevent influenza virusinfection [18,19]. In Kenya, a country of 39 million people, only30,000 doses of seasonal influenza vaccine are administered annu-ally; HCWs are seldom vaccinated routinely [20].
The first case of pH1N1 was confirmed in Kenya in June 2009
kers willing to receive the pandemic influenza vaccine? Results from, attitudes and practices concerning infection with and vaccination016/j.vaccine.2011.01.063
[21]. Since then, more than 1200 cases have been identified through 54
hospital-based and population-based surveillance. The introduc- 55
tion of pandemic influenza to Kenya was of concern to the Kenyan 56
Ministry of Health and the Kenyan public [21,22]. In November 57
2009, WHO announced that Kenya and Togo would be the first two 58

ING
J
2 cine x
c59
v60
H61
(62
t63
c64
65
f66
k67
v68
269
70
h71
J72
m73
c74
a75
h76
o77
t78
o79
d80
i81
82
o83
t84
t85
C86
s87
p88
d89
290
91
s92
i93
s94
w95
m96
t97
i98
o99
a100
a101
f102
t103
p104
a105
e106
c107
i108
t109
110
t111
v112
A113
w114
b115
t116
w117
c118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
ARTICLEModel
VAC 11407 1–6
P.A. Oria et al. / Vac
ountries in Sub-Saharan Africa to receive WHO-donated pH1N1accines. The government of Kenya, through the Ministry of Publicealth and Sanitation (MoPHS) and the Ministry of Medical Services
MoMS) subsequently adopted a plan that prioritized vaccinatinghe country’s 120,000 HCWs with donated vaccine. The pH1N1 vac-ination campaign was launched in April 2010.
In order to inform a campaign to promote pH1N1 vaccinationor HCWs, we conducted a cross-sectional survey to assess HCWs’nowledge, attitudes and practices (KAP) about infection with andaccination against pH1N1.
. Materials and methodology
We conducted a cross-sectional survey of HCWs in selectedealth care facilities in Kenya from January 11, 2010 through
anuary 26, 2010. We used qualitative and quantitative researchethods including a questionnaire and focus group discussions. We
hose this mixed-methods approach because pairing quantitativend qualitative components of a study can generate more compre-ensive data, corroborate findings, and allow the use of results fromne method to enhance insights attained with the complemen-ary method [23]. Data collection instruments included questionsn knowledge and attitudes about pH1N1, pH1N1 vaccination,emographics of respondents and sources used for health-related
nformation.Prior to the KAP assessment, the study team, which consisted
f communications specialists, clinicians and epidemiologists fromhe Kenyan MoPHS and MoMS, the Kenya medical research insti-ute/centers for disease control and prevention (KEMRI/CDC) andDC-Atlanta, received a two-day training from communicationspecialists from CDC-Atlanta and KEMRI/CDC in survey design andurpose, questionnaire administration, and facilitating focus groupiscussions.
.1. Survey sites
We targeted HCWs at 20 health facilities in three of Kenya’seven provinces and the capital, Nairobi. Provinces were selectedn order to achieve geographic and demographic diversity in theurvey. In each province, five different types of healthcare facilitiesere selected: a provincial general hospital, a private hospital, aission hospital, a district hospital and an outpatient health cen-
er. Except for the provincial general hospital, of which there is onen each province, facilities in each province were selected basedn convenience. All HCWs in the facility were eligible and encour-ged to complete the questionnaire. In addition, because hospitaldministrative and support staff were included in the target groupor pandemic vaccine by the Kenyan Ministry of Health, we includedhem in the quantitative and qualitative parts of our study. Partici-ation was voluntary and we set out to recruit as many participantst each site as possible. HCWs were broadly defined as employ-es who participated either directly or peripherally in deliveringlinical services and ranged from physicians and nurses to admin-strative and support staff. At each site, we engaged head clinicianso recruit participants.
The study team visited each area of the hospital and explainedhe study to the staff in each area. The team only distributed the sur-ey to HCWs who expressed an interest in completing the survey.fter 5–10 min the team collected the questionnaires. No incentives
Please cite this article in press as: Oria PA, et al. Are Kenyan healthcare wora cross-sectional survey of healthcare workers in Kenya about knowledgeagainst 2009 pandemic influenza A (H1N1), 2010. Vaccine (2011), doi:10.1
ere provided. No HCWs refused to complete the questionnaire,ut not everyone in the hospital expressed an interest in filling outhe questionnaire. No information was collected from people whoere told about the questionnaire but did not express interest in
ompleting it. All surveys were completed and collected.
PRESSxx (2011) xxx–xxx
At the 16 hospital sites, we worked together with the medicalsuperintendent to identify 6–12 HCWs for the focus group discus-sions, stressing the importance of having representation from abreadth of healthcare workers. Focus group discussions typicallyincluded doctors, clinical officers, nurses, laboratory techniciansand periodically administrators and support staff. Clinical officersare health care providers trained for 3 or 4 years and hold a diplomaor a bachelors degree in clinical medicine.
2.2. Data collection tools
We distributed a structured, self-administered, anonymous,paper questionnaire. The questionnaire included 25 questionsabout demographics, knowledge and attitudes about pH1N1 ingeneral and in Kenya specifically, pH1N1 vaccine, and sourcesof health-related information. Most questions were closed-ended,allowing participants to choose from a pre-existing set of answers.
We collected qualitative data through focus group discussionswith HCWs. Two assessment team members conducted the focusgroup discussions; one moderated the group discussion while theother took notes. The moderator’s main objective was to facilitatediscussion between respondents. Group discussions lasted 1–2 h,were audio recorded, and trained teams later generated verbatimtranscripts. The group discussion guide included general questionsand probes.
The questionnaire and group discussion guide used in this studywere developed by the study team. The team initially conducted aliterature search to identify key issues related to vaccine acceptanceof influenza and other vaccines that had previously been described.In addition, stakeholders at the Kenyan Ministry of Health wereasked what questions they thought should be included. We pilotedthe questionnaires with local public health workers and we madeadditional modifications based on the feedback we received.
2.3. Data analysis
Qualitative and quantitative data were analyzed separately withthematic and statistical analyses, respectively. Questionnaire datawere entered into a Microsoft Access database and analyzed withSTATA Statistical Software: Release 10 [24]. We used bivariatelogistic regression analysis to identify predictors of the HCW’swillingness to receive the pH1N1 vaccine. A multivariate logisticregression model that included all variables with p-values <0.05 inbivariate analysis was fitted; we selected the variables significantlyassociated with accepting the pH1N1 vaccine through backwardelimination.
All focus group discussion recordings were transcribed verba-tim. Using a full transcript, we conducted a content analysis of thedocument. From this review and analysis, we summarized the data,coded the data by identifying clusters, and generated a list of keythemes, according to previously described methods for qualitativedata analysis [25].
2.4. Ethical review
This assessment was determined to be exempt from ethicalreview by the Kenyan MoPHS, which considered it to be part ofthe Kenyan government’s public health practice. The protocol wasalso reviewed for human subjects protection concerns and neces-sity of IRB review by both the CDC national center for immunization
kers willing to receive the pandemic influenza vaccine? Results from, attitudes and practices concerning infection with and vaccination016/j.vaccine.2011.01.063
and respiratory diseases (NCIRD) human subjects contact and the 173
NCIRD Associate Director of Science and was determined to be part 174
of the emergency public health practice response to the pandemic 175
and was not deemed to be research. Interviewers obtained verbal 176
consent from all survey participants. 177
ARTICLE IN PRESSG Model
JVAC 11407 1–6
P.A. Oria et al. / Vaccine xxx (2011) xxx–xxx 3
Table 1Characteristics of healthcare workers who completed knowledge, attitudes, andpractices survey about infection with and vaccination against 2009 pandemicinfluenza A (H1N1), Kenya, 2010.
N/total (%) or mean SD
ProvinceCentral 165/659 (25.0)Coast 158/659 (24.0)Nairobi 200/659 (30.4)Nyanza 136/659 (20.6)
Facility typeFaith-based facility 118/659 (17.9)Private facility 102/659 (15.5)Public facility 439/659 (66.6)
Age (mean, SD) 34.5 (9.4)Sex
Male 252/659 (38.2)Female 407/659 (61.8)
Patient contactNo 78/649 (12.0)Yes 571/649 (88.0)
Hospital rolePhysician/medical officer 29/647 (4.5)Clinical officer 74/647 (11.4)Nurse 205/647 (31.7)Laboratory staff 49/647 (7.6)Pharmacy staff 33/647 (5.1)Physiotherapist 13/647 (2.0)Support staff 59/647 (9.1)Health records officer 44/647 (6.8)Other 141/647 (21.8)
Child(ren) < 5 years old at home 246/659 (37.3)Pregnant 26/659 (3.9)
3178
3179
3180
181
i182
p183
f184
r185
[186
a187
c188
h189
h190
3191
192
c193
5194
3195
r196
a197
o198
p199
w200
(201
p202
r203
f204
t205
r206
Table 2Healthcare workers’ knowledge and attitudes towards infection with and vaccina-tion against 2009 pandemic influenza A (H1N1), Kenya, 2010.
N/total (%) or mean SD
What symptoms are associated with pandemic H1N1 flu?Cough 481/659 (73.0)Runny nose 558/659 (84.7)Diarrhea 72/659 (10.9)Fever 575/659 (87.3)Shortness of breath 224/659 (34.0)Sore throat 357/659 (54.2)Who is at high risk for complications from pandemic H1N1 flu?Healthcare workers 488/659 (74.1)People over 60 years old 298/659 (45.2)Pregnant women 332/659 (50.4)Young children less than 5 years 406/659 (61.6)People with chronic diseases like asthma 323/659 (49.0)People with HIV/AIDS 340/659 (51.6)Young, healthy adults 112/659 (17.0)Do not know 15/659 (2.3)Have there been cases of pandemic H1N1 flu in Kenya?Yes 598/652 (91.7)No 34/652 (5.2)Do not know 20/652 (3.1)Have there been cases of pandemic H1N1 flu in your hospital or clinic?Yes 171/643 (26.6)No 366/643 (56.9)Do not know 106/643 (16.5)Can pandemic H1N1 flu be severe enough to cause a person to be
hospitalized?Yes 613/650 (94.3)No 24/650 (4.6)Do not know 13/650 (2.0)Can people die from pandemic H1N1 flu?Yes 594/656 (90.5)No 37/656 (5.6)Do not know 25/656 (3.8)If a pandemic H1N1 flu vaccine were available for free in Kenya, would
you get it?Yes 575/645 (89.1)No 43/645 (6.7)Do not know 27/645 (4.2)If yes, what would be your main reason for getting the vaccine?to protect myself from pandemic H1N1 flu 485/565 (85.8)To protect my patients from pandemic H1N1
flu22/565 (3.9)
To protect my family members from pandemicH1N1 flu
30/565(5.3)
Other 28/565(5.0)Is pandemic H1N1 flu vaccine effective in protecting people from
pandemic H1N1 flu?Yes 380/631 (60.2)No 36/631 (5.7)Do not know 216/631 (34.2)Can vaccinating healthcare workers with pandemic H1N1 flu vaccine
prevent the spread of pandemic H1N1 flu to patients?Yes 521/647 (80.5)No 77/647 (11.9)Do not know 49/647 (7.6)Where do you get current information on health-related matters?Media (newspapers, radio, television) 497/645 (77.0)Internet 268/645 (41.6)Other health care employees 308/645 (47.8)Communications from the ministry of health
or continuing education430/645 (66.7)
Community/religious leaders 168/645 (26.0)Where have you learned the most about pandemic H1N1 flu?Media (newspapers, radio, television) 474/645 (73.4)Internet 268/645 (41.6)Other health care employees 138/645 (21.4)Communications from the ministry of health
or continuing education319/645 (49.5)
Community/religious Leaders 68/645 (10.5)
Someone in household is pregnant 19/659 (2.9)Chronic medical condition such as, asthma,
chronic lung disease, chronic heart disease,liver disease, or HIV/AIDS
24/659 (3.6)
. Results
.1. Quantitative results
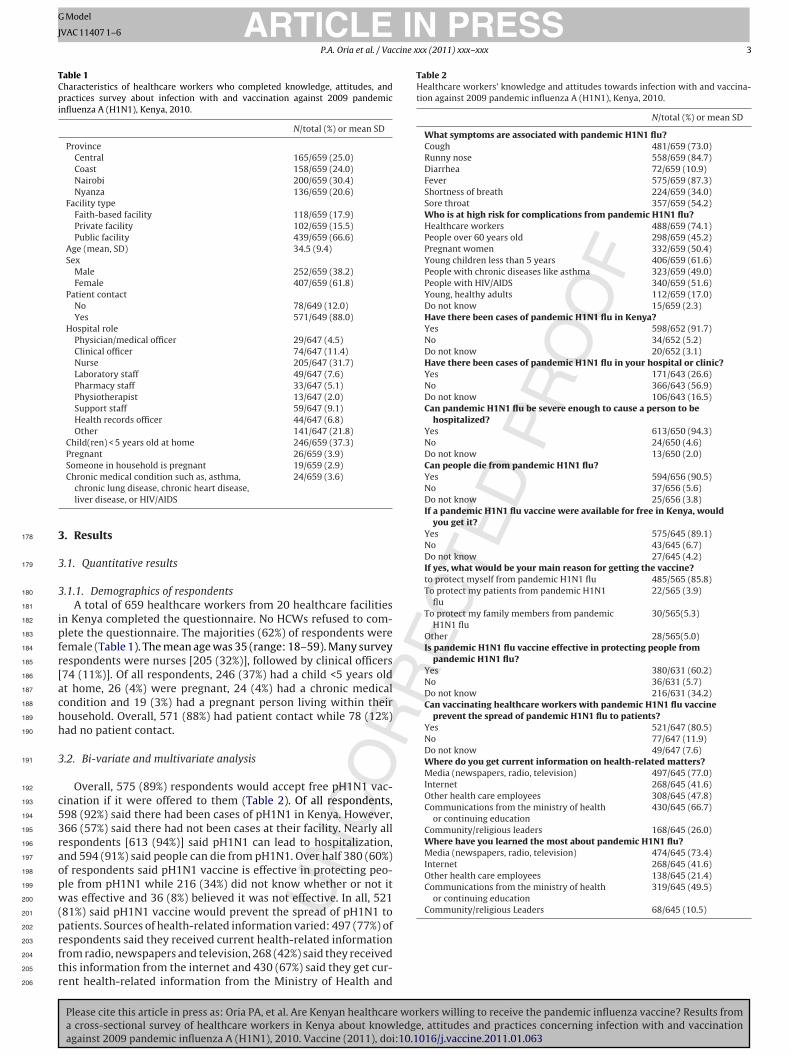
.1.1. Demographics of respondentsA total of 659 healthcare workers from 20 healthcare facilities
n Kenya completed the questionnaire. No HCWs refused to com-lete the questionnaire. The majorities (62%) of respondents wereemale (Table 1). The mean age was 35 (range: 18–59). Many surveyespondents were nurses [205 (32%)], followed by clinical officers74 (11%)]. Of all respondents, 246 (37%) had a child <5 years oldt home, 26 (4%) were pregnant, 24 (4%) had a chronic medicalondition and 19 (3%) had a pregnant person living within theirousehold. Overall, 571 (88%) had patient contact while 78 (12%)ad no patient contact.
.2. Bi-variate and multivariate analysis
Overall, 575 (89%) respondents would accept free pH1N1 vac-ination if it were offered to them (Table 2). Of all respondents,98 (92%) said there had been cases of pH1N1 in Kenya. However,66 (57%) said there had not been cases at their facility. Nearly allespondents [613 (94%)] said pH1N1 can lead to hospitalization,nd 594 (91%) said people can die from pH1N1. Over half 380 (60%)f respondents said pH1N1 vaccine is effective in protecting peo-le from pH1N1 while 216 (34%) did not know whether or not itas effective and 36 (8%) believed it was not effective. In all, 521
81%) said pH1N1 vaccine would prevent the spread of pH1N1 to
Please cite this article in press as: Oria PA, et al. Are Kenyan healthcare workers willing to receive the pandemic influenza vaccine? Results froma cross-sectional survey of healthcare workers in Kenya about knowledge, attitudes and practices concerning infection with and vaccinationagainst 2009 pandemic influenza A (H1N1), 2010. Vaccine (2011), doi:10.1016/j.vaccine.2011.01.063
atients. Sources of health-related information varied: 497 (77%) ofespondents said they received current health-related informationrom radio, newspapers and television, 268 (42%) said they receivedhis information from the internet and 430 (67%) said they get cur-ent health-related information from the Ministry of Health and
ARTICLE IN PRESSG Model
JVAC 11407 1–6
4 P.A. Oria et al. / Vaccine xxx (2011) xxx–xxx
Table 3Likelihood of agreeing to receive free 2009 pandemic influenza A (H1N1) vaccineaccording to other responses among healthcare workers in Kenya.
Number (n) OR (95% CI)
ProvinceNairobi 186 RefCentral 156 2.00(0.80–5.00)Coast 145 0.95(0.44–2.06)Nyanza 131 1.67(0.66–4.17)
Sex of respondentMale 238 RefFemale 380 0.85(0.44–1.62)
Age of respondent18–34 yrs 337 Ref35–49 yrs 223 1.81(0.89–3.71)50 yrs and over 46 1.35(0.39–4.62)
Cadre of respondentPhysician 27 2.48(0.32–19.45)Clinical officer 72 1.62(0.53–5.00)Nurse 195 RefLaboratory staff 45 0.99(0.31–3.06)Physiotherapist 13 1.15(0.14–9.36)Health records officer 40 1.81(0.40–8.19)Other 217 1.38(0.66–2.89)
Do you have direct contact with patients?No 71 RefYes 541 1.00(0.38–2.64)
Have there been cases of pandemic H1N1 flu in Kenya?No 37 RefYes 529 3.57(1.38–9.29)
Can pandemic H1N1 flu be severe enough to cause a person to behospitalized?No 20 RefYes 537 2.01(0.57–7.07)
Can people die from pandemic H1N1 flu?594No 28 RefYes 523 4.27(1.81–10.06)
Is there specific medication available to treat from pandemic H1N1 flu?No 172 RefYes 309 1.28(0.65–2.55)Do not know 87 1.08 (0.43–2.76)
Is pandemic H1N1 flu vaccine effective in protecting people frompandemic H1N1 flu?599No 29 RefYes 345 4.63(1.79–11.98)Do not know 183 2.60(0.99–6.81)
Can vaccinating HCW with pandemic H1N1 flu vaccine prevent the spreadof pandemic H1N1 flu to patients?No 61 RefYes 478 5.60(2.74–11.43)Do not know 31 1.09(0.40–2.95)
Do you get current information on health-related matters from otherHCWs?No 202 RefYes 416 2.08(1.08–4.02)
Do you get current information on health-related matters from
c207
s208
i209
n210
t211
212
K213
v214
S215
p216
g217
n218
p219
Table 4Multivariate logistic regression analysis of select variables associated with accep-tance to receive free 2009 pandemic influenza A (H1N1) vaccine among healthcareworkers in Kenya (N = 538).
Adjusted OR (95% CI) p-Value
Have there been cases of pandemic H1N1 flu in Kenya?No RefYes 3.94(1.21–12.76) 0.022
Can people die from pandemic H1N1 flu?No RefYes 3.83(1.25–11.77) 0.019
Is pandemic H1N1 flu vaccine effective in protecting people frompandemic H1N1 flu?No RefYes 1.91(0.51–7.23) 0.339
Can vaccinating HCWs with pandemic H1N1 flu vaccine prevent thespread of pandemic H1N1 flu to patients?No RefYes 4.73(2.12–10.58) <0.001
Would you advise patients to get pandemic H1N1 flu vaccine if it wereavailable in Kenya?No RefYes 32.60(9.08–116.97) <0.001
Do you get current information on health related matters from otherHCWs?No RefYes 1.22(0.49–3.01) 0.670
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
sneezing, runny nose, muscle pains, sore throat, headache, general 249
community/religious leaders?No 453 RefYes 165 2.93(1.13–7.58)
ontinuous medical education (CME). Overall, 86% of respondentsaid protecting themselves from pH1N1 was their main reason forntent to receive pandemic vaccine, 5% said they would get vacci-ated mainly to protect their families and 4% said they would gethe vaccine mainly to protect their patients.
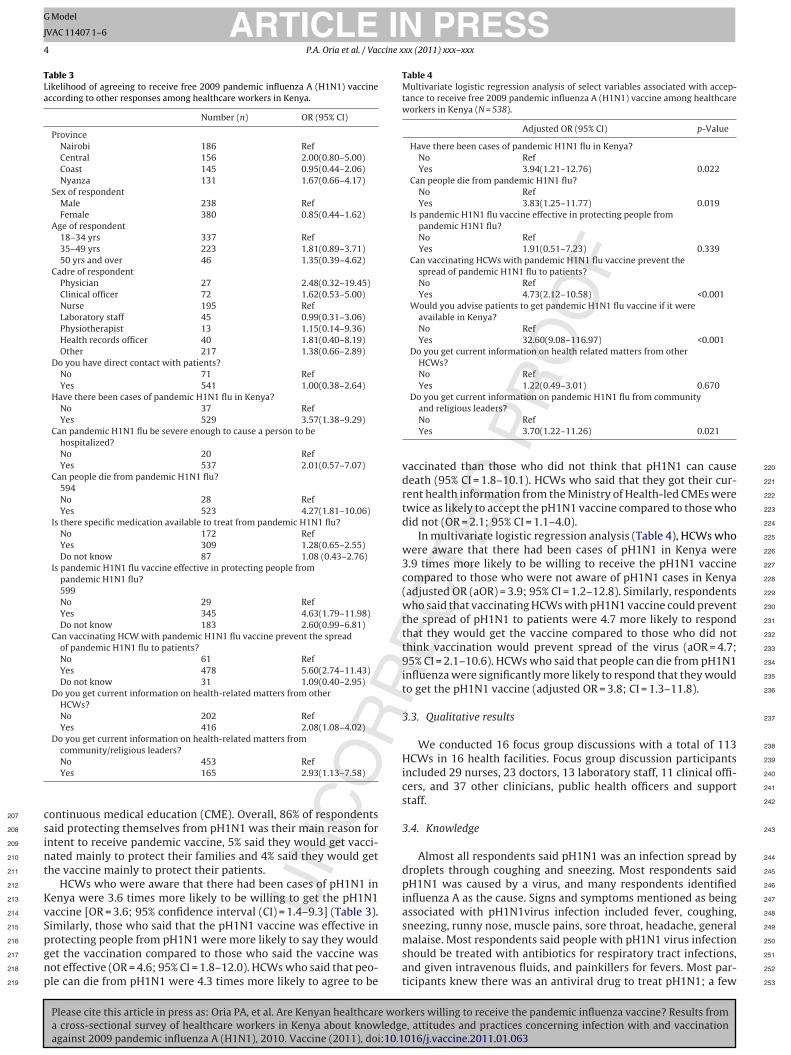
HCWs who were aware that there had been cases of pH1N1 inenya were 3.6 times more likely to be willing to get the pH1N1accine [OR = 3.6; 95% confidence interval (CI) = 1.4–9.3] (Table 3).imilarly, those who said that the pH1N1 vaccine was effective in
Please cite this article in press as: Oria PA, et al. Are Kenyan healthcare wora cross-sectional survey of healthcare workers in Kenya about knowledgeagainst 2009 pandemic influenza A (H1N1), 2010. Vaccine (2011), doi:10.1
rotecting people from pH1N1 were more likely to say they wouldet the vaccination compared to those who said the vaccine wasot effective (OR = 4.6; 95% CI = 1.8–12.0). HCWs who said that peo-le can die from pH1N1 were 4.3 times more likely to agree to be
Do you get current information on pandemic H1N1 flu from communityand religious leaders?No RefYes 3.70(1.22–11.26) 0.021
vaccinated than those who did not think that pH1N1 can causedeath (95% CI = 1.8–10.1). HCWs who said that they got their cur-rent health information from the Ministry of Health-led CMEs weretwice as likely to accept the pH1N1 vaccine compared to those whodid not (OR = 2.1; 95% CI = 1.1–4.0).
In multivariate logistic regression analysis (Table 4), HCWs whowere aware that there had been cases of pH1N1 in Kenya were3.9 times more likely to be willing to receive the pH1N1 vaccinecompared to those who were not aware of pH1N1 cases in Kenya(adjusted OR (aOR) = 3.9; 95% CI = 1.2–12.8). Similarly, respondentswho said that vaccinating HCWs with pH1N1 vaccine could preventthe spread of pH1N1 to patients were 4.7 more likely to respondthat they would get the vaccine compared to those who did notthink vaccination would prevent spread of the virus (aOR = 4.7;95% CI = 2.1–10.6). HCWs who said that people can die from pH1N1influenza were significantly more likely to respond that they wouldto get the pH1N1 vaccine (adjusted OR = 3.8; CI = 1.3–11.8).
3.3. Qualitative results
We conducted 16 focus group discussions with a total of 113HCWs in 16 health facilities. Focus group discussion participantsincluded 29 nurses, 23 doctors, 13 laboratory staff, 11 clinical offi-cers, and 37 other clinicians, public health officers and supportstaff.
3.4. Knowledge
Almost all respondents said pH1N1 was an infection spread bydroplets through coughing and sneezing. Most respondents saidpH1N1 was caused by a virus, and many respondents identifiedinfluenza A as the cause. Signs and symptoms mentioned as beingassociated with pH1N1virus infection included fever, coughing,
kers willing to receive the pandemic influenza vaccine? Results from, attitudes and practices concerning infection with and vaccination016/j.vaccine.2011.01.063
malaise. Most respondents said people with pH1N1 virus infection 250
should be treated with antibiotics for respiratory tract infections, 251
and given intravenous fluids, and painkillers for fevers. Most par- 252
ticipants knew there was an antiviral drug to treat pH1N1; a few 253

ING
J
cine x
p254
a255
t256
257
w258
a259
h260
c261
p262
a263
f264
s265
3266
267
t268
fi269
H270
t271
i272
h273
d274
t275
w276
a277
t278
t279
s280
s281
t282
m283
284
w285
l286
p287
p288
t289
O290
o291
a292
b293
3294
295
b296
w297
a298
m299
o300
k301
c302
k303
r304
v305
t306
307
c308
H309
t310
t311
t312
g313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
ARTICLEModel
VAC 11407 1–6
P.A. Oria et al. / Vac
eople specified Tamiflu (the trade name for oseltamivir) as thentiviral. Few respondents knew that Tamiflu was available fromhe provincial general hospitals to treat confirmed cases of pH1N1.
Respondents mentioned hand washing, use of handkerchiefshen coughing or sneezing, isolating and treating sick people,
voiding congested areas, dusting surfaces, wearing masks whenandling confirmed pH1N1 patients, and conducting health edu-ation with community members as preventive measures forandemic influenza. Very few respondents mentioned vaccinations a means of prevention. Most respondents said that the main dif-erence between pH1N1 and seasonal flu was that pH1N1 is moreevere than seasonal flu.
.5. Risk perception
Most respondents said pH1N1 is not a problem in Kenya becausehere have been no deaths in the country and suspected and con-rmed cases of the disease in Kenya have been mild so far. SomeCWs thought that Caucasians were more prone to complica-
ions and death from pH1N1. “The impression is that [pandemicnfluenza] is a racist kind of disease”, said a nurse at a missionospital. “People call it ugonjwa ya wazungu to mean white man’sisease”. One clinical officer at a mission hospital said, “In Kenyahis disease is affecting people but not killing them, but with thehites we have heard they are dying so I don’t know if in Kenya
nd Africa we are more immune to the virus”. Some HCWs saidhat pH1N1 “was not big” in their community, and said they trustedheir immune systems to fight the virus alone. “Nobody has died”,aid a respondent at one provincial hospital. “We have not seen theeriousness of the condition. If there were people that died, two orhree people, then (I) would say I’d better be careful here, this thing
ay kill us”.Some respondents thought that risk of pH1N1 virus infection
as tied to travel outside of the country and since Kenyans traveless they are less likely to get infected. One medical officer at arivate hospital said, “Since Kenya is not in the high risk zones (forH1N1 infection), the vaccine should be given to visitors comingo Kenya such as tourists and people coming from other nations”.ne nurse at a national referral hospital said, “Rich people are thenes who travel. They go to the airport and get into a plane andlong the way they get (pH1N1). Poor people rarely or never travely plane”.
.6. Acceptability, benefits and risks of vaccination
While most of the respondents said they would be willing toe vaccinated if a free vaccine were available, most also said theyould need more information about the vaccine before they would
gree to get vaccinated. Most respondents said they needed infor-ation about the vaccine’s efficacy, safety, benefits, and duration
f protection. “We have not seen (the vaccine); we don’t evennow its components, we don’t know the mode of action, so youannot just bring the vaccine and we accept it . . .you need (tonow) some effects after the outcome”, said a district hospitalespondent. Many respondents who said they would not get theaccine were concerned that the vaccine campaign was a clinicalrial.
In contrast to questionnaire respondents, most focus group dis-ussion participants had not heard of a vaccine against pH1N1.
Please cite this article in press as: Oria PA, et al. Are Kenyan healthcare wora cross-sectional survey of healthcare workers in Kenya about knowledgeagainst 2009 pandemic influenza A (H1N1), 2010. Vaccine (2011), doi:10.1
owever, most participants said that if a vaccine were availablehey would get the vaccine in order to avoid getting infected byheir patients. A few others said they would get immunized to pro-ect their families as well. Very few respondents said they wouldet vaccinated to protect their patients.
PRESSxx (2011) xxx–xxx 5
3.7. Sources of information and knowledge gaps
Most HCWs said they receive current health-related informa-tion from the internet and continuing medical education lecturesat their health facility. Almost all the HCWs said they had receivedmost of their information about pH1N1 from the media and theMinistries of Health. The Ministries of Health were the most trustedsources of health-related information.
4. Discussion and conclusion
We found that although most surveyed HCWs in Kenyaexpressed willingness to get the pH1N1 vaccine if it were offeredfor free, many group discussion respondents said they would behesitant to be vaccinated because of lack of information aboutpH1N1 vaccine safety and efficacy. According to our question-naire, the overall reported willingness to accept the vaccine amongKenyan HCWs was much higher than reported acceptance levelsof HCWs towards pH1N1 vaccine in other more developed coun-tries [26–28]. In a recent survey of HCWs in Greece, an acceptancerate of 17% for pH1N1 vaccine was reported; in that survey, theprincipal reason for refusing vaccination was fear of side effects, afear that was more common among people who received informa-tion about the safety of the vaccine mainly from mass media [28].A 2009 study of HCWs in Hong Kong about willingness to accepta pre-pandemic influenza vaccine found that the major barriersto acceptance were fear of side effects and doubts about efficacy[27]. The greater willingness to get vaccinated among HCWs inKenya may reflect a higher degree of general trust in vaccination inKenya and a more immediate appreciation of the utility of vaccinesin preventing disease and responding to outbreaks. Indeed, out-breaks of vaccine-preventable diseases, such as measles and polio,have occurred recently in Kenya, and vaccination campaigns wereprominent aspects of both outbreak responses [29,30].
While over 90% of Kenyan HCWs expressed willingness toaccept vaccine, in discussion groups many HCWs expressed con-cerns about pH1N1 safety and effectiveness and expressed doubtabout the severity of pH1N1 disease. These concerns are similarto concerns about pH1N1 vaccine raised by HCWs in more devel-oped countries [31–35], which found that doubts about the risk ofside effects and concerns about vaccine efficacy were barriers toinfluenza vaccination. Recognizing that responding to a question-naire may not reflect practice when it comes to actually receivingthe vaccine to ensure widespread uptake of this voluntary vaccine,clear messages must be relayed to the country’s HCWs about thebenefits of influenza vaccination, and the safety and effectiveness ofthe vaccine. The United States Advisory Committee on Immuniza-tion Practices recommends annual vaccination of healthy healthcare providers and persons in training for health care professions[36]. Influenza vaccines are effective in reducing cases of influenza,especially when the components of the vaccine match circulatinginfluenza strains and circulation is high [37]. Well matched sea-sonal influenza vaccine has been shown to prevent serologicallyconfirmed influenza by 85–90%, may reduce worker absenteeism,and can indirectly protect patients in some settings [19]; however,it is not clear that HCWs in Kenya are aware of these data. A recentstudy of patients who received pH1N1 vaccine in the United Statesof America found no substantial differences between the pH1N1vaccine and seasonal influenza vaccines in the proportion or typesof serious adverse events reported [38].
kers willing to receive the pandemic influenza vaccine? Results from, attitudes and practices concerning infection with and vaccination016/j.vaccine.2011.01.063
We found that HCWs who knew that pH1N1 cases had occurred 371
in Kenya and who believed that pH1N1 could cause hospitaliza- 372
tion and death were much more likely to accept vaccination. Those 373
who were not convinced of the severity of pH1N1 among Africans 374
were more skeptical of vaccination; during group discussions, some 375

ING
J
6 cine x
H376
d377
D378
n379
a380
s381
m382
i383
2384
o385
[386
[387
388
m389
t390
t391
c392
t393
394
a395
t396
d397
n398
s399
t400
d401
H402
n403
v404
i405
f406
o407
v408
d409
p410
c411
p412
c413
414
w415
c416
v417
w418
f419
t420
e421
p422
l423
A424
425
a426
f427
i428
a429
a430
R431
432
433
434
435
436
437
Q3 438
439
440
441
442
443
444
445
446
447
448
[ 449
450
451
[ Q4 452
453
[ 454
455
[ 456
457
458
[ 459
460
461
[ 462
463
464
465
[ 466
467
[ 468
[ 469
470
471
[ 472
473
[ 474
[ 475
476
[ 477
[ 478
479
[ 480
481
[ 482
483
[ 484
485
486
[ 487
488
489
[ 490
491
492
[ 493
494
[ 495
496
497
[ 498
499
500
[ 501
502
[ 503
504
505
[ 506
507
[ 508
509
[ 510
511
[ 512
ARTICLEModel
VAC 11407 1–6
P.A. Oria et al. / Vac
CWs doubted the ability of pH1N1 to cause severe disease andeath in Africans and therefore doubted the need for vaccination.espite limited surveillance for influenza on the African conti-ent, pH1N1 virus infection has been found to cause morbiditynd mortality in Kenya and throughout Africa [39]. In most ofub-Saharan Africa, surveillance for influenza is relatively limited,aking it difficult to compare the relative impact of the pandemic
n Africa with other regions of the world. In Kenya, as of April 24th010, 1283 cases of laboratory-confirmed pH1N1 were identified,f which 15.3% were hospitalized, and two pH1N1 patients died40]. In South Africa, 12,640 cases and 93 deaths have been reported41].
Results of the survey were shared with the Kenya MoPHS andembers of the National Taskforce on Influenza – the two groups
hat directed the pH1N1 vaccination awareness campaign – prior tohe onset of the campaign. On the basis of our findings, communi-ations messages and materials were developed and disseminatedo inform HCWs about pH1N1 virus infection and vaccine.
Our investigation had limitations. First, because the quantitativend qualitative parts of the survey were administered simul-aneously, we could not use our findings from the qualitativeiscussions to inform the development of the survey question-aire. In addition, both components of this assessment relied onelf-reported behavior. However, while we administered a ques-ionnaire with closed-ended questions, we also used focus groupiscussions to obtain more detailed answers. Our study includedCWs at a limited number of healthcare facilities in Kenya, and mayot be generalizable to all HCWs in Kenya. However, we included aariety of HCWs from public, private and mission healthcare facil-ties – the three different kinds of facilities that exist in Kenya – inour of the eight provinces in Kenya. We also included all the typesf healthcare workers in Kenya who were eligible to receive theaccine. Therefore, we believe that our data reflect the intentions ofiverse groups regarding pH1N1 vaccination. Finally, our surveyedopulation was limited to HCWs. Therefore, direct comparisonsannot be made to people with chronic medical conditions andregnant women, the other two groups targeted for pH1N1 vac-ination in the initial phase of the vaccination campaign in Kenya.
Our investigation shows that while most Kenyan HCWs seemilling to get a free pH1N1 vaccine, they still have a number of
oncerns, which could lead to reduced vaccine uptake during theaccination campaign. We found that the Kenya Ministry of Healthas one of the most common sources of health-related information
or HCWs. Sharing more information from trusted sources, such ashe Kenya Ministry of Health and Community and religious lead-rs, with Kenyan HCWs about the safety and effectiveness of theH1N1vaccine, and more data about pH1N1 infections in Kenya, is
ikely to improve the uptake of vaccine among HCWs in Kenya.
cknowledgements
The authors wish to thank Rosalia Kalani, Abdirizack Mohamed,nd Joseph Njau from the Ministry of Public Health and Sanitationor participating in data collection. We also thank all the 20 facil-ty administrators who arranged for the data collection sessionsnd all the respondents who participated in this study. We alsocknowledge CDC-Kenya for funding this study.
eferences
Please cite this article in press as: Oria PA, et al. Are Kenyan healthcare wora cross-sectional survey of healthcare workers in Kenya about knowledgeagainst 2009 pandemic influenza A (H1N1), 2010. Vaccine (2011), doi:10.1
[1] MMWR. Swine Influenza A(H1N1) infection in two children—Southern Califor-nia, March–April 2009. MMWR Dispatch 2009;58:1–3.
[2] WHO. World now at the start of 2009 influenza pandemic; 2009.[3] WHO. WHO recommendations on pandemic (H1N1) 2009 vaccines. Pandemic
(H1N1) 2009 briefing note 2; 2009.
513
[
[[
[
PRESSxx (2011) xxx–xxx
[4] Suspected nosocomial influenza cases in an intensive care, unit. MMWR MorbMortal Wkly Rep 1988;37(1). p. 3–4, 9.
[5] Salgado CD, et al. Influenza in the acute hospital setting. Lancet Infect Dis2002;2(3):145–55.
[6] Maltezou HC, Drancourt M. Nosocomial influenza in children. J Hosp Infect2003;55(2):83–91.
[7] Chironna M, et al. A nosocomial outbreak of 2009 pandemic influenza A (H1N1)in paediatric oncology ward in Italy, October–November 2009. Eurosurveil-lance 2009;15(1).
[8] Elizabeth PF, James G, J. JE. Healthcare personnel and nosocomial transmissionof pandemic 2009 influenza. Crit Care Med 2010;38:e98–102.
[9] Balkovic ES, et al. Nosocomial influenza A (H1N1) infection. Am J Med Technol1980;46(5):318–20.
10] Voirin N, et al. Hospital-acquired influenza: a synthesis using the outbreakreports and intervention studies of nosocomial infection (ORION) statement. JHosp Infect 2009;71(1):1–14.
11] Cunha BA, Thekkel V, Krilov L. Nosocomial swine influenza (H1N1) pneumonia:lessons learned from an illustrative case. J Hosp Infect 74(3):278–81.
12] Van Voris LP, Belshe RB, Shaffer JL. Nosocomial influenza B virus infection inthe elderly. Ann Intern Med 1982;96(2):153–8.
13] Pachucki CT, et al. Influenza A among hospital personnel and patients.Implications for recognition, prevention, and control. Arch Intern Med1989;149(1):77–80.
14] Hammond GW, Cheang M. Absenteeism among hospital staff during aninfluenza epidemic: implications for immunoprophylaxis. Can Med Assoc J1984;131(5):449–52.
15] CDC. Influenza vaccination of healthcare personnel: Recommendations of theHealthcare Infection Control Practices Advisory Committee (HICPAC) and theAdvisory Committee on Immunization (ACIP), 2006. Morb Mort Wkly Rep2006;55.
16] Schoub BD. Surveillance and management of influenza on the African continent.Expert Rev Respir Med 4(2): 167–9.
17] Yazdanbakhsh M, Kremsner PG. Influenza in Africa. PLoS Med 2009;6(12).18] CDC. Prevention and control of influenza: recommendations of the advisory
committe on immunization practices (ACIP), 2008. Morb Mort Wkly Rep2008;57(RR-7):1–59.
19] Jordan R, Hayward A. Should healthcare workers have the swine flu vaccine?BMJ 2009:339.
20] Mwangi M. Personal communication 2010; Sanofi Co.: Nairobi.21] MMWR. Introduction and Transmission of 2009 pandemic influenza A (H1N1)
virus—Kenya, June–July 2009. MMWR Wkly 2009;58(41):1143–6.22] Nation D. Alert over Kenya’s first case of H1N1 flu; 2009.23] Creswell JW, Fetters MD, Ivankova NV. Designing a mixed methods study in
primary care. Ann Fam Med 2004;2(1):7–12.24] StataCorp. Statistical software: release 7.0. College Station, TX: Stata Corpora-
tion; 2001.25] Beyea SC, Nicoll LH. Collecting, analyzing, and interpreting focus group data.
AORN J 2000;71(6). p. 1278, 1281–3.26] Pareek M, et al. Willingness of healthcare workers to accept volun-
tary stockpiled H5N1 vaccine in advance of pandemic activity. Vaccine2009;27(8):1242–7.
27] Chor JS, et al. Willingness of Hong Kong healthcare workers to acceptpre-pandemic influenza vaccination at different WHO alert levels: two ques-tionnaire surveys. BMJ 2009;339:pb3391.
28] Rachiotis G, et al. Low acceptance of vaccination against the 2009 pan-demic influenza A(H1N1) among healthcare workers in Greece. Eur Surveill2010;15(6).
29] MMWR. Progress in measles control—Kenya 2002–2007. MMWR Wkly2007;56(37):969–72.
30] WHO. Polio in Sudan—high risk of international spread;2009 [cited 2009 30 March, 2010]; Available from:http://www.who.int/csr/don/2009 03 02a/en/index.html.
31] Castella A, Argentero PA, Lanszweert A. Factors influencing uptake of influenzavaccination in healthcare workers. Findings from a study in a general hospital.Ann Ig 2009;21(1):35–40.
32] Tabbarah M, et al. What predicts influenza vaccination status in older Ameri-cans over several years? J Am Geriatr Soc 2005;53(8):1354–9.
33] Talbot TR. Improving rates of influenza vaccination among healthcareworkers: educate; motivate; mandate? Infect Control Hosp Epidemiol2008;29(2):107–10.
34] Tapiainen T, et al. Influenza vaccination among healthcare workers in a univer-sity children’s hospital. Infect Control Hosp Epidemiol 2005;26(11):855–8.
35] Thomas RE, Jefferson T, Lasserson TJ. Influenza vaccination for healthcare work-ers who work with the elderly. Cochrane Database Syst Rev. 2: p. CD005187.
36] Fiore A, Recommendations of the Advisory Committee on Immunization Prac-tices (ACIP) 2010; 59: p. 1–62.
37] Jefferson TO, et al. Vaccines for preventing influenza in healthy adults. CochraneDatabase Syst Rev 2007;(2):CD001269.
kers willing to receive the pandemic influenza vaccine? Results from, attitudes and practices concerning infection with and vaccination016/j.vaccine.2011.01.063
38] MMWR. Safety of influenza A (H1N1) 2009 monovalent vaccines—United 514
States, October 1–November 24, 2009. MMWR Wkly 2009;58(48):1351–6. 515
39] WHO. Pandemic (H1N1) 2009—update 97; 2010. 516
40] Osoro E. Hospitalized cases of 2009 Pandemic A (H1N1) in Kenya; submitted Q5 517
for publication. 518
41] NICD; 2009. 519
Copyright © 2022 FDOKUMEN




















