
AnnualReport09 CFNI.pdf (3.058Mb) - IRIS PAHO
77
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of AnnualReport09 CFNI.pdf (3.058Mb) - IRIS PAHO

To: The Director and Staff of the Pan American Health Organization andMember Countries of the Caribbean Food and Nutrition Institute
I have the honour to submit the Annual Report of
the Caribbean Food and Nutrition Institute for the
year ending 31 December 2009.
Respectfully yours,
Fitzroy J. HenryDirector, CFNI


iii
Contents
Director’s Note . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .v
PART I: TECHNICAL COOPERATION — REGIONAL
Planning and Policy Formulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
National Plans of Action on Nutrition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Food and Nutrition Security . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Food Safety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Institutional Dietetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Surveillance/Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
Surveillance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
• Training in Food-Borne Disease Surveillance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
• Training in Survey Methods – 24-hour Dietary Recall . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
• Training in Data Entry, Analysis and Reporting in Nutrition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
Evaluation Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
• Evaluation of School Lunch Program in Montserrat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
• Evaluation of School Meal Options in Trinidad and Tobago . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
Policy Oriented Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
• School-Based Behavioural Intervention in Food in Four Caribbean Countries . . . . . . . . . . . . . . . .13
• Development of Regional Population Dietary Goals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
• Application of Nutrient-Cost Analysis in the Revision of Poverty Lines . . . . . . . . . . . . . . . . . . . . .16
• Nutrition Information on Food Labels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
• A Comparison of the Nutrient Content and Cost of Commercial vs. Homemade Complementary Foods in Jamaica . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .20
Human Resource Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
Summary of CFNI Training Programs - 2009 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
HIV/AIDS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
Awards/Partnerships/Collaborations/Technical Consultations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
Major Presentations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27
iv
Promotion and Dissemination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Promoting Healthy Lifestyles in Schools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
2009 Caribbean Nutrition Day . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Food-Based Dietary Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Anaemia Prevention and Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Nutrition Displays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Promotion of Young Child Nutrition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Regional Nutrition Competitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Nyam News and Cajanus. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
PART II: CFNI DEVELOPMENT
Staff ...................................................................................................................53
Security.....................................................................................................................................................53
Staff Development and Achievement ...............................................................................................54
Budget and Finance ...............................................................................................................................54
Audit....................................................................................................................55
CFNI Building.......................................................................................................55
Information and Technology Services..............................................................................................55
Library ................................................................................................................55
Materials Production Unit ..................................................................................................................58
ANNEXES
Annex I: Organization Chart....................................................................................................................64
Annex II: CFNI Operating Budget 2009 .................................................................................................65
If the food crisis in 2008 was about soaring prices,the financial crisis of 2009 is about lowerpurchasing power. When combined, these
unleash devastating consequences to poor countriesand communities, particularly on nutrition in chil-dren. But the Food-Fuel-Finance crises of the last fewyears were also instructive and compel us to scale upthe nutrition capacity to buffer countries againstfuture shocks. The vulnerability of small islanddeveloping states is even greater and calls for syner-gies among health systems, social protection, foodsecurity and poverty reduction.
The Caribbean is prone to natural disasters, particu-larly hurricanes. Between June and November eachyear the region is threatened by several tropicalstorms which often bring with them floods and landslides. The region also experiences regular periods ofdrought and, less frequently, earthquakes.Hurricanes, floods and drought often devastate thecrops and the agriculture base of the Caribbeaneconomies. This has a direct effect on domestic foodsupplies and also foreign exchange earnings whichare required to buy food, among other needs.
Hurricanes and floods directly affect food availabilitybut not all sudden-onset disasters produce food short-ages severe enough to cause harmful changes in nutri-tional status. Sudden-onset disasters, however, causedisruption of transportation and communicationsystems and distortions in social and economicactivities. Countries that have food stocks may findthem inaccessible due to the disruptions in the distribu-tion system or loss of income with which to buy food.
In the Caribbean, prolonged crises affect the avail-ability and access to food through the erosion oflivelihoods resulting from crop failure, depletion offood stocks, market failure, among others. This inturn affects how the limited food is allocated within thefamily. Breastfeeding and complementary feeding prac-tices are usually maintained during Caribbean crisesand young children are given priority at feeding time.
How then can we preserve nutrition with theserepeated challenges?
Despite the repeated assaults of hurricanes, droughtand floods, the undernutrition rates in the region stillshow a declining trend. Interestingly, the percentageof overweight children increased. Clearly otherfactors drive the overweight trend upwards. But whydid the underweight population continue to declinedespite these repeated shocks? It is contended herethat three fundamental and robust programs act as abuffer to these crises.
1. Maternal and Child Health programs that protectthe health and wellbeing of women, particularlypregnant and lactating women; family planning;breast feeding and complementary feedingprograms, child health and immunization; and ironand food supplementation of mothers and youngchildren.
v
PRESERVING NUTRITION IN CRISES
2. School feeding programs that alleviate short-termhunger in undernourished and well-nourishedschoolchildren and avoid micronutrient deficien-cies. There are also other benefits. In Jamaica,providing breakfast to primary school studentssignificantly increased attendance and arithmeticscores.
3. Fortified foods are currently available across theCaribbean. With the exception of iron, micro-nutrient deficiency is low. The Caribbean popula-tion is currently being targeted through thefortification of flour with iron and vitamins. Theflour products are widely eaten by the adult popu-lation and the challenge is to ensure that the ironlevel is monitored so that standards are adheredto. Another challenge is to ensure that suitablefortified flour products are eaten widely by youngchildren as well. There is much scope to encour-age this in promoting improved young child feed-ing practices.
A good way to preserve nutrition in crises is tostrengthen nutrition infrastructure and programs innon-crisis times. CFNI therefore firmly advocates 6lines of programmatic action:
1. Support the establishment of national food andnutritional goals so that the sub-region’s agricul-ture and food systems can deliver adequate andnutritionally appropriate quantities of food, espe-cially to low-income and vulnerable groups. Toachieve this requires:
• The recognition by the health sector thatprevention strategies have to be a collabora-tion with partners from many sectors (multi-sectoral);
• A recognition at the national level that the foodand agriculture sector is one of the crucial part-ners in any policy aimed at addressing theregion’s main public health problem;
2. Support multi-sectoral interventions that would:
(a) reduce diets high in fats and sugars in total
energy intake and increase intakes of fruitsand vegetables in diets;
(b) reduce relative food energy from animalsources;
(c) monitor food imports relative to health goals;and
(d) develop a food-price policy that takes intoaccount all components of food security.
3. Assist in the process of galvanizing official (political)support for, and facilitate the passage through toCabinets, of National Food Policies, National Plansof Action for Food and Nutrition Security andmulti-sectoral coordinating mechanisms.
4. Explore the development of appropriate incen-tives that encourage the production andconsumption of regionally produced foods,particularly fruits and vegetables. These actionsmust be supported by national food-based dietaryguidelines with adequately-funded promotionstrategies.
5. Support for the establishment of formal planninglinkages between the agriculture sector and othersectors (especially, health, tourism, trade andplanning) in order to ensure a more integratedand coordinated approach to policy and programdevelopment.
6. The development of a regional Food SecurityStrategy to address emerging food security issues,the prevention and control of NCDs, and themonitoring and evaluation of the 2007 Heads ofGovernment and Caribbean AgricultureMinisters’ Declarations.
Most of these actions are highlighted in this annualreport. The support of national and regional partnersis gratefully acknowledged.
Dr. Fitzroy HenryDirector, CFNI
vi
vii
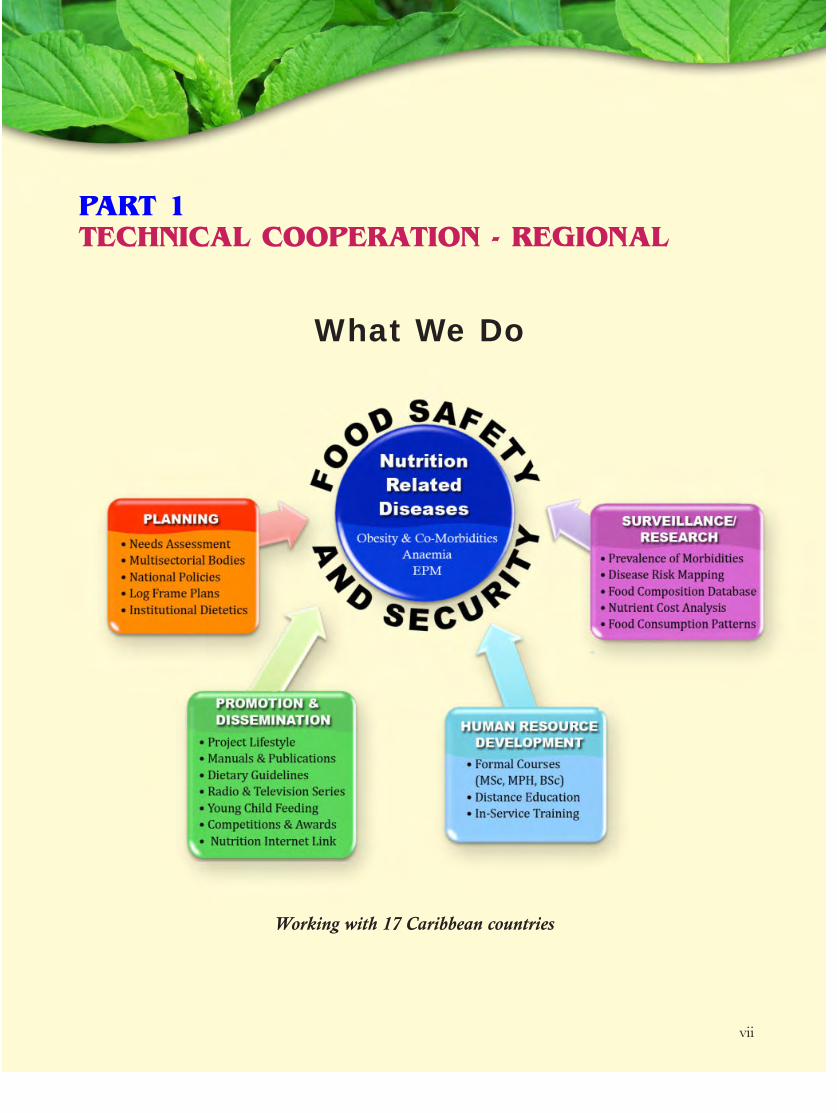
PART 1TECHNICAL COOPERATION - REGIONAL
What We Do
Working with 17 Caribbean countries


1
National Plans of Action on Nutrition In 2009, CFNI continued to assist countries in review-ing their existing Food and Nutrition Policy and Plans ofAction for Nutrition documents. CFNI submitted thedraft Food and Nutrition Policy and Plan of Action tothe Permanent Secretary, Ministry of Health, Antiguafor a country review and update. The review was doneand further assistance was requested for the revision ofthe document. For Dominica, the draft policy docu-ment was submitted to the Permanent Secretary andthe Chairperson of the Dominica Food and NutritionCouncil for an in-country review. CFNI will later draftthe final revision of the document for submission toCabinet. This is expected to occur in 2010. Belize wasassisted with the revision of their Food and NutritionPolicy and Plan of Action. The review was used as partof the continued training of the members of theNational Food and Nutrition Security Commission. Afirst draft was submitted to the Chairman of theCommission to be used in a National Workshop toaddress the CFNI comments and missing data.
The policy for Trinidad and Tobago is still in a firstdraft stage. The information now needs updating andplans were made to have multisectoral meetings tocomplete the second draft. The Ministryof Agriculture, Jamaica requested assis-tance from CFNI to develop a NationalFood and Nutrition Security Policy. Onemeeting was held and a draft conceptpaper entitled: “Towards a Food andNutrition Security Policy for Jamaica”was prepared and submitted.
The Bahamas is expected to reschedulethe National Consultation for the finaliza-tion of the policy and plan of action soon.The Turks and Caicos Islands andAnguilla are still awaiting ratification oftheir revised policies by Cabinet. Whenthis is completed further assistance wouldbe given to enhance the members of theCouncil for effective co-ordination of thePlan. A request was made by Anguilla
for CFNI to conduct the training of the Councilmembers in early 2010.
CFNI also continued to support the multisectoralapproach to planning and implementation by enhancingcapacities of the members of the existing and new nationalFood and Nutrition Councils. Training was conductedwith the Councils in Montserrat and Belize.
In Montserrat, training of the members of the NationalFood and Nutrition Council was done during the period 28– 30 July 2009 following the official launch of the Council.
Twelve persons participated. At the end of the sessionthe following outputs were achieved:
• A strengthened National Food and NutritionCouncil
• A first draft Food and Nutrition Security Bulletin
• First draft of the Strategic/Operational Plan for theCouncil.
These training sessions will continue in 2010 with thecompletion of the first Food and Nutrition SecurityBulletin and the finalization of the Operational Plan forthe Council.
PLANNING AND POLICY FORMULATION
Dr Ballayram, CFNI, presenting at the Training Workshop on Food and Nutrition Policy,in Montserrat.

2
The training of the Food and Nutrition SecurityCommission members in Belize was conducted duringthe revision of the Belize National Food and NutritionPolicy document, 9-12 November 2009. Approximately30 persons participated in the three days of training. Atthe end of the session the following outputs wereachieved:
• A strengthened National Food and NutritionSecurity Commission.
• Updated information for the collation of theNational Food and Nutrition Policy and Plan ofAction.
Training will also commence in Anguilla, Dominicaand possibly the Bahamas when they are ready. CFNIis still awaiting feedback from the British VirginIslands for continued training of the Food andNutrition Council members.
Country Status of Food and Nutrition PolicyStatus of Food and Nutrition
Council/Commission/Committee
Anguilla Policy with the Ministry of Health since2008
Policy not taken to Cabinet so no formal Councilyet. Expected to be done soon. Request madefor training of the Council in early 2010.
Antigua and Barbuda Document submitted to the PermanentSecretary, Ministry of Health
No formal Council yet. Once the policy iscompleted and ratified by Cabinet, training of theCouncil members will commence.
Bahamas Document with the Ministry of Healthsince 2008
Policy not taken to Cabinet so no formal Councilyet. National Consultation to be done.
Barbados No request made No Council exists.
Belize Awaiting dates for training.Policy also needs reviewing
Council present and functioning.
British Virgin Islands Policy ratified by Cabinet since 2007 Council ratified but not functioning. The names ofthe Council members have not been submitted toCFNI. There exists a Chronic Diseases Committeewhich may be expected to take up the functions ofthe Council. The makeup of the Committee mayneed to be revised to ensure it is multidisciplinaryand not solely Health.
Cayman Islands No request made No Council exists.
Dominica The Policy is in draft form Council present and functioning.
Grenada CFNI submitted the final draft in 2007 The Grenada Food and Nutrition Council contin-ues to operate in the same format.
Guyana No request made No Council exists.
Jamaica Policy to be written. Concept paper drafted
No Council exists.
Montserrat Policy accepted by Cabinet/ ExecutiveCouncil.
Council present and functioning.
Status of Food and Nutrition Policies and Councils In Member Countries - 2009

3
Food and Nutrition SecurityCFNI’s mandate is to enhance the quality of life of thepeople in the Caribbean through the promotion of goodnutrition and healthy lifestyle behaviors. As an integralpart of this mandate, the Institute continues to advancethe food and nutrition security and poverty alleviationagenda in member countries through advocacy, technicalcooperation, and program implementation. As in previ-ous years, this agenda was particularly relevant in 2009,especially in light of several critical food and nutritionissues that continue to attract the attention and responseof the Institute.
In particular, increasing world commodityprices, contributed to high domestic food andnon-food prices, thereby constraining the abil-ity of the population, especially the poor andvulnerable groups, to purchase food and basicnon-food items. The household level conse-quences of these high prices are most acutelyfelt in low income households. For foodimporting countries it is estimated that a 50%rise in staple food prices causes a 21% increasein total food expenditure, increasing thesefrom 50 to 60% of income, compared to highincome countries where this rise in pricescauses a 6% rise in retail food expenditure with
income expenditure on food rising from 10 to 11%.These world price changes have impacted with varyingdegrees on Caribbean economies. Since 2000, theConsumer Price Index (CPI) has increased by 16-18%(Antigua, Bahamas, Dominica), 22-30% (Belize,Grenada, St. Lucia, St. Vincent and the Grenadines, St.Kitts and Nevis), 59-63% (Trinidad and Tobago,Guyana) and 133-230% (Jamaica, Dominican Republic,Suriname, and Haiti). These rising prices (which reducethe ratio of wages to prices), constrain the ability of thepopulation, especially the poor and vulnerable groups, topurchase food and basic non-food items. Estimates from
Country Status of Food and Nutrition PolicyStatus of Food and Nutrition
Council/Commission/Committee
St. Kitts and Nevis Policy submitted since 2004. No response from country to date
No Council to date.
St. Lucia No request made No Council exists.
St. Vincent and theGrenadines
Policy accepted a few years ago Council present and functioning.
Suriname No request made No Council exists.
Trinidad and Tobago Draft completed but will be used as aworking document for a multi-sectoral team to review
No Council exists.
Turks and Caicos Islands Policy with the Ministry of Health No Council exists. Policy not sent to Cabinet as yet.
• Antigua• Bahamas • Dominica
• Belize • Grenada• St. Lucia• St. Vincent
& theGrenadines
• St. Kitts &Nevis
• Trinidad &Tobago
• Guyana
• Jamaica• Dominican
Republic• Suriname• Haiti
Consumer Price Index 2000 - 2009
4
CFNI’s nutrient cost analysis1 demonstrate that for mostcountries studied, rising food prices are reversing gainsmade in the past in the ability of the minimum wage topurchase a minimum cost balanced diet.
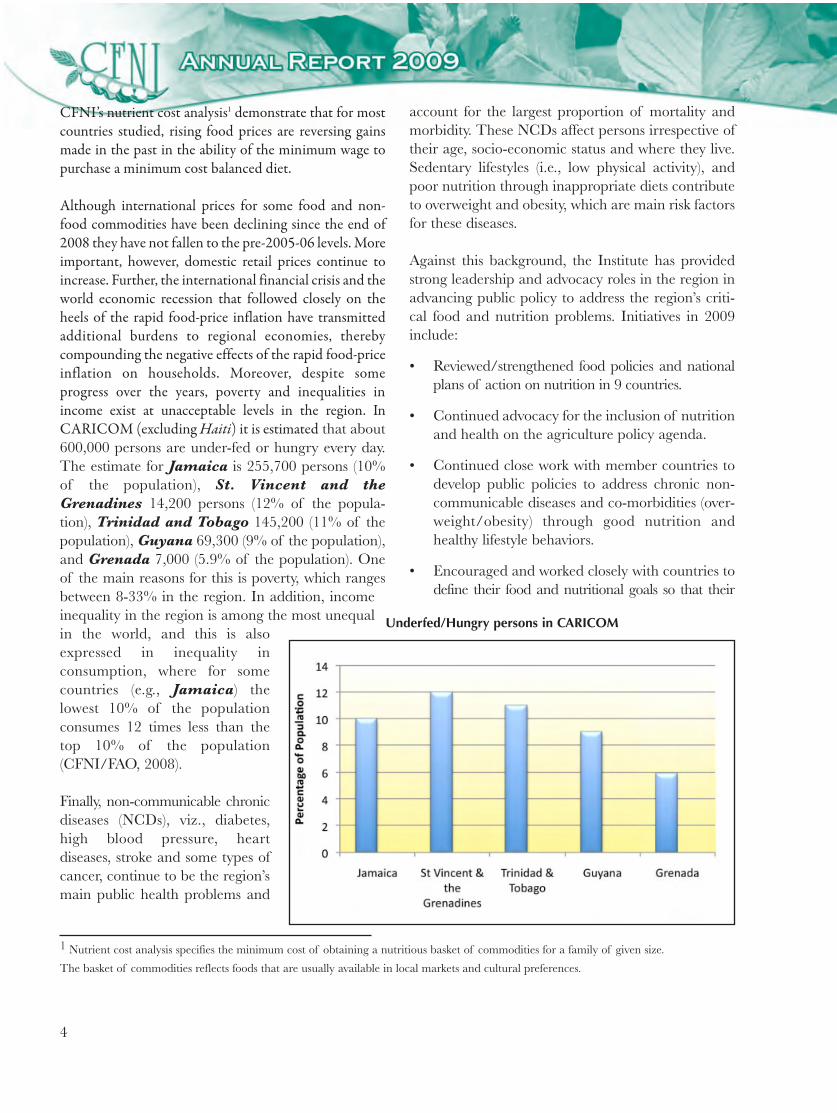
Although international prices for some food and non-food commodities have been declining since the end of2008 they have not fallen to the pre-2005-06 levels. Moreimportant, however, domestic retail prices continue toincrease. Further, the international financial crisis and theworld economic recession that followed closely on theheels of the rapid food-price inflation have transmittedadditional burdens to regional economies, therebycompounding the negative effects of the rapid food-priceinflation on households. Moreover, despite someprogress over the years, poverty and inequalities inincome exist at unacceptable levels in the region. InCARICOM (excluding Haiti) it is estimated that about600,000 persons are under-fed or hungry every day.The estimate for Jamaica is 255,700 persons (10%of the population), St. Vincent and theGrenadines 14,200 persons (12% of the popula-tion), Trinidad and Tobago 145,200 (11% of thepopulation), Guyana 69,300 (9% of the population),and Grenada 7,000 (5.9% of the population). Oneof the main reasons for this is poverty, which rangesbetween 8-33% in the region. In addition, incomeinequality in the region is among the most unequalin the world, and this is alsoexpressed in inequality inconsumption, where for somecountries (e.g., Jamaica) thelowest 10% of the populationconsumes 12 times less than thetop 10% of the population(CFNI/FAO, 2008).
Finally, non-communicable chronicdiseases (NCDs), viz., diabetes,high blood pressure, heartdiseases, stroke and some types ofcancer, continue to be the region’smain public health problems and
account for the largest proportion of mortality andmorbidity. These NCDs affect persons irrespective oftheir age, socio-economic status and where they live.Sedentary lifestyles (i.e., low physical activity), andpoor nutrition through inappropriate diets contributeto overweight and obesity, which are main risk factorsfor these diseases.
Against this background, the Institute has providedstrong leadership and advocacy roles in the region inadvancing public policy to address the region’s criti-cal food and nutrition problems. Initiatives in 2009include:
• Reviewed/strengthened food policies and nationalplans of action on nutrition in 9 countries.
• Continued advocacy for the inclusion of nutritionand health on the agriculture policy agenda.
• Continued close work with member countries todevelop public policies to address chronic non-communicable diseases and co-morbidities (over-weight/obesity) through good nutrition andhealthy lifestyle behaviors.
• Encouraged and worked closely with countries todefine their food and nutritional goals so that their
1 Nutrient cost analysis specifies the minimum cost of obtaining a nutritious basket of commodities for a family of given size.
The basket of commodities reflects foods that are usually available in local markets and cultural preferences.
Underfed/Hungry persons in CARICOM

5
agriculture and food systems could deliver adequateand nutritionally appropriate quantities of food, espe-cially to low-income and vulnerable groups.
• Advocated for a structured food import replace-ment program and a re-orientation of foodimports and the food distribution system, toincrease the availability of good quality-nutritiousfoods in member countries.
• Conducted and disseminated nutrient cost analy-ses for 8 member countries.
• As an integral part of its poverty alleviationagenda, the Institute sourced funds and imple-mented its Small Grants Program in St. Kittsand Nevis. These small grants provided anopportunity for displaced sugar workers andother community-based groups to design andimplement sustainable small projects to enhancefood and nutrition security and reduce poverty.Six community-based groups in the twin-islandstate benefited from grants totaling $120,000.The grants were given to projects that: (i) engagedin production activities for home-consumptionand income generation; (ii) strengthened existingproductive initiatives and improved productivityand competitiveness; and (iii) implemented tech-nologies appropriate for the production andprocessing of food.
Food SafetyDuring 2009, CFNI expanded its technical coopera-tion to work with member countries to strengthentheir national plans of action on matters related tofood and nutrition. Specifically, the Institute, takinginto account the strides made by its involvement withcountries over the past few years to strengthen theirrespective Food Policy and Plan of Action, embarkedon focusing on the formulation of a National FoodSafety Policy and Plan of Action. The pilot work wasdone with Grenada after CFNI initiated discussionwith the PAHO Representation of the EasternCaribbean Countries to lend support to this islandstate for formulating the policy. The principal focuswas on addressing policy issues on food safety exclu-sively. While acknowledging that food security, foodsafety and food quality issues are often dealt with in
tandem to each other, food safety, as defined by theCodex Alimentarius, is the “assurance that food willnot cause harm to the consumer whether it isprepared or eaten according to its intended use”. Thechallenge was to have experts at CFNI working incollaboration with CAREC and joining forces withnational experts in Grenada to develop the nationalfood safety policy framework.
The objectives were to (a) apply food safety principlesand practices throughout the food and produceindustry; (b) consider the role of key players in themanagement and implementation of food safety; and(c) identify monitoring mechanisms to ensure compli-ance. The combined team examined and revieweddocuments essential to the formulation of theproposed National Food Safety Policy, using as theelements deemed most essential to the design anddevelopment of the policy document, three levels ofsystems, namely:
• How the organizations, groups and individualsthat are involved in food safety and quality oper-ate in Grenada. In this context, discussions wereheld on existing policies, legislation and relation-ships among critical stakeholders on the farm totable continuum.
• The existing resources, information, proceduresand protocols, structures, decision-makingprocesses, and overall infrastructure in governmentagencies, the food inspectorate in general, foodindustries, food laboratories and consumer interests.
• The knowledge, skills, competencies, work ethicsof food inspectors, producers, processors, manu-facturers, distributors and the consumers.
A draft policy was prepared for Grenada and is nowreceiving the attention of the national authorities.CFNI intends to continue this work with otherCaribbean member countries building on the successthat has been dependent upon the ability to use amultisectoral approach incorporating the main stagesof the food supply chain by giving consideration toagricultural inputs (pesticides, fertilizers, animalfeeds, veterinary drugs and antibiotics, etc.); primaryproduction (farmers, growers, fisherfolks, etc.);primary food processing operations (abattoirs, dairies,
6
grain mills, etc.); secondary food processing opera-tions (freezing, drying, food preservation, canning, etc.);food distribution for import, export and domesticconsumption; food retailing (grocers, supermarkets,etc.); food catering (street food vending, restaurants,workplace and school environment, nursing homes,etc.); and preparation of foods within households.
Institutional Dietetics As countries continued to engage in planning todefine and address their health problems, the contri-bution of nutrition in the control and management ofthe chronic diseases epidemic and to the overallhealth and well being of persons utilizing public insti-tutions remained an area of national and regionalconcern. In 2009, ten countries: Anguilla,Antigua and Barbuda, Barbados, Belize,British Virgin Islands, Guyana, Jamaica,Montserrat, St. Vincent and the Grenadines, andTrinidad and Tobago requested technical coopera-tion from CFNI to support improvements in variousaspects of their institutional dietetics services. The tech-nical support requested by these countries related tothree main areas:
1. development and or revision of institutionalnorms/standards for the improvement of dieteticservices and nutrition programs;
2. assessments of dietetic services in public institu-tions in CFNI member countries; and
3. strengthening of the delivery of dietetic servicesin public institutions.
At end of 2009, CFNI supported it member countriesin developing several sub-regional institutionalstandards for improving planning and delivery ofdietetic services. The sub-regional standards initiatedincluded: establishing nutrient and meal standards;standardization of menu (to meet health needs);reporting dietetics services; training of foodserviceworkers for health related institutions; standards ofcare for selected clinical dietetic services in primaryand secondary care; standards for administrativedietetic services in primary and secondary care; andimproving quality of care through centralized meal
service. Additionally, evaluation was planned andconducted on the institutional dietetics services,specifically related to school meals in Trinidad andTobago and Montserrat. Additional informationof these activities are provided in the surveillanceand research section of this report. Several activitiesthat contributed to the strengthening of dieteticservices in public institutions were undertaken inAnguilla, Antigua, Barbados, Dominica,Guyana, Montserrat, Jamaica, St Vincent andthe Grenadines, Trinidad and Tobago. Theserelated specifically to:
1. Recommendation for nutrient analysis softwarefor the development of production standards(menus and recipes) for both Anguilla andMontserrat.
2. Initiation of data collection towards the develop-ment and implementation of a of a structureddietary reporting system in Guyana andMontserrat.
3. Analysis of data to develop nutrient and mealstandards for selected institutions in Anguilla,Antigua and Montserrat.
4. Revision of and preparation of menus to meetnutrient standards in Anguilla, Antigua andMontserrat.
5. Training of foodservice supervisors and other keypersonnel in Barbados, Trinidad and Tobagoand Guyana.
6. Preparation of a framework for incrementaltraining of food service staff and exploration offoodservice supervisors training in Montserratand Barbados.
7. Preparation and initial review of the menus inkeeping with nutrient and meal standards.
8. Development and testing of nutrition screeningtool and standards of care in Montserrat andJamaica.
9. Consultations on dietetics services in St Vincentand the Grenadines, Barbados and Trinidadand Tobago.

7
10. Definitions of the roles and functions of nutritionofficers and dietitians for Dominica.
Development of Sub-RegionalStandards
Over the last decade of interaction between CFNIand its member countries, primary components ofinstitutional dietetic services have been identified thatmust be provided in order to foster and support opti-mal health in the users of these facilities. During thatperiod, the dietetics services provided by key institu-tions in several countries were assessed to determinethe extent to which these core components of dietet-ics services were adequately provided. These assess-ments indicated a lack of appropriate standardswhich continued to impede the effectiveness and effi-ciency of the delivery of dietetics services. Thesedata have shown that there is still a need for evidence-based dietetics services in the Caribbean region. Sincethen, many countries under CFNI technical guidancehave embarked on a process of seeking to structure, anddeliver dietetic services in a systematic, scientific and costeffective way that meet the needs of their population.
Data supplied to or generated by the dietary depart-ments are potentially powerful sources of informationto improve both the targeting and planning atnational and institutional levels as well as the dailydelivery of these services. It can also provide usefulinsight in the need for and allocation of resources todietetic services. Accordingly, efforts have been initi-ated to assist countries in identifying key indicators tomonitor, develop or strengthen the system. Thesystem will collect, analyze, interpret and use appro-priate dietetics data to establish appropriate/relevantnorms and standards for effective and efficient deliveryof dietetics services. This activity includes the use oftwo main sets of data:
• Needs oriented data – these provide informationby manipulating data related to the nutritionalstatus of the clientele/patients or inmates.
• Service oriented data – these provide informationon the service delivered and resources required by
the department based on the types and quantitiesof meals and diets requested.
Needs Oriented Data
Needs oriented data were used to ascertain the nutri-tional requirements of the population, estimate nutri-ent requirements and establish nutrient and mealstandards. Datasets inclusive of the nutritionalassessment criteria, that is, age, gender, body size,medical condition and mobility form the basis forgenerating the needs oriented data. Three countries,Anguilla, Antigua and Montserrat engaged inthe collection of these data in 2009 and submitted thedata to CFNI where it is being analyzed to generatenutrient standards. The nutrient standards will thenbe used to develop culturally appropriate mealstandards inclusive of menus and standardizedrecipes. One country, Guyana, is in the process ofstrengthening its system in four hospitals in fourregions to capture these data.
In most hospitals and other related institutions. Thedata collected are used to establish general kilocaloricstandards that are applied across the board. As morespecificity is required based on the diversity of dietorders, additional data will be collected specific topatients with these conditions. Montserratexpanded their dataset to include persons with hyper-tension and or diabetes. Montserrat is faradvanced in the preparation of a technical documenton the development of their nutrient standards andthe supporting elements to establish meal standardsfor their dietetic department.
Nutrient standards are the primary outcome ofcollecting and analyzing needs oriented data. Thedocument being prepared by Montserrat is beingused to guide the development of sub regional stan-dard on the process used to develop nutrient stan-dards for health related institutions.
Service Oriented Data
The types and quantity of meals ordered from thedietary departments or school canteens are a directreflection of the technical expertise required andgeneral workload of the department. These data
8
have direct implications for the level and number oftechnical to non-technical persons as well as the levelof expertise and training required to deliver theseoutputs (number and types of meals). Diet and mealcensus data are fundamental to the understanding ofservice oriented data. They must be collated andinterpreted in relation to food items and recipes sothat when constituted will provide the appropriatemix of nutrients in the meals provided to the recipi-ent. This is the only concept of a balanced diet thatcan be measured during this process.
Overall production data are important aspects ofservice-oriented data based on the total numbers ofmeals required; the food and time resources used toproduce these meals must be monitored to optimizethe forecasting and management of the resources bythe dietary department. Additional aspects related toservice are productivity indicators such as labourhours, number of meals produced per staff, meal costper patient/client, per diet and per day.
Reporting Dietary Services
Ongoing monitoring of service data provides thebasis for dietary reports that are needed at manage-rial and governmental levels to guide planning forand evaluation of dietary services. Very fewCaribbean countries collect, collate and generatereports of their dietetic services with a quantitativecomponent that can be used as quick references to theservices provided and their impact on the populationserved. Through discussions with Guyana andMontserrat a structured reporting format has beendevised. This addresses the core aspects of dieteticservices and is being refined and introduced for test-ing in these two countries. Systematic retraining wasinitiated in Guyana with foodservice supervisorsfrom four regional hospitals to facilitate the genera-tion and collection of relevant data to prepare peri-odic dietary report. Through this process usefulquantitative and qualitative data on dietetic serviceswill be provided to management, to serve as evidencefor the allocation of resources and the developmentof core norms and standards.
Menu Standardization
The menu is the nucleus of the dietetic department.It serves as a backbone or foundation against whichdiet prescriptions are rapidly converted to meals. Itallows for forward planning and acquisition ofsupplies, utensils and equipment to be used in theproduction of meals as well as the expertise of thepersonnel required to produce these meals. Menusfor the hospitals in Anguilla and Montserrat andthe senior citizen home in Antigua were submittedfor review to determine if there are appropriate tomeet the meals and nutrient standards in these insti-tutions. These menus must be nutritionally adequateand also culturally appropriate. Therefore standardrecipes are being generated for each of the menuitems. Two countries, Montserrat and Anguilla,have sought and received advice on appropriate soft-ware to analyze these recipes for appropriate nutrientcontent in keeping with the established nutrient stan-dards based on the reference nutritional profile oftheir populations.
Training of Dietary Staff
All members of staff working in institutional dieteticservices such as hospitals, school feeding programs,day care facilities, nursing homes and prisons shouldbe appropriately trained in basic principles requiredto provide nutritionally adequate meals that arewholesome and aesthetically appealing to the client.Upward mobility from entry level to positions ofsupervision requires that these persons take on addi-tional responsibility and more technical aspects of theservices. The need has been recognized for personsemployed to these services to receive appropriatebasic training at entry level address health implica-tions of the meals being in order to support thepreparation and service of the meals. Additionally,incremental training in relevant principles of nutri-tion and dietetics is needed as persons advance/orare promoted to foodservice supervisor. This trainingis necessary to ensure adequate performance of addi-tional functions in selected aspects of meal produc-tion and service in keeping with the health needs ofthe population group being served.

9
Currently there are no universally accepted compe-tencies with subsequent training programs to equippersons at the entry or advance levels for foodserviceoperation in health-related institutions. While thereare many hospitality-related training, there is a dearthof training in institutional dietetic services thataddress the application of foodservice subsystems tothe health status of the target population. Thereforepersons that are employed as foodservice workers andcooks to the health-related foodservice operations areunable adequately apply nutrient and meal standardsto their duties. Similarly, they do not use standardoperation procedures in the performance of theirduties in the various foodservice subsystems. Hence,many of these institutions are unable to deliver andmonitor the appropriateness of nutrition and dieteticservices to ensure cost effectiveness.
Both Barbados and Montserrat initiated discus-sions in 2009 to implement structured trainingprograms to address these issues. Barbados is focus-ing on a formal foodservice supervisors’ course thatcan be upgraded over time to a technical or profes-sional course in dietetics. Montserrat explored theintroduction of a structured accredited in-servicetype training program. A training plan was draftedfor the dietetic staff for finalization and implementa-tion in 2010 in Montserrat. The training plan willbe used to prepare in-service training manuals oncore standards and procedures for implementation ofmeal standards – production and procurement.
Preparation of Standards of Care andGuidelines for Administrative andClinical Dietetics Services
Two countries, Barbados and Jamaica, embarkedon the documentation of standards and or guidelinestowards the standardization of both administrativeand clinical dietetics services. The NationalNutrition Centre in the Ministry of Health inBarbados prepared a draft document entitled“Nutritious and Healthy Foods in Schools:Nutritional and Practical Guidelines for Barbados”.CFNI provided technical input and reviewed thisdocument.
Since the ending of 2008, the Nutrition Unit of theMinistry of Health has initiated the development ofadministrative and clinical dietetics standards forprimary and secondary care with the support ofCFNI. These standards were reviewed in 2009 and amethodology prepared to test, finalize and dissemi-nate these standards. The aim is that there will benational implementation of these standards in 2010.It is also hoped that the standards of care developedin Jamaica will be disseminated to the othermember countries. In addition plans are in place toinvolve technical persons from other countries in thedevelopment of standards that may not have beenaddressed in Jamaica.
In Montserrat, a nutrition screening toolkit wasdeveloped and testing initiated.
Assessment of Dietetic Services inPublic Institutions
Assessment of aspects of dietetic services wasconducted in schools in two countries: Montserratand Trinidad and Tobago. The research method-ology and findings used are detailed under thesurveillance and research section of the report.
Discussions continued with Grenada and theBritish Virgin Islands regarding the evaluation oftheir school feeding program. Although muchpreparatory work was done with these countries, theevaluation was not conducted for varying reasons.
A three-day workshop was held in St Vincent andthe Grenadines to present and discuss findings andrecommendations of the evaluation of the NationalSupplemental Feeding Program/Nutrition SupportProgram. On one day, the workshop focused on thecomponent of the assessment of the findings relatedto the preschool population, the second day focusedon health care workers and the third day focused onprimary schools. Several working groups reviewedthe findings and recommendations by CFNIand identified the way forward for each group. It wasagreed that these recommendations would becompiled by a technical team in country andsubmitted to the responsible governmental agencies.

10
Up to the end of 2009, work was still ongoing on thecompilation of these recommendations.
Strengthening of Dietetic Services inPublic Institutions
Technical cooperation was provided to several coun-tries towards strengthening of their institutionaldietetic services. This was provided mainly in theform of training sessions conducted in Barbadosand Guyana; preparation of Terms of Reference forimplementing nutritional standards in Jamaica; andpreliminary assessment of a regional hospital inTrinidad and Tobago.
In Barbados, a 2-day in-service training workshopfor foodservice supervisors, assistants and other corestaff was held to equip the relevant staff to interpretdiet prescription and produce diets for selected situa-tions. The focus of this training was on nutrition forthe elderly with special emphasis on diets for hyper-tension, diabetes, renal, high protein, and ‘no wheat’being prescribed by physicians. At the end of thetraining several recommendations were made forimproving the services in these homes and discussionswere held between senior dietitians responsible forthese services in primary care in Barbados andCFNI on how these could be implemented.
In addition to training conducted with the foodser-vice supervisors on collecting and compiling relevantdietetics data, another training of staff was held withover 20 participants from a range of private andpublic institutions to discuss the importance of thedata to nutritional standards and the core standards
necessary for the improvement of the services. Manyparticipants expressed an interest in participatingwith the main project hospitals in improving systemsto strengthen the contribution of dietetics services tothe overall quality of care provided to the users oftheir institutions.
Jamaica continued to work towards implementationof nutritional standards in Early ChildhoodInstitutions, to this end a Terms of Reference wasdeveloped and submitted for funding to supportnational implementation of these standards
There was a preliminary exploratory visit to conductexpert analysis of the foodservice facility in SanFernando Hospital in Trinidad and Tobago inorder to analyze the efficiency and effectiveness ofthe current meal service system. The department isexploring a proposed change from a decentralizedsystem toward the introduction of centralized mealservices. Discussions were initiated on the proposedlayout, design and operations procedure for central-ization of meal services and a list of required equip-ment generated. In order to implement centralizedmeal services it was evident that the hospital neededto ensure the implementation of appropriate opera-tional standards and procedures. This would alsohave implications for reassignment and training ofstaff to implement this improved meal distributionsystem. There was a subsequent visit to sensitizesenior management in the hospital to the advantagesand implications of these changes. The team in SanFernando Hospital in Trinidad and Tobagoexpressed their support to improving these services in2010.
11
SURVEILLANCE
Training in Food-Borne DiseaseSurveillanceCFNI collaborated with two other PAHO Centres –Caribbean Epidemiology Center (CAREC) and thePan American Center for Foot-and-Mouth Disease(PANAFTOSA) to assist in capacity building for food-borne disease surveillance in the Caribbean sub-region. It was important for CFNI to join in thispartnership as the fight against food-borne diseasesinvolves several aspects of food safety. CFNI remainsconscious about the inter-relatedness between safe,nutritious and healthy food and its availability to theconsuming public, and recognizes that food lossesarising from condemnations or disposal of diseased,unsafe food automatically raise the potential forreduction in the availability of food to the consumingpublic. Consequently, through a strong surveillancenetwork that embraces several aspects of the foodchain, it is potentially more beneficial to know theindividual status of the various foods and food groupsand to plan more effectively to address any gaps. Theinstitute was therefore pleased to align itself to assistin facilitating at the Integrated Foodborne DiseaseSurveillance (WHO GFN, formerly GlobalSalmonella Surveillance) Workshop and the Burdenof Illness Workshop held in Barbados in November2009. Interestingly, the workshop participants fromAntigua and Barbuda, The Bahamas,Barbados, Belize, Dominica, Grenada,Guyana, Jamaica, St. Lucia, Suriname,Trinidad and Tobago and Turks and CaicosIslands all endorsed the five pillars of a food safetysystem as enunciated by WHO to include (a) develop-ment of food control programs, (b) laws and regula-tions, (c) inspection services, (d) food-borne diseasesurveillance and (e) social education and communica-tion. All countries developed draft Action Plans thatare to be approved by the National Authorities and beused to strengthen their national food-borne diseasesurveillance programs.
Training in Survey Methods – 24-hourDietary Recall
As part of CFNI’s World Diabetes Foundation (WDF)supported project in schools in the region, theInstitute planned and conducted the collection of 24-hour recall data from school-children in Form 2 ofproject schools in the relevant countries. This datacollection forms part of the baseline data which willbe used in evaluating the impact of this interventionon children’s eating behaviours.
A sample of children from each project school wasselected, instruments and training manual developedand a detailed schedule for data collection developedfor Grenada, Trinidad and Tobago, St. Kittsand Nevis and St. Vincent and the Grenadines.
Nutrition and other personnel were trained in thecollection of 24-hour recall data over a 3-day periodand this training involved training in general inter-viewing techniques, training in collecting food recalldata, and practical exercises in collecting data fromthe target age group. The training also involved theproduction of food models that would be used in theinterviews.
Data collection was done over a 3-week period in theschools.
Training in Data Entry, Analysis andReporting in NutritionAs part of the Institute’s ongoing initiatives to buildcapacity in the management and analysis of foodand nutrition surveillance data CFNI in collabora-tion with the PAHO ECC office planned and facili-tated basic and advanced training in the use of EpiInfo for data entry, analysis and reporting.
SURVEILLANCE/RESEARCH

12
The basic training was conducted in Grenada andSt. Kitts and Nevis. In Grenada training wasconducted for approximately 20 public health profes-sionals including environmental health officers, nursesurveillance officers, laboratory technologists, and apharmacist, in addition to staff of the Grenada Foodand Nutrition Council. The training was aimed athelping participants to apply skills to their work situ-ation and therefore participants built databases fordata that they collect routinely at work.
Training in St. Kitts was conducted primarily fordata management staff of the Ministry of Health ofSt. Kitts and Nevis, 10 of whom were trained. Inaddition two staff members from the Ministries ofHealth and Education in Montserrat also partici-pated. The contents of this course was adapted based onthe experience gained in Grenada and was re-struc-tured to include some basic Statistics and Epidemiology,in order that participants could better understand theapplication of certain features of Epi Info and theoutput generated by the program.
As a follow up to the in-country training a regionaltraining course was held in Barbados in Decemberthat was aimed more specifically at capacity buildingin data management and analysis relating to the foodand nutrition situation. Some 10 persons participatedfrom Barbados, Grenada, Montserrat,Dominica, Antigua, St. Lucia, and St Vincentand the Grenadines. The workshop also aimed toimpart skills to other health workers, many of whomprofessionally support national nutrition officers such asepidemiologists.
EVALUATION RESEARCH
Evaluation of School Lunch Program inMontserrat The Director of Education and the Nutrition Officer inMontserrat requested the assistance of CFNI in theplanning for a breakfast program in Montserrat. Aspart of this planning process it was agreed that theInstitute in collaboration with the Ministries of
Education and Health would conduct an evaluation ofthe existing lunch program and in so doing ascertain thefeasibility of a breakfast program for students. Theobjectives for the evaluation were:
1. To identify and describe the existing meal optionsthat are available to students on a school mealsprogram in Montserrat.
2. To determine the perception of participantstowards meal options.
3. To determine the perception of officials from theMinistry of Education (education officer, principal,teachers) and parents towards meal options.
4. To assess the quality and nutrient content ofsample meals.
5. To examine operations management with respectto cost effectiveness.
6. To examine aspects of the operations including:facilities, production, procurement, food safety,monitoring and control, adherence to standards.
7. To determine the cost effectiveness of mealoptions and operations.
8. To identify resources, policy/program changesnecessary for the improvement of meal options.
All students attending Government schools wereselected (717) and a sample of parents were alsoselected (334). Instruments were developed, pre-tested and training was conducted over a four dayperiod (November 2-5) at the GovernmentHeadquarters Training Room in Brades, with 11enumerators in attendance. Data collectioncommenced the week of November 16, 2009. Dataentry will be done in country by trained personnelusing the Epi-Info Program. Analysis will be done atCFNI’s office in Jamaica. This collaborationinvolved the Ministries of Education and Health(Montserrat) in conjunction with CFNI. CFNI alsofacilitated the participation of the Nutritionist fromAntigua who undertook the assessment of the foodservice facilities. A report is expected by mid year2010.
13
Evaluation of School Meal Options inTrinidad and TobagoA combination of methods was used in data collec-tion viz: Focus Groups, Observations, Key InformantInterviews and a Quantitative Survey. The finalsample was some 5,000 children from primary andsecondary schools in Trinidad and Tobago.
The main findings were:
1. While there are a number of school meal optionsavailable at the primary and secondary level, thegovernment run School Nutrition Program (SNP)is the most popular option at the primary leveland to a lesser extent at the Secondary level.
2. Students, parents and teachers are generally posi-tive about the SNP in terms of the types of foodavailable, taste and general operations.
3. The other school meal options (canteens, tuckshops, restaurants etc.) play a more importantrole in the secondary schools as some studentsappear to have the ability to leave the compound.
4. There is a very wide range of food and meal itemsavailable from the different school meal options andthe students’ preferences also cover a wide range ofitems. However, the fact that many students areconsuming soft drinks and a range of snack items inthe school setting is cause for concern.
5. The availability of fruit, vegetables and to a lesserextent legumes in the school meals observed isinadequate. This is also a concern raised byteachers and some parents.
6. The nutritional status of the children in primaryand secondary schools is also cause for greatconcern with some 25% of the students classifiedas either overweight or obese. Another 14% of allstudents surveyed were classified as underweight.
7. Record keeping as it relates to the food service oper-ations needs to be strengthened and restructured.
8. The status of the food service facilities at theschools needs to be more closely evaluated
especially in the area of eating facilities and someareas of food safety and sanitation.
These findings and their implications will be furtherdiscussed with the Government of Trinidad andTobago with a view to developing a program ofspecific interventions to address issues of concern.
POLICY ORIENTEDRESEARCH
School-Based Behavioural Intervention inFour Caribbean CountriesThis report presents the baseline findings for this4-year study.
Baseline data collected were collected and analyzedfrom schools participating in the World DiabetesFoundation (WDF) funded project “PreventingDiabetes and Other Chronic Diseases through aSchool-based Behavioural Intervention”. Data werecollected from 1,916 students in Grades 7 (Forms 1)in Intervention and Control schools in Grenada, St.Kitts and Nevis, St. Vincent and theGrenadines, and Trinidad and Tobago. Themean age of the cohort was 12 years with 56%females and 44% of male respondents.
The data collected included:
• Students’ Knowledge Attitude and Practices(KAP) related to nutrition and physical activity.
• Heights and Weights.
• Fitness levels.
• Blood Pressure.
Summary of Main Findings
Students’ knowledge and awareness of correct dietbehaviour and physical activity were tested. Theresults indicated that across both intervention and
14
control schools, response rates were high, with morethan half of the students identifying the correct dietbehaviour(s) for each nutrition question posed. Thispercentage was higher in intervention than controlschools (though not significantly). However, students’correct responses to physical activity questions were notas high and students activity levels were low with almosthalf of the students (47%) reportedly being inactive for2 hours or more on an average school day and approxi-mately 75% on weekends
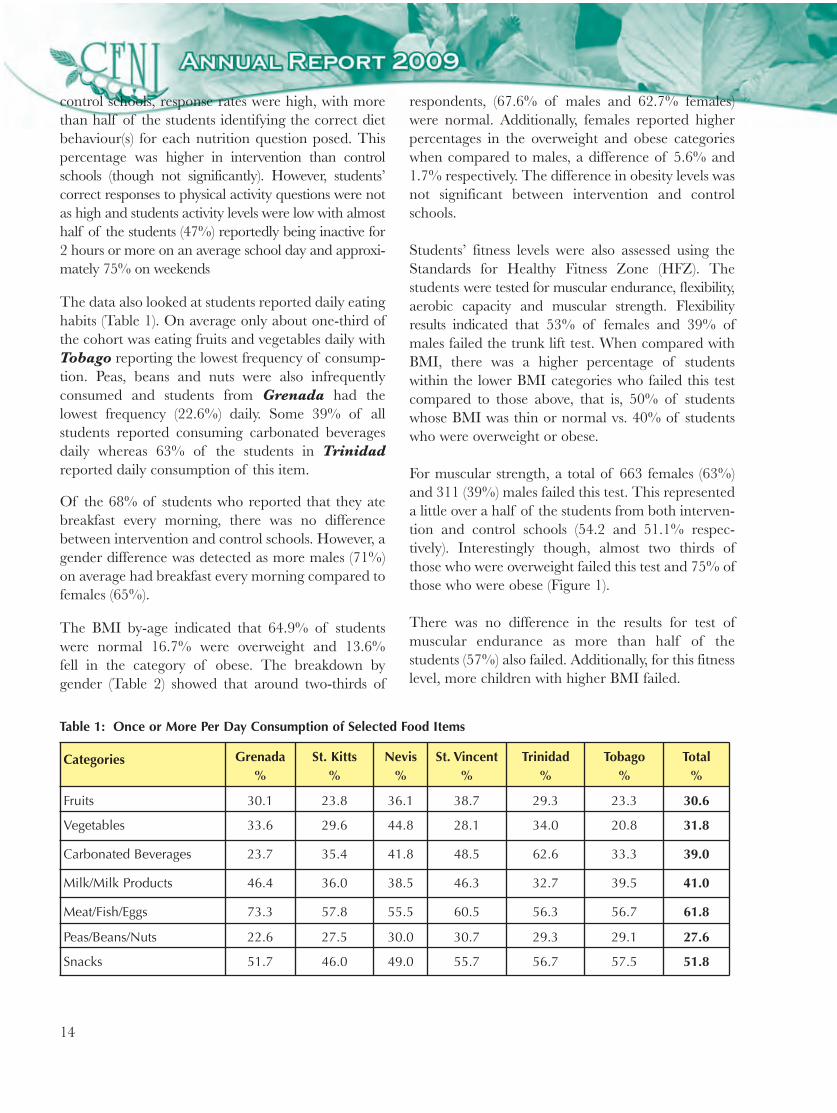
The data also looked at students reported daily eatinghabits (Table 1). On average only about one-third ofthe cohort was eating fruits and vegetables daily withTobago reporting the lowest frequency of consump-tion. Peas, beans and nuts were also infrequentlyconsumed and students from Grenada had thelowest frequency (22.6%) daily. Some 39% of allstudents reported consuming carbonated beveragesdaily whereas 63% of the students in Trinidadreported daily consumption of this item.
Of the 68% of students who reported that they atebreakfast every morning, there was no differencebetween intervention and control schools. However, agender difference was detected as more males (71%)on average had breakfast every morning compared tofemales (65%).
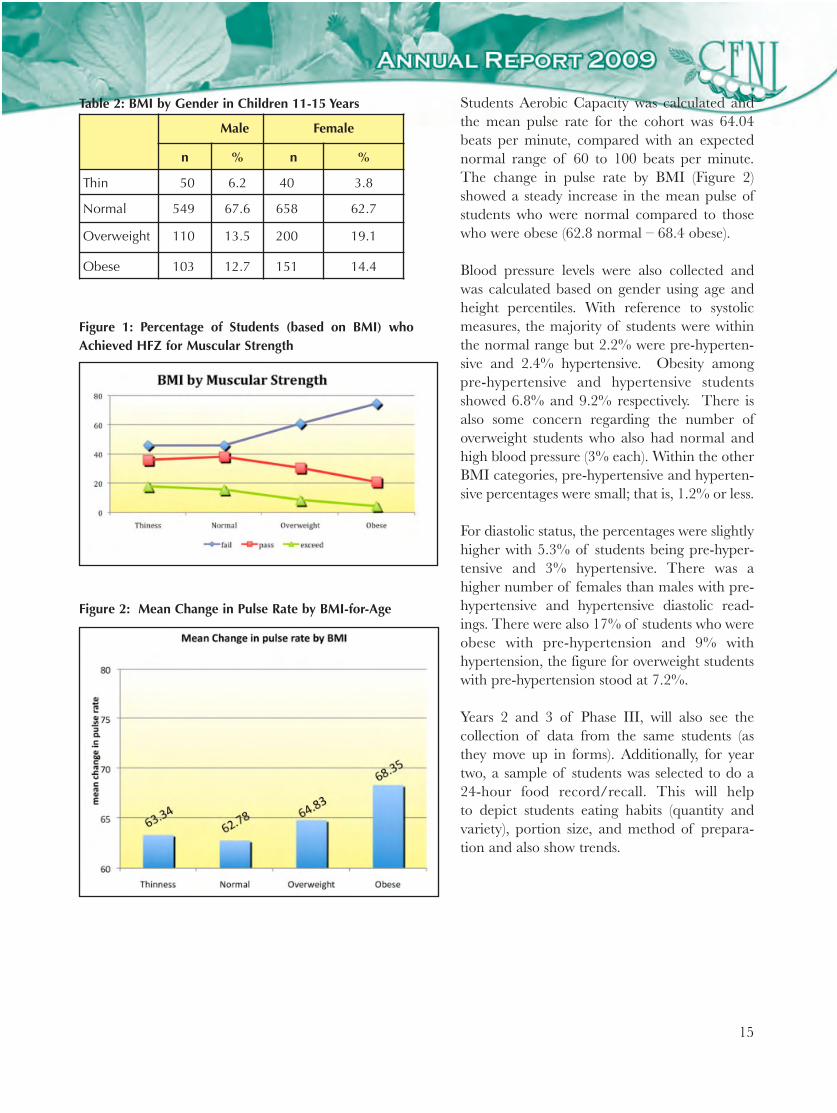
The BMI by-age indicated that 64.9% of studentswere normal 16.7% were overweight and 13.6%fell in the category of obese. The breakdown bygender (Table 2) showed that around two-thirds of
respondents, (67.6% of males and 62.7% females)were normal. Additionally, females reported higherpercentages in the overweight and obese categorieswhen compared to males, a difference of 5.6% and1.7% respectively. The difference in obesity levels wasnot significant between intervention and controlschools.
Students’ fitness levels were also assessed using theStandards for Healthy Fitness Zone (HFZ). Thestudents were tested for muscular endurance, flexibility,aerobic capacity and muscular strength. Flexibilityresults indicated that 53% of females and 39% ofmales failed the trunk lift test. When compared withBMI, there was a higher percentage of studentswithin the lower BMI categories who failed this testcompared to those above, that is, 50% of studentswhose BMI was thin or normal vs. 40% of studentswho were overweight or obese.
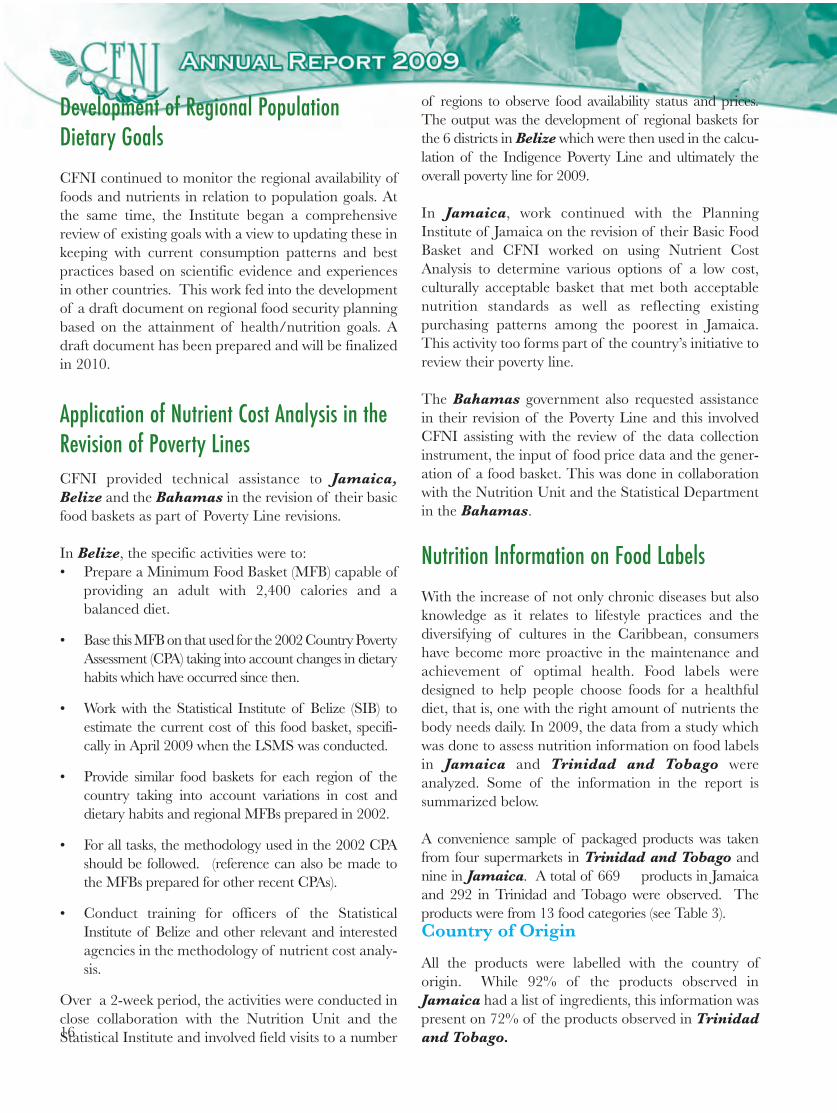
For muscular strength, a total of 663 females (63%)and 311 (39%) males failed this test. This representeda little over a half of the students from both interven-tion and control schools (54.2 and 51.1% respec-tively). Interestingly though, almost two thirds ofthose who were overweight failed this test and 75% ofthose who were obese (Figure 1).
There was no difference in the results for test ofmuscular endurance as more than half of thestudents (57%) also failed. Additionally, for this fitnesslevel, more children with higher BMI failed.
Categories Grenada%
St. Kitts%
Nevis%
St. Vincent%
Trinidad%
Tobago %
Total%
Fruits 30.1 23.8 36.1 38.7 29.3 23.3 30.6
Vegetables 33.6 29.6 44.8 28.1 34.0 20.8 31.8
Carbonated Beverages 23.7 35.4 41.8 48.5 62.6 33.3 39.0
Milk/Milk Products 46.4 36.0 38.5 46.3 32.7 39.5 41.0
Meat/Fish/Eggs 73.3 57.8 55.5 60.5 56.3 56.7 61.8
Peas/Beans/Nuts 22.6 27.5 30.0 30.7 29.3 29.1 27.6
Snacks 51.7 46.0 49.0 55.7 56.7 57.5 51.8
Table 1: Once or More Per Day Consumption of Selected Food Items
15
Table 2: BMI by Gender in Children 11-15 Years
Male Female
n % n %
Thin 50 6.2 40 3.8
Normal 549 67.6 658 62.7
Overweight 110 13.5 200 19.1
Obese 103 12.7 151 14.4
Figure 1: Percentage of Students (based on BMI) whoAchieved HFZ for Muscular Strength
Students Aerobic Capacity was calculated andthe mean pulse rate for the cohort was 64.04beats per minute, compared with an expectednormal range of 60 to 100 beats per minute.The change in pulse rate by BMI (Figure 2)showed a steady increase in the mean pulse ofstudents who were normal compared to thosewho were obese (62.8 normal – 68.4 obese).
Blood pressure levels were also collected andwas calculated based on gender using age andheight percentiles. With reference to systolicmeasures, the majority of students were withinthe normal range but 2.2% were pre-hyperten-sive and 2.4% hypertensive. Obesity amongpre-hypertensive and hypertensive studentsshowed 6.8% and 9.2% respectively. There isalso some concern regarding the number ofoverweight students who also had normal andhigh blood pressure (3% each). Within the otherBMI categories, pre-hypertensive and hyperten-sive percentages were small; that is, 1.2% or less.
For diastolic status, the percentages were slightlyhigher with 5.3% of students being pre-hyper-tensive and 3% hypertensive. There was ahigher number of females than males with pre-hypertensive and hypertensive diastolic read-ings. There were also 17% of students who wereobese with pre-hypertension and 9% withhypertension, the figure for overweight studentswith pre-hypertension stood at 7.2%.
Years 2 and 3 of Phase III, will also see thecollection of data from the same students (asthey move up in forms). Additionally, for yeartwo, a sample of students was selected to do a24-hour food record/recall. This will helpto depict students eating habits (quantity andvariety), portion size, and method of prepara-tion and also show trends.
Figure 2: Mean Change in Pulse Rate by BMI-for-Age
16
Development of Regional PopulationDietary GoalsCFNI continued to monitor the regional availability offoods and nutrients in relation to population goals. Atthe same time, the Institute began a comprehensivereview of existing goals with a view to updating these inkeeping with current consumption patterns and bestpractices based on scientific evidence and experiencesin other countries. This work fed into the developmentof a draft document on regional food security planningbased on the attainment of health/nutrition goals. Adraft document has been prepared and will be finalizedin 2010.
Application of Nutrient Cost Analysis in theRevision of Poverty LinesCFNI provided technical assistance to Jamaica,Belize and the Bahamas in the revision of their basicfood baskets as part of Poverty Line revisions.
In Belize, the specific activities were to:• Prepare a Minimum Food Basket (MFB) capable of
providing an adult with 2,400 calories and abalanced diet.
• Base this MFB on that used for the 2002 Country PovertyAssessment (CPA) taking into account changes in dietaryhabits which have occurred since then.
• Work with the Statistical Institute of Belize (SIB) toestimate the current cost of this food basket, specifi-cally in April 2009 when the LSMS was conducted.
• Provide similar food baskets for each region of thecountry taking into account variations in cost anddietary habits and regional MFBs prepared in 2002.
• For all tasks, the methodology used in the 2002 CPAshould be followed. (reference can also be made tothe MFBs prepared for other recent CPAs).
• Conduct training for officers of the StatisticalInstitute of Belize and other relevant and interestedagencies in the methodology of nutrient cost analy-sis.
Over a 2-week period, the activities were conducted inclose collaboration with the Nutrition Unit and theStatistical Institute and involved field visits to a number
of regions to observe food availability status and prices.The output was the development of regional baskets forthe 6 districts in Belize which were then used in the calcu-lation of the Indigence Poverty Line and ultimately theoverall poverty line for 2009.
In Jamaica, work continued with the PlanningInstitute of Jamaica on the revision of their Basic FoodBasket and CFNI worked on using Nutrient CostAnalysis to determine various options of a low cost,culturally acceptable basket that met both acceptablenutrition standards as well as reflecting existingpurchasing patterns among the poorest in Jamaica.This activity too forms part of the country’s initiative toreview their poverty line.
The Bahamas government also requested assistancein their revision of the Poverty Line and this involvedCFNI assisting with the review of the data collectioninstrument, the input of food price data and the gener-ation of a food basket. This was done in collaborationwith the Nutrition Unit and the Statistical Departmentin the Bahamas.
Nutrition Information on Food LabelsWith the increase of not only chronic diseases but alsoknowledge as it relates to lifestyle practices and thediversifying of cultures in the Caribbean, consumershave become more proactive in the maintenance andachievement of optimal health. Food labels weredesigned to help people choose foods for a healthfuldiet, that is, one with the right amount of nutrients thebody needs daily. In 2009, the data from a study whichwas done to assess nutrition information on food labelsin Jamaica and Trinidad and Tobago wereanalyzed. Some of the information in the report issummarized below.
A convenience sample of packaged products was takenfrom four supermarkets in Trinidad and Tobago andnine in Jamaica. A total of 669 products in Jamaicaand 292 in Trinidad and Tobago were observed. Theproducts were from 13 food categories (see Table 3).Country of Origin
All the products were labelled with the country oforigin. While 92% of the products observed inJamaica had a list of ingredients, this information waspresent on 72% of the products observed in Trinidadand Tobago.
17
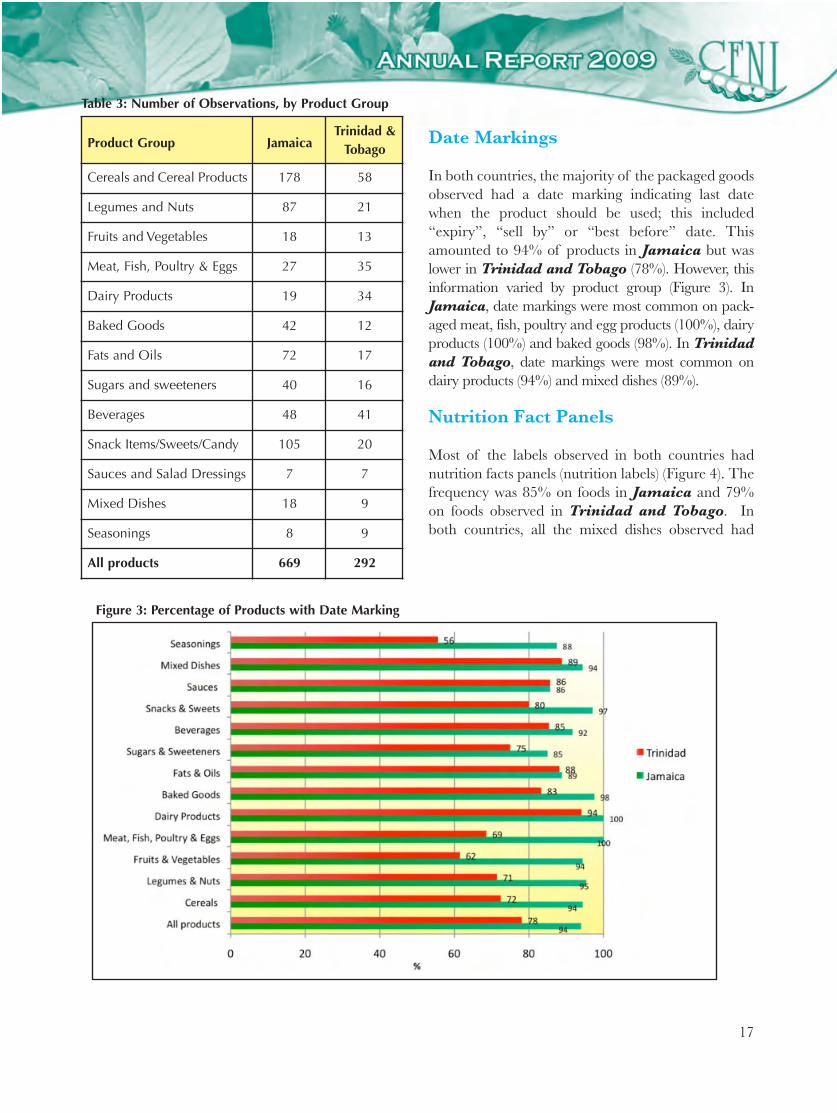
Date Markings
In both countries, the majority of the packaged goodsobserved had a date marking indicating last datewhen the product should be used; this included“expiry”, “sell by” or “best before” date. Thisamounted to 94% of products in Jamaica but waslower in Trinidad and Tobago (78%). However, thisinformation varied by product group (Figure 3). InJamaica, date markings were most common on pack-aged meat, fish, poultry and egg products (100%), dairyproducts (100%) and baked goods (98%). In Trinidadand Tobago, date markings were most common ondairy products (94%) and mixed dishes (89%).
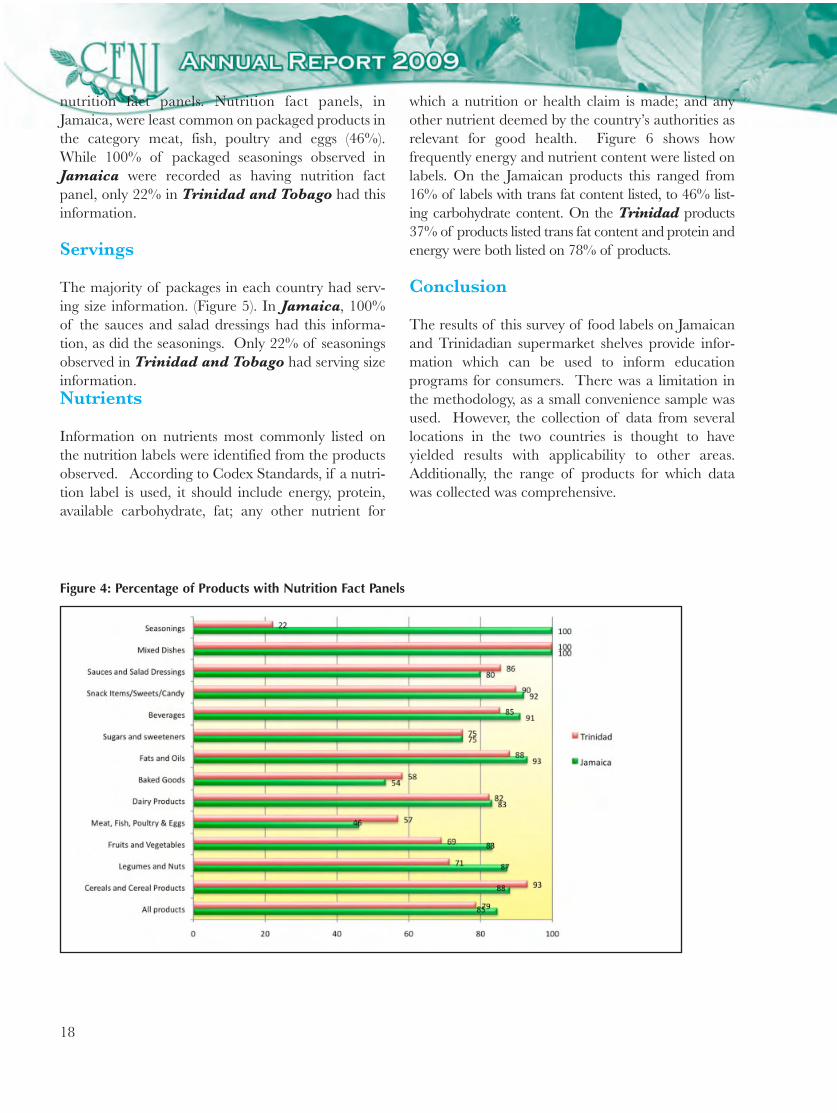
Nutrition Fact Panels
Most of the labels observed in both countries hadnutrition facts panels (nutrition labels) (Figure 4). Thefrequency was 85% on foods in Jamaica and 79%on foods observed in Trinidad and Tobago. Inboth countries, all the mixed dishes observed had
Product Group JamaicaTrinidad &
Tobago
Cereals and Cereal Products 178 58
Legumes and Nuts 87 21
Fruits and Vegetables 18 13
Meat, Fish, Poultry & Eggs 27 35
Dairy Products 19 34
Baked Goods 42 12
Fats and Oils 72 17
Sugars and sweeteners 40 16
Beverages 48 41
Snack Items/Sweets/Candy 105 20
Sauces and Salad Dressings 7 7
Mixed Dishes 18 9
Seasonings 8 9
All products 669 292
Table 3: Number of Observations, by Product Group
Figure 3: Percentage of Products with Date Marking
18
nutrition fact panels. Nutrition fact panels, inJamaica, were least common on packaged products inthe category meat, fish, poultry and eggs (46%).While 100% of packaged seasonings observed inJamaica were recorded as having nutrition factpanel, only 22% in Trinidad and Tobago had thisinformation.
Servings
The majority of packages in each country had serv-ing size information. (Figure 5). In Jamaica, 100%of the sauces and salad dressings had this informa-tion, as did the seasonings. Only 22% of seasoningsobserved in Trinidad and Tobago had serving size information.Nutrients
Information on nutrients most commonly listed onthe nutrition labels were identified from the productsobserved. According to Codex Standards, if a nutri-tion label is used, it should include energy, protein,available carbohydrate, fat; any other nutrient for
which a nutrition or health claim is made; and anyother nutrient deemed by the country’s authorities asrelevant for good health. Figure 6 shows howfrequently energy and nutrient content were listed onlabels. On the Jamaican products this ranged from16% of labels with trans fat content listed, to 46% list-ing carbohydrate content. On the Trinidad products37% of products listed trans fat content and protein andenergy were both listed on 78% of products.
Conclusion
The results of this survey of food labels on Jamaicanand Trinidadian supermarket shelves provide infor-mation which can be used to inform educationprograms for consumers. There was a limitation inthe methodology, as a small convenience sample wasused. However, the collection of data from severallocations in the two countries is thought to haveyielded results with applicability to other areas.Additionally, the range of products for which datawas collected was comprehensive.
Figure 4: Percentage of Products with Nutrition Fact Panels

19
At the time of the survey, the CARICOM RegionalStandard for Labelling of Pre-packaged Foods hadnot yet been finalized. However, it was clear thatmost of the products surveyed were already adheringto some of the aspects of that standard.
Despite the fact that use of the nutrition label is notmandatory, except if claims are made, most packagedfoods had nutrition labels. Some of the foods thatwere without nutrition labels could have been retailedproducts; that is, packaged by the establishment, ordue to some degree of interviewer error. This waslikely due in parts to efforts to meet standards of trad-
Figure 5: Percentage of Products with Serving Size
Figure 6: Percentage of Products with Energy and Nutrient Content listed
20
ing partners such as the USA, if these products arebeing exported. There has also been consumereducation by various entities such as the Ministries ofHealth and CFNI, which may have resulted indemand for such information on products. Furtherresearch on consumer use of the information on foodlabels is now warranted.
A Comparison of the Nutrient Content andCost of Commercial vs. HomemadeComplementary Foods in JamaicaDuring the first two years of life, good nutrition iscrucial as a child undergoes a period of rapid growthand development. Studies have indicated that aninfant’s nutritional intake is a determinant of healthyeating habits, pattern and status in childhood andadulthood.
The World Health Organization recommends that aninfant should be fed exclusively with breast milk forthe first six months after which time the child shouldbe introduced to appropriate complementary foods inorder to fill the child’s growing needs.
Complementary (weaning) foods consist of differenttypes of liquid, semi-solid and solid foods so as tosmooth the transition from a breast milk diet to thatof an adult.
There are two types of complementary foods;commercially made and homemade. For years, nutri-tionists and economists have long advocated the use ofhomemade foods instead of commercial product due tonutrient density and cost. This report compares the cost,calorie and nutrient content of twenty commercialcomplementary foods available in Jamaica againsttwenty homemade complementary foods.
Methods
A list of twenty randomly selected commercialcomplementary foods was created by visiting sixsupermarkets in the urban areas of Kingston and St.Andrew and one rural town – Morant Bay, betweenJuly 2008 and December 2009. The list included infor-
mation on the cost, nutrient content per serving, list ofingredients and net weight per container. The cost ofeach item was verified/updated in December 2009.
Items for homemade recipes were purchased during themonth of December 2009 from two of the six super-markets above as well as the major wholesale market inJamaica – the Coronation Market in Kingston.
Homemade Recipes
Homemade recipes were developed and tested in theFood Demonstration Kitchen of CFNI. Theserecipes were based on the major ingredients listed oncommercial foods labels except in case of availabilityand cultural acceptance e.g. turkey meat was substitutedby fish fillet due its unavailability locally. The texture,appearance and taste of each commercial product werealso considered in establishing homemade recipes.
Nutrient Calculation: Nutrient values were based on 100 gedible portions using primarily CFNI’s FoodComposition Tables for Use in the English-speakingCaribbean (1998) and to a lesser extent nutritiondata.com. Calculations were done for kilocalories (kcal),macronutrients (total carbohydrate, protein and fat) andthree micronutrients (iron, vitamin C and sodium).
Findings
The majority of homemade items appear to providesimilar energy and nutrient values at a lower costthan commercial complementary foods. However, amore detailed analysis is required for comparing thevitamin C and iron content of the two types ofcomplementary foods. In addition imputed labourcosts will have to be applied to the homemaderecipes. These and other revisions will be incorpo-rated into a final version of this study during 2010.HIV/AIDSTwo training sessions were conducted: one in StVincent and the Grenadines and the other inJamaica for health care workers on improving thenutritional care offered to persons with HIV/AIDS.
21
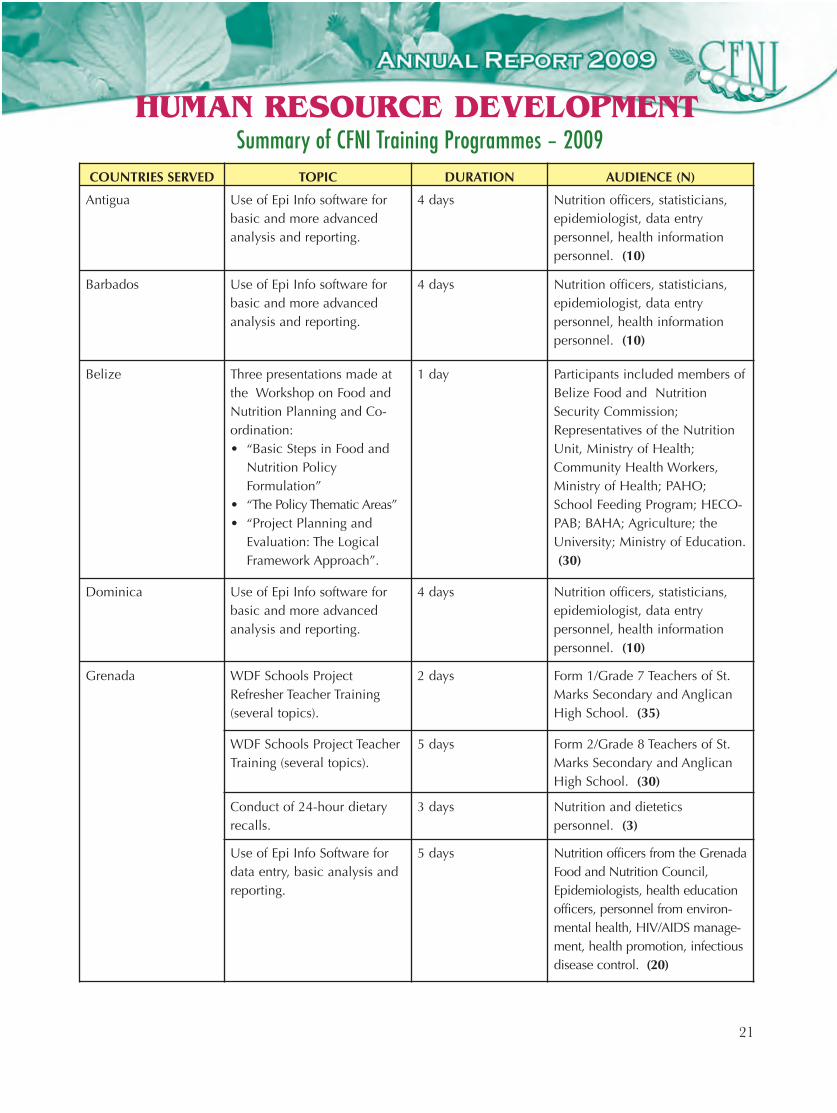
HUMAN RESOURCE DEVELOPMENT
COUNTRIES SERVED TOPIC DURATION AUDIENCE (N)
Antigua Use of Epi Info software forbasic and more advancedanalysis and reporting.
4 days Nutrition officers, statisticians,epidemiologist, data entrypersonnel, health informationpersonnel. (10)
Barbados Use of Epi Info software forbasic and more advancedanalysis and reporting.
4 days Nutrition officers, statisticians,epidemiologist, data entrypersonnel, health informationpersonnel. (10)
Belize Three presentations made atthe Workshop on Food andNutrition Planning and Co-ordination:• “Basic Steps in Food and
Nutrition PolicyFormulation”
• “The Policy Thematic Areas”• “Project Planning and
Evaluation: The LogicalFramework Approach”.
1 day Participants included members ofBelize Food and NutritionSecurity Commission;Representatives of the NutritionUnit, Ministry of Health;Community Health Workers,Ministry of Health; PAHO;School Feeding Program; HECO-PAB; BAHA; Agriculture; theUniversity; Ministry of Education.(30)
Dominica Use of Epi Info software forbasic and more advancedanalysis and reporting.
4 days Nutrition officers, statisticians,epidemiologist, data entrypersonnel, health informationpersonnel. (10)
Grenada WDF Schools ProjectRefresher Teacher Training(several topics).
2 days Form 1/Grade 7 Teachers of St.Marks Secondary and AnglicanHigh School. (35)
WDF Schools Project TeacherTraining (several topics).
5 days Form 2/Grade 8 Teachers of St.Marks Secondary and AnglicanHigh School. (30)
Conduct of 24-hour dietaryrecalls.
3 days Nutrition and dietetics personnel. (3)
Use of Epi Info Software fordata entry, basic analysis andreporting.
5 days Nutrition officers from the GrenadaFood and Nutrition Council,Epidemiologists, health educationofficers, personnel from environ-mental health, HIV/AIDS manage-ment, health promotion, infectiousdisease control. (20)
Summary of CFNI Training Programmes – 2009
22
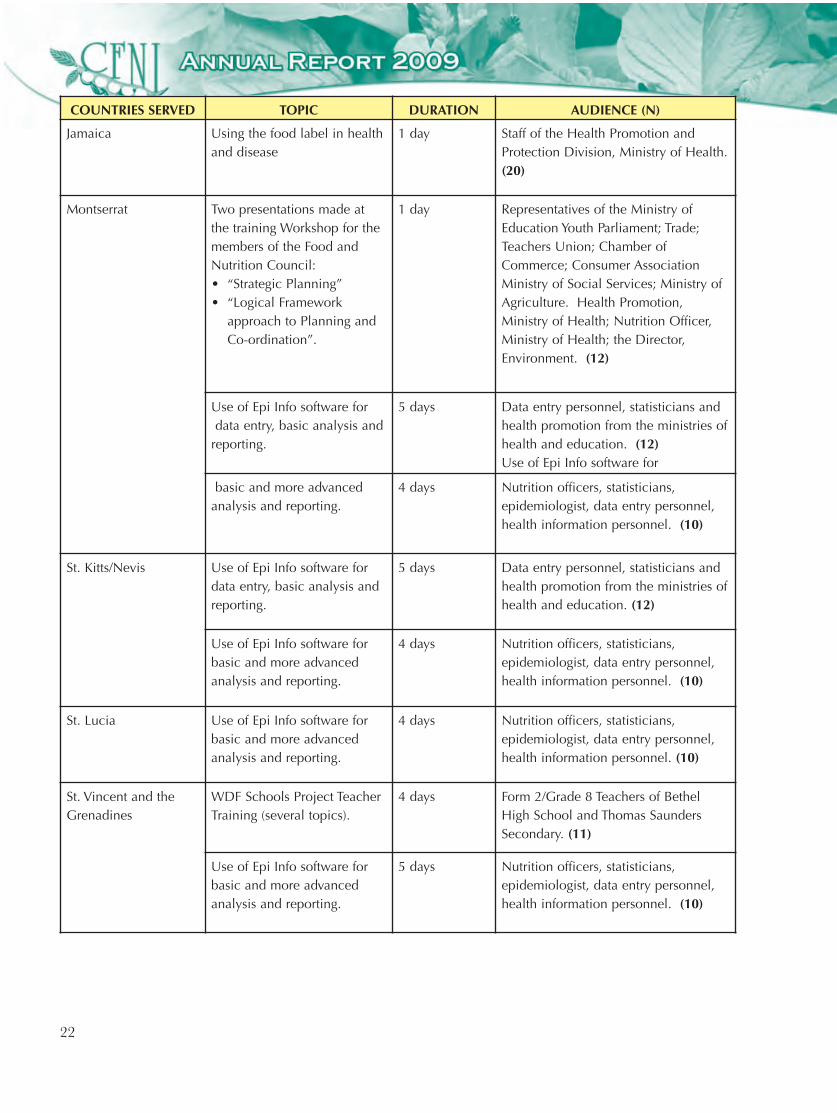
COUNTRIES SERVED TOPIC DURATION AUDIENCE (N)
Jamaica Using the food label in healthand disease
1 day Staff of the Health Promotion andProtection Division, Ministry of Health.(20)
Montserrat Two presentations made atthe training Workshop for themembers of the Food andNutrition Council:• “Strategic Planning”• “Logical Framework
approach to Planning andCo-ordination”.
1 day Representatives of the Ministry ofEducation Youth Parliament; Trade;Teachers Union; Chamber ofCommerce; Consumer AssociationMinistry of Social Services; Ministry ofAgriculture. Health Promotion,Ministry of Health; Nutrition Officer,Ministry of Health; the Director,Environment. (12)
Use of Epi Info software fordata entry, basic analysis and
reporting.
5 days Data entry personnel, statisticians andhealth promotion from the ministries ofhealth and education. (12)Use of Epi Info software for
basic and more advancedanalysis and reporting.
4 days Nutrition officers, statisticians,epidemiologist, data entry personnel,health information personnel. (10)
St. Kitts/Nevis Use of Epi Info software fordata entry, basic analysis andreporting.
5 days Data entry personnel, statisticians andhealth promotion from the ministries ofhealth and education. (12)
Use of Epi Info software forbasic and more advancedanalysis and reporting.
4 days Nutrition officers, statisticians,epidemiologist, data entry personnel,health information personnel. (10)
St. Lucia Use of Epi Info software forbasic and more advancedanalysis and reporting.
4 days Nutrition officers, statisticians,epidemiologist, data entry personnel,health information personnel. (10)
St. Vincent and theGrenadines
WDF Schools Project TeacherTraining (several topics).
4 days Form 2/Grade 8 Teachers of BethelHigh School and Thomas SaundersSecondary. (11)
Use of Epi Info software forbasic and more advancedanalysis and reporting.
5 days Nutrition officers, statisticians,epidemiologist, data entry personnel,health information personnel. (10)

23
The training in St Vincent and the Grenadinesinvolved over 20 participants from the Milton CatoHospital, while in Jamaica the participants wereselected from all of the regions and involved a rangeof health care workers form both primary andsecondary care. The team training approach wasused for both workshops with local persons supportedby CFNI officers. Many of the local trainers wereparticipants in previous training conducted by CFNIin this project.Nutrition algorithms were developed and plans areon stream for their pretesting and eventual launch ofthe algorithms and guidelines in 2010. Pretesting willtake place in three (3) territories among health careworkers.
Awards/Partnerships/ Collaborations/Technical Consultations1. CFNI was the recipient of Wellness and Lifestyle
Award from the Environmental HealthFoundation (Jamaica) for outstanding contribu-tion to wellness and healthy lifestyles.
2. CFNI was the recipient of the award from theEmpowering Lives for the Future Ministries andMinistry of Health for outstanding commitmentand support to Jamaica’s National Infant andYoung Child Feeding Program.
3. Collaborated with the Ministry of Health and theMinistry of Education in implementing a project“Evaluation of School Meal Options in Trinidad and
COUNTRIES SERVED TOPIC DURATION AUDIENCE (N)
Trinidad and Tobago WDF Schools Project RefresherTeacher Training (several topics)– Trinidad.
2 days Form 1/Grade 7 Teachers of SanFernando East Secondary. (10)
WDF Schools Project RefresherTeacher Training (several topics)– Tobago.
2 days Form 1/Grade 7 Teachers ofRoxborough Composite Secondary.(20)
WDF Schools Project TeacherTraining (several topics) –Trinidad.
5 days Form 2/Grade 8Teachers of SanFernando East Secondary. (8)
WDF Schools Project TeacherTraining (several topics) –Tobago.
5 days Form 2/Grade 8 Teachers ofRoxborough Composite Secondary. (8)
“Food and Nutrition PolicyDevelopment”.
1 day UWI BSc Nutrition Final YearStudents. (30)
“Food Security, Nutrition andHealth in the Caribbean:Perspectives from CFNI”.
1 day Representatives from: FAO; IICA;CARDI; Ministry of Agriculture;University of the West Indies;UNECLAC; CARIRI; KAIRI Consultants.(25)
Conduct of 24-hour dietaryrecalls – Trinidad.
3 days WDF Project Country coordinator andnutrition and dietetics graduates. (4)
Conduct of 24-hour dietaryrecalls Tobago.
3 days WDF Project Country coordinatorand school feeding personnel. (4)
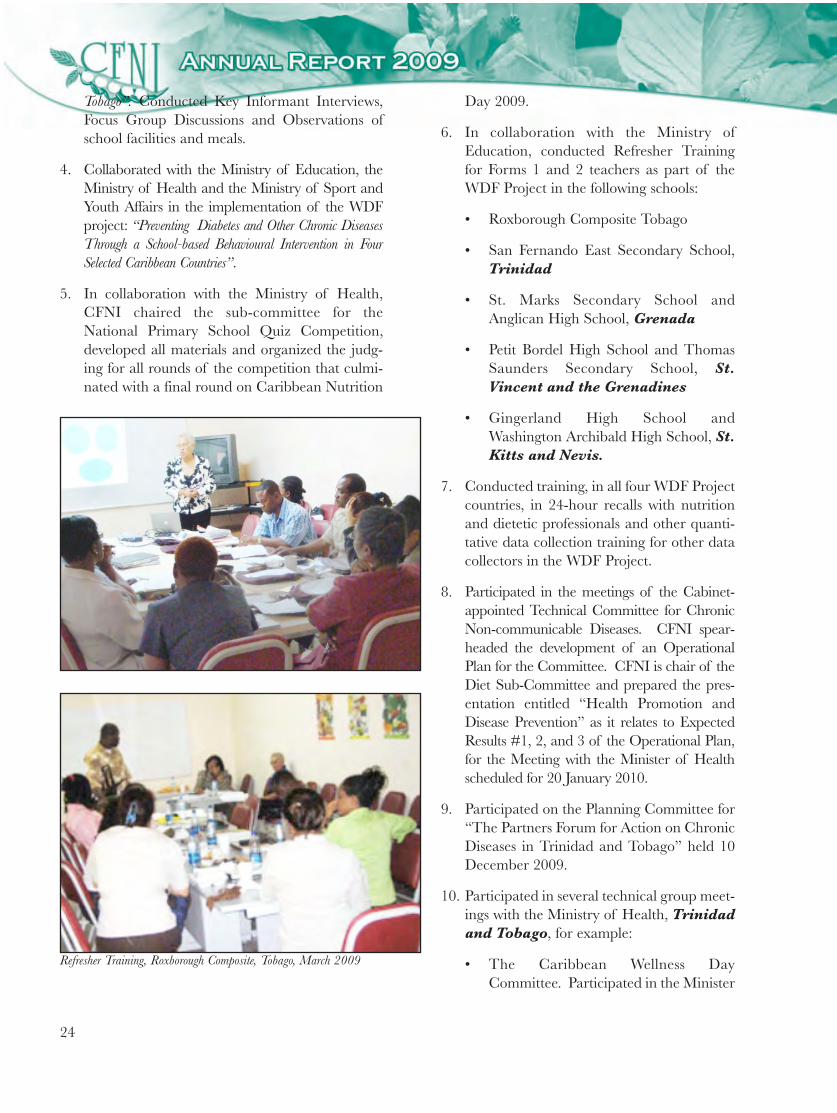
24
Tobago”. Conducted Key Informant Interviews,Focus Group Discussions and Observations ofschool facilities and meals.
4. Collaborated with the Ministry of Education, theMinistry of Health and the Ministry of Sport andYouth Affairs in the implementation of the WDFproject: “Preventing Diabetes and Other Chronic DiseasesThrough a School-based Behavioural Intervention in FourSelected Caribbean Countries”.
5. In collaboration with the Ministry of Health,CFNI chaired the sub-committee for theNational Primary School Quiz Competition,developed all materials and organized the judg-ing for all rounds of the competition that culmi-nated with a final round on Caribbean Nutrition
Refresher Training, Roxborough Composite, Tobago, March 2009
Day 2009.
6. In collaboration with the Ministry ofEducation, conducted Refresher Trainingfor Forms 1 and 2 teachers as part of theWDF Project in the following schools:
• Roxborough Composite Tobago
• San Fernando East Secondary School,Trinidad
• St. Marks Secondary School andAnglican High School, Grenada
• Petit Bordel High School and ThomasSaunders Secondary School, St.Vincent and the Grenadines
• Gingerland High School andWashington Archibald High School, St.Kitts and Nevis.
7. Conducted training, in all four WDF Projectcountries, in 24-hour recalls with nutritionand dietetic professionals and other quanti-tative data collection training for other datacollectors in the WDF Project.
8. Participated in the meetings of the Cabinet-appointed Technical Committee for ChronicNon-communicable Diseases. CFNI spear-headed the development of an OperationalPlan for the Committee. CFNI is chair of theDiet Sub-Committee and prepared the pres-entation entitled “Health Promotion andDisease Prevention” as it relates to ExpectedResults #1, 2, and 3 of the Operational Plan,for the Meeting with the Minister of Healthscheduled for 20 January 2010.
9. Participated on the Planning Committee for“The Partners Forum for Action on ChronicDiseases in Trinidad and Tobago” held 10December 2009.
10. Participated in several technical group meet-ings with the Ministry of Health, Trinidadand Tobago, for example:
• The Caribbean Wellness DayCommittee. Participated in the Minister

25
of Health Press Conference on CaribbeanWellness Day, 19 September 2009.
• National Health Promotion Committee.
11. Participated on a sub-committee set up by theMinistry of Legal Affairs, Consumer AffairsDivision to develop a Position Paper “FactorsInfluencing Food Consumption Patterns inTrinidad and Tobago”. The completed final draftdocument is to be presented to the Minister earlyin 2010.
12. Participated in the meetings of the NationalAgricultural Advisory Commission set up by theMinister of Agriculture Land and MarineResources. The main goal of the Commission isto “provide advisory, monitoring, evaluating and reporting
services to the Minister of Agriculture Land and MarineResources and his/her nominees, on all matters relating tothe preparation and implementation of the National Foodand Nutrition Security and Agri-business CompetitivenessPlan”.
13. Participated in CARICOM meeting on“Implementing the CARICOM CommunityAgricultural Policy: Issues, Options and Process”,Cascadia Hotel.
14. Participated in IICA, Trinidad and TobagoAnnual Accountability Meeting.
15. Participated in the Roundtable Launchof IICA/CARDI Awards for Excellencein Agriculture Journalism held 6 October2009. The Roundtable meeting focusedon “The Role of the Media in PromotingFood Security in Trinidad and Tobago”The main objectives of the roundtablewas to:
• Foster a greater understanding of thefood security issues among the mediain Trinidad and Tobago.
• Increase the interaction between theagricultural sector and the media.
• Encourage more informed reportingon food security issues.
• Encourage awareness of food securityissues among citizens of Trinidadand Tobago.
• Create new partnerships betweenagricultural sector stakeholders andthe media.
16. Participated on an IICA sub-committeeto develop the proposed AgriculturalAgencies Communications Networkas a follow-up mechanism from the
Roundtable Launch of theAgricultural Media Awards. CFNI devel-oped a draft program and materials to
guide the development of a strategic planRefresher Training, San Fernando East Secondary School, Trinidad, March 2009

26
19. Participated in the CARICOM/UNICEF Healthand Family Life Education (HFLE) in St. Lucia,28 September – 2 October 2009. The mainpurpose of the meeting was to: “Review and updatethe CARICOM-led HFLE Strategy with the aim ofinfusing Drug Prevention in the Regional HFLECurriculum”.
20. Participated in the CARICOMBiosafety Meeting, 17-18March, Barbados. The meet-ing was held to reactivate theRegional Working Group and towork on the GMO-Biotechnology Regional Policyand Strategy.
21. Participated in the University ofthe West Indies, St Augustine,launch of their EmployeeHealth and Wellness Program.CFNI literature was displayedand distributed to persons inattendance.
22. Participated in a Nutrition andHIV/AIDS workshop forselected health care profession-als 14 and 15 July, Trinidadand Tobago. This two dayprogram was aimed at improv-ing the quality of life of peopleliving with HIV/AIDS byimplementing an integratedapproach to nutritional treat-ment care and support.
23. Participated in a Gender Mains-treaming in Health trainingWorkshop 30 September – 2October 2009. This workshopsought to enhance the skillsof the PAHO sub-regional staffin the Caribbean on gendermainstreaming in health as partof the implementation of the
Organization’s Gender EqualityPolicy and also to promote genderresponsive technical cooperation,
for the proposed Network. CFNI will play a keyrole in that Strategic Planning Workshopplanned for February 2010.
17. CFNI was represented at the IICA DayCelebrations held on 7 October 2009.
18. Participated on IICA Working/Technical Groupfor the IICA/CARDI Project “EnhancingInformation and Communication for Food Securityin Trinidad and Tobago”. Brochures, Copy Bookswith Food Security information; and a Poster weredeveloped.
WDF Year 2 Teacher Training, Petit Bordel High School and Thomas Saunders Secondary School, St. Vincent and The Grenadines
Refresher Training, St. Marks Secondary School and Anglican High School, Grenada, March2009

27
ensuring that differential issues and needs of thewomen and men are recognized, taken intoaccount, and addressed in health programs, policiesand projects.
24. Prepared a paper for UNICEF on Estimates ofCost of Feeding 0-4 Year Olds in Jamaica.
25. Participated in meetings of Jamaica’s NationalInfant and Young Child Feeding Committee andsupported the Committee’s work in research intoinfant feeding practices, promotion of breastfeed-ing and development of policy documents.
26. Participated in Ministry of Health and UNICEFmeeting to disseminate baseline results fromExclusive Breastfeeding Pilot in Clarendon andSt. Catherine, Jamaica.
27. Collaborated with the Bureau of Standards Jamaicain the development and revision of standards,through representation on the National StandardsCommittee, National Food Standards Committee,National Codex Committee and LabellingCommittee.
28. Collaborated with the National AgriculturalHealth and Food Safety Coordinating Committeein the coordination of food safety programs inJamaica.
29. Participated in the National Physical ActivityStakeholders meeting, Technical Working Groupon Physical Activity and advocacy/policysubcommittee (Jamaica).
30. Collaborated with the Early Child Commissionin Jamaica in the setting of standards, and coor-dination of early childhood and nutritionprograms.
31. Participated in stakeholders meeting for the post-graduate Dietetic/Nutrition Internship Programin Jamaica.
32. Participated in the Fifth Ministerial Meeting ofthe Inter-American Board of Agriculture (IABA)held in Jamaica. The theme of the meeting wasBuilding Capacity for Enhancing Food Securityand Rural Life in the Americas.
33. Participated in meeting on Salt Consumption inthe Americas. The meeting, held in Miami,Florida, USA was organized by PAHO and thePublic Health Agency of Canada. The purposewas to document the policies and initiatives in theAmericas Region aimed at reducing dietary saltto prevent and control chronic non-communica-ble diseases, and to feature relevant experiencesin CARMEN countries, other countries andWHO regions.
Major Presentations1. Eradication: A Hemispheric Mission - Presentation at
the 4th Steering Committee Meeting ofCaribVET, Trelawny, Jamaica, 16 March 2009.
2. Report on the Assessment of Veterinary Needs in theCaribbean Sub-region – Presentation at the ChiefVeterinary Officers Meeting, Trelawny,Jamaica, 18 March 2009.
3. Proposed Guidelines for Port Health Surveillance Systems.Presentation at Chief Veterinary OfficersMeeting, Trelawny, Jamaica, 18 March 2009.
4. School-based Nutrition Programs a Caribbean Experience.Presentation at the Sub-regional Workshop onHealth Promotion Policy, Canada, 25-27 March2009.
5. Food & Nutrition in Natural Disasters: Key Issues for theHealth Sector in Disaster Preparedness and Management.Presentation to students in the Masters in PublicHealth (MPH) program at the University of theWest Indies, Mona, Jamaica, 25 March 2009.
6. Caribbean Food Crisis: Implications andResponses. Presentation to PAHO representativesand CARICOM officials and senior technicalofficers in the Bahamas Ministry of Health. TheBahamas, April 2009.
7. An International Health Regulations Perspective forHealth and Tourism. Presentation at the FirstPAHO Caribbean Sub-Regional Working GroupMeeting on Health and Tourism, GrandBarbados Hotel, Barbados, 2-3 April 2009.
28
8. Food Security, Nutrition and Health in the Caribbean:Perspectives from CFNI. Presentation at Round TableDiscussion on the FAO Project “Promoting CARI-COM/CARIFORUM Food Security” (projectGTFS/RLA/141/ITA), University of the WestIndies, Trinidad and Tobago, 23 April 2009.
9. International Health Regulations (IHR) in Jamaica.Presentation at The National Ship SanitationTraining Workshop for Port Health Officers,Ocho Rios, Jamaica, 28 April 2009.
10. Health Promoting Schools: A systematicApproach to Support Healthy Eating inCaribbean Schools. Presentation to jointCOHSOD Ministers of Health and Education.Jamaica. June 3, 2009.
11. The concept and rationale of WorkplaceWellness. Presentation made to Chief ExecutiveOfficers of various public, private and academicenterprises. Grenada, 10 June, 2009.
12. Developing an Effective Food Safety Policy for Grenada.Presentation at the Working Group Meeting forFormulating a Food Safety Policy, Grenada, 24August 2009.
13. Preventing Diabetes and Other DiseasesThrough a School-Based Behavioral Interventionin Four Countries. Presented to representatives ofthe World Diabetes Foundation. Jamaica.September 2009.
14. The implementation of Workplace WellnessPrograms. Presentation made to Chief ExecutiveOfficers of various public, private and academicenterprises. Grenada, 15 September 2009.
15. Food and Nutrition Policy Development. Lecture to theThird Year BSc in Nutrition and DieteticsStudents,UWI, St Augustine Campus, Trinidad
and Tobago 9 October 2009.
16. Developing a Food Security Policy for Jamaica.Presentation made to the Minister of Agriculture,Permanent Secretary and other senior technicalofficers of the Ministry of Agriculture. Jamaica.15 October 2009.
17. Participated in the 7th Global Conference onHealth Promotion. Worked with the WDF teamto prepare Position Paper on Diabetes which wasused as an advocacy tool for inclusion in the “Callfor Action” Nairobi, Kenya, 26-30 October2009.
18. Food Safety in the PAHO Region: Emphasis on theCaribbean Sub-region Presentation at the IntegratedFoodborne Disease Surveillance Workshop,Grand Barbados Hotel, Barbados, 22-29November 2009.
19. Developing Regional and National Food SecurityPolicies. Presentation made to senior technicalofficers in Agriculture and Health across theCaribbean. Georgetown, Guyana. 30 November2009.
20. Nutrition and Hypertension. Presentation to secondyear associate degree students at ExcelsiorCommunity College, Jamaica, 1 December2009.
Promoting Healthy Lifestyles in Schools
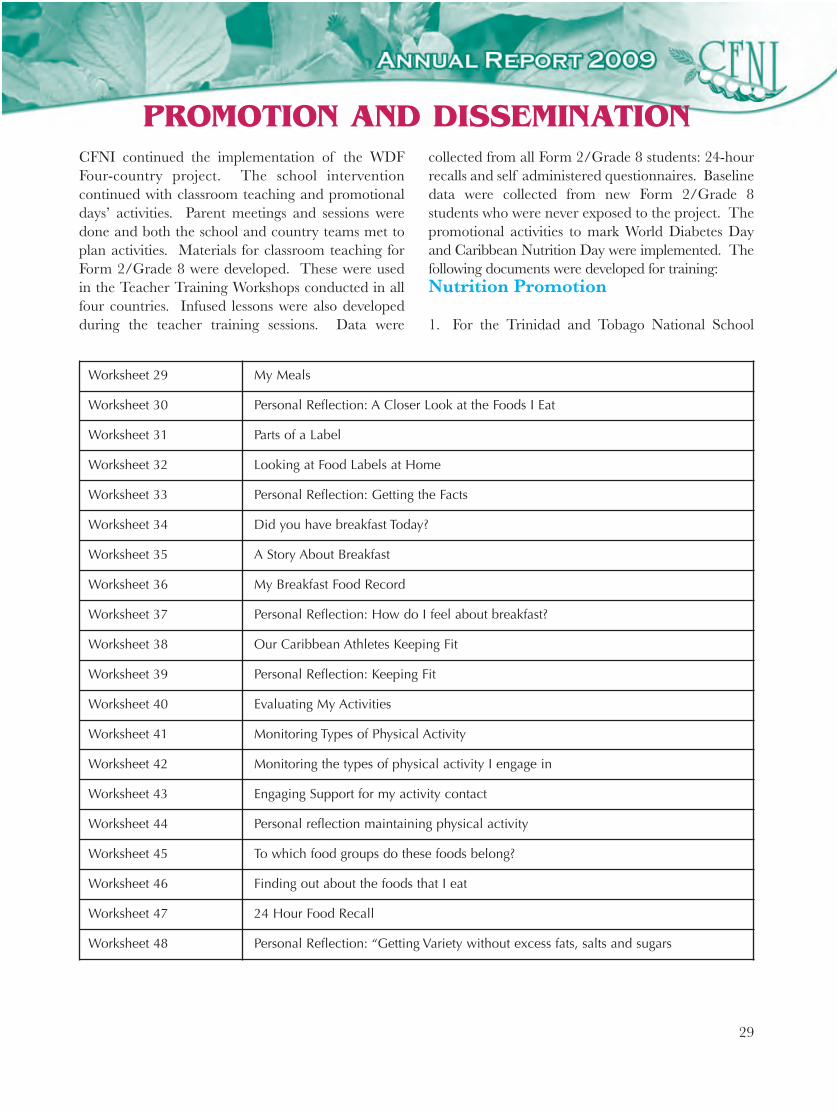
29
CFNI continued the implementation of the WDFFour-country project. The school interventioncontinued with classroom teaching and promotionaldays’ activities. Parent meetings and sessions weredone and both the school and country teams met toplan activities. Materials for classroom teaching forForm 2/Grade 8 were developed. These were usedin the Teacher Training Workshops conducted in allfour countries. Infused lessons were also developedduring the teacher training sessions. Data were
collected from all Form 2/Grade 8 students: 24-hourrecalls and self administered questionnaires. Baselinedata were collected from new Form 2/Grade 8students who were never exposed to the project. Thepromotional activities to mark World Diabetes Dayand Caribbean Nutrition Day were implemented. Thefollowing documents were developed for training:Nutrition Promotion
1. For the Trinidad and Tobago National School
PROMOTION AND DISSEMINATION
Worksheet 29 My Meals
Worksheet 30 Personal Reflection: A Closer Look at the Foods I Eat
Worksheet 31 Parts of a Label
Worksheet 32 Looking at Food Labels at Home
Worksheet 33 Personal Reflection: Getting the Facts
Worksheet 34 Did you have breakfast Today?
Worksheet 35 A Story About Breakfast
Worksheet 36 My Breakfast Food Record
Worksheet 37 Personal Reflection: How do I feel about breakfast?
Worksheet 38 Our Caribbean Athletes Keeping Fit
Worksheet 39 Personal Reflection: Keeping Fit
Worksheet 40 Evaluating My Activities
Worksheet 41 Monitoring Types of Physical Activity
Worksheet 42 Monitoring the types of physical activity I engage in
Worksheet 43 Engaging Support for my activity contact
Worksheet 44 Personal reflection maintaining physical activity
Worksheet 45 To which food groups do these foods belong?
Worksheet 46 Finding out about the foods that I eat
Worksheet 47 24 Hour Food Recall
Worksheet 48 Personal Reflection: “Getting Variety without excess fats, salts and sugars
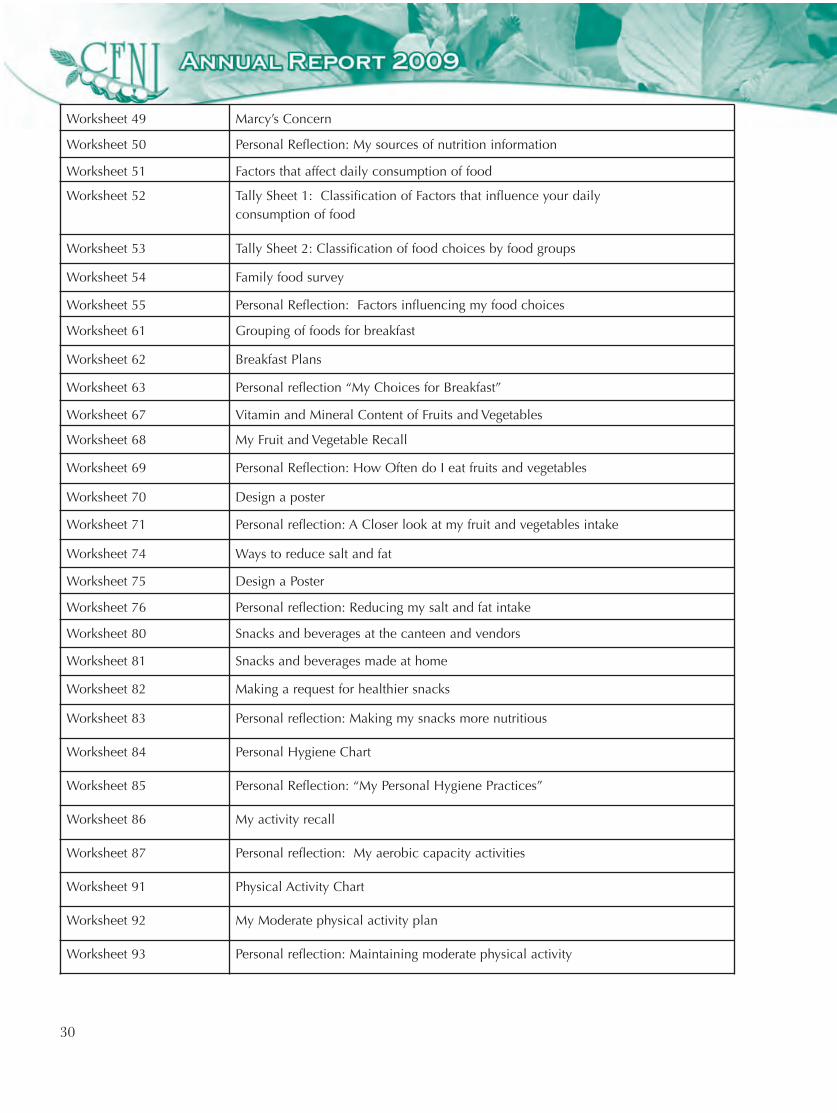
30
Worksheet 49 Marcy’s Concern
Worksheet 50 Personal Reflection: My sources of nutrition information
Worksheet 51 Factors that affect daily consumption of food
Worksheet 52 Tally Sheet 1: Classification of Factors that influence your daily consumption of food
Worksheet 53 Tally Sheet 2: Classification of food choices by food groups
Worksheet 54 Family food survey
Worksheet 55 Personal Reflection: Factors influencing my food choices
Worksheet 61 Grouping of foods for breakfast
Worksheet 62 Breakfast Plans
Worksheet 63 Personal reflection “My Choices for Breakfast”
Worksheet 67 Vitamin and Mineral Content of Fruits and Vegetables
Worksheet 68 My Fruit and Vegetable Recall
Worksheet 69 Personal Reflection: How Often do I eat fruits and vegetables
Worksheet 70 Design a poster
Worksheet 71 Personal reflection: A Closer look at my fruit and vegetables intake
Worksheet 74 Ways to reduce salt and fat
Worksheet 75 Design a Poster
Worksheet 76 Personal reflection: Reducing my salt and fat intake
Worksheet 80 Snacks and beverages at the canteen and vendors
Worksheet 81 Snacks and beverages made at home
Worksheet 82 Making a request for healthier snacks
Worksheet 83 Personal reflection: Making my snacks more nutritious
Worksheet 84 Personal Hygiene Chart
Worksheet 85 Personal Reflection: “My Personal Hygiene Practices”
Worksheet 86 My activity recall
Worksheet 87 Personal reflection: My aerobic capacity activities
Worksheet 91 Physical Activity Chart
Worksheet 92 My Moderate physical activity plan
Worksheet 93 Personal reflection: Maintaining moderate physical activity
31
Quiz Competition, CFNI prepared a brief pres-entation for the attending secondary school chil-dren and teachers about CFNI’s Regional SchoolNutrition Quiz Competition.
2. In collaboration with the Ministry of Health,CFNI chaired the sub-committee for the NationalPrimary School Quiz Competition, developed allmaterials and organized the judging for all roundsof the competition that culminated with a finalround on Caribbean Nutrition Day 2009.
2009 Caribbean Nutrition DayCaribbean Nutrition Day 2009 was celebrated underthe theme “Healthy Eating and Active Living: AFamily Affair”. A poster/flyer was designed for theoccasion and disseminated to member countries inaddition to other relevant posters available at CFNI.Countries were encouraged to involve their ownMinisters of Health and other officials to prepare anddeliver messages in keeping with the theme. Severalcountries shared their plans and activities for the dayand these were posted on the CFNI website. TheCFNI family focused on increasing physical activitythrough their steps to health initiative which culmi-nated on PAHO Wellness Day.
Food-Based Dietary Guidelines
CFNI continued to work with member countries onthe development, implementation and promotion ofFood-Based Dietary Guidelines, which are used togive simple dietary advice to help the populationmake healthy choices that promote healthy lifestyles.
Dominica
Following on CFNI’s technical assistance in the devel-opment of guidelines in Dominica in collaborationwith the Institute of Nutrition of Central Americaand Panama (INCAP) and the Food and AgricultureOrganization (FAO), that country was assisted furtherin the promotion of the guidelines. The 10-point setof guidelines had previously been launched,supported by a package of promotional materialsbranded with the image of the country’s national bird‘Sisserou’ an umbrella symbol for the multi mediamessages. Ongoing monitoring and assessment of thepromotion initiatives underscored the need for furthercapacity building in social communication generally andmessage development and dissemination specifically.
Against this background, CFNI, in collaboration withthe Ministry of Health, facilitated a two-day work-shop in Dominica in May. The goal of the workshopwas to develop and strengthen the capabilities ofparticipants, which included health education, envi-ronment, nutrition and communication officers, inthe skills and strategies needed to design and promote
the FBDGs. A mixture of presentationsand working groups was used to achievethe objective of enabling participants to:
1. Understand key guidelines inmarketing a health product.
2. Undertake a basic analysis of marketaudience(s), channels and messages.
3. Identify key elements in preparing amarketing strategy.
4. Produce a creative brief to guide thedevelopment of a communication inter-vention aimed at promoting key messagesin the new FBDGs for Dominica. Students viewing a CFNI display

32
The workshop targeted nutrition, health educationand communication/information officers responsiblefor planning, implementing and evaluating healthcommunication programs, specifically Dominica’sFood-Based Dietary Guidelines. The 25 participantsin attendance came from a wide variety of publicsector entities, including agriculture, health andeducation, media/information and NGOs.
Belize
Belize’s food-based dietary guidelines are being devel-oped under the auspices of the National Food andNutrition Security Commission. In November, incollaboration with the Government of Belize andPAHO, CFNI facilitated a workshop for the multisec-toral committee, the objectives of which were to:
1. Present the health and nutrition situation of Belize.
2. Discuss implications of the health and nutritionsituation and strategies for alleviating them.
3. Determine priority problems and set nationalobjectives to be addressed through Food BasedDietary Guidelines.
The 28 participants included representatives from theCommission, the Ministries of Health, Education,and Agriculture and Fisheries, and the BelizeAgricultural Health Authority. Various presentationswere made by local presenters to describe the food,nutrition and health situation of the country. TheCFNI facilitators, as well as informing participants ofthe process of developing food-based dietary guide-lines and highlighting some critical food and nutritionsecurity issues in Belize, guided them through work-ing group discussions, the outputs of which was aprioritized list of nutrition problems in the country,which should be addressed by the guidelines.
The process will continue with the development oftechnical guidelines which will define the nutritionalgoals for the population and convert these into typesand quantities of food.
Jamaica
Jamaica is at the stage of development of food-based dietary guidelines and has now compiled a listof draft guidelines and proposed illustrativediagrams. CFNI continues to provide technical inputthrough the task force meetings and developmentalworkshops being used to further the process.
Anaemia Prevention and Control
Iron deficiency anaemia, particularly in pregnantwomen and young children, continues to be a prob-lem in some Caribbean countries. Recommendedstrategies for prevention and control of micronutrientdeficiencies such as this include supplementation,use of fortified foods, modifying the diet to optimizeiron intake and absorption, and other public healthmeasures. To guide the implementation of thesestrategies, CFNI has developed a RegionalProtocol for the Detection, Prevention andTreatment of Anaemia in Maternal and ChildHealth Clinics in the Caribbean. These guide-lines, still in draft form, will be made available tomember countries once finalized.
A country-specific protocol has already beencompleted for Guyana, and in 2009, this was furtherdeveloped into a training package, with accompany-ing trainer’s guide, activities booklet and PowerPointslides, which have all been made available to thecountry.
During the year, Guidelines for Detection,Prevention and Treatment of Iron DeficiencyAnaemia in Children were also drafted forAnguilla. These guidelines, which are under review,are intended to help health care workers to imple-ment effective screening and management proce-dures for the prevention and control of irondeficiency anaemia in children from birth to 12 yearsold through use in health centres and schools. Theguidelines take into account current programs andrecent research and international recommendationswhich apply to children, and place emphasis onscreening, supplementation and use of iron-rich andfortified foods as well as public health measures such

33
as control of parasites.
Nutrition DisplaysNutrition messages along various themes werepromoted through displays at expositions and confer-ences throughout the year. These include:
• Ministry of Agriculture’s Production andMarketing Organization Conference at TrelawnyMulti-purpose Stadium, Jamaica.
• Ministry of Agriculture and Fisheries’ CorporateWellness Program celebration at the Ministry ofAgriculture head office, Hope Gardens, Jamaica.
• Display on food labelling and the sugar and saltcontent of commonly eaten foods at the officialmedia launch of Caribbean Wellness Day at theoffice of the Prime Minister of Jamaica.
• Display on Careers in Nutrition and Dietetics atNational Science and Technology Exposition atthe University of Technology, Jamaica.
• World Food Day Display at Garvey Maceo HighSchool in Clarendon, Jamaica. The theme wasAchieving Food Security in Times of Crisis.
Promotion of Young Child Nutrition Capacity building for implementing recommenda-tions of the Global Strategy for Infant and YoungChild Feeding remained the main focus of technicalcooperation activities related to the improvement ofyoung child nutrition. Support was given in thefollowing areas: development of national policies oninfant and young child feeding; introduction of thenew WHO child growth standards; and, training oftrainers with regard to equipping health workers withknowledge/ skills for counselling and assisting moth-ers with adopting recommended feeding practices.
Development of National Infant andYoung Feeding Policy
In Jamaica, CFNI participated in discussions on the
revision and updating of the draft national Infant andYoung Child Feeding Policy. The 1-day multi-stake-holder consultation involved small group discussionson specific sections of the draft document. Pertinentissues from the group reports were discussed in theplenary session and a broad consensus reached on anumber of proposed policy actions. CFNI also partic-ipated in a small working group with members of thenational Infant and Young Child Feeding Committeeto prepare the revised draft of the policy document.After a final review by the Committee, the documentwill be submitted for Cabinet approval.
CFNI assisted the National Infant and Young ChildNutrition Committee of the Ministry of Health inSt. Vincent and the Grenadines with planningand conducting a national consultation for the devel-opment of their Infant and Young Child FeedingPolicy. Participants included personnel fromMinistries of Health, Education, and Finance, theDepartment of Gender Affairs, Community HealthServices, representatives of the National Associationof Early Childhood Educators, Medical, Nursing andPharmacist Associations and the St Vincent Save theChildren Fund (VINSAVE). After presentations onthe situation on young child nutrition in the countryand the Global Strategy for IYCF, the participants, inworking group sessions, reviewed IYCF practices andcurrent policies and programs with a view to identify-ing areas for improvement. They also defined objec-tives for the policy and priority strategies/actions forachieving these objectives. In addition, they maderecommendations on responsibilities for policy imple-mentation, mechanisms for monitoring and evalua-tion and strategies for mobilizing resources in supportof policy implementation.
Introduction of the New WHO ChildGrowth Standards
Preparations for the introduction of the new WHOChild Growth Standards remained a major focusof child health services in many countries. Incollaboration with the PAHO office for the EasternCaribbean, CFNI assisted the Ministries of Health inAntigua and Barbuda, Barbados, Dominica,Montserrat and St. Vincent and the

34
Grenadines in planning and conducting workshopsfor trainers. Participants included nutrition anddietetic personnel, supervisors from hospital andcommunity health services, nursing tutors, coordina-tors of early childhood development programs in theMinistry of Education and technical officers from theMinistry of Health. The workshop agenda includedpresentations on the development of the new growthstandards, demonstrations of measuring techniquesfollowed by practice by the participants, and practicalexercises on the plotting and interpretation of growthtrends and counselling mothers. Each participantreceived a copy of the training manual which was devel-oped to guide health workers in the use of the revisedrecords. In the final workshop session, training planswere discussed with the participants who were expectedto conduct training for the other health and child careworkers in their respective work settings.
Similar workshops were also conducted in Jamaicaand Guyana. In Jamaica, nutrition and dieteticpersonnel as well as public health nurses attended the4-day training program. As part of the roll-out of train-ing for the introduction of the revised child healthrecords country-wide, tutors in health training institu-tions in Guyana were trained by CFNI in the plottingand interpretation of the new child growth standards.
Upgrading Skills for Protecting,Promoting and SupportingAppropriate Infant and YoungFeeding Practices
A 2-day workshop on the International Code ofMarketing of Breastmilk Substitutes was conductedin St. Vincent and the Grenadines in collabora-tion with the National Infant and YoungChild Nutrition committee. Participants includedmedical and nursing personnel, community healthnursing supervisors, community nutrition officers andpersonnel from early childhood development/educa-tion services. The objectives of the workshop were toexplain the objectives, scope and provisions of theInternational Code and the ways in which the
marketing of breastmilk substitutes can underminethe effectiveness of breastfeeding promotion efforts,and to identify practices in local settings which werein violation of the Code.
Twenty-four participants including public healthnurses, supervisors of early childhood centers andnutrition and dietetic personnel attended a trainingworkshop conducted by CFNI in collaboration withthe South West Regional Health Authority,Trinidad and Tobago. The training program wasaimed at upgrading participants’ knowledge onrecommended infant and young child feeding prac-tices; and improving skills in monitoring key aspectsof nutrition services in day care and early childhoodcentres. The agenda included presentations onimportant aspects of young child nutrition and prac-tical exercises which focused on the application oftheoretical principles.
Training activities were also conducted under theextension phase of the Government of Guyana/Inter-American Development Bank (GOG/IDB)Basic Nutrition Program. A 2-day workshopwas conducted for tutors from the three nursingschools and the University of Guyana. The workshopfocused on the knowledge/skill areas that health work-ers require for counseling and supporting mothers inimproving young child feeding practices. CFNI alsoconducted a workshop on maternal and young childnutrition for physicians working in primary care serv-ices in Guyana. Topics discussed in presentationsand case study discussions related to strategies forimproving nutrition in pregnancy and lactation; scien-tific evidence on the benefits of exclusive breastfeeding,and the application of principles of lactation manage-ment; the development, use and interpretation of thenew WHO child growth standards; and the recom-mended protocol for prevention and management ofiron-deficiency anemia in maternal and child healthservices.
Another related activity under the Basic Nutrition
35
Box 1: List of National Teams/Countriesparticipating in the Caribbean Schools Food andNutrition Quiz Competition, 2009
• Albena Lake Hodge Comprehensive School, Anguilla
• Clare Hall Secondary and Christ the King HighAntigua & Barbuda
• Queen’s College, Bahamas
• Christ Church Foundation School, Barbados
• Sacred Heart College, St Viator High School & Orange WalkTechnical High , Belize
• Bregado Flax Educational Centre & Elmore Stoutt HighSchool, British Virgin Islands
• Bishop’s College (Carriacou), Grenada
• St Catherine High School, Jamaica
• Vieux Fort Comprehensive, Leon Hess Comprehensive, StJoseph’s Convent and Castries Comprehensive, St. Lucia
• Barrouallie Secondary, Emmanuel High, Bequia CommunityHigh School, St. Joseph’s Convent (Kingstown), St. Vincent & the Grenadines
• Bishop’s High School (Tobago), Trinidad & Tobago
• HJ Robinson High School, Turks and Caicos Islands
Program in Guyana was the preparation offive instructional videos on topics related toyoung child nutrition which will be used inhealth training institutions.
Regional Nutrition Competitions 2009 Caribbean Schools’ Food& Nutrition Quiz Competition
The objectives of the quiz competitionwere:
1. to improve the image of food and nutri-tion within the region;
2. to promote good nutrition and healthylifestyles in schools and communities;and
3. to help students in their preparation forlocal and regional examinations in Foodand Nutrition.
Twelve countries participated in the prelim-inary rounds (up to Semi-finals) of the 2009competition which was conducted onOctober 21 – 22, 2009 through theUniversity of the West Indies (UWI) OpenCampus facilities which allowed directcontact with eleven of the twelve participat-ing countries. CFNI provided fundingsupport for the team from Turks andCaicos Islands to access the UWI OpenCampus system via the telephone.
A list of the 12 national teams, and theschools and countries they represented, isshown in Box 1. The preliminary rounds were conducted on aknock-out basis as follows: Round 1; Round 2and Semi-finals. An outline of the proceed-ings up to the Semi-Final round of the compe-
CFNI’s Kimberly Ashby-Mitchell (left) conducts thecoin toss for the start of the Caribbean Schools Foodand Nutrition Quiz Competition Finals in KingstonJamaica.
36
tition is given in Box 2.
The finals of the 2009 competition took the form of aface-to face contest which was staged on Monday,November 16, at the Mona Visitors Lodge andConference Centre, Kingston, Jamaica. The two final-ist teams from British Virgin Islands and St. Lucia,along with their coaches were awarded a free trip toJamaica to take part. Approximately 250 students andteachers from secondary schools in Jamaica were thereto witness the contest, which was videotaped for circula-tion to audiences around the region.
The team from the British Virgin Islands took thelead early, scoring 120 points to their opponents’ 80points in the first round. In the second round, St Luciascored 190 to the British Virgin Islands’ 250. Thelast round ended with the British Virgin Islandsscoring 75 points and St. Lucia scoring 90 points. Theteam from the British Virgin Islands emerged victo-rious in the 2009 Caribbean Schools Food and NutritionQuiz Competition, defeating St. Lucia 445 to 360.
The individual champion of the 2009 competitionwas Claudine Martinez from Orange Walk TechnicalHigh School, Belize.Evaluation questionnaires were sent to all focal/contact persons in participating countries seekingtheir views on the organization and conduct of the
Box 2: Summary of the proceedings ofthe 2009 Caribbean Schools’ Food &Nutrition Quiz Competition – up to theSemi-Final Round
ROUND 1: 12 Teams At the end of Round 1, the four lowest scoring teamswere eliminated. The eight teams going forward were:
Belize – 11 pointsBritish Virgin Islands – 11 pointsGrenada – 11 points St. Lucia – 11 pointsSt. Vincent – 10 pointsTurks & Caicos Islands – 10 pointsAntigua – 9 points Bahamas – 8 points
At the end of Round 1, four students participated intie breakers before Claudine Martinez from OrangeWalk Technical High School, Belize emerged victo-rious with the highest individual score to becomethe Individual Champion of the competition.
ROUND 2: 8 TeamsThe scores at the end of Round 2 were:
St. Lucia – 9 pointsAntigua – 8 pointsBelize – 8 pointsBritish Virgin Islands – 8 points Bahamas – 7 points Grenada – 7 points St. Vincent– 5 points Turks & Caicos Islands – 4 points
The teams from Bahamas, Grenada, St. Vincent andTurks and Caicos Islands were eliminated and thefour other teams moved on to the Semi-final.
SEMI-FINAL ROUND: 4 TeamsThe scores at the end of this round were:
British Virgin Islands - 6 pointsSt. Lucia - 6 pointsAntigua - 5 pointsBelize – 4 points
The team from Antigua emerged as the third placewinner. The teams from British Virgin Islands andSt. Lucia moved on to the final round.
The winning team from The British Virgin Islands along with theircoaches, Mrs. Heida Joyles-Selwood and Mrs. Camille Gumbs posewith the first prize trophy, book and medal prizes.

37
2009 competition. Seven persons completed thequestionnaire. The feedback received indicated thatrespondents were generally satisfied with the organi-zation and conduct of the competition and thoughtthat the standard attained should be maintained inthe future. They also made some useful suggestionsfor future improvement of the competition.
In addition to CFNI, the Dominica CoconutProducts and the Caribbean Association of HomeEconomists (CAHE) were the main sponsors of the2009 Caribbean Schools Food & Nutrition QuizCompetition.2009 Caribbean Nutrition Promotion
Individual champion, Claudine Martinez, of Orange Walk Technical,Belize collects her trophy from Ms. Cynthia Perriel-Clarke (CAHERepresentative)
Mrs. Julie Augustin-Charlery (centre) and her team from St. Luciaproudly accept the 2nd place trophy from Dr. Gillian Smith, AssistantRepresentative, FAO
Competition
The objectives of the competition are:• To provide visibility to exemplary projects or
activities aimed at improving food and nutrition.
• To promote the sharing of information on effortsto improve food and nutrition in the Caribbean.
A call for entries was issued in the first quarter of theyear. This was in the form of a promotionalbrochure in which the rules of the competition andguidelines for submission of entries were outlined.The brochure was disseminated throughout thecountries served by CFNI.
Eleven entries were received from 9 countries, repre-senting a range of governmental and non-govern-mental agencies and organizations. It is of note thatthree entries were received from Grenada. The titleof entries and the agencies making the submissionsare listed in Table 4.
The judges of the competition were: Professor JulieMeeks-Gardner, Nutritionist/Director, ChildDevelopment Centre, Ms. Clare Forrester, SocialCommunication Consultant and Mrs. BeverlyLawrence, Food Policy Analyst, CFNI. Entries werejudged on the following criteria: relevance of objec-tives; creativity; appropriateness of communicationstrategies and channels; and achievements/impact inrelation to stated objectives.
As in previous years, a variety of projects weresubmitted both in terms of the topics addressed andthe types of activities undertaken. A range ofcommunication approaches was utilized andactivities were implemented in different settings,targeting various population groups. The judgeswere impressed with the level of networking andpartnership building strongly evident in submittedentries. They also commented on the clearer defini-tions of objectives and target groups. But theyremained critical of the limited information providedon impact assessments. The judges’ comments on the
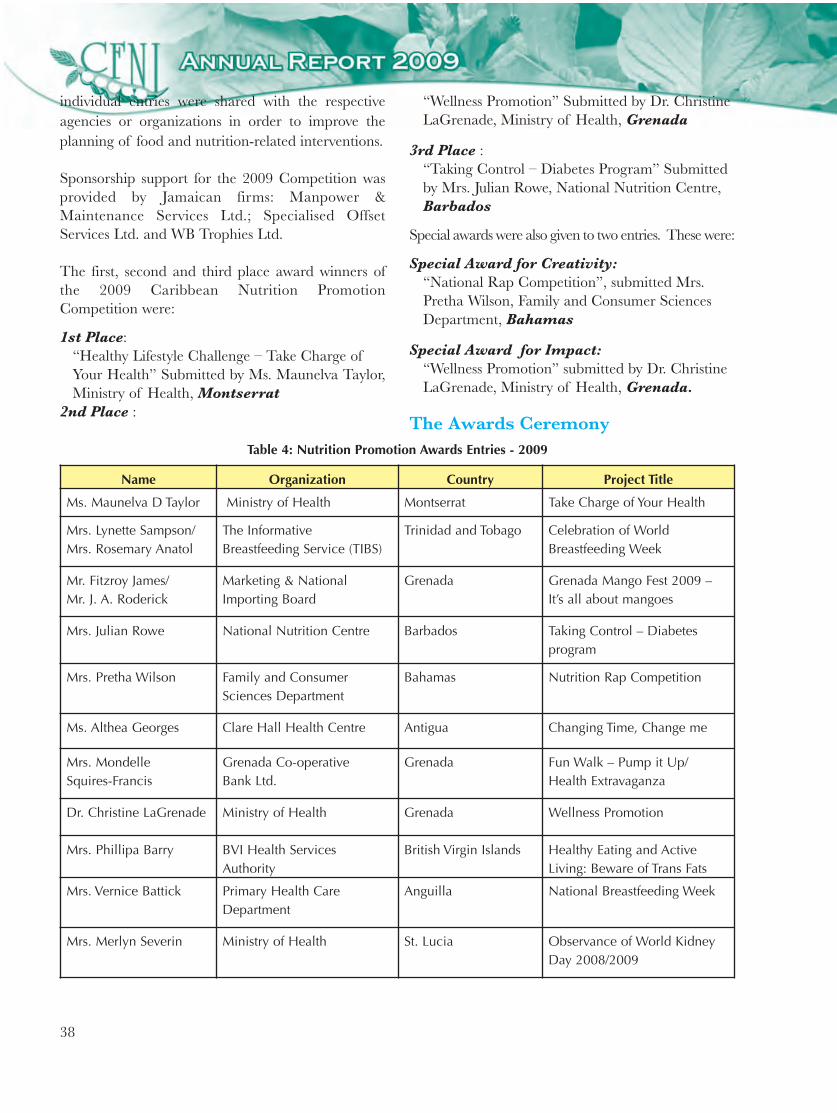
38
Name Organization Country Project Title
Ms. Maunelva D Taylor Ministry of Health Montserrat Take Charge of Your Health
Mrs. Lynette Sampson/Mrs. Rosemary Anatol
The InformativeBreastfeeding Service (TIBS)
Trinidad and Tobago Celebration of WorldBreastfeeding Week
Mr. Fitzroy James/ Mr. J. A. Roderick
Marketing & NationalImporting Board
Grenada Grenada Mango Fest 2009 –It’s all about mangoes
Mrs. Julian Rowe National Nutrition Centre Barbados Taking Control – Diabetesprogram
Mrs. Pretha Wilson Family and ConsumerSciences Department
Bahamas Nutrition Rap Competition
Ms. Althea Georges Clare Hall Health Centre Antigua Changing Time, Change me
Mrs. Mondelle Squires-Francis
Grenada Co-operative Bank Ltd.
Grenada Fun Walk – Pump it Up/Health Extravaganza
Dr. Christine LaGrenade Ministry of Health Grenada Wellness Promotion
Mrs. Phillipa Barry BVI Health ServicesAuthority
British Virgin Islands Healthy Eating and ActiveLiving: Beware of Trans Fats
Mrs. Vernice Battick Primary Health CareDepartment
Anguilla National Breastfeeding Week
Mrs. Merlyn Severin Ministry of Health St. Lucia Observance of World KidneyDay 2008/2009
Table 4: Nutrition Promotion Awards Entries - 2009
individual entries were shared with the respectiveagencies or organizations in order to improve theplanning of food and nutrition-related interventions.
Sponsorship support for the 2009 Competition wasprovided by Jamaican firms: Manpower &Maintenance Services Ltd.; Specialised OffsetServices Ltd. and WB Trophies Ltd.
The first, second and third place award winners ofthe 2009 Caribbean Nutrition PromotionCompetition were:
1st Place:“Healthy Lifestyle Challenge – Take Charge ofYour Health” Submitted by Ms. Maunelva Taylor,Ministry of Health, Montserrat
2nd Place :
“Wellness Promotion” Submitted by Dr. Christine LaGrenade, Ministry of Health, Grenada
3rd Place :“Taking Control – Diabetes Program” Submitted by Mrs. Julian Rowe, National Nutrition Centre, Barbados
Special awards were also given to two entries. These were:
Special Award for Creativity:“National Rap Competition”, submitted Mrs. Pretha Wilson, Family and Consumer Sciences Department, Bahamas
Special Award for Impact:“Wellness Promotion” submitted by Dr. Christine LaGrenade, Ministry of Health, Grenada.
The Awards Ceremony

39
The awards dinner provided the forum for highlight-ing the accomplishments of the winners of the tworegional nutrition competitions. The function washeld on Wednesday, November 18, 2009 at the TerraNova Hotel, Kingston, Jamaica, and was attendedby a multi-sectoral gathering including food andnutrition planners and practitioners, education andhealth personnel, teachers and schoolchildren.
In his opening remarks as chairperson of theevening’s proceedings, Dr Fitzroy Henry, Director,CFNI, welcomed the guests and offered congratula-tions to the winners in both competitions. He thankedthe sponsors who had faithfully supported the activi-ties over the years and reminded the audience aboutthe objectives of the regional competitions and theircontinuing relevance to efforts towards improvingfood and nutrition in the region. The Director alsopraised the contributions of the teachers and otherresource persons in all participating countries whoorganize the national quiz competitions in prepara-tion for participation at the regional level.
Representatives from CFNI’s three main partneragencies in the UN system, the United NationsChildren’s Fund (UNICEF), the Food andAgriculture Organization (FAO) and the PanAmerican Health Organization (PAHO) also broughtgreetings on behalf of their respective organizations.
Over and above the prize trip to Jamaica, the final-
ist teams and the individual champion of theCaribbean Schools’ Food and Nutrition QuizCompetition received trophies, cash awards, medalsand book prizes, as well as a tour to places of interestin Jamaica. The third place winners were alsoawarded a trophy, cash prize and books. Coaches ofthe individual champion and the first, second andthird place winners received cash awards, while bookprizes were given to the twelve teams that partici-pated in the regional competition. Copies of theDVD of the final round of the competition will alsobe distributed to all countries.
The winner of the top award in theNutrition Promotion Competition wasawarded a prize trip, to attend the speciallyconvened awards ceremony in Jamaica.The sponsored prize also included hotelaccommodation, a trophy, cash prize and atour to places of interest in Jamaica.Awards to the other winners includedtrophies, plaques and cash prizes.
Nyam News and Cajanus
Ms. Maunelva Taylor of the Ministry of Health,Montserratreceiving her prize from Dr. Fitzroy Henry, Director, CFNI for thewinning entry in the 2009 Nutrition Promotion Competition.
Students in performance at the Awards Ceremony

40
Nyam News Issues Disseminated toMember Countries in 2009
The themes addressed were:
1. Physical Activity
Recognizing that diet and physical activity are thetwin pillars of a healthy lifestyle. Seven issues ofNyam News were dedicated to this topic on phys-ical activity during the publication period.
The first Nyam News article in the series sought todefine physical activity, present the benefits ofengaging in physical activity and present somerecommendations. Physical activity refers to anybodily movement produced by the skeletal musclethat increases energy expenditure above the basallevel. It includes such activities as walking, aerobicsand weight lifting. While the term physical activity isoften used interchangeably with exercise, there is adifference between the two. Exercise is a sub-cate-gory of physical activity that is planned, structured,repetitive and purpose driven.
• The health benefits of physical activityinclude:
• Building of lean muscle and reducing fat
• Improving overall energy level
• Improving strength and endurance
• Strengthening of bones and joints
• Reducing anxiety and stress
• Increasing self esteem
• Preventing disease.
It is recommended that everyone should start bydoing moderate physical activity for at least 30minutes, most or all days of the week. Sedentarypersons may start slowly with short periods of activ-ity and gradually increase the level and durationover time. While engaging in physical activity, it isimportant to keep its three components in mind –frequency, intensity and time (FIT).
As a follow up to the first issue on Understanding
Physical Activity the second issue continued theseries by showing how physical activity can bepromoted.
Physical activity should be promoted at the indi-vidual, community and national level and in bothformal and informal settings e.g. at school andcommunity meetings. The general public can bereached via the mass media or by the use ofposters, flyers and brochures. While fitness clubsand gyms have gained popularity in the past fewyears, trained instructors who can give properguidance is essential to ensure that injuries areavoided, especially by those who are new to theworld of structured exercise.
When planning a physical activity promotioncampaign we must consider the psychological barri-ers that must be addressed – perception of bodyimage, lack of confidence, absence of immediaterewards. Physical activity should be promoted to theextent that persons with negative perceptions canfeel comfortable with it and are encouraged toinclude it in their daily lives. In the promotion ofany exercise program, everyone should be encour-aged to set goals that are achievable.
Subsequent issues of Nyam News looked at the rela-tionship between physical activity and chronicdisease:
(a) Obesity – Obesity has become a majorpublic health concern in the Caribbean and isknown to decrease life expectancy in bothchildren and adults. It affects more than aquarter of the adult population, particularlyour women.
Lack of physical activity is a clear and signifi-cant contributing factor to obesity. Normalregulation of body weight occurs when energyinput is equal to energy output. The control ofobesity is a lifelong undertaking and to make themost effective use of physical activity in the fightagainst this condition must become a way oflife. Physical activity affects body compositionand weight in that it promotes the loss of fatwhile preserving lean body mass.

41
(b) Cancer – Cancer is one of the leadingcauses of death in the Caribbean. Some ofthe more well-known are breast cancer,prostate cancer, cancers of the colon, cervix,stomach, rectum and lung cancer.
There is a body of evidence which suggeststhat physically active women have up to 40%reduced risk of developing cancer. There isalso a positive association between breastcancer and obesity. Physical activity and exer-cise are therefore important keys in reducingbreast cancer through the role they play infighting obesity.
Individuals who are physically active can alsoreduce their risk of developing colon cancerby 40-50%, with the greatest reduction in riskamong those who are most active.Additionally some studies have found thatphysically active persons may have a 30-40%reduced risk of developing lung cancer.Results of the relationship between physicalactivity and prostate cancer are inconsistent.While several studies indicate it is probable thatphysical activity decreases the risk of developingprostate cancer by 10-30%, others have foundno evidence to support this finding.
While we may not know exactly what physio-logical mechanisms can reduce the cancer riskin our bodies, it seems clear that increasing ourlevel of physical activity is a wise strategy.
(c) Diabetes – The incidence of diabetescontinues to increase in the Caribbean.Studies have shown that exercise and ahealthy diet can prevent the development ofType II diabetes in people with ImpairedGlucose Tolerance (IGT) and in persons with“pre-diabetes”.
Physical activity may prevent the onset ofType II diabetes because it improves generalfitness and cardiovascular endurance, lowersblood pressure and lipids; and because ithelps reduce total body fat, specifically intra-abdominal fat distribution – a known riskfactor for insulin resistance.
Studies in several developed countries suggestthat moderate reduction in weight and walk-ing each day for half an hour reduces theincidence of diabetes by more than half inoverweight individuals. Thus, regular physi-cal activity is a primary preventive measurefor individuals who may be susceptible to thecondition.
Persons with Type I diabetes must, however,exert caution when engaging in physicalactivity. The most common problem theymay encounter during exercise is hypogly-caemia (low blood sugar level), which canoccur during, immediately after, or manyhours after physical activity. However,depending on the nature of the activity andits timing relative to the individual’s meal andinsulin schedule, hypoglycaemia can beprevented.
Some information that persons with diabetesshould bear in mind with regard to diabetesand physical activity include:
• Ensure blood glucose monitoring equip-ment is available at all physical activitysites
• Check blood glucose levels as required
• Be prepared to treat hypoglycaemia
• Drink extra water as hydration is important.
(d) Cardiovascular Disease – the majorcardiovascular diseases include coronaryheart disease, cerebrovascular disease, hyper-tension, heart failure and rheumatic heartdisease.
Regular physical activity prevents or delaysthe development of high blood pressureand reduces blood pressure in people withhypertension. Physical activity can also lowerblood cholesterol levels which will eventuallydecrease the risk of developing cardiovascu-lar disease.

42
Physical inactivity is a major risk factor forheart disease and stroke and is linked tocardiovascular mortality. Studies have shownthat people who modify their behaviour andstart regular physical activity after heartattack have better rates of survival. Thus,individuals who already have heart diseaseare recommended to engage in regular phys-ical activity (exercise).
The risk of developing heart disease e.g.angina or heart attack is remarkably reducedin people who are physically active whencompared to sedentary individuals.
A physically active lifestyle reduces the risk ofsudden cardiac deaths, even among personswith advanced coronary arteriosclerosis.
In the final issue of Nyam News in the physi-cal activity series, the main evidence for thevarious health indicators was collated and theinfluence of physical activity on improvinghealth and well-being and therefore quality oflife emphasized.
2. The Impact of Select Vitamins, Mineralsand Foods on Health
Several articles were dedicated to address theimpact of certain key vitamins, minerals andfoods on health.
(a) Vitamin E and Your Health – Vitamin Ebelongs to the group of fat-soluble vitamins,i.e. it dissolves and remains in the fatty tissuesof the body. Vitamin E, is in fact, a term for amixture of eight compounds which can beclassified into two sub-groups – tocopherolsand tocotrienols. The most common andmost active of these in the body is alpha-toco-pherol. Vitamin E is primarily derived fromplant sources.
Vitamin E functions as an antioxidant and helpsprevent oxidative stress by working togetherwith other food substances such as vitamin C,glutathione, selenium and vitamin B3 in anattempt to regulate overactive molecules.
Studies have shown that vitamin E:
• Protects the skin from UV light whenapplied externally (to the skin);
• Appears to prevent the formation ofblood clots and so prevents heart attacks;
• Protects and ensures permeability of thecapillary system, protects vitamin A andessential fatty acids from oxidation in thecells and prevents breakdown of bodytissues.
• Stimulates the body’s immune response.
However, supplementation with too muchvitamin E on the other hand may interferewith the action of vitamin K and high dosestaken daily over a long period has been foundto increase the risk of death.
(b) Chromium and Your Health –Chromium is one of the most commonelements that exist in the environment.Naturally occurring dietary chromium isfound in a variety of foods e.g. meats, driedbeans and spices. It is an essential nutrientwith very low toxicity.
There is no recommended dietary allowancefor chromium. However, adequate intakeshave been established. Chromium’s primaryfunction is in carbohydrate and lipid (fat)metabolism. It is thought that it is the activecomponent of the Glucose Tolerance Factor(GTF). Chromium’s role appears to be inimproving insulin sensitivity thus aiding inpreventing insulin resistance. Chromium mayalso play a role in fat and cholesterol metabo-lism by lowering LDL levels while increasingconcentrations of apolipoprotein A, a compo-nent of high density lipoprotein cholesterol(HDL).
Supplementation with chromium has beenfound to reverse insulin resistance and signs ofdiabetes in persons being intravenously fed.However, supplements should be taken withcaution as chromium interacts with some

43
medications, especially if they are taken on aregular basis. Possible toxicity can also resultif consumed in excessive amounts.
(c) Cranberries and Your Health –Cranberries are scarlet red, tart berries thatgrow widely in Europe, Asia and the UnitedStates. In the Caribbean however we rarelyencounter the fresh fruit and our interactionwith cranberries is usually limited to the juice,drink or the dried fruit.
Cranberries are low in saturated fat andsodium and are a good source of vitamin C.
Some of the strongest scientific evidencerelated to the health benefits of cranberries islinked to its ability to reduce the risk ofurinary tract infections. They reduce the riskof bladder infections by acidifying the urineand preventing bacteria from sticking to thewalls of the bladder.
While cranberries do provide some otherbenefits, they also contain measureableamounts of oxalates which when concen-trated in body fluids can crystallize and causehealth problems e.g., oxalate kidney stonesand impaired calcium absorption.
(d) Sugar and Your Health – Sugar refers to aclass of carbohydrates made up of one or twomolecule structures or units.Monosaccharides e.g. glucose, fructose andgalactose are the simplest sugars and the finalbreakdown products of carbohydrate diges-tion in humans. Among the disaccharides,sucrose is the most common but other exam-ples include lactose and maltose.
There are both physiological and commercialuses of sugars. Glucose is the body’s mainsource of energy. Commercially, sugar isused in foods to enhance flavor and appeal.
Many sugary foods and drinks are often low inother nutrients and provide little satiation.Excessive consumption of these energy densefoods encourages further eating to satisfy
perceived needs and actual functional require-ments. This increases the likelihood of indis-criminate eating leading to weight gain andobesity.
A few tips for reducing sugar intake include:
• Reading food labels and choosing lesssweet alternatives.
• Reducing the amount of sugar added tobeverages.
• Using more fruits and less sugar in cakes.
• Choosing sweet snacks less often.
(e) Coffee and Your Health – The coffeebeverage is made from coffee berries that arepicked when ripe then processed and dried.The coffee beans are roasted and used tomake the coffee in beverages and other foods.Coffee impacts on health in a variety of ways:
It contains a highly active anti-cancercompound which is believed to boost theactivity of the enzymes thought to preventcolon cancer.
Although the evidence is weak, coffee hasbeen reported to reduce the risk ofAlzheimer’s disease, gall bladder and gall-stone disease, Parkinson’s disease and Type IIdiabetes.
It is thought that the caffeine in coffee blocksa receptor in the liver giving it a protectiveproperty against liver disease.
Caffeine acts as a diuretic and as a laxative.This has led to its use in enemas for coloncleansing.
Caffeine is a stimulant and is widely used as ameans of staying awake. It also affects thecentral nervous system. Studies show thatsignificant amounts of caffeine can lead toconstipation, high cholesterol levels, anxiety andsleep changes. It can also cause irritability insome individuals with excessive consumptionand even withdrawal symptoms.

44
Overall, coffee consumption should be nomore than two cups per day to minimize thepossible adverse effects of the caffeine.
(f) Herbs, Food and Health – A two part seriesabout the food and medicinal uses herbs.
In the first issue we examined how herbs areused in foods and medicine, their nutrientcontent and some tips to ensuring that theyare used safely.
Colloquially herb is a broad term referring tovarious parts of plants that are useful tohumans. But, strictly speaking, herbs are theleaves of certain plants that grow in temper-ate climates used for flavouring while spicesare the buds, fruits, flowers, bark, seeds androots of plants, many of which grow in tropi-cal climates.
Herbs are generally added during foodpreparation to improve the taste of cookeddishes making them more palatable. Herbsmay be used fresh or dried, whole or ground.
Most herbs contribute very little, if any calo-ries, or nutrients. However, there are a fewherbs that may contribute a significantamount of vitamins and minerals e.g. thymeis an excellent source of iron, manganese andvitamin K, chives are rich in vitamins A andC and dill seed is a good source of calcium.
At present there is renewed interest in the useof herbal remedies. While herbal remediesmay relieve the symptoms of some disordersand conditions, they have not been shownscientifically to cure them. Tips for whenusing herbs as food or medicine includetelling your doctor the herbal products orover the counter drugs you are using to avoiddrug interactions and not using herbal medi-cines as a replacement for medicationprescribed by your healthcare provider totreat serious medical problems such as cancer,diabetes or heart disease.
The second Nyam News issue on herbs detailedthe traditional use of specific herbs as medicinesto help the public better understand theirpurported biological or medicinal benefits.
(g) Green Tea and Your Health – Green teaoriginated in China and is prepared from theleaves, leaf buds and internodes of the teaplant Camellia senensis.
Green tea contains nutrients such as vitaminC and alkaloids including caffeine which giveit a stimulant effect.
Green tea has been reported to:
• Protect against a range of cancers e.g.cancers of the lung, prostate and breast, byinactivating oxidants before cell damageoccurs, reducing the size of tumors andinhibiting the growth of cancer cells with-out harming healthy tissue.
• Play a role in weight loss by increasingmetabolic rates and speeding up fatoxidation.
• Control blood sugar levels in diabeticpersons. Studies also suggest that theremay be a link between tea drinking andreduced risk of Type II diabetes.
• Help to inhibit the growth of bacteriathat cause bad breath and tooth decay.
• The possible negative effects about greentea center around its high fluoridecontent which could cause neurologicaldamage, renal damage, osteoporosis,arthritis and other bone disorders.
3. Highlights of Specific Foods
Three Nyam News issues were devoted to specificfood items. These food items were:
(a) Cheese – Cheese is a commonly consumedfood in the Caribbean that is made from thecurdled milk of cows, goats, sheep or othermammals.
45
There are three basic steps that are commonto all cheese making. First, proteins in milkare transformed into solid lumps called curds.Second, the curds are separated from themilky liquid, called the whey, and shaped orpressed into molds. Finally, the shaped curdsare ripened using a variety of aging andcuring techniques.
Cheese can be classified based on moisturecontent, ripening methods or whether theyare natural or processed.
Cheese is a concentrated source of protein,vitamins and minerals, as well as fat andcholesterol. The fat and cholesterol content,however, varies depending on the milk used.Cheese is a calcium-rich food, providing 20-25% of the daily amount needed to build andmaintain bone mass. Its inclusion in the dietis also said to reduce the risk of osteoporosis,help regulate blood pressure, reduce the riskof colon cancer development and reducesymptoms of premenstrual syndrome.
(b) Chocolate – The bitter seeds/beans of the cocoa are used to make chocolate. The cocoabean is 31% fat of which 60% is saturated.Two-thirds of the fat is in the form of stearicacid and the remainder is in the form of oleicacid. The protein from the cocoa plant is richin the essential amino acids tryptophan andphenylalnine as well as tyrosine. There aremany different types of chocolate: unsweet-ened chocolate/bitter chocolate, bittersweet/semi-sweet chocolate, sweet chocolate (dark),milk chocolate and white chocolate.
The underlying reasons for chocolate crav-ings are not clearly understood but arebelieved to center around:
• Its taste, smell and texture which arerelated to its high fat and sugar content.
• Its link to pleasurable physiological andpsychological sensations.
• Its role in balancing low levels of neuro-transmitters that work in the regulation
of mood, food intake or compulsivebehaviours.
• Its association with monthly hormonalcycles and mood swings in women.
So far, studies involving chocolate havesuggested that its health benefits are derivedfrom its flavanoid content. Flavanoids arereported to have potential beneficial effectson human health including anti-viral, anti-allergy, anti-inflammatory and anti-oxidanteffects. Usually, however, chocolate is impli-cated in many conditions e.g. acne, dentalcaries, and migraines. Evidence for theseremains inconclusive. However, it should benoted that chocolate does have a role to playin a healthful diet as it can offer some healthbenefits, but it is high in calories due to itshigh fat content and should be consumed inmoderation and also chosen wisely.
(c) High Fructose Corn Syrup – High fruc-tose corn syrup (HFCS) is a sweetener madefrom corn and is found in numerous foodsand beverages. The “high fructose” in thename of the product refers to a higher fructosecontent than corn syrup, which contains onlyglucose. It is produced by converting cornstarchto a syrup with high dextrose (glucose) content.Conversion of much of this glucose to fructoseresults in a syrup with a structure similar tosucrose (table sugar), and which is called highfructose corn syrup.
It is estimated that food companies purchaseHFCS at prices up to 70% less than sugar. Inaddition to its cheap cost, HFCS is purportedto enhance the natural flavours of manybeverages, fruit fillings and dairy products,while maintaining their freshness and flavour.
Since the emergence of HFCS as a sweetenerin many foods, consumption of the producthas drastically increased. At around the sametime as this increase, the prevalence ofobesity has doubled – Is HDCS to blame? Itis safer to say that the increase in HFCSconsumption has contributed to the obesity

46
epidemic, just like any other refined sugarconsumed in large amounts. HFCS gives thesame effect as sucrose (normal table sugar) inthe sense that if you eat too much of it youwill accumulate too much calories in anunbalanced way. Moderation is the key and itis recommended that we consume sugars andsweets sparingly. Consumers should thereforebe watchful, read food labels for sugar in anyform and choose a balanced diet with foodsfrom the six Caribbean food groups.
4. Eating to Live or Living to Eat
Our desire to eat is not just governed by hungerbut also by the body’s control system, environ-mental influences, emotional factors, social influ-ences, health status, medication and sensoryaspects.
Hunger and appetite both encourage eating.Hunger is an inborn stimulus – the physiologicalneed to eat. Appetite, on the other hand, is alearned response which is usually associated withsensory aspects of food. The feeling of fullnessafter we have eaten usually lasts for a while. Thisfeeling of fullness is what is called satiety. Hunger,appetite and satiety are the three main factors thatdetermine whether we eat to live or live to eat. Weneed to let hunger have greater influence on oureating behaviours and stop eating when we are full.
(Our bodies were made with sensitive systemsthat prompt us when to eat and when to stopeating.) After we have identified the situationsthat cause us to eat, we can modify our responsesto those situations so that we eat in response tohunger and not other external factors.
5. Healthy Eating Amidst Rising Food Prices
There is no doubt that households in the Caribbeanare currently experiencing challenges in the area ofdollar management in light of the impact of globaloccurrences that are affecting food prices.
To ensure good nutrition, food selection shouldbe based on using a variety of foods in the sixCaribbean food groups. One way of helping to
balance food expenditure and still pay attentionto your health is to return to home gardening. Inthis way, savings from not purchasing whateveryou grow can be used to help purchase what youneed.
To avoid wastage, consumers should always bearin mind the quantity as well as the value of fooditems needed so that each family member will getsuitable amounts according to their needs. Somehelpful tips are:
• Plan before you purchase.
• Prepare a shopping list and stick to it.
• Use food labels to compare brands, weight,price and nutrient content of foods beforemaking the decision to purchase.
• Use peas and beans more often and reducethe amount of meat.
• Purchase less convenience foods and eat outless often.
6. Gluten Intolerance
Gluten is a protein commonly found in grainssuch as wheat, barley and rye. Gluten is a dairy-free, sodium-free, cholesterol-free, fat-free proteinalternative that may be used by vegetarians.
When dough made with wheat flour is kneaded,the gluten formed contributes to the viscosity andability of the mixture to extend, stretch, or rise,once a leavening agent is present. The moredeveloped the gluten, the chewier the productsuch as pizza and bagels, while less developedgluten gives tender baked goods e.g. cookies.
Gluten intolerance is a broad term that describesa disorder in which some persons may suffer fromabdominal pain, bloating or diarrhea when theyeat certain specific foods. The immune systemdetects gluten as a threat and puts its defensivemechanism into action by producing antibodiesto get rid of the foreign element. The antibodiesthat are produced attack the lining of the smallintestines.

47
Once someone has gluten intolerance it is virtuallyincurable but it can be controlled. The treatment isto completely remove gluten form the diet. Fooditems that do not contain gluten include groundprovisions, rice, corn, tapioca and peas, beans andnuts.
7. Calcium: Beyond Bones
Calcium is an essential nutrient and the mostabundant mineral in the body. It is found in awide variety of foods e.g. milk, cheese, cannedfish, beans and nuts. During the period of skele-tal growth and maturation calcium accumulatesin the skeleton resulting in increased bone mass.
Calcium serves several beneficial roles in thebody:
• It is essential for muscle contraction.
• Calcium in nerve cells stimulates the releaseof neurotransmitters which carry impulses totarget tissues.
• Calcium, vitamin K and a protein calledfibrinogen help blood platelets to form clots.
• Calcium is needed for the action of enzymeswhich regulate chemical reactions essential forlife.
• Findings from some clinical studies suggestthat a diet rich in calcium and low in energymay play a role in the prevention and treat-ment of obesity as it leads to a greater reduc-tion in body fat, specifically abdominal fat.
• Research also indicates that high dietarycalcium intakes may help to prevent coloncancer as well as the recurrence of pre-cancerous colon polyps which may lead tocolon cancer.
• There is evidence that calcium may have arole in the regulation of blood pressure andthat supplemental calcium decreases theseverity of pre-menstrual symptoms (PMS).
8. Fortified Water
Fortification is the addition of one or more essen-tial nutrients to a food, whether or not it isnormally contained in the food, for the purpose ofpreventing or correcting a demonstrated deficiencyof one or more nutrients. Fortified water, alsoknown as enhanced or functional water, has beenmodified to incorporate not only nutrients butalso other dietary factors such as fruit andvegetable extracts, electrolytes, herbal supple-ments, caffeine and antioxidants.
Some of the benefits of fortified water are that itencourages persons to be hydrated and is able toreplace electrolytes lost after 60 minutes or moreof high intensity physical activity. Noteworthy toois the fact that at the 1992 InternationalConference on Nutrition (ICN), among thestrategies recommended to alleviate micronutri-ent deficiencies was the fortification of water withnecessary micronutrients when feasible, if exist-ing food supplies fail to provide adequateamounts in the diet. Consumers, though, must beaware that many of these waters are sweetenedusing sugar and can contribute to health prob-lems such as high blood sugar levels.
Overall, the decision to regularly consume forti-fied water is a personal choice and one thatshould be made only after knowing all the accu-rate facts.

48
CAJANUS Issues Disseminated toMember Countries in 2009
1. New Child Growth Standard
The article “The New WHO Child GrowthStandard” explains why these standards wereneeded, reviews the methodology and results ofthe Multicentre Growth Reference Study(MGRS) from which the standards were devel-oped and outlines the status of implementation inthe Americas. The following article “The WHOMulticentre Growth Reference Study: Planning,Study Design and Methodology” provided insightsinto the complexity of the MGRS and the chal-lenges faced in conducting the project of this nature.This article provided an overview of the differentphases of the project from its inception in 1990 to itsexpected completion in 2010.
Guidelines for the implementation of the newgrowth standards at country level are outlined ina report of the Technical Advisory Group (TAG)convened by CFNI and the Office of theCaribbean Program Co-ordination (OCPC/PAHO) in November 2005. The recommenda-tions focused on replacement of the existingGrowth Charts as well as increased attention toimproving the quality of child health services.
A brief review of the progress in implementations ofsome of the key recommendations of the GlobalStrategy for Infant and Young Child Feedingendorsed by the World Health Assembly in 2002 isalso included in this issue. This review emphasizesthe need for renewed commitment to increasedaction for improving child feeding practices.
In this context, a short extract by the WHO on“The Optimal Duration of ExclusiveBreastfeeding: A systematic Review (Abstract)”was the final article in this issue of the Cajanus.
The news briefs in this issue covered a range oftopics including foods marketed to children, fibreand magnesium intakes and the development ofType II diabetes, the impact of exercise on bodyfat in boys and girls, and dispelling the myth thatbreastfeeding creates sagging breasts.
2. Gender, Obesity and HIV/AIDS
The articles in this issue are derived from a studyof the existence and effects of a number of socialdeterminants on the chronic disease andHIV/AIDS risks of men and women in ninevaried Jamaican communities. Quantitative andqualitative assessments of responses in interviewsamong 367 men and women focused on theimportance of gender in relationships dynamicsat household and community levels and theresulting effects on food intake, sexual relationsand health risks.
The opening article covered the concept relatedto gender, sex and inequity in health.Elaborations on the social determinants of healthincluding wealth and income and work werefeatured as well as gender as a social determinantof health, which was discussed extensively. Thiswas followed by an article on the methodologyused in the study emphasizing that a comparativeapproach (male vs. females) was taken to under-score the strength of gender as the predominantdriving factor within the study population.
The findings of the study were presented in threearticles. The first “Findings 1: Male and FemalePatterns of Sexual Relationships” focused on theimpact of socially constructed roles on male/female patterns of sexual relationships, sexualactivity, relationship status and partnering andpartner influences and sexual efficacies: male vs.female dominance.
The second article, “Findings II: Exposure andVulnerability Especially of Women toHIV/AIDS and Chronic Diseases” covered theeffects of media and entertainment, foodpurchase storage and safety, physical activity andtelevised immobility. “Findings III : MaleDifferences in Health Status, Perceptions andHealth-Seeking Behaviours” discussed health-seeking behaviours, concepts of health and healthbehaviours, satisfaction with life, health status,obesity, nutritional status, perceptions and
49
satisfaction, the chronic diseases and sexual activ-ity: a significant area of health risk.
The final article of this issue presented the conclu-sions and recommendations from this study includ-ing a call to refocus attention on gender normsspecifically those that marginalize females.
3. Public Policies in Agriculture for Healthand Nutrition
This issue of Cajanus presented the keynotepresentations of The Symposium on Food andAgriculture Policies and Obesity organized byCFNI, in collaboration with the Food andAgriculture Organization (FAO). This sympo-sium gathered several agriculture ministers,senior agriculture and food specialists in theregion to identify clear guidelines on how agricul-ture/food policies can impact on obesity andNCDs through the availability of healthy foods,the behaviour of consumers to make healthy foodchoices and how these in turn can stimulategrowth in the food and agriculture sectors.
The presentations were as follows:
• How do Agriculture Policies Impact on Obesity andNon-Communicable Diseases: Experience from OtherCountries ~ Prakash Shetty (a visiting professorof public health nutrition at the Institute ofHuman Nutrition, University of SouthHampton, United Kingdom, and editor-in-chief of the European Journal of ClinicalNutrition). Highlights included the drivers oflifestyle related diseases, the challenge ofurbanization and globalization to foodsystems, food and agriculture policies thatincrease the risk of obesity and NCDs andfood and agriculture policies that promotebetter health outcomes.
• The Importance of Caribbean Agriculture FoodPolicies in Obesity Control ~ Fitzroy Henry(Director, CFNI). Highlights includedrethinking the agriculture/ food policydiscussions on incentives that subsidize theproduction of local nutritious foods andpolicy recommendations.
• Refocusing Agri-Tourism on Healthy Lifestyles ~Carolyn Hayle (Lecturer, UWI, Mona,Jamaica on sustainable tourism and market-ing). Highlights included imperatives to refo-cus agri-tourism, changes and the Caribbeanregion, the wellness industry and understand-ing the global tourism system.
• Food Trade, Food Security and Health in theCaribbean ~ Deep Ford (Senior Economist andLeader of the Trade and DevelopmentGroup in Commodities and Trade Division,FAO, Rome). Highlights included food secu-rity and trade linkages in the Caribbean, agri-culture trade policy and food security,national and global policies changes and foodsecurity in the Caribbean and improved tradepolicy for the Caribbean.
• Opportunities to Modify Agricultural Trade Policy inCARICOM to Counter the Rise in Obesity andChronic Non-Communicable Disease ~ VincentAtkins (Senior Research Professional in theAgricultural Trade Negotiating Program ofthe Caribbean Regional NegotiatingMachinery). Highlights included implicationsof the market access commitments for health,health implication of domestic supportreduction commitments for Caribbean coun-tries, health implications of the commitmentson export subsidies for Caribbean countriesand recommendations for policy actions.
4. Food Based Dietary Guidelines
This issue of the Cajanus highlights the efforts ofseveral Caribbean countries that have developedguidelines that will encourage the selection,preparation and consumption of healthy foods.These Food Based Dietary Guidelines (FBDGs)focus on risk reduction and health promotion andare expected to not only guide the general publicbut also the development of food policy andnutrition education programs.
Articles in this issue discussed the rationale for theFBDGs as well as provided a background for theirdevelopment in the Caribbean. An explanation of
50
the guidelines and the process of developing theFBDGs are also explored in subsequent articles.
The reader is shown pictorial renderings of selectFBDGs in Caribbean countries as well as exam-ples of the promotional materials developed forthe FBDGs by some countries. A table is used tohighlight the common messages between coun-tries; this complements the article highlightingthe key recommendations of the FBDGs forCaribbean Countries.
The article preparation and use of Food basedDietary Guidelines discussed the underlyingassumption for FBDG, key principles for theirdevelopment including the nutrition conceptsand also the implementation, preparation and theuse of FBDGs.
News briefs continued the theme of FBDGs byhighlighting stories from St Vincent and theGrenadines and Guyana. Other topics coveredincluded “Obesity Linked to Fat not Calories”and “Stress Promotes Abdominal Fat”.

Part II
CFNI Development
Miss Sharon Locke, PAHO Long Service Awardee, listensattentively as Mr. Marlon Martin reads her citation at thePAHO/CFNI Awards Luncheon, Kingston , Jamaica
Mrs. Janice Welch, PAHO Long Service Awardee (2nd left) poses with Dr. CarolBoyd-Scobie (3rd left), PAHO/WHO Representative, Trinidad and Tobago, andother staff of the Trinidad and Tobago Representation.
Miss Paula Trotter accepts her PAHO Long Service Award fromDr. Leahcim Semaj, guest speaker at the PAHO/CFNI AwardsLuncheon, Kingston , Jamaica


53
StaffThe staff complement for the Institute stationed inJamaica and Trinidad and Tobago comprised thefollowing for 2009:
Technical Staff: 11Administrative Staff: 18Total: 29
Please see Organization Chart – Annex 1.Three PAHO consultants were recruited in 2009 toassist with the technical cooperation program of theInstitute. These were Dr. Candace Simpson-Smithlocated at the Trinidad Centre and Misses KimberlyAshby-Mitchell and Renelle Aarons located inJamaica.
The Institute contracted several persons to assist withthe technical program. The areas of assistanceincluded the CFNI/IDB project, World DiabetesFoundation project, Trinidad and Tobago SchoolMeals Project, food security and health promotion.
SecurityCFNI, as a UN office, is expected to comply with theUN’s Minimum Operating Security Standards(MOSS) developed for Jamaica. In order to meetsome of these requirements, the following documentswere produced in 2009:
• Business Continuity Plan
• CFNI Office Safety and Security Manual
• CFNI Emergency Evacuation Plan.
Business Continuity Plan
In 2009, CFNI developed a Business Continuity Plan(BCP) with the capacity to maintain continuity ofhighly critical operations during, and subsequent to, adisaster and/or critical incident.
The Business Continuity Plan for CFNI included,among other things, information on:
• Processes during normal operation
• Processes and critical operational services
• Impact analysis matrix on critical processes
• Prioritization matrix on critical processes
• Mitigation strategies definition on criticalprocesses weaknesses/implementation
• Critical Processes Management and LogisticalSupport Team.
A Crisis Management Team was formed whichundertook the responsibility of steering the develop-mental process of the BCP.
Emergency Evacuation Plan
During the year in review, the Emergency EvacuationPlan (EEP) was finalized. It applies to all emergen-cies where employees may need to evacuate thebuilding for personal safety and thus minimizethreats to life and property. This EEP communi-cates the policies and procedures for employees tofollow in an emergency situation. This Plan hasbeen circulated to all employees.
Under this Plan, employees have been informed of:
• Preferred means of reporting fires and otheremergencies
• Emergency escape procedures
• Procedures to account for all employees afteremergency evacuation has been completed
• The alarm system.
CFNI Development

54
Office Safety and Security Manual
This document outlines basic security procedures tobe followed in the workplace and includes informa-tion on fire prevention, security issues to considerwhen working late, preventing fall injuries, preventingmachine accidents, preventing cuts and punctures,earthquake, hurricane preparation and bomb threatprocedures. It also contains key contact numbers forsecurity personnel at the University of the WestIndies, Jamaica, the UN Department of Safety andSecurity in Jamaica and a Communication Tree.
Staff Development and Achievement
Awards
PAHO Long Service awards were given to the follow-ing personnel in the year under review:
Mrs. Janice Welch, Administrative – 30 yearsAssistant, (Trinidad)
Miss Sharon Locke, Director’s Assistant – 20 years
Miss Paula Trotter, Nutritionist – 15 years
Mr. Rupert Burrell, Pressman – 15 years
Training
Training activities included:
• Michelle Tappin-Lee and Jacinth Waugh:First Aid Training conducted by UNDSS, Jamaica
• All Staff:Functions and use of Elluminate (in-house)
• All Staff:International Public Sector AccountingStandards (IPSAS) Training (in-house)
• All Staff:Crime Mitigation Lecture by the UNDSS,Jamaica (in-house)
• Administrative Staff, Jamaica:Use of AMPES, Obligation creation and prepar-ing documents for printing (in-house)
• Marlon Martin and Michelle Tappin-Lee:PAHO Procurement Workshop which high-lighted new procurement policies of the organi-zation conducted by Procurement Unit, PAHO,Washington.
• Sharon Locke:Human Resources Training conducted byHRM, PAHO, Washington.
• Enett Noble:Workshop on Electronic Digitization and BookRepair Workshop, Jamaica
• Candace Simpson-Smith: Nutrition and HIV/AIDS workshop for selected health care profes-sionals in Trinidad and Tobago.
• Candace Simpson-Smith and Janice Welch:Training Workshop on Gender Mainstreaming inHealth, Trinidad and Tobago.
Budget and Finance
The total operating budget for 2009 wasUS$2,444,393.00. See Annex 2 for further informa-tion on the breakdown of the budget by expendituretypes.
Quota contributions from CFNI member countriestotaled US$392,636.00.
Extra-budgetary funding accounted for 25% of theoperating budget with a total of US$615,957.00.
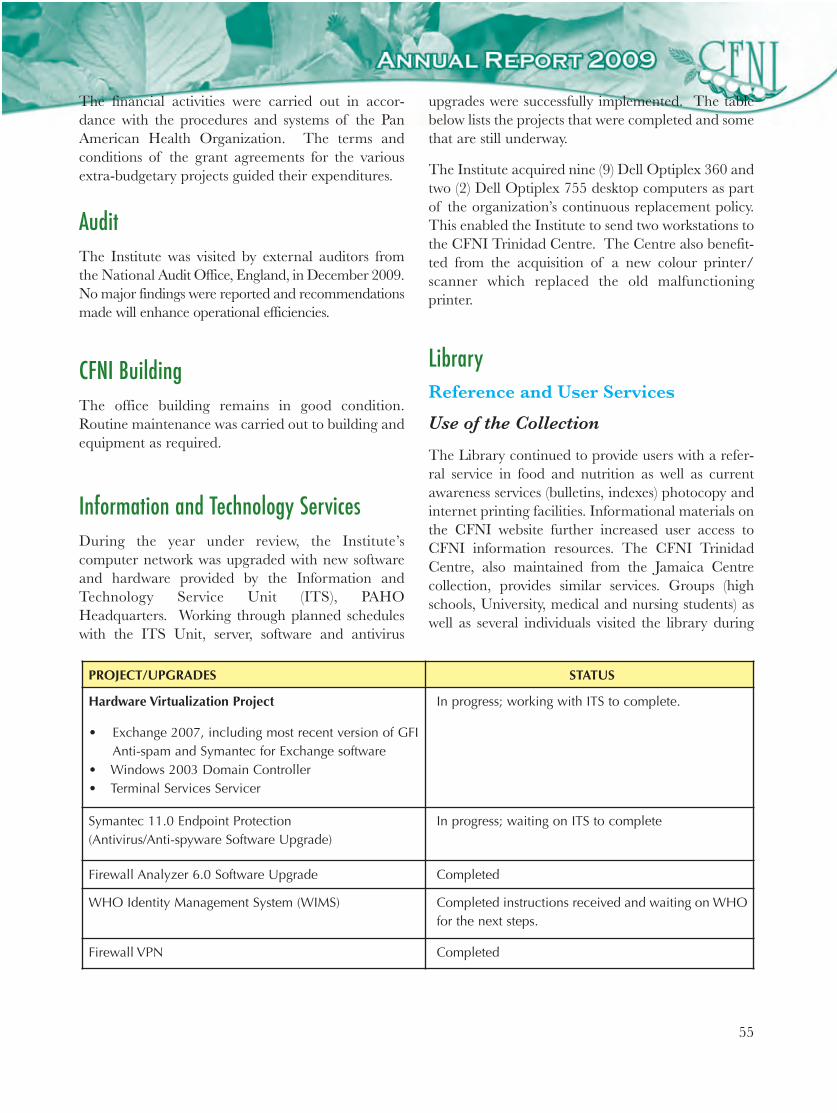
55
The financial activities were carried out in accor-dance with the procedures and systems of the PanAmerican Health Organization. The terms andconditions of the grant agreements for the variousextra-budgetary projects guided their expenditures.
AuditThe Institute was visited by external auditors fromthe National Audit Office, England, in December 2009.No major findings were reported and recommendationsmade will enhance operational efficiencies.
CFNI BuildingThe office building remains in good condition.Routine maintenance was carried out to building andequipment as required.
Information and Technology ServicesDuring the year under review, the Institute’scomputer network was upgraded with new softwareand hardware provided by the Information andTechnology Service Unit (ITS), PAHOHeadquarters. Working through planned scheduleswith the ITS Unit, server, software and antivirus
upgrades were successfully implemented. The tablebelow lists the projects that were completed and somethat are still underway.
The Institute acquired nine (9) Dell Optiplex 360 andtwo (2) Dell Optiplex 755 desktop computers as partof the organization’s continuous replacement policy.This enabled the Institute to send two workstations tothe CFNI Trinidad Centre. The Centre also benefit-ted from the acquisition of a new colour printer/scanner which replaced the old malfunctioningprinter.
LibraryReference and User Services
Use of the Collection
The Library continued to provide users with a refer-ral service in food and nutrition as well as currentawareness services (bulletins, indexes) photocopy andinternet printing facilities. Informational materials onthe CFNI website further increased user access toCFNI information resources. The CFNI TrinidadCentre, also maintained from the Jamaica Centrecollection, provides similar services. Groups (highschools, University, medical and nursing students) aswell as several individuals visited the library during
PROJECT/UPGRADES STATUS
Hardware Virtualization Project
• Exchange 2007, including most recent version of GFIAnti-spam and Symantec for Exchange software
• Windows 2003 Domain Controller• Terminal Services Servicer
In progress; working with ITS to complete.
Symantec 11.0 Endpoint Protection (Antivirus/Anti-spyware Software Upgrade)
In progress; waiting on ITS to complete
Firewall Analyzer 6.0 Software Upgrade Completed
WHO Identity Management System (WIMS) Completed instructions received and waiting on WHOfor the next steps.
Firewall VPN Completed
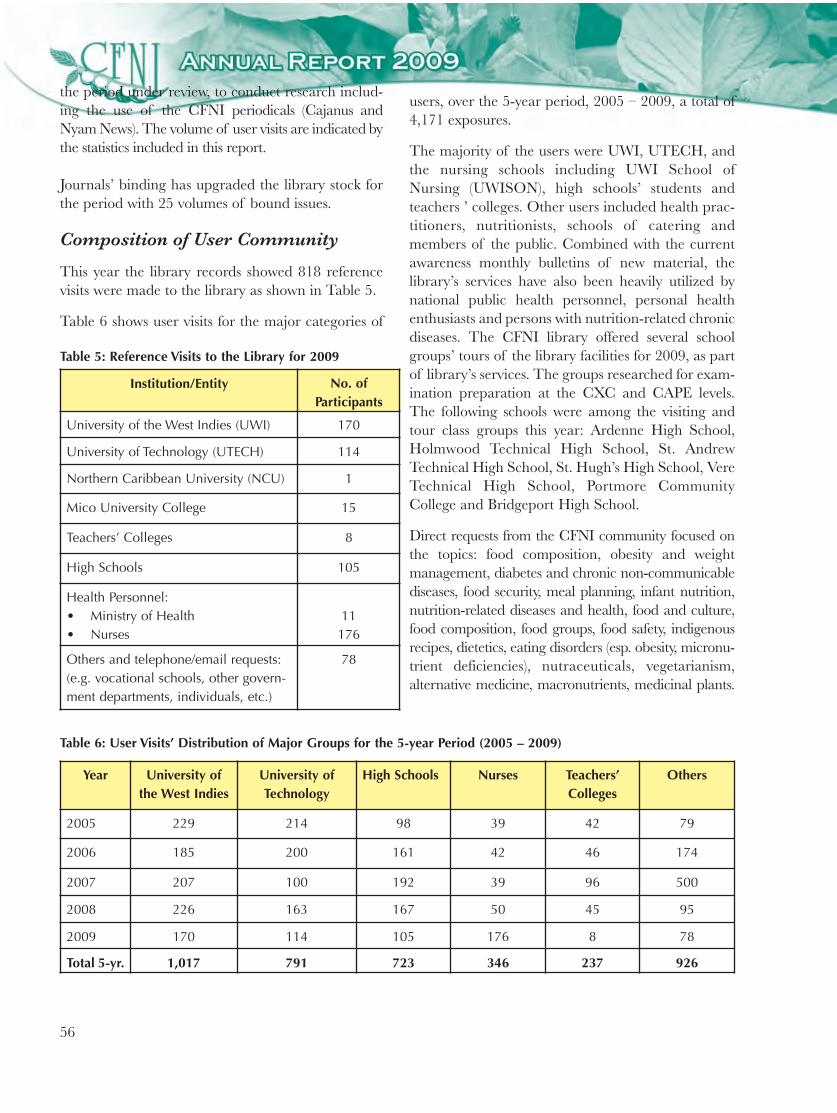
56
the period under review, to conduct research includ-ing the use of the CFNI periodicals (Cajanus andNyam News). The volume of user visits are indicated bythe statistics included in this report.
Journals’ binding has upgraded the library stock forthe period with 25 volumes of bound issues.
Composition of User Community
This year the library records showed 818 referencevisits were made to the library as shown in Table 5.
Table 6 shows user visits for the major categories of
Institution/Entity No. of Participants
University of the West Indies (UWI) 170
University of Technology (UTECH) 114
Northern Caribbean University (NCU) 1
Mico University College 15
Teachers’ Colleges 8
High Schools 105
Health Personnel:• Ministry of Health• Nurses
11176
Others and telephone/email requests:(e.g. vocational schools, other govern-ment departments, individuals, etc.)
78
Year University ofthe West Indies
University ofTechnology
High Schools Nurses Teachers’Colleges
Others
2005 229 214 98 39 42 79
2006 185 200 161 42 46 174
2007 207 100 192 39 96 500
2008 226 163 167 50 45 95
2009 170 114 105 176 8 78
Total 5-yr. 1,017 791 723 346 237 926
Table 6: User Visits’ Distribution of Major Groups for the 5-year Period (2005 – 2009)
users, over the 5-year period, 2005 – 2009, a total of4,171 exposures.
The majority of the users were UWI, UTECH, andthe nursing schools including UWI School ofNursing (UWISON), high schools’ students andteachers ’ colleges. Other users included health prac-titioners, nutritionists, schools of catering andmembers of the public. Combined with the currentawareness monthly bulletins of new material, thelibrary’s services have also been heavily utilized bynational public health personnel, personal healthenthusiasts and persons with nutrition-related chronicdiseases. The CFNI library offered several schoolgroups’ tours of the library facilities for 2009, as partof library’s services. The groups researched for exam-ination preparation at the CXC and CAPE levels.The following schools were among the visiting andtour class groups this year: Ardenne High School,Holmwood Technical High School, St. AndrewTechnical High School, St. Hugh’s High School, VereTechnical High School, Portmore CommunityCollege and Bridgeport High School.
Direct requests from the CFNI community focused onthe topics: food composition, obesity and weightmanagement, diabetes and chronic non-communicablediseases, food security, meal planning, infant nutrition,nutrition-related diseases and health, food and culture,food composition, food groups, food safety, indigenousrecipes, dietetics, eating disorders (esp. obesity, micronu-trient deficiencies), nutraceuticals, vegetarianism,alternative medicine, macronutrients, medicinal plants.
Table 5: Reference Visits to the Library for 2009

57
Further, from existing reference resources subject bibli-ographies and reference guides (library pathfinders)have been supplied to user clientele.
CFNI staff utilized the reference research facilitiesand the new journals received by the library. Internsand assistant consultants made good use of the retro-spective nutrition research resources maintained inthe library collection.
Information Outreach
Public information was enhanced by displaysmounted in 2009 (30 displays). Exhibitions anddisplays for the year also increased public awarenesson the importance of nutrition to lifestyle practices; invarious cases, in support of health ministries’ activities.
The Library participated in the displays and othercommunity events with provision of educationalresources and materials. In October, one very success-ful out-of-town display was presented at the GarveyMaceo High School to celebrate World Food Day.Other successful display events were the 4-H Clubs(Denbigh, Clarendon) and UWI exhibitions.
The library provided presentations to visiting healthgroups, several large high school groups and the publicin an endeavour to strengthen and enhance the functionof information provision to the user community.CFNI Website
The CFNI website carried issues of Cajanus 2007and Nyam News to 2008. The new activities of theschools’ competitions, food-based dietary guidelinesand information on the new CARPHA are nowavailable for access on the site. Website URL:http://www.paho.org/cfni.
UWI Network
The Library was participant in the launch of a UWILibrary Network in March 2009, by the UWI LibraryPublic and Outreach Services. The purpose of thenetwork was to open shared resources between thelibraries located on the Campus in the areas of:
• Fostering co-operation
• Duplication avoidance
• Shared training opportunities.
• Standardization of cataloguing and book processing
• Facilitate access to the facilities of the UWILibrary services
• A manual to be compiled on paraprofessionaltraining, copyright and uploading
• Aim for teams on digitization, internet work, usereducation, cataloguing.
New Title Acquisitions
A total of five hundred (500) new items includingjournals, books and pamphlets updated CFNI’scollection this year. New Journals Bulletins/NewBooks Bulletins are regularly issued to facilitate userresearch.
Materials Production Unit
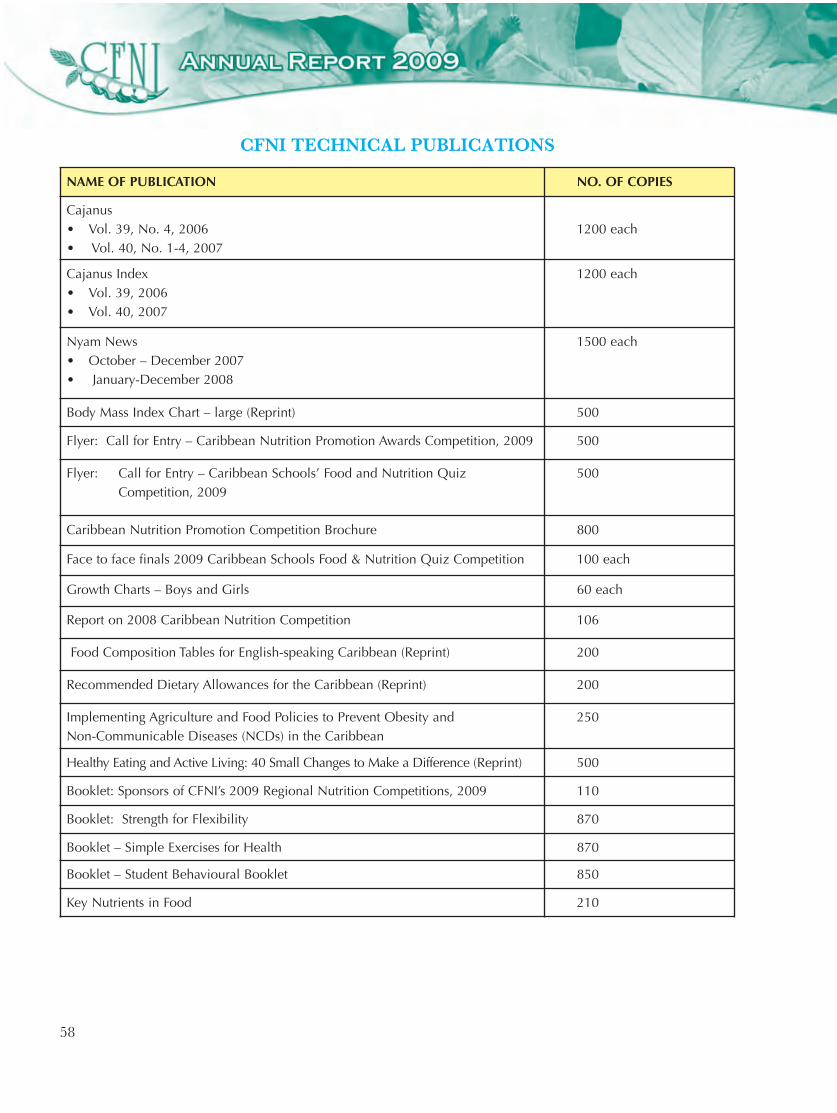
58
NAME OF PUBLICATION NO. OF COPIES
Cajanus • Vol. 39, No. 4, 2006 • Vol. 40, No. 1-4, 2007
1200 each
Cajanus Index• Vol. 39, 2006• Vol. 40, 2007
1200 each
Nyam News • October – December 2007• January-December 2008
1500 each
Body Mass Index Chart – large (Reprint) 500
Flyer: Call for Entry – Caribbean Nutrition Promotion Awards Competition, 2009 500
Flyer: Call for Entry – Caribbean Schools’ Food and Nutrition QuizCompetition, 2009
500
Caribbean Nutrition Promotion Competition Brochure 800
Face to face finals 2009 Caribbean Schools Food & Nutrition Quiz Competition 100 each
Growth Charts – Boys and Girls 60 each
Report on 2008 Caribbean Nutrition Competition 106
Food Composition Tables for English-speaking Caribbean (Reprint) 200
Recommended Dietary Allowances for the Caribbean (Reprint) 200
Implementing Agriculture and Food Policies to Prevent Obesity and Non-Communicable Diseases (NCDs) in the Caribbean
250
Healthy Eating and Active Living: 40 Small Changes to Make a Difference (Reprint) 500
Booklet: Sponsors of CFNI’s 2009 Regional Nutrition Competitions, 2009 110
Booklet: Strength for Flexibility 870
Booklet – Simple Exercises for Health 870
Booklet – Student Behavioural Booklet 850
Key Nutrients in Food 210
CFNI TECHNICAL PUBLICATIONS
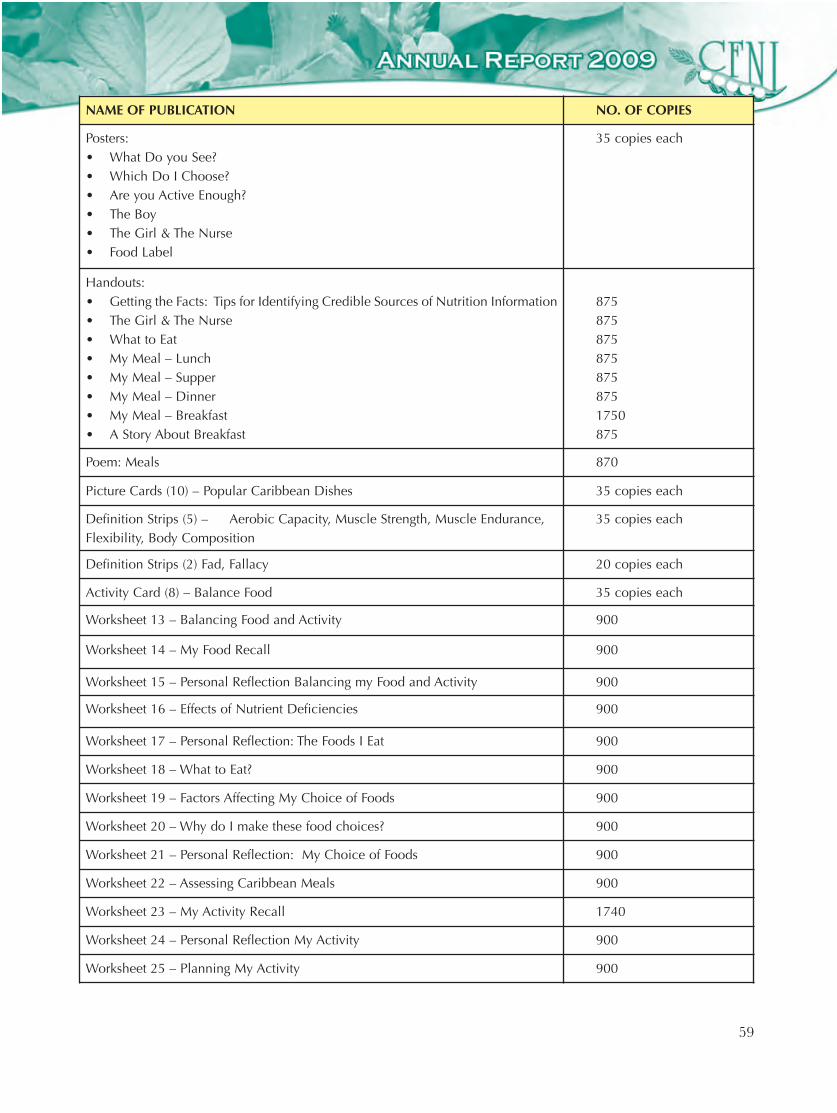
59
NAME OF PUBLICATION NO. OF COPIES
Posters: • What Do you See?• Which Do I Choose?• Are you Active Enough?• The Boy• The Girl & The Nurse• Food Label
35 copies each
Handouts: • Getting the Facts: Tips for Identifying Credible Sources of Nutrition Information• The Girl & The Nurse• What to Eat• My Meal – Lunch• My Meal – Supper• My Meal – Dinner• My Meal – Breakfast• A Story About Breakfast
875 8758758758758751750875
Poem: Meals 870
Picture Cards (10) – Popular Caribbean Dishes 35 copies each
Definition Strips (5) – Aerobic Capacity, Muscle Strength, Muscle Endurance,Flexibility, Body Composition
35 copies each
Definition Strips (2) Fad, Fallacy 20 copies each
Activity Card (8) – Balance Food 35 copies each
Worksheet 13 – Balancing Food and Activity 900
Worksheet 14 – My Food Recall 900
Worksheet 15 – Personal Reflection Balancing my Food and Activity 900
Worksheet 16 – Effects of Nutrient Deficiencies 900
Worksheet 17 – Personal Reflection: The Foods I Eat 900
Worksheet 18 – What to Eat? 900
Worksheet 19 – Factors Affecting My Choice of Foods 900
Worksheet 20 – Why do I make these food choices? 900
Worksheet 21 – Personal Reflection: My Choice of Foods 900
Worksheet 22 – Assessing Caribbean Meals 900
Worksheet 23 – My Activity Recall 1740
Worksheet 24 – Personal Reflection My Activity 900
Worksheet 25 – Planning My Activity 900
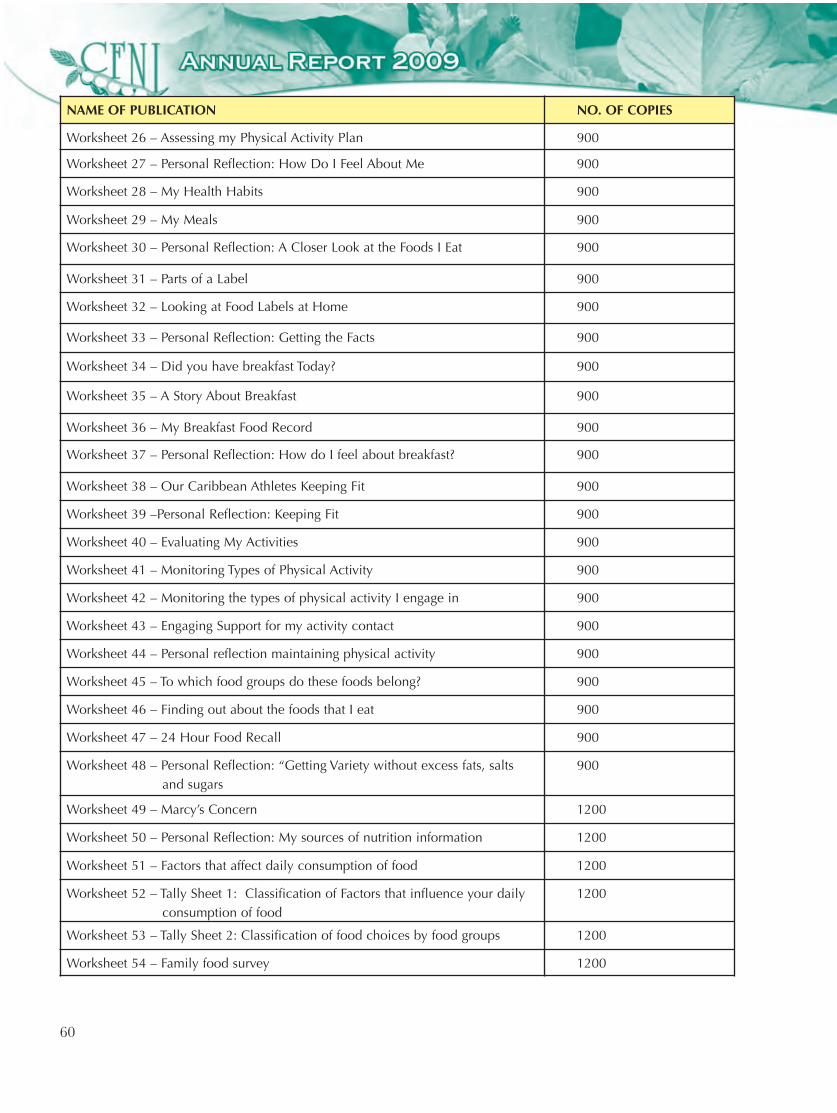
60
NAME OF PUBLICATION NO. OF COPIES
Worksheet 26 – Assessing my Physical Activity Plan 900
Worksheet 27 – Personal Reflection: How Do I Feel About Me 900
Worksheet 28 – My Health Habits 900
Worksheet 29 – My Meals 900
Worksheet 30 – Personal Reflection: A Closer Look at the Foods I Eat 900
Worksheet 31 – Parts of a Label 900
Worksheet 32 – Looking at Food Labels at Home 900
Worksheet 33 – Personal Reflection: Getting the Facts 900
Worksheet 34 – Did you have breakfast Today? 900
Worksheet 35 – A Story About Breakfast 900
Worksheet 36 – My Breakfast Food Record 900
Worksheet 37 – Personal Reflection: How do I feel about breakfast? 900
Worksheet 38 – Our Caribbean Athletes Keeping Fit 900
Worksheet 39 –Personal Reflection: Keeping Fit 900
Worksheet 40 – Evaluating My Activities 900
Worksheet 41 – Monitoring Types of Physical Activity 900
Worksheet 42 – Monitoring the types of physical activity I engage in 900
Worksheet 43 – Engaging Support for my activity contact 900
Worksheet 44 – Personal reflection maintaining physical activity 900
Worksheet 45 – To which food groups do these foods belong? 900
Worksheet 46 – Finding out about the foods that I eat 900
Worksheet 47 – 24 Hour Food Recall 900
Worksheet 48 – Personal Reflection: “Getting Variety without excess fats, salts and sugars
900
Worksheet 49 – Marcy’s Concern 1200
Worksheet 50 – Personal Reflection: My sources of nutrition information 1200
Worksheet 51 – Factors that affect daily consumption of food 1200
Worksheet 52 – Tally Sheet 1: Classification of Factors that influence your daily consumption of food
1200
Worksheet 53 – Tally Sheet 2: Classification of food choices by food groups 1200
Worksheet 54 – Family food survey 1200
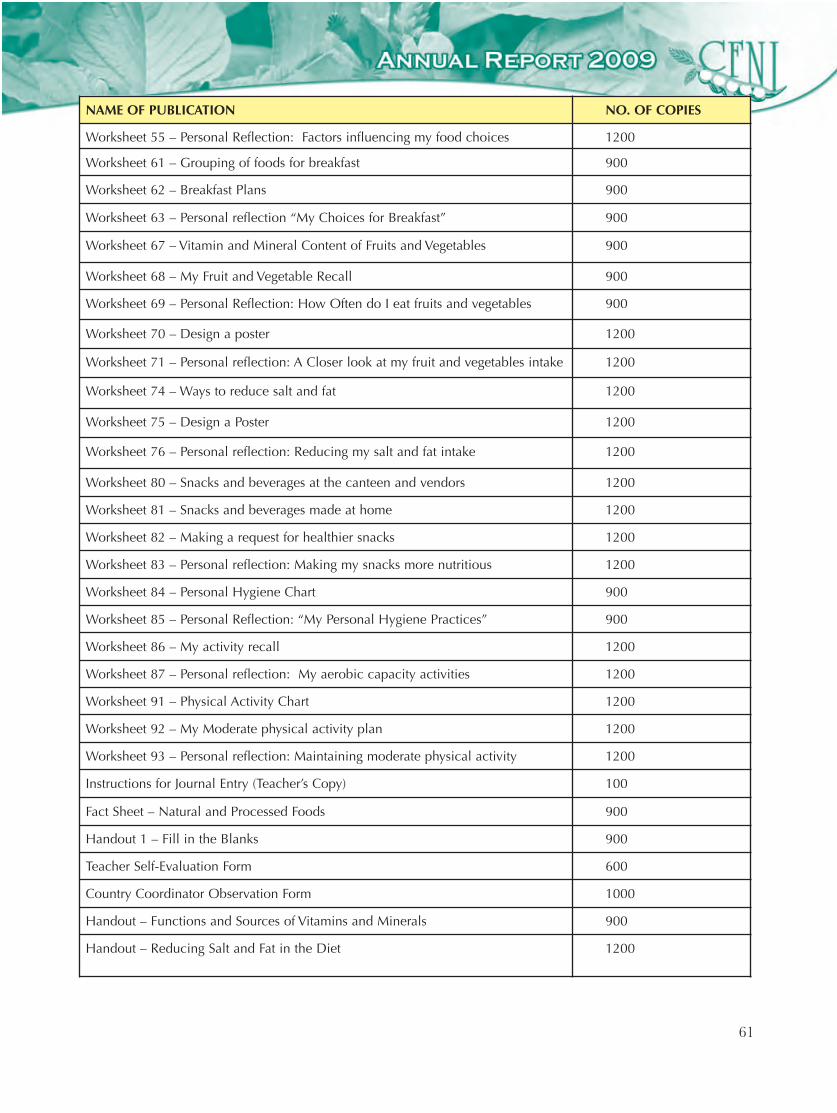
61
NAME OF PUBLICATION NO. OF COPIES
Worksheet 55 – Personal Reflection: Factors influencing my food choices 1200
Worksheet 61 – Grouping of foods for breakfast 900
Worksheet 62 – Breakfast Plans 900
Worksheet 63 – Personal reflection “My Choices for Breakfast” 900
Worksheet 67 – Vitamin and Mineral Content of Fruits and Vegetables 900
Worksheet 68 – My Fruit and Vegetable Recall 900
Worksheet 69 – Personal Reflection: How Often do I eat fruits and vegetables 900
Worksheet 70 – Design a poster 1200
Worksheet 71 – Personal reflection: A Closer look at my fruit and vegetables intake 1200
Worksheet 74 – Ways to reduce salt and fat 1200
Worksheet 75 – Design a Poster 1200
Worksheet 76 – Personal reflection: Reducing my salt and fat intake 1200
Worksheet 80 – Snacks and beverages at the canteen and vendors 1200
Worksheet 81 – Snacks and beverages made at home 1200
Worksheet 82 – Making a request for healthier snacks 1200
Worksheet 83 – Personal reflection: Making my snacks more nutritious 1200
Worksheet 84 – Personal Hygiene Chart 900
Worksheet 85 – Personal Reflection: “My Personal Hygiene Practices” 900
Worksheet 86 – My activity recall 1200
Worksheet 87 – Personal reflection: My aerobic capacity activities 1200
Worksheet 91 – Physical Activity Chart 1200
Worksheet 92 – My Moderate physical activity plan 1200
Worksheet 93 – Personal reflection: Maintaining moderate physical activity 1200
Instructions for Journal Entry (Teacher’s Copy) 100
Fact Sheet – Natural and Processed Foods 900
Handout 1 – Fill in the Blanks 900
Teacher Self-Evaluation Form 600
Country Coordinator Observation Form 1000
Handout – Functions and Sources of Vitamins and Minerals 900
Handout – Reducing Salt and Fat in the Diet 1200
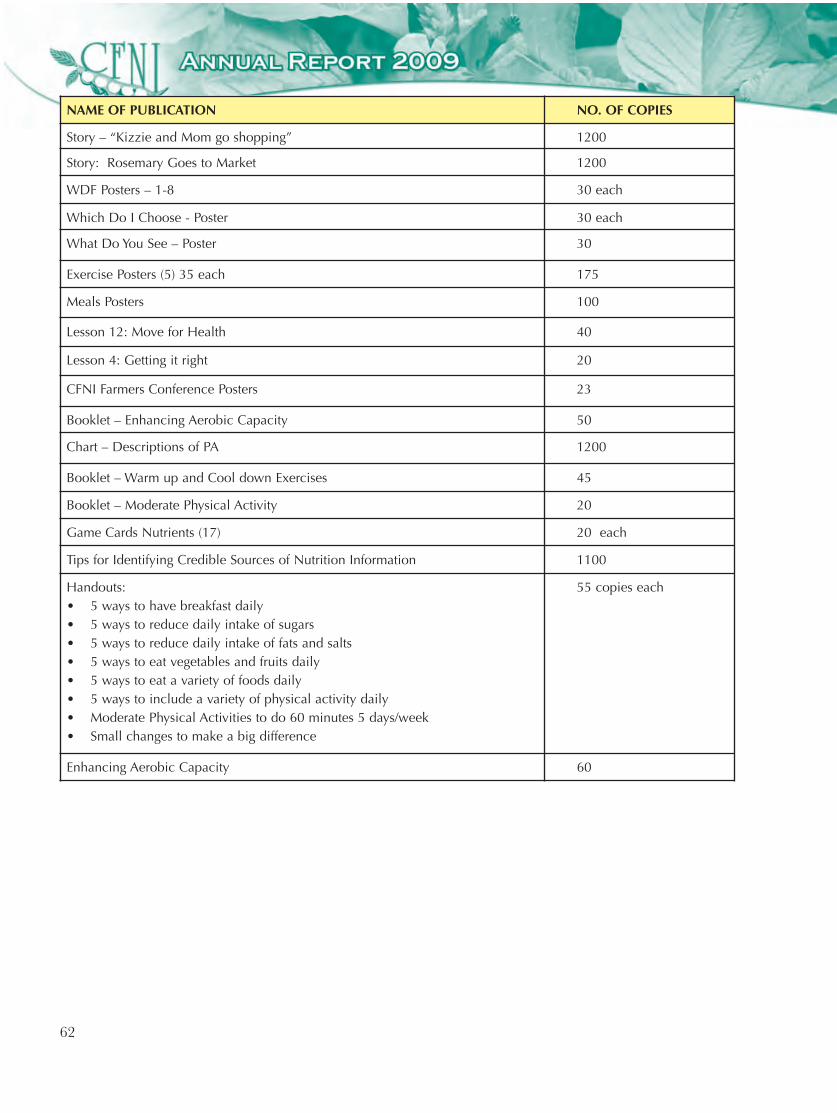
62
NAME OF PUBLICATION NO. OF COPIES
Story – “Kizzie and Mom go shopping” 1200
Story: Rosemary Goes to Market 1200
WDF Posters – 1-8 30 each
Which Do I Choose - Poster 30 each
What Do You See – Poster 30
Exercise Posters (5) 35 each 175
Meals Posters 100
Lesson 12: Move for Health 40
Lesson 4: Getting it right 20
CFNI Farmers Conference Posters 23
Booklet – Enhancing Aerobic Capacity 50
Chart – Descriptions of PA 1200
Booklet – Warm up and Cool down Exercises 45
Booklet – Moderate Physical Activity 20
Game Cards Nutrients (17) 20 each
Tips for Identifying Credible Sources of Nutrition Information 1100
Handouts: • 5 ways to have breakfast daily• 5 ways to reduce daily intake of sugars• 5 ways to reduce daily intake of fats and salts• 5 ways to eat vegetables and fruits daily• 5 ways to eat a variety of foods daily• 5 ways to include a variety of physical activity daily• Moderate Physical Activities to do 60 minutes 5 days/week• Small changes to make a big difference
55 copies each
Enhancing Aerobic Capacity 60
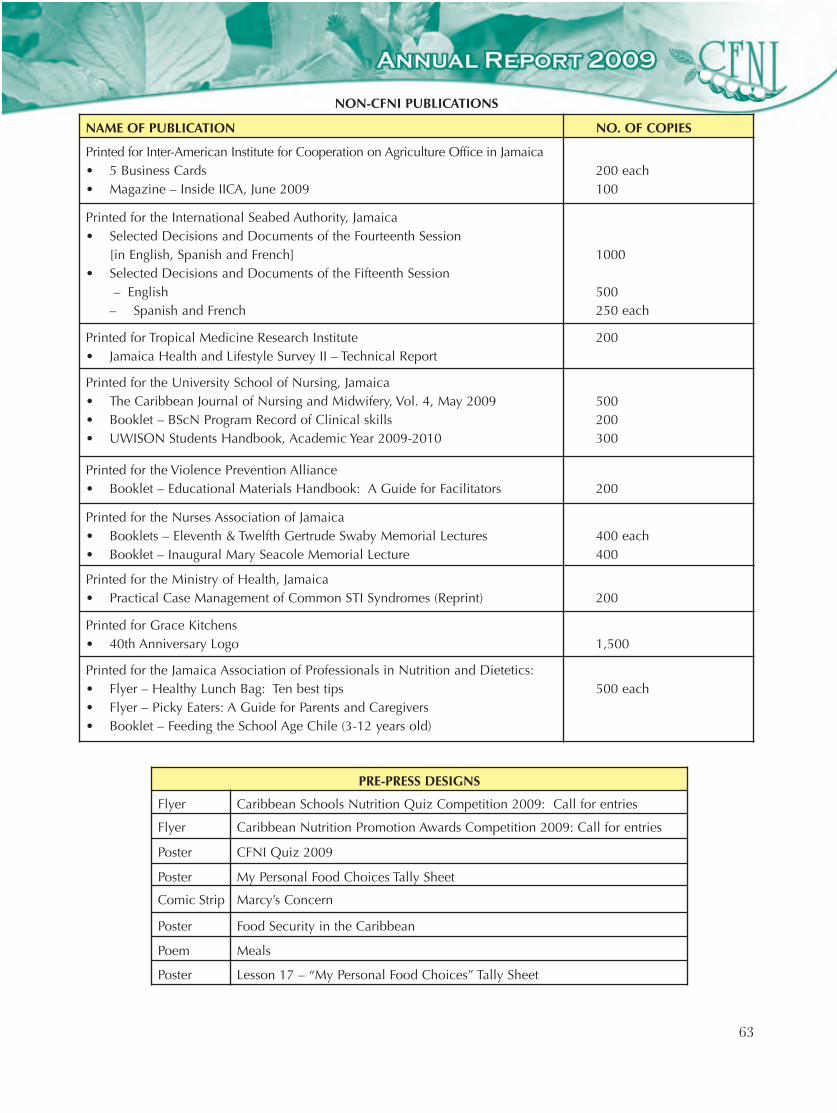
63
NAME OF PUBLICATION NO. OF COPIES
Printed for Inter-American Institute for Cooperation on Agriculture Office in Jamaica• 5 Business Cards • Magazine – Inside IICA, June 2009
200 each100
Printed for the International Seabed Authority, Jamaica• Selected Decisions and Documents of the Fourteenth Session
[in English, Spanish and French]• Selected Decisions and Documents of the Fifteenth Session
– English– Spanish and French
1000
500 250 each
Printed for Tropical Medicine Research Institute• Jamaica Health and Lifestyle Survey II – Technical Report
200
Printed for the University School of Nursing, Jamaica• The Caribbean Journal of Nursing and Midwifery, Vol. 4, May 2009• Booklet – BScN Program Record of Clinical skills • UWISON Students Handbook, Academic Year 2009-2010
500200300
Printed for the Violence Prevention Alliance• Booklet – Educational Materials Handbook: A Guide for Facilitators 200
Printed for the Nurses Association of Jamaica• Booklets – Eleventh & Twelfth Gertrude Swaby Memorial Lectures • Booklet – Inaugural Mary Seacole Memorial Lecture
400 each400
Printed for the Ministry of Health, Jamaica• Practical Case Management of Common STI Syndromes (Reprint) 200
Printed for Grace Kitchens • 40th Anniversary Logo 1,500
Printed for the Jamaica Association of Professionals in Nutrition and Dietetics:• Flyer – Healthy Lunch Bag: Ten best tips• Flyer – Picky Eaters: A Guide for Parents and Caregivers• Booklet – Feeding the School Age Chile (3-12 years old)
500 each
NON-CFNI PUBLICATIONS
PRE-PRESS DESIGNS
Flyer Caribbean Schools Nutrition Quiz Competition 2009: Call for entries
Flyer Caribbean Nutrition Promotion Awards Competition 2009: Call for entries
Poster CFNI Quiz 2009
Poster My Personal Food Choices Tally Sheet
Comic Strip Marcy’s Concern
Poster Food Security in the Caribbean
Poem Meals
Poster Lesson 17 – “My Personal Food Choices” Tally Sheet
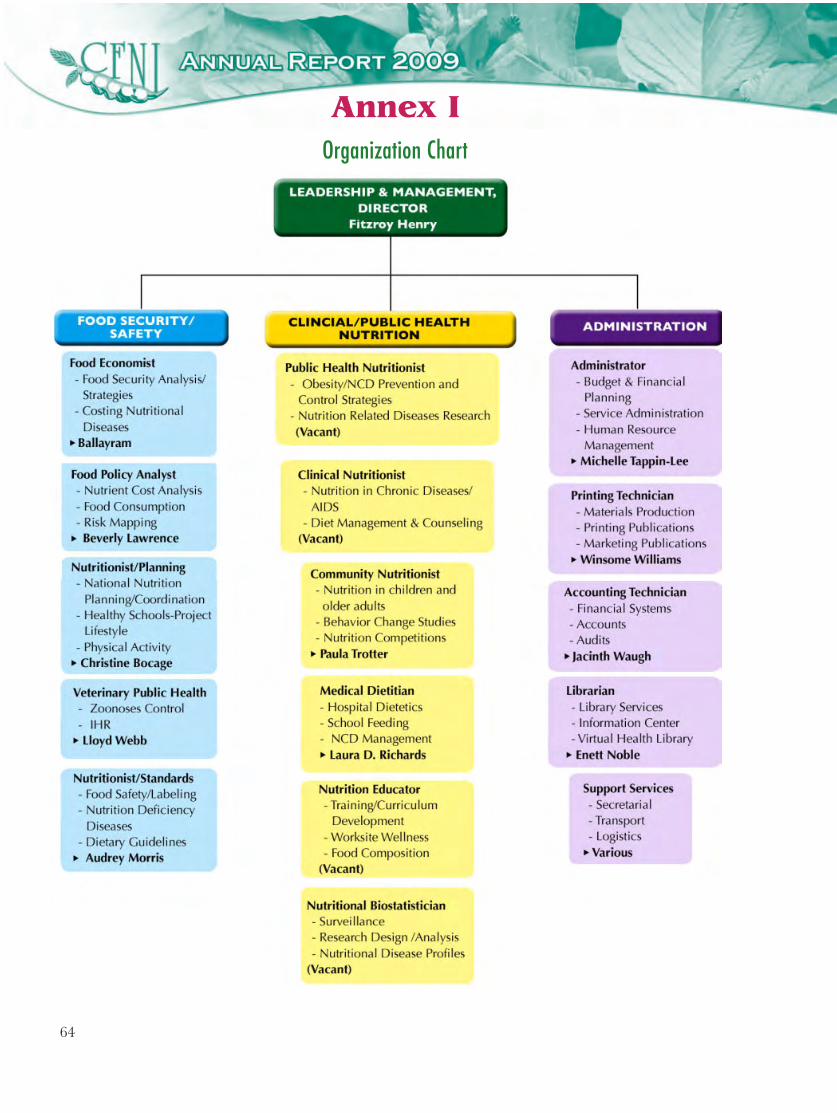
64
Organization Chart
Annex I

65
Expenditure Type/Funding Source
Core Funding ExtrabudgetaryFunding
TotalExpenditure
Total(%)
PAHO/WHO Govt. Quota
Personnel Costs 606,400 340,007 42,378 988,785 40%
General Project Costs 829,400 52,629 573,579 1,455,608 60%
Total 1,435,800 59%
392,636 16%
615,957 25%
2,444,393 100%
2,444,393 100%
CFNI Operating Budget 2009 (US$)
Annex II










![S]l1~I~cek: - IRIS PAHO Home](https://static.fdokumen.com/doc/165x107/631510f36ebca169bd0b0b21/sl1icek-iris-paho-home.jpg)










