II ' IIrI :i E ¡li 'III~a11 :J 11 l - IRIS PAHO
199
II ' IIrI :i E ¡li 'III~ a11 :J 11 l
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of II ' IIrI :i E ¡li 'III~a11 :J 11 l - IRIS PAHO

II ' IIrI :i E ¡li 'III~ a11 :J 11 l

QUADRENNIAL REPORT OF THE DIRECTORof the
PAN AMERICAN SANITARY BUREAU
REGIONAL OFFICE FOR THE AMERICAS
of the
WORLD HEALTH ORGANIZATION
1966-1969
Official Document No. 101* August 1970
PAN AMERICAN HEALTH ORGANIZATIONPan American Sanitary Bureau, Regional Office of the
WORLD HEALTH ORGANIZATION525 Twenty-fhird Street, N. W.
Washington, D. C. 20037
* This report is a companion volume to Official Document No. 102, Annual Report of the Director,1969, and to Scientific Publication No. 207, Health Conditions in the Americas-1965-1968.
*To the
States Members
of the
Pan American Health Organization
I have the honor to transmit herewith the Quadrennial Report on
the work of the Pan American Sanitary Bureau, Regional Office for
the Americas of the World Health Organization, for the years 1966-
1969. This Report summarizes the activities at Headquarters and in
the countries; greater detail is presented in the Annual Report for
1969, which is submitted separately, and in the Annual Reports for the
first three years of the quadrennium.
Respectfully,
Abraham Horwitz
Director
TABLE OF CONTENTS
INTRODUCTION - - - - - -
I. HIGHLIGHTS OF THE PERIOD 1966-1969Historic Events _Prevailing Current Problems -
II. THE EXTERNAL RELATIONS OF THE ORGANIZATIONThe Organization within the Inter-American System _Relations with the United Nations System _Relations with National and International Institutions _Scientific and Public Communications _
III. INTERNAL DEVELOPMENTS IN THE ORGANIZATIONConstitutional QuestionsOrganizational StructureFinancial Questions -Administrative Questions _
IV. THE PROGRAMS OF THE ORGANIZATIONGeneral Activities
Health Statistics -Health Planning _Administrative Methods and Practices _Health Legislation -Evaluation
Control or Eradication of Diseases _ _ _Yellow Fever _ - -Aedes aegypti -MalariaSmallpoxTuberculosisPoliomyelitisLeprosyVenereal DiseasesYawsPlagueInfluenzaArbovirus Infections _Parasitic Diseases _Chronic and Degenerative Diseases _- -
Zoonoses
_ vii
13
- 19- 21- 24- 26
_ 31- 33_ 35_ 40
43-_ _-_ _ _43-_ _-_ _ _48
50-..... _ _ 50-_ _-_ _ _52
5353
-_ _-_ _ _54-_ _-_ _ _56-_ _-_ _ _60-_ _ _-_ _63-_ _-_ _ _66- _ _-_ _ 67-_ _-_ _ _70-..... _ _ 72-_ _-_ _ _72
74-_ _-_ _ _76
78- -- _ -82
- _ _-_ _ _ 84Sanitary Engineering and Environmental Sciences _ 93
Environmental Sanitation _ - 93Water Supply _ - 94Water Supply in Rural Areas _ _ _ _ 97Administration and Management of Water Services _ _ _ 99Sewerage and Water Pollution - - 100Collection and Disposal of Solid Wastes _ _ 101Pan American Sanitary Engineering and Environmental
Sciences Center - - 102
iii
Promotion of HealthGeneral Health Services _ _ _- -
Medical Care and Rehabilitation _- -
NursingMaternal and Child Health _ _ _NutritionMental Health _Dental Health _Veterinary Public Health _- - - -
Other Health Services .Public Health Laboratories _ _ _Drug Control _Food Hygiene _Health and Radiation _Health and Education _
Research Development and Coordination _Advisory Committee on Medical ResearchResearch and Research Training ProjectsMultinational Programs _Biomedical Communication - - - -
Operations Research _Nutrition Research
1041041_ _ _ 106
- _-_ _ _ 1.15-... -_ _ 117-.... -__120
-1_ _ _ _ 126128
-.... _ _ __1,30-. .... _-_ 131-1_ _ _ _ _ 1.31….... …_ _ 1.33- _ _ _ _ 135-1_ _ _ _ _ 1.37…1_ _ _ 1__l38-1_ _ _ _ _ 1.40- _ _ _ _ 141-1_ _ _ _ _ 142-.... -__143-. .... _- 144-.... -__146-.... _-__146
Programs of the Pan American Zoonoses Center _ _- - 150Programs of the Pan American Foot-and-Mouth Disease
Center - _ _152Sanitary Engineering Research _ _ - 152Tuberculosis Research - _153Other Research Activities _ - 153
Human Resources Development _ - - 154Special Studies -_ 155Strengthening of Teaching Institutions _ _ - 156Other Training Programs - - - - - 163Fellowships - - -169
Publications and Reference Services _ _ _ 171
FINAL COMMENTS _ _
Index
_ _ _ 173
_ _ _ 175
iv
i
i
ACRONYMS AND CORRESPONDING AGENCIES
AID
AIDIS
CARE
CEPIS
CFNI
CIAP
CINVA
CLAM
CREFAL
ECLA
EXIMBANK
FAO
IAEA
IACC
IA-ECOSOC
IDB
ILO
INCAP
NCDC
OAS
PAHO
PASB
UN
UNDP
UNDP-SF
UNESCO
UNICEF
WHO
Agency for International Development (USA)
Inter-American Association of Sanitary Engineering
Cooperative for American Relief to Everywhere
Pan American Sanitary Engineering and Environmental SciencesCenter
Caribbean Food and Nutrition Institute
Inter-American Committee on the Alliance for Progress
Inter-American Housing and Planning Center
Latin American Center for Medical Administration
Regional Center for Functional Literacy in Rural Areas for LatinAmerica
Economic Commission for Latin America (UN)
Export-Import Bank (USA)
Food and Agriculture Organization (UN)
International Atomic Energy Agency
Inter-American Cultural Council
Inter-American Economic and Social Council (OAS)
Inter-American Development Bank
International Labour Organisation
Institute of Nutrition of Central America and Panama
National Communicable Disease Center (USA)
Organization of American States
Pan American Health Organization
Pan American Sanitary Bureau
United Nations
United Nations Development Program
United Nations Development Program, Special Fund
United Nations Educational, Scientific, and Cultural Organization
United Nations Children's Fund
World Health Organization
EXCERPT FROM THE REPORT OF THEMEETING OF AMERICAN CHIEFS OF STATE
C. HealthImprovement of health conditíons is fundamental to the economic and social devel-
opment of Latín America.Available scientific knowledge makes it possible to obtain specific results, whlch, in
accordance with the needs of each country and the provisions of the Charter of Puntadel Este, should be utilized to attain the following objectives:
a. Control of communicable diseases and eradication of those for whích methods fortotal elimination exíst. Pertinent programs shall receive international coordinationwhen necessary.
b. Acceleration of programs for providing drinking-water supplies, sewerage, andother services essential to environmental sanitation in rural and urban areas, givingpreference to lower-income groups. On the basis of studies carried out and withthe cooperation of international financing agencies, national revolving fund systemsshall be used to assure the continuity of such programs.
c. Greater and more rapid progress in improving nutrition of the neediest groups ofthe population, takíng advantage of all possibilitíes offered by national effort andinternational cooperation.
d. Promotion of intensive mother and child welfare programs and of educationalprograms on overall family guidance methods.
e. Priority for basic and advanced training of professíonal, technical, administrative,and auxiliary personnel, and support of operational and administrative research inthe field of health.
f. Incorporation, as early as the preinvestment phase, of national and regional healthprograms into general development plans.
The Presidents of the member states of the OAS, therefore, decide:
1. To expand, within the famework of general planning, the preparation and imple-mentation of national plans that will strengthen infrastructure in the field of health.
2. To mobilize internal and external resources to meet the needs for financing theseplans. In this connection, to call upon CIAP, when analyzing the health sector innational development programs, to take into account the objectives and needs indicated.
3. To call upon the Pan American Health Organization to cooperate with the govern-ments in the preparation of specific programs relating to these objectives.
April 1967
INTRODUCTION
The political decisions directly affecting the health ofthe inhabitants of the Americas during the four-yearperiod 1966-1969 are part of a sequence of historicalevents which have taken place during the decade 1960-1969. The Declaration of the Presidents of Americain April 1967 reaffirmed and widened in scope thepronouncements and objectives of the Charter of Puntadel Este. The first Special Meeting of Ministers ofHealth of the Americas, in April 1963, which gave aframe of reference and a functional content to theCharter, was followed by a second, held in Buenos Airesin October 1968, at which the statements of the Chiefsof State were translated into practical measures.
What has been achieved during-the four-year period1966-1969 in regard to health cannot be dissociatedfrom these outstanding events of the decade. The pro-found changes which have taken place during thisperiod in ideas, behavior and customs, and in the aspira-tions of both men and Governments, have been particu-larly marked in the health field.
The most noteworthy change-which has given riseto a whole body of doctrine-is the acceptance of thenotion of health as a component of economic andsocial development. The strength of the convictionheld in regard to the relationship involved here still hasto be demonstrated further. However much it ought tobe so, the fact is that moral arguments are not sufficient,even though they do point to the obligation on any so-ciety to prevent and cure the ills of its inhabitants. Con-crete cases show that it is possible to demonstrate thevital importance of a healthy population for the growthof the economy and the improvement of well-being. Itis essential to investigate such cases in increasing num-bers, to the point where we can formulate a theory ofthe interdependence of health and development. Thisis another way of saying that the complex process ofhealth protection, promotion, and restoration does notdepend exclusively on medical technology; this is ofcourse essential, but it must be supplemented by all thefactors which make for individual and collective well-being.
This way of thinking has had a series of consequencesof the utmost importance, which have been taking place
throughout the decade of the 1960's. We see them inthe various methods of adjusting needs to availableresources; in the structuring and administration ofhealth services; in the development of manpower re-sources; and the investigation of problems, with em-phasis on the relatively more frequent ones. In otherwords, the doctrine referred to has been followed bypolicies, principles, norms, and procedures designedto give it form and put it into practice. Thus an imagehas taken shape of the purposes that guide the Govern-ments of the Americas in regard to health, and a seriesof concrete measures have been taken to achieve them;all this with due regard to the way of life, the customs,and the traditions which give societies their distinctivecharacteristics that differentiate them from others intheir reaction to a given situation.
The decade under discussion, and particularly the lastfour years of the decade, witnessed the acceptance andcrystallization of the idea of planning as a system ofinvestment in accordance with priorities. Thus we findthe allocation of funds reflected in the methods adoptedfor the formulation of health plans. The basis of alloca-tion may be the amount of damage caused, for example,the level of the mortality figures; or the choice may bebetween various techniques; between services and instrú-ments, including education, research, and capital invest-ment; between levels of health as expressed in life ex-pectancy at birth or other indicators; or again betweensectors, e.g., public versus private. The delimitation ofspheres of action is after all the essence of politicaldecision, without which planning is devoid of purpose.Without continuity here, the process is lacking whichleads from formulation to implementation, evaluation,and periodic readjustment of the objectives of individualprograms and projects. Planning helps to rationalizethe series of decisions leading to stages worked out inadvance, since there is a constant reinfusion of the ex-perience acquired through successive activities as eachis carried out.
During the previous decade, positive achievementstook place in the Hemisphere in the identification ofpriority problems (the diagnosis phase); in the formula-tion of national plans or specific programs and the im-
vii
plementation of both; and in the training of planners.No less important was the recognition of the limitingfactors, the real obstacles to the process, and theurgency of coping with them. But all in all, we mustagree that all this took place at the subsectoral level, asregards both the institutions involved and the functionsincluded. In other words, not all health services admin-istered by Governments today form part of their plans;nor do the many functions carried out at present by thevarious public and private bodies. If we seek an ex-planation for this state of affairs, it comes down to adispersal of efforts, which is the same as saying failureto achieve coordination of resources. Time and timeagain, statements by the Governing Bodies of the Or-ganization have brought out this point and have recom-mended concrete measures for correcting it and so im-proving the output and productivity of services, inother words, increasing the number of beneficiaries andadding to their well-being.
It has been felt indispensable to enlist the participa-tion of the universities, on the grounds that they arewanted as a factor in development. Teaching of thehealth sciences is basic to the achievement of the goals ofeach and every plan and program, which throw light onchanges projected and enabling those actually made tobe evaluated. Science and technology constantly intro-duce new interpretations of vital phenomena and of thehealth problems of societies, and different ways of cop-ing with them. This alone would justify joint action byGovernments and universities in an area so vital forsocial progress.
The topic for the Technical Discussions at the XIXMeeting of the Directing Council of the Pan AmericanHealth Organization, XXI Meeting of the RegionalCommittee of the World Health Organization, was"Financing of the Health Sector." ' The discussion ofthis topic brought out the need for a study in depth ofthe nature of the situation in each country in the face ofthe relative shortage of funds, the multiplicity of budgetsources not properly coordinated, and the urgent needto increase the productivity of the various services. Onthe basis of the findings of the study, it will be possibleto determine what are the major investments needed bythe health sector to extend the coverage and includepopulation groups not enjoying permanent care servicesso far. External financing was considered to be a sup-plement-at times indispensable-to domestic re-sources for specific projects, but not a regular and ordi-nary source for capital equipment.
This brief sketch of the situation is prompted by thestatement made above that health planning as carriedhitherto has been subsectoral in scope. Plans have
1 Scientific Publication PAHO 208, 1970.
tended to concentrate on activities designed to attaingoals which vary in nature according to the methodselected. They do not ordinarily include investmentprograms, programs for the training of professionalsand auxiliaries, for the improvemen: of the administra-tive infrastructure, and for research, among others.We should bear in mind that even in the countries witha relatively high per-capita income there is an evidentimbalance between what is needed and what is feasible,immediately or over the long term. Statesmen are con-stantly called upon to decide matters of priority andalternative procedures or solutions.
In the last few years, a series of missions organizedby the Inter-American System or the United Nationshave studied the trend of the economy of the LatinAmerican countries and the Caribbean area, with spe-cial reference to external capital needs. Inclusion ofhealth in these missions has been exceptional. Othersocial sectors too have been neglected, at a time whenwe are preaching developrnent for well-being. Theurgency of systematic programming of investment hasbecome manifest. In other words, while investnmentshave played a highly important role in speeding up thesolution of certain outstanding problems, they have notalways been part of national health plans. They havetended rather to reflect the credit policy of certain Gov-ernments or lending institutions. If investments areprogrammed-and there is a well-defined and well-triedtechnique for this-I feel sure that the inflow of externalcapital can be increased; and the prospects are evenbetter if this is done through joint action by the interna-tional credit and health bodies, working together withthe State.
The same procedure should be followed in regard tothe other components I have mentioned, namely, thetraining of manpower, the expansion and modernizationof the technical and administrative infrastructure, andresearch.
The task of consolidating over-all health planning inthe Americas and making it viable must be an item ofthe agenda for the decade beginning in 1970. Greatas is its complexity, its prospective effect on individualand collective well-being is even greater.
The action which must be taken to bring about cer-tain improvements in the economy and social progress,as set forth in the political pronouncements of thedecade, has triggered off a reaction against the status quoand emphasis on change as a way of life. This has beenreflected in the reorganization of health ministries andinstitutions, in the revision of current legislation, inthe adaptation of structures to the requirements oftechnology, and in the situation of the universities.
Time and time again during this period, Govern-
viiI
ments and international bodies, public and private,have recognized that the two essential constants forprogress in the health sector are the existence in everycountry of services having the widest possible coverage,and the training of professionals and auxiliaries tocarry out the aims of individual programs and of theplan as a whole. In other words, there has been aconsensus to the effect that no health project is feasibleunless there is a stable infrastructure.
Linked with the foregoing is the rural question andwhat has been called the ruralization of the urbanenvironment in the Americas. This embraces theareas where the inhabitants have little or no access toeven minimum health services. There are no preciseestimates on this point, but there must be at least 30million persons in the countries of Central America,South America, and the Caribbean area in that situa-tion. To put it another way, 57 per cent of communitieswith under 10,000 inhabitants have virtually no medicalcare, either for prevention or for cure. It may well bethat this calls for heavier investment and greater in-genuity than any other problem on the part of thoseresponsible for health in the Americas. Yet it cannotbe solved on traditional lines within a period acceptablefrom the human point of view. Nor is it conceivablethat health can be left to the professionals, since thesewill not be forthcoming in adequate numbers, even bythe end of this century, to meet the present needs andfuture needs as they arise constantly from the popula-tion increase. No success has been achieved with sys-tems deriving from other cultures and grafted ontocustoms and ways of life which in the long run rejectthem. New formulas must be sought for the solutionof each problem as it arises, based on the best informa-tion available.
This is another basic agenda item for the 1970's andsucceeding decades. It is a matter for Governments andtheir various institutions in the health field, for universi-ties and all their branches which teach subjects andfunctions relating to health, and for international bodiesset up to promote over-all and sectoral development.If they continue to go their separate ways, the resultsthey achieve will be only partial and limited in scope.If they coordinate among themselves and within them-selves, the prospects increase enormously and the con-sequences reach out into the future. This is cor-roborated by experience.
The Technical Discussions 2 at the XVII Meeting ofthe Directing Council, held in Port-of-Spain, Trinidad
2 Final Report of the Technical Discussions: "Methods forIncreasing Health Service Coverage in Rural Areas." Pub-lished in the English edition of the Boletín de la OficinaSanitaria Panamericana-Selections from 1968.
and Tobago, referred to this rural problem and to theways and means of coping with it over a period. Men-tion was made of various approaches for differentecological situations, designed to increase coverageand at the same time to achieve nation-wide solutions.The movement has continued, but not at the speedthat Governments would like to see. Two factors tendto slow down the process: shortage of funds and lackof technical manpower. External capital is indispen-sable if the entire population is to be provided withminimum services, at any rate in regard to the com-monest diseases. It must be pointed out that as far aswater supply is concerned, not less than 20 million ruralinhabitants now have installations, either communityfacilities or house connections, and this has happenedwithin the last ten years.
Whatever the system applied, in all the countries theproportion of the national revenue earmarked forhealth is insufficient for the present population. If eventhe simplest installations have to be constructed, asis the case in the rural areas, the magnitude of theinvestment increases enormously. To put into practicewhat we have proclaimed, namely, that health is aright and not a privilege, we must create the necessaryconditions to make it come true. This is the essentialhumanitarian background of our entire operation. Ifthe present policy of international credit bodies doesnot give or intend to give priority to investment forrural health services, other machinery will have to beestablished for this purpose; it is inescapable, because itinvolves human beings.
In order to convince the decision-making authoritiesof the need for increasing health budgets, both thespending and duplication or lack of coordination ofnational resources must be reduced to a minimum, withthe help of a rational planning process.
It is not surprising that in the course of the decadeit was not found possible to make use of all the knowl-edge resulting from the new contributions of scienceand technology in the countries of the Americas.Whether it is because there were no services, or prop-erly trained technicians, or essential equipment, theplain fact is that only some of the inhabitants, and thosemostly in the larger cities, enjoyed the benefit of up-to-date medical care, preventive or curative.
The Governments agreed as to the urgency of im-proving the organization and administration of in-stitutions to attain the general and specific targets ofindividual programs and of national plans. Of the initia-tives promoted by the Pan American Health Organiza-tion over the last ten years, few are as important asthat designed to give administration the status itdeserves, to modernize administrative techniques prop-
ix
erly, and to give administrators the prestige their workmerits. Administration comprises a series of disciplineswhich until fairly recently were either ignored or under-estimated by health specialists, who failed to realizethat without them the goals of their programs could notbe attained. As has often been said, no less importantthan deciding what to do is deciding how to do it. Theplanning process has revealed the weaknesses on theadministrative side. The science and art of administra-tion have not been static; on the contrary, administra-tive techniques have taken advantage of the latest scien-tific developments as embodied in systems analysis, andtoday use is made of computers. The volume of healthinvestments in the Americas, the complexities of theprocedures used, and the number of officials devotedto the task, are reason enough for this. For the develop-ing countries of the Region, perhaps the main prob-lem is that of deciding what computers should really beused for, which means balancing the cost against thebenefits to be derived. There is no denying the impor-tance of information which is provided at the right timeand is as accurate and complete as possible. But itdoes not follow that it must always be compiled,analyzed, and distributed, unless the data are indispen-sable to the recipients in the exercise of their duties.In other words, we must pay attention to what sciencehas to offer, but we must adapt it to the actual capacityof institutions to solve the problems that occur mostfrequently.
It would appear that in the decade now beginning,and in those that will follow, greater and greater usewill be made of the technique we call systems analysis,in the investigation of the phenomena underlyinghealth and sickness, in the application of methods ofreducing morbidity and mortality, and in the adminis-tration of the services involved. The Computer Centerin Health, officially inaugurated in April 1970 in BuenosAires, under the auspices of the Government of Argen-tina and this Organization, will help in the training ofprofessionals and the study of problems, and over thelong term it will cooperate with Governments in deter-mining the areas in which the use of computers isjustified.
This practical reform will be given impetus bymodernization of the traditional health administrationmethods. Progress here has been substantial in anumber of countries over the last ten years. It can beseen in program budgeting, in accounting and financeprocedures, in the structuring of personnel and supplydepartments, and elsewhere. There is still much to bedone to reach a level of efficiency where expenditurewill be reduced to a minimum and unnecessary opera-tions and costly, inefficient duplication avoided. This is
directly bound up with the training of professionalsand technicians in administration, and the investigationof problems where the solution will help in the formula-tion and execution of alternatives. Even in the eventof a decision to use computers, the basic data must beof first-rate quality if they are to reflect the real stateof affairs.
The Organization has promoted and itself providedactive collaboration in this field and will continue todo so in the light of its significance for better health.
A feature of the 1960's was the :marked interest inuniversity teaching in the field of medical education.The growing imbalance between the palpable needs ofsociety and the lack of manpower-especially profes-sionals-to meet them is at the root of this situation,one that has been experienced throughout the world.The concentration of physicians and other health profes-sionals in the large urban centers to the detriment of therural environment is common. At the same time, therehas been haphazard migration from the country to thecities, and shantytowns lacking even minimum serviceshave sprung up on the periphery of the cities, thusaggravating the general problem in all the countries.Where the problem has been studiedl in some depth-a noteworthy example being the study of human re-sources in Colombia a-it is found that the teachingand learning process must be looked at closely, sinceit has shortcomings which need to be remedied. Norcan we fail to mention that the students themselveshave voiced the urgency of university reform, some-times in no half-hearted way. There are those whobelieve that this problem cannot be dissociated frompolitical structures, while others feel that strictlyeducational components are involved which it wouldbe well to analyze and to reform where necessary.
The present Report describes how the Organizationover the last four years has sponsored a study of 130medical schools in Central and South America, a realsociological investigation of the process of trainingphysicians. A preliminary analysis indicates that thereis a clear dissociation between secondary educationand medical education, between medical education anduniversity education, and between the university andthe government bodies-in this instance the ministriesof health-and public and private institutions concerned
3 Study on Health Manpower and Medical Education inColombia, Parts 1, II, and III. Sponsored by the Ministry ofPublic Health of Colombia, the Colombian Association ofMedical Schools, and the Pan American Health Organization,1967.
x

with the prevention and cure of disease. What is per-haps most serious is that the teaching process is not inkeeping with the actual situation the students will haveto live with when they have graduated. They aretaught in more or less great detail the make-up of ahuman being, from the cells to the various organs andsystems, and they are required to build these up intothe synthesis represented by the individual as a biologi-cal unit and a social entity. Curricula and technicaland administrative structures are closely interde-pendent, and hence rigid. The transmission of knowl-edge is thus done piecemeal. On the same principle,there is a tendency to compartmentalize communitiesand not to relate problems as they exist and evolve tothe human and material resources available to solvethem. The various types of health professionals aretrained separately, and they therefore tend to go theirseparate ways and the greater the specialization, theworse the isolation.
The idea has emerged of creating faculties of healthsciences, where the teaching would be multidisciplinaryand cover the various professions simultaneously, sub-ject of course to such variations as derive from thespecific responsibilities of each in the social environ-ment and the knowledge needed to fulfill those respon-sibilities. A scheme on these lines is being developed atthe University of Brasilia. Other universities in theAmericas have likewise expressed an interest in in-troducing such schemes. Here, I think, is another basicitem for the agenda of the decade now beginning andfor later decades. Needless to say, the training inmedical studies and kindred disciplines must be ini-tensified; it seems likely that other methods will bedevised for making the teaching more effective thanit is today. In any event, between teachers and students,for whom the goal is after all the same, there must bean atmosphere of mutual understanding, a constructivedialogue accompanied by a steady improvement of themethods of achieving real knowledge. This is theprinciple underlying the "laboratories of human rela-tions and medical teaching" sponsored by the Organiza-tion in the last eight years and held in 15 countries ofthe Region with the participation of about 2,000teachers.
Over the last decade the need has become manifest toapply the educational sciences to the teaching of thehealth sciences. It implies a knowledge of a series ofdisciplines which must be acquired by those interestedin specializing exclusively in this field. They must ofcourse be teachers with a considerable amount of ex-perience. Their presence is essential today to catalyzeand shape the new ideas on the university in relationto development as referred to above. The World
Health Organization and the Pan American HealthOrganization have an important contribution to makehere.
Whatever appears most ill-timed in our societies isinvariably explained by its background. The wordecology has come into fashion in the last few years, andrightly so. It emphasizes the subtle process of adapta-tion of living beings to the surrounding environment ofwhich they are part. The environment changes, eitherthrough the designs of nature or the intervention ofmen, as a consequence of economic development. Itis possible to differentiate in the environment com-ponents of a chemical, physical, biological, psychological,and social character. All of these, alone or in combina-tion, give rise to health problems-either by direct ac-tion (as in the case of microorganisms); because theyreach concentrations which have harmful effects (as inthe case of water, air and soil pollutants); because theyupset the balance of species (as for example insecti-cides); or because they are factors causing psychologicaldisturbance and interfering with social harmony.
The Director-General of WHO, speaking at the45th Session of the Executive Board, said that "Thephrase 'environmental factors affecting man' had cometo mean all things to all men, since it concerned boththe qualitative and the quantitative aspects of man'ssocial and physical environment and ranged from arelatively narrow concern with pollutants to all aspectsof ecology and the biosphere. Neither of those oppos-ing lines of approach were fitting from the point ofview of WHO's operations: the first because pollutants,although admittedly of great importance, representedonly one of the major external factors affecting man'shealth and the second because it was too comprehen-sive." 4
Discussions are going on at the present time, withunusual vehemence in the technologically advancedcountries, concerning the urgency of environmental con-trol, especially in regard to factors whose actual andpotential effect is calculated to interfere seriously withthe lives of more and more people. A strong publicawareness has developed on this question, and it hasaroused the concern of Governments and universities.The solution of the manifest problems and the avoid-ance or reduction of their impact alike constitute avast field of research, since the number of variablesis enormous.
In virtually all the developing societies in the
4 Official Records of the World Health Organization 182(Part II), p. 40 1970.
xi
Americas, although in differing degrees, situations areemerging which will inevitably lead to that found atpresent in the developed countries. Hence we mustforestall the state of affairs described above.
Meanwhile the deficiency in basic sanitation-in-stallation of water supply services, solid waste disposal,food protection, and occupational medicine-persists.So long as there are families and communities withoutthese basic elements of well-being, this and nothingelse should be the priority of Governments, as re-flected in the level of investment of domestic resourcesand external capital. The progress made in the Amer-icas in the last decade is undoubtedly considerable asfar as water supply is concerned, but a great deal hasstill to be done, especially in the rural areas, and itsimportance is vital.
As I have said, Governments cannot afford to beindifferent to the visible consequences of industrializa-tion, urbanization, and internal migration. Many of thelarge cities in Latin America and the Caribbean areahave concentrations of air pollutants injurious to healthand living conditions; and the same is occurring inregard to other components of the environment. Itwould appear to be vital to devise a policy to be re-flected in urgent direct action, identification of newproblems, and education. This is yet another itemfor the health agenda of the 1970's and subsequentdecades, and it can help to determine the functions ofWHO and PAHO as laid down by their GoverningBodies.
As has been aptly said, there is a need not onlyfor new methods and programs to prevent or controlpollution, but for ideas and values designed to make thefuture world safe to live in, a world where life will bemeasured rather in terms of improved human relationsthan of increased gross national product. The restora-tion of the natural environment of the earth and thediscovery of how to live peacefully on it will becomethe national goal.
Because health is a right, the population increasing,and social demand growing, all matters relating totimely medical care of the sick continue to be vitalissues. In accordance with the traditional approach, wemust try to prevent disease; and if this cannot be done,we must try to reduce its scope and to prolong life. Thishas led to the creation of a complex process, involvinghuge investments in all the countries, in the form ofmedical services. Since over 80 per cent of the na-tional health budgets are earmarked for curativemedicine, and since also we still cannot meet the needs
of all those requiring such medicine, the urgent necessityhas been felt for other systems calculated to producehigher output from the installed capacity. It is well tobear in mind that no society has so far attained theideal of providing the best possible medical care to allthe inhabitants all the time.
We find in the Americas the paradoxical situationwhere hospitals of high quality, wilh the latest equip-ment, have empty beds while at the same time there aresick persons without access to these or other institutions.This basic problem of an imbalance between needs andresources is aggravated by a variety of factors, includingnot only a shortage of beds, but their deficient geo-graphic distribution and the poor state of repair ofthe establishments. Some are antiquated, over 50 yearsold, yet here is where physicians are being trained.
Other deficiencies are the poor level of utilization andlow output of the establishments available. The formeris seen in the use of extremely costly equipment foronly a few hours a day; the latter in the fact that forvarious reasons, many professionals, technicians, andauxiliaries do not furnish, either in quality or inquantity, the medical care which in principle couldbe expected of them. In addition to this, there arefactors which are not always easy to cope with, suchas economics, average income, relationship betweenprivate practice and State medical care.
Apart from the fact that coverage is limited andthe facilities concentrated largely in the main urbancenters, there is a shortage of both professionals andhealth auxiliaries. As is well known, the deficit ismuch greater in the case of nurses than of doctors, butthere is also a shortage of maintenance engineers,technicians, and other specialists.
Finally, there is the rising cost of the entire operation.Wages are increasing, equipment is more complex andmore indispensable, construction costs are rising at aparallel rate, so that all in all the investment mountsup, as 1 have said, to represent over 80 per cent of thehealth budgets of the individual countries. It is nowonder that Governments are anxious to get the bestpossible output from the installed capacity and tokeep construction of new establishments down to theabsolutely essential minimum. This is precisely whatoperational research tries to do, and hospital careprovides it with a wide field of application which needsto be developed.
Nevertheless, there are other possibilities to beachieved by better organization of the whole process.Under the heading of national health systems, a func-tional structure would be built up in an attempt toconcentrate all the available resources on the existingproblems, so as to reach fixed targets which would be
xii
evaluated periodically. According to the legislation inforce, the system could take the form of a single serviceor represent a combination of various institutions. Inany case it calls for the formulation and implementationof a policy, the delivery of services, financing, anddevelopment of manpower resources. I need hardlyrepeat that the system, whatever its structure, mustoperate in terms of the health plan.
This is the background underlying the activities ofWHO and PAHO in regard to medical care. Theseactivities are concentrated in areas where they havea catalyzing effect, e.g., direct advisory services, educa-tion, and research. But the problem as a whole isanother important item for the agenda of Governmentsand international organizations over the present andsucceeding decades. Not all the experience of the pastis useful today; it must be brought up to date in thelight of experiments which stray from the beaten trackin search of ways and means of serving patientspromptly and efficiently.
* * *
Notable advances have been made in the control ofcommunicable diseases, acute and chronic; but thesestill warrant priority in the Americas. Between 1956and 1967 the mortality rate in children under 5 yearsof age from infectious diseases dropped by some 52per cent, from diseases of the respiratory system by 35per cent, from those of the digestive apparatus (largelygastroenteritis) by 48 per cent, and from ill-definedcauses by 42 per cent. This progress, which we havereason to believe has continued, is the consequence ofthe application of preventive measures, in particularimmunization, installation of water supply services andbasic sanitation, and health education. But in spite ofthe knowledge we have today, there is still too higha level of mortality which could be avoided.
"A careful study of the reasons for this situation hasshown that one of the main causes lies in shortcomingsin the administration of vaccination programs, princi-pally in the form of ill-defined objectives, activitiesthat are not conducted at useful levels, inadequateorganization, and lack of continuity of the programs.Another factor is the use of vaccines which are of poorquality as a result of defective production methods orloss of potency due to poor preservation." 5
This opinion was given in the Final Report of theSeminar on Administrative Methods for 'VaccinationPrograms held in Montevideo, Uruguay, in November1968. A complete system was sketched out, to be
5 Document SMAPV/18, 16 November 1968, p. 1.
supplemented by evaluation of targets and epidemio-logical surveillance, the responsibility in this last instancebeing all the greater where the incidence of the particu-lar disease is reduced.
There should be no smallpox or poliomyelitis bythe end of the 1970's. The incidence of the com-municable diseases frequent in early childhood shoulddecline even more rapidly. This will, of course, dependlargely on the extent to which malnutrition is reduced.If the targets of the Charter of Punta del Este are to beattained, the present figures for deaths from tuberculosisshould be cut by one half. In regard to malaria, anendeavor must be made to bring 99 per cent of thearea exposed to risk today into the maintenance phase;this will mean the introduction of techniques to solvethe problem of resistance of the anopheles mosquitoto chlorinated insecticides and the regularity of financ-ing and political decisions.
It is likewise to be hoped that the countries andterritories which today are free of Aedes aegypti willtake due steps to avoid all reinfestation; that wherethis has taken place, they will succeed in once againeliminating the vector; and that where infestationexists today, a systematic program will be undertakento eradicate it.
The entire group of communicable diseases for whichcontrol or eradication methods exist should, and Ithink will, lose the unenviable primacy they havetoday in the Hemisphere.
Here is another item of the agenda for the 1970'sand succeeding decades.
"What happens to children in their first five yearsmarks them for the rest of their lives ... people areprisoners of their nutritional past." 6
This single statement should be enough to reveal theseriousness of the malnutrition problem in the Ameri-cas; but the situation is even worse. A mere glance atthe mortality rate in infants and children under 5 yearsshowing malnutrition as the underlying cause, bearstragic witness to what is occurring in virtually all thecountries to a greater or lesser degree. Underregistra-tion, as we well know, at times applies to a considerableproportion of both deaths and malnutrition cases. Thiscan be seen clearly in the Inter-American Investigationof Mortality in Childhood, sponsored by the Organi-zation. A preliminary analysis of 6,519 deaths 7 cover-
6 "René Dubos," by Anthony Bailey. Horizon, Vol. XII(3), p. 58 (Summer, 1970).
xiii
ing 13 areas in eight countries provides sound argumentsto corroborate this.
If it is true that health is a right, every human beingshould have a biologically balanced diet. This is not amere national goal but one which transcends frontiersand embraces the whole of mankind. We cannot re-main unmoved in the face of death by inanition oraccept arguments which merely help to perpetuate astate of affairs repugnant to our conscience. We can-not go on being divided into two groups, those whoeat properly-the privileged ones-and those whohardly eat enough to subsist. We must not wait forresearch to confirm the fact that malnutrition is a con-dition contributing to mental retárdation, or at leastinhibits the learning process in children. We must act,making use of the resources available in each country,and supplementing them with imported resources. Thiswas appreciated and accepted by the Governments whenthey decided to formulate a food and nutrition policyprimarily to meet the biological needs of the popula-tion and as far as possible those of the economy aswell. The ministries of health and agriculture havetaken a decision to this effect,8 and a Group of Expertsset up by FAO and our Organization 9 has definedbases and practices to this end. We are aware thatthis is an extremely complex task. The interests, in-grained habits, traditions, and customs to be taken intoconsideration are many. The problem involves Govern-ments as a whole; hence the absolute necessity forcoordination to achieve goals which, we repeat, mustbe principally concerned with feeding the population.The statistics are incomplete; the technology is any-thing but modern; practices are in many instancesantiquated; land is unproductive; and there is anenormous shortage of professionals and auxiliaries.Although it may seem paradoxical, at the present timethere is a great waste of food. I should like to stresshere, since it is a matter of direct interest to us, the lossof proteins through the zoonoses and foot-and-mouthdisease, which also gravely affects the economy. Thecost-benefit relationship between immunization and itseffects is measurable in monetary indicators; but what-
7 See "Progress Report on the Inter-American Investigationof Mortality in Childhood," submitted to the Ninth Meetingof the Advisory Committee on Medical Research, DocumentPAHO/ACMR 9/18, 15 June 1970, p. 2.
8 Resolution IX, "Nutrition Program in the Americas," IXMeeting of the Directing Council of PAHO, Final Report,Official Document PAHO 99, p. 59. Resolution IV, "NationalFood and Nutrition Policies," III Inter-American Meeting onFoot-and-Mouth Disease and Zoonoses Control. Final Report,Document RICAZ3/26, p. 13.
9 Elements of a Food and Nutrition Policy in Latin America.Scientific Publicarion PAHO 194 (English edition in prepara-tion).
ever the magnitude of these indicators, they do notproperly reflect what the loss of life signifies. Rodents,insects, and other species likewise destroy vast quanti-ties of foodstuffs.
The formulation and steady implementation of thefood and nutrition policy is an urgent item on theagenda for the decade now beginning and those whichwill follow. Governments and international organiza-tions, public and private, must join forces to respond tothis ineluctable challenge to our consciences, to reducemalnutrition in children, pregnant women, and adults,and to help to ensure that each of these tasks is fulfilled.As I have said, nothing would appear to be impossiblein the Americas today, however great the undertaking.
The debate on the relationship between populationand development has been one of the outstandingevents of the decade. It has gone on the world over,and it has been crystallized in declarations by Govern-ments and in the resolutions of international bodies. TheChurches have interpreted it in terms of the basic tenetsof their particular faith. For many it is the mostimportant of all questions for the future of mankind.Clearly, the very discussion of "family planning" isaffecting customs and shaking deep-rooted convictions-and even more so, the application of any system forthe spacing of children.
In the Americas, the Governments have establishedtheir policies and the terms under which advisory ser-vices can be obtained on request from WHO andPAHO. They have told us that we must concentrateon achieving health objectives and not demographicobjectives. Our task is not the size and structure ofthe population, but the reduction of the impact of dis-ease and death, and assistance to ensure that everyhousehold is properly informed and can make its owndecision as to the number of children it wants. To thisend family planning activities must be an integral partof health services, especially those aimed at maternaland child protection.
The experience gained up to now in the countriescarrying out this type of activities shows that there arestill great gaps in the knowledge of the physiology ofhuman reproduction, and that the contraceptive meth-ods in use are deficient and in some cases harmful.Hence the importance of intensifying basic and appliedresearch. The teaching of these matters is limited inthe universities, which makes it difficult, where there isa definite population policy, to put it into practice.
There is likewise a lack of knowledge of the relation-ship between the various sectors of the economy and
xiv
the size and structure of communities. Programming ofthe manpower resources required by a given countryfor its economic and social development is complicatedby the fact that there are no bases for forecasting howmany people are in need of training and how they shouldbe trained in each undertaking, whether government orprivate. There is not sufficient information available asyet to justify an objective assessment of what the num-ber of children means for a family in terms of incomeand the prospects of ensuring them a normal growth andgiving them the opportunity for becoming what theywant to become.
Here is another field of action for the 1970's andlater decades. International cooperation, given in ac-cordance with the views of Governments which considerit necessary, can play a very important role in educa-tion, in research, and in providing advisory services forthe formulation and execution of programs.
"The development of science and the use of scienceto aid man depends more on an understanding societythan on an affluent society. The most fundamentalproblem confronting the development of science-in-cluding biomedical science-in Latin America relatesnot to any specific deficiency but to a complex of socialattitudes that result in a nonscientific or an antiscientificattitude on the part of the population generally andoften on the part of political leaders. Leaders of sciencein Latin America bear a heavy responsibility to changethese attitudes." 10
While this argument can still be substantiated, definiteprogress has been made in the Latin American countriesand the Caribbean area in the last decade. The UnitedStates of America continues to be the world center forscientific research and, in our own field, particularlyfor research in molecular biology.
During the past decade, the Pan American HealthOrganization endeavored to coordinate and systematizestudies relating to priority health problems. It set upa Department for the purpose, and it had the valuableexperience of the Advisory Committee on Medical Re-search. The work done can be seen from the AdvisoryCommittee's reports, 1l the publications of PAHO, andthe analysis of projects.
An over-all view indicates that valuable contribu-tions have been made to the knowledge and understand-
10 Science Policy in Latin America. Scientific PublicationPAHO 119, p. 5, 1966.
11 Research in Progress, 1970. Publication RD/49/5(9)-R,June 1970.
ing of certain phenomena which occur in human beingsand societies, in both normal and pathological states.Among the more important are those in nutrition in itsvarious aspects; the dynamics of child and adult mor-tality and its many causes; certain zoonoses and theirprevention; malaria, in regard both to vectors and toplasmodia; and education with a view to the measure-ment of manpower resources.
This applies both to problems which require re-search for their solution and also to budgetary sources.A considerable proportion of our funds do not derivefrom the regular budget, that is to say, from governmentcontributions, as laid down in our Constitution; theyrepresent voluntary grants made by public, or privateinstitutions but earmarked for specific purposes. Henceit has been stated that "Latin American countries mightwell set as a goal the investment in research of .5 to1 per cent of the gross national product, depending onthe relative wealth of the nation. Biomedical researchis essential to the intellectual and cultural advancementof nations and to the attainment of both humanitarianand economic goals." 12
This is a goal we should like to see attained in thecourse of the decade, at any rate insofar as it relatesto the health sciencies.
It would be useful to evaluate what has been done;to identify other areas which have emerged as a conse-quence of the progress made; to determine what ma-chinery should be put into motion to institutionalizeresearch in the individual countries and throughout theHemisphere; and to link all this effort closely with theuniversities with a view to the training of professionalsand the further training of graduates; in short, to formu-late and introduce a new plan of study in the biomedicalsciences as a contribution to the knowledge of the nor-mal processes of human life, and to the treatment andprevention of pathological conditions. Here is yetanother item for our agenda which, by its nature andpurposes, extends its present horizons to the end of thecentury.
The spiraling growth of the technology and indus-trialization of health equipment, materials, and drugsmakes the prospect for the 1970's somewhat disquiet-ing. The difficulty will be not so much to formulatepossible alternatives as to select those best calculatedto attain the targets set. At the same time, the 1970'swill be a decade of opportunity if we are able to makeproper use of the lessons of the last decade, to benefitfrom past mistakes, and to put our faith in the innateability, the good intentions, and the heartfelt and legiti-mate aspirations of the people. Hence the responsi-
12 Science Policy in Latin America. Op. cit., p. 5.
xv
bilities of those with the decision-making power toreduce the impact of mortality and morbidity are greatand will be still greater.
In the preceding pages I have identified some of thebasic health problems whose solution should form partof an agenda for the coming decade. They are relatedboth to the situation in the health sector in respect ofthe dynamics of disease and to the resources employed-human, financial, or material. The account does notclaim to be complete, but it does include what is re-vealed by the progress made over the last few years,what is identified in social demand, and what tech-nology tells us it is vital to apply. The Governmentsdecide, and the international bodies that advise them,including PAHO and WHO, must amend or mold theirpolicy accordingly. The more clearly defined the plan,and its programs and projects, the more coordinatedand efficient the work of these bodies will be. If we
seek complementarity, the pivot must be the humanbeings; the means, national investmnients of every kind;and international coordination and external capital mustbe complementary.
"Man and the earth are two complementary compo-nents of an indivisible system. Each shapes the otherin a wonderfully creative symbiotic and cybernetic com-plex. The theology of the earth has a scientific basis inthe simple fact that man ennerged from the earth andthen acquired the ability to modify it and shape it, thusdetermining the evolution of his own future social lifethrough a continuous act of creation." 13
This is the continuing theme of our agenda, as soprofoundly expressed by René Dubos: the protectionof health and the prolongation of life.
13 Dubos, René. A Theology of the Earth (Lecture deliveredon 2 October 1969 at the Smithsonian Institution, Washington,D. C.). U. S. Government Printing Office, 1969, p. 16.
xvi
1. HIGHLIGHTS OF THE PERIOD 1966-1969
HISTORIC EVENTS
Cooperation in the field of public health in the Hemi-sphere during the quadrennium 1966-1969 was markedby the signature of three important documents: theProtocol of Buenos Aires of 1967, which contains theamendments to the Charter of the Organization ofAmerican States, signed in Bogotá in 1948; the Declara-tion of the Presidents of America, signed at Punta delEste on 14 April 1967; and the Final Report of theSpecial Meeting of Ministers of Health of the Americas,approved in Buenos Aires on 18 October 1968.
NEW CHARTER OF THE OAS
The Act of Rio de Janeiro, adopted in November1965, laid down general guidelines to be followed inthe preparation of amendments to the Charter of theOAS and recognized the imperative need to make theInter-American System more dynamic. The Economicand Social Act of Rio de Janeiro, also approved at theSecond Special Inter-American Conference, reaffirmedthe principles of the Declaration and the Charter ofPunta del Este of 1961 as a fundamental policy of theOAS and of the Governments of the Member States.The Organization took part in that meeting, in the ensu-ing meetings in Panama and Washington, D. C., in1966, and in the Third Special Inter-American Confer-ence of Buenos Aires in 1967, which approved theProtocol of Amendments to the Charter of Bogotá. Theoriginal purposes of the Charter were institutional, legal,and political and the amendments were an attempt tobring the Inter-American System closer to the problemsof the present, among which economic and social devel-opment, economic integration, and political security areuppermost in importance.
The health objectives of the new Charter of the OASare essentially the same as those already recognized inthe Charter of Bogotá, although they are proclaimedmore broadly and couched in more comprehensiveterms. The provisions on specialized inter-Americanorganizations, which include the Pan American HealthOrganization as the agency responsible for advising the
OAS in matters of public health and medical care, werealso left virtually unchanged.
The relations between the OAS and our Organizationhave undergone no change: they continue to be gov-erned by the Agreement signed in 1950 and by a spiritof full cooperation which has been evident whenever thetwo institutions came together to attend to matters ofcommon interest.
DECLARATION OF THE PRESIDENTS OF AMERICA
The Meeting of American Chiefs of State in 1967was preceded by careful planning, and the Organizationparticipated in its preliminary stages to ensure that theagenda would include those problems of health which,by reason of their nature and scope, required solutionsat the highest level, as recommended by the XVII PanAmerican Sanitary Conference in October 1966. Theresults achieved were such as to lead the Directing Coun-cil in 1967 to "express its satisfaction with the fullrecognition given the health sector in the Declaration ofthe Presidents of America and in the Action Programapproved by them at Punta del Este on 14 April 1967,and to incorporate into the policy of the Organizationthe proposals in that document that are directly or in-directly related to health."
In the Declaration of the Presidents we should liketo emphasize a general principle, a major objective,and a method of action. The principle is the recognitionof the fundamental role of health in the economic andsocial development of Latin America. The objective isfound in the reaffirmation of the goals set forth in 1961in the Charter of Punta del Este. And the method ofaction is the cooperation of the Organization with theGovernments in the preparation of programs relatingto the specific problems pointed out by the Chiefs ofState. The latter point is deserving of special attentionbecause it sets forth in clear and unequivocal terms theresponsibility of our Organization to cooperate with andassist the Governments of the Americas in matters ofhealth, thereby designating PAHO as the agency charged
1
-r -- FSpecial Meeting of __nisters of Health of the Americas, Buenos Ai.es, Argenti i 1 '
Special Meeting of Ministers of Health of the Amnericas, Buenos Aires, Argentina, 14-18 October 1968.
with helping the Governments to prepare specific pro-grams for attaining the health objectives laid down bythe Presidents of America.
Health, as a social function and service, satisfiesvital needs of society. It influences production andproductivity and the improvement of the physical envi-ronment. This socioeconomic value of health in noway detracts from its moral significance as a factorof well-being for individuals and of harmonious rela-tions and development for the community. This is thelesson to be learned from the Declaration of the Presi-dents, which has been made an integral part of thepolicy of the Organization and has, in effect, governedour activities during the four-year period under review.
The specific health problems mentioned in the Decla-ration will be discussed in the relevant portions of thisReport.
FINAL REPORT OF THE SPECIAL MEETING OFMINISTERS OF HEALTH
The Special Meeting of Ministers of Health of theAmericas, held in Buenos Aires in October 1968, wasthe second gathering of the highest national healthauthorities held in the Hemisphere. The Ministers ofHealth of the Signatory Governments of the Charter ofPunta del Este had met in April 1963 and had de-clared, after a careful analysis, that the Ten-Year
Public Health Program of the Alliance for Progress wasfeasible provided that its objectives were integrated withthe national goals in the field of health. The principlesand recommendations set forth by the Ministers in1963 were incorporated into our program by virtue ofResolution XXXII of the XIV Meeting of the DirectingCouncil and into our general policy in 1968, by Resolu-tion XXVI, in which the Council resolved to "incorpo-rate into the general policy of the Pan American HealthOrganization all the recommendations emanating fromthe Special Meeting of Ministers of Health of theAmericas."
As a result of the trend which has been gainingstrength in the last 20 years, and particularly in the lastdecade, health has come to be considered an integralpart of development. Public health has acquired a newdimension transcending the narrow limits which confinedits action to dealing with major epidemics; it has becomea basic instrument of economic growth and social de-velopment and an integral part, from the preinvestmentphase, of every undertaking required by the people in theinterest of an equitable distribution of national income.Such are the conclusions at which we arrive in examiningthe Ten-Year Public Health Program of 1961, theReport of the Ministers of Health in 1963, the Declara-tion and Action Program of the Presidents in 1967, andthe recommendations of the Ministers of Health in
2
1968. A continuing line of thought is observablethrough all these documents. And a continuous line ofaction is also followed because they are all based on the
same fundamental principles and pursue the same ends:health as the immediate goal, and development andsocial well-being as the longer-range objective.
PREVAILING CURRENT PROBLEMS
Latin America has certain general problems whichremained essentially unchanged during 1966-1969. Thisexplains the parallel line followed in the four docu-ments mentioned above.
These are the same problems which are today ofvital concern to nations throughout the world. Whilethere are certain features which are common to all theAmericas and others peculiar to each political societyin the Hemisphere, the problems are essentially thesame. In spite of the profound differences betweenindustrialized countries and nations in process of indus-trialization, the same concerns, although in differentdegrees, have been imposed on both groups of countriesby the demands of modern times.
Some of these matters are not confined to the field ofhealth and their solution must be sought beyond itslimits, although the health sector is an essential factorthat must be taken into consideration both in definingthe problems and in determining how to resolve them.
Prior to discussing certain prevailing current problemswithin the context of the four-year period under review,we shall examine a number of questions directly relatedto our activities in the field of health.
SALIENT HEALTH MATTERS
During the four-year period, certain communicablediseases for which effective control methods are nowavailable occurred in epidemic form in countries of LatinAmerica and the Caribbean area, in contrast to thesituation in the more developed countries, especiallythe United States of America, where only sporadiccases occurred. This indicates a failure to transfer toour countries the benefits of advances made availableby modern science and technology.
It is true that sorne of the great pestilential diseasesappear to be on the road to extinction. No cases ofcholera have been reported in the Americas during thepresent century except two laboratory-acquired infec-tions in the United States of America in 1965. Urbanyellow fever is also effectively under control, the mostrecent cases having been reported in Trinidad in 1954.In contrast, jungle yellow fever, firmly based in theAmazon, Orinoco, and Magdalena River Basins, hasappeared further south since the epizootic outbreak of
1964 and 1965 and extended as far as the 30th parallelsouth in 1966.
In the case of plague, the high incidence in Ecuadorand Peru in 1965 and 1966 was significantly reducedin 1967 and 1968, but dormant foci continue to pose athreat to the populations concerned. Louse-borne typhusis circumscribed at the present time to the mountainousparts of Mexico and the Andean highlands in Boliviaand Peru.
In 1966 the World Health Organization launched aworld-wide smallpox eradication campaign which hasled to the gradual elimination of the disease from theHemisphere except in Brazil, where a massive immuni-zation effort justifies a confident outlook.
Poliomyelitis, for which a vaccine of proven effective-ness is available, emerged in epidemic form during thelast four years in Argentina, Brazil, Colombia, Ecuador,Guatemala, Mexico, Nicaragua, Peru, and Venezuela.
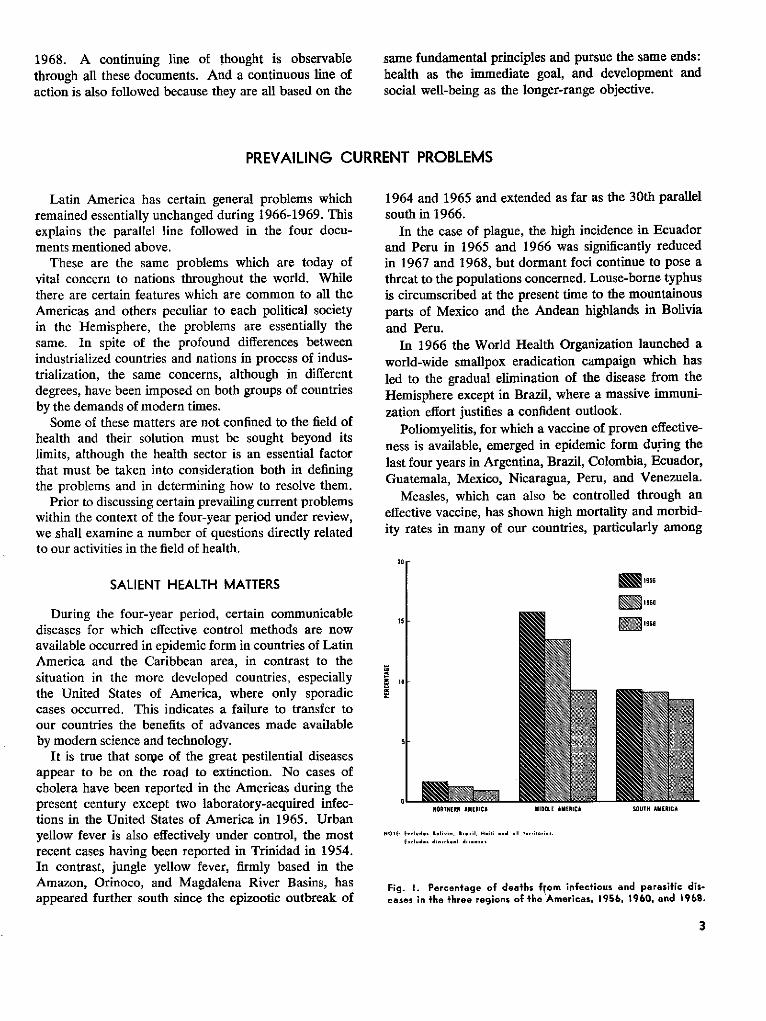
Measles, which can also be controlled through aneffective vaccine, has shown high mortality and morbid-ity rates in many of our countries, particularly among
20r
i
r
1956
2 1960
liB86
NORTHIERi AMERICA MIDOLE AMERICA SOUTH AMERICA
NOTE Elu.d.,s eolivBa, Broi;, Haili and aIl ter.ldoi
Eiiluder dj. diel dis.ase
Fig. 1. Percentage of deaths from infectious and parasitic dis-eases in the three regions of the Americas, 1956, 1960, and 1968.
3
01
the lowest income sectors in which malnutrition is afrequent problem.
In 1965, 1966, and 1968 there were epidemic out-breaks of dengue fever, a disease transmitted by Aedesaegypti, throughout the Caribbean area, particularly inPuerto Rico, Jamaica, Venezuela, and Curaçao. Trini-dad and Tobago had eradicated the vector and wastherefore free of disease. During the same period therewere outbreaks of Venezuelan equine encephalitis in thenorthern part of South America, particularly Colombiaand Venezuela, and in certain countries of CentralAmerica, indicating a need to conduct more intensiveresearch into possible means of controlling this diseasein the future.
Tuberculosis mortality has declined, but the diseasecontinues to afflict the population in many parts of theHemisphere. Leprosy, parasitic diseases, and Chagas'disease, the incidence of which is not precisely known,are taking a heavy toll in our countries.
Venereal diseases have shown a marked increase inthe Americas, particularly among the young, whichmakes them a serious social problem.
Nutritional deficiencies, which are becoming increas-ingly widespread because of population growth and theloss of protein brought about by the zoonotic diseases,especially foot-and-mouth disease, are an added com-plication in the health conditions of the Americas.
Also, a better knowledge of the prevalence of certainzoonoses, such as rabies, brucellosis, and hydatidosis,has confirmed the serious effect these have on man'shealth.
These conditions are reflected in something which inour opinion is even more serious: the phenomenon wehave referred to as "excess deaths," that is to say,deaths which could have been avoided by timely ap-plication of safe and effective means that science affordsfor their prevention or control. This is particularlysignificant in the case of children under 5 years of age,whose death, apart from weighing heavily on the con-science, represents an incalculable economic and socialloss.
The Pan American Health Organization/WorldHealth Organization, in cooperation with the Govern-ments, has given its attention to all these problems, butthe need remains to intensify in all the countries theuse of effective vaccines and other available preventivemethods so as to prevent the appearance of further out-breaks and the consequent suffering of our population.
ECONOMIC INTEGRATION
Lafin American Common Markef
The American Presidents assumed a number ofsolemn commitments regarding this matter, the impor-
tance of which is increasing with the passage of time.The Latin American Free Trade Association (LAFTA)and the Central American Common Market (CACM)are to evolve and converge by gradual stages, beginningin 1970, toward a Latin American Common Market,which should be substantially in operation within aperiod of no more than 15 years. The idea of a com-mon market had been put forth in the Economic andSocial Act of Rio de Janeiro and included in the Proto-col of Buenos Aires, so that today it is one of the funda-mental objectives of the Inter-American System.
"This great task," said the Presidents, "will reinforcehistoric bonds, will promote industrial development andthe strengthening of Latin American industrial enter-prises, as well as more efficient production and newopportunities for employment, and will permit the regionto play its deservedly significant role in world affairs.The ties of friendship among the peoples of the Conti-nent will thus be strengthened."
Economic integration demands a vigorous and sus-tained effort to facilitate the movement of persons andgoods throughout the Hemisphere; to increase foreigntrade, a matter of vital importance to the economy andprosperity of the Latin American countries; to moder-nize rural life so as to offer the majority of the peoplethe social well-being they demand and are entitled to;and to foster industrialization as an essential element ofeconomic development. But the basic role of healthmust be taken into account in all these efforts.
The Ministers of Health noted certain specific prob-lems inherent in the establishment of a common market:problems arising from trade in food and drugs; frompopulation movements and the increasing demands forhealth services; from the role and use of medical. andparamedical personnel; and from the lack of a harmoni-ous and uniform body of inter-American health legisla-tion. All these problems will be discussed in the relevantsections of this Report.
GEOGRAPHY AND HEALTH
The world has witnessed a vertiginous growth of airtransportation, to a point where the farthest regions ofthe Hemisphere are today in continuous communicationone with the other and with the rest of the world, pri-marily through the movement of persons and mail, butalso through freight traffic, which includes an increas-ingly large variety of goods. At the same time, highlyimportant changes in overland transportation havebrought or are bringing into contact regions of theHemisphere between which there was formerly no con-tinuing interchange. These substantial communica-tion links are posing serious health problems becauseof the proximity of the jungle, the emergence of new or
4
enlarged communities, and the movement of people andgoods. During the period 1966-1969, the Organizationfollowed with interest the work on the construction ofthe Bolivarian Highway and its junction with the Trans-Chaco Highway, and the entire network of roads beingbuilt in the Continent with the assistance of foreigncapital. This new highway structure will radicallychange human and ecological relationships in the re-gions traversed and will give rise to health problems towhich we must be consistently alert.
River Basins
The river basins in which a number of countries orregions are joining efforts to further the economic de-velopment of an area served by a major waterway areof key importance to public health.
It was in recognition of this that the Organization,in the early part of the period, sponsored the First Re-gional Symposium on River Basin Development, towhich it invited representatives of the basic developmentsectors and of the principal economic and financial insti-tutions of the Region. Through this and subsequentseminars, agreement was reached on the concepts andtechniques for the analysis and, as appropriate, develop-ment of the great potential wealth of the river basins.As an outcome of these activities the Organization re-ceived a large number of requests for information andtechnical assistance in this field.
The Organization participated in various projectsduring 1966-1969, notably: the project for the develop-ment of the River Plate Basin, encompassing five coun-tries; the study of the Santa Lucía River Basin in Uru-guay; the study of the Guayas River Basin in Ecuador;the project for the development of the Bogotá RiverBasin in Colombia; the project for the development ofthe Huallaga, Chiriyacu, and Nieva River Basins inPeru; and the project to control pollution of the LermaRiver in Mexico.
Project for the Development of the River Plate Basin
In 1968 an agreement was signed by Argentina, Bo-livia, Brazil, Paraguay, and Uruguay, under the sponsor-ship of the Inter-American Development Bank (IDB),the OAS, and the Economic Commission for LatinAmerica (ECLA), for integrated development of theRiver Plate Basin.
The signatory countries established an internationalcommission to examine the problems and projects relat-ing to this Basin, and each has appointed a nationalcommission composed of representatives of agencies ofthe national Government. The Ministers of Health ofthe River Plate countries have met from time to time
during the past few years to consider health problemsof mutual interest. During their sixth meeting, held inAugust 1968, in the arrangements for which the ZoneVI Office played a very active part, they examined thehealth aspects of the integrated program for the devel-opment of the River Plate region. The Organizationreceives guidance from the Ministers of Health, con-ducts activities recommended by them, and proposesmatters which the Ministers may individually or collec-tively submit to the national commissions for considera-tion or for presentation to the Coordinating Commission.By following this procedure, the Organization conductsits activities through the channels established by thecountries themselves.
A meeting of laboratory directors was held in SaoPaulo, Brazil, to agree on standard procedures to as-sure that the data collected by the five countries will besimilar and comparable, and studies have begun on thequality of water in the Basin. Basic data on water qualityare being gathered through a network of laboratoriesorganized at the beginning of the four-year period. Uni-form analytical methods, established by mutual agree-ment, are used to assess the quality of the water anddetermine its acceptability in terms of criteria laiddown by the countries.
Study of the Santa Lucía River Basin
This study was planned under an agreement signed inMay 1968 between the Government of Uruguay, theOrganization of American States, and our Organiza-tion. Its principal aim is to foster optimum use of waterresources in the Basin, as determined in accordance withrelevant criteria and guidelines supplied by the country.At the same time, a detailed work program was pre-pared, professional personnel were recruited, an ad-ministrative organization was developed, and projectoperations were initiated within a few months. Thestudy is expected to be completed around the end of1970. The Organization's responsibilities include engi-neering studies on future water needs for municipal andindustrial use, treatment of waste materials, water pol-lution, and quality requirements for each of the principaluses to which water is put. The health studies assignedto the Organization refer primarily to the public healthimplications and cost-benefit ratios of proposed changesin the water resources of the Basin. These changes mayhave secondary effects such as colonization and resettle-ment of population groups, which can create healthproblems.
The Santa Lucía agreement is the first of such tripar-tite arrangements in which the Organization has takenpart. It sets an important precedent for agreements oncooperation and development of methodology, one that
5
Signing of an agreement for a study of hydraulic resources in the Santa Lucta River Basin in Uruguay. Those signing,from leff to right: Mrs. Pura Sasco de Sundblad, Acting Representative of Uruguay to the Council of the OAS;Mr. Galo Plaza, Secretary General of the OAS; and the Director of the Pan American Sanitary Bureau.
can be highly useful in similar projects in the Region.The first stage of the project has been completed on orahead of schedule.
Development of the Guayas River Basin
The Organization is cooperating in the health andwater quality aspects of this study at the request of theEcuadorean health authorities and the Director of theExecutive Commission for Study of the Development ofthe Guayas River Basin. It has provided four short-term consultants, in addition to making available theservices of the engineering consultant assigned to theRiver Plate project. A plan of operations for subsequentactivity has been developed.
Huallaga, Chiriyacu, and Nieva River Basins
The FAO, as executing agency for the projects ofthe United Nations Development Program (UNDP)relating to agricultural development in these three riverbasins, has requested our cooperation. The Organiza-tion's technical assistance will deal primarily with thesanitation and health services necessary for the coloniza-tion and establishment of rural communities and withphysical planning and rural housing.
Pollution Problems in the Lerma River
The Director of the water supply program of theMexican Ministry of'Hydraulic Resources has requested
our assistance in the planning and implementation of aprogram to control water pollution in this Basin. Pre-liminary advisory services have been rendered andplans prepared for initial activities.
Development of the Amazon Basin
In July 1968 a meeting of representatives of theAmazon countries, called by the Government of Brazil,met in Manaus and examined a program for the develop-ment of the Amazon Basin. This program includes thehealth sector and affords us an opportunity to cooperatein the health aspects as such and in regard to their inte-gration into the plans for economic and social develop-ment of the Basin.
Coordination of Border Activities
Coordination of border activities poses a number ofspecial problems and is of great importance from thestandpoint of health. A frontier region, where twocountries come together geographically, is also oftena region in which two cultures and civilizations blendinto distinct social patterns in which elements of thetwo neighboring countries are present side by side.
The sheer length of the border between Mexico andthe United States of America-more than 1,800 miles-and the intensive flow of people and goods acrossthe boundary, led to the establishment of the UnitedStates-Mexico Border Public Health Association, which
6
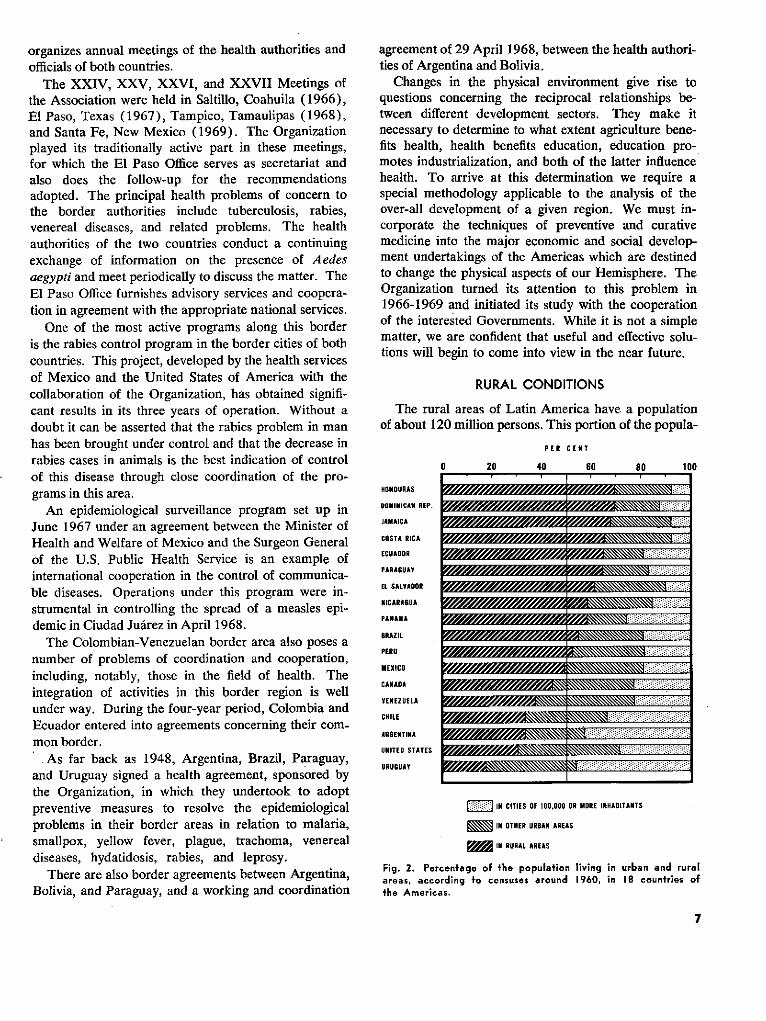
organizes annual meetings of the health authorities andofficials of both countries.
The XXIV, XXV, XXVI, and XXVII Meetings ofthe Association were held in Saltillo, Coahuila (1966),El Paso, Texas (1967), Tampico, Tamaulipas (1968),and Santa Fe, New Mexico (1969). The Organizationplayed its traditionally active part in these meetings,for which the El Paso Office serves as secretariat andalso does the follow-up for the recommendationsadopted. The principal health problems of concern tothe border authorities include tuberculosis, rabies,venereal diseases, and related problems. The healthauthorities of the two countries conduct a continuingexchange of information on the presence of Aedesaegypti and meet periodically to discuss the matter. TheEl Paso Office furnishes advisory services and coopera-tion in agreement with the appropriate national services.
One of the most active programs along this borderis the rabies control program in the border cities of bothcountries. This project, developed by the health servicesof Mexico and the United States of America with thecollaboration of the Organization, has obtained signifi-cant results in its three years of operation. Without adoubt it can be asserted that the rabies problem in manhas been brought under control and that the decrease inrabies cases in animals is the best indication of controlof this disease through close coordination of the pro-grams in this area.
An epidemiological surveillance program set up inJune 1967 under an agreement between the Minister ofHealth and Welfare of Mexico and the Surgeon Generalof the U.S. Public Health Service is an example ofinternational cooperation in the control of communica-ble diseases. Operations under this program were in-strumental in controlling the spread of a measles epi-demic in Ciudad Juárez in April 1968.
The Colombian-Venezuelan border area also poses anumber of problems of coordination and cooperation,including, notably, those in the field of health. Theintegration of activities in this border region is wellunder way. During the four-year period, Colombia andEcuador entered into agreements concerning their com-mon border.
As far back as 1948, Argentina, Brazil, Paraguay,and Uruguay signed a health agreement, sponsored bythe Organization, in which they undertook to adoptpreventive measures to resolve the epidemiologicalproblems in their border areas in relation to malaria,smallpox, yellow fever, plague, trachoma, venerealdiseases, hydatidosis, rabies, and leprosy.
There are also border agreements between Argentina,Bolivia, and Paraguay, and a working and coordination
agreement of 29 April 1968, between the health authori-ties of Argentina and Bolivia.
Changes in the physical environment give rise toquestions concerning the reciprocal relationships be-tween different development sectors. They make itnecessary to determine to what extent agriculture bene-fits health, health benefits education, education pro-motes industrialization, and both of the latter influencehealth. To arrive at this determination we require aspecial methodology applicable to the analysis of theover-all development of a given region. We must in-corporate the techniques of preventive and curativemedicine into the major economic and social develop-ment undertakings of the Americas which are destinedto change the physical aspects of our Hemisphere. TheOrganization turned its attention to this problem in1966-1969 and initiated its study with the cooperationof the interested Governments. While it is not a simplematter, we are confident that useful and effective solu-tions will begin to come into view in the near future.
RURAL CONDITIONS
The rural areas of Latin America have a populationof about 120 million persons. This portion of the popula-
HONODURAS
OOMINICAr REP.
JAMAICA
COSTA RICA
ECUAOOR
PARAGUAY
EL SALVADOR
NICARAGUA
BRAZIL
PERU
MEXICO
CANADA
VENEZUELA
CHILE
ARGENTINA
UNITED STATES
URUGUAY
PER CENT
D 20 40 60 80 100
~N'~N, ~NNNNNNN."~iiiitiiiiitiiiiiiiii[i!iiiii:ii/\\\\.:...~,NNZ~/// ~NNNNNNNNNNNNNNNN~ ,~ifitii: .iiiU:ii~!?i:: .i:tiitiiii[itii:.:..» » m m » g ... .... ~~~~~~~~~~~~~~:::::::::-::-::'i\i\\\\\\\\ : .. .....iiiiii
:: IN CITIES OF 100,000 OR MORE INHABITANTS
_ IN OTHER URBAN AREAS
_ IN RURAL AREAS
Fig. 2. Percentage of the population living in urban and ruralareas, according fo censuses around 1960, in 18 countries ofthe Americas.
7
- - - - - - -
�II�III·:·II9 :77
:itiiiii::':
:á, :.:::iijiiii
í: : . :..:::::W = 31 ~ 71 . ..~~~:::::I::I:ii�iiii':i
-�:�j'iii:i��iii�ii
. . . : .::: z.::: :
iiiiiiiiliii�iiiF

tion is denied the benefits of modern living conditions,which are concentrated in the urban environment. Aclear indication of the neglect in which they live is thefact that mortality rates in the rural areas are three anda half times as high as in urban centers.
This is perhaps the basic problem in Latin America.It is a problem of giant proportions, and one againstwhich progress is slow. We have not even managed toagree on a precise definition of what constitutes ruralpopulation. Moreover, the matter is rendered extremelycomplex in the rural areas by the combination of a seriesof social and cultural factors. Living conditions in therural environment are shaped by the prevailing systemsof land tenure and exploitation, human resources andcommunications, crop and livestock production, workmethods, electrification, credit facilities, and social andcultural characteristics.
The health infrastructure in rural areas is often inade-quate to provide minimum health care or preventiveservices, which places the local inhabitants at a disad-vantage. Rural life, which borders in certain cases onthe primitive, is no longer lived out in isolation, giventhe development of communications and the penetrationof the outside world by means of radio.
Migrafion from the Rural Areas
All these conditions combine to spur the movement ofrural dwellers to the cities at a rate which in certaincountries has reached 5 per cent of the population peryear and brought about the establishment of crowdedsettlements around the major cities, with their attendantsocial and health problems. This is the phenomenonwhich has been graphically described as the "ruraliza-tion" of the urban environment.
The fact that this phenomenon is basically related toindustrialization does not reduce our responsibility forendeavoring to find the solution, for it would seem to beundeniable that if the rural dweller were able to satisfyhis needs and find an adequate level of social well-beingin his own environment he would not be forced by cir-cumstances to emigrate to the cities. In order to alle-viate this problem we proposed some years ago theestablishment of a rural welfare fund, a proposal whichunfortunately failed to find sufficient response, but theneed for which is being made increasingly evident bycircumstances.
Motivation of fhe Community
Two aspects of the rural problem have particularlyheld our attention: motivation of the rural dweller andthe establishment of revolving funds. We have alwaysbelieved that the charges of apathy and indifference
Village dwellers collaborate in the installation of polyethylenepipes for a community water supply system.
levelled against the rural population were simply pre-texts to justify its neglect. The facts have shown thatwe were right. The rural communities have contributedtheir own labor and materials for the construction offacilities to provide them with water or sewage disposalservices. This contribution has been enthusiasticallygiven by the rural population when proper motivationwas provided in advance.
Revolving Funds
In regard to revolving funds, the initial reaction,which was to question their economic feasibility, hasradically changed. A number of Governments havewelcomed the idea and received tecinical advisory ser-vices for the establishment of such funds. The Presi-dents of America supported the concept through theirDeclaration that "national revolving fund systemsshall be used to assure the continuity" of programs forproviding drinking-water supplies, sewerage, and otherservices essential to environmental sanitation in ruraland urban areas. The Ministers of Health, for theirpart, recommended at their meeting in Buenos Airesthat PAHO/WHO expand its assistance to the Govern-ments in the establishment and utilization of revolvingfund systems. The Department of Engineering andEnvironmental Sciences has devoted special attention tothis activity and has also continued its examination ofrevolving fund systems that will operate more simplyand effectively. A certain satisfaction can be taken in
8
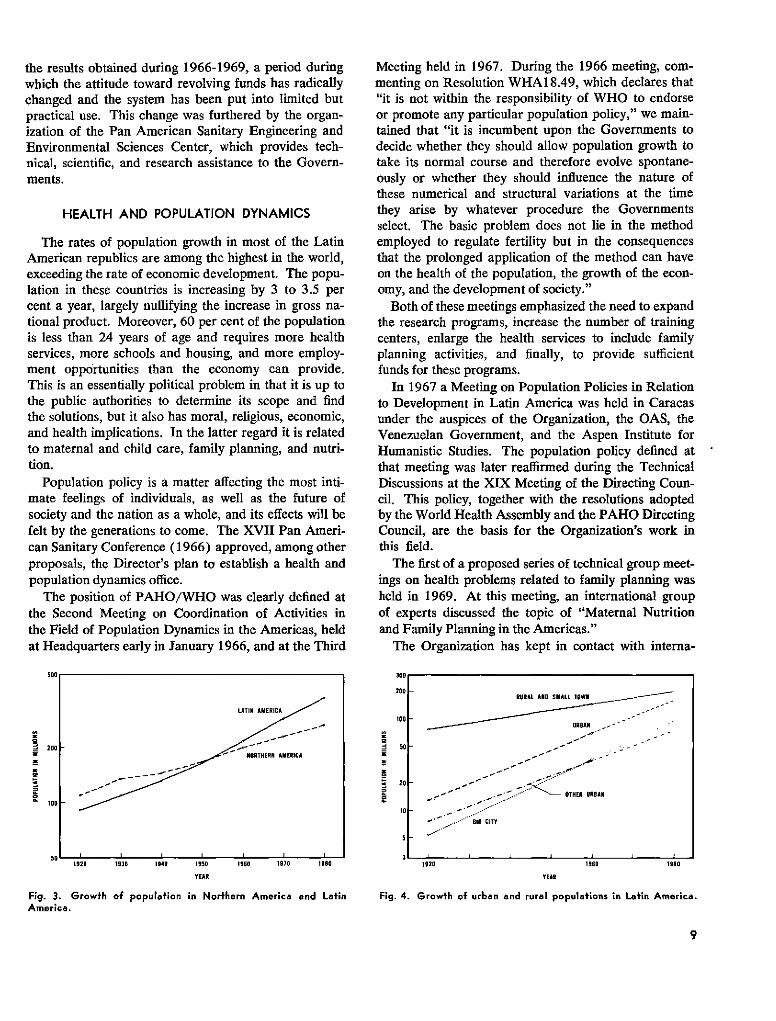
the results obtained during 1966-1969, a period duringwhich the attitude toward revolving funds has radicallychanged and the system has been put into limited butpractical use. This change was furthered by the organ-ization of the Pan American Sanitary Engineering andEnvironmental Sciences Center, which provides tech-nical, scientific, and research assistance to the Govern-ments.
HEALTH AND POPULATION DYNAMICS
The rates of population growth in most of the LatinAmerican republics are among the highest in the world,exceeding the rate of economic development. The popu-lation in these countries is increasing by 3 to 3.5 percent a year, largely nullifying the increase in gross na-tional product. Moreover, 60 per cent of the populationis less than 24 years of age and requires more healthservices, more schools and housing, and more employ-ment opportunities than the economy can provide.This is an essentially political problem in that it is up tothe public authorities to determine its scope and findthe solutions, but it also has moral, religious, economic,and health implications. In the latter regard it is relatedto maternal and child care, family planning, and nutri-tion.
Population policy is a matter affecting the most inti-mate feelings of individuals, as well as the future ofsociety and the nation as a whole, and its effects will befelt by the generations to come. The XVII Pan Ameri-can Sanitary Conference (1966) approved, among otherproposals, the Director's plan to establish a health andpopulation dynamics office.
The position of PAHO/WHO was clearly defined atthe Second Meeting on Coordination of Activities inthe Field of Population Dynamics in the Americas, heldat Headquarters early in January 1966, and at the Third
Meeting held in 1967. During the 1966 meeting, com-menting on Resolution WHA18.49, which declares that"it is not within the responsibility of WHO to endorseor promote any particular population policy," we main-tained that "it is incumbent upon the Governments todecide whether they should allow population growth totake its normal course and therefore evolve spontane-ously or whether they should influence the nature ofthese numerical and structural variations at the timethey arise by whatever procedure the Governmentsselect. The basic problem does not lie in the methodemployed to regulate fertility but in the consequencesthat the prolonged application of the method can haveon the health of the population, the growth of the econ-omy, and the development of society."
Both of these meetings emphasized the need to expandthe research programs, increase the number of trainingcenters, enlarge the health services to include familyplanning activities, and finally, to provide sufficientfunds for these programs.
In 1967 a Meeting on Population Policies in Relationto Development in Latin America was held in Caracasunder the auspices of the Organization, the OAS, theVenezuelan Government, and the Aspen Institute forHumanistic Studies. The population policy defined atthat meeting was later reaffirmed during the TechnicalDiscussions at the XIX Meeting of the Directing Coun-cil. This policy, together with the resolutions adoptedby the World Health Assembly and the PAHO DirectingCouncil, are the basis for the Organization's work inthis field.
The first of a proposed series of technical group meet-ings on health problems related to family planning washeld in 1969. At this meeting, an international groupof experts discussed the topic of "Maternal Nutritionand Family Planning in the Americas."
The Organization has kept in contact with interna-
1960 1970 19s0
Fig. 3. Growth of population in Northern America and LatinAmerica.
300.
200
100
50
20
o10
5
1920 1960 1980
YEAR
Fig. 4. Growth of urban and rural populations in Latin America.
9
arE
1z
W:
SOO
LATIN AMERICA
200 'NORTHER AMERICA
100
q0r
RURAL AND SMALL TOWN
URBAN
v ~'~'-~'~'~"~", .OTHER UReAN
. ...- '"" 1IG CITY
1920 1930 1940 1950
YEAR
QL
o
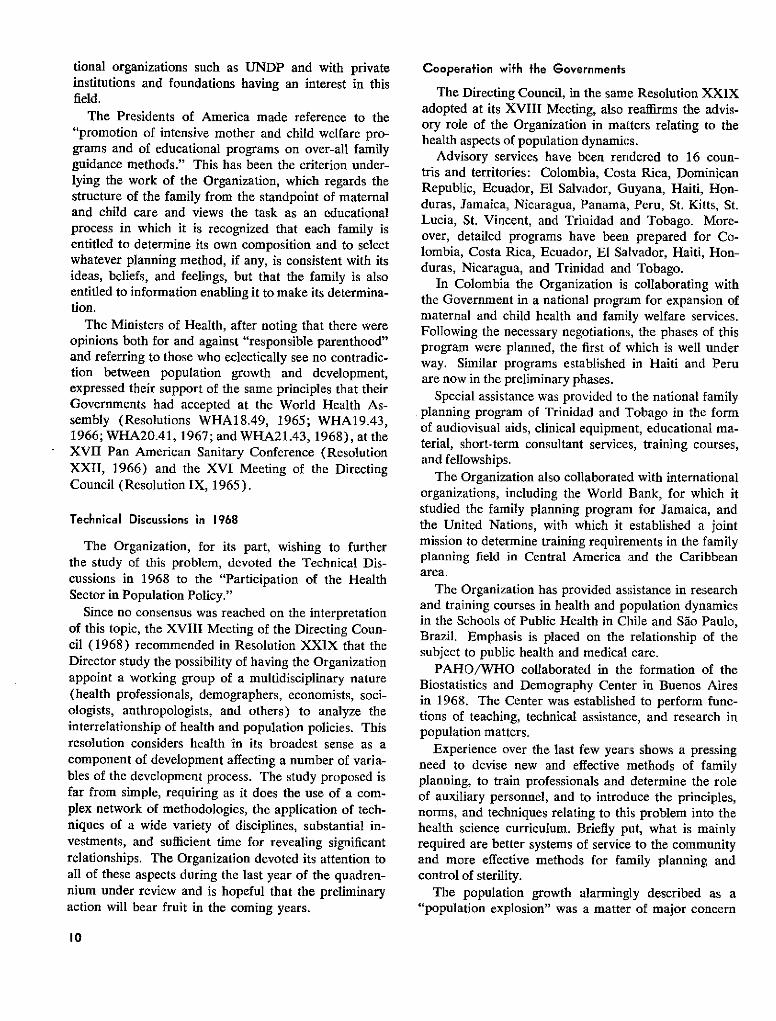
tional organizations such as UNDP and with privateinstitutions and foundations having an interest in thisfield.
The Presidents of America made reference to the"promotion of intensive mother and child welfare pro-grams and of educational programs on over-all familyguidance methods." This has been the criterion under-lying the work of the Organization, which regards thestructure of the family from the standpoint of maternaland child care and views the task as an educationalprocess in which it is recognized that each family isentitled to determine its own composition and to selectwhatever planning method, if any, is consistent with itsideas, beliefs, and feelings, but that the family is alsoentitled to information enabling it to make its determina-tion.
The Ministers of Health, after noting that there wereopinions both for and against "responsible parenthood"and referring to those who eclectically see no contradic-tion between population growth and development,expressed their support of the same principles that theirGovernments had accepted at the World Health As-sembly (Resolutions WHA18.49, 1965; WHA19.43,1966; WHA20.41, 1967; and WHA21.43, 1968), at theXVII Pan American Sanitary Conference (ResolutionXXII, 1966) and the XVI Meeting of the DirectingCouncil (Resolution IX, 1965).
Technical Discussions in 1968
The Organization, for its part, wishing to furtherthe study of this problem, devoted the Technical Dis-cussions in 1968 to the "Participation of the HealthSector in Population Policy."
Since no consensus was reached on the interpretationof this topic, the XVIII Meeting of the Directing Coun-cil (1968) recommended in Resolution XXIX that theDirector study the possibility of having the Organizationappoint a working group of a multidisciplinary nature(health professionals, demographers, economists, soci-ologists, anthropologists, and others) to analyze theinterrelationship of health and population policies. Thisresolution considers health in its broadest sense as acomponent of development affecting a number of varia-bles of the development process. The study proposed isfar from simple, requiring as it does the use of a com-plex network of methodologies, the application of tech-niques of a wide variety of disciplines, substantial in-vestments, and sufficient time for revealing significantrelationships. The Organization devoted its attention toall of these aspects during the last year of the quadren-nium under review and is hopeful that the preliminaryaction will bear fruit in the coming years.
Cooperafion with the Governments
The Directing Council, in the same Resolution XXIXadopted at its XVIII Meeting, also reaffirms the advis-ory role of the Organization in matters relating to thehealth aspects of population dynamics.
Advisory services have been rendered to 16 coun-tris and territories: Colombia, Costa Rica, DominicanRepublic, Ecuador, El Salvador, Guyana, Haiti, Hon-duras, Jamaica, Nicaragua, Panama, Peru, St. Kitts, St.Lucia, St. Vincent, and Trinidad and Tobago. More-over, detailed programs have been prepared for Co-lombia, Costa Rica, Ecuador, El Salvador, Haiti, Hon-duras, Nicaragua, and Trinidad and Tobago.
In Colombia the Organization is collaborating withthe Government in a national program for expansion ofmaternal and child health and family welfare services.Following the necessary negotiations, the phases of thisprogram were planned, the first of which is well underway. Similar programs established in Haiti and Peruare now in the preliminary phases.
Special assistance was provided to the national familyplanning program of Trinidad and Tobago in the formof audiovisual aids, clinical equipment, educational ma-terial, short-term consultant services, training courses,and fellowships.
The Organization also collaborated with internationalorganizations, including the World Bank, for which itstudied the family planning program for Jamaica, andthe United Nations, with which it established a jointmission to determine training requirements in the familyplanning field in Central America and the Caribbeanarea.
The Organization has provided assistance in researchand training courses in health and population dynamicsin the Schools of Public Health in Chile and Sao Paulo,Brazil. Emphasis is placed on the relationship of thesubject to public health and medical care.
PAHO/WHO collaborated in the formation of theBiostatistics and Demography Center in Buenos Airesin 1968. The Center was established to perform func-tions of teaching, technical assistance, and research inpopulation matters.
Experience over the last few years shows a pressingneed to devise new and effective mnethods of familyplanning, to train professionals and determine the roleof auxiliary personnel, and to introduce the principles,norms, and techniques relating to this problem into thehealth science curriculum. Briefly put, what is mainlyrequired are better systems of service to the communityand more effective methods for family planning andcontrol of sterility.
The population growth alarmingly described as a"population explosion" was a matter of major concern
10
during 1966-1969 and one to which the Organizationdevoted continuous attention within the frameworkestablished by the World Health Assembly and thePAHO Governing Bodies.- We have followed the courseof action prescribed by the Member Governments andhave provided them with advisory services wheneverthey have requested them.
FOOD AND NUTRITION POLICY
In 1967 a study on the nutrition program in theAmericas was placed before the Directing Council. Thisstudy noted that "an analysis of the work done by PAHOin the field of nutrition in the last 10 years shows thatit has followed a logical pattern, satisfying the mosturgent needs, and following the guidelines proposed inthe Charter of Punta del Este, the recommendation ofthe Task Force on Health, and the resolution of the XVIPan American Sanitary Conference." Referring to theemerging awareness of nutrition problems among thepopulation and the public authorities, the study recalledthat the Declaration of the Presidents of America hadpointed to nutrition as one of the three principal healthproblems having the highest priority, the others beingthe eradication of infectious diseases and the provisionof water to rural communities. This study led to the pro-posal of a new program in which PAHO/WHO wouldtake the leading role within a coordinated system forapproaching national nutrition problems from a highpolicy level.
The Directing Council adopted a resolution instruct-ing the Director to "continue to develop all aspects ofthe nutrition program in progressive steps consonant
with the development of the over-all program of PASB"and calling for closer collaboration with FAO and otherinternational and bilateral organizations. The resolutionalso emphasized "the importance, for nutrition programplanning, of the close collaboration of all national insti-tutions in the agriculture, industry, education, andhealth fields."
The Ministers of Health, at their Special Meeting inBuenos Aires, examined the many aspects of the prob-lem of food production. They noted that progress hadclearly been made in the diagnosis and treatment ofnutritional diseases but not in their prevention, and thatthis was due to a lack of information concerning thesupply of protective and energy-yielding food for meet-ing the vital needs of each population group. Theystated that in all countries of the Americas there is anurgent need to define a national policy for systematicaction against the problems of food and nutrition tomake it possible to assure an adequate nutritional levelto the population while also meeting the needs ofeconomic development.
Infant Morfality
Nutrition is an important contributing factor in thehigh rates of mortality among infants and children under5 years of age in the less developed areas of all the coun-tries in the Hemisphere. Protein and calorie deficien-cies go hand in hand with infectious diseases, ignorance,overcrowding, unhealthful living conditions, and theshortage of medical services. The result is that 44 percent of all those who die in Latin America are childrenunder 5 years of age and that, on the basis of a com-
An effort is made to provide adequate food for school groups as part of a food and nutrition policy.
II
parison of the average rates of infant mortality in theUnited States of America and Canada with those forLatin America and the Caribbean, it is found that some741,000 of these children could be saved if they wereproperly nourished and in a condition to withstand theonslaught of the environment and of disease. This is anextremely serious moral problem which imposes anobligation on all of us to contribute to its solution. It isalso a source of concern and shame and is perhaps thesalient index of underdevelopment in the field of health.An essential step toward the solution of this problem wastaken during the period under review with the com-mencement on 1 July 1968 of the Inter-American In-vestigation of Mortality in Childhood, which will bediscussed further on.
Loss of Essential Profeins
In a society suffering from malnutrition and whereundernutrition is chronic among the low-income sectors,the loss of essential proteins is a health problem, aneconomic problem, and a problem of development ingeneral. This problem is made even worse by certainanimal diseases such as foot-and-mouth disease, bovinetuberculosis, rabies, brucellosis, and parasitosis, for thesolution of which significant amounts of national re-sources and the assistance of foreign capital are re-quired. It should be noted in this regard that both theIDB and the World Bank have a policy of extendingfinancial assistance, under certain conditions, for pro-grams directed to the control of various zoonoses.
These programs, because of the biological nature ofthe problem with which they deal, require constant re-search and the training of personnel. The Pan-Ameri-can Foot-and-Mouth Disease Center and the Pan Amer-ican Zoonoses Center are engaged in such research andtraining activities, in addition to providing advisoryservices to Governments.
Future Action
The XIX Meeting of the Directing Council (1969)recommended to the PASB that it continue to give highpriority to the nutrition program and that it assigncorresponding resources to provide the services re-quired for effective action, especially in the formulationof national food and nutrition policies. It further rec-ommended to the Governments that "national food andnutrition policies be formulated according to suggestedguidelines as soon as possible with the objective ofcontrolling the problem of malnutrition, thus reducingthe costs of health care and allowing reassignment andmore efficient use of resources."
This course of action, followed by the Governments
and the Organization, will result ini a concerted multi-disciplinary effort.
MODERN SCIENCE AND TECHNOLOGY
It has been truthfully said that humanity has pro-gressed more in the last 50 years than in all the preced-ing centuries. The advances of science and moderntechnology have provided us with effective weaponsfor the eternal battle against disease. These advancesare but forerunners of even greater progress that offersthe prospect of a stunning dleveloprnent of science andtechnology by the year 2000.
The Presidents of America recognized in 1967 that"science and technology offer genuine instruments forLatin American progress and must be given an unpre-cedented impetus at this time. This effort calls for inter-American cooperation, in view of the magnitude of theinvestments required and the level attained in suchknowledge. In the same way, their organization andimplementation in each country cannot be effected with-out a properly planned scientific and technologicalpolicy within the general framework of development."
Research
These ideas were the basis upon which the Ministersof Health defined the national and international healthresearch policy. The Ministers conceived of research asan essential factor for the development of the Americas,which requires the modernization of institutions andsystems.
The health sciences, which operate within a spectrumranging from molecular biology to social biology, in-cluding economics, must be placed at the service of all.They are the property of humanity. Every country andevery person must contribute to the extent of his ability,vocation, and means to their development and applica-tion.
Science and technology and their discoveries andinventions are universal. Ideas have no particular coun-try, and eminent scientists are citizens of the world.But each environment imposes its laws and makes itnecessary to take the cultural characteristics, history,way of life, public opinion, and traditions, as well asbeliefs and superstitions of each society, into account,lest scientific and technological progress fail to find aresponse and its benefits be lost.
The Scientific and Cultural Community
Along with their distinct characteristics, the Americashave certain basic features that make it possible andeven imperative to carry out a Hemisphere-wide pro-gram of scientific and technological research. This was
12
said by the Presidents of America in their Declarationand recognized by the Ministers of Health at theirSpecial Meeting in 1968.
Moreover, as far as we are concerned, any effectiveeconomic community in Latin America must be basedon a scientific and cultural community. It is this con-viction which has guided the research policy of theOrganization to an ever-increasing extent in the last10 years, a policy to which an average of 33 per cent ofthe total budget was devoted in 1966-1969, or aboutUS$3,000,000 in 1969.
Research Policy
The XVI Pan American Sanitary Conference (1962)noted the need to increase our research activities. Thiswas done, with the assistance of the Advisory Commit-tee on Medical Research, with the result that the XVIIPan American Sanitary Conference (1966) was able toexamine a report summarizing 90 projects in progressor completed.
The research program had been directed principallyinto those areas of biomedical investigation and train-ing for research that were related to the objectives ofthe Organization. This explains why there were a num-ber of research projects in certain fields: 17 on nutri-tion, 6 on malaria eradication, 13 on foot-and-mouthdisease, and 11 on environmental sanitation.
The XVII Conference authorized the Director toestablish a Special Fund for Research in order to expandthis program. Contributions to this Fund were pledgedby Argentina, Brazil, and Uruguay.
The Organization's research activities during 1966-1969 closely followed the guidelines established bythe Conference. In order to make these activities morecohesive, the Research Unit was raised in 1968 to therank of a Department, while its services were increasedand its technical personnel enlarged. The program ofPAHO/WHO has played an important part in thedevelopment and consolidation of biomedical researchresources and possibilities in the Americas.
Fifth Meeting of the PAHO AdvisoryCommittee on Medical Research heldaf Headquarters in Washington, D.C.,13-17 June 1966.
Multinational Centers
The Conference also called for a study on means forexpanding and augmenting the number of multinationalcenters for training and research in the life sciences andmedicine. A few months later the Presidents of Americaproposed "that multinational technological and scientifictraining and research institutions at the postgraduatelevel be established, and that institutions of this naturealready existing in Latin America be strengthened" aspart of the Regional Scientific and Technological Devel-opment Program. The XVII Meeting of the DirectingCouncil, convinced that the development of cooperativeprograms to strengthen multinational activities in thefield of higher education and research in the healthsciences in Latin America was identical in purpose andmethods with the original program, confirmed that"PAHO is the logical international organization in theWestern Hemisphere to sponsor and coordinate cooper-ative multinational programs for research and graduateeducation in the health sciences" and requested theDirector "to continue to take this position." ResolutionXXIV, in which this paragraph appears, also estab-lished the future guidelines, particularly as regardsfinancing, which together with the recommendations ofthe Ministers of Health have been the basis for subse-quent action by the Organization.
The XIX Meeting of the Directing Council, followinga recommendation of the 61st Meeting of the ExecutiveCommittee, declared that multinational centers areneeded and useful and requested the appointment of astudy group to draw up a set of general guidelines forthe establishment and operation of such centers. TheCouncil further recommended that the Governmentsstudy the possibility of assuming a progressively largershare of the operating budget of centers located in theircountries and of extending the services of those centersto the countries of the Hemisphere, in the first place toother countries in the Zone to which they belong.Finally, the Council recommended to the Director thatthe funds made available be primarily used, subject to
13
certain conditions, for aiding the countries that requestmore assistance.
Migration of Professionals
A discussion of research and of university educationwill generally bring up the problem of the exodus ofhealth personnel, scientists, and engineers from LatinAmerica. The XVII Pan American Sanitary Confer-ence examined a report which proposed the strengthen-ing of existing research centers and recognized the needfor continued United States support of scientific workin Latin America, together with an Organization-spon-sored program of visiting professorships directed to theformation of a cadre of Latin American researchers whowould later continue their activities. The report alsorecommended that PAHO/WHO conduct a study onthe status of' research in Latin America and establish acenter to provide information on the migration of scien-tific personnel.
In Resolution XVII the Conference requested theGovernments to take appropriate measures to strengthennational policies leading to research and training pro-grams in health and, the sciences which would provideincentives for nationals to remain at home. This wouldexpand the capacity. of countries to develop economi-cally and culturally, strengthen universities, and facili-tate the provision of more adequate health services inthe countries concerned. The Special Meeting of Min-isters also recommended the establishment of conditionsto encourage a greater number of physicians and healthscientists to remain in their countries.
Migration is a biological process occurring in everyliving species. Not all of its causes are economic, al-though in certain cases the latter play a predominantrole, as exemplified by the migratory movements ofworkers who leave their country in search of employ-ment and better living conditions. In the case of scien-tists, professionals, and technicians, the lack of encour-agement and opportunities is often the decisive factorthat prompts them to move to a place where they canfind the means of advancing in their work.
The Organization has carefully followed this prob-lem, a precise assessment of which has not been possiblebecause of the lack of complete information. A researchpolicy such as that which is sought by the GoverningBodies of the Organization would undoubtedly reducethe migration of health professionals to a substantialdegree.
HUMAN RESOURCES
In 1966 we stated: "There has been a renewal ofeffort in the Americas, in all fields of science and tech-
nology, aimed at training professional and auxiliaryhealth workers. It is realized that they are essentialfactors in development and that its slow pace is in largemeasure due to the shortage of manpower at the mana-gerial, intermediate, and operational levels. This short-age is clearly evident in the health field, where thegreat diversity of functions calls for a great diversity oftechnicians. In addition to knowledge and experience,they must possess a spirit of understanding and toler-ance which is rooted in a feeling of empathy with, anddevotion to, all other human beings." This assessment,which reflects the actual situation during the period1966-1969, has guided the work of the Organization.
Specifically, the policies and activities of the Organi-zation have focused on both the qualitative and quanti-tative aspects of the problem, for along with more per-sonnel there is a need for improved instruction and abroader curriculum. During the last 25 years the num-ber of medical schools has more than doubled, but theratio of physicians to total population has remainedconstant at about 6.5 per 10,000 inhabitants, most ofthe physicians being concentrated in the city and manylacking an awareness of their social function.
In Latin America the schools of medicine, which forhistoric and economic reasons are financially dependentupon the State, are not providing uniform instructionand in many cases the curriculum they offer has internalinconsistencies and is unresponsive to the present-dayconcept of education for development, a concept stem-ming from the major political, economic, and socialdecisions of the last 10 years and recognized in theCharter of Punta del Este, which recommended thateducation be planned to conform to the trends of eco-nomic and social development. The university cannotafford to remain aloof from the problems affecting manand society, particularly in matters dealing with individ-ual human life and social well-being. Instruction must bein line with the social realities. It was in recognition ofthis that the Presidents of America declared: "We willvigorously promote education for development." In sodeclaring they imbued the process of education with awell-defined purpose and emphasized the importance ofa search for new patterns and schemes of instruction inthe universities of the Hemisphere. Medical educationis no exception. We have a clear awareness today thatthe medical profession has important responsibilities inthe process of satisfying the essential aspirations of man.
The Crisis in the Universities
The period 1966-1969 witnessed a growth of themovement arising in recent times to free the universitiesfrom the attitude of indifference and "business as usual"and place them at the service of vital ideas circulating
14
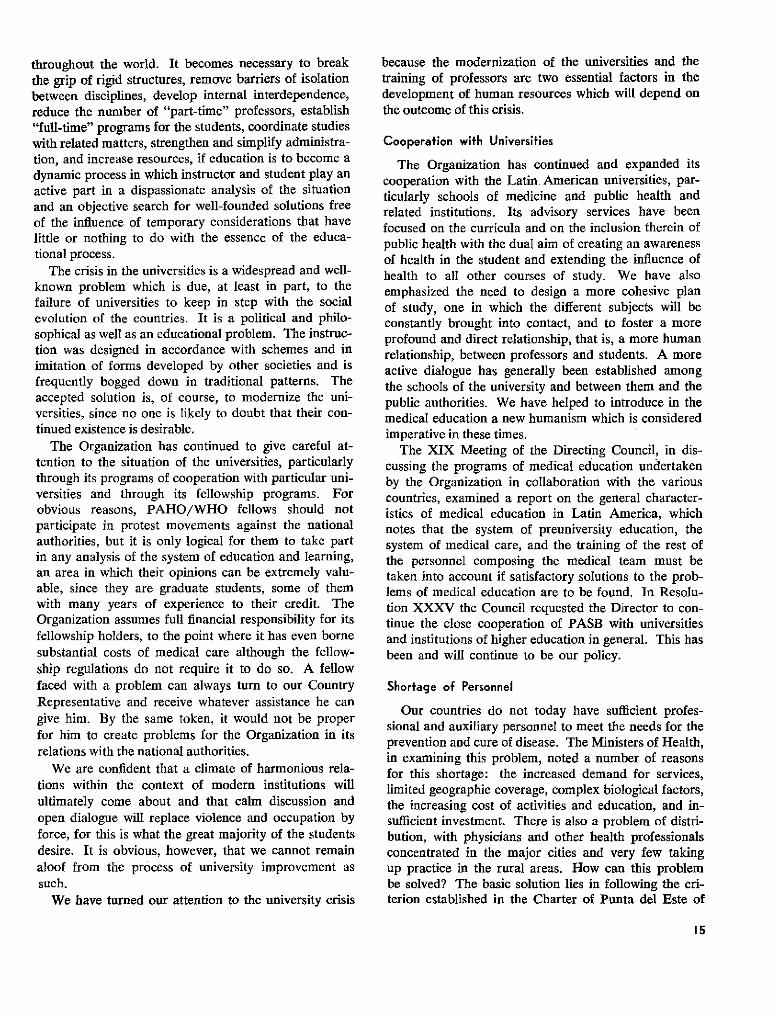
throughout the world. It becomes necessary to breakthe grip of rigid structures, remove barriers of isolationbetween disciplines, develop internal interdependence,reduce the number of "part-time" professors, establish"full-time" programs for the students, coordinate studieswith related matters, strengthen and simplify administra-tion, and increase resources, if education is to become adynamic process in which instructor and student play anactive part in a dispassionate analysis of the situationand an objective search for well-founded solutions freeof the influence of temporary considerations that havelittle or nothing to do with the essence of the educa-tional process.
The crisis in the universities is a widespread and well-known problem which is due, at least in part, to thefailure of universities to keep in step with the socialevolution of the countries. It is a political and philo-sophical as well as an educational problem. The instruc-tion was designed in accordance with schemes and inimitation of forms developed by other societies and isfrequently bogged down in traditional patterns. Theaccepted solution is, of course, to modernize the uni-versities, since no one is likely to doubt that their con-tinued existence is desirable.
The Organization has continued to give careful at-tention to the situation of the universities, particularlythrough its programs of cooperation with particular uni-versities and through its fellowship programs. Forobvious reasons, PAHO/WHO fellows should notparticipate in protest movements against the nationalauthorities, but it is only logical for them to take partin any analysis of the system of education and learning,an area in which their opinions can be extremely valu-able, since they are graduate students, some of themwith many years of experience to their credit. TheOrganization assumes full financial responsibility for itsfellowship holders, to the point where it has even bornesubstantial costs of medical care although the fellow-ship regulations do not require it to do so. A fellowfaced with a problem can always turn to our CountryRepresentative and receive whatever assistance he cangive him. By the same token, it would not be properfor him to create problems for the Organization in itsrelations with the national authorities.
We are confident that a climate of harmonious rela-tions within the context of modern institutions willultimately come about and that calm discussion andopen dialogue will replace violence and occupation byforce, for this is what the great majority of the studentsdesire. It is obvious, however, that we cannot remainaloof from the process of university improvement assuch.
We have turned our attention to the university crisis
because the modernization of the universities and thetraining of professors are two essential factors in thedevelopment of human resources which will depend onthe outcome of this crisis.
Cooperation witfh Universities
The Organization has continued and expanded itscooperation with the Latin American universities, par-ticularly schools of medicine and public health andrelated institutions. Its advisory services have beenfocused on the curricula and on the inclusion therein ofpublic health with the dual aim of creating an awarenessof health in the student and extending the influence ofhealth to all other courses of study. We have alsoemphasized the need to design a more cohesive planof study, one in which the different subjects will beconstantly brought into contact, and to foster a moreprofound and direct relationship, that is, a more humanrelationship, between professors and students. A moreactive dialogue has generally been established amongthe schools of the university and between them and thepublic authorities. We have helped to introduce in themedical education a new humanism which is consideredimperative in these times.
The XIX Meeting of the Directing Council, in dis-cussing the programs of medical education undertakenby the Organization in collaboration with the variouscountries, examined a report on the general character-istics of medical education in Latin America, whichnotes that the system of preuniversity education, thesystem of medical care, and the training of the rest ofthe personnel composing the medical team must betaken into account if satisfactory solutions to the prob-lems of medical education are to be found. In Resolu-tion XXXV the Council requested the Director to con-tinue the close cooperation of PASB with universitiesand institutions of higher education in general. This hasbeen and will continue to be our policy.
Shorfage of Personnel
Our countries do not today have sufficient profes-sional and auxiliary personnel to meet the needs for theprevention and cure of disease. The Ministers of Health,in examining this problem, noted a number of reasonsfor this shortage: the increased demand for services,limited geographic coverage, complex biological factors,the increasing cost of activities and education, and in-sufficient investment. There is also a problem of distri-bution, with physicians and other health professionalsconcentrated in the major cities and very few takingup practice in the rural areas. How can this problembe solved? The basic solution lies in following the cri-terion established in the Charter of Punta del Este of
15
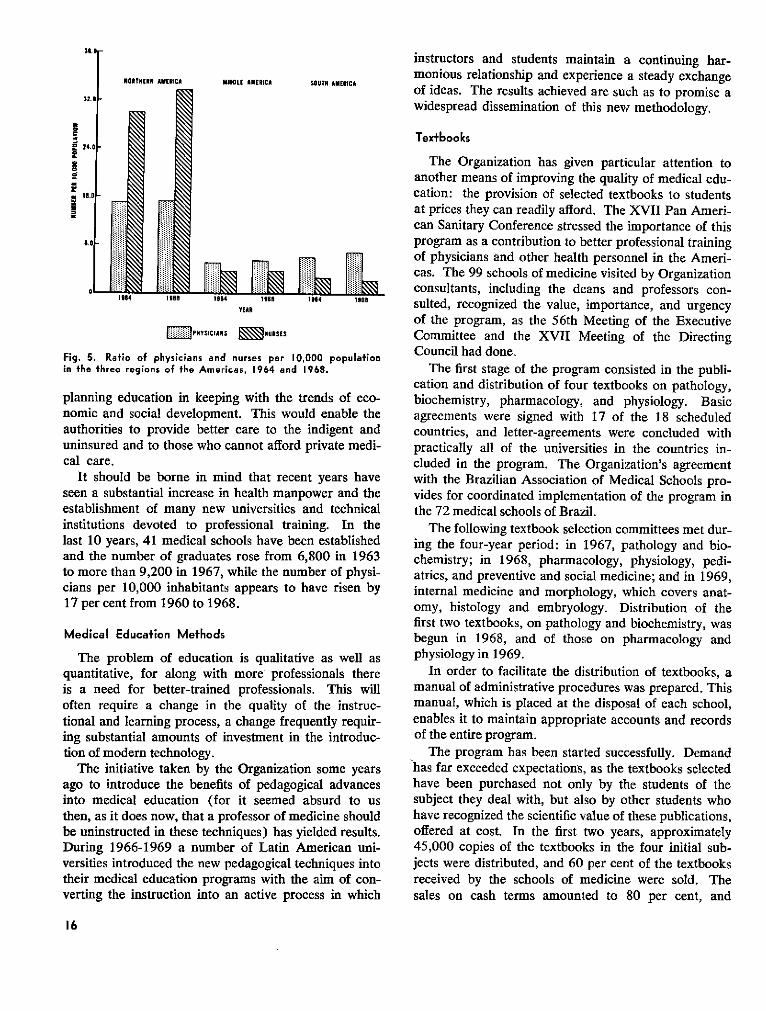
32.0
u
du
p
Ema1
NOlAnHElN ANERICA
iii
ii ii
24.0-
16.0
.
0.-5
MIDDLE AMERICA SOUTH AMERICA
Dbr%1964 1966 1964 ;196
YEAR
E::PHYSICIANS NURSES
Fig. 5. Ratio of physicians and nurses per 10,4in the three regions of the Americas, 1964 and I
planning education in keeping with the trnomic and social development. This woulauthorities to provide better care to theuninsured and to those who cannot afford ]cal care.
It should be borne in mind that recenseen a substantial increase in health manpcestablishment of many new universities ainstitutions devoted to professional trainlast 10 years, 41 medical schools have beeand the number of graduates rose from 6,to more than 9,200 in 1967, while the numcians per 10,000 inhabitants appears to h17 per cent from 1960 to 1968.
Medical Education Methods
The problem of education is qualitativquantitative, for along with more profesis a need for better-trained professionaloften require a change in the quality oftional and learning process, a change freqiing substantial amounts of investment in ttion of modern technology.
The initiative taken by the Organizatiojago to introduce the benefits of pedagogiinto medical education (for it seemed athen, as it does now, that a professor of mebe uninstructed in these techniques) has yiDuring 1966-1969 a number of Latin Aversities introduced the new pedagogical teetheir medical education programs with theverting the instruction into an active proc
instructors and students maintain a continuing har-monious relationship and experience a steady exchangeof ideas. The results achieved are such as to promise awidespread dissemination of this new methodology.
Textbooks
The Organization has given particular attention toanother means of improving the quality of medical edu-cation: the provision of selected textbooks to studentsat prices they can readily afford. The XVII Pan Ameri-can Sanitary Conference stressed the importance of thisprogram as a contribution to better professional trainingof physicians and other health personnel in the Ameri-cas. The 99 schools of medicine visited by Organizationconsultants, including the deans and professors con-
1904 19S5 sulted, recognized the value, importance, and urgencyof the program, as the 56th Meeting of the ExecutiveCommittee and the XVII Meeting of the Directing
000 populafion Council had done.968. The first stage of the program consisted in the publi-
cation and distribution of four textbooks on pathology,rends of eco- biochemistry, pharmacology, and physiology. Basic[d enable the agreements were signed with 17 of the 18 scheduledindigent and countries, and letter-agreements were concluded withprivate medi- practically all of the universities in the countries in-
cluded in the program. The Organization's agreementIt years have with the Brazilian Association of Medical Schools pro-ower and the vides for coordinated implementation of the program inLnd technical the 72 medical schools of Brazil.iing. In the The following textbook selection committees met dur-n established ing the four-year period: in 1967, pathology and bio-,800 in 1963 chemistry; in 1968, pharmacology, physiology, pedi-ber of physi- atrics, and preventive and social medicine; and in 1969,have risen by internal medicine and morphology, which covers anat-
omy, histology and embryology. Distribution of thefirst two textbooks, on pathology and biochemistry, wasbegun in 1968, and of those on pharmacology and
'e as well as physiology in 1969.sionals there In order to facilitate the distribution of textbooks, as. This will manual of administrative procedures was prepared. This
the instruc- manual, which is placed at the disposal of each school,iently requir- enables it to maintain appropriate accounts and recordsthe introduc- of the entire program.
The program has been started successfully. Demandn some years has far exceeded expectations, as the textbooks selectedcal advances have been purchased not only by the students of theabsurd to us subject they deal with, but also by other students whodicine should have recognized the scientific value of these publications,elded results. offered at cost. In the first two years, approximatelymerican uni- 45,000 copies of the textbooks in the four initial sub-chniques into jects were distributed, and 60 per cent of the textbooks
aim of con- received by the schools of medicine were sold. The:ess in which sales on cash terms amounted to 80 per cent, and
16
3.Or
collections have been very satisfactory on the creditsales. As instructed by the Directing Council, the Organ-ization has persisted in its efforts to obtain extra-budgetary funds for intensifying and expanding its pro-gram of education and training. Although no financialassistance arrangements were actually concluded dur-ing the four-year period, the highly favorable recep-tion accorded the textbook program in its initial stageswarrants the expectation that financial support will bereceived from institutions concerned with the improve-ment of professional and medical education in theAmericas, enabling the Organization to achieve one ofthe basic objectives of the textbook program, namely,establishment within four years of a self-sustaining fundpermitting the program to be financed indefinitely withincome derived from the sale of textbooks.
EXTERNAL FINANCIAL RESOURCES
The demand for health services is increasing day byday as a result of public demands to share in the bene-fits of scientific and technological advance now beyondthe reach of low-income and even moderate-incomegroups. Modern preventive and curative medicine, in-cluding rehabilitation, offers valuable and highly effec-tive therapeutic methods, techniques, and equipmentwhich often require substantial amounts of investmentbeyond the financial possibilities of the great majorityof persons who need them. The Governments them-selves are finding it impossible to meet the requirementsof economic development and social progress out oftheir budgetary resources. This raises the problem ofhow to strengthen the sources of national income withthe help of external financing to expand the financialcapacity of the public sector and enable it to meet justand imperative social demands. Only with the coopera-tion of foreign capitai is it possible to speed the solutionof certain health problems affecting a large number ofpersons or a particular region of basic interest forsocial development.
Recent years, particularly those since the meeting ofthe Task Force on Health in 1963, have been markedby renewed interest of the Governments in gainingaccess to new sources of international financing, particu-larly for the health sector. During 1966-1969 thistrend became even more pronounced and our Organiza-tion attempted to provide advisory services to countriesrequesting them for this purpose.
International Financial Insfitutions
The institutions providing loans for the health sectorin the Americas are the Inter-American DevelopmentBank, the World Bank, the Agency for International
Development, and EXIMBANK. Each of these has itsown criteria to govern its loans, which are not restrictedto national Governments but are extended also to politi-cal subdivisions, autonomous agencies, and under cer-tain conditions to private concerns.
In addition to these institutions, the Governments ofcertain countries, including Canada, the German FederalRepublic, and the United States of America, have shownan interest in programs of hospital construction andequipment, water supply, malaria eradication, sanitationservices, and rural health units, among others.
The Inter-American Development Bank holds a lead-ing position in this field. In 1968 it defined the type ofhealth programs that were eligible for loans from itsFund for Special Operations. With the consent of thePresident of the Bank, the document setting forth itscredit policy was distributed to the Ministers of Healthas a means of familiarizing them with the procedure fordrawing up and for submitting loan applications meet-ing the Bank's requirements.
The Ministers of Health in Buenos Aires, commentingon the document, noted that it reflected "the experienceof the Bank, which envisions the development of theAmericas as a harmonious process of economic growthand social welfare."
Among the social investments of the IDB are thosefor water supply and sewage disposal programs. Theseservices, essential to individual health and economic andsocial well-being, were given priority in the Charter ofPunta del Este and were emphasized by the Presidentsof America and the Ministers of Health in 1963 and1968. The IDB loans in this field have served as acatalyst to local investment. By June 1968 $1.4 billionhad been devoted to water supply and sewerage servicesin Latin America. Of this amount, $800 million repre-sented national funds and $550 million, of which 75 percent was provided by the IDB, was derived from loansof international organizations. The technical servicesof the Organization have worked in close relationshipwith the relevant national services and those of the IDBin implementing these programs.
In addition to the programs indicated above, theFund for Special Operations has extended credit assist-ance to medical and health education, the constructionof university hospitals, and the control of foot-and-mouth disease.
An important program in which the IDB collaboratesthrough loans is the control and prevention of foot-and-mouth disease in the countries of South America,which to date amount to US$30,000,000. Likewise, theOrganization has cooperated closely with the IDB as thetechnical advisory body in the evaluation of loan re-quests and at present participates in the development
17

and execution of these programs. The IDB has broad-ened its policy in animal health through the grantingof loans for the control of other animal diseases, espe-cially the zoonoses.
Loans from the World Bank require extensive prepar-atory arrangements often lasting several months andincluding exploratory studies and preliminary assess-ments of the borrower and the project. In recent yearsthe Bank has extended its operations into two healthareas: foot-and-mouth disease control and populationgrowth. The Organization has furnished advisory ser-vices whenever the Governments or the Bank have sorequested it.
The AID has not established a standard procedurefor the processing and granting of loans. The projectsare generally selected by its Mission in the applicantcountry. In their many years of cooperation, the Organ-ization and AID have established a mutually beneficialtechnical relationship .
EXIMBANK follows conventional banking proce-dures and gives special importance to the managementaspects of a project. The Organization has not beendirectly involved in any loan operation of EXIMBANK.
Technical Discussions in 1969
These Discussions, held during the XIX Meeting ofthe Directing Council, dealt with the topic "Financingof the Health Sector." The Final Report of the Discus-sions, in referring to external financing, states that it"should be used solely for developing the health infra-
structure, in its broadest sense; that is, not only forfinancing the construction of water supply and seweragesystems and health establishments, but also for man-power training, operations research, and promotingmodern administration. In this way productivity andoperating capacity can be increased. However, externalfinancing must be used as a 'takeoif' resource, not as aregular and continuous source of funds."
The Report further suggests "that external fundsshould preferably be channeled through multilateralagencies because they are true instruments of interna-tional solidarity."
Finally, the Report states that "the financial re-sources at present available to the health sector cannotsatisfy the growing demand for services; at the sametime, any increase in external or internal financingshould be used to deal with problems in a rationalmanner; that is, with due attention to priorities andby means of technically sound projects that reflect awell-defined health policy, thereby enabling optimumuse to be made not only of funds but also of manpowerand physical resources in all health sector institutions."
In regard to this aspect of the Technical Discussions,the XIX Meeting of the Directing Council recommendedto the Director, in Resolution XXXIX, that he study thepossibility of the Organization's organizing a regionalstudy for the purpose of improving the machinery, con-ditions, and terms for external funds for developing thehealth infrastructure, in the broadest sense.
This activity was begun during the final quarter of1969.
18
II. THE EXTERNAL RELATIONS OF THE ORGANIZATION
THE ORGANIZATION WITHIN THE INTER-AMERICAN SYSTEM
THE GENERAL SECRETARIAT OF THE OAS
A continuing and cordial relationship has existed formany years between the OAS and our Organization, ex-tending into the period following the election of Mr.Galo Plaza, in 1968, to the post of Secretary General.
Speaking at the inaugural session of the XIX Meetingof the Directing Council in 1969, Mr. Plaza remarked:"It is heartening to examine the coordination arrange-ments established between the OAS and the Pan Ameri-can Health Organization and to discover that the twobodies maintain the desired coordination at both thedirecting and the technical level, without duplication."This coordination has extended to a number of fields,as will be seen below.
Operafion Relief
On 24 April 1965, a political movement, subse-quently leading to armed strife between opposing po-litical forces, began in the Dominican Republic. Thesocial disruption stemming from the violent confronta-tion of political parties prompted the Tenth Meeting ofConsultation, upon the proposal of the Special Commit-tee it had designated to deal with the parties at conflict,to establish a relief operation known as "OperaciónSocorro." The participation of the American countriesin this operation placed in evidence, once again, thespirit of brotherly solidarity that has traditionally unitedtheir people in critical times.
The Organization placed at the disposal of OperationSocorro its entire complement of available medicalstaff. Referring to this assistance, the Secretary Generalof the OAS later said that "the cooperation of PAHOwas highly effective, particularly in the supervision ofhospital services and the adoption of measures to avoidpossible epidemics."
Emergency Situation in El Salvador and Honduras
In July 1969 a border incident led to a confrontationbetween the armed forces of El Salvador and Honduras,
causing profound concern in the inter-American com-munity and leading the OAS to offer its peaceful media-tion through the Eleventh Meeting of Consultation ofMinisters of Foreign Affairs.
The machinery of the Inter-American EmergencyAid Fund, administered by a committee consisting of theSecretary General of the OAS, the Chairman of theInter-American Committee on the Alliance for Progress(CIAP), and the Director of PASB, was called intoplay. Our Organization was given the task of coordi-nating all health aspects, including contributions by theGovernments, international organizations, and the Funditself. PAHO/WHO consultants stationed in the twocountries or assigned to Zone III cooperated with theMinisters of Health and the agencies created by the twoGovernments concerned in efforts to ease the tragicsituation.
The Secretary General of the OAS, speaking at theXIX Meeting of the Council, referred in the followingterms to our cooperation: "I should nevertheless liketo make very special mention of the splendid help givenby PAHO, through the Inter-American EmergencyAid Fund, in the recent conflict between the two sisterRepublics of El Salvador and Honduras. Dr. Horwitzwas in constant contact with me during the emergency,and his presence on the actual scene of the conflict atcritical times helped to speed up the dispatch of themedicines needed to relieve human suffering. Now thatthe military stage of the conflict is fortunately over, weare working together to assist the affected Governmentsin their rehabilitation efforts."
The meeting of the Council, in Resolution XI, tooknote of the establishment of the Fund, thanked the Sec-retary General of the OAS for promptly making avail-able the necessary resources, and the Governments fortheir effective assistance in the form of manpower ormaterial resources for improving health conditions inthe areas affected by the emergency, expressed its satis-faction for the action taken by the Director, and author-ized him to make an advance of up to $100,000 fromthe Working Capital Fund for the purpose of providing
19
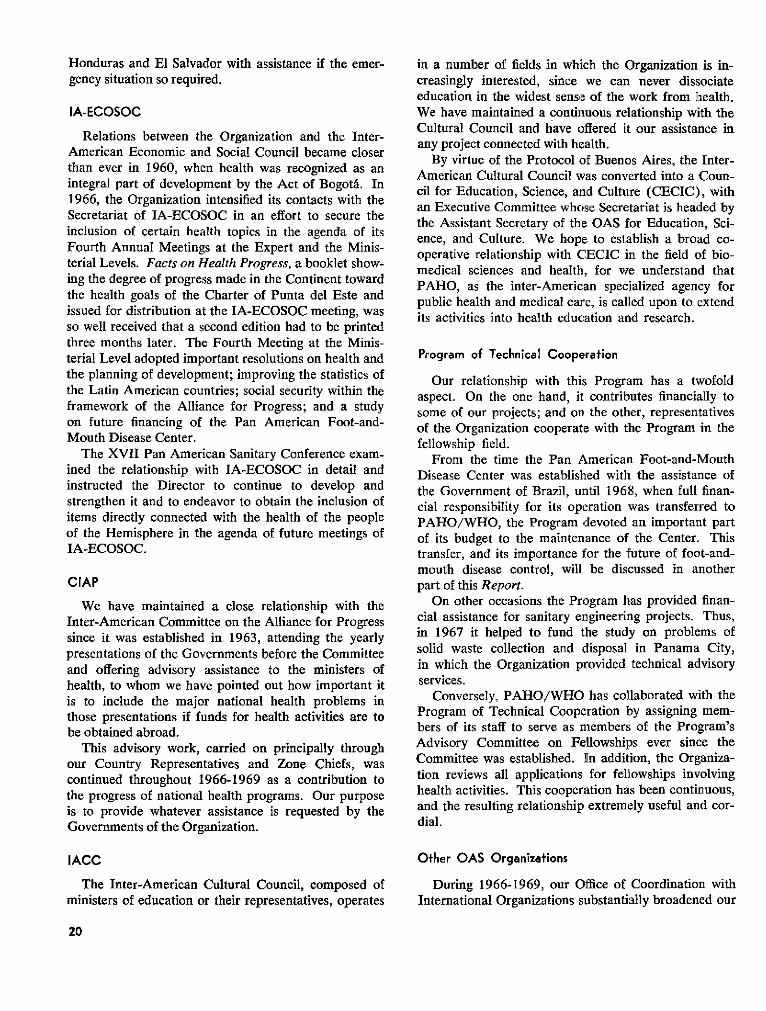
Honduras and El Salvador with assistance if the emer-gency situation so required.
IA-ECOSOC
Relations between the Organization and the Inter-American Economic and Social Council became closerthan ever in 1960, when health was recognized as anintegral part of development by the Act of Bogotá. In1966, the Organization intensified its contacts with theSecretariat of IA-ECOSOC in an effort to secure theinclusion of certain health topics in the agenda of itsFourth Annual Meetings at the Expert and the Minis-terial Levels. Facts on Health Progress, a booklet show-ing the degree of progress made in the Continent towardthe health goals of the Charter of Punta del Este andissued for distribution at the IA-ECOSOC meeting, wasso well received that a second edition had to be printedthree months later. The Fourth Meeting at the Minis-terial Level adopted important resolutions on health andthe planning of development; improving the statistics ofthe Latin American countries; social security within theframework of the Alliance for Progress; and a studyon future financing of the Pan American Foot-and-Mouth Disease Center.
The XVII Pan American Sanitary Conference exam-ined the relationship with IA-ECOSOC in detail andinstructed the Director to continue to develop andstrengthen it and to endeavor to obtain the inclusion ofitems directly connected with the health of the peopleof the Hemisphere in the agenda of future meetings ofIA-ECOSOC.
CIAP
We have maintained a close relationship with theInter-American Committee on the Alliance for Progresssince it was established in 1963, attending the yearlypresentations of the Governments before the Committeeand offering advisory assistance to the ministers ofhealth, to whom we have pointed out how important itis to include the major national health problems inthose presentations if funds for health activities are tobe obtained abroad.
This advisory work, carried on principally throughour Country Representatives and Zone Chiefs, wascontinued throughout 1966-1969 as a contribution tothe progress of national health programs. Our purposeis to provide whatever assistance is requested by theGovernments of the Organization.
IACC
The Inter-American Cultural Council, composed ofministers of education or their representatives, operates
in a number of fields in which the Organization is in-creasingly interested, since we can never dissociateeducation in the widest sense of the work from health.We have maintained a continuous relationship with theCultural Council and have offered it our assistance inany project connected with health.
By virtue of the Protocol of Buenos Aires, the Inter-American Cultural Council was converted into a Coun-cil for Education, Science, and Culture (CECIC), withan Executive Committee whose Secretariat is headed bythe Assistant Secretary of the OAS for Education, Sci-ence, and Culture. We hope to establish a broad co-operative relationship with CECIC in the field of bio-medical sciences and health, for we understand thatPAHO, as the inter-American specialized agency forpublic health and medical care, is called upon to extendits activities into health education and research.
Program of Technical Cooperation
Our relationship with this Program has a twofoldaspect. On the one hand, it contributes financially tosome of our projects; and on the other, representativesof the Organization cooperate with the Program in thefellowship field.
From the time the Pan American Foot-and-MouthDisease Center was established with the assistance ofthe Government of Brazil, until 1968, when full finan-cial responsibility for its operation was transferred toPAHO/WHO, the Program devoted an important partof its budget to the maintenance of the Center. Thistransfer, and its importance for the future of foot-and-mouth disease control, will be discussed in anotherpart of this Report.
On other occasions the Program has provided finan-cial assistance for sanitary engineering projects. Thus,in 1967 it helped to fund the study on problems ofsolid waste collection and disposal in Panama City,in which the Organization provided technical advisoryservices.
Conversely, PAHO/WHO has collaborated with theProgram of Technical Cooperation by assigning mem-bers of its staff to serve as members of the Program'sAdvisory Committee on Fellowships ever since theCommittee was established. In addition, the Organiza-tion reviews all applications for fellowships involvinghealth activities. This cooperation has been continuous,and the resulting relationship extremely useful and cor-dial.
Other OAS Organizations
During 1966-1969, our Office of Coordination withInternational Organizations substantially broadened our
20
Signing of the agreement for thetransfer of responsibility for the PanAmerican Foot-and-Mouth DiseaseCenter, formerly under the Program ofTechnical Cooperation of the OAS,to the Pan American Health Organiza-tion. Signing are Mr. Galo Plaza,Secretary General of the OAS, andthe Director of the Pan American Sani-tary Bureau.
contacts with the various organs and specialized organi-zations of the OAS, particularly with the Council and itsCommittees during the period of negotiation of theamendments to the Charter. With the special purpose ofassuring the continuing presence of the health sector inthese deliberations, the Organization was represented inmany meetings and also presented its points of view tothe General Secretariat, which invariably received themsympathetically.
The Organization also cooperated actively with thePermanent Secretariat of the Inter-American TravelCongress on standards for the international transporta-tion of human remains; with the Permanent Inter-American Social Security Committee in matters relatingto the coordination of medical services; with the Inter-American Housing and Planning Center (CINVA) inhousing programs; and with the Inter-American Chil-dren's Institute on programs of maternal and childhealth. Our cooperation with these and other agencieswill be dealt with in other sections reviewing the activi-ties of PAHO/WHO.
MEETINGS OF MINISTERS OF HEALTH OF CENTRALAMERICA AND PANAMA
The Organization has maintained a very active andproductive relationship with the Ministers of PublicHealth of Central America and Panama, whose annualmeetings during the four-year period were attended bythe Director of the Bureau, accompanied by the Chiefof Zone III and advisers. Of particular importancewas the XII Meeting in this series (San Salvador, 23-25August 1967), which was also the first regular meetingof the Central American Public Health Council.
The Organization has a long record of cooperationwith the Ministers of Public Health of Central Americaand Panama, which began their annual meetings in 1945as the Superior Public Health Council to examine publichealth problems of mutual interest. In addition, theOrganization, through its Zone III Office, CountryRepresentatives, and consultants, has advised the meet-ings of Ministers whenever requested to do so and hascooperated in the preparation and implementation ofthe resolutions adopted. This tradition of cooperationin the improvement of Central American health condi-tions was continued in 1966-1969.
RELATIONS WITH THE UNITED NATIONS SYSTEM
THE DEVELOPMENT DECADE
The period reviewed in this report marked the endof the Development Decade instituted in 1961 by theXVI United Nations Assembly. Development, under-stood to mean economic growth and also social progress,was the subject of continuing discussion during the lastdecade. The impetus given to this concept by the inter-national community has undoubtedly helped to mobilizepublic opinion and has induced national authorities to
give increasing importance to measures designed tofoster economic and social progress.
The prevailing opinion at first was that economicprogress was first and foremost in importance and thatsocial, cultural, and health advances would naturallyfollow in its wake. Under this criterion it was only logi-cal that industrial development was considered para-mount. But the need for balanced development came tobe recognized more and more as it became apparent thatpeople were interested in other things besides increasing
21
their income. As we have said on other occasions, justas health progress is impossible in an economic vacuum,economic growth cannot be expected in countries withexcessively high rates of mortality and morbidity, par-ticularly from diseases for which effective methods ofprevention and treatment are available.
Our relationship with the United Nations familystems from the fact that the Organization, through thePan American Sanitary Conference and the DirectingCouncil, acts as Regional Committee of the WorldHealth Organization for the Americas. The WorldHealth Organization's policies are determined by WHOand the Director-General and carried out with ourfullest cooperation in matters of interest to the healthof the Continent.
UNDP
In the latter part of 1965 the United Nations Assem-bly, by Resolution 2029 (XX) combined the ExpandedProgram of Technical Assistance with the Special Fundto establish what is now the United Nations Develop-ment Program. This program has Resident CountryRepresentatives with which our own Representativesmaintain close working relations while, of course, alsomaintaining direct communication with the ministers ofhealth, in keeping with our responsibility for advisingthem, upon request, in connection with their efforts toinclude health activities within the general developmentplans and stimulating increasing contributions from na-tional sources and also from international programssuch as UNDP.
In the period following the merging of the TechnicalAssistance Program with the Special Fund, we en-deavored to interest the Resident Representatives ofUNDP in our own activities and to encourage the Gov-ernments to prepare projects that could be financed bythe Special Fund. There were then four programs thatwere considered of possible interest to UNDP. Two ofthem (the program for coordination of sanitary engi-neering instruction offered by the four Venezuelan uni-versities, and a similar program at the University ofGuanabara) were strictly national in scope; the thirdwas the Latin American Center for Occupational Medi-cine; and the fourth was the Pan American ZoonosisCenter, a five-year program involving a total of $1.5million. In addition, there were the Pan AmericanHealth Planning Program, then in its early stages, andthe Hospital Maintenance and Engineering Center inVenezuela.
In 1967 the system for the formulation of projects forfinancing by the Technical Assistance component ofUNDP was changed to a system of continuous program-ming in which a ceiling figure is set for each country and
any funds not used by the beneficiary government arereturned and reallocated. The new system was put intoeffect in 1969.
In March of that same year the Resident Representa-tives met in Santiago, Chile, and devoted the first halfof their meeting to an over-all review of the develop-ment programs, with the second half given over to acountry-by-country examination of programs underway. Among the salient aspects of the meeting were itscharacterization of the Organization's cooperation withthe Latin American Institute for Economic and SocialPlanning (ILPES) in the planning of health courses asan outstanding example of international collaboration;the mention made of the success achieved in sanitaryengineering programs, particularly at the University ofGuanabara; and the suggestion that it might be advisableto eliminate regional programs entirely, retaining onlynational programs.
Since 1966, the Organization has been attempting toarouse the interest of the Governments in securing thefinancing of programs by UNDP. By the beginning of1969 the Special Fund had spent more than $900 mil-lion throughout the world, of which only $23 millionhad been devoted to health. In the Americas the UNDPhas allocated a total of $7,062,717 to country, regional,and intercountry programs.
This level of contribution can be substantially im-proved, particularly if we find the means of includingthe health component in all development programs, in-cluding agriculture programs, approved by the UNDP.
UNICEF
The United Nations Children's Fund, established forthe protection of children, has been concerned withproblems of health since the commencement of its ac-tivity and has participated iii many programs of ourOrganization. In 1966, UNICEF moved its RegionalOffice for the Americas to Santiago, Chile.
In December of the same year the Organization par-ticipated in the Meeting of Area Representatives ofUNICEF held in Guatemala. During that meeting wehad occasion to examine the traditional programs, par-ticularly the malaria program, in which UNICEF hadparticipated. We also presented some new programs, in-cluding the following: water supply systems for com-munities of less than 5,000 inhabitants; textbooks onnursing; public health laboratories; applied nutrition;and training of auxiliary personnel, all of which webelieved of possible interest to UNICEF. During 1968and 1969 we endeavored to interest UNICEF in theprograms of infrastructure and the training of auxiliarypersonnel as possible means of furthering its policy forthe economic and social development of Latin America.
22
UNICEF continued to provide assistance during1966-1969, especially for programs related to malariaeradication, nutrition, and health services.
ECLA
The work of the Economic Commission for LatinAmerica has been a source of continuing interest to theOrganization. ECLA's annual reports on the LatinAmerican economy provide information and point uptrends and directions that are very useful to us in gain-ing a complete understanding of economic developmentprograms in Latin America.
As we have frequently said, economics and health areindissolubly combined in their influence on the wayof life of individuals and nations. No economy canprosper in an unhealthy environment, for a man who isill does not produce; conversely, health cannot be ex-pected to flourish in a poor environment, for healthprograms cost money. It is this which leads us to con-tinue paying attention to the work of ECLA as a sourceof sound information for our own studies.
For our own part, we have cooperated with ECLAin the health aspects of its activities dealing with hous-ing, natural resources and power, planning, and indus-trial development. These are programs in which otherinternational organizations have also participated.
FAO
PAHO/WHO has extensive areas of cooperationwith the Food and Agriculture Organization of theUnited Nations. Many problems of agriculture andnutrition are so closely related to health that the twoaspects are all but inseparable. The community ofinterests is made evident by the many joint FAO/WHOcommittees or working parties that have been formed.
The Organization continued to cooperate with FAOin applied nutrition programs, in which the aim is toincorporate present knowledge in this field to com-munity activities. UNICEF also takes part in theseprograms. But the most noteworthy support is pro-vided by the Caribbean Food and Nutrition Institute,which began operations on 1 January 1967. Furtherreference to the Institute will be made in a subsequentsection.
WORLD FOOD PROGRAM
This is a multilateral program whose food resourcesderive especially from surpluses of the participatingcountries, from which it also receives financial assistancefor its operations. It was established by the UnitedNations and FAO in late 1962; it began operations in
1963 with an experimental project, and was firmlyestablished in 1965. Its aim is to utilize the distributionof food as an incentive to development and welfareprograms.
From the very beginning we have studied the possi-bilities of appealing to the WFP as a means of support-ing programs of supplementary feeding of vulnerablegroups, particularly mothers and children, improvinghospital diets; supporting administration of antimalariadrugs and in leprosy work; and as a stimulus in programsfor the utilization of local manpower in projects ofcommunity interest. Among the latter, rural watersupply programs deserve special mention.
In 1969 we studied in more detail the utilization ofthe World Food Program in the health sector andcollaborated with its member countries in the formula-tion of projects that finalized with the approval of sixrequests for projects in Colombia, Dominican Republic,Ecuador, El Salvador, and Peru. Another 19 projectsin various countries were in different stages of prepara-tion in December 1969.
Preliminary reports on these activities were presentedto the 61st Meeting of the Executive Committee andthe XIX Meeting of the Directing Council (1969) andthe Governments expressed an interest that the use ofthese resources continue to be promoted and that theOrganization cooperate with them in the study andpreparation of plans for their utilization.
UNESCO
The programs for the economic and social develop-ment of aboriginal population groups have given riseto coordination of the activities of a number of inter-national organizations. An attempt has been made toestablish a method that will avoid duplication of effortsand ensure harmonious development of programs re-quiring multidisciplinary action for the accomplishmentof their purposes. o
In 1966-1969, WHO continued its cooperation withUNESCO in the Regional Center for Functional Liter-acy in Rural Areas for Latin America (CREFAL) byorganizing a regular yearly course on health as a com-ponent of community development as part of the Cen-ter's 14th to 17th programs of short courses on nutri-tion, courses for the training of specialized personnel,and seminars. FAO, the United Nations, the OAS, andthe ILO also cooperated in the work of the Center.
The textbook La salud en el proceso de desarrollo dela comunidad, prepared for use in the regular yearlycourses of CREFAL, was published by the Organiza-tion.
The book entitled Planeamiento de la educación sani-
23

taria en las escuelas, widely distributed to the countriesof the Continent, was published jointly by WHO andUNESCO.
ILO
The Organization was in frequent contact during1966-1969 with the International Labour Organisation'sliaison office in Washington, D. C., for Latin Americanactivities.
In September 1966 we participated in the 8th Con-ference of American States Members of ILO and fol-lowed with interest the professional training programsand occupational surveys conducted in various LatinAmerican countries by that Organization. In the early
part of 1967 we attended a meeting on coordination ofsocial security activities conducted by various interna-tional organizations in the Americas. The meeting washeld in Geneva at ILO headquarters. During the sameyear, PAHO/WHO, together with the United Nationsand ILO, extended advisory services at the request ofthe Government of Venezuela to the committee estab-lished to organize a unified health service in that coun-try.
The ILO cooperated in some of our programs andit is reasonable to assume that with the advance of in-dustrialization in the Americas new fields of activitywill emerge in which the two organizations can usefullycooperate.
RELATIONS WITH NATIONAL AND INTERNATIONAL INSTITUTIONS
The Organization frequently conducts activities withfinancial assistance from private or public institutions.Conversely, it also provides subsidies and assistance ofvarious kinds to associations or societies active in thefield of health. In certain cases, such as those of thePan American Medical Confederation and the PanAmerican Federation of Associations of MedicalSchools, relations have been established by the Govern-ing Bodies of the Organization. In other cases it is theWHO which has entered into consultative and coopera-tive arrangements with the international nongovern-mental organizations concerned. A large number ofsuch nongovernmental organizations attend the meetingsof the Regional Committee; for example, at the XVIIPan American Sanitary Conference, XVIII Meeting ofthe Regional Committee, 16 nongovernmental organ-izations were represented.
THE FOUNDATIONS
An important role in the life of PAHO/WHO isplayed by foundations, which provide support for thehealth program by furnishing grants for specific pur-poses. Mention should be made first of three UnitedStates foundations because of their very importantrelationships with the Organization. The W. K. KelloggFoundation was primarily interested in the training ofpersonnel in hospital statistics, progressive patient care,and nutrition. The Williams-Waterman Fund of theResearch Corporation contributed to the establishmentof the Caribbean Food and Nutrition Institute and toresearch on nutritional anemias and endemic goiter.The Milbank Memorial Fund participated in programs
on manpower and medical education and the teachingof preventive and social medicine.
A number of other private groups became interestedin the Organization's program during the same period.The Anna Fuller Fund participated in a study in 1967of patients with certain forms of malignant neoplasmshospitalized in Buenos Aires. The Josiah Macy, Jr.,Foundation aided various programs to strengthen pedi-atric education in Latin America. The NutritionFoundation cooperated in the nutrition program, theWellcome Foundation in the joint research program ofthe Pan American Zoonoses Center, and the Rocke-feller Foundation also expressed an interest in the afore-mentioned Caribbean Institute.
Of interest for special reasons was the collaborationof the Brother's Brothers Foundation in a program ofvaccination against smallpox, tuberculosis, and polio-myelitis in Nicaragua in 1966, and that provided by theSpecial Public Health Service Foundation of Brazil,through the Evandro Chagas Institute, in a study toassess the effectiveness of poliomyelitis vaccine in tropi-cal zones.
ASSOCIATIONS AND UNIVERSITIES
In Latin America there are many groups-variouslycalled associations, societies, leagues, unions, etc.-whose purpose is to bring together persons who for pro-fessional reasons or because of shared convictions wishto unite their efforts behind a common cause. Exam-ples are the medical, hospital, and nursing associationsand the leagues against tuberculosis, alcoholism, andvenereal diseases. All of these groups perform an
24
important social function by helping to enlist the sup-port of public opinion, without which a public healthactivity is difficult to carry out or loses its effect. Weknow-and experience has repeatedly borne this out-that a highly motivated community participating withfull awareness and volution is a prerequisite to thesuccessful accomplishment of the objectives of anyhealth program.
There is thus continuing contact between the Organi-zation and associations having objectives in the healthsector. It is only natural that a community of pur-poses will lead to related activities. The period from1966-1969 was no exception in this regard, and therewere many associations with which we entered intocontact. Salient among these was the American PublicHealth Association, at whose annual meetings it hasbecome traditional for PAHO/WHO to present ex-hibits which in these past years have dealt with watersupply programs, medical care in the Americas, PAHO/WHO publications, and the use of health statistics innational health programs. We also collaborated withthe World Health Foundation of the United States ofAmerica and with the United States Association for theUnited Nations, as well as mounting an exhibit on"Health and Peace" in the Headquarters building inobservance of United Nations Day and Week in 1967.
The Organization expanded its relations with theuniversities of the Hemisphere, particularly with theschools of public health. This was a natural outgrowthof the increased emphasis on training and research. Wehave already mentioned both of these matters in a gen-eral way and will do so in greater detail when discussingthe relevant activities of the Organization.
PAHO/WHO's relations with universities are of vari-ous kinds and generally involve one of the five followingtypes of activities: (1) grants to a university to enableit to expand its facilities or improve its instruction oractivities; (2) the supply of equipment for the installa-tion or modernization of technical services; (3) theprovision of technical assistance, usually through aspecialized consultant who serves as adviser in the per-formance of specific research projects or coordinateswork of this kind; (4) assistance in the organization ofadvanced training and short-term courses; and (5)direct provision of advisory services and fellowships. Allof these contributions to the process of university edu-cation are centered on the field of health and are car-ried forward within the general framework of the funda-mental purposes defined by the Constitution and byresolutions of the Governing Bodies. We must neverforget that if the fundamental purpose of our Organiza-tion is "to promote and coordinate efforts of the coun-tries of the Western Hemisphere to combat disease,
lengthen life, and promote the physical and mentalhealth of the people," the university education and re-search in the health sciences have a vital place in ourOrganization.
Particular emphasis was placed during 1966-1969 onthe establishment of useful contacts between universitiesand ministries of health, which have often operatedseparately as if there were no connection between theeducational process and public action in the field ofhealth. We have endeavored to correct this tendencyby taking advantage of every opportunity to establishlinks between the two kinds of institutions. The par-ticipation of a university or group of universities in cer-tain projects has brought them into joint activities withthe ministries of health. While bringing about the estab-lishment of adequate relations between educationalinstitutions and health authorities is a slow and diffi-cult task, involving as it does the altering of traditionaladministrative patterns, it is one that will result in betterservice to people and the community and which ourexperience shows we can accomplish if we persevere.
OTHER INSTITUTIONS
PAHO/WHO's relations in 1966-1969 includedthose with a number of other public and private institu-tions. Some of these were public national agencieswhose over-all sphere of activity includes the healthsector. A case in point is the United States Agency forInternational Development (AID), from which wecontinued receiving financial support for various pro-grams, including two that were started in 1966: theInter-American Investigation of Mortality in Childhoodand the Program of Training for Research in Healthand Population Dynamics.
The group of public and national institutions alsoincludes agencies directly concerned with health andtherefore interested in our activities. First and fore-most in this group were the National Institutes ofHealth of the U. S. Public Health Service, which con-tinued to provide assistance to virological research andother programs. Two of the programs assisted by theseInstitutes (salt fluoridation and mental health) con-cluded in 1967, and others, involving epidemiologicalstudies, concluded in 1968. The U. S. Public HealthService participated in other programs, as did theNational Communicable Disease Center and the Inter-national Influenza Center in Atlanta, Georgia (USA).
The Organization, for its part, furnished advisoryservices, grants, and fellowships to health institutions ofvarious kinds. In Brazil, for example, it cooperatedwith the Adolfo Lutz Institute by assisting in the organ-
25
A modern building housing part of theyellow fever vaccine laboratory at theOswaldo Cruz Institute in Rio deJaneiro, Brazil.
ization of courses dealing with the laboratory diagnosis in tropical areas. The Oriof smallpox; with the Oswaldo Cruz Institute, by pro- sistance to the Nutrition Inviding equipment, materials, and advisory services for tan Institute, the Institutethe production of dried smallpox vaccine; and with the National Institute of RuralEvandro Chagas Institute, by helping to carry out a Institute of Rehabilitationstudy to assess the effectiveness of poliomyelitis vaccine Paulo.
SCIENTIFIC AND PUBLIC COMMUNICATIONS
Rapid development of the modern science of com-munication is a distinctive feature of our times, born ofthe need to provide persons, institutions, and communi-ties with information enabling them to reach agree-ments or adopt decisions on a logical and suitablefoundation.
PAHO/WHO has continuously expanded its servicesfor communication to and among other organizationsand persons interested in matters of health. This ex-pansion is plainly evident, a fact which merits particu-lar emphasis as it reflects the performance of one of theprincipal functions of the Organization. It should beessentially a forum for matters of health. Indeed, itsConstitution, in specifically listing the functions of thePan American Sanitary Conference provides that it shall"serve as a forum for the interchange of informationand ideas relating to the prevention of disease, thepreservation, promotion and restoration of mental andphysical health, and the advancement of sociomedicalmeasures and facilities for the prevention and treatmentof physical and mental diseases in the Western Hemi-sphere."
ganization also rendered as-istitute of Recife, the Butan-of Sanitary Engineering, theI Endemic Diseases, and then of the University of Sao
SCIENTIFIC INFORMATION
Scientific information is a multifaceted concept. Theterm "scientific," as used here, refers to a wide varietyof activities, professional and technical as well asscientific. Thus, "scientific information" is conceivedof as embracing information on the health sciences, themedical profession, and health methods alike.
The Organization performs its information functionby various means, principally those described below.In the field of science, PAHO/WHO prepared andorganized the First International Conference on Viraland Rickettsial Diseases of Man (Washington, D. C.,7-11 November 1966), which was attended by 280scientists from 27 countries and whose proceedings,published in English in 1967, provide an over-view ofpresent knowledge in this field. In sanitary engineering,the Organization participates in the annual congressesof the Inter-American Association of Sanitary Engi-neering (AIDIS), with which it has maintained a closerelationship since its establishment. The Organizationalso attends international meetings with the aim of
26
informing them of its activities. A case in point was theInternational Conference on Water for Peace, held in1967 and attended by more than 5,000 persons fromsome 100 countries, to which the Organization presentedreports on the present status of the water supply pro-gram in Latin America, the financing of water supplysystems, and the hemisphere-wide program of personneltraining, as well as submitting a proposed program forproviding impetus to water supply programs in theAmericas. Documents of this Conference of potentialinterest to members of the PAHO/WHO professionalstaff in connection with their duties were distributedto them.
The scientific information activities described abovecan be considered of a general nature. In addition tothem there are also other, more intensive activities, ofmore limited scope, to which the Organization devotesits attention. We refer to the seminars on varioushealth problems which are held annually for the purposeof providing a group of professionals or technicians withup-to-date information and the opportunity of exchang-ing ideas on these problems and solutions so that theycan later apply them to the performance of their work.Three examples of such activities are:
(1) The Seminar on Nursing Education, held in
;i ?M VACM &t&IjMO 13 MW 13sj.~ bb S . 141
the University of the Western Indies (Jamaica) in1966 and attended by 19 instructors from the area whoexamined the needs for personnel and for training andformulated the general outlines of a program for thetraining of professional nurses in comprehensive nursingcare; (2) the Seminar on the Teaching of Psychiatryand Mental Health in Latin American Schools of Medi-cine, held in Lima late in 1967 and attended by 44 pro-fessionals from 19 American republics, who examinedthe teaching of these subjects as part of the basic medi-cal course in the schools of medicine; and (3) theSeminar on Administrative Methods for Leprosy Con-trol Programs, held in Guadalajara (Mexico) in mid-1968, and attended by persons from 46 American coun-tries who examined specific aspects and programs ofleprosy control in Latin America.
The work in the field of scientific communicationsincludes the issuance of publications designed to guidethe activities of health workers in the broadest senseof the term. Examples of such publications are A Guidefor the Identification of the Snail Intermediate Hosts ofSchistosomiasis in the Americas, published in 1967 andintended for use by personnel engaged in control activi-ties, either in the laboratory or in the field; and aSpanish translation of the American Dental Associa-
. o.. " .
I
27
tion's dental materials guide prepared in 1967 withthe assistance of the University of Mérida (Venezuela)and distributed throughout Latin America. Also partof this group of publications are a number of manualsof work procedures, of which the following were issuedin 1966: an updated Spanish version of a trainingmanual issued in English by the U.S. Public HealthService on basic protection procedures against ionizingradiations; a Spanish translation of the manual on theuse of X rays in medicine and dentistry and the controlof radiation hazards, issued in English by the AmericanCollege of Radiology-the Spanish version was widelydistributed by PAHO/WHO in Latin America, andcopies in English were sent to Jamaica and Trinidad andTobago; (a Spanish translation of the book publishedin 1964 by the Venereal Disease Research Laboratoryof the U. S. National Communicable Disease Center) onSerologic Tests for Syphilis, which was distributed onlyto health services for use as a reference document intesting and control programs; and a Spanish translationof a U. S. Public Health Service publication ClinicalHandbook on Economic Poisons. Also included in thesame group is a Spanish translation of a book by Dr.D. B. Jelliffe on Child Health in the Tropics, written toserve as a practical manual for medical and paramedi-cal personnel and covering the principal aspects ofchild health in tropical regions in general. In preparingthe translation, the text was adapted to reflect specifichealth conditions in the Americas.
In 1967 the Organization published Spanish andPortuguese versions of a handbook on the operation,maintenance, and minor repair guide of jet injectorsissued in English by the National Communicable Dis-ease Center (U. S. Public Health Service). These ver-sions were made available to the field personnel ofsmallpox eradication programs in Latin America. Alsopublished in 1967 was a second Spanish edition ofProcedure for the Investigation of Foodborne DiseaseOutbreaks, an adaptation of a handbook issued by theInternational Association of Milk, Food, and Environ-mental Sanitarians and intended for public healthworkers who have no special training or experience inepidemiological research.
In 1968 a single volume edition was published con-taining the Spanish versions of a U. S. Public HealthService handbook on the guide for laboratory animalfacilities and care and of a guide for shipments of smalllaboratory animals issued by the National Academy ofSciences, U. S. National Research Council. The sameyear saw the publication of the third edition of theManual for the Microscopic Diagnosis of Malaria, byDr. A. J. Walker, and the publication of Profilaxia dasdoenVas transmissíveis, a Portuguese version of the
APHA publication Control of Communicable Diseasesin Man.
This section would not be complete without a briefgeneral reference to the Technical Discussions held eachyear during the meeting of the Directing Council or theConference. These Discussions serve as a means forproviding information on a pre-selected health topic, ofinterest to the Americas, to a group of professionalscomposed mainly of public health officials.
Although some of the topics discussed have beenmentioned above and all will be touched upon in thesections dealing with the relevant activities of the Organ-ization, it is believed appropriate to list here the topicsdealt with during the four years covered by this report.The XVII Pan American Sanitary Conference examinedthe "Means for Promoting and Making Effective theCoordination between the Services and Programs ofMinistries of Health, Social Security Institutes, andOther Institutions that Conduct Activities Related toHealth"; and the Directing Council discussed "Methodsfor Increasing Health Service Coverage in Rural Areas"at its XVII Meeting, "Participation of the Health Sec-tor in Population Policy" at its XVIII Meeting, and"Financing of the Health Sector" at its XIX Meeting.The Final Report of each year's Technical Discussionsand the papers submitted to them are published in theBoletín and serve as a valuable source of technicalinformation.
PUBLIC INFORMATION
As an international organization, PAHO/WHO isduty-bound to keep the public informed of its basicpurposes, goals, activities, and available resources.This is accomplished in part by means of the AnnualReports submitted to the Council or the Conference, asthe case may be, and the Quadrennial Report, whichcovers in broader detail the progress of the Organizationbetween one Pan American Sanitary Conference and thenext.
But public information, as understood today, is in-formation transmitted through the media of the press,radio, and television. The Organization uses the massmedia as frequently as its budget permits, preparing alarge number of articles or reports on matters of interestto the general public for publication or broadcast. Dur-ing 1966-1969, the Organization issued 664 press re-leases, organized press conferences and interviews dur-ing meetings or other special events sponsored byPAHO/WHO, and lent films to civic and voluntarygroups.
Contacts with Latin American radio stations wereconsiderably enlarged. In 1968 the Organization in-
28
augurated a new series of filmed news broadcasts inSpanish entitled "Salud para las Américas." Each filmhas four 51/2 minute broadcasts, so that the stations canschedule an entire sequence in advance. Five com-plete programs were put on film and distributed to 300stations in Spanish-speaking countries.
Television and motion picture production, requiring,as they do, specially-trained staff and substantial re-sources, have not been within the reach of the Organiza-tion.
An illustrated newsletter entitled Gazette, printed inSpanish and English, first appeared in 1969, with aninitial pressrun of 10,000 copies. Its purpose is tomake the work of the Organization and its Governmentsbetter known to public officials outside the field ofhealth and to the general public. Each number containsvarious bulletins and news items about projects, meet-ings, and other matters considered to be of interest.
The Public Information Service aims to provide in-formation in nontechnical language on the programs,activities, and objectives of the Organization, a serviceto which considerable importance is attached, since inthe last analysis the prestige of an institution is foundedon public opinion.
WOR H IAL
TWENTIETH ANNIVERSARY OF WHOWORLD HEALTH DAY
On April 7, observed each year as World Health Day,an attempt is made to focus public attention on a currenthealth event or a serious health problem. The topicschosen by WHO for worldwide attention and dissemi-nated by us in the Americas during 1966-1969 were:"Man and His Cities," in 1966; "Partners in Health,"in 1967; "Health in the World of Tomorrow," in 1968;and "Health, Labor and Productivity," in 1969. Ma-terial prepared by WHO, accompanied by a messagefrom the Director-General is distributed on these occa-sions throughout the Continent, along with remarks ofthe Director of the Bureau underlining the significanceof the day. This material is used by teachers in theirclassrooms, as well as by health authorities and officersin their work. April 7 is one of the few occasions onwhich the Organization's activities in behalf of healthand well-being in the Americas are brought to the at-tention of the general public.
In 1968, World Health Day coincided with the Twen-tieth Anniversary of WHO. (For the record, PAHO hadcompleted its 65th year of existence.) A special effortwas made to encourage the organization of a recordnumber of commemorative events in the countries,Zones, and Headquarters. An illustrated pamphlet en-titled An Approach to Health (Un enfoque en la salud)was prepared and distributed to 2,000 newspapers inthe United States of America, 900 in Canada, and 650in Latin America. A special radio program was broad-cast to 35 stations in Spanish-speaking countries, and athree-minute television newscast, the first TV programever produced by PAHO/WHO, was sent on tape to300 stations throughout the Continent, with separatescripts in English, Spanish, and Portuguese.
A highly significant event took place at Headquarters:Dr. Joshua Lederberg spoke in our Council Chamberon "Health in the World of Tomorrow." This, in ouropinion, was an eminently fitting way of celebrating theTwentieth Anniversary of WHO.
29
:
---- 7777~~~~~~--7--777~~~~

u
o
o
E
o
-a0
c
E
o
c>
-
-_-
oo
O
XE
oo
-o
co
=1
o
I,
III. INTERNAL DEVELOPMENTS IN THE ORGANIZATION
CONSTITUTIONAL QUESTIONS
NEW MEMBERS
Two countries, Barbados and Guyana, became mem-bers of the Pan American Health Organization on 2October 1967, by unanimous decision of the XVII Meet-ing of the Directing Council, increasing the roster of theOrganization to 28, including 25 Member Govern-ments-Argentina, Barbados, Bolivia, Brazil, Chile,Colombia, Costa Rica, Cuba, the Dominican Republic,Ecuador, El Salvador, Guatemala, Guyana, Haiti, Hon-duras, Jamaica, Mexico, Nicaragua, Panama, Paraguay,Peru, Trinidad and Tobago, the United States of Amer-ica, Uruguay, and Venezuela-and three ParticipatingGovernments, France, Kingdom of the Netherlands,and the United Kingdom.
AMENDMENT OF THE CONSTITUTION
In view of the increase in the number of Govern-ments making up the Organization and the desirabilityof providing for broader representation in the ExecutiveCommittee, the XVIII Meeting of the Directing Councilamended Article 15-A of the Constitution of the Organi-zation to read as follows:
The Executive Committee shall be composed of nineMember Governments of the Organization elected by theConference or the Council for overlapping periods of threeyears. Each of the elected Member Governments shall beentitled to designate one representative to the ExecutiveCommittee. Each representative may be accompanied byone or more alternates and advisers. A Member Govern-ment shall not be eligible for re-election to the ExecutiveCommittee until one year has elapsed since the expirationof its term of office.
The Council also approved a transitional article read-ing as follows:
On the entry into force of the amendment to Article15-A, the vacancies on the Executive Committee shall. befilled and two additional members shall be elected to bringthe membership to nine. At subsequent elections a suffi-
cient number of vacancies shall be filled to keep the mem-bership of the Executive Committee at nine Member Gov-ernments of the Organization and, if necessary, the termsof office of the Governments elected shall be adjusted, pro-vided that in no instance shall a Government be entitled tobe a member of the Executive Committee for more thanthree successive years.
ELECTION OF THE DIRECTOR
One of the functions residing exclusively in the Con-ference is to elect the Director of the Pan AmericanSanitary Bureau (Article 4-E of the Constitution). On29 September 1966, the Conference elected Dr. Abra-ham Horwitz by virtue of Article 21-A of the Constitu-tion and Rule 42 of its Rules of Procedure (ResolutionV). Pursuant to Article 4 of the Agreement betweenPAHO and WHO and Articles 49 and 52 of the WHOConstitution, the Director-General of WHO was noti-fied of the election for purposes of the appointment ofthe Regional Director for the Americas.
EXECUTIVE COMMITTEE: ELECTION OFGOVERNMENTS AND EXPIRATION OF
TERMS OF OFFICE
During the four-year period, the Governments of thefollowing countries were elected to membership in theExecutive Committee: Colombia and the United Statesof America (1966); Nicaragua, Trinidad and Tobago,and Uruguay (1967); Argentina, Brazil, Costa Rica,and Mexico (1968); and Guyana, Peru, and Venezuela(1969).
During the same period, the Governments of the fol-lowing countries completed their periods of office andreceived a vote of thanks from the Conference or theDirecting Council: Brazil and Mexico (1966); Jamaica,Panama, and Venezuela (1967); Ecuador and Guate-mala (1968); and Brazil, Colombia, and the UnitedStates of America (1969).
31
RULES OF PROCEDURE OF THEGOVERNING BODIES
The Directing Council, at its XVII Meeting, amendedRule 30 of its Rules of Procedure to read as follows:
Resolutions, amendments and substantive motions shallnormally be introduced in writing and handed to the Direc-tor who shall circulate copies to the representatives. As ageneral rule, no proposal shall be discussed or put to thevote unless copies of it have been circulated to all repre-sentatives not later than the session preceding the meeting.The President may, however, under special circumstances,permit the discussion and consideration of such resolutions,amendments or substantive motions even though they havenot been previously circulated.
Proposals shall be voted on in the order in which theyare presented, except when the Council decides to the con-trary. Parts of a proposal or of an amendment shall bevoted on separately if any representative so requests.
The Council also requested the Director to examinethe Rules of Procedure of the Governing Bodies with aview to adapting them to the number of members of theOrganization and to submit the proposed amendmentsto the Executive Committee. The Committee, at its 61stMeeting, approved the amendments to its own Rules ofProcedure and transmitted to the Directing Councilthose relating to the Rules of Procedure of the Counciland the Conference. The XIX Meeting of the DirectingCouncil approved the proposed amendments to its Rulesof Procedure with only one change and referred to theConference, together with its favorable report and withchanges in two articles, the proposals for amending theRules of Procedure of the Conference. The amend-ments consisted essentially in providing for the additionof a Rapporteur to the Secretariat of the meetings, withdirect participation in the preparation of draft resolu-tions and the Final Report.
MEETINGS OF THE GOVERNING BODIES
The XVII Pan American Sanitary Conference washeld in 1966, and the XVII, XVIII, and XIX Meetingsof the Directing Council in the three following years.These were also the XVIII to XXI Meetings, inclusive,of the Regional Committee of WHO for the Americas.The first and last were held at Headquarters, the secondin Port-of-Spain, Trinidad and Tobago, and the third inBuenos Aires, Argentina, pursuant to Article 7-A and12-A of the Constitution and Resolutions XL of theXVII Conference and XII of the Directing Council in1967.
The meetings were attended by the highest publicauthorities of the Governments of the Organization andby many specialists in public health, generally officials of
national health services as required by Article 5-B of theConstitution. Thus, the Conference was attended by 14ministers of health, four undersecretaries of health, andone director general of health, and the correspondingfigures for the meetings of the Directing Council were11, 5, and 5; 6, 2, and 2; and 7, 4, and 4, respectively.
The Executive Committee held 10 meetings, the 54ththrough the 63rd, during the period under review. Inaccordance with Article 17 of the Constitution, the 57thand 58th Meetings took place in Port-of-Spain and the60th in Buenos Aires.
All of these meetings are specifically provided for inthe Constitution, which specifies their function in Arti-cles 4, 9, and 14, with respect to the Conference, theDirecting Council, and the Executive Committee, re-spectively. The relevant documents, including the pro-posed program and budget estimates, the Annual Reportof the Chairman of the Executive Committee, the An-nual and Quadrennial (in the case of the Conference)Reports of the Director, and the Financial Report andReport of the External Auditor, were submitted to allof these meetings and received the approval of the ap-propriate Governing Body, which commended theBureau on its work.
In addition to considering administrative and financialmatters, the meetings of the Governing Bodies examinedand discussed every aspect of the technical activities ofthe Organization with a view to assisting the Govern-ments in establishing the health policies of the Organi-zation. The XVII Conference approved resolutions onthe programs of research, mental health, medical care,and medical textbooks, among other matters, andadopted a declaration and standards concerning theinternational transportation of human remains. TheXVII Meeting of the Directing Council approved resolu-tions on poliomyelitis, water supply, fellowships, andChagas' disease, in addition to one relating to the PanAmerican Foot-and-Mouth Disease Center designatingthe Organization as the agency responsible technicallyand administratively for the Center, establishing its fi-nancing through a quota system, and authorizing theDirector to convene annually, beginning in 1968, ameeting of Ministers of Agriculture or their representa-tives, to review the program of the Center and to con-sider matters of mutual interest. Salient among theresolutions of the XVIII Meeting of the Directing Coun-cil were those on the Institute of Nutrition of CentralAmerica and Panama, the development of the RiverPlate Basin, and teaching and research in the healthsciences, as well as Resolution XXVI, which incorpo-rated all the recommendations of the Special Meeting ofMinisters of Health of the Americas into the policy ofPAHO/WHO. At the XIX Meeting of the Council
32
54th Meeting of the Executive Committee of the Pan AmericanHealfth Organization, April 1966.
resolutions were approved on the nutrition program,Aedes aegypti, malaria eradication, long-term planningand evaluation, the Regional Library of Medicine, inaddition to one concerning the emergency situation inHonduras and El Salvador.
The Executive Committee, at its meetings during1966-1969, continued to perform its role as an advisorybody to the Directing Council and the Conference and
played an extremely active part in the examination ofthe proposed program and budget estimates preparedby the Director of the Bureau, which was examined itemby item at the 56th, 59th, and 61st Meetings. The 57thMeeting (September 1967) devoted particular attentionto the financing of the Pan American Foot-and-MouthDisease Center and to Official Document 76, containingthe proposed program and budget estimates of PAHOfor 1968 and the WHO Region of the Americas for1969 and the provisional draft of the proposed programand budget of PAHO for 1969. The Chairman of theExecutive Committee declared this document to be "per-haps superior to the program and documents of anyother international organization." It is a genuine pro-gram budget in which the complex activities of inter-national health are presented in an orderly functionalarrangement representing definite progress toward theobjective of offering the Governments as much informa-tion as possible to guide them in the very basic matter ofdetermining the apportionment of available funds forthe performance of health activities in the Americas.This progress is part of a continuous process that wasstarted some years ago and is gradually being perfectedthrough experience with a view to improving the serviceto the Governments of the Organization.
ORGANIZATIONAL STRUCTURE
THE CONCEPT OF HEALTH
The general concept of health is summarized in thefundamental purposes of PAHO/WHO: to combatdisease, lengthen life, promote health, and contribute tothe well-being and development of nations. The de-mands of the time requires the placement of health inan economic and social context, as a fundamental com-ponent of development, a concept which has been gain-ing increasing acceptance in the Americas since theadoption of the Act of Bogotá (1960), which recognizedthe thesis upheld by our Organization that health is tobe regarded in the Americas as an integral part of theprocess of economic growth, taken to mean the adoptionof a series of measures directed to increasing the wel-fare of the individual, his family, and his community.Individual and collective health are part of economicdevelopment, which influences and is in turn influencedby them. This thesis later received the support of theAmerican Chiefs of State and of the Ministers of Healthof the Hemisphere, as can be seen in this Report.
THE STRUCTURE OF SERVICES
The structure of the services is determined by thearrangements considered necessary for the protection,promotion, and restoration of health and for the devel-opment of human resources through health activitieswhich are well designed, properly organized and ad-ministered, and coordinated and integrated with pro-grams for the economic and social development of thecommunity.
These services are performed in the Organization atthree levels: central, zonal, and national, with a viewto meeting the needs of the Governments as effectivelyas possible. This organizational structure remained un-changed: the six Zone Offices, Country Representa-tives, and the El Paso Field Office continued to provideliaison between Headquarters and the Governments.This division of functions is based on the principle ofdecentralization of program planning and execution,combined with centralization of administrative functionsin Washington, a principle adopted some years ago and
33
applied since with satisfactory results, including thereduction of costs for operations and personnel. Thedivision into three levels has been shown in practice tobe an effective arrangement for the performance of thefunctions of the Pan American Health Organization/World Health Organization. But we must never forgetthat an administrative structure is a working mechanismwhich is in constant activity and whose constituent ele-ments are continuously interacting on one another. Andwe must always keep in mind that health is indivisibleand that only the complexity and diversity of its mani-festations has led us to design a multiple structureadapted to them.
In order to bring the administrative structure moreinto line with the needs, the central services were re-aligned under an arrangement in which the "traditional"departments (communicable disease control, malariaeradication, health statistics, among others) were re-tained; the objectives of some of them (environmentalsciences and sanitary engineering, scientific and publiccommunications) were expanded; certain units (medi-cal care administration, human resources development,research promotion and coordination and evaluation),were raised to departmental rank; a new department(general and special technical services) and a new sec-tion (computer science) were created, along with fivenew units (poliomyelitis, chronic diseases, cancer, para-sitic diseases, and the office for liaison with internationalorganizations).
ADVISORY COMMITTEES
Advisory committees and working groups are estab-lished as part of the administrative structure and aregiven responsibility for examining a particular field ofactivity or exploring new activities so as to offer theOrganization and the Bureau, through their reports, newguidelines and critical appraisals that will enable them todevelop a more efficient and suitable health policy.
In 1966 the Advisory Group on Pediatric Educationwas convened and the Research Group on the Chemo-therapy of Chagas' Disease held its Second Meeting.The Fourth Meeting of the Regional Advisory Commit-tee on Health Statistics held its Fourth Meeting in 1966and its Fifth in 1968. The Advisory Committee onMedical Research held its Fifth, Sixth, Seventh, andEighth Meetings during the four-year period. TheAdvisory Committee on the Teaching of Preventive andSocial Medicine in Latin America held a meeting in1967, and the Technical Advisory Committee on Nutri-tion met for the first time in 1968.
The Scientific Advisory Committee of the Pan Ameri-can Zoonoses and Foot-and-Mouth Disease Centers, ap-pointed by the Director of PASB to review the work
programs of the Centers, especially those related to re-search, held its First Meeting in 1967. The Commit-tee's recommendations in the past three years have hadan important impact on the activities of the Centers and,consequently, on the zoonoses control and researchprograms carried on by the countries.
In addition to these committee meetings, the StudyGroup on Coordination of Medical Care Services ofMinistries of Health, Social Security Institutes, and Uni-versities, sponsored jointly by the OAS and the Organi-zation, met in August 1969, and the Scientific AdvisoryCommittee on the Regional Library of Medicine met in1968 and 1969. Other committees, such as those onmalaria and Aedes aegypti, will be mentioned in therelevant portion of this Report.
CENTERS
Also a part of the Organization are a number of cen-ters established to deal with health problems and needswhich are common to several countries and requireparticular research activities and specially trained per-sonnel. The Institute of Nutrition of Central Americaand Panama, the Latin American Center for Classifica-tion of Diseases, the Health Sciences Education Infor-mation Center, and the Pan American Zoonoses Centercarried forward their regular programs during the four-year period, as did the Pan American Foot-and-MouthDisease Center, which in 1968 was transferred com-pletely to the Organization.
The PAHO/WHO Immunology Research and Train-ing Center, with headquarters in Sáo Paulo, the LatinAmerican Center for Medical Administration, and thePopulation Information Center were established in1966, and the Caribbean Food and Nutrition Institutein 1967. The Pan American Sanitary Engineering andEnvironmental Sciences Center, the Regional Libraryof Medicine, and the Pan American Health PlanningProgram were organized in 1968, and the ComputerCenter in Health (Argentina) and the PAHO/WHOImmunology Research and Training Center (Mexico)were established in 1969.
All these centers constitute a network of facilities fordealing with important aspects of the health sector.They have generally been established at the initiative ofa given country which has provided facilities, installa-tions, services, and contributions of every kind for theiroperation. Such has been the case with the PanAmerican Foot-and-Mouth Disease Center, sponsoredby Brazil, the Zoonoses Center, by Argentina, and theCaribbean Food and Nutrition Institute, by Jamaica.In certain instances, however, a proposal of a particularGovernment has been supported by other countries witha view to obtaining assistance from the United Nations
34

Main building of the Pan AmericanFoot-and-Mouth Disease Center, Riode Janeiro, Brazil.
Development Program, as in the case of the Pan Ameri-can Health Planning Program. As for INCAP, all ofthe Central American countries and Panama are itsmembers by virtue of an agreement.
Each center has a specific field of activity, generallyindicated by its name, and all are at the service of theentire membership of the Organization. Their researchfindings are made available to all the countries, andtheir laboratories and training courses are open to na-tionals of any member of the Organization. Centers areestablished in response to the need for a given activityand the desirability of decentralizing so as to renderbetter service to the Governments.
CONSULTANTS
Short- and long-term consultants and temporary ad-visers are a key component of the operational structure.They are generally charged with examining a particularproblem in the field and suggesting a means of solving it.
The number of consultants and advisers has grown asthe Governments have turned to the Organization formore and more services. This trend was strongly ac-centuated during the four-year period, as reflected bythe following figures: in 1966, 517 consultants andadvisers were designated; in 1967, 627; in 1968, 759;and in 1969, 752. The results have amply justified thepolicy applied in this respect, which enables the Organ-ization to reduce the number of staff appointments,obtain the services of experienced, high-level specialistswho, in any event, are generally available for only ashort period, and render better service to the Govern-ments.
An evaluation of advisory services provided to theGovernments through temporary consultants was madein 1967. Its findings and recommendations served as abasis for preparing a manual -setting forth in broad out-line the duties of consultants and guidelines for the sub-mission of their reports.
FINANCIAL QUESTIONS
PROGRAMS
An increasingly larger number of programs, dealingwith a widening variety of subjects, were approved eachyear during the period under review. Two-thirds ofthem can be described as "on-going programs" becausethey are designed to cope with major health problemswhich are still in process of solution. The remainingthird is made up in part of new initiatives of the Gov-ernments in which the Organization has been asked to
collaborate. We say "in part" because many such re-quests (149 in 1966, 172 in 1967, 239 in 1968, and303 in 1969) could not be complied with for lack offunds. In 1967 the unsatisfied demand for additionalservices represented more than $4,000,000.* The in-creasing interest of the Governments in enlisting ourcooperation is a clear sign of the vitality and efficiency
* All references to dollars in this Report are to United Statescurrency.
35
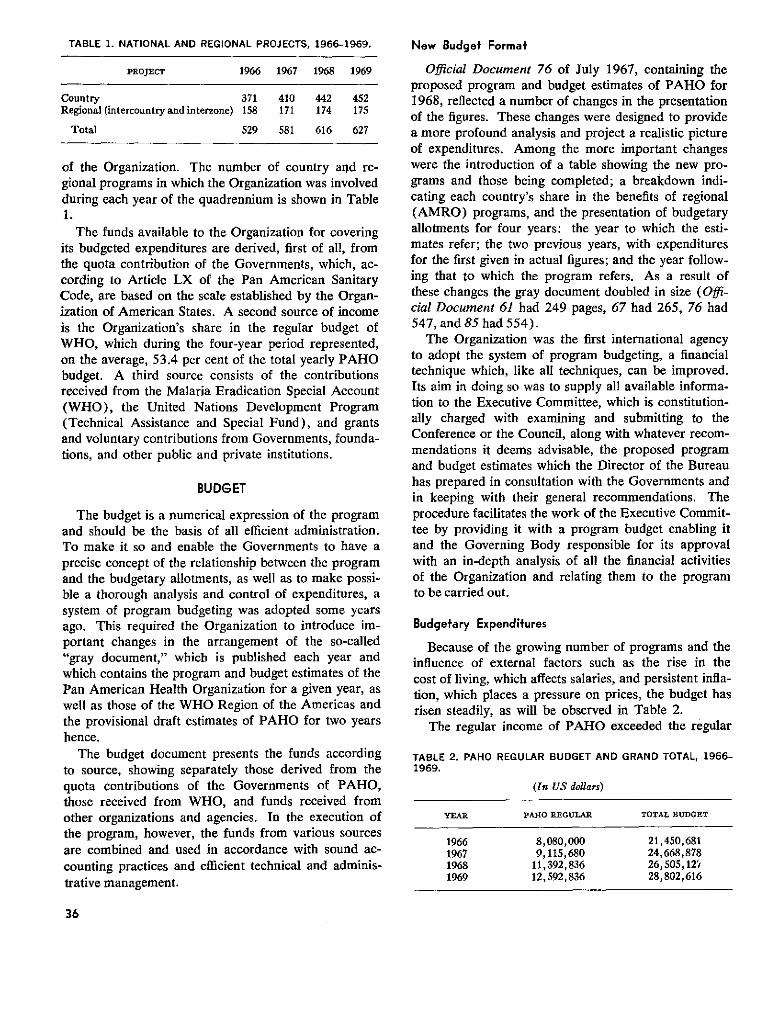
TABLE 1. NATIONAL AND REGIONAL PROJECTS, 1966-1969.
PROJECT 1966 1967 1968 1969
Country 371 410 442 452Regional (intercountry and interzone) 158 171 174 175
Total 529 581 616 627
of the Organization. The number of country and re-gional programs in which the Organization was involvedduring each year of the quadrennium is shown in Table1.
The funds available to the Organization for coveringits budgeted expenditures are derived, first of all, fromthe quota contribution of the Governments, which, ac-cording to Article LX of the Pan American SanitaryCode, are based on the scale established by the Organ-ization of American States. A second source of incomeis the Organization's share in the regular budget ofWHO, which during the four-year period represented,on the average, 53.4 per cent of the total yearly PAHObudget. A third source consists of the contributionsreceived from the Malaria Eradication Special Account(WHO), the United Nations Development Program(Technical Assistance and Special Fund), and grantsand voluntary contributions from Governments, founda-tions, and other public and private institutions.
BUDGET
The budget is a numerical expression of the programand should be the basis of all efficient administration.To make it so and enable the Governments to have aprecise concept of the relationship between the programand the budgetary allotments, as well as to make possi-ble a thorough analysis and control of expenditures, asystem of program budgeting was adopted some yearsago. This required the Organization to introduce im-portant changes in the arrangement of the so-called"gray document," which is published each year andwhich contains the program and budget estimates of thePan American Health Organization for a given year, aswell as those of the WHO Region of the Americas andthe provisional draft estimates of PAHO for two yearshence.
The budget document presents the funds accordingto source, showing separately those derived from thequota contributions of the Governments of PAHO,those received from WHO, and funds received fromother organizations and agencies. In the execution ofthe program, however, the funds from various sourcesare combined and used in accordance with sound ac-counting practices and efficient technical and adminis-trative management.
New Budget Formaf
Official Document 76 of July 1967, containing theproposed program and budget estimates of PAHO for1968, reflected a number of changes in the presentationof the figures. These changes were designed to providea more profound analysis and project a realistic pictureof expenditures. Among the more important changeswere the introduction of a table showing the new pro-grams and those being completed; a breakdown indi-cating each country's share in the benefits of regional(AMRO) programs, and the presentation of budgetaryallotments for four years: the year to which the esti-mates refer; the two previous years, with expendituresfor the first given in actual figures; and the year follow-ing that to which the program refers. As a result ofthese changes the gray document doubled in size (Offi-cial Document 61 had 249 pages, 67 had 265, 76 had547, and 85 had 554).
The Organization was the first international agencyto adopt the system of program budgeting, a financialtechnique which, like all techniques, can be improved.Its aim in doing so was to supply all available informa-tion to the Executive Committee, which is constitution-ally charged with examining and submitting to theConference or the Council, along with whatever recom-mendations it deems advisable, the proposed programand budget estimates which the Director of the Bureauhas prepared in consultation with the Governments andin keeping with their general recommendations. Theprocedure facilitates the work of the Executive Commit-tee by providing it with a program budget enabling itand the Governing Body responsible for its approvalwith an in-depth analysis of all the financial activitiesof the Organization and relating them to the programto be carried out.
Budgetary Expendifures
Because of the growing number of programs and theinfluence of external factors such as the rise in thecost of living, which affects salaries, and persistent infla-tion, which places a pressure on prices, the budget hasrisen steadily, as will be observed in Table 2.
The regular income of PAHO exceeded the regular
TABLE 2. PAHO REGULAR BUDGET AND GRAND TOTAL, 1966-1969.
(In US dollars)
YEAR PARO REGULAR TOTAL BUDGET
1966 8,080,000 21,450,6811967 9,115,680 24,668,8781968 11,392,836 26,505,12'11969 12,592,836 28,802,616
36
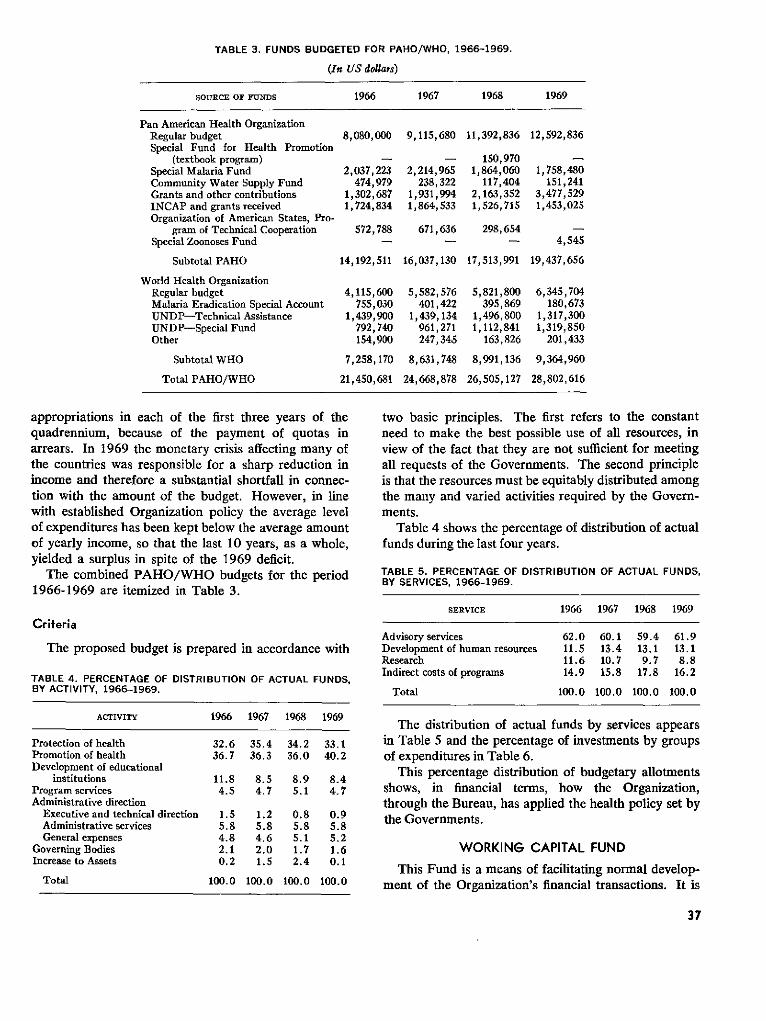
TABLE 3. FUNDS BUDGETED FOR PAHO/WHO, 1966-1969.
(In US dollars)
SOURCE OF FUNDS 1966 1967 1968 1969
Pan American Health OrganizationRegular budget 8,080,000 9,115,680 11,392,836 12,592,836Special Fund for Health Promotion
(textbook program) - - 150,970Special Malaria Fund 2,037,223 2,214,965 1,864,060 1,758,480Community Water Supply Fund 474,979 238,322 117,404 151,241Grants and other contributions 1,302,687 1,931,994 2,163,352 3,477,529INCAP and grants received 1,724,834 1,864,533 1,526,715 1,453,025Organization of American States, Pro-
gram of Technical Cooperation 572,788 671,636 298,654Special Zoonoses Fund - - - 4,545
Subtotal PAHO 14,192,511 16,037,130 17,513,991 19,437,656
World Health OrganizationRegular budget 4,115,600 5,582,576 5,821,800 6,345,704Malaria Eradication Special Account 755,030 401,422 395,869 180,673UNDP-Technical Assistance 1,439,900 1,439,134 1,496,800 1,317,300UNDP-Special Fund 792,740 961,271 1,112,841 1,319,850Other 154,900 247,345 163,826 201,433
Subtotal WHO 7,258,170 8,631,748 8,991,136 9,364,960
Total PAHO/WHO 21,450,681 24,668,878 26,505,127 28,802,616
appropriations in each of the first three years of thequadrennium, because of the payment of quotas inarrears. In 1969 the monetary crisis affecting many ofthe countries was responsible for a sharp reduction inincome and therefore a substantial shortfall in connec-tion with the amount of the budget. However, in linewith established Organization policy the average levelof expenditures has been kept below the average amountof yearly income, so that the last 10 years, as a whole,yielded a surplus in spite of the 1969 deficit.
The combined PAHO/WHO budgets for the period1966-1969 are itemized in Table 3.
Criferia
The proposed budget is prepared in accordance with
TABLE 4. PERCENTAGE OF DISTRIBUTION OF ACTUAL FUNDS,BY ACTIVITY, 1966-1969.
ACTIVITY 1966 1967 1968 1969
Protection of health 32.6 35.4 34.2 33.1Promotion of health 36.7 36.3 36.0 40.2Development of educational
institutions 11.8 8.5 8.9 8.4Program services 4.5 4.7 5.1 4.7Administrative direction
Executive and technical direction 1.5 1.2 0.8 0.9Administrative services 5.8 5.8 5.8 5.8General expenses 4.8 4.6 5.1 5.2
Governing Bodies 2.1 2.0 1.7 1.6Increase to Assets 0.2 1.5 2.4 0.1
Total 100.0 100.0 100.0 100.0
two basic principles. The first refers to the constantneed to make the best possible use of all resources, inview of the fact that they are not sufficient for meetingall requests of the Governments. The second principleis that the resources must be equitably distributed amongthe many and varied activities required by the Govern-ments.
Table 4 shows the percentage of distribution of actualfunds during the last four years.
TABLE 5. PERCENTAGE OF DISTRIBUTION OF ACTUAL FUNDS,BY SERVICES, 1966-1969.
SERVICE 1966 1967 1968 1969
Advisory services 62.0 60.1 59.4 61.9Development of human resources 11.5 13.4 13.1 13.1Research 11.6 10.7 9.7 8.8Indirect costs of programs 14.9 15.8 17.8 16.2
Total 100.0 100.0 100.0 100.0
The distribution of actual funds by services appearsin Table 5 and the percentage of investments by groupsof expenditures in Table 6.
This percentage distribution of budgetary allotmentsshows, in financial terms, how the Organization,through the Bureau, has applied the health policy set bythe Governments.
WORKING CAPITAL FUND
This Fund is a means of facilitating normal develop-ment of the Organization's financial transactions. It is
37
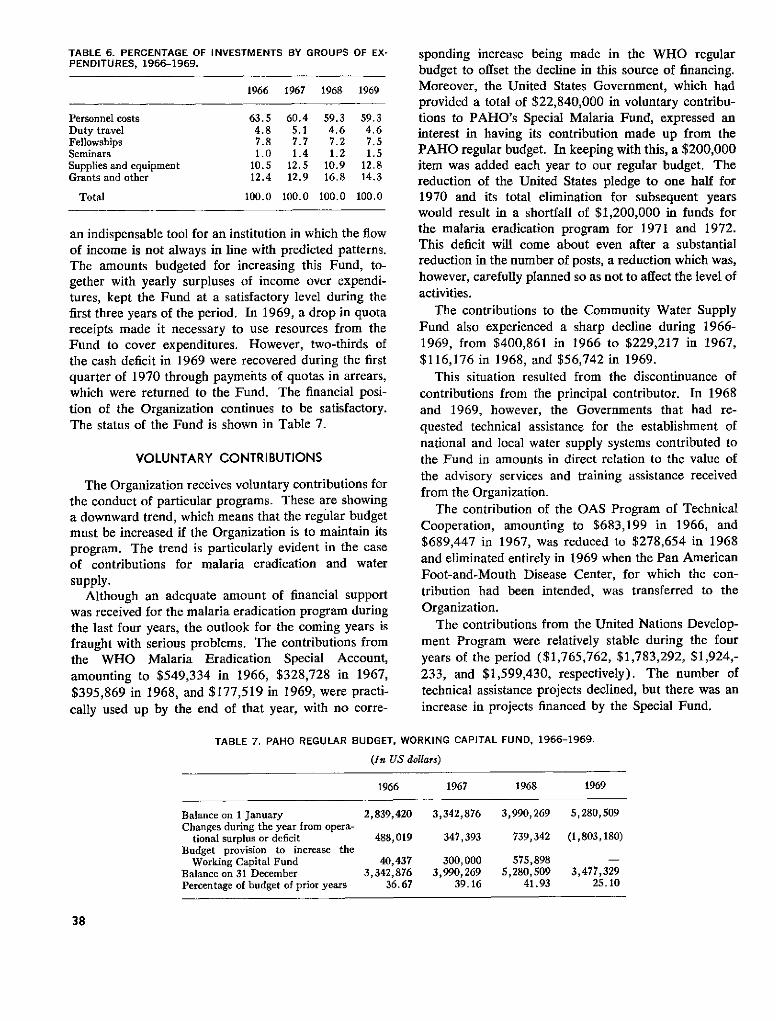
TABLE 6. PERCENTAGE OF INVESTMENTS BY GROUPS OF EX-PENDITURES, 1966-1969.
1966 1967 1968 1969
Personnel costs 63.5 60.4 59.3 59.3Duty travel 4.8 5.1 4.6 4.6Fellowships 7.8 7.7 7.2 7.5Seminars 1.0 1.4 1.2 1.5Supplies and equipment 10.5 12.5 10.9 12.8Grants and other 12.4 12.9 16.8 14.3
Total 100.0 100.0 100.0 100.0
an indispensable tool for an institution in which the flowof income is not always in line with predicted patterns.The amounts budgeted for increasing this Fund, to-gether with yearly surpluses of income over expendi-tures, kept the Fund at a satisfactory level during thefirst three years of the period. In 1969, a drop in quotareceipts made it necessary to use resources from theFund to cover expenditures. However, two-thirds ofthe cash deficit in 1969 were recovered during the firstquarter of 1970 through payments of quotas in arrears,which were returned to the Fund. The financial posi-tion of the Organization continues to be satisfactory.The status of the Fund is shown in Table 7.
VOLUNTARY CONTRIBUTIONS
The Organization receives voluntary contributions forthe conduct of particular programs. These are showinga downward trend, which means that the regular budgetmust be increased if the Organization is to maintain itsprogram. The trend is particularly evident in the caseof contributions for malaria eradication and watersupply.
Although an adequate amount of financial supportwas received for the malaria eradication program duringthe last four years, the outlook for the coming years isfraught with serious problems. The contributions fromthe WHO Malaria Eradication Special Account,amounting to $549,334 in 1966, $328,728 in 1967,$395,869 in 1968, and $177,519 in 1969, were practi-cally used up by the end of that year, with no corre-
sponding increase being made in the WHO regularbudget to offset the decline in this source of financing.Moreover, the United States Government, which hadprovided a total of $22,840,000 in voluntary contribu-tions to PAHO's Special Malaria Fund, expressed aninterest in having its contribution made up from thePAHO regular budget. In keeping with this, a $200,000item was added each year to our regular budget. Thereduction of the United States pledge to one half for1970 and its total elimination for subsequent yearswould result in a shortfall of $1,200,000 in funds forthe malaria eradication program for 1971 and 1972.This deficit will come about even after a substantialreduction in the number of posts, a reduction which was,however, carefully planned so as not to affect the level ofactivities.
The contributions to the Community Water SupplyFund also experienced a sharp decline during 1966-1969, from $400,861 in 1966 to $229,217 in 1967,$116,176 in 1968, and $56,742 in 1969.
This situation resulted from the discontinuance ofcontributions from the principal contributor. In 1968and 1969, however, the Governments that had re-quested technical assistance for the establishment ofnational and local water supply systems contributed tothe Fund in amounts in direct relation to the value ofthe advisory services and training assistance receivedfrom the Organization.
The contribution of the OAS Program of TechnicalCooperation, amounting to $683,199 in 1966, and$689,447 in 1967, was reduced to $278,654 in 1968and eliminated entirely in 1969 when the Pan AmericanFoot-and-Mouth Disease Center, for which the con-tribution had been intended, was transferred to theOrganization.
The contributions from the United Nations Develop-ment Program were relatively stable during the fouryears of the period ($1,765,762, $1,783,292, $1,924,-233, and $1,599,430, respectively). The number oftechnical assistance projects declined, but there was anincrease in projects financed by the Special Fund.
TABLE 7. PAHO REGULAR BUDGET, WORKING CAPITAL FUND, 1966-1969.
(In US dollars)
1966 1967 1968 1969
Balance on 1 January 2,839,420 3,342,876 3,990,269 5,280,509Changes during the year from opera-
tional surplus or deficit 488,019 347,393 739,342 (1,803,180)Budget provision to increase the
Working Capital Fund 40,437 300,000 575,898 -Balance on 31 December 3,342,876 3,990,269 5,280,509 3,477,329Percentage of budget of prior years 36.67 39.16 41.93 25.10
38

Grants to INCAP declined as a result of a smalleramount of contributions from United States sources.
Conversely, the total of all funds received by theOrganization in the form of grants and subsidies frompublic and private organizations showed a substantialincrease, from $2,371,690 in 1966 to $2,429,350 in1967, $2,843,750 in 1968, and $3,300,725 in 1969.
TAX EQUALIZATION FUND
This Fund, established on 1 January 1969 by virtueof Resolution VII of the XVIII Meeting of the Direct-ing Council, is credited each year with the proceeds ofwithholdings under the Staff Assessment Plan.
The credits to the Fund are recorded in subaccountsof the Fund, in the name of Governments in the pro-portion of their assessments for the financial year con-cerned. These individual credits are then reduced bythe amounts which the Organization sets aside to coverthe liabilities in respect of taxes levied by each Govern-ment on emoluments received by staff members fromPAHO/WHO. The resulting amounts are taken intoaccount in determining the contribution due from theGovernments for the fiscal year.
In the succeeding fiscal year, the credits allowed eachGovernment are re-examined to take account of theactual charges made in respect of amounts reimbursedto staff who are subject to national taxes. Should suchcharges exceed the available credit of any Government,the excess shall be added to the contribution of thatGovernment for the second succeeding year.
This system, which is also applied to the UnitedNations, the OAS, and WHO, is designed to ensurethat Governments exempting their nationals on thestaff of the Organization from the payment of tax ontheir salaries are accorded equal financial treatment tothat extended Governments levying such taxes.
PROCUREMENT FUND
The Organization's procurement activities repre-sented an increase in workload over the previous four-year period. The number of purchase orders issuedrose by 20 per cent, line items by 3 per cent, and thedollar value by 45 per cent. The proforma invoicesrendered to Governments showed a decrease of 50 percent in terms of line items but the dollar value remainedsubstantially the same. Purchases on behalf of Gov-ernments rose 29.4 per cent in comparison with 1962-1965.
Beginning in 1966, the WHO undertook to do its. ownpurchasing in the Americas except where circumstancesmade it necessary to use the services of PAHO. In
TABLE 8. SUPPLY SERVICE, 1966-1969.
NO. OF NO. OF VALUE IN
ACTIVITY ORDERS ITEMS US DOLLARS
Purchases for PAHO projects 3,597 14,560 2,642,215Purchases for WHO projects 1,921 12,955 3,027,701Purchases for WHO Headquarters 355 1,808 646,619Purchases for operations of PAHO
Headquarters, Washington 881 3,207 820,996Purchases made through WHO
Headquarters 401 1,907 1,744,380Contractual services 961 1,448 662,933Purchases made on behalf of
Governments 1,399 7,446 1,774,081
Total 9,515 43,331 11,318,925
Price quotations for Member 7,556 10,803,360Governments
50,887
TABLE 9. SUPPLY SERVICE, SUMMARY BY YEAR, 1966-1969.
PURCHASES PROFORMA TOTAL SHIP- PRINTED
YEAR (LINE INVOICES (LINE MENTS ITEMS
ITEMS) (LINE ITEMS) ITEMS)
1966 12,134 1,875 14,009 2,186 9391967 10,110 1,939 12,049 1,913 8791968 9,613 2,617 12,230 1,845 9841969 11,474 1,125 12,599 1,722 753
spite of this, net procurement by PAHO increased by1,622 orders and 1,224 line items.
Purchasing activities are detailed in Tables 8 and 9.
EMERGENCY PROCUREMENT REVOLVING FUND
This Fund, established in 1949 to enable the Organi-zation to provide service to the Governments in emer-gency situations, has been used substantially, especiallyin recent years. It was accordingly decided to increasethe Fund in 1963 from $50,000 to $75,000 and againin 1966, by decision of the XVII Pan American SanitaryConference, to $100,000.
In 1968 the Executive Committee at its 59th Meet-ing made a careful review of the status of the Fund andrecommended to the Directing Council that its amountbe increased to $125,000, urging once again that Gov-ernments receiving assistance from the Fund repay theamounts advanced as soon as possible. This recom-mendation was accepted by the XVIII Meeting of theDirecting Council in Resolution VIII.
Table 10 shows the status of the Fund during thefour-year period.
The Fund has been used to meet requests from 15countries and one territory, generally for combatingepidemic outbreaks or conducting vaccination cam-paigns in the case of hurricanes, earthquakes, floods,
39
TABLE 10. STATUS OF THE EMERGENCY PROCUREMENT RE-VOLVING FUND, 1966-1969.
(To 31 December of each year)
1966 1967 1968 1969
Cash in banks 59,972 28,772 48,411 71,992Invoices to be collected 40,028 71,228 76,589 53,008
Authorized amount 100,000 100,000 125,000 125,000
and other catastrophies. In most cases the assistancehas consisted in the purchase and shipment of vaccines.
The Fund, limited though its amount may be, is agenuine manifestation of inter-American mutual assist-ance and solidarity in the face of emergencies.
SPECIAL FUND FOR RESEARCH
The XVII Pan American Sanitary Conference author-ized the Director to establish a Special Fund for Re-search to strengthen the PAHO/WHO researchprogram. Two years later (1968) the Special Meetingof Ministers of Health recommended to the Govern-ments that they contribute to that Fund in order tofacilitate the achievement of the social, economic, andhealth objectives described in the Declaration of thePresidents of America.
During the period under review, a number of Gov-ernments pledged contributions to the Special Fund anda part of the amounts so pledged was received.
SPECIAL FUND FOR HEALTH PROMOTION
The Organization has made a yearly budget alloca-tion of $250,000 to this Fund pursuant to an agreementof October 1962 with the W. K. Kellogg Foundation.These annual allotments are credited to the Fund inlieu of reimbursement of the 20-year interest-free loanof $5,000,000 received from the Foundation for theconstruction of the Headquarters building.
The Directing Council at its XIX Meeting, recogniz-ing the desirability of augmenting the size and scope ofthe Fund, with the objective of further strengthening thehealth programs of the Americas, decided in Resolu-tion XXXIII to expand the scope of the Fund, initiallyused only for water supply, nutrition, and education,to include other health activities. The Council alsoauthorized the Director to increase the amount of regu-lar budget contributions to the Fund in years whenthere were budgetary surpluses; and to transfer to theFund any portion of such surpluses not needed to keepthe Working Capital Fund at an adequate level. TheDirector was also requested to seek extrabudgetarysources of funds, including voluntary contributions frompublic and private agencies.
Resources from the Special Fund for Health Pro-motion have been used since 1968 to finance the text-book program, which is ultimately expected to pay foritself out of proceeds from the sale and rental of books.
ADMINISTRATIVE QUESTIONS
QUOTAS
The collection of quota contributions is a matter ofcontinuing concern to the Governing Bodies. The XVIIPan American Sanitary Conference, in Resolution VI,again drew the attention of Governments "to the needfor quotas to be paid as soon as possible, within thecourse of each financial year, and especially to the needfor plans for the payment of arrears within stipulatedperiods to be strictly adhered to." The Directing Coun-cil made similar recommendations in Resolutions V ofits XVII Meeting and VI of its XVIII Meeting. In thelatter resolution, the Council expressed satisfaction atthe achievement of "a sound financial position throughthe consistent application over the years of the policiesnecessary for maintaining budgetary expenditures withinincome, building up the Working Capital Fund, andcreating reserves for termination costs." At its XIXMeeting, the Council thanked the Governments
"for the success achieved in reducing arrears to thelowest level in many years," but also expressed con-cern about the number of Governments in arrearsmore than two years and requested the Director tobring to their attention "the importance of unanimoussupport of the program of the Organization throughthe full and prompt payment of quota contributions."The situation can and should be improved to a pointwhere there are no more quotas in arrears and quotasare paid in the year for which they are assessed.
The percentage of quota collections during 1966-1969 is shown in Table 11.
TABLE 11. PERCENTAGE OF QUOTA COLLECTIONS BY FISCALYEAR, 1966-1969.
YEAR PER CENT YEAR PER CENT
1966 80.68 1968 81.721967 81.74 1969 74.22
40
APPOINTMENT OF EXTERNAL AUDITOR
The XVII Meeting of the Directing Council, afternoting with regret the resignation of Mr. Uno Brunskogas External Auditor, for reasons of age, and expressingits appreciation for his services, appointed Mr. LarsBreie, External Auditor of WHO, to succeed Mr.Brunskog.
PERSONNEL
The role of the staff in the accomplishment of theOrganization's program is fundamental and self-evident.Administrative efficiency requires that the staff beproperly qualified and sufficiently large to discharge allthe technical and administrative duties. The staff mustalso reflect the inter-American and international char-acter of the Organization to the greatest practicableextent.
The administrative rationalization carried out be-tween 1962 and 1964 made it possible to keep the sizeof the staff within proper limits while placing increasingemphasis on activities in the field, where the closestcooperation can be given the national health authorities.
Table 12 gives the size of the staff, with a breakdownby categories and by duty stations.
The staff is composed of persons from nearly all thecountries in the Hemisphere and many non-Americancountries and can therefore be considered amply repre-sentative.
SALARY INCREASE
The professional staff was granted a salary increasein 1966 and a further increase, along with a largereducation allowance, effective 1 January 1969, as hadbeen approved by the United Nations General Assem-bly. The latest salary increase involved a total cost of$375,000 and represented, on the average, a 5 per centrise.
Just as the salaries of the international staff are based
TABLE 12. PAHO/WHO STAFF, 1966-1969.
1966 1967 1968 1969
HeadquartersProfessional 103 105 113 117Local 157 171 182 180
Zone Offices and CountriesProfessional 407 417 412 416Local 401 407 455 478
TotalProfessional 510 522 525 533Local 558 578 637 658
Grand total 1,068 1,110 1,162 1,191
on the scale established by the United Nations, those ofthe local personnel are set in line with prevailing levelsof compensation in each duty station. The local staff atHeadquarters received salary adjustments in 1966,1967, 1968 and in July 1969, an increase of approxi-mately 8 per cent.
Local employees in the Zone Offices served undervarying salary conditions over the four-year period butreceived in every instance a salary at least as large asthe best prevailing locally for a similar job.
PROPERTY HOLDINGS
The Organization acquired a number of new build-ings during the period under review. In 1967 it pur-chased new quarters for the Zone IV Office, and in1968 it acquired half of one floor in an office buildingin Guatemala City to house the Zone III offices. Addi-tional space adjacent to the Zone VI offices in BuenosAires was also acquired. All of this was in keeping withthe policy of providing suitable quarters for the opera-tion of our Zone Offices. Negotiations were also under-taken for the purchase of premises in Caracas.
The Pan American Foot-and-Mouth Disease Center,the Institute of Nutrition of Central America andPanama, and the Pan American Zoonoses Center areall operating in quarters donated by the host Govern-ments, Brazil, Guatemala, and Argentina, respectively.
The Executive Committee instructed the Director atits 56th Meeting to report to the next meeting of theDirecting Council on short- and long-range plans formeeting space requirements, particularly in the Head-quarters area, where land is becoming increasinglyhard to get. The Director submitted a report to theXVII Meeting of the Directing Council, which com-mended him on his efforts to obtain favorable accom-modations for the Zone Offices and on his long-rangeplans and urged him to continue the study of possiblesolutions to the long-range needs at Headquarters.
In 1969, after receiving the authorization of theExecutive Committee, a building was acquired in theimmediate vicinity of the present Headquarters buildingto meet long-range space requirements of the Organiza-tion. The XIX Meeting of the Directing Council, inResolution XXIX, expressed its approval of the pur-chase and satisfaction at the favorable terms andconditions obtained.
According to financial projections made, the prop-erty that was purchased-the Governor ShepherdApartments at 2121 Virginia Avenue, N.W.-shouldyield sufficient revenue to repay the investment withina reasonable short time. It will also enable the Organ-ization to meet additional space requirements bygradually converting apartments into offices as the need
41
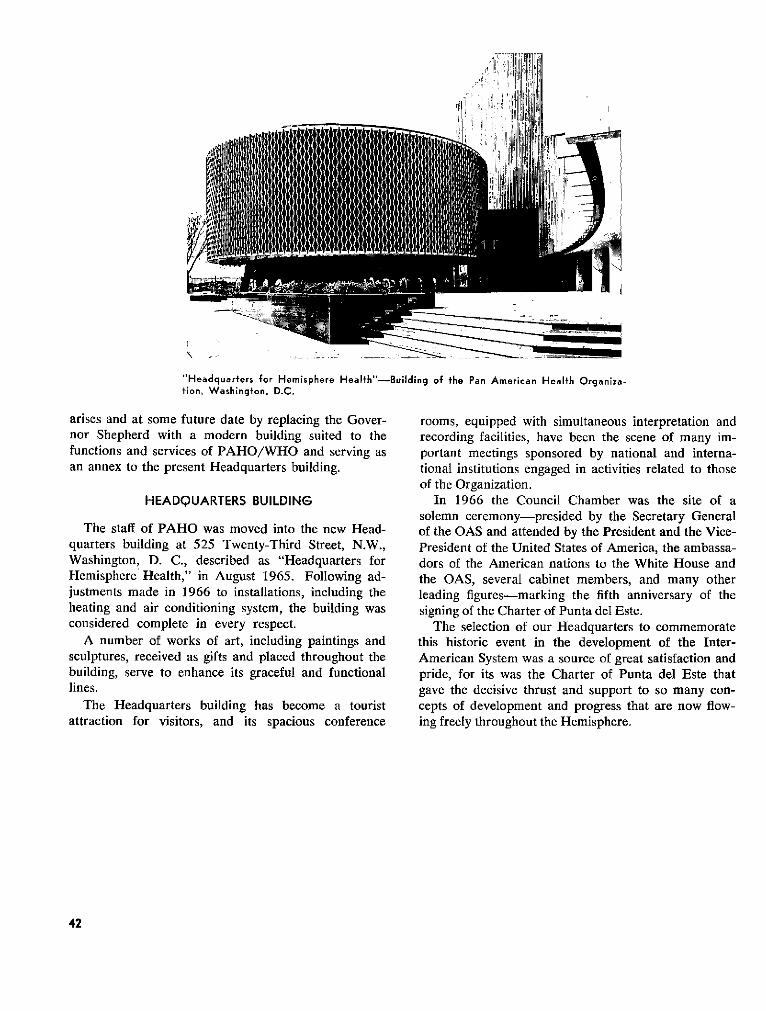
"Headquarters for Hemisphere Health"-Building of the Pan American Health Organiza-tion, Washington, D.C.
arises and at some future date by replacing the Gover-nor Shepherd with a modern building suited to thefunctions and services of PAHO/WHO and serving asan annex to the present Headquarters building.
HEADQUARTERS BUILDING
The staff of PAHO was moved into the new Head-quarters building at 525 Twenty-Third Street, N.W.,Washington, D. C., described as "Headquarters forHemisphere Health," in August 1965. Following ad-justments made in 1966 to installations, including theheating and air conditioning system, the building wasconsidered complete in every respect.
A number of works of art, including paintings andsculptures, received as gifts and placed throughout thebuilding, serve to enhance its graceful and functionallines.
The Headquarters building has become a touristattraction for visitors, and its spacious conference
rooms, equipped with simultaneous interpretation andrecording facilities, have been the scene of many im-portant meetings sponsored by national and interna-tional institutions engaged in activities related to thoseof the Organization.
In 1966 the Council Chamber was the site of asolemn ceremony-presided by the Secretary Generalof the OAS and attended by the President and the Vice-President of the United States of America, the ambassa-dors of the American nations to the White House andthe OAS, several cabinet members, and many otherleading figures-marking the fifth anniversary of thesigning of the Charter of Punta del Este.
The selection of our Headquarters to commemoratethis historic event in the development of the Inter-American System was a source of great satisfaction andpride, for its was the Charter of Punta del Este thatgave the decisive thrust and support to so many con-cepts of development and progress that are now flow-ing freely throughout the Hemisphere.
42
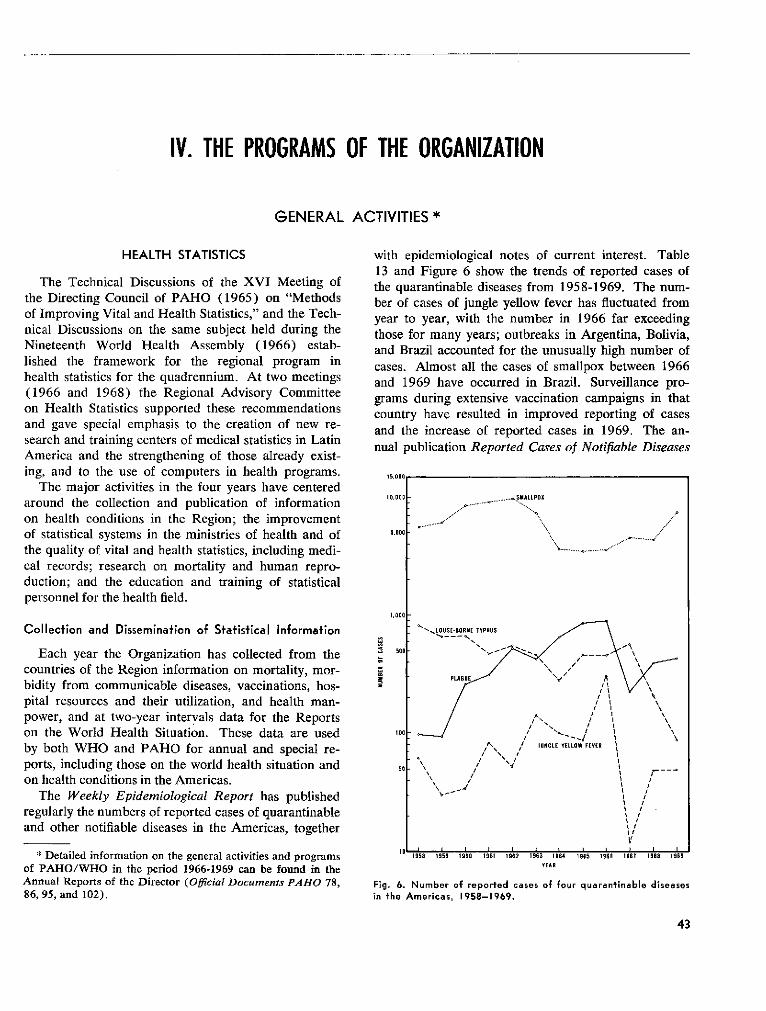
IV. THE PROGRAMS OF THE ORGANIZATION
GENERAL ACTIVITIES *
HEALTH STATISTICS
The Technical Discussions of the XVI Meeting ofthe Directing Council of PAHO (1965) on "Methodsof Improving Vital and Health Statistics," and the Tech-nical Discussions on the same subject held during theNineteenth World Health Assembly (1966) estab-lished the framework for the regional program inhealth statistics for the quadrennium. At two meetings(1966 and 1968) the Regional Advisory Committeeon Health Statistics supported these recommendationsand gave special emphasis to the creation of new re-search and training centers of medical statistics in LatinAmerica and the strengthening of those already exist-ing, and to the use of computers in health programs.
The major activities in the four years have centeredaround the collection and publication of informationon health conditions in the Region; the improvementof statistical systems in the ministries of health and ofthe quality of vital and health statistics, including medi-cal records; research on mortality and human repro-duction; and the education and training of statisticalpersonnel for the health field.
Collection and Dissemination of STatisTical Information
Each year the Organization has collected from thecountries of the Region information on mortality, mor-bidity from communicable diseases, vaccinations, hos-pital resources and their utilization, and health man-power, and at two-year intervals data for the Reportson the World Health Situation. These data are usedby both WHO and PAHO for annual and special re-ports, including those on the world health situation andon health conditions in the Americas.
The Weekly Epidemiological Report has publishedregularly the numbers of reported cases of quarantinableand other notifiable diseases in the Americas, together
* Detailed information on the general activities and programsof PAHO/WHO in the period 1966-1969 can be found in theAnnual Reports of the Director (Oficial Documents PAHO 78,86, 95, and 102).
with epidemiological notes of current interest. Table13 and Figure 6 show the trends of reported cases ofthe quarantinable diseases from 1958-1969. The num-ber of cases of jungle yellow fever has fluctuated fromyear to year, with the number in 1966 far exceedingthose for many years; outbreaks in Argentina, Bolivia,and Brazil accounted for the unusually high number ofcases. Almost all the cases of smallpox between 1966and 1969 have occurred in Brazil. Surveillance pro-grams during extensive vaccination campaigns in thatcountry have resulted in improved reporting of casesand the increase of reported cases in 1969. The an-nual publication Reported Cases of Notifiable Diseases
IO.000
5.000
I.000
500
100
50
1958 1959 1960 19l1 1962 1963 1964 1965 1966
YEAR1967 1596 1959
Fig. 6. Number of reported cases of four quaran+inable diseasesin the Americas, 1958-1969.
43
. SMALLPOX
....'"''"' ......
-_LOUSE-BORNE TYPHUS
UNL YELO FE\\
i IU NtLE YELLOW FEVER\"S---2/ 1
I \\ //
Q\\ *I /
II
71I
t I
I0 I .... .. .I ... ...
t2
ii
a11
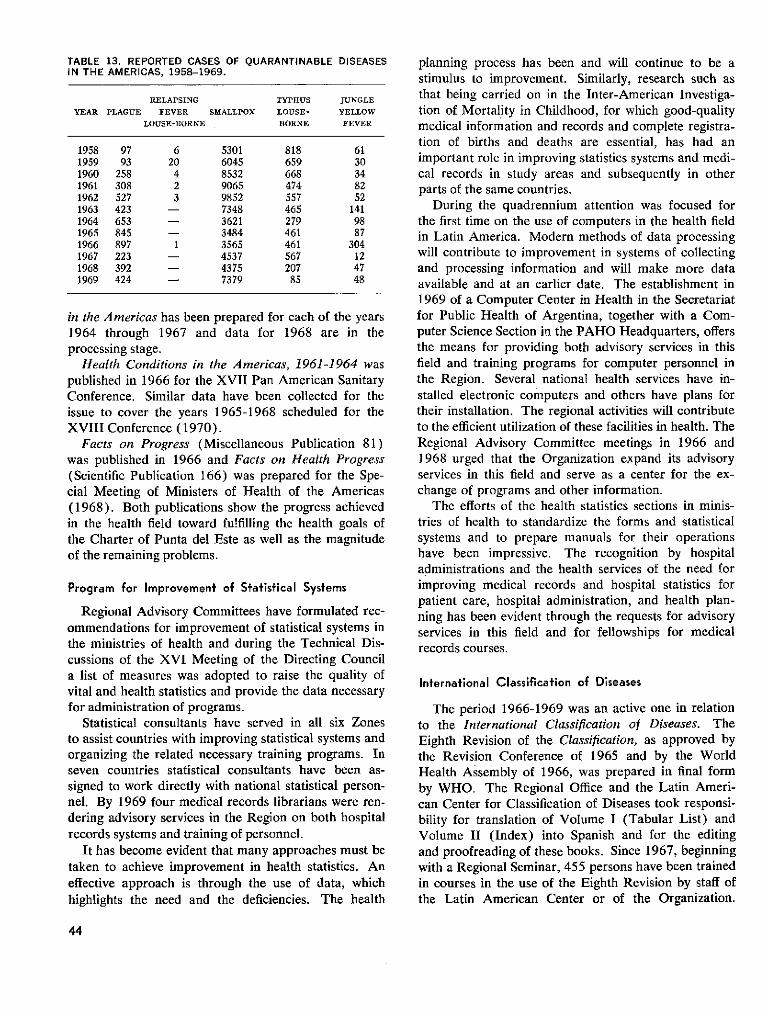
TABLE 13. REPORTED CASES OF QUARANTINABLE DISEASESIN THE AMERICAS, 1958-1969.
RELAPSING TYPHUS JUNGLE
YEAR PLAGUE FEVER SMALLPOX LOUSE- YELLOW
LOUSE-BORNE BORNE FEVER
1958 97 6 5301 818 611959 93 20 6045 659 301960 258 4 8532 668 341961 308 2 9065 474 821962 527 3 9852 557 521963 423 - 7348 465 1411964 653 - 3621 279 981965 845 - 3484 461 871966 897 1 3565 461 3041967 223 - 4537 567 121968 392 - 4375 207 471969 424 - 7379 85 48
in the Americas has been prepared for each of the years1964 through 1967 and data for 1968 are in theprocessing stage.
Health Conditions in the Americas, 1961-1964 waspublished in 1966 for the XVII Pan American SanitaryConference. Similar data have been collected for theissue to cover the years 1965-1968 scheduled for theXVIII Conference (1970).
Facts on Progress (Miscellaneous Publication 81)was published in 1966 and Facts on Health Progress(Scientific Publication 166) was prepared for the Spe-cial Meeting of Ministers of Health of the Americas(1968). Both publications show the progress achievedin the health field toward fulfilling the health goals ofthe Charter of Punta del Este as well as the magnitudeof the remaining problems.
Program for Improvemenf of Statistical Sysfems
Regional Advisory Committees have formulated rec-ommendations for improvement of statistical systems inthe ministries of health and during the Technical Dis-cussions of the XVI Meeting of the Directing Councila list of measures was adopted to raise the quality ofvital and health statistics and provide the data necessaryfor administration of programs.
Statistical consultants have served in all six Zonesto assist countries with improving statistical systems andorganizing the related necessary training programs. Inseven countries statistical consultants have been as-signed to work directly with national statistical person-nel. By 1969 four medical records librarians were ren-dering advisory services in the Region on both hospitalrecords systems and training of personnel.
It has become evident that many approaches must betaken to achieve improvement in health statistics. Aneffective approach is through the use of data, whichhighlights the need and the deficiencies. The health
planning process has been and will continue to be astimulus to improvement. Similarly, research such asthat being carried on in the Inter-American Investiga-tion of Mortality in Childhood, for which good-qualitymedical information and records and complete registra-tion of births and deaths are essential, has had animportant role in improving statistics systems and medi-cal records in study areas and subsequently in otherparts of the same countries.
During the quadrennium attention was focused forthe first time on the use of computers in the health fieldin Latin America. Modern methods of data processingwill contribute to improvement in systems of collectingand processing information and will make more dataavailable and at an earlier date. The establishment in1969 of a Computer Center in Health in the Secretariatfor Public Health of Argentina, together with a Com-puter Science Section in the PAHO Headquarters, offersthe means for providing both advisory services in thisfield and training programs for computer personnel inthe Region. Several national health services have in-stalled electronic computers and others have plans fortheir installation. The regional activities will contributeto the efficient utilization of these facilities in health. TheRegional Advisory Committee meetings in 1966 and1968 urged that the Organization expand its advisoryservices in this field and serve as a center for the ex-change of programs and other information.
The efforts of the health statistics sections in minis-tries of health to standardize the forms and statisticalsystems and to prepare manuals for their operationshave been impressive. The recognition by hospitaladministrations and the health services of the need forimproving medical records and hospital statistics forpatient care, hospital administration, and health plan-ning has been evident through the requests for advisoryservices in this field and for fellowships for medicalrecords courses.
Infernational Classificafion of Diseases
The period 1966-1969 was an active one in relationto the International Classification of Diseases. TheEighth Revision of the Classification, as approved bythe Revision Conference of 1965 and by the WorldHealth Assembly of 1966, was prepared in final formby WHO. The Regional Office and the Latin Ameri-can Center for Classification of Diseases took responsi-bility for translation of Volume I (Tabular List) andVolume II (Index) into Spanish and for the editingand proofreading of these books. Since 1967, beginningwith a Regional Seminar, 455 persons have been trainedin courses in the use of the Eighth Revision by staff ofthe Latin American Center or of the Organization.
44
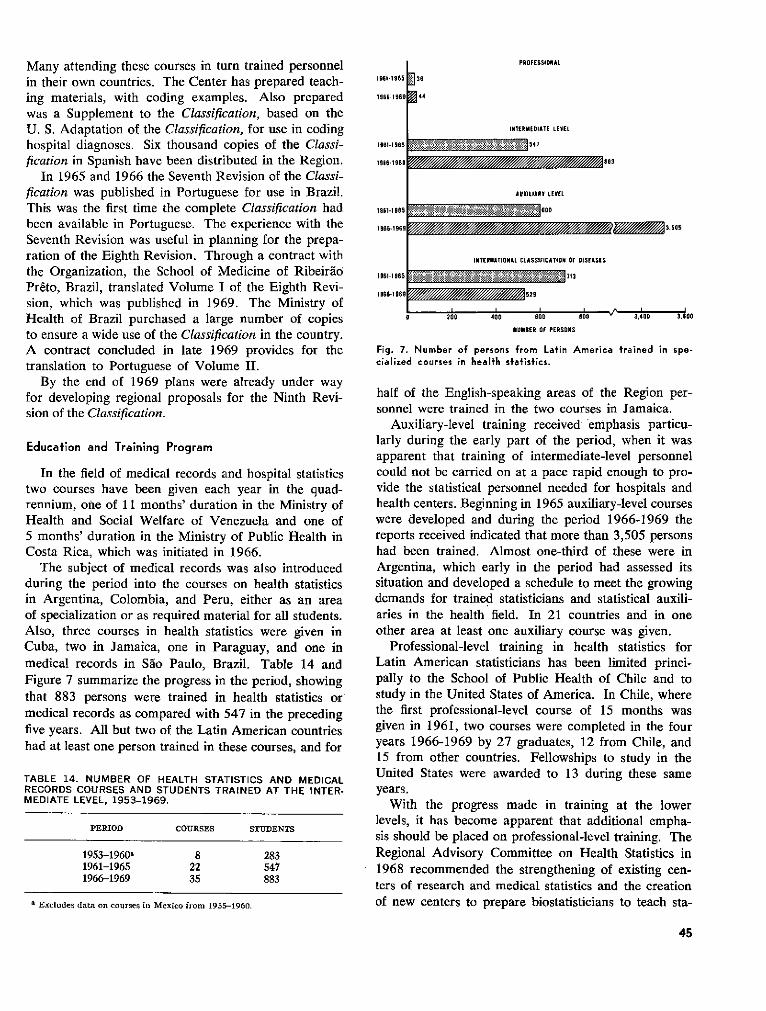
Many attending these courses in turn trained personnelin their own countries. The Center has prepared teach-ing materials, with coding examples. Also preparedwas a Supplement to the Classification, based on theU. S. Adaptation of the Classification, for use in codinghospital diagnoses. Six thousand copies of the Classi-fication in Spanish have been distributed in the Region.
In 1965 and 1966 the Seventh Revision of the Classi-fication was published in Portuguese for use in Brazil.This was the first time the complete Classification hadbeen available in Portuguese. The experience with theSeventh Revision was useful in planning for the prepa-ration of the Eighth Revision. Through a contract withthe Organization, the School of Medicine of RibeiráoPréto, Brazil, translated Volume I of the Eighth Revi-sion, which was published in 1969. The Ministry ofHealth of Brazil purchased a large number of copiesto ensure a wide use of the Classification in the country.A contract concluded in late 1969 provides for thetranslation to Portuguese of Volume II.
By the end of 1969 plans were already under wayfor developing regional proposals for the Ninth Revi-sion of the Classification.
Educafion and Training Program
In the field of medical records and hospital statisticstwo courses have been given each year in the quad-rennium, one of 11 months' duration in the Ministry ofHealth and Social Welfare of Venezuela and one of5 months' duration in the Ministry of Public Health inCosta Rica, which was initiated in 1966.
The subject of medical records was also introducedduring the period into the courses on health statisticsin Argentina, Colombia, and Peru, either as an areaof specialization or as required material for all students.Also, three courses in health statistics were given inCuba, two in Jamaica, one in Paraguay, and one inmedical records in Sáo Paulo, Brazil. Table 14 andFigure 7 summarize the progress in the period, showingthat 883 persons were trained in health statistics ormedical records as compared with 547 in the precedingfive years. All but two of the Latin American countrieshad at least one person trained in these courses, and for
TABLE 14. NUMBER OF HEALTH STATISTICS AND MEDICALRECORDS COURSES AND STUDENTS TRAINED AT THE INTER-MEDIATE LEVEL, 1953-1969.
PERIOD COURSES STUDENTS
1953-1960 8 2831961-1965 22 5471966-1969 35 883
a Excludes data on courses in Mexico from 1955-1960.
1961-1965
1966-1969
1961-1965
PROFESSIONAL
] 36
INTERMEOIATE LEVEL
: 1.!1.:: : :1;.8 511 1 547
196-196 3/////////
19611965
1966-1969 // 3505
1961-1965
1966-1969
AUXILIARY LEVEL
::::::~.~ _ 6 ;00
INTERNATIONAL CLASSIFICATION OF OISEASES
I .L 13. i .k ./71
529
0 200 400 600
NUMBER OF PERSONS
Bu ' 3,4UU J.UU
Fig. 7. Number of persons from Latin America trained in spe-cialized courses in health statistics.
half of the English-speaking areas of the Region per-sonnel were trained in the two courses in Jamaica.
Auxiliary-level training received' emphasis particu-larly during the early part of the period, when it wasapparent that training of intermediate-level personnelcould not be carried on at a pace rapid enough to pro-vide the statistical personnel needed for hospitals andhealth centers. Beginning in 1965 auxiliary-level courseswere developed and during the period 1966-1969 thereports received indicated that more than 3,505 personshad been trained. Almost one-third of these were inArgentina, which early in the period had assessed itssituation and developed a schedule to meet the growingdemands for trained statisticians and statistical auxili-aries in the health field. In 21 countries and in oneother area at least one auxiliary course was given.
Professional-level training in health statistics forLatin American statisticians has been limited princi-pally to the School of Public Health of Chile and tostudy in the United States of America. In Chile, wherethe first professional-level course of 15 months wasgiven in 1961, two courses were completed in the fouryears 1966-1969 by 27 graduates, 12 from Chile, and15 from other countries. Fellowships to study in theUnited States were awarded to 13 during these sameyears.
With the progress made in training at the lowerlevels, it has become apparent that additional empha-sis should be placed on professional-level training. TheRegional Advisory Committee on Health Statistics in1968 recommended the strengthening of existing cen-ters of research and medical statistics and the creationof new centers to prepare biostatisticians to teach sta-
45
*A
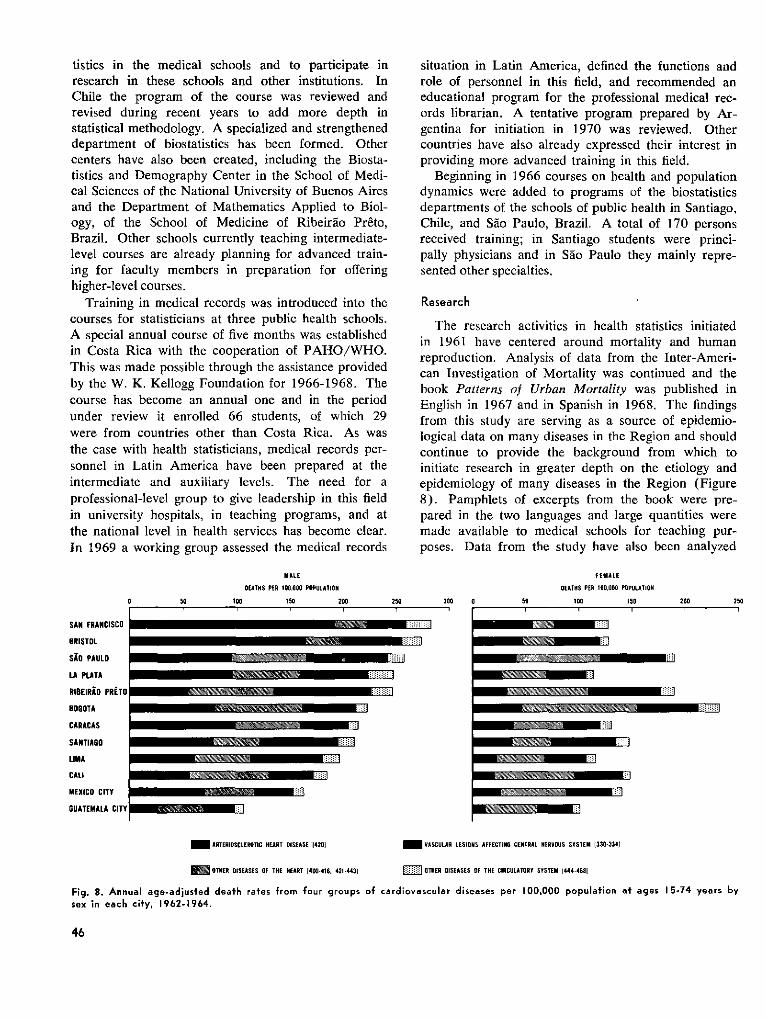
tistics in the medical schools and to participate inresearch in these schools and other institutions. InChile the program of the course was reviewed andrevised during recent years to add more depth instatistical methodology. A specialized and strengtheneddepartment of biostatistics has been formed. Othercenters have also been created, including the Biosta-tistics and Demography Center in the School of Medi-cal Sciences of the National University of Buenos Airesand the Department of Mathematics Applied to Biol-ogy, of the School of Medicine of Ribeiráo Preto,Brazil. Other schools currently teaching intermediate-level courses are already planning for advanced train-ing for faculty members in preparation for offeringhigher-level courses.
Training in medical records was introduced into thecourses for statisticians at three public health schools.A special annual course of five months was establishedin Costa Rica with the cooperation of PAHO/WHO.This was made possible through the assistance providedby the W. K. Kellogg Foundation for 1966-1968. Thecourse has become an annual one and in the periodunder review it enrolled 66 students, of which 29were from countries other than Costa Rica. As wasthe case with health statisticians, medical records per-sonnel in Latin America have been prepared at theintermediate and auxiliary levels. The need for aprofessional-level group to give leadership in this fieldin university hospitals, in teaching programs, and atthe national level in health services has become clear.In 1969 a working group assessed the medical records
situation in Latin America, defined the functions androle of personnel in this field, and recommended aneducational program for the professional medical rec-ords librarian. A tentative program prepared by Ar-gentina for initiation in 1970 was reviewed. Othercountries have also already expressed their interest inproviding more advanced training in this field.
Beginning in 1966 courses on health and populationdynamics were added to programs of the biostatisticsdepartments of the schools of public health in Santiago,Chile, and Sáo Paulo, Brazil. A total of 170 personsreceived training; in Santiago students were princi-pally physicians and in Sao Paulo they mainly repre-sented other specialties.
Research
The research activities in health statistics initiatedin 1961 have centered around mortality and humanreproduction. Analysis of data from the Inter-Ameri-can Investigation of Mortality was continued and thebook Patterns of Urban Mortality was published inEnglish in 1967 and in Spanish in 1968. The findingsfrom this study are serving as a source of epidemio-logical data on many diseases in the Region and shouldcontinue to provide the background from which toinitiate research in greater depth on the etiology andepidemiology of many diseases in the Region (Figure8). Pamphlets of excerpts from the book were pre-pared in the two languages and large quantities weremade available to medical schools for teaching pur-poses. Data from the study have also been analyzed
MALE
DEATHS PER 100,000 POPULATI0N
0 00 100ISO 200
SAN FRANCISCO
BRISTOL
SiO PAULO
LA PLATA
RIBEIRiO PRETO
BOGOTA
CARACAS
SANTIAGO
LIMA
CALI
MEXICO CITY
GUATEMALA CITY
250 300 0
FEMALE
DEATHS PER 100.000 POPULATION
50 100 150
_ ARTERIOSCLEROTIC HEART DISEASE 1420)
OTHER DISEASES OF THE HEART 1400-416. 421-4431
M VASCULAR LESIONS AFFECTING CENTRAL NERVOUS SYSTEM 1[30-3341
= OTHER DISEASES OF THE CIRCULATORY SYSTEM (444-468l
Fig. 8. Annual age-adjusted deafh rates from four groups of cardiovascular diseases per 100,000 population at ages 15-74 years bysex in each city, 1962-1964.
46
200 250
1 � � 1 � 1 � � 1 i 1
MENERMEN~~~~~~~riiir
"WIM~
11
liiiiiaI�
R�B�
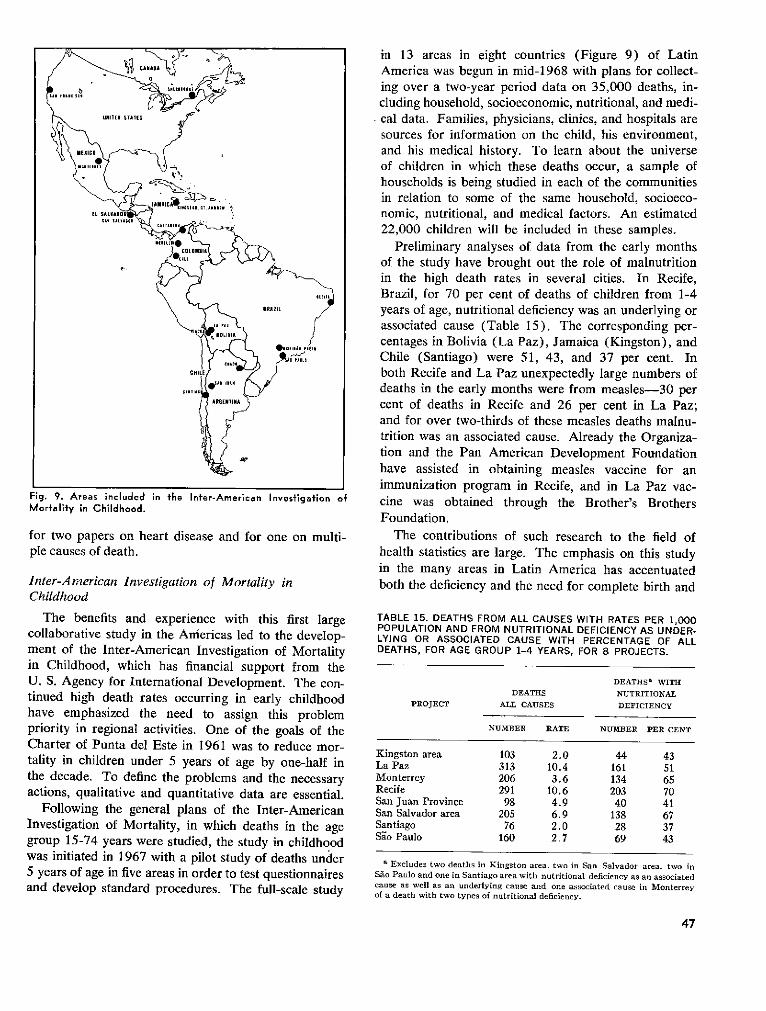
Fig. 9. Areas included in the Inter-American Investigation ofMortality in Childhood.
for two papers on heart disease and for one on multi-ple causes of death.
Inter-American Investigation of Mortality inChildhood
The benefits and experience with this first largecollaborative study in the Americas led to the develop-ment of the Inter-American Investigation of Mortalityin Childhood, which has financial support from theU. S. Agency for International Development. The con-tinued high death rates occurring in early childhoodhave emphasized the need to assign this problempriority in regional activities. One of the goals of theCharter of Punta del Este in 1961 was to reduce mor-tality in children under 5 years of age by one-half inthe decade. To define the problems and the necessaryactions, qualitative and quantitative data are essential.
Following the general plans of the Inter-AmericanInvestigation of Mortality, in which deaths in the agegroup 15-74 years were studied, the study in childhoodwas initiated in 1967 with a pilot study of deaths under5 years of age in five areas in order to test questionnairesand develop standard procedures. The full-scale study
in 13 areas in eight countries (Figure 9) of LatinAmerica was begun in mid-1968 with plans for collect-ing over a two-year period data on 35,000 deaths, in-cluding household, socioeconomic, nutritional, and medi-cal data. Families, physicians, clinics, and hospitals aresources for information on the child, his environment,and his medical history. To learn about the universeof children in which these deaths occur, a sample ofhouseholds is being studied in each of the communitiesin relation to some of the same household, socioeco-nomic, nutritional, and medical factors. An estimated22,000 children will be included in these samples.
Preliminary analyses of data from the early monthsof the study have brought out the role of malnutritionin the high death rates in several cities. In Recife,Brazil, for 70 per cent of deaths of children from 1-4years of age, nutritional deficiency was an underlying orassociated cause (Table 15). The corresponding per-centages in Bolivia (La Paz), Jamaica (Kingston), andChile (Santiago) were 51, 43, and 37 per cent. Inboth Recife and La Paz unexpectedly large numbers ofdeaths in the early months were from measles-30 percent of deaths in Recife and 26 per cent in La Paz;and for over two-thirds of these measles deaths malnu-trition was an associated cause. Already the Organiza-tion and the Pan American Development Foundationhave assisted in obtaining measles vaccine for animmunization program in Recife, and in La Paz vac-cine was obtained through the Brother's BrothersFoundation.
The contributions of such research to the field ofhealth statistics are large. The emphasis on this studyin the many areas in Latin America has accentuatedboth the deficiency and the need for complete birth and
TABLE 15. DEATHS FROM ALL CAUSES WITH RATES PER 1,000POPULATION AND FROM NUTRITIONAL DEFICIENCY AS UNDER-LYING OR ASSOCIATED CAUSE WITH PERCENTAGE OF ALLDEATHS, FOR AGE GROUP 1-4 YEARS, FOR 8 PROJECTS.
DEATHSa WITHDEATHS NUTRITIONAL
PROJECT ALL CAUSES DEFICIENCY
NUMBER RATE NUMZBER PER CENT
Kingston area 103 2.0 44 43La Paz 313 10.4 161 51Monterrey 206 3.6 134 65Recife 291 10.6 203 70San Juan Province 98 4.9 40 41San Salvador area 205 6.9 138 67Santiago 76 2.0 28 37Sao Paulo 160 2.7 69 43
a Excludes two deaths in Kingston area, two in San Salvador area, two inSao Paulo and one in Santiago area with nutritional deficiency as an associatedcause as well as an underlying cause and one associated cause in Monterreyof a death with two types of nutritional deficiency.
47
death registration systems and for medical records ofgood quality in hospitals and clinics. In the study areasspecial efforts have been made to assure improvementin these data, and the procedures initiated shouldbe extended beyond the study areas. Similarly thecontributions of research to medical education andmedical practice should also be great. In several coun-tries where there is more than one study area, coordi-nating meetings of national groups from the associationof medical schools, the ministry of health, the localcollaborators, and the PAHO/WHO staff of'the In-vestigation have been held to ensure that the findingsof the study will have the broadest possible use inmedical education and the greatest application in thehealth field. As a result of these meetings, autopsyservices have been expanded in some areas.
In 1969 an area in California was added to the study.This project is supported by the Children's Bureau ofthe U.S. Department of Health, Education, and Wel-fare. At the beginning of 1970 an area in the Provinceof Quebec, Canada, is to enter the study and will havefinancial support from the National Health Service.
Research on multiple causes of death was carriedout with the study of records from two cities in theInter-American Investigation of Mortality in adults,supported by funds from the National Center for HealthStatistics of the U.S. Public Health Service. Plans arebeing made for analysis of multiple causes from theInvestigation of Mortality in Childhood and also fromsamples of death certificates in the countries of theRegion. Such research will contribute to the planningfor the Ninth Revision of the International Classifica-tion of Diseases.
Other Studies
In 1966 two longitudinal investigations of humanreproduction were begun in the Americas with thesupport of PAHO and WHO. One was in Peru intwo communities of under 3,000 population (Lurín onthe coast, and Masma in the highlands). Followinginitial censuses of the population, monthly visits weremade to all households with women in the child-bearingages and at three-month intervals to all other house-holds. At each visit data were obtained on births,deaths, migration, pregnancies, fetal deaths, breastfeeding, and condition of live-born children in thehousehold. Each community is being followed for athree-year period. Already provisional data showdifferences in birth rates, birth weights, and intervalsbetween pregnancies.
In Sao Paulo, Brazil, a prospective fertility study in1966-1967 covered a sample of women previouslyinterviewed in a retrospective study. The women were
interviewed at four-month intervals over a one-yearperiod.
A working group in Santiago, Chile, in 1968 re-viewed the methodology of these two studies and ofother research in Chile and Colombia. Recommenda-tions were made for a collaborative longitudinal studyof human reproduction with the participation of severalLatin American countries, which would encompassinvestigation of biological phenomena of reproduction,health characteristics of the mother, and the product ofconception including growth and development of thechild.
Studies of this kind, as they progress toward theachievement of their objectives, and other measuressuch as the use of computers for health data, will con-tribute greatly in future years toward the improvementof statistical systems, which form the basis for allsound planning in the health sector. The period 1966-1969 was one of intensive activity in the healthstatistics field, and the advances made promise muchfor the future.
HEALTH PLANNING
The countries of the Hemisphere, in cooperationwith the Organization, continued their work in thefield of health planning within the framework of na-tional economic and social development plans.
In the quadrennium activities were directed mainlyto establishing a methodology for planning in the healthsector, training personnel through national and inter-national courses, and formulating and later evaluatingplans. An analysis of the development of the healthplanning process during the period reveals a clearlymarked tendency in a considerable number of coun-tries to use planning as an instrument for improvinginstitutional and intrasectoral coordination, for ensur-ing better utilization of resources and their allocationto the true requirements of the health situation, andfor promoting research aimed at increasing knowledgeof the health situation and the investment of resources.It is to be noted, however, that this tendency is en-countering two fundamental obstacles which are af-fecting not only the health sector but also the moregeneral development process: these are deficiencies inthe decision-making process, and the limited operatingcapacity of the administrative systems that have toimplement these decisions.
It can be said that, in the health sector, planninghas followed the lines of general planning and develop-ment. In the first stage emphasis was laid on the de-velopment and application of over-all methods drawnlargely from econometrics, and on the formulation ofplans of a general nature, with institutional coverage
48
most often limited to the ministries of health. Theexperience gained and the results observed in theevaluations of implementation programs point to theneed to widen the objectives and attempt to strengthenthe administrative and information systems and co-ordination between institutions, as well as to plan thedevelopment of the infrastructure and promote greatereffectiveness of the decision-making machinery. Theseconcerns are evident in the change in the content of newhealth plans, in the reformulations derived from theevaluation of older plans, and in the modifications madein training programs, with the inclusion of new disci-plines and new knowledge relevant to the developmentof the planning process and its administration.
Pan American Health Planning Program
Along these same lines, the methodology developedunder the auspices of the Organization was revised bya working group of consultants in this field. At theirmeeting in March 1967, the group examined the statusof health planning in the Americas and, following acritical analysis, recommended a number of basicimprovements and additions to the methodology, stress-ing the need to perfect it through systematic research.A review of the period showed that both methodo-logical and operational research and the investigationof health as a component of economic and socialdevelopment merited immediate and preferential at-tention. In this context, it was gratifying to note that,in accordance with the recommendation of the XVIIPan American Sanitary Conference (Resolution XXI)and as a result of the interest displayed by the coun-tries of the Hemisphere, assistance was received fromthe United Nations Development Program in estab-lishing the Pan American Health Planning Program.This Program has made it possible to consolidate andextend the training activities that the Organization hadbeen carrying out since 1962 in conjunction with theLatin American Institute for Economic and SocialPlanning.
The Program has as its objects the development ofhuman resources, the implementation of a researchprogram, and the dissemination of technical and scien-tific knowledge. The establishment of the Program isan effective response to the need for training of per-sonnel and for research in line with the planningsituation in the countries. The efforts made by theGovernments are evident from the fact that 12 coun-tries currently have health plans with a nationalcoverage, at various stages of execution. Eight of theseplans have been periodically evaluated and revised. Ofthe 12 countries that were considered to be fully en-gaged in the planning process, five had reached the stage
of consolidating the measures for the execution of theirplans at the local operational level. The remainingseven countries were in the initial stages of the process.
As a result of the training program, the countrieshave been able to train some 2,000 workers. In addi-tion, 226 health specialists have attended the interna-tional courses organized by the Pan American HealthPlanning Program. It should be noted that five coun-tries have provided systematic training in planningtechniques through regular courses given at theirschools of public health.
Quadrennial Projections
In order to implement the recommendations madeby the Governing Bodies of the Organization, a pro-cedure for the long-term planning of PAHO/WHOactivities in cooperation with national Governmentswas designed and put into practice. This method,known as the PAHO/WHO Quadrennial Projections,enables the various factors that are directly or indi-rectly involved in the assistance provided to Govern-ments of the Organization to be considered within thecontext of a single process. It is based on the estab-lishment of a common frame of reference within whichthe major health problems are examined, health policyis considered in the light of the stage reached in eco-nomic and social development, goals and priorities areestablished, and the sectors are identified in whichPAHO/WHO assistance is required in order to realizethese priorities and reach the goals set.
The suggested procedure was approved by the XIXMeeting of the Directing Council (Resolution XXVII)and has begun to be adopted by the countries. Withthis method, which permits joint planning with thecountries, it is hoped to arrive in 1970 at a first approxi-mation of the program for cooperation with the Govern-ments, and of the budget for a four-year period startingin 1972. Refinements to the method should make itpossible to set up a permanent and more dynamicprocess.
In short, during the quadrennium we have remainedtrue to the principle laid down in the Charter of Puntadel Este that planning is "an instrument for establish-ing priorities in an objective manner, for increasingthe output of available resources, and for making in-vestments to achieve measurable objectives. The WorldHealth Assembly, the Pan American Sanitary Con-ference, and the Directing Council of PAHO havedecided to make health planning part of the policy.For planning is a means, not an end; a process, not anendpoint; a path of action, not a terminus. The methodused in preparing the plan is of no importance. Theessential thing is the decision to draw up a plan and
49
the achievement of its objectives," as was stated by theMinisters of Health in 1968.
ADMI N ISTRATIVE METHODS AND PRACTICES
Among the international agencies, our Organizationhas taken a leading position in recognizing the im-portance of administration and incorporating advisoryservices and training in this subject as an integral partof its program of collaboration with and assistance toGovernments. The increasing demand for consultantservices in this subject arises from the consciousnessin the Americas of the possibilities for more productiveutilization of resources, through. organizing and ad-ministering them in a more effective manner.
Advisory services provided to the health ministrieshave proved not only that effective improvement inprocedures and performance can be made within exist-ing national regulations, but also that administrativeadvances in one ministry can complement, and evenstimulate, national administrative reform.
Cooperation of the Organization directed towardpromoting improvement of administration in general,and administrative services in particular includes:
a) Promotion and advice in regard to administrationas an integral part of the totality of activities whichconstitute planning in the health sector.
b) Promotion and advice in regard to the imple-mentation of systems, comprising the best structuralorganization and procedures to assure efficient use ofresources for dynamic health services.
c) Promotion and advice in regard to training inadministration for health personnel at all levels.
Advisory services and fellowships in administration,for ministries of health as well as for special programssuch as malaria eradication and water supply, have
Fourth Seminar on Organization andAdministration of Health Servies,Maracay, Venezuela, November 1969.
been provided to 24 countries, and a series of seminarsand courses have been organized.
Under this heading, special reference should be madeto the work of computerization and mechanizationthat has been carried out in the Organization. Theactivities of the data processing unit were greatlyexpanded during the quadrennium in both administra-tive and technical program areas, and in 1969 a Com-puter Science Section was established in the HealthStatistics Department.
Computerization, which allows great quantities ofdata to be stored and processed, has been applied since1967 in the finance and accounts areas, and a co-operative arrangement was made with the Pan Ameri-can Union for the use of the IBM 360/30 Computer,which made it possible to institute new methods thatcould not be employed before because of their highcost. At the end of 1969 a start was made on thestandardization of data for the computer so as to per-mit exchange of information between WHO andPAHO.
The methods and procedures used for reproducingand distributing the Organization's publications havealso been modernized. The equipment acquired in1969 included a Cheshire labeling machine, two photo-offset machines, and a collecting machine. Two Xerox3601 and 3603 machines were also put into use toreduce the typing workload in the Departments.
Modernization of the reproduction and distributionfacilities-a requirement of the present age-has en-abled the Organization to handle an increased volumeof work at reasonable cost.
HEALTH LEGISLATION
The advisory services to Governments in the reviewand modernization of their health legislation were
50
broadened and extended to include a study of the rela-tionship between health and law, in compliance withResolution XXIII of the XVII Meeting of the DirectingCouncil.
Group of Experts
A study group was convened in April 1968 to definethe technical, practical, and financial aspects of thisrelationship. The report submitted by this group pointsout the scope of the relationship between health andlaw in the national, regional, and international spheresand examines aspects such as nutrition, water supply,pharmaceutical products, industrial hygiene, and others.The report also deals with education, public adminis-tration, international cooperation, economic integra-tion, and the establishment of community legislation,with special emphasis on the general development plansfor integration of frontier areas or joint utilization ofregional resources. The 59th Meeting of the ExecutiveCommittee recommended that the Directing Councilapprove the preliminary report of the Director, whichwas based on the expert group report, and that a studyof the problem be presented to the XVIII Pan AmericanSanitary Conference. For its part, the Special Meetingof Ministers of Health devoted a special chapter oftheir Final Report to health legislation and recom-mended that the laws be revised to bring them intoline with scientific advances and the requirements ofeconomic and social development. The Ministers alsoemphasized the need to achieve a certain uniformity inthe national health legislations or to give them sufficientflexibility to facilitate international cooperation. Theyalso placed renewed stress on the need for an in-depthstudy of the Pan American Sanitary Code.
Study on Health Legislafion
A study on health legislation was also completed,the first stage of which covered the information avail-able for the period 1948-1966 on 20 Latin Americancountries: Argentina, Bolivia, Brazil, Chile, Colombia,Costa Rica, Cuba, Dominican Republic, Ecuador, ElSalvador, Guatemala, Haiti, Honduras, Mexico, Nica-ragua, Panama, Paraguay, Peru, Uruguay, and Vene-zuela. The legal systems of the countries listed arecomparable since they have, in general, a commonorigin. Three sectors were defined for the purposesof the study: constitutions, special legislation, andpenal codes. The constitutions were examined toidentify aspects relating to health. Special health legis-lation, including health codes, was then analyzed.Finally, the sections of the penal codes dealing withhealth were examined. The second stage of the study
will cover an analysis of similar features of health legis-lation in the English-speaking countries; it is hoped tocomplete this in 1970.
Pan American Sanilary Code
It has been pointed out that this Code, which wassigned in Cuba in 1924, together with its AdditionalProtocols of October 1927 and September 1952, canno longer be generally said to be relevant to the healthsituation in the Western Hemisphere. Moreover, thenew Member States of the Organization (Barbados,Guyana, Jamaica, and Trinidad and Tobago) are notparties to this international treaty, which was concludedbetween the 21 American Republics that originallysigned and ratified it. Nonetheless it should be notedthat the Governments mentioned in the precedingparagraph have undertaken to apply the provisions ofthe Code in their respective territories. Once the com-parative study of health legislation in the countries ofthe Americas (called for in Resolution XXVIII of theXIX Meeting of the Directing Council) has been com-pleted, work will start on analyzing the Pan AmericanSanitary Code in the light of advances in science andtechnology, present-day problems, and projections ofeconomic and social development. A draft study hasbeen prepared, which will be submitted to the Con-ference for its consideration, in order to determinewhether it is desirable to amend the Code or to replaceit by a dynamic and flexible instrument that will allowperiodic updating of its various provisions and be inharmony with the laws of each country.
International Transportation of Human Remains
It is of interest to note that the V Meeting of theTechnical Committee on the Removal of Travel Bar-riers (Managua, Nicaragua, 18-21 July 1967) recom-mended the national application of the standards forthe international transportation of human remains, ap-proved by the XVII Pan American Sanitary Conference(Resolution XXIX). The following countries haveimplemented these standards or modified their nationalregulations accordingly: Argentina, Barbados, Brazil,Colombia, Costa Rica, Dominican Republic, Guate-mala, Mexico, and Nicaragua. While not supportedby a special legislative or regulatory act, the standardsare being applied in Guyana, Antigua, Dominica, Gre-nada, Montserrat, St. Kitts, Nevis and Anguilla, St.Lucia, St. Vincent, and the Virgin Islands (UnitedKingdom). In British Honduras, Jamaica, Trinidadand Tobago, and Venezuela the implementation ofthese standards is awaiting the enactment of the neces-sary legislation. This has been the first time that the
51
Organization has endeavored to establish juridicalnorms, through the Conference, with regard to ahealth problem, while at the same time leaving theGovernments at perfect liberty to incorporate them intheir own legislative systems or not.
Future Activities
The developments that have taken place in this newactivity and the many and varied juridical questionsraised by economic integration and the future LatinAmerican Common Market have highlighted,.as wasstated by the Ministers of Health in 1968, the lack ofa harmonious and uniform inter-American healthlegislation. The future activities of our Organizationwill have to develop in this direction.
EVALUATION
The work of the Organization in this field has beenguided by the policies laid down by the GoverningBodies and by the instructions contained in the WHOManual.
At its XV Meeting (1964) the Directing Councildecided, in Resolution XIII:
To request the Director to continue the evaluation of theOrganization's program, to extend it to all country projectsin which the Organization cooperates, and to make a con-tinuing review of the project activities in all stages of theirdevelopment.
At its XIX Meeting (1969) the Council examinedthe report on the evaluation process and in ResolutionXXVI reiterated the earlier resolution and called uponnational personnel to participate in the process of pro-gram and project evaluation.
A revised version of the principles of project evalua-tion, dated 15 June 1967, is to be found in the WHOManual. The Manual requires, among other things, aquantitative and qualitative appraisal of the achieve-ment of each project in relation to its objectives and anassessment of the degree to which the different pro-grams of the Organization are developing in accord-ance with needs and policies. It places particularemphasis on the description of the impact of eachproject within its specific field, on public health ingeneral, and in the socioeconomic sphere.
In pursuit of these purposes the Department ofEvaluation was created at Headquarters at the end of1967. It was decided, as a first step, to concentrateupon the measurement of project "effectiveness," that isto say, to determine the degree of accomplishment ofpredetermined objectives. A working paper on evalua-tion was prepared in April 1968 explaining in detailthe procedure that was proposed. After thorough dis-
cussion of this document with staff in the field and atHeadquarters, general instructions on project evalua-tion were issued in July 1968. According to theseinstructions every project in operation was to be re-viewed and a basic document prepared, containing adescription of the problem that gave rise to the projectand of the baseline situation, the project objectivesclearly defined in terms of time and coverage, thesignificant activities, and appropriate indicators. Tocomplement the basic document, those responsible foreach project were to formulate and report their annualtargets early each year, to keep a record of the activitiescarried out, and to prepare evaluation sheets at the endof the year in the form specified.
There have been four main features of the work ofthe Organization in this field during the quadrennium:first, a vigorous effort to apply the evaluation procedureto all the projects; second, the utilization of the resultsof evaluation; third, the incorporation of the evalua-tion procedure in the Quadrennial Projections of thecooperative activities of the Organization; and, finally,the intensive orientation of the staff in all aspects ofthe work.
In 1968 and 1969 a series of meetings were heldwith the staff at Headquarters, in the Zones, and in thecountries to promote the utilization of the process ofevaluation as a working tool at all levels of operation,select appropriate technical criteria for project evalua-tion in the various specialized fields of work, andprepare model basic documents.
In 1969 the incorporation of the evaluation proce-dure in the preparation of the Quadrennial Projectionsfirmly established project evaluation as a continuousprocess, indispensable for determining the extension ortermination of projects and for deciding upon changesin the program and budget. This facet of the policyenvisaged in Resolution XXVI of the XIX Meeting ofthe Directing Council was thereby implemented.
When evaluation documents arrived at the Head-quarters Office the following criteria were applied:
1) Was there an adequate definition of the baselinesituation?
2) Was the interrelationship among the various en-tities (problem, purpose, objectives, activities) clearlyestablished?
3) Were the objectives clearly defined?4) Was there an appropriate selection of indices?5) Were the annual targets adequate in relation to
the duration of the project and its objectives?6) In general, were the documents prepared in such
a way as to facilitate the measurement of attainment ofobjectives?
7) Was there an adequate appraisal of the impact
52
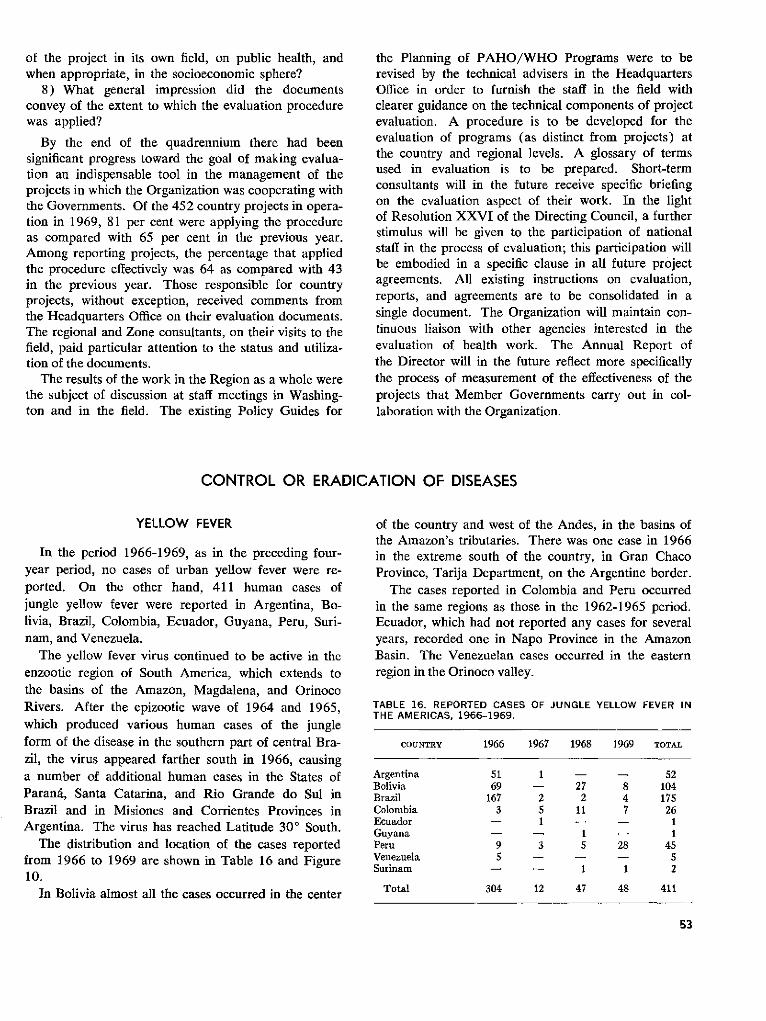
of the project in its own field, on public health, andwhen appropriate, in the socioeconomic sphere?
8) What general impression did the documentsconvey of the extent to which the evaluation procedurewas applied?
By the end of the quadrennium there had beensignificant progress toward the goal of making evalua-tion an indispensable tool in the management of theprojects in which the Organization was cooperating withthe Governments. Of the 452 country projects in opera-tion in 1969, 81 per cent were applying the procedureas compared with 65 per cent in the previous year.Among reporting projects, the percentage that appliedthe procedure effectively was 64 as compared with 43in the previous year. Those responsible for countryprojects, without exception, received comments fromthe Headquarters Office on their evaluation documents.The regional and Zone consultants, on their visits to thefield, paid particular attention to the status and utiliza-tion of the documents.
The results of the work in the Region as a whole werethe subject of discussion at staff meetings in Washing-ton and in the field. The existing Policy Guides for
the Planning of PAHO/WHO Programs were to berevised by the technical advisers in the HeadquartersOffice in order to furnish the staff in the field withclearer guidance on the technical components of projectevaluation. A procedure is to be developed for theevaluation of programs (as distinct from projects) atthe country and regional levels. A glossary of termsused in evaluation is to be prepared. Short-termconsultants will in the future receive specific briefingon the evaluation aspect of their work. In the lightof Resolution XXVI of the Directing Council, a furtherstimulus will be given to the participation of nationalstaff in the process of evaluation; this participation willbe embodied in a specific clause in all future projectagreements. All existing instructions on evaluation,reports, and agreements are to be consolidated in asingle document. The Organization will maintain con-tinuous liaison with other agencies interested in theevaluation of health work. The Annual Report ofthe Director will in the future reflect more specificallythe process of measurement of the effectiveness of theprojects that Member Governments carry out in col-laboration with the Organization.
CONTROL OR ERADICATION OF DISEASES
YELLOW FEVER
In the period 1966-1969, as in the preceding four-year period, no cases of urban yellow fever were re-ported. On the other hand, 411 human cases ofjungle yellow fever were reported in Argentina, Bo-livia, Brazil, Colombia, Ecuador, Guyana, Peru, Suri-nam, and Venezuela.
The yellow fever virus continued to be active in theenzootic region of South America, which extends tothe basins of the Amazon, Magdalena, and OrinocoRivers. After the epizootic wave of 1964 and 1965,which produced various human cases of the jungleform of the disease in the southern part of central Bra-zil, the virus appeared farther south in 1966, causinga number of additional human cases in the States ofParaná, Santa Catarina, and Rio Grande do Sul inBrazil and in Misiones and Corrientes Provinces inArgentina. The virus has reached Latitude 30 ° South.
The distribution and location of the cases reportedfrom 1966 to 1969 are shown in Table 16 and Figure10.
In Bolivia almost all the cases occurred in the center
of the country and west of the Andes, in the basins ofthe Amazon's tributaries. There was one case in 1966in the extreme south of the country, in Gran ChacoProvince, Tarija Department, on the Argentine border.
The cases reported in Colombia and Peru occurredin the same regions as those in the 1962-1965 period.Ecuador, which had not reported any cases for severalyears, recorded one in Napo Province in the AmazonBasin. The Venezuelan cases occurred in the easternregion in the Orinoco valley.
TABLE 16. REPORTED CASES OF JUNGLE YELLOW FEVER INTHE AMERICAS, 1966-1969.
COUNTRY 1966 1967 1968 1969 TOTAL
Argentina 51 1 - - 52Bolivia 69 - 27 8 104Brazil 167 2 2 4 175Colombia 3 5 11 7 26Ecuador - 1 - - 1Guyana - - 1 - 1Peru 9 3 5 28 45Venezuela 5 - - - 5Surinam - 1 1 2
Total 304 12 47 48 411
53

Fig. 10. Reported cases of jungle yellow fever, by maior political division of each country, 1966 and 1967-1969.
At the end of 1968 the Organization extended up to31 December 1971 its agreement with the BrazilianHealth Ministry, by which it makes an annual contribu-tion of US$10,000 to the Oswaldo Cruz Institute; andit maintained the agreement with Colombia's PublicHealth Ministry on the execution of programs andactivities related to yellow fever epidemiology and con-trol, through cooperation between PAHO/WHO andthe Colombian National Institute of Health. Both insti-tutes produce and distribute 17D yellow fever vaccineand provide free diagnostic services to all countries ofthe Americas.
AEDES AEGYPTI
The eradication of Aedes aegypti both made ad-vances and suffered setbacks during the quadrennium.At the beginning of the period the A. aegypti problempersisted in the extreme north of South America, in theUnited States of America, and in the Caribbean area.At the same time Argentina, Guatemala, Mexico, Bra-zil, Honduras, and Panama were reinfested. The rein-festations in the first three countries were quicklyeliminated, but not in the other three, despite the factthat eradication campaigns were actively reorganized.The question of the eradication of A. aegypti in theCaribbean islands is receiving close attention. The cam-paign has been intensified in Barbados, Guyana, andSurinam and preparations have been made for startingit in Antigua, Grenada, the Cayman Islands, and Mont-serrat, while studies for the organization of the program
in the Netherlands Antilles, Jamaica, and St. Vincenthave been conducted. Campaigns have also beenstarted in Guadeloupe, French Guiana, and Martinique.The campaign in the United States, Puerto Rico, andthe Virgin Islands (USA) was interrupted in 1969.These setbacks are helpful in that they oblige us all tolook afresh at the problem of the eradication of A.aegypti, which on many occasions has not been con-sidered in all its seriousness and vital importance forthe health of the Hemisphere.
All the necessary authority has been received fromthe Governing Bodies for extending effective supportto programs for the eradication of A. aegypti. Thevalidity of the eradication certificate does not extendfor longer than three years, and visits, which in factrepresent full-scale inspection, are authorized. Resolu-tion XVIII of the XVII Meeting of the Directing Coun-cil covers, from the administrative point of view, therequirements of a Hemisphere-wide eradication pro-gram. The basis for the resolution was furnished bythe reports of the Conference on Aedes aegypti Eradi-cation in the Americas and of the Study Group on thesame subject, and also the report of the Working Groupon Laboratory Colonies of Aedes aegypti, as approvedat the meetings held at Headquarters in 1967 underthe auspices of the Organization.
A ctivities
The following activities are worthy of mention:
1 ) Technical cooperation for the development and
54
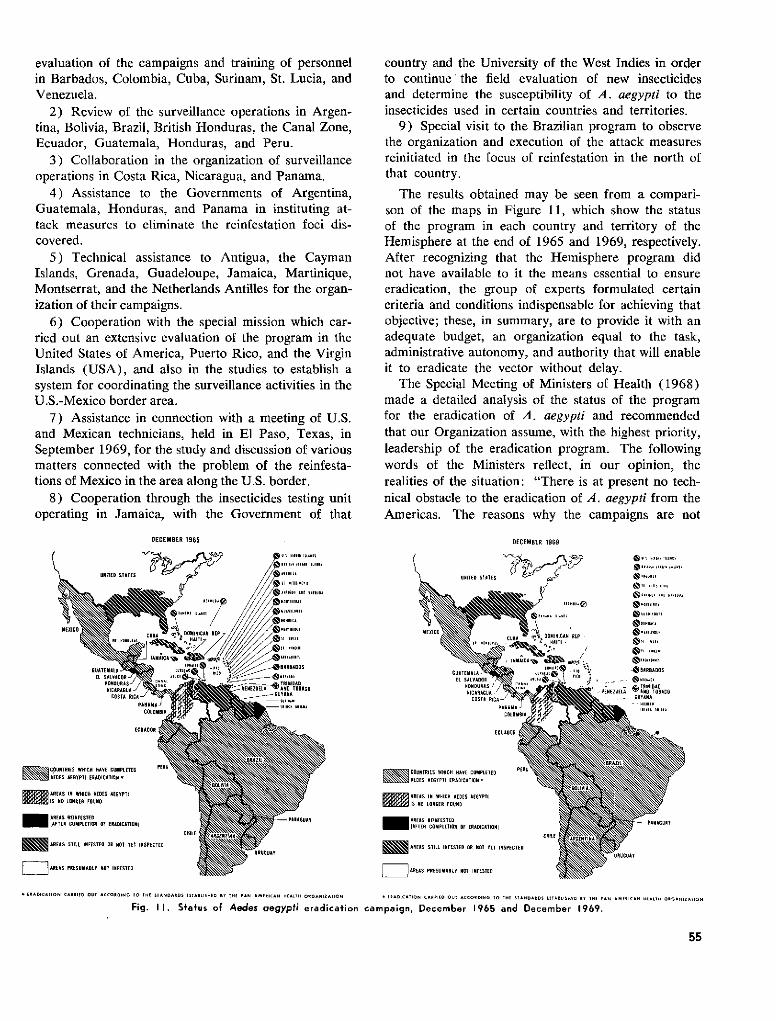
evaluation of the campaigns and training of personnelin Barbados, Colombia, Cuba, Surinam, St. Lucia, andVenezuela.
2) Review of the surveillance operations in Argen-tina, Bolivia, Brazil, British Honduras, the Canal Zone,Ecuador, Guatemala, Honduras, and Peru.
3) Collaboration in the organization of surveillanceoperations in Costa Rica, Nicaragua, and Panama.
4) Assistance to the Governments of Argentina,Guatemala, Honduras, and Panama in instituting at-tack measures to eliminate the reinfestation foci dis-covered.
5) Technical assistance to Antigua, the CaymanIslands, Grenada, Guadeloupe, Jamaica, Martinique,Montserrat, and the Netherlands Antilles for the organ-ization of their campaigns.
6) Cooperation with the special mission which car-ried out an extensive evaluation of the program in theUnited States of America, Puerto Rico, and the VirginIslands (USA), and also in the studies to establish asystem for coordinating the surveillance activities in theU.S.-Mexico border area.
7) Assistance in connection with a meeting of U.S.and Mexican technicians, held in El Paso, Texas, inSeptember 1969, for the study and discussion of variousmatters connected with the problem of the reinfesta-tions of Mexico in the area along the U.S. border.
8) Cooperation through the insecticides testing unitoperating in Jamaica, with the Government of that
DECEMBER 1965
ARDS 111 R I NSEUEIIEDA STATES B//T ILSPT D
iR DI NICARNA / NPRSAL 1 0 S
GUATEMNL A RI? L : o '/ / ANDASEl SALVADOR\*- \ iE _
M COUNTRIES WHICH HAVE COMPLETED
AREAS IN WHICH AEOES AGYPI
AREAS STIL IHEESTED OR EOT YET INSPECTED
..E.S R.......... o I..ETE.SI
country and the University of the West Indies in orderto continue the field evaluation of new insecticidesand determine the susceptibility of A. aegypti to theinsecticides used in certain countries and territories.
9) Special visit to the Brazilian program to observethe organization and execution of the attack measuresreinitiated in the focus of reinfestation in the north ofthat country.
The results obtained may be seen from a compari-son of the maps in Figure 11, which show the statusof the program in each country and territory of theHemisphere at the end of 1965 and 1969, respectively.After recognizing that the Hemisphere program didnot have available to it the means essential to ensureeradication, the group of experts formulated certaincriteria and conditions indispensable for achieving thatobjective; these, in summary, are to provide it with anadequate budget, an organization equal to the task,administrative autonomy, and authority that will enableit to eradicate the vector without delay.
The Special Meeting of Ministers of Health (1968)made a detailed analysis of the status of the programfor the eradication of A. aegypti and recommendedthat our Organization assume, with the highest priority,leadership of the eradication program. The followingwords of the Ministers reflect, in our opinion, therealities of the situation: "There is at present no tech-nical obstacle to the eradication of A. aegypti from theAmericas. The reasons why the campaigns are not
DECEMBER 1969
iUA TENMAL A -
..... ... .1 ,,.,",
D. OOMINICAN REP .HAITI . ''"
Y 1"iTN. U. OA1íí1..í."'" 0 1 *í' -NBARBADOS
, VENEZUELA AND TODADO
DOlABAr
ECUADOR
COUNTRIES WHICH HAVE COMPLETED PERAS AEGYPTI ERADICATION *
= AREAS IN WHICH AEDES EOYPTIIS NO LONGER FOUNO
- AREAS REINFESTED_IATER COMPLETION ODE ERAOICATIONI
AREAS STILL INrESTED OR NT YET INSPECTED
= AREAS PRESOABLY NOT INFESTED
-PA RAGUAY
CHIIE
URUGUAY
. I[ADIC*AION CA-.lAD OUI ACCO OING -O TH SIA-NDAADS ASTA-LIlSHR BY 1EA PAN AMERICAN HEATOH OCOANIZNTION * RAODICATIONN CAAlDO OUT CCOODBINO .1 IA SI.TANDAODS ATABlISDO B*Y I.E PA- N A-NiCA- HALI O.GACNIZAION
Fig. II. Status of Aedes aegypti eradication campaign, December 1965 and December 1969.
55
t
El SALVADOR
llllUHONIURAS 1COSTL RlCNcolores
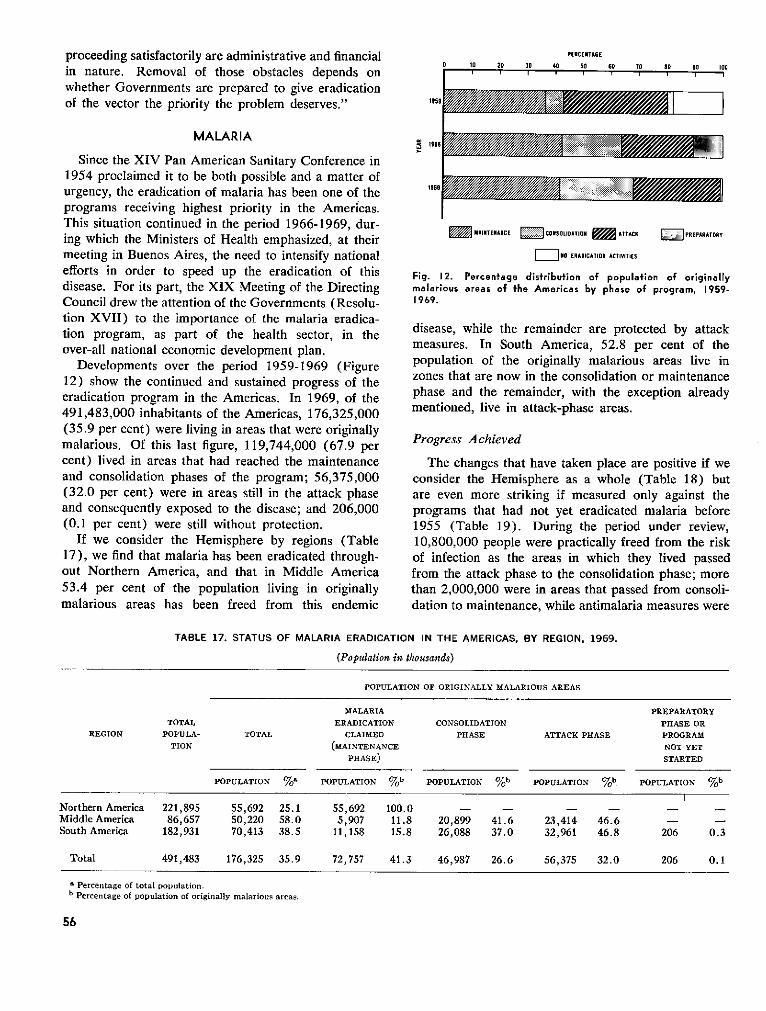
proceeding satisfactorily are administrative and financialin nature. Removal of those obstacles depends onwhether Governments are prepared to give eradicationof the vector the priority the problem deserves."
MALARIA
Since the XIV Pan American Sanitary Conference in1954 proclaimed it to be both possible and a matter ofurgency, the eradication of malaria has been one of theprograms receiving highest priority in the Americas.This situation continued in the period 1966-1969, dur-ing which the Ministers of Health emphasized, at theirmeeting in Buenos Aires, the need to intensify nationalefforts in order to speed up the eradication of thisdisease. For its part, the XIX Meeting of the DirectingCouncil drew the attention of the Governments (Resolu-tion XVII) to the importance of the malaria eradica-tion program, as part of the health sector, in theover-all national economic development plan.
Developments over the period 1959-1969 (Figure12) show the continued and sustained progress of theeradication program in the Americas. In 1969, of the491,483,000 inhabitants of the Americas, 176,325,000(35.9 per cent) were living in areas that were originallymalarious. Of this last figure, 119,744,000 (67.9 percent) lived in areas that had reached the maintenanceand consolidation phases of the program; 56,375,000(32.0 per cent) were in areas still in the attack phaseand consequently exposed to the disease; and 206,000(0.1 per cent) were still without protection.
If we consider the Hemisphere by regions (Table17), we find that malaria has been eradicated through-out Northern America, and that in Middle America53.4 per cent of the population living in originallymalarious areas has been freed from this endemic
1959
' 1966
1969
PERCENTACE
O 10 20 30 40 50 60 Tn in on n.,u
MAINTE iANC i C ONSOLIDATION ATT ACK PREPARATORY
[ NO ERADICATION ACTIVITIES
Fig. 12. Percentage distribution of population of originallymalarious areas of the Americas by phase of program, 1959-1969.
disease, while the remainder are protected by attackmeasures. In South America, 52.8 per cent of thepopulation of the originally malarious areas live inzones that are now in the consolidation or maintenancephase and the remainder, with the exception alreadymentioned, live in attack-phase areas.
Progress Achieved
The changes that have taken place are positive if weconsider the Hemisphere as a whole (Table 18) butare even more striking if measured only against theprograms that had not yet eradicated malaria before1955 (Table 19). During the period under review,10,800,000 people were practically freed from the riskof infection as the areas in which they lived passedfrom the attack phase to the consolidation phase; morethan 2,000,000 were in areas that passed from consoli-dation to maintenance, while antimalaria measures were
TABLE 17. STATUS OF MALARIA ERADICATION IN THE AMERICAS, BY REGION, 1969.
(Population in thousands)
POPULATION OF ORIGINALLY MALARIOUS AREAS
MALARIA PREPARATORYTOTAL ERADICATION CONSOLIDATION PHASE OR
REGION POPULA- TOTAL CLAIMED PHASE ATTACK PHASE PROGRAMTION (MAINTENANCE NOT YET
PHASE) STARTED
POPULATION %a POPULATION %b POPULATION %b POPULATION %b POPULATION %b
Northern America 221,895 55,692 25.1 55,692 100.0 - - - - -Middle America 86,657 50,220 58.0 5,907 11.8 20,899 41.6 23,414 46.6 - -South America 182,931 70,413 38.5 11,158 15.8 26,088 37.0 32,961 46.8 206 0.3
Total 491,483 176,325 35.9 72,757 41.3 46,987 26.6 56,375 32.0 206 0.1
^ Percentage of total population.b Percentage of population of originally malarious areas.
56
1 1 1 1 1 1
r1 1
............1..... 1......1V0,"--- 11/
i'/////////////////////////////1/// :-:1:i·-:i: ::r:::ji:: :::::::::: ' :::::
�:-:::::·:::::-:-:-:-:-:-:::-:::::::::i:
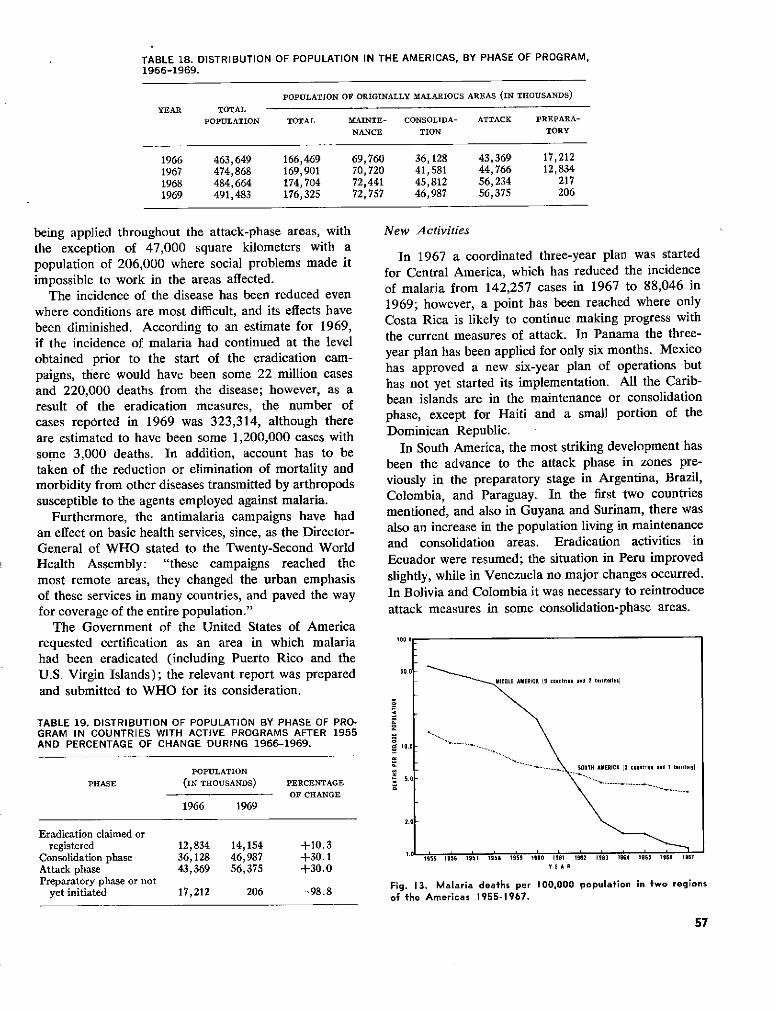
TABLE 18. DISTRIBUTION OF POPULATION IN THE AMERICAS, BY PHASE OF PROGRAM,1966-1969.
POPULATION OF ORIGINALLY MALARIOUS AREAS (IN THOUSANDS)
YEAR TOTALPOPULATION TOTAL MAINTE- CONSOLIDA- ATTACK PREPARA-
NANCE TION TORY
1966 463,649 166,469 69,760 36,128 43,369 17,2121967 474,868 169,901 70,720 41,581 44,766 12,8341968 484,664 174,704 72,441 45,812 56,234 2171969 491,483 176,325 72,757 46,987 56,375 206
being applied throughout the attack-phase areas, withthe exception of 47,000 square kilometers with apopulation of 206,000 where social problems made itimpossible to work in the areas affected.
The incidence of the disease has been reduced evenwhere conditions are most difficult, and its effects havebeen diminished. According to an estimate for 1969,if the incidence of malaria had continued at the levelobtained prior to the start of the eradication cam-paigns, there would have been some 22 million casesand 220,000 deaths from the disease; however, as aresult of the eradication measures, the number ofcases reported in 1969 was 323,314, although thereare estimated to have been some 1,200,000 cases withsome 3,000 deaths. In addition, account has to betaken of the reduction or elimination of mortality andmorbidity from other diseases transmitted by arthropodssusceptible to the agents employed against malaria.
Furthermore, the antimalaria campaigns have hadan effect on basic health services, since, as the Director-General of WHO stated to the Twenty-Second WorldHealth Assembly: "these campaigns reached themost remote areas, they changed the urban emphasisof these services in many countries, and paved the wayfor coverage of the entire population."
The Government of the United States of Americarequested certification as an area in which malariahad been eradicated (including Puerto Rico and theU.S. Virgin Islands); the relevant report was preparedand submitted to WHO for its consideration.
TABLE 19. DISTRIBUTION OF POPULATION BY PHASE OF PRO-GRAM IN COUNTRIES WITH ACTIVE PROGRAMS AFTER 1955AND PERCENTAGE OF CHANGE DURING 1966-1969.
POPULATION
PHASE (IN THOUSANDS) PERCENTAGE
OF CHANGE
1966 1969
Eradication claimed orregistered 12,834 14,154 +10.3
Consolidation phase 36,128 46,987 +30.1Attack phase 43,369 56,375 +30.0Preparatory phase or not
yet initiated 17,212 206 -98.8
New Activities
In 1967 a coordinated three-year plan was startedfor Central America, which has reduced the incidenceof malaria from 142,257 cases in 1967 to 88,046 in1969; however, a point has been reached where onlyCosta Rica is likely to continue making progress withthe current measures of attack. In Panama the three-year plan has been applied for only six months. Mexicohas approved a new six-year plan of operations buthas not yet started its implementation. All the Carib-bean islands are in the maintenance or consolidationphase, except for Haiti and a small portion of theDominican Republic.
In South America, the most striking development hasbeen the advance to the attack phase in zones pre-viously in the preparatory stage in Argentina, Brazil,Colombia, and Paraguay. In the first two countriesmentioned, and also in Guyana and Surinam, there wasalso an increase in the population living in maintenanceand consolidation areas. Eradication activities inEcuador were resumed; the situation in Peru improvedslightly, while in Venezuela no major changes occurred.In Bolivia and Colombia it was necessary to reintroduceattack measures in some consolidation-phase areas.
100.0
50.o
" .IOOL . .AiRIC co untries anid t. riito.r-.l
2.0
I955 5956 195 1959 595 199I0 19ER 19 196 5 1964 I 1966 1961as 1956 1957 1958 ls9 1950 19651 1962 1 963 1i4 1965 l96 7
Fig. i3. Malaria deaths per 100,000 population in two regionsof the Americas 1955-1967.
57
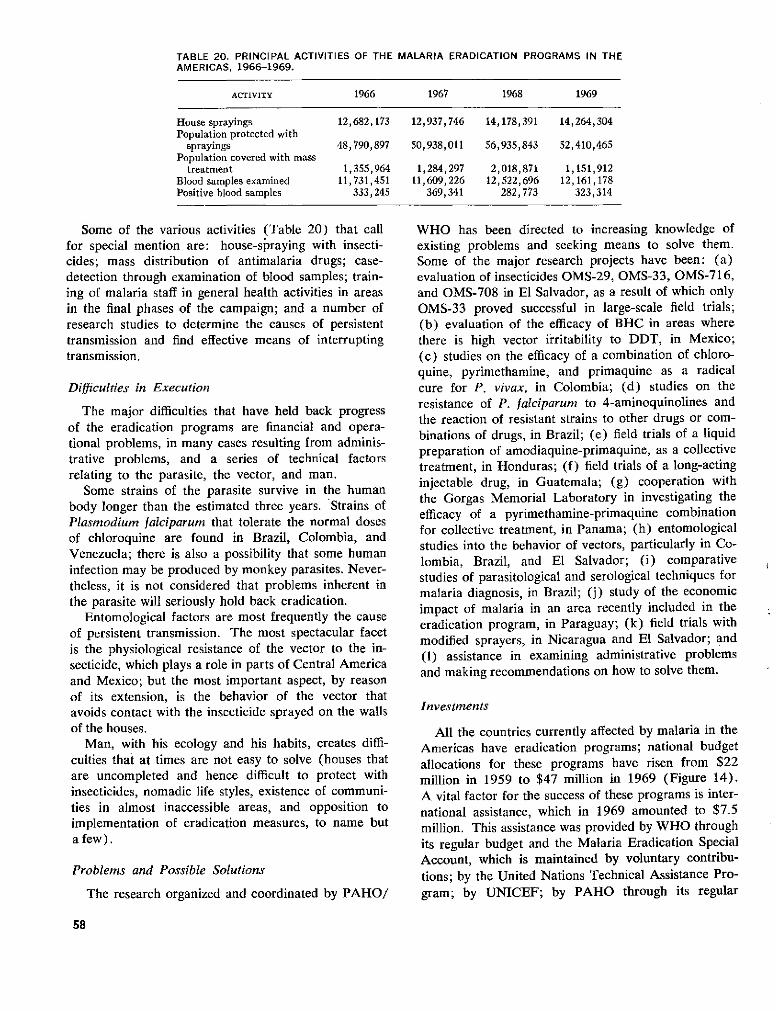
TABLE 20. PRINCIPAL ACTIVITIES OF THEAMERICAS, 1966-1969.
MALARIA ERADICATION PROGRAMS IN THE
ACTIVITY 1966 1967 1968 1969
House sprayings 12,682,173 12,937,746 14,178,391 14,264,304Population protected with
sprayings 48,790,897 50,938,011 56,935,843 52,410,465Population covered with mass
treatment 1,355,964 1,284,297 2,018,871 1,151,912Blood samples examined 11,731,451 11,609,226 12,522,696 12,161,178Positive blood samples 333,245 369,341 282,773 323,314
Some of the various activities (Table 20) that callfor special mention are: house-spraying with insecti-cides; mass distribution of antimalaria drugs; case-detection through examination of blood samples; train-ing of malaria staff in general health activities in areasin the final phases of the campaign; and a number ofresearch studies to determine the causes of persistenttransmission and find effective means of interruptingtransmission.
Difficulties in Execution
The major difficulties that have held back progressof the eradication programs are financial and opera-tional problems, in many cases resulting from adminis-trative problems, and a series of technical factorsrelating to the parasite, the vector, and man.
Some strains of the parasite survive in the humanbody longer than the estimated three years. Strains ofPlasmodium falciparum that tolerate the normal dosesof chloroquine are found in Brazil, Colombia, andVenezuela; there is also a possibility that some humaninfection may be produced by monkey parasites. Never-theless, it is not considered that problems inherent inthe parasite will seriously hold back eradication.
Entomological factors are most frequently the causeof persistent transmission. The most spectacular facetis the physiological resistance of the vector to the in-secticide, which plays a role in parts of Central Americaand Mexico; but the most important aspect, by reasonof its extension, is the behavior of the vector thatavoids contact with the insecticide sprayed on the wallsof the houses.
Man, with his ecology and his habits, creates diffi-culties that at times are not easy to solve (houses thatare uncompleted and hence difficult to protect withinsecticides, nomadic life styles, existence of communi-ties in almost inaccessible areas, and opposition toimplementation of eradication measures, to name buta few).
Problems and Possible Solutions
The research organized and coordinated by PAHO/
WHO has been directed to increasing knowledge ofexisting problems and seeking means to solve them.Some of the major research projects have been: (a)evaluation of insecticides OMS-29, OMS-33, OMS-716,and OMS-708 in El Salvador, as a result of which onlyOMS-33 proved successful in large-scale field trials;(b) evaluation of the efficacy of BHC in areas wherethere is high vector irritability to DDT, in Mexico;(c) studies on the efficacy of a combination of chloro-quine, pyrimethamine, and primaquine as a radicalcure for P. vivax, in Colombia; (d) studies on theresistance of P. falciparum to 4-aminoquinolines andthe reaction of resistant strains to other drugs or com-binations of drugs, in Brazil; (e) field trials of a liquidpreparation of amodiaquine-primaquine, as a collectivetreatment, in Honduras; (f) field trials of a long-actinginjectable drug, in Guatemala; (g) cooperation withthe Gorgas Memorial Laboratory in investigating theefficacy of a pyrimethamine-primaquine combinationfor collective treatment, in Panama; (h) entomologicalstudies into the behavior of vectors, particularly in Co-lombia, Brazil, and El Salvador; (i) comparativestudies of parasitological and serological techniques formalaria diagnosis, in Brazil; (j) study of the economicimpact of malaria in an area recently included in theeradication program, in Paraguay; (k) field trials withmodified sprayers, in Nicaragua and El Salvador; and(1) assistance in examining administrative problemsand making recommendations on how to solve them.
Investments
All the countries currently affected by malaria in theAmericas have eradication programs; national budgetallocations for these programs have risen from $22million in 1959 to $47 million in 1969 (Figure 14).A vital factor for the success of these programs is inter-national assistance, which in 1969 amounted to $7.5million. This assistance was provided by WHO throughits regular budget and the Malaria Eradication SpecialAccount, which is maintained by voluntary contribu-tions; by the United Nations Technical Assistance Pro-gram; by UNICEF; by PAHO through its regular
58
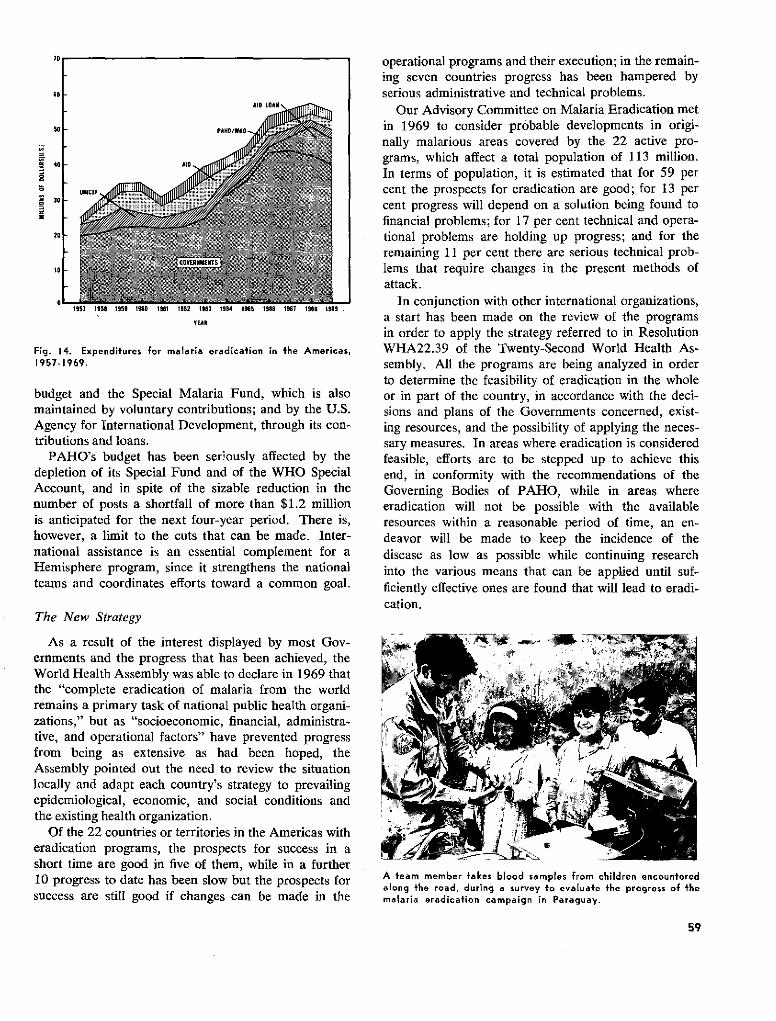
0
401
o
30L-¡
20
10
I0
VEAR
Fig. 14. Expenditures for malaria eradication in the Americas,1957-1969.
budget and the Special Malaria Fund, which is alsomaintained by voluntary contributions; and by the U.S.Agency for International Development, through its con-tributions and loans.
PAHO's budget has been ser!ously affected by thedepletion of its Special Fund and of the WHO SpecialAccount, and in spite of the sizable reduction in thenumber of posts a shortfall of more than $1.2 millionis anticipated for the next four-year period. There is,however, a limit to the cuts that can be made. Inter-national assistance is an essential complement for aHemisphere program, since it strengthens the nationalteams and coordinates efforts toward a common goal.
The New Strategy
As a result of the interest displayed by most Gov-ernments and the progress that has been achieved, theWorld Health Assembly was able to declare in 1969 thatthe "complete eradication of malaria from the worldremains a primary task of national public health organi-zations," but as "socioeconomic, financial, administra-tive, and operational factors" have prevented progressfrom being as extensive as had been hoped, theAssembly pointed out the need to review the situationlocally and adapt each country's strategy to prevailingepidemiological, economic, and social conditions andthe existing health organization.
Of the 22 countries or territories in the Americas witheradication programs, the prospects for success in ashort time are good in five of them, while in a further10 progress to date has been slow but the prospects forsuccess are still good if changes can be made in the
operational programs and their execution; in the remain-ing seven countries progress has been hampered byserious administrative and technical problems.
Our Advisory Committee on Malaria Eradication metin 1969 to consider probable developments in origi-nally malarious areas covered by the 22 active pro-grams, which affect a total population of 113 million.In terms of population, it is estimated that for 59 percent the prospects for eradication are good; for 13 percent progress will depend on a solution being found tofinancial problems; for 17 per cent technical and opera-tional problems are holding up progress; and for theremaining 11 per cent there are serious technical prob-lems that require changes in the present methods ofattack.
In conjunction with other international organizations,a start has been made on the review of the programsin order to apply the strategy referred to in ResolutionWHA22.39 of the Twenty-Second World Health As-sembly. All the programs are being analyzed in orderto determine the feasibility of eradication in the wholeor in part of the country, in accordance with the deci-sions and plans of the Governments concerned, exist-ing resources, and the possibility of applying the neces-sary measures. In areas where eradication is consideredfeasible, efforts are to be stepped up to achieve thisend, in conformity with the recommendations of theGoverning Bodies of PAHO, while in areas whereeradication will not be possible with the availableresources within a reasonable period of time, an en-deavor will be made to keep the incidence of thedisease as low as possible while continuing researchinto the various means that can be applied until suf-ficiently effective ones are found that will lead to eradi-cation.
A team member takes blood samples from children encounteredalong the road, during a survey to evaluate the progress of themalaria eradication campaign in Paraguay.
59
[
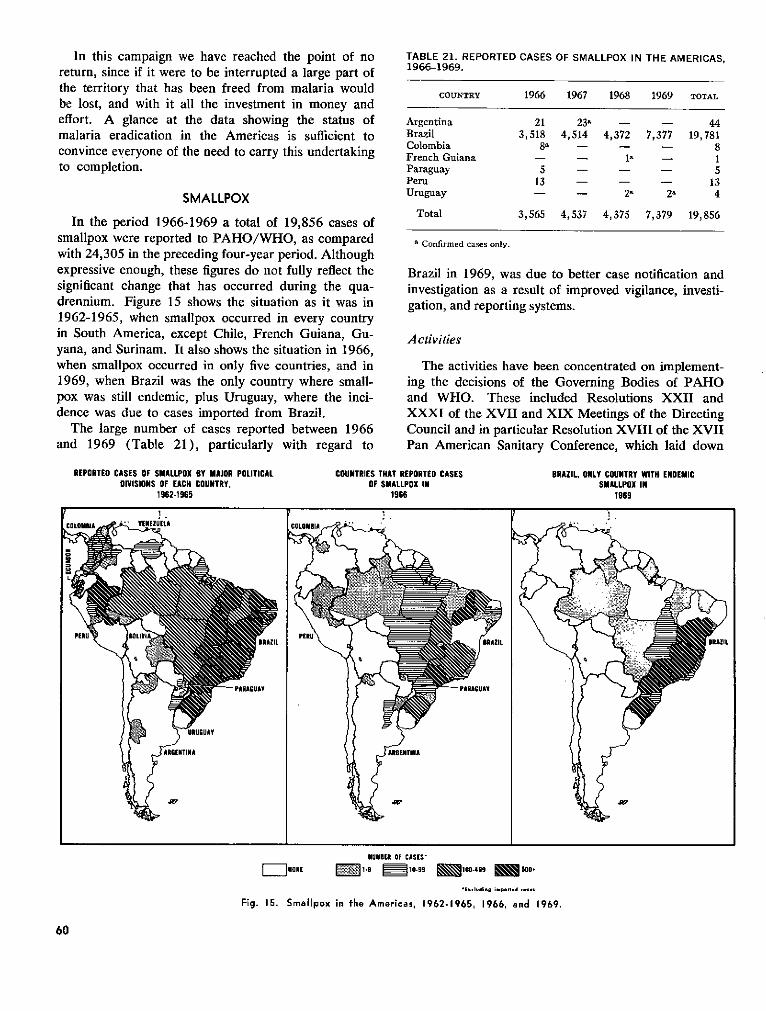
In this campaign we have reached the point of noreturn, since if it were to be interrupted a large part ofthe territory that has been freed from malaria wouldbe lost, and with it all the investment in money andeffort. A glance at the data showing the status ofmalaria eradication in the Americas is sufficient toconvince everyone of the need to carry this undertakingto completion.
SMALLPOX
In the period 1966-1969 a total of 19,856 cases ofsmallpox were reported to PAHO/WHO, as comparedwith 24,305 in the preceding four-year period. Althoughexpressive enough, these figures do not fully reflect thesignificant change that has occurred during the qua-drennium. Figure 15 shows the situation as it was in1962-1965, when smallpox occurred in every countryin South America, except Chile, French Guiana, Gu-yana, and Surinam. It also shows the situation in 1966,when smallpox occurred in only five countries, and in1969, when Brazil was the only country where small-pox was still endemic, plus Uruguay, where the inci-dence was due to cases imported from Brazil.
The large number of cases reported between 1966and 1969 (Table 21), particularly with regard to
TABLE 21. REPORTED CASES OF SMALLPOX IN THE AMERICAS,1966-1969.
COUNTRY 1966 1967 1968 1969 TOTAL
Argentina 21 23a - - 44Brazil 3,518 4,514 4,372 7,377 19,781Colombia 8a - - - 8French Guiana - - 1- 1Paraguay 5 - - - 5Peru 13 - - - 13Uruguay - - 2 2 4
Total 3,565 4,537 4,375 7,379 19,856
' Confirmed cases only.
Brazil in 1969, was due to better case notification andinvestigation as a result of improved vigilance, investi-gation, and reporting systems.
Activities
The activities have been concentrated on implement-ing the decisions of the Governing Bodies of PAHOand WHO. These included Resolutions XXII andXXXI of the XVII and XIX Meetings of the DirectingCouncil and in particular Resolution XVIII of the XVIIPan American Sanitary Conference, which laid down
REPORTED CASES OF SMALLPOX BY MAJOR POLITICAL COUNTRIES THAT REPORTED CASES BRAZIL, ONLY COUNTRY WITH ENDEMICDIVISIONS OF EACH COUNTRY, OF SMALLPOX IN SMALLPOX IN
1962-1965 1966 1969
i . P r 1.
NIUMBER OF CASES'
=I]NON[ 1-'9 0910-99 1 00-499 E 500+
5*Ex.Idino A~po5ed - 9s9s
Fig. 15. Smallpox in the Americas, 1962-1965, 1966, and 1969.
60
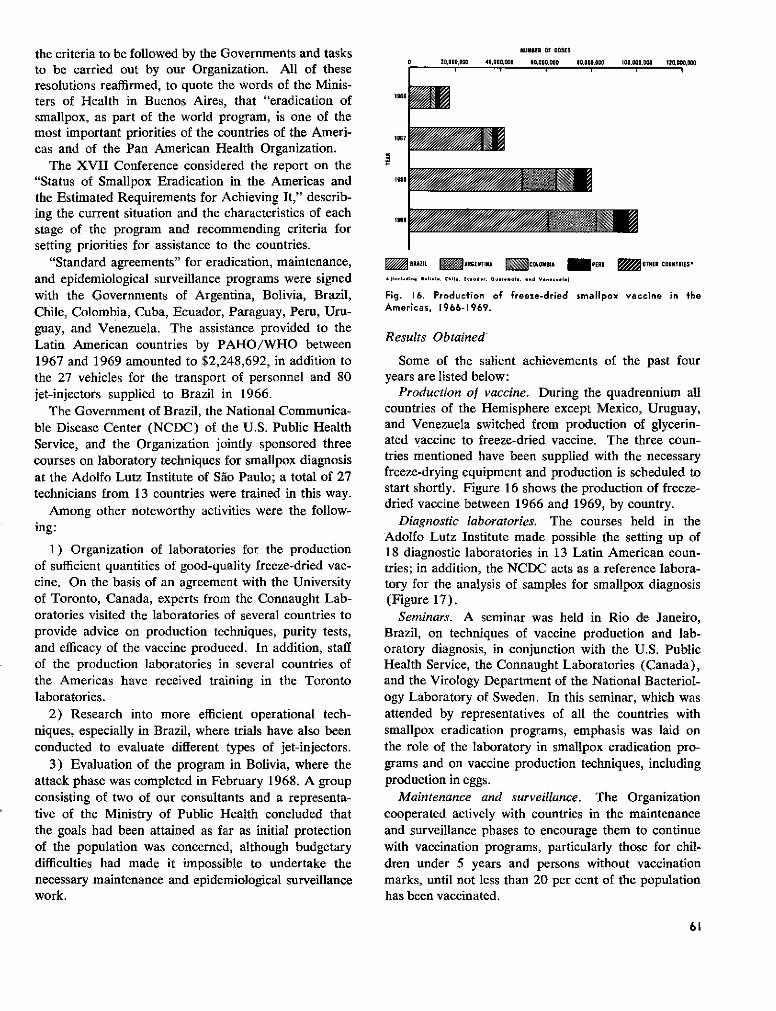
the criteria to be followed by the Governments and tasksto be carried out by our Organization. All of theseresolutions reaffirmed, to quote the words of the Minis-ters of Health in Buenos Aires, that "eradication ofsmallpox, as part of the world program, is one of themost important priorities of the countries of the Ameri-cas and of the Pan American Health Organization.
The XVII Conference considered the report on the"Status of Smallpox Eradication in the Americas andthe Estimated Requirements for Achieving It," describ-ing the current situation and the characteristics of eachstage of the program and recommending criteria forsetting priorities for assistance to the countries.
"Standard agreements" for eradication, maintenance,and epidemiological surveillance programs were signedwith the Governments of Argentina, Bolivia, Brazil,Chile, Colombia, Cuba, Ecuador, Paraguay, Peru, Uru-guay, and Venezuela. The assistance provided to theLatin American countries by PAHO/WHO between1967 and 1969 amounted to $2,248,692, in addition tothe 27 vehicles for the transport of personnel and 80jet-injectors supplied to Brazil in 1966.
The Government of Brazil, the National Communica-ble Disease Center (NCDC) of the U.S. Public HealthService, and the Organization jointly sponsored threecourses on laboratory techniques for smallpox diagnosisat the Adolfo Lutz Institute of Sao Paulo; a total of 27technicians from 13 countries were trained in this way.
Among other noteworthy activities were the follow-ing:
1) Organization of laboratories for the productionof sufficient quantities of good-quality freeze-dried vac-cine. On the basis of an agreement with the Universityof Toronto, Canada, experts from the Connaught Lab-oratories visited the laboratories of several countries toprovide advice on production techniques, purity tests,and efficacy of the vaccine produced. In addition, staffof the production laboratories in several countries ofthe Americas have received training in the Torontolaboratories.
2) Research into more efficient operational tech-niques, especially in Brazil, where trials have also beenconducted to evaluate different types of jet-injectors.
3) Evaluation of the program in Bolivia, where theattack phase was completed in February 1968. A groupconsisting of two of our consultants and a representa-tive of the Ministry of Public Health concluded thatthe goals had been attained as far as initial protectionof the population was concerned, although budgetarydifficulties had made it impossible to undertake thenecessary maintenance and epidemiological surveillancework.
NUMBER OF DOSES
BRAZIL WAR GENTINA = COLOMSIA / PERU M OTHER COUNTRIES'
*(Including Bolivioa Cile , Eiuodo* OuG ala.., and Vene.uel.)
Fig. 16. Production of freeze-dried smallpox vaccine in theAmericas, 1966-1969.
Results Obtained'
Some of the salient achievements of the past fouryears are listed below:
Production of vaccine. During the quadrennium allcountries of the Hemisphere except Mexico, Uruguay,and Venezuela switched from production of glycerin-ated vaccine to freeze-dried vaccine. The three coun-tries mentioned have been supplied with the necessaryfreeze-drying equipment and production is scheduled tostart shortly. Figure 16 shows the production of freeze-dried vaccine between 1966 and 1969, by country.
Diagnostic laboratories. The courses held in theAdolfo Lutz Institute made possible the setting up of18 diagnostic laboratories in 13 Latin American coun-tries; in addition, the NCDC acts as a reference labora-tory for the analysis of samples for smallpox diagnosis(Figure 17).
Seminars. A seminar was held in Rio de Janeiro,Brazil, on techniques of vaccine production and lab-oratory diagnosis, in conjunction with the U.S. PublicHealth Service, the Connaught Laboratories (Canada),and the Virology Department of the National Bacteriol-ogy Laboratory of Sweden. In this seminar, which wasattended by representatives of all the countries withsmallpox eradication programs, emphasis was laid onthe role of the laboratory in smallpox eradication pro-grams and on vaccine production techniques, includingproduction in eggs.
Maintenance and surveillance. The Organizationcooperated actively with countries in the maintenanceand surveillance phases to encourage them to continuewith vaccination programs, particularly those for chil-dren under 5 years and persons without vaccinationmarks, until not less than 20 per cent of the populationhas been vaccinated.
61
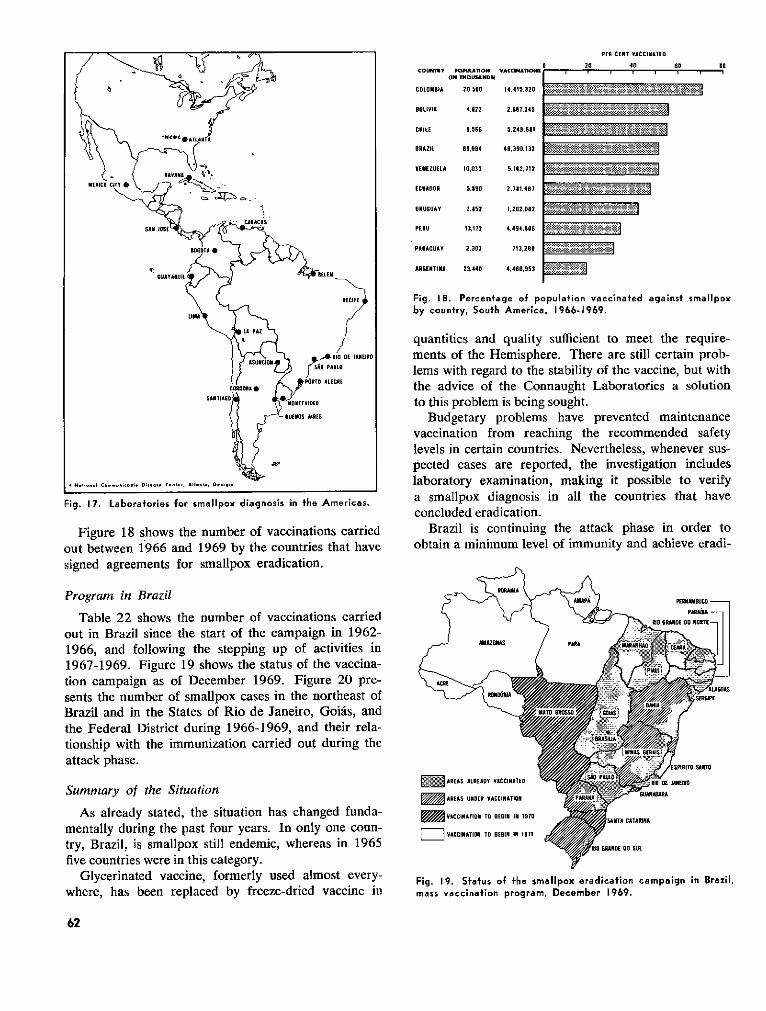
Fig. 17. Laboratories for smallpox diagnosis in the Americas.
Figure 18 shows the number of vaccinations carriedout between 1966 and 1969 by the countries that havesigned agreements for smallpox eradication.
Program in Brazil
Table 22 shows the number of vaccinations carriedout in Brazil since the start of the campaign in 1962-1966, and following the stepping up of activities in1967-1969. Figure 19 shows the status of the vaccina-tion campaign as of December 1969. Figure 20 pre-sents the number of smallpox cases in the northeast ofBrazil and in the States of Rio de Janeiro, Goiás, andthe Federal District during 1966-1969, and their rela-tionship with the immunization carried out during theattack phase.
Summary of the Situation
As already stated, the situation has changed funda-mentally during the past four years. In only one conn-try, Brazil, is smallpox still endemic, whereas in 1965five countries were in this category.
Glycerinated vaccine, formerly used almost every-where, has been replaced by freeze-dried vaccine in
COUNTnY KIlPl^AON(,N T4OUSANDS)
COLOMBIA 20.500
BOLIVIA 4,.22
CHILE 9.566
BRAZIL 69.604
VENEZUELA 10,035
ECUADOR 5.890
URUGUAY 28052
PERU 13,172
PARAGUAY 2,303
ARGENTINA 23,440
14,415,320
2.67.,345
5,24.6 81
46,390.132
5,162,712
2.781.487
1.202,082
4,494.606
713,289
4,466,953
PER CENT VACCINATEO
20 40 0S 0
Fig. 18. Percentage of population vaccinated against smallpoxby country, South America, 1966-1969.
quantities and quality sufficient to meet the require-ments of the Hemisphere. There are still certain prob-lems with regard to the stability of the vaccine, but withthe advice of the Connaught Laboratories a solutionto this problem is being sought.
Budgetary problems have prevented maintenancevaccination from reaching the recommended safetylevels in certain countries. Nevertheless, whenever sus-pected cases are reported, the investigation includeslaboratory examination, making it possible to verifya smallpox diagnosis in all the countries that haveconcluded eradication.
Brazil is continuing the attack phase in order toobtain a minimum level of immunity and achieve eradi-
Fig. 19. Status of the smallpox eradication campaign in Brazil,mass vaccination program, December 1969.
62
VACClNAT Is .
m~m~ffl=
W~B��~1
~Í-m 1, � NIONEM
o~
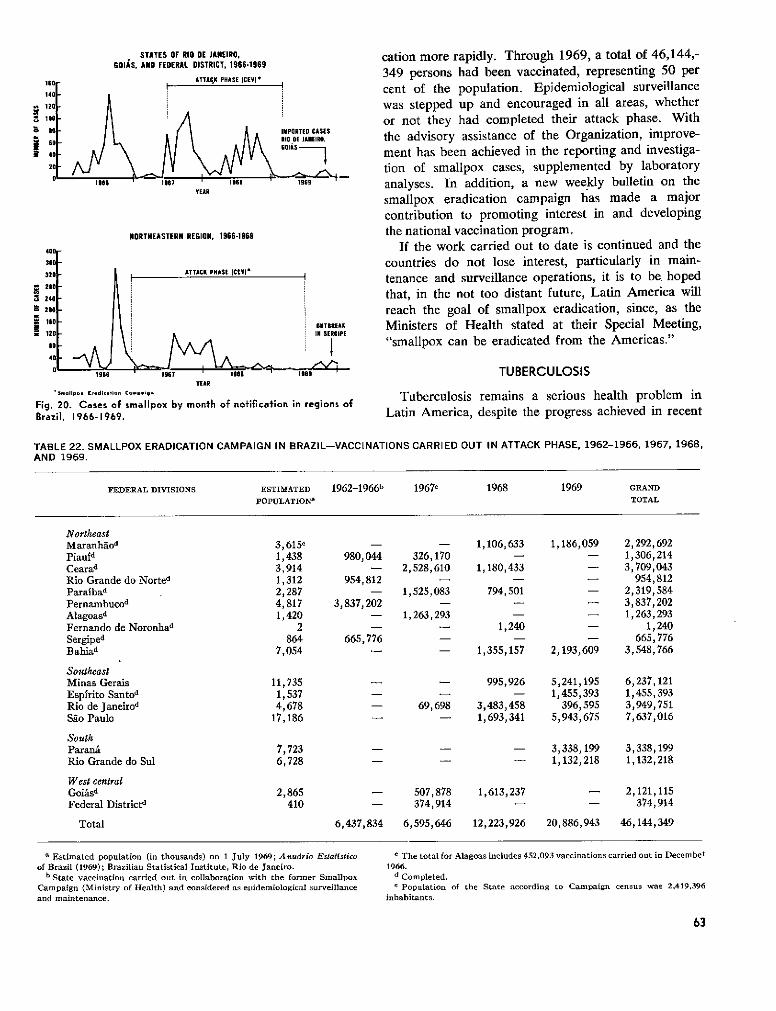
118140
12(
r #o
z 60I 40
20
STATES OF RIO DE JANEIRO,601GOIS, AND FEDERAL DISTRICT, 1966-1969
ATTACK PHASE ICEVlI
UIII
h ~~~~~~~~~~~~~~~~~~~~~~~61966 1967
YEAR
IPORTED CASES10 DE JANEIRO,
COIÁ -1965
HORTHEASTERN REGION, 1966-1969
ATTACK PHASE tCEVl*
OUTBREAKIN SERGIPE
VEARSaIillpo. Erdit.ion Co..ien
Fig. 20. Cases of smallpox by month of notification in regions ofBrazil, 1966-1969.
cation more rapidly. Through 1969, a total of 46,144,-349 persons had been vaccinated, representing 50 percent of the population. Epidemiological surveillancewas stepped up and encouraged in all areas, whetheror not they had completed their attack phase. Withthe advisory assistance of the Organization, improve-ment has been achieved in the reporting and investiga-tion of smallpox cases, supplemented by laboratoryanalyses. In addition, a new weekly bulletin on thesmallpox eradication campaign has made a majorcontribution to promoting interest in and developingthe national vaccination program.
If the work carried out to date is continued and thecountries do not lose interest, particularly in main-tenance and surveillance operations, it is to be hopedthat, in the not too distant future, Latin America willreach the goal of smallpox eradication, since, as theMinisters of Health stated at their Special Meeting,"smallpox can be eradicated from the Americas."
TUBERCULOSIS
Tuberculosis remains a serious health problem inLatin America, despite the progress achieved in recent
TABLE 22. SMALLPOX ERADICATION CAMPAIGN IN BRAZIL-VACCINATIONS CARRIED OUT IN ATTACK PHASE, 1962-1966, 1967, 1968,AND 1969.
FEDERAL DIVISIONS ESTIMATED 1962-1966b 19670 1968 1969 GRAND
POPULATIONa
TOTAL
NortheastMaranháod 3,615e - - 1,106,633 1,186,059 2,292,692Piaufd 1,438 980,044 326,170 - - 1,306,214Cearad 3,914 - 2,528,610 1,180,433 - 3,709,043Rio Grande do Norted 1,312 954,812 - - - 954,812
Parafbad 2,287 - 1,525,083 794,501 - 2,319,584Pernambucod 4,817 3,837,202 - - - 3,837,202
Alagoasd 1,420 - 1,263,293 - - 1,263,293
Fernando de Noronhad 2 - - 1,240 - 1,240
Sergiped 864 665, 776 - - - 665,776
Bahiad 7,054 - - 1,355,157 2,193,609 3,548,766
SoutheastMinas Gerais 11,735 - - 995,926 5,241,195 6,237,121Espfrito Santod 1,537 - - - 1,455,393 1,455,393
Rio de Janeirod 4,678 - 69,698 3,483,458 396,595 3,949,751Sáo Paulo 17,186 - - 1,693,341 5,943,675 7,637,016
SouthParaná 7,723 - - - 3,338,199 3,338,199
Rio Grande do Sul 6,728 - - - 1,132,218 1,132,218
West centralGoiásd 2,865 - 507,878 1,613,237 - 2,121,115Federal Districtd 410 - 374,914 - - 374,914
Total 6,437,834 6,595,646 12,223,926 20,886,943 46,144,349
a Estimated population (in thousands) on 1 July 1969; Anudrio Eslatlstico
of Brazil (1969); Brazilian Statistical Institute, Rio de Janeiro.b State vaccination carried out in collaboration with the former Smallpox
Campaign (Ministry of Health) and considered as epidemiological surveillance
and maintenance.
c The total for Alagoas includes 452,093 vaccinations carried out in December
1966.d Completed.
e Population of the State according to Campaign census was 2,419,396
inhabitants.
63
n o _ _ - -..^^
^·
1
i_=

years as a result of modern chemotherapy, BCG vac-cination, and greater knowledge of the facts concerningthe disease by the public. The lack of personnel quali-fied to use modern methods and techniques, the short-comings in the planning of the control programs, andinadequate utilization of health services with consequentpoor performance of existing resources, are factorswhich help to aggravate the harm caused by the disease.
Despite the substantial reduction in the mortalityand morbidity rates, tuberculosis has not been elimi-nated as a public health problem in any country in theAmericas.
The inadequacy of the information available in vari-ous countries hampers a precise evaluation of thepresent epidemiological situation of the disease. It isestimated that in Latin America there are 85 millionpersons with the infection and 1,250,000 active cases.
According to the latest data, the mortality per100,000 inhabitants is 22 in South America and 18 inCentral America and the Caribbean, and the respectiverates for new cases are 92 and 45 per 100,000.In Northern America, where mortality is 3.5 andthe rate for new cases 21.4 per 100,000, in addition tothe annual occurrence of 50,000 cases there are manymillions of infected persons and each year the reactiva-tion of tuberculosis is confirmed in thousands of persons.
Figures 21 and 22 show, respectively, the deaths fromtuberculosis in all its forms per 100,000 population andthe number of reported cases in the three regions of theAmericas between 1953 and 1968.
PAHO/WHO Programn
In prior years, the principal assistance furnished by
9
i
2
9
2
!s
the Organization was in the form of collaboration withthe Governments in BCG vaccination campaigns. Theradical changes which have come about in tuberculosiscontrol techniques and methods have meanwhile hadtheir inevitable repercussions on the programs, whichwere initially directed to:
a) Training of national personnel in new methodsand techniques, through the provision of fellowships forcourses, participation in seminars, and inservice train-ing.
b) Assistance in the establishment of national proj-ects in pilot areas, including prevalence surveys, thedetection and treatment of cases, and BCG vaccination.
c) Surveys on the tuberculosis problem in the coun-tries in order to study the mortality and morbiditytrends, ascertain the availability of personnel, installa-tions and equipment, determine the needs and formu-late possible recommendations for meeting them.
The Organization has reviewed and brought up todate its policy, standards, basic concepts, and generalorientation on tuberculosis control, and has drawn up afour-year projection of the operations to be carried out.
In the past few years the program has been directedtoward the promotion of effective and economical tu-berculosis control by means of the systematic applica-tion of the knowledge and resources available.
In accordance with this policy, the Organization paysspecial attention to the bacteriological diagnosis ofcases; incorporation of antituberculosis programs ingeneral health services; determination of priorities inthe program, among which emphasis should be givento suitable chemotherapy as the basis of any controleffort; establishment of limited areas in which the
zu0 .
It
1
t
1
YEAR
Fig. 21. Deaths from tuberculosis per 100,000 population inthree regions of the Americas, 1953-1967.
1953 1954 1955 1958 1957 195a 1959 1960 1961 1962 1963 1964 1995 1966 1967 196s
YEAt
Fig. 22. Reported cases of tuberculosis per 100,000 populationin the three regions of the Americas, 1953-1968.
64
_ SUT AMERICA
IDsDOLE AMERICA
' ..... ̀-.`~~--..................
20
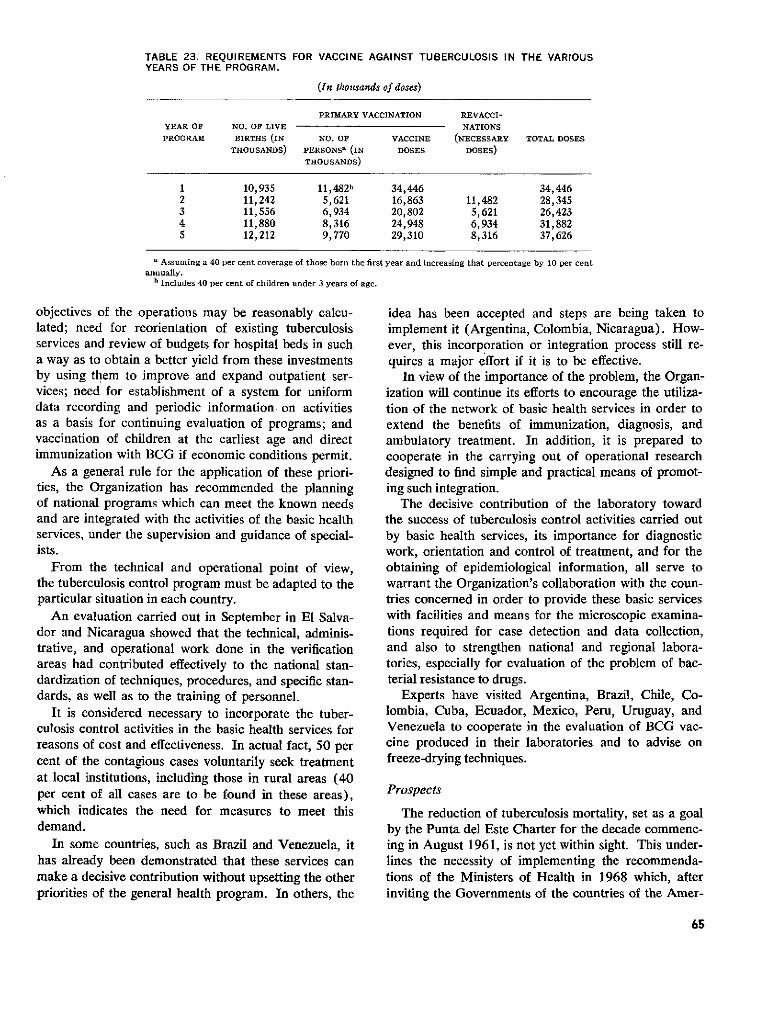
TABLE 23. REQUIREMENTS FOR VACCINE AGAINST TUBERCULOSIS IN THE VARIOUSYEARS OF THE PROGRAM.
(In thousands of doses)
PRIMARY VACCINATION REVACCI-YEAR OF NO. OF LIVE NATIONSPROGRAM BIRTHS (IN NO. OF VACCINE (NECESSARY TOTAL DOSES
THOUSANDS) PERSONSa (IN DOSES DOSES)THOUSANDS)
1 10,935 11,482b 34,446 34,4462 11,242 5,621 16,863 11,482 28,3453 11,556 6,934 20,802 5,621 26,4234 11,880 8,316 24,948 6,934 31,8825 12,212 9,770 29,310 8,316 37,626
a Assuming a 40 per cent coverage of those born the first year and increasing that percentage by 10 per centannually.
h Includes 40 per cent of children under 3 years of age.
objectives of the operations may be reasonably calcu-lated; need for reorientation of existing tuberculosisservices and review of budgets for hospital beds in sucha way as to obtain a better yield from these investmentsby using them to improve and expand outpatient ser-vices; need for establishment of a system for uniformdata recording and periodic information on activitiesas a basis for continuing evaluation of programs; andvaccination of children at the earliest age and directimmunization with BCG if economic conditions permit.
As a general rule for the application of these priori-ties, the Organization has recommended the planningof national programs which can meet the known needsand are integrated with the activities of the basic healthservices, under the supervision and guidance of special-ists.
From the technical and operational point of view,the tuberculosis control program must be adapted to theparticular situation in each country.
An evaluation carried out in September in El Salva-dor and Nicaragua showed that the technical, adminis-trative, and operational work done in the verificationareas had contributed effectively to the national stan-dardization of techniques, procedures, and specific stan-dards, as well as to the training of personnel.
It is considered necessary to incorporate the tuber-culosis control activities in the basic health services forreasons of cost and effectiveness. In actual fact, 50 percent of the contagious cases voluntarily seek treatmentat local institutions, including those in rural areas (40per cent of all cases are to be found in these areas),which indicates the need for measures to meet thisdemand.
In some countries, such as Brazil and Venezuela, ithas already been demonstrated that these services canmake a decisive contribution without upsetting the otherpriorities of the general health program. In others, the
idea has been accepted and steps are being taken toimplement it (Argentina, Colombia, Nicaragua). How-ever, this incorporation or integration process still re-quires a major effort if it is to be effective.
In view of the importance of the problem, the Organ-ization will continue its efforts to encourage the utiliza-tion of the network of basic health services in order toextend the benefits of immunization, diagnosis, andambulatory treatment. In addition, it is prepared tocooperate in the carrying out of operational researchdesigned to find simple and practical means of promot-ing such integration.
The decisive contribution of the laboratory towardthe success of tuberculosis control activities carried outby basic health services, its importance for diagnosticwork, orientation and control of treatment, and for theobtaining of epidemiological information, all serve towarrant the Organization's collaboration with the coun-tries concerned in order to provide these basic serviceswith facilities and means for the microscopic examina-tions required for case detection and data collection,and also to strengthen national and regional labora-tories, especially for evaluation of the problem of bac-terial resistance to drugs.
Experts have visited Argentina, Brazil, Chile, Co-lombia, Cuba, Ecuador, Mexico, Peru, Uruguay, andVenezuela to cooperate in the evaluation of BCG vac-cine produced in their laboratories and to advise onfreeze-drying techniques.
Prospects
The reduction of tuberculosis mortality, set as a goalby the Punta del Este Charter for the decade commenc-ing in August 1961, is not yet within sight. This under-lines the necessity of implementing the recommenda-tions of the Ministers of Health in 1968 which, afterinviting the Governments of the countries of the Amer-
65
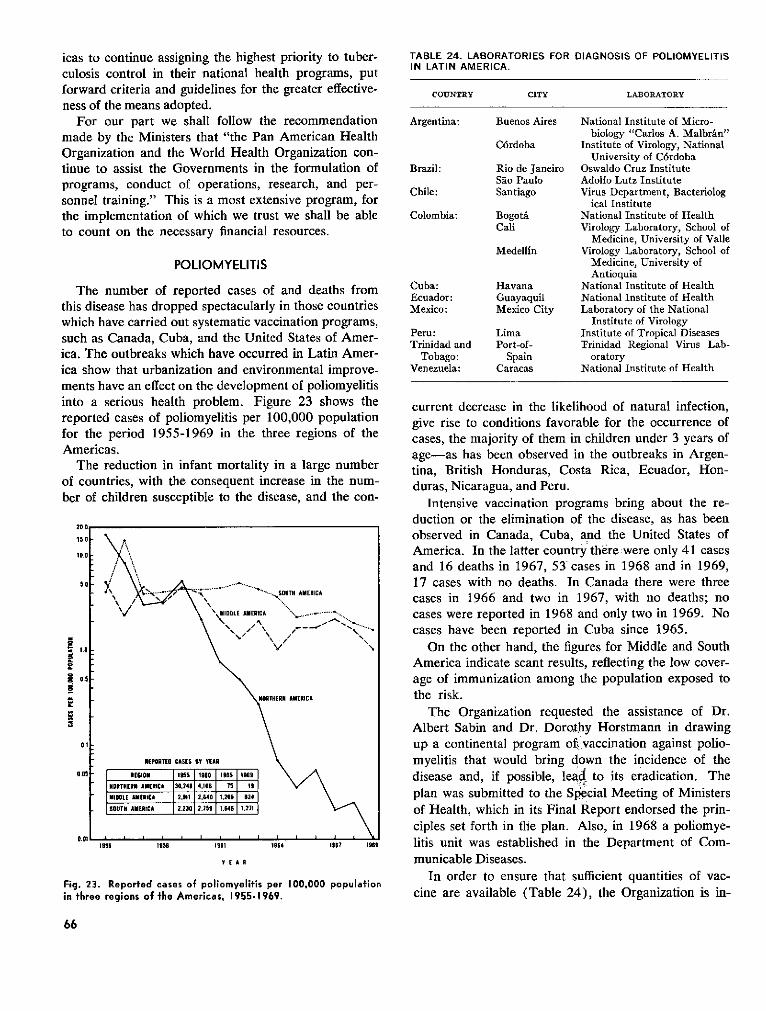
icas to continue assigning the highest priority to tuber-culosis control in their national health programs, putforward criteria and guidelines for the greater effective-ness of the means adopted.
For our part we shall follow the recommendationmade by the Ministers that "the Pan American HealthOrganization and the World Health Organization con-tinue to assist the Governments in the formulation ofprograms, conduct of operations, research, and per-sonnel training." This is a most extensive program, forthe implementation of which we trust we shall be ableto count on the necessary financial resources.
POLIOMYELITIS
The number of reported cases of and deaths fromthis disease has dropped spectacularly in those countrieswhich have carried out systematic vaccination programs,such as Canada, Cuba, and the United States of Amer-ica. The outbreaks which have occurred in Latin Amer-ica show that urbanization and environmental improve-ments have an effect on the development of poliomyelitis
into areport(for theAmeri
Theof couber of
118
a
E2
11
Fig. 23in three
TABLE 24. LABORATORIES FOR DIAGNOSIS OF POLIOMYELITISIN LATIN AMERICA.
COUNTRY CITY LABORATORY
Argentina: Buenos Aires National Institute of Micro-biology "Carlos A. Malbrán"
Córdoba Institute of Virology, NationalUniversity of Córdoba
Brazil: Rio de Janeiro Oswaldo Cruz InstituteSao Paulo Adolfo Lutz Institute
Chile: Santiago Virus Department, Bacteriological Institute
Colombia: Bogotá National Institute of HealthCali Virology Laboratory, School of
Medicine, University of ValleMedellín Virology Laboratory, School of
Medicine, University ofAntioquia
Cuba: Havana National Institute of HealthEcuador: Guayaquil National Institute of HealthMexico: Mexico City Laboratory of the National
Institute of VirologyPeru: Lima Institute of Tropical DiseasesTrinidad and Port-of- Trinidad Regional Virus Lab-
Tobago: Spain oratoryVenezuela: Caracas National Institute of Health
serlous nealtn proolem. rigure 2j snows tne current decrease in the likelihood of natural infection,ed cases of poliomyelitis per 100,000 population give rise to conditions favorable for the occurrence ofe period 1955-1969 in the three regions of the cases, the majority of them in children under 3 years oficas. age-as has been observed in the outbreaks in Argen-reduction in infant mortality in a large number tina, British Honduras, Costa Rica, Ecuador, Hon-
intries, with the consequent increase in the num- duras, Nicaragua, and Peru.children susceptible to the disease, and the con- Intensive vaccination programs bring about the re-
duction or the elimination of the disease, as has beenobserved in Canada, Cuba, and the United States ofAmerica. In the latter country there were only 41 casesand 16 deaths in 1967, 53 cases in 1968 and in 1969,
*1y .\\ A .NC17 cases with no deaths. In Canada there were three; *-· · ·. * suT"^ rwticr cases in 1966 and two in 1967, with no deaths; no
\/.DDLE AMERICA . "_. ... cases were reported in 1968 and only two in 1969. No
cases have been reported in Cuba since 1965.
On the other hand, the figures for Middle and SouthAmerica indicate scant results, reflecting the low cover-age of immunization among the population exposed to
ORTHERNR AERICA the risk.The Organization requested the assistance of Dr.
Albert Sabin and Dr. Dorothy Horstmann in drawingup a continental program of. vaccination against polio-
REPORTED CASES Y 1EAR \ myelitis that would bring down the incidence of theIECION I955 1SSD60 1 -9S ISSS \ Adisease and, if possible, lead to its eradication. The
HORTHERN AMERICA 30,248 4.106 75 1 .,
MIDDEE AMERICA 2,94 2,640 1.266 834 plan was submitted to the Special Meeting of MinistersSDUTH AYERICA 2.230 2.159 .U46 1.271 \ of Health, which in its Final Report endorsed the prin-
ciples set forth in the plan. Also, in 1968 a poliomye-19ss 1i95 1961 1964 1967 1969 litis unit was established in the Department of Com-
Y E A R municable Diseases.
In order to ensure that sufficient quantities of vac-Reported ericases of poliomyelitis per 100,000 populrganization is i-eregions of the Americas. 1955-1969. cine are available (Table 24), the Organization is in-
66
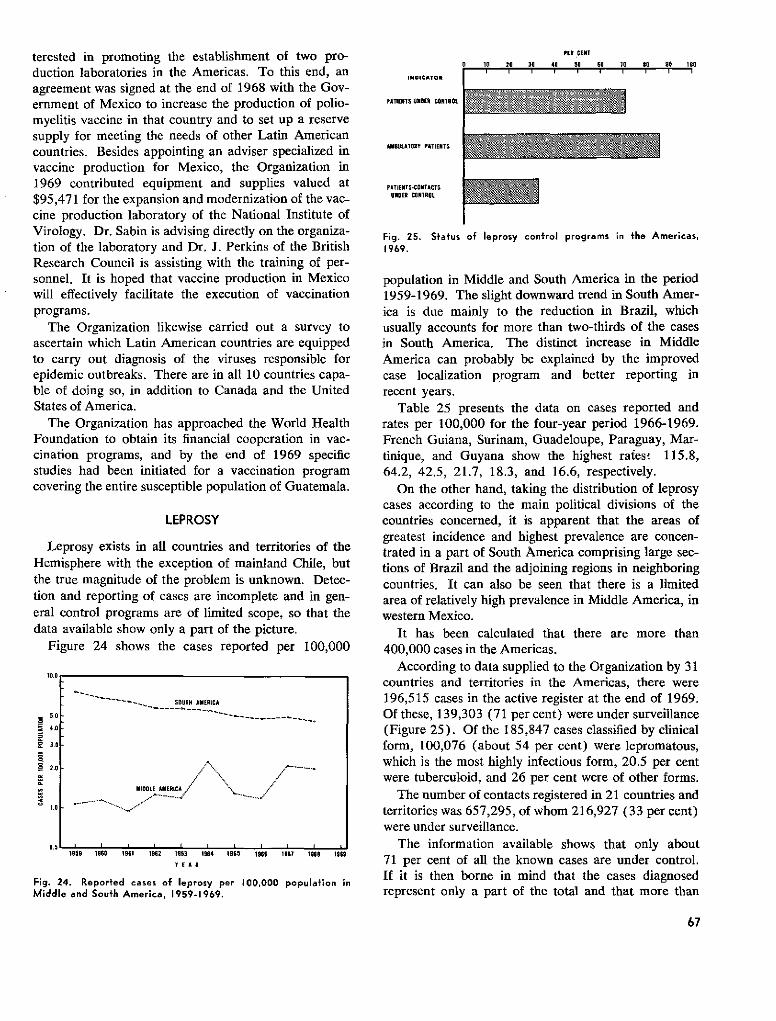
terested in promoting the establishment of two pro-duction laboratories in the Americas. To this end, anagreement was signed at the end of 1968 with the Gov-ernment of Mexico to increase the production of polio-myelitis vaccine in that country and to set up a reservesupply for meeting the needs of other Latin Americancountries. Besides appointing an adviser specialized invaccine production for Mexico, the Organization in1969 contributed equipment and supplies valued at$95,471 for the expansion and modernization of the vac-cine production laboratory of the National Institute ofVirology. Dr. Sabin is advising directly on the organiza-tion of the laboratory and Dr. J. Perkins of the BritishResearch Council is assisting with the training of per-sonnel. It is hoped that vaccine production in Mexicowill effectively facilitate the execution of vaccinationprograms.
The Organization likewise carried out a survey toascertain which Latin American countries are equippedto carry out diagnosis of the viruses responsible forepidemic outbreaks. There are in all 10 countries capa-ble of doing so, in addition to Canada and the UnitedStates of America.
The Organization has approached the World HealthFoundation to obtain its financial cooperation in vac-cination programs, and by the end of 1969 specificstudies had been initiated for a vaccination programcovering the entire susceptible population of Guatemala.
LEPROSY
Leprosy exists in all countries and territories of theHemisphere with the exception of mainland Chile, butthe true magnitude of the problem is unknown. Detec-tion and reporting of cases are incomplete and in gen-eral control programs are of limited scope, so that thedata available show only a part of the picture.
Figure 24 shows the cases reported per 100,000
IO.O r
5.0L-
4.0
3.0
I.0
f IDo
1959 1960 1961 1962 1903
E A
1964 1965 1 1966 196 1968 1969
Fig. 24. Reported cases of leprosy per 100,000 population inMiddle and South America, 1959-1969.
INDICATO!
PATIENTS UNDER CONTROL
AUIBUtTORY PATIENTS
PATIENTS-CONTACTSUNDER CONTROL
PER CENT
0 10 20 30 4 50 SO 70 o0 0S 100
Fig. 25. Status of leprosy control programs in the Americas,1969.
population in Middle and South America in the period1959-1969. The slight downward trend in South Amer-ica is due mainly to the reduction in Brazil, whichusually accounts for more than two-thirds of the casesin South America. The distinct increase in MiddleAmerica can probably be explained by the improvedcase localization program and better reporting inrecent years.
Table 25 presents the data on cases reported andrates per 100,000 for the four-year period 1966-1969.French Guiana, Surinam, Guadeloupe, Paraguay, Mar-tinique, and Guyana show the highest rates! 115.8,64.2, 42.5, 21.7, 18.3, and 16.6, respectively.
On the other hand, taking the distribution of leprosycases according to the main political divisions of thecountries concerned, it is apparent that the areas ofgreatest incidence and highest prevalence are concen-trated in a part of South America comprising large sec-tions of Brazil and the adjoining regions in neighboringcountries. It can also be seen that there is a limitedarea of relatively high prevalence in Middle America, inwestern Mexico.
It has been calculated that there are more than400,000 cases in the Americas.
According to data supplied to the Organization by 31countries and territories in the Americas, there were196,515 cases in the active register at the end of 1969.Of these, 139,303 (71 per cent) were under surveillance(Figure 25). Of the 185,847 cases classified by clinicalform, 100,076 (about 54 per cent) were lepromatous,which is the most highly infectious form, 20.5 per centwere tuberculoid, and 26 per cent were of other forms.
The number of contacts registered in 21 countries andterritories was 657,295, of whom 216,927 (33 per cent)were under surveillance.
The information available shows that only about71 per cent of all the known cases are under control.If it is then borne in mind that the cases diagnosedrepresent only a part of the total and that more than
67
-SOUT AMERICA____- .-------
MIDOLE AMERICA .'
-ERS-REg
>~~~~~~0-
', ' '11 ' Ala'', .. > `1w"-, - 1, 11 k . MI, �
u.5' ' i i I I I . I I I,---
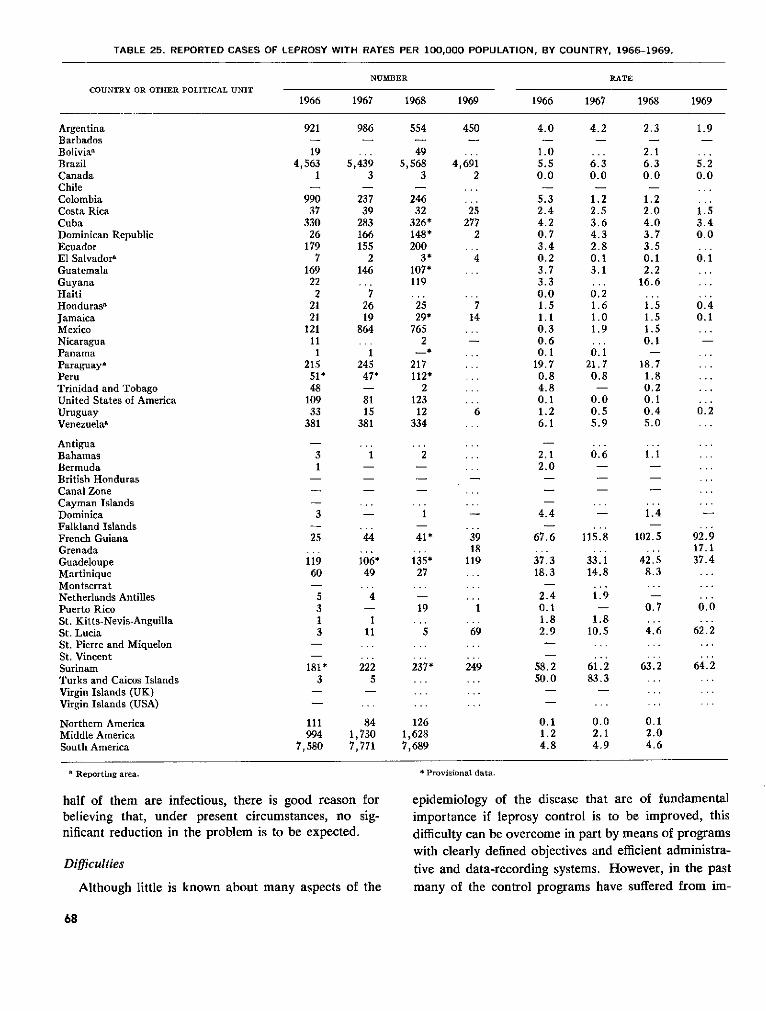
TABLE 25. REPORTED CASES OF LEPROSY WITH RATES PER 100,000 POPULATION, BY COUNTRY, 1966-1969.
NUMBER
COUNTRY OR OTHER POLITICAL UNIT
ArgentinaBarbadosBolivia,BrazilCanadaChileColombiaCosta RicaCubaDominican RepublicEcuadorEl Salvador,GuatemalaGuyanaHaitiHondurasaJamaicaMexicoNicaraguaPanamaParaguay,PeruTrinidad and TobagoUnited States of AmericaUruguayVenezuelaW
AntiguaBahamasBermudaBritish HondurasCanal ZoneCayman IslandsDominicaFalkland IslandsFrench GuianaGrenadaGuadeloupeMartiniqueMontserratNetherlands AntillesPuerto RicoSt. Kitts-Nevis-AnguillaSt. LuciaSt. Pierre and MiquelonSt. VincentSurinamTurks and Caicos IslandsVirgin Islands (UK)Virgin Islands (USA)
Northern AmericaMiddle AmericaSouth America
1966 1967 1968 1969
921
194,563
1
99037
33026
1797
169222
2121
121111
21551*48
10933
381
31
3
25
11960
5313
181*3
111994
7,580
986
5,4393
23739
283166155
2146
72619
864
1245
47*
8115
381
1
44
106*49
4
111
2225
841,7307,771
554
495,568
3
24632
326*148*200
3*107*119
2529*
7652
217112*
2123
12334
2
1
41*
135*27
19
5
237*
1261,6287,689
450
4,6912
25277
2
4
714
6
3918
119
1
69
249
. . .
RATE
1966 1967 1968 1969
4.0
1.05.50.0
5.32.44.20.73.40.23.73.30.01.51.10.30.60.1
19.70.84.80.11.26.1
2.12.0
4.4
67.6
37.318.3
2.40.11.82.9
58.250.0
0.11.24.8
4.2
6.30.0
1.22.53.64.32.80.13.1
0.21.61.01.9
0.121.70.8
0.00.55.9
0.6
115.8
33.114.8
1.9
1.810.5
61.283.3
0.02.14.9
2.3
2.16.30.0
1.22.04.03.73.50.12.2
16.6
1.51.51.50.1
18.71.80.20.10.45.0
1.1
1.4
102.5
42.58.3
0.7
4.6
63.2
0.12.04.6
1.9
5.20.0
1.53.40.0
0.1
0.40.1
0.2
92.917.137.4
0.0
62.2
64.2
. . .
a Reporting area. * Provisional data.
half of them are infectious, there is good reason forbelieving that, under present circumstances, no sig-nificant reduction in the problem is to be expected.
Difficulties
Although little is known about many aspects of the
epidemiology of the disease that are of fundamentalimportance if leprosy control is to be improved, thisdifficulty can be overcome in part by means of programswith clearly defined objectives and efficient administra-
tive and data-recording systems. However, in the pastmany of the control programs have suffered from im-
68
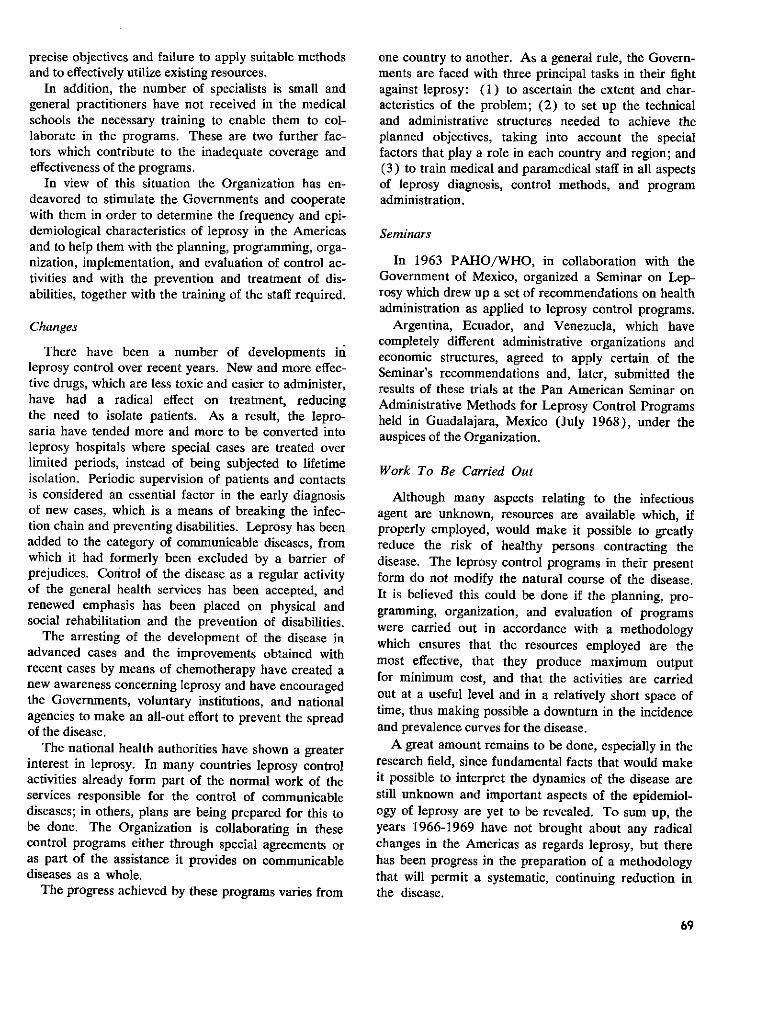
precise objectives and failure to apply suitable methodsand to effectively utilize existing resources.
In addition, the number of specialists is small andgeneral practitioners have not received in the medicalschools the necessary training to enable them to col-laborate in the programs. These are two further fac-tors which contribute to the inadequate coverage andeffectiveness of the programs.
In view of this situation the Organization has en-deavored to stimulate the Governments and cooperatewith them in order to determine the frequency and epi-demiological characteristics of leprosy in the Americasand to help them with the planning, programming, orga-nization, implementation, and evaluation of control ac-tivities and with the prevention and treatment of dis-abilities, together with the training of the staff required.
Changes
There have been a number of developments inleprosy control over recent years. New and more effec-tive drugs, which are less toxic and easier to administer,have had a radical effect on treatment, reducingthe need to isolate patients. As a result, the lepro-saria have tended more and more to be converted intoleprosy hospitals where special cases are treated overlimited periods, instead of being subjected to lifetimeisolation. Periodic supervision of patients and contactsis considered an essential factor in the early diagnosisof new cases, which is a means of breaking the infec-tion chain and preventing disabilities. Leprosy has beenadded to the category of communicable diseases, fromwhich it had formerly been excluded by a barrier ofprejudices. Control of the disease as a regular activityof the general health services has been accepted, andrenewed emphasis has been placed on physical andsocial rehabilitation and the prevention of disabilities.
The arresting of the development of the disease inadvanced cases and the improvements obtained withrecent cases by means of chemotherapy have created anew awareness concerning leprosy and have encouragedthe Governments, voluntary institutions, and nationalagencies to make an all-out effort to prevent the spreadof the disease.
The national health authorities have shown a greaterinterest in leprosy. In many countries leprosy controlactivities already form part of the normal work of theservices responsible for the control of communicablediseases; in others, plans are being prepared for this tobe done. The Organization is collaborating in thesecontrol programs either through special agreements oras part of the assistance it provides on communicablediseases as a whole.
The progress achieved by these programs varies from
one country to another. As a general rule, the Govern-ments are faced with three principal tasks in their fightagainst leprosy: (1) to ascertain the extent and char-acteristics of the problem; (2) to set up the technicaland administrative structures needed to achieve theplanned objectives, taking into account the specialfactors that play a role in each country and region; and(3) to train medical and paramedical staff in all aspectsof leprosy diagnosis, control methods, and programadministration.
Seminars
In 1963 PAHO/WHO, in collaboration with theGovernment of Mexico, organized a Seminar on Lep-rosy which drew up a set of recommendations on healthadministration as applied to leprosy control programs.
Argentina, Ecuador, and Venezuela, which havecompletely different administrative organizations andeconomic structures, agreed to apply certain of theSeminar's recommendations and, later, submitted theresults of these trials at the Pan American Seminar onAdministrative Methods for Leprosy Control Programsheld in Guadalajara, Mexico (July 1968), under theauspices of the Organization.
Work To Be Carried Out
Although many aspects relating to the infectiousagent are unknown, resources are available which, ifproperly employed, would make it possible to greatlyreduce the risk of healthy persons contracting thedisease. The leprosy control programs in their presentform do not modify the natural course of the disease.It is believed this could be done if the planning, pro-gramming, organization, and evaluation of programswere carried out in accordance with a methodologywhich ensures that the resources employed are themost effective, that they produce maximum outputfor minimum cost, and that the activities are carriedout at a useful level and in a relatively short space oftime, thus making possible a downturn in the incidenceand prevalence curves for the disease.
A great amount remains to be done, especially in theresearch field, since fundamental facts that would makeit possible to interpret the dynamics of the disease arestill unknown and important aspects of the epidemiol-ogy of leprosy are yet to be revealed. To sum up, theyears 1966-1969 have not brought about any radicalchanges in the Americas as regards leprosy, but therehas been progress in the preparation of a methodologythat will permit a systematic, continuing reduction inthe disease.
69
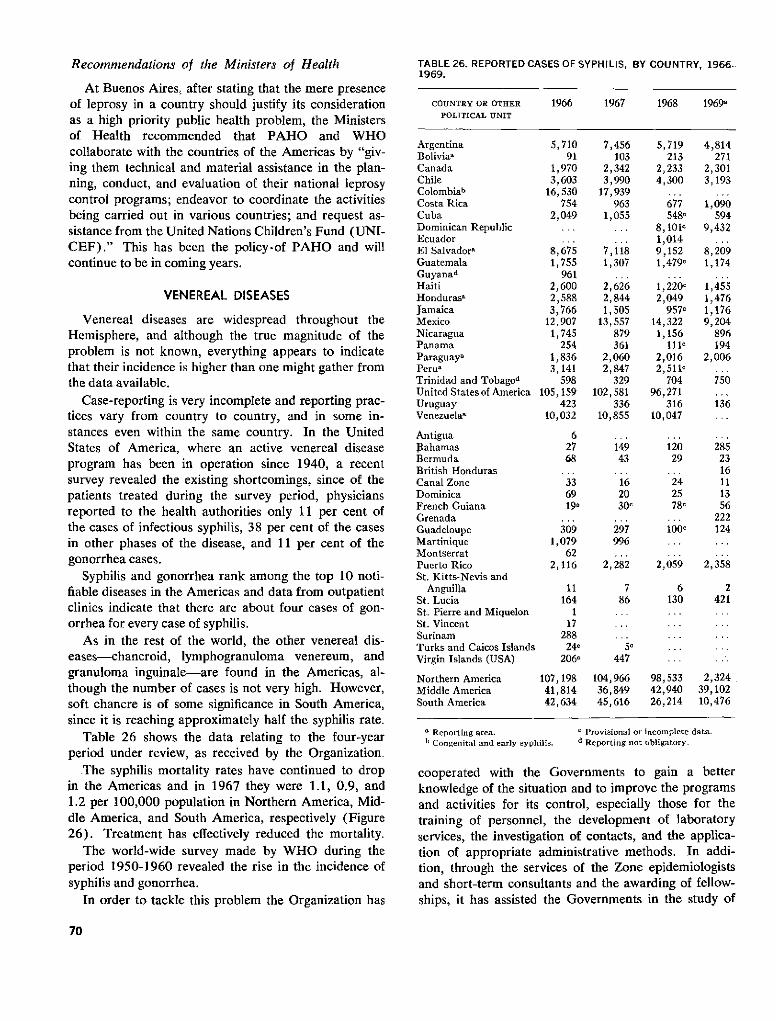
Recommendations of the Ministers of Health
At Buenos Aires, after stating that the mere presenceof leprosy in a country should justify its considerationas a high priority public health problem, the Ministersof Health recommended that PAHO and WHOcollaborate with the countries of the Americas by "giv-ing them technical and material assistance in the plan-ning, conduct, and evaluation of their national leprosycontrol programs; endeavor to coordinate the activitiesbeing carried out in various countries; and request as-sistance from the United Nations Children's Fund (UNI-CEF)." This has been the policy-of PAHO and willcontinue to be in coming years.
VENEREAL DISEASES
Venereal diseases are widespread throughout theHemisphere, and although the true magnitude of theproblem is not known, everything appears to indicatethat their incidence is higher than one might gather fromthe data available.
Case-reporting is very incomplete and reporting prac-tices vary from country to country, and in some in-stances even within the same country. In the UnitedStates of America, where an active venereal diseaseprogram has been in operation since 1940, a recentsurvey revealed the existing shortcomings, since of thepatients treated during the survey period, physiciansreported to the health authorities only 11 per cent ofthe cases of infectious syphilis, 38 per cent of the casesin other phases of the disease, and 11 per cent of thegonorrhea cases.
Syphilis and gonorrhea rank among the top 10 noti-fiable diseases in the Americas and data from outpatientclinics indicate that there are about four cases of gon-orrhea for every case of syphilis.
As in the rest of the world, the other venereal dis-eases-chancroid, lymphogranuloma venereum, andgranuloma inguinale-are found in the Americas, al-though the number of cases is not very high. However,soft chancre is of some significance in South America,since it is reaching approximately half the syphilis rate.
Table 26 shows the data relating to the four-yearperiod under review, as received by the Organization.
The syphilis mortality rates have continued to dropin the Americas and in 1967 they were 1.1, 0.9, and1.2 per 100,000 population in Northern America, Mid-dle America, and South America, respectively (Figure26). Treatment has effectively reduced the mortality.
The world-wide survey made by WHO during theperiod 1950-1960 revealed the rise in the incidence ofsyphilis and gonorrhea.
In order to tackle this problem the Organization has
TABLE 26. REPORTED CASES OF SYPHILIS, BY COUNTRY, 1966-1969.
COUNTRY OR OTHER 1966 1967 1968 19690POLITICAL UNIT
Argentina 5, 710Boliviaa 91Canada 1,970Chile 3,603Colombiab 16,530Costa Rica 754Cuba 2,049Dominican Republic . ..EcuadorEl Salvadora 8,675Guatemala 1,755Guyanad 961Haiti 2,600Hondurasa 2,588Jamaica 3,766Mexico 12,907Nicaragua 1,745Panama 254Paraguaya 1,836Perua 3,141Trinidad and Tobagod 598United Statesof America 105,159Uruguay 423Venezuelaa 10,032
Antigua 6Bahamas 27Bermuda 68British HondurasCanal Zone 33Dominica 69French Guiana 19aGrenadaGuadeloupe 309Martinique 1,079Montserrat 62Puerto Rico 2,116St. Kitts-Nevis and
Anguilla 11St. Lucia 164St. Pierre and Miquelon 1St. Vincent 17Surinam 288Turks and Caicos Islands 240Virgin Islands (USA) 206c
Northern America 107,198Middle America 41,814South America 42,634
a Reporting area.' Congenital and early syphilis.
7,456103
2,3423,990
17,939963
1,055
7,1181,307
2,6262,8441,505
13,557879361
2,0602,847
329102,581
33610,855
14943
162030 c
297996
2,282
786
5c447
104,96636,84945,616
5,719213
2,2334,300
6775480
8,10101,0149,1521,479c
1,220,2,049
957e14,3221,156
111l2,0162,5110
70496,271
31610,047
12029
2425780
100l
2,059
6130
98,53342,94026,214
4,814271
2,3013,193
1,090594
9,432
8,2091,174
1,4551,4761,1769,204
896194
2,006
750
136
2852316111356
222124
2,358
2421
2,32439,10210,476
c Provisional or incomplete data.d Reporting not obligatory.
cooperated with the Governments to gain a betterknowledge of the situation and to improve the programsand activities for its control, especially those for thetraining of personnel, the development of laboratoryservices, the investigation of contacts, and the applica-tion of appropriate administrative methods. In addi-tion, through the services of the Zone epidemiologistsand short-term consultants and the awarding of fellow-ships, it has assisted the Governments in the study of
70
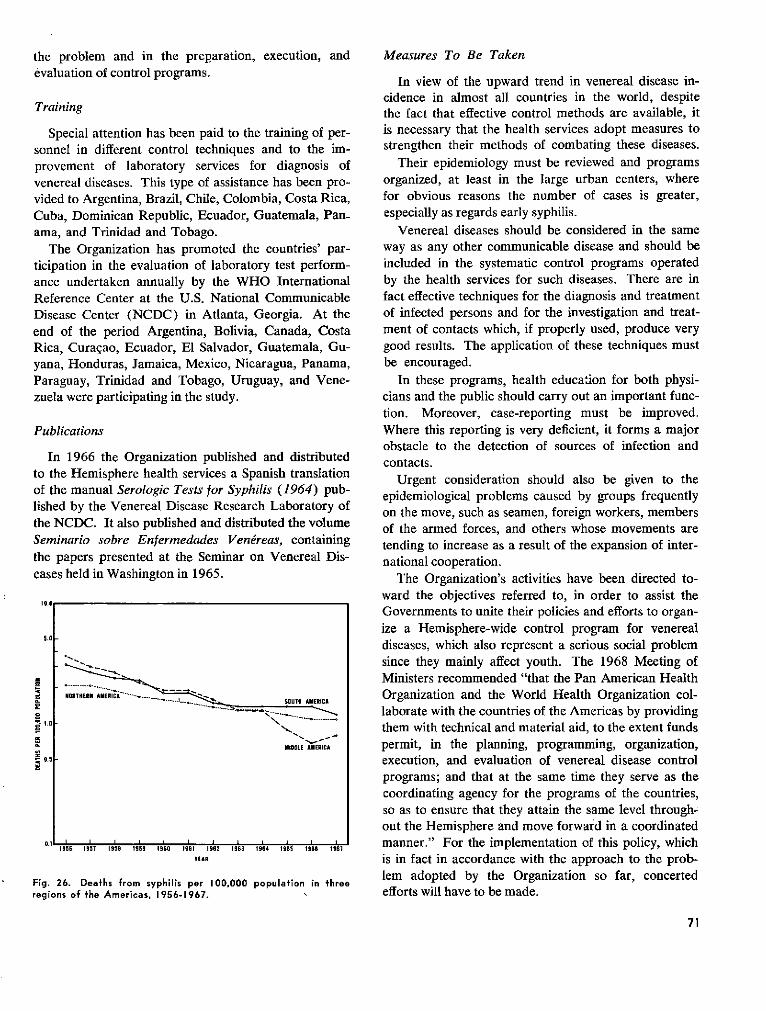
the problem and in the preparation, execution, andevaluation of control programs.
Training
Special attention has been paid to the training of per-sonnel in different control techniques and to the im-provement of laboratory services for diagnosis ofvenereal diseases. This type of assistance has been pro-vided to Argentina, Brazil, Chile, Colombia, Costa Rica,Cuba, Dominican Republic, Ecuador, Guatemala, Pan-ama, and Trinidad and Tobago.
The Organization has promoted the countries' par-ticipation in the evaluation of laboratory test perform-ance undertaken annually by the WHO InternationalReference Center at the U.S. National CommunicableDisease Center (NCDC) in Atlanta, Georgia. At theend of the period Argentina, Bolivia, Canada, CostaRica, Curaçao, Ecuador, El Salvador, Guatemala, Gu-yana, Honduras, Jamaica, Mexico, Nicaragua, Panama,Paraguay, Trinidad and Tobago, Uruguay, and Vene-zuela were participating in the study.
Publications
In 1966 the Organization published and distributedto the Hemisphere health services a Spanish translationof the manual Serologic Tests for Syphilis (1964) pub-lished by the Venereal Disease Research Laboratory ofthe NCDC. It also published and distributed the volumeSeminario sobre Enfermedades Venéreas, containingthe papers presented at the Seminar on Venereal Dis-eases held in Washington in 1965.
109.
1956 1951 1958 1959 1960 19t1 1962 1963 1964 1965 1966 1967
YEAR
Fig. 26. Deaths from syphilis per 100,000 population in threeregions of the Americas, 1956-1967.
Measures To Be Taken
In view of the upward trend in venereal disease in-cidence in almost all countries in the world, despitethe fact that effective control methods are available, itis necessary that the health services adopt measures tostrengthen their methods of combating these diseases.
Their epidemiology must be reviewed and programsorganized, at least in the large urban centers, wherefor obvious reasons the number of cases is greater,especially as regards early syphilis.
Venereal diseases should be considered in the sameway as any other communicable disease and should beincluded in the systematic control programs operatedby the health services for such diseases. There are infact effective techniques for the diagnosis and treatmentof infected persons and for the investigation and treat-ment of contacts which, if properly used, produce verygood results. The application of these techniques mustbe encouraged.
In these programs, health education for both physi-cians and the public should carry out an important func-tion. Moreover, case-reporting must be improved.Where this reporting is very deficient, it forms a majorobstacle to the detection of sources of infection andcontacts.
Urgent consideration should also be given to theepidemiological problems caused by groups frequentlyon the move, such as seamen, foreign workers, membersof the armed forces, and others whose movements aretending to increase as a result of the expansion of inter-national cooperation.
The Organization's activities have been directed to-ward the objectives referred to, in order to assist theGovernments to unite their policies and efforts to organ-ize a Hemisphere-wide control program for venerealdiseases, which also represent a serious social problemsince they mainly affect youth. The 1968 Meeting ofMinisters recommended "that the Pan American HealthOrganization and the World Health Organization col-laborate with the countries of the Americas by providingthem with technical and material aid, to the extent fundspermit, in the planning, programming, organization,execution, and evaluation of venereal disease controlprograms; and that at the same time they serve as thecoordinating agency for the programs of the countries,so as to ensure that they attain the same level through-out the Hemisphere and move forward in a coordinatedmanner." For the implementation of this policy, whichis in fact in accordance with the approach to the prob-lem adopted by the Organization so far, concertedefforts will have to be made.
71
SOUT0 AMERICA
..OC '~1.0 - 1
MIDDLE AMERICA
0.5
0.1 . 1 . . . 1 .
1
E
o
g
,
a
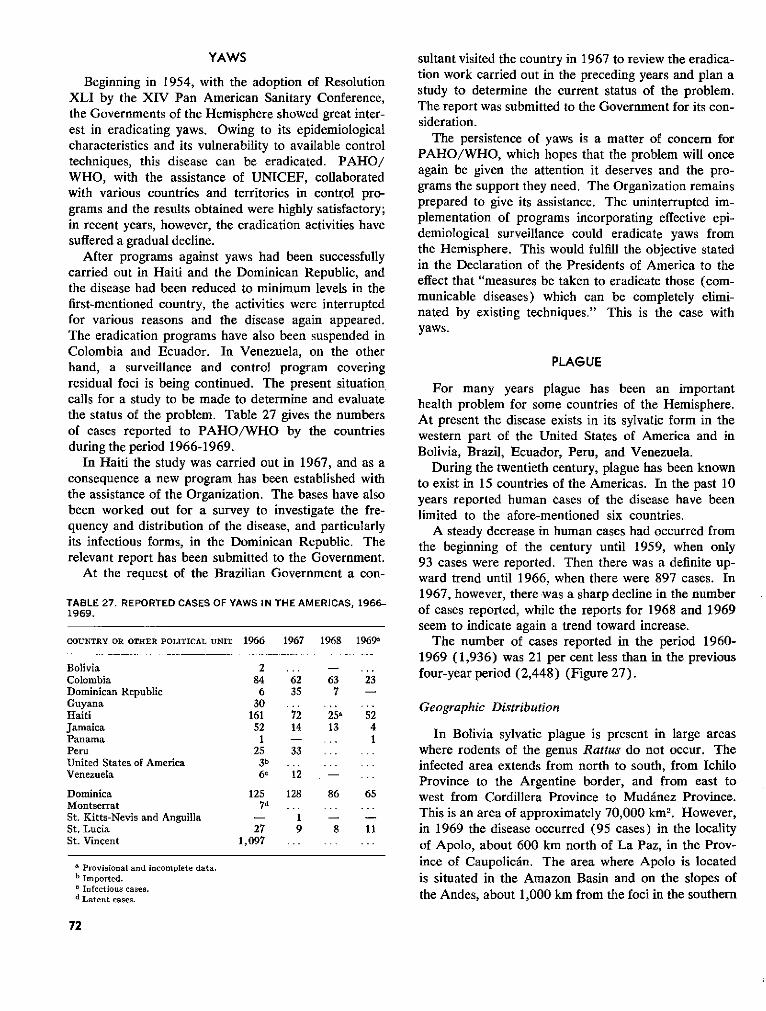
YAWS
Beginning in 1954, with the adoption of ResolutionXLI by the XIV Pan American Sanitary Conference,the Governments of the Hemisphere showed great inter-est in eradicating yaws. Owing to its epidemiologicalcharacteristics and its vulnerability to available controltechniques, this disease can be eradicated. PAHO/WHO, with the assistance of UNICEF, collaboratedwith various countries and territories in control pro-grams and the results obtained were highly satisfactory;in recent years, however, the eradication activities havesuffered a gradual decline.
After programs against yaws had been successfullycarried out in Haiti and the Dominican Republic, andthe disease had been reduced to minimum levels in thefirst-mentioned country, the activities were interruptedfor various reasons and the disease again appeared.The eradication programs have also been suspended inColombia and Ecuador. In Venezuela, on the otherhand, a surveillance and control program coveringresidual foci is being continued. The present situationcalls for a study to be made to determine and evaluatethe status of the problem. Table 27 gives the numbersof cases reported to PAHO/WHO by the countriesduring the period 1966-1969.
In Haiti the study was carried out in 1967, and as aconsequence a new program has been established withthe assistance of the Organization. The bases have alsobeen worked out for a survey to investigate the fre-quency and distribution of the disease, and particularlyits infectious forms, in the Dominican Republic. Therelevant report has been submitted to the Government.
At the request of the Brazilian Government a con-
TABLE 27. REPORTED CASES OF YAWS IN THE AMERICAS, 1966-1969.
COUNTRY OR OTHER POLITICAL UNIT 1966 1967 1968 1969·
Bolivia 2 - .Colombia 84 62 63 23Dominican Republic 6 35 7 -Guyana 30Haiti 161 72 25a 52Jamaica 52 14 13 4Panama 1 - ... 1Peru 25 33United States of America 3b ...Venezuela 6E 12
Dominica 125 128 86 65Montserrat 7dSt. Kitts-Nevis and Anguilla - 1St. Lucia 27 9 8 11St. Vincent 1,097 ... ...
a Provisional and incomplete data.b Imported.o Infectious cases.d Latent cases.
sultant visited the country in 1967 to review the eradica-tion work carried out in the preceding years and plan astudy to determine the current status of the problem.The report was submitted to the Government for its con-sideration.
The persistence of yaws is a matter of concem forPAHO/WHO, which hopes that the problem will onceagain be given the attention it deserves and the pro-grams the support they need. The Organization remainsprepared to give its assistance. The uninterrupted im-plementation of programs incorporating effective epi-demiological surveillance could eradicate yaws fromthe Hemisphere. This would fulfill the objective statedin the Declaration of the Presidents of America to theeffect that "measures be taken to eradicate those (com-municable diseases) which can be completely elimi-nated by existing techniques." This is the case withyaws.
PLAGUE
For many years plague has been an importanthealth problem for some countries of the Hemisphere.At present the disease exists in its sylvatic form in thewestern part of the United States of America and inBolivia, Brazil, Ecuador, Peru, and Venezuela.
During the twentieth century, plague has been knownto exist in 15 countries of the Americas. In the past 10years reported human cases of the disease have beenlimited to the afore-mentioned six countries.
A steady decrease in human cases had occurred fromthe beginning of the century until 1959, when only93 cases were reported. Then there was a definite up-ward trend until 1966, when there were 897 cases. In1967, however, there was a sharp decline in the numberof cases reported, while the reports for 1968 and 1969seem to indicate again a trend toward increase.
The number of cases reported in the period 1960-1969 (1,936) was 21 per cent less than in the previousfour-year period (2,448) (Figure 27).
Geographic Distribution
In Bolivia sylvatic plague is present in large areaswhere rodents of the genus Rattus do not occur. Theinfected area extends from north to south, from IchiloProvince to the Argentine border, and from east towest from Cordillera Province to Mudánez Province.This is an area of approximately 70,000 km2. However,in 1969 the disease occurred (95 cases) in the localityof Apolo, about 600 km north of La Paz, in the Prov-ince of Caupolicán. The area where Apolo is locatedis situated in the Amazon Basin and on the slopes ofthe Andes, about 1,000 km from the foci in the southern
72
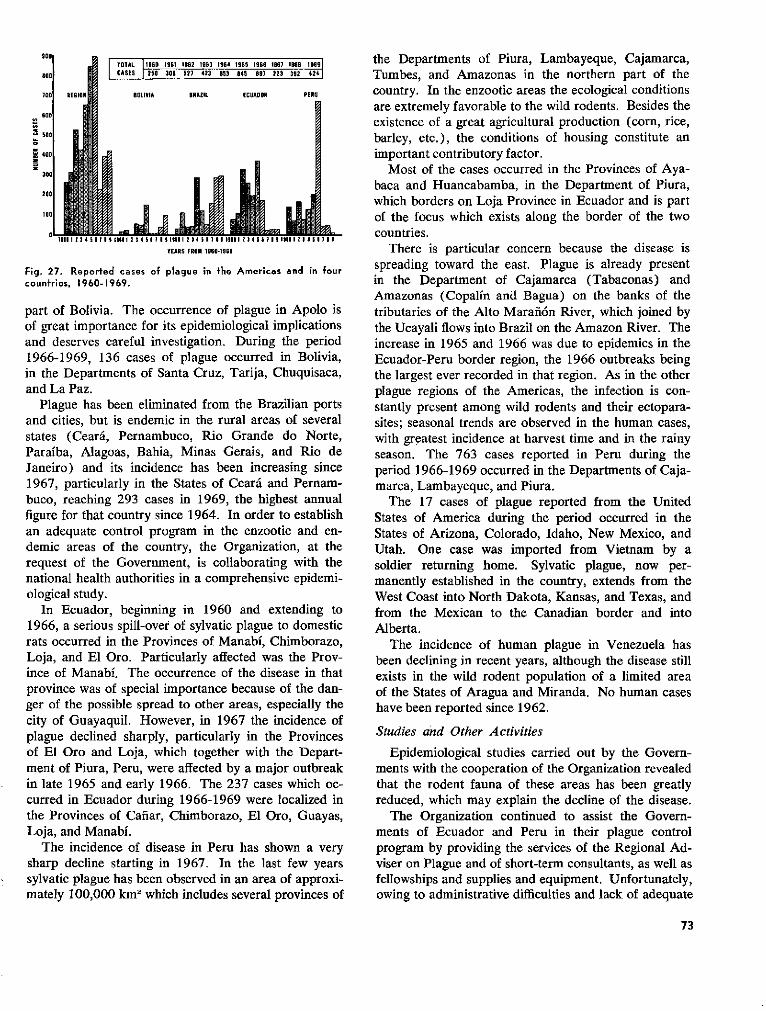
900
900
70
600
500
400
3
20
100
o0
TOTAL 1960 1961 1962 1963 1964 1965 1966 1967 196 19681CASES 258 308 527 423 653 945 897 223 392 424
BOLIVIA BRAZIL ECUADOR PERU
. lLi ¡YEARS FROM 1960-1969
Fig. 27. Reported cases of plague in the Americas and in fourcountries, 1960-1969.
part of Bolivia. The occurrence of plague in Apolo isof great importance for its epidemiological implicationsand deserves careful investigation. During the period1966-1969, 136 cases of plague occurred in Bolivia,in the Departments of Santa Cruz, Tarija, Chuquisaca,and La Paz.
Plague has been eliminated from the Brazilian portsand cities, but is endemic in the rural areas of severalstates (Ceará, Pernambuco, Rio Grande do Norte,Paraíba, Alagoas, Bahia, Minas Gerais, and Rio deJaneiro) and its incidence has been increasing since1967, particularly in the States of Ceará and Pernam-buco, reaching 293 cases in 1969, the highest annualfigure for that country since 1964. In order to establishan adequate control program in the enzootic and en-demic areas of the country, the Organization, at therequest of the Government, is collaborating with thenational health authorities in a comprehensive epidemi-ological study.
In Ecuador, beginning in 1960 and extending to1966, a serious spill-over of sylvatic plague to domesticrats occurred in the Provinces of Manabí, Chimborazo,Loja, and El Oro. Particularly affected was the Prov-ince of Manabí. The occurrence of the disease in thatprovince was of special importance because of the dan-ger of the possible spread to other areas, especially thecity of Guayaquil. However, in 1967 the incidence ofplague declined sharply, particularly in the Provincesof El Oro and Loja, which together with the Depart-ment of Piura, Peru, were affected by a major outbreakin late 1965 and early 1966. The 237 cases which oc-curred in Ecuador during 1966-1969 were localized inthe Provinces of Cañar, Chimborazo, El Oro, Guayas,Loja, and Manabí.
The incidence of disease in Peru has shown a verysharp decline starting in 1967. In the last few yearssylvatic plague has been observed in an area of approxi-mately 100,000 km2 which includes several provinces of
the Departments of Piura, Lambayeque, Cajamarca,Tumbes, and Amazonas in the northern part of thecountry. In the enzootic areas the ecological conditionsare extremely favorable to the wild rodents. Besides theexistence of a great agricultural production (corn, rice,barley, etc.), the conditions of housing constitute animportant contributory factor.
Most of the cases occurred in the Provinces of Aya-baca and Huancabamba, in the Department of Piura,which borders on Loja Province in Ecuador and is partof the focus which exists along the border of the twocountries.
There is particular concern because the disease isspreading toward the east. Plague is already presentin the Department of Cajamarca (Tabaconas) andAmazonas (Copalín and Bagua) on the banks of thetributaries of the Alto Marañón River, which joined bythe Ucayali flows into Brazil on the Amazon River. Theincrease in 1965 and 1966 was due to epidemics in theEcuador-Peru border region, the 1966 outbreaks beingthe largest ever recorded in that region. As in the otherplague regions of the Americas, the infection is con-stantly present among wild rodents and their ectopara-sites; seasonal trends are observed in the human cases,with greatest incidence at harvest time and in the rainyseason. The 763 cases reported in Peru during theperiod 1966-1969 occurred in the Departments of Caja-marca, Lambayeque, and Piura.
The 17 cases of plague reported from the UnitedStates of America during the period occurred in theStates of Arizona, Colorado, Idaho, New Mexico, andUtah. One case was imported from Vietnam by asoldier returning home. Sylvatic plague, now per-manently established in the country, extends from theWest Coast into North Dakota, Kansas, and Texas, andfrom the Mexican to the Canadian border and intoAlberta.
The incidence of human plague in Venezuela hasbeen declining in recent years, although the disease stillexists in the wild rodent population of a limited areaof the States of Aragua and Miranda. No human caseshave been reported since 1962.
Studies and Other Activities
Epidemiological studies carried out by the Govern-ments with the cooperation of the Organization revealedthat the rodent fauna of these areas has been greatlyreduced, which may explain the decline of the disease.
The Organization continued to assist the Govern-ments of Ecuador and Peru in their plague controlprogram by providing the services of the Regional Ad-viser on Plague and of short-term consultants, as well asfellowships and supplies and equipment. Unfortunately,owing to administrative difficulties and lack of adequate
73
OI
1 a11 ( 1111 1
financial support, the progress has been slowed downand it has not been possible to attain the goals estab-lished in the plan of operations. The details of this as-sistance can be found in the Annual Reports of theDirector for the years 1966 to 1969.
While current control and containment measures havebeen more successful, it has become evident that beforefurther progress can be made against plague it will benecessary to undertake a thorough study of the natureof the disease.
On the basis of a detailed examination and evaluationof the information on plague in the Americas, containedin the technical literature, officiál reports and othersources, a series of ecological research studies weredesigned.
This program includes ecological studies, researchon the natural infection of wild rodents and fleas, onsensitivity to plague of different species of rodents, studyof the strain of plague bacillus isolated, and researchon the flea fauna and methods of control.
Investigations of this kind may reveal the existenceof species of prime importance for the maintenance ofplague, and possibly even of limited foci where the in-fection persists and from which it is apt to break outwhenever an increase in the wild rodent and Lago-morpha population provides adequate fuel for a spreadof the disease. Though admittedly requiring great ini-tial efforts, such investigations will in the long runfacilitate a watch over the trend of sylvatic .plague inthe Americas.
These studies, which are of great importance for anational approach to the effective control of the disease,are being carried out in Brazil, where a very activeresearch program on plague has been under way since1966 with the cooperation of the Organization.
Similar studies were planned to be initiated in 1968in Peru and Ecuador and later in Bolivia. However,owing to lack of resources in the first two countries theinitiation of this program had to be postponed indefi-nitely.
INFLUENZA
Because of the rapid spread of this disease fromcountry to country, WHO established an influenza pro-gram in 1947. Since then it has collected and dissemi-nated laboratory and epidemiological information onthe nature and extent of epidemics, in collaboration withnational health authorities, two international centers(the World Influenza Center at the National Institutefor Medical Research in London, England; and theInternational Influenza Center for the Americas, at theU.S. National Communicable Disease Center in At-lanta, Georgia), and recognized national influenza
laboratories, of which there are now 80 in 55 coun-tries. Of these, 16 are located in the Region of theAmericas (Argentina 2, Brazil 2, Canada 1, Chile 1,Jamaica 1, Mexico 1, United States of America 6, Uru-guay 1, and Venezuela 1).
The functions of the two international centers are asfollows:
1) To obtain, characterize, and preserve representa-tive strains from outbreaks in different parts of theworld and distribute them to research and productionlaboratories.
2) To recommend upon request, the strains thatshould be included in influenza vaccines.
3) To arrange for the training of research workersin specialized techniques.
4) In collaboration with WHO, to collect and dis-tribute information on the strains of influenza virusprevalent in different parts of the world.
5) To assist national centers in the solution of tech-nical problems.
6) To collaborate with WHO in the field and labora-tory studies.
National influenza centers are designated by nationalhealth authorities and are recognized by WHO on thebasis of technical ability, willingness to send firstly iso-lated strains to one of the international influenza cen-ters, and willingness to send virological and epidemio-logical information to WHO and the internationalcenters.
Epidemics, Outbreaks, and Virus
As in previous years, the Organization continued toassist the countries of the Hemisphere by providinginformation on influenza outbreaks throughout theworld, reagents for early diagnosis of the disease, tech-nical assistance for control activities, and in certaininstances, vaccines.
The epidemics reported to WHO during the periodOctober 1965 to September 1966 were of small tomoderate extent. The clinical forms of this diseasewere generally mild. In this Region, strains of virus A2were isolated from Canada, Panama, the United Statesof America, and Venezuela. Virus B was isolated fromArgentina, Canada, and the United States. Only sero-logic evidence of virus A2 was obtained in Trinidad andTobago. Periods of increased influenza morbidity,without laboratory confirmation, were reported by ElSalvador, Guatemala, and Honduras.
Laboratory studies of the antigenic evolution of virusA2 showed gradual shifts away from the 1957 proto-type. The strains isolated during the 1965-1966 influ-enza season constituted a relatively homogenous group,
74

SANTIAGO
BRISTOL
MEXICO CITY
BOGOTA
RIBEIRAO PRETO
Sio PAULO
LIMA
LA PLATA
CARACAS
SAN FRANCISCO
CAUl
GUATEMALA CITY
MAtE
DEATHS PER 100,000
0 20 40 60 0O, . ¡ V , i ,
=INFLUENZA ANO PHEUMONIA
= BRONCHITIS
FEMALE
POPULATION
0 20 40 60
" .....1 .... .; 1
M, ASTHMA
M OTHER
Fig. 28. Annual age-adiusted death rates from influenza andpneumonia, bronchitis, asthma, and other respiratory diseasesper 100,000 population. by sex, at 15-74 years, in each city,1962-1964.
and were readily differentiated from the variants foundbefore 1962.
In 1967 epidemics of influenza-like disease werereported in Argentina, Canada, Chile, Jamaica, Trini-dad and Tobago, and the United States. As in theprevious epidemic season, the disease was generallymild.
In the United States outbreaks of influenza-like dis-ease were reported in 29 of the 37 states in the easternand central regions of the country. Although outbreakswere reported from Colorado, Montana, New Mexico,Utah, and Wyoming, activity in that mountain regiondid not appear to be widespread as in the eastern andcentral states.
Laboratory studies indicated that the prevalentviruses in 1967 constituted a homogenous group ofstrains related to the isolates from the 1966-1967season.
Influenza viruses are known to undergo continualantigenic change. Minor variations, as discerned bylaboratory procedures, occur frequently. Moderatechanges can result in increased number of influenzacases, presumably on the basis of the population'sheightened susceptibility to the variant. Major anti-genic shifts occur infrequently. When they do, theymay produce widespread or even pandemic disease, asin 1957 when the A2 (Asian) strain first appeared.
Hong Kong Strain. In 1968 a new strain of influenzaappeared. The first outbreak caused by this new strainof influenza virus A2/Hong Kong/68 was reported inmid-July by the health authorities in Hong Kong and
the virus was isolated by the National Influenza Centerthere. The strain was immediately dispatched to theWHO World Influenza Center, Mill Hill, London,where it was found to be sufficiently different fromprevious strains of the A2 virus to inform WHO Head-quarters that the WHO influenza emergency plan shouldbe put into action.
Each of the 80 National Influenza Centers which co-operate with WHO in 55 countries were immediatelyinformed about the emergence of the new strain and itsavailability at the World Influenza Center and theInternational Influenza Center for the Americas fordistribution to them and to vaccine producers andlaboratories interested in working with it.
The Hong Kong strain of influenza virus A2 causeda very large epidemic in Hong Kong and spread rapidlyto countries as far as India and the northern territoryof Australia, as had happened in the 1957 epidemic.Later its progress slowed down, but epidemics occurredin many countries of the northern hemisphere in thewinter 1968-1969. In all these countries, except theUnited States, the disease was mild and not associatedwith a large increase in deaths. In the United States,however, the number of "excess deaths" was similar tothe number in 1957-1958. This experience of wide-spread infection associated with a high level of excessmortality was unique. It did not occur in the othertemperate-climate countries in the Americas. Canada,for example, experienced a relatively slight increase inincidence of disease and practically no excess deaths.
With the exception of Canada, the United States,and Puerto Rico, no outbreaks of influenza caused bythe Hong Kong strain were reported in the Americasduring 1968.
Low levels of antibodies against the A2/Hong Kong/68 strain were demonstrated in 1968 in the sera of per-sons who had documented influenza during the previousepidemic. Similar observations were made in a groupof persons vaccinated with the previously availablecommercial vaccines.
Because the new strain differed quite considerablyfrom the older A2 strain, which it displaced, previouslyexisting supplies of vaccine A2 Singapore provided littleprotection against the Hong Kong strain.
Thanks to early warning given through the WHOnetwork of influenza centers, biological products labora-tories were able to set up their production lines quickly.
The Organization kept the Governments continuouslyinformed about the development of the epidemicthrough cables and the Weekly Epidemiological Report,and provided them with viral reagents for the earlydiagnosis of influenza, strains of A2/Hong Kong/68virus for the preparation of vaccines, assistance in
75
�S�E$�h��:�
g�g�-�
9g�i��
�WI�o��j��g�-·f��
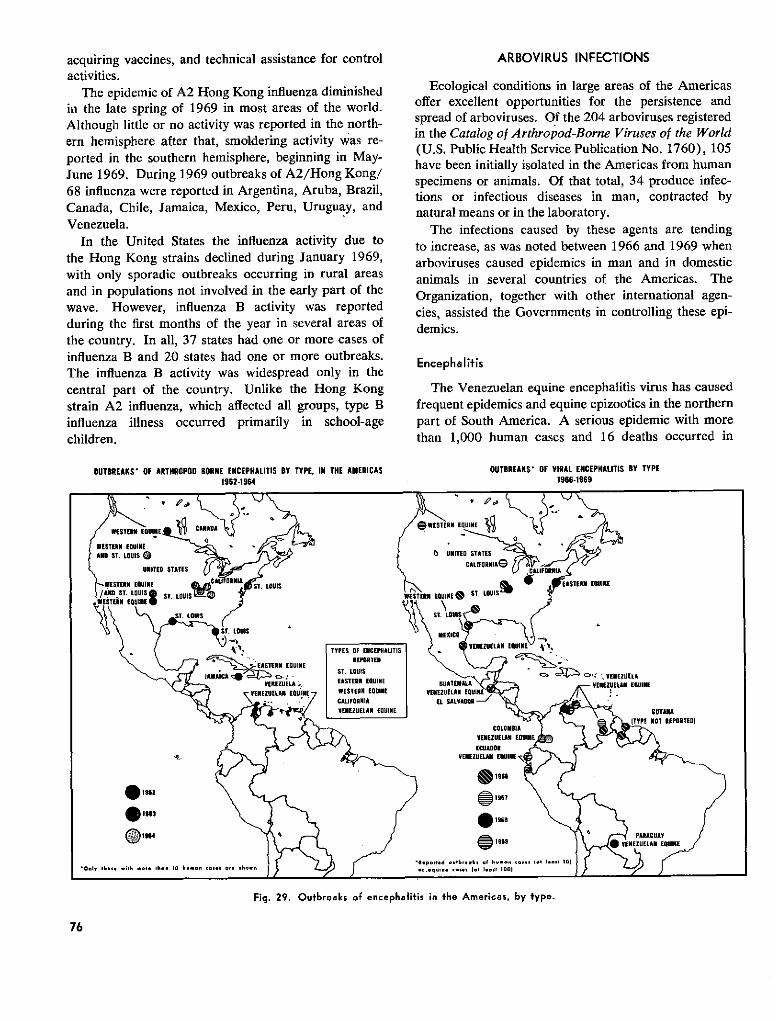
acquiring vaccines, and technical assistance for controlactivities.
The epidemic of A2 Hong Kong influenza diminishedin the late spring of 1969 in most areas of the world.Although little or no activity was reported in the north-ern hemisphere after that, smoldering activity was re-ported in the southern hemisphere, beginning in May-June 1969. During 1969 outbreaks of A2/Hong Kong/68 influenza were reported in Argentina, Aruba, Brazil,Canada, Chile, Jamaica, Mexico, Peru, Uruguay, andVenezuela.
In the United States the influenza activity due tothe Hong Kong strains declined during January 1969,with only sporadic outbreaks occurring in rural areasand in populations not involved in the early part of thewave. However, influenza B activity was reportedduring the first months of the year in several areas ofthe country. In all, 37 states had one or more cases ofinfluenza B and 20 states had one or more outbreaks.The influenza B activity was widespread only in thecentral part of the country. Unlike the Hong Kongstrain A2 influenza, which affected all groups, type Binfluenza illness occurred primarily in school-agechildren.
OUTBREAKS' OF ARTHROPOD BORNE ENCEPHALITIS BY TYPE, IN THE AMERICAS1962-1964
ARBOVIRUS INFECTIONS
Ecological conditions in large areas of the Americasoffer excellent opportunities for the persistence andspread of arboviruses. Of the 204 arboviruses registeredin the Catalog of Arthropod-Borne Viruses of the World(U.S. Public Health Service Publication No. 1760), 105have been initially isolated in the Americas from humanspecimens or animals. Of that total, 34 produce infec-tions or infectious diseases in man, contracted bynatural means or in the laboratory.
The infections caused by these agents are tendingto increase, as was noted between 1966 and 1969 whenarboviruses caused epidemics in man and in domesticanimals in several countries of the Americas. TheOrganization, together with other international agen-cies, assisted the Governments in controlling these epi-demics.
Encephalifis
The Venezuelan equine encephalitis virus has causedfrequent epidemics and equine epizootics in the northernpart of South America. A serious epidemic with morethan 1,000 human cases and 16 deaths occurred in
OUTBREAKS' OF VIRAL ENCEPHALITIS BY TYPE1966-1969
Fig. 29. Outbreaks of encephalitis in the Americas, by type.
76
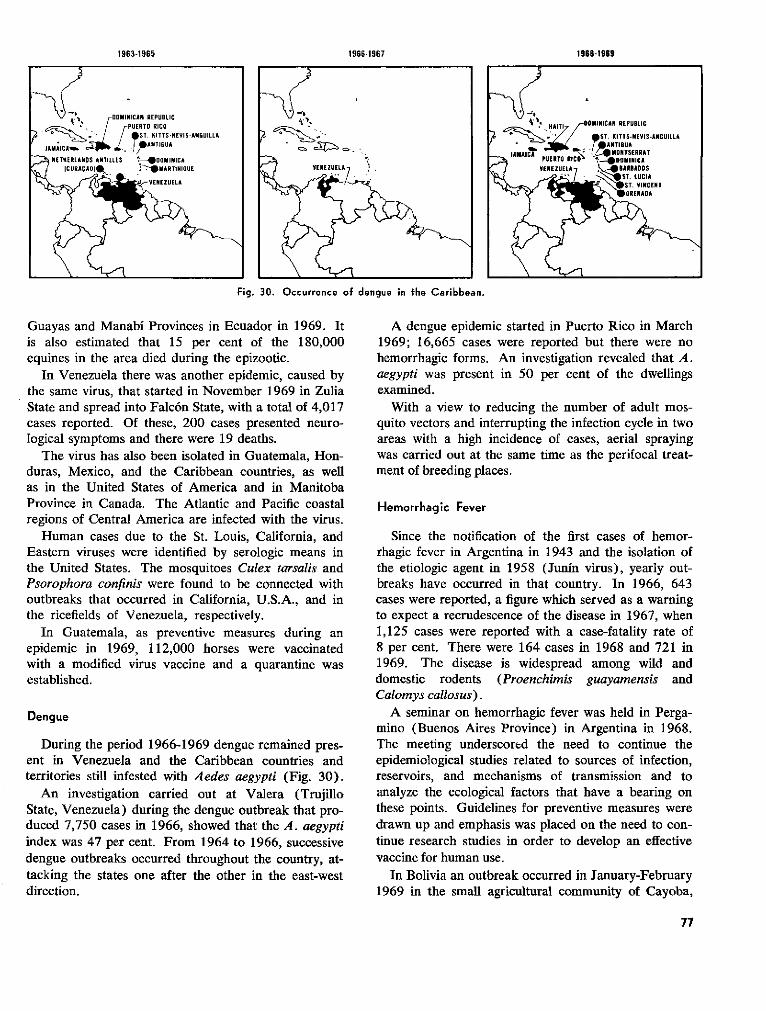
1966-1967
Fig. 30. Occurrence of dengue in the Caribbean.
Guayas and Manabí Provinces in Ecuador in 1969. Itis also estimated that 15 per cent of the 180,000equines in the area died during the epizootic.
In Venezuela there was another epidemic, caused bythe same virus, that started in November 1969 in ZuliaState and spread into Falcón State, with a total of 4,017cases reported. Of these, 200 cases presented neuro-logical symptoms and there were 19 deaths.
The virus has also been isolated in Guatemala, Hon-duras, Mexico, and the Caribbean countries, as wellas in the United States of America and in ManitobaProvince in Canada. The Atlantic and Pacific coastalregions of Central America are infected with the virus.
Human cases due to the St. Louis, California, andEastern viruses were identified by serologic means inthe United States. The mosquitoes Culex tarsalis andPsorophora confinis were found to be connected withoutbreaks that occurred in California, U.S.A., and inthe ricefields of Venezuela, respectively.
In Guatemala, as preventive measures during anepidemic in 1969, 112,000 horses were vaccinatedwith a modified virus vaccine and a quarantine wasestablished.
Dengue
During the period 1966-1969 dengue remained pres-ent in Venezuela and the Caribbean countries andterritories still infested with Aedes aegypti (Fig. 30).
An investigation carried out at Valera (TrujilloState, Venezuela) during the dengue outbreak that pro-duced 7,750 cases in 1966, showed that the A. aegyptiindex was 47 per cent. From 1964 to 1966, successivedengue outbreaks occurred throughout the country, at-tacking the states one after the other in the east-westdirection.
A dengue epidemic started in Puerto Rico in March1969; 16,665 cases were reported but there were nohemorrhagic forms. An investigation revealed that A.aegypti was present in 50 per cent of the dwellingsexamined.
With a view to reducing the number of adult mos-quito vectors and interrupting the infection cycle in twoareas with a high incidence of cases, aerial sprayingwas carried out at the same time as the perifocal treat-ment of breeding places.
Hemorrhagic Fever
Since the notification of the first cases of hemor-rhagic fever in Argentina in 1943 and the isolation ofthe etiologic agent in 1958 (Junín virus), yearly out-breaks have occurred in that country. In 1966, 643cases were reported, a figure which served as a warningto expect a recrudescence of the disease in 1967, when1,125 cases were reported with a case-fatality rate of8 per cent. There were 164 cases in 1968 and 721 in1969. The disease is widespread among wild anddomestic rodents (Proenchimis guayamensis andCalomys callosus).
A seminar on hemorrhagic fever was held in Perga-mino (Buenos Aires Province) in Argentina in 1968.The meeting underscortd the need to continue theepidemiological studies related to sources of infection,reservoirs, and mechanisms of transmission and toanalyze the ecological factors that have a bearing onthese points. Guidelines for preventive measures weredrawn up and emphasis was placed on the need to con-tinue research studies in order to develop an effectivevaccine for human use.
In Bolivia an outbreak occurred in January-February1969 in the small agricultural community of Cayoba,
77
1963-1965 1968-1969
25 miles north of Magdalena, in Beni Department.There were 10 cases with six deaths. The Machupovirus was isolated in the rodents Calomys callosus cap-tured underneath the houses. During the outbreak 100inhabitants fled and the rest were transferred to anotherarea to permit extermination of the rodents at Cayoba.The rodent population rises during the corn harvest, afact that is frequently linked with the outbreaks. In1968 an earlier date was set for the corn harvest andthis resulted in the outbreak also occurring earlier,hence reconfirming the generally held view that therodents are virtual reservoirs of the disease.
PARASITIC DISEASES
The parasitic diseases are among the most importantpublic health problems in the Americas. From the pointof view of both public health and economic develop-ment, parasitic diseases stand out as massive problemswhich remain essentially unsolved. They create a tre-mendous drain on the health and economic efficiencyof a large part of the population in almost all countriesof the Americas. They also affect the health of domesticanimals and so have an important influence on the foodsupply and the general level of human nutrition. Thusthe parasitic diseases are important handicaps to pro-grams for social and economic progress.
The magnitude of the problem is evident from rec-ords of prevalence of the more important diseases inthis category. In a recent report the approximate num-ber of persons in Brazil with schistosomiasis was statedto be over 6 million. Of this number, about 1.5 mil-lion are partially disabled by the disease and 119,000totally disabled. The economic loss due to this dis-ability is great; according to one estimate it exceeds$60 million per year. Over-all data for Chagas' diseaseare not available, but in Venezuela about 20 per cent ofthe rural population is infected and of these about half,or 280,000 persons, have significant heart damage dueto the infection. In those infected persons, heart diseasewas four times more common than in uninfected per-sons of the same area.
In Argentina 400,000 persons currently have signifi-cant heart damage due to the disease. Up to 82 percent of the heart lesions found in sampled populationswere due to Chagas' disease.
Schistosomiasis and Chagas' disease have been givenpriority in the Organization's parasitic diseases programbecause they produce the greatest amount of injury.Other parasitic diseases also take their toll, however.Onchocerciasis affects a significant portion of the popu-lation in Mexico, Guatemala, and Venezuela. Toxo-plasmosis is undoubtedly of great importance in manycountries. Leishmaniasis in its various forms occurs in
numerous areas. Amebiasis, cysticercosis, and theintestinal worms also demand attention because of themorbidity they cause.
Although national programs vary greatly with respectto the relative emphasis they place on the parasiticdiseases, it can be said without hesitation that thesediseases are almost universally underestimated. Whilestriking progress has been made against some of themore important communicable diseases in recent years,very little real progress has been made against theparasitic diseases.
During the past four years there has been an increasein interest in the parasitic diseases and a greater recog-nition of their importance and of the need to controlthem. There has also been considerable progress inthe development of more effective control measures.Nevertheless, it must be admitted that there has beenlittle increase in the size and scope of national programsand little concrete evidence that most countries areready to give higher priority to control of the parasiticdiseases, even when they have been clearly demon-strated to be national scourges of great social and eco-nomic significance.
One reason often given for the weakness of anti-parasitic programs has been the purported lack ofeffective and economical means to control them. To adegree this has been justified in the past, but advancesin knowledge have begun to make that point of viewobsolete, at least for some of the parasites.
The program of the Organization has been designedprimarily to stimulate countries to improve their con-trol programs. In order to assist progress in thatdirection, encouragement has also been given to im-provement in collection of prevalence and morbiditydata and in procedures for evaluation of control pro-grams. In addition, support has been given to programsfor training, exchange of technical information, andresearch related to control programs.
A Regional Adviser on Parasitic Diseases was placedon the staff of the Organization to plan and coordinatethe program in this field.
As part of a broad program to increase the ex-change of technical information among workers in theAmericas, publications and references on the principalproblems in this field were collected and selected infor-mation was distributed. One of the projects of this typeincluded the distribution of information and materialsfor the Kato thick-film technique for the diagnosis ofintestinal worm infections and schistosomiasis. Thetechnique is rapid, easy, accurate, and inexpensive,and is being recommended for routine laboratory diag-nosis and for survey and evaluation work.
78
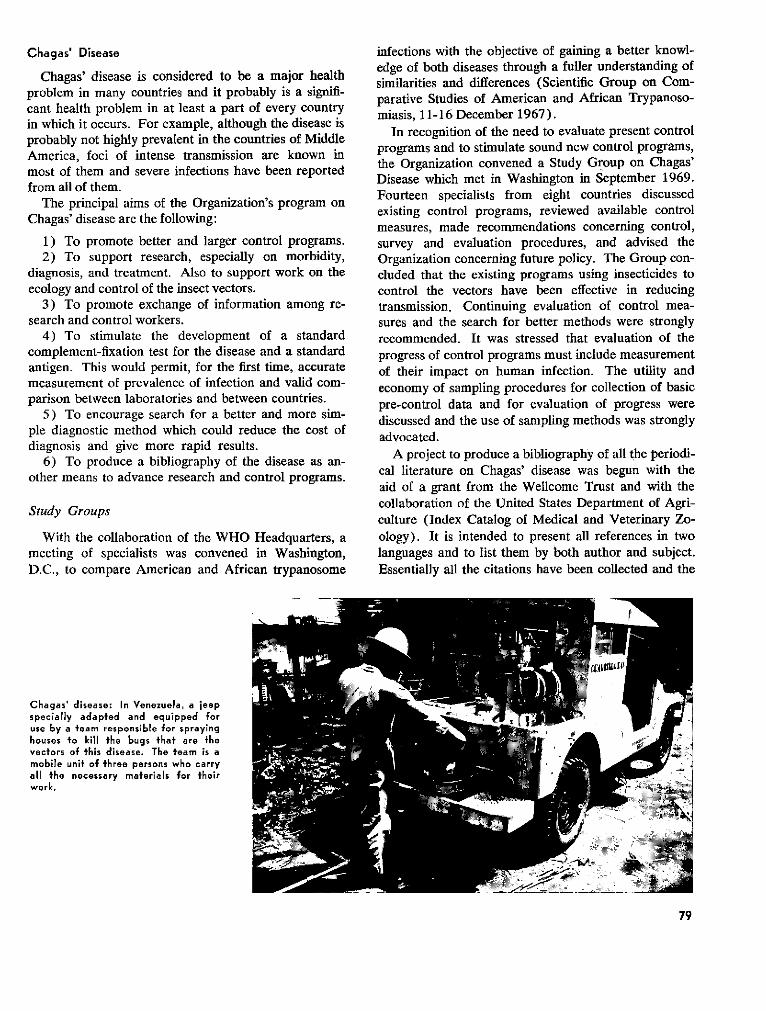
Chagas' Disease
Chagas' disease is considered to be a major healthproblem in many countries and it probably is a signifi-cant health problem in at least a part of every countryin which it occurs. For example, although the disease isprobably not highly prevalent in the countries of MiddleAmerica, foci of intense transmission are known inmost of them and severe infections have been reportedfrom all of them.
The principal aims of the Organization's program onChagas' disease are the following:
1) To promote better and larger control programs.2) To support research, especially on morbidity,
diagnosis, and treatment. Also to support work on theecology and control of the insect vectors.
3) To promote exchange of information among re-search and control workers.
4) To stimulate the development of a standardcomplement-fixation test for the disease and a standardantigen. This would permit, for the first time, accuratemeasurement of prevalence of infection and valid com-parison between laboratories and between countries.
5) To encourage search for a better and more sim-ple diagnostic method which could reduce the cost ofdiagnosis and give more rapid results.
6) To produce a bibliography of the disease as an-other means to advance research and control programs.
Study Groups
With the collaboration of the WHO Headquarters, ameeting of specialists was convened in Washington,D.C., to compare American and African trypanosome
Chagas' disease: In Venezuela, a jeepspecially adapted and equipped foruse by a team responsible for sprayinghouses to kill the bugs that are thevectors of this disease. The team is amobile unit of three persons who carryall the necessary materiais for theirwork.
infections with the objective of gaining a better knowl-edge of both diseases through a fuller understanding ofsimilarities and differences (Scientific Group on Com-parative Studies of American and African Trypanoso-miasis, 11-16 December 1967).
In recognition of the need to evaluate present controlprograms and to stimulate sound new control programs,the Organization convened a Study Group on Chagas'Disease which met in Washington in September 1969.Fourteen specialists from eight countries discussedexisting control programs, reviewed available controlmeasures, made recommendations concerning control,survey and evaluation procedures, and advised theOrganization concerning future policy. The Group con-cluded that the existing programs using insecticides tocontrol the vectors have been effective in reducingtransmission. Continuing evaluation of control mea-sures and the search for better methods were stronglyrecommended. It was stressed that evaluation of theprogress of control programs must include measurementof their impact on human infection. The utility andeconomy of sampling procedures for collection of basicpre-control data and for evaluation of progress werediscussed and the use of sampling methods was stronglyadvocated.
A project to produce a bibliography of all the periodi-cal literature on Chagas' disease was begun with theaid of a grant from the Wellcome Trust and with thecollaboration of the United States Department of Agri-culture (Index Catalog of Medical and Veterinary Zo-ology). It is intended to present all references in twolanguages and to list them by both author and subject.Essentially all the citations have been collected and the
79
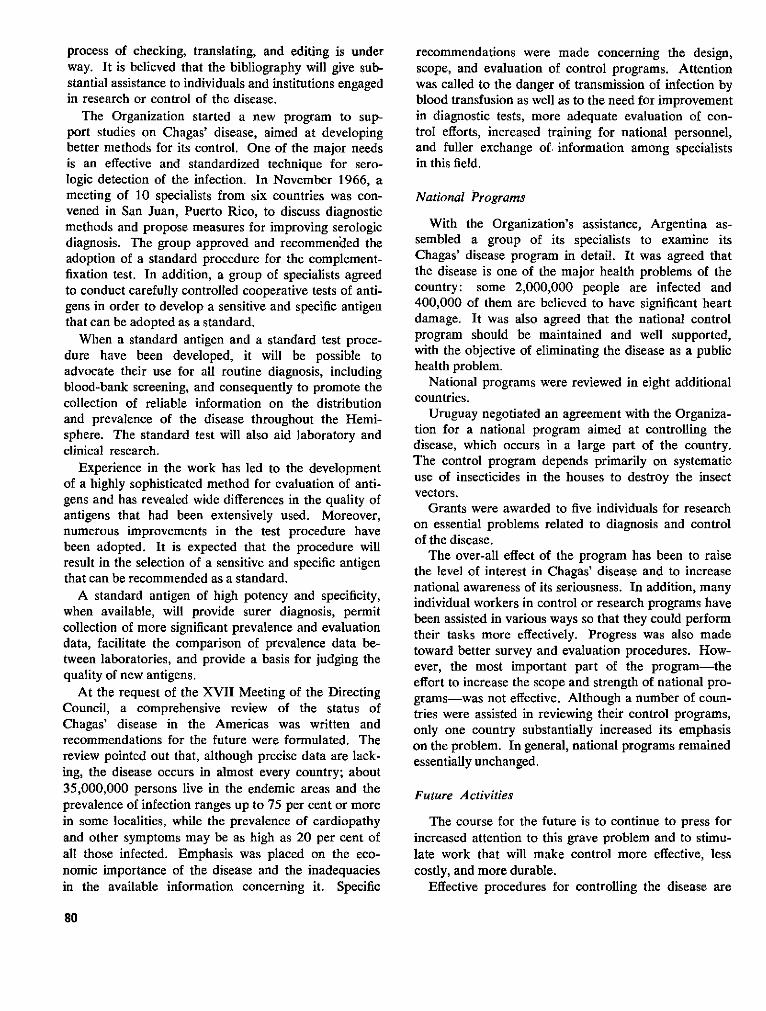
process of checking, translating, and editing is underway. It is believed that the bibliography will give sub-stantial assistance to individuals and institutions engagedin research or control of the disease.
The Organization started a new program to sup-port studies on Chagas' disease, aimed at developingbetter methods for its control. One of the major needsis an effective and standardized technique for sero-logic detection of the infection. In November 1966, ameeting of 10 specialists from six countries was con-vened in San Juan, Puerto Rico, to discuss diagnosticmethods and propose measures for improving serologicdiagnosis. The group approved and recommended theadoption of a standard procedure for the complement-fixation test. In addition, a group of specialists agreedto conduct carefully controlled cooperative tests of anti-gens in order to develop a sensitive and specific antigenthat can be adopted as a standard.
When a standard antigen and a standard test proce-dure have been developed, it will be possible toadvocate their use for all routine diagnosis, includingblood-bank screening, and consequently to promote thecollection of reliable information on the distributionand prevalence of the disease throughout the Hemi-sphere. The standard test will also aid laboratory andclinical research.
Experience in the work has led to the developmentof a highly sophisticated method for evaluation of anti-gens and has revealed wide differences in the quality ofantigens that had been extensively used. Moreover,numerous improvements in the test procedure havebeen adopted. It is expected that the procedure willresult in the selection of a sensitive and specific antigenthat can be recommended as a standard.
A standard antigen of high potency and specificity,when available, will provide surer diagnosis, permitcollection of more significant prevalence and evaluationdata, facilitate the comparison of prevalence data be-tween laboratories, and provide a basis for judging thequality of new antigens.
At the request of the XVII Meeting of the DirectingCouncil, a comprehensive review of the status ofChagas' disease in the Americas was written andrecommendations for the future were formulated. Thereview pointed out that, although precise data are lack-ing, the disease occurs in almost every country; about35,000,000 persons live in the endemic areas and theprevalence of infection ranges up to 75 per cent or morein some localities, while the prevalence of cardiopathyand other symptoms may be as high as 20 per cent ofall those infected. Emphasis was placed on the eco-nomic importance of the disease and the inadequaciesin the available information concerning it. Specific
recommendations were made concerning the design,scope, and evaluation of control programs. Attentionwas called to the danger of transmission of infection byblood transfusion as well as to the need for improvementin diagnostic tests, more adequate evaluation of con-trol efforts, increased training for national personnel,and fuller exchange of. information among specialistsin this field.
National Programs
With the Organization's assistance, Argentina as-sembled a group of its specialists to examine itsChagas' disease program in detail. It was agreed thatthe disease is one of the major health problems of thecountry: some 2,000,000 people are infected and400,000 of them are believed to have significant heartdamage. It was also agreed that the national controlprogram should be maintained and well supported,with the objective of eliminating the disease as a publichealth problem.
National programs were reviewed in eight additionalcountries.
Uruguay negotiated an agreement with the Organiza-tion for a national program aimed at controlling thedisease, which occurs in a large part of the country.The control program depends primarily on systematicuse of insecticides in the houses to destroy the insectvectors.
Grants were awarded to five individuals for researchon essential problems related to diagnosis and controlof the disease.
The over-all effect of the program has been to raisethe level of interest in Chagas' disease and to increasenational awareness of its seriousness. In addition, manyindividual workers in control or research programs havebeen assisted in various ways so that they could performtheir tasks more effectively. Progress was also madetoward better survey and evaluation procedures. How-ever, the most important part of the program-theeffort to increase the scope and strength of national pro-grams-was not effective. Although a number of coun-tries were assisted in reviewing their control programs,only one country substantially increased its emphasison the problem. In general, national programs remainedessentially unchanged.
Future Activities
The course for the future is to continue to press forincreased attention to this grave problem and to stimu-late work that will make control more effective, lesscostly, and more durable.
Effective procedures for controlling the disease are
80
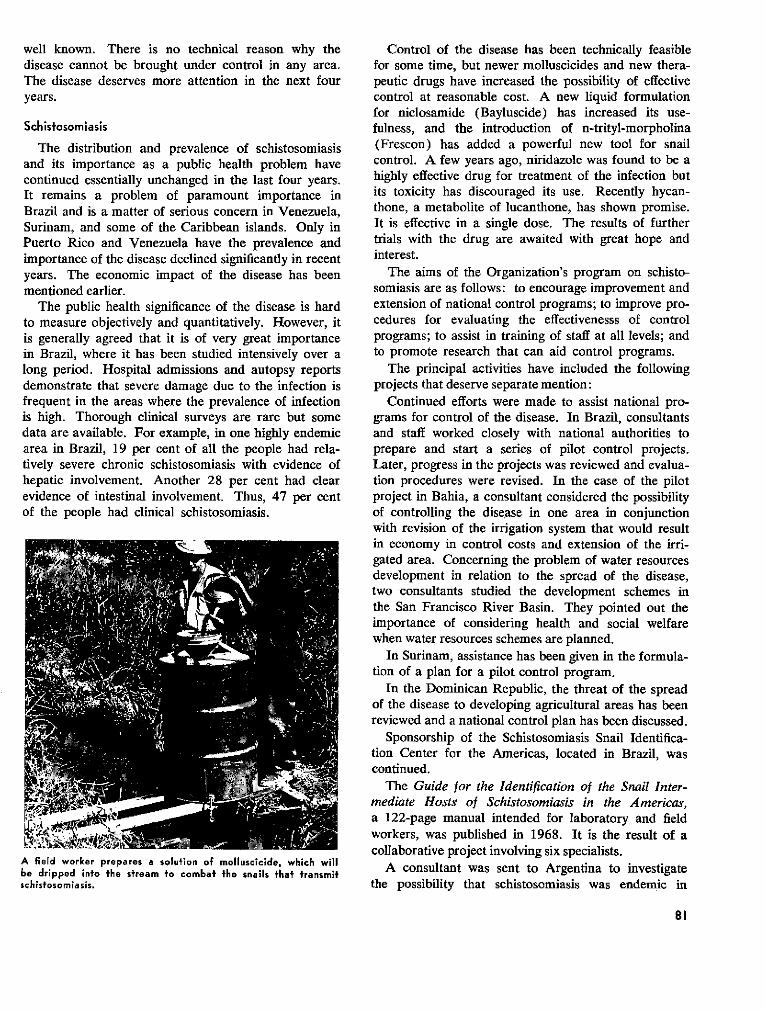
well known. There is no technical reason why thedisease cannot be brought under control in any area.The disease deserves more attention in the next fouryears.
Schistosomiasis
The distribution and prevalence of schistosomiasisand its importance as a public health problem havecontinued essentially unchanged in the last four years.It remains a problem of paramount importance inBrazil and is a matter of serious concern in Venezuela,Surinam, and some of the Caribbean islands. Only inPuerto Rico and Venezuela have the prevalence andimportance of the disease declined significantly in recentyears. The economic impact of the disease has beenmentioned earlier.
The public health significance of the disease is hardto measure objectively and quantitatively. However, itis generally agreed that it is of very great importancein Brazil, where it has been studied intensively over along period. Hospital admissions and autopsy reportsdemonstrate that severe damage due to the infection isfrequent in the areas where the prevalence of infectionis high. Thorough clinical surveys are rare but somedata are available. For example, in one highly endemicarea in Brazil, 19 per cent of all the people had rela-tively severe chronic schistosomiasis with evidence ofhepatic involvement. Another 28 per cent had clearevidence of intestinal involvement. Thus, 47 per centof the people had clinical schistosomiasis.
A field worker prepares a solution of molluscicide, which willbe dripped into fhe stream to combat the snails that transmitschistosomiasis.
Control of the disease has been technically feasiblefor some time, but newer molluscicides and new thera-peutic drugs have increased the possibility of effectivecontrol at reasonable cost. A new liquid formulationfor niclosamide (Bayluscide) has increased its use-fulness, and the introduction of n-trityl-morpholina(Frescon) has added a powerful new tool for snailcontrol. A few years ago, niridazole was found to be ahighly effective drug for treatment of the infection butits toxicity has discouraged its use. Recently hycan-thone, a metabolite of lucanthone, has shown promise.It is effective in a single dose. The results of furthertrials with the drug are awaited with great hope andinterest.
The aims of the Organization's program on schisto-somiasis are as follows: to encourage improvement andextension of national control programs; to improve pro-cedures for evaluating the effectivenesss of controlprograms; to assist in training of staff at all levels; andto promote research that can aid control programs.
The principal activities have included the followingprojects that deserve separate mention:
Continued efforts were made to assist national pro-grams for control of the disease. In Brazil, consultantsand staff worked closely with national authorities toprepare and start a series of pilot control projects.Later, progress in the projects was reviewed and evalua-tion procedures were revised. In the case of the pilotproject in Bahia, a consultant considered the possibilityof controlling the disease in one area in conjunctionwith revision of the irrigation system that would resultin economy in control costs and extension of the irri-gated area. Concerning the problem of water resourcesdevelopment in relation to the spread of the disease,two consultants studied the development schemes inthe San Francisco River Basin. They pointed out theimportance of considering health and social welfarewhen water resources schemes are planned.
In Surinam, assistance has been given in the formula-tion of a plan for a pilot control program.
In the Dominican Republic, the threat of the spreadof the disease to developing agricultural areas has beenreviewed and a national control plan has been discussed.
Sponsorship of the Schistosomiasis Snail Identifica-tion Center for the Americas, located in Brazil, wascontinued.
The Guide for the Identification of the Snail Inter-mediate Hosts of Schistosomiasis in the Americas,a 122-page manual intended for laboratory and fieldworkers, was published in 1968. It is the result of acollaborative project involving six specialists.
A consultant was sent to Argentina to investigatethe possibility that schistosomiasis was endemic in
81
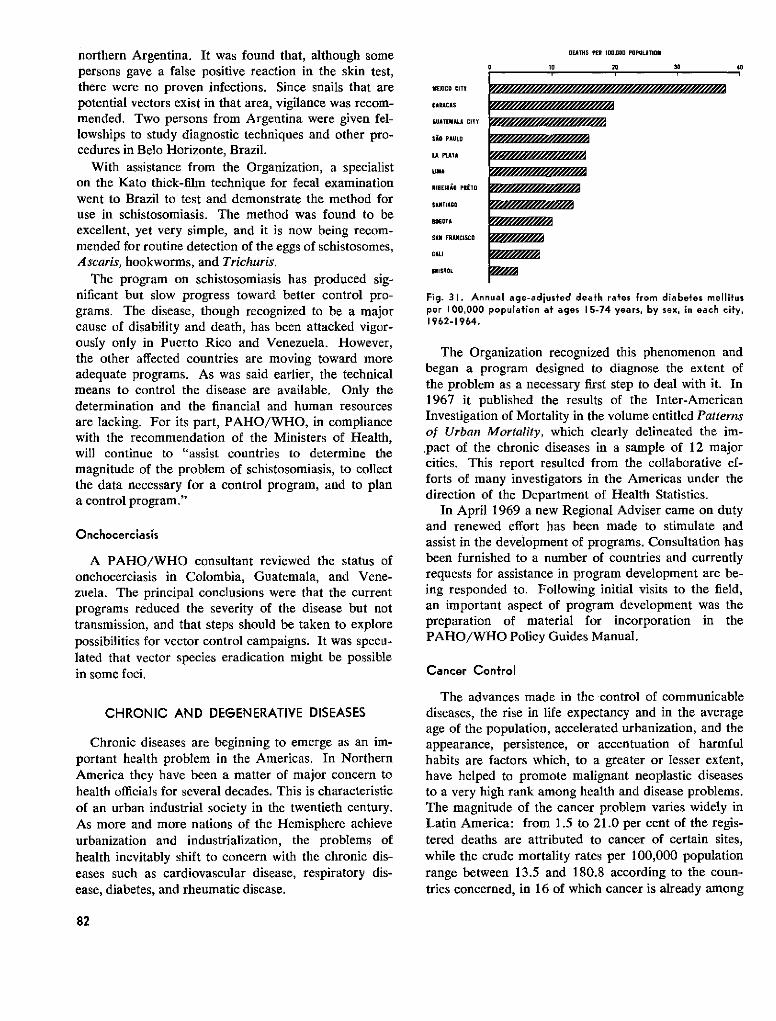
northern Argentina. It was found that, although somepersons gave a false positive reaction in the skin test,there were no proven infections. Since snails that arepotential vectors exist in that area, vigilance was recom-mended. Two persons from Argentina were given fel-lowships to study diagnostic techniques and other pro-cedures in Belo Horizonte, Brazil.
With assistance from the Organization, a specialiston the Kato thick-film technique for fecal examinationwent to Brazil to test and demonstrate the method foruse in schistosomiasis. The method was found to beexcellent, yet very simple, and it is now being recom-mended for routine detection of the eggs of schistosomes,Ascaris, hookworms, and Trichuris.
The program on schistosomiasis has produced sig-nificant but slow progress toward better control pro-grams. The disease, though recognized to be a majorcause of disability and death, has been attacked vigor-ously only in Puerto Rico and Venezuela. However,the other affected countries are moving toward moreadequate programs. As was said earlier, the technicalmeans to control the disease are available. Only thedetermination and the financial and human resourcesare lacking. For its part, PAHO/WHO, in compliancewith the recommendation of the Ministers of Health,will continue to "assist countries to determine themagnitude of the problem of schistosomiasis, to collectthe data necessary for a control program, and to plana control program."
Onchocerciasís
A PAHO/WHO consultant reviewed the status ofonchocerciasis in Colombia, Guatemala, and Vene-zuela. The principal conclusions were that the currentprograms reduced the severity of the disease but nottransmission, and that steps should be taken to explorepossibilities for vector control campaigns. It was specu-lated that vector species eradication might be possiblein some foci.
CHRONIC AND DEGENERATIVE DISEASES
Chronic diseases are beginning to emerge as an im-portant health problem in the Americas. In NorthernAmerica they have been a matter of major concern tohealth officials for several decades. This is characteristicof an urban industrial society in the twentieth century.As more and more nations of the Hemisphere achieveurbanization and industrialization, the problems ofhealth inevitably shift to concern with the chronic dis-eases such as cardiovascular disease, respiratory dis-ease, diabetes, and rheumatic disease.
MEXICO CITY
CARACAS
GUATEMALA CITY
Si0 PAULO
LA PULATA
LlMA
RIBEI1RO PRÉTO
SANTIAGO
BOGOTA
SAN FRANCISCO
CALI
BRISTOL
1D
DEATHS PER I00.000 POPULATION
20 30 40
Fig. 31. Annual age-adjusted death rates from diabetes mellitusper 100,000 population at ages 15-74 years, by sex, in each city,1962-1964.
The Organization recognized this phenomenon andbegan a program designed to diagnose the extent ofthe problem as a necessary first step to deal with it. In1967 it published the results of the Inter-AmericanInvestigation of Mortality in the volume entitled Patternsof Urban Mortality, which clearly delineated the im-.pact of the chronic diseases in a sample of 12 majorcities. This report resulted from the collaborative ef-forts of many investigators in the Americas under thedirection of the Department of Health Statistics.
In April 1969 a new Regional Adviser came on dutyand renewed effort has been made to stimulate andassist in the development of programs. Consultation hasbeen furnished to a number of countries and currentlyrequests for assistance in program development are be-ing responded to. Following initial visits to the field,an important aspect of program development was thepreparation of material for incorporation in thePAHO/WHO Policy Guides Manual.
Cancer Control
The advances made in the control of communicablediseases, the rise in life expectancy and in the averageage of the population, accelerated urbanization, and theappearance, persistence, or accentuation of harmfulhabits are factors which, to a greater or lesser extent,have helped to promote malignant neoplastic diseasesto a very high rank among health and disease problems.The magnitude of the cancer problem varies widely inLatin America: from 1.5 to 21.0 per cent of the regis-tered deaths are attributed to cancer of certain sites,while the crude mortality rates per 100,000 populationrange between 13.5 and 180.8 according to the coun-tries concerned, in 16 of which cancer is already among
82
I I I I
givi9 //~7////~'7//////7//
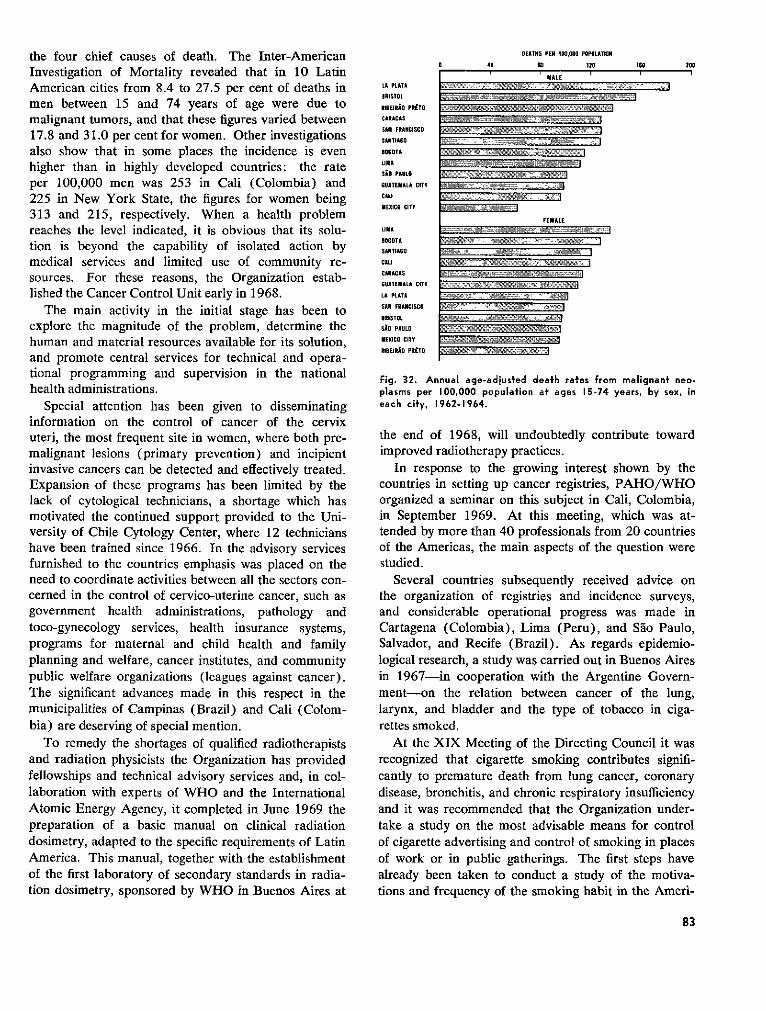
the four chief causes of death. The Inter-AmericanInvestigation of Mortality revealed that in 10 LatinAmerican cities from 8.4 to 27.5 per cent of deaths inmen between 15 and 74 years of age were due tomalignant tumors, and that these figures varied between17.8 and 31.0 per cent for women. Other investigationsalso show that in some places the incidence is evenhigher than in highly developed countries: the rateper 100,000 men was 253 in Cali (Colombia) and225 in New York State, the figures for women being313 and 215, respectively. When a health problemreaches the level indicated, it is obvious that its solu-tion is beyond the capability of isolated action bymedical services and limited use of community re-sources. For these reasons, the Organization estab-lished the Cancer Control Unit early in 1968.
The main activity in the initial stage has been toexplore the magnitude of the problem, determine thehuman and material resources available for its solution,and promote central services for technical and opera-tional programming and supervision in the nationalhealth administrations.
Special attention has been given to disseminatinginformation on the control of cancer of the cervixuteri, the most frequent site in women, where both pre-malignant lesions (primary prevention) and incipientinvasive cancers can be detected and effectively treated.Expansion of these programs has been limited by thelack of cytological technicians, a shortage which hasmotivated the continued support provided to the Uni-versity of Chile Cytology Center, where 12 technicianshave been trained since 1966. In the advisory servicesfurnished to the countries emphasis was placed on theneed to coordinate activities between all the sectors con-cerned in the control of cervico-uterine cancer, such asgovernment health administrations, pathology andtoco-gynecology services, health insurance systems,programs for maternal and child health and familyplanning and welfare, cancer institutes, and communitypublic welfare organizations (leagues against cancer).The significant advances made in this respect in themunicipalities of Campinas (Brazil) and Cali (Colom-bia) are deserving of special mention.
To remedy the shortages of qualified radiotherapistsand radiation physicists the Organization has providedfellowships and technical advisory services and, in col-laboration with experts of WHO and the InternationalAtomic Energy Agency, it completed in June 1969 thepreparation of a basic manual on clinical radiationdosimetry, adapted to the specific requirements of LatinAmerica. This manual, together with the establishmentof the first laboratory of secondary standards in radia-tion dosimetry, sponsored by WHO in Buenos Aires at
LA PLATA
SRISTOL
iIBEIRiO PRETO
CARACAS
SAN FRANCISCO
SANTIAGO
BOGOTA
LIMA
SAO PAULO
GUATEMALA CITY
CALI
MEXICO CITY
LIMA
BOGOTA
SANTIAGO
CALI
CARACAS
GUATEMALA CITY
LA PLATA
SAN FRANCISCO
BRISTOL
SAi PAULO
MEXICO CITY
RIBEIRiO PRETO
DEATHS PER 100,000 POPULATION
O 40 80 120 1S0 200
IMALE
,~ °
, - ay'
7 lx W Y WYIY
~IN^I-- 2ww 10 i --F«- -a =
~ _" ' ~' . ¥i
·Iy .» =;^ 2 i- ·:ay ·-- ·]-
]~ <·~~· 1 ·~´ 0 a mix Y 7
Fig. 32. Annual age-adjusted death rates from malignant neo-plasms per 100,000 population at ages 15-74 years, by sex, ineach city, 1962-1964.
the end of 1968, will undoubtedly contribute towardimproved radiotherapy practices.
In response to the growing interest shown by thecountries in setting up cancer registries, PAHO/WHOorganized a seminar on this subject in Cali, Colombia,in September 1969. At this meeting, which was at-tended by more than 40 professionals from 20 countriesof the Americas, the main aspects of the question werestudied.
Several countries subsequently received advice onthe organization of registries and incidence surveys,and considerable operational progress was made inCartagena (Colombia), Lima (Peru), and Sao Paulo,Salvador, and Recife (Brazil). As regards epidemio-logical research, a study was carried out in Buenos Airesin 1967-in cooperation with the Argentine Govern-ment-on the relation between cancer of the lung,larynx, and bladder and the type of tobacco in ciga-rettes smoked.
At the XIX Meeting of the Directing Council it wasrecognized that cigarette smoking contributes signifi-cantly to premature death from lung cancer, coronarydisease, bronchitis, and chronic respiratory insufficiencyand it was recommended that the Organization under-take a study on the most advisable means for controlof cigarette advertising and control of smoking in placesof work or in public gatherings. The first steps havealready been taken to conduct a study of the motiva-tions and frequency of the smoking habit in the Ameri-
83
( _ ii A .E=3= .......................... a _b.9.= .................. X
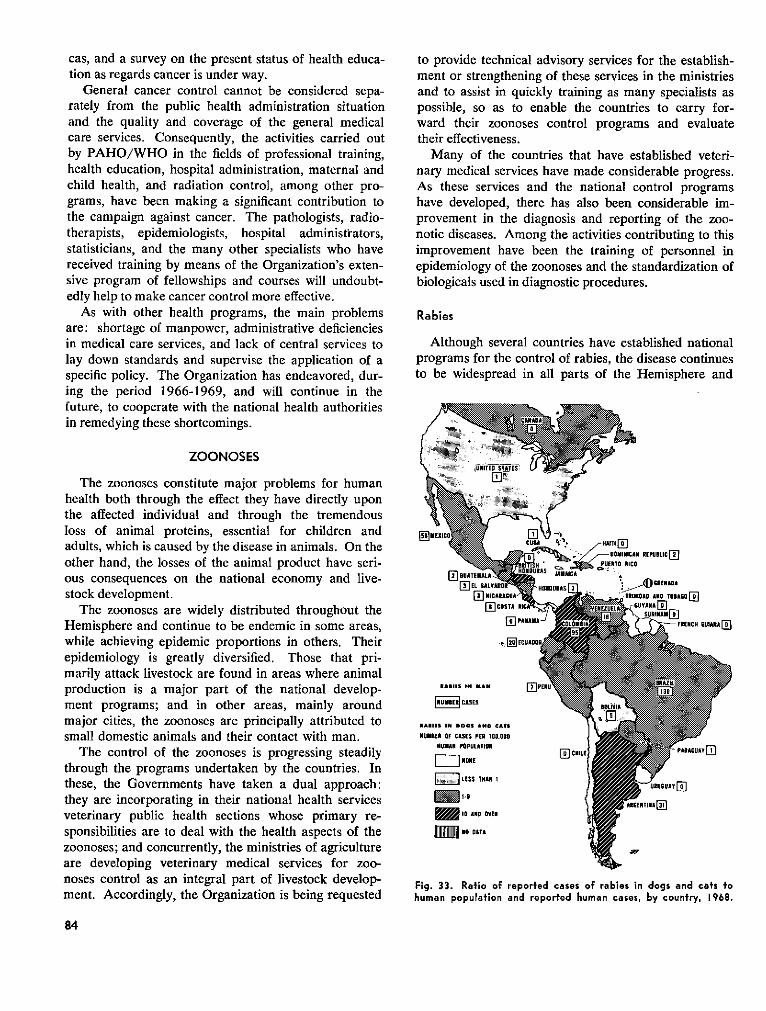
cas, and a survey on the present status of health educa-tion as regards cancer is under way.
General cancer control cannot be considered sepa-rately from the public health administration situationand the quality and coverage of the general medicalcare services. Consequently, the activities carried outby PAHO/WHO in the fields of professional training,health education, hospital administration, maternal andchild health, and radiation control, among other pro-grams, have been making a significant contribution tothe campaign against cancer. The pathologists, radio-therapists, epidemiologists, hospital administrators,statisticians, and the many other specialists who havereceived training by means of the Organization's exten-sive program of fellowships and courses will undoubt-edly help to make cancer control more effective.
As with other health programs, the main problemsare: shortage of manpower, administrative deficienciesin medical care services, and lack of central services tolay down standards and supervise the application of aspecific policy. The Organization has endeavored, dur-ing the period 1966-1969, and will continue in thefuture, to cooperate with the national health authoritiesin remedying these shortcomings.
to provide technical advisory services for the establish-ment or strengthening of these services in the ministriesand to assist in quickly training as many specialists aspossible, so as to enable the countries to carry for-ward their zoonoses control programs and evaluatetheir effectiveness.
Many of the countries that have established veteri-nary medical services have made considerable progress.As these services and the national control programshave developed, there has also been considerable im-provement in the diagnosis and reporting of the zoo-notic diseases. Among the activities contributing to thisimprovement have been the training of personnel inepidemiology of the zoonoses and the standardization ofbiologicals used in diagnostic procedures.
Rabies
Although several countries have established nationalprograms for the control of rabies, the disease continuesto be widespread in all parts of the Hemisphere and
ZOONOSES
The zoonoses constitute major problems for humanhealth both through the effect they have directly uponthe affected individual and through the tremendousloss of animal proteins, essential for children andadults, which is caused by the disease in animals. On theother hand, the losses of the animal product have seri-ous consequences on the national economy and live-stock development.
The zoonoses are widely distributed throughout theHemisphere and continue to be endemic in some areas,while achieving epidemic proportions in others. Theirepidemiology is greatly diversified. Those that pri-marily attack livestock are found in areas where animalproduction is a major part of the national develop-ment programs; and in other areas, mainly aroundmajor cities, the zoonoses are principally attributed tosmall domestic animals and their contact with man.
The control of the zoonoses is progressing steadilythrough the programs undertaken by the countries. Inthese, the Governments have taken a dual approach:they are incorporating in their national health servicesveterinary public health sections whose primary re-sponsibilities are to deal with the health aspects of thezoonoses; and concurrently, the ministries of agricultureare developing veterinary medical services for zoo-noses control as an integral part of livestock develop-ment. Accordingly, the Organization is being requested
iURITEDSTATES U
[- NICARAGUA HUN
ElTOSTA RIC
~ PANAMA-'
'. nI-EC°UA° O
AIIMS IN MAN I-lPERI
NUE CASES
e'- ¥ -HAITI E[
%"' / " DOMINICAN REPUSLICjP" OERTO RICO
JAMAICA
HDUsoSmo .iICRESNADA- .TRINIDAD ADO TOSAOI'T]
ENEZUEAiLA G<UYANA ]Ei
COLMIA, ' FRENCH GUIANA[]
AE111S IN 0005 ANO CATS
MNUMER OF CASES PER IO,OO000HUMAN POPULATION
[i LESS THAN 1 U E
Dlo AND OVER
Fig. 33. Ratio of reporfed cases of rabies in dogs and cats tohuman population and reported human cases, by country, 1968.
84
jy r 1 i'
_ ~ ~ ~~~~~~~é . -,t
Vaccination clinics as a control for urban rabies.
causes about 210 human deaths each year. The majorpublic health problem arises from the association ofdogs and humans in the urban areas, principally themajor cities. The mass migration of the populationfrom the rural to urban environments has broughtabout large increases in the dog populations in themetropolitan areas, where the dog is allowed to runfreely in search of food and reproduce without control.Canine population studies in many of the major citiesof South America have revealed an average of approxi-mately two dogs per family. This high density of thedog population contributes greatly to the frequency ofanimal bites and subsequent human cases of rabies.
In areas where adequate rabies control programs donot exist, it is not unusual for 25 per cent of the personsbitten to receive the antirabies treatment. The rabiescontrol programs usually consist of three phases. Thefirst is to conduct massive vaccination campaigns inorder to immunize the majority of the owned dogs.The second is to capture and sacrifice as many of thestray dogs as possible with the aim of reducing theirnumber to the level where transmission of the virus isgreatly diminished. In the third phase, animals thathave bitten persons are held for clinical observation todetermine whether they have rabies.
One of the more significant programs in the controlof canine rabies has been the project designed to con-trol the disease in dogs in 12 cities on the Mexico-United States border. This project, initiated in January1966, has set as its objective the progressive reductionof canine rabies in this border area over a five-yearperiod, until it is eventually eliminated. An evaluationof the project in 1969 revealed some significant achieve-
ments. In the three years of its operation no humancases of rabies have been reported. Epidemics ofcanine rabies have been eliminated, and cases in dogshave been reduced to a negligible number. More than80 per cent of the owned dogs have been vaccinatedand about 30 per cent of the estimated number of un-vaccinated dogs have been captured and sacrificed.One of the most outstanding results has been thetremendous reduction in the number of bitten personsreceiving the antirabies treatment. In some cities thisnumber has been reduced to well under 19 per cent, afact which indicates the effectiveness of the captureand observation of the biting animals and the extentto which the need for indiscriminate use of the anti-rabies treatment has been reduced.
The second aspect of the rabies problem in the Amer-icas is that concerned with wildlife, including bats andterrestrial mammals.
A major wildlife problem has existed in Grenada,where the mongoose is the principal reservoir andvector of rabies. The Organization has been providingassistance in Grenada's program since 1966 throughthe services of short-term consultants, training of per-sonnel for field and laboratory services, and provisionof supplies and equipment. With the implementation ofrecommendations made by the consultants, the rabiescontrol program has been progressing satisfactorily.With respect to the public health aspects, no humancases of rabies have been reported and the cases in dogshave been virtually eliminated. A program of vaccina-tion of dogs and elimination of stray dogs has beenfunctioning properly. A rabies diagnostic service wasestablished on the island, but the problem in wildlife
85
is still a major concern. Since the control of this situa-tion requires constant and expensive efforts to keep themongoose population down to a level where the dis-ease will not be transmitted to domestic animals andto man, constant poison-bait programs have been ineffect. Ecological studies of the mongoose have beenundertaken to determine means for preventing transmis-sion of the disease within this population.
Although there has been an increase in the numberof national programs to control rabies, an expansion ofdiagnostic and reporting services, and a greater effortby health authorities to control the problem in urbanareas, the incidence of rabies continues to rise in theAmericas. During the four-year period, PAHO/WHOconsultants assisted the health authorities of Argentina,Brazil, Grenada, Peru, Uruguay, and several CentralAmerican countries with the planning and developmentof control programs. The Organization also sponsoredmany courses on the epidemiology, diagnosis, and con-trol of rabies in several countries and in the Pan Ameri-can Zoonoses Center. In September 1967, the FirstInternational Seminar on Rabies in the Americas washeld at the Center in Buenos Aires, under the jointsponsorship of the Argentine Government and theOrganization. There were 102 participants from mostof the countries of the Hemisphere and representativesfrom some European countries attended as observers.Through the cooperative efforts of the health authori-ties of the countries and the Pan American ZoonosesCenter, the Rabies Surveillance System for the Ameri-cas has been established. The monthly report of theSystem is published by the Center and distributed tothe Governments and interested agencies. To sum-marize the current situation, it can be said that, ingeneral, programs for the immunization of owned dogsand the reduction of the stray dog population have notachieved the levels desired for protection or safety ofhuman health, but rather are operated more on anemergency basis in response to an outbreak of thedisease. Until continuity in the programs is achieved,the breaking of the transmission cycle can never beachieved.
Brucellosis
Because of the human health problem to which itgives rise, the economic losses it causes, and its widedistribution in the various animal species, brucellosis isundoubtedly the most important zoonosis in the Ameri-cas. If accurate reports on brucellosis cases could beobtained in the countries, they would reveal tremendouslosses to cattle production and productivity. For ex-ample, an estimate in only five countries reveals that
direct losses due to bovine brucellosis alone amount toabout $155 million each year.
Human Brucellosis
During the period of this report, the highest occur-rence of human cases of brucellosis was reported fromArgentina, Mexico, and Peru, which together notifiedannually more than 5,000 cases.
In 1967 an outbreak occurred in the greater Limaarea in Peru in which 2,286 cases were reported withina period of approximately four months, producing acase-rate for those sectors which reported the disease of36.08/100,000. Brucella melitensis caused 97 per centof the 360 cases studied in this epidemic, goats beingthe main source of infection; it was discovered thatthe principal means of transmission was through theconsumption of fresh unpasteurized goat cheese. Fol-lowing this epidemic, the Organization gave assistanceto the Peruvian authorities by furnishing technical ad-visory services, equipment, and vaccine to control thedisease in the goat population, the principal reservoirof the disease in that country.
The three countries reporting the highest incidence ofhuman brucellosis also have a high prevalence of cap-rine brucellosis in their large goat herds. While muchof the transmission to man is due to ingestion of con-taminated milk and milk products, transmission alsooccurs by contact with the animals by persons workingwith them.
Bovine Brucellosis
From the financial standpoint of losses in productionand productivity and to livestock development, bovinebrucellosis is undoubtedly the most important mani-festation of this disease. Recent serologic surveys con-ducted in many of the South American countries haverevealed the high incidence of reactors, predominantlyin dairy cattle. Most of these dairy herds supply milkto the large metropolitan cities of South America, andin these areas the percentage of infected herds some-times exceeds 60 per cent. However, in other parts ofSouth and Central America and Panama low infectionrates have been reported in both the herds and individ-ual animals. Some countries are conducting serologicsurveys in conjunction with calf vaccination programsto control the disease, but this is done only sporadicallyin South America. Wide-scale control campaigns areyet to be initiated.
Uruguay has had a national campaign to controlbrucellosis since 1964, and recently Argentina ap-proved regulations making brucellosis vaccination com-pulsory, a measure that will serve as a basis for the
86
Animals being assembled for examina-tion in a brucellosis control program.
national campaign to begin in 1970. Many of the coun-tries have increased their requests for assistance fromthe Pan American Zoonoses Center in the planning,execution, evaluation, and coordination of the cam-paigns against the disease. These programs encompassdiagnosis, production and control of diagnostic antigensand vaccines, and training of personnel in the epidemi-ology of brucellosis.
In several countries swine brucellosis is a majorproblem. Goat brucellosis represents a serious publichealth problem in Argentina, Mexico, and Peru.
Bovine Tuberculosis
A high prevalence of bovine tuberculosis is foundin most of the South American countries, except Vene-zuela, and the highest infection rates are found in dairycattle in the milk sheds of the major cities. Althoughthe disease is also a problem in beef cattle, it affectsthem much less than it does the dairy herds that supplythe milk for human consumption in the large metropoli-tan areas. On the basis of a recent sample survey con-ducted in 11 areas in Argentina, it was estimated thatannual losses due to bovine tuberculosis amount to$60,000,000.
While infection rates are high in most of SouthAmerica, the prevalence of the disease in Central Amer-ica and the West Indies is very low.
In the dairy herds around the large cities of Argen-tina, Brazil, Chile, Paraguay, Peru, and Uruguaybovine tuberculosis is one of the chief animal healthproblems. Control and eradication programs are di-rected primarily at these areas because of the publichealth implications and because the animals are main-tained in the dairy herds for many years, unlike thoseused for meat production, which usually have ashorter economic life and where the turnover of newreplaceable animals is more frequent. Although studies
have revealed that in some zones the infection rate isconsiderable in some of these meat-producing animals,they are discovered very easily in the slaughterhouseand subsequently destroyed. Insidious infection in thedairy cow, with constant transmission of the tubercu-losis bacillus in the milk, is more difficult to control.
A very effective tuberculosis eradication campaignhas been carried out in Venezuela, where animal dis-ease reporting data indicate a reduction in the infectionrate to only 0.11 per cent, with a simultaneous reduc-tion in human cases caused by bovine tuberculosisbacillus.
Uruguay conducted a tuberculosis eradication cam-paign in the milk sheds around Montevideo; subsidieswere paid to producers participating in the program,which reached 75 per cent of the dairies in the area.By this method, the rate of tuberculin positive animalswas reduced to less than 1 per cent in those establish-ments participating in the program.
To summarize, as is the case with the other majorzoonoses, effective programs are conducted by certaincountries, but wide-scale campaigns to achieve thelevel of protection necessary to solve the public healthproblems do not exist in the Americas.
Total animal health programs, under the direction ofgovernment veterinary medical services, will be neces-sary in order to achieve the results required to controlthe economic and public health losses due to this dis-ease.
Hydafidosis
This disease, which produces serious human healthproblems, also causes tremendous economic losses inboth the public health sphere and in the livestock in-dustry of the Americas. In South America, the highprevalence of hydatidosis is found in the countries thathave large numbers of sheep, such as Argentina, Chile,
87
1

and Uruguay. The economic losses it causes in publichealth are very difficult to evaluate; however, it hasbeen estimated that in these three countries alone theannual cost is approximately $650,000. This figure doesnot include the subsistence or welfare payments toaffected individuals or the loss of man-hours affectingthe economy of these countries. For example, in Chileand Uruguay from 500 to 800 human cases are re-ported annually, with a mortality of about 7 per cent.Uruguay has reported that 995 patients required atotal of 34,262 days of hospitalization because of thedisease. Most of the patients are in the age groupfrom 20 to 40 years, which is the most highly produc-tive segment of the population, and they usually comefrom the sheep-raising areas. The agricultural lossesdue to hydatidosis in Argentina, Chile, and Uruguayare reported to be no less than $10,000,000, but thisfigure is probably conservative since the exact lossesare difficult to measure. For example, of the 13,000,000head of cattle and 13,000,000 sheep slaughtered yearlyin those three countries and in Rio Grande do Sul,Brazil, approximately 3,500,000 are condemned be-cause of hydatidosis. In the national slaughterhouse ofMontevideo, 205,122 bovine livers weighing almost750 tons were condemned during one year. This de-struction of animal tissue represents a serious loss ofhigh-protein food destined for human consumption.Furthermore, in all of the slaughterhouses in Uruguay,more than 60 per cent of the livers processed are con-demned for the same reason. Campaigns against thedisease have thus far been largely unsuccessful. Con-trol procedures aimed at breaking the transmissioncycle between the dog and the sheep have been appliedin association with concentrated health education ef-forts, but in the majority of cases these programs have
Natural cycle of the parasite that causes hydatidosis.
been ineffective. The legislative measures applied in anattempt to control the disease have had similar results.Basic knowledge of the epidemiology of the diseaseand of ecologic aspects of the parasite has been far fromcomplete, and this has contributed to the lack of suc-cess in many of these programs.
Pan American Zoonoses Center
Since its establishment in 1956 under an agreementbetween the Government of Argentina and the Organ-ization, the Pan American Zoonoses Center has con-tinued to develop its services. The assistance extendedby the United Nations Development Program for thestrengthening of the Center has enabled it to achieve afull complement of scientific staff with which to under-take programs covering many of the major zoonosesin the Americas. The broadening of its activities andthe development of new ones have led to an increasein the number and variety of requests from the Govern-ments for the Center's assistanice. It has thus come tooccupy an important place as a regional institution.
During the period, the Center was transferred fromits former location in Azul, Argentina, to new premisesin the National Institutes of Health of Argentina inRamos Mejía, Buenos Aires, where the facilities wereremodeled to accommodate the staff and additionalbasic equipment was installed.
The principal activities of the Center in support ofzoonoses control programs are:
1) Training of personnel in field and laboratorywork.
2) Advice on the planning, execution, and evalua-tion of programs, standardization of reagents and diag-nostic tests, reference tests on vaccines and sera, tech-nical assistance in the supply of reference strains andreagents, and for the production of biologicals.
3) Research work to develop the most adequatediagnostic and control methods for the Hemisphere.
Significantly contributing to the increase in the Cen-ter's activities was the Final Report of the Special Meet-ing of the Ministers of Health of the Americas. In therecommendations concerning the zoonoses, emphasiswas laid on the agricultural, economic, and publichealth significance of these diseases and the countries'responsibility for controlling them; and the role andobjectives of the Center in its future programs of as-sistance to the countries were clearly defined. Subse-quently, similar recommendations and resolutionswere adopted by the Ministers of Agriculture of theAmericas at the II Inter-American Meeting on Foot-and-Mouth Disease and Zoonoses Control (Rio deJaneiro, Brazil, 14-17 May 1969).
88
Pan American Zoonoses Center.
During the quadrennium the authorities of the Gov-ernment of Argentina expressed satisfaction with theexpansion of activities achieved by the Center, whichhas led to a productive exchange of scientists and infor-mation and the development of new technology. Theygave continuous support to the Center and made manyrequests to the Organization for increased assistancein training and field activities for existing and newprograms in Argentina.
Technical Services
Technical advisory services were rendered to Argen-tina, Bolivia, Brazil, Chile, Colombia, Cuba, Ecuador,Mexico, Panama, Paraguay, Peru, Uruguay, Venezuela,and the Central American countries on problems ofthe zoonoses and other aspects of veterinary publichealth related to brucellosis, rabies, hydatidosis, hemor-rhagic fever, encephalitis, and laboratory animal careand management. Laboratory services were providedin connection with the production and distribution ofstandardized biologicals, control of vaccines and anti-gens, typing of strains of various microorganisms, andadditional reference diagnostic services. For example,in 1966 the staff of the Center examined 35,158 speci-mens for diagnosis, 158 biological products for studyand control, and 914 whole animals for diagnosis andtaxonomic classification. Specialists of the Centervisited several countries to provide assistance in rabiesvaccine production; in Colombia they collaborated inthe planning of control programs against goat brucello-sis; in Peru, in the program against rabies; and in Uru-guay and Argentina, in the bovine tuberculosis controlprograms. They also participated in many meetings onzoonoses control held in Argentina, Guatemala, Pan-ama, Uruguay, and Venezuela.
The Center provided technical advice on rabies vac-cine production and control and supplied standardizedvirus for the production of vaccines to institutions and
laboratories in Argentina, Brazil, Colombia, Cuba,Mexico, Peru, Uruguay, and Venezuela during 1967.Assistance was also given, in collaboration with theArgentine Government, in the implementation of na-tional programs for the control of rabies, brucellosis,and bovine tuberculosis.
During the period, the Center established itself as areference laboratory offering its services to the healthauthorities of Latin America in connection with rabies,brucellosis, hydatidosis, leptospirosis, hemorrhagicfever, and tuberculosis. A major contribution towardan understanding of the epidemiology of rabies wasmade with the establishment by the Center, in collabo-ration with the health and agricultural authorities of thecountries, of the Rabies Surveillance System for theAmericas. Each Government reports monthly to theCenter on the cases of human and animal rabies intheir respective territory and the Center compiles, ana-lyzes, and reproduces this information for distributionto all the national health and agriculture authorities andother interested agencies. The basic information of theSurveillance System includes occurrence of human andanimal cases, rabies diagnosis, antirabies treatment inman, and data on postvaccinal neuroparalytic reactions.
Studies were initiated by the staff of the Center incooperation with the Argentinian animal health authori-ties to detect microbiological contaminations of meatfor exportation. These are being conducted in slaugh-terhouses in the Buenos Aires area to determine thedegree of infection by Salmonella and other entericorganisms in the animals before slaughter and con-tamination of the meat product following the slaughterprocess. The Center assisted Colombia's animalhealth authorities to design and prepare an investigationof the prevalence of hydatidosis in sheep-raising areasand to establish preventive measures for reducing therisk of its introduction into non-affected areas. Assist-ance was also given in the production of antigens andvaccines for control of brucellosis in that country.
In order to provide technical advisory services on abroad and diversified basis, new scientists were addedto the professional staff, which reached full capacity bythe end of 1969.
The Scientific Advisory Committee
Of great significance for the promotion, implementa-tion, and evaluation of the programs of the Center wasthe establishment of this Committee, which held its firstmeeting from 20 to 25 November 1967 at the newsite in Ramos Mejía. After a careful review and ap-praisal of the Center's programs and activities, theCommittee made recommendations for improvementin the three basic areas of technical advisory services,
89
-- T?-
research, and training. This Committee, comprising adiversified group of medical scientists with the highestqualifications, has continued to play a role in thedevelopment of the Center's work.
Publications
The Center continued to improve its quarterly bul-letin entitled Zoonoses, which has achieved wider dis-tribution and a position of prestige among the scientificpublications in this field.
The activities of the Center in research and trainingare described in the section of this Report on researchdevelopment and coordination and development ofhuman resources.
Pan American Foot-and-Mouth Disease Center
Foot-and-mouth disease is the most important animaldisease in the countries that it affects, and is a constantthreat to the other countries in the Hemisphere thatare free of it. Its great economic significance and thedifficulty and complex measures required for its con-trol are the main reasons for the establishment of theCenter. The chief factors to be considered in connec-tion with foot-and-mouth disease may be summarizedas follows:
1 ) The highly contagious nature of the disease andthe rapidity with which it spreads among cattle, swine,sheep, and other cloven-hooved animals.
2) The financial losses suffered by agriculture as aresult of the disease.
3) The damage it does to the production of animalprotein and the relation between this and the severeproblem of protein malnutrition in the growing humanpopulation of the Americas.
4) The losses suffered by national economiesthrough the closing of export markets, since countriesthat are free of the disease cannot run the risk of im-porting animals and animal products from affectedcountries.
In the four-year period there has been a full recogni-tion of the effect of the disease on the economies anddevelopment of countries that are in a large measuredependent upon livestock production, and of the urgentneed to launch national and multinational campaignsfor foot-and-mouth disease control.
The impact of the disease on economic developmentin the countries of the Hemisphere has been pointedout many times by the Governments and by scientistsconcerned with its control. The serious losses in termsof essential proteins necessary for human nutrition,the consequences for the agricultural economy, and theeffects on animal production and productivity have all
been taken into consideration in the development of aunified approach to the control and prevention of foot-and-mouth disease. Of special importance to the in-creased efforts to bring the disease under control weretwo major events affecting the Center's future activitiesand its relationship to the Governments of affectedcountries in the execution of their control programs.The first was the transfer of complete administrativeresponsibility for the Center to the Organization, whichhas led to greater autonomy and proficiency in thedevelopment and conduct of the Center's activities andprograms. The second was the decision by the Inter-American Development Bank to grant financial assist-ance to the countries in their campaigns against foot-and-mouth disease. With the cooperation of otheragencies interested in the control of the disease, theOrganization convened a working group to considerthe problem in the Americas. This group developed a"Guide for the preparation of projects for the controlof foot-and-mouth disease" and a special document oncriteria for the analysis and evaluation of loan requestsfor such projects. Both of these documents have beenused by many countries in preparing their applicationsto the Inter-American Development Bank. The Centerhas assisted several countries in the preparation of theserequests.
The Center has greatly intensified its efforts to bringabout more effective coordination among the countriesin order to develop multinational activities for the con-trol of the disease in affected areas. It has stronglyrecommended that stringent restrictions be adopted inconnection with the movement of animals and has pro-moted the development of regulations and barriersagainst the entry of the disease into countries alreadyfree of it.
During the quadrennium the Center made importantscientific contributions to the identification of the typesand new subtypes of foot-and-mouth disease viruses.It also prepared inactivated vaccines derived from themodified live virus. Of great significance to the appli-cation of diagnostic procedures was the method devel-oped for identification of carriers by a technique that isrelatively easy to perform and is available to the coun-tries. The Center developed a broader orientation andcloser coordination in its program of education andadvanced training for professional personnel who willspecialize in the prevention and control of foot-and-mouth disease.
Field Advisory Services
The staff travelled to all the countries of LatinAmerica to review and offer assistance in the foot-and-mouth disease control programs. Discussions were held
90
Field and laboratory investigation of foot-and-mouth disease.
with the animal health authorities for the purposeof establishing the Inter-American Foot-and-MouthDisease Epidemiological Surveillance System. Such areporting system is essential in order to ascertain thestatus of the disease in the countries and to obtainmore basic knowledge concerning its epidemiology. Atthe present time, no foot-and-mouth disease is foundnorth of the Darién area in Panama, which in essenceconstitutes a "buffer zone" of protection between theaffected areas of South America and the non-affectedregions to the north.
In 1967 an outbreak of the disease was diagnosedfor the first time in the Argentine portion of Tierra deFuego, and northward into the Patagonia. In 1969there was a small outbreak in the Punta Arenas area ofChile, for the first time since the 1920's. The occur-rence of these two outbreaks in non-affected or disease-free areas underscores the need for constant surveil-lance against animal diseases, for epidemics of thiskind could also occur in the disease-free area north ofPanama where exportation of animals and animalproducts to other disease-free countries is of greateconomic importance.
Since 1968 Argentina, Chile, and Paraguay havereceived loans from the IDB for the financing of cam-paigns against foot-and-mouth disease and have alreadyinitiated programs for its control and possible eradica-tion. Uruguay started its national campaign with thecontrol of vaccines on a national scale and the applica-tion of compulsory vaccination in the northern districtsbordering on Rio Grande do Sul in Brazil.
Diagnostic and Reference Services
During the period 1966-1969 the Center studiedand diagnosed 2,060 specimens of epithelial tissue, ofwhich 1,748 were positive for foot-and-mouth disease.The type and subtype of each isolate was determined.Resultant new subtypes were prepared and sent to theWorld Reference Laboratory in Pirbright, England, foridentification and taxonomic designation.
Through the characterization studies at the Center,it was determined that type C virus, which first ap-peared in Colombia in 1967 near Leticia on the Ama-zon River, raised a problem of special importance tothe animal health authorities, since this new type couldspread rapidly throughout the Region. However, con-trol measures adopted by the Ministry of Agriculture,including application of slaughter techniques, vaccina-tion measures, and continued quarantine and observa-tion, brought the outbreak under control.
Studies conducted in 1969 on the typing and sub-typing of virus isolates led to the identification of fivenew subtypes, which were subsequently submitted tothe World Reference Laboratory.
Another major contribution by the Center's Diag-nostic and Reference Section is the production ofhyperimmune serum for use by the Center itself and bythe national laboratories of the countries in their diag-nostic and research work. For example in 1969, theCenter produced 2,315 ml of hyperimmune serum, ofwhich 822 ml were sent to 11 different countries foruse in their laboratories. The Center also sent 102 mlto the World Reference Laboratory.
91
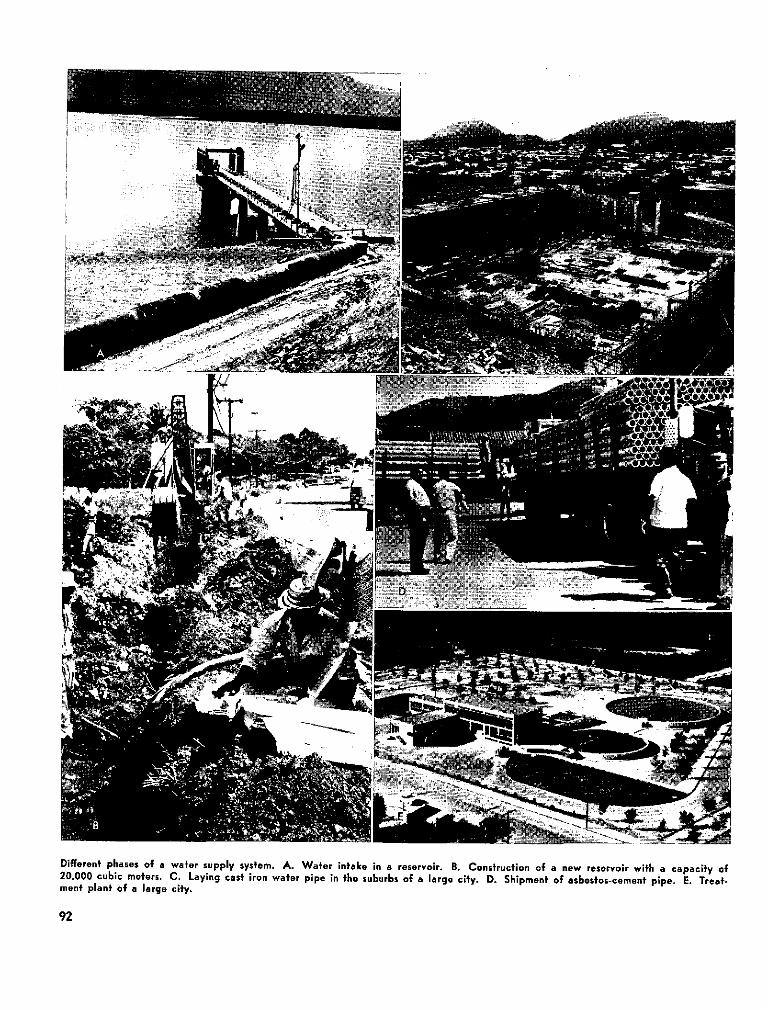
r
Different phases of a water supply system. A. Water intake in a reservoir. B. Construction of a new reservoir with a capacity of20,000 cubic meters. C. Laying cast ¡ron water pipe in the suburbs of a large cify. D. Shipment of asbesfos-cemenf pipe. E. Treat-ment plant of a large cify.
u:~~~~~~~~~~~~~~~~~~~~~~,~. *c.Z,-l~~~ ?
:II ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~.
,1~~~~~~~~~~~~~~~~~~~~~e
r~~~~~~~~~~~~~~~~~~
Dífferenf phases of a wator supply system. A. Watar infake ¡n a reservoir. B. Construcfion of a new reservoir wifh a capacify of20.000 cubic meters. C. Laying cast iran water pipe in the suburbs of a large city. D. Shipment of asbastos-cement pipe. E. Treat-ment planf of a largo city.
92

To summarize, with the complete transfer of theCenter to the Organization, the convening of annualmeetings of Ministers of Agriculture or their repre-sentatives to examine its program and activities, andthe broadening of the loan policies of both IDB and
the World Bank to include foot-and-mouth diseaseprograms, the Center has embarked on a new erawhich will enable it to further increase its services tothe Governments of the Americas.
SANITARY ENGINEERING AND ENVIRONMENTAL SCIENCES
ENVIRONMENTAL SANITATION
Transition was the most characteristic aspect ofenvironmental activities in the quadrennium. Transi-tion from primary emphasis on traditional activitiessuch as water supply and sewerage to newer and emerg-ing problems such as air pollution, industrial healthhazards, solid wastes, water pollution, industrial wastes,and river basin development. Transition also from em-phasis on improving undergraduate education to thedevelopment of graduate centers for education and re-search and to continuing professional education. Thesechanges in emphasis required corresponding changes inthe deployment and utilization of our resources-and,significantly, the establishment of a new resource, thePan American Sanitary Engineering and EnvironmentalSciences Center (CEPIS).
Water supply activities continued to be the largest.During the latter part of the four-year period increasedattention was devoted to sewerage, with the purpose ofapplying to this important field the organizational, ad-ministrative, financial, and technical methodology thathas been so successful in the water supply field. At thesame time we sought to decrease our traditional activi-ties in these fields in view of the developed compe-tence in the countries to maintain the momentumachieved. As the quadrennium closed our emphasisin water supply was focused on new technology, es-pecially that related to water treatment; on pre-feasi-bility studies; on the securing of external financial as-sistance; on executive administration; and on designparameters and construction programming.
The Pan American Air Pollution Surveillance Net-work was established mid-way in the quadrenniumand now includes 22 stations. Several of the cities haveadded a number of stations to the initial one estab-lished with the Organization's assistance. Reportscovering the operation of the Network have been pre-pared for distribution. Increased interest in air pollu-tion control was reflected also in the number of requestsfor technical assistance in developing new or strength-ened programs. The First Regional Seminar on Air
Pollution was held under the Organization's sponsor-ship.
Other problems resulting from intensified urbaniza-tion and industrialization received increased attention.Short-term consultants were furnished to several coun-tries to help in assessing solid wastes problems andworking out solutions. Industrial hazards grew as in-dustry expanded, and more countries requested evalua-tions of existing programs and aid in establishing newor improved ones. A First Regional Seminar on Sili-cosis was held and the proceedings were prepared forpublication. The Institute of Occupational Health andAir Pollution Research in Chile concluded five yearsof operation with UNDP assistance, and was incorpo-rated into the permanent health structure of thatcountry.
Severe water pollution problems plagued severalcities and the need for control programs became muchmore evident. Organization staff, supplemented byshort-term consultants, responded to requests for as-sistance. Important new authorizations and organiza-tions for water and air pollution activities emerged atboth state and national levels. Several studies of thepollution of major important bodies of water were ini-tiated. Sewage and industrial waste treatment receivedmore attention in technical training courses and semi-nars as cities became more aware of the need to curbwater pollution.
The hemisphere-wide attention to planning mani-fested itself in several environmental areas. Amongthe more important of these was river basin develop-ment planning. Sponsored jointly by the University ofSao Paulo and the Organization, the First RegionalSymposium on River Basin Planning was held in thatcity. Two more symposia were held subsequently.The proceedings of these meetings contain valuabledescriptions and discussions of the new concepts andnew processes for solving river basin developmentproblems.
With environment in a rapid stage of transition,there was need for a parallel transition in the trainingand utilization of manpower. Curricula modifications,
93
reflecting the newer problems and public concerns,were made. More emphasis was placed on quality anddepth of teaching related to these more difficult prob-lems. Graduate programs were extended and strength-ened; research was accented. Programs of teachingand research, with UNDP-SF assistance, were expandedin Venezuela and Brazil.
The adjustments in the Organization's resources tomeet the new requirements were substantial. Country,Zone, and Headquarters environmental sciences andengineering staff were reoriented to place greater em-phasis not only on the newer problems, but also onnational and regional planning, policy, and program-ming and on coordination with national and regionaldevelopment plans-in both traditional areas of activityand new areas. Finally, in recognition of the need forimproving capability to render expert technical assist-ance to Member Countries, a new resource was devel-oped, largely by reshaping existing resources-the PanAmerican Sanitary Engineering and EnvironmentalSciences Center. This resource, established in 1968,is expected to render important assistance in the pro-vision of technical information materials, expert con-sultant services, support for university-based teachingand research institutions, and ultimately, in researchand technical training methodology.
WATER SUPPLY
The Presidents of America, at their meeting inPunta del Este, and the Ministers of Health, at theirmeeting in Buenos Aires, again emphasized the needto continue assigning the highest priority to programsfor water supply and sewerage systems in order tomaintain the high level of progress achieved since 1961.The two meetings bore witness to the fact that, duringthe quadrennium, programs designed to provide thepeoples of the Hemisphere with more and better sanita-tion services continued to receive maximum attention,as they had during the preceding four years. Theperiod was one of effective and resolute progress onthe part of the Governments, working with the collab-oration of international lending and technical assist-ance agencies.
Several countries continued contributing to the Com-munity Water Supply Fund, established in 1959 tosupport the Organization's program in this field. Table28 shows the contributions made in the past fouryears. As can be seen, the countries have increasedtheir contributions, except for the United States ofAmerica, as a result of the programs of technical as-sistance in the administration and management of waterand sewerage services, assisted by loans from the
TABLE 28. CONTRIBUTIONS TO THE PAHO COMMUNITY WATERSUPPLY FUND.
(In US dollars)
COUNTRY 1966 1967 1968 1969
Bolivia 9,950Brazil 3,000 4,698Dominican Republic 25,000Ecuador 12,000Jamaica 21,835Nicaragua 1,000 24,000Peru 17,460 2,183Trinidad and Tobago 20,235 25,000United States of America 300,894 115,000 1,906Uruguay 25,000Venezuela 4,721
Total 300,894 148,235 94,201 70,552
Inter-American Development Bank (see also ChapterIII, p. 38).
One of the chief recommendations of the GoverningBodies with reference to water programs was theestablishment by the countries of agencies or institu-tions able to plan, construct, manage, and direct waterand sewerage services in an efficient and rational man-ner. This concept has gained much ground, and at theend of 1969 most of the countries had organizations of.their own which could already look back on consider-able achievements; the advances made warrant the ex-pectation that in a few years' time highly efficientagencies will be operating in this field.
Invesfmenfs and Resulis
During the period 1966-1969, the internationalcredit agencies and the Governments were very activein supporting programs for the construction or expan-sion of water services (Table 29). Investments by in-ternational credit agencies together with those of thecountries totaled $945.42 million, $323.41 of whichrepresented international loans and the remaining$622.01 million were national funds. These figuresreflect an increase in investment compared with thepreceding four-year period. Table 30 presents thefunds allocated from January 1966 through December1969, broken down by country and by internationalagency. It is estimated that both national and inter-national investments made through December 1969will benefit a total of 70 million persons, an increase of26 million over the corresponding figure at the end of1965.
Figure 34 shows that at the end of the period cov-ered by this Report the countries reported that 72 percent of the urban population had access to water suppliesthrough house connections or public hydrants and that16 per cent of the rural population had adequate water
94
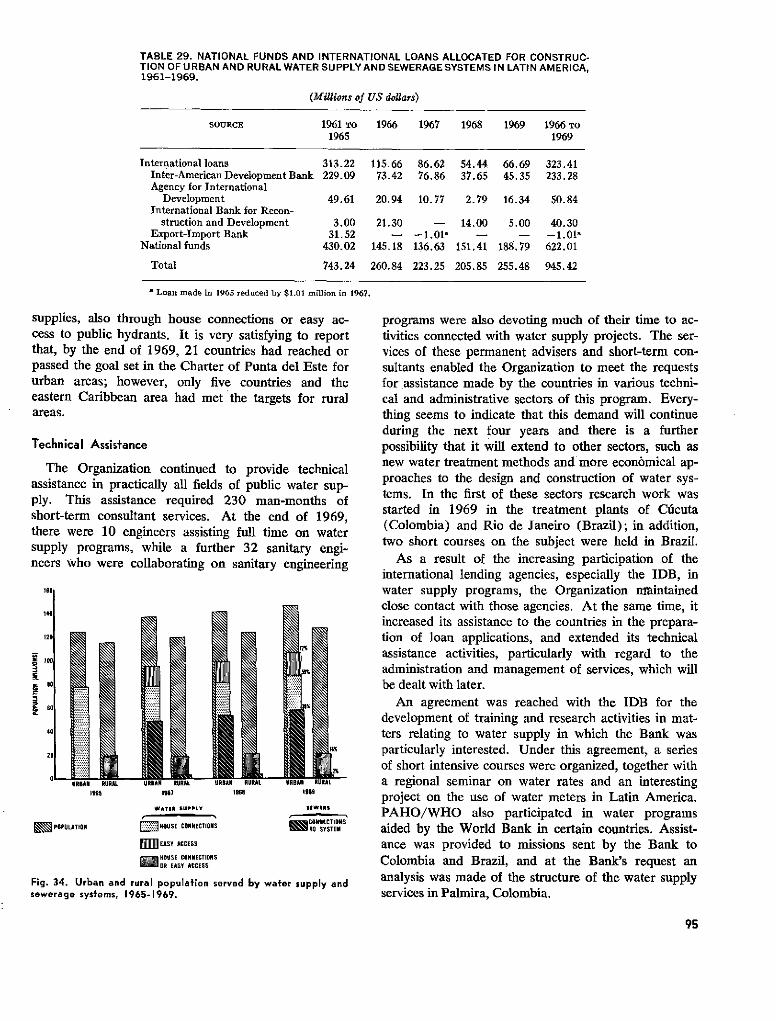
TABLE 29. NATIONAL FUNDS AND INTERNATIONAL LOANS ALLOCATED FOR CONSTRUC-TION OF U RBAN AND RURAL WATER SUPPLY AND SEWERAGE SYSTEMS IN LATIN AMERICA,1961-1969.
(Millions of US dollars)
SOURCE 1961 To 1966 1967 1968 1969 1966 TO1965 1969
International loans 313.22 115.66 86.62 54.44 66.69 323.41Inter-American Development Bank 229.09 73.42 76.86 37.65 45.35 233.28Agency for International
Development 49.61 20.94 10.77 2.79 16.34 50.84International Bank for Recon-
struction and Development 3.00 21.30 - 14.00 5.00 40.30Export-Import Bank 31.52 - - - - -1.011
National funds 430.02 145.18 136.63 151.41 188.79 622.01
Total 743.24 260.84 223.25 205.85 255.48 945.42
a Loan made in 1965 reduced by $1.01 million in 1967.
supplies, also through house connections or easy ac-cess to public hydrants. It is very satisfying to reportthat, by the end of 1969, 21 countries had reached orpassed the goal set in the Charter of Punta del Este forurban areas; however, only five countries and theeastern Caribbean area had met the targets for ruralareas.
Technical Assisfance
The Organization continued to provide technicalassistance in practically all fields of public water sup-ply. This assistance required 230 man-months ofshort-term consultant services. At the end of 1969,there were 10 engineers assisting full time on watersupply programs, while a further 32 sanitary engi-neers who were collaborating on sanitary engineering
195ss 1987 19s8 1969
WATEt SUPPLY SW9*S
E POPULATION E'NOUSE CONNECTIONS =CON" ECTIONS
mO lEASY ACCESS
8OUSE CONNECTIONS"OR EASY ACCESS
Fig. 34. Urban and rural population served by water supply andsewerage systems, 1965-1969.
programs were also devoting much of their time to ac-tivities connected with water supply projects. The ser-vices of these permanent advisers and short-term con-sultants enabled the Organization to meet the requestsfor assistance made by the countries in various techni-cal and administrative sectors of this program. Every-thing seems to indicate that this demand will continueduring the next four years and there is a furtherpossibility that it will extend to other sectors, such asnew water treatment methods and more economical ap-proaches to the design and construction of water sys-tems. In the first of these sectors research work wasstarted in 1969 in the treatment plants of Cúcuta(Colombia) and Rio de Janeiro (Brazil); in addition,two short courses on the subject were held in Brazil.
As a result of the increasing participation of theinternational lending agencies, especially the IDB, inwater supply programs, the Organization nmaintainedclose contact with those agencies. At the same time, itincreased its assistance to the countries in the prepara-tion of loan applications, and extended its technicalassistance activities, particularly with regard to theadministration and management of services, which willbe dealt with later.
An agreement was reached with the IDB for thedevelopment of training and research activities in mat-ters relating to water supply in which the Bank wasparticularly interested. Under this agreement, a seriesof short intensive courses were organized, together witha regional seminar on water rates and an interestingproject on the use of water meters in Latin America.PAHO/WHO also participated in water programsaided by the World Bank in certain countries. Assist-ance was provided to missions sent by the Bank toColombia and Brazil, and at the Bank's request ananalysis was made of the structure of the water supplyservices in Palmira, Colombia.
95
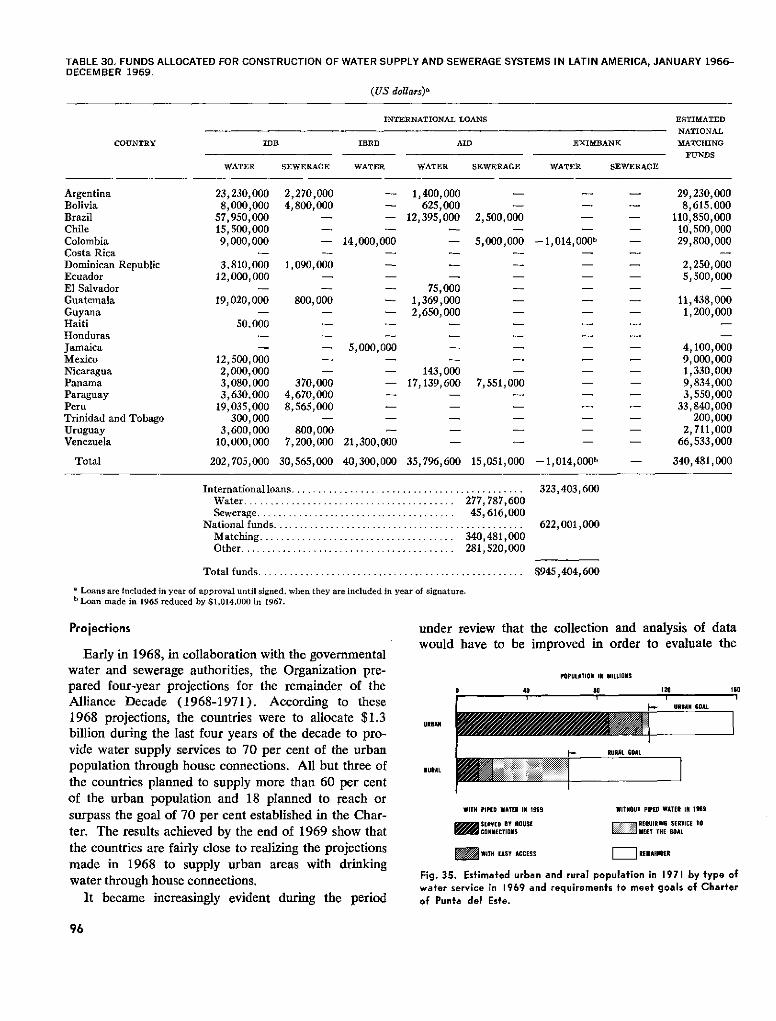
TABLE 30. FUNDS ALLOCATED FOR CONSTRUCTION OF WATER SUPPLY AND SEWERAGE SYSTEMS IN LATIN AMERICA, JANUARY 1966-DECEMBER 1969.
(US dollars),
INTERNATIONAL LOANS ESTIMATED
NATIONAL
COUNTRY IDB IBRD AID EXIMBANK MATCHING
FUNDS
WATER SEWERAGE WATER WATER SEWERAGE WATER SEWERAGE
Argentina 23,230,000 2,270,000 - 1,400,000 - - - 29,230,000Bolivia 8,000,000 4,800,000 - 625,000 - - - 8,615,000Brazil 57,950,000 - - 12,395,000 2,500,000 - - 110,850,000Chile 15,500,000 - - - - - 10,500,000Colombia 9,000,000 - 14,000,000 - 5,000,000 -1,014,000b - 29,800,000Costa Rica -
Dominican Republic 3,810,000 1,090,000 - - - - - 2,250,000Ecuador 12,000,000 - - 5,500,000El Salvador - - - 75,000 .Guatemala 19,020,000 800,000 - 1,369,000 - - - 11,438,000Guyana - - - 2,650,000 -- - 1,200,000Haiti 50,000 -Honduras -
Jamaica - - 5,000,000 - - - - 4,100,000Mexico 12,500,000 - - - 9,000,000Nicaragua 2,000,000 - - 143,000 - - - 1,330,000Panama 3,080,000 370,000 - 17,139,600 7,551,000 - 9,834,000Paraguay 3,630,000 4,670,000 - - - 3,550,000Peru 19,035,000 8,565,000 - 33,840,000Trinidad and Tobago 300,000 - - 200,000Uruguay 3,600,000 800,000 - 2,711,000Venezuela 10,000,000 7,200,000 21,300,000 - - 66,533,000
Total 202,705,000 30,565,000 40,300,000 35,796,600 15,051,000 -1,014,000b - 340,481,000
International loans ............................................Water ...................................... 277,787,600Sewerage ...................................... 45,616,000
National funds ................................................Matching ..................................... 340,481,000Other ........................................ 281,520,000
323,403,600
622,001,000
Total funds ................................................... $945,404,600
' Loans are Included in year of approval until signed, when they are included in year of signature.b Loan made in 1965 reduced by $1,014.000 in 1967.
Projecfions
Early in 1968, in collaboration with the governmentalwater and sewerage authorities, the Organization pre-pared four-year projections for the remainder of theAlliance Decade (1968-1971). According to these1968 projections, the countries were to allocate $1.3billion during the last four years of the decade to pro-vide water supply services to 70 per cent of the urbanpopulation through house connections. All but three ofthe countries planned to supply more than 60 per centof the urban population and 18 planned to reach orsurpass the goal of 70 per cent established in the Char-ter. The results achieved by the end of 1969 show thatthe countries are fairly close to realizing the projectionsmade in 1968 to supply urban areas with drinkingwater through house connections.
It became increasingly evident during the period
under review that the collection and analysis of datawould have to be improved in order to evaluate the
40
POPULATION IN MILLIONS
#o
L,.
120
URBAN GOAL
URAN
Ih- RURAL GOAL
RURAL
WITH PIPED WATER IN 1969
SERVED BY HOUSEi -0 tCONNECTIONS
WITHOUT PIPEO WATER IN 1969
.El REQUIRING SERVICE TOMEET THE GOAL
= WITH EASY ACCESS Z REMAINDER
Fig. 35. Estimated urban and rural population in 1971 by type ofwater service in 1969 and requirements to meet goals of Charterof Punta del Este.
96
sO'I
. 1 PAF~
O 1
1
progress being made in public water supply and sewer-age programs and provide an adequate basis forexpanding those programs. The Organization con-sequently prepared a manual on methodology of datacollection programs for community water and seweragesystems in Latin America and assisted in analyzing thedata-collection procedures in Argentina, Brazil, CostaRica, and Mexico as a preliminary step for providingincreased advisory services in this field in coming years.
Program for Surinam
In 1969 the UNDP-SF approved a project for anational water supply and sewerage program in Suri-nam. By the year's end exploratory drilling operationshad started, together with the compilation of hydro-logic data, in the lower part of the Surinam RiverBasin. This project is the first of its kind to be financedby the United Nations in the Americas, and containspractical elements for providing water and sewerageservices to communities in which it is expected thatthe Government will undertake major economic devel-opment activities.
WATER SUPPLY IN RURAL AREAS
In April 1967 the goal of supplying potable waterand sewerage to 50 per cent of the rural populationwas reaffirmed by the American Chiefs of State atPunta del Este. In October 1968 the Ministers ofHealth, in their final Declaration, stated: "We havegiven special attention to the problems of populationsliving in rural areas, because of their seriousness andbecause of the need to bring these people into the main-stream of modem life and economic progress." Theywent on to say: "We propose to encourage themodernization of rural life .... " Thus it can be seenthat this quadrennium has been one in which therehas been a growing awareness of the rural community,and an increasing desire to further accelerate themodernization of rural life that was started in prioryears.
To assist the countries in meeting this challenge, theOrganization has strongly supported the development,expansion, and strengthening of national and local waterand sanitation programs in the rural areas. Theseefforts have been based on the concept that while strongviable water and sanitation programs constitute animportant measure for the protection and improvementof health, they can also serve as the focal point for thedevelopment of a host of related health services andprograms.
The driving philosophy behind the development ofthese programs has been to assist the countries to ap-
proach the goals of: (1) providing the inhabitants ofthe rural areas with adequate quantities of potablewater-piped, where possible, into the house; and (2)providing basic sanitation programs that will ensure asafe and sanitary environment. To this end, the Organ-ization has sought to promote national institutionsthat would furnish administrative, technical, and finan-cial support to viable, long-range and locally-basedprograms.
PAHO/WHO has rendered technical, administrative,and financial advice in these activities. In addition tothe traditional methods, it has sought to assist the coun-tries to promote, demonstrate, and establish such con-cepts as:
Maximum community participation in the establish-ment and operation of the required systems.
Use of revolving funds to strengthen program financ-ing.
Use of simplified design, construction, and manage-ment techniques to reduce program time and costs whileincreasing program coverage.
To give assistance in organizing and obtaining themaximum utilization of the resources available to thecountries, the Organization has supplied staff members,short-term consultants, and fellowships to the variousprograms. In addition, it has actively collaborated withthe various international organizations such as UNI-CEF, the World Food Program, the Canadian Interna-tional Development Agency (CIDA), the Organiza-tion of American States, and CARE for the supply offunds and materials to the countries of the Americas.
While it appears that not all the countries will
97
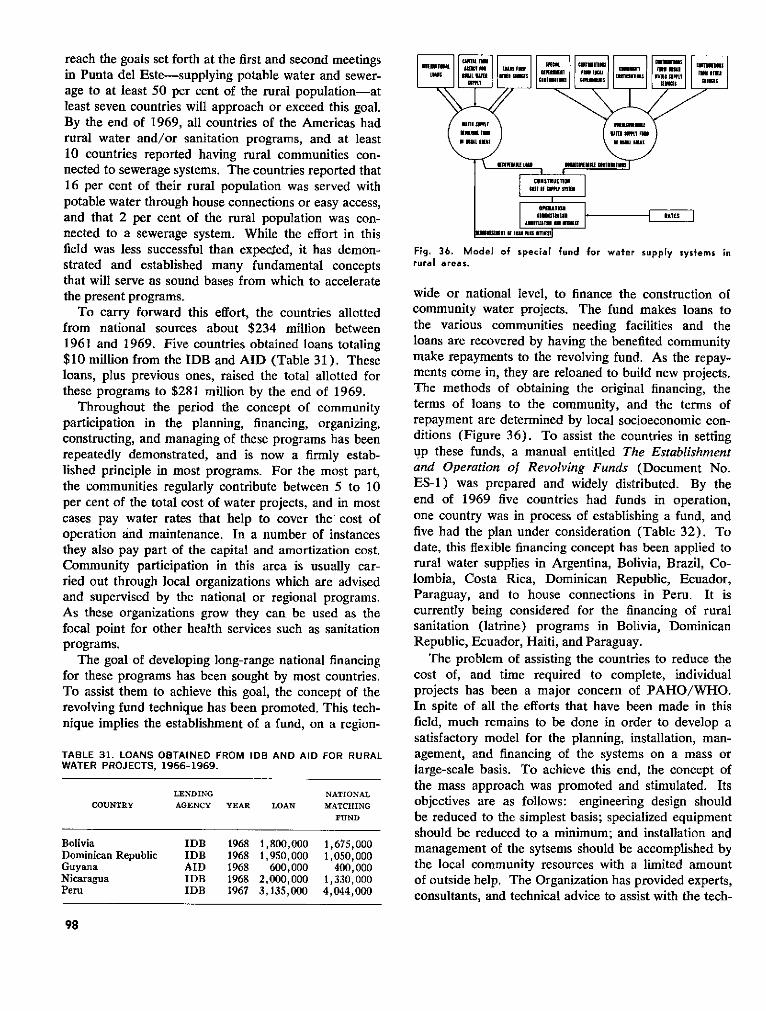
reach the goals set forth at the first and second meetingsin Punta del Este-supplying potable water and sewer-age to at least 50 per cent of the rural population-atleast seven countries will approach or exceed this goal.By the end of 1969, all countries of the Americas hadrural water and/or sanitation programs, and at least10 countries reported having rural communities con-nected to sewerage systems. The countries reported that16 per cent of their rural population was served withpotable water through house connections or easy access,and that 2 per cent of the rural population was con-nected to a sewerage system. While the effort in thisfield was less successful than expecIed, it has demon-strated and established many fundamental conceptsthat will serve as sound bases from which to acceleratethe present programs.
To carry forward this effort, the countries allottedfrom national sources about $234 million between1961 and 1969. Five countries obtained loans totaling$10 million from the IDB and AID (Table 31). Theseloans, plus previous ones, raised the total allotted forthese programs to $281 million by the end of 1969.
Throughout the period the concept of communityparticipation in the planning, financing, organizing,constructing, and managing of these programs has beenrepeatedly demonstrated, and is now a firmly estab-lished principle in most programs. For the most part,the communities regularly contribute between 5 to 10per cent of the total cost of water projects, and in mostcases pay water rates that help to cover the' cost ofoperation and maintenance. In a number of instancesthey also pay part of the capital and amortization cost.Community participation in this area is usually car-ried out through local organizations which are advisedand supervised by the national or regional programs.As these organizations grow they can be used as thefocal point for other health services such as sanitationprograms.
The goal of developing long-range national financingfor these programs has been sought by most countries.To assist them to achieve this goal, the concept of therevolving fund technique has been promoted. This tech-nique implies the establishment of a fund, on a region-
TABLE 31. LOANS OBTAINED FROM IDB AND AID FOR RURALWATER PROJECTS, 1966-1969.
LENDING NATIONALCOUNTRY AGENCY YEAR LOAN MATCHING
FUND
Bolivia IDB 1968 1,800,000 1,675,000Dominican Republic IDB 1968 1,950,000 1,050,000Guyana AID 1968 600,000 400,000Nicaragua IDB 1968 2,000,000 1,330,000Peru IDB 1967 3,135,000 4,044,000
Fig. 36. Model of special fund for water supply systems inrural areas.
wide or national level, to finance the construction ofcommunity water projects. The fund makes loans tothe various communities needing facilities and theloans are recovered by having the benefited communitymake repayments to the revolving fund. As the repay-ments come in, they are reloaned to build new projects.The methods of obtaining the original financing, theterms of loans to the community, and the terms ofrepayment are determined by local socioeconomic con-ditions (Figure 36). To assist the countries in settingup these funds, a manual entitled The Establishmentand Operation of Revolving Funds (Document No.ES-1) was prepared and widely distributed. By theend of 1969 five countries had funds in operation,one country was in process of establishing a fund, andfive had the plan under consideration (Table 32). Todate, this flexible financing concept has been applied torural water supplies in Argentina, Bolivia, Brazil, Co-lombia, Costa Rica, Dominican Republic, Ecuador,Paraguay, and to house connections in Peru. It iscurrently being considered for the financing of ruralsanitation (latrine) programs in Bolivia, DominicanRepublic, Ecuador, Haiti, and Paraguay.
The problem of assisting the countries to reduce thecost of, and time required to complete, individualprojects has been a major concern of PAHO/WHO.In spite of all the efforts that have been made in thisfield, much remains to be done in order to develop asatisfactory model for the planning, installation, man-agement, and financing of the systems on a mass orlarge-scale basis. To achieve this end, the concept ofthe mass approach was promoted and stimulated. Itsobjectives are as follows: engineering design shouldbe reduced to the simplest basis; specialized equipmentshould be reduced to a minimum; and installation andmanagement of the sytsems should be accomplished bythe local community resources with a limited amountof outside help. The Organization has provided experts,consultants, and technical advice to assist with the tech-
98
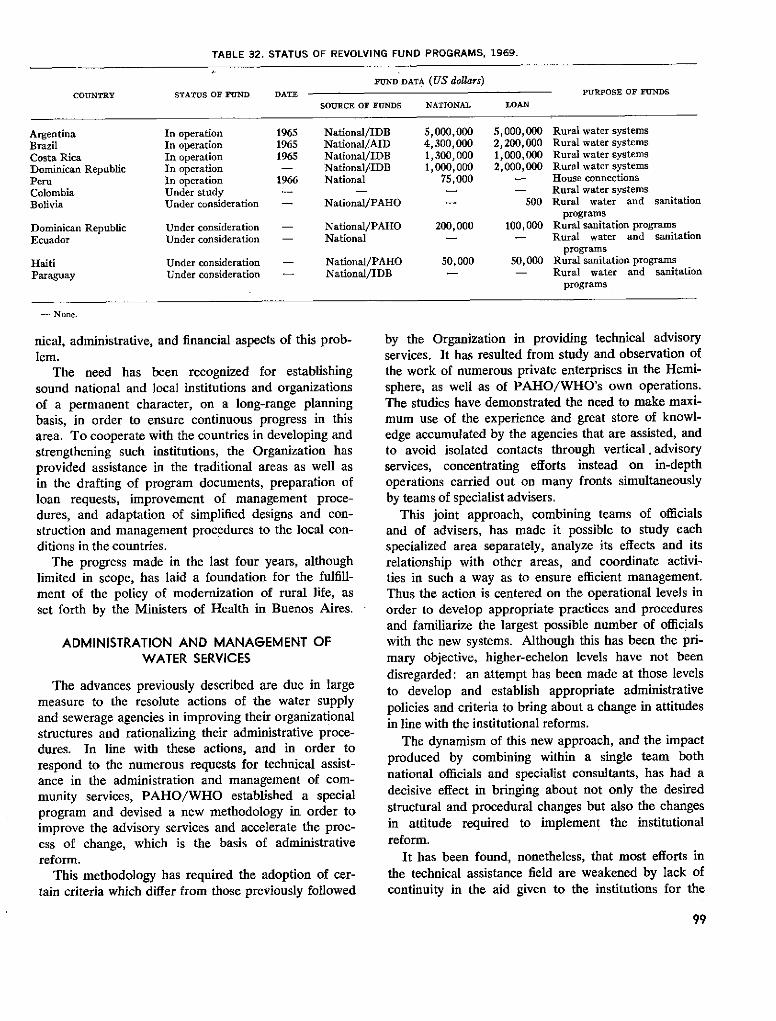
TABLE 32. STATUS OF REVOLVING FUND PROGRAMS, 1969.
FUND DATA (US dollars)
COUNTRY STATUS OF FUND DATE PURPOSE OF FUNDS
SOURCE OF FUNDS NATIONAL LOAN
Argentina In operation 1965 National/IDB 5,000,000 5,000,000 Rural water systemsBrazil In operation 1965 National/AID 4,300,000 2,200,000 Rural water systems
Costa Rica In operation 1965 National/IDB 1,300,000 1,000,000 Rural water systemsDominican Republic In operation - National/IDB 1,000,000 2,000,000 Rural water systemsPeru In operation 1966 National 75,000 - House connectionsColombia Under study - - - - Rural water systems
Bolivia Under consideration - National/PAHO - 500 Rural water and sanitationprograms
Dominican Republic Under consideration - National/PAHO 200,000 100,000 Rural sanitation programsEcuador Under consideration - National - - Rural water and sanitation
programsHaiti Under consideration - National/PAHO 50,000 50,000 Rural sanitation programsParaguay Under consideration - National/IDB - - Rural water and sanitation
programs
- None.
nical, administrative, and financial aspects of this prob-lem.
The need has been recognized for establishingsound national and local institutions and organizationsof a permanent character, on a long-range planningbasis, in order to ensure continuous progress in thisarea. To cooperate with the countries in developing andstrengthening such institutions, the Organization hasprovided assistance in the traditional areas as well asin the drafting of program documents, preparation ofloan requests, improvement of management proce-dures, and adaptation of simplified designs and con-struction and management procedures to the local con-ditions in the countries.
The progress made in the last four years, althoughlimited in scope, has laid a foundation for the fulfill-ment of the policy of modernization of rural life, asset forth by the Ministers of Health in Buenos Aires.
ADMINISTRATION AND MANAGEMENT OFWATER SERVICES
The advances previously described are due in largemeasure to the resolute actions of the water supplyand sewerage agencies in improving their organizationalstructures and rationalizing their administrative proce-dures. In line with these actions, and in order torespond to the numerous requests for technical assist-ance in the administration and management of com-munity services, PAHO/WHO established a specialprogram and devised a new methodology in order toimprove the advisory services and accelerate the proc-ess of change, which is the basis of administrativereform.
This methodology has required the adoption of cer-tain criteria which differ from those previously followed
by the Organization in providing technical advisoryservices. It has resulted from study and observation ofthe work of numerous private enterprises in the Hemi-sphere, as well as of PAHO/WHO's own operations.The studies have demonstrated the need to make maxi-mum use of the experience and great store of knowl-edge accumulated by the agencies that are assisted, andto avoid isolated contacts through vertical. advisoryservices, concentrating efforts instead on in-depthoperations carried out on many fronts simultaneouslyby teams of specialist advisers.
This joint approach, combining teams of officialsand of advisers, has made it possible to study eachspecialized area separately, analyze its effects and itsrelationship with other areas, and coordinate activi-ties in such a way as to ensure efficient management.Thus the action is centered on the operational levels inorder to develop appropriate practices and proceduresand familiarize the largest possible number of officialswith the new systems. Although this has been the pri-mary objective, higher-echelon levels have not beendisregarded: an attempt has been made at those levelsto develop and establish appropriate administrativepolicies and criteria to bring about a change in attitudesin line with the institutional reforms.
The dynamism of this new approach, and the impactproduced by combining within a single team bothnational officials and specialist consultants, has had adecisive effect in bringing about not only the desiredstructural and procedural changes but also the changesin attitude required to implement the institutionalreform.
It has been found, nonetheless, that most efforts inthe technical assistance field are weakened by lack ofcontinuity in the aid given to the institutions for the
99
application of recommendations and the solution ofproblems that arise. Therefore, an essential feature ofthe new approach is to continue our services for a suf-ficient length of time to bring about the changes pro-posed. Furthermore, assistance programs with no pro-vision for personnel training have proved ineffectual.Consequently, the greatest concern of the teams hasbeen to prepare personnel to use and handle the opera-tional machinery established during the period of as-sistance.
The collaboration of the Organization in the pasthas included the provision of teams of two to threeadvisers, in successive stages, to cover a series ofclosely interrelated aspects, such as rates, billing andcollection, and public relations. Countries whose insti-tutions were larger and had more staff have also re-ceived, in successive stages, groups of five to 10 con-sultants for periods of six to eight weeks each. Duringthese periods, operational manuals were prepared toserve as guides for the daily operations of the institu-tion; at the same time, a basic document was preparedfor programming the application of recommendationsand gradually implementing improvements in the systemaccording to the absorptive capacity of the institution.
Among the sectors commonly covered by advisoryprograms of the type mentioned are: organizationalstructure; organization and methods; staff planning andadministration; budgets, accounting, auditing, suppliesadministration, billing and collecting; public relations;transportation and workshops; meters; operation and
Planning and drafting office in a nationalsewerage institute.
maintenance; construction planning and control; andother factors required to promote improved manage-ment, build up a cadre of executives, and introduceeconomic criteria in the development of water andsewerage projects.
The Organization's efforts have proved insufficient toattain its objective; consequently it has turned to themultiplying effect of training public service officials toserve as advisers in other countries. The results thusobtained have widened the scope of assistance and theapplication of reforms and improvements.
The advances achieved by the countries in applyingthe recommendations are expressly reflected in thestatistics for the past four years. Group missions weresent to 13 countries (Bolivia, Colombia, DominicanRepublic, Ecuador, El Salvador, Guatemala, Hon-duras, Jamaica, Mexico, Nicaragua, Peru, Trinidadand Tobago, and Uruguay); 22 countries received otherforms of technical assistance; 118 manuals were pre-pared for the agencies receiving assistance; and anannual average of 90 consultant-months were providedboth in the form of consultant teams and for supple-mentary and follow-up work; approximately 200 of-ficials of water and sewerage agencies were trainedeach year in management and administration; and asum of $939,813 was received to defray the costs ofthe technical assistance provided during the period1965-1969.
The improvements made by the water and sewerageorganizations throughout the Hemisphere show clearlythat the administrative reform has taken firm root andthat this has made possible the investment of $945.42million over the past four years.
The interest of the Governments has been main-tained on an unprecedented level. For 1970 and 1971,PAHO/WHO has received requests from 18 institu-tions that wish to carry out programs for institutionalimprovements and administrative reform and have of-fered cash contributions to finance a large part of thetotal cost of these projects.
SEWERAGE AND WATER POLLUTION
The countries continued to work toward the targetsset in the Charter of Punta del Este for sewerage pro-grams. The results obtained, particularly in rural areas,still fall far short of the goals. The available data showthat only 22 per cent of the total population (urbanand rural) of the countries of the Americas are servedby sewerage systems. In urban areas, 39 per cent ofthe population have such services, whereas in ruralareas only 2 per cent are estimated to have propersewerage services or individual disposal systems.
100

Digging of trench for installation of sewerage for a town of10,000 inhabitants.
Loans and Technical Assistance
The international credit agencies assisted the coun-tries in this program through the granting of loans.Loans granted during the period 1966-1969 totaled$45.6 million, the major portion of which came fromthe Inter-American Development Bank, which providedapproximately $30.5 million, representing 67 per centof the total funds from banks and credit agencies. Loanswere granted to Argentina, Bolivia, Brazil, Colombia,Dominican Republic, Guatemala, Panama, Paraguay,Peru, Uruguay, and Venezuela. National counterpartfunds are estimated to have matched or equaled theamount of the loans. Most of the works financed withthese funds were designed to extend or improve existingsewerage services in cities and communities of somesize.
The Organization continued to collaborate with thecountries in solving certain specific problems relating tosewerage and pollution of water bodies. Assistance ofthis type was fumished by the permanent staff of engi-neers or by short-term consultants to the following
countries and localities: Brazil, Brasília and Sáo Paulo;Colombia, Bogotá; Ecuador, Guayas River Basin; Ja-maica, Montego Bay; Mexico, Acapulco and LermaRiver Basin; Uruguay, Montevideo; Peru, Lima; Haiti,Port-au-Prince. In Cuba, assistance was given withexperimental studies on oxidation ponds for the primarytreatment of sewage, and a considerable number ofthese were successfully developed.
A major educational effort was made in the fields ofsewerage, treatment of sewage and industrial wastes,and water pollution through the organization of alarge number of short intensive courses. Similarly,seven university research projects on matters relatingto treatment of liquid wastes of household or industrialorigin were completed or were under way. A detailedaccount of these various activities is given in the sec-tions dealing with manpower development and research.
Projections
As with water supply systems, four-year projectionsfor the period 1968-1971 were drawn up in 1968 inconjunction with the national authorities. The goal ofserving 42 per cent of the urban population throughproper sewerage systems in 1971 is reasonably close tobeing achieved if one takes into account that, at theend of 1969, 40 per cent of the urban populationalready had access to such systems. The projectionsfor rural areas, on the other hand, are rather modest, inline with the results obtained during this period.
COLLECTION AND DISPOSAL OF SOLID WASTES
PAHO/WHO continued its policy of cooperatingwith and providing technical assistance to countriesfor the organization and operation of national ormunicipal agencies responsible for the collection anddisposal of garbage and solid wastes. The importanceof public cleaning services for environmental healthhas been recognized ever more clearly. A series ofhighly complex factors are aggravating the problemsin this area: growing urbanization and industrializa-tion, rural migration to the cities, a vast increase in thequantities of waste materials produced, and the diffi-culty of finding proper sites for waste disposal facilities.
Short-term consultants gave assistance in a numberof cities-Buenos Aires, Caracas, Panama City, Lima,Santiago, and Tegucigalpa and San Pedro Sula in Hon-duras-in various aspects of the problem, from theselection of sites for incinerators to the use of sanitarylandfills and the establishment of specifications forrefuse-collecting vehicles and equipment. Most of thecountries were assisted in studying and solving prob-lems relating to the collection and disposal of solid
101

wastes, and in many cases considerable progress wasmade in improving the quality of the services.
Training and educational activities in subjects con-nected with this field received special attention. Eightshort intensive courses were organized and were at-tended by more than 250 officials, professional work-ers, and university professors. During these courses,excellent manuals were written which will serve asreference texts in the countries.
PAN AMERICAN SANITARY ENGINEERINGAND ENVIRONMENTAL SCIENCES CENTER
The principal purpose of the Center, which becameoperational early in 1968, is to render expert technicaland scientific assistance to the countries, especially inconnection with the new environmental problems aris-ing from increased urbanization, industrialization, andtechnological development. It also serves as an inter-national reference and information agency. The prepa-ration and distribution of technical information ma-terials is an important function and serves to extend andmultiply the technical assistance services which can beprovided by the limited staff of expert consultants serv-ing on a Regional basis. In addition to these functions,it is expected that, when the necessary resources be-come available, the Center will play a key role in thesupport of training and research activities.
The current staff provides expert assistance in thefields of air pollution, water supply, water pollution,housing, urbanization, physical planning, industrialhygiene, and rural community development. A libraryhas been established and the preparation of technicalinformation has begun. Equipment for printing andreproduction has been installed and is in use.
Administrative and operational guides for the Cen-ter were prepared and issued.
During the first year of operation, advisory servicesin the fields of specialization covered by the Centerwere rendered to 14 countries of the Region.
Air Pollufion and Industrial Hygiene
Development of the Pan American Air PollutionSurveillance Network continued under the auspices ofthe Center. At the end of the quadrennium 22 stationssituated in Argentina, Brazil, Chile, Colombia, Mexico,Peru, Uruguay, and Venezuela were in normal opera-tion. The first report of the Network was distributed inMarch 1969.
Evaluations of the air pollution programs were madein Argentina, Colombia, and Cuba. Assistance wasgiven to Peru in conducting a course on air pollution,and to the Institute of Occupational Health and AirPollution Research of Chile, where classes were givenon the same subject. Seven fellowships were grantedto professionals from four countries for the study ofair pollution.
The final report of the UNDP project on the Instituteof Occupational Health and Air Pollution Research wasprepared by the Center staff. It covers the organizationand development of the Institute, the objectives at-tained, an evaluation of the project, and sets forth rec-ommendations and conclusions.
Assistance was given to El Salvador in the selectionand briefing of a short-term consultant for the study ofindustrial hygiene legislation in the country. The Cen-ter also helped to conduct the following short courses:mine ventilation (University of Oruro, Bolivia); (Uni-versity of Nuevo León, Mexico); and industrial hygiene(National University of Colombia). The followingcountries were visited one or more times in connectionwith industrial hygiene studies: Argentina, Bolivia,Colombia, Chile, Cuba, El Salvador, and Mexico.
- - 11- . -
Industrial hygiene. Left: A miner (suffering from silicosis) uses wef drill fo damp down dust. Right: Example of a mask used againstdust in a crusher mill.
102

Chile was assisted in conducting a seminar held atthe Institute of Occupational Health for 70 industrialhygiene workers of the National Health Service. Thisseminar, which included conferences, round tables, andshort courses, should make an important contributionto upgrading the activities in this field both in Chileand in other Latin American countries, since the Insti-tute serves as a training center for the Hemisphere.Advisory services were rendered to the Governmentof Cuba in connection with its program of industrialhygiene, and in particular the problems arising from themassive use of pesticides, which are applied to rice andsugarcane fields by airplane. A consultant from theOrganization spent a month in the country advisingthe national officials on the pesticide problem and onlaboratory techniques employed for pesticide analysis.The Government was also given advice on the planningof a short industrial hygiene course to be presented in1970 and on the training of professional staff in thisfield.
The programs in occupational health in Argentinaand Colombia were reviewed at the request of thesecountries, since both programs are undergoing majorchanges.
Housing
The general housing situation in Latin America hastended to worsen in spite of all the efforts made by thecountries to overcome the existing deficiencies. It isapparent that the designs, systems, and procedures cur-rently employed are not properly adjusted to the socialand economic conditions prevailing in most of theareas.
Housing programs in general still suffer from a basicdefect: they do not provide an adequate proportion ofsolutions for low-income families, and existing projectsconcentrate principally on construction in the largercities. Small towns and villages, as well as rural areas,receive only scant help.
Consequently, low-cost housing development schemesin Latin America, both official and private, cover lessthan 10 per cent of the housing needs. Most of thepopulation continues to build traditionally by self-help.However, lacking the necessary programming, technicalassistance, or orientation through adequate minimumstandards, this tremendous effort often culminates inprecarious dwellings like those which form the notori-ous shanty-towns of the big cities. These difficult con-ditions may continue for years to come, or as long asthe present approach to the problem remains un-changed.
The determining influence of the environment onman's physical and mental health is an undisputed and
A modern housing project in Venezuela.
universally accepted fact. Housing is part of this en-vironment and consequently affects the health and wel-fare of the whole population. A case in point in LatinAmerica is the connection between Chagas' disease andhousing. The disease, whose transmission is intimatelyassociated with the structural design of dwellings, oc-curs in almost all countries of the Region and perhapsas many as 10 million people are infected by it (seealso pp. 79-81).
The establishment of the Pan American SanitaryEngineering and Environmental Sciences Center, whosefield of activity includes housing in its broader context,has enabled the Organization to intensify its work inregard to the residential environment and has led tohigher efficiency in the programs related to this field.
The Organization's participation in housing, origi-nally limited to the purely sanitation aspects, has beenextended in recent years to cover a wide range of re-lated problems, such as urban development, commun-ity facilities, and physical planning, all of which havebecome of vital interest to health authorities. This hasbeen accompanied by an increased demand for special-ized advisory services from the Organization.
Activities in which the Center is participating includethe pilot projects in rural housing organized by the OASInter-Agency Committee on Housing and Urban De-velopment and to be carried out in Colombia, Ecuador,and Venezuela; the publishing of minimum standardsof urbanization in collaboration with the Inter-Ameri-can Housing and Planning Center (CINVA), and theexperimental housing project (PREVI) in Lima, Peru.
103

Advisory services in rural housing and physical plan-ning were also given to the FAO/UNDP-SF project forthe development of the Huallaga River Basin in Peru.
Other Activities
During the first year of its operations three meetingswere held at the Center: one of the Executive Boardof the Inter-American Association of Sanitary Engi-neering (AIDIS); a meeting of PAHO staff to discusshousing; and a meeting of PAHO Zone engineers anddepartmental staff. Reports covering these two lastmeetings were prepared by the Center.
In addition to collaboration in matters concerning
fellowships, assistance was given in training programsfor professionals working in specialized fields of inter-est to the Center.
The Center was designated by the World HealthOrganization as a WHO Reference Center on wastesdisposal. This will enable it to participate in a world-wide network of collaborating institutions which ex-change information and consider solutions to technicalproblems in this field.
A water supply specialist was added to the staff atthe close of the period. The Center will thus be ableto provide expert services in relation to the newestdevelopments, especially in water treatment technology.
PROMOTION OF HEALTH
GENERAL HEALTH SERVICES
The countries' determination to improve and expandtheir national health services as instruments for healthpromotion, protection, restoration, and rehabilitationwithin the framework of national development wasunequivocally incorporated in the Punta del Este reso-lutions relating to the Hemisphere as a whole.
One of the factors leading up to this decision was anawareness of the deficiencies of the health services atdifferent levels of national administration, as regardsboth organization in general and their main components-human resources, installed capacity, investments, andexpenditures-and also their functional aspect andoperational effectiveness. Added to this was the stimu-lus provided by demonstration projects, many of whichwere still in progress.
The 1962 Annual Report included the followingstatement: "As a continuation of past efforts, assist-ance was given in 1962 to 21 demonstration projectsin 19 countries. The purpose of these projects both atthe national and at the local level was to apply ap-proved standards for preventive and curative activitiesand for health promotion." In that same year, eight ofthe 21 projects outlined specific objectives and actionfor establishing and implementing national health plans.In 1966 this figure went up to 15 out of 38, and in1968 to 23 out of 48.
Thus health-service development projects passed inthis way from the demonstration to the general applica-tion stage. This led the Governments to promote thedevelopment of a process placing emphasis on system-atic planning in the socioeconomic sectors and onaction considered necessary in order to accomplish the
established objectives and goals. Ministries of health,as the leaders in their sector, began to formulate na-tional analyses and plans of action in collaboration withother sectors, aiming, on the one hand, to increase theoutput of goods and services and, on the other, to makethese accessible to the majority of the population.
At this stage of expansion, with efforts being made tospeed up the process and broaden its scope, the short-comings of the health service system were made all themore evident-some already well known and others stillunder investigation. These have been and will continueto be a field for action in the health service projects.
The variety and complexity of these deficiencies werethe main factors that prompted ministries to continuedeveloping these projects. An examination of the proj-ects shows how each different situation has beentackled with different approaches and different em-phases, while at the same time they have maintainedthe basic objectives and principles of health serviceorganization and administration that continued togovern their structure and functioning and which hadbeen proved valid in the earlier demonstration stage.
During the period 1966-1969 the number of health-
TABLE 33. NUMBER OF COUNTRIES AND TERRITORIES RE-CEIVING ADVISORY SERVICES THROUGH PROJECTS FOR DE-VELOPMENT OF GENERAL HEALTH SERVICES, 1966-1969.
NO. OF COUNTRIES AND TERRITORIES
YEAR PROJECTS
COUNTRIES TERRITORIES TOTAL
1966 38 23 4 271967 41 23 4 271968 45 26 6 321969 48 26 11 37
104
service development projects rose from 38 to 48, andthe number of countries and territories where theywere in progress rose from 27 to 37, as can be seenfrom Table 33.
The most steady progress is to be seen in those proj-ects where the improvement and expansion of the healthsystem was based on a health plan which, even if notnational or general, at least operated on a ministeriallevel and provided basic services. A good example ofthis was the obvious improvement in the statisticsunits of health ministries or services in a number ofcountries, such as El Salvador, northeast Brazil, Chile,Colombia, Peru, and Panama, where the systems andforms of organization employed were being adapted tothe needs of the established plans.
Another noteworthy example was the progress madein the regionalization of health services, introduced asa result of certain regional development plans, as in thecase of Paraguay, which established a VI Region inorder to provide health services in a new settlementarea; Brazil, which had projects in the northeast,southern, and Amazon regions; Argentina, which setup eight health regions to serve the eight principalsocioeconomic development areas; and Honduras,which established the III Health District in the SanPedro Sula region, among others.
Thus it has been possible to institute or strengthenan entire regional technical and administrative systemdesigned to serve the needs of the plan and providedwith the necessary budgetary and legal support andwith the authority to take decisions, the absence ofwhich has been and continues to be one of the difficul-ties facing the regional health service system.
This tendency to "regionalize development" in thecountries is also reflected in the scope of the healthservice projects receiving assistance from the Organiza-tion, as can be seen in Table 34.
At the beginning of the quadrennium, 11 out of 38projects (29 per cent) were operating on a regionalscale and in 1969, 18 out of 48 (37 per cent). In somecases these projects also received assistance from otherintemational agencies such as UNDP, UNICEF, FAO,UNESCO, and ILO, thus resulting in multidisciplinary
TABLE 34. DISTRIBUTION OF PROJECTS ACCORDING TO TYPE,1966-1969.
YEAR TOTAL NATIONAL REGIONAL INTERCOUNTRY(AMRO)
1966 38 27 11 -1967 41 19 20 21968 45 30 14 11969 48 28 18 2
advisory services, no longer of a demonstration andvertical nature but integral in character.
At the same time, projects on a national scale, whilestressing their health promotion, protection, and re-covery activities, improved or undertook studies onother components of the system at a central level, in-cluding organization of technical and administrativedepartments, standards for program activities, opera-tional methods and procedures, present and futureneeds as regards funds and fund sources, legal bases,relationships with other agencies within and outsidethe sector, and plans for programs under way orscheduled for execution.
The Organization's assistance in these projects,which encompass such a wide variety of activities, hasbeen reflected in the make-up of the advisory servicesto meet the countries' needs in increasingly specializedhealth fields. This diversification of advisory serviceshas in some cases been achieved by means of permanentstaff members, but more often by short-term advisers.In terms of budgetary expenditures, PAHO/WHO'sassistance is shown in Table 35.
The relative importance of general health servicesprojects within the Organization's total budget is par-tially reflected in the more or less constant proportionof 11 per cent, which was maintained during the four-year period. Although this was the proportion main-tained in budgetary terms, the number of projects in-creased in 1969 by 26 per cent, as compared with1966.
The progress made in terms of intra-, extra-, andparasectoral coordination, as regards both its accept-ance as a means for obtaining more rational utilizationof funds and the measures taken to achieve it, hashelped to strengthen health services at all levels ofadministration. The action taken to make health plan-ning a part of the over-all development process facili-tated contact among institutions that organized groupsto study and assess health needs and high-level com-mittees to give guidance on matters affecting healthpolicy. Projects in 14 countries concentrated on themethods of coordination, from the action taken by dif-ferent sectoral agencies to identify common aims and
TABLE 35. BUDGET FOR GENERAL HEALTH SERVICES PROJECTS(No. 3100), 1966 to 1969.
(In thousands)
TOTAL PAHO/WHO TOTAL 3100 PROJECTSYEAR
DOLLARS % DOLLARS %
1966 19,690 100.0 2,317 11.81967 22,099 100.0 2,475 11.21968 24,033 100.0 2,494 10.41969 24,780 100.0 2,787 11.2
105
TABLE 36. NUMBER OF OFFICERS TRAINED AT THE LOCALLEVEL, AVERAGES PER PROJECT AND PER CENT INCREASE.
OFFICERS PER PROJECT
YEAR NO. OF NO. OF OFFICERS
PROJECTSa
TRAINED AVERAGE PER CENT
INCREASE
1966 19 4,061 213.7 -1967 24 11,123 463.5 1171968 15 6,568 437.9 1051969 19 11,597 610.4 186
a This information does not include all the projects.
objectives for preventive and curative medical care, tothe adoption of legal measures for the almost completeintegration of health and care services under the admin-istration of the ministry of health.
The ministries have thus been strengthened by thisregionalization and coordination process. If to thisprogress one adds the work done in training personnelat the local level through the health services projects-this being another field in which advances were made-satisfaction is warranted regarding the over-all activitiesof the countries, although there is still much to be doneto expand the coverage of basic health services, espe-cially in the rural areas, and this therefore remains agoal for future years.
It should be noted that the average number of per-sonnel trained locally, per project reporting, rose from213.7 in 1966 to 610.4 in 1969 (Table 36). Theemphasis placed on training is therefore clearly evident.
To sum up, the Governments, with the support of
the Organization's advisory services, have continued tomake progress in the development of general healthservices projects, in keeping with the principle thathealth is a unified whole and health activities shouldbe integrated.
MEDICAL CARE AND REHABILITATION
In the previous four-year period the Organizationdefined a medical care policy that had been progres-sively formulated at a series of meetings convened forthat purpose.
The field of action of medical care is linked withrelated activities in other sectors of economic and socialdevelopment, so that medical care policy has to beconsidered in conjunction, and in close coordination,with other interested groups. Medical care, in fact,uses human and other resources ranging far beyond thesphere of action of the health sector, and it thereforemust establish relations with other sectors, such associal security, whose close administrative and financialconnection with medical care cannot be denied. Onthe other hand, the setting up of a system of medicalcare requires the simultaneous implementation of aninfrastructure program together with the installation ofhighly specialized equipment, all of which necessitatesinvestments that affect the availability of funds for othersocial and economic development projects. Lastly, butno less important, the decisive role to be played by theorganized medical profession and other related profes-sional groups in the provision of medical services to the
Exhibif on medical care in the Americas.
106
community must be taken into account. The medicalcare program therefore has to be 'adapted to the require-ments and characteristics of all these groups and sectorsif it is to prove successful.
In the 1966-1969 period the Organization's medicalcare policy, as defined by the Governing Bodies, re-ceived the support of other organizations of the Inter-American System. In fact, the Inter-American Eco-nomic and Social Council (IA-ECOSOC), at its FourthAnnual Meeting at the Ministerial Level, adopted reso-lutions which, in essence, recommended to the Govern-ments that the "social security plans and programs formedical services be improved and coordinated withdevelopment plans, and particularly with the healthplans in each country," and also that the Governments"incorporate activities relating to the prevention andcure of diseases in the development efforts, particularlyin the land settlement, city planning, and industrialdevelopment programs."
The Permanent Inter-American Social Security Com-mittee, the Pan American Medical Conference, andthe VIII Conference of the American States Membersof the International Labour Organisation passed reso-lutions which, in one form or another, supported thoseadopted by PAHO/WHO. By virtue of these recom-mendations, organizations representing the social secu-rity institutions, the organized medical profession, andlabor groups showed themselves to be in favor of anintegral medical care policy as an essential element ofnational health plans.
This action at the international level culminated atthe Special Meeting of Ministers of Health of theAmericas, at which "there was general agreement thatthe coordination of health resources is essential andthat it would be pointless to continue to talk abouthealth planning unless there is mutual understandingamong institutions in the health sector to coordinatetheir resources."
Medical Care Policy
By drawing on the experience gained and taking intoaccount the opinions and interests of all the groupsinvolved, the Organization has brought up-to-date itsmedical care policy, which can now be summarized inthe following points:
a) Intrasectoral coordination of the institutions pro-viding health services, whether preventive or curative,as an essential step toward the integral planning ofhealth services.
b) Adaptation of the hospital system to meet therequirements of integrated health programs and cooper-ate effectively in the training of professional and techni-cal health personnel.
c) Improvement of hospital administration to raisethe quality of the medical care provided and increasethe productivity of the hospital-bed resources available.
d) Development of a progressive program of train-ing in health service administration designed to incor-porate instruction in the basic principles of adminis-tration in the curricula for medical students and traineesfor the paramedical professions, to provide inservicetraining for professional staff holding senior positions,and to train future specialists in health service adminis-tration and, most particularly, future instructors andresearchers in administration.
Coordination of Medical Care Services
The Organization has been fostering the policy ofinstitutional and intrasectoral coordination since 1962.Regarding this subject, the Ministers of Health declaredthat "coordination will make it possible to raise thelevel of medical care, expand coverage as much aspossible, and promote the active participation of thelocal community in the planning and administration ofservices." They further pointed out: "Systems shouldbe set up in each country without delay for the effectivecoordination of the health services of ministries ofhealth with those of social security institutions,.univer-sities, and other private and public bodies. To assurethat coordination is effective, it should be a permanentactivity of all those who participate in the process ofplanning, administration, and provision of servicesunder the guidance of the health ministries or the cor-responding agencies. In this way, closer institutionallinks will be forged at the central level, regionalizationwill be achieved at the intermediate level, and integra-tion of curative and preventive services at the locallevel."
This recommendation introduced a new element intothe coordination process: participation by the universi-ties in the planning, administration, and execution ofhealth programs. There are two reasons which fullyjustify this. Not only do the universities train healthprofessionals-their basic and essential function-butthey also own and administer, on an ever-growing scale,hospitals and other health establishments which, ofnecessity, have to be included in the process of coordi-nation of regional health programs.
In accordance with the recommendation of the Min-isters' Meeting and in implementation, moreover, ofanother formulated by the XVII Meeting of the Direct-ing Council, the Organization, in cooperation with theOAS, organized a Study Group on the Coordinationof Medical Care Services, composed of five experts fromministries of health, five from social security institu-tions, and five from schools of medicine. It was also
107

attended by observers from the ILO, the InternationalSocial Security Association, the Permanent Inter-American Social Security Committee, and the PanAmerican Federation of Associations of MedicalSchools. The Group, so constituted, included amplerepresentation of national and international institu-tions concerned with the administration and financingof health services and the training of the personnelneeded to provide such services.
The Group discussed in detail the mechanismsthrough which intrasectoral coordination of healthinstitutions could be achieved in order to define acommon health policy, and administrative methods forincreasing the utilization and productivity of availableresources and for making the services accessible to thosewho need them.
From the point of view of manpower development,the Group analyzed the need to utilize general hospi-tals, including outpatient clinics, suburban and ruralservices, and even home services, for teaching purposes,thus bringing medical students into contact with themedico-social reality of the environment in which theywill have to exercise their profession. Special emphasiswas laid on using the installed capacity of social secu-rity hospitals for teaching, since these hospitals usuallyhave the best buildings, equipment, and installations.
As regards financing, the Group made a study of theoperational costs of medical care and of capital invest-ments for medical care services. It decided in favor ofmultilateral financing and the mobilization of nationaland international resources for the remodeling andadaptation of health establishments, with technical-and probably financial-assistance from organizationsof the Inter-American System. It recognized that "ifthe whole range of preventive, curative, and social ser-vices necessary for maintaining health is to be madeavailable, and considering the high level attained bythe cost of health care, it cannot be expected for thetime being that any single institution or body will bein a position to finance them in their entirety, and itwill, therefore, be necessary in the meantime to haverecourse to multilateral financing and to coordinatedadministration under a national health system."
Continuing its policy of coordination in the inter-national field and with a view to ensuring the widestpossible dissemination of the principles and thinkingbehind it, the Organization participated in a largenumber of national and international meetings dealingwith coordination of medical care services, among whichthe following were of special importance:
VIII Conference of American States Members of theILO (Ottawa, Canada, September 1966)
IX Medico-Social Congress of the Pan American Medi-cal Confederation (Lima, Peru, April 1966)
XV Conference on Social Security in the Americas(Lima, Peru, September 1967)
First Salvadorean Social Security Congress (San Salva-dor, El Salvador, December 1967)
First Venezuelan Seminar on Hospitals (Caracas, Vene-zuela, August 1968)
XXXVII Costa Rican National Medical Congress (SanJosé, Costa Rica, November 1968)
Second Regional Conference of Hospitals of the Inter-national Hospital Federation (San José, Costa Rica, No-vember 1968)
First American Congress on Social Security Medicine(Mexico City, January 1969)
World Round-Table Conference on the Contribution ofSocial Security Systems to Public Health Programs (Oax-tepec, Mexico, January 1969)
Greater Colombian Seminar on Social Security andMedical Education (Quito, Ecuador, November 1969).
Annual courses on the organization and operation ofmedical services of social security institutions, organizedby the Inter-American Center for Social Security Studies,in Mexico City.
Technical assistance was rendered to countries re-questing it in the fields of hospital regionalization, co-ordination of preventive and curative services at thelocal level, plans for establishing integrated health ser-vices, and study and collection of basic data needed forsetting up national health insurance schemes. Argen-tina, Brazil, Cuba, the Dominican Republic, Guatemala,Guyana, Panama, Peru, Trinidad and Tobago, Uru-guay, and Venezuela all received assistance in one ormore of these fields.
Hospifal Planning and Administration
The hospital-a key component of the medical caresystem, because of its administrative complexity, thevariety of services it provides, and its high operatingcost-has had high priority in the Organization's pro-grams during the four-year period.
The Special Meeting of Ministers of Health definedthe problem in the following terms.
The regionalization and coordination of programs forthe building of hospitals and other health facilities is evenmore important when such programs are covered by theinvestment plan which, in turn, is one of the componentsof the national health plan and of the economic and so-cial development plan. The enormous capital investmentnecessary to implement a construction program has amajor impact on the distribution of financial resources,and its effect on the national economy is such that it mustreflect a strictly functional and economic standpoint, sincethe capital invested in hospitals could, as an alternative,be invested in schools, roads, or industrial machinery,
108
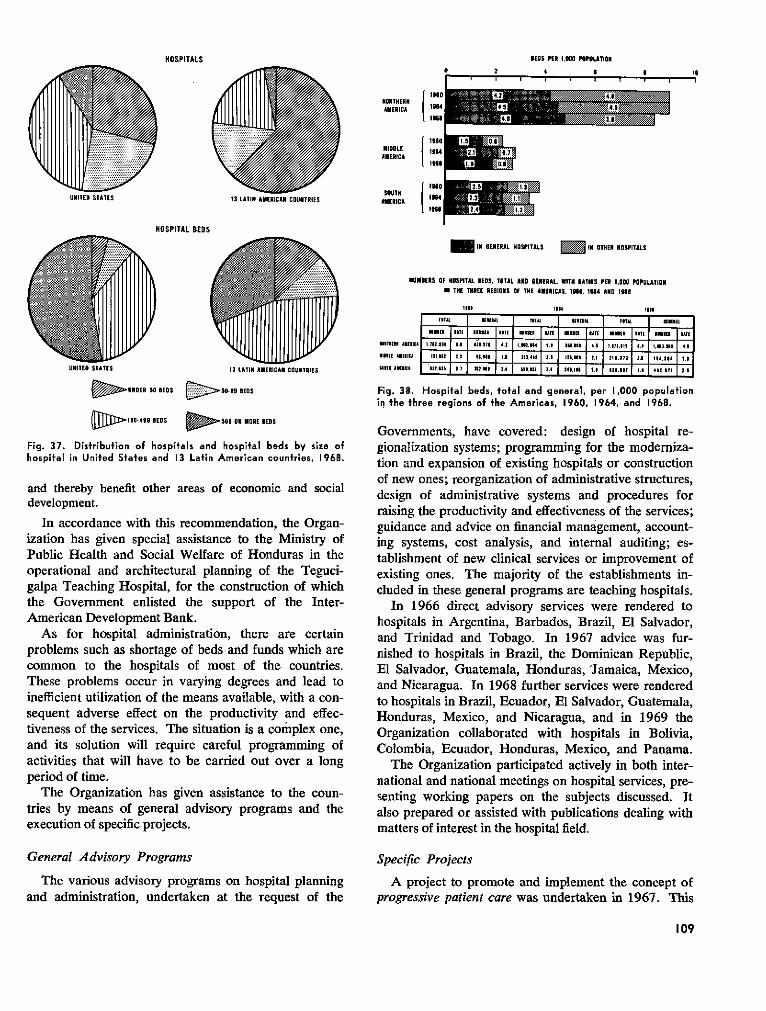
ORTHER 19AMERICA I
lsel
MIDD LE HAMERICA 1
1 8'4
AMERICA 1H :1 aR .
HOSPITAL BEDS
D STATES 13 LATIN
> UNOER SO REDS '->5- 50-99 BEDS
> 100- 499 BEDS o O500 OR MORE BEDS
Fig. 37. Distribution of hospitals and hospital beds by size ofhospital in United States and 13 Latin American countries, 1968.
and thereby benefit other areas of economic and socialdevelopment.
In accordance with this recommendation, the Organ-ization has given special assistance to the Ministry ofPublic Health and Social Welfare of Honduras in theoperational and architectural planning of the Teguci-galpa Teaching Hospital, for the construction of whichthe Government enlisted the support of the Inter-American Development Bank.
As for hospital administration, there are certainproblems such as shortage of beds and funds which arecommon to the hospitals of most of the countries.These problems occur in varying degrees and lead toinefficient utilization of the means available, with a con-sequent adverse effect on the productivity and effec-tiveness of the services. The situation is a complex one,and its solution will require careful programming ofactivities that will have to be carried out over a longperiod of time.
The Organization has given assistance to the coun-tries by means of general advisory programs and theexecution of specific projects.
General Advisory Programs
The various advisory programs on hospital planningand administration, undertaken at the request of the
M IHM GENERAL HOSPITALS 3 IN OTHER IOSPITALS
HUMNERS OF HOSPITAL EODS, TOTAL AOD GENERAL, WITH RATIOS PER 1,000 POPULATION
IN THE TRIRE REGIONS OF THE AMERICAS. IN10, 18G4 ANOD 198
losl 1934 los
I RATEa BATE *lo lATE ama1 lATE f|laumA
mn o II ,1,3 I3 3 ,lIE3 4 2 .1 3 1. 3,3 _,il4 tE 4 .6 3,)3I 3. I3,4, .3
NI1B 11 3ElC I3LEl 31, 3.33 3l 4 1. 3 211,44E 3 .I 1 3l 3 33 .31 3 3.3l 1
senolTd lI , 1 E. ' EL 2.4, _ s Sl 3.4 lta E. 4ElIT!
Fig. 38. Hospital beds, total and general, per 1,000 populationin the three regions of the Americas, 1960, 1964, and 1968.
Governments, have covered: design of hospital re-gionalization systems; programming for the moderniza-tion and expansion of existing hospitals or constructionof new ones; reorganization of administrative structures,design of administrative systems and procedures forraising the productivity and effectiveness of the services;guidance and advice on financial management, account-ing systems, cost analysis, and internal auditing; es-tablishment of new clinical services or improvement ofexisting ones. The majority of the establishments in-cluded in these general programs are teaching hospitals.
In 1966 direct advisory services were rendered tohospitals in Argentina, Barbados, Brazil, El Salvador,and Trinidad and Tobago. In 1967 advice was fur-nished to hospitals in Brazil, the Dominican Republic,El Salvador, Guatemala, Honduras, 'Jamaica, Mexico,and Nicaragua. In 1968 further services were renderedto hospitals in Brazil, Ecuador, El Salvador, Guatemala,Honduras, Mexico, and Nicaragua, and in 1969 theOrganization collaborated with hospitals in Bolivia,Colombia, Ecuador, Honduras, Mexico, and Panama.
The Organization participated actively in both inter-national and national meetings on hospital services, pre-senting working papers on the subjects discussed. Italso prepared or assisted with publications dealing withmatters of interest in the hospital field.
Specific Projects
A project to promote and implement the concept ofprogressive patient care was undertaken in 1967. This
109
HOSPITALS REDS PER 1,000 POPULATION
4 eir i i
G 30
4.2
4. 11.5
p�� .8
0 21 T 1
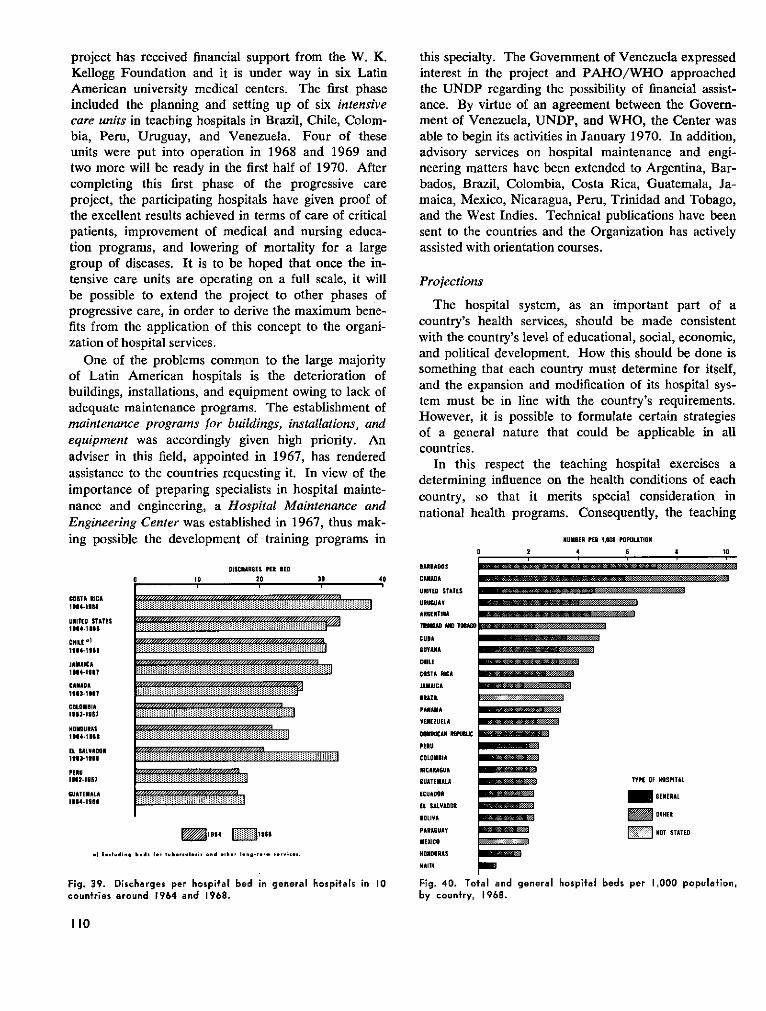
project has received financial support from the W. K.Kellogg Foundation and it is under way in six LatinAmerican university medical centers. The first phaseincluded the planning and setting up of six intensivecare units in teaching hospitals in Brazil, Chile, Colom-bia, Peru, Uruguay, and Venezuela. Four of theseunits were put into operation in 1968 and 1969 andtwo more will be ready in the first half of 1970. Aftercompleting this first phase of the progressive careproject, the participating hospitals have given proof ofthe excellent results achieved in terms of care of criticalpatients, improvement of medical and nursing educa-tion programs, and lowering of mortality for a largegroup of diseases. It is to be hoped that once the in-tensive care units are operating on a full scale, it willbe possible to extend the project to other phases ofprogressive care, in order to derive the maximum bene-fits from the application of this concept to the organi-zation of hospital services.
One of the problems common to the large majorityof Latin American hospitals is the deterioration ofbuildings, installations, and equipment owing to lack ofadequate maintenance programs. The establishment ofmaintenance programs for buildings, installations, andequipment was accordingly given high priority. Anadviser in this field, appointed in 1967, has renderedassistance to the countries requesting it. In view of theimportance of preparing specialists in hospital mainte-nance and engineering, a Hospital Maintenance andEngineering Center was established in 1967, thus mak-ing possible the development of training programs in
COSTA RICA10l4-100l
UlITED STATES1964-1668
CHILE '1I64-1601
JAMAICA11U4-1S7
CANADAR113-10l7
CDLOMBIAU3$-1 RB7
HONDURASIRU4.1UUU
EL SALVADOR1OR3-tIll
PERU16112 1S7
GUATEMALA1114-1AR
I1DISCHARGES PER RED
20 20 40
21964 m a19S1
.) E..lu.din . b.d. t1 be loi, ofnd t,h., lon-i-e-- i - *. .
Fig. 39. Discharges per hospital bed in general hospitais in 10countries around 1964 and 1968.
this specialty. The Government of Venezuela expressedinterest in the project and PAHO/WHO approachedthe UNDP regarding the possibility of financial assist-ance. By virtue of an agreement between the Govern-ment of Venezuela, UNDP, and WHO, the Center wasable to begin its activities in January 1970. In addition,advisory services on hospital maintenance and engi-neering matters have been extended to Argentina, Bar-bados, Brazil, Colombia, Costa Rica, Guatemala, Ja-maica, Mexico, Nicaragua, Peru, Trinidad and Tobago,and the West Indies. Technical publications have beensent to the countries and the Organization has activelyassisted with orientation courses.
Projections
The hospital system, as an important part of acountry's health services, should be made consistentwith the country's level of educational, social, economic,and political development. How this should be done issomething that each country must determine for itself,and the expansion and modification of its hospital sys-tem must be in line with the country's requirements.However, it is possible to formulate certain strategiesof a general nature that could be applicable in allcountries.
In this respect the teaching hospital exercises adetermining influence on the health conditions of eachcountry, so that it merits special consideration innational health programs. Consequently, the teaching
lUMBER PER 1,000 POPULATION
2 4 6 a 10
AURBADOS
CARADA
UlNITED TATES
URUGUAY
ARGENTINACARAETll t
T~AO AH TOACO /
CUGA YCUYAA ,
CHILECOSTA RICA
JAMAICA
BRAZIL
VElNEZUELA
lUtMCAN RPSCPERU
COLOMBIA
NICARAGUA
rUATEMALA _ TYPE OF NOSPITAL
ECUDOR GEERAL
EL SALVADOR I
ROLIVA OTHER
PARAGUAY IOT STATEDMEXICO
HONlDURAS R
HAITI
Fig. 40. Total and general hospital beds per 1,000 population,by country, 1968.
¡o10
iliiiiiliiiiiiiijii;iiijiiiiii
liiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiii
iiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiii
iiiiiiiiiiiciiiiiiiiiiiiiiiiijiiiiiiiiii
iiliijiiliijiiiiiiliijlIiiiIlIiiijiIijlI
iiIlIiiiIlIiiiIiIiIiIiiIjiiiiiiIiIiiiIlI
iIlIiiiIiIiiiIlIii
·'·'·'·'·:·'·'·:
II
hospital almost always has, or should have, excellentmedical staff who are responsible for the developmentof both the medical care and the teaching programs.The teaching hospital creates an image for the studentwho tomorrow may possibly be in charge of setting upor directing new hospital services. This multiplicationfactor alone would be sufficient justification for thepriority accorded advisory programs to assist teachinghospitals. Notwithstanding this priority, Governmentsmay of course designate nonteaching hospitals foradvisory assistance.
Among the projects that could be undertaken are thefollowing:
1. In agreement with each Government concerned,selection of one or more hospitals, teaching or non-teaching, with a view to converting them into pilot ormodel hospitals in each country, both for the care ofpatients and for the development of teaching programs,and all operated under the most efficient administrationprinciples.
2. Carrying out of a census of teaching hospitals,to be continued and updated at regular intervals.
3. Evaluations of architectural features and of theefficiency of installations and equipment in hospitalswhich each Government considered to be of nationalimportance, in order to assess the requirements interms of modernization, expansion, or replacement bynew buildings. Only in this way will it be possible toobtain a quantitative idea of the investments in build-ings and equipment needed for hospitals of nationalimportance in the countries of the Hemisphere.
4. Once the needs were known, and with the activeinterest of the Government concerned, continuation andexpansion of the Organization's cooperation in con-nection with the channeling of national and internationalfunds to finance improvement programs for hospitalbuildings, installations, and equipment.
5. Continuation of the project to apply the progres-sive patient care concept to other phases in hospitalswhich have already made a start with the establishmentof intensive care units. Extension of this project toother hospitals in countries where this type of servicehas not yet been established.
6. Cooperation with hospital maintenance programsthrough the training of specialist personnel at the Hos-pital Maintenance and Engineering Center in Caracas,and the provision of direct advisory services by con-sultants.
7. Improvement of hospital administration throughthe application of operating procedures and systemsdesigned to increase productivity. Work systems andschemes should be based on analysis of the results of
IV
Intensive care unit in the San Juan de Dios Hospital in Bogotá,Colombia.
time and activity studies conducted in each of thehospitals participating in this type of project.
Education and Training of Personnel
During the four-year period, the varied and complexproblems faced by the hospital establishments-whichin Latin America and the Caribbean area number al-most 13,000-posed a major difficulty for educationand training designed to produce a rational administra-tion system, and they will continue to do so in thefuture. The importance of the administrative functionis increasing from day to day, especially as regards theadoption and implementation of decisions leading toimprovement in the efficiency and productivity of hos-pitals and health establishments.
The Organization has carried out extensive activitiesfor education and training in medical care and hospitaladministration in the Americas; these have included:
1. Determination of the need for training in healthadministration.
2. Planning of education and training courses to meetthat need.
3. Training of teachers and instructors capable ofinstilling attitudes conducive to effective learning.
4. Evaluation of training programs, basically fromthe threefold angle of (a) curriculum evaluation, (b)evaluation of the instruction process, and (c) evalua-tion of the product of the instruction, i.e., the impact ofcourse graduates on their environment, in terms of theirability to change the existing situation.
Activities in this field included the First Symposiumon the Teaching of Administration of Medical Services,organized in 1967 by PAHO/WHO with the coopera-
III
1
tion of the School of Public Health of Antioquia Uni-versity, Colombia. This meeting, attended by profes-sors of medical care administration from the eightprojects existing at the time, together with hospitaldirectors who acted as tutors during the Symposium,outlined a training policy that stressed the urgent neednot only for training specialists in medical care andhospital administration, together with intermediate-levelstaff, but also for incorporating the principles of publichealth administration and hospital administration in thecurricula of medical students. The latter is consideredfundamental, in order to make the clinical physicianaware of the need for his active participation in theadministration of the health institution in which heworks.
Also in 1967, the Fifth Conference of Directors ofSchools of Public Health of Latin America was held inBuenos Aires, Argentina. This Conference endorsedthe recommendations of the Symposium in theirentirety.
The Organization cooperated closely, through theministries of health, with the institutions responsible forthe education and training of medical care administra-tion personnel. This cooperation was extended pri-marily to the regular public health administration andmedical care and hospital administration courses of theSchools of Public Health of the Universities of BuenosAires, Argentina, and of Sao Paulo, Brazil; the Founda-tion for Specialized Teaching in Public Health in Riode Janeiro, and the Health Ministry of the State ofMinas Gerais, Brazil; the University of Chile; the Uni-versity of Antioquia, Colombia; the Ministry of Healthand Welfare of Mexico; the Ministry of Public Healthof Peru; the Central University of Venezuela; and theNational Department of Higher Education of Cuba.
Assistance was rendered to all these institutions inconnection with the formulation of aims and objectives,program content, teaching methods, and evaluation ofthe training courses and plans.
Similar assistance was given in the medical care andhospital administration programs of the Catholic Uni-versity in Rio de Janeiro, the Hospital Fund of Cun-dinamarca Department in Bogotá, Colombia, the Inter-American Center for Social Security Studies (CIESS)in Mexico, and the Cayetano Heredia University inLima, Peru.
The number of regular medical care and hospitaladministration programs in Latin America rose fromeight to 17 during the four-year period. The programsare not all the same as regards duration, attendanceand entrance requirements, type of degree awarded,course content, and teaching-learning methodology.
To improve the practice stage of the training in ad-
ministration for medical directors, the First VenezuelanSymposium on Residencies in Hospital Administrationwas held in 1969. The 25 participants were professorsfrom the School of Public Health, directors of the majorhospitals in the country who acted as course tutors,and officials of the Ministry of Health and Social Wel-fare. They made an in-depth study of the objectives,duration, and purpose of residencies and also the re-sponsibilities of the instructor, the resident, the Schoolof Public Health, and the Ministry.
In order to assist with the inclusion of educationalprograms on health service and hospital administrationin the curricula of medical schools, advisory serviceswere rendered to several schools, in close cooperationwith the respective associations of schools of medicine.In addition, the first seminar for teachers of preventiveand social medicine, directors of university hospitals,and teachers responsible for clinical services was heldin November 1969 at the Latin American Center forMedical Administration (CLAM), with 15 participantsfrom the universities in Buenos Aires and Rosario (Ar-gentina), Santiago and Concepción (Chile), Asunción(Paraguay), and Montevideo (Uruguay).
The graduate courses in health and hospital admin-istration have become the main source of training fordirectors and senior administrative staff of hospitalsand health and medical care establishments in LatinAmerica. As the importance of effective administra-tion of health programs and hospitals has come to berecognized in recent years, attention has been focusedon the responsibilities of training programs for ad-ministrators. The chief responsibility of graduate pro-grams is that they should constantly review their ob-jectives, principles, content, and role in such a way asto provide the students with training that will makethem best suited to contribute toward the improve-ment of health in the countries of the Americas.
The need for research and advanced training in theparticular fields of medical care and hospital adminis-tration has become increasingly apparent in LatinAmerica. The Latin American Center for Medical Ad-ministration was set up in Buenos Aires, Argentina, in1967 to meet this need. CLAM was established as astudy and advanced training institution as the outcomeof a joint effort by the Secretariat for Health of Argen-tina, the University of Buenos Aires, and the Organiza-tion. It therefore plays an important role in the ex-change and training of senior staff, with special emphasison research into the medical care problems which healthinstitutions and hospitals are faced with today.
Among CLAM's activities special attention shouldbe drawn to its course on hospital maintenance and
112
engineering and its participation in the teaching of thehospital administration course at the School of PublicHealth. During 1969 CLAM laid the groundwork forthe execution of four teaching and two research pro-grams in the course of 1970. One of the researchprograms relates to the financing and cost of medicalcare in Argentina, and the other to the quality of themedical care provided in the Buenos Aires hospitals.
A point worthy of special mention is the growing par-ticipation by teaching hospitals in community medicalcare programs. Teaching hospitals (owned by univer-sities or affiliated with schools of medicine) have con-siderable, effective influence. They make up 4 per centof all hospitals, with 20 per cent of the beds availablein Latin America. Through being located in the mostpopulous cities and taking in a high proportion of themost complicated cases, they account for more than50 per cent of the operating cost of all hospital beds.They are moreover usually large, with more than 300beds as a rule. Their placement between the medicalschool with its research laboratories, on the one hand,and the community with its resources, on the other,means that they are able to translate the results ofresearch and medical education into new and bettertechniques of medical care.
The medical schools' greater awareness of the needto create suitable fields for pregraduate and postgradu-ate training in medicine makes the teaching hospitalthe keystone of the medical care systems of the future.It must therefore be presumed that every effort made toimprove the human resources involved, and especiallytheir organization and rational administration, will havea significant impact and could conceivably bring abouta profound change in medical care in the Hemisphere.It is accordingly incumbent upon those in charge ofmedical education and responsible for administeringthat key resource known as the "teaching hospital" toestablish a dynamic relationship between the universityand its school of medicine-the peak of professionaland academic authority-and the Governments-thehighest political authority of the community and of thepeople.
Rehabilifafion
During recent years, the health authorities have cometo recognize that rehabilitation forms an essential partof good medical care. It has also been increasinglyunderstood that rehabilitation services in some form oranother may be required by any patient, with the pos-sible exception of the short-term, acute case.
Thus there is a growing demand for appropriate ser-vices for cardiac and respiratory problems, problemsof communication, mental problems, and many others.
It is no longer satisfactory to think of rehabilitation asbeing synonymous with the physical restoration oflocomotor cases; the concept has come to mean that alllong-term patients should be returned to society asphysically, socially, and economically independent aspossible.
In accordance with this concept, progress has beenmade in two directions:
1) Integration of rehabilitation services into pro-grams of public health.
2) Training of personnel in the specific techniquesneeded to provide these services. This personnel in-cludes medical rehabilitation specialists, physical andoccupational therapists, prosthetists, psychologists, so-cial workers, and workers in vocational rehabilitation.
During the years under review, PAHO/WHO hasassisted with both these aspects. Consultations, semi-nars, and meetings have been organized for the purposeof giving orientation to administrators and health per-sonnel on the purpose of rehabilitation services, andalso specific training courses have been arranged.
Perhaps the most important activity of the first typewas the meeting of a study group in 1969 to discuss thetraining of medical specialists in physical medicine andrehabilitation.
It had been apparent for some time that there werein Latin America many different approaches as to theway in which physicians should be prepared to provideor supervise rehabilitation services. Some were only
A technician in prosthesis.
113
receiving traditional training in orthopedics, some werebeing trained exclusively in physical medicine, somewere being trained abroad, while others were not re-ceiving any specific training. At the request of severalleading rehabilitation specialists, it was decided to setup a study group to investigate these points and makeappropriate recommendations.
Nine experts were invited (five from South America,four from North and Central America) to discuss whatthey considered should be the type of postgraduatetraining that a physician should receive in order to pre-pare him to give services as a specialist in physicalmedicine and also to advise upon and coordinate suchother rehabilitation services as pafients might require(occupational therapy, prosthetics services, services ofsocial or vocational rehabilitation, etc.).
The group produced a report which was later sub-mitted to a meeting attended by about 40 Latin Ameri-can physicians specializing in this field, who unani-mously accepted the recommendations made. It is nowtherefore hoped that this document will provide a guide-line to all health authorities in the Hemisphere wishingto prepare suitably trained physicians to execute andsupervise rehabilitation services.
With regard to specific training, PAHO/WHO co-operated with several programs. The occupationaltherapy training course in Sao Paulo, Brazil, has con-tinued its activities. Two special six-week courses weregiven in Pórto Alegre and Recife for the training oflocal physicians. Training of occupational therapistsand prosthetic technicians was continued in Santiago,Chile, and a special course was given to nurses in re-habilitation techniques. In Caracas, Venezuela, thetraining school for physical therapists, established in1965, graduated its first 13 students and the trainingof occupational therapists was added by the school. Aschool of prosthetics was established in Buenos Aires,Argentina. The training of teachers for deafmute chil-dren was started in Santiago. Special short-term train-ing for auxiliary emergency physical therapists wascarried out in Guayaquil, Ecuador, following a polio-myelitis epidemic there. A survey was conducted at therequest of the Central American Public Health Councilto establish the feasibility of organizing the training ofmedical and paramedical rehabilitation personnel ona regional basis in Central America.
During 1969 the first course was given in this area totrain paramedical personnel as teachers. In the nine-month course, given in Mexico City, 19 physical thera-pists from physical therapy schools in eight countries(Argentina, Brazil, Chile, Colombia, Guatemala, Mex-ico, Uruguay, and Venezuela) were prepared in modernteaching techniques as they apply to physical therapy.
During the course, all students were required to pre-pare two monographs, one on the administrative aspectsof schools of physical therapy and one giving an outlinefor the teaching schedule of a given scientific aspect ofthe subject. The monographs were then produced astwo volumes, one administrative and one scientific,which it is felt will be of considerable assistance tohealth authorities wishing to train this type of personnel.
Countries to which consultant services were providedduring these years (other than those in which there wereestablished projects) included: Bolivia, Cuba, theDominican Republic, Ecuador, Haiti, and Peru. Closecooperation was maintained with other internationalagencies in this field, such as the Rehabilitation Unit ofthe United Nations, the International Labour Organi-sation, Rehabilitation International, and the WorldRehabilitation Fund.
With regard to future activities, it is anticipated thatpublic health authorities will continue to become in-creasingly aware of the need for automatically ensuringthat rehabilitation services are provided within theirprograms so that the mentally and physically disabledpatients may systematically complete their therapy andreturn to a productive economic and social life. Thisin turn will probably entail increasing need for consulta-tive services and the preparation of personnel.
Forecasts for the Coming Decade
The trend shown by medical services in Latin Amer-ica as well as in other regions of the world makes itpossible to predict the direction in which these serviceswill develop during the decade starting in 1970. Theneed to institute national health systems, the complexi-ties of medical diagnosis and treatment, and the needto step up the training of health professionals andtechnicians are together forcing an urgent reorganiza-tion of hospital structures to adapt to recent advancesin medicine and public health.
As a result of scientific progress and social change,hospitals will have to modify the structure of theirinternal and external services in order to perform fullytheir tasks in preventive and curative medicine, reha-bilitation of the disabled, and medical teaching. Thesefunctions, which are inherent in every hospital, will bedeveloped to a greater or lesser extent depending on thesize, location, and degree of specialization of each par-ticular hospital. It is, nonetheless, to be hoped thatevery hospital will participate, each to the extent it isable, in providing comprehensive services to the com-munity, particularly through outpatient departmentsand home care services, and in giving comprehensiveinstruction in medicine to physicians and other healthprofessionals and technicians.
114
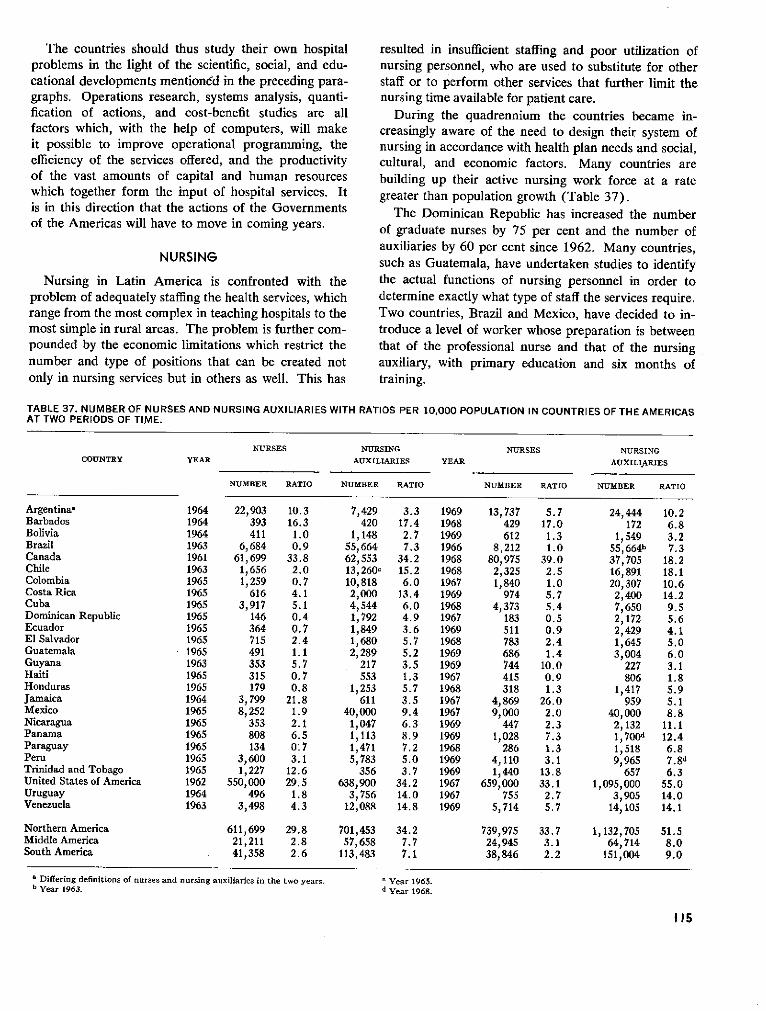
The countries should thus study their own hospitalproblems in the light of the scientific, social, and edu-cational developments mentioned in the preceding para-graphs. Operations research, systems analysis, quanti-fication of actions, and cost-benefit studies are allfactors which, with the help of computers, will makeit possible to improve operational programming, theefficiency of the services offered, and the productivityof the vast amounts of capital and human resourceswhich together form the input of hospital services. Itis in this direction that the actions of the Governmentsof the Americas will have to move in coming years.
NURSING
Nursing in Latin America is confronted with theproblem of adequately staffing the health services, whichrange from the most complex in teaching hospitals to themost simple in rural areas. The problem is further com-pounded by the economic limitations which restrict thenumber and type of positions that can be created notonly in nursing services but in others as well. This has
resulted in insufficient staffing and poor utilization ofnursing personnel, who are used to substitute for otherstaff or to perform other services that further limit thenursing time available for patient care.
During the quadrennium the countries became in-creasingly aware of the need to design their system ofnursing in accordance with health plan needs and social,cultural, and economic factors. Many countries arebuilding up their active nursing work force at a rategreater than population growth (Table 37).
The Dominican Republic has increased the numberof graduate nurses by 75 per cent and the number ofauxiliaries by 60 per cent since 1962. Many countries,such as Guatemala, have undertaken studies to identifythe actual functions of nursing personnel in order todetermine exactly what type of staff the services require.Two countries, Brazil and Mexico, have decided to in-troduce a level of worker whose preparation is betweenthat of the professional nurse and that of the nursingauxiliary, with primary education and six months oftraining.
TABLE 37. NUMBER OF NURSES AND NURSING AUXILIARIES WITH RATIOS PER 10,000 POPULATION IN COUNTRIES OF THE AMERICASAT TWO PERIODS OF TIME.
NURSES NURSING NURSES NURSINGCOUNTRY YEAR AUXILIARIES YEAR AUXILIARIES
NUMBER RATIO NUM-BER RATIO NUMBER RATIO NUMBER RATIO
Argentinaa 1964 22,903 10.3 7,429 3.3 1969 13,737 5.7 24,444 10.2Barbados 1964 393 16.3 420 17.4 1968 429 17.0 172 6.8Bolivia 1964 411 1.0 1,148 2.7 1969 612 1.3 1,549 3.2Brazil 1963 6,684 0.9 55,664 7.3 1966 8,212 1.0 55,664b 7.3Canada 1961 61,699 33.8 62,553 34.2 1968 80,975 39.0 37,705 18.2Chile 1963 1,656 2.0 13,260c 15.2 1968 2,325 2.5 16,891 18.1Colombia 1965 1,259 0.7 10,818 6.0 1967 1,840 1.0 20,307 10.6Costa Rica 1965 616 4.1 2,000 13.4 1969 974 5.7 2,400 14.2Cuba 1965 3,917 5.1 4,544 6.0 1968 4,373 5.4 7,650 9.5Dominican Republic 1965 146 0.4 1,792 4.9 1967 183 0.5 2,172 5.6Ecuador 1965 364 0.7 1,849 3.6 1969 511 0.9 2,429 4.1El Salvador 1965 715 2.4 1,680 5.7 1968 783 2.4 1,645 5.0Guatemala 1965 491 1.1 2,289 5.2 1969 686 1.4 3,004 6.0Guyana 1963 353 5.7 217 3.5 1969 744 10.0 227 3.1Haiti 1965 315 0.7 553 1.3 1967 415 0.9 806 1.8Honduras 1965 179 0.8 1,253 5.7 1968 318 1.3 1,417 5.9Jamaica 1964 3,799 21.8 611 3.5 1967 4,869 26.0 959 5.1Mexico 1965 8,252 1.9 40,000 9.4 1967 9,000 2.0 40,000 8.8Nicaragua 1965 353 2.1 1,047 6.3 1969 447 2.3 2,132 11.1Panama 1965 808 6.5 1,113 8.9 1969 1,028 7.3 1,700d 12.4Paraguay 1965 134 0.7 1,471 7.2 1968 286 1.3 1,518 6.8Peru 1965 3,600 3.1 5,783 5.0 1969 4,110 3.1 9,965 7.8dTrinidad and Tobago 1965 1,227 12.6 356 3.7 1969 1,440 13.8 657 6.3United States of America 1962 550,000 29.5 638,900 34.2 1967 659,000 33.1 1,095,000 55.0Uruguay 1964 496 1.8 3,756 14.0 1967 755 2.7 3,905 14.0Venezuela 1963 3,498 4.3 12,088 14.8 1969 5,714 5.7 14,105 14.1
Northern America 611,699 29.8 701,453 34.2 739,975 33.7 1,132,705 51.5Middle America 21,211 2.8 57,658 7.7 24,945 3.1 64,714 8.0South America 41,358 2.6 113,483 7.1 38,846 2.2 151,004 9.0
a Differing definitions of nurses and nursing auxiliaries in the two years. V Year 1965.b Year 1963. d Year 1968.
115

A committee studies standards for levels of nursing care. In a surgical pediatrics ward two nurses discuss care to begiven to a recently admitted young patient.
In some countries such as Brazil, El Salvador,Panama, and Paraguay nursing has had an active rolein the planning process, but in most countries progressin incorporating the nurse into the team has been slow.
Brazil, Chile, and Peru, through short courses, haveprepared several nurses in the methodology of planning,but considering the Region as a whole and the role thenurse should play, the number of nurses trained in thisspecialty is wholly insufficient.
There is an increasing consciousness of the need touse nursing resources more efficiently and effectively.To identify the problem, studies on the activities ofnursing personnel have been carried out in Brazil, Cuba,the Dominican Republic, Guatemala, Guyana, Jamaica,and Peru. The findings indicate that from 40 to 60per cent of nursing personnel time is spent on non-nursing activities. Figure 41 shows the classification ofactivities of nursing personnel.
The amount of nursing time spent on non-nursing
COUNTRY ANURSES AND NURSING AUXILIARIES
COUNTRY BSTAFF NURSES
= PATIENT CARE M ADMINISTRATIVE . OTNER
Fig. 41. Classification of activities of nursing personnel.
activities can be diminished only through the improve-ment of both over-all administration and nursing serviceadministration. Increased emphasis has been placed onthe training of nursing auxiliaries working in the serviceswho have not had formal preparation. Table 38 indi-cates the progress made in some countries of LatinAmerica.
The organization of continuing education programsfor nurses in the services was stepped up during thefour-year period. In these programs major emphasiswas given to nursing service administration, specialcourses having been organized for all countries ofCentral America and for Bolivia, the Dominican Repub-lic, Ecuador, and Peru with the Organization's assist-ance. In 1969 64 per cent of nursing personnel in theDominican Republic received some type of inservice orcontinuing education.
There has been an increasing interest in the improve-ment of the nursing-midwifery component of maternaland child health services. Nursing care for prematureswas improved in Córdoba, Argentina, and pediatricnursing as well as over-all nursing-midwifery care werestrengthened in Brazil. Costa Rica, the Dominican
TABLE 38. PERCENTAGE OF NURSING AUXILIARIES WITHTRAINING WORKING IN HEALTH SERVICES IN CENTRALAMERICA AND PANAMA, 1965 AND 1969.
COUNTRY 1965 1969
Costa Rica 55 78El Salvador 67 79Guatemala 56 72Honduras 91 93Nicaragua 91 73Panama 11 70
116
-
[ /
1
L, . . .1
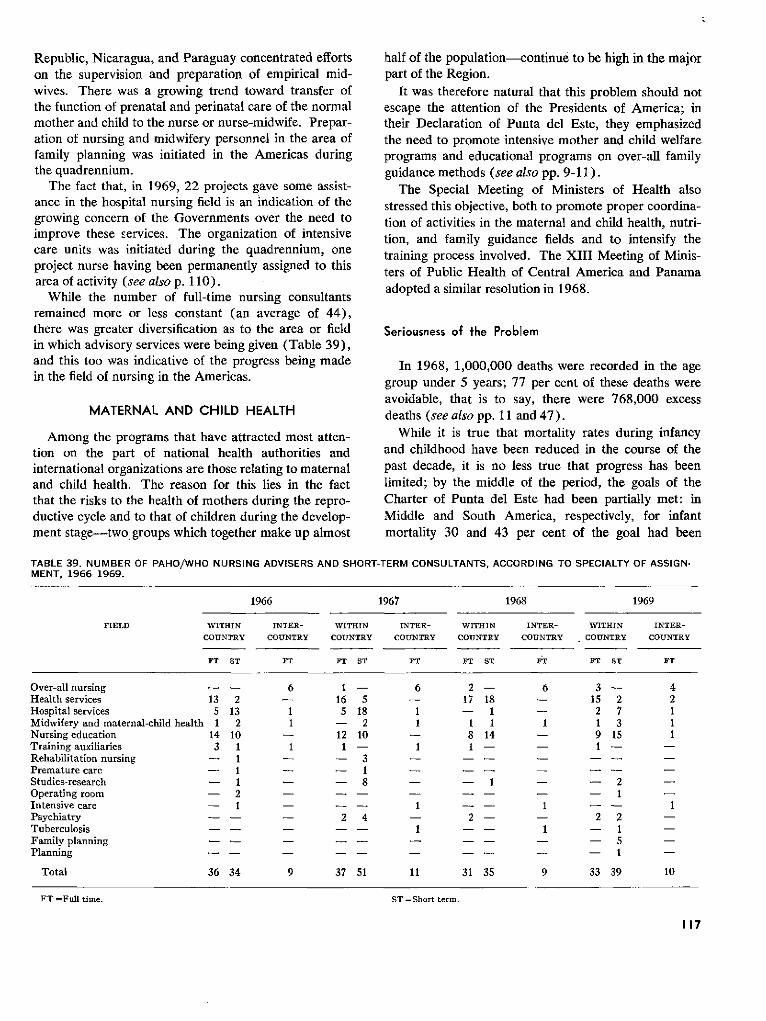
Republic, Nicaragua, and Paraguay concentrated effortson the supervision and preparation of empirical mid-wives. There was a growing trend toward transfer ofthe function of prenatal and perinatal care of the normalmother and child to the nurse or nurse-midwife. Prepar-ation of nursing and midwifery personnel in the area offamily planning was initiated in the Americas duringthe quadrennium.
The fact that, in 1969, 22 projects gave some assist-ance in the hospital nursing field is an indication of thegrowing concern of the Governments over the need toimprove these services. The organization of intensivecare units was initiated during the quadrennium, oneproject nurse having been permanently assigned to thisarea of activity (see also p. 110).
While the number of full-time nursing consultantsremained more or less constant (an average of 44),there was greater diversification as to the area or fieldin which advisory services were being given (Table 39),and this too was indicative of the progress being madein the field of nursing in the Americas.
MATERNAL AND CHILD HEALTH
Among the programs that have attracted most atten-tion on the part of national health authorities andinternational organizations are those relating to maternaland child health. The reason for this lies in the factthat the risks to the health of mothers during the repro-ductive cycle and to that of children during the develop-ment stage-two groups which together make up almost
half of the population-continue to be high in the majorpart of the Region.
It was therefore natural that this problem should notescape the attention of the Presidents of America; intheir Declaration of Punta del Este, they emphasizedthe need to promote intensive mother and child welfareprograms and educational programs on over-all familyguidance methods (see also pp. 9-11).
The Special Meeting of Ministers of Health alsostressed this objective, both to promote proper coordina-tion of activities in the maternal and child health, nutri-tion, and family guidance fields and to intensify thetraining process involved. The XIII Meeting of Minis-ters of Public Health of Central America and Panamaadopted a similar resolution in 1968.
Seriousness of the Problem
In 1968, 1,000,000 deaths were recorded in the agegroup under 5 years; 77 per cent of these deaths wereavoidable, that is to say, there were 768,000 excessdeaths (see also pp. 11 and 47).
While it is true that mortality rates during infancyand childhood have been reduced in the course of thepast decade, it is no less true that progress has beenlimited; by the middle of the period, the goals of theCharter of Punta del Este had been partially met: inMiddle and South America, respectively, for infantmortality 30 and 43 per cent of the goal had been
TABLE 39. NUMBER OF PAHO/WHO NURSING ADVISERS AND SHORT-TERM CONSULTANTS, ACCORDING TO SPECIALTY OF ASSIGN-MENT, 1966-1969.
1966 1967 1968 1969
FIELD WITHIN INTER- WITHIIIN INTER- WITHIN INTER- WITHIN INTER-
COUNTRY COUNTRY COUNTRY COUNTRY COUNTRY COUNTRY COUNTRY COUNTRY
FT ST FT FT ST FT FT ST ET FT ST FT
Over-all nursing -- 6 1 - 6 2 - 6 3 - 4Health services 13 2 - 16 5 - 17 18 - 15 2 2Hospital services 5 13 1 5 18 1 - 1 - 2 7 1Midwifery and maternal-child health 1 2 1 - 2 1 1 1 1 1 3 1Nursing education 14 10 - 12 10 - 8 14 - 9 15 1Training auxiliaries 3 1 1 1 - 1 1 - 1 - -Rehabilitation nursing - 1 - - 3 - - - - - -Premature care - 1 1 - - - - -Studies-research - 1 - - 8 - - 1 - - 2 -Operating room - 2 - - - - - 1 -
Intensive care - 1 - - 1 1 - - 1Psychiatry - - - 2 4 - 2 - - 2 2 -Tuberculosis - - -- 1 -- 1 - 1 -
Family planning - - - - - - - 5Planning -- - -- - -- - - 1
Total 36 34 9 37 51 11 31 35 9 33 39 10
FT =Full time. ST =Short term.
117
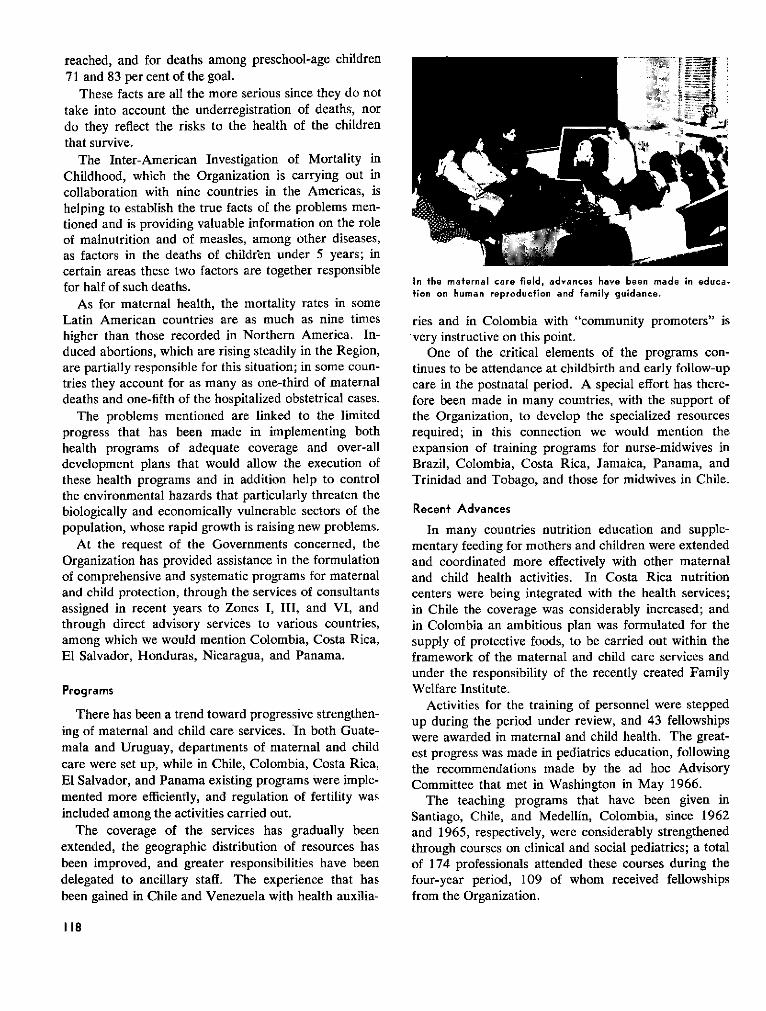
reached, and for deaths among preschool-age children71 and 83 per cent of the goal.
These facts are all the more serious since they do nottake into account the underregistration of deaths, nordo they reflect the risks to the health of the childrenthat survive.
The Inter-American Investigation of Mortality inChildhood, which the Organization is carrying out incollaboration with nine countries in the Americas, ishelping to establish the true facts of the problems men-tioned and is providing valuable information on the roleof malnutrition and of measles, among other diseases,as factors in the deaths of children under 5 years; incertain areas these two factors are together responsiblefor half of such deaths.
As for maternal health, the mortality rates in someLatin American countries are as much as nine timeshigher than those recorded in Northern America. In-duced abortions, which are rising steadily in the Region,are partially responsible for this situation; in some coun-tries they account for as many as one-third of maternaldeaths and one-fifth of the hospitalized obstetrical cases.
The problems mentioned are linked to the limitedprogress that has been made in implementing bothhealth programs of adequate coverage and over-alldevelopment plans that would allow the execution ofthese health programs and in addition help to controlthe environmental hazards that particularly threaten thebiologically and economically vulnerable sectors of thepopulation, whose rapid growth is raising new problems.
At the request of the Governments concerned, theOrganization has provided assistance in the formulationof comprehensive and systematic programs for maternaland child protection, through the services of consultantsassigned in recent years to Zones I, III, and VI, andthrough direct advisory services to various countries,among which we would mention Colombia, Costa Rica,El Salvador, Honduras, Nicaragua, and Panama.
Programs
There has been a trend toward progressive strengthen-ing of maternal and child care services. In both Guate-mala and Uruguay, departments of maternal and childcare were set up, while in Chile, Colombia, Costa Rica,El Salvador, and Panama existing programs were imple-mented more efficiently, and regulation of fertility wasincluded among the activities carried out.
The coverage of the services has gradually beenextended, the geographic distribution of resources hasbeen improved, and greater responsibilities have beendelegated to ancillary staff. The experience that hasbeen gained in Chile and Venezuela with health auxilia-
In the maternal care field, advances have been made in educa.tion on human reproduction and family guidance.
ries and in Colombia with "community promoters" isvery instructive on this point.
One of the critical elements of the programs con-tinues to be attendance at childbirth and early follow-upcare in the postnatal period. A special effort has there-fore been made in many countries, with the support ofthe Organization, to develop the specialized resourcesrequired; in this connection we would mention theexpansion of training programs for nurse-midwives inBrazil, Colombia, Costa Rica, Jamaica, Panama, andTrinidad and Tobago, and those for midwives in Chile.
Recent Advances
In many countries nutrition education and supple-mentary feeding for mothers and children were extendedand coordinated more effectively with other maternaland child health activities. In Costa Rica nutritioncenters were being integrated with the health services;in Chile the coverage was considerably increased; andin Colombia an ambitious plan was formulated for thesupply of protective foods, to be carried out within theframework of the maternal and child care services andunder the responsibility of the recently created FamilyWelfare Institute.
Activities for the training of personnel were steppedup during the period under review, and 43 fellowshipswere awarded in maternal and child health. The great-est progress was made in pediatrics education, followingthe recommendations made by the ad hoc AdvisoryCommittee that met in Washington in May 1966.
The teaching programs that have been given inSantiago, Chile, and Medellín, Colombia, since 1962and 1965, respectively, were considerably strengthenedthrough courses on clinical and social pediatrics; a totalof 174 professionals attended these courses during thefour-year period, 109 of whom received fellowshipsfrom the Organization.
118
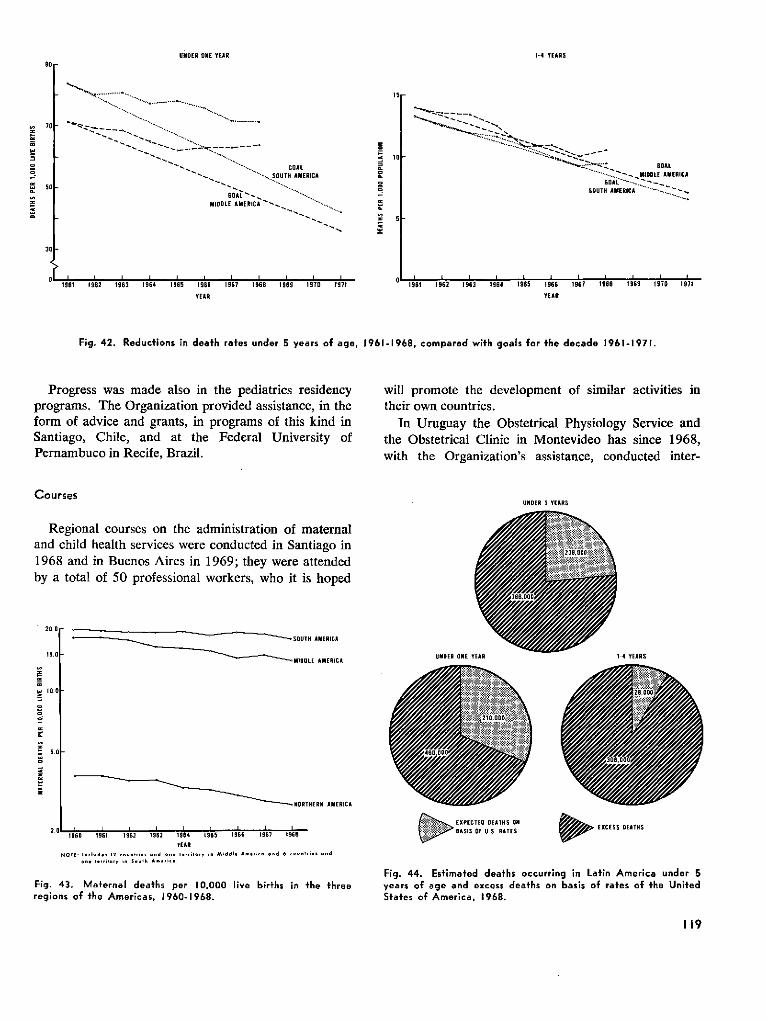
UNDER ONE YEAR
__' _____ e.GOAL9.**" . SOUTH AMERICA
MIDDL AMERIC . ..........-
___~~~~~~~~~~~~~~~~GA
.-_MIDLE AMERICA
. .... ---_SoUTH AMERIC ...........
1961 1 962 19163 1 916 1 965 19166 1967 1968 1969 1970 1971
VEARl
,961 1962 1963 1964 1965 1966 1967 1968 1969 1970 1971
YEAR
NORTHERN AMERICA
1960 1961 1962 1963 1964 1965 1966 1967 1968
VEAR.01E: 'nl ,... l---, i·< .d ...· ii.i i. *iddl· .. _¡_.. .a 6 ~i~ ... ..d
... i. 5...hloih n·i<
1-4 YEARS90
70
1:í
19
-t
i
31
Fig. 42. Reductions in death rafes under 5 years of age, 1961-1968, conipared wifh goals for fhe decade 1961-1971.
Progress was made also in the pediatrics residencyprograms. The Organization provided assistance, in theform of advice and grants, in programs of this kind inSantiago, Chile, and at the Federal University ofPernambuco in Recífe, Brazil.
will promote the development of similar activities intheir own countries.
In Uruguay the Obstetrical Physiology Service andthe Obstetrical Clinic in Montevideo has since 1968,with the Organization's assistance, conducted inter-
Courses
Regional courses on the administration of maternaland child health services were conducted in Santiago in1968 and in Buenos Aires in 1969; they were attendedby a total of 50 professional workers, who it is hoped
.20.Or --
UNDER 5 YEARS
~ ~~_~~~~___YIOOLÍ L------*I M' D R L EA`MICRlL15.1 UNDER ONE YEAR 1-4 YEARS
Y 1-1tzS,
1
.
1a
0.0
EXPECTEO DE 'TNS ON EXCESS DEANS
> BASS OF U.S. RATES2.
Fig. 44. Esfirnafed deafhs occurring in Lafin Arnerica under 5years of age and excess deafhs on basis of rates of fhe UnifedSfafes of Arnerica, 1968.
Fig. 43. Mafernal deafhs per 10,000 ¡¡ve birfhs in *he fhreeregions of ¡he Arnericas, 1960-1968.
119
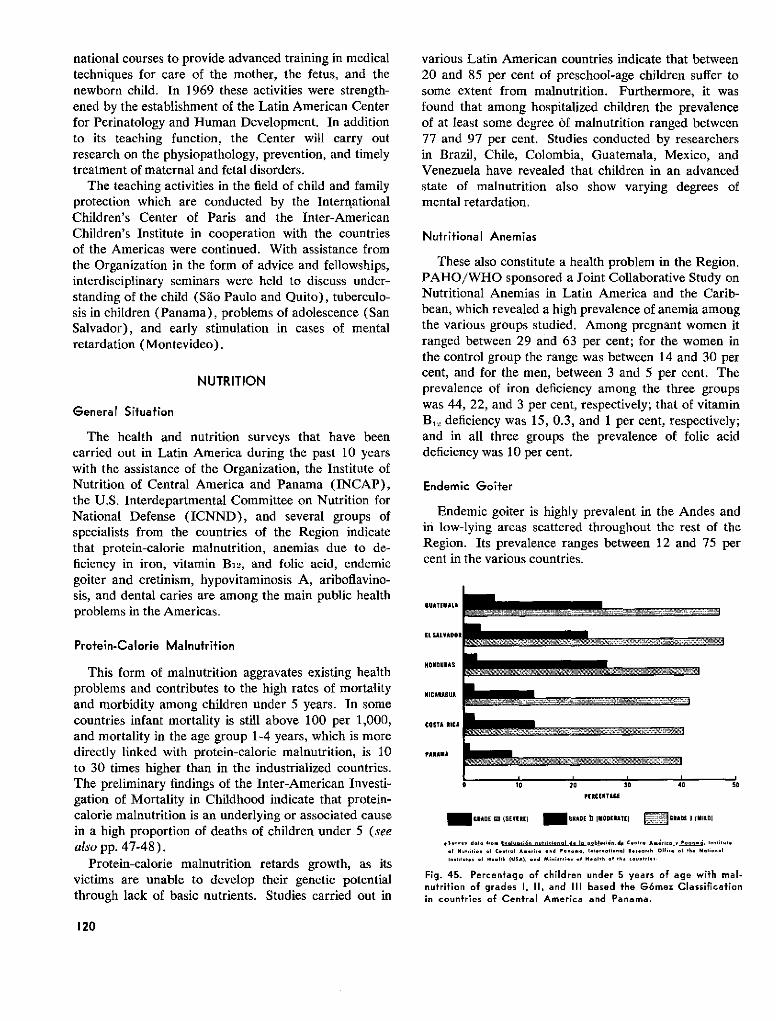
national courses to provide advanced training in medicaltechniques for care of the mother, the fetus, and thenewborn child. In 1969 these activities were strength-ened by the establishment of the Latin American Centerfor Perinatology and Human Development. In additionto its teaching function, the Center will carry outresearch on the physiopathology, prevention, and timelytreatment of maternal and fetal disorders.
The teaching activities in the field of child and familyprotection which are conducted by the InternationalChildren's Center of Paris and the Inter-AmericanChildren's Institute in cooperation with the countriesof the Americas were continued. With assistance fromthe Organization in the form of advice and fellowships,interdisciplinary seminars were held to discuss under-standing of the child (Sáo Paulo and Quito), tuberculo-sis in children (Panama), problems of adolescence (SanSalvador), and early stimulation in cases of mentalretardation (Montevideo).
NUTRITION
General Situation
The health and nutrition surveys that have beencarried out in Latin America during the past 10 yearswith the assistance of the Organization, the Institute ofNutrition of Central America and Panama (INCAP),the U.S. Interdepartmental Committee on Nutrition forNational Defense (ICNND), and several groups ofspecialists from the countries of the Region indicatethat protein-calorie malnutrition, anemias due to de-ficiency in iron, vitamin B12, and folic acid, endemicgoiter and cretinism, hypovitaminosis A, ariboflavino-sis, and dental caries are among the main public healthproblems in the Americas.
Protein-Calorie Mainutrition
This form of malnutrition aggravates existing healthproblems and contributes to the high rates of mortalityand morbidity among children under 5 years. In somecountries infant mortality is still above 100 per 1,000,and mortality in the age group 1-4 years, which is moredirectly linked with protein-calorie malnutrition, is 10to 30 times higher than in the industrialized countries.The preliminary findings of the Inter-American Investi-gation of Mortality in Childhood indicate that protein-calorie malnutrition is an underlying or associated causein a high proportion of deaths of children under 5 (seealso pp. 47-48).
Protein-calorie malnutrition retards growth, as itsvictims are unable to develop their genetic potentialthrough lack of basic nutrients. Studies carried out in
various Latin American countries indicate that between20 and 85 per cent of preschool-age children suffer tosome extent from malnutrition. Furthermore, it wasfound that among hospitalized children the prevalenceof at least some degree of malnutrition ranged between77 and 97 per cent. Studies conducted by researchersin Brazil, Chile, Colombia, Guatemala, Mexico, andVenezuela have revealed that children in an advancedstate of malnutrition also show varying degrees ofmental retardation.
Nutritional Anemias
These also constitute a health problem in the Region.PAHO/WHO sponsored a Joint Collaborative Study onNutritional Anemias in Latin America and the Carib-bean, which revealed a high prevalence of anemia amongthe various groups studied. Among pregnant women itranged between 29 and 63 per cent; for the women inthe control group the range was between 14 and 30 percent, and for the men, between 3 and 5 per cent. Theprevalence of iron deficiency among the three groupswas 44, 22, and 3 per cent, respectively; that of vitaminB,, deficiency was 15, 0.3, and 1 per cent, respectively;and in all three groups the prevalence of folic aciddeficiency was 10 per cent.
Endemic Goiter
Endemic goiter is highly prevalent in the Andes andin low-lying areas scattered throughout the rest of theRegion. Its prevalence ranges between 12 and 75 percent in the various countries.
UATEMA LA
EL SAL VADOR
HONDURAS
NICARAGUA
COSTA l ICA
PANAMA
0 10 20 30 40 50
PERCENTAGE
1 GRADE m (SEVERE) GRAOE 11 MODlEATEl IRADE 1 I llDI
Suvrvey daleo Iro Evluui&f nutri<ional de la pobla<ién de Caniro Am ri<c v Pennm~ In<tiltvt
of Nulrition ol Cln;ral Ameria and tnooam, Iniernatienal Researh< Ollice oal ik NationalInslituts of NeeRlb IUSA), and Ministti·e al Health of Ihe auflirles.
Fig. 45. Percentage of children under 5 years of age with mal-nutrition of grades 1, II, and III based the G6mez Classificationin countries of Central America and Panama.
120
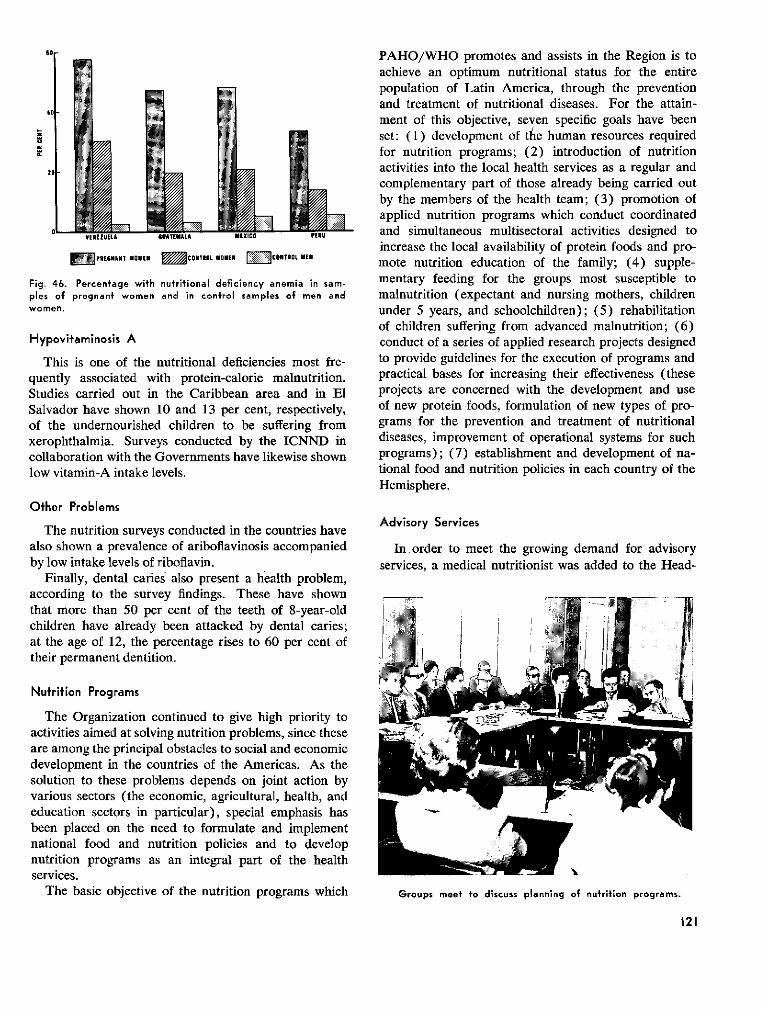
Sor
40
1r:
m
81
MPREGAIAT WOMEN = NTRCOITIL UMEN MCONTROE UEN
Fig. 46. Percentage with nutritional deficiency anemia in sam-ples of pregnant women and in control samples of men andwomen.
Hypovitaminosis A
This is one of the nutritional deficiencies most fre-quently associated with protein-calorie malnutrition.Studies carried out in the Caribbean area and in ElSalvador have shown 10 and 13 per cent, respectively,of the undernourished children to be suffering fromxerophthalmia. Surveys conducted by the ICNND incollaboration with the Governments have likewise shownlow vitamin-A intake levels.
Other Problems
The nutrition surveys conducted in the countries havealso shown a prevalence of ariboflavinosis accompaniedby low intake levels of riboflavin.
Finally, dental caries also present a health problem,according to the survey findings. These have shownthat more than 50 per cent of the teeth of 8-year-oldchildren have already been attacked by dental caries;at the age of 12, the percentage rises to 60 per cent oftheir permanent dentition.
Nufrition Programs
The Organization continued to give high priority toactivities aimed at solving nutrition problems, since theseare among the principal obstacles to social and economicdevelopment in the countries of the Americas. As thesolution to these problems depends on joint action byvarious sectors (the economic, agricultural, health, andeducation sectors in particular), special emphasis hasbeen placed on the need to formulate and implementnational food and nutrition policies and to developnutrition programs as an integral part of the healthservices.
The basic objective of the nutrition programs which
PAHO/WHO promotes and assists in the Region is toachieve an optimum nutritional status for the entirepopulation of Latin America, through the preventionand treatment of nutritional diseases. For the attain-ment of this objective, seven specific goals have beenset: (1) development of the human resources requiredfor nutrition programs; (2) introduction of nutritionactivities into the local health services as a regular andcomplementary part of those already being carried outby the members of the health team; (3) promotion ofapplied nutrition programs which conduct coordinatedand simultaneous multisectoral activities designed toincrease the local availability of protein foods and pro-mote nutrition education of the family; (4) supple-mentary feeding for the groups most susceptible tomalnutrition (expectant and nursing mothers, childrenunder 5 years, and schoolchildren); (5) rehabilitationof children suffering from advanced malnutrition; (6)conduct of a series of applied research projects designedto provide guidelines for the execution of programs andpractical bases for increasing their effectiveness (theseprojects are concerned with the development and useof new protein foods, formulation of new types of pro-grams for the prevention and treatment of nutritionaldiseases, improvement of operational systems for suchprograms); (7) establishment and development of na-tional food and nutrition policies in each country of theHemisphere.
Advisory Services
In order to meet the growing demand for advisoryservices, a medical nutritionist was added to the Head-
Groups meet to discuss planning of nutrition programs.
121
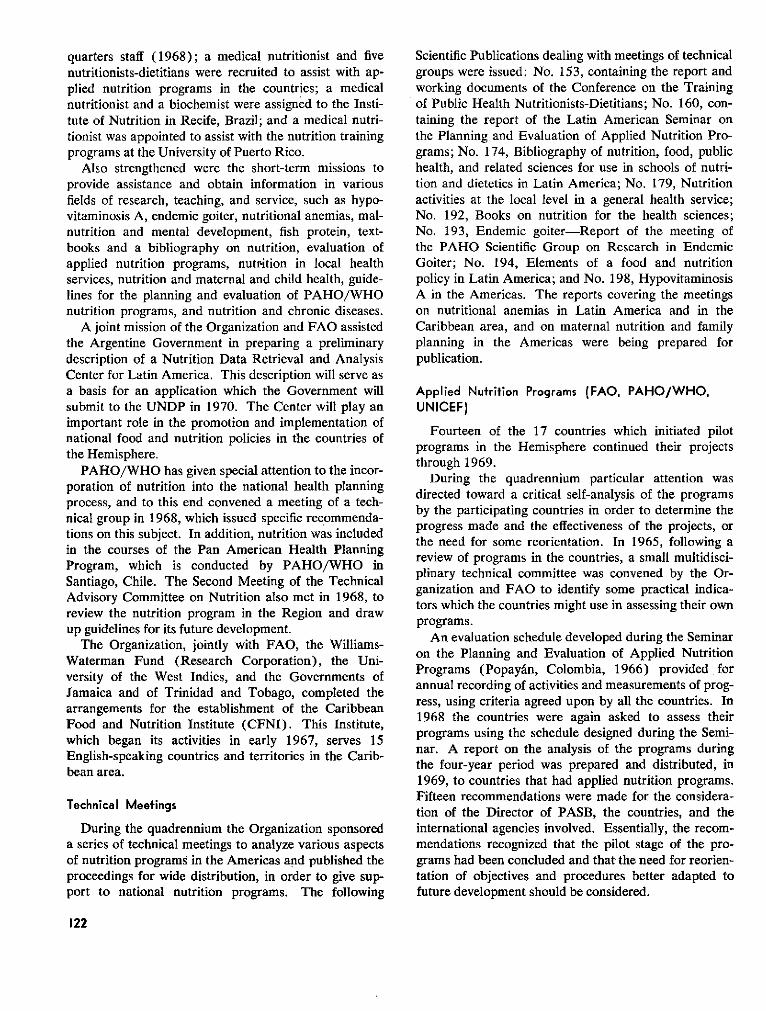
quarters staff (1968); a medical nutritionist and fivenutritionists-dietitians were recruited to assist with ap-plied nutrition programs in the countries; a medicalnutritionist and a biochemist were assigned to the Insti-tute of Nutrition in Recife, Brazil; and a medical nutri-tionist was appointed to assist with the nutrition trainingprograms at the University of Puerto Rico.
Also strengthened were the short-term missions toprovide assistance and obtain information in variousfields of research, teaching, and service, such as hypo-vitaminosis A, endemic goiter, nutritional anemias, mal-nutrition and mental development, fish protein, text-books and a bibliography on nutrition, evaluation ofapplied nutrition programs, nutrition in local healthservices, nutrition and maternal and child health, guide-lines for the planning and evaluation of PAHO/WHOnutrition programs, and nutrition and chronic diseases.
A joint mission of the Organization and FAO assistedthe Argentine Government in preparing a preliminarydescription of a Nutrition Data Retrieval and AnalysisCenter for Latin America. This description will serve asa basis for an application which the Government willsubmit to the UNDP in 1970. The Center will play animportant role in the promotion and implementation ofnational food and nutrition policies in the countries ofthe Hemisphere.
PAHO/WHO has given special attention to the incor-poration of nutrition into the national health planningprocess, and to this end convened a meeting of a tech-nical group in 1968, which issued specific recommenda-tions on this subject. In addition, nutrition was includedin the courses of the Pan American Health PlanningProgram, which is conducted by PAHO/WHO inSantiago, Chile. The Second Meeting of the TechnicalAdvisory Committee on Nutrition also met in 1968, toreview the nutrition program in the Region and drawup guidelines for its future development.
The Organization, jointly with FAO, the Williams-Waterman Fund (Research Corporation), the Uni-versity of the West Indies, and the Governments ofJamaica and of Trinidad and Tobago, completed thearrangements for the establishment of the CaribbeanFood and Nutrition Institute (CFNI). This Institute,which began its activities in early 1967, serves 15English-speaking countries and territories in the Carib-bean area.
Technical Meefings
During the quadrennium the Organization sponsoreda series of technical meetings to analyze various aspectsof nutrition programs in the Americas and published theproceedings for wide distribution, in order to give sup-port to national nutrition programs. The following
Scientific Publications dealing with meetings of technicalgroups were issued: No. 153, containing the report andworking documents of the Conference on the Trainingof Public Health Nutritionists-Dietitians; No. 160, con-taining the report of the Latin American Seminar onthe Planning and Evaluation of Applied Nutrition Pro-grams; No. 174, Bibliography of nutrition, food, publichealth, and related sciences for use in schools of nutri-tion and dietetics in Latin America; No. 179, Nutritionactivities at the local level in a general health service;No. 192, Books on nutrition for the health sciences;No. 193, Endemic goiter-Report of the meeting ofthe PAHO Scientific Group on Research in EndemicGoiter; No. 194, Elements of a food and nutritionpolicy in Latin America; and No. 198, HypovitaminosisA in the Americas. The reports covering the meetingson nutritional anemias in Latin America and in theCaribbean area, and on maternal nutrition and familyplanning in the Americas were being prepared forpublication.
Applied Nufrifion Programs (FAO, PAHO/WHO,UNICEF)
Fourteen of the 17 countries which initiated pilotprograms in the Hemisphere continued their projectsthrough 1969.
During the quadrennium particular attention wasdirected toward a critical self-analysis of the programsby the participating countries in order to determine theprogress made and the effectiveness of the projects, orthe need for some reorientation. In 1965, following areview of programs in the countries, a small multidisci-plinary technical committee was convened by the Or-ganization and FAO to identify some practical indica-tors which the countries might use in assessing their ownprograms.
An evaluation schedule developed during the Seminaron the Planning and Evaluation of Applied NutritionPrograms (Popayán, Colombia, 1966) provided forannual recording of activities and measurements of prog-ress, using criteria agreed upon by all the countries. In1968 the countries were again asked to assess theirprograms using the schedule designed during the Semi-nar. A report on the analysis of the programs duringthe four-year period was prepared and distributed, in1969, to countries that had applied nutrition programs.Fifteen recommendations were made for the considera-tion of the Director of PASB, the countries, and theinternational agencies involved. Essentially, the recom-mendations recognized that the pilot stage of the pro-grams had been concluded and that the need for reorien-tation of objectives and procedures better adapted tofuture development should be considered.
122

Preschool-age children receivesupplementary food in a nutri-tion center as part of an appliednutrition program.
PAHO/WHO continued to promote and assist withthe incorporation of nutrition activities into the localhealth services, both through the multisectoral appliednutrition programs and other programs conducted sepa-rately by the health sector. Special attention was givento the utilization of the resources of the World FoodProgram (WFP) in food supplementation projectsundertaken by the health services to assist the mostvulnerable population groups (mothers and childrenunder 5 years). For this purpose, PAHO/WHO hasestablished liaison with the WFP and the bases havebeen laid for considerably increasing the use of this foodassistance both in health services and hospital foodservices.
The nutrition rehabilitation services represent anotheractivity complementary to the regular health services towhich special attention has been given. Notable prog-ress in the organization of such services has been madein Central America and in Brazil, Colombia, Ecuador,Peru, and Venezuela.
Institute of Nutrition ofCentral America and Panama
Nutritional deficiencies are among the most serioushealth problems confronting the peoples of the CentralAmerican Isthmus and of other countries that havesimilar ecologic conditions. Although there has been adecided increase in the incidence of severe forms ofmalnutrition in recent years, the light or moderate forms,which frequently pass unnoticed, continue to affect largesegments of the population, principally small children.The reduction of the severe forms is considered to bedue primarily to the prevention and recuperation pro-grams undertaken by the health services. The reductionof the chronic, subclinical forms, however, requires
coordinated action by other sectors involved in theproblem, such as agriculture, economy, and education.These subclinical forms constitute a serious obstaclebecause, directly or indirectly, they bring about retarda-tion of the growth and physical and mental developmentof children and low productivity of the adult workingpopulation. Thus they represent an important limitingfactor in the efforts being made by the Governments tospeed up the process of social and economic develop-ment.
In fulfillment of its general purpose of assisting themember countries in the study of their nutrition prob-lems and in the search for and application of practicalmeasures for solving them, INCAP continued to developits activities in the three phases of its work program:research, education, and advisory services. The follow-ing is a summary of the most important work carriedout in the 1966-1969 period in the last of these areas;the other two are discussed under the sections dealingwith research and development of human resources.
Nutrition and Public Health
At the beginning of the period, a seminar attendedby officials from the Central American countries andPanama made a study of the nutrition situation in orderto determine the order of priorities for the action to betaken. On basis of the magnitude and seriousness ofthe various problems, the availability and effectivenessof control measures, and the resources available fortheir implementation, two activities of the health sectorwere singled out as being of the highest priority froma nutrition point of view: (a) control of endemic goiter,and (b) adequate and timely treatment of childrensuffering from protein-calorie malnutrition.
INCAP accordingly redoubled its efforts to assist the
123
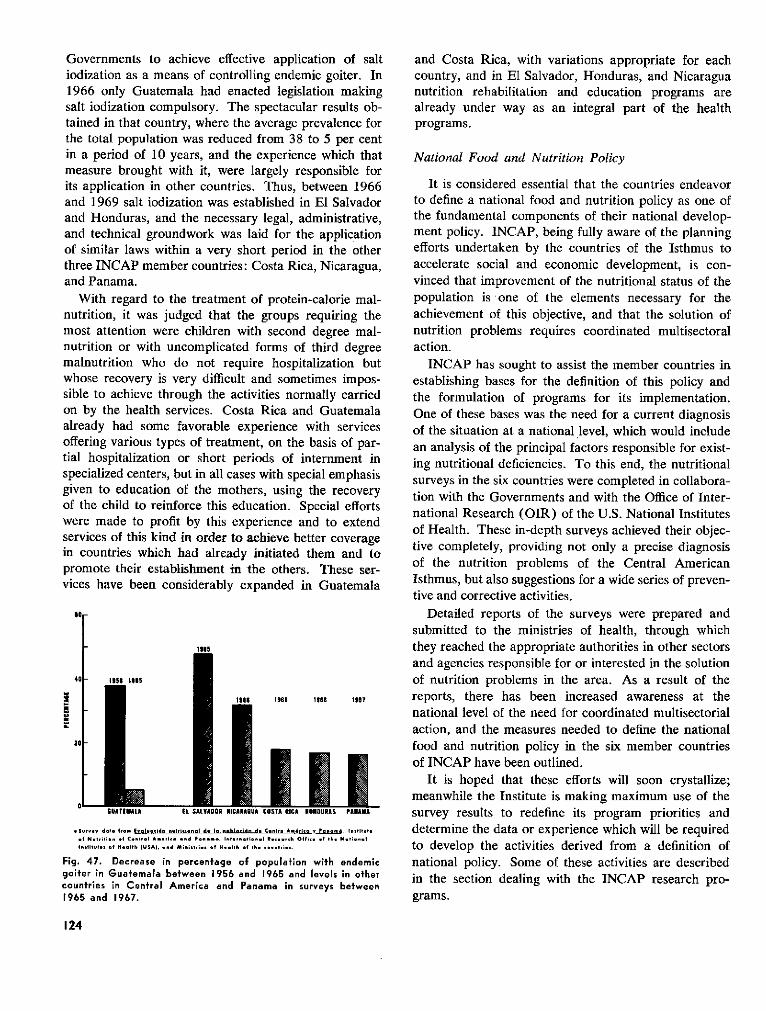
Governments to achieve effective application of saltiodization as a means of controlling endemic goiter. In1966 only Guatemala had enacted legislation makingsalt iodization compulsory. The spectacular results ob-tained in that country, where the average prevalence forthe total population was reduced from 38 to 5 per centin a period of 10 years, and the experience which thatmeasure brought with it, were largely responsible forits application in other countries. Thus, between 1966and 1969 salt iodization was established in El Salvadorand Honduras, and the necessary legal, administrative,and technical groundwork was laid for the applicationof similar laws within a very short period in the otherthree INCAP member countries: Costa Rica, Nicaragua,and Panama.
With regard to the treatment of protein-calorie mal-nutrition, it was judged that the groups requiring themost attention were children with second degree mal-nutrition or with uncomplicated forms of third degreemalnutrition who do not require hospitalization butwhose recovery is very difficult and sometimes impos-sible to achieve through the activities normally carriedon by the health services. Costa Rica and Guatemalaalready had some favorable experience with servicesoffering various types of treatment, on the basis of par-tial hospitalization or short periods of internment inspecialized centers, but in all cases with special emphasisgiven to education of the mothers, using the recoveryof the child to reinforce this education. Special effortswere made to profit by this experience and to extendservices of this kind in order to achieve better coveragein countries which had already initiated them and topromote their establishment in the others. These ser-vices have been considerably expanded in Guatemala
40 1r
5
GUATEMALA EL SALVADOR NICARAmUA COSTA RICA HOlDURAS PANAIA
,Srv-y data Ir Ivluaidn nulrilional * l Bbln*iHn d. Cinto A&rlc 1 Panam, Instlitul
Insitm i s If Health UI, ind pinistries i o He pl a lh wO¡t nh im.
Fig. 47. Decrease in percentage of population with endemicgoiter in Guatemala between 1956 and 1965 and levels in othercountries in Central America and Panama in surveys between1965 and 1967.
and Costa Rica, with variations appropriate for eachcountry, and in El Salvador, Honduras, and Nicaraguanutrition rehabilitation and education programs arealready under way as an integral part of the healthprograms.
National Food and Nutrition Policy
It is considered essential that the countries endeavorto define a national food and nutrition policy as one ofthe fundamental components of their national develop-ment policy. INCAP, being fully aware of the planningefforts undertaken by the countries of the Isthmus toaccelerate social and economic development, is con-vinced that improvement of the nutritional status of thepopulation is one of the elements necessary for theachievement of this objective, and that the solution ofnutrition problems requires coordinated multisectoralaction.
INCAP has sought to assist the member countries inestablishing bases for the definition of this policy andthe formulation of programs for its implementation.One of these bases was the need for a current diagnosisof the situation at a national level, which would includean analysis of the principal factors responsible for exist-ing nutritional deficiencies. To this end, the nutritionalsurveys in the six countries were completed in collabora-tion with the Governments and with the Office of Inter-national Research (OIR) of the U.S. National Institutesof Health. These in-depth surveys achieved their objec-tive completely, providing not only a precise diagnosisof the nutrition problems of the Central AmericanIsthmus, but also suggestions for a wide series of preven-tive and corrective activities.
Detailed reports of the surveys were prepared andsubmitted to the ministries of health, through whichthey reached the appropriate authorities in other sectorsand agencies responsible for or interested in the solutionof nutrition problems in the area. As a result of thereports, there has been increased awareness at thenational level of the need for coordinated multisectorialaction, and the measures needed to define the nationalfood and nutrition policy in the six member countriesof INCAP have been outlined.
It is hoped that these efforts will soon crystallize;meanwhile the Institute is making maximum use of thesurvey results to redefine its program priorities anddetermine the data or experience which will be requiredto develop the activities derived from a definition ofnational policy. Some of these activities are describedin the section dealing with the INCAP research pro-grams.
124
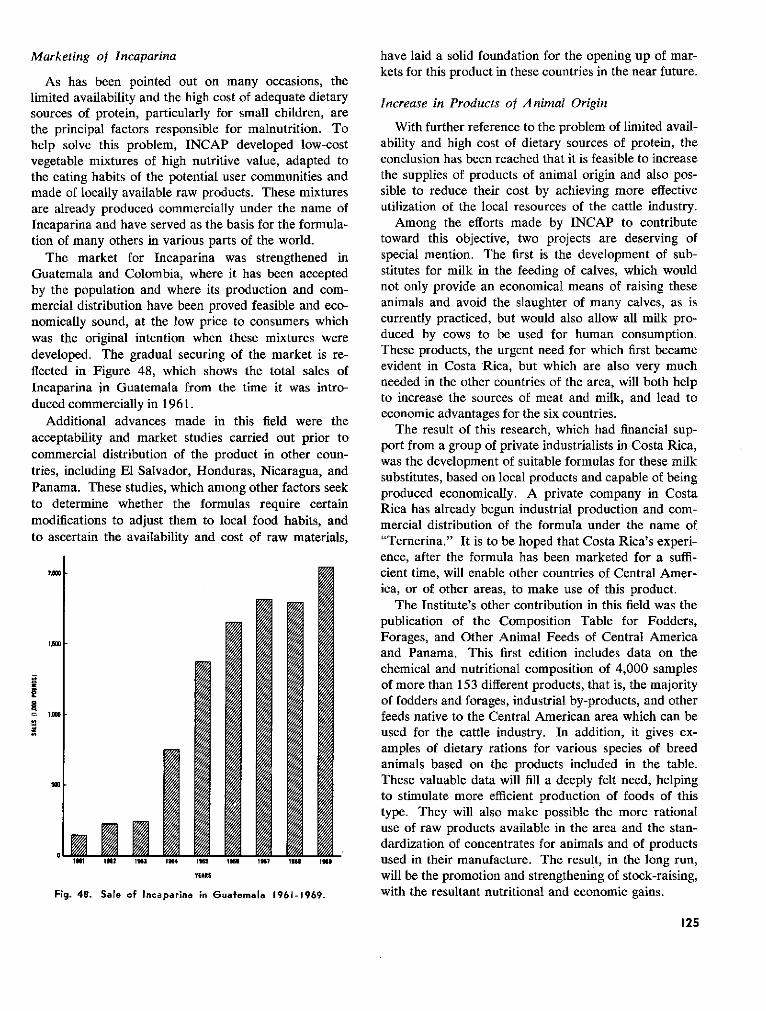
Marketing of Incaparina
As has been pointed out onlimited availability and the high cosources of protein, particularly fcthe principal factors responsiblehelp solve this problem, INCA1vegetable mixtures of high nutritithe eating habits of the potential imade of locally available raw procare already produced commerciallIncaparina and have served as thetion of many others in various pai
The market for IncaparinaGuatemala and Colombia, whereby the population and where itsmercial distribution have been prcnomically sound, at the low pricewas the original intention whendeveloped. The gradual securingflected in Figure 48, which sho,Incaparina in Guatemala from tlduced commercially in 1961.
Additional advances made inacceptability and market studiescommercial distribution of the prtries, including El Salvador, HoncPanama. These studies, which amto determine whether the formmodifications to adjust them to 1lto ascertain the availability and c
1Ri 12z INU 1N4 In5
YEIARS
Fig. 48. Sale of Incaparina in Gu
many occasions, the)st of adequate dietary)r small children, are
have laid a solid foundation for the opening up of mar-kets for this product in these countries in the near future.
Increase in Products of Animal Origin
for malnutrition. To With further reference to the problem of limited avail-P developed low-cost ability and high cost of dietary sources of protein, theive value, adapted to conclusion has been reached that it is feasible to increaseuser communities and the supplies of products of animal origin and also pos-lucts. These mixtures sible to reduce their cost by achieving more effectively under the name of utilization of the local resources of the cattle industry.basis for the formula- Among the efforts made by INCAP to contributerts of the world. toward this objective, two projects are deserving ofwas strengthened in special mention. The first is the development of sub-it has been accepted stitutes for milk in the feeding of calves, which wouldproduction and com- not only provide an economical means of raising these)ved feasible and eco- animals and avoid the slaughter of many calves, as iseto consumers which currently practiced, but would also allow all milk pro-these mixtures were duced by cows to be used for human consumption.of the market is re- These products, the urgent need for which first became
ws the total sales of evident in Costa Rica, but which are also very muchhe time it was intro- needed in the other countries of the area, will both help
to increase the sources of meat and milk, and lead toeconomic advantages for the six countries.this field were the
The result of this research, which had financial sup-port from a group of private industrialists in Costa Rica,
*oduct in other coun-was the development of suitable formulas for these milk
duras, Nicaragua, and s substitutes, based on local products and capable of beinglong other factors seek produced economically. A private company in Costaiulas require certain Rica has already begun industrial production and com-ocal food habits, and mercial distribution of the formula under the name ofcost of raw materials, "Ternerina." It is to be hoped that Costa Rica's experi-
ence, after the formula has been marketed for a suffi-cient time, will enable other countries of Central Amer-ica, or of other areas, to make use of this product.
The Institute's other contribution in this field was thepublication of the Composition Table for Fodders,Forages, and Other Animal Feeds of Central Americaand Panama. This first edition includes data on thechemical and nutritional composition of 4,000 samplesof more than 153 different products, that is, the majorityof fodders and forages, industrial by-products, and otherfeeds native to the Central American area which can beused for the cattle industry. In addition, it gives ex-amples of dietary rations for various species of breedanimals based on the products included in the table.These valuable data will fill a deeply felt need, helpingto stimulate more efficient production of foods of thistype. They will also make possible the more rationaluse of raw products available in the area and the stan-dardization of concentrates for animals and of products
,IM -7 ~ , s i#used in their manufacture. The result, in the long run,will be the promotion and strengthening of stock-raising,
uatemala 1961-1969. with the resultant nutritional and economic gains.
125
i-* -- ------- ---o 1
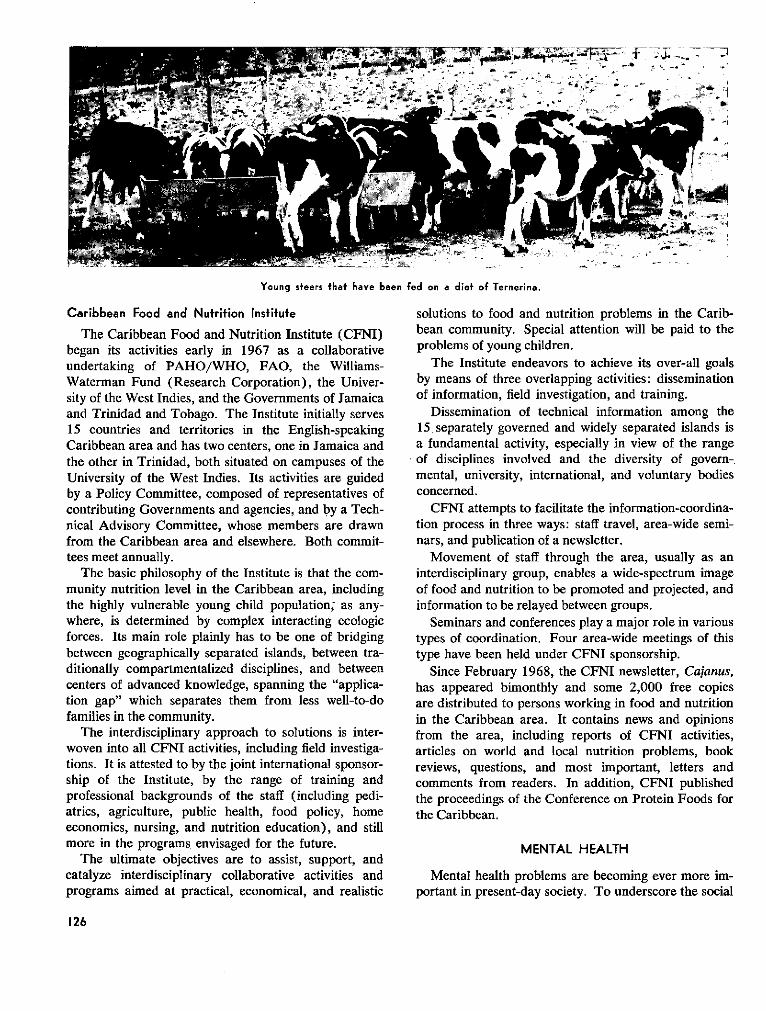
x.~~~ -
¡ A ' ~~.-i
Young steers that have been fed on a diet of Ternerina.
Caribbean Food and Nutrifion Institute
The Caribbean Food and Nutrition Institute (CFNI)began its activities early in 1967 as a collaborativeundertaking of PAHO/WHO, FAO, the Williams-Waterman Fund (Research Corporation), the Univer-sity of the West Indies, and the Governments of Jamaicaand Trinidad and Tobago. The Institute initially serves15 countries and territories in the English-speakingCaribbean area and has two centers, one in Jamaica andthe other in Trinidad, both situated on campuses of theUniversity of the West Indies. Its activities are guidedby a Policy Committee, composed of representatives ofcontributing Governments and agencies, and by a Tech-nical Advisory Committee, whose members are drawnfrom the Caribbean area and elsewhere. Both commit-tees meet annually.
The basic philosophy of the Institute is that the com-munity nutrition level in the Caribbean area, includingthe highly vulnerable young child population; as any-where, is determined by complex interacting ecologicforces. Its main role plainly has to be one of bridgingbetween geographically separated islands, between tra-ditionally compartmentalized disciplines, and betweencenters of advanced knowledge, spanning the "applica-tion gap" which separates them from less well-to-dofamilies in the community.
The interdisciplinary approach to solutions is inter-woven into all CFNI activities, including field investiga-tions. It is attested to by the joint international sponsor-ship of the Institute, by the range of training andprofessional backgrounds of the staff (including pedi-atrics, agriculture, public health, food policy, homeeconomics, nursing, and nutrition education), and stillmore in the programs envisaged for the future.
The ultimate objectives are to assist, support, andcatalyze interdisciplinary collaborative activities andprograms aimed at practical, economical, and realistic
solutions to food and nutrition problems in the Carib-bean community. Special attention will be paid to theproblems of young children.
The Institute endeavors to achieve its over-all goalsby means of three overlapping activities: disseminationof information, field investigation, and training.
Dissemination of technical information among the15 separately governed and widely separated islands isa fundamental activity, especially in view of the rangeof disciplines involved and the diversity of govern-mental, university, international, and voluntary bodiesconcerned.
CFNI attempts to facilitate the information-coordina-tion process in three ways: staff travel, area-wide semi-nars, and publication of a newsletter.
Movement of staff through the area, usually as aninterdisciplinary group, enables a wide-spectrum imageof food and nutrition to be promoted and projected, andinformation to be relayed between groups.
Seminars and conferences play a major role in varioustypes of coordination. Four area-wide meetings of thistype have been held under CFNI sponsorship.
Since February 1968, the CFNI newsletter, Cajanus,has appeared bimonthly and some 2,000 free copiesare distributed to persons working in food and nutritionin the Caribbean area. It contains news and opinionsfrom the area, including reports of CFNI activities,articles on world and local nutrition problems, bookreviews, questions, and most important, letters andcomments from readers. In addition, CFNI publishedthe proceedings of the Conference on Protein Foods forthe Caribbean.
MENTAL HEALTH
Mental health problems are becoming ever more im-portant in present-day society. To underscore the social
126
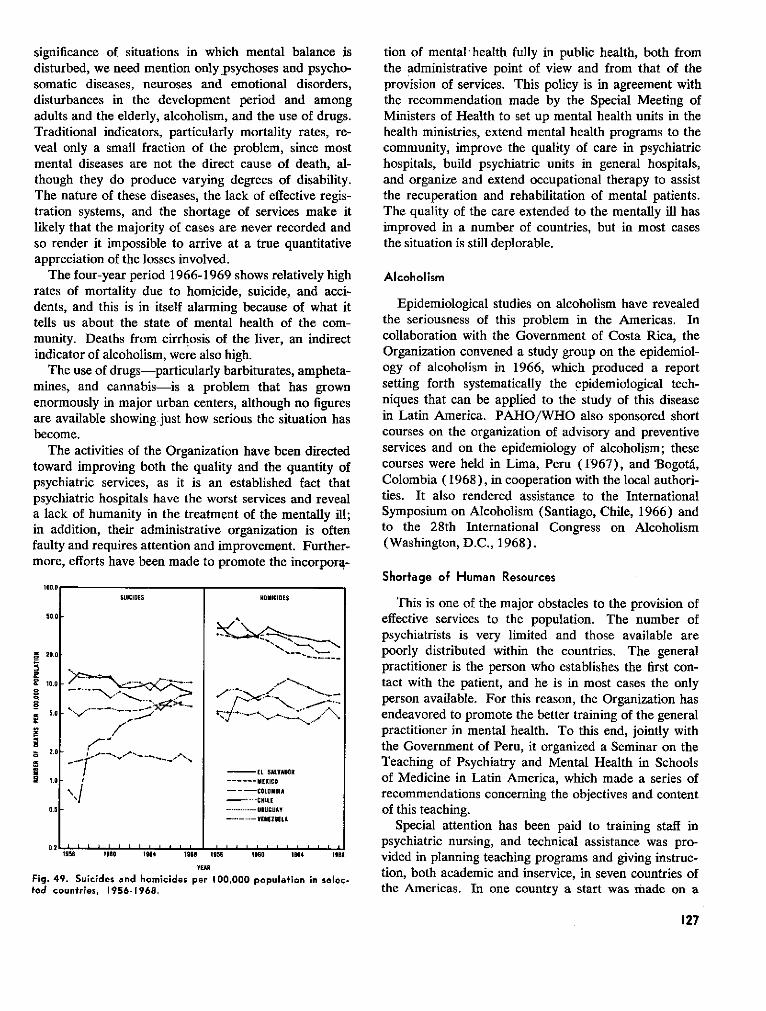
significance of situations in which mental balance isdisturbed, we need mention onlypsychoses and psycho-somatic diseases, neuroses and emotional disorders,disturbances in the development period and amongadults and the elderly, alcoholism, and the use of drugs.Traditional indicators, particularly mortality rates, re-veal only a small fraction of the problem, since mostmental diseases are not the direct cause of death, al-though they do produce varying degrees of disability.The nature of these diseases, the lack of effective regis-tration systems, and the shortage of services make itlikely that the majority of cases are never recorded andso render it impossible to arrive at a true quantitativeappreciation of the losses involved.
The four-year period 1966-1969 shows relatively highrates of mortality due to homicide, suicide, and acci-dents, and this is in itself alarming because of what ittells us about the state of mental health of the com-munity. Deaths from cirrhosis of the liver, an indirectindicator of alcoholism, were also high.
The use of drugs-particularly barbiturates, ampheta-mines, and cannabis-is a problem that has grownenormously in major urban centers, although no figuresare available showing just how serious the situation hasbecome.
The activities of the Organization have been directedtoward improving both the quality and the quantity ofpsychiatric services, as it is an established fact thatpsychiatric hospitals have the worst services and reveala lack of humanity in the treatment of the mentally ill;in addition, their administrative organization is oftenfaulty and requires attention and improvement. Further-more, efforts have been made to promote the incorpora-
u
Fictec
tion of mental health fully in public health, both fromthe administrative point of view and from that of theprovision of services. This policy is in agreement withthe recommendation made by the Special Meeting ofMinisters of Health to set up mental health units in thehealth ministries, extend mental health programs to thecommunity, improve the quality of care in psychiatrichospitals, build psychiatric units in general hospitals,and organize and extend occupational therapy to assistthe recuperation and rehabilitation of mental patients.The quality of the care extended to the mentally ill hasimproved in a number of countries, but in most casesthe situation is still deplorable.
Alcoholism
Epidemiological studies on alcoholism have revealedthe seriousness of this problem in the Americas. Incollaboration with the Government of Costa Rica, theOrganization convened a study group on the epidemiol-ogy of alcoholism in 1966, which produced a reportsetting forth systematically the epidemiological tech-niques that can be applied to the study of this diseasein Latin America. PAHO/WHO also sponsored shortcourses on the organization of advisory and preventiveservices and on the epidemiology of alcoholism; thesecourses were held in Lima, Peru (1967), and Bogotá,Colombia (1968), in cooperation with the local authori-ties. It also rendered assistance to the InternationalSymposium on Alcoholism (Santiago, Chile, 1966) andto the 28th International Congress on Alcoholism(Washington, D.C., 1968).
Shortage of Human Resources100.0
SUICIOES HOMICIDES This is one of the major obstacles to the provision of,0.0 - effective services to the population. The number of
psychiatrists is very limited and those available are20.0 -_.... . - poorly distributed within the countries. The general
practitioner is the person who establishes the first con-,oo10.0 . ... -~ .. ... * /"~.. tact with the patient, and he is in most cases the only
_ /--.~',*. -~ ./ _... person available. For this reason, the Organization has.0 ., -. .\..........7 endeavored to promote the better training of the general
practitioner in mental health. To this end, jointly withr/'-"2.0 _ ,'rthe Government of Peru, it organized a Seminar on the
r S ALVO R Teaching of Psychiatry and Mental Health in Schools1.0 _. ."------MEXICO of Medicine in Latin America, which made a series of
· | --- COLOMIA recommendations concerning the objectives and content0.5 _ ................. URUGUAY of this teaching.
Special attention has been paid to training staff in0.2 .. l. . l . g L. I N ..... 14 9 psychiatric nursing, and technical assistance was pro-
195S 19W6 1.4 les. 1s ISSO ISS4 I968 vided in planning teaching programs and giving instruc-r9ER tion, both academic and inservice, in seven countries ofg. 49. Suicides and homicides per 100,000 population in selec-
d countries, 1956-1968. the Americas. In one country a start was made on a
127
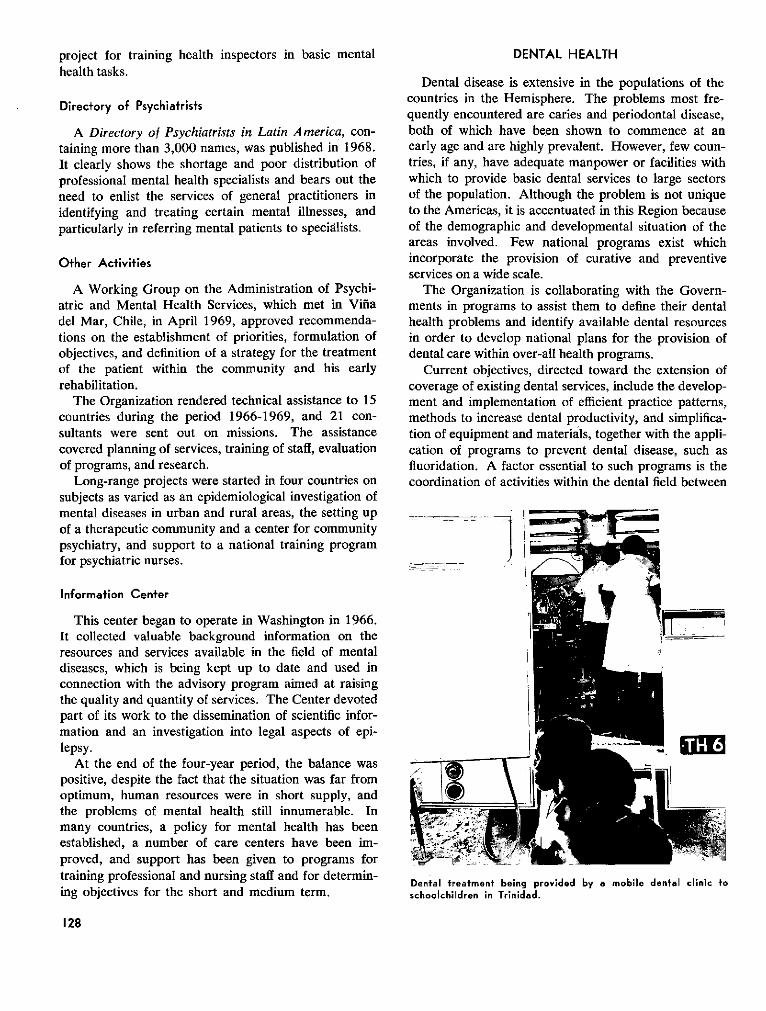
project for training health inspectors in basic mentalhealth tasks.
Direcfory of Psychiatrists
A Directory of Psychiatrists in Latin America, con-taining more than 3,000 names, was published in 1968.It clearly shows the shortage and poor distribution ofprofessional mental health specialists and bears out theneed to enlist the services of general practitioners inidentifying and treating certain mental illnesses, andparticularly in referring mental patients to specialists.
Other Activities
A Working Group on the Administration of Psychi-atric and Mental Health Services, which met in Viñadel Mar, Chile, in April 1969, approved recommenda-tions on the establishment of priorities, formulation ofobjectives, and definition of a strategy for the treatmentof the patient within the community and his earlyrehabilitation.
The Organization rendered technical assistance to 15countries during the period 1966-1969, and 21 con-sultants were sent out on missions. The assistancecovered planning of services, training of staff, evaluationof programs, and research.
Long-range projects were started in four countries onsubjects as varied as an epidemiological investigation ofmental diseases in urban and rural areas, the setting upof a therapeutic community and a center for communitypsychiatry, and support to a national training programfor psychiatric nurses.
Information Center
This center began to operate in Washington in 1966.It collected valuable background information on theresources and services available in the field of mentaldiseases, which is being kept up to date and used inconnection with the advisory program aimed at raisingthe quality and quantity of services. The Center devotedpart of its work to the dissemination of scientific infor-mation and an investigation into legal aspects of epi-lepsy.
At the end of the four-year period, the balance waspositive, despite the fact that the situation was far fromoptimum, human resources were in short supply, andthe problems of mental health still innumerable. Inmany countries, a policy for mental health has beenestablished, a number of care centers have been im-proved, and support has been given to programs fortraining professional and nursing staff and for determin-ing objectives for the short and medium term.
DENTAL HEALTH
Dental disease is extensive in the populations of thecountries in the Hemisphere. The problems most fre-quently encountered are caries and periodontal disease,both of which have been shown to commence at anearly age and are highly prevalent. However, few coun-tries, if any, have adequate manpower or facilities withwhich to provide basic dental services to large sectorsof the population. Although the problem is not uniqueto the Americas, it is accentuated in this Region becauseof the demographic and developmental situation of theareas involved. Few national programs exist whichincorporate the provision of curative and preventiveservices on a wide scale.
The Organization is collaborating with the Govern-ments in programs to assist them to define their dentalhealth problems and identify available dental resourcesin order to develop national plans for the provision ofdental care within over-all health programs.
Current objectives, directed toward the extension ofcoverage of existing dental services, include the develop-ment and implementation of efficient practice patterns,methods to increase dental productivity, and simplifica-tion of equipment and materials, together with the appli-cation of programs to prevent dental disease, such asfluoridation. A factor essential to such programs is thecoordination of activities within the dental field between
Dental treatment being provided by a mobile dental clinic toschoolchildren in Trinidad.
128
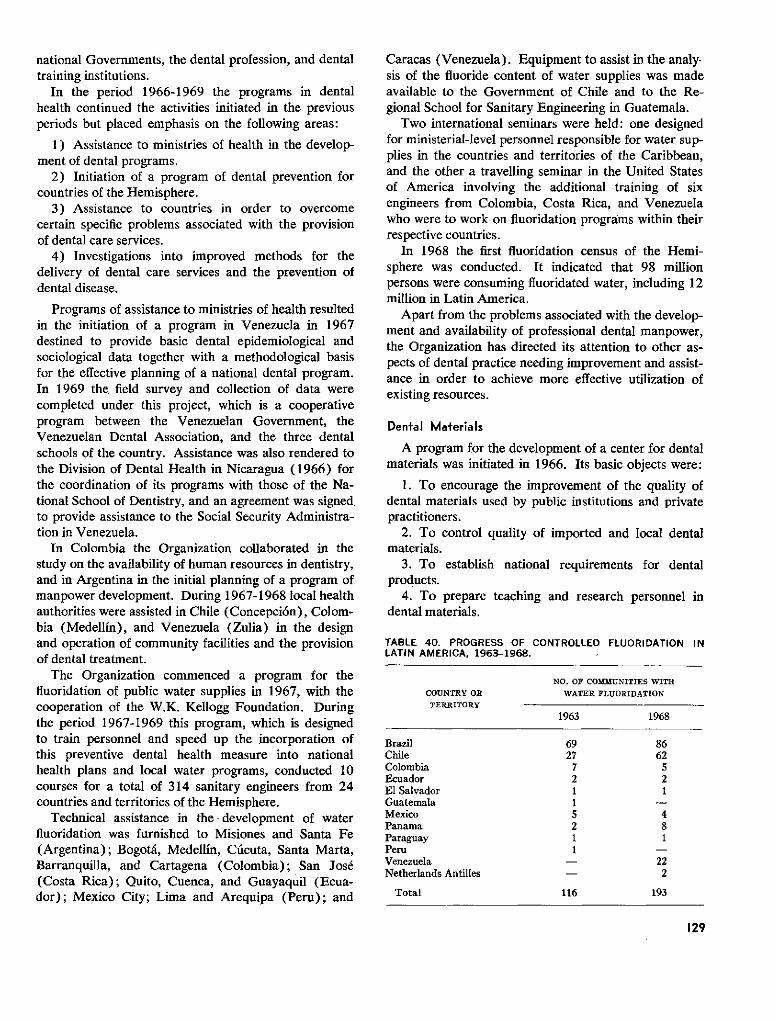
national Governments, the dental profession, and dentaltraining institutions.
In the period 1966-1969 the programs in dentalhealth continued the activities initiated in the previousperiods but placed emphasis on the following areas:
1) Assistance to ministries of health in the develop-ment of dental programs.
2) Initiation of a program of dental prevention forcountries of the Hemisphere.
3) Assistance to countries in order to overcomecertain specific problems associated with the provisionof dental care services.
4) Investigations into improved methods for thedelivery of dental care services and the prevention ofdental disease.
Programs of assistance to ministries of health resultedin the initiation of a program in Venezuela in 1967destined to provide basic dental epidemiological andsociological data together with a methodological basisfor the effective planning of a national dental program.In 1969 the field survey and collection of data werecompleted under this project, which is a cooperativeprogram between the Venezuelan Government, theVenezuelan Dental Association, and the three dentalschools of the country. Assistance was also rendered tothe Division of Dental Health in Nicaragua (1966) forthe coordination of its programs with those of the Na-tional School of Dentistry, and an agreement was signedto provide assistance to the Social Security Administra-tion in Venezuela.
In Colombia the Organization collaborated in thestudy on the availability of human resources in dentistry,and in Argentina in the initial planning of a program ofmanpower development. During 1967-1968 local healthauthorities were assisted in Chile (Concepción), Colom-bia (Medellín), and Venezuela (Zulia) in the designand operation of community facilities and the provisionof dental treatment.
The Organization commenced a program for thefluoridation of public water supplies in 1967, with thecooperation of the W.K. Kellogg Foundation. Duringthe period 1967-1969 this program, which is designedto train personnel and speed up the incorporation ofthis preventive dental health measure into nationalhealth plans and local water programs, conducted 10courses for a total of 314 sanitary engineers from 24countries and territories of the Hemisphere.
Technical assistance in the development of waterfluoridation was furnished to Misiones and Santa Fe(Argentina); Bogotá, Medellín, Cúcuta, Santa Marta,Barranquilla, and Cartagena (Colombia); San José(Costa Rica); Quito, Cuenca, and Guayaquil (Ecua-dor); Mexico City; Lima and Arequipa (Peru); and
Caracas (Venezuela). Equipment to assist in the analy-sis of the fluoride content of water supplies was madeavailable to the Government of Chile and to the Re-gional School for Sanitary Engineering in Guatemala.
Two international seminars were held: one designedfor ministerial-level personnel responsible for water sup-plies in the countries and territories of the Caribbean,and the other a travelling seminar in the United Statesof America involving the additional training of sixengineers from Colombia, Costa Rica, and Venezuelawho were to work on fluoridation programs within theirrespective countries.
In 1968 the first fluoridation census of the Hemi-sphere was conducted. It indicated that 98 millionpersons were consuming fluoridated water, including 12million in Latin America.
Apart from the problems associated with the develop-ment and availability of professional dental manpower,the Organization has directed its attention to other as-pects of dental practice needing improvement and assist-ance in order to achieve more effective utilization ofexisting resources.
Dental Materiais
A program for the development of a center for dentalmaterials was initiated in 1966. Its basic objects were:
1. To encourage the improvement of the quality ofdental materials used by public institutions and privatepractitioners.
2. To control quality of imported and local dentalmaterials.
3. To establish national requirements for dentalproducts.
4. To prepare teaching and research personnel indental materials.
TABLE 40. PROGRESS OF CONTROLLED FLUORIDATION INLATIN AMERICA, 1963-1968.
NO. OF COMMUNITIES WITH
COUNTRY OR WATER FLUORIDATION
TERRITORY
1963 1968
Brazil 69 86Chile 27 62Colombia 7 5Ecuador 2 2El Salvador 1 1Guatemala 1Mexico 5 4Panama 2 8Paraguay 1 1Peru 1Venezuela - 22Netherlands Antilles - 2
Total 116 193
129
5. To initiate applied research in dental materials,especially as related to large population groups.
The plan for the center was developed in conjunctionwith the W.K. Kellogg Foundation, the Dental HealthCenter of the United States Public Health Service, andthe Ministry of Public Health and Social Welfare andthe dental schools of Venezuela. The $500,000 project,with a contribution of $153,000 from the Kellogg Foun-dation, was dedicated at the Central University inCaracas in 1969. In conjunction with this project asurvey of the utilization of dental materials and theteaching of this subject in dental schools of LatinAmerica was also begun in 1969.
The development of auxiliary dental manpower con-tinues to be of prime interest, and in 1967-1968 theOrganization conducted a survey on the availability andutilization of such personnel in Latin America. TheGovernment of Jamaica was completing the constructionof a school, the first of its kind in the Americas, to traindental auxiliaries to provide dental services to school-children. This joint project has had the cooperation ofUNICEF, which provided dental equipment for theschool. The Organization also gave assistance in pro-grams for the training of dental auxiliaries at the Uni-versities of Zulia in Venezuela and Antioquia in Colom-bia.
Since Latin America does not produce dental equip-ment on an extensive scale, many countries have toimport such equipment. In an effort to facilitate theacquisition of equipment and introduce modern conceptsin regard to its specifications and use, the Organizationgave assistance to the Municipality of Medellín and theUniversity of Antioquia in the design and demonstrationof simplified dental equipment. Such equipment hasbeen subsequently tried out in Colombia and Venezuela.Assistance was also given in the setting up of a clinic inArgentina designed to increase the productivity of dentalservices. In conjunction with this project, a trainingcourse was held for some 10 auxiliary workers fromall parts of the Province of Buenos Aires.
Research
The research on the effectiveness of salt as a vehicleof fluoride, initiated in the period 1962-1966 in coop-eration with the U.S. Public Health Service and theGovernment of Colombia, was continued during thequadrennium. To date the studies have demonstratedthat salt can serve as a vehicle for fluoride compounds;it has proved acceptable in a community preventivedental program involving four communities (some28,000 persons) in Antioquia, Colombia.
In conjunction with the dental epidemiology programin Brazil, studies were initiated in 1967 on the effective-ness of certain self-applied topical fluoride agents in
the prevention of dental caries. This project has beenconducted in collaboration with the Dental Health Cen-ter of the U.S. Public Health Service, for the purpose ofinvestigating the efficacy of such agents as an adjunctto the fluoridation of water supplies or for use in areaswhere the fluoridation of water supplies is impractical.
Investigations have been started in connection withthe program on dental materials. These investigationsinvolve four studies, and a new concept in the preven-tion of dental caries-utilizing pit and fissure sealants-which in cooperation with the University of Zulia will betested in the first community experience in the world.Protocols and final arrangements for the project havebeen completed. An additional project to test the appli-cation of intermediate simple dental materials, utilizingauxiliary personnel, at the University of Zulia and inMedellín, Colombia, was prepared in 1969 for initiationin 1970. Both investigations are being conducted inconjunction with the Division of Dental Health of theU.S. Public Health Service.
To summarize, PAHO/WHO activities in dentalhealth have developed at a satisfactory pace, if availablemanpower is taken into account, and they will be carriedforward in the future in collaboration with the Govern-ments, in an attempt to solve the problems of dentaldisease in the Hemisphere.
VETERINARY PUBLIC HEALTH
The development of veterinary public health serviceswithin the ministries of health of many countries of theHemisphere has brought about significant changes inthis specialty. These services have generated increasedrequests from the countries for the Organization's tech-nical advisory services, consultation on the design,preparation, and implementation of zoonoses controlprograms, and specifically, the organization of programsfor training veterinarians as specialists in zoonoses con-trol, food hygiene, and other aspects of veterinary publichealth.
Of outstanding importance to the activities of theseservices were the recommendations of the Special Meet-ing of Ministers of Health, which recognized the impactof the zoonoses on the economy and on food productionin the Americas and the measures that should be takenby the Governments to organize programs for the con-trol of these diseases. Subsequently, the Ministers ofAgriculture, at their II Meeting, adopted resolutionsconcerning the zoonoses and the execution of nationalprograms for their control, and also proposals for thelong-term financing of the Pan American ZoonosesCenter so as to cooperate in the activities being carriedout by the countries.
The requests from the Governments have been metthrough the assignment of consultants to the different
130
Zone Offices. Veterinary public health consultants arecurrently attached to the Zone II, III, IV, and V Officesand the Field Office in El Paso, Texas. Consultation inZone VI is provided by the professional staff of the PanAmerican Zoonoses Center. Since the assignment ofthese Zone consultants, broad programs of assistance inveterinary public health and veterinary medical educa-tion have been developed in many of the countries. Asthese programs progress, the countries recognize theneed for greater expansion of veterinary medical serviceswithin their ministries of health and agriculture, andaccordingly request assistance on a more extensive scalefrom the Organization.
Considerable progress has been made in many of thenational rabies control programs with the help of theseconsultants, who have also provided advisory servicesand training assistance in the areas of brucellosis andbovine tuberculosis control and the epidemiology ofzoonoses. Advances have also been made in under-standing the problems of food hygiene and in the prep-aration and development of national and local programsto solve some of these problems. As part of its activitiesin the food hygiene field, the Organization sponsoredand conducted the Annual Seminar on Food and DrugControl for Central America and Panama.
The results achieved in the rabies control programconducted along the U.S.-Mexico border and coordi-nated by the veterinary public health consultant in theEl Paso Office were of major significance. Prior to thatprogram, El Paso as well as Juárez, Mexico, had re-ported more cases of canine rabies than any two citiesin the Hemisphere. Human cases of rabies and largenumbers of bites by animals, particularly the stray dogswhich were so numerous there, occurred all along theborder. As a consequence of this program, started threeyears ago, no human cases have been reported, noepidemics of canine rabies have occurred, well over 80per cent of the owned dogs have been vaccinated, andapproximately 30 per cent of the estimated stray dogpopulation has been captured and destroyed.
One of the important contributions to rabies controlin the Americas has been the advisory assistance fur-nished by the Organization for the establishment ofnational rabies diagnostic laboratories and the trainingof many specialists in the fluorescent antibody techniqueas a routine procedure in rabies diagnosis. Also, a
better understanding of zoonoses control was gained asa result of the International Symposium on Health As-pects of the International Movement of Animals, held inSan Antonio, Texas (28-30 August 1968) under thesponsorship of the Organization and the Conference ofPublic Health Veterinarians. More than 160 partici-pants representing 18 countries reviewed in detail theproblems associated with the movement of animals andanimal products and their implications for public health.
To further strengthen the programs of zoonoses con-trol, a Seminar on the Epidemiology of Zoonoses washeld at the Pan American Zoonoses Center (August1968) for 29 veterinarians and four physicians, repre-senting 14 countries.
The veterinary public health consultant in Zone IVassisted the Government of Ecuador in coordinating theactivities and mobilizing the resources of health andagriculture sectors in the campaign to control the out-break of Venezuelan equine encephalitis. This epidemiccaused thousands of clinical cases in horses, resulting inthe death of many animals. Several human cases anddeaths occurred. The consultant also helped with thecoordination of the work between epidemiologists, vi-rologists, veterinarians, and laboratory and hospitalmedical services.
The assignment of the veterinary public health con-sultant to Zone V, in January 1969, led to an increasein the activities undertaken in fields of zoonoses control,food hygiene, veterinary medical education, and otherrelated services in cooperation with the federal authori-ties of Brazil. Assistance was rendered, in conjunctionwith the health authorities of Sao Paulo, in the designand preparation of a canine rabies control program.The consultant also helped to prepare and conduct acourse on rabies diagnosis and production and controlof rabies vaccine, which was sponsored by the Organiza-tion and held at the School of Veterinary Medicine inBelo Horizonte, Brazil, with 23 participants from theregional laboratories of the Ministry of Agriculture.
This brief account of PAHO/WHO activities inveterinary public health reflects the steady advancesthat have been made, and it is to be hoped that infuture years the rate of progress will be even greater asthe Governments intensify their efforts to curb the lossescaused by zoonotic diseases to both individuals and theeconomy.
OTHER HEALTH SERVICES
PUBLIC HEALTH LABORATORIES
During the four-year period reasonable progress wasmade in the improvement of health laboratory servicesin Latin America. While the need for these services is
well recognized, the development of adequate laborator-ies is still lagging. Some advances have been made inextending health services to the rural areas, but in manycountries concomitant laboratory services have notbeen provided to support the available medical services.
131
The Organization has attempted to assist the Govern-ments by providing fellowships for training specialistpersonnel from almost all the countries of the Americas,and by assigning regular staff members and short-termconsultants to furnish technical advice on the organiza-tion and strengthening of central laboratories and tocooperate in specific activities such as the productionand control of biological products for the treatment andprevention of infectious diseases, establishment of ani-mal colonies, organization of virological diagnostic lab-oratories, and improvement of immunological tech-niques. Other services have included the provision ofbiological reagents, reference services for the assay ofvaccines, sponsoring of courses on bacteriological andserological techniques, and advice on the selection oflaboratory equipment and methods.
In 1966 advisory services were rendered to Colombia,to assist in the planning of a new building for theNational Institute of Health. A consultant was madeavailable to Brazil to assist in the establishment of avirological diagnostic laboratory at the Oswaldo CruzInstitute in Rio de Janeiro, where studies on entericviruses were pursued. The laboratory played an im-portant part in the investigation of outbreaks of polio-myelitis and other paralytic diseases in the States ofGuanabara and Rio Grande do Norte. An agreementwas signed with Venezuela to extend assistance in thedevelopment of the Laboratories Division of the Minis-try of Health and Social Welfare.
Some countries recognized their inability to strengthentheir national laboratories utilizing solely their ownresources and sought outside assistance for this purpose.Advice was furnished to Peru on the preparation of aplan and application for assistance from the Inter-
American Development Bank for financing and buildinga new National Institute of Health. Advice was alsogiven on the preparation of applications to the UNDPfor assistance in modernizing the National Institutes ofHygiene, Epidemiology, and Microbiology in Cuba andthe National Health Laboratories in Mexico. The plansfor both projects were completed and were submitted tothe UNDP for consideration.
Perhaps the most significant progress has been madein the production and control of biologicals. In 1966the Organization assisted the National Institute of Micro-biology in Buenos Aires by providing technical informa-tion and equipment, including a freeze-drying unit. Along-term consultant was assigned to the National Insti-tute of Health of Colombia to assist in the preparationof pertussis and diphtheria vaccine.
Smallpox Vaccine
Past failures to meet the goals of the continent-widesmallpox campaign were due largely to the lack ofadequate supplies of good-quality vaccine. To over-come this problem an agreement was concluded withthe Connaught Laboratories (Canada) to furnish con-sultant services for the following purposes:
1) Assessment of the status of all laboratories inLatin America producing smallpox vaccine, in regard tophysical facilities, procedures in force, staff, and testingfacilities.
2) Recommendations for improvements in facilities,staff, and procedures.
3) Making available the services of a standard refer-ence laboratory in Toronto.
This program was begun in 1967. All laboratories
Extensive drug control work isdone in the Central FederalControl Laboratory in Brazil.
;í
132
producing smallpox vaccine were visited and recom-mendations made for their improvement, and they wereencouraged to submit samples of all smallpox vaccineproduced to the Connaught Laboratories for testing. Asa result of the program, the quality of vaccine hasmarkedly improved. Most countries are now producinga good quality freeze-dried vaccine which meets theminimum requirements established by WHO.
Otfher Vaccines
Although considerable progress has been made inthe preparation of a good-quality smallpox vaccine bythe various countries, similar progress has not beenrealized in the production and control of other vaccines.Beginning in 1969, the Connaught Laboratories agreedto extend their advisory services to include all types ofvaccines produced by the official laboratories of LatinAmerica.
The production of biologicals for the treatment andprevention of infectious diseases is an important functionthat may be required of a national laboratory when otherfacilities are not available, but a significant number ofLatin American countries do not produce such bio-logicals. Although they are needed for immunizationprograms, the demand in some countries is insufficientto permit production on an economical basis.
For many years the Organization has collaboratedwith Brazil and Colombia in the production of theyellow fever vaccines needed for control of yellow feverin Latin America. In 1967 a short-term consultantstudied the production of this vaccine in Colombia withthe objective of standardizing the techniques in use inLatin America in accordance with WHO recommenda-tions. Brazil, in addition to producing yellow fevervaccine needed for its own use, maintains a stock ofnearly 5 million doses which are available for shipmentto any country when needed. The Organization is alsocollaborating with Mexico with the aim of producingpoliomyelitis vaccine in sufficient amounts to meet theneeds of all the Latin American countries. It has alsobeen assisting the Government of Guatemala in planninga project for the production of biologicals for all ofCentral America. This project, approved by all theMinisters of Health of the area, has reached the finalstages of a feasibility study. If this study proves to besatisfactory, the project will be financed by the CentralAmerican Bank for Economic Integration.
DRUG CONTROL
The people of Latin America are spending, directlyor indirectly (through taxes, etc.), more than $1,500,-000,000 per year for drugs. Until recently, the countries
imported most of these drugs, but as the result ofnational laws enacted to stimulate domestic drug pro-duction, they now manufacture approximately 90 percent of the drugs consumed in their territories. Thus,the drug manufacturing industry of Latin America hasexpanded greatly within the last few years and willcontinue to do so in order to satisfy the increasingrequirements of the population.
There are many technical problems involved in manu-facturing drugs, some of which are very difficult toovercome. It is for this reason that health officials,particularly those in countries that are only now develop-ing a strong technical base, are concerned over thequality of the drugs distributed.
The Organization has pointed out on a number ofoccasions that in order to ensure good drug quality, acountry should have a modern drug control law which isadministered by a well-coordinated agency staffed byhighly trained administrators, inspectors, and analystsand supplied with adequate funds to carry out a highlevel of drug control activity.
In order to assess the situation in the variouscountries, PAHO/WHO conducted a continental surveyin 1968 which produced the data shown in Table 41.This information, along with the Organization's sug-gestions for improvement, was presented in a report tothe Special Meeting of the Ministers of Health. Thatmeeting adopted a number of important decisions which,together with the report, provide a comprehensive set ofprinciples that will serve as a guide for the drug controlactivities of the countries and the Organization inforthcoming years.
PAHO/WHO continued its program of assistanceboth to individual countries and to groups of countrieson a regional basis. Experts were sent to make com-prehensive studies of the drug control situation in Brazil,Costa Rica, and Uruguay, and to study the governmentdrug testing laboratories in Mexico, Peru, and Vene-zuela. The results of these studies were submitted informal reports to the Governments concerned.
The Organization made a rapid survey of the drugcontrol situation in Jamaica, Guyana, and Trinidad andTobago at the beginning of February 1969, and on thebasis of the partial information obtained made recom-mendations to the Conference of Health Ministersof the Caribbean (Trinidad, 11-14 February 1969),concerning the possibility of intergovernmental actionto deal with the drug control problems of the countriesof that area.
Since 1965 the Organization has sponsored annualseminars for the food and drug control officials of thecountries of Central America and Panama. Theseseminars are useful for providing information to such
133
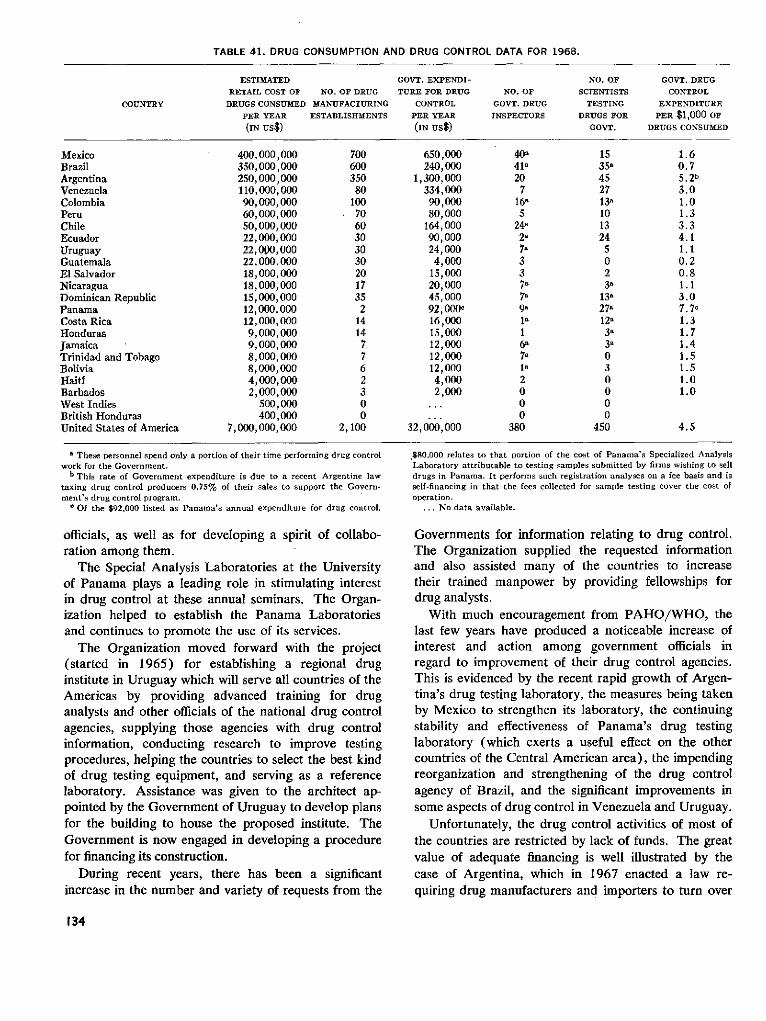
TABLE 41. DRUG CONSUMPTION AND DRUG CONTROL DATA FOR 1968.
ESTIMATED
RETAIL COST OF NO. OF DRUG
DRUGS CONSUMED MANUFACTURING
PER YEAR ESTABLISHMENTS
(IN us$)
GOVT. EXPENDI-
TURE FOR DRUG
CONTROL
PER YEAR
(IN us$)
NO. OF
GOVT. DRUG
INSPECTORS
NO. OF
SCIENTISTS
TESTING
DRUGS FOR
GOVT.
GOVT. DRUG
CONTROL
EXPENDITURE
PER $1,000 OFDRUGS CONSUMED
MexicoBrazilArgentinaVenezuelaColombiaPeruChileEcuadorUruguayGuatemalaEl SalvadorNicaraguaDominican RepublicPanamaCosta RicaHondurasJamaicaTrinidad and TobagoBoliviaHaitíBarbadosWest IndiesBritish HondurasUnited States of America
' These personnel spend only a portion of their time performning drug controlwork for the Government.
b This rate of Government expenditure is due to a recent Argentine lawtaxing drug control producers 0.75% of their sales to support the Govern-ment's drug control program.
c Of the $92,000 listed as Panama's annual expenditure for drug control,
officials, as well as for developing a spirit of collabo-ration among them.
The Special Analysis Laboratories at the Universityof Panama plays a leading role in stimulating interestin drug control at these annual seminars. The Organ-ization helped to establish the Panama Laboratoriesand continues to promote the use of its services.
The Organization moved forward with the project(started in 1965) for establishing a regional druginstitute in Uruguay which will serve all countries of theAmericas by providing advanced training for druganalysts and other officials of the national drug controlagencies, supplying those agencies with drug controlinformation, conducting research to improve testingprocedures, helping the countries to select the best kindof drug testing equipment, and serving as a referencelaboratory. Assistance was given to the architect ap-pointed by the Government of Uruguay to develop plansfor the building to house the proposed institute. TheGovernment is now engaged in developing a procedurefor financing its construction.
During recent years, there has been a significantincrease in the number and variety of requests from the
.$80,000 relates to that portion of the cost of Panama's Specialized AnalysisLaboratory attributable to testing samples submitted by firms wishing to selldrugs in Panama. It performs such registration analyses on a fee basis and isself-financing in that the fees collected for sample testing cover the cost ofoperation.
... No data available.
Governments for information relating to drug control.The Organization supplied the requested informationand also assisted many of the countries to increasetheir trained manpower by providing fellowships fordrug analysts.
With much encouragement from PAHO/WHO, thelast few years have produced a noticeable increase ofinterest and action among government officials inregard to improvement of their drug control agencies.This is evidenced by the recent rapid growth of Argen-tina's drug testing laboratory, the measures being takenby Mexico to strengthen its laboratory, the continuingstability and effectiveness of Panama's drug testinglaboratory (which exerts a useful effect on the othercountries of the Central American area), the impendingreorganization and strengthening of the drug controlagency of Brazil, and the significant improvements insome aspects of drug control in Venezuela and Uruguay.
Unfortunately, the drug control activities of most ofthe countries are restricted by lack of funds. The greatvalue of adequate financing is well illustrated by thecase of Argentina, which in 1967 enacted a law re-quiring drug manufacturers and importers to turn over
134
COUNTRY
400,000,000350,000,000250,000,000110,000,00090,000,00060,000,00050,000,00022,000,00022,000,00022,000.00018,000,00018,000,00015,000,00012,000,00012,000,0009,000,0009,000,0008,000,0008,000,0004,000,0002,000,000
500,000400,000
7,000,000,000
700600350
8010070603030302017352
141477623
02,100
650,000240,000
1,300,000334,00090,00080,000
164,00090,00024,0004,000
15,00020,00045,00092,000 c
16,00015,00012,00012,00012,0004,0002,000
32,000,000
40,41'207
1685
2482'7,337,7,9,
16'7a
1a2OOO
380
1535,45271381013245O23'
13'27'12'3a
3,O3ooOO
450
1.60.75.2b3.01.01.33.34.11.10.20.81.13.07.7o1.31.71.41.51.51.01.0
4.5
to the Government 1 per cent of their gross sales. Ofthe money so obtained, one-fourth is used by theGovernment for supporting basic medical research, andthe remainder for drug control purposes. The amplefunds obtained by means of this law have enabledArgentina to develop an excellent laboratory base forassuring high quality drug production in that country.
It is to be hoped that with the establishment in thenear future of a regional drug institute in Uruguay, animportant step forward will have been taken in this field,which deserves ever-increasing attention by the healthauthorities.
FOOD HYGIENE
Food-borne diseases continue to be a constanthealth hazard for man. The threat of transmission ofthese diseases has increased steadily in the Hemisphereduring the last decade because of the mass migration ofpopulations from rural areas to urban centers, the rapidtransporting of animals and foodstuffs, environmentalpollution, concentration of animals for feeding andhandling, and changes in food habits and food-prepara-tion techniques. Among the social, cultural, and eco-nomic effects of this population movement has been thedevelopment of food-handling conditions which areoften less sanitary than those in the interior or ruralareas themselves. The overcrowded conditions, the lessnatural environmental influences, and the problem ofquantity of available food have created further hazardsfor this population in its efforts to re-establish itselfunder better economic conditions.
Food hygiene continues to be the responsibility andan important activity of the health services of thecountries and of the Organization, because:
1) It is a duty to prevent foodstuffs from serving asvehicles for toxin-carrying infective agents and non-infectious chemicals.
2) It is a duty to preserve food, especially theprotein-rich food of animal origin, essential for humannutrition.
Such was our thinking when, at the II Inter-AmericanMeeting on Foot-and-Mouth Disease and ZoonosesControl, we stated:
The Governments of the Americas have clearly decidedprogressively to reduce the incidence of foot-and-mouthdisease because it means the loss of proteins essential tochildren under 5 years of age whose mortality annuallyaccounts for 45 per cent of all deaths. Evidence has beenrepeatedly produced to show that well-nourished childrenresist environmental assaults, especially infectious diseasesand those of a psychological nature, whereas the mal-nourished child-a by-product of underdevelopment-
rapidly falls victim to them. Among the survivors there isa growing proportion whose impaired intellectual develop-ment is reflected in the inability to learn and to grow.Malnutrition in the final months of pregnancy and in thefirst six months of life gives rise to as much as a 30 per centreduction in the number of brain cells; these are the findingsof research studies being carried out with the collaborationof our Organization.
In most countries there are no programs adequateto protect the population from infected or contaminatedfoods or to control the abuse of food additives orpreservatives. Nor do many of the countries have foodanalysis laboratories or trained personnel for field orlaboratory work. Meat inspection programs are re-stricted to large slaughterhouses or warehouses in themajor cities and are usually understaffed. Milk ormilk-products control services carry out only limitedsampling and the analysis is generally for economic andnot for health purposes. For example, the 1967 out-break of brucellosis involving more than 2,000 humancases in Lima, Peru, resulted from the ingestion ofunpasteurized goat cheese containing the Brucellamelitensis agent.
With the use of modern technology, the food industryhas developed rapidly in recent years in Latin America.This technology has been the result of scientific prog-ress, but the control of the food as a public healthservice has failed to keep pace with these technologicaladvances. The use of antibiotics as additives to pre-serve meat and fish, or of toxic preservatives andadditives that may be carcinogenic, underscores the need
*, -i·" WP;o-
Technicians take samplesverify quality.
in retail food establishments to
135
for adequate control of food processing, preparation,and preservation.
Some countries, such as Argentina, Brazil, and Vene-zuela, are making efforts to improve their food controlservices in regard to registration and analysis of pro-cessed products. However these countries, like manyothers, are confronted with a serious problem owing tothe lack of trained personnel for the supervision andtechnical observation of food production, preparation,warehousing, and retail distribution.
Seminars
One of the significant achievements in food hygienewas the adoption by the Governments of the CentralAmerican countries, in 1966, of sanitary standards forfood and drugs. Consultants from the Organizationcooperated with these Governments in the III Seminaron Food and Drug Control for Central America andPanama (San José, Costa Rica, June 1967). Thediscussions and conclusions dealt with the need for legis-lation on food and drug control, for the establishmentof standards, for the licensing and analysis of products,and for competent inspection procedures.
A regional food-analysis reference laboratory forCentral America and Panama has been proposed toassist in meeting these countries' requests for assistancein food hygiene.
The IV Seminar on Food and Drug Control forCentral America and Panama (San Salvador, ElSalvador, June 1968) reviewed the accomplishments ofeach country in implementing the recommendations ofthe three previous Seminars, especially in regard to theuse of minimum food standards prepared by the Organ-ization and the licensing and analysis of foodstuffs.Included in these standards were principles of labeling,laws and regulations for the use of food additives, con-trol of pesticide residues in food, and basic principlesfor the standardization of laws and regulations con-cerning importation of food.
Educational and procedural activities in food hygienewere reinforced at the international, regional, and na-tional levels during the quadrennium. Contributing tothis progress was the WHO-sponsored InterregionalSeminar on Food-Borne Diseases and Intoxications andFood Hygiene Practices (Copenhagen, Denmark,August 1969), which was attended by eight professionalworkers from Latin American countries (Argentina,Brazil, Colombia, Costa Rica, Mexico, Peru, and Vene-zuela). The participants, drawn from the medical,veterinary medical, and other professions related topublic health and food hygiene, discussed the majorfood-borne diseases and intoxications in both the Amer-icas and the European Region.
In 1969 the V Seminar for Central America andPanama was held in Managua, Nicaragua, under theOrganization's sponsorship and in collaboration withthe Nicaraguan Ministry of Public Health. The Organ-ization provided the advisory services of Headquartersand Zone III staff. The main topics of discussion werefood intoxication, use of gas chromatography equipmentin food analysis, drug standards, use of plastic con-tainers, and standardization of food colors.
Consultation on food hygiene was furnished to Argen-tina, Brazil, British Honduras, Colombia, Guatemala,Honduras, and Uruguay. The Governments of Braziland Colombia were assisted with the organization, prep-aration, and conduct of two training courses.
Through the Zone Veterinary public health consul-tants, assistance was rendered to the countries of theRegion in various aspects of food hygiene, especiallythose related to inspection, processing, and preservationof foods of animal origin. Technical information onfood hygiene was furnished to health and agriculturalagencies throughout Latin America.
During this period the greatest obstacle to the achieve-ment of objectives in food hygiene in general was thelack of trained professional and technical personnel toassume responsibility for inspection and surveillance.
Gas chromatography unit for analysis of residues of pesticidesin foods, in the food analysis section af INCAP.
136
1 -1F., -- - TIP
In addition to the health hazard of transmission ofdiseases through food, great wastage and deteriorationof food have been observed in countries which areexperiencing losses of animal protein and where foodproduction itself is insufficient. Although there has beenimprovement in food hygiene in the Americas as aresult of the legislation adopted in some countries, thishas not been enough to accomplish what is reallynecessary to solve the problems and adequately protectthe public. Great efforts are needed for the training ofprofessional and technical staff in food hygiene practicesin order to bring about closer cooperation between thehealth services and those engaged in the food industryand food trade.
HEALTH AND RADIATION
The application of nuclear technology and radiationin the field of medicine has resulted in spectacularprogress, as it has in industry, agriculture, and research.This progress has brought with it the responsibility forevaluating and taking measures to avoid the hazards tohealth which the use of these tools entails. This is atask for the public health services, and one in which theOrganization has been providing assistance and supportfor a number of years.
PAHO/WHO has cooperated with the countries inthe formulation of radiation protection, hygiene andsurveillance programs, fostering their application in theinterests of public health and encouraging the adoptionof adequate safeguards. Special attention has beenpaid to the following points in the drawing up of theseprograms:
a) Identification of sources of radiation and ofenvironmental contamination.
b) Drafting of legislation and regulations.c) Training of personnel.d) Coordination of the programs of national and
international agencies that carry out related activities.e) Promotion and coordination of research in the
field of radiobiology.
During the period 1966-1969 the Organization gaveassistance in these activities to Argentina, Bolivia,Brazil, Chile, Colombia, Costa Rica, Ecuador, Guyana,Jamaica, Nicaragua, Peru, Trinidad and Tobago, Uru-guay, and Venezuela.
A survey was started with the aim of standardizingnomenclature for the presentation of data and layingthe bases for evaluating the existing and planned man-power and material resources at the regional level. Theprogram for the surveillance of radioactivity levels inair, water, and food was continued in order to detectpossible risks to health from radioactive fallout produced
by the detonation of nuclear devices. This study is beingundertaken in cooperation with the USPHS NationalCenter for Radiological Health and is utilizing a networkof air sampling stations located in Buenos Aires, La Paz,Santiago, Bogotá, Guayaquil, Quito, Cuenca, George-town, Kingston, Lima, Caracas, and Trinidad. Thestudy also includes measurements of samples of milkobtained from stations in Bogotá, Santiago, Guayaquil,Montego Bay, Lima, and Caracas.
The Organization also assisted with the installation offilm dosimetry laboratories to measure exposure levelsin persons exposed to radiation by reason of their work;such assistance was given to Bolivia, Chile, Colombia,Ecuador, and Peru.
Some countries of the Americas have already enactedlegislation governing radiation protection. The Organ-ization's health and radiation unit prepared a modellaw of this type and also gave advice to one country onthe preparation of the pertinent provisions of its healthcode.
Training and Courses
The course for the training of physicians in theclinical use of radioisotopes continued to be given at theLatin American Center established in the El SalvadorHospital, connected with the University of Chile. Theprogram is sponsored by the University, the ChileanNational Health Service, the W.K. Kellogg Foundation,and the Organization. By the end of 1969, nine annualcourses had been held for a total of 34 physicians fromdifferent Latin American countries.
The Organization assisted with the annual basic train-ing courses at the national level organized in Argentina,Chile, Colombia, Costa Rica, Ecuador and Nicaragua,and in 1966, jointly with WHO and the U.S. PublicHealth Service, it organized an international course onradiological inspection.
Assistance has also been given to candidates fromdifferent countries in obtaining fellowships, thus helpingwith the training of radiophysicists and radiotherapists.
Coordinafion
Particular emphasis has been placed on coordinationof the programs of national and international agenciesworking in the radiation field, in order to achieve betterutilization of available manpower and equipment and toproperly channel, without duplication, the resourcesfurnished through international technical assistance.Close cooperation is maintained with WHO Head-quarters, and there is constant contact also with theInternational Atomic Energy Agency (IAEA) withrespect to programs under way in the Americas.
137
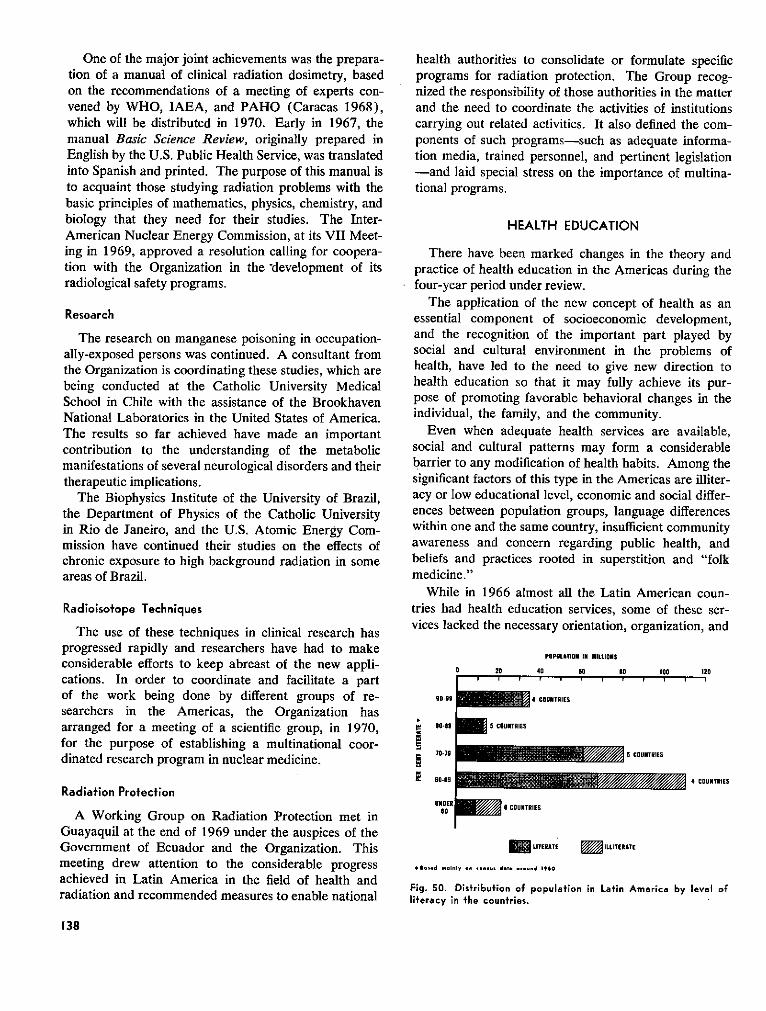
One of the major joint achievements was the prepara-tion of a manual of clinical radiation dosimetry, basedon the recommendations of a meeting of experts con-vened by WHO, IAEA, and PAHO (Caracas 1968),which will be distributed in 1970. Early in 1967, themanual Basic Science Review, originally prepared inEnglish by the U.S. Public Health Service, was translatedinto Spanish and printed. The purpose of this manual isto acquaint those studying radiation problems with thebasic principles of mathematics, physics, chemistry, andbiology that they need for their studies. The Inter-American Nuclear Energy Commission, at its VII Meet-ing in 1969, approved a resolution calling for coopera-tion with the Organization in the development of itsradiological safety programs.
Research
The research on manganese poisoning in occupation-ally-exposed persons was continued. A consultant fromthe Organization is coordinating these studies, which arebeing conducted at the Catholic University MedicalSchool in Chile with the assistance of the BrookhavenNational Laboratories in the United States of America.The results so far achieved have made an importantcontribution to the understanding of the metabolicmanifestations of several neurological disorders and theirtherapeutic implications.
The Biophysics Institute of the University of Brazil,the Department of Physics of the Catholic Universityin Rio de Janeiro, and the U.S. Atomic Energy Com-mission have continued their studies on the effects ofchronic exposure to high background radiation in someareas of Brazil.
Radioisotope Techniques
The use of these techniques in clinical research hasprogressed rapidly and researchers have had to makeconsiderable efforts to keep abreast of the new appli-cations. In order to coordinate and facilitate a partof the work being done by different groups of re-searchers in the Americas, the Organization hasarranged for a meeting of a scientific group, in 1970,for the purpose of establishing a multinational coor-dinated research program in nuclear medicine.
Radiation Protection
A Working Group on Radiation Protection met inGuayaquil at the end of 1969 under the auspices of theGovernment of Ecuador and the Organization. Thismeeting drew attention to the considerable progressachieved in Latin America in the field of health andradiation and recommended measures to enable national
health authorities to consolidate or formulate specificprograms for radiation protection. The Group recog-nized the responsibility of those authorities in the matterand the need to coordinate the activities of institutionscarrying out related activities. It also defined the com-ponents of such programs-such as adequate informa-tion media, trained personnel, and pertinent legislation-and laid special stress on the importance of multina-tional programs.
HEALTH EDUCATION
There have been marked changes in the theory andpractice of health education in the Americas during thefour-year period under review.
The application of the new concept of health as anessential component of socioeconomic development,and the recognition of the important part played bysocial and cultural environment in the problems ofhealth, have led to the need to give new direction tohealth education so that it may fully achieve its pur-pose of promoting favorable behavioral changes in theindividual, the family, and the community.
Even when adequate health services are available,social and cultural patterns may form a considerablebarrier to any modification of health habits. Among thesignificant factors of this type in the Americas are illiter-acy or low educational level, economic and social differ-ences between population groups, language differenceswithin one and the same country, insufficient communityawareness and concern regarding public health, andbeliefs and practices rooted in superstition and "folkmedicine."
While in 1966 almost all the Latin American coun-tries had health education services, some of these ser-vices lacked the necessary orientation, organization, and
0 20 41
90.99
00-89
70.79
90-69
UNDER0so
POPULATION IN MILLIONS
, 90 1l0 100 120
4 COUNTRIES
5 COUNTRIES
COUNTRIES
4 COUNTRIES
98 COUITRIES
EL'TERATE M'"ITERATE
*Based .oinl o.n .e.su. dot a..und 1960
Fig. 50. Distribution of population in Latin America by level ofliteracy in the countries.
138
ENERENERREM5:i
5
resources with which to fulfill their basic functionssatisfactorily. For various reasons, their activitiesamounted to little more than provision of information orpublic relations. They usually operated without liaisonwith similar activities conducted in other sectors such asgeneral education, land reform, social service, com-munity development, and agricultural cooperatives andextension work. In the Caribbean area only threecountries had health education services.
The educational functions and responsibilities of thedifferent professional members of the health team werenot clearly defined. Everything was usually left to thespecialists, little attention being given to the responsi-bility of the entire staff for health education work.There were, moreover, not enough specialists (Table42) and a good proportion of the personnel of thehealth agencies had not received appropriate training.
The Organization's efforts, therefore, were directedprimarily to assisting the Governments to review theorientation of their health education services. To thisend it sponsored a series of meetings on a Hemispherescale. One of them, the Latin American Seminar onHealth Education in relation to Health Planning (Para-cas, Peru, 20-26 April, 1969), discussed the mostfeasible means of strengthening and integrating thesocial and educational components in the health plan-ning process, and sought to define those areas in whichresearch was most urgently needed in order to facilitatethis process and establish indicators to assist with theevaluation of education campaigns in the health andbehavioral sciences and their inclusion in the healthplanning methodology. The Seminar also defined therole of educators as members of the health team.
The Regional Seminar on Postgraduate Preparationof Health Workers in Health Education and Behavioral
Sciences (Buenos Aires, Argentina, 28 August-5 Sep-tember 1969) reviewed health education policy andsuggested changes in the curricula in this discipline atschools of public health in the light of present-dayrequirements.
For the purpose of demonstrating quantitatively thespecific value of health education as an essential part ofhealth programs, a small working group convened byPAHO/WHO prepared the bases for conducting anevaluation of the educational component of some of thehealth projects undertaken by various countries with theOrganization's assistance. The intention was to developsuitable instruments and indices with which to assessbehavioral changes in individuals and groups subjectedto health education.
Several Governments were assisted with the analysisof administrative structures within the health ministriesat the various levels of operation, in order to identifykey points where health education specialists couldexercise greater influence over the orientation and super-vision of educational activities conducted by health andrelated services and to increase the effectiveness ofhealth education among the different population groups.Special attention was paid to the countries of the CentralAmerican Isthmus and of the English-speaking Carib-bean area, where effective coordination between officialand voluntary agencies and community groups has beenachieved through local health committees. The Organ-ization also helped to reformulate the organizational andoperational bases of health education services in Bolivia,Brazil, Colombia, Cuba, the Dominican Republic, andPeru.
Health education has been made part of over-allfamily guidance within the maternal and child healthprograms, with a view to encouraging proper health
TABLE 42. PERSONNEL IN HEALTH EDUCATION IN THE AMERICAS, 1967./
OTHER
MINISTRIES OR DEPARTMENTS OF HEALTH GOVERNMENTAL
AND VOLUNTARY
INSTITUTIONSAREAS OF TRE REGION
SPECIALISTS IN OTHER PERSONNEL IN HEALTH
HEALTH EDUCATION EDUCATION SERVICES EXISTING
SPECIALISTS
EXISTING LMINIMUM EXISTING MINIMUMNECESSARY NECESSARY
Canada 7 1 11 11 27United States of America 511b 714 860 40 33Latin America 232 740 210 565 40Caribbean 8 28 17 20 5
Total 758 1,483 324 636 105
a According to PAHO/WHO survey.b In the case of the U.S.A. the information (including Puerto Rico) was
obtained from the shools of public health according to the places of employ-
ment of the graduates in health education. The information applicable toColumbia University is not included because of lack of data.
c Data available only for Puerto Rico.
139
habits in the family group and inducing parents to helpensure, as far as they are able, a healthy and productivelife for their children. Advisory services in these activi-ties were rendered to the Governments of Colombia,Jamaica, and Trinidad and Tobago.
It is evident that, from the health point of view, aproperly structured, organized, and supervised schoolsystem constitutes a most valuable tool for directlyinfluencing not only the families of schoolchildrenbut also the entire population of the district, especiallyin rural areas, through effective health education pro-grams. In most countries, however, schools had notbeen effectively and systematically used for this purpose.The basic facts about health were not always taught inthe schools and the pupils' needs and interests in regardto both local and national health problems were nottaken into account. For this reason the Organizationhas encouraged and assisted the Governments to givedue attention to health education activities but in theschools and in teacher-training institutions. In thisconnection, WHO and UNESCO jointly published themanual Planning of Health Education in Schools, whichwas distributed to the Governments concerned, andPAHO prepared and distributed in Spanish a healtheducation guide on rabies, the first of a series of suchguides on major health problems in the Americas de-signed especially for teachers. Several countries, includ-ing Argentina and Brazil, requested the Organization'sassistance in reviewing their school health educationprograms.
As a result of the intensified community promotionactivities in rural water supply programs in Central andSouth America, carried out with PAHO/WHO assist-
ance, the benefited communities in some areas arecontributing between 10 and 20 per cent of the construc-tion costs of the systems, plus their contribution towardfinancing their operation and administration. In thesame way, the educational activities in the malariaeradication campaigns in the Central American Isthmusand Surinam have promoted extensive voluntary co-operation by local communities in the collection of bloodspecimens from febrile cases and in collective treatment.The most typical example is Surinam where, despite thediversity of ethnic and cultural groups, the population'sinitial resistance has been overcome, due in no smallpart to good health education work.
By the end of the quadrennium, some of the Carib-bean countries and territories that had lacked healtheducation services had begun to organize such servicesand to recruit suitable staff for them. This was particu-larly the case in Barbados, Dominica, Grenada, andSt. Vincent. For their part, Jamaica, Guyana, andTrinidad and Tobago drew up plans to strengthen andextend their services so as to achieve greater coverage.
The establishment of a Health Education WorkingGroup that meets annually and whose conclusions andrecommendations are endorsed by the Central AmericanPublic Health Council has facilitated the joint action bythe Governments and the Organization to increase theeffectiveness of these services in the Central AmericanIsthmus.
Although there is much that remains to be done, theprogress made in health education in the period 1966-1969 has laid a foundation for further advances in theyears to come.
RESEARCH DEVELOPMENT AND COORDINATION
In response to the new policy directions for researchset forth by the Presidents of America in 1967, anexpanded PAHO/WHO research program was con-ceived and put into operation during the quadrennium.It is based on the following broad aims:
*To increase the capacity of the peoples of the Ameri-cas to protect themselves against the major diseases thataffect them.
*To help improve the effectiveness of health expendi-tures in the nations of the Hemisphere.
*To elevate, through close association with research,the quality of the training of physicians and biomedicalresearch workers and to strengthen the institutions thateducate them.
*To establish conditions that will encourage more
physicians and health-related scientists to remain intheir own countries.
*To promote and support health research in priorityareas and to coordinate these programs with activitiessponsored by other international and national bodies.
*To strengthen the existing capacity for biomedicalresearch and research training of institutions in LatinAmerica, and to tie them together more effectively.
Research is an indispensable means of uncoveringthe causes of disease, finding remedies, and guiding theuse of resources. The inclusion of research in a totalhealth program is ultimately justified because of itsfavorable effects on levels of health. In earlier yearsit was argued that a health agency, especially one thatdeals primarily with countries in which many disease
140
Medical research laboratory in Trinidad.
problems can be resolved by applying known remedies,should concern itself not with securing new knowledgebut rather with making use of the vast body of informa-tion already available but not being applied. This argu-ment is no longer accepted; experience has shown thatactive research efforts must be carried on to ensure,among other things, that existing knowledge is effec-tively used.
Thus, the Organization is committed to expanding itsprogram of research and to helping the Governments tostrengthen their own programs in this area. In order todeliver its services more effectively, it established a De-partment of Research Development and Coordination.
ADVISORY COMMITTEE ON MEDICAL RESEARCH
Guidelines for the Organization's research programare provided by this Advisory Committee, which meetsonce a year to review the needs and resources forbiomedical research in Latin America and to suggestthe fields of research that the Organization mightproperly cultivate. Its counsel and recommendationsare taken carefully into consideration in the setting ofpriorities.
In response to specific suggestions by the AdvisoryCommittee, and often in connection with its annualmeetings, panels of distinguished scientists are convened
to explore a variety of topics of current interest. In1966, in a special session on life at high altitudes, con-sideration was given to the problem of man's naturaland acquired acclimatization to anoxic environments-a subject of special significance in the Western Hemi-sphere, where several million people reside at altitudesof over 10,000 feet. The following year, attention wasdirected to the immunologic aspects of parasitic infec-tions, including the outstanding problems in the host-parasite relationship in these infections and the com-plexity of the antigenic structure of the parasite and ofthe response of the host. In addition, a special sym-posium was held on drug resistance in human malaria.A 1968 panel reviewed the biomedical challengespresented by the American Indian and stressed theurgency of studying such populations from a multidisci-plinary perspective-drawing upon ecology, anthro-pology, medicine, and genetics-before these primitivegroups disappear entirely or become acculturated. Theperinatal factors affecting human development-themany factors that may act during pregnancy, labor, andearly life and can interfere with the normal developmentof the infant-were examined at the special session ofthe Advisory Committee in 1969, and a symposium alsoheld in conjunction with that meeting dealt with thesubject of iron metabolism and anemia, with presenta-tions on topics ranging from the basic concepts of thechemistry and biochemistry of iron to the epidemio-
141

logical and therapeutic aspects of the anemia problem.The proceedings of each of these scientific meetingswere published in the Organization's Scientific Publica-tions Series.
In 1966 the Advisory Committee also devoted specialattention to the problem of the migration of healthpersonnel, scientists, and engineers from Latin America.A report on this subject, prepared at its request (Scien-tific Publication PAHO 142), reviewed the importanceof these professional groups to the national economiesand to the intellectual, cultural, and political future ofthe countries concerned. In particular, the study identi-fied the characteristics and size of the migrating groups,analyzed the forces leading to migration, and recom-mended measures that would reconcile the legitimateaspirations of highly trained individuals with the needsof the countries for trained manpower.
During its more recent meetings, the Advisory Com-mittee has also given consideration to studies in nutri-tion, physical growth, and mental development; compar-ative childhood mortality in the Americas; leprosy; fieldstudies with long-acting antimalaria drugs; dentalhealth; geographic distribution and possible northwardmovement of Venezuelan encephalitis virus in CentralAmerica and Mexico; and the role of molecular biologyin health and medicine.
Finally, the Committee maintains under continuousreview the progress of research funded by both theOrganization and outside sources in such broad fields asnutrition, communicable diseases, environmental health,reference and training center activities, health man-power, and medical education.
The expanded research program endorsed by theAdvisory Committee in 1968 calls for the work to becarried out through the following means: implementa-tion of research and research training projects in fields
Special session on perinatal factors held during the 1969 Meetingof the Advisory Committee on Medical Research.
that are directly relevant to health problems in theHemisphere; promotion of multinational cooperativeefforts among biomedical scientists so as to make thebest possible use of existing resources for research andresearch training; strengthening of communicationamong biomedical scientists in the Hemisphere; andimprovement of the effectiveness of health expendituresthrough the application of operations research method-ologies to the planning and administration of publichealth programs.
These phases of activity, taken together, form theframework of the Organization's current research pro-gram. Under each of them, specific undertakings havebeen initiated-and some of them carried to completion-during the quadrennium.
RESEARCH AND RESEARCH TRAINING PROJECTS
The Organization uses several approaches for sup-porting and implementing these efforts. It has beenlearned, for example, that financial assistance to inde-pendent investigators for projects of their own selectionis a highly effective means of promoting research. Ac-cordingly, a research grants program offers assistancein areas related to the general objectives of the Organiza-tion. The research projects in which it is interestedmay be supported by the Organization itself or by out-side sources. There were exactly 100 such undertakingsin progress at the end of 1967. A volume entitledResearch in Progress, containing summaries of theseactivities, is published regularly. Its most recent edition,with information as of December 1969, will appear in1970.
The program on virology offers an example of resultsachieved from a PAHO/WHO-coordinated researchactivity. Devoted to the study of the ecology of arbo-viruses, especially the role of migratory birds in thespread of these viruses in temperate and tropical areas inthe northern part of the Hemisphere, this effort hasbeen focused on the study of encephalitis viruses trans-mitted by arthropods in Mexico and Central America.
During the period 1966-1969, seven arboviruseswere isolated for the first time from Mexico, includingVenezuelan encephalitis and St. Louis encephalitisviruses (Table 43). In 1967 Venezuelan encephalitisvirus was isolated from British Honduras and from theAtlantic and Pacific lowlands of Guatemala, and in thesame year eastern encephalitis virus was isolated fromthe Petén in northern Guatemala. The isolations estab-lished the endemicity of these important human andequine pathogens in areas where they were previouslyunknown. The dramatic success of the field programis due in large part to the discovery that the hamster is
142
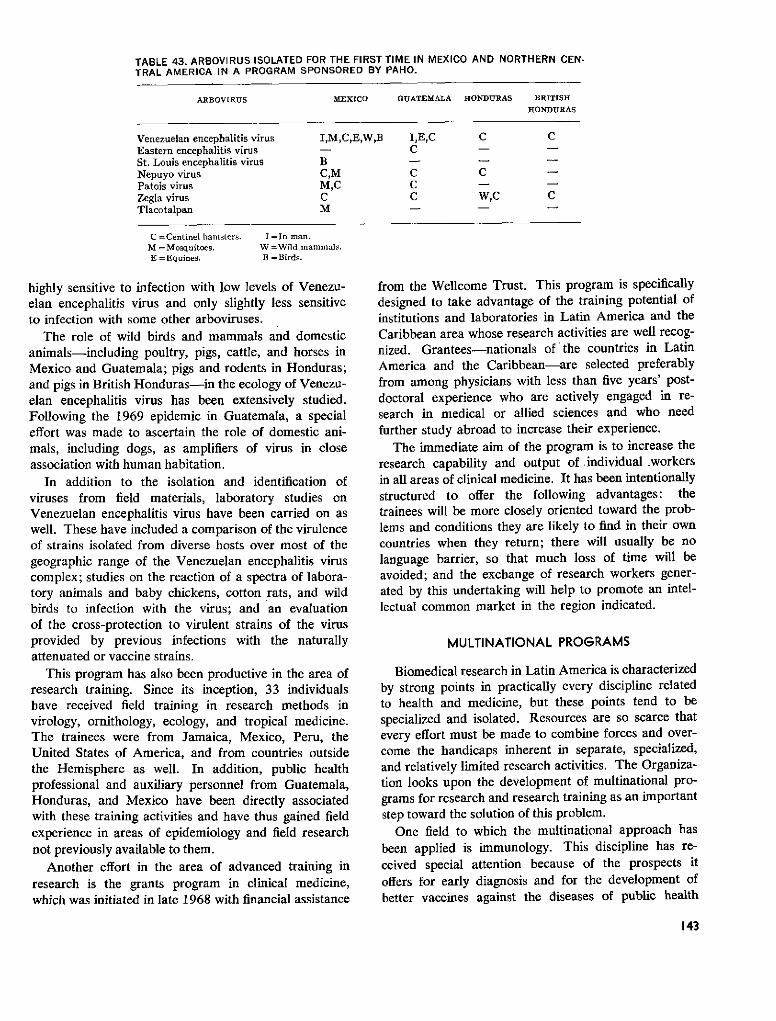
TABLE 43. ARBOVIRUS ISOLATED FOR THE FIRST TIME IN MEXICO AND NORTHERN CEN-TRAL AMERICA IN A PROGRAM SPONSORED BY PAHO.
ARBOVIRUS MEXICO GUATEMALA HONDURAS BRITISHHONDURAS
Venezuelan encephalitis virus I,M,C,E,W,B I,E,C C CEastern encephalitis virus - CSt. Louis encephalitis virus B - -Nepuyo virus C,M C CPatois virus M,C CZegla virus C C W,C CTlacotalpan M - -
C =Centinel hamsters.M = Mosquitoes.E= Equines.
I =In man.W =Wild mammals.B = Birds.
highly sensitive to infection with low levels of Venezu-elan encephalitis virus and only slightly less sensitiveto infection with some other arboviruses.
The role of wild birds and mammals and domesticanimals-including poultry, pigs, cattle, and horses inMexico and Guatemala; pigs and rodents in Honduras;and pigs in British Honduras-in the ecology of Venezu-elan encephalitis virus has been extensively studied.Following the 1969 epidemic in Guatemala, a specialeffort was made to ascertain the role of domestic ani-mals, including dogs, as amplifiers of virus in closeassociation with human habitation.
In addition to the isolation and identification ofviruses from field materials, laboratory studies onVenezuelan encephalitis virus have been carried on aswell. These have included a comparison of the virulenceof strains isolated from diverse hosts over most of thegeographic range of the Venezuelan encephalitis viruscomplex; studies on the reaction of a spectra of labora-tory animals and baby chickens, cotton rats, and wildbirds to infection with the virus; and an evaluationof the cross-protection to virulent strains of the virusprovided by previous infections with the naturallyattenuated or vaccine strains.
This program has also been productive in the area ofresearch training. Since its inception, 33 individualshave received field training in research methods invirology, ornithology, ecology, and tropical medicine.The trainees were from Jamaica, Mexico, Peru, theUnited States of America, and from countries outsidethe Hemisphere as well. In addition, public healthprofessional and auxiliary personnel from Guatemala,Honduras, and Mexico have been directly associatedwith these training activities and have thus gained fieldexperience in areas of epidemiology and field researchnot previously available to them.
Another effort in the area of advanced training inresearch is the grants program in clinical medicine,which was initiated in late 1968 with financial assistance
from the Wellcome Trust. This program is specificallydesigned to take advantage of the training potential ofinstitutions and laboratories in Latin America and theCaribbean area whose research activities are well recog-nized. Grantees-nationals of'the countries in LatinAmerica and the Caribbean-are selected preferablyfrom among physicians with less than five years' post-doctoral experience who are actively engaged in re-search in medical or allied sciences and who needfurther study abroad to increase their experience.
The immediate aim of the program is to increase theresearch capability and output of individual .workersin all areas of clinical medicine. It has been intentionallystructured to offer the following advantages: thetrainees will be more closely oriented toward the prob-lems and conditions they are likely to find in their owncountries when they return; there will usually be nolanguage barrier, so that much loss of time will beavoided; and the exchange of research workers gener-ated by this undertaking will help to promote an intel-lectual common market in the region indicated.
MULTINATIONAL PROGRAMS
Biomedical research in Latin America is characterizedby strong points in practically every discipline relatedto health and medicine, but these points tend to bespecialized and isolated. Resources are so scarce thatevery effort must be made to combine forces and over-come the handicaps inherent in separate, specialized,and relatively limited research activities. The Organiza-tion looks upon the development of multinational pro-grams for research and research training as an importantstep toward the solution of this problem.
One field to which the multinational approach has
been applied is immunology. This discipline has re-ceived special attention because of the prospects itoffers for early diagnosis and for the development ofbetter vaccines against the diseases of public health
143
A scientist examining cultures at the Microbiology Laboratory ofINCAP.
importance in the Americas. In particular, it is hopedthat research in this field will lead to ways of immunizingagainst parasitic diseases such as malaria and that itwill provide insights into the problems of autoimmuneand other immunopathological disorders and cancer.
The Organization has established two ImmunologyResearch and Training Centers, one in Sáo Paulo andthe other in Mexico City, which operate in coordinationwith three other WHO centers outside the Hemisphere.The students, who come from all parts of Latin America,are exposed to a research atmosphere and learn byexample how research of high quality is conducted.Whenever possible, diseases of local public healthimportance are used as models for the training given.
The center at Sao Paulo was established in 1966 atthe Paulista School of Medicine and in January 1969was transferred to the Butantan Institute. To date, fourannual eight-month courses have been given at thepostgraduate level, and in 1970 it is planned to offer aprogram of four months' duration, which will receivestudents from Brazil and other countries as well. Itsresearch activity has included work on the responses ofpatients with Brazilian pemphigus foliaceus to treatmentwith immunosuppressive drugs; on the biological signifi-cance of the heterogeneity of immunoglobulins for thepurpose of determining which ones afford protectionagainst infectious agents and which ones contribute totissue damage by hypersensitivity reactions (allergy andimmunopathology); and on the mechanism of hemor-rhagic reaction produced in the skin of normal labora-tory animals by the sera of Brazilian pemphigus folia-ceus patients. Future research will concentrate on theimmunochemistry of venoms and antivenoms of the
two major groups of snakes in Brazil: Crotalus andBothrops.
The center in Mexico City began combined opera-tions during 1969 using the laboratory facilities andpermanent staff of seven cooperating institutions. Itoffers a unique three-year training program leadingtoward the Master's or Ph.D. degree, and it also givesshorter courses and seminars at the postgraduate level.Research is being carried on in the following areas:immunochemical analysis of carbohydrate antigens inmycobacteria; immunoglobulin levels in malnutrition;the role of the common antigen (Kunin) of E. coli ininfant diarrheas; antigenicity of IgG in various states ofaggregation, and its implications in immunological toler-ance and rheumatoid arthritis; complement componentsin rabbits in relation to immune responses, includingrejection of transplants; immunochemical properties ofpolysaccharides from M. tuberculosis, M. leprae, N.brasiliensis, N. asteroides, and K. rhinoscleromatis;systemic lupus; anti-enzyme antibodies; laboratorymodels of anaphylaxis; erythrocyte groups and othergenetic markers in normal and atopic populations; cell-mediated immunity in lepromatous and tuberculoidleprosy; anti-DNA antibodies in collagen diseases; ex-perimental induction of anti-nuclear antibodies by differ-ent pharmocological agents; collagen antigenicity; de-layed hypersensitivity with special reference to cytotoxiceffectors; and production of antibodies to guinea pigmacrophages.
It is hoped that the provision of initial PAHO/WHOsupport to these centers of excellence will lead to theireventual establishment as a continuing feature in therespective host institutions.
BIOMEDICAL COMMUNICATION
As part of the effort to promote communicationamong biomedical scientists in the Hemisphere, a con-tinuing program of scientific meetings and symposia isbeing carried on. In addition to the special sessionsheld in conjunction with the annual meetings of theAdvisory Committee on Medical Research, interna-tional conferences have been convened on a number ofsubjects of broad and immediate public health im-portance.
The PAHO/WHO International Conference on Vac-cines against Viral and Rickettsial Diseases of Man heldat the end of 1966, brought together 280 scientists from27 countries. The Conference reviewed current knowl-edge in this field and called attention to directions andneeds in vaccine research. It also reported on the latestresults from chemotherapeutic and other approaches tothe control of these diseases. The proceedings of the
144
Conference were published in a special volume early in1967 (Scientific Publication PAHO 147).
In preparation for an international symposium onmycoses, a consultant from the Organization visitedinstitutions in Argentina, Brazil, Colombia, Mexico, andVenezuela in late 1969 to determine the status of workin the field of medical mycology as carried on in thesecountries.
Another facet of the communications effort is theseries of PAHO/WHO Lectures on the BiomedicalSciences. In 1967 Professor Abel Wolman spoke onthe theme "The Unreasonable Man," and in 1968Professor Joshua Lederberg dealt with the subject of"Health in the World of Tomorrow." The texts ofthese two lectures were issued as Scientific PublicationsPAHO 152 and 175, respectively.
The Organization also has the commitment to im-prove communication through the occasional publica-tion of research findings in fields of special public healthinterest in the Americas. In this connection, a mono-graph summarizing current knowledge on Argentinehemorrhagic fever was published and distributed in 1969(Scientific Publication PAHO 183).
Regional Library of Medicine
The exchange of information among biomedicalscientists in the Hemisphere has been enhanced greatlyby the activities of the Regional Library of Medicinein Sao Paulo, Brazil. The Library was established inresponse to an urgent need for improved medical libraryresources and services in South America.
A survey conducted by the Organization in 1965 hadrevealed serious deficiencies in the supply of informa-tion to the biomedical community, a shortage of trained
"- : I;.j'
Regional Library of Medicine, SaoPaulo, Brazil.
library personnel, and a lack of awareness of modernprocedures for the analysis and retrieval of scientificinformation. At a meeting of the U.S. National Libraryof Medicine attended by representatives of PAHO/WHO and of other institutions interested in this field,it was recommended that a central core of bibliographicresources be developed to better serve the Latin Ameri-can biomedical community. Finally, with support fromthe Brazilian Ministries of Health and of Education andCulture, the U.S. National Library of Medicine, andthe Commonwealth Fund, the Regional Library wasformally opened in April 1967 on the premises of thePaulista School of Medicine. In January 1968 a full-time director was appointed.
From an initial collection of approximately 15,000volumes, including journals and monographs, the Li-brary doubled the size of its holdings to 30,000 volumeswithin two years. Acquisition by subscription increasedfrom 400 titles in 1967 to 1,200 in 1968 and 1,300 in1969. During the same three years, a total of 25,202journal issues were received from the U.S. Book Ex-change and added to the collection. By using theseissues to fill gaps in the serials holdings, the Library atthe end of 1969 was well on the way to its goal of acomplete collection of 1,200 selected periodicals from1960 onward.
Seven subcenters in Brazil-Fortaleza, Recife, Salva-dor, Brasilia, Rio de Janeiro, Belo Horizonte, andPorte Alegre-have been identified as the basis of aninterlibrary network within the country. Once theselibraries' resources are pooled and operations through-out Brazil are fully established, the Regional Librarywill cooperate with national centers elsewhere in SouthAmerica. Already in 1969 gift and exchange activities
145
were conducted with 188 libraries in Brazil and 363similar institutions in other South American countries.
Interlibrary loan services were initiated within Brazilin January 1969, and in the course of the year 12,085requests from 90 Brazilian libraries were processed:approximately 51 per cent were satisfied from theLibrary's own resources, 14 per cent by other librariesin the Sao Paulo area, and 35 per cent by the U.S.National Library of Medicine. During the same period,66 reference requests were received for special biblio-graphies; of these, 41 were fulfilled using the resourcesat,the Regional Library and 25 were submitted to theNational Library of Medicine for retrieval by the com-puter-based Medical Literature Analysis and RetrievalSystem (MEDLARS). With the experience gainedfrom its operations in 1969, the Regional Library hopesto have the necessary base for extending interlibraryloan services to other South American countries on a fullscale in 1970.
The Directing Council has requested the Director tostudy ways of increasing the financial and technicalresources of the Library and to explore the possibilityof partial self-financing. It has also pointed out the needto begin the program for training staff in modern pro-cedures for the collection, classification, and use ofbibliographic information in the biomedical sciences.
This is a program whose future development willhelp to accelerate and improve both teaching and re-search in the biomedical sciences in Latin America.
OPERATIONS RESEARCH
One of the chief problems faced by health adminis-trators in Latin America is how to make the most effec-tive use of the limited resources available to them.Operations research supplies the scientific methodologiesso that administrators can arrive at the best possiblesolutions for establishing orders of priorities, determin-ing the bases upon which choices can be made, anddeveloping objective means for deciding on the relativeeffectiveness of different programs.
Accordingly, in November 1968 a unit was estab-lished within the Department of Research Developmentand Coordination to promote the application of opera-tions research methodologies to the description andsolution of public health problems so as to obtain maxi-mum returns on investments in this sector. Thesemethodologies are currently being applied to healthplanning, blood bank operations, manpower studies,and the determination of a typology for the countriesof the Americas based on mortality structures. Ad-visory services in this field are available to the Govern-ments.
NUTRITION RESEARCH
Endemic Goiter
Nine laboratories and research units in eight coun-tries (Argentina, Brazil, Chile, Colombia, Ecuador,Mexico, Peru, and Venezuela) are now participatingin the PAHO/WHO Collaborative Study on EndemicGoiter and Cretinism. Epidemiological and socioeco-nomic data were collected and the use of intramuscularinjections of iodized oil as a means of preventing goiterwas investigated in Ecuador and Peru. Interim ap-praisals were made of the thyroid status of adult popu-lation treated with iodized oil by intramuscular injection.Preliminary results showed substantial reduction inprevalence of goiter and in the size of enlarged glandsin the communities.
The Third Meeting of the PAHO Scientific Group onEndemic Goiter took place in Puebla, Mexico, in June1968. The meeting reviewed the status of this publichealth problem in the Americas and analyzed the resultsof the various research projects under way, giving specialattention to the results obtained with iodized oil inEcuador and Peru. On the basis of these findings aprotocol was formulated detailing the conditions of useand the methodology of this alternate form of prophy-laxis for endemic goiter and cretinism. This informationhas been made available to the Governments. Thereport of the Scientific Group was published and dis-tributed by the Organization (Scientific PublicationPAHO 193). This compendium of 34 scientific papersincludes the significant research on endemic goiter andrelated defects carried out by the participants in thepast two years.
The Iodine Reference Laboratory in Santiago, Chile,was completed in 1966 and started its training activitieslate in the year. During the quadrennium it continuedto strengthen its program of endemic goiter studiesthrough the checking of duplicate samples from collabo-rating laboratories, and helped to improve the tech-niques through training of personnel. The Laboratorytrained six technicians and undertook 2,138 determina-tions of 1127 in biological samples.
Nutritional Anemias
The PAHO/WHO Collaborative Study on NutritionalAnemias was continued actively with the collaborationof research units in Argentina, Brazil, Colombia, Guate-mala, Mexico, Paraguay, Peru, Trinidad and Tobago,the United States of America, and Venezuela.The Reference Laboratory for the study of nutritionalanemias at the Venezuelan Scientific Research Institutetrained research workers from seven collaborating lab-oratories in hematological techniques and completed
146

more than 2,000 laboratory determinations of hemato-logical indices for national and international investiga-tors.
The Second Meeting of the PAHO Scientific Groupon Nutritional Anemias took place in August 1968 inCaracas, Venezuela. The data on the epidemiology ofthis group of diseases collected in collaborating labora-tories in recent years was analyzed and discussed.Specific recommendations were made for preventivemeasures through local health services; gaps in knowl-edge were identified; and future research areas weredefined. The report was prepared and distributed in1969.
Hypovifaminosis A
Hypovitaminosis A and its severe ocular manifesta-tions of xerophthalmia and keratomalacia have beenidentified as public health nutrition problems in variousparts of the Hemisphere. A complete analysis of allavailable data on vitamin A intake in the Americas wasundertaken for the purpose of defining the extent of theproblem of vitamin A deficiency.
A Technical Group was convened by PAHO/WHOin November 1968 to define the nature of the problemand make recommendations for specific preventive mea-sures. It also identified gaps in scientific knowledge anddefined areas in need of further research. The reportof this Group was prepared for publication in 1970.
Maternal Nutrition and Family Planning
Relatively little information is available to healthservices in the Americas on the subject of maternalnutrition and its relationship to patterns of reproduction.A Technical Group was therefore convened to considercritically different aspects of the problem, taking intoaccount biological, socioeconomic, and cultural factorsand the interrelations of program activities in nutritionand family planning. The report of the Group sum-marized the evidence reviewed and conclusions reached.Since several gaps in knowledge were identified, recom-mendations for research were made that will help toorient future investigations. The report was preparedfor publication and distribution in 1970.
Nutrition and Mental Development
In recent years increasing attention has been paidto the relationship between nutrition and mental devel-opment, and a number of studies on this subject areunder way or planned in Latin America. PAHO/WHOhas assisted by providing short-term consultants andtraining fellows for the development of project Chile-4201, on brain development in malnourished children.
The current interest in studies on the interrelationshipof nutrition and development has led to an increasingdemand for the training of Latin American scientists inbasic and clinical research in this subject area. To meetthese requests, a training program for professional per-sonnel is being planned by the Organization in close
-1
ffiPsychological tests are an important part of the longitudinal study to determine the effect of nutrition on mental growth anddevelopment.
147
i 1l 1 11. k,l� L *
11'1 ik

cooperation with the Government of Chile, the Uni-versity of Chile, and Cornell University (U.S.A.)
In 1968 the nutrition component of the Inter-Ameri-can Investigation of Mortality in Childhood was activelydeveloped during the planning and pilot study stagesof that project. By placing considerable emphasis onnutrition status prior to and at the time of death inpreschool-age children, it is expected that more quantita-tive estimates of the contribution of malnutrition tochildhood morbidity and mortality can be made in thefuture. Preliminary reports indicate that up to 70 percent of the preschool deaths in some areas miay beassociated with malnutrition.
Nufrifion and Chronic Diseases
The Organization's publication Patterns of UrbanMortality identified chronic diseases as a public healthproblem of considerable magnitude. Recent epidemio-logical research has identified nutritional aspects ofthese diseases as being of particular importance. Obe-sity, diabetes, and arteriosclerotic heart disease havesignificant nutritional aspects. Relatively little informa-tion is available on the interrelationship of nutrition andchronic diseases in the Caribbean area and LatinAmerica. A consultant was appointed to visit 10 repre-sentative countries of the Hemisphere: Argentina(Buenos Aires); Brazil (Sáo Paulo); Chile (Santiago);Colombia (Bogotá and Cali); Guatemala City; Jamaica(Kingston); Mexico City; Peru (Lima); Uruguay(Montevideo); and Venezuela (Caracas). The purposewas to collect information on nutrition-related chronicdiseases, particularly obesity, diabetes, and arterioscle-rotic heart disease. The report will be available fordistribution during 1970.
Nutrifion Surveys
At the request of the Ministry of Public Health andSocial Welfare of the Dominican Republic, a nationalnutrition survey was carried out by the Research Cor-poration with the close cooperation and advice ofPAHO/WHO technical staff. The general objectivewas to reveal the principal food and nutrition problemsthat affect the most vulnerable population groups, inorder to establish practical measures for their solution.A report will be prepared during 1970.
The research and training programs of the Instituteof Nutrition of the Federal University of Pernambuco(Recife, Brazil) were further strengthened with a viewto meeting the local needs and promoting nutritionactivities in the health services of northeastern sectorof the country.
Investigations were continued for the modification
and improvement of Incaparina-type foods and theimprovement of cereal food crops. PAHO/WHO fieldstaff participated in clinical and acceptability testing ofprotein-rich foods in Brazil, Peru, and Trinidad andTobago.
Operations research aimed principally at evaluatingthe functioning of nutrition rehabilitation centers wasconducted in Brazil (Recife), Colombia, Guatemala,and Haiti and plans were made for similar studies inPeru.
As a means of strengthening nutrition research, theOrganization rendered assistance to the recently createdLatin American Nutrition Society and to its quarterlyjournal Archivos Latinoamericanos de Nutrición, thefirst issue of which was published in December 1966.
That same year the Organization again sent to Chilea short-term consultant to cooperate in the updating ofthe protocol for the research project on the biodynamicsof vitamin D in osteomalacia, which was submitted tothe U.S. National Institutes of Health for financialsupport.
INCAP Research Programs
The research activities of INCAP were reoriented andthe order of priorities adjusted in accordance with theneeds uncovered by the nutrition surveys in the membercountries, the progress in scientific knowledge, and thetechnical resources available for solving the majorproblems in the Central American area.
Special attention has been given to research aimed atimproving the quality of the diet. Among the significantstudies are those on both experimental animals andchildren to establish the nutritive value of geneticallyimproved varieties of corn, in particular Opaco-2. It
Corn, basic cereal used in food for large segments of thepopulation of the Central American area, is studied for thepurpose of improving its nutritional value.
148
-,A
4
1 ~ i''' 1 '
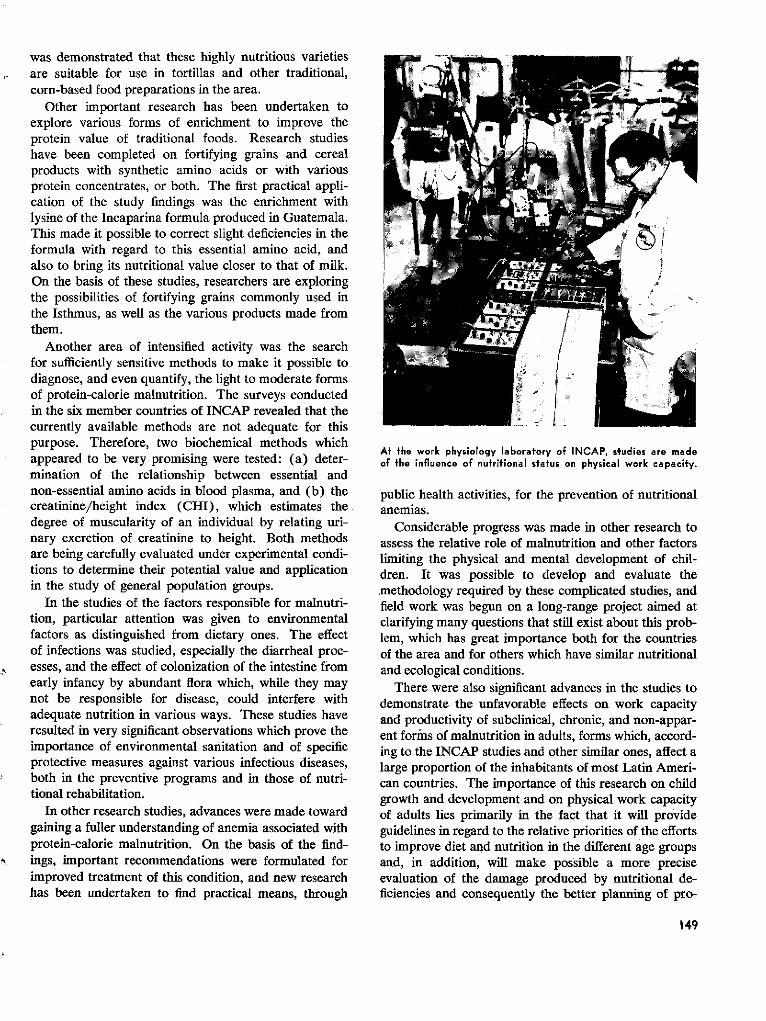
was demonstrated that these highly nutritious varietiesare suitable for use in tortillas and other traditional,corn-based food preparations in the area.
Other important research has been undertaken toexplore various forms of enrichment to improve theprotein value of traditional foods. Research studieshave been completed on fortifying grains and cerealproducts with synthetic amino acids or with variousprotein concentrates, or both. The first practical appli-cation of the study findings was the enrichment withlysine of the Incaparina formula produced in Guatemala.This made it possible to correct slight deficiencies in theformula with regard to this essential amino acid, andalso to bring its nutritional value closer to that of milk.On the basis of these studies, researchers are exploringthe possibilities of fortifying grains commonly used inthe Isthmus, as well as the various products made fromthem.
Another area of intensified activity was the searchfor sufficiently sensitive methods to make it possible todiagnose, and even quantify, the light to moderate formsof protein-calorie malnutrition. The surveys conductedin the six member countries of INCAP revealed that thecurrently available methods are not adequate for thispurpose. Therefore, two biochemical methods whichappeared to be very promising were tested: (a) deter-mination of the relationship between essential andnon-essential amino acids in blood plasma, and (b) thecreatinine/height index (CHI), which estimates thedegree of muscularity of an individual by relating uri-nary excretion of creatinine to height. Both methodsare being carefully evaluated under experimental condi-tions to determine their potential value and applicationin the study of general population groups.
In the studies of the factors responsible for malnutri-tion, particular attention was given to environmentalfactors as distinguished from dietary ones. The effectof infections was studied, especially the diarrheal proc-esses, and the effect of colonization of the intestine fromearly infancy by abundant flora which, while they maynot be responsible for disease, could interfere withadequate nutrition in various ways. These studies haveresulted in very significant observations which prove theimportance of environmental sanitation and of specificprotective measures against various infectious diseases,both in the preventive programs and in those of nutri-tional rehabilitation.
In other research studies, advances were made towardgaining a fuller understanding of anemia associated withprotein-calorie malnutrition. On the basis of the find-ings, important recommendations were formulated forimproved treatment of this condition, and new researchhas been undertaken to find practical means, through
At the work physiology laboratory of INCAP, studies are madeof the influence of nutritional status on physical work capacity.
public health activities, for the prevention of nutritionalanemias.
Considerable progress was made in other research toassess the relative role of malnutrition and other factorslimiting the physical and mental development of chil-dren. It was possible to develop and evaluate the.methodology required by these complicated studies, andfield work was begun on a long-range project aimed atclarifying many questions that still exist about this prob-lem, which has great importance both for the countriesof the area and for others which have similar nutritionaland ecological conditions.
There were also significant advances in the studies todemonstrate the unfavorable effects on work capacityand productivity of subclinical, chronic, and non-appar-ent forms of malnutrition in adults, forms which, accord-ing to the INCAP studies and other similar ones, affect alarge proportion of the inhabitants of most Latin Ameri-can countries. The importance of this research on childgrowth and development and on physical work capacityof adults lies primarily in the fact that it will provideguidelines in regard to the relative priorities of the effortsto improve diet and nutrition in the different age groupsand, in addition, will make possible a more preciseevaluation of the damage produced by nutritional de-ficiencies and consequently the better planning of pro-
149
grams of both the health sector and other sectors aswell.
The results of INCAP research activities were circu-lated through 253 scientific articles published in widelyrecognized journals, and they served also as the basisof various reports and documents presented to interestedGovernments and organizations. These studies haveenabled INCAP to maintain the scientific standing re-quired for its effective functioning as a center of ad-vanced education and as an advisory and collaborativeagbncy in the nutrition field.
Program of the Caribbean Food and Nutrition Insfitute
The Institute's research activities are related to prac-tical problems of high priority. They are interdiscipli-nary and collaborative in character and are designed topromptly feed back data for planners and for the initia-tion, orientation, modification, and evaluation of preven-tive programs.
Where clinical or laboratory research is required inconnection with a research project in the field, the Insti-tute seeks the cooperation of existing centers, preferablythose in the Caribbean area. Whenever possible, itsresearch is carried out in active collaboration with thestaff of relevant governmental departments, voluntarybodies, and international agencies. It cooperates withcenters, units, and schools in the Caribbean or abroadto develop joint projects of short or long duration.
The following collaborative studies have been com-pleted: a rapid survey of childhood malnutrition inSt. Vincent; an investigation of cultural concepts ofmarasmus in rural Jamaica; the cost-availability of foodsin the Caribbean; the arm circumference as a publichealth index of malnutrition; the financial cost ofmalnutrition; and the interrelationship of nutrition andschistosomiasis in St. Lucia.
At the request of the Government of Barbados, afull-scale national food and nutrition survey was carriedout in May 1969 jointly by staff of the ministries ofhealth, agriculture, and education of Barbados, by CFNIstaff and students, and by PAHO/WHO and FAOcolleagues. The survey was based on the home-visitingof a randomly selected 1 per cent sample of the house-holds of the country, and included biomedical examina-tions (clinical, anthropometric, hematologic, biochemi-cal); dental examination and sociocultural inquiries(knowledge and beliefs concerning nutrition, health, andyoung child feeding practices); socioeconomic data(household characteristics, family income and expendi-ture); food consumption (families and vulnerablegroups); food production and economics (national,local, and family levels).
Rapid analysis of the 750,000 items of informationwas undertaken by computer and the preliminary resultswere presented four weeks after the end of the survey.A complete analysis of the data will be presented inearly 1970.
At the request of the Government of Trinidad andTobago, a national food consumption survey was initi-ated by the Institute, jointly with the National NutritionUnit and the Ministries concerned with this field. Datacollection will be completed in early 1970.
Collaborative investigation of current methods ofyoung-child feeding in the Caribbean was continued byCFNI staff and students, and by other national andinternational staff in the area. Results will be availablefrom Antigua, Barbados, Dominica, Grenada, Guyana,Jamaica, Montserrat, St. Kitts-Nevis-Anguilla, St. Lucia,St. Vincent, and Trinidad and Tobago for a CFNItechnical group meeting to be held in 1970, and theywill form the basis of a publication to be entitled "Guide-lines to Young-Child Feeding in the ContemporaryCaribbean."
As a follow-up of the CFNI Conference on ProteinFoods in the Caribbean (Georgetown, Guyana, July1968), a joint FAO/WHO-PAHO/CFNI team under-took a two-month survey (October-November 1969) toassess the feasibility of producing and marketing withinthe Caribbean area, a protein-base processed food de-rived mostly from locally grown ingredients, for use byfamilies, and especially young children.
PROGRAMS OF THE PAN AMERICANZOONOSES CENTER
This Center, although a relatively new institution,has made marked progress in laboratory and field re-search activities that seek to throw further light on thecomplexities of the zoonoses. There is a great potentialfor further advances in this field. As a result of itsexpansion and the extension of its activities on a re-gional scale, the Center possesses a staff with a widerange of experience as well as the necessary facilities toenable it to develop research programs in greater depth.
Brucellosis
The work undertaken in connection with this diseasehas taken the form of both laboratory and field research,directed primarily to the isolation of Brucella strains inhuman and animal cases from various Latin Americancountries. Some of the field investigations have includedserum agglutination tests on large numbers of animals todetermine the prevalence of the disease in areas in whichthere are large concentrations of livestock, especiallycattle, sheep, and goats. Research on phages associated
150
1
-
with strains of Brucella has been carried out with a viewto determining strain-specific bacteriophage which willaid in the identification of the new Brucella isolates.
Other laboratory procedures were studied in order todevelop a rapid diagnostic test for use in the detectionof ram epididymitis. Vaccine study trials have beenconducted with a live attenuated vaccine of Brucellaabortus in combination with a heat-killed culture ofB. suis to determine the efficacy of this product againstswine brucellosis. The Argentine Zoonoses Institutecooperated with the Center in this project. Other vac-cine trials were conducted, using safety tests on differentstrains of B. abortus employed in the production ofvaccine.
In two large dairy establishments where 9,500 ani-mals were kept solely for milk production, a brucellosiseradication program was undertaken in association withthe Government of Argentina as part of the Center'sresearch activities. The program included vaccinationof calves between 3 and 6 months of age using B.abortus strain 19 vaccine and the serum agglutinationtest to detect reactors, with subsequent isolation andslaughtering. This program made it possible to reducethe prevalence of the disease from 26 per cent in 1960to less than 1 per cent in 1969.
Rabies
Most of the research undertaken by the Center inthe past four years has been on rabies. Outstanding inthis program were the studies evaluating the variousvaccines available for the protection of cattle. Theirpurpose was to find a method of protection againstparalytic rabies in cattle transmitted by vampire bats.The presence of this disease has been confirmed in allbut two or three countries of the Americas. It is a majorproblem in Bolivia, Brazil, Mexico, Paraguay, and Vene-zuela and in the northern part of Argentina. Large-scaleoutbreaks have occurred in many parts of Paraguay,and in Mexico the annual losses from this disease arein the neighborhood of $10,000,000. The total lossesin all the countries affected in the Americas are of theorder of $50,000,000 a year. The studies of variousvaccines for the protection of cattle included a compari-son of levels of neutralizing antibodies developed incattle over periods of one, two, and three years. Inconjunction with these studies, research was under-taken on the transfer of neutralizing antibodies againstrabies from the vaccinated cows to their calves, in orderto determine whether passive immunity was acquired bythese young animals as a short-term protection.
At the same time, other investigations were conductedin which 17 heterogeneous strains of rabies virus from17 different countries were examined to determine their
L
Extensive research on rabies is conducted at the Pan AmericanZoonosis Center.
virulence and immunogenicity for the purpose of select-ing one of them for vaccine use and serum productionand possibly for challenge purposes in research.
Probably the most outstanding contribution to rabiesepidemiology and control was the continuing effort madeby the Center to improve diagnostic procedures, such asthe preparation of biological reagents for fluorescentantibody tests and the standardization of diagnosticagents and antigens for vaccine production. Determinedefforts were also made to improve the quality control ofrabies vaccine.
Studies were made on purification of the virus bycentrifugation and chromatography with a view to de-veloping an antigen free of undesirable substances.Other rabies research studies were those concerned withreference control of vaccines, development of a sero-logic test for rabies, interference between rabies andother viruses, nonfatal rabies in dogs, ecological andvirological studies of bat rabies, comparative studies ofdifferent schedules of postexposure antirabies vaccina-tion in humans, sensitivity of tissue culture systems forthe isolation of latent rabies virus, and evaluation of acorneal test as an ante-mortem laboratory method forrabies diagnosis.
The ecological studies initiated in northern Argentinaon vampire bats have a very important bearing on theproblem of bovine rabies in South America. Biotelem-etry measurements of these bats were made in orderto obtain a better understanding of their ecology. Forthese studies, miniature radio transmitters weighing lessthan 10 grams were used; these were attached to thebats, which were then set free. A radio receiver pre-pared especially for this purpose was employed to detectand record the direction and distance of the bats' flight.For the first time it was possible to determine by mea-
151
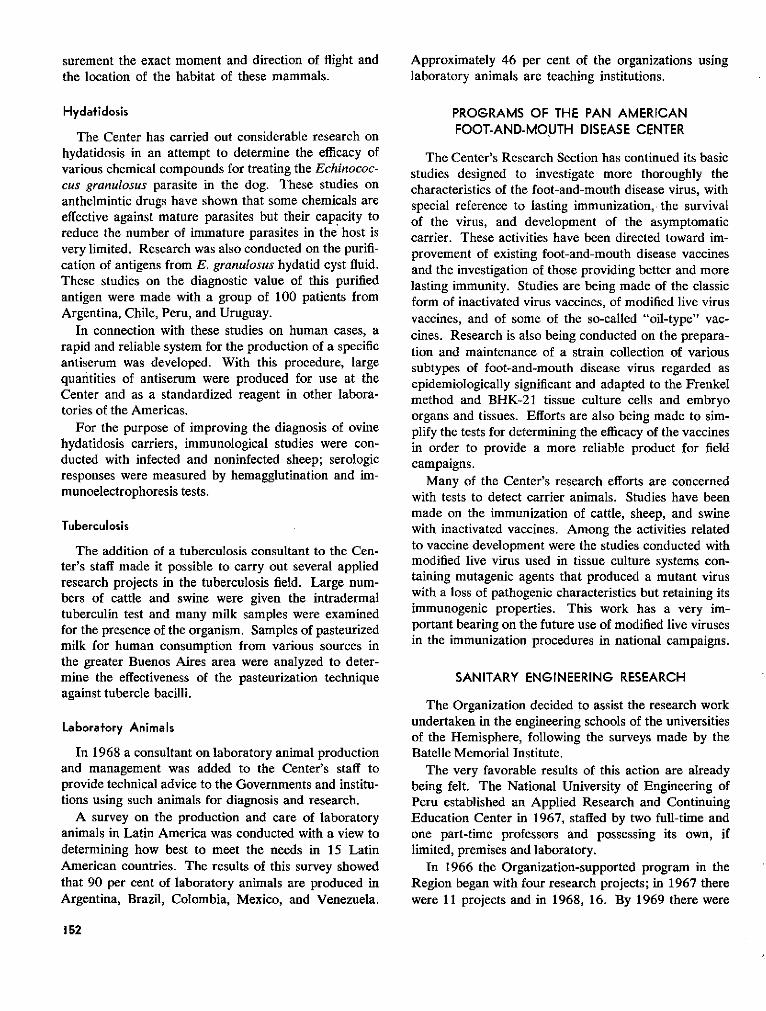
surement the exact moment and direction of flight andthe location of the habitat of these mammals.
Hydatidosis
The Center has carried out considerable research onhydatidosis in an attempt to determine the efficacy ofvarious chemical compounds for treating the Echinococ-cus granulosus parasite in the dog. These studies onanthelmintic drugs have shown that some chemicals areeffective against mature parasites but their capacity toreduce the number of immature parasites in the host isvery limited. Research was also conducted on the purifi-cation of antigens from E. granulosus hydatid cyst fluid.These studies on the diagnostic value of this purifiedantigen were made with a group of 100 patients fromArgentina, Chile, Peru, and Uruguay.
In connection with these studies on human cases, arapid and reliable system for the production of a specificantiserum was developed. With this procedure, largequantities of antiserum were produced for use at theCenter and as a standardized reagent in other labora-tories of the Americas.
For the purpose of improving the diagnosis of ovinehydatidosis carriers, immunological studies were con-ducted with infected and noninfected sheep; serologicresponses were measured by hemagglutination and im-munoelectrophoresis tests.
Tuberculosis
The addition of a tuberculosis consultant to the Cen-ter's staff made it possible to carry out several appliedresearch projects in the tuberculosis field. Large num-bers of cattle and swine were given the intradermaltuberculin test and many milk samples were examinedfor the presence of the organism. Samples of pasteurizedmilk for human consumption from various sources inthe greater Buenos Aires area were analyzed to deter-mine the effectiveness of the pasteurization techniqueagainst tubercle bacilli.
Laboratory Animais
In 1968 a consultant on laboratory animal productionand management was added to the Center's staff toprovide technical advice to the Governments and institu-tions using such animals for diagnosis and research.
A survey on the production and care of laboratoryanimals in Latin America was conducted with a view todetermining how best to meet the needs in 15 LatinAmerican countries. The results of this survey showedthat 90 per cent of laboratory animals are produced inArgentina, Brazil, Colombia, Mexico, and Venezuela.
Approximately 46 per cent of the organizations usinglaboratory animals are teaching institutions.
PROGRAMS OF THE PAN AMERICANFOOT-AND-MOUTH DISEASE CENTER
The Center's Research Section has continued its basicstudies designed to investigate more thoroughly thecharacteristics of the foot-and-mouth disease virus, withspecial reference to lasting immunization, the survivalof the virus, and development of the asymptomaticcarrier. These activities have been directed toward im-provement of existing foot-and-mouth disease vaccinesand the investigation of those providing better and morelasting immunity. Studies are being made of the classicform of inactivated virus vaccines, of modified live virusvaccines, and of some of the so-called "oil-type" vac-cines. Research is also being conducted on the prepara-tion and maintenance of a strain collection of varioussubtypes of foot-and-mouth disease virus regarded asepidemiologically significant and adapted to the Frenkelmethod and BHK-21 tissue culture cells and embryoorgans and tissues. Efforts are also being made to sim-plify the tests for determining the efficacy of the vaccinesin order to provide a more reliable product for fieldcampaigns.
Many of the Center's research efforts are concernedwith tests to detect carrier animals. Studies have beenmade on the immunization of cattle, sheep, and swinewith inactivated vaccines. Among the activities relatedto vaccine development were the studies conducted withmodified live virus used in tissue culture systems con-taining mutagenic agents that produced a mutant viruswith a loss of pathogenic characteristics but retaining itsimmunogenic properties. This work has a very im-portant bearing on the future use of modified live virusesin the immunization procedures in national campaigns.
SANITARY ENGINEERING RESEARCH
The Organization decided to assist the research workundertaken in the engineering schools of the universitiesof the Hemisphere, following the surveys made by theBatelle Memorial Institute.
The very favorable results of this action are alreadybeing felt. The National University of Engineering ofPeru established an Applied Research and ContinuingEducation Center in 1967, staffed by two full-time andone part-time professors and possessing its own, iflimited, premises and laboratory.
In 1966 the Organization-supported program in theRegion began with four research projects; in 1967 therewere 11 projects and in 1968, 16. By 1969 there were
152
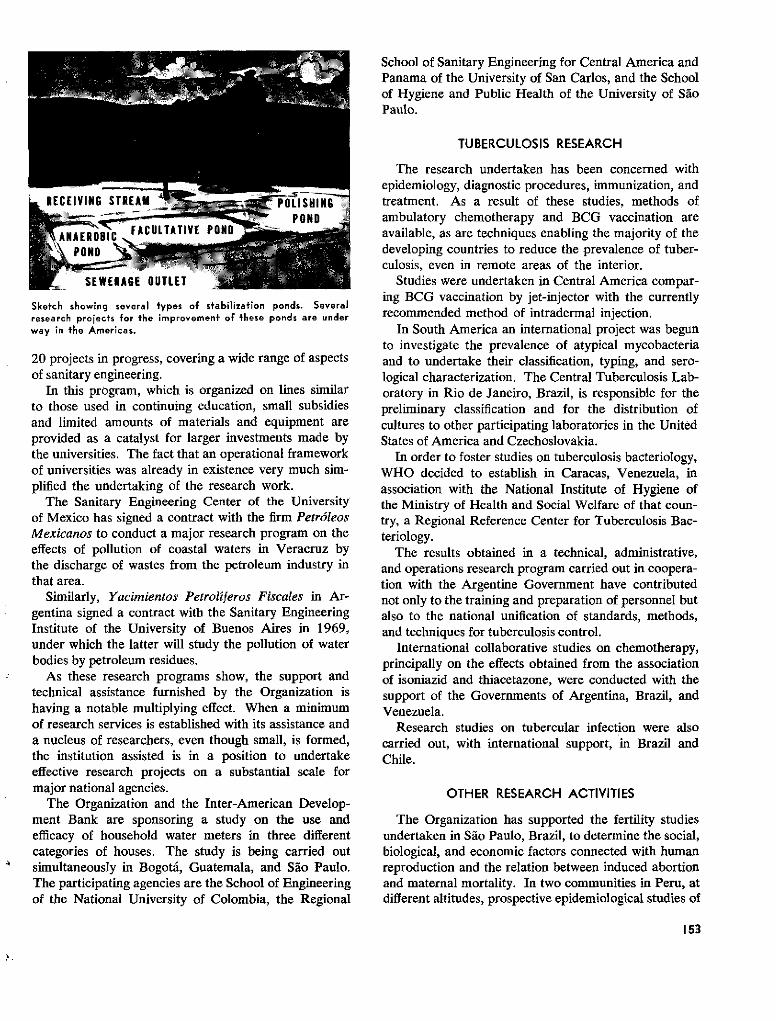
RECEIVING STR
NAERBI FACULTATIVE PON
SEWERAGE OUTLET
Sketch showing several types of stabilization ponds. Severalresearch projects for the improvemenf of these ponds are underway in the Americas.
20 projects in progress, covering a wide range of aspectsof sanitary engineering.
In this program, which is organized on lines similarto those used in continuing education, small subsidiesand limited amounts of materials and equipment areprovided as a catalyst for larger investments made bythe universities. The fact that an operational frameworkof universities was already in existence very much sim-plified the undertaking of the research work.
The Sanitary Engineering Center of the Universityof Mexico has signed a contract with the firm PetróleosMexicanos to conduct a major research program on theeffects of pollution of coastal waters in Veracruz bythe discharge of wastes from the petroleum industry inthat area.
Similarly, Yacimientos Petrolíferos Fiscales in Ar-gentina signed a contract with the Sanitary EngineeringInstitute of the University of Buenos Aires in 1969,under which the latter will study the pollution of waterbodies by petroleum residues.
As these research programs show, the support andtechnical assistance furnished by the Organization ishaving a notable multiplying effect. When a minimumof research services is established with its assistance anda nucleus of researchers, even though small, is formed,the institution assisted is in a position to undertakeeffective research projects on a substantial scale formajor national agencies.
The Organization and the Inter-American Develop-ment Bank are sponsoring a study on the use andefficacy of household water meters in three differentcategories of houses. The study is being carried outsimultaneously in Bogotá, Guatemala, and Sao Paulo.The participating agencies are the School of Engineeringof the National University of Colombia, the Regional
School of Sanitary Engineering for Central America andPanama of the University of San Carlos, and the Schoolof Hygiene and Public Health of the University of SáoPaulo.
TUBERCULOSIS RESEARCH
The research undertaken has been concerned withepidemiology, diagnostic procedures, immunization, andtreatment. As a result of these studies, methods ofambulatory chemotherapy and BCG vaccination areavailable, as are techniques enabling the majority of thedeveloping countries to reduce the prevalence of tuber-culosis, even in remote areas of the interior.
Studies were undertaken in Central America compar-ing BCG vaccination by jet-injector with the currentlyrecommended method of intradermal injection.
In South America an international project was begunto investigate the prevalence of atypical mycobacteriaand to undertake their classification, typing, and sero-logical characterization. The Central Tuberculosis Lab-oratory in Rio de Janeiro, Brazil, is responsible for thepreliminary classification and for the distribution ofcultures to other participating laboratories in the UnitedStates of America and Czechoslovakia.
In order to foster studies on tuberculosis bacteriology,WHO decided to establish in Caracas, Venezuela, inassociation with the National Institute of Hygiene ofthe Ministry of Health and Social Welfare of that coun-try, a Regional Reference Center for Tuberculosis Bac-teriology.
The results obtained in a technical, administrative,and operations research program carried out in coopera-tion with the Argentine Government have contributednot only to the training and preparation of personnel butalso to the national unification of standards, methods,and techniques for tuberculosis control.
International collaborative studies on chemotherapy,principally on the effects obtained from the associationof isoniazid and thiacetazone, were conducted with thesupport of the Governments of Argentina, Brazil, andVenezuela.
Research studies on tubercular infection were alsocarried out, with international support, in Brazil andChile.
OTHER RESEARCH ACTIVITIES
The Organization has supported the fertility studiesundertaken in Sao Paulo, Brazil, to determine the social,biological, and economic factors connected with humanreproduction and the relation between induced abortionand maternal mortality. In two communities in Peru, atdifferent altitudes, prospective epidemiological studies of
153
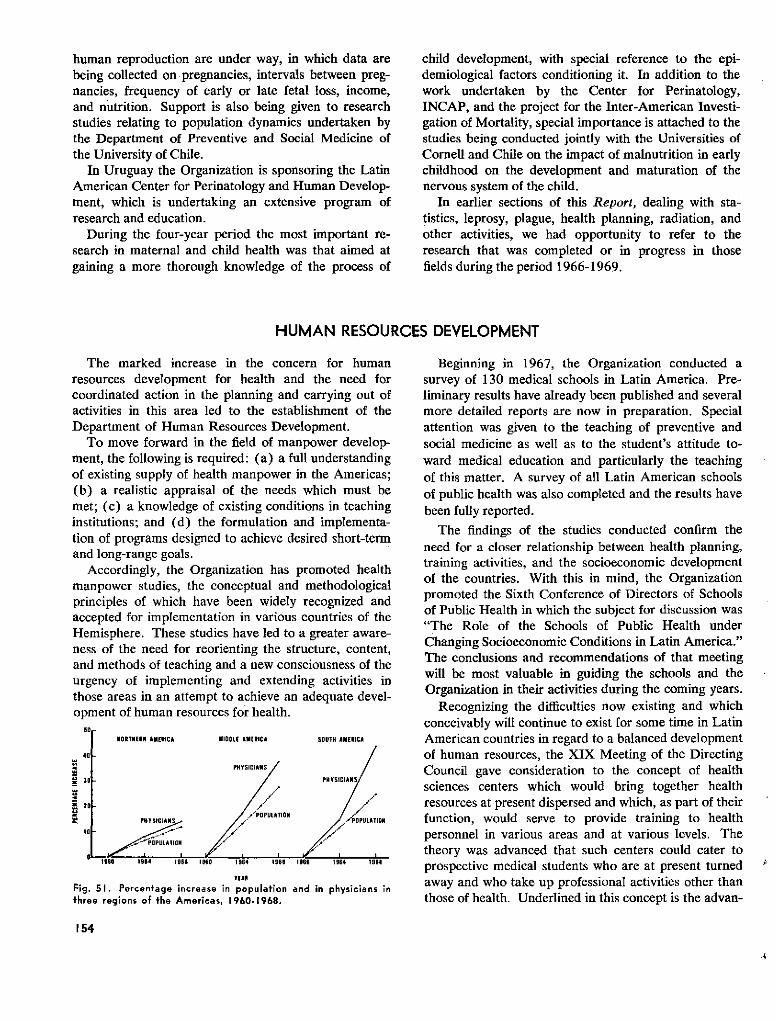
human reproduction are under way, in which data arebeing collected on pregnancies, intervals between preg-nancies, frequency of early or late fetal loss, income,and nutrition. Support is also being given to researchstudies relating to population dynamics undertaken bythe Department of Preventive and Social Medicine ofthe University of Chile.
In Uruguay the Organization is sponsoring the LatinAmerican Center for Perinatology and Human Develop-ment, which is undertaking an extensive program ofresearch and education.
During the four-year period the most important re-search in maternal and child health was that aimed atgaining a more thorough knowledge of the process of
child development, with special reference to the epi-demiological factors conditioning it. In addition to thework undertaken by the Center for Perinatology,INCAP, and the project for the Inter-American Investi-gation of Mortality, special importance is attached to thestudies being conducted jointly with the Universities ofCornell and Chile on the impact of malnutrition in earlychildhood on the development and maturation of thenervous system of the child.
In earlier sections of this Report, dealing with sta-tistics, leprosy, plague, health planning, radiation, andother activities, we had opportunity to refer to theresearch that was completed or in progress in thosefields during the period 1966-1969.
HUMAN RESOURCES DEVELOPMENT
The marked increase in the concern for humanresources development for health and the need forcoordinated action in the planning and carrying out ofactivities in this area led to the establishment of theDepartment of Human Resources Development.
To move forward in the field of manpower develop-ment, the following is required: (a) a full understandingof existing supply of health manpower in the Americas;(b) a realistic appraisal of the needs which must bemet; (c) a knowledge of existing conditions in teachinginstitutions; and (d) the formulation and implementa-tion of programs designed to achieve desired short-termand long-range goals.
Accordingly, the Organization has promoted healthmanpower studies, the conceptual and methodologicalprinciples of which have been widely recognized andaccepted for implementation in various countries of theHemisphere. These studies have led to a greater aware-ness of the need for reorienting the structure, content,and methods of teaching and a new consciousness of theurgency of implementing and extending activities inthose areas in an attempt to achieve an adequate devel-opment of human resources for health.
.0 -HORTHERN AMERICA MIDOLE AMERICA SOUTH AMERICA
40 -
- PHYSICIANS
30 - PHYSICIANS
POPULATIONPHYSICIANS /POPULATION
Beginning in 1967, the Organization conducted asurvey of 130 medical schools in Latin America. Pre-liminary results have already been published and severalmore detailed reports are now in preparation. Specialattention was given to the teaching of preventive andsocial medicine as well as to the student's attitude to-ward medical education and particularly the teachingof this matter. A survey of all Latin American schoolsof public health was also completed and the results havebeen fully reported.
The findings of the studies conducted confirm theneed for a closer relationship between health planning,training activities, and the socioeconomic developmentof the countries. With this in mind, the Organizationpromoted the Sixth Conference of Directors of Schoolsof Public Health in which the subject for discussion was"The Role of the Schools of Public Health underChanging Socioeconomic Conditions in Latin America."The conclusions and recommendations of that meetingwill be most valuable in guiding the schools and theOrganization in their activities during the coming years.
Recognizing the difficulties now existing and whichconceivably will continue to exist for some time in LatinAmerican countries in regard to a balanced developmentof human resources, the XIX Meeting of the DirectingCouncil gave consideration to the concept of healthsciences centers which would bring together healthresources at present dispersed and which, as part of theirfunction, would serve to provide training to healthpersonnel in various areas and at various levels. Thetheory was advanced that such centers could cater toprospective medical students who are at present turnedaway and who take up professional activities other thanthose of health. Underlined in this concept is the advan-
154
YEAR
Fig. 51. Percentage increase in population and in physicians in
three regions of the Americas, 1960-1968.
tage which can ensue from a properly integrated andorganized curriculum envisaged to produce categoriesof health personnel stratified at increasingly high levels.This structure could absorb at the outset larger numbersof candidates who may later switch their initial interestin studying medicine to other related fields. This newmovement, which is a departure from traditional think-ing in medical education, is now being carefully pro-moted, supported, and evaluated by the Organization.
In addition to long-range plans for the integration ofhealth sciences, the Organization addresses its activitiesto the immediate need for strengthening teaching insti-tutions and their personnel as paramount instrumentsfor the development of human resources. Seminars onthe administration of medical schools are organized aswell as laboratories and workshops, thus complementingthe continuing assistance provided through the Organi-zation's fellowship program, which in the period 1966-1969 made awards to 731 faculty members from schoolsof medicine and related sciences.
PAHO/WHO's contribution to the expansion of edu-cational activities in support of health manpower is alsoevidenced in the number of additional faculty memberswho have attended the courses entitled "Laboratory ofHuman Relations and Medical Teaching," sponsoredwith a view to raising the level of instruction. Underthis program the participant, through proper applicationof group dynamics, gains first-hand knowledge of stu-dent's motivations, expectations, and experience as wellas of factors acting on interpersonal relations as theyrelate to the teaching-learning process.
Short courses on epidemiology for public health per-sonnel in service were conducted as a new approach toextend the training facilities to those who had not hadthe opportunity of formal public health training. Similarprograms were developed to acquaint professors inclinical departments of medical schools with generalprinciples and applications of clinical epidemiology.
Of particular importance has been the assistance pro-vided through and with the cooperation of the nationalassociations of medical schools and other similar asso-ciations. To the extent possible, the Organization hasattempted to channel its assistance to medical schoolsthrough the national associations in order to achieve ahigher degree of coordination at the national level.
To further strengthen institutions of learning, PAHO/WHO established in 1967 a textbook program, designedto make quality textbooks available at prices compatiblewith the financial situation of medical students, and thushelp to remove one of the fundamental obstacles con-fronting medical education in Latin America. Today,more than 100 medical schools are incorporated to thisprogram (see Chapter I, p. 16).
Of no less importance are the efforts to alleviate thecritical need for auxiliary personnel. Studies are beingconducted to determine in what measure nonprofes-sional workers can relieve high-level personnel of someof the duties they are now called upon to perform. It isestimated that nonprofessionals can be trained in greaternumbers and at lower costs than professional staff. TheOrganization has therefore encouraged the countries andoffered them assistance to develop local resoúrces forthe training of auxiliary staff in accordance with theirparticular needs.
Broad support and assistance are provided to a varietyof other health-related projects for the development ofhuman resources through short- and long-term con-sultants and specialists.
The Organization publishes in Spanish-with sum-maries in Portuguese, French, and English-a quarterlyjournal, Educación médica y salud, which is particularlyaddressed to teaching personnel in the health sciencesin Latin America but is also widely distributed to librar-ies in the United States of America and Canada.
SPECIAL STUDIES
During the past four years the trend toward planningfor national development by means of broad integratedprograms has been gaining momentum and has de-manded a careful re-examination of existing needs andavailable resources. To achieve this end, the Organiza-tion sponsored or conducted surveys and studies whichhave yielded invaluable information for the formulationof programs and projects for the development of humanresources.
A two-year study of health manpower and medicaleducation was completed in Colombia in 1966, under
155
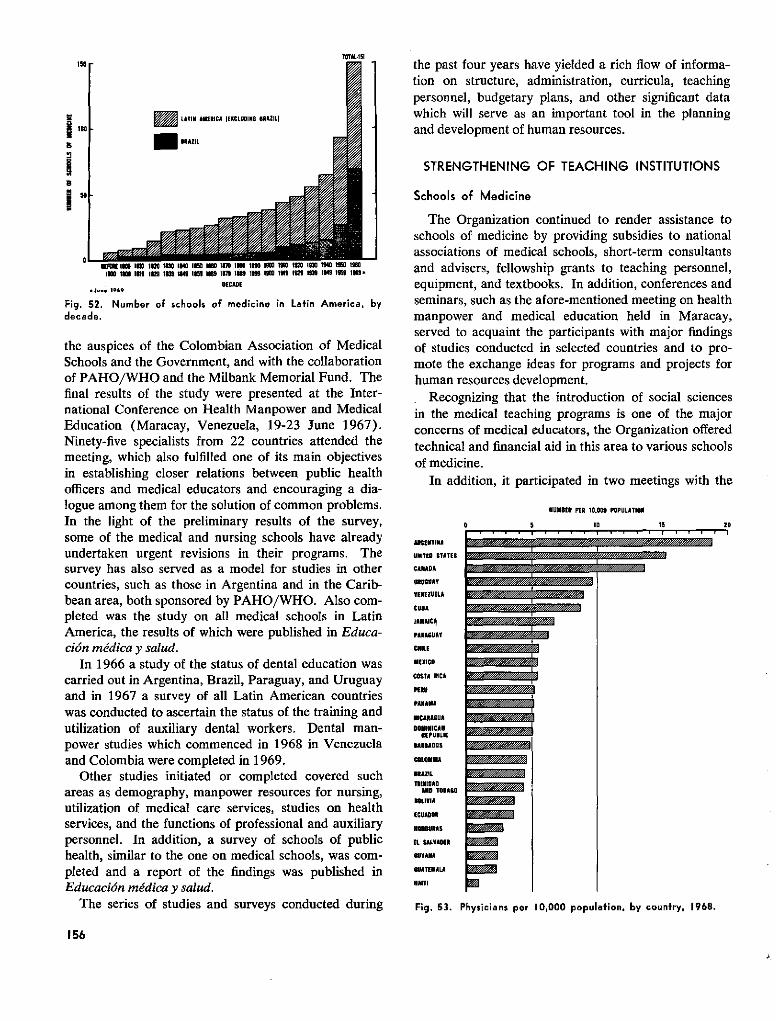
loo
rS
i
lTO-l5A
E LATll AMERICA IEXCLUDIi 11RAZILI
- ---
m Ia
i UI 0 l I I io l o im 0 I uE 160 uN ll 10 lIO 0 l ls ll In IIIW 1 II 11 1nc iL io IXn lO ios iora IX c 1 o inc 1 o9o 1io 1c" i-
DECADE.J.. 1969
Fig. 52. Number of schools of medicine in Latin America, bydecade.
the auspices of the Colombian Association of MedicalSchools and the Government, and with the collaborationof PAHO/WHO and the Milbank Memorial Fund. Thefinal results of the study were presented at the Inter-national Conference on Health Manpower and MedicalEducation (Maracay, Venezuela, 19-23 June 1967).Ninety-five specialists from 22 countries attended themeeting, which also fulfilled one of its main objectivesin establishing closer relations between public healthofficers and medical educators and encouraging a dia-logue among them for the solution of common problems.In the light of the preliminary results of the survey,some of the medical and nursing schools have alreadyundertaken urgent revisions in their programs. Thesurvey has also served as a model for studies in othercountries, such as those in Argentina and in the Carib-bean area, both sponsored by PAHO/WHO. Also com-pleted was the study on all medical schools in LatinAmerica, the results of which were published in Educa-ción médica y salud.
In 1966 a study of the status of dental education wascarried out in Argentina, Brazil, Paraguay, and Uruguayand in 1967 a survey of all Latin American countrieswas conducted to ascertain the status of the training andutilization of auxiliary dental workers. Dental man-power studies which commenced in 1968 in Venezuelaand Colombia were completed in 1969.
Other studies initiated or completed covered suchareas as demography, manpower resources for nursing,utilization of medical care services, studies on healthservices, and the functions of professional and auxiliarypersonnel. In addition, a survey of schools of publichealth, similar to the one on medical schools, was com-pleted and a report of the findings was published inEducación médica y salud.
The series of studies and surveys conducted during
the past four years have yielded a rich flow of informa-tion on structure, administration, curricula, teachingpersonnel, budgetary plans, and other significant datawhich will serve as an important tool in the planningand development of human resources.
STRENGTHENING OF TEACHING INSTITUTIONS
Schools of Medicine
The Organization continued to render assistance toschools of medicine by providing subsidies to nationalassociations of medical schools, short-term consultantsand advisers, fellowship grants to teaching personnel,equipment, and textbooks. In addition, conferences andseminars, such as the afore-mentioned meeting on healthmanpower and medical education held in Maracay,served to acquaint the participants with major findingsof studies conducted in selected countries and to pro-mote the exchange ideas for programs and projects forhuman resources development.
Recognizing that the introduction of social sciencesin the medical teaching programs is one of the majorconcerns of medical educators, the Organization offeredtechnical and financial aid in this area to various schoolsof medicine.
In addition, it participated in two meetings with the
AIIENTINA
UNITED STATES
CANADA
URUGUAY
VENEZUELA
CURA
LAMAICA
PAIRAGUAY
CHILE
MEXICO
COSTA ICA
PERU
PANANA
NICARAGUADOMINICAN
REPUBLICBARBADOS
COLONMIA
BRAZILTRINIDIOAO
AOD TOBACOBOLIVIA
ONOEDURAS
EL SALVADOR
GUYANA
GUATEMALA
HAITI
MUMBER PER 10.000 POPULATION
10 15 20
Fig. 53. Physicians per 10,000 population, by country, 1968.
156
�´·�í�·���F�i�.�?·�
�ii�"//////�l//�"��
m
~~~ 9~~~~~·~~~~~·~~~~~·~~~~~ i~~~~
Ea·~~
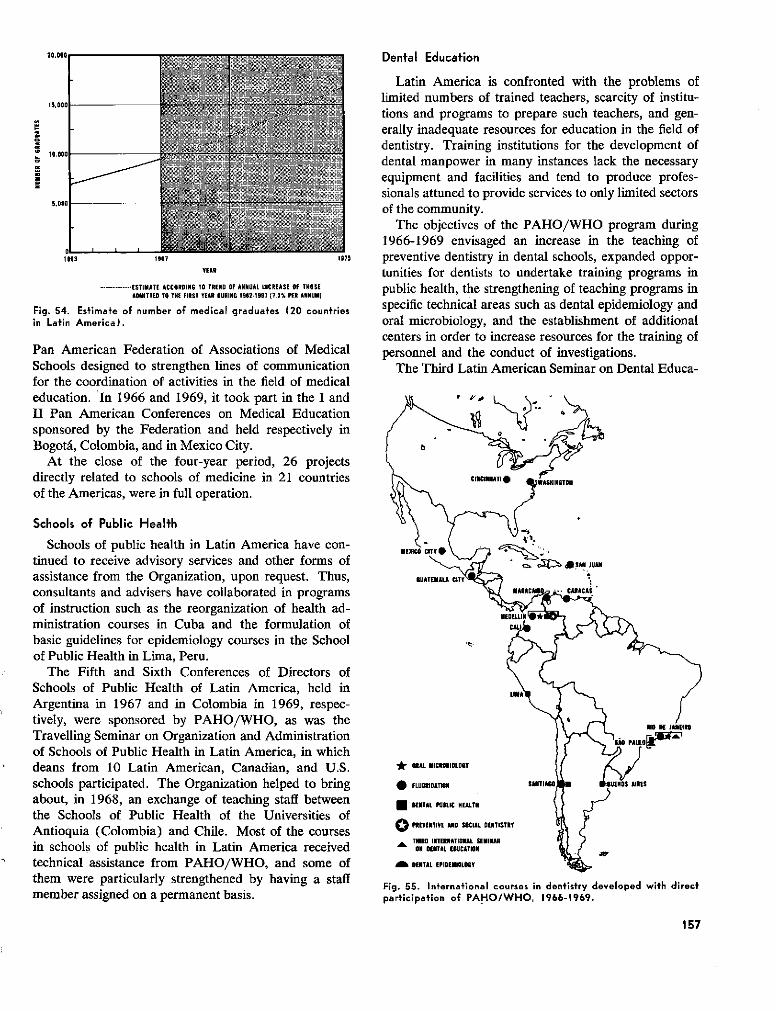
Dental Education
1.oo000
11g! 10,0011
1963 1967 1975
YEAR
.................. ESTIMATE ACCOROING TO TRENO OF ANNUAL INCREASE OF TMHSEADMITTED TO THE FIRST YEAR OURING 1962-1967 (7.3% PER ANNUM)
Fig. 54. Estimate of number of medical graduates (20 countriesin Latin America).
Pan American Federation of Associations of MedicalSchools designed to strengthen lines of communicationfor the coordination of activities in the field of medicaleducation. In 1966 and 1969, it took part in the I andII Pan American Conferences on Medical Educationsponsored by the Federation and held respectively inBogotá, Colombia, and in Mexico City.
At the close of the four-year period, 26 projectsdirectly related to schools of medicine in 21 countriesof the Americas, were in full operation.
Schools of Public Health
Schools of public health in Latin America have con-tinued to receive advisory services and other forms ofassistance from the Organization, upon request. Thus,consultants and advisers have collaborated in programsof instruction such as the reorganization of health ad-ministration courses in Cuba and the formulation ofbasic guidelines for epidemiology courses in the Schoolof Public Health in Lima, Peru.
The Fifth and Sixth Conferences of Directors ofSchools of Public Health of Latin America, held inArgentina in 1967 and in Colombia in 1969, respec-tively, were sponsored by PAHO/WHO, as was theTravelling Seminar on Organization and Administrationof Schools of Public Health in Latin America, in whichdeans from 10 Latin American, Canadian, and U.S.schools participated. The Organization helped to bringabout, in 1968, an exchange of teaching staff betweenthe Schools of Public Health of the Universities ofAntioquia (Colombia) and Chile. Most of the coursesin schools of public health in Latin America receivedtechnical assistance from PAHO/WHO, and some ofthem were particularly strengthened by having a staffmember assigned on a permanent basis.
Latin America is confronted with the problems oflimited numbers of trained teachers, scarcity of institu-tions and programs to prepare such teachers, and gen-erally inadequate resources for education in the field ofdentistry. Training institutions for the development ofdental manpower in many instances lack the necessaryequipment and facilities and tend to produce profes-sionals attuned to provide services to only limited sectorsof the community.
The objectives of the PAHO/WHO program during1966-1969 envisaged an increase in the teaching ofpreventive dentistry in dental schools, expanded oppor-tunities for dentists to undertake training programs inpublic health, the strengthening of teaching programs inspecific technical areas such as dental epidemiology andoral microbiology, and the establishment of additionalcenters in order to increase resources for the training ofpersonnel and the conduct of investigations.
The Third Latin American Seminar on Dental Educa-
GUATEMALA CITVY'
* ORAL MICRORIOLORY
FLUORIDATION
a DENTAL PUJLIC NEALTH
O PREVENTIVE D SOCIAL DENTISTRY
THIRD INTERATIONAL SEMINARON DENTAL EDUCATION
DENTAL EPIDENIOLOGY
A IES
Fig. 55. International courses in dentistry developed with directparticipation of PAHO/WHO, 1966-1969.
157
20,000,
, ¿

tion was held in Petrópolis, Brazil, in November 1966,with the collaboration of the Government of Brazil andthe W. K. Kellogg Foundation. It was attended byrepresentatives of the 47 schools in Argentina, Brazil,Paraguay, and Uruguay and by 80 observers from coun-tries of the Hemisphere. Other international seminarswere held in Maracaibo, Venezuela, to determine thestructure of the dental curriculum, and in Caracas in1967 on standardization, control, investigation, andtraining in dental materials, and in 1969 on the teachingof'pedodontics. National seminars in which the Organi-zation collaborated were also held in Venezuela and inEcuador, where the dental education program for thethree dental schools was discussed and the Associationof Dental Schools for Ecuador was founded.
The Organization assisted in the design and planningof the new dental school in Panama and in the develop-ment of its teaching program. A special program wasarranged for professors of the new school to visit otherschools of dentistry. Departments of preventive den-tistry were assisted in several countries and an inter-national course for teachers of this discipline was or-ganized at the University of Antioquia (Colombia) inNovember 1967; it was attended by 15 participantsfrom eight countries.
A course on dental epidemiology was conducted atthe University of Sao Paulo, Brazil, in 1967 and courseson oral microbiology were held at the Oswaldo CruzInstitute (Rio de Janeiro) in 1966 and at the Universityof Antioquia in 1968. In the period 1968-1969 theprogram for the introduction of simplified dental equip-ment was initiated and courses were held in Medellín(2 courses) and Maracaibo for national personnel. As-sistance in the preparation of auxiliary personnel wasrendered to the Province of Buenos Aires in Argentina,
* i-X~~~~~~~~
Building (under construction) of the School of Dental Nurses inJamaica.
where a course was given for 10 persons responsible forthe training of auxiliaries.
During the four-year period facilities for the teachingof public health to dentists were increased and theOrganization gave assistance for this purpose to theUniversities of Sáo Paulo and Antioquia, the NationalUniversity of San Marcos in Lima, and the Universityof Chile. The University of Antioquia initiated defini-tive programs in dental public health in 1968 and theUniversity of San Marcos did so in 1969.
The collection of information on matters related todental education and dental health has been pursued. Asurvey was conducted on the status of dental educationin the 50 dental schools of Brazil, in six schools inArgentina, and in those in Paraguay and Uruguay. Thesurvey findings were incorporated in a working docu-ment used at the afore-mentioned seminar on dentaleducation in Petrópolis. The national surveys on dentaleducation and the availability of human resources cur-rently being conducted in Colombia and Venezuela havealso received support from the Organization. In 1969 asurvey on teaching in the field of dental materials wasinitiated in Latin America; the results will be utilized inthe over-all program for dental materials in the Hemi-sphere and by the Center for dental materials establishedat the Central University in Caracas in that same year.
The preparation and training of auxiliary personnelhas been supported in Jamaica, where the Governmentconstructed the first school in the region to train schooldental auxiliaries. At the University of Antioquia, aprogram in 1968-1969 demonstrated that it was possibleto train such personnel to perform expanded functionsin dentistry, and at the University of Zulia, Venezuela,additional programs for the training of auxiliary per-sonnel to discharge such functions are being undertaken.Two surveys on the present situation of dental auxiliarypersonnel and their training were conducted and thesehave provided data for two publications.
A center for the development of training programs indental epidemiology was established in Sao Paulo, andanother for applied research in social dentistry was setup in Pórto Alegre, Brazil, in 1967.
The Organization, in collaboration with the AmericanDental Association, has continued to assist the develop-ment of activities of the Latin American Association ofDental Schools (ALAFO). Specific support was pro-vided for the third annual meeting held in Petrópolis in1966 and for the Seminar on the Teaching of Pedodon-tics (Caracas, 1969). A system was established in 1968to facilitate the interchange of information among the91 schools of dentistry in Latin America.
During 1968 surveys were conducted to provide infor-mation for three directories: Schools of Dentistry in the
158
Americas, Dental Auxiliary Education Programs inLatin America, and Latin American Dental Journals.Other publications prepared include a Guide to DentalMaterials (in Spanish), Guidelines for the Dévelopmentof Dental Curricula, and Current Situation of DentalA uxiliary Personnel in Latin A merica. A manual on thedesign and construction of simplified dental equipmenthas been prepared for publication.
In the field of fluoridation, the laboratory manualFluoride Determinations in Water was published inEnglish and Spanish. An updated Spanish edition ofthe Manual of Water Fluoridation Practice was preparedfor publication, as was a technical manual for the fluori-dation of public water supplies (see also p. 128-130).
Training in Sanitary Engineering
Considerable progress was made with education insanitary engineering in the four-year period. In 1967the Sanitary Engineering Department of the Central Uni-versity in Caracas was opened, providing postgraduateeducational facilities, and in the same year the post-graduate course in sanitary engineering was establishedin the Polytechnical School at the Catholic University inPernambuco (Brazil). In 1968 the School of SanitaryEngineering in Buenos Aires was raised to the levelof Sanitary Engineering Institute. In the following yearthe University of Antioquia introduced full five-yearcourses in sanitary engineering and in Peru the universityreforms included the School of Sanitary Engineering ofthe National University of Engineering.
Seminars and Meetings
In 1966 a Regional Symposium on Administration ofWater Supply and Sewerage Services was held in SanSalvador, El Salvador, and in 1967 a Symposium onRiver Basin Development took place in Sáo Paulo,Brazil. In addition, an international course on waterfluoridation engineering techniques was organized inCincinnati, Ohio, under the joint sponsorship of theOrganization, the W. K. Kellogg Foundation, and theUnited States Public Health Service. Also in 1967 anInternational Seminar on Water Rates was held inQuito, Ecuador, under the auspices of the Organizationand the Inter-American Development Bank.
In 1968 a Regional Seminar on the Teaching of Sani-tary Engineering in Latin America was held in Quito,Ecuador; and in Rio de Janeiro a Seminar on WaterQuality Control was organized. In view of its impor-tance, mention should also be made of the Symposiumon the Development of Water Resources held in Mara-caibo, Venezuela.
At a graduate school of engineering, tesis are performed withequipment provided for the posigraduate courses for engineersspecializing in the design and operation of water supply systems.
Collaboration with Universities
The Organization has carried on an intensive programto assist in strengthening the schools of engineering inwhich sanitary engineering is taught at various levels.These schools are faced with a shortage of laboratoryfacilities, due to the high cost of installations and equip-ment, which hinders them in their teaching work. It isencouraging to note that the countries are making sub-stantial efforts to set up, expand, and improve labora-tories in order to overcome these difficulties. For thispurpose they have sought financial assistance from inter-national agencies or from other Governments throughbilateral agreements. For their part, several voluntaryfoundations are giving assistance with the installation oflaboratories and UNDP is providing similar support.During the quadrennium Brazil, Colombia, Guatemala,Mexico, Paraguay, Peru, and Venezuela received assist-ance from some of these institutions and agencies. TheOrganization, within the limits of its budgetary re-sources, has also given positive support to the countriesof the Americas through the provision of materials andequipment and through programs of continuing edu-cation.
PAHO/WHO has also furnished technical assistanceto Argentina, Bolivia, Chile, Guatemala, Peru, andTrinidad and Tobago for the review of sanitary en-gineering curricula in some of their engineering schools.
The School of Engineering of the Central Universityof Venezuela was given assistance in improving its ad-ministrative practices, and it is hoped that the Organi-zation's support will lead to effective modernization ofits over-all administration, which would go side-by-sidewith the progress made in the improvement of studyprograms.
159
The program for improving the teaching of sanitaryengineering in four Venezuelan universities was activelycontinued. Financial assistance for the program hasbeen provided by the UNDP, and the Organization hasserved as executing agency. The universities in questionare the Central University and the Andrés Bello CatholicUniversity in Caracas, the University of Zulia in Mara-caibo, and the University of Los Andes in Mérida. As aresult of the program, the sanitary engineering curriculain these universities have been consolidated, laboratorieshave been expanded through the provision of addit.ionallecture classrooms and teaching materials, and fellow-ships and travel grants have been awarded for the addi-tional training of teaching staff.
One purpose of the project was to introduce a post-graduate program of studies at the Central Universitywhich, in addition to the teaching activities, wouldconcentrate on research into water and air pollution,radioactivity, and biological, chemical, and other prob-lems of environmental health. This objective wasachieved in 1967 when the postgraduate course of theDepartment of Sanitary Engineering was established.
This program has been extended until June 1970.Meanwhile, a new program to support research projectsin sanitary engineering in the same four universitieswas prepared and submitted to UNDP for its considera-tion. This program, if approved, will commence in mid-1970.
In the four years under review, UNDP has helpedto finance the plan for improvement and expansionof the Institute of Sanitary Engineering of SURSAN(Superintendency of Urbanization and Sanitation) inBrazil. The Institute is located at the University ofGuanabara in Rio de Janeiro, where it is conductingtraining programs in sanitary engineering. In additionto its teaching activities, it is organized to undertakeresearch and also to provide services. The Institute'slaboratories have been expanded and improved, as hasits library. Furthermore, its personnel receive travelgrants for further professional training. An importantpart of the Institute's educational activities are theshort intensive courses of which, in the 1966-1969period, it offered 31 on various aspects of sanitaryengineering.
With the Organization's support, exchanges of infor-mation and of visits by professionals were arrangedbetween the School of Hygiene and Public Health ofthe University of Sao Paulo and the School of SanitaryEngineering of the National University of Engineeringof Peru; between the Institute of Sanitary Engineeringof Buenos Aires University and the School of Hygieneand Public Health in Sao Paulo; and between theSchool of Engineering of the University of the West
Indies in Trinidad and Tobago and the Central Uni-versity of Venezuela.
Progress was also made in interuniversity coopera-tion within countries. Such associations developedbetween the Universities of Sao Paulo, and of Paraíbain Brazil; the Universities of Buenos Aires and ofRosario in Argentina; the National University of En-gineering and the University of Ica in Peru; and theUniversities of Chile and of Concepción in Chile.
Continuing Education
The program of continuing education in sanitaryengineering, initiated in the preceding period, was con-tinued during 1966-1969 with a marked expansion ofactivities. The countries' response to this program wasimmediate and their interest has steadily increased.
The Organization has furnished assistance throughshort-term consultants who have acted as advisers andalso through the assignment of lecturers; the provisionof limited amounts of equipment and materials forimproving laboratories, installations, teaching facilities,and printing services; small grants to pay local lecturers,coordinators, and auxiliary staff; and assistance forimproving libraries and printing technical manuals.
In the four-year period, 225 courses and 23 seminarsand symposia, totaling 17,542 instruction hours, wereheld. There were 7,161 participants and 1,566 na-tional and 530 international lecturers served in theprogram (Table 44). These figures alone indicate theextent to which the program has been accepted by thecountries.
The courses covered a wide range of subjects. Mostof them dealt with water supply and water treatment, inall their many phases, but many other subjects were alsocovered, such as use of computers, solid wastes disposal,administration and finance, emergency services, swim-ming pool operation, and industrial hygiene, thus in-dicating the remarkable adaptability of this program.It can confidently be stated that, as a result of thisactivity, the universities participate much more inten-sively than in the past in the formulation and study ofnational problems.
Special Programs
In 1967 an agreement was signed with IDB underthe terms of which that institution gave financial sup-port to a number of the short intensive courses whichwere held in that year. Those selected related to sub-jects in which the Bank was particularly interested.Under the same agreement, the International Seminaron Water Rates was held in Quito, Ecuador, in 1967.
A further agreement was signed with IDB underwhich the Organization undertook to carry out a special
160
r
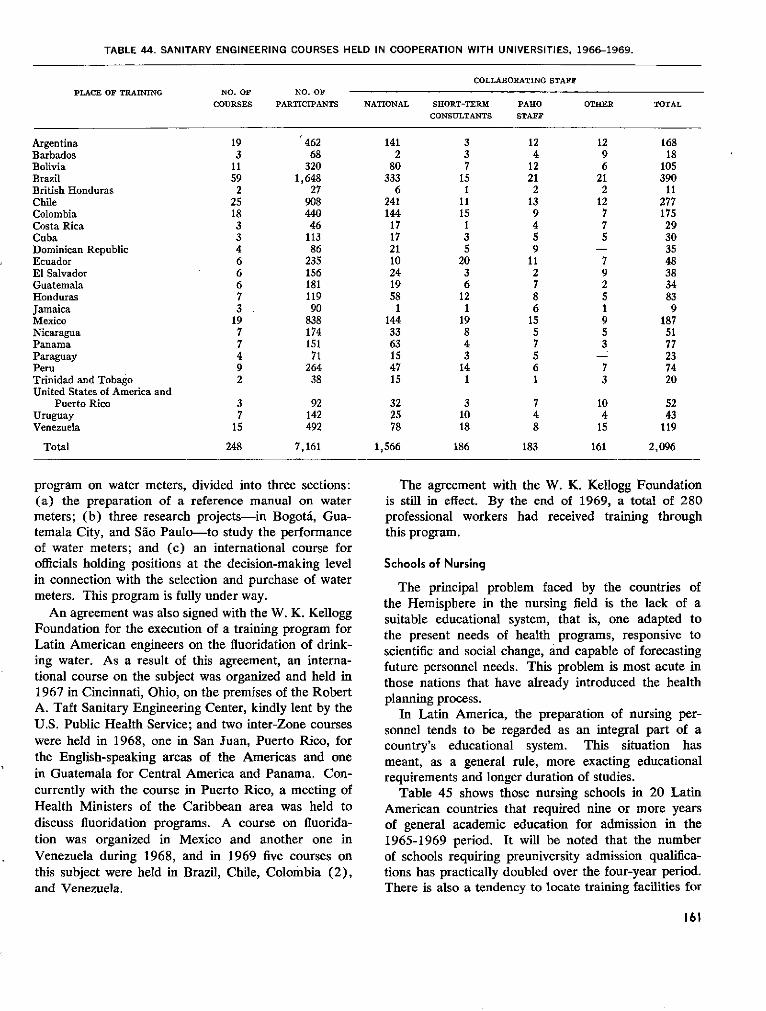
TABLE 44. SANITARY ENGINEERING COURSES HELD IN COOPERATION WITH UNIVERSITIES, 1966-1969.
COLLABORATING STAFFPLACE OF TRAINING NO. OF NO. OF
COURSES PARTICIPANTS NATIONAL SHORT-TERM PARO OTHER TOTALCONSULTANTS STAFF
Argentina 19 462 141 3 12 12 168Barbados 3 68 2 3 4 9 18Bolivia 11 320 80 7 12 6 105Brazil 59 1,648 333 15 21 21 390British Honduras 2 27 6 1 2 2 11Chile 25 908 241 11 13 12 277Colombia 18 440 144 15 9 7 175Costa Rica 3 46 17 1 4 7 29Cuba 3 113 17 3 5 5 30Dominican Republic 4 86 21 5 9 - 35Ecuador 6 235 10 20 11 7 48El Salvador 6 156 24 3 2 9 38Guatemala 6 181 19 6 7 2 34Honduras 7 119 58 12 8 5 83Jamaica 3 90 1 1 6 1 9Mexico 19 838 144 19 15 9 187Nicaragua 7 174 33 8 5 5 51Panama 7 151 63 4 7 3 77Paraguay 4 71 15 3 5 - 23Peru 9 264 47 14 6 7 74Trinidad and Tobago 2 38 15 1 1 3 20United States of America and
Puerto Rico 3 92 32 3 7 10 52Uruguay 7 142 25 10 4 4 43Venezuela 15 492 78 18 8 15 119
Total 248 7,161 1,566 186 183 161 2,096
program on water meters, divided into three sections:(a) the preparation of a reference manual on watermeters; (b) three research projects-in Bogotá, Gua-temala City, and Sao Paulo-to study the performanceof water meters; and (c) an international course forofficials holding positions at the decision-making levelin connection with the selection and purchase of watermeters. This program is fully under way.
An agreement was also signed with the W. K. KelloggFoundation for the execution of a training program forLatin American engineers on the fluoridation of drink-ing water. As a result of this agreement, an interna-tional course on the subject was organized and held in1967 in Cincinnati, Ohio, on the premises of the RobertA. Taft Sanitary Engineering Center, kindly lent by theU.S. Public Health Service; and two inter-Zone courseswere held in 1968, one in San Juan, Puerto Rico, forthe English-speaking areas of the Americas and onein Guatemala for Central America and Panama. Con-currently with the course in Puerto Rico, a meeting ofHealth Ministers of the Caribbean area was held todiscuss fluoridation programs. A course on fluorida-tion was organized in Mexico and another one inVenezuela during 1968, and in 1969 five courses onthis subject were held in Brazil, Chile, Colombia (2),and Venezuela.
The agreement with the W. K. Kellogg Foundationis still in effect. By the end of 1969, a total of 280professional workers had received training throughthis program.
Schools of Nursing
The principal problem faced by the countries ofthe Hemisphere in the nursing field is the lack of asuitable educational system, that is, one adapted tothe present needs of health programs, responsive toscientific and social change, and capable of forecastingfuture personnel needs. This problem is most acute inthose nations that have already introduced the healthplanning process.
In Latin America, the preparation of nursing per-sonnel tends to be regarded as an integral part of acountry's educational system. This situation hasmeant, as a general rule, more exacting educationalrequirements and longer duration of studies.
Table 45 shows those nursing schools in 20 LatinAmerican countries that required nine or more yearsof general academic education for admission in the1965-1969 period. It will be noted that the numberof schools requiring preuniversity admission qualifica-tions has practically doubled over the four-year period.There is also a tendency to locate training facilities for
161
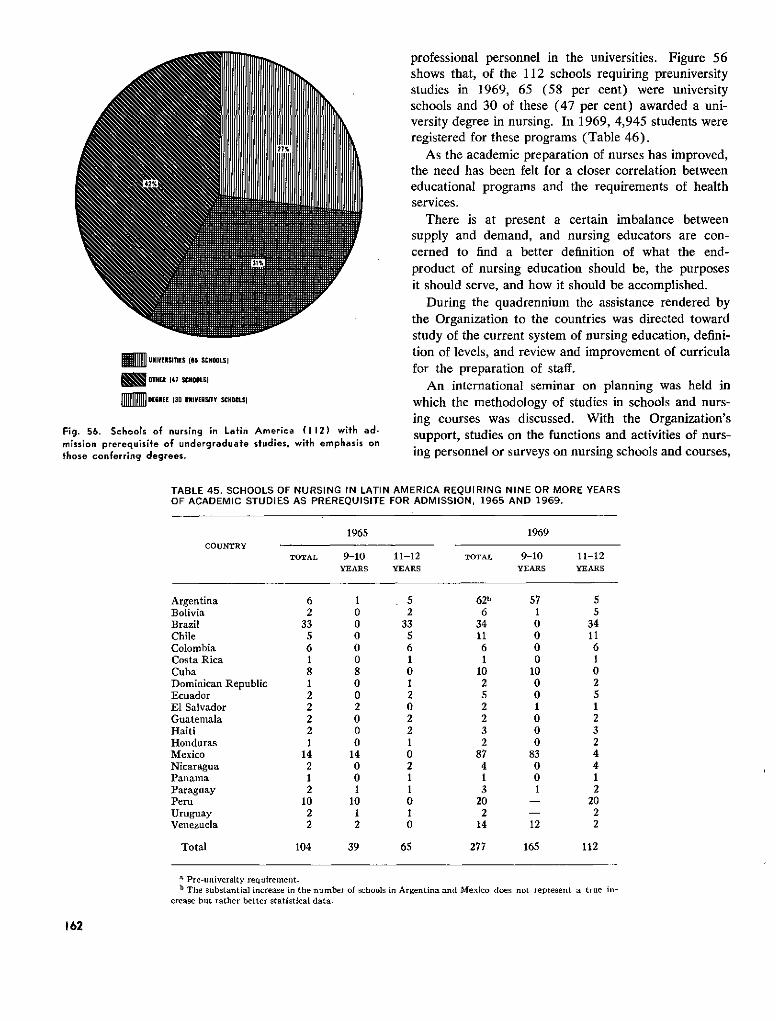
K m UNIVERSITIES (65 SCHOOLSI
OTHER 147 SCHOOLSI
mml DEGREE 130 UrOVERSITY SCHOOLSI
Fig. 56. Schools of nursing in Latin America (112) with ad-mission prerequisite of undergraduate studies, with emphasis onthose conferring degrees.
professional personnel in the universities. Figure 56shows that, of the 112 schools requiring preuniversitystudies in 1969, 65 (58 per cent) were universityschools and 30 of these (47 per cent) awarded a uni-versity degree in nursing. In 1969, 4,945 students wereregistered for these programs (Table 46).
As the academic preparation of nurses has improved,the need has been felt for a closer correlation betweeneducational programs and the requirements of healthservices.
There is at present a certain imbalance betweensupply and demand, and nursing educators are con-cerned to find a better definition of what the end-product of nursing education should be, the purposesit should serve, and how it should be accomplished.
During the quadrennium the assistance rendered bythe Organization to the countries was directed towardstudy of the current system of nursing education, defini-tion of levels, and review and improvement of curriculafor the preparation of staff.
An international seminar on planning was held inwhich the methodology of studies in schools and nurs-ing courses was discussed. With the Organization'ssupport, studies on the functions and activities of nurs-ing personnel or surveys on nursing schools and courses,
TABLE 45. SCHOOLS OF NURSING IN LATIN AMERICA REQUIRING NINE OR MORE YEARSOF ACADEMIC STUDIES AS PREREQUISITE FOR ADMISSION, 1965 AND 1969.
1965 1969COUNTRY
TOTAL 9-10 11-12 TOTAL 9-10 11-12YEARS YEARS YEARS YEARS
Argentina 6 1 5 62b 57 5Bolivia 2 0 2 6 1 5Brazil 33 0 33 34 0 34Chile 5 0 5 11 0 11Colombia 6 0 6 6 0 6Costa Rica 1 0 1 1 0 1Cuba 8 8 0 10 10 0Dominican Republic 1 0 1 2 0 2Ecuador 2 0 2 5 0 5El Salvador 2 2 0 2 1 1Guatemala 2 0 2 2 0 2Haiti 2 0 2 3 0 3Honduras 1 0 1 2 0 2Mexico 14 14 0 87 83 4Nicaragua 2 0 2 4 0 4Panama 1 0 1 1 0 1Paraguay 2 1 1 3 1 2Peru 10 10 0 20 - 20Uruguay 2 1 1 2 - 2Venezuela 2 2 0 14 12 2
Total 104 39 65 277 165 112
a Pre-university requirement.b The substantial increase in the number of schools in Argentina and Mexico does not represent a true in-
crease but rather better statistical data.
162
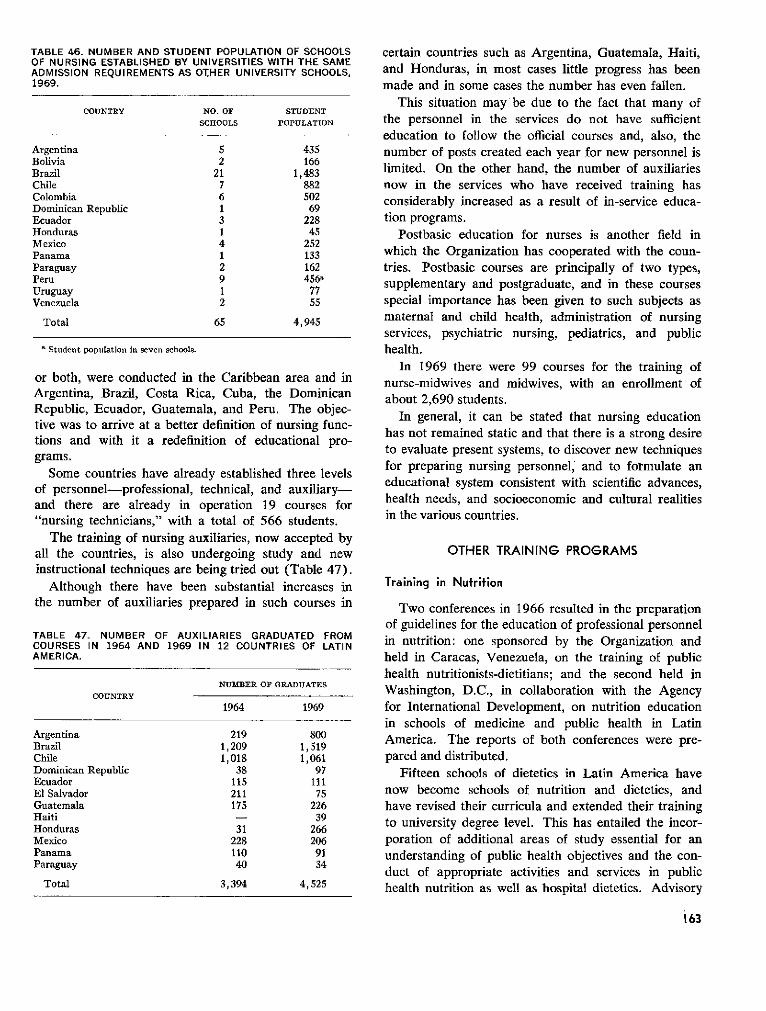
TABLE 46. NUMBER AND STUDENT POPULATION OF SCHOOLSOF NURSING ESTABLISHED BY UNIVERSITIES WITH THE SAMEADMISSION REQUIREMENTS AS OTHER UNIVERSITY SCHOOLS,1969.
COUNTRY NO. OF STUDENT
SCHOOLS POPULATION
Argentina 5 435Bolivia 2 166Brazil 21 1,483Chile 7 882Colombia 6 502Dominican Republic 1 69Ecuador 3 228Honduras 1 45Mexico 4 252Panama 1 133Paraguay 2 162Peru 9 456'Uruguay 1 77Venezuela 2 55
Total 65 4,945
a Student population in seven schools.
or both, were conducted in the Caribbean area and inArgentina, Brazil, Costa Rica, Cuba, the DominicanRepublic, Ecuador, Guatemala, and Peru. The objec-tive was to arrive at a better definition of nursing func-tions and with it a redefinition of educational pro-grams.
Some countries have already established three levelsof personnel-professional, technical, and auxiliary-and there are already in operation 19 courses for"nursing technicians," with a total of 566 students.
The training of nursing auxiliaries, now accepted byall the countries, is also undergoing study and newinstructional techniques are being tried out (Table 47).
Although there have been substantial increases inthe number of auxiliaries prepared in such courses in
TABLE 47. NUMBER OF AUXILIARIES GRADUATED FROMCOURSES IN 1964 AND 1969 IN 12 COUNTRIES OF LATINAMERICA.
NUBER OF GRADUATESCOUNTRY
1964 1969
Argentina 219 800Brazil 1,209 1,519Chile 1,018 1,061Dominican Republic 38 97Ecuador 115 111El Salvador 211 75Guatemala 175 226Haiti - 39Honduras 31 266Mexico 228 206Panama 110 91Paraguay 40 34
Total 3,394 4,525
certain countries such as Argentina, Guatemala, Haiti,and Honduras, in most cases little progress has beenmade and in some cases the number has even fallen.
This situation may be due to the fact that many ofthe personnel in the services do not have sufficienteducation to follow the official courses and, also, thenumber of posts created each year for new personnel islimited. On the other hand, the number of auxiliariesnow in the services who have received training hasconsiderably increased as a result of in-service educa-tion programs.
Postbasic education for nurses is another field inwhich the Organization has cooperated with the coun-tries. Postbasic courses are principally of two types,supplementary and postgraduate, and in these coursesspecial importance has been given to such subjects asmaternal and child health, administration of nursingservices, psychiatric nursing, pediatrics, and publichealth.
In 1969 there were 99 courses for the training ofnurse-midwives and midwives, with an enrollment ofabout 2,690 students.
In general, it can be stated that nursing educationhas not remained static and that there is a strong desireto evaluate present systems, to discover new techniquesfor preparing nursing personnel, and to formulate aneducational system consistent with scientific advances,health needs, and socioeconomic and cultural realitiesin the various countries.
OTHER TRAINING PROGRAMS
Training in Nufrifion
Two conferences in 1966 resulted in the preparationof guidelines for the education of professional personnelin nutrition: one sponsored by the Organization andheld in Caracas, Venezuela, on the training of publichealth nutritionists-dietitians; and the second held inWashington, D.C., in collaboration with the Agencyfor International Development, on nutrition educationin schools of medicine and public health in LatinAmerica. The reports of both conferences were pre-pared and distributed.
Fifteen schools of dietetics in Latin America havenow become schools of nutrition and dietetics, andhave revised their curricula and extended their trainingto university degree level. This has entailed the incor-poration of additional areas of study essential for anunderstanding of public health objectives and the con-duct of appropriate activities and services in publichealth nutrition as well as hospital dietetics. Advisory
163

services are being provided to these schools by theOrganization.
In accordance with the recommendations of theCaracas conference, a comprehensive bibliography oftexts and teaching materials available in Spanish, Por-tuguese, and English was compiled and distributed(Scientific Publication PAHO 174). The insufficientnumber of texts in Spanish and Portuguese presents aproblem for faculty members and students. A technicalgroup meeting in Washington, D.C., in 1969 made rec-ommendations to the Organization for the translationof certain textbooks on nutrition. It also establishedguidelines for the selection of such texts for schools ofnutrition and dietetics, schools of medicine, schools ofnursing, and schools of public health (Scientific Publica-tion PAHO 192).
No information is currently available on the totalnumber of medical schools or schools of public healththat have departments of nutrition or specific courseson nutrition.
A new program, granting a Master of Science degreein Public Health Nutrition, was initiated in Puerto Ricoin 1967, with advisory services from the Organization.In 1969, there were students from Brazil, Canada,Colombia, Ecuador, Peru, and Venezuela, as well asthe United States of America. This graduate course isopen to physicians and public health nutritionists hold-ing university degrees.
Advisory services were also furnished to the Schoolof Public Health of the Central University of Venezuelain the development of their department of nutrition, aswell as to the two schools of nutrition and dietetics inthat country.
Another postgraduate course leading to a Masterof Science degree with emphasis on nutrition wasopened in 1969 at the School of Hygiene and PublicHealth in Sao Paulo. The School also offers a shortcourse for physicians in alternate years; and the Institute
. ~w, .a
' /~~ &d&
-i ,ril-i.
of Nutrition in Recife conducts a short course annually.Both courses are assisted by the Organization.
The Organization has provided technical assistanceand actively participated in the nine-month course inpublic health nutrition for graduate dietitians offeredby the School of Public Health, Lima, Peru; in thetraining programs for personnel of hospital dietaryservices in the Dominican Republic; and in short coursesfor teachers, health personnel, and agricultural workersin Barbados, Brazil, Costa Rica, Dominica, Guyana,Jamaica, Paraguay, Peru, St. Kitts, St. Lucia, Trinidadand Tobago, and Venezuela.
It has continued its collaboration with FAO andUNICEF in the five-month course on food economy andapplied nutrition offered especially for agricultural andhome economics personnel. This course, formerly heldat the La Molina Agrarian University in Lima, Peru,was transferred to Bogotá, Colombia, and is being con-ducted under the joint sponsorship of the NationalUniversity, the Ministry of Agriculture, and the Nutri-tion Department of the Colombian Institute of FamilyWelfare. Known as "CRECENA," the course trained atotal of 47 persons in 1968-1969 from 16 Central andSouth American countries.
Training Activities at INCAP
The shortage of professional and technical staffadequately trained in nutrition and related disciplines,which has for many years been facing the membercountries of INCAP, is one of the limiting factors inthe conduct of applied nutrition programs. For thisreason, the Institute has, from its outset, devoted amajor part of its efforts to assisting in every possibleway to overcome this limitation through the trainingof personnel, not only from Central America andPanama but also from the other countries of theRegion and even other parts of the world. In the past,in keeping with the countries' requirements and avail-
4Senior-year students at the INCAPSchool of Nutrition receive instructionon practical work in dietetics.
164
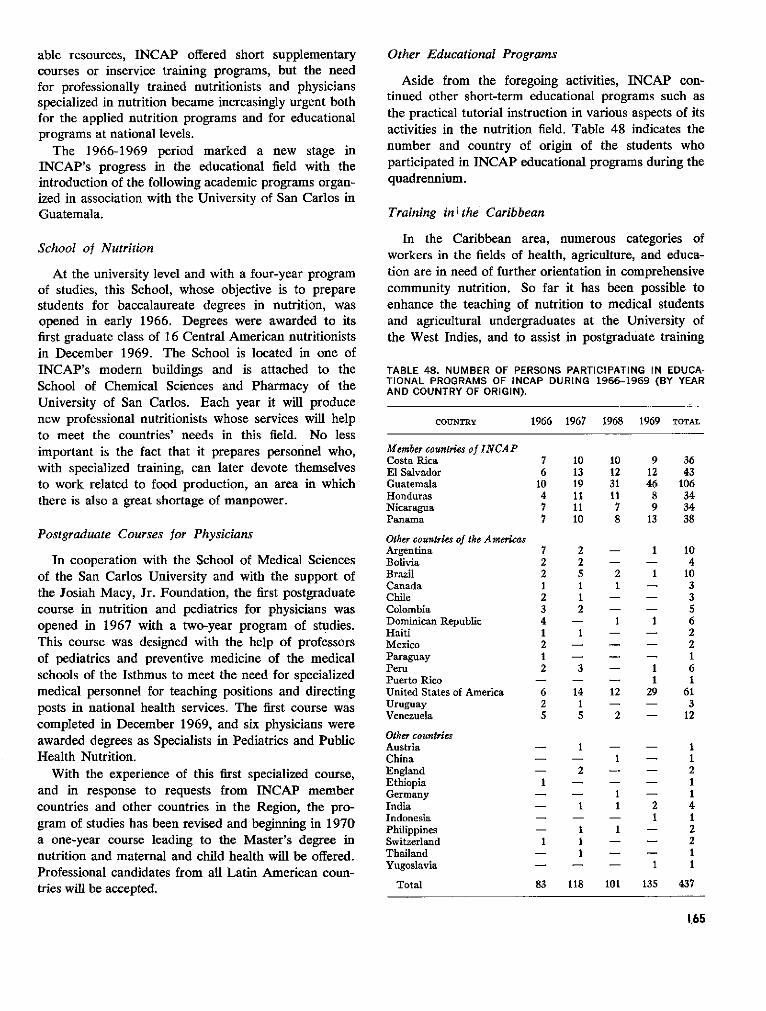
able resources, INCAP offered short supplementarycourses or inservice training programs, but the needfor professionally trained nutritionists and physiciansspecialized in nutrition became increasingly urgent bothfor the applied nutrition programs and for educationalprograms at national levels.
The 1966-1969 period marked a new stage inINCAP's progress in the educational field with theintroduction of the following academic programs organ-ized in association with the University of San Carlos inGuatemala.
School of Nutrition
At the university level and with a four-year programof studies, this School, whose objective is to preparestudents for baccalaureate degrees in nutrition, wasopened in early 1966. Degrees were awarded to itsfirst graduate class of 16 Central American nutritionistsin December 1969. The School is located in one ofINCAP's modern buildings and is attached to theSchool of Chemical Sciences and Pharmacy of theUniversity of San Carlos. Each year it will producenew professional nutritionists whose services will helpto meet the countries' needs in this field. No lessimportant is the fact that it prepares personnel who,with specialized training, can later devote themselvesto work related to food production, an area in whichthere is also a great shortage of manpower.
Postgraduate Courses for Physicians
In cooperation with the School of Medical Sciencesof the San Carlos University and with the support ofthe Josiah Macy, Jr. Foundation, the first postgraduatecourse in nutrition and pediatrics for physicians wasopened in 1967 with a two-year program of studies.This course was designed with the help of professorsof pediatrics and preventive medicine of the medicalschools of the Isthmus to meet the need for specializedmedical personnel for teaching positions and directingposts in national health services. The first course wascompleted in December 1969, and six physicians wereawarded degrees as Specialists in Pediatrics and PublicHealth Nutrition.
With the experience of this first specialized course,and in response to requests from INCAP membercountries and other countries in the Region, the pro-gram of studies has been revised and beginning in 1970a one-year course leading to the Master's degree innutrition and maternal and child health will be offered.Professional candidates from all Latin American coun-tries will be accepted.
Other Educational Programs
Aside from the foregoing activities, INCAP con-tinued other short-term educational programs such asthe practical tutorial instruction in various aspects of itsactivities in the nutrition field. Table 48 indicates thenumber and country of origin of the students whoparticipated in INCAP educational programs during thequadrennium.
Training in ithe Caribbean
In the Caribbean area, numerous categories ofworkers in the fields of health, agriculture, and educa-tion are in need of further orientation in comprehensivecommunity nutrition. So far it has been possible toenhance the teaching of nutrition to medical studentsand agricultural undergraduates at the University ofthe West Indies, and to assist in postgraduate training
TABLE 48. NUMBER OF PERSONS PARTICIPATING IN EDUCA-TIONAL PROGRAMS OF INCAP DURING 1966-1969 (BY YEARAND COUNTRY OF ORIGIN).
COUNTRY 1966 1967 1968 1969 TOTAL
Member countries of INCAPCosta Rica 7 10 10 9 36El Salvador 6 13 12 12 43Guatemala 10 19 31 46 106Honduras 4 11 11 8 34Nicaragua 7 11 7 9 34Panama 7 10 8 13 38
Other countries of the AmericasArgentina 7 2 - 1 10Bolivia 2 2 - - 4Brazil 2 5 2 1 10Canada 1 1 1 - 3Chile 2 1 - - 3Colombia 3 2 - - 5Dominican Republic 4 - 1 1 6Haiti 1 1 - - 2Mexico 2 - - - 2Paraguay 1 - - - 1Peru 2 3 - 1 6Puerto Rico - - - 1 1United States of America 6 14 12 29 61Uruguay 2 1 - - 3Venezuela 5 5 2 - 12
Other countriesAustria - 1 - - 1China - - 1 - 1England - 2 - - 2Ethiopia 1 - - - 1Germany - - 1 - 1India - 1 1 2 4Indonesia - - - 1 1Philippines - 1 1 - 2Switzerland 1 1 - - 2Thailand - 1 - - 1Yugoslavia - - - 1 1
Total 83 118 101 135 437
1,65
programs for home economists, public health inspectors,and nurses.
One difficulty in the Caribbean area is the insufficientnumber, at all levels, of personnel trained to deal withpractical aspects of community nutrition geared to theactual problems and resources.
A major activity of the Caribbean Food and Nutri-tion Institute (CFNI) was the implementation in 1969of the new course leading to the Diploma in CommunityNutrition of the University of the West Indies. It isdesigned primarily for key middle-level personnel fromministries of agriculture, health, education, and com-munity development. The first cotirse, which is for oneacademic year (nine months), was completed in Octo-ber 1969. The training program was mobile: the firstthree months were spent in Jamaica, followed by sixweeks' field experience in selected Caribbean countriesand six weeks' experience in Trinidad Followingexaminations, the second part of the course consistedof three months of supervised field investigation carriedout in the students' home country and detailed by thestudents in an analytical report on the project.
The course was interdisciplinary, practical, andrelated to the problems and background of the Carib-bean area. The sequence in the presentation of its mainsubject matter was as follows: the human scene andecology, the diet and its production, malnutrition (itscausation and recognition), techniques for the assess-ment of food and nutrition status, and methods of com-bating malnutrition.
Twenty-nine Government-sponsored students re-ceived PAHO fellowships for the course. In addition,two public health physicians from the Philippines wereawarded WHO fellowships.
The Caribbean students were from the followingcountries: Antigua (2), Barbados (8), Grenada (2),Guyana (3), Jamaica (6), Montserrat (1), St. Kitts-Nevis-Anguilla (1), St. Lucia (1), St. Vincent (1),and Trinidad (4). The students' fields of specializa-tion were the following: health (11), agriculture (5),home economics education (9), community develop-ment or social welfare (4).
The ultimate aim of CFNI is to develop a network ofinformed influential officers and policy-makers andtechnically trained personnel throughout the area, inorder to facilitate the implementation of practical in-terdisciplinary programs and activities directed towardthe solution of food and nutrition problems in theCaribbean.
Training in Zoonoses
This activity of the Pan American Zoonoses Centerhas been the one most requested by the Governments.
One of the major deficiencies in the national healthprograms is the lack of specialists trained in the controland prevention of the zoonoses. The health authoritiesof the Latin American countries have recognized thecapability of the Center for providing high-level train-ing. Special attention has therefore been given to thisactivity and some outstanding achievements have beenmade, although the lack of adequate space and of afull staff of professionals at the Center had a limitingeffect on the number of trainees that were received.
In response to the requests from the Governmentsduring the four-year period, 114 professional workersfrom all the countries of Latin America received in-dividual training of short- and long-term duration.
Many international courses and seminars were con-ducted by the Center, including the First InternationalSeminar on Rabies in the Americas (September 1967),with 102 participants from almost all countries of theHemisphere and observers from European countries(see also p. 86). Immediately following the Seminar,the Center offered an international course on rabiesdiagnosis and vaccine production, which was attendedby specialists from eight Central and South Americancountries. In 1968 three international courses wereconducted at the Center: one on epidemiology andlaboratory methods related to leptospirosis (for 17professionals from eight countries); in August, a two-week seminar on the epidemiology of the zoonoses (33participants from 14 countries); and in November acourse on ram epididymitis (eight participants fromfive countries). During 1969 the Center offered threeinternational courses: one on the production of B.abortus strain 19 vaccine and antigens for brucellosisdiagnosis (for 17 fellows from seven countries); inAugust, one on the breeding and handling of laboratoryanimals (17 participants from eight countries); andin November, a seminar on production and control ofrabies vaccine (24 participants from 11 countries).Professional staff of the Center participated in manymeetings, courses, seminars, and symposia sponsoredby other agencies and Governments in many countriesof the Hemisphere.
Training in Foof-and-Mouth Disease
During the quadrennium the training programs of thePan American Foot-and-Mouth Disease Center havebeen very helpful to the Governments in their cam-paigns to combat this disease. From the time of theCenter's establishment to the end of 1969, 25 inter-national courses were conducted. Individual trainingin various aspects of research, control, and preventionof foot-and-mouth disease was provided for more than500 veterinarians. The subjects in which instruction
166
Course on diagnosis of vesicular diseases held at the PanAmerican Foot-and-Mouth Disease Center.
was given included laboratory techniques and methodsfor diagnosis of vesicular diseases, planning and admin-istration of prevention and control campaigns, epi-demiology and statistics, production and control offoot-and-mouth disease vaccines, and animal healthplanning programs. Many national training coursesand seminars sponsored by the Organization were con-ducted each year through the Center and in cooperationwith the national authorities. Some of them were heldin countries free of foot-and-mouth disease and dealtwith the prevention of the disease in those areas, andothers were held in affected countries for the trainingof personnel in control methods.
For example, in 1969 a course on the diagnosis ofvesicular diseases was held at the Center during May-June for 14 fellows from 12 countries. In Septembera course on the prevention of foot-and-mouth diseasewas held in Guayaquil, Ecuador, for 14 fellows fromeight Spanish-speaking countries free of the disease.In December a similar course was presented in Englishat Maracay, Venezuela.
The Center's Training Section prepares and dis-tributes two publications: the Epidemiological Reportof the Center, and the periodical Cuadernos, bothdealing with the epidemiology of foot-and-mouthdisease in Latin America and with research, technicaladvisory services, and training in this field. The recentaddition of reproduction equipment and qualified staffhas made it possible to improve the effectiveness ofthis information.
Training in Tuberculosis
Tuberculosis control calls for administrators andsupervisors who have been trained in epidemiology,planning, evaluation, and operations research. Totrain personnel of this category, the Organization hasawarded fellowships to officials of national health ser-vices, enabling them to attend international courses ontuberculosis control in Prague and Rome, and haspromoted the training of personnel at the nationallevel.
In addition, in order to more rapidly reduce theshortage of expert personnel capable of formulatingand coordinating programs and to ensure the inclusionof tuberculosis control activities in national healthservices, the Organization, in association with the Gov-ernment of Venezuela, organized in Caracas, on apermanent basis, an international course on epidemiol-ogy of tuberculosis and administration of control pro-grams, with special consideration given to the epi-demiological, social, and economic conditions prevailingin the countries of the Americas. The first course washeld in 1969 and was attended by 20 physicians fromArgentina, Bolivia, Brazil, Chile, Colombia, theDominican Republic, Ecuador, El Salvador, Guate-mala, Honduras, Nicaragua, Mexico, Panama, Para-guay, Peru, and Venezuela.
To provide personnel with training in bacteriologicalmethods and techniques and to emphasize their impor-tant bearing on epidemiological reporting, treatmentcontrol, and program evaluation, the Organization alsocooperated with the Government of Venezuela in con-ducting three regional courses on tuberculosis bacteri-ology. Held in Caracas, these courses were attendedby physicians and technicians from various LatinAmerican countries.
Assistance continued to be given in the trainingof nurses and other health personnel with the aim ofstandardizing techniques, ensuring comparability ofresults, and facilitating the execution of tuberculosiscontrol programs as part of the activities of local healthservices. A program of this kind was carried out inBrazil, in which some 180 nurses and nursing auxilia-ries were trained.
Training in Population Dynamics
Since 1966 the Organization has been cooperatingwith the Universities of Sáo Paulo and of Chile in theestablishment of centers for research and training inhealth and population dynamics. The first courses wereheld in Chile in 1966 and in Brazil in 1967, and sincethen each of these schools has organized an annualcourse for national and foreign students.
The Biostatistics and Demography Center in Buenos
167
Aires, which was established in 1968 through the col-laboration of the School of Medicine of the Universityof Buenos Aires, the Government of Argentina, andPAHO/WHO, will also conduct a training program.
In 1968 a survey was made of the centers in LatinAmerica which provided opportunities for educationin family planning and population dynamics. Thiscomprehensive survey covered research, clinical instruc-tion, and the administration of population programs.The results were used as a basis for discussion by aWorking Group which met at Headquarters to makerecommendations on educational requirements in thisfield.
The six schools of medicine of Central America andPanama undertook a study on the teaching of demog-raphy, physiology of reproduction, obstetrics, andrelated subjects.
In 1968 the Organization sponsored, together withother agencies, a meeting on the teaching of demog-raphy in schools of medicine. It also organized twocourses on family planning and population dynamicsfor nurses and midwives, which were attended by 85students from 23 countries; and it sponsored a seminaron the educational components in population dynamics,at which there were 72 participants. Assistance wasalso furnished to the Latin American Course onMaternal and Child Health, at which an integratedplan of studies in maternal and child health and familyplanning was presented.
Training has been considered an important part ofthe program development in this field; in Colombia,for example, training activities were accomplishedwithin the national program in 1969.
Veferinary Medical Education
The development of veterinary medical serviceswithin the ministries of health and of agriculture inthe countries of the Hemisphere has resulted from thedemand for greater participation by veterinarians inprograms of community health. The national publichealth and animal health authorities, recognizing theeconomic losses to health and livestock developmentcaused by the zoonoses and foot-and-mouth disease,have requested the training of larger numbers ofspecialists in these diseases, at both undergraduate andcontinuing-education levels.
The countries have suffered for years from a seriousshortage of veterinarians, and now that the demandfor their services is increasing, the problem has becomeparticularly acute. The progress of the profession invarious Latin American countries has been affectedby such factors as the scarcity of schools of veterinarymedicine, the short time in which some have been in
operation, the professional competence of veterinar-ians, and other social, cultural, and economic condi-tions. Another very important factor in veterinarymedical education in Latin America is the tremendousloss of students during the professional academic cur-riculum. For example, in North America, of thestudents admitted to the professional curriculum, ap-proximately 72 per cent are graduated, while in LatinAmerica the proportion is only about 29 per cent.Directly influencing this rate are the absence of em-ployment opportunities upon graduation, the lack ofincentives for the student, and personal financial re-sponsibilities during the academic programs.
The Organization has attempted to strengthen veteri-nary medical education at the international, national,and local levels during the four-year period.
In Latin America the activities of the veterinarianupon graduation are different from those in NorthAmerica. Most of the Latin American graduates areemployed full time by the Governments in activitiesrelated to animal health, public health, and preventivemedicine. At present, more than 50 per cent of theveterinarians are in service with the Governments, incontrast to the United States of America, where 23per cent are full-time employees of the federal, state, ormunicipal agencies. At the present time, there are 70schools of veterinary medicine in the Americas, 21 ofthem in the United States of America and Canada.The total enrollment in all schools is about 14,000, withapproximately 4,800 attending schools in the U.S. andCanada.
The Organization's efforts to strengthen its programof support to schools of veterinary medicine havecentered primarily on the provision of consultant ser-vices, teaching materials, and equipment and the spon-soring of courses for continuing education in epidemiol-ogy, veterinary public health, and preventive medicine.Seminars, symposia, and other meetings on the teachingof preventive medicine and public health in veterinarymedical schools have been organized in different areasof the Hemisphere.
Meetings and Publications
In March 1967 the III Seminar on the Teaching ofPreventive Medicine and Public Health in Schools ofVeterinary Medicine in Latin America, was held at theSan Marcos University in Lima, Peru. Fifty personsrepresenting most of the countries of Latin Americaattended. The data obtained from a survey of teachingprograms conducted by the Organization in 42 schoolsof veterinary medicine in Latin America were used toprepare the basic working document of the meeting.The subjects discussed included the minimum content
168
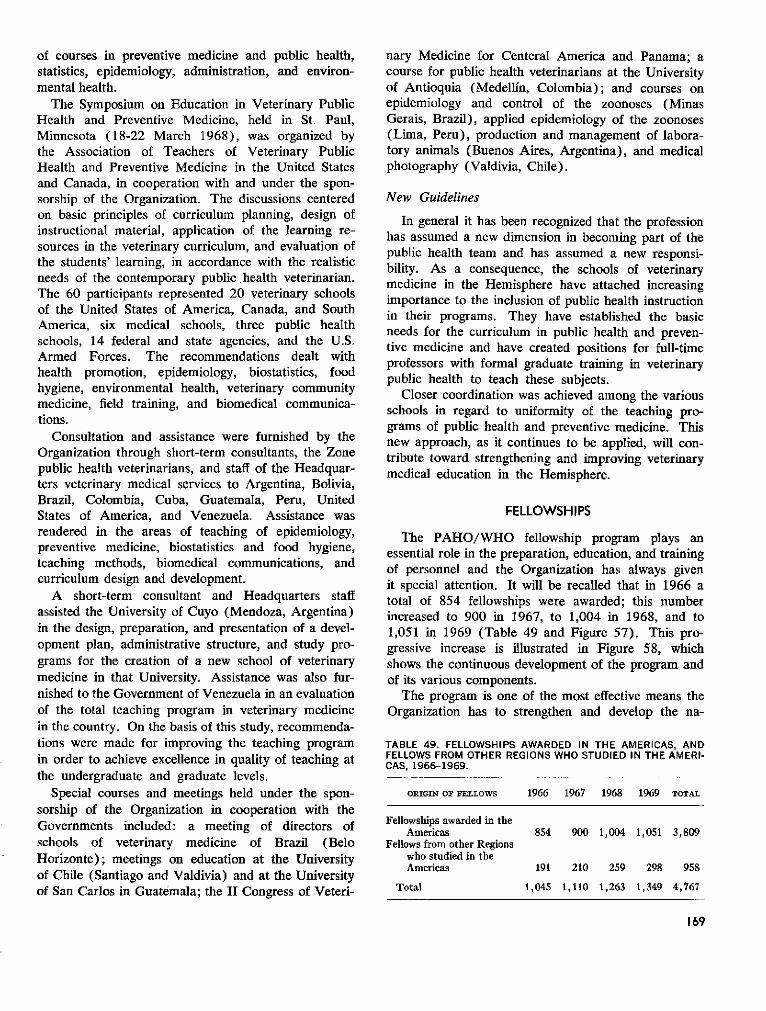
of courses in preventive medicine and public health,statistics, epidemiology, administration, and environ-mental health.
The Symposium on Education in Veterinary PublicHealth and Preventive Medicine, held in St. Paul,Minnesota (18-22 March 1968), was organized bythe Association of Teachers of Veterinary PublicHealth and Preventive Medicine in the United Statesand Canada, in cooperation with and under the spon-sorship of the Organization. The discussions centeredon basic principles of curriculum planning, design ofinstructional material, application of the learning re-sources in the veterinary curriculum, and evaluation ofthe students' learning, in accordance with the realisticneeds of the contemporary public health veterinarian.The 60 participants represented 20 veterinary schoolsof the United States of America, Canada, and SouthAmerica, six medical schools, three public healthschools, 14 federal and state agencies, and the U.S.Armed Forces. The recommendations dealt withhealth promotion, epidemiology, biostatistics, foodhygiene, environmental health, veterinary communitymedicine, field training, and biomedical communica-tions.
Consultation and assistance were furnished by theOrganization through short-term consultants, the Zonepublic health veterinarians, and staff of the Headquar-ters veterinary medical services to Argentina, Bolivia,Brazil, Colombia, Cuba, Guatemala, Peru, UnitedStates of America, and Venezuela. Assistance wasrendered in the areas of teaching of epidemiology,preventive medicine, biostatistics and food hygiene,teaching methods, biomedical communications, andcurriculum design and development.
A short-term consultant and Headquarters staffassisted the University of Cuyo (Mendoza, Argentina)in the design, preparation, and presentation of a devel-opment plan, administrative structure, and study pro-grams for the creation of a new school of veterinarymedicine in that University. Assistance was also fur-nished to the Government of Venezuela in an evaluationof the total teaching program in veterinary medicinein the country. On the basis of this study, recommenda-tions were made for improving the teaching programin order to achieve excellence in quality of teaching atthe undergraduate and graduate levels.
Special courses and meetings held under the spon-sorship of the Organization in cooperation with theGovernments included: a meeting of directors ofschools of veterinary medicine of Brazil (BeloHorizonte); meetings on education at the Universityof Chile (Santiago and Valdivia) and at the Universityof San Carlos in Guatemala; the II Congress of Veteri-
nary Medicine for Centeral America and Panama; acourse for public health veterinarians at the Universityof Antioquia (Medellín, Colombia); and courses onepidemiology and control of the zoonoses (MinasGerais, Brazil), applied epidemiology of the zoonoses(Lima, Peru), production and management of labora-tory animals (Buenos Aires, Argentina), and medicalphotography (Valdivia, Chile).
New Guidelines
In general it has been recognized that the professionhas assumed a new dimension in becoming part of thepublic health team and has assumed a new responsi-bility. As a consequence, the schools of veterinarymedicine in the Hemisphere have attached increasingimportance to the inclusion of public health instructionin their programs. They have established the basicneeds for the curriculum in public health and preven-tive medicine and have created positions for full-timeprofessors with formal graduate training in veterinarypublic health to teach these subjects.
Closer coordination was achieved among the variousschools in regard to uniformity of the teaching pro-grams of public health and preventive medicine. Thisnew approach, as it continues to be applied, will con-tribute toward strengthening and improving veterinarymedical education in the Hemisphere.
FELLOWSHIPS
The PAHO/WHO fellowship program plays anessential role in the preparation, education, and trainingof personnel and the Organization has always givenit special attention. It will be recalled that in 1966 atotal of 854 fellowships were awarded; this numberincreased to 900 in 1967, to 1,004 in 1968, and to1,051 in 1969 (Table 49 and Figure 57). This pro-gressive increase is illustrated in Figure 58, whichshows the continuous development of the program andof its various components.
The program is one of the most effective means theOrganization has to strengthen and develop the na-
TABLE 49. FELLOWSHIPS AWARDED IN THE AMERICAS, ANDFELLOWS FROM OTHER REGIONS WHO STUDIED IN THE AMERI-CAS, 1966-1969.
ORIGIN OF FELLOWS 1966 1967 1968 1969 TOTAL
Fellowships awarded in theAmericas 854 900 1,004 1,051 3,809
Fellows from other Regionswho studied in theAmericas 191 210 259 298 958
Total 1,045 1,110 1,263 1,349 4,767
169
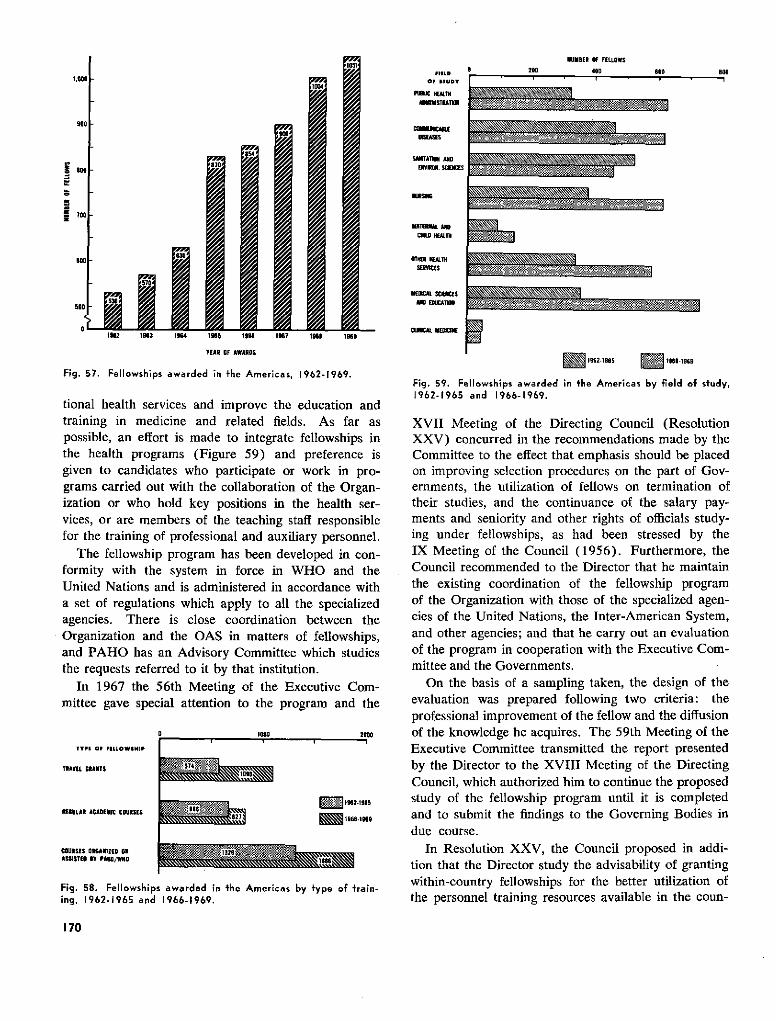
HUMBER OF FELLOWS.--
.00
1#62 1963 1964 195 1968 197 1968 1i9
VEAR OF AWAROS
Fig. 57. Fellowships awarded in fthe Americas, 1962-1969.
tional health services and improve the education andtraining in medicine and related fields. As far aspossible, an effort is made to integrate fellowships inthe health programs (Figure 59) and preference isgiven to candidates who participate or work in pro-grams carried out with the collaboration of the Organ-ization or who hold key positions in the health ser-vices, or are members of the teaching staff responsiblefor the training of professional and auxiliary personnel.
The fellowship program has been developed in con-formity with the system in force in WHO and theUnited Nations and is administered in accordance witha set of regulations which apply to all the specializedagencies. There is close coordination between theOrganization and the OAS in matters of fellowships,and PAHO has an Advisory Committee which studiesthe requests referred to it by that institution.
In 1967 the 56th Meeting of the Executive Com-mittee gave special attention to the program and the
O 1000 2000
TYPI OF FILLOWSHIP
TIAVEL GRANTS
1OEULAR ACADEIIC COUISES 1 2
COURSIS OIOAIZEO 01ASSITEOU BY PAHO/WN6
Fig. 58. Fellowships awarded in the Americas by type of 'rain-ing, 1962-1965 and 1966-1969.
fllgO zuu 450 0 800
LIC H. H103*ALmSTURA.
OIDSEASE CEINS
OICAL SODNCE
ernments, the utilization of fellows on termination of
E E 1962195 19C6.186 9
Fig. 59. Fellowships awarded in the Americas by field of sfudy,192- 1965persnne and 196- 1969.
XVII Meeting of the Directing Council (ResolutionXXV) concurred in the recommendations made by theCommittee to the effect that emphasis should be placedon improving selection procedures on the part of Gov-ernments, the utilization of fellows on termination oftheir studies, and the continuance of the salary pay-ments and seniority and other rights of officials study-ing under fellowships, as had been stressed by theIX Meeting of the Council (1956). Furthermore, theCouncil recommended to the Director that he maintainthe existing coordination of the fellowship programof the Organization with those of the specialized agen-cies of the United Nations, the Inter-American System,and other agencies; and that he carry out an evaluationof the program in cooperation with the Executive Com-mittee and the Governments.
On the basis of a sampling taken, the design of theevaluation was prepared following two criteria: theprofessional improvement of the fellow and the diffusionof the knowledge he acquires. The 59th Meeting of theExecutive Committee transmitted the report presentedby the Director to the XVIII Meeting of the DirectingCouncil, which authorized him to continue the proposedstudy of the fellowship program until it is completedand to submit the findings to the Governing Bodies indue course.
In Resolution XXV, the Council proposed in addi-tion that the Director study the advisability of grantingwithin-country fellowships for the better utilization ofthe personnel training resources available in the coun-
170
tries themselves. The 61th Meeting of the Committeeapproved the general criteria presented by the Directorfor granting within-country fellowships and asked thatthe Governments be consulted on the matter. TheXIX Meeting of the Council (Resolution XXXVIII)
approved provisionally the proposed criteria and askedthat it be informed of the experience obtained after theprogram has been in operation for one year.
That was the status of the fellowship program at theend of 1969.
PUBLICATIONS AND REFERENCE SERVICES
During the quadrennium, measures were taken tostrengthen and plan on a coordinated basis all of theHeadquarters services concerned with publications andreference services, in order to fulfill the function of theOrganization as a "collection and distribution center"of health information in the Americas.* These includepublications and editorial services, distribution, visualaids, translations, and library and reference services.
The program is designed as a complement to thework of the technical divisions, and as a means of dis-seminating to as wide an audience as possible informa-tion on the work of the Governments and the Organiza-tion in reducing disease and promoting individual andcommunity well-being, as well as the knowledge gainedand new techniques developed in the health and medicalsciences.
*Pan American Sanitary Code, Chap. IX, Art. 55.
Exhibit of publications in the PAHOLibrary. i
PUBLICATIONS
The principal technical organ-the monthly Boletínde la Oficina Sanitaria Panamericana-continued thework for which it was created 49 years ago by theSixth International Sanitary Conference (Montevideo,1920). As the number of readers increased, themonthly pressrun rose from 11,100 copies in 1966 tomore than 14,300 by the end of 1969. In the four-yearperiod some 280 main articles were published, fromauthors in all parts of the Americas as well as otherregions of the world, in addition to the sections devotedto medical and health news and reports on items ofcurrent interest.
In 1967 the Organization introduced the new one-volume English edition of the Boletín, published onceeach year and containing a selection of the articles andreports featured in the regular monthly journal during
171
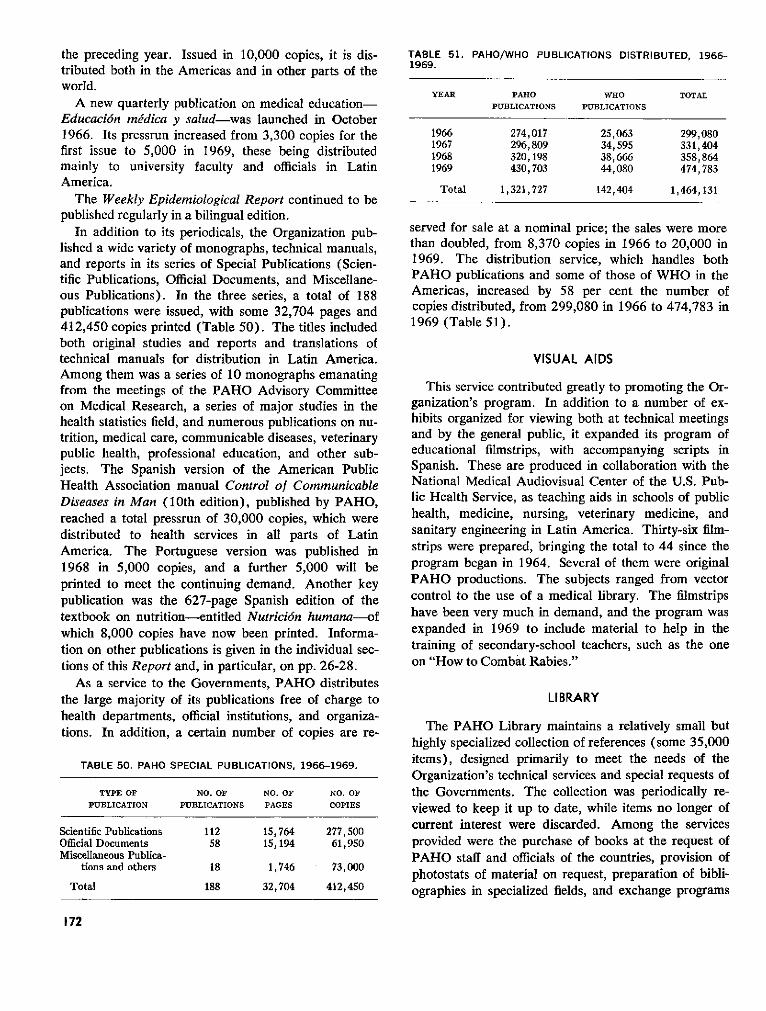
the preceding year. Issued in 10,000 copies, it is dis-tributed both in the Americas and in other parts of theworld.
A new quarterly publication on medical education-Educación médica y salud-was launched in October1966. Its pressrun increased from 3,300 copies for thefirst issue to 5,000 in 1969, these being distributedmainly to university faculty and officials in LatinAmerica.
The Weekly Epidemiological Report continued to bepublished regularly in a bilingual edition.
In addition to its periodicals, the Organization pub-lished a wide variety of monographs, technical manuals,and reports in its series of Special Publications (Scien-tific Publications, Official Documents, and Miscellane-ous Publications). In the three series, a total of 188publications were issued, with some 32,704 pages and412,450 copies printed (Table 50). The titles includedboth original studies and reports and translations oftechnical manuals for distribution in Latin America.Among them was a series of 10 monographs emanatingfrom the meetings of the PAHO Advisory Committeeon Medical Research, a series of major studies in thehealth statistics field, and numerous publications on nu-trition, medical care, communicable diseases, veterinarypublic health, professional education, and other sub-jects. The Spanish version of the American PublicHealth Association manual Control of CommunicableDiseases in Man (10th edition), published by PAHO,reached a total pressrun of 30,000 copies, which weredistributed to health services in all parts of LatinAmerica. The Portuguese version was published in1968 in 5,000 copies, and a further 5,000 will beprinted to meet the continuing demand. Another keypublication was the 627-page Spanish edition of thetextbook on nutrition-entitled Nutrición humana-ofwhich 8,000 copies have now been printed. Informa-tion on other publications is given in the individual sec-tions of this Report and, in particular, on pp. 26-28.
As a service to the Governments, PAHO distributesthe large majority of its publications free of charge tohealth departments, official institutions, and organiza-tions. In addition, a certain number of copies are re-
TABLE 50. PAHO SPECIAL PUBLICATIONS, 1966-1969.
TYPE OF NO. OF NO. OF NO. OFPUBLICATION PUBLICATIONS PAGES COPIES
Scientific Publications 112 15,764 277,500Official Documents 58 15,194 61,950Miscellaneous Publica-
tions and others 18 1,746 73,000
Total 188 32,704 412,450
TABLE 51. PAHO/WHO PUBLICATIONS DISTRIBUTED, 1966-1969.
YEAR PAHO WHO TOTALPUBLICATIONS PUBLICATIONS
1966 274,017 25,063 299,0801967 296,809 34,595 331,4041968 320,198 38,666 358,8641969 430,703 44,080 474,783
Total 1,321,727 142,404 1,464,131
served for sale at a nominal price; the sales were morethan doubled, from 8,370 copies in 1966 to 20,000 in1969. The distribution service, which handles bothPAHO publications and some of those of WHO in theAmericas, increased by 58 per cent the number ofcopies distributed, from 299,080 in 1966 to 474,783 in1969 (Table 51).
VISUAL AIDS
This service contributed greatly to promoting the Or-ganization's program. In addition to a number of ex-hibits organized for viewing both at technical meetingsand by the general public, it expanded its program ofeducational filmstrips, with accompanying scripts inSpanish. These are produced in collaboration with theNational Medical Audiovisual Center of the U.S. Pub-lic Health Service, as teaching aids in schools of publichealth, medicine, nursing, veterinary medicine, andsanitary engineering in Latin America. Thirty-six film-strips were prepared, bringing the total to 44 since theprogram began in 1964. Several of them were originalPAHO productions. The subjects ranged from vectorcontrol to the use of a medical library. The filmstripshave been very much in demand, and the program wasexpanded in 1969 to include material to help in thetraining of secondary-school teachers, such as the oneon "How to Combat Rabies."
LI BRARY
The PAHO Library maintains a relatively small buthighly specialized collection of references (some 35,000items), designed primarily to meet the needs of theOrganization's technical services and special requests ofthe Governments. The collection was periodically re-viewed to keep it up to date, while items no longer ofcurrent interest were discarded. Among the servicesprovided were the purchase of books at the request ofPAHO staff and officials of the countries, provision ofphotostats of material on request, preparation of bibli-ographies in specialized fields, and exchange programs
172
with other libraries. Some 3,200 readers and visitors also regularly performed language services during meet-were received in the Library in 1969. ings of the Governing Bodies and technical conferences.
Translations done by the regular staff in four languages(English, Spanish, Portuguese, and French) totalled
This service met the needs of all the publications and 47,858 pages during the four years (an average ofinformation activities, and at the same time those of 11,965 per year), apart from work performed duringthe technical departments at Headquarters. The staff the meetings and that done under outside contract.
FINAL COMMENTSThe period from 1966 to 1969 which we have reviewed in the preceding pages
from the standpoint of health conditions and progress in the Americas and the workof PAHO/WHO emerges as one of consolidation and further application of thepolicy, initiated in 1961, of integrating health into economic and social development.
The picture described is likely to remain essentially unchanged throughout thenext few decades, with certain trends becoming, perhaps, more pronounced, as faras the Region as a whole is concerned, although in terms of individual countriesconditions will, of course, continue to vary with the degree of industrializationattained in each. Indeed, even within a single country there are sharp ecologicaldifferences which are reflected in widely varying ways of life in urban versus ruralenvironments, tropical versus highland areas, autochthonous versus industrializedcommunities, and so on.
In spite of a deeply-felt obligation to solve the existing problems and attenuatetheir harmful effects, the national health authorities are prevented by a lack ofsufficient resources from taking effective action against every negative aspect of thesituation. And their task is made even more difficult by the paucity of trained per-sonnel, by scarcity or inadequacy of facilities and services, and by insufficient fund-ing, problems which are in turn accentuated by economic conditions and by historicand cultural patterns that are often a hindrance to social progress.
The health of the people is primarily a concern of the Governments. Determin-ing the problems that need to be tackled and the ways and means of doing the jobis a matter within the purview of each Government. In every phase of this work,however, they can count on receiving the help of PAHO/WHO to the extent thatthey so request and its budget allows.
A salient feature of our entire pattern of collaboration with the Governments isthe importance attached to research and manpower development. This task, inwhich the universities, other teaching institutions, and special centers play a vitalrole, must be expanded and extended while continued efforts are also made to com-bat disease with the knowledge and methods placed in our reach by the healthsciences and modern technology. The multidisciplinary approach is an imperativeof the times.
As we continue-in the words of our Constitution-to "promote and coordinateefforts of the countries of the Western Hemisphere to combat disease, lengthen life,and promote the physical and mental health of the people," we are buoyed by theknowledge that Latin America has achieved the conditions necessary for sustainedeconomic and social development and that, where health is concerned, there is nowawareness of what needs to be done, how to accomplish it, and how to predictresults. In all this activity to improve the material conditions and well-being of theAmerican nations, the Pan American Health Organization is proud to be at theservice of all the countries of the Hemisphere.
173
i
INDEX
Administrative methods and practices, 50Administrative questions, 40-43
appointment of External Auditor, 41Headquarters building, 42personnel, 41
table, 41property holdings, 41-42quotas, 40
table, 40salary increase, 41
Adolfo Lutz Institute (Brazil), 25, 61Aedes aegypti, 54-56
status of the campaign (figure), 55(see also Yellow fever)
Advisory Comm'ittee on Medical Research, 141-142Advisory Committees of PAHO, 34Agency for International Development (AID), 17, 18, 25,
47, 95, 96, 98, 99, 163Air pollution and industrial hygiene, 93, 102-103Alcoholism, 127American Public Health Association, 25Anemias, nutritional, 120, 121
research, 146-147Anna Fuller Fund, 24Arbovirus infections, 76-78
arbovirus isolated in Mexico and Central America(table), 143
dengue, 77encephalitis, 76-77hemorrhagic fever, 77-78
Associations, PAHO relations with, 24-25
Biomedical communications, 144-146Bovine
brucellosis, 86-87tuberculosis, 87, 152
Brother's Brothers Foundation, 24, 47Brucellosis, 86-87
research, 150-151Budget, 36-38
tables, 36, 37, 38Butantan Institute (Brazil), 26, 144
Canadian International Development Agency (CIDA), 97Cancer, 82-84
mortality from malignant neoplasms (figure), 83CARE, 97Caribbean Food and Nutrition Institute, 34, 126
research, 150training, 165-166
Centers of PAHO, 34-35Chagas' disease, 79-81
future activities, 80-81national programs, 80study groups, 79-80
Charter of Bogotá, 1Charter of Punta del Este, 1, 11, 17, 20, 42, 47, 96, 97Chronic and degenerative diseases, 82-84
cancer, 82-84diabetes mellitus, mortality (figure), 82
Commonwealth Fund, 145Communicable diseases, 53-76
A edes aegypti, 54-56Arbovirus infections, 76-78chronic and degenerative diseases, 82-84influenza, 74-76leprosy, 67-70malaria, 56-60parasitic diseases, 78-82plague, 72-74poliomyelitis, 66-67smallpox, 60-63tuberculosis, 63-66venereal diseases, 70-71yaws, 72yellow fever, 53-54zoonoses, 84-93
Computer Center in Health, 34Connaught Laboratories (Canada), 61, 62, 132, 133Constitutional questions, 31-33
amendments to the Constitution, 31election of the Director, 31Executive Committee, election of Governments, 31
new Members, 31Governing Bodies, rules of procedure, and meetings, 32-
33Control or eradication of diseases, 53-93
arbovirus infections, 76-78chronic and degenerative diseases, 82-84communicable diseases, 53-76parasitic diseases, 78-82zoonoses, 84-93
Current problems, 3-18economic integration, 4external financial resources, 17-18food and nutrition policy, 11-12geography and health, 4-7health and population dynamics, 9-11human resources, 14-17modern science and technology, 12-14rural conditions, 7-9salient health matters, 3-4
Deaths (see Mortality)Declaration of the Presidents of America, 1, 1-2, 97Dengue, 77
occurrence in the Caribbean (figure), 77Dental health, 128-130
fluoridation in Latin America (table), 129
175
research, 130training, 157-159
courses (figure), 157Development Decade of the United Nations, 21-22Diabetes mellitus, mortality (figure), 82Directing Council, 32Diseases (see Control or education of diseases)Drug control, 133-135
data on drug consumption and control (table), 134
Economic Commission for Latin America (ECLA), 5, 23Economic integration, 4Economic and Social Act of Rio de Janeiro, 1Education (see Human resources and Training)Emergency situation in El Salvador and Honduras, 19-20Encephalitis, 76-77
outbreaks (figure), 76Endemic goiter, 120-121, 124
research, 146Environmental sanitation, 93-94
(see also Sanitary engineering and environmentalsciences)
Evaluation, 52-53Evandro Chagas Institute (Brazil), 24, 26Executive Committee, 33EXIMBANK (Export-Import Bank, USA) 17, 18, 95, 96External relations of PAHO, 19-29
with national and international institutions, 24-26scientific and public communications, 26-29with the United Nations system, 21-24within the Inter-American system, 19-21
Fellowships, 169-171figures and table, 169-170
Financial questions, 35-40budget, 36-38
tables, 36, 37, 38Emergency Procurement Revolving Fund, 39-40
table, 40Procurement Fund, 39programs, 35-36Special Fund for Health Promotion, 40Special Fund for Research, 40supply service (tables), 39Tax Equalization Fund, 39voluntary contributions, 38-39Working Capital Fund, 37-38
Financial resources, external, 17-18international financial institutions, 17-18Technical Discussions (1969), 18
Fluoridation, 129, 159Food hygiene, 135-137Food and nutrition policy, 11-12Foundations, PAHO relations with, 24Funds, PAHO (see under Financial questions)
General activities, 43-53administrative methods and practices, 50evaluation, 52-53health legislation, 50-52health planning, 48-50health statistics, 43-48
General health services, 104-106budget (table), 105country projects (tables), 104, 105, 106
Geography and health, 4-7coordination of border activities, 6-7river basins, 5-6, 93, 159
Goiter (see Endemic goiter)Governing Bodies, PAHO, 30-33
Health education, 138-140personnel (table), 139
Health legislation, 50-52future activities, 52group of experts, 51international transportation of human remains, 51-52Pan American Sanitary Code, 51study on, 51
Health planning, 48-50Pan American Health Planning Program, 34, 35, 49quadrennial projections, 49-50
Health and population dynamics, 9-10training, 167-168
Health and radiation, 137-138research, 138training, 137
Health Sciences Education Information Center, 34Health services, other, 131, 140
drug control, 133-135food hygiene, 135-137health education, 138-140health and radiation, 137-138public health laboratories, 131-133
Health statistics, 43-48collection and dissemination of information, 43-44
quarantinable diseases (figure and table), 43, 44education and training, 45-46
figure and table, 45improvement of systems, 44International Classification of Diseases, 44-45research, 46-47
Hemorrhagic fever, 77-78Highlights of the period, 1-18
historic events, 1-3prevailing problems, 3-18
Historic events (1966-1969), 1-3Declaration of the Presidents of America, 1, 1-2, 97OAS, new Charter of the, 1Special Meeting of Ministers of Health of the Americas,
2-3, 56, 70, 97, 107, 108, 117, 130Hospital Maintenance and Engineering Center (Vene-
zuela), 110, 111Hospitals, 108-111
distribution of, and beds in (figure), 109, 110general advisory programs, 109projections, 110-111specific projects, 109-110
Housing, 103-104Human reproduction, investigations of, 48Human resources, 14-17, 154-171
cooperation with universities, 15crisis in the universities, 14-15fellowships, 169-171medical education methods, 16shortage of personnel, 15-16strengthening of teaching institutions, 156-169textbooks, 16-17(see also Training)
176
Hydatidosis, 87-88research, 152
Hypovitaminosis A, 121research, 147
Immunology Research and Training Center (Brazil), 34,144
Immunology Research and Training Center (Mexico), 34,144
Industrial hygiene, 102-103Influenza, 74-76
deaths (figure), 75epidemics, outbreaks, and virus, 74-76
Institute of Nutrition of Central America and Panama, 34,35, 123-125
research, 148-150training, 164-165
Institute of Occupational Health and Air Pollution Re-search (Chile), 93, 102, 103
Institute of Rehabilitation of the University of Sao Paulo(Brazil), 26
Institute of Sanitary Engineering (Brazil), 26, 160Inter-American Association of Sanitary Engineering
(AIDIS), 26, 104Inter-American Children's Institute, 21, 120Inter-American Committee on the Alliance for Progress
(CIAP), 20Inter-American Cultural Council (IACC), 20Inter-American Development Bank, 5, 17, 18, 94, 95, 96,
98, 99, 101, 109, 132, 153, 159, 160Inter-American Economic and Social Council (IA-
ECOSOC), 20, 107Inter-American Housing and Planning Center (CINVA),
21, 103Inter-American Investigation of Mortality, 47, 83, 154
in Childhood, 47-48, 118, 119figure and table, 47
Inter-American Meeting on Foot-and-Mouth Disease andZoonoses Control, 135
Inter-American System, PAHO within the, 19-21General Secretariat of the OAS, 19-21Meetings of Ministers of Health of Central America
and Panama, 21Internal developments in PAHO, 31-42
administrative questions, 40-42constitutional questions, 31-33financial questions, 35-40organizational structure, 33-35
International Atomic Energy Agency, 137International Bank for Reconstruction and Development
(World Bank), 10, 17, 18, 95, 96International Classification of Diseases, 44-45International Conference on Vaccines against Viral and
Rickettsial Diseases of Man, 144International Influenza Center for the Americas, 25, 74, 75International Labour Organisation (ILO), 24, 105, 107,
108International transportation of human remains, 51-52
Josiah Macy, Jr., Foundation, 24, 165
Kellogg Foundation, W. K., 24, 40, 46, 110, 129, 130,137, 158, 159, 161
Laboratories (see Public health laboratories)Laboratory animals, 152Latin American Center for Classification of Diseases, 34Latin American Center for Medical Administration, 34,
112, 113Latin American Center for Perinatology and Human
Development, 154Latin American Common Market, 4Latin American Institute of Economic and Social Planning,
22Leprosy, 67-70
changes in the control, 69recommendations of the Ministers of Health, 70reported cases (figure and table), 67, 68seminars, 69status of the programs (figure), 67
difficulties, 68-69work to be carried out, 69-70
Library, 172-173
Malaria, status of the eradication, 56-60difficulties, 58figures and tables, 56, 57, 58, 59investments, 58-59new activities, 57-58new strategy, 59-60problems and solutions, 58progress achieved, 56-57
Malnutrition, 120children with (figure), 120
Maternal and child health, 117-120, 154Medical care and rehabilitation, 106-115
coordination of services, 107-108education and training, 111-113hospitals, 108-111
distribution of, and beds (figure), 109, 110general advisory programs, 109projections, 110-111specific programs, 109-110
policy, 107rehabilitation, 113-115
Medical education (see Human resources)Mental health, 126-128
research, 147-148suicides and homicides (figure), 127training, 127-128
Milbank Memorial Fund, 24, 156Ministers of Health of the Americas, Special Meeting, 2-3,
14, 17, 56, 70, 97, 107, 108, 117, 130Ministers of Health of Central America and Panama,
Meetings of, 21Mortality
cardiovascular diseases (figure), 46in childhood, 47-48, 118, 119diabetes mellitus (figure), 82encephalitis, 76-77infectious and parasitic diseases (figure), 3malaria (figure), 57malignant neoplasms (figure), 83maternal (figure), 119nutritional deficiency (table), 47respiratory diseases (figure), 75syphilis (figure), 71tuberculosis (figure), 64
177
National Communicable Disease Center (USA), 25, 61,71,74
National Institute of Rural Endemic Diseases (Brazil), 26National Institutes of Health (USA), 25, 124Nursing, 115-117
schools of, 161-163training, 115-116, 161-163
staff (figures and tables), 16, 115, 116, 117Nutrition, 120-126
advisory services, 121-122Caribbean Food and Nutrition Institute, 34, 126, 150,
165-166and chronic diseases, 148endemic goiter, 120-121and family planning, 147hypovitaminosis A, 121INCAP, 34, 35, 123-125, 148-150and mental development, 147-148nutritional anemias, 120, 146-147
figure, 121policy, 11-12programs, 121, 122-123protein-calorie malnutrition, 120research, 146-150survey, 148training, 163-166
Nutrition Foundation, 24Nutrition Institute of Recife (Brazil), 26Nutritional deficiency, deaths from (table), 47
OAS (see Organization of American States)Onchocerciasis, 82Organization of American States, 5, 9, 97, 103, 107
new Charter of the, 1PAHO relations with the, 19-21
CIAP, 20emergency situation in El Salvador and Honduras,
19-20IACC, 20IA-ECOSOC, 20Operation Relief, 19other OAS organizations, 20-21Program of Technical Cooperation, 20
Organizational structure, 33-35advisory committees, 34centers, 34-35concept of health, 33consultants, 35structure of health services, 33-34
Oswaldo Cruz Institute (Brazil), 26, 132, 158
Pan American Air Pollution Surveillance Network, 93, 102Pan American Development Foundation, 47Pan American Foot-and-Mouth Disease Center, 34, 90-93
research, 152training, 166-167
Pan American Health Planning Program, 34, 35, 49Pan American Sanitary Code, 51Pan American Sanitary Conference, 30, 32Pan American Sanitary Engineering and Environmental
Sciences Center, 34, 93, 102-104Pan American Zoonoses Center, 34, 88-90, 130
research, 150-152training, 166
Parasitic diseases, 78-82Chagas' disease, 79-81mortality from (figure), 3onchocerciasis, 82schistosomiasis, 81-82
Personnel, PAHO/WHO, 41Plague, 72-74
geographic distribution, 72-73reported cases (figure), 73studies, 73-74
Poliomyelitis, 66-67laboratories for diagnosis (table), 66reported cases (figure), 66
Pollution (see Air pollution and industrial hygiene andWater supply)
Population dynamics (see Health and population dynam-ics)
Population Information Center, 34Program of Technical Cooperation of the OAS, 20Programs of PAHO, 35-36, 43-173
control or eradication of diseases, 53-93general activities, 43-53health services, other, 131-140human resources, 14-17, 154-171promotion of health, 104-131publications and reference services, 171-173research, 12-14, 140-154sanitary engineering and environmental sciences, 93-104
Projects, national and regional (table), 36Promotion of health, 104-131
dental health, 128-130general health services, 104-106maternal and child health, 117-120medical care and rehabilitation, 106-115mental health, 126-128nursing, 115-117nutrition, 120-126veterinary public health, 130-131
Public health laboratories, 131-133Publications, 171-173
distributed (table), 172number of (table), 172
Quarantinable diseases, reported cases (figure and table),43, 44
Rabies, 84-86in dogs and cats (figure), 84research, 151-152
Rabies Surveillance System for the Americas, 86Radiation and health, 137-138Reference services, 171-173Regional Center for Functional Literacy in Rural Areas
for Latin America (CREFAL), 23Regional Library of Medicine, 34, 145Rehabilitation, 113-115
(see also Medical care)Research, 12-14, 140-154
Advisory Committee on Medical Research, 141-142biomedical communications, 144-146brucellosis, 150-151cancer, 83
178
Chagas' disease, 79dental health, 130foot-and-mouth disease, 152health statistics, 46-47human reproduction, 48hydatidosis, 152manganese poisoning, 138migration of professionals, 14mortality, 46-47multinational centers, 13-14multinational programs, 143-144nutrition, 146-150operations, 146other activities, 153-154plague, 73-74policy, 13rabies, 151-152radiations, 146sanitary engineering, 152-153scientific and cultural community, 12-13smallpox, 61Special Fund, 40training in, 142-143tuberculosis, 152, 153zoonoses, 150-152
Respiratory diseasesdeath rates from (figure), 75
River basins, 5-6, 92, 159development of the Amazon Basin, 6development of the Guayas River Basin, 6development of the River Plate Basin, 5Huallaga, Chiriyacu, and Nieva River Basins, 6pollution in the Lerma River, 6study of the Santa Lucía River Basin, 5-6
Rockefeller Foundation, 24Rural areas
conditions, 7-9water in, 97-99
Sanitary engineering and environmental sciences, 93-104collection and disposal of solid wastes, 101-102environmental sanitation, 93-94loans and technical assistance, 101Pan American Sanitary Engineering and Environmental
Sciences Center, 102-104air pollution and industrial hygiene, 102-103housing, 103-104other activities, 104
research, 152-153revolving fund programs (table), 99sewerage and water pollution, 100training, 159-161
courses (table), 161water supply, 94-100
Schistosomiasis, 81-82Scientific and public communications, 26-29
anniversary of WHO (20th), 29public information, 28-29scientific information, 26-28World Health Day, 29
Schools of medicine, 156-157number of (figure), 156number of medical graduates (figure), 157physicians per 10,000 population (figure), 16, 156
Schools of nursing, 161-163figures and tables, 162, 163
Schools of public health, 157Sewerage services, 100
figures and tables, 95, 96, 99Silicosis, 93Smallpox, 60-63
activities, 60-61campaign in Brazil, 62
figure and table, 62, 63laboratories for diagnosis (figure), 62population vaccinated, (figure), 62production of vaccine (figure), 61reported cases (figure and table), 60, 63results obtained, 61-62summary of the situation, 62-63vaccine against, 61, 63, 132
Special Inter-American Conference (2nd and 3rd), 1Special Public Health Service Foundation (Brazil), 24Staff (see Personnel)Syphilis
deaths from (figure), 71reported cases (table), 70
Technical Discussions, PAHO Directing Council, 10, 18Textbooks, PAHO program, 16-17Training
dental health, 157-159foot-and-mouth disease, 166-167health and population dynamics, 167-168health statistics, 45-46immunology, 144maternal and child health, 119-120medical care, 111-113mental health, 127-128nursing, 115-116, 161-163nutrition, 163-166radiation, 137research, 142-143sanitary engineering, 159-161tuberculosis, 64, 167venereal diseases, 71veterinary medicine, 168-169zoonoses, 166-167
Translation services, 173Tuberculosis, 63-66
deaths from (figure), 64reported cases (figure), 64research, 153training, 64, 167vaccine
against, 64, 65requirements (table), 65
(see also Bovine tuberculosis)
United Nations Children's Fund (UNICEF), 22-23, 58,70, 72, 97, 105, 130, 164
United Nations Development Program (UNDP), 6, 22, 34,93, 94, 97, 102, 104, 105, 110, 122, 132, 159, 160
United Nations Educational, Scientific and Cultural Orga-nization (UNESCO), 23-24, 105, 140
United Nations Food and Agriculture Organization (FAO),6, 11, 23, 104, 105, 122, 126, 150, 164
179
United Nations, PAHO relations with, 21-24Development Decade, 21-22ECLA, 23FAO, 23ILO, 24UNDP, 22UNESCO, 23-24UNICEF, 22-23World Food Program, 23
United States Association for the United Nations, 25Universities, PAHO relations with, 24-25U.S. Public Health Service, 25, 48, 61, 130, 159
Vaccines (see under name of disease)Venereal diseases, 70-71
measures to be taken, 71publications on, 71syphilis
reported cases (table), 70training, 71
Veterinary public health, 130-131training, 168-169
Visual aids, 172
Water supply, 94-100administration of services, 99-100figures and tables, 94, 95, 96, 98, 99pollution, 100
in rural areas, 97-99status of revolving fund programs (table), 99
Wellcome Foundation, 24Wellcome Trust, 79, 143Williams-Waterman Fund of the Research Corporation,
24, 122, 126World Bank (see International Bank for Reconstruction
and Development)World Food Program, 23, 97, 123World Health Foundation of the U.S.A., 25World Influenza Center, 74, 75
Yaws, 72reported cases (table), 72
Yellow fever, 53-54reported cases (figure and table), 53, 54(see also A edes aegypti)
Zoonoses, 84-93bovine tuberculosis, 87brucellosis, 86-87hydatidosis, 87-88rabies, 84-86research, 150-152training, 166-167(see also Pan American Foot-and-Mouth Disease Center
and Pan American Zoonoses Center)
180
Photograph by:Alcides Almada, Paul Almasy, Eli Finer, Carl Frank, INCAP, James B. Johnson,P. Larsen, E. Loureiro, Armando Matiz (Bogotá, Colombia), Ministry ofHydraulic Resources, Mexico, Pan American Foot-and-Mouth Disease Center,PAHO Flash WHO, Pan American Union, Pan American Zoonoses Center,E. Rice, Robert Schafer, Eric Schwab.

















![S]l1~I~cek: - IRIS PAHO Home](https://static.fdokumen.com/doc/165x107/631510f36ebca169bd0b0b21/sl1icek-iris-paho-home.jpg)


