18262.pdf - IRIS PAHO Home
166
Ti~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~~~~~~~~~~~i · it :~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ .i .~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~[ _1._ -~~~~~~~~ ~~ .: . _ _ = ._ ~~~ ~~. . . .. _ . . _ .. _ ~~~~~~~~~~______ _ _ _ _ __ A"_ ;; ;~~~; ; ;; ; ; ;; ; ; ;; __- ;; .~~~~ ~~~~~~__ _-_ _- _-_ _- .~~~~~ ~~~~~~~_- _- _- _ _- _- -_ ~~~~...-_ _ =.=-_ _ __ i-~~~~~~ ! ! !! ! m ! ! m! _ ! mm ! ! [] !! .- _ _- _ -. _ ._=_
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of 18262.pdf - IRIS PAHO Home
Ti~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~~~~~~~~~~~i ·it
:~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ .i
.~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~[ _1._
-~~~~~~~~ ~~ .: . _ _ =
._ ~~~ ~~. . . . . _ . . _ .. _
~~~~~~~~~~______ _ _ _ _ __
A"_ ;; ;~~~; ; ;; ; ; ;; ; ; ;; __- ;;
.~~~~ ~~~~~~__ _-_ _- _-_ _-__;;.~~~~~ ~~~~~~~_- _- _- _ _- _- -___-_-
~~~~...-_ _ =.=-_ _ __
i-~~~~~~ ! ! !! ! m ! ! m! _ ! mm ! ! [] !!
.-_ _-
_ -. _
._=_
Cover design by Judith Mays
annual reportof the director1980
Official Document No. 177July 1981
PAN AMERICAN HEALTH ORGANIZATIONPan American Sanitary Bureau * Regional Office of theWORLD HEALTH ORGANIZATION525 Twenty-third Street, N.W.Washington, D.C. 20037, U.S.A.
ISBN 92 75 17177 7
© Pan American Health Organization, 1981
Publications of the Pan American Health Organization enjoy copyright protection in accordancewith the provisions of Protocol 2 of the Universal Copyright Convention. For rights of reproductionor translation of PAHO publications, in part or in toto, application should be made to the Office ofPublications, Pan American Health Organization, Washington, D.C. The Pan American Health Orga-nization welcomes such applications.
The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part of the Secretariat of the Pan American HealthOrganization concerning the legal status of any country, territory, city, or area of its authorities, orconcerning the delimitation of its frontiers or boundaries.
The mention of specific companies or of certain manufacturers' products does not imply that theyare endorsed or recommended by the Pan American Health Organization in preference to others of asimilar nature that are not mentioned.
Contents
INTRODUCTION vii
Chapter 1: GENERAL DIRECTION OF THE ORGANIZATION 1Governing Bodies 3
Directing Council 3Executive Committee 6
American Region Programming and Evaluation System (AMPES) 8Long-Term Planning 8Management 8Relations with Other Organizations 11
PAHO and the international cooperation system 12PAHO and the inter-American system 13Subregional groups 13Bilateral agencies 14Foundations 15
Chapter2: HEALTH SERVICE SYSTEMS 17Medical Care Systems 17Health Planning 21National Health Information Systems 22Management Systems 24Financing Health Services 24Health Facilities Maintenance 25Health Education 26Maternal and Child Health and Family Welfare 27Nutrition 31Health Service Research 37
Chapter3: DISEASE PREVENTION AND CONTROL 39Communicable Diseases 41
Expanded Program on Immunization 41Tuberculosis 47Acute respiratory infections 49Leprosy 50Diarrheal diseases 51Bacterial diseases 54Sexually transmitted diseases 54
iii
Rickettsial and viral diseases 55Aedes aegypti eradication 57Malaria 59Other parasitic diseases 64
Blindness Prevention 66Noncommunicable Diseases 67
Cancer 67Other noncommunicable diseases 70
Mental Health 70Dental Health 73Laboratory Services 75Epidemiologic Surveillance 77Biologicals 78
Vaccine control 78Drug quality control 79Blood banking 80
Radiation Health 81Accident Prevention 83
Chapter4: ENVIRONMENTAL HEALTH AND PROTECTION 85Water Supply and Basic Sanitation 87Institutional Development 90Solid Waste Management 92Control of Pollution and Other Environmental Health Hazards 95Occupational Health 99Food Protection 99
Chapter 5: HUMAN RESOURCES AND RESEARCH 103Infrastructure Development and Manpower Planning 104Education and Training 104
Medicine 104Public health and social medicine 105Health care administration 106Nursing 107Mental health 108Dentistry 108Engineering and environmental sciences 109Veterinary medicine 110Continuing education 111Technical and auxiliary personnel 111
Fellowships 114Educational Technology and Technologic Resources 116Regional Library of Medicine and the Health Sciences 118Research Promotion and Coordination 119
Advisory Committee on Medical Research 122Research grants 122
iv
Chapter 6: SPECIAL PROGRAMS 125Zoonoses and Animal Health 125Emergency Preparedness and Disaster Relief Coordination 134Statistical Services 141Publications 142
Index 149Acronyms and Corresponding Agencies or Programs 157
v
"It is today accepted that health is an end for each human beingand a means for the society to which he belongs."
Ten-Year Health Plan forthe Americas, 1971-1980
u -
.- 1 I
(Photos by J. Vizcarra Brenner/PAHO, except bottom left photo, by R. Blessing)
Introduction
A new decade-and a new era in Pan American health-have begun.During the year this report covers, the Ten-Year Health Plan for the Americas
conceived at Santiago in 1972 ended, its successes and failures were analyzedand lessons drawn from them, and the Americas started out toward a new anddifficult but not impossible goal: health for all by the end of this century.
Within the process of attaining the goal of health for all by the year 2000,basic national and regional health strategies were worked out and, in manycountries, put into effect. Those strategies are predicated on certain fundamen-tal concepts in whose validity health care specialists around the world generallyagree. Outstanding among them are primary care in order to upgrade the levelsof well-being and extend health services to all people, the participation of thecommunity in health sector matters, the use of technologies appropriate to localconditions, and the necessity of technical cooperation among developing coun-tries and between them and the international organizations at their service.Equally important is the role of women as consumers and providers of healthcare.
Attaining the goal of health for all by the year 2000 as defined by thehemisphere's countries has obvious but far-reaching implications in economicand social development. In our view it must be regarded not as an isolated sec-toral objective but as part of the broader aim that the governments have alreadyendorsed in the United Nations by establishing the New International Develop-ment Strategy, the New International Economic Order, and the War on Ex-treme Poverty. Whether the goal can be attained depends on the extent towhich governments introduce changes in their approach and in their systems, aswell as on many technical and economic factors and, more importantly, onpolitical conditions and social situations. It is also necessary to strengthen thedialogue between the social and production sectors, which, though longrecognized as important, has been delayed by a series of situations to the detri-ment of the very purpose of development.
For PAHO, 1980 marked a transition from earlier- and what now seem quiteconventional-ways of carrying out its mission to new and often experimentalmodes of technical cooperation with its member countries. Long and carefulthought went into elaborating the strategies, but they offer the possibility ofproviding all citizens of the Americas with adequate health care by the year2000.
C/Héctor R. Acuña
Director
Chapter 1
GENERAL DIRECTIONOF THE ORGANIZATION
The opening year of the twentieth cen-tury's ninth decade marked a further reorien-tation in the activities of the Pan AmericanHealth Organization toward universal healthin the hemisphere by the end of the century.
The goal of health for all by the year 2000springs from two statements of purpose. Oneis a World Health Assembly resolution(WHA30.43) of 1977 proclaiming that the mainsocial target of governments and the WorldHealth Organization should be "attainmentby all citizens of the world by the year 2000of a level of health that will permit them tolead a socially and economically productivelife." The other is the Declaration of Alma-Ata, adopted a little over a year later at theInternational Conference on Primary HealthCare at Alma-Ata, U.S.S.R., which said thatprimary health care is the key to the attain-ment of health for all.
For the Americas, universal health is a goallong sought. The first hemispheric resolutionto improve health and health care was theCharter of Punta del Este, which was signedin Uruguay in 1961 and led to the Ten-YearPublic Health Program of the 1960s. Thenext, formulated at the Third Special Meetingof American health ministers at Santiago in1972, was the Ten-Year Health Plan for theAmericas which ended in 1980.
These two decennial plans, which ended inboth successes and failures, are now being
continued through a far more ambitious re-gional strategy and plan of action based onnational strategies and plans intended to giveeach of the hemisphere's citizens access tohealth services within the next two decades.
During the year, 24 nations formulated na-tional health strategies, which naturallyvaried according to individual countries.Some gave highest priority to the rural or ur-ban poor; others focused on the elderly andways of caring for them, a reflection ofpopulation aging thanks to advances in com-municable disease control; still others stressedthe need to form new and stronger links be-tween the health sector and other develop-mental spheres. These were only some of theemphases in national health strategies, manyof which combined many themes.
Generally speaking, all the countries aswell as PAHO now accept certain premises asessential to advancing health care.
Among them are the extension of healthservices to the entire population; the basicimportance of primary health care as thestrategy for achieving complete coverage; theneed for technical cooperation amongdeveloping countries, between developedand developing countries, and between thelatter and the international organizations ser-ving them rather than the older concept of"technical assistance" from extranational andoften paternalistic agencies; linkages among
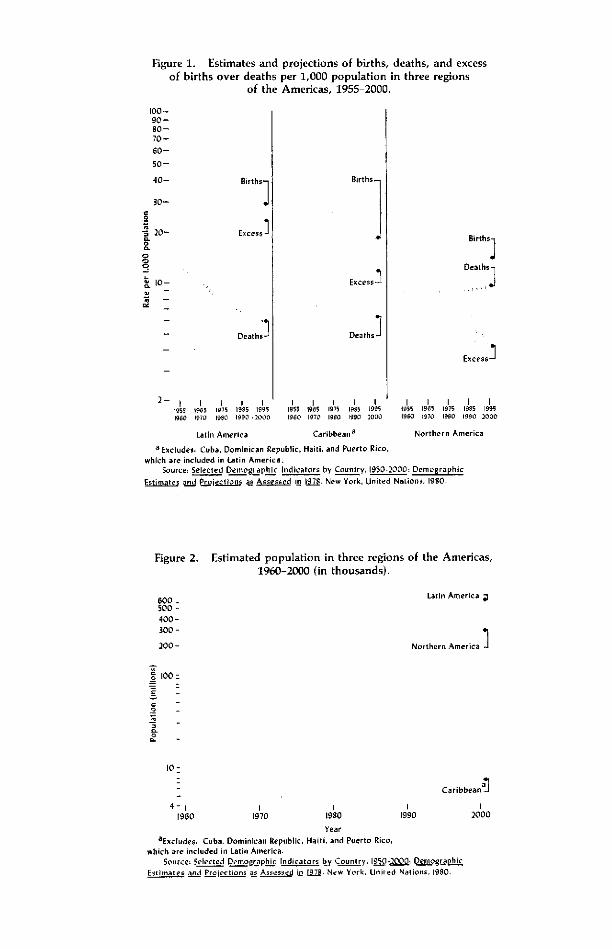
Figure 1. Estimates and projections of births, deaths, and excessof births over deaths per 1,000 population in three regions
of the Americas, 1955-2000.
Births 1
Excess-
Deaths-
1 1 ¡* I I I I i1955 1965 ¡975 1985 19951960 1970 1980 1990 ,2000
Latin America
Births-
Excess -
Deaths]
I I i I1955 1965 1975 19S5 19951960 1970 1990 t990 1000
Caribbean a
Birthsj
Deaths
1 .i s i
Excess
¡ 1 l1955 1965 1975 1985 19951960 1970 1990 1990 2000
Northern America
a Excludes Cuba, Dominican Republic, Haiti., and Puerto Rico,
which are included in Latin America.Source Selected Demographic Indicators by Country, 1950-2000 Demographic
Estimates and eLojection as Assessed ¡in 197S. New York, United Nations. 1980.
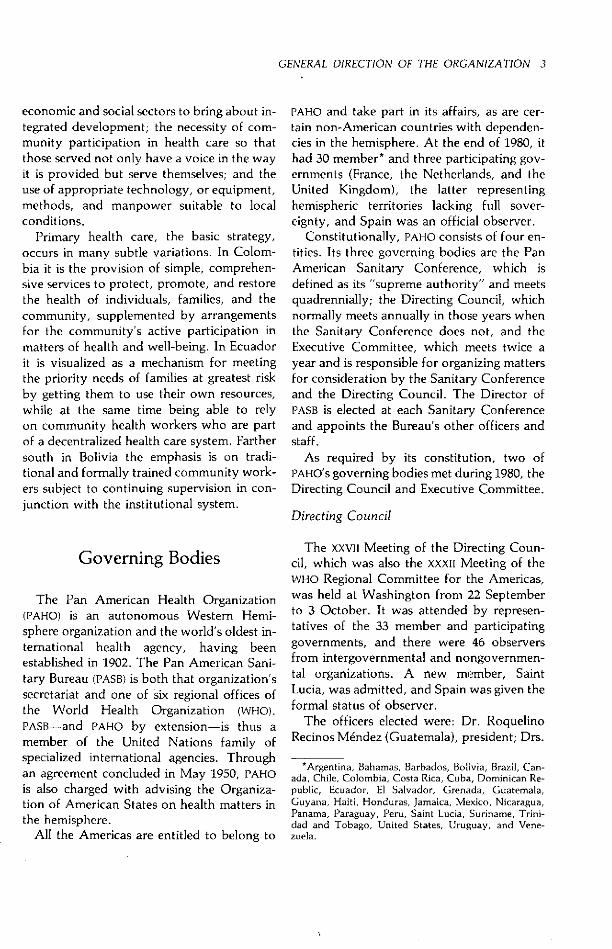
Figure 2. Estimated population in three regions of the Americas,1960-2000 (in thousands).
600 _ Latin America500 -
400 -300-
Northern America 1
4- I1960 19701970
191980
19901990
Caribbeanal
20002000
Year
aExcludes, Cuba. Dominican Republic, Haiti. and Puerto Rico,which are included in Latin America.
Source Selected Demographic Indicators by Country. 1950-2000 Demographic
Estimates and Projections as Assessed in 1979. New York, Uniled Nations. 1980.
00 -90-80-70-
60-
50-
40-
30-
20-e.'Z
o
I08,
rlo-
2-
2-
200 -
100:
o _
o.
E
_ _
r0
0 -
GENERAL DIRECTION OF THE ORGANIZATION 3
economic and social sectors to bring about in-tegrated development; the necessity of com-munity participation in health care so thatthose served not only have a voice in the wayit is provided but serve themselves; and theuse of appropriate technology, or equipment,methods, and manpower suitable to localconditions.
Primary health care, the basic strategy,occurs in many subtle variations. In Colom-bia it is the provision of simple, comprehen-sive services to protect, promote, and restorethe health of individuals, families, and thecommunity, supplemented by arrangementsfor the community's active participation inmatters of health and well-being. In Ecuadorit is visualized as a mechanism for meetingthe priority needs of families at greatest riskby getting them to use their own resources,while at the same time being able to relyon community health workers who are partof a decentralized health care system. Farthersouth in Bolivia the emphasis is on tradi-tional and formally trained community work-ers subject to continuing supervision in con-junction with the institutional system.
Governing Bodies
The Pan American Health Organization(PAHO) is an autonomous Western Hemi-sphere organization and the world's oldest in-ternational health agency, having beenestablished in 1902. The Pan American Sani-tary Bureau (PASB) is both that organization'ssecretariat and one of six regional offices ofthe World Health Organization (WHO).PASB-and PAHO by extension-is thus amember of the United Nations family ofspecialized international agencies. Throughan agreement concluded in May 1950, PAHOis also charged with advising the Organiza-tion of American States on health matters inthe hemisphere.
All the Americas are entitled to belong to
PAHO and take part in its affairs, as are cer-tain non-American countries with dependen-cies in the hemisphere. At the end of 1980, ithad 30 member* and three participating gov-ernments (France, the Netherlands, and theUnited Kingdom), the latter representinghemispheric territories lacking full sover-eignty, and Spain was an official observer.
Constitutionally, PAHO consists of four en-tities. Its three governing bodies are the PanAmerican Sanitary Conference, which isdefined as its "supreme authority" and meetsquadrennially; the Directing Council, whichnormally meets annually in those years whenthe Sanitary Conference does not, and theExecutive Committee, which meets twice ayear and is responsible for organizing mattersfor consideration by the Sanitary Conferenceand the Directing Council. The Director ofPASB is elected at each Sanitary Conferenceand appoints the Bureau's other officers andstaff.
As required by its constitution, two ofPAHO's governing bodies met during 1980, theDirecting Council and Executive Committee.
Directing Council
The XXVII Meeting of the Directing Coun-cil, which was also the XXXII Meeting of theWHO Regional Committee for the Americas,was held at Washington from 22 Septemberto 3 October. It was attended by represen-tatives of the 33 member and participatinggovernments, and there were 46 observersfrom intergovernmental and nongovernmen-tal organizations. A new member, SaintLucia, was admitted, and Spain was given theformal status of observer.
The officers elected were: Dr. RoquelinoRecinos Méndez (Guatemala), president; Drs.
*Argentina, Bahamas, Barbados, Bolivia, Brazil, Can-ada, Chile, Colombia, Costa Rica, Cuba, Dominican Re-public, Ecuador, El Salvador, Grenada, Guatemala,Guyana, Haiti, Honduras, Jamaica, Mexico, Nicaragua,Panama, Paraguay, Peru, Saint Lucia, Suriname, Trini-dad and Tobago, United States, Uruguay, and Vene-zuela.

4 REPORT OF THE DIRECTOR
The 1980 Directing Council. Seated ondais are Dr. Héctor R. Acuñia, Director
.and secretar/ ex officio; Dr. RoquelinoRecinos Méndez (Guatemala), President;Dr. S. Paul Ehrlich, Ir., Deputy Director;Mr. Donald E. Miller (Jamaica), Rap-porteur; and Mr. Michel Careau (Canada)Chairman, 84th Executive Committee.(1'hoto: R. Molina/PAHO)
Jorge Michelsen (Colombia) and RodolfoGirón Flores (El Salvador), vice presidents;and Mr. Donald E. Miller (Jamaica), rap-porteur. Dr. Héctor R. Acuña, Director ofthe Pan American Sanitary Bureau, served assecretary ex officio.
Argentina, Jamaica, and Nicaragua wereelected to serve on the Executive Committee,replacing Brazil, Canada, and Venezuela.
The Director opened the meeting with anaddress that set the stage for the deliberationsthat followed over the next 10 days. Inpresenting his annual report for 1979, hepointed to the dominant theme of health forall by the year 2000. He went on to state thatPAHO is working in collaboration with thegovernments to assess progress made towardfulfilling the objectives of the Ten-YearHealth Plan for the Americas. The resultinginformation is to serve as a basis for planningand carrying out health care programs overthe next two decades.
The Council extensively consideredregional strategies for attaining universalhealth in the Americas by the end of the cen-tury. The discussion focused on the adapta-tion of primary health care to the special and
widely differing needs of the American na-tions. Emphasis was placed on extendinghealth service coverage, environmental im-provement, community organization andparticipation, better mechanisms for intersec-toral linkage, development of research andappropriate technologies, manpower devel-opment, establishment of national systemsfor financing the health sector, and reorienta-tion of international cooperation. As a resultof these discussions, the Director was askedto prepare an action plan for the Americasencompassing all the strategies agreed on.The plan will include technical and ad-ministrative support measures, means foridentifying and mobilizing resources, researchpromotion, development of appropriatetechnologies, and information exchange, andit will provide for further intra- and intersec-toral coordination as well as an overallsystem for monitoring and evaluation.
The "Study of WHO's Structures in Light ofits Functions" addressed the issues ofmultidisciplinary and intersectoral planningand programming, technical cooperationamong developing countries, and interactionbetween the countries and PAHO. Discussion

GENERAL DIRECTION OF THE ORGANIZATION 5
of this study led to the adoption of measuresto improve the flow of resources for priorityprograms, synchronization of planning cy-cles, strengthening PAHO's contribution to thereview process of WHO's World HealthAssembly and Executive Board, and expan-sion of the role and responsibilities of countryrepresentatives (CD27.10).
During the year multidisciplinary teams ofinternational experts evaluated five PanAmerican Centers-the Pan American Foot-and-Mouth Disease and Zoonosis Centers,Caribbean Food and Nutrition Institute, In-stitute of Nutrition of Central America andPanama, and Caribbean Epidemiology Cen-tre. The Centers and the evaluations of themwere the subject of detailed discussion. TheDirecting Council approved resolutions call-ing for consolidation of their programs on thebasis of country priorities and, in general, in-creased shifting of responsibility for theCenters to the countries, with PAHO actingprimarily as the Centers' coordinator andmanager (CD27.18, .26, .27, .29).
Consideration of the role of women indevelopment resulted in a resolution stressingequality of the sexes in education, the specialneeds of disabled women, monitoring prog-ress in the United Nations' World Plan of Ac-tion for women, and the advancement ofwomen in decision-making positions in thehealth sector, both generally and withinPAHO (CD27.17).
The Director was commended on thespeedy execution of PAHO's program to con-trol diarrheal diseases, and the Councilrecommended that the program continue tobe emphasized as an essential component ofprimary health care (CD27.9).
Recognizing the deteriorating malaria situ-ation in the Americas, PAHO has drawn up aplan for the disease's ultimate eradication.The Council urged the governments to pressforward with several antimalaria measures,among them coordinated control in borderareas, training for program personnel, and in-tegration of malaria operations into primary
health care systems (CD27.13).
The Council took note of the progressmade in carrying out the Expanded Programon Immunization (EPI), which PAHO launchedin 1977 in order to reduce child morbidity andmortality from communicable diseases in-cluded in the program, foster self-reliance inproviding immunization services, and buildup facilities for vaccine production and qual-ity control. Consideration was given to waysto increase PAHO's vaccine purchase revolv-ing fund and to vaccine quality control,training, and cold-chain maintenance(CD27.15).
The Council recognized the increasing im-pact of noncommunicable diseases on mor-bidity and mortality, with an attendant rise indemand for related care, and pointed to theaging trend in the population. Its resolutioncalled on the governments to include mea-sures within their programs and strategies toprevent chronic. noncommunicable diseases.
A Jamaican technician uses a simpledevice for diagnosing nutritional anemiadeveloped by PAHO's Caribbean Food
and Nutrition Institute at Kingston.
(P rle - -vi RAr ---- e/p H
6 REPORT OF THE DIRECTOR
Particular mention was made of hyperten-sion, rheumatic fever and rheumatic heartdisease, diabetes mellitus, and cervicalcancer, for which effective control methodsexist (CD27.16).
Several of the countries cited the benefitsto be gained through technical cooperationamong developing countries, and the Counciladopted a resolution stressing that program'svalue in making the countries "nationally andcollectively self-reliant" (CD27.14).
Fully cognizant of the important roleplayed by nurses in providing primary healthcare, the Council recommended that they begiven broader responsibilities in treating com-mon diseases, health planning and adminis-tration, and basic decision making. It alsocalled for upgraded training for nurses andnursing auxiliaries to include instruction insuch subjects as epidemiology, the socialsciences, community health, primary care,and evaluation and research methods(CD27.19).
Among other subjects the Council dealtwith, drug abuse was recognized to be an in-creasingly serious problem, and the govern-ments were urged to incorporate programsfor its prevention in their health systems(CD27.41). Because of the hemisphere's vulner-ability to so many kinds of catastrophe,disaster relief was of special interest, and theCouncil noted PAHO's efforts to build up anemergency preparedness system locally, na-tionally, and regionally (CD27.40). The Coun-cil also noted progress made under themedium-term human resources developmentprogram (CD27.22).
For the first time, owing to the changeoverfrom annual to biennial budgeting, PAHO'sbudget was not on the agenda. There wasdebate, however, about the collection ofquota contributions and other financial mat-ters. The Council commended the Directoron PAHO's sound financial. position (CD27.25).
The Council's two-day technical discus-sions dealt with "Community Health Educa-tion: Evaluation of Present Programs, NewApproaches, and Strategies." The resolution
based on the discussions (CD27.34) urged thegovernments to promote community healtheducation more vigorously, provide for com-munity participation in national health plansand in developing primary health care techni-ques, include community education in allhealth care training, apply operations re-search techniques to this important field,prepare guidelines for educational activities,and exchange information on the subject."Managerial Analysis of Health Systems" wasthe topic chosen for the 1982 technicaldiscussions.
Executive Committee
The 84th Meeting of the Executive Com-mittee, held at Washington from 23 to 27June, was attended by representatives ofBrazil, Canada, Chile, Guatemala, Guyana,Mexico, Peru, United States, and Venezuela,with observers from Colombia, Cuba, Nic-aragua, and Trinidad and Tobago. The of-ficers were Mr. Michel Careau (Canada),chairman; Dr. Carlos Luis de Paredes Soley(Guatemala), vice-chairman; Dr. Luis DavidMarcial (Mexico), rapporteur; and Dr.Héctor Rodríguez (Chile), rapporteur protempore. Dr. Héctor R. Acuña served assecretary ex officio.
The 24 resolutions adopted over the fivedays of deliberation reflected the Commit-tee's interest in a wide range of subjects. Ofspecial interest was the formulation of re-gional strategies for attaining health for all bythe year 2000.
Progress in several programs was reviewed.The Committee's proposals and recommen-dations were reflected in the decisions madeby the Directing Council, as noted above. Inparticular, the following activities were stud-ied: the diarrheal disease control program,whose fast pace was noted; the hemisphericmalaria control program against a disease thathas recrudesced and demands total eradica-tion; the noncommunicable disease controlprogram, which deals with conditions that
GENERAL DIRECTION OF THE ORGANIZATION 7
f'nlOtO i.. IVlolina/'AHO)
The 84th Meeting of the ExecutiveCommittee. Dr. Héctor R. Acuña,
Director, left, and Mr. Michel Careau(Canada), Chairman, sign the Final
Report.
are causing major changes in American mor-bidity and mortality and proposes measuresfor combating them; and the Expanded Pro-gram on Immunization, whose strategieswere endorsed and for which additionalfinancing was proposed. Evaluations of thePan American Centers were also reviewed.
The Committee called on the governmentsto formulate programs to meet the healthneeds of adolescents and youth. In addition,it examined the abuse of narcotic andpsychotropic substances, to be included onthe agenda of the Directing Council, andmalnutrition and nutrient deficiency-inducedmental retardation.
Specific consideration was given to meansof strengthening WHO's regional structuresand functions. The Committee recommendedthe subject to the Directing Council for fulldebate, asking that it consider ways of linking
regional strategies to efforts to strengthenWHO's structures and, in general, that it con-template actions that will help further thedecisions and policies of the World HealthAssembly. The Committee entrusted prepa-ration of a full study of the matter to a work-ing group.
The provisional draft of WHO's 1982-83biennial program budget for the Americaswas reviewed and forwarded to the DirectingCouncil with the recommendation that it beapproved.
Note was taken of the decision to grant the1980 PAHO Award for Administration to Dr.Jair de Oliveira Soares of Brazil.
The 85th Meeting of the Executive Com-mittee, held in Washington on 3 October,was attended by representatives of Argen-tina, Chile, Guatemala, Guyana, Jamaica,Mexico, Nicaragua, Peru, and the UnitedStates, as well as observers from Brazil,Cuba, and the Dominican Republic. The of-ficers were Dr. Ramón Alvarez Gutiérrez(Mexico), chairman; Dr. Augusto SchusterCortés (Chile), vice-chairman; and Dr. OscarH. Gonzáles Carrizo (Argentina), rapporteur.Dr. Héctor R. Acuña was secretary ex officio.
The Committee took note of the resolu-tions approved by the xxvII Meeting of theDirecting Council and commented on pointsto be discussed in its future debates. Jamaicaand Nicaragua were designated a subcommit-tee to examine the World Plan of Action forwomen. Argentina was elected to replaceBrazil on the PAHO Award for Administrationcommittee. Jamaica was designated to replaceVenezuela on the Standing Subcommittee onInter-American Nongovernmental Organiza-tions. Mexico took Canada's place on theSubcommittee on Long-Term Planning andProgramming.
In a resolution on buildings and installa-tions, a working group of the representativesof Chile, Jamaica, and the United States wascreated to study and make recommendationson the Governor Shepherd building, theheadquarters annex in Washington.
8 REPORT OF THE DIRECTOR
American RegionProgramming and Evaluation
System (AMPES)
This system has been designed for pro-gramming, monitoring, and evaluatingPAHO's technical cooperation as requested byits member governments. AMPES is an instru-ment of PAHO as a whole, with methods thatallow an objective dialogue with the coun-tries in specifying their health goals togetherwith the allocation of PAHO resources whichcontribute to achieving those goals. It is alsoa uniform procedure for describing PAHO'sresources and its regional programs as derivedfrom resolutions of its governing bodies.
The system, which in 1980 began its thirdyear of operation, underwent a variety of im-provements in both methods and structure.A complete draft reference manual wasprepared and is expected to be distributed in1981. The manual modified most documentformats, simplified the preparation of materi-als, and introduced medium-term program-ming to coincide with PAHO's two-yearbudget cycle.
An Operations Manager's data unit wasfully established for data entry, maintenance,and selected retrieval using PAHO's digitalcomputer and word-processing equipment.Internal controls and work flow procedureswere initiated to facilitate accurate logging,data entry, verification, and retrieval, anddistribution of all AMPES documents andreports.
Long-Term Planning
A long-term planning office was estab-lished in January. Reporting to the Directorand acting under his immediate supervision,it is responsible for coordinating and par-ticipating in strategic and operational analy-ses and preparing proposals to the Director
about various long-term PAHO activities. Itsprincipal functions are to:
. Analyze the implications for the governmentsand PAHO of global, regional, and nationalpolicies, situations, and trends with respect to thedevelopment of strategies and their plans of actionfor attaining the goal of health for all by the year2000.
* Study and propose new analytic methods andpossible solutions to problems that affect or in themedium or long term may affect PAHO's policiesor strategies for cooperating with the countries inachieving those purposes.
* Coordinate monitoring and evaluation ofregional strategies and plans of action to achieveuniversal health.
* Program, organize, and supervise, in accor-dance with the Director's instructions, the work ofsuch internal or external interdisciplinary groupsas may be created to perform such studies andanalyses.
During 1980 the office focused on cooper-ating in the evaluation of the Ten-YearHealth Plan for the Americas and assisting thegovernments and PAHO in formulating re-gional strategies for achieving health for all,designing a method for developing the rele-vant action plan, preparing PAHO's contribu-tion to the document being drafted by theUnited Nations Economic Commission forLatin America on economic and socialdevelopment strategies for that area in the1980s, and aiding the Inter-American Devel-opment Bank in drawing up the health sectorchapter of its study of its role in thehemisphere during the same decade.
Management
A number of significant changes occurredin PAHO's management during the year. Someof the highlights were:
* Execution of recommendations by the ad-visory committee of international banking expertson shifting certain local currency assets into highinterest accounts and establishing local currencyconversion plans for minimizing losses due tomonetary fluctuation.
(Photos: S. Siefken/pAHO)
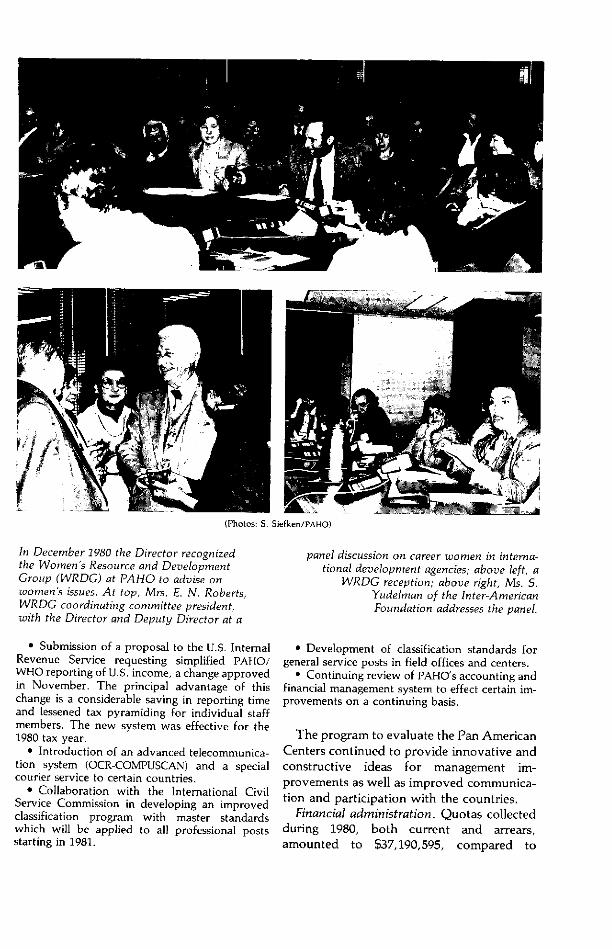
In December 1980 the Director recognized panel discussion on career womnen in interna-the Womnen's Resource and Development tional development agencies; above left, aGroup (WRDG) at PAHO to advise on WRDG reception; above right, Ms. S.women's issues. At top, Mrs. E. N. Roberts, Yudelman of the Inter-AmericanWRDG coordinating committee president, Foundation addresses the panel.with the Director and Deputy Director at a
* Submission of a proposal to the U.S. InternalRevenue Service requesting simplified PAHO/WHO reporting of U.S. income, a change approvedin November. The principal advantage of thischange is a considerable saving in reporting timeand lessened tax pyramiding for individual staffmembers. The new system was effective for the1980 tax year.
* Introduction of an advanced telecommunica-tion system (OCR-COMPUSCAN) and a specialcourier service to certain countries.
* Collaboration with the International CivilService Commission in developing an improvedclassification program with master standardswhich will be applied to all professional postsstarting in 1981.
* Development of classification standards forgeneral service posts in field offices and centers.
* Continuing review of PAHO's accounting andfinancial management system to effect certain im-provements on a continuing basis.
The program to evaluate the Pan AmericanCenters continued to provide innovative andconstructive ideas for management im-provements as well as improved communica-tion and participation with the countries.
Financial administration. Quotas collectedduring 1980, both current and arrears,amounted to $37,190,595, compared to
10 REPORT OF THE DIRECTOR
$33,828,098 for 1979. Though the totalamount collected exceeded that of theprevious year, the ratios of collections toamounts due on January 1 of each yeardecreased slightly.
Total miscellaneous income, mostly frominterest on investments, amounted to$1,533,508, compared to $1,415,485 for theprevious year-an increase of approximately8.34 percent. Expenditures from trust fundscontinued to increase, from $7,897,102 in1979 to $9,406,581.
Personnel. At the end of 1980, PAHO's staffnumbered 1,337 (including 60 temporary em-ployees), as compared with 1,317 (including36 temporary employees) a year earlier. Ofthe 1,277 regular staff, 459 were assigned toheadquarters, 90 to area and field offices, 490to intercountry projects, and 238 to countryprojects.
In accordance with 1980 Directing Councilrecommendations (CD27.17), renewed effortswere made to increase the proportion ofwomen on the staff and enhance their status.Among these measures were urging thegovernments to nominate more women forprofessional positions in PAHO and establish-ing hemispherewide contact with professionalwomen's organizations and universities toenlist their cooperation in advertising vacan-cies. Plans are underway to expand the use ofa computerized roster of applicants to ensureidentification of all possible candidates foreach vacant post. As far as possible, ar-rangements will be made to have womenrepresented in selection committee proceed-ings.
Conference services. The conference ser-vices supported 229 PAHO, subregional, ornational meetings in Washington or else-where. A total of 436 man-days of transla-tion, editing, and précis-writing and 635 man-days of interpretation were needed to servicethese meetings. Through staff or contractorsthe language services unit translated a total of14,566 pages in four working languages(Spanish, 60.5 percent; English, 30.4 percent;
Portuguese, 8.6 percent, and French, 0.5percent).
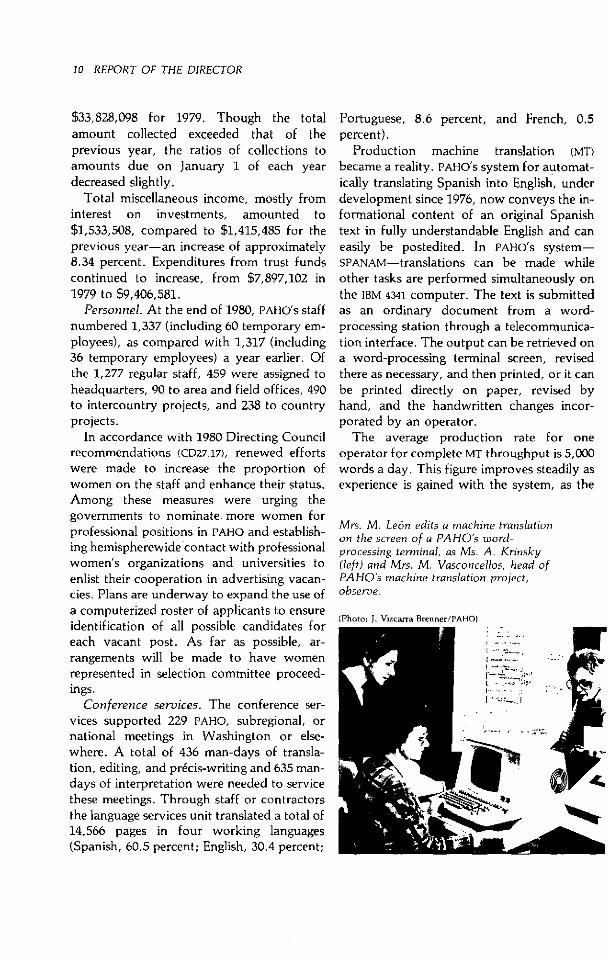
Production machine translation (MT)became a reality. PAHO's system for automat-ically translating Spanish into English, underdevelopment since 1976, now conveys the in-formational content of an original Spanishtext in fully understandable English and caneasily be postedited. In PAHO's system-SPANAM- translations can be made whileother tasks are performed simultaneously onthe IBM 4341 computer. The text is submittedas an ordinary document from a word-processing station through a telecommunica-tion interface. The output can be retrieved ona word-processing terminal screen, revisedthere as necessary, and then printed, or it canbe printed directly on paper, revised byhand, and the handwritten changes incor-porated by an operator.
The average production rate for oneoperator for complete MT throughput is 5,000words a day. This figure improves steadily asexperience is gained with the system, as the
Mrs. M. León edits a machine translationon the screen of a PAHO's word-processing terminal, as Ms. A. Krinsky(left) and Mrs. M. Vasconcellos, head ofPAHO's machine translation project,observe.
(Photo: J. Vizcarra Brenner/PAHO)

GENERAL DIRECTION OF THE ORGANIZATION 11
MT dictionary is enlarged, and as continuedenhancements are made in the basic software.
Management and computer services. Con-tinued emnphasis was placed on reviewingPAHO activities at headquarters and in thefield to ensure that efficient managementsystems are established and practiced andthat management information systems alloweffective information flow. To achieve this,management studies and surveys were con-ducted, new technologies evaluated, and,when feasible, advanced microprocessorsystems installed.
As a result of studies completed during theyear, field activities were improved throughcontinued decentralization. Examples werean increase in local purchase ceilings, in-service training sessions for staff, installationof a pilot Country Representative ad-ministrative filing system in Trinidad andTobago, and the complete revision of thePAHO/WHO field operations manual.
Technologic advances included the in-stallation of microfiche equipment to savespace and retrieval time, the introduction ofoptical character-recognition equipment tospeed and simplify the dissemination of telexcommunications to the field, linking head-quarters word-processing and computersystems, and the introduction of a data basecapability in the computer system.
PAHO also continued its advice to healthministries on developing their computerizedinformation systems.
Health information and documentation.The health information and documentationcenter at headquarters concentrated mainlyon providing basic information and scientificsupport to PAHO's technical divisions. Re-quests for bibliographic searches continued tobe processed through MEDLINE/ELHILL III andDIALOG computer terminals. A total of 1,005bibliographies were compiled, three-quartersof them for field staff. More than 10,000photocopies of articles in scientific journalswere supplied at the request of various of-ficers. By the end of the year the number of
technical or scientific documents prepared byWHO, PAHO, other regional offices, and thegovernments stored in the PAHO documenta-tion system (PAHODOC) data bank totaledmore than 11,000.
Relations with OtherOrganizations
PAHO maintains close working relationswith a variety of other United Nations,hemispheric, subregional, and private orga-nizations in carrying out its many missions.Many, such as international lending agencies,are not directly involved in health mattersand use PAHO to manage programs in whichthey invest; others are interested in special-ized areas of health and channel fundsthrough PAHO in their fields of concern.
This section covers only the highlights ofPAHO's relations with other organizations.Because of their specific nature, most suchrelationships are described in the later pro-gram chapters of this report.
The United Nations held its second high-level meeting to review technical cooperationamong developing countries (TCDC) in Ge-neva in late May and early June. PAHOprepared and submitted to the meeting aprogress report on TCDC in health as WHO'sglobal focal point for TCDC activities.
Since extrabudgetary funding is becomingever more important to PAHO's programs,senior PAHO staff and their counterparts fromthe Inter-American Development Bank (IDB)and United Nations Development Program(UNDP) met in Washington and New Yorkduring the year. The meetings with IDB al-lowed the two organizations to develop astrategy for complementary action in techni-cal cooperation programs in the Americas.The meetings with UNDP were to review pro-posals for four regional programs preparedby PAHO to be included in UNDP's 1982-86work cycle.

12 REPORT OF THE DIRECTOR
PAHO and the international cooperationsystem
United Nations Childrens Fund (UNICEF).
PAHO and UNICEF continued 20 years of jointactivities by holding a workshop to discussfurther collaboration in developing drinkingwater supply and basic sanitation programsfor dispersed rural inhabitants. In addition,the two organizations worked with a WorldBank-sponsored project in Paraguay to ex-pand coverage of its village water program.
United Nations Development Program(UNDP). UNDP continued to finance manyprojects-particularly in environmental con-trol and community health and veterinarypublic health training-in which PAHO acts.as its executing agency.
PAHO assisted in designing and organizingthree subregional and eight country projectsto be funded by UNDP which are to begin in1981 and in which PAHO will act as executingagency. The main content of these projects ismanagement development in health servicesand defining the development and mainte-nance of their physical infrastructure. Indesigning them, PAHO emphasized the con-cepts of mutual support and technical coop-eration among developing countries.
United Nations Disaster Relief Office(UNDRO). During 1980 the Caribbean sufferedthe ravages of one of the most devastatinghurricanes of the century. PAHO and UNDROworked together to help Barbados, Haiti, andJamaica carry out relief and rehabilitationoperations.
United Nations Economic Commission forLatin America (ECLA). Joint PAHO/ECLA ac-tivities have expanded as a result of the Inter-national Drinking Water Supply and Sanita-tion Decade. PAHO cooperated with ECLA inpreparing a document on Latin Americanfinancial requirements for achieving WaterDecade goals. It also took part in planning aLatin American seminar, to be held in early1981, on horizontal Water Decade coopera-tion in identifying and defining approaches,mechanisms, and proposals for activities in
the water and sanitation sector.PAHO participated in a meeting early in the
year to draft the action plan for a jointUNEP/ECLA project for environmental man-agement in the wider Caribbean at whichstaff presented an overview of environmentalhealth in the area.
United Nations Environment Program(UNEP). PAHO and UNEP continued to col-laborate in planning and executing regionalactivities related to the human environment,as set out in their memorandum of under-standing signed in 1977 and due to be re-viewed in 1981. UNEP served as the focus ofcooperation among more than 20 interna-tional and inter-American organizations andin that role sponsored two workshops. Thefirst was on environmental training andresulted in plans to prepare an inventory oftraining activities and programs. The seconddealt with environmental informationsystems.
United Nations Food and AgricultureOrganization (FAO). PAHO increased its col-laboration with the Joint FAO/WHO CodexAlimentarius Commission and JointFAO/WHO Food and Animal Feed Contamina-tion Monitoring Program. The senior officerof FAO's food science, control and consumerprotection group visited Washington to pro-mote greater cooperation between FAO andPAHO in food protection activities of mutualinterest.
United Nations Fund for Population Ac-tivities (UNFPA). PAHO officials held an impor-tant meeting in Washington with seniorUNFPA policy and technical staff to conduct adetailed review of the two organizations'joint policies and operations, inasmuch asPAHO is the executing agency for variousUNFPA-funded projects in the hemisphere.
European Economic Community (EEC).Contact was established with EEC to discussits interest in financing a multidisciplinaryproject under which PAHO would assistBolivia, Colombia, Ecuador, and Peru indevising comprehensive development and in-tegration of selected primary health care

GENERAL DIRECTION OF THE ORGANIZATION 13
projects.League of Red Cross Societies. The League
aided several of PAHO's disaster managementand relief projects.
World Bank. The World Bank and PAHOworked closely in the health field, exchanginginformation and reports and holding con-sultative meetings. Much of the Bank's in-terest was in preparatory studies for the Inter-national Drinking Water Supply and Sanita-tion Decade which PAHO helped carry out.
World Food Program (WFP). Close relationscontinued between PAHO and this United Na-tions affiliate, which has food distributionprojects in several countries of the Americas.
PAHO and the inter-American system
Organization of American States (OA5).The tenth regular session of the OAS GeneralAssembly, at which PAHO was represented,was held at Washington in November. PAHOrepresentatives took part in the ad hoc coun-try review meeting of the Permanent Com-mission of the Inter-American Economic andSocial Council on Paraguay and Guatemalain April and June, respectively, and attendedthe Inter-American Economic and SocialCouncil meeting at Washington in October.
PAHO staff participated in an OAS-sponsored June meeting of representatives ofthe small island territories of the Caribbean atSan Juan, Puerto Rico, to review major oil-spill risks and identify cooperative needs andoil-spill control technologies. Staff likewisetook part in a followup meeting of represen-tatives from throughout the wider Caribbeanin Barbados in November to draw up an oil-spill contingency plan for the islands and con-sider means for putting it into effect.
Inter-American Development Bank (IDB).IDB is the international financial agency sup-plying the largest share of funding for healthinfrastructure development projects in theAmericas. Each loan is normally accom-panied by a technical cooperation compo-nent to assist the country in making the im-provements in technical and administrative
systems required for developing health ser-vices. PAHO generally assumes responsibilityfor technical cooperation in projects of thistype at the request of the country concernedand with IDB's approval.
PAHO continued to serve as executingagency for technical cooperation projectsfinanced by IDB, particularly institutionaldevelopment programs associated with loansfor developing health services, as well asstudies to determine the feasibility of projectsfor investment in health. During 1980, workunder such projects continued in seven coun-tries, four new projects were initiated, andfive additional cooperation projects to beginin 1981 were approved and the relevantagreements signed.
To plan future cooperative activities, PAHOenvironmental health staff participated in ajoint PAHO/IDB working session during whichthey briefed IDB officials on future healthneeds in the water and sanitation sector. Anexpansion began of the IDB-sponsored watersupply and sewerage agency operation andmaintenance project at PAHO's Pan AmericanCenter for Sanitary Engineering and En-vironmental Sciences at Lima.
IDB continued to play an important role infoot-and-mouth disease control programs inLatin America in which PAHO acts as ex-ecuting agency.
Inter-American Institute for Cooperationon Agriculture. PAHO cooperated with thisorganization in an advanced training coursefor Caribbean veterinarians in Guyana.
Subregional groups
Conference of Ministers Responsible forHealth in the Caribbean. The sixth meeting ofCommonwealth Caribbean health ministerswas held in Grenada in mid-July. PAHO wasrepresented and a senior staff member gavean address. The areas discussed in whichPAHO's technical cooperation was requestedwere food safety, control of sexually trans-mitted diseases, cancer, smoking, medical
14 REPORT OF THE DIRECTOR
education, and continuing education inhealth care.
Caribbean Community (CARICOM). A jointmeeting between PAHO and Caribbean Com-munity secretariat staff was held in Grenadain mid-July. The main items discussed werefunding for a subregional primary health careworkshop in 1981, food safety, health infor-mation systems, and disaster preparedness.
Caribbean Development Bank (CDB). CDBagreed to finance two joint activities, a leakdetection survey in connection with theCaribbean basin water management projectand a seminar on water supply projectpreparation and financing. CDB and PAHOjointly funded a seminar for 18 managers andsenior engineers of Caribbean water utilitieswhich provided technical information on im-proving project preparation and helpedfamiliarize the participants with the policiesand procedures of lending institutions.
CDB cooperated with PAHO in carrying outwater supply and sanitation sector studies inAntigua, British Virgin Islands, Grenada, andSt. Vincent.
Ministers of Health of the Andean PactCountries. The Director General of WHO andthe Director of PAHO attended the seventhmeeting of the Andean health ministers atQuito in June. The main health topics withimplications for PAHO were the training anduse of family medical practitioners, themanufacture of pharmaceutical and biologi-cal products, the production of oral rehydra-tion salts, a basic environmental plan for theAndean subregion, and technical cooperationin health care and food and nutrition amongthe Andean countries.
Foreign Ministers of River Plate BasinCountries. The PAHO Area Representative at-tended the annual meeting of the foreignministers of the River Plate countries atBuenos Aires in December. Five areas of in-terest to PAHO were reviewed: schistosomiasiscontrol, Aedes aegypti surveillance pro-grams, foot-and-mouth disease campaigncoordination, food and nutrition programs,and training of nutrition professionals.
Ministers of Health of Central America andPanama. The Director addressed the simulta-neous meetings of health ministers and direc-tors general of health of Central America andPanama at their meetings in Tegucigalpa inAugust. The meetings' subjects of major in-terest to PAHO were communicable diseasecontrol, extension of health care coverage,control of sexually transmitted diseases,analysis of community health problems, ur-ban and periurban health problems, andhealth care standards.
Bilateral agencies
Canadian International DevelopmentAgency (CIDA). CIDA, PAHO, and 10 Carib-bean countries signed a memorandum ofunderstanding to extend the Caribbean basinwater management project through the endof 1981, with a CIDA contribution of Cana-dian $370,000. CIDA has also been supportinga PAHO-managed continuing health careeducation project in Bolivia, Colombia,Cuba, Dominican Republic, Ecuador,Guatemala, and Honduras since 1978 andveterinary assistant training for the Carib-bean at Georgetown.
Canadian International DevelopmentResearch Centre (IDRC). IDRC agreed to con-tinue support to the Pan American Networkfor Information and Documentation onSanitary Engineering and EnvironmentalSciences (REPIDISCA) at Lima. Having sup-ported the network's first phase, in whichsystem tools were designed to improve ac-cessibility of information on sanitary engi-neering and the environment, IDRC signed anagreement for a two-year operational phasegrant to test the design, improve user accessto information, and exchange that informa-tion among participating institutions.
The Canadian agency also expressed in-terest in following up a previous IDRC-fundedresearch project to evaluate the engineeringefficiency of the San Juan stabilization pondsnear Lima where wastewater treatment andreuse are being tested. The prospects are

GENERAL DIRECTION OF THE ORGANIZATION 15
good for ever greater use of reclaimed waterin agriculture and fish culture. The proposednew project would determine implied poten-tial health hazards by quantifying thepresence of toxic compounds and pathogenicbacteria and carrying out related sociologicand epidemiologic studies.
German Technical Cooperation Agency(GTZ). The second phase of the FederalRepublic of Germany's International WaterSupply and Sanitation Decade national plan-ning project began. The 10 participatingcountries throughout the world include threein the Americas-Bolivia, Haiti, andParaguay. GTZ provided $300,000 to covercosts of PAHO technical assistance in the threecountries, which includes specialized con-sultants, planning workshops, and certain ad-ministrative support costs. The general aimsof the project are to promote and advise onplanning for extending water supply andsanitation services to underserved com-munities, encourage faster development ofthe sector, and increase the flow of externalresources to it.
U.S. Agency for Internaticnal Develop-ment (USAID). Numerous meetings,workshops, and seminars were held to helpcoordinate and expand the technical coopera-tion services of PAHO and USAID to the coun-tries. During the disaster relief efforts follow-ing Hurricane Allen in the Caribbean, PAHOand USAID collaborated to ensure coordina-tion in bilateral actions and those of theUnited Nations agencies.
U.S. Centers for Disease Control (CDC).This major component of the U.S. PublicHealth Service collaborated with PAHO inseveral laboratory development projects andas a biologicals reference center.
U.S. National Institutes of Health (NIH).NIH, the foremrnost biomedical research centerin the United States, cooperated extensivelywith PAHO in several investigative programs.An agreement with NIH enabled PAHO to con-
tinue its cooperation with Brazil, Colombia,and Peru in their primatology programs. Aworkshop on managing and breeding simiansin their native habitats was held at Iquitos,Peru, under NIH auspices.
Foundations
Pan American Health and Education Foun-dation (PAHEF). A continuing PAHO col-
laborator, PAHEF supported 36 PAHO-
administered projects. In addition to trustfunds carried forward from 1979, PAHEFreceived $940,000 from 19 public organiza-tions, private foundations, corporations, andindividuals for use in Latin American healthendeavors. Major donors or grantors in-cluded the W. K. Kellogg Foundation, IBM,United Kingdom overseas developmentministry, and various pharmaceutical com-panies. The projects supported are mainly ineducation (dental, medical, nursing, andnutrition) and disease control (cardiovasculardisease, leprosy, and leptospirosis).
The PAHO/PAHEF textbook and instruc-tional materials program, financed by IDBloans to PAHEF, continued its expansion frommedicine and nursing into other health fieldsas well as into materials for technicians andcommunity health care workers.
W. K. Kellogg Foundation. Relations be-tween the W. K. Kellogg Foundation andPAHO continued and close contacts weremaintained. Execution of the two main jointprograms-coordination and support ofhealth care administration education in LatinAmerica and the Caribbean, and the regionalprogram of perinatal and maternal and childcare with emphasis on primary healthcare-advanced satisfactorily. A jointmeeting between representatives of the Foun-dation and PAHO was held in October at Bat-tle Creek, Michigan, where current programswere examined and ways to improve coor-dination considered..
%a ppf D
1~~~~~
* -~~~~~~
e:*
Chapter 2
HEALTH SERVICE SYSTEMS
PAHO's collaboration with the countries indeveloping health services focuses on theprimary health care strategy for doing so.Given its components and the variety ofways in which the countries are carrying itout, PAHO has grouped its activities in healthservice development into three major areas.These are:
Development of health services. Particularattention is being given to defining the prior-ity components of primary care. Special em-phasis is placed on identifying the needs ofunserved groups, applying techniques to in-clude intersectoral linkages and communityparticipation in primary care programming,developing appropriate technology for ad-ministering and delivering services, and up-dating health worker training. PAHO alsoseeks to organize health care levels to meetthe requirements of primary care and to im-prove the quantity, quality, and accessibilityto care levels of greater complexity.
Technology in health and service to specialgroups. This category includes promotionand development of such areas as nutrition,family health, and health education. It alsoinvolves new fields of cooperation such aspromoting the participation of women ineconomic and social development, care of theelderly, and development of appropriatehealth care technologies.
Development of health systems. Because ofthe need to expand the capacity of healthsystems and make systematic evaluations oftheir use, impact, and efficiency, PAHO also
supports health planning and the develop-ment of methods for programming intersec-toral activities to regionalize health caresystems and expand installed capacity, andpromotes administrative development andstrengthened national health informationsystems.
Medical Care Systems
The hemisphere's medical care systems-despite significant recent changes-still re-quire substantial reform and reorientation toadjust their organization and operating pro-cedures to the new and expanded objectivesof health for all.
The changes required are of many kinds.Essentially, the contents of service programsneed to be revised to include primary careand community participation. It is imperativeto reexamine and strengthen their institu-tional structure to achieve equitable accessfor different groups according to their healthcare needs, and rationalize and optimizeresource use, both in planning and develop-ing health facilities and within the facilitiesthemselves in using personnel and technol-ogy. The latter are often expensive and exerta decisive influence on overall costs, which inturn largely determine how much services canbe extended.
17
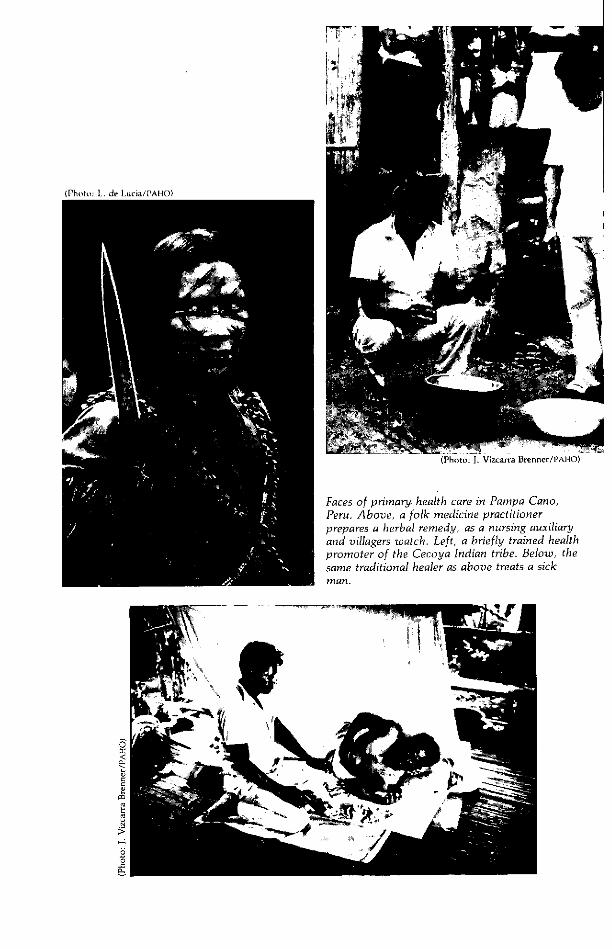
(Photo: J. Vizcarra Brenner/PAHO)
Faces of primarj health care in Pampa Cano,Peru. Above, a folk medicine practitionerprepares a herbal remedy, as a nursing auxiliaryand villagers watch. Left, a briefly trained healthpromoter of the Cecoya Indian tribe. Below, thesame traditional healer as above treats a sickman.
o
r:1
m1
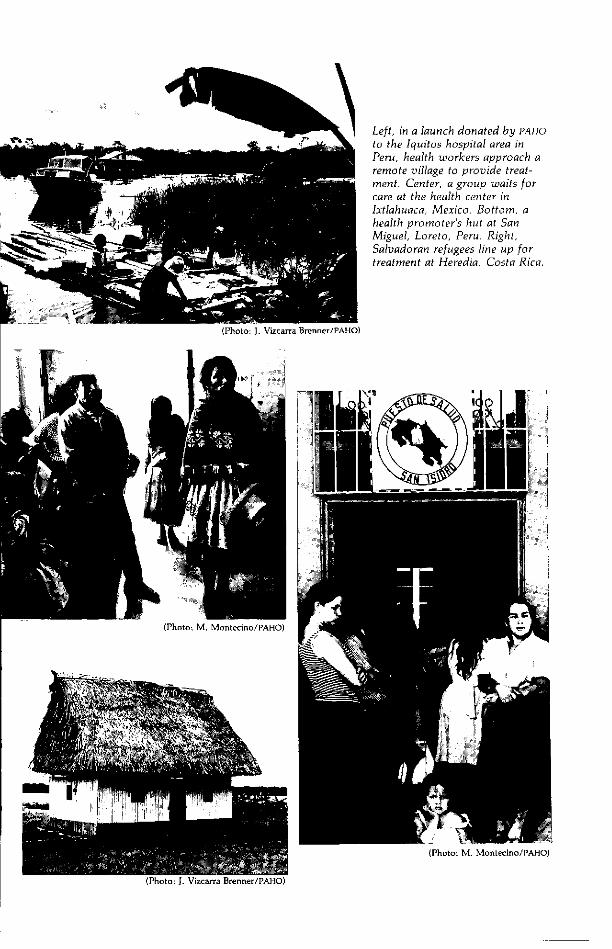
Left, in a launch donated by PAHO
to the Iquitos hospital area inPeru, health workers approach aremote village to provide treat-ment. Center, a group waits forcare at the health center inIxtlahuaca, Mexico. Bottom, ahealth promoter's hut at SanMiguel, Loreto, Peru. Right,Salvadoran refugees line up fortreatment at Heredia, Costa Rica.
aLlUd :j :
~~~~~~~~~~~~~~~~~~~~~~~~~~ 1 4| ' ix
(Photo: M. Montecino/PAHO)
20 REPORT OF THE DIRECTOR
Most of the countries are trying to bringabout these changes. PAHO's technicalcooperation in support of these efforts fallsinto three main areas: (1) optimizing resourceuse in developing health facilities, (2)strengthening coordination between healthministries and social security agencies, in-cluding technical assistance to the latter, and(3) promoting alternative forms of serviceorganization to make them more accessibleand efficient.
Development of health facilities. PAHOassisted the Andean countries in preparingfinal documents for five national serviceorganization and plant management projects.In addition, a subregional interdisciplinaryseminar on health facilities programming, de-velopment, and maintenance was conductedin Venezuela for 72 health officers from 14American countries. These activities werecarried out by a group of experts from the fiveAndean countries. PAHO and the secretariatof the Hipólito Unanue Agreement providedoverall coordination, and the work was car-ried out under the auspices of UNDP, withwhich funding negotiations were initiated.
In the same area, cooperation in teachingand research was initiated with the HealthFacilities Research Center of the University ofBuenos Aires, and further support was pro-vided to the hospital development projects inGuatemala, Guyana, and Trinidad and To-bago. Work to strengthen and develop the in-frastructure of the Ecuadoran social securityinstitute's various health services continued,and assistance was given in formulating andinitially executing a preinaugural plan for theGuayaquil Children's Hospital.
Technical cooperation with social securityagencies. PAHO continued to encourage andstrengthen working relations with nationalsocial security institutions. Highlights in thisfield were its collaboration with Ecuadordescribed above and the initiation of atechnical cooperation agreement with thePeruvian social security institute to review itshealth care programs and recommend im-
provements in the technical and admin-istrative procedures of its operating units.The agreement also calls for assistance indesigning and executing health educationprograms for social security beneficiaries,manpower development and training, partic-ularly at management levels, and dissemina-tion of scientific information for refresher andcontinuing education courses for the in-stitute's technical staff.
PAHO also helped make a comprehensiveanalysis of the Costa Rican social security in-stitute to identify aspects of the organizationand its general service policies that mightneed to be adjusted to the government'sdevelopment and administrative reformpolicies.
PAHO participated in various regionalsocial security meetings. These included aweek-long seminar on the role of socialsecurity in coverage extension programs atLima and the Inter-American Social SecurityConference at Santo Domingo.
General improvement of medical caresystems. In this third area of technicalcooperation, PAHO supported specific proj-ects in various countries to program servicesby ascending levels of care. It advised on thepreparatory work and design of such a proj-ect in Chile and collaborated with Peru'shealth ministry in preparations for nationalseminars at which echeloned care underspecific conditions in various parts of thecountry will be discussed and analyzed.PAHO worked with Uruguay's health ministryin the same field and studied the possibility ofintroducing the concept of levels of care at alarge hospital in Montevideo.
It also continued promoting and support-ing improvements in hospital organizationand operation as part of coverage extensionprograms, ambulatory care schemes, andemergency services, particularly in metropoli-tan areas.
In the hospital field, a compilation oforganizational and operating standards in thedifferent countries was begun. Cooperation

HEALTH SERVICE SYSTEMS 21
was provided to the Bahamas, Costa Rica,Ecuador, El Salvador, Honduras, and Nic-aragua in organizing and programming med-ical records and statistical services in newhospitals. The Dominican Republic andGuyana received assistance in preparing proj-ects to improve their medical and statisticalrecords in order to create national health in-formation systems. In Costa Rica, PAHOcooperated in following up the developmentof the national cancer registry.
The medical care systems of the Americashave undergone significant changes in recentyears.
The first such change has been the increas-ing participation of social security agencies inhealth care. An important development inthis regard was the almost complete initiationof a program of basic health services for 10million farmers in Mexico. This program,undertaken by the federal government andthe Mexican social security institute, is of far-reaching importance because of its nationalimpact and its possible adoption in othercountries. It represents a substantial changein the ways in which social security is funded,and it is designed to provide health care notonly to the working population but also topeople who do not contribute to socialsecurity. This is accomplished through con-tributions by the government to the institute.
This initiative, together with those ofBrazil, Costa Rica, Panama, and other coun-tries that have adopted similar policies, willbe highly influential in speeding universalsocial security coverage and thus the greaterparticipation of social security in health care.
A second change is the integration ofhealth care programs. In several countries,more emphasis is being put on determiningways to achieve more efficient resource usethrough gradual amalgamation of previouslyvertical programs into integrated agencieswhich provide a comprehensive package ofservices. As this trend toward programmaticand operational integration has advanced,the need has become apparent to strengthen
central medical care organizations so as to en-dow them with enough capacity to enablethem to supervise, guide, and evaluate thecomprehensive delivery of services.
A third change is the countries' greaterconcern with finding effective solutions tothe problem of delivering services in urbanareas, particularly in the poor fringes of ma-jor cities. Developments in this area were theinitiation of research on selected metropolitanhealth services at the Health FacilitiesResearch Center in Buenos Aires and a na-tional seminar on this subject at Medellín inwhich an attempt was made to establish tiesbetween health service and general urbanplanning.
Health Planning
Planning health services that are more effi-cient and effective and provide equitablecoverage for all continues to be a fundamen-tal concern.
Most of the countries have explicit policiesand strategies to guide the formulation oftheir health plans and programs. Some haveformulated programs to extend health servicecoverage, others have prepared necessary in-stitutional plans, and still others havedeveloped sectoral plans in which all agenciesproviding health services participate.
Some inconsistency is apparent betweenpolicies and activities to carry them out. Forexample, general development policies com-monly provide for multisectoral projects em-bracing health services, housing, education,agriculture, and other sectors, but health ser-vices often continue to perform their tradi-tional activities in isolation from the othersectors.
The present situation must be replaced byone in which the different parts of the healthinfrastructure (planning, administration, in-formation systems, human resources, invest-ment projects) are considered together in
22 REPORT OF THE DIRECTOR
planning the development of services so thatthey will be properly balanced.
These were some of the events that occur-red in health planning in the Americas duringthe year:
* Argentina's health ministry sponsored an11-week course in health planning and program-ming. It also began applying nationally a unifiedguide containing technical, programming, infor-mation, and administrative standards.
* In Brazil the major development was the for-mulation of the PREVSAUDE draft project for in-vesting more than $3 billion over six years inestablishing 11,000 health posts, 17,000 healthcenters, 10,000 beds, and 3,700 emergency unitsand training 300,000 health workers. PREVSAUDEinvolves all agencies in the country providinghealth services in one way or another.
* Chile's health ministry is now transformingthe entire sectoral structure and developing newways of financing services based on a larger rolefor the private sector and greater userresponsibility.
* In Colombia the national integration plan, in-cluding chapters devoted to the health sector, waspublished in March. The government reachedagreement with WHO on a program, to be fundedby the Netherlands, to develop the plan's primaryhealth care aspects. Numerous health planning ac-tivities are underway in Colombia, including a na-tional health survey which will provide informa-tion of fundamental importance for carrying outand revising the national plan.
* In Dominica a team of PAHO consultantshelped formulate a national health plan.
* Grenada, with assistance from PAHO,established a planning group which prepared aguide for and then began formulating a nationalhealth plan.
* Guatemala, with PAHO assistance, continuedto carry out its 1978-82 health plan and extendedservice coverage, a project being financed by IDB.A project was formulated and a new IDB loannegotiated for building three hospitals at a com-bined cost of $50 million.
* In Honduras, the annual health operationsplan, based on the 1979-83 national plan, was car-ried out. The country's record in coverage exten-sion has been one of systematic advances, such asan increase in yearly consultations per capita from0.2 in 1975 to 1.0 in 1980 and a rise in hospitaldischarges from 2.6 to 7.2 per 100 inhabitants overthe same period. The Netherlands is supportingcoverage extension by providing funds for equip-ment and training.
* In Paraguay, PAHO provided technical adviceand IDB financed planning to carry out coverageextension. The health ministry also programmedhealth services in the area of the Yacyretáhydroelectric dam between Paraguay andArgentina.
* In Peru the health ministry issued an emer-gency health sector plan. Immediately thereafter,participants in a seminar at Paracas on health sec-tor management coordination drew up com-prehensive short-term guidelines for reorganizingthe sector. As a result, a national health plan for1980-85 was prepared in the last quarter. PAHOprovided continuing support to Peru's endeavors.
National HealthInformation Systems
The countries are endeavoring to establishnational health information systems to pro-duce the data required for effective healthcare decision making.
PAHO supports these efforts in accordancewith governing body resolutions (WHA30.46,WHA32.2, WHA32.8, and CD27.20). Its assistanceis based on the need to overcome limitationsin the health statistics infrastructure and theuse of statistics by programming and manage-ment organizations. It aids in strengtheningnational health statistics systems, improvingdata registration and storage, adjusting dataprocessing to the needs and capabilities of thecountries, developing reporting systems pro-viding necessary information for control andevaluation, training, and related matters.
Before 1979 PAHO oriented its statisticaltraining activities toward data producers. Inthat year it reoriented its training towardstatistics users in health ministry manage-ment. Since then, four workshops-inGrenada (in conjunction with CARICOM),Guyana, Jamaica, and Paraguay-have beenconducted for senior health officials.
Argentina received assistance in revisingand preparing teaching materials for the threehealth information courses conducted in thatcountry. In Bolivia, El Salvador, and

HEALTH SERVICE SYSTEMS 23
Area health chiefs meet at the Costa Ricanhealth ministry in San José to discuss uniformstatistical procedures.
IPho--os M Monteino/PAHO)
Nicaragua, PAHO provided instructors for ageneral course on medical records andstatistics. In Chile, it collaborated in a criticalanalysis of the present course and maderecommendations for improving it so it willmeet Chile's needs and those of other LatinAmerican countries. It helped Costa Rica andPeru conduct special refresher courses forpersonnel who had completed regular medi-cal records courses and were called upon toassume responsibilities in meeting the newdemands on the health services. Eleven fel-lows from Cuba, Honduras, Mexico, Nica-ragua, and Panama attended the refreshercourse in Costa Rica. In Venezuela it helpedanalyze three existing intermediate and aux-iliary courses in order to restructure them andplan for a university-level course.
A total of 315 students completed the 1980courses, compared with an average of 258 ayear from 1970 through 1979, an indication ofPAHO's increased emphasis on training.
In redesigning their information systems,certain countries sought to develop modularinformation procedures. Thus, Costa Ricafully integrated information collection for itsrural health, health care for the underservedurban population, and nutrition programsand introduced "balance sheets" to adjustprogramming to their actual needs. Similar
A staff member records a baby's medicalhistory at the Ramón González Coro Mother
and Child Hospital in Havana.
redesign activities were carried out in Chile,Colombia, Dominican Republic, Ecuador,Guyana, Honduras, Jamaica, Nicaragua,Paraguay, and Turks and Caicos.
Regional activities to stimulate the im-provement of basic programs in vital healthstatistics and medical and health records con-tinued in nearly all the countries. In this area,PAHO cooperated with Ecuador and Nicara-gua in developing general guidelines fororganizing medical records and statisticalunits in new hospitals as part of their cover-age extension programs. In the Bahamas,Costa Rica, El Salvador, and Honduras ithelped improve existing services to develop
24 REPORT OF THE DIRECTOR
adequate health information systems. In theDominican Republic and Guyana, it aided indeveloping country projects to improvemedical and health records (includingstatistical records) to design health informa-tion systems. With PAHO's assistance, thematernal and child health departments ofCosta Rica and Panama began to standardizeperinatal clinical history forms.
Management Systems
Achieving health for all by the end of thiscentury calls for further adjustment in PAHO'stechnical cooperation in improving the ad-ministrative efficiency and effectiveness ofhealth services and assuring that their benefitsare distributed more equitably.
PAHO's management advisory activitiesembraced most of the countries through proj-ects financed regularly or extrabudgetarily.Administrative development programs havegradually been integrated as far as possibleinto broader institutional development ef-forts within the context of extending healthservice coverage.
This has been possible primarily in large-scale development programs carried out withexternal financial assistance. In such cases ad-ministrative improvements are generallysought in planning, service regionalization,financial management, supply administra-tion, personnel management, and legislation.PAHO provided technical assistance in contin-uing or starting projects of this type inBolivia, Costa Rica, Dominican Republic,Ecuador, El Salvador, Guatemala, Guyana,Haiti, Nicaragua, and Paraguay. A widerange of activities-from the preparation ofmanuals for standardizing procedures tocomprehensive health system studies-wascarried out in these projects.
PAHO continued to advise on resource ad-ministration, especially in basic health ser-vices. Case studies were made in Ecuador and
Panama of drug supply management athealth posts and centers and communityhospitals. Analyses of financing, accounting,cost control, and budgets were intensified inGuyana and Jamaica.
In Ecuador, Honduras, and Panama, PAHO
provided assistance in designing, equipping,and staffing new hospitals. This was sup-plemented by advice on specific medicalrecords, information systems, financing,maintenance, and nursing problems.
Problems in administering regional servicenetworks, and especially relations betweeninstitutions, took shape as a new field of col-laboration. PAHO began revising its publishedmaterials on referral systems, patient flow,appointment and admission procedures, andmulti-institution administration.
It also collaborated with the Costa Ricansocial security institute in a comprehensiveanalysis to identify that agency's priorityproblems. In Colombia the last touches wereput on a broad administrative developmentproject embracing supply, administration, fi-nance, maintenance, and institutional man-agement with a strong emphasis on training.This project is receiving UNDP financialassistance. Organizational behavior investi-gations were initiated in Chile and Brazil.
Financing Health Services
Financial limitations have traditionallybeen one of the main obstacles to extendinghealth services to meet coverage targets fully.These constraints will become even morecritical during the 1980s and 1990s when allthe countries will have to make extraordinaryefforts to finance capital and operating costs.
Briefly summarized, the financial con-straints the countries face are: an insufficientproportion of gross national product devotedto the public health sector, inadequaterevenue generation within the sector, ine-
HEALTH SERVICE SYSTEMS 25
quitable distribution of funds among healthsubsectors, management problems in op-timizing resource use, inflation, and of courseincreasing demand for services.
The countries are trying to strengthen thehealth sector financially in various ways.Among them are external financing todevelop physical and institutional infrastruc-tures; institutional integration to achieve abetter socioeconomic balance in generating,distributing, and using the sector's financialresources; revision of health plans to speedgrowth and facilitate development projectfinancing; improvements in financial ad-ministration, cost containment, and op-timization of resource use; and advances inintersectoral linkage and community par-ticipation as means of sharing financialresponsibilities, reducing costs, and assuringbetter use of common resources.
PAHO cooperated with the countries in thefollowing areas directly or indirectly dealingwith service financing:
* In nine countries it participated in feasibilitystudies to establish alternatives for physical in-frastructure development projects and facilitatetheir external financing.
* In four countries it initiated or continued itsassistance in improving the financial administra-tion of health services, with emphasis onbudgetary programming techniques, and indesigning ways to monitor productivity, revenues,and costs in highly complex health systems.
. In four countries it helped secure externalloans for development projects, especially for in-stitutional development and strengthening unitsresponsible for carrying out the projects.
. It improved coordination among financialagencies operating in the health field and helpedobtain funds from nontraditional sources.
Health Facilities Maintenance
During the 1970s PAHO concentrated oncreating an awareness of the importance ofhealth facilities maintenance because of its ef-fect on the quality and cost of health care. In-
creasing investment in infrastructure and theprogressive introduction of sophisticated in-stallations and equipment have resulted in theparalysis of a high proportion of installedcapacity because of poor maintenance.
Still, there were advances during thedecade. Mexico and Venezuela led the way inestablishing national maintenance systems, amovement that gradually spread to othercountries.
In 1980 PAHO's primary emphasis shifted todeveloping simple methods for detecting andanalyzing maintenance problems in healthservices largely devoted to primary care.These methods are a tool for determiningways to prevent and correct such problems.A start was also made in formulating simplermeans of solving the most common problemsthrough training and the use of guides. Someprogress along these lines was made in Cen-tral America and Jamaica.
With less PAHO participation than in thepast, the national maintenance centers,especially in Colombia, Costa Rica, Ecuador,El Salvador, Mexico, and Venezuela, took onmore substantial training functions. In severalcountries the national centers began to offertraining in hospital maintenance to skilledand technical personnel.
Health care has traditionally been regardedas a labor-intensive sector requiring relativelylittle capital investment. This situation hasbeen changing, and the sector is now bothlabor- and capital-intensive because of itsgrowing reliance on technology. Appropriatetechnology is an excellent means of ra-tionalizing maintenance program priorities.The magnitude of this task makes it necessaryto have close collaboration between thepublic and private sectors and between pro-ducers and users of equipment andinstallations.
To discuss this issue, PAHO, the AmericanSociety of Hospital Engineering, and Partnersof the Americas participated in the annualmeeting of the International Society ofHospital Engineering. This new relationship

26 REPORT OF THE DIRECTOR
among the three organizations marked thebeginning of a major effort to includeengineering associations and schools in theanalysis and solution of the increasinglyserious problems in biomedical and healthengineering.
The growing impact of energy costs hasspurred initial efforts to examine unconven-tional energy alternatives. In Barbados, an in-itial cooperative project was begun. To con-tain costs, Costa Rica started a major experi-ment in using simple technology to recoversilver from x-ray plate development. Such ex-periments may become demonstrations forother countries.
In Ecuador, El Salvador, Honduras, andPanama, PAHO collaborated in developingmaintenance programs in advanced medicalcenters where a variety of problems are pos-ing increasing challenges to technicians andadministrators.
PAHO continued its cooperation with thePan American Development Foundation indistributing emergency equipment to hospi-tals, with emphasis on maintenance compo-nents.
Efforts in 1981 will be concentrated ondeveloping methods for maintaining equip-ment in basic health services, making betteruse of national training and vocational educa-tion centers, conducting appropriate technol-ogy experiments, and particularly on increas-ing the interaction of experts in this fieldthrough a collaborative network of centersand programs.
Health Education
Health education has been an essentialcomponent of programs to promote healththrough extension of primary care servicesand community participation to improvehealth and development conditions. As an in-tegral part of programs to prevent or reduce
Community leaders meet in a convertedrailroad car in a Panama City suburb todiscuss local health problems.
health risks, health education efforts werestrengthened in programs to better the healthof families, with particular emphasis onchildren, adolescents, and mothers.
To reaffirm the major role of health infor-mation and education in achieving health forall and increasing awareness among Americangovernments that primary health care cannotbe attained without adequate health educa-tion, the Directing Council began the newdecade by devoting its 1980 technical discus-sions to community health education. Studieswere made in 23 countries to determine thecurrent status of such education and indicatenew strategies and techniques.
Health education activities were includedin 18 major maternal and child health andfamily planning projects, and training in anddevelopment of family life education ac-tivities were conducted under UNFPA sponsor-ship in Antigua, Bolivia, Dominica, Panama,St. Kitts-Nevis, and Saint Lucia.
PAHO worked with USAID and the Univer-sity of the West Indies to include health edu-cation in the curricula of primary schoolstudents in Antigua, Barbados, Belize, BritishVirgin Islands, Dominica, Grenada, Montser-
rat, St. Kitts-Nevis, Saint Lucia, and St.Vincent.
A health education workshop was held inJuly in conjunction with the University of theWest Indies. Participants from Bermuda,Haiti, Jamaica, and Trinidad and Tobagodeveloped a provisional strategy for healtheducation in the Caribbean, drafted a con-stitution for a Caribbean health educationassociation, and planned a Caribbean healtheducation newsletter. The first nationalhealth education council in the Carib-bean-an autonomous body of 60 voluntaryagencies, clubs, and cooperating governmen-tal departments-was established in theBahamas.
PAHO provided fellowships to train healtheducators from Antigua and the Bahamas inmaster's degree programs in the UnitedStates.
In the area of community participation inhealth and development, PAHO participatedwith USAID, the American Public HealthAssociation, World Bank, and IDB in plan-ning strategies for community participation inprimary health care projects. In the UnitedStates, PAHO also collaborated with the Na-tional Council for International Health inplanning a program to train and supportprimary health care workers to start in 1981.
Maternal and Child Health andFamily Welfare
In carrying out its maternal and childhealth program, PAHO places special em-phasis on applying epidemiologic methods indetecting and preventing risks to mothers andchildren, particularly in poor urban and ruralfamilies which are considered especiallyvulnerable to health problems.
Priority was given to developing com-prehensive activities encouraging inter-disciplinary solution of health problems and
The Havana Pediatric Hospital encouragesparents to spend time with their sick children(above). And a mother comforts a sick babyat the gastroenteritis ward of the Bustamante(Children's) Hospital in Kingston.
(Photo: J. Vizcarra Brenner/PAHO)
28 REPORT OF THE DIRECTOR
(Photo: M. Montecino/PAHO)
(Photo: J. Vizcarra Brenner/PAHO)
Children require much care and training ingood health practices. Counterclockwise,starting at left, a girl is just inmmunized atCarrizal, Costa Rica; a boy is examined at theSan José Children's Hospital; a motherreceives instruction in feeding her baby atHarbour View Health Center, Kingston; apupil at the Education and Nutrition Centerin Carrizal; a boy learns to wash his hands atthe center; a mother and child at HarbourView.
(Photo: M. Montecino/PAHO) (Photo: M. Montecino/PAHO)

30 REPORT OF THE DIRECTOR
promoting intersectoral linkages. Thus,maternal and child health and family plan-ning programs were coordinated with ac-tivities in nutrition, mental health, and healtheducation and community participation, andlinks were established with other develop-ment sectors such as education, agriculture,planning, and labor.
PAHO acted as executing agency for mater-nal and child health and family planning pro-grams to which UNFPA contributed $8,972,401in 23 countries and territories (Anguilla, An-tigua, Bolivia, British Virgin Islands, CaymanIslands, Chile, Colombia, Cuba, Dominica,Ecuador, El Salvador, Haiti, Honduras,Jamaica, Mexico, Nicaragua, Panama, Peru,St. Kitts-Nevis, Saint Lucia, St. Vincent,Trinidad and Tobago, and Uruguay). Inalmost all of them, family planning andmaternal and child care activities were coor-dinated with coverage extension and primaryhealth programs. PAHO provided technicaland administrative support to countries withprojects already underway and those thatbegan formulating proposals.
In addition, UNFPA contributed $1,961,620for such regional and subregional activities asfamily health and population dynamics,studies on mortality and indicators of healthand well-being, health and youth, continuingeducation in family health program ad-ministration, and studies of the linkage offamily planning with primary mother-and-child care. It began evaluating the regionalprojects it supported from 1974 to 1980, andwith PAHO held eight meetings to evaluateprojects in Cuba, Dominica, Ecuador, Haiti,Mexico, Panama, St. Kitts-Nevis, andUruguay.
PAHO cooperated with UNICEF in nationalmother-and-child health programs and infollowing up regional activities begun in 1979to mark the International Year of the Child.In some countries it and UNICEF were coex-ecuting agencies for UNFPA-financed maternaland child health programs. Since the healthof children is adversely affected by un-
wholesome environmental conditions,UNICEF provided funds for building ruralwater supply and excreta disposal systems invarious countries.
A perinatal and maternal and child careprogram with emphasis on primary care,financed largely by the W. K. Kellogg Foun-dation, was launched early in the year. Theprogram's purpose is to create demonstrationareas where primary care, training, andepidemiologic and health service research canbe associated. Twelve such projects began inBrazil, Colombia and Uruguay, and pro-posals were initiated for similar projects in theDominican Republic and Mexico.
Regionally, PAHO supported studies on in-dicators of family health and well-being. Aworking group on mortality in children andindicators of health and well-being represent-ing 10 countries met at Brasilia, and as a resultvarious national programs undertook studiesor improved the research designs of their ex-isting maternal and child health projects. Fourcountries (Argentina, Bolivia, Trinidad andTobago, and Uruguay) initiated studies ongeneral morbidity and mortality amongchildren and mothers according toPAHO/WHO methodologic guidelines.
Several countries started studies of risk fac-tors in mother-and-child care as a tool fordeveloping prediction models based on riskprinciples and extending coverage. A groupof experts met at Washington in October anddrew up guidelines for using the risk conceptin extending coverage through primary care.
PAHO's training activities relating to thehealth of women and children ranged fromcourses for midwives and community healthworkers to those for administrators of na-tional maternal and child health programs.The latter included a maternal and childhealth seminar on for 40 professionals fromeight countries, a course on pediatric primaryhealth care for 26 professionals from ninecountries, and an international course onperinatal public health for 52 participantsfrom 12 countries.
HEALTH SERVICE SYSTEMS 31
PAHO's Latin American Perinatology andHuman Development Center at Montevideohas long been a leader in perinatal research,perinatologist training, and promotingknowledge of the underlying principles ofobstetrics. In recent years the Center hasfocused its efforts on simplifying perinatalcare, developing appropriate technologies forprimary care, and investigating obstetric ser-vices to further the extension of theircoverage.
The Center provided advisory and trainingservices to the countries, conducted coursesand seminars, and coordinated Latin Ameri-can collaborative research projects.
In the training area it conducted 14 coursesand seminars on subjects ranging from ap-propriate technologies for nurses and mid-wives to the scientific principles of fetal,maternal, and newborn care for more than300 participants. In research, it further ex-panded the standardization of perinatal carerecords to a total of 15 countries. In the LatinAmerican collaborative survey of standardsfor managing premature infants, it began totabulate the findings from maternity clinics in12 countries in order to establish generalstandards of care in the future.
Nutrition
Despite the political commitment andfinancial effort of the governments to in-crease programs of major social impact, 1980did not necessarily reflect a significant ad-vance in solving the hemisphere's food andnutrition problems. The situation continuedto be characterized by clear imbalances in theproduction, distribution, and consumptionof basic foods, especially among the urbanand rural poor.
As a result of this imbalance, energy-
protein malnutrition affects about 60 percentof children under age five, endemic goiter af-fects about 20 percent of the population insome countries, and iron-deficiency anemiasaffect 29 to 63 percent of pregnant womenand other susceptible age groups. In contrast,the number of people affected by vitamin A
deficiency decreased significantly in thosecountries where vitamin A-fortified sugar wasintroduced. Other countries began studies ofthe prevalence of hypovitaminosis A and for-mulated means of controlling it.
Serious problems related to the physical,social, and cultural environment also per-sisted which help aggravate the situationbecause of their negative effect on food in-take and the use of essential nutrients.Among these problems are the highprevalence of diarrheal and acute respiratorydiseases, inadequate potable water and ex-creta disposal, lack of sanitation in handlingand consuming food, prejudices about thenutritive value of certain foods, and er-roneous practices in feeding infants and veryyoung children as seen in the decline inbreastfeeding in urban areas and the influenceof commercial advertising that may causepeople to spend money they cannot afford onexpensive foods of questionable nutritionalvalue.
Though it is not as critical in its acutenessand severity as in other parts of the world,the nutritional panorama in most of LatinAmerica contrasted unfavorably with thesituation in nations such as Argentina,Canada, some Caribbean countries, and theUnited States, where the main nutrition prob-lem was excessive energy consumption withresulting overweight and obesity, conditionscommonly associated with chronic and de-generative diseases such as diabetes mellitus,hypertension, and coronary insufficiency.
In addition, chronic malnutrition afflictedcountries with great potential for satisfyingdomestic food needs or for developing otherunexploited resources and so employ under-or unused labor and thus increase the ability
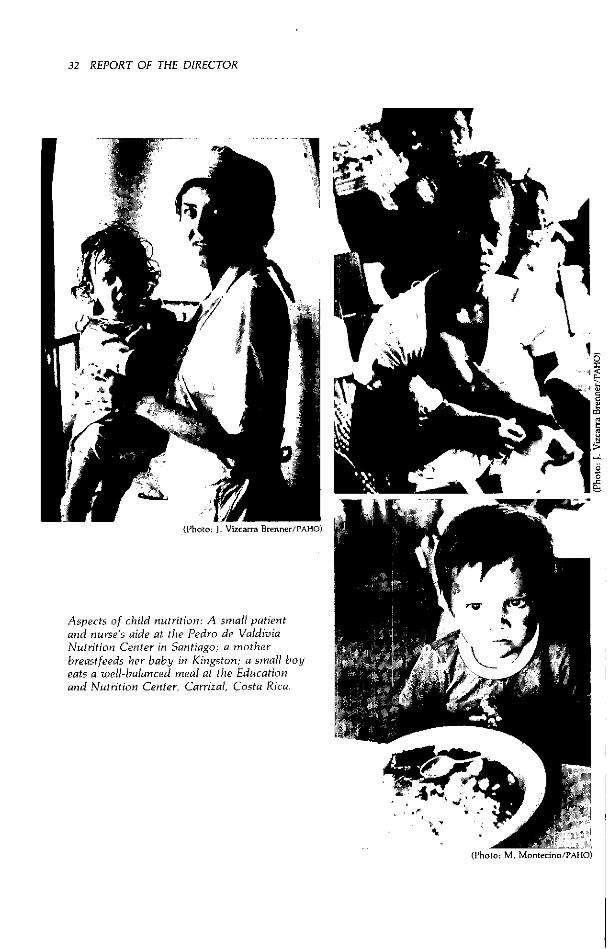
32 REPORT OF THE DIRECTOR
(Photo: 1. Vizcarra Brenner/PAHO)
Aspects of child nutrition: A smnall patientand nurse's aide at the Pedro de ValdiviaNutrition Center in Santiago; a motherbreastfeeds her baby in Kingston; a small boyeats a well-balanced meal at the Educationand Nutrition Center, Carrizal, Costa Rica.
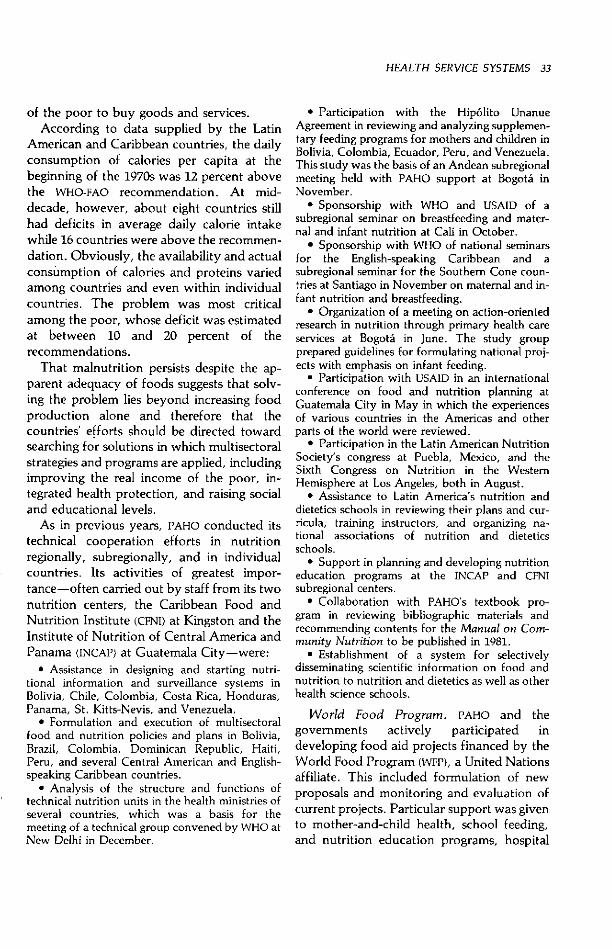
HEALTH SERVICE SYSTEMS 33
of the poor to buy goods and services.According to data supplied by the Latin
American and Caribbean countries, the dailyconsumption of calories per capita at thebeginning of the 1970s was 12 percent abovethe WHO-FAO recommendation. At mid-decade, however, about eight countries stillhad deficits in average daily calorie intakewhile 16 countries were above the recommen-dation. Obviously, the availability and actualconsumption of calories and proteins variedamong countries and even within individualcountries. The problem was most criticalamong the poor, whose deficit was estimatedat between 10 and 20 percent of therecommendations.
That malnutrition persists despite the ap-parent adequacy of foods suggests that solv-ing the problem lies beyond increasing foodproduction alone and therefore that thecountries' efforts should be directed towardsearching for solutions in which multisectoralstrategies and programs are applied, includingimproving the real income of the poor, in-tegrated health protection, and raising socialand educational levels.
As in previous years, PAHO conducted itstechnical cooperation efforts in nutritionregionally, subregionally, and in individualcountries. Its activities of greatest impor-tance-often carried out by staff from its twonutrition centers, the Caribbean Food andNutrition Institute (CFNI) at Kingston and theInstitute of Nutrition of Central America andPanama (INCAP) at Guatemala City-were:
* Assistance in designing and starting nutri-tional information and surveillance systems inBolivia, Chile, Colombia, Costa Rica, Honduras,Panama, St. Kitts-Nevis, and Venezuela.
* Formulation and execution of multisectoralfood and nutrition policies and plans in Bolivia,Brazil, Colombia, Dominican Republic, Haiti,Peru, and several Central American and English-speaking Caribbean countries.
* Analysis of the structure and functions oftechnical nutrition units in the health ministries ofseveral countries, which was a basis for themeeting of a technical group convened by WHO atNew Delhi in December.
* Participation with the Hipólito UnanueAgreement in reviewing and analyzing supplemen-tary feeding programs for mothers and children inBolivia, Colombia, Ecuador, Peru, and Venezuela.This study was the basis of an Andean subregionalmeeting held with PAHO support at Bogotá inNovember.
* Sponsorship with WHO and USAID of asubregional seminar on breastfeeding and mater-nal and infant nutrition at Cali in October.
* Sponsorship with WHO of national seminarsfor the English-speaking Caribbean and asubregional seminar for the Southern Cone coun-tries at Santiago in November on maternal and in-fant nutrition and breastfeeding.
* Organization of a meeting on action-orientedresearch in nutrition through primary health careservices at Bogotá in June. The study groupprepared guidelines for formulating national proj-ects with emphasis on infant feeding.
* Participation with USAID in an internationalconference on food and nutrition planning atGuatemala City in May in which the experiencesof various countries in the Americas and otherparts of the world were reviewed.
* Participation in the Latin American NutritionSociety's congress at Puebla, Mexico, and theSixth Congress on Nutrition in the WesternHemisphere at Los Angeles, both in August.
* Assistance to Latin America's nutrition anddietetics schools in reviewing their plans and cur-ricula, training instructors, and organizing na-tional associations of nutrition and dieteticsschools.
* Support in planning and developing nutritioneducation programs at the INCAP and CFNIsubregional centers.
* Collaboration with PAHO's textbook pro-gram in reviewing bibliographic materials andrecommending contents for the Manual on Com-munity Nutrition to be published in 1981.
* Establishment of a system for selectivelydisseminating scientific information on food andnutrition to nutrition and dietetics as well as otherhealth science schools.
World Food Program. PAHO and thegovernments actively participated indeveloping food aid projects financed by theWorld Food Program (WFP), a United Nationsaffiliate. This included formulation of newproposals and monitoring and evaluation ofcurrent projects. Particular support was givento mother-and-child health, school feeding,and nutrition education programs, hospital
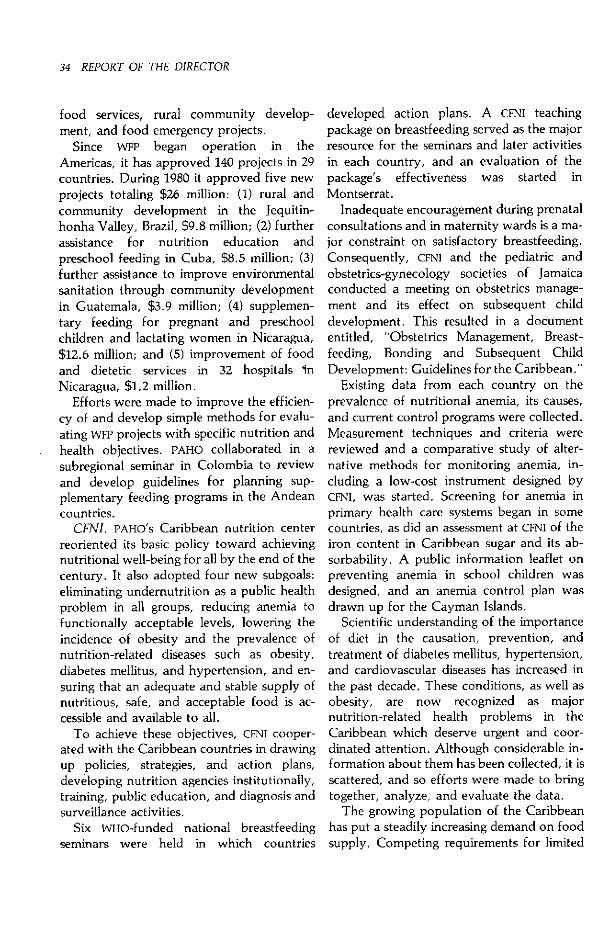
34 REPORT OF THE DIRECTOR
food services, rural community develop-ment, and food emergency projects.
Since WFP began operation in theAmericas, it has approved 140 projects in 29countries. During 1980 it approved five newprojects totaling $26 million: (1) rural andcommunity development in the Jequitin-honha Valley, Brazil, $9.8 million; (2) furtherassistance for nutrition education andpreschool feeding in Cuba, $8.5 million; (3)further assistance to improve environmentalsanitation through community developmentin Guatemala, $3.9 million; (4) supplemen-tary feeding for pregnant and preschoolchildren and lactating women in Nicaragua,$12.6 million; and (5) improvement of foodand dietetic services in 32 hospitals InNicaragua, $1.2 million.
Efforts were made to improve the efficien-cy of and develop simple methods for evalu-ating WFP projects with specific nutrition andhealth objectives. PAHO collaborated in asubregional seminar in Colombia to reviewand develop guidelines for planning sup-plementary feeding programs in the Andeancountries.
CFNI. PAHO's Caribbean nutrition centerreoriented its basic policy toward achievingnutritional well-being for all by the end of thecentury. It also adopted four new subgoals:eliminating undernutrition as a public healthproblem in all groups, reducing anemia tofunctionally acceptable levels, lowering theincidence of obesity and the prevalence ofnutrition-related diseases such as obesity,diabetes mellitus, and hypertension, and en-suring that an adequate and stable supply ofnutritious, safe, and acceptable food is ac-cessible and available to all.
To achieve these objectives, CFNI cooper-ated with the Caribbean countries in drawingup policies, strategies, and action plans,developing nutrition agencies institutionally,training, public education, and diagnosis andsurveillance activities.
Six WHo-funded national breastfeedingseminars were held in which countries
developed action plans. A CFNI teachingpackage on breastfeeding served as the majorresource for the seminars and later activitiesin each country, and an evaluation of thepackage's effectiveness was started inMontserrat.
Inadequate encouragement during prenatalconsultations and in maternity wards is a ma-jor constraint on satisfactory breastfeeding.Consequently, CFNI and the pediatric andobstetrics-gynecology societies of Jamaicaconducted a meeting on obstetrics manage-ment and its effect on subsequent childdevelopment. This resulted in a documententitled, "Obstetrics Management, Breast-feeding, Bonding and Subsequent ChildDevelopment: Guidelines for the Caribbean."
Existing data from each country on theprevalence of nutritional anemia, its causes,and current control programs were collected.Measurement techniques and criteria werereviewed and a comparative study of alter-native methods for monitoring anemia, in-cluding a low-cost instrument designed byCFNI, was started. Screening for anemia inprimary health care systems began in somecountries, as did an assessment at CFNI of theiron content in Caribbean sugar and its ab-sorbability. A public information leaflet onpreventing anemia in school children wasdesigned, and an anemia control plan wasdrawn up for the Cayman Islands.
Scientific understanding of the importanceof diet in the causation, prevention, andtreatment of diabetes mellitus, hypertension,and cardiovascular diseases has increased inthe past decade. These conditions, as well asobesity, are now recognized as majornutrition-related health problems in theCaribbean which deserve urgent and coor-dinated attention. Although considerable in-formation about them has been collected, it isscattered, and so efforts were made to bringtogether, analyze, and evaluate the data.
The growing population of the Caribbeanhas put a steadily increasing demand on foodsupply. Competing requirements for limited

HEALTH SERVICE SYSTEMS 35
landspace-particularly in the island ter-ritories-create a need to integrate policiesfor food, nutrition, and economic develop-ment.
Responsibility for collecting data on totalfood availability, market flows, and house-hold consumption rests on the governmentagencies concerned, and in particular ontrade and agriculture ministries. CFNI com-piled food import and production data fromGrenada, Montserrat, and St. Kitts-Nevis in aformat suitable for nutrition planning andtested a simplified food balance sheet in thelast country.
In December 1977, two of the 17 countriesand territories sponsoring CFNI had nationalfood and nutrition policies. At the end of1980 the figure stood at nine. National foodand nutrition councils provide the institu-tional framework for controlling multidisci-plinary food and nutrition plans and pro-grams. A CFNI workshop in May pooled ideason elaborating and developing councilactivities.
Developing food and nutrition manpoweris an important CFNI objective. This includescurriculum development and training oftrainers. CFNI gave its second three-month in-tensive course on food and nutrition planningand two short refresher courses for graduatesof its diploma in community nutritionprogram.
Considerable improvement in nutritiontraining for nurses was achieved. Guidelinesfor basic nursing curricula were developed,and similar nutrition guidelines for publichealth nurse training are being compiled. Atwo-week nutrition module to train familynurse practitioners for the smaller territoriesin a course in St. Vincent was developed andtaught by CFNI's staff.
Three national workshops were held at therequest of the governments to train people inplanning and carrying out community nutri-tion education.
INCAP. INCAP carried out its customarytraining, technical assistance, and research
activities for the benefit of the CentralAmerican countries and Panama.
INCAP's training activities and academiccourses were carried out through the Centerfor Higher Studies in Nutrition and FoodScience in cooperation with the University ofSan Carlos at Guatemala City. One hundredtwenty-two students-about a sixth of themfrom hemispheric countries outside CentralAmerica-were enrolled in the nutritionschool, food science and technology andfood science and animal nutrition courses,and the postgraduate courses on publichealth with a specialization in nutrition andmaternal and child health and on biochem-istry and human nutrition. Twenty-seven ofthe students graduated.
Thirteen professionals participating in theINCAP/United Nations University advancedtutorial training program were in residence,along with 66 persons who received tutorialtraining in specific areas and techniques. The13 professionals who participated in the ad-vanced tutorial program represented a totalof 86 fellowship-months and came from ninecountries, including Japan and the Philip-pines.
INCAP provided technical assistance to allsix countries it serves.
In Costa Rica it advised the national nutri-tion program on defining, programming, andmaintaining the quality of its data processingsystems. In addition, INCAP supported thecountry's multisectoral food and nutritionplanning in its preliminary stages and col-laborated with the Costa Rican Nutrition andHealth Research and Training Institute indeveloping cooperative projects to be carriedout in 1981.
In El Salvador a member of INCAP's profes-sional staff was stationed until September atthe agriculture ministry's livestock develop-ment center to assist in a medium-sized andsmall farmers' program to produce foods ofanimal origin intensively. The country alsocontinued to receive assistance in improvingand updating its food balance sheets.
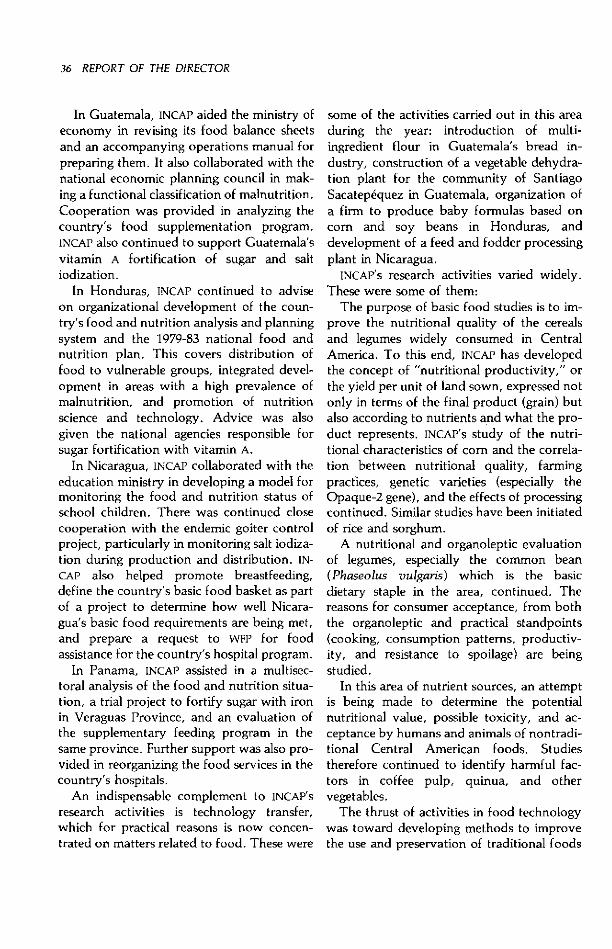
36 REPORT OF THE DIRECTOR
In Guatemala, INCAP aided the ministry ofeconomy in revising its food balance sheetsand an accompanying operations manual forpreparing them. It also collaborated with thenational economic planning council in mak-ing a functional classification of malnutrition.Cooperation was provided in analyzing thecountry's food supplementation program.INCAP also continued to support Guatemala'svitamin A fortification of sugar and saltiodization.
In Honduras, INCAP continued to adviseon organizational development of the coun-try's food and nutrition analysis and planningsystem and the 1979-83 national food andnutrition plan. This covers distribution offood to vulnerable groups, integrated devel-opment in areas with a high prevalence ofmalnutrition, and promotion of nutritionscience and technology. Advice was alsogiven the national agencies responsible forsugar fortification with vitamin A.
In Nicaragua, INCAP collaborated with theeducation ministry in developing a model formonitoring the food and nutrition status ofschool children. There was continued closecooperation with the endemic goiter controlproject, particularly in monitoring salt iodiza-tion during production and distribution. IN-CAP also helped promote breastfeeding,define the country's basic food basket as partof a project to determine how well Nicara-gua's basic food requirements are being met,and prepare a request to WFP for foodassistance for the country's hospital program.
In Panama, INCAP assisted in a multisec-toral analysis of the food and nutrition situa-tion, a trial project to fortify sugar with ironin Veraguas Province, and an evaluation ofthe supplementary feeding program in thesame province. Further support was also pro-vided in reorganizing the food services in thecountry's hospitals.
An indispensable complement to INCAP's
research activities is technology transfer,which for practical reasons is now concen-trated on matters related to food. These were
some of the activities carried out in this areaduring the year: introduction of multi-ingredient flour in Guatemala's bread in-dustry, construction of a vegetable dehydra-tion plant for the community of SantiagoSacatepéquez in Guatemala, organization ofa firm to produce baby formulas based oncorn and soy beans in Honduras, anddevelopment of a feed and fodder processingplant in Nicaragua.
INCAP's research activities varied widely.These were some of them:
The purpose of basic food studies is to im-prove the nutritional quality of the cerealsand legumes widely consumed in CentralAmerica. To this end, INCAP has developedthe concept of "nutritional productivity," orthe yield per unit of land sown, expressed notonly in terms of the final product (grain) butalso according to nutrients and what the pro-duct represents. INCAP's study of the nutri-tional characteristics of corn and the correla-tion between nutritional quality, farmingpractices, genetic varieties (especially theOpaque-2 gene), and the effects of processingcontinued. Similar studies have been initiatedof rice and sorghum.
A nutritional and organoleptic evaluationof legumes, especially the common bean(Phaseolus vulgaris) which is the basicdietary staple in the area, continued. Thereasons for consumer acceptance, from boththe organoleptic and practical standpoints(cooking, consumption patterns, productiv-ity, and resistance to spoilage) are beingstudied.
In this area of nutrient sources, an attemptis being made to determine the potentialnutritional value, possible toxicity, and ac-ceptance by humans and animals of nontradi-tional Central American foods. Studiestherefore continued to identify harmful fac-tors in coffee pulp, quinua, and othervegetables.
The thrust of activities in food technologywas toward developing methods to improvethe use and preservation of traditional foods
HEALTH SERVICE SYSTEMS 37
and byproducts nutritious to humans oranimals. Thus INCAP continued to developappropriate technologies to prevent thehardening and biodeterioration of commonbeans and other legumes. Technical advicewas given to farmer groups interested inpreserving and packing vegetables bydehydrating, pickling, and canning them.Studies were also initiated of the use ofbananas and their wastes as animal feed andof the fruit itself for human consumption.
An analysis of findings from a study of theprotein-energy requirements of preschoolchildren made in 1979 was completed. Theresults indicate that well-nourished pre-schoolers meet their protein-energy needsand grow satisfactorily when their diet in-cludes sufficient amounts of basic foods(beans, corn, bread) to satisfy their appetite,a greater energy density through the additionof oil or sugar to certain foods, and thepresence of an older person to encourage orhelp the child to eat. A new phase in the proj-ect was begun to determine if foods normallyavailable in poor households and preparedand served traditionally can provide sourndnutrition to such children, and whether thepreliminary findings are applicable to chil-dren with mild or moderate malnutrition.
In collaboration with Guatemala's childnutrition agency, INCAP began designing asystem for the early diagnosis, prevention,and correction of malnutrition in childrenand pregnant women in poor urban areas.The system includes much community par-ticipation and close coordination with localhealth services.
INCAP collaborated in a Central Americanbreastfeeding workshop at Tegucigalpa inMarch. As a result, guides for promotingbreastfeeding and improving mother andchild nutrition were prepared, published, anddistributed to pediatricians, obstetricians,and various public and private institutions inCentral America and Panama. Work alsowent forward on developing methods todetermine infant feeding practices before and
after weaning in developing countries. Trialswere carried out to determine the feasibilityof using strained black beans and corn mealor bread as a supplement to mother's milk.These trials indicated that the formulas aretolerated by children between four and sixmonths of age, do not interfere withbreastfeeding practices, and are accepted bymothers.
Health Service Research
The many and varied problems confront-ing American health services in their effort toobtain the goals of universal accessibility andcoverage require systematic research to createnew thinking about health service problemsand how to solve them.
This research is multi- and interdisciplinaryin nature and embraces systems analysis, in-dustrial engineering, and other disciplines, allof which must form a harmonious whole tosupport decision making in health care.
PAHO's governing bodies, after consideringpolicies and strategies for attaining universalhealth by the end of the century, have madespecific recommendations for promoting andusing health service research.
Serious problems arise in executing theserecommendations. Generally speaking, LatinAmerica and the Caribbean lack the criticalmass of investigators required to carry outsuch research meaningfully. Communicationbetween health workers who confront realdaily problems and researchers is generally in-efficient, and there is still a shortage oftrained operations researchers with thenecessary understanding of health andmedical care systems. Health service staff re-quire more information and greater motiva-tion to accept and develop this type ofresearch systematically. Moreover, in most ofthe countries areas of major interest forresearch have not been completely identified

38 REPORT OF THE DIRECTOR
and the funding needed to finance it isunavailable.
Despite these constraints, some importantadvances have been made. Several postgrad-uate health administration training programshave included operations research, and someundergraduate programs in industrial andsystems engineering have participated indeveloping operations research on health ser-vices. Though still on a limited scale, some ofthe countries are carrying out coverage exten-sion programs which include researchcomponents.
PAHO has initiated a health service researchprogram whose general goal is to promoteand collaborate in developing and coor-dinating this type of research. In furtheranceof this goal, support has been providedmainly in encouraging and strengtheninglocal capacity to conduct operations researchon health services, and promoting and sup-porting the transfer and adaptation of opera-tions research techniques in various healthservice fields.
In the former area, assistance was fur-nished in conducting a survey to identifyhealth areas and personnel involved in healthservice research in the industrial engineeringand operations research programs of LatinAmerica and the Caribbean, and support wasprovided in designing various research pro-
tocols. These included operations research ondrug administration in hospitals, develop-ment of supply administration, sterilizationcenters, and infection control centers inhospitals, and investigations of appropriatetechnology in health facility maintenance. Inthe latter area, issues of health serviceresearch were discussed during meetings onthe development of physical infrastructuresof health institutions in Venezuela and of aworking group on the risk approach to ma-ternal and child health care at Washington.
PAHO prepared and distributed the finalreports on a regional operations researchseminar, training in health operationsresearch in Latin America, health serviceoperations research in Latin America, and in-formation systems and decision making onadministrative research in the health services,and a bibliography on health service opera-tions research.
It also cooperated in intercountry healthservice research and introducing operationsresearch into the regional programs in thisfield. A health service research workshop isscheduled for January 1981 at Washington.Specialists in epidemiology, sociology, sys-tems engineering, economics, health admin-istration, teaching and research programs,and health services will attend.
Chapter 3
DISEASE PREVENTIONAND CONTROL
Communicable diseases continue to beamong the principal health problems in mostcountries of Latin America and the Carib-bean. They are responsible for high morbid-ity and mortality, especially among the poor,for whom they are an obstacle tosocioeconomic development. Endemic infec-tious or parasitic diseases place a heavyburden on health during individual growthand development and the productive years.They are responsible for a wide variety ofdisabilities and lessen work capacity.
Cases of several diseases subject to interna-tional regulation occurred in 1980: jungleyellow fever in the Andean countries andBrazil, plague in Bolivia, Brazil, and theUnited States, and imported cases of cholerain Canada and the United States.
The resistance of the vectors of malaria andother parasitoses to insecticides and ofPlasmodium falciparum to certain drugs con-tinued to be a problem.
Noncommunicable diseases such as car-diovascular conditions, diabetes, and cancerare a major cause of mortality in most of thecountries. Others such as rheumatic fever andchronic allergies are common causes of mor-bidity and disability. Accidents, especiallyoccupational and vehicular, continued togrow in importance and were another impor-tant cause of death.
On thepositive side, the Latin Americanand Caribbean countries made significantprogress in formulating and developing
disease prevention and control programs,especially in integrating such activities intotheir regular health services as part of primarycare and in training personnel at variouslevels for those activities.
In the years ahead an increase in theprevalence of chronic diseases and accidentsis foreseen, as well as a need for greater em-phasis on hospital infections control and thereliability and adequate transportation ofbiologicals. Promising advances are apparentin immunology and the production of newvaccines, drugs, and insecticides for the fightagainst bacteria and other pathogenic agents,reservoirs, and vectors.
In both its direct cooperation with in-dividual countries and its regional activities,PAHO gave priority to helping programsagainst those diseases or groups of diseasesthat affect the largest numbers of people andfor which effective means of prevention andcontrol are available, and to services support-ing such programs. These diseases includeddiarrheas, tuberculosis and acute respiratoryinfections, diseases preventable by vaccina-tion, malaria, and preventable or controllablechronic conditions.
PAHO participated in efforts by healthministries to develop their epidemiologic ser-vices so as to improve their operationalcapability through better program organiza-tion and administration and integration ofspecialized activities into the primary careprovided by existing health services. The
39
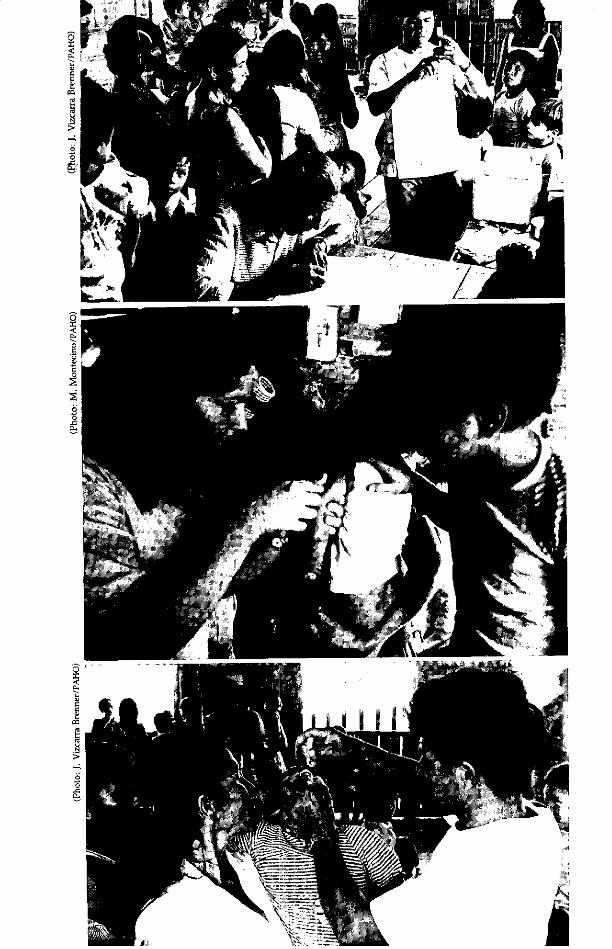
o5
o
-oo-
ç-!~~~~~~~~~~~~~~~~~~~~~~~~.. i
vs
?F A
DISEASE PREVENTION AND CONTROL 41
development of support programs, such asthose involving morbidity and mortality in-formation, epidemiologic surveillance, labo-ratory services, research, and training, wasalso promoted. Assistance was extended inprocuring effective, high-quality supplies forprevention, diagnosis, and treatment andsuch other critical items as biologicals, drugs,insecticides, reagents, and equipment.
PAHO also continued its assistance in carry-ing out intercountry programs to control cer-tain diseases that are highly prevalent or areassuming greater importance in specific areas.This was to demonstrate the efficacy andfeasibility of preventive and therapeuticmeasures and gain experience helpful in set-ting up permanent control programs withwider coverage. A modular short course onthe principles of epidemiology in preventingand controlling disease was developed duringthe year after trials in three countries; it isscheduled for wide dissemination in 1981.
Publication of the Epidemiological Bulletinin Spanish and English was initiated in 1980.This pragmatically oriented newsletter isbased essentially on information supplied bythe countries.
The goal of the Expanded Program on Im-munization is to vaccinate all children andpregnant women against six common preven-table diseases by 1990. Top and bottom, vac-cination at a health center at Miraflores,Loreto, Peru; center, a vaccinator atwork in a home in Carrizal, Costa Rica.
Communicable Diseases
Expanded Program on Immunization
As the 1980s begin, the Americas arevigorously carrying out the 1977 resolutionsof the World Health Assembly and PAHO'sDirecting Council (WHA30.53, WHA30.54, andCD25.27) on developing the Expanded Pro-gram on Immunization (EPI). The program'sgoal is to provide immunization for allchildren in the world by 1990, especiallyagainst diphtheria, tetanus, whooping cough,poliomyelitis, measles, and tuberculosis, andto reduce morbidity and mortality from otherselected diseases of public health importancefor which safe and effective vaccines exist orwill become available.
According to available information, of themore than 80 million children born in thedeveloping world each year, about 5 milliondie of the common contagious childhooddiseases, largely because less than 10 percentof them are protected through immunization.
EPI's primary target diseases are diphtheria,tetanus, whooping cough, poliomyelitis,measles, and tuberculosis. This high priorityprogram is directed toward high-risk infantsand pregnant women and rests on integratingimmunization activities in general health ser-vices if such services are available. As statedin the Declaration of Alma-Ata of September1978, immunization is an essential componentof primary health care and should be viewedas the starting point for extending health ser-vice coverage.
Although immunization was one of thepriorities of the Ten-Year Health Plan for theAmericas established at Santiago in 1972, fewcountries have shown any real progress incontrolling vaccine-preventable diseases asthe plan nears its end. When EPI waslaunched in the Americas in 1977, PAHO'sDirecting Council identified some of the ma-jor problems hindering the expansion of im-munization activities. These problems were

42 REPORT OF THE DIRECTOR
related to planning, management and evalua-tion of immunization activities, vaccine pro-curement, the availability of suitable cold-chain equipment, and logistics. The fact thatnational information and epidemiologic sur-veillance systems are still undeveloped has ex-acerbated the difficulties of evaluating the im-pact of immunization activities nationallyand regionally.
PAHO's technical cooperation thus focuseson five major activities: training, operation ofa revolving fund to buy vaccines and relatedsupplies, developing and testing cold-chainequipment, information systems and pro-gram operation evaluation, and informationdissemination.
Training. In 1980 the second phase of train-ing activities, which followed the regionalworkshop held at Lima in 1979, included na-tional middle management EPI workshops inArgentina, Brazil, Chile, Honduras, Nicara-gua, and Paraguay which 300 participants at-tended. Some of these countries have alreadystarted a third phase of training for localworkers organized and conducted by personswho participated in the national workshops.In the English-speaking Caribbean, the firstsubregional workshop was held at Port-of-Spain in June with one or two participantsfrom each country and territory in the area.National workshops followed in Belize,British Virgin Islands, Cayman Islands,Guyana, and Jamaica. The total number ofnational workshops held was 17 at the end ofthe year, and it is expected that all countriesparticipating in the program will have heldworkshops by the end of 1982.
Another result of the national workshopshas been the preparation, publication, anddistribution of national standards and opera-tions manuals. By the end of the year thehealth ministries in Bolivia, Colombia, Ecua-dor, Honduras, and Peru had distributedsuch manuals throughout their countries.
EPI training materials were also presentedto a regional meeting at Washington ofrepresentatives of Latin American public
health schools to encourage the schools to in-clude such materials in their regular curricula.Some schools have already done so and arealso taking part in training workers for im-munization activities.
The training materials are included inPAHO's expanded textbook and instructionalmaterials program. More than 1,200 sets havebeen requested and distributed to variouscountries, evidence of their interest in carry-ing out this component of the program.
Revolving Fund. Since the establishment ofthe EPI Revolving Fund in 1979, its member-ship has gradually increased to embracealmost all countries and territories in thehemisphere. During its first year of opera-tion, 23 members bought their EPI vaccinesthrough the Fund. Nine new countries andterritories joined the Fund in 1980, bringingits membership to 30.
Figure 3 shows the number of doses of eachtype of vaccine purchased through the Fundin 1979 and 1980. A total of 41.8 million doseswere acquired through the Fund in 1980, 1.8million or 4.5 percent more doses than in1979.
A problem the Fund experienced duringthe year was that two countries cancelledtheir quarterly orders a month or two afterplacing them. Another was that some coun-tries were slow in paying their invoices. Dur-ing the third quarter of the year 20 of the 30Fund participants were delinquent for morethan two months in their payments, and as ofyear's end total arrears were $575,843.
Operating costs were approximately $3million, an increase of 11.1 percent over 1979.
Together, increased operations, delinquentreimbursements, and limited capitalization ofthe Fund resulted in delays in placing orderswith vaccine suppliers averaging about amonth until funds became available.
New vaccine purchase contracts wereissued for the period June 1980 to July 1981.The price of measles vaccine, usually thecostliest of the four EPI vaccines (measles,poliomyelitis, DPT, and BCG), decreased an
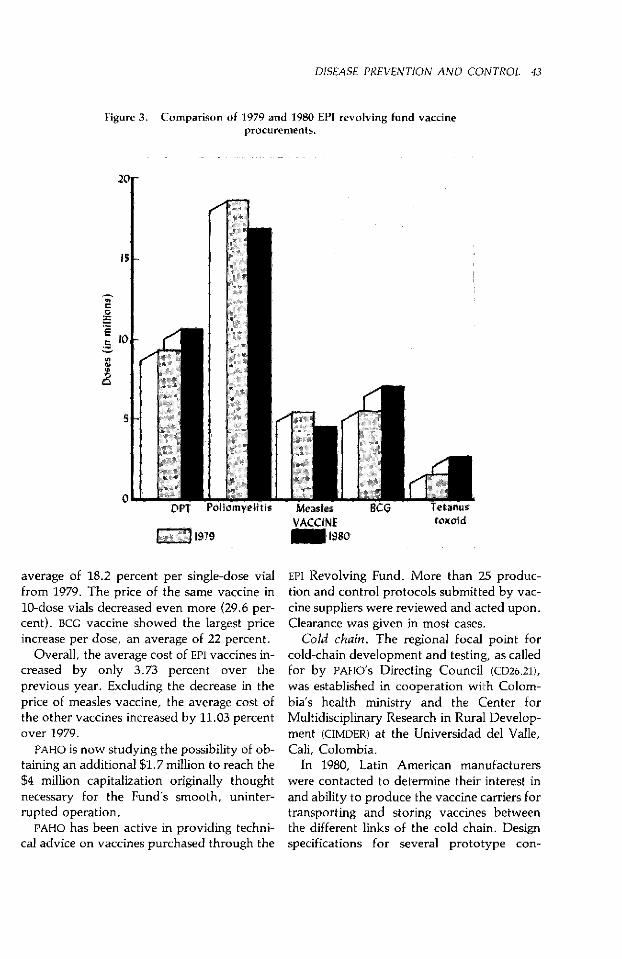
DISEASE PREVENTION AND CONTROL 43
Figure 3. Comparison of 1979 and 1980 EPI revolving fund vaccineprocurements.
20r
151-
o
o lo0- <-
s5
oDPT Pc
1979
Ivica..y.
VACCINE1980
.Ltoxoid
average of 18.2 percent per single-dose vialfrom 1979. The price of the same vaccine in10-dose vials decreased even more (29.6 per-cent). BCG vaccine showed the largest priceincrease per dose, an average of 22 percent.
Overall, the average cost of EPI vaccines in-creased by only 3.73 percent over theprevious year. Excluding the decrease in theprice of measles vaccine, the average cost ofthe other vaccines increased by 11.03 percentover 1979.
PAHO is now studying the possibility of ob-taining an additional $1.7 million to reach the$4 million capitalization originally thoughtnecessary for the Fund's smooth, uninter-rupted operation.
PAHO has been active in providing techni-cal advice on vaccines purchased through the
EPI Revolving Fund. More than 25 produc-tion and control protocols submitted by vac-cine suppliers were reviewed and acted upon.Clearance was given in most cases.
Cold chain. The regional focal point forcold-chain development and testing, as calledfor by PAHO's Directing Council (CD26.21),was established in cooperation with Colom-bia's health ministry and the Center forMultidisciplinary Research in Rural Develop-ment (CIMDER) at the Universidad del Valle,Cali, Colombia.
In 1980, Latin American manufacturerswere contacted to determine their interest inand ability to produce the vaccine carriers fortransporting and storing vaccines betweenthe different links of the cold chain. Designspecifications for several prototype con-
DWV
44 REPORT OF THE DIRECTOR
A vital link in any immuniza-tion programn is a proper coldchain with an adequate vac-cine supply, as seen here inthe central cold room atSan José.
([Jhoto: M. MontecinlO/lA-lu)
tainers were transmitted to them and those
interested were invited to submit bids. Based
on these tenders, a certain number of coldboxes and vaccine carriers will be producedfor testing at the Cali center to determinetheir suitability for EPI use.
In conjunction with the Universidad del
Valle's thermal sciences laboratory, CIMDER
built an environmental testing chamber,which was tested with excellent results and
fully meets PAHO/WHO specifications.One of the many problems in the EPI cold
chain is that of continuously monitoring thetemperatures at which vaccines are stored.
To assure that suitable instruments are
available for monitoring the temperature ofvaccine storage refrigerators daily, PAHO/
WHO has designed a thermometer for EPI use.Water resistant, it consists of liquid crystalsaffixed to a paper backing with a strip of
foam. Samples were distributed to all coun-tries in the hemisphere and are already in usein several.
The cold chain, an integral though oftensilent and unperceived part of immunizationactivities, is one of the components that go
wrong most frequently. It is therefore essen-tial to have personnel who are proficient in
understanding and running the cold chain
and others who can repair and maintain ex-isting equipment.
Peru, in collaboration with PAHO, orga-nized a six-week course on cold-chain equip-
ment maintenance at Chiclayo in August and
September. The 12 participants reviewed EPI
goals and standards, studied the principles of
refrigeration thermodynamics, examined dif-
ferent refrigeration systems, and participatedin several laboratory exercises with differentkinds of equipment.
Since the Peruvian cold-chain course was
the first of its kind, PAHO is reviewing its cur-riculum and evaluating the feasibility of of-
fering a similar course in other countries.Information systems and evaluation. Prog-
ress in developing information systems and
evaluation remains slow, not only because of
constraints imposed by the scarcity of EPI
management staff nationally and withinPAHO but also because national health infor-
mation systems are maturing slowly. Duringthe year PAHO initiated an EPI informationsystem in which participating countries sub-mit information to it, particularly about theprogram's high-priority target groups-in-fants and pregnant women. Of particular im-
portance are information systems for measur-ing vaccination coverage and morbidity and
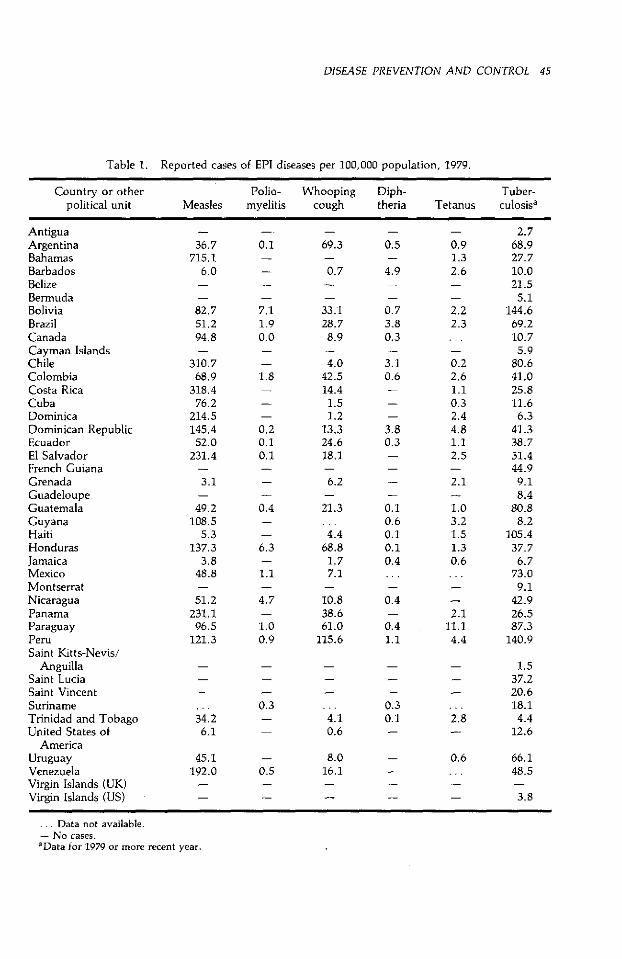
DISEASE PREVENTION AND CONTROL 45
Table 1. Reported cases of EPI diseases per 100,000 population, 1979.
Country or other Polio- Whooping Diph- Tuber-political unit Measles myelitis cough theria Tetanus culosisa
AntiguaArgentinaBahamasBarbadosBelizeBermudaBoliviaBrazilCanadaCayman IslandsChileColombiaCosta RicaCubaDominicaDominican RepublicEcuadorEl SalvadorFrench GuianaGrenadaGuadeloupeGuatemalaGuyanaHaitiHondurasJamaicaMexicoMontserratNicaraguaPanamaParaguayPeruSaint Kitts-Nevis/
AnguillaSaint LuciaSaint VincentSurinameTrinidad and TobagoUnited States of
AmericaUruguayVenezuelaVirgin Islands (UK)Virgin Islands (US)
36.7715.1
6.0
82.751.294.8
310.768.9
318.476.2
214.5145.452.0
231.4
3.1
49.2108.5
5.3137.3
3.848.8
51.2231.196.5
121.3
34.26.1
45.1192.0
0.1
7.11.90.0
1.8
0.20.10.1
0.4
6.3
1.1
4.7
1.00.9
0.3
69.3
0.7
33.128.7
8.9
4.042.514.4
1.51.2
13.324.618.1
6.2
21.3
4.468.8
1.77.1
10.838.661.0
115.6
4.10.6
- 8.00.5 16.1
... Data not available.- No cases.aData for 1979 or more recent year.
0.5
4.9
0.73.80.3
3.10.6
3.80.3
0.10.60.10.10.4. . .
0.4
0.41.1
0.30.1
0.91.32.6
2.22.3
0.22.61.10.32.44.81.12.5
2.1
1.03.21.51.30.6. . .
2.111.1
4.4
2.8
0.6
2.768.927.710.021.5
5.1144.669.210.75.9
80.641.025.811.66.3
41.338.751.444.99.18.4
80.88.2
105.437.7
6.773.0
9.142.926.587.3
140.9
1.537.220.618.1
4.412.6
66.148.5
3.8
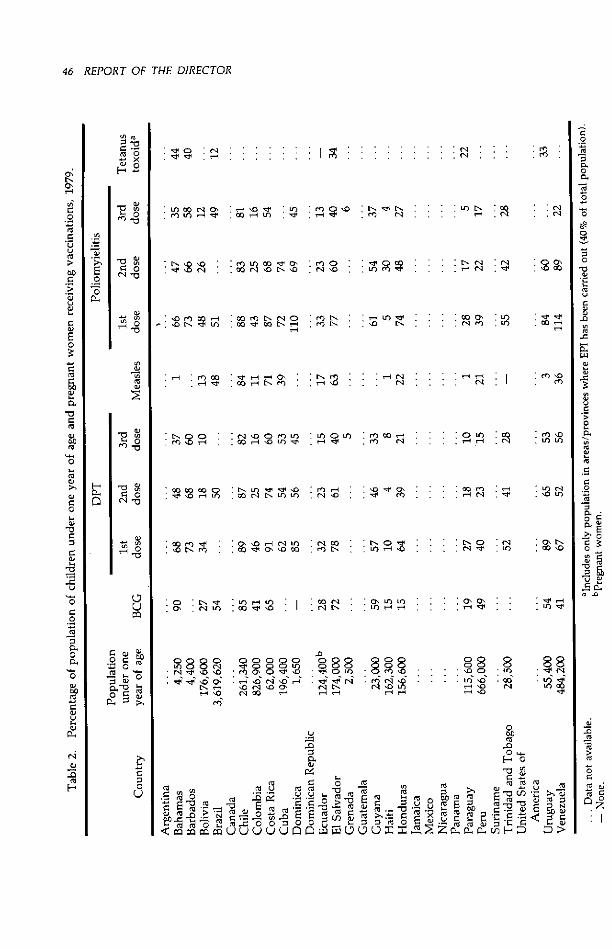
46 REPORT OF THE DIRECTOR
o
C rn n Ln 00 --- 0n ' Dv U 'f D 'n N :-l E
.C * Er eU)HI :m: :N : : : : : : : '
u~~ ~ ~ c> lo o4 . o N 00 l o g' lo cl lo Ln ro N lo U .os
E ~ C, oo ~ «"<, to soN o. o rn L N . m ....... o 0 U,)
0',
O r n .N olo O o 00 rqsO rn u) U or U)*e°Oe «. W eU
'-4 ~ ~ -0~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
'~ ~ rC 8 X o X o, ' ' p ~ m 0 , ' ' p n lo
c> ~ >~ ' ,-- L qH o .. .... N , N _
c .~ c
u~~~~~~~~~~~~~~~~~~~~~~~~~~~
,~~~~~~o
e u ° > to'o LOo) I ' rts :- oX Nr- :) oc O.. E <S f 'ON sD 0E O N O 'O c O lo O m U) U') - lo
.9 -.n9-- o -~oL N . ..'
o) ~ ~ ~ ~ ~ 0 oc tL o no o U -,r 0
O _ ou O- o ri L0 u) u) rD oS cn i0 lo LnS r S9 u s
w '
1ç o 5) ~ O r z H «'
_0 b D
m- rq ' ... .. .. ...
c0 o o mo -Id, oloo ro o
o u C> u D 0 C u U u a C> 0C C C 0 C > 0 ;L .
-~~~~~~~~~~~~~~~~~ ~~~~~~~.9
<, 'm oo ---
''
bo r oL 1l nC
~ ~ ~~~~ 0
.w'~
oj~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~oo> 0
-o o-o>~~o0 ,c `
O 0~~~<uu CN ~ - U U *O'LO:O : A> z - ' - )

DISEASE PREVENTION AND CONTROL 47
mortality. Putting such systems into effectwill allow EPI programs to be evaluated.
Program evaluation is taught in EPI trainingcourses. Emphasis is on reviewing operationsthrough frequent supervisory trips to guideperipheral staff and on performing samplesurveys, either for routine use in assessingvaccination coverage or for exceptional useto estimate the incidence of clinical disease orperform serologic studies.
Other aspects of evaluation which receivedincreased emphasis were comprehensive pro-gram reviews (or "audits") using independentstaff and strengthened disease surveillance.
A comprehensive and more general pro-gram evaluation methodology was elabo-rated and tested in collaboration with thehealth ministries in Bolivia and Colombia latein the year. In the multidisciplinarymethodology, a group of eight to 10 profes-sionals from various health ministry depart-ments and two to four international staffmembers work together for two weeks, dur-ing which they examine all aspects of the na-tional program and its relationship to othercomponents of primary health care at alllevels.
The experiences in Bolivia and Colombiaproved highly productive. Observers fromother countries who were present during theevaluations are already planning to use thesame methods for evaluating their own pro-gram activities.
Another major activity was the prepara-tion and publication in December of a docu-ment entitled "Surveillance Guidelines for theExpanded Immunization Program" whoseSpanish version is to be published in 1981. Itoutlines simple methods of data collection,analysis, and use often applicable locally.The manual will be distributed to the coun-tries in early 1981.
Tables 1 and 2 show the status of thehemisphere's immunization programs andreported cases of EPI diseases per 100,000population. These data are an index of theregional program's progress, though it is
recognized that their incompleteness is itself areflection of the immaturity of differentcountries' information systems.
Information dissemination. The EPINewsletter, which first appeared in May 1979and is published bimonthly in English andSpanish, is distributed throughout thehemisphere to health personnel working inimmunization services at all levels. Its func-tion is to report on the new procedures,techniques, and practices constantly beingdeveloped in the various EPI fields. It alsoserves as a forum for exchanging informationand new ideas about how to solve problemsidentified in national programs.
Information on the availability of cold-chain equipment and its suitability for use innational programs is periodically distributedto program managers throughout theAmericas to enable them to choose the bestequipment for their programs.
Periodic regional meetings of national pro-gram managers, the first of which will takeplace in 1981, will maintain the interest of im-munization workers and keep them up todate on the latest knowledge and techniquesin the field.
Tuberculosis
Tuberculosis is still a serious health prob-lem which causes 40,000 deaths annually inthe hemisphere. Despite the decline in mor-tality during the decade 1969-78 in theAmericas (Figure 4), 200,000 new cases arereported every year. Though tuberculosismortality is declining at about 5 percentyearly, this is still far below what can be ex-pected from current treatment.
Within the last decade, all countries in thehemisphere have integrated tuberculosis con-trol activities into their general health ser-vices, though many must still quantify theactivities' objectives and improve the super-vision and evaluation of tuberculosis control.The progress made in integrating diagnostic
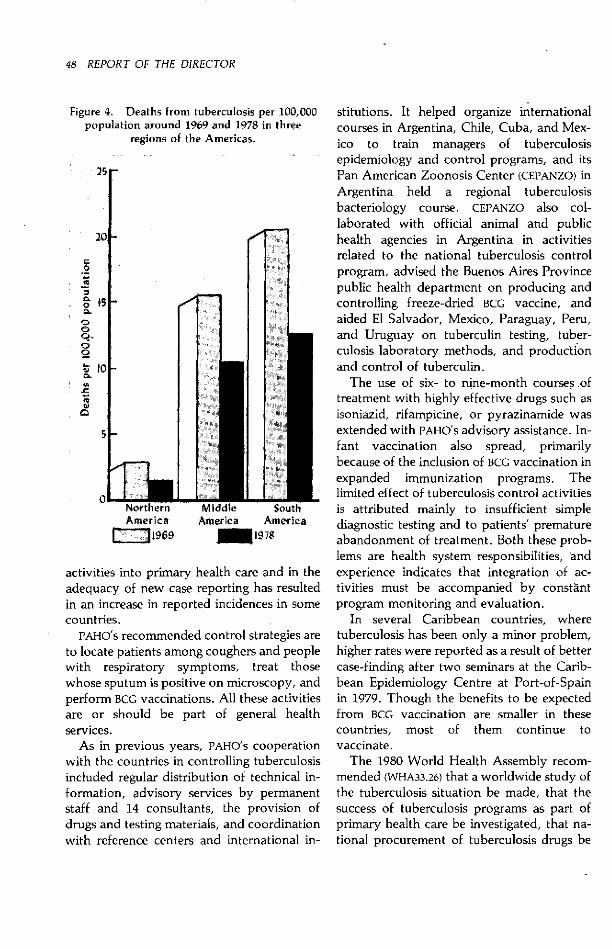
48 REPORT OF THE DIRECTOR
Figure 4. Deaths from tuberculosis per 100,000population around 1969 and 1978 in three
regions of the Americas.
25r
201-
o
M
ooo.o
0 10
5
0 Northern Middle SouthAmerica America Amefica
1969 Q 197
activities into primary health care and in theadequacy of new case reporting has resultedin an increase in reported incidences in somecountries.
PAHO's recommended control strategies areto locate patients among coughers and peoplewith respiratory symptoms, treat thosewhose sputum is positive on microscopy, andperform BCG vaccinations. All these activitiesare or should be part of general healthservices.
As in previous years, PAHO's cooperationwith the countries in controlling tuberculosisincluded regular distribution of technical in-formation, advisory services by permanentstaff and 14 consultants, the provision ofdrugs and testing materials, and coordinationwith reference centers and international in-
stitutions. It helped organize internationalcourses in Argentina, Chile, Cuba, and Mex-ico to train managers of tuberculosisepidemiology and control programs, and itsPan American Zoonosis Center (CEPANZO) inArgentina held a regional tuberculosisbacteriology course. CEPANZO also col-laborated with official animal and publichealth agencies in Argentina in activitiesrelated to the national tuberculosis controlprogram, advised the Buenos Aires Provincepublic health department on producing andcontrolling freeze-dried BCG vaccine, andaided El Salvador, Mexico, Paraguay, Peru,and Uruguay on tuberculin testing, tuber-culosis laboratory methods, and productionand control of tuberculin.
The use of six- to nine-month courses oftreatment with highly effective drugs such asisoniazid, rifampicine, or pyrazinamide wasextended with PAHO's advisory assistance. In-fant vaccination also spread, primarilybecause of the inclusion of BCG vaccination inexpanded immunization programs. Thelimited effect of tuberculosis control activitiesis attributed mainly to insufficient simplediagnostic testing and to patients' prematureabandonment of treatment. Both these prob-lems are health system responsibilities, andexperience indicates that integration of ac-tivities must be accompanied by constantprogram monitoring and evaluation.
In several Caribbean countries, wheretuberculosis has been only a minor problem,higher rates were reported as a result of bettercase-finding after two seminars at the Carib-bean Epidemiology Centre at Port-of-Spainin 1979. Though the benefits to be expectedfrom BCG vaccination are smaller in thesecountries, most of them continue tovaccinate.
The 1980 World Health Assembly recom-mended (WHA33.26) that a worldwide study ofthe tuberculosis situation be made, that thesuccess of tuberculosis programs as part ofprimary health care be investigated, that na-tional procurement of tuberculosis drugs be

DISEASE PREVENTION AND CONTROL 49
Testing for tuberculosis, San ]osé.
facilitated, and that more money be providedfor tuberculosis control. The suggested studywas initiated in the Americas with twosurveys, one on the incidence of the diseaseand the other on the status of tuberculosisprograms. Their findings are to be submittedto PAHO's governing bodies in 1981 andanalyzed by a panel of experts to be con-vened by WHO and the International UnionAgainst Tuberculosis.
Two WHO study groups analyzed the un-favorable results of a BCG vaccination studyin south India. A controlled trial of a Danishand a French BCG vaccine was made in anarea of 360,000 people just west of Madrasbetween July 1968 and March 1971, and 7.5years later its preliminary followup showedthat vaccination conferred no protection onthose who had received it. WHO's expertsconcluded that the preliminary findings werenot directly applicable to BCG vaccination ofchildren, the control measure should be con-tinued, and epidemiologic surveys need to bemade in individual countries so that expectedbenefits can later be compared with those ac-tually achieved through the vaccination ofchildren. Epidemiologic conditions warrantBCG vaccination of newborns and infants in
all Latin American countries, which continueto apply this policy as recommended byPAHO.
Acute respiratory infections
Because of the considerable morbidity andmortality from acute respiratory infections inchildren and the serious health andsocioeconomic problems caused by acute andchronic respiratory diseases in adults, the1979 World Health Assembly recommended(WHA32.33) a program against such infections.
Though few of the Americas have reliableincidence data because acute respiratory in-fections are not reportable, data from themid-1970s suggest that infant mortality due tosuch infections may vary from 50 per 100,000population in Canada and the United Statesto 1,052 in continental Middle America.More than 22 percent of infant deaths in con-tinental Middle America were caused bypneumonias or, to a lesser extent, influenza.According to those data, acute respiratory in-fections were one of the three commonestcauses of death in infants in 19 and in childrenunder five years in 18 in 24 countries.
Since acute respiratory infections are a

50 REPORT OF THE DIRECTOR
leading cause of infant and child mortalityand technical resources are available todiminish such deaths, PAHO has given thisproblem high priority. Together with ex-panded immunization and diarrhea controlprograms, appropriate technology can dimin-ish child and infant mortality if carried outextensively through primary health care sys-tems.
Several of the Americas declared their in-terest in this program. In April PAHO spon-sored three consecutive meetings in Rio deJaneiro on this subject: a course for virolo-gists on diagnosing respiratory viruses, aregional seminar on acute respiratory infec-tions, and a meeting of experts from variouscountries to prepare a research protocol onthe etiology, clinical treatment, behavior,and course of pneumonia in children seen inhealth services.
With PAHO support, Brazil and Mexicobegan research on the program's epidemio-logic and operational aspects to obtain datanecessary for organizing national control pro-grams. Other countries, such as Argentina,Bolivia, and Venezuela, have startedepidemiologic surveys and programmingactivities.
Leprosy
Leprosy continues to be a major publichealth problem in Latin America and theCaribbean, where a quarter-million cases areregistered in 31 countries and territories andalmost 20,000 new cases are reported yearly.Half of all new cases are of the lepromatousor infectious type.
Although leprosy control is still hamperedby the low efficacy of available measuresagainst it, significant advances in treatmentwere made during 1980 thanks to the in-troduction of a new drug (rifampicine), in-tegration of case-finding and therapy intoprimary health care, coordination with tuber-culosis control programs, and developmentof a promising vaccine.
In 1972 the health ministers of theAmericas recommended at their Santiagomeeting that leprosy surveillance and controlactivities be further developed and improvedas integral parts of general health services andthat a regional leprosy training and researchcenter be established to help define uniformcontrol methods. These recommendations,reinforced by several WHO and PAHO resolu-tions (WHA29.70, WHA32.39, CD26.37), havegradually been carried out.
PAHO provided advisory services throughits regular staff and consultants. Five nationalcontrol programs were provided drugs, andfive others received grants for various fieldactivities.
It also provided training to eight fellowsfrom several countries in the yearly leprpsycontrol course conducted at the PanAmerican Center for Research and Trainingin Leprosy and Tropical Diseases (CEPIALET)in Caracas and through a seminar in SaintLucia for 17 participants from three Carib-bean countries. An Andean subregionalseminar on leprosy control at which the na-tional programs of Bolivia, Colombia,Ecuador, Peru, and Venezuela were analyzedwas held at Lima in July.
PAHO signed two important leprosy agree-ments during the year, one with Venezuelafor further research and training at CEPIALETand the other with the Dominican Republicto provide advice on a combined leprosy-tuberculosis control program in that country.
In the area of research, CEPIALET continuedto develop a leprosy vaccine mixing live BCGand killed leprosy bacilli.
Voluntary organizations continued to sup-port leprosy control, either directly to thecountries or through PAHO. A contributionby the Japanese Shipbuilding Industry Foun-dation (JSIF) allowed a regional post for anurse to develop training aids and programsto be created and the second meeting of thestanding committee on leprosy control in theCaribbean to be held. JSIF and the GermanLeprosy Relief Association financed asubregional seminar at Lima in which
DISEASE PREVENTION AND CONTROL 51
representatives from Bolivia, Colombia,Ecuador, Peru, and Venezuela participated.The Damien Foundation contributed fundsfor a special combined leprosy and tuber-culosis control program in the DominicanRepublic. A PAHO program for the Caribbeanreceived support from the InternationalLeprosy Association (ILA), JSIF, and EmmausSuisse, and several other countries in thehemisphere received program support fromILA and its national affiliates.
Diarrheal diseases
Although acute diarrheal diseases remain aleading cause of childhood morbidity andmortality in most of the Americas, prospectsfor their control are steadily improving. In-tensive research in recent years into almost allaspects of diarrheal diseases has led to anumber of breakthroughs and technical in-novations which, added to traditionalprevention and control measures, provide abasis for controlling them.
Diarrheal diseases are the leading cause ofdeath in children under five years in 10 of 24Latin American countries (Table 3). Rates forLatin America range from 75.9 in the Carib-bean to 381.5 in continental Middle America.
Initiated by the 1978 World HealthAssembly (WHA31.44) as a global high priorityand further supported by the PAHO DirectingCouncil (CD26.38, CD27.9), the diarrheal diseasecontrol program relies on five majorstrategies: early treatment of acute diarrhealepisodes through oral rehydration therapyand suitable dietary management; improvedchild care practices, including promotion ofbreastfeeding, proper weaning, and personalhygiene; health education; improved watersupply, environmental sanitation, and foodhygiene; and epidemiologic surveillance.
The program's medium- and long-term ob-jectives are to reduce diarrheal disease mor-tality and morbidity by integrating its ac-tivities in existing primary health caresystems. Such integration is now underway
in several member countries, while othersplan to begin it in 1981.
The program has two main components,operations and research. In the former area,PAHO has sponsored several regional andsubregional planning meetings over the pastthree years in which representatives frommore than 30 countries have participated.Two regional training centers, in Costa Ricaand Jamaica, have been designated andreceive PAHO support. Technical cooperationin national programming or manpower train-ing has been provided to 12 countries. In-creased activity is expected in this area in1981, particularly as new training manualsand course materials become available andare adapted to the needs of specific countries.Subregionally, two courses for national pro-gram managers are planned for 1981.
In planning their national programs, PAHOurges countries to adopt as their medium-term goal the reduction of diarrheal casefatality rates to less than 1 percent. Othersuggested goals are reducing hospital diar-rheal admissions by half and, as an indicationof the cost-effectiveness of oral rehydrationtherapy, reducing annual government ex-penditures to treat acute diarrheal diseases by50 percent or more. Preliminary results in-dicate that several countries have achieved orsurpassed these goals in the last two years.
To maximize therapeutic benefits, PAHOhas adopted the goal of regional self-reliancein producing oral rehydration salts by 1984.In close coordination with UNICEF and WHO,PAHO consultants have so far advised 17countries on local production and qualityassurance, and at least 15 are now producingthe salts. Colombia has announced its inten-tion to start production in sufficient quan-tities to satisfy national and, eventually,subregional requirements. UNICEF and WHOwill contribute equipment and raw materialsto this project. To ensure that local formula-tions conform to WHO/UNICEF specifications,a regional production workshop will be heldat Bogotá in 1982.
To complement program operations,
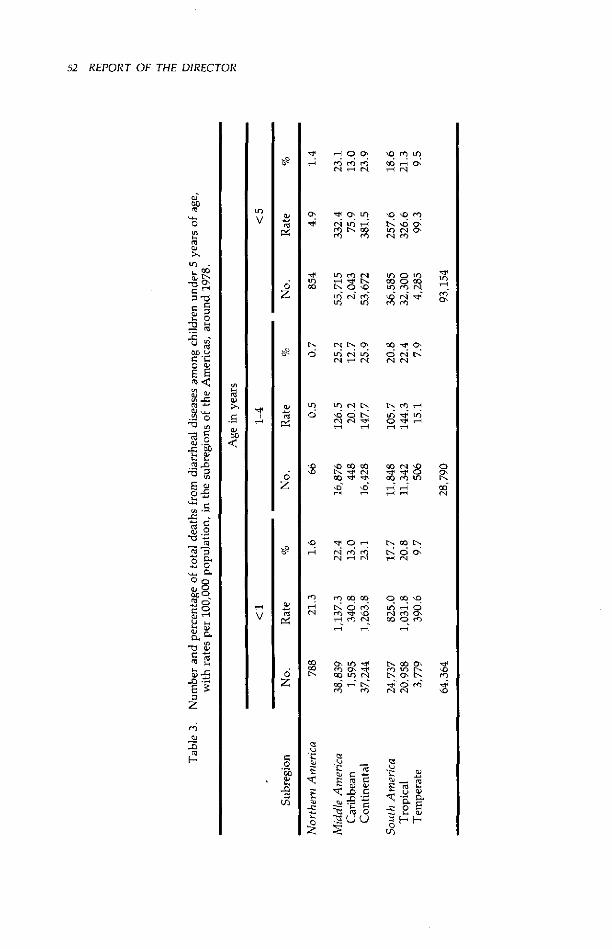
52 REPORT OF THE DIRECTOR
li 9 os Iq re U1e" *n c0 0L
0~ ~0'LO 0'Olo 0
co io n ro 0
Q EN o ' U) L Lf
co lo LLu n rel en
r mS-o o srqr o
'OO L osfS
' U) U ) N' eo) lo o> LN vn Ln
lo ci 0o
D u0 00 00 Lo Lo E
EN N oN ENO 'EO
Lo Lo ri1U4 0 cn in1
H Srn co cS O
«) oE U) 01 t «
" N
u :
EJ-~
._u (U OHHF
.' mcu r - ;. .
U1
.5CUEJEJ
EJ
00
o
O0
3 a0
C E
CJo
_'~
~o <-'
E~ c
E o-CE
E'Jo o
C 0
.X .9
--oo
CJd
u, c
EJS
z
CE
o
Zz
oz
Lo
Loo')
oo-,
lo
lo
CE'
'0
o
05
'oo
V)
EJEZ
E-z1-
z
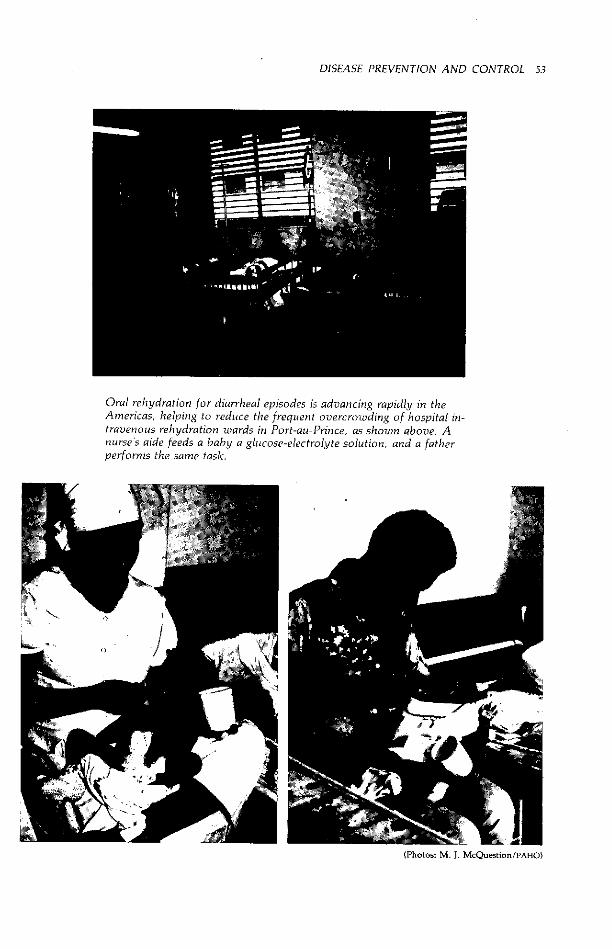
DISEASE PREVENTION AND CONTROL 53
Oral rehydration for diarrheal episodes is advancing rapidly in theAmericas, helping to reduce the frequent overcrowding of hospital in-travenous rehydration wards in Port-au-Prince, as shown above. Anurse's aide feeds a baby a glucose-electrolyte solution, and a fatherperforms the same task.
(Photos: M. J. McQuestion/PAHO)

54 REPORT OF THE DIRECTOR
regional research activities are shifting fromthe major clinical studies of the past twoyears toward operations research in the field.WHO awards grants for basic diarrheal diseaseresearch, while each regional office ad-ministers funds for operations research. Dur-ing 1980, PAHO provided technical or finan-cial support for research in nine countries,and assistance for at least four more projectsis planned in 1981. Most of these projectsfocus on refining program delivery methods;others deal with behavioral, fiscal, clinical,and training problems in specific countries.
Finally, human rotavirus enzyme-linkedimmunosorbent assay reagents were distrib-uted to more than 30 regional laboratories,each of which currently participates in alaboratory proficiency-testing system ad-ministered by PAHO's Institute of Nutrition ofCentral America and Panama at GuatemalaCity. This system will considerably enhancethe diagnostic capabilities of major nationallaboratories, since rotaviruses have recentlybeen found to account for almost half of allinfant diarrheas.
Bacterial diseases
The chief aim of PAHO's bacterial diseaseprogram is to provide technical expertise inresponse to national requests, particularly inemergency or epidemic situations. Thediseases of principal interest are plague, me-ningococcal meningitis, and typhoid fever.
Sporadic cases of plague occurred in atleast three countries (Bolivia, 23; Brazil, 91,and the United States, 18), though it isthought that most cases go unrecognized. Asa result of a PAHO-sponsored subregionalcourse at Piura, Peru, revised surveillanceprocedures using domestic sentinel animals asindicators of local plague activity were in-troduced in Peru and will be initiated inBolivia in 1981. An international plague con-sultation is planned for early 1982 at PAHOheadquarters.
Although endemic in the hemisphere, me-ningococcal meningitis occurred in small out-breaks in Cuba, Panama, and Paraguay inlate 1979. PAHO provided technical coopera-tion for the resulting epidemiologicinvestigations.
A large-scale prospective trial of an ex-perimental oral typhoid vaccine in Chile con-tinued to receive PAHO support, but last-minute problems in producing the vaccine setthe study back a year. Several collateralstudies on the basic epidemiology of typhoidand the role of carriers were conducted or areplanned for 1981 in connection with this vac-cine trial. Their composite findings maybecome the basis for a nationwide typhoidcontrol effort.
Sexually transmitted diseases
The magnitude of the problem of sexuallytransmitted diseases (STD) remains essentiallyunknown throughout the Americas. Somecountries such as Canada, Costa Rica, Cuba,and the United States have relatively reliabledata on the incidence of gonorrhea andsyphilis. No information is collected, how-ever, on the incidence of other STD such aschlamydia-associated nongonococcal urethri-tis, trichomoniasis, Herpes simplex infec-tions, hepatitis B, amebiasis, and salmonellainfections.
Most of these diseases are importantbecause of their serious, debilitating, long-term complications, foremost among which ispelvic inflammatory disease (PID). PID isresponsible for sterility, ectopic pregnancy,and chronic pelvic pain. The magnitude ofthis problem is only now being recognized inthe United States, where 600,000 to 900,000cases occur each year at an economic cost of$1.25 billion. The severity of PID as a publichealth problem throughout the Americas isunknown. In April, PAHO cosponsored an in-ternational PID symposium at CDC.
With the exception of the four nationsmentioned above, few countries have well-

DISEASE PREVENTION AND CONTROL 55
organized STD control programs. Althoughmost countries have developed guidelinesand standards for diagnosis and treatment,few have undertaken the epidemiologicstudies needed to define high-risk groups,identify priority areas for intervention, andcarry out disease control strategies. Eachcountry must decide the most suitable mix-ture of case-finding, screening, contact trac-ing, surveillance, and laboratory techniquesfrom knowledge of STD epidemiology in itspopulation. It is clear, however, that the in-terventions chosen must be provided throughexisting primary health care systems.
PAHO again sponsored an international STDtraining course in Chile and assisted indeveloping and carrying out a research pro-tocol to assess the efficacy of several treat-ment regimens for gonococcal infection andthe susceptibility of Neisseria gonorrhoeae toantibiotics. It also encouraged surveillance ofspecial penicillin-resistant (penicillinase-producing) N. gonorrhoeae strains. Isolateshad earlier been identified in Argentina,Canada, Mexico, and the United States, andin 1980 the strain was identified in Panamaand the United States reported an upsurge inisolations.
PAHO's policy is to strengthen availablehuman resources through clinical, labora-tory, epidemiologic, and managerial training.The United States has established a Spanish-language STD training center in Puerto Rico.PAHO has helped organize the first world con-gress on STD, to be held in Puerto Rico in1981.
Rickettsial and viral diseases
PAHO's basic approach to rickettsial andviral diseases has been to develop adequatelaboratory diagnostic capabilities throughtraining programs, reagent provision, con-sultations, manual development, and profi-ciency testing. It conducts surveillance pro-grams for diseases that can be effectively con-
trolled and distributes information bulletinsabout several.
Rickettsia. Two important rickettsialdiseases in the Americas are louse-borneepidemic typhus and Rocky Mountain spot-ted fever. Although they are endemic in cer-tain areas, little is known about the true ex-tent of the morbidity and mortality theycause.
In 1980 five countries (Bolivia, Costa Rica,Ecuador, Peru, and Trinidad and Tobago)reported 67 cases of louse-borne epidemictyphus, of which Peru accounted for two-thirds. Rocky Mountain spotted fever occurssporadically throughout North and SouthAmerica. It was suspected to exist in MiddleAmerica as well, but confirmation did not oc-cur until 1980 when three fatal cases in CostaRica were carefully investigated and Rickett-sia rickettsii was isolated from one.
Influenza. Nine laboratories in theAmericas monitored influenza as col-laborating centers in WHO's global influenzasurveillance program. These laboratories arelocated in Argentina, Brazil, Canada, Chile,Colombia, Guyana, Jamaica, Peru, and theUnited States. Much more information on theepidemiology of influenza viruses in countriesother than Canada and the United States isneeded to formulate vaccination and controlpolicies.
Hepatitis. The three forms of hepatitis-A,B, and non-A/non-B-are a major publichealth problem in rural and urban areasthroughout the world. Two hundred millionpeople are chronically infected with type Balone. The magnitude of the problem in LatinAmerica and the Caribbean is not wellunderstood for lack of systematic, labora-tory-based serologic studies, but 1.2 to 1.5million cases of type A and a half-millioncases of type B are thought to occur yearly.The non-A/non-B type probably occurs, butits extent is unknown.
It is now clear that sexual transmission maybe primarily responsible for the spread oftype B in certain populations. A successfulhuman field trial of a new hepatitis B vaccine

56 REPORT OF THE DIRECTOR
in the United States produced 96 percentserum conversion rates and an efficacy rate of92 percent.
Hemorrhagic fever. Several viral hemor-rhagic fevers continue to be focal problems insome countries. A special project conductedby Argentina's National Center for the Studyof Argentinian Hemorrhagic Fever atPergamino, advised by PAHO's Pan AmericanZoonosis Center and financed by UNDP, todevelop a vaccine against Junín virus, theagent causing Argentinian hemorrhagic fever,has progressed satisfactorily and will con-tinue until human field trials can be com-pleted. A seed virus has been developed as acandidate vaccine.
Dengue. Dengue, like yellow fever, isspread by the Aedes aegypti mosquito. Thedengue type 1 pandemrnic that occurred in theCaribbean in 1977 and continued there thefollowing year has now tapered off. In 1980there were between 8,500 and 9,000 reportedcases, mostly of type 1-a sharp contrast tothe almost half-million cases reported in 1977.
The disease spread northward throughMexico as anticipated. Late in the year theUnited States reported the first indigenouscontinental transmission of dengue since1945. Seventeen persons who had not trav-eled abroad developed the disease. Onlythree countries (Colombia, El Salvador, andHonduras) reported more than 1,000 caseseach. Surveillance was strengthened to detectdengue hemorrhagic fever, but no cases werereported.
Yellow fever. Since 1972 the incidence ofjungle yellow fever has been upward. Thedisease peaks in two- or three-year cycles andis gradually spreading to areas where no caseswere previously reported. In 1980 sevenAmerican countries-Bolivia, Brazil, Colom-bia, Ecuador, Peru, Trinidad and Tobago,and Venezuela-together reported 116 cases.
Following a 1979 outbreak in humans andsimians in Trinidad and Tobago, PAHO col-laborated with that country's health ministryin a study to determine the extent of yellow
fever virus in monkeys. This included anassessment of the simians and theirmovements, monkey capture, and virologicsampling. Virus was isolated from sick andapparently healthy Alouatta palliata.
In response to the relatively large numberof cases of jungle yellow fever in 1978 and1979, PAHO sponsored an internationalmeeting on yellow fever at Belém, Brazil, inApril.
PAHO is acting to ensure that adequate sup-plies of 17-D yellow fever vaccine are availablefor routine and emergency use. Production oflyophilized yellow fever vaccine in theAmericas ranges from 8 to 13 million doses
Vaccination against yellow feverin Colombia.
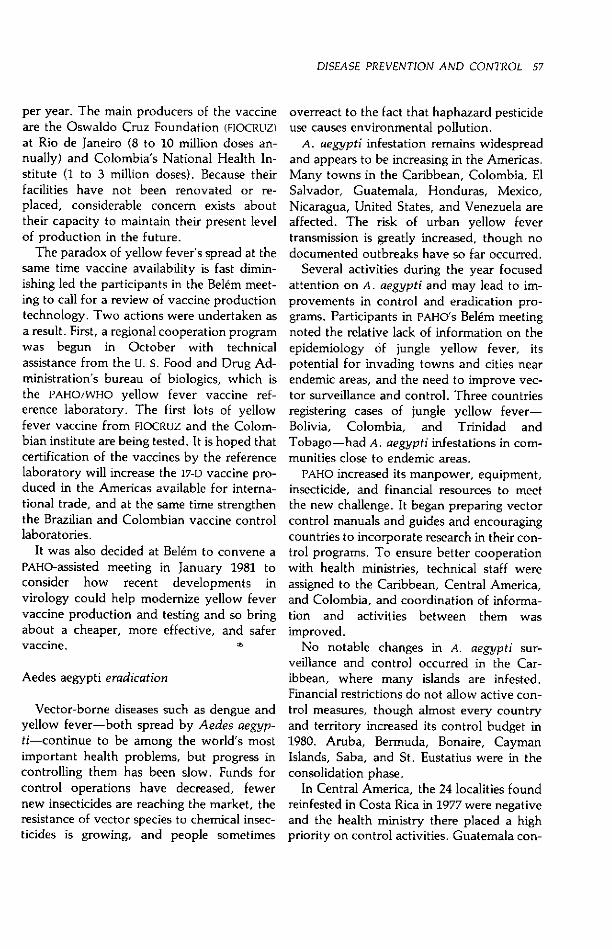
DISEASE PREVENTION AND CONTROL 57
per year. The main producers of the vaccineare the Oswaldo Cruz Foundation (FIOCRUZ)at Rio de Janeiro (8 to 10 million doses an-nually) and Colombia's National Health In-stitute (1 to 3 million doses). Because theirfacilities have not been renovated or re-placed, considerable concern exists abouttheir capacity to maintain their present levelof production in the future.
The paradox of yellow fever's spread at thesame time vaccine availability is fast dimin-ishing led the participants in the Belém meet-ing to call for a review of vaccine productiontechnology. Two actions were undertaken asa result. First, a regional cooperation programwas begun in October with technicalassistance from the u. s. Food and Drug Ad-ministration's bureau of biologics, which isthe PAHO/WHO yellow fever vaccine ref-erence laboratory. The first lots of yellowfever vaccine from FIOCRUZ and the Colom-bian institute are being tested. It is hoped thatcertification of the vaccines by the referencelaboratory will increase the 17-D vaccine pro-duced in the Americas available for interna-tional trade, and at the same time strengthenthe Brazilian and Colombian vaccine controllaboratories.
It was also decided at Belém to convene aPAHO-assisted meeting in January 1981 toconsider how recent developments invirology could help modernize yellow fevervaccine production and testing and so bringabout a cheaper, more effective, and safervaccine.
Aedes aegypti eradication
Vector-borne diseases such as dengue andyellow fever-both spread by Aedes aegyp-ti-continue to be among the world's mostimportant health problems, but progress incontrolling them has been slow. Funds forcontrol operations have decreased, fewernew insecticides are reaching the market, theresistance of vector species to chemical insec-ticides is growing, and people sometimes
overreact to the fact that haphazard pesticideuse causes environmental pollution.
A. aegypti infestation remains widespreadand appears to be increasing in the Americas.Many towns in the Caribbean, Colombia, ElSalvador, Guatemala, Honduras, Mexico,Nicaragua, United States, and Venezuela areaffected. The risk of urban yellow fevertransmission is greatly increased, though nodocumented outbreaks have so far occurred.
Several activities during the year focusedattention on A. aegypti and may lead to im-provements in control and eradication pro-grams. Participants in PAHO's Belém meetingnoted the relative lack of information on theepidemiology of jungle yellow fever, itspotential for invading towns and cities nearendemic areas, and the need to improve vec-tor surveillance and control. Three countriesregistering cases of jungle yellow fever-Bolivia, Colombia, and Trinidad andTobago-had A. aegypti infestations in com-munities close to endemic areas.
PAHO increased its manpower, equipment,insecticide, and financial resources to meetthe new challenge. It began preparing vectorcontrol manuals and guides and encouragingcountries to incorporate research in their con-trol programs. To ensure better cooperationwith health ministries, technical staff wereassigned to the Caribbean, Central America,and Colombia, and coordination of informa-tion and activities between them wasimproved.
No notable changes in A. aegypti sur-veillance and control occurred in the Car-ibbean, where many islands are infested.Financial restrictions do not allow active con-trol measures, though almost every countryand territory increased its control budget in1980. Aruba, Bermuda, Bonaire, CaymanIslands, Saba, and St. Eustatius were in theconsolidation phase.
In Central America, the 24 localities foundreinfested in Costa Rica in 1977 were negativeand the health ministry there placed a highpriority on control activities. Guatemala con-
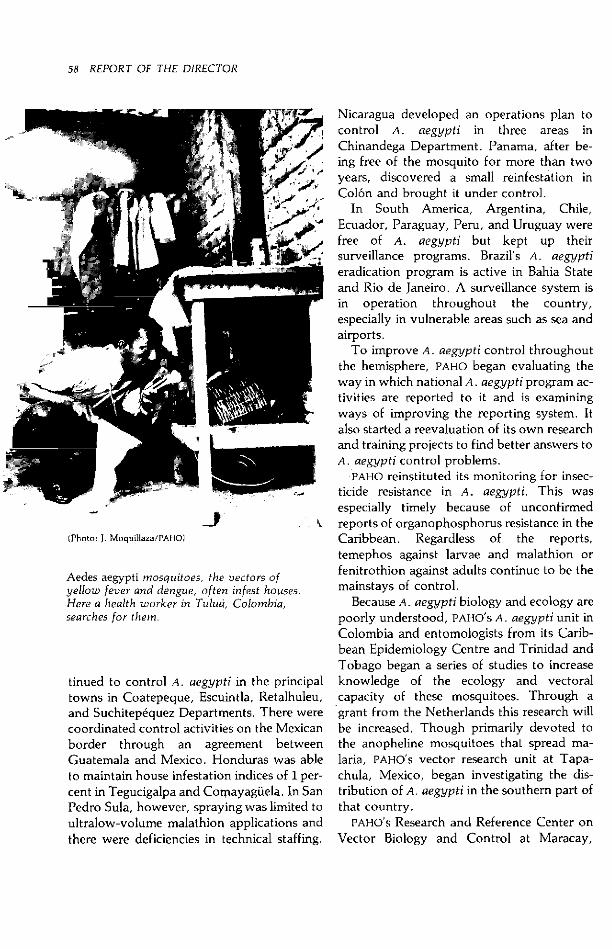
58 REPORT OF THE DIRECTOR
-J(Photo: J. Moquillaza/PAHO)
Aedes aegypti mosquitoes, the vectors ofyellow fever and dengue, often infest houses.Here a health worker in Tuluá, Colombia,searches for them.
tinued to control A. aegypti in the principaltowns in Coatepeque, Escuintla, Retalhuleu,and Suchitepéquez Departments. There werecoordinated control activities on the Mexicanborder through an agreement betweenGuatemala and Mexico. Honduras was ableto maintain house infestation indices of 1 per-cent in Tegucigalpa and Comayaguela. In SanPedro Sula, however, spraying was limited toultralow-volume malathion applications andthere were deficiencies in technical staffing.
Nicaragua developed an operations plan tocontrol A. aegypti in three areas inChinandega Department. Panama, after be-ing free of the mosquito for more than twoyears, discovered a small reinfestation inColón and brought it under control.
In South America, Argentina, Chile,Ecuador, Paraguay, Peru, and Uruguay werefree of A. aegypti but kept up theirsurveillance programs. Brazil's A. aegypti
eradication program is active in Bahia Stateand Rio de Janeiro. A surveillance system isin operation throughout the country,especially in vulnerable areas such as sea andairports.
To improve A. aegypti control throughoutthe hemisphere, PAHO began evaluating theway in which national A. aegypti program ac-tivities are reported to it and is examiningways of improving the reporting system. Italso started a reevaluation of its own researchand training projects to find better answers toA. aegypti control problems.
PAHO reinstituted its monitoring for insec-ticide resistance in A. aegypti. This wasespecially timely because of unconfirmedreports of organophosphorus resistance in theCaribbean. Regardless of the reports,temephos against larvae and malathion orfenitrothion against adults continue to be themainstays of control.
Because A. aegypti biology and ecology arepoorly understood, PAHO's A. aegypti unit inColombia and entomologists from its Carib-bean Epidemiology Centre and Trinidad andTobago began a series of studies to increaseknowledge of the ecology and vectoralcapacity of these mosquitoes. Through agrant from the Netherlands this research willbe increased. Though primarily devoted tothe anopheline mosquitoes that spread ma-laria, PAHO's vector research unit at Tapa-chula, Mexico, began investigating the dis-tribution of A. aegypti in the southern part ofthat country.
PAHO'S Research and Reference Center onVector Biology and Control at Maracay,

DISEASE PREVENTION AND CONTROL 59
Venezuela, tested the insect growth regulatormethoprene as an A. aegypti attractant inovitraps, and Anguilla initiated an islandwidecontrol program using it.
To be truly effective, research informationmust be broadly disseminated. To accomplishthis, courses on modern insecticide and massimmunization equipment were given in Col-ombia. PAHO's vector control unit in Colom-bia's National Health Institute at Bogotá andthe Maracay center trained entomologists,parasitologists, and vector control specialistsfrom throughout the Americas. This union ofresearch and training will be expanded andadditional courses are in preparation.
Research and the development of newways to control vector-borne diseases havebeen severely hampered by the lack of pro-fessional medical entomologists. To improvethis situation, a degree course in medical en-tomology has been offered at Valle Universityin Guatemala and master's degree courses arebeing planned in Panama and Venezuela.
As training of vector control specialists andmedical entomologists expands, certain rou-tine activities such as monitoring develop-ing resistance, vector distribution studies,and equipment and insecticide evaluation willbecome national responsibilities.
Malaria
The number of malaria cases recorded inthe Americas continued to rise. While somecountries were able to keep malaria undercontrol, the situation deteriorated in others.No significant change occurred in relation tothe population in areas of different phases oferadication.
Of the 230,366,000 people living in thehemisphere's originally malarious areas at theend of the year, 58,659,000 (25.4 percent)were in areas where transmission still occur-red (attack phase), 57,087,000 (25.1 percent)were in areas where malaria transmission hadbeen interrupted (consolidation phase), and114,620,000 (49.5 percent) were in areas
where malaria had been eradicated (main-tenance phase).
The malaria situation at the end of the year(Figure 5) can be summarized by dividing thecountries into four groups to describe theprogress achieved, problems encountered,and projects for improvement (Table 4).
Group 1. Twelve countries or territorieswith a population of 72,844,000, or 31.5 per-cent of the population in the hemisphere'soriginally malarious area, had eradicated thedisease (Chile, Cuba, Dominica, Grenadaand Carriacou, Guadeloupe, Jamaica, Mar-tinique, Puerto Rico, Saint Lucia, Trinidadand Tobago, mainland United States, and theU.S. Virgin Islands). More cases wereregistered in this group in 1980 in comparisonwith previous years, but all were importedand there was no evidence of transmission.
Group II. Eight countries or territories witha total of 15,002,000 people, or 6.5 percent ofthose in the originally malarious area, had in-terrupted or almost eliminated malariatransmission, with the exception of Belize,Dominican Republic, and Guyana where thenumber of cases increased. The epidemiologicsituation deteriorated in those countries, duemainly to the importation of more cases fromneighboring countries, insufficient coverage,or untimely application of antimalarial mea-sures and inadequate budgeting for equip-ment, materials, and transportation. In pre-vious years, however, the situation in thethree countries had responded favorably toattack measures.
Group III. The five countries in this groupcontinued their antimalarial activities butmade little progress during the year. In Brazil,DDT spraying was suspended in an area of47,481 km2 with 680,671 inhabitants, andanother area of 11,641 km 2 with 58,297 in-habitants was transferred from the consolida-tion to the maintenance phase. More malariacases were registered in the country becauseof outbreaks in new human settlements in theAmazon basin. The epidemiologic situationin Suriname deteriorated due to an outbreak
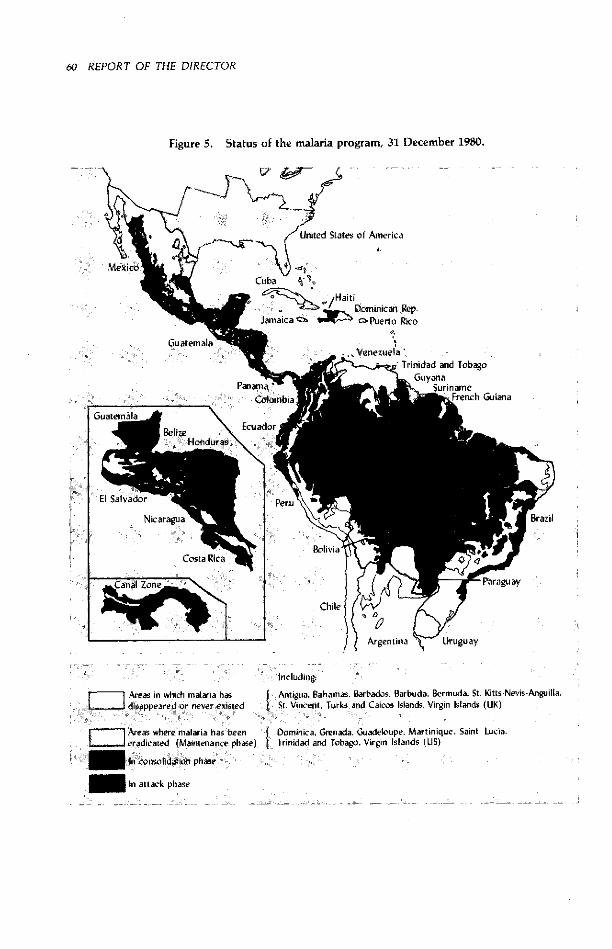
60 REPORT OF THE DIRECTOR
Figure 5. Status of the malaria program, 31 December 1980.
L;# - -- -
Cuba - A'1
G Hi tDominican Rep.Jamaica <~ rPuerlo Rico
.. . Venezuela 'i~,i -- ~ -~,a.-%Trinidad and Tobago
'e F'~M ra{' _ ~GuyanaBamna ' _I1~ , ~ ̂Suriname
Crnbloiha UFr iFre nch Guiana
El Salvado rP
Nicaragua . Brazil
BoliviaCosta Rica
Canal Zone P araguay
Chile C 2 [
Argentina uguay
Including
Areas in which malanria has Antigua. Bahamas. Barbados, Barbuda, Bermuda, St. Kitts-Nevis-Anguilla,. .. disappeared or never existed St. Vincent, Turks and Caicos Islands, Virgin Islands (UK)
W" Areas where malaria has been { Dominica, Grenada. Guadeloupe, Martinique, Saint Lucia,eradicated (Maintenance phase) Trinidad and Tobago. Virgin Islands (US)-_ n consolidation phase
In attack phase
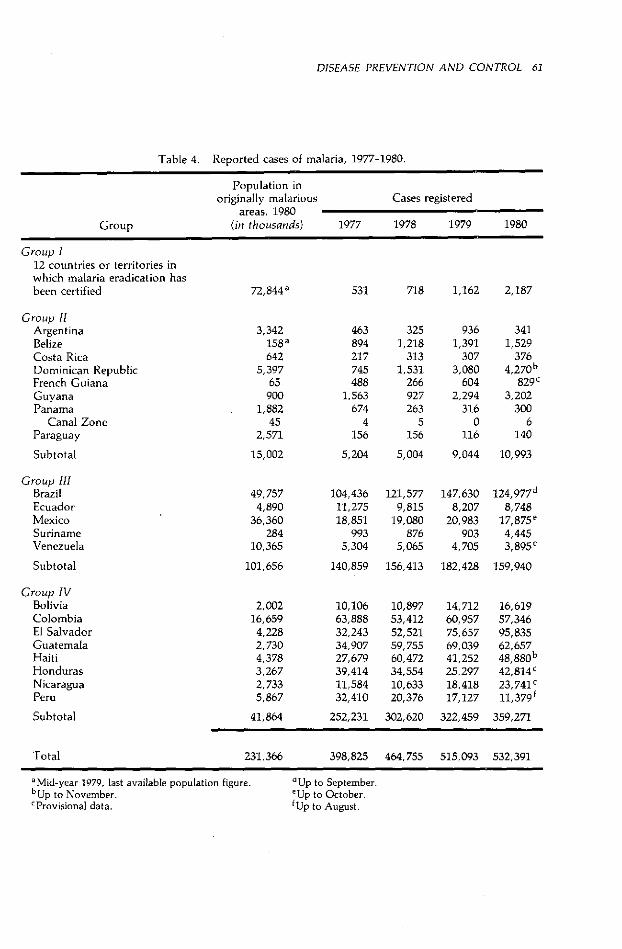
DISEASE PREVENTION AND CONTROL 61
Table 4. Reported cases of malaria, 1977-1980.
Population inoriginally malarious Cases registered
areas, 1980Group (in thousands) 1977 1978 1979 1980
Group I12 countries or territories inwhich malaria eradication hasbeen certified
Group IIArgentinaBelizeCosta RicaDominican RepublicFrench GuianaGuyanaPanama
Canal ZoneParaguay
Subtotal
Group IIIBrazilEcuadorMexicoSurinameVenezuela
Subtotal
72,844 a
3,342158 a642
5,39765
9001,882
452,571
15,002
49,7574,890
36,360284
10,365
101,656
531 718 1,162 2,187
463894217745488
1,563674
4156
3251,218
3131,531
266927263
5156
9361,391
3073,080
6042,294
3160
116
3411,529
3764,270b
829 c3,202
3006
140
5,204 5,004 9,044 10,993
104,43611,27518,851
9935,304
121,5779,815
19,080876
5,065
147,6308,207
20,983903
4,705
124,977 d
8,74817,875e4,4453,895C
140,859 156,413 182,428 159,940
10,10663,88832,24334,90727,67939,41411,58432,410
10,89753,41252,52159,75560,47234,55410,63320,376
14,71260,95775,65769,03941,25225,29718,41817,127
16,61957,34695,83562,65748,880 b
42,814c23,741c11,379 f
252,231 302,620 322,459 359,271
398,825 464,755 515,093 532,391
aMid-year 1979, last available population figure.bUp to November.'Provisional data.
'Up to September.eUp to October.fUp to August.
Group IVBoliviaColombiaEl SalvadorGuatemalaHaitiHondurasNicaraguaPeru
Subtotal
2,00216,6594,2282,7304,3783,2672,7335,867
41,864
Total 231,366

62 REPORT OF THE DIRECTOR
along an interior river. No major changeswere observed in the other three countries.
Group IV. There was general deteriorationin the remaining eight countries. The problemof vector resistance to all common insec-ticides used along the Pacific coast of CentralAmerica obliged El Salvador, Guatemala,and Nicaragua to use costly and geographi-cally limited alternative antimalarial mea-sures. Honduras had serious administrativeand operational problems in addition to vec-tor resistance. Since 1979, when the malariaprogram was integrated into Honduras' gen-eral health services, antimalarial measureshave not been applied with enough coverageand supervision.
In Haiti, vector resistance to DDT was con-firmed. Peru merged its malaria program in itsgeneral health service in 1978, and since thenno systematic antimalarial measures havebeen applied. Epidemiologic information pro-vided by a network of voluntary col-laborators has decreased so much that preciseevaluation of Peru's malaria status is notpossible, but the situation appears to havedeteriorated seriously. Colombia continuedto carry out antimalarial activities accordingto its new policy of stratifying malariousareas and concentrating resources and effortsin accordance with malaria endemicity and itseffect on socioeconomic development.
The lack of progress in malaria control hasaroused the concern of American govern-ments during the past two years. In 1978 thePan American Sanitary Conference adopteda resolution reaffirming that eradication is thefinal goal of the malaria program in theAmericas. The Directing Council reviewedthe malaria program in 1980 and asked thegovernments and PAHO to reformulate na-tional malaria plans according to each coun-try's specific situation, give high priority tofinancing and executing such plans, exploreall possible sources for supporting malaria ac-tivities nationally and regionally, strengthentraining, and increase field research.
In compliance with these resolutions, PAHO
and the governments have carried out thefollowing major activities: a review and refor-mulation of the national malaria plans in 12countries; elaboration of a hemispheric planin support of the malaria programs andpresentation of the plan at the subregionalplanning meetings in Buenos Aires, Guate-mala City, Lima, and Port-of-Spain; studiesof training needs, existing teaching institu-tions, and possible sources of training fundsin seven countries (Brazil, Colombia, Cuba,Guatemala, Mexico, Peru, and Venezuela);and promotion of national research activitiesand reorientation of PAHO's research projectat Tapachula, Mexico.
Despite several constraints, the followingresearch activities were in progress during theyear:
In insecticide field trials, extensive studiesof mosquito susceptibility to new insecticideswere conducted in El Salvador to design com-binations of multiple attack measures. Con-tact bioassays with moderately and highlyresistant A. albimanus strains showed accept-able mortalities for up to 40 days on woodsurfaces, while noncontact bioassays showedpractically no fumigant effects.
Residual house spraying with deltamethrinwas tested in Guatemala. Furniture, hangingobjects, and household articles were notsprayed. Preliminary bioassay results showedA. albimanus mortalities of 98.3 percent onwood and 85.9 percent on block surfacesseven months after spraying. Residents of thetest houses showed some irritation to thesprays which is being quantified.
A field trial began in February in Haiti tocompare the relative efficacy of DDT,malathion, and fenitrothion under local con-ditions in 11,000 to 13,000 houses. Althoughit is still too early to evaluate the results,bioassays of fenitrothion-sprayed surfacesshowed 100 percent A. albimanus mortalitythroughout the three-month cycle, whereasmortality was considerably reduced with DDTand malathion by the end of the cycle. In atrial of fenitrothion in Les Cayes, one of the
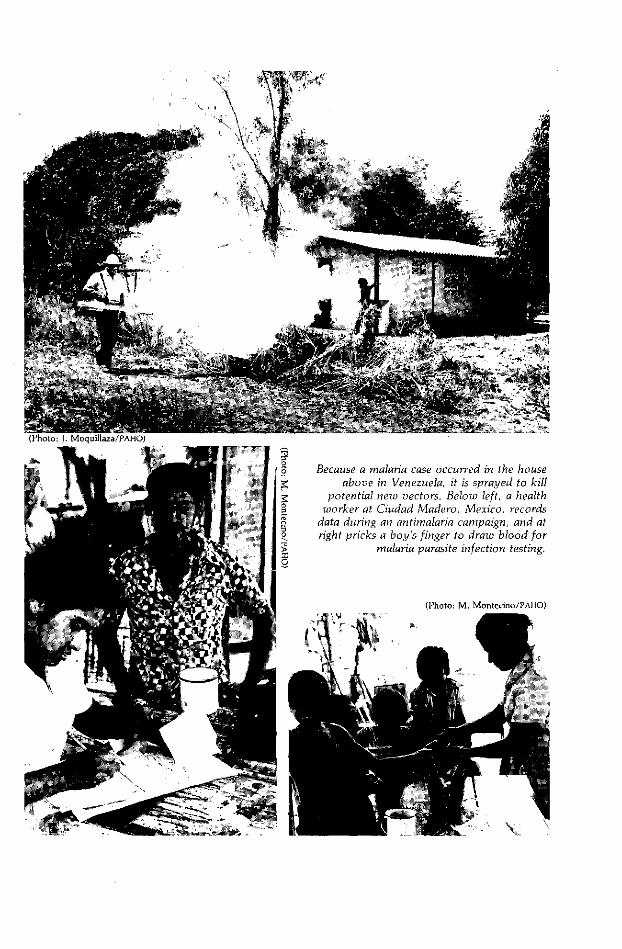
oBecause a malaria case occurred in the house
above in Venezuela, it is sprayed to killpotential new vectors. Below left, a health
worker at Ciudad Madero, Mexico, records. data during an antimalaria campaign, and ato right pricks a boy's finger to draw blood for
malaria parasite infection testing.o
(Photo: M. Montecino/PAHO)
1;l I1 1 I

64 REPORT OF THE DIRECTOR
two most important foci in the country,malaria transmission was considerably re-duced after six four-month cycles.
The biologic control agent Bacillus thur-ingiensis israeliensis was used in a small fieldtrial against anopheline larvae in Venezuela.
In the area of immunology, the malariaunit at Colombia's National Health Instituteat Bogotá is carrying out primate investiga-tions to help develop a malaria vaccine. It isdeveloping suitable simian models for study-ing human malaria and evaluating simianhosts for their usefulness in testing malariaantigens and the optimal methods for collect-ing, reproducing, and preserving parasites forantigen preparation. The unit has developedimmunologic tests such as continuous in vitrocultivation and serologic and immune com-plex techniques. It has also typed SouthAmerican plasmodial parasite strains accord-ing to their response to antimalarial drugsand started preliminary research tocharacterize such strains biochemically andantigenically.
In the area of chemotherapy, in vitroassessment of Plasmodium falciparum sen-sitivity to chloroquine showed that 80 per-cent of isolates studied in Brazil, Colombia,Ecuador, and Panama are resistant to 1.5nanomoles or more of chloroquine diphos-phate per milliliter of blood.
In Haiti, isolates showed that P. falciparummaintains great susceptibility to the samelevels observed in 1971. In El Salvador andHonduras no indication of resistance hasbeen observed. Results in Nicaragua weresomewhat different since 1.25 nMol ofchloroquine per milliliter of blood were re-quired to inhibit schizont maturation insteadof the 0.75 nMol/ml observed in 1976.
Clinical and routine followup observationsin Brazil and Colombia suggest an increasingnumber of failures to treat falciparum infec-tions with combined pyrimethamine andsulfadoxine.
Brazil, with PAHO cooperation and finan-cial support from the Special Program for
Training and Research in Tropical Diseases,completed the second phase of an investiga-tion of the efficacy, tolerance, and phar-macodynamics of mefloquine, an alternateantimalarial belonging to the quinolinometh-anol group. Analysis of the clinical and phar-macologic data produced at the Barros Bar-reto Hospital in Belém, Brazil, is underway.
Other parasitic diseases
Diseases caused by protozoan and helmin-thic infections, a serious public health prob-lem in the Americas, are advancing ratherthan receding despite efforts to control them.Several reasons explain this situation, most ofwhich are social and economic rather thanmedical. Rapid urbanization increases thetransmission of water- and food-borne dis-eases, including parasitic infections, becausecities are ill equipped to provide safe waterand sanitary facilities to large influxes of peo-ple. Migrations to open new lands foragriculture, animal husbandry, and mineraland oil prospecting as well as the seasonalmovements of agricultural workers are alsorecognized factors in the spread of parasitism.
Because of the importance of socioeco-nomic factors in the transmission of para-sitic diseases, existing technology, howeveradvanced, has not been able to cope withthese problems, particularly in tropical andsubtropical climates.
Recognizing this situation, PAHO promotesintegrated parasitic disease control. TheSpecial Program for Research ancd Training inTropical Diseases (TDR) sponsored by WHO,UNDP, and the World Bank also cooperates inthis effort. Among TDR's target diseases areChagas' disease, schistosomiais, filariasis,and leishmaniasis.
Chagas' disease. Trypanosoma cruzi, thecausative agent of Chagas' disease, occurs in avariety of mammals to such an extent that anequilibrium has been established between theparasite and the host and the disease is con-sidered a typical zoonosis.

DISEASE PREVENTION AND CONTROL 65
Humans become naturally infected whentheir skin or mucous membranes come incontact with feces of infective triatomine vec-tors. This situation is more likely to happenwhen housing conditions allow insects tobreed in homes and when animal reservoirsare close by. After an acute period, thedisease enters a chronic stage in which theheart and other organs are affected. Suddendeath may occur in young persons, and thosewho survive may have shortened lives.
Ten to 15 million people in the Americasare infected. Because of migration from ruralto metropolitan areas, blood transfusiontransmission is becoming a problem in addi-tion to natural infection.
Control measures are based on short-termvector control though insecticiding and long-term housing improvements. Chemotherapyis effective in acute cases, which are difficultto detect, but treatment is less effective inchronic cases.
The health ministries are becoming increas-ingly aware of the problem, to the extent thatArgentina, Brazil, Uruguay, and Venezuelahave established national control programs,while Ecuador, Paraguay, and Peru haveestablished similar programs in high-preva-lence areas.
Epidemiologic studies and pilot control ac-tivities are being carried out in Bolivia andChile. In addition, Colombia, Costa Rica,Cuba, El Salvador, Guatemala, Mexico, andPanama are carrying out basic epidemiologicwork on this problem. Some countries-bothindustralized and developing-are carryingout basic parasite and chemotherapy research(Argentina, Brazil, Federal Republic of Ger-many, United Kingdom, United States, andVenezuela, among others).
Through its Research and Reference Centeron Vector Biology and Control at Maracay,Venezuela, PAHO supported studies on hous-ing, parasite strain characterization, and vec-tor ecology and insecticide screening, as wellas training in vector taxonomy and biology.
The study of the effect of house modifica-
tion on the transmission of T. cruzi continuedin Trujillo State, Venezuela. The countryallotted a substantial budget to supplementthe Edna McConnell Clark Foundation'sgrant to this project. A site was chosen forbuilding experimental houses to test varioussurface plastics and other constructionmaterials. The better materials will be used invillage trials.
The Maracay center also continued itsevaluation of insecticides against Rhodniusprolixus. Field trials with fenitrothion andpirimephos-methyl were begun and gavegood results during the first three months.The field trial of bendiocarb which began inAugust 1979 was terminated in June when 30percent of the treated houses becamereinfested. A new trial using another formula-tion is planned.
With TDR support, PAHO sponsored orhelped organize meetings on serodiagnosis(Sao Paulo), clinical epidemiology (Brasilia),and the epidemiologic, social, and economicaspects of present and future methods ofChagas' disease control (Mexico City).
Schistosomiasis. Of the three major flukesthat cause schistosomiasis in tropical and sub-tropical parts of the world, only one-Schistosoma mansoni-occurs in the Ameri-cas. Transmitted by snail hosts, the diseaseoccurs in Brazil, Dominican Republic, Gua-deloupe, Martinique, Puerto Rico, SaintLucia, St. Martin, Suriname, and Venezuela.
Chemotherapeutic agents against thedisease are effective and relatively safe, butbecause it is difficult to cure all cases inendemic areas, chemotherapy must be com-plemented by other measures, particularlyadequate water and excreta sanitation andthe use of molluscicides where there is majorhuman-snail contact.
PAHO's activities were geared toward ob-taining better knowledge of the disease'sdistribution and epidemiology. It also sup-ported training in epidemiologic surveillanceof areas hitherto free of schistosomiasis butwhere snails are potential intermediate hosts
66 REPORT OF THE DIRECTOR
and there is an influx of migrants from knownendemic foci. Areas where large hydroelectricdams are being built, particularly in SouthAmerica, warrant special surveillance.
Leishmaniasis. A protozoan parasite infec-tion, leishmaniasis exists in all Latin Americancountries except Chile. The visceral form ofthe disease (kala-azar) causes high mortality,particularly among children. Mucocutaneousleishmaniasis is chronic in evolution andcauses deformity, especially of the nose andpharynx. Diffuse cutaneous leishmaniasis isalso chronic and incapacitating, and theanergic form produces a marked granulo-matous reaction and lepromatoid lesions.This last form has been found in Brazil,Dominican Republic, Mexico, and Vene-zuela.
PAHO and Venezuela's health ministrysponsored an international seminar onleishmaniasis diagnosis and treatment atCEPIALET in Caracas for 25 participants fromBrazil, Colombia, Cuba, Mexico, Nicaragua,Peru, and Venezuela.
Blindness Prevention
It is estimated that between 20 and 40million people in the world are blind, if thedefinition of blindness is a visual acuity of lessthan 3/60 or its equivalent, and that three-quarters of them live in developing countries.Two-thirds of the causes are preventable, andone-fifth of the world's blind can be cured.
The Americas have all six of the blindingconditions WHO identifies as important toprevent-trachoma, glaucoma, cataracts,traumatic eye injuries, xerophthalmia, andonchocerciasis.
Onchocerciasis, a filarial disease, is pre-dominantly rural. Eye lesions and blindnessmay result if it goes untreated. The diseaseoccurs in well-defined parts of Africa and, inthe Americas, where it was first discoveredin Guatemala in 1915, in that country and
Brazil, Colombia, Ecuador, Mexico, andVenezuela.
Antionchocerciasis measures are aimedfirst at preventing blindness, second at con-trolling the Simulium black flies that vectorOnchocerca volvulus, the parasitic wormthat causes the disease, and third at control-ling and eventually eradicating the parasite.Blindness prevention is based on medicallysupervised chemotherapy and nodule re-moval.
PAHO continued to emphasize the need tointegrate blindness prevention in generalhealth services and especially in primaryhealth care activities. The regional advisorycommittee on blindness prevention met atBelo Horizonte, Brazil, in July.
National programs exist in Brazil, Canada,Colombia, Guatemala, Panama, and theUnited States. The programs in Peru andVenezuela are pilot ones, but it is expectedthat they will be expanded into national pro-grams. In eight other countries from whichinformation is available there are scatteredblindness prevention activities, but as yettheir governments have not formulated or ac-cepted national programs.
PAHO stressed establishing national blind-ness prevention committees in all countries.Such committees must represent the entirespectrum of interested governmental (health,agriculture, industry, and other ministries)and nongovernmental organizations (oph-thalmologists, epidemiologists, other healthcare professionals, media leaders, and thecommunity).
Coordination of PAHO's blindness preven-tion program with the activities of non-governmental organizations was deemeddesirable not only to use available resourcesbetter but to convene and support regionalworkshops in training, program planning andresource assessment and mobilization-areasin which such organizations have particularexpertise.
In addition to these considerations of pro-gram development, recommendations for

DISEASE PREVENTION AND CONTROL 67
training included development of healtheducation materials for eye care and blind-ness prevention programs, inclusion of in-structional material in medical school andpostgraduate curricula, and provision ofPAHO fellowships for training in primary eyecare and blindness prevention.
PAHO supported training in the diagnosisand treatment of onchocerciasis in Guatemalaand Mexico. Guatemala's National Commit-tee for the Blind and Deaf held a regionalseminar on primary eye care training tech-niques. Conclusions from these meetingsrelated to the use of Snellen notation forrecording visual acuity, need for eye ex-amination of all children beginning school,continued prophylaxis of ophthalmia neo-natorum, and a major emphasis on com-munity education. Along these lines, it isnoteworthy that educational and trainingmaterials used in primary eye care weredeveloped for PAHO by the International EyeFoundation.
The highest priority for the future is train-ing workers for various levels of eyecare-administrators responsible for develop-ing and executing national programs,ophthalmic assistants, technicians, andprimary health care workers in villages. Thistraining is being conducted with the help ofWHO's five blindness prevention col-laborating centers in the Americas, one inGuatemala City, one in Lima, and three inthe United States.
Noncommunicable Diseases
Noncommunicable diseases are growing inpublic health importance in most of thehemisphere's countries. This trend resultsprincipally from the gradual control of com-municable diseases, increases in life expec-tancy at birth, and environmental changes.
In response to the concerns expressed bythe countries, PAHO has in recent years con-
siderably increased its cooperation with thegovernments in developing criteria and plan-ning adequate programs to control noncom-municable and chronic diseases.
PAHO's program and activities focus mainlyon cancer, hypertension and rheumatic fever,chronic rheumatic diseases, diabetes mellitus,and chronic allergies. This program wasreviewed at length and endorsed at the 1980Directing Council meeting (CD27.16).
Cancer
Malignant neoplasms have been identifiedas the second most frequent cause of death in30 of 37 American countries and territories.Age-adjusted death rates for malignantneoplasms in the Americas range from 38.5 incontinental Middle America to 80.8 intemperate South America. Hemispheric mor-tality rates from cancer are shown in Table 5,together with death rates for cancers ofselected sites in males and females.
Health ministries are paying increasing at-tention to cancer as an important publichealth problem and creating comprehensivecontrol and treatment programs. A 1978survey revealed 62 institutions in 16 countriesin Latin America and the Caribbean ex-clusively devoted to cancer research andtreatment.
PAHO continued its efforts to obtain ex-trabudgetary funds to strengthen cancer con-trol institutions in the Americas. It also pro-moted the training of junior medical and aux-iliary personnel, gathering and studyingepidemiologic data, and collecting anddisseminating cancer research information.Much of this activity is conducted throughthe Latin American Cancer Research Infor-mation Project (LACRIP), a joint PAHO-U.S.National Cancer Institute (NCI) effort.
LACRIP provided 981 custom CANCERLINEsearches requested by 255 oncologiststhroughout Latin America and the Carib-bean. NCI's CANCERLINE data base providesworldwide coverage of published and currentcancer research activities.
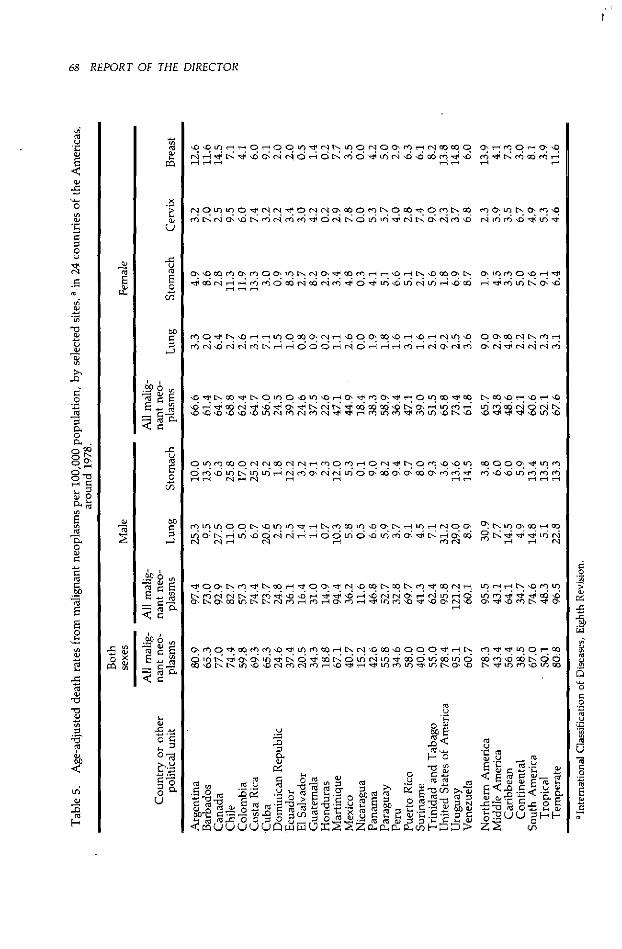
68 REPORT OF THE DIRECTOR
o O lL 1- ) 0- O iO " e r t- U)O 0 r O O'LO e- rq ob 00 OrN Z ' O oI r) rq O < O (S to O (' LO ri 'O ' O e, LO ¿O'-H '-e '
O' -' cl O c-l O' 'Om " m m m L -
0' OO L- O ¿ LOOO'LO~ r -1N O' r~ t -4 -riL'O t- N 'O~O Nl O' LOLO0'1O Iz ~ l
¡-4909Cl '-49O ~L~r ~ Z 9f~_ i1 l l 9c ~L~O~U l 9l
" e, O111 mC m0O mNm :t '" nlo ) ') o 0O' "CI U ¡-¡ l
'O X O O O O ' O L O ' O -4 0 S' L O O ' t ° O \ L O m'o -4 oq t'1 rq 9 rq o ' rq rq Cr O rq o" 'O O LO LO *nOO O 'O m 'O Lt lo L rq L O rN rq " m LO 0O LO c LO LO LO rO '0
O L Oq n r N <' 0' N " O LO 40 m 0l O m '0 '0 LOÓÑÑL<ÓOqCOO'COO'LOLO1
Ls cO 'O - 'O -4 '0
o *n d, rq lo rq lo
CoO 000 O' LO LOeO lo lo Ln On L L
¡-U r U-
LOLBOLOrOLOLOrlOCOLO LOO¡eUTr'lOO' O'.lxuOs'CO-4n C; t, -- *n lOo rq rqi N O O- * n O lo Ln m O; " li~ - oQ "6 -, -, zt z ui rq
rq rq r rq <' -U rq- ,- ,- rq
ll:r O Oe tl re t tl q li ll O O:X etz rq 1O oO tlo oO tl r9 " oO rq - In -1 _ 19 ro e IL, R rq rq C t~ "Z in " lo) lo 1 " -0 l"o oc rq °o, =s1 NrO L; q csO ui r) $ " v o oX
'-4
O' L O o ol LO )O N *o LO mO t Ls rq 'O cO 0 00 U) m Ln s
O lo 1L tL LO 'O 'o " LO <U o o- l O *n - 4 LOn LO LO Ir Ln rs O' lOoO~oN 0 ~ ~ ~000 q~HXOv ~u O ZtsOvLs <ul LO LO O LO c ooonNocoZ Usool 0
w m lo m tu c
ca
=~~~~ ._
Co m u o'- z- X Ce
a>
EW.
_cama>
pn
u-x
U_>camEo
(n
wrC
bo
¿O
b°- ° e
E c~ -2
¢ -C
E-O
r-
. z$o u
-1
U
<0a
O
'Eoo.=
ou
"0ra
,o
~.9-O
cho
"0
-aOd
o°
o
EEO
ca
ca
ta
-o
ca
a>
CJ
a>
-oo
1-
.go 6
<=
._.
-oUOu0 -oiJ CU
.:o
a>
-i
-o
-c
.gp
a..OO.2
u
.cca
ooa>
z
uCz
.E
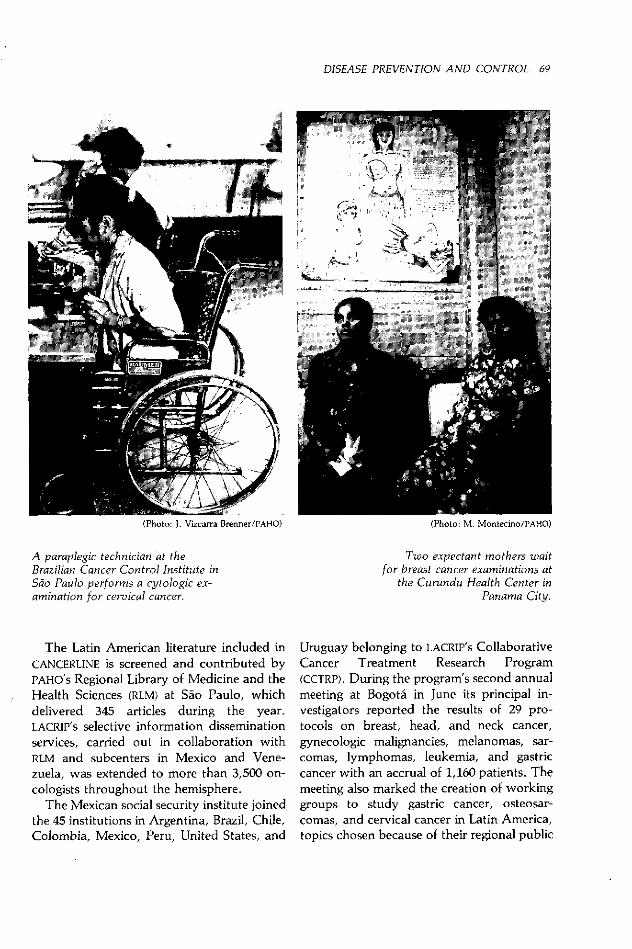
DISEASE PREVENTION AND CONTROL 69
(Photo: J. Vizcarra Brenner/PAHO)
A paraplegic technician at theBrazilian Cancer Control Institute inSao Paulo performs a cytologic ex-amination for cervical cancer.
The Latin American literature included inCANCERLINE is screened and contributed byPAHO's Regional Library of Medicine and theHealth Sciences (RLM) at Sáo Paulo, whichdelivered 345 articles during the year.LACRIP's selective information disseminationservices, carried out in collaboration withRLM and subcenters in Mexico and Vene-zuela, was extended to more than 3,500 on-cologists throughout the hemisphere.
The Mexican social security institute joinedthe 45 institutions in Argentina, Brazil, Chile,Colombia, Mexico, Peru, United States, and
(Photo: M. Montecino/PAHO)
Two expectant mothers waitfor breast cancer examinations at
the Curundu Health Center inPanama City.
Uruguay belonging to LACRIP'S CollaborativeCancer Treatment Research Program(CCTRP). During the program's second annualmeeting at Bogota in June its principal in-vestigators reported the results of 29 pro-tocols on breast, head, and neck cancer,gynecologic malignancies, melanomas, sar-comas, lymphomas, leukemia, and gastriccancer with an accrual of 1,160 patients. Themeeting also marked the creation of workinggroups to study gastric cancer, osteosar-comas, and cervical cancer in Latin America,topics chosen because of their regional public
; � ' p---- ' 1 �11.111^
l�, 1,1 1 'J~ � ��- - - -

70 REPORT OF THE DIRECTOR
health importance. The results of the threestudies will be compared with experiencefrom other areas of the world.
CCTRP also awarded research traininggrants to nine junior oncologists and nurses,financed the exchange of 18 principal in-vestigators, provided drugs for treating pa-tients, and gave grants of $6,000 to $14,000 tothe Latin American centers.
PAHO's cancer program expanded to in-clude a comprehensive four-year project todetermine the possible carcinogenic andteratogenic effects of pesticides in humans.This project is a collaborative effort betweenPAHO, Colombia's National Health Institute,University of Miami, U.S. Environmental Pro-tection Agency, NCI, and WHO's InternationalAgency for Research on Cancer at Lyons,France.
Other noncommunicable diseases
Cardiovascular disease (particularly hyper-tension and rheumatic and coronary heartdisease), diabetes, and chronic rheumaticdiseases are being given high priority in theAmericas. The Directing Council approved aresolution (CD27.16) urging that health min-istries include programs and strategies intheir national health plans to counter the riskfactors causing increased morbidity and mor-tality from these diseases. The resolution alsorecommended that the countries promotegeneral health service activities to preventand control such diseases, with special atten-tion to conditions that can be effectively con-trolled such as hypertension, rheumatic feverand heart disease, and diabetes.
The resolution also asked the Director tosupport improved geriatric care programs;continue to support national noncom-municable disease prevention and controlprograms and cooperative activities amongthe countries, and continue efforts to obtainextrabudgetary funds for such programs.
The PAHO working group on hypertensioncontrol, composed of representatives from
Argentina, Bolivia, Brazil, Chile, Colombia,Cuba, Ecuador, Mexico, Peru, and Vene-zuela, met at Bogotá to discuss the results ofthe first three years of collaborative hyper-tension studies and plan future activities, in-cluding draft guidelines for community hy-pertension control which are now beingedited.
Representatives of the countries takingpart in PAHO's rheumatic fever and rheumaticheart disease prevention program (Argentina,Bolivia, Brazil, Chile, Ecuador, Peru, andVenezuela) met at Santiago to discuss prog-ress during its fourth year. The final registryof patients after a five-year followup wasmade in September, and results of the col-laborative study will be analyzed in 1981.
The final version of an operating manualfor community-based programs to preventand control rheumatic fever and diabetes is inpress and will be published in 1981.
The disability caused by chronic rheumaticdiseases and their burden on health serviceshave been under joint study since 1978 byArgentina, Brazil, Chile, Mexico, Uruguay,and Venezuela. The advisory study groupmet at Washington to discuss preliminaryresults and future activities, includingpreparation of guidelines for adequatelytreating some of the most common rheumaticconditions by nonspecialized medical andparamedical personnel.
Argentina, Brazil, Chile, Colombia, Mex-ico, Peru, Uruguay, and Venezuela have beenparticipating since 1979 in a study of the mor-bidity and disability caused by chronicallergies, their relation to various risk factors,and the burden they place on medical ser-vices. Its results will be analyzed in 1981-82.
Mental Health
There is a substantial gap between themagnitude of mental health problems and thehuman and material resources available for

DISEASE PREVENTION AND CONTROL 71
dealing with them in the Americas. Thissituation is particularly critical in rural andmarginal urban areas where there is a highprevalence of psychologic disorders andanomalous behaviors stemming from theadverse conditions in which their inhabitantslive. The rates of suicide, homicide, ac-cidents, and voluntarily inflicted injuries arerising steadily in various countries. More-over, epidemiologic surveys reveal a high in-cidence of neuroses, alcoholism, drugdependency, and behavioral problems inchildren. Psychiatric and mental healthfacilities are not meeting the clear demand forcurative services, and health promotion anddisease prevention activities are barely under-way in the major cities.
A growing interest is apparent in the studyof psychosocial factors that influence healthand well-being and in developing measures tohelp control harmful factors and promotebeneficial ones.
PAHO's governing bodies have dealt withmental health several times (CSP15.13,csP16.15, CD16.21, CE84.6). At the DirectingCouncil's 1979 meeting, a resolution (CD26.17)was approved recommending that updatedinformation be obtained on the influence ofsuch factors as malnutrition and otheradverse environmental conditions on thedevelopment of children. Another resolutionfrom the same meeting recommended that, inpreparing their health programs, govern-ments take account of the psychosocial fac-tors in child development and includemeasures in such programs to foster har-monious maturation.
During 1980 PAHO continued to cooperatewith the countries in developing ways tomodernize psychiatric services, includingmental health activities in general health pro-grams, and for injecting psychosocial con-siderations into the programs. Furtherassistance was provided in organizing mentalhealth, alcoholism, and drug dependency ser-vices, disseminating technical information,and extending support to mental health train-
ing and research centers.The Executive Committee asked the Direc-
tor (CE84.11) to draw up a report of drug abuseprograms in the hemisphere. In its laterdiscussion of the report, the Directing Coun-cil emphasized the need for further and con-tinuous updating of epidemiologic data aboutdrug abuse and for strengthening multisec-toral efforts to reduce illicit drug demand.
Two technical meetings at PAHO head-quarters helped to reorient the mental healthprogram both regionally and in specific coun-try projects.
The first of these PAHO-sponsored meet-ings, in March and April at Washington, wasof a working group on the inclusion ofpsychosocial components in primary healthcare. Representatives of Bolivia, Brazil, Co-lombia, Guatemala, Honduras, Panama,Peru, United States, and Venezuela attended.The functions of the primary health workeras a mental health agent were discussed, andrecommendations were made for developingtraining materials.
The second meeting, in May in Washing-ton, was of a group studying the influence ofmalnutrition and other environmental factorson child development. Seven specialists fromChile, Colombia, Guatemala, Jamaica, Mex-ico, United States, and Uruguay participated.The group's working documents and finalreport have been distributed.
Closer ties were developed with the WHOcollaborating centers on mental health,alcoholism, and drug dependency in Canada,Colombia, Mexico, and the United States,and a neurologic sciences collaborating centerwas designated in Colombia. Twenty-twospecialists from 10 countries met at one of thecollaborating centers (Cali, Colombia) toreview ways to extend mental health services.Another technical group, which met atWashington, discussed problems pertainingto a classification of mental diseases multiax-ially-or biologically, psychologically, andsociologically-in which criteria based on thesocial environment and its psychologic conse-
72 REPORT OF THE DIRECTOR
Occupational rehabilitation activitiesat the Pavas Psychiatric Hospital inSan José.
(Photo: M. Montecino/PAHO)A _
quences and attendant disabilities as well aspurely medical criteria were considered.
A mental health team visited Brazil to assistone of its states in developing plans for ex-tending mental health services and integratingthem into the primary care system.
PAHO cooperated with new mental healthofficials in Argentina, Dominican Republic,and Ecuador in analyzing those countries'revised mental health programs, all of whichare based on developing community care ser-vices as an alternative to traditional institu-tionalization. Consultants worked with themental health departments of Chile,Grenada, and St. Vincent in evaluating theirservices.
Modernization of psychiatric nursing ser-vices and a shift in the role of the nurse tothat of active community agent was one ofthe cooperative activities PAHO undertookwith Argentina, Colombia, Dominican Re-public, and the English-speaking Caribbeancountries. Staff members and consultantsmade visits and conducted workshops.
Surveys of the epidemiology of alcoholismin Ecuador and Honduras and a study ofcommunity responses to alcoholism problemsin Mexico were completed. Groundwork waslaid for developing a system of epidemiologicsurveillance of drug abuse and traffic ac-cidents in Argentina, Mexico, and Peru.
Service support, training, and researchprograms were started in Bolivia and Peruwith financial assistance from the United Na-tions Fund for Drug Abuse Control (UNF-DAC). New drug abuse project agreementswere signed with Colombia and Ecuador.
A seminar on the safe use of psychotropicsubstances and narcotic drugs was held atBuenos Aires under the auspices of theArgentine government, UNFDAC, and PAHO
to examine problems and propose practicalsolutions in carrying out the 1961 Single Con-vention on Narcotics and the entry into forceof the 1971 Agreement on PsychotropicSubstances. Ten countries and five interna-tional organizations were represented:

DISEASE PREVENTION AND CONTROL 73
In the future, PAHO's cooperative activitieswill be aimed primarily at extending mentalhealth services as part of general health ser-vices and at using primary care workers ascommunity mental health agents.
Dental Health
Dental disease continues to plague theAmericas. There has been little improvementin the situation or in the resources availableto prevent and arrest the two most prevalentdental ailments, caries and periodontaldisease.
The availability of dental services is still thealmost exclusive domain of the dental profes-sional and the untrained practitioner, andonly limited numbers of dental professionalsare to be found in rural and marginal urbanareas where needs are greatest. With the ex-ception of the English-speaking Caribbeancountries and Suriname where school pro-grams using dental auxiliaries have beendeveloped, little emphasis has been placed ontraining auxiliary or intermediary workers toprovide dental services in underserved areasand extend services where professionals arepresent.
Despite the increase in dental schools toapproximately 120 and increases in their classsize, little if any change has occurred in thedentist-population ratio in most LatinAmerican countries. The ratio of dentists inthe public health sector to the population tobe served is often more than 1 to 100,000.The estimate that 90 percent of the dentalmanpower in many countries provide serviceto 10 percent of the population likewisereveals the extent of the problems and theburden on the public sector.
Dental disease affects almost everyone inLatin America. National epidemiologicstudies in the 1970s in Colombia andVenezuela demonstrated the early onset ofdental disease in children and the need to em-
phasize preventive programs. Similarly, datafrom many countries show the lack ofrestorative care, particularly in younger agegroups.
Dental health appears to receive little at-tention in national health service planningand, in view of the universal nature of thedisease involved, little priority. This is oftenseen in the financial support allocated to den-tistry in the public sector.
The 1970s also showed the need for ap-plication of modern concepts and technologyin providing dental services and the problemsassociated with a shortage of dental mainte-nance and denture technicians.
During 1980 PAHO collaborated with na-tional health authorities in developing dentalhealth programs in the Bahamas, Cuba,Dominican Republic, Ecuador, Guyana, Ja-maica, Nicaragua, Peru, Suriname, Trinidadand Tobago, and Venezuela. Attention wasdirected to problems associated with the ex-tensive periodontal disease in the countries,particularly those of the Caribbean and nor-thern South America where its extent is beingidentified.
At their annual meeting, the Andeanhealth ministers again expressed interest indeveloping a dental program for and increas-ing the use of auxiliaries in that area. Con-tinued progress was made in carrying out theresolutions passed by the CommonwealthCaribbean health ministers.
A complete review of existing dental ser-vices was made in Nicaragua and changeswere made in them to increase the availabilityof care, particularly in rural areas. Continuedemphasis was placed on improving thedelivery of dental services in Mexico andVenezuela, together with systems for analyz-ing extended coverage and providing primarycare. Advice was given to Ecuador on devel-oping methods for collecting oral epidemio-logic data, and a simplified system for gath-ering dental disease data was instituted incertain Caribbean countries.
Until an effective vaccine or other new
74 REPORT OF THE DIRECTOR
(Photo: M. Montecino/PAHO) (Photo: M. Montecino/PAHO)
A dentist and her assistant extract atooth at Ciudad Netzahualcóyotl The dental unit at Ciudad Net-Hospital on the outskirts of Mexico zahualcóyotl Hospital can treat manyCity. patients at the same time.
mass preventive agent is developed, fluoridewill continue to be the mainstay in prevent-ing caries because it has proved remarkablyeffective when administered in differentvehicles. The two principal ones are drinkingwater and table salt, and through themfluoridation is easy to carry out and inexpen-sive. In the absence of mass measures or ascomplementary dental care procedures, A saturation-suspension cone such as
,. .1 I r 11 1 . . I . ~~~~A saturation-suspension cone such asfluoride may be usefully administered in this one in Brazil can be used totablets, solutions, gels, and pediatric drops. fluoridate water in towns of 2,000 toSpecial school fluoridation programs are also 150,000 population.possible.
Drinking water is fluoridated in about 15 (Photo: G. R. Roviralta/PAHO)
countries. The total population with access tofluoridated water supplies in Latin America ,and the Caribbean at the end of the year was l W --estimated at 40 million. Fluoridation of com-munity water supplies was promoted in areaswhere the measure appears most feasible ormost acceptable. l
PAHO emphasized training professional andtechnical staff in standard fluoridation tech-'niques. This included promotional activities,preliminary studies, project preparation andexecution, surveys of fluoridation system op-
DISEASE PREVENTION AND CONTROL 75
eration and maintenance, and research. Thedevelopment and use of simply designed andinexpensive dosing equipment was promotedand information disseminated about it.
Naturally overfluoridated drinking water isa serious problem in some parts of Argentina,El Salvador, Mexico, and Peru. Argentina isnow the only country where part of thefluoride is removed from water as a regularpractice. Other countries voiced interest inadopting this practice.
Special emphasis was put on preventiveprograms in response to the Directing Coun-cil's 1979 resolution (CD26.39) on salt fluorida-tion to prevent dental caries. This measurewill especially benefit rural areas and smallcommunities where water fluoridation is im-practical. Salt fluoridation has been studiedin Colombia and proposals were made for itswide use there. Initial reviews were made anddiscussions held with governments interestedin carrying out this preventive measure insuitable places, and Mexico, Nicaragua, St.Kitts-Nevis, and Saint Lucia began consider-ing its feasibility.
Laboratory Services
Laboratory services are a set of structuredprocedures to produce data for improvingpatient diagnosis and treatment, determinethe prevalence of pathogenic agents in thecommunity, and identify their presence in theenvironment. As health programs develop,laboratories play a more important role insupporting them.
The problems in carrying out health plans,including training and infrastructure develop-ment, are reflected in miniature in laboratoryactivities.
PAHO continued to cooperate in establish-ing laboratory systems able to meet the grow-ing demand for them. As executing agency ina project to strengthen laboratory systems inthe smaller English-speaking Caribbean
islands which UNDP approved during theyear, PAHO will provide assistance in improv-ing existing hospital laboratories, training,and setting up programs to service biomedicalequipment and maintain quality control.These laboratories will also begin clinicalchemistry, pathology, microbiology, andsimilar studies in collaboration with the largercentral laboratories in Barbados, Guyana,Jamaica, and Trinidad and Tobago.
Chile, with PAHO and UNDP assistance,pressed forward with its program tostrengthen its public health laboratory andconsolidate and expand peripheral labora-tories in the national network. The Domini-can Republic, with assistance from PAHO,prepared a request for UNDP aid to strengthenand expand laboratory services throughoutthe country. Ecuador received PAHOassistance in formulating a plan to strengthenits National Institute of Hygiene and TropicalMedicine and extend its regional and locallaboratory network. Mexico, with PAHOassistance, planned to establish a nationallaboratory system to satisfy increasingdemands in medical care and environmentalprotection. The authorities there are seekingUNDP financial support for a 1982-86 programto strengthen central reference laboratories,establish 14 regional laboratories, and pro-vide minimal laboratory facilities in health in-stitutions requiring them. Uruguay, which re-quested PAHO technical advice in preparing arequest for UNDP financial aid, strengthenedits regionalized laboratory system, includingits central laboratory and departmental andlocal facilities. Venezuela asked PAHO's helpin converting its laboratories into a nationalnetwork.
Representatives of 23 countries attended aregional seminar on biologic reagent produc-tion and control held by PAHO and the Mexi-can health and welfare secretariat at Oaxte-pec in November. The participants reviewedprocurement and use of biologic reagents anddrew up recommendations to establish qual-ity control laboratories in each country,
76 REPORT OF THE DIRECTOR
designate laboratories as collaborating centersto produce and distribute reagents, and ap-point a permanent regional committee tooversee the recommendations' execution.
PAHO continued its program of externalquality control in bacteriology in Caribbeanlaboratories and in serology in all the coun-tries as part of CDC's worldwide program toevaluate syphilis serology. Also in coopera-tion with CDC, the national laboratories ofArgentina, Chile, and Colombia began evalu-ating serologic techniques for diagnosinghepatitis B. CDC participation in these pro-grams and its expansion into other areas, in-cluding hematology, will ensure that data ob-tained by laboratories in different countriesare comparable and reliable and make possi-ble more precise assessments of health condi-tions.
Following up a course conducted at Mardel Plata, Argentina, in late 1979 on qualitycontrol in clinical chemistry, PAHO initiatedarrangements to include Argentina, Bar-bados, Belize, Colombia, Costa Rica, Cuba,Ecuador, Guyana, Honduras, Panama, Uru-guay, and Venezuela in a new WHO clinicalchemistry quality control program centeredat Birmingham, England.
Laboratory work entails exposure tobiologic, chemical, and physical agents, withconsequent risk of work-related infections orlesions. The risk is especially high inmicrobiology, where infections continue tobe reported frequently. To institute safetymeasures to help control this risk, WHO spon-sored a meeting of representatives from allparts of the world at which the global situa-tion was reviewed and recommendationsmade. PAHO thereafter developed plans fortwo regional courses, in English and Spanish,to train instructors who in turn will give na-tional courses on returning to their owncountries. A manual of safety standards andprocedures-to be distributed to all the coun-tries in the hemisphere-was prepared for usein the regional courses, which will be offeredin cooperation with CDC and NIH.
PAHO cooperated with the countries inorganizing seminars, courses, and othermeetings by providing experts, scholarships,and teaching materials. In cooperation withthe University of Sao Paulo's institute oftropical medicine, a two-month course on theserodiagnosis of parasitic diseases was givenfor 15 Brazilians and two participants fromother countries. PAHO also provided an ex-pert to Chile for a course on the same subjectfor provincial laboratory directors. A courseon quality control was organized in conjunc-tion with Uruguay for staff of its clinicalmedicine laboratories.
In cooperation with WHO, PAHO designed athree-phase pilot program to determine thelaboratory tests, materials, manpower, logis-tics, and supervision necessary to supportprimary health care programs. The programwill be tested in Honduras and Mexico todetermine its worldwide applicability.
PAHO continued to supply materials tofacilitate the transfer of appropriate technol-ogy, including manuals, reference antigensand antisera, cell lines, and standardsubstances.
It also coordinated the cooperative projectfinanced by Merck Sharp & Dohme to deter-mine the prevalence of various antigenictypes of pneumonia streptococci in 10 coun-tries. The study is to identify the types mostprevalent in the hemisphere's clinical syn-dromes and include them in a widely usedvaccine. Four hundred fifty strains with an-tigenic types different from those in the vac-cine have so far been identified, and it ishoped that the project can be completed in1981.
The role of immunology in the diagnosis ofcommunicable and noncommunicable dis-eases, the pathogenesis of degenerative andtumoral diseases, and the treatment of certainclinical syndromes has given this discipline animportance that calls for establishing specialimmunology laboratories.
PAHO has been helping develop laboratorymanpower, diagnostic services, and research
DISEASE PREVENTION AND CONTROL 77
programs through two collaborating centers,one at the Butantan Institute in Sao Pauloand the PAHO/WHO immunology collaborat-ing center comprising several laboratories inMexico City.
Increasing interest in immunology prompt-ed the establishment of a network of immu-nology centers in the Caribbean with theassistance of the Netherlands. This program,which began in 1977 with training at theWHO Collaborating Center for ImmunologyTraining and Research (ITR) in Amsterdam,has been carried out in Cuba, Jamaica, Suri-name, and Trinidad and Tobago. A Dutchand PAHO evaluation team verified the pro-gram's benefits in diagnosis, foreign exchangesavings through local reagent production,and training.
Costa Rica, Guatemala, and Hondurashave already expressed interest in participat-ing in the program, which may ultimately beextended to other countries.
An advisory group consisting of im-munologists from Cuba, Jamaica, Suriname,and Trinidad and Tobago met at PAHO head-quarters in February to plan a Caribbean im-munology seminar in 1981 to establish stan-dards for extending the Caribbean programto other countries.
Vigorous action continued in training im-munology personnel. ITR trained 29 scientistsfrom Cuba (14), Jamaica (7), Suriname (6),and Trinidad and Tobago (2). The Sáo Paulocenter conducted its annual basic im-munology course, which is designed for in-structors, and its counterpart in Mexico of-fered a course on clinical immunology.Venezuela's National Clinical ImmunologyCenter in Caracas initiated training coursesfor physicians (three years), scientists (twoyears), and technicians (nine months). Incooperation with Switzerland and WHO,identical courses in French and in English onthe immunology of infectious diseases wereoffered at WHO's immunology training andresearch center in Lausanne. Three par-ticipants from the Americas attended.
Correct diagnosis of an immunologic syn-drome is important since adequate treatmentdepends on it. To standardize procedures andobtain comparable and reliable data, PAHOinvited the countries to participate in CDC'simmunodiagnosis proficiency testing pro-gram. It is planning to organize regionalrefresher courses on immunology methods toenable participants to evaluate the efficiencyof their laboratories.
Epidemiologic Surveillance
PAHO made several improvements in itsepidemiologic surveillance program throughits headquarters and field staff. The mecha-nism for weekly and annual collection ofepidemiologic data was strengthened to meetthe operational requirements of the variousdisease prevention and control programs andautomated data processing will be introducedin 1981. Its new Epidemiological Bulletinbegan to appear in Spanish and English, withpressruns of 5,500 copies per issue.
A modular short course on the epidemio-logic principles of disease prevention andcontrol was prepared with Rockefeller Foun-dation support to train health service profes-sionals. The preliminary material was testedin Uruguay and later Cuba and Mexico, andthen revised in light of results from the trialcourses. The course will be distributedgenerally in 1981 and, as a complement,preliminary steps will be taken to reformulatethe program for training intermediateepidemiologists.
To bring the Pan American Sanitary Codeinto consonance with the InternationalHealth Regulations, the code's disease-reporting chapter will be revised and updatedin 1981.
Eleven epidemiologists and three associatedexperts assigned to PAHO country programs,as well as the staff of the CaribbeanEpidemiology Centre, worked with national
78 REPORT OF THE DIRECTOR
counterparts to strengthen epidemiologicsystems and develop various disease preven-tion and control programs.
PAHO's Caribbean Epidemiology Centre(CAREC) at Port-of-Spain was established atthe beginning of 1975 after having beenoperated by the Rockefeller Foundation andUniversity of the West Indies as the TrinidadRegional Virus Laboratory. It is sponsoredand financed by the English- and Dutch-speaking governments of the Caribbean.
USAID awarded CAREC a $1,160,000 grantin 1979 to develop national surveillancesystems and supporting laboratories. During1980 CAREC used funds from the grant toestablish a training unit and develop newmodular training manuals for physicians,students, public health nurses and inspectors,and statistical surveillance officers. These willbe a vital tool in introducing simple epi-demiologic techniques, including graphicpresentation of how to measure health andthe provision of primary care.
CAREC's program was revised in detail byits scientific advisory committee and counciland endorsed by the Commonwealth Carib-bean health ministers at their July conferencein Grenada.
Since 1979 CAREC's program has been oneof consolidation. There are now 18 interna-tional and 80 local staff. The national pro-grams are based on annual workshops for-mulated by national epidemiologists whomeet at CAREC in May. The annual work-shops for epidemiologists, laboratory direc-tors, and statistical surveillance officers are offundamental importance in developing thesurveillance system. Special emphasis was puton laboratory management and on-the-jobtraining in laboratory techniques in thesmaller islands using USAID funds. CARECworked closely with the Trinidad publichealth laboratory.
Dissemination of information is a key com-ponent of the program. The CAREC Surveil-lance Report was published monthly with acirculation of 2,500 copies. There was an en-
couraging rise in the number of consultationsby the countries without an increase in the re-quests for on-site epidemic assistance. Ameeting to review disease in the Caribbeanwas convened in association with PAHO head-quarters to plan a reassessment of Caribbeanhealth priorities.
The outbreak of yellow fever in Trinidadin 1978-79 and the continuing threat ofdengue have highlighted the need for goodarbovirology diagnostic facilities and tech-niques. During the year a joint project wasdesigned by Trinidad and Tobago, CAREC,and Canada's IDRC to develop the uses of in-sect cell lines in viral isolation and diagnosis.
Malaria remains indigenous in Belize,Guyana, and Suriname, and infections -c-curred throughout the year. Because CAREC's
laboratory proficiency testing had indicated alack of diagnostic expertise in malaria, twocourses for technicians were conducted.
Communicable disease cannot be geo-graphically isolated. Continuing efforts aremade to improve contacts with surroundingcountries. CAREC has particularly strong linkswith CDC, which seconds staff to it. Newlinks are being established with the Canadiannational surveillance system.
The appointment of a West Indian aslaboratory superintendent and training of-ficer was a major step in carrying out thepolicy to train West Indies nationals for allthe senior posts at CAREC.
CAREC research programs continued instreptococcal disease, filariasis, leptospirosis,and ischemic heart disease. Support camefrom the British Medical Research Council,NIH, IDRC, and a grant from PAHO for yellowfever research.
Biologicals
Vaccine control
Vaccine control in Latin America variesgreatly and in general is advancing very
DISEASE PREVENTION AND CONTROL 79
slowly. Though most vaccine producers testtheir own products, very few have testinglaboratories that are independent from pro-duction. The concept of national controllaboratories as part of governmental biologicsregulation is still nascent. At its 1980 meetingthe Directing Council reminded governments(CD27.15) of the importance of national con-trol laboratories and urged more vigorous ac-tion to strengthen them.
In Argentina, the control department ofthe Carlos A. Malbrán Microbiology In-stitute, which was modernized during theyear, tests the protective potency of pertussisvaccine. Through a collaborative study withthe u.s. Food and Drug Administration'sbureau of biologics, PAHO's designated per-tussis reference laboratory, the efficiency ofthe Malbrán laboratory is being evaluated.PAHO is providing services to the newBrazilian federal laboratory being built at Riode Janeiro for testing biologicals and vac-cines, particularly those supplied to the na-tional immunization program through thefederal drug supply agency.
In Chile, the Institute of Public Health'svaccine control laboratory at Santiago wasgiven responsibility for testing vaccines pro-duced in and outside the country, a task thatwill require better premises, improved equip-ment, and a larger staff. In Colombia, a newcontrol laboratory separate from productionhas been established, though it has far to gobefore it can effectively support the NationalHealth Institute's vaccine production. Thesedevelopments culminated the consultationsPAHO had provided in the last two years.
A new agreement between PAHO and Mex-ico provides for PAHO assistance in convert-ing the control department of that country'spublic health laboratory into a nationalvaccine-testing facility. In time the laboratorywill also assume responsibility for testing vac-cines from neighboring countries, a functionnow carried out by the National Virology In-stitute under the Directorate General ofBiological and Reagent Production.
PAHO provided testing advice to Chile,Colombia, and Venezuela about pertussisvaccines and to Peru about tetanus and per-tussis vaccines because those countries'laboratories continue to face problems withthe antigenic quality of the pertussis pro-duced in submerged culture.
Recognizing the importance of viral vac-cine surveillance in expanded immunizationprograms, the Directing Council recom-mended (CD27.15) that national controllaboratories be strengthened so they cantitrate live viral vaccines. As a result, PAHO isestablishing a collaborative program to buildtechnical skill and help national laboratoriesacquire experience in assaying the potency ofviral vaccines. Yellow fever vaccine is also in-cluded in this program because of thatdisease's importance in many countries.Apart from direct technical advice by a vac-cine expert, laboratories eligible for participa-tion in the program will receive trainingassistance, laboratory manuals in English orSpanish on standard testing procedures, andreagents and reference preparations. Argen-tina, Brazil, Colombia, Cuba, DominicanRepublic, Ecuador, and Mexico have voicedtheir interest in joining the program.
To build up vaccine-testing experience,PAHO encourages national control labora-tories to have their tests verified by an out-side reference laboratory it designates. Dur-ing the year such a laboratory provided DPTvaccine reference testing to Argentina,Bolivia, Brazil, Colombia, Ecuador, Guate-mala, Peru, and Venezuela. In the light ofresults reported by the laboratory, fresh seedshave been provided to replace old ones andreference vaccine was made available to mostnational laboratories. Another laboratoryprovided reference services for testing yellowfever vaccine produced in Brazil andColombia.
Drug quality control
Despite rapidly growing national expen-

80 REPORT OF THE DIRECTOR
ditures on pharmaceutical products in LatinAmerica and the Caribbean (more than $7billion in Latin America in 1980, a 22 percentincrease over 1979), the public health sectorcontinues to suffer from a scarcity of essentialdrugs needed for extending health care to themedically underserved.
To assist governments in overcoming thesedifficulties, the Directing Council instructedthe Director (CD27.23) to study the establish-ment of a revolving fund or other mecha-nisms for collectively purchasing large quan-tities of selected drugs. An internal workinggroup undertook a preliminary study ofpossible financing mechanisms for andPAHO's role in the acquisition of criticalhealth supplies. The group's findings andrecommendations will be presented to the Ex-ecutive Committee in June 1981.
To strengthen the infrastructure requiredto deliver medicaments, particularly in pri-mary health care, an interdisciplinary opera-tions research project was begun to assess themanagement and use of drugs in health centerhospitals and health posts. Preliminary find-ings showed deficiencies in all areas of thepharmaceutical supply systems studied-from selection and procurement through dis-tribution and use. A 1981 meeting is plannedto analyze these problems and develop solu-tions to them.
Information on drug safety and efficacy isbeing provided regularly through a specialquarterly section of the Boletín de la OficinaSanitaria Panamericana. This information isparticularly useful to government agenciesconcerned with regulating the use of drugs inboth the private and public sectors.
Recruitment of professional staff broughtthe Caribbean Regional Drug Testing Labora-tory at Kingston a step closer to full opera-tion. The start of specialized microbiologicand pharmacologic analyses of phar-maceutical products the English-speakingCaribbean islands produce or import waspostponed to 1981 because of delays in thearrival of necessary equipment contributedby CIDA.
In Brazil, the PAHO-assisted Drug QualityInstitute (DQI) at Sáo Paulo, which isoperated by the Oswaldo Cruz Foundation,worked closely with a UNDP project todevelop an integrated national drug controlsystem and build and staff the Foundation-operated federal laboratory at Rio de Janeiro,whose construction was almost complete atyear's end. The training and advisory servicesprovided by DQI during the year includedspecialized analytic courses, seminars onevaluating drug combinations, and a sym-posium on national drug policies.
Through its permanent staff and tem-porary consultants, PAHO also providedtechnical collaboration to drug control pro-grams and courses in Argentina, Chile, Co-lombia, Costa Rica, Cuba, El Salvador,Guatemala, Peru, Trinidad and Tobago, andVenezuela.
The demand for pharmaceuticals is ex-pected to increase in the foreseeable futuredue among other things to expanding healthcoverage and rapid urbanization. PAHO's ef-forts will be directed toward closer collabora-tion with government agencies responsiblefor the control and use of drugs to ensuretheir reliable supply at affordable prices. Topromote comprehensive regional and na-tional pharmaceutical supply policies andidentify areas for intercountry cooperation,PAHO will hold a regional meeting on drugpolicies and management in late 1981.
Blood banking
Blood is in short supply in most LatinAmerican and Caribbean countries. Bloodcomponents and plasma derivatives are rarecommodities which must be imported at highcost for lack of necessary technology to pro-cess blood. In the absence of regulatorysystems to control the quality and safety ofblood products, it is difficult to protect blooddonors and recipients adequately.
The dependence of many existing bloodcenters on the remunerated donors who pro-vide more than 60 percent of Latin American

DISEASE PREVENTION AND CONTROL 81
and Caribbean blood requirements has ab-normally increased the risk of hepatitis B in-fection. This situation could also result in anincrease in the incidence of liver cancer.
The change from whole blood administra-tion to blood component therapy in treatingvarious clinical illnesses is progressing veryslowly, largely because the complexity ofplasma component fractionation and freeze-drying technology has hampered the availa-bility of such components for clinical pur-poses. Large blood banks in capital cities areproducing a quite limited amount of bloodcomponents, but most of what is required hasto be imported. Fractionation facilities able toproduce large amounts of serum exist inArgentina (1), Brazil (2), and Mexico (3).Only the plants at Córdoba, Argentina, andthe Mexican Institute of Hygiene are non-commercial.
Governing body resolutions in 1975(WHA28.72 and CE74.21) urged health ministriesto establish national policies to ensure thatblood and its products are safe, of goodquality, and available in adequate quantities.In 1980 PAHO therefore decided to invite thehemisphere's governments to begin planninglong-term national blood programs. Cubaand Nicaragua have national policies andprograms; Brazil, Uruguay, and Venezuelahave blood banking laws; and other coun-tries are drafting or should soon pass suchlegislation.
The first regional planning meeting willtake place at Bogotá in 1981 with financialassistance from WHO and the League of RedCross Societies.
The International Society of Blood Trans-fusion (ISBT) gave PAHO permission totranslate four of its guides into Spanish, andso far PAHO has distributed more than 100sets free to blood banks in all Latin Americancountries. A generous contribution by theAmerican Association of Blood Banks ena-bled PAHO to distribute 120 sets of books onblood transfusion to 75 educational institu-tions and national blood banks in LatinAmerica and the Caribbean.
During 1981 PAHO will increase its coopera-tion with the League of Red Cross Societiesand ISBT in extending blood program cover-age to provincial areas while strengtheningthe supportive role of national blood banks.
Radiation Health
Radiation health deals with the develop-ment and use of medical ionizing radiationand protection from radiation hazards,whatever their source. Radiation medicinecomprises three distinct areas: diagnosticradiology, radiotherapy, and nuclear medi-cine.
In rural and marginal urban areas of LatinAmerica and the Caribbean most people donot have access to diagnostic radiology,which has become the most important andexpensive single method of clinical diagnosisin modem medicine. Many hospitals do nothave the most basic x-ray equipment or staffadequately trained to use it. When it isavailable, x-ray equipment is often over-sophisticated and prone to breakdown. Inmost countries medical students receive noexperience in radiologic services before begin-ning their careers. There are few schools forradiologic technicians and no organized train-ing programs for other professionals such asmedical physicists or dosimetry specialists.
The situation in radiotherapy and nuclearmedicine is similar in most American coun-tries. In a well-developed cancer control pro-gram it is estimated that at least half of all pa-tients will benefit from radiation therapy, yetin many countries adequate staff and equip-ment are not available. In addition, there areextremes between the very modern and ad-vanced equipment in a few medical centersand the obsolete equipment in most otherhospitals.
In the area of radiation protection, manypatients, health workers, and communitymembers are exposed to unnecessarily highrisks due to faulty diagnostic x-ray equip-

82 REPORT OF THE DIRECTOR
ment. High-intensity radiation sources areused in industry and agriculture, and seriousaccidents have been reported. Nuclearresearch reactors have been built in Argen-tina, Brazil, Chile, Colombia, Mexico, andVenezuela. Power reactors are in operation orunder construction in Argentina, Brazil, andMexico, and are being considered in othercountries. National radiation protection ser-vices have been established in 13 healthministries and some countries have such ser-vices in their labor ministries or nuclearenergy agencies, but even where they existmost are understaffed and unable to copewith the problems noted above.
Mindful of the need to support primaryhealth services, PAHO's efforts in radiationmedicine in 1980 focused on developing abasic x-ray system for health centers andfront-line hospitals. The system includes notonly a simplified x-ray machine, which hasbeen designed according to PAHO/WHO
specifications and is easily installed, rugged,and simple to maintain, but also three-monthtraining of community operators and instruc-tion of local general practitioners in how toevaluate the images the equipment produces.Meetings were held with x-ray manufacturersand national authorities, and the plan for aclinical field trial of the basic radiologysystem was completed. Pending the deliveryof satisfactory prototypes by the manufac-turer, the field trial is scheduled to begin inColombia in 1981.
In the radiotherapy area, quality assurancewas promoted through the IntercomparisonStudy for Cobalt-60 Teletherapy Units car-ried out in collaboration with WHO and theInternational Atomic Energy Agency (IAEA)in Vienna. This study involves comparison ofthe radiation output of a cobalt-60 telether-apy unit, which is calculated by the par-ticipating national center, with the radiationdose as actually measured by a ther-moluminescent dosimeter. The measurementis made by the IAEA laboratory which pro-vides the necessary dosimeters and acces-
sories, laboratory instruments, and technicallaboratory staff. PAHO and WHO cooperateby coordinating the participation of nationalauthorities. PAHO provided followuptechnical cooperation to identify sources ofdosimetry errors through a radiologicphysicist's visits to radiotherapy centers inChile, Colombia, Ecuador, Peru, andUruguay.
Collaboration to strengthen radiotherapyservices was also provided through consulta-tion with Chilean and Haitian authorities andthrough PAHO participation in the third con-gress of the Circle of Ibero-Latin AmericanRadiotherapists at Mexico City and a subre-gional radiotherapy workshop at Santiago.
In the nuclear medicine area, qualityassurance was stimulated through coopera-tion with the Federated Council of NuclearMedicine Organizations in organizing aworkshop to be held at PAHO headquarters inApril 1981, and with Colombia in organizinga regional quality assurance workshop to beheld at Bogotá in May 1981.
Technical advice on radiation protectionwas provided in PAHO staff and consultantvisits to Barbados, Chile, Mexico, and Peru.Topics about which guidance was providedwere the organization of protection services,instrumentation and methods for radiationmeasurement, calculation of radiation shield-ing, personal dosimetry services for workers,radiation control regulations and inspections,courses, and preparation for radiation ac-cidents and emergencies.
The cooperative pilot program with Argen-tina, Colombia, Educador, Guyana, Jamaica,Mexico, Peru, and Venezuela to measure en-vironmental radiation levels was completedand the final report prepared. Informa-tion was provided to radiologic specialiststhroughout the hemisphere through monthlydistribution of the Bibliography of RecentPublications containing author and titleentries in 16 journals and through distributionof the newsletter of the Latin AmericanAssociation of Societies of Biology and
DISEASE PREVENTION AND CONTROL 83
Nuclear Medicine. Arrangements were madewith the American Association of Physicistsin Medicine to provide the scientific literatureit publishes free of charge to WHO's radiationhealth collaborating centers in Latin America.In cooperation with the u.s. Food and DrugAdministration's bureau of radiologicalhealth, the bureau's scientific literature wasmade available free to radiologic workersthroughout the Americas.
Contact was also maintained with variousauthoritative international radiologic organi-zations such as the International Commissionon Radiation Units and Measurements andthe International Commission on Radiologi-cal Protection to assure relevance and uni-formity in PAHO's efforts to promote the useof internationally accepted radiologic stan-dards throughout the hemisphere.
Accident Prevention
Accidents as a group are one of the fiveprincipal causes of death in all age groups in26 of 36 American countries and territories.In addition, the overall accident rate has in-creased in all but one of the Americansubregions-temperate South America. Theuse of hospital services also reflects the im-portance of accidents as a health problem. Insix of the 10 countries providing reliablehospital discharge data, accidents are theprincipal reason for hospitalization. In allcountries, accidents rank no lower than sec-ond as the major cause of hospitalization.
Motor vehicle injuries will become a critical
problem for the Americas during the 1980s asroad networks and vehicle densities increase.An exacerbating problem is that many of thehemisphere's countries have difficulty obtain-ing automotive spare parts because they donot manufacture their own, and hence vehi-cle maintenance lags and contributes to highaccident rates. Legislation, education, androad and vehicle safety design have so far notkept pace with these problems.
PAHO continued to collect statistical infor-mation on traffic accidents for inclusion in aWHO survey to determine the magnitude andnature of traffic accidents in the developingworld. Eight American countries took part inthe survey-Argentina, Chile, Colombia,Guatemala, Jamaica, Mexico, Peru, andVenezuela. The survey data will be the basisof a WHO meeting in Mexico City inNovember 1981 on the same subject, ameeting in whose planning and organizationPAHO continued to participate. Health, lawenforcement, road planning, construction,and maintenance specialists will represent 60countries.
At the request of the Caribbean Commu-nity, PAHO assigned a short-term consultantto study the traffic accident situation in An-tigua, Barbados, Belize, Guyana, and SaintLucia. Data collection and analysis will con-tinue through 1981 to help develop plans andprograms to reduce the magnitude of thisserious problem.
In the field of national activities, Mexicoand Peru created intersectoral national com-missions to analyze their traffic accidentproblems and highway safety education ex-periences.
r1 y . -1 ~
jM e^ Z'
y~~~~~
t*
(Photo: J. Vizcarra Brenner/PAHO)
mmqwvp"- --
~ l_.4 .-1
1
Chapter 4
ENVIRONMENTAL HEALTHAND PROTECTION
Socioeconomic development in LatinAmerica and the Caribbean has in recentyears resulted in exponential urbanizationand industrialization. More than 600 millionpeople-twice the population of 1970-willinhabit the hemisphere by the close of thecentury. Migration to urban areas is expectedto result in a population of 450 million incommunities of more than 20,000 people bythe year 2000. Now burgeoning industrializa-tion will multiply many times over. Thesefactors-population growth, migration totowns and cities, and increased industrializa-tion-will characterize and aggravate en-vironmental health concerns in the Americasin the years to come.
Water supply and sanitation continued tobe a major problem in most countries during1980. In urban areas at the end of 1979, 157.2million people had house connections or easyaccess to water supply systems, and in ruralareas only 41.4 million had these services.
These data are shown in Figure 6, togetherwith the most recent estimates of populationserved by sewage disposal systems. Thoughdata about sewerage are less complete, thepopulation served is less than 86 million ur-ban and 1.3 million rural residents.
The International Drinking Water Supplyand Sanitation Decade (1981-90), officiallylaunched in November at a special session of
the United Nations General Assembly, aimsto provide these basic needs to the rural andurban poor. The Water Decade grew out ofthe United Nations Water Conference at Mardel Plata, Argentina, in March 1977 and is aglobally coordinated effort to ensure that allthe world's peoples have adequate drinkingwater and basic sanitation by 1990. Toachieve this goal, strategies to combat themajor constraints of the past will have to beadopted. These strategies include planning,manpower training, institutional develop-ment, appropriate technology, and financ-ing.
Management of solid wastes poses increas-ing problems, despite the efforts of publichealth authorities to deal with them. Solidwaste collection was especially critical in sev-eral large metropolitan areas where garbageproduction actually outpaced the urbangrowth rate. This often requires the insti-tution of emergency measures to avert ma-jor environmental disasters. Nevertheless,greater awareness of the problem and its im-plications has led to national solid wastemanagement planning and the allotment ofnational or external funds.
Cities, particularly industrial ones, are ex-periencing increasing air, water, and soilpollution and food contamination. Thoughmany governments have applied or are con-
85
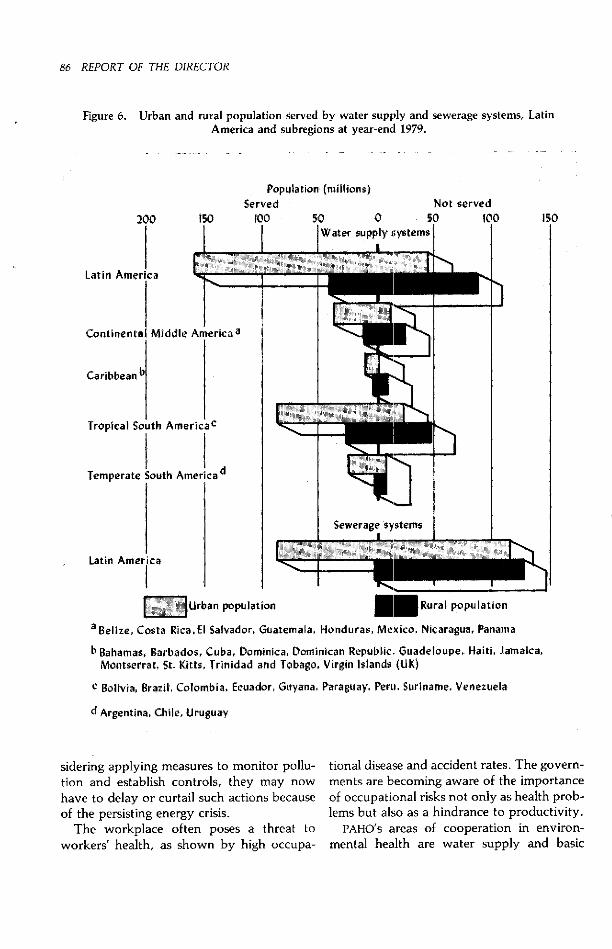
86 REPORT OF THE DIRECTOR
Figure 6. Urban and rural population served by water supply and sewerage systems, LatinAmerica and subregions at year-end 1979.
200 150
Latín America
IContinental Middle Americaa
Caribbean b
Tropical South AmericaC
Temperate outh AmercaTmeaesouth Americad
Population (millions)Served
l00
IN
50 0 50
Water supply systemsI I s;S;il \ aRSDU;iau e- 77
_ --4f-
ot served100
Latin America
[II Urban population B Rural population
aBelize, Costa Rica,EI Salvador, Guatemala, Honduras, Mexico, Nicaragua, Panama
bBahamas, Barbados, Cuba, Dominica, Dominican Republic, Guadeloupe, Haiti, Jamaica,Montserrat, St. Kitts, Trinidad and Tobago, Virgin Islands (UK)
c Bolivia, Brazil, Colombia, Ecuador, Guyana, Paraguay, Peru, Suriname, Venezuela
d Argentina, Chile, Uruguay
150
sidering applying measures to monitor pollu-tion and establish controls, they may nowhave to delay or curtail such actions becauseof the persisting energy crisis.
The workplace often poses a threat toworkers' health, as shown by high occupa-
tional disease and accident rates. The govern-ments are becoming aware of the importanceof occupational risks not only as health prob-lems but also as a hindrance to productivity.
PAHO's areas of cooperation in environ-mental health are water supply and basic

ENVIRONMENTAL HEALTH AND PROTECTION 87
sanitation, solid waste management, institu-tional development, environmental and otherhealth hazards and pollution control, oc-cupational health, fluoridation, and foodprotection.
Water Supply andBasic Sanitation
The provision of adequate safe drinkingwater and basic sanitation measures such asimproved excreta disposal and housing havelong been recognized as keystones inestablishing and maintaining a healthful en-vironment in which families can live andwork. When the International DrinkingWater Supply and Sanitation Decade waslaunched, the world's nations rededicatedthemselves to the principle that the universalprovision of these basic health services is at-tainable. They committed themselves to pro-viding safe water supply and adequate sanita-tion service to all by 1990, with special atten-tion to underserved peoples in rural andmarginal urban areas.
This effort will mean that 254 million addi-tional people in the Americas will need ade-quate safe drinking water and about 390million will require excreta disposal servicesbetween 1981 and 1990. The estimated cost ofthis effort will be $50 billion, which roughlyequals the combined gross national productsof Peru and Venezuela for 1979.
The actual cost and the coverage achievedwill depend greatly on the technologic mix(the number of house connections as com-pared to public standpipes, or latrines tosewerage systems) and the type of service(low-cost, simplified technology) the coun-tries adopt.
This will be the third time the Americashave set special water and sanitation goals.Each time they have focused their attentionon different targets within the sector. In the1960s it was water supplies for urbanresidents; in the 1970s, water supplies andsewerage for urban areas and drinking water
and sanitation for villages; in the 1980s it is tobe safe drinking water and adequate basicsanitation measures for rural and marginal ur-ban areas.
To prepare for this massive effort, theAmericas have worked hard in recent yearsto maximize their use of existing resourcesand find ways to focus their water and basicsanitation efforts on programs to strengthentheir primary goal of health for all by the endof the century. In 1980, for example, theyemphasized strengthening national planningcapabilities by establishing national WaterDecade action committees in seven countries,with five more about to be established; con-tinued their efforts to develop sector studies(22 country studies covering 99 percent of thehemisphere's population have now beencompleted), and worked closely with techni-cal cooperation agencies to help identify anddevelop realistic programs and projects forfinancing.
Bolivia, Haiti, and Paraguay were includedin an international cooperation project spon-sored by the Federal Republic of Germany'stechnical cooperation agency (Gesellschaftfur Technische Zusammenarbeit, or GTZ) andWHO for planning the Water Decade. Projectactivities were initiated late in the year andwill continue through 1981. Agreements weresigned for two new rural water and sanitationprojects in El Salvador-one for nationalplanning financed by USAID and the other fordesigning expanded rural water programsfinanced .by UNDP. In Chile and Mexico theauthorities initiated actions to reformulatesectoral plans to reflect Water Decade goals.In Argentina, Bolivia, Colombia, Guatemala,and Peru meetings were held to review thesectoral situation in light of the WaterDecade. Together with the Caribbean Devel-opment Bank, PAHO and the World Bankconducted project preparation and executionactivities.
In examining the needs of the Americas,the countries looked beyond the WaterDecade's cost to the very real human conse-
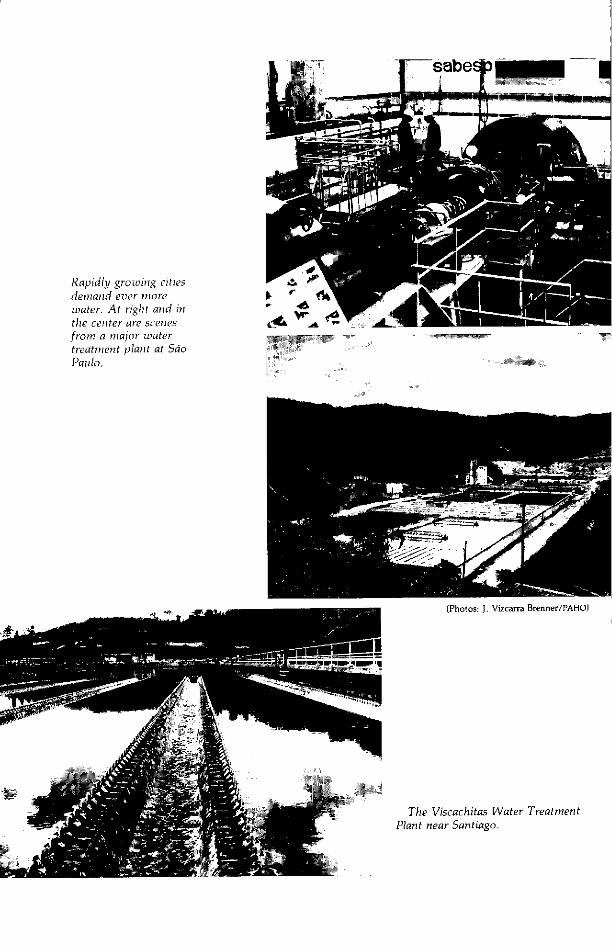
1-sabe P _-iijlmí_
Rapidly growing citiesdemnand ever miorewater. At right and inthe center are scenesfromn a major watertreatment plant at SaoPaulo.
(Photos: J. Vizcarra Brenner/PAHO)
The Viscachitas Water TreatmentPlant near Santiago.
k -
NF _

ENVIRONMENTAL HEALTH AND PROTECTION 89
1T1Urbanization oftenoutstrips water-main lay-ing. Here a tank truckdelivers potable water toresidents of a marginal SaoPaulo suburb.
(Photo: J. Vizcarra Brenner/PAHO)
quences that result from the lack of thesebasic services. It has been estimated that diar-rheal diseases alone account for 200,000deaths a year. To this must be added thehours of personal drudgery spent in obtainingpitiful amounts of water, often of dubiousquality. Recognizing that 39 of every 100people still lack access to drinking watersystems and 76 lack adequate excretadisposal, the countries sought to do threethings: (1) improve existing services byupgrading the quality of available human andtechnical resources; (2) construct new ser-vices to expand existing ones, and (3)strengthen current operation and mainte-nance capabilities.
To carry out the strategies established bythe Directing Council in 1979 (CD26.22),
PAHO's water and basic sanitation programfocused on four kinds of activity: (1) assistingcountries in preparing for the Water Decade;(2) identifying and developing programs andprojects for presentation to financing agen-cies; (3) carrying out activities to increase thenumber, type, and quality of the sector'smanpower; and (4) executing projects to im-prove the quality of drinking water andsanitation services.
Special Water Decade activities includedjoint efforts with ECLA to prepare tworegional meetings to discuss horizontalcooperation, the first to be held at Santiago
in early 1981 and the second a few monthslater. In addition, planning went forwardwith ECLA to launch the Water Decade in theAmericas during its meeting at Montevideo inMay 1981.
To strengthen national capacities for pro-gram or project identification and develop-ment, PAHO continued its cooperative pro-gram with the World Bank. Technical advicewas also given to Costa Rica, Panama, andUruguay on water tariffs and to Montevideoon a sewerage project expected to cost $100million which it is anticipated will be financedby IDB. Aid was also given to Argentina inpreparing a multicity water supply projectwhich will cost $600 million and be financedby the World Bank.
Recognizing that the countries' resourcesvary widely, PAHO emphasized developingnetworks of water and sanitation institutionswhich can collaborate on common problems,exchange experiences, and share resources.This concept was furthered when the newlyfounded Association of Water and SanitationInstitutions of Central America and Panamaagreed to support the Costa Rican water andsewerage authority's La Uruca training centeras the focal point for training trainers whowill in turn develop the thousands of techni-cians needed throughout the subregion.Financing for this project was discussed withGTZ and IDB. As this concept is applied and
._ ��� - 1
90 REPORT OF THE DIRECTOR
proved in Central America, it will be ex-panded to other subregions.
A prerequisite for preparing and carryingout country programs is the availability at alllevels of skilled personnel who understandand are able to execute governmental and in-stitutional policies. To help increase the poolof these technicians, engineers, and mana-gers, PAHO helped the countries create thebasis for an increased regional training effort.Through the Pan American Center for
Sanitary Engineering and EnvironmentalSciences (CEPIS) at Lima, it continued tocooperate with Peru to ensure that thematerials and results of the IDB-sponsoredproject for technologic development of sectorinstitutions (DTIAPA) are made available to allwater and sanitation agencies in the hemi-sphere.
To help countries develop technologiesthat more realistically reflect local human,technical, and financial resources, severaloperations research projects were established.To improve the quality of the water being
Water leak detection inBridgetown.
(Photo: J. Vizcarra Brenner/PAHO)- --- r--: -~
provided, investigations of the technical andmanagerial aspects of simplified disinfectiontechniques were conducted with waterauthorities in Argentina, Colombia, CostaRica, and Peru. CEPIS research results onsimplified, low-cost water treatment plantswere adapted to conditions in Costa Rica andHonduras, and in the future will be extendedto other countries.
Awareness of the need to resolve opera-tional problems was reflected in an increase inthe number of projects to help countriesreduce the unaccounted-for water lossesmany are suffering. An agreement was signedwith CIDA and the Caribbean DevelopmentBank to cosponsor a leakage detection train-ing program based in Barbados. Trinidad andTobago's water and sewerage authoritystarted its joint IDB- and UNDP-sponsoredproject to improve various technical areassuch as distribution system maintenance andleak detection. A UNDP-sponsored project inUruguay helped that country's public worksagency conduct studies to reduce unac-counted-for water lost because of leakage.
Institutional Development
The strengthening of water supply andsanitation institutions and the sector itself hasbeen recognized as a crucial element for at-taining the goals of environmental health ser-vices and programs. Through its institutionaldevelopment program, PAHO collaboratedwith 13 countries in establishing andstrengthening their environmental health in-stitutions. This will enable them to help thesector attain the goal of water and sanitationfor all by 1990.
Cooperating with 34 national and local in-stitutions responsible for both rural and ur-ban area services, PAHO functioned as acatalyst in carrying out sound managementtechniques. Through a holistic system ap-proach, staff members and short-term con-sultants worked in close collaboration with

ENVIRONMENTAL HEALTH AND PROTECTION 91
institutional staff, establishing organizationaland information systems to support manage-ment in decision making. This includeddevelopment of human resources as well aslegal, financial, and organizational aspects.
These planned changes improve the effec-tiveness of the institutions and results in anincrease of coverage and better quality of ser-vices. Among the principal goals of institu-tional development projects are: improve-ment of planning, operation, and mainte-nance, project preparation and execution,and institution of adequate tariffs and com-mercial systems to increase revenues.
In addition to the use of PAHO resources,these projects are financed by the agenciesthemselves or by loans and contributionsfrom national and international financialorganizations such as IDB, the World Bank,and UNDP.
To support national institutional develop-ment projects and programs, CEPIS preparedand executed the first of five modularworkshops to train trainers in the commercialaspects of water supply and sanitation agen-cies. PAHO adapted the models prepared byBrazil's National Housing Bank (BNH) withPAHO's technical cooperation to develop thatcountry's state water and sewerage authori-ties institutionally. This five-year project,completed in July, carried out most of itsscheduled activities in cooperating withBrazil's 21 participating state water andsewerage authorities. BNH incorporated theproject in its regular programs and created aunit to run it, as well as lines of credit tofinance the state agencies in executing similarprojects including training. To assist BNH incarrying out the program nationally, Brazilrequested a two-year PAHO cooperative pro-gram, which began in July.
Barbados, with PAHO advice, completedthe establishment of its new national waterand sewerage authority, a project begun in1978.
In Colombia, PAHO cooperated with theNational Institute for Municipal Develop-
(Photo: M. Montecino/PAHO)
Local labor and materials are keys tothe rapid expansion of rural water sup-
ply systems, as shown above inUtive, Panama.
ment in several continuing environmentalprograms in such areas as water supply andsanitation, solid waste management, markets,and training.
In Haiti, PAHO continued the technicalcooperation project it started in 1977 with thenational water service in setting up manage-ment, operation, and maintenance systemsand developing water sources. On comple-tion of bidding procedures, work began onwater supply systems for 10 medium-sizedcities.
Two main projects were underway in ruralwater supply and sanitation. One, datingfrom 1977, was to develop and strengthen theexecutive unit of Guatemala's rural watersupply program. The unit's organizationalstructure was created and improvementswere made in promoting community par-ticipation, which gave the communitiesserved a share in the responsibility foroperating and maintaining their watersystems. Other achievements were new data

92 REPORT OF THE DIRECTOR
processing systems, simplified operating pro-cedures, and improved information for deci-sion making.
The other project, also started in 1977, wascarried out by Paraguay's environmentalsanitation agency with PAHO cooperation. Itspurpose is to improve the agency's mana-gerial and operational capability in executinga $6 million World Bank loan for rural watersupply and sanitation works, as well as toprepare the institution and rural communityboards for managing, operating, and main-taining the systems.
PAHO expanded its institutional develop-ment program to solid waste disposal andpollution control agencies. The continuationof the CEPIS workshop modules for trainingtrainers will be strengthened by assigning astaff member responsibility for these ac-tivities. Finally, workshops and pilot ex-periments were programmed to foster com-munity participation and health education,mainly in rural and slum areas.
Solid Waste Management
During the second half of the 1970s, solidwaste collection and disposal came to berecognized as a critical problem in LatinAmerican and Caribbean cities.
Most municipal sanitation services in thehemisphere were organized 20 to 50 years agowhen the cities they served were muchsmaller than accelerating urbanization hasmade them today. In 1960, for example, 21cities in Latin America and the Caribbean hadmore than a half-million population, but in1980 there were 50 such cities. As a citygrows, it has been found, each of its residentsgenerates more daily waste. It has beenestimated that each of the 1,200 LatinAmerican towns and cities with more than20,000 inhabitants generated 137,000 tons ofsolid waste daily in 1980, and that in 1990they may each generate 230,000 tons a day,an increase of almost 70 percent. The prob-
lem worsens in direct relation to the size ofcities, since in Latin America towns withfewer than 20,000 inhabitants generate only 5percent of total urban solid waste.
Present urban sanitation is far fromsatisfactory in the hemisphere. Thirty percentof the paved streets in Latin American andCaribbean cities are not regularly cleaned; athird of the trash in those cities is not col-lected; and only 40 percent of the waste thatis collected is disposed of in sanitary landfills.Nineteen of 20 towns and cities with 20,000or more inhabitants still dispose of theirdetritus in open dumps.
That the hemisphere's cities can control thesolid wastes they produce is seen in Rio deJaneiro, whose Companhia Municipal deLimpeza Urbana (COMLURB) has becomeperhaps the best urban sanitation system inthe area in the past 15 years through in-tegrated operations, administration, financ-ing, and training. Rio de Janeiro's $10 percapita annual expenditures on solid wastemanagement and COMLURB's $52 million an-nual budget are considerably less than thosein many major cities of the industrializedworld, yet thanks to good management theresults are better.
Other cities with improving solid wastemanagement systems have adopted measuresto suit their specific conditions, an example ofwhich is Buenos Aires' metropolitan ecologicprotection scheme (cinturón ecológico), a cir-cumferential forest belt. During the last threeor four years several cities such as BuenosAires, Rio de Janeiro, and Sáo Paulo havetried to control air pollution resulting fromtrash burning by prohibiting building in-cinerators and increasing refuse collection.
Despite these advances, solid waste man-agement remains a critical problem in thehemisphere.
The phenomenal growth of large metropol-itan areas in Latin America-Lima's popula-tion is now estimated at 5 million, Bogotá's at4 million, and Guayaquil's at 1 million, for in-stance-makes them particularly susceptible
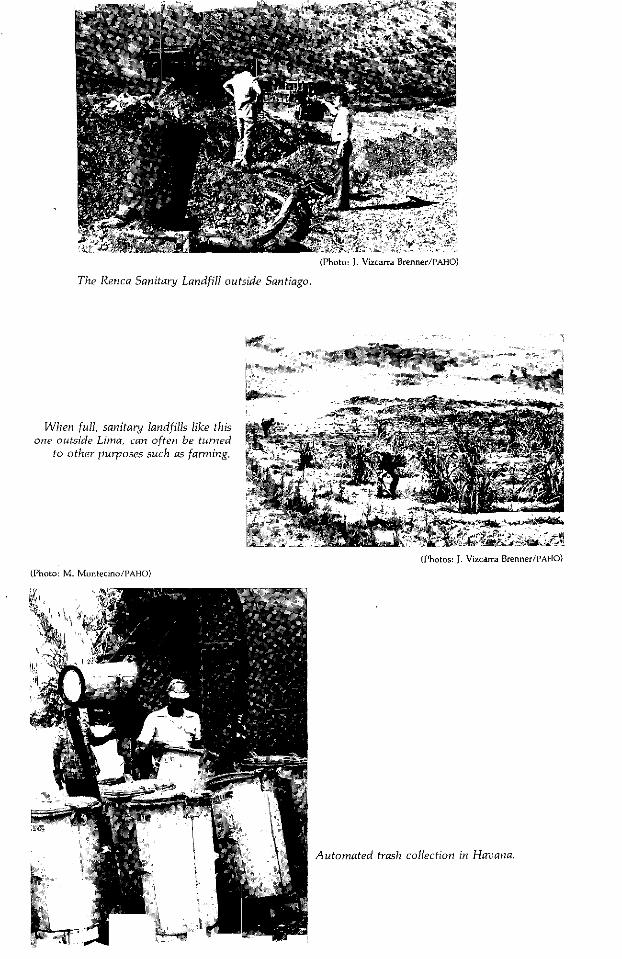
(Photo: J. Vizcarra Brenner/PAHO)
The Renca Sanitary Landfill outside Santiago.
When full, sanitary landfills like thisone outside Lima, can often be turned
to other purposes such as farming.
(Photos: J. Vizcarra Brenner/PAHO)
(Photo: M. Montecino/PAHO)
Automated trash collection in Havana.
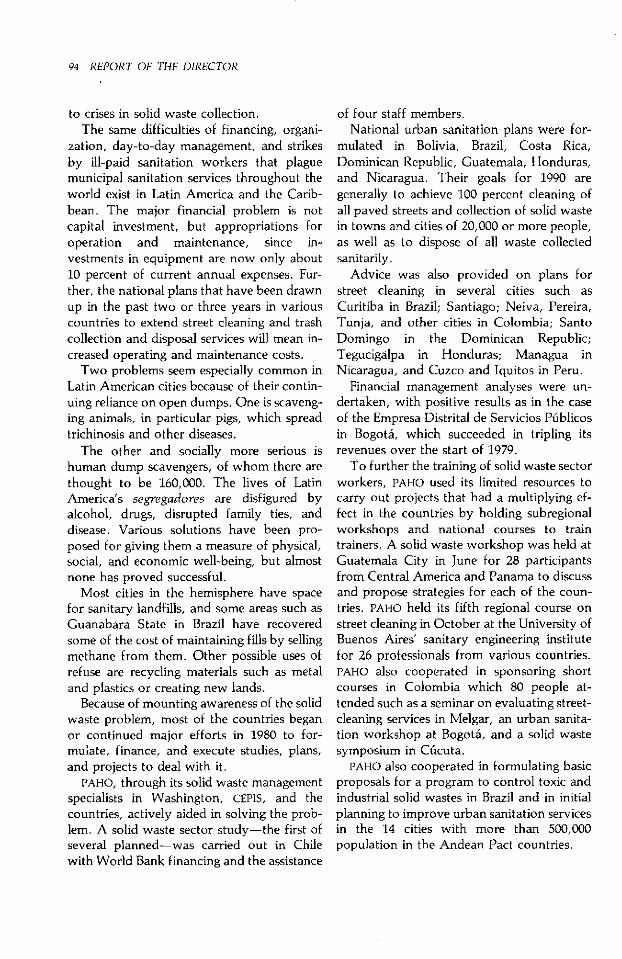
94 REPORT OF THE DIRECTOR
to crises in solid waste collection.The same difficulties of financing, organi-
zation, day-to-day management, and strikesby ill-paid sanitation workers that plaguemunicipal sanitation services throughout theworld exist in Latin America and the Carib-bean. The major financial problem is notcapital investment, but appropriations foroperation and maintenance, since in-vestments in equipment are now only about10 percent of current annual expenses. Fur-ther, the national plans that have been drawnup in the past two or three years in variouscountries to extend street cleaning and trashcollection and disposal services will mean in-creased operating and maintenance costs.
Two problems seem especially common inLatin American cities because of their contin-uing reliance on open dumps. One is scaveng-ing animals, in particular pigs, which spreadtrichinosis and other diseases.
The other and socially more serious ishuman dump scavengers, of whom there arethought to be 160,000. The lives of LatinAmerica's segregadores are disfigured byalcohol, drugs, disrupted family ties, anddisease. Various solutions have been pro-posed for giving them a measure of physical,social, and economic well-being, but almostnone has proved successful.
Most cities in the hemisphere have spacefor sanitary landfills, and some areas such asGuanabara State in Brazil have recoveredsome of the cost of maintaining fills by sellingmethane from them. Other possible uses ofrefuse are recycling materials such as metaland plastics or creating new lands.
Because of mounting awareness of the solidwaste problem, most of the countries beganor continued major efforts in 1980 to for-mulate, finance, and execute studies, plans,and projects to deal with it.
PAHO, through its solid waste managementspecialists in Washington, CEPIS, and thecountries, actively aided in solving the prob-lem. A solid waste sector study-the first ofseveral planned-was carried out in Chilewith World Bank financing and the assistance
of four staff members.National urban sanitation plans were for-
mulated in Bolivia, Brazil, Costa Rica,Dominican Republic, Guatemala, Honduras,and Nicaragua. Their goals for 1990 aregenerally to achieve 100 percent cleaning ofall paved streets and collection of solid wastein towns and cities of 20,000 or more people,as well as to dispose of all waste collectedsanitarily.
Advice was also provided on plans forstreet cleaning in several cities such asCuritiba in Brazil; Santiago; Neiva, Pereira,Tunja, and other cities in Colombia; SantoDomingo in the Dominican Republic;Tegucigalpa in Honduras; Managua inNicaragua, and Cuzco and Iquitos in Peru.
Financial management analyses were un-dertaken, with positive results as in the caseof the Empresa Distrital de Servicios Públicosin Bogotá, which succeeded in tripling itsrevenues over the start of 1979.
To further the training of solid waste sectorworkers, PAHO used its limited resources tocarry out projects that had a multiplying ef-fect in the countries by holding subregionalworkshops and national courses to traintrainers. A solid waste workshop was held atGuatemala City in June for 28 participantsfrom Central America and Panama to discussand propose strategies for each of the coun-tries. PAHO held its fifth regional course onstreet cleaning in October at the University ofBuenos Aires' sanitary engineering institutefor 26 professionals from various countries.PAHO also cooperated in sponsoring shortcourses in Colombia which 80 people at-tended such as a seminar on evaluating street-cleaning services in Melgar, an urban sanita-tion workshop at Bogotá, and a solid wastesymposium in Cúcuta.
PAHO also cooperated in formulating basicproposals for a program to control toxic andindustrial solid wastes in Brazil and in initialplanning to improve urban sanitation servicesin the 14 cities with more than 500,000population in the Andean Pact countries.

ENVIRONMENTAL HEALTH AND PROTECTION 95
Control of Pollutionand Other Environmental
Health Hazards
Accelerated population growth, industrial-ization, and socioeconomic development ingeneral have resulted in greater pollution ofthe air, water, and soil throughout theAmericas. Unfortunately, this growing prob-lem has not been coupled with increased con-struction of pollution treatment facilities orexecution of pollution prevention programs.Since pollution is known to be detrimental tohuman health and well-being, PAHO providestechnical cooperation to the countries inpollution monitoring, prevention, andcontrol.
Strong environmental protection programsrequire broad national policies and financialand manpower commitments. These are be-ing stimulated by individual projects in thecountries and the Global EnvironmentalMonitoring System (GEMS), carried out byUNDP, UNESCO, World Meteorological Orga-nization, and WHO. As part of GEMS, airmonitoring data began to be collected in 1978and water quality data a year later in theAmericas.
CEPIS is the regional focus for monitoringactivities. .As such it relays informationreceived from GEMS stations to WHO,distributes technical information on monitor-ing, responds to country requests, andcooperates in system operation and deter-mination of equipment needs through mis-sions to the various stations.
PAHO also provides assistance in evaluatingand improving national pollution controlprograms, formulating and preparing projectproposals to be submitted to lending agen-cies, identifying human resources, and defin-ing terms of reference for air and water qual-ity monitoring activities.
In Brazil, PAHO has collaborated in devel-oping several UNDP-funded environmentalpollution control projects. In Rio de Janeiro a
project to develop the state's environmentalcontrol program, carried out by the state'sEnvironmental Engineering Foundation andwith PAHO as UNDP's executing agency, wascompleted in 1980. Its final report recom-mended the restoration of Lake Rodrigo deFreitas, used for recreation but badlypolluted, control of air pollution, manage-ment of solid wastes, improvement of heavilycontaminated Guanabara Bay, and preven-tion and control of pollution in the Paraibado Sul River, the major water supply sourceof the city of Rio de Janeiro. To complementthat project, UNDP financed an additionalsmall project late in the year to study ways tocontrol air, water, and soil pollution due totoxic chemicals.
In support of environmental pollution con-trol carried out in Sáo Paulo by the StateCompany for Technology in Basic Sanitation(CETESB), PAHO assisted as executing agencyin a UNDP-funded project to develop aresearch and environmental pollution controlprogram. It included assistance in institu-tional development, water pollution control,establishment of a water quality monitoringnetwork, air pollution monitoring, solidwaste disposal, urban noise control, andtraining in environmental pollution controlmethods. As followup to that project, CETESBand PAHO signed an agreement to carry out awater, soil, and air pollution control programfor Sáo Paulo State, to be financed byCETESB.
In the area of pollution control in the cityof Sáo Paulo and its environs, CETESB willconduct a three-year World Bank-financedindustrial pollution control project for whichPAHO technical cooperation is planned toreduce industrial particulate emissions, in-dustrial discharges of toxic substances intorivers, and health risks, as well as treating in-dustrial wastes and strengthening CETESB'scapacity to plan and carry out a long-termpollution control program.
PAHO also collaborated in a UNDP-fundedproject to formulate a plan for restoring Lake
(Photos: J. Vizcarra Brenner/PAHO)
Lake Paranoá, a once badly pollutedartificial recreational lagoon in Brasilia,is now being restored to its formerquality. Above, technicians from thelocal water utility take samples of thelagoon's water.
Industrial air pollution, Sao Paulo.

ENVIRONMENTAL HEALTH AND PROTECTION 97
Paranoá, an artificial lagoon in Brasilia whosewater quality has deteriorated because ofdomestic and agricultural pollution, andmaintain the water quality of Lake Desco-berto, which is to serve as Brasília's source ofdrinking water.
Recife was the site of a seminar, attendedby Brazilian and foreign participants, onwater resources in arid and semiarid locales,the purpose of which was to analyze short-and medium-term solutions for water re-source use in northeastern Brazil.
In Colombia, several pollution controlprojects have been underway. As part of aproject to develop the Cauca River water-shed, PAHO arranged travel seminars and pro-vided advisory services in designing andlocating industrial waste treatment plants andusing chromatography equipment to analyzepesticides.
PAHO provided advice and support to aproject for researching, monitoring, and con-trolling pollution in Cartagena Bay and sur-rounding areas, especially attempts to definealternative and economical technical solu-tions to the problem.
PAHO and Colombia signed an agreementfor technical cooperation in protecting theBogotá savanna water resources, includingadvisory services in the organization requiredfor integrated control and management of thebasin of the Bogotá and Suárez Rivers as wellas establishment of water quality criteria andstandards. Collaboration began on studies ofindustrial liquid waste pollution, especiallythat resulting from tanning.
A wastewater treatment and disposal proj-ect in the city of Bogotá received PAHO sup-port through advisory services in analysis ofalternatives to wastewater treatment and inwater chlorination and through training fromtravel seminars.
In Costa Rica, technical cooperation inpreparing an environmental protection pro-gram has focused on advisory services in col-lecting information on water and air pollu-tion and in soil pollution control with em-
phasis on pesticides and fertilizers.In Venezuela, PAHO executed a UNDP-
financed environmental pollution researchproject to develop and strengthen the na-tional environmental research directorate;establish norms, strategies, and activities forenvironmental preservation; evaluate the im-pact of development on the environment;and investigate pollution. Activities includedstudy of water quality and pollution dis-charge in Lakes Maracaibo and Valencia andall their tributaries, sediment analysis, andevaluation of eutrophication in the two lakes.
Air pollution in the Caracas Valley,development of a sanitary landfill on Marga-rita Island, research on stabilization lagoons,and the environmental effect of petroleumextraction and refining were other activitiesin Venezuela. Decision makers have used theresults of these studies to determine suitablecourses of action.
Human illness and death from exposure toenvironmental health hazards continue to in-crease in frequency and severity.
PAHO has for many years been meeting na-tional requests for information about chemi-cal safety. In the 1970s, for instance, it col-laborated with Argentina, Barbados, Bolivia,Brazil, Chile, Colombia, Costa Rica,Dominican Republic, Ecuador, Mexico,Trinidad and Tobago, and the United Statesin their attempts to resolve problems associ-ated with the continued indiscriminate use oftoxic substances. Because such use of toxicsubstances is a worldwide problem, theWorld Health Assembly voted to create aninternational chemical safety program.
The program, a joint activity of severalUnited Nations specialized agencies, aims to:(1) make and disseminate evaluations of theeffects of chemicals on human health and en-vironmental quality; (2) develop guidelineson exposure limits for all types of chemicalssuch as acceptable daily intakes and max-imum permissible or desirable levels in air,water, food, and the working environment;(3) develop guidelines on methods for toxic-

98 REPORT OF THE DIRECTOR
ity testing, epidemiologic and clinical studies,and risk and hazard identification, quan-tification, and evaluation; (4) coordinate in-ternational laboratory testing and epidemi-ologic studies when suitable, and promoteresearch on dose-response relations andmechanisms of the biologic effects of chemi-cals; and (5) develop information for copingwith chemical accidents and promote effec-tive international cooperation and trainingand manpower development in this field.
About 50 nations are interested in theglobal program, including Canada, Mexico,the United States, and possibly Brazil.
PAHO cooperates in the program in theWestern Hemisphere through its head-quarters and the Pan American Center forHuman Ecology and Health (ECO), which wasfounded at Mexico City in 1975 and in Junemoved to its new center at Metepec, 80 kmwest of the Mexican capital. In addition to itstoxic substance control research and advisoryservices, ECO's staff also counsels nationalauthorities on the health effects likely toresult from activities which may produce ma-jor ecologic changes, such as colonization ordam construction.
Interior of the Pan American Center forHuman Ecology and Health, Metepec,Mexico.
(Photo: M. Montecino/PAHO)
During the year ECO finished a criticalreview of organochlorine pesticide residues inhuman milk and the health risks they poseand began an inventory of human resourcesin toxicology in the hemisphere. Since ECO islocated close to a Mexican agricultural re-search and extension center, joint effortshave begun with local officials to developSpanish-language correspondence and class-room courses for agricultural extensionworkers on the safe handling of pesticides.When finished, the courses will be tested inthe state of Mexico and later made availableregionally. Another ECO activity related totoxic substance control was a visit to advisethe Nicaraguan Institute of Natural and En-vironmental Resources on hazards associatedwith mercury contamination in Lake Mana-gua resulting from gold ore refining.
The WHO environmental health criteriaprogram, established in 1973 with UNEP sup-port, published six more criteria documentsduring the year. PAHO disseminated thesematerials and completed plans for translatingthem into Spanish, while translating andpublishing three other criteria documents inthat language. The purposes of the WHO pro-gram are to assess existing information on therelationship between exposure to environ-mental agents and human health, and to pro-vide guidelines for setting exposure limitsconsistent with health protection.
Also part of the GEMS programs sponsoredby WHO and UNEP is a pilot project, begun in1978, to assess human exposure to metallicand organochlorine pollutants through bio-logic monitoring. Because of the nature of thestudy and financial constraints, the project'smetals component is limited to 10 countriesand its organochlorine compounds compo-nent to 12 countries.
Mexico and the United States participate inboth of the program's components, and Peruhas joined the metals component in order tomonitor pollution in the Mantaro River,which is to serve as Lima's water source.PAHO's main interest in the new GEMS pro-gram is in encouraging hemispheric govern-
ENVIRONMENTAL HEALTH AND PROTECTION 99
ments to develop an understanding of theirown problems and start monitoring pro-grams, and it has provided some equipmentfor the latter activity.
Occupational Health
The labor force of Latin America and theCaribbean is now estimated to number be-tween 100 and 110 million workers. It hasbeen conservatively estimated that theseworkers suffer 10 million occupational ac-cidents and 50,000 fatalities annually. Oc-cupational diseases are also widespread andincreasing. Studies carried out in variouscountries show that disability due to in-dustrial accidents and occupational diseasesmay average about 10 percent of the annualgross national income of developing coun-tries, including direct and indirect costs ofbonuses, reduced working hours, extendedvacations, and early retirements.
The Third Special Meeting of Americanhealth ministers at Santiago in 1972 includedprotection of 70 percent of workers exposedto occupational risks in the 14 countries withfully operating occupational health programsand of 50 percent of workers in countrieswithout well-developed programs among thegoals in the Ten-Year Health Plan for theAmericas (1971-80).
Although those goals were not reached,many countries have made major progress inprotecting their workers. The Andean coun-tries are developing a subregional occupa-tional health program, and the English-speaking Caribbean countries have begundefining the problem in their islands andorganizing programs to deal with it. Thesocial security institutes of most of the coun-tries have also interested themselves in oc-cupational health, and occupational healthtraining institutions have been established orare being established in at least six countries.
In 1980 CEPIS sent representatives toHipólito Unanue Agreement meetings on oc-
cupational health, responded to national re-quests for information and advice on the sub-ject, and organized a programming workshopintended to have a multiplier effect once par-ticipants return to their own countries. In theCaribbean, it and ILO cooperated in planningan early 1981 workshop for that subregion'soccupational health program.
PAHO also advised the health ministries ofBolivia, Chile, Ecuador, and Paraguay on thecreation or improvement of their occupa-tional health programs.
Food Protection
Food protection lags seriously in LatinAmerica and the Caribbean since perhapsonly a half-dozen countries have organizedfood inspection programs. Some are financednationally and others are supported in wholeor part by UNDP, which has received more re-quests for aid in this area than it can im-mediately finance.
Though the food protection problemsnoted in previous years persisted in 1980, atleast half the hemisphere's countries showedsome degree of interest in establishing or im-proving their food protection programs. Twofactors principally account for this increasedinterest. First, morbidity and mortality fromfood-borne diseases continue to be a signifi-cant percentage of the reported hospitaldischarges and deaths in most of the coun-tries. And second, the increasing cost of foodin domestic and world commerce has led toawareness that reducing domestic food lossesaveraging 30 percent from wastage due tocontamination and inadequate distributioncould help a country's balance of paymentsand lower the expenses of treating patientswith food-borne infections and intoxications.The developing countries are producing lessfood, particularly nutritive protein, thanthey could and are losing more than theyshould.
In consequence, the health ministers have
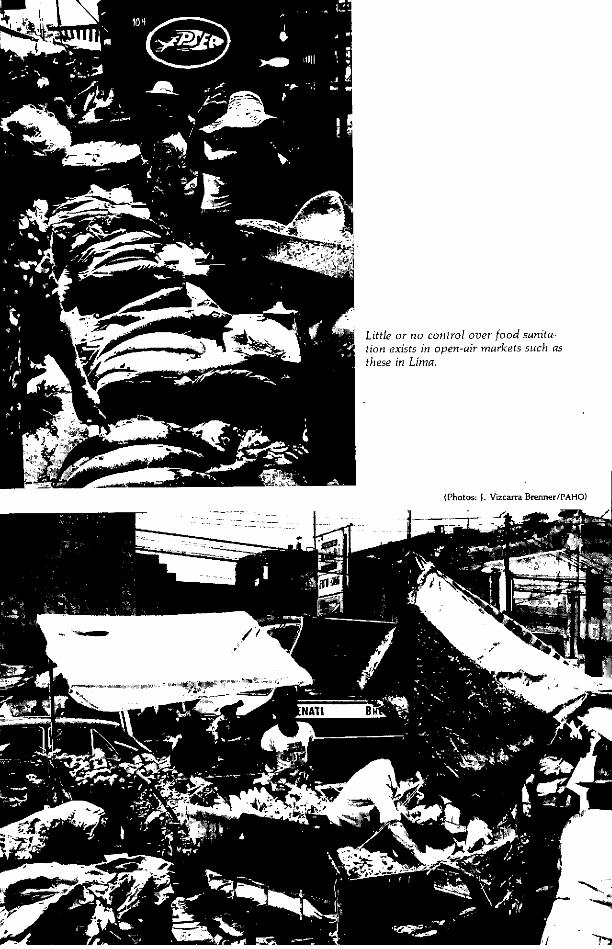
Little or no control over food sanita-tion exists in open-air markets such asthese in Lima.
(Photos: J, Vizcarra Brenner/PAHO)
---i ~--Y _
P. I Id, -
ENVIRONMENTAL HEALTH AND PROTECTION 101
adopted resolutions at several of theirsubregional meetings asking PAHO to help inplanning, designing, and carrying out foodprotection programs. As an example, theCommonwealth Caribbean health ministersrecommended at their 1980 annual meetingthat each country in the English-speakingCaribbean develop a food safety policy andthat, with PAHO's help, a technical group beformed to draw up a subregional food safetypolicy and guidelines. An initial planningmeeting for the Caribbean food safety pro-gram was held in Barbados in September.
Often through its Pan American ZoonosisCenter (CEPANZO) in Argentina, PAHO ad-vised national food control services in Argen-tina, Bolivia, Brazil, Chile, Colombia, Ecua-dor, Honduras, Panama, Peru, and Trinidadand Tobago. These are examples of some ofPAHO's advisory services to the countries:
* CEPANZO continued its research on microbi-ologic criteria for controlling Argentine cheese andcompleted its studies of soft and semihard cheeses,developed microbiologic criteria for controllingArgentine curds, and conducted counts ofStaphylococcus aureus in powdered milk.
* Under an agreement with the Dairy IndustryTechnology Research Center (CITIL) of Colom-bia's National Institute of Industrial Technology,CEPANZO continued to cooperate in organizingand developing CITIL's dairy products microbi-ology laboratories. It also continued its assistanceto Colombia in organizing a national food controllaboratory network.
* Honduras' meat inspection service, whichwas operating only in export packing plants, ex-tended its oversight to municipal slaughterhousesprocessing meat for domestic consumption. In-spectors were also stationed at poultry slaughter-houses and sausage plants. Quarantine services arebeing extended as technical improvements aremade in the program, with strict surveillancemaintained at overland checkpoints and sea andairports to prevent the importation of diseasesharmful to the country's livestock industry.
* In Trinidad and Tobago, PAHO provided fur-ther assistance under the milk control and slaugh-terhouse quality evaluation programs. Assess-ments of the government slaughterhouses atPrinces Town, Roxborough, San Juan, Scar-borough, and Tunapuna were completed on thetwo islands. The desirability of centralizing theslaughtering facilities for both islands to improve
the sanitary quality of meat was pointed out.
PAHO was particularly active in helpingtrain food inspection workers of varyingdegrees of seniority during 1980. The hemrni-spheric educational program in food protec-tion, in collaboration with Colombia's Schoolof Public Health at Medellín, graduated 22food inspectors from its 22-week food protec-tion course. Four of the students were fromother countries. The Medellín school also of-fers five or six month-long internationalcourses in various countries for professionalsevery year using its own faculty and short-term consultants.
Specialized national courses in food pro-tection for professionals were conductedjointly with national authorities at Barran-quilla, Colombia, and in Panama.
In addition, PAHO cooperated with thepublic health school at Tulane University inNew Orleans, Louisiana, in training veteri-narians and lay health workers from theEnglish- and Dutch-speaking Caribbean tobecome public health inspectors with a strongemphasis on food inspection. Such studentsare first entered in the school's core publichealth master's degree program as auditorsand then assigned to on-the-job training posi-tions in the New Orleans area suitable to theirprevious education. Supported by fellow-ships from PAHO's country programs, theygenerally receive five or six months oftraining.
Cooperation also continued with two jointWHO/FAO bodies, the Codex AlimentariusCommission and Food and Animal Feed Con-tamination Monitoring Program. A seniorFAO food protection specialist visited PAHO
headquarters to discuss activities of mutualinterest.
PAHO staff and consultants gathered infor-mation from selected countries to prepare theworking document for the technical discus-sions of the 1981 Directing Council meeting.The first draft of the document was reviewedby several experts representing regulatoryagencies, international organizations, andacademic institutions.

1
1
Chapter 5
HUMAN RESOURCES AND RESEARCH
Planning and training the personnel neededfor coverage extension programs based onprimary care was the main focus of humanresource development in the Americas in1980. Programs to train technical and aux-iliary personnel received special emphasis. Inuniversity programs, an effort was made toinclude new primary care concepts andpractices.
Just as health care organization requiresdetermining levels and areas in which pro-grams are to operate, so must the types ofhealth workers to be used in them be deter-mined. This makes it possible to allocate bet-ter roles in meeting program requirementsand staffing facilities and to evaluate perfor-mance. Rising service costs, inflation, andunderuse of health professionals in manycountries make it imperative that humanresource development be taken properly intoaccount in any coverage extension effort,since labor costs account for more than 60percent of health sector budgets.
Practical training in medicallaboratory technology at Commu-nity College, Bridgetown.(Photos: J. Vizcarra Brenner/PAHO)
These problems have prompted efforts todevelop human resource programs that pro-mote retraining with continuing education inorder to solve shortcomings detected throughsupervision. Indeed, an effort is being madeto modernize all training in accordance withthe latest principles of health administration.
A marked discrepancy nevertheless existsbetween manpower requirements and outputas a result of inadequate planning. In addi-tion, overall development planning is notproviding an adequate framework for educa-tional and particularly human resource plan-ning. This is due to weak organizational tiesbetween the two levels of planning, theoreti-cal disagreements as to the proper place ofeducation in general planning, and the manypractical obstacles confronting planning inunstable environments with few and fluc-tuating resources. Special attention is accord-ingly being given to supporting healthministry manpower units to help them sur-mount these obstacles.
The development of coverage extensionprograms requires the development of scien-tific research as well. During the year,therefore, health service investigations werepromoted in order to develop action-orientedresearch to provide continuous scientificsolution to the problems of health services.PAHO also continued to support biomedicaland socioepidemiologic research, particularlyin its priority fields of work.
103

104 REPORT OF THE DIRECTOR
The Advisory Committee on MedicalResearch increased its interest in specificareas, among which were health service,socioepidemiologic, nutrition, and diarrhealdisease research. Finally, the Special Programfor Research and Training in TropicalDiseases has stimulated the development ofresearch institutions and investigations deal-ing with the diseases the program covers.
Infrastructure Developmentand Manpower Planning
PAHO continued to provide technicalassistance to the countries in developinghealth care training institutions and pro-grams. This included institutional analysis,problem identification, and preparation ofremedial plans which in some cases gobeyond training alone and envisage changesin administrative and physical infrastructure.
The establishment of training project net-works has led to extensive exchanges of ex-perience among representatives of nationalplans and programs and the institutions mak-ing up those networks. Initial evaluations ofnetworks of subcenters in nursing educationtechnology, advanced health administrationstudies, public health schools and graduateschools of preventive and social medicine,continuing education programs, and thesupervisor training program show the valueof such networks in developing the hemi-sphere's health schools and programs.
Special mention should be made of the firstintercountry technical cooperation programsin health education. One is between theUniversities of Santiago, Cuba, and Guadala-jara, Mexico, and the other is between Cubaand Nicaragua. Both train middle-level tech-nical personnel.
PAHO continued its projects to strengthentraining institutions comprehensively withthe support of IDB and other lending agencies.In the Dominican Republic it assisted the
Catholic University of Santiago; in Hondurasit resumed its support of the development ofthe medical school and its teaching hospital,and continued its program to train personnelat other levels of the health ministry, and inNicaragua it provided further assistance tothe university development and technical andauxiliary personnel training program. In thecommunity health training program for Cen-tral America and Panama (PASCCAP), itsought to provide comprehensive support totraining centers in their efforts to producehealth workers better equipped to serve incoverage extension programs.
In the area of human resources planring,PAHO collaborated with the health ministryof Barbados in a survey to identify the man-power needed to carry out that country'sproposed national health insurance scheme.In Trinidad and Tobago, it worked withhealth and finance ministry officials toprepare a report on present and projectedmanpower needs for that country's healthservices.
In collaboration with the Colombianhealth ministry, PAHO sponsored a second in-ternational course on manpower planning for-18 participants from 10 countries. A followupcourse was designed which will give par-ticipants the specific skills needed to developnational health manpower plans.
Education and Training
Medicine
PAHO's main regional activity in medicaleducation during 1980 was a joint effort withthe Pan American Federation of MedicalSchool Associations (FEPAFEM) to define mini-mal requirements for new medical schools.As a result of the explosive growth in thenumber of medical schools in Latin Americaand the Caribbean in recent years, there arenow nearly 300 with more than 250,000

HUMAN RESOURCES AND RESEARCH 105
students. This growth will probably con-tinue.
PAHO and FEPAFEM therefore suggested thatminimal requirements be established to guidecountries in authorizing the creation of newschools. A set of such requirements, essen-tially based on providing the personnel healthservices needed to respond to the needs of thepopulation, was developed in preliminarymeetings at Caracas and in Brazil.
PAHO initiated country activities in con-junction with national medical school associ-ations. A guide for evaluating schools ofmedicine previously used in all six Peruvianmedical schools and in proposals forestablishing new schools was the basic docu-ment for the first national meeting, held inPeru in September. At the meeting, whichwas attended by participants from all Peru-vian schools of medicine, observers from theassociations of Ecuador, Colombia, and Mex-ico, and FEPAFEM, and delegates from thePeruvian health ministry and social securityinstitute, conclusions and recommendationswere reached on ways of rationalizing theestablishment of medical schools by takingexisting health plans and overall health man-power planning into account to ensure fulland gainful physician employment.
PAHO continued to support individualcountries' medical education programs on re-quest, mainly to achieve closer integrationbetween training and service institutions, asthe primary care strategy dictates. Teaching-service integration seminars were held inChile, Paraguay, and Peru. Communityhealth-oriented medical education programscontinued in Brazil, Colombia, Cuba,Jamaica, Mexico, and Venezuela. Special sup-port was extended to IDB-funded medicaleducation programs at the Catholic Univer-sity of Santiago in the Dominican Republicand in Mexico.
Guatemala's school of medicine receivedassistance in reforming its curriculum anddeveloping an audiovisual unit, for whichPAHO's Latin American Health Education
Technology Center (CLATES) at Rio de Janeirosupplied educational video cassettes. Supportwas given to the University of Honduras'medical school in solving the problems of itsrelationship with its teaching hospital. InPeru, audiovisual instruction and educationaltechnology support was provided to themedical schools of San Marcos and CayetanoHeredia universities.
The University of Panama's medical schoolreceived assistance in pedagogic training. Inthe same area, professors of medicine con-tinued to receive advanced training in educa-tional methods at CLATES.
PAHO provided support to the Universityof Costa Rica's medical school for an epide-miology training program which, though be-gun as a national activity, had participantsfrom all of Central America.
In Colombia, the Military School ofMedicine and Social Sciences, established in1979 with PAHO's advice, inaugurated a newbuilding to house a regional pathologycenter, library, and basic science laboratory.The school also received audiovisual aidsfrom CLATES.
The schools of medicine of Santiago,Cuba, and Guadalajara, Mexico, conductedjoint activities in curricular improvement andinstructor retraining. They also jointly pro-duced a mother-and-child care textbook. Thecoordinational arrangements were developedin periodic meetings, the last of which, heldat Guadalajara in December, determined thefinal composition of the textbook.
Public health and social medicine
Educational programs in public health andsocial and preventive medicine are now re-quired to assume greater responsibility formeeting the training needs of present healthworkers and new personnel who will be ac-tive in the 1980s and 1990s.
A revision of public health structures andprograms to adjust them to the countries'
106 REPORT OF THE DIRECTOR
needs began in 1980. Schools of public healthinitiated plans to decentralize their instruc-tion through regionalization of basic coursesinvolving interaction between health servicesand universities. Impressive initial resultswere achieved in Brazil, Colombia, andVenezuela. While continuing their graduateprograms, public health schools and depart-ments of social medicine are trying to in-stitute a wide variety of short-term programs,seminars, and workshops in priority areas ofadministration, planning, and research onteaching methods. Such projects were par-ticularly active in Chile, Colombia, Ecuador,and Mexico.
The Latin American Association of PublicHealth Schools (ALAESP), which comprisesgraduate public health and social medicineprograms, continued its activities with PAHOsupport. Its headquarters was moved fromthe National School of Public Health atMedellín to that at Rio de Janeiro.
In December the public health school atSao Paulo sponsored a meeting on health ser-vice research methods as a followup to thepromotional activities ALAESP had initiated.The public health schools of Colombia andVenezuela revised their structures and pro-grams. In Cuba, a health development in-stitute continued to organize and conduct itstraining and research programs, including aninternational health program. A seminar forprovincial heads of epidemiologic serviceswas held with PAHO assistance. Mexico'sSchool of Public Health continued to offer itstraining course for health administrators andplanners in collaboration with PAHO.
PAHO continued to prepare in-serviceepidemiology training materials which werefield-tested in Cuba, Mexico, and Uruguay.After they are revised, they will be madeavailable to countries requesting them.
Health care administration
One of PAHO's concerns, particularly dur-ing the last three years, has been to support
health administration training programs inLatin America and the Caribbean. The ex-isting programs in the hemisphere were iden-tified jointly with the W. K. Kellogg Founda-tion and, subsequently, subregional meetingswere held in Puerto Rico in 1976 and Braziland Colombia in 1977 to lay the groundworkfor strengthening schools responsible for suchtraining and eventually expanding their train-ing capacity.
In March a new stage in this program wasinaugurated. Its goals are to: (1) develop asystem to provide information on and fostereffective communication among health ad-ministration training programs, (2) improvesuch programs' procedures and content, (3)develop continuing education programsbased on health service requirements, (4) pro-mote research to integrate education andhealth services, and (5) establish new healthadministration training programs.
Between March and December visits weremade to the programs in Brazil, Chile, Co-lombia, Costa Rica, Dominican Republic,Ecuador, Mexico, and Venezuela.
All the training programs were used asvehicles to promote health service research todevelop new and alternative care models andencourage teaching-service integration. Thefollowing studies were undertaken with PAHOsupport: (1) a medical care model for under-served urban residents, (2) the organizationalbehavior at the University of Sao Paulo'smedical school and its teaching hospital, (3) areview of the literature on health care costsand their control, (4) a similar review onhealth service evaluation and planning, and(5) another literature review on organiza-tional behavior in health services.
Workshops were conducted to improvethe procedures and content of the health ad-ministration training programs in variouscountries. They covered training in organiza-tional behavior, health service evaluation andplanning, and the economic and financialaspects of health cost containment.
The program increased its commitment toassist in training executive and middle-
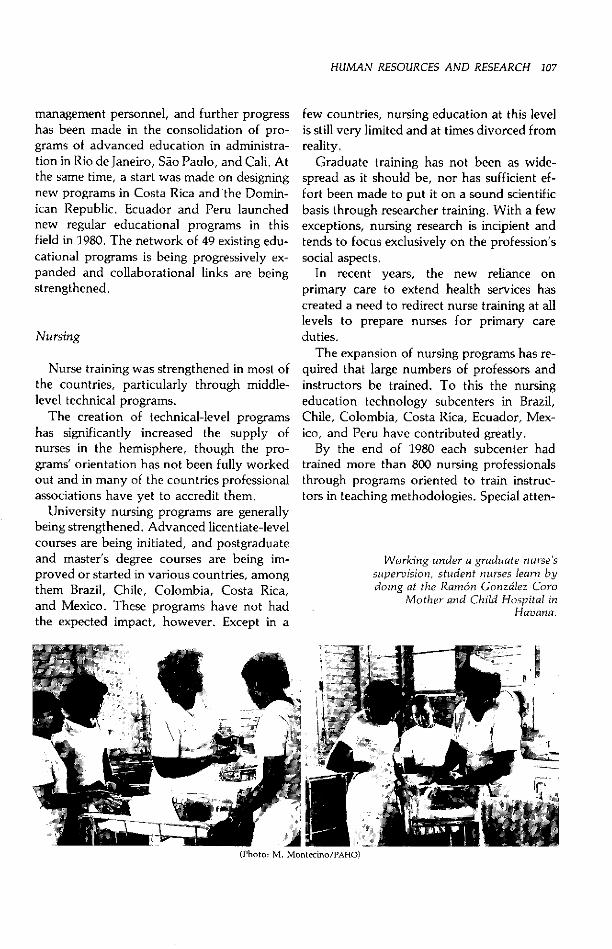
HUMAN RESOURCES AND RESEARCH 107
management personnel, and further progresshas been made in the consolidation of pro-grams of advanced education in administra-tion in Rio de Janeiro, Sao Paulo, and Cali. Atthe same time, a start was made on designingnew programs in Costa Rica and the Domin-ican Republic. Ecuador and Peru launchednew regular educational programs in thisfield in 1980. The network of 49 existing edu-cational programs is being progressively ex-panded and collaborational links are beingstrengthened.
Nursing
Nurse training was strengthened in most ofthe countries, particularly through middle-level technical programs.
The creation of technical-level programshas significantly increased the supply ofnurses in the hemisphere, though the pro-grams' orientation has not been fully workedout and in many of the countries professionalassociations have yet to accredit them.
University nursing programs are generallybeing strengthened. Advanced licentiate-levelcourses are being initiated, and postgraduateand master's degree courses are being im-proved or started in various countries, amongthem Brazil, Chile, Colombia, Costa Rica,and Mexico. These programs have not hadthe expected impact, however. Except in a
few countries, nursing education at this levelis still very limited and at times divorced fromreality.
Graduate training has not been as wide-spread as it should be, nor has sufficient ef-fort been made to put it on a sound scientificbasis through researcher training. With a fewexceptions, nursing research is incipient andtends to focus exclusively on the profession'ssocial aspects.
In recent years, the new reliance onprimary care to extend health services hascreated a need to redirect nurse training at alllevels to prepare nurses for primary careduties.
The expansion of nursing programs has re-quired that large numbers of professors andinstructors be trained. To this the nursingeducation technology subcenters in Brazil,Chile, Colombia, Costa Rica, Ecuador, Mex-ico, and Peru have contributed greatly.
By the end of 1980 each subcenter hadtrained more than 800 nursing professionalsthrough programs oriented to train instruc-tors in teaching methodologies. Special atten-
Working under a graduate nursessupervision, student nurses learn bydoing at the Ramón Gonzalez Coro
Mother and Child Hospital inHavana.
(Photo: M. Montecino/PAHO)
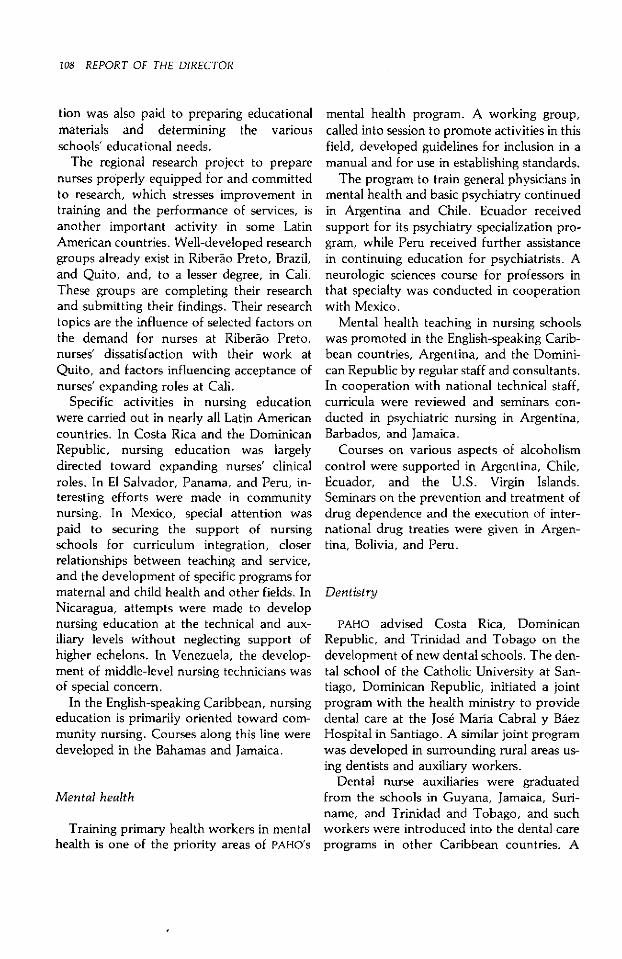
108 REPORT OF THE DIRECTOR
tion was also paid to preparing educationalmaterials and determining the variousschools' educational needs.
The regional research project to preparenurses properly equipped for and committedto research, which stresses improvement intraining and the performance of services, isanother important activity in some LatinAmerican countries. Well-developed researchgroups already exist in Riberao Preto, Brazil,and Quito, and, to a lesser degree, in Cali.These groups are completing their researchand submitting their findings. Their researchtopics are the influence of selected factors onthe demand for nurses at Riberao Preto,nurses' dissatisfaction with their work atQuito, and factors influencing acceptance ofnurses' expanding roles at Cali.
Specific activities in nursing educationwere carried out in nearly all Latin Americancountries. In Costa Rica and the DominicanRepublic, nursing education was largelydirected toward expanding nurses' clinicalroles. In E1 Salvador, Panama, and Peru, in-teresting efforts were made in communitynursing. In Mexico, special attention waspaid to securing the support of nursingschools for curriculum integration, closerrelationships between teaching and service,and the development of specific programs formaternal and child health and other fields. InNicaragua, attempts were made to developnursing education at the technical and aux-iliary levels without neglecting support ofhigher echelons. In Venezuela, the develop-ment of middle-level nursing technicians wasof special concern.
In the English-speaking Caribbean, nursingeducation is primarily oriented toward com-munity nursing. Courses along this line weredeveloped in the Bahamas and Jamaica.
Mental health
Training primary health workers in mentalhealth is one of the priority areas of PAHO's
mental health program. A working group,called into session to promote activities in thisfield, developed guidelines for inclusion in amanual and for use in establishing standards.
The program to train general physicians inmental health and basic psychiatry continuedin Argentina and Chile. Ecuador receivedsupport for its psychiatry specialization pro-gram, while Peru received further assistancein continuing education for psychiatrists. Aneurologic sciences course for professors inthat specialty was conducted in cooperationwith Mexico.
Mental health teaching in nursing schoolswas promoted in the English-speaking Carib-bean countries, Argentina, and the Domini-can Republic by regular staff and consultants.In cooperation with national technical staff,curricula were reviewed and seminars con-ducted in psychiatric nursing in Argentina,Barbados, and Jamaica.
Courses on various aspects of alcoholismcontrol were supported in Argentina, Chile,Ecuador, and the U.S. Virgin Islands.Seminars on the prevention and treatment ofdrug dependence and the execution of inter-national drug treaties were given in Argen-tina, Bolivia, and Peru.
Dentistry
PAHO advised Costa Rica, DominicanRepublic, and Trinidad and Tobago on thedevelopment of new dental schools. The den-tal school of the Catholic University at San-tiago, Dominican Republic, initiated a jointprogram with the health ministry to providedental care at the José María Cabral y BáezHospital in Santiago. A similar joint programwas developed in surrounding rural areas us-ing dentists and auxiliary workers.
Dental nurse auxiliaries were graduatedfrom the schools in Guyana, Jamaica, Suri-name, and Trinidad and Tobago, and suchworkers were introduced into the dental careprograms in other Caribbean countries. A
HUMAN RESOURCES AND RESEARCH 109
meeting of auxiliaries and dentists from Bar-bados, Dominica, Grenada, Guyana, Jamai-ca, St. Kitts-Nevis, Saint Lucia, and Trini-dad and Tobago was held to evaluate the useof dental auxiliaries in the English-speakingCaribbean. The participants agreed that gov-ernments must prepare adequately for thereturn of auxiliaries from training programsto ensure their rapid incorporation intohealth care activities and that the health andeducation sectors should collaborate to de-velop dental programs for school children.
Interest in training auxiliary workers con-tinued in Colombia, Mexico, Nicaragua,Panama, and Peru.
A course on dental equipment mainte-nance was planned in conjunction with theInstitute of Dental Resources in Quito for theAndean countries, and training programs fordental equipment maintenance technicianswere arranged in conjunction with commer-cial companies in several other countries.
PAHO's first course on social periodonticswas conducted in Spanish at Chicago andWashington in conjunction with the Univer-sity of Illinois. Advice was also provided tocountries such as Brazil, Chile, Ecuador, andPeru on conducting continuing educationprograms emphasizing the prevention andcontrol of dental diseases.
Engineering and environmental sciences
The trend toward subregional training ac-tivities in lieu of national short courses con-tinued. Of particular note were the followingactivities, all oriented to the goals of the In-ternational Drinking Water Supply andSanitation Decade:
* A 10-day course on controlling and measur-ing water wastage through leaks in water distribu-tion networks. Organized by CEPIS, the coursewas attended by 30 professional engineers.
* A three-week course on water supply systemoperation and maintenance for installation man-agers and supervisors. The course was cosponsoredby the Peruvian health ministry's environmental
sanitation division, Peru's industrial worker train-ing service, and CEPIS. Twenty-four Peruvianwaterworks supervisors and one each from Boliviaand Ecuador attended.
* Preparation, publication, and distribution inall 10 courses participating in the Caribbean basinwater management project of performance-ori-ented training manuals and guides geared to localconditions and the scholastic preparation of thetrainees. These publications were prepared bylocal engineers, technicians, and water utilitymanagers.
Foremost among the national educationalactivities carried out by local universities, en-gineering schools, and environmental engi-neering institutions were a week-long seminaron human ecology, development, and en-vironmental protection in San José sponsoredby the Costa Rican health ministry's en-vironmental sanitation division and PAHO'sPan American Center for Human Ecologyand Health in Mexico, and a symposium onwastewater reuse sponsored by the NationalAutonomous University of Mexico withPAHO's cooperation.
The proceedings of the symposium on en-vironmental manpower development held atRio de Janeiro in November 1979 werepublished as a three-part manual. The firstpart describes the symposium's objectives andrecommendations, the second discusses threetechnical topics related to manpower devel-opment, and the third contains informationon current successful environmental man-power development in the hemisphere andelsewhere.
The symposium's methods were used inorganizing two educational activities, in Co-lombia and Guatemala. PAHO collaborated ina review of Colombia's program to trainwater and sanitation workers, focusing onhuman resource development rather thanmerely training. In cooperation with PAHO,the Regional School of Sanitary Engineeringand the Standing Committee on DrinkingWater and Sanitation Coordination in Guate-mala sponsored a two-day seminar on man-power for the Water Decade.
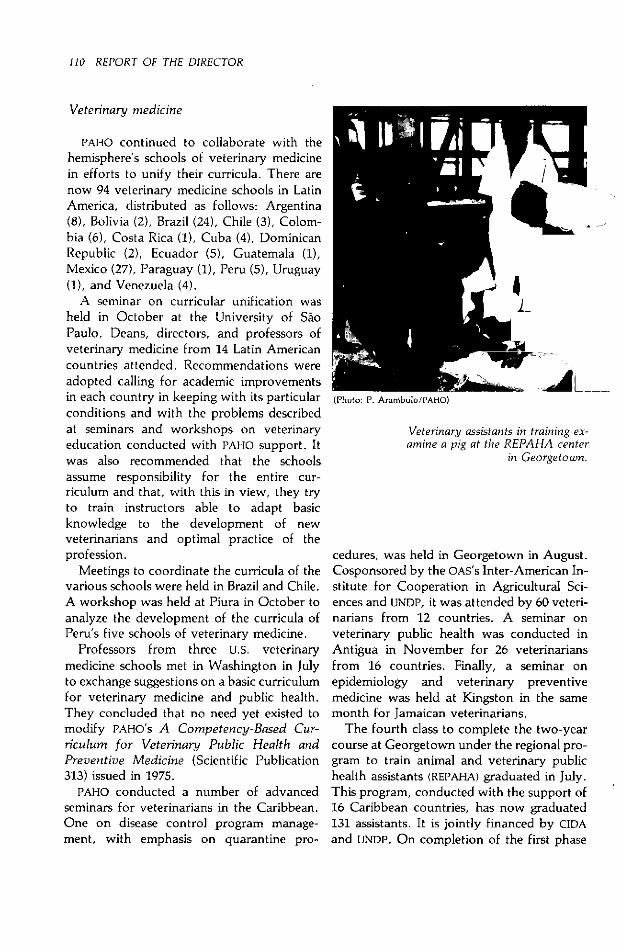
110 REPORT OF THE DIRECTOR
Veterinary medicine
PAHO continued to collaborate with thehemisphere's schools of veterinary medicinein efforts to unify their curricula. There arenow 94 veterinary medicine schools in LatinAmerica, distributed as follows: Argentina(8), Bolivia (2), Brazil (24), Chile (3), Colom-bia (6), Costa Rica (1), Cuba (4), DominicanRepublic (2), Ecuador (5), Guatemala (1),Mexico (27), Paraguay (1), Peru (5), Uruguay(1), and Venezuela (4).
A seminar on curricular unification washeld in October at the University of SaoPaulo. Deans, directors, and professors ofveterinary medicine from 14 Latin Americancountries attended. Recommendations wereadopted calling for academic improvementsin each country in keeping with its particularconditions and with the problems describedat seminars and workshops on veterinaryeducation conducted with PAHO support. Itwas also recommended that the schoolsassume responsibility for the entire cur-riculum and that, with this in view, they tryto train instructors able to adapt basicknowledge to the development of newveterinarians and optimal practice of theprofession.
Meetings to coordinate the curricula of thevarious schools were held in Brazil and Chile.A workshop was held at Piura in October toanalyze the development of the curricula ofPeru's five schools of veterinary medicine.
Professors from three U.S. veterinarymedicine schools met in Washington in Julyto exchange suggestions on a basic curriculumfor veterinary medicine and public health.They concluded that no need yet existed tomodify PAHO's A Competency-Based Cur-riculum for Veterinary Public Health andPreventive Medicine (Scientific Publication313) issued in 1975.
PAHO conducted a number of advancedseminars for veterinarians in the Caribbean.One on disease control program manage-ment, with emphasis on quarantine pro-
(Photo: 1-'. Arambulo/PAHO)
Veterinary assistants in training ex-amine a pig at the REPAHA center
in Georgetown.
cedures, was held in Georgetown in August.Cosponsored by the OAS's Inter-American In-stitute for Cooperation in Agricultural Sci-ences and UNDP, it was attended by 60 veteri-narians from 12 countries. A seminar onveterinary public health was conducted inAntigua in November for 26 veterinariansfrom 16 countries. Finally, a seminar onepidemiology and veterinary preventivemedicine was held at Kingston in the samemonth for Jamaican veterinarians.
The fourth class to complete the two-yearcourse at Georgetown under the regional pro-gram to train animal and veterinary publichealth assistants (REPAHA) graduated in July.This program, conducted with the support of16 Caribbean countries, has now graduated131 assistants. It is jointly financed by CIDAand UNDP. On completion of the first phase

HUMAN RESOURCES AND RESEARCH 111
of the program, UNDP and PAHO agreed on asecond phase, to run from January 1981 toDecember 1984, after which it is anticipatedthat the Caribbean countries will assume fullresponsibility for the program in 1985.
A continuing education course for REPAHAgraduates on poultry industry problems wasconducted in Georgetown in September.Eighteen animal and veterinary public healthassistants from 11 countries participated.
PAHO's Pan American Zoonosis Center(CEPANZO) in Argentina also continued itsprofessional and technical training program.This included both individual training andintra- and extramural courses, the latter heldin the countries with the cooperation of na-tional authorities and institutions. Fellow-ships for intramural courses were providedby PAHO and such international agencies asFAO, USAID, UNDP, 1DB, and national govern-ments and universities. One hundred eightyprofessionals were trained during the year.Forty-two from 16 countries received in-dividual training at CEPANZO, and 44 par-ticipated in intramural and 94 in extramuralcourses.
Continuing education
After a year devoted essentially to organiz-ing national programs and streamlining re-gional and subregional coordination, PAHO's
continuing education program recorded itsfirst accomplishments in 1980 in most of theeight countries participating in the program'sfirst stage. Continuing education activitieswere carried out in Bolivia, Colombia, Cuba,Dominican Republic, Ecuador, Guatemala,and Honduras, in every case with CIDA finan-cial assistance. The Canadian agency hasbeen supporting continuing education pro-grams in Latin America since 1978.
Activities in Colombia continued unabatedas the health ministry's human resourcesdirectorate gradually increased its personnel,and more than 9,000 health professionals and
technicians participated in the program. Thedirectorate's audiovisual aids center wasstrengthened, especially in educational televi-sion.
In Cuba, where the program is part of thevice ministry of education and research,significant progress was made. The programbranched out in new directions, including avideo cassette course in tropical medicine.The first national continuing educationworkshop, a three-day meeting in Novem-ber, reviewed the program and recommendednew activities.
PAHO signed an agreement with theDominican Republic at mid-year for a pro-gram that was later organized and launched.
In Guatemala the thrust was on continuingeducation for health ministry rural auxiliariesthrough self-instruction and periodic groupevaluation modules. In Honduras, where theprogram is closely tied to training in supervi-sion, the emphasis was on developing contin-uing education for individual and entireteams of health workers. A PAHO/CIDAevaluation team made a field inspection ofthe programs in these two countries andrecommended continued financial and tech-nical assistance to both programs as well astheir possible future expansion. In December,CIDA agreed to Nicaragua's admission to theprogram and to provide the necessary finan-cial assistance. PASCCAP was designated theproject's reference center.
Technical and auxiliary personnel
Programs to extend health service coverageare underway in various countries. In somecases their financing is almost entirely na-tional, while in others the programs are sup-ported by outside agencies.
The extent of coverage varies widely fromcountry to country and depends on the initialsituation and magnitude of the effort tospread it. Many countries have yet to defineclearly the personnel they need for their
112 REPORT OF THE DIRECTOR
Future middle-level techniciansreceive instruction in Havana.
(Photo: M. Montecino/PAHO)
coverage extension programs, and this isespecially true of auxiliary and middle-leveltechnical health workers.
The existing structure of health servicesmade it necessary to create a new type of in-termediate technical worker equipped tocarry out new kinds of health practice inunderserved urban and rural areas. Twotypes of technicians are now found in bothhealth services and training centers-"monovalent" technicians, whose work islimited to aiding professional personnel, and"polyvalent" technicians who work in coor-dination with university-trained profession-als.
Programs to train middle-level techniciansare underway in a number of countries,notably Chile, Costa Rica, Cuba, DominicanRepublic, Ecuador, Mexico, Nicaragua, Peru,and Venezuela. PAHO continued to supportthe programs for training intermediate techni-cians in the Dominican Republic, Mexico,and Venezuela, and in Cuba and Nicaragua,which have a technical cooperation agree-ment specifically providing for such training.
As an outcome of the first technicalcooperation workshop on developing mid-dle-level technical personnel, in 1979 atCamaguey, Cuba, an intercountry programwas started to train this kind of worker.
The second such workshop was held inApril at Cumaná, Venezuela, with par-ticipants from Bolivia, Colombia, Cuba,Dominican Republic, Nicaragua, Peru, andVenezuela. PASCCAP and Hipólito UlnanueAgreement representatives also attended.The objectives of the second workshop wereto determine the extent of compliance withthe first workshop's resolutions and ensuretheir continuity and feasibility, and reviewthe program's progress and the use of in-termediate technical personnel in light of theexperience of the various countries par-ticipating in it.
The second workshop's participants rec-ommended that instructor training programsbe conducted to assure the development andcontinuing education of middle-level tech-nical personnel, that documentation centersbe organized and training materials be pro-duced to facilitate selective dissemination ofinformation about continuing education, andthat the scientific and technical knowledgepossessed by the countries be placed at thedisposal of students.
In Brazil, the health worker training pro-gram begun in 1975 was reorganized to in-clude the social welfare ministry in additionto the ministries of health and of educationand culture. The program's objectives now

HUMAN RESOURCES AND RESEARCH 113
include improving manpower training andplanning methods and activities to formulatea comprehensive human resources develop-ment plan, improving the integration ofteaching and service, fostering continuousimprovement in the quality of health caretraining through curriculum evaluation andrevision as well as the application of modernpedagogic techniques, promoting the prepa-ration and supply of better teaching and self-training materials, and upgrading service,training, and research personnel through bet-ter coordination among graduate health caretraining centers.
In the Caribbean, PAHO and the secretariatof the Caribbean Community have beenendeavoring to improve coordination amongCaribbean schools training technical and aux-iliary health workers. The special projectorganized for this purpose in 1975 completedits second phase in 1980.
Pursuant to recommendations included inan evaluation made in 1979, a proposal wasprepared for the project's third phase, tobegin in January 1981 and last two years. Theproject is financed by CIDA, UNDP, whichgranted $600,000 to cover its regular staff andconsultant requirements during the thirdphase, and UNICEF, which continued tofinance the training of community auxiliariesand their use in primary health care activities.As executing agency, PAHO provides supportfor the project's programs and centers whennecessary, though it began making ar-rangements to transfer its training activities tothe Caribbean Community.
In January, PAHO convened a meeting ofinternational agencies operating in the Carib-bean to provide them information on re-quirements for training technical and aux-iliary personnel.
In Central America, the technical advisorycouncil of the community health workertraining program for Central America andPanama (PASCCAP) met for the second time,at San José in February, and approved theprogram's 1980 action plan. This covered the
following subprograms: health services re-search and development, educational re-search and development, social and epidemi-ologic research, continuing education andtraining in supervision, training in coverageextension administration, research on anddevelopment of intermediate technical per-sonnel, planning human resources forcoverage extension, production of educa-tional materials, and development of an in-formation and documentation center.
The action plan was carried out in thecountries and at PASCCAP's headquarters inSan José. Through its health ministry, CostaRica made available a building including of-fices, a meeting room, a print shop, andaudiovisual aids and information and docu-mentation rooms.
Two courses for representatives from thecountries were held as part of the health ser-vices research subprogram, one in San Joséand the other in Panama City. Visits weremade to national groups to determine theirresearch support requirements. Research pro-tocols were prepared and put into effect incollaboration with groups in Costa Rica,Guatemala, and Honduras. In Nicaragua, agroup of subprogram advisers held a meetingand defined activities to be carried out in thisand other countries.
In the educational research and develop-ment subprogram, work began on develop-ing self-instruction modules and incorporat-ing in them the basic strategies of primarycare, community participation, appropriatetechnology, intersectoral linkage, and theprinciples of pedagogic methodology.
Activities were also carried out in in-dividual countries. In El Salvador, the com-munity nursing school received support, andadvice was provided on developing educa-tional methods for training auxiliary andtechnical personnel. In Guatemala, assistancewas furnished in educational developmentand review of curricula for training auxiliaryand community health workers. In Hon-duras, university faculty in the health area

114 REPORT OF THE DIRECTOR
received assistance in educational develop-ment and technology.
As part of the continuing education andsupervision training subprogram, technicaladvice was given to Guatemala and Hon-duras on continuing education and to all theCentral American countries and Panama ontraining in supervision. With the participa-tion of an advisory group, a subregional con-tinuing education program was conducted inGuatemala. The national coordinators of thesupervision program met at Guatemala Cityin November.
Programs to train local health service unitsupervisors and advisers were started inBolivia, Brazil, Panama, and Peru.
Coordinated by CLATES, a meeting washeld at Lima in May to organize the activitiesto be carried out in Bolivia, Brazil, and Peru.Five representatives from each of the coun-tries and PAHO consultants participated. InBolivia, it was only in the latter part of theyear that educational activities closely tied tothe continuing education program wereresumed. In Brazil, two activities were carriedout, one coordination among the variousparticipating states and the other an attemptto define the national program. Peru's healthministry approved a supervision modeldesigned by the program's multidisciplinaryteam. Educational activities were initiated,including workshops for metropolitan Limaand the health areas chosen for this stage ofthe program, Cuzco, Iquitos, and Puno.
In Panama, the program was started atmid-year in accordance with an existingsupervision model developed by the healthministry. Several activities were carried outto upgrade the methods used by instructorsproviding training in supervision at variouslevels.
Fellowships
PAHO's fellowship program provides thefinancial and administrative means by whichhealth workers in the Americas may further
their academic development, obtain practicaltraining, attend short courses, or visit institu-tions or colleagues abroad in any field ofstudy or activity related to health. The gov-erning bodies set priorities, but the govern-ments make final determinations of fields ofstudy and candidates.
In 1980 there was a small decrease in thetotal number of fellowships awarded and inthe total number of fellowship months used.Awards declined from 1,289 in 1979 to 1,216(5.7 percent) and the number of months from5,250 to 4,330 (17.5 percent).
The total cost of the fellowships awardedincreased from $4,400,865 in 1979 to$4,533,620 (3 percent). The average cost of along-term award (over six months) for studyin Canada or the United States rose from$9,448 to $11,362 (20 percent), while long-term training elsewhere rose from an averageof $5,970 to $6,789 (14 percent). Short-termfellowships (six months or less) and groupfellowships for organized courses increased incost by 18 percent. The overall average in-crease in cost per fellowship month rose from$838 in 1979 to $1,047 in 1980 (25 percent).These increases are due to escalating costs oftransportation, living, and training. Stipendrates, which had been held back in recentyears to restrain the impact of inflation, fi-nally had to be revised to more realistic levelsto keep the program alive.
Although the number of awards decreased,total activity in the fellowship program ac-tually increased. This was largely due to a 26percent rise in the number of fellows fromother parts of the world placed for studies inthe Americas. In addition, a large number oflong-term fellows who had received awardsin previous years continued their studies in1980 under PAHO's administrative and techni-cal responsibility.
Of the 1,216 fellowships requested by thegovernments in 1980 (Table 6), 21 percentwere in public health administration, 8 per-cent in environmental sanitation, 5 percent innursing, 11 percent in maternal and childhealth, 24 percent in other health services, 20
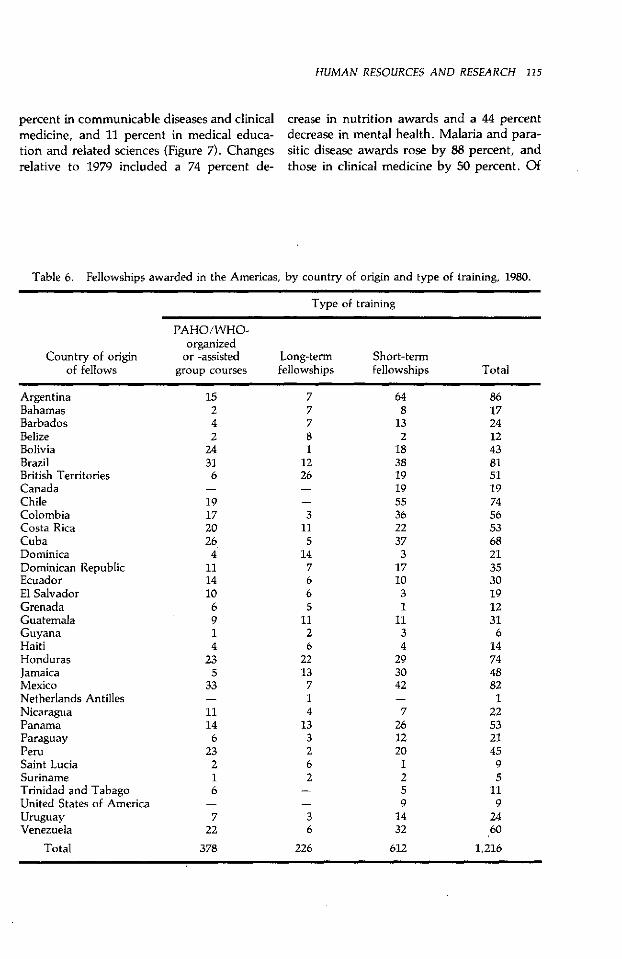
HUMAN RESOURCES AND RESEARCH 115
percent in communicable diseases and clinical crease in nutrition awards and a 44 percentmedicine, and 11 percent in medical educa- decrease in mental health. Malaria and para-tion and related sciences (Figure 7). Changes sitic disease awards rose by 88 percent, andrelative to 1979 included a 74 percent de- those in clinical medicine by 50 percent. Of
Table 6. Fellowships awarded in the Americas, by country of origin and type of training, 1980.
Type of training
PAHO/WHO-organized
Country of origin or -assisted Long-term Short-termof fellows group courses fellowships fellowships Total
Argentina 15 7 64 86Bahamas 2 7 8 17Barbados 4 7 13 24Belize 2 8 2 12Bolivia 24 1 18 43Brazil 31 12 38 81British Territories 6 26 19 51Canada - - 19 19Chile 19 - 55 74Colombia 17 3 36 56Costa Rica 20 11 22 53Cuba 26 5 37 68Dominica 4 14 3 21Dominican Republic 11 7 17 35Ecuador 14 6 10 30El Salvador 10 6 3 19Grenada 6 5 1 12Guatemala 9 11 11 31Guyana 1 2 3 6Haiti 4 6 4 14Honduras 23 22 29 74Jamaica 5 13 30 48Mexico 33 7 42 82Netherlands Antilles - 1 - 1Nicaragua 11 4 7 22Panama 14 13 26 53Paraguay 6 3 12 21Peru 23 2 20 45Saint Lucia 2 6 1 9Suriname 1 2 2 5Trinidad and Tabago 6 - 5 11United States of America - - 9 9Uruguay 7 3 14 24Venezuela 22 6 32 60
Total 378 226 612 1,216
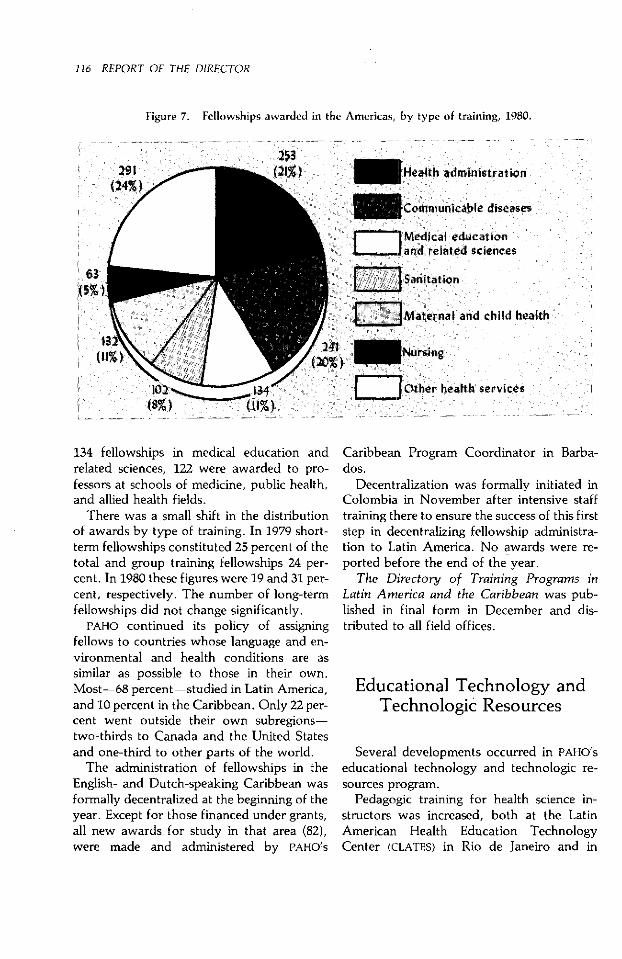
116 REPORT OF THE DIRECTOR
Figure 7. Fellowships awarded in the Americas, by type of training, 1980.
253Health administration
- Communicable diseases
W- -- Medical education.!Jandi related sciences
[jZ Sanitation
[ m M aternal and child health
(20%>vNursing
Other health services
63i5%
134 fellowships in medical education andrelated sciences, 122 were awarded to pro-fessors at schools of medicine, public health,and allied health fields.
There was a small shift in the distributionof awards by type of training. In 1979 short-term fellowships constituted 25 percent of thetotal and group training fellowships 24 per-cent. In 1980 these figures were 19 and 31 per-cent, respectively. The number of long-termfellowships did not change significantly.
PAHO continued its policy of assigningfellows to countries whose language and en-vironmental and health conditions are assimilar as possible to those in their own.Most-68 percent-studied in Latin America,and 10 percent in the Caribbean. Only 22 per-cent went outside their own subregions-two-thirds to Canada and the United Statesand one-third to other parts of the world.
The administration of fellowships in theEnglish- and Dutch-speaking Caribbean wasformally decentralized at the beginning of theyear. Except for those financed under grants,all new awards for study in that area (82),were made and administered by PAHO's
Caribbean Program Coordinator in Barba-dos.
Decentralization was formally initiated inColombia in November after intensive stafftraining there to ensure the success of this firststep in decentralizing fellowship administra-tion to Latin America. No awards were re-ported before the end of the year.
The Directory of Training Programs inLatin America and the Caribbean was pub-lished in final form in December and dis-tributed to all field offices.
Educational Technology andTechnologic Resources
Several developments occurred in PAHO'seducational technology and technologic re-sources program.
Pedagogic training for health science in-structors was increased, both at the LatinAmerican Health Education TechnologyCenter (CLATES) in Rio de Janeiro and in
HUMAN RESOURCES AND RESEARCH 117
various countries with CLATES' support. Atthe request of the National Autonomous Uni-versity of Mexico, the former Latin AmericanHealth Education Technology Center in Mex-ico City was converted to a purely nationalinstitution, though it continues to maintainlinks with PAHO.
Headquarters was made responsible forproviding methodologic support to all re-gional, subregional, and national meetingsthat PAHO coordinates or supports financiallyand technically. This made it possible toorganize meetings more effectively andachieve better results through continuingevaluation. A quarterly directory of PAHO
meetings was started and distributed to thecountries.
From 1976 to 1980 the W. K. Kellogg Foun-dation supported PAHO's Latin AmericanProgram for Educational Development inHealth (PLADES) to bridge the gap betweenhealth and education systems. At the begin-ning of the year PAHO presented a new pro-posal to the Foundation to develop anevaluation system applicable not only toPLADES but to other Kellogg service-trainingintegration projects. The Foundation agreed,and CLATES began preparing a general assess-ment of PLADES.
In the educational technology field,CLATES and the countries continued their ac-tivities. Work in this field has recently beenstrengthened through the participation ofPASCCAP, which has an educational researchand development subprogram, a unit for pro-ducing educational materials, and a healthscience and technology information center.Following startup CLATES support, PASCCAP
is expected to begin meeting CentralAmerica's educational technology require-ments.
CLATES offered nine health educationcourses and seminars at Rio de Janeiro be-
tween January and July. These meetings dealtwith health science curricula, evaluation ofhealth sciences instruction, audiovisual aids,group dynamics in education, human
resource planning, teaching-service integra-tion, didactics applied to the health sciences,MUMP/MIIS computer programming languagefor education, and training instructors incomprehensive medicine. More than 500health science instructors attended these five-to ten-day courses with the help of fellow-ships awarded by PAHO, their own countries,or Brazil's Superintendency for InternationalTechnical Cooperation.
It also continued to participate in the mas-ter's degree program in educational technol-ogy at the Federal University of Rio deJaneiro and provided courses and advisoryservices in Bolivia, Chile, Colombia, Ecua-dor, Honduras, Nicaragua, Paraguay, andPeru.
Within PAHO, CLATES supported the Ex-panded Program on Immunization (EPI) inproducing filmstrips on the cold chain andrefrigerators for EPI regional and nationaltraining programs, and the emergency pre-paredness program in adapting filmstrips andtranslating and adapting disaster relief simula-tion exercises. It and PAHO's Latin AmericanCenter for Perinatology and Human Devel-opment at Montevideo reached an agree-ment to collaborate in the latter's new ma-ternal and child health and communityprograms.
Nursing education technology activitiescontinued to be carried out through a net-work of nine national subcenters which pro-vided training to students from other schoolsand in some cases from fields other thannursing.
The newest subcenter is that in Lima,where the nursing school of Children'sHospital, operated by Peru's health ministryin conjunction with the University of SanMarcos, began operations. Several courses onpedagogy and modular instruction were of-fered for instructors in nursing, medicine, anddentistry. The first courses were conductedwith the support of CLATES. The subcenteralso collaborated with the health ministry'ssupervision training program in preparing

118 REPORT OF THE DIRECTOR
specific modules and training future instruc-tors for the program.
The other subcenters, in Brazil (Bahia andBelo Horizonte), Chile, Costa Rica, Colom-bia (Bogotá and Cali), Ecuador, and Mexico,continued to work in their respective areas.They produced educational materials invarious formats, mainly modular and ori-ented toward integration between nursingschools and health services. All the centersoffered courses and seminars on educationaltechnology, in some cases with direct supportfrom CLATES.
Regional Library ofMedicine and theHealth Sciences
PAHO's Regional Library of Medicine andthe Health Sciences (RLM) in Sao Paulo coor-dinates a health information network inwhich it is the regional center for LatinAmerica and the Caribbean, national centerfor Brazil, and subcenter for Sao Paulo State.
RLM carried out highly diversified service,training, and administration programs duringthe year. Its activities included expansion andstrengthening of the Brazilian and LatinAmerican health information networks,research, analysis and indexing of LatinAmerican publications, selective informationdissemination, publishing, advanced biomed-ical librarian training, bibliography searches,interlibrary loans, and service to users in theSao Paulo area.
At its meeting in May 1979, RLM's scientificadvisory committee suggested the establish-ment of a long-range working group toundertake a detailed study of further expan-sion of the Latin American health informa-tion network. As a consequence of the com-mittee's suggestion, the group was estab-lished. With Rockefeller Foundation support,it held four meetings and retained consultants
in 1980 to visit various countries and examinethe current situation. A proposal to create thehealth information network was developedfor submission to funding agencies.
Plans and studies were made to expandRLM's network of users through betteremployment of the technology and facilitiesavailable in the Latin American countries. Ex-tending and improving bibliographic searchservices through online telex access to theMEDLINE system and the Latin American In-dex Medicus data base, at a cost within thereach of the countries, is a short-term pros-pect.
In 1979, RLM began evaluating the circula-tion of biomedical periodicals locally, inBrazil, and in Latin America to determine thecharacteristics of users and their requirementsin order to guide periodicals acquisitionpolicies and pinpoint reasons for nonfulfill-ment of periodicals requests.
Continued analysis of the findings of theevaluation furthered administrative planning.Information on titles requested that wereavailable or unavailable at RLM was highlyuseful in making subscription renewal deci-sions for 1981 so as to improve its collectionwithout burdening its budget. The data ob-tained reflect local demand and that fromother libraries in the Brazilian and LatinAmerican networks, and so provide a repre-sentative profile of the actual use of the avail-able collection.
The semiannually published Latin Ameri-can Index Medicus is making a significantcontribution to biomedical information byproviding a central source of data on articlesin approximately 250 Latin Americanpublications. As the work on this publicationgoes forward, increasing information be-comes available on the output of health in-stitutions and professionals in Latin America,and hence exchanges and cooperation amongthem are facilitated. The two volumes dis-tributed or prepared during the year covered6,000 articles.
RLM's programs to disseminate selected in-
HUMAN RESOURCES AND RESEARCH 119
formation about cancer (LACRIP), nutrition(INAN), and public health continued theirregular operations.
LACRIP provided cancer information to3,272 professionals in 18 countries (including1,336 in Latin America) and distributed32,266 photocopies of articles requested byparticipating libraries. INAN furnished 5,775copies of nutrition articles produced in LatinAmerica or published by international agen-cies to 517 users active in nutrition in Brazil.The Sao Paulo health department, in chargeof the public health bibliography program,compiled bibliographies on 69 subjects.
Under an agreement with the University ofSáo Paulo's public health school, RLM initi-ated a new publication to disseminate infor-mation on public health and related disci-plines. "Alerta Bibliografico-Serie I-SaúdePública" is a quarterly containing summariesof periodicals, books, theses, and otherdocuments.
Two advanced training courses were con-ducted for biomedical librarians from Braziland other Latin American countries. Twoother courses were offered on the use ofRLM's facilities.
Four computer terminals, at RLM and theBelo Horizonte, Rio de Janeiro, and Salvadorsubcenters, are used to compile bibliog-raphies to meet requests from Brazil andother Latin American countries. During theyear, 3,673 searches of the u.s. NationalLibrary of Medicine's MEDLINE data base werecarried out, including 1,166 made by thesubcenters and 2,507 by RLM.
Forty thousand requests for photocopies ofscientific articles were received, slightly lessthan a third of them from countries otherthan Brazil. RLM was able to fill 82 percent ofthe requests from its own or the Brazilian net-work's collections.
A "List of Current Periodicals Available atRLM" was prepared. Some of the titles listedwere not available at RLM but were held bylibraries in the Brazilian network. This wasexpected to be a valuable tool in improving
the exchange of information among thelibraries in the network.
RLM's library department provides basicsupport to Sao Paulo-area users, especiallythose at the Sao Paulo School of Medicine,which accounted for 50,591 or 73 percent ofall local users of its services in 1980. A total of9,657 books were loaned or consulted and81,310 requests for publications were re-ceived, three-quarters of which were filled lo-cally.
Research Promotionand Coordination
The governments have become more con-scious of the significance, relevance, andnecessity of scientific and technologic ad-vances in solving current practical problemsof public health. PAHO has therefore ex-panded its research activities by continuouslysupporting its network of 10 research centers,
Results of research on mosquitocontrol are schemratized on a bulletin
board at the National Institute ofHygiene and Epidemiology in
Havana.
(Photo: M. Montecino/PAHO)
� 1
L#f@!# Jsi&
S1k rWáffl":.'5 > ¡'O r w
(Photo: J. Moquillaza/PAHO)
Larvivorous fish such as these at an experimental station inColombia are often used to control mosquitoes.
promoting and funding health service in-vestigations and biomedical research, andbacking a number of independent investi-gators and research teams throughout thehemisphere.
It has also advised the governments on ef-forts to develop national health researchpolicies. During 1980 it sponsored a meetingalong these lines at Montevideo of delegatesfrom Argentina, Chile, Paraguay, and Uru-guay. In addition, the bases of future na-tional meetings on health research policies inBrazil and Venezuela were set up during theyear.
As a followup to a 1979 meeting in Argen-tina, a second meeting was held at which theintersectoral study group on the ethical
aspects of research presented a draft code ofethics for that country. Work on draftingcodes of ethics for research using human sub-jects also proceeded in other countries. InColombia and Costa Rica the drafts were welladvanced.
PAHO believes that fostering research ac-tivities will require development of a criticalmass of national institutions. Thus, a pro-gram has been initiated to identify andstrengthen national research centers havingclose links with PAHO which will become anetwork to be used not only as regional train-ing centers and to promote and conductresearch projects within PAHO's priorities butalso to stimulate technical cooperation amongdeveloping countries.
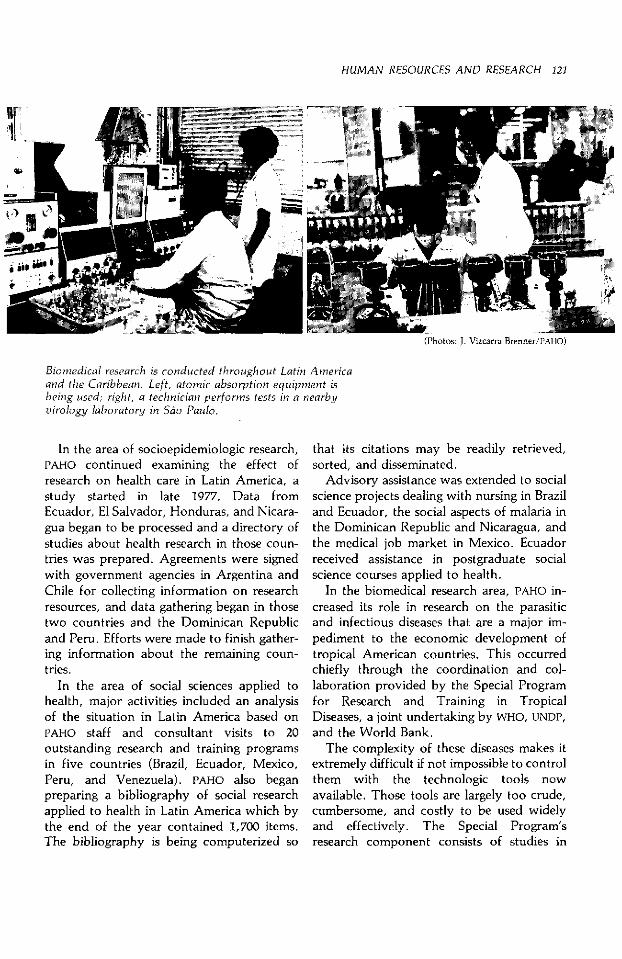
HUMAN RESOURCES AND RESEARCH 121
(Photos: J. Vizcarra Brenner/PAHO)(Photos: J. Vizcarra Brenner/PzAHO)
Biomedical research is conducted throughout Latin Amrericaand the Caribbean. Left, atomic absorption equipment isbeing used; right, a technician performs tests in a nearbyvirology laboratory in Sio Paulo.
In the area of socioepidemiologic research,PAHO continued examining the effect ofresearch on health care in Latin America, astudy started in late 1977. Data fromEcuador, El Salvador, Honduras, and Nicara-gua began to be processed and a directory ofstudies about health research in those coun-tries was prepared. Agreements were signedwith government agencies in Argentina andChile for collecting information on researchresources, and data gathering began in thosetwo countries and the Dominican Republicand Peru. Efforts were made to finish gather-ing information about the remaining coun-tries.
In the area of social sciences applied tohealth, major activities included an analysisof the situation in Latin America based onPAHO staff and consultant visits to 20outstanding research and training programsin five countries (Brazil, Ecuador, Mexico,Peru, and Venezuela). PAHO also beganpreparing a bibliography of social researchapplied to health in Latin America which bythe end of the year contained 1,700 items.The bibliography is being computerized so
that its citations may be readily retrieved,sorted, and disseminated.
Advisory assistance was extended to socialscience projects dealing with nursing in Braziland Ecuador, the social aspects of malaria inthe Dominican Republic and Nicaragua, andthe medical job market in Mexico. Ecuadorreceived assistance in postgraduate socialscience courses applied to health.
In the biomedical research area, PAHO in-creased its role in research on the parasiticand infectious diseases that are a major im-pediment to the economic development oftropical American countries. This occurredchiefly through the coordination and col-laboration provided by the Special Programfor Research and Training in TropicalDiseases, a joint undertaking by WHO, UNDP,and the World Bank.
The complexity of these diseases makes itextremely difficult if not impossible to controlthem with the technologic tools nowavailable. Those tools are largely too crude,cumbersome, and costly to be used widelyand effectively. The Special Program'sresearch component consists of studies in

122 REPORT OF THE DIRECTOR
tropical countries to develop new and effec-tive tools to control six diseases: malaria,schistosomiasis, leishmaniasis, trypanosomi-asis (including Chagas' disease), filariasis, andleprosy.
One of the Special Program's componentsis institutional development to build and rein-force the ability of selected universities andresearch institutions to carry out investiga-tions. Nine research centers in Argentina,Bolivia, Brazil, Cuba, Peru, and Venezuelareceived institutional development grants forcapital equipment and long-term support. Inaddition, advanced training through researchtraining or visiting scientist grants was pro-vided to scientists from institutions in Argen-tina, Brazil, Mexico, Paraguay, and Vene-zuela.
Investigators in 15 American countries con-ducted research on the six target diseases. Inall, 192 projects supported by grants totalingmore than $4 million were active during theyear.
Advisory Committee on Medical Research
PAHO's Advisory Committee on MedicalResearch (ACMR), composed of 18 distin-guished scientists chosen for their wide ex-perience and knowledge of health problemsin the Americas, met at San José in June. Thehost institution was Costa Rica's newlyestablished Nutrition and Health Researchand Training Institute. ACMR's members hadan opportunity to visit this and other scien-tific institutions in the country, familiarizethemselves with their work, and make con-tact with their researchers.
The ACMR meeting was largely devoted todiscussion of the reports of various subcom-mittees. The diarrheal disease research sub-committee reported on the recommendationsfrom its meeting in Panama in which scien-tists from 10 countries participated. Thehealth service research subcommittee's reporthighlighted the social research being con-ducted in Latin American health services.
Dr. Sune Bergstrom, chairman, ACMR.
The nutrition research subcommittee re-ported on a proposed regional research pro-gram which was later extensively discussed ata PAHO-sponsored meeting of prominent nu-tritionists at Bogotá. ACMR's members alsoheard a report from their subcommittee onthe ethical aspects of research using humansubjects.
As in earlier ACMR meetings, two of PAHO'sresearch and advisory units, the LatinAmerican Center for Perinatology andHuman Development at Montevideo and thecommunity health training program at SanJosé, reported on their research activities.The committee also heard and discussed apresentation on malnutrition, mental devel-opment, behavior, and learning, papers onthe history of health research centers in LatinAmerica, and a progress report on tropicaldisease research and malaria in the Americas.
Research grants
PAHO continued to carry the program ofgrants for research and research training that

HUMAN RESOURCES AND RESEARCH 123
began in 1970 to support the development ofresearch in priority health areas.
Research applications are rated on the basisof the scientific merit and expected results,the extent to which the proposed research isrelated to PAHO's priorities, and the availabil-ity of funds. Training grant applications areevaluated on the basis of qualifications,working and research conditions at the pro-posed study site, and the relevance of thetraining requirements to the needs of theirhome countries.
As a matter of policy, PAHO gives prefer-
ence to projects presented by researchersfrom Latin America and the Caribbean inorder to encourage research in those coun-tries. Whenever possible, it also promotescollaborative studies involving institutions intwo or more countries.
Sixty proposals were received during theyear, by the end of which 39 had beenevaluated and 20 grants totaling $125,015 hadbeen awarded to applicants from Brazil, Co-lombia, Costa Rica, Jamaica, Mexico, Pan-ama, Peru, United States, Uruguay, and Ven-ezuela.

DYL- -Á1-
I i;\L
-4
1
se fl
/e - wrre ,
i� � , 1
� j! 1
1-v
Chapter 6
SPECIAL PROGRAMS
Zoonoses and Animal Health
Disease is a major constraint on thedevelopment of the livestock industry inLatin America and the Caribbean. Amongthe many diseases affecting Latin Americanand Caribbean herds today, foot-and-mouthdisease (FMD) and zoonoses are especially im-portant because, in addition to limiting cattleraising, they place restraints on livestock andmeat marketing. Zoonoses are diseases com-mon to man and animals in which animals arehosts of pathogenic agents, direct or in-termediary vectors, or sources of environ-mental contamination.
As it has for several decades, PAHO con-tinued to advise the countries on their animalhealth programs. It did so through head-
A game warden inspects PadreIsland in the Amazon River nearIquitos, Peru, where moustachedtamarins (Saguinus mystax) are bredfor primate studies and medicalresearch.
quarters staff, specialists assigned to area orcountry offices, and its two animal healthresearch units, the Pan American ZoonosisCenter (CEPANZO) at Ramos Mejía, Argen-tina, established in 1956, and the PanAmerican Foot-and-Mouth Disease Center(PANAFTOSA) at Rio de Janeiro, established in1951.
With CEPANZO's technical cooperation, thecountries have made substantial progress indeveloping the infrastructure of their veteri-nary public health services. These were someof CEPANZO's advisory activities during theyear:
In Bolivia the ministry of rural andagricultural affairs' FMD, rabies, and brucello-sis control service (SENARB) made appreciableprogress in building its laboratory and centraloffice, 12 veterinary centers, and 12 quaran-tine stations. Because of the economic condi-tions the country faces, SENARB and Bolivia'szoonosis control programs will require con-tinued support from PAHO and specificallyCEPANZO and PANAFTOSA.
At the request of Brazil's health ministry,PAHO redesigned the ministry's veterinarypublic health activities. As priority areas, itwas agreed to institute a zoonosis controlprogram in the ministry, which began asurvey to identify the country's principalzoonoses as a basis for establishing indicators,and to establish intersectoral cooperation to
125
126 REPORT OF THE DIRECTOR
use human and material resources better.CEPANZO advised Sao Paulo's four-year-oldmunicipal Urban Zoonosis Center on design-ing a system for collecting statistical data,preparing sampling surveys, and performingperiodic evaluations of and making ad-justments in such activities. The Center hasalready been quite successful in controllingrabies and is now developing programs tobring rodents and other zoonoses undercontrol.
In Guatemala, CEPANZO provided assis-tance in developing field statistical systems, aproject which was approved and began to beput into operation, and cooperated with thedirectorate general of animal health in plan-ning its new structure and specific functions.
In Honduras the organization of the animalhealth program, begun in 1975, was com-pleted. It consists of 10 central units whosefunctions are executed by seven area agricul-tural offices, for each of which buildings wereconstructed to house laboratory and ad-ministrative staff.
In Mexico, a technical and administrativereorganization continued in the animal healthdirectorate general of the agriculture andwater resources secretariat. The main thrust iscentralization of policy, standards, strategies,and program supervision and decentraliza-tion of their execution, including the prepara-tion of local programs.
PAHO also assisted various national animalhealth diagnostic and production labora-tories. CEPANZO and PANAFTOSA continuedto supply the countries reference biologicalsfor their diagnostic and biological productionprograms and to check biologicals preparedin national laboratories. CEPANZO suppliedlaboratory animals (guinea pigs, rabbits,hamsters, gerbils, mice, and rats) to enablethe countries to start or renew their colonies.
In Brazil, PAHO advised on the installationof a national animal health reference andtraining laboratory in Belo Horizonte fundedby the ministry of agriculture. All construc-tion was completed and equipment imported,
and the laboratory is to go into service in1981. PAHO signed an agreement with theParaná State Technical Institute to provideCEPANZO advisers and short-term consultantsfor improving animal experimentation, virol-ogy, and immunology laboratories engagedin biological research and production. PAHO'stechnical assistance is funded by a grant fromthe state government. CEPANZO also gave ad-vice on serology procedures to the UrbanZoonosis Center in Sao Paulo.
The eastern English-speaking Caribbeanveterinary laboratory project, which wasbegun in March 1977 and is financed by CIDA
and UNDP with PAHO as executing agency,continued its activities in the smaller islands.Now headquartered in Saint Lucia, the proj-ect includes eight laboratories, in Antigua,Dominica, Grenada, Montserrat, St. Kitts-Nevis, Saint Lucia, and St. Vincent. Ac-tivities in 1980 included the organization of apermanent network of laboratories to servethe islands' animal and veterinary publichealth services. At the governments' request,CIDA agreed to consider supporting the proj-ect's second phase.
PAHO also acted as executing agency in aUNDP-sponsored project to aid Guyana in set-ting up a veterinary diagnostic laboratory inGeorgetown. The laboratory will not onlystrengthen Guyana's animal health programbut also, in conjunction with PAHO's17-country veterinary assistant training proj-ect (REPAHA) at Georgetown, help producesuch assistants for Guyana and the rest of theCaribbean. Four experts will participate in theGuyana project. The project director arrivedin late 1980, and the other three specialists areto report during the first half of 1981.
Honduras' laboratory unit was reorganizedinto three departments: diagnosis, biologicalproduction control, and research and train-ing. PAHO helped oversee the construction ofthe central and seven regional laboratories.Equipment layout was planned and thenecessary equipment, materials, and reagentswere chosen. Training programs for labora-
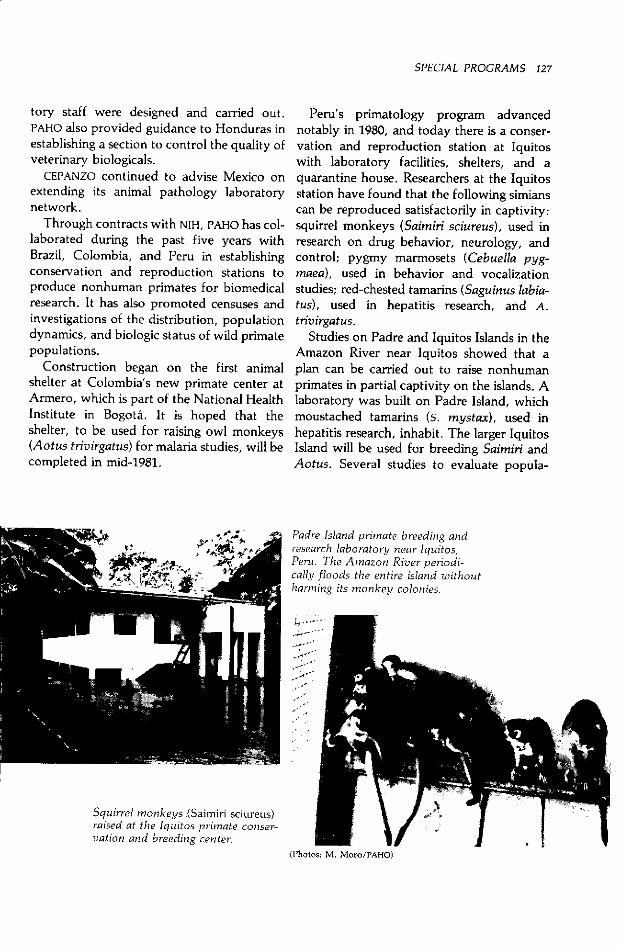
SPECIAL PROGRAMS 127
tory staff were designed and carried out.PAHO also provided guidance to Honduras inestablishing a section to control the quality ofveterinary biologicals.
CEPANZO continued to advise Mexico onextending its animal pathology laboratorynetwork.
Through contracts with NIH, PAHO has col-laborated during the past five years withBrazil, Colombia, and Peru in establishingconservation and reproduction stations toproduce nonhuman primates for biomedicalresearch. It has also promoted censuses andinvestigations of the distribution, populationdynamics, and biologic status of wild primatepopulations.
Construction began on the first animalshelter at Colombia's new primate center atArmero, which is part of the National HealthInstitute in Bogotá. It is hoped that theshelter, to be used for raising owl monkeys(Aotus trivirgatus) for malaria studies, will becompleted in mid-1981.
Peru's primatology program advancednotably in 1980, and today there is a conser-vation and reproduction station at Iquitoswith laboratory facilities, shelters, and aquarantine house. Researchers at the Iquitosstation have found that the following simianscan be reproduced satisfactorily in captivity:squirrel monkeys (Saimiri sciureus), used inresearch on drug behavior, neurology, andcontrol; pygmy marmosets (Cebuella pyg-maea), used in behavior and vocalizationstudies; red-chested tamarins (Saguinus labia-tus), used in hepatitis research, and A.trivirgatus.
Studies on Padre and Iquitos Islands in theAmazon River near Iquitos showed that aplan can be carried out to raise nonhumanprimates in partial captivity on the islands. Alaboratory was built on Padre Island, whichmoustached tamarins (s. mystax), used inhepatitis research, inhabit. The larger IquitosIsland will be used for breeding Saimiri andAotus. Several studies to evaluate popula-
Padre Island primate breeding andresearch laboratory near Iquitos,Peru. The Amazon River periodi-cally floods the entire island withoutharming its monkey colonies.
Squirrel monkeys (Saimiri sciureus)raised at the Iquitos primate conser-vation and breeding center.
128 REPORT OF THE DIRECTOR
tions, capture, animal marking, and popula-tion monitoring were carried out during theyear.
A workshop was held under NIH auspicesat Iquitos in November on the managementand production of primates in their nativecountries which 56 scientists from 18 African,American, Asian, and European countries at-tended. The participants recognized thatprimate research is and will continue to beessential to many biomedical studies benefit-ing man. They also discussed subjects relatedto research on preserving and breedingnonhuman primates. Their papers will even-tually appear as a proceedings.
The following was the animal disease situa-tion in the Americas during the year:
African swine fever. This disease, firstidentified in Africa in 1910 and unrelated tohog cholera, entered the Americas in 1971in an outbreak in Cuba which was quicklycontrolled, though at the cost of 500,000hogs. An outbreak in Cuba in early 1980 wasquickly brought under control and laterended. African swine fever has persisted inBrazil, Dominican Republic, and Haiti since1978. PAHO continued to collaborate withFAO through PANAFTOSA in monitoring thedisease.
Brucellosis. CEPANZO assisted in controllingbrucellosis in Argentina under an agreementwith the national agriculture ministry andSan Luis Province on various aspects of apilot project to control brucellosis in goats. InBolivia, with PAHO advice, SENARB progress-ed in controlling brucellosis in Cochabambaand Santa Cruz Departments. Surveys weremade in both departments to determine theprevalence of the disease.
CEPANZO continued to advise Colombia'sbovine brucellosis control program andlaboratories on controlling brucellosis vac-cine and antigen production. A number ofworking sessions on freeze-dried vaccineswere held. It also supplied brucellosis an-tigens to Ecuador for diagnostic activities atthe veterinary laboratories in Guayaquil and
(Photo: M. Montecino/PAHO)
National Veterinary Biological Pro-duction Company, Mexico City.
the research program of the Central Univer-sity.
PAHO continued to assist Paraguay'sbrucellosis program. The central laboratory'sbrucellosis and bovine rabies control labora-tories were installed and vaccination againstbrucellosis was started. CEPANZO continuedto advise Mexico on increasing the NationalVeterinary Biological Production Company'scapacity to produce brucellosis antigens andvaccines and improve their quality.
In research, CEPANZO continued its studiesto identify Brucella strains isolated fromhumans and animals in Latin America.Studies were also conducted of the factors af-fecting the preservation of Brucella vaccine.
Equine encephalitides. Though there havebeen outbreaks of Venezuelan and otherequine encephalitides in recent years, 1980saw relatively few cases in animals. Brazilreported 177 cases, Colombia 11, andNicaragua two. Belize, Brazil, Colombia, ElSalvador, Guatemala, Mexico, and Nicara-gua together immunized 897,570 horses withvarious kinds of vaccine.

SPECIAL PROGRAMS 129
The only country to report human caseswas the United States, which reported 840cases of primary encephalitides withoutspecification of the causal agent. Mostdiagnoses of cases in man and animals con-tinue to be reported as "virus unidentified"because in many countries samples are nottaken for laboratory examination or thenecessary technology for adequate examina-tion is absent.
Foot-and-mouth disease. FMD continues tobe one of the animal health problems of mostserious concern to the Americas. Its impor-tance lies in its ease of dissemination, its effectin raising production costs because afflictedherds produce less meat and milk, and par-ticularly in the barriers it creates to the sale ofcattle and cattle products in internationalmarkets.
The Americas north of the Panamanian-Colombian border and the former Guianasare FMD-free, a status they strive to maintain.No outbreaks occurred in those countries in1980, but vesicular stomatitis, a diseaseclinically similar to FMD and distinguishablefrom it only through laboratory analysis, oc-curred nonepidemically in Mexico (119cases), all the Central American countries(234 cases), and Panama (12 cases) to aboutthe same extent as in previous years. PANAF-TOSA provided diagnostic services to CentralAmerica and Panama pending the inaugura-tion of a laboratory built by Panama and theUnited States on PANAFTOSA's proposal. Thelaboratory is expected to begin operation in1981.
In Panama, a project to monitor vesiculardiseases epidemiologically was begun withUNDP funding and PAHO as executing agency.Its main objective is to develop national in-formation systems for FMD prevention pro-grams in Central America and Panama.Guatemala and Nicaragua reorganized theirFMD control programs and prepared applica-tions for IDB financial assistance with PAHO's
technical advice.In 1964 the South American countries af-
fected by FMD decided to undertake con-tinental control, and today all those affectedhave national control and eradication pro-grams. FMD morbidity in South America hasgenerally declined in that the number of af-fected herds has decreased, though in somecountries the desired abatement has not beenachieved. In certain cases, indeed, outbreaksof epidemic proportion have occurred, as in1980 in parts of Brazil, Colombia, Ecuador,and Uruguay.
The national programs are coordinatedthrough the South American Foot-and-Mouth Disease Control Commission (CO-SALFA), which meets once a year to evaluatethe status of the disease and the programs.PANAFTOSA acts as COSALFA's ex officio sec-retariat.
During the year PANAFTOSA disseminatedoil-adjuvant vaccine, which provides signifi-cantly longer immunity and so needs to beemployed less often than vaccines now ingeneral use. It produced 1.5 million doses,which were used to inoculate 700,000 cattlein Argentina, Bolivia, Brazil, Colombia, Par-aguay, Peru, and Venezuela.
To emphasize further the execution of FMDcontrol strategies, PANAFTOSA conducted athree-month course on animal health pro-gram development attended by 25 veteri-narians from 14 Latin American countries. Toassess the effectiveness of procedures recom-mended for eradicating a possible FMD out-break, a simulation exercise was carried outin Guyana with the participation of English-speaking Caribbean countries. As followup,PANAFTOSA prepared a "Guide for theEradication of Animal Diseases, with SpecialEmphasis on Foot-and-Mouth Disease." ASpanish translation will be distributed in1981.
In services to specific countries, PANAF-TOSA reached a preliminary agreement withArgentina, Brazil, and Uruguay to unify theirFMD activities in order to eradicate the diseasefrom the River Plate basin.
This decision was based on the experience
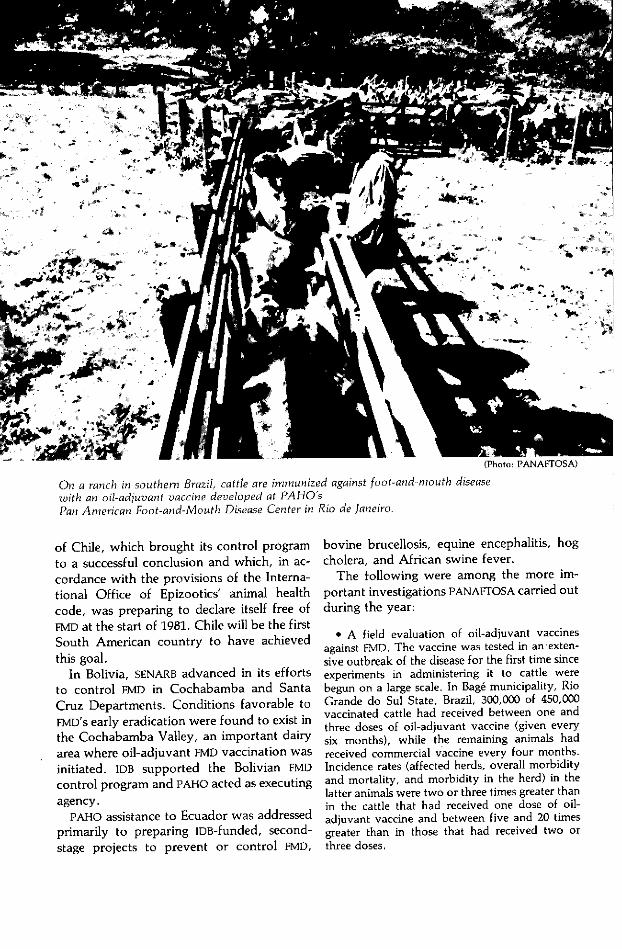
On a ranch in southern Brazil, cattle are immunized against foot-and-mouth diseasewith an oil-adjuvant vaccine developed at PAHOsPan American Foot-and-Mouth Disease Center in Rio de Janeiro.
of Chile, which brought its control program
to a successful conclusion and which, in ac-
cordance with the provisions of the Interna-
tional Office of Epizootics' animal health
code, was preparing to declare itself free of
FMD at the start of 1981. Chile will be the first
South American country to have achieved
this goal.In Bolivia, SENARB advanced in its efforts
to control FMD in Cochabamba and Santa
Cruz Departments. Conditions favorable to
FMD's early eradication were found to exist in
the Cochabamba Valley, an important dairy
area where oil-adjuvant FMD vaccination was
initiated. IDB supported the Bolivian FMD
control program and PAHO acted as executing
agency.PAHO assistance to Ecuador was addressed
primarily to preparing IDB-funded, second-
stage projects to prevent or control FMD,
bovine brucellosis, equine encephalitis, hog
cholera, and African swine fever.
The following were among the more im-
portant investigations PANAFrOSA carried out
during the year:
* A field evaluation of oil-adjuvant vaccinesagainst FMD. The vaccine was tested in an exten-sive outbreak of the disease for the first time sinceexperiments in administering it to cattle werebegun on a large scale. In Bagé municipality, RioGrande do Sul State, Brazil, 300,000 of 450,000vaccinated cattle had received between one andthree doses of oil-adjuvant vaccine (given everysix months), while the remaining animals hadreceived commercial vaccine every four months.Incidence rates (affected herds, overall morbidityand mortality, and morbidity in the herd) in thelatter animals were two or three times greater thanin the cattle that had received one dose of oil-adjuvant vaccine and between five and 20 timesgreater than in those that had received two orthree doses.
SPECIAL PROGRAMS 131
* Development of methods to control thepotency of oil-adjuvant FMD vaccine for swine. Alarge-scale test was performed to evaluate thequality of the first commercial oil-adjuvant vac-cine for hogs, and it was shown to have high im-munogenic value.
* Development of a simplified method formaintaining surveillance of latent FMD virus incarrier cattle. The test is made in order to isolateFMD virus from pools of throat swabs fromslaughterhouses. The preliminary results demon-strated the method's efficacy in identifying FMDviral strains prevalent in various geographic areas.
* Cooperation with the Federal University ofMinas Gerais' veterinary school in studying therisk of spread and endemicity mechanisms of FMDin the Mato Grosso swamps.
* Development of mathematical models ofepidemiologic risk.
* Analysis of classification errors in the immunestatus of animal herds determined by indirectserologic methods.
* Studies of the pathogenesis and epidemiologyof vesicular stomatitis.
* Continued research to characterize FMD fieldvirus strains anti- and immunogenically and FMDgeographically on the basis of statistics from thecountries and the continuous epidemiologic sur-veillance system. The study of animal losses fromFMD also continued, and preliminary results willappear in mid-1981.
Hydatidosis. CEPANZO continued its col-laboration with the hydatidosis control pro-grams of Brazil, Peru, and Uruguay. Reagentsfor immunodiagnosis of human hydatidosiswere tested for CDC and two East Africanmedical institutions.
CEPANZO conducted a study of the seroepi-demiology of human hydatidosis in BuenosAires Province and Neuquén and ChubutTerritories, Argentina, and the mountains ofPeru. It was shown that seroepidemiologicsurveys to detect asymptomatic carriers pro-duce basic data useful for evaluating theprogress of hydatidosis control programs.Several limitations on hydatidosis epidemio-logic surveillance were identified and neces-sary changes in such surveillance were intro-duced.
CEPANZO's evaluation of a pilot hydati-dosis control program in Neuquén showedthat the prevalence of hydatidosis infection in
humans, sheep, and dogs there was continu-ing to decline. Under working agreementswith various Argentine provincial govern-ments, CEPANZO provided further advice onapplying immunology techniques in diagnos-ing human hydatidosis, conducting serologysurveys to detect carriers with hydatid cysts,and developing laboratories to produce an-tigens and antisera for immunodiagnosis.
In Peru's hydatidosis control program, ac-tivities were extended to Arequipa, Cuzco,and Puno Departments, where health person-nel were trained in control methods, andwork continued at the Túpac Amaru andPachacútec agricultural cooperatives in JunínDepartment.
Leptospirosis. CEPANZO carried out studiesof the prevalence of leptospiral antibodies instray dogs in Argentina. Seventy-three (51percent) of 143 randomly obtained serumspecimens produced results indicating theanimals had been in contact with leptospirasin which agglutinins against the canine sero-variant predominated (37 percent). Studieswere also conducted of leptospirosis preva-lence in Argentina's wild animals.
Rabies. CEPANZO cooperated with Argen-tina's rabies control commission, whose workhas led to a striking reduction in the numberof rabies cases in the country. No humancases occurred in 1980.
PAHO provided assistance to the Bolivianhealth ministry's rabies control program,mainly in the cities of Cochabamba, La Paz,and Santa Cruz. Canine surveys throughoutthe country were the basis for dog vaccina-tion and destruction campaigns begun in thelast quarter of the year. It was necessary toimport canine rabies vaccine to cover re-quirements, but mouse breeding colonieswere enlarged and this should lead to in-creased vaccine production in 1981.
Further technical assistance was providedto Brazil's national rabies control program,which was extended nationwide with strikingresults in most states and territories. As aresult of activities carried out by Sáo Paulo's
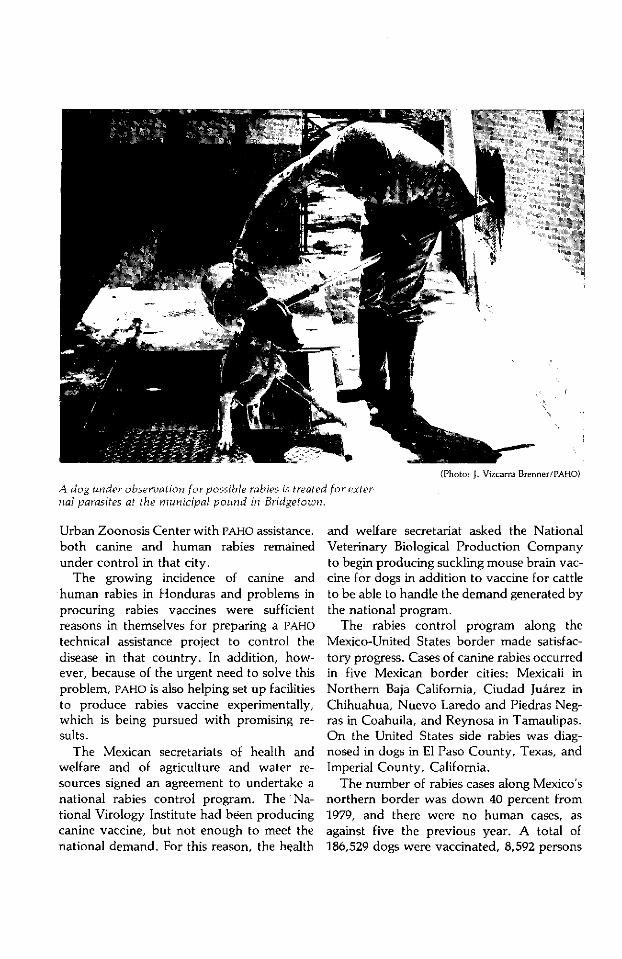
(Photo: J. Vizcarra Brenner/PAHO)
A dog under observation for possible rabies is treated for exter-nal parasites at the municipal pound in Bridgetown.
Urban Zoonosis Center with PAHO assistance,both canine and human rabies remainedunder control in that city.
The growing incidence of canine andhuman rabies in Honduras and problems inprocuring rabies vaccines were sufficientreasons in themselves for preparing a PAHOtechnical assistance project to control thedisease in that country. In addition, how-ever, because of the urgent need to solve thisproblem, PAHO is also helping set up facilitiesto produce rabies vaccine experimentally,which is being pursued with promising re-sults.
The Mexican secretariats of health andwelfare and of agriculture and water re-sources signed an agreement to undertake anational rabies control program. The Na-tional Virology Institute had been producingcanine vaccine, but not enough to meet thenational demand. For this reason, the health
and welfare secretariat asked the NationalVeterinary Biological Production Companyto begin producing suckling mouse brain vac-cine for dogs in addition to vaccine for cattleto be able to handle the demand generated bythe national program.
The rabies control program along theMexico-United States border made satisfac-tory progress. Cases of canine rabies occurredin five Mexican border cities: Mexicali inNorthern Baja California, Ciudad Juárez inChihuahua, Nuevo Laredo and Piedras Neg-ras in Coahuila, and Reynosa in Tamaulipas.On the United States side rabies was diag-nosed in dogs in El Paso County, Texas, andImperial County, California.
The number of rabies cases along Mexico'snorthern border was down 40 percent from1979, and there were no human cases, asagainst five the previous year. A total of186,529 dogs were vaccinated, 8,592 persons
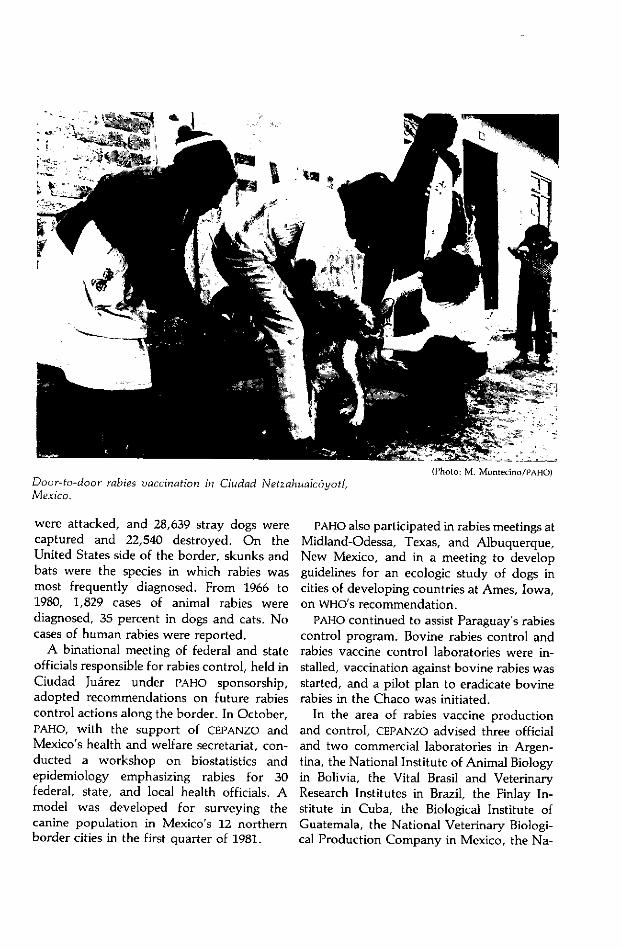
Door-to-door rabies vaccination in Ciudad Netzahualcóyotl,Mexico.
were attacked, and 28,639 stray dogs werecaptured and 22,540 destroyed. On theUnited States side of the border, skunks andbats were the species in which rabies wasmost frequently diagnosed. From 1966 to1980, 1,829 cases of animal rabies werediagnosed, 35 percent in dogs and cats. Nocases of human rabies were reported.
A binational meeting of federal and stateofficials responsible for rabies control, held inCiudad Juárez under PAHO sponsorship,adopted recommendations on future rabiescontrol actions along the border. In October,PAHO, with the support of CEPANZO andMexico's health and welfare secretariat, con-ducted a workshop on biostatistics andepidemiology emphasizing rabies for 30federal, state, and local health officials. Amodel was developed for surveying thecanine population in Mexico's 12 northernborder cities in the first quarter of 1981.
PAHO also participated in rabies meetings atMidland-Odessa, Texas, and Albuquerque,New Mexico, and in a meeting to developguidelines for an ecologic study of dogs incities of developing countries at Ames, Iowa,on WHO's recommendation.
PAHO continued to assist Paraguay's rabiescontrol program. Bovine rabies control andrabies vaccine control laboratories were in-stalled, vaccination against bovine rabies wasstarted, and a pilot plan to eradicate bovinerabies in the Chaco was initiated.
In the area of rabies vaccine productionand control, CEPANZO advised three officialand two commercial laboratories in Argen-tina, the National Institute of Animal Biologyin Bolivia, the Vital Brasil and VeterinaryResearch Institutes in Brazil, the Finlay In-stitute in Cuba, the Biological Institute ofGuatemala, the National Veterinary Biologi-cal Production Company in Mexico, the Na-
v
134 REPORT OF THE DIRECTOR
tional Health Institute in Peru, and the Na-tional Hygiene Institute in Venezuela. Thisadvisory assistance led to recommendationsfor improving the production of sucklingmouse brain vaccines and to promotion ofNIH's technique for testing inactivated vac-cines.
CEPANZO continued its investigations toevaluate the immunity conferred by inac-tivated rabies vaccines on cattle. The inac-tivated tissue culture vaccine CEPANZO devel-oped (PV-BHK-EI), which had protected 89 per-cent of dogs for three years after vaccination,was used in these studies. Solid protectionlasting for two years was obtained in all cattleimmunized with aluminum hydroxide vac-cine. The effect of the dose and route of in-oculation of rabies vaccine as seen in theserologic response of cattle was also investi-gated.
CEPANZO also continued studies of humanimmune response after suckling mouse brainvaccination. One group of test subjectsreceived 14 daily doses of the vaccine plusbooster doses on days 10 and 20, whileanother received seven daily doses followedby three boosters on days 10, 20, and 90. Therapid appearance of high IgG antibody levelssuggests the possibility of reducing still fur-ther the number of suckling mouse brain vac-cine doses used in treating patients exposed torabies.
Tuberculosis. CEPANZO supplied PPD fordiagnostic activities at the National HygieneInstitute's veterinary laboratory in Guayaquiland the Central University in Quito. PAHOcontinued to cooperate with Jamaica in its ef-forts to declare the country free of bovinetuberculosis. Eradication of the disease wasclose at hand.
In research, CEPANZO continued to analyzethe results of various tuberculin tests usingbovine PPD in Argentine cattle, the bacterio-logic diagnosis of nonpulmonary tuberculo-sis, and atypical mycobacteria in BuenosAires Province.
Emergency Preparednessand Disaster Relief
Coordination
The impact of natural and man-madedisasterson the hemisphere's countries andtheir health services was significant in 1980,though of lesser magnitude than in 1979.
Hurricanes were a persistent threat in theCaribbean, and one-Hurricane Allen-severely affected Haiti, Jamaica, and SaintLucia. Disasters small enough not to requiremassive international assistance, such asfloods, moderate earthquakes, and localdroughts, seriously impeded development.
The health consequences of disasters arelikely to increase in the future. Although thefrequency and strength of earthquakes andhurricanes will not change, mounting popula-tion density, progressive settlement of vul-nerable flood-prone and coastal areas, andthe continuing construction of health facili-ties and housing without proper risk analysisand engineering precautions will increase theeffect of disasters on public health in the nextdecade.
Man-made disasters, including those result-ing from industrialization and social progressdue to greater urbanization, creation ofhazardous industries, increased air traffic,and safety legislation that lags behind suchadvances, are increasingly frequent. Ex-amples of "technologic catastrophes" in re-cent years in Latin America are a serious firein a Bogotá skyscraper in 1974, continuingfactory-produced chlorine gas contaminationof Colombia's Cartagena Bay, and mercurycontamination in several parts of Nicaraguaresulting from gold ore processing.
Although many vulnerable countries in thehemisphere still lack standing disaster prepar-edness programs and health sector foci foremergency relief coordination, some coun-tries made considerable progress in 1980. Co-
SPECIAL PROGRAMS 135
lombia and Ecuador established units in theirhealth ministries to prepare and updatedisaster plans and train necessary personnel.In the Caribbean, following the catastrophic1979 hurricane season, awareness grew of theneed for action. Hurricane Allen caughtHaiti, Jamaica, and Saint Lucia better pre-pared. Haiti's health ministry held severalcoordination meetings with international andbilateral aid agencies; the Jamaican healthministry activated its emergency plan, whichresulted in far more effective relief than after
earlier disasters; and Saint Lucia mobilized itsstrengthened high-level emergency coordi-nating committee to manage the hurricane'saftermath.
To reflect the countries' increasing concernabout emergency preparedness, the DirectingCouncil adopted a resolution (CD27.40) askingthe Director to seek extrabudgetary fundingto strengthen PAHO's regional and areatechnical cooperation in emergency prepar-edness and disaster relief.
Toward this end, grant negotiations were
Chilean disaster preparedness workers inspect an emergencymedical relief team supply container in Santiago.
(Photo: J. Vizcarra Brenner/PAHO)
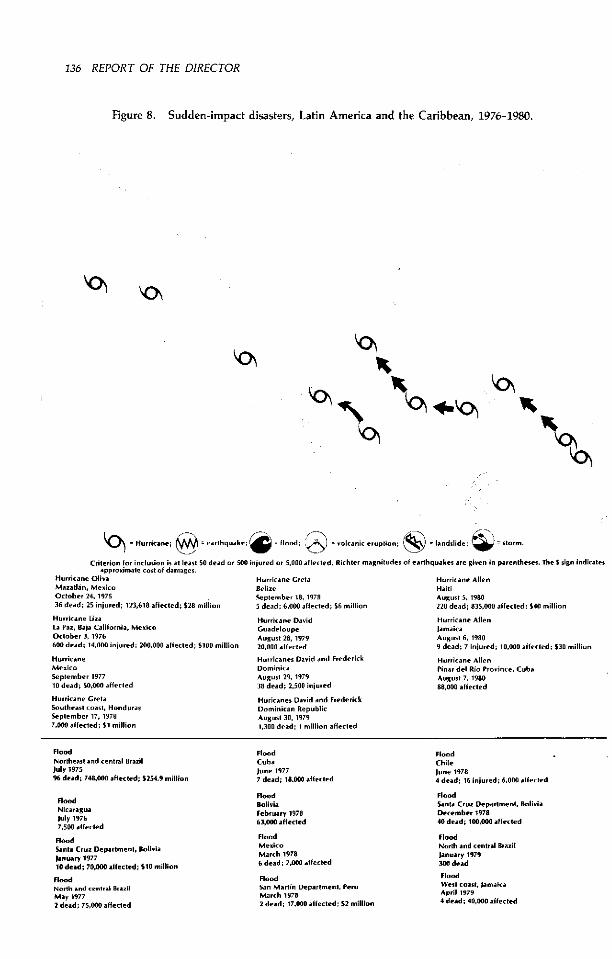
136 REPORT OF THE DIRECTOR
Figure 8. Sudden-impact disasters, Latin America and the Caribbean, 1976-1980.
bj 0
4 = H-.ri.ane; @ earthq.ake: 4 lood.d; volcan¡c e--plion ; = Iandslide ; = --orm-
Criterion lot inclusion i at easI 50 dead or 500 injuired or 5,000 affected. Richler magniludes ol earthquakes are given in parentheses. The $ sign indicatesapproximate cost ol damages.
Hurricane Oliva Hurr¡ic.ane Greta Hurricane AllenMazatin, Mexico Belize HaitiOctober 24 1975 September 18. 1978 August 5. 198036 de.d; 25 injured; 123,618 affeced; $28 milioin 5 dead; 6,000 affected; $6 million 220 dead; 835,000 affected; $40 million
Hurricane Liza[a Paz, Baja California, MexicoOctober 3, 1976600 dead; 14,000 injured; 200,000 alfecled; $100 million
HurricaneMexicoSeplember 197710 dead; 50.000 aIfecled
Hurricane GrelaSoutheast coast, HondurasSeplember 17. 19787.000 alfected; $1 million
Hurricane DavidGuadeloupeAugust 28. 197920.000 affected
Hurricanes David and FrederickDominicaAugust 29, 197938 dead; 2,500 injured
Huricanes David and FrederickDominican RepublicAugust 30, 19791.300 dead; 1 million affecled
Hurricane AllenJamaicaAugust 6, 19809 dead; 7 injured; 108000 affected; $30 million
Hurricane AllenPinar del Rio Province. CubaAugusl 7, 198088,000 aifecled
FloodNortheast and central BrazilJuly 197596 dead; 748,000 affected; $254.9 million
FloodNicaraguaJuly 19767,500 affected
FloodSanta Cruz Department, Bolivialanuary 197710 dead; 70,000 affected; $10 million
FloodNorth and central BrazilMay 19772 dead; 75,000 affected
FloodCubajune 19777 dead; 18.000 affected
FloodBoliviaFebruary 197863,000 affected
FloodMexicoMarch 19786 dead; 7,000 affected
FloodSan Martin Department., PeruMarch 19782 dead; 17,000 affected; $2 million
FloodChileJune 19784 dead; 16 injured; 6,000 aflected
FloodSanta Cruz Department. BoliviaDecember 197840 dead; 100.000 aIffected
FloodNorth and central BrazilJanuary 1979300 dead
FloodWest coast, JamaicaApril 19794 dead; 40,000 affected
lí>
Y4y%.
1<� 4.0
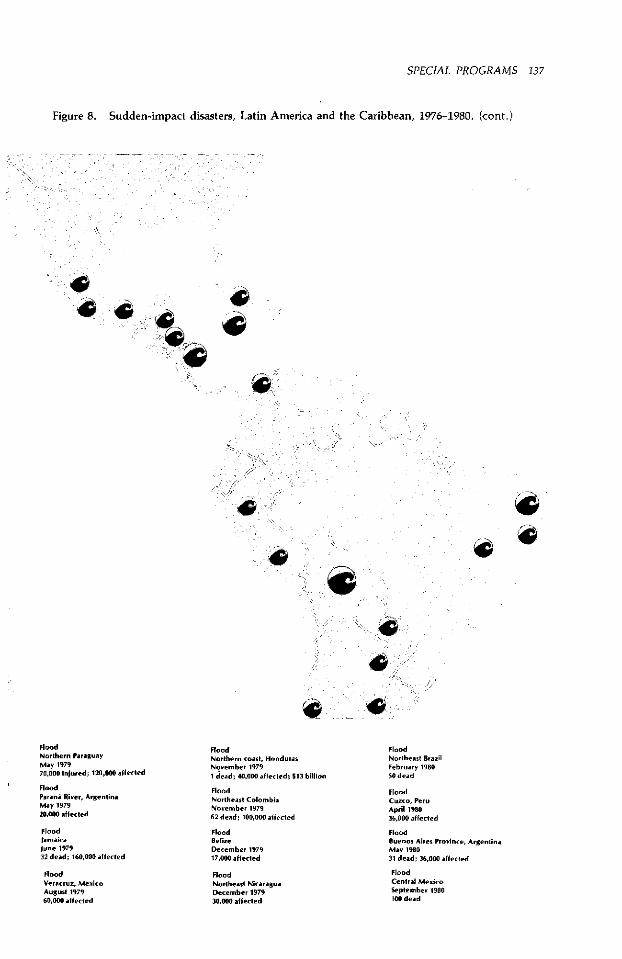
SPECIAL PROGRAMS 137
Figure 8. Sudden-impact disasters, Latin America and the Caribbean, 1976-1980. (cont.)
4 _ .,
FloodNorthern ParaguayMay 197970,000 injured; 120,000 affecled
FloodParana River, ArgentinaMay 197920,000 aMfeled
FloodJamaicaIune 197932 dead; 160,000 affected
FloodVeracruz, MexkicoAugust 197960,000 affected
FloodNorthern coast, HondurasNovember 19791 dead; 40,000 affected; $13 billion
FloodNortheast ColombiaNovember 197962 dead; 100,000 affected
FloodBelizeDecember 197917,000 alffected
FloodNortheast NicaraguaDecember 197930.000 alffected
FloodNortheast BrazilFebruary 198050 dead
FloodCuzco, PeruApril 198036,000 alffected
FloodBuenos Aires Province, ArgentinaMay 198031 dead; 36,000 aifected
FloodCentral MexkicoSeptember 1980100 dead
1 ,(A01111
w
lo
4
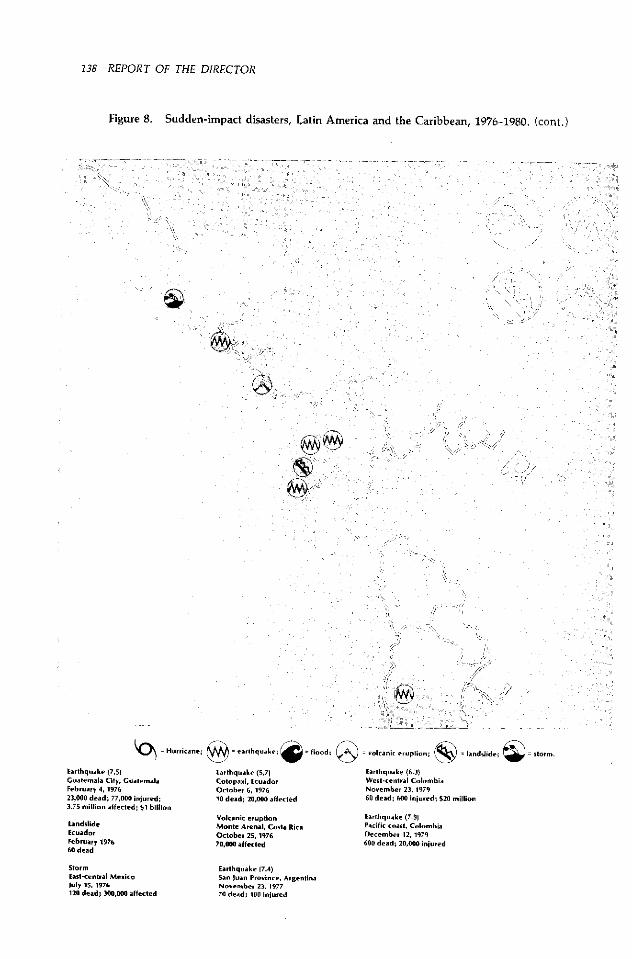
138 REPORT OF THE DIRECTOR
Figure 8. Sudden-impact disasters, Latin America and the Caribbean, 1976-1980. (cont.)
_ 37 y S__Xr-7X 0g-_o ®;7_ : ¡_
Hricane; = earthquake;
Earthquake (7.5) Earthquake (5.7)Guatemala City, Guatemala Cotopaxi, EcuadorFebruary 4,1976 October 6, 197623,000 dead; 77,000 injured; 10 dead; 20,000 alfected3.75 million alfected; $1 billion
Volcanic eruptionbndslide Monte Arenal, Costa RicaEcuador October 25,1976February 1976 70,000 affected60 dead
StormEast-central MexicoJuly 15, 1976120 dead; 300,000 affected
lloodi; ) = volcani erption; = landslde; = sto..m.
Earthquake (6.3)West-central ColombiaNovember 23, 197960 dead; 600 injured; $20 million
Earthquake (7.9)Pacific coast, ColombiaDecember 12,1979600 dead; 20,000 injured
Earthquake (7.4)San luan Province, ArgentinaNovember 23, 197770 dead; 100 inijured
�s _5,�� 1 . ',
1
successfully completed with the EuropeanEconomic Community (EEC) and USAID. EECapproved a five-year, $1.5 million grant tohelp develop national emergency prepared-ness programs in Latin America. Simul-taneous negotiations with several agencieswere pursued to secure funding for a com-parable five-year program in the Caribbean.USAID committed $99,358 for preparingand disseminating guidelines, manuals, andtraining aids throughout the hemisphere andpledged an initial $100,000 to strengthenPAHO's disaster preparedness activities in theCaribbean.
The Swedish International DevelopmentAuthority approved an initial $110,000 grantto underwrite disaster preparedness activitiesin the Caribbean. PAHO will receive the fundsearly in 1981.
PAHO organized or cosponsored fourdisaster preparedness meetings during theyear. The first was a Caribbean nurses'workshop on their role in disaster prepared-ness and relief in Barbados in May. Several ofthe workshop participants began activitiesafter returning to their own countries. Thenext meeting was a Caribbean disasterpreparedness conference organized by PAHO,USAID, the United Nations Disaster Relief Of-fice (UNDRO), League of Red Cross Societies,and other agencies at Santo Domingo later inMay 1980. Officials of various countries andagencies identified 55 possible preparednessprojects and formulated a comprehensivefive-year preparedness program to be con-sidered by potential funding agencies.
The third meeting was a disaster reliefmanagement seminar for 35 senior Caribbeanofficials at Montego Bay, Jamaica, in June.The last was a three-day meeting of Andeandisaster experts jointly sponsored by PAHOand the Hipólito Unanue Agreement atBogotá in November. The working groupreviewed disaster preparedness in the healthsector in their countries. Among its most im-portant recommendations was establishmentof a special high-level unit with its own
(Photo: J. Vizcarra Brenner/PAHO)
Houses destroyed by a flood in cen-tral Peru.
budget in each health ministry to improvedisaster preparedness and coordinate reliefactivities.
One of PAHO's most important activities indisaster preparedness was to contract theUniversity of the West Indies to prepare asimulation exercise to train disaster reliefcoordinators, for decision making understress and in uncertainty cannot be taught inlectures or conferences. Tested during theJamaica seminar, the day-long exercise re-produced the strain of postdisaster manage-ment.
After reading a brief profile of an imagi-nary country, participants were told that"Hurricane Goliath" had just struck "Cariba"and were assigned roles as members of its na-tional emergency committee. In rapid fire,
140 REPORT OF THE DIRECTOR
the coordinator then fed the participants anunwieldy succession of reports on damage,medical and sanitation problems, and thestatus of food, transport, and communica-tions. Much of the information was deliber-ately unreliable and contradictory so as toreproduce the rumors and confusion of an ac-tual disaster. The exercise room was hot,telephones rang, communication lines wentdown, and no breaks to relieve the tensionwere allowed. At the end of the seven-hoursimulation the participants agreed they knewfar more about how to manage a crisis thanbefore.
A similar exercise entitled "Earthquake inTocuy" was written for Latin American con-ditions with the cooperation of PAHO's LatinAmerican Health Education TechnologyCenter in Rio de Janeiro. It will be tested in1981.
Technical manuals also received priorityattention. Emergency Health ManagementAfter Natural Disasters was edited, trans-lated, and sent for publication. Drafts ofpostdisaster management manuals on com-municable disease surveillance and control,emergency environmental health manage-ment, evaluation and control of vectors,rodents, and pests, and medical supplymanagement were completed in English andwill be translated and published in 1981 and1982.
It also prepared eight instructional slideshows with English captions covering the ma-jor aspects of emergency health management.Initiated in 1979, the shows were tested at theJamaica seminar and WHO's October course inBrussels on postdisaster health care and reliefmanagement, and revised in light of com-ments from other organizations such as UN-
DRO, UNICEF, and the League of Red CrossSocieties. Spanish captions will be preparedin 1981.
Other PAHO activities were support ofshort-term travel fellowships for health of-ficials from Barbados, Cuba, Ecuador, andJamaica, and promotion, technical support,
1
(Photo: J. Vizcarra Brenner/PAHO)
Adobe slum houses overlooking theRímac River in Lima would topplein an earthquake.
and funding of two research projects (a studyof health problems caused by HurricaneDavid in Dominica in 1979 through a $10,000grant to the University of the West Indies,and a morbidity and mortality survey follow-ing the 1979 earthquake in Tumaco, Colom-bia, through another $10,000 grant to thatcountry's health ministry).
The Directing Council reviewed the pro-posed medium-term plan for PAHO's disasterpreparedness program. The plan includesstrengthening PAHO's technical ability to helpcountries prepare for man-made disasters,which are an increasing threat to publichealth; increasing its cooperation in organiz-ing multidisciplinary health ministry seminarsand workshops as part of national emergencypreparedness programs in the health sector;
SPECIAL PROGRAMS 141
including emergency preparedness in trainingmeetings and materials organized by otherPAHO technical units, as in a module onhospital disaster planning for health servicemanagement courses or postdisaster rehabili-tation of water and sanitation systems duringa regional sanitary engineering meeting;organizing short and refresher courses fordisaster relief coordinators alternately inEnglish and Spanish to transmit new researchfindings; and increasing PAHO support ofscientific evaluations of postdisaster relief ac-tivities and epidemiologic surveys.
Experience from Hurricanes David (1979)and Allen (1980) in the Caribbean indicatesthe need for PAHO to have in reserve a self-sufficient and multidisciplinary team ready tohelp assess needs and coordinate interna-tional health assistance if asked for by adisaster-affected country. Countries vulner-able to disaster have been urged to facilitatethe team's entry after a disaster by givingprior consent.
PAHO provided emergency medical sup-plies and equipment totaling $43,000 to Haiti,$10,000 to Jamaica, and $4,000 to Saint Luciaafter Hurricane Allen. These donations re-sulted from reallocation of savings in coun-try-or regional programs.
The lack of contributions to PAHO's naturaldisaster relief fund prevented the shipment ofadditional relief supplies. Because PAHO is notas well equipped to buy and ship largeamounts of medical supplies on short noticeas specialized bilateral and international agen-cies, it concentrates on assessing needs andgiving advice to the international communityon the most effective health assistance.
Statistical Services
To monitor health conditions in theAmericas, PAHO collects data from the coun-tries and processes, analyzes, and dissemi-nates them. The information collected willbe used to determine the potential impact of
the health improvement measures and strate-gies PAHO and the governments are adoptingto bring about universal health and gaugethe effectiveness of programs to carry outthose measures and strategies.
The first priority of PAHO's statistical ser-vice during the year was to design a com-puterized data base to allow wide flexibilityin accessing information and analyzing vari-ous types of data. A consulting firm washired to do so and is expected to submit itsfinal design report in early 1981.
Discussions were also initiated withinPAHO to ascertain information requirementsfor monitoring and evaluating different pro-grams. This led to the design of new forms forcollecting data on vaccinations, epidemio-logic surveillance, leprosy, and mortality.Discussions of forms for gathering informa-tion on human resources, hospitals, andhealth service use are underway, as aremethods and procedures for collecting dataon health expenditures and health servicecoverage.
Data on mortality, communicable diseases,human resources, and hospitals were updatedfor internal use and in reports and specificpublications, including Health Conditions inthe Amnericas, to be published in 1982.
PAHO supplied mortality statistics to WHOand the United Nations Statistics Office, andstatistics on communicable diseases, hospi-tals, and human resources to WHO.
As the focal point for information onhealth in the hemisphere, PAHO receives andanswers numerous queries from governmentsand training and research centers in theAmericas and other WHO regions and frominternational organizations.
Much of the information PAHO collects andpublishes is not internationally comparable.A priority activity in 1981 will be to identifyvariant areas and promote the developmentof more uniform international data collec-tion, processing, and dissemination stand-ards.
To promote use of the International

142 REPORT OF THE DIRECTOR
Classification of Diseases (ICD), PAHO re-tained two consultants to support theVenezuelan Classification Center (CEVECE) inCaracas in its activities as WHO's Spanish-language classification center.
CEVECE is preparing the Spanish translationof the International Classification of Pro-cedures in Medicine, which is to be publishedin 1981, and issued its first quarterly newslet-ter to apprise national disease classificationofficials of problems and possible solutions inapplying the Classification and of relevantpublications, and to answer queries it re-ceives. The first international course ondisease classification for producing morbidityand mortality statistics was held in July andAugust. Nineteen students from nine LatinAmerican countries attended.
CEVECE's highest priority in 1981 and 1982will be to support the countries in extendinghealth service coverage through primary careby helping them develop classifications ofsymptoms or health problems suitable fortreatment by nonmedical personnel. Suchclassifications will aid in designing informa-tion systems for programming, controlling,and evaluating primary care programs.
The Brazilian Center for Disease Classifica-tion published and distributed the revisedversion of volumes 1 and 2 of the Classifi-caçao Internacional de Doenças after testingand correcting a trial edition published in1979. The Portuguese translation of volume 1of the International Classification of Pro-cedures in Medicine was finished, and thework will be distributed in 1981. The centeralso decided to publish a thrice-yearlynewsletter. Its first issue included explana-tions of coding and other aspects of ICD'sninth revision and information on ICDcourses.
Publications
Through its publications program PAHOdisseminates scientific and technical informa-
tion of international interest on health pro-motion, disease prevention, and allied sub-jects.
The PAHO/WHO publications coordinationworking group held its sixth annual meetingin November to discuss mutual policy, plan-ning, and communications problems. Thepresence of a representative from WHO'sEuropean regional office added a new view-point to the discussions, especially in theareas of interregional cooperation and possi-ble copublishing.
Periodical publications
The monthly Boletín de la Oficina Sani-taria Panamericana entered its 58th year ofpublication as PAHO's main Spanish-languagescientific and technical periodical. It featured77 original articles on public health, healthcare research, disease control, animal health,health manpower, health administration, en-vironmental health, and many other subjectsby authors from the Americas as well as otherparts of the world. A new quarterly section inspecial format entitled "Information on Phar-macology" began to appear in the July issue.
The quarterly Bulletin of PAHO entered-its14th year and included 34 original articles andnews on such subjects as rural health,primary health care, ambulatory care, nutri-tion, family health, maternal and childhealth, immunology, microbiology and virol-ogy, mental health, cancer, and environmen-tal health.
Educación Médica y Salud, also a quarterlyin its 14th year, devoted its first issue of 1980wholly to nursing, as had its last issue of1979. The two nursing issues later appearedtogether in Spanish as Scientific Publication393. The other three 1980 issues included ar-ticles and abstracts on varied manpowertopics such as university medical tutoring,technology evaluation, curricular reforms,research in hospitals, teaching through simu-lation, medical specialization trends, and
SPECIAL PROGRAMS 143
j i -___ s~ mv
(Photos: J. Vizcarra Brenner/PAHO)
teaching in nutrition and health admin-istration.
The bimonthly Epidemiological Bulletin,which appeared for the first time in 1980, pro-motes the exchange of epidemiologic infor-mation among the Americas. It periodicallypublishes short accounts of and comments onthe epidemiologic activity of important com-municable and noncommunicable diseases aswell as information from the countries andPAHO field research activities and technicalaspects of disease surveillance, prevention,and control programs. Each issue also in-cludes a section on diseases subject to interna-tional health regulation and a calendar ofcourses and meetings. The newsletter'spressrun was 3,000 copies in Spanish and2,000 in English.
Scientific publications and official documents
The selections approved for the 1980special publications program, comprisingscientific publications and official and other
documents, were edited and produced by thestaff at headquarters and at the PAHO/WHOpublications and documentation service inMexico. These comprised 27 titles totaling5,081 printed pages and 61,160 copies.
The most important volume published dur-ing the year was Zoonoses and Com-municable Diseases Common to Man andAnimals (Scientific Publication 354) by PedroAcha and Boris Szyfres, originally issued inSpanish in 1977. It contains detailed descrip-tions of diseases transmitted from vertebrateanimals to man and those common to manand animals. The book, of special interest tostudents, technical staff, and professionals inthe human and animal health sciences, com-bines up-to-date information in a singlevolume on both the medical and veterinaryaspects of diseases that have traditionallybeen dealt with in different texts.
The proceedings of the xII Inter-AmericanMeeting, at the Ministerial Level, on Foot-and-Mouth Disease and Zoonoses Controlwere published as Animal Health in theAmericas, 1979 (Scientific Publication 391).
:
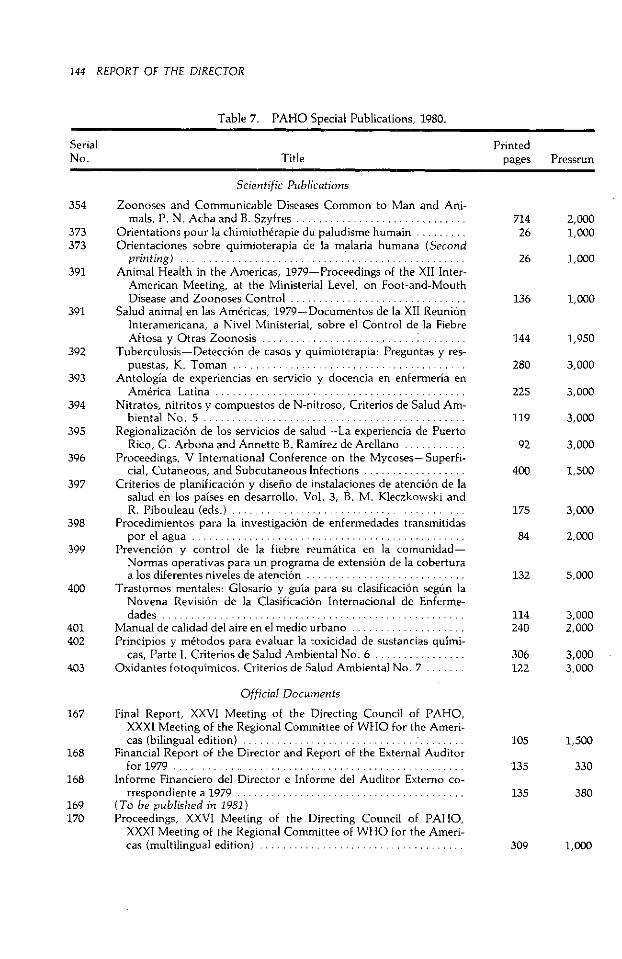
144 REPORT OF THE DIRECTOR
Table 7. PAHO Special Publications, 1980.
Serial PrintedNo. Title pages Pressrun
Scientific Publications
354 Zoonoses and Communicable Diseases Common to Man and Ani-mals, P. N. Acha and B. Szyfres .............................
373 Orientations pour la chimiothérapie du paludisme humain .........373 Orientaciones sobre quimioterapia de la malaria humana (Second
printing) ................ ..................................391 Animal Health in the Americas, 1979-Proceedings of the XII Inter-
American Meeting, at the Ministerial Level, on Foot-and-MouthDisease and Zoonoses Control ...............................
391 Salud animal en las Américas, 1979-Documentos de la XII ReuniónInteramericana, a Nivel Ministerial, sobre el Control de la FiebreAftosa y Otras Zoonosis ........................... ........
392 Tuberculosis-Detección de casos y quimioterapia: Preguntas y res-puestas, K. Toman .. .............. .... ... ..................
393 Antología de experiencias en servicio y docencia en enfermería enAmérica Latina ...........................................
394 Nitratos, nitritos y compuestos de N-nitroso, Criterios de Salud Am-biental No. 5 ..............................................
395 Regionalización de los servicios de salud-La experiencia de PuertoRico, G. Arbona and Annette B. Ramírez de Arellano ...........
396 Proceedings, V International Conference on the Mycoses-Superfi-cial, Cutaneous, and Subcutaneous Infections ..................
397 Criterios de planificación y diseño de instalaciones de atención de lasalud en los países en desarrollo, Vol. 3, B. M. Kleczkowski andR. Pibouleau (eds.) .........................................
398 Procedimientos para la investigación de enfermedades transmitidaspor el agua ................................................
399 Prevención y control de la fiebre reumática en la comunidad-Normas operativas para un programa de extensión de la coberturaa los diferentes niveles de atención ............................
400 Trastornos mentales: Glosario y guía para su clasificación según laNovena Revisión de la Clasificación Internacional de Enferme-dades .....................................................
401 Manual de calidad del aire en el medio urbano ....................402 Principios y métodos para evaluar la toxicidad de sustancias quími-
cas, Parte I. Criterios de Salud Ambiental No. 6 ................403 Oxidantes fotoquímicos. Criterios de Salud Ambiental No.7 .......
Official Documents
167 Final Report, XXVI Meeting of the Directing Council of PAHO,XXXI Meeting of the Regional Committee of WHO for the Ameri-cas (bilingual edition) ..........................
168 Financial Report of the Director and Report of the External Auditorfor 1979 ....................................................
168 Informe Financiero del Director e Informe del Auditor Externo co-rrespondiente a 1979 .. .. ... .... ... ..........................
169 (To be published in 1981)170 Proceedings, XXVI Meeting of the Directing Council of PAHO,
XXXI Meeting of the Regional Committee of WHO for the Ameri-cas (multilingual edition) ....................................
714 2,00026 1,000
26 1,000
136 1,000
144 1,950
280 3,000
225 3,000
119 3,000
92 3,000
400 1,500
175 3,000
84 2,000
132 5,000
114 3,000240 2,000
306 3,000122 3,000
105 1,500
135 330
135 380
309 1,000
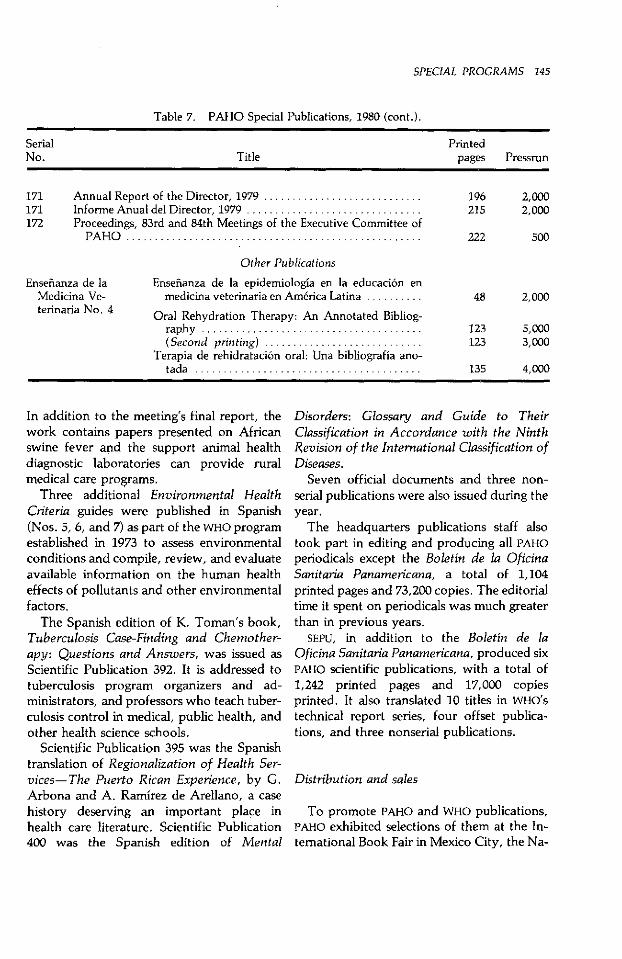
SPECIAL PROGRAMS 145
Table 7. PAHO Special Publications, 1980 (cont.).
Serial PrintedNo. Title pages Pressrun
171 Annual Report of the Director, 1979 ............................ 196 2,000171 Informe Anual del Director, 1979 ............................... 215 2,000172 Proceedings, 83rd and 84th Meetings of the Executive Committee of
PAHO .................................................... 222 500
Other Publications
Enseñanza de la Enseñanza de la epidemiología en la educación enMedicina Ve- medicina veterinaria en América Latina .......... 48 2,000terinaria No. 4 Oral Rehydration Therapy: An Annotated Bibliog-
raphy ....................................... 123 5,000(Second printing) ............................ 123 3,000
Terapia de rehidratación oral: Una bibliografía ano-tada ....................................... 135 4,000
In addition to the meeting's final report, thework contains papers presented on Africanswine fever and the support animal healthdiagnostic laboratories can provide ruralmedical care programs.
Three additional Environmental HealthCriteria guides were published in Spanish(Nos. 5, 6, and 7) as part of the WHO programestablished in 1973 to assess environmentalconditions and compile, review, and evaluateavailable information on the human healtheffects of pollutants and other environmentalfactors.
The Spanish edition of K. Toman's book,Tuberculosis Case-Finding and Chemother-apy: Questions and Answers, was issued asScientific Publication 392. It is addressed totuberculosis program organizers and ad-ministrators, and professors who teach tuber-culosis control in medical, public health, andother health science schools.
Scientific Publication 395 was the Spanishtranslation of Regionalization of Health Ser-vices-The Puerto Rican Experience, by G.Arbona and A. Ramírez de Arellano, a casehistory deserving an important place inhealth care literature. Scientific Publication400 was the Spanish edition of Mental
Disorders: Glossary and Guide to TheirClassification in Accordance with the NinthRevision of the International Classification ofDiseases.
Seven official documents and three non-serial publications were also issued during theyear.
The headquarters publications staff alsotook part in editing and producing all PAHOperiodicals except the Boletín de la OficinaSanitaria Panamericana, a total of 1,104printed pages and 73,200 copies. The editorialtime it spent on periodicals was much greaterthan in previous years.
SEPU, in addition to the Boletín de laOficina Sanitaria Panamericana, produced sixPAHO scientific publications, with a total of1,242 printed pages and 17,000 copiesprinted. It also translated 10 titles in WHO'stechnical report series, four offset publica-tions, and three nonserial publications.
Distribution and sales
To promote PAHO and WHO publications,PAHO exhibited selections of them at the In-temational Book Fair in Mexico City, the Na-

146 REPORT OF THE DIRECTOR
tional Council for International Health con-ference in Washington, and the annualmeetings of the American Veterinary MedicalAssociation in Washington and the AmericanPublic Health Association in Detroit, Michi-gan.
Emphasis throughout the year was on in-creasing the paid distribution of PAHO pub-lications, as a result of which $77,444 was in-voiced, an increase of 41 percent over 1979.The amount collected was $72,624. A newsystem for maintaining and updating PAHO'sseveral mailing lists by computer was alsodesigned and put into effect, and the nec-essary computer terminal was installed in thedistribution and sales unit.
The numbers of publications distributedduring the year were: periodicals, 217,637;scientific publications, 72,203; official docu-ments and other publications, 37,943, andWHO publications, 6,558. The grand total was334,341.
Filmstrips
In the filmstrip program, 82 titles havebeen completed to date on a variety of sub-jects including environmental sanitation, nu-trition, maternal and child care, food hy-giene, laboratory procedures, communityhealth, slaughterhouse hygiene, and eye care.A total of 4,573 filmstrip copies weredistributed, 2,958 gratis to educational in-stitutions and 1,615 sold to individuals. In ad-dition, 1,037 sets of the printed materials onprimary eye care were distributed.
Textbook and instructional materialsprogram
In 1979 PAHO expanded its textbook pro-gram to provide high quality textbooks andother instructional materials to all fields andlevels of study in the health sciences. The ex-pansion was financed by a $5 million IDB loan
to the Pan American Health and EducationFoundation and a $1.5 million PAHO con-tribution. PAHO acts as the project's loanguarantor and executing agency.
The program's principal emphasis is ontraining primary health workers in accord-ance with PAHO and WHO priorities for ex-tending basic health services to the urban andrural poor. In August, in compliance with arequest from the health ministers of CentralAmerica and Panama, PAHO brought to-gether staff from the ministries at San José toreview each country's nursing auxiliarypriorities and needs and make recommenda-tions regarding the preparation of manualsand instructional modules for training auxil-iaries.
After the meeting, three short-term con-sultants were retained to begin preparation ofthe first manual, on maternal and child care,and by December a pilot version was readyfor review by the ministerial working group.It is expected that this and other manuals andaudiovisual materials will be completed in1981.
PAHO financed the production of a set ofinstructional modules for training healthworkers in various aspects of communicabledisease and immunization strategies and pro-cedures. These materials are now availablethrough PAHO's expanded immunization pro-gram office, and distribution through text-book program channels is expected to beginin 1981.
By the end of the year, the program in-cluded five professional-level textbooks inthe basic sciences, five in dentistry, four innutrition, three in nursing, and two each inveterinary medicine and environmentalhealth. Seventeen of the 19 Spanish- andPortuguese-speaking countries in the hemi-sphere had signed basic agreements permit-ting purchase and sale of materials.
Total sales of medical textbooks wereabout the same volume as in the previous twoyears, with considerable gains in severalcountries being partially offset by losses in

SPECIAL PROGRAMS 147
others due to strikes and university closures.No new titles were added, though the Por-tuguese version of Sabiston's surgery text-book became available to participatingschools in Brazil for the first time. Manuals incertain medical specialties will be consideredfor inclusion in 1981.
A number of administrative changes weremade in medical textbook distribution, in-cluding consolidation of export shipmentsfrom different Mexican publishers. It is hopedthat by anticipating medical school re-quirements throughout the hemisphere andmaking consolidated sea shipments, stock-outs can be avoided and sales increased.
The interest of nursing schools participat-ing in the program grew in 1980. Sales weresignificantly higher in most countries, andover 19,000 books were sold by the end ofthe year. Three titles are now available inPortuguese to Brazilian students. The secondSpanish editions of several books whosetranslations PAHO commissioned for exclusivesale in the Americas will appear in 1981. Aseries of self-instructional perinatal caremodules for university nursing students isalso planned.
Considerable progress was made in bring-ing other health science schools into the pro-gram. About 40 percent of eligible dental
schools had signed memoranda of under-standing, and the conclusion of a basic agree-ment with Brazil toward the end of the yearpromised to double the number of dentalschools participating in the first few monthsof 1981. In nutrition, most students now haveaccess to books through the program, eitherdirectly or through participating medicalschools. Less progress was made in veterinarymedicine and sanitary engineering, mainlybecause unforeseen delays in negotiating text-book purchases from publishers made it dif-ficult to give potential participants a clearidea of what materials would be available. Itis expected that negotiations for several addi-tional books in these areas will be completedin early 1981 and that most veterinary andsanitary engineering schools will be par-ticipating by the end of the year.
The sale of stethoscopes, sphygmomanom-eters, and diagnostic sets continued at aboutthe same rate as in the previous two years.The chance of a significant increase in salesin 1981 seems good, since several schools inBrazil and Mexico plan to order instrumentsfor the first time. Sales were extended to in-clude nursing schools, and it appears that anumber of dental schools will also be able tomake use of the materials offered.
Index
A
Accidents, 39, 83Acute respiratory infections (see Respiratory infections,
acute)Administration, health care, 24
training in, 106-107Aedes aegypti, 14, 57-59African swine fever, 128Air pollution (see Pollution)Alcoholism, 71Allergies, 70American Association of Blood Banks, 81American Association of Physicists in Medicine, 83American Public Health Association, 27, 146American Region Programming and Evaluation System
(AMPES), 8American Society of Hospital Engineering, 25American Veterinary Medical Association, 146AMPES (see American Region Programming and Evalua-
tion System)Andean Pact
disaster preparedness, 139health facilities, 20health ministers, meeting of, 14nutrition, 33occupational health, 99
Anemias, iron-deficiency, 31Animal health, 125-134Animal Health in the Americas, 1979, 143-144Antigua, 14, 26, 27Argentina
elected to PAHO Executive Committee, 4food protection, 101Health Facilities Research Center (University of Buenos
Aires), 20, 21information systems, health, 22Malbrán Microbiology Institute, Carlos A., 79National Center for the Study of Argentinian Hem-
orrhagic Fever, 56planning, health, 22wastes, solid, 92water and sanitation, 90
Association of Water and Sanitation Institutions ofCentral America and Panama, 89
Auxiliaries and technicians. health. 111-114
B
Bahamashealth education, 27hospitals, 21information systems, health, 23-24
Barbadosdisaster relief, 12health facilities maintenance, 26manpower planning, 140water and sanitation, 90, 91
Belizehealth education, 26malaria, 59
Biologicals, 78-81Blindness prevention, 66-67Blood banks, 80-81Boletín de la Oficina Sanitaria Panamericana, 80, 142,
145Bolivia
animal health, 125health education, 26information systems, health, 22-23plague, 54primary health care, 3rabies, 131water and sanitation, 87yellow fever, 56
BrazilAedes aegypti situation, 58animal health, 125-126Butantan Institute, 77Center for Disease Classification, 142Companhia Municipal de Limpieza Urbana, 92Environmental Engineering Foundation, 95health workers, 112-113laboratories, 77National Housing Bank, 91nutrition, 34plague, 54planning, health, 22pollution control, 95primate production, 127rabies, 131-132respiratory infections, acute, 50State Company for Technology in Basic Sanitation, 95
149
150 REPORT OF THE DIRECTOR
Superintendency for International Technical Coop-eration, 117
Urban Zoonosis Center (Sao Paulo), 126, 132wastes, solid, 92yellow fever, 56
British Virgin Islands (see Virgin Islands, British)Brucellosis, 128Buildings and installations, PAHO, 7Bulletin of PAHO, 142
C
CanadaInternational Development Agency (CIDA), 14, 80, 90,
110, 113, 126International Development Research Centre (IDRC),
14-15, 78Cancer, 6, 13, 67-70CANCERLINE (computerized bibliographic searches), 67-
70CAREC Surveillance Report, 78Caribbean, English-speaking
animal health, 126education, family life, 26-27health workers, 113nutrition, 34-35water management project, 12, 14
Caribbean Community (CARICOM), 14, 22, 113Caribbean Regional Drug Testing Laboratory, 80health ministers, meeting of, 13-14information systems, health, 22
Caribbean Development Bank, 14, 90Caribbean Epidemiology Center (CAREC), 5, 48, 58,
77-78Caribbean Food and Nutrition Institute (CFNI), 5, 33,
34-35Cataract (see Blindness prevention)Catholic University of Santiago (Dominican Republic),
104, 105, 108Cayman Islands, 34Center for Higher Studies in Nutrition and Food Science
(Guatemala City), 35Center for Multidisciplinary Studies in Rural Develop-
ment (CIMDER, Cali), 43Central University (Ecuador), 134CEPANZO (see Pan American Zoonosis Center)CEPIS (see Pan American Center for Sanitary Engineer-
ing and the Environmental Sciences)CFNI (see Caribbean Food and Nutrition Institute)Chagas' disease, 64-65Chemical safety (see Pollution)Children (see Maternal and child health/family plan-
ning)Chile
information systems, health, 23Institute of Public Health, 79laboratories, 76planning, health, 22typhoid fever, 54
Cholera, 39Circle of Ibero-Latin American Radiotherapists, 82Clark Foundation, Edna McConnell, 65CLATES (see Latin American Health Education Tech-
nology Center)Cold-chain vaccine equipment (see Expanded Program
on Immunization)Collaborative Cancer Treatment Research Program,
69-70Colombia
Center for Multidisciplinary Studies in Rural Devel-opment (Cali), 43
continuing education, 111diarrheal diseases, 51Empresa Distrital de Servicios Públicos (Bogota), 94food protection, 101health facilities maintenance, 25information systems, health, 23laboratories, 76malaria, 62, 64National Health Institute, 57, 59, 64, 70, 79, 127National Institute for Municipal Development, 91planning, health, 22pollution control, 97primary health care, 3primate production, 127water and sanitation, 90yellow fever, 56
Communicable diseases (see Diseases, comminunicable)Community health training program for Central Amer-
ica and Panama (PASCCAP), 104, 112-113, 117Community participation in health, 3, 4, 17Conference services, PAHO, 10-11COSALFA (see South American Foot-and-Mouth Disease
Control Commission)Costa Rica
diarrheal diseases, 51health facilities maintenance, 25, 26information systems, health, 23-24nutrition, 35pollution control, 97social security institute, 20water and sanitation, 90
Cruz Foundation, Oswaldo, 57, 80Cuba
continuing education, 111nutrition, 34
D
Damien Foundation (Belgium), 51Declaration of Alma-Ata, 1Dengue, 56Dental health, 73-75
education (see Education and training, dentistry)Diabetes, 6, 70Diarrheal diseases, 5, 6, 51-54, 89Diet (see Nutrition)Diphtheria (see Expanded Program on Immunization)Directing Council PAHO (see under Pan American
Health Organization)
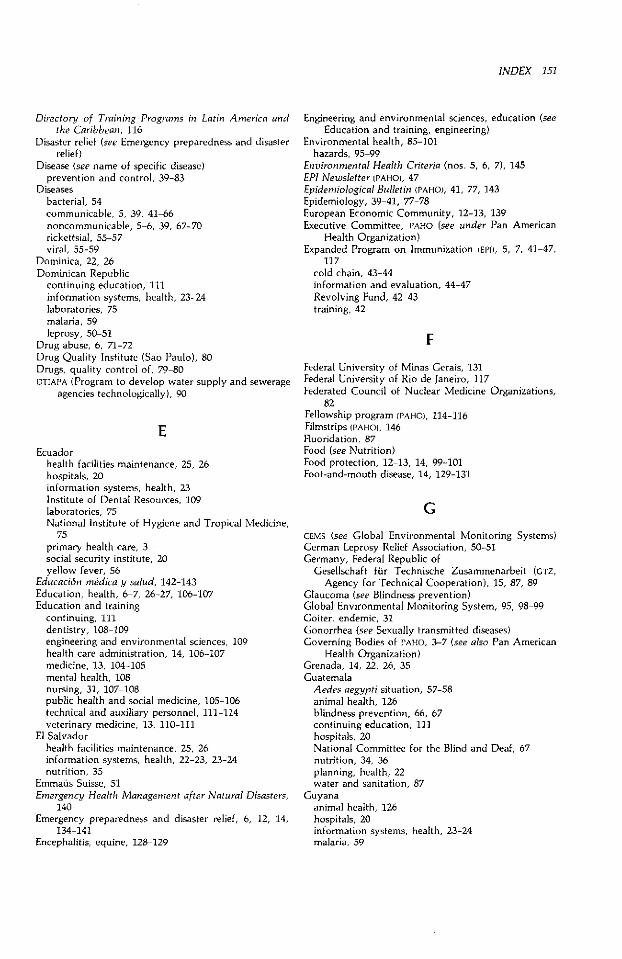
INDEX 151
Directory of Training Programs in Latin America andthe Caribbean, 116
Disaster relief (see Emergency preparedness and disasterrelief)
Disease (see name of specific disease)prevention and control, 39-83
Diseasesbacterial, 54communicable, 5, 39, 41-66noncommunicable, 5-6, 39, 67-70rickettsial, 55-57viral, 55-59
Dominica, 22, 26Dominican Republic
continuing education, 111information systems, health, 23-24laboratories, 75malaria, 59leprosy, 50-51
Drug abuse, 6, 71-72Drug Quality Institute (Sao Paulo), 80Drugs, quality control of, 79-80DTIAI'A (Program to develop water supply and sewerage
agencies technologically), 90
EEcuador
health facilities maintenance, 25, 26hospitals, 20information systems, health, 23Institute of Dental Resources, 109laboratories, 75National Institute of Hygiene and Tropical Medicine,
75primary health care, 3social security institute, 20yellow fever, 56
Educación médica y salud, 142-143Education, health, 6-7, 26-27, 106-107Education and training
continuing, 111dentistry, 108-109engineering and environmental sciences, 109health care administration, 14, 106-107medicine, 13, 104-105mental health, 108nursing, 31, 107-108public health and social medicine, 105-106technical and auxiliary personnel, 111-114veterinary medicine, 13, 110-111
El Salvadorhealth facilities maintenance, 25, 26information systems, health, 22-23, 23-24nutrition, 35
Emmaus Suisse, 51Emergency Health Management after Natural Disasters,
140Emergency preparedness and disaster relief, 6, 12, 14,
134-141Encephalitis, equine, 128-129
Engineering and environmental sciences, education (seeEducation and training, engineering)
Environmental health, 85-101hazards, 95-99
Environmental Health Criteria (nos. 5, 6, 7), 145EPI Newsletter (PAHO), 47Epidemiological Bulletin (PAHO), 41, 77, 143Epidemiology, 39-41, 77-78European Economic Community, 12-13, 139Executive Committee, PAHO (see under Pan American
Health Organization)Expanded Program on Immunization (EPI), 5, 7, 41-47,
117cold chain, 43-44information and evaluation, 44-47Revolving Fund, 42-43training, 42
F
Federal University of Minas Gerais, 131Federal University of Rio de Janeiro, 117Federated Council of Nuclear Medicine Organizations,
82Fellowship program (PAHO), 114-116Filmstrips (PAHO), 146Fluoridation, 87Food (see Nutrition)Food protection, 12-13, 14, 99-101Foot-and-mouth disease, 14, 129-131
G
GEMS (see Global Environmental Monitoring Systems)German Leprosy Relief Association, 50-51Germany, Federal Republic of
Gesellschaft fir Technische Zusammenarbeit (GTZ,Agency for Technical Cooperation), 15, 87, 89
Glaucoma (see Blindness prevention)Global Environmental Monitoring System, 95, 98-99Goiter, endemic, 31Gonorrhea (see Sexually transmitted diseases)Governing Bodies of PAHO, 3-7 (see also Pan American
Health Organization)Grenada, 14, 22, 26, 35Guatemala
Aedes aegypti situation, 57-58animal health, 126blindness prevention, 66, 67continuing education, 111hospitals, 20National Committee for the Blind and Deaf, 67nutrition, 34, 36planning, health, 22water and sanitation, 87
Guyanaanimal health, 126hospitals, 20information systems, health, 23-24malaria, 59
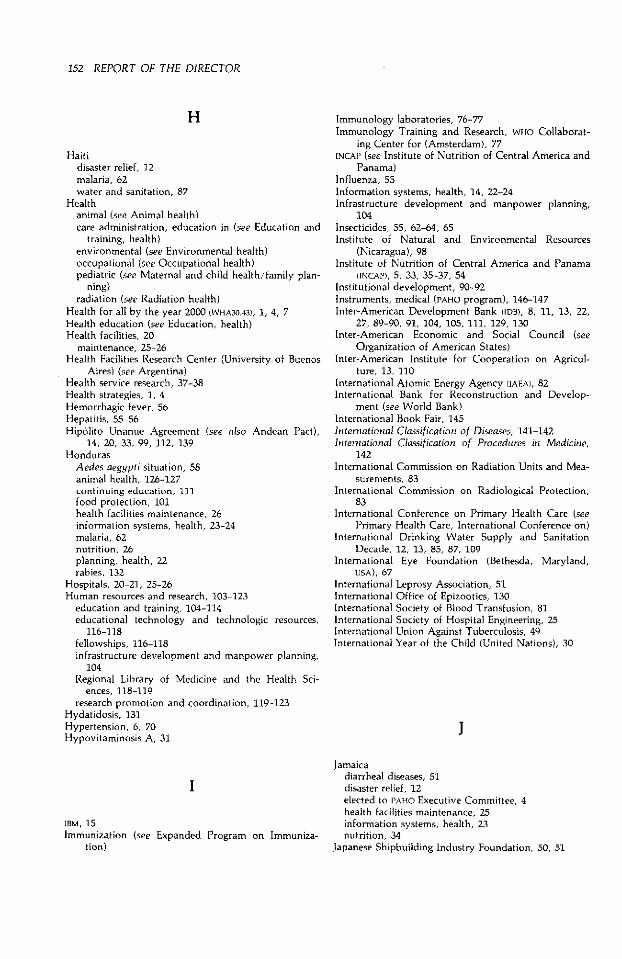
152 REPORT OF THE DIRECTOR
H
Haitidisaster relief, 12malaria, 62water and sanitation, 87
Healthanimal (see Animal health)care administration, education in (see Education and
training, health)environmental (see Environmental health)occupational (see Occupational health)pediatric (see Maternal and child health/family plan-
ning)radiation (see Radiation health)
Health for all by the year 2000 (WHA30.43), 1, 4, 7Health education (see Education, health)Health facilities, 20
maintenance, 25-26Health Facilities Research Center (University of Buenos
Aires) (see Argentina)Health service research, 37-38Health strategies, 1, 4Hemorrhagic fever, 56Hepatitis, 55-56Hipólito Unanue Agreement (see also Andean Pact),
14, 20, 33, 99, 112, 139Honduras
Aedes aegypti situation, 58animal health, 126-127continuing education, 111food protection, 101health facilities maintenance, 26information systems, health, 23-24malaria, 62nutrition, 26planning, health, 22rabies, 132
Hospitals, 20-21, 25-26Human resources and research, 103-123
education and training, 104-114educational technology and technologic resources,
116-118fellowships, 116-118infrastructure development and manpower planning,
104Regional Library of Medicine and the Health Sci-
ences, 118-119research promotion and coordination, 119-123
Hydatidosis, 131Hypertension, 6, 70Hypovitaminosis A, 31
IBM, 15
Immunization (see Expanded Program on Immuniza-tion)
Immunology laboratories, 76-77Immunology Training and Research, WHO Collaborat-
ing Center for (Amsterdam), 77INCAP (see Institute of Nutrition of Central America and
Panama)Influenza, 55Information systems, health, 14, 22-24Infrastructure development and manpower planning,
104Insecticides, 55, 62-64, 65Institute of Natural and Environmental Resources
(Nicaragua), 98Institute of Nutrition of Central America and Panama
(INCAP), 5, 33, 35-37, 54Institutional development, 90-92Instruments, medical (PAHO program), 146-147Inter-American Development Bank (IDB), 8, 11, 13, 22,
27, 89-90, 91, 104, 105, 111, 129, 130Inter-American Economic and Social Council (see
Organization of American States)Inter-American Institute for Cooperation on Agricul-
ture, 13, 110International Atomic Energy Agency (IAEA), 82International Bank for Reconstruction and Develop-
ment (see World Bank)International Book Fair, 145International Classification of Diseases, 141-142International Classification of Procedures in Medicine,
142International Commission on Radiation Units and Mea-
surements, 83International Commission on Radiological Protection,
83International Conference on Primary Health Care (see
Primary Health Care, International Conference on)International Drinking Water Supply and Sanitation
Decade, 12, 13, 85, 87, 109International Eye Foundation (Bethesda, Maryland,
USA), 67International Leprosy Association, 51International Office of Epizootics, 130International Society of Blood Transfusion, 81International Society of Hospital Engineering, 25International Union Against Tuberculosis, 49International Year of the Child (United Nations), 30
1
Jamaicadiarrheal diseases, 51disaster relief, 12elected to PAHO Executive Committee, 4health facilities maintenance, 25information systems, health, 23nutrition, 34
Japanese Shipbuilding Industry Foundation, 50, 51
INDEX 153
K
Kellogg Foundation, W. K., 15, 30, 106, 117
L
Laboratories, 75-77LACRIP (see Latin American Cancer Research Informa-
tion Project)Latin American Association of Public Health Schools,
106Latin American Association of Societies of Biology and
Nuclear Medicine, 82-83Latin American Cancer Research Information Project
(LACRIP), 67-70, 119Latin American Center for Perinatology and Human
Development (Montevideo), 31, 117, 122Latin American Health Education Technology Center
(CLATES, Rio de Janeiro), 105, 114, 116-117, 140Latin American Index Medicus, 118Latin American Nutrition Society, 33Latin American Program for Educational Development
in Health (PLADES), 117League of Red Cross Societies, 13, 81, 139, 140Leishmaniasis, 66Leprosy, 50-51Leptospirosis, 78, 131
Military School of Medicine and Social Sciences (Co-lombia), 105
Ministers of Health of the AmericasThird Special Meeting of (September 1972), 1
Montserrat, 26, 34, 35
N
Narcotics (see Drug abuse)National Autonomous University of Mexico, 109, 117National Council for International Health (U.S.), 27,
145-146Nicaragua
Aedes aegypti situation, 58continuing education, 111elected to PAHO Executive Committee, 4information systems, health, 23nutrition, 34, 36
Noncommunicable diseases (see Diseases, noncom-municable)
Nongonococcal urethritis (see Sexually transmitteddiseases)
Nurses and nursing, 6education (see Education and training, nursing)
Nutrition, 14, 31-38
o
M
Malaria, 5, 6, 39, 59-64Malnutrition, 7, 31-32Management, PAHO, 9-11Management systems, health, 24Maternal and child health/family planning, 27-31Measles (see Expanded Program on Immunization)Medical care systems, 17-21Medical education (see Education and training, medi-
cine)Medical Research Council (UK), 78MEDLINE (computerized bibliographic searching), 11,
118-119Meningitis, meningococcal, 54Mental health, 70-73
education in (see Education and training, mentalhealth)
Mexicoanimal health, 126dengue, 56health facilities maintenance, 25Institute of Hygiene, 81laboratories, 75National Virology Institute, 79, 132primary health care, 21rabies, 132-133respiratory infections, acute, 50
Occupational health, 86, 99Oral rehydration therapy (see Diarrheal diseases)Onchocerciasis (see Blindness prevention)Organization of American States
PAHO, relations with, 3, 13
P
PAHEF (see Pan American Health and Education Founda-tion)
Pan American Center for Human Ecology and Health(ECO), 98, 109
Pan American Center for Research and Training inLeprosy and Tropical Diseases (Caracas), 50, 66
Pan American Center for Sanitary Engineering and En-vironmental Sciences (CEPIS, Lima), 13, 90, 91, 92,94, 95, 99, 109
Pan American Centers (PAHO), 5-7Pan American Development Foundation (PADEF), 26Pan American Federation of Medical School Associa-
tions, 104-105Pan American Foot-and-Mouth Disease Center (PANAF-
TOSA, Rio de Janeiro), 5, 125, 126-129Pan American Health and Education Foundation
(PAHEF), 15, 146
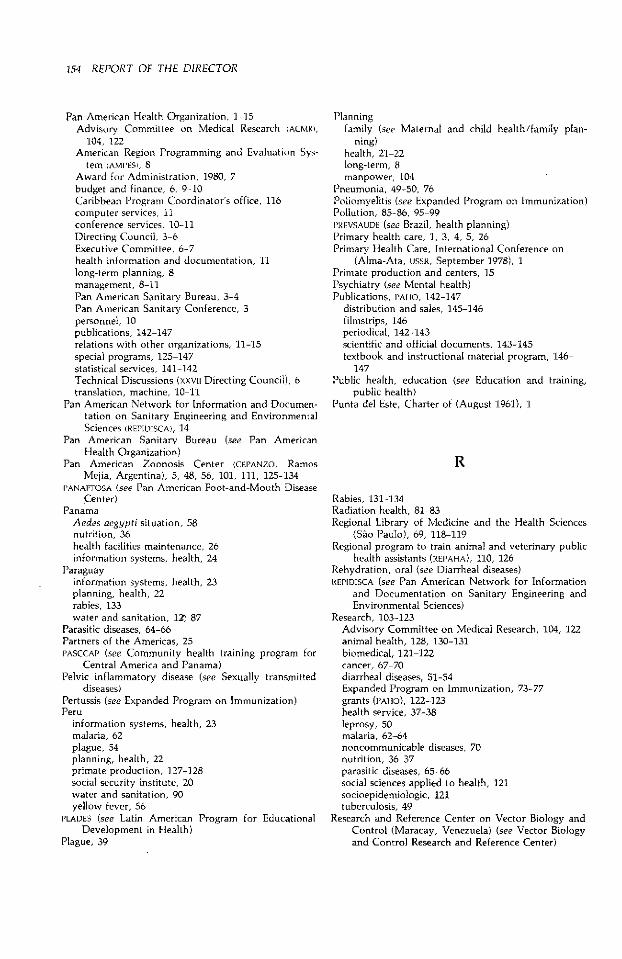
154 REPORT OF THE DIRECTOR
Pan American Health Organization, 1-15Advisory Committee on Medical Research (ACMR),
104, 122American Region Programming and Evaluation Sys-
tem (AMI'ES), 8Award for Administration, 1980, 7budget and finance, 6, 9-10Caribbean Program Coordinator's office, 116computer services, 11conference services, lO-11Directing Council, 3-6Executive Committee, 6-7health information and documentation, 11long-term planning, 8management, 8-11Pan American Sanitary Bureau, 3-4Pan American Sanitary Conference, 3personnel, 10publications, 142-147relations with other organizations, 11-15special programs, 125-147statistical services, 141-142Technical Discussions (xxvli Directing Council), 6translation, machine, 10-11
Pan American Network for Information and Documen-tation on Sanitary Engineering and EnvironmentalSciences (REPIDISCA), 14
Pan American Sanitary Bureau (see Pan AmericanHealth Organization)
Pan American Zoonosis Center (CEP'ANZO, RamosMejía, Argentina), 5, 48, 56, 101, 111, 125-134
PANAFTOSA (see Pan American Foot-and-Mouth DiseaseCenter)
PanamaAedes aegypti situation, 58nutrition, 36health facilities maintenance, 26information systems, health, 24
Paraguayinformation systems, health, 23planning, health, 22rabies, 133water and sanitation, 12Z 87
Parasitic diseases, 64-66Partners of the Americas, 25PASCCAP (see Community health training program for
Central America and Panama)Pelvic inflammatory disease (see Sexually transmitted
diseases)Pertussis (see Expanded Program on Immunization)Peru
information systems, health, 23malaria, 62plague, 54planning, health, 22primate production, 127-128social security institute, 20water and sanitation, 90yellow fever, 56
PLADES (see Latin American Program for EducationalDevelopment in Health)
Plague, 39
Planningfamily (see Maternal and child health/family plan-
ning)health, 21-22long-term, 8manpower, 104
Pneumonia, 49-50, 76Poliomyelitis (see Expanded Program on Immunization)Pollution, 85-86, 95-99I'PREVSAUDE (see Brazil, health planning)Primary health care, 1, 3, 4, 5, 26Primary Health Care, International Conference on
(Alma-Ata, USSR, September 1978), 1Primate production and centers, 15Psychiatry (see Mental health)Publications, PAHO, 142-147
distribution and sales, 145-146filmstrips, 146periodical, 142-143scientific and official documents, 143-145textbook and instructional material program, 146-
147Public health, education (see Education and training,
public health)Punta del Este, Charter of (August 1961), 1
R
Rabies, 131-134Radiation health, 81-83Regional Library of Medicine and the Health Sciences
(Sao Paulo), 69, 118-119Regional program to train animal and veterinary public
health assistants (REPAHA), 110, 126Rehydration, oral (see Diarrheal diseases)REPIDISCA (see Pan American Network for Information
and Documentation on Sanitary Engineering andEnvironmental Sciences)
Research, 103-123Advisory Committee on Medical Research, 104, 122animal health, 128, 130-131biomedical, 121-122cancer, 67-70diarrheal diseases, 51-54Expanded Program on Immunization, 73-77grants (PAHO), 122-123health service, 37-38leprosy, 50malaria, 62-64noncommunicable diseases, 70nutrition, 36-37parasitic diseases, 65-66social sciences applied to health, 121socioepidemiologic, 121tuberculosis, 49
Research and Reference Center on Vector Biology andControl (Maracay, Venezuela) (see Vector Biologyand Control Research and Reference Center)
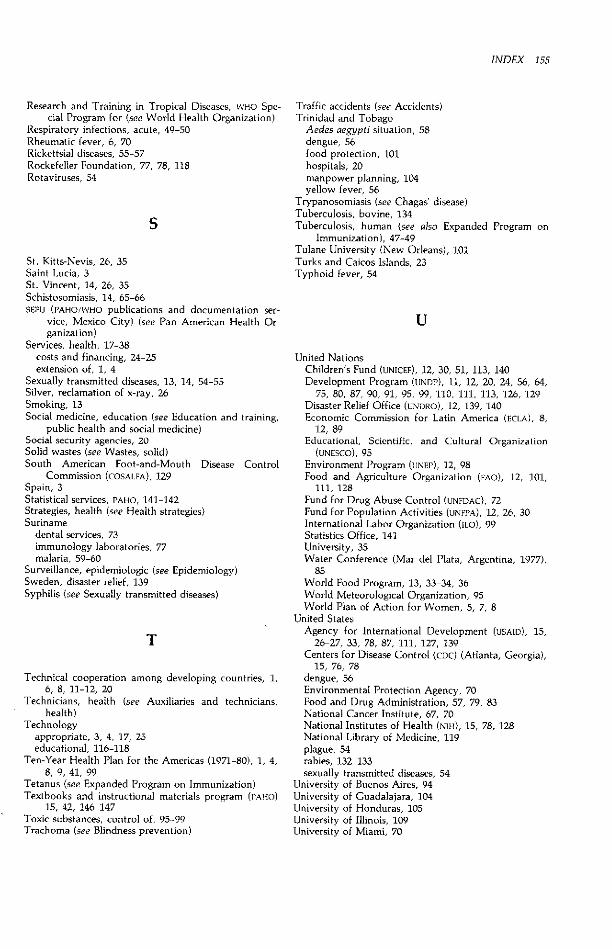
INDEX 155
Research and Training in Tropical Diseases, WHO Spe-cial Program for (see World Health Organization)
Respiratory infections, acute, 49-50Rheumatic fever, 6, 70Rickettsial diseases, 55-57Rockefeller Foundation, 77, 78, 118Rotaviruses, 54
S
St. Kitts-Nevis, 26, 35Saint Lucia, 3St. Vincent, 14, 26, 35Schistosomiasis, 14, 65-66SEPU (PAHO/WHO publications and documentation ser-
vice, Mexico City) (see Pan American Health Or-ganization)
Services, health, 17-38costs and financing, 24-25extension of, 1, 4
Sexually transmitted diseases, 13, 14, 54-55Silver, reclamation of x-ray, 26Smoking, 13Social medicine, education (see Education and training,
public health and social medicine)Social security agencies, 20Solid wastes (see Wastes, solid)South American Foot-and-Mouth Disease Control
Commission (COSALFA), 129Spain, 3Statistical services, PAHO, 141-142Strategies, health (see Health strategies)Suriname
dental services, 73immunology laboratories, 77malaria, 59-60
Surveillance, epidemiologic (see Epidemiology)Sweden, disaster relief, 139Syphilis (see Sexually transmitted diseases)
T
Technical cooperation among developing countries, 1,6, 8, 11-12, 20
Technicians, health (see Auxiliaries and technicians,health)
Technologyappropriate, 3, 4, 17, 25educational, 116-118
Ten-Year Health Plan for the Americas (1971-80), 1, 4,8, 9, 41, 99
Tetanus (see Expanded Program on Immunization)Textbooks and instructional materials program (PAHO)
15, 42, 146-147Toxic substances, control of, 95-99Trachoma (see Blindness prevention)
Traffic accidents (see Accidents)Trinidad and Tobago
Aedes aegypti situation, 58dengue, 56food protection, 101hospitals, 20manpower planning, 104yellow fever, 56
Trypanosomiasis (see Chagas' disease)Tuberculosis, bovine, 134Tuberculosis, human (see also Expanded Program on
Immunization), 47-49Tulane University (New Orleans), 101Turks and Caicos Islands, 23Typhoid fever, 54
U
United NationsChildren's Fund (UNICEF), 12, 30, 51, 113, 140Development Program (UNDP), 11, 12, 20, 24, 56, 64,
75, 80, 87, 90, 91, 95, 99, 110, 111, 113, 126, 129Disaster Relief Office (UNDRO), 12, 139, 140Economic Commission for Latin America (ECLA), 8,
12, 89Educational, Scientific, and Cultural Organization
(UNESCO), 95Environment Program (UNEP), 12, 98Food and Agriculture Organization (FAO), 12, 101,
111, 128Fund for Drug Abuse Control (UNFDAC), 72Fund for Population Activities (UNFPA), 12, 26, 30International Labor Organization (ILO), 99Statistics Office, 141University, 35Water Conference (Mar del Plata, Argentina, 1977),
85World Food Program, 13, 33-34, 36World Meteorological Organization, 95World Plan of Action for Women, 5, 7, 8
United StatesAgency for International Development (USAID), 15,
26-27, 33, 78, 87, 111, 127, 139Centers for Disease Control (CDC) (Atlanta, Georgia),
15, 76, 78dengue, 56Environmental Protection Agency, 70Food and Drug Administration, 57, 79, 83National Cancer Institute, 67, 70National Institutes of Health (NIH), 15, 78, 128National Library of Medicine, 119plague, 54rabies, 132-133sexually transmitted diseases, 54
University of Buenos Aires, 94University of Guadalajara, 104University of Honduras, 105University of Illinois, 109University of Miami, 70
156 REPORT OF THE DIRECTOR
University of Panama, 105University of San Carlos (Guatemala City), 35University of San Marcos, 117University of Santiago (Cuba), 104University of Sao Paulo, 76, 106, 110, 119University of the West Indies (Kingston), 26-27, 78,
139, 140Uruguay
hospitals, 20laboratories, 75
V
Vaccines (see also Expanded Program on Immuniza-tion), 54-57, 64, 78-79, 130-134
Valle University (Guatemala), 59Vector biology and control, 58-59Vector Biology and Control Research and Reference
Center (Maracay, Venezuela), 58-59, 65Venezuela
Center for the Classification of Diseases, 142health facilities maintenance, 25information systems, health, 23laboratories, 75leprosy, 50National Clinical Immunology Center (Caracas), 77pollution control, 97yellow fever, 56
Vesicular disease, 129Veterinary education and training (see Education and
training, veterinary)Virgin Islands, British, 14, 26Vitamin A deficiency, 31
W
Wastes, solid, 85, 86, 92-94Wastewater, 14-15Water pollution (see Pollution)Water supply and sanitation, 85, 87-90Whooping cough (see Expanded Program on Immuniza-
tion)Women, 5, 7, 8World Bank, 12, 13, 27, 64, 87, 91, 92, 94, 95World Food Program (see United Nations)World Health Organization
environmental health criteria program, 98, 145International Agency for Research on Cancer, 70Special Program for Research and Training in Tropi-
cal Diseases, 64, 104, 121"Study of WHO'S Structures in Light of its Functions,"
4-5World Meteorological Organization, 95
X,Y,Z
X rays (see Radiation health)Xerophthalmia (see Blindness prevention)Yellow fever, 39, 56-59Zoonoses (see Animal health)Zoonoses and Communicable Diseases Common to
Man and Animals, 143
ACRONYMS AND CORRESPONDING AGENCIES OR PROGRAMS
ACMRAMPESCARECCARICOMCDCCEPANZOCEPIALET
CEPIS
CFNICIDACLAP
CLATESCOSALFAECLAECOEECEPIFAOIAEAIBRD
IDBIDRCIICAILOINCAPLACRIPNIHOASOIRSA
PADEFPAHEFPAHOPANAFTOSAPASBPASSCAP
PLADES
RLMUNUNDPUNDROUNEPUNFDACUNFPAUNICEFUNUUSAIDWFPWHO
PAHO Advisory Committee on Medical ResearchAmerican Region Programming and Evaluation SystemCaribbean Epidemiology CenterCaribbean CommunityCenters for Disease Control (USA)Pan American Zoonosis CenterPan American Center for Research and Training in Leprosy and
Tropical DiseasesPan American Center for Sanitary Engineering and Environ-
mental SciencesCaribbean Food and Nutrition InstituteCanadian International Development AgencyLatin American Center for Perinatology and Human Develop-
mentLatin American Center for Educational Technology in HealthSouth American Foot-and-Mouth Disease Control CommissionEconomic Commission for Latin America (UN)Pan American Center for Human Ecology and HealthEuropean Economic CommunityExpanded Program on ImmunizationFood and Agriculture Organization (UN)International Atomic Energy AgencyInternational Bank for Reconstruction and Development
(World Bank)Inter-American Development BankInternational Development Research Center (Canada)Inter-American Institute for Cooperation on AgricultureInternational Labor OrganizationInstitute of Nutrition of Central America and PanamaLatin American Cancer Research Information ProjectNational Institutes of Health (USA)Organization of American StatesInternational Regional Organization for Health in Agriculture
and LivestockPan American Development FoundationPan American Health and Education FoundationPan American Health OrganizationPan American Foot-and-Mouth Disease CenterPan American Sanitary BureauProgram on Health Training of the Community of Central
America and PanamaLatin American Program for Educational Development in
HealthRegional Library of Medicine and the Health SciencesUnited NationsUnited Nations Development ProgramUnited Nations Office of the Disaster Relief CoordinatorUnited Nations Environment ProgramUnited Nations Fund for Drug Abuse ControlUnited Nations Fund for Population ActivitiesUnited Nations Children's FundUnited Nations UniversityU.S. Agency for International DevelopmentWorld Food ProgramWorld Health Organization