Q /¢ IF.1 - IRIS PAHO Home
327
WORLD HEALTH ORGANIZATION DISTR.: LIMITEO DISTR.: LIMITEE tu Q /¢ IF.1 ORGANISATION MONDIALE DE LA SANTE ACHR33/95.14 (Report) ORIGINAL: ENGLISH ADVISORY COMMITTEE ON HEALTH RESEARCH REPORT TO THE DIRECTOR-GENERAL on its thirty-third session held at WHO headquarters, Geneva 17-20 October 1995 CONTENTS AND AGENDA * Report of the thirty-third session of ACHR * Report of Working Group of ACHR: Information requirements of Health Policy Research (Annex 1) a Report of Working Group of ACHR: DALY Review Group (Annex 2) * Report of ACHR Peer Review Group on the Ad Hoc Committee on Health Research relating to future intervention options (Annex 3) * Report of the Ad Hoc Committee: Investing in health research and development: an Agenda to address problems of the poor (Draft 2.0) (Annex 4) * Activity reports from the Regions (Annex 5) a Appendix: Report on first ACHR workshop held at Schloss Reisensburg (3 - 7 April 1995) This document is not issued to the general public, and all rights are reserved by the World Health Organization (WHO). The document may not be reviewed, abstracted, quoted, reproduced or translated, in part or in whole, without the prior written permission of WHO. No part of this document may be stored in a retrieval system or transmitted in any form or by any means - electronic, mechanical or other - without the prior written permission of WHO. The views expressed in documents by named authors are solely the responsibility of those avthb '° Ce document n'est pas destiné á etre distribué au grand public et tous les droits y afférents sont réservés par I'Organisation mondiale de la Santé (OMS). 11 ne peut etre commenté, résumé, cité, reproduit ou traduit, partiellement ou en totalité, sans une autorisation préalable écrite de l'OMS. Aucune partie ne doit etre chargée dans un systéme de recherche documentaire ou diffusée sous quelque forme ou par quelque moyen que ce soit - électronique, mécanique, ou autre - sans une autorisation préalable écrite de 'OMS. Les opinions exprimées dans les documents par des auteurs cités nommément n'engagent que lesdits auteurs.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Q /¢ IF.1 - IRIS PAHO Home
WORLD HEALTH ORGANIZATIONDISTR.: LIMITEO
DISTR.: LIMITEEtu Q /¢ IF.1
ORGANISATION MONDIALE DE LA SANTE
ACHR33/95.14 (Report)
ORIGINAL: ENGLISH
ADVISORY COMMITTEE ON HEALTH RESEARCH
REPORT TO THE DIRECTOR-GENERAL
on its thirty-third sessionheld at WHO headquarters, Geneva
17-20 October 1995
CONTENTS AND AGENDA
* Report of the thirty-third session of ACHR
* Report of Working Group of ACHR: Information requirements of HealthPolicy Research (Annex 1)
a Report of Working Group of ACHR: DALY Review Group (Annex 2)
* Report of ACHR Peer Review Group on the Ad Hoc Committee on HealthResearch relating to future intervention options (Annex 3)
* Report of the Ad Hoc Committee: Investing in health research anddevelopment: an Agenda to address problems of the poor (Draft 2.0)(Annex 4)
* Activity reports from the Regions (Annex 5)
a Appendix: Report on first ACHR workshop held at Schloss Reisensburg(3 - 7 April 1995)
This document is not issued to the general public, and all rightsare reserved by the World Health Organization (WHO). Thedocument may not be reviewed, abstracted, quoted, reproduced ortranslated, in part or in whole, without the prior written permissionof WHO. No part of this document may be stored in a retrievalsystem or transmitted in any form or by any means - electronic,mechanical or other - without the prior written permission ofWHO.
The views expressed in documents by named authors are solely theresponsibility of those avthb ' °
Ce document n'est pas destiné á etre distribué au grand public et tousles droits y afférents sont réservés par I'Organisation mondiale de laSanté (OMS). 11 ne peut etre commenté, résumé, cité, reproduit outraduit, partiellement ou en totalité, sans une autorisation préalableécrite de l'OMS. Aucune partie ne doit etre chargée dans un systéme derecherche documentaire ou diffusée sous quelque forme ou par quelquemoyen que ce soit - électronique, mécanique, ou autre - sans uneautorisation préalable écrite de 'OMS.
Les opinions exprimées dans les documents par des auteurs citésnommément n'engagent que lesdits auteurs.
U; I,,.. - ,--- , vi L ~ U"~ ~WORLD HEALTH ORGANIZATION DISTR RESTREINTE
ORGANISATION MONDIALE DE LA SANTE~~x~ ~~ ~~~~~~ ~~~~ zyACHR33/95.1 Rev.2
ORIGINAL: ENGLISH
ADVISORY COMMITTEE ON HEALTH RESEARCH
Thirty-third session
Geneva, 17 - 20 October 1995
Opening: Tuesday 17 october 1995
Executive Board Room, 09h30
DRAFT AGENDA
1. Opening of the session
2. Election of officers
3. Adoption of the agenda and programme of work
4. Introductory statement by the Director-General
5. Introductory statement by the Chairman
6. Report of Working Groups of ACHR:6.1 Health Research Policy6.2 Health Policy Research
7. Ad Hoc Committee on Health Research relating to future intervention
options
8. Review of research plans and activities at global level
8.1 Review on on-going programmes
8.2 Report on new WHO-Research initiatives
9. Review of research plans and activities at regional level
10. Future directions for ACHR activities
11. Collaborative research activities with:
11.1 the Council for International Organizations of Medical Sciences
11.2 other groups and organizations
12. Other business
13. Review and adoption of the report
14. Closure of the session
The contents of this restricted document may not be divulged to Lecontenuduprésentdocumentádistributionrestxeintenedoitpasetrepersons other than those to whom it has been originally addressed. It divulgué a des personnes autres que celles a quiil était initialement des-may not be further dístributed nor reproduced in any manner and tiné. II ne saurait faire I'objet d'uneredistribution oud'une reproductionshould not bereferenced in bibliographical matter or cited. quelconques et ne doit pas figurer dans une bibliographie ni etre cité.

-3-
LIST OF MEMBERS AND OTHER PARTICIPANTS
Members
Professor T.M. Fliedner, Director, Institute of Occupational and Social Medicine,University of Ulm, Ulm (Donau), Germany (Chairman)
Professor J.M. Borgono, Head of Department of Public Health, Faculty of Medicine,University of Chile, Santiago de Chile, Chile (Vice-Chairman)
Professor L. Malcolm, Professor Emeritus and Consultant A.H., Lyttelton, New Zealand,(Vice-Chairman)
Professor P.G. Svensson, Director, Centre for Public Health Research, Karlstad, Sweden(Rapporteur)
Dr Bernadine P. Healy', Cleveland Clinic Foundation, Cleveland, United States of America
Professor Ju. F. Issakov, Vice-President, Russian Academy of Medical Sciences, Moscow,Russian Federation
Professor L. Kaptué, Inspecteur général, Ministére de la Santé publique, Yaoundé,Cameroon
Professor W.A. Karczewski, Former Minister of Science and Technology, Warsaw, Poland
Professor J. Lederberg, University Professor, President Emeritus, The RockefellerUniversity, New York, United States of America
Professor M. Manciaux, Ecole de Santé Publique, Faculté de Médecine, Vandoeuvre lesNancy, France
Professor Niu Shiru, Director, Institute of Environmental Health and Engineering, ChineseAcademy of Preventive Medicine, Beijing, China
Professor Charas Suwanwela, President, Chulalongkorn University, Bangkok, Thailand
Chairmen of the regional Advisory Committees on Health Research
Professor Mireille David, Biologiste des H6pitaux, Médecin Chef Microbiologie,Départment des Sciences Fondamentales et Biologiques, Faculté de Médecine, Universitédu Bénin, Lomé, Togo (Chairman, African Advisorv Committee on Health Research)
' Unable to attend.
-4-
Dr N.M. de Almeida Filho, Department of Preventive Medicine, Federal University ofBahia, Bahia, Brazil (Chairman, PAHO Advisory Committee on Health Research)
Professor M.E. Chatty, Minister of Health, Ministry of Health, Damascus, Syrian ArabRepublic (Chairman, Eastern Mediterranean Advisorv Committee on HealthResearch)
Professor J. Rantanen, Director-General, Institute of Occupational Health, Helsinki, Finland(Chairman, European Advisory Committee on Health Research)
Professor Aree Valyasevi, Dean, Faculty of Medicine, Thammasaat University, Rangsit,Nondabur, Thailand (Chairman, South-East Asia Advisory Committee on HealthResearch)
Professor A.N. Herrin, School Economics, University of the Philippines, Diliman, QuezonCity, Philippines (Chairman, Western Pacific Advisorv Committee on HealthResearch)
Temporary Advisers
Dr N. Bailey, Lauenen, Switzerland
Professor C. Cabrol, Service de Chirurgie Cardio-vasculaire, Hópital La Pitié, Paris,France
Professor B.M. Dickens, Faculty of Law, University of Toronto, Toronto, Canada
Professor M. Gabr, Former Chairman, ACHR, Head, Pediatric Department, Faculty ofMedicine, Cairo, Egypt
Professor A. Jablensky, The University of Western Australia, Department of Psychiatryand Behavioural Science, Medical Research Foundation Building, Perth, Australia
Professor D.T. Jamison, UCLA Center for Pacific Rim Studies, Los Angeles, United Statesof America
Dr M. Kerker, Technical Advisor Human Resources/Health, Federal Ministry of ForeignAffairs, Swiss Development Cooperation (SDC), Bern, Switzerland
Dr C.H.G. Oldham', Science and Technology Adviser to the President of the InternationalDevelopment Research Center (IDRC), Ottawa, Canada
' Unable to attend.
-5-
Professor B. O. Osuntokun*, Former Chairman ACHR, University of Ibadan, Ibadan,Nigeria
Mr V. Oviatt, Cail, Fife, United Kingdom
Professor B. McA. Sayers, Former Dean, Imperial College of Science, Technology andMedicine, Director, Centre for Cognitive Systems, William Penney Laboratory, ImperialCollege, London, United Kingdom
Professor E.Thorbecke', H.E. Babcok Professor of Economics and Food Economics,Cornell University, Ithaca, New York, United States of America
Professor M. Usui, Faculty of Policy Management, Keio University (SFC), Endo, FujisawaCity, Japan
Dr P. Vahl, Medical Director, Medical Devices Agency, London, United Kingdom
Council for International Organizations of Medical Research (CIOMS)
Dr Z. Bankowski, Executive Secretary, CIOMS, Geneva, Switzerland
Council on Health Research for Development (COHRED)
Dr Y. Nuyens', Coordinator, Palais des Nations, Geneva, Switzerland
International Agency for Research on Cancer (IARC)
Dr P. Kleihues, Director, IARC, Lyon, France
International Council of Scientific Unions (ICSU)
Professor Y. Verhasselt', Geografisch Instituut, Vrije Universiteit Brussel, Brussels,Belgium
United Nations
Mr S. Khmelnitski, External Relations and Inter-Agency Officer, United Nations, Palaisdes Nations, Geneva, Switzerland
* Deceased on 21 September 1995.
' Unable to attend.
-6-
United Nations Educational, Scientific and Cultural Organization (UNESCO)
Mr V. Kotchetkov, Chief, Science, Technology and Society Unit, United NationsEducational, Scientific and Cultural Organization (UNESCO), Paris, France
Representatives from the WHO regional offices
Regional Office for Africa: Dr L.G. Sambo, Acting Director, HSC
Regional Office for the Americas: Dr A. Pellegrini, Chief, Research Coordination
Regional Office for the Eastern Mediterranean: Dr El-Sheikh Mahgoub', RegionalAdviser, Research Promotion and Development
Regional Office for Europe: Dr J. Bury', Regional Adviser, Training and Research inPublic Health
Regional Office for South-East Asia: Dr S.P. Tripathy, Director, Research and FamilyHealth
Regional Office for the Western Pacific: Regional Adviser, RPD'
WHO headquarters Secretariat
Dr H. Nakajima, Director-General
Dr A. Piel, Director, Cabinet of the Director-General
Mr D.G. Aitken, Assistant Director-General
Dr F.S. Antezana, Assistant Director-General
Dr R.H. Henderson, Assistant Director-General
Dr Hu Ching-Li, Assistant Director-General
Dr A. Kone-Diabi, Assistant Director-General
Dr S. Lyagoubi-Ouahchi, Acting Assistant Director-Genral
Dr N.P. Napalkov, Assistant Director-Genral
' Unable to attend.
-7-
Dr W. Kreisel, Executive Director
Dr T. Turmen, Executive Director
Dr M.A. Belsey, Programme Manager, Maternal and Child Health and Family Planning
Dr C.G. Bolis, Division of Mental Health
Mr S.S. Fluss, Division of Publishing, Language and Library Services
Dr T. Godal, Director, Special Programme for Research and Training in Tropical Diseases
Dr E.H.T. Goon, Director, Division of Development of Human Resources for Health
Dr A. Issakov, Division of Strengthening of Health Services
Dr A. Kalache, Chief, Aging and Health Programme
Dr T. Kjellstrom, Director, Office of Global and Integrated Environmental Health
Dr U Ko Ko, Special Adviser to the Director-General
Dr B. Mansourian, Director, Research Policy and Strategy Coordination (Secretary)
Dr L.L. Prilipko, Division of Mental Health
Dr C. Romer, Programme Manager, Safety Promotion and Injury Control
Dr J. Szczerban, Vice-Chairman, Council for Science and Technology
Dr J.L. Tulloch, Director, Division of Diarrhoeal and Acute Respiratory Disease Control
Dr D. Yach, Chief, Policy Action Coordination
-8-
1. OPENING OF THE SESSION (Agenda item 1)
The Chairman, Professor T.M. Fliedner, opened the thirty-third session of the Advisory
Committee on Health Research, and welcomed members to Geneva. A minute of silence was
observed in memory of Professor B.O. Osuntokun, who passed away on 21 September 1995.
2. ELECTION OF OFFICERS (Agenda item 2)
Professors Borgono and Malcolm were elected vice-chairmen, and Professor P. Svensson,
rapporteur.
3. ADOPTION OF THE AGENDA AND PROGRAMME OF WORK (Agenda item 3)
The draft agenda (ACHR33/95.1 Rev.2) and the Programme of Work (ACHR33/95.2 Rev.1)
were adopted.
4. INTRODUCTORY STATEMENTS (Agenda items 4 and 5)
In their opening remarks, the Director-General and the Chairman stressed several points
amongst which, that: (a) ACHR being concerned by definition with the health policy debate,
there should be greater synergy with the Governing Bodies. (b) The whole ACHR system,
including all regions, should contribute to updating the research agenda in support of WHO's
health development strategy. (c) The unavoidable inter-dependence between different parts of the
"global village" is becoming widely recognized, for example, with respect to changes in human
ecology, migration problems and the growth of mega-cities. (d) The international scientific
community represents a vast reservoir of knowledge, not only in the biomedical sciences, but in all
disciplines of potential relevance to health: it should be sensitized and exploited for the benefit of
global health development.
A development of particular interest, noted by the chairman, was the first ACHR workshop
on strategic planning, held at the International Institute for Scientific Cooperation, at Schloss
Reisensburg near Ulm (cf. Appendix). The workshop used new conceptual and technical
approaches to identify the global R&D agenda in order to complement the WHO efforts on
renewing the HFA strategy.
-9-
The Director of the Cabinet, Dr A. Piel, recalling recent WHO achievements in control of
epidemics, elimination of diseases and promotion of health, emphasized the current efforts in the
"renewal of Health for All" strategy. The guidance of ACHR, as the highest research policy body,
was sought to help answer at least four questions: (a) What direction should future scientific
research take? (b) What are the "gaps" in knowledge and technology that need to be filled to carry
out the Health for All strategy? (c) What are the research priorities that WHO itself and/or
scientific and other institutions should undertake? (d) Is it possible to create an interactive network
of scientific institutions, WHO and other collaborating partners, drawing on the newly available
telematics technology?
In summary, WHO is calling on the ACHR to devise a strategy that would "mobilize brains
to serve humanity".
5. ACHR WORKING GROUPS (Agenda item 6)
The update on Health Research Policy constituted an extension of previous work which was
started 10 years ago both at global and at regional levels. The Chairman reiterated the
Committee's intention to consolidate all these efforts and translate them into an operationally-
viable strategic plan.
With regard to Health Policy Research, the Committee, recalling an earlier discussion of the
subject at its 32nd session, as well as other contributions by the regional ACHRs, accepted the
background paper on Information Requirements (Annex 1) as a timely input which will be
complemented by other material and by further studies.
The committee endorsed the Chairman's plan for another workshop in the spring of 1996, to
develop further concepts and methods, as well as to explore ways and means to harmonize research
efforts between global and regional levels.
- 10-
6. ACHR REVIEW GROUPS (Agenda items 6 and 7)
6.1 Report of the ACHR DALY Review Group:
The findings of the DALY Review Group, which was set up at the thirty-second meeting
of the ACHR in response to concerns expressed about the validity of the DALY as a health
indicator, were reported in a Conference Room Paper (Annex 2).
The ACHR endorsed the conclusions and accepted the recommendations of the Review
Group. The risks involved in using this - as yet invalidated - tool were emphasized by several
committee members. The ACHR believes that a unidimensional indicator of DALY-type is
fundamentally inappropriate for general purposes.
The DALY should not be used for setting health research priorities. Further, use of the
DALY in resource allocation is dangerous: it diverts attention from the original determinants of
disease that dictate whether - and if so, which - policy measures should get resources.
The concerns of the ACHR should be drawn to the attention of funding agencies at national,
regional and global levels. It was also recommended that the findings of the Review Group should
be published in appropriate scientific journals.
6.2 Report of the ACHR Peer Review Group on the work of the "Ad Hoc Committee on
Health Research relating to future intervention options" (Annex 3):
Members of the Peer Review Group (set up by the ACHR at its 32nd session) outlined the
reasons behind their recommendations concerning the draft Report 2.0 (28 August 1995) of the Ad
Hoc Committee which, it was understood, was not yet in final form. The Peer Review Group
appreciated the efforts of the Ad Hoc Committee (Annex 4) in collecting and assembling a
comprehensive amount of data but found substantial flaws in concepts and weaknesses of
methodology in the draft Report. The Peer Review Group observed with concern that major
conclusions and recommendations in the Report seemed to be independent of, and not logically
derived from, the analysis of the data presented. A particular source of concern was the proposal
of the Ad Hoc Committee to establish a Consortium for Health Research, the effect of which
would be to weaken the institutional integrity of WHO and to subsume WHO's mandate as the UN
organization with responsibility to all Member Countries for Health Research.
- 11 -
The Committee noted Professor D.T. Jamison's reply, speaking as Chairman of the Ad Hoc
Committee. In thanking the ACHR for its work, and expressing his reservations about a few of
the recommendations, he agreed to take account of the verbal and written comments and
recommendations in revising the Ad Hoc Committee's Report which was scheduled for completion
by spring 1996.
The ACHR accepted and endorsed the 10 conclusions and recommendations of the Peer
Review Group's Report and proposed that they should be drawn to the attention of the Director-
General. The Peer Review Group was asked to monitor further developments of the work of the
Ad Hoc Committee and its reports.
7. REVIEW OF RESEARCH PLANS AND ACTIVITIES AT GLOBAL LEVEL
(Agenda item 8)
7.1 Review of on-going programmes:
AGING AND HEALTH PROGRAMME
In view of the increasing numbers of elderly people worldwide, WHO is urged to explore
innovative ways of increasing the regular budget allocation to the programme and involve
the Regional Offices more closely; the Aging and Health programme is encouraged to
supplement meagre resources by developing an enlarged network.
EURO and PAHO are urged to fill their vacancies in respect of focal points for their aging
and health programmes.
A high priority should be given to training of manpower, in ways that take into account the
cultural and social diversities in health service needs among the elderly.
MATERNAL AND CHILD HEALTH AND FAMILY PLANNING
The overall assessment of the MCH programme was very favourable; its linkages to a
variety of relevant agencies and WHO Collaborating Centres were noted as particular
strengths.
- 12 -
The research performed by, and in collaboration with, the programme was evaluated as
relevant and valid to its strategy and an appropriate proportion of the budget was spent on
research.
It is recommended that a research agenda should be created for the next decades, to take due
account of developing demographic trends. Where applicable in the light of social and
cultural circumstances, the use of technology should be carefully scrutinised for possible
misuse; prenatal screening and subsequent procedures are two of several sources of
potential concern, arising both from ethical and practical considerations.
It is recommended that ACHR should continue its review of the MCH programme,
especially the adolescent health component, which the ACHR was unable to review
thoroughly, because of time constraints.
NEUROSCIENCES AND MENTAL HEALTH
This programme area was strongly supported. Taking into account the rapidly growing
importance of neurosciences, and their relevance to other fields of health (particularly in the
context of the elderly) the ACHR emphasized their importance within WHO's activities. It
recommended that support to neurosciences be strengthened with special attention to
research on neuroepidemiology, problems of therapy resistance and side-effects in neurology
and psychiatry as well as pain control, epilepsy and brain injury.
It is recommended that the consultative role of the programme should be strengthened,
especially in support of the Decade of the Brain and other initiatives of the United Nations
system. This may attract extrabudgetary funding.
The aim of the programme should be to promote mental health despite population increase
and social and economic turbulence.
SAFETY PROMOTION AND INJURY CONTROL
The committee recommended that a progressive research agenda be developed, to provide a
basis for useful discussions at interprogrammatic fora and that a strategy paper be published
- 13 -
in the Bulletin or another appropriate journal. This would contribute to
expanding the perceived scope of public health to include safety promotion and injury
control.
The research agenda should address: concepts and definitions; the design and validation of
indicators and other instruments to clarify the nature of the problems encountered; and the
development and application of methods of analysis that take account of psychosocial and
behavioural parameters in safety, from which interventions can be designed - for instance, to
prepare health care services likely to be needed as a result of injury such as those resulting
from ethnic, domestic, organized violence, etc. ACHR's advice is that activity in this field
is timely; it both deserves and requires full WHO support in advocacy of its importance.
ACHR should receive a Report on activities in this field at its next meeting. The topic is a
proper topic of concern for the Renewed Health for All programme and the ACHR input to
it - perhaps in raising the profile of the field and contributing backup in planning its
development.
The performance of this programme shows that it is possible to perform efficiently even
with one professional staff who is able to attract enough support from outside.
ACHR supports the strategy of a HQ-based role for the Safety Promotion and Injury Control
Programme; it would continue to co-ordinate relevant work in different programmes.
7.2 Report on new WHO-Research initiatives:
a) Global and integrated Environmental Health
Having listened with interest to the presentation, the ACHR supported the proposal that, in
order to strengthen links between it and the Global and Integrated Environmental Health
Programme, members with an interest in environmental issues should become, through the ACHR
Secretariat, more closely linked with the research promotion activities of the Programme with,
where appropriate, a view to active participation in its activities.
b) WHO Kobe centre for Health Development
Following the presentations on the Kobe centre which is established, ACHR members
expressed their appreciation for this novel initiative and the wish to be actively involved in the
- 14 -
further development of the work of this Centre, as well as in the promotion of analogous
initiatives. ACHR stressed the need for scientific rigour to be kept in mind both in the recruiting
process and in the operation of the Centre. It therefore recommended that ACHR appoint a small eworking group in order to assist in monitoring and assessing this process.
8. REVIEW OF RESEARCH PLANS AND ACTIVITIES AT REGIONAL LEVEL
(Agenda item 9)
In reviewing research plans and activities at regional level (Activity reports, Annex 5), the
ACHR heard with concern that the European Advisory Committee on Health Research (EACHR)
had not been able to meet during the biennium due to financial constraints, which also made WHO
- sponsored and coordinated research within the region impossible. It recognized both the
importance of the European infrastructure for research, the fruits of which could be made generally
available; and the role of health and health policy research for central and Eastern countries and
newly independent states, from which, without such support, there was a danger of brain-drain in
coming years.
It therefore strongly recommended that an operational budget be allocated to the EACHR, in
order to enable it to meet annually, and that a EURO focal point be identified to coordinate the
different Health Research efforts within the Region.
In considering matters arising from the presentation about work of the Western Pacific
Advisory Committee on Health Research (WPACHR) the ACHR strongly recommended that WHO
support trans-regional initiatives. Particular reference was made to research into lifestyle - related
health status and research into health sector reforms, and particularly into alternative health
insurance schemes.
9. FUTURE DIRECTIONS FOR ACHR ACTIVITIES (Agenda item 10)
In discussing "Future Directions for ACHR Activities", the ACHR took note of and
deliberated on medical, organizational, social, cultural, religious, economic, ethical, legal and
related aspects of the growing gap between the demand for organs suitable for transplantation and
their availability. Committee members found these matters to be of concern to all regions of the
world, and to countries at all stages of economic development, since they embody the universal
- 15 -
challenge of relating the effective use of medical technology to its economic and social costs. The
ACHR recommends that:
* WHO be encouraged to take a role of international leadership in promoting study and
resolution of the full range of issues raised by expanding medical potentials to recover and
transplant organs from people following their deaths;
* A Task Force be established, co-ordinated by RPS, to identify and structure the medical,
social, economic, ethical and related issues implicated in the potential advance in health care that
cadaveric organ recovery and transplantation represent; and
* WHO collaborates with CIOMS, UNESCO, Council of Europe, the Transplantation Society,
International Trans Ethics Forum, and other appropriate non-governmental organizations to collect
and share information on practices of organ recovery and distribution, in order to develop
guidelines sensitive to the values and practical considerations that must be respected to achieve
acceptable policies and effective practices that close the gap between the recovery and
transplantation of organs. The potential future use of xenografts, and the associated ethical and
cultural issues, could also be examined in the course of this endeavour.
These recommendations would assist the Director-General to give effect to World Health
Assembly resolution WHA44.25. This resolution endorsed the Guiding Principles on Human
Organ Transplantation proposed by the Director-General, and in Article 4(1) requested that the
Director-General:
review the Guiding Principles from time to time in the light of national experience in their
implementation and of developments in the field of human organ transplantation.
Professor Lederberg drew attention to the health consequences of the proliferation of
biological weapons. The Committee agreed to include this matter in the next agenda.
- 16 -
10. COLLABORATION WITH NGOs AND OTHER ORGANIZATIONS
(Agenda item 11)
10.1 With the Council for International Organizations of Medical Sciences (CIOMS)
Dr Bankowski, Secretary-General of CIOMS, made a brief presentation to the Committee on
the activities of the Council. References were made to the follow-up activities of the CIOMS
Conference on "Poverty, Vulnerability and the Value of Human Life", held at Ixtapa, Mexico, and
the emerging declaration on "A global Agenda for Bioethics". CIOMS would continue to
coordinate international activities in bioethics and ethics of health care and is organizing in 1996,
in the framework of its programme entitled "An International Dialogue on Health Policy, Ethics
and Human Values", a series of international and intercultural consultations. The main goal of
these broad consultations is to provide ethical background for a new global health policy based on
the concepts of equity and solidarity in the context of the "Renewing the Health-for-All Strategy"
of WHO. In addition, CIOMS would continue to mobilize, through its broad membership, the
scientific medical community for a closer collaboration with ACHR and WHO.
ACHR welcomed the report and emphasized the importance of close collaboration with
CIOMS, particularly in the field of ethics.
The ACHR was highly appreciative of CIOMS activities in the field of bioethics, expressed
support for the CIOMS Programme "An International Dialogue on Health Policy, Ethics
and Human Values", and the CIOMS initiative on the Global Agenda for Bioethics.
In addition, ACHR strongly supports CIOMS activities aimed to provide ethical background
for the new global health policy of WHO which is based in equity and solidarity, and
recommended that WHO provide both technical and financial support to assist CIOMS in carrying
out its programme on bioethics.
10.2 As regard to UNESCO, the ACHR was impressed with the work being undertaken by
UNESCO in the field of global scientific communications, especially in relation to its pilot project
for information technology and networking in Sub-Saharan Africa. It recommended that WHO
should collaborate with UNESCO and other relevant agencies in the area of scientific connectivity
and information technology.

- 17 -
10.3 The earlier presentation of Dr Kerker, on behalf of the Council for Health Research for
Development (COHRED), was also noted with interest.
11. REVIEW AND ADOPTION OF THE REPORT (Agenda item 13)
ACHR reviewed and adopted the summary report of its thirty-third session subject to its
finalization by the chairman, the rapporteur and the secretary.
12. CLOSURE OF THE SESSION (Agenda item 14)
Dr Piel made some closing remarks on behalf of the Director-General who was on duty
travel in Bogota and Cartagena, Colombia, in connection with the Non-Aligned Movement
Summit. The Director-General was also dealing with the new Pattaroyo vaccine, a much-needed
"magic bullet" in the war on malaria, that was currently undergoing trials. But "magic bullets"
also had to be delivered, in the context of each society, based on an understanding of the complex
of interrelated determinants of health. While WHO welcomed the opportunity of network
communication among scientific institutions as proposed by ACHR, the same degree of
competence and confidence did not necessarily pertain to certain of the media and political or
commercial interest groups. For example, certain media had gone to extravagant lengths to
discredit WHO's actions in cholera control, child vaccination and primary health care, but
developing countries and partners fortunately trusted WHO. From these experiences it wa~itex
that:
1. WHO was science-based;
2. WHO was not "just another health organization";
3. There were no "quick fixes" in public health.
Dr Piel said that the Director-General welcomed the activism of the ACHR, and its guidance
for the future health research agenda that should be part of the renewal of Health for All. It
should be possible to agree on a general intellectual framework of the major determinants of health
- behavioural, environmental, biological, medical, social, etc. - and use that framework as a starting
point for defining health research strategies in concert with the renewal of HFA, health monitoring
and evaluation. ACHR had agreed to examine the feasibility of creating an interactive network
among existing scientific institutions, WHO, and other partners, and to explore the use of modem
telematics technology.
18 -
It was agreed that the thirty-fourth session of the global ACHR would be held from
15 to 18 October 1996 in Geneva. _
e
e
O
ANNEX 1
DISTR.: RESTRICTEDOISTR.: RESTREINTEo 'm ~ WORLD HEALTH ORGANIZATION
ORGANISATION MONDIALE DE LA SANTE''ORGANISATION MONDIALE DE LA SANTEACHR33/95.6
ADVISORY COMMITTEE ON HEALTH RESEARCH
Thirty-third session
Geneva. 17 - 20 October 1995
Agenda item 6
REPORT OF WORKING GROUPS OF ACHR
HEALTH POLICY RESEARCH
The contents of this restricted document may not be divulged topersons other than those to whom it has been originally addressed. Itmay not be further distributed nor reproduced in any manner andshould not be referenced in bibliographical matter or cited.
Le contenu du présent document á distribution restreinte ne doit pas itredivulgué á des personnes autres que celles a qui il était initialement des-tiné. II ne saurait faire l'objet d'une redistribution ou d'une reproductionquelconques et ne doit pas figurer dans une bibliographie ni etre cité.
ORIGINAL: ENGLISH
A.1
achr4.docjune.95
Information requirements of Health Policy Research
Ronnev B. Panera¡, Ph.D.Department of Medical Physics,University of LeicesterLeicester LE1 5WW - UK
1. Introduction
Health Policy Research (HPR) has been defined as the process of scientific investigation insetting policies, leading to the formulation of strategies, priorities and plans for heaithdevelopment [1]. Health development is considered as a positive change in health satuswhere health benefits are maximized and health hazards are minimized.
The importance of HPR cannot be overemphasized. Most countries are undergoing aperiod of overwhelning transformation of their social and economic sectors with directimplications on health levels [2-4]. Health services are under strain, on one hand becauseof cost containment policies and, on the other, because of increased demands resulingfrom population ageing, technological innovations, and the resurgence of communicablediseases (H1IV, tuberculosis) [5-7]. In particular, developing countries, which have notbeen able to overcome infectious and parasitic diseases and other conditions associated topoverty, such as malnutrition, are now facing an epidemiological transition which bringsthe additional burden of chronic and degenerative diseases [8-10]. In this scenario. theformulation, implementation and evaluation of health policies that can promote healthdevelopment while coping with the process of change, become a top priority. To achievethis goal the following framework has been proposed for health policy planning [I I]:
a) Identifying and defining the problemb) Identifying and priority ranking of objectives within the framework
of a valid value system.c) Identifying resources, as well as the groups competing for these resources.d) Considering altemative solutions.e) Choosing the optimal system for implementation of the chosen solution.f) Synthesis of the system.g) Updating concepts, equipment, characteristics, and data.h) Testing the system.i) Refining the design based on a correlation of test data and requirements.
1
The above steps involve three basic "building blocks" of health policy research:data/information collection, analysis/assessment, and decision-making. This paperdiscusses the information needs of HPR, in particular the requirements for problemidentification and assessment of the impact of different interventions and policies. Futurework will concentrate on the role of analysis and decision-making. A rigorous defliirion ofInformation is not adopted and in many instances the term can be confounded with Data.Broadly, some form of preliminary analysis is performed on raw data to generate somne'information" but this kind of analysis usually relies on procedures which are of rouineuse and will not be described in detail here.
2. The information challenge
In an ideal world, health policy making should attempt to promote health development byjudicious use of the existing knowledge about the determinants of health and disease. Fora number of reasons this ideal still lies a long way ahead. Knowledge is still limited mmany key areas such as in the understanding of physiopathological processes. Adequateinformation to descnrbe health conditions and to support resource allocation is notgenerally available. We are only beginning to develop large-scale quantitative models thatare essential to cope with the dimensions and complexity of health service researchproblems. Explicit policy making is frequently muddled by lack of consensus onappropriate criteria for what is best for society or for different sub-groups; individual andsocietal values are at the heart of the problem Finally, political and financial interests arealways present and often dominate the entire process. Given these difficulties, the extentto which health policy-making can be transformed into an entirely rational exerciseremains to be established. On the other hand, areas for improvement in the currentsituation can be easily identified and these constitute the mission of HPR. The productionand dissemination of information to support the formulation, implementation andevaluation of health policy are amongst these areas. In the absence of reliable information,policy and decision-making will be dominated by political interests or, with the bes ofintentions, will be a 'jump in the dark". Absence of adequate information is the mostfrequent excuse for maintaining the status quo of arbitrary and politically biased de-ision-making as observed in many developing countries. Why more and better information arenot readily available ? The answer is largely to do with the low priority given to theproduction of relevant information. In other words, because there are implicit policies ofnot improving the availability of information. Consequently, progress in the identification,production and dissemination of better information for health policy rmaking represents amajor challenge requiring concerted actions at the political, technical, and organizantionalspheres.
The complexity and multidimensionality of the concepts of health and disease, themultiplicity of their determinants, together with the diversity of resources required forhealth prevention and care pose an almost infinite demand on the amount of informationthat would be required under ideal circumstances. In fact, information is just anotherresource required for achieving health development and therefore it has its limitations andits own costs. As a consequence, its demand has to be put into perspective and, ultimately,
2
A. 1
it has to be subjected to cost-effectiveness analysis. Despite this caveat though hiertothe main problem with the information requirements of HPR is its limited availabi'irv. Thisis particularly the case of developing countries. Sadly, the same distortions that affect theallocation of resources for health also affect the production/distribution of healthinformation. Very limited information is normally available at community level forexample on sanitation, nutrition, education, environment, or income. The same appies forinformation that could be obtained by primary care services: incidence/prevalence ofcomnmon diseases, disability, family planning, immunization, and so on. However. moreclinical and epidemiological information becomes available as we progress along thehierarchy of the health care system, particularly at tertiary/quaternary level. In otherwords, the pyramid is inverted for the production and availability of information for HPR1
The difficulties involving the availability of information in developing countries to szpportHPR is well illustrated by a WHO/UNDP project developed in Brazil (Federal Universityof Rio de Janeiro) in collaboration with the University of Virginia (Prof E.O. Attinger)and the Imperial College, Univ. of London (Prof£ B.McA. Sayers). A large effort ;asconducted during several years to collect data that could characterize the multiple impactsof different sectors of society on health levels. Because of the time lags frequentlyobserved in the relationship between social/economic/environmental determninants andhealth levels, a dynamic approach was favoured and this required sequential data forseveral years. The year 1960 was selected as the ideal beginning of the time series becauseof the accelerated industrialization and urbanization observed during the 60's. Although itwould have been ideal to collect data that could reflect inner city differences in heaihhlevels, this was clearly impossible and, as a compromise, data had to be aggregated for awhole town. A total of 60 different towns, covering about 50 % of the urban populationof the country were selected for the study. In its initial phase, which run until 1985. 60different variables and indicators were selected and data were collected from differentsources, in an attempt to obtain complete time series from 1960 to 1983. Given thenumber of towns, variables and years involved, the final target was therefore about60x60x23 = 82,800 data values. In fact only approximately 21,000 values were collcted,or 25 % of the desired total. Despite this disappointing result, it became evident that moredata were becoming available in more recent years and this was confirmed when a s.¿conddata collection was performed in 1990/91, this time involving as many as 106variables/indicators [12,13 ].
Developing and maintaining comprehensive information systems that can cope with thedemand of information for HPR represents a major investment and a long-termcommitment for any country. This task is almost insurmountable for developing coountriesbecause ofthe lack of tradition in systematic data collection, resource imitations. and theunderstandable dominance of short-term approaches to policy-making. The criticalsituation of population health levels and quality of life in most of these countries requiresdetermined action and imaginative approaches to improve policy making. Beforeconsidering this particular situation though, it is important to explore whether theidentification and selection of information for HPR can be placed within a rationalframework which can guide fuiture developments in this area.
3

. Approaches to information identification and selection.
The framnework proposed for health policy planning, listed in Section 1 above [ 11] gives ageneral idea of the information needs of HPR, in particular steps a,b,c,d,e,and g. For eachof these steps however, the identification of the specific data/information required is mind-blowing given the dimensions which the problem assumes for policy-making at a nationalor international scale.
Existing systems for the production/dissemination of information that can be useful oreven essential for HPR are uncoordinated and of very low specificity. Characteristically,different organizations and structures produce masses of data for multiple users. This isthe case of demographic information, vital statistics, infrastructure (water supplh.transportation, electricity), environmental risks, health services, food production and soon. In developed countries large volumes of data are produced in some sectors. such ashealth services statistics [14] co-existing with critical gaps such as information on theefficacy/effectiveness of health programmes and interventions [6,15,16]. This unbalance inthe production/dissemination of information needs to be addressed. On one hand theoverproduction of some kinds of information, in an open ended fashion, suggests thatresources are being wasted. On the other hand, the scarcity of essential pieces ofinformation highlights areas where research efforts should be concentrated.
An interesting theoretical question arises from the quest to identify the informationrequired for HPR Is it possible to identify the information needed by any objectivemethod ? If the answer is positive, then the next question is really thorny By whatmethods exactly ? Attempts to answer this question in more limited contexts haveresulted in proposals such as the "waterfall approach" suggesting that information shouldbe sought by first identifying the decisions that need to be made in a certain problem-area.By working backwards, step-by-step, it should be possible then to identify theanalysis/information/indicators/data required to support that particular decision-makingprocess. Although highly complex and demanding for large scale problems, this approachis nevertheless feasible in well defined areas such as resource allocation [17,18]. In otherareas the waterfall approach could also be used but it tends to become irrelevant wxtenhealth policy making is dominated by political interests or, as frequently happens. n istrapped by value-laden considerations. Although these situations are not devoid ofinformation needs (e.g. people's acceptance of I-V screening) their ephemeral andchanging focus may not justify the effort required to generate routine information.
The main problem with the waterfall approach though is the distance separating decision-mrnaking and the generation of corresponding improvements in health levels as the uhimategoal of HPR. The cognitive crisis arises from the fact that at macro-level most decisionsaffect multiple health problems. Conversely, improvements in any health problem dependon multiple decision-making. This comnplication is a direct consequence of the ecologicalnature of the determinants of health: there is not a well established input-output structure,the system is an aggregate of multiple interacting sub-systems. Policy. decisions affectingone such sub-system. e.g. industrial development or distribution of income, spread through
4
A.1
the other sub-systems and the final impact on health levels is the cumulative effectchannelled through different pathways: housing, employment, infrastructure, nutriion,environmental conditions, access to health care, etc. Analytical models to identifv dme mostsignificant pathways and to estimate their relative contribution are obviously needed. Oneadditional contribution of such models is to work as a guide to the appropriate andrelevant information for HPR_ Focusing on health development as the goal of HPR. theidentification of the determinants of health can offer a shortcut to the informnation neededto formulate policies that will maximise health as a single entity or any of its multipiecomponents. However, it is unlikely that we will be able to separate the data/informationneeded from the conceptual/analytical model used to identify the relative contnbumon ofdifferent determinants of health. Consequently, model selection should take into accountnot only performance but also parsimony towards information demands. In addition.modelling can also give an indication of the value of different variables/data/information. Itis well known and accepted that one the main uses of quantitative models in this context isto answer questions of the 'What if?..." type. This is usually understood as the attempt tosimulate the effect of selective interventions, such as the impact of increasing maternaleducation on infant mortality for example. What is suggested here however is an euensionofthis approach to explore the impact of missing data or of not having certain variables atall In other words, a sensitivity analysis of the value of information.
Despite these possibilities to improve the rational identification of the information requiredfor HPR, the political and ethical components of the health arena have to be kept in mimndwhen assessing the cost-effectiveness of information gathering efforts. Important researchopportunities exist along these lines though. In this direction, a characterization of the"epidemiology" of policy and decision-making can be enlightening. Similar to medicalpractices, which have been shown to vary considerably from one region to another. policy-making will probably show large differences between regions/countries. What are thereasons behind these differences ? What are the objective criteria and information adoptedin different scenarios ? Above all, what impacts have been obtained in each case ? Suchstudies are likely to point out towards significant differences in organization, efficiency,and accountability, as well as the influence of cultural and socio-economic factors.However, the political nature of this line of inquiry cannot be denied. For how long :andifferent societies tolerate uninformed choice ?
From the steps listed in the Introduction (Section 1) it is clear that policy-making requiresinformation that allows the identification of health problems, priorities, resourcesavailable, alternative solutions, and the likely impacts of different interventions. Adequateinformation is not available in several of these areas, e.g. the cost-effectiveness of medicalinterventions. In other areas there is still limited understanding of the way the informationavailable should be incorporated in the policy-making process. Thiis s the case ofinformation that can express the duality of health and disease. The problems invohked inthis specific area are discussed in the following sections.
5
4. The measurement of health and disease.
Both steps of problem identification and assessment of the impacts of interventions and/orhealth policies require the ability to measure health status and the burden of disease. Thedifficulties facing the absolute measurement of socially and culturally produced conceptssuch as health and disease have been object of extensive discussions [2,19,20]. The-re iswidespread consensus that such measurement is in fact almost impossible and that atmost, we have to do with indirect measures or 'indicators" of health (or disease). Despitea very large number of such indicators in use for multiple aspects of the health-diseaseprocess, there is no agreement about which indicators are more appropriate underdifferent circumstances. The multiplicity of indicators available reflects the complexity ofthe determinants of health and the fact that each medical speciality tends to adoptindicators and scales which are specific to the conditions under their care [14,21-23].
The most reliable and easily available information reflecting health conditions are mortalitydata. In developing countries it is relatively simple to identify health problems by thepremature mortality observed in relation to the corresponding situation of more developedcountries. This can give a strong basis for health policy, e.g. involving immunization.family planning, allocation of obstetric and emergency services, etc. [8]. The limitations ofmortality data become apparent though when more refined allocation of resources isdesired or in situations in which the indicator adopted looses the sensitivity to reflecthealth gains. In addition, there are many conditions which carry a large burden of mfferingbut which are not proportionally reflected by mortality data. Obvious examples are polio, emalaria, and mental disease. A large number of indicators of morbidity have beenproposed in addition to the classical measures of incidence and prevalence of disease.Some examples are indicators of risk, disease staging, prognosis, and outcome [2_-28]. Asmentioned above, the diversity of such indicators in part results from thecompartmentalization of medical practice and the proliferation of sub-specialities tach asneonatology and neurosurgery, but also reflects the difficulty to obtain more generalindicators of health. For HPR, indicators that can be applied to a single conditioni diseaseare of limited use because they can only be applied to a handful of individuals at an- onetime. The main challenge then is to find indicators that can be used across multiple healthproblems in order to characterize the health status of a whole population. As mentionedabove, an aggregated measure such as life-expectancy would satisfy some of theseconditions, but, on the other hand. it does not have the sensitivity to reflect the burden ofdisease of all conditions and populations. To overcome the intrinsic limitation of usmgonly mortality data, attempts have been made to construct multidimensional indicators thatcan reflect the physical, social, and psychological dimensions of health. An important sub-group is comprised of health status indicators (HSI) which attempt to classify eachperson's present state of health according to some ordinal scale. Examples are theSickness Profile Index (SP), EuroQol, Nottingham Health Profile (NHP), Qualitn of LifeIndex (QLI), Rosser Index, and Quality of Well Being Scale (QWB) [21,29-33].
The most common approach adopted for the construction of HSI is the application ofquestionnaires involving the assessment of the individual's rating along several dimensions
6
A. 1
such as physical capacity/disability, social adaptation, satisfaction, psychological wIlbeing/distress, pain, and others. Each of these dimensions is then weighed according topre-determined sets of values to yield a single number reflecting the individual' s healthstatus. The final nunerical values are usually standardized to lie in the interval 0-1corresponding to death/permanent coma in one extreme and perfect health in the catrer.Important metihodological characteristics can distinguish between these indicators. Themain ones are the information extracted from the individual, how this information isweighed, and, above all, the method used to validate the results against well estabEishedstates of health. The latter is directly related to the derivation of the set of weights oy aprocess of adjustment. An extensive literature is available describing the constructon andvalidation of these indicators. Notably, other HSI follow different principles. One .~ampleis the Rosser Index [32,34] which classifies the individual into one of 29 different statesof health. These states are described by two main dimensions, disability and distres& whichare subdivided into 8 and 4 categories, respectively. Figure 1 contains the correspondingnumerical values for each health level. It can be observed that there are states con.sderedworse than death. To obtain the values given in Fig. 1, a group of 70 subjects were askedto make a judgement about the relative severity of pairs of health states, keeping in mindthe resource implications represented by treating different numbers of patients in thedifferent states. This was achieved by establishing the point of indifference between thehypothesis of curing one patient in the more severe state or curing a larger number ofpatients in the less severe state. The successive ratios between pairs of states were thenused to construct a single scale leading to the values in Fig. 1.
In a class of its own is the application of the concept of utility, as developed b vonNeumann and Morgestern [35] as an indicator of health status. Rather than expressing thevalue of different goods and products to a consumer, the measure of utility attenmpts toexpress the value of different states of health to one individual, based on the assumptionthat this would guide his decision-making and behaviour in the face of uncertainty. Theoutstanding characteristic of the concept of utility is its axiomatic properties and the largevolume of both theoretical and applied work that has shown its consistency to desinbehuman preferences. Similarly to other HSI, utilities are expressed between 0 (death) and 1(perfect health). For an individual at a state of less than perfect health, e.g. hypertension,the estimation of the corresponding utility is obtained by what is known as the standardgamble. The person is offered a gamble of undergoing a hypothetical therapy which willrestore perfect health ( with a certain probability, say p = 90 %) or suffering immediatedeath, with the complementary probability, ( 1- p = 0.1, in this case). If the individualdoes not accept the gamble, the probabilities are readjusted and another gamble is offereduntil a point of indifference is reached. At this point, the probability p represents theutility of the particular health state considered. It might be possible then that a similar stateof health might have different utility for different individuals. Not surprisingly, one of themain applications of this concept has been as an outcome measure for clinical decision-making for individual patients [36]. Although utilities have been elicited from real patientsin some studies, in the m ajority of cases studies have adopted proxies which have notpersonally experienced the health states considered.
7
For health policy making it is necessary to have indicators of health that can be apiied topopulations rather than to a single person. In this regard it is important to note thautilities have been aggregated to represent "group utilies", although, from a theormicalstandpoint, very restrictive axioms are required to support this approach [37].
The HSI mentioned above reflect the heaklth condition of one individual (or group ; at acertain moment in time. The extension of this individual's life is also important. Txpically,during one's life there will be sudden reductions in health status, represented by episodesof disease, with return to full health (HSI = 1.0) or to a reduced value. Throughour the lifespan, the average health status will then be given by the area under the curve of uiity Vs.time. This concept, that both quality and duration of life have to be considered has beenadopted by a number of analysts in the past giving way for what is nowadays callea thequality-adjusted life years (QALY) approach In this context the term "quality of fe" isused as a synonym of health status, it differs from the more general concept and esimatorsadopted in socio-economic studies which usually include other dimensions such as livingconditions, ownership of certain goods, access to services, and so on [38].
In principle, any of the HSI mentioned above, standardized to the 0-1 scale, can be used asthe quality adjustment for the life-years remaining to one individual/population orgainedulost as the result of some intervention/policy. Afer multiplication the indinidualfactors are usually lost, the resulting number of QALYs reflects the intrinsic assumntion ofthis approach, that quality and extension of life are interchangeable quantities. Thevalidity of this assumption across different populations remains to be established. Other echaracteristics of the QALY indicator have also troubled analysts. One is the fact that aQALY gained as the result of some intervention is independent of the individual's age.Moreover, the same QALY can either be gained by two individuals which improve theirhealth status by a value of 0.5 during one year or by ten other individuals improving theirquality of life by a factor of 0.1. These limitations of the QALY approach generateconsiderable ethical concerns and the possiblity that the resulting policies will lead toinequity.
One modification of the QALY indicator is the disability-adjusted life-years (DALY) inwhich a measure of disability is used to express severity of disease and "life-years"expresses potential years of life lost, that is the difference between the age at death and lifeexpectancy. Consequently the DALY is a negative indicator of health expressing theburden of disease. As noted before, most HSI include disability as one of the dimensionsconsidered, but this is usually comnplemented by other relevant dimensions thatcharacterize the universe of an individual's quality of life. The Rosser Index for exampleincludes distress as its second dimension (Fig. 1). By only considering disability, D.ALYscan be regarded as a more limited version of QALY while suffering from the sameproblems such as the intrinsic assumption that individuals are willing to interchange lessdisability by a shorter life span. As some of the other indices, DALYs can also lead tosignificant distortions when used across non-uniform populations. For an individual with aphysical disability requiring the use of a wheelchair, it makes an enormous differencewhether he/she is middle class, living in an industrialized country, or in a poor comunity
8
A.1
of a less developed country. Since DALYs are usually estimated by standardizedprocedures (e.g. using ICD codes) [39], both individuals could end up having the samennmber of DALYs although they would certainly require different policies adapted to theirparticular circumstances.
The attraction of using the QALY/DALY indicators for health policy-making is thepossibility of identifying health problems and assessing the impact of different policies witha single number that can be used across different population groups, health problems. andmedical specialities. Several studies have shown this possibility by estimnating the cost perQALY of different health interventions or medical procedures. Some of these resurs haveimmediate clear-cut implications for policy-making. As an example, Boyle et aL [40] haveshown that neonatal intensive care costs US$ 2,800/QALY (1978 values) for neonateswith birthweight 1000-1499 g but increases to US$ 19,600/QALY for the birthweightgroup 500-999 g. Much larger differences in cost/QALY have been obtained in otherareas [37].
For the large majority of health problems, the benefits accruing from health careinterventions are likely to be small using as reference the usual health status scale rangingfrom 0 to I [16]. As shown by the values in Figure 1, a very significant improvement in anindividual's quality of life would be represented by an intervention which would movehim/her from V.C to III.B . This represents a gain of 0.972-0.900 = 0.072 QALY for eachyear of additional life. On average, looking across the whole spectrum of health care, notmany interventions are likely to have more significant effects [16]. This observation callsattention to the risks of comparing QALY studies using different HSI for expressmg thequality of life factor. The scales are not the same and one individual who is at Q = 0.9 inthe Rosser scale might be either at 0.95 or 0.70 in another scale. This can introducesubstantial distortions for inter-study comparisons which use different HSI for calculatingQALY/DALY. Therefore, accuracy is an essential requirement for QALY/DALYindicators and, hitherto, there is not enough evidence that this can be satisfactorihlachieved. Many studies dealing with clinical decision-making or health technolonyassessment use sensitivity analysis [15,36] as a tool to characterize the degree ofuncertainty of their results. This approach should become mandatory in any studiesinvolving estimations of QALY/DALYs such as the calculation of cost/QALY. Evenbetter, the statistical distribution of these indicators should be taken into account andestimated values should always be quoted with their 95 % confidence limits to avoid themisleading impression of accuracy given by the number of decimal places frequentlyquoted in these estimations (Fig. 1).
One recent application of the DALY method, which can be criticized from the aboveargument, is the World Development Report [39]. Usming mortality data according to theICD groups, analysts estimated the corresponding level of disability for each cause ofdeath using a 6 level disability scale. To begin with, it is highly questionable whether 6levels give enough discrimination and accuracy to describe the whole spectrum of qualityof life. Secondly, whether it is reasonable to classify all individuals with the same condition(or cause of death in fact) with a uniform level of disabilty. It could be argued that, in an
9
attempt to overcome the limitations of mortality data to express the burden of disdase, theDALY method is in fact introducing distortions which end up destroying the reliableinformation represented by mortality statistics. The same risk obviously also affe=sQALYs with whatever HSI adopted to estimate quality of life. Once more North-Southdifferences have to be considered because the distortions that can be introduced areproportional to the variability of life expectancy of different populations. In counties withvery uniform populations and long life expectancies, such as Japan and the Scandinaviancountries, the benefits of adopting the QALY/DALY approach might outweigh the risksmentioned above. This is certainly not the case in countries with population sub-groupsshowing differences in life expectancy of up to 20-30 years as frequently observed in thedeveloping world [39].
5. Alternative approaches to the characterization of health
The search for a single indicator that can express the complexity of the phenomena ofhealth/disease results from an intrinsic difficulty of collecting/analysinglinterpretingmultidimensional data. The same difficulty applies to other variable/dimensions: populationsub-groups, geography, or the effect of time. As a consequence, one frequent simpiifyingapproach is to pool data from different individuals, regions, periods of time. Thelimitations of this procedure are well known, it is important however to highlight theinformation "destroying" characteristics of pooling data for health policy-makiing. This isparticularly relevant for countries with large socio-economic disparities which shouldrequire a more refined and disaggregated process of health policy-making taldng mratoaccount regional and cultural specificities. Consequently, the role of the local versus thecentral level of planning and the choice of the appropriate degree of data/informationaggregation are important topics to be tackled by HPR. Interestingly enough,technological developments might have a strong influence on this dilemma with theappearance of Geographical Information Systems (GIS). The enthusiasts of this approachclaim that all future health information systems will be GIS. This might actuallv be true insome areas such as primary health care [41-42]. Ifthis is the case, GIS might have aradical impact on current dynamics of health planning and policy-making. The linkbetween geography and health has long been established [19] but it is only relativelvrecently that computer technology has allowed usefuil dynamic applications of spaio-temporal analysis [43]. Initial applications have focused on rural epidemiological orepizootic problems but the same approach can be extended to urban areas with thepossibility of representing individual dwellings and the corresponding health records of itsinhabitants. For cities/regions with large disparities in infrastructure such as water supply,sewage, health services, schools, and so on, GIS are clearly a very powerfil tool for healthpolicy-making and will probably dictate the way information will be collected and analysedfor this purpose.
Other technological developments also have to be considered. In particular, analvticdevelopments in systems analysis and cognitive sciences allow several alternatives for the
10
A.1
analysis and interpretation of multivariate and multiattribute information. These methodshave considerable potential for HPR but require a concerted research effort to expioretheir applicability and limitations. A pioneer study in this direction was performed bvAttinger and Ahuja on the effects of socio-economic change on health levels [3]. Withreference to the World Bank study mentioned previously [39], there is no reason 4why theanalysts could not have kept the two dimensions, disability and life-years lost, as separatevariables throughout the study without altering its objectives. The advantages wouid betwo-fold: In the first place this would avoid the risk of corrupting the mortality dira withless exact estimations of disability. Secondly, by keeping the two dimensions separated, itwould be easier to formulate health policies which are more specific to each dimenion indifferent countries. The same can be extended to the information used to obtain QALYsusing utility, the Rosser index, SIP, or other HSI. In this case some indices, such as SIPwill generate more than 2 or 3 dimensions but this can be easily accommodated byanalytical techniques.
The most conspicuous technological development of the last decade is certainlv th.affordability of microcomputers of high computational power and data storage capacity.This is already having a dramatic effect on the way health data is collected at the locallevel, but other applications on HPR are lagging behind. Limiting our discussion to theinformation requirements of HPR, it is not too farfetched to imagine a scenario in whichcomputer based records will be available for each individual and will be used both for PHCat the local level and integrated for analysis and policy-making at more central levelswithout the need to pool and destroy information. No technical difficulties lie in th. wayfor this approach. Optical disk technology allows storage of individual records (iithread/write possibility) for less than US$ 1 per person. The major difficulties, andadditional costs, lie with the social engineering aspect of this project, that is the necessarymanpower, infrastructure, and organization [44]. Against opposition and lack of politicalwill, it should be argued that the health sector deserves at least the same tools used by theInland Revenue services, including those of some developing countries.
The possibility of having computerized individual health records for each citizen bringsadditional problems of data confidentiality but also opens new avenues for research onhealth policy. As an example, it should be possible to explore the feasibility of a healthhneeds based approach where the gross national requirements are obtained as thesumnation of individual needs. The knowledge required for this enterprise is not entirelyavailable, more research is needed on forecasting health service and multisectorial needsfrom personal data comprising the individual's health history, age, socio-economicconditions, and genetic risks. One clear advantage of this approach though is on thedevolution stage when the same records can be regionally disaggregated until the actualdelivery of services is provided. Intermediate levels of decision-making, e.g. on the controlof children's immunization, can improve the efficiency of the system.
11
Undoubtedly, this scenario of integrated personal computer health records is more realisticfor industrialized countries, not only because of the resources required, but mainIv becauseof the difficulties of acquiring the appropriate data in developing countries. Furthermore,because of the alienation of the most socially deprived sectors of the population in thesecountries, there are serious risks of exacerbating existing problems of inequity by underrepresenting the health needs of these sub-groups of the population. Developing countriesneed immediate action regarding policy-making to improve resource allocation to promoteimprovements in health conditions. As mentioned previously, in many of these countriesmortality data can still be the main source of information, for example by calculatingpotential years of life lost in comparison with more developed countries. However.disaggregating these data at the neighbourhood level will remain a problem for someconsiderable time until more efficient information systems can be implemented. On-epossibility to improve upon this situation, which remains almost unexplored in the healthfield, is the use of a new group of techniques belonging to the emerging field ofKnowledge Based Engineering.
For a moment let's return to the estimation of utility described previously to express thequality of life factor of the QALY indicator. Torrance and Feeny (37) have emphasizedthe importance of interviewing expertise to elicit consistent estimates of utility from agiven individuaL This experience is important, for example, to conduct the standardgamble exercise. If probabilities/utilities of say, 0.8 and 0.9 have not been previouslyaccepted, the interviewer will have to judge, from previous answers, whether to offer thenext gamble at probabilities of 0.825, 0.850, or 0.875. Furthermore, he/she will have todetect when the point of indifference, which will determine the definitive expression ofutility, is reached. As a result, lack of experience can lead to gross errors in technique.This example shows that the calculation of QALY for a person or a group of persons, isnot an absolute measurement, but an estimate which depends on the person's values andpreferences and, also, on the interviewer's experience, knowledge, and ability to interpretsemantic information as manifested by the individual/patient. We should not be shocked bythis observation since the interpretation of semantic information as expressed by thepatient has a long history in the evolution of Medicine [45]. In the 17th centurv ph.yxsiciansused to conduct anamnesis by only listening to their patients or even by only reading theirletters [45]. Despite the technological revolution in diagnostic armamentarium. patient'ssymptoms are still an important element of the clinical interview. The physician's role inthe process is one of acquiring, analysing, and interpreting information of different nature,including semantic and visual information, to classify his/her patient in a particular state ordiagnostic category. Therapeutic management of this patient will depend ofthisclassificatory process.
On a different level of the hierarchy of living systems, when dealing with a population ofindividuals, or a community, the same principles apply to health policy making ashighlighted in Section 3 above: we need to classify this community and select theappropriate policies to move from state A (e.g. poor health level) to state B ( improved
12
A.1
health level). Ideally we would like to conduct the most objective and accuratemeasurement of the health status of this community. However, as discussed at the outset,this is not possible, and we have to resort to HSI which work by either interpretingsemantic information ( iLe. questionnaires), subjective judgement (Rosser index), or expertinterpretation of individual preferences (utilities). Therefore, to a considerable exint, weare already making use of information that is not entirely objective and not generamd by adirect method of measurement. Can we complete the many gaps in the informantionavailable by "asking" this community where it "hurts" and how its pains are affected byother factors ? Can visual/convivial information be added and extended by ComnnmityHealth Workers with experience in this community ? The answer to these questions is aresearch hypothesis well worth pursuing. The mnain reason is the situation of developingcountries as discussed before, in which availability of data/informnation to support healthpolicy making is still a considerable problem. A Comnunmty Health Worker might not beable to put precise numbers on the incidence/prevalence of different conditions in his/hercommunity but he/she will be able to describe into words its deficiencies, needs. resources,strengths, and to rank different problems. Knowledge Based Engineering techniques cantransform these statements into attributes which will allow the characterization of thatcommunity. The expected benefit of different interventions can also be ranked andpriorities can then be identified [46]. It is important to stress that the methods requiredfor this exercise have been available for some time now and are increasingly used inindustry and business applications.
The possibility of automating medical diagnosis by feeding patient's data into a computerhas been shown for a number of different conditions with very convincing results in termsof diagnostic accuracy [47-48]. Different mathematical techniques can be adopted for thispurpose, some examples are decision-trees, bayesian statistics, expert systems. naurallanguage processing, and neural networks. One important distinction among thesemethods is the amount of data required. In one extreme is bayesian statistics, requiringmassive amounts of data for most realistic applications and, in the other, expert systems,which can rely mainly on information extracted from one or more experts thus mmnnizingthe dependence on external information. The same analytical tools could be used forcommunity-wide applications. Other related methods, such as operations research [17,18]and qualitative clustering would also be of value, for example to support resourceallocation [15]. In fact, although the reasoning above has concentrated on the "diagnostic"stage, there is no theoretical reason to dismiss the possibility of using Knowledge BasedEngineering methods to all nine steps of the health policy planning process outlined insection 1. Although there is growing interest in the application of these methods tomedical decision-malking, HPR has not received a fraction of the attention it desen es.
13

6. Conclusions
Research on Health Policy requires a very large effort to collect and disseminateinformation that can be used as a basis for a more rational process of planning anddecision-making. Characteriing different levels of health/disease is one aspect ofparticular importance to allow the appropriate identification of health problems. priortiesfor action, and the assessment of the impact of interventions. Attempts to express themultidimensional concept of health by single indicators, such as QALY/DALYs need to becarefully assessed. Such indicators are based on assumptions that are not generliable,can be objected on ethical grounds, and can lead to distortions because of liitations inaccuracy. Advances in Systems Science pre-empt the use of such indicators andmultivariate techniques can be used to manage the complexity of the representation ofhealth/disease while leading to more specific policies. The scarcity and historicaldifficulties of collecting/disseminating appropriate information in developing countiesneeds to be urgently addressed. Knowledge Based Engineering techniques offerconsiderable potential as an alternative approach that can lead to short-term improvemrnentsin policy-making in these countries.
7. References
1. WHO (1994) Report to the Director General, Advisory Comnmittee on HealthResearch. Report 32/94.22, Geneva, World Health Organization.
2. WHO (1993) Researchfor Health Principles, Perspectives and Strategies. AdvisoryCommittee on Health Research, Geneva: World Health Organization.
3. Attinger EO and Ahuja DR (1980) Health and Socieconomic Change, IEEE Trans,Syst. Man, Cybern. 10:781-796 e
4. Brenner MH (1979) Mortality and the national economy, Lancet 568-573
5. Restrepo HE and Rozental M (1994) The social impact of aging populations:Some major issues. Soc. Sci. Med. 39:1323-1338
6. Evans RW (1983) Health care technology and the inevitability of resource allocationand rationing decisions. JAMA 249:2047-2053
7. Doll R (1987) Major epidemics of the 20th Century: from Coronary Thrombois toAIDS. J.R. Statist. Soc. A 150(4):373-395
8. Walsh JA and Warren KS (1979) Selective primary care. An interim strategy for l
14
A.1
disease control in developing countries. NEJM 301:967-974
9. McKeown T (1983) Abasisforhealth strategies. BritishMed J. 287:594-5%.
10. Frenk J, Bobadilla JL, Sepúlveda J, Cervantes ML (1989) Health transition in middle-income countries: new challenges for health care. Health Policy and Planzung 4:29-39.
11. Attinger EO (1988) Societal systems, technology and health. Geneva: WorldHealth Organization
12. Panerai RB (1985) Multisectorial Determinants of Health in Brazil. Progress Report.Division of Biomedical Engineering, Charlottesville, VA: University of Vrmia.
13. Gismondi RC, Almeida RMVR, Infantosi AFC, Panerai RB (1994) Interactivecomputer-aided system for health determinants modelling. Physics in Medicine andBiology 39a:536
14. Department of Health (1989) Health Service Indicators Guidance: Dictionz,-..London: Her Majesty's Stationery Office.
15. Panerai RB and Pena-Mohr J (1989) Health Technology Assessment Methodologiesfor Developing Countries. Washington, DC: Pan American Health Organization,pp 109
16. Bunker JP, Frazier HS, Mosteller F (1994) Improving Health: Measuring Eff-ects ofMedical Care. The Milbank Quarterly, 72:225-258
17. Chen MM and Bush JW (1976) Maxmizing health system output with political andadministrative constraints using mathematical programming. Inquiry XIII:215-227
18. Portela MC and Panerai RB (1989) - Decision support system for resourceallocation in perinatal care. Proc. MEDINFO 89 Conference, Amsterdam' NorthHolland, pp 317-321.
19. Dubos R (1965) Man Adapting. New Haven: Yale University Press.
20. Illich I (1976) Medical Nemesis. The Expropiation of Health.New York: Random House
21. Hollandsworth Jr JG (1988) Evaluating the impact of medical treatment on thequality of life: A 5-year update. Soc. Sci. Med. 26:425-434
22. Falotico-Taylor J, McClellan M and Mosteller F (1989) The use of quality of lifemeasures in technology assessment. In Quality of Life and Technology Assessment.Washington DC: National Academy Press, pp 7-44
15
23. Palta M, Gabbert D, Fryback D et al (1990) Development and validation of an indexfor scoring baseline respiratory disease in the very low birth weight neonate.Pediatrics 86:714-721
24. Ross MG, Hobel CJ, Bragonier JR et al (1986) A simplified risk-scoring s-stemfor prematurity. Amer. J. Perinat. 3:339-344.
25. Langfitt TW (1978) Measuring the outcome from head injuries.J. Neurosurg. 48:673-678.
26. Cullen DJ, Civetta JM, Briggs BA et al (1974) Therapeutic intervention scortlasystem A method for quantitative comparison of patient care.Crit. Care Med. 2:57-65
27. Knauss WA, Draper EA, Wagner DP, Zimrmernman JE (1985) APACHE II: Aseverity of disease classification. Crit. Care Med. 13:818-828
28. Pollack M, Ruttiman E, Getson PR (1987) Accurate prediction of the outcomeof pediatric intensive care: A new quantitative method. NEFM 316:134-139.
29. Bergner M, Bobbit RA, Pollard WE, Martin D and Gilson BS (1976) The SicknessImpact Profile: validation of a health status measure. Med Care 14:57-67 e
30. The EuroQol Group (1990) A new facility for the measurement of health-relatedquality of life. Health Policy 16:199-208
31. Padilla GV, Presant C, Grant MM et aL (1983) Quality of life index for patientswith cancer. Research in Nursing and Health 6:117-126
32. Rosser R and Kind P (1978) A scale of valuation of states of illness: Is there asocial consensus ? Int. J. Epidem. 7:347-358.
33. Kaplan RM and Anderson JP (1988) A general health model: Update andapplications. Health Services Research 23:203-235.
34. Gudex C and Kind P. The QALY toolkit. Discussion Paper 38, Centre for HeahhEconomics, University of York.
35. von Neumann J and Morgenstemn O (1944) Theory of gamnes and economic behavior.Princeton, NJ: Princeton University Press.
36. Weinstein MC, Fineberg HC et al. (1980) Clinical Decision Analysis.Philadelphia. PA: WB Saunders.
16
A.1
37. Torrance GW and Feeny D (1989) Utilities and quality adjusted life years.Int. J. Techn. Assess. Health Care, 5:559-575.
38.McGranahan DV, Richard-Proust C, Sovani NV et al (1972) Contents andMeasurements of Socioeconomic Development. New York: Praeger.
39. World Bank (1993) World Development Report 1993. Investment in Health.Oxford: Oxford University Press.
40. Boyle MH, Torrance GW, Sinclair JC and Horwood SP (1983) Economic evahiationof neonatal intensive care of very low birth-weight infants. NEFM 308:1330-1337.
41. Nobre FF, Lahtermaher D, Macedo MMA (1991) A geographical information systemfor epidemiological surveillance. Proc. Annual International Conference of the EEEEngineering in Medicine and Biology Society 13:1208-1209.
42. Matos HJ, Nadal J, Panerai RB (1994) A geographic information system fornutritional surveillance in primary health care. Physics in Medicine andBiology 39a:552
43. Sayers BMcA, Mansourian BG, Phan Tan T, Bogel K (1977) A pattern-analysis studyof a wild-life rabies epizootic. Medical Informatics 2:11-34.
44. Ayres RU (1985) Social technology and economic development.TechrL Forecasting Soc. Change 28:141-157.
45. Reiser SJ (1978) Medicine and the reign of technology.- Cambridge: Cambridge University Press.
46. Panerai RB, Almeida RT, Portela MC et aL (1991) Estimating the effectiveness ofperinatal care technologies by expert opinion. Int J Techn Assess Health Care7:367-378.
47. de Dombal FT, Leaper DJ, Staniland JR et al. (1972) Computer-aided diagnosis ofacute abdominal pain. BMJ 2:9-13.
48. Shortliffe EH (1976) Computer based medical consultations: MYCIN.New York: Elsevier Publishing Co.
17
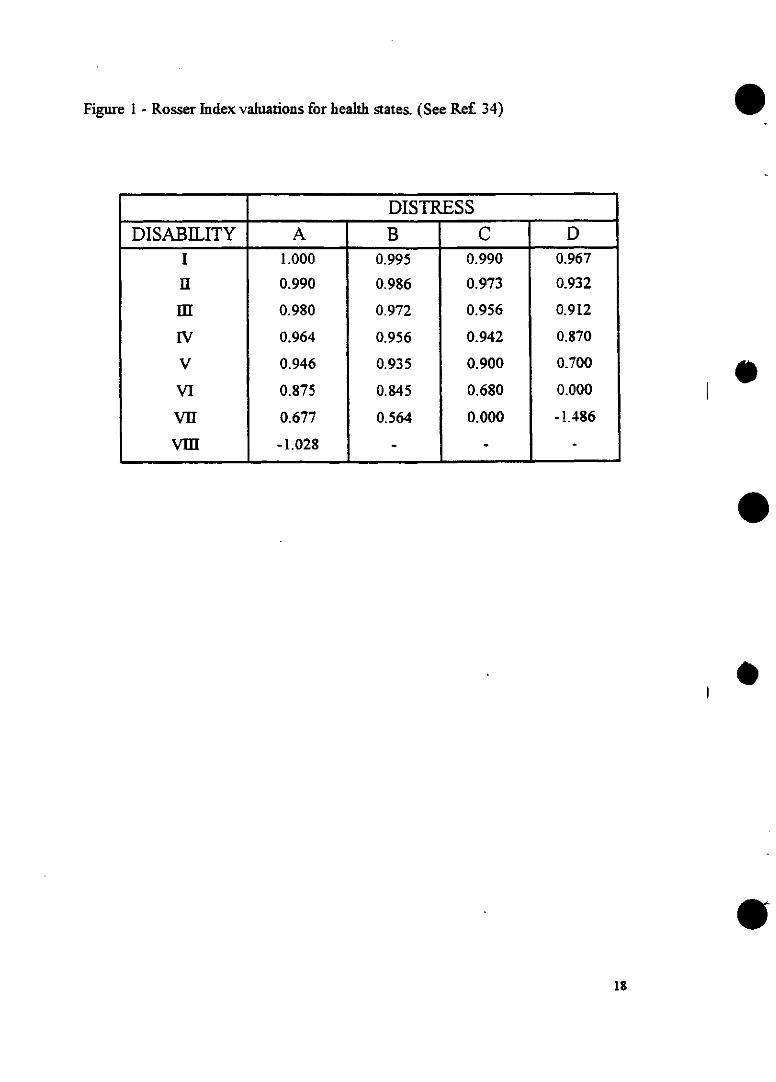
Figure 1 - Rosser Index valuations for health states. (See Ref 34) 0
9
DISTRESSDISABILITY A B C D
I 1.000 0.995 0.990 0.967
uI 0.990 0.986 0.973 0.932
111 0.980 0.972 0.956 0.912
IV 0.964 0.956 0.942 0.870
V 0.946 0.935 0.900 0.700
VI 0.875 0.845 0.680 0.000
VII 0.677 0.564 0.000 -1.486
VIII -1.028 - -
e
0
18
,y 3 WORLD HEALIH ORGANIZATION
'~ 4~ ORGANISATION MONDIALE DE LA SANTE
> ADVISORY COMMITTEE ON HEALTH RESEARCH
Thirty-third session
Geneva, 17 - 20 October 1995
ANNEX 2 DISTR.: RESTREINTE
ACHR33/CRP/95.1
ENGLISH ONLY
Agenda item 6
REPORT OF WORKING GROUPS OF ACHR
DALY REVIEW GROUP
The contents of this restricted document may not be divulged topersons other than those to whom it has been originally addressed. Itmay not be further distributed nor reproduced in any manner andshould not be referenced in bibliographical matter or cited.
Le contenu du présent document á distribution restreinte ne doit pas étredivulgué á des personnes autres que celles á qui ii était initialement des-tiné. II ne saurait faire I'objet d'une redistribution ou d'une reproductionquelconques et ne doit pas figurer dans une bibliographie ni etre cité.
A.2
Commentary on the DALY concept
General observations
1. Health and disease are complex phenomena; but the practical problems ofcollecting, analysing and interpreting the multidimensional data needed toexpress their complexity are severe. This is the reason behind the search for asingle indicator that will capture the important elements contributing to thetotal burden of ill-health.
2. The DALY is a new indicator purporting to express the burden of diseaseand disability in quantitative terms. It attempts to assess the totality of yearsof life lost due to premature mortality, combined with the years "lost" due toliving with a disability. It employs life tables to estimate expected years of lifelost by premature death; incorporates the supposed "social value" of timelived at different ages by a time-related weighting system; makes time livedwith a disability comparable with time lost due to mortality by defining sixclasses of severity of disability; and utilises a "discount rate" in respect ofexpected future health benefits. It pools much data on different types ofdisease and disability, on many individuals in different regions and socialenvironments, and consequently obtains the benefits and suffers the defectsof information aggregation.
3. The development of the DALY methodology is a considerable technicalachievement. The detailed debate which its appearance has generated isevidence of the wide range of ideas, concepts and mathematical elements thathave been utilised. A detailed discussion has been published to explain thechoices involved in formulating the descriptive equations and the parametervalues selected. As an attempt to produce a single coherent index from twomajor health status variables, it evidently constitutes a potential advance thatrequires serious examination.
4. The DALY approach incorporates disability (which is not handled, exceptas the final outcome, by mortality measures) in the overall burden of diseaseassessment; insofar as a single indicator is desirable, this is practicallyadvantageous because the disability contribution is claimed to be significant(Murray et al. estimate 34%). It necessitates expressing disability on the samebasis as mortality; however, for somrne critics, this raises both ethical andpractical difficulties. These matters are resolved by some in pragmatic terms,on the grounds that decisions on the rational use of money resources for theprovision of health care commonly assume a unidimensional description ofhealth outcomes; however, there are other viewpoints (see below).
5. Equally, the procedure of weighting the "value" of years lost, by prematuredeath or the onset of disability, according to age is a focus of much debate.The argument in favour is not yet convincing. Murray's view of this issue issimplistic, adopting unequal age-weights to "capture different social roles atdifferent ages", accepting the relevance of "the concept of dependency andsocial role" but "not linked to total income levels". But adopting this position,
A.2
the weighting to be assigned to different disabilities is then determined on anoperational basis that uses "... limited ability to perform activities in one/twoor more/ all of the following areas: recreation, education, procreation oroccupation." This suffices, together with the age-weighting used, in thepresent formulation of the DALY, to account for the effect of the disability.But it classifies all individuals with the same condition with a uniform level ofdisability, which has yet to be justified, and it does not include the economicfactor attributable to resource cost.
6. Indicators that refer only to a single disease or disability are of limited usesince they can be applied to few individuals at any one time. What is neededis an indicator that can accommodate multiple health problems and soprovide a picture of health status of a population. There have been manyattempts to overcome the intrinsic limitation of using only mortality data, bydevising multi-dimensional indicators that can reflect the physical, social andpsychological dimensions of health, although most of these are applicableprimarily to individuals. Some of these health status indices attempt toclassify on each dimension quantitatively: they include the Sickness ProfileIndex, Euroqol, Nottingham Health Profile, Quality of Life Index, RosserIndex, Quality of Well Being Scale. Most employ a questionnaire approach toestimating in each dimension, then a weighting of dimensions to achieve asingle number.
7. Many health status indices include disability as one of their dimensions,and in some cases these are also complemented by other relevant dimensionsthat characterise the universe of an individual's quality of life. However, forhealth policy making and resource allocation it is both desirable to have aunidimensional (single number) indicator and necessary that the indicatorcan be applied to populations rather than to individuals.
8. The QALY is one of the population health indicators which, in acceptingthat both quality (in the health context) and duration of life have to beconsidered, utilise one or other of the health status indices mentioned above;it assumes that quality and extension of life are interchangeable quantities.The validity of this assumption across different populations remains to beestablished. The same QALY figure can be gained by two individualsimproving their health status by a value of 0.5 (on a scale 0-1) during oneyear, or by ten other individuals improving their quality of life by 0.1; doesthis generate confidence in decision-making? These limitations of the QALYapproach generate considerable ethical concerns and the possibility that theresulting policies (for intervention) will lead to inequity.
9. The DALY is a restricted modification of the QALY approach. It stillinvolves the implicit assumption that individuals are willing to interchangeshorter life span and less disability and, like the QALY, suffers fromdifficulties as discussed below; nevertheless, it constitutes a usefuldevelopment.
2
A.2
Some problems with the DALY
10. There are several difficulties with the DALY, in concept and in practice.First, it is a combination of unlike elements (due to mortality and todisability). Social value is attached to years lost due to death, and years "lost"due to life with a disability. But one should not disregard the intendedapplications of DALYs in thinking about their structure and legitimacy. It is afundamental feature of the DALY approach that: (Murray, p430) "To theextent possible, any health outcome that represents a loss of welfare shouldbe included in an indicator of health status ..... In other words, if society wouldbe willing to devote some resources to avert or treat a health outcome, thatoutcome should be included in the total estimated burden". The resource costof the "health outcome" should then enter into this calculation.
11. The resource cost alters with the nature of the disability and thelocal/regional/country circumstances. For instance, a health outcome thatdisables a young adult may prevent him from gainful employment. In anyevent, there is a welfare cost for the individual's support; and if employmentwould have been available to an able-bodied individual, then the nett resourcecost of the disability must also take account of the loss of his contribution toGDP. (This position is reflected in the so-called human capital theory, whichregards humans as machines with costs of maintenance on the one hand andproductive output on the other.) In view of the way the DALY is intended tobe used for resource allocation, economic value is associated with these twoelements and the DALY needs to be improved to incorporate nett resourcecost estimates.
12. When applied in heterogeneous populations, DALYs may producesignificant distortions that may lead to poor policy-making or resourceallocation. Individuals with particular disabilities, for instance, may be quitedifferently disadvantaged in poor communities of a less developed countryby comparison with those within more prosperous groups in anindustrialised country. Pursuing the point, is it reasonable to classify allindividuals with the same condition as having a fixed level of disability, andin any case, is it adequate to limit the classification of disability to six levels?
13. Those who prefer to consider resource consequences rather than ethicalimplications see no difficulty in combining the two elements of mortality anddisability as predicated for the DALY. However, there would be advantagesin keeping the two elements separate. It is accepted that mortality data isboth easier to obtain than disability data, even disregarding the problems ofturning the latter into their DALY contribution, and of better quality.Separating the two elements would prevent inevitably inexact estimates ofdisability from corrupting mortality data. Technically, keeping separate thetwo elements: years lost due to mortality; years "lost" due to life with adisability: is easily achieved. By keeping the two elements separate, it wouldbe easier to formulate health policies which are more specific to each elementin different countries. Further, there are circumstances in which the raweconomic "cost" of a death is small, whilst that due to a disabling but not life-
3
A.2
threatening condition may be large, and doubtless vice versa in othercircumstances. For some applications, maintaining this separation could bedistinctly advantageous, and would remove one of the existing sources ofdifficulty with the DALY.
14. But even so, the mortality data of various countries are not yet fullyreliable as far as the causes of death are concerned: these causes are oftenintricate. Assessment of disability is even more problematical for severalreasons: poor existing epidemiological basis; great variability as to possiblecompensation; perception and personal response to the disability by thedisabled, by the family, by neighbours and by the community. The poorquality and extremely limited availability of data may prove to be an over-riding factor.
15. Second, the DALY approach does not yet accept a multi-determinantorigin or a multi-pathology character of disease. Even communicablediseases are complex, occurring in individuals with different health,nutritional and social status before the onset. In non-communicable diseasesthe situation is even more complicated because this multifactorial character isthe rule, as it is for injuries. Moreover, especially in the poor, in the elderlyand even more so in developing countries, a given disease is seldom isolated;multi-pathology is common.
16. The same difficulty occurs when the DALY is employed to estimate theburden of disease attributable to a variety of risk factor exposures. How doesone use a DALY approach to translate epidemiological knowledge onmortality and morbidity into the needed intervention without taking intoaccount powerful determinants of psy.chosocial, economic and legal kinds?Limiting the DALY, as an indicator of health status, to immediatedeterminants of disease or disability does not accommodate the more remotebut not necessarily less powerful contributions due to such factors as poverty,poor education, inadequate housing, undesirable social conditions, socialsupport and community participation in care programmes.
17. Third, the structure of the indicator and the precise weighting to beattached to the so-called "discount" by which the "value" of later years isincreasingly reduced, is subject to uncertainty and debate. Different cultureswould undoubtedly take different views on this matter, and even within apopulation, very different attitudes will be taken to disability and verydifferent problems will be experienced by comparably disabled individuals indifferent communities, regions or countries. Again in economic terms, are allDALYs equivalent across a population with economically active and inactivepopulation groups? The fundamental difficulty here is another effect ofheterogeneity, a difficulty which is rarely well handled in theoreticalepidemiology. In consequence, while detailed improvements in formulationof the DALY through adjustment of its various parameters can be made, it -would still be difficult to justify comparisons of DALY counts betweencommunities, regions or across country boundaries.
4
A.2
Utilisation of the DALY approach
18. The attraction of using a DALY type indicator for policy-making is thepossibility of identifying health problems and priorities, and assessing theimpact of different policies with a single number that can be used acrossdifferent population groups and health problems. Resource allocationdepends upon policies that identify priorities in the light of complexcircumstances and demands, including specific health needs. So primaryapplication areas for a DALY-type indicator are in assisting resourceallocation, internationally and nationally, to achieve effective interventions atthe public health level, and in supporting research to improve policies andrefine the resource allocation process.
19. But applying any methodology, including the DALY, for decision-makingrequires good-quality data, and this is likely to remain a major problem: forinstance because official country data is often highly unrepresentative andsubstantial regional differences often exist within countries, while redefinitionof categories and diagnoses in the pursuit of accuracy creates difficulties ininterpreting serial data. Not surprisingly, a substantial proportion of the dataused so far has been generated by modelling or by expert guesswork.
20. If suitable data were to become available to allow the DALY to beapplied, then verification, validation and utility can be considered: does theapplication work as intended; is it possible to validate the results; and howeffective is the method in comparison with any alternative? It is not yet clearhow any of these questions can be answered. However, there may be a placefor simulation in testing the utility of the approach.
5
A. 2
Conclusions and Recommendations
21. The Review Group submits the following conclusions and recommendations tothe ACHR:
i. The DALY is a methodology for aggregating data about health outcomes -specifically, mortality and disability - into a single number which is proposed as,
in principle, a guide for decision-making about cost effective and prioritiesinterventions. The calculation of the DALY is carried out, in effect, in economicterms.
ii. The development of the DALY is a considerable technical achievement.Its conceptual basis and structure have been, for the most part, clearly laid out.This reveals that there are many points of technical detail which needreconsideration. Certain of the assumptions are controversial and still in debate.The formulation of the DALY is, therefore, not yet mature.
In particular, the technique purports to assign a "value" to human life, a"value" which varies according to age in a complex manner. If the intended useof the DALY is to calculate financial implications for society of the incidence ofdeath or disability, this technique might be defended. If the "value" is intendedto express a "social" concept, as appears to be true for the current form of theDALY, then ethical issues must be involved. The Review Group recommendsthat CIOMS be asked to investigate the ethical aspects involved.
iii. Suppression of information always accompanies data "pooling". In theDALY, "pooling" takes place in two ways: by aggregating healthy life years lostdue to mortality with those due to disability; and by aggregating data acrossregions of a country which may experience quite different physical and socio-economic environments. The DALY methodology could be extended to allow itstwo elements (mortality and disability) to be carried separately through thecalculations
and presented in a way that is clear to, and readily handled by, users. This wouldsignificantly improve the potential practical utility of the DALY-type approach.
The distorting effect of heterogeneity of the population on the DALY inits present form risks poor policy-making or resource allocation. This difficultymight be resolved by the design of multi-dimensional indicators and if researchon the DALY-type methodology were to be continued, the scope for suchdevelopments should be considered, as a basis for more illuminating descriptionsof health status.
iv. A major hurdle yet to be overcome is the insufficient availability of theextensive, good quality data needed by the methodology. On the other hand,attempting notionally to use the DALY in practical situations may help to definethe data most urgently needed.
6

A.2
v. The Review Group strongly discounts the value of the DALY for settingresearch priorities. Furthermore, verification of the methodology (that it doeswhat it purports to); validation of the underlying concept (that the DALYindicator does provide a valid basis for decision-making); and assessment of itsutility in practice (in comparison with other methodologies); are all yet to beachieved. There is a case for continuing research on DALY-type indicators forpurposes of describing health status, or different forms, for research prioritisation;such work would require multidisciplinary contributions.
vi. A DALY-type methodology would need very careful and well-informeduse. Its users need to understand that, in its present form, it fails to accommodatethe multi-factorial nature of disease, the existence of long-standing as well asimmediate determinants of disease, or to recognise the common situation thatmultiple pathologies can and do co-exist.
vii. Subject to the above, the ACHR could commend this technical advance.ACHR could properly encourage the refinement, development and extension ofthe DALY-type approach, based on appropriate research, and the verification andvalidation - in practice - of the result. It should positively discourage use of theDALY in its present form, without full cognisance of the limitations expressed,especially those in iii and vi above; it should also discourage the untimely use ofthe DALY for allocation of resources for the attempted improvement of health.
Acknowledgement
In discussing the DALY concept and preparing this Report, the ReviewGroup appreciated the assistance of detailed reviews by technical experts: inparticular, Dr Norman T.J. Bailey (Geneva); Professor N.E. Day (Cambridge),Professor J. Doroszewski (Warsaw); Dr Donald F. McGranahan (Geneva); and DrRonney B. Panerai (Leicester)
7
1 NWUKLDL HEALIH URUANIlAIIUN
ORGANISATION MONDIALE DE LA SANTE
ADVISORY COMMITTEE ON HEALTH RESEARCH
t ~Thirtv-third session
Geneva. 17 - 20 October 1995
DISTR.: RESTREINTE
ACHR33/95.7
ENGLISH ONLY
Agenda item 7
AD HOC COMMITTEE ON HEALTH RESEARCH RELATING
TO FUTURE INTERVENTION OPTIONS
REPORT OF ACHR PEER REVIEW GROUP
The contents of this restricted document may not be divulged topersons other than those to whom it has been originally addressed. Itmay not be further distributed nor reproduced in any manner andshould not be referenced in bibliographical matter or cited.
Le contenu du présent document a distribution restreinte ne doit pas étredivulgué a des personnes autres que celles á qui il était initialement des-tiné. II ne saurait faire I'objet d'une redistribution ou d'une reproductionquelconques et ne doit pas figurer dans une hibliographie ni étre cité.
ANNEX 3
A.3
REPORT OF THE ACHR PEER REVIEW GROUP
on Draft 2.0
of the Report of the Ad Hoc Committee on
Health Research Relating to Future Intervention Options
1. INTRODUCTION AND BACKGROUND
2. SUMMARY OF CONTENTS
3. DISCUSSION
3.1 Scope and Concepts
3.2 Approaches and Methods
3.3 Proposals and Recommendations
4. CONCLUSIONS
APPENDIX
A.3
-2-
1. INTRODUCTION AND BACKGROUND
This peer review has been commissioned by the Global Advisory
Committee on Health Research (ACHR) at its Thirty-second session in
October 1994. The report of that session had been endorsed by the
Director-General and the Executive Board in January 1995. ACHR had
formally adopted the following statement:
"The ACHR supports research initiatives which promote WHO's programme
objectives. The ACHR equally recognized that it plays an advisory
role to the Director-General and through the Director-General to the
governing bodies. Such advice must be based on scientific merit and
preserve the institutional integrity of WHO.
The ACHR, however, expressed its concern over the process by which
the Ad Hoc Committee on Health Research was formed. It is in WHO's
interest that all initiatives regarding research be coordinated in
order to achieve maximum impact and authority and avoid overlapping.
WHO has mandated the ACHR to perform this coordinating function. By
launching the Ad Hoc Committee without prior consultation with ACHR,
the objective of WHO to have coordinated activities in health
research has been compromised.
However, given the fact that the Ad Hoc Committee has commenced its
work and is under pressure to complete its report by June, 1995, the
ACHR would not wish to cause delays and, as it supports such
activities in principle, offers and recommends to peer review the
report before its publication and endorsement by WHO. It is
recommended that the ACHR appoint a group of experts to undertake
this task" (p. 24 of ACHR32/94.22 Report).
The Ad Hoc Committee, since it first met in March 1994, produced
several working papers and drafts, the latest (but not last one) of which -
draft 2.0 - was formally conveyed for ACHR information and review, on
29 August 1995. Chairman ACHR, Professor T.M. Fliedner, convened the Peer
Review Group (PRG) consisting, in addition to the Chair, ACHR, of
Professor W. Karczewski (member), Professor M. Manciaux (member),
Professor B.McA. Sayers (former member, co-opted) and
Professor A. Jablensky (former Chairman, EUR/ACHR), co-opted).
It is understood that the Ad Hoc Committee report is not to be
considered as a final product and is likely to undergo further
transformations. For this reason, the PRG has difficulty in expressing a
categorical opinion and thus reserves its definitive judgment until a final
report is available.
A.3
- 3-
The PRG carried out its work in the knowledge that a wealth of
background material in WHO had formally dealt with health research
policies. For example, the 9th General Programme of Work (GPW) (para. 64)
states that WHO: "will continue to promote and support health research and
technological development in accordance with its policies and in response
to the health problems in countries. It will identify important bioethical
issues in certain aspects of health research and in their clinical
applications, and will stimulate the exchange of opinion and the sharing of
information in that regard. It will stimulate and support the
strengthening of health research capacity in countries, with emphasis on
affordability and sustainability. By monitoring and analysing advances in
medical, biological and behavioural sciences and health technology it will
seek to identify existing technology that could be used directly or be
further developed to solve significant problems in health care; to assess
new and emerging science and technology for future application in solving
health problems; and to catalyse research to meet known and emerging
needs." And (para. 65): "It will strengthen the collection, assessment
and dissemination of information on cost-effective new methods for health
development. It will explore new ways of intensifying cooperation with the
scientific community and promoting more active involvement and
collaboration."
Prior to adopting the 9th GPW, the World Health Assembly, in 1990,
called for a clearly enunciated health research strategy in order to
translate the research goals, priorities and programmes into coherent and
coordinated action in support of health for all (resolution WHA43.19). To
fulfil this, the Advisory Committee on Health Research (ACHR), drawing on
the work of its own task forces and subcommittees, considered that new
dimensions were needed to give proper emphasis to the infrastructural,
economic, environmental and socio-behavioural aspects of the health
research strategy given in 19861. The earlier statementl interpreted the
goal of "health for all by the year 2000" as aiming to achieve a
substantial improvement in health in all countries, particularly those
where the need is greatest. It stressed that "it is not unrealistic to
define more precisely a level of health below which it is hoped that no
country will fall: infant mortality below 50 (per 1000 live births) and
life expectation at birth of 60 years."'1 These levels were reached in the
middle of this century by the developed countries and more recently in some
developing countries.
The determinants of the global health picture were also described and
the consequential approaches to research planning were discussed,1 based on
the following key observations:
Advisory Committee on Health Research. Health research strategy.
Unpublished document WHO/RPD/ACHR(HRS)/86, 1986.
A.3
- 4 -
* The human genetic constitution is much the same today as it was a
hundred thousand years ago, before the advent of any form of pastoral or
agricultural activity. That is to say, we now face vastly changed
conditions of life with the same genetic equipment of our ancestors who
were hunter-gatherers.
* The modern transformation of health in the developed countries and
the associated increase of populations, which began more than a century
before effective medical intervention was possible, is to be attributed
largely to improvements in living conditions.
* Research has shown us the nature of infectious disease and the
possibility of its prevention by environmental measures and immunization.
e* It has been recognized in the last few decades that most
noncommunicable diseases are also preventable by changes in living
conditions and behaviour; the most striking evidence is the recent decline
of coronary deaths and the findings that most cancers are potentially
preventable.
Specific research efforts should now be focused on: O
control of diseases associated with poverty using well-known,
effective measures and applying existing knowledge;
° control of both infectious and noncommunicable diseases, which are
specific to the tropics, using all available resources including
basic, clinical and epidemiological research;
° control of diseases associated with affluence, using applied research
or, when the influences are unknown, epidemiological research into
the disease's origins;
° treatment and care of the sick, based on biomedical research, O
science and technology;
O delivery of health services (by working with policy-makers and
communities) through the process of assessing needs, planning,
financing and implementing programmes and evaluating them in terms of
coverage, efficiency and effectiveness.
Countries with very limited resources should give higher priority to
research and services in nutrition, immunization and sanitation.
In order to further elaborate the formulation of a WHO health
research strategy, ACHR drew on the work of its own Task Forces and
Subcommittees namely, the Task Force on Science and Technology, the Task
Force on Health Development Research, the Task Force on Evolving Problems
of Critical Significance to Health, the Subcommittee on Health and the
Economy and the Subcommittee on Research Capability Strengthening. The
ACHR considered that although the Health Research Strategy adopted in 1988
is a valid cornerstone of WHO's research strategy, new dimensions should be
A.3
- 5 -
added to give proper emphasis to infrastructural, economic, environmental
and behavioural aspects. The revised strategy focused on the relevance of
economic environment to health, global problems and global solutions,
health research and human development, science and technology policies, the
emergence of new ethical issues and research capability strengthening in
developing countries. It further emphasized the context in which health
research is to be developed: a world in transition, the changing scene of
science and technology, and the importance of identifying research needs on
the basis of health needs. Research capability strengthening at country
level is badly needed, and international cooperation in the field of
constrained resources, that makes it necessary to carefully define health
research priorities. A resume of the report has been published in World
Health Bulletin, 1994, 72(4): 533-538.
2. SUMMARY OF CONTENTS
The report "Investing in health research and development: An agenda
to address problems of the poor" - Draft 2.0 - starts with its own summary,
stressing the benefits of past research and advocating further investments.
It underlines the relationship between health and poverty and illustrates
the task ahead with statistical data on communicable, nutritional and
maternal conditions. Four problems are emphasized:
(a) Emerging and re-emerging diseases are given due visibility and the
case is made for expanding research efforts to tackle them.
(b) It is argued that R&D is needed for the coming epidemic of
noncommunicable diseases and injuries, particularly in relation to
epidemiological studies and the development of cost-effective
clinical algorithms.
(c) Understanding and improving health systems represent a third area of
concern: the social and behavioural sciences should assume a greater
role, to clarify the interaction between "demand" and "supply".
(d) Finally the report recommends a range of policies to strengthen
institutional networking. More adequate cooperation between industry
and governments should be promoted, including a reconsideration of
the present patent system and stimulation of the private sector in
product development by the "provision" of global markets.
The concluding proposal is the creation of a "Consortium on
International Health Research and Development"l, representing "the
governments of developing countries, the major donors, the principal
research programmes, important research centres and the private sector".
2.1 Introduction
Reference is made to previous efforts in documenting global health
problems, particularly of the World Bank (WDR 93). The report is

A.3
-6-
considering health R&D as a "segment" within the health sector, rather thanpart of all R&D. Three types of activity are distinguished: fundamentalresearch (to contribute to basic knowledge), strategic research, (definedas "research whose purpose is primarily to increase - and publish -knowledge and understanding of a significant health problem, but with aview eventually to solving or reducing the impact of the problem throughfurther development and evaluation"), and development activities: products(drugs, vaccines, equipment, prostheses and diagnostics), interventions(public health, personal health) and instruments of government policy.
In respect of resource allocation, the report argues that factorsaffecting public health should be taken into consideration asquantitatively and as systematically as possible. The DALY methodology ispresented and used as a way of doing this and allows the quantitativeestimation and projection of disease burden.
The introduction ends with a consideration of the roles of differentdisciplines and their expected contribution in resolving the four healthproblem areas identified by the report.
2.2 Why invest in health research?
The contribution of scientific and technological progress to advancesin health is discussed and the case is made to justify the cost-
effectiveness of past R&D.
The future promises of science are sketched out and it is assumedthat health research has tremendous potential to solve some of the mostpressing problems of the low and middle-income countries, providedinvestors choose to take advantage of the opportunities before them.
2.3 Health and poverty: the unfinished agenda
The chapter reviews available data on disease burdens, comparingdifferent geographic regions and, assessing past achievements and currentprogress. It discusses the modalities and costs of possible interventions
and their likely outcomes.
Projections are also calculated for years of life lost due to variousgroups of conditions, in the light of existing data on disease burdens.The needs for strategic research are assessed, and the case is made tostrengthen the role of behavioural research and health systems and policysciences, in order to overcome the barriers to the effective implementation
of existing tools.
Examples are given to illustrate the contribution of variousdisciplines (biomedical science, population sciences, health systems andpolicy research) to the solution of important diseases or health problems,
A.3
-7 -
such as diarrhoeal diseases, vaccine preventable diseases, and reproductive
health.
2.4 Emerging and re-emerging microbes
The title covers a number of large groups of infections:
a) common, well-known agents such as Mycobacterium tuberculosis and
Plasmodium falciparum;
b) pathogens having recently entered human populations such as HIV;
c) bacteria which have become drug-resistant, such as Shigella
dysenteriae and Staphylococcus aureus; and
d) newly recognized pathogens, such as E. coli 0157 and hantavirus.
Examples of general and specific factors are given which have
contributed to the emergence of infectious diseases.
Tuberculosis, HIV and other STDs, Malaria, Pneumococcal disease and
drug-resistant shigella dysenteriae are discussed in some detail, and
projections of HIV incidence are plotted by region through year 2020.
The case is made for promoting strategic research in this domain and
examples are given of cost-effective interventions for alleviating the
burden of these diseases. Priorities for the development of certain
interventions in AIDS, TB, STDs, Malaria and Pneumococcal infections are
also suggested.
2.5 The coming epidemic of noncommunicable diseases and iniuries
Whereas the global population is growing at the rate of 1.7% p.a.,
the share of that population over the age of 65 is growing at 2.5% p.a.
Those aged 80 years or more constituted 16% of the world's total elderly
population in 1992. Middle-income and low-income countries are aging most
rapidly, and are experiencing the demographic transition within much more
compressed time frames than it has been the case for the established market
economies. This will necessarily increase the burden of NCDs everywhere.
In addition, the "patterns of exposure to certain risks associated with ill
health are altering in all populations": for example tobacco use (8% of
all lost DALYs), diets and patterns of physical activity.
Projected years of healthy life lost for certain countries and
regions are shown, by broad cause group, 1990 - 2020. The chapter
emphasizes measurement of the burden of diseases by risk factors, and
advocates the need for strategic research. For example, estimates are
presented, under both optimistic and pessimistic scenarios, of averted,
avertable, and unavertable global burden attributable to tobacco use with
existing interventions, 1990. Opportunities for intervention development
and evaluation are consequently outlined.
A.3
-8 -
2.6 In pursuit of equitable and efficient health services: learning fromexperience
This chapter discusses the interaction between "real" people and
their "real" health systems. It advocates policy-oriented research that
aims to close the gaps between what can technically be achieved (efficacy)
and what is actually achieved (effectiveness).
A typology of health research by levels of analysis is presented as:
(i) Biomedical research (subindividual level); (ii) clinical research
(individual level); (iii) Behavioural research (individual and household
levels); (iv) Epidemiological research (population level); and (v) Health
systems research (institutional level). The latter is further classified
into health services research (micro level) and health policy research
(macro level).
The needs for strategic research are assessed, at the level of
populations, households and individuals, as well as at the level of health
systems and policies. It is argued that a single indicator of health
status would be needed, combining the impact of mortality, morbidity and
disability, in order to set priorities for intervention and for measuring
the effects of interventions, some of which save lives while others improve
the quality of life. Research is needed to test the transportability of
the DALY - and that of other indicators - to different cultural settings.
Several research topics are also identified in relation to health
systems and policies, such as: (i) setting priorities for the allocation
of public resources, (ii) health services financing, (iii) translating
policy into plans and action, (iv) health needs assessment and monitoring
systems as well as information management, (v) decentralization (transfer
of functions, resources and authority to peripheral levels of government),
(vi) mix of public and private health services provision and financing,
(vii) standards and quality of care, and (viii) community organizations.
The chapter concludes that there is a striking shortage of research
efforts into the functioning of health systems and the behaviours of the
populations served by them. Research into the "supply" and "demand" sides
of a country's health system - and the interactions between them - can
produce significant findings that result in major improvements in the
quality and coverage of services and reduction in excess cost. It is
argued that investors should devote resources to turning research results
into action, for example through the development and evaluation of cost-
effective instruments of public policy and practical tools for health
workers. "These may include essential drugs lists, model legislation,
priority intervention packages, insurance benefit lists, pricing and
taxation policies, practical manuals for use by health workers, and
summaries of research results for use by health workers and decision
makers".
A.3
-9 -
2.7 Responding to needs: institutions, incentives and finance for futurehealth R&D
This chapter "examines the options for organizing the institutional
and financial framework for global health R&D in such a way that it can
meet those challenges"...
Three levels are distinguished: the operational level (basic cells
of research), the resource allocation level (Research Councils,
Foundations, NGOs, Governments and Programmes), and the advocacy level
(e.g. COHRED).
The discussion focuses on building capacity for research in low and
middle-income countries and outlines the key factors for success: (i)
capable, committed leadership, (ii) stable long-term linkage with other
institutions, (iii) the ability to attract young, talented researchers and
give them freedom to pursue their ideas, (iv) the securing of adequate
resources for long-term and dependable support, (v) the capacity to train a
large number of individuals from whom subsequent leaders can emerge.
The subsequent major argument is about linking public and private
sectors, in order to provide industry with incentives to engage its
expertise in alleviating their problems. (Since the costs of bringing a
new pharmaceutical product from laboratory bench to market have been
estimated at as high as $359 million).
Financing of health research is however the main focus for this
chapter, under the title "Investment in health R&D: trends, prospects and
proposed solutions". It is first argued that research is a "poor relation
within the health sector", no government according research more than 4.5%
of its total domestic health spending (e.g. U.S.) while for many, it is a
fraction of 1% (e.g. Mexico, 0.5%), the world average being 3.2% (1992).
The next problem is that support for health research is stagnating
and in some cases falling. The example of NIH is cited, where the annual
budget is expected to fall by 9% over the next four years (from $11.3
billion to $10.7 billion). Another area of concern is the "inadequate
coordination" which has resulted in important gaps within health research
efforts, as illustrated in chapters 5 and 6.
Possible reasons are given for the neglect of health research, one of
which is that "the arguments for research are not being put clearly enough
to those who must make decisions about how to invest shrinking resources".
The chapter makes a series of recommendations to both government and
donors, for example in respect of capacity building, incentives for the
private sector, (e.g. subsidies, extended patent protection, guaranteed
markets) and reallocation of health sector resources to R&D.
A.3
- 10 -
Some of the recommendations are of more direct concern to WHO: the
case is made for a new "Programme for Research and Training on Healthy
Aging and Noncommunicable Diseases" to be "hosted" by "existing candidates"
such as IARC, WHO or a national government...
A second proposal is for a "Programme for Research and Training on
Health Systems and Policy" to be formed from the existing institutions and
groups conducting research and training in these areas (e.g. IHPP network).
Last but not least, it is recommended that a "Consortium on
International Health R&D" be formed to provide a forum for review of needs
and opportunities for global health R&D. The Consortium would consist of
"governments of developing countries, the major donors, and the research
community". It is suggested that the Consortium concept be tested,
initially, as an "informal gathering of interested parties" (June 1996).
3. DISCUSSION
3.1 Scope and concepts
3.1.1 The title of the report: "Investing in health research and
development: an agenda to address problems of the poor" has undergone a
revealing development. In November 1993, the task of the Committee was
described as an "ad hoc review on health research priorities with special
reference to developing countries". In January 1994 the group described
its task as a "Study of international health related research priorities"
and subsequently as an "Ad hoc study of international health research
priorities". In May 1994, the concept was even broader: "The foundation
of the future: research for global gains in health in the 21st century".
The April and June 1995 drafts were entitled: "Investing in health
research and development" and in August 1995 the scope was again modified:
"Investing in health research and development: an agenda to address
problems of the poor".
Thus, one has to notice that the committee went a long way from a
very broad scope - research for global gains in health - to a much more
restricted scope such as "Investing in health research and development: an
agenda to address the problems of the poor". Indeed, the key issues of the
report address "health and poverty: the unfinished agenda", "emerging and
re-emerging microbes", "preparing for the non-communicable diseases and
injuries" and "equitable and efficient health services".
It should be pointed out that the Committee has collected and
digested for its report data and other material which have an objective
value and are useful in discussing the relationship between health
development and scientific research.
A.3
- 11 -
However, in reviewing the Ad Hoc Committee report, the PRG identified
a number of conceptual and methodological problems which seriously
undermine the report's credibility as a framework for evaluating priorities
for health research and development investment. Even within its present
circumscribed scope, the selection of issues to be discussed in the report
does not reflect adequately the spectrum of problems affecting "the poor"
throughout the world's regions. Several documents previously presented by
the ACHR system (regionally as well as globally) have emphasized that a
global perspective on the "health problem landscape" should include other
dimensions. The "health problem landscape" is not a static situation, but
a dynamic process. As various WHO documents (including ACHR reports) have
argued, diseases are not the only factors affecting the "productive life
span" that is necessary for sustainable human development. Productive life
and health in the "global village" are co-determined by dynamic changes in
the natural and man-made environment, population growth and migration,
nutrition, industrial expansion and economic factors, and the consequences
of energy and raw material consumption. The ongoing revolution in
communication technology is also likely to have a major impact.
In considering the potentialities of scientific and technological
research, as a report on "Investing in health research and development"
should do, it is further necessary to adopt a forward looking perspective.
The impact of scientific advances on future health was most recently
considered by a joint ACHR and CIOMS meeting (Charlottesville, 1994), the
report of which has been published.
All these aspects are barely acknowledged, and certainly not
adequately reflected in the report of the Ad Hoc Committee. The PRG
therefore does not consider the content and recommendations of the report
an adequate basis for identifying priority areas for investing in health
research and development.
3.1.2 A major criticism of the report was that it lacks an explicit
conceptual framework for "health problems". It appears to rely upon an
implicit concept of health which is regressive by the standards of the
definition inscribed in the WHO constitution as long ago as 1948 - namely
that "health is not merely the absence of disease but a state of complete
physical, mental and social well-being". Although the introduction of
DALY's adds the dimension of disability to the conventional measure of
mortality and does represent a conceptual step forward (notwithstanding the
provisional status and lack of validation of the actual DALY measures used
at present), health in the report is practically equated with reductions in
specific morbidity. The four "globally significant clusters of health
problems": the continuing spread of infectious diseases, undernutrition
and excess fertility, the rising incidence of noncommunicable diseases, and
the inefficiencies and inequities in health systems, are effectively
A.3
- 12 -
separated from their social, economic, ecological and political context.
Although the authors of the report do acknowledge inter alia that many of
the determinants of these clusters of problems lie outside the health
sector, the main thrust of the report and its recommendations is the
proposition that increased allocations to specific health research will be
a cost-effective way of improving health conditions in low-and middle-
income countries.
The paradox of the changing world at the end of the millennium - that
the global increases in life expectancy are parallelled by unremitted
poverty, a deteriorating environment, population increases, a global rise
in violence, ethnic conflicts and uprooting on a mass scale - suggests that
simplified definitions of health problems and proposals for their solution
by a mere reallocation of resources, or by the creation of yet another
international "forum", are extremely unlikely to provide a credible basis
for concerted international action by governments, donors and international
organizations. Projections of health needs and the formulation of options
for appropriate research and development will not result in meaningful
action unless the boundaries between health and other global problems are
effectively removed and innovative research strategies are set in place
which address the interlocked problems of the environment, population
dynamics, and the political economy of health simultaneously with those of
biomedical research and health system design.
It is unfortunate that the report's conclusions and recommendations
seem to point in the precisely opposite direction - not towards a more
effective integration of health research into a multisectoral strategy for
tackling global problems, but towards a virtual separation of health
research from health programmes as well as from the more general
developments in science and technology. The need for an integrated,
multisectoral approach to global health problems has been a major
preoccupation of WHO for decades. There can be no denial of the
difficulties encountered on the way to its realization. However,
abandoning this objective would be a retrograde step. On the contrary,
ways and means should be found to mobilize the scientific community
everywhere for a greater and more active involvement in research on global
health development.
3.1.3 The report is burdened with relatively trivial facts and
declarative statements, giving insufficient information on sources or
references and their reliability. In this sense, the report is unlikely to
impress the scientific community. It contains unsubstantiated assertions
and generalizations, such as "the window of opportunity may be closing" ...
"economic and political factors have created a climate hostile to research"
(p. 2, lines 1-3); "governments accord R&D for health only a low priority"
A.3
- 13 -
(p. 2, para. 2); (however see, per contra, Science, June 30, July 21,
August 11). It fails universally to follow a logical progression from
facts to conclusions through complete threads of argument.
The use of "journalese" language obscures the failure to translate
the substantial data collection exercise presented in the report into
properly supported conclusions about research priorities. Statements about
the needs for strategic research and its priorities often take the form of
unsupported assertions. For example, the recommendation about resource
reallocations to health R&D is not supported by any systematic comment on
how such resource reallocation could be accommodated within health systems,
or within the national context. This is not a trivial problem. Even if a
need for new means of attacking health problems is recognized and accepted
at the political level, the actual intervention options are not necessarily
achievables.
For instance, in allocating research funding to particular new
initiatives in the field of biomedical R&D, how does one integrate factors
like development period, cost of research, risk of failure, cost of
implementation, potential DALYs saved, use of scarce human resources,
availability of personnel for implementation and the cost of their
training, collateral health and economic benefits, consonance with
government policies and so on? Similar considerations apply to the
planning of health systems development. These are factors that decision-
makers need to handle and strategic R&D in the field of decision support
technology is needed. This has repeatedly been pointed out in ACHR
deliberations.
In thinking about priorities, it needs to be recognised that specific
health problems have attributes like "importance", possible "interventions"
have attributes like "cost" and "likelihood", which are subject to
political realities. Many believe that sustained government action on
policies aiming first to improve the socio-economic conditions for the poor
segment of the population would be a more potent factor impacting health
than many other interventions. But in any case, recognising what R&D
investments would be consistent and synergistic with government economic
policies is a key factor in the definition of priorities. What is,
therefore, needed is a "knowledge map" of the interactions and forces that
must be considered when planning interventions. This is where strategic
research is needed, in the sense of developing methodologies for better
informed and effective decision-making recognising political and socio-
economic realities. Interventions have consequences and some of these are
likely to be undesirable and perhaps delayed in their effect. Decision-
making techniques that take account of constraints (e.g. limited.rate of
input of resources) and of the time-course of both desired and unwanted
effects are now being used in other fields; they should be adapted for use
in the health area.
A.3
- 14 -
These examples show the need for strategic methodological research
which the ACHR has been advocating. This research would be strategic in
the sense that it would enable the scientific community to undertake a new
range of "tactical" R&D making the best possible use of limited resources.
The PRG also noted that other research areas of seminal relevance do
not receive adequate attention in the report. For example, information and
communication technology will have an impact on epidemiological information
acquisition, compilation and interpretation, in telemedicine, at the level
of PHC and in secondary or tertiary health care centres. It also includes
important computer-based "tools" for management of large projects, like
organisational redevelopment or control of cost and schedule in the
industrial production of health care equipment. Similarly, biomedical
engineering research is not mentioned; it has much to offer towards an
integrated R&D policy.
3.2 Approaches and Methods
3.2.1 The report aims to present a quantitative base for decision-
making about health research needs and priorities, using the DALY concept
as its cornerstone. However, the report fails to highlight adequately the
present limitations on the use of the DALY which make the concept an, as
yet, invalidated index. This results in a mismatch between the attempt to
achieve, at the input stage, a quantitative definition of the scale of
health problems, and the lack of objectivity at the stage of interpretation
and judgment.
As an indicator, the DALY concept reaches beyond mortality measures
in an attempt to take account of morbidity and disability. It may be
regarded as a step along the pathway towards indicators that will also
assess economical factors and, subsequently, quality of life elements. At
present, however, there are three types of difficulty with the DALY
concept. First, it is a combination of very different elements: years
lost due to death and years "lost" due to a life with disability to which
an economic loss in value is attributed. Secondly, there is a continuing
debate about the structure of the indicator and about the precise weights
attached to the so-called discount element - by which the "value" of later
years of life is increasingly reduced. (In different cultures, different
discount "weights" will certainly be needed and single intercountry DALY
comparisons may thus be invalid). Thirdly, there are circumstances in
which the "cost" attributable to a death may be economically small whilst
that due to a disabling but not life-threateing condition may be
economically large. (DALYs gained by a specific intervention that, for
instance, reduces mortality cannot easily be compared, for economic cost-
effectiveness, with DALYs gained by increasing years lived with a
disability). And, again in economic terms, are all DALYs equivalent across
a population with economically active and inactive population groups?
Ethics and economics are mixed uneasily in the DALY in its present form.
A.3
- 15 -
The PRG does not accept the reduction of research priority identification
to an estimation of DALYs; it is believed that such a reduction will be
unacceptable to the scientific community at large.
3.2.2 The DALY concept and specific diseases need a special mention.
What is a "specific" disease? It refers to the very simple situation when
a given agent causes a well defined pathological event with foreseeable
consequences: this, at least theorically, is the case in most communicable
diseases. Yet these diseases occur in various patients, with different
health, nutritional and social status prior to the onset of the disease.
Even these communicable diseases are complex and often multifactorial in
their determinants. The problem is much more difficult in the
noncommunicable diseases, where multifactorial causation is the rule, as it
is for injuries. Moreover, especially in the poor, in the elderly, and
even more in developing countries, a given disease is very seldom isolated:
comorbidity and "polypathology" are common. In these circumstances, the
DALY will be of limited use.
Throughout the report there is a confusion between the cost-
effectiveness of an intervention eventually resulting in a reduction of the
disease burden and the cost-effectiveness of the R&D resulting in the
intervention technology. The cost of the needed research is not included
into the calculation of DALY. For these reasons also, as acknowledged by
the report, the DALY indicator is still open to considerable debate; and
it seems premature to use it as the tool for making priority decisions in
the field of R&D, or even more broadly, in the full range of health
interventions. Other indicators - either single (like the infant mortality
rate, IMR) or aggregated, as proposed by ACHR - should not be forgotten:
they could be more accurate than DALY in many instances.
The burden of diseases associated with selected risk factors is
touched upon in Chapter 5 and expanded in Annex 1. After the presentation
of some basic concepts, the model of tobacco is discussed at length, since
it is regarded a suitable case for the DALY approach. Yet the report is
quite silent on such determinants as the social image of smoking, the
behavioural aspects of the smoking habit, the role of the advertisement
through media, or the price. How does one translate epidemiological
knowledge on morbidity and mortality into the needed intervention without
taking into account these psychosocial, economic, legal determinants? DALY
does not seem convincingly useful in this approach, even more so when we
consider that the same risk factor may lead to different - sometimes
combined - ill-effects, whereas several risk factors often combine their
action in producing the same disease.
Tobacco is, nevertheless, a good model of risk factor. When the
report deals with alcohol, water supply, personal hygiene, matters become
fuzzy and the report concludes that "Estimating the burden of disease and
A.3
- 16 - _
injury attributable to exposure to risk factors is intrinsically very
problematic" and "There are major obstacles to reliably quantifying the
burden of ill-health due to risk factor exposures".
3.2.3 The DALY concept considers the consequences of disease in terms
of mortality and disability. While mortality should be a relatively
straightforward indicator, in actual fact the mortality data of many
countries - even developed ones - are not reliable as far as the causes of
deaths are concerned. Disability measurement is even more open to
criticism for several reasons: poor epidemiological basis; great
variability as to the possible compensations; perception, representation
and the subjective weighting of the disability by the disabled and by the
family, neighbours, coworkers or the community at large. All these factors
make the estimation of the D of DALY very questionable.
Subject to the difficulties already discussed, DALY is applicable in
the ideal situation where a single agent (or risk factor) determines a
given, well identified disease or case of ill health. However, this is
rarely the situation: many illnesses are multifactorial. By limiting the
model the to the immediate determinants of ill-health one fails to take
into account the more remote but powerful determinants such as poverty,
poor education, housing, social conditions and social support and community
participation. Many diseases of poverty are plural, combining
malnutrition, communicable diseases, parasitosis, etc. In these multirisk
and/or multipathogenic situations, is the DALY reliable and credible? It
is open to discussion and to further intensive research, before
consideration is given to routine applications.
3.2.4 In relation to "research priorities", the report argues
implicitly in a very simple way: where there is a relative mismatch
between non-avertable burden of ill health (expressed in DALY) and existing
R&D activity, there is a case for research investment: the greater the
mismatch the higher the priority. But research needs resources. In the
context of, say, a developing country, many factors enter into the
allocation of resources, even within the health sector. The report accepts
DALY-accounting as the basis for estimating needs, choosing interventions
and optimising choices. Disregarding the present imperfection of the DALY
concept, this is a tempting idea. However, it needs careful evaluation.
The implied goal is to reduce the count of DALYs lost by applying
interventions directed at specific health problems. But an intervention to
improve the DALY-count may create unwanted side effects which, at the very
least, deserve attention, or at worst, may run contrary to government
economic policy. For example, it is not unknown for mortality due to one
disease to "mask" concurrent evidence of another disease which may be at
A.3
- 17 -
least as potent in generating lost DALY-counts. Therefore, any system of
prioritising research and interventions must be questioned if it is
exclusively based on DALY-accounting.
3.3 Proposais and Recommendations
The report of the "Ad Hoc Committee" culminates with some proposals
and solutions intended to better respond to health research needs. The PRG
felt that they are neither fully convincing nor neutral. Some are
irrealistic (for example researchers in developing countries being freed
from civil service management procedures).
A better coordination between public and private sectors is rightly
advocated; however its difficulties are underestimated. Serious
philosophical divergence makes the collaboration uneasy (e.g. health
effects of tobacco). As to the proposal to "support the costs of the early
stages of product development", it is difficult to reconcile it with the
general contention that research funds are already scarce and therefore
they could hardly be invested in product development running at
ca. 360 million USD, per product (op. cit.).
WHO is mentioned as a "major player" in health research; yet the
report argues that WHO, as other international agencies, has a number of
other concerns besides research and can only focus on its own mandate.
Such statements pave the way to the Ad Hoc Committee's final proposal: the
creation of a "Consortium".
The major concern of the PRG is that adopting the recommendations of
the report regarding the creation of a Consortium for International Health
Research and Development would be tantamount to relinquishing the role of
WHO in promoting health research as defined in its Constitution. The
statement (page 146) that "existing international health organizations,
such as WHO, have a number of other concerns besides research, and can
focus only on their own mandates" is either ill-informed, or misleading.
This statement is a revealing sign of the basic assumptions and intentions
of the report. Although WHO is not a primarily research organization,
health research ranging from the molecular level to the population and
health system level has always been an indispensable part and parcel of the
activities of the Organization. Special programmes such as HRP and TDR are
widely regarded as world leaders in their respective fields, and the
majority of the WHO programmes have a strong research component. The
integration of research with service or specific intervention delivery
programmes has always been a particular strength of WHO, and examples of
success, such as the smallpox eradication programme, bear witness to this.
The proposed consortium is obviously meant to replace WHO's most
important commitments (p. XV); it is planned to create a new "forum" that
would decide about priorities and funding of health research. However, as
A.3
- 18 -O
the authors of the report themselves admit, "The conclusions (of the
report) are the products not of the analysis per se, but of the committee's
judgments informed by data and analysis" (p. 10). This self-acknowledged
judgmental, "top-down" approach is proposed to replace the existing formal
WHO research structures at regional and global level. It is evident that
the implications of the Ad Hoc Committee's recommendation could be
disastrous: neither the governments nor the scientific community will be
keen to accept "orders", the more that the present version of the report is
disputable both from the scientific and the political point of view.
4. CONCLUSIONS
The Peer Review Group, having considered and discussed draft 2.0 of
the report, takes note and thanks the "Ad Hoc Committee" for providing it.
The PRG also notes that the "Ad Hoc" report had not been commissioned by
either the WHO's governing bodies nor by the ACHR.
As regards the substance of the report, the PRG is of the following
opinion:
1. It recognizes that considerable effort has been expended in preparing
the material and appreciates the extent of work involved.
2. The draft report contains a number of interesting views and a
compilation of valuable data.
3. The paper as a whole cannot be considered as an original study, but
rather as an expanded review of existing information and an eloquent
advocacy platform.
e4. Scientific rigour would require that relevant sources and references
be systematically quoted for all appropriate information and
arguments.
5. A number of pertinent and essential science policy documents,
(including WHO material at regional and global levels) are either
ignored or occluded in the development of the Committee's thesis, so
raising doubts about its objectivity.
6. The approaches and methods appear to be unidimensional in so far as
the prime criteria for judgment about health intervention and R&D
priorities seem to be accountability in a merely monetary sense.
7. Despite stated precautions, the whole construction is based on DALYs,
a still untested indicator for the intended purposes. Other
alternatives are deliberately excluded.
A.3
- 19 -
8. The report explicitly takes health R&D out of the context of overall
R&D efforts (thus downplaying, inter alia, the universality of
Science).
9. The ethical dimension deserves more than a passing remark and any
consideration of resource allocation scenarios should take it into
account. Such an omission weakens the overall credibility of the
proposed scheme and lends a mechanistic - if not simplistic - profile
to health problems.
10. The report culminates with a proposal for new institutional
arrangements. However this conclusion does not arise logically from
the arguments developed throughout the analysis.
A.3
- 20 -
APPENDIX
Individual Members of the PRG had a number of discrete remarks on
specific points of the report and whereas all of them have not been
compiled, the small sample below illustrates the type of concerns which
were aired by the Group.
Paragraph Comment
Are the individuals listed under WHO Secretariat with their
nationalities participating in this study in their capacity of
WHO officers or as nationals?
3 from top
2 from top
1 a) and b)
3 from top
top
4 from top
Meta-analysis has recently been
criticized and found to be of limited
use in health research.
The statement that disease burdens are
"both a consequence and a cause" of
poverty is simplistic.
Reduction of behaviour and
environmental influences on health to
trivial examples.
Sequencing of the genome of a pathogen,
failure to complete a course of
chemotherapy, etc. are heterogeneous
problems, difficult to subsume under
"strategic research".
Uncritical acceptance of DALYs as
unquestionably valid.
The impact of treatments for
phenylketonuria or childhood leukaemia
on population health indices is
marginal - both are rare conditions.
e
Page
vii
x
xii
5
o
7
12
20
e
A.3
- 21 -
21 top "... Such as whether community care is
appropriate in severely mentally ill
patients in specific settings" - the
meaning is unclear.
bottom The reference to naltrexone in
alcoholism leaves the false impression
that this is a routine cost-effective
treatment: it is not.
22-23 Fig. 2.3 "1972:... Biochemical basis of bipolar
affective disorder discovered" - such a
basis is not known up to date.
"1986:... Key discoveries in neurology"
- what are they?
24 bottom Gene therapy for atherosclerosis is at
present beyond the most optimistic
projections into future developments.
25 top The basis for the assumption that
"research alone explains the increase
in life expectancy" is not made
explicit and remains questionable.
26-27 Fig. 2.4 and 2.5 The difference between these two
figures is not clear: both have
million's of years of healthy life as
the ordinate.
31 top It is not clear how scanning
technologies are used in
epidemiological research into
Alzheimer's disease that may lead to
preventive treatments (if the authors
are referring to the UK study on
aluminium in the drinking water, its
methodology and conclusions have been
severely criticised).
A.3
- 22 -
Fig. 5.17 & 5.18
bottom
No data source is given for the
estimates about avertable and
unavertable global burden of
schizophrenia and major affective
disorders. The percentages are
arbitrary and suggest a spurious
precision.
What are the safety + ethical
implications of
"streamlining the regulatory controls"?
top The statement under "Major players in
health research" that "the World Health
Organization has a mandate..." etc.,
and that it invests $223 million into
health research contradicts the
statement on p.146 (2nd para. from top)
that "existing international
organizations, such as the WHO, have a
number of other concerns besides
research...", etc. Which of the two
statements represents the view of the
authors?
115
e
154
160
e
o
Annex 4
DISCUSSION DRAFTNOT FOR QUOTATION
Draft 2.028 August 1995
Investing in health research and development:An agenda to address problems of the poor
WORLD HEALTH ORGANIZATION
Ad Hoc Committee on Health ResearchRelating to Future Intervention Options
This draft of the Committee's Report was prepared for discussion andreview by a subcommittee of the Ad Hoc Committee at Cape Town,South Africa, 11-13 September 1995.
Contents
Study participants ............................................................................................................ viii
Summary .............................................................................................................................. x
Chapter 1: Introduction ....................................................................................................... 11.1 Preamble ..................................................................................................................................... 11.2 The background to this Report: antecedent activities ................................................................ 31.3 Scope and focus .......................................................................................................................... 51.4 M ethods .................................................................................................................................... 10
Chapter 2: Why invest in health research? Historical experience and thepromise of science ..................................................................................................... 16
2.1 The scientific underpinnings of past health improvement ....................................................... 192.2 Investments that paid off: the cost-effectiveness of past R&D ................................................ 212.3 Looking ahead: research tools for the future ............................................................................ 242.4 Chapter summary ...................................................................................................................... 32
Chapter 3: Health and poverty: The unfinished agenda ................................................. 343.1 Assessing th e burden ................................................................................................................ 343.2 Projecting the burdens ahead .................................................................................................... 403.3 Assessing needs for strategic research ............................................................ 51......................... 13.4 Opportunities for intervention development and evaluation .................................................... 543.5 Chapter summary and recommendations ................................................................................. 62
Chapter 4: Emerging and re-emerging microbes: the continually changingthreat of infectious disease ....................................................................................... 64
4.1 Change in the global village: factors in the emergence of disease .......................................... 644.2 Four major threats to public health .......................................................................................... 674.3 Responding to emerging diseases ............................................................................................. 784.4 Assessing needs for strategic research ..................................................................................... 804.5 Opportunities for intervention development and evaluation .................................................... 824.6 Chapter summary and recommendations ................................................................................. 89
Chapter 5: Preparing for the coming epidemic of noncommunicablediseases and injuries ................................................................................................. 90
5.1 Projecting the future ................................................................................................................. 945.2 Measuring the burden of diseases by risk factors .................................................................. 1065.3 Assessing needs for strategic research ................................................................................... 1095.4 Opportunities for intervention development and evaluation .................................................. 1135.5 Chapter su mmary and recommendations ............................................................................... 118
iii
WHO Ad Hoc Health R&D Report, Draft 2.0
Chapter 6: In pursuit of equitable and efficient health services:learning from experience ......................................................................................... 119
6.1 The framework for analysis ......................................................................................... 1206.2 Reaping the benefits of research ............................................................................... 1256.3 Assessing needs for strategic research ................................................................................... 1236.4 Assessing ongoing research activity ....................................................................................... 1426.5 Chapter summary and recommendations ............................................................................... 144
Chapter 7: Responding to needs: institutions, incentives andfinance for future health R&D .................................................................................. 145
7. I Building capacity for research in low- and middle-income countries: current status andpossible solutions .................................................................................................................. 149
7.2 Working together: in search of better links between public and private sectors ................... 1537.3 Investment in health R&D: trends, prospects and proposed solutions ................................... 1577.4 Chapter summary and recommendations ............................................................................... 166
Bibliographical note and references .............................................................................. 168
List of tables, figures and boxes .............................................................................. 169
The WHO Ad Hoc Committee: Review participants and study schedule .................... 173Review participants ...................................................................................................................... 173Study schedule .............................................................................................................................. 184
Annexes [Not included in this draft]1. Global patterns of cause of death and burden of disease in 1990, with alternative projections
to the year 2020-by Christopher J. L. Murray and Alan D. Lopez
2. Estimates of disease burden due to selected imnportant risk factors-by Christopher J. L. Murray and Alan D. Lopez
3. The CGIAR system and its relevance for international health R&D-by Rajiv Misra
4. The pharmaceutical industry and health needs of developing countries-by William Comanor
5. Aggregate levels and trends in expenditure on health R&D--by Catherine Michaud and Christopher J. L. Murray
6. The International Center for Diarrhoeal Disease Research, Bangladesh: -
experiences and implications for the future-by Demissie Habte
7. From investigation to eradication: Beyond the first 20 years of the TDR-by Tore Godal
8. The development of priorities for research relating to households and populations-by David Evans
9. The development of priorities for research relating to health policy and systems-by Katja Janovsky
iv
Contents v
Supplementary PapersA: Estimating and projecting the burden of diseases and risk factors
A. 1 Health resource allocation and disease burden measurement: Issuesconcerning late fetal and early childhood death-by Dean T. Jamnison and Julian C. Jamison
A.2 Estimated disease burden reduction from implementation of minimumessential intervention packages-by Claude Nanjo and Dean T. Jamison
B: R&D institutions and institutional developmentB. 1. Institutional development options for international health R&D
-by Rajiv Misra and Joel AlmeidaB.2 Incentives for private sector involvement in vaccine development: HIV-1 vaccines as a
case study-by Seth Berkley
C: Health R&D expenditures: case studiesC. 1 Expenditures on health R&D in India
-by Joel Almeida and Rajiv MisraC.2 Expenditures on health R&D in Mexico
-by Beatriz ZuritaC.3 Expenditures on health R&D in South Africa
-by D. YachD: Health systems research-status and priorities
D. 1 Health policy and systems research: A framework for assessing priorities-by Andrew Cassels
D.2 Needs assessment and monitoring systems-by Richard Cibulskis and John Izard
D.3 Quality of health services-papers by James R. Heiby and Enrique Ruelas
D.4 The "public-private mix"-papers by Peter Berman and Sara Bennett
D.5 Assessment of health needs and health system performance-by Martin McKee
D.6 Human resources policies and systems-papers by Fred Abbatt and Peter Hornby
D.7 Priority setting for health-by Chris Ham
D.8 Financing-by Barbara McPake
D.9 The policy process-papers by Anne-Marie Foltz and Gill Walt
D. 10 Decentralization-papers by Thomas Bossert and Charles Collins
9

WHO Ad Hoc Health R&D Report, Draft 2.0
E: Health R&D needs and opportunities for selected conditionsE. 1 Acute respiratory infections
-by James Tulloch and colleaguesE.2 Coronary artery disease
-by T. Pearson and P. JhaE.3 Malaria
-by David Evans and colleaguesE.4 Tuberculosis
-by Christopher J. L. Murray, P. Nunn and colleagues
e
e
eI
vi
Study participants
Committee members
Professor Dean T. Jamison, USA(Committee Chair)
Professor Kamini Mendis, Sri Lanka(Committee Co-Chair)
Dr. Adenike O. Abiose, NigeriaDr. A. Asamoa-Baah, GhanaDr. Sune Bergstrom, SwedenDr. Seth Berkley, USAProfessor Barry Bloom, USAProfessor David Bradley, UKProfessor Gelia T. Castillo, PhilippinesDr. Chunming Chen, P.R.C.Dr. Mercedes Concepcion, PhilippinesProfessor Gertrude B. Elion, USADr. Richard Feachem, UKDr. Julio Frenk, Mexico
(Co-Chair, Working Group II)Dr. Baron Paul Janssen, BelgiumDr. Maureen Law, CanadaDr. Philippe Lazar, FranceDr. Sverre O. Lie, NorwayDr. Juan Luis Londoño, Colombia
(Co-Chair, Working Group II)Dr. Mahmoud M. Mahfouz, EgyptDr. Anthony B. Miller, CanadaMr. Rajiv L. Misra, India
(Chair, Working Group III)Dr. Carlos Morel, BrazilProfessor A.S. Muller, The NetherlandsProfessor Christopher J. L. Murray, New
Zealand (Chair, Working Group I)Dr. Plutarco Naranjo, EcuadorDr. Sir Gustav J.V. Nossal, AustraliaDr. B.O. Osuntokun, NigeriaProfessor Richard Peto, UKDr. Jean-Pierre Poullier, BelgiumDr. Srinath K. Reddy, IndiaDr. Susanna Sans, SpainProfessor Norman Sartorius, RomaniaDr. Jaime Sepúlveda, MexicoDr. Vladimir P. Sergiev, RussiaDr. Yukiko Sugino, JapanDr. Derek Yach, South Africa
WHO Secretariat
Dr. Tore Godal, Norway(Study Co-Director)
Dr. James Tulloch, Australia(Study Co-Director)
Dr. David B. Evans, AustraliaDr. Katja Janovsky, The Czech RepublicDr. Alan D. Lopez, AustraliaDr. Thomas C. Nchinda, Cameroun
Committee staff
Dr. Joel Almeida, IndiaMs. Phyllida Brown, UKMr. Leslie Evans, USADr. Catherine Michaud, SwitzerlandDr. Beatriz Zurita, MexicoMr. Claude Nanjo, Japan
Addresses, phone numbers and briefbiographical sketches of the study partici-pants may be found beginning on p. 173.
vii
-
3-
WHO Ad Hoc Health R&D Report, Draft 2.0
e
e
e
viii
Summary
Why invest in health research? The benefits of past research andits promise for the future
The health of the world's peoples has improved. more in the past four generations than in the preced-ing 400. Between 1950 and 1990 alone, life expectancy at birth in the low- and middle-income coun-tries has grown by more than two decades-from 40 to 63 years. And, even in Sub-Saharan Africa,where the gain has been slowest and smallest, the pace of improvement has still been faster thananything experienced by the rich countries in their own periods of demographic transition in the lastcentury.
The reasons for the transformation are complex. Higher incomes, which lead to better dietsand increase people's control over their household environment, are strongly associated with betterhealth-but the improvement in the world's health has gathered pace faster than the growth in in-comes during the second half of the 20th century, indicating that other factors are also at play. Edu-cation is key amnong these: In many studies, mother's education is the strongest determinant of childsurvival in developing countries.
But in addition to these well-known explanations, health research has been an important-and possibly underestimated-factor. Research has brought two different types of tangible benefit tohealth. On the one hand, it has resulted in cost-effective products and interventions to deal with im-portant health problems. For example, vaccines have revolutionized preventive medicine, and nowavert an estimated 3.2 million child deaths per year at a relatively low cost of $1.4 billion (CVI 1993,p. 23). The eradication of polio is within sight, and smallpox is a fading memory. New drugs, power-ful and inexpensive diagnostic tests, and improved equipment also add to the list of cost-effectiveways to improve health. These new products make expenditures on health services potentially pro-ductive; and income growth allows those expenditures to be made.
Research has also benefited health in a second tangible way-by bringing the scientificknowledge that people and governments can use to change their behaviour. In the early 20th century,growing public knowledge of the germ theory of disease, first put forward by Pasteur and Koch, en-abled individual households to improve their health by adopting safer behaviours, such as handwash-ing and the boiling of milk (Preston and Haines 1991)
iThe discovery in the 1950s that smoking causes lung cancer, and the discovery that it in-creases the risk of heart disease and stroke, have been widely understood by the public in the estab-lished market economies; public knowledge combined with governmental taxation and regulatorypolicies to discourage tobacco use have led to a steady downturn in smoking in these countries. Edu-cated individuals change their behaviour relatively rapidly in response to new information; hence theproductive uptake of scientific knowledge relevant to health has been accelerated by steadily improv-ing education levels worldwide.
ix
WHO Ad Hoc Health R&D Report, Draft 2,0
Less tangibly, but just as important, research for health has established a culture of inquirythat is of great value to a complex society reliant on up-to-date information and critical appraisal. Ithas increasingly encouraged health providers-doctors, nurses, managers and community workers-to base their practice on evidence.
Research and development hold equally great promise for improving health in the future.This is true in part because the R&D enterprise itself is becoming steadily more productive; impor-tant reasons for this include:
* Computers and developments in data analysis technology are enabling researchers to buildhealth databases and perform meta-analyses of large numbers of clinical trials, both pub-lished and unpublished, on a scale that would have been impracticable in earlier years. Theresults of meta-analyses have led, for examnple, to improved treatments for breast cancer-adisease with major impact in all regions.
* Communications technology is enabling health-care providers to update their knowledge viaon-line databases, to seek their colleagues' advice in other cities or other continents as theymake a difficult diagnosis, and to alert colleagues to suspected outbreaks of infections.
* Recombinant DNA technologies have exploded in the past 20 years, enabling the design ofvaccines and diagnostics and opening the way for gene therapies.
* Scanning technologies are revolutionizing the study of the brain, as well as enhancing thepossibilities for noninvasive diagnosis of a wide range of conditions, including certain infec-tions.
* Improved diagnostic technologies underpin not only improved treatment but, also, rapid ad-vances in epidemiology and, hence, public health.
* Combinatorial chemistry is enabling scientists to screen thousands of compounds as potentialdrugs within a fraction of the time traditional techniques required. Synthetic peptide chemis-try has enabled, for the first time, the development of a candidate vaccine for malaria in Co-lombia that shows promise in early trials.
This Report addresses the question of how these increasingly potent R&D tools can be usedto confront four globally significant clusters of health problems: an unfinished agenda of infection,undernutrition and excess fertility among the poor, the threat of emerging microbes; the rising epi-demic of noncommunicable disease and injury in developing countries; and inefficiencies and ineq-uities in health systems. Tight budgets and constrained institutional capacity limit the extent to which '
potentially productive R&D investments can be made; hence the importance of allocating R&D re- C '
sources to where the ultimate payoff in health is likely to prove highest. While no algorithm can peintto optimal allocations, the analyses undertaken for this Report seek systematically to inform resourceallocation decisions: by assessing the disease burden expected to be associated with a problem; byidentifying reasons for the remaining disease burden (e.g. lack of tools or lack of efficient use ofavailable tools); by assessing (through subjective judgements of scientists) the extent to which thecurrent knowledge base is adequate to underpin development of improved interventions (and hence tojudge the relative priority to be attached to additional research efforts relative to development ef-forts); and, finally, in light of the preceding, by assessing the extent to which current R&D alloca-tions to dealing with the problem are reasonable in terms of level and composition.
In light of this background analytic effort, the Report comes to a number of recommenda-tions concerning priorities for R&D to address health problems in the four clusters discussed. Box 1
x
Summary
summarizes these recommendations and related recommendations for institutional change and devel-opment.
[Box 1 about here]
Health and poverty: The unfinished agenda
Despite the dramatic improvements of past decades, poor maternal health, undernutrition and thecommunicable diseases of childhood remain major causes of ill health. In 1990, communicable, ma-ternal and perinatal conditions were responsible for a third of all deaths in the world as a whole, andmore than two-thirds of all deaths in Sub-Saharan Africa (Annex 1). Some 12 million children stilldie every year of diseases that are essentially controllable with existing tools. Immunization pro-grammes have been highly successful-yet current efforts still fail to avert roughly half of the burdenof ill health from vaccine-preventable diseases in children. Women in low-income countries continueto suffer unacceptably from the preventable adverse effects of pregnancy and childbirth; maternalcomplications are estimated to claim some 430 000 lives a year.
In addition, many women who want to limnit their famnily size currently lack the means to doso. An estimated 120 million fecund women around the world are not using contraception eventhough they want to avoid becoming pregnant. The consequences of excess fertility for health can besevere: for example, some 60 000 women die from unsafe abortions each year.
An analysis of the priorities for health research in communicable and maternal conditionssuggests that there are two overwhelming categories of need. One is for new products: no vaccinesyet exist for those diseases that cause some 70% of the infectious disease burden in children. Betterversions of existing products are also needed, such as a measles vaccine that can be given to veryyoung infants. Among the "best buys" identified by this review is research that is aimed at improvingthe efficiency of immunization schedules in low-income and middle-income countries, principally byreducing the number of necessary contacts between health workers and children, and thus increasingthe chances of successfully immunizing the highest possible proportion of children in a population.And in the field of reproductive health, there remains a need for additional male methods of contra-ception.
xi
WHO Ad Hoc Health R&D Report, Draft 2.0
Box 1. Recommendations of this Report
Analyses in this Report lead to a number of specific recommendations. Fourpairs of recommendations identify needs and opportunities associated with the fourproblem areas of global health upon which the Report focuses; the final five recom-mendations address the institutional and financial responses appropriate for both do-nors and governments.
Health and poverty: The unfinished agenda1. Despite the existence of cost-effective interventions, communicable dis-
eases, poor reproductive health and undemutrition continue to account for unneces-sarily high disease burdens in most low-income and some middle-income countries.These burdens fall overwhelmingly on the poor and are both a consequence and acause of their poverty. Recent analyses suggest that integrated packages of interven-tions (such as a package for the integrated management of the sick child) could sub-stantially increase the managerial and financial feasibility of reducing those burdens.Govemrments and donors should shift resources into developing and evaluating suchpackages further in different settings and, if their benefits are confirmed, invest inthem as a highly cost-effective means to improve health. i
2. A significant portion of the burdens of infectious diseases and poor repro-ductive health still cannot be addressed by existing tools. New tools are needed-e.g.to increase the effectiveness of vaccination schedules by reducing the number of oc-casions when children must come into contact with health workers, to allow measlesimmunization at earlier ages, and to provide a wider choice of contraceptive methods.Current efforts, both in strategic research and in new product development, are inade-quate to deal with these challenges. Investment in these areas now holds the promisenot only of improving health but also of reducing costs.
Emerging and re-emerging microbes: the continually changing threat ofinfectious disease
3. Economic, social and environmental changes have created the conditions inwhich emerging and re-emerging microbes can spread rapidly, with potentially disas-trous impact on human health. Greater use (and frequent misuse) of antimicrobialsand other control measures has encouraged the emergence of drug-resistant strainsof lethal microorganisms in regions where they were previously controlled. Althoughthe developing regions are bearing the brunt of these problems, countries at all in-come levels are at risk. Two lines of strategic research should be implemented and fi-nancially supported: (a) study of the relation between the emergence of resistantstrains and pattems of use (and misuse) of existing antimicrobials; and (b) the evalua-tion and enhancement of international capacity to detect and monitor emerging ordrug-resistant pathogens in any region.
xii
Summary
(Box 1 continued)
4. Malaria, HIV, TB and pneumococcal infections are four emerging or re-emerging diseases that significantly affect global health status now and are likely tocause further widespread and costly damage if current trends continue. The obviousshortage of existing tools to deal with these threats calis for investment in biomedicalR&D at levels appropriate to the scale of the threats. The potential payoffs from vac-cines against pneumococcal infections and malaria, from female-controlled methodsof preventing HIV infection, and from simplified algorithms for control of TB are particu-larly high.
Dealing with the coming epidemic of noncommunicable disease and injuries5. Faced with growing numbers of cases of noncommunicable diseases and
injuries, developing countries should increase their relevant strategic research in epi-demiology, demography, behavioural science and health policy. Particular attentionshould be given to understanding country- and region-specific levels and determinantsof environmental and behavioural risk factors for these conditions-for example de-terminants of smoking pattems or understanding prevalence levels and risk factors forepilepsy. Biomedical science relevant to these conditions is already comparatively wellsupported in the established market economies and is not therefore a priority. How-ever, some middle- and lower-income countries may need to maintain or develop theirown biomedical research because of the possibility of genuine differences in the char-acteristics of environments and populations (e.g. with respect to the currently unex-plained high risk in South Asians of diabetes and heart disease).
6. The development of drugs to deal with noncommunicable diseases shouldclaim a low priority on the resources of low- and middle-income countries because ofmassive investment in the established market economies. However, the design ofpreventive algorithms (including behaviour change programmes) and cost-effective di-agnostic methods, treatments and rehabilitation to respond to NCDs and injuriesshould be a porioty for support by donors and govemrnments worldwide. Implementa-tion of these recommendations will require both additional funding and strengtheningof the institutions that do the work.
xii
WHO Ad Hoc Health R&D Report, Draft 2.0
(Box 1 continued)
In pursuit of equitable and efficient health policies: leaming from experience7. There is a striking shortage of research effort into the functioning of health
systems and the behaviours of the populations served by them. Yet, from the availableevidence, it is clear that research into both the 'supply" and the "demand" sides of acountry's health system-and the interactions between them-can produce significantfindings that result in major improvements in the quality and coverage of services andreduction in excess costs. Although in some cases the findings of research will bespecific to a particular location, many govemments seek information on how levelsand trends in key indicators in their own countries compare with other countries. Thisprovides a strong argument for systematic development of intemationally comparabledata sets on health finance, disease burden, system characteristics and interventioncost-effectiveness. A global analytic effort to make use of such data could, in addition,dramatically strengthen health policy by enabling countries to leam from each other'sexperience.
8. Investors should devote resources to tuming research results into action, forexample through the development and evaluation of cost-effective instruments of pub-lic policy and practical tools for health workers. These may include essential drugslists, model legislation, priority intervention packages, insurance benefit lists, pricingand taxation policies, practical manuals for use by health workers, and summaries ofresearch results for use by health workers and decision makers.
Responding to the challenges: institutions, incentives and financingfor health R&D
To advance the recommendations above, institutional change and financialcommitment will be required by both govemments and donors. The following recom-mendations are addressed to both: clearly, some are more particularly the concem ofgovemrments and some are more the concem of donors. The recommendations out-line some steps that might be taken to proceed, first in terms of the operation of re-search at national and international levels, and finally in terms of resources and inter-national coordination. These proposais, by emphasizing mechanisms that shift re-sources from nonproductive institutions to productive ones, would inevitably lead tounevenness in the geographical and national distributions of effort. This is no causefor concem as long as the aggregate productivity of R&D to address problems of thepoor steadily increases.
xiv
Summaiy
(Box 1 continued)
9. Governments have much to gain from the development of national agendasfor health research that focus resources into areas of research and institutions withhigh potential and away from those with low potential. Govemrnments and donors mayfurther increase the efficiency of R&D by strengthening national and regional researchcapacity, through, for example, improvements in the quality of training, incentives toreverse the brain drain, policies that require research posts to be competitive andbased on the peer-reviewed allocation of funds; and competitive core support for insti-tutions. The payoffs from investment in good standards are likely to be significant,while poor-quality or repetitive research is wasteful and may have serious conse-quences for health.
10. Govemrnments and donors may profitably explore the development of newinstruments-beyond the current patents system-for engaging the skills and energyof the private sector, including existing industry in low- and middle-income countries,in the development of vaccines, antimicrobiais and other drugs, diagnostic tests,prostheses and equipment. These incentives could include development subsidies,extended patent protection, guaranteed markets, streamlined regulatory requirements,improved market information (including certification of product quality) and contractingfor specific tasks. Clearly, govemments will need to lead in the development of newinterventions to deal with the health needs of the poorest; yet they can achieve thistask efficiently only by bringing in the competence and capacity of the private sector.
11. Two new initiatives are recommended to fill major gaps in current R&D ac-tivity. First, a new Programme for Research and Training on Healthy Aging and Non-communicable Diseases should be formed, based on the models of existing interna-tional programmes such as HRP and TDR. The host institution for this programmeshould be chosen from existing candidates such as IARC, WHO or a national govern-ment on the basis of the demonstration of the necessary resources and capacity toprovide effective leadership. Secondly, a strong Programme for Research and Train-ing on Health Systems and Policy should be formed from the existing institutions andgroups conducting research and training in these areas. The potential payoff fromthese programmes would be high for countries in all income levels; hence not only aiddonors but, also, the health ministries and research councils of high-income countrieshave much to gain from investing in them.
12. A Consortium on International Health R&D should be formed to provide aforum for review of needs and opportunities for global health R&D-making use ofanalytic data on disease burden, R&D opportunities and the level of ongoing efforts.The Consortium would bring together the govemrnments of developing countries, themajor donors, and the research community. Analytic work undertaken by and for theConsortium would provide improved information for decentralized decisions on fundingand resource allocation. The Consortium concept might, initially, be tested as an in-formal gathering of interested parties.
XV
WHO Ad Hoc Health R&D Report, Draft 2.0
(Box 1 continued)
13. Given the high retums to R&D in health improvement and the currently lowpriority accorded to health research by most govemments, a modest reallocation ofhealth sector resources to R&D is recommended as a means to bring substantial netgains in health, particularly the health of the poor. Given that much of R&D providesan intemational public good, there is a particularly strong case for donors to reallocatetheir health portfolios to increase R&D funds. The institutional capacity for supportinghealth R&D that many donors possess strengthens the case for them to increase thisform of assistance, while the globalization of health problems and the solutions re-quired suggests that sources of investment in international health R&D should be di-versified to include high-income countries' ministries of health and research councils.Govemments of low- and middle-income countries are likely to find increased alloca-tions to appropriate health R&D to be both a cost-effective way of improving healthconditions in their country and, potentially, an investment in the infrastructure for po-tentially productive national industries.
9
e
xvi
Summary
But a second-and equally important-set of priorities on this unfinished agenda for com-municable and maternal conditions lies in improving the effectiveness of existing interventions andtreatments. Another of the "best buys" for health research is the evaluation and development of inte-gratedpackages of interventions. For example, growing numbers of countries are adopting a packageknown as the Integrated Management of the Sick Child (IMSC), which the WHO estimates could cutchild deaths in high mortality areas by 50% if uptake of the service were good. The package, which isprojected to be among the most cost-effective interventions in low- and middle-income countries,aims to provide case management of five disease clusters (diarrhoeal diseases, acute respiratory in-fections, measles, acute malnutrition and malaria) which together account for seven out of every 10child deaths each year. Implementation of the package demands that health workers at primaryhealth-care centres are trained to assess the whole child, not to single out specific diseases, and totake appropriate action for treatment which is clearly set out in standard guidelines adapted to eachcountry or region. The challenge to research lies in determining how to increase coverage with thepackage by convincing the population to make greater use of the services and by extending the serv-ices to more of the health system in both the public and private sectors.
Other packages relevant to the unfinished agenda are the Mother-Baby Package (WHO,1994) and the Healthy Women Counselling Guide. The Mother-Baby Package aims to meet the needsof women by providing integrated, high-quality health services for family planning and during preg-nancy, delivery and immediately after birth. It also provides health services for newborn babies. Thepackage treats the mother and her infant together because the factors that cause maternal deathsoverlap with those that cause ill health in pregnancy, stillbirths and deaths among newborn babies.The goals of the package are to reduce maternal deaths by half and perinatal and neonatal deaths by30 to 40% of 1990 levels by the turn of the century. The Healthy Women Counselling Guide, cur-rently under development, aims to provide simple health messages to the most neglected sectoramong poor populations in the low-income and middle-income countries: rural, illiterate women whoare the main health providers in households. At a somewhat broader level, efforts are being made toidentify clusters of interventions (and intervention packages) that constitute an essential minimum forbuilding up a country's primary health care system; the Tanzanian government-with Canadian col-laboration-has initiated a development and evaluation effort (TEHIP-the Tanzanian EssentialHealth Intervention Project) along these lines.
Developing and evaluating packages in different contexts are major goals for health researchin the coming decades. Greater understanding is needed of the incentives that encourage health-careproviders to implement such packages and the disincentives that prevent them from doing so; equallyimportant is a better knowledge of the factors that determine their uptake by households and indi-viduals. Properly implemented and responding to the grassroots needs of communities, these pack-ages could represent some of the most cost-effective ways to gain DALYs in low-income and mid-dle-income countries.
Emerging and re-emerging diseases: the continually changingthreat of infectious disease
In the past 15 years, the world has been forced to accept that infectious diseases are not the spentforce they were once believed to be. Some 20 newly recognized pathogens have emerged since the1970s (CDC Atlanta, 1994). Perhaps more significantly, old enemies such as TB and malaria are re-surging in certain regions of the world. Equally worrying, a growing list of bacteria are developing
xvii
xviii WHO Ad Hoc Health R&D Report, Draft 2.0
resistance to one or more antibiotics; they include Pneumococcus, Staphylococcus aureus and Shi-gella dysenteriae. This Report focuses on four emerging or resurgent pathogens whose impact onpublic health is currently judged to be greatest and for which existing tools are currently inadequateor are expected soon to become so. They are: Pneumococcus, malaria, HIV (clustered for assessmentand intervention purposes with other STDs) and TB.
Multidrug-resistant TB drew widespread public attention in the United States in the early1990s, but the possibility of worldwide emergence of drug-resistant strains is of much greater con-cern to public health. Although data are scarce, the WHO estimates that as many as 50 million peopleworldwide may now carry strains of TB that are resistant to one or more of the common drugs. Thecost of treating a patient who is infected with drug-resistant strains may be several orders of magni-tude greater than the cost of treating drug-sensitive strains. In addition, the number of new cases ofTB disease is expected to rise sharply in endemic communities where HIV is also prevalent. Mul-tidrug-resistant strains of the malaria parasite P. falciparum have severely hampered malaria treat-ment and control efforts in parts of South-East Asia, and drug resistance is increasing in parts of Sub-Saharan Africa. Malaria has thrived on uncoordinated economic development, dilatory control ef-forts, changing land use and the mass movements of people that are increasing worldwide. The emer-gence of drug-resistant strains of Pneumococcus bacteria have caused widespread concern. Amongsingle infectious organisms, Pneumococcus is second only to TB in the number of deaths it causesworldwide. Research is required not only to determine the extent of the problem but also to betterunderstand the clinical significance of laboratory-detected resistance with respect to the therapeuticefficacy of the antibiotics concerned. Even more important is research to determine the effect of dif-ferent dosage schedules and macro patterns of antibiotics on the emergence of resistant strains.Strategies to slow the emergence of resistance need to be developed and carefully evaluated.
An assessment of the priorities for tackling the emerging and re-emerging problems suggeststhat biomedical research is still urgently needed to develop better products and interventions. For ex-ample, the WHO and other agencies are supporting efforts to develop a vaginal microbicide thatwomen could use to protect themselves from HIV and other STDs without having to rely on theirpartners to use condoms. Simple, effective diagnostics and better antibiotics are needed for STDs.The possibility of developing a time-release antibiotic formulation for TB chemoprophylaxis coulddramatically change global TB control strategies. Vaccines against pneumococcal infections areamong the most needed interventions-and among those that represent the "best buys" for health re-search in this area; likewise, although the goal of achieving an effective malaria vaccine has re-mained elusive, a new generation of approaches shows promise.
The threat from these four diseases or disease clusters is clear. Yet an analysis of researchspending conducted for this Report suggests that current efforts to tackle them are wholly inadequate.Malaria, which accounted for almost 11 per cent of Sub-Saharan Africa's total disease burden in1990, receives less than $58 million a year in research spending (Annex 5). Research on TB in devel-oping countries, the leading infectious killer of adults, receives at most some $33 million. In a worldthat spends almost $55 billion on health research overall, these figures-which are both of the orderof 0.1 per cent of all health research spending-highlight the mismatch of current priorities and cur-rent and future needs. The cost of neglecting research and development on these conditions nowcould be disastrous: Suppose, for example, no new antimalarials are developed and multidrug-resistant strains of the parasite spread much more extensively than at present; or that multidrug-resistant TB emerges and spreads rapidly in endemic communities where 1HIV prevalence is alsohigh. In order to address these problems, donors, researchers and in particular the governments ofmiddle-income countries will have to make important choices about R&D investment. [Note: ex-penditure estimates still undergoing revision.]
Summary
R&D needs for the coming epidemic of noncommunicable diseasesand injuries
Projections for this Report indicate that noncommunicable diseases will together account for morethan three-quarters of all deaths in developing regions by 2020, compared with the (already high)50% in 1990. Given that many of these conditions cause chronic illness for which there are currentlyfew cost-effective interventions (although many costly ones), the implications for health-care provi-sion are immense and the challenges to researchers clear. Among the noncommunicable diseases, themain causes of lost DALYs will be ischaemic heart disease, stroke, psychiatric conditions and can-cers, many of which currently lack cost-effective responses.
Demographic change and changes in the patterns of risk exposure in developing regions willalso result in other changes in the health profiles of countries. Injuries, both unintentional and inten-tional, will overtake communicable and maternal conditions in many low- and middle-income re-gions as the second biggest cause of lost years of life. Yet the health sector has so far barely evenbegun to respond to this new reality. A key priority for researchers is to learn more about the propor-tion of disease burden for selected conditions that can be attributed to specific risk factors, such assmoking, alcohol consumption and air pollution. This Report provides somrne of the first attempts toestimate these proportions.
Research on NCDs that is relevant to the particular needs of developing countries is scant,with only a few nations-notably China-taking significant initiatives. Research on injuries is se-verely neglected worldwide. Assessments for this Report suggest that priorities for research in non-communicable diseases should focus on the development of cost-effective clinical algorithms (e.g.inexpensive but responsive protocols for treatment of heart attacks, manic depressive illness, or epi-lepsy) and health promotion packages designed to prevent or postpone disease by encouraginghealthy eating, exercise and the avoidance of risk factors linked with these diseases, most notablysmoking. Evaluation of these protocols in multi-centre trials will both provide evidence on their effi-cacy and begin the process of disseminating best practice. Biomedical research into the physiology ofthese diseases is well covered already by efforts in the high-income economies and appears not there-fore to be a priority for new efforts, except in cases where there may appear to be genuine differencesin the characteristics of environments and populations as, for example, with cardiovascular disease inSouth Asia. But there will be a major need for epidemiological studies to establish the prevalence ofdisease and risk factors in different groups and to enable health systems to plan the provision of care.
A key recommendation of this Report is the creation of a new Special Programme of Train-ing and Research in Healthy Aging and Noncommunicable Diseases, to be based on existing modelssuch as the special programmes on tropical diseases and reproductive health.
In pursuit of equitable and efficient health services: Learning fromexperience
The discussion so far has focused on health research into specific diseases and health needs. But im-provements in human health will not be achieved simply by finding better ways to deal with specificdiseases. Major goals for health research are to understand and improve the health systems withinwhich health services for various needs are provided, and the needs and behaviours of the popula-
xix
.
xx WHO Ad Hoc Health R&D Report, Draft 2.0
tions that use those health systems. The performance of health systems varies enormously betweencountries in terms of the health outcomes achieved, the percentage of GNP consumed, the percentageof the population covered, and the quality of care as measured by popular satisfaction with the serv-ices. The challenge to research is to extract pattems from this diverse experience that can informpolicy choices in the decades to come.
Research in the social and behavioural sciences can shed light on the interaction between the"demand" side (the users) and the "supply" side (the service providers) within a health system; theimpact of different pricing policies on people's uptake of services; the impact of decentralizing aservice; the impact of different methods of paying health-care providers on their incentive to meettheir clients' needs or to over- or misprescribe services; or the impact of making intensive efforts toput new research findings into clinical practice. Research in these disciplines is clearly not confinedto specific diseases but involves broader concerns: for example, a system whose health-care provid-ers are paid a fee for each service they offer is likely to drive costs upwards and create incentives forunnecessary and cost-ineffective treatments for a whole range of specific conditions.
Research needs on the demand side include the development of rapid and low-cost methodsof measuring and monitoring population health status to create national estimates of disease burden;information about the social determinants of behaviours that increase or decrease the risks of certaindiseases and conditions; studies of the interactions between households and their local health sys-tems, including the development of cheap and reliable methods of monitoring the patterns of use ofhealth-care services; and studies of decision making on health matters within households, particularlyconcerning gender-specific issues.
On the supply side, work needs to be done at the country level to assess the particular na-tional and local factors determining the performance of health systems in terms of cost, coverage andquality of health systems; studies need to be done of national health accounts, including measurementof resource flows; and estimates need to be made of intervention cost and effectiveness (particularlyin the evaluation of integrated packages). At the international level there is a need for comparativestudies of expenditures, fmance and efforts to reform health systems in different settings; and, moregenerally, studies of needs, opportunities and resource flows in health research.
These areas of research are likely to become much more influential as health systems aroundthe world reform and increasingly require information about what works and what does not. Invest-ment in well-designed studies in these areas may become highly cost-effective. One estimate sug-gests that improvements in the performance of health systems could reduce the total burden of illhealth by at least 10% in developing countries, and by up to 50% in the poorest countries if moneycurrently spent on high-cost services were diverted to cost-effective interventions. Individual studieshave already demonstrated their worth: for example, health services researchers in Mexico Cityfound that a training package for physicians on the treatment of acute diarrhoea significantly cut thewasteful and erroneous prescription of antibiotics and increased the use of more appropriate oral re-hydration therapy. The strategy was calculated to save up to $173 per patient treated; every institu-tion that paid for a practitioner to attend a training workshop recouped the cost three times over intwo years, simply through the savings on its drugs bill (Gutierrez et al. 1994).
Yet despite the undoubted potential of such research for enhancing health care and prosper-ity, it is a neglected field, receiving minimal support from the major donors. An analysis for this Re-port suggests that together, the major funding agencies' spending on health systems and health policyresearch did not amount to more than $50 million in 1993-less than 0.1 per cent of the world's totalhealth research spending (Annex 5).
Summary
Among the "best buys" identified for R&D investment in this area is the development ofstrong national data sets that will both improve local decision-making and enable internationallycomparative studies of health system performance, population needs, disease burden, and the cost-effectiveness of different interventions in different settings. Such data would enable countries tolearn from each other's experience, reduce waste in research and appreciate the complexity of localand national factors in determining policy. Data that will enable international comparisons of reformsand the quality of services will be essential to both the developed and developing countries in effortsto improve health. Such data will be valuable also in helping to take account of the influence on cost-effectiveness of changes in scale and the location of the intervention. Another major priority is fordonors and governmnents in developing countries to provide specific support for evaluation researchand the systemrnatic dissemination of research results to health-care providers. The Report recom-mends that one mechanism for implementing these proposals would be the creation of a Special Pro-gramme (or Network) of Research and Training for Health Services and Health Policy Research.
Building stronger institutions for global health
Despite many laudable efforts by individual research programmes and institutions, the sum of theworld's effort in health research for developing countries is inadequate to the tasks it faces. Indi-viduals and institutions are hampered by isolation, while a lack of coordination means that resourcesare wasted in some areas of research by excessive repetition between different teams and other areasare neglected totally. Noncompetitive resource allocation, civil-service personnel policies and lack of
concern for peer-reviewed publication lead to wasteful expenditures on duplicative research of oftenmodest quality. Too few systematic efforts exist to translate health research results into action-todevelop new products or procedures---or to develop a culture of evidence-based practice amonghealth service providers.
The "brain drain" is an acute reality. Leading health researchers everywhere operate in aglobal labour market in which there may be strong financial and professional incentives to leave theirregion of origin. Salaries within the public sector in many developing countries are barely sufficientto support individuals, and in some disciplines, such as economics, the health sector is unable tocompete with other sectors. Not surprisingly, the quality of research is highly variable: there arethriving centres of excellence in a number of low- and middle-income countries, but there are alsomany unproductive centres whose resources are allocated on a noncompetitive basis or on nonmeritconsiderations. The overall efficiency of utilization of scarce R&D resources can be markedly en-hanced by rewarding institutions that solve these problems by reallocating resources in their favor; aninevitable consequence will be uneven geographic distribution of facilities and effort.
This Report advances a range of policies to strengthen and develop centres that will attractand support productive research scholars. These centres (or the networks that link them) could alsoserve key training functions-perhaps best through drawing heavily on modern communicationstechnologies to offer "external degrees" as has been pioneered by the Mexican National Institute of
Public Health. An important element of this policy will be to combine national commitment with theinternationalization of aspects of finance, staffing and substantive mandate.
Another problem lies in the inadequate cooperation of industry and governments. The privatesector has unrivalled capacity and skills to offer, particularly in the development of new drugs, diag-nostics and medical equipment. Yet the present patent system offers too few incentives to encourageprofit-motivated involvement on a large scale in the health needs of poor people in developing coun-
xxi
WHO Ad Hoc Health R&D Report, Draft 2.0
tries. Conversely, the public sector currently lacks the experience and the capacity to move in wherethe private sector is absent. To date, there have been only very limited efforts made to explore newincentives and ways to increase cooperation between the two sectors. This Report points to ways ofimproving market information (including information on product quality), market guarantees, ex-tended patents, selectively reduced regulation (based on risk-benefit analysis), and up-front subsidiesas directions for the public sector to explore to stimulate greater involvement of the private sector inproduct development. Certain strategies that have already proved successful should be pursued fur-ther: for example, the provision of global markets for manufacturers, such as IJNICEF's global vac-cines market and the PAHO revolving fund in the Americas, both of which have helped to provideincentives to manufacturers to meet global needs.
This Report makes several specific proposals for strengthening the international health re-search system. Theflavor of our recommendations lies in improving the information and incentiveenvironment in which decentralized resource allocation decisions are taken; little role isforeseenforcentralized decision-making. One proposal is the creation of a Consortium on International HealthResearch and Development, representing the governments of developing countries, the major donors,the principal research programmes, important research centres and the private sector. The Consor-tium would act as a forum for the analysis and review of needs and opportunities for health R&D; itwould be informed by a scientific advisory group, among others, and would base its reviews on dataprovided by a trends analysis group and advice on national research priorities. The Consortiumn'saims would include the advocacy of health research as an international public good, and the trackingof resource flows to R&D.
Conclusion
Global challenges demand, in some sense, a global response. The fruits of R&D are shared by all na-tions: each country may invest a relatively modest sum, but the aggregate may benefit all. Collectiveaction is the economically rational response to "public goods" such as R&D; here, collective actionlies principally in the hands of the global community. Among the many competing demands on thefunds allocated to international assistance for health, those that serve to generate new products andinterventions that can be shared by all claim special merit. If the international system collectivelyfails to invest in productive R&D then, in all likelihood, great opportunities to improve the welfare ofthe peoples of the developing world will be missed entirely. Yet R&D commitments have been de-clining: The challenge to donors in times of budgetary stringency is to recognize their own compara-tive advantage in the generation and dissemination of knowledge.
e
xxii
Chapter 1: Introduction
Human health stands at a crossroads with formidable challenges ahead. First, despite tremendousprogress, poverty's friends-the traditional major killers of developing countries-have not goneaway. Acute respiratory infections, diarrhoeal disease, undernutrition, malaria and a clutch of vac-cine-preventable diseases such as measles continue to kill millions of children every year. Women,meanwhile, continue to suffer the health consequences of unwanted or unsafe pregnancy and child-birth. While spectacular gains have been made against these old enemies to health, there is no roomwhatever for complacency. Indeed, some of the gains of recent decades on this unfinished agenda arenow being threatened in the poorest countries by widening economic gaps, deepening poverty, rapidpopulation growth and economic and social instability.
Secondly, emerging and re-emerging microbes such as HIV, Mycobacterium tuberculosis(the cause of TB) and a growing list of drug-resistant pathogens threaten all communities in a worldthat is experiencing rapid ecological and demographic change. Thirdly, thanks to steep declines infertility and improved life expectancy, the entire world's population is aging, leading to a dramaticrise in the prevalence of age-related diseases in developing countries. And fourthly, health-care costsare rising, while in many communities people are failed by inefficient, inequitable health systemswhose services are of poor quality or beyond their reach.
Since the greatest burden of ill health is borne by the people of the developing world, thisReport focuses on them. But this is not a report for the developing world alone. In an increasinglyconnected planet, no region can consider itself immune to the problems of others; the challengesahead are global. This Report assesses investmnent in research and development as a critical instru-ment for meeting these global challenges.
1.1 Preamble
Daunting as the world's future health needs may sound, the opportunities today for seizing betterhealth may never have been greater. There are already grounds for hope: more children are survivingto school age, more couples have control of their fertility, and more people are enjoying a healthy oldage, than at any time in the past. The reasons for these improvements are generally well known:among them the most fundamental are rising incomes and more widespread education. Income's cen-sequences in better nutrition, safe water and sanitation have each, of course, made major contribu-tions. But in addition, research has brought an extraordinary stream of benefits over the past century,ranging from immunization and antibiotics to the knowledge of germ theory that has enabled parentsto give safe care to their infants. In its relatively short history, the culture of research in health hasmade a powerful impact already, and its greatest benefits may be yet to come. Developments in biol-ogy, in computers and communications technology have transformed the landscape in which re-searchers work. Already those technologies are bringing new dividends: for example in diagnostics,imaging and the rapid dissemination of information.
Despite these achievements, intensive work lies ahead if the world is to rise to the challengesit faces and if the dividends of research are to be shared equitably by the world's populations. Indeed,
1
WHO Ad Hoc Health R&D Report, Draft 2.0
the window of opportunity created by recent gains in health and technology may be closing. In manycountries, both developed and developing, economic and political factors have created a climate thatis often indifferent, and sometimes arguably even hostile, to research. Although funding for R&Dincreased steadily worldwide in both the public and private sectors from the mid-970s to the early1990s, that growth now appears to have peaked in many countries. In 1992, total funding for healthresearch, including basic science, reached a total of about $55 billion (Annex 5). Projections for thisReport, based on an assessment of recent trends, indicate that funds for R&D will decline during thelate 1990s in the public sector, while in the pharmaceuticals industry growth has already declinedsharply. This decline may well lead to a real decrease in the total amount of private funding forhealth research by the end of the decade. In this context, research intended to solve the world's mostpressing health problems is particularly vulnerable. Official development assistance (ODA) from theestablished market economies (EMEs) is at an all-time low, despite most bilateral donors' pro-claimed priority for poverty reduction, and the proportion of ODA that is devoted to health has fallenfrom more than 5% to just 3.4%. Within this meagre sum, only a fraction goes to health research anddevelopment.
Governments accord R&D for health only a low priority. None spends more than 4.5% oftheir health budget on it; most of the established market economies spend less than half of this(Annex 5). Available data from the middle-income countries in the late 1980s and early 1990s showsimilarly low levels of support. For example, South Africa spends between 1.5% and 1.7% of its totalhealth budget on R&D and Mexico spends between 0.3% and 0.5% of its total health budget onR&D. Health research is also a poor relation in the total R&D portfolio of many developing coun-tries. Since the late 1980s India, for example, has consistently devoted less than 2% of its R&Dbudget to health, whereas defence, industry, space and agriculture all receive much larger allocations.Yet, even as funding falters, the health challenges ahead demand urgent action. Many of the gains ofrecent years against communicable diseases could be compromised if drug-resistant strains of M tu-berculosis and other agents were to become more widespread than current estimates suggest (WHOTB Programme 1995). And, whereas the established market economies are able to adjust gradually tothe health needs of their aging populations, some developing countries face an increase of between200% and 400% in their elderly populations in the next 30 years (U.S. Bureau of the Census 1992).Indeed, the increase in the elderly populations in low-income and middle-income countries will farexceed that of their general populations in the period.
Governmnents, donors and health researchers at the crossroads must decide now how theyshould invest in research to bring better health in future. This Report explores how they might do so,and offers some suggestions for key choices ahead. It begins with the case for R&D: Past researchhas delivered spectacular benefits to health and new technologies promise more for the future. Thereport then takes each of the four coming challenges to the world's health in turn, starting with theunfinished agenda on communicable and maternal conditions. In the case of specific diseases and -conditions, the Report shows the projected burdens of those conditions between 1990 and 2020 and,for selected examples, analyzes the nature and extent of research efforts and intervention develop-ment to tackle them
Where the challenge concerns the inefficiency and poor quality of health systems rather thanspecific diseases or conditions, assessments of the key problems and priorities for research in futureare presented. In many cases, the report identifies a mismatch between the scale of a given healthproblem and the research effort that is being put into dealing with it. The report offers suggestions asto how to set priorities for the rational allocation of resources for R&D in future. And finally, it dis-cusses the options for change in the international system of health R&D, including ways tostrengthen capacity for research in developing countries.
e
2
Chapter 1: Introduction
The process of research involves multiple steps, not all of which can be captured by a sim-plistic picture. Initial discoveries-sometimes by accident-have led to the understanding of broaderconcepts that then triggered new concepts and new discoveries in different directions. Figure 1.1 il-lustrates this process with selected examples from biomedicine.
[Figure 1.1 about here]
This Report excludes from its remit fundamental research, and focuses on strategic researchand intervention development and evaluation as a means to solving practical problems. This is not inany way to underestimate the value of fundamental research, which has an intrinsic value of its ownand also generates the knowledge base that can be applied through strategic research and develop-ment and evaluation. The decision to exclude fundamental research was reached because it was con-sidered that judgements about its priorities are governed by a number of considerations other thanthose of health needs and opportunities, and are beyond the scope of this Report. The Report, then,takes the products of fundamental research as a base from which investments in more applied healthR&D can be made.
1.2 The background to this Report: antecedent activities
This study was initiated in response to several recent requests for a broad-based review of needs andopportunities for R&D in the health sector. It builds on the World Bank's World Development Report1993: Investing in Health (WDR 93). The public health and clinical control packages identified bythe WDR-on the basis of disease burden and intervention cost-effectiveness--reasonably reflect theminimum potential of today's technology, and the WDR's analysis of health systems and policyprovides an appropriate starting point for country-based plans of action. WDR 93 suggests an ap-proach to priority assessment for R&D using information on disease burden, existing interventionsand ongoing efforts-that foreshadows the efforts reported here.
The study also builds on the work of the WHO's Advisory Committee on Health Researchand the strategic orientations, both global and regional, given by the ACHR system. In particular, thestudy draws on the important contribution made by the WHO's Technical Discussions on health re-search at the 43rd World Health Assembly (Research Strategiesfor Health, A.M. Davies and B.P.Mansourian, 1992). It also owes a considerable debt to the Commission on Health Research for De-velopment, whose influential report Health Research: Essential Link to Equity in Development hasset the agenda for the past five years, especially in developing the concept of essential national healthresearch (ENHR). The Commission identified a "gross mismatch" between health needs and researchinvestment in the developing countries and found that many countries neglect the research needed toinform decisions on health policy. To fill the gap, the Commission argued for research at a nationallevel for each country to understand its own problems, make the best use of limited resources, im-prove health policy and management, foster innovation and experimentation, and provide the foun-dation for a stronger voice from developing countries in setting international priorities (Task Forceon Health Research for Development 1991). Now, given the global gains in health that can be confi-dently expected from R&D, the present study seeks to build on these efforts by pointing to a numberof key specific areas where international efforts could have high payoffs and by suggesting limitedbut important institutional changes that could help redirect limited R&D resources toward the topicsand the institutions where their payoff would be highest.
3
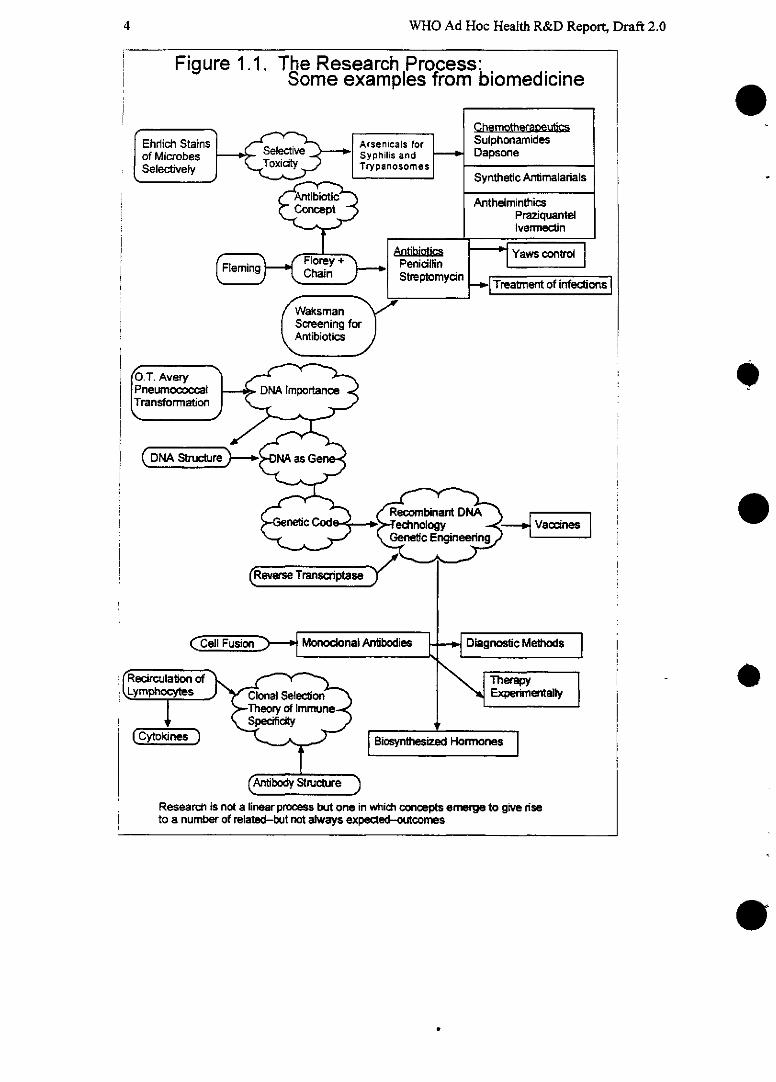
WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 1.1. The Research Process:Some examples from biomedicine
Chemotherapeuticsh Stains Arsenicais for Suiphonamideshaobes Select -v Syphilis and Dapsone¡ObeS Toxicity ~TrypanosomeshivelyJtveiT a Trypanosomes Synthetic Antimalariais
•Antibiotic AnthelminthicsPraziquantelIvermectin
ti~ _ Antibiotics~FleminC ~ _ Florey + Yas ctPenicillinro
~ Chan ~ StriSeptomycíS~n Treatmrent of infections
smcreening forAntibiotics
Cel Fusion Monoclona Antibodies Diagnostic Methods
rmation _
3 0As re as Gi
Ef 5 ^ 9 ~Genei Engineeigw
(Reverse Transcits
_ _ ~~~~ _ > Dia~[~g7nostic Mwethods|
'FK)i \ ro Therapy
(Antibody Structure )
Research is not a linear process but one in which concepts emerge to give riseto a number of related-but not always expected-outcones
4
Chapter 1: Introduction
1.3 Scope and focus
This Report is concerned with research for health. It takes as its starting point the recognition thatgood health is achieved not merely by avoiding disease and gaining access to good health care, butalso by escaping from poverty and receiving a good education. These broader socio-economic de-terrninants of health are well established and this Report fully acknowledges their importance. It ac-knowledges that interventions in many domains outside the traditional health sector, such as educa-tion or housing, may have crucial impact on the health of households, populations and individuals.However, in the interests of focus and clarity, the Committee has sought to narrow its attention on theimmediate, or proximal, determinants of good and ill health which may be better understood andmodified as a result of research and development (R&D). These determinants are taken to be:
a) behaviours that place an individual at risk of poor health outcomes-such as smoking orunsafe sexual activity;
b) environmental influences such as contaminated water or smoke emitted by a cookingstove;
c) theavailability and application of health interventions. Health interventions are defmned asactions that reduce the incidence or severity of adverse health conditions (for a fullerdefinition see Box 1.1); and
d) the health system within which such interventions are provided and which determines ac-cess to services.
[Box 1.1 about here]
Wherever the allocation of resources is concerned, the Report has chosen to focus on health R&D asa segment within the health sector, rather than health R&D as a segment within all R&D. This is be-cause other components of the health sector such as disease control, health promotion and clinicalservices are intimately linked with research activities. That said, country-specific analyses of the roleof R&D for health will appropriately look at the overall R&D context as well as the health sectorcontext.
The Committee has taken a comparatively simple approach to assessing needs and opportu-nities for research and development in health. It has begun by identifying four broad challenges toglobal health in the coming decades which are amenable to R&D. The first is the "unfinishedagenda" of the diseases and conditions traditionally linked to poverty, which include: undernutrition,the major childhood killers including respiratory infections, diarrhoeal diseases and the vaccine-preventable cluster of childhood diseases; and poor maternal and reproductive health. The second isthe emerging and re-emerging infectious diseases including Pneumococcus, malaria and thetropical cluster, HIV and STDs, and TB-that pose growing threats to communities worldwide orwithin particular regions. Within this group, many diseases have never truly been conquered, and arenow resurging as a result of antimicrobial resistance, demographic and environmental change andother factors. The third challenge is the coming epidemic of noncommunicable diseases and inju-ries that is appearing with the aging of the world's population and the changing patterns of exposureto certain health risk factors. The fourth is the inequity, inefficiency and poor quality of health sys-tems worldwide, whose costs are spiraling while many remain without access to their services or dis-satisfied with unsatisfactory care.
5
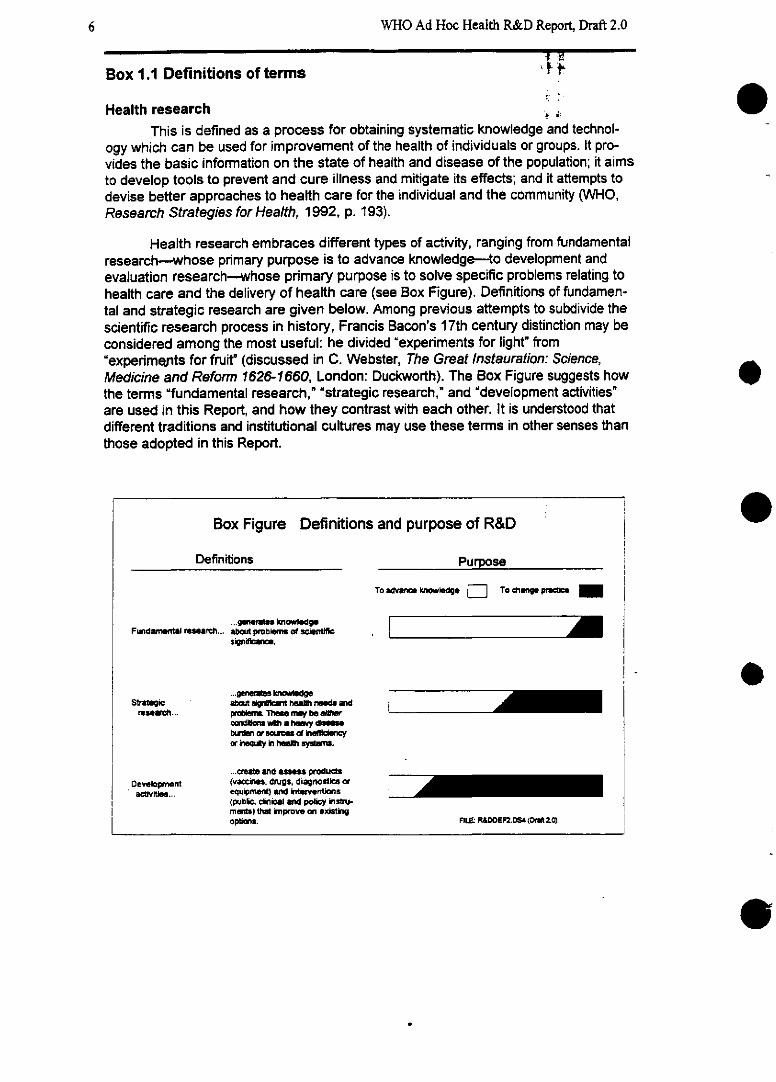
WHO Ad Hoc Health R&D Report, Draft 2.0
Box 1.1 Definitions of terms
Health researchThis is defined as a process for obtaining systematic knowledge and technol-
ogy which can be used for improvement of the health of individuals or groups. It pro-vides the basic information on the state of health and disease of the population; it aimsto develop tools to prevent and cure iliness and mitigate its effects; and it attempts todevise better approaches to health care for the individual and the community (WHO,Research Strategies for Health, 1992, p. 193).
Health research embraces different types of activity, ranging from fundamentalresearch-whose primary purpose is to advance knowledge- to development andevaluation research--whose primary purpose is to solve specific problems relating tohealth care and the delivery of health care (see Box Figure). Definitions of fundamen-tal and strategic research are given below. Among previous attempts to subdivide thescientific research process in history, Francis Bacon's 17th century distinction may beconsidered among the most useful: he divided "experiments for light" from'experimep.ts for fruit' (discussed in C. Webster, The Great Instauration: Science,Medicine and Reformn 1626-1660, London: Duckworth). The Box Figure suggests howthe terms "fundamental research," 'strategic research," and "development activities"are used in this Report, and how they contrast with each other. It is understood thatdifferent traditions and institutional cultures may use these terms in other senses thanthose adopted in this Report.
Box Figure Definitions and purpose of R&D
Definitions Purpose
To advnce kn, edge ] To change p¡oetie
/J
/I/
Fundamentl rseanrf...
Statag~cresae~t ...
Developmentactvities...
...gmi iknowldgeabut problen~ of sceificsigni 1,.
...* p ns g~a~ut si ant hea~ nee~s andprem. Tle nwy be eWrond-- wlh a hesy diabwdan orms~ of inencyor iequty in hea~h sys~TI.
a...nts and _s producta(va cns. dnugs, diagnostics orequipment) and hteventons(pubic, dlical and policy insat-ments) that improve on existingopions. FIL RO&DDEF2.D64 (Dt 2.zO)
e
e
e
e
l
r-
L
6
.
Chapter 1: Introduction
(Box 1.1 Continued)
It is clear that each stage of research is to some extent dependent upon oth-ers, and that a linear model of the different stages of research is unhelpful in under-standing the process. The diagonal line in the above diagram seeks to stress the inter-relatedness of each stage and the fact that there is likely to be substantial movementback and forth between stages. Nevertheless, it is generally true that the proportion ofthe research objective that is defined as being "for fruit" (to change practice) ratherthan "for light" (to advance knowledge) will increase with the spread of the dark sec-tion towards the left side of the bar.
Fundamental researchThis has been defined as research whose purpose is principally to increase
knowledge about problems of scientific significance. This review does not deal with re-source allocation to or within fundamental research except to note that the products offundamental research serve as a foundation for strategic reseach and intervention de-velopment.
Strategic researchThis has been defined as research whose purpose is primarily to increase (and
publish) knowledge and understanding of a significant health problem, but with a vieweventually to solving or reducing the impact of the problem through further develop-ment and evaluation. The relative importance of the knowledge-gaining componentand the problem-solving component will vary depending on the type of project and thenature of the problem. Importantly, the definition of strategic research adopted by thisReport is not purely biomedical but encompasses also the work of behavioural scien-tists, epidemiologists, demographers and health policy scientists. Specific healthproblems worthy of strategic research within each discipline might include, for exam-ple, sequencing the genome of an important pathogen; ascertaining the factors de-termine the biting behaviour of anopheles mosquitoes; why most people fail to com-plete a course of chemotherapy once their symptoms disappear; what proportion ofthe burden of a given disease can be attributed to a specific risk factor in a specificpopulation; and what effects the decentralization of health services have on the cover-age of a given service within a given population.
Development activities: products, interventions and policy instruments1. Products. These are defined to encompass five basic groups of health-
related material products: drugs, vaccines, equipment, prostheses and diagnostics.
2. Interventions. These may be combinations of products, algorithms, infor-mation or policies that reduce the risk, duration or severity of an adverse health condi-tion (Jamison et al. 1993). They may be usefully subdivided as either:
7
.
WHO Ad Hoc Health R&D Report, Draft 2.0
(Box 1.1 Continued)
* Public health interventions-those that are sought of or directed towardentire populations or subgroups, including immunization, mass chemoprophylaxissuch as the addition of iodine or medications to salt or the fluoridation of water,nutritional interventions, such as encouraging all pregnant and pre-conceptionwomen to take folic acid supplements; or
* Personal health service interventions-those that are provided at facilities andusually to individuals; these include in- and outpatient medical treatments, screening and re-habilitation.
3. Instruments of govemrnment policy. These encourage or discourage spe-cific health interventions, e.g. pricing and/or taxing policies on tobacco, pricing policiesfor health services; essential drugs lists; policies for paying health workers accordingto the type and range of services they offer.
Biomedical sciencesThis term includes all strategic biological, medical and clinical sciences.
Population sciencesFor the purpose of this Report, this term covers epidemiology, demography
and the behavioural sciences. It is not intended to denote solely that part of health re-search concemrned with fertility, family planning and population control.
Health policy sciencesThis term includes health policy research and health systems research, includ-
ing health services research.
Disability-adjusted life year (DALY)This is a unit of currency for measuring the burden of disease that, unlike tradi-
tional mortality statistics, allows researchers and health policy-makers to assess thenonfatal consequences of ill health and injuries as well as premature death (WDR 93,Murray and Lopez 1994). Each lost DALY indicates the loss of a year's healthy life-that is, the time lived with a disability and the time lost through premature death. The -
assumptions on which the DALY is based are not universally accepted, and remain amatter for continued ongoing debate. However, the advantage of this currency is that,as a single indicator, it provides a comparable measure of the outcome of health inter-ventions for a wide range of particular health problems and diseases. For an explana-tion of the uses of the DALY to measure disease burden, see Box 1.2.
e
8
Chapter 1: Introduction 9
(Box 1.1 Continued)
Essential national health research (ENHR)This concept, first set out by the Commission on Health Research for Devel-
opment, aims to achieve equity in health and development. It holds that each develop-ing country should establish and strengthen an appropriate health research base to'understand its own problems; improve health policy and management; enhance theeffectiveness of limited resources; foster innovation and experimentation; and providethe foundation for a stronger developing country voice in setting international prionties"(Commission on Health Research for Development 1990, OUP).
WHO Ad Hoc Health R&D Report, Draft 2.0
Clearly, the boundaries between the infectious diseases discussed under the "unfinishedagenda" and those considered to be re-emerging are somewhat arbitrary. For example, malaria is animportant cause of child morbidity and mortality in the poorest regions of the world, and could there-fore be considered a part of the unfinished agenda; but because drug-resistant strains are emerging inmany regions, it has been treated as a re-emerging disease. Diarrhoeal disease is a large part of theunfinished agenda; but the special case of drug-resistant Shigella dysenteriae requires discussion un-der re-emerging diseases. However, the distinction between the two categories is felt to be valid intermns of the different needs and opportunities for R&D that they present.
1.4 Methods
A numnber of criteria are clearly important in thinking about the claims on R&D resources that a par-ticular problem area or approach might make. Is the problem big? (The world lost 70 times as manyDALYs from TB as from lymphatic filariasis in 1990.) Do we already have good tools for dealingwith the problem? (The availability of multi-drug therapy-MDT-for leprosy attenuates the case forinvesting in development of a leprosy vaccine.) Is the science base good? If so, one might proceedrapidly to pi'oduct development and testing (as with pneumoccocal vaccine); if not, strategic researchto develop the knowledge base might be required (as with HIV vaccine). Are the high-income coun-tries already spending a lot on the problem? (R&D money available to low- and middle-incomecountries could add little to what is already being spent by rich countries to study atherogenesis or todevelop new drugs for controlling hypertension or hyperlipidemia.)
Few would disagree that consideration of resource allocation within health R&D for develop-ing countries should, in some way, take the above considerations into account. This Report argues,simply, that we should attempt to take these factors into account as quantitatively and systematicallyas possible. Sometimes this will not be possible. Even when it is possible, the resulting informationcan only inform---not determine---resource allocation decisions. Yet the Committee has been struckby how often these considerations are ignored: R&D money goes to diseases of little signficancewhile major killers (e.g. TB) are neglected; attention goes to marginal improvements in already goodproducts while major opportunities are missed (e.g. heat stable polio vaccine relative to efforts to re-duce the number of contacts requred to fully immnunize a child).
This Report provides much new information on current and projected levels of disease bur-den; on current levels of R&D spending; on the reasons for remaining disease burden for selectedconditions; and, also, for selected conditions, on scientists' judgements about development opportu-nities and strategic research needs. These analyses point us in the direction of a number of specificconclusions although-always and inevitably-the conclusions are the products not of the analysisper se but of the Committee's judgements informed by data and analysis. For the longer term, one ofthe Committee's main recommendations is to put in place a process for continually informing R&Ddecision making by improving the information environment in which those decisions are taken.
1.4.1 Steps to inform R&D resource alUocation
We suggest four steps to inform thinking about allocation of R&D resources to and within aproblem area (e.g. TB or malnutrition).
e
10
Chapter 1: Introduction
i) Calculate the burden of disease to be addressed; Annexes 1 and 2 provide the detailed re-sults of our work in this area; Box 1.2 provides a brief sunmmary.
[Box 1.2 about here]
ii) Identify the reasons why the disease burden persists. Figure 1.2 indicates the analyticalapproach applied. Using data supplied by experts in each field, it is possible to estimate what portionof the total burden of each disease or condition is now being averted, what could be averted withbetter use of existing interventions, and what cannot be averted with existing interventions but re-quires new ones. The analysis is intended to identify where the greatest needs lie, and thereby guideassessment of the priorities for different types of research. The unit of currency employed for thisanalysis is the disability-adjusted life year.
[Figure 1.2 about here]
The whole square represents the total estimated disease burden (in DALYs) from a givencondition, such as diarrhoeal disease. The horizontal axis represents the coverage of the population-that is, how far into the population the appropriate mix of interventions is currently penetrating. Thevertical axis represents the combined efficacy of this mix. The subdivisions within that square repre-sent different portions of the burden: (1) that which is being averted now by the existing mix of cost-effective interventions among the people that the intervention is reaching; (2) that which could beaverted if the existing interventions were used more efficiently; (3) that which could be averted withexisting tools, but not cost-effectively; and (4) that which is not avertable with existing interventions.Calculations of the relative share occupied by each subdivision, based on data supplied by experts ineach field, can help to spell out the priorities for research . For example, where it is calculated that alarge portion of the total burden of a certain disease cannot be averted with the existing cost-effectivetools, then there is a strong case for biomedical R&D. Where it is calculated that a large portion ofthe burden could be averted if fmances were distributed differently, there is a strong case for strategicresearch into health policies and health systems to analyze the reasons for an apparent mismatch be-tween needs and investment. Where it is calculated that a large portion of the total burden could beaverted if the existing tools were applied with greater technical efficiency, then there is a strong casefor strategic research into the behaviour of service users and providers to learn how coverage couldbe increased and efficiency maximized.
iii) Judge the adequacy of the current knowledge base. This undertaking relies, of course, onthe subjectivejudgement of informed scientists. If the knowledge base is adequate to support devel-opment of specific interventions, then the (estimated) cost-effectiveness of those interventions rela-tive to those currently available can be assessed. The desirability of intervention development willthen depend on its cost, estimated probability of success and extent of improvement offered over -
available alternatives. If the knowledge base doesn't allow development of new interventions-judged to be attractive in the way indicated-there is a suggestion of the desirability for strategic re-search to strengthen the knowledge base. Clearly this process could conclude that multiple ap-proaches are desirable-particularly if the relevant disease burden is large.
11
WHO Ad Hoc Health R&D Report, Draft 2.0
Box 1.2 Measuring the global burden of disease: Progress and con- estraints
Lost DALYs (or diasbility-adjusted life years-see Box 1.1) can be used to in-dicate the burden of diseas-c in the whole world, in a specific group or population, orfrom a particular condition. For example, Sub-Saharan Africa lost 575 DALYs per1000 people in 1990, compared with the established market economies, which lostjust 117 DALYs per 1000. Neuropsychiatric disease lost the developing world 72 mil-lion DALYs in 1990; respiratory infections cost the developing world 119 million. TheWorld Bank's WDR 1993 provided the first attempt to measure the global burden ofdisease-by age, sex, region and cause for 1990-and used the DALY as its meas-ure. A major reassessment of the WDR's estimates has been undertaken for this Re-port along with projection of disease burden into the future (Annex 1).
In order to assess disease burden, the World Bank and the WHO began byassigning all deaths worldwide in 1990 to the 109 intemationally recognized categoriesof disease, subdividing by age, sex and demographic region (such as the establishedmarket economies, or Latin America and the Caribbean). The number of years of lifelost was assessed as the difference between the actual age at death and the age towhich the person could have expected to live from t hat age, given the mortality levelsin a post-transition country, that is, 82.5 years life expectancy for women and 80 formen. Next, the incidence of disability due to disease or injury within each gender, ageand demographic region was estimated from the available information within eachcommunity and from expert opinion. The expected duration of the disabling condi-tion-to remission or death-was multiplied by a weighting factor that allowed the se-verity of the condition to be taken into account. For example, a severely disablingcondition that stops the person from doing basic activities, such as eating unaided,was assigned more weight than a condition that limits solely one nonessential activity,such as recreation. Finally, the researchers incorporated a discounting system to allowfuture years of life to become gradually less valuable, and assigned different relativevalues to years at different stages in a person's life. A year of life at birth is relativelylow in value, rises rapidly to age 25, when the person is likely to have older andyounger dependents, and then declines slowly.
It is important to note that the DALY construct involves explicit underlying as-sumptions. Their very explicitness makes it possible to undertake "sensitivity analy-ses' of how estimates of disease burden vary with respect to age-weighting, discountrates and disability weights; the results of analyses that have been undertaken doshow an effect on estimates of disease burden but, reassuringly, the effects are smallover the reasonable range of assumptions. Extension and exploration of the DALYconcept continues, and some potential lines of change explicitly introduce burden as-sociated with late fetal death and would increase the estimated relative burden of non-communicable diseases in developing countries-reinforcing one of the main mes-sages of this Report (Supplementary Paper A. 1).
e
12
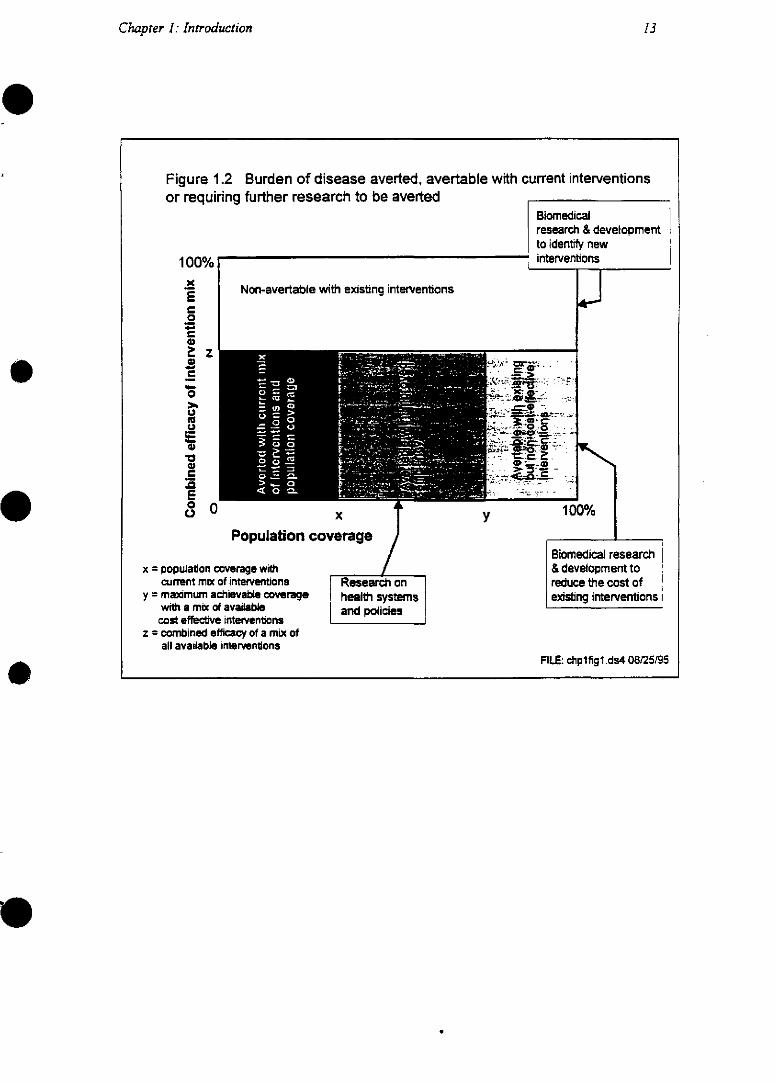
Chapter 1: Introduction
Figure 1.2 Burden of disease averted, avertable with current interventionsor requiring further research to be averted
Biomedicalresearch & development 1to identify new
- interventions
Non-avertable with existing interventions
Population co
x = population coverage withcurrent mix of interventions
y = maximum achievable coveragewith a mix of availablecost effective inteventiona
z = combined efficacy of a mix ofall available interventons
x
verage
Research onhealth systemsand policies
y
Biomedical research& development toreduce the cost ofexisting interventions i
FILE: chplfigl.ds4 08/25/95
100%
Z
Eo
)e2 Z-2
ou.u
uee
3
Ec a 1
WHO Ad Hoc Health R&D Report, Draft 2.0
iv) Finally, assess the adequacy of the current level of effort Annex 5 reports the Commit-tee's attempts to describe ongoing levels of resource allocation. Problems of data availability makethis effort a difficult one; additional attention is required on an ongoing basis. In light of what is nowbeing spent, and of the attractiveness of development and strategic research possibilities identified instep (iii), judgements about appropriate changes in the level or composition of resources allocation tothe problem area can be made.
The Committee views this systematic approach to informing decision-making as a way of in-formingjudgement-not replacing it. Our experience in applying the approach suggests that neglect-ing one or more of the above steps is both frequent and distorts resource allocation; hence our con-clusion about the desirability of more generally adopting a systematic approach.
1.4.3 The roles of different disciplines
Since health problems have broad origins and impacts, different disciplines within health re-search-from biomedical scientists to health policy analysts-must contribute to addressing them.The Committee divided up health research into three very broad disciplinary aggregates to assist as-sessments of priority activities and ongoing activities. These domains (defined in Box 1.1) are: bio-medical sciences; population sciences-which include demography, epidemiology and behavioural osciences; and health policy sciences-which include social and economic sciences and health sys-tems research. Each makes an essential contribution to assessing need and developing interventionsand each is to some extent dependent on ithe others. Tools for health are useless unless they are suc-cessfully implemented. Take the following examples:
* malaria: biomedical researchers study the immune response of individuals to malaria para-sites at the molecular level; population scientists (epidemiologists) study the proportion ofpeople in a given population with some natural immunity to the parasites; sociobehaviouralresearchers study the factors that determine whether people use bednets or other protectivedevices or not; economists study the pricing and policy factors that determine whether peopleshould be asked to buy their own bednets or have them provided free; and health systems re-searchers study the advantages and disadvantages of different approaches to organizing theprevention and treatment of malaria. These could include the promotion of bednets as part ofthe job of local health centres, or by a central, vertically organized malaria programme.
* contraception: biologists research and develop contraceptive methods, epidemiologists in-vestigate contraceptive safety and efficacy of methods in use, sociobehavioural researchersinvestigate couples' perceived unmet needs and the relationships between clients and provid-ers, systems researchers investigate factors that limit access to contraceptive services.
* smoking: biomedical scientists study the mechanisms by which cigarette smoking can causecancers of various types; population scientists study the evidence linking tobacco use withvarious diseases and estimate the burden of those diseases that can be attributed to smoking;sociobehavioural researchers focus on why certain groups take up smoking and how theymay be persuaded to stop; and economists study how policies such as tobacco taxation caninfluence smoking behaviour.
The analysis of resource allocation priorities has sought to identify, within each of the fourmajor health problem areas, the balance of disciplinary effort that is most relevant. Table 1. 1 pro-
14
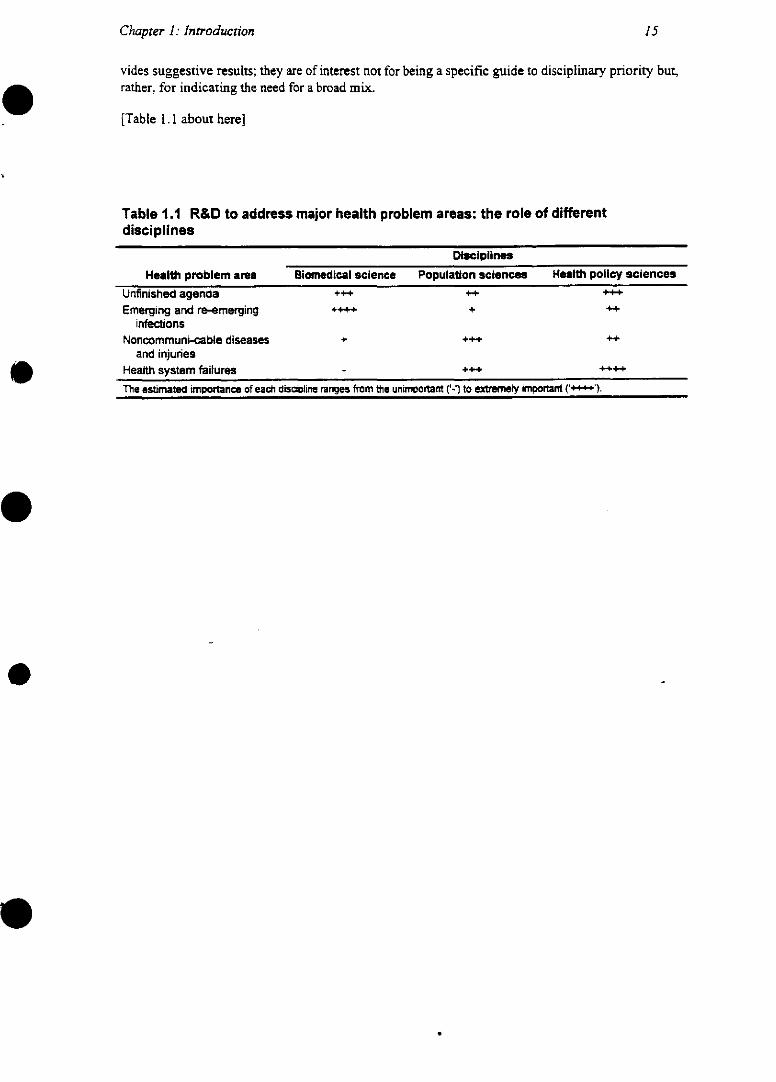
Chaprer 1: Introduction
vides suggestive results; they are of interest not for being a specific guide to disciplinary priority but,rather. for indicating the need for a broad mix.
[Table 1.1 about here]
Table 1.1 R&D to address major health problem areas: the role of differentdisciplines
Disciplines
Heali problem area Biomnedical science Population sciences Health poUnfinished agenda +++ ++Emerging and re-emerging ++++ +
infectionsNoncommuni-cable diseases +++
and injuriesHealth system failures - +++The estimated importane of each disacIline ranges from the unimportant ('-') to extremely impDortant (:: .
olicy sciences
++-
++--d
-
15
eChapter 2: Why invest in health research? Historical
experience and the promise of science
The health of the world's peoples has improved more in the past four generations than in the preced-ing 400. In China in 1950, the odds that a child would not live to reach school age were as high asone in three. For those children's children, just 30 years later, the odds had fallen to about one in 15,and they are expected to reach one in 28 by the year 2000 (WDR 1993: 203).
The scale and pace of the change are unprecedented. In the middle-income and low-incomecountries overall, life expectancy at birth has risen sharply from 40 years in 1950 to 63 years in 1990(Figure 2.1) and the trend is still upward. Even in Sub-Saharan Africa, where the improvement hasbeen slowest and smallest, the gain has been greater over the past four decades than it was over acomparable period in Europe in the 19th century.
[Figure 2.1 about here]
The reasons for the dramatic improvements are complex. First, incomes have risen in a num-ber of countries, allowing households to escape from poverty, eat a better diet, and gain greater con-trol over their environment and their lives. But income growth alone cannot explain all of the in-crease. People in any given income bracket are healthier now than they were 100 years ago atequivalent incomes (see Figure 2.2). In other words, income x buys better health now than it did 30years before. Therefore, other factors must help to explain why people live longer and healthier lives.
[Figure 2.2 about here]
Environmental changes such as clean water, sanitation and improved housing, are recognizedto have played an important role (McKeown 1962, 1976). These changes, together with increasedfood intake (Fogel 1994), are perhaps dithe principal routes through which higher incomes enhancepeople's health. Education, particularly mother's education, is crucial: in many developing countriesparental education levels are the strongest determinant of child survival even after controlling forhousehold income and access to health services (Caldwell 1993). On the whole, educated women arealso more likely to limit family size, and children born into smaller families are more likely to sur-vive than children born into large ones. Other major determinants of health beyond income include _ethnic origin, immigration and mobility. Studies conducted largely in high-income countries indicatethat, independent of income, such factors play a statistically significant part in increasing the rates.ofdisease and disability in populations (Pincus et al. 1987; Chirikos and Nickel 1986; Verbrugge 1979;Davey Smith and Egger 1992). Social disadvantage appears to have an adverse effect on the health ofhouseholds even where a wide range of health services are free and universally available (Report of aResearch Working Group, "The Black Report", 1980).
16
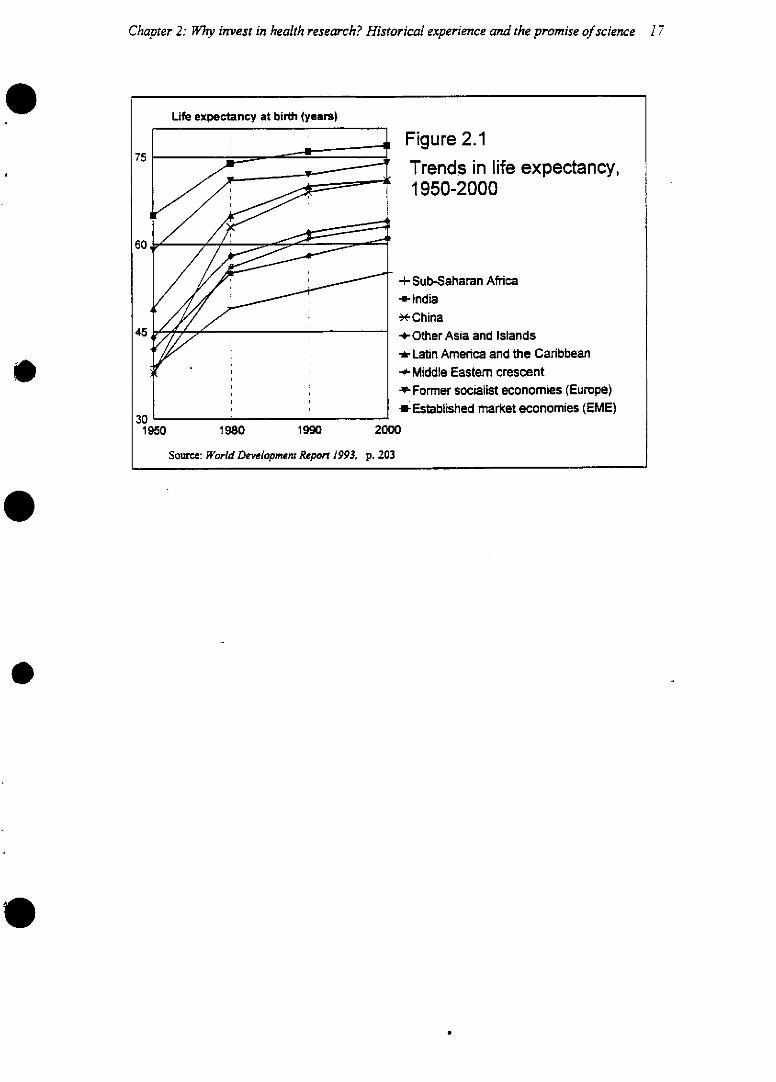
Chapter 2: WIhy invest in health research? Historical experience and the promise of science 17
Life expectancy at birth (years)
Figure 2.175
,_~~ ~ ~Trends in life expectancy,
60 /X~/~~ :=1950-200060
/ : /ó -i- Sub-Saharan Africa-*-India-*- C h inaa
45 +Other Asia and Islandsi/~ I ts~--Latin Amenrica and the Caribbean
,~~ I( < ' i SF~-+M iddle Easterm crescent/ I, i+ I ~--Former socialist economies (Europe)
~~l30 ~- ol*Established market economies (EME)1950 1980 1990 2000
Source: World Development Report 1993. p. 203
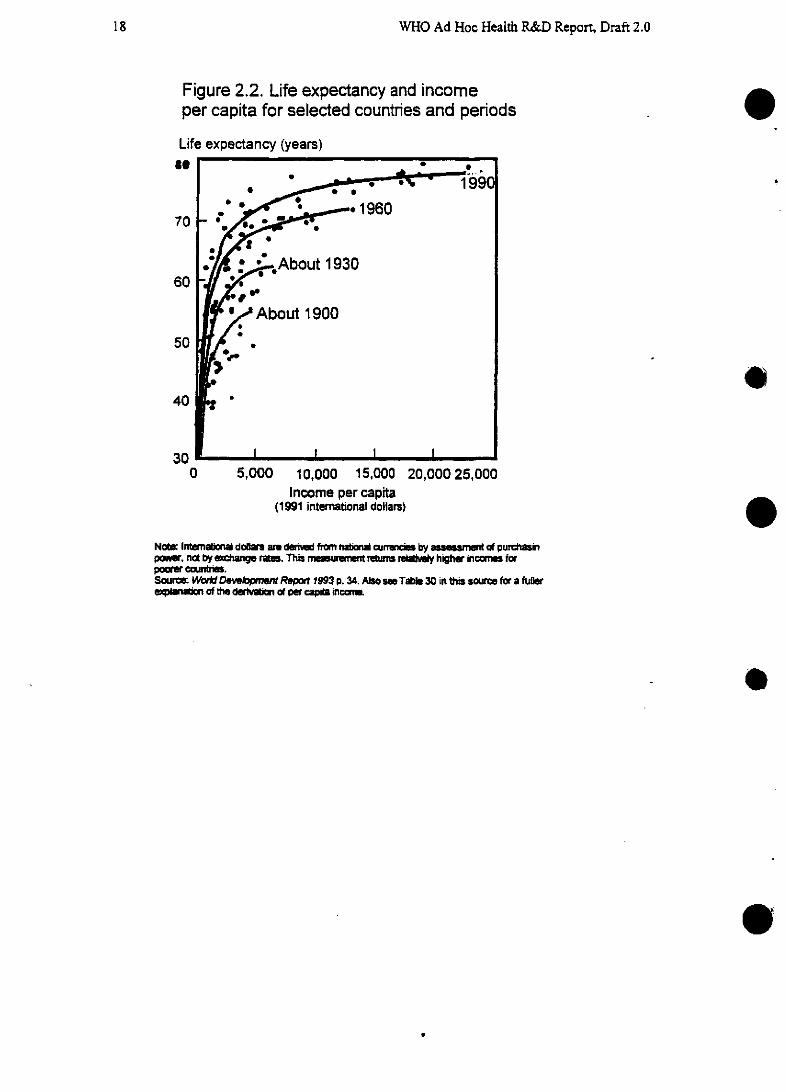
WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 2.2. Life expectancy and incomeper capita for selected countries and periods
Life expectancy (years)e 1
70
60
50
40
30
o
e0 5,000 10,000 15,000 20,000 25,000
Income per capita(1991 international dollars)
No: Interna~n a d~al are derid from nat curnci by assrmt « purchasinpor~. not by exhange rate. This mewre~ returns rdi~ y higher intornas forpoarer couwtn.Sourmc Wor Devepment Rep 1993 p. 34. Also se Tl~ 30 in this soa e for a fullerepman of the deran of par capia mcm
0
18
Chapter 2: Wl7y invest in health research? Historical experíence and thepromise of science 19
2.1 The scientific underpinnings of past health improvement
However, these factors together account for only a portion of the enormous gains in health status seenduring the past century. Another factor-the impact of scientific research-may have been underes-timated. Scientific research has triggered improvements in health in two tangible ways: by bringingknowledge that households can use to live healthier lives, and by producing direct medical and healthinterventions such as vaccines and clinical algorithms. Beyond those tangible benefits, it has alsobrought a culture of inquiry and an understanding that practice should be based on evidence-both ofwhich are of direct value to any society.
The importance of household knowledge as an outcome of research may only now be gainingrecognition. On the basis of studies of the U.S. censuses in 1900 and 1910, Preston and colleagues(1991) showed that parents' education made relatively little difference to children's survival untilscientific knowledge became available that enabled households to improve their health. Once thegerm theory of disease was widely understood, Preston argues, households adopted healthier behav-iours, such as boiling water for infants or washing their hands regularly. Education came into its ownas an imnportant health determinant once that new knowledge was available: the better educatedhouseholds were able to acquire the new knowledge more rapidly in order to change their own behav-iour and to seek professionals' advice or help. Researchers have argued that modemrn, pro-scienceeducation enables people in the low- and middle-income countries today to make the best use of cur-rent medical knowledge (Caldwell 1993). Meanwhile the products of technological development-radio and television, telephones and commnunications networks-ensure that information about healthis disseminated more rapidly than ever before. [Material from Mushkin and Weisbrod to be added onrole of R&D in improving health in the United States.]
Science has also had a direct-and dramatic-impact on health. Research has led to bettervaccines, medicines, diagnostic and therapeutic equipment and procedures and to rational means ofevaluating, selecting and deploying these innovations. In the past century and a quarter, there havebeen revolutionary changes in our concepts of disease, our understanding of the nature of life andbiology, our ability to intervene effectively in the course of disease and our ability to prevent it fromarising. And, while the gradual declines in mortality that were experienced by most of the industrial-ized countries may be attributed pardly to wealth, a safer environment and better diet, the situation isdifferent in many low-income countries. The reduction in mortality in these countries has been sorapid, and in many Sub-Saharan African countries has taken place amid so little economic improve-ment, that they cannot reasonably be ascribed purely to socioeconomic changes. Improved educationhas played a major role, but largely because it has enabled people to make good use of the preventiveand therapeutic interventions available to them. Much of the improvement in health must, therefore,be attributed to health research.
The greatest of the tangible advances since the 1 880s have been in the war against communi-cable diseases and have largely flowed from the demonstration of the microbial origins of infections,which were most clearly exemplified by the work of Louis Pasteur, but were dependent on manyother people, as towards the end of the l9th century scientists rapidly sorted microbial infectionsfrom noncommunicable diseases. From thec discovery of the microbial agents of communicable dis-eases flowed two main approaches-chemotherapy, or the search for Paul Ehrlich's "magic bullet"-and immunoprophylaxis, or the quest for vaccines.
The great flowering of chemotherapy dates from the late 1930s with the production of thesulphonamides, the outcome of a pharmaceutical company's research, and then penicillin, discovered
WHO Ad Hoc Health R&D Report, Draft 2.0
earlier by Fleming and developed by Florey and Chain in academrnic laboratories within the publicsector. Subsequent discoveries have also come from varied origins, with both streptomycin andcephalosporin originating in university laboratories and many other antimicrobials emerging from theprivate sector. During the Second World War, the benefits of this research were powerfully demon-strated when antibiotics and antimalarials transformed the prospects and the morale of the Alliedtroops, bringing a sharp reduction in the proportion of losses that were due to disease as comparedwith those due to enemy action (Vannevar Bush: Science: The Endless Frontier, Washington, D.C.:National Science Foundation).
The development of vaccines against human diseases began 200 years ago with Jenner's in-oculation against smallpox. The past century has seen the introduction of effective vaccines againstseveral of the major childhood diseases and conditions, particularly polio, diphtheria, pertussis, teta-nus, measles and Haemophilus influenzae, and their refinement and improvement continues. Whilethe first generation of vaccines relied mainly on empirical research, modern approaches employequally great creativity and more technological sophistry. Now, genetically engineered vaccines arecoming into use, for example against hepatitis B virus, while the rate of progress in this area points toan increasing payoff for genetic engineering in the near future. Even the use of synthetic peptides tomake vaccines, once regarded as futile by many, has now received encouragement from the devel-opment in Cclombia of Spf66, a synthetic candidate vaccine for malaria.
Beyond antimicrobials and vaccines against communicable diseases, there are many moretangible benefits of research which continue to be improved and developed. Anaesthesia has evolvedfrom a relatively crude process to a highly sophisticated one. With the discovery of insulin the effec-tive treatment of diabetes began; with X-ray, the first of the scanning technologies now comple-mented by ultrasound, positron emission tomography and others to enable noninvasive diagnosis fora wide range of conditions. The link between tobacco smoking and lung cancer was f-rst made in the1950s as a result of epidemiological research, resulting, eventually, in policy changes.to restrictsmoking in public places and a downturn in smoking in the established market economies.
The benefits of research have continued and the pace of development has intensified. Hor-monal contraception has given women greater control over their fertility. New endoscopic surgicaltechniques, properly implemented, have dramatically reduced the inconvenience to patients and thenumber of days that they must spend in hospital; and the early diagnosis and Ueatment of certaincongenital malformations, and metabolic disorders such as phenylketonuria, have enabled many oth-erwise disadvantaged children to live normal lives. Oral rehydration therapy has saved many morefrom dying of diarrhoeal disease. The treatment of childhood cancers in the industrialized countries isone of the great success stories of the past 30 years, with 80% of childhood leukaemias now cured.
Another great advance has been the randomized clinical trial (RCT), which enables physi-'cians and researchers to assess the efficacy of interventions in a rational manner. Meta-analyses ofmany RCTs enable researchers to detect the benefits-and disadvantages--of interventions whoseeffects are comparatively modest but which may be of great importance in the treatment of com mondiseases. The identification of genes responsible for single-gene diseases such as cystic fibrosis hasopened up the possibilities of devising genetic therapies for some conditions, and trials for certain ofth ese th erapies are now under way. The roles of multiple genes in more complex disorders from car-diovascular disease to schizophrenia are now being actively sought.
Health research, however, goes further than the biomedical sciences. Researchers in healtheconomics and epidemiology have developed measures of the cost-effectiveness of health interven-tions that enable governments and other authorities to plan the best use of health-care resources.
e
20
Chapter 2: Why invest in health research? Historical experience and the promise of science 21
Health services researchers have identified the most effective models of care for a wide range ofconditions, such as whether community care is appropriate in severely mentally ill patients in specificsettings. Such research has been instrumental, for examnple, in demonstrating that programmes ofprimary health care and nutrition care in poor rural areas can be highly cost-effective in reducing in-fant and child mortality.
All these tangible benefits of health research have emerged within a broader scientific con-text which has itself delivered more persuasive and complex contributions. Most importantly, theculture of research has provided a rational, knowledge-based framnework for progress in health. Bothmedical practice and health policy have been the prey of ineffective remedies and fashions in policyfor centuries, and a scientific framework has provided as much for eliminating the irrational and inef-fective as for the development of new ways to improve health. Systematic reviews of clinical re-search, such as those now being produced by the Cochrane Collaboration, and the dissemination ofresearch findings to practitioners are at last creating a climate for evidence-based medicine that islong overdue. Changes in therapy or health services that have ignored rational analysis have retardedprogress.
[Figure 2.3 about here]
2.2 Investments that paid off: the cost-effectiveness of past R&D
As a proportion of all health spending, R&D's share is very small indeed. Worldwide in1992, it accounted for just over 3% of total health expenditure (Annex 6). Yet its impact has beendisproportionately high. It has led, for example, to affordable interventions (defined as those that costless than $100 for each year of healthy life they save) for 8 out of the 10 main causes of disease bur-den in young children in developing countries (WDR 93: 222). Thus, for example, acute respiratoryinfections, which kill more children than any other disease or disease-cluster in low-income andmiddle-income countries, can be managed at a cost of $30 per year of healthy life gained (HarvardCenter for Population and Development Studies 1995) and measles vaccine buys DALYs for as littleas $2 to $15 each (Jamison et al. 1993).
Data from the United States indicate that for every $1 I spent on the diphtheria-tetanus-pertussis vaccine, $6 in direct costs are saved; for every $1 spent on the measles-mumps-rubellavaccine, $16.34 in direct costs are saved; and for every $1 spent on oral polio vaccine, $3.40 aresaved (EJ. Hatziandreu, et al., CDC 1995).
Analyses of the cost-effectiveness of specific research investrnments are rare, at least to date.However, data from the U.S. National Institutes of Health for selected areas indicate that the payofffrom investment can be very high indeed. For example, research into drug addiction has produced anumber of cost-effective and life-saving treatments. Conservative estimates indicate that for every $1invested in addiction treatment programmes, there is a return of between $4 and $7 in reduced drug-related crime, criminal justice costs and theft alone. When savings related to health care are included.total savings can exceed costs by 12 to 1. Similarly, research into alcoholism has led to the use in theUnited States of naltrexone, an opiate antagonist that reduces craving for alcohol for those in treat-ment, and the subsequent demonstration that use of the drug reduces relapse rates by between 58%and 72%.
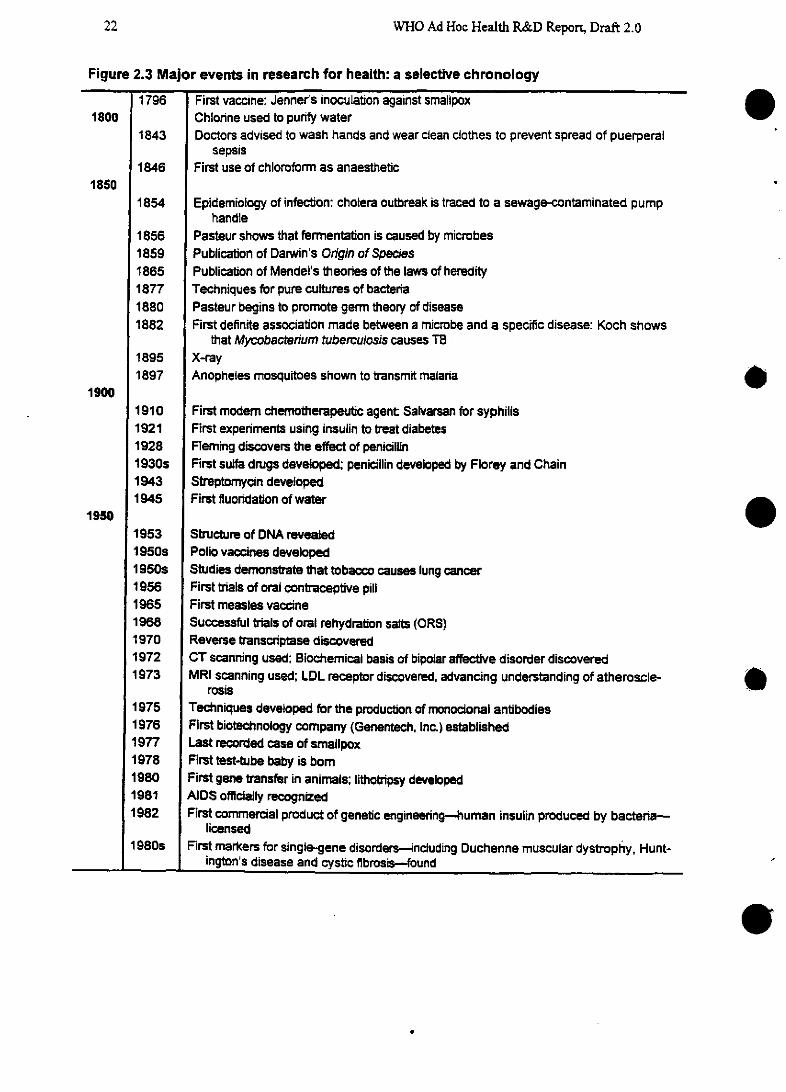
WHO Ad Hoc Health R&D Reponrt, Draft 2.0
Figure 2.3 Major events in research for health: a selective chronology
1796 First vaccine: Jennerts inoculation against smallpox1800 Chlorine used to punfy water
1843 Doctors advised to wash hands and wear clean clothes to prevent spread of puerperalsepsis
1846 First use of chloroform as anaesthetic1850
1854 Epidemiology of infection: cholera outbreak is traced to a sewage-contaminated pumphandie
1856 Pasteur shows that fermentation is caused by microbes1859 Publication of Darwin's Origin of Species1865 Publication of Mendel's theories of the laws of heredity1877 Techniques for pure cultures of bacteria1880 Pasteur begins to promote germ theory of disease1882 First definite association made between a microbe and a specific disease: Koch shows
that Mycobactenrium tuberculosis causes TB1895 X-ray1897 Anopheles mosquitoes shown to transmit malaria
19001910 First modem chemrnotherapeutic agent Salvarsan for syphilis1921 First experiments using insulin to treat diabetes1928 Fleming discovers the effect of penicillin1930s First suifa drugs developed; penicillin developed by Florey and Chain1943 Streptomycin developed1945 First fluoridation of water
19501953 Structure of DNA revealed1950s Polio vaccines developed1950s Studies demonstrate that tobacco causes lung cancer1956 First trials of oral contraceptive pill1965 First measles vaccine1968 Successful triais of oral rehydration salts (ORS)1970 Reverse transcriptase discovered1972 CT scanning used; Biochemical basis of bipolar affective disorder discovered1973 MRI scanning used; LDL receptor discovered, advancing understanding of atheroscle-
rosis1975 Techniques developed for the production of monocional antibodies1976 First biotechnology company (Genentech, Inc.) established1977 Last recorded case of smallpox1978 First test-tube baby is bom1980 First gene transfer in animals; lithotripsy developed1981 AIDS officially recognized1982 First commercial product of genebtic engineering-human insulin produced by bacteria-
licensed1980s First markers for single-gene disorders--including Duchenne muscular dystrophy, Hunt-
ington's disease and cystic fibrosis-found
22
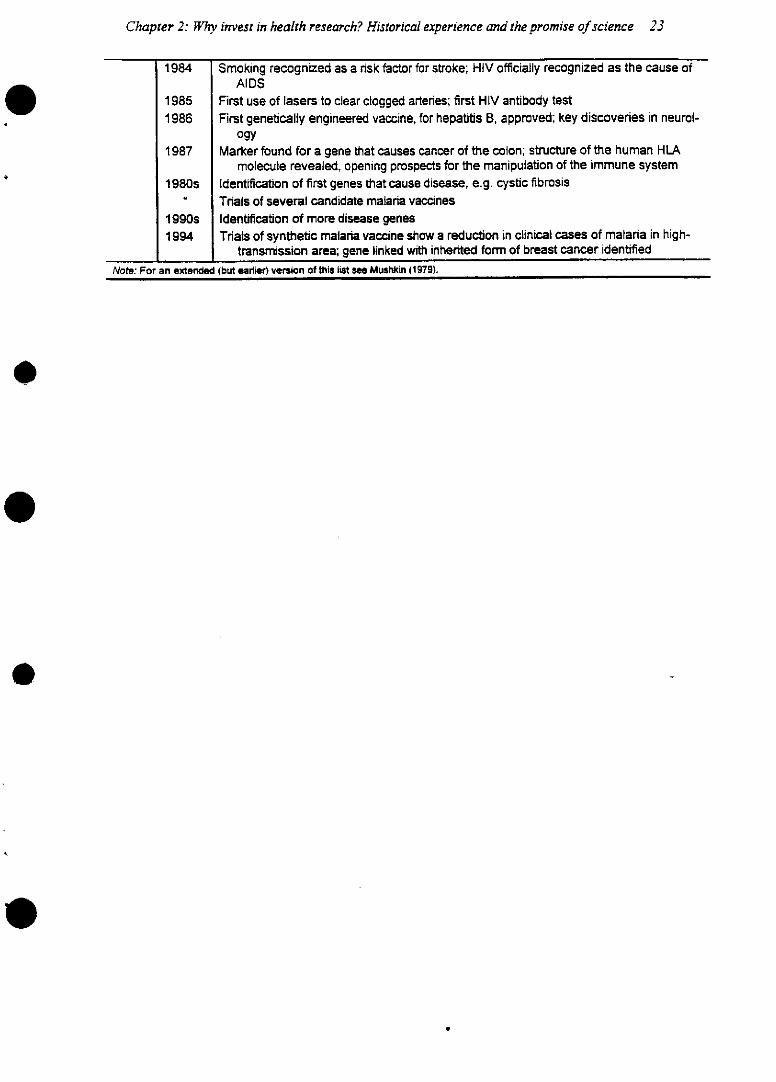
Chapter 2: Why invest in health research? Historical experience and the promise of science 23
1984 Smoking recognized as a nsk factor for stroke; HIV officially recognized as the cause ofAIDS
1985 First use of lasers to clear clogged arteries; first HIV antibody test1986 First genetically engineered vaccine, for hepatitis B, approved; key discoveries in neurol-
ogy1987 Marker found for a gene that causes cancer of the colon; structure of the human HLA
molecule revealed, opening prospects for the manipulation of the immune system1980s Identification of first genes that cause disease, e.g. cystic fibrosis
Trials of several candidate malaria vaccines1 990s Identification of more disease genes1994 Trials of synthetic malaria vaccine show a reduction in clinical cases of malaria in high-
transmission area; gene linked with inherited form of breast cancer identified
Note: For an extended (but earlier) version of this list see Mushkin (1979).
.
WHO Ad Hoc Health R&D Report, Draft 2.0
Alcohol abuse is of paramount importance as a risk factor for disease and injuries worldwide;the overall economic cost of alcohol abuse, in lost productivity, treatment costs, damage to property,social and administrative costs and crime has been estimated at $98.6 billion per year in the U.S.alone. Research played a crucial role in demonstrating that increasing the minimum legal drinkingage in the various states of the United States from 18 to 21 would reduce the number of road trafficincidents and related fatalities significantly. Since 1988 all states have imposed a minimum age of 21years, saving many lives and an estimated financial savings of up to $600 million per year.
There are many more examples from the United States. R&D has produced a sputum test forPneumocystis carinii pneumonia for an outlay of $440 000 that is now estimated to save around $50million per year by removing the need for invasive diagnostic procedures. Studies of donated bloodconfirmed that it was not necessary to screen all donated blood in the U.S. for HIV antigens-a muchmore expensive and laborious process than that of screening for antibodies to the virus. The studiescost $500 000, and enabled the Federal government to save an estimated $37 million to $49.4 millionper year by avoiding the purchase of a costly antigen test kit.
It may be argued that over the past 30 years, health R&D as a whole has been highly cost-effective. Estimates for this Report indicate that DALYs can be bought through research at relativelylow cost (see Box 2.1).
[Box 2.1 about here]
2.3 Looking ahead: research tools for the future
The lessons of the past make an already strong case for health R&D but the opportunities offered bynew developments in science and technology add weight to that case. Research is now progressing atunprecedented speed, enabled by a range of research technologies that have transformed the envi-ronment in which science is done.
Recombinant DNA technology has made it possible for scientists to manipulate the expres-sion of genes in microorganisms to create components for vaccines-for example against Salmonellatyphimurum--and to devise gene therapies. Whereas so far gene therapy is being developed only forsingie-gene disorders such as cystic fibrosis and is primarily beyond the reach of all but the wealthi-est economies, its nature and cost are likely to change in future so that it can tackle more complexdisorders, such as atherosclerosis, and so that it becomes a cost-effective form of intervention in low-and middle-income countries. Recombinant DNA technology and the techniques of DNA amplifica-tion have also transformed the possibilities for diagnosing infections, such as chlamydia, and certainmetabolic conditions by detecting minuscule quantities of indicator substances in saliva and otherfluids, thus reducing the need for more inconvenient and expensive invasive tests.
24
Chapter 2: Why invest in health research? Historical experience and the promise of science 25
Box 2.1 Estimating the cost-effectiveness of past health R&D and the im-pact of neglecting research in future
The overall cost-effectiveness of R&D has been estimated, within certain as-sumptions, for the period 1960-1990. Under this model, R&D has been highly cost-effective, saving DALYs for under $50 each. The model assumes that research aloneexplains the increase in life expectancy over and above that associated with rising in-comes, illustrated in Figure 2.2. This is clearly an oversimplification but, even if theimpact of research is weaker than the model assumes, it is still cost-effective. Figures2.4 and 2.5 show that research has averted the loss of a highly significant number ofDALYs in the past 30 years.
The calculation is made by comparing trends in mortality rates over the past 30years with what they would have been expected to be, had the relationship betweenincome and ¡¡life expectancy remained at its 1960 level. The difference between ex-pected and observed mortality rates is then converted into a measure of the numberof healthy years of life lost. The cost of health R&D-which includes all health re-search from genetics to sociology--is estimated from the available data on researchspending by the public and private sectors since 1960. The cost of research per yearof healthy life gained is then calculated. The model takes into account the increasedhealth expenditure that is likely to be attributed to health research.l (Comparable fig-ures for other health expenditures will be available for the next draft).
It is clear that the cost-effectiveness of R&D could be improved further if wastewere reduced. For example, unnecessary duplication between laboratories and over-lap in programmes may account for a substantial proportion of limited funds that mightbe better used on other research activities. At present, there is neither an oversightmechanism for reducing overlap and duplication, nor a tracking system to monitor re-source flows. Many research efforts are not translated into policy nor taken up byhealth-care providers; future challenges will demand such systematic efforts to in-crease efficiency.
Assumptions of the model:
1. In this model, research expenditures were set as a fixed percentage (2.9%) of global expenditure onheaith (in 1990 U.S. dollars).
2. This global expenditure on health was determined from a regression equation used for the Worfd Deve/-opment Report 1993 study of global health expenditures.
3. Effectiveness (DALYs Gained) was determined by comparing DALY projections with projected total DA-LYs that would have been incurred without research from 1960 to 1990.
4. Both sets of DALY projections are based on the relationship between GDP and life expectancy at birth. asthis relationship was presented in the WDR 1993. This relationship in 1990 differs from that in 1960; thatis, controlling for GDP, LEB is greater in 1990 than in 1960.
5. Benefits were discounted at 3% and only benefits gained before the year 2050 were included.6. This model assumed the increase in total health spending that is likely to be attributable to health re-
search to be a ratio of 1:1.
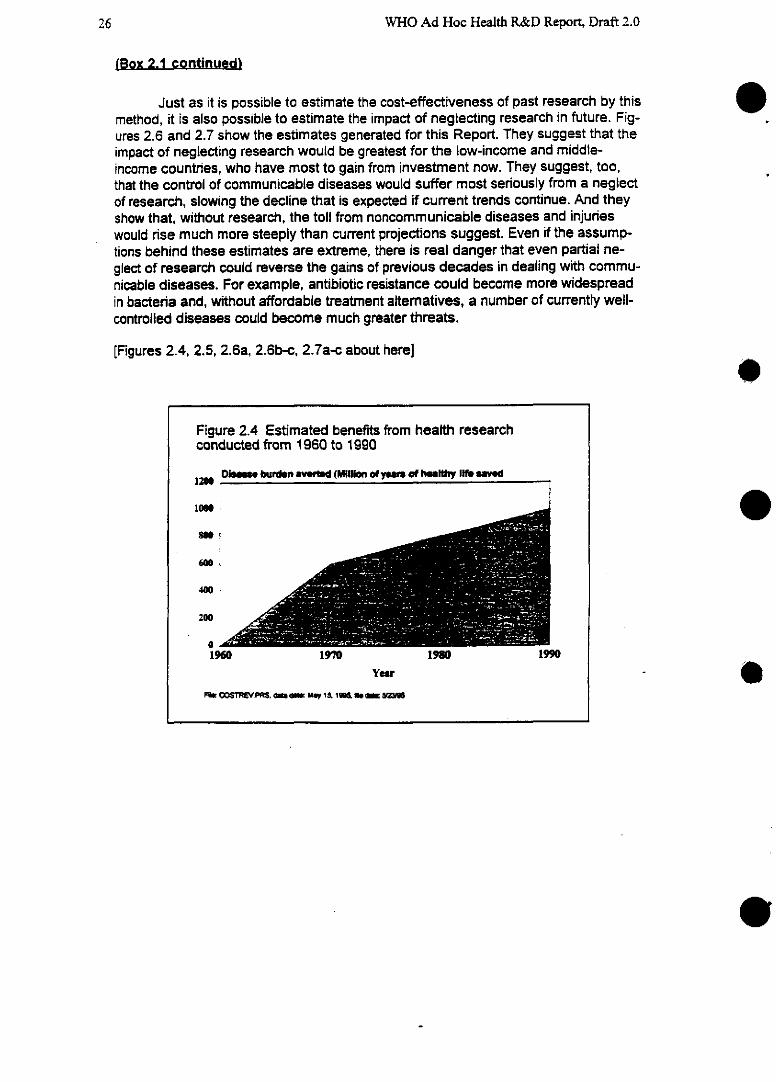
WHO Ad Hoc Health R&D Report, Draft 2.0
(Box 2.1 continued)
Just as it is possible to estimate the cost-effectiveness of past research by thismethod, it is also possible to estimate the impact of neglecting research in future. Fig-ures 2.6 and 2.7 show the estimates generated for this Report. They suggest that theimpact of neglecting research would be greatest for the low-income and middle-income countries, who have most to gain from investment now. They suggest, too,that the control of communicable diseases would suffer most seriously from a neglectof research, slowing the decline that is expected if current trends continue. And theyshow that, without research, the toll from noncommunicable diseases and injurieswould rise much more steeply than current projections suggest. Even if the assump-tions behind these estimates are extreme, there is real danger that even partial ne-glect of research could reverse the gains of previous decades in dealing with commu-nicable diseases. For example, antibiotic resistance could become more widespreadin bacteria and, without affordable treatment altematives, a number of currently well-controlled diseases could become much greater threats.
[Figures 2.4, 2.5, 2.6a, 2.6b-c, 2.7a-c about here]
eFigure 2.4 Estimated benefits from health researchconducted from 1960 to 1990
i Dke* burdn avytd (Miion of yearn of hultly If muved
400
200oe
o19601960 19Y0 1980 1990
Year
FM COSTr~evPRS. ~ My 15. ,
26
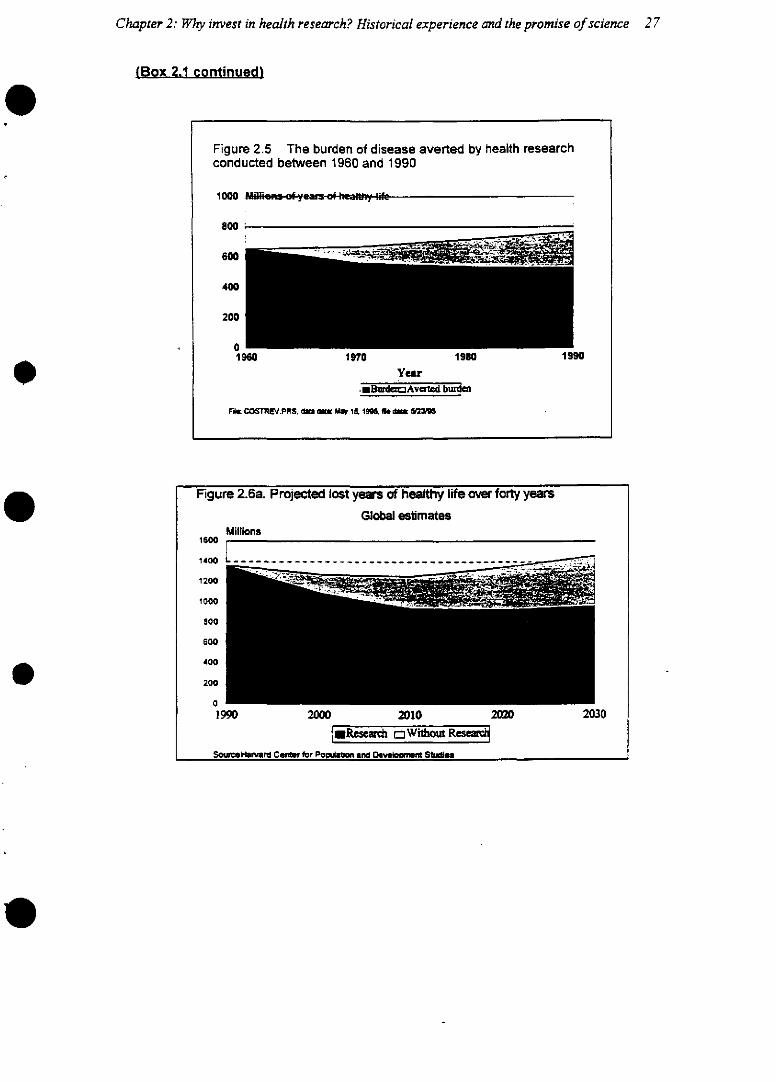
Chapter 2: Wlry invest in health research? Historical experience and the promise of science 27
(Box 2.1 continued)
F¡gure 2.5 The burder, of disease averted by health research
Figure 2.5 The burden of disease averted by health researchconducted between 1960 and 1990
1000 if'is . ; . f
800
600
400
200
1960 1970 1980 1990
Year
mBzda2Avaed burde
F« COSTREV.PRS. da ~, May 15. 19~ fk ~
Figure 2.6a. Projected lost years of healthy life over forty years
Global estimatesMillions
1600
1400 ..................... -. '"~ -'
12Wj
1000
800
600
400
200
1990 2000 2010 2 20 2030
S eRescah rWitroutRs
SouuHarmrd Ce for Pobuma and DeOveWn S1ubos
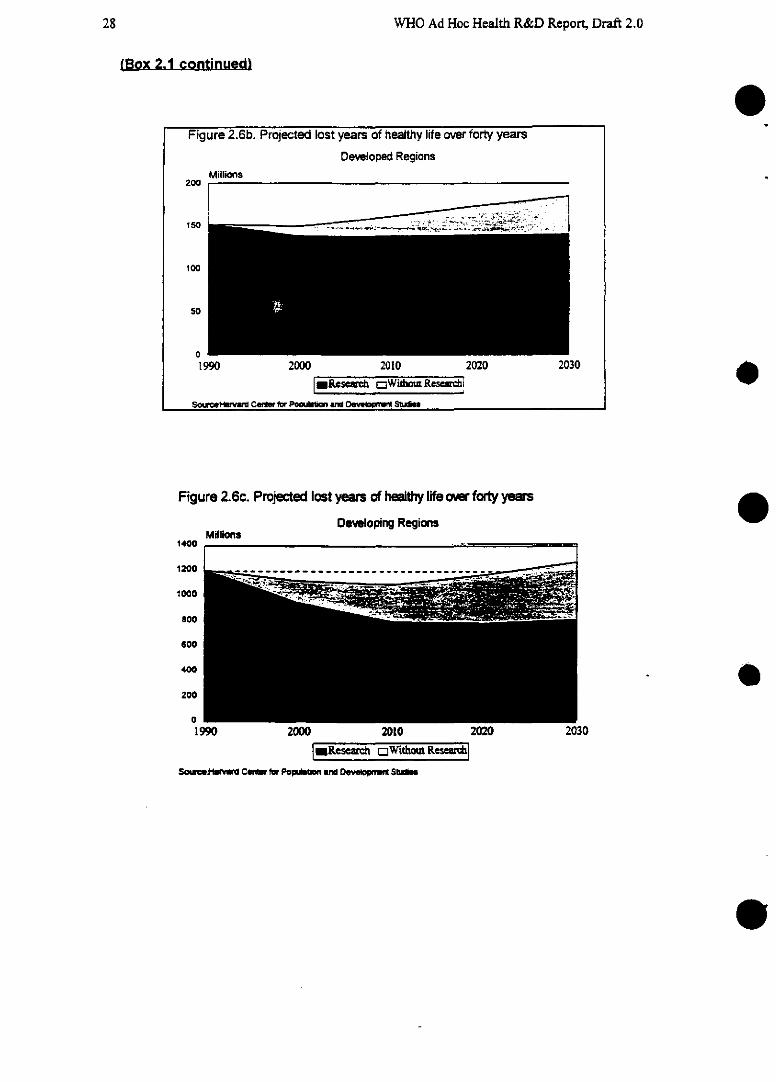
WHO Ad Hoc Health R&D Report, Draft 2.0
(Box 2.1 continued}
Figure 2.6c. Projected lost years of healthy lfe over forty years
DeMeloping RegionsMi#llans
1400
1200
1000
800
600
400
200
1900NuU ¿ZIO
m.Resa~ rC=Witho~R Kese~
Sourc.j-fmnu~ Cen.f fo~ PoumW ad Don=~ s$idn
0Figure 2.6b. Projected lost years of healthy l¡fe over forty years
Developed RegionsMillions
200
100
50
01990 2000 2010 2020 2030
m*Re,.~ cWi hout R¢se~ !i
e
e2030
--- 1--- --- -- _~--- .-
---
28
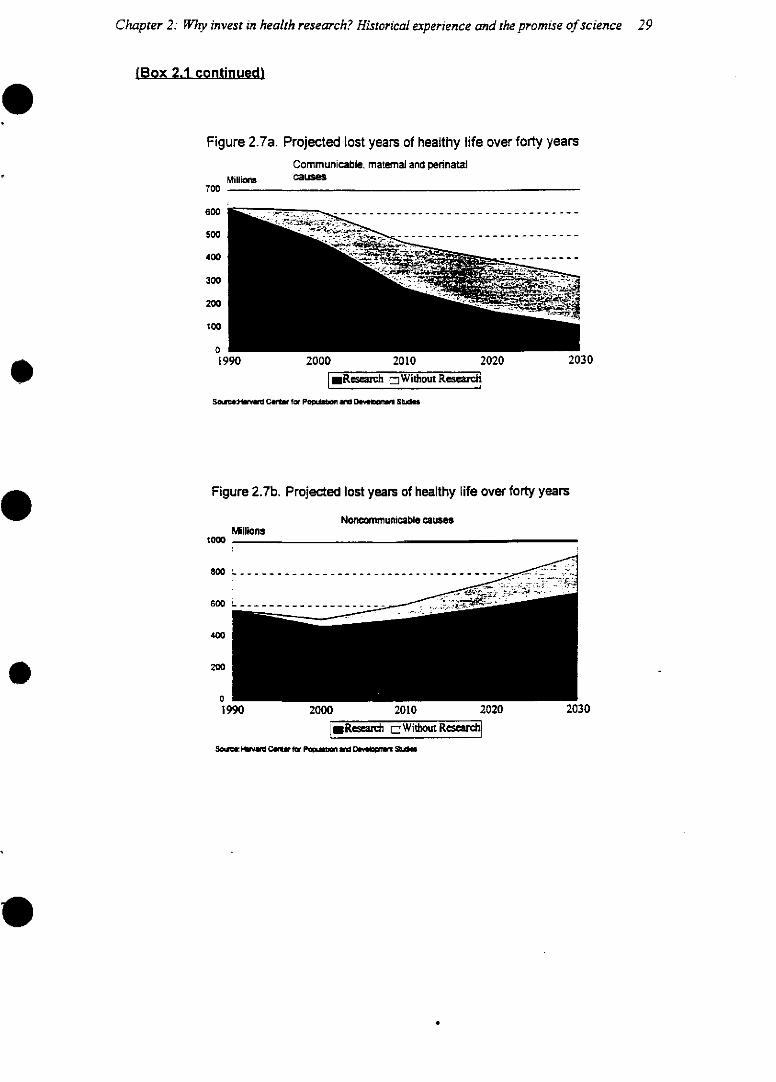
Chapter 2: Why invest in health research? Historical experience and the promise of science 29
(Box 2.1 continued}
Figure 2.7a. Projected lost years of healthy life over forty years
0 I
Communicable. maternal and pennatalMilins Cases
20301990 2000 2010 2020
lResearch =Without Restar
S~~avu CUr for Po~.on aM Dev~u, S~gk
Figure 2.7b. Projected lost years of healthy life over forty years
Noncomnmunicable causesMillions
800 …...... … _-- - - - - - - -.- .-. - r, .
600 L- ....
400
200
1YUJ ZUU ZULU ¿
Rsea rch a Without Renr
S5~ w Ca~ fo Po on uc De~ Sk~
700
600
500
400
300
200
100
1000
.
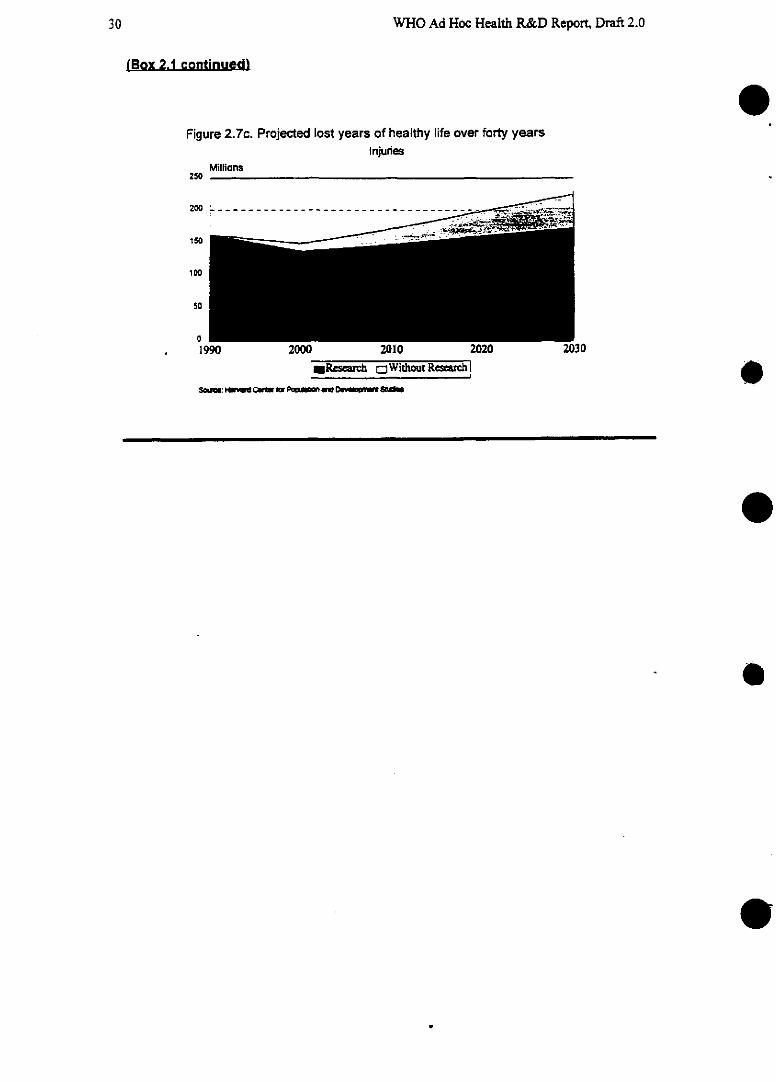
WHO Ad Hoc Health R&D Report, Draft 2.0
(Box 2.1 continued)
Figure 2.7c. Projected lost years of healthy life over forty yearsInjurdes
Millions250
200 -. - - - - - - - - -
150 _
1 Oso-
01990 2000 2010 2
i.Reach tWithoutRc~sw !bS5~. áFiad ClW br P u 0~ 0_~ S
0
0
0
e
.
30
Chapter 2: Wly invest in health research? Historical experience and the promise of science 31
Structural biology, using crystallography, recombinant DNA technologies and the increasedpower of computer technology, has enabled the first steps towards rational drug design and the iden-tification of targets for drug action, exemplified in the development of the anti-HIV drug nevirapine.Combinatorial chemistry-a technique for the rapid building of a complete library of compounds forscreening as potential chemotherapeutic agents against a specific target-has made it possible to doin a week what once took a year. The various technologies for scanning, particularly computerizedtomography, ultrasound, magnetic resonance imaging and positron emission tomography, are onlynow beginning to yield some of their most exciting benefits. Using PET, for example, researchers arediscovering that they can visualize the site and action of psychoactive drugs in the brain, the proc-esses of cognition and memory, and the motor control of specific movements. Scanning technologiesare also being used to reveal structural abnormalities associated with disorders such as Alzheimer'sdisease, enabling not only more accurate diagnosis but also better epidemiological research that mayhelp to pin down risk factors for these disorders and lead to preventive treatrnents.
The explosion in computer technologies and the vastly enhanced capacity that they bring todata analysis are altering forever thec relationships between health providers and the information theyneed for effective performance. Physicians and nurses can now access databases for the most up-to-date information on which treatmnents and care models are most effective; data from numerous clini-cal trials can be assembled and submitted to meta-analysis to detect small but important effects ofinterventions. Computers are also enabling health managers to store and network records on patients,prescriptions, supplies and to monitor performance indicators such as waiting list times.
It is not only health-care providers who benefit from all this information, however. Patientscan access databases and electronic information about their conditions. People providing highlytechnical care at home, either to themselves or to relatives or friends, may soon be aided by a com-puter set up to answer questions and provide information. While most of the beneficiaries of comput-ers in health are likely to be in the rich countries for the short-terrn future, the middle-income andlow-income countries are unlikely to be excluded in the longer term. The falling costs and increasingpower and reliability of personal computers are already enabling small groups of health activists andcommunity workers in low-income countries to produce educational materials for a fraction of thecost of old typesetting and printing technologies.
The communications revolution and the technologies that have driven it promise more forhealth than perhaps any other recent innovation. In the established market economies networks ofpatients are taking advantage of electronic mail and the Internet to keep themselves informed and toorder medical supplies through buyers' groups. Research journals are beginning to publish their pa-pers on line, particularly in the area of clinical trials, and teams of researchers increasingly use elec-tronic mail to consult each other informally and for peer review (see Box 2.2).
Physicians and surgeons are beginning to use computer communications technology to shareskills and consult each other for information and advice, for example in diagnosing complex or rareconditions. A digitized image, for example from a CT scan, may be transmitted electronically fromthe treating physician to another thousands of miles away for comments. Surgeons in remoter regionswill even be able to take advice in real time from more experienced colleagues in other cities whocan watch on video monitor and give instructions by telephone. Computer networks and telecommu-nications will also transform the potential of distance learning and training for health-care providersand health managers and in the continuing education that has become essential for all professionals inthe fast-moving field of health.
WHO Ad Hoc Health R&D Report, Draft 2.0
None of these developments will deliver their full potential, however. unless investment inresearch continues. Assessments for this Report indicate that research funding is faltering in manyareas, and particularly in relation to the needs of people in the low- and middle-income countries(Annex 6). At a time when the potential for research to deliver benefits to health has never beengreater, the need for investnent in it has clearly not been persuasively argued.
[Box 2.2 about here]
2.4 Chapter summary
Improvements in income, education and sanitation have brought about a steady transformation inhuman health in the 20th century which continues today. However, health research has also broughtunprecedented developments whose contribution to the overall improvement may have been under-estimated. Health research has brought solutions to some of the most pressing health problems of thelow- and middle-income countries and has tremendous potential to do so further in future, providedinvestors choose to take advantage of the opportunities before them.
e
e
e
32

Chapter 2: Wly invest in health research? Historical experience and the promise of science 33
Box 2.2 A peer review network for biomedical science
The future of international health and medicine may be shaped by two recentinnovations: a global revolution in electronic communication, and a worldwide exten-sion of organized processes of scientific self-criticism for evaluating medical scienceand practice. Through critical peer review, experts in a particular field (peers) assessthe validity and menrit of research produced by others in the field. This process of self-criticism and quality assurance has been thus far based in medical journmais. Whilethere are thousands of joumrnals, the extent to which they use peer review varies. Re-search published in peer-reviewed joumrnals helps shape the clinical decisions made byphysicians and other health professionals, the kinds of therapies and technologiesused, and the strategies adopted by nations to promote health and prevent disease. Ascience of peer review is emerging at the same time that new communication tech-nologies have extended the reach of information and reduced the costs of its dissemi-nation.
The potential impact of the digital information age on the science and practiceof medicine, and particularly on extending the culture of science through the practiceof peer review, is well recognized by organizations that promote health intemationallyand by medical joumrnals. In many regions a scientifically robust medical profession ismatunring or just emerging. Participation in self-critical scientific dialogue and peer re-view promotes a professional culture in medicine that may be as important to sustain-able improvements in clinical practice and public health as the delivery of medicaleducation, technology and supplies. Access to the world medical literature and identi-fication with peer review (as a joumal reader, author or reviewer) may contribute sub-stantially to increasing professional self-identity and the development of professionalinstitutions and culture. Decreasing scientific isolation by bringing more scientists andclinicians into the world biomedical community is key to achieving change.
A consortium of medical joumrnal editors, led by JAMA and BMJ, in partnershipwith Project HOPE, a nonproflt nongovemrnmental organization, are now planning aglobal dissemination of biomedical information through new technologies. This effortwas launched at a meeting in Bellagio, Italy, in April 1995 that brought together editorsof major medical joumals from both the high-income and low- and middle-incomecountries. A lasting system of communication between medical scientists and practi-tioners across national boundaries and diverse cultures, based on access to peer re-view literature and publishing but evolving to other telemedical and tele-distanceleaming applications, is envisioned. The goal is to improve worldwide access to bio-medical peer review systems and information and the practice of peer review in allelements of health care from research to clinical care. The next major step will be aCongress on Global Biomedical Communication to e held in Prague in 1997 to launcha worldwide electronic biomedical peer review network.
eChapter 3: Health and poverty: The unfinished agenda
The previous chapter reviewed the broad achievements of health research in the past century andlooked ahead at the potential of new research technologies to bring further cost-effective improve-ments to people's physical and mental well being in the coming decades. In this chapter, the first offour assessing particular challenges ahead, we focus on a group of three broad health problems ofdeveloping countries that make up the unfinished agenda for the late 20th century. They are: thecommnunicable diseases of childhood (including diarrhoeal disease, respiratory infections and thecluster of vaccine-preventable diseases); undernutrition; and poor reproductive health, particularlyunwanted fertility and unsafe pregnancy and childbirth. Although there have been significant ad-vances in dealing with some of these so-called traditional problems, their persistence is a stark re-minder of the unacceptable levels of poverty found in much of the developing world and of the wid-ening gap between the poorest nations and the richest. There is an urgent need for more research intothese problems-research that will yield both new interventions and better ways to use the existingknowledge and tools.
3.1 Assessing the burden
In 1990, communicable, maternal and perinatal conditions were together responsible for more thanfour out of every 10 deaths in developing countries. In Sub-Saharan Africa, however, these condi-tions accounted for more dthan two-thirds of all deaths (Figure 3.1).
[Figures 3.1 a-c about here]
And whereas the gap in infant mortality between thec rich countries and the developing coun-tries narrowed by half between 1960 and 1993, from 133 to 54 per 1000 live births, the gap betweenall developing countries and the least developed actually widened (, 1995). These "traditional" healthproblems of developing countries have thus become increasingly concentrated in the poorest popula-tions of the world whose capacity to deal with them is weakest
e3.1.1 Childhood conditions
Somrne 12.2 million children under the age of five still die in developing countries every year,most of them from diseases that are essentially preventable with existing tools. Seven out of every 10of these child deaths are linked with just five conditions: diarrhoea, pneumonia, measles, malaria ormalnutrition (World Health Report, WHO, 1995). In many cases, a child will be affected by morethan one factor at the same time (see Figure 3.2).
[Figure 3.2 about here]
34
.
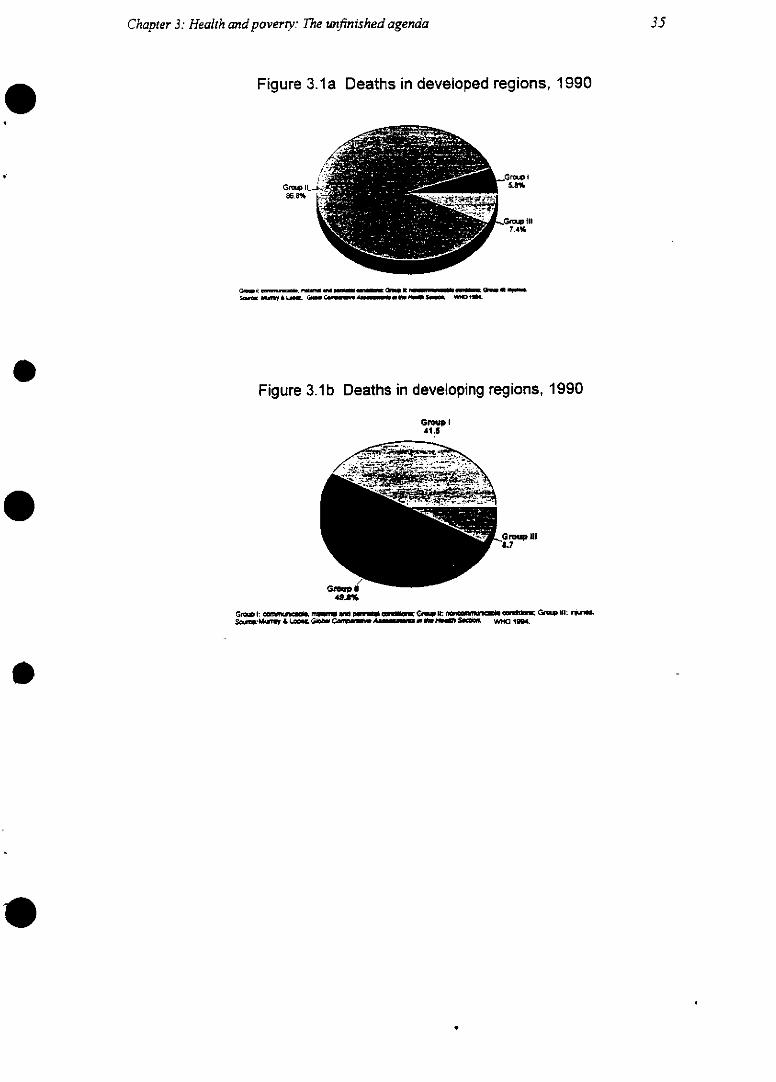
35Chapter 3: Health and poverrty: The unfinished agenda
Figure 3.1a Deaths in developed regions, 1990
Gr~ (II8.6%
IG~ 1I7.4%
S &,OMIldfl& LA9.GOLC~elM .eU l PSg. WHO ISB4
Figure 3.1b Deaths in developing regions, 1990
Gmup I41 5
/ -A De.v.. ':s De~~~~~~~~~~~~~~tf
G, á4l%
Gem wmfts~. i~ l ~ ~ .~.. C. 1U: nun-míuo as -_ G~ NI: wq~u.50g~MUTW 4. Lozu. Ge Con__.A ~ ge Cs _3 S iO 1994.
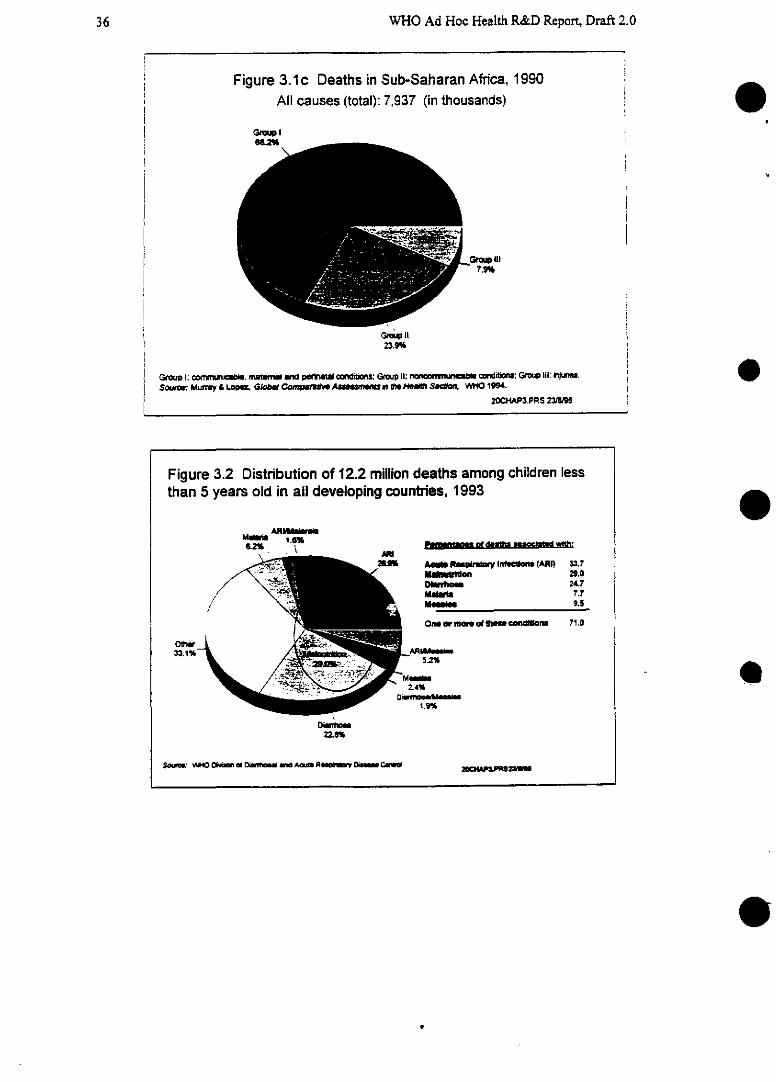
WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 3.1c Deaths in Sub-Saharan Africa, 1990Al causes (total): 7,937 (in thousands)
G~Ies.Z
7.9%
GMt23.9%
Gmup I: ca11/JnKlt~e, maernal atid pefulatal ¢o ts: Gp I1: nommnvn cd~l: Group iii: mira'ms.So~e: Mun'y & LOwm. G/omlt , 4numJe o'm D $4~1t. WHO 1994.
20CHAP3.PRS 23/9
20CIN~~
o
Figure 3.2 Distribution of 12.2 million deaths among children lessthan 5 years old in all developing countries, 1993
M B U ' W m v 2 1.0Dlafflmoe 24.7MMIIIm 7.7
9.5
oneoelmo.m 0< le ac andion 71.0
· ~~~~~~AR/L5.2%
2.4%Dá ntomad eaml.s
1.9%
o-m22.11
e
e
36
i
i
i1
Chapter 3: Health and poverty: The unfinished agenda
For example, infection with measles virus may be found alongside an acute respiratory in-fection. Altogether, since the decade began, somrne 42 million children have already died from diar-rhoea, pneumonia, measles, malaria or malnutrition. Others have survived, but have suffered damagethat will remain with them all their lives. The resulting disabilities may lower their quality of life, putthem at a disadvantage in responding to the demrnands of society, and even, in some cases, hasten therate at which they age.
Dietary insufficiency takes different forms. One is protein-energy malnutrition (PEM), whichcauses wasting-low weight for a given height-in up to 11% of children in low-incomrne countries,and 27% in India. Infections and parasitic diseases, particularly intestinal helminths, may play a sig-nificant role in wasting, too. A second form of dietary insufficiency is inadequate intake of micronu-trients, particularly of vitamin A, iron and iodine. Taken together, these different types of dietary in-sufficiency may account for as much as a quarter of the total disease burden in children worldwide(WDR 93 p. 77). Vitamin A deficiency is estimnated to cause eye damage in 13.8 million childrenworldwide with up to 500 000 of these children going blind each year. Two out of three of those whogo blind die. Children who lack adequate vitamin A are also more vulnerable to infections such asmeasles and diarrhoeal diseases. Epidemiological research is also beginning to suggest that undernu-trition in utero and in infancy may be linked with chronic diseases such as cardiovascular disease inadulthood IDJP Barker et al., 198x)
For some of these conditions, the necessary lifesaving interventions exist already---such as,for example, vaccines against the childhood cluster of diseases (diphtheria, tetanus, polio, and mea-sles). The potential of the existing interventions is clearly high. For example, in the two decadessince the Expanded Programmne on Immunization (EPI) was founded, the proportion of children im-munized has risen impressively from just 5 per cent to more than 75 per cent (GPV data in WorldHealth [Jan.-Feb. 1995]: p. 4), with immunization costing as little as $15 per child in the low-incomecountries. By the early 1990s, the EPI was preventing an estimated 2.9 million deaths from measles,neonatal tetanus and whooping cough, plus 560 000 cases of polio, each year, at a cost of betweenjust $12 and $17 for each year of healthy life purchased in low-income countries. Similarly, re-searchers have established that vitamin A supplementation is capable of reducing deaths from mea-sles and diarrhoeal disease by as much as 30 per cent and that, when given through the sarne distri-bution schedule as an immunization programme, it can be highly cost-effective (WDR 93, p. 81).
But the tremendous achievements of the past three decades are not good enough; it is clearthat the full potential of the existing interventions is not being realized. There is a simple lack of ac-cess to, or under utilization of, simple affordable treatnents for the main killers of children. Immuni-zation rates in some countries are actually falling and in at least 18 countries, coverage remains atless than half of the relevant child population. Every year, the WHO estimates, measles is linked vwththe deaths of more than I million children; 500 000 babies die from neonatal tetanus because of fail-ure to immunize their mothers with tetanus toxoid; and more than 110 000 children are still crippledby polio virus-neven with the goal of its eradication within sight. It has been estimated that roughlyhalf the burden of ill health from vaccine-preventable diseases in children is still not being averted(CVI 1993, p. 1). In addition, vaccines are simply not available yet for many infectious organisms; novaccines exist against those microbes that cause some 70% of the infectious disease burden in chil-dren (GPV 1995).
37
0
WHO Ad Hoc Health R&D Report, Draft 2.0
3.1.2 Poor reproductive health
As if the burden from these childhood conditions were not great enough, poor reproductivehealth is another major impediment to the development and productivity of individuals, householdsand economies.
Disparities in the health of boys and girls begin at birth in many cultures, where girls receiveless food, health care and economic opportunities than boys. Many girls enter puberty already mal-nourished, and this is exacerbated by early pregnancy and childbirth, putting the adolescent's growthand health into competition with her unborn fetus. Women's health throughout the reproductive yearsis also compromised by anemia and undernutrition, putting them at risk of other diseases.
Among the conditions for good reproductive health are the right of men and women to learnabout and obtain safe, effective, affordable and acceptable methods of family planning, and the rightof women to have appropriate health services to enable them to go through a safe pregnancy and birth(Challenges in Reproducntive Health Research, WHO 1994). Yet all too few women in the poorestcountries find these services within their reach. The consequences are unacceptably high rates of un-wanted pregnancies, unsafe abortions, and complications of pregnancy and delivery. Beyond the im-mediate health implications, rapid population growth is unsustainable and a cause for global concern.In addition, although it is treated elsewhere in the Report, STDs and HIV/AIDS impact reproductivehealth, particularly in the form of infants born infected.
An estimated 120 million fecund women are not using contraception even though they wantto avoid becoming pregnant (Population Reports, Series M, 11, 1992, p. 23). Surveys within individ-ual countries suggest that most women want smaller families: the average actual number of births perwoman is higher than the desired number (Figure 3.3).
[Figure 3.3 about here] O
In the poorest countries, the capacity of the services is inadequate to meet need; in manySub-Saharan African countries, for example, family-planning services are able to meet less than athird of the potential demand. As well as desiring fewer children, many couples want to space theirbirths better. Evidence suggests that babies born within 24 months of an older sibling are more likelyto suffer ill health, and even to die, before they reach five years of age (Challenges in ReproductiveHealth Research, WHO 1994).
Unwanted pregnancies not only carry heavy emotional and practical costs to women andtheir families; they may also be dangerous and impose a heavy economic burden on the population asa whole. Worldwide, it is estimated that 25 million of the 55 million abortions performed each year eare done under unsafe conditions. The complications kill some 60 000 women (WDR 1993, p. 84). Astudy in Tanzania found that conditions diagnosed as likely to be due to the complications of abortionwere the most common reasons for admission to gynaecological wards, with a cost for treatment ofabout $7.50 per day (G.S. Mpangile et al., Reproductive Health Marters 1993, 2:21-31).
38
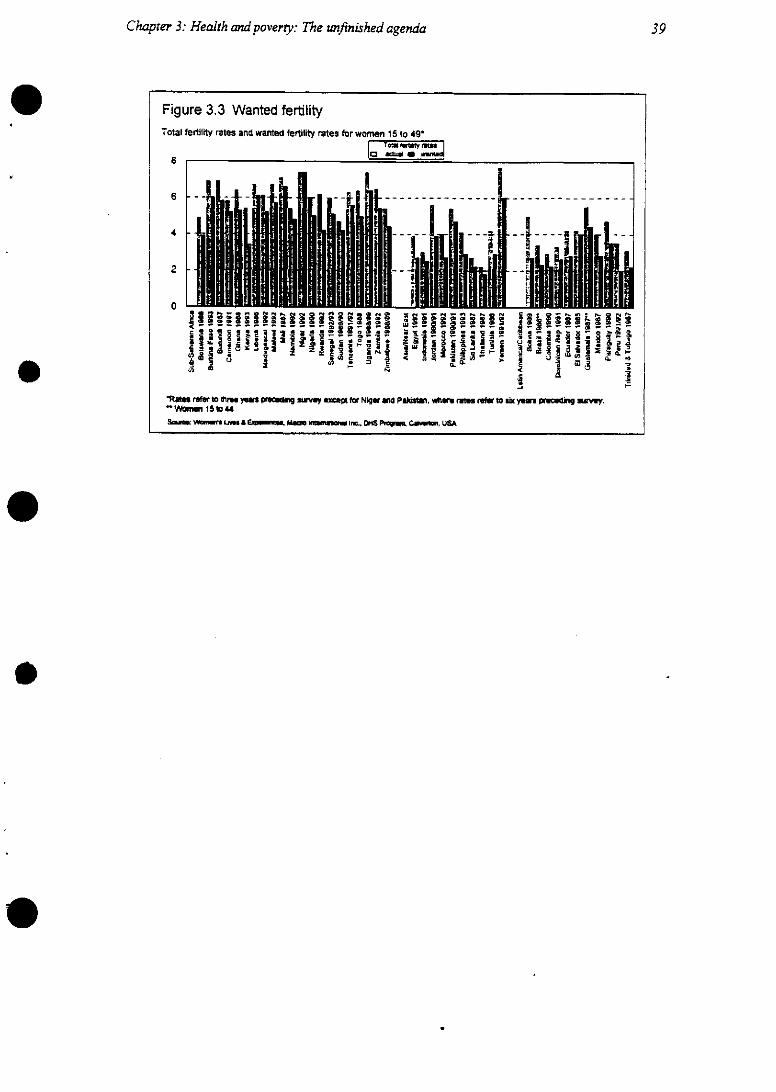
Chapter 3: Health andpoverty: The unfinished agenda
Figure 3.3 Wanted fertilityTotal fertility rates and wanted fertility rates for women 15 to 49*
Ic foxpt, m. j8
6
4
2
o
i - .e o ° E 1 ;
i M i 1 z f ,N|In a1 Ji ~ -
1~ mfar 10to Ua ye.s pmcmdmj s exmg< fu Níger u~l plaasta. wfiere rtes i4. to um yea1 iru:m~mj mVey.Wmn 15t o44
Sae~ WNon Lm & E.nn. aOHS~ memgm inec o0S Pem.a Ca~n. USA
39
WHO Ad Hoc Health R&D Report, Draft 2.0
Pregnancy and childbirth are not free of risk in the healthiest populations, but the differencein the degree of risk to women in developed and developing countries is amnong the starkest of theglobal gaps in health. In the established market economies, only one in 2700 women will die as a re-sult of the complications of pregnancy or birth (WDR 1993). In low-income countries the risk is atleast an order of magnitude higher. Almost no family or community can go untouched by thisscourge. The death of a womrnan puts her surviving children at risk, too: those under the age of five are50 per cent more likely to die themselves than if their mother had survived.
3.2 Projecting the burdens ahead
To the extent that poverty recedes, or that known cost-effective interventions are more fully imple-mented. it is reasonable to expect that the major communicable diseases of childhood and the conse-quences of undernutrition will gradually reduce their share of the world's total burden of il health(Annex 1). However, projections made for this report offer no grounds for complacency. Indeed, theexpectation that there will be real declines in the prevalence of the major childhood killer diseases isbased on the assumption that the gains of recent decades will continue. However, it is by no meanscertain that this assumption is reasonable. There are disturbing preliminary indications that in certaindeepening pockets of poverty the long decline in infant mortality may even be reversing [data tocome]. This finding is not without precedent: in Brazil in the 1970s, during the country's "economicmiracle", the concentration of poverty led to an increase in the infant mortality rate in the populationas a whole, but borne almost entirely by the poorest section of the population. Meanwhile, infantmortality in the higher-income groups improved substantially (Yunes, J. PAHO, full reference tocome). Similar trends may be emerging in the former socialist economies. And, as the next chapterwill show, the epidemiology of communicable diseases can and does change rapidly for a number ofreasons. Moreover, the burden of unwanted fertility and its consequences is expected to continue forsome years, even if fertility is reduced, simply because a high proportion of the populations of devel-oping countries are or will be entering their reproductive years during the period 1990-2025 (Figure3.4).
[Figure 3.4 about here]
And, in certain countries, rapid population growth may threaten some of the health gains ofthe 20th century (HRPI 1995).
The projections shown here (Table 3.1 and Figure 3.5) estimate the cumulative years of lifethat have been lost, and are expected to be lost, through premnature death from different causes duringthe entire period between 1990 and 2020. The method enables weighting to allow for year-to-yearfluctuations in the prevalence of diseases and gives a more meaningful estimate of the overall burdenin the period than a projection curve based on a single year could do (Annex l).[ NOTE: becausethese projections cover only years of life lost, and not disability, they underestimate the impactof certain conditions such as neurological and psychiatric diseases. Projections that incorporatedisability are in the process of being completed aud will be available with the final draft.]
[Table 3.1 about here]
[Figure 3.5 about here]
e
40
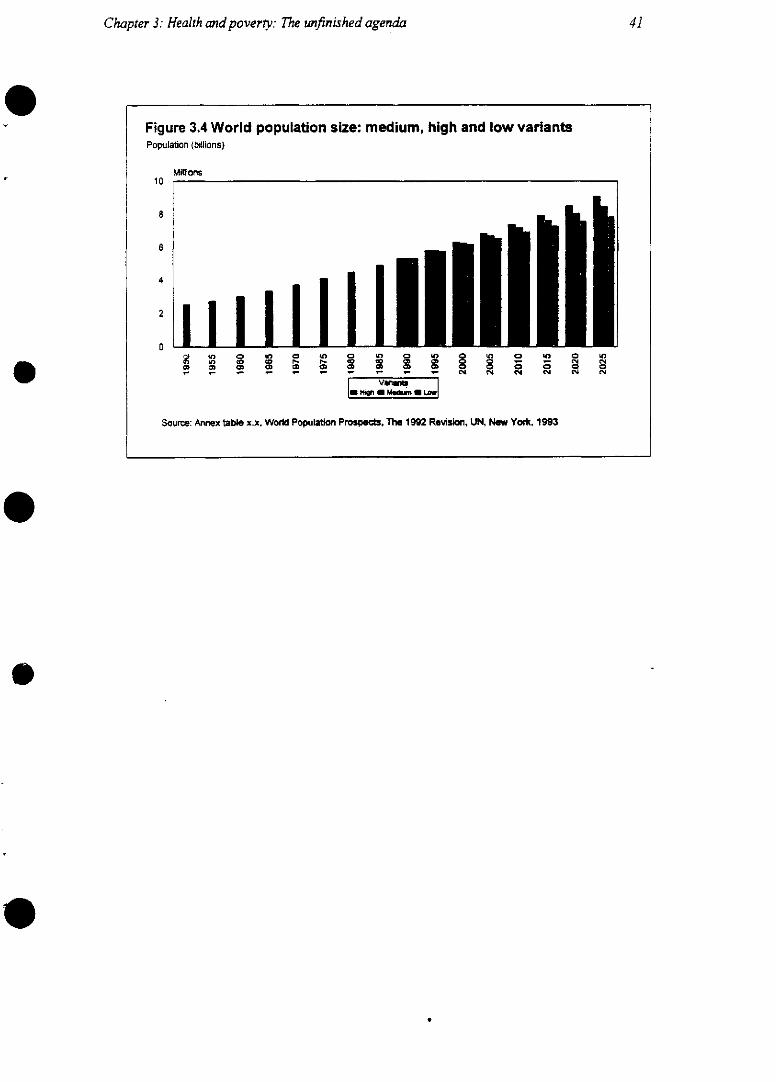
41Chapter 3.: Health andpoverty: The unfinished agenda
Figure 3.4 World population size: medium, high and low variantsPopulation (billions)
10Millions
Source: Annex table x.x. World Population Prospect, The 1992 Revision~, UN, New York, 1993
O < O 0- 1 0 0 0 0 0 0 - -2 c' e.0nW>c 0 ` 0 0 0 0 0 0 0 000
- i z, i i z 11 C4 11 11 CM. <ol
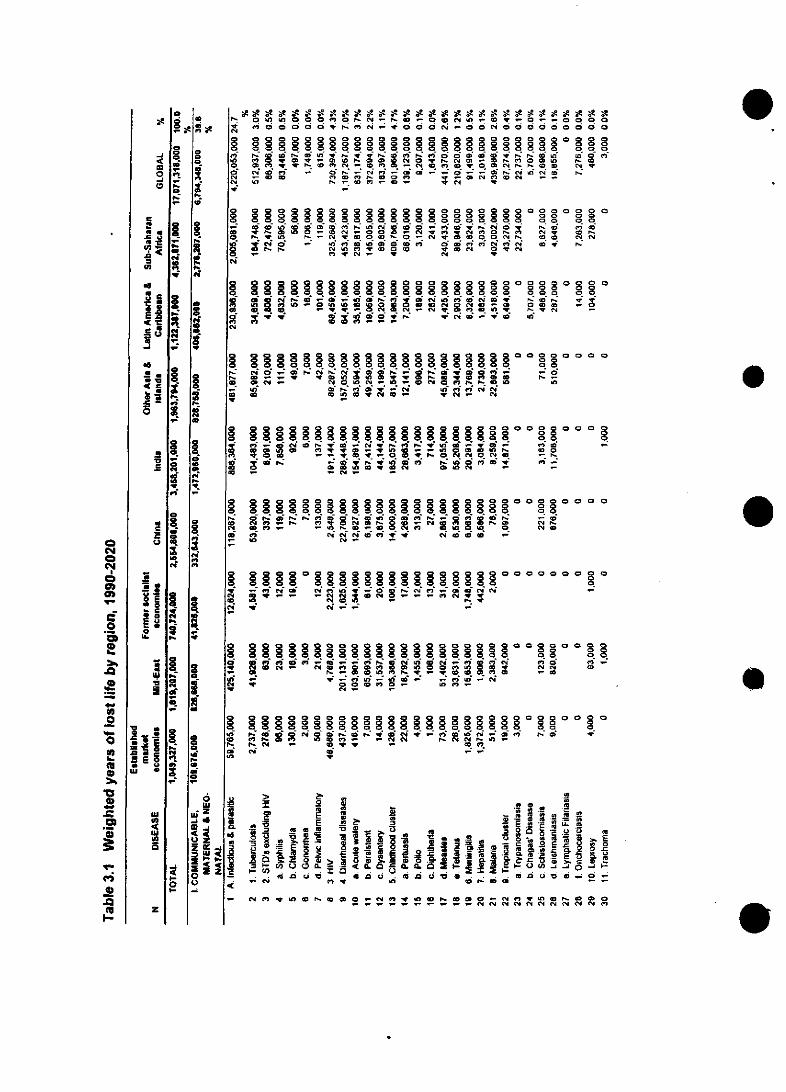
oa
8eCi
Q
y O- e, Na - q a - a eN 1- ea Q t a a a _ O
0°-.'.' O - e O ,y O O 0° O- O O O 0 e 0° 0
C, ck Ç n -t Nl IR e«M ck "l O c4 N 1 Cr
O-~~~~~~~~~~ P. _ e__O ;NN8 MIe ID e- ra D- a- O n t _ Cl4 N o cm
CMOXQn1* N4 t m _ N m 0u, ~ ~ o c c !14 a c
- > 'r - .' e a M 0 OO M l C S 4N e e t ID O E1 t ZD N O t N~C
u, esP. U W.: ,uauuu, ca er a4d e rae-iI e -v a v -ra e O cm i r a N S _-. . -V@ .- -c.
cee,-CM -
o o o.,,,,,,,,,,,o o,.... e-Nr. Oaa _ ¡_N1N -_e bO
u, ee-,q- u~~~~~~~~~~~~, cl c,4 rae Neva _uN 0 ID N _ n _ ZD 0ra- cm
Cd e e-y e- e u _- e, 10 e u, Nce u> _ ey e- utu Ne 3 _ _ -
2 o8 8 8 8 o °o 8 o o o° o 8 o8 88 81 8 8 8 1 88i - ew e-e- - cN, r d P.: r _ e-
~~~~~~ - N _ _ 0 &0 N _~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~l 04
ea e, a. e- e, qa o a e- c- a Xc e- o 7Nor o eDcN .^u _-e caae u u,0 a u, a DDN 0 Nai d, cuece -a, N -
a a a0 0
e eea C
0 0 Q
8 8a, o _e
oo
co
§a§etr~
q aN a
e-cet cm
Q o, X _
y e-la *ne u,~ 1<
a a0 a a aa a
- ae -
, o o o o o88
e, -
el¡
e 0o o,
Na D
o; 8l 8l 8¡ ol e 8 8 . . . . o° . .o o' o 4 04 8 ole3 C-4 l ;1, eraO--e cuy.'< e_ Eq N X N N N D P, _ we
lé ci _: _: -
N<' c' _ N Q , 0 u, u, e - - e, u, , 0u aeeea R , _ -O <q c _ e, q
le C 0 0 d U> 2 - i; m i - N
o o o oa a a
* _ae
o8 8 §s 8 o § §§§ M o 8 so0 oel r- - e2' - c " , zD cm - 0 Na N _ ck e _ DN4 Q > _
Eu5¿ea.o
_it 1Z~ al
", <5 s e n u 0 s
ai. u, c nu e - ncoe --
- N en Q un , c a 0 _ N « v -a e D' ° N Ñ N m N n N N N N…raeararar~0 0 0 C ca c4 0raea me
`c. .o
e -
e- CMsus
-e g o
lo «) 0
ca eg, WA3Iara
e < U,- . ..,
eaqetP,
ot
01e-
E.a-fi
e3-
e,1
Cd
esiioqm
E<e.
ao¡!Iret
-1h-e
E
i
E
14
1NCk
a
CduN
4.e-ucau
¿ eIDi
uu 9-'
=
o
-J
uo-Jo
'u-u.c umt
u,-
o,
a.
u-a
.6
*0
o
u
c
ue
u
a'
uuI�a1
1:
iiiBEOu uw e
uu>
uo
z
eo0z
«<4Q
Cb._1-C
0
.>
-
I..
01 1
.0
e
.2
I
I
0
ñ..0
0
2wi
e-
4
a.2m r
0 3 z=i S- l
J ca- Ca,
u
e
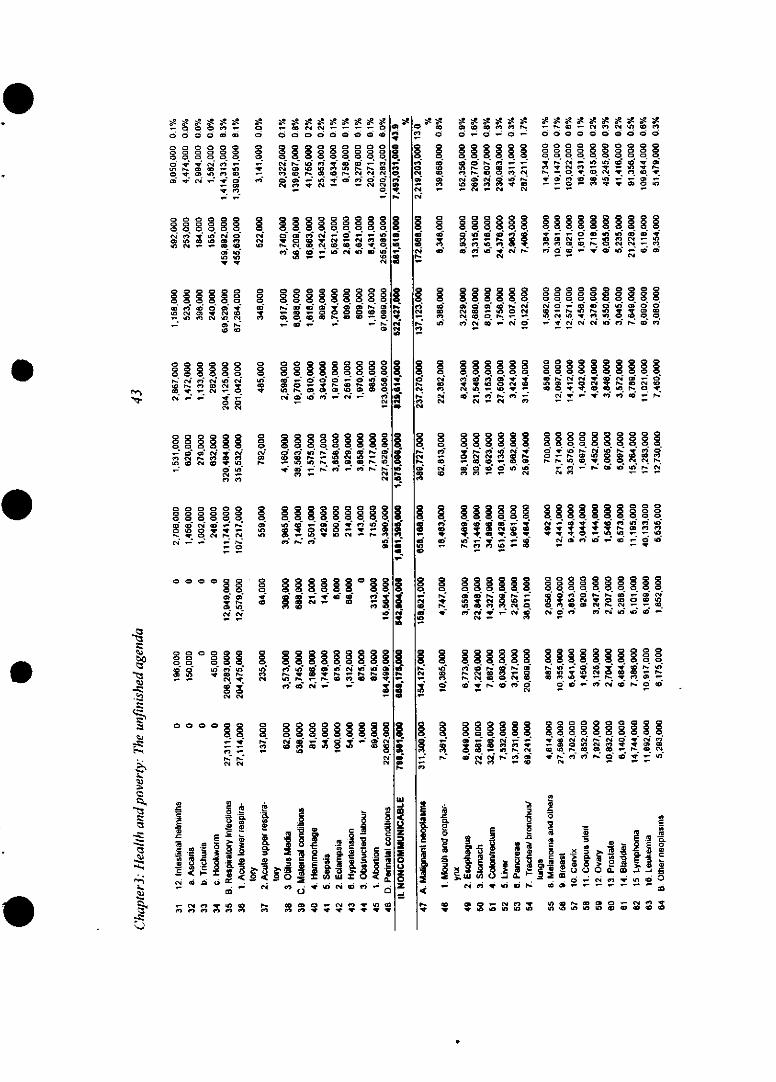
- o ae e, -
o o o o a ao o o a a ao o o a o oo . s ea e, -
o 4. o a e, a»
- O4. e,
No a oaa NO
=0 1
a a
o O o oao
ci ci w oo
_, e, ea a eaN
a a
oh a o N aogeae w a _ eaae-.
N Noc4C
_(O ed0 e N a
e, ceq- aa^Na _
o o o o,
e, e
000
O k IDo q
N a - e-
4. e.a a
S
c,
§
§
88
N
w
o§%
,w<
10
N
00 aaa8 p
W 0
<'9 01114 ea
- 8.
e, _
Na N:
c:
toJ
M
Rcq r- n a q t
rfc, rvX X No i _.ii v C4 o oo
N 0 e t N _N e I»
aq al a - a7 a aoe
ean a,-e- e,
g eO O, O O Oe
C4 M
_ 2 e . .
e,- oo_ ea
_, Noo
.0 |XP E X-
- so ro N , as X r I
7 !? - t wi í cm W, °8 8
el;i
d
e-4. U _. e- - e e. a--le. r ¡
la - o 2NeS,~~~~~~~e
u 0
-. m -- N00XZtll
P._
_N 0 _ -te W
.c; E - - - -
2.
o -~~~~~~~l ,)w ó Q á.c . -~ C O Z O a
- - ea e, * . a c e -a ea
0,.4».
o,¡
4.e.
1.a¡
u
e*,.C4
u1
04
ur
SSe ek a
ft 0
_ a»- z!ea -
d0°9<'ue.-
V
P.:e,
1e¡
<'4
Np'am.
I100
2W
1
2'a-ai
¡i
,rt
a aD a e, < r.a o - o -
C.C4ea a ea a_ a -
N 10nd01
o ° o 4 o°
O1 ele ew
e4 a
. _ cm. eo
M e a - aO.
a - , e- _ , -
ea-ea e
aa. - -
e, e a y- « tea-OO e,
o o o ea8
D .-De d
ea
a n _
eaqe, _-D
- r- aD - eaNe e, a 1 e,a a a a a o a o a a
oaaaaa aao
y . e , u, a ae, 4. N e,10 e 4 - ' 4 1*. - N l a0 N 4 y e, a
o .o o(o co
e, _, a a e. a eaea- e,
elu
ID o a N _ - N 10
aaa aaaaa00
cao oa a oc ,N
aao 888 ° a
a o - an a 4. e.a ea
a0 AIo 4.al a e-a 4
N *n l cln- Q DoO
0--a 0 . 0 aeDaear-,sO- e, - . a a «a _-e
° -a aoO oa ua a r
aa1 a 0
e l e c¿ (D O N
4.N _a ID <' a 4. ea1 e,
ai a ei ao a a e_ O ea
0 e- e, e, N a a - - a
N Oea k z1-
° 8 88z
-50
o o
o O E nw1 O - N 0q
- 2 1W
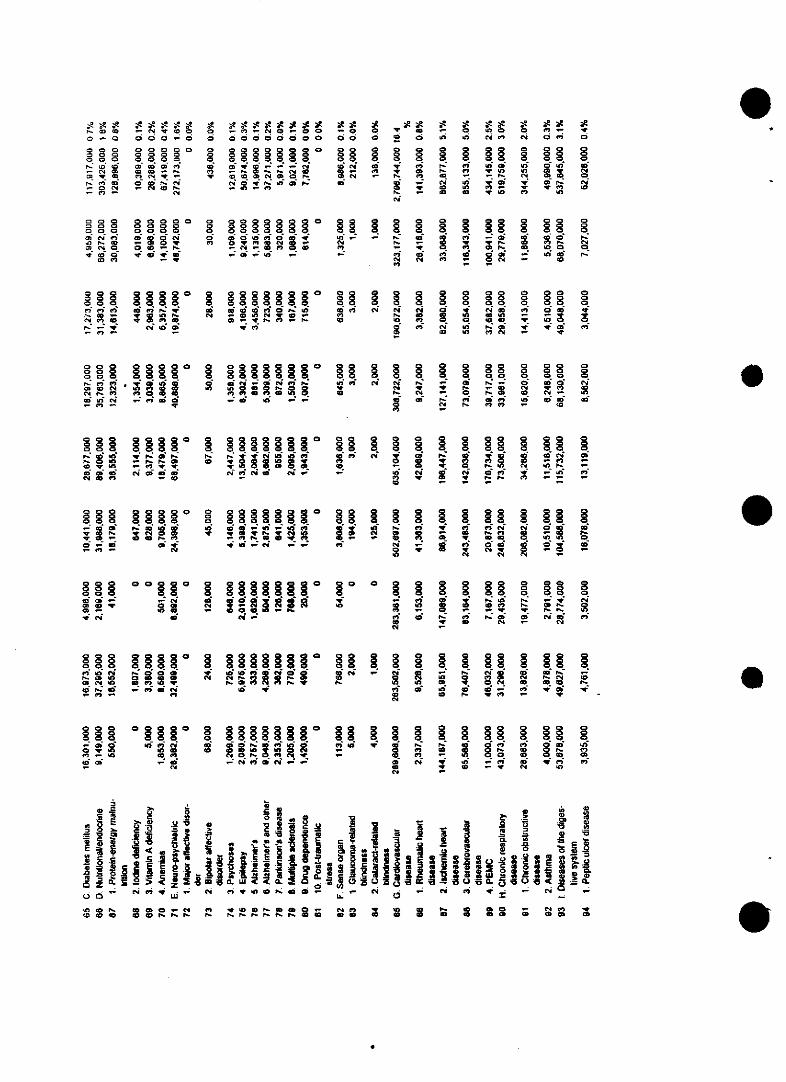
, -N T eo.-o o o 0 o
_N0 C4 w,a, t e ,<4*'-e o D OE
- O N _ N «0 1b_~~¿.
S
0
o
8,D
_ le, _4 0_ e oo o o o o o o o
88 §~888 §C
N O a ¿4 10 v-_ d _ e.
X0 N Y 'a00 d 0
80§0 § §lDc¡ * y _
el¡
_ e e oO °O O Ol70 U)4e
0
'a i ;! ,<D rtD cowv-
o¿.40oO
N>u,w.
m
o, -
00 g
O e,
q. eck .
leeC408cmw
alC.0 0c2o» od o oa 8 34cN0, O, a- _
q . . _ t
0
8ci
y _ N 0 -n - _
N cmmj
8 8° °8 8°88°°e- 0 -* q L §N e, - -- -_ ) 0 P. IrO
§8.e j~~~~ e j~~~~ e : e j ~~~ e,0 8 8 § § 9 1 C, °o o8 ° §8 88 R 8 C,
_ e e, Oac lO e a l_- lo m q° 10 el <N
OR o§ §8§ §§ 0,. ,q . . .
~ m elN ' 2 i e01 ID _7_.4e-, e m o!! < - C,>D00r
0 y l¿ 0 e,
yo t e-
o - o4 CD C>
,lo Oi_o- e -
_ -
y cm
, r o: is_: r r-_ c1 t lo e- e- e- al
§D C0,eD 20 PE_ %
a,O U
e
08
o
so
(46
D
8
N!
. . .l ..
N eN e-e 5
°*,¿.4 8 -- ° o
§§§§§§o
§§ 1 1. §~o r° 8 4
N o N
1 1 1. 1. 1
O O cm 0 0;
_ 1 14N0 l
35 0 e- e,C»- - a 9
ej-
§O 0 §*;i 9 i?
°O OO
mlo
0011
0o eN
-N
cmN
¿.4 cod~~
lo y ej o
§ § ¡ ¡ f ¡ § r e O 1.1 1. 1. 1, e ; o¡ cm - e o y oN O , t * - e,
_ NO- ¿.4 , al .4 -
1. 1. q NO 0 O N0 e- le
i -yle > _ en
at
1
80q0-l
1.§ju e.
e0ylal
yk °8
ye,W
1.
8e,>(ncc
A;~~~~~~~< j . u l|||sj C ^S|Ag-. . U . C ' - v · 0 a -· · ¿. e, y - -
uM Ne M_ e M- e , ¡ _ N . * alO^@ O _ X _ : - N. 1 '
V c e o c e e - e - e - e - e -e -e -e -e - e- e U * U U e W a a l a l a l
o 0 00Ck8 a88
e, ! 8 cO> - O N
800d
O8.e-r-
0
e,
§ §
O c
tle
e,
0° °8 ¿Cw O 2
_c¡ xiw
e
9cl
el¡
°8 8 °o88
_ o ( _
- al e--
-O e-al
e, ale,
<.4 ; e- ee
4.
1 N1- 3 e-e,8 y N N
o, 0 8y S o y¿. e .N
o8
N0
8
o8.
cN
8.
e-
8 8ue-e-
_S o
1.123 ; ti e
o o o8 8oeq al Nal ¿.4 lO
- e, -
al"
0 y ue, -4
o °- y
¿.4
e
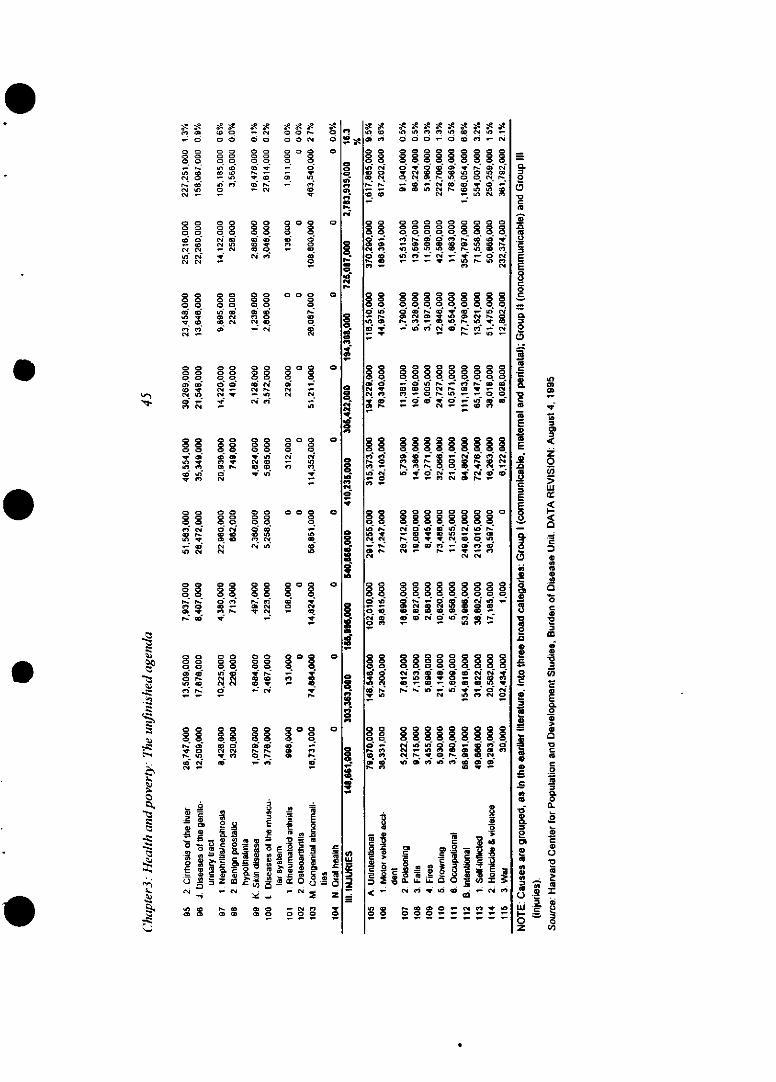
e, s
- o
0 00 o
N O
N 0-.0
el.q 4
.0 00 00 0
0 00 0
q q-
0 0 0 00>0 0 0
q q N D=0 In44
4- c1t N! .
cm N _
O Oo O
q q
yo
N _!
- N.. O00
0000q00
m4 _
-r N~
o 0 8000o o_ 0
_-o enOD
0 0 0 000b0 02 0
0 0D 0 00 e, 0
00 - 0
80 0 800 0 00
u) <0 Ob= r4 e,k N N OR
CD- _4N
Oo
0d(.4
0 8 8 o >0 0 0 0
C0 O 0 N4 O _q: i Nt _t N 1i N -O o0 2 < - .45 _-1 N N R _0, N
<27 N - N n _
0 c 0
'. o
00< 0 00 0 0 0
-t -M N a
z;0 CM44 ( 4 (.4
8 O O 0111
4.44 (. eT:¿8 4 C1" 4 4:; ,
0 00 0
0 0
N 4
8.
°a400n
0 0 0 0 0 8 8 8-,_y. oe P.-, e N _ wel 0 0- 0 c4 e N.Ck 4q e, y. q - O T ct c
co " - E'
r- ci .440 0 7-44.er oq N
08c ov 0
N0 _
0 0
04t - §C( 4 4.
,E'e, O0 8 0 0 8ct . o , § rF C,e _ In q D, ,
o>£ 0i
O 4> 40lcm o
ef
19o
8
a
o
a
8
o10
e,
a
'au-m3
3i
<» e)44 e, e, r 0 " 44 -
o o o - o o M .- N
8 0 8 c8 8880 0 0 00 0 0 N O
800 8 8c o $ 88°°-y 0.0 0 0
o- 0o o o0 o ooo8 8 8
0o el rq , In*a ag _ D<
o 8 0 0c so
O a O D 1 D * X Ucm " O l neON 1<0
4n Ck r, X _ n MI o "t diIDt _ )n cl 0D PX
_ 8 1 c_ n _8
Ne¡ <. u_ P. ei _ _OO
C4 " oo _! N z « N
°o 8° 8 a° Oo
i Ri CRO_ D_ D w
090 000000000DPw I
14 ~ ~ ~ ~ C N N_ OND e>N
_ S O 8 _ 8 CS C 1
_e r z e « -le le rf 21
co It O o« D
o c m O e ° 0 2 - (.
ftei m R cm .
oo oo oe .
5 N D _D _4 4 > 4D
Og c d N d O N
Oso so§ eeXor. a
E q
< c4 -e c> j ó <L
o 1 So «019:: v :! 11
_ o
rizZojor3
ru-z.i2
z:
i�
1..111,1zZ.
,I.2z:u
-zZ:u�u
:2z
L�
e
0
o
o
,0
C»
oz
m
uj
1-
lo<e
o
.O
0-,
,s
o
ooo
D
00
o
C Q
0
oio
s o
1u)
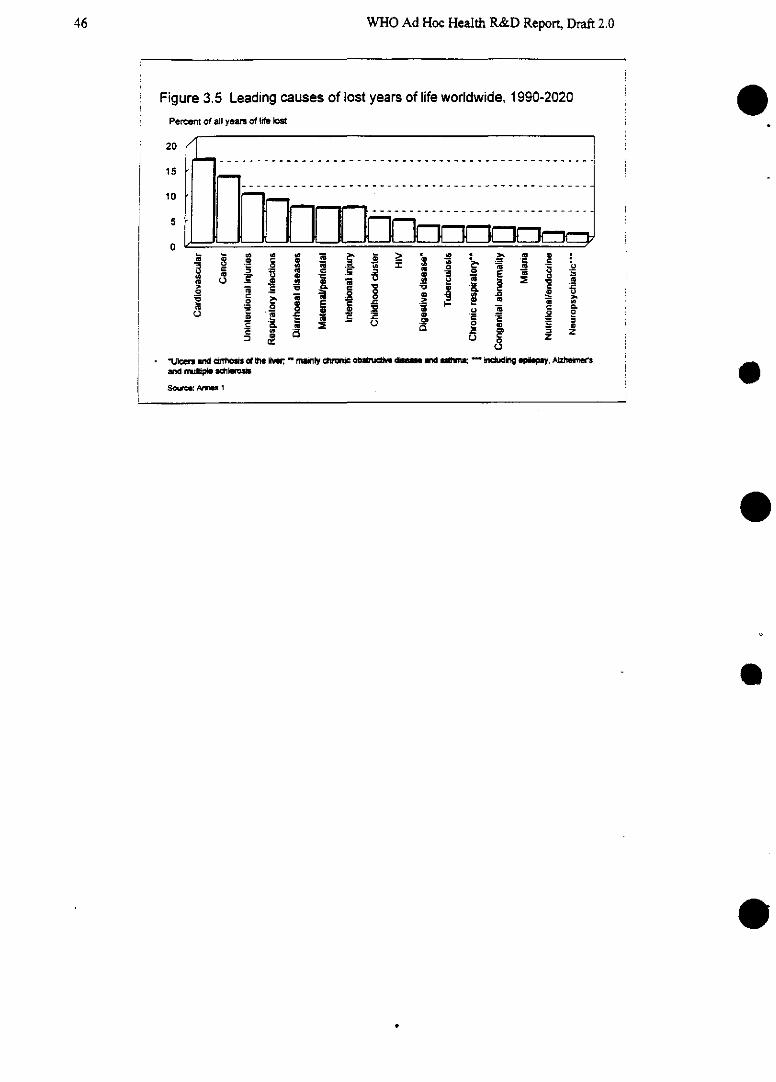
WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 3.5 Leading causes of lost years of life worldwide, 1990-2020Percent of all years of life lost
20
15
« Nueces~- -S -ihOi -e - -l -a - -D - -S - -_
10
5
0
Jo
gL
soufi Arlnl l o ~ .~ ~ u e
e
46
Chapter3: Health andpoverty: The unfinished agenda
Over the period 1990-2020, more than a quarter of the world's total lost years of life will befrom just this handful of causes-the causes that make up the unfinished agenda.
* The share of years of life lost from respiratory infections will be 8.3% of the total-thefourth leading cause of premature death worldwide and the leading cause amnong children.
* Diarrhoeal diseases will be responsible for another 7% of the total, and
* The childhood cluster of vaccine-preventable diseases (pertussis, polio, diphtheria, measlesand tetanus) another 4.7%.
* Maternal and perinatal conditions together will claim a further 6.8% of the lost years of life.
Taken together, therefore, these conditions will account for almost 27% of years lost throughpremature deaths worldwide. [Final draft will also include estimates of burden from disability]. Theneeds for research and opportunities for intervention related to these conditions are discussed later inthe chapter.
3.2.1 The burden of disease attributable to risk factors
Most efforts to assess the causes of ill health have focused on the diseases or injuries thatthey produce. However, there are a number of behavioural and environmental factors, to which indi-viduals and populations are exposed to different degrees, that influence the likelihood of experienc-ing those diseases and injuries. For example, exposure to poor sanitation and poor personal hygieneincrease the risk of infections; tobacco smoking increases the risks of circulatory diseases and lungcancer. The extent to which specific disease burdens can be attributed to particular risk factors is ob-viously an important question because reduction in exposure to the risk may substantially reduce theincidence of the disease. Epidemiologists are therefore working to measure as accurately as possiblethe proportion of the burden for specific diseases, conditions and injuries that can be attributed tospecific risk factors (Annex 2). The categories by which disease burden can be measured are set outin Figure 3.6. This shows the importance not only of disease and premature mortality but also dis-ability, as a consequence of disease or injury. Disabilities that profoundly affect a person's quality oflife and productivity, such as partial mental retardation due to undernutrition, but which have nottraditionally been taken into account in health statistics, can be incorporated by this approach.
[Figure 3.6 about here]
For this Report, the contributions of selected risk factors to disease burden in 1990 have been[or will be] assessed, including water and sanitation and malnutrition. (Tables 3.2 and 3.3)
[Table 3.2 about here]
[Table 3.3 about here]
47
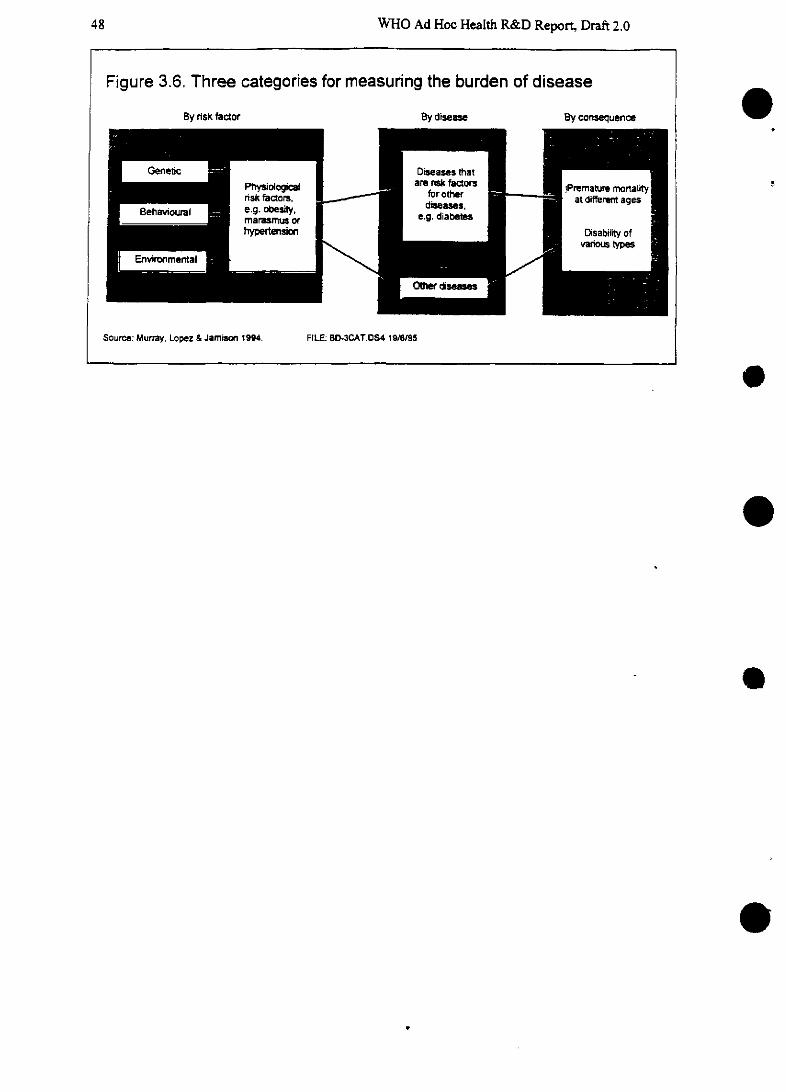
WHO Ad Hoc Health R&D Report, Draft 2.0
e
e
e
e
e
Figure 3.6. Three categories for measuring the burden of disease
By risk factor By disease By consequence
Geneti Diseass thatPhysioogica l are rsk factorsare TiaR factara Premature mortalnrisk factors, for other atut
Behavioural e.g. o sity.diseases, at dif t agee u _ g. ~marasmusor _ e.g. diabetes
hypertension ¡ Disability of_ ~ MryLe&a 19I. - . 9vanous types
Sounvironmental m \ F
Source: Murray, LopeZ & Jamiso 1994. FILE: BD-3CAT.OS4 1ste/s5
48
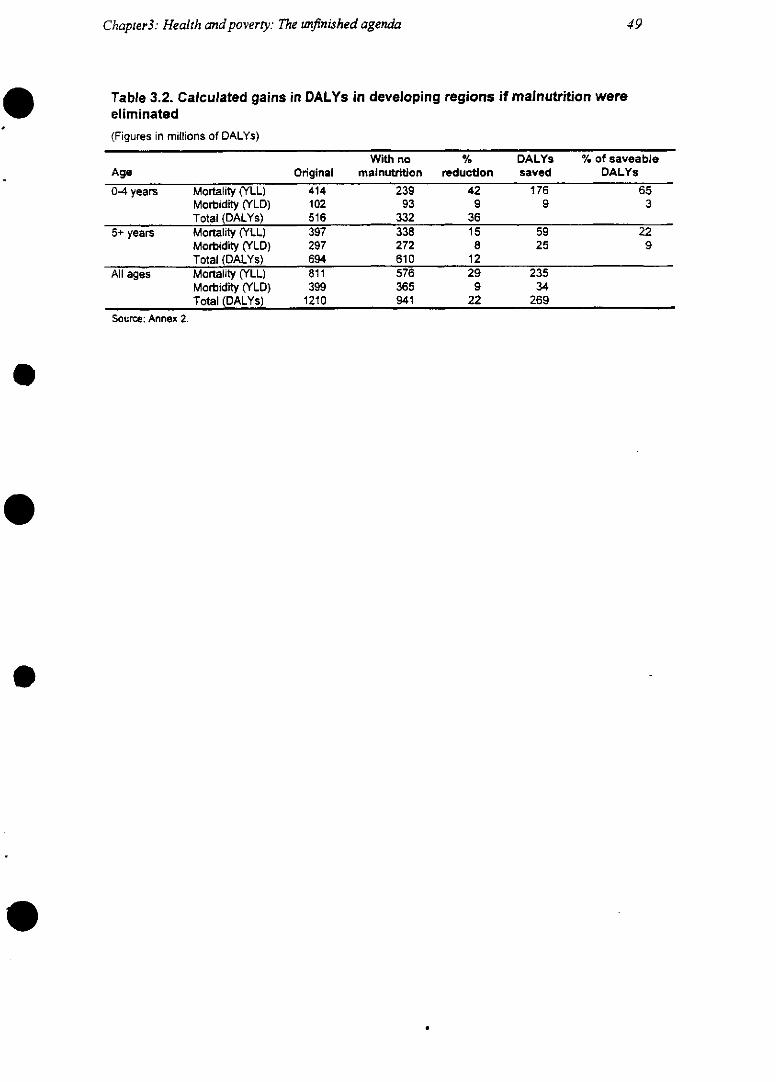
Chapter3: Health andpoverty: The unfinished agenda 49
Table 3.2. Calculated gains in DALYs in developing regions if malnutrition wereeliminated(Figures in millions of DALYs)
With no % DALYs % of saveableAge Original mainutrition reduction saved DALYs
0-4 years Mortality (YLL) 414 239 42 176 65Morbidity (YLD) 102 93 9 9 3Total (DALYs) 516 332 36
5+ years Mortality (YLL) 397 338 15 59 22Morbidity (YLD) 297 272 8 25 9Total (DALYs) 694 610 12
All ages Mortality (YLL) 811 576 29 235Morbidity (YLD) 399 365 9 34Total (DALYs) 1210 941 22 269
Source: Annex 2.
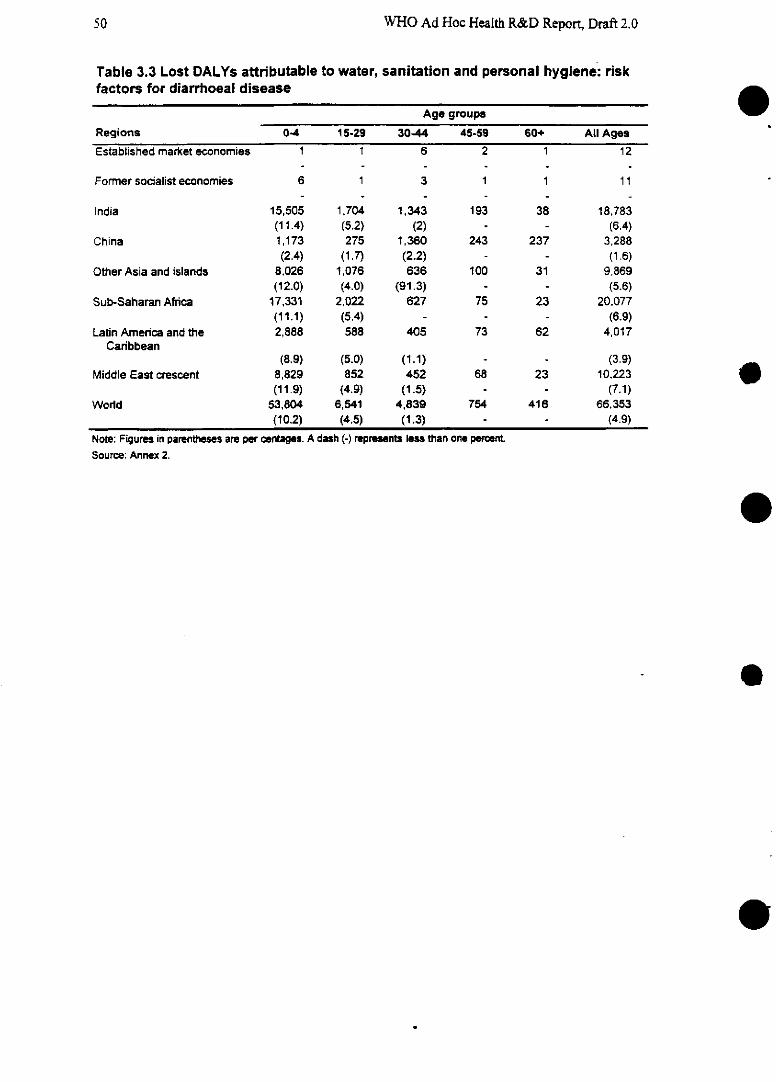
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 3.3 Lost DALYs attributable to water, sanitation and personal hygiene: riskfactors for diarrhoeal disease
Age groups
Regions 0-4 15-29 30-44 45-59 60+ All Ages
Established market economies 1 1 6 2 1 12
Former socialist economies 6 1 3 1 1 11
India 15,505 1,704 1,343 193 38 18,783(11.4) (5.2) (2) - - (6.4)
China 1,173 275 1,360 243 237 3,288(2.4) (1.7) (2.2) - - (1.6)
Other Asia and islands 8,026 1,076 636 100 31 9,869(12.0) (4.0) (91.3) - - (5.6)
Sub-Saharan Africa 17,331 2,022 627 75 23 20,077(11.1) (5.4) - - - (6.9)
Latin Amenrica and the 2,888 588 405 73 62 4,017Caribbean
(8.9) (5.0) (1.1) - - (3.9)Middle East crescent 8,829 852 452 68 23 10,223
(11.9) (4.9) (1.5) (7.1)World 53,804 6,541 4,839 754 416 66,353
(10.2) (4.5) (1.3) - - (4.9)
Note: Figures in parentheses are per centages. A dash (-) represents less than one percent
Source: Annex 2.
e
e
e
e
50
Chapter3: Health and poverty: The unfinished agenda
Table 3.2 shows the very major reduction in disease burden that would result from eliminat-ing malnutrition. Yet, in discussions of the importance of malnutrition as a risk factor for disease,attention needs to shift to assessments of the relative contributions of dietary insufficiency and infec-tion to various types of malnutrition. For only by understanding the origins of malnutrition can ap-propriate preventive strategies be devised. While there is strong evidence that the origins of vitaminA deficiency and iodine deficiency are principally dietary, there is evidence that iron deficiency maybe due much more substantially to infections, such as from malaria parasites and helminths.
Understanding the origins of the two other major forms of malnutrition-failure to grow inheight (stunting) or failure to grow in weight (wasting)-is less well developed. Both diarrhoeal andrespiratory infections are of documented importance; parasitic infections and dietary quality areprobably also important; and insufficient energy content in the diet may play a major role in somecases. Where risk factors interact positively, estimates of the number of lost DALYs that could besaved by eliminating each risk factor one by one will produce a total number of saveable DALYsgreater than the number that would be obtained if all the risk factors were eliminated together. A keypriority for researchers is to clarify the patterns of attributable risk-and therefore the potentialpoints of intervention-for this massively important set of conditions.
3.3 Assessing needs for strategic research
There can be little doubt, then, that the dramatic progress of the 20th century has not yet suc-ceeded in eliminating the "old" health problems of developing countries. So, what are the prioritiesfor strategic research? What does the health sector still need to know before it can go about develop-ing new interventions and making better use of existing ones? As set out in Chapter l, the Committeehas attempted to explore some answers through a two-step process of (a) analyzing the magnitude ofdifferent types of need and (b) assessing the level of ongoing research in an attempt to define the big-gest gaps between need and action. It should be stressed, once again, that by strategic research wemean research that will generate knowledge relevant to these problems, whether that knowledge bebiomedical, epidemiological, behavioural or relevant to the performance of health systems (seeDefinitions of termins, Chapter 1).
3.3.1 Analyzing the magnitude of research needs
The Committee has taken selected specific health problems from the unfinished agenda formore detailed analysis [THIS SECTION TO BE AMPLIFIED WHEN FURTHER DATA AVAIL-ABLE; SEE BELOW]. As set out in Chapter 1, section 1.4, it has attempted to analyze what portionof the total burden of each disease or condition is now being averted, what could be averted withbetter use of existing interventions, and what cannot be averted with existing interventions but re-quires new ones. The analysis is intended to identify where the greatest needs lie, and thereby guideassessment of the priorities for different types of research.
Two examples of this analysis are provided with this draft for illustration [based on prelimi-nary calculations] (see Figures 3.7 and 3.8). [NOTE: these figures are based on intermediate cal-culations and, as readers will see, they do not correspond with the analysis set out in Chapter 1in Figure l.x. They are included for illustration only; updated figures will be available shortly.An updated version of the analysis is available in this draft for TB (Chapter 4).]
51
.
WHO Ad Hoc Health R&D Report, Draft 2.0
[Figure 3.7 about here]
[[Figure 3.8 about here]
These analyses show, first, just how much of the total existing disease burden from theseconditions could be averted with already existing technologies but is not being averted; and secondly,they indicate the magnitude of the need for investment in research into household and populationneeds and health service delivery that could lead to the imnproved use of existing tools. In the case ofdiarrhoeal diseases, just 7% of the existing burden is estimated to be unavertable with currentlyavailable technologies. Fully 43% of the burden could be averted with improved allocative effi-ciency---that is, with better use of money in the health portfolio. In the case of pneumonia, by con-trast, there is a clear need for more biomedical research: some 29% of the existing burden of pneu-monia cannot be averted with existing interventions. [These and other health problems will be ana-lyzed for final draft when revised, with more expansive discussion of the types of opportunities forresearch identified by each analysis.]
In the field of human reproduction, strategic behavioural research is needed to understandwhat factors influence people's perceptions of need for contraception, to learn more about their pre-ferred methods, and to understand the policies that influence the provision of family planning serv-ices so that more of the potential demand can be met. However, it is clear that women and men alsowant a greater choice of contraceptive methods and that existing methods are not acceptable to eve-ryone. There is therefore a need for biomedical research that will lead eventually to new methods.
3.3.2 Assessing ongoing research activity
The Comnmittee has made efforts to estimate the world's investment in research into a num-ber of selected health problems in an attempt to gauge the levels of activity relative to the diseaseburden that these problems cause. Research funding data are notoriously difficult to establish withany accuracy when the usual methods -such as collecting figures from the annual reports of organi-zations-are used and significant funds from a large numnber of sources, such as small charities, maybe missed, leading to biased results. This potential source of inaccuracy has been addressed bysampling at random the literature on specific subject areas and identifying the sources of funds on alarge sample of papers published between 1992 and 1994 as a basis for estimating funding (Annex x,Murray et al.).
For the current draft, research spending in the unfinished agenda has been assessed for twoconditions: acute respiratory infections and diarrhoeal diseases. The results indicate quite clearly thebroad mismatch between activity and need. In 1992, total funding for health research-from basicscience to health policy research--reached about $55 billion. But of that total just $32 million-farbelow a tenth of one per cent-was spent on diarrhoeal diseases, which will account for a full 7% ofthe burden of lost years of life in the next 25 years. Similarly, research expenditure on acute respira-tory infections was little better. It has been estimated at between $48 million and $68 million,whereas the condition is expected to account for more than 8% of the burden of lost years of life inthe next 25 years.
e
52
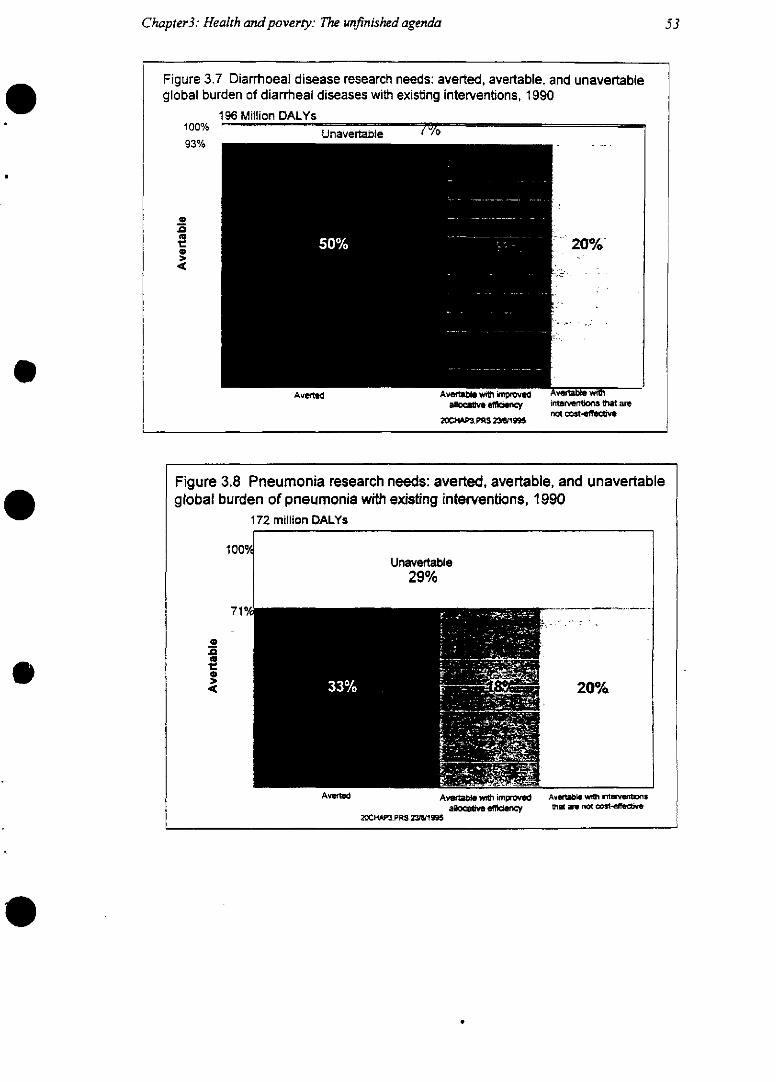
Chapter3: Health and poverty: The unfinished agenda
Figure 3.7 Diarrhoeal disease research needs: averted, avertable, and unavertableglobal burden of diarrheal diseases with existing interventions, 1990
196 Million DALYs100%
93%
o<ut2o»
U In2vertabhi 1 -/0
20%
AvWtUi~ wit wllpmprveallcve effaewcy
20C.3~.PRS 238/1995
..
Av~rbe wiñhintervenions 8at arenot co tffetve
20~C .PRS 2W1995
Averted
Figure 3.8 Pneumonia research needs: averted, avertable, and unavertableglobal burden of pneumonia with existing interventions, 1990
172 million DALYs
1000/CUnavertable
29%
71 O/
_e .0~~~~~~~~~~~~~~~~
u
< 20%
AvertaUs wft impoved Avwrtabbe w iMwenl~ sallocabve effiency at am not cost-~ ve
53
AV~
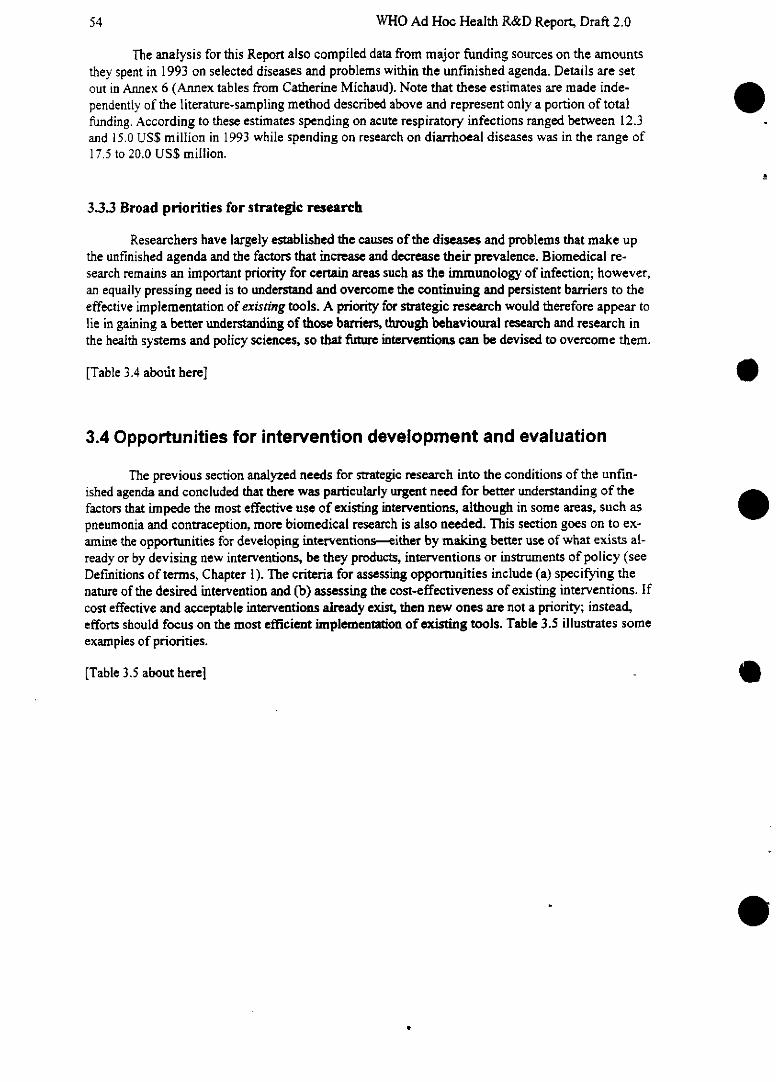
WHO Ad Hoc Health R&D Report, Draft 2.0
The analysis for this Report also compiled data from major funding sources on the amountsthey spent in 1993 on selected diseases and problems within the unfinished agenda. Details are set
out in Annex 6 (Annex tables from Catherine Michaud). Note that these estimates are made inde-pendently of the literature-sampling method described above and represent only a portion of totalfunding. According to these estimates spending on acute respiratory infections ranged between 12.3and 15.0 US$ million in 1993 while spending on research on diarrhoeal diseases was in the range of17.5 to 20.0 US$ million.
3.3.3 Broad priorities for strategic research
Researchers have largely established the causes of the diseases and problems that make upthe unfinished agenda and the factors that increase and decrease their prevalence. Biomedical re-search remains an important priority for certain areas such as the immunology of infection; however,an equally pressing need is to understand and overcome the continuing and persistent barriers to theeffective implementation of existing tools. A priority for strategic research would therefore appear tolie in gaining a better understanding of those barriers, through behavioural research and research inthe health systems and policy sciences, so that future interventions can be devised to overcome them.
[Table 3.4 about here]
3.4 Opportunities for intervention development and evaluation
The previous section analyzed needs for strategic research into the conditions of the unfin-ished agenda and concluded that there was particularly urgent need for better understanding of thefactors that impede the most effective use of existing interventions, although in somrne areas, such aspneumonia and contraception, more biomedical research is also needed. This section goes on to ex-amine the opportunities for developing interventions-either by making better use of what exists al-ready or by devising new interventions, be they products, interventions or instruments of policy (seeDefinitions of terms, Chapter 1). The criteria for assessing opportunities include (a) specifying thenature of the desired intervention and (b) assessing the cost-effectiveness of existing interventions. Ifcost effective and acceptable interventions already exist, then new ones are not a priority; instead,efforts should focus on the most efficient implementation of existing tools. Table 3.5 illustrates sornmeexamples of priorities.
[Table 3.5 about herel
e
54

Chapter3: Health andpoverty: The unfinished agenda
Table 3.4 Broad priorities for strategic research in the unfinished agenda (illustrativeexamples)
Population sciences(demography,
Disease or health epidemiology, Health systems and policyproblem Biomedical science behavioural sciences) research
Diarrhoeal disease ++ +++ ++++(Example): strategic re- (Example): determi- (Example): Studies of workc-search towards vaccines nants of mothers' deci- place policies on breastfeed-for Shigella dysentenae, sions to abandon ing and matemity leaverotavirus breastfeeding
Vaccine preventable ++ + ++++diseases (Example): Studies to- (Example): Studies of options
wards mutiple- for reducing the number ofimmunogen vaccines; chtild contacts in the EPI-plusstudies of infant immune immunization scheduleresponses
Reproductive health ++ +++ ++++(Example): Mechanisms (Example): Studies of (Example): Comparativeof spermatogenesis, tar- perceived need for fer- studies of quality of caregets for contraceptive tility regulation, and of given to women in Mother-vaccines, drugs provider behaviour in Baby package with aim of
FP ciinics identifying targets for im-provement
Note: Assessed prionrity ranges from low (+) to 'very high (+: +).
55
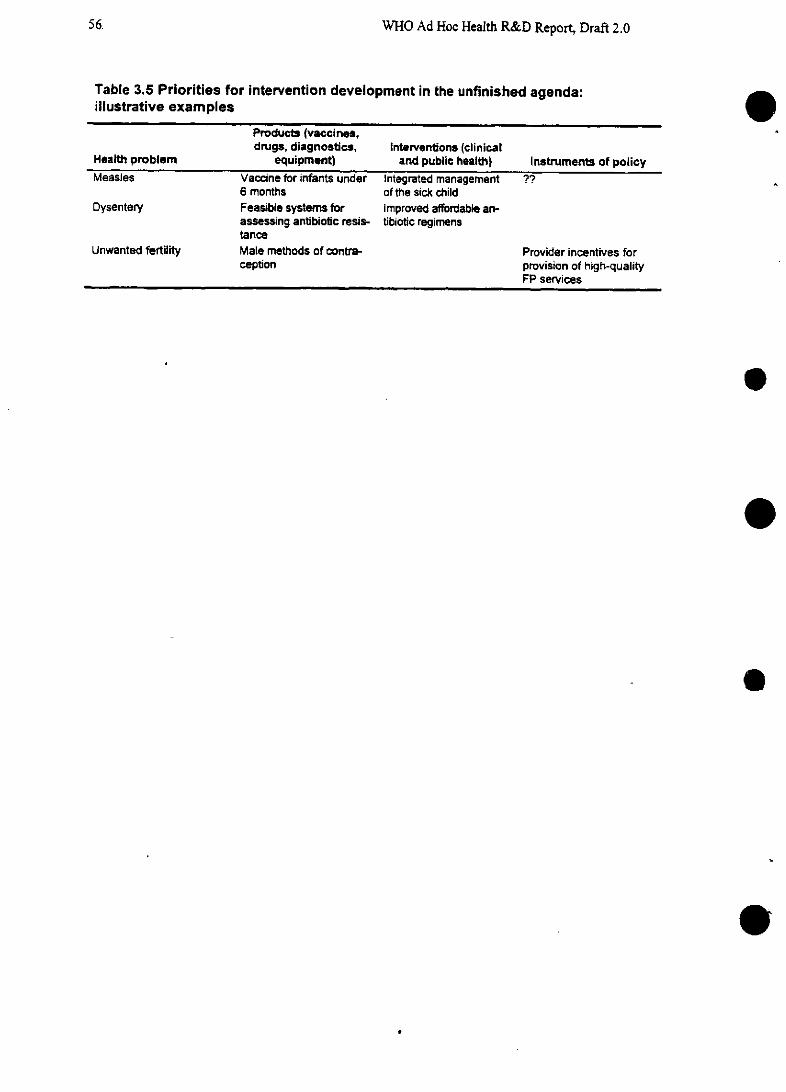
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 3.5 Priorities for intervention development in the unfinished agenda:illustrative examples
Products (vaccines,drugs, diagnostics, Interventions (clinical
Health problem equipment) and public health) Instruments of policyMeasles Vaccine for infants under Integrated management ??
6 months of the sick childDysentery Feasible systems for Improved affordable an-
assessing antibiotic resis- tibiotic regimenstance
Unwanted fertility Male methods of contra- Provider incentives forception provision of high-quality
FP services
e
e
e
56.
.
Chapter3: Health and poverty: The unfinished agenda
3.4.1 Opportunities for research on minimum essential packages
Governments around the world are already working to implement certain essential clinicalpackages of health services that together have the potential to avert a high proportion of the total bur-den of disease worldwide. In particular, five groups of comparatively simple interventions have beenidentified (WDR 93, p. 112) as essential to an effective, equitable health service: prenatal and deliv-ery care; family planning services; management of the sick child; treatment of tuberculosis; and casemanagement of sexually transmitted diseases. All five are highly cost-effective; implementing eachof them costs less than $50 for each year of healthy life purchased in the low-income countries wherethe greatest burden remains to be averted (Figure 3.9):
[Figure 3.9 about here]
The first three of these groups of interventions relate to the unfinished agenda. Projectionsfor this Report [not available with this draft] will show the impact of implementing the minimumessential packages on the burden of the unfinished agenda, contrasted with the trends that can be ex-pected if the packages are not implemented.
The findings of our analysis for this Report suggest that key priorities for intervention devel-opment lie in evaluating and improving the implementation of these packages. However, these stepsdepend on a variety of complex factors at the level of individual districts such as the capacity of thehealth system locally to deliver them, the availability of data to monitor needs and intervention cost-effectiveness at local level, and so on. Steps are now being taken to evaluate packages and how toimplement them at district level, in two rural districts in Tanzania (Box 3. 1).
More specific research priorities identified by experts within each package are summarizedbelow.
[Box 3.1 about here]
Package 1: Integrated Management of the Sick Child (IMSC)
Three out of four children seeking health care every day suffer from one of the five condi-tions discussed above: pneumonia, diarrhoea, measles, malaria and malnutrition. As the discussionabove has outlined, many of these children will be suffering from more than one condition, and diag-nosis is not necessarily simple. As a result, treatment guidelines have been developed to cover themost common potentially fatal conditions, enabling health workers tofocus on the whole child ratherthan on specific diseases and reducing duplication of effort (WHO Division of Diarrhoeal and AcuteRespiratory Disease Control, 1995). The health worker assesses every child for a set of signs andsymptoms, including cough or difficulty in breathing, diarrhoea, fever, or ear problems, and assessesthe child's nutrition and immunization status. Depending on the findings, the health worker can thenallocate the child either for urgent referral, or specific medical treatment and advice, or simple advicefor home treatment. The guidelines are printed in wallcharts and booklets for use in remote health-care settings. Health workers are trained in the use of the guidelines. Properly implemented, thepackage has been assessed to be the intervention likely to have the greatest impact in reducing theglobal burden of disease (WDR 93). Clearly, as yet that potential has not been met. The key to betterimplementation lies in evaluation research and the refinement of the package.
57
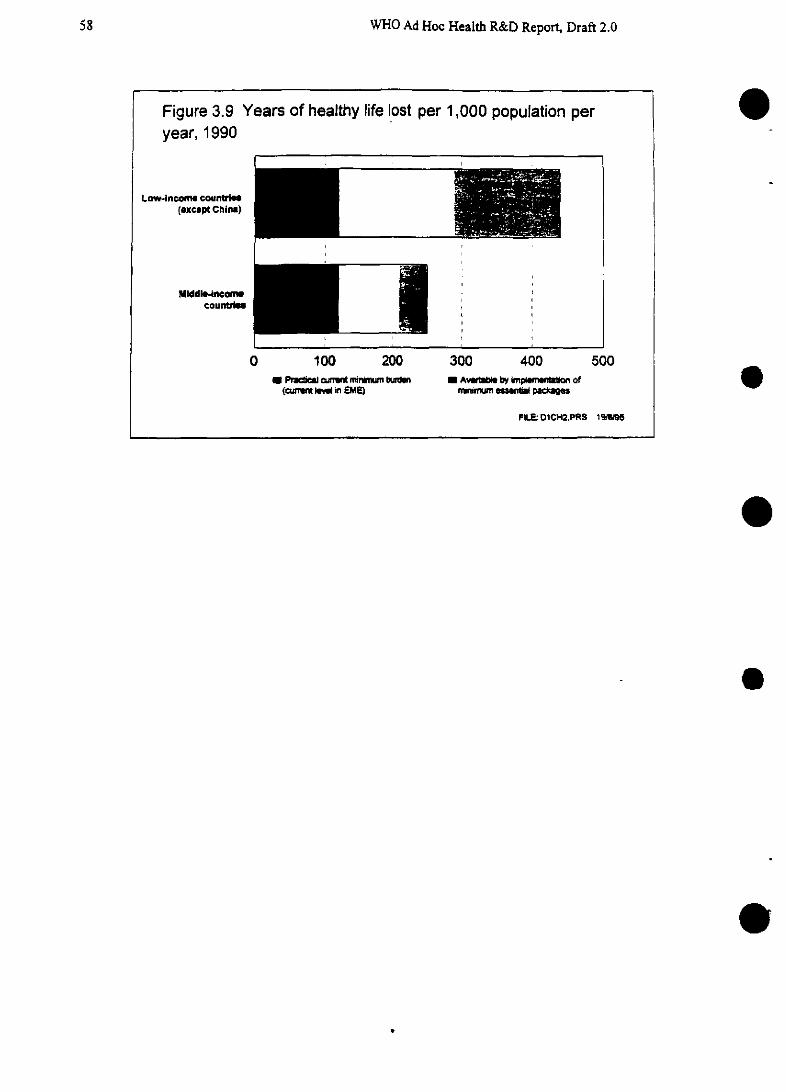
WHO Ad Hoc Health R&D Report, Draft 2.0
e
e
e
.
58
Chapter3: Health andpoverty: The unfinished agenda
Box 3.1 The Tanzanian Essential Health Intervention Project (TEHIP)
The development of a common currency for measuring the global burden ofdisease and the cost-effectiveness of interventions has, in principle, enabled countriesto establish health intervention priorities. However, the adoption and implementation ofa minimal essential package of health interventions as recommended by WDR 93 en-tails some difficulties such as a health system's capacity to effectively plan and im-plement the package and access to the necessary information needed in the planningprocess. To assess the feasibility and impact of such an approach, at district level,International Development Research Center supported the creation of the EssentialHealth Interventions Project (EHIP). It is EHIP's hypothesis that health interventionprioritization and resource allocation should be made on the basis of burden of dis-ease and cost-effectiveness analysis carried out at the district level. EHIP has identi-fied several steps as necessary for achieving this end:
* to assess "the District Health Management Teams' capacity to establish priori-ties and plan the allocation of resources according to local estimates of bur-den of disease and knowledge of cost-effectiveness'.
* to determine the extent to which district health plans can be translated intoeffective delivery of and use of the essential health interventions
* to assess the cost as well as impact of the essential health intervention pack-age on the burden of disease.
In an effort to promote the implementation of EHIP, the International Develop-ment Research Centre and the Tanzanian Ministry of Health organized a twelve-dayworkshop in Summer 1995 in Morogoro, Tanzania, with representatives from WHO,the World Bank, and from the districts of Morogoro Rural and Rufiji. The objectives ofthe Tanzanian Essential Health Intervention Project (TEHIP) Workshop were to:
· provide the background and introduction to the main concepts behindTEHIP so as to provide all participants with a basic understanding on theproject objectives.
* through a simulation exercise based on the burden of disease currentlyknown for Morogoro Rural and Rufiji, identify potential cost-effective es-sential packages of health interventions.
* develop the TEHIP workplace for the first year of the project.
* widen and reinforce partnerships for TEHIP.
TEHIP will be implemented in the districts of Morogoro Rural and Rufiji.
59
WHO Ad Hoc Health R&D Report, Draft 2.0
(Box 3.1 continued)
The meeting reviewed the state of the Tanzanian health sector and introducedthe concepts behind the determination of the burden of disease and cost effective-ness. Thereafter, several potential interventions were reviewed. An important part ofthe workshop consisted of cost-effectiveness simulations whereby three small groups(Morogoro District, Rufiji District, and the national level) estimated the fixed and vari-able costs needed for cost-effectiveness calculations. Six interventions were costed insuch a manner. the integrated management of the sick child, the mother-baby pack-age, EPI-plus, STD control, impregnated bednets, and tuberculosis management. Thesimulations served to solidify the concepts underlying cost-effectiveness calculationsand also provided some comparisons of costs between districts and at the nationallevel. A fourth group looked at burden of disease calculations and identified potentialhealth interventions to be included in the package.
The workshop concluded with the determination of the TEHIP workplan andbudget for year one (July 1995 through June 1996) of the project. The aim of theworkshop was to determine the feasibility of evaluating the cost-effectiveness of po-tential interventions at the district and national level, and assessing the policy, plan-ning, and management processes needed to implement TEHIP. The research compo-nent of the project aims at investigating supply and demand aspects of the healthsystem. It hopes to determine the current health system capacity and to identify thoseareas that need capacity-building. Its two main components are health system re-search and demographic and epidemiological research. The research component ofTEHIP aims at strengthening the districts information base so as to assist the DistrictHealth Management Teams establish priorities and plan the allocation of resourcesbased on local burden of disease estimations, cost-effectiveness, system capacity,and community preferences.
The EHIP steering committee is chaired by IDRC and indcludes representativesfrom Tanzania, WHO, World Bank, UNICEF, CIDA and the Clark Foundation. How-ever, IDRC is committed to establishing full intellectual partnership with the recipientcountry and leaves all in-country management and planning to the host country.
.
60
Chapter3: Health and poverty: The unfinished agenda
Selected research prioritiesfor IMSC
The WHO's Division or Diarrhoeal and Acute Respiratory Disease Control has identified anumber of priorities for research on IMSC. They include:
* Improving the adequacy of clinical management, including studies of the classifications andtreatments given by health workers compared with those given by expert paediatricians withaccess to diagnostic aides such as x-ray radiology and laboratory services;
* Improving treatment for dysentery and pneumonia, with the development of affordable alter-native antibiotic regimens and feasible methods for surveillance of antibiotic resistance;
* Improving the clinical diagnosis of malaria and anemia possibly assisted by simply diagnos-tic tests;
* Improving delivery of the package to young infants, through the development of the simplestset of clinical signs to detect serious bacterial infection and studies into the feasibility oftraining health workers to assess and correct feeding problems such as poor breastfeedingattachment and suckling.
Package 2: The Mother-Baby package
This package, which is currently under development, incorporates the provision of familyplanning services, antenatal care, including the diagnosis and treatment of STDs, clean and safe de-livery and essential obstetric care. It is based on the principles that every womnan has the right to equi-table, high-quality care, including primary health care and basic maternity care, in the interests of ahealthy pregnancy and the safe delivery of a healthy infant. The World Bank has estimated that theextension of prenatal, delivery and postpartum care to 80%/o of the world's population would reduceby 40% the burden of disease associated with unsafe childbirth, at a cost of between $90 and $255per birth attended-no more than $9 per capita (WDR 93).
Research priorifies for the Mother and Baby package
The WHO's Division of Family Health has identified a number of research priorities for thepackage as it evolves. Among them are:
* Research into the delivery of services to women with the aim of identifying targets for irn-provements in quality of care;
* The assessment of appropriate technologies, such as a simple partograph that can be used tomonitor labour outside the hospital environment or the adaptation of simple sterile pre-loaded injection capsules, such as Uniject, to enable health workers in remote settings to giveoxytocin in stage III of labour, with the aim of reducing post-parmum haemorrhage andminimizing the risk of sepsis.
61
WHO Ad Hoc Health R&D Report, Draft 2.0
Healthy Women Counselling Guide
This package, which is currently being developed by 13 WHO programmes, will provide esimple health messages to womrnen, the main providers in the farnily, about many health conditions,their treatment and prevention. It is aimed at the most neglected sector arnong poor populations indeveloping countries: illiterate women in rural areas. It focuses on women's health in a holistic way,including both reproductive and nonreproductive health. As no other such guide exists, this is de-signed to make a unique contribution to women's health, with spin-offeffects for the health of theirfamilies and communities. We know that women spend a large proportion of their earnings on farnilynutrition and health care, but lack of knowledge of appropriate sources of treatment often means thatthese resources are poorly allocated or wasted. The guide, it is hoped, will help to reduce such prac-tices by advising on appropriate treatnent at home, as well as what to expect from health services.
Research prioritiesfor the Healthy Women Counselling Guide
* Form (pictures, clinic talks, stories) and medium (books, radio, support groups) in whichhealth messages should be provided;
* Development of additional messages not included so far (e.g. eye problems, drug abuse, vio-lence);
* Impact of the guide on women's health;
* Impact of the guide on health of other family members, male and female.
3.5 Chapter summary and recommendations
The major killer diseases of childhood, malnutrition, and poor reproductive health will remain sig-nificant challenges to research for at least the next 25 years. Taken together, these conditions willaccount for more than a quarter of the total years of life lost over the period and if poverty deepens orexisting interventions cease to be effective, their impact could become even more severe. Researchexpenditure on these conditions does not begin to approach need as assessed by the share of the bur-den of premature death attributable to them. Cost-effective interventions already exist for many ofthese conditions, but their implementation so far has fallen short of potential. Priorities for researchfocus on the implementation, evaluation and improvyement of existing interventions and interventionpackages, and the development of new tools where necessary. The "best buys" for R&D investment,include the evaluation of the minimum essential packages and research aimed at reducing the numberof contacts needed between health workers and children in the immunization schedule of EPI.
1. Despite the existence of cost-effective interventions, communicable diseases, poor reproductivehealth and undernutrition continue to account for unnecessarily high disease burdens in mostlow-income and some middle-income countries. These burdens fall overwhelmingly on the poorand are both a consequence and a cause of their poverty. Recent analyses suggest that integratedpackages of interventions (such as a package for the integrated management of the sick child)could substantially increase the managerial and financial feasibility of reducing those burdens.Governments and donors should shift resources into developing and evaluating such packages
62
Chapter3: Health and poverty: The unfinished agenda 63
further in different settings and, if their benefits are confirmed, invest in them as a highly cost-effective means to improve health.
2. A significant portion of the burdens of infectious diseases and poor reproductive health still can-not be addressed by existing tools. New tools are needed--e.g. to increase the effectiveness ofvaccination schedules by reducing the number of occasions when children must come into con-tact with health workers, to allow measles immunization at earlier ages, and to provide a widerchoice of contraceptive methods. Current efforts, both in strategic research and in new productdevelopment, are inadequate to deal with these challenges. Investment in these areas now holdsthe promise not only of improving health but also of reducing costs.
.
eChapter 4: Emerging and re-emerging microbes: the
continually changing threat of infectious disease
In the 50 years since the Second World War, the development of antimicrobial drugs, immunizationprogrammes and the better nutritional status enjoyed by the populations of the established marketeconomies had increasingly led to a widespread perception that infectious diseases were a recedingthreat that had largely been brought under control. It was widely assumed that the technologies thathad succeeded in controlling diseases such as tuberculosis in the EMEs would succeed worldwide,given timne. However, over the past two decades, there have been a growing number of reasons tochallenge that perception. The emergence of HIV has forcefully reminded the industrialized worldthat not all communicable diseases are easily treated or cured, and the spread of multidrug-resistantTB in the urban United States drew international attention to the threat posed by a pathogen that haslong been a major killer in the poor world. Antibiotic-resistant strains of a number of bacteria, suchas Pneumococcus, seriously threaten to undermine treatment in a number of countries, rich and poor.Meanwhile many low- and middle-income countries have experienced setbacks in the control of agrowing list of communicable diseases, mainly due to rapid demographic and economic changes, thespread of drug-resistant strains of pathogens and the breakdown of health systems.
This chapter focuses on the threats to global health posed by emerging and re-emerging dis-eases and the challenges they create for research and development.
4.1 Change in the global village: factors in the emergence of dis- lease
During the 1990s there has been intense public interest in the emergence of exotic "new" infectiousagents such as Ebola virus, which recently reappeared after almost two decades to cause a widelyreported epidemic in Zaire, and hantavirus in the United States. However, for all their high profile,these agents have to date contributed very little to the global burden of disease. Further, they are onlyone part of the very broad conceptual "umbrella" of emerging diseases. The concept includes severallarge and overlapping categories:
* common, well-known pathogens that had been thought to be under control in many (thoughnot all) parts of the world but which, for a number of reasons, are now in dramatic resur- -
gence, such as Mycobacterium tuberculosis, the cause of TB, and Plasmodiumfalciparum,the cause of life-threatening malaria;
* pathogens that have entered human populations comparatively recently and spread to becomeepidemic as a result of changes in human behaviour, principally HIV;
* pathogens that have become resistant to many, even most, of the available drugs againstthem, including Shigella dysenteriae and Staphylococcus aureus;
* pathogens that are newly recognized, such as E. coli 0157 and hantavirus.
64
Chapter 4: The continually changing threat of infectious disease
In the past, pandemics of plague, smallpox, cholera and syphilis have been associated with periods ofrapid economic change or population growth (Addressing Emerging Infectious Disease Threats: APrevention Strategyfor the United States, Atlanta: CDC, p. 2). Growing migration, internationaltravel and commerce in the late 20th century have made it possible for local outbreaks of infection tospread around the world within days, forcing governments to recognize that international borders areno barrier to microbes.
The factors that influence the emergence and re-emergence of disease are complex and inter-related. They include changes in the genome of the organisms themselves that alter their relationshipswith their hosts; the selection for, and spread of, drug-resistant strains as a result of inappropriate useof antimicrobials; and changes in human behaviour and ecology. Table 4.1 sets out some of the mostsignificant examples, both of new emerging diseases and old diseases resurging or re-emerging.
[Table 4.1 about here]
In the past 15 years, a number of important communicable diseases have emerged or re-emerged on a scale sufficient to attract international interest. They include:
* tuberculosis;
* pneumococcal disease in children;
* malaria;
* HIV and other STDs, such as Chlamydia trachomatis;
* cholera in Latin America;
* yellow fever,
* diphtheria in Russia and Ukraine;
* multidrug-resistant Shigella dysenteriae, the most virulent of the Shigella bacteria, which arethe most frequent cause of bloody diarrhoea (dysentery);
* African trypanosomiasis in Zaire (in the case of this example, it should be noted that whilethe impact of the disease may be low worldwide, it is of enormous importance in Zaire,where 90 % of the world's cases are concentrated);
* Ieishmaniasis in Sudan;
* filariasis
* plague in India.
65
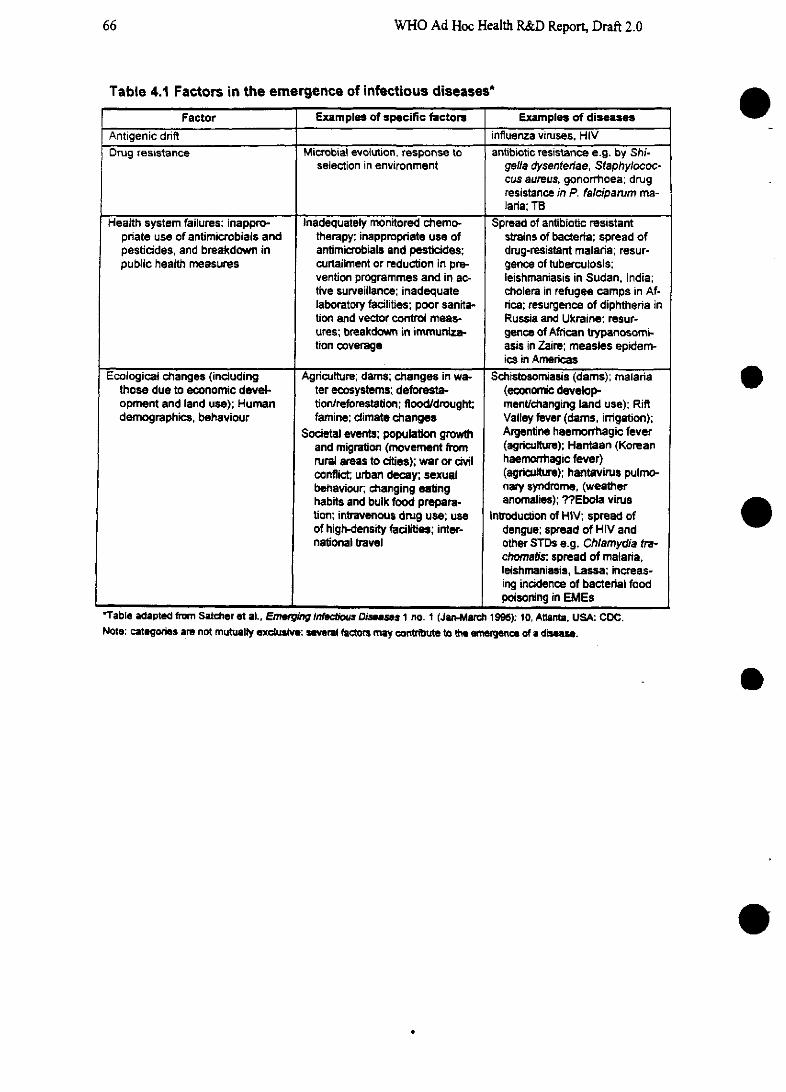
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 4.1 Factors in the emergence of infectious diseases*
Factor Examples of specific factore Examples of diseasesAntigenic drift influenza viruses, HIVDrug resistance Microbial evolution, response to antibiotic resistance e.g. by Shi-
selection in environment gella dysenteriae, Staphylococ-cus aureus, gonorrhoea; drugresistance in P. falciparum ma-laria; TB
Health system failures: inappro- Inadequately monitored chemo- Spread of antibiotic resistantpriate use of antimicrobials and therapy; inappropriate use of strains of bacteria; spread ofpesticides, and breakdown in antimicrobials and pesticides; drug-resistant malaria; resur-public health measures curtailment or reduction in pre- gence of tuberculosis;
vention programmes and in ac- leishmaniasis in Sudan, India;tive surveillance; inadequate cholera in refugee camps in Af-laboratory facilities; poor sanita- rica; resurgence of diphthenria intion and vector control meas- Russia and Ukraine; resur-ures; breakdown in immuniza- gence of African trypanosomi-tion coverage asis in Zaire; measles epidem-
ics in AmericasEcological changes (including Agriculture; dams; changes in wa- Schistosomiasis (dams); malaria
those due to economic devel- ter ecosystems; deforesta- (economic develop-opment and land use); Human tion/reforestation; flood/drought; mentchanging land use); Riftdemographics, behaviour famine; climate changes Valley fever (dams, irrigation);
Societal events; population growth Argentine haemorrhagic feverand migration (movement from (agriculture); Hantaan (Koreanrural areas to cities); war or civil haemorrhagic fever)conflict; urban decay; sexual (agriculture); hantavirus pulmo-behaviour; changing eating nary syndrome, (weatherhabits and bulk food prepara- anomalies); ??Ebola virustion; intravenous drug use; use Introduction of HIV; spread ofof high-density facilities; inter- dengue; spread of HIV andnational travel other STDs e.g. Chlamydia tra-
chomais; spread of malaria,leishmaniasis, Lassa; increas-ing incidence of bacterial foodpoisoning in EMEs
'Table adapted fromn Satcher et al., Emergng Infectfous Dases 1 no. 1 (Jan-Marc~ 1995): 10, Atlanta. USA CDC.Note: categones are not mutualty exclusive: several fctomr muy contribute to the emergence of a disease.
e
o
e
e
66
Chapter 4: The continually changing threat of infectious disease
In addition, somrne 20 pathogens have been newly identified since 1973, including rotavirus;Cryptosporidium parvum, the cause of an acute form of enterocolitis; hepatitis C virus; and severalspecies of Campylobacter (Satcher et al. 1995). However, this Report has chosen to focus on fouremerging and re-emerging diseases and disease clusters with a major contribution to the global bur-den of disease. They are: HIV and other STDs; tuberculosis; pneumococcal disease; and malaria andthe other diseases in the tropical cluster. These four diseases or disease clusters form the main subjectof the remainder of this chapter. They have been singled out because (1) they all have significant dis-ease burdens; (2) they are amenable to research, in contrast to the many as-yet unknown emergingdiseases; and (3) each of them shows unstable epidemic patterns due, at least in part, to the geneticand ecological characteristics of the causative organisms, which are known to change rapidly in theirrelationships with their hosts and with the existing control measures against themrn. For further dis-cussion of the Committee's reasons for including these diseases in this chapter, rather than in the pre-ceding one, please see Chapter 1, Scope and Focus.
According to cumulative projections for this Report, which allow weighting for changes inprevalence over time, these four diseases and disease clusters will together account for some 15 percent of the total loss of years of life between 1990 and 2020 (see Table 3.1 in previous chapter).
4.2 Four major threats to public health
4.2.1 Tuberculosis
Among infectious diseases, tuberculosis is the single biggest killer of adults, and is responsible formore than a quarter of avoidable adult deaths. Within a decade, some 30 million people will havedied because of it (WHO Report on the Tuberculosis Epidemic, 1995). At any one time around theworld, some 20 million people are sick with TB. The currently available vaccine, BCG, is useful inpreventing somrne forms of childhood TB but is ineffective in adults. Short-course chemotherapy cancure up to 95 per cent of patients, but failures in the admninistration of that therapy make its actualeffectiveness much lower in many settings. The emergence of multidrug-resistant strains of M tuber-culosis in New York during the early 1990s drew widespread attention to the disease, but the scale ofthe problem of drug resistance may be much greater elsewhere. Data are scant, but the WHO esti-mates that more than 50 million people are already infected with strains that are resistant to one ormore drugs.
The spread of HIV has created a new urgency to the threat from TB. A person infected withboth organisms is about 30 times more likely to develop TB disease than one who is infected with TBalone. In 1994, an estimnated 5.6 million people were infected with both pathogens and TB is now theleading cause of death among HIV-infected people. As a result, deaths from TB may rise as high as 4million a year by 2005. If TB cases were properly handled, the total costs of caring for people withAIDS could be cut by as much as half(WHO 1995).
Weighted projections for this Report indicate that IB will account for fully 3% of total yearsof life lost before 2020. (NB: projections to follow for various scenarios, e.g.: MDR TB becomesmore widespread, DOTS is implemented in 80% of countries, etc.)
67
WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 4.1 indicates how the remaining burden of TB might best be addressed through re-search of different types.
[Figure 4.1 about here]
4.2.2 HIV and other STDs
The HIV pandemic which began in the late 1970s has now affected every inhabited conti-nent. Every day, an estimated 6000 people become infected (World Health Report 1995, WHO, p.29). By the year 2000, it is estimated that there will be some 26 million people living with HIV in-fection worldwide, the vast majority of them in Sub-Saharan Africa and Asia. By that time, somrne 40million people will have been infected in total since the pandemic began. Although AIDS is lessprevalent than somrne other diseases such as malaria in most developing countries, its economic impactis higher because it incapacitates and kills young and middle-aged adults who are at their most pro-ductive, and to date it has also disproportionately affected skilled and managerial workers (WDR 93,p. 20). In the short history of the pandemic to date, few genuinely promising antiviral drugs havebeen developed and none that is affordable by low-income countries. The search for vaccines has sofar brought more frustrations than successes, and is restricted in the case of study of potential liveattenuated vaccines by risk-benefit issues in industrialized countries.
The costs of caring for people with AIDS are high. Studies from a range of developing coun-tries have indicated that the costs of direct medical care alone ranged from between 60% and 80% ofper capita GNP to several times per capita GNP (AIDS in the World, Mann, Tarantola and Netter,eds., Harvard University Press 1992, p. 484). The average is about 150% of GNP per capita (WDR93). In addition, family members of people with AIDS are affected; young children who lose theirmothers to AIDS are more likely to die themselves and even older offspring are disadvantaged; in astudy in Tanzania, teenagers' school attendance dropped by half if they had lost an adult femalemember to AIDS.
Projections of the course of the IV pandemic up to 2020 have been generated for this Re-port for eight regions (Figures 4.2 to 4.9).
[Figures 4.2 to 4.9 about here]
The projections show the time lag between incidence of infection and death from AIDS, in-dicating that the number of AIDS cases in most regions will continue to rise steeply until between2005 and 2010, after which it will continue at a relatively high level, imposing the heaviest cost bur-den on those regions least equipped to pay: gross domestic product for India and Sub-Saharan Africais projected to grow scarcely at all over the period whereas in the Established Market Economies it isprojected to climb steeply (Figure 4.10).
[Figure 4.10 about here]
68
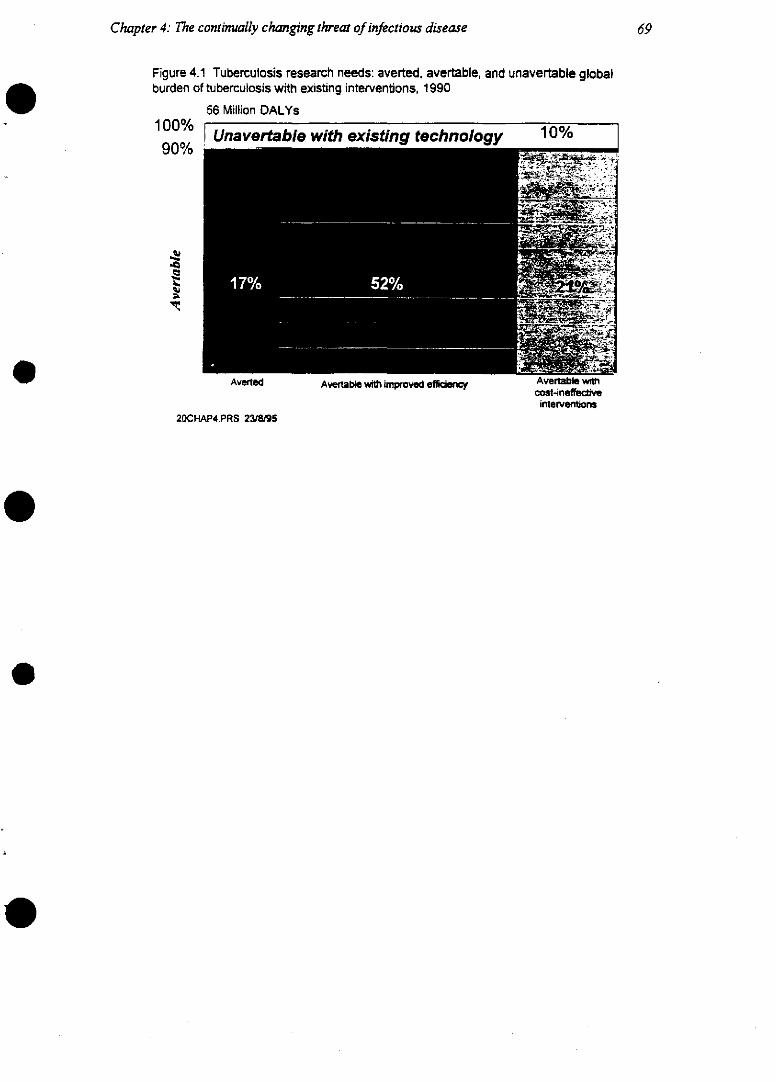
Chapter 4: The continually changing threat of infectious disease
Figure 4.1 Tuberculosis research needs: averted, avertable, and unavertable globalburden of tuberculosis with existing interventions, 1990
56 Million DALYs
1 00% Unavertable with existing technology 10%90% ....
Averted Avertable with ~ipmved efficent Avertable wtcost-ineffectNe
interventions20CHAP4.PRS 23/8/95
69
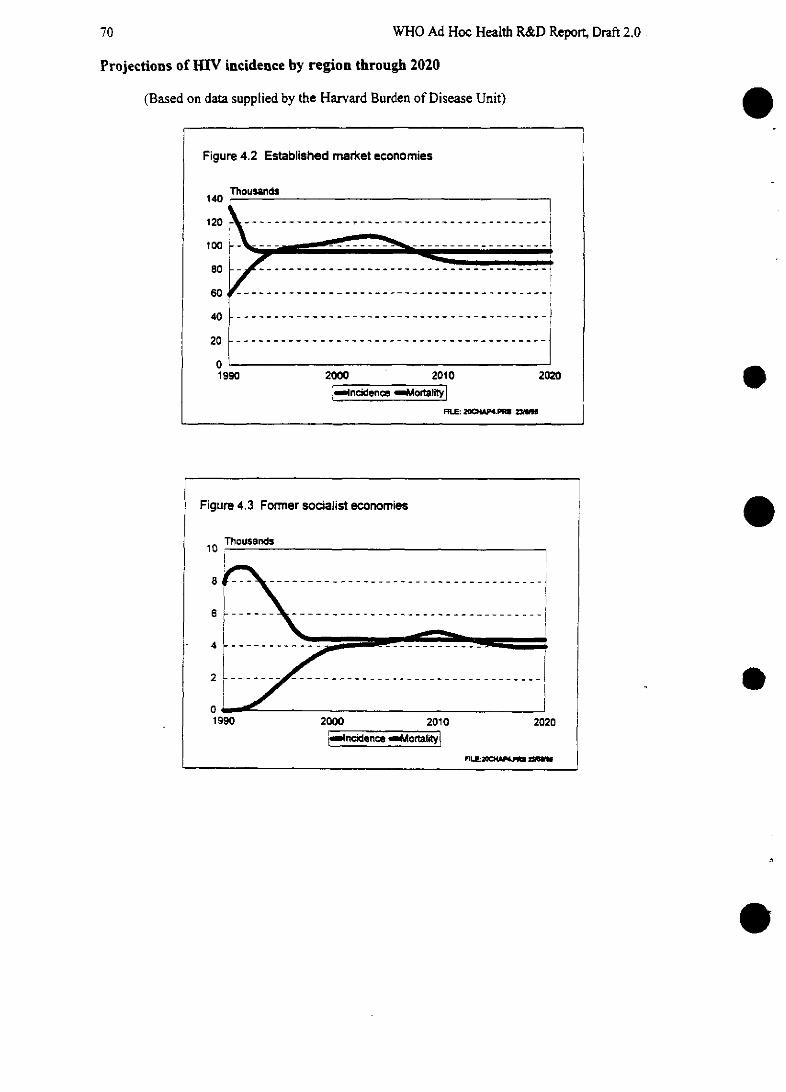
70 WHO Ad Hoc Health R&D Report, Draft 2.0
Projections of HIV incidence by region through 2020
(Based on data supplied by the Harvard Burden of Disease Unit)
Figure 4.2 Established market economies
140Thousands
1200 --- 21 ------------ 2---1 00 - -L - - - ~ --------- -- _ _____
80« __-----------------
40 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
20 ---- L------------------!~ ------------------
100
Fiues . oresoaltecnms1990 2000 2010 2020.
_~ncídenee * ortaÉ_
MUE: 2~CP.PRU Z
1
Figure 4.3 Former socialist economies^
40 ..........................
0 _
1990 2000 2010 2020
I~ ncidín *c y
rLL-OM U~
i~,=~.=.,Molne

Chapter 4.: The continually changing threat of infectious disease
Figure 4.4 Developing countries in Asia exctluding India and China
Thousands4UU
300
200
100
01990 2000 2010
!-ncidence -Mortality i'as iK>d. dW~ of PboffC ad Ind~a o
Figure 4.5 Latin Arnerica and the Caribbean
250 r-
200 L -
150
100 -
50 -
19901 990
2020
FuI. . 2CPS 4 M,
2000 2010 2020
ncidence -~MortaityFL 23n,~Z~ -
- -
71
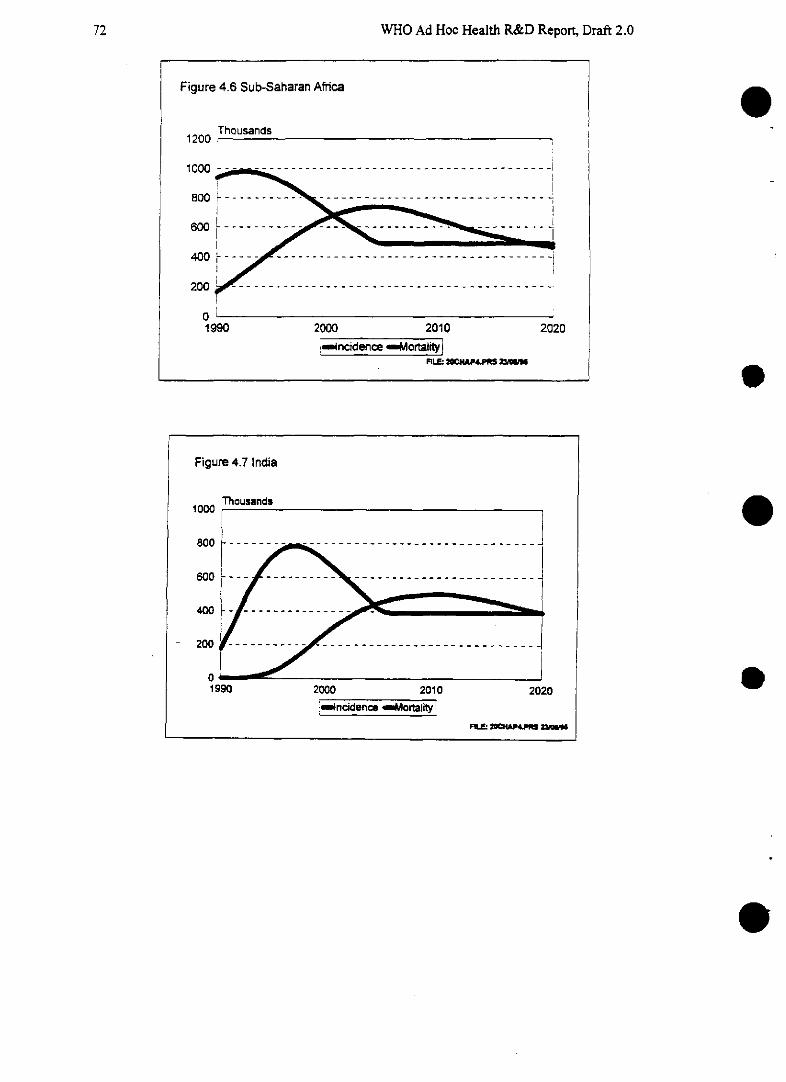
WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 4.7 IndiaFigure 4.7 India
incidence -Mortality !Fur" al P as Z~
e
e
e
e
72
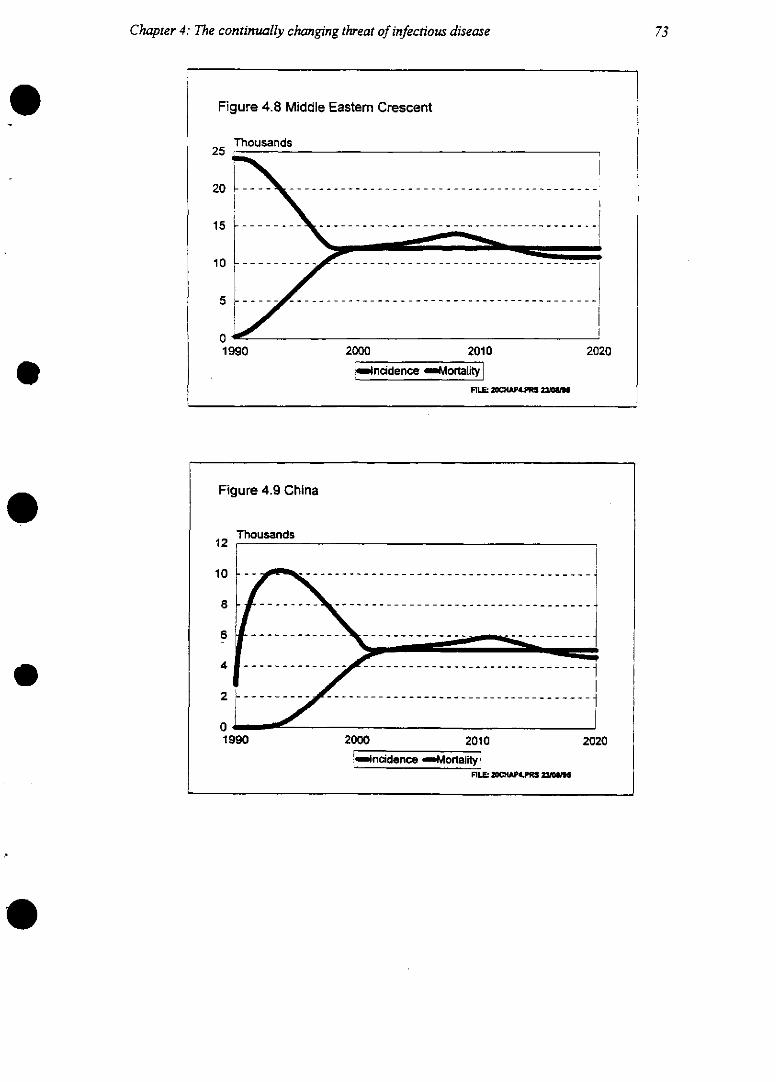
Chapter 4: The continually changing threat of infectious disease 73
Figure 4.8 Middle Eastem Crescent
Thousands25
0
1990 2000 2010 2020
imncidenc MraltPIIL =M14P4.PMt ~GI
Figure 4.9 China
Thousands12
1990 2000 2010 20206----d---- . -- -- o- -- -
FILL: ZO~AP.PI ~
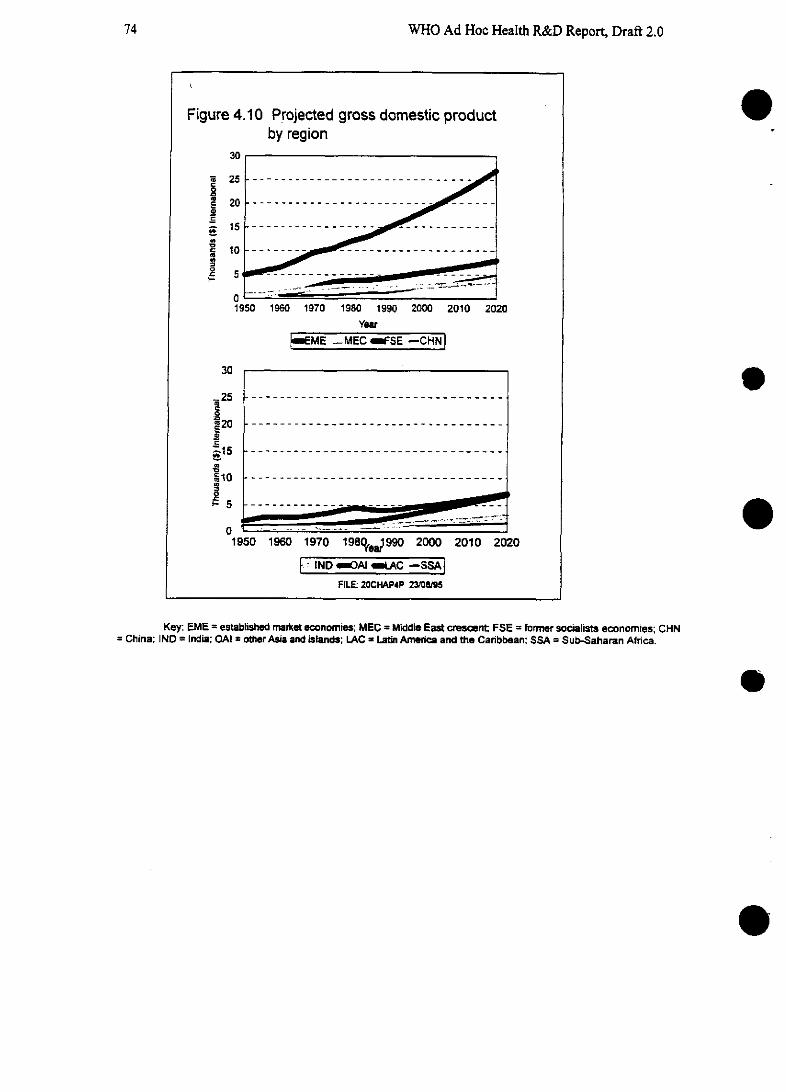
74 WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 4.10 Projected gross domestic productby region
30
20
15
03
1950 1960 1970 1980 1990 2000 2010 2020
Year
EME -MEC FSE -CHN
30
.- 25 -....-..-..-..-..-..-..-..-..-..-..-..-..-..-..-..-.
i 20 -....-..-..-..-..-..-..-..-..-..-..-..-..-..-..-..-.
20
1950 1960 1970 198%er990 2000 2010 2020
IND ~OAI LAC -ssA
FILE: 20CHAP4P 23/0895
Key: EME -established market economies; MEC = Middle East cresent FSE = former socialists economíes; CHN- China; IND -- India: OAI = other Asia and islands; LAC = Latin America and the Caribbean: SSA = Sub-Saharan Africa.
e
e

Chapter 4: The continually changing threat of infectious disease
Even after the first wave of the epidemic in each region has peaked. the incidence of HIV in-fection in developing regions will remain steady and at significantly higher levels than in the EMEsor the former socialist economies. By 2005, the incidence of HIV infection is expected to settle ataround 500 000 infections per year in Sub-Saharan Africa overall, and in India at 400 000 infectionsper year. The costs of the pandemic to the world will therefore remain unprecedentedly high for gen-erations to come. The assumptions on which these projections are based are explained in Annex 1.
Other STDs are much cheaper to treat and most are more easily treated, but they must first bediagnosed and in many people-particularly women-STDs can go undiagnosed for years, for acombination of reasons. These include the stigma that prevents people from seeking medical atten-tion and the tendency to regard as normal symptoms, such as vaginal discharge, which may indicateinfection. The health burden from STDs worldwide is enormous; they are estimated to cause up to 15per cent of the disease burden in the urban populations of developing countries (Challenges in Re-productive Research, WHO 1994, p. 83).
[Table 4.2 about here]
STDs may be considered part of the problem of emerging and re-emerging diseases for sev-eral reasons. There is increasing evidence to suggest that HIV, the biggest of the newly identifiedpathogens, spreads more easily from person to person through sexual contact when one or both par-ties are also infected with other STDs. Drug resistance is also a problem with several STDs; andrapid social and demographic change has been associated with epidemics of several sexually trans-mitted infections. Penicillin-resistant strains of Neisseria gonorrhoeae, the cause of gonorrhoea, havebeen identified in up to 60 per cent of samples tested in some developing countries (P. J. Rowe,Challenges in Reproductive Health Research, WHO 1994) and Chlamydia trachomatis has becomerecognized as an emerging disease with significant impact on the health of women and children. Theemergence of chlamydial infections has been attributed to increased sexual activity (Institute ofMedicine 1992, p. 36) and also to increased recognition of the disease.
Women-and children---bear a disproportionately heavy share of the burden of STDs and aremore likely to suffer long-termn effects than men. Chlamrydial infection during pregnancy can result ininfant pneumonia and blindness (trachoma), and prolonged untreated infection in women can lead tosterility. Eight out of 10 womnen with ectopic pregnancy have serological evidence of past chlamnydialpelvic infection. Even in Sweden, where the health facilities and information available to women areamong the best in the world, up to a quarter of cases of a single episode of upper genital tract infec-tion end in tubal occlusion even when treated promptly. Researchers believe that the incidence oftubal occlusion must be much higher in environments where prompt diagnosis and treatment are notavailable (Challenges in Reproductive Health Research, WHO, 1994, p. 85). Cancer of the cervix isthe most common malignancy in women in developing countries; at least four human papilloma vi-ruses have been associated with this malignancy.
Taken together, HIV and other STDs are expected to account for 4.8% of the global total ofyears of life lost over the coming 25 years (Table 3. 1). [As above, need details of assumptions andbreakdown by different scenarios, e.g. with and without effective STD diagnostics, with and withoutaffordable HIV vaccine.]
75
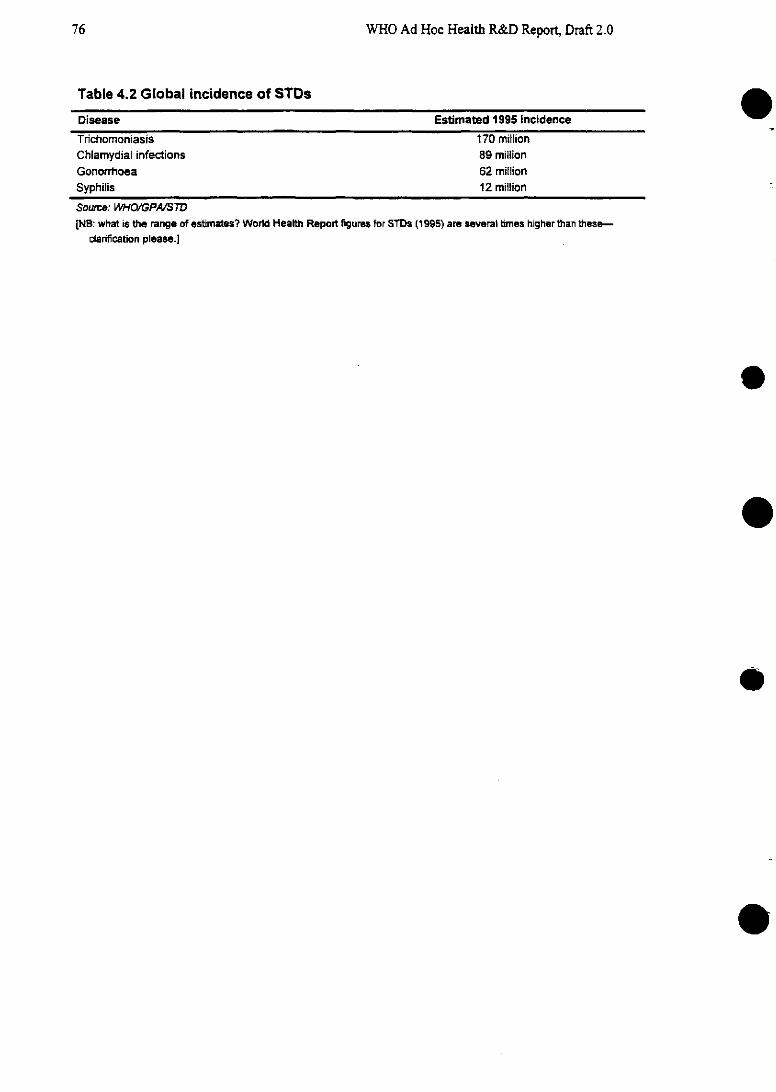
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 4.2 Global incidence of STDs
Disease Estimated 1995 incidence
Trichomoniasis 170 millionChlamydial infections 89 millionGonorrhoea 62 miillionSyphilis 12 million
Source: WHO/GPA/STD[NB: what is the range of estimates? World Health Report figures for STDs (1995) are several times higher than these-
clarification please.]
e
.
o
e
76
Chapter 4: The continually changing threat of infectious disease
4.2.3 Malaria
Every year, worldwide, up to 500 million people fall sick with malaria, 90% of them in Af-rica (WHO TDR 20-year review, 1995). Outside Africa, more than two-thirds of reported cases areconcentrated in just six countries: India, Brazil, Sri Lanka, Afghanistan, Viet Nam and Colombia.Twenty years ago, malaria had been eradicated from 37 countries including the former USSR, theU.S., and most of Europe and Australia. The number of cases annually had fallen as low as 90 millionafter an intensive eradication effort based largely on spraying houses with insecticide (WHO TDR20-year review 1995). Reasons for the gradual comeback of the disease in the mid 1970s are com-plex: they include the cost of eradication teams, loss of motivation in the face of a seemingly declin-ing threat, and, to a lesser extent, the development of insecticide resistance by the vectors and drugresistance by the parasites.
In the 1980s and 1990s, malaria has undoubtedly returned as a major threat to world health.The number of countries regarded as malarious by WHO increased from 90 in 1992 to 140 in 1994(WHO TDR 20-year review) [are data available to graph this curve?]. In 1987, the estimated directand indirect costs of malaria to Africa annually were estimated at $800 million; by 1995, they wereexpected to exceed $1 800 million. Drug-resistant strains of malaria parasites have become increas-ingly prevalent, particularly in South-East Asia in Cambodia and Myanmar, and in the Brazilian rain-forest where mining and changing land use is exposing nonimmune adults to areas of high risk andintense transmission. Malaria has thrived on uncoordinated and rapid economic development, rapidurbanization, mass migration and wars. In the Eastern Mediterranean region, malaria is worst incountries where wars have destabilized communities: Sudan, Somralia, Iraq, Afghanistan and Dji-bouti. A rising number of travellers from the EMEs are also being exposed to malaria.
Projections for this Report which allow weighting for changing prevalence indicate that ma-laria alone will account for a highly significant 2.6% of total lost years of life in the period 1990-2020-more than the combined total from cancers of the stomach and bowel. Taken together with theother diseases of the tropical cluster, including schistosomiasis, trypanosomiasis and the remainder,the total will be 3%/--as much as TB. In Sub-Saharan Africa, the burden is expected to be muchhigher [detailed projections to come; projections for different scenarios including the further spreadof drug-resistant strains]; in 1990 malaria alone accounted for 11 per cent of the region's disease bur-den and the tropical cluster together was the leading cause of disease burden (Global ComparativeAssessments in the Health Sector, WHO 1994).
4.2.4 Pneumococcal disease
Acute respiratory infections (ARI) are the leading cause of death among young children inthe developing world (see Chapter 2). Of more than 12 million in 1990, almost a quarter were fromARI. The biggest single cause of these ARI was the Pneumococcus bacterium, which also causesmeningitis. Pneumococcus has rarely hit the headlines, but it should have. It kills 1.9 million people ayear-compared with 2 million killed by TB. This makes it the second most important single infec-tious cause of death worldwide (B. Schwartz and S. Gove, PIDJ supplement, in press). Alarmingly,there are now increasing reports of multidrug-resistant strains of pneumococcal bacteria both in de-veloping and developed countries around the world (for example, Addressing Emerging InfectiousDisease Threats: A Prevention Strategy for the United States; CDC Atlanta, p. 2). These strains arealready complicating treatment for meningitis. [More here on projections when further data avail-able.]
77
WHO Ad Hoc Health R&D Report, Draft 2.0
4.2.5 Drug-resistant Shigella dysenteriae
An important cause of epidemics of dysentery, often with high fatality rates, S. dysenteriae,is now giving cause for concern in many low-income countries. While this organism is excludedfrom the four major threats, it merits increased attention in the immediate future. Studies in Bangla-desh between 1982 and 1990 showed that resistance to a range of antibiotics grew sharply during theperiod. In 1983 13% of isolates were resistant to ampicillin, 23.5% were resistant to trimethoprim-sulfamethoxazole (TMP-SMZ), and 0.8% to both. By 1990, 51.2% of isolates studied were resistantto ampicillin, 47.7% were resistant to TMP-SMZ, and 40.5% were resistant to both. Resistance to athird antibiotic, nalidixic acid, rose from 0.8% in 1985, when studies began, to 20.2% in 1990. TypeI strains of the bacterium developed resistance particularly rapidly, with more than two-thirds resis-tant to both ampicillin and TMP-SMZ by 1990 and 57.9% resistant to nalidixic acid. Neither drug isnow of use in treating any strains of the bacterium in Bangladesh, and nalidixic acid is no longer ofany use for Type I strains (Bennish et al., ICDDRB and others, Clinical Infectious Diseases 1992,14:1055-60). At district level in many countries where diarrhoeal diseases are a major cause of childmortality, facilities for assessing drug sensitivity do not exist.
[Figure 4.10 about here]
e4.3 Responding to emerging diseases
As the above sections have shown, there is a high price to pay for ignoring or misinterpreting eventhe early signs of epidemics of emerging or re-emerging pathogens. However, the Committee doesnot consider that it is a cost-effective use of research money for every country in the world to de-velop state-of-the-art facilities for microbiological research and surveillance. International expertiseand international communications are of sufficient quality that a rapid response should be possible byresearchers between countries and even between regions. Instead, the Committee considers it impor-tant that all countries have the capacity to respond quickly to control outbreaks, using infection con-trol methods, while regional centres should be strengthened to perform the necessary microbiologicalanalyses. Investment in research may be more profitably directed to developing new tools for tack-ling the major emerging and re-emerging threats, as later discussions in this chapter argue further.
The lesson from TB should be clear enough: in New York City in the 1990s, the cost oftreating TB was estimated at around $2000; the cost of treating multidrug-resistant TB rose as high as$250 000 (WHO Report on the Tuberculosis Epidemrnic 1995). In countries with fewer resources thanthe US, the effects of drug-resistant microbes becoming epidemic may be incalculable.
In part because of the political interest generated by emerging diseases, a number of agencieshave been asked to prepare action plans. The WHO has already identified key research priorities forthe area of emerging diseases in general (WHO BVI 1995). USAID, under the guidance of the Na-tional Science and Technology Council's CISET committee, has also recommended a range of re-sponses (Global Microbial Threats in the 1990s, USAJD 1995). Together, and with other nationalagencies, NGOs and donors, these bodies have identified key priorities for addressing emerging in-fectious diseases.
78
79Chapter 4. The continually changing threat of infectious disease
[Figure 4.10: LESLIE I have attached a fax copy of the paper for data to bemade into a possible graph, NOT next week but before Draft 2 mails if possible-PB]
WHO Ad Hoc Health R&D Report, Draft 2.0
4.4 Assessing needs for strategic research
e4.4.1 Broad priorities for strategic research
A clear requirement for the health sector as a whole in the prevention of the major emerging and re-emerging diseases is to imnprove basic public health facilities, both to ensure surveillance of new out-breaks and to encourage and regulate the appropriate use of antimicrobials. However, for health re-search, the subject of this Report, investmnent in biomedical research-and, to a lesser extent, popu-lation sciences-must now claim a high priority if the world is to acquire the necessary knowledge toenable the future development of a range of new tools and interventions and to broaden its defencesagainst these diseases. In addition, the new technologies that enable rapid communication of suchoutbreaks (such as electronic mail, the Internet, radios, etc.) should be exploited to the full. Strategicresearch needs have been assessed, as in Chapter 3, through a two-step process of (a) analyzing themagnitude of different types of need and (b) assessing the level of ongoing research in an attempt todefine the biggest gaps between need and action. Table 4.3 cites some examples of priority areasdrawn from the four diseases/disease clusters on which the chapter has focused. [Table for illustra-tion only: improvements/additions/corrections sought ASAP please.]
[Table 4.3 about here]
4.3.3 Strategic research priorities for TB, HIV and other STDs, malaria andpneumococcal disease: analyzing the magnitude of research needs
As in the previous chapter, research needs have been [or will have been by final draft] ana-lyzed for selected diseases or disease clusters with the aim of identifying where the greatest needs lie.The examnple of TB was shown in Figure 4.1.
In the case of TB, a substantial portion of the burden of disease remains unavertable with thecurrently available cost-effective technologies. Indeed, the currently averted burden is comparativelysmall. The analysis suggests that there is a clear need for biomedical research to build up knowledgethat could lead to tools to avert the currently unavertable burden. In addition, there is a need for re-search into health policies that would increase allocative efficiency, and health systems research thatwould increase the technical efficiency of current interventions. [THIS SECTION TO BE AMPLI-FIED CONSIDERABLY TO EXPAND AROUND THE RESEARCH NEEDS RELATED TOEACH COMPONENT OF THE DIAGRAM]
e
80
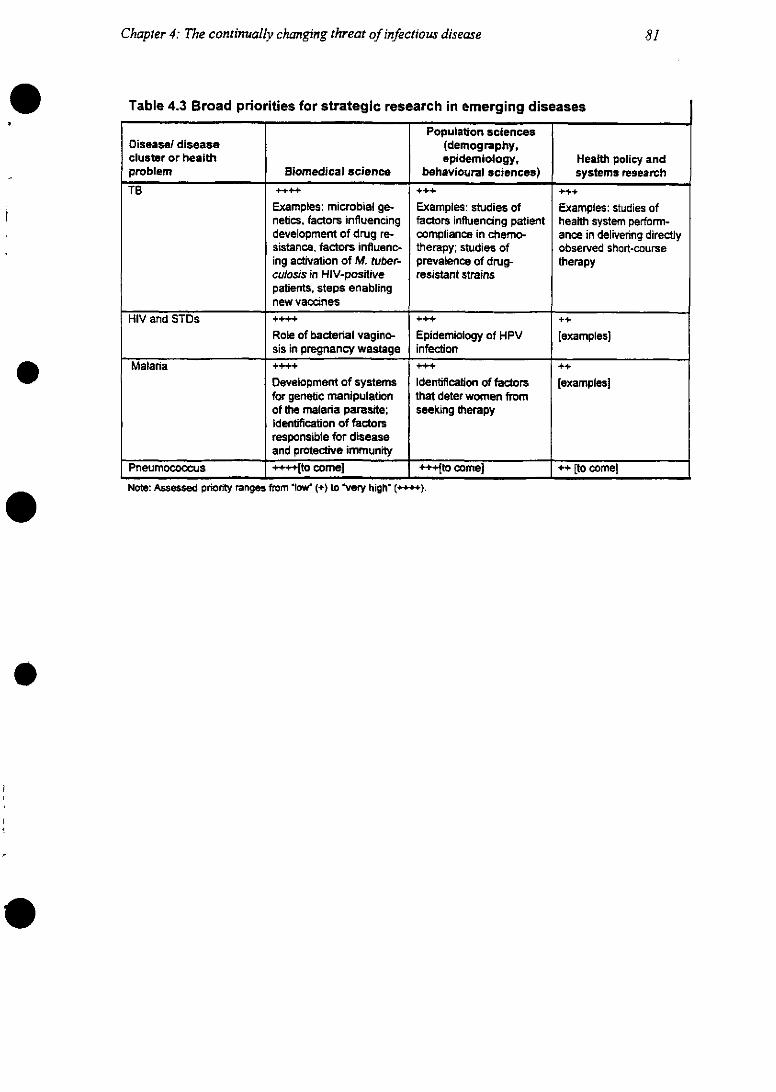
Chapter 4: The continually changing threat of infectious disease
Table 4.3 Broad priorities for strategic research in emerging diseases
Population sciencesDiseasel disease (demography,cluster or health epidemiology, Health policy andproblem Biomedical science behavioural sciences) systems research
TB . +++ ..Examples: microbial ge- Examples: studies of Examples: studies ofnetics, factors influencing factors influencing patient health system perform-development of drug re- compliance in chemo- ance in delivenring directlysistance, factors influenc- therapy; studies of observed short-courseing activation of M. tuber- prevalence of drug- therapyculosis in HIV-positive resistant strainspatients, steps enablingnew vaccines
HIV and STDs ++++. +++ ++Role of bacterial vagino- Epidemiology of HPV [examples]sis in pregnancy wastage infection
Malanria ++++ +++ ++Development of systems Identificatioban of factors [examples]for genetic manipulation that deter women fromof the malaria parasite; seeking therapyIdentification of factorsresponsible for diseaseand protective immunity
Pneumococcus ++++[to come) +++[to come) ++ [to come]
Note: Assessed priority ranges from 'low' (+) to 'very high' (++TT).
81
WHO Ad Hoc Health R&D Report, Draft 2.0
4.3.4 Assessing ongoing strategic research activity
As in the previous chapter, this Report has analyzed the level of research activity for specificemerging and re-emerging diseases. Using the sampling method of funding sources in the publishedliterature described in Chapter 2, it was found that TB receives between $19 million and $33 milliona year in total, and malaria $58 million a year. Once again, the extent of investment in these diseasesas a fraction of all health research spending is extraordinarily small in relation to the scale of theirimpact. The mismatch is particularly acute in view of the current instability in the epidemiology ofthese diseases and the degree of uncertainty about fuiture trends. HIFV has received a much greaterlevel of funding, now well in excess of $1 billion a year [exact figure still being revised], but thatinvestment is still not large.
[More information on specific spending on these diseases by different agencies to comefrom Catherine Michaud].
4.5 Opportunities for intervention development and evaluation
Having identified the areas of greatest need for strategic research and the current overall amount ofongoing effort, we turn to the development of products and interventions. Without new products-drugs, vaccines and diagnostic technologies-and other interventions, such as clinical algorithmns,successful control of these emerging and re-emerging diseases will be impossible. But, as was set outin Chapter 2, the assessment of how best to invest funds in development must be guided not only byneed, but also by specifying the nature of a new desired intervention and measuring its likely cost-effectiveness relative to existing ones. If, for example, a new intervention is likely to cost as much asan existing one, and yet offer little qualitative advantage over it, then it might be argued that the de-velopment of the intervention is not worth investing in.
4.4.1 Assessing relative cost-effectiveness: the example of malaria
In the preparation of this Report, specific analyses of the relative cost-effectiveness of differ-ent interventions for malaria were conducted. Cost-effectiveness was measured in ternms of the cost indollars for each year of healthy life gained. Analyses of this type can be helpful in giving guidanceabout the characteristics that a product must have if it is to compete with existing interventions, andthe nature of the research that needs to be undertaken to develop and evaluate that product. So far,few such analyses have been conducted because they require data on the cost-effectiveness of currentinterventions, which are rarely available. In the case of malaria, however, there are good data fromThe Gambia for at least some of the intervention types compared (see for example, Picard et al. 1993and Greenwood et al. 1988) and additional studies under way in Burkina Faso, Ghana and Egypt.
The analyses compared the cost-effectiveness, under different scenarios, of using vaccines,insecticide-impregnated bednets and drugs (chemoprophylaxis) to prevent malaria. The results areshown in Tables 4.4, 4.5, 4.6 and 4.7, both for the inherent interest of the information and to illustratethe methodology.
[Tables 4.4, 4.5, 4.6, and 4.7 about here]
e
82
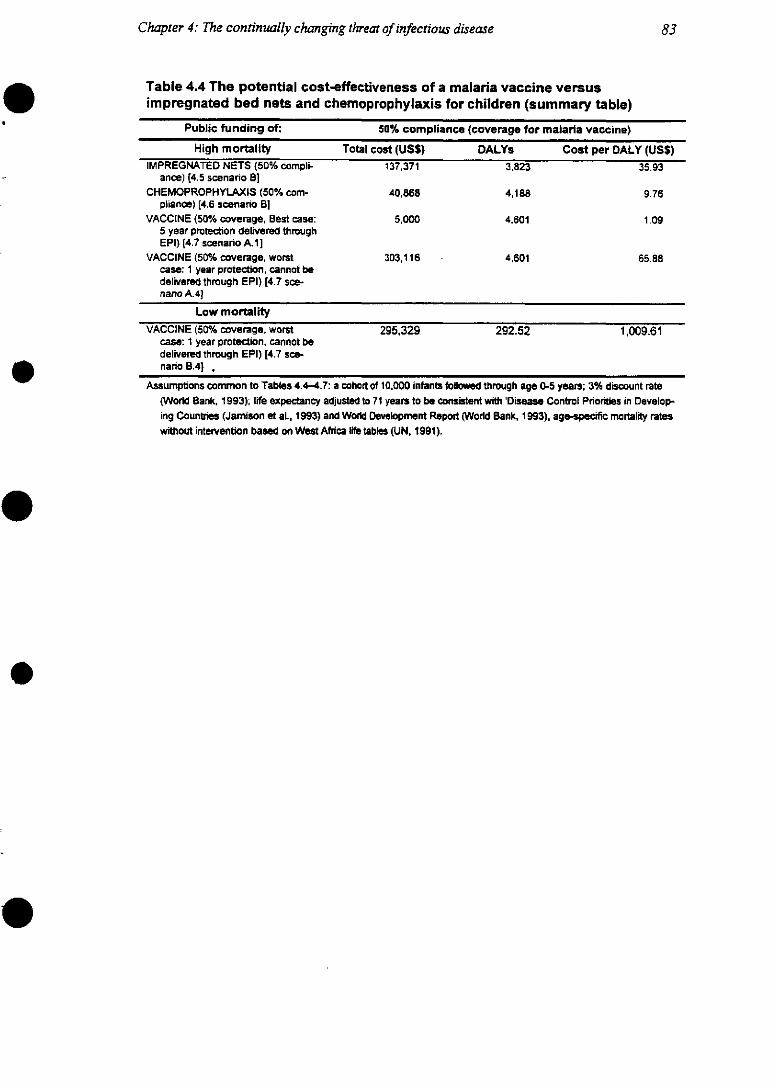
Chapter 4: The continually changing threat of infectious disease
Table 4.4 The potential cost-effectiveness of a malaria vaccine versusimpregnated bed nets and chemoprophylaxis for children (summary table)
Public funding of: 50% compliance (coverage for malaria vaccine)
High mortality Total cost (USS) DALYs Cost per OALY (USS)IMPREGNATED NETS (50% compli- 137,371 3,823 35.93
ance) [4.5 scenanrio B]CHEMOPROPHYILAXIS (50% com- 40,868 4,188 9.76
pliance) [4.6 scenanrio 1B]VACCINE (50% coverage, Best case: 5,000 4,601 1.09
5 year protection delivered throughEPI) [4.7 scenanrio A. 11
VACCINE (50% coverage, worst 303,116 4,601 65.88case: 1 year protection, cannot bedelivered through EPI) [4.7 sce-nano A.41
Low mortalityVACCINE (50% coverage, worst 295,329 292.52 1,009.61
case: 1 year protection, cannot bedelivered through EPI) [4.7 sce-nario B.4],
Assumptions common to Tables 4.4-4.7: a cohort of 10,000 infants followed through age 0-5 years; 3% discount rate(World Bank, 1993); life expectancy adjusted to 71 years to be consistent with 'Disease Control Priorities in Develop-ing Countries (Jamnison et al., 1993) and World Development Report (World Bank, 1993), agespecific mortality rateswithout intervention based on West Africa ife tables (UN, 1991).
83
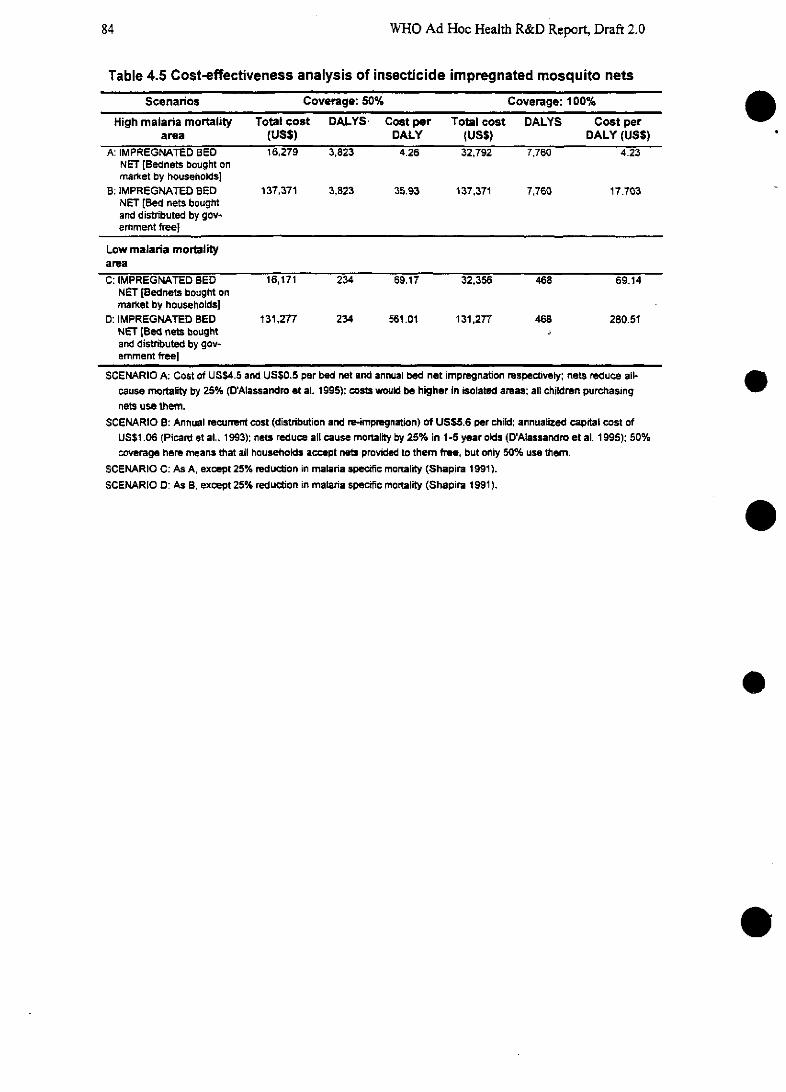
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 4.5 Cost-effectiveness analysis of insecticide impregnated mosquito nets
Scenarios Coverage: 50% Coverage: 100%
High malaria mortality Total cost DALYS Cost per Total cost DALYS Cost perarea (USS) DALY (USS) DALY (USS)
A: IMPREGNATED BED 16,279 3,823 4.26 32,792 7,760 4.23NET [Bednets bought onmarket by households]
B: IMPREGNATED BED 137,371 3,823 35.93 137,371 7,760 17.703NET [Bed nets boughtand distributed by gov-emrnment free]
Low malaria mortalityareaC: IMPREGNATED BED 16,171 234 69.17 32,356 468 69.14
NET [Bednets bought onmarket by households]
D: IMPREGNATED BED 131,277 234 561.01 131,277 468 280.51NET [Bed nets bought oand distributed by gov-emment freel
SCENARIO A: Cost of US$4.5 and US$0.5 per bed net and annual bed net impregnation respectiveiy; nets reduce ail-cause mortaity by 25% (D'Alassandro et al. 1995); costs would be higher in isolated amreas; all children purchasingnets use them.
SCENARIO B: Annual recurrent cost (distribution and re-impregnation) of USS5.6 per child: annualized capital cost ofUS$1.06 (Picard et al., 1993); nets reduce all cause mortality by 25% in 1-5 year olds (D'Alassandro et al. 1995); 50%coverage here means that all households accept nets provided to them free, but only 50% use them.
SCENARIO C: As A, except 25% reduction in malaria specific mortality (Shapira 1991).SCENARIO D: As B, except 25% reduction in malaria specific mortality (Shapira 1991).
e
e
e
elo
84
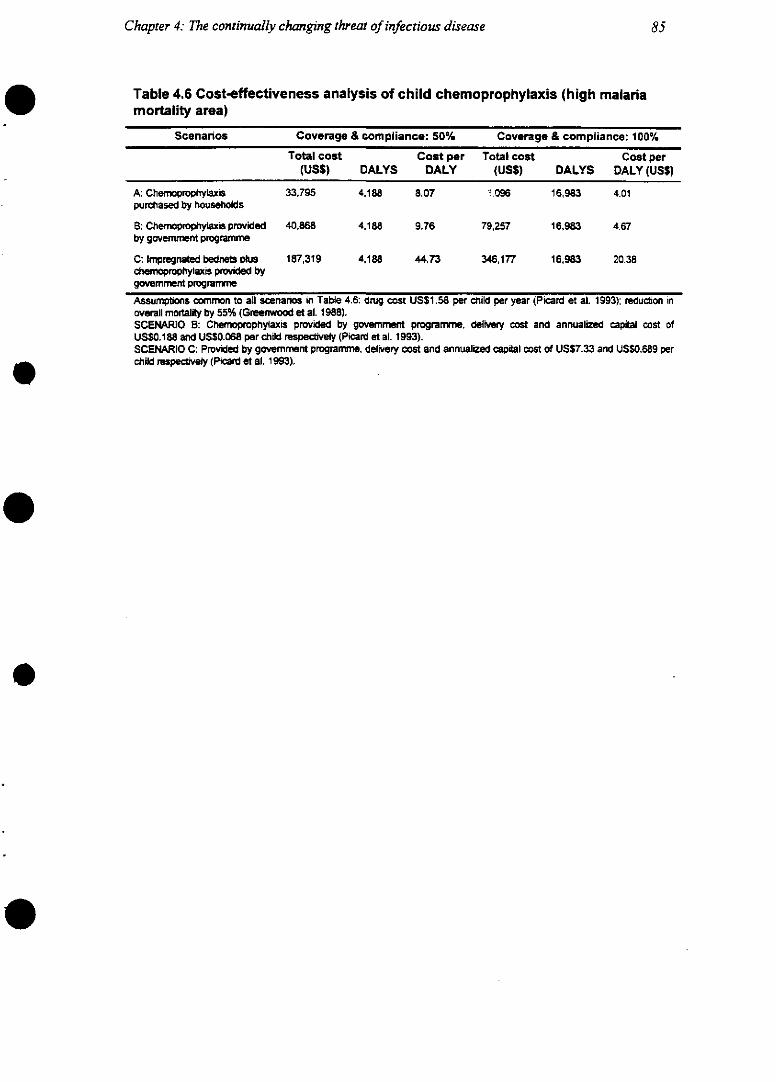
Chapter 4: The continually changing threat of infectious disease
Table 4.6 Cost-effectiveness analysis of child chemoprophylaxis (high malariamortality area)
Scenarios Coverage & compliance: 50% Coverage & compliance: 100%
Total cost Cost per Total cost Cost per(USS) DALYS DALY (USS) DALYS DALY (USS)
A: Chemoprophylaxis 33.795 4.188 8.07 096 16,983 4.01purchased by households
B: Chemrnoprophylaxis provided 40,868 4.188 9.76 79,257 16,983 4.67by government programme
C: Impregnated bednets plus 187,319 4,188 44.73 346,177 16,983 20.38chem~oprophylaxis provided bygovemment programme
Assumptions common to all scenarnos in Table 4.6: drug cost US$1.58 per chiild per year (Picard et al. 1993); reducton inoverall mortality by 55% (Greenwood et al. 1988).SCENARIO B: Chemoprophylaxis provided by government programmne, delivery cost and annualized capital cost ofUS$0.188 and US$0.068 per child mspecively (Picard et al. 1993).SCENARIO C: Provided by govemrnment programme, delivery cost and annualized capital cost of USS7.33 and US$0.689 perchild rspe~ vely (Picard et al. 1993).
85

WHO Ad Hoc Health R&D Report Draft 2.0
Table 4.7 Cost-effectiveness analysis of malaria vaccine
Malaria control options Coverage: 50% Coverage: 100%
Cost per Cost perTotal cost DALY Total cost DALY
(USS) DALYS (USS) (USS) DALYS (USS)A: HIGH MORTAL- 1. Best 5,000 4,601 1.09 10,000 9,367 1.07
ITY AREA (30%reduction in allcause mortality)
2. Most 43,019 4,601 9.35 88,867 9,367 9.49likely
3. Poor 119,058 4,601 25.88 246,600 9,367 26.334. Worst 303,116 4,601 65.88 623,201 9,367 66.53
B: LOW MORTAL- 1. Best 5,000 292.52 17.09 10,000 585.74 17.07rrY AREA (30%redudction in ma-lanria specificmortality of62/1000 deathsin 1-5 year olds(Shapira 1991)
2. Most 41,722 292.52 142.63 83,613 585.74 142.75likely
3. Poor 115,165 292.52 393.70 230,839 585.74 394.10
4. Worst 295,329 292.52 1,009.61 591,678 585.74 1,010.14
SCENARIO A. 1: Vaccine delivered through EPI; marginal cost of US$1 per child; 5 year duration of protection.
SCENARIO A.2: First dose delivered through EPI; marginal cost of US$1 per child; annual cost per child of USS2.50, 1 yearduration of protection; subsequent 3 doses to age 5.
SCENARIO A.3: First dose delivered through EPI; marginal cost of US$1 per child; annual cost per child of USS7.50, 1 yearduration of protedction; subsequent 3 doses to age 5.
SCENARIO A.4: Cannot be delivered through EPI; 1 year duration of protection; annual doses costing US$15 per immunized
child.
SCENARIO B.1: As A.1, except 30% reduction in malaria specific mortality.
SCENARIO B.2: As A.2, except 30% reduction in malanria specific mortality.
SCENARIO B.3: As A.3, except 30% reduction in malana specfic mortality.
SCENARIO B.4: As A.4, except 30% reduction in malanria specfic mortality.
o
e
o
e
e
86
Chapter 4: The continually changing threat of infectious disease
The calculations show, perhaps surprisingly, that a vaccine could be a highly cost-effectiveintervention relative to others, at a cost of about $1 for each year of healthy life gained. This wouldrepresent an extremely high payoff from research. The finding holds even where only modest protec-tion is induced. This is particularly interesting in light of the results of a recent trial of Spf66, a syn-thetic peptide vaccine developed in Colombia that was shown to cut clinical cases of the disease inrural Tanzania by up to one-third (The Lancet, xx Dec. 1994). The critical determinants of cost-effectiveness are the duration of protection provided by the vaccine, and whether or not its deliverycan be designed to take full advantage of the existing mechanisms of the Extended Programme onImmunization. As the tables show, a vaccine whose protection lasts only for a short period and whichrequires special delivery mechanisms would not be worth developing. This type of analysis givesparticularly useful guidance about the kind of questions vaccine developers need to be asking: forexample, the vaccine's effectiveness should be determined in children of the samne age as the childrento whom the EPI system delivers vaccines rather than in children of a theoretically "optimal" age.
[Similar analyses are being developed for HIV vaginal microbicides/vaccines and pneumo-coccus vaccines; these will show the estimated marginal cost effectiveness of the desired interven-tions i.e., taking into consideration the effectiveness of the existing tools.]
4. 4.2 Broad priorities for intervention development
The magnitude of the threats from the four diseases discussed above--to high-income coun-tries as well as developing countries--should not be underestimated. Currently, research investmentis wholly inadequate to the tasks of preventing and containing those threats. However, there are ma-jor opportunities for investors in research to make a difference, by supporting the timely developmentof products and other interventions that could rein in, or even overcome, these diseases. Table 4.8provides some illustrative examples.
[Table 4.8 about here]
87
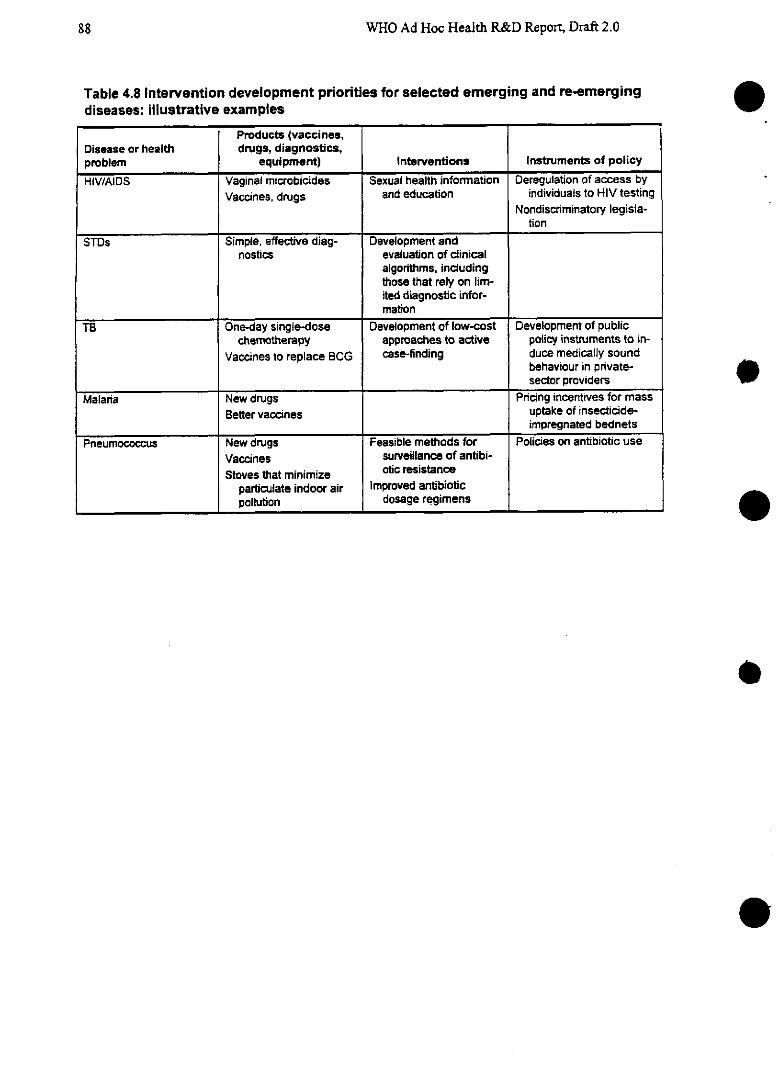
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 4.8 Intervention development priorities for selected emerging and re-emergingdiseases: illustrative examples
Products (vaccines,Disease or health drugs, diagnostica,problem equipment) Interventions Instruments of policy
HIV/AIDS Vaginal microbicides Sexual health information Deregulation of access byVaccines, drugs and education individuals to HIV testing
Nondiscriminatory legisla-tion
STDs Simple, effective diag- Development andnostics evaluation of clinical
algorithms, includingthose that rely on lim-ited diagnostic infor-mation
TB One-day single-dose Development of low-cost Development of publicchemotherapy approaches to active policy instruments to in-
Vaccines to replace BCG case-finding duce medicaly soundbehaviour in private-sector providers
Malaria New drugs Pricing incentives for massBetter vaccnes .uptake of insecticide-
impregnated bednets
Pneumococcus New drugs Feasible methods for Policies on antibiotic useVaccines surveillance of antibi-
Stoves that minimize otic resistancepartculate indoor air Improved antibiobcpollution dosage regimens
e
o
e
e
88
Chapter 4: The continually changing threat of infectious disease
4.6 Chapter summary and recommendations
Economic, behavioural and environmental changes have created the conditions in which emergingand re-emerging microbes can spread rapidly with potentially disastrous impact on human health.Greater use-and frequently inappropriate use-of antimicrobials is fostering the emergence of drug-resistant strains of lethal microorganisms that were thought to have been conquered. Four emergingand re-emerging diseases or disease clusters together account for around one-sixth of the total pro-jected lost years of life between 1990 and 2020: they are, TB, HIV and other STDs, malaria andpneumoccocal infections. The future course of these four is uncertain and requires considerable newinvestment in biomedical R&D.
1. Economic, social and environmental changes have created the conditions in which emerging andre-emerging microbes can spread rapidly, with potentially disastrous impact on human health.Greater use (and frequent misuse) of antimicrobials and other control measures has encouragedthe emergence of drug-resistant strains of lethal microorganisms in regions where they werepreviously controlled. Although the developing regions are bearing the brunt of these problems,countries at all income levels are at risk. Two lines of strategic research should be implementedand financially supported: (a) study of the relation between the emergence of resistant strainsand patterns of use (and misuse) of existing antimicrobials; and (b) the evaluation and enhance-ment of international capacity to detect and monitor emerging or drug-resistant pathogens in anyregion.
2. Malaria, HIV, TB and pneumnococcal infections are four emerging or re-emerging diseases thatsignificantly affect global health status now and are likely to cause further widespread and costlydamage if current trends continue. The obvious shortage of existing tools to deal with thesethreats calls for investment in biomedical R&D at levels appropriate to the scale of the threats.The potential payoffs from vaccines against pneumococcal infections and malaria, from female-controlled methods of preventing HIV infection, and from simplified algorithms for control ofTB are particularly high.
89
Chapter 5: Preparing for the coming epidemic ofnoncommunicable diseases and injuries
The world's population is aging. While the global population is growing at 1.7% per year, the shareof that population aged over 65 is growing faster, at 2.5% per year. In many countries, the "oldestold"-those aged 80 years or more, who are most likely to need support-are the fastest-growinggroup, already constituting 16% of the world's total elderly population in 1992. In the United States,for example, the absolute number of over-80s is expected to more than double from its 1990 level of7 million by 2030 (An Aging World II, International Population Reports P95/92-3, U.S. Bureau of theCensus, 1992).
But it is the middle-income and low-income countries that are aging most rapidly, as the re-sult of steep declines in fertility, a fall in infant mortality and improvements in life expectancy overthe past four decades. These countries are experiencing the demographic transition within much morecompressed time frames than the EMEs. In many middle-income countries and some low-incomecountries, the proportion of the population aged over 65 is expected to increase by between 200% and400% between 1990 and 2030 (Figure 5.1). Thus the growth in this age group will be much greaterthan for the rest of the population. In most European countries, the transition took between two andthree times as long. In absolute numbers, the developing countries are already home to most of theworld's elderly: more than 200 million of the 356 million people over the age of 65 live in develop-ing regions (Epidemiology and OldAge, Ebrahim and Kalache, eds., BMJ Publishing Group, forth-coming). These changes will impose new and profound demands on countries' health systems if theyare to find affordable and equitable ways of meeting the competing needs of all age groups. So far,however, health research has devoted relatively little attention to these problems.
It is important to make explicit that the aging of populations results not only in an increasedrelative proportion of elderly in the population, but, earlier, in an increased proportion of adults rela-tive to children. This changed proportion also carries epidemiological implications: Injury and psy-chiatric disease, to take two examples, fall heavily on this age group.
[Figure 5.1 about here]
Two separate processes are driving the rapid changes in health needs that the world's popu-lation now faces. The first is a demographic shift towards older populations, which will bring with ita massive rise in the number of cases of many noncommunicable diseases -such as ischaemic heartdisease, cerebrovascular disease, diabetes, neurological and psychiatric diseases and cancers-thatare associated with older age groups. This will result in a much heavier relative burden of NCDs inevery population. The numbers of people with disabilities and impairments associated with age, in-cluding visual and hearing impairmnents, will also increase.
90
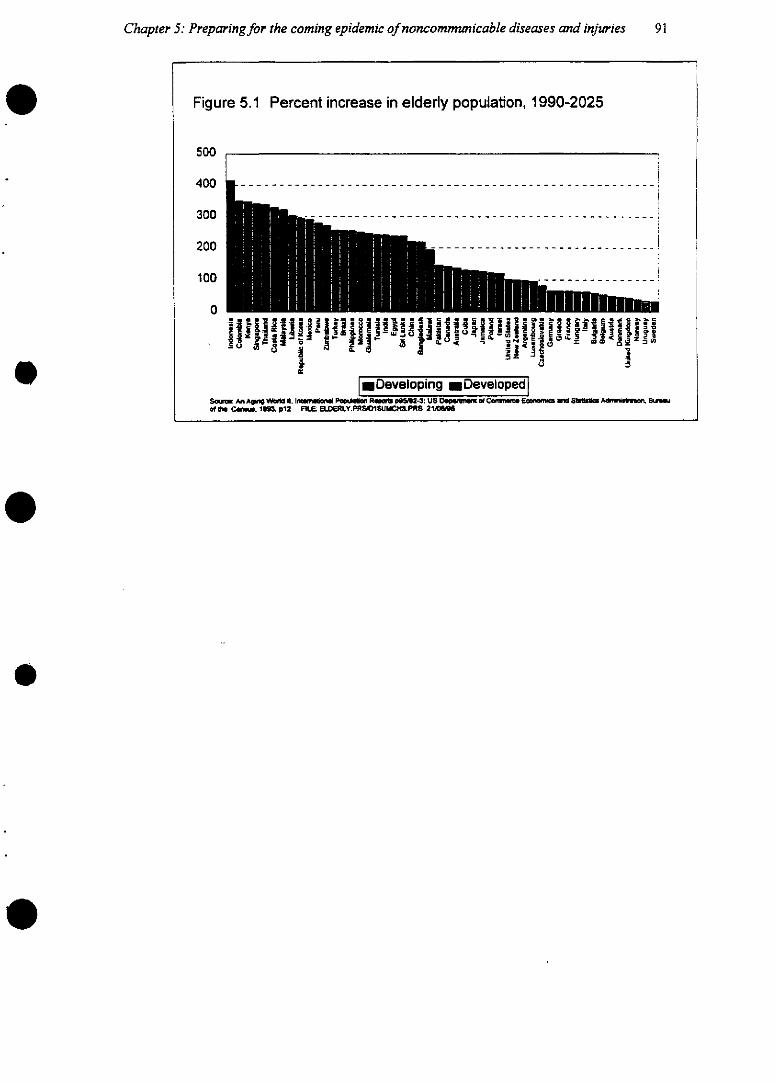
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries
Figure 5.1 Percent increase in elderly population, 1990-2025
500 r
200
10
&~ ~ L-- 1 <30, -1 z ? 1
*lDeveloping UDevelopediSae,~:m AgnWl Al Intoureai PCJlaim Aw~%g P~152.3: US Dl~pmiu WCw cm~ ¢ Adwmus llof @i Caiguá. 1U. p12 FRLE. ELDERLY.PRS.VISUMCH~ PRS 2116/9
91
-- - - - - - -1i
-- - - - - - !i
ii
1
i-- - - - - - -
WHO Ad Hoc Health R&D Report, Draft 2.0
The second process-which is inherently more complex-is that patterns of exposure tocertain risks associated with ill health are altering in all populations. For example, the number ofDALYs lost through tobacco use-by far the single greatest risk factor associated with lung cancer,acute myocardial infarction and strokc -is expected to double or even treble by 2020 to at least 8%of all lost DALYs. Diets are also changing, with widespread increases in the amounts of saturated fatand salt consumed by populations whose intake was traditionally lower. Patterns of physical activityalso change with increased urbanization; infections with certain viruses, such as hepatitis B and hu-man papilloma viruses, are now known to be linked with particular cancers and some bacterial infec-tions play a role in heart disease. The relationships between these risk factors and disease is only par-tially understood. Equally important, it is likely that further risk factors exist that are as yet unknown.Much of the variation in current patterns of noncommunicable diseases cannot be explained byknown risk factors.
While the demographic shift may have a relatively simple effect in increasing the number ofcases of age-related diseases, the changes in patterns of exposure to risk are much more complex andtheir effects more difficult to interpret. The prevalence of risky behaviours linked with several non-communicable diseases, and with some injuries, is rising-as, for example, in increased use of motorvehicles worldwide-but there is little reliable evidence that age-specific rates of particular non-communicable diseases are increasing anywhere. Indeed, in the rich countries, the rates of sornmeNCDs appear to have been falling for decades. Data from the middle-income and low-income coun-tries are much scarcer. In the relatively short term of the projections made for this Report, however,there is no question that the absolute numbers of cases of NCDs will rise sharply as a direct result ofaging.
A complex crisis
The challenges posed by population aging are acute. The aging of the world has been de-scribed as a triumph of social development and public health (Aging and Health, WHO BackgroundReport 1995). Healthy, active and independent old age is a goal increasingly attained by people in theEMEs; elders contribute much to society, and forward-thinking businesses are increasingly realizingthe value of employing older people in flexible working pattemrns. However, the world's "older"countries-Europe, Scandinavia, North America and Japan-are already deeply troubled by the costsof providing health care for the increasingly frail "older old", the costs of providing for a growingelderly population in economies whose active workforces are shrinking, and other questions of inter-generational equity. How much more acute, then, will these problems be for countries experiencingthe transition in the space of barely two generations, and without the full range of resources that theEMEs have evolved? The widening gaps in GDP per capita between the richest and poorest regionswill only intensifythe problems (see Figure 4.10).
This problem is clearly illustrated by the case of Brazil. The country has experienced rapiddemographic transition-with fertility declining by about two-thirds in just 15 years. A report for theWorld Bank in the late 1980s concluded that by the middle of that decade, the 9% of the Brazilianpopulation aged 55 and over was absorbing 44% of the social benefits provided by the governent,mostly in the form of pensions and health care. By contrast, the 36% of the population aged 15 andunder received only 28% of social benefits. Not surprisingly, the distribution of benefits was alsoskewed towards the richest in the population, with only one-fifth of the benefits reaching the 41% ofhouseholds whose income was below half the level of the minimum wage (World Bank 1989). With
92
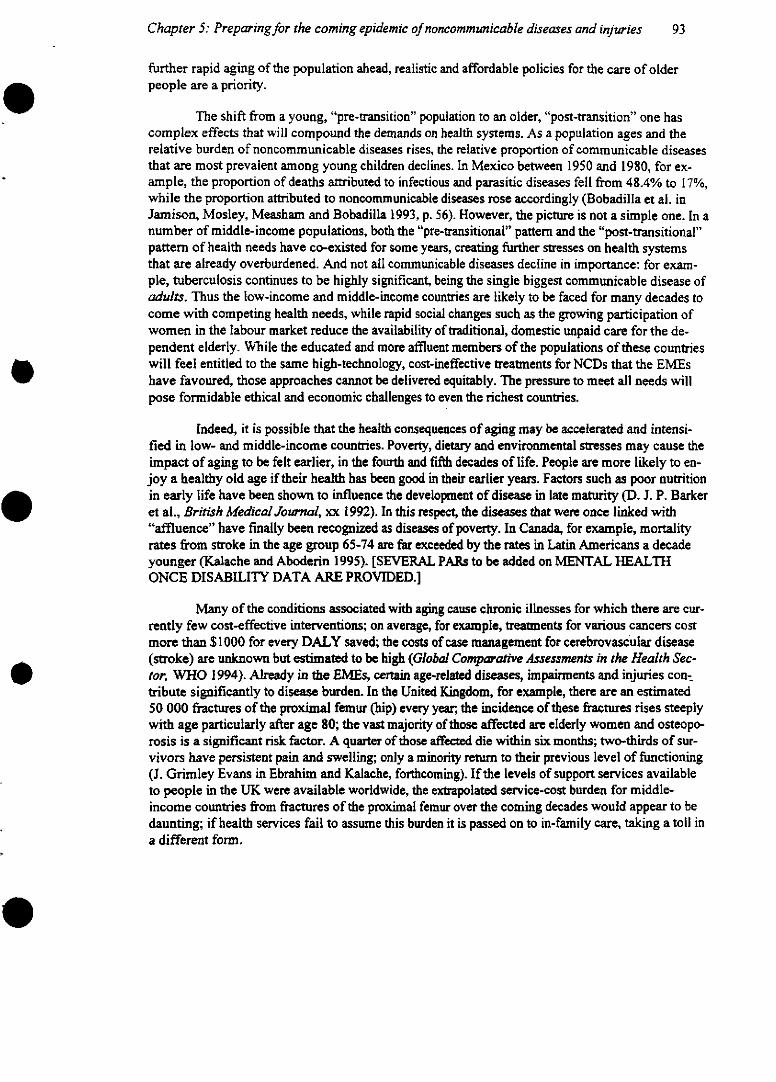
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries
further rapid aging of the population ahead, realistic and affordable policies for the care of olderpeople are a priority.
The shift from a young, "pre-transition" population to an older, "post-transition" one hascomplex effects that will compound the demands on health systems. As a population ages and therelative burden of noncommunicable diseases rises, the relative proportion of communicable diseasesthat are most prevalent among young children declines. In Mexico between 1950 and 1980, for ex-ample, the proportion of deaths attributed to infectious and parasitic diseases fell from 48.4% to 17%,while the proportion attributed to noncommunicable diseases rose accordingly (Bobadilla et al. inJamison, Mosley, Measham and Bobadilla 1993, p. 56). However, the picture is not a simple one. In anumber of middle-income populations, both the "pre-transitional" pattern and the "post-transitional"pattern of health needs have co-existed for some years, creating further stresses on health systemsthat are already overburdened. And not all communicable diseases decline in importance: for exam-ple, tuberculosis continues to be highly significant, being the single biggest communicable disease ofadults. Thus the low-income and middle-income countries are likely to be faced for many decades tocome with competing health needs, while rapid social changes such as the growing participation ofwomen in the labour market reduce the availability of traditional, domestic unpaid care for the de-pendent elderly. While the educated and more affluent members of the populations of these countrieswill feel entitled to the same high-technology, cost-ineffective treatments for NCDs that the EMEshave favoured, those approaches cannot be delivered equitably. The pressure to meet all needs willpose formidable ethical and economic challenges to even the richest countries.
Indeed, it is possible that the health consequences of aging may be accelerated and intensi-fied in low- and middle-income countries. Poverty, dietary and environmental stresses may cause theimpact of aging to be felt earlier, in the fourth and fifth decades of life. People are more likely to en-joy a healthy old age if their health has been good in their earlier years. Factors such as poor nutritionin early life have been shown to influence the development of disease in late maturity (D. J. P. Barkeret al., British Medical Journal, xx 1992). In this respect, the diseases that were once linked with"affluence" have finally been recognized as diseases of poverty. In Canada, for example, mortalityrates from stroke in the age group 65-74 are far exceeded by the rates in Latin Americans a decadeyounger (Kalache and Aboderin 1995). [SEVERAL PARs to be added on MENTAL HEALTHONCE DISABILITY DATA ARE PROVIDED.]
Many of the conditions associated with aging cause chronic illnesses for which there are cur-rently few cost-effective interventions; on average, for example, treatments for various cancers costmore than $1000 for every DALY saved; the costs of case management for cerebrovascular disease(stroke) are unknown but estimated to be high (Global Comparative Assessments in the Health Sec-tor. WHO 1994). Already in the EMEs, certain age-related diseases, impairnents and injuries con-tribute significantly to disease burden. In the United Kingdom, for example, there are an estimated50 000 fractures of the proximal femur (hip) every year, the incidence of these fractures rises steeplywith age particularly after age 80; the vast majority of those affected are elderly women and osteopo-rosis is a significant risk factor. A quarter of those affected die within six months; two-thirds of sur-vivors have persistent pain and swelling; only a minority return to their previous level of functioning(J. Grimley Evans in Ebrahim and Kalache, forthcoming). If the levels of support services availableto people in the UK were available worldwide, the extrapolated service-cost burden for middle-income countries from fractures of the proximal femur over the coming decades would appear to bedaunting; if health services fail to assume this burden it is passed on to in-family care, taking a toll ina different form.
93
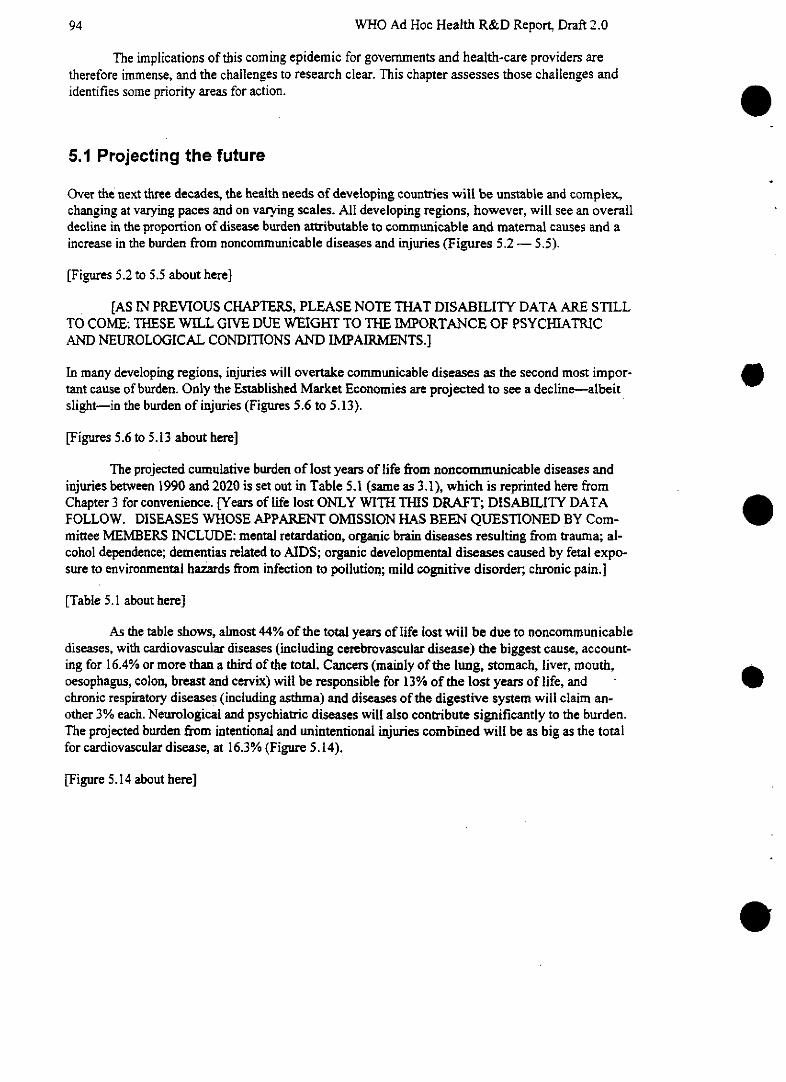
WHO Ad Hoc Health R&D Report, Draft 2.0
The implications of this coming epidemic for governments and health-care providers aretherefore immense, and the challenges to research clear. This chapter assesses those challenges andidentifies some priority areas for action.
5.1 Projecting the future
Over the next three decades, the health needs of developing countries will be unstable and complex,changing at varying paces and on varying scales. All developing regions, however, will see an overalldecline in the proportion of disease burden attributable to communicable and maternal causes and aincrease in the burden from noncommunicable diseases and injuries (Figures 5.2 - 5.5).
[Figures 5.2 to 5.5 about here]
[AS IN PREVIOUS CHAPTERS, PLEASE NOTE THAT DISABILITY DATA ARE STILLTO COME: THESE WILL GIVE DUE WEIGHT TO THE IMPORTANCE OF PSYCHIATRICAND NEUROLOGICAL CONDITIONS AND IMPAIRMENTS.]
In many developing regions, injuries will overtake communicable diseases as the second most impor-tant cause of burden. Only the Established Market Economies are projected to see a decline-albeitslight-in the burden of injuries (Figures 5.6 to 5.13).
[Figures 5.6 to 5.13 about here]
The projected cumulative burden of lost years of life from noncommnunicable diseases andinjuries between 1990 and 2020 is set out in Table 5.1 (samne as 3.1), which is reprinted here fromChapter 3 for convenience. [Years of life lost ONLY WITH THIS DRAFT; DISABILITY DATAFOLLOW. DISEASES WHOSE APPARENT OMISSION HAS BEEN QUESTIONED BY Com-mittee MEMBERS INCLUDE: mental retardation, organic brain diseases resulting from trauma; al-cohol dependence; dementias related to AIDS; organic developmental diseases caused by fetal expo-sure to environmental hazards from infection to pollution; mild cognitive disorder;, chronic pain.]
[Table 5.1 about here]
As the table shows, almost 44% of the total years of ¡¡life lost will be due to noncommunicablediseases, with cardiovascular diseases (including cerebrovascular disease) the biggest cause, account-ing for 16.4% or more than a third of the total. Cancers (mainly of the lung, stomach, liver, mouth,oesophagus, colon, breast and cervix) will be responsible for 13% of the lost years of life, and -
chronic respiratory diseases (including asthma) and diseases of the digestive system will claim an-other 3% each. Neurological and psychiatric diseases will also contribute significantly to the burden.The projected burden from intentional and unintentional injuries combined will be as big as the totalfor cardiovascular disease, at 16.3% (Figure 5.14).
[Figure 5.14 about here]
94
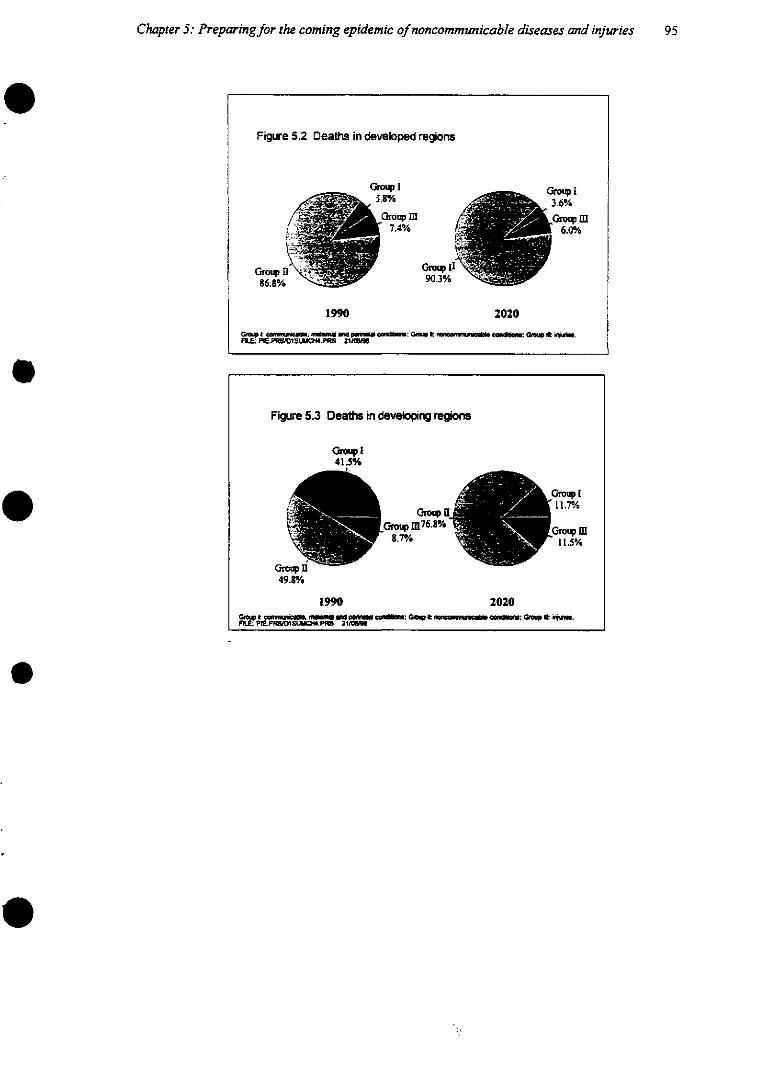
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries
Figure 5.2 Deaths in developed regions
G°.oup 1
. r 5.83% 3.6%6.0%
~lil
1990 2020
Gst t. campe. no urd _w t : Ge t oc cu o~u, an au_.FU.!. PW.PRWOS~IQ# .PRS 211W
Fígure 5.3 Deaths in developing regions
41_~%41.5%
a.tupn~~~~~~~~~~~~~~Gru8.7%/ 15
49.8%
1990 2020GF mt ca s nmw aM 0UU _ ~e m: G, t e _mun~a _~: C~ t 'u.FlLU: PI!E.PRS/tSO4.P1W 2116lW
95
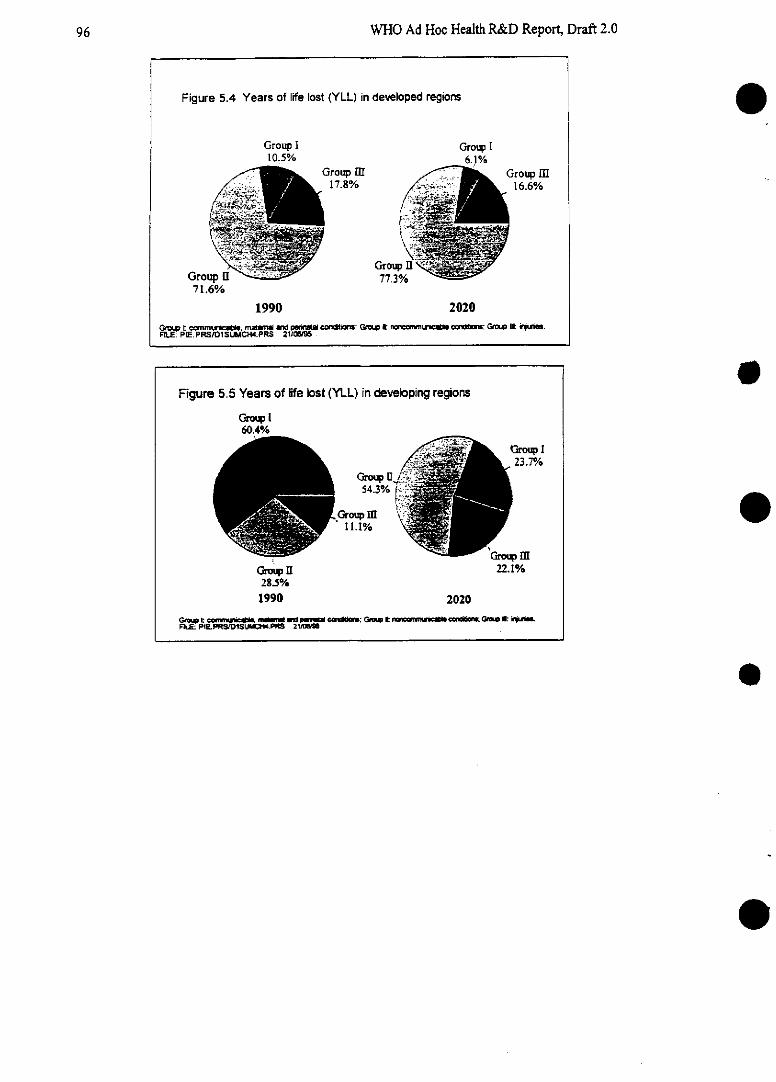
WHO Ad Hoc Health R&D Report, Draft 2.0
e
e
e
e
e
Figure 5.4 Years of life lost (YLL) in developed regions
Group I Group I10.5% 6.1%
/ _ ~~Group M Group I17.8% 16.6%
Grouhpou m G77pII
71.6%
1990 2020
Gnaimwmuae muU ad pe cz~: GsI t nw~u~ o~: GQw Ukt qi.FiE. P'E PRS/D1SU"IOCH4.PRS 21¡ai96
Figure 5.5 Years of ¡ife lost (YLL) in developing regions
Grop I60.4%/o
3roup I23.7%/
54.3% 0/ ''/ i i
G_,roup M11.1% ~ ~ ~ ~ 2.1
Gro~ II 22.1%28.5%
1990 2020
GaMe21: a m 1 _ _: Gnem t I __ro: Gie e qjv_FulE PlEpRSfD15UMI pR5 21i~I
96
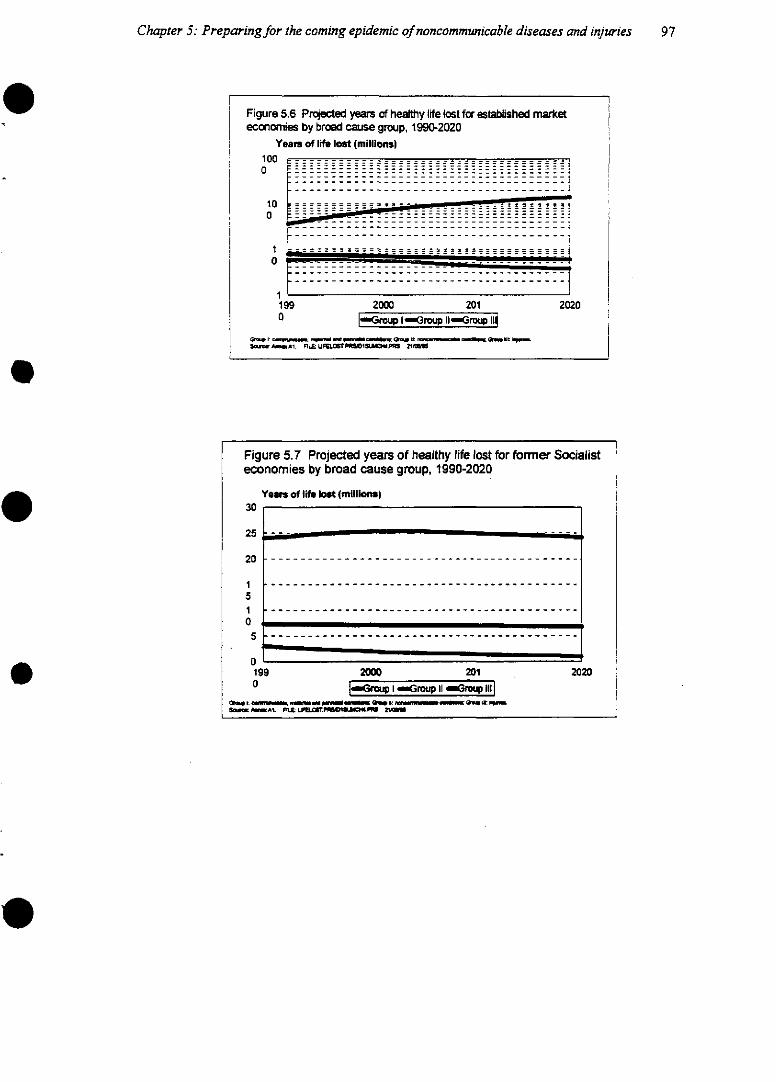
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries
Figure 5.6 Projected years of healthy iife lost for estabilished marketeconomies by broad cause group, 1990-2020
Yearn of Ife Iost (millions)lo O .- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -o0
10o
10
1;199 2000 201 20:O -, roup 1-Grou Irou l
G~1 : ce ,e. e l li l t ~-Ñ _^1. F;UL UFqLT.I1#I.PRF; 21r;;
20
Figure 5.7 Projected years of healthy life lost for former Socialisteconomies by broad cause group, 1990-2020
Yeas of lif bst (millionm)30
25 ---
20 ....................
1 ------------------------------------------
510
0199 2000 201 . 202° 1 I roup 11 dreq 11l3
geja e~t .g m - Qe, o,.:__qeu .Sel 1. kq P.IL .LmmtPCI&Ll_ 2l
- - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - ---
- - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
97
20
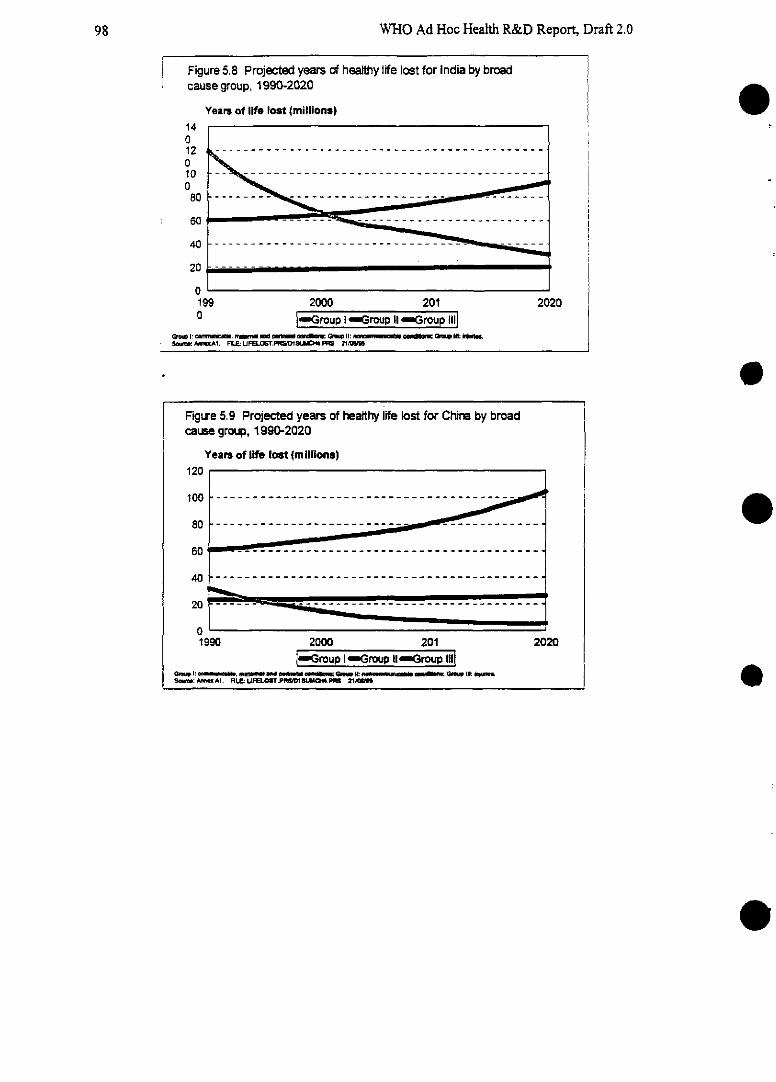
WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 5.8 Projected years of healthy life lost for India by broadcause group, 1990-2020
Years of life lost (milliona)14o12o10o
80
60
40
20
o19'o
2000 201[Group ¡ Group II Grou II
~'1 m~VI* ~f. -M.4~miW - ~ ~ll Q ~ mImll.t- Gm IIU tr.oa 1 n L: R . ~ U 1S , e~ _ : .0 ~ les:5UEC:MW~. .M 21.
2020
e
e
e
e
Figure 5.9 Projected years of healthy life lost for China by broadcause group, 1990-2020
Years of life lost (m llions)120
100 --- - ----------- --- -- ------ ~~
60 -- - - - - - - - - - - - - - -
40 - - - - - - - - - - - - - - - - - - - - - - - - -
20
01990 2000 201 2020
-Group -. Group I--roup ¡ilGc l: MW. MU UIF MLM lS ... I(M W M : al W I1S: i1.So:~ bAI RI.E:UFELO'TPN.PR1DlMIII4.1N 21M Z
------------
98
r
9
--- _~ --------------------------------------
---------------------------------------
- - - - - - - - - - - - - - - - - - -
----------------------
----------------- --
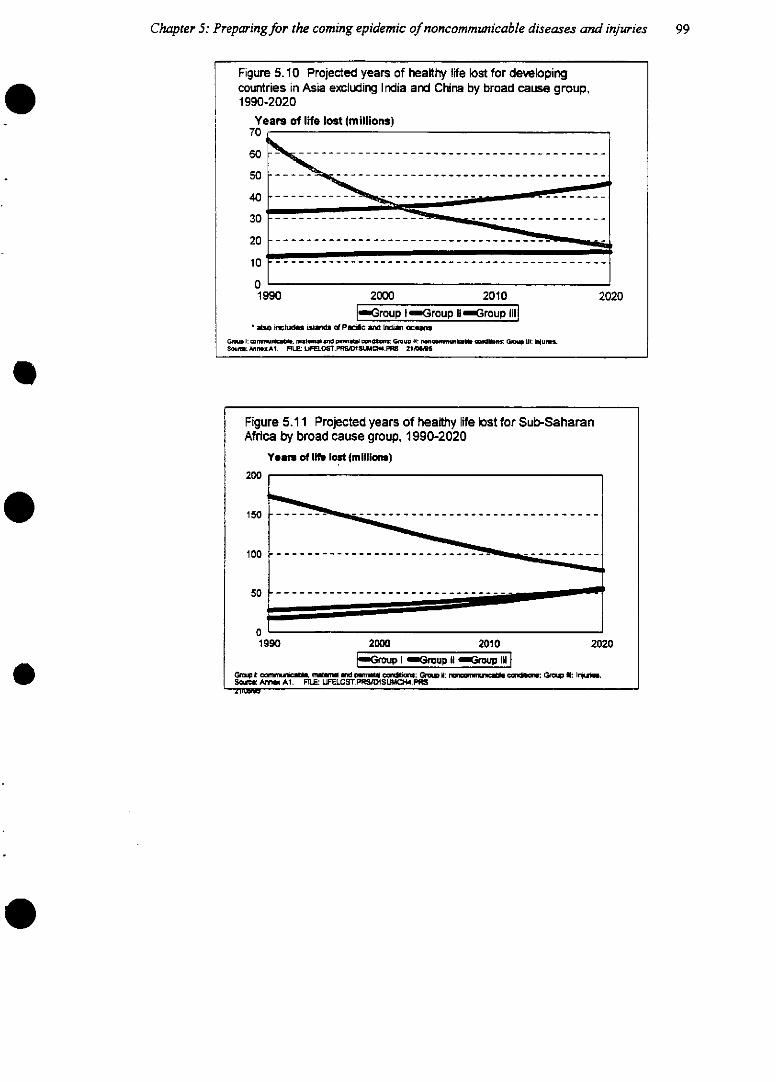
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries 99
Figure 5.10 Projected years of healthy life lost for developingcountries in Asia excluding India and China by broad cause group,1990-2020
Yearn of ife lost (millions)70 j
60 - - - - - - - - - - - - - - - - - - - -
50 _- - - - - -
40 --
20 _-----------------------
10 ............................................--
01990 2000 2010 2020
|Group 1 Group II Group IIIal* ao cud í si~lid PueH Tnd Inbm~ oceum
~ID í: amnAlll. mirotml aTd Cn wiUlNPS GnMupj I1: fiQloP.ne, undcS2 ¡I: C l UwlS.ShOa:. MnlxA1. FlíE: LIFE.OSTPRSD1SUIC4.PIIS 211ID$S
Figure 5.11 Projected years of healthy life blost for Sub-SaharanAfrica by broad cause group, 1990-2020
Year of lif lost (milliona)s
200
150 - - - - - - - - - - - - - - - - - - - - - -
100 - - ----- - - - - - - -
5o01990 2000 2010 2020
,roup -Group il Group lilG:t cnv, mn Ud p,, C~.mia,: Grp #: :,, Gm.. tx ieru~.
SoUa mAl X £ A1 U. UFELOST.P~ S~DL .PFRSnr1
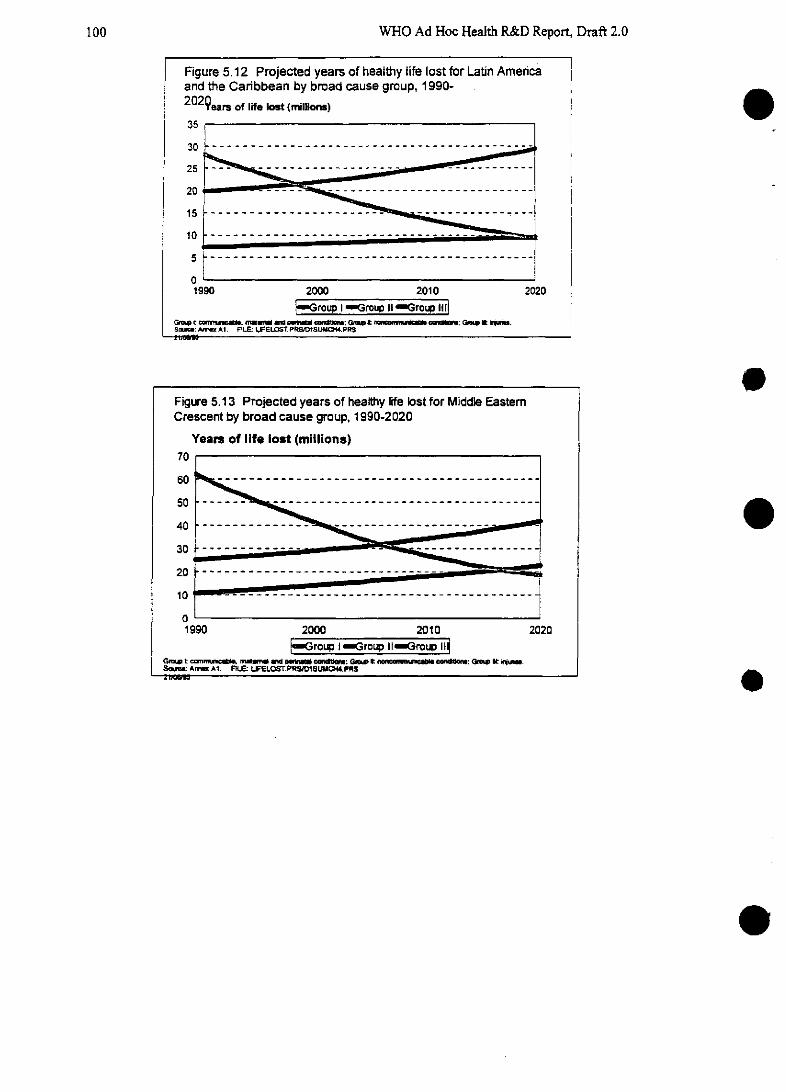
100 WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 5.12 Projected years of healthy life lost for Latin Americaand the Caribbean by broad cause group, 1990-2 02 9 ears of life ost (miions)
35
30 _ ---------------- ~~~~~ ;á,25 .-
20 . . - - -
1510 __ - __-- ___-- __ __ -- - - -- - - _ -j
10 ------------------------ _-I
01990 2000 2010 2020
mGroup 1 Group II Group IIIG~. c m m~ el . omlga* ctn~: G. e r nwmmm~ic.lg G lt G aS~ A. A1. FILE: LIFELOST.PRS/DISUMO. PRS
oFigure 5.13 Projected years of healthy life lost for Middle EasternCrescent by broad cause group, 1990-2020
Years of life lost (millions)70
60 - -- - - - - - --- ---- - ------- ____ ----- ---- ----
40 _ _ _ _______ _ -
30 ---------------
20
1990 2000 2010 2020"Group I-roup IGroup 1i
Glou cemm~r m~ aed w d --- : Gm' t _=auuI edm: Gp e i.SmWM A AI. L WELOS'. PRSOlSUMC 4.PR$
e
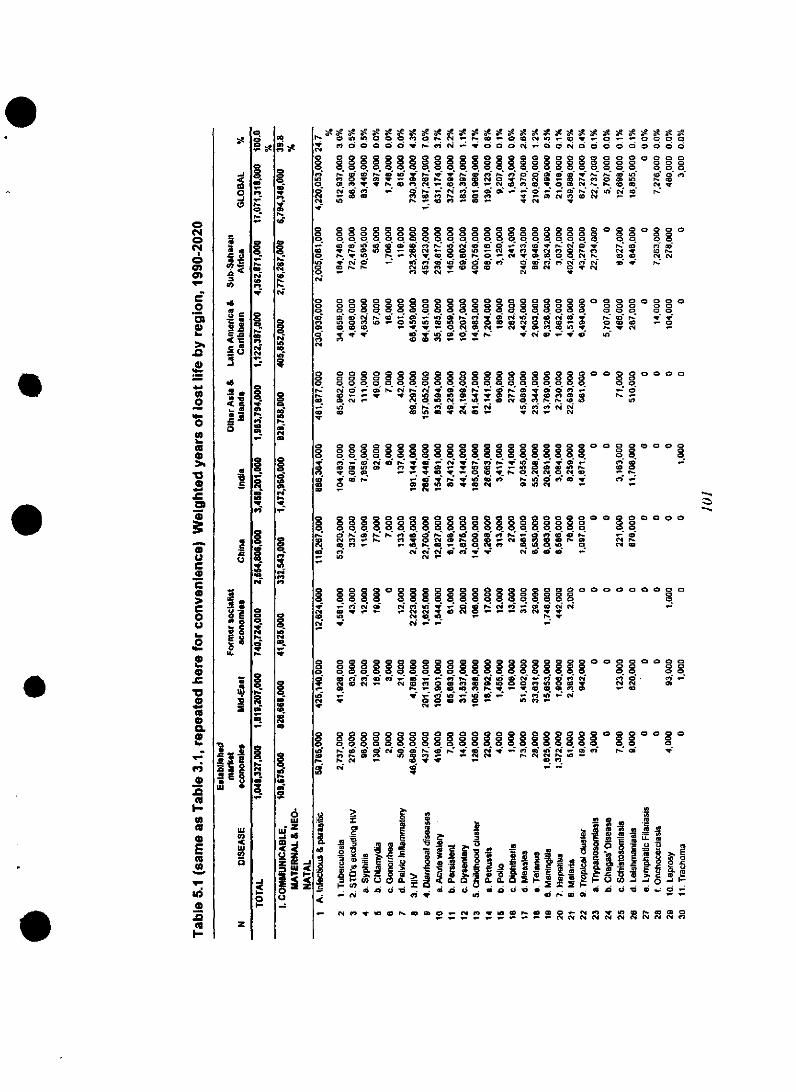
., . .e~ -. 0e 0 g . 400z . g,In HIHn o= o> > C> r, <M o- co C o C4 1 <p $ S S S
* e7 000 000000000_00 « _ t O O O di 00 O O OO 0O0O 00OO00OO0 OO O OO OO OO O 0000
O ~ ~ ~ ~~b O4 Ol O OOOOOO Oi O OO<4 1 COD el co Zo ID 0 t- C, e, co eiev IZ1 _r
-n c s o NN t 02m
CN Iq Z cl 0 -R R R R O 0vu s1s
o> o 0 o g o 8 oo oooo o o og o o o-0o o0 o o0 olo 0 o @ lo o o4 omoo o o
°O ÑvXOS ae_ O _ 't0e ^ (d o °> >o s ,- N
<' t.00 N>0 O>e - -H00 e> C OIDe>W 0 q IN f -- tOu _> n I n _ 0 N
Ñ .. ~0 N.'<'4w C0U>cmO>M 0ge> C<eC4>' o
O 0 ( D O O - O Ot e ' O 4 > 0 ( 0 q
> O Oe 0 -e U O > 0 0 0 0 0 (4 0 0 4 0 -GDCl{0 _ t - N O . N NCl ok c1 t 2 . ID , N
" s c Ir U)Oiiaz *. eCmO- * se> 0 0 m ~
8 82 o 8 g 8 °2 ° 8 008 °°oU. o0 o 8o. o
l:D C N N 1* eb < V. _ h le N *oa o lIn 0 f N 1N -_e m
lo ca -ne xz _ No Ui C4
N 0
0 --Oi <'40n
888800000000000 00 0
e>
004 O < V O O O V 0. O > 0O 0 0t.O O1 -0 > 0 . 0 =1 0 O N C 4 c, 0
'- 4 -f g « » D 4. CO O -k ., c . . .O1 q vO«NONI
CD llY- _ v0 w 1 Z 1,0 1, I o 0, IDreo t e 8 8 w 8 N cm
O OO O OO OPOOOO - O 0< 0 > <O O88g g o 8 g o° 8 8 . . . 8
oe> p r f i o r « «<'j<'¡.e .,_ * o oo «O, -v, 0 0n N N N e n t t N «> zla ID~§§§§§§§§§§§§§~§§~§§op CD
0>C00~O O O O
,- 0a<'4'L
o o0 N00q
<'> 0*<o <('4 <N
0080000
° 2 8 ° 0 ° 0
q , oi
- o_ -
° O 8 ° ° °0 020
O O2
- oe> -
o8.
o o o o o o o
oo8N r.<'4 e-
o c, 0 o o § § o so Bso o o11 < 0 -NN
- N;;
0°8 8° 888 o8° 8C08 8° 80 o8o (o o- o o-0 0 -V o-o
t N _ D '40 _ - « -
<-< - D O N D 0 1 t - N0N10 >
Ñ N 0 _ _P.t. cm
= 0 0 a 0 0 30 8 0 o
e o e>_Ct 0
088008000
N. mi q
D-
o -~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
i ; w di 4 = * e 0 * 4 6 = * c = wi od p] .: dfi*a _ _
_» N 10 0 e Co h io e o N 0 u) IDrO O_ N I 0 C- _ _ _ _ _ _ _ _ _ N N~~c N cm N- <N N N N N el
O
e>
N
co
('4
,ol
a
a
O
C>
1
u
CID
a
te
¡
O
,0w
.o,«R,1
o°
o,,
oe-
ce
O
5
a
c,3
z
i
o.-o.
$
*"c
o C
c ,
E= u
e>,
.6
a
.ce
aO
Sz
'-
ot1locm
'U-
,oE'
>1
.0
0
0
0A-
00,>b
Co
>1
o
oC0
0u
A..
'0
oomm<l
Eb.
o
m
I-,0m
Ela
o
m
.-1-
e
41

-o o o o o o o ~{o o o a o ao o o o o o o o o
--o 8 o°e ° 8o>o o o oo o o o o o o o o
o0 _ o o 0 o o o
0 0 0 0 0 o _
*0 fW _ _ D0 l 1_ 0 0 N 0 0 «0 0 a
cn e ci C=i q t e o _ .o i ce ct e
04 ee - C>9UC.e
wk ew . mj _.- _> eae>a
o o o o oe o o o o o- o o o oo o o o o o oooooo*8n 0 000 oo 0 o0
-) ey ,k N q In N. c1 CDOL cDX1t <k cq-- 00 In _, D> _D _ _
ej
<D 0 200 0
D s 0 N o eb o _> * Q o
co c)t _ N uD 0 <» S 0D 10 da cmSw2 _ C» _ l _" cm .1 5 l C V. _ 1 . _
: o o o ° ° ° ° ° 2 ° ° ° ° °
oao ooo o o ov o oo oo
(oaO Op oa a ao
o o o o o o o o o
O, 8 a 0 a < Dsx
- c -iu>e > NL _1 1 c- eo~~~~~oao N _a a <o S aa a _
000000 o o oo o oc a o aoo
e-ejes Nu>ft CM u>_a00_ au>e
c/) c~ r ~)Q /Q _v-e- o 00O oooo, o oo, ooa, o, o
ej~ ~~~~~~~e
· ~ ~ ~ ~ ~ ~ ~ ~ ~ c . 'L-.
o
_ -t I_ tO- O tO N t -
8 8 ° 00 8 8
00 00 0 0 0c
°D 14. °'° e n c *wt't 1 ot
,tt a ,un to a . _ aco el C C
u>~ ~ ~ Nj -e:u-0
C.)~~~~~~~~~~~~~C
©
a aca a ooao ao ao
oa a , a a ooo o a , aa oa o
~' ~ _0 m'ro2 -i
- D- N C 4 ej u>3se-Ue>U
_ cS ' ni n ..... e -Oe- u e-
Z ca 0> U> t* e> e -l> o ° - o - ° -
SSooooooooo_ 0 <O _ N .! N _.e Co cno o o - ej e> e O > cm O > o
O o oa o o 0 0 0 0 a 0 0 0 o o 0o oo o o O o 000 oo o8 8888o8o1o8o o O o o o oq o ok o
uo z O -_ N ej - >0 u >tto té C AO MN N " - O ON wtqt tt
u>- .0 u> .--
t u> eu tj >m O ( 0 qt tS tS tO tO i _ _ tS -
.e joanej6.de. .C >u . . .o > o, ce *
e> ~- u>>>>u ... ~--0evva
0 tO In _ f. tt M O t i 0b N -..
roCtejej ej cn - -qt Dt 9 qt
c, §e 12 1o 12 C, C, C, ei «i _ , C, <i e' i _
8 88888 8 8g8 88 88gg8 8g°8 8
ei NCi qqq qi q NN N O ID O 'O C So ie0 l v_ i _ N- oi _J o N N S id e ; -S <S e ,_
o co O , o O le Ow O» m
N(O (O c* 0 V M (Ci la NF N e) t- i_ 1
0n 000000e t _ ee O s > so e 0 s o = No o o o o o > ooo ,uoeoej-ouo
IS fN Si N . osq R qX R N qq Ck Ci Cli
4 « e co _ <o N s rvS> e o u o o e N r
No .. .i . e Ct
uO> UeU . veje. __
ej - - ej-
8 o t, M ° 8°°°°
o 00000 00o 0 0 0 0 g 8 g 8 o 8 cm
u> eju>.- Oe u>eu e >va e.....~
0i 00 _ _ - e000 0N 0 0 0 0 0o o 00e> r os vv e _ ce S - ovej
o) o cm ° ° ° cm 8 P- ° ° °°
o'4 °o oo o p, o el j m) o oe o oooej Xa ej oe e> f- -< I R miN ee -i
N e* ee « c2 , O, O -ce (D N ) 1 N _ <e
ck - - - aM i N- ik . . i C-i N i ( .(&e i _ s
0 00000~~0 00000 0
8 8 88 8 88 0088ggg8 8 800g88
o cD o cl o o o 8 o oeo o Coo o In oo o rN l«uO «1 -
O (_-CU O- u> a y- u> u> 0 _ e j Ce ju 0
Ci i t - « S Ci i (D; ES i ci C'i mi C>
; z i f_ ib t i N N - t- N dD C4 _
Cu O D _ek N q0 . c j e> -- Ne
(4 ei N í Ñ r S i cS v¡ m o 0 « v eq
X~~~~~~~~~c aa ci c i
s tX8 § X< e"8 gc E m8c888 E8 2
c1t - - - --C
- - CO o,¡ ci cí -v
0 000000N e t e « 1 c 0 00 0 0 N0 t ITP: a e e e0 0~~~~0
u> eu>e-~~~~~~~ séW
r4m ic ~ m0---- - -j - -
eje> -u> ej -~W> -- -O c
e
e
e
.
e
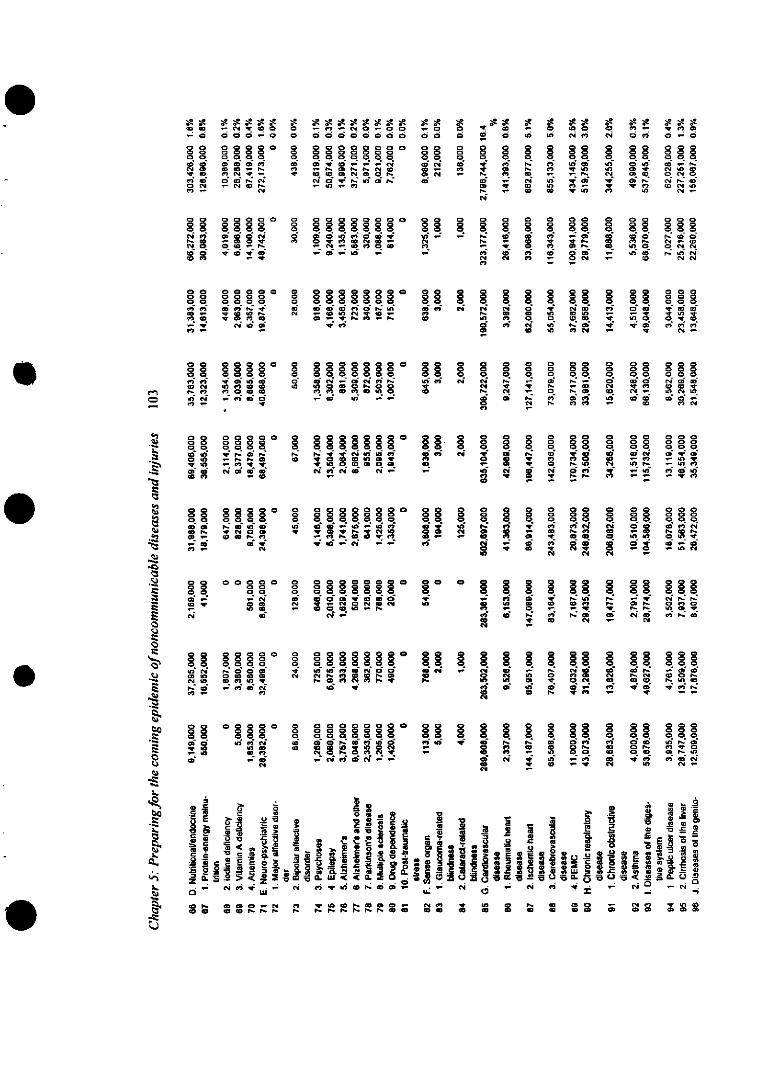
O O
" aa aa a
m O
O amw0
-.e,- g" Ir O _
o. a a- a0 0 e-0O O O, . -
dce:lolO D0 O 1em N Ir _O Ci Nú P.N
C40N
88§ 883880e¡i MiUOC. .Ñ" O> co acmN=, O00 ._ej a,-e- Z
88 8 o888°0 C> O eq C
t"e>o .90e> r
; el 010U0
T OT C
> e-e e>ao D o<D cmt
a
co
0,q
R0
o.9
ao
o0,
n
- se> -° S aS a a
_ u) _ N O a O-
j a .9 e- u O e -
- O - e > O
- V « > a -
O 8 8 8 8 o 8oo o e> a, e- o,
- o 0 N .90 _O _ e- e. - e
e
8 00003 8 a
u>a o a e- aoe> o o o> o a
0 0_RqqUZ _q
a ao o a S > o e le
Og O aO 0 81 8 8
oea o .N, D e > oaOC e l e- e In _ 9
0 -1
o e- e> v e _
o o o ~ ~ M o - o~ o
8 a 8 8 8 8 8 8810 _ ; D 0 0 -
C-4 ej - a.N, -_
O 0 1 «1 g 8 8 *e> e- 0 0 0 02
O O O> a ID oOi e> a *n -aO CD D 4 co N
8o a R 0 8 8>
e- ts e- _ o -a C ea e- e >
e> N - « oO1 le 1 r-N% _1 i C
a a 0 a 0 ao c m e - o
1 ao _ rs ta aoe - .9 -M <o
D -O 0e e>
0j
88 a°8go
09 000
N D
o
0
goalau,
0ej
8 8 8 88 88 o. 1 ¡, o 1 ,o S g 0 8 80 o°°cq C g <k 0 .9 a e _O
Ñ N eo CM- - o e. N .el - - -
. .° e- .° ° - °'
* M - N - -
8 ° S 1s so 8 11§ 18o 1 M e- .; j e e> f,M- e -o **> *; 2 _ ZD CW O
D: I N Cla cm3 A
a o g a a a a0 0 a a= O a o a § Q8 8 8 8 8 °° 8 8 8 o
la --SE;eÑ .- NiN e-.(4 - ~el; b - M
a0 0 80 o aa2 8 ao ° o o a ° ac o °o °o ° g o 8° 8 80 8° o 8 g oN eJ O .M . . .i NJ . R R e c O O o0 0) a , c a ej > e e l e > 0 4 a- < 9 a u o
,_ jo _ e O. e a0 ea N, ° e> j °i 8° 8i 8 °d M oe8>8 o o ° oo o u o 8 ,
a -a alo In ti 0 N a a a aOl N N__N N8 1 a ¡ ¡ 8 a 8 8 a a a 8 8 1 8 1 8 1 8 1 8~~~~~~~~~~~~~~~~~~~~~~~~~~~~~"D
ela-
1D a a aCa2o
c oo eo
_o _ *e -
OD e* In <NCD rtt m 0
800 8 8 g
o oo
o_ t N 1i N:«
e -e 0 0 . 9
ej. e,e-0
o W 0 8 0a a a o
.9 N -D
a, ae-o , 4.9 e e > o D N
a 0 u
5 .' ~ ~g~ . w~ ,. ~ o- ~2 C'4E 2- j - .Sj .a- 5' E> . -b' 5e S
Mo6 CL w 0. .t_ : ta; ~ .. ~ , , _ )OrZ - E N C) - N , _ N f1 o e o o _ e> . eje> . 0 0 e-_ N c0 e> . 9 O O _0 N
00 b o e-e- m e -e MI - r e- - - 0 0G O : 0 CM m Ow ur-r-P 'r~' , oG D D c co ~ ,o~ ~ C>Cb
aej
8.n
eN
e> -O «mce,8 8o aia le
" u00
a a
O N e-
CD cm !gN_
e 8 0
e- S a
qN .Ncm-
a m cm
0 0 00 oaCD cDO0
CD Iq O_ u0 s0
0
a
g
MiCt
N
C-
.9
a
88g 888g0i . Oi O O
_ i le o UZ o
° 8 °888oj oeooN , _ 4 N 100 0 0 0
ID ? ID
.i
-oL.E0
.3..
-o
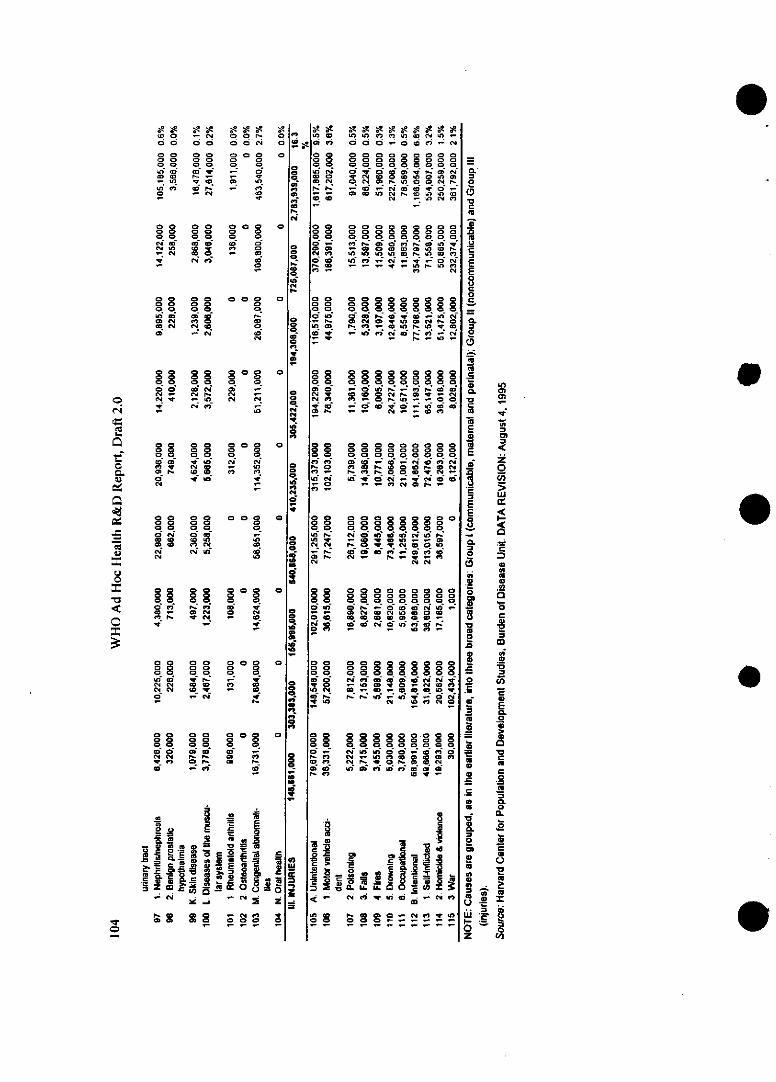
c o
0 0
o oo o8 8_) eq
o o_ 8
v cmcwI
- Co No oo o0 8
rD oo e.o Co
o o
o o<N
ca ca
Cc¡ l
o
0
o
ca
0crI!s
O
Oca
o
0
o
o
00<o
o0
caca>0
8,8 c88 , 80 CMO C OXIR Na Nl c 0* -_ N (O
(N
o o88M- t-o
8 8 0 0
oce
Ci
sg0 ea 02
<o lo a
cm. cmuSOCMd
0 0 C0G
ca OeaO b e w«
o, o
8 oC>DC
_o_ Oca ca
o oN NN, N',c
00 00 c
lt tl O,88 8 8
0o2oiO>0MNM
o.
CMci0,t
Nz
O O0O-
D CMel ca
0*kca
oo
oca-
oo
rs
o
8caca
0 8qo,
NCkz
os 80
yca
oor-
00
oca~
2 o E U s~J.r c°g7Rta R=
2iD E oo 2ENp, 0 C 0 Cke
0 . 1
1a'1ca
caCCLaet1"ma
caCLa0u!i
0tez
ocea e e sa ca *n uc N Ia) -
0000000 0
a c o o o _ o ci c - ci
O O O O O O O O O O OO O O O O O O O O O8... oo oo o OOOO OM 0 O O O O> O O. O Ocao tcc O ca o n>f O > er-- -ca ce o0 - O c , CM rO ca uN O , ca
0000 00000
0000 0000000
c- - _ a .caID O
§§ e C0 0_ 0
<» 000 o0000
0000000000~00000000000
Ck ui ct-c~acc
c2 00 O0
Io oo oo oooog
0 , oo ,8, 8 o 8, o,
O 0 02 c Lc r aO Z e_. _ _. .- ._ . ca
00 000000000
_ D _0 0 _0 _0
Cm ca e, - O, q - S. O, O
00000000 8 00 I
r o e ca 1 ca o ca r- ca e
_ 0 0 0c 00-
- e ca ca aei ci ca c_ e. CM -ol _ . -
CM 0 C, C C C
OuO O O O0O O O O
oe, ~ ~ c - - cae,0I 00 0 000N0
C ca - c ca O _
8° °o o o ° 8 °8 o°8 o °8 o
I- e C> aa c c ca c o eaO c, aM e= e a c I -
N: 40 QD C=i - O
c, > .7 C..1-
l ~ w o, o0 o
1c N D -s q .D c t
<o- e.I_ 1 e¡ _W W fá - C N
oI88oo
°°°°°°!°
I g O0 0ii o~ °o o§
e
e
e
e
ew WJoz
r-
o
o.
cC
as
u
o
m
IC
o
=
oE3
o
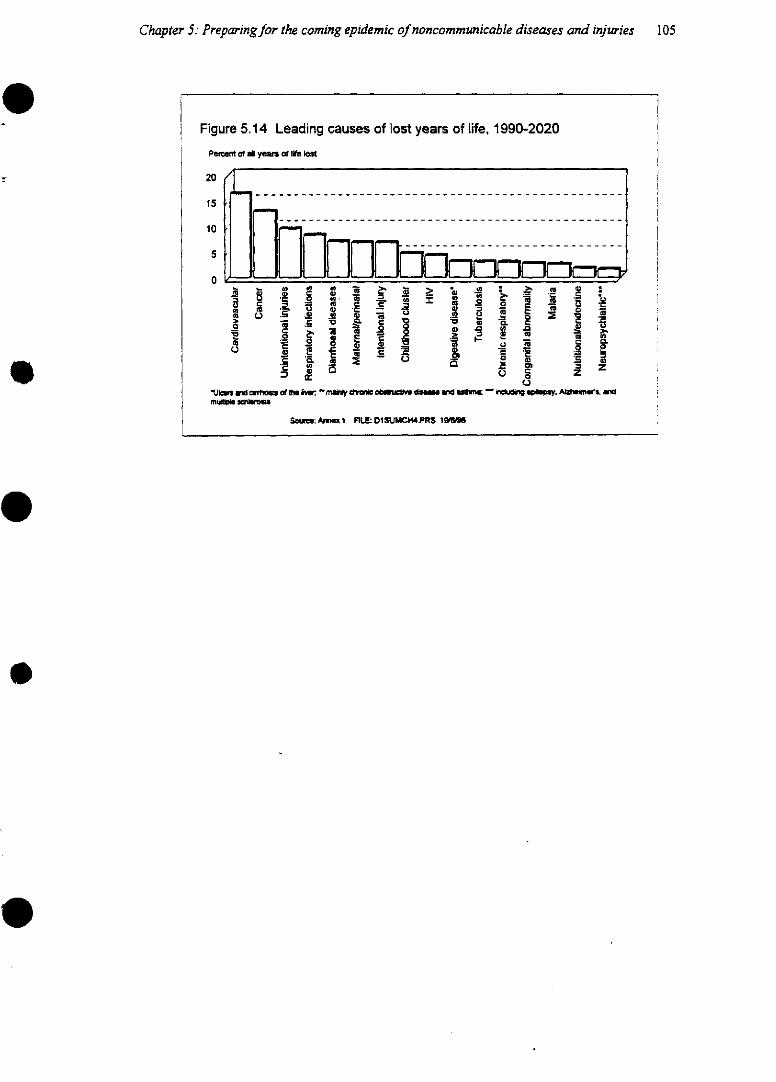
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries
Figure 5.14 Leading causes of lost years of life, 1990-2020
Pert of all year al ife Iaos
20
15
10
5
0
·- - m _ La 't - O í0ú i l a
zUIcus a*d cirnoms ofi aw t: maar drwc ob~INIJ/ da~ fUd acl n -U , cud m, AJz!umes.
S :Anmm*i FILE:DlSUMC.4.PRS lg9~'
105
WHO Ad Hoc Health R&D Report, Draft 2.0
5.2 Measuring the burden of diseases by risk factors
Most efforts to assess the causes of ill health have focused on the diseases or injuries that they pro-duce. However, as was discussed above, there are a number of behavioural and environmental fac-tors, to which individuals and populations are exposed to different degrees, which influence the like-lihood of experiencing those diseases and injuries. Half of all smokers will eventually be killed bytheir habit, and deaths due to tobacco consumption are projected to increase from 3 million in 1990 to10 million by 2020 (Peto and Lopez 1994). Alcohol increases the risk of injuries through road trafflicincidents and, to some extent, other injuries; in France, an estimated 50% of people occupying hospi-tal beds have conditions related to alcohol misuse (see Box 5.1 on Alcohol and road injuries in SouthAfrica); air pollution contributes to respiratory disease.
For this Report, estimates have been made of the proportion of the burden of noncommuni-cable diseases that may be attributed to specific known risk factors. Smoking is presented here (Table5.2). As with the risk factors for communicable diseases discussed in Chapter 3, there is much inher-ent uncertainty in this exercise. Much of the literature on attributable risk, such as the estimates of theproportion of deaths attributable to smoking (Peto, Lopez et al.) is based on estimating the currentburden that can be attributed to past exposure. Attempts to calculatefiuture burden are even moredifficult, especially where there is a lag between exposure to risk and the onset of the disease. As aresult, the exercise has focused on current burden and not on projected burden.
It is important to distinguish the different types of risk factor. At least three can be identified.The first is category of risks are those to which people are genuinely "exposed", either through riskybehaviours or through the environment in which they live: smoking, alcohol, physical activity, sexualactivity, air pollution, and others. The second category consists of physiological states that predisposeto disease: hypertension, nutritional status and others, which are themnselves the consequence of othertrue exposure. For example, high blood pressure is the result of a complex interplay of genes, devel-opmental factors, salt intake and other factors. A third category is social states-such as unemploy-ment, poverty or gender-all of which may play significant roles in disease but none of which can beeasily measured (see Annex 2, Lopez and Murray, for further discussion).
Attributable risks may, of course, overlap. A death from heart attack could be attributed tohypertension, smoking or high alcohol intake, so it is not surprising that the sum of the burden at-tributable to all three factors is higher than the actual measured burden. This means that all estimatesmust be treated with caution.
[Table 5.2 about here]
[Box 5.1 about here]
e
106
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries 107
Box 5.1 Alcohol as a risk factor: the South African experience
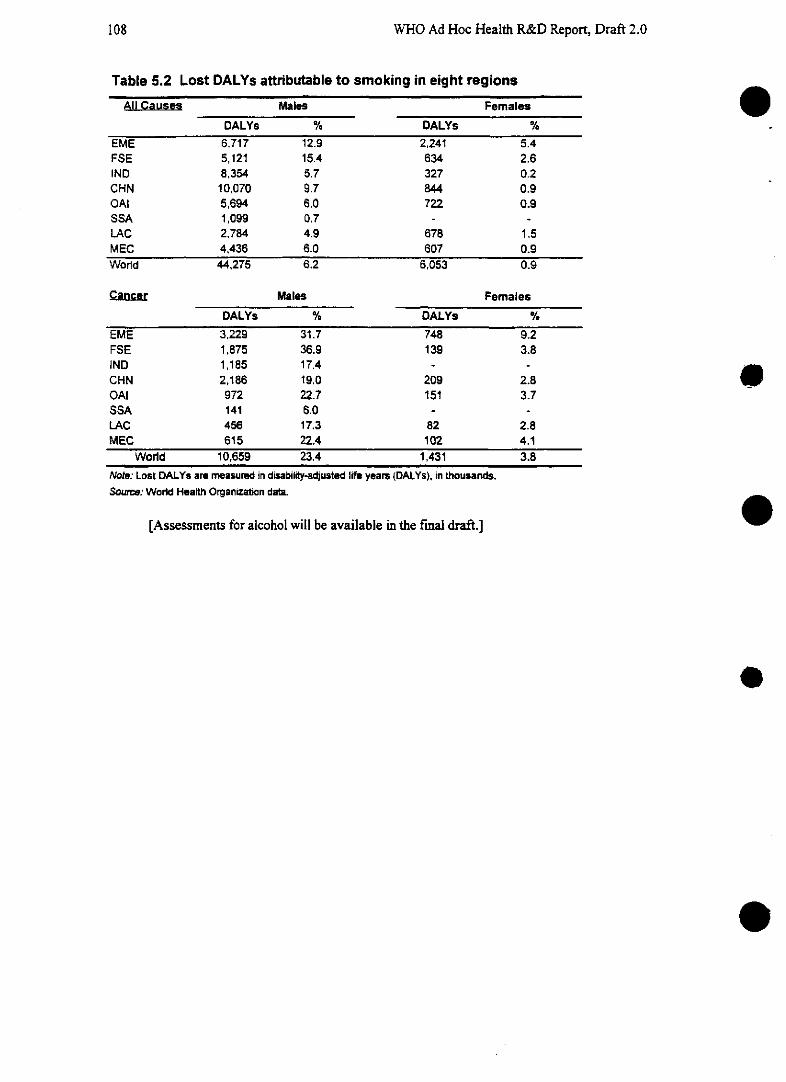
8WHO Ad Hoc Health R&D Report, Draft 2.0
Table 5.2 Lost DALYs attributable to smoking in eight regions
All Causes Males Females
DALYs % DALYs %
EME 6,717 12.9 2,241 5.4FSE 5,121 15.4 634 2.6IND 8,354 5.7 327 0.2CHN 10,070 9.7 844 0.9OAI 5,694 6.0 722 0.9SSA 1,099 0.7 - -LAC 2,784 4.9 678 1.5MEC 4,436 6.0 607 0.9World 44,275 6.2 6,053 0.9
Cancer Males Females
DALYs % DALYs %
EME 3,229 31.7 748 9.2FSE 1,875 36.9 139 3.8IND 1,185 17.4 - -CHN 2,186 19.0 209 2.8OAI 972 22.7 151 3.7SSA 141 6.0 - -LAC 456 17.3 82 2.8MEC 615 22.4 102 4.1
World 10,659 23.4 1,431 3.8
Note: Lost DALYs are measured in disability-adjusted life years DALYs), in thousands.Sourc: World Health Organization data.
[Assessments for alcohol will be available in the fmal draft.]
e
O
o
108
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries 109
5.3 Assessing needs for strategic research
As in preceding chapters, the following section provides an analysis of needs for strategic research by(a) analyzing the magnitude of different types of need and (b) assessing the level of ongoing researchin an attempt to define the biggest gaps between need and investnent. For this draft an analysis ofresearch needs on tobacco use is presented. The burden from smoking that is unavertable, and theburden that could be averted with better use of existing interventions-principally health promotionand smoking prevention activities-is set out under optimistic and pessimistic assumptions (Figures5.15 and 5.16.
[Figures 5.15 and 5.16 about here]
[Note: The figures on which these diagrams are based are currently under revision; the as-sumptions on which they are based will be detailed in Annex 2].
[Final draft will contain further squares for selected other NCDs or their risk factors, whichare currently under revision.]
5.3.1 Assessing ongoing research activity
Noncommunicable diseases have long been a priority for the developed countries, althoughinjuries remain a neglected area of health research. In developing regions, certain countries, notablyChina and a small number of middle-income countries, have begun intensive efforts to study thesediseases and conditions, but most countries have yet to devote significant resources to them.
This Report has sought to assess the subset of research activity in the area of NCDs that isconducted in, or supported by, the EMEs but is relevant worldwide. All biomedical research is as-sumed to be relevant worldwide; other disciplines have been subdivided to assess the amount spenton research relevant specifically to developing countries. The methodology is explained in Annex x.
An analysis of funding sources in the literature between 1992 and 1994 (as described inChapter 3) was conducted for selected diseases and risk factors: cardiovascular disease(epidemiological research only); asthma; motor vehicle accidents; and smoking.
Asthma, which accounts for a projected 0.3% of lost years of life between 1990 and 2020, re-ceived between $127 million and $158 million a year. Epidemiological studies of cardiovascular d/s-ease, which accounts for 16.4% of projected YLL, received $100 million a year. (Epidemiology rele-vant to the EMEs received more support, but is seen as irrelevant to the needs of low-income andmiddle-income countries and has therefore been excluded from the analysis.) Motor vehicle acci-dents, by far the biggest source of unintentional injuries and alone the cause of 3.6% of YLL, appearto be the most severely neglected of the areas studied, receiving between $24 and $33 million a year.Smoking, probably the biggest single preventable risk factor for disease, received between $148 mil-lion and $164 million. [THIS SECTION MUST BE EXPANDED TO DISCUSS WHAT IS HAP-PENING TO THE MONEY THAT IS NOT BEING SPENT ON ANY OF THE DISEASES IDEN-TIFIED; NEED EXAMPLES OF THE "OVERSPENDING" DISEASES TO EXPLAIN THE MIS-MATCH BETTER.]
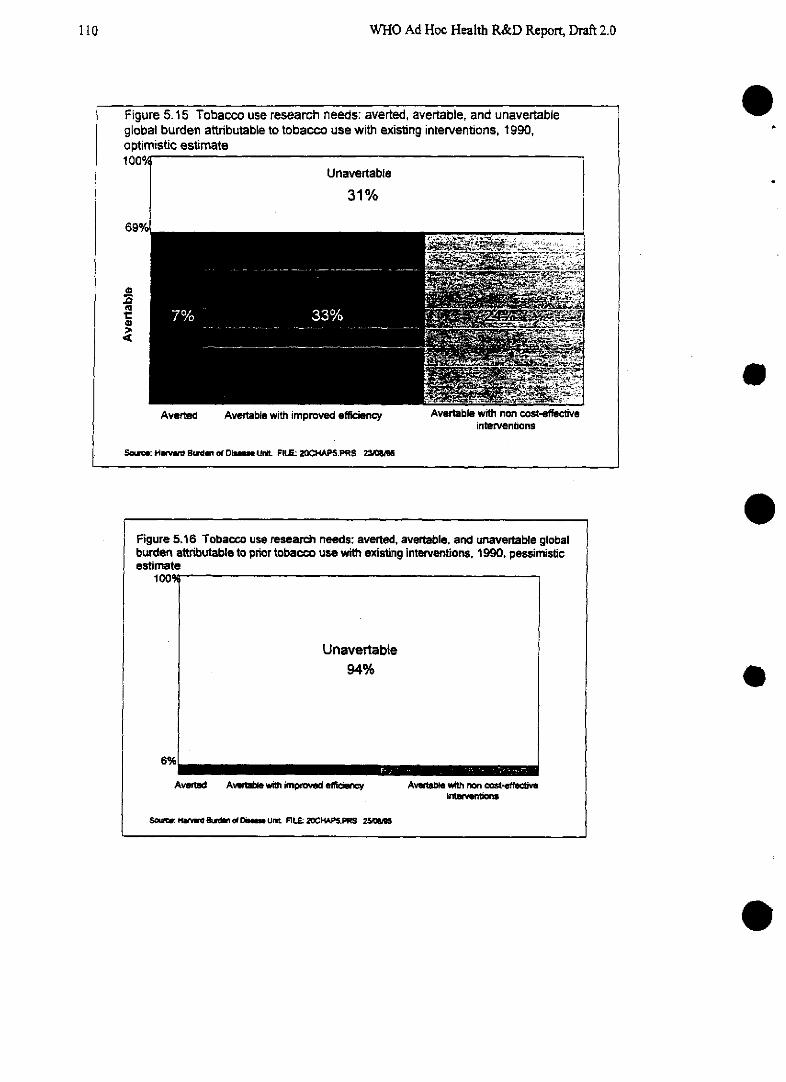
WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 5.15 Tobacco use research needs: averted, avertable, and unavertableglobal burden attributable to tobacco use with existing interventions, 1990,optimistic estimate
Avertable with improved efficiency
So~ce: HM N~ Burd of D0i_ Und FILE: 20CHAPS.PRS 23»A
AverUIle wnn non fcos[interventons
e
Figure 5.16 Tobacco use research needs: averted, avertable, and unavertable globalburden attributable to prior tobacco use with existing interventions, 1990, pessimisticestimate
100
Unavertable94%
6%
Aved Avwbie with improved effciency Avewab with non cot-efftveSo~: M t intervenlPn2
Sme: HWn4, hi*dmn al DiaO_ Un. FILE: 2OCHAPS.PRS 255
e
e
llO
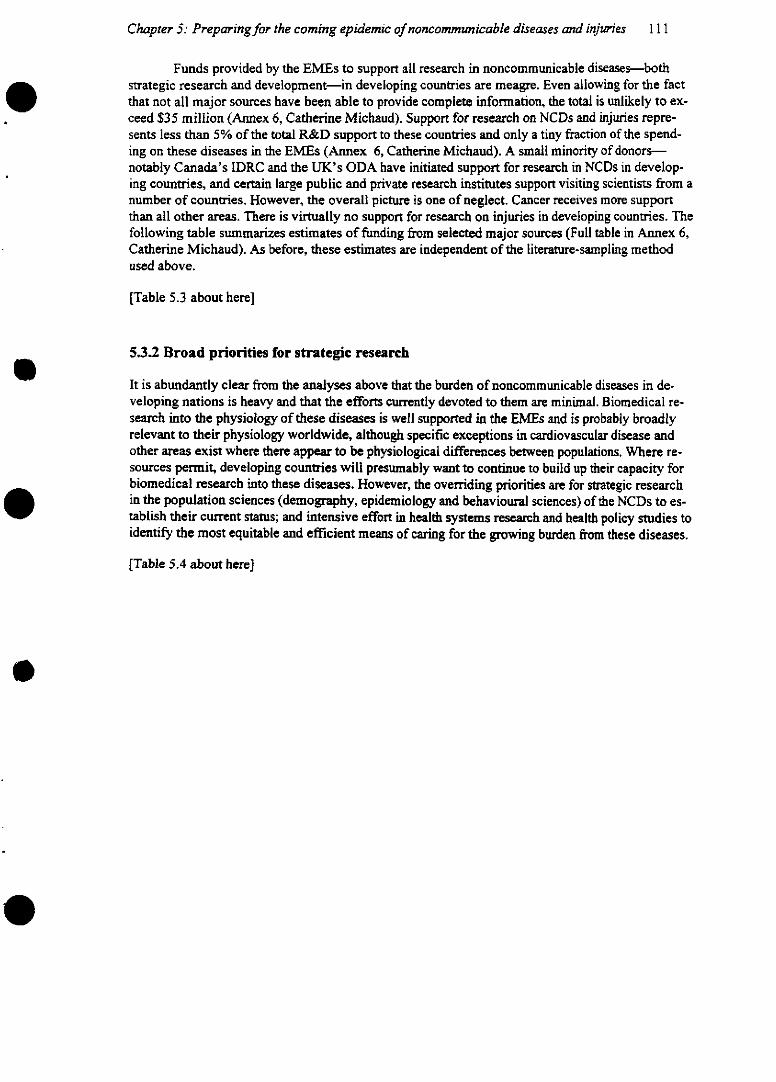
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries 111
Funds provided by the EMEs to support all research in noncommunicable diseases-bothstrategic research and development-in developing countries are meagre. Even allowing for the factthat not all major sources have been able to provide complete information, the total is unlikely to ex-ceed $35 million (Annex 6, Catherine Michaud). Support for research on NCDs and injuries repre-sents less than 5% of the total R&D support to these countries and only a tiny fraction of the spend-ing on these diseases in the EMEs (Annex 6, Catherine Michaud). A small minority of donors-notably Canada's IDRC and the UK's ODA have initiated support for research in NCDs in develop-ing countries, and certain large public and private research institutes support visiting scientists from anumber of countries. However, the overall picture is one of neglect. Cancer receives more supportthan all other areas. There is virtually no support for research on injuries in developing countries. Thefollowing table summarizes estimates of funding from selected major sources (Full table in Annex 6,Catherine Michaud). As before, these estimates are independent of the literature-sampling methodused above.
[Table 5.3 about here]
5.3.2 Broad priorities for strategic research
It is abundantly clear from the analyses above that the burden of noncommunicable diseases in de-veloping nations is heavy and that the efforts currently devoted to them are minimal. Biomedical re-search into the physiology of these diseases is well supported in the EMEs and is probably broadlyrelevant to their physiology worldwide, although specific exceptions in cardiovascular disease andother areas exist where there appear to be physiological differences between populations. Where re-sources permit, developing countries will presumably want to continue to build up their capacity forbiomedical research into these diseases. However, the overriding priorities are for strategic researchin the population sciences (demography, epidemiology and behavioural sciences) of the NCDs to es-tablish their current status; and intensive effort in health systems research and health policy studies toidentify the most equitable and efficient means of caring for the growing burden from these diseases.
[Table 5.4 about here]
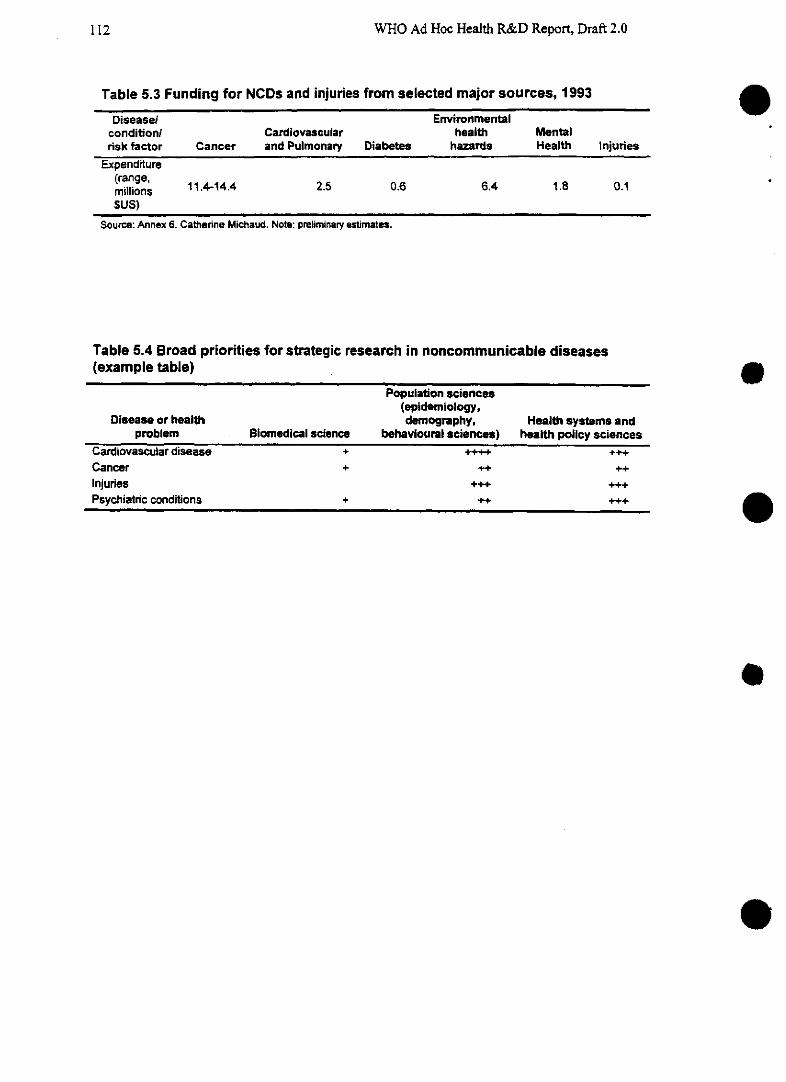
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 5.3 Funding for NCDs and injuries from selected major sources, 1993
Disease/ Environmentalcondition/ Cardiovascular health Mentalrisk factor Cancer and Pulmonary Diabetes hazards Health Injuries
Expenditure(range,m¡lliíons 11.4-14.4 2.5 0.6 6.4 1.8 0.1
SUS)Sources) Annex Catherne Michau Note preina estiate
Source: Annex 6. CaUsefine Michaud. Note: preliminary estimates.
Table 5.4 Broad priorities for strategic research in noncommunicable diseases(example table)
Population sciences(epidemiology,
Dlsease or health demography, Health systems andproblem Blomedical science behavioural asciences) health policy sciences
Cardiovascular disease + 4 +++Cancer + ++ ++Injuries +. +++
Psychiatric conditions + ++ +++
e
o
e
e
e
112
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries 113
5.4 Opportunities for intervention development and evaluation
The assessment of research activity above suggests that this area requires urgent attention. As inprevious chapters, the opportunities for intervention development have been assessed by (a) specify-ing the nature of the desired intervention and (b) measuring the cost-effectiveness of existing inter-ventions. Unlike the diseases and problems of the unfinished agenda set out in Chapter 2, there are
few cost-effective interventions available in this area except certain prevention programmes, such astobacco or alcohol control, where DALYs can be saved for an estimated $35-55 each (Global Com-
parative Assessments in the Health Sector, WHO 1994, p. 174). By contrast, most treatments fornoncommunicable diseases have been developed with the EMEs in mind and are far beyond the reachof most countries. In the U.S., for example, the cost-effectiveness of treating patients with acute
myocardial infarction (heart attack) using tissue plasminogen activator was recently calculated at$32,678 per year of life saved (Mark et al., New England Journal of Medicine, May 25 1995). How-ever, affordable interventions are possible: aspirin, for example, has been shown capable of saving
23% of lives when given after a first acute myocardial infarction (ISIS-2 trial). In India, the cost perlife saved (calculated for the drug alone) would be less than $5 (K. S. Reddy, personal communica-tion). However, there are key questions about the practicalities of maintaining therapy, such as pa-tient compliance, and further research will be needed to establish the effectiveness of aspirin therapyin community settings. Selected desired interventions are illustrated here. Assessments for this report
suggest that priorities should focus on the development of cost-effective clinical algorithms (such asinexpensive but responsive protocols for the management of heart attacks), improved methods forearly diagnosis of cancers, and health promotion packages designed to elicit healthy eating, exerciseand, where possible, the avoidance of risk factors linked with disease, most notably smoking.
Some suggestions of areas of potential intervention and product development can be seen inTable 5.5 and in Figures 5.17 and 5.18
[ESTIMATES OF COST-EFFECTIVENESS OF SELECTED DESIRED INTERVENTIONS RELATIVE TOEXISTING APPROACHES ARE BEING DEVELOPED AND WILL BE AVAILABLE FOR FINAL DRAFT.]
[Table 5.5 about here]
[Figures 5.17 and 5.18 about herel
The examples shown above indicate the need for better algorithms, preventive care and prod-ucts to address a major-and badly neglected-challenge ahead. Equally important, however, will bethe need for research into health policies and action to develop legislative and f'mancial tools to err-able the most effective, high-quality care for the greatest number of the population. The cultural andsocioeconomic changes that are happening alongside aging in the low-income and middle-incomecountries will demand careful sociobehavioural and economic research, as well as epidemiology, ifcountries are to establish population needs and prepare to provide an adequate range of services. Thisimportant issues form the focus of the next chapter.
[Box 5.2 about here]
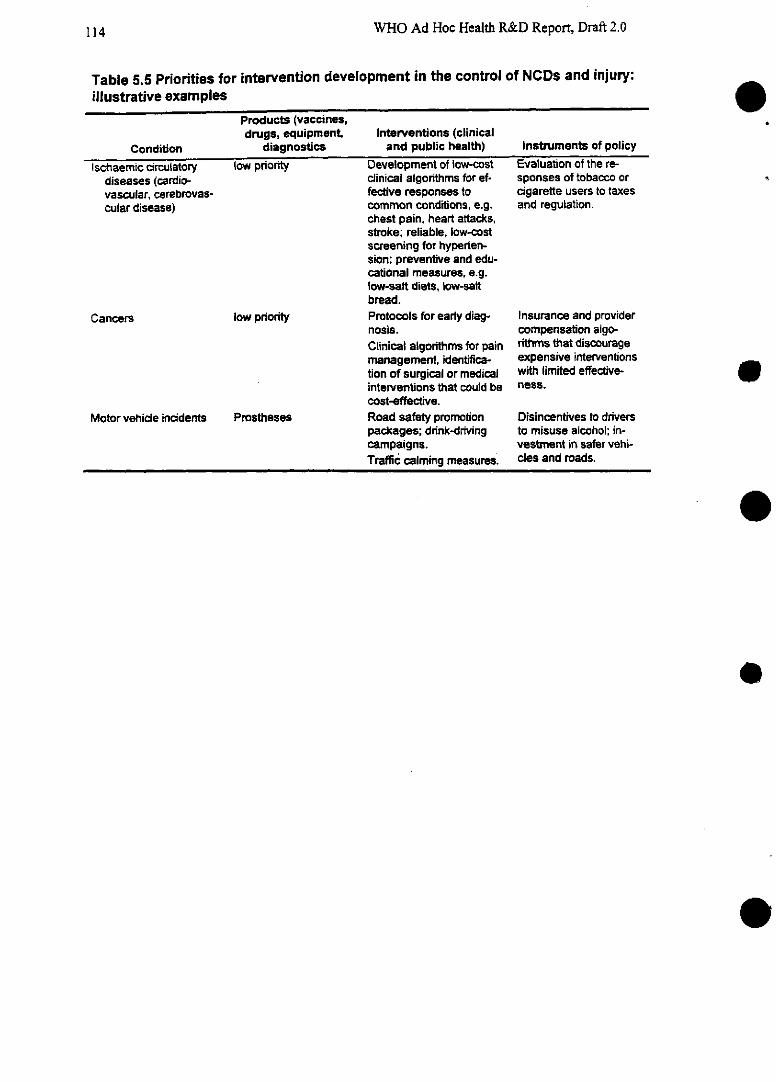
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 5.5 Priorities for intervention development in the control of NCDs and injury:illustrative examples
Products (vaccines,drugs, equipment, Interventions (clinical
Condition diagnostics and public health) Instruments of policy
Ischaemic circulatory low pnriority Development of low-cost Evaluation of the re-diseases (cardio- clinical algorithms for ef- sponses of tobacco orvascular, cerebrovas- fective responses to cigarette users to taxescular disease) common conditions, e.g. and regulation.
chest pain, heart attacks,stroke; reliable, low-costscreening for hyperten-sion; preventive and edu-cational measures, e.g.Iow-salt diets, low-saltbread.
Cancers low prority Protocols for earty diag- Insurance and providernosis. compensation algo-Clinical algorithms for pain rithms that discouragemanagement, identifica- expensive interventionstion of surgical or medical with limited effective-interventions that could be ness.cost-effective.
Motor vehicle incidents Prostheses Road safety promotion Disincentives to driverspackages; drink-driving to misuse alcohol; in-campaigns. vestment in safer vehi-Traffic calming measures. cles and roads.
e
o
e
e
114
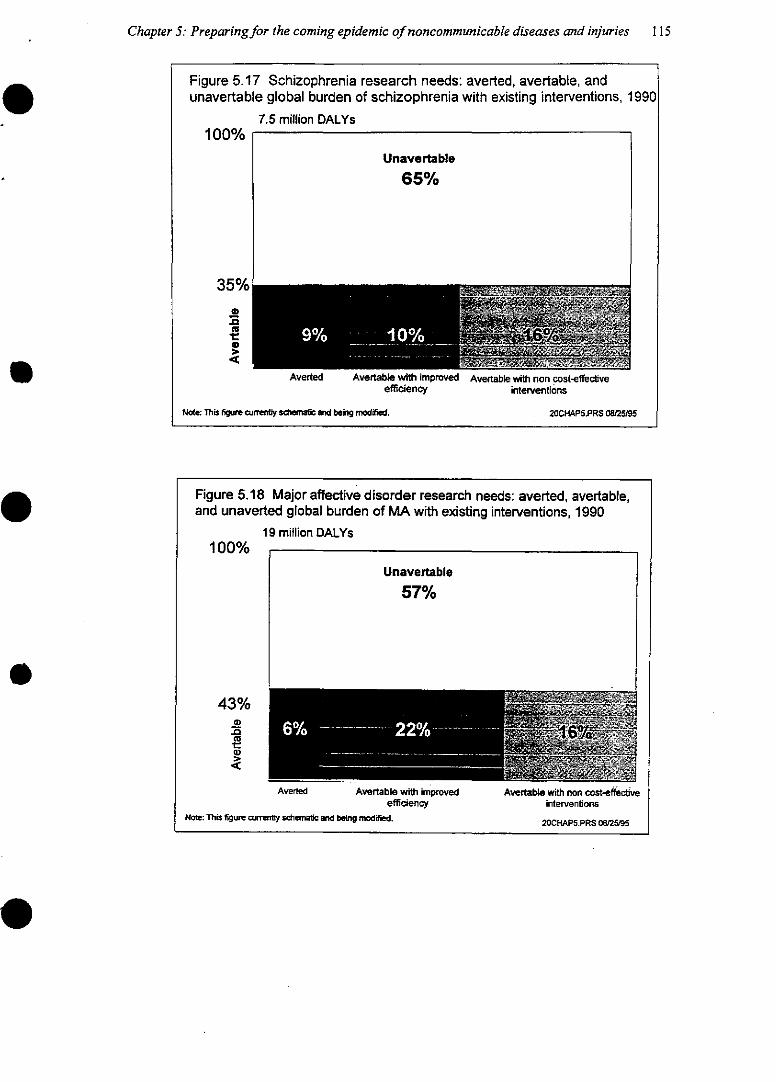
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries 115
20CHAP5.PRS 08/25/95
Figure 5.17 Schizophrenia research needs: averted, avertable, andunavertable global burden of schizophrenia with existing interventions, 1990
7.5 million DALYs100%
Unavertable
65%
35%
e
Averted Avertable with improved Avertable with non cost-effectiveefficiency interventions
Note: This figure cu~ny sdemaic and being modified. 20CHAP5.PRS 08/25/95
Figure 5.18 Major affective disorder research needs: averted, avertable,and unaverted global burden of MA with existing interventions, 1990
19 million DALYs100%
Unavertable
57%
43%mmm
4 3 OYo
8Ñ il
Averted Avertable with improved Avertable with non cost-effectveefficiency interventions
Note: This figure curly sotematic and being modifed.
WHO Ad Hoc Health R&D Report, Draft 2.0
Box 5.2 Traditional medicine: Alternative or complement?
Traditional medicine has been practiced by many Asian countries for as longas 5000 years. The two most popular forms of traditional medicine are traditional Chi-nese medicine (TCM) and Ayurvedic Medicine. Traditional Chinese medicine includesthe practice of herbal medicine, acupuncture, acupressure and moxibustion. Ayurvedicmedicine includes herbal medicine, massages and various relaxing exercises such asmeditation and deep breathing.
Traditional medicine promotes healthy aging. It recommends low-fat diets andexercises to stimulate the body and mind. The philosophy of traditional medicine is tomaintain physical and mental well-being to prevent the onset of disease. The recom-mendation of a healthy lifestyle along with herbal treatment and relaxing exercisesmay be a valuable component of healthy aging. People who use traditional therapiesclaim that traditional medicine can relieve stress, cure disease, and produce anes-thetic effects. Some herbs have been proven effective against diseases that modernmedicine at present does not have adequate treatments for. For example, xinghaosu(artemesin) is used as an anti-malaria medication.
Although traditional medicine is practiced extensively, some techniques andherbs are unsafe. The U.S. Food and Drug Administration has found toxic substancesin the herbs used in some concoctions. Possible toxic ingredients in the patents aremercury, arsenic, and camphor. Furthermore, practitioners prescribe substances thatmay be harmful rather than helpful in treating illnesses. For example, dong gui is pre-scribed as a post partum strengthener, yet it actually causes bleeding. There is also aquestion of cleanliness of the needies used in acupuncture. The lack of regulation oftraditional practices has resulted in the use of untested herbs and has fostered unli-censed practitioners to exploit patients.
There is a need for research on TCM and Ayurveda to establish which treat-ments are efficacious against which conditions. One obstacle to research is that pre-scriptions are tailored to the individual's needs. There is no one technique or herb thatcures a disease, thus making it difficult to show the effects of each of the componentsof the treatment. Traditional medicine practitioners argue that traditional medicine hasalready undergone clinical trial-by trial and error- over many centuries; what existstoday is a refined product of those years of experience. Nevertheless, there is a needfor research to prove these claims. The literature has limited data on TCM, even morelimited on Ayurveda, since the rich source of written research from India and China isnot being translated into other languages. The studies that have been done need to beanalyzed for confounding factors and problematic experimental design.
Four areas need further investigation:
* translation of available studies from China and India into English andother languages.
* intervention trials to test for the efficacy of herbal use and various tradi-tional practices.
e
116
Chapter 5: Preparingfor the coming epidemic of noncommunicable diseases and injuries I 17
(Box 5.2 continued)
* population/epidemiological studies to compare the health status ofpopulations that use traditional medicine to populations that use mod-ernm medicine.
* how to integrate appropriate traditional interventions into health systemfinance and service delivery.
WHO Ad Hoc Health R&D Report, Draft 2.0
5.5 Chapter summary and recommendations
Noncommunicable diseases and injuries are rapidly becoming the leading sources of disease burdenin developing countries as their populations age. Despite the trends, the ongoing research devoted tothese conditions is wholly inadequate in most regions and specific support for them from donors tothe developing countries is embryonic at best. Better understanding of the epidemrniology of theseconditions and of the risk factors that influence them is urgently needed, as are cost-effective inter-ventions.
1. Faced with growing numbers of cases of noncommunicable diseases and injuries, developingcountries should increase their relevant strategic research in epidemiology, demography, behav-ioural science and health policy. Particular attention should be given to understanding country-and region-specific levels and determinants of environmental and behavioural risk factors forthese conditions-for example determinants of smoking patterns or understanding prevalencelevels and risk factors for epilepsy. Biomedical science relevant to these conditions is alreadycomparatively well supported in the established market economies and is not therefore a prior-ity. However, some middle- and lower-income countries may need to maintain or develop theirown biomedical research because of the possibility of genuine differences in the characteristicsof environments and populations (e.g. with respect to the currently unexplained high risk inSouth Asians of diabetes and heart disease).
2. The development of drugs to deal with noncommunicable diseases should claim a low priorityon the resources of low- and middle-income countries because of massive investment in the es-tablished market economies. However, the design of preventive algorithms (including behaviourchange programmes) and cost-effective diagnostic methods, treatments and rehabilitation to re-spond to NCDs and injuries should be a priority for support by donors and governments world-wide. Implementation of these recommendations will require both additional funding andstrengthening of the institutions that do the work.
e
e
118
Chapter 6: In pursuit of equitable and efficient healthservices: learning from experience
Chapters 3, 4 and 5 focused on the research challenges of specific diseases or health problems, suchas unsafe childbirth, malaria, cardiovascular disease and injuries. This chapter has a different scope.It concerns the health systems within which services are provided, the people who use those systems,and the interaction between them. The success of this interaction is crucial to the health of a nation.And, at a time when many countries around the world are reforming their health systems, knowledgeabout what policies work best has never been so badly needed.
Research has the potential to meet two major and growing challenges in this area. First, thebeliefs, behaviours and decisions of households are of increasingly great importance in determiningthe ways in which health systems are used. People are taking increased responsibility for their health,both as their knowledge increases, and as governments and others devolve responsibility to them. Forexample, in the established market economies, many pharmaceutical preparations that were once is-sued only on prescription are now made available over the counter. In the middle- and low-incomecountries, self-medication has always been an important feature of health care, but this is only nowbeing acknowledged by the research commnunity. Behavioural science can provide vital knowledgeabout the choices people make. Secondly, health systems around the world are being reformed, fre-quently with decentralization, user charges, managed competition and splits between the roles of pur-chaser and provider. Yet to date, information on the performance of different systems is in shortsupply, both within countries and between countries.
This chapter, then, is about the interaction between real people and their real health systems.It is about the policy-oriented research that aims to close the gaps between what can technically beachieved and what is actually achieved. These gaps can have profound impact on human health, bothat the level of specific diseases or conditions and at the broader level of access to the system as awhole. And efforts to close these gaps can have an enormous payoff in controlling the high and rap-idly rising expenditures that households and countries commit to health.
For example, no matter how good a treatment for malaria may be, it is useless if most of thepeople in a region see no value in it and would sooner treat themselves or seek alternative therapies.In the case of TB, cure rates can be as high as 90% in ideal conditions but will fall below 40% wherepeople see no reason to continue taking their tablets after their symptoms stop, or find it too expen-sive to attend a clinic, or where health workers have no motivation to supervise therapy. The differ-ence between the efficacy of the intervention under controlled conditions and its effectiveness in realsituations can be reduced by learning what the problems are and remedying them. But the gap be-tween an inefficient, poor-quality service and an efficient, high-quality service has implications for amuch broader range of health consequences than simply improving the control of any specific dis-ease. An ineffective system will have consequences on the health of whole groups of people: for ex-ample, no matter how technically proficient the services in clinics may be, they are useless to thevery poor-whose need is often greatest-ifthis strata cannot afford to use them.
Countries pay dearly for failing to understand their people's perceived health needs and be-liefs, and for failing to organize health services that provide high-quality care efficiently and equita-bly. The costs-both to the health of their population and to their public purse-are extraordinarily
119
WHO Ad Hoc Health R&D Report, Draft 2.0
high. It has been estimated, for example, that a saving of just 10% in the efficiency with which exist-ing tools are used by health systems in the low- and middle-income countries could result in anoverall reduction of 10% in the total burden of disease in their populations, and a reduction of up to50% in the poorest countries. And an inefficient system may consume as much as 5% more of acountry's GNP than an efficient one. Evidence on health expenditures (Table 6.1) and health out-comes across the OECD countries vividly illustrates this point (Schieber, Poullier and Greenwald[sp?] 1994).
[Table 6.1 about here]
In the case of the United States, waste is estimated to account for between 25% and 30% ofthe current bill of $800 billion spent on health care each year. This is waste that no country, howeverwealthy, can afford. If only 1% of the waste were eliminated as a result of behavioural and healthsystems research, it would represent savings of $2 billion per year. R&D built up from the global di-versity of experiences about the interactions between health systems and their users has already re-sulted in major changes in certain settings and the policy implications have been discussed. In theUK, for example, where some $50 billion is spent every year on patient care, it has been estimatedthat a 1% gain in cost-effectiveness through improved decision making on the basis of the results ofhealth services research would recoup $50 million in a single year (R. Lilford, et al., Health ServicesManagement Research, vol. 7 [November 1994] p. 214-19). Yet perhaps surprisingly, it attracts onlyminimal interest and funding-even in a period in which many countries are reforming their healthsystems and need accurate information more than ever. This chapter discusses the opportunities anddirections for investment in research that will systematically assemble data and evidence that willallow health systems to learn from the policy successes and mistakes not only of their own past, butfrom the experience of others.
6.1 The framework for analysis
6.1.1 Making sense of a complex picture
Studies of the ways in which people seek and receive health services can be divided, for con-venience, into studies of the "demand" side-the needs and behaviours of the households and popu-lation-and the "supply" side-the providers of services and the organizational, legal and politicalframrnework within which they work. Clearly, however, it is the interaction between the two sides thatis of most importance.
In studying this system, it is helpful to think in terms of a progression from the narrowest fo-cus of health research-biomedical research at the level of cells and systems-up through clinicalresearch at the level of the individual, to behavioural research at level of the individual and thehousehold, and on to epidemiological research at the population level. Above this is health systemsresearch-at the level of whole institutions. This latter can further be subdivided between the microlevel (health services research) and the macro level--the broadest focus, on health policies. This isset out below (Figure 6.1 and Table 6.2).
e
120
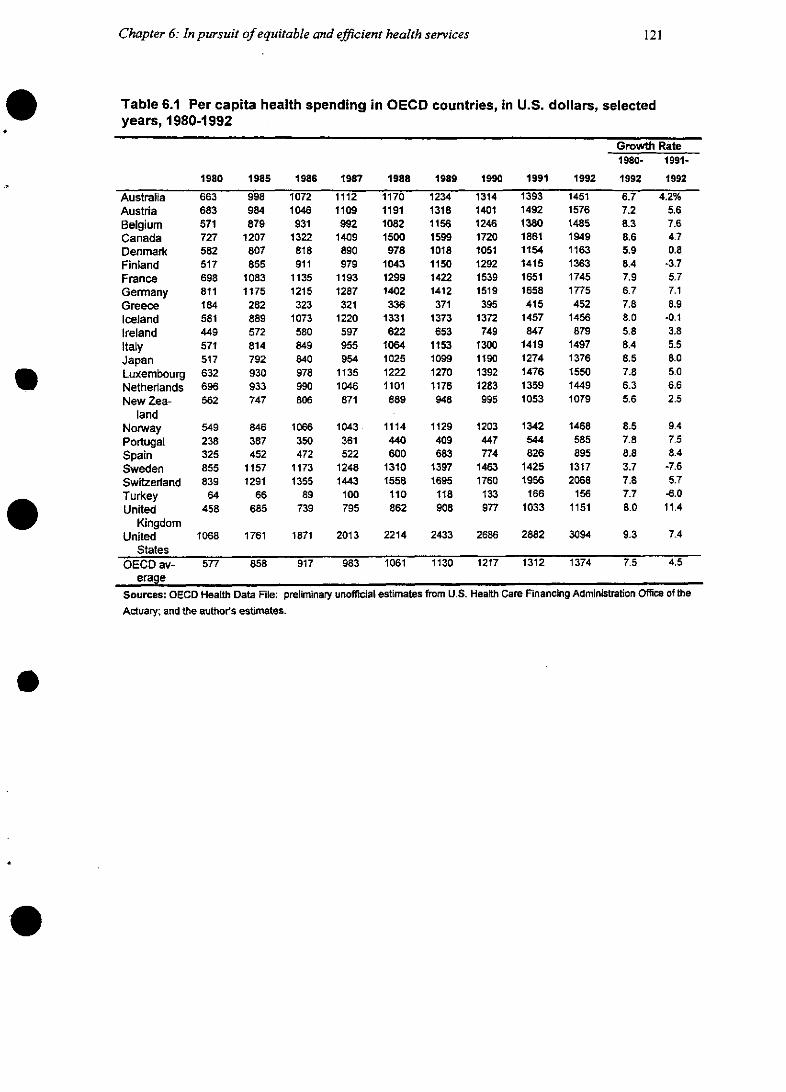
Chapter 6: In pursuit of equitable and efficient health services
Table 6.1 Per capita health spending in OECD countries, in U.S. dollars, selectedyears, 1980-1992
Growth Rate1980- 1991-
1980 1985 1986 1987 1988 1989 1990 1991 1992 1992 1992
Australia 663 998 1072 1112 1170 1234 1314 1393 1451 6.7 4.2%Austria 683 984 1046 1109 1191 1318 1401 1492 1576 7.2 5.6Belgium 571 879 931 992 1082 1156 1246 1380 1485 8.3 7.6Canada 727 1207 1322 1409 1500 1599 1720 1861 1949 8.6 4.7Denmark 582 807 818 890 978 1018 1051 1154 1163 5.9 0.8Finland 517 855 911 979 1043 1150 1292 1415 1363 8.4 -3.7France 698 1083 1135 1193 1299 1422 1539 1651 1745 7.9 5.7Germany 811 1175 1215 1287 1402 1412 1519 1658 1775 6.7 7.1Greece 184 282 323 321 336 371 395 415 452 7.8 8.9Iceland 581 889 1073 1220 1331 1373 1372 1457 1456 8.0 -0.1Ireland 449 572 580 597 622 653 749 847 879 5.8 3.8Italy 571 814 849 955 1064 1153 1300 1419 1497 8.4 5.5Japan 517 792 840 954 1025 1099 1190 1274 1376 8.5 8.0Luxembourg 632 930 978 1135 1222 1270 1392 1476 1550 7.8 5.0Netherlands 696 933 990 1046 1101 1176 1283 1359 1449 6.3 6.6New Zea- 562 747 806 871 889 948 995 1053 1079 5.6 2.5
landNorway 549 846 1066 1043 1114 1129 1203 1342 1468 8.5 9.4Portugal 238 387 350 361 440 409 447 544 585 7.8 7.5Spain 325 452 472 522 600 683 774 826 895 8.8 8.4Sweden 855 1157 1173 1248 1310 1397 1463 1425 1317 3.7 -7.6Switzerland 839 1291 1355 1443 1558 1695 1760 1956 2068 7.8 5.7Turkey 64 66 89 100 110 118 133 166 156 7.7 -6.0United 458 685 739 795 862 908 977 1033 1151 8.0 11.4elo ~ ~ KingdomUnited 1068 1761 1871 2013 2214 2433 2686 2882 3094 9.3 7.4
StatesOECD av- 577 858 917 983 1061 1130 1217 1312 1374 7.5 4.5
erageSources: OECD Health Data File: preliminary unofficial estimates from U.S. Health Care Financing Administration Office of theActuary; and the author's estimates.
121
WHO Ad Hoc Health R&D Report, Draft 2.0
[Figure 6.1 about here]
[Table 6.2 about here] O
Within this framework, the type of R&D conducted depends on the area of focus: Figure 6.2sets out a simplified typology.
[Figure 6.2 about here]
On the demand side, researchers in the behavioural sciences study individual and householdbeliefs and knowledge-t-4he determinants of risky or care-seeking behaviours-for example, what arethe relative effects on tobacco use of raising taxes, legislating limitation of use or simply educatingpeople about the risks? At the interface, health services research assesses the effects of differentmethods of service delivery, for example, whether a minor surgical operation is best delivered as anoutpatient procedure or an inpatient procedure, or whether certain medical procedures actually domore harm than good; and behavioural science studies the way health providers make choices aboutthe type of services they provide. Further "up" the scale on the supply side, health systems research-ers study the effects of general financing schemes on service provision or, for example, cross nationalcomparisons of performance as a function of different financial and organizational arrangements. Onthe largest scale, researchers analyze the political, economic and legal influences on a nation's healthpolicies and structures. Their findings can assist policy makers in deciding how resources could bebetter allocated within the health sector, the best methods of obtaining the political and administra-tive commitment to resource reallocation, and the best mechanisms by which legislation can createan appropriate system for the delivery of services. These may include factors outside the traditionalhealth sector whose influence on health may be profound, such as the availability or nonavailabilityof old-age pensions, sickness and injury benefits and maternity benefits. Clearly, interactions at alllevels make the reality more complex than this framework suggests.
6.1.2 Measures for research
As the previous three chapters showed, it is possible to measure the impact of people's be-haviour and of better or worse health services and health policies on the control and prevention of aspecific disease. The example of TB in Chapter 3 showed that much of the currently unaverted bur-den of the disease could be reduced if existing tools were better used-greater "technical effi-ciency"-and if resources were better spent---greater "allocative efficiency". However, research intothe needs of people and the functioning of health systems cannot restrict itself to measuring the bur-den of specific diseases. A badly functioning system will have an impact on numerous health condi-tions. Long waiting lists will delay treatments for many different problems. A broken-down truckwill affect the delivery of supplies for a whole range of needs, with consequent effects across aspectsof health as diverse as child immunization, maternal health and rehabilitation for disabled or injuredpersons. Lack of education and information about health within households may deny their membersaccess to a broad range of services. Indeed, many of the factors that influence the interaction betweenhealth systems and their users are outside the traditional control of the health sector-women's edu-cation, for instance, has a major impact on health in households, and outside factors such as housing,energy supply and others can have wide ranging effects (see Box 6.1 on electrification and health inSouth Africa). Because of these broader effects, researchers need other yardsticks beyond the meas-urement of disease burden to assess needs and the performance of health systems.
e
122

Chapter 6: In pursuit of equitable and efficient health services
Figure 6.1 Typology of health research by levels of analysis
Health systems research (institutional level Health services research (micro level)Health policy research (macro level)
Table 6.2 Elements of the health system
Demand sideHouseholds and populations
InteractiqonAgencies in sectors outside health
Institutional purchasers
The State
People acting individually or as households who canproduce health benefits by individual or collective ac-tion and behaviour, as seekers of health care and aspurchasers of care. People forming groups (e.g. usergroups, village committees, trade unions) can influ-ence the form, cost, quality and content of healthservices. Behavioural choices influence risk exposureand prevention of disease.
Produce benefits indirectly as a result of the goods orservices they provide (e.g. agriculture, education,housing, employment, communications, water supply).Organizations such as insurance funds, district healthauthorities or health maintenance organizations whichdefine health needs for defined populations and pur-chase clinical and support services from providersusing a variety of contractual mechanisms.
Aggregates resources and interests from the popula-tion and channels them to the providers. Many institu-tional providers are state agencies. Govemrnment insti-tutions are responsible for the financing, regulation,purchasing and provision of health care
Supply sideResource institutions
Service providers
Produce the human and material resources for healthcare-concemed with basic and in-service training ofhealth personnel and health-related R&D. These willinclude universities, medical schools, schools of publichealth, R&D departments of private companies, foun-dations, etc.)In the public, private, NGO or traditional sectors. Manyindividuals give informal unpaid care at home. Otherswork in some kind of institutional setting such as ahospital, health centre or primary health facility. Serv-ices include clinical and support services.
Source: Frenk 1994 (adapted).
123
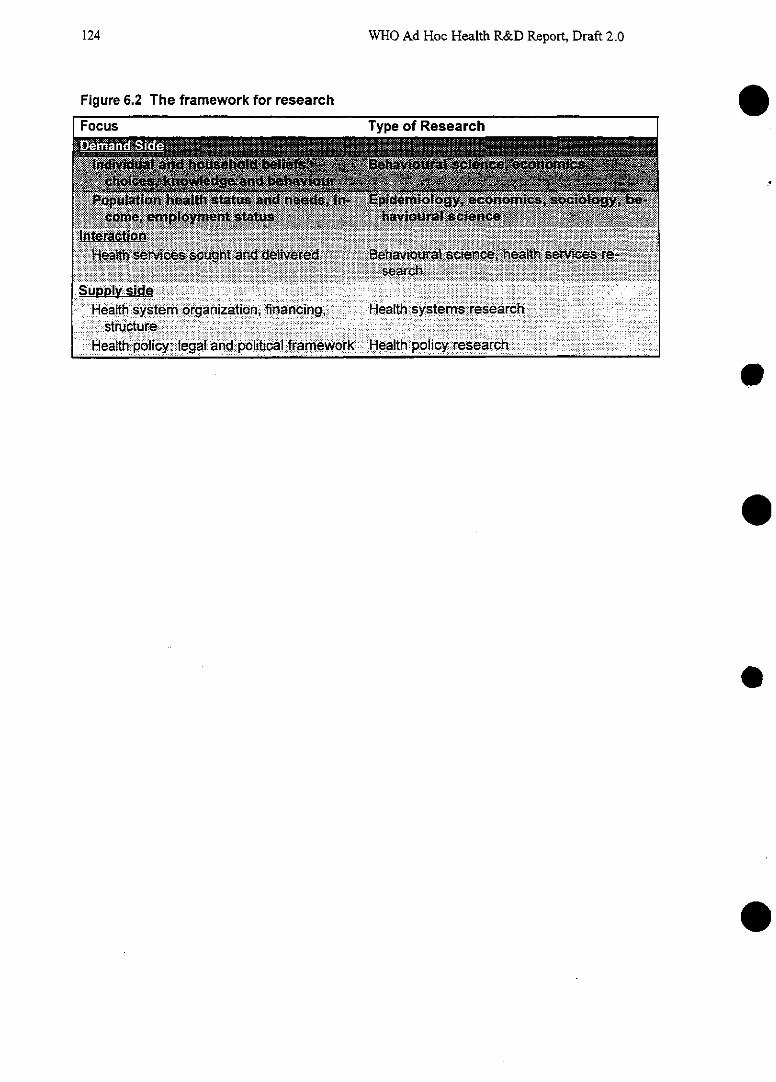
WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 6.2 The framework for research
1 Focus TvDe of Researche
e
e
0
09
124
Chapter 6: In pursuit of equitable and efficient health services
Some of those yardsticks will be qualitative, based on behavioural research to identify peo-ple's beliefs and choices about health. Some will be quantitative: the efficiency of a health systemcan be measured in terms of the share of the country's GNP that it consumes, and sometimes usinganalysis of the cost-effectiveness of different interventions; the equity of the system can be measured,at least in part, by the degree of access and coverage it provides for a population relative to its healthneeds. Some yardsticks will be both qualitative and quantitative. The quality of care provided by asystem may often be measured in terms of its efficiency and equity, but also in terms of the satisfac-tion of those who use it.
6.2 Reaping the benefits of research
The findings of such research have already made significant impacts on the prevention and control ofa number of specific diseases and conditions. For example, behavioural scientists found that in mostsettings, more than half of people with malaria-like symptoms chose not to attend the official healthservices as a first line of treatment, but instead prefer to treat themselves. These findings have ledhealth providers in these communities to rethink their strategies so that, rather than simply improvethe delivery of malaria treatment services, they have tried to educate communities to make appropri-ate choices about when and how to seek treatment for the disease. In the case of TB treatment, it waseconomic research that first showed that, contrary to health workers' opinion, short-course chemo-therapy was more cost-effective than the traditional longer course of cheaper medicines becausepeople found it easier to comply with the shorter course, and were more likely to be cured at the endof it. Beyond specific diseases, these types of research are also beginning to influence decision mak-ers. Health policy research into the effects of introducing charges for services in a number of Africancountries has produced important early insights into some of the factors that can affect the success orfailure of such reforms (McPake 1994). Further studies of the effects of different types of health in-surance scheme are also beginning to throw light on the best ways to finance health services.
It should be emphasized that health policy research is a relatively new field, which beganaround the turn of the century and entered a phase of rapid expansion in the 1970s. Its methods aremade more complex by the complexity of the subject. Many studies are subject to confounding vari-ables and other methodological uncertainties: for example, how does a country that wants to assessthe impact of one component of its recently introduced reforms (such as decentralization) distinguishthat component from all the others? Despite such uncertainties, these early studies represent the firstserious attempts to introduce rational behaviour into the hitherto often chaotic environment withinwhich health services have been organized and delivered. In the current context of health-system re-form, there is preliminary evidence that service outputs and performance initially deteriorate whenfinancial and organizational reforms are introduced. Further evidence based on research will be cru-cial in determining the shape of future reforms; the current reforms may be seized as an opportunityfor that research.
There are many examples of such research and no single review can hope to assess them all.But to illustrate the field and the types of impact such studies can have, some examples have beenprovided in the three following tables. The first, Table 6.3, concentrates on the behavioural sciencesshowing results of studies into the behaviours of both providers and their clients; the second, 6.4, fo-cuses on examples from the field of health services research; the third, 6.5, sets out examples fromthe fields of health systems and health policy research.
125
WHO Ad Hoc Health R&D Report, Draft 2.0
[Table 6.3 about here]
[Table 6.4 about here]
[Table 6.5 about here]
[Box 6.1 about here]
6.2.1 Comparisons between countries: pitfalls and benefits
Research into what makes for effective health services is an international public good. Itsscope is far too great for any single country to manage every aspect of it. There are important bene-fits that one country can gain from another's experience-particularly in planning and implementinghealth reforms. However, there is an important caveat with the study of health systems and healthpolicies. Although there are often broad trends, what is true for one system and environment may notbe true for another (Cassels 1994). For example, the impact of user fees on attendance rates in healthsettings has been mixed, and there is a risk that overly simplistic international comparisons-oftenbased on studies with widely disparate designs-will produce a diluted picture of chaotic variationrather than produce lessons that all countries can build on. Thus, individual nations have much to elearn from focusing on their own studies. However, where broad trends and patterns can safely beextracted, these are likely to be of exceptional value to international health research. They have thepotential to guide policy makers, and also to maximize the efficiency of research by reducing repeti-tion and overlap.
6.2.2 Translating results into action
The growing appreciation of the potential payoffs from research into the performance ofhealth systems is matched by an understanding that this research in these areas is useless unless itamounts to something that health providers and managers can use. Research becomes valuable whenits outcomes are practical products such as essential drugs lists (see Box 6.3), insurance benefit lists,fee schedules, architectural designs and translations of academic findings into formats accessible topolicy makers (Frenk 1992).
[Box 6.3 about here]
6.3 Assessing needs for strategic research
The earlier sections of this chapter have shown the potential for a high payoff from investment inresearch in the behavioural sciences and in health services, systems and policy research. This rein-forces the conclusions of Chapters 3, 4 and 5 which revealed that, for many specific diseases andconditions, attempts to reduce disease burden by closing the gaps between efficacy and effectivenesswould depend heavily on research into health services and systems. However, there is also an urgentneed to set priorities in the broader areas of household behaviour, health policy and health systemsthat cannot be measured purely in terms of specific diseases.
e
126
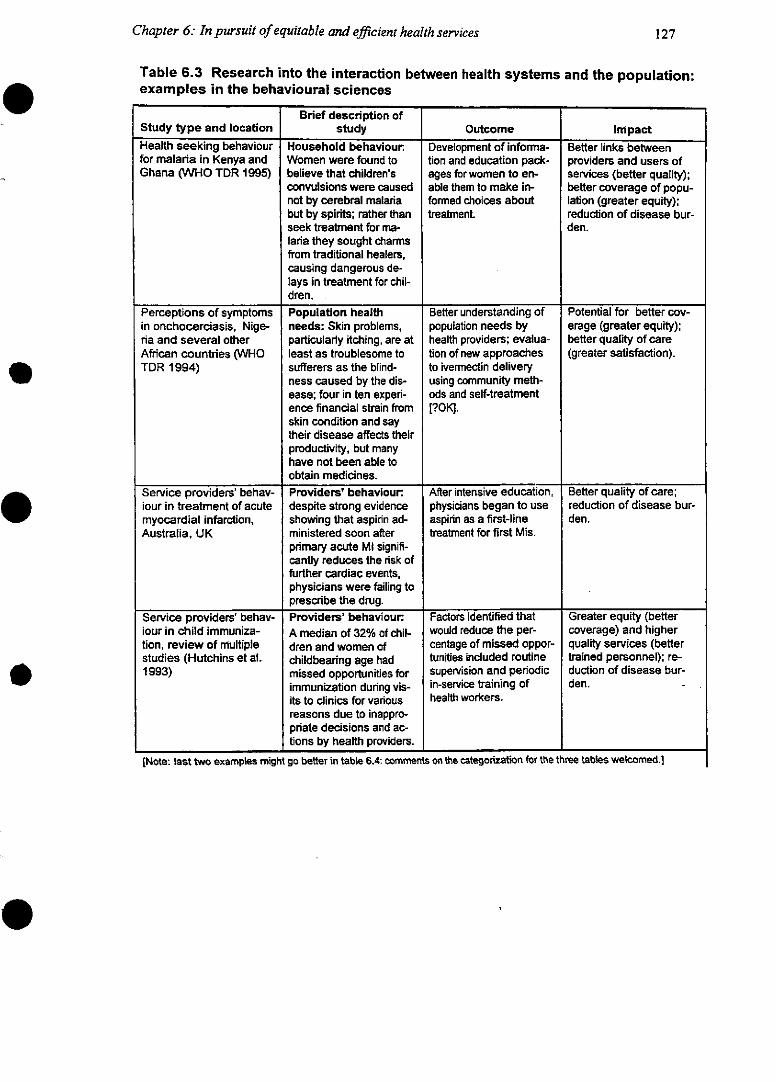
Chapter 6: In pursuit of equitable and efficient health services
Table 6.3 Research into the interaction between health systems and the population:examples in the behavioural sciences
Brief description ofStudy type and location study Outcome Impact
Health seeking behaviour Household behaviour Development of informa- Better links betweenfor malaria in Kenya and Women were found to tion and education pack- providers and users ofGhana (WHO TDR 1995) believe that children's ages for women to en- services (better quality);
convulsions were caused able them to make in- better coverage of popu-not by cerebral malaria formed choices about lation (greater equity);but by spirits; rather than treatment. reduction of disease bur-seek treatment for ma- den.laria they sought charmsfrom traditional healers,causing dangerous de-lays in treatment for chil-dren.
Perceptions of symptoms Population health Better understanding of Potential for better cov-in onchocerciasis, Nige- needs: Skin problems, population needs by erage (greater equity);ria and several other particularly itching, are at health providers; evalua- better quality of careAfrican countries (WHO least as troublesome to tion of new approaches (greater satisfaction).TDR 1994) sufferers as the blind- to ivermectin delivery
ness caused by the dis- using community meth-ease; four in ten experi- ods and self-treatmentence financial strain from [?OK].skin condition and saytheir disease affects theirproductivity, but manyhave not been able toobtain medicines.
Service providers' behav- Providers' behaviour. After intensive education, Better quality of care;iour in treatment of acute despite strong evidence physicians began to use reduction of disease bur-myocardial infarction, showing that aspirin ad- aspirin as a first-line den.Australia, UK ministered soon after treatment for first Mis.
primary acute Ml signifi-cantly reduces the risk offurther cardiac events,physicians were failing toprescribe the drug.
Service providers' behav- Providers' behaviour. Factors identified that Greater equity (betteriour in child immuniza- A median of 32% of chil- would reduce the per- coverage) and highertion, review of multiple dren and women of centage of missed oppor- quality services (betterstudies (Hutchins et al. childbearing age had tunities included routine trained personnel); re-1993) missed opportunities for supervision and periodic duction of disease bur-
immunization during vis- in-service training of den.its to clinics for various health workers.reasons due to inappro-priate decisions and ac-tions by health providers.
[Note: last two examples might go better in table 6.4: comments on the categorization for the three tables welcomed.]
127
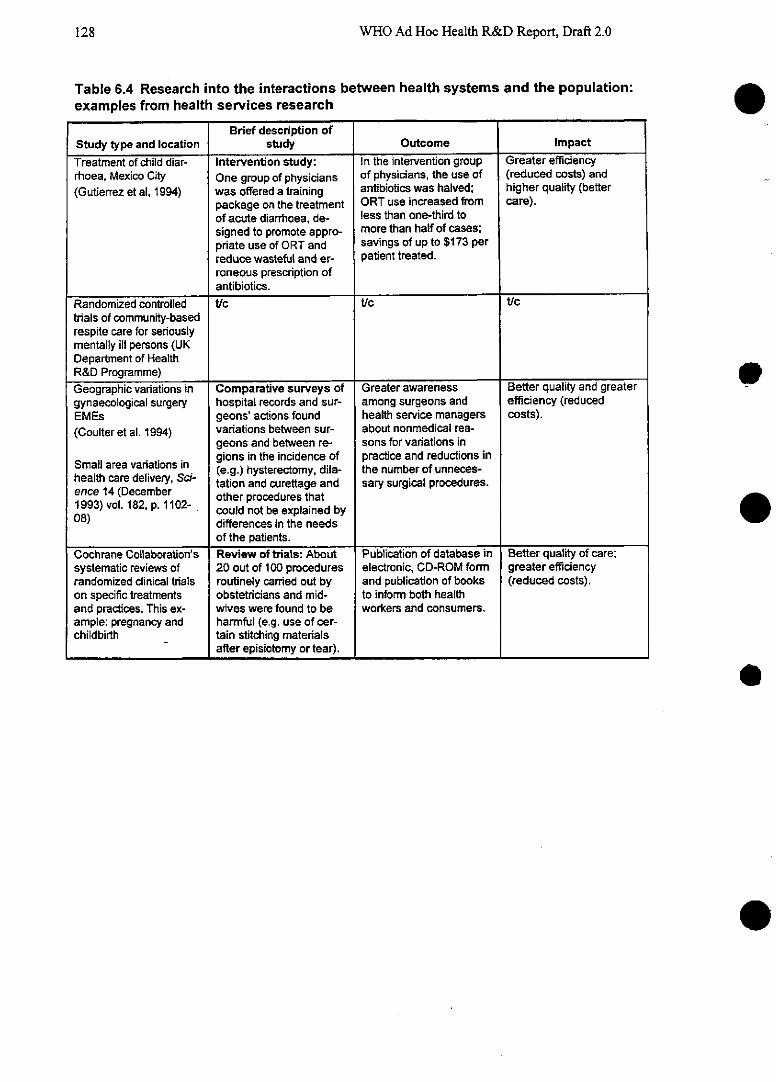
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 6.4 Research into the interactions between health systems and the population:examples from health services research
Brief description ofStudy type and location study Outcome ImpactTreatment of child diar- Intervention study: In the intervention group Greater efficiencyrhoea, Mexico City One group of physicians of physicians, the use of (reduced costs) and(Gutierrez et al, 1994) was offered a training antibiotics was halved; higher quality (better
package on the treatment ORT use increased from care).of acute diarrhoea, de- less than one-third tosigned to promote appro- more than half of cases;priate use of ORT and savings of up to $173 perreduce wasteful and er- patient treated.roneous prescription ofantibiotics.
Randomized controlled t/c tic t/ctrials of community-basedrespite care for seriouslymentally ill persons (UKDepartment of HealthR&D Programme)Geographic variations in Comparative surveys of Greater awareness Better quality and greatergynaecological surgery hospital records and sur- among surgeons and efficiency (reducedEMEs geons' actions found health service managers costs).(Coulter et al. 1994) variations between sur- about nonmedical rea-
geons and between re- sons for variations inm a .. gions in the incidence of practice and reductions in
Small area vanadeiy S (e.g.) hysterectomy, dila- the number of unneces-health care delvr S- tation and curettage and sary surgical procedures.19)oence 14 (Dec -er other procedures that1993) vol. 182, . 1102- .could not be explained by08) differences in the needs
of the patients.Cochrane Collaboration's Review of trials: About Publication of database in Better quality of care;systematic reviews of 20 out of 100 procedures electronic, CD-ROM form greater efficiencyrandomized clinical trials routinely carried out by and publication of books (reduced costs).on specific treatments obstetricians and mid- to inform both healthand practices. This ex- wives were found to be workers and consumers.ample: pregnancy and harmful (e.g. use of cer-childbirth tain stitching materials
after episiotomy or tear).
e
e
e
.
128
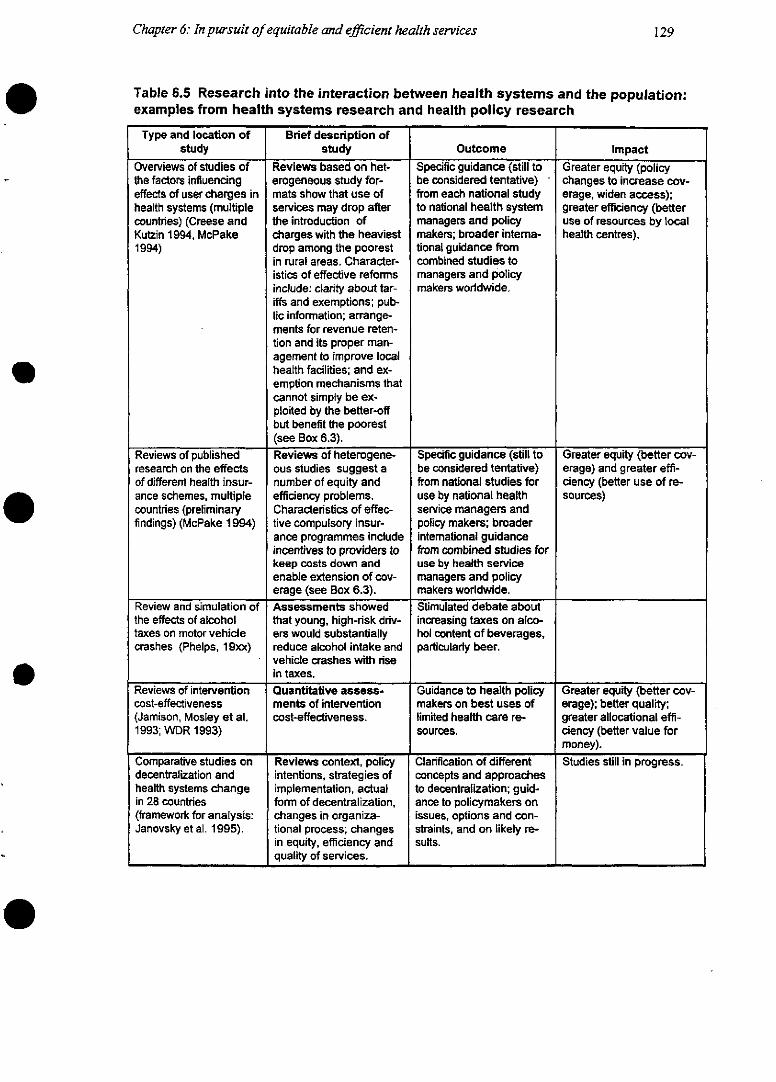
Chapter 6: In pursuit of equitable and efficient health services
Table 6.5 Research into the interaction between health systems and the population:examples from health systems research and health policy research
Type and location of Brief description ofstudy study Outcome Impact
Overviews of studies of Reviews based on het- Specific guidance (still to Greater equity (policythe factors influencing erogeneous study for- be considered tentative) changes to increase cov-effects of user charges in mats show that use of from each national study erage, widen access);health systems (multiple services may drop after to national health system greater efficiency (bettercountries) (Creese and the introduction of managers and policy use of resources by localKutzin 1994, McPake charges with the heaviest makers; broader intemrna- health centres).1994) drop among the poorest tional guidance from
in rural areas. Character- combined studies toistics of effective reforms managers and policyinclude: clarity about tar- makers worldwide.iffs and exemptions; pub-lic information; arrange-ments for revenue reten-tion and its proper man-agement to improve localhealth facilities; and ex-emption mechanisms thatcannot simply be ex-ploited by the better-offbut benefit the poorest(see Box 6.3).
Reviews of published Reviews of heterogene- Specific guidance (still to Greater equity (better cov-research on the effects ous studies suggest a be considered tentative) erage) and greater effi-of different health insur- number of equity and from national studies for ciency (better use of re-ance schemes, multiple efficiency problems. use by national health sources)countries (preliminary Characteristics of effec- service managers andfindings) (McPake 1994) tive compulsory insur- policy makers; broader
ance programmes include international guidanceincentives to providers to from combined studies forkeep costs down and use by health serviceenable extension of cov- managers and policyerage (see Box 6.3). makers worldwide.
Review and simulation of Assessments showed Stimulated debate aboutthe effects of alcohol that young, high-risk driv- increasing taxes on alco-taxes on motor vehicle ers would substantially hol content of beverages,crashes (Phelps, 19xx) reduce alcohol intake and particularly beer.
vehicle crashes with risein taxes.
Reviews of intervention Quantitative assess- Guidance to health policy Greater equity (better cov-cost-effectiveness ments of intervention makers on best uses of erage); better quality;(Jamison, Mosley et al. cost-effectiveness. limited health care re- greater allocational effi-1993; WDR 1993) sources. ciency (better value for
money).Comparative studies on Reviews context, policy Clarification of different Studies still in progress.decentralization and intentions, strategies of concepts and approacheshealth systems change implementation, actual to decentralization; guid-in 28 countries form of decentralization, ance to policymakers on(framework for analysis: changes in organiza- issues, options and con-Janovsky et al. 1995). tional process; changes straints, and on likely re-
in equity, efficiency and sults.quality of services.
129
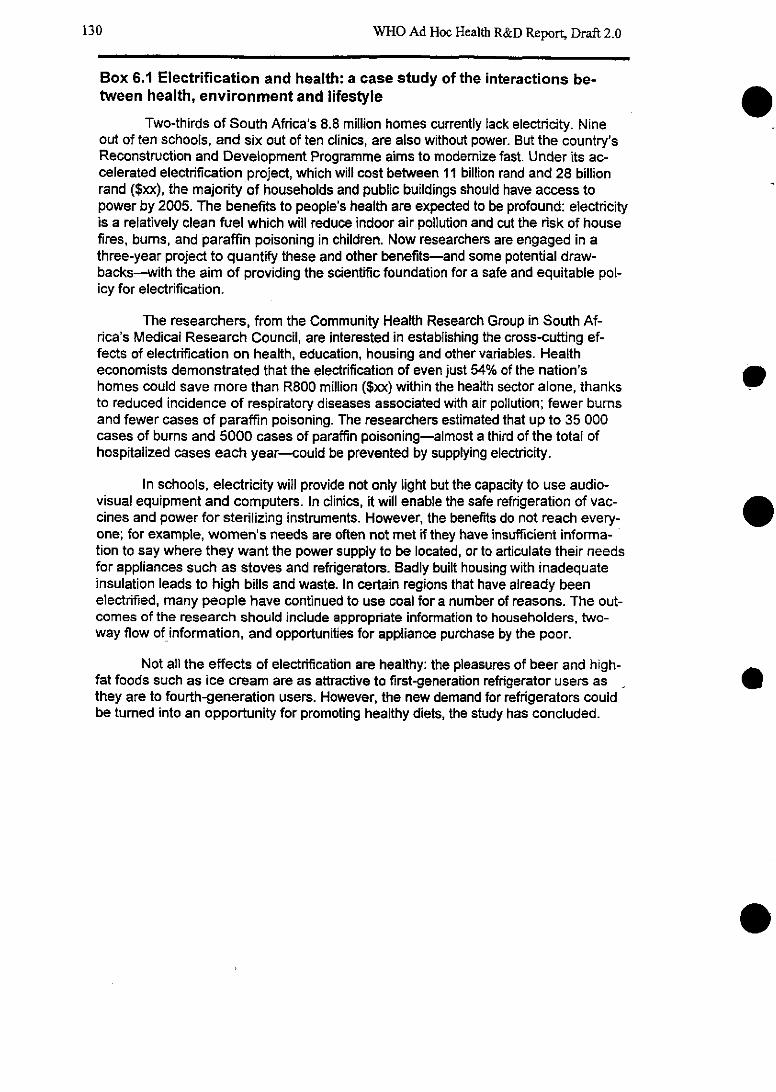
WHO Ad Hoc Health R&D Report, Draft 2.0
Box 6.1 Electrification and health: a case study of the interactions be-tween health, environment and lifestyle
Two-thirds of South Africa's 8.8 million homes currently lack electricity. Nineout of ten schools, and six out of ten clinics, are also without power. But the country'sReconstruction and Development Programme aims to modemize fast. Under its ac-celerated electrification project, which will cost between 11 billion rand and 28 billionrand ($xx), the majority of households and public buildings should have access topower by 2005. The benefits to people's health are expected to be profound: electricityis a relatively clean fuel which will reduce indoor air pollution and cut the risk of housefires, bums, and paraffin poisoning in children. Now researchers are engaged in athree-year project to quantify these and other benefits-and some potential draw-backs-with the aim of providing the scientific foundation for a safe and equitable pol-icy for electrification.
The researchers, from the Community Health Research Group in South Af-rica's Medical Research Council, are interested in establishing the cross-cutting ef-fects of electrification on health, education, housing and other variables. Healtheconomists demonstrated that the electrification of even just 54% of the nation'shomes could save more than R800 million ($xx) within the health sector alone, thanksto reduced incidence of respiratory diseases associated with air pollution; fewer bumsand fewer cases of paraffin poisoning. The researchers estimated that up to 35 000cases of bums and 5000 cases of paraffin poisoning-almost a third of the total ofhospitalized cases each year-could be prevented by supplying electricity.
In schools, electricity will provide not only light but the capacity to use audio-visual equipment and computers. In clinics, it will enable the safe refrigeration of vac-cines and power for sterilizing instruments. However, the benefits do not reach every-one; for example, womrnen's needs are often not met if they have insufficient informa-tion to say where they want the power supply to be located, or to articulate their needsfor appliances such as stoves and refrigerators. Badly built housing with inadequateinsulation leads to high bilis and waste. In certain regions that have already beenelectrified, many people have continued to use coal for a number of reasons. The out-comes of the research should include appropriate information to householders, two-way flow of information, and opportunities for appliance purchase by the poor.
Not all the effects of electrification are healthy: the pleasures of beer and high-fat foods such as ice cream are as attractive to first-generation refrigerator users as lthey are to fourth-generation users. However, the new demand for refrigerators couldbe tumed into an opportunity for promoting healthy diets, the study has concluded.
130
Chapter 6: In pursuit of equitable and efficient health services 131
(Box 6.1 continued)
The MRC study concluded that electrification's benefits for health were broad,that it was pivotal to intersectoral development and that it should be supported by na-tional and international agencies as part of an integrated energy policy. The study rec-ommended that sensitivity be required to understand the implications of electrificationfor the very poor, the marginalized and the underserved. It recommended that stan-dardized and sustainable pollution monitoring protocols, electricity consumption dataand energy-related morbidity data should be included as part of the national healthinformation system to help to quantify the health benefits of electrification. National,regional and local goals should be set for reducing particulate air pollution levels andincentives should be created for the building of energy-efficient homes. Information onthe health benefits of electrification should be disseminated at national and interna-
tional le.V.S t Comparisons between countries: pitfalls and benefits
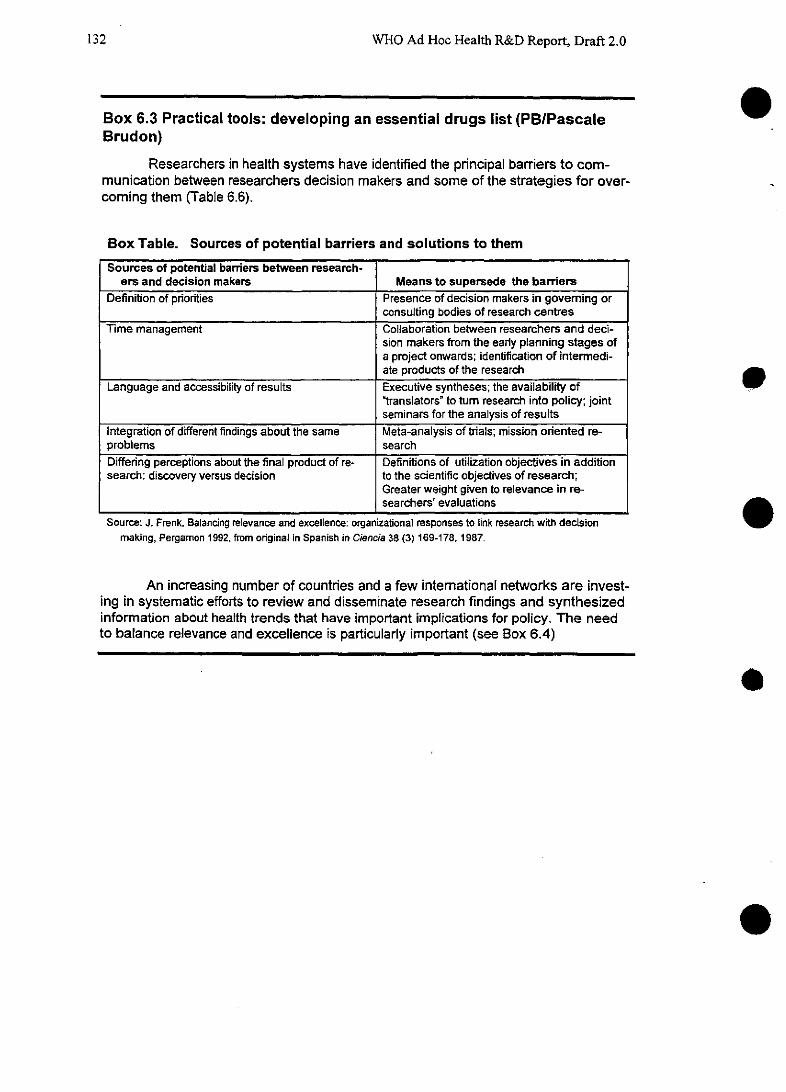
WHO Ad Hoc Health R&D Report, Draft 2.0
Box 6.3 Practical tools: developing an essential drugs list (PBIPascaleBrudon)
Researchers in health systems have identified the principal barriers to com-munication between researchers decision makers and somrne of the strategies for over-coming them (Table 6.6).
Box Table. Sources of potential barriers and solutions to themSources of potential barriers between research-
ers and decision makers Means to supersede the barriersDefinition of priorities Presence of decision makers in govemrning or
consulting bodies of research centresTime management Collaboration between researchers and deci-
sion makers from the early planning stages ofa project onwards; identification of intermedi-ate products of the research
Language and accessibility of results Executive syntheses; the availability of'translators' to turn research into policy; jointseminars for the analysis of results
Integration of different findings about the same Meta-analysis of triais; mission oriented re-problems searchDiffering perceptions about the final product of re- Definitions of utilization objectives in additionsearch: discovery versus decision to the scientific objectives of research;
Greater weight given to relevance in re-searchers' evaluations
Source: J. Frenk. Balancing relevance and excellence: organizational responses to link research with decisionmaking, Pergamon 1992, from original in Spanish in Ciencia 38 (3)169-178, 1987.
An increasing number of countries and a few international networks are invest-ing in systematic efforts to review and disseminate research findings and synthesizedinformation about health trends that have important implications for policy. The needto balance relevance and excellence is particularly important (see Box 6.4)
.
e
e
o
e
132
Chapter 6: In pursuit of equitable and efficient health services
To assist this process, the Committee assessed needs and opportunities for R&D in thesefields, as in previous chapters, relying more on qualitative assessments than on the quantitative as-sessments used in earlier chapters. Two separate studies were conducted: one focused on populations,households and individuals, the other on health systems and policies.
6.3.1 Populations, households and individuals
The process used to develop priorities for research on populations, households and individuals in-volved three complementary elements. First, opinions concerning the need for research were solicitedfrom selected health policy makers, systems managers and researchers through the medium of aquestionnaire. Respondents were asked to score research areas in terms of need, giving highest prior-ity to those they believed would lead to the greatest improvements in health status, efficiency, equityor consumer satisfaction. Second, background papers were commissioned from authors who wereasked to consider both needs and opportunities for research. Opportunities were said to exist wherethere is an identified need, the questions are amenable to research, an no (or little) previous researchhas addressed the problem. The background papers and the results of the questionnaires were fed intoa series of consultations with small groups of researchers and decision makers designed to considerthe meaning of the earlier work and to incorporate the results into a final set of research priorities. Afuller description of the methodology is to be found in Annex 8, David Evans.
There was a high degree of consensus that the overall purpose of research relating to popula-tions, households and individuals should be to design and test interventions that, directly or indi-rectly, improve health status. However, it is often not possible to assess the need for interventions, ortheir impact, because the current ways of collecting data on mortality, morbidity and disability-vitalregistration systems, census and population surveys-are time consuming and costly. This is illus-trated by the fact that accurate data on mortality by age, sex and major causes are still not availablefor large parts of the world, and data on disease and disability even harder to find.
6.3.1.1 Prioritiesfor research relating topopulations
For the reasons outlined above, the most important global research priority in the area ofpopulations identified for this Report involves the development of rapid, low-cost methods for meas-uring and monitoring population health status. The full agenda for population research is shown inTable 6.6.
[Table 6.6 about here]
Beyond the need for measuring methods, three more of the priorities identified also concernthe development of methodologies: topics 2, 4 and 5. For Topic 2, it was agreed, indicators thatcombine the impact of mortality, morbidity and disability into a single measure of health status arecritical for setting priorities for intervention and for measuring the effects of interventions, some ofwhich save lives while others improve the quality of life. The DALY indicator is one useful indicatorin this direction, but further work is needed to test its transportability-and that of other indicators-to different cultural settings. Another need is to reduce the complexity of the measure and the cost ofusing it at country level. Somrne research of this type has already begun, with the World Bank and theIDRC sponsoring studies to adapt use of the DALY to different settings (see Chapter 3, Box 3.1 onTEHIP).
133
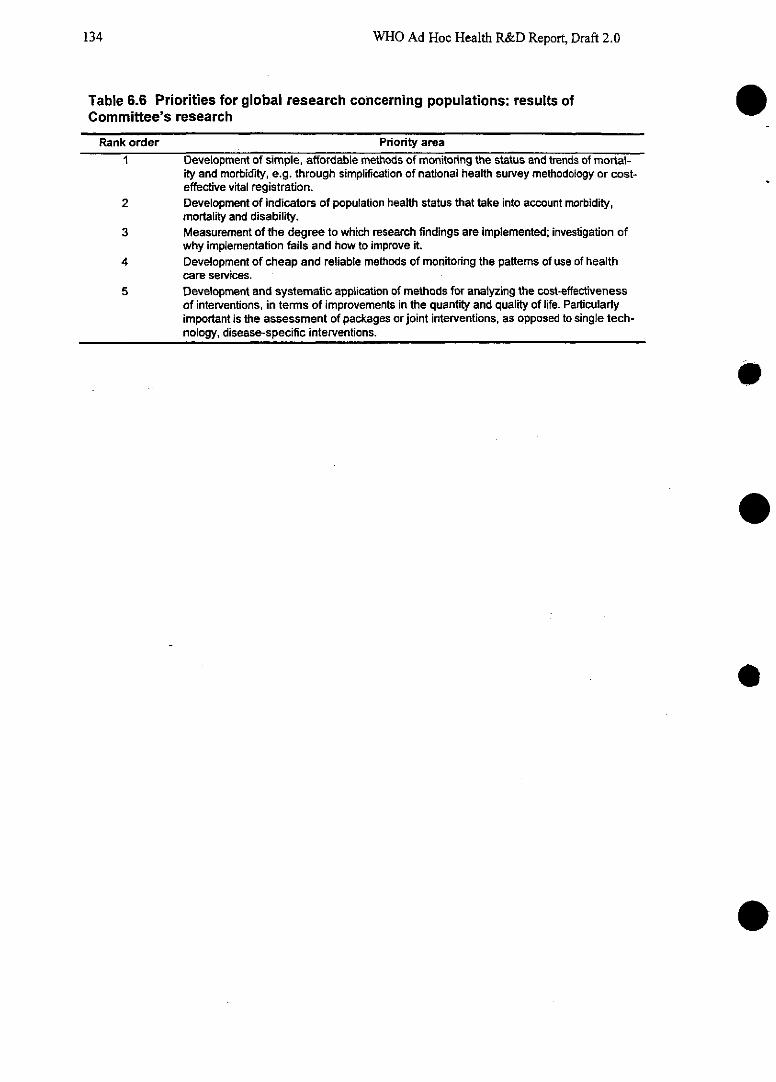
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 6.6 Priorities for global research concerning populations: results ofCommittee's research
Rank order
0Priority area
1 Development of simple, affordable methods of monitoring the status and trends of mortal-ity and morbidity, e.g. through simplification of national health survey methodology or cost-effective vital registration.
2 Development of indicators of population health status that take into account morbidity,mortality and disability.
3 Measurement of the degree to which research findings are implemented; investigation ofwhy implementation fails and how to improve it.
4 Development of cheap and reliable methods of monitoring the pattems of use of healthcare services.
5 Development and systematic application of methods for analyzing the cost-effectivenessof interventions, in terms of improvements in the quantity and quality of life. Particularlyimportant is the assessment of packages or joint interventions, as opposed to single tech-nology, disease-specific interventions.
e
e
o
134
Chapter 6: In pursuit of equitable and efficient health services 135
Box 6.4 on strategies for dissemination developed by National Institute ofPublic Health, Mexico, with examples of "executive syntheses" of find-ings
-PB with material from Julio Frenk).
WHO Ad Hoc Health R&D Report, Draft 2.0
Topic 4 identified the need for research to develop rapid, low-cost ways of monitoring thepattems of health service use. This is important to many forms of behavioural research, while furtheranalysis of the methodologies used in analyses of cost-effectiveness would help to shed light onstudies of the impact of combined interventions on multiple diseases. Such combined interventionsmight include packages, such as a package for healthy school children involving micronutrients andtreatments for helminths and other parasitic infections-all of which together could improve healthand cognition. They might also include combinations of approaches to treat single diseases, such as acombination of treated bednets and drugs to treat malaria. Until now, cost-effectiveness analyseshave been used largely to compare single interventions aimed at single diseases.
The choice of Topic 3-on ways to implement research and turn it into action-reflects thefrustrations of both policy makers and researchers that the results of studies in the population sci-ences are often not made available to policy makers, and often not translated into action, as discussedabove.
The priorities identified in Table 6.6 are all important in enabling countries to improve theirhealth status. Some of them can be undertaken at national level, but for others-particularly the de-velopment of methodologies-there are significant economies of scale and clear logical reasons forinternational collaboration. Sharing between countries can ensure that critical research is undertakenin a variety of settings and that the results of work done in one country are made available to others.
6.3.1.2 Households and individuals
The importance of research into understanding the determinants and consequences of house-hold and individual behaviours affecting health cannot be underestimated. In almost every country inthe world, the household is the place where key health decisions are made. In the high-income coun-tries, people are changing their relationship with the formal health sector and taking increasing re- esponsibility for their own health. This is illustrated by the fact that more and more medicines are nowmade available over the counter, while many people also choose to use alternative therapies. Peoplein middle- and low-income countries, meanwhile, have traditionally financed a higher proportion oftheir own health-care costs than people in the North (WDR 1993) and they are being asked to takeeven more responsibility in many countries as governments seek to shift the burden of financinghealth services more toward the private sector. As a result, the beliefs, choices and behaviours of in-dividuals and households will become even more important in determining their health.
Much of the existing research to date has been linked to particular diseases, conditions andrisk factors, as earlier examples have shown. Often it is relevant and specific to a particular contextwithin a particular country, confirming the need for national-level approaches. However, there aresome broader "generic" questions that cut across diseases and which are often best asked in morethan one context and more than one country.
The generic topics in household and individual behaviours that were identified by the exer-cises are shown in Table 6.7.
[Table 6.7 about here]
e
136
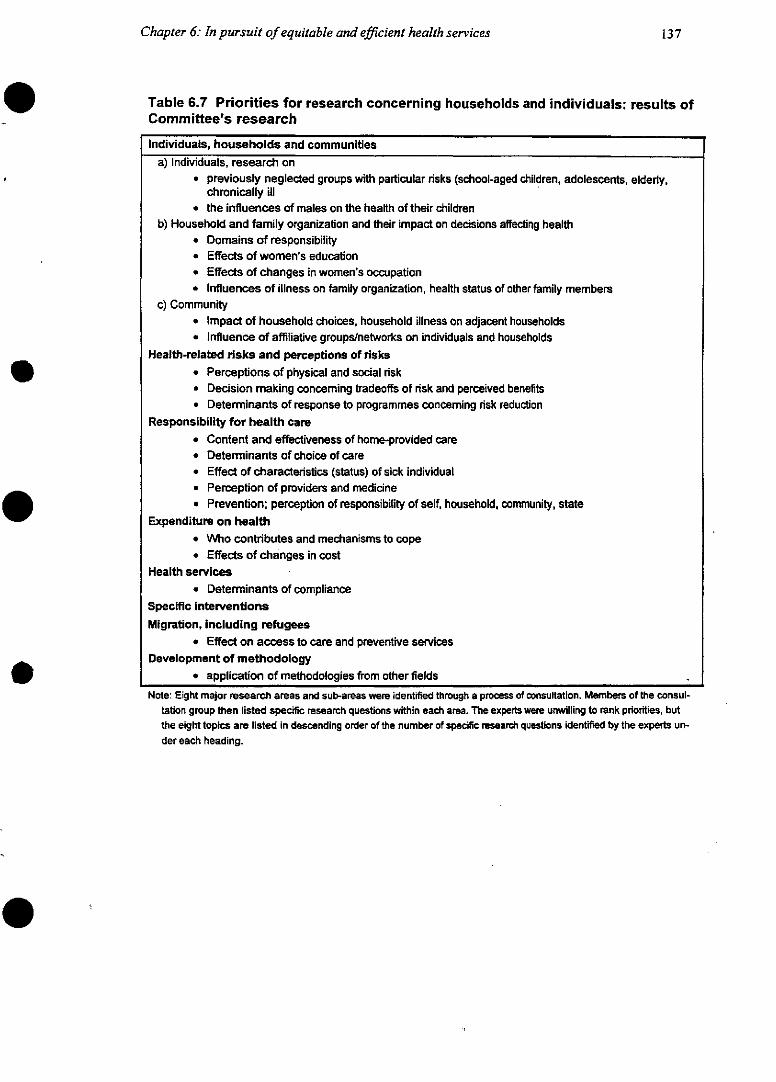
Chapter 6: In pursuit of equitable and efficient health services
Table 6.7 Priorities for research concerning households and individuals: results ofCommittee's research
Individuals, households and communitiesa) Individuals, research on
* previously neglected groups with particular risks (school-aged children, adolescents, elderty,chronically ill
* the influences of males on the health of their childrenb) Household and family organization and their impact on decisions affecting health
* Domains of responsibility* Effects of women's education* Effects of changes in women's occupation* Influences of illness on family organization, health status of other family members
c) Community* Impact of household choices, household illness on adjacent households* Influence of affiliative groups/networks on individuals and households
Health-related risks and perceptions of risks* Perceptions of physical and social risk* Decision making conceming tradeoffs of risk and perceived benefits* Determinants of response to programmes conceming risk reduction
Responsibility for health care* Content and effectiveness of home-provided care* Determinants of choice of care* Effect of characteristics (status) of sick individual* Perception of providers and medicine* Prevention; perception of responsibility of self, household, community, state
Expenditure on health* Who contributes and mechanisms to cope* Effects of changes in cost
Health services* Determinants of compliance
Specific interventionsMigration, including refugees
* Effect on access to care and preventive servicesDevelopment of methodology
* application of methodologies from other fieldsNote: Eight major research areas and sub-areas were identified through a process of consultation. Members of the consul-
tation group then listed specific research questions within each area. The experts were unwilling to rank priorities, butthe eight topics are listed in descending order of the number of specific resarch questions identifed by the experts un-der each heading.
137
WHO Ad Hoc Health R&D Report, Draft 2.0
Despite the difficulties of reaching consensus in an area whose scope is so broad and whosemethodologies so diverse, two related themes emerged strongly. The first is the need to widen thefocus of research from narrow consideration of the determinants of specific health-related behaviours eor the risk factors that contribute to a specific disease, to a broader examination of the social contextin which risky or disease-preventive behaviours occur. For example, research has now clarified thatsomrne of the breeding sites for mosquitoes that transmit dengue fever are in domains of householdspace that women control (washing basins and pet feeding dishes) while others are in spaces con-trolled by men (spare tyres and bottles saved for various purposes). The implication is that interven-tions aimed at vector control for dengue will not be effective unless they develop ways to engageboth womrnen and men in their activities. Similarly, household behavioural research has shown thatparents' decisions about where to allow their children to go to sleep in the evenings influence thechildren's risk of malaria.
The second major theme that emerged was the need for explicit consideration of the changing natureof the social context and how it influences health and the efficiency of the system that provideshealth services. For example, it is now clear that people's perceptions of the meaning of the word"community"-that is, who actually belongs to their community and who they will cooperate with-will change when those people migrate, move to a city, and so on. This means that the traditionalmodels of "community participation" that health workers have relied upon in stable, rural areas needto be reconsidered and reevaluated in urban areas or in areas of rapid population movements. Re- esearch aimed at improving the technical or allocative efficiency of health interventions cannot beproperly designed without a better understanding of these social influences on people's decisions.
Three further issues emerged as priorities for research on households and individuals. First,there is an urgent need for greater communication among researchers, both within and across geo-graphic areas and disciplines. Researchers from one discipline are often unaware of studies carriedout in another discipline on topics that are of common interest to both. Secondly, a proportion of theresearch that has been undertaken in this area is of poor quality: in particular, there has been a degreeof repetition, such as asking questions that have already been answered, and there has been a degreeof poor design-such as using research methods that cannot answer the questions the study set out toask. The participants in these exercises identified the need to develop mechanisms to ensure goodstandards when research funds are allocated, such as peer review of study proposals to ensure thathigh technical quality is maintained. The third further priority identified by the exercises was a list oftopics for research that cut across the categories by which health research has traditionally been di-vided. For example, the behaviour of health workers-their advice, preventive care and treatments-in both public and private sectors is of key importance in determining the health behaviours ofhouseholds and has an impact on the economic efficiency of the whole system. Yet there has beenlittle research into these cross-cutting issues, especially in the low- and middle-income countries.
Three further issues emerged as priorities for research on households and individuals. First,there is an urgent need for greater communication among researchers, both within and across geo-graphic areas and disciplines. Researchers from one discipline are often unaware of studies carriedout in another discipline on topics that are of common interest to both. Secondly, a proportion of theresearch that has been undertaken in this area is of poor quality: in particular, there has been a degreeof repetition, such as asking questions that have already been answered, and there has been a degreeof poor design-such as using research methods that cannot answer the questions the study set out toask. The participants in these exercises identified the need to develop mechanisms to ensure goodstandards when research funds are allocated, such as peer review of study proposals to ensure thathigh technical quality is maintained. The third further priority identified by the exercises was a list oftopics for research that cut across the categories by which health research has traditionally been di-
138
Chapter 6: In pursuit of equitable and efficient health services
vided. For example, the behaviour of health workers-their advice, preventive care and treatments-in both public and private sectors is of key importance in determining the health behaviours ofhouseholds and has an impact on the economic efficiency of the whole system. Yet there has beenlittle research into these cross-cutting issues, especially in the low- and middle-income countries.
The other topics for research identified by the exercise (Table 6.8) fall outside the bounds ofhealth research as it is usually defined. They could, however, have even more influence on the healthstatus of populations, households and individuals than more narrowly defined health research. Butbecause they fall outside the traditional areas, it is difficult to attract funding for them. Like healthagencies and programmes, funding agencies are often organized in a "vertical" fashion, with the sec-tion that covers health having no connections with those that cover other sectors such as education.Investors in health research may have much to gain from strengthening their collaborations withother investors.
[Table 6.8 about here]
6.3.2 Health systems and policies
A questionnaire, structured in line with the major components of the health system, was developedand tested with members of the WHO Forum for Health Sector Reform. The responses of this groupformed the basis for commissioning a series of expert reviews (background papers) on major topicsof interest. A revised questionnaire was then sent to health policy makers, systems managers, bilat-eral and international agencies and researchers worldwide to obtain a range of view on priorities forhealth system development in general, and for health policy and systems research in particular.
The topics identified as priorities for research are necessarily very broad (Table 6.9).
[Table 6.9 about here]
Topics considered of critical importance by members of the WHO Forum for Health SectorReform that did not appear under the top 10 priorities of the subsequent review included human re-sources development, employment structures and civil service reform; provider payment mecha-nisms; content, mix and packaging of services; and the influence of other sectors on health outcomes.
A number of topics were considered important for health system development, but not assubjects for research. These included drug management, planning and budgeting, financial manage-ment and personnel management. However, six of the top ten priorities for research were also listedamong the top ten priorities for health-system development.
Research topic 1, settingprioritiesfor the allocation ofpublic resources, is concerned withthe criteria governing the allocation of public funds between different geographical regions, differentlevels and types of care. Questions about criteria for setting priorities, principles of eligibility forservices, the minimum package to which all should have access, and cost-effectiveness are includedunder this heading.
139
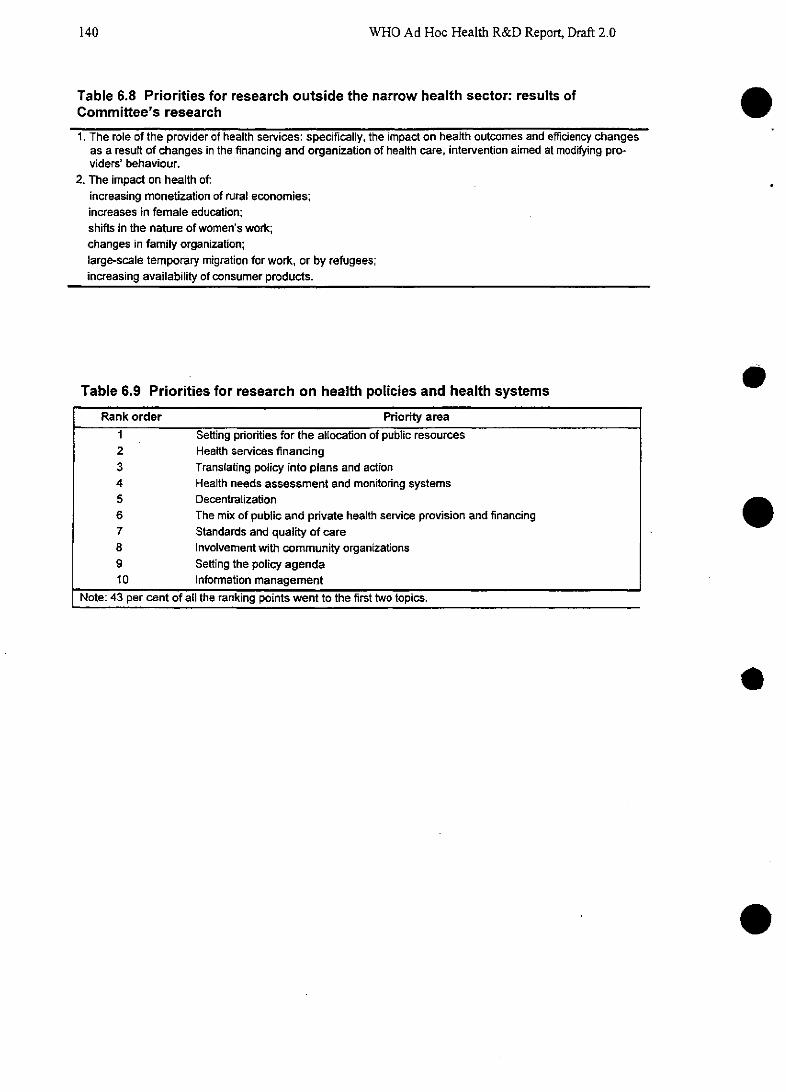
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 6.8 Priorities for research outside the narrow health sector: results ofCommittee's research
1. The role of the provider of health services: specifically, the impact on health outcomes and efficiency changesas a result of changes in the financing and organization of health care, intervention aimed at modifying pro-viders' behaviour.
2. The impact on health of:increasing monetization of rural economies;increases in female education;shifts in the nature of women's work;changes in family organization;large-scale temporary migration for work, or by refugees;increasing availability of consumer products.
Table 6.9 Priorities for research on health policies and health systems
Rank order Priority area1 Setting priorities for the allocation of public resources2 Health services financing3 Translating policy into plans and action4 Health needs assessment and monitoring systems5 Decentralization6 The mix of public and private health service provision and financing7 Standards and quality of care8 Involvement with community organizations9 Setting the policy agenda10 Information management
Note: 43 per cent of all the ranking points went to the first two topics.
e
e
140
Chapter 6: In pursuit of equitable and efficient health services
Research topic 2, health servicesfinancing, focuses on levels and sources of health expendi-ture, covering the entire range of financing options, including national and local taxes, user fees andhealth insurance. It also explores progressive/regressive trends in health-care financing. An expertreview (McPake 1994) analyzed existing studies and, where possible, drew broad conclusions (seeTables 6.3 and Box 6.1). In the area of user charges, these included the need to provide clear infor-mation, exemption mechanisms and local rewards for health centres to avoid a steep and prolongeddecline in use of health services by the poorest. In the area of health insurance, the reviews concludedthat compulsory insurance schemes are likely to be cost-effective only if there are strong incentivesto providers to keep costs down.
Research topics 3 and 9, translatingpolicy into plans and action, and setting the policyagenda, are concerned with the policy process, raising questions about the adoption of policy issues,the identification and appraisal of options, different ways of turning policies into plans, legislationand action, and means of controlling, monitoring and supporting the implementation of policy. Ex-pert review revealed the need to move away from the traditional linear concept of policy formulation,which assumes a unitary rational actor and pays more attention to policy analysis than to policy im-plementation, to a model where multiple streams of problems, solutions and politics affect policychange (Walt 1995, Foltz 1995, Porter 1995).
Research topics 4 and 10, health needs assessment and monitoring systems and informationmanagement, addressed questions about epidemiological systems for analyzing data, surveillancesystems, and systems for monitoring key indicators of performance.
Research topic 5, decentralization-defined as the transfer of functions, resources andauthority to peripheral levels of government-identified five key areas for future research (Collins1995). These were the theoretical and conceptual background to understanding decentralization; theconditions for effectiveness; the study of decentralization to hospitals and health centres; the internalorganization of hospitals; and the operation of public-sector markets. It was argued that internationalcomparative research on decentralization is well worth undertaking, but stressed that care should betaken to avoid its potential limitations and problems. There was strong emphasis on the need forcomplementarity between national and international research. Further detail on the remaining topicsis outlined in greater detail in a background paper accompanying this Report.
Research topic 6, on the mix ofpublic and privare health services provision andfinancing,covered a wide spectrum of concerns on the balance between public and private providers, on regu-lations and contracts governing relationships between public and private agencies, and on the effectsof different forms of public and private financing.
Research topic 7, on standards and quality of care, sought to better understand definitions ofstandards and quality, review mechanisms and processes for monitoring standards; and analyze ex-periences with quality assurance and medical audit.
Research topic 8 is about community organizations, considering public involvement in theplanning, management and monitoring of services, and the means through which civil organizationsare able to influence the form, content, cost or quality of care.
There was strong emphasis on the need for complementarity between national and interna-tional research. Further detail on research priority topics is outlined in a background document onhealth policy and systems research.
141
WHO Ad Hoc Health R&D Report, Draft 2.0
In all these domains, the Committee felt that one important key to progress lies in the sys-tematic generation and utilization of data that are (at least partially) internationally comparable. Forwithout information on how levels and trends in key indicators in their own countries compare withother countries, national reformers will lack benehmarks forjudging performance. Likewise, analystsof health policies will lack the empirical basis forjudgeing which policies work-and which do not.A clear "best buy" for research in this domain will be institutionalization of continued efforts to gen-erate and analyze internationally comparable data sets.
6.4 Assessing ongoing research activity
The foregoing sections of this chapter have discussed the high potential payoffs from research intothe interactions between health systems and the population-from the understanding of individualand household behaviour through to the economic and legal policies that determine national healthstatus. Because of its broader nature, much of the payoff from these areas of research is likely to bediffuse, at least at first, and its benefits less sharply visible than the effects of, say, biomedical re-search into the efficacy of a vaccine or a drug. Yet, as the early part of the chapter argued, there ismuch to be gained-both in financial and health terms-from investing in these areas of health re-search. To date, however, only the most minor resources have been devoted to them. While certainmiddle- and low-income nations (Mexico, South Africa, the Philippines, for example) are conductinghigh-quality research in relevant areas, their contributions alone are unable to match the scale of theneed. Even within the EMEs, support is extremely patchy. The UK government has recently imposeda levy for R&D on the budgets of major service providers. The Canadian government's Medical Re-search Council has recently completed a strategic planning exercise, as a result of which it is nowcommitted to increasing the proportion of funding for health systems research to about half of its to-tal grants. However, these are rare steps. As for the major donors, the current level of investment isminimal. An analysis conducted for this Report could identify at most $50 million invested by the emajor donors in broad behavioural research, health systems research and health policy sciences (seeTable 6.10).
[Table 6.10 about here]
In preceding chapters, this Report identified a number of mismatches between need and thelevel of ongoing research effort in specific health conditions. It would appear, however, that thegreatest deficit of all between need and activity is here in the fields of behavioural, health systemsand health policy research. Beyond the measurement of investment in this area of research, it is clearthat, so far, there has been too little activity to generate results. Most apparent is the lack of either -strong national data or internationally comparable data on the outcomes of health system reform; theabsence of simple and low-cost methods for obtaining population data on mortality, morbidity anddisability; inadequate attention to household behaviours in an era when households are taking in-creasing responsibility for their health; the absence of national health accounts; a shortage of compa-rable data on the cost and effectiveness of different interventions for particular health needs in differ-ent settings (as, for example, with the malaria interventions described in Chapter 4); and a shortage ofdata on needs, opportunities and resource flows in health research.
e
142
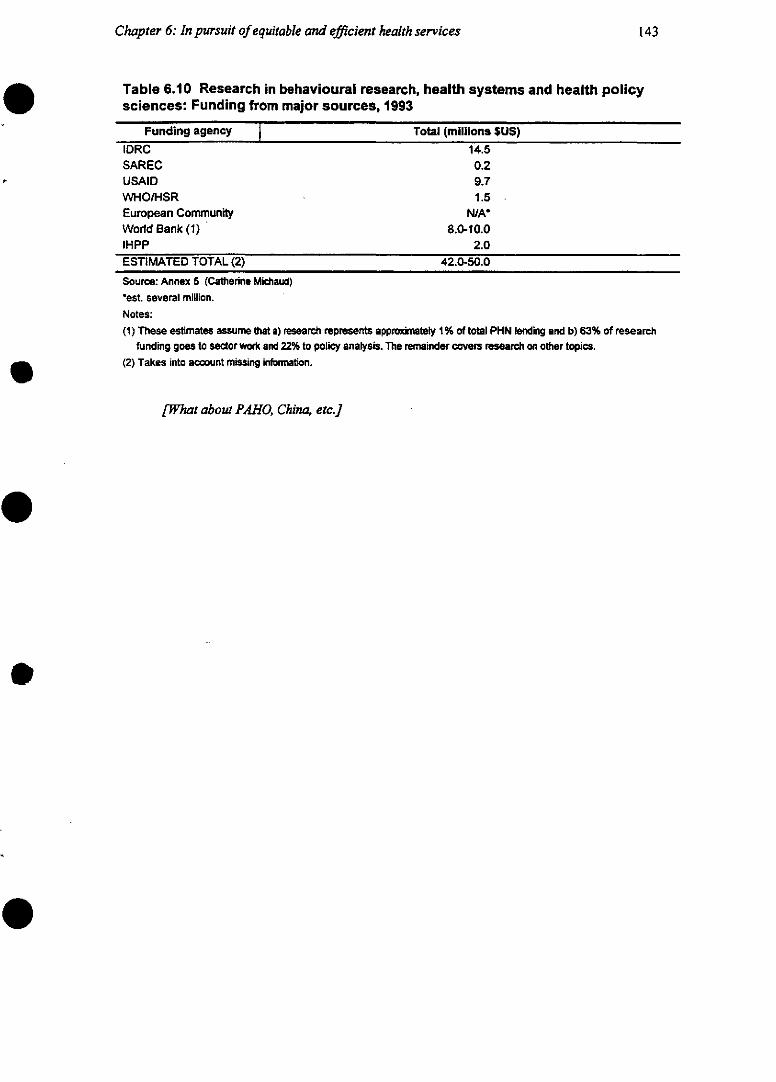
Chapter 6: In pursuit of equitable and efficient health services
Table 6.10 Research in behavioural research, health systems and health policysciences: Funding from major sources, 1993
Funding agency Total (millions SUS)
IDRC 14.5SAREC 0.2USAID 9.7WHO/HSR 1.5European Community N/AWorld Bank (1) 8.0-10.0IHPP 2.0ESTIMATED TOTAL (2) 42.0-50.0
Source: Annex 5 (Catherine Michaud)*est. several million.Notes:(1) These estimates assume that a) research represents appromately 1% of total PHN lending and b) 63% of research
funding goes to sector work and 22% to policy analysis. The remainder covers research on other topicas.(2) Takes into account missing information.
[What about PAHO, China, etc.]
143
WHO Ad Hoc Health R&D Report, Draft 2.0
6.5 Chapter summary and recommendations
The health-and prosperity-of nations is strongly influenced by the health behaviours and decisionsmade by households, individuals and populations and their interaction with the health systems thatserve them. Yet this Report has identified a marked shortage of research effort relevant to this crucialaspect of health, even at a time when health reforms are under way worldwide and governments needinformation more acutely than ever before. Expert consultations conducted for the Report indicatethat the priorities for research include the development of simple, affordable measures of healthstatus at national level and for international comparison, of the degree to which research findings areimplemented, and of the cost-effectiveness of different interventions in different settings. Despite thecomplexity and potential pitfalls of making international comparisons between health systems, thismust increasingly be a goal for health researchers who wish to maximize the use of resources, shareexperience and enable countries to learn from each other.
1. There is a striking shortage of research effort into the functioning of health systems and the be-haviours of the populations served by them. Yet, from the available evidence, it is clear that re-search into both the "supply" and the "demand" sides of a country's health system-and the in-teractions between them-can produce significant findings that result in major improvements inthe quality and coverage of services and reduction in excess costs. Although in somrne cases thefindings of research will be specific to a particular location, many governments seek informationon how levels and trends in key indicators in their own countries compare with other countries.This provides a strong argument for systematic development of internationally comparable datasets on health finance, disease burden, system characteristics and intervention cost-effectiveness.A global analytic effort to make use of such data could, in addition, dramatically strengthenhealth policy by enabling countries to learn from each other's experience.
2. Investors should devote resources to turning research results into action, for example throughthe development and evaluation of cost-effective instruments of public policy and practicaltools for health workers. These may include essential drugs lists, model legislation, priorityintervention packages, insurance benefit lists, pricing and taxation policies, practical manualsfor use by health workers, and summaries of research results for use by health workers anddecision makers.
e
144
Chapter 7: Responding to needs: institutions, incentivesand finance for future health R&D
This Report has so far focused on identifying needs and opportunities for R&D within four specificchallenges to global health-the unfinished agenda, emerging and re-emerging diseases, aging andnoncommunicable diseases, and the challenge of improving health systems. The current chapter ex-amines the options for organizing the institutional and financial framework for global health R&D insuch a way that it can meet those challenges.
There can be little doubt that the current institutions and networks for health R&D-particularly R&D relevant to the needs of low- and middle-income countries-are inadequate for thedemands placed upon them. Resource allocation and institutional development for global health re-search has never been planned or coordinated but has instead evolved a set of networks and collabo-rations that have grown up, haphazardly and in piecemeal fashion. This decentralization confers im-portant advantages: flexibility and freedom from domination by a single paradigm are chief amongthem. Yet, as we have discussed in preceding chapters, lack of an overview of the system has led toimportant needs remaining unmet, imnportant opportunities unpursued, and an incentive environmentthat fails to provide for the R&D needs relevant to diseases of the very poor. A number of other re-views (for example, the Commission on Health Research for Development, 1987) have highlightedthese problems, and they are familiar to most researchers, investors and policy makers within thefield. This Report, however, was not intended to be a rehearsal of well-known problems. Instead, theCommittee has chosen to look at realistic and practical solutions to those problems. The flavor ofthese solutions lies in improving the information and incentive environment in which decentralizedR&D resource allocation decisions are taken; little role is foreseen for strongly centralized planning.
Problems at three levels
At the most basic level-the level at which research is actually conducted, in laboratories, inother institutions and within communities--those problems include an imbalance of researchers,funds and capacity in favour of the rich countries and at the expense of the poor. An acute problem isthe continuing haemorrhage of much-needed talent away from the poorer countries-not only to theEstablished Market Economies but also to neighbouring countries in the region, where higher salariesare offered-as, for example, between southern African countries and South Africa. (While no onewould argue that scientists from low-income countries should be denied rights to work where theyhave opportunities-rights long enjoyed by scientists from high-income countries-the globalizationof labour markets for the highly skilled does pose important policy challenges to low-income coun-tries.) The relationships between public and private sectors are not being exploited effectively, andthe public sector has so far largely failed to appreciate how it must change to adapt to new needs.Within most countries, the quality of research is held back by inadequate training, insufficient staffmotivation and a lack of competition; by lack of leadership, by the instability of short-term funding,and by isolation from peers, poor access to the research literature and an inability to respond rapidlyto changing demands.
Beyond the actual conduct of research, at the level of resource allocation, there are furtherproblems. Largely because of a lack of coordination between those who finance health research, there
145
WHO Ad Hoc Health R&D Report, Draft 2.0
are major gaps in certain areas of health need, and overlaps and wasteful duplication within others.The scale of need for specific health problems is not matched by the levels of research resources al-located to them. Meanwhile, there is an extraordinary dearth of information either about resourceflows into different areas of health R&D, or about the outcomes of research investment.
Finally-and perhaps critically-there is a disturbing lack of advocacy for health research atthe highest political levels. There is no collective voice for health research, no forum by which inves-tors in research can share information, analyze needs or identify priorities. Existing internationalhealth organizations, such as the WHO, have a number of other concerns besides research, and canfocus only on their own mandates. Overall, research relevant to the health problems of the poor re-ceives just a fraction of all health research spending, and, as a share of the total, it is falling. The fal-ling levels of investment in health research today are a disturbing signal that the information con-veyed in Chapter 2-on the high returns to investment in health R&D-has failed to reach decision-makers.
This chapter discusses options for arguments for injecting energy, leadership, capacity andquality into research institutions in the low- and middle-income countries. It examines options forenhancing cooperation between the public and private sectors; and it puts forward proposals for thecreation of a Consortium for International Health R&D that would act as an advocate for researchand a forum for periodic review of needs, opportunities and institutional capacity. The Committeebelieves that these steps would begin to create the climate in which the unfinished agenda could betackled, and in which the world could respond to rapid changes in the status of infectious diseasesand the growing importance of noncommunicable diseases and injuries. Perhaps most importantly,these steps would enable countries to build up their national research on health needs and healthpolicies in such a way that the widespread current reforms of the health sector can be turned into anopportunity for sharing knowledge across international boundaries.
The following three sections of the chapter discuss these proposals in somewhat more depth.A more detailed descriptive overview of the framneworks within which research is done is set out inBox 7.1.
[Box 7.1 about here]
e
146
Chapter 7: Responding to needs: institutions, incentives andfinanceforfuture health R&D 147
Box 7.1 The current framework for health research: a descriptive back-ground
The operational levelThe basic cell of research is a laboratory or unit headed by a senior scientist.
Senior scientists gather to work in university departments or research institutes; atypical institute might employ 30 senior scientists. The whole department or institute'sinterests will tend to be multidisciplinary, while each basic cell will focus on one disci-pline or a small set of closely related ones. Crucial to the success of research is theability to respond quickly to change-both at the level of the individual cell and the in-stitute as a whole. The basic cell must respond by acquiring new technologies andskilis; the institute must respond by acquiring new or more developed disciplines.
The basic core funding for such research institutes usually comes from gov-emrnments. In most countries, civil-service personnel policies tend to push researchinstitutions too heavily towards tenure, thereby creating institutions that become un-productive and unable to respond to new challenges. Over time, core budgets tend tobe eaten up by salaries, reducing manoeuvrability still further. In order to overcomethese structural weaknesses in institutions, a third level of institution has recentlyevolved, known as a network centre. These network centres are functionally linkedand share common resources, but are often physically disparate units.
The resource allocation levelThe next level of research organization is that of the agencies and pro-
grammes that sponsor and develop research and research capacity. This resourceallocation level represents a heterogeneous group; its most important members are:
* national research councils;
* foundations and nongovemmental organizations;
* ministries of health;
* dedicated NGOs ( for example, the cancer funds); and
* programmes, national or international, with a mandate dedicated to a particu-lar field. Support for the international programmes comes from multilateral andbilateral funds and private foundations.
These organizations often fund work on the basis of peer review, on a com-petitive, time-limited basis.
WHO Ad Hoc Health R&D Report, Draft 2.0
(Box 7.1 continued)
The forum and advocacy levelThis exists only patchily at present. Dedicated organizations such as the
Council on Health Research for Development (see Box 7.4) support countries in set-ting their own priorities for Essential National Health Research and share informationbetween countries. Specific programmes and foundations act as advocates for theirown areas. But there is currently no coordination or common voice for investors andscientists in health research at international level.
e
e
e
e
148
Chapter 7: Responding to needs: institutions, incentives andfinancefor future health R&D 149
7.1 Building capacity for research in low- and middie-income coun-tries: current status and possible solutions
7.1.1 The problem
It comes as no surprise to the health community that researchers in low- and middle-income countriesface undue difficulties. Salaries are poor; rewards to productivity are hampered by nonnerit consid-erations in the appointment and promotion of senior staff and by restrictive personnel policies; coresupport for the maintenance of libraries, databases, equipment and buildings is inadequate; andcommunications between scientists at the regional and international levels are poor. Few laboratoriesor teams have the facilities, or have achieved a critical mass of capacity, to work at the speed nowrequired for success, nor the wherewithal to update and share skills. Not surprisingly, there is often alack of leadership and many of the best scientists leave for better-paid, more stimulating posts in theEMEs or for positions of administrative imhportance in government or the private sector.
While there is substantial capacity for high-quality research in the EMEs, only a small frac-tion of it is focused on the health problems of the people who bear the overwhelming burden of dis-ease. Also, there are too few incentives for good scientists to focus on the health problems of the low-and middle-income countries. As this Report has already pointed out, it is important to question theimplicit assumption that these health problems are qualitatively different from those of the industrial-ized world, particularly as the distinction is being gradually blurred by demographic and epidemiol-ogical changes. However, in practice, there are important distinctions. In particular, the responsesthat are appropriate to the emerging epidemic of noncommunicable diseases in developing countriesmust necessarily be different: more cost-effective solutions must be developed that can be applied inresource-poor societies. Moreover, solutions to the health problems that affect developing countriesare more likely to be found by high-quality researchers who have regular access to the affectedpopulations. Thus the existence of plenty of high-quality health research in the EMEs seems unlikelyto be enough.
Meanwhile, developing countries are left with a fraction of the human and technical re-sources of the EMEs, while their health problems are many times greater. While this is, of course, tosome extent inevitable the Committee has concluded that it is both feasible and worthwhile to ad-dress this issue directly. Given that scientists operate in an international market, it might be arguedthat the relative share of the total pool of scientists in any particular region was irrelevant to the con-duct of good research worldwide. However true this might be for certain other domains of science,the practice of health research relies heavily on close contact with other areas of the health sector, onthe local epidemiological environment, and on clinical, behavioural and social sciences that arerooted in local and national frameworks. In addition, the development of research capacity dependscritically on good training and teaching, which must be done at least in large part through strongleaders within local structures and by concentrating resources on productive institutions while freeingthe resources committed to nonproductive ones.
Comparative data on human capital and research output for different regions are difficult toobtain and subject to bias and the effects of highly incomplete data. However, estimates from theUNESCO World Science Report 1996 (forthcoming) suggest that R&D scientists of an disciplines,
WHO Ad Hoc Health R&D Report, Draft 2.0
including health, are overwhelmingly concentrated in the OECD countries (about half of the total),and Asia-principally Japan and the newly industrialized economies of Southeast Asia. Africa-including South Africa-has only 6% of the world's scientists, Latin America only 4% and thecountries of the near and Middle East only 3% (see Table 7.1).
[Table 7.1 about here]
Measures of the output of researchers also exist, but these are even more fraught with diffi-culty. Analyses that rely solely on indicators such as the number of published papers or patentsgranted per region are open to criticism for failing to reflect the true nature of scientific research; inparticular, they fail to capture the importance of translating published research into real interventions.They are also subject to a heavy bias towards anglophone researchers because the available databasesof published research are overwhelmingly restricted to English-language publications. However, forall their imperfections, they may provide some indication of the worldwide imbalances in activity inthe absence of other indicators (see Table 7.2).
[Table 7.2 about here]
The need to build capacity is urgent and rarely disputed; the best means for doing so is lessclear. This Report advances a number of proposals that could enable better national-level researchand thus improved international links. These proposals, by emphasizing mechanisms that shift re-sources from nonproductive institutions to productive ones, will inevitably lead to unevenness ingeographical and national distributions of effort. The Committee views this as no cause for concernas long as aggregate capacity for R&D to address problerms of the poor steadily increases.
7.1.2 Proposed solutions
Individual teams, institutions and programmes have demonstrated that it is possible to dofirst-rate research in low-income and middle-income countries. Their advice (see, for examnple,Twenty Years of Progress, TDR 1995) and investigations by the Committee overwhelmingly suggestthat certain factors are key for success. These include:
* capable, committed leadership;
* stable long-term linkage with other institutions, particularly in the North but also with otherSouthern collaborators;
* the ability to attract young, particularly talented researchers and give them freedom to pursuetheir ideas;
* the securing of adequate resources for long-term and dependable support;
* the capacity to train a large number of individuals from whom subsequent leaders canemerge. The number must be large enough to allow for wastage and other losses.
e
150
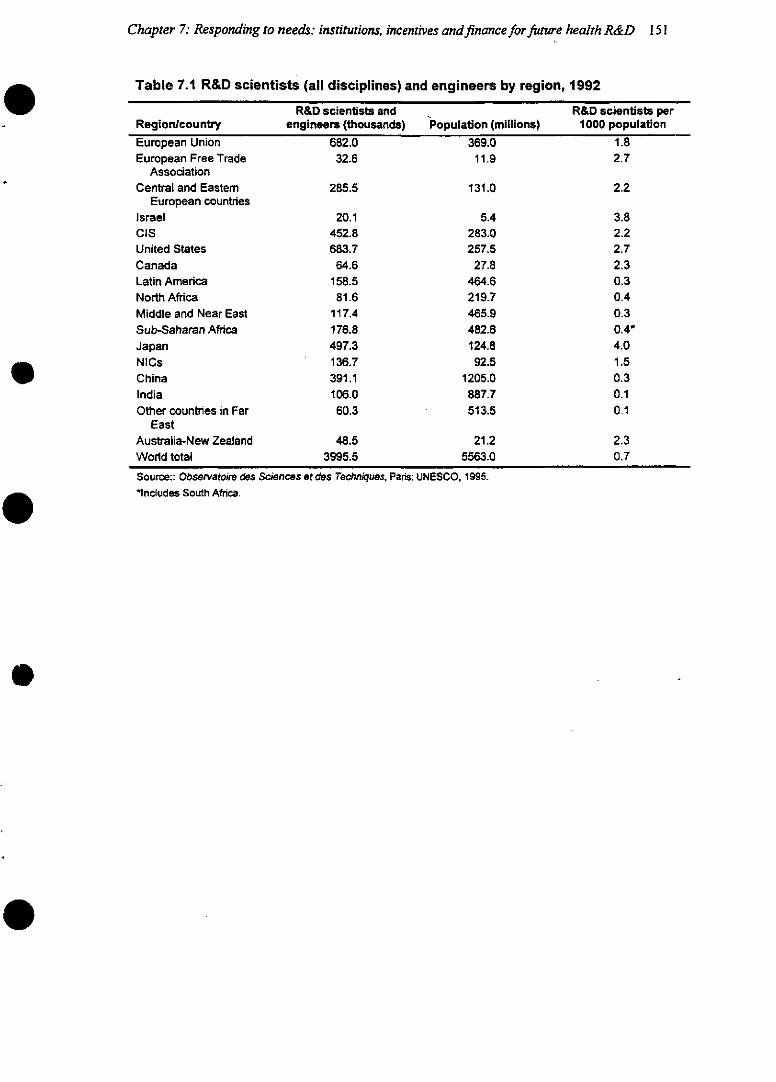
Chapter 7: Responding to needs: institutions, incentives andfinanceforfuture health R&D 151
Table 7.1 R&D scientists (ail disciplines) and engineers by region, 1992
R&D scientists andRegion/country engineers (thousands) Population (nEuropean Union 682.0 369.0European Free Trade 32.6 11.9
AssociationCentral and Eastem 285.5 131.0
European countriesIsrael 20.1 5.4CIS 452.8 283.0United States 683.7 257.5Canada 64.6 27.8Latin America 158.5 464.6North Africa 81.6 219.7Middle and Near East 117.4 465.9Sub-Saharan Africa 176.8 482.6Japan 497.3 124.8NICs 136.7 92.5China 391.1 1205.0India 106.0 887.7Other countries in Far 60.3 513.5
EastAustralia-New Zealand 48.5 21.2World total 3995.5 5563.0
Source:: Observatoire des Sciences et des Techniques, Pars: UNESCO, 1995.Includes South Africa.
illions)R&D scientists per
1000 population1.82.7
2.2
3.82.22.72.30.30.40.30.4*4.01.50.30.10.1
2.30.7
-
-
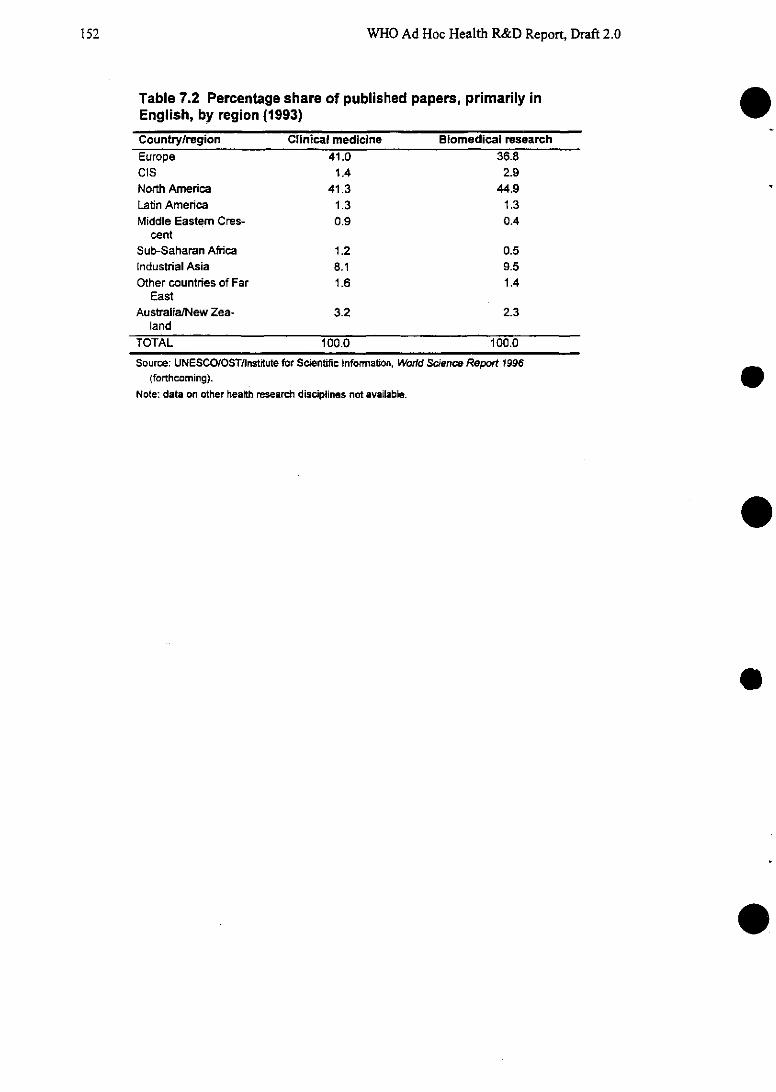
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 7.2 Percentage share of published papers, primarily inEnglish, by region (1993)
Country/region Clinical medicine Biomedical researchEurope 41.0 36.8CIS 1.4 2.9North America 41.3 44.9Latin America 1.3 1.3Middle Eastem Cres- 0.9 0.4
centSub-Saharan Africa 1.2 0.5Industrial Asia 8.1 9.5Other countries of Far 1.6 1.4
EastAustralia/New Zea- 3.2 2.3
land
TOTAL 100.0 100.0
Source: UNESCO/OST/Institute for Scientific Information, World Science Report 1996(forthcoming).
Note: data on other health research disciplines not available.
e
.
e
e
e
152
Chapter 7: Responding to needs: institutions, incentives andfinanceforfuture health R&D 153
In order to facilitate the achievement of these factors for success, the Committee proposes certainpractical steps should be taken which may be of interest to governments, donors and other investors.First, institutions in low- and middle-income countries should be freed from civil-service manage-ment procedures to enable them to offer salary scales that will give them a competitive advantage andbegin to combat the brain drain. To secure good staff, institutions should be enabled to recruit by ac-tive search and on the basis of peer-reviewed competition. Institutions should make a proportion ofthe work they support extramural to encourage competition. Some institutions, such as the OswaldoCruz Foundation in Brazil, have already moved in these directions with great success, for example byfreeing up intrarnural resources for competitive allocation between groups and within the institution,with assessments being made by an external review group.
Second, an international element to institutions is increasingly seen as essential for the per-formance of cutting-edge research. Since the market for researchers is international, institutionsshould expect that some of their staff will be foreign nationals, although restrictive policies in somecountries may, at present, prevent this. Where foreigners may not be employed, it is at least prefer-able for the scientific advisory board of the institution to contain some international representation.Staff should be enabled to participate in international fellowship schemes, exchanges and othermechanisms that foster long-term links with other institutions. Links between institutions are increas-ingly essential; no single institution can expect to have within its teams all the research skills neededfor a rapid response to a continually changing set of problems and goals.
Third, governments should develop national and regional agendas for health research basedon assessments of needs and scientific opportunities, thereby focusing limited resources on areaswhere payoff is likely to be highest.
7.2 Working together: in search of better links between public andprivate sectors
The contribution of the private sector to health research, in the traditional pharmaceuticals (drugs,vaccines, diagnostics) industries and in a growing list of other health products such as health educa-tion materials, has been highly significant in recent decades. Health researchers in the public sectorneed industry for many reasons, including its expertise in development, its efficiency as a manufac-turer and distributor, and, not least, its financial power. But both private and public sectors recognizethat the health problems of the world's poorest are comparatively neglected by the industry.
7.2.1 The problem
The poor are effectively excluded from the world's economic markets and there are few orno incentives for industry to engage its expertise with their problems. The costs of bringing a newpharmaceutical product from laboratory bench to market have been estimated at as high as $359 mil-lion and the process may take 10 years (Harvard Business Review, Jan.-Feb. 1994). These costs mustbe recovered through pricing the resulting product at levels far above the (often quite small) marginalcost of production and packaging; for this reason, the industry is unlikely to develop products formarkets whose purchasing power is extremely limited. It is possible that some markets in the middle-income countries will grow extensively in coming decades and that this will encourage the pharma-
WHO Ad Hoc Health R&D Report, Draft 2.0
ceuticals companies to invest in them. However, this prospect seems unlikely for the poorest regions,particularly Sub-Saharan Africa and South Asia, whose health needs are currently greatest and pro-jected to remain so for the foreseeable future (see Table 7.3).
[Table 7.3 about here]
As a result, national and international research programmes in the public sector, and withsupport from the private foundations, have increasingly accepted that they must take some respon-sibility for researching and developing products themselves, through new mechanisms of collabora-tion with industry (Godal, T., Science 263 (1994): 1864). At the samrne time, the pharmaceuticals in-dustry is itself adapting to recession and other factors to turn itself more into an integrated organiza-tional framework that is comparable to some of the international R&D progranmmes financed by thepublic sector. This is partly because of the growing interdependence of different types of skill andcapacity in the industry, as, for example, in the relationships between the small biotechnology com-panies and the larger, more stably resourced, pharmaceuticals companies. The industry increasinglycontracts out its research and manufacturing components, locating each component in the most eco-nomically and technically suitable location rather like an assembly industry. The increasing integra-tion has been described as a move towards an "extended farnily" network (Scrip 23 [Sept. 1994]:12). See Figure 7.1.
[Figure 7.1 about here]
7.2.2 Possible solutions
The skills, energy and capacity of the private sector must be better harnessed by the publicsector if health research, and particularly product development, for the needs of people in lowest-income countries is to improve. The Committee suggests a number of mechanisms for doing so,based on existing experience where successes have been achieved:
* by supporting the costs of the early stages of product development, from compound screen-ing right through to phase II trials if necessary, and offering to support post-marketing sur-veillance.
· by providing the industry with detailed analyses of the potential market and of the risks andbenefits of introducing a product.
* by providing the industry with guaranteed markets for new products, such as vaccines. Insuch schemes, national governments agree to purchase a known quantity of a specified prod-uct, raising the finance either from their national budget or through special loans. For exanm-ple, UNICEF's Independent Vaccine Initiative is a system that lends funds for vaccinesagainst the childhood cluster of diseases at low interest rates to certain countries that meet itsspecific qualifications.
* by streanmlining the regulatory controls imposed by the public sector on the industry to theminimum necessary for good standards, in order to cut the industry's costs.
by carefully designed tax relief schemes.
154
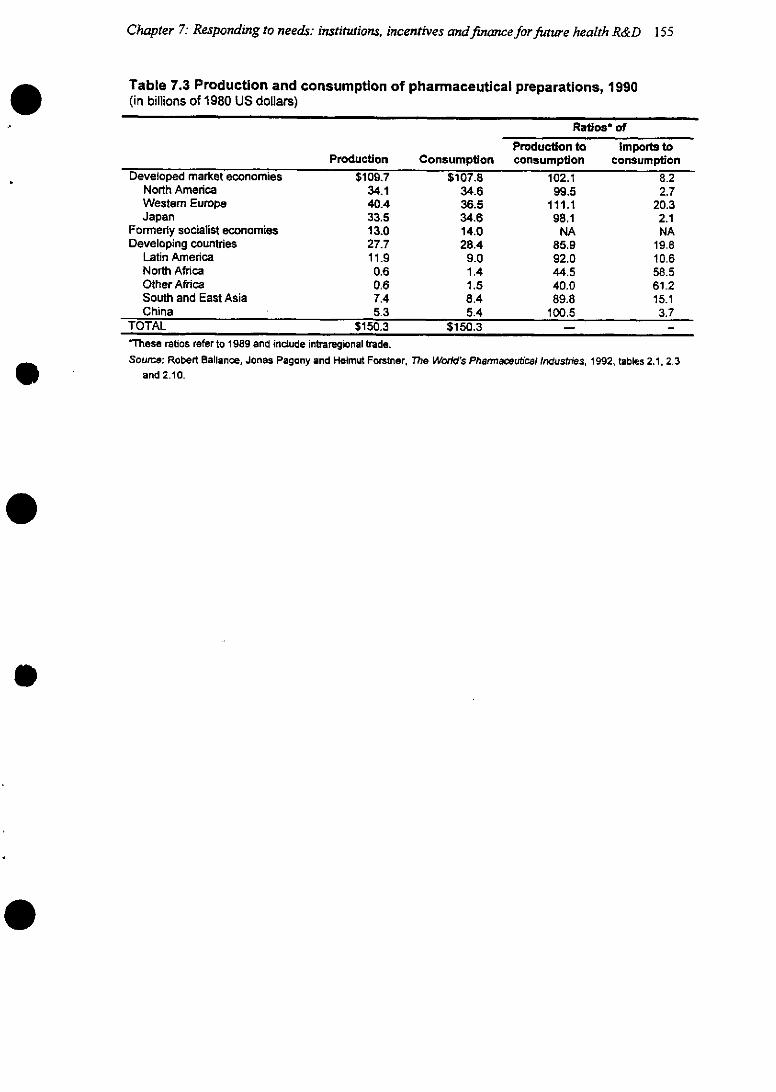
Chapter 7: Responding to needs: institutions, incentives andfinanceforfuture health R&D 155
Table 7.3 Production and consumption of pharmaceutical preparations, 1990(in billions of 1980 US dollars)
Ratios ofProduction to Importe to
Production Consumption consumption consumptionDeveloped market economies $109.7 $107.8 102.1 8.2
North America 34.1 34.6 99.5 2.7Westem Europe 40.4 36.5 111.1 20.3Japan 33.5 34.6 98.1 2.1
Formerly socialist economies 13.0 14.0 NA NADeveloping countries 27.7 28.4 85.9 19.8
Latin America 11.9 9.0 92.0 10.6North Africa 0.6 1.4 44.5 58.5Other Africa 0.6 1.5 40.0 61.2South and East Asia 7.4 8.4 89.8 15.1China 5.3 5.4 100.5 3.7
TOTAL $150.3 $150.3 - -'These ratios refer to 1989 and indcude intraregional trade.Source: Robert Ballance, Jonas Pagony and Helmut Forstner, The World's Pharmaceutical Industries, 1992, tables 2.1, 2.3
and 2.10.
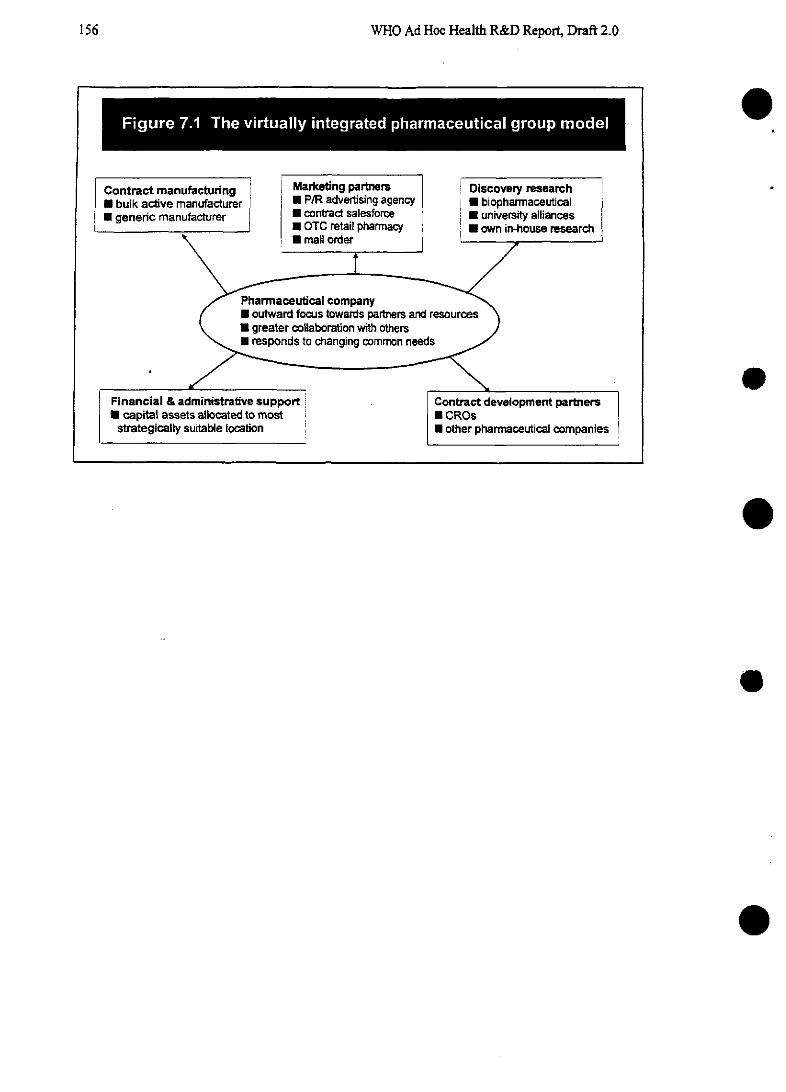
WHO Ad Hoc Health R&D Report, Draft 2.0
- - - -e * *.0 . . - . e e e.-
Contract manufacturing Marketing partners Discovery research i* bulk active manufacturer * P/R advertising agency j E biopharmaceutical* generic manufacturer contract salesforce a university alliances
* OTC retail pharmacy E * own in-house research\ mail order
Pharmaceutical companygrate * oa outward focus towamis partners and resources )
• greater collaboration vwith othersJ\ *~ responds to changing common needs /
Financial & administrative support Contract development partnersO capital assets allocated to most ! CROs
strategically suitable location E other pharmaceutical companies
o
o
o
e
e
156
Chapter 7: Responding to needs: institutions, incentives andfinanceforfuture health R&D 157
* by financial incentives within the patents system. A number of attempts to modify the patentsystem have been attempted, such as the Orphan Drug Act of 1983 in the United States. Thisgives companies tax breaks and lengthened exclusivity rights for drugs with small markets.However, the act has not reversed the downward trend in R&D on drugs for diseases that areprevalent in developing countries and further extension of the period of patent protection-beyond the 20 years recently internationally agreed in the Uruguay round-is unlikely tosubstantially affect incentives.
* by making the best use of the extraordinary commitment of individuals and particular com-panies within the private sector. Some have already demonstrated themselves willing to un-dertake research and development, production and supply of drugs on a break-even or de-fined-profit basis; more may be encouraged to do so, for example in the field of AIDS vac-cine research (see Box 4.2 in Chapter 4 on HIV vaccines).
7.3 Investment in health R&D: trends, prospects and proposed so-lutions
The current financial climate for global health research gives cause for concern and demonstrates thecurrent lack of high-level advocacy for a vital and cost-effective investment. Before moving on todiscuss possible solutions, this section discusses the resource allocation level of global health re-search, beginning with an overview of overall investnent trends, and moving on to discuss the gapsin research needed to meet the challenges identified in earlier chapters.
7.3.1 Problem 1: Research is a poor relation within the health sector
Governmnents and other investors have clearly not been persuaded of the value of healthR&D. No government, whether in developed or developing regions, accords research more than 4.5%of its total domestic health spending, and for most the share is considerably lower. The United Statesspends more than any other country, at 4.5%; but for many established market economies the figureis considerably lower, ranging between 0.3% in Finland and 3.5% in Denmark [can have the wholetable here or refer (Annex 6)]. Available data from middle-income countries suggest that R&D has anequally low claim on health resources. For example, South Africa spends no more than 1.7% of itstotal health budget on R&D, while for Mexico the figure is no more than 0.5%. As a share of theworld's total expenditure on health, research claimed just 3.2% in 1992 (see Figure 7.2).
[Figure 7.2 about here]
Research into the health of people in low- and middle-income countries is particularly ne-glected, despite the fact that these countries bear by far the greatest share of the world's total diseaseburden. Of an estimated $55 billion invested in R&D worldwide in 1992, just $2 billion-or 3.6/%--was devoted to problems that overwhelmingly burden developing countries. Of this total, the gov-ernments of the low- and middle-income countries invested some $800 million (or 40%), a sum thatwas matched by the EME governments. The private sector provided the remainder.
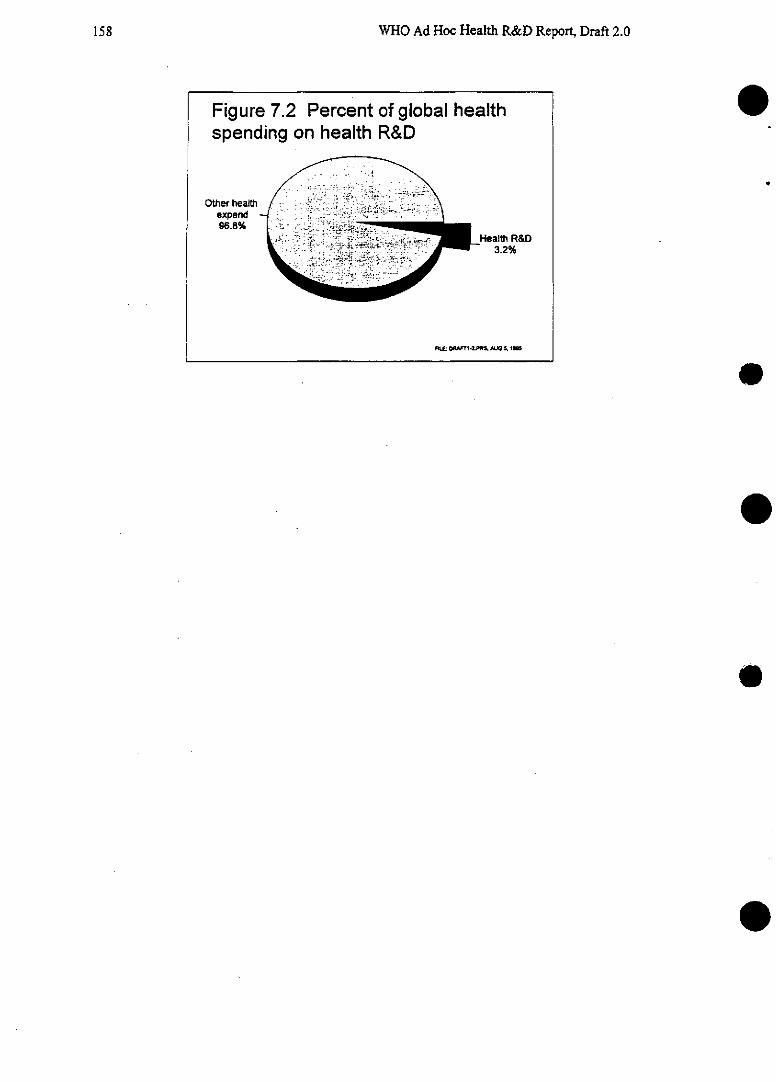
158 WHO Ad Hoc Health R&D Report, Draft 2.0
Figure 7.2 Percent of global healthspending on health R&D
Other healthexpend96.8%
Health R&D3.2%
F!.É 0M NT1 *2.PWR AUG St
e
e
e
Chapter 7: Responding to needs: institutions, incentives andfinanceforfuture health R&D 159
73.2 Problem 2: Support for health research is stagnating and in some cases falling
After two decades of growing investment, health research is now in deep jeopardy. Duringthe 1970s and 1980s, many of the governments of the EMEs expanded investment into health R&Dbut that growth has slowed right down and is now expected to fall in real terms. For example in theUnited States, the country whose health R&D alone accounts for most of the worldwide investment,the budget for the National Institutes of Health is expected to fall by 9% in the next four years from$11.3 billion to $10.7 billion. Basic biomedical research, which lays the groundwork for the strategicresearch and intervention development covered by this Report, is facing cutbacks by the U.S. Con-gress (Annex 5).
The pharmaceuticals industry, which during the 1980s expanded its investment in R&D morerapidly than the public sector in the United States, has recently sharply contracted its investment be-cause of the soaring costs of health care in the EMEs, which have led the industry to project a de-crease in its profit margins. Because of the projected decrease, the rate of growth in R&D investmnentin the pharmaceuticals industry has tumbled from 17.4% in 1992 to less than 7.7% in 1995 in theU.S.
The decline in investment in official development assistance from the EMEs to the rest of theworld is even more serious. Official Development Assistance (ODA) for health (which includeshealth research) is at an all time low, with governments in the EMEs allocating it on average just3.6% of GDP-halfthe target set by the OECD-in 1994. The share of this total allocated to healthhas declined too, falling to 3.6% by 1993. Within this health budget, just $170 million went to sup-port R&D-less than a tenth of the health allocation.
ODA is given in two basic ways-as bilateral assistance directly from one government toanother; or as multilateral assistance, from a government to an international agency which acts as anintermediary and passes it on to a recipient country. About 44% of ODA for health R&D is given asbilateral funds, the rest as multilateral funds. Bilateral ODA to the health sector has fallen by 27%since 1988.
Trends in multilateral funds for health R&D are more difficult to assess because of the ac-counting systems of the donors and recipients of these funds (Annex 6). The principal agencies thatreceive multilateral funds are the UN organizations, but multinational, nongovernmnental organiza-tions such as the Council on Health Research for Development (COHRED) and the InternationalHealth Policy Program (ITHPP) also receive multilateral support. As well as providing regular, budg-etary support to the international organizations, many governments choose to provide additional dis-cretionary (or extrabudgetary) funds to specific research programmes. These extrabudgetary fundsare classified as multilateral aid and it is possible to get a partial picture of multilateral investmenttrends by examining extrabudgetary contributions to particular research programmes. See Box 7.2 foran overview of the major organizations in the arena of world health research.
[Box 7.2 about here]
WHO Ad Hoc Health R&D Report, Draft 2.0
Box 7.2 Major players in health research
This study is rooted within the work of the health research community world-wide. The structure of that community is summarized here. At national level, researchis carried out by universities, institutes, in health-care settings and the pharmaceuti-cais industry. Health research is funded by govemrment ministries, research councils,private funds and the private sector. At the international level, the major players sup-porting research are the UN agencies, private foundations, development agencies andprivate sector multinationais. As a specialized agency for health, the World Health Or-ganization has a mandate in its constitution 'to promote and conduct research in thefield of health". A substantial proportion ($223 million) of its extrabudgetary resourcesof over $600 million is invested in health research [information on research allocationwithin regular budget to come]. The Advisory Committee on Health Research advisesthe WHO Director-General on the Organization's policy for health research.
Other UN agencies and funds involved in health research include the UNPopulation Fund, the UN Development Programme, UNICEF, and, on the key issue ofnutrition, the ACC/SCN.
The World Bank has given increased attention to health research in recentyears. It is now the biggest contributor to the United Nations Development Pro-grammelWorld BankNVHO Special Programme for Research and Training in TropicalDiseases (TDR)($xxx). Its expertise in health research is increasing, especially inhealth financing and topics related to other sectors. Its potential to mobilize resourceshas been clearly documented in the field of agricultural research through the Consul-tative Group on International Agricultural Research (CGIAR).
Private foundations have been pioneers in international health research, oftenwith origins that extend back before the existence of the UN. They include: theRockefeller Foundation, the Wellcome Trust, the McArthur Foundation, the EdnaMcConnell Clark Foundation, the Sasakawa Memorial Health Foundation, the AgaKhan Foundation, the Pew Charitable Trusts and the Ford Foundation. Many of thesefoundations support specially designed programmes or networks such as the Interna-tional Health Policy Program (IHPP) and the International Clinical Epidemiology Net-work (INCLEN).
In the past two decades, the overseas development agencies of a number ofdeveloped countries have been pioneers in international health R&D, particularly thosewith dedicated agencies for research, such as the IDRC and SAREC. In addition, anumber of nongovernmental organizations are involved in supporting and enablinghealth research. These include the International Planned Parenthood Federation,Family Health International, the Population Council and the Program for Applied Tech-nology in Health (PATH). Another key player is COHRED, the Council on Health Re-search for Development, which has assisted countries engaged in national priority-setting for health research. It is registered as a nongovemrmental organization in Swit-zerland and focuses its work on building capacity for essential national health re-search.
e
160
Chapter 7: Responding to needs: institutions, incentives andfinanceforfuture health R&D 161
(Box 7.2 continued)
Finally, the govemments of a number of middle-income countries, and somelow-income countries, are taking a growing interest in health R&D. Among them, Bra-zil, China, India, Indonesia, [Mali??,] Mexico, South Africa and Thailand are some ofthose already demonstrating particular leadership. Their decisions and investment ac-tivities in the coming decades will be critical in determining the progress of research,and there is every reason to believe their already considerable influence within the in-temational health research community will rapidly grow.
[Note: This box will be revised to reflect the division of players into investors,R&D networks, and R&D institutions as in Figure 7.3. Additional institutions will beadded e.g. CELADE, INCAP, CFNI.]
WHO Ad Hoc Health R&D Report, Draft 2.0
Two particular programmes, the Special Programme of Research, Development and ResearchTraining in Human Reproduction (HRP) and the Special Programme for Research and Training inTropical Diseases (TDR) are discussed here. The support of a number of investors, including smallcountries such as Denmark, Sweden and Norway, has been critical in enabling these programmes tobecome highly effective and in improving the health of millions. Table 7.4 shows cumulative ex-trabudgetary support from a number of countries and international programmes to two such pro-grammes, HRP and TDR. It is worth noting that, because of the international nature of health re-search, a large portion of these investments return to certain donor countries whose scientists are en-gaged in research projects supported by the programmes.
[Table 7.4 about here]
However, despite the achievements of special programmes such as these, there is now dis-turbing evidence that even they are losing support. Investment in the special programmes has begunto show some downward trends, with the contributions of many donors declining in the early 1990s(Annex 6). These trends indicate that multilateral support for health research may be no more healthythan bilateral support.
The only organizations to increase their investment in health R&D in the 1990s are the pri-vate research foundations, such as the Wellcome Trust and the Rockefeller Foundation (Annex 6).Their contribution to overall research funding is significant, but comparatively small.
7.3.3 Problem 3: Inadequate coordination has resulted in important gaps within healthresearch efforts
The major challenges to health that were identified in the foregoing chapters include two forwhich the current institutional arrangements are wholly inadequate. As discussed in Chapter 5, thereis insufficient effort in research into noncommunicable diseases, aging and the changing exposure ofpopulations to various risk factors associated with disease. As discussed in Chapter 6, there is an ex-traordinary shortage of research and coordination into the health needs, beliefs and behaviours ofpopulations and households, and of the impact of health policies, particularly at a time when healthsystems are under reform in most countries.
7.3.4 Possible reasons for the neglect of health research
The reasons for declining investment in health R&D are complex. One is of course the worldrecession, which has tempted governments to focus inwards and on short-term solutions. Another isthe frustration of investors at the current mechanisms for conducting and coordinating health re-search. Investors may not always be confident that their funds are being put to best use or that theyare not overlapping with other investors on similar work. They may be unable to track the outcomesof their investment or see the benefits of their work, partly because of the lack of good data monitor-ing systems and data on resource flows. A third reason is simply that the arguments for research arenot being put clearly enough to those who must make decisions about how to invest shrinking re-sources.
e
162
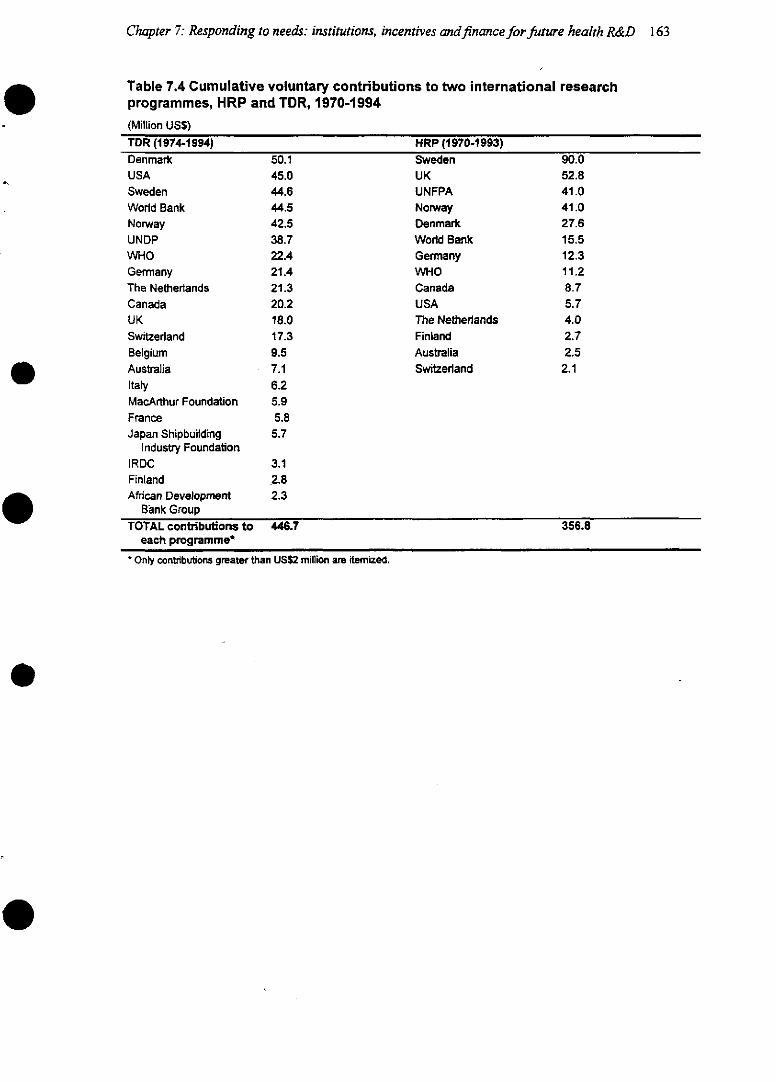
Chapter 7: Responding to needs: institutions, incentives andfinanceforfuture health R&D 163
Table 7.4 Cumulative voluntary contributions to two international researchprogrammes, HRP and TDR, 1970-1994
(Million US$)TDR (1974-1994) HRP (1970-1993)Denmark 50.1 Sweden 90.0USA 45.0 UK 52.8Sweden 44.6 UNFPA 41.0World Bank 44.5 Norway 41.0Norway 42.5 Denmark 27.6UNDP 38.7 World Bank 15.5WHO 22.4 Germany 12.3Germany 21.4 WHO 11.2The Netherlands 21.3 Canada 8.7Canada 20.2 USA 5.7UK 18.0 The Netherlands 4.0Switzerland 17.3 Finland 2.7Belgium 9.5 Australia 2.5Australia 7.1 Switzerland 2.1Italy 6.2MacArthur Foundation 5.9France 5.8Japan Shipbuilding 5.7
Industry FoundationIRDC 3.1Finland 2.8African Development 2.3
Bank GroupTOTAL contributions to 446.7 356.8
each programme*
Only contributions greater than US$2 million are iternized.
WHO Ad Hoc Health R&D Report, Draft 2.0
7.3.5 Proposed solutions
The capacity exists within existing health research structures to create a global forum forgovernments, donors and scientists and to act as an advocate for health research at the highest politi-cal levels. The forum, which could be called the Consortium for International Health Research, couldreview needs, opportunities and resource flows in health R&D, basing its reviews on analytic data onthe health needs of countries and regions. Its aims would be to fill important existing gaps in healthresearch, reduce overlap, and generate and disseminate between countries data on national healthsystem performance, disease burden, health needs and intervention priorities. It would take advicefrom a scientific advisory group and from bodies already involved in enabling health research at na-tional and international levels, such as COHRED. Its data would be commissioned from a TrendsAnalysis Group, to be built up out of existing expertise, which would provide for international com-parison structured analyses of resource flows, global burden of disease, the cost-effectiveness of in-terventions in different communities and data on the performance of individual countries' healthsystems, particularly where possible with the aim of sharing experience on the best ways to conducthealth sector reform. This Consortium has the potential to demonstrate at national and internationallevels the benefits of health research, and, because of the data on resource flows and performancethat it could generate and monitor, to convince investors of the high payoffs that research can bring(see Figure 7.3).
[Figure 7.3 about here]
In order to strengthen resources for research in noncommunicable diseases and injuries andin health needs and health systems, two new initiatives are suggested. A Special Programme of Re-search and Training on Healthy Aging and Noncommunicable Diseases should be formed, modelledon existing special programmes. Its goals should include greater understanding of the risk factors anddeterminants of these diseases in different settings and the development of affordable and sustainableinterventions to deal with this growing epidemic. New, sustainable and affordable interventions arevital for the health of whole populations and must counterpoint, not duplicate, the interventions al-ready developed in the EMEs, many of which cannot be imported directly into low-income settings.In addition, a Special Programme of Research and Training on Health Services and Health PolicyResearch should be developed. Its goals should include the development of methodologies for studiesthat will enhance understanding of the impact of different health policies in different settings on theefficiency, equity and the quality of systems.
o
164
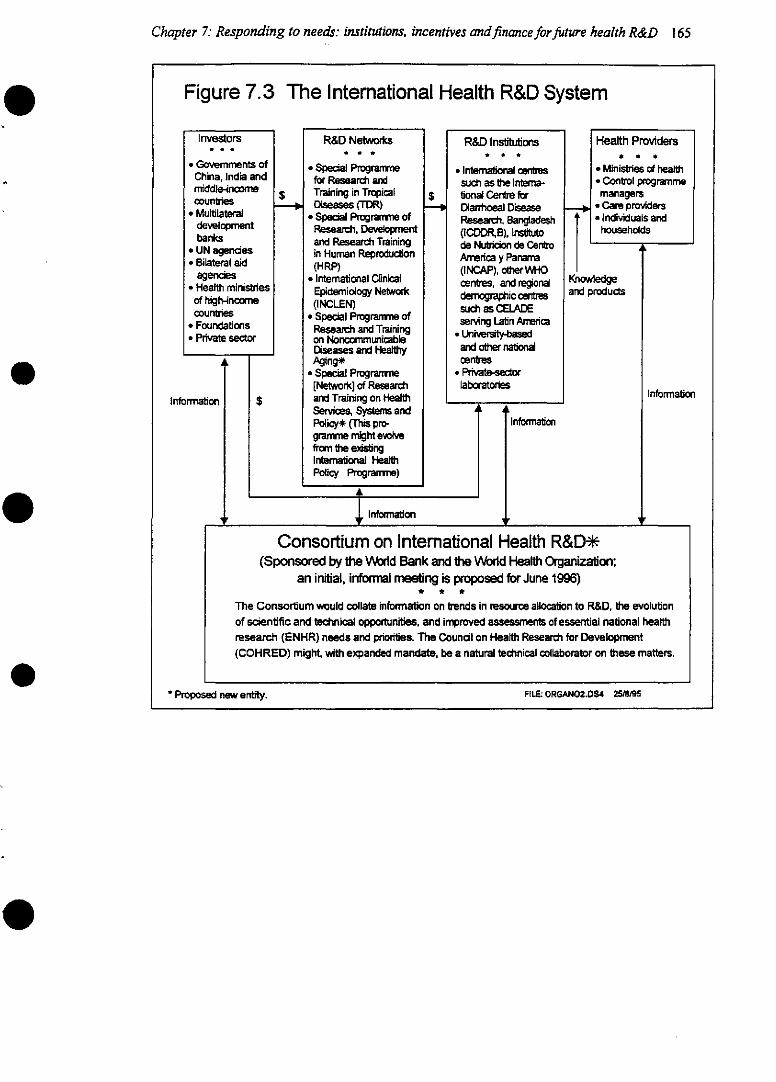
Chapter 7: Responding to needs: institutions, incentives andfinancefor future health R&D 165
Figure 7.3 The Intemational Health R&D System
Investors
Governments ofChina, India andmiddle-incarmecounties
* Multilateraldevelopmentbanks
* UN agencies* Bilateral aid
agencies* Health ministries
of high-inc~mecountlies
* Foundations* Private sector
Infomation
$
$
R&D Networks
* Special P gramefor Research andTraining in TropicalDiseases (TDR)
* Special Progranmne ofResearch, Developentand Research Trainingin Human Reproduction(HRP)
* International ClinicalEpidemiology Network(INCLEN)
* Special Progranmme ofResearch and Trainingon NoncomrnmunicableDiseases and HealthyAging*
* Special Progra e[Network] of Researchand Training on HealthServices, Systems andPolicy* (This pro-gramme might evolvefromn the exisüngInternatonal HealthPolicy Programne)
4
S
1 Information
R&D Institutions
* International centessuch as the Interna-tional Centre forDiarrhoeal DiseaseReseath, Bangladesh(ICDDR,B), Ins~utode Nu~icion de CentroAmerica y Panama(INCAP), o~~erWHOcentres, and regionaldo~aphic oentressuch as CELADEserving Latin Amrerica
* Universi~ybedaid otwer nationalcentres
* Privatedrlaboratories
tInformation
Health Providers* * *
. Ministries of health* Control progranmemanagers
. Care providers*Individuals and
households
iedgeroducts
Information
Proposed new entity. FILE: ORGANO2.0S4 2518195
Consortium on International Health R&D*(Sponsored by the World Bank and the Worid Healt Organization;
an initial, infonral meeting is proposed for June 1996)* * *
The Consortium would collate information on trends in resource allocation to R&D, he evolutionof scientific and technical opportunities, and improved assessments of essential national healthresearch (ENHR) needs and priorities. The Coundl on Health Researd for Development(COHRED) might, with expanded mandate, be a natural technical collaborator on these matters.
A
q r
' Prop~ new enfdy- FILE: ORGAN02.DS4 25/89
WHO Ad Hoc Health R&D Report, Draft 2.0
7.4 Chapter summary and recommendations
Current arrangements for the conduct and financing of global health research are inadequate for theworld's current and changing health needs. In particular, a lack of capacity at national and regionallevel is hampering the performance of high-quality research, while inadequate collaboration betweenprivate and public sectors is preventing either from directing their respective skills best toward im-proving the health of poorer populations. At the resource allocation level, there is insufficient coordi-nation, with particular gaps around research into noncommunicable diseases and research into thefactors that ensure the best interaction between people and health systems. Resources for health re-search are falling at a time when research has more than ever to give---a decline which suggests thatdecision makers have not been persuaded of the need for research.
The following recommendations are addressed to both governments and donors: clearly,some are more particularly the concem of governments and some are more the concern of donors.The recommendations outline some steps that might be taken to proceed, first in terms of the opera-tion of research at national and international levels, and finally in terms of resources and internationalcoordination. ·1. Governments have much to gain from the development of national agendas for health research
that focus resources into areas of research and institutions with high potential and away fromthose with low potential. Governments and donors may further increase the efficiency of R&Dby strengthening national and regional research capacity, through, for example, improvements inthe quality of training, incentives to reverse the brain drain, policies that require research poststo be competitive and based on the peer-reviewed allocation of funds; and competitive core sup-port for institutions. The payoffs from investment in good standards are likely to be significant,while poor-quality or repetitive research is wasteful and may have serious consequences forhealth.
2. Governments and donors may profitably explore the development of new instruments-beyondthe current patents system-for engaging the skills and energy of the private sector, includingexisting industry in low- and middle-income countries, in the development of vaccines, antimi-crobials and other drugs, diagnostic tests, prostheses and equipment. These incentives could in-clude development subsidies, extended patent protection, guaranteed markets, streamnlinedregulatory requirements, improved market information (including certification of product qual-ity) and contracting for specific tasks. Clearly, governments will need to lead in the developmentof new interventions to deal with the health needs of the poorest; yet they can achieve this taskefficiently only by bringing in the competence and capacity of the private sector.
3. Two new initiatives are recommended to fill major gaps in current R&D activity. First, a newProgramme for Research and Training on Healthy Aging and Noncommunicable Diseasesshould be formed, based on the models of existing international programmes such as HRP andTDR. The host institution for this programme should be chosen from existing candidates such asIARC, WHO or a national government on the basis of the demonstration of the necessary re-sources and capacity to provide effective leadership. Secondly, a strong Programme for Re-search and Training on Health Systems and Policy should be formed from the existing institu-tions and groups conducting research and training in these areas. The potential payoff from theseprogrammes would be high for countries in all income levels; hence not only aid donors but,
166
Chapter 7: Responding to needs: institutions, incentives andfinanceforfuture health R&D 167
also, the health ministries and research councils of high-income countries have much to gainfrom investing in them.
4. A Consortium on International Health R&D should be formed to provide a forum for review ofneeds and opportunities for global health R&D-making use of analytic data on disease burden,R&D opportunities and the level of ongoing efforts. The Consortium would bring together thegovernments of developing countries, the major donors, and the research community. Analyticwork undertaken by and for the Consortium would provide improved information for decentral-ized decisions on funding and resource allocation. The Consortium concept might, initially, betested as an informal gathering of interested parties.
5. Given the high returns to R&D in health improvement and the currently low priority accorded tohealth research by most governments, a modest reallocation of health sector resources to R&D isrecommnended as a means to bring substantial net gains in health, particularly the health of thepoor. Given that much of R&D provides an international public good, there is a particularlystrong case for donors to reallocate their health portfolios to increase R&D funds. The institu-tional capacity for supporting health R&D that many donors possess strengthens the case forthem to increase this form of assistance, while the globalization of health problems and the so-lutions required suggests that sources of investment in international health R&D should be di-versified to include high-income countries' ministries of health and research councils. Govern-ments of low- and middle-income countries are likely to find increased allocations to appropri-ate health R&D to be both a cost-effective way of improving health conditions in their countryand, potentially, an investment in the infrastructure for potentially productive national indus-tries.
0Bibliographical note and references
e
0
0
168
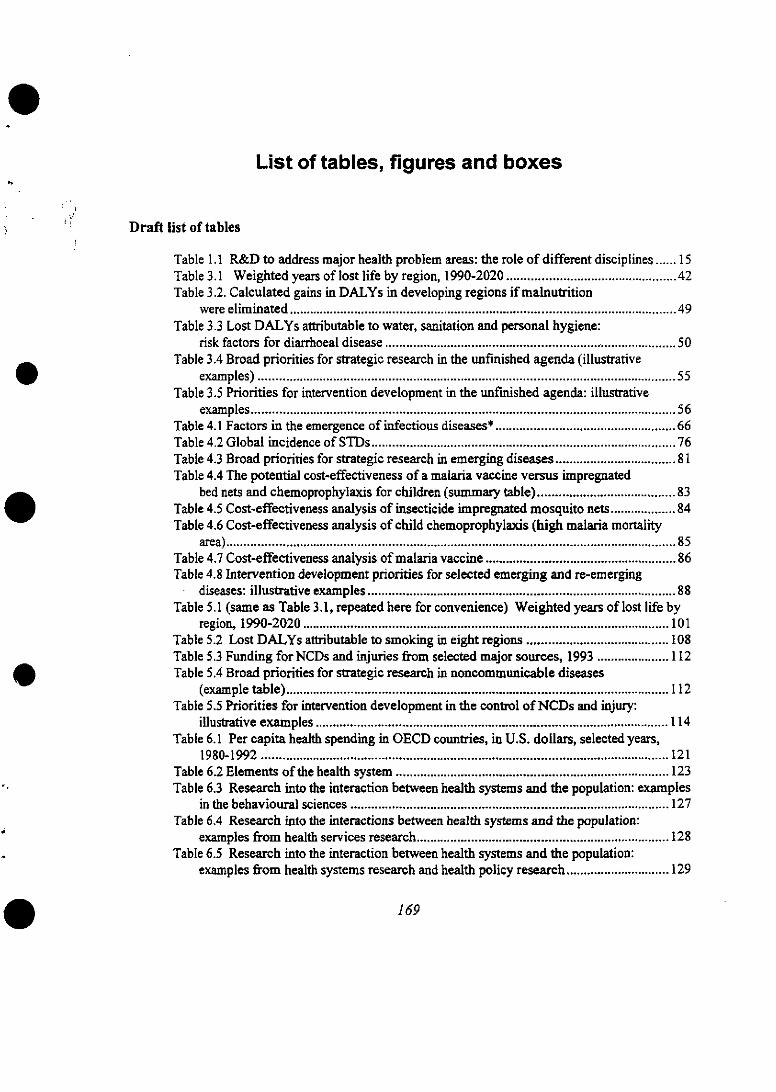
List of tables, figures and boxes
Draft list of tables
Table 1.1 R&D to address major health problem areas: the role of different disciplines ...... 15Table 3.1 Weighted years of lost life by region, 1990-2020 ................................................. 42Table 3.2. Calculated gains in DALYs in developing regions if malnutrition
were eliminated ................................................................................................................ 49Table 3.3 Lost DALYs attributable to water, sanitation and personal hygiene:
risk factors for diarrhoeal disease ............................................................. ...................... 50Table 3.4 Broad priorities for strategic research in the unfinished agenda (illustrative
examples) ......................................................................................................................... 55Table 3.5 Priorities for intervention development in the unfinished agenda: illustrative
examples ........................................................................................................................... 56Table 4.1 Factors in the emergence of infectious diseases* .................................................... 66Table 4.2 Global incidence of STDs ........................................................................................ 76Table 4.3 Broad priorities for strategic research in emerging diseases ................................... 81Table 4.4 The potential cost-effectiveness of a malaria vaccine versus impregnated
bed nets and chemoprophylaxis for children (sumnmary table) ........................................ 83Table 4.5 Cost-effectiveness analysis of insecticide impregnated mosquito nets ................... 84Table 4.6 Cost-effectiveness analysis of child chemoprophylaxis (high malaria mortality
area) .................................................................................................................................. 85Table 4.7 Cost-effectiveness analysis of malaria vaccine ....................................................... 86Table 4.8 Intervention development priorities for selected emerging and re-emerging
dise ases: illustrative examples ......................................................................................... 88Table 5.1 (same as Table 3.1, repeated here for convenience) Weighted years of lost life by
region, 1990-2020 .......................................................................................................... 101Table 5.2 Lost DALYs attributable to smoking in eight regions ......................................... 108Table 5.3 Funding forNCDs and injuries from selected major sources, 1993 ..................... 112Table 5.4 Broad priorities for strategic research in noncommunicable diseases
(example table) ............................................................................................................... 112Table 5.5 Priorities for intervention development in the control of NCDs and injury:
illustrative examples ...................................................................................................... 114Table 6.1 Per capita health spending in OECD countries, in U.S. dollars, selected years,
1980-1992 ...................................................................................................................... 121Table 6.2 Elements of the health system ............................................................................... 123Table 6.3 Research into the interaction between health systems and the population: examples
in the behavioural sciences ............................................................................................ 127Table 6.4 Research into the interactions between health systems and the population:
examples from health services research ......................................................................... 128Table 6.5 Research into the interaction between health systems and the population:
examples from health systems research and health policy research .............................. 129
169
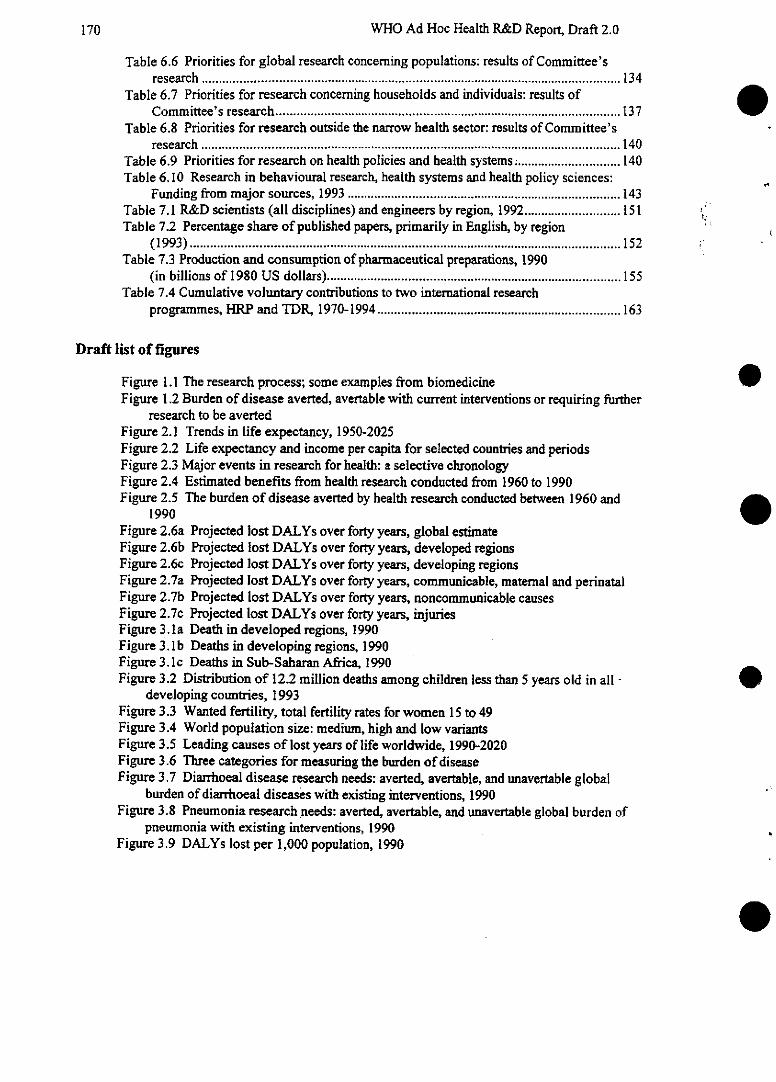
WHO Ad Hoc Health R&D Report, Draft 2.0
Table 6.6 Priorities for global research concerning populations: results of Committee'sresearch .......................................................................................................................... 134
Table 6.7 Priorities for research concerning households and individuals: results ofCommittee's research ............................................................................................ 137
Table 6.8 Priorities for research outside the narrow health sector: results of Committee'sresearch .......................................................................................................................... 140
Table 6.9 Priorities for research on health policies and health systems ............................... 140Table 6.10 Research in behavioural research, health systems and health policy sciences:
Funding from major sources, 1993 ................................................................................ 143Table 7.1 R&D scientists (all disciplines) and engineers by region, 1992 ............................ 151Table 7.2 Percentage share of published papers, primarily in English, by region
(1993) ............................................................................................................................. 152Table 7.3 Production and consumption of pharmaceutical preparations, 1990
(in billions of 1980 US dollars) ...................................................................................... 155Table 7.4 Cumulative voluntary contributions to two international research
programinmes, HRP and TDR, 1970-1994 ....................................................................... 163
Draft list of figures
Figure 1.1 The research process; some examples from biomedicineFigure 1.2 Burden of disease averted, avertable with current interventions or requiring further
research to be avertedFigure 2.1 Trends in life expectancy, 1950-2025Figure 2.2 Life expectancy and income per capita for selected countries and periodsFigure 2.3 Major events in research for health: a selective chronologyFigure 2.4 Estimated benefits from health research conducted from 1960 to 1990Figure 2.5 The burden of disease averted by health research conducted between 1960 and
1990Figure 2.6a Projected lost DALYs over forty years, global estimateFigure 2.6b Projected lost DALYs over forty years, developed regionsFigure 2.6c Projected lost DALYs over forty years, developing regionsFigure 2.7a Projected lost DALYs over forty years, communicable, maternal and perinatalFigure 2.7b Projected lost DALYs over forty years, noncommunicable causesFigure 2.7c Projected lost DALYs over forty years, injuriesFigure 3.1a Death in developed regions, 1990Figure 3. lb Deaths in developing regions, 1990Figure 3.1c Deaths in Sub-Saharan Africa, 1990Figure 3.2 Distribution of 12.2 million deaths among children less than 5 years old in all -
developing countries, 1993Figure 3.3 Wanted fertility, total fertility rates for women 15 to 49Figure 3.4 World population size: medium, high and low variantsFigure 3.5 Leading causes of lost years of life worldwide, 1990-2020Figure 3.6 Three categories for measuring the burden of diseaseFigure 3.7 Diarrhoeal disease research needs: averted, avertable, and unavertable global
burden of diarrhoeal diseases with existing interventions, 1990Figure 3.8 Pneumonia research needs: averted, avertable, and unavertable global burden of
pneumrnonia with existing interventions, 1990Figure 3.9 DALYs lost per 1,000 population, 1990
170
List of tables, figures and boxes
Figure 4.1 Tuberculosis research needs: averted, avertable and unavertable global burden oftuberculosis with existing interventions, 1990
Figure 4.2 Established market economies (projections of the HIV pandemic)Figure 4.3 Former socialist economies (Projections of the HIV pandemic)Figure 4.4 Developing countries in Asia excluding India and China (projections of the HIV
pandemic)Figure 4.5 Latin America and the Caribbean (projections of the HIV pandemic)Figure 4.6 Sub-Saharan Africa (projections of the HIV pandemic)Figure 4.7 India (projections of the HIV pandemic)Figure 4.8 Middle Eastern Crescent (projections of the HJV pandemic)Figure 4.9 China (Projections of the HIV pandemic)Figure 4.10 Projected gross domestic product by regionFigure 5.1 Percent increase in elderly population, 1990-2025Figure 5.2 Deaths in developed regionsFigure 5.3 Deaths in developing regionsFigure 5.4 Years of life lost (YLL) in developed regionsFigure 5.5 Years of life lost (YLL) in developing regionsFigure 5.6 Projected DALYs lost for established market economies by broad cause group,
1990-2020Figure 5.7 Projected DALYs lost for former socialist economies by broad cause group, 1990-
2020Figure 5.8 Projected DALYs lost for India by broad cause group, 1990-2020Figure 5.9 Projected DALYs lost for China by broad cause group, 1990-2020Figure 5.10 Projected DALYs lost for developing countries in Asia excluding India and
China by broad cause group, 1990-2020Figure 5.11 Projected DALYs lost for sub-Saharan Africa by broad cause group, 1990-2020Figure 5.12 Projected DALYs lost for Latin Amnerica and the Caribbean by broad cause
group, 1990-2020Figure 5.13 Projected DALYs lost for Middle Eastern Crescent by broad cause group, 1990-
2020Figure 5.14 Leading Causes of lost years of life, 1990-2020Figure 5.15 Tobacco use research needs: averted, avertable, and unavertable global burden
attributable to tobacco use with existing interventions, 1990, optirnistic estimnateFigure 5.16 Tobacco use research needs: averted, avertable, and unavertable global burden
attributable to tobacco use with existing interventions, 1990, pessimrnistic estimnateFigure 5.17 Schizophrenia research needs: averted, avertable and unavertable global burden
of schizophrenia with existing interventions, 1990Figure 5.18 Major affective disorder research needs: averted, avertable and unavertable -
global burden of MAD with existing interventions, 1990Figure 6.1 Typology of health research by levels of analysisFigure 6.2 The framework for researchFigure 7. I The virtually integrated pharmaceutical group modelFigure 7.2 Percent of global health spending on health R&DFigure 7.3 The international health R&D system
171
WHO Ad Hoc Health R&D Report, Draft 2.0
Draft list of boxes
Summary1. Recommendations
Chapter 1.1.1 Terms and definitions1.2 Measuring the global burden of disease: progress and constraints [IN]1.3 Health interventions across disease groups: transverse issues (Matthias Kerker)
Chapter 2.2.1 The cost-effectiveness of research [IN]2.2 A peer review network for biomedical science: the implications of the digital information
age (George Gellert) [IN]Chapter 3.
3.1 Making packages work for people: The Essential Health Interventions Project (ClaudeNanjo) [IN]
3.2 Planning interventions to promote safe infant feeding and weaning in Pakistan(PB in consultation with John Mason)
Chapter 4.4.1 New diagnostics for STDs needed: specifying the nature of a product (Seth Berkley)4.2 AIDS vaccines: needs and opportunities (Seth Berkley)
Chapter 5.5.1 Alcohol as a risk factor: the South African experience (PB/Derek Yach)5.2 Ayurvedic and traditional Chinese medicine in the treatment of noncommunicable
diseases (My La) [INChapter 6.
6.1 Electrification and health: a case study of the interactions between health, environmentand lifestyle [PB in consultation with Derek Yach] [IN]
6.2 Health care financing: the lessons with user charges and health insurance (KatjaJanovsky)
6.3 Practical outcomes of research: developing an essential drugs policy (PB in consultationwith Pascale Brudon)
6.4 Practical outcomes of research: "executive syntheses" of research findings (PB inconsultation with Julio Frenk)
6.5 Building research capacity in South Africa (PB with information from Dr. Ramashala,South African MRC)
Chapter 7.-7.1 The organizational framrnework: a descriptive background [IN1]7.2 Major players in health research7.3 Capacity building: the TDR experience7.4 Capacity building: the INCLEN experience (Seth Berkley) [IN]7.5 The Council on Health Research for Development (Yvo Nuyens) [IN]7.6 New Products for the Poor (Beatriz Zurita)7.7 Success stories: ivermectin and praziquantel (material from Michael Reich, TDR)7.8 Ethics in health research (Derek Yach)
172
The WHO Ad Hoc Committee:Review participants and study schedule
Review participants
Committee members
Professor Dean T. Jamison(COMMTrrEE CHAIR)
Professor of Public Health andDirector, Center for Pacific Rim
Studies11292 Bunche HallUniversity of CaliforniaLos Angeles, CA 90095-1487Tel: (310) 206-0223Fax: (310) 206-4018
DEAN T. JAMISON studied at ...
Professor Karnini Mendis(COMMrITrrEE CO-CHAIR)
Departmnent of ParasitologyFaculty of MedicineUniversity of Sri LankaPO Box 271, Kynsey RoadColombo 8, Sri LankaTel: (94-1) 69-9284Fax: (94-1) 69-9284
Dr. Adenike O. AbioseMedical DirectorNational Eye CentreNational Institute of OphthalmologyPMB 2267Off Express By-PassKaduna, NigeriaTel: (23-46) 221-3131Fax: (23-46) 221-5642
173
WHO Ad Hoc Health R&D Report, Draft 2.0
Dr. A. Asamnoa-BaahDirectorPolicy, Planning, Monitoring and
Evaluation DivisionMinistry of HealthP.O. Box M44Accra, GhanaTel: (233-21) 66-54-21 ext. 4208Fax: (233-21) 66-38-10
Dr. Sune BergstromKarolinska InstituteSolnavagen 1P.O. Box 6025010401 Stockholm 60, SwedenTel: (46-8) 611-8587Fax: (46-8) 611-1733
Dr. Seth BerkleyAssociate DirectorDivision of Health SciencesThe Rockefeller Foundation420 Fifth AvenueNew York, NY 10018Tel: (212) 852-8324Fax: (212) 764-3468
Professor Barry BloomChainnrmanDepartment of Microbiology and
ImmunologyAlbert Einstein College of MedicineForchheimer Bldg., Room 4111300 Morris Park AvenueNew York, NY 10461Tel: (718) 430-2221 or 2889Fax: (718) 904-1473
Professor David BradleyProfessor of Tropical HygieneLondon School of Hygiene andTropical Medicine
Keppel StreetLondon WC 1 E 7HT, United KingdomTel: (44-171) 927-2216Fax: (44-171) 580-9075
e
174
The WHO Ad Hoc Committee: Review participants and study schedule
Professor Gelia T. CastilloProfessor of Rural SociologyDepartment of Agricultural Education
and Rural StudiesCollege of AgricultureUniversity of the PhilippinesLaguna, PhilippinesTel: (63-2) 596-813Fax: (63-2) 521-1036 c/o IRR
Dr. Chunming ChenSenior AdvisorChinese Academy of Preventive
Medicine27 Nan Wei RoadBeijing, 100050 P.R.C.Tel: (86-10) 318-6655 ext. 2411Fax: (86-10) 317-0892
Dr. Mercedes Concepcion2423 Zamora StreetPasay, Metro-Manila 1300,
PhilippinesTel: (63-25) 218-421Fax: (63-25) 211-036Professor Gertrude B. ElionScientist EmeritusBurroughs Wellcome Co.3030 Cornwallis RoadResearch Triangle Park, NC 27709Tel: (919) 248-3000Fax: (919) 315-8375
Dr. Richard FeachemSenior Population, Health and
Nutrition AdviserThe World BankRoom S-10451818 H Street, NWWashington, DC 20433Tel: (202) 473-0632Fax: (202) 522-3234
[When the Committee was formed Dr.Feachem was Dean, London School ofHygiene and Tropical Medicine.]
175
WHO Ad Hoc Health R&D Report, Draft 2.0
Dr. Julio Frenk(CO-CHAI, WORKING GROUP II)
Executive Vice President of theMexican Health Foundation andDirector of the Center for Health andthe Economy
Fundación Mexicana para la SaludPeriférico Sur 480914610 México D.F.MéxicoTel: (52-5) 655-9011Fax: (52-5) 655-8211
Baron Dr. Paul JanssenPresidentJanssen PharmaceuticalTurnhoutseweg 30B-2340 Beerse, BelgiumTel: (32-14) 602-111 OFax: (32-14) 602-841
Dr. Maureen LawDirector GeneralHealth Sciences DivisionInternational Development Research
CenterP.O. Box 8500Ottawa Ontario, KIG3H9 CanadaTel: (613) 236-6163Fax: (613) 567-7748
Dr. Philippe LazarDirector-GeneralINSERM101 mrue Tolbiac-75656 Paris cedex 13, FranceTel: (33-14) 423-6000Fax: (33-14) 423-6065
Dr. Sverre O. LieChairmanDepartment of PediatricsRikshospitalet0027 Oslo, NorwayTel: (47-22) 869-006 or 005Fax: (47-22) 422-822
e
176
The WHO Ad Hoc Committee: Review participants and study schedule
Dr. Juan Luis Londoño(CO-CHAIR, WORKING GROUP II)
Principal Health EconomistTechnical Department for Latin
Americaand the Caribbean
The World Bank1818 H Street, N.W.Washington, DC 20433Tel: (202) 458-5634Fax: (202) 522-3234
[When the Committee was formed Dr.Londoño was the Minister of Health ofColombia.]
Dr. Mahmoud M. MahfouzProfessor of Radiation Oncology and
Nuclear Medicine15b Sherif StreetCairo, EgyptTel: (20-2) 392-6670Fax: (20-2) 392-3726
Dr. Anthony B. MillerDepartment of Preventive Medicine
and BiostatisticsUniversity of TorontoMc Murrich Building12 Queens Park, Crescent West 4th
FloorToronto, Ontario, M5S 1A8 CanadaTel: (416) 978-2040Fax: (416) 978-8299
Mr. Rajiv L. Misra(CHAIR, WORKING GROUP III)
c/o World Health OrganizationRegional Office for Southeast Asia,
World Health HouseIndraprastha Estate, Mahatma Gandhi
RoadNew Delhi 110002, IndiaTel: (91-11) 331-7804, ext. 442Fax: (91-11) 331-8607 or 332-7972
177

WHO Ad Hoc Health R&D Report, Draft 2.0
Dr. Carlos MorelPresidentOswaldo Cruz FoundationAv. Brasil 4365, ManguinhosCaixa Postal 926Rio de Janeiro 21045-900, BrazilTel: (55-21) 270-2496Fax: (55-21) 260-6707
Professor A.S. MullerDepartment of Social MedicineAcademic Medical CentreMeibergdreef 151105 AZ Amsterdam, The
NetherlandsTel: (31-20) 566-4602Fax: (31-20) 697-2316
Professor Christopher J. L. Murray(CHAIR, WORKING GROUP I)
Harvard Center for Population andDevelopment Studies
Roger and Ellen Revelle Building9 Bow StreetCambridge, MA 02138Tel: (617) 495-8498Fax: (617) 496-3227
Dr. Plutarco NaranjoAvenida 12 de Octubre 2206Quito, EcuadorTel: (59-32) 225-632Fax: (59-32) 568-114
Dr. Sir Gustav rV. NossalDirectorWalter and Eliza Hall Institute of
Medical ResearchThe Post OfficeRoyal Melbourne HospitalMelbourne Victoria, 3050 AustraliaTel: (61-3) 345-2555Fax: (61-3) 345-2508
e
178
The WHO Ad Hoc Committee: Review participants and study schedule
Dr. B.O. OsuntokunUniversity of IbadanDepartment of MedicineNeurology UnitP.M.B. 9388 Ibadan, NigeriaTel: (23-422) 810-4745Fax: (23-422) 241-0489
Professor Richard PetoClinical Trial Service Unit & ICRFCancer Studies Unit
Radcliffe InfirmaryUniversity of OxfordOxford, OX2 6BR United KingdomTel: (44-186) 457-241Fax: (44-186) 558-817
Dr. Jean-Pierre PoullierHead, Health Policy StudiesOrganisation for Economic
Cooperationand Development (OECD)
2 Rue Andre-Pascal75775 Paris Cedex 16, FranceTel: (33-14) 524-9186Fax: (33-14) 524-9098
Dr. Srinath K. ReddyDepartment of CardiologyCardio-thoracic CentreAll India Institute of Medical SciencesAnsari Naar, New Delhi, 110029 IndiaTel: (91-11) 685-2899Fax: (91-11) 686-2663
Dr. Susanna SansInstitute of Health StudiesU.D. Hospital Sant TanPavello del Convent 20 P167 Avenida Sant Antonio ClaretBarcelona, 8025 SpainTel: (34-3) 456-3612Fax: (34-3) 433-1572
179
WHO Ad Hoc Health R&D Report, Draft 2.0
Professor Norman SartoriusI chemin Gilbert Trolliet1209 Geneva, SwitzerlandTel: (41-22) 740-1538Fax: (41-22) 734-3469
Dr. Jaime SepúlvedaDirector GeneralInstituto Nacional de Salud PúblicaAv. Universidad No 655 - 2o. PisoCol. Sta. Ma. Ahuacatitlán62508 Cuernavaca, Morelos, MexicoTel: (52-73) 17-57-34Fax: (52-73) 11-24-72
[When the Committee was formed Dr.Sepúlveda was Undersecretary,Department of Health, Republic ofMexico.]
Dr. Vladimir P. SergievDirectorMartsinovsky Institute of Medical
Parasitology and Tropical Medicine20, Malaya PyrogovskayaMoscow, 119435 RussiaTel: (70-95) 246-8049 or 0644Fax: (70-95) 246-9047
Dr. Yukiko SuginoAdviserTakeda Chemical Industries, Ltd.3-6 Doshomachi 2-chome Chuo-kuOsaka, JapanTel: (81-6) 204-2027Fax: (81-6) 204-2168
Dr. Derek YachGroup ExecutiveCommunity Health Research GroupMedical Research Council1 Soutpansberg RoadPrivate Bag X385Pretoria 0001, South AfricaTel: (27-12) 324-1680Fax: (27-12) 324-1695
e
180
The WHO Ad Hoc Committee: Review participants and study schedule
WHO Secretariat
Dr. Tore Godal(STUDY CO-DIRECTOR)
Director, Special Programme forResearch and Training in TropicalDiseases (TDR)
World Health OrganizationCH-1211 Geneva 27, SwitzerlandTel: (41-22) 791-3802Fax: (41-22) 791-4854
Dr. James Tulloch(STUDY CO-DIRECTOR)
Director, Division of Diarrhoeal andAcute Respiratory Disease Control(CDR)
World Health. OrganizationCH-1211 Geneva 27, SwitzerlandTel: (41-22) 791-2632Fax: (41-22) 791-4853
Dr. David B. EvansEconomistSpecial Programme for Research and
Training in Tropical Diseases (TDR)World Health Organization20, Avenue AppiaCH-1211 Geneva 27, SwitzerlandTel: (41-22) 791-3767Fax: (41-22) 791-4854
Dr. Katja JanovskySocial Scientist-National Health Systems and PoliciesWorld Health Organization20, Avenue AppiaCH-1211 Geneva 27, SwitzerlandTel: (41-22) 791-2568Fax: (41-22) 791-0746
181
WHO Ad Hoc Health R&D Report, Draft 2.0
Dr. Alan D. LopezScientistProgramme on Substance AbuseWorld Health Organization20, Avenue AppiaCH-1211 Geneva 27, SwitzerlandTel: (41-22) 791-2374Fax: (41-22) 791-4851
Dr. Thomas C. NchindaMedical OfficerSpecial Programme for Research and
Training in Tropical Diseases (TDR)World Health OrganizationCH-1211 Geneva 27, SwitzerlandTel: (41-22) 791-3808Fax: (41-22) 791-4854
eCommittee staff
Dr. Joel Almeida(Research Associate)c/o GTBWorld Health OrganizationCH-1211 Geneva 27, SwitzerlandTel: (41-22) 791-2655Fax: (41-22) 791-4199
Ms. Phyllida Brown(Science Writer)28 Archbishops PlaceLondon SW2 2AJ, United KingdomTel: (44-181) 674-5140Fax: (44-181) 244-8260
Mr. Leslie Evans(Technical Editor)Center for Pacific Rim Studies11290 Bunche HallUniversity of CaliforniaLos Angeles, CA 90095-1487Tel: (310) 206-3556Fax: (310) 206-4018
182

The WHO Ad Hoc Committee: Review participants and study schedule
Dr. Catherine Michaud(Research Associate)Harvard Center for Population and
Development StudiesRoger and Ellen Revelle Building9 Bow StreetCambridge, MA 02138Tel: (617) 495-0419Fax: (617) 496-3227
Mr. Claude Nanjo(Research Associate)Center for Pacific Rim Studies11288 Bunche HallUniversity of CaliforniaLos Angeles, CA 90095-1487Tel: (310) 206-8984Fax: (310) 206-4018
Dr. Beatriz Zurita(Research Associate)Fundacion Mexicana Para La Salud
PeriféricoSur No. 4809Col. El Arenal TepepanDeleg. Tlalpan, 14610, México, D.F.Tel: (52-5) 655-9011Fax: (52-5) 655-8211
183

WHO Ad Hoc Health R&D Report, Draft 2.0
Study schedule e
e
e
e
e
184
Annex 5
REVIEW OF RESEARCH PLANS AND ACTIVITIES AT REGIONALLEVEL (Agenda item 9)
AFR/ACHR
1. INTRODUCTION
1.1 African Health Policies and research Priorities
The regional policy on health development has served as a framework for countries informulating and/or improving their respective health policies. It emphasized the tripod ofstrengthening the managerial capacity of the health system, human resources development andhealth research as the cornerstone of health development. Priority health programmes that havebeen adopted by the Regional Committee are the basis for identifying the priority areas forresearch.
Despite existing modest research infrastructure, weak research coordination, severefinancial constraints and inadequate health information support, several countries are conductingresearch in health. Nevertheless, individual capacities and research proposals are still weak in mostof the countries. Most of research activities are externally funded. The dissemination of researchresults and related information are not adequately managed by decision makers.
Consequently the review of national health policies in 1994 indicates the need to makepolicies on health research more explicit.
1.2 Revitalizing Research in the Region
Early in 1995, efforts to revitalize research in the Region were initiated through thesemeasures:
a) redesignation of Regional staff responsible for research in AFRO;b) designation of membership of the African Advisory Committee on Health
Development;c) reconstitution of the AFRO Research Development Committee;d) revival of the quarterly technical series on public health;e) updating and re-organizing of the Regional Expert's Panel;f) establishment of the inventories of research activities, institutions and
extrabudgetary - funded projects.
A Medium Term Plan for Research Policy and Strategy Coordination for 1996-1997 in theAfrican Region was prepared, taking into consideration the constraints described in the introductionand the 9GPW. It aims to collaborate with countries in preparing and implementing nationalresearch policies and plans, better utilization and coordination of resources and results, promoting aresearch culture among health sciences institutions and personnel.
-2-
1.3 Financial Support to Health Research
To implement the 1990 African ACHR recommendation on the progressive allocation ofhealth sector funds for research, countries were encouraged to identify activities and allocate fundsin the health research budget line of the AFRO Programme Operations Coordination (AFROPOC)system. For the 1994-1995 biennium, the total allocation by all countries was nearly one percent.These activities fall into four categories research preparation conduct and dissemination, training,technical support, materials support. While these activities involve the WHO regular budget, manyothers are undertaken with extrabudgetary-funding.
1.4 Research Activities
Research activities were integrated into health programmes in the areas of:
a) appropriate technology for example solar power laboratory equipment in 3countries, vaccine virus monitoring;
b) land-based sources of population;c) effectiveness of insecticide impregnated materials in reducing malaria, and insect
sensitivity to insecticides in refugee camps;d) preparation of a distribution map on A. Gambiae in each country in the Region;e) studies related to ARI, CDD, EPI, LEPROSY, TB;
In relation to district health systems, the following activities have been implemented:
a) establishment of baseline on district health profiles involving 1071districts in 30 countries
b) development and testing of a protocol on the rapid assessment of the managementof district health systems
c) review of experiences on monitoring the progress of community health
2. RESEARCH TRAINING CAPACITY STRENGTHENING
2.1 HSR Project
This was initiated in 1987 with support from the WHO, the Dutch Technical Cooperation(DGIS) and the Royal Tropical Institute (RTI) to promote and apply HSR results in decision-making. A proposal for Phase 3 (1996-2000) has been submitted to donors with WHO/AFRO asthe executing agency and covering 18 Eastern and Southern African and Lusophone countries. Itwill be country-focused with emphasis on sustainability of the HSR process, the strengthening ofrelevant structures and mechanisms and coordination among external partners. The following keystrategies in previous Phases remain valid for the third Phase: i) advocacy, ii) capacity buildingthrough HSR training, training of trainers and integration of HSR in selected curricula, iii)technical and financial support to the conduct of research and use of results, iv) strengthening ofHSR institutions, v) networking through intercountry meetings, publications, TCDC andvi) linkages with institutional and international agencies and other donors.
e
-3-
2.2 Research training
The HSR Project has developed 5 training modules which have been translated into threelanguages, widely disseminated and used including in the training of 800 provincial and districthealth workers through workshops since 1987. Of these, 200 received further training asfacilitators. The HSR Project has supported 100 studies evolved from these HSR workshops; 50%of results had been fully implemented. Summaries have been published and disseminated.Networking was successful in sharing country experiences among the participants of the HSRProject. An intercountry HSR Newsletter has been published twice a year. Three universities havepartially achieved the integration of HSR into various university curricula.
Other research-related training provided in the Region were as follows: i) 28 scientists (10countries) participated in 2 workshops on epidemiological research methodology organized by theRegional Centre for Training in Reproductive Health, ii) epidemiology and invermectin distributionas part of the Onchocerciasis Control Project devolution scheme, iii) epidemiology for districthealth teams (4 countries). By 1994, 355 senior level health officials have been trained inepidemiology over a 10 year period Programming by the countries of 24 national courses for 1995reflected their interest in this activity.
Other research-related training have provided in the Region, namely on epidemiology.
2.3 Research Structures and Institutions
As of 1994, there were 46 registered WCCs in the region. Five institutions weredesignated as WCCs during the 1993-94 biennium in the areas of: Blindness Prevention (Malawi,Mali, Nigeria), Mental Health (Nigeria, Zimbabwe) and Oral Health (South Africa). Assistancewas provided to the Network of African Postgraduate Public Health Training and ResearchInstitutions (NAPHTRIP).
2.4 Health Information Support to Research
In response to an identified need for the availability of, and improved access toinformation on health research in the Region, the collection of data on research activities incountries towards the establishment of a Health Research Information System for Africa (HERISA)was revived in 1995. All Member states have started compiling on-going research which will beorganized into a regional data base.
Additional information support was provided by the WHO/AFRO library with the regularpublication of the African index Medicus commencing in 1993, in collaboration with the WHO/HQlibrary in Geneva.
3. RESEARCH MEETINGS AND CONSULTATIONS
In line with the approach of integrating management improvement with training andresearch, the AACHD could not meet in 1994 due to the social and political climate in Brazzaville.A Consultation on Health Research and Development took place later in the year. The 1993meeting discussed a document on Research and Monitoring of Community Health using
-4-
27 indicators and based on the analysis of household surveys (conducted in 41 countries from 1988to 1992) to measure progress in community health.
The 1994 Consultative Meeting on Health Research and Development reviewed research inlight of the 9th General Programme of Work (9GPW). More specifically, it:a) assessed the relevance of research policies to the prevailing health problems and b) evaluatedprogress on research, related fellowships and overall support to research. It recommended: i)institutionalization of research inventories and mechanisms for health research; ii) strengtheningand increasing essential health research and iii) strengthening national mechanisms for reviewingand awarding research implementation and collaboration.
PAHO/ACHR
The 33rd meeting of AMRO/ACHR took place on 19-21 April 1995, in Salvador, Brazil.In the absence of the chairman, Dr Adolpho Martinez-Palomo, Dr Naomar de Almeida Filhopresided this meeting.
Four topics of the agenda should be highlighted: the role of the research in theimplementation of the PAHO's Strategic Programmatic Orientations (SPO); the situation of healthresearch in Latin America and the Caribbean; new PAHO initiatives for promoting andstrengthening research capabilities in the Region and the structure and function of the RegionalACHR:
1. The Directors of the five divisions of AMRO, each of them acting as focal point for one ofthe SPOs, have participated in the last ACHR meeting and presented the regional situation of theircorrespondent area, the strategies of technical cooperation and their views about the role ofresearch to implement these strategies.
In relation to this topic the main discussions and recommendations of the ACHR were thefollowing:
- The emergence of the health promotion approach present a series of conceptual andmethodological challenges. It is necessary to define what is understood by "promotion" and by"health" as well as other related concepts such as quality of life and lifestyles. The concept ofrisk, which is basic for epidemiology related to disease prevention, cannot continue as the basis foran epidemiology geared toward health promotion. The shift from disease prevention to healthpromotion would entail no longer research or activities to prevent a specific, clinically defineddisease, but rather studying a complex social process that is taking place in order to redirect it forthe sake of a health concept that is still being developed.
- Until recently, ecological studies were considered of secondary importance in the area ofepidemiology. This position is currently being revised. PAHO, which in the 1950s and 1960spromoted a more conceptual ecological perspective when methodological developments were justbeginning, should promote them once again--this time, however, with greater prospects for successdue to current methodological advances.
- The Committee considered the significance of the problem posed by re-emerging andemerging diseases, particularly the need for surveillance systems for early detection. Also noted as
-5-
necessary was the capability to monitor changes in infectious agents, which should be theresponsibility of the competent institutions of the Region, through a network of CollaboratingCentres established for this purpose.
- Need for strengthening Health Systems and Services Research (HSSR). For some timePAHO/WHO has been carrying out a series of activities including training, support for projects,dissemination of information in order to promote HSSR in the Region. The Committee recognizesthe pressing need to coordinate these activities with other agencies working in this field in order toachieve the greatest possible results.
2. In relation to the situation of health research in the Region, a study made by the secretariatwas presented in the ACHR meeting about the scientific production of six Latin Americancountries in the period 1972-1992 (Argentina, Brazil, Chile, Cuba, Mexico, and Venezuela). Thedata were collected from the database of the Institute for Scientific Information (ISI). Thisdatabase does not provide a complete inventory of
scientific production in the countries under consideration, but it affords an inventory of the highestquality research published internationally.
Among the findings of this study the following should be mentioned:
- for the entire period 1972-1992, there were 41,238 articles published by authors residingin one of the six countries. These countries are the source of nearly 90% of total scientific outputof Latin America and the Caribbean, both in general and in the health sciences in particular.
- the concentration of scientific output among these six countries is increasing, with theproportional share from Brazil and Argentina having grown from 57% in 1973 to 68% in 1992.The concentration has varied according to the types of research; clinical research is the mosthomogeneously distributed, public health research the most concentrated (60.7% of these articlesare from Brazil). This last point raises grounds for concern because public health research requiresgreater decentralization, given the diversity of problems faced and their influence on decision-making affecting health care.
- there is also an imbalance between the types of research, since public health research(epidemiology and health systems research) accounts for only 2.7% of the articles. The averagenumber of citations for an article whose first author resides in one of the six countries studied isthree (3) per article, less than half of the average citations per article for the total number on theISI database (7.78%). This average is not uniform for different types of research. The averagenumber of research citations of a biomedical article were 4.03, whereas public health articles were
1.61.
In the discussion on the health research situation in the Region, recommendations weremade by the ACHR that the secretariat should continue studies on scientific output, expand thesources of consultation, and combine qualitative and quantitative analyses in order to betterunderstand the actual situation in the Region.
The Committee reiterated its concern about understanding better what is happening withresearch funding in the Region, particularly the analysis of funding amounts, sources, andmechanisms and recommended studies about this topic. It also noted that even though research is
-6-
basically carried out with public funds, its orientation does not respond to the major public healthproblems.
The Committee mentioned the need to promote a "publication culture" in the Region,particularly in the area of public health research, because many of the results are not published inwidely circulated journals. PAHO should also step up the activities of the Latin American andCaribbean Center on Health Sciences Information (BIREME) that are currently in progress toimprove the quality of journals published in the Region and have them included in internationaldatabase.
3. In the presentation of the new initiatives and lines of cooperation put in place by PAHO in1994/95 it was emphasized:
- Cooperative activities in policy-making and management of research institutions. Thedegree of institutionalization of scientific activity in health and the complexity of the S&T systemhave made it necessary for research institutions in the Region to define more precisely theirinstitutional policies and priorities. Studies, models of analysis and meetings with researchers,administrators and policy makers have been developed in order to support the strategic planning ofthese institutions;
- In the areas of public health research and biotechnology, new mechanisms have beenlaunched combining training, support for research projects, institutional development, andstrengthening ties between institutions in the United States, Canada, and Europe and those in LatinAmerica and Caribbean. Through an agreement with the National Institutes of Health (NH),research grants are awarded annually for research projects using biotechnology techniques. Thegrants include a 3-month training period at NH (or an affiliate institution) and at least onesupervisory visit by an NH researcher to the LAC institution in which the project is under way.An agreement with the Canadian International Development Research Center (ICRC) will allow toaward nine grants each year for public health research training. For 1-year period, LACresearchers could complete their education at post-doctoral level in institutions in the United States,Canada, or Europe. By the end of the year, the researchers should present a project to theResearch Grants Program in order to obtain a grant on returning home.
- In respect to the Research Grants Program new strategies for the administration of theprogram are in place with the objective to increase and diversify the demand and to improve thequality of proposals. PAHO is promoting several "research competitions", focused in the RGPpriority areas. The award candidates are preselected to participate in workshops where theyreceive technical support from experts to improve their projects. The proposals are then submittedto ad hoc committees integrated by experts in the area.
In the discussion of those activities, the Committee imparted a positive response tocompetitions and workshops as new forms of promotion and support for projects. It was suggestedthat the scale of projects be reviewed, but with the recognition of the importance of continuing tofill the niche of medium-size projects costing between US$20,000 and US$30,000. Taking intoconsideration this recommendation, after the meeting, PAHO's Director decided to expand therange of projects. By the end of this year it will be launched a Research Grants subprogram tosupport doctoral theses. This subprogram should encourage new vocations to study subjects ofinterest to the Organization. The quality of the projects would be ensured because they would beundertaken under the responsibility of a thesis adviser. On the other hand, support will be given
-7-
also to larger projects, involving several institutions, which will allow comparative analyses ofsubjects of interest selected by the Organization according to its criteria. The call for proposals,which will be taken under a common protocol, will be made on a case by case basis in due course.In 1995, a multi-institutional project of this type is on preparation on the subject of violence andhealth. The practice of shared financing in partnership with other funding sources will bestrengthened in order to support projects of greater scale.
4. Finally, in relation to the structure and role of ACHR the principal recommendationsfavour a more active profile for the Committee and its members in the work of the Organization,more frequent meetings, maintenance of current subcommittees (Biotechnology and Health Systemsand Services Research).
PAHO's Director stressed that the Committee cannot simply endorse what PAHO does andserve as a rubber stamp; that would be a waste of time and resources. The Committee shouldfocus its efforts on orienting PAHO research policies, along with other technical cooperationactivities of the Organization and for the next four years should be concentrated in the five areasselected by the Governing Bodies as SPOs.
He announced his decision to return to hold annual meetings, to expand the number ofACHR members from 12 to 15 and to maintain the two existing subcommittees, emphasizing theneed to energize the HSSR Subcommittee. Following the meeting of the ACHR the HSSRSubcommittee met on September 14-15 in the University of North Carolina and a Plan of Actionto promote and strengthen HSSR was discussed and recommended to be implemented in 1996.
EMR/ACHR
I. Highlights of Regional "ACHR-Related" activities since the 32nd Session of theGlobal ACHR.
1.1 The 18th Session of the EM/ACHR, Riyadh, Saudi Arabia, 20 - 22 March 1995.
1. The session was inaugurated by H.E. The Minister of Health, Saudi Arabia, Mr Faisal AlHujailan, who stressed the important role played by the EM/ACHR in supporting health research inthe Region. He noted that it was not possible to identify priority health problems and providesolutions for them without promotion of health research capabilities in the different countries. Asregards Saudi Arabia, he mentioned that the health research
projects supported by the MOH were based on the national health policies and priorities with PHCbeing the comrner stone.
2. Dr Hussein A. Gezairy, Regional Director, in his address to the meeting, explained theworking of the ACHR both globally and regionally. The EM/ACHR assists in developing regionalresearch programmes and advises the RD on ongoing and planned research activities in the EMR.He mentioned that since the previous session the research programme at EMRO has been activeand included: support of research projects particularly with respect to health systems research(HSR) and diseases of modemr lifestyles, technical and financial support to various nationalactivities, and continuation of the visits of the Task Force on Health Research.
-8-
3. A report on the Progress of the EMR Research Programme was presented by De El SheikhMahgoub, acting RPS. He mentioned the various activities that have been initiated by EMROduring the past two years i.e. since the last session of the Committee.
4. The experience of the MOH Saudi Arabia in health research was presented by Dr OthmanA.A. Al-Rabieah, Adviser to the Minister of Health. The following comments emerged at thediscussion:
* The Saudi Ministry of Health programme was a success because it was backed by politicalcommitment, a viable health research structure and a committed budget.
* The establishment of peripheral health research structures was an important step incomprehensive health research promotion in the Kingdom.
* The positive impact of the short research training courses at the Colleges of HealthSciences was apparent.
* The continuity of leadership of the Saudi Ministry of Health shows the importance of thisfactor in health development in general, including health research.
* WHO input in Saudi Arabia is technical rather than financial, which underlies theimportance of this aspect of WHO support.
5. The following four topics were presented as selected technical papers:
5.1 Dissemination and Utilization of Research Results
The importance of the topic was stressed and the various methods and target groups werescanned. It was recommended:
(a) that Member States should consider the establishment of a national body to be responsiblefor the dissemination of research results,
(b) strengthening networking between different research centres in the Region and institutingregional mechanisms for dissemination of research results.
5.2 Viral Hepatitis C and E
Following a general consideration of the topic, the situation of viral hepatitis in Pakistanwas presented. The discussion revealed that the Pakistan experience was similar tot hat of someother countries in the Region, e.g. Egypt and Sudan. Further information on the matter wasneeded from all the countries; in this respect WHO was launching a large scale survey to beginsoon. It was recommended:
(a) that research priorities in this field include mode of transmission,
(b) WHO considers holding an Intercountry meeting on hepatitis in order to prepare relevantprotocols and set priorities for research in this field.
-9-
5.3 Ethical Considerations in Health Research
The impact of recent advances in sciences and technology on the ethics of health researchwas noted. The ethical codes and guidelines prepared by the Council for InternationalOrganizations of Medical Sciences (CIOMS) were mentioned. It was pointed out that the sourcesof health ethics were drawn from various value systems - and that religion was particularlyimportant in the EM Region. The following recommendations emerged from the discussion:
(a) EMRO should have its regional ethical review committee or at least develop guidelines forbenefit of Member States;
(b) Member States be encouraged to set up ethical review committees;
(c) research projects submitted for funding whether at WHO/HQ or its Regional Officesshould have ethical clearance;
(d) a special committee or group to be established to look into the problem of clinical trials incountries of the Region for new drugs and vaccines that have not been comprehensivelytested in industrialized countries where they have been developed first;
(e) trials of non-medical interventions which have indirect effect on human beings, e.g.insecticides, should also be considered seriously; and
(f) this topic should also be presented at the next meeting of National Officer Responsible forHealth Research in Member States.
5.4 Psychological Aspects of Hereditary Diseases and Genetic Counselling
It was mentioned that hereditary disorders are involved in a significant number of mentaland physical diseases. Because of the advances on medical genetics, guidelines for counselling andconduct of genetic services become necessary. The recommendations included:
(a) those aspects that have greater health related impact to be given due priority in theRegion's health research projects;
(b) orienting research towards training of health workers, counsellors and teachers and in thedevelopment of curriculum material; and
(c) whenever possible, research on mental health and noncommunicable diseases to includesections related to genetic aspects of these disorders.
6. Report on the Progress of the UNDP/World Bank/WHO Special Programme forResearch and Training in Tropical Diseases (TDR)
This was presented by Dr J. Hashmi, Medical Officer, TDR. He stated that the researchand development component of TDR had been restructured as of early 1994. The disease specificsteering committees have been disbanded and three new components established:
- 10-
i. Strategic Research (SR)
ii. Product Research and Development (PRD)
iii. Applied Field Research (AFR).
He also presented some highlights of TDR activities related to filariasis, leishmaniasis,leprosy, malaria and schistosomiasis. He informed the meeting that a new grant format "RegionalLinkage Grant for Research Training" was established in 1993. He also referred to the JointEMRO/TDR/CTD Small Grants Programme initiated in 1992 to promote control-related researchon leishmaniasis, malaria and schistosomiasis. It was recommended that (a) TDR/RCS to continueto provide funds for EMR/CTD/TDR Small Grants programme, (b) Member States be advised byEMRO to utilize WHO fellowship fund for training of promising young scientists in TDR relatedfields.
7. Highlighting of the Global ACHR, 32nd Session, 10-14 October 1994
This was presented by Dr B. Mansourian, Director RPS/WHO Geneva. He mentioned thatthis session was marked by a return to the Global ACHR cycle of annual meetings. For the firsttime a report on the ACHR was formally presented by the Director-General to the Executive Boardat its January 1995 Session. Discussion was focused on three main items (i) the impact ofscientific advances on future health - the committee urged developing countries to participateactively in the use of new developments and advances in science and technology, (ii) healthresearch policy - where several studies were made and compiled in a reference monograph entitled"Research for Health: Principles, Perspectives and Strategies",(iii) health policy research - presented to the ACHR for the first time although closely linked withHSR - considered as the process of scientific investigation in setting policies leading to formulationof strategies, priorities and plans for health development.
8. The general recommendations on research promotion to Member States were:
8.1 To countries. Countries should:
i. Send their newly appointed national focal points to EMRO for orientation on regionalresearch activities and opportunities for research grants, (ii) establish national review committeesfor health research from experienced researchers in order to help young or new researchers inpreparing research protocols and even guiding them in the research activities, (iii) give priority toresearch programmes in country allocations from the regular budget of WHO, (iv) encourageholding workshops for training in research methodology for health personnel, (v) give dueattention for training in research methodology in undergraduate and postgraduate curricula, (vi)encourage the establishment of national research institutions in countries that do not already havethem, (vii) promote positive relations between ministries of health and universities and otherscientific agencies and Collaborating Centres, (viii) set up a national research agenda which shouldbe prioritized, (ix) national research bodies should get actively involved in the dissemination ofresearch results.
e
- 11 -
8.2 WHO should:
i) promote research: the Regional Director will contact countries asking them to give dueattention for national research programmes, ii) include the subject of research as a topic fortechnical discussion at a forthcoming session of the RC, iii) disseminate information about researchopportunities available in WHO, iv) promote positive relations between ministries of health anduniversities and other scientific agencies and collaborating centres, v) establish and strengthennetworking between research centres in the Region, vi) compile abstracts of research in the Regionand disseminate to researchers and decision makers in the countries? vii) The Regional Office couldadopt some commissioned research suggested, and near consensus on it brought about, by thecountries.
1.2 Follow-Up of the Recommendations of the 17th Session of the EM/ACHR
These pertained to three topics: Diseases of Modem Lifestyles, Health of Adolescents,Human Reproduction. The fellow up included:
a. strengthening national capacities e.g. through sponsorship to attend conferences,preparation of protocols and manuals, partial support of research proposals and offering oftechnical advice.
b. motivation and support for Member States to develop relevant national programmes.
II. Regional Research Activities
11.1 Review of Research and Development Activities in the Region
11. 1.1 Support for Research Projects (EMR Research Grants)
During the past year a total of US$81 662 was spent on support of 7 research projectscovering areas on HSR, epidemiological research, clinical studies on non communicable diseases,community participation, MCH and environmental issues. They formed about 1/3 of the totalapplications. The two main factors for rejection were (a) not choosing researchable problemswithin EMR priorities, (b) inability to develop research protocols.
II.1.2 EMRO/TDR/CTD Small Grants Programmefor Control-Oriented Research in TDR-targeted Diseases
An amount of US$100 000, contributed by RD/EMRO (50%), TDR/HQ (30%) andCTD/HQ (20 %) has been allocated annually to support research of an operative nature in TDR-targeted diseases. In 1994/95 these grants were earmarked for malaria, six being awarded, eightother proposals referred for improvement and nine rejected. Since the launching of this scheme in1992, 30 such grants were awarded, the quality of research being good and the projects well-managed.
- 12 -
II. 1.3 EMRO Prizesfor Health Research and Health Systems Research
The EMRO prize scheme was launched in 1991 to encourage young scientists to undertakehealth research and health systems research. In 1994 there were 64 submissions from 39applicants representing 8 Member States. It was a strong competition with stringent criteria forrating and selection. Hence it was gratifying to find that 15 submissions were rated as "A".
II. 1.4 Technical and Financial Support to National Health Research and Development Activities
These centred mainly on support for various national meetings and consultations to developpolicies and strategies and convene scientific conferences.
II. 1.5 Visits of the Task Force (TF) for Health Research
The TF mechanism has been in operation in the EMR for more than a decade now. It hasproved very useful in activating research in Member States and getting researchers from variousinstitutions and decision-makers in the MOH to sit together and agree on a sustainable system forhealth research and development activities.
The terms of reference of the TF were as in previous visits with emphasis on theidentification of a health research policy and strategy especially in relation to the development ofPHC system. The missions were undertaken through visits to policy makers, researchers andvarious institutions engaged in health or health-related research. The Minister of Health and theWR were kept informed of the findings and of the proposed recommendations.
During the past year three TF visits were undertaken: (i) to Syrian Arab Republic (3-9December 1994), (ii) to Lebanon (10-14 December 1994) and (iii) to Libyan Arab Jamahiriya (3-10 June 1995).
At the 1 8th session of the EM/ACHR the following recommendations were made withrespect to the TF visits:
i. since the TF mechanism has proven its worth, Member States that have not yet made useof it are to be encouraged to do so. ii. EMRO to compile, analyze and publish the experiencearising out of the TF visits so as to highlight details of both regional and national policies andstrategies and to make this novel experience adopted by EMRO available to WHO/HQ and itsother Regions.
II.2 Research Training and Related Institution Capability Strengthening
II.2.1 EMR Research Training Grants
One grant has been awarded to a researcher to visit an advanced centre for researchtraining in connection with his research project.
e
- 13 -
II.2.2 National Training Activities
i. three national training activities on HSR were held in Egyptii. a training course on HSR development was held in Jordaniii. a national training workshop on health research and HSR was held in Yemen
II.2.3 WHO Collaborating Centres
EMRO encourages the establishment of these centres to boost institutional capabilities and
activate the implementation of WHO programmes. Hence it is gratifying to see a growing interest
among Member States in this respect. During the past year five new centres were designated,bringing the total number of WHO Collaborating Centres in the EMR to 48.
11.3 Research-Related Meetings and other Consultation Type Activities
11.3.1 Sixth Intercountry Meeting of National Officers Responsiblefor Health Research (Cairo,27-29 August 1994)
This meeting was attended by both MOHs focal points for research and others in charge of
health research. It adopted the following recommendations:
a. WHO to conduct a study to evaluate the HSR development processes and networkingmethods in Member States,
b. MOHs to develop mechanisms for allocation of funds for HSR in their own budgets,
c. each country to identify a more permanent national focal point for HSR in order to achieve
a more efficient follow-up of country programmes through implementation ofrecommendations made in previous meetings,
d. sustain efforts in HSR orientation because of the continuing development in this field and
the relatively rapid turn-over of managers and policy makers,
e. EMRO to continue with its TF mechanism and motivate countries to benefit from it in
developing and evaluating their HSR programmes,
f. EMRO to evaluate the impact of the WHO Collaborating Centres int he development ofhealth research in general and HSR in particular,
g. EMRO to compile and disseminate information about the organizational setups of healthresearch and HSR in Member States.
II.3.2 Intercountry Workshop on Reproductive Health Research Methodology (Dubai, UAE, 25-
29 March 1995)
The RA/RPS participated in this workshop where he acted as a resource person to help
participants in developing protocols in MCH. Several protocols were developed by the
- 14-
participants; these are to be further refined at EMRO and sent to Member States to select anddevelop as appropriate.
II.3.3 Global Activity
The Regional Adviser, RPS, participated in the "Workshop on New Approaches for HealthResearch Strategy", held be the WHO Collaborating Centre for Global Modelling of HealthPerspectives, at the International Institute for Scientific Cooperation at Schloss Reisensburg nearUlm, Germany, from 2 to 8 April 1995. The workshop concentrated on (a) quantifying researchpriority areas for both developing and developed countries (b) building new approaches forinteractive research planning processes using modern technology.
EUR/ACHR
The stringent economic situation of the Region and consequently of the WHO RegionalOffice for Europe has continued and worsened since the last meeting. This has prevented theRACHR from convening, and otherwise the activity has been extremely low due to low prioritygiven to health research by the EURO Office under the pressures from many other compellingpriorities such as the assistance in the former Yugoslavia and the RACH also propose that theother bodies active in the Region will take care of health research policy. There is an idea that theextensive research programmes of the European Union will cover part of the activity needed andthe European Science Foundation the rest. It is however not likely that this will happen. Eventhough the activities mentioned above are most valuable in their own jurisdictions, all regionalresearch policy needs are not covered by those mechanisms. This is particularly true in the case ofhealth research needed in the non-EU Europe. WHO/EURO should have and keep the leadershipin regional health research policy and of course collaborate in relevant issues with EU, ESF andother relevant bodies. Only the WHO/EURO policy in health research can be expected to beeffectively integrated and coordinated with the global health research policy of WHO, whilethough desirable, this cannot be automatically expected from the other health research activitiescarried out in Europe.
It should also be noted that no other body in the Region has that mandate with suchgeographic and substantive coverage as that of WHO/EURO. This implicitly also means thatleaving the responsibility to others automatically leaves holes in the coverage of this mostimportant activity. It also implies handing over the leadership to the limited group of countrieswhich do not and cannot represent the interests of all 51 European States. To state this is notmeant to prejudice the most important role of EU research policy and of ESF in the healthresearch of Western Europe; it just refers to variation in the research needs in different parts of theRegion. WHO/EURO would have an important role to balance the gap between East and West inhealth research and also in transfer of research results to the Eastern parts of the Region.
In spite of the low profile of the EACHR and of the low priority given to its activities,much relevant research activity and important developments have taken place within or incollaboration with the framework of WHO/EURO programmes. EACHR has however not playeda major role in those activities. Probably, the most active element among those programmes hasbeen the European programme for the environment and health, some details of which are describedhere.
- 15 -
Dialogue of Research with Policy-Makers
A WHO/EURO meeting was held last spring in Leeds, United Kingdom, to discuss theDialogue on Research Policy Links in Public Health, where all parts of the Region wererepresented. The meeting particularly concentrated in the dialogue and link between public healthresearch and policy-makers and financiers, particularly the R&D organizations, using the UK as astudy case. The conclusions and report on how new possibilities to develop such dialogue andsimultaneously raise funding for health research will be published by the end of 1995.
The European Environmental Health Programme and Action Plan
Due to growing of Europeans about their environment, environmental health research (EH)has been a major component of the WHO/EURO programme. The EH activities have beensubstantially strengthened by the establishment of the European Centre for Environment andHealth which, with the help of financial and political support of the Dutch, Italian and FrenchGovernments, was founded as a follow-up of the Frankfurt Environment and Health Conference(1989), and has Units in Bilthoven, Rome and Nancy. These Units have research and collection,analysis, and dissemination of information on the European EH situation as the main elements intheir activities.
As was described in the report for the 32nd Session of the GACHR, the EuropeanEnvironment and Health Action Plan, which was adopted in 1994 by 47 ministers of environmentand health, has been the most important guideline for WHO/EURO activities in EH. The officehas concentrated in the implementation of the 100 recommendations adopted by the MemberGovernments for the subsequent 5-year period. Due to severe economic constraints, theprogramme particularly for its research elements has been substantially constricted (some projectspostponed), but still a remarkable portion of about 20 research elements are under implementationunder the European Committee on Environment and Health. National programmes forenvironment and health are actively prepared by the Member Countries. The following activitieswith research elements have been given highest priority (Table 1):
- Environment and respiratory diseases- Accidents and injuries of all kind- Reproductive disorders and environment- Food safety and veterinary health- Urban development- Water hygiene- Physical and psychological consequences of nuclear contamination of the
environment.
Research in these areas is initiated and carried out as part of the other public health actionsand it is mainly very applied by nature. Synchrony and synergism are seeked for with the relevantresearch programmes and the EU and other bodies. Financial support and practical collaboration isalso obtained from the World Bank, particularly for projects in the CCEE and NIS.
A major effort was put forward in research, surveys and data collection for the documentConcern for Europe's Tomorrow, a 537 page book, which was published recently. The bookcontains the results of so far the most comprehensive study on health and environment ofEuropeans. It indicates the occurrence, distribution, intensity, trends and priorities of the EH
- 16 -
problems in Europe and proposes state-of-the-art solutions for their prevention and control. Thedata collected in the project also give guidance for further implementation of the EuropeanEnvironment and Health Action Plan and Programme. Though pan-European in character, due tothe urgent needs for environment and health in the Eastern parts of the Region, the most intensiveparts of the Programme are directed to the CCEE and particularly NIS.
The Fourth Framework Programme and BIOMED 2 of the European Union
The 12.3 billion ECU 4th Framework Research Programme of EU contains the BIOMED 2part with funding of 336 million ECU. This programme is designed to give a response to theactual and expected future health needs of the union countries. The BIOMED 2 reflects the majoradvancements and possibilities for the health sector provided by the modem biomedical research,new morbidity patterns seen in Europe, including new infections, re-emerging infections andgrowing prevalence of chronic diseases among the aging populations. Also the possibilities todevelop competitive industry providing products to the health sector, have been considered.
The priority research areas of BIOMED 2 are the following:
1. Pharmacology and development of new drugs2. Medical technology and technics3. Brain research4. Socio-economically important diseases5. Genetics research6. Research on public health and health services research7. Medical ethics.
The number of project applications in the year 1995 was about 7,700 and about 1/10 ofthem were given funding.
The 4th Framework Programme also contains a substantial elements for training youngscientists and also elements for promoting mobility of more senior scientists.
The Role of the European Science Foundation (ESF)
The collaborative organ of the European Research Councils, the ESF, has so far beenactive with very limited financial resources, but now the collaboration within the frames of the 4thFramework Programme of EU, it has now possibilities to strengthen its activities.
The ESF has offered EU and interesting proposal for its scientific contribution to the EUprogrammes, including BIOMED 2.
EU and WHO/EURO
The Environmental Health Action Plan was prepared in collaboration betweenWHO/EURO and the EU. WHO has recently produced a report on the health of the populationsof the EU countries. Numerous individual programmes are also carried out together. The recentlyestablished European Environment Agency in Copenhagen will substantially improve the practicalpossibilities for collaboration.
- 17 -
Situation in Eastern Europe
An extensive study on health status and on the state of the environment was carried out inconnection with CET Project. The study indicated the urgent needs for health and environmentactions in the most Eastern parts of the Region. Also, the needs for the development ofregistration, monitoring, and data systems, service infrastructures, methodology and qualityassurance, as well as for certain aspects of research, and training of experts are evident.
While some excellent research projects on health have been initiated, there is much workleft to develop health research as a research infrastructure providing continuously scientific-basedand a reliable picture on health development and research activity, which can provide sufficientsupport for policy-making on health, for methods development and for expert training. Theresources of WHO/EURO are not sufficient to meet those needs, but by creating productivecollaborative links and networks, some progress has already been demonstrated.
SEAR/ACHR
The participants in the meeting were the Directors of Medical Research Councils orAnalogous Bodies of countries in South-East Asia regions, the Regional Director and officers ofWHO/SEARO as well as special invitees.
The main objectives of the meeting are as follows:
- review the current status of and exchange information on research promotion,development, co-ordination and management;
- develop guidelines required for further improvement of national mechanisms;- develop an over all strategy for promotion technical cooperation;- outline the role of WHO in promoting the development of national research
mechanisms
A. The RPD activities were reviewed as follows:
(a) Regional Collaborative Studies on Drug Resistant P. falciparum malaria tochoroquine and others. A situation analysis is being conducted in 8 countries of the region(Bangladesh, Bhutan, India, Indonesia, Myanmar, Nepal, Sri Lanka and Thailand:
(b) Multicentre study of the process and out come of collaboration between the nursingservices and education in three countries (India, Myanmar and Thailand) in 1993, the study isdirected primarily towards the improvement of the quality of nursing care and secondarily toimproving the quality of nursing education.
(c) Development of a vaccine for Dengue Haemorrhagic Fever (DHF) has progressedto a stage of industrial production of monovalent vaccine which will be able to phase III trial inearly 1994. The formulation of tetra valent vaccine for children aged 5-9 years still requiredfurther requirement to obtain the optimal dose.
(d) Review of WHO/RPD Programmes in countries of the region in reference todevelopment of research activities in the country; impact on the national health research policies,
- 18 -
program and health development.
Urgent needs for fellowships for training for research capability strengthening such asEpidemiology was stressed especially among weaker countries.
B. Matters arising out of the 19th and 20th SEA/ACHRs for consideration of MRCswere discussed as follows:
1. Research for the improvement of Health Care Delivery System: SEA/ACHRacknowledged and supported the importance of HSR at the district level and the type of researchshould be operational and problem solving in nature.
2. Strategic Plan for promoting and strengthening Health Economic Research (HER):SEA/ACHR agreed that HER is essential for the development of health programmes in view offinancial and other resources constraints and the need to secure adequate resources inputs fordevelopment of health care systems. At the national level (macro) HER deals with prioritization ofresources; where as, at local or operational level, HER will deal with distribution of resourceswithin the health sector. Regarding the strategies to promote HER, ACHR took up the issue ofestablishing national training capacity to produce competent professionals to do HER. ACHR alsorecommended HER receive emphasis in the revised health research strategy of WHO/SEARO.
3. Health Policy Research (HPR) is the application of scientific methods in theformulation of policy options and the description of consequences or implications of each option.It is recommended HPR should be considered a priority area for promotion and support by WHO.
4. Strategies for research on Health Behaviour (HBR)
HBR is a part of health system research in its scope and purpose and it is based on bio-psycho-social model of health. It is presently recognized that undesirable health behaviour and lifestyle whether that be smoking, eating habits, lack of adequate exercise and others may lead tochronic degenerative diseases. Research evidences show that modification of undesirable todesirable behaviours can reduce the incidence of these diseases. Research findings also show thatinformation dissemination and awareness building do not necessarily lead to behavioral changes.Therefore, there is need to strengthen HBR in member countries of the South-East Asia region.
eC. Report on Special and Global Programmes:
1. A progress report on the research activities related to leishmaniasis, leprosy,lymphatic filariasis and malaria was made. Particular attention on the treatment of complicatedP.falciparum malaria by using artemesinin derivatives was mentioned in more details.
2. Research, Development and Research Training in Human Reproduction (HRP)Now, the program has extended its activities to cover wider field of reproductive health. Itaddresses the reproductive processes, functions and systems at all stages of life. Progress in thisdirection has been made in some member countries.
- 19 -
3. Acquired Immune-Deficiency Syndrome (AIDS) - WHO research strategy onHIV/AIDS includes biomedical, social and behavioral research and prevention research. Vaccinedevelopment has received the major part of WHO support. Clinical trial has already beenconducted in Thailand and India.
4. Operational Research on Tuberculosis Control: TB is a re-emerging diseases inmany regions of the world. It was generally agreed that the following studies will be carried outin SEA region:
- Development of Methods to enhance adherence to anti-TB chemo therapy, the roleof NGO/Private sector in the management of TB.
- Studies on surveillance of drug resistance in TB patients.- Research on the interaction of HIV and tuberculosis.
D. Health Future Trend Assessment:
The objectives of this study include:
- to predict future developments;- to provide early warning of potentially threatening developments or potential
opportunities;- to stimulate learning processes, imaginative thinking and creative design for the
future;- to enable people to determine the future they prefer;- to explore a range a alternative options;- to support strategic policy developments.
It is useful to have in mind some basis definitions of health futures and related items.
There are four types of future:
a. possible future, that is what may happen;b. plausible future, that is what could happen;c. probable future, that is what is likely to happen;d. preferable future, that is what we want to happen.
It was agreed that Health Futures Research conceptually and methodologically would be auseful tool as part of the health policy, planning and managerial process both at the national andprogram levels.
The work of ACHR during the past year in the context of Regional RPD Programme*
The Advisory Committee on Health Research, has been advising the Regional Director onformulating an effective Regional Health Research Policy and Strategies for the past two decades.This year, the SEA/ACHR celebrated the 20th anniversary. The twenty-first session of the South-East Asia Advisory Committee on Health Research (SEA/ACHR) was held at the WHO RegionalOffice for South-East Asia, New Delhi, from 10-13 April 1995 to review research promotion and
- 20 -
development activities of the Region. The meeting was attended by SEA/ACHR members specialinvitees from RPS/HQ, TDA, HRP, Vice Chairman of Global ACHR and WHO Secretariat.
Regional Health Research Strategies
The health research strategies of the Region were defined very clearly in 1993. Researchpromotion and development activities are being carried out in line with the said strategies, viz:
* Dr Tripathy kindly supplied the information Research is related to the eight elements primaryhealth care and researchable areas had been identified and prioritized within the framework of theeight elements of primary health care. Differential emphasis was given on health systems researchand that health research system is being developed as a whole and linked to the health care system.Inter-sectoral research and research beyond the health domain in matters affecting health has alsobeen promoted.
Summary of RPD activities during the preceding year
The research activities undertaken with the WHO country budget support for ResearchPromotion and Development were:
- Recruiting of short-term consultants in fields such as Health Systems Research,molecular biology, biotechnology, demography, nutrition, demography and healthstatistics, use of Rapid Assessment Procedures (RAP) in nutrition surveys, tobaccorelated diseases, population genetics, laboratory techniques such as pathogenesis ofDHF, medical sociology, health economics, etc.
- Improving institutional facilities by the acquisition of supplies and equipment.
- Publication of research bibliographies and abstracts and periodicals related toresearch.
- meetings of policy makers, administrators and researchers for the assessment ofresearch needs and priorities and development of plan of action for nationalresearch programmes.
- Conducting workshops to impart training in research methodologies anddevelopment of research project proposals.
- Provision of grants to research workers, including post-graduate students forstudies on identified national priority topics.
- Award of fellowships in diverse fields related to research. These includedmolecular biology including genetic engineering, cancer epidemiology, biomedicalstatistics, health management research, maintenance of biomedical equipment,advanced computer technology, library services, research administration andmanagement, clinical research, HIV infection and AIDS, clinical genetics, organtransplantation, nutrition, environmental health and health behaviour.
- 21 -
The activities carried out under the WHO inter-country RPD were - direct support forresearch, research training grants and visiting scientist grants, institutional strengthening grants,workshops, consultancy services, scientific meetings, WHO Collaborating Centres, and ExpertAdvisory Panels.
In relation to RPD activities, WHO/SEARO has already embarked on the:
a. Mechanisms to disseminate information on important outcomes of major research projects.
b. Assessment of research needs jointly by scientists, policy makers and administration.
c. Improvement of the quality of incoming research proposals by conducting workshops inthe countries. Follow up action had been built into the system for feed back in order tohave continuity. The balance between the social science workshops and biomedicalscience workshops has also been taken into account.
Health Policy Analysis/Research
Health Policy Analysis/Research (HPA/R) Proposals for a Promotional Framework werediscussed in the context of the role of WHO on HPA/R at the country level. The need tostrengthen the capabilities of countries inthis aspect was also discussed.
WHO/SEARO has already planned to embark on HPR activities along the following line:
a. Advocacy for Health Policy Analysis and Research will be receiving the highest priority invarious fora including ministers, parliamentarians, administrators, educationists, healthpersonnel and media community.
b. A Health Policy Analysis Advocacy kit will be developed, incorporating, among others,successful country experiences.
c. Capacity strengthening in Health Policy Analysis and Research will be built throughsupport initially to institutions already engaged in such activities and through traininggrants.
Global ACHR and ACHRs of other Regions
The principal terms of reference of the ACHR were recalled, mainly the general orientationof research activities, priority setting on the basis of policy guidelines emanating from theGoverning bodies and from the regions, review, of programmes in terms of scientific and technicalpolicy, formulation of ethical criteria applicable to research, and harmonization.
Three major items were discussed as follows:
a. the impact scientific advances on future health with special attention to emerginginfections, to information technology and to promoting awareness of global problems ofcritical significance to health;
- 22 -
b. health research policy; and
c. health policy research as the process of scientific investigation in setting policies,formulating strategies, prioritizing and planning for health development.
Attention would be given to the problems of equity and social development is insufficientand needs augmentation. The dialogue between the regional and global ACHR offices would alsobe strengthened.
Special and Global Programmes
UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases(TDR)
In this area, SEA/ACHR recommended to support research relating to:
a. finding suitable macrofilariacides,b. Promote Research in the use of DEC-fortified salt, andc research on drug resistant malaria and integrated malaria control on a priority basis.
Special Programme of Research Development and Research Training in HumanReproduction (HRP)
In the field of HRP, SEA/ACHR recommended to promote:
a. Studies to increase male responsibilities in reproductive health should be encouraged.b. The research to develop male methods of fertility regulation should be further
strengthened.
Research on Newer Strategies for Vector Control
Research on newer strategies for vector control was discussed and in line with therecommendations agreed upon, WHO/SEARO would support:
a. Research to promote sibling species complex - distribution, response to insecticides,vectorial capacity and biting rhythm, etc.
b. Studies on the role of insecticide impregnated bednets in the control of malaria and othervector borne diseases.
In addition, Regional Office would examine the possibility of developing and advancedresearch facility in the region for the collection, identification and characterization of insects ofpublic health importance. Regional Office would also encourage intercountry linkages among thecore research groups for coordinated research and experience sharing.
Research on Human Resources for health (HRH)
SEA/ACHR noted the need for HRH issues in the context of the wider maco-dimensionand bring different sector into a functional relationship. It was agreed that the countries would besupported for a further period of at least six years so that they would be able to develop the
- 23 -
capacity essential to undertake HRI-H research.
A programme of research would be developed to predict or identify the characteristics andattributes of health and health related personnel who will provide general health care in the firsttwo decades of the 21st Century in SEA countries at different stages of development.
Future Research Agenda "Research Direction of RPD Programme of SEARO (Medium-Term)"
In keeping with the ongoing development and activities of global and regional researchscenario, and the research objectives and strategies, the members of the SEA/ACHR felt that therewas a need to set the future research agenda for the region which should include:
1. The research agenda/direction for the SEA/RPD Programme should be selective, catalyticand have sufficient momentum. Accordingly, the following are the broad and priorityareas identified for implementation within the next three biennia.
- Research on the behavioral, socio-economic and cultural aspects and determinantsof health and disease.
- Research on the development of Human Resources for Health with respect to allcategories of health personnel at all levels of the health care system.
- Research to facilitate assessment and rapid application of existing and emerginghealth and information communication technologies in health programmes of SEAcountries.
- Health policy research and health promotion research.
- Research to identify constraints to implementation of health programmes as theyaffect clients, providers of health care, and policy and managerial apparatus.
2. The Regional Office may establish appropriate mechanisms, including Working Groupsthat will enable implementation of the above research agenda within the next three biennia.
WPR/ACHR
1. INTRODUCTION
WHO's involvement in health research stems from article 2(n) of its Constitution,which calls on the Organization "to promote and conduct research in the field of health".The WHO research programme ensures substantial participation by regions and countries.WHO's policy has been to support the building up of national research capabilities,particularly in developing Member States. It has also endeavoured to promote effectiveand efficient systems for health research management, including information support for
research. The emphasis has been on applied or operational research rather than on basic orfundamental research.
- 24 -
WHO's research programmes generally have two interrelated purposes: to obtainresults that are relevant and applicable, and to strengthen the research capacity of thecountries themselves. These two purposes are evident in the work of the globalprogrammes such as the programmes for control of diarrhoeal diseases and control of acuterespiratory infections, special programme of research, development and research training inhuman reproduction, and special programme for research and training in tropical diseases.In addition, these purposes underlie all the research programmes of WHO to a greater orlesser extent.
2. MAJOR ACTIVITIES
2.1 Development of strategic plan for health research
A joint meeting of the Western Pacific Advisory Committee on Health Research(WPACHR) and the Directors of Health Research Councils or Analogous Bodies(HRC/AB), held in August 1994, requested that a task force be established to develop astrategic plan for health research in the Region over the next five years. This task forcemet from 29 August to 1 September 1995.
The task force considered various background factors, including the history ofresearch priority setting within the Region and the guidelines proposed by the Newhorizons in health concept. It was considered that more input was required to this processbefore the strategic plan could be finalized. It is expected that the process will becompleted by the time of the combined meeting with the members of WPACHR and thedirectors of HRC/AB in August 1996.
2.2 National health research management mechanisms
Member States have been encouraged by the Regional Committee, WPACHR andthe working group meetings of HRC/AB to develop adequate mechanisms for coordinatingtheir research activities. These should link research priorities to the solution of majorhealth or health-related problems. Focal points to coordinate and manage activities havenow been established in 14 countries: Australia, Brunei Darussalam, China, Fiji, LaoPeople's Democratic Republic, Malaysia, New Zealand, Papua New Guinea, thePhilippines, the Republic of Korea, Samoa, Singapore, Solomon Islands and Viet Nam.
2.3 Strengthening of national research capability
National workshops on research design and methodology are organized to provide abroad framework of research methodology for use in biomedical or health systemsresearch. Seventeen workshops have been held since 1981, with the latest in Beijing,China, (September 1994) and Chengdu, Sichuan, China (August 1995).
The manual on Health research methodology. a guide for training in researchmethods is currently being translated into the Laotian language.
Since August 1994, three research training grants were awarded to researchers fromMalaysia, the Republic of Korea and Viet Nam. Thirteen contracts for research projectshad been supported by WHO.
- 25 -
2.4 Collaborating centres
The network of WHO collaborating centres is an important and useful mechanismfor carrying out activities in support of the Organization's programmes at all levels. As of1 August 1995, the number of collaborating centres in the Region totalled 215. Themajority are located in China (67), Japan (52), and Australia (40). The programmes withthe most centres include clinical, laboratory and radiological technology (21), othercommunicable disease prevention and control activities (17) and human reproductionresearch (14).
The second annual meeting of the heads of all WHO collaborating centres inMalaysia was held in December 1994, during which the activities of the four centres werereviewed and discussed.
The second national meeting of WHO collaborating centres in Japan was held inFebruary 1995. The meeting discussed the roles of the centres and the future directionsfor improvement of work, communication and coordination of WHO collaborating centres.
The fifth meeting of the heads of all WHO collaborating centres in China was heldin Shanghai from 24 to 26 July 1995. The agenda included discussions on the currentstatus of WHO collaborating centres globally and in the Western Pacific Region; how towrite annual reports; and the "New horizons in health".
The heads of WHO collaborating centres for health education, occupational health,traditional medicine and primary health care in China also held meetings, strengtheningcollaboration and communication among the centres within the same WHO programme.
The heads of all collaborating centres (18) in Shanghai met in July 1995 to discusshow they can get involved in multidisciplinary research among themselves.
To strengthen the information exchange and coordination among WHOcollaborating centres, their activities based on 1993 annual reports reviewed in 1994 weresummarized and printed dissemination.
2.5 WHO Regional Centre for Research and Training in Tropical Diseases andNutrition
The WHO Regional Centre for Research and Training in Tropical Diseases andNutrition, located at the Institute for Medical Research in Kuala Lumpur, Malaysia, hascontinued to undertake numerous research projects; perform many specialized diagnostictests; train large number of individuals from both within and outside of Malaysia; andprovide many consultative and advisory services. It was involved in regional collaborativeresearch projects with Brunei Darussalam and Lao People's Democratic Republic(nutrition); China (malaria); and Viet Nam (control of diarrhoeal diseases).
- 26 -
3. ACTIVITIES CARRIED OUT BY THE GLOBAL PROGRAMMES
3.1 Programmes for Control of Diarrhoeal Diseases (CDD) and Control of Acute eRespiratory Infections (ARI)
Between July 1993 and June 1995, four CDD-supported research projects werefunded and one proposal development workshop was conducted in the Region, with a totalbudget of US$ 122 200. Approximately 31% of that amount was allocated tostrengthening research capability (the workshop), with the balance going to the followingfour research projects: evaluating the impact of the national diarrhoeal diseases controlprogramme on childhood mortality in the Philippines; determining the factors influencingthe duration of exclusive breast-feeding in China; a multicentre study to evaluate the safetyand efficacy of reduced-osmolarity oral rehydration salt solution in children with acutewatery diarrhoea in Viet Nam; and a focused ethnographic study on the control ofdiarrhoeal diseases at community level among the Kinh population in Viet Nam.
Acute respiratory infections, particularly pneumonia, are among the leading causesof morbidity and mortality in children in the developing countries in the Region. Everyyear 300 000 deaths from acute respiratory infections are estimated to occur in childrenunder five years of age in the Region. In view of this, case management and behaviouralresearch continue to be priorities and increasing emphasis is given to research related topreventive interventions and health systems. During the period 1993-1994, 12 researchprojects were supported by the Programme in Australia, China Papua New Guinea, thePhilippines and Viet Nam for improvement of case management. Focused ethnographicstudies were conducted in China and the Philippines in order to develop methods whichcan be used in developing home care messages.
3.2 Special Programme of Research, Development and Research Training inHuman Reproduction (HRP)
The activities of this Special Programme may be categorized as: (1) research inhuman reproduction; and (2) strengthening of national research capacities in reproductivehealth.
During 1993-1994, 157 grants were provided with a budget of US$ 2 418 832. Ofthis, 76.4% was for research projects. The majority of the studies concerned the safetyand efficacy of existing contraceptive methods and the development of new birth controltechnologies. Other studies included psychosocial factors affecting family planningacceptance, epidemiology of infertility, health service aspects of family planning,information management, maternal death surveillance, prevalence of sexually transmitteddiseases, gender power relations, risk factors of pelvic inflammatory disorders anddevelopment of home-based maternal records.
The remaining funds were allocated to strengthening research capability inreproductive health, including family planning. Institutions were supported by provision ofsupplies and equipment, as well as research training, and by collaborating in developingexpertise and planning research.
.
- 27 -
3.3 Special Programme for Research and Training in Tropical Disease (TDR)
Of the diseases covered by the Programme, malaria, schistosomiasis, filariasis andleprosy continue to be public health problems within the Region. Leishmaniasis is ofconcern in certain areas only in China, while trypanosomiasis and Chagas disease do notoccur in the Region.
During 1993-1994, 125 projects were supported by TDR, with a budget of aboutUS$ 3.7 million. Approximately 44% of the total amount was allocated to institutionstrengthening and training activities. The balance was allocated to research projects.
Long-term support was provided to institutions in China (6), the Philippines (4) andViet Nam (1).
The Malaria Control Service of the Philippines through WHO continues to produceand distribute globally in vitro kits for testing the sensitivity of malaria parasites toantimalarial drugs as well as low-cost portable incubators, which can be used where aconstant temperature is required.
4. RESEARCH ACTIVITIES WITHIN THE REGIONAL PRIORITY AREAS
4.1 Environmental health
Studies were carried out in China, Malaysia and Viet Nam to compile existinginformation on urban health and environmental problems and formulate plans forenvironmental health risk management and improving the health of the urban population.
4.2 Eradication and control of selected diseases
The Department of Virology, National Institute of Health, Tokyo, Japan, a regionalreference laboratory for poliomyelitis eradication, continued to develop and assess the Lalpha tissue culture cell lines. It is expected that use of these cells will make it easier forthe poliomyelitis diagnostic laboratories in the Region to detect and grow wild poliovirusisolates.
It is important that operational research in malaria remains relevant to the controlprogramme objectives and does not cause an additional burden on routine activities and thecommunity. Research is being actively pursued in areas of Plasmodium falciparum drugresistance monitoring (Cambodia, the Lao People's Democratic Republic and Viet Nam);methods of improving malaria diagnosis and treatment through the private sector(Cambodia); developing single treatment packets for treating mosquito nets in Papua NewGuinea and Cambodia; and improving methods of P. falciparum diagnosis in the absenceof a microscope (nine malarious countries in the Region).
A study on the treatment of bamboo curtains with permethrin in Viet Nam hasprovided good control of the main vector or dengue haemorrhagic fever, Aedes aegypti. Areduction in human cases also occurred. These results have practical application andindicate that treatment of curtains and different fabrics inside houses can provideprotection against the bites of dengue vectors in other countries.
- 28 -
4.3 Health promotion
A project to assess health promotion needs in the Republic of Korea wasundertaken to form the basis for the development of the health promotion programme.This research activity is to be divided into two phases. During the first phase, from Juneto September 1992, a survey on health promotion needs was conducted, involving330 patients, 2600 households and 176 health centre professionals. In the proposed secondphase, in-depth data analysis will be performed to find common needs and suitable typesof health care and health promotion programmes. Persons with high-risk behaviours willbe interviewed.
The WHO Collaborating Centre for Health Promotion through Research andTraining in Sports Medicine (Department of Preventive Medicine and Public Health,Tokyo Medical Centre, Japan) has conducted various studies on the effect of strenuousexercise (triathlon) on the different aspects of the human body in order to identify thelimitations of exercise and thereby determine the optimal volume and level of exercise forhealth promotion. The topics of these studies can be categorized under the followinggeneral headings: cardiac function, muscle aerobic capacity, the immune system, moodstate profiles, serum vitamin E and blood hormones.
4.4 Strengthening management
A fourteen-county study is being conducted in China to provide information thatcan be used to formulate national policy on health insurance schemes for rural areas. Thefourteen-county sample is stratified by economic level and type of insurance scheme. It isanticipated that this research will enable policymakers to guide the development ofinsurance programmes in rural areas more effectively by highlighting what may be thesignificant factors which influence successful insurance programmes.
Collaborative research continues with the Korea Institute of Health ServicesManagement to develop policy and management analysis frameworks in the area of healthcare financing and health insurance. The purpose of these frameworks is to structuredebates, research, analysis and policy decision-making in such a way as to focus adecision's impact more effectively on identified development goals to learn more from thedecisions that are subsequently made.
4.5 Other areas
The study on the epidemiology and characterization of Neisseria gonorrhoeaeisolates in China was begun in June 1994. Of these, 30.6% were resistant to penicillin;9.8% to tetracycline; 5.9% to spectinomycin; and 4.8% to ceftriaxone. The 17penicillinase-producing N. gonorrhoeae were identified by iodometric method. Plasmidanalysis has shown that different sizes of plasmids related to different antibiotics. Thework is still continuing.
A study of coronary heart disease in a Chinese population is being carried on inBeijing, China, to measure the possible causal factors that are likely to increase the risk ofcoronary heart disease in the study population currently living in Beijing, and to comparetrends and determinants of coronary heart disease between China and other Asian nations.
- 29 -
Research on intervention treatment of Impaired Glucose Tolerance (IGT), as a partof a programme on "Five-year diabetes prevention and management in nine provinces anddistricts in China (1994-1999)" is being carried out in China. The expected 6000 IGTpersons diagnosed in a survey from different ethnic groups, geographic areas andeconomic classes are randomized to a control group or one of three treatment groups: dietonly, exercise only or diet and exercise. It will be determined whether these interventionstrategies are associated with a reduction in the incidence of diabetes. The initial studyshows positive results, demonstrating that diabetes can be prevented by lifestylemodifications.
A multicentre study on childhood accidents involving China, Hong Kong, Japan,the Philippines and the Republic of Korea is ongoing. The multicentre study on evaluationof psychosocial rehabilitation in Japan, the Lao People's Democratic Republic, Malaysiaand Singapore started in 1995. Evaluation of psychoeducation with neuroleptics forschizophrenia and with low-dose maintenance for prevention of its relapse in the Chineserural areas has been conducted in Shandong, China. A bio-psychosocial study onsubtyping of schizophrenia is being carried out by the Tokyo Medical and DentalUniversity, Japan.
In June 1994, a Working Group met in Aomori, Japan, to finalize the Guidelinesfor clinical research methodology for acupuncture, which is the first of its kind in theworld. These guidelines integrate basic principles and methods of modern scientificresearch with the nature and characteristics of traditional medicine.
All 12 WHO Collaborating Centres for Traditional Medicine in the Region wereactively involved in the following areas of research: mechanism of acupuncture treatment;effectiveness of acupuncture treatment for pain relief, coronary health disease, etc.; safetyand efficacy of traditional herbal medicine; and pharmacological, toxicological andphytochemical studies on medicinal plants.
Projects on the use of herbal medicine for malaria, cancer and other diseases wereconducted in China, the Lao People's Democratic Republic and Viet Nam. A survey onmedicinal plants was performed in selected provinces in the Lao People's DemocraticRepublic.
Evaluation methodology is being developed by the College of Nursing, Universityof the Philippines, to measure the level and effectiveness of HIV-related content in thenursing curriculum. A comparison will be made between the integration of the content inselected rural and urban nursing universities and colleges.
Over the last decade, a number of knowledge, attitude, behaviour and practicesurveys, and studies of HIV risk behaviours have been undertaken in the countries of theRegion. A critical analysis of these existing studies will assess the comparative risk ofHIV infection in the countries, determine the current levels of AIDS knowledge andidentify gaps in existing research.
~~,b WORLD HEALTH ORGANIZATION
le, A..' ORGANISATION MONDIALE DE LA SANTE
ADVISORY COMMITTEE ON HEALTH RESEARCH
Thirty-third session
Geneva, 17 - 20 October 1995
Aqenda item 5
STRATEGIC PLANNING IN HEALTH RESEARCH
Report on Meeting
held at Schloss Reisensburg
3 - 7 April 1995
The contents of this restricted document may not be divulged topersons other than those to whom it has been originally addressed. Itmay not be further distributed nor reproduced in any manner andshould not be referenced in bibliographical matter or cited.
Le contenu du présent document a distribution restreinte ne doit pas étredivulgué á des personnes autres que celles á qui il était initiaiement des-tiné. II ne saurait faire l'objet d'une redistribution ou d'une reproductionquelconques et ne doit pas figurer dans une bibliographie ni etre cité.
Appendix
DISTR.: RESTRICTEDDISTR.: RESTREINTE
ACHR33/INF.DOC./95.1
ORIGINAL: ENGLISH
Appendix
Strategic Planningin
Health Research
Report from the
ACHR Workshop:'New Approaches for Health Research Strategy Planning'
of the
WHO Collaborating Centre forGlobal Modelling of Health Perspectives
held at the
International Institute for Scientific Cooperation,Schlofl Reisensburg near Ulm, Germany
April 3 - 7, 1995
Appendix
Table of Contents
1. INTRODUCTORY REMARKS 2
2. BACKGROUND 3
3. GOALS AND OBJECTIVES 3
4. HEALTH DETERMINANTS 4
5. HEALTH STATUS AND RESEARCH PRIORITIES 5
5.1 OUTCOME OF RESEARCH 55.2 DEFINING HIEALTH STATUS 5
5.3 TtHE NEED FOR PERSUASIVE RESEARCH 5
5.4 THE HEALTH PROFILE 6
5.5 HEALTH PROFILES AND DEFICITS 6
5.6 HEALTH SECTORS AS COMPONENTS OF TiE 'HEALTH PROFILE' 6
5.7 THE HEALTH PROFILE APPROACH 6
5.8 NEEDS ASSESSMENT 8
6. METHODOLOGICAL AND IMPLEMENTATIONAL ASPECTS 8
6.1 NEED FOR CONSENSUS AND COOPERATION 8
6.2 TIHE ROLE OF INFORMATION TECHNOLOGY 8
6.3 THE HEALTH RESEARCH PLANNING PROCESS 8
6.4 STUDY TEAMS 9
6.5 BENEFITS 10
7. CONCLUSIONS AND RECOMMENDATIONS 10
ANNEX 1 12ANNEX 2 13ANNEX 3 14
LIST OF PARTICIPANTS 15
2
1. Introductory Remarks
The mission of the World Health Organization (WHO) is to improve the health of humanpopulations throughout the world's many and varied regions. To achieve this goal in the futureseveral important steps must be undertaken:
. Population health status indicators must be identified, analysed and the correspondingproblems clearly delineated,
• Population health indices (profiles) must be created and research priorities set,* Research targets must be specified, dates set, and progress measures established,. Research activities must be initiated and health programs developed, implemented and
evaluated.
To assess the important issues and to explore new approaches for health research strategyplanning within WHO, an ACHR-Workshop was organized by the WHO Collaborating Centerfor Global Modeling of Health Perspectives at SchloB3 Reisensburg. The participants of thisworkshop agreed to initiate new activities which would include a process of health statusassessment identification of needed research and continue with a selected subsequent programimplementation. It was agreed that success in this initiative will depend on strong input fromacadenmia, governments, WHO, health professionals and other stakeholders.
Undertaking the above steps will be facilitated by a cyclical process which will be sponsored bythe WHO's Advisory Committees for Health Research (ACHR). This approach is intended tohelp overcome the methodological barriers which often prevent a developing country' smeaningful participation in the 'Health for All' strategy. Since the planning and execution ofsuch research will require more resources than are readily available, especially in developingcountries, it was seen as an important task of the WHO-ACHR system to address this issue.
It was agreed that WHO and its ACHR system as a promoter of research and as the adviser tothe Director General and, through him, the Ministers of Health worldwide, should use itscatalytic power to establish the methodological foundation and to promote the cooperativeclimate for this important initiative. The various steps must be designed and carried out notonly at global and regional levels, but also, and perhaps more important, at the level ofindividual countries and regionsL. To this end, it was agreed that member countries,international organizations, the scientific community and other interested parties must bemobilized to take part in this increasingly urgent undertaking.
Accordingly the Global ACHR initiated a process of consultation with the Regional ACHRs,the WHO Collaborating Centers, and expert groups to develop a plan of action for identifyinghealth research priorities and strategies needed for promoting research of critical significanceto human populations world-wide. This process is targeted to be in operation by the year 2000.
Utilization of new information technologies can make a major contribution in solving manyhealth research problems, especially with regard to the development of an integrated andcomprehensive profile of health needs. The increasing reliance on multidisciplinary andmultiprofessional elements within public health research and the multisectoral input into such
i to be distinguished from the six official WHO Regions
Appendix3
research activities require the full use of modern communication technologies at the globallevel.
A consensus regarding research goals, priorities and strategies should be attempted. Such anagreement (or at least consensus on the smallest common denominator) requires extensiveconsultation world-wide. This report summarizes the results of an ACHR workshop (April 3 to7, 1995, at Schlo3 Reisensburg near Ulm) which recommended both a process and thesupporting technology to achieve this goal.
2. Background
Scientific communities including universities, research institutes, academies of sciences,academies of engineering, etc., are important sources of new information and sources foradvanced technologies. The expertise of these institutions must be included in efforts to solveproblems of critical significance to local, regional, national and global health.
Recent scientific and technological advances in informatics and telecommunications have apotential for reducing the 'gap' between industrialized and developing countries. Thus it isimportant that developing countries are participants rather than mere observers in thedevelopment of scientific and technological advances for health care and human development.
All nations have the rights to benefit from scientific and technological progress. There aremany advances in the health field which are well-supported by scientific research but notaccepted and implemented by governments and communities. The weak linkages betweenscience and technology and their application have important consequences for the future. Themajor reasons why scientific knowledge and available information are not incorporated intoprograms and strategies designed to solve major health problems should be identified. Effortsdesigned to assess such barriers should consider how scientists can function better in theircapacity of generating basic scientific knowledge and as advisors, as well as how they canbetter cooperate with policy makers, health services leaders and educators in solving healthproblems at. the local, regional, national and global levels. Furthermore, it is important toencourage the latter to involve the full support of the relevant scientific bodies, rather thanattempt to address major health issues independently.
3. Goals and Objectives
The goals of the workshop were:
* To review a new system's planning approach allowing the following:* to easily communicate among health systems planners, the research community, and
WHO,. to identify key issues for improving the global health status despite existing
constraints,• to continuously update and monitor the health research priorities,• to increase the awareness of long and short term action plans by establishing a broad
consensus regarding the actions to be undertaken.· To evaluate concepts for describing the multiple components, factors and issues determining
local, regional, national and global health.
4
. To formulate specific plans for implementing the recommendations developed by theparticipating members in order to bring forward ideas, recommendations and suggestionsfor future action.
. To pave the methodological way for updating the research priorities within WHO in itseffort to implement the health-for-all strategy.
In the context of addressing the above goals and objectives, the workshop set out to define theprocess with which
I local2 , regional 3, national or global health indicators can be structured,
• community health problems can be identified,
* research priorities can be established on the basis of an index (the health profile), and
* appropriate methodological approaches can be reviewed which may be relevant to suchACHR research planning activities.
The intention of the workshop was to underline the reiterated commitment to narrow the gapbetween the research capacities of developed and developing countries (research transfer)because the community health problems may in fact be ubiquitous but the research resourcesrequired to investigate and cope with them are far from equally distributed.
Therefore, it is now necessary to
* identify equivalent problem types,* define specific problems common to several economic, ecological or geographical regions,* set research priorities which deal with health problems of global significance.
4. Health Determinants
To provide a general framework in which the objectives of the workshop could be discussed,four overview presentations were made which addressed four different issues: public health,disease, social, and environmental issues. The speakers emphasized the multifactorial nature of'health', 'disease', 'well-being', 'disability' and the interrelationships among the social,political, cultural, educational, economic, biological, chemical and physical environments. Itwas argued that any singular measure of population's health is, by itself incomplete. Whiledefining 'disease' is difficult, the concept of 'impairment - disability - handicap' serves as thecurrent basis for the WHO classification. The effort to conceptualize 'disease' includes thedimensions of clinical syndrome, structural/functional abnormalities, etiology, comorbidity, andsocial dysfunction. However, it was also recognized that problems will arise when, as isincreasingly the case, the differences between disease and non-disease become blurred: e.g.HIV positivity, genetic predisposition, mental retardation, personality disorders, drug abuse,etc.
e2 local = town, community
3 regional = administrative or geographical areas with common problems;does NOT necessarily refer to WHO Regions
~~~5 ~Appendix
Information was presented which shows that, at low income levels, improvements in health canbe achieved through investment in education, selective government intervention, increased jobopportunities, the transfer of information and technology, the individual life style behavior,nutrition, quality of housing and improvement in communication within and amongcommunities.
Local, regional, national, and global health is determined by complex factors includingpopulation growth, migration, industrialization, energy consumption, culture, food availabilityand depletion of natural resources, and by the disruption of the equilibrium of the local andregional ecological systems. Negative results include the contamination of air, soil and water.Also, the accumulation of toxic substances in the human food chain has become a major healthconcern. More information and knowledge is needed about global eco-system dynamics andtheir relationships to human health and well-being. A globally-integrated chemical andbiological monitoring system could provide the scientific basis for future 'models' forpredicting the health effects of environmental degradation on future generations.
5. Health Status and Research Priorities
The process of making positive changes in the global health picture is complex. It is useful tolist some key aspects which such a process must include.
5.1 Outcome of researchThe most important target outcomes of any health research planning effort must, in the finalanalysis, be the provision of information and knowledge support for the implementation andmanagement (incl. evaluation) of effective and efficient health programs; and that theseprograms must be targeted on a country's biggest (by some accepted criteria) health problems,which must also be amenable to correction.
5.2 Defining health statusBefore work can begin on programin development, delivery and management, there is a need toidentify the problem areas which such programs are to address. Thus it was recognized that thevast majority of these problem areas, while unique in their details to specific countries, areshared (in more general terms) by many countries, and can be defined in terms of commonlyrecognized surrogates: health status indicators. Apart from some tailoring, research to measureand define health status indicators, and thus to define and compare health status, can also bereadily 'shared' between and among countries. Shared problems - shared solutions, with dueadaptation to local conditions.
5.3 The need for persuasive researchWhile the objective determinnation of population health status, in countries, regions orcommunities, is largely a scientific matter, the formulation, resourcing and implementation ofsolutions is a very practical and political matter. Unfortunately, too often health research hasbeen allowed to progress to the publication of fine and thorough papers without then beingpushed to a more useful conclusion: the acceptance by those whose job it is to manage,govern, act. It was therefore recognized that the ACHR process must incorporate a mechanismto make academic findings more persuasive and hence more useful.
6
The power of health research findings to persuade at the political and bureaucratic levels isvery much facilitated by recent technological advances in informatics. Routinely available data(e.g. health status indicators) can be combined into a holistic picture summarizing a country'shealth situation, essentially by creating a composite measure (an index) for the visualization ofhealth status and the demonstration of progress toward certain goals. Such a tool may be moreuseful than a profusion of papers for persuading decision-makers to take the necessary steps toimprove health. Involving the community leaders and health care providers in formulatingresearch policies is another necessity to be reflected in such a development process. (seeAnnex 1: Illustration of Health Profile Diagram).
5.4 The health profileOne of the workshop's outcomes was the finding that work should commence on thedistillation of health determinants and indicators into a 'health profile'. While the profile isbased on parameters measured in terms of 'deficits', the actual intent is to describe thepresence or absence of 'Good Health'. While the absence of disease, malnutrition, pollution,education, etc., does not automatically imply good health, a reduction of 'deficits' will be inmost cases a prerequisite for improving the health status within a community. At the politicaland administrative levels (i.e. where the real work has to be done) the health profile wouldallow:
* the demonstration of the existence of health deficits,* the comparison between health systems,* the prioritization of problems for action, and• the recognition of progress or decline.
5.5 Health profiles and deficitsThe complexity of a country's health situation makes it difficult for it to be illustrated in acomprehensive and meaningful way. The proposed health profile offers one solution. Bypermitting the simultaneous visualization of the current health profile and the hoped-for healthprofile, it is possible to identify and visually represent the gap between the current state-of-affairs and a target state: i.e. the already-mentioned 'health deficit'. This deficit then becomesthe visible target for action in that it can be reduced. The reduction can be measured, andcredit can be taken for the research and health programming steps to achieve the desiredreductions.
5.6 Health sectors as components of the 'health profile'Health determinants and status indicators at local, regional, national and global levels were,provisionally, grouped into five sectors as follows: (see Annex 2)
5.7 The health profile approachA 'health profile' was proposed which consists of a circle with radial segments (see Figure 1)representing the various health profile sectors. Each segment is itself composed of related(therefore contiguous) health determinants and status indicators (see 5.6 above). The
7 Appendix
composition of the parameters within these sectors will differ slightly from region to region.The health profile was considered to be the most effective manner with which to illustrate, onthe basis of one simple visual device, the health status of a community or region.
The radius of the profile 'circle' is constant and represents the 100% level of the target state.The length of each 'spoke' describing a health determinant (within a specific sector) wouldrepresent an actual parameter value (%) in relation to the desired target level. The parametersand their target levels would be initially set by WHO in cooperation with the scientific andlocal, regional and national health sector communities. Health 'deficits' within a region couldthus be easily identified. A time sequence of this model could also be used to demonstrateimproving, as well as deteriorating, trends. Furthermore, a model could be used to describeemerging opportunities for scientific investigation in the sense of a scenario analysis.
There are two underlying premises which are important to note when using the health profilemethod to identify research opportunities. First, in most situations the research opportunitieswill not be limited to a single 'spoke', but will require interventions involving the simultaneoustargeting of several health determinants, often in different sectors. Second, changes in healthstatus in one area may well be accompanied by changes (not necessarily positive) in a numberof additional areas. In assessing the value of research proposals it is necessary to sum potentialbenefits and risks in all areas.
Using this approach the procedure would be as follows:
* to identify a health 'deficit' or major area of poor health from the health status profile ofthe selected community or region;
* to identify the key contributing factors amenable to scientific intervention and to estimatethe proportion of the total benefit which a modification of each factor would likelycontribute;
* to assess the research opportunity via a comprehensive review of the available data andinformation as well as through a consensus of those scientists who are expert in this area;
* to attribute the benefit obtained through a modification of each contributing factor to theappropriate major health determinant within the health profile;
* to assess the effect of each intervention on the total health profile so as to estimate thetotal benefit to the community or region; and
* to apply existing and gained knowledge in implementing new programs.
A research program based on this approach may lead to an increase in some of the areas ofscientific activity currently under way but may also decrease the priority in other areas ofcurrent activity. It may, therefore, be necessary in some cases to assess the impact of such achange in research activity rather than to assess only the impact of the new proposal in total.Using the health profile 'model' to determine health research priorities will require access to acomprehensive data base in order
* to achieve a more reliable measure of the health status within a community,* to be able to obtain an estimate of the actual research opportunity, and* to be able to estimate the effect of the proposed interventions on the critical health
deficiencies within the selected community or region.
8
5.8 Needs assessmentThis proposed approach for identifying research priorities can best be carried out ifsophisticated methods of data storage, retrieval, multiple access and analysis are available.Furthermore, the assessment of research opportunities is possible when user-friendly andsophisticated methods of communication are available to the scientists and health professionalswho are experts in the selected fields. Identifying research priorities in those countries wheresuch facilities do not exist at present should not be postponed. An interim approach should beidentified until more advanced communication technology is made available, which in itself is apriority.
6. Methodological and Implementational Aspects
It should be noted that in this context the idea of 'health research planning' is to suggest theexercise of preparing for and organizing the research process, and is not in any way meantto imply that health research creativity will be reduced. On the contrary, it is anticipated thatwith adequate and imaginative research planning the outcome of the research process will besignificantly enhanced.
6.1 Need for consensus and cooperationSuccessful implementation of a large-scale targeted research program requires the consensus,cooperation and collaboration among researchers and research groups as well as concernedorganizations and institutions. As demonstrated by means of a national health research plan(USA) the experience has shown that the scientific community cannot be 'confronted' withprogram goals and objectives developed 'outside'. The scientists themselves in cooperationwith community leaders and health care providers must be mobilized to develop their owngoals and priorities with the identified global health needs.
A consensus approach such as the Delphi method or the consensus development conference(CDC) may turn out in practice to be a successful tool for integrating the interests andexperiences of different cooperating partners taking into account the global view as well aslocal requests and needs.
e6.2 The role of information technologyThe consultation process requires intensive communication and would benefit from newinformation technology. The participants of the workshop agreed that the health researchplanning could substantially benefit from the immediate application of new technologies. Thiswould not only speed up information transfer but would also reduce the need to travel and thuslower costs.
This combination of advantages will provide an opportunity for the developing countries tobenefit from new information and knowledge as quickly as industrialized nations. On the otherhand they can effectively bring in their particular interests. Thus the application of newinformation technology may help to bridge the gap between developed and developingcountries.
9 Appendix
6.3 The health research planning processOne of the basic tasks of research planning is to analyze the critical processes and to definecooperation partners in relation to the specific problem. A structure for these processes wasoutlined in the workshop.
The planning process involves several phases and different actors from within and outsideWHO in a continuing process of consultation and consensus building as illustrated in Annex 3.
The first step in the planning process will be the identification of issues, drawing uponknowledge from the ACHR system, experts from academia, governments, the United Nationssystem, NGOs and the national academies of science and medicine.
The second step following the identification of priority issues is a consensus building processto forge a research agenda around each major issue. The result will produce research agendasfor both basic research (knowledge development) and applied research for problem solving(including the utilization of existing knowledge).
6.4 Study teamsTo take advantage of the wide range of knowledge and expertise available world-wide, it willbe necessary in the consensus building process to include members from a wide spectrum ofscientific and professional organizations. The process should be carried out by small,multidisciplinary teams. Members should bring in diverse scientific expertise, the perspectivesand concerns of the regions of the world that are most affected and concerned with theproblem under consideration.
The study teams will create outcomes which will be highly selective and focused such that clearstatements regarding the potential impact of scientific research on the health profile model canbe made. It is expected that the study teams will review and synthesize relevant data and on-going research, identify the significant gaps in knowledge and potential payoffs for researchinvestments, and identify research opportunities, suggesting methods and potential areas fornew research where that may be appropriate. The findings and recommendations of the studyteams will be their own, independent of the organizational affiliations of individual members.
The study teams will make extensive use of electronic communication technology wherebyaccess to data-bases throughout the world will be desirable and will play an important part ingathering appropriate information.
The recommended research agendas developed by these teams will then be circulated withinthe scientific communities, the UN system, member countries, donor agencies and through theWHO regions. The resulting projects to address significant health 'deficits' will generateinformation and experiences that will add to the knowledge base which can then be used infuture considerations.
10
6.5 BenefitsThe benefits of a clearly structured process of research planning include the following:
. it provides the basic scientific and management program guidelines for decisions andactions;
* it provides the framework for the dialogue among the WHO/ACHR, the scientificcommunity and governments concerning research priorities and actions;
* it provides the visibility of program activities and progress for the participants;
* it allows to focus and relate multidisciplinary scientific approaches;* it permits the incorporation of a great number of participants from different fields of
research; and· it provides a feed back process and permits the incorporation of new ideas and allows
redirection when unforeseen problems occur.
7. Conclusions and Recommendations
A Health Research Strategy Planning Concept must take full advantage of the knowledge base
and research experiences available within the scientific communities world-wide. The ACHRmembers can provide the appropriate infrastructure for establishing a consensus finding systemto determine research priorities within WHO.
Therefore, the participants of the workshop agreed to support the development andimplementation of:
* a framework within the ACHR system which will allow the identification and continuousupdating of research priorities, based on a computer assisted consultation process to advisethe Director General and, through him, the Ministers of Health worldwide, and to install a
cyclical mechanism for interaction with the research and scientific communities,· a plan of action to promote research and to incorporate technology within WHO for
renewing the Health for All strategy and to provide selected world-wide access to databases of WHO and other UN institutions,
* a communication network, based on currently available communication technology throughwhich all regional members of the Global and Regional ACHRs, and the WHO officersresponsible for research promotion and development, will participate actively andcontinuously in the development and updating of a global health research priority settingprocess. (An INTERNET-based communications system is suggested which allows ACHRsmembers to interact with collaborating researchers and scientific organizations world-wide).
The following action-plan to achieve these goals was proposed:
* The creation of a communications network should begin immediately with theestablishment of a data base including the addresses and telephone, fax, e-mail contacts ofmembers within the ACHR system.
* The WHO Collaborating Center for Global Modelling of Health Perspectives, in closecooperation with the Research Institute for Applied Knowledge Processing at theUniversity of Ulm, should serve as the initial network coordinator.
~1 ~~~1 ~Appendix
* An attempt will be made to initiate a communication network involving as many membersas possible within the global ACHR system including the active support of the RegionalOffices. In addition, two ACHR Regions will be selected to develop appropriateexperiences in establishing the communication network for research priority setting: Oneregion which is well equipped in network facilities (e.g. PAHO) and one region which haslimited access to INTERNET (e.g. AFRO)
The technical details associated with the implementation of the information technology forsetting research priorities will be up-dated and refined in conjunction with the overalldevelopment of the ACHR health research strategic planning process.
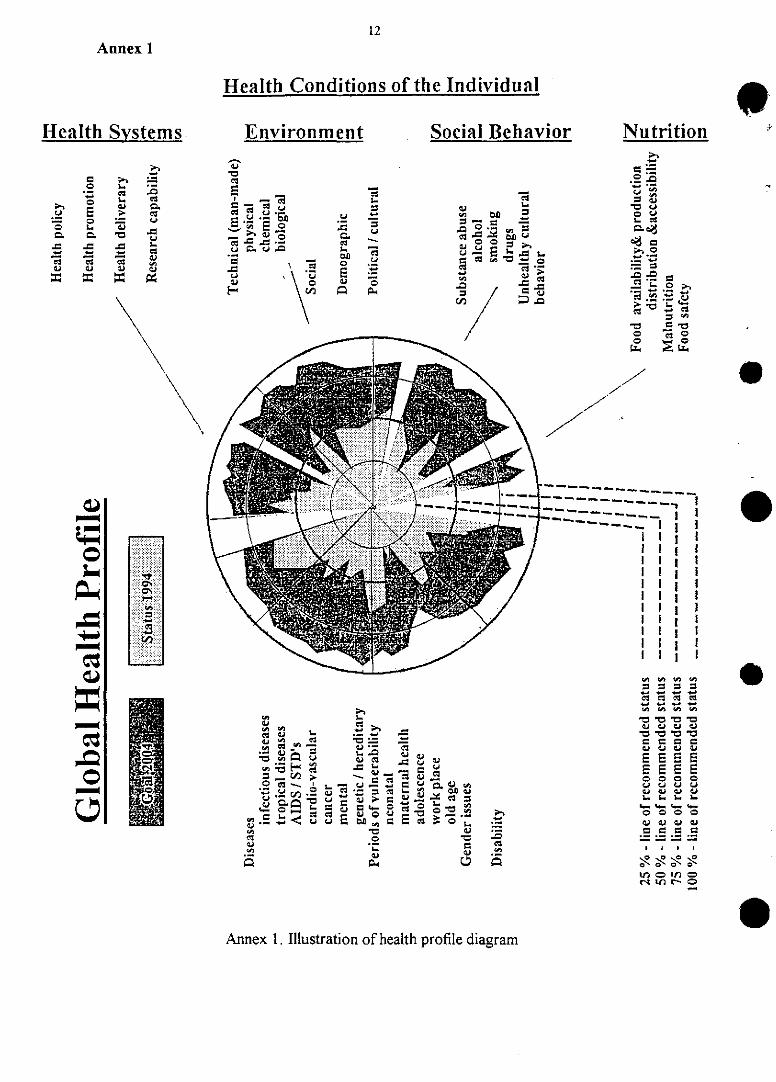
12Annex 1
Health Conditions of the Individual
Health Systems. Environment Social Behavior Nutrition
ig ~ ~ go~~~~~~ ~~~~~~~~ >~ {3a "a ¢3
¢3 - - - - - -- - -
c .. ..... -
....... g . . g 'c= _ _ = ...
.~~~~~~~ oo
4 .W . . ...... :issi nd .. / t , . v.. .- _ .. .Q t' :j ,........,., '. __ ... .........
1t l- -a __ I Ig . ci O =
_~~~~~~~~~~~~o = L- , 1= g L- C. g. c EE
0 o o C C C C4
V)~~~~~~~ *q 0 V : *
_ Q _ S S S S~~~o
Annex 1. Illustration of health profile diagram
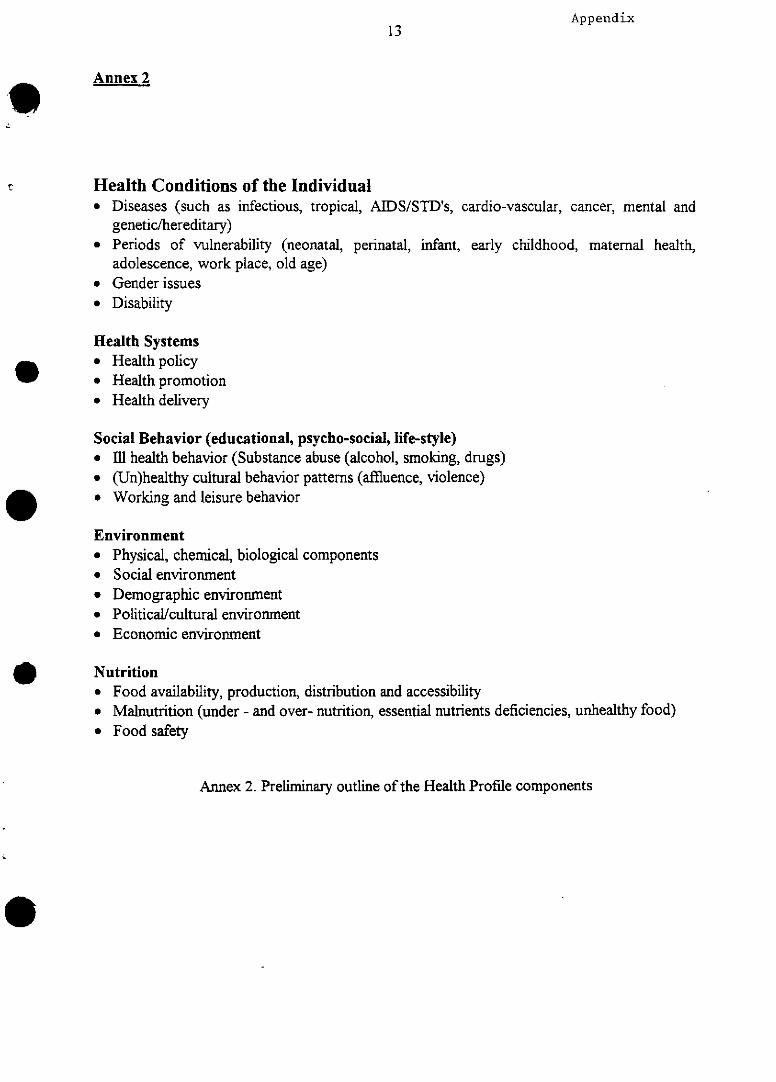
Appendix13
Annex 2
Health Conditions of the Individual• Diseases (such as infectious, tropical, AIDS/STD's, cardio-vascular, cancer, mental and
genetic/hereditary). Periods of vulnerability (neonatal, perinatal, infant, early childhood, maternal health,
adolescence, work place, old age)• Gender issues. Disability
Hlealth Systems* Health policy* Health promotion* Health delivery
Social Behavior (educational, psycho-social, life-style)* Ill health behavior (Substance abuse (alcohol, smoking, drugs)* (Un)healthy cultural behavior patterns (affluence, violence)* Working and leisure behavior
Environment• Physical, chemical, biological components* Social environment* Demographic environment• Political/cultural environment• Economic environment
Nutrition• Food availability, production, distribution and accessibility* Malnutrition (under - and over- nutrition, essential nutrients deficiencies, unhealthy food)* Food safety
Annex 2. Preliminary outline of the Health Profile components
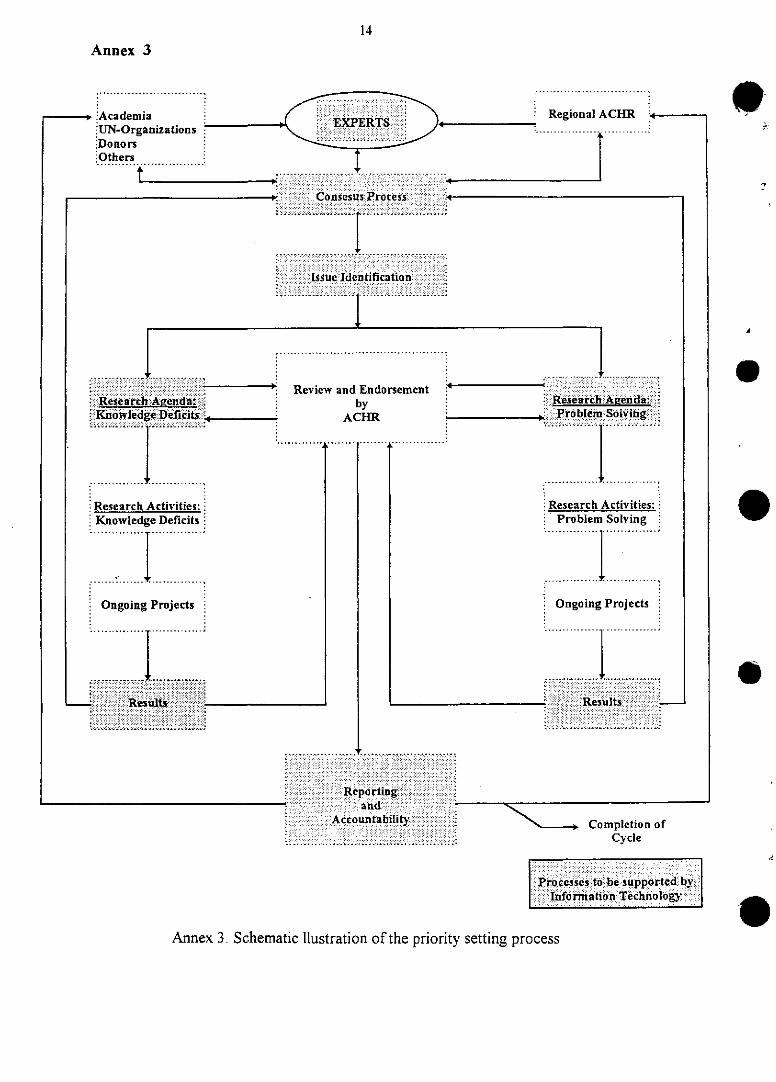
14
Annex 3
.............................
'Academia , Regional ACHR * -
:UN-Organizations . .:.....,Donors:Others1
.Others ,................~ ~ ~ ~ ~ ~ ...............
i.Ot.h~~~~~~~~~~~~. .. .....................t~~~~~~~~~~~~~~~. . .. .. . . ... ... .
Ie. .t a..t.... . .i.n...
....Issue Ideotificst niiii1111i!ii ii!iii!i iiiiiii ........! ......! ..iii
:; ,~~~~~~~~~~~~..,.. ';........ .. ....... .......... . . . . . . .
........ ...... ..................,8
::::::::: ~ Review and EndorsementG:.:Reseá iihAAenday: by
K no wl dge efici s .4 A C H R
Research Activities:Knowledge Deficits
iiii..............i ...............iOngoing Projects
'.............................
~~~~~~~~.....,..."
~~~~~~~~............. . . , , : .
.... ... ....... .... ...,. .
« '' :::::.~~~~~:iiR : 'e':'ti D'c h ::~A gertd:.!::: i:i.Research. Aenda.
: . :Problem Solvi'g ,',
........ .................. ...... 1........ .iT
Research Activities: :Problem Solving
Ongoing Projects
......... ...............
:^-- -- - -::::::::::::::::::::::::::::::::
",..''.'i::111¢11!: iiiiiiii:::?:1ii!?!:.:es lts ii .' ! ? : ~:
. .:.i:i%:a. iid i:.. -..-. , .' :.. .... ..... .... :.
......~~~~~~~~Réporlin
:iAccountability'.. :iii : i:.....
....................... .. ...
Completion ofCycle
-E':000-',-,0'-. .i .:d.- ESE.;iiii;: E. 0 EfD -;..... -........
r:i ' ncnss:srto be supportedh byTu ' . Ifo rmatio n 'Technology. , " .
Annex 3. Schematic llustration of the priority setting process
e
.4
e
e
Appendix15
List of Participants
Dr. Isabel R. AletaRegional Officer for Health ResearchWorld Health OrganizationRegional Office for AfricaP.O. Box 6Brazz7avileRepublic of the CongoTel.: 00242-839-111Fax: 00242-839-400E-mail: [email protected] (group account)
Prof. Dr. K. BallschmiterLeiter der Abteilung AnalytischeChemie und Umweltchemieder Universitae [t UlmOberer Eselsberg89070 UlmTel.: 0049-731-502-2750Fax: 0049-731-502-2763E-mail: [email protected]
Dr. Ibrahim Bet El MalWorld Health OrganizationRegional Office for the Eastern MediterraneanP.O. Box 3252, BenghaziLibyenFax: 00218-61-95829-25
Prof. Dr. J.M. BorgonoHead of Department of Public HealthFaculty of MedicineUniversity of ChileGran Avenida 3100Santiago de ChileChileTel.: 0056-2-555 27 16Fax: 0056-2-556 32 11
16
Prof. A.J. Campbell, MD, FRACP 9Head Department of MedicineMedical SchoolUniversity of OtagoP.O. Box 913DunedinNew ZealandTel.: 0064-3-474-7641Fax: 0064-3-474-7641E-mail: john.campbell(stonebow.otago.ac.nz
Dr. Yamina ChakkarWorld Health OrganizationBureau de Liaison del'Oms pour L'Algerie4, Chemin El-Bakr EI-BiarAlgerAlgeriaTel: 00213-291-16-86Fax: 00213-291-16-86
eProf. Dr. M.E. Chatty *)Minister of HealthDamascusSyriaTel.: 00963-11-2233111Fax: 00963-11-2223085
Dr. Chen KenResponsible OfficerResearch Promotion and DevelopmentRegional Office for the Western PacificWorld Health OrganizationUnited Nations Avenue1099 Manila, PhilippinesTel.: 00632-521-8421Fax: 00632-521-1036E-mail: Address unknown
Prof. Dr. Dr. J. EdrichCentral Institut for Biomedical TechniquesUlm University, Uni-West89070 Ulm, GermanyTel.: 0049-731-502-5300Fax: 0049-731-502-5309
Appendix17
Dr. E1-Sheikh MahgoubRegional Adviser, RPSc/o EMROWorld Health OrganizationRegional Office for Eastern MediterraneanP.O. Box 1517Alexandria 21511EgyptTel.: 00203-48-38-0090Fax: 00203-48-38-8916
Prof Dr. M. Feinleib, M.D., Ph.D.Georgetown University Medical Center2233 Wisconsin Ave. N.W.Suite 525Washington, D.C. 20007U.S.A.Tel.: 001-202-687-0880Fax: 001-202-687-5229E-mail: [email protected]
Prof£ Dr. J.M. ForsytheProfessorial Fellow in Public HealthCentre for Health Services StudiesGeorge Allen WingThe University CanterburyKent CT2 7NFUnited KingdomTel.: 0044-1227-764000Fax: 0044-1227-475477E-mail: j.m.forsythe-2~ukc.ac.uk
Prof. Dr. Dr.h.c.mult. T.M. FliednerDirector of the WHO-Collaborating Centre forGlobal Modelling of Health PerspectivesandChairman of the Advisory Committee for Health Researchc/o Institue for Occupational and Social Medicineof the University of Ulm89070 UlmGermanyTel.: 0049-731-502-3400Fax: 0049-731-502-3415E-mail: [email protected]
18
Prof. Dr. M. Gabr162 Tahrir StreetCairoEgyptTel.: 0020-2-393-02-67Fax: 0020-2-393-07-50
Dr. R. GellertDepartment of Internal MedicineWarsaw Medical AcademyBanacha la02-097 WarsawPolandTel.: 0048-2-658-36-30Fax: 0048-22-22-7496E-mail: [email protected]
C. GreinerResearch Institute of Applied KnowledgeProcessing (FAW)University of Ulm89070 UlmTel.: 0049-731-501-950Fax.: 0049-731-501-999E-mail: greiner®faw.uni-ulm.de
Dr. Myint HtweAg. Regional Adviserin Medical ResearchWorld Health OrganizationRegional Office for South East AsiaWorld Health HouseNew Delhi - 110002, IndiaTel.: 0091-11-33-17-804Fax: 0091-11-33-18-607E-mail: [email protected]
Prof. Dr. I. HawryszkiewyczSchool of Computing SciencesUniversity of TechnologyP.O Box 123 BroadwaySydney, NSW 2007AustraliaTel.: ++61-2-3301809Fax: ++61-2-3301807
Appendix
E-mail: [email protected]. M.A. Ibrahim, M.D. *)DeanSchool of Public HealthThe University of North Carolinaat Chapel HillChapel Hill, N.C. 27599-7400USATel.: 001-919-966-3215Fax: 001-919-966-7678
Prof. Dr. Witold A. Karczewski *)State Committe for Scientific Researchul. Wspolna 1/300-529 WarszawaRepublic of PolandTel.: 0048-2-628-19-44Fax: 0048-2-628-09-22E-mail: wak~frodo.nask.org.pl
Dr. Tord KjellstroemDirectorOffice of Global andIntegrated Environmental HealthWorld Health Organization20, Avenue AppiaCH-1211 Geneva27Tel.: 0041-22-791-2111Fax: 0041-22-791-4123E-mail: [email protected]
Prof. Dr. M. ManciauxUniversité Henri PoincareFaculté de MedecineEcole de Sante Publique de Nancy54505 Vandoeuvre les Nancy CedexTel.: 0033-83-59-2500 (poste 2134)Fax: 0033-83-59-2690E-mail: [email protected]
Dr. B. MansourianDirectorOffice of Research Policyand Strategy CoordinationWorld Health Organization29 Avenue AppiaCH-1211 Geneva27Tel.: 0041-22-791-2785
19
20
Fax: 0041-22-791-4169
Dr. A.Martinez-PalomoCentro de Investigacion Y de Estudios Avanzados DelipnDpto. Patologia ExperimentalAve. Instituto Politecnico NacionalMexico, D.F. C.P. 07000Tel.: 00525-754-8708Fax: 00525-754-8708
Prof Dr. B.O. OsuntokunUniversity of IbadanP.O. Box 9388IbadanNigeriaTel.: 00234-22-414-745Fax: 00234-22-410-489
Dr. A. PielDirector, Cabinet of theDirector GeneralWorld Health Organization29 Avenue AppiaCH-1211 Geneva27Tel.: 0041-22-7912111Fax: 0041-22-7910746
Prof. Dr. Dr. F.J. RadermacherDirectorResearch Institute ofApplied Knowledge Processingand Professor for Computer ScienceUniversity of Ulm89070 UlmTel.: 0049-731-501-100Fax: 0049-731-501-999E-mail: rademac(faw.uni-ulm.de
Dr. U. ReischlInstitute for Occupationaland Social MedicineUniversity of Ulm89070 UlmTel.: 0049-731-502-3400Fax: 0049-731-502-3415
Appendix21
E-mail: [email protected]
Dr. Rebecca de los RiosRegional Advisor on Health ResearchPan American Sanitary BureauRegional Office of the World Health Organization525 Twenty-Third Street, N.W.Washington, D.C. 20037-2895USATel.: 001-202-861-4303Fax: 001-202-861-8472E-mail: [email protected]
Dr. T. RoseResearch Institute of Applied Knowledge Processingand Professor for Computer ScienceUniversity of Ulm89070 UlmTel.: 0049-731-501-617Fax: 0049-731-501-999E-mail: [email protected]
Dr. U. RiekertResearch Institute of Applied Knowledge Processingand Professor for Computer ScienceUniversity of Ulm89070 UlmTel.: 0049-731-501-500Fax: 0049-731-501-999E-mail: [email protected]
Marlis Schabacker-Bock, Dipl.-Soz.Institute for Occupational and Social MedicineUniversity of Ulm89070 UlmTel.: 0049-731-54045Fax: 0049-731-552642E-mail: [email protected]
Dr. Salah Salem Al Haithamic/o EMROWorld Health OrganizationP.O. Box 543Sana ta, YemenTel.: 00967-1-252191
22
Fax: 00967-1-251637
Dr. Susanne StoiberActing Deputy AssistantSecretary for HealthDepartment of Health and Human ServicesHubert H. Humphrey Building200 Independence Avenue. S.W.Washington D.C. 2021USATel.: 001-202-205-0152Fax: 001-202-690-7054E-mail: [email protected]
eProf. Dr. P.G. SvenssonDirector of theCentre for Public Health Researchs-650 09 KarlstadSwedenTel.: 0046.54-88-55-00Fax: 0046-54-88-55-23E-mail: per-gunnar. svensson@hks. se
Dr. J. SzczerbanVice-ChairmanCouncil for Science and TechnologyWorld Health Organization29 Avenue AppiaCH-1211 Geneva27Tel.: 0041-22-791-2786Fax: 0041-22-791-0746E-mail: [email protected]
Prof. Dr. A. ValyaseviFaculty of MedicineThammasat UniversityRangsit Campus, Klong-LuangPrathum-thanee 12120ThailandTel.: 0066-2-516-4548Fax: 0066-2-516-9403

23 Appendix
T. WiedmannAbteilung AnalytischeChemie und Umweltchemieder Universitae[t UlmOberer Eselsberg89070 UlmTel.: 0049-731-502-2751Fax: 0049-731-502-2763
*) unable to attend