
Passing the torch - Yale School of Medicine - Yale University
Upload
khangminh22Category
view
0download
0
2019A N N U A L R E P O R T
D E P A R T M E N T O FE M E R G E N C Y M E D I C I N E
Alberta Health Services
Our Vision
Our Mission To provide a patient-focused, quality health system that is accessible and sustainable for all Albertans.
Our Values
To provide a patient- focused quality health system that is accessible and sustainable for all Albertans.
We show kindness and empathy for all in our care, and
for each other.
We are honest, principled and transparent.
We treat others with respect and dignity.
We strive to be our best and give our best.
We place safety and quality improvement at the
centre of all our decisions.
Cumming School of Medicine University of Calgary ________________________________________________________
DEAN'S OFFICE CUMMING SCHOOL OF MEDICINE STRATEGIC PLAN 2015 – 2020 ______________________________________________________
VISION
We partner with University leaders to support the "Eyes High" vision.
"Eyes High" is the University of Calgary's bold and ambitious vision to become one of Canada's top five research universities, grounded in innovative learning and teaching and fully integrated with the community of Calgary, by the university's 50th anniversary in 2016.
MISSION
By creating and delivering exemplary human resources services, processes, and outcomes
VISION
Creating the future of health
MISSION
We must fulfill our social responsibility to be a school in which the common goal of improved health guides service, education and research. We must foster the collective pursuit of knowledge and its translation, through education and application, to better the human condition.
VALUES
Excellence |Collaboration| Engagement| Respect
we contribute to and share in the University's mission and goals to:
Sharpen focus on research and scholarship; Enrich the quality and breadth of learning; Fully integrate the university with the
community.
VALUES
The strategy also articulates eight core values shared by the university community; curiosity; support; collaboration; communication; sustainability; globalization; balance and excellence.
EMERGENCY DEPARTMENT MISSION STATEMENT
2019 ANNUAL REPORT
Calgary Emergency Medicine is committed to
Providing High Levels of Patient Care
that Involve Integrated Clinical and Academic Leadership.
TABLE OF CONTENTS
EXECUTIVE SUMMARY MESSAGE FROM DEPARTMENT HEAD ................................................................................................................. 1 EMERGENCY DEPARTMENT ACCOMPLISHMENTS .................................................................................................... 4
EMERGENCY MEDICINE DEPARTMENT OPERATIONS
DEPARTMENT STRUCTURE AND ORGANIZATION .................................................................................................... 11 EMERGENCY MEDICINE COMMITTEES ................................................................................................................. 13
MANPOWER AND WORKFORCE PLANNING
MD RECRUITMENT AND TRAINING ..................................................................................................................... 14 RETENTION STRATEGIES ................................................................................................................................... 15 GOALS AND STRATEGIES .................................................................................................................................. 15 IMPACT ON OTHER DEPARTMENTS AND AHS RESOURCES ........................................................................................ 15
EMERGENCY PHYSICIAN LEADERSHIP GROUP ........................................................................................ 16
SITE UPDATES FOOTHILLS MEDICAL CENTRE ........................................................................................................................ 26
ROCKYVIEW GENERAL HOSPITAL .................................................................................................................... 28 SOUTH HEALTH CAMPUS .............................................................................................................................. 30 PETER LOUGHEED CENTRE ............................................................................................................................ 32 CLINICAL INFORMATICS ................................................................................................................................ 34
DEPARTMENT PROGRESS AND NEWS
CAEP 2019 SUMMARY AND HIGHLIGHTS ........................................................................................................... 35 EMERGENCY PHYSICIAN LEAD (EPL) PROJECT UPDATE .......................................................................................... 36 CALGARY ED DISASTER REPORT ......................................................................................................................... 38 OPIOIDS/HARM REDUCTION ............................................................................................................................. 41 PHARMACY UPDATE ...................................................................................................................................... 42 HEALTH LINK ................................................................................................................................................ 43 REHABILIITATION UPDATE ....................................................................................................................... 44 DISTRIBUTED LEARNING AND RURAL INITIATIVES (DLRI) UPDATE .............................................................................. 47 EMERGENCY DEPARTMENT GLOBAL HUB UPDATE ................................................................................................. 48 FRIDAY NEWSLETTER STATISTIC UPDATE ............................................................................................................. 49 MIKE HODSMAN MEMORIAL LECTURE ................................................................................................................. 50 EMERGENCY ULTRASOUND ............................................................................................................................... 50 CLINICAL PHARMACOLOGY AND TOXICOLOGY ...................................................................................................... 51 SOCIAL MEDIA UPDATE ................................................................................................................................... 52 AIRWAY MANAGEMENT PAUSE (AMP) .............................................................................................................. 52 PHYSICIAN SUPPORT FUND (PSF) ....................................................................................................................... 53 ACH PEDIATRIC EMERGENCY RESEARCH TERM (PERT) ........................................................................................... 54 PATIENT SAFETY & QUALITY ASSURANCE ............................................................................................................. 55 SHOCK TRAUMA AIR RESCUE SOCIETY (STARS) UPDATE ........................................................................................... 56 ED GALA ....................................................................................................................................................... 57
ANNUAL OPERATIONAL DATA ANNUAL LOS DATA ......................................................................................................................................... 65
MEDICAL EDUCATION
CCFP – EM PROGRAM ..................................................................................................................................... 69 FRCPC PROGRAM ............................................................................................................................................ 71 OFF-SERVICE AND ELECTIVE MEDICAL EDUCATION ................................................................................................ 73 UNIVERSITY OF CALGARY EMERGENCY MEDICINE CLERKSHIP .................................................................................... 74 GRAND ROUNDS ............................................................................................................................................ 75 SIMULATION ................................................................................................................................................. 76
EMERGENCY MEDICINE RESEARCH
EMERGENCY RESEARCH SUMMARY .................................................................................................................... 77 RENAL COLIC PROJECT ..................................................................................................................................... 84 PRIHS PROJECTS ............................................................................................................................................. 87 THE SUMMER OF E-SCCOTER ........................................................................................................................... 88 CUMMING SCHOOL OF MEDICINE ACTIVITY PROFILE ............................................................................................... 89 2019 LIST OF GRANTS AWARDED ..................................................................................................................... 93 PUBLICATIONS IN 2019................................................................................................................................... 95 ABSTRACTS IN 2019 ..................................................................................................................................... 101
MESSAGE FROM DEPARTMENT HEAD
2019 ANNUAL REPORT 1
The 2019 year presented a number of challenges to our mission of providing excellent emergency care but also saw a number of novel and unique initiatives that are allowing us to meet the challenges created by ED access block and overcrowding and the need to optimize efficiency in our use of resources. Our department is fortunate to have a cadre of dedicated leaders, both established and up and coming who have contributed to our successes and has helped us to excel in both the clinical operations and academic realm.
A Selection of Top Departmental Achievements for 2019: 1. The launch of the Emergency Physician Lead pilot undertaken for separate three-month periods at the PLC and FMC. The
initiative emerged as one of the key projects developed through the zone-wide EMS flow initiative and was associated with improved outcomes for EMS park patients, better operational flow and excellent feedback from nearly all medical and nursing staff who were affected.
2. Significant progress has been made in regards to the CPSA mandate of communicating relevant outcomes from episodic care (including EM care) to relevant family physicians. Sincere thanks to Dr. Neil Collins who served as the acting Department Head from July to December for leading this initiative.
3. ConnectCare was an important AHS achievement in 2019 but a portion of the credit for successful emergency implementation can be ascribed to clinical informatic leaders in our department who have contributed to this outcome for years, including the important Clinical Knowledge Content Management system that was the precursor of current order sets across the province.
4. The need to optimize resources through reductions in stretcher hours is a key priority for our department. Dr. Shawn Dowling, newly recruited GFT and Effectiveness Coordinator for our department has worked collaboratively with our colleagues in DI and General Surgery to eliminate the need for oral contrast in cases of suspected appendicitis being evaluated with CT, achieving a safe and patient-preferred improvement in diagnosis with significant gains in operational efficiency.
5. A highly successful internal review of our very popular and highly sought after Royal College Residency training program in Emergency Medicine as well as Royal College Fellowship in Clinical Pharmacology and Toxicology. Congrats to Drs. Patocka, Francis, Lucyk and to support from Madhavi Talasila for the FR program success.
6. The creation and filling of a novel EM and mental health liaison position for the FMC funded through the Calgary Health Trust and the Calgary Mental Health Association. Congrats to Dr. Jen Nicol on the role and to FMC physician leadership for facilitating.
7. Expanded clinical analytics and reporting to MDs (72-hour revisit resulting in admission alert and Tableau-based reports on numerous metrics mailed out to all MDs) as well as growing participation at MD facilitated audit and feedback sessions.
8. Extensive remodeling and innovation for Intake Zones and Minor Treatment at the PLC in late 2019. 9. Physician retention strategies including the introduction of new scheduling software across two sites that can better
incorporate shift preferences and time off requests. 10. Launch of a specialist direct referral pathway that addresses previous safety risks and sees a higher degree of involvement
by emergency physicians in high-risk transitions in care. 11. Improved practice patterns in these areas: near elimination of urine toxicology, coags in chest pain, renal colic imaging,
probenecid use in soft tissue infections. 12. Favorable and improving operational metrics when compared to similar Alberta hospitals, especially time to MD, LWBS and
72 hour returns (see http://focus.hqca.ca) 13. Favorable EIP statistics compared to other Canadian jurisdictions (see: https://yourhealthsystem.cihi.ca/hsp/?lang=en 14. Ongoing support for a myriad of activities by the Physician Support Fund supported by MD contributions. 15. Adam Oster’s leadership of a robust Quality Assurance program highlighted by multiple polcy changes made after Safety
Reviews. 16. Development of a new recruitment and interview process (Walker) that makes our Department more attractive to
prospective candidates. 17. New Parental leave Policy championed by Dr. Margaret Greidanus.

MESSAGE FROM DEPARTMENT HEAD
2019 ANNUAL REPORT 2
Academic / Faculty Development / Recognition:
1. Drs. Marshall Ross and Fareen Zaver Top 40 under 40 in Calgary for 2019 2. Dr. Shawn Dowling ED Emergency Physician of the Year for the Canadian Association of Emergency Physicians –
urban category for 2019. 3. Sarah McPherson – CSM PGME award for 2019. 4. Highly successful and stable PGME with CBD introduced and running smoothly (McPherson, Francis, Fedwick,
Patocka) 5. Calgary ED MDs taking over/leading large zone, provincial or national mandates in health in Alberta and beyond:
Collins (ED operational lead / Interim DH), Baker (AZMD), Rich (Associate CMIO), Patocka (RCPSC PD), Dowling (Assistant Dean CME - PLP/AMA), Abbi (AMA), Barkhurst (Calgary Zone EMS), Brulotte (EMS), DelCastilho (SHC FD), Moussadji (Medical Affairs – complaints/disaster), Johnston (Director of DLRI at the U of C), Yarema (PADIS), Head (CSART), Lazarenko (AHS Pharmacy). Vipond (CAPE).
6. High involvement in securing the 2025 ICEM conference for Canada (4000 delegates anticipated) 7. Expanding and increasingly stable research department with a number of CIHR (McRae) and PRIHS (Andruchow)
grants held by departmental clinician scientists. 8. Fifteen faculty successfully promoted to Assistant and Associate Professor in 2019 9. Physician Wellness and recognition: MD gala now in its’ fifth year 10. Innovation: AMP (Huffman), INFO Sessions (Rose) 11. Launch of the Calgary Health Trust Research Fund supporting the Grant Innes Resident Research award. 12. Vibrant Simulation and Ultrasound programs (McNeil, Peterson) 13. Mike Hodsman annual lecture series 14. Ongoing and enhanced communications to the department via Friday newsletter 15. Launch of the Professional Development Hubs – most active include MD Wellness (Dr. Huma Ali) and Global
Emergency Medicine (Dr. Andrew Battison) 16. PRIHS IV funding. “Improving Acute Care for Long-Term Residents: A Better Way to Care for the Frail Elderly in
Times of Medical Urgency” (Hair, Zuzic, Baker, Collins, Grigat, Wang, Andruchow, Szava-Kovats, Lang, Holroyd-Leduc, Spackman) $1.2M

MESSAGE FROM DEPARTMENT HEAD
2019 ANNUAL REPORT 3
Challenges / Threats:
1. Unfavorable time to MD statistics compared to others in Canada (see: https://yourhealthsystem.cihi.ca/hsp/?lang=en
2. Strain on AHS and U of C funding envelopes – always asked to do more with less 3. Severe EIP issues and access block at key periods of the year i.e. flu and particularly severe at SHC at times. 4. No departmental “Academic Medicine Health Services Plan - AMHSP” (ARP) to support up and coming and some
established leaders in our department. 5. Limited leadership development opportunities for young faculty with significant academic interest and credentials. 6. Largely ineffective surge strategy 7. GFT position remains unfilled (new recruitment profile approved this month) 8. Variable support among MDs for the research / innovation mission of the department 9. Sustainability of research program given few GFTs and no ARP (AMHSP). 10. Limited dedicated support for resident and junior faculty research 11. Managing engagement in a very large physician group 12. No annual CME conference that we can call our own. 13. No Faculty Development leadership and minimal engagement with U of C offerings by our staff. 14. Continuous increases in ED MD staff numbers which has added complexity and created challenges for coordination.
While still reasonably cohesive some site-specific silos of activity and culture exist.
Dr. Eddy Lang, MDCM CCFP(EM) CSPQ Zone Clinical Department Head January-June, 2019
Dr. Neil Collins, MD, CCFP (EM) Zone Clinical Department Head July-December, 2019

EMERGENCY DEPARTMENT ACCOMPLISHMENTS
2019 ANNUAL REPORT 4
Academic Appointment Promotions
Clinical Professor Dr. Mark Yarema
Clinical Associate Professor Dr. Aaron Johnston
Clinical Assistant Professor
Dr. Jennifer Puddy Dr. Coleen Carey Dr. Anjali Pandya Dr. Katherine Bateman
Dr. Chris Bond Dr. Ashlea Wilmott Dr. Kathryn Crowder Dr. Scott Seadon
FMC Physician of the Year Award
Dr. James Andruchow Presented annually by the FMC Medical Staff Association in recognition of an individual's outstanding commitment to patients, staff, and learners within the Foothills Hospital community they serve. James is the first ER doctor to receive this prestigious award! The selection committee was most impressed by his research and interdisciplinary work with Cardiology and Radiology, as well as his commitment to furthering the next generation of learners.
UME EM Clerkship Behind-the-Scenes Award Dr. Erik Saude Contributions to the Clerkship, such as coordination of curriculum innovation, re-development of examinations, faculty development, student and preceptor feedback.
CAEP Urban Emergency Physician of the Year Dr. Shawn Dowling Shawn has brought a number of innovations to our department and continues to lead in many areas including the facilitated audit and feedback sessions he runs in conjunction with leads at a number of sites.
2019 CAEP Research Grant Recipient Dr. Fareen Zaver
2019 CAEP Research Grant Recipient & New FRCP Program Director Dr. Catherine Patocka
EMERGENCY DEPARTMENT ACCOMPLISHMENTS
2019 ANNUAL REPORT
Post Graduate Clinical Education Award for Clinical, Adjunct and Research Faculty Dr. Sarah McPherson
Urgent Care Medical Director and Section Chief Under Department of Family Medicine & Department of Rural Medicine, Calgary Zone Dr. Charles Wong He is a Family Physician with his CCFP (EM) designation currently practicing Emergency Medicine at the Rockyview Hospital. In that role he has focused on quality improvement initiatives for physicians and patient care and has worked with the third year Emergency Medicine program in a leadership capacity.
2019 Ian Steill Researcher of the Year (CAEP) Dr. Andrew McRae
Canadian Association of Emergency Physicians Alan Drummond Advocacy Award Dr. Joe Vipond
APPETITE - AHS President's Award for Outstanding Achievement in Innovation & Research Excellence Dr. Stephen Freedman
Commitment to Comfort QI Collaborative Team - AHS President's Award for Outstanding Achievement in Innovation & Research Excellence Dr. Jennifer Thull-Freedman
CPoCUS Research Award for Staff Clinicians Dr. Charles Wong
Canadian Certified Physician Executive (CCPE) Credential Dr. Gerald Lazarenko
ACH ED Medical Informatics Lead / Connect Care Provincial Physician Trainer - EM Track Dr. Ashlea Wilmott
ARCH (Addiction Recovery & Community Health) Consultants Drs. Meira Louis & Mark Scott
Emergency Adult Knowledge Lead Dr. Ryan Chung
Dr. Colin DelCastilho participated in the annual Race to the Top stair challenge at South Health Campus in support of Heart Month. Watch the highlight video here: https://www.youtube.com/watch?v=5_EFK1LyVtQ&feature=youtu.be
5

EMERGENCY DEPARTMENT ACCOMPLISHMENTS
2019 ANNUAL REPORT
Honorable Mentions: Class of 2018 Clerkship Awards Dr. Mark Bromley Dr. Tony Chad Dr. Ping-Wei Chen Dr. Cathy Dorrington Dr. Andrew Fagan Dr. Mardelle Gamble Dr. James Huffman Dr. Eileen Kabaroff
Dr. David Lendrum Dr. Andre Michalchuk Dr. Jennifer Nicol Dr. Christopher Rebus Dr. Paul Tourigny Dr. Stuart Turner Dr. Phil Ukrainetz Dr. Bryan Young
Gold Star Award: Class of 2020 Preclerkship Awards (AEBM course) Dr. Eddy Lang
Gold Star Award: Class of 2020 Preclerkship Awards (Medskills course) Dr. Ian Wishart
End of an Era Award (Admissions) Dr. Ian Walker
Honour Roll recipients: Class of 2020 Preclerkship Award Dr. Tony Chad Dr. Mark Scott
Gold Award: Class of 2018 Clerkship Awards Dr. Puja Chopra Dr. Mike Su
6

EMERGENCY DEPARTMENT ACCOMPLISHMENTS
2019 ANNUAL REPORT
Recruitment:
Dr. Catherine Patocka assumed the role of FRCPC Resident Director effective April 1, 2019. Catherine graduated from the McGill Royal College EM Residency Program in 2013, and has worked as an emergency physician in Calgary since then.
She holds the rank of Clinical Assistant Professor at the University Of Calgary Cumming School Of Medicine. In addition to her clinical duties, Catherine holds leadership positions including the Calgary EM Competence by Design (CBD) Lead for EM, and provincially she serves as the Clinical Knowledge and Content Management (CKCM) Lead for Emergency Medicine. Catherine also serves as a Board Member with the (CAEP) Canadian Association of Emergency Physicians Board of Directors.
Educational leadership and scholarship are strong areas of interest for Catherine and as a result, she obtained a Diploma in Health Sciences Education through the McGill Centre for Medical Education, a Diploma in Educational Design through the Academic Life in Emergency Medicine (ALiEN), and a thesis-based Masters of Health Professions Education (MHPE) from Maastricht University in Netherlands.
Catherine completed her Doctor of Medicine degree at McGill University, and her Bachelors of Science Honors in Pharmacology at the University of Alberta.
The Calgary Department of Emergency Medicine would also like to thank Dr. Sarah McPherson for doing an exceptional job as FRCPC Resident Director, as well as various other roles she's had in leading and supporting the FRCPC Residency Program for the past 10 plus years. Sarah has made many outstanding contributions to the Residency Program, and she will be missed.
Dr. Shawn Dowling appointed as the new QI Scientist position effective September 1, 2019. Shawn will be leveraging his impressive achievements by continuing with the Physician Learning Program in a leadership role as well as staying on our Clinical Effectiveness Coordinator where he will provide oversight for a number of improvement initiatives that will have impact well beyond our zone.
Dr. Anjali Pandya is the new CBD Lead for the FRCPC residency program - active with the CBD program since its inception last year both as a committee member and the assessment lead. She will now take the lead on all issues related to CBD including implementation, evalution and faculty development.
Dr. Brad Granberg is the new Disaster Coordinator.
Dr. Scott Lucyk is the Program Director Clinical Pharmacology & Toxicology.
Dr. Jennifer Nicol is the Emergency Physician Liasion Lead for Mental Health.
7

EMERGENCY DEPARTMENT ACCOMPLISHMENTS
2019 ANNUAL REPORT
Dr. Marshall Ross - Recipient of Calgary's Top 40 under 40 for 2019
Dr. Marshall Ross created a new protocol for addressing opioid addiction in Calgary emergency rooms that has formed the basis for ER treatment of overdoses throughout the province.
Age: 35
Job title: Emergency Physician, Alberta Health Services; Clinical Lecturer, Department of Emergency Medicine, Cumming School of Medicine, UCalgary.
Why he’s a 2019 Top 40 under 40: Dr. Marshall Ross created a new protocol for addressing opioid addiction in Calgary emergency rooms that has formed the basis for ER treatment of overdoses throughout the province.
Dr. Marshall Ross doesn’t need much sleep. We should all be grateful for that.
It’s partly how he has managed to help overhaul treatment of opioid addiction in emergency rooms across Alberta, work as an on-call physician for STARS air ambulance and maintain long hours in his career as an emergency room doctor, all while making time for his young family. He also somehow manages to fit in time for research.
The ongoing opioid crisis, which has killed more than 2,000 Albertans since the provincial government started reporting opioid-related deaths in 2016, has been
a constant and worsening shadow during his time in the ER. “Pretty much every shift, I come in and see someone overdosing on opioids,” says Ross. “It’s just a huge part of what we do.” But “what we do” — reversing an overdose, then sending
addicts back out into the world — struck Ross as insufficient. “I was just giving them a pamphlet and sending them on their way. It didn’t seem like we were doing anything to change things.”
So he set about changing things himself. He had read a Yale study that showed the ER is one of the most underused places to help someone break an opioid addiction — for many suffering addiction, it’s their only contact with health professionals. Ross developed an emergency room protocol for the use of suboxone, a drug that binds to opioid receptors in a way that limits its potential for abuse. By preventing overdosing and withdrawal symptoms, suboxone is the “best chance at getting off opiates,” Ross says.
After Calgary ER physicians started using Ross’s protocol, it gained traction and has formed the basis for a province-wide protocol. There’s a lot of stigma around addiction, and Ross acknowledges that medical professionals aren’t immune to it. Some doctors and nurses were resistant to the new approach. “They’re not thinking of it as a disease, they’re thinking of it as a behavioural problem.”
But in a deadly crisis, it’s hard to argue with what works. “We’ve got to do this,” says Ross. “It would be crazy not to do this. I don’t see anyone else doing it, so I’m going to take it on and champion it.”
Source: Avenue Magazine Calgary, October 29, 2019
Photograph: Avenue Magazine Calgary, October 29, 2019
8

EMERGENCY DEPARTMENT ACCOMPLISHMENTS
2019 ANNUAL REPORT
Dr. Fareen Zaver - Recipient of Calgary's Top 40 under 40 for 2019
Dr. Fareen Zaver is changing medical education in ways that will help new doctors in Canada and around the world.
Age: 34
Job title: Emergency Physician, Peter Lougheed Centre and South Health Campus; Clinical Assistant Professor, Department of Emergency Medicine, Cumming School of Medicine, UCalgary.
Why she’s a 2019 Top 40 under 40: Dr. Fareen Zaver is changing medical education in ways that will help new doctors in Canada and around the world.
Dr. Fareen Zaver always wanted to be a doctor in her hometown of Calgary. But, she wasn’t initially accepted into medical school in Canada. Instead, she completed her medical degree at a school in the Caribbean. That made her an international medical graduate, limiting her options for getting back to Canada to do a residency in emergency medicine. So she moved to Washington D.C., to complete four years of residency and a fifth year at the Mayo Clinic. In her last year there, while studying for her Canadian certification exams, she built an online education curriculum for emergency medicine residents.
Today, Zaver is an emergency physician at the Peter Lougheed Centre and the South Health Campus and her medical curriculum is used around the world. She could have returned to Canada earlier if she had been willing to train in a different specialty, but that wasn’t an option she would consider.
“Emergency medicine is the place where you get to hold someone’s hand, look them in the eyes and tell them that you’re going to try to provide safety for them on what might be their worst day,” she says.
She hopes her story inspires others who struggle with unexpected obstacles on their career path. “It’s about working hard and being resourceful and not giving up when things get really difficult,” she says.
Inspired by her own difficult experiences in training, Zaver developed a virtual online community for residents and directs a fellowship for physicians who want to create online training programs. Her online emergency medicine curriculum is now used in 10 countries, making her an international leader in medical education.
She is currently pursuing a master’s degree in medical education. For her thesis, she is creating a curriculum to help new doctors as they transition from trainees to independent practice. “I don’t want someone else to have to go through those same struggles I did,” she says. “I want to build something so the next generation of people experience it differently.”
Source: Avenue Magazine Calgary, October 29, 2019
Photograph: Avenue Magazine Calgary, October 29, 2019
9

EMERGENCY DEPARTMENT ACCOMPLISHMENTS
2019 ANNUAL REPORT
Dr. Eddy Lang is the successful candidate for the University of Calgary Scientific Director, University Liaison position for the Alberta Health Services Strategic Clinical Networks. This position will be assumed as part of his Scientific Director position and will be enabled by his position in the Faculty of Medicine at the University of Calgary.
The need for this position comes out of recent stakeholder consultations for the Strategic Clinical Network roadmap where improved two-way communications with Alberta’s Universities was noted to be critical.
Eddy is well placed to take on the major responsibilities of this role including to streamline SCN/University communications, liaising with Alberta’s Universities to foster collaborations, find synergies in scientific activities and to increase research funding coming into Universities in areas aligned with SCN priorities. Eddy will serve as a communications lead to Scientific Directors to ensure that they are aware of the University initiatives that may impact SCNs and he will serve as a key conduit and ambassador helping promote a stronger relationship between the networks and Universities.
10

EMERGENCY MEDICINE DEPARTMENT OPERATIONS
2019 ANNUAL REPORT 11
Departmental Structure and Organization
Governance:
Physician leads within the Department of Emergency Medicine include a Department Head -Eddy Lang (January-June 2019), Interim Academic Department Head – Grant Innes (July-December 2019), Interim Clinical Department Head & Operations Lead - Neil Collins (July-December 2019), Deputy Department Head & Operations Lead- Neil Collins (January-June 2019) and Deputy Department Head & Operations Lead-Ian Walker (July-December 2019).
Site Chief at each hospital (RGH – Nancy Zuzic; PLC – Richard Morris, SHC – Cameron McGillvray, and FMC – Ian Walker (January-June 2019), FMC (Interim) - David Lendrum (July-December 2019).
Assistant Site Chief at each hospital (FMC – David Lendrum and Interim- Alyssa Morris and Andrea Boone (July-December 2019), PLC – Cathy Dorrington, RGH – Grant Kennedy, SHC – Dan Joo).
Royal College Residency Director - Sarah McPherson (January-March 2019) and Catherine Patocka (April 2019 onwards), Assistant FRCPC Residency Program Director - Marc Francis, CCFP-EM Residency Director -Jason Fedwick, Clerkship Director -Gavin Greenfield, Director of Off Service Resident Education and Undergraduate Education - Meira Louis.
Senior Researcher - Dr. Grant Innes, Research Chief - Stephanie Vandenberg, Junior Researcher -James Andruchow.
ED Ultrasound Coordinator - Danny Pederson, Simulation Coordinator - Gord McNeil, Informatics Lead - Matthew Grabove, Effectiveness Coordinator - Shawn Dowling, Quality Improvement & Safety Lead - Adam Oster, Disaster Planning Coordinator - Kevin Hanrahan (January-June 2019) and Brad Granberg (July 2019 onwards), Department Section Chief of Toxicology - Mark Yarema and Clinical Pharmacology & Toxicology Director- Scott Lucyk. .
Scott Banks, Zone Department Manager, oversees budget, physician recruitment and management.

EMERGENCY MEDICINE DEPARTMENT OPERATIONS
2019 ANNUAL REPORT 12
EMERGENCY MEDICINE DEPARTMENT OPERATIONS
2019 ANNUAL REPORT 13
EM Committees:
Seven main DEM committees meet monthly or bi-monthly.
The Physician Executive Committee:
The Physician Executive Committee provides leadership, direction and support for all physician-related activities. The Committee is a decision-making body for physician resources, scheduling, operational, and quality, safety and financial aspects of the Zone Department of Emergency Medicine (ZDEM).
The ZDEM Operations Committee:
The Operations Committee is a multi-disciplinary committee including Physician, Nursing and administrative representatives. Duties include strategic planning, prioritization, quality, safety, innovation and oversight of all ED systems and processes.
The Academic Steering Committee:
The Academic Steering Committee guides the development of the EM academic program. Primary agenda items for the 2019 year included strategic planning towards short term and long-term academic goals, faculty development, recruitment to academic positions and educational programming.
The Promotions Committee:
This committee processes faculty appointments and promotion requests for the Academic Department of Emergency Medicine.
The ZDEM Physician Resources Committee:
The Physician Resources Committee is a subcommittee of the Physician Executive Committee. It provides leadership and makes decisions with respect to physician resource needs, search and selection, and physician hiring in the Department of Emergency Medicine.
The Quality Assurance Committee:
This committee reports to the ZDEM Operations Committee. It is one of the few departmental QAC’s that have been allowed to continue within the new AHS Safety framework.
The Calgary Physician Support Fund Oversight Committee:
This committee is comprised of 6 emergency physicians who oversee a fund that was set up to support education, development and research in the Calgary Emergency Department. Funding for this committee is provided exclusively by emergency physicians who have agreed to support the fund. The average emergency physician contributes $1,800 annually to this fund.
Department Membership:
The Department of Emergency Medicine currently employs 210+ plus active physician staff and treats approximately 300,000 patient visits per year (annualized value based on current and projected inflow volumes). Historically there were two main “practice-groups” (The Foothills-PLC group and the Rocky view group), but an increasingly zone focus and multi-site practice has changed this model. We now have extensive physician cross-coverage of sites, with a variety of site combinations. Currently all our Emergency Medicine physicians have academic appointments.
MANPOWER AND WORKFORCE PLANNING
2019 ANNUAL REPORT 14
MD Recruitment and Training
We currently have 210 MD’s working in the Calgary Zone at four adult hospitals.
A full time equivalent (FTE) “line” is usually between 12 and 14 shifts per 28 days.
Physicians are scheduled between 0.5 and 1.0 of an FTE.
Physician Resource involves anticipating reductions in physician supply due to parental leaves, international medical work, sabbaticals, illness, retirement, resignation and reduction in FTE requested (both for personal reasons and to accommodate non-clinical work).
Increased in operations created by the addition of shifts also requires adding new physicians. One new shift requires just over 2 new MD’s to staff it.
We have currently 10 locums working to fill short term shortages in manpower during the period July 2018 to July 2019. Some of those physicians may continue to work in the region as permanent members when their locum period expires, expanding our permanent group further.
We also hired 10 locums for temporary work in the summer of 2019.
Hiring summer locums gives much needed tertiary care experience to new graduates and allows time off for permanent ED staff. We aim for no more than 20% of the shifts being covered by locums.
Turnover and expansion of operations usually results in the hiring of between 2 and 8 new permanent Emergency Physicians per year.

MANPOWER AND WORKFORCE PLANNING
2019 ANNUAL REPORT 15
Retention Strategies
AHS Calgary Zone Emergency Departments represent the largest single group of ED physicians in Canada. We have on staff 210 physicians with 0-46 years of service in the region. The Calgary Zone provides highly coordinated and well-organized care to a catchment area that includes 1.2 million patients.
Calgary Zone Emergency Physicians staff the Emergency Departments of 4 adult hospitals, and some are cross appointed at the tertiary care Alberta Children’s Hospital. There is a wide variety of work available. Shifting is flexible with most physicians getting time off when they request it. Sabbaticals, parental leave and leaves for international medical work are usually accommodated.
Seniority is currently recognized with enhanced scheduling flexibility including exclusion from nights, or increased holiday time during the summer. Planning is in progress to provide further scheduling flexibility based on seniority, and to rationalize the scheduling process at Christmas and in the summer.
Job satisfaction is enhanced by a collegial atmosphere, and a robust academic program. High level Grand Rounds occur on a weekly basis and in-house procedural skills sessions are offered semi-annually. A robust simulation program is offered at all Calgary hospitals. Staff physicians have expert simulation sessions available to them where they can practice their resuscitation skills and crisis resource management in a non-threatening collegial atmosphere.
Goals and Strategies
Our underlying primary goal is to provide safe and efficient care to all patients that present to a Calgary Zone Emergency Department. We have increased physician resources and continue to modify ED shift scheduled so that we can better match physician capacity to patient demand. This requires ongoing reassessment of demand, but it is also dependent on modifying operations so that added physicians are effective (i.e. able to examine patients in care spaces). Our “surge strategy” takes effect when patient demand exceeds physician resources and a minimum
number of assessment spaces are available, the departments proceed with a physician call out to assist in the department. This strategy has had some success and we anticipate that it will continue to be better utilized in 2020.
The increased number of admitted patients remaining in the ED because of a shortage of available inpatient beds in 2019 in the Calgary Zone, has been extremely challenging and has crippled many of our previously successful ED in-patient process changes (i.e. creation of intake area in all adult ED’s; Over Capacity Plan (OCP) triggering and implementation to name a few).
ED overcrowding is not the root of the current crisis rather it is the result of the limited number of available inpatient beds stemming primarily from the province’s shortage of long-term care beds. Although AHS and the province of Alberta continue to try and find measures to improve access, until more acute care and long-term beds are created, we anticipate the situation may worsen over the coming year.
Impact on other Departments and AHS Resources
Hiring Emergency Department physicians has an impact on the provincial physician budget (payments are fee for service billings though the Physician Services Branch), but minimal impact on other Calgary departments and the CMO (Medical Affairs) budget, as the physician are fee for service workers increasing in response to growing patient demand. We have required and will continue to require some additional resources for ongoing advertising and physician recruitment until this active initiative winds down in June 2020.
Scott Banks, Emergency Department Calgary Zone Manager

EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 16
Dr. Eddy Lang, Zone Clinical Department Head (January-June 2019) Dr. Eddy Lang is a Professor and Department Head for Emergency Medicine at Cumming School of Medicine- University of Calgary and Alberta Health Services, Calgary Zone. His areas of interest are knowledge translation, evidence-based medicine and operations research. He is a member of the GRADE working group and has led the development of GRADE-based clinical practice guidelines in pre-hospital care in the US as well as with the International Liaison Committee for Resuscitation. Dr. Lang is also an award-winning educator having received recognition at both the university, national and international levels. He also serves as Senior Editor for the Canadian Journal of Emergency Medicine, Associate Editor for both ACP Journal Club and the International Journal of Emergency Medicine. In addition, he is a member of the Canadian Task Force on Preventive Health Care (CTFPHC). Dr. Lang chaired the Canadian Association of Emergency Physicians Conference (CAEP) 2018 and he was appointed as the Scientific Director of the Emergency Strategic Clinical Network ESCN in Alberta.
Dr. Grant Innes, Acting Zone Academic Department Head (July-December 2019)
Dr. Grant Innes is a full professor at the Cumming School of Medicine and served as Clinical Department Head for Emergency Medicine at Alberta Health Services, Calgary Zone from 2008 to 2013. During his tenure as department head, the academic department of Emergency Medicine at the University of Calgary was created, becoming the 7th academic department of this specialty in Canada.
After his success reducing patients’ length of stay in the ED of St. Paul Hospital in Vancouver, Dr. Innes served as the principal architect for the Alberta Overcapacity Program (OCP) launched in December 2010. This program led to dramatic reductions in emergency inpatients and, through collaborative approaches with inpatient services, realized gains in reduced length of inpatient stay. The impact of OCP has been felt province wide and led to improved quality of care and working conditions across sixteen of Alberta’s busiest emergency departments. This program gained the top prize at an
international research competition with over 800 projects presented.
Dr. Innes is the founding Editor-in-Chief of The Canadian Journal of Emergency Medicine (CJEM). In his honour, the Canadian Association of Emergency Physician grants annually the Grant Innes Research Paper and Presentation award that recognizes the most significant contributions to Emergency Medicine research. Dr. Innes is a nationally known researcher and opinion leader in this specialty having published over 116 publications listed in pubmed.org. His research interests are health services and operations, flow and access, acute coronary syndrome diagnosis, and renal colic management.
EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 17
Dr. Neil Collins, Acting Zone Clinical Department Head (July-December 2019) Dr. Neil Collins graduated from the University of Calgary in 1990, followed with Family Medicine in 1992. He practiced urban and rural family medicine in British Columbia and Alberta prior to completion of his CCFP(EM) training in Calgary in 1996, where he has been working clinically for 23 years. He has previously held the administrative positions of CCFP (EM) Residency Program Director and Peter Lougheed Centre Emergency Department Site Chief. Since November 2017 Dr. Collins has held the position of Calgary Zone Emergency Deputy Department Head. His administrative interests include ED Resource utilization, ED Flow and Physician Metrics and Evaluation.
Dr. Ian Walker, Acting Zone Clinical Department Deputy Head
(July-December 2019)
Dr. Ian Walker was the Site Chief at Foothills Medical Centre until July 1st 2019 when he temporarily assumed the role of Acting Deputy Department Head for six months. He will be returning to his role at FMC as of Jan 1st, 2020. He completed medical school at the University of Calgary, Family Medicine training at the University of Ottawa and the CCFP (EM) program at University of Calgary. He has been a member of the department since 2001. The majority of his extra clinical roles have been educational in nature, including a prolonged term as Director of Admissions.

EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 18
Dr. David Lendrum, FMC Site Chief, STARS Transport Physician (July-December 2019) Dr. David Lendrum completed his medical degrees at the University of Calgary and Emergency Medicine residency and Masters of Medical Education at the University of Toronto. He has since worked in Calgary since graduating in 2008 and currently split his clinical time between Foothills Medical Centre and Alberta Children’s Hospital. He took the role of Assistant Site Chief of FMC Emergency in early 2018. His extra clinical roles includes working as a transport physician for STARS, as an on-hill medical provider at Sunshine and Lake Louse with an urban search and rescue team known as CANTF2.
Dr. Rick Morris, PLC Site Chief
Dr. Rick Morris is the site chief of Peter Lougheed Centre. He graduated from McMaster University in 1998, and obtained his certification through the CCFP program at the University of Calgary with a joint academic appointment in Family Medicine. He has been a department member since 2001. Past administrative positions have included RMES director and Regional Manpower Lead.
Dr. Cathy Dorrington, PLC Assistant Site Chief
Dr. Cathy Dorrington graduated from medical school in 1994 at McMaster University, and subsequently completed her FRCPC Emergency Medicine residency in 1999 at the University of Calgary. She has worked in Calgary since then, currently at the PLC and FMC sites.
Dr. Dorrington was the Emergency Department Site Chief at Foothills Medical Centre from 2012-2015 and has held the position of Emergency Department Assistant Site Chief at Peter Lougheed since 2017.

EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 19
Dr. Nancy Zuzic, RGH Site Chief
Dr. Nancy Zuzic continues as the Site Chief at the Rockyview General Hospital. Dr. Zuzic received her MD at the University of Ottawa in 1997 and then completed her CCFP-EM residency in Calgary in 2000, working clinically at the Rockyview ED ever since. Nancy is fortunate to work with a cohesive and supportive administration team at the RGH ED that continues to find innovative ways to improve flow and patient care.
Dr. Grant Kennedy, RGH Assistant Site Chief
Dr. Grant Kennedy graduated from the University of Manitoba in 2006 followed by his doctorate in Emergency Medicine via the CCFP program in 2009. In his spare time Dr. Kennedy enjoys spending time with his wife and three kids. He also enjoys writing and performing music.

EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 20
Dr. Cameron McGillivray, SHC Site Chief
Dr. Cameron McGillivray completed an undergraduate degree in Physics in 1996 from Whitworth University in Washington State while on an athletic scholarship. Prior to medical school, he worked as a Paramedic in Vancouver and taught for UBCO in their Adult Basic Education and Engineering Technology Programs. He attained his Medical Doctorate from the University of British Columbia in 2004, and proceeded through the CCFP Program with Family Medicine, graduating in 2006. He worked on Vancouver Island before returning to UBC to complete the CCFP-EM in 2008. He then worked in Ontario until coming to the Calgary Emergency Department in 2013. Dr. McGillivray has been the South Health Campus Site Chief since 2017 and was the Assistant Site Chief from 2015-2016.
Dr. Daniel Joo, SHC Assistant Site Chief
Dr. Daniel Joo completed his medical degree at the University of Calgary in 2008 and his Emergency Medicine Residency (CCFP-EM) in 2011. After working in emergency departments in Vancouver and Ottawa, he moved home and joined the department in Calgary in 2014. Dr. Joo took on a new role as Deputy Chief of the SHC Emergency Department in August 2018. His extra-clinical interests include residency education primarily in the areas of ultrasound and simulation. In his spare time, Dr. Joo enjoys spending time with his wife and kids, and stays active playing sports, running, and biking.
Dr. Matthew Grabove, Medical Informatics Physician Lead
Dr. Matthew Grabove has been in the Calgary Zone ED Medical Informatics Physician Lead since 2017. He graduated from Memorial University of Newfoundland in 2004 and completed his residency training in family medicine in Toronto in 2006. He then worked as a family physician in Toronto and Yellowknife before completing his CCFP-EM certification. Dr. Grabove practiced as an ER physician in Saint John and Brampton before joining the department in Calgary in 2013.
Having a background in computer science, Dr. Grabove has a keen interest in the intersection of medicine and technology with a focus on the impacts of technology in the ED.

EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 21
Dr. Adam Oster, Quality Improvement and Safety Lead
Dr. Adam Oster graduated from the RCPS EM Program via University of Calgary in 2006, through the FRCPC program. He enjoys cross-country skiing and biking in his spare time.
Dr. Tom Rich, Associate Chief Medical Information Officer
Dr. Tom Rich graduated from the University of British Columbia in 1991, then completed his inner city Family Practice Residency at St. Pauls Hospital in Vancouver. He then moved to Calgary to complete his CCFP-EM residency in 1994 and has been working in Calgary as an Emergency Physician ever since. Over the past 25 years he has been actively involved in numerous administrative interests such as Patient Safety and Quality Improvement. The last 10 years he has been focused on Clinical Informatics providing leadership roles within the Calgary Zone, and I snow on the provincial Connect Care project. His interests and involvements included STARS, CAEP, McMahon Stadium events, FIS World Cup Ski racing Lake Louise, and Vancouver Olympics 2010.
Dr. Jason Fedwick, Division Chief CCFP(EM) Calgary Zone ED
Dr. Jason Fedwick graduated from the University of British Columbia in Family Medicine after starting residency in General Surgery. He then completed the EM program in Calgary where he has since worked in the Calgary Zone Emergency Departments. He was the South Health Campus site chief from 2014 to 2016. Currently he is the CCFP-EM Program Director, a Transport Physician for STARS and a member of Canada Task Force 2. In his spare time, Dr. Fedwick enjoys mountain biking, snowboarding and climbing.

EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 22
Dr. Catherine Patocka, FRCPC (ED) Medical Education Program Director
Born and raised in Edmonton, Catherine came to Calgary in 2013 after completing medical school and FRCP residency training at McGill University. She works clinically at the FMC and PLC and has a special interest in medical education. She became the FRCPC residency program director in April 2019 and continues to have a strong interest in medical education scholarship and research. Outside of medicine she likes to hike, ski and spend time in the mountains with her husband Stephane and 3 children Juliette, Samuel and Dominic.
Dr. Marc N. Francis MD, FRCPC-EM, Assistant Program Director FRCPC Emergency Medicine
Dr. Marc Francis was born at the Foothills Hospital (and may die there too) He was raised in Calgary. He completed his undergraduate and his medical school training at Queen’s University in Kingston Ontario. He returned home to Calgary to complete his FRCPC Emergency Medicine in 2008 with a special focus in Pediatric Emergency Medicine. Currently Marc splits clinical time between the FMC and the ACH and works as a STARS Transport Physician. Marc has been the Assistant Program Director for the last 5 years and loves connecting with the resident group. Marc and his wife Jennifer have 3 children and in what little spare time he has, Marc plays basketball, drives kids to activities, and goofs around on the guitar.
EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 23
Dr. Meira Louis, Under Graduate Student and Off – Service Resident Coordinator
Originally from Toronto, I finished an undergraduate and masters in Ontario before moving to Calgary for my MD and FR residency in emergency medicine. I have worked as a staff physician at the PLC and FMC since graduating in 2014. Soon after starting work, I took over as the coordinator of Elective and Off Service Education. Recently I have also taken over as course chair for electives in the Undergraduate Medical Education program. In my spare time I help my amazing husband juggle our four kids.
Dr. Antonia Stang, Section Chief Pediatric Emergency Medicine
Dr. Antonia Stang completed her medical degree, pediatric residency and pediatric emergency medicine fellowship at McGill University in 2008. She joined the section of pediatric emergency medicine at the Alberta Children’s Hospital in the same year as graduating. Her research interests are in health services research with a focus on quality improvement and patient safety. She is a member of Pediatric Emergency Research Canada (PERC), a national network of pediatric emergency researchers.
Dr. Stephanie Vandenberg, Research Director
Dr. Stephanie Vandenberg is an emergency physician in the Calgary Zone, Research Director for the Department of Emergency Medicine (@uofcemresearch) and Clinical Lecturer at the Cumming School of Medicine. She received her MD from the University of Toronto and holds a Bachelor of Arts & Science from McMaster University with a Minor in Biochemistry and a thesis in Paediatric HIV. She completed a Master’s of Science in Epidemiology at the London School of Hygiene and Tropical Medicine and performed a subgroup analysis of the WOMAN trial data (tranexamic acid in postpartum hemorrhage) for her graduate project.
Stephanie uses a “research for advocacy” framework to engage discussions on health systems, harm reduction, and ways to improve vulnerable populations’ health outcomes using principles of social entrepreneurship and information design/visualization.

EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 24
Dr. Gavin Greenfield, Emergency Medicine Clerkship Director Cumming School of Medicine, University of Calgary
Dr. Gavin Greenfield graduated from medical school at the University of Western Ontario in 1998. He completed his Family Medicine training (Calgary) in 2000 and after working in various places for a year completed his CCFP(EM) training in 2002 (also in Calgary). He was the Site Chief at the Foothills Medical Centre from 2006 to 2012. In addition to his current role as Clerkship Director he is also the Medical Director of Education at STARS where he has worked as a Transport Physician since 2005. He has a special interest in education around Airway, Mechanical Ventilation and Blood Gases. In addition to his Canadian career he enjoys International Medicine and has spent time in Haiti as well as the Philippines.
Dr. Scott Lucyk, Program Director, Royal College Clinical Pharmacology and Toxicology Program
Scott Lucyk is a Clinical Assistant Professor and works as an Emergency physician with AHS-Calgary Zone and as a Medical Toxicologist with PADIS. He is the Associate Medical Director at PADIS and the Program Director of the RCPSC Clinical Pharmacology and Toxicology subspecialty program. He obtained his FRCPC in Emergency Medicine from the University of Alberta, followed by a Medical Toxicology fellowship at the New York City Poison Control Centre.
EMERGENCY MEDICINE PHYSICIAN EXECUTIVE MEMBERS
2019 ANNUAL REPORT 25
Scott Banks, Emergency Medicine Zone Department Manager
Scott is the Calgary Zone Department Manager for Emergency Medicine, Critical Care Medicine & Obstetrics & Gynecology. Scott assumed the Critical Care portfolio in Sept 2017, Obstetrics & Gynecology in July 2018 and has continued to serve as the Zone Manager in Emergency Medicine since 2008. Scott completed his Master of Business Administration degree (MBA) at the University of Calgary in 1993 specializing in Human Resources and International Management, and his Bachelor of Arts Honors degree in 1989 from the University of Regina. Scott is a 23 year Chartered Professional in Human Resources (CPHR) in Alberta, and holds a Certified International Trade Professional Designation (CITP) in Canada. Previously Scott served as the Vice President of Operations & Human Resources at The Brenda Strafford Foundation, and as Senior Vice President & Chief Operating Officer at a for profit healthcare college in Oahu, Hawaii. He has also served as an International Development Consultant with the Canadian International
Development Agency in Guyana, Manager of the Mount Royal University Small Business Training Centre, and as a Market Intelligence Research Officer for the Canadian Federal Government at the Canadian High Commission in Trinidad. In addition, he served as the Manager of Business Training & Commercial Accounts with the Business Development Bank of Canada. Scott has lived and/or worked in Hawaii, Canada, Trinidad, Guyana, Haiti, and Dominica. Scott is married and has very active six and nine year old boys. He enjoys spending quality time with his family, his French bulldog, jogging, travelling, and volunteering with World Vision.

FOOTHILLS MEDICAL CENTRE UPDATE
2019 ANNUAL REPORT 26
Department 2019 was our first successful full year utilizing the recently opened B pod treatment area. This new treatment space houses our intake patient treatment area, which we have had in various iterations for almost 10 years now in the Foothills Hospital Emergency Department, but this version is a significant improvement over any other previous intake areas. This current version has better patient assessment spaces, better patient confidentiality and a dramatically better physical environment for the physicians and nurses to work in. The intake area is based on the clinical idea that a patient does need to be assessed by the nursing and physician teams on a proper examination stretcher, but the patient does not need to stay on an examination stretcher to receive their care. This approach allows patients who are waiting for diagnostic tests to do so in a chair instead of occupying a patient stretcher. Similarly, patients who meet certain clinical criterial are able to receive their care while resting in a reclining chair instead of a stretcher. Having the physical infrastructure to facilitate efficient patient assessments in stretchers and then the delivery of care in alternative treatment spaces continues to improve the efficiency of the Emergency Department. Furthermore, the intake area has allowed the department to continue to manage arriving patients despite having the majority of our treatment stretchers occupied by admitted patients. Leadership Over the past year Dr. Ian Walker took on the role as interim Deputy Department Head to support Dr. Eddy Lang’s (Emergency Department Head) sabbatical. As such, Dr. David Lendrum took on the role as interim Site Chief at the Foothills Hospital Emergency Department and Dr. Andrea Boone and Dr. Alyssa Morris were hired as interim assistant site chiefs. These changes in leadership were very successful and we are very thankful to all the physicians who took on extra administrative roles over the past year. The physician leadership team works in partnership with the nursing leadership team on a daily basis. The incredibly hard-working and effective nursing leadership team is led by Sharleen Luzny who is supported by
patient care managers Erin Bugbee and the newest edition to their team, Julie Meyer. Manpower As like the previous year, several new physicians were added to the FMC physician group in 2019 due to some physicians choosing to practice at different Emergency Departments in Calgary and from MD attrition. No new shifts were added to the physician roster during 2019.
In response to a noted sharp increase in the time patients wait in a care to see a physician between 1 am and 5 am, a third dedicated night physician was introduced on a trial basis in the summer of 2018. This was a successful trial and the third night shift was incorporated into the regular schedule. In 2019, the start time of the three-night shifts was examined and subsequently adjusted to ensure physician resources best matched patient wait times.
The physician administration group continually assesses the need for further adjustments of the physician schedule. As 2019 comes to a close, we are not planning on adding any further clinical shifts to the roster at this time.
At this time, there are 18 shifts per day, for a total of 127 hours of scheduled physician coverage per day. Peak coverage occurs between 16:00 and 22:00 when there are either 7 or 8 physicians on duty. By comparison, in 2014, there were 14 shifts for a total of 108 of physician coverage. This represents not only an increase in coverage, but also a universal transition to 7-hour physician shifts on both days and nights in keeping with local consensus about ideal length of shifts to support physician wellness and productivity.
There are currently over 100 physicians scheduled to work at the FMC however, none of whom work exclusively at this site. While this does provide excellent cross pollination with other sites, it also has the deleterious effect of limiting the sense of ownership that physicians have of the department.

FOOTHILLS MEDICAL CENTRE UPDATE
2019 ANNUAL REPORT 27
To address the concerns raised in 2018 regarding physician shifts being left unfilled due to physician illness or emergencies, a physician back-up schedule was created. The implementation of the physician back-up schedule was quickly adopted by all and has decreased the number of unfilled physician shifts significantly. Given our large physician group we are currently able to manage most physician emergencies in both the short and long term.
Occupational Therapist in the ED As part of the enhanced patient flow initiatives across the zone having a dedicated Occupational Therapist in the ED was trialed. FMC received support to provide Occupational Therapy coverage 7 days a week and most felt the addition of these professionals was hugely beneficial to both patient care patient safety. In the latter half of 2019 this trial came to an end and we are hopeful for future funding to have these excellent patient advocates back in the department.
HELO During 2019, the Hospital EMS Liaison Officer (HELO) medics worked closely with the nursing staff to ensure the most efficient and effective patient movement in the Emergency Department. Most felt the HELO paramedics were an effective addition to FMC ED operations in decreasing patient wait-times and addressing patients waiting in the Emergency Department hallways. The funding for this trial position is complete and we are hopeful to have future funding available to bring the HELO medics back into the department CTAS 1 PHYSICIAN and RAAPID/ECG SCHEDULE We have had a full year of using the CTAS 1 and RAAPID/ECG schedule. The implementation of this schedule has led to less confusion regarding which physician is responsible for the many critical and time-sensitive tasks. Furthermore, this schedule has dramatically reduced the number of over-head pages in the department and also ensured that all physicians working in the department have equitable access to managing the most critically unwell patients. We continue to adjust this physician task schedule to maximize physician workflow and foresee it being used in future.
SPECIALIST TRANSFER PATIENTS AND PRIVATE PATIENTS A major change was implemented in late 2019 to address the numerous safety concerns that were raised concerning patients that were transferred from another facility to see a specialist physician (Specialist Transfer Patients) and patients that arrived at triaged to be seen by their own specialist physician (Private Patients). In the past these patients were triaged upon arrival and the specialist physicians were notified. The specialist physicians were the most responsible physician for these patients, and they were not assessed or managed by an Emergency Physician. As the specialist physicians were at times not immediately available to manage their patients in the Emergency Department due to other responsibilities, patient care was at times compromised. As such, the Emergency Department has undergone an extensive process to move towards a goal that any patient presenting to the department have an assigned Emergency Physician as the patient’s most responsible physician until the patient is admitted to the hospital.
We continue to build the processes and implementation strategies to best maximize patient safety while balancing the needs of the Emergency Department Physicians and those of the specialist physicians.
Plans for 2020 Major priorities for the coming year include:
• Implement and develop the Specialist and Private patient referral process.
• Continually re-evaluate the most efficient and effective use of the clinical treatment spaces.
• Re-evaluation, in conjunction with Trauma Services, of our current level 1 trauma processes.
Dr. Ian Walker & Dr. David Lendrum
FMC Emergency Site Leadership Team

ROCKYVIEW GENERAL HOSPITAL UPDATE
2019 ANNUAL REPORT 28
Capacity RGH ED volume increased from 79, 455 in 2018 to 82, 734 in 2019. RGH ED saw a daily average of 227 patients including an average of 62 EMS visits per day. Distribution of patients throughout the ED remains consistent with 34% treated in the Main ED, 42% in Intake and 24% in the Minor Treatment Area. Nursing and physicians continue to monitor patient arrivals and capacity adjusting or adding shifts to attempt to match arrival times and decrease patient wait times. Chest Pain Process RGH ED continues to make improvements to the chest pain process, in order to improve Triage to ECG times for patients presenting with cardiac chest pain or cardiac type pain. Patients presenting with cardiac chest pain/type pain are triaged directly to a touch down ECG stretcher where the patient is simultaneously registered, assessed by a nurse and an ECG is completed. The ECG is reviewed by the RN and a physician is consulted if there is any question or abnormality noted on the ECG. The patient is then moved from the ECG touch down stretcher to an appropriate location within the ED. Prior to implementation, median triage to ECG time was 36 minutes and only 3% of patients received an ECG within the 10-minute target time. For 2019, the median triage to ECG time was 7 minutes, with 66% of patients receiving an ECG under the 10-minute target. This has been an effective, sustained process change at RGH ED. Stat Stroke Process Since 2018, the Stat Stroke Process has aimed to expedite stroke identification, treatment and transfer for patients presenting with acute neurological deficits. Patients presenting with an acute neurological deficit are immediately triaged to a location and a physician is overhead paged to the bedside. This process is well received by nurses and physicians and is consistently utilized to expedite physician assessment for query stroke patients. Recently enhancements were made to the process to ensure robust communication to all services involved. For example, Unit Clerks provide a repeat overhead page for a physician to the bedside and the bedside nurse communicates with CT as soon as the physician decides to order a CT scan.
Capacity RN As a part of the EMS Park initiatives and funding, RGH ED added a Capacity RN position to the staffing model. The Capacity RN role was funded from October 15, 2018 to September 20, 2019. The Capacity RN worked during peak demand hours (1100-2300) and was responsible for improving stretcher capacity and flow throughout the department, as well as supporting the chest pain process. The Capacity RN improved movement out of stretchers, assisted with expediting discharges and admissions in order to open up space for EMS and patients requiring a stretcher space. Since implementing these EMS Park initiatives, RGH ED demonstrated improved EMS Offload times.
OT/PT in ED As a part of the EMS Park initiatives and funding, RGH ED received dedicated PT and OT coverage, 7 days per week. In addition to the existing role of completing functional assessments, a pathway for patients presenting with low back pain was implemented. This low back pain initiative aimed to provide physiotherapy assessment and intervention for patients presenting with low back pain prior to physician assessment. When able, the ED pharmacist was also consulted to prescribe early non-opioid analgesic. The primary goal of this initiative was to assist with patient flow and reduce ED length of stay, therefore improving EMS offload. Secondary goals included reduced time to analgesic, reduced diagnostic imaging, decreased opioid use and improved patient care by providing condition specific education and access to community resources. When a patient was seen by PT and a Pharmacist prior to physician assessment, results showed that ED length of stay decreased from 4 hours to 3 hours, opioid prescriptions decreased from 49% to 17%, diagnostic imaging decreased from 49% to 33% and 0 patients returned to the ED within 72 hours compared to 7% that did not see PT and Pharmacy. Despite these results, funding for these positions ended September 30, 2019. A PRIHS grant has been submitted to continue the OT/PT work in the ED, with notification of acceptance expected sometime later this year.

ROCKYVIEW GENERAL HOSPITAL UPDATE
2019 ANNUAL REPORT 29
ED Treatment Plan
The ED Treatment Plan team continues to develop consistent and supportive care plans for vulnerable patients who have a high volume of ED visits. In addition to physicians, this multidisciplinary team has dedicated members from nursing, social work and EMS. With leadership support to expand to zone-wide oversight, a total of 15 physicians from across the zone have been involved in this project. Five physicians, representing all adult sites, sit on the committee and the remaining physicians have authored plans or are involved in plan authorship now. The team continues to develop linkages with resources and services in the community including a new partnership with the Chronic Pain Centre.
There are currently 15 active ED Treatment Plans and 5 plans under development. There are 10 priority candidates who are on an immediate “wait list,” and at least 100 additional patients who have been nominated that would benefit from a treatment plan. Patients are prioritized based on ED/EMS usage and the nature of their presentations.
Preliminary data shows a significant reduction in average monthly visits across the group of Treatment Plan patients and a QI project is underway. The current goal is to improve uptake across the Calgary Zone and to ensure sustainability for this project as the case load increases. This requires having MD and RN representatives at each site. The committee received a $6000 grant from the Physician Support Fund to pay small honoraria to treatment plan authors. Ongoing monitoring and updating of plans is increasingly labor intensive as more plans are created. There is currently no dedicated funding for any team members. All members participate either as volunteers or as an extension of their existing roles. Resources needed to sustain this work are protected time and funding for team members and continued access to assigned office administrative support.
RAAPID Call Schedule RGH ED implemented a new RAAPID call schedule to ensure continuity for patients being transferred to the ED for physician assessment. ED MDs beginning their shift become the designated RAAPID MD responsible for taking RAAPID calls/referrals. At peak times of day, the designated RAAPID MD rotates through several MDs to spread the workload. When the referred patient arrives at Triage, the ED MD who took the call (or designate, if MD has handed over) is paged and will assign themselves to see that patient.
Mental Health and Parallel Clearance ED Nursing Management, QI and Site Chief began meeting regularly with Mental Health to improve relationships and process with Psychiatry and Psych Emerg staff. In the summer a revised Parallel Clearance process was launched which aims to improve flow and efficiency for patients presenting with mental health complaints. Dr. Nancy Zuzic, RGH Emergency Site Chief Ashley Murakami, RGH ED Quality Improvement Lead

SOUTH HEALTH CAMPUS UPDATE
2019 ANNUAL REPORT 30
The South Health Campus daily ED visits have slowed their
year over year growth despite continued incremental
growth in population in Calgary’s southeast. In terms of
demographics, patients over the age of 65 placed a higher
demand on the hospital and the Emergency Department
with an increase in admissions from 3934 patients to 4255
patients (~8%). This is largely due to the opening and growth
of several seniors’ lodges and assisted living facilities in the
immediate vicinity to the hospital. There also continues to
be a significant number of pediatric visits to the SHC ED,
which is reflected by the large proportion of young families
in the area.
Admitted patient capacity has been an ongoing issue at the
South Health Campus which has stressed the hospital’s
resources and led to many admitted patients being
temporarily housed in the emergency department. This has
resulted in longer ED wait times.
The South Health Campus has continued to support its four
foundational pillars of collaborative practice, innovation,
patient and family centered care, and wellness while
attempting to mitigate the increased demands placed on
the emergency department. Several key strategies were
initiated by the emergency department, hospital
administration, and zone administration over the past year,
with the intent of improving ED wait times and lowering EHS
offload times.
Achievements of 2019
1. SHC Peak Capacity Escalation Plan. A characteristic
essential to a functioning emergency department is the
ability to be flexible and adaptable to variations in
patient volume and acuity. In response to a significant
increase in Emergency Boarded Inpatients (EIPs), the
SHC Administration in partnership with the Emergency
Department Administration has collaborated to develop
an innovative and novel overcapacity protocol. A
stepwise, integrated, laddered response to defined
triggers allows the ED and hospital to anticipate and
react early to offset potential higher demands on the
SHC Emergency Department without disrupting care.
Since implementation, the ED has improved its
capability to deliver uncompromised patient care at all
times. The SHC Capacity Committee meets monthly and
has revised its escalation triggers over the year to better
mitigate the negative effects of EIP burden.
2. Several Quality Improvement Initiatives including the
SHC STEMI and Acute Stroke projects have significantly
improved the door to intervention times for SHC
patients. Also, the oral vs iv medication and the EMS
Rapid Patient exchange projects have led to improved
delivery of health care to SHC ED patients. A GI Food
Bolus project was initiated by the Emergency
Department with collaboration with the
Gastroenterology Department to improve the
experience and outcome for patients presenting to the
SHC ED with a food bolus. It has been well received.
3. The Pediatrics Pod was completed at the end of the
summer and saw its first patients in September. Its
innovative design enables the department to
proactively meet the diverse needs of the pediatric
patient population and to provide unparalleled care
while managing costs and reducing overall risk. With its
opening, the SHC Emergency Department anticipates
becoming a leader in future delivery of pediatric
emergency care in Alberta. In the few months since
seeing its first patient, there appears to be a rise in
pediatric visits to the SHC Emergency Department and
families have welcomed the improved care and
experience.
4. The South Health Campus ER has become a leader in
providing emergency care to seniors in Alberta. As
mentioned earlier, the SHC ED has experienced a
significant increase in seniors’ visits and admissions
compared to the previous years. Research has shown
that time spent in an emergency department setting
significantly increases delirium rates (8% increase over
baseline for 8 hours spent in the ED) in patients over the
age of 65. Experiencing delirium significantly increases
mortality and considerably increases the hospital
admission length of stay. Unfortunately, due to hospital
capacity levels (often above 110%) the 90%ile for ED

SOUTH HEALTH CAMPUS UPDATE
2019 ANNUAL REPORT 31
LOS for patients 65 and older is currently 43.13 hrs. We
identify the impact of the delay of transfer to the
inpatient ward and anticipate it will influence the
patient experience and outcome as well as compound
the EIP burden. Our Senior Friendly ED Committee has
initiated several projects/programs for the benefit of
our senior’s population, one being to mitigate the risk of
developing delirium. An ongoing QI project, the
“Implementation of the CAM assessment tool” (for
delirium screening) by the bedside RN has had an
increased uptake. In addition the committee has
developed a robust senior specialized volunteer
programme termed the SUPER volunteers. SUPporting
seniors in the ER. These volunteers have undergone
specialized training that will allow them to optimally
support vulnerable and isolated seniors in the SHC ER by
reorienting, assisting, and improving their hospital
experience. Similar programs have demonstrated a
lower rate of delirium in admitted patients over the age
of 65.
5. Implementation of SHC site specific guidelines to the
Emergency Fast Track. The demands and resource
imbalance at SHC have necessitated the adoption of
optimized Fast Track guidelines with the intent to
enhance patient flow and improve patient safety.
6. Implementation of a five bed holding/transition pod
within the department to cohort patients with
appropriate resources. Staff and patients have credited
this innovation with improving patient care and leading
to less negative outcomes experienced within the
department. Measured metrics such as reported falls
within the department have supported the positive
impact of this initiative.
7. South Health Campus Emergency Department Wellness
Committee. A joint, collaborative partnership between
physicians, nurses, ancillary care staff, and paramedicals
to improve working conditions, the emergency
environment, and promote care giver wellness.
8. Dedicated ER OT/PT. Early ambulation and
physiotherapy have been identified as key factors to
prevent deconditioning and the development of
delirium, both of which add to an increase in patient
length of stay. After losing funding to support this
innovative and beneficial program, the SHC
administration reallocated resources to continue to
offer PT/OT services in the Emergency Department,
albeit in a slightly decreased capacity.
9. SHC ED monthly case rounds/modified M&M rounds
Staff has continued to recognize the SHC ED as a young,
exciting, innovative, and supportive place to work.
Dr. Cameron McGillivray, SHC Site Chief

PETER LOUGHEED CENTRE UPDATE
2019 ANNUAL REPORT 32
Emergency InPatient (EIPs) Bed Block
Ongoing struggles this year with our ED having, ON AVERAGE, and 50% of our 34 care space stretchers occupied by admitted patients. Fortunately, we have made progress in a few areas that will, eventually, help to alleviate this long standing problem.
Progress Achieved:
1. Women’s Health Clinic (WHC) space acquisition: This space, just adjacent to our Current Minor Treatment area, has been allocated to our ED space after many years of lobbying. We have had multiple meetings along with a full planning day with all ED Team members to develop our new patient flow processes. Movement into the new areas will occur over late November and early December of this year. It is expected that a portion of the WHC will be our new Minor Treatment area with the remainder of the space being used for a Department Results / Re-assessment / Discharge area. Our current Minor Treatment area will become our new Assessment/ Intake Treatment area with the old Intake Hallway space becoming EMS Park / Touchdown to allow proximity to Triage. Clearly, we would like to eliminate EMS Park but it will still be a reality for now. This move allows the entire ED patient space to undergo “lock down”. Additionally, our current D area and Intake 8/9 will be combined with increased stretchers spaces in D and recliners in 8/9.
2. Modification of Surge Criteria: The PLC Surge Criteria is now more appropriately aligned with the other Region EDs. Our Surge trigger is now >12 EIPs instead of the previous 20. Additionally, over the next 4 months, we are tracking the ability of our Charge RNs to appropriately and safely identify Surge Appropriate patients 24/7 so we are able to move past our current 12 hrs daily of Surge ability.
3. Addiction Recovery & Community Health (ARCH)
program was launched at the end of 2018. Through this last year, it has been instrumental in supporting our patients with addictions challenges along with increasing our staff’s familiarity with treatment options available for this patient population.
4. Completion of the Emergency Physician Lead project
completed at the end of February and was found to be beneficial by the majority of our ED team members. Further funding was not forthcoming and the project has been terminated. No news currently on having this position return to our ED.

PETER LOUGHEED CENTRE UPDATE
2019 ANNUAL REPORT 33
New additions to our ED team:
Donna Kelly and Barb Jensen have completed their administrative terms and have retired. We thank them for their years of hard work and service. Suzanne Wickware has been appointed as interim Patient Care Manager for the PLC. It has been a busy year and Suzanne has been working hard on multiple new initiatives some of which include RN shifting changes, department flow processes and keeping her finger on the pulse of the new WHC development. Additionally, Maria Vera has been added to our Administrative team and has been essential support in many areas in our ED.
Pediatrics: Drs. Hilary Ambrose and Brit Sunderani have been instrumental in reviewing areas of improvement for our Pediatric population (approx 8%
of our patient volumes). We are becoming more closely linked to the ACH to align our two department’s processes. A needs survey has been sent out to our ED MDs and we will continue to work towards a goal of high level pediatric care at the PLC.
Psychiatry: We have tightened our relationship with our Psychiatry Emergency Services over the last several years. The resident and on-call MD will see appropriate patients throughout the night, allowing earlier decisions on dispositions with resultant bed space savings. Additionally, when able, our PES RN team has been parallel evaluating patients prior to ED MD assessment. Finally, we are further forward in developing an Urgent Psychiatry outpatient option at the PLC with meetings going forward with our Mosaic PCN group as the eventual site.
Dr. Rick Morris, PLC Site Chief
CLINICAL INFORMATICS
2019 ANNUAL REPORT 34
Clinical Informatics
2019 has been a busy year for the ED informatics team! Continuing their roles were: Dr. Tom Rich as ACMIO for the Calgary Zone, Dr. Matthew Grabove as ED Informatics Physician Lead and Dr. Ashlea Wilmott as Peds ED Informatics Lead and Provincial ED Connect Care Physician Training Lead.
Notable achievements from 2019:
• A transformative change occurred in Alberta healthcare with the launch of Connect Care Wave 1 at the University of Alberta Hospital system in Edmonton on Nov 3. The CMIO will be conducting a detailed analysis of launch, taking lessons learned to improve implementation of subsequent waves.
• Drawing on our experience with the Sunrise EMR in the Calgary zone, our departmental members have been crucial to the development of many aspects of the new provincial CIS. We continue to be involved in this project via the Connect Care ED area council, Pediatrics area council, and various other working groups.
• Farewell to Sunray, hello EDSP. The new EDSP terminals deployed throughout the zone in the summer replacing the aging Sunray terminals. The user experience has generally been positive, although, as with any new technology, there have been a few hiccups along the way. EDSP offers many advantages including enhanced security and performance and has now been rolled out to most major ED’s across the province.
• The SCM 18.4 upgrade in September was a challenging experience due to the extended downtime across the zone. Given that these major upgrades only happen every couple of years, this may be the last one for most sites! Meetings with IT are ongoing to improve the downtime experience and avoid unexpected system outages.
• Recognizing the IT staffing shift to Connect Care, changes to SEC have been kept to a minimum. However, we were able to implement a communication pathway in SEC between nurses and volunteers as part of the Senior-Friendly ED project at SHC.
Looking forward to 2020:
• Connect Care will begin Calgary zone deployment at the urban UCC’s in May of next year followed by the PLC and ACH in October.
• Ongoing commitment to the further configuration and development of Connect Care. • Various events are planned to introduce Connect Care to our department with formal training starting for
physicians at PLC/ACH mid-year. • Recruitment of Connect Care ED super users and area trainers will begin in earnest in early 2020. • Maintenance of SEC/SCM until Connect Care arrives at all Calgary sites. Due to limited staffing and resources,
the only changes to SEC will be critical break fixes and order set updates but no new functionality.
Dr. Matthew Grabove Physician Project Lead Clinical Informatics

CAEP 2019 SUMMARY & HIGHLIGHTS
2019 ANNUAL REPORT 35
Congrats to our Sim Team who made a very valiant effort against
eventual Sim Olympiad champions from the University of Manitoba.
Kudos for stepping up go to Miles Hunter, Sean Crooks, Dirk Chisolm
and Dana Stewart.
Educational researchers from the U of C also in the spotlight with posters
presented and / or supervised by our med ED leaders Aaron Johnston Anoop Manocha hard at work rehearsing over the last few days to make sure tonight’s Doc that Rock / Emergency Medicine Advancement Fundraiser is a huge success.
Congrats to all the great submissions from our research division including great work by our trainees.
https://caep.ca/research/grant-competition/grant-winners/
Congratulations to Huma Ali for an impressive achievement. On April 27 and 28 Huma used some remarkable facilitation and leadership skills to achieve consensus and direction among 30 academic EM MDs from across Canada. Under the auspices of CAEP, the group developed a bid that, if successful, would see Canada hosting the International Conference on Emergency Medicine in Montreal in 2025. Her contributions were exemplary and contributed to what will hopefully be a winning effort.
Kudos to Andrew McRae and the research team for this contribution to our understanding of latent PE in patients presenting with syncope to the ED. Important work just published in the Annals of Emergency Medicine.
The research program also has excellent representation from Calgary and includes lightning oral 83 on POCUS education presented by Conor McKaigney.
Congrats as well to Andrew McRae, CAEP research chair for leading an impressive research program.

EMERGENCY PHYSICIAN LEAD (EPL) TRIAL 2018/2019
IN THE CALGARY ZONE
2019 ANNUAL REPORT 36
THE BELOW DATA IS FROM UNPUBLISHED RESEARCH AND IS FOR INTERNAL USE ONLY. NO REPRODUCTION WITHOUT PERMISSION.
Rising patient volumes and hospital-wide crowding have been difficult to address from within the emergency department (ED), but have significant negative implications for ED such as increasing time waiting to be seen by a physician, increasing EMS Park length of stay (EMS LOS), and increasing ED length of stay (ED LOS). Interventions such as the implementation of an emergency physician lead (EPL) role to assist in managing overall ED throughput have been widely studied. The Calgary EPL worked with the triage nurses, emergency charge nurse, departmental ED MDs, consultants and allied health professionals to collaboratively manage patient flow in the ED by matching patient demand to resources, initiating early investigations, treatments and consulting services as needed, identifying situations related to workload, and attending to issues that cause access block.
The Emergency Physician Lead (EPL) role was trialed in the Calgary Zone at the Peter Lougheed Centre and Foothills Medical Centre from December 3, 2018 - February 28, 2019 (PLC) and March 1 - May 31, 2019 (FMC). There were two EPL shifts per day, 0700-1400 and 1400-2100. The EPL role was evaluated for flow-specific outcomes and acceptability and feedback from ED staff.
Specific outcomes that were evaluated included: ED LOS, EMS LOS, physician initial assessment time (PIA), time-to-consult, left without being seen rates (LWBS), and ED revisits with admission within 72 hours. Comparison periods to each of the EPL trial periods were the immediate 90 days prior to the EPL presence, and the same three months prior to the EPL presence, in an effort to account for potential seasonal variation in ED volume and acuity, temporal co-interventions (such the presence of additional ED resources introduced in November 2018 i.e. HELO, additional nursing hours, PT in the ED, etc.) and year-to-year changes in ED resources, volumes and hospital capacity variations.
The results of the EPL evaluation were mixed but generally positive, with the PLC site appearing to benefit most from the implementation of the EPL role. ED LOS saw a 6.4% relative reduction and an impressive 25% relative reduction was seen in EMS LOS compared to the 3 months prior at the PLC. This translates to 4379 ED bed-hours gained and 1171 fewer hours of EMS units parked in the ED over the three months of the EPL trial. The LOS data for the FMC did not demonstrate the same change. The ED LOS saw a relative increase of 2.4%. Unfortunately, a relative increase in EMS LOS of 15.7% was also seen at FMC compared to the 3 months prior to EPL. Of note, the daily ED volume increased at FMC during the EPL period by 7.1%, while the other sites all experienced stable or declining ED daily volumes during the same time. EMS volume also increased at the FMC during this time. It is unclear whether the burden of this late seasonal surge in ED and EMS volume at FMC, possibly related to an anecdotal late-running flu season, affected the effectiveness of the EPL on LOS measures.
PIA time was decreased by 5.8% at PLC and by 17.5% at FMC. These values are for patients admitted to hospital only, so this reflects ED physician initial assessment sooner for those patients ultimately higher acuity/requiring hospitalization. Patients requiring hospitalization were consulted sooner compared to previous at both sites. Each of these incremental gains in ED minutes of treatment time by assessing and consulting patients sooner leads to gains in ED bed hours that improve overall access to care for ED patients and flow in the ED.

EMERGENCY PHYSICIAN LEAD (EPL) TRIAL 2018/2019
IN THE CALGARY ZONE
2019 ANNUAL REPORT 37
Qualitative feedback was also collected via surveys from ED MDs, ED RNs, EMS professionals and consultants on the effect of the EPL on optimizing throughput, the effect of the EPL on timeliness of admissions and discharges, the extent to which the EPL was a resource to other professionals, and the effect of the EPL on participants’ workload. Many comments focused on the benefits to patient care, with many anecdotal comments stating front-line staff including ED RNs, EMS and department ED MDs felt that the interactions with the EPL made patients and families feel the quality of care was expedited and improved. Constructive feedback was collated and will be considered for any further trial of an EPL.
Lastly, case examples of patient-specific timely diagnoses made by the EPL (at triage, in EMS Park or in the ED waiting room) were reviewed. Examples included cases of bedside-ultrasound diagnosed ruptured ectopic pregnancies, intracranial hemorrhages requiring urgent neurosurgical intervention, impending respiratory collapse, and sepsis from ascending cholangitis.
Dr. Kathryn Crowder

CALGARY EMERGENCY DEPARTMENT DISASTER REPORT
2019 ANNUAL REPORT 38
Transition in leadership: Dr. Kevin Hanrahan stepped down as Disaster Coordinator in June 2019 and accepted a larger role within EMS. Dr. Brad Granberg; who completed his Disaster Management/Medicine training here at the University of Calgary, has taken over the role. We are grateful for all the hard work Kevin has put in over the past few years to continually improve our hospital emergency preparedness systems and look forward to working with him in his new role.
Disaster Communication System (DCS): After years of work we are pleased to announce the creation of the Disaster Communication System, which replaces the old fan-out procedures in the event of a Code Orange. The app is a custom two-way text communication system that significantly improves system efficiency and patient safety during an external disaster. The system has been tested and rolled out as of December 1, 2019 across five Calgary Hospitals. Several other clinical groups (ICU, Trauma etc) have shown interest in the application and are looking at ways to support their Code Orange process as well.
Disaster Medicine Fellowship: We are pleased to have both Dr. Robyn Roger (Winnipeg EM R4) and Dr. Kelsey Ragan (Calgary EM R4) join us this year as Disaster Medicine Fellows. The focus of their fellowship includes Hospital emergency preparedness, Simulation, HUSAR search and rescue, International Health and disaster relief, Mass gathering medicine, and resident disaster day training among others. We are excited to have such talented MDs that will look to develop and lead Disaster Medicine in Calgary for years to come.
CODE ORANGE Duty MD Cheat Sheet: After years of work we are pleased to roll out the ED MD Duty MD Cheat Sheet. After the Code Orange simulation in 2016, it was uncovered that our current process was overly cumbersome and confusing. As a result we have created a new 1-page checklist of ED MD responsibilities during a Code Orange. This sheet has been tested and reviewed by AHS Human Factors to ensure efficiency and clarity. We will be conducting a brief 1-on-1 training session (5min) for each MD in the new-year as well as providing PDF versions that can be easily stored on phones in the event of a Code Orange.
Simulations/table tops: There are no current plans for a large-scale exercise in the near future however we are planning several small tabletop disaster exercises in Calgary over the next year to test out our new processes and supporting material. To date, there has not been a City-wide event since June 2016. This is a significant challenge to disaster preparedness and the system will require a significant investment in resources by Alberta Health Services, at many levels, to fully realize the potential gains and hard work that our planners have undertaken.

CALGARY EMERGENCY DEPARTMENT DISASTER REPORT
2019 ANNUAL REPORT 39
Disaster Planning Groups:
1) ED MD Disaster Planning Group: The ED MD/RN Disaster Planning group for all sites continues to meet quarterly to discuss the plans and approaches to Code Orange (external disaster) event management in the City. This group is comprised of the Disaster Coordinator (Dr. Granberg), MD and RN representatives from each Calgary ED (Dr. Brulotte RGH, Dr. Rodger PLC, Dr. Unwalla ACH, Dr. Cram FMC, Dr. Rebus SHC) a representative from E/DM, ED Administration and Medical Affairs.
2) EDM Disaster Working Group: Regular meetings with EMS/RAAPID/Emergency Disaster Management (E/DM) in order to better manage the notification and activation of Code Orange between agencies has been, and continues to be an ongoing challenge. We continue to advocate for a clear and concise call out that allows front line staff (ED MD and RN) to have input in the decision to active a Code Orange. We continue to work with and push AHS E/DM regarding the improvement of this critical piece of disaster preparedness.
3) FERA TRAUMA Activation Group: Is an ongoing project between Trauma, ICU and the FMC ED that is a specific foothills trauma response to multiple Level 1 activations at any given time. The idea being that the “FERA trauma” activation will occur when multiple level 1 patients present simultaneously requiring additional surgeons, anesthetists and ORs. As we continue to work with our colleagues in ICU and Trauma in developing the process, we will be updating and training the FMC ED MD group in the near future. There is no definite start date at this time.
Mass Gathering Medicine: The University of Calgary’s annual “Bermuda Shorts Day” was provided a field hospital. Calgary Emergency staff physicians and residents assisted EMS during this event. This initiative dramatically reduces the number of patients transferred to Calgary EDs. A similar facility has been in existence with the Calgary Stampede Parade, Chasing Summer festivals etc. previously, significantly assisting EMS, decreasing ED presentations and preparing for potential large-scale disasters at these venues. Additionally, a requirement for FRCPC residents to complete MGM experiences was added to the FRCPC curriculum this year and will be supported by interested ED staff.
Canada Task Force 2 (CANTF2): Drs. Hanrahan, Granberg, Seadon, Fedwick and Bateman continue to be involved with the Provincial Disaster Team, Canada Task Force 2 (CAN-TF2), with various exercises and preparedness initiatives including the week-long Disaster Medical Specialist Course in October. Both Dr. Ragan and Dr. Rodgers are also members on this team as a component of their Disaster Medicine training.

CALGARY EMERGENCY DEPARTMENT DISASTER REPORT
2019 ANNUAL REPORT 40
Resident Training: “Disaster Days” for our Emergency Residents will be held in March and June 2020 involving EMS, TEMS, IRP and CANTF2 and faculty members. This learning opportunity was well received by all involved in 2018 and has become a bi-annual event for all the residents. This is also an excellent opportunity for a (limited) number of staff to see exactly what our rescue teams do on a daily basis. But a note of caution, it is exhausting and will push your limits, so is not for the faint of heart.
Physician staff N95: Testing is near 100% and some members have taken the opportunity to do CBRNE training with our nursing colleagues. E/DM has helped to make this a regular occurrence. There is now a process in place to track compliance and the members of our Department have been exceptional at maintaining their N95 compliance.
Dr. Brad Granberg, ED Disaster Coordinator

OPIOID CRISIS/HARM REDUCTION IN ALBERTA
2019 ANNUAL REPORT 41
Opioid use disorder is a chronic, relapsing illness/condition that continues to be a major public health crisis affecting many Albertans. On average, 2 individuals die every day in Alberta as a result of an apparent accidental opioid poisoning. Two of the main causes are the rise of potent illicit opioids (such as fentanyl), and the overuse and misuse of prescription opioids for the last few decades.
• In the first quarter of 2019, there were 2,620 emergency and urgent care visits related to opioid misuse.
• In 2019, the Calgary and Edmonton Zones had the highest number of ED visits related to opioids and other drug use.
Buprenorphine/Naloxone (Suboxone®) Initiative in Alberta Emergency Departments
For many individuals who live with opioid use disorder, there are prescription medications available that can help, such as buprenorphine/naloxone (Suboxone®). When taken as prescribed, this medication reduces cravings and withdrawal symptoms. It helps people feel normal and use opioids less often and in smaller amounts. Once on a stable dose, some people can stop taking their substance altogether.
This crisis is complex and will continue to require more efforts from all areas of healthcare and society. Many individuals who live with opioid use disorder visit emergency departments because of an overdose, withdrawal symptoms, or other issues related to opioid use.
Since 2018, emergency departments across the province, including the Calgary zone, are playing a major role in helping patients who live with opioid use disorder by implementing a patient-centered, evidence-based care approach to screen and initiate buprenorphine/naloxone for eligible emergency department patients. Our Calgary zone physician lead, Dr. Marshall Ross has been particularly passionate and committed in spreading this new initiative. The project takes a harm reduction approach and combines the initiation of medication treatment for eligible patients at the ED, with rapid and effective transfers to specialized community clinics or primary care.
Since the launch of the program in 2018, it is now live at 79 emergency departments/urgent care clinics across the province. The goal is to have it implemented at all 107 adult sites across the province during this fiscal year. Within the Calgary zone, all 17 sites are live with the program.
Ken Scott, Senior Project Manager

PHARMACY UPDATE
2019 ANNUAL REPORT 42
The Pharmacy ED team is now into its second year of deployment to all ED centers across Calgary. It has again been a busy year.
Pharmacists and Pharmacy Technicians working at each site have taken part in a number of initiatives aimed at addressing the medication needs of patients in the ED. In addition, the pharmacy team has been actively participating in various committees and projects. Pharmacists continue to play a large role in reviewing microbiology results (Ab Labs) and working with the ED results physicians to promote antimicrobial stewardship practices and ensure that patients receive appropriate management. Pharmacy technicians work within the EDs across the zone to complete best possible medication histories (BPMH) for patients, improving accuracy and safety for patients in the ED. Across the zone, pharmacy has also been involved with the ESCN Suboxone initiation program, which has now been fully implemented at all sites within Calgary. The RGH emergency team is now involved in the multidisciplinary ED Treatment Plan Committee, which formulates a specific treatment strategy for recurrent ED patients in order to identify unmet needs in the community. The PLC emergency team, inspired by the work done at RGH, recently piloted a Physio + Pharm team to provide assessment and care to patients with lower back pain. All sites continue to find unique ways to provide
consistent clinical pharmacist services in ED, with the ACH now entering its second year of clinical deployment.
Other highlights include a student led quality improvement project at FMC, examining ways to improve our contact with patients post discharge, as part of our abnormal labs process. SHC is in the initiation stages for the COBBRA trial, a head-to-head randomized controlled trial (RCT) between apixaban and rivaroxaban, comparing the safety (rates of major and/or clinically relevant non-major bleeding) between these agents for the treatment of acute venous thromboembolism. This study is led by the FMC Thrombosis Clinic.
The ED pharmacy team has seen a number of changes in staffing at various Calgary centers, with some familiar faces returning from temporary positions. As part of expanding practice within the ED, we are now accepting more students and resident rotations through our ED’s. In the past year, ED pharmacists precepted 8 PharmD students and 2 pharmacy residents, providing valuable training and experience for future ED practitioners.
The pharmacy ED team continues to proudly support patients within the Calgary region and looks forward to another year of collaboration with the ED team.
Philippe Boilard, Clinical Pharmacist

HEALTH LINK
2019 ANNUAL REPORT 43
In the past year, Health Link answered 694,313 calls. Of those calls, 530,216 were answered by the nurse triage line. The remaining calls were answered by our other services, including health care navigation, addictions and mental health services and Alberta Quits smoking cessation line.
The breakdown of nursing triage advice is shown below for Calgary zone and provincially. 19% of callers from Calgary Zone were advised to seek care in an ED, whereas 45% were give advice to care for themselves at home without seeing a health care professional.
Of the callers referred to the ED, 60% followed through with the advice within 24 hours. This does not include callers who were told to call 911 as their demographics are not collected. Including those callers would increase the follow-through rate to 72%. Of the patients who were advised to seek care in a non-ED setting or care for themselves at home, 35% still went to the ED within 24 hours. Health Link referrals accounted for 3.9% of all ED visits provincially.
Health Link operates Dementia Advice, a service to support people living with dementia and their caregivers,
staffed by senior’s health nurses. In the past year, 2700 people were helped by this service, most commonly for caregiver stress and service referral. ED physicians can refer patients to this service. Check the Alberta Referral Directory for instructions.
Health Link has referral relationships with several Primary Care Networks in Alberta. Callers who are attached to a PCN, or unattached but live in the designated area, can be referred to a physician on-call or an After-Hours clinic where they receive a same-day appointment. In the past year, almost 13,000 callers were referred to one of these services, potentially avoiding an ED visit.
You may have noticed the health information and prevention videos playing in the ED waiting rooms. These are created by Health Link and HUTV. Any feedback or ideas on future topics are welcome.
Dr. Denise Watt Medical Director, Health Link
45% 46%
36% 33%
19% 21%
0%
20%
40%
60%
80%
100%
Calgary Zone Provincial
Perc
enta
ge o
f Cal
ls
Health Link Disposition - Triage CallsApril 1, 2018 - March 31, 2019
Advised to Seek Care in EDAdvised to See Doctor/Talked to Other Health Care ProvidersSelf Care/Treat at Home

REHABILITATION UPDATE
2019 ANNUAL REPORT 44
From November 1st, 2018 to September 30th, 2019, rehabilitation expanded its role in the Emergency Department (ED) in Calgary’s urban adult acute care sites as part of a funded pilot project sponsored by the systems flow initiative. The goal was to improve flow into, through, and out of the ED by partnering with staff to prevent unnecessary admissions, connect patients with community resources and provide timely assessment, treatment and discharge planning for admitted patients.
Shared Successes
3 common Key Performance Indicators (KPI) were identified for the urban adult acute care sites (FMC, PLC, RGH, SHC). Throughout the project period ALL 4 adult acute care sites realized significant improvements across all KPIs.
Key Performance Indicator #1:
Performance Indicator #2:
233
170
245 246 261205
250
178132
189153
050
100150200250300
Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Total Number of Emergency In-Patient Referrals
RGH PLC FMC SHC Zone Total
170 190 189 196 217 209 194229
254 258225
050
100150200250300
Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Total Number of Emergency Outpatient Referrals
RGH PLC FMC SHC Zone Total

REHABILITATION UPDATE
2019 ANNUAL REPORT 45
Performance Indicator #3:
DIMER was contracted to survey patients and staff about the effectiveness of Rehabilitation’s role in the ED over the course of the trial period at the 4 acute care sites.
• 86.5% of patients agreed or strongly agreed that they felt supported by PT/OT and were satisfied with their
care.
• 94% of physicians and staff working in the ED agreed or strongly agreed that PT/OT improved patient flow
through the ED.
82 103 96 82 77 103 94167 162 175 178
0
100
200
Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Total Number of Community Referrals
RGH PLC FMC SHC Zone Total

REHABILITATION UPDATE
2019 ANNUAL REPORT 46
Site Specific Successes
Given each site in the Calgary zone has its own unique challenges, we were able to realize some site specific improvements as we worked to optimize our contribution to improving system flow.
Foothills Medical Centre • Occupational Therapy (OT) assisted in preventing an average of 32 admissions per month during the pilot period from
November 2018 through September 2019; with the total number of admissions avoided over the 11 month trial being 350 patients. Over the pilot period our OTs had 1109 referrals or patient interactions.
• Total number of Emergency Outpatient Referrals over the pilot period increased 126%, from 49 patients the first month to 111.
• Total number of Community Referrals (e.g. home care/equipment/outpatient clinics) from the ED increased by 235% from the first month to the last month of the pilot, with a high of 67 referrals in a month.
Rockyview General Hospital • The addition of Physiotherapy and Pharmacy screening low back pain (LBP) patients prior to the emergency MD
assessment has reduced, on average: diagnostic imaging by 16%, opioid prescriptions by 32.5% and LOS in the ED by 1 hour.
• Ability to directly admit 9 patients to Acute Geriatric Unit (AGU) from the Emergency Department. LOS of patients directly admitted to AGU is 14.2 days less than a patient who comes to the AGU program from an acute inpatient unit. Previous inappropriate admissions are being avoided by maximizing referrals to Community Resources (Urgent Referral to Senior’s Health, Home Care, Alberta Healthy Living, etc.)
Peter Lougheed Centre • Presence of Rehabilitation in the ED assisted in preventing admissions in 69% of the patients in which OT/PT were
consulted. • Length of stay for ED out-patients with an OT/PT referral decreased by approximately 5 hours compared to patients
not seen by rehab in the previous year.
South Health Campus • Total hospital length of stay reduced by 2.15 days in patients seen by Rehabilitation upon admission in the ED when
compared to a similar time period in the previous year. • Total hospital length of stay reduced by 4.08 days in patients who waited > 24 hours for transfer to an in-patient bed
from the ED when Rehabilitation was initiated immediately upon admission • Presence of Rehabilitation in the ED assisted in preventing admissions in 52% of the ED patients in which OT/PT were
consulted.
Dr. Laurie-Ann Baker

DISTRIBUTED LEARNING AND RURAL INITIATIVES (DLRI) UPDATE
2019 ANNUAL REPORT 47
The Office of Distributed Learning and Rural Initiatives (DLRI) at the Cumming School of Medicine believes in providing quality healthcare to the people of rural Alberta. We strive to accomplish this goal through fostering meaningful relationships between medical educators, health-care professionals in training and individuals and families in rural Alberta. Our vision is to engage communities, inspire social accountability and create opportunities. We believe that our commitment to education and research in rural Alberta is a key part of developing skilled and dedicated rural physicians.
DLRI manages two large Government of Alberta grants that support rural education for medical students, clinical clerks, and residents. Our office coordinates rural placements for learners at all levels from pre-clinical medical students to residents. We support medical student placements that can be as short as a single day of shadowing and as long the entire clerkship for our University of Calgary Longitudinal Integrated Clerkship. We support residency programs in both Family Medicine and wide variety of specialties to place resident physicians in rural training environments. DLRI also supports our rural preceptors and educators through our Faculty Development and Cabin Fever conferences.
Over the past year DLRI has updated its website https://cumming.ucalgary.ca/ruralmedicine and communication strategy. Our monthly newsletter reaches over 200 dedicated rural physicians who are part of our clinical teaching faculty and has been key to building the community of rural medical educators. Through our website, Facebook, Twitter and Instagram we are connecting with medical students and residents and helping to share the story of rural medicine in Alberta.
Over the upcoming year we are looking forward to some updates to our conference offerings. At this year’s Cabin Fever, our flagship conference, we will highlight some of the scholarly work done by our office as well as scholarly work happening across rural Alberta. We also look forward to rolling out our Foundational Skills for Medical Teachers course at N*62, our northern Faculty Development conference held in Yellowknife.
As a medical school we have a responsibility to train physicians who will provide care for all Albertans. At DLRI we make the links between learners and interesting rural opportunities, and support rural physicians as cutting edge medical educators. We believe that exposing learners to rural practice, and supporting rural physicians in a clinical faculty is an important part of the future of rural healthcare in our province.
Dr. Aaron Johnston Director of Distributed Learning & Rural Initiatives

EMERGENCY DEPARTMENT GLOBAL HEALTH HUB
2019 ANNUAL REPORT 48
The Global EM (GEM) hub is dedicated to enhancing opportunities for engagement, collaboration, and education in fields such as refugee, northern, tropical, wilderness, and disaster medicine as well as public health. Our goal is for Calgary to become a beacon for GEM by harnessing our collective experiences and offering a variety of ways to expand them. Thus far, more than 50 emergency physicians in Calgary have joined the GEM hub. After the success of our inaugural GEM grand rounds last March with Dr. Megan Landes, we are grateful to have received another grant for $2500 from the Physicians’ Support Fund towards our annual global EM speaker series. We are thrilled to announce that Dr. James Maskalyk will be coming to Calgary next fall. Dr. Maskalyk is the author of the bestselling and critically acclaimed books “Six Months in Sudan” and “Life on the Ground Floor.” He will be giving a grand rounds presentation and attending a GEM social event September 24, 2020. He will be speaking on his experiences with humanitarian relief with Médecins San Frontiers, his work as faculty in the department of emergency medicine at Addis Ababa University, and the future of global emergency medicine in Canada. It is anticipated that his visit will galvanize further interest and collaboration within GEM here in Calgary.
We have been working on several projects for members to get involved with both locally and internationally. We are cementing ties with the Mbarara University of Science and Technology (MUST) and their department of emergency medicine to help support their new emergency medicine fellowship program, the first in Uganda. We were fortunate to receive a grant from the McLaughlin Travelling Medical Education Fund to help fund this new project, named the Calgary-Mbarara Emergency Medicine (CMEM) Collaboration. The goal is to provide an opportunity for interested faculty and trainees to contribute to the development of emergency medicine at MUST. As well, we are working on a study in collaboration with Canadian Physicians for Aid and Relief and the University of Maryland to study the prevalence, risk factors, and mortality of sepsis in the North Shoa region of Ethiopia. We have also been in talks with the University of Manitoba and the Federal Government to develop a program where Calgary ED physicians could fly-in to provide weekend coverage at the Garden Hill First Nation, a community with many high-acuity medical issues and in need of assistance.
We are excited for the future of the GEM hub! Dr. Andrew Battison
Dr. James Maskalyk

TUESDAY NEWSLETTER STATISTICS
2019 ANNUAL REPORT 49
The Emergency Department administration department moved the distribution date for the weekly newsletters from Friday to Tuesday this year. The rationale was that Tuesdays are a more active day for physicians to be checking emails, and would result in an increase in readership and engagement. The newsletter remains well-received with an average of 78% of recipients opening the email every week. The content of the newsletters varies week by week, but generally contains topics such as:
• SCM Updates
• FMC Project Updates
• Clinic Updates
• Upcoming Promotions/Awards/Grants
• Academic Appointment Updates
• Publications of Note
• Previous Grand Rounds Links
• Research News
• Upcoming events
• Teaching Sessions
Engagement with the newsletter has increased with an average of 32.8% of readers clicking on at least one link within the newsletter each week (an increase of over 10% from last year).
Meghan Prevost
MIKE HODSMAN MEMORIAL LECTURE
2019 ANNUAL REPORT 50
The Mike Hodsman Memorial lecture celebrates the life of our late colleague, Dr. Mike Hodsman and his great love of learning. The fifth annual lecture took place May 2, 2019 in the Foothills Auditorium. The event was well attended by emergency medicine residents, physicians, nurses and pediatric emergency medicine physicians. Our keynote speaker was Dr. Andrew Petrosoniak from St. Michael’s Hospital in Toronto. He spoke on Elite Performance in Medicine and Resuscitation Economics. Complementary speakers included Dr. Christopher Hicks who appeared by videoconference to present on Psychological Safety in Dynamic Team Environments and Dr. Vincent Grant who presented on Using Simulation for the Bigger Picture. Dr. Stuart Rose finished off the morning with a video presentation on the INFO debriefing program and a panel discussion on how to optimize feedback in team environments. Approximately 90 people attended the lecture live or by videoconference.
The evening prior to the event, Dr. Petrosoniak and emergency physician staff and residents enjoyed a casual catered dinner at the home of Dr. Colleen Carey. Following the lecture, Dr. Petrosoniak joined our emergency medicine residents and program directors for lunch.
This event was funded through the Physician Support Fund, KidsSim, and the resident and clerk electives account.
There was widespread positive feedback from the event. We look forward to the 2020 lecture featuring Dr. Gregory Luke Larkin on Mental Health and Addictions.
Dr. Colleen Carey
POCUS in Calgary is alive and well. This year has seen us increase our number of machines at RGH and soon to be another at FMC. There are two endocavitary probes available for use at FMC with a protocol for cleaning finally approved and up and running.
Education continues to be a focus for POCUS in Calgary. We delivered our first ever, locally developed Resident Introductory Course this summer (rather than outsourcing to the EDE folks). The Junior resident ultrasound course continues to thrive and we hope to introduce a senior ultrasound block for the residents soon. Special thanks to Kasia Lenz for spear heading the resident ultrasound education program.
For staff ED, the PSF has approved funding for hands-on POCUS sessions with the first session being held December 12th. We plan to cover a variety of topics during these sessions in order for staff to brush up on current skills and develop new ones. Hopefully with ongoing support from the PSF, we can make these sessions happen regularly.
Dr. Danny Peterson, ED Ultrasound Coordinator
ULTRASOUND UPDATE

CLINICAL PHARMACOLOGY AND TOXICOLOGY
2019 ANNUAL REPORT 51
The Poison and Drug Information Service (PADIS) and Section of Clinical Pharmacology and Toxicology (CPT) in Calgary had another successful year in 2019. In July, our CPT residency program welcomed its second fellow, Dr. Riley Hartmann from the U of S Emergency Medicine program. The program will be undergoing its mandatory 18 month internal accreditation review in December 2019. In September, our Clinical Pharmacology physician consultation service turned one year old. The service celebrated by reaching the 100th consult milestone the same month. The mandate of this service is to provide advice on Clinical Pharmacology patient scenarios such as adverse drug events, drug interactions, de-prescribing, and unusual responses to medications. We also welcomed Dr. Kathryn Watson as one of the physicians taking call for this service in the spring of 2019. An educational ‘CPT Pearl of the Week’ has also been included in the Emergency Medicine weekly newsletter to educate staff and residents about clinical issues pertaining to Clinical Pharmacology and Toxicology. In the 2019 academic year, PADIS welcomed 50 residents from Emergency Medicine, Internal Medicine, Anesthesia, Psychiatry, Pathology and Critical Care Medicine for our popular Medical Toxicology rotation. This rotation involves a combination of bedside medical toxicology consultations in Calgary hospitals and small-group teaching sessions on management of common poisonings. We also continue to have Saskatchewan RCPSC and CCFP-EM residents take call from Regina and Saskatoon, and our annual “Toxicology Skills Days” continued in both Edmonton and Regina. Our medical toxicology clinic continues to see patients monthly at the Holy Cross Ambulatory Care Centre in the Rockyview Hospital. This monthly clinic was developed to provide evaluation, diagnosis, and management of adult patients in Alberta with toxic exposures, adverse drug events, follow care after hospitalization for poisonings, and interpretation of toxicology tests performed in the community.
In April 2019, a leadership change at the Poison and Drug Information Service occurred. Melissa McDougall is the Acting PADIS Manager and Tricia Chambers is the Director of both PADIS and Health Link, replacing Heather Gallant and John Montpetit. This leadership change allows both PADIS and the Section of CPT to benefit from the resources available at Health Link to improve our service to Albertans.
Dr. Eric McGillis joined our PADIS toxicologist group in November 2019. Eric completed his toxicology fellowship training in Minnesota. In addition to his work at PADIS, he will be working clinical shifts at the Rockyview Hospital ED. He has been a welcome addition to our staff.
Dr. Mark Yarema was promoted to Clinical Professor in the University of Calgary Departments of Emergency Medicine, Physiology and Pharmacology, Critical Care Medicine, and Medicine in July 2019. The year 2020 will see the Section embark on a 6 month strategic planning process to develop its plan for the next 3 years. Stakeholders will include section members, referring physicians, Undergraduate and Postgraduate Medical Education, and patient advisors.
Dr. Mark Yarema Section Chief Clinical Pharmacology and Toxicology

SOCIAL MEDIA
2019 ANNUAL REPORT 52
The departmental website contains details of previous Grand Rounds as well as summaries of journal clubs for those who were unable to attend. There is also information on QPath, departmental ultrasound and clinical cases. The resident website, Calgaryem.com, contains helpful information for prospective students, residents and schedule information.
The @UCalgaryEM Twitter account now has over 1000 followers. Follow the account for details of departmental events as well as useful medical education links and sites. Other Calgary Twitter accounts to follow include:
Eddy Lang @EddyLang1
Nadim Lalani @ERmentor
Fareen Zaver @FZaver
Chris Bond @socmobem
Catherine Patocka @PatockaEM
Shawn Dowling @shawnkdowling
Mark Yarema @mcyarema
Stephanie Vandenberg @StephVDBG
James Huffman @JamesLHuffman
Dr. Chris Bond
Through 2019, interest in the Airway Management Pause (AMP) both within Calgary Emergency Medicine and beyond has continued to grow. One of the most significant developments of the past year was the adoption of newest version of the tool by the Department of Critical Care Medicine (DCCM) for use within the adult ICU’s, the CVICU and the Outreach (Code 66) teams. The airway experts from the DCCM had input in the newest versions of the tool (Version 10.2) which was also updated to align and integrate with the new Difficult Airway Management (DAM) Carts and the departmental algorithm for difficult airway management in an unconscious patient.
Results of the ED implementation study showed the introduction of the AMP to a group of highly skilled healthcare professionals working in adult emergency departments was associated with: 1. A more calm and organized environment during
airway management 2. Increased role-clarity among team members. 3. Higher team effectiveness scores
All three of these associations held true when team members assessed themselves and also when they were observed by independent, trained observers. The manuscript of this study is currently being written with plans to submit for publication in 2020.
Dr. James Huffman
Airway Management Pause
PHYSICIAN SUPPORT FUND (PSF)
2019 ANNUAL REPORT 53
The Physician Support Fund would like to thank all contributing members in good standing for their ongoing support. Your contributions make it possible for members of our department to pursue extra-clinical projects that benefit our department and our specialty.
Mandate: • To support initiatives brought forward to the committee by individual members or departmental leadership which are
likely to improve the intellectual, clinical and/or working environment of emergency physicians practicing within the Calgary area
• To provide top-up funding for the residency programs when appropriate other funding is not available. Both the Department of Emergency Medicine and the Support Fund committee group will continue to explore and advocate for appropriate level funding from the appropriate sources.
Some of the projects that have been fully or partially funded by the PSF in 2019 are as follows:
Annual Global EM Speaker Series
Physician Support Fund Resident Research Award (PSF-RR)
ED Staff Ultrasound Continuing Education Session
ED Research Day
Connect Care Optimization Lead
ED Treatment Plans
Procedural Skills Workshops
Interdisciplinary Simulation Program
Emergency Physician Wellness Metrics Program Access
Physician Social Nights
Emergency Medicine Hub Budget Funding
Grand Rounds Support
Hodsman Lecture Series
SHC Emergency Case Rounds
ED Staff Direct Physician Observation
FRCPC Program and Assistant Program Director Top up Funding
CCFP EM Program Director Top up Funding
Residency Program Budget Support

ACH PEDIATRIC EMERGENCY RESEARCH TEAM (PERT)
2019 ANNUAL REPORT 54
SummaryOver the past 12 months the emergency department (ED) at the Alberta Children’s Hospital (ACH) cared for over 75,000 ill and injured children. Children are cared for 24 hours a day, seven days a week. The high volume and diversity of patients seen in the ED provides a unique opportunity for generating new knowledge and improving the quality of pediatric care. Our research team is one of the largest pediatric emergency research teams in Canada. In the past year we generated new knowledge with the potential to improve the outcomes for patients with diarrheal illnesses, severe infections, trauma, abdominal pain, respiratory emergencies and painful injuries. Our team members contributed to the science of resuscitation, precision medicine, quality improvement and simulation. In the past year we have 63 peer reviewed publication and received substantial funding from local, national and international sources.
Over 900 patients enrolled Research
Exceptional care for
over 89,000 children
Provided by a team of
63 physicians
Clinical
and 63 publications
With grant funding totalling
$5,706,107
Education
and over 200
nurses
With grant funding totalling
$3,847,680
$5,796,091 co-
investigator/collaborator
334 medical trainees
PERT Team
Physicians: Angelo Mikrogianakis Section Lead
Antonia Stang Research Lead
Graham Thompson Medical Director PEMRAP
David Johnson Senior Medical Director, Alberta Health Services Maternal Newborn Child & Youth Strategic Clinical Network (MNCY SCN)
Stephen Freedman Alberta Children’s Hospital Foundation Professor, Child Health and Wellness, ACHRI, Healthy Outcomes, Theme Lead
Jennifer Thull-Freedman Quality and Safety Lead
Adam Cheng Simulation Research Lead
Kelly Millar Education Lead
Vincent Grant Simulation Medical Director
50+ Emergency Department Physicians
Coordinators/Research Assistants Karen Lowerison Jianling Xie Sarah Williamson-Urquhart Kelly Kim Rebecca Emerton Kassi Shave
Ashley Jones
50+Volunteer Research Assistants (Pediatric Emergency Medicine Research Assistant Program (PEMRAP)
Research Trainees
Gillian Tarr Eyes High Post-Doctoral Scholar
Thomas Kellner Graduate Student
Chu Yang Lin Graduate Student
Yiqun Lin PhD Student
Administration: Julie Slinn Shayla Baier Gertrud VanDerMey Mona Bechervaise
Research Nurses: Jen Crotts (PEMRAP Lead)
Clare Howland Jelena Komanchuk Ruza Goulden 200+ Emergency Department nurses
You can view the complete report at: https://www.ucalgary.ca/paed/files/paed/pert-2017-annual-report.pdf

PATIENT SAFETY & QUALITY IMPROVEMENT
2019 ANNUAL REPORT 55
Patient Safety
Highlights for the 2019 year in ED Patient Safety included projects in the following areas.
1. EMS Park Expedited Transfer of Care
This pilot project demonstrated a significant reduction in EMS Park utilization (both in terms of number of patients in EMS Park as well as EMS Park patient LOS). The key mechanisms that accounted for this improvement were likely a combination of many novel factors including the RN Liaison, EMS HELO improved site-wide movement of boarded patients and improved understanding of our own internal departmental capacities.
While the funding for the above positions was temporary and not renewed we know have a much better understanding of how to reduce EMS Park utilization and this is something that we can leverage in the near future to continue to drive down care delivered in this area.
2. Direct Referral Process Change
As you know many adverse events occurred in this patient group. Thank you for reporting these. Mainly, adverse events were attributable to the Most Responsible Healthcare Practitioner being unavailable or delayed in providing patient care and markedly extended ED LOS.
Previous work had been done in this area to address prolonged consultations and delayed disposition decision-making. The ED QAC formed a working group that looked at the entire process of Direct Referral, taking into consideration the many RLS reports in this area and the repeated areas of risk that had been identified through Quality Assurance Reviews.
The new process proposed by this working group and the process that is largely now in its early phase of operationalization, is one where the ED MD is the MRHP and, where feasible, is involved on the phone during the referral-consultation discussion. We hope this change in accountability, de-risks to some extent the Transition in Care of the Direct Referral patient. Thank you again to the members of the Working Group and to all those involved in helping troubleshoot the new process. Thank you for supporting this new process – even when it is additional work for you.
Please continue to use the RLS system to let us know about close calls or adverse events. This is the best and most efficient way to report an issue and will let us quickly feed back to you what action(s) are being taken. All of the major initiatives that have come out of our QAC started as an RLS.
Dr. Adam Oster, Patient Safety Lead Co-Chair, RDEM QAC

SHOCK TRAUMA AIR RESCUE SOCIETY (STARS)
2019 ANNUAL REPORT 56
2019 has been an extremely busy year for STARS as we received and have implemented a brand new airframe in the Airbus H145. This is a modern replacement for our aging BK117s which are being phased out entirely over the next few years. It’s an exciting time at STARS and we appreciate the hard work of all of our staff and the support of all of our donors.
We continue to be tasked with patients of increasing complexity both medically and logistically. Our cohort of 28 active Transport Physicians (composed of 25 Emergency Physicians and 3 Anesthesiologists) have continued to do an outstanding job triaging, providing medical direction, as well as attending on the most complex of missions. In addition, our seasoned group of critical care RNs and Paramedics continued to distinguish themselves in the procurement of outstanding care.
We also have an established and successful STARS Transport Medicine Fellowship program with our 6th fellow currently training with us. These folks represent the next generation of Transport Physicians and are well prepared to advance our patient care capabilities going forward.
From Sept 2018 to Sept 2019 we’ve flown 467 patients. 362 of these were interfacility transfers and 204 were scene calls. We did 1 search and rescue related mission. On 22 of our missions, blood products were administered (total 47 units). Our air medical crew continue to perform at a very high level with 43 of 43 patients requiring intubation, being successfully intubated on 1st or 2nd attempt (42/43 were on the 1st attempt!).
The above missions represent a small portion of the cases our Transport Physicians actually provide medical advice on with a large number of Red Referral calls either being managed in the sending community after the provision of medical advice, or being transferred to Calgary and other receiving sites like Red Deer, Lethbridge, or Medicine Hat in the south, by both ground and fixed wing resources. Many patients bypass the Emergency Departments entirely due to the excellent call flow systems we have through RAAPID and the STARS Emergency Link Centre, going direct to CCU, ICU, and surgical services at times. Flight call has become busier and busier with the huge variety of interesting challenges presented to us on a daily basis. My Transport Physician colleagues continue to do a superb job providing support to these patients and their sending medical providers.
Michael Betzner, Medical Director
STARS Calgary

2019 ANNUAL REPORT 57
ED GALA 2019

2019 ANNUAL REPORT 58
2019 ANNUAL REPORT 59

2019 ANNUAL REPORT 60

2019 ANNUAL REPORT 61

ED GALA WINNERS
2019 ANNUAL REPORT 62
On behalf of the ED Gala planning committee:
Gala 2019 has been deemed a success!!
Thank you to all who attended and to all who worked and allowed many others to participate.
Congratulations to all of our nominees once again!
Humanitarian
Stan Mayer - Stan continues to be one of our most active global health contributors and has sacrificed months if not years to this work. He is a strong patient advocate and works hard clinically to ensure his patients are well cared for and his practice remains current. Stan is a well-respected colleague who often goes out of his way to help the department and its members.
Michelle Simonelli - Michelle has been an important advocate for pediatric injury prevention. Through her work with CHIRPP (Canadian Hospital Injury Reporting and Prevention Program) and The City of Calgary, Michele has made significant strides in having changes made to National Building Codes that would make second story windows safer in an effort to prevent window falls in young children.
Joe Vipond – Joe has worked tirelessly around the advocacy work pertaining to the coal phase-out and Canadian Association of Physicians for the Environment. He is willing to take a stand publically for what he believes is right and often has to manage the media as a result. His dedication to community is admiral.
WINNER: DR. JOE VIPOND
Mike Hodsman Lifelong learning
Jonathan Guilfoyle - Jonathan not only stays up to date with all the latest literature himself, but makes an effort to share new learning with his colleagues and challenge them with difficult cases he's seen. Jonathan has also been key to ensuring that pediatric trauma patients in our city get the best evidence based care possible. He is well respected among his colleagues and a favorite among a number of learners that are privileged to work with him.
Andrew McRae - Andrew is nothing short of a research superstar at CSM and AHS. His work is practical and clinically relevant e.g. Troponin, and he has been very productive with CIHR and PRIHS grants and publications. Andrew is a quiet colleague who clinically strives to provide good patient care and advocate for his patients.
Stu Turner - Despite being almost 40 years into his career, Stu is continues to work hard and remains passionate and committed to Evidence based medicine. His knowledge is up to date and his attitude is refreshingly keen and positive. Stu regularly listens to podcasts and reviews journals and is frequently used as a resource to many of our colleagues. Over the years, Stu has taken on many roles within the ED and more recently, he has had an active role in organizing site specific emergency medicine rounds at the site.
WINNER: DR. JONATHAN GUILFOYLE
ED GALA WINNERS
2019 ANNUAL REPORT 63
Physician of the Year- FMC
Cory Brulotte – Cory is an excellent clinician who goes the extra mile to do what’s right for his patients. He remains current in his practice and is described as an excellent friend and colleague. Cory continues to contribute extra-clinically to EMS and is more than willing to lend a hand to help out the department and his colleagues.
Dave Lendrum - Dave is great clinician who also manages to juggle many extra clinical activities such as STARS and more recently taking on an administrative role as assistant and site lead at FMC. He has an obvious passion for medicine and helps make Calgary an excellent place to practice.
Catherine Patocka - Catherine single-handedly led a high profile randomized controlled trial on optimal learning design for CPR training. The study was published this month in the prestigious journal Resuscitation and it will unquestionably shape how CPR classes will be taught around the globe. The fact that she completed this trial without any protected time or financial support is truly remarkable. Catherine is a hard working clinician who has now more recently stepped into the role as program director for the FRCP Emergency Medicine program.
WINNER: DR. CORY BRULOTTE
ROOKIE: DR. PATTI LEE
Physician of the Year- PLC
Neil Collins – Neil emulates what all of us should strive for when it comes to patient care. Long established as a solid clinician who strongly advocates for his patients, in recent years Neil has also taken on many demanding leadership roles within the department. Previously serving as co-program director for the CCFP(EM) program alongside Ian Walker, Neil then moved over to administration first serving as site chief at the PLC then taking over the role as deputy department head in 2017. More recently Neil has willingly taken on the role of department head while Eddy is away on sabbatical. Most importantly in all of this, Neil firmly emulates that good patient care should always be the number one priority.
Margriet Greidanus – Margriet is described as quietly just doing what is required. She is a well-respected clinician who’s past roles include program director for the EM program here in Calgary. Margriet is quick to help out where she can and often volunteers her time on committees both at the site and zone level. More recently Margriet can be credited with helping establish a parental leave policy within the department of emergency medicine.
Leigh Morris – Has worked tirelessly as a scheduler through many changes and manpower demands. Has reviewed and managed multiple IT solutions to help streamline physician scheduling. Leigh genuinely cares about and takes the time to speak with his patients. It makes all the difference when people feel heard and understood and the physician has taken the time to answer their questions – Leigh emulates what all of us should be doing.
WINNER: DR. NEIL COLLINS
ROOKIE: DR. KARL PHILIPS

ED GALA WINNERS
2019 ANNUAL REPORT 64
Physician of the Year- RGH
Christine East – Although relatively new in her career, Christine has been determined to become involved in many site and zone wide projects. Her most recent work alongside Scott Farquharson has been her relentless time and effort around establishing patient specific care plans for some of our more challenging patients. Christine is a well-respected clinician who is enjoyed by her colleagues and other members of the ED team. Her passion for medicine and her will to do the right thing has made her a rising star within our department.
Ayesha Khory - Previously assistant site chief at RGH, now co-ordinates monthly case rounds (originally with Stu Turner and now with Dave Fu and Christine East), Ayesha has been leading the project on physio/ pharmacy and low back pain in the ED. She is described as a great team member, the social coordinator for the business group and has an excellent rapport with all allied health and consultants.
Kari McFarlane – Has worked tirelessly as a scheduler through many changes and manpower demands. Provides valuable input to the manpower committee, volunteers hours at the med school working as a preceptor for such things as procedural skills. Kari is a patient advocate who takes pride in providing good clinical care to her patients.
WINNER: DR. CHRISTINE EAST
ROOKIE: DR. NATASHA WRIGHT
Physician of the Year- SHC
Huma Ali - Huma has dedicated hundreds of hours to developing the peer support network that was recently announced (Wellness hub project). Partnering with Dr. Jane Lemaire, she has put our department on the map of MD wellness across Canada with this unique program. Huma was also instrumental in getting Canada (Montreal) to secure the ICEM meeting for 2025 which is expecting 4K delegates. At a retreat in Montreal, she facilitated a planning process which helped create the winning details for the bid.
Kathryn Crowder - Kathryn has volunteered countless hours in support of the evaluation of EPL project. It is felt that without that analysis, the EPL would not be perceived as well as it is within senior AHS leadership. Other projects have included her strong commitment to QI at SHC over the last few years with projects including the TLP pilot and audit and feedback to reduce IV therapies in Intake. Kathryn is well respected by her colleagues and consistently works hard at maintaining a high level of care.
Matthew Grabove – Matt is a strong clinician who willingly helps his colleagues and department whenever the need arises. Prior to taking on his official role in IT, Matt was quick to volunteer for site based committees to assist in any way he could. He continues to work hard in his non-clinical role while still maintaining a solid clinical practice. Matt is described as a great physician who shows much kindness to his patients and an outstanding colleague to those that work with him.
WINNER: DR. HUMA ALI
ROOKIE: DR. PAUL MCKENNA
Physician of the Year- ACH
Ping Chen
Roger Galbraith
Bella Sztukowski
WINNER: DR. ROGER GALBRAITH
ROOKIE: DR. MELANIE WILLIMAN

ANNUAL OPERATIONAL (LOS) DATA
2019 ANNUAL REPORT 65

ANNUAL OPERATIONAL (LOS) DATA
2019 ANNUAL REPORT 66

ANNUAL OPERATIONAL (LOS) DATA
2019 ANNUAL REPORT 67
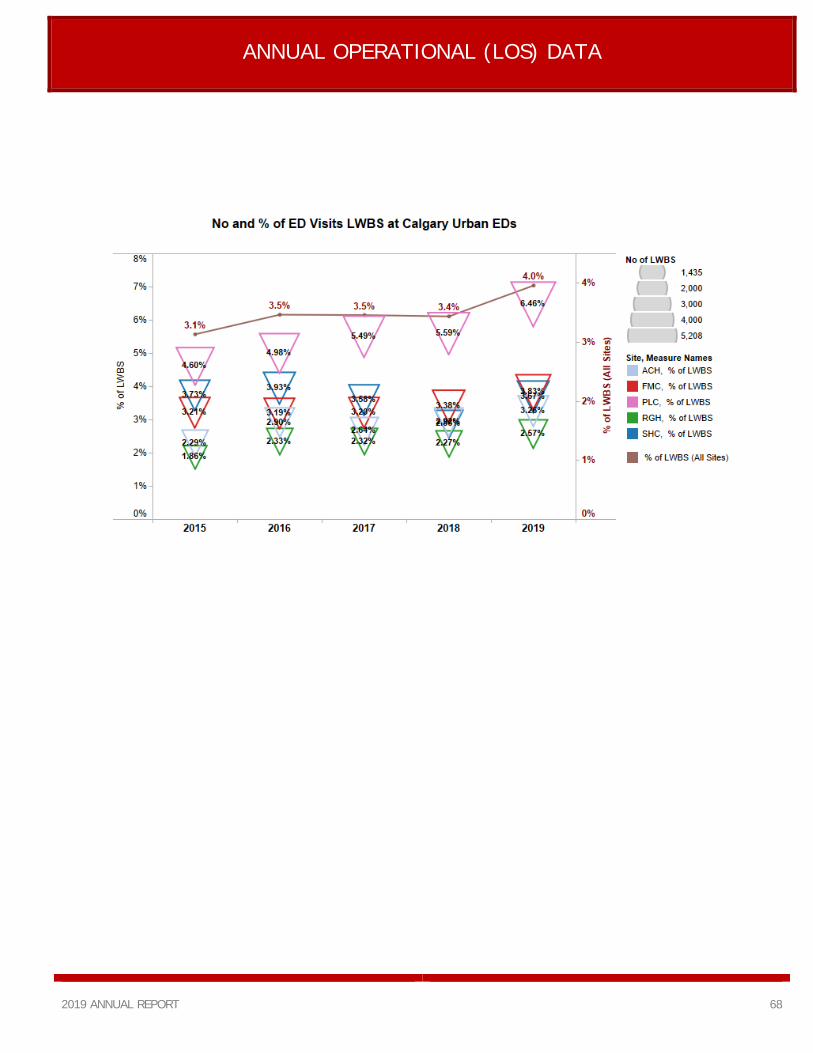
ANNUAL OPERATIONAL (LOS) DATA
2019 ANNUAL REPORT 68

CCFP-EM PROGRAM
2019 ANNUAL REPORT 69
The CCFP-EM program is having a fantastic year thanks to the continued support of our staff and residents. I am truly humbled when considering the number of people involved in resident education. It has been a privilege to be a part of this program and I want to extend a sincere thanks to all the dedicated educators working on shift, at academic day, and behind the scenes to train our future colleagues.
The Current Resident Team
Please welcome our 2019/2020 resident team, if you see one of these hard working residents on shift, please feel free to include them in any and all cases.
Updates
New Classroom
Academic teaching sessions will be moving to a new space. Thanks to PGME funding, the residency program will be moving to a space within the Emergency Department (F Pod). It’s hoped the new classroom will be a welcoming environment for the expanding program and bring learners in to closer contact with the emergency team. Feel free to check out the teaching schedule at http://www.calgaryem.com/ and drop by for any sessions of interest. The residents really enjoy having staff at their teaching sessions.
Competency Based Evaluations
The CCFP-EM program is transitioning to a competency based medical education model. Residents will be asking for overall shift evaluations and more specific feedback on certain professional activities. Please direct any questions to me as we make this transition.
CCFP-EM PROGRAM
2019 ANNUAL REPORT 70
The Core EM Team
Madhavi Talasila, Tris Malasani, Lilian Prudencio These amazing administrators go above and beyond on a daily basis to support the residents and are key to the success of the program.
Simulation
Scott Seadon
The simulation program continues to be a resident favorite involving countless hours of preparation and the contribution of many allied staff.
Ultrasound, Airway Skills, Central Line Course, Advanced Procedural Skills, ECG Rounds, Ventilator Workshop
Dan Joo, Danny Peterson, Bryan Weber, Gavin Greenfield, Stefan DaSilva, Rob Hall, Colleen Carey, Paul Tourigny , Kasia Lenz
The CCFP-EM program is lucky to have a dedicated and talented group of educators that contribute to the curriculum and pass on the skills needed to become successful Emergency Physicians.
Competency Committee
Todd Peterson, Leigh Morris, Eileen Kabaroff, Marge McGillivray, Justin LeBlanc, Christine East, Jamie McLellan, Dave Fu
These wonderful staff physicians are involved in reviewing evaluations and making sure residents are on track for success in the program.
Research
Stephanie VandenBerg The residents are involved in a variety of research projects facilitated by a great group of clinician-researchers.
Longitudinal Preceptors
Jen Puddy, Phil Ukrainetz, Margriet Greidanus, Anoop Manocha, Dan Joo, Mike Su, Rob Lafreniere
These dedicated physicians are paired with individual residents and act as mentors, teachers, colleagues and friends as the resident’s progress through the year.
CaRMS
Shelly Chopra, Ben Shepphard, Dan Metcalfe, Dan Joo, Gavin Greenfield, Stuart Rose, Scott Seadon, Collen Carey, Eileen Kabaroff, Jamie McLellan The program continues to attract talented residents from across the country and received 118 applications for 8 spots this year. This tireless group volunteered to review files and interview our future EM residents.
Exam Preparation
Christine East To prepare for the final exams a large group of staff volunteer to administer practice oral and written exams throughout the year. Staff continually update the curriculum and exams to ensure the success of our residents.
The FRCPC Program
Catherine Patocka, Marc Francis, the FRCPC residents The CCFP-EM program benefits immensely from a close relationship with the Royal College Program. From team building days to weekly academic sessions, the FRCP staff and residents work tirelessly to produce one of the most intense and well received educational programs in the country.
Dr. Jason Fedwick Program Director CCFP – EM Calgary Zone ED

FRCPC PROGRAM SUMMARY
2019 ANNUAL REPORT 71
This year saw a change in the educational leadership for the FRCPC program director. Dr. Sarah McPherson, who did an outstanding job leading and supporting the program for over 10 years decided it was time to pursue other interests and Dr. Catherine Patocka has taken on the role as of April 2019. The education leadership team including assistant program director Dr. Marc Francis, CCFP program director Dr. Jason Fedwick and administrative support team Madhavi Talasila and Tris Malasani have done an exceptional job ensuring a seamless transition.
In the 2019 CaRMS match, we recruited four candidates: Cody Dunne, Jason Elzinga, Cara McCulloch and Natasha Goumeniouk. The program is already busy preparing for another busy CaRMS season as Emergency Medicine in Calgary continues to be a highly desired postgraduate training program among medical students from across the country. The program recently underwent an internal review process through the postgraduate medical education (PGME) office. Although the official report has not been received, the reviewers were clearly impressed by many aspects of the program and expressed a desire to integrate many of the innovations into their own programs. This review is an important steppingstone to the external accreditation review which will happen in a few years.
A major focus of the program this year continues to be the ongoing implementation of the Royal College’s competency-based medical education framework “Competence by Design”. CBD lead, Dr. Anjali Pandya, and the CBD committee continue to work to implement necessary curricular and assessment changes including stage-based simulation, new assessment tools, updated rotation templates and faculty development. We are tremendously fortunate to have an incredible group of educators who have been engaged and interested in making this complete curricular overhaul successful. CBD aims to ensure that all trainees have the opportunity to develop and demonstrate competence in the skills necessary to function as specialist in emergency medicine. Because it can be difficult to ensure consistent access to low-frequency, high-stakes events such as resuscitations and Level 1 traumas our program has had to dramatically increase our use of simulation for formative and summative assessment. We are incredibly fortunate to have a highly skilled team of simulation educators who can provide high quality simulation and debriefing experiences. We would like to especially thank the nursing operations and educator leads at the FMC for their continued enthusiasm and commitment to helping organize interprofessional, in-situ simulation for our residents at the FMC. These are incredibly valuable experiences for our residents and contribute substantially to their learning. Over the past few years as our residency programs have grown, it has become increasingly difficult to find consistent, appropriate space in which to host our academic full day sessions. We are pleased to announce that Dr. Jason Fedwick was successful in securing a PGME infrastructure grant to provide equipment and furniture for the F-pod space at the Foothills Medical Centre to serve as the programs education space on Thursdays. Renovations are currently underway and we expect the space to be useable by early next year. We would like to highlight some of our major programs and the people who have helped to make them a success The Residency Training Committee – meets monthly to review the program and to develop improvements and policy.

FRCPC PROGRAM SUMMARY
2019 ANNUAL REPORT 72
Members: Meira Louis, Lisa Campfens, David Fu, Bryan Weber, Conor McKaigney, Andrew Robinson, Bela Sztukowski, Ryan Wilkie, Greg Bellar, Tahara Bhate, Sarah McPherson, Meaghan McKenzie, Jen Puddy The CBD Committee – meets monthly to design and implement changes required for CBD Members: Anjali Pandya (chair), Geoff Lampard, Fareen Zaver, Kelsey Ragan, Steve Liu, Ken Chan, Katie Anker, Sean Fair, Sean Crooks, Natasha Goumeniouk The Clinical Competency Committee - Meets quarterly to provide a transparent review of resident performance and to make promotions decisions Members: Aaron Johnston (chair), Geoff Lampard, Ryan Deedo, Jason Lord, Healther Patterson, Fareen Zaver & Andrea Boone
Simulation programs – Multidisciplinary simulation provided bimonthly for junior residents, monthly for senior residents and in modules for specific CBD teaching and assessment
Junior simulation – Patricia Lee-Nobbee
Senior simulation – Jen Puddy
CBD stage specific simulation – Anjali Pandya
Ultrasound and procedural skills: Includes annual basic ultrasound training, certification of beginner and advanced ultrasound skills, 2 annual airway workshops, annual CVC workshop, casting and splinting
workshops and an annual advanced procedures cadaver lab session. Members: Danny Peterson, Kasia Lenz, Rob Hall, Bryan Weber, Gavin Greenfield, Stefan DaSilva EMS and disaster medicine – redesign of the EMS rotation Katherine Bateman, Brad Granberg Wellness and Coaching – Faculty development of coaches for residents, wellness and resiliency training for the residents Nadim Lalani, Mark Bromley Longitudinal Preceptors – Teachers and mentors who are paired with individual residents throughout the year Ryan Deedo, Todd Peterson, Alyssa Morris, Cathy Dorrington, Ian Rigby, Jen Nicol, Bruce MacLeod, Lester Mercur, James Huffman, Sarah McPherson, Andrea Boone, Gord McNeil, Art Tse, Brad Granberg, Geoff Lampard, Lisa Campfens, Marshall Ross, Conor McKaigney, Mike Betzner, Anjali Pandya, Rhonda Ness, Fareen Zaver, Andrew Robinson, Mardelle Gamble and Kip Rodgers
The FRCP program is exceptionally grateful to have a fantastic group of hardworking residents and dedicated staff educators who continued to support and improve our training program.
Dr.Catherine Patocka, Division Chief Education

OFF-SERVICE & ELECTIVE MEDICAL EDUCATION IN THE
DEPARTMENT OF EMERGENCY MEDICINE 2018-2019
2019 ANNUAL REPORT 73
Rotations in the Calgary Zone adult emergency departments continue to be highly sought after by University of Calgary residents and their home training programs. The Department of Emergency Medicine hosted 91 mandatory off-service learners during the 2018-2019 academic year. This represents approximately 10,100 hours of direct 1:1 learner supervision by our teaching faculty. The majority of these resident physicians were from the family medicine residency training program (70 learners), while the remainder came from programs as diverse as plastic surgery, orthopedic surgery, general surgery, neurology, dermatology, pathology, internal medicine, cardiac surgery, vascular surgery, and psychiatry. Our Department continues to handle this demand while maintaining a 1:1 preceptor to learner ratio for most shifts.
Since emergency medicine remains popular among Canadian medical students and family practice residents, the demand for medical student and resident electives in our Department continues to grow. In the 2018-2019 academic year, the Department of Emergency Medicine received elective requests from 86 residents (mostly family medicine) and 78% of these residents were offered electives. We hosted 49 elective residents (up from 43 in 2017-2018) with requests from the University of Calgary (41 residents), UBC (15 residents), U of A (5 residents), U of T (8 residents), McMaster (8 residents), and other Canadian schools. Notably, we hosted 2 senior residents from other FR training programs in Canada this year, showcasing the popularity of Calgary as a teaching site and possible future employment prospect.
On the medical student side, in the 2018-2019 academic year the Department of Emergency Medicine received elective requests from 144 medical students and 80% of these students were offered electives.
We hosted 87 elective students (down from 96 in 2016-2017) with requests from the University of Calgary (37 clerks), UBC (24 clerks), U of A (12 clerks), U of T (12 clerks), UWO (9 clerks), U of O (14 clerks), McMaster (3 clerks), Queens (5 clerks), U of M (9 clerks), U of S (5 clerks), Dalhousie (2 clerks), as well as a few requests from each of the other Canadian schools. The 139 elective learners we hosted in 2018-2019 represent over 10,000 hours of direct 1:1 learner supervision by our teaching faculty. We were also able to host 20 students from the U of C for their “med 440” block. Calgary emergency department has always been able to accommodate all interested 440 students due to the strong support our staff gives to these junior learners. The rotation continues to have strongly positive reviews from the students.
Overall, both the mandatory and elective adult emergency medicine rotations are highly regarded by our learners, who appreciate the diversity of patients, high quality bedside teaching, and one-on-one direct staff supervision around the clock. In total, our teaching faculty provided well over 30,000 hours of direct 1:1 learner supervision in the 2018-2019 academic year, and this figure does not include the hundreds of hours our faculty spent on the direct supervision of pre-clerkship level students through the University of Calgary summer pre-clerkship elective program as well as the many U of C medical students who request informal shadowing of an emergency physician throughout the year.
Dr. Meira Louis Coordinator of Elective & Off-service Learners
UNIVERSITY OF CALGARY EMERGENCY MEDICINE CLERKSHIP
2019 ANNUAL REPORT 74
The Class of 2019 completed their Emergency Medicine mandatory clerkship rotation in April 2019. 149 students completed their mandatory Emergency Medicine rotation in Calgary. These students worked 3 shifts at the Foothills Medical Centre and 4 shifts at one of the other adult sites. The remainder completed their Emergency Department rotations through their UCLIC sites. The overall ranking for the mandatory Calgary based emergency rotation was 4.5, higher than the Class of 2017 (4.1) and the Class of 2018 (4.0). The 4.5 ranking was tied with O&G for the #1 highest ranked clerkship rotation. We continued to use “One45” for the daily in-training evaluation reports (ITER). This allows more efficient completion of the final ITER and likely makes the final ITER more accurate. The completion rate for the in-training evaluation reports by our staff is greater than 95%. Students have moved away from the SunRay cards and now use their proximity cards to access SCM/SEC and other resources. There were a few hiccups (mostly around training) early on however these seem to have been resolved.
The Class of 2019 saw the introduction of the “Observed History and Physical” teaching session. This involves a staff preceptor observing the performance of a history and physical exam by the clerk on an actual emergency department patient. The duration is usually about 45 minutes. This activity has been very well received. Student identified strengths of the rotation include the quality of on-shift teaching (the vast majority of shifts involve working directly with the staff physician with no other team members), the quality of scheduled teaching sessions and the balance of responsibility and supervision. Further, the administrative organization and the core document were seen as strengths. There were no specifically identified weaknesses. Of course, our Undergraduate Medical Education Hub and the Emergency Department Clerkship Committee are continuing to look for ways to improve the rotation. With the addition of the “Nursing Block” session along with the maintenance of the rest of the outstanding teaching sessions we plan to further improve the educational experience for clerks in the Class of 2020.
Dr. Gavin Greenfield Undergraduate Medical Education (UME)

GRAND ROUNDS
2019 ANNUAL REPORT 75
Grand Rounds Presentations in
2019
2019 has seen a successful year for Grand Rounds presentations. Emergency Medicine Department Grand Rounds are held weekly on Thursday at 9:00am in the Coombs theatre of the Foothills Medical Centre. This program meets the accreditation criteria of the College of Family Physicians of Canada and has been accredited for 1.0 MainPro-M1 credits. This program is also approved as an accredited group learning activity as defined by the maintenance of certification program of the Royal College of Physicians and Surgeons of Canada.”
“We have continued the Quality Assurance & Educational Rounds (QAER) now pairing residents with staff mentors for QI mentorship. We have continued recording the weekly grand rounds to allow staff to watch presentations they were unable to attend in person. We continue to host content experts from other specialties to ensure the highest quality content and have improved the content of the grand rounds topics with stricter guidelines and more robust topic choices.”
Past Grand Round presentations can be found online at www.ucalgary/ermedicine
Past Grand Round recordings can be found as podcasts at www.albertaplp.ca/podcasts
Dr. Fareen Zaver

SIMULATION
2019 ANNUAL REPORT 76
The Emergency Medicine Simulation Program continues to progress. The Simulation Education Advisory Committee (SEAC) helps oversee the simulation activity for medical students, residents, physicians and nurses working in the Emergency department.
SEAC consists of:
Medical Director: Gord McNeil
Medical Student Lead: Kevin Haley
FRCP Junior Residents Lead: Patty Lee and Andrea Boone
CCFP-EM Resident Leads: Scott Seadon and Stuart Rose
FRCP Residents Lead: Jen Puddy
Staff Simulation Lead: Gord McNeil
Nurse Educators from 4 Adult Emergency Departments
STARS representative: James Huffman
This committee continues to work together to bring resources of each of these programs under one umbrella. All programs are continuing to develop more facilitators and scenarios to enhance the education of medical students, residents and staff.
The Emergency Medicine Staff Interdisciplinary Simulation Program continues to thrive and grow. These weekly sessions gather physicians, nurses, respiratory therapists and pharmacists to participate in sessions that focus on teamwork skills, practicing procedural skills and expanding knowledge bases. Over 160 different physicians and 600 nurses have participated in approximated 300 sessions in the last 9 years. The team is exposed to critical care scenarios and is encouraged to practice, in real time, the skills they will need for their daily practice in Emergency Medicine. Our team of facilitators are now well recognized as valuable teachers for a variety of simulation courses and have become speakers at international conferences.
Dr. Gord McNeil
Medical Director of Simulation

EMERGENCY MEDICINE RESEARCH UPDATE
2019 ANNUAL REPORT 77
The 2019 academic year has been a period of continued research excellence. We worked closely with our new Research Coordinator, Dr. Hina Walia and the research assistants at the Rockyview General Hospital to complete two large multi-centre studies at that site. We have since transitioned our research infrastructure to Foothills Medical Centre ED exclusively which has allowed us to centralize our research focus and collaborate with other departments in an effort to optimize care for our emergency department patients with seven ongoing studies.
The Research Group hosted its first strategic vision planning session with great success. Representation from emergency physicians, nurses, paramedicine, allied health, the Emergency Strategic Clinical Network and emergency medicine administration contributed to a fruitful conversation on how to advance and support emergency medicine-based research in Calgary (please see outline of Strategic Vision below). We eagerly anticipate the launch of our new research website!
We continue to employ four research assistants who work at one adult emergency medicine site (Foothills Medical Centre) screening, consenting and recruiting emergency medicine patients to national, provincial and local research studies.
We were happy to support and build the research capacity of our trainees and supported various emergency medicine researchers in applications to CIHR, PRIHS, ESCN, Alberta Health Innovates and other relevant funding opportunities. Our researchers continue to contribute to evidence and knowledge translation practices around Choosing Wisely, Audit & Feedback practices, Quality Improvement and cutting-edge studies evaluating the use of imaging for renal colic, concussion and pulmonary embolism; biomarkers in cardiac disease, in addition to supporting the work of the Emergency Strategic Clinical Networks focus on opioid
misuse and opioid replacement therapies (suboxone). Ongoing partnerships within the University of Calgary with the Divisions of Cardiology, Neuro-radiology, Neurology, Gastro-enterology, Hematology and Orthopedics and Spinal Surgery allows us to participate in timely, relevant, patient centred research that aims to improve the health of Albertans.
Finally, we bade a fond farewell to Ms. Katrina Koger, administrative assistant, who provided exemplary support to the research program during her four years with the Research Group. We are grateful for leadership she has provided and wish her luck with her future career. We also thank Dr. Hina Walia, our interm research coordinator, for her contribution to research excellence, especially at the Rockyview site. Dr. Walia transition to a different role within AHS in August.
Research Day 2019
The Department of Emergency Medicine’s 9th Annual Research Half Day, entitled “Transform: The Science of Health Improvement” on April 11, 2019 was an immense success, with 112 participants in attendance, celebrating research excellence in Emergency Medicine across healthcare areas: staff and resident physicians, nurses, respiratory therapists, medical students, social workers, paramedics, plastic surgery residents, emergency strategic clinical network representatives and researchers. An engaging keynote was provided by Dr. Lucas Chartier who invited us to re-envision the role quality improvement has in improving patient and systems level care. Additionally, eight oral research presentations, fifteen academic posters, and twelve Pechakucha presentations occurred. The event was tweeted on social media under the handle #ResearchDay2019
Dr. Stephanie Vandenberg Research Director

EMERGENCY MEDICINE RESEARCH UPDATE
2019 ANNUAL REPORT 78
Current Studies
1. Age-Adjusted D-dimer cut-off levels to rule out deep vein thrombosis: A prospective outcome study (Adjust-DVT) Start Date: July 2017 End Date: July 2021 Number Enrolled: 40 Utilization of age-adjusted d-dimer (10 ug/L x age in years) to guide DVT care pathway. Patients with a Wells <2 will only have an ultrasound if d-dimer exceeds age-adjusted cutoff. Patients 50 and over with Wells ≥2 will receive an initial ultrasound at ED visit. If initial ultrasound is negative, patients will only receive a serial ultrasound if d-dimer exceeds age-adjusted cutoff.
2. Plastic cling wrap as an interim burn dressing
Start Date: August 2017 End Date: August 2020 Number Enrolled: 1 Standardized questionnaires will be used to measure both patient and ED staff/Outpatient Burn Unit staff impressions on plastic wrap, such as the ease of plastic wrap removal, pain scores, and healing time. Training for plastic wrap application and removal will be provided. Follow-up within 24h will be provided by the burn clinic.
3. ED Ultrasonographic Regional Anesthesia to Prevent Incident Delirium in Hip Fracture Patients
Complete Number Enrolled: 50 To test whether a knowledge to practice intervention to train, facilitate and encourage ED physicians to use ultrasound-guided regional anesthesia can reduce new cases of delirium following hip fractures.
4. Predicting Emergency Department Delirium with an Interactive Customizable Tablet to Prevent Repeat Visits
Complete Number Enrolled: 280 Eligible participants will play the “serious game” on the tablet at initial enrolment, as well as an interview on health, independence, current thinking, reasoning, and risk factors for becoming delirious. The patient will then participate in 6 initial follow-up visits if they are admitted to hospital where they will re-play the tablet game. At 7 days, the patient will be contacted for the final follow up which will take place on the unit (if admitted) or on the phone (if discharged) which will include an interview on their current health status and independence.
5. LEAD study – Paul ([email protected])
LEAD. FMC Site. Validation of clinical prediction rule for investigation of suspected DVT in pregnant patients. Lead site is McMaster University. Calgary PI Dr. P Wilson (Internal Medicine). Eligible patients are referred to LEAD study coordinator/team. ED RAs can complete enrolments on weekends.

EMERGENCY MEDICINE RESEARCH UPDATE
2019 ANNUAL REPORT 79
6. Comparison of Bleeding Risk between Rivaroxaban and Apixaban for the treatment of acute venous thromboembolism (COBBRA) Comparison of Bleeding Risk between Rivaroxaban and Apixaban for the treatment of acute venous thromboembolism. Background To address the clinical equipoise of which DOAC has the best risk to benefit ratio, a head-to-head randomized controlled trial between Apixaban and Rivaroxaban with safety as primary outcome is needed. Primary Objective is to compare the safety of Apixaban and Rivaroxaban in terms of bleeding for treatment of VTE. Study Intervention Patients will be randomized to one of 2 groups: 1. Apixaban group: 10 mg PO BID for 1 week, then 5 mg PO, BID for 3 months of treatment, or 2. Rivaroxaban group: 15 mg PO BID for 3 weeks, then 20 mg PO OD for 3 months of treatment. Eligibility & Recruitment: All acute non-cancer VTE adult patients that are DOAC candidates are eligible for the study. The window for recruitment is 72 hours after diagnosis Follow Up: All patient sent to the clinic will be followed by thrombosis clinic; even if they decline enrollment in to the study.
7. SCIATIA
Sciatica is a condition referring to the irritation of the sciatic nerve, forming a ‘shooting pain’ at the lumbar vertebrae of the spine and travelling down one leg. Most of the time, this irritation is due to one of the intervertebral discs herniating and impinging this nerve. Fortunately, a vast majority (75%) of patients recover within 12 weeks. Past this point it is difficult to determine if a patient will recover. This extended prognosis timeline can be both discouraging to the patient and expensive to the health care system. This study aims to gain a better understanding of who will recover and who will require surgery. Can systemic inflammatory profiles of a patient with sciatica collected at repeated times help us predict the natural history of lumbar disc herniations on a patient specific basis? We will be screening and recruiting patients with acute sciatica at the earliest signs of onset to collect a serum sample. We will continue to follow up with them at 4 and 16 weeks, comparing varying inflammatory markers. Accurate prognostication could improve the patient experience, aid in the better allocation of health care resources, and provide significant cost-savings to health care payers.
8. E-Scooter (City of Calgary Collaboration) Background: The introduction of electronic scooters (e-scooters) in Calgary as of July 13, 2019 has prompted investigation into the health impact of this new mode of transportation. Preliminary ED data in Calgary reveals up to 199 scooter related injuries in the period of July 10-August 13, 2019, as inferred from instances where the term scooter appeared on the ED triage note. Aim: This study aims to quantify the incidence and characteristics of moderate to severe injuries associated with the use of e-scooters in Calgary between June 2019 – October 2019. Methods: Retrospective review of paper medical records of all patients presenting to Foothills Medical Centre Emergency Departments who arrive via emergency medical services (EMS) to with the term “scooter” included in the triage note. Sample Size: 40
Research Personnel
FMC Research Assistant Group (As of November 1, 2019): Jessica Kuehne Daniel Andruchow Daniel Major Ashley Clarke Coverage: Monday through Friday 08h00-15h00

EMERGENCY MEDICINE RESEARCH UPDATE
2019 ANNUAL REPORT 80
Ongoing Partnerships/Collaborations
1. Partnership for Research and Innovation in Health System (PRIHS)
1.1. Reassessment of Clinical Practices for Patient Presenting to the Emergency Department with Upper Gastrointestinal Bleeding.
To optimize the management of patients presenting to emergency with non-variceal upper gastrointestinal bleeding (UGIB), the Emergency Strategic Clinical Network is leading a provincial quality improvement initiative. This project aims to optimize several key areas of UGIB management: (1) the use of a Glasgow-Blatchford based pathway for the disposition of patients, (2) increased access to urgent outpatient endoscopy, and (3) increased adherence to transfusion guidelines.
Within the past year this project has undertaken an evaluation at Foothills Medical Centre which found a 6.3% drop in the admission of low acuity UGIB patients. An evaluation of Dr. Dowling’s changes to UGIB order sets found a 33% decrease in pantroprazole infusion orders. An “Iron Summit” was held in Calgary bringing together 45 clinical leaders from 9 departments to advance the appropriate management of iron deficiency anemia patients through increased access to outpatient IV Iron and to streamline the referral process. Work is underway in collaboration with Day Medicine to execute these objectives. The Emergency SCN has begun collaboration discussions with the Digestive Health SCN focused on advancing best clinical practices within the final year of this grant, as well as legacy research and clinical sustainability.
1.2 Evaluation of the Connect 2 Care (C2C) Team for Vulnerable Patients with Complex Needs
Researchers at the University of Calgary’s O’Brien Institute for Public Health have partnered with Calgary Urban Project Society (CUPS) and Alpha House to evaluate the Connect 2 Care (C2C) intervention for socially vulnerable patients with complex health needs. Socially vulnerable individuals, including those experiencing homelessness, have higher acute care utilization compared with the general population. Despite available primary care and social services, many have significant challenges accessing the services they need in the community. The C2C (formerly the Coordinated Care Team [CCT]) intervention aims to improve care coordination for socially vulnerable patients by bridging the gap between acute care and community services. This novel intervention combines elements of intensive case management with community outreach and navigation.
Initially launched November 1, 2015, C2C consists of 2 registered nurses, to be supplemented by first 2, then 4 navigators. Referrals are accepted from emergency departments, hospital units and community partners. The team will have expertise in chronic disease management, mental health and addictions, and extensive knowledge around social programs, community health, housing, and financial, transportation and legal resources. Population

EMERGENCY MEDICINE RESEARCH UPDATE
2019 ANNUAL REPORT 81
Referrals are accepted from emergency departments (ED), hospital units and community partners, for patients meeting the following criteria:
1. ≥18 years of age AND 2. Homeless or unstably housed AND 3. ≥ 3 ED/Urgent Care (UC) presentations, or ≥ 2 hospitalizations within the past year, AND 4. A history of one or more high-risk conditions (used by partner – Anansi Health):
Substance use disorder; mental illness with functional impairment (depression, anxiety disorder, bipolar disorder, psychotic disorder); congestive heart failure; diabetes with HbA1c>9%; chronic obstructive pulmonary disease; asthma; cardiovascular disease; uncontrolled hypertension with end-organ damage; end-stage liver disease; end-stage kidney disease.
Evaluation/Objectives
We will evaluate the C2C intervention using the Donabedian framework of structure, process, and outcome. To assess structure, we will document the program’s context, resources, and partner supports. Process indicators include: referrals to primary care, housing, addiction and mental health programs. Outcome measures include: ED visits, hospitalizations, costs, quality of life, self-reported health status, patient, staff, and partner experiences.
The objectives of this evaluation are:
1. To document the structure and process of the C2C model of care throughout the phases of implementation. 2. To determine the effectiveness of the C2C program in reducing acute care utilization and improving patient-
reported outcomes. 3. To assess patient, staff, and partner experience with the C2C. 4. To explore the links among structure and processes that lead to health and program outcomes, both positive
and negative.
1.3 Improving Acute Care for Long-Term Care Residents: A Better Way to Care for the Frail Elderly in Times of Medical Urgency
The aim of this PRIHS application to is improve the care provided to long-term care (LTC) residents who develop an acute health issue, focusing on a patient-centered approach that provides the appropriate treatment in the right location. Specifically, we will optimize, standardize and evaluate the current processes followed when considering transfer of residents from LTC to an emergency department (ED). Our proposed solution is evidence-informed and aims to better optimize and integrate the use of current healthcare resources.
Objectives
1) To implement and evaluate an evidence-informed standardized care process for the care of LTC residents experiencing an acute change in health status 2) To scale and spread the standardized care process for the care of LTC residents experiencing an acute change in health status.

EMERGENCY MEDICINE RESEARCH UPDATE
2019 ANNUAL REPORT 82
Methodology
This is an integrated knowledge translation (iKT) project that has been informed by the knowledge to action (KTA) cycle <37>. Specifically, we have identified an evidence-informed solution to address a care gap and have engaged with relevant stakeholders. We will implement this change initiative, considering both local LTC context and barriers to implementation. The implementation strategy can be modified to address these identified barriers. Although the INTERACT® tools used will remain consistent, the care and referral pathway can also be adapted to address contextual factors unique to each AHS zone. We will evaluate the initial implementation in the Calgary zone using a rigorous evaluation plan, and continue to monitor the sustainability and provincial spread using a provincial LTC-ED transfer dashboard developed as part of this initiative.
1.2 Emergency Medicine Strategic Clinical Network (ESCN) Collaborations
1.2.1 ED Buprenorphine/Naloxone (Suboxone) Initiation: a province wide strategy to improve access to opioid replacement therapy for patients with substance misuse disorder
1.2.2 Improving the patient intake experience: a patient centred partnership with AHS Human Factors and Wayfinding experts to improve the experience of patients in the emergency department intake areas.
1.2.3 ESCN Systematic Review Awards Competition
Clinical risk prediction scores and high-sensitivity cardiac troponin assays for the prediction of major adverse cardiac events in emergency department patients with chest pain: A systematic review and meta-analysis - Dr. Andrew McRae Many clinical risk scores can accurately identify patients at low risk of short-term major adverse cardiac events (MACE). However, existing scores were derived prior to the availability of highsensitivity cardiac troponin (hs-cTn) assays, and as such they incorporate less sensitive contemporary cTn results. The goal of the proposed review will be to summarize the evidence on the performance of existing risk prediction scores for MACE and coronary artery disease when combined with hs-cTn assay results. Appropriate use of risk prediction scores can guide clinicians to better match follow up strategy to a patient’s risk for MACE.
1.2.4 ESCN Summer Studentship Awards Competition
Student: Kiran Grant Supervisor: Dr. Grant Innes Project Title: Throughput interventions to reduce ED crowding: a systematic review Student: Luke Green-Harrison Supervisor: Dr. Catherine Patocka and Eddy Lang Project Title: The emergency physician leader: A realist evaluation of the impact of a new physician role on ED overcrowding in the Calgary area

EMERGENCY MEDICINE RESEARCH UPDATE
2019 ANNUAL REPORT 83
EMERGENCY MEDICINE RESEARCH GROUP 5 – YEAR STRATEGIC VISION
Mission: The Emergency Medicine Research Group exists to improve patient and family care and health system efficiency through actionable research, collaboration, and mentorship. Vision: In five years, we will become a nationally recognized leader in meaningful emergency research, and have a growing cohort of researchers and a stable research infrastructure enabling further growth and success.
Strategic Goals Strategic Initiatives G1: “Becoming a nationally recognized leader in emergency research”
G2: “Achieve sustainable growth of the research group”
G3: “Meaningful engagement of patients and families in emergency research”
I1 “Leverage our senior researchers, health systems research, decision support and analytical experience to use the staged implementation of EPIC/ConnectCare as an unprecedented opportunity for research, knowledge translation, and clinical practice improvement across the province” I2 “Use access to and relationships with the 4 adult sites to increase staff engagement across the Calgary zone” I3 “Recruit, mentor, and support junior researchers” I4 “Use access to and relationships with the Calgary EM zone leadership/operations to identify and continuously evaluate priority projects and procure dedicated funding” I5 “Use previous materials and plans to create a central research funding opportunity database” I6 “Leverage available infrastructure to promote emergency research within Calgary” I7 “Develop a comprehensive system for multi-center projects” I8 “Engage with the provincial government to identify shared priority projects.” I9 “Identify key competencies needed and secure permanent funding for them”
I10 “Integrate patient and family experience in EM research” I11: “Identify key scholarly areas for our group”
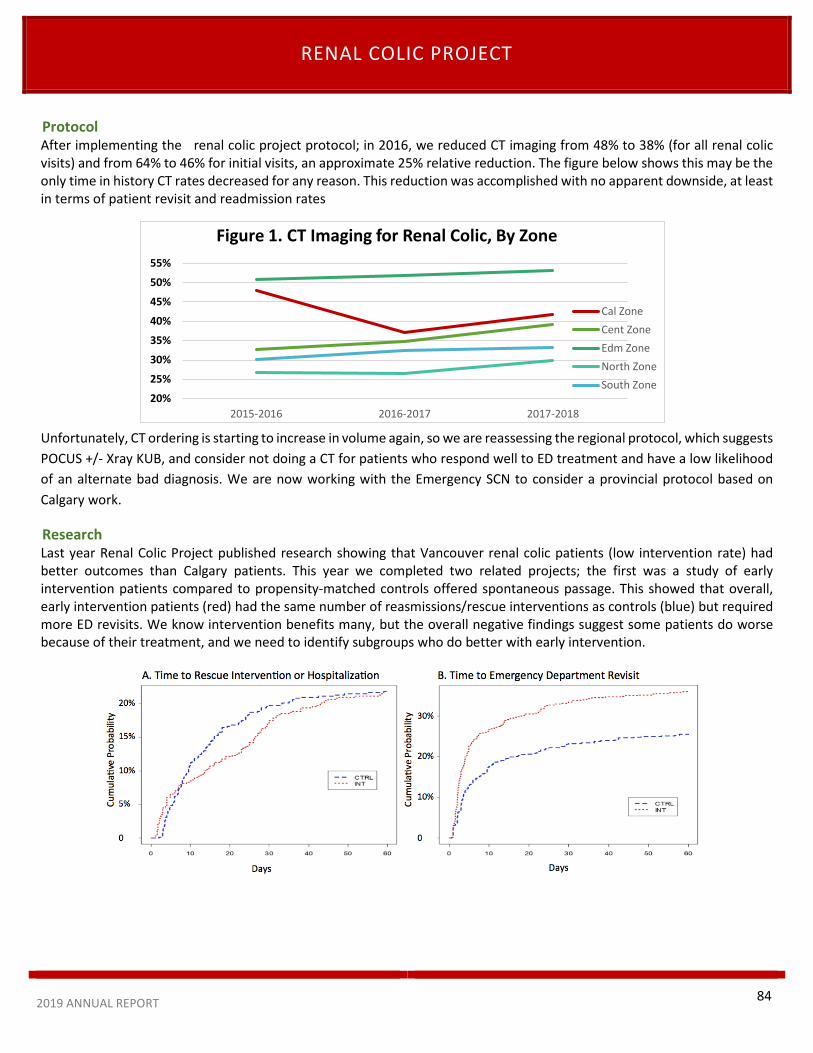
RENAL COLIC PROJECT
2019 ANNUAL REPORT
ProtocolAfter implementing the renal colic project protocol; in 2016, we reduced CT imaging from 48% to 38% (for all renal colic visits) and from 64% to 46% for initial visits, an approximate 25% relative reduction. The figure below shows this may be the only time in history CT rates decreased for any reason. This reduction was accomplished with no apparent downside, at least in terms of patient revisit and readmission rates
Unfortunately, CT ordering is starting to increase in volume again, so we are reassessing the regional protocol, which suggests POCUS +/- Xray KUB, and consider not doing a CT for patients who respond well to ED treatment and have a low likelihood of an alternate bad diagnosis. We are now working with the Emergency SCN to consider a provincial protocol based on Calgary work.
Research Last year Renal Colic Project published research showing that Vancouver renal colic patients (low intervention rate) had better outcomes than Calgary patients. This year we completed two related projects; the first was a study of early intervention patients compared to propensity-matched controls offered spontaneous passage. This showed that overall, early intervention patients (red) had the same number of reasmissions/rescue interventions as controls (blue) but required more ED revisits. We know intervention benefits many, but the overall negative findings suggest some patients do worse because of their treatment, and we need to identify subgroups who do better with early intervention.
20%
25%
30%
35%
40%
45%
50%
55%
2015-2016 2016-2017 2017-2018
Figure 1. CT Imaging for Renal Colic, By Zone
Cal ZoneCent ZoneEdm ZoneNorth ZoneSouth Zone
84

RENAL COLIC PROJECT
2019 ANNUAL REPORT
The second study was a subgroup analysis to answer this question. See next.
In this figure, the bottom line is that stone width and location nare the primary outcome determinants. The data suggests there is a low-risk group (all stones <5mm) who do better with spontaneous passage, a high-risk group (all stones >7mm and proximal or middle stones >5mm) who do better with early intervention, and an intermediate risk group (5.0-6.9mm distal stones) who have similar outcomes regardless of treatment. There are hopes that Dr. Grant Innes will present a Grand Rounds presentation in the future on this topic.
Other research In a recently published paper,1 we reported that the average level of ED access block in Canadian EDs (i.e. the cumulative number of hours that arriving high acuity patients are blocked from care because of overcrowding) is 46,000 hours per ED per year, but that this value is only ~1% of the available inpatient bed capacity at the corresponding hospitals. This means the size of the problem is very small relative to the size of the potential solution, and that, if access block was viewed as a ‘whole hospital’ problem, it could be solved by hospital capacity or efficiency improvements in the range of 1-2%.
In a recent collaborative study2 looking at 1009 ED fentanyl overdoses (most who received prehospital naloxone), only 1.6% required repeat naloxone dosing after arrival. Among 752 low-risk patients with clear mentation and normal vital signs, only 3 (0.4%) required repeat naloxone, none were admitted, and median ED length of stay was 168 minutes. The bottom line: Fentanyl overdoses can be managed much like heroin overdoses: Patients who are clinically stable usually require only brief observation periods.
In another recent collaborative study3 we followed 834 ED patients with prolonged QTc intervals (female>460 ms; male>440 ms) and compared these to 417 matched patients with normal QTc. 30-day mortality was 4.7% in the prolonged group and 5.0% in the normal group, with no patients suffering nonfatal cardiac arrest. Findings were similar in the subgroup with very prolonged QTc >500msec. This suggests that, in ED patients, current definitions of QT prolongation are not associated with measurable outcome differences and may not be appropriate for ED risk stratification purposes.
0%
10%
20%
30%
40%
50%
60%
70%
<5mm 5-6.9mm >7mm <5mm 5-6.9mm >7mm
Distal Stones Proximal-Middle Stones
Control
Intervention
85

RENAL COLIC PROJECT
2019 ANNUAL REPORT
Some of our other recently published work suggested that physician payment mechanisms have little effect on ED operational performance,4 and that the development of hospital accountability frameworks defining clear program operational expectations, along with demand-driven overcapacity protocols would go a long way to improving access to care. 5
1. Emergency department overcrowding and access block: A smaller problem than we think. Can J Emerg Med 2018; Nov 8:1-9. doi:10.1017/cem.2018.446. [Epub ahead of print].2. Safety of a Brief Emergency Department Observation Protocol for Patients With Presumed Fentanyl Overdose. Ann Emerg Med 2018;72(1):1-83. Emergency department patients with a prolonged QT interval do not have increased thirty-day mortality. Ann Emerg Med 2019;73: in press4. Impact of Physician Payment Mechanism on ED Operational Performance. Can J Emerg Med 2018:20(2):183-905. Accountability: A Magic Bullet for Emergency Care Delays and Healthcare Access Blocks. Healthcare Management Forum. 2018;3:172-77
Dr. Grant Innes, Senior Researcher
86

PRIHS PROJECT
2019 ANNUAL REPORT 87
PRIHS IV: Improving Acute Care for Long Term Care Residents: A Better Way to Care for the Frail Elderly in Times of Medical Urgency.
This is a 3 year PRIHS (Partnership for Research and Innovation in the Health System) project funded by Alberta Innovates and Alberta Health Services. The original project started in the Calgary Zone as a CMO quality improvement seed grant in which the care and referral pathway was successfully implemented on a limited bases. Led by Dr. Jayna Holroyd Leduc (Principal Investigator) and Heather Hair (Operational Lead), in partnership with the Emergency Strategic Clinical Network (SCN) and the Seniors Health SCH, the mail goal of this project is to reduce the rate of resident/patient transfers from Long Term Care (LTC) facilities to emergency departments (ED).
The Problem
This initiative intends to optimize the care for LTC residents in times of medical urgency, and reduce unnecessary risks associated with transfers to ED and hospital admissions. Transfers to ED and hospital admissions are associated with increased risk of hospital-acquired infections, falls, delirium, and functional decline. Additionally, evidence indicates that LTC residents and families would prefer to receive care for acute issues at the LTC site where possible.
The Proposed Solution
A centralized and standardized LTC-ED care and referral pathway is being implemented with support from RAAPID (Referral, Access, Advice, Placement, Information and Destination) and Mobile Integrated Healthcare (MIH) (previously known as Community Paramedics). RAAPID will arrange a conversation between the LTC site and the ED (and with community paramedics as required) to discuss the best plan of care, and to facilitate direct communication between
relevant physicians if transfer to ED is appropriate. Additionally, if appropriate and able, the MIH will support treatment of the medical concern at the LTC site, thus avoiding an ED transfer.
Two tools from INTERACT (Interventions to Reduce Acute Care Transfers) will help support LTC staff (i.e. HCAs and nurses) to detect, communicate and address acute changes in residents’ health sooner. Identifying changes in a resident’s condition sooner will better enable LTC staff and physicians to manage these health issues onsite.
Outcomes expected
Overall, this project is focused on ensuring the right care at the right time in the right place for LTC residents. In addition to reducing transfers to the ED, there are a number of secondary outcomes expected from this intervention:
• Change the rate of admissions of LTC residents to hospital
• More LTC residents will be cared for at their LTC sites, with the support of MIH (community paramedicine) when needed
• To improve the outcomes and quality of life of residents of LTC in times of medical urgency by detecting issues sooner and managing them at the LTC site if possible, instead of transferring them to the ED.
• To improve communication between the LTC site and the emergency department when a transfer to the emergency department is required
The Plan
Using a randomized step-wedge design, 4-5 Calgary-zone LTC sites will be supported every 3 months to implement this LTC-ED pathway and the INTERACT tools, eventually bringing 38 LTC sites on board over the next 2 years. Beginning in 2021, selected LTC sites in Central Zone will also be included.
Heather Hair, RN MBA Executive Director (ESCN)
Emergency Strategic Clinical Network

THE SUMMER OF THE E-SCOOTER
2019 ANNUAL REPORT 88
The Summer of the E-Scooter
Calgary’s Emergency Departments came into the national and international spotlight as one of the only international jurisdictions that could report on the Emergency Department and thus the public health and injury prevention implications of motorized rental scooters. Calgary, as it turns out logged over 750 000 rides over the 2019 season, making it the second most popular jurisdiction for E-scooter use for the population with access.
Data reporting on E-scooter visits to the Emergency Department is currently hampered by the lack of an ICD-10 code dedicated to the identification of riders and pedestrians who sustain injuries related to e-scooter transport. Fortunately, our uniquely linked electronic health records made it possible to gather information on E-scooter related visits by searching the term E-scooter and scooter from the triage note across all 5 Calgary EDs and the two Urgent Care centers using Sunrise Clinical Manager.
The City of Calgary commissioned a research project led through our division which linked ED visits to individuals transported to by EMS for E-scooter related injuries. This project led to recommendations presented to City Council on December 18, 2019 and where a recommendation to lower the inherent E-scooter speed limit by 5km/hour to 15km/hour as it was noted that high speed was a contributing factor to the more serious injuries encountered.
Overall, we saw 671 ED visits related to e-scooter use with upper extremity injury, lower extremity injury and head trauma being the most common presentations. Fortunately, no deaths of ICU admissions were recorded although there have been fatalities associated with E-scooter use.
E-scooter activities resulted in a fair amount of media attention to the role that our EDs provide in caring for the injured and our contribution to important public health initiatives and policy.
Dr. Eddy Lang Zone Clinical Department Head

89
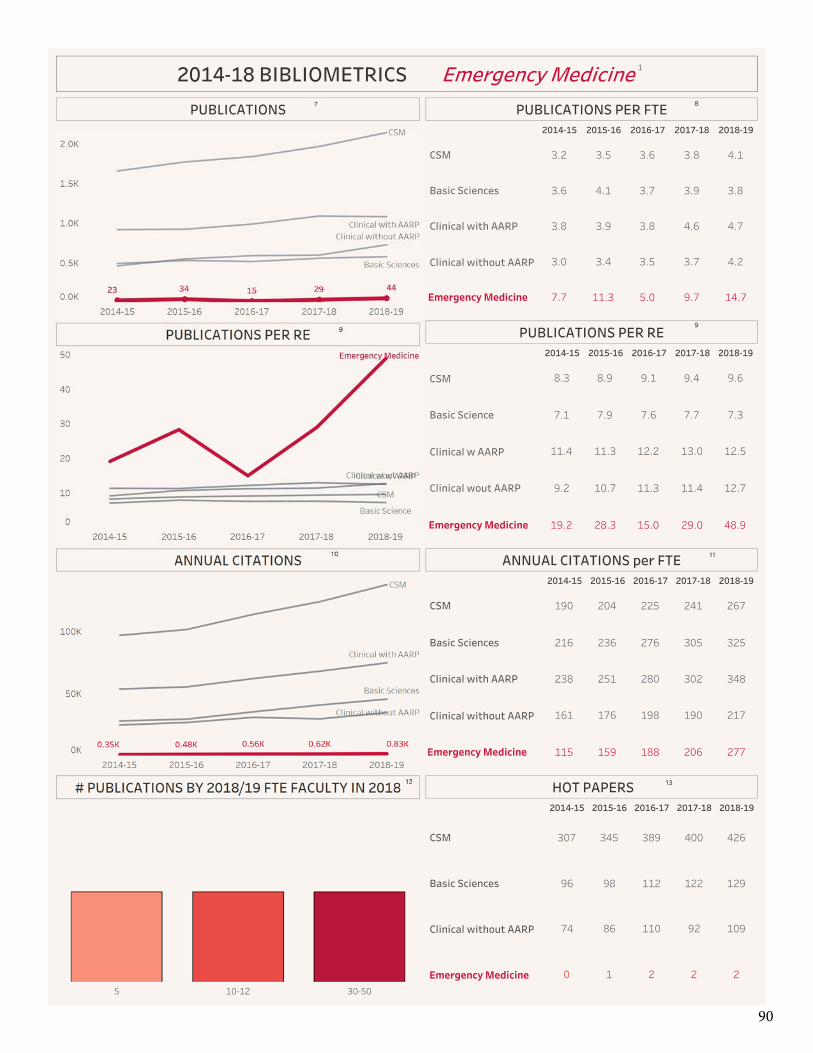
90

91

92

2019 LIST OF GRANTS AWARDED
2019 ANNUAL REPORT 93
1. Project: Simulated scenarios to receive real-time feedback: does feedback in SIM facilitate more effective attainment
of pediatrics competencies for Emergency Medicine residents
Investigators: Meaghan Mackenzie PI: Dr. Doshi Agency: Office of Health and Medical Education Scholarship (OHMES) Total Funds: $2040 Period: January 2019
2. Project: Can we improve the use of gastroscopy to investigate dyspepsia in otherwise healthy adults in Alberta? Sharing Choosing Wisely guidelines, current practice patterns and resources to optimize appropriate use
Investigators: Co-investigator. S. Dowling PI: Dr. Kerri Novak. Agency: Choosing Wisely Alberta Grant Total Funds: $95,177 Period:
3. Project: Integrating Quality Improvement & Value-Base Healthcare in Emergency Department Processes. Investigators: S. Dowling Agency: Campus Alberta Meeting Grant Total Funds: $4000 Period: 2019
4. Project: De-implementing Low Value Care: A Research Program of the Choosing Wisely Canada Implementation Research Network.
Investigators: S. Dowling Agency: Canada Institutes of Health Research, Innovative Clinical Trials Stream Total Funds: $1,400,000 + $1,400,000 in matching funds Period: 2019
5. Project: Novel risk prediction tools for emergency department patients with suspected coronary artery disease. Investigators: PI: Andrew McRae Agency: Canadian Institutes of Health Research Project Grant Total Funds: $123,212 Period: 2019 - 2021
6. Project: Risk prediction tools for emergency department patients with suspected coronary disease in the high-sensitivity troponin era
Investigators: PI: Andrew McRae Agency: Alberta Health Services Emergency Strategic Clinical Network Systematic Review Grant Total Funds: $12,700 Period: 2019
7. Project: Understanding frequent emergency department visitors in Alberta and Ontario through advanced statistical modeling techniques.
Investigators: PI: Scott Fielding and Rhonda Rosychuk. Co-I Andrew McRae Agency: CIHR Secondary Analysis Operating Grant Total Funds: $70,000 Period: 2018 -2019
2019 LIST OF GRANTS AWARDED
2019 ANNUAL REPORT 94
8. Project: Calgary-Mbarara Emergency Medicine Collaboration (CMEM).
Investigators: Andrew Battison, Ian Wishart, Jason Fedwick, Heather Baxter, Kelsey Ragan Agency: The McLaughlin Travelling Medical Education Fund Total Funds: $10,000 per year x 3 years Period: 2019 - 2021
9. Project: Community Based Naloxone Kits: Using design methods to transform complex user needs into innovative community partner project” Academy for Design Innovation Management Conference 2019 June 20, 2019 London, United Kingdom.
Investigators: Stephanie VandenBerg Agency: Faculty Conference Travel Grant Total Funds: $1500 Period: May 2019

PUBLICATIONS IN 2019
2019 ANNUAL REPORT 95
1. Bond C, et al. Hot Off the Press: SGEM #218. Excited Delirium: A Systematic Review. Acad Emerg Med. 2019 Jan 26;26(1):106-108.
2. Hersi, Mona, Traversy, Gregory, Thombs, Brett D, Beck, Andrew, Skidmore, Becky, Groulx, Stéphane, Lang, Eddy, et al. Effectiveness of Stop Smoking Interventions among Adults: Protocol for an Overview of Systematic Reviews and an Updated Systematic Review. 2019. Web.
3. Hamel, Candyce, Lang, Eddy, et al. Screening for Depression in Women during Pregnancy or the First Year Postpartum and in the General Adult Population: A Protocol for Two Systematic Reviews to Update a Guideline of the Canadian Task Force on Preventive Health Care. 2019. Web.
4. Heitz, Corey, Justin Morgenstern, Christopher Bond, et al. "Hot Off the Press: Validation of the Pediatric NEXUS II Head Computed Tomography Decision Instrument for Selective Imaging of Pediatric Patients with Blunt Head Trauma." Academic Emergency Medicine: Official Journal of the Society for Academic Emergency Medicine 26.2 (2019): 246-49. Web.
5. Raman, Maitreyi, Sara Lukmanji, Ian Walker, et al. "Does the Medical College Admission Test (MCAT) Predict Licensing Examination Performance in the Canadian Context?" Canadian Medical Education Journal 10.1 (2019): E13-19. Web.
6. Williams, Kenneth, Eddy S Lang, et al. "Evidence-Based Guidelines for EMS Administration of Naloxone." Prehospital Emergency Care 23.6 (2019): 749-63. Web.
7. Bond, Christopher, et al. "Hot off the Press: SGEM #226. I Want a New Drug—One That Doesn't Cause an Adverse Drug Event." Academic Emergency Medicine 26.4 (2019): 447-50. Web.
8. Francis, Marc N, Ian M Wishart, et al. "Use of Pharmacologic Sleep Aids and Stimulants Among Emergency Medicine Staff Physicians In a Canadian Tertiary Care Setting: A Web-Based Survey." Annals of Emergency Medicine 73.4 (2019): 325-29. Web.
9. Daraz, Lubna, Starr Webb, Rob Kunkle, Mohammad Hassan Murad, and Eddy Lang. "Training Curriculum to Help Patient Representatives Participate Meaningfully in the Development of Clinical Practice Guidelines." BMJ Evidence-based Medicine 24.6 (2019): 227-230. Web.
10. Morgenstern, Justin, Corey Heitz, Chris Bond, et al. "Hot Off the Press: Comparison of Emergency Medicine Malpractice Cases Involving Residents to Nonresident Cases." Academic Emergency Medicine 26.5 (2019): 556-58. Web.
11. Morgenstern, Justin, Corey Heitz, Chris Bond, et al. "Hot Off the Press: Assessing Risk of Future Suicidality in Emergency Department Patients." Academic Emergency Medicine 26.12 (2019): 1388-390. Web.
12. Blanchard, Ian E., Ryan Kozicky, Dana Dalgarno, Justin Simms, Stacy Goulder, Tyler S. Williamson, Susan Biesbroek, Lenore Page, Karen Leaman, Suzanne Snozyk, Lyle Redman, Keith Spackman, Christopher J. Doig, Eddy S. Lang, et al. "Community Paramedic Point of Care Testing: Validity and Usability of Two Commercially Available Devices." BMC Emergency Medicine 19.1 (2019): 30. Web.
13. Morgenstern, Justin, Corey Heitz, Chris Bond, et al. "Hot Off the Press: Hospital Observation Upon Reversal (HOUR) With Naloxone: A Prospective Clinical Prediction Rule Validation Study." Academic Emergency Medicine 26.6 (2019): 680-83. Web.

PUBLICATIONS IN 2019
2019 ANNUAL REPORT 96
14. Heitz, Corey, Justin Morgenstern, Christopher Bond, et al."Hot Off the Press: SGEM #257-EMTALA: It's the Law of the Land." Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine (2019): Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine, June 17, 2019. Web.
15. Dimitropoulos, Gina, Elizabeth Morgan-Maver, Brooke Allemang, Kyleigh Schraeder, Shannon D. Scott, Jorge Pinzon, Gail Andrew, Gregory Guilcher, Lorraine Hamiwka, Eddy Lang, et al. "Health Care Stakeholder Perspectives regarding the Role of a Patient Navigator during Transition to Adult Care." BMC Health Services Research 19.1 (2019): 390. Web.
16. Reay, Gudrun, Jill M Norris, Lorelli Nowell, K Alix Hayden, Katherine Yokom, Eddy S Lang, et al. "Transition in Care from EMS Providers to Emergency Department Nurses: A Systematic Review." Prehospital Emergency Care : Official Journal of the National Association of EMS Physicians and the National Association of State EMS Directors (2019): 1-13. Web.
17. Heitz, Corey, Justin Morgenstern, Christopher Bond, et al. "Hot Off the Press: A Systematic Review And Meta-analysis of Ketamine as an Alternative to Opioids for Acute Pain in the Emergency Department." Academic Emergency Medicine 26.8 (2019): 946-48. Web.
18. Bond, Christopher, et al. "Hot Off the Press: SGEM #237. Screening Tool for Child Sex Trafficking." Academic Emergency Medicine 26.7 (2019): 823-25. Web.
19. Chartier, Lucas B, Shawn E Mondoux, Antonia S Stang, Adam M Dukelow, Shawn K Dowling, Edmund S H Kwok, Sachin V Trivedi, Joshua Tepper, and Eddy Lang. "How Do Emergency Departments and Emergency Leaders Catalyze Positive Change through Quality Improvement Collaborations?" CJEM 21.4 (2019): 542-49. Web.
20. Morgenstern, Justin, Corey Heitz, Chris Bond, et al. "Hot Off the Press: Prospective Validation of a Checklist to Predict Short-term Death in Older Patients After ED Admission in Australia and Ireland." Academic Emergency Medicine 26.11 (2019): 1289-291. Web.
21. Girotti, Jorge A, Chanatry, Julie A. Clinchot, Daniel M, McClure, Stephanie C, Sein, Aubrie Swan, Walker, Ian W, et al. A Investigating Group Differences in Examinees’ Preparation for and Performance on the New MCAT Exam. Academic Medicine: August 13, 2019 - Volume Publish Ahead of Print
22. Hunter, Miles, Nicholas Packer, and Shawn Dowling. "Does the CATCH Clinical Decision Rule Adequately Determine Which Children with Minor Head Injury Require Computed Tomography (CT) Imaging?" CJEM (2019): 1-3. Web.
23. Zaerpour, Farzad, Diane P Bischak, Mozart B C Menezes, Andrew Mcrae, and Eddy S Lang. "Patient Classification Based on Volume and Case-mix in the Emergency Department and Their Association with Performance." Health Care Management Science (2019): 1-14. Web.
24. Mahajan, Amita, Anne Kemp, T Lee-Ann Hawkins, Amy Metcalfe, Shawn Dowling, et al.. "Postpartum Hypertensive Disorders in the Emergency Department - A Retrospective Review of Local Practice in Calgary, Alberta." Pregnancy Hypertension (2019): Pregnancy Hypertension, 20 December 2019. Web.
25. Heitz, Corey, Justin Morgenstern, Christopher Bond, et al. "Hot Off the Press: Low-dose Magnesium Sulfate Versus High Dose in the Early Management of Rapid Atrial Fibrillation: Randomized Controlled Double-blind Study." Academic Emergency Medicine 26.9 (2019): 1093-095. Web.
26. Heitz, Corey, Justin Morgenstern, Christopher Bond, et al. "Hot Off the Press: SGEM #264-Hooked on A Feeling? Opioid Use and Misuse Three Months After Emergency Department Visit for Acute Pain." Academic Emergency Medicine :
PUBLICATIONS IN 2019
2019 ANNUAL REPORT 97
Official Journal of the Society for Academic Emergency Medicine (2019): Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine, September 14, 2019. Web.
27. Bond, Christopher, Justin Morgenstern, Corey Heitz, and William K Milne. "Hot Off the Press: Please Stop, Prescribing - Antibiotics for Viral Acute Respiratory Infections." Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine (2019): Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine, September 4, 2019. Web.
28. Johnston, Aaron, Kylie Booth, Jim Christenson, David Fu, Shirley Lee, Yasmine Mawji, Doug Myhre, Etienne Van Der Linde, and Eddy Lang. "Building and Strengthening Relationships between Academic Departments/divisions of Emergency Medicine and Rural and Regional Emergency Departments." CJEM 21.5 (2019): 595-99. Web.
29. Collier, Amanda, Gregory Marton, Shannon Chun, Cheri Nijssen-Jordan, Susan A Bartels, Simon Pulfrey, Eddy Lang, et al. "CAEP 2018 Academic Symposium: Recommendations for Developing and Supporting Global Emergency Medicine in Canadian Academic Emergency Departments and Divisions." CJEM 21.5 (2019): 600-06. Web.
30. Bond, Christopher, Justin Morgenstern, Corey Heitz, and William K Milne. "Hot Off the Press: Chemical Versus Electrical Cardioversion for Atrial Fibrillation." Academic Emergency Medicine: Official Journal of the Society for Academic Emergency Medicine (2019): Academic Emergency Medicine: Official Journal of the Society for Academic Emergency Medicine, October 18, 2019. Web.
31. Bond, Christopher, et al. "Hot Off the Press: She Works Hard for the Money—Time's Up in Health Care." Academic Emergency Medicine 26.10 (2019): 1177-180. Web.
32. Dowling S, Hair H, Boudreau D, Grigat D, Rice C, Born KB, VandenBerg S. A Patient-focused Information Design Intervention to Support the Minor Traumatic Brain Injuries (mTBI) Choosing Wisely Canada Recommendation. Cureus. 2019 Oct 9;11(10):e5877. doi: 10.7759/cureus.5877. PMID: 31763100; PMCID: PMC6834108.
33. Simon Berthelot, Eddy S. Lang, et al. "Canadian In-hospital Mortality for Patients with Emergency-sensitive Conditions: A Retrospective Cohort Study." BMC Emergency Medicine 19.1 (2019): 1-9. Web.
34. Morgenstern, Justin, Corey Heitz, Chris Bond, et al. "Hot Off the Press: The Effect of Financial Incentives on Patient Decisions to Undergo Low-value Head CT Scans." Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine (2019): Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine, November 14, 2019. Web.
35. Packer, Nicholas, Miles Hunter, and Shawn Dowling. "Does the Tonicity or Rate of Intravenous Fluid Infusion Affect Neurologic Outcomes in Children with Diabetic Ketoacidosis?" CJEM 21.6 (2019): 710-12. Web.
36. Cheng, Amy H Y, Sam Campbell, Lucas B Chartier, Shawn Dowling, et al "Choosing Wisely Canada's Emergency Medicine Recommendations: Time for a Revision." CJEM 21.6 (2019): 717-20. Web.
37. James E. Andruchow, M., Timothy Boyne, Grant Innes, Shabnam Vatanpour, Isolde Seiden-Long, Dongmei Wang, Eddy Lang, and Andrew D. Mcrae. "Low High-Sensitivity Troponin Thresholds Identify Low-Risk Patients With Chest Pain Unlikely to Benefit From Further Risk Stratification." CJC Open 1.6 (2019): 289-96. Web.
38. Soar J, Lang E, et al. "2019 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support;
PUBLICATIONS IN 2019
2019 ANNUAL REPORT 98
Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task..." Circulation 140.24 (2019): E826-880. Web.
39. Chan, Kenneth, and Eddy Lang. "In Pregnant Women, the Pregnancy-adapted YEARS Algorithm Ruled out PE, with a Low Rate of VTE at 3 Months." Annals of Internal Medicine 171.4 (2019): JC19. Web.
40. McRae AD, Andruchow JE et al. CJEM Debate: #TropandGo—Negative high-sensitivity troponin test is safe as a final test for most emergency departments patients with chest pain. Can J Emerg Med. 2019; in press.
41. Thiruganasambandamoorthy V, Sivilotti MLA, Rowe B, McRae A, et al. "Prevalence of Pulmonary Embolism Among Emergency Department Patients With Syncope: A Multicenter Prospective Cohort Study." Annals of Emergency Medicine 73.5 (2019): 500-10. Web.
42. Thiruganasambandamoorthy, Sivilotti, McRae, et al. "Duration of Electrocardiographic Monitoring of Emergency Department Patients With Syncope." Circulation 139.11 (2019): 1396-406. Web.
43. McRae A, Graham M, Abedin T, Ji Y, Yang H, Wang D, Southern D, Andruchow J, Lang E, Innes G, et al. "Sex-specific, High-sensitivity Cardiac Troponin T Cut-off Concentrations for Ruling out Acute Myocardial Infarction with a Single Measurement." CJEM : Journal of the Canadian Association of Emergency Physicians 21.1 (2019): 26-33. Web.
44. Kavsak, McRae, et al. "A Multicenter Assessment of the Sensitivity and Specificity for a Single High-Sensitivity Cardiac
Troponin Test at Emergency Department Presentation for Hospital Admission." The Journal of Applied Laboratory Medicine 4.2 (2019): 170-79. Web.
45. Stiell, Ian G, M Sean Mcmurtry, Andrew Mcrae, et al. "The Canadian Cardiovascular Society 2018 Guideline Update for Atrial Fibrillation - A Different Perspective." CJEM 21.5 (2019): 572-575. Web.
46. Stiell, Ian G, M Sean McMurtry, Andrew McRae, et al. "Safe Cardioversion for Patients With Acute-Onset Atrial Fibrillation and Flutter: Practical Concerns and Considerations." The Canadian Journal of Cardiology 35.10 (2019): 1296-300. Web.
47. Lucyk S. Decontamination Principles: Prevention of Dermal, Ophthalmic, and Inhalational Absorption. In: Nelson LS,
Howland MA, Lewin N, Smith S, Goldfrank L, Hoffman R, editors. Goldfrank’s Toxicologic Emergencies, 11e. New York: McGraw-Hill Education; 2019.
48. Perry, Birnie, Macle, Vadeboncoeur, Thiruganasambandamoorthy, Borgundvaag, Brison, Hohl, McRae. et al.. "PL02: A Randomized, Controlled Comparison of Electrical versus Pharmacological Cardioversion for Emergency Department Patients with Recent-onset Atrial Fibrillation." CJEM : Journal of the Canadian Association of Emergency Physicians 21.S1 (2019): S5. Web.
49. Patocka, Catherine, et all. "A Randomized Education Trial of Spaced versus Massed Instruction to Improve Acquisition and Retention of Paediatric Resuscitation Skills in Emergency Medical Service (EMS) Providers." Resuscitation 141 (2019): 73-80. Web.
50. Scheuermeyer FX, Norena M, Innes G et al. "Decision Aid for Early Identification of Acute Underlying Illness in Emergency Department Patients with Atrial Fibrillation or Flutter." CJEM (2019): 1-8. Web.
51. Innes, Grant D. "Can a HEART Pathway Improve Safety and Diagnostic Efficiency for Patients With Chest Pain?" Annals of Emergency Medicine 74.2 (2019): 181-84. Web.
PUBLICATIONS IN 2019
2019 ANNUAL REPORT 99
52. Innes, Grant, et al. "CJEM Debate Series: #HallwayMedicine - Our Responsibility to Assess Patients Is Not Limited to
Those in Beds; Emergency Physicians Must Assess Patients in the Hallway and the Waiting Room When Traditional Bed Spaces Are Unavailable." CJEM 21.5 (2019): 580-86. Web.
53. Helman A, Ovens H, Campbell S, Innes GD. Episode 129 ED Overcrowding and Access Block – Causes and Solutions.
Emergency Medicine Cases. September, 2019. https://emergencymedicinecases.com/ed-overcrowding-access-block-causes-solutions. Accessed [August 19,2019]
54. Campbell, Samuel G, Grant D Innes, Kirk D Magee, Manal O Elnenaei, and Brian H Rowe. "A Five-step Program for Diagnostic Test Addiction." CJEM 21.5 (2019): 576-79. Web.
55. Innes, Grant D, et al. "Emergency Overcrowding and Access Block: A Smaller Problem than We Think." CJEM 21.2 (2019): 177-185. Web.
56. Stewart D, Lang E, Wang D, Innes G. Are emergency medical services offload delay patients at increased risk of adverse outcomes? CJEM. Cambridge University Press; 2019;21(4):505–12.
57. Scheuermeyer, Frank X, Hubert Wong, Tyler W Barrett, Jim Christenson, Eric Grafstein, Brian Grunau, Matt Wiens, and Grant Innes. "Active Management of Atrial Fibrillation or Flutter in Emergency Department Patients with Renal Impairment Is Associated with a Higher Risk of Adverse Events and Treatment Failure." CJEM 21.3 (2019): 352-60. Web.
58. Scheuermeyer, Frank X, Innes, Grant, Grafstein, Eric, Chard, Ryan, Vandenberg, Stephanie, et al. "Emergency Department Patients With a Prolonged Corrected QT Interval Do Not Have Increased Thirty-day Mortality." Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine 26.7 (2019): 818-22. Web.
59. Yeung, Matthew, Christina Schweitzer, Dongmei Wang, Colin Weaver, and Eddy Lang. "Orthomageddon: A Retrospective Cohort Study of Weather-dependent Variations in Emergency Department Volume in a Canadian City." The American Journal of Emergency Medicine (2019): The American Journal of Emergency Medicine, 11 December 2019. Web.
60. Samuel, Susan, Gina Dimitropoulos, Kyleigh Schraeder, Scott Klarenbach, Alberto Nettel-Aguirre, Greg Guilcher, Daniele Pacaud, Jorge Pinzon, Eddy Lang, et al. "Pragmatic Trial Evaluating the Effectiveness of a Patient Navigator to Decrease Emergency Room Utilisation in Transition Age Youth with Chronic Conditions: The Transition Navigator Trial Protocol." BMJ Open 9.12 (2019): E034309. Web.
61. Patrick M, Holroyd B, and Eddy Lang. "Emergency Strategic Clinical Network: Advancing Emergency Care in Alberta through Collaborative Evidence-informed Approaches." CMAJ : Canadian Medical Association Journal = Journal De L'Association Medicale Canadienne 191.Suppl (2019): S24-S26. Web.
62. Murad, M Hassan, Robert I Liem, Eddy S Lang, et al.. "2019 Sickle Cell Disease Guidelines by the American Society of Hematology: Methodology, Challenges, and Innovations." Blood Advances 3.23 (2019): 3945-950. Web.
63. Arora, Nikita, Clarissa Hjalmarsson, Eddy Lang, et al. "CJEM Debate Series: #DomesticViolence - We Should Routinely Screen for Domestic Violence (intimate Partner Violence) in the Emergency Department." CJEM 21.6 (2019): 701-05. Web.

PUBLICATIONS IN 2019
2019 ANNUAL REPORT 100
64. Geocadin, Callaway, Fink, Golan, Greer, Ko, Lang, et al. "Standards for Studies of Neurological Prognostication in Comatose Survivors of Cardiac Arrest: A Scientific Statement From the American Heart Association." Circulation 140.9 (2019): E517-542. Web.
65. Optimal Strategies for the Diagnosis of Acute Pulmonary Embolism: A Health Technology Assessment [Internet].
Sinclair A, Peprah K, Quay T, McInnis M, Lang E, et al. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2018 Jan. PMID: 30896896
66. Klil-Drori, Adi J., Dwip Prajapati, Zhiying Liang, Meng Wang, Dominique Toupin, Latifah Alothman, Eddy Lang, et al. "External Validation of ASPECT (Algorithm for Suspected Pulmonary Embolism Confirmation and Treatment)." Medical Care 57.8 (2019): E47-52. Web.

ABSTRACTS IN 2019
2019 ANNUAL REPORT 101
1. Innes GD, Grafstein E, McRae A, et al. Which patients with acute ureteral colic should have early intervention, Presented at the University of Calgary Emergency Medicine Research Day, April 2019.
2. Innes GD. Recent research into the emergency care of patients with acute renal colic, at Alberta Strategic Clinical Network Quality Improvement Forum, Red Deer, AB. February 28.
3. Innes GD, McRae A, Lang E, Wang D, Andruchow J. Predictors of appropriate hospitalization in elderly patients presenting to the ED. Can J Emerg Med 2019; 21 (Suppl 1): S12-13
4. Innes GD, Grafstein E, McRae A, et al. Which patients with acute ureteral colic should have early intervention? Can J Emerg Med 2019; 21 (Suppl 1): S15-16
5. Innes GD, Grafstein E, McRae A, et al. Does early intervention improve outcomes for patients with acute ureteral colic? Can J Emerg Med 2019; 21 (Suppl 1): S45-46
6. McRae A, Innes GD, Schull M, Lang E, et al. Association between ED Crowding Metrics and 72-hour Emergency Department Revisits. Can J Emerg Med 2019; 21 (Suppl 1): S1
7. Stackhouse S, Innes GD, Grafstein, E. Does triage assignment correlate with outcomes for ED patients with chest pain. Can J Emerg Med 2019; 21 (Suppl 1): S37
8. Johnston L, Innes GD. Significance of asymptomatic oxygen desaturation in elderly ED patients. Can J Emerg Med 2019; 21 (Suppl 1): S87
9. Hayward J, Innes GD. Unexplained variation in “to-go” opioid dispensing across emergency departments in a large Canadian cohort. Can J Emerg Med 2019; 21 (Suppl 1): S17
10. McRae A, Vatanpour S, Ma J, Lang E, Innes GD, et al. Development and diagnostic performance of a kidney function adjustment score for a single high-sensitivity cardiac Troponin T measurement in emergency department patients with chest pain. Can J Emerg Med 2019; 21(Suppl 1): S6-7
11. Podcast. EM Cases Episode 128 Low Risk Chest Pain and High Sensitivity Troponin – A Paradigm Shift. July. 2019. Emergency Medicine Cases Audio Eddy Lang Program.Pdcast downloaded 49,076 times worldwide. https://emergencymedicinecases.com/low-risk-chest-pain-high-sensitivity-troponin/
12. Hari B, Palmer N, Johnston A “Using Banff as a Model to Develop Simulation Programs in Rural and Regional Settings A Descriptive Study” 2019 Family Medicine Forum, Vancouver BC
13. Johnston A.T, Varughese J “Change Management in Family Medicine Education” Peer reviewed oral presentation, 2019 Family Medicine Forum, Vancouver BC
14. Penner K, Johnston AT “Simulation [RM1] of a successful rural faculty development event” 2019 Peer reviewed oral presentation, Rural and Remote Medicine Conference Halifax, NS
15. Charina I, Johnston AT “Greg’s Wings workshop facilitator” 2019 Cabin Fever Conference. Banff, AB 16. Johnston AT, Wyman R, Fowler N “From Enhanced Skills to Enhanced Competence: Triple C and Enhanced Skills Residency Training”
2018 Family Medicine Forum Toronto, ON 17. Johnston AT, Graves L, Eyre A, Wong E, Antao V, Bethune C, Oandasan I “Building Leadership Skills in Family Medicine Educators:
One-day Workshop” 2019 Family Medicine Forum, Toronto, ON 18. CAEP 2018/19 Grant Competition titled Does a 72-hour re-admission alert notification foster physician reflection? A mixed methods
realist evaluation Catherine Patocka 2019 19. VandenBerg, S “Community Based Naloxone Kits: Using design methods to transform complex user needs into innovative community
partner project” Academy for Design Innovation Management Conference 2019 June 20, 2019 London, United Kingdom 20. Vipond J, “MD advocacy on climate change”; “Practical MD Advocacy”; ““Evidence-based Analgesia” The 27th Annual Rural and
Remote Medicine Course April 4/5, 2091, Halifax, NS 21. Vipond J, “MD advocacy on climate Change” Anaesthesia Resident Rounds July 4, 2019 Calgary 22. Vipond J, Sullivan B. Citizen Climate Advocacy”. Campus Alberta Student Conference on Health Oct 5, 2019 Edmonton 23. Vipond J, Urgent Care Pearls: “Evidence-based Analgesia” Fam Med Symposium Nov 28, 2019, Calgary 24. Vipond J, “MD Advocacy on Climate Change” O'Brien Institute for Public Health Seminar Series Dec 6, 2019, Calgary 25. Al Fawaz S, Al Deeb M, Huffman JL, Kholaif NA, Garlich F, Chuang R. A Case of Status Epilepticus and Transient Stress Cardiomyopathy
Associated with Smoking the Synthetic Psychoactive Cannabinoid, UR-144, Am J Case Rep. Dec 20, 2019. 26. Geocadin RG, Callaway CW, Fink EL, Golan E, Greer DM, Ko NU, Lang E, Licht DJ, Marino BS, McNair ND, Peberdy MA, Perman SM,
Sims DB, Soar J, Sandroni C. Standards for Studies of Neurological Prognostication in Comatose Survivors of Cardiac Arrest: A Scientific Statement From the American Heart Association. Circulation. 2019 Aug 27;140(9):e517-e542. doi: 10.1161/CIR.0000000000000702. Epub 2019 Jul 11.

ABSTRACTS IN 2019
2019 ANNUAL REPORT 102
27. Lefebvre, Dennis, Kathryn Dong, Erica Dance, Rhonda Rosychuk, Mark Yarema, Danielle Blouin, Jennifer Williams, and Brian Rowe.
"Resident Physician Wellness Curriculum: A Study of Efficacy and Satisfaction." Cureus 11.8 (2019): E5314. Web. 28. Mullins, Michael E, Mark C Yarema, Marco L A Sivilotti, Margaret Thompson, Michael C Beuhler, D Adam Algren, and Christopher P
Holstege. "Comment on "transition to Two-bag Intravenous Acetylcysteine for Acetaminophen Overdose"." Clinical Toxicology (Philadelphia, Pa.) (2019): 1-3. Web.
29. Mutsaers, Adam, Jason P Green, Marco L. A Sivilotti, Mark C Yarema, Dylan Tucker, David W Johnson, Daniel A Spyker, and Barry H Rumack. "Changing Nomogram Risk Zone Classification with Serial Testing after Acute Acetaminophen Overdose: A Retrospective Database Analysis." Clinical Toxicology 57.6 (2019): 380-86. Web.
30. Al Fawaz, Sarah, Mohammad Al Deeb, James L Huffman, Naji A Al Kholaif, Fiona Garlich, and Ryan Chuang. "A Case of Status Epilepticus and Transient Stress Cardiomyopathy Associated with Smoking the Synthetic Psychoactive Cannabinoid, UR-144." The American Journal of Case Reports 20 (2019): 1902-906. Web.
31. Avery-Cooper, Geordon, and Scott Seadon. "Does Bag-mask Ventilation between Induction and Laryngoscopy Reduce the Incidence of Hypoxemia during Intubation of Critically Ill Patients?" CJEM 21.6 (2019): 713-14. Web.
32. Colmers-Gray, Isabelle N., Keeth Krishnan, Teresa M. Chan, N. Seth Trueger, Michael Paddock, Andrew Grock, Fareen Zaver, and Brent Thoma. "The Revised METRIQ Score: A Quality Evaluation Tool for Online Educational Resources." AEM Education and Training 3.4 (2019): 387-92. Web.
33. Thoma, Brent, Alison Turnquist, Fareen Zaver, Andrew K Hall, and Teresa M Chan. "Communication, Learning and Assessment: Exploring the Dimensions of the Digital Learning Environment." Medical Teacher 41.4 (2019): 385-90. Web.
Copyright © 2022 FDOKUMEN




















