
yalemedicine - Yale School of Medicine
52
Keeping up with Dr. Spock 12 Snails, parasites and progress 18 Yale training pays off at sea 4 summer 2005 y ale m edicine Spreading the gospel How Yale faculty teamed up with the federal government, a local hospital, community groups and churches to improve health in New Haven and the Naugatuck Valley. 24
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of yalemedicine - Yale School of Medicine
Keeping up withDr. Spock
12
Snails, parasites and progress
18
Yale training paysoff at sea
4
summer 2005
yalemedicine
Spreading the gospelHow Yale faculty teamed up with the federalgovernment, a local hospital, community groups and churches to improve health in New Haven and the Naugatuck Valley.
24


s u m m e r 2 0 0 5CO N T E N T S
yale medicine
on the coverThe Rev. Audrey Tinsley is the pastor of the Pentecostal AssemblyChurch of Deliverance in NewHaven, a community health advisorand a diabetic. All these aspects of her life come together in one ofthe projects of the Yale-GriffinPrevention Research Center, whichis working to reduce diabetesamong African-Americans.
backgroundLow-fat cooking is key to preventingand managing diabetes, one ofthe messages from the PreventionResearch Center.
Photographs by Gale Zucker
On the Web yalemedicine.yale.eduOn our website, readers can submit class notes or a change of address,check the alumni events calendar, arrange for a lifelong Yale e-mail aliasthrough the virtual Yale Station and search our electronic archive.
2 Letters4 Chronicle8 Rounds
10 Findings12 Books & Ideas16 Capsule
18 The silent scourge of development”More than two decades ago Yale public health experts warned that dams along the Senegal River would bring disease.A Yale medical student’s research finds their predictions have come true. A letter from Senegal.By Kohar Jones, m.d. ’05
24 Promoting health, from the ground upPart of a national effort to create community health partnerships,a Yale center is working with New Haven churches to preventdiabetes and with suburban school nurses to stop teen smoking.The goal? Healthier communities invested in their own outcomes.By Jennifer Kaylin
31 Essay32 Faculty34 Students42 Alumni47 In Memoriam48 Follow-Up48 Archives49 End Note
“

yale
med
icin
esu
mm
er20
052 letters
yale medicineAlumni Bulletin of the Yale University School of MedicineSummer 2005, Volume 39, No. 3
Editor in ChiefMichael Kashgarian, m.d. ’58, hs ’63Professor of Pathology and Molecular,Cellular and Developmental Biology
EditorMichael FitzsousaDirector of Publications
Managing EditorJohn Curtis
Contributing EditorsJanet Emanuel, ph.d.Peter FarleyJennifer KaylinSharon McManusKaren PeartCathy ShufroJacqueline WeaverMarc Wortman, ph.d.
ContributorsTerry DagradiJohn DillonNora Groce, ph.d.Rhea HirshmanKohar Jones, m.d.Alla KatsnelsonJill MaxPat McCaffreyColleen Shaddox
Copy EditingAnne Sommer
Office Manager/Editorial AssistantClaire M. Bessinger
Senior Administrative Assistant/Website CoordinatorCheryl R. Violante
DesignDaphne Geismar
PrintingThe Lane Press
Yale Medicine is distributed to alumni,faculty, students and friends of the School of Medicine, as well as leaders in Yale University alumni activities.
Abbreviations commonly used in YaleMedicine include hs to denote the finalyear of residency for house staff, fw forthe final year of a fellowship, eph for theDepartment of Epidemiology and PublicHealth and School of Public Health andynhh for Yale-New Haven Hospital.
Postal permit held by Yale University,155 Whitney Ave., New Haven, CT 06520
Copyright © 2005Yale University School of MedicineAll rights reserved.
address correspondence to Editor, Yale MedicineP.O. Box 7612New Haven, CT 06519-0612Telephone: 203-785-5824Facsimile: 203-785-4327Electronic mail: [email protected]: http://yalemedicine.yale.edu
how to reach usYale Medicine welcomes news andcommentary. Please send lettersto the editor (250 words or less)and news items to Yale Medicine,P.O. Box 7612, New Haven, CT 06519-0612, or via electronicmail to [email protected], andinclude a daytime telephone num-ber. Submissions may be editedfor length, style and content.
visit us on the webyalemedicine.yale.edu
Well-rested residentsmake fewer mistakes“Recreating the Residency” byPeter Farley [Fall/Winter 2004]contains a large amount ofpalaver garnered from second-ary sources. The grand juryfound insufficient evidence toreturn an indictment of murderagainst the attending physician.Instead they indicted the systemof graduate medical education.
Ms. Zion did not die from an overdose of cocaine. She diedfrom hyperpyrexia—her lastrecorded temperature was 108degrees.
The Accreditation Council forGraduate Medical Educationrules governing residents’ workhours are based on New Yorkstate regulations enacted in1989. Yale will find, as have manyprograms in New York state, thateliminating sleep deprivationand chronic fatigue will improvethe physical and mental healthof young doctors and reducemedical errors in patient care.Bertrand M. Bell, m.d.,Distinguished University Professor,Professor of Medicine, AlbertEinstein College of Medicine ofYeshiva University
The writer was chair of the com-mission now known as the Bell Commission, formed by NewYork state health commissioner David Axelrod, m.d., after LibbyZion’s death to investigate issues surrounding patient care and the training of physicians in NewYork hospitals.
The cause of Libby Zion’s deathremains a subject of debate, andindeed, no consensus emergedamong investigating agencies asto what went wrong. A jury in acivil trial split the blame for herdeath between Cornell MedicalCenter’s New York Hospital andZion herself. An autopsy foundtraces of cocaine in her nasalpassages, but subsequent teststurned out negative. A grand juryblamed the death on inadequatecare and numerous mistakes,including a mishandled diagno-sis, made by unsupervisedinterns and residents. —Eds.
Zaccagnino to retire as ceo of ynhhAs this issue of Yale Medicinewas being prepared, Joseph A.Zaccagnino, m.p.h. ’70, presidentand ceo of Yale-New HavenHospital (ynhh) and the YaleNew Haven Health System since1991, announced his retirementafter 35 years at the hospital. Hewill retire effective September 30.
“My decision to retire wasnot an easy one, but it wasmade with the recognition thatas time passes, the opportuni-ties for new experiences andchallenges as well as the flexi-bility to spend more time with family cannot be deferredindefinitely,” Zaccagnino said in a statement at the end ofMay. “I plan to continue toactively serve in the health care sector as an advisor to senior management and gov-erning boards, by lecturing atthe graduate level more fre-quently than has been possiblerecently and by serving on additional corporate boards.”
Zaccagnino began workingat the hospital in 1970 under thementorship of John D. Thompson,r.n., m.s., professor and direc-tor of the Program in HospitalAdministration at the School ofPublic Health. By 1978, when hewas 32, Zaccagnino had becomeexecutive vice president andchief operating officer of ynhh.
Over the next 27 years,under Zaccagnino’s leadership,the medical school’s primaryteaching hospital grew into ahealth care system that oper-ates three hospitals in Connecti-cut, has annual revenues of $1.5billion, has 1,500 acute care bedsand serves one out of every fivehospitalized patients in the state.At ynhh Zaccagnino also over-saw construction of the Children’sHospital and the renovation ofadult patient care areas.
A search committee repre-senting both the hospital andthe health system is already at work seeking a successor, anda new ceo is expected to benamed this summer.

3from the editor
S E CO N D O P I N I O N BY S I D N EY H A R R I S
Small answers to big questions
They say an ounce of prevention is worth a pound of cure,but changing unhealthy behaviors is not always a simplematter—as anyone who has tried to stop smoking or loseweight can tell you. It’s that much more complicated whenthe goal is encouraging healthy choices for an entire com-munity. The public health work of the Yale-Griffin Preven-tion Research Center, described by Jennifer Kaylin in thisissue’s cover story (“Promoting Health, From the GroundUp,” page 24), is even more ambitious in that its goal is tohelp not just one community but a half-dozen New Haven-area towns. When you consider that Yale-Griffin is one of 28 such centers across the United States, you get a true ideaof the scale and scope of the undertaking.
Nonetheless, the guiding principles of the projects arethat the solutions to some national public health challengesare local, rather than global or grandiose, and that people willsolve their own problems when aided by solid informationderived from careful research. The community-academic part-nership has already produced results: close to half the subur-ban high school students enrolled in the center’s smokingcessation program quit cigarettes, and in New Haven a dozenchurches have educated their parishioners about diabetes prevention through a partnership with Yale-Griffin.
The other feature article this summer (“The SilentScourge of Development,” page 18) looks at a public healthcrisis in Africa that evolved predictably but without restraint
over several decades and has affected hundreds of thousandsof people. Here, too, the prevention of disease—in this caseschistosomiasis spread by freshwater snails in the SenegalRiver—was a key goal championed by Yale researchers hiredin the 1970s to evaluate the public health impact of damconstruction. Unfortunately, their recommendations wereignored. Kohar Jones, m.d. ’05, who wrote her medicalschool thesis on this topic after several trips to Senegal, doesa skillful job of describing the economic and cultural back-drop to the crisis and telling a story that connects severalgenerations of Yale scholars.
On a sad note, we received the news that the formermanaging editor of Yale Medicine, Marjorie B. Noyes, died onMay 7. A 1953 graduate of the School of Art and Architecture,Noyes kept the magazine on the mark and on schedule from1971 to 1986, according to former Editor and Deputy DeanArthur Ebbert Jr., m.d., now a professor emeritus of medicine.“She was a very careful, very meticulous editor,” says Ebbert.“We would discuss what we wanted to put in each issue, andthen she made sure it all got done.” Noyes’ history of NewHaven industry, co-edited with Preston Maynard, was pub-lished in January. This issue of Yale Medicine is dedicated toher memory.
Michael [email protected]

Yale trauma trainingpreps Navy corpsmen In two-day workshops at Yale theNavy’s independent duty corpsmenlearn the basics of trauma care.
When the Navy submarine uss SanFrancisco struck an uncharted, under-sea mountain in early January, respon-sibility for the dozens of injured sailors fell to James H. Akin, the ves-sel’s medical corpsman. For 22 hours,Akin triaged the wounded—whoseinjuries ranged from bruises andpulled muscles to a fatal blow to thehead—and put sailors and officers to work cleaning and irrigating lacera-tions until he could suture them.
As he stitched up the wounded,Akin’s main concern was machinist’smate Joseph A. Ashley, who had struck his head during the impact.Akin immoblilized Ashley, checked his airway, breathing and circulation,and inserted an IV. He showed other
4 chronicle news from cedar streetya
lem
edic
ine
sum
mer
2005
During their yearlong medical training,the Navy’s independent duty corpsmenspend two days at Yale, where they learnthe basics of trauma care. Among the Yale faculty teaching the corpsmen wastrauma surgeon Lewis Kaplan.
joh
n c
urt
is (
2)
sailors how to monitor Ashley’s airwaywhile he tended to other patients. Asrescue vessels approached the strickensubmarine, Navy doctors on ships andbases around the Pacific advised themedical corpsman by radio. But whenthe rescuers arrived, heavy seas madeevacuations impossible. Ashley ulti-mately died of his injuries.
In March, Akin received a Meritori-ous Service Medal for his performanceduring the crisis. And he credited his ability to handle the medical emer-gency to the trauma training hereceived at Yale, under the direction of Reuven Rabinovici, m.d., professorof surgery and chief of the Section of Trauma, Surgical Critical Care andSurgical Emergencies.
For the past several years, Rabinovicihas directed a course in the basics oftrauma treatment for the Navy’s inde-pendent duty corpsmen, or idcs, givenby trauma surgeons at Yale. It’s part ofthe 56 weeks of training the corpsmenreceive before they’re assigned to sub-
marine duty and the care of crews ofbetween 130 and 170 men.
“Their scope of practice is very narrow—primary care medicine foradult males, 20 to 45 years old,” said Lt. Donald Harris, pa-c, clinicalprogram manager at the Naval Opera-tional Medicine Institute Detach-ment. The detachment is stationed 50 miles east of New Haven at the NavalUndersea Medical Institute (numi) at the Naval submarine base in Groton,Conn. (In May the base appeared on a Pentagon list of military facilities tobe considered for closing.)
In addition to medical duties, theidc monitors shipmates for exposureto radiation, practices preventive medicine and is responsible for envi-ronmental and occupational health.Corpsmen are also responsible for the mental health of the crew, not anunlikely concern in a cramped, self-contained environment that recycles its own air, converts sea water into drinking water and can stay under-water for as long as food supplieslast—up to 65 days.
“They’re the doctor, nurse, chaplainand psychologist,” said Capt. Paul C.Kelleher, m.d., director of education atnumi. Their emergency medical sup-plies and equipment, Kelleher said,roughly correspond to what is availableon a paramedic’s ambulance. And their

5
training at Yale covers different kindsof trauma, including blunt injuries as well as gunshot and stab wounds. One classroom scenario involves awounded Navy seal coming on boardfor emergency treatment.
The sessions at Yale began threeyears ago when numi sought toenhance trauma training. Yale’s in-house program that teaches resi-dents advanced trauma life supportwas adapted for idcs. “This program is less than what the doctor needs, but it’s what the idcs need,” saidHarris. As the first line of care, idcslearn how to stabilize patients untilthey can be evacuated to definitivemedical facilities.
The training starts with classroomsessions that cover the initial evalu-ation and resuscitation of a traumapatient. Then corpsmen move on to ananimal lab to practice basic surgicaltechniques such as intravenous access,chest tube placement, opening a surgical airway and emergency ampu-tations. “They are all basic lifesaving procedures that the idc may need toperform on board,” said Rabinovici.
The next day the idcs attend inter-active sessions with Yale trauma surgeons who pose real-life scenarios—such as a stab wound in the neck—and expect the idcs to describe theappropriate treatment. The idcs also rotate through clinical electives in surgery and anesthesia at Yale-New Haven Hospital.
The training made a difference forAkin when the uss San Francisco collided with the uncharted mountain350 miles southeast of its base inGuam. According to Harris, the pro-gram manager in Groton, “he feltconfident in his knowledge and man-agement of the injuries to his crewbecause of the trauma training hereceived” from Yale surgeons.
Rabinovici said he was glad to learnthat the training had paid off. “It is notthat we said we could help—indeed, wedid help. I feel very good about that.”
—John Curtis
Drugmaker invests in New Haven facility and joint projects at Yale
Like many enterprises with interna-tional reach, Pfizer makes its corporatehome in New York. But the companyhas deep roots in southeastern Connect-icut, having built what was then theworld’s largest manufacturing plant forantibiotics in Groton in 1946. Today,more than 6,000 Pfizer scientists andpersonnel work in drug discovery inGroton and at the company’s GlobalResearch and Development headquar-ters in nearby New London.
With the April opening of the $35million New Haven Clinical ResearchUnit (cru), a 50-bed dedicated facilityfor Phase I drug trials, Pfizer furtherstrengthened its ties to Connecticutand added new luster to a three-year-old research alliance with Yale.
At the cru, volunteers will partici-pate in trials of potential medicinesthat have cleared several years of safetystudies in the laboratory. Pfizer willcollaborate with bioimaging experts atthe School of Medicine, who will usepositron emission tomography (pet)and other technologies to track theaction of drugs in the human body,especially in the brain.
Diane K. Jorkasky, m.d., Pfizer’svice president of clinical pharma-cology, said that the ability to draw onthe expertise of Yale scientists figuredheavily in the company’s decision to locate the cru in New Haven. Butthose collaborations are just one exam-ple of Pfizer’s partnerships with Yale.
In 2003, the company established a fellowship in memory of the latePatricia S. Goldman-Rakic, ph.d., a
renowned Yale neurobiologist, to sup-port a graduate student in neurosci-ence in Yale’s Combined Program inBiological and Biomedical Sciences.Through Pfizer Faculty Developmentgrants, five assistant and associate professors in the School of Medicinehave been granted up to $50,000worth of research time at the medicalschool’s Magnetic Resonance ResearchCenter. And in a new joint effort ofPfizer’s Women Leaders Network andthe medical school’s Office for Womenin Medicine, a female medical schoolfaculty member will spend 12 weeksworking alongside Pfizer researchersin Groton and New London each year.
“The relationship is one of win-win for Yale and Pfizer,” said Jorkasky,“and the biggest winners will be thepatients who will benefit from the sci-ence that the partnership explores.”
—Peter Farley

yale
med
icin
esu
mm
er20
056 chronicle
Cells culled from mouse bone marrow differentiate into blood cells.
dia
ne
krau
se
For stem cell researcher,Connecticut’s initiative offers a new avenue for progress
In her Yale laboratory in 2001, Diane S.Krause, m.d., ph.d., surprised the sci-entific community with her discoverythat adult stem cells taken from thebone marrow of mice can produce liver,lung, intestine and skin cells. To her dismay, her studies and similar findingshave provided ammunition to oppo-nents of embryonic stem cell research,who have used her results to argue thatresearch with stem cells derived fromhuman embryos is unnecessary.Speaking in January at a hearing of theConnecticut General Assembly, theassociate professor of laboratory medi-cine and pathology said, “To close offthis avenue of research based on theearly promise of adult stem cells is toplay the odds with people’s lives.” Shecalled upon the legislature to supportboth adult and embryonic stem cellresearch in the state.
In May the state legislature did justthat as it approved a bill to commit$100 million to embryonic stem cellresearch over 10 years. At a ceremonyin Farmington a few weeks later, with
Krause and medical school Dean RobertJ. Alpern, m.d., looking on, Gov. M.Jodi Rell signed the bill into law. Thebill’s passage is expected to boost this research at Yale and the Univer-sity of Connecticut. The legislationestablishes a two-step process in whichexperts in both science and ethicsreview requests for funding.
Unlike adult stem cells, which haveshown a limited ability to develop intoother cells, embryonic stem cells cangenerate virtually any type of cell in thebody. Biologists believe they have thepotential to help treat diseases such asdiabetes and Alzheimer’s and to repairthe spine, heart and other organs.Along with Alpern, Krause advised theGeneral Assembly as it drafted legisla-tion to make Connecticut a “safe haven”for embryonic stem cell research.
This field of study has been limitedin the United States by guidelinesestablished by President Bush thatrestrict federal funding exclusively tospecific embryonic stem cell linesestablished prior to August 9, 2001.Supporters of the research contendthat many of those pre-existing lineshave been tainted by cells from otheranimals, such as mice, and that thelimited number of lines hampersopportunities for study.
The controversial research receiveda major boost last year after Californiavoters approved $3 billion in fundingfor stem cell research over 10 years.New Jersey’s acting governor, RichardJ. Codey, announced in January thathis state would invest an additional$150 million in its stem cell institute,created in 2004 with $11.5 million instartup funding.
In her Yale office, Krause pointed toan increasingly competitive researchenvironment. “I’ve been contacted bystates that have announced funding tosee if I’d be willing to move,” she said.“Connecticut doesn’t want to lose theopportunity and researchers.”
Krause is spearheading the effort toestablish a stem cell program at Yale,and is one of more than 20 scientistsacross the university doing stem cell-related work. Recruitment of a seniorleader for the Yale program began thispast winter with an internationalsearch and will likely be followed bythe recruitment of five to seven addi-tional faculty members whose work isfocused solely on stem cell biology.
Once established, the new programwill likely have investigators perform-ing both adult and embryonic stem cellresearch, with separate laboratories for any research using embryonic celllines not approved for federal funding.“No one can predict,” Krause said,“which lines of investigation will leadto development of effective and safetreatments. We can say with 100 per-cent certainty, though, that what welearn from embryonic stem cells willbe useful for developing new thera-pies.” Although she does not currentlywork with embryonic stem cells, shesaid, “I want the freedom to useembryonic stem cells as a tool when I need to use that tool.”
—Marc Wortman

7
et cetera • • •C I R A O P E N S O F F I C E I N I N D I A
President Richard C. Levin inaugurated a newoffice for the Center for InterdisciplinaryResearch on aids (cira) in India in January.Joining him in the city of Chennai werecira’s director, Michael H. Merson, m.d., andUniversity Secretary Linda K. Lorimer, j.d. ’77.
The new office will initially administerthree projects. Project Parivartan, which issupported by a three-year grant from the Bill& Melinda Gates Foundation, will study community interventions designed to reducehiv risk among sex workers, truckers andinjection drug users.
A second project, supported by theChildren’s Investment Fund Foundation, willevaluate a model program that providesmedical, psychosocial and nutrition servicesto families with a child infected with oraffected by hiv/aids. The third project is aresearch and training program that willstudy the influence of religious and culturalfactors on the mental health and transmis-sion risk behavior of hiv-infected persons.
—John Curtis
C I S CO N T R AC T R E N E W E D
The National Cancer Institute (nci) hasrenewed a five-year, $5 million contract withthe Yale Cancer Center to operate the nci’s Cancer Information Service (cis) in NewEngland. The cancer center has operated the New England service since it was createdin 1976 to provide up-to-date cancer infor-mation to the American public. The cis part-ners with state and regional organizations to develop education efforts for people lack-ing access to cancer information and serv-ices, provide current scientific information inunderstandable language and study ways to promote healthy behaviors.
“The cis is a critical resource for theAmerican public, and we feel privileged to be able to continue to provide this service,”said Linda Mowad, r.n., program director for the cis at Yale.
The contract also includes a researchcomponent covering New England and sevenother states to help the cis educate the public about cancer and contribute to thenation’s cancer control efforts.
—J.C.
more than 30 tons of medical suppliesto hospitals overseas. “Each of thesepieces of material,whether it be a suture,a glove or a sponge, is going to wind upin another part of the world and be use-ful,” said Rosenblatt. The program hasalso saved the hospital over $30,000 in disposal costs since its inception, at a cost of about $200 per year for disinfecting and bagging the supplies.
Today, remedy trains hospitals toorganize their own programs and has helped 358 hospitals begin recov-ery activities. The organization pro-vides teaching packets free of charge,and with Yale’s Office of Interna-tional Health, has developed a noti-fication program called aire-mail, in which medical supplies donated byhospitals and vendors are advertisedvia e-mail to 125 participating non-profit humanitarian organizations. It has also developed a catalog calledremedy Atlas, consisting of the 240 supplies most often recovered, which will help ensure that recipi-ents are getting supplies they need.
Meanwhile, the collecting, sorting,packing and shipping of surplus medical supplies has largely beentaken over by students. In 2001, rysa(remedy at Yale Students Association)was started by Jonathan S. Cohen, pa ’04, who is now a pa surgical resi-dent at The Johns Hopkins Hospital.
“It’s been incredible to see all thisstuff come from what would have beenthe garbage in New Haven and end up being packaged and shipped all overthe world,” said Cohen. Between lastAugust and January, rysa volunteersshipped 3,500 pounds of supplies fromthe New Haven area to eight countries.
For rysa volunteers, long hoursorganizing medical supplies has itsrewards. “The volunteers are having a direct effect with everything that they do,” said Rosenblatt.
—Jill Max
Alumni interested in starting a local REMEDY program may contact Silvia Botero at [email protected]. ra
nd
all
eno
s
From the operating room to hospitals in need, remedyprovides surgical supplies
In 1991, after several volunteer mis-sions to Latin America, William H.Rosenblatt, m.d., hs ’90, fw ’91, pro-fessor of anesthesiology and surgery(otolaryngology) at the School ofMedicine, made an observation that was to have far-reaching effects: many of the hospitals he visited were in dire need of medical supplies, while at Yale-New Haven Hospital(ynhh) many of those same supplieswere discarded without being used.
Thus was born remedy (RecoveredMedical Equipment for the Develop-ing World), a nonprofit committed torecovering surplus medical supplies and teaching others how to do it.
What started as a local program at ynhh to collect opened but unused surgical supplies—which have never touched a patient but can’t bereprocessed due to liability concerns—has grown into a grass-roots organiza-tion involving hundreds of hospitalsaround the United States. From Yalealone, the remedy program has donated

yale
med
icin
esu
mm
er20
058 rounds medicine and health at yale
Psychiatry, the law and the death penalty For more than 30 years a Yale program has examined the interfaceof law and psychiatry.
Although death penalty decisions arealways controversial, the case of con-victed serial murderer Michael B. Rosshas proven to be one of the most com-plex legal battles seen in Connecticutin recent years. Ross, who was foundguilty of murdering six young womenin the early 1980s, was sentenced todeath 18 years ago. Since then, a seriesof appeals, hearings and overturneddecisions has involved not only thecourts but also two of Yale’s forensicpsychiatrists. Howard V. Zonana, m.d.,professor of psychiatry, interviewedRoss before his 1987 trial, and MichaelA. Norko, m.d., associate clinical pro-fessor of psychiatry, evaluated Ross in 1995, in 2004 and again in Marchwhen Ross attempted to waive his right to appeal. Norko found no evi-dence that Ross suffered from “deathrow syndrome” or that he was incom-petent to waive his right to appeal.Ross was executed on Friday, May 13.
The Ross case is one of about 1,000 consultations for court casesboth local and national that the Law and Psychiatry Division at theSchool of Medicine tackles each year. What began in 1973 as an elec-tive for residents examining the interface between law and psychiatryhas grown into a division of five units and 23 staff members thatoffers a one-year fellowship in foren-sic psychiatry, as well as courses for psychiatric residents.
“Forensic psychiatry is defined asthe use of psychiatric expertise to aid in the resolution of legal problems,and it also deals with patients in settings like prisons, where there are special needs that have to be accountedfor,” explained Zonana, who directs the division.
That definition brings forensic psy-chiatrists into the courtroom as well asthe clinic. They consult on everythingfrom insanity defenses to the termina-tion of parental rights. As part of theirtraining, law and psychiatry fellowsrotate through various settings: theywork with law students in the JeromeN. Frank Legal Services Organiza-tion, they see the victim’s perspectivethrough postings with the state’s attorney and they may work in the fed-eral public defender’s office or at theConnecticut Juvenile Training Schoolrun by the Department of Childrenand Families.
The division also contracts with thestate of Connecticut to evaluate thecompetency of defendants in the NewHaven region to stand trial—almost200 cases a year. Under close facultysupervision, residents conduct evalu-ations, write reports and testify in court.
“We try to get them to approacheach case from an objective, criticalviewpoint, which may be differentfrom the objective in clinical work,where you’re trying to establish a rap-port with the patient,” said Norko. “In forensic psychiatry that’s not neces-sarily the goal, because the outcome of your evaluation may or may not behelpful to the person.”
On a broader scale, the division frequently examines legal issues suchas a statute on the competency of
juveniles to stand trial or the legal regu-lation of psychiatry. “Psychiatry is themost legally regulated subspecialty inmedicine because of the fact that wecan detain people against their will,”explained Zonana. The division alsocreated a jail diversion project in 1995that places a clinician in the court toassess defendants charged with drug-related misdemeanors and developtreatment plans as alternatives to incar-ceration. Thanks to the success of theproject, the Connecticut legislature hassince expanded it to all lower criminalstate courts.
“It’s a very diverse program, whichI think is probably one of our biggeststrengths,” said Norko, who is the divi-sion’s deputy training director. “Theother is that we make a consciouseffort to present more than one view-point about how forensic psychiatryshould be done.”
—Jill Max
jim
fra
zier

9
et cetera • • •M O L E C U L E L I N K E D TO I M M U N E AT TAC K
A Yale scientist has found that blocking a keymolecule protects implants, pacemakers,artificial joints and other foreign biomateri-als from attack by the immune system.
“Implantation of biomaterials, devices,and tissue-engineered constructs into tissues causes the development of a foreign-body reaction that can lead to implantfailure,” said Themis R. Kyriakides, ph.d.,assistant professor of pathology and biomedical engineering, a member of the interdepartmental program in VascularBiology and Transplantation and lead authorof a study published in December in TheAmerican Journal of Pathology.
Kyriakides and his team focused on areas where tissue and implants meet andforeign body giant cells form. In studies with mice, the team genetically eliminatedthe molecule, CC chemokine ligand 2 (ccl2),or blocked its action with decoy proteins.
The success of the experiments with mice opens up the possibility of finding tar-gets for drugs to sustain implants.
—John Curtis
YA L E TO L E A D ST R O K E ST U DY
The School of Medicine will lead a $33 million trial to examine a novel approach for preventing stroke—the Insulin Resist-ance Intervention after Stroke (iris) trial.Sponsored by the National Institute ofNeurological Disorders and Stroke, the iristrial will test the effectiveness of reducinginsulin resistance with pioglitazone, com-pared with placebo, for preventing recurrentstroke and myocardial infarction amongnondiabetic stroke patients with a recentischemic stroke and insulin resistance.
“This is the first trial that will look atthe effect of this drug specifically to preventclinically significant vascular events in non-diabetic patients,” said principal investigatorWalter N. Kernan, m.d., associate professorof medicine.
Researchers at Yale designed the studyand will coordinate its conduct at more than60 research sites in the United States andCanada, recruiting more than 3,000 nondia-betic men and women over 45 who haveinsulin resistance and have had a recentischemic stroke.
—J.C.
Complex congenital heartpatients live longer, need newtreatment paradigm
“Sometime in the next decade,” saidJames C. Perry, m.d., professor of pediatrics (cardiology) and chief of theSection of Pediatric Cardiology, “therewill be, for the first time, more peopleover 18 living with congenital heartdisease than people under 18.”
Congenital heart disease (chd), the most common of birth defects,affects 0.8 percent of all live births inany given year in the United States.Thanks to advances in surgical andmedical management techniques fortreating children born with structuralabnormalities of the heart, many children for whom chd would once have been an early death sentence cannow expect to live well into adulthood.
That fact underlies the work of the Yale-New Haven Adult CongenitalHeart Program, the first of its kind inConnecticut and one of only two dozenin the country. The outpatient clinic isstaffed by Perry and coordinator NicoleK. Boramanand, a.p.r.n. ’99, and the
program provides a collaborative andmultidisciplinary approach to moni-toring and treating adult survivors ofpediatric chd. The most commonproblems experienced by these patientsare arrhythmias and heart failure.
“Pediatric heart patients in the pastwere often discharged from pediatriccare based on age, but adult cardiolo-gists are not usually trained to managecongenital heart disease. Those patientshad nowhere to go,” Perry said. “Ourprogram offers access to pediatric and adult cardiologists, heart failurespecialists, pulmonologists, transplantspecialists, specialists in high-riskobstetrics and other medical staff withessential expertise.”
Patient education is also critical.“Our focus is on preventive mainte-nance,” Boramanand said. “What treatments and lifestyle adjustmentscan increase the length and quality of life? For instance, we emphasize toour patients that the old notion that all people with adult chd should avoidexercise is no longer accepted.”
Boramanand notes that anotheraspect of education and prevention isobtaining extensive diagnostic informa-tion up front. “If we get readings earlyand track them regularly, we can see situations that may require treatment.”
Perry points out that individualswho survive into adulthood with chdalso experience the full range of healthconcerns, from catching the flu todeveloping arthritis to managing preg-nancy and childbirth, and notes thatthe center helps clinicians learn moreabout this population.
As of this spring the Yale-NewHaven Adult Congenital HeartProgram, which began in July of2004, had seen nearly 100 patientsranging in age from 17 to their late50s. “Life expectancies vary,” saidPerry, “and this is a group of patientswe are just beginning to learn about.But to see people with complex congenital heart defects going stronginto middle age is remarkable.”
—Rhea Hirshmanein
at p
eled

activated when the body mounts animmune response against commoninfections, may cause prions to replicateand spread. But no one knew how far.
Ruddle’s team was working withmouse models of inflammation in thekidneys, pancreas and liver. Her workhad shown that in chronic immunediseases, T and B cells can form out-posts outside of the immune systemthat are very similar to lymph nodes.Since prion levels are known to behigh in lymph nodes, the internationalteam hypothesized that the organizedoutposts may allow spread of prions to other organs of the body beyond thenervous and immune systems. Sureenough, the researchers reported in January in the journal Science thatwhen Ruddle’s mice were infected with prions, their inflamed kidneys,pancreases and livers carried enor-mous prion levels—as high as thosefound in diseased spleens.
“It was thought that even if a cow was infected (with bse), what wasmost important was that the brain didn’t get into the feed. But if you havea chronic infection in that animal, youneed to think about that, too,” Ruddlesaid. The work may have far-reachingimplications, such as the need forincreased monitoring of farm animals,says Ruddle. Although cattle are rou-tinely checked for fever, some inflam-matory conditions such as early formsof diabetes, she notes, would not necessarily have visible symptoms.
—Alla Katsnelson
yale
med
icin
esu
mm
er20
0510 findings from the bench
Prions found outsidenervous system Finding suggests more stringentmonitoring of farm animals may beneeded to protect the public.
Nancy H. Ruddle, ph.d. ’68, the John Rodman Paul Professor ofEpidemiology and Public Health andprofessor of immunobiology, is thefirst to admit that she’s no expert onmad cows. Her laboratory studies the human lymphoid system and howit mediates chronic infection and autoimmune diseases such as diabetesand multiple sclerosis. But Ruddle’srecent collaboration with pathologistAdriano Aguzzi, m.d., ph.d., in Swit-zerland has overturned one of the major tenets of public health efforts to curb mad cow disease.
More formally known as bovinespongiform encephalopathy (bse), mad
cow disease is caused by prions—mis-folded protein fragments that clumptogether and destroy the brain. Otheranimals, such as sheep, goats andmink, are also susceptible to prion dis-eases. In fact, researchers believe thatthe mad cow epidemic started becauseanimal feed was contaminated with the brains of sheep infected with theprion disease scrapie. In humans, contraction of the variant Creutzfeldt-Jakob Disease has been attributed toeating bse-infected beef—specifically,the animals’ brain, spinal cord andimmune system tissues such as thespleen and lymph nodes. Experts have assumed that other parts of theanimal were safe to eat.
Aguzzi, a professor of neuropathol-ogy and molecular biology at the Uni-versity of Zurich, has long been on the trail of prion diseases. In 1997 histeam showed that the immune system’s B cells, or B lymphocytes, which are

11
et cetera • • •M I C R O R N A L I N K E D TO O N CO G E N E
A Yale scientist has identified a microrna,let-7, that controls an oncogene implicated in about 20 percent of cancers, includinglung cancer. The finding, reported in Marchin the journals Cell and Developmental Cell,presents new possibilities for diagnosis andtreatment, according to Frank J. Slack, ph.d.,assistant professor of molecular, cellular and developmental biology.
Oncogenes are segments of dna thatcan induce uncontrolled cell growth and,ultimately, the formation of canceroustumors. Micrornas regulate gene expres-sion. Let-7, said Slack, stops the oncogeneknown as Ras from producing the Ras pro-tein. In the absence of let-7 rna, cells in thenematode C. elegans continued to divideinstead of differentiating normally. Let-7 inhumans, Slack said, is almost identical to the worm sequence.
Lung cancer has a poor prognosis, saidSlack, “but gene therapy with let-7 may be a way to alleviate it or slow it down.”
—John Curtis
SMOKI NG TU RNS RECEPTOR ON AN D OFF
Cigarette smoking turns on and then inacti-vates brain receptors that are critical to the effectiveness of antidepressants, accord-ing to a study published by Yale scientists in Biological Psychiatry last fall.
Finding a way to manipulate those recep-tors could make antidepressants work more quickly—most now take up to threeweeks to bring emotional relief. “This finding has implications for those patientswho are depressed to the point of being suicidal and for the 30 percent of peoplewho are not responsive to antidepressantsthat are now available,” said Marina R.Picciotto, ph.d., associate professor of psy-chiatry, pharmacology and neurobiology,and senior author of the study.
The next step, Picciotto said, will be tostudy the role of these nicotine receptors,nAChRs, in regulating behavioral and cellularresponses to antidepressants. The recep-tors may have a direct effect in mediatingresponses or they may act indirectly, bymodulating neurotransmission in other cell types.
—J.C.
Yale scientists find a genetic connection to age-related macular degeneration
Biomedical research into the geneticbasis of disease has progressed at arapid clip since the sequence of thehuman genome was announced in2000, but this past March 10 saw thescientific equivalent of a triple play.
Three research teams, includingone led by Josephine J. Hoh, ph.d.,an assistant professor in Yale’s Depart-ment of Epidemiology and PublicHealth, simultaneously announcedthat they had identified a gene variantassociated with a greatly increased risk of age-related macular degenera-
tion (amd), a progressive disease lead-ing to blindness that affects more than10 million elderly Americans.
The human genome can be thought of as a vast string of 3 billionletters in which each letter representsone of the four nucleotides that pro-vide instructions to the body’s protein-building machinery. The genome is99.8 percent identical among humans,but after every 100- to 300-letter stretchon average are single nucleotide poly-morphisms, or snps (pronounced“snips”), sites where one letter is substi-tuted for another. Scientists believe thatsnps may help explain why some peo-ple are predisposed to certain diseasesor respond differently to drug therapies.
Remarkably, all three of the teamswho published their findings in March
On this genome map of a subject with age-related macular degeneration, red and white squares represent strong matches withprobes that find gene variants.
independently zeroed in on preciselythe same snp, a spot on chromosome 1 that is home to a gene that codes foran immune system protein known ascomplement factor H (cfh). In itsusual form, cfh acts as a brake on thecomplement system, a component of the body’s innate immune response.
According to Hoh, whose groupscanned the full genomes of 96 individ-uals with AMD and those of 50 controls,those who carry two copies of the newlyidentified variant in the cfh gene arenearly 7.5 times more likely than therest of the population to develop amd.“This is only an association,” Hohemphasized. “It doesn’t really tell youthat this is the cause of the disease.”
Nonetheless, a faulty version of cfhmay indeed be a culprit in amd. Forexample, yellowish deposits at the backof the eye known as drusen, the clini-cal hallmark of amd, contain comple-ment proteins.
Hoh credits the Raymond andBeverly Sackler Fund for the Arts andSciences for making the study pos-sible. “This particular kind of study isexpensive, not the normal thing a junior faculty member can perform,”she said. “I am extremely grateful forthe support from the Sackler Family.”
Michael B. Bracken, m.p.h. ’70,ph.d. ’74, the Susan Dwight BlissProfessor of Epidemiology and Hoh’scollaborator, adds that the work repre-sents an entirely new way of doing epidemiology. “For the past 100 years,we’ve used a hypothesis-testingapproach, where hypotheses were gen-erated from animal studies or smallhuman studies and then we did largeepidemiology studies.”
By contrast, whole-genome searchesfor snps are “hypothesis-free”: “Theassociation between a gene and diseaseis established first, and the biology isdone after,” Bracken said. “This takesall that we’ve thought about doing science and turns it on its head, andit’s likely to have major payoffs in the future.”
—Peter Farley
shei
la w
estm
an

12 books & ideas bookshelfya
lem
edic
ine
sum
mer
2005
A radical notion of child rearingFollowing in the footsteps of Dr. Spock,a Yale alumnus updates the classic guide for parents.
as Spock’s views on TV: “There seems to be very little simi-larity between the world the electronic babysitter is selling to our children and the world we would like to see.”
Raised in Chicago in a household with the 1958 editionof Spock’s book on the shelf, Needlman coincidentally followed Spock’s career path. Both majored in English atYale College. Both attended medical school at Yale, althoughSpock transferred to Columbia. After training in pediatrics at Boston University, Needlman took a job at Case Westernin the same clinic where Spock had worked.
Needlman has found his own experience of the parent-child relationship endlessly interesting. He has a 16-year-olddaughter, Grace, with his wife, Carol F. Farver, m.d. ’85, asurgical pathologist he met on their first day at Yale medicalschool. As a father and a doctor, he has observed that chil-dren can be both predictable and surprising. “A wonderfulmystery of parenting is that there are some qualities thatshow a lot of continuity. You can look at a child at two andthen at 15 and say, ‘I recognize that.’ But there are a lot ofthings that you can’t recognize: the same kid who wasunhinged at five can be amazing, interested, interesting andcapable of handling things beautifully at 15.” Six monthsafter its publication by Pocket Books in June 2004, the Spock-Needlman edition of Dr. Spock’s Baby and Child Care hadsold nearly 100,000 copies. Not bad for a subversive littlebook that’s been around since 1946.
—Cathy Shufro
Bookshelf is a column focusing on matters related to books and authors at the School of Medicine. Send ideas to Cathy Shufro [email protected].
According to Robert D. Needlman, m.d. ’85, Dr. Spock’sBaby and Child Care—which has found a place on the book-shelves of 50 million parents across three generations—is “subversive.”
Benjamin M. Spock, m.d., med ’29, initiated a revolu-tion, said Needlman, with the first words of his 25-cent book,published in 1946. “Trust yourself,” Spock told parents. “You know more than you think you do.”
“Those famous lines were subversive to the doctor asexpert,” says Needlman, who revised and expanded the bookfor its eighth edition, the first revision since Spock died in 1998 at age 94. In Spock’s day, pediatricians dictated rigidschedules for sleeping and feeding and warned parents toresist the temptation to pick up fussy children for fear of spoil-ing them. Spock, in contrast, encouraged parents to discoverwhat their children needed as individuals and to foster rela-tionships of mutual affection and respect. This model of par-enting is now so unexceptional that contemporary Americansmay not appreciate how much of it originated with Spock.“We understand that it’s no longer optimal, or even appropri-ate, to dictate to people what to do,” said Needlman.
An associate professor at Case Western Reserve Univer-sity in Cleveland, Needlman incorporated his own insights in the new 992-page edition. He discusses gay and lesbianparents, how to stimulate a love of reading, how childrenrespond to disaster and how young adults react when theyleave home for college.
Needlman felt no qualms when he disagreed with Spock’srecommendations. “I changed them—it was easy,” he saidwith a laugh. For instance, he eliminated the suggestion thata woman with postpartum blues cheer herself up by buying a new outfit. Instead, he suggests exercise, renewed contactwith friends, talking to one’s partner—and seeking medicalhelp if the change of mood is severe.
The book combines the practical with the abstract, hesaid. “Some of it is very nuts-and-bolts: How do you changea diaper? A lot is philosophical: How do you raise children to be responsible citizens?” Needlman preserves Spock’sexact words in short passages labeled “Classic Spock,” such
Pediatrician Robert Needlmanspent two years revising andupdating the classic Dr. Spock’sBaby and Child Care. The eighthedition of the guide, the first revi-sion since Benjamin Spock died in 1998, was published last year.
jan
ine
ben
tive
gn
a

13book notes
Sighting Anton Pavlovichby Elizabeth Loewald, m.d., fw’77 (Hermitage Publishers) Theauthor considers Chekhov’s lifeas a doctor and writer, describ-ing how his chronic tuberculosis,interests and talents affected his character, life choices and lit-erary work.
Preventive Cardiology:A Practical Approach, 2nd ed.edited by Nathan D. Wong,m.p.h. ’85, ph.d. ’87, Henry R.Black, m.d., fw ’74, hs ’75, andJulius M. Gardin, m.d. (McGraw-Hill Professional) This updatedsource provides clinically rel-evant information about theprevention of coronary heartdisease, including risk factorsand screening guidelines.
Radiology Illustrated:Gynecologic Imagingby Seung Hyup Kim, m.d., BruceL. McClennan, m.d., professorand chair of diagnostic radiology,and Eric K. Outwater, m.d. (W.B.Saunders) Over 3,000 imagesand brief descriptions of clinicaldisorders and diseases followedby case studies demonstrate the spectrum of benign andmalignant gynecologic disordersand the optimal modality forimaging each condition.
Guide to Publishing a Scientific Paperby Ann M. Körner, ph.d. ’74(Bioscript Press) This bookexplains how to produce, submitand revise a scientific paper for publication and offers adviceabout applying for funding.
Pathology & Genetics:Tumours of the Breast andFemale Genital Organsedited by Fattaneh A. Tavassoli,m.d., professor of pathology, and Peter Devilee, ph.d. (OxfordUniversity Press) This guidedescribes the pathology andgenetics of each lesion, alongwith its epidemiology, etiology,clinical features, prognosis and predictive factors.
50 Signs of Mental Illness:A User-Friendly AlphabeticalGuide to Psychiatric Symptomsand What You Should KnowAbout Themby James W. Hicks, m.d. ’91, hs’95 (Yale University Press) Fromanger to sexual preoccupations,from cravings to obsessions,this volume describes the cluesthat may signal mental illness.Starting each topic with avignette to illustrate a symp-tom, the author considerswhether it arises from illness orconstitutes a normal responseto stress. The book outlinesavailable treatments and copingstrategies for each symptom.
Parent Management Training:Treatment for Oppositional,Aggressive, and AntisocialBehavior in Children andAdolescentsby Alan E. Kazdin, ph.d., direc-tor of the Child Study Center and the John M. Musser Professorof Psychology (Oxford UniversityPress) This manual covers thebackground, principles and theory of parent managementtraining and discusses tech-niques for treating children and adolescents who displayoppositional, aggressive andantisocial behavior.
Sharing the Land of Canaan:Human Rights and the Israeli-Palestinian Struggleby Mazin B. Qumsiyeh, ph.d.,associate professor of genetics(Pluto Press) Qumsiyeh docu-ments the core issues in theconflict between Israelis andPalestinians and articulates a road map for peace based onhuman rights and a sharedfuture rather than apartheid.
American Dreaming and Other Storiesby Doris M. Iarovici, m.d. ’92(Novello Festival Press) Theauthor explores the Americanideal of success based on self-reliance and draws upon herown immigrant childhood tocreate stories of people in tran-sition. She tells of their trials,resilience, empathy and hope.
The Breast Cancer Book:What You Need to Know toMake Informed Decisionsby Ruth H. Grobstein, m.d.,ph.d. ’57, fw ’63 (Yale Univer-sity Press) This guide provides the tools women and men facing breast cancer need tomake informed decisions.
I’m Your Father, Boy:A Family Memoir of Barbadosby Ezra E.H. Griffith, m.d., professor of psychiatry andAfrican American Studies (HatsOff Books) The author talks of father-son relationships, the cultural changes involved inmoving to New York City in 1956and the impact of moderniza-tion and globalization on hismemories of his father.
A Field Guide to North AtlanticWildlife: Mammals, Seabirds,Fish, and Other Sea Lifeby Noble S. Proctor and Patrick J.Lynch, director of the MedMediaGroup at the School of Medicine(Yale University Press) Withrange maps and text on pagesdirectly opposite full-color illus-trations, this guidebook providesconcise information that facili-tates quick identification ofmore than 200 species of wild-life on or near the Atlantic coast.
The Synaptic Organization of the Brain, 5th ed.edited by Gordon M. Shepherd,m.d., ph.d., professor of neurobiology and neuroscience(Oxford University Press) Thisbook covers new advances in the study of the neural basis ofbrain function resulting fromthe mouse and human genomeprojects, biochemical analysesand laser microscopy of den-drites. Each chapter highlightsthe principles common to allregions and the adaptationsunique to each.
Carotenoids in Health and Diseaseedited by Norman I. Krinsky,ph.d., Susan T. Mayne, ph.d.,professor of epidemiology, and Helmut Sies, ph.d. (MarcelDekker) Carotenoids such asbeta carotene and lycopene are a focus of research on therelationship between plantnutrients and human health.This reference reviews studieson the latest biochemicalresearch and reports findingsregarding the use of carot-enoids in preventing cancers and sunburn, as well as eye,heart, vascular and photo-sensitivity diseases.

yale
med
icin
esu
mm
er20
05in circulation
The descriptions above are based on information from the publishers.
send notices of new books toCheryl Violante, Yale Medicine,
P.O. Box 7612, New Haven, CT 06519-0612, or via e-mail to [email protected]
As the library enters cyberspace,patrons still arrive to read, write,research—and listen to music
14 books & ideas book notes
Medical Physiology: A Cellularand Molecular Approachby Walter F. Boron, m.d., ph.d.,professor of cellular and molecu-lar physiology, and Emile L.Boulpaep, m.d., professor of cel-lular and molecular physiology(W.B. Saunders) This textbooklinks molecular and cellularbiology to the study of humanphysiology and disease andincludes new material on hemo-stasis and fibrinolysis.
Health and the IncomeInequality Hypothesis:A Doctrine in Search of Databy Nick Eberstadt and Sally L.Satel, m.d., hs ’88, lecturer in psychiatry (AEI Press) While a number of recent studies suggest that inequality inincome—not poverty per se—is bad for people’s health, therich included, this volume offersanother view of this hypoth-esis. By controlling relevantvariables, the authors suggestthat income distribution is less a determinant of popula-tion health than the inequalityhypothesis would suggest.
Dietary Supplements andMultiple Sclerosis:A Health Professional’s Guideby Allen C. Bowling, m.d. ’88,ph.d. ’88, and Thomas M.Stewart, j.d., pa-c, m.s. (DemosMedical Publishing) Health professionals knowledgeableabout complementary and alter-native medicine can guide MSpatients away from possiblyharmful therapies and towardlow-risk, possibly effective thera-pies. The supplements selectedfor inclusion are those with spe-cific relevance to MS that arepopular among the general pub-lic or known to have seriousadverse effects.
Listening to Fear: Helping Kids Cope, from Nightmares to the Nightly Newsby Steven Marans, m.s.w., ph.d.,the Harris Associate Professor ofChild Psychoanalysis in the ChildStudy Center (Owl Books) Thistext seeks to equip readers withhands-on tools: specific wordsand actions to elicit informationand ease distress. The book isorganized by age group, frominfancy to adolescence.
Diagnostic Atlas of RenalPathologyby Agnes B. Fogo, m.d., andMichael Kashgarian, m.d. ’58, hs’63, professor of pathology andmolecular, cellular and develop-mental biology (W.B. Saunders)This new atlas covers all majorinflammatory, infectious, pre-neoplastic and neoplastic dis-eases of the kidney. More than600 illustrations help readersto recognize the pathologic fea-tures and clinical manifestationsof both common and rare renaldisorders and to formulate con-fident and accurate diagnoses.
Arthur E. Broadus, m.d., ph.d., Ensign Professor of Medicine, hesitatesto advertise his not-so-private sanctuary: Yale’s Medical HistoricalLibrary. He is hoping the crowds won’t catch on.
“I escape over here for about an hour a day when I can, becauseit’s peaceful and lovely and I can think and read, and sometimeswrite—and mostly get away from the din,” said Broadus, sectionchief in endocrinology.
Down the hall and past the rotunda, in the Information Roomof the Harvey Cushing/John Hay Whitney Medical Library, medical student Tejaswini More is studying from Robbins Pathologic Basis ofDisease while listening to Haydn through earphones. The library computers have a really good music program, says More, and she getsmore done here than in her room.
Just a few years ago, ophthalmology resident Amir Ahmadi, m.d.,would have been a more typical library visitor: he has come to look upan article. But now Ahmadi is the exception, because patterns of libraryuse have changed radically. Where annual electronic visits number inthe millions, those who walk in the door just top 500,000, a ratio of18 remote users for every person who walks in. And yet, said Director R.Kenny Marone, m.l.s., “Come in here in the afternoon, and you can’tfind a seat.”
Medical students come to use the conference rooms for studygroups, to seek guidance from a reference librarian or to borrow a laptop. Residents and students bring their personal digital assistantsto a workstation in the Information Room, where they install appli-cations such as InfoPOEMs, eMedicine and Griffith’s 5-Minute ClinicalConsult, which provide information about drugs and diagnoses.Students isolate themselves in carrels. Researchers read journals in the sun-drenched Morse Periodical Room. Downstairs, students click away in the Computer Resource Laboratory (crl), night and day.“We used to have people leave at quarter of twelve, and they were unhappy,” says Marone. “So we decided to make the crl a 24-hour facility.”
The library is also open to the general public. “They have access:It’s Yale’s way of giving back to the greater New Haven community,”said Marone. Sometimes patients or parents drop in to look up infor-mation after a visit to the doctor or hospital.
When library service assistant George Moore began working atthe library in 1978, “the furniture was dark, very heavy, very male,and there were heavy drapes on the windows. It was really a very forbidding place. Now we have carpeting, comfortable furniture,plants and better lighting. It’s warm, it’s alive. It’s a very pleasantplace to be—a livable space.”
—Cathy Shufro

15on campus
ST E V E N M I L E SSilence among doctors in the face of torture
Even as fbi agents and intelli-gence officers were warningtheir superiors that interroga-tions of detainees in Iraq andAfghanistan and at GuantanamoBay in Cuba had gone terriblywrong, military doctors andnurses remained silent. “I havereviewed 14,000 pages of docu-ments and can find only twoinstances of health care pro-fessionals trying to stop thisabuse,” said Steven H. Miles,m.d., director of the Center forBioethics at the University ofMinnesota, in a talk at medicalgrand rounds in March.
Those whose duty it was tosee to the well-being of pris-oners, he said, often failed: Theyprovided inadequate health care. They supplied confidentialmedical data to interrogatorsand oversaw coercive interroga-tions. They filed false reports tocover up torture. And they failedto report abuses.
“I think we can look at thefailure in two ways,” Miles said.“There was a policy environ-ment going down the chain ofcommand authorizing theabuse. And there was a failure of accountability going up.”
—J.C.
M A R G R É T O D D S D ÓT T I RIceland’s national health service provides for all
In Iceland, universal access tohealth care is enshrined in law.As a result the country has noprivate health insurance and theisland’s 290,000 residents relyon a national health service—state-run hospitals and primaryhealth care centers—at minimalcharge. If they see specialists in private practice, about 75 per-cent of the fees are reimbursedby the government.
Margrét Oddsdóttir, m.d., hs’92, professor and chief of sur-gery at Landspitali UniversityHospital in Reykjavik, describedthe Icelandic health system inMarch at the 50th annualSamuel Clark Harvey Lecturesponsored by the Departmentof Surgery. Most surgical pro-cedures, she said, can be donein Iceland, but patients travelabroad for heart operations ininfants, solid organ transplanta-tion (other than living-relatedrenal transplantation) and allogenic bone marrow trans-plantation. The national healthsystem has a waiting list forsurgery, but if waiting timeexceeds six months, patientsmay travel abroad for treat-ment at government expense.Today, the only waiting listlonger than six months is forcataract eye surgery.
Such a health system—which accounts for 10 percent ofthe country’s gross domesticproduct—is possible in a small,homogeneous population,Oddsdóttir said, adding, “I don’tknow if it’s possible in a large,heterogeneous population likethe United States.”
—J.C.
B I L L M c K I B B E NHumans change their world,with no end in sight
Over the last 20 years writer Bill McKibben has looked at theways humans have altered theworld around them, and he hascome away worried. “Withoutquite realizing it,” he said ata talk in February sponsored bythe Yale Divinity School andYale’s Interdisciplinary BioethicsProject, “we had grown so largethat there was nothing excepttectonic and volcanic forces that remained outside our deepinfluence. … Humans havealways interfered with the worldaround them, but their altera-tions have always had an edge.We live in a world where, all of a sudden, that is not true. Thereis no longer any edge to oureffects on the world around us.”
With the advent of geneticengineering, the influence ofhumans has turned inward and,McKibben said, it is importantto draw a moral line.“I would saywe draw it at germ line manipu-lation of human embryos, whata layman would call the crea-tion of designer babies,” saidMcKibben, author of The End ofNature and Long Distance andscholar-in-residence at Middle-bury College. “It is a line thatis very real and very palpable,yet allows room for humantherapy.”
—John Curtis
J E F F R E Y S AC H SThe poor need help from the rich
You don’t get much health carefor $4 per person. That’s whatIndia spends on public healtheach year, far too little to con-front its growing aids crisis, saideconomist Jeffrey D. Sachs,ph.d., author of The End ofPoverty: Economic Possibilities forOur Time and director of theEarth Institute at ColumbiaUniversity.
India must increase healthspending 10-fold, and to do so,Sachs argued at a February con-ference, “Health Crisis in SouthAsia,” it needs help from thedeveloped world. As its economygrows, India will be able tofinance its own health systemwithin a decade, but until thenit requires assistance. That pro-posal is among the recommen-dations of the U.N.’s MillenniumProject, directed by Sachs, a planto meet the MillenniumDevelopment Goals, includinghalving the world’s extremepoverty by 2015.
Sachs points out that in2002, 22 donor countries includ-ing the United States promisedto give 0.7 percent of their grossnational product annually asdevelopment assistance to poorcountries. The United States’rate is now only 0.15 percent.
“In many cases governmentsare ready to take action butneed the donor countries to givethe help they promised,” saidSachs.
—Cathy Shufro
16 capsule
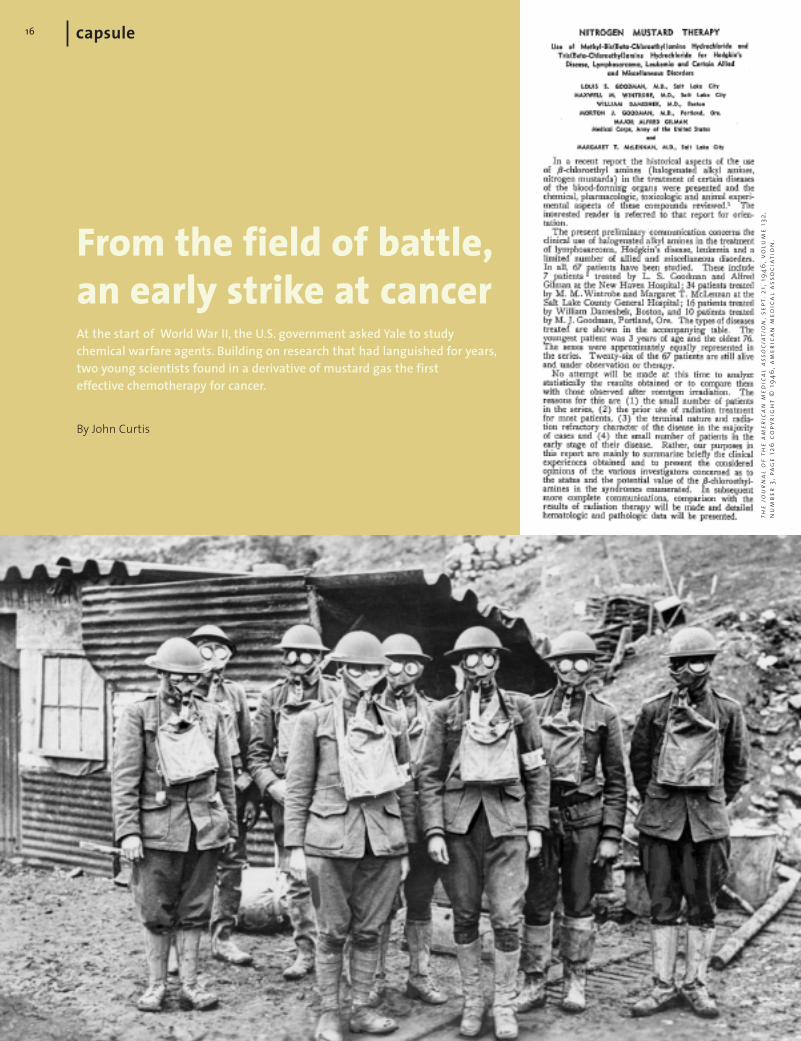
From the field of battle,an early strike at cancerAt the start of World War II, the U.S. government asked Yale to study chemical warfare agents. Building on research that had languished for years,two young scientists found in a derivative of mustard gas the firsteffective chemotherapy for cancer.
By John Curtis
the
jou
rnal
of
the
amer
ican
med
ical
ass
oci
atio
n,s
ept.
21,1
946
,vo
lum
e 13
2,n
um
ber
3,pa
ge
126
copy
rig
ht
© 1
946
,am
eric
an m
edic
al a
sso
ciat
ion
.

Early in 1942 two young assistant professors in Yale’s new Department of Pharmacology, Louis S. Goodman,m.d., and Alfred Gilman, ph.d., tookon the study of nitrogen mustard. This agent was derived from a lethalgas used in the trenches of World War I, and the United States, whichhad just entered World War II, feared it might again be used in battle.By year’s end, the two young scien-tists had found in an agent of death amedicine with lifesaving possibilities.Their use of nitrogen mustard with ahuman patient ushered in a new era ofcancer treatment. “This was the firstpatient in the world treated by chemo-therapy,” said David S. Fischer, m.d.,clinical professor of medicine, whogave a talk on the history of chemo-therapy for the Beaumont MedicalClub in March.
Scientists had been seeking a“magic bullet” for cancer since ancienttimes—the Romans practiced mas-tectomy, and Egyptians used topicalpreparations derived from medicinalherbs. By the 11th century the Arabphysician Ibn Sina, known in the Westas Avicenna, was using arsenicaltherapy systemically. The use of arseni-cals in an effort to treat cancer con-tinued for centuries, but without effect,said Fischer. “Until about 1900, theonly real therapy for cancer was to cutit out,” he said. “Cancer, by definition,was a surgical disease.” FollowingWilhelm Conrad Roentgen’s discoveryof the X-ray in 1895, medicine addedradiation, which could shrink tumors,to its arsenal of cancer therapies.
After World War I, however, medi-cal researchers noticed an interestingeffect of mustard gas—it destroyed
17
lymphatic tissue and bone marrow.Perhaps, they reasoned, it could alsokill cancer cells in the lymph nodes.But, Fischer said, this idea wentnowhere. “They saw the relationship,but they didn’t do anything about it.”
Some experiments in this area continued and revealed that topicalapplications of nitrogen mustard,derived from the sulfa mustard used in battle, caused tumors in mice toregress. But that line of research alsolanguished for a decade, until 1942,when the government’s Office ofScientific Research and Developmentcontracted with institutions around the country, including Yale, to studychemical warfare agents. Goodmanand Gilman, who had recently pub-lished the first edition of what wouldbecome a classic text, The Pharmaco-logical Basis of Therapeutics, began tostudy the effects of nitrogen mustardon lymphoma.
“They did their studies mainly inmice,” Fischer said. “They foundabsolutely dramatic regression of thelymphoma.” Further studies in rabbitswere equally encouraging. Goodman,Gilman and their team decided it wastime for a clinical trial. Gustaf E.Lindskog, m.d., an assistant professorof surgery, recommended a patient,J.D., a 48-year-old silversmith in theterminal stages of lymphosarcoma.Radiation no longer had any effect onhis tumors.
“As his condition seemed hopeless,he was offered experimental therapywith nitrogen mustard,” Fischer said.“In December of 1942, this 48-year-oldpatient was given 10 consecutive dosesof nitrogen mustard, a 10th of a milli-gram to a milligram per kilogram of
body weight, roughly 2.5 times whatbecame the standard dose. Nobody hadany idea of what dose to give him.”(The scientists had decided that therewas a safe distance between a lethaldose and a therapeutic dose of nitro-gen mustard.)
Within two days they noted a soften-ing of the tumor masses. By the end of treatment the tumors disappeared.A month later, however, the patientrelapsed, and subsequent courses oftreatment were less effective. Never-theless the scientists were encouraged.“This was proof,” said Fischer, “thatcancer could be treated by chemicals.”
Further trials followed. Around thecountry, 67 patients, including sevenat Yale, were treated with nitrogenmustard. The clinical trials remained a military secret, even from caregivers,until 1946—the first Yale patients’charts said only, “0.1 mg. per kg. compound X given intravenously.”
By 1943 the team responsible for the first successful clinical trial of chemotherapy had disbanded. Goodman continued his research inSalt Lake City. Gilman entered theArmy. Lindskog went on to becomechair of surgery at Yale. But they had made a major contribution to cancer therapy by proving the worthof nitrogen mustard. Scientists began to look at other alkylatingagents—which can attack cells at anypoint in their life cycle. And nitro-gen mustard, which was incorporatedinto multidrug chemotherapy forHodgkin’s disease, remains a potentagent against cancer today.
John Curtis is the managing editor of Yale Medicine.
Alfred Gilman and Louis Goodman (far left andleft) had just published a pharmacology text-book when they were asked to study nitrogenmustard, a version of the sulfa mustard used in World War I gas attacks. In survivors thegas was found to destroy lymphatic tissue andbone marrow. The scientists believed it couldalso attack lymphoma. Their findings remaineda military secret until 1946, when they werepublished in The Journal of the American Medi-cal Association.
nat
ion
al l
ibra
ry o
f m
edic
ine
(2)
ap/w
ide
wo
rld
yale
med
icin
esu
mm
er20
0518
In the Senegalese village of Mbagam, health worker FatouKine Manga fines those who enter the waters of the SenegalRiver. Despite her warnings to others, Manga admits tobreaking her own rule. “Even me, I go to the river!”
Snails that carry parasites lurk there, threateninginfection with schistosomiasis. This debilitating chronic disease attacks the poorest of the poor—those who, like Manga, lack access to clean water and sanitation and rely oninfected water for drinking, cooking, cleaning and bathing.Poverty and schistosomiasis are rampant in Mbagam, bothdespite and because of the dams along the Senegal River.
I arrived in the West African nation of Senegal inSeptember 1998, on my 21st birthday, to examine the healtheffects of the dams for my senior essay at Yale. This researchwould later become the topic of my medical school thesis, as well. For two months I lived in the capital city of Dakar,
the westernmost point of Africa. Described by a friend as aminiature version of Paris—after a bombing—downtownDakar had multistory apartments with ornate wrought-ironrailings and crumbling facades. Outside the skyscraper that housed the West African Bank, I dropped change on theblankets of beggars with polio. At the West African ResearchCenter, as part of my study abroad program, I studied thecountry’s economics, politics and culture.
For my monthlong field project, my instructor inthe indigenous language of Wolof encouraged me to followin a Yale tradition and study schistosomiasis along theSenegal River. Twenty-one years earlier, he proudly told me,he had been the interpreter for a Yale team studying thepotential effects of the dams on human disease. Wilbur G.Downs, m.d., m.p.h., led the team, which included HerbertS. Sacks, m.d., hs ’53; George A. Silver, m.d., m.p.h.;
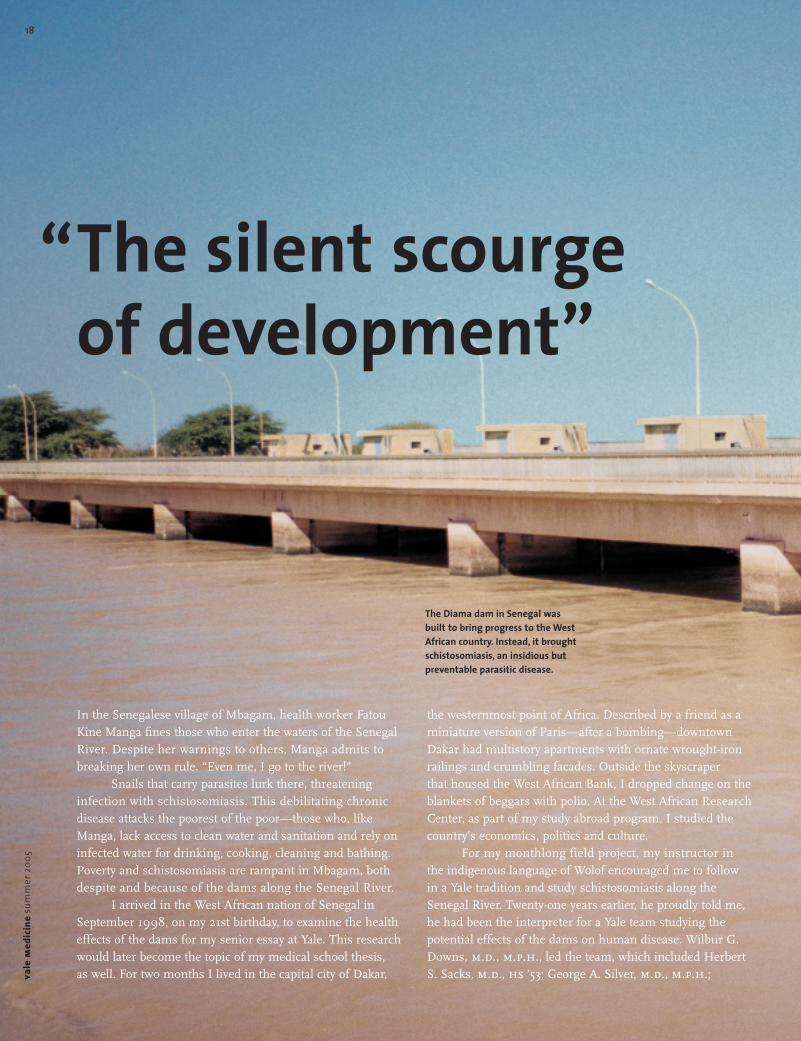
The silent scourgeof development”
The Diama dam in Senegal wasbuilt to bring progress to the WestAfrican country. Instead, it broughtschistosomiasis, an insidious butpreventable parasitic disease.
“

19
Eric W. Mood, m.p.h. ’43; Robert B. Tesh, m.d.; and Curtis L.Patton, ph.d. My Wolof teacher’s enthusiasm sparked myown. When the director of the nongovernmental organiza-tion Environment and Development Action in the ThirdWorld asked me to conduct an informal field survey onwhether schistosomiasis would limit the socioeconomicdevelopment of the Senegal River region, I gladly agreed.
Sugar fields, rice paddies and near-desertThat November, I left the city for the Sahel, the region southof the Sahara, to begin my survey. Two months after therainy season, the Sahel was already tan and dry. Herderswearing the traditional wraparound headdresses of thePulaar people drove thin cattle over the land. Barbed wireprevented the herds from encroaching on the irrigated plots that nurtured dreams of agricultural development.
From the sugar cane boomtown of Richard Toll I con-tinued a few kilometers downstream to Mbagam, a rice-farming village. My hosts were a prosperous farming family,wealthy enough to own a latrine and a mosquito net forguests. There was no electricity, but at night we gatheredwith villagers in a neighboring compound to watch televi-sion—powered by wires connected to a car battery—underthe stars on a dirt floor next to cows. A relative of theseneighbors lived in France, where he washed dishes and senthis wages home to support the family, pay the taxes and buy the car that provided power for the flickering imagesthat allowed the villagers to dream of a different life.
The dams along the Senegal River also fed hopes of a new life. Omar Niang, president of the village farmingcooperative, praised the dams for doubling the rice harvest.But standing next to a pump that transported water from
More than two decades ago Yale public health experts warned that dams along the Senegal River would bring disease.A Yale medical student’s research finds that their predictions have come true.
A letter from Senegal.
Article and photographs byKohar Jones, m.d. ’05
20ya
lem
edic
ine
sum
mer
2005
the river to the rice paddies, he noted the negative aspects.Workers wore uncomfortable plastic boots for protection frominfected water, and they all took the anti-schistosome drugpraziquantel. “Everything has a good side and a bad,” he said.
Schistosomiasis, named “the silent scourge of devel-opment” by the World Health Organization in 1998, is thebad side of dams. It follows water development projects thatcreate the perfect habitat for the snails that carry the disease(See sidebar, p. 21).
In 1994, less than 10 years after the dams were com-pleted, Mbagam had a disease prevalence of 91 percent.About 2,500 villagers joined the estimated 200 million peo-ple worldwide who are infected with schistosomiasis. Theother 9 percent joined 400 million people around the worldat risk of infection.
The dams and the disease they brought emerged from Senegal’s colonial legacy. Senegal, the former jewel inthe crown of colonial French West Africa, became independ-ent in 1960 but maintained close trading ties with France.In 1968, however, France stopped subsidizing the dominantpeanut economy just as a drought hit sub-Saharan Senegal.Both peanut farmers and nomadic herders saw theireconomies and lives devastated. Villagers flooded the capitalcities in search of work, and starving masses threatened to
undermine political stability. In 1972, amid widespreadfamine, Senegal adopted French colonial plans to dam andirrigate land along the Senegal River.
With its neighbors Mali and Mauritania, Senegalformed the Senegal River Development Organization(Organisation pour la Mise en Valeur du fleuve Sénégal—omvs). Dams provided hope for a desperate population. The massive hydroelectric Manantali Dam in Mali promisedboth electricity and a link between landlocked Mali andAtlantic trade routes. The small Diama Dam at the mouth of the river, between Senegal and Mauritania, would pre-vent salt water from creeping up the river bed during the dry season, allowing for two harvests of rice each year.Unfortunately, reality never matched the hopes.
By 1988 the dams were completed, but the promisednew civilization never came to be. Following the dictates of Structural Adjustment Programs (saps) of the World Bankand International Monetary Fund, which demanded a bal-anced budget, Senegal dismantled and privatized its nationalhealth system and agricultural agencies just as they wereneeded most. Senegalese economists wryly renamed thesaps “the Suffering of the African People.”
Disease comes to Richard TollDuring my month surveying schistosomiasis, my base was in Richard Toll, home to the Senegal Sugar Company(Compagnie Sucrière Sénégalaise—css). My new homebecame the gated Cité Cadre, where electricity generated bythe burning of sugar cane stalks powered the air condi-tioners of the expatriate and Senegalese managers of the css, who directed development in the region. It was a city on a hill, separated from the center of town by a scattering ofneighborhoods and the tall green waving stalks of irrigatedsugar cane.
Trucks carrying molasses and sugar cubes to Dakar rumbled along the paved, two-lane National Route, dodging horse-drawn carriages, pedestrians and the occasional cow. The paychecks of the sugar cane workers supported a bustling market, a regional economic mag-net. Electric lines strung overhead connected cementblock homes. Two water towers were under construction. A latrinisation program promised to sanitize the town.Richard Toll was the model of agroindustrial developmentfor the nation.
In 1998 author Kohar Jones, then a senior at Yale College, traveled to Senegal to investigate the linksbetween dams and the spread of schistosomiasis.
ein
at p
eled
“The silent scourge of development”

2121
A disease of poverty and progress
No disease is as clearly linked withdevelopment as schistosomiasis.Nicknamed the “germ of progress”in the 1970s for its close associationwith water development projectsthat allowed freshwater snails tothrive, schistosomiasis remains the“silent scourge of development.”Though preventable and treatable,it flourishes throughout the devel-oping world. It has infected 200million people worldwide, andthreatens an additional 400 mil-lion, primarily in Africa, Asia andLatin America. Of those infected,120 million people are sympto-matic, 20 million have severe com-plications and 200,000 die eachyear, more than the number ofdeaths from aids, diabetes, kidneydisease, pneumonia and influenzacombined in the United States.
Humans are at risk when theyenter freshwater sources infestedwith snails that release fork-tailedparasites called cercariae. Cercar-iae burrow through skin and growinto worms that inhabit the capil-laries of the intestines or bladder.The worms mate and lay barb-tailed eggs that cut through vesselwalls, eventually leaving the bodyin the feces or urine. When peoplerelieve themselves near snail-infested water, the eggs enter thewater and hatch, then grow intoparasites called miracidia thatlodge in the shells of specific snailhosts. Each miracidium gives riseto thousands of cercariae, and thecycle explodes.
An initial acute infection withschistosomiasis is followed bychronic debilitating disease. Afteran initial itchy rash at the site ofcercaria entrance, accompanied byfever, weeks go by with minimalsymptoms. The cercariae grow intoworms that use molecular mimicryto evade detection by the immunesystem. Schistosome eggs, not the
worms, bring disease. Anemia—often severe, sometimes deadly—accompanies blood loss indiarrhea or urine. In many regionswith endemic urinary schistoso-miasis, a boy is considered to be a man after blood appears in hisurine, thought to be a form ofmale menstruation.
Severe complications ensuewhen excess eggs wash deeperinto the body, eliciting an inflam-matory immune response. Liverscarring clogs the return of bloodto the heart. Initial heavy infectionwith intestinal schistosomiasis can kill with bloody diarrhea, orcause irreversible paralysis if eggsare washed into the spinal cord.
Communitywide access to cleanwater, sanitation and snail eradi-cation programs can prevent schis-tosomiasis outbreaks. Praziquantel,a miracle drug discovered in the1970s, kills both the worms andtheir eggs in a single dose withminimal side effects. It does notprevent reinfection, but it doesprevent serious complications ofheavy infection. Unfortunately, allthese measures to prevent andtreat schistosomiasis are costly,often beyond the means of devel-oping communities. (Happily,the cost of praziquantel recentlydropped considerably, increasingaccess worldwide.)
Schistosomiasis is a disease ofpoor sanitation, contaminatedwater, ineffective health systemsand unaffordable medications.It threatens impoverished com-munities struggling to build better lives.
—Kohar Jones
Without clean water and sanita-tion, the river becomes kitchen,laundry and bathroom, promotingan ongoing cycle of infection andreinfection.

yale
med
icin
esu
mm
er20
0522
estimated that all but two had schistosomiasis. “If people don’tdo anything, then in 10 years they are indisposed, and in 30years they are dead,” he said.
Return to the StatesFrom Mbagam, I took a donkey cart to the main road to catcha car rapide to the regional capital of Saint-Louis to take asept place (a seven-seated old Peugeot) back to Dakar to catchmy plane home—a century’s worth of development com-pressed into 24 hours. Descending through the cloud coverover New York City, I appreciated the rains that watered the gardens that provided food for farmers and industrial workers alike. I returned to New Haven, where librariesserve as cathedrals of knowledge and the sum of humanexperience could be consulted to shape future planning.medline provided information about schistosomiasis anddisease outbreak in Senegal. Patton, a professor of epidemi-ology (microbiology) and one of the original Yale researchers,provided the team’s reports.
The schistosomiasis epidemic, I learned, could havebeen prevented. In 1972, when the omvs decided to developthe Senegal River, the link between dams and disease waswell-established. Nevertheless, dam planning progressedwith minimal attention to public health concerns.
In 1978, the Yale researchers warned developmentplanners that schistosomiasis was a “serious public healthproblem” that, without adequate control measures, “might beaggravated by irrigated agriculture. … inhibiting both agri-cultural and economic development.” They recommended adisease surveillance team to track outbreaks and implementimmediate control measures. They “strongly urged” thatSenegalese groups with “considerable experience” as well as“the necessary trained personnel and mobile units to carryout such work” conduct the health surveys. The only reasonthe Senegalese weren’t already doing this work was that theywere “rather short of funds and supplies.”
Unfortunately, as budgets contracted under the saps,the recommendations were ignored. Nothing was done toavert the preventable outbreak of schistosomiasis. And ageneration later, I arrived in Senegal to ask if schistosomia-sis would limit the socioeconomic development of the riverregion. After my first visit in 1998, I made three moretrips to Senegal, with support from the Fund for Investi-gative Journalism and the medical school’s Office of Student
But development had already brought disease. In1986, the completion of the Diama Dam blocked the saltwater tongue of the Atlantic. Freshwater snails migratedfrom a nearby lake through a sugar company canal and intothe fresh water of the Senegal River, where their populationexploded. The human population of the sugar boomtownwas also exploding. From 10,000 when the css was foundedin 1972, Richard Toll’s population had more than quintupledby 1988, to an official 50,000 (but closer to 75,000) resi-dents, largely due to immigration. Urban amenities had notkept up. An infected migrant worker is believed to havebrought the parasite to Richard Toll. The css canals becameground zero in a massive schistosomiasis outbreak.
Although there had been 50 isolated cases of intes-tinal schistosomiasis among migrant workers between 1970and 1980, before the dam was built, in January 1988 DiokelDieng, a government health worker in Richard Toll, diag-nosed a new case of intestinal schistosomiasis along theSenegal River. By the end of the year, he had found 29 cases.By the end of 1989, there were nearly 2,000. By August1990, a full 60 percent of the population of Richard Toll wasinfected with intestinal schistosomiasis. And it spread. By1998, schistosomiasis had infected hundreds of thousandsof people in the Senegal River region. In many towns andvillages, as in Richard Toll, the prevalence rates were just shyof 100 percent—only the youngest children, who had not yet had extensive contact with infected water, remained freeof disease. It was the largest public health problem facingthe region, greater than the looming threat of aids and theconstant presence of malaria—and all because of the ecologi-cal changes wrought by dams and irrigation.
Still, when I asked Aboubakry Gassama, m.d., the headof the css health services, whether schistosomiasis would limitsocioeconomic development, he said no. Although most work-ers were sick with schistosomiasis, there were enough healthymigrant workers desperate for a paycheck to replace them.The limiting factor, he said, was the lack of financial resourcesto irrigate the land around the river. (Of the 600,000 acresthat planners had hoped to irrigate by 2000, only 75,000 werein use—the same number that had been irrigated 10 yearsearlier). This was not to say that schistosomiasis wasn’t a prob-lem. Of every 100 workers waiting on benches that lined theclinic’s long concrete hallway, nursing machete wounds fromthe fields or parasitic lesions from the Senegal River, Gassama
“The silent scourge of development”
In Mbagam, a rice-farming villageon the Senegal River, workerswear awkward rubber boots andtake yearly doses of praziquantelto ward off infection with schistosomiasis.
Research, to explore this question. There was no easy answer,I found. It depended on how you defined development.
For individuals struggling to become masters of theirown destiny, schistosomiasis severely limited their progress to greater personal and economic freedom. Sick, they couldnot work. Without work, they could not pay for health care,school expenses for their children or even food.
For industries struggling to make a profit, schistoso-miasis had little impact. There were always healthy workersto replace the sick. The limiting factor for economic develop-ment was simply the lack of local money to invest in irriga-tion, factories and industry. Foreign investors shied awayfrom supporting further irrigation at the edge of a desert.
Instead of boosting macroeconomic indicators, thedams ushered in an era of epidemic infectious disease.Poverty trapped villagers in an endless cycle of infection andreinfection. In retrospect, Patton described it as an “extraor-dinary example of poor planning.”
23
A drought in the 1960s and 1970sdrove cattle herders off the dryplains of the Sahel and into thecities. In response, the Senegalesegovernment and its neighbors
Senegal at a glance
hiv/aids prevalence 0.8 percent (7.4 in sub-Saharan Africa)
Infant mortality 56.53 deaths per 1,000 live births (6.5 in the U.S)
Religion Muslim, 94 percentChristian, 5 percentindigenous beliefs, 1 percent
Industries fish processing, agriculture, phosphate mining,fertilizer production, petroleum refining,construction materials
Population 10,852,147
Population living 54 percent (12 in the U.S.)
below poverty line
Unemployment 48 percent (urban youth, 40 percent)
Literacy 40.2 percent
Area 117, 714 square miles (slightly smaller than South Dakota)
Arable land 12.78 percent
The Yale team’s recommendations—disease surveil-lance, strengthened health systems, implementation of available measures to control disease—remain apt today.Health planning must be part of all development planning.
In Mbagam, where four spigots provided water for up to 3,000 people, Manga continued to violate the very rules she had set to protect the health of the villagers. “Only four flasks a day,” said Manga, bemoaning the daily ration—about eight gallons for each household of up to 30 people. “That’s not enoughwater for sure. You have no choice but to enter the river. It’s the financial means that we’re missing. Aboveall, the means.” YM
Kohar Jones, m.d. ’05, is a resident in family practice at Middlesex Hospitalin Middletown, Conn. She plans to publish her medical school thesis under the title Germs of Progress: Schistosomiasis in Senegal and the Ethics,Politics and Economics of International Health Research and Developmentin the 20th Century.
resolved to spur agriculture andeconomic development by building dams along the SenegalRiver. Development, however,remains elusive.
s o u rc e : c i a w o r l d fac t b o o k

yale
med
icin
esu
mm
er20
05
Healthy eating is the linchpin ofdiabetes prevention and control.At a March workshop communityhealth advisors got some lessonsin preparing low-fat dishes.
25
Part of a national effort to create communityhealth partnerships, a Yale center is workingwith New Haven churches to prevent diabetesand with a suburban school to stop teensmoking. The goal? Healthier communitiesinvested in their own outcomes.
Promotinghealth, from the ground up
By Jennifer KaylinPhotographs by Gale Zucker
In 1997, when Veronica Puleo, r.n., became the nurse atAmity High School in the New Haven suburb of Woodbridge,she was prepared to handle the fevers, sore throats, head-aches, sprained ankles and other ailments that routinelyafflict students, but there was one health problem that confounded her.
Cigarette smoking was so rampant that school offi-cials imposed a $65 fine on any student caught smoking in the school. The hard-core smokers chose to try their luck in“Marlboro Country,” a secluded area behind the school wherestudents gathered to light up. If caught there, they faced anafter-school detention, with Puleo sometimes presiding.
“For three hours we’d sit and talk,” she says. “They’dtell me how they were coughing up blood, or that they feltawful in the morning until they’d had their first cigarette, orthat they couldn’t fall asleep at night until they had a cigarette.They were almost pleading with me. They were so addicted,but had no way to stop.”

yale
med
icin
esu
mm
er20
0526
took charge of the situation and helped me out,” Puleorecalls. Katz introduced her to scientists doing research on adolescent smoking. He joined her at meetings with students and helped her write a news bulletin for parents.Eventually, their work became a research project on theeffectiveness of tailored behavioral interventions and thedrug Zyban in fighting adolescent nicotine addiction.Although Zyban has helped adults quit smoking, Puleo saysit proved ineffective with her study group. Study findingswere published in the journal Behavior Modification last year.
What did work was the eight-week program she andKatz developed. Each week focused on a different topic—from what cigarette smoking does to the body and identifyingwhy students smoke to preparing them for withdrawal.Students received gum, pencils and water bottles to fulfill theoral fixation that cigarettes satisfy. Puleo and Katz set out toidentify what incentives work best with adolescents. “We gavethem a choice: money or pizza and soda at our weekly meet-ings,” Puleo says. The answer provided some insight intowhy adult treatment models don’t necessarily work with ado-lescents. “The money meant nothing; they just use it to buymore cigarettes,” Puleo says. “The pizza and soda was frontand center. It allowed them to socialize, which is so impor-tant for young people, and gave them something to look forward to from week to week.” Katz, a nutrition expert, wassomewhat reluctant to go the pizza and soda route. “But I am a practical guy,” he notes. “I try very hard not to make‘perfect’ the enemy of ‘good.’ I figured we could get to dietary detox once we helped these kids quit smoking.”
There are now about 60 students enrolled in the program. Katz estimates that between a third and a halfeither quit smoking or cut back significantly. The prc stayedinvolved with the Amity smoking cessation program forabout four years, until it could run on its own. “This is thekind of thing we’re hoping to achieve on a larger scale,” Katz says. “A big part of what our center does is to take theknowledge we acquire and translate it into a real-world setting until it can become self-sustaining.”
The Yale-Griffin prc has generated studies and publi-cations in the area of smoking cessation for adults, andinvented a novel behavior modification technique Katz terms“impediment profiling,” which identifies barriers to behaviorchange. “Then we tailor the intervention components to cor-respond,” Katz says. “We’ve had success with this approach
Promoting health, from the ground up
Puleo knew she had to do something, but with limitedresources and no program geared for adolescents, she was at aloss. “I was spinning my wheels,” she says. Then she learnedabout the Yale-Griffin Prevention Research Center (prc).
The prc is a partnership between the Department ofEpidemiology and Public Health at Yale and Griffin Hospitalin Derby, where it is headquartered. It was established in1998 with a $350,000-a-year grant from the Centers forDisease Control and Prevention (cdc). That allotment grewto $800,000 annually in the second funding cycle, whichbegan last October. Funding from other sources brings theprc budget to between $2 million and $2.5 million each year.
One of 28 such centers nationwide, the Yale-Griffinprc collaborates with the community to develop innovativeapproaches to health promotion and disease prevention.Collectively, the national prc network conducts about 500research projects a year on such topics as aging, arthritis,asthma, job safety, nutrition, cardiovascular health, tobaccocontrol, obesity, diabetes prevention and control, schoolhealth and violence prevention.
“The prc model, which was developed about 20 yearsago, grew out of a productive period in the history of publichealth,” says Eduardo J. Simoes, m.d., m.sc., m.p.h., programdirector of the cdc’s prevention research centers. “We had conquered a lot of diseases through immunizations. We weremaking progress in the areas of occupational and environmen-tal health, so the logical next step was to invest in preventionresearch at the community level.” Besides funding the prcs,the cdc provides oversight and makes periodic site visits.
Michael H. Merson, m.d., the former dean of publichealth and the Anna M.R. Lauder Professor of PublicHealth, is the principal investigator of the cdc grant. Hecalls the prc program “one of the most important initiativesthe cdc has in this country.” Too often, he says, there’s adivide between academic research and real-world applica-tion. “These centers are really critical in bringing the twotogether, in taking the best in public health knowledge andapplying it in a field setting.”
Pizza, soda and cigarettesWhen Puleo contacted the Yale-Griffin prc, she was put intouch with the director, David L. Katz, m.d., m.p.h. ’93, asso-ciate clinical professor of epidemiology and public health,who, along with Merson, founded the prc. “He immediately
At weekly Bible Study meetings,the Rev. Audrey Tinsley, pastor ofthe Pentecostal Assembly Churchof Deliverance in New Haven,spends a few minutes discussingdiabetes. “It affects people of color disproportionately,” saysTinsley, herself a diabetic.
27
in smoking cessation and physical activity promotion, andjust received notice of our first grant award to develop the technique for dietary change and weight control as well.”
Another prc study found positive results with congestive heart failure patients who received a treadmilland access to a cardiac rehab nurse to help them use it. “The participants really liked it, which is proof of principle,”Katz says. “Now we’re looking for collaborators to help us study whether this could reduce the number of hospitali-zations and mortality.”
A randomized trial just completed by the prc foundthat massage therapy was highly effective for patients with osteoarthritis of the knee. Katz says the next step is tocrunch the financial numbers. “Given all the press about the dangers of anti-inflammatory medicine, what if massageis as good, or better? This could lead to a significant policychange. But to get there requires showing not only that itworks, but that it’s cost-effective.”
Partnering with the communityBeth P. Comerford, m.s., the prc’s deputy director, saysprcs focus on different health issues, depending on theneeds of the community, but their basic approach is always
the same: partnering with the community. “Everybody at thetable holds an equal place and is involved in the decisionsbeing made.” This is a time-consuming and, at times, frus-trating process, Comerford concedes, but because the goal is real-world application, it can also be rewarding.
“With the traditional clinical trial model, you’re basi-cally saying, ‘You’re the subject, we do things to you.’ Thenwe leave,” Comerford says. While researchers may develop theperfect scientific protocol, if it requires test subjects to do some-thing that makes them uncomfortable, such as take a medica-tion or have blood drawn, they may refuse to participate. Andany scientific results may not be lasting in real-world settings.“What we do,” Comerford says, “is go to the community at thestart and ask them, ‘What are your priorities? What would workto address them? What would people be willing to do?’ This iskey for participation and sustainability.”
In 2002, the Yale-Griffin prc embarked on a long-term project called predict (Partners Reducing Effects ofDiabetes: Initiatives through Collaboration & Teamwork).While researchers want to determine why information aboutdiabetes isn’t reaching the at-risk population, they know that for this project to succeed, there are side issues theymay have to tackle first. “Before you can focus on the health

yale
med
icin
esu
mm
er20
0528
issue, you may need to work with people on issues related tojobs, child care, housing,” Comerford says.
While it may seem digressive for public healthresearchers to address such social ills as unemployment, Katzsays it’s essential. “If you tell a group of people you want to talk to them about diabetes and they say they’re more con-cerned about finding jobs and you say, ‘Yeah, well that’s not our thing,’ they’re going to show you the door,” he says.He offers an example from his clinical work: A patientcouldn’t quit smoking. The resident physician kept focusingon smoking cessation, but Katz found out she was homeless,and the focus shifted to the patient’s more pressing needs.Three months after she’d moved into a new home, she wasready to quit smoking.
The predict project will evaluate the CommunityHealth Advisor model for getting people at risk to adopthealthier lifestyles. This method identifies natural leaders in a community and trains them to serve as surrogates forhealth care professionals. “Rather than the traditional we’re-here-to-help-you model,” Katz says, “members of thecommunity spread the gospel.” New Haven will be the testcommunity and Bridgeport will be the delayed control—meaning it won’t get any intervention until after the study is over. A related pilot study seeks to improve the patient-doctor relationship by coaching patients who have beennewly diagnosed with diabetes on how to talk to their doctors.
For predict, researchers initially planned to workthrough the public schools to disseminate information aboutdiabetes, but an advisory committee of community mem-bers felt it should be a church-based initiative. “We helpedthem tweak their structure,” says committee memberSharon Bradford. “We decided they should work through thereligious community. We felt there was a captive audience in the churches.” The committee also put researchers intouch with local ministers and helped select and hire a localoutreach coordinator to serve as a liaison between the com-munity and the prc.
That outreach worker is Maurice Williams, who alsosaw that working through the schools wouldn’t be effective.“When parents go to a school they’re thinking about howtheir child is doing in school, not about health issues,” hesays. “Plus, if you work through the churches the message is flowing from the parent down. The child isn’t carrying all the weight of bringing the information home.”
Twelve African-American churches in New Havenwere chosen for the study. Two volunteers from each wererecruited as community health advisors. During 10 weeks oftraining they learned about the causes, symptoms and treat-ment options for diabetes. They also learned about nutrition,how to read food labels, low-fat cooking techniques and different methods they might use to educate their congrega-tions. Church members were then given a baseline survey to see how much they know about diabetes. The next step,which is under way, is for the community health advisors to go back to their churches and educate their congregationsabout diabetes. Church members will then be surveyedagain to see whether their understanding about diabetes has increased.
“Why don’t they serve fruits and vegetables?”The Rev. Audrey Tinsley, the pastor of the PentecostalAssembly Church of Deliverance, signed up as a communityhealth advisor because she has diabetes. “I wanted to learn ways I could keep my diabetes from escalating into some-thing worse, and I wanted to help keep other people fromgetting the disease,” she says. She spends 15 minutes ofevery Bible Study period sharing information about diabetesand passes out diabetes literature at her church.
Tinsley now talks about diabetes with a convert’s zeal. “It affects people of color disproportionately,” she says. “It affects us more because of the food we eat. Fast food,junk food, something quick. Diet is the number one thingthat causes diabetes.”
When the conversation turns to school lunches,Tinsley’s voice takes on an angry edge. “Pizza, chickennuggets,” she says. “There’s nothing nutritional here! Why don’t they serve fruits and vegetables? Why don’t thekids have decent food?”
Tinsley isn’t alone. At a meeting of community healthadvisors in the basement of Bethel ame Church, everyonehad stories to tell. Several people talked about their ownexperiences with diabetes. Food was a recurring subject ofconversation—low-fat ways to prepare favorite dishes, thebenefits of Mrs. Dash salt substitutes, the merits of cookingcollard greens with smoked turkey instead of pork. At onepoint, someone suggested putting together a cookbook of healthy recipes. One health advisor wrote a skit about dia-betes she hoped the group could present at a community
Promoting health, from the ground up
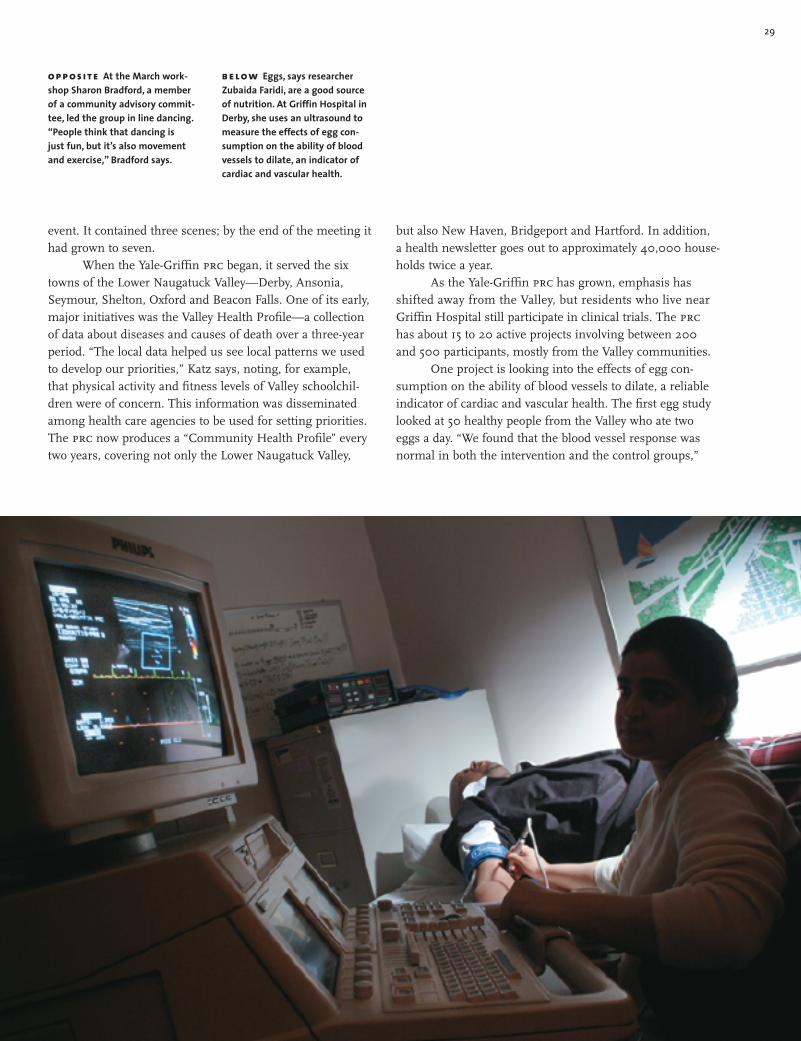
29
but also New Haven, Bridgeport and Hartford. In addition, a health newsletter goes out to approximately 40,000 house-holds twice a year.
As the Yale-Griffin prc has grown, emphasis hasshifted away from the Valley, but residents who live nearGriffin Hospital still participate in clinical trials. The prchas about 15 to 20 active projects involving between 200 and 500 participants, mostly from the Valley communities.
One project is looking into the effects of egg con-sumption on the ability of blood vessels to dilate, a reliableindicator of cardiac and vascular health. The first egg studylooked at 50 healthy people from the Valley who ate twoeggs a day. “We found that the blood vessel response wasnormal in both the intervention and the control groups,”
event. It contained three scenes; by the end of the meeting ithad grown to seven.
When the Yale-Griffin prc began, it served the sixtowns of the Lower Naugatuck Valley—Derby, Ansonia,Seymour, Shelton, Oxford and Beacon Falls. One of its early,major initiatives was the Valley Health Profile—a collectionof data about diseases and causes of death over a three-yearperiod. “The local data helped us see local patterns we usedto develop our priorities,” Katz says, noting, for example,that physical activity and fitness levels of Valley schoolchil-dren were of concern. This information was disseminatedamong health care agencies to be used for setting priorities.The prc now produces a “Community Health Profile” everytwo years, covering not only the Lower Naugatuck Valley,
o p p o s i t e At the March work-shop Sharon Bradford, a memberof a community advisory commit-tee, led the group in line dancing.“People think that dancing is just fun, but it’s also movementand exercise,” Bradford says.
b e l o w Eggs, says researcherZubaida Faridi, are a good sourceof nutrition. At Griffin Hospital inDerby, she uses an ultrasound tomeasure the effects of egg con-sumption on the ability of bloodvessels to dilate, an indicator ofcardiac and vascular health.

yale
med
icin
esu
mm
er20
0530
says clinical research associate Zubaida Faridi, m.d., m.p.h.This means egg consumption did not have a negative effecton the endothelium—the inner lining of the blood vessel—nor did it raise serum cholesterol levels. Faridi is now repli-cating the study on test subjects with elevated cholesterollevels. “We see this study as having practical applications fora large element of the population,” Faridi says. “Eggs are a very commonly used food, with an excellent nutrition pro-file, and their exclusion from the diet comes at a cost.”
Katz believes the move toward community-basedresearch models represents a sea change in public healthresearch. “It’s health with and for communities, rather thanthe paternalistic, ‘Trust us, we’re from an academic environ-ment,’” he says. “Gertrude Stein had it right: ‘A difference,to be a difference, must make a difference.’ For research tomake a difference, it must be put to use in the real world.”While Katz says research universities are slow to deviatefrom their time-tested ways, he sees the prc’s methodologyas the wave of the future, from the standpoint of both public acceptance and financial support.
“I’m hoping we’re tossing a pebble in the pond andthat the ripples go to the far shore.” YM
Jennifer Kaylin is a writer in New Haven.Gale Zucker is a photographer in Branford, Conn.
Like other once-thriving industrialtowns in the Naugatuck Valley,Derby has fallen on hard times.Health issues in the Valley werethe initial focus of the Derby-based Yale-Griffin PreventionResearch Center, led by David Katz,which promotes self-sustainingprojects for better health.
From medicine to media,a doctor extends his reach
After becoming an expert in nutri-tion, obesity and chronic-diseaseprevention, David L. Katz, m.d.,m.p.h. ’93, wasn’t satisfied treat-ing patients in his office; hewanted to get the message out tothe widest possible audience.That led to his now-flourishingsecond career as a media star.
It began in 1997 with a healthcolumn in the New Haven Register,followed by appearances on localTV, and then a monthly health column in O, The Oprah Magazine.He contributed articles to maga-zines and newspapers and wassoon appearing on Good MorningAmerica, the Today show, 48 Hoursand 20/20. Most recently, he wasnamed medical correspondent forthe abc network, and he will soonbegin a nutrition/health columnfor The New York Times.
“I was drawn to the media forthe same reason I was drawn topublic health: to have the greatestimpact on the health of the popu-lation,” he says.
A self-described multitasker—Katz, 42, typically works at least10 hours a day, seven days a week,and once juggled three bookdeadlines simultaneously—he recognizes that his expandingmedia obligations will require himto cut back on his clinical and academic duties. He plans to teacha bit less and relinquish his postas director of medical studies inpublic health at the School ofMedicine, which he has held foreight years. He will continue tosee patients and to direct Yale’sPrevention Research Center.
“What’s mattered to me fromthe start,” he says, “is making adifference. I’m interested in real-world impact, as soon as possible.”That’s why he sees his work in themedia as worthwhile. “We couldall but eradicate heart disease,
and greatly reduce the toll of can-cer, just by implementing what wealready know,” he says. “So thequestion is: how do we get peopleto make changes in their lives?One thing that’s clear, you need toreach them. Through my work inthe media, I can reach many morepeople in one day than I couldhope to reach treating patients inmy office over the span of myentire career.”
Besides teaching, treatingpatients, writing and making public appearances, Katz is also a successful inventor and poet.Among his inventions—he holdsfive patents—are an anatomicallyappropriate bicycle seat, a multi-use winter sport boot for childrenand a child-safe nail clipper. As an antidote to all his medical writ-ing he turns to poetry, which hasbeen published in anthologies andjournals ranging from the strictlyliterary to JAMA: The Journal of theAmerican Medical Association.
Katz, who has five children,says that when he’s not workinghe enjoys cooking, horseback riding, hiking, skiing and carpen-try. His wife, Catherine, a neuro-scientist, is collaborating with himon a book about nutrition.
He attributes his productivityto passion for the things he does.“Loving what you do makes all thedifference,” he notes.
—Jennifer Kaylin
Promoting health, from the ground up

31
we welcome submissionsDo you have an opinion to share on a vitaltopic in medicine, health or science? Send your thoughts to Essay, Yale Medicine, P.O. Box 7612, New Haven, CT 06519-0612,or via e-mail to [email protected].
essay nora e. groce, ph.d.
An assumption withdeadly consequencesThroughout the world, health workers find it hard to believe that thedisabled are at risk for hiv/aids.
Because of the strange sores that hadbegun to appear on the inside of James’mouth and on his arms, the 28-year-old finally decided to get tested forhiv. Heterosexual, with more than onegirlfriend, and living in a region ofsouthern Africa where almost 40 per-cent of the population is hiv-positive,James had good reason to worry. Hebegged a neighbor for a ride into townto avoid walking seven hours to thehiv clinic, and once there he waitedthree hours for his name to be called.As soon as he stepped to the frontdesk, however, he was dismissed; thenurse had been watching James while he waited, and right away shetold him, “You don’t need a test; youcouldn’t possibly have hiv.”
When I spoke with James six monthslater, the wasting caused by the aidsvirus had already begun to take its toll.Like millions of other Africans, thisyoung man would soon die of aids.James was different from them in onlyone way: James was deaf.
The vulnerability to hiv/aids of theworld’s 600 million disabled peoplehas been virtually ignored. Conven-tional wisdom dictates that people withdisabilities are unlikely to be at risk—unlikely to have sex, use drugs or bevulnerable to rape. Yet disabled indi-viduals are at equal or increased riskfor all known aids risk factors. Highrates of poverty and illiteracy and thestigma associated with disability only
increase these risks for the millions of people who live with a physical dis-ability or psychiatric illness or who are blind, deaf or mentally retarded.
As a researcher on disability issues, I suspected that the impact of aidson those with pre-existing disabilitieswas being overlooked. I was unpre-pared, however, for how little attentionthis issue had received. A search of the global literature yielded only 38short articles on the topic.
I wanted to fill this gap. In 2003,with funding from the World Bank Iundertook a global survey on hiv/aidsand disability. We sent it to 5,500 aidsresearchers, rehabilitation programs anddisability advocacy groups worldwide.Responses came from 57 countries.
Worldwide, the data showed, aidseducation and outreach programs areextremely unlikely to reach disabledindividuals. aids radio campaigns donot educate the deaf. Billboard andnewspaper campaigns do not reach theblind. With global literacy rates for disabled adults averaging as low as 3 percent (and around 1 percent fordisabled women), many disabled indi-viduals can’t understand complicatedaids education messages. For thosewho do seek testing or medical care,accessibility remains a problem: stairsimpede entrance to clinics for thosewith physical mobility problems.
Concerns do not end there. Theassumption that people with disabilitiesare virgins endangers lives in twoways. In dozens of countries, individ-uals with disabilities are turned awayfrom testing centers by health workerswho assume that they are neither sexu-ally active nor hiv-positive. In manycountries they are targeted for rape by
hiv-positive people who believe in “vir-gin cleansing.” Even those diagnosedwith hiv are at the bottom of lists formedical care and social support; theirlives are considered less valuable thanthose of people without disabilities.
These results carry a message for clinicians worldwide: they must beaware of the risks that their disabledpatients face. Yet people with disabil-ities find that doctors rarely ask themwhether they are sexually active or dis-cuss safer sex, even though their risk ofphysical abuse and rape is significantlyhigher than for nondisabled people, par-ticularly in group homes or institutions.
The survey results have fosteredincreased awareness of hiv/aids anddisability, and over the past year, a consortium of UN agencies has joinedthe World Bank and disability advo-cacy organizations to press for inclu-sion of a disability component in aidsoutreach and education. My colleaguesand I have begun a new series of stud-ies to better identify and evaluate pro-grams for disabled individuals at risk. I hope it will make a difference: theneed is immediate, and millions oflives are at stake.
For more information, visitwww.cira.med.yale.edu/globalsurvey.
The American Sign Language symbols above spell aids.
Nora E. Groce, ph.d., is an associate professor of public health and anthropology in the GlobalHealth Division of the School of Public Health.

yale
med
icin
esu
mm
er20
0532 faculty notes
Thomas GillDavid Leffell Kim Bottomly Steven Hebert Stefan Somlo Hal Blumenfeld
Three Yale scientists have receivedclose to $1 million each from the Ellison Medical Foundation topursue research into infectiousdisease. The three are among the10 Senior Scholars in GlobalInfectious Disease announced in December.
Jorge E. Galán, ph.d., d.v.m.,the Lucille P. Markey Professor of Microbiology and chair of the Section of Microbial Patho-genesis, will study the bac-terium Campylobacter jejuni,one of the most common causesof gastrointestinal infectionworldwide.
John R. Carlson, ph.d., theEugene Higgins Professor ofMolecular, Cellular and Develop-mental Biology, will explore new approaches to the design of repellents and traps for disease-carrying insects.
Ruslan Medzhitov, ph.d., pro-fessor of immunobiology and aHoward Hughes Medical Insti-tute investigator, will examinehow immune system responsesto one infectious agent affectthe body’s defenses against con-current infections.
Thomas M. Gill, m.d., fw ’94,associate professor of medicine(geriatrics), and Michael Cappello,m.d., fw ’95, associate professorof pediatrics and epidemiology,have been elected to the Ameri-can Society for Clinical Investi-gation (asci), one of the nation’soldest and most respectedmedical honor societies. Theasci membership includesphysician-scientists elected fortheir achievements in biomedi-cal research.
Two Yale physician-scientistswere honored with majorawards in the field of kidneyresearch at the World Congress
of Nephrology meeting inSingapore in June.
Steven C. Hebert, m.d., thechair and c.n.h. Long Professorof Cellular and Molecular Physi-ology and professor of medicine,and Stefan Somlo, m.d., fw ’91,the c.n.h. Long Professor ofMedicine and chief of the Sectionof Nephrology, are being recog-nized for important discoveries.
Hebert will receive the A.N.Richards Award, which carries a$10,000 cash prize, from theInternational Society of Nephrol-ogy (isn) for three discoveries inthe field of ion transport and ionsensing. Somlo will share theLillian Jean Kaplan InternationalPrize for Advancement in theUnderstanding of PolycysticKidney Disease for his work in dis-covering genes that cause poly-cystic kidney and liver diseases.Somlo and co-recipient Gregory G.Germino, m.d., hs ’87, of the JohnsHopkins School of Medicine willreceive $50,000 each from Thepkd Foundation and the isn.
A third Yale nephrologist,Walter F. Boron, m.d., ph.d., pro-fessor of cellular and molecularphysiology, has been selected to receive the Homer W. SmithAward, the American Society ofNephrology’s top honor for basicresearch. The award, which carries a $10,000 cash prize, willbe presented at the society’sannual meeting in November in Philadelphia.
Two Yale psychiatrists receivedthe American Psychiatric Asso-ciation’s apire/Kempf FundAward for Research Developmentin Psychobiological Psychiatry atthe association’s annual meetingin Atlanta in May.
John H. Krystal, m.d. ’84, theRobert L. McNeil Jr. Professor of Clinical Pharmacology and
Bottomly nameddeputy provost for science, technologyh. kim bottomly, ph.d., hasbeen named deputy provost forscience, technology and facultydevelopment, effective July 1.Bottomly, who has been at Yalesince 1980, is professor of immuno-biology, dermatology and molecu-lar, cellular and developmentalbiology. She also served as actingchair of the Section of Immuno-biology. Provost Andrew D.Hamilton, ph.d., announced theappointment in April.
As deputy provost, Bottomlywill help shape and implementpolicies in the natural sciences,anthropology, psychology, statis-tics and linguistics. She will over-see Yale Engineering, the School ofForestry & Environmental Studies,the Peabody Museum of NaturalHistory, the Yale Institute for Biospheric Studies and the Yale-affiliated Haskins Laboratories.Bottomly will also work on initia-tives to increase faculty diversity,improve recruitment and reten-tion of women and underrepre-sented minorities in science, andenhance career developmentfor faculty.
As deputy dean,Leffell moves practiceinto 21st centuryWith his appointment as deputydean for clinical affairs in February,david j. leffell, m.d., hs ’86,continues a task he began almost10 years ago, when he added anew portfolio to his work in theclinic and laboratory. As associatedean for clinical affairs and direc-tor of what was then called theYale Faculty Practice, Leffell soughtto improve the business side ofmedicine. The faculty practice isnow the Yale Medical Group (ymg),where recent surveys showimproved patient satisfaction, aswell as areas where improvementis needed. Most importantly,the ymg has begun to introducechanges in the practice of medi-cine, helping it move outside traditional departmental bounda-ries into interdisciplinary,disease-based teams that includeresearchers as well as physicians.
“Because our knowledge of disease is so much more refined,we understand that solutions to illness are not limited to a particu-lar organ in which the disease isexpressed,” said Leffell, who willoversee the growth and develop-ment of the clinical practice. Amonghis goals are strengthening tiesbetween clinical care and medicalresearch and spreading the wordabout Yale’s faculty expertise. Healso hopes to improve the clinicalinfrastructure by making it easierfor patients to make appointmentsand by ensuring close communica-tions between referring physiciansand specialists.
“To teach medical students tobe doctors of the 21st century,to take care of patients with newtechnology and medications ofthe 21st century, you have to havea clinical practice of the 21stcentury,” Leffell said.

33
send faculty news toClaire M. Bessinger, Yale Medicine,
P.O. Box 7612, New Haven, CT06519-0612, or via e-mail to [email protected]
John MacMickingRonald Breaker Stephen WaxmanLinda Degutis Robert UdelsmanVincent DeVita Jr. Bruce McClennan Anna Marie Pyle
deputy chair for research in theDepartment of Psychiatry, andDaniel H. Mathalon, m.d., ph.d.,assistant professor of psychiatry,were recognized for providingnew insights into the neurobiol-ogy and treatment of cognitiveimpairments associated withschizophrenia.
In March Sidney J. Blatt, ph.d.,professor of psychiatry and psy-chology and chief of psychologyin the Department of Psychiatry,in collaboration with colleaguesin Belgium, published a book,The Theory and Treatment ofDepression: Towards a DynamicInteractionism Model, that grewout of a collaboration begun in 2003. Blatt spent a monththat year at the Catholic Univer-sity of Leuven as a visiting pro-fessor. A colleague at Yale, Paul L.Errera, m.d., hs ’57, professoremeritus of psychiatry and anative of Belgium, sent greet-ings via videotape.
Hal Blumenfeld, m.d., ph.d.,fw ’98, assistant professor ofneurology, neurobiology andneurosurgery, has received theDreifuss-Penry Epilepsy Awardfrom the American Academy ofNeurology. The award recognizesphysicians in the early stages of their careers who have con-tributed to epilepsy research.
Ronald R. Breaker, ph.d., associ-ate professor of molecular, cellu-lar and developmental biology,has been named a HowardHughes Medical Institute inves-tigator and the Henry Ford IIProfessor of Molecular, Cellularand Developmental Biology.Breaker’s lab explores the “rnaworld,” the idea that the Earth’sfirst life forms were composedof rna rather than dna. His
studies have led him to discoverdozens of regulatory struc-tures, known as riboswitches,which might be used to controlthe activity of genes insertedinto cells during the course ofgene therapy.
David C. Cone, m.d., associate pro-fessor of surgery (emergencymedicine) and public health, wasinstalled as president-elect ofthe National Association of emsPhysicians at the group’s annualmeeting in January.
Linda C. Degutis, m.s.n. ’82,dr.ph. ’94, associate professor of surgery (emergency medicine)and epidemiology and publichealth, was elected chair of theexecutive board of the AmericanPublic Health Association, theprimary association for publichealth professionals.
Vincent T. DeVita Jr., m.d., hs ’66,the Amy and Joseph PerellaProfessor of Medicine, has beennamed editor in chief of a newjournal for oncologists, NatureClinical Practice Oncology. DeVitapreviously served as head of theYale Cancer Center and directorof the National Cancer Institute.
Marie L. Landry, m.d., hs ’77, fw’81, professor of laboratory medi-cine and director of the ClinicalVirology Laboratory at Yale-NewHaven Hospital, received the2005 Diagnostic Virology Awardfrom the Pan American Societyfor Clinical Virology in May for outstanding contributions tothe field.
Robert J. Levine, m.d., hs ’63, pro-fessor of medicine and co-chairof the Yale Bioethics Project, hasreceived the Health ImprovementInstitute’s Lifetime Achievement
Award for Excellence in HumanResearch Protection. Levine hascontributed to the literature ofthe field of protection of humanresearch subjects by publishingover 200 articles and one majormonograph and by founding andediting irb: A Review of HumanSubjects Research.
John D. MacMicking, ph.d., assist-ant professor in the Section of Microbial Pathogenesis, hasbeen selected as a 2005 SearleScholar as part of a programthat supports the independentresearch of young faculty in the biomedical sciences andchemistry. In 2004 MacMickingalso received the MallinckrodtFoundation Program ScholarAward, given annually to youngscientists starting their careers.He studies host innate immu-nity, with an emphasis on therole played by interferon path-ways against intracellular infec-tions like tuberculosis.
Bruce L. McClennan, m.d., profes-sor and chair of diagnostic radiology, was elected presidentof the American Roentgen RaySociety, effective May 15. The oldest radiology society in theUnited States, it has advancedradiology through annual scien-tific and educational meetingsand the American Journal ofRoentgenology.
Stephanie S. O’Malley, ph.d., pro-fessor of psychiatry and directorof the department’s Division ofSubstance Abuse Research, hasreceived the 2004 Dan AndersonResearch Award. The award,sponsored by the Butler Centerfor Research at the HazeldenFoundation, honors researcherswho have advanced the study ofaddiction recovery.
Anna Marie Pyle, ph.d., has beenappointed the William EdwardGilbert Professor of MolecularBiophysics and Biochemistry.Her research explores how rnafolds and organizes itself to catalyze reactions. Since 2002,Pyle has also been a HowardHughes Medical Institute investigator.
The Bayer Pharmaceuticals Corp.has given the 2004 Bayer Awardto Raymond R. Russell, m.d., ph.d.,fw ’00, assistant professor ofmedicine (cardiology). Russellstudies cardiac function andmetabolism and the changesassociated with disease states.
Robert Udelsman, m.d., m.b.a.,the Lampman Professor ofSurgery and Oncology and chairof surgery, was elected presi-dent of the American Associa-tion of Endocrine Surgeons.Membership includes surgeonswho devote significant portionsof their practice or research toendocrine surgery and who arecertified by the American Boardof Surgery.
Stephen G. Waxman, ph.d., m.d.,professor and chair of neurol-ogy and professor of pharma-cology and neurobiology, has been named the Bridget MarieFlaherty Professor of MolecularNeurology. Waxman, a renownedneurologist and molecular neuroscientist, studies the rolesof sodium channels in multiplesclerosis, spinal cord injury andneuropathic pain.

The Class of ’05
yale
med
icin
esu
mm
er20
0534 students
terr
y d
agra
di
(3)
a b ov e Medical students sported toy stethoscopes as a symbol of their calling.
o p p o s i t e l e f t Graduates Mariah Ruth and Michael Shapiro joked with Associate Dean Nancy Angoff before the procession to the main campus.
o p p o s i t e r i g h t Helena Hansen, whograduated from the m.d./ph.d. program,took her daughter, Kirin, onstage as shereceived her diploma.

35
An unfinished agenda:keeping people healthy At Commencement, a former surgeon general urges access tohealth care and sex education.
Growing up in a small town in Arkansas,M. Joycelyn Elders, m.d., never saw aphysician until she went to college. Butin 1993 she became the nation’s topdoctor, and as surgeon general her out-spoken support of sex education pro-voked controversy. Access to knowledgeabout sexual health issues was a themeshe echoed in her Commencementaddress at the School of Medicine inMay, and the crowd loved it.
Elders told the 96 graduating stu-dents—who offered standing ovations atthe beginning and end of her address—that an increase in hiv infections, ris-ing rates of sexually transmitted diseasesand the highest teenage pregnancy ratesin the industrialized world prove thatthere’s an important place for sexual-health education in schools. “You can’t
keep people healthy if you don’t educatethem,” said Elders, professor emeritusof pediatric endocrinology at the Univer-sity of Arkansas for Medical Sciences.“And you can’t educate them if they’renot healthy.”
Although she has long advocatedabstinence, she also feels that youngpeople need to know about safe sex.“The vows of abstinence,” she told thecheering crowd, “break far more easilythan a latex condom.”
She also cautioned the graduatesthat, despite having the best medicaleducation, the best training, the besthospitals and the best colleagues in theworld, they have a huge unfinishedagenda. “We need to make sure we haveimproved access to care for all of ourpeople,” she said, noting that more than40 million people in the United Stateslack health insurance. Elders ended on anote of optimism, asking the graduatesto use their power, prestige and positionin their communities to effect change.
At the Commencement onHarkness Lawn, the Class of 2005
joh
n c
urt
is
The Class of 2005 chose Joycelyn Elders,who served as surgeon general under President Clinton, as its keynote speaker.

yale
med
icin
esu
mm
er20
0536 students
An “old-fashioned” idea:nothing is more importantthan the public health
Fast Food Nation author Eric Schlosserpeered at the 107 public health studentsgathered for Commencement in BattellChapel on May 23 and called them“strange.” In a culture that insists that“everything is better when it’s forprofit,” he said, these new graduates ofthe School of Public Health believe in “incredibly old-fashioned” ideas: thepublic good, the public interest andpublic service.
“There is nothing more importantthan the public health,” said Schlosser, a journalist whose bestselling bookdescribes how the fast food industry hastransformed America’s diet and itseconomy. “We have lost sight of thisbasic truth, and the greed and the self-ishness of the past two decades haveobscured it.” Even the wealthiest willnot be safe from what Schlosser calls“the great levelers of mankind: theviruses and microbes that don’t reallycare where you went to school.”
Good public health saves money inthe long run, said Schlosser. Just as disease mapping helped pioneering epi-demiologist John Snow, m.d., discoverthe water pump responsible for muchof a London cholera outbreak in 1854, modern maps would locate theAmerican public health crisis in thepoorest neighborhoods. “It is an illu-sion—a dangerous illusion—to thinkthat the poor health of the poor can be ignored. We will all pay for it oneway or another,” said Schlosser, notingthat microbes from a sick busboy can find their way into the finest ofgourmet meals.
honored Robert D. Auerbach, m.d., hs ’87, lecturer in obstetrics, gynecol-ogy and reproductive sciences, with the Francis Gilman Blake Award foroutstanding teaching. Jennifer M.Gaudiani, m.d., a resident in internalmedicine, received the Betsy WintersHouse Staff Award, given to the resi-dent who has made the most signifi-cant contribution to the education of medical students. This year’s class gift was the largest ever: $2,000 wasgiven to the Society for DistinguishedTeachers, and $2,000 was pledged to the medical school’s endowment forscholarships, an amount that will bematched by the university.
The Bohmfalk Prize for teachingbasic sciences was awarded to a husband-and-wife team for the firsttime: Marie L. Landry, m.d., hs ’77, fw ’81, professor of laboratory medi-cine, and Peter S. Aronson, m.d.,fw ’75, the c.n.h. Long Professor ofMedicine and professor of cellular and molecular physiology. The BohmfalkPrize for teaching clinical sciencewent to Michael K. O’Brien, m.d.,ph.d., assistant clinical professor ofsurgery (gastroenterology). Sharon K.Inouye, m.d., m.p.h. ’89, professor ofmedicine, received the Leonard TowHumanism in Medicine Award, whileCatherine Chiles, m.d., associate clini-cal professor of psychiatry, won theLeah M. Lowenstein Prize, which rec-ognizes faculty who promote humaneand egalitarian medical education.The first annual Alvin R. FeinsteinAward for outstanding clinical skillswas awarded to Ronald R. Salem,m.d., associate professor and chief of surgery (oncology).
—Jill Max
to p Stephanie Colegio-Eisenbarth celebratedwith her husband, Oscar Colegio, who gradu-ated from the medical school last year.
a b ov e Inna Landres and Michele Flaggebefore the university ceremony on Old Campus.
terr
y d
agra
di
joh
n c
urt
is

37
In closing, Schlosser told the gradu-ates, “We need more strange people likeyou. I have enormous respect for thepath you have chosen.”
Also speaking was graduate ReshmaTrasi, who told her classmates to persist despite barriers and to listen.“The next time you want to say some-thing, try stopping yourself and let-ting the other person talk. … It willopen your mind.”
The students chose Elizabeth H.Bradley, m.b.a., ph.d. ’96, associateprofessor of public health, for theAward for Excellence in Teaching, herthird in her nine-year career at Yale.
Other awardees included Lisa M.DiFedele, Farnoosh Hashemian, AsaMargolis and Bonnie E. Gould Rothberg,m.d. ’94, hs ’96, each of whomreceived a Dean’s Prize for outstandingmaster’s thesis.
The Wilbur G. Downs InternationalHealth Prize went to Anna Beitin; theHenry J. (Sam) Chauncey Jr. InspirationAward to Elinor Schwimmer; and theCortlandt Van Rensselaer Creed Awardto Edward Magee and Anika Hines.
—Cathy Shufro
c l o c k w i s e f r o m to p l e f t
Before the ceremony on Old Campus, publichealth student Koren Odierna helped ArunaDhara adjust her stole as Nabila Alibhaiwatched.
Fast Food Nation author Eric Schlosser, left, withpublic health Dean Brian Leaderer, said in hisCommencement address that the health of thepoor cannot be ignored. Viruses and microbes,he said, are “the great levelers of mankind.”
Elizabeth Bradley received the award for excel-lence in teaching.
Kevin Neill waited with classmates for the procession into Battell Chapel.
Reshma Trasi, who gave the student address,was joined by her family at the ceremony atBattell Chapel.
joh
n c
urt
is (
5)

yale
med
icin
esu
mm
er20
0538 students
Match Day sees more bound for New Haven residencies andtraining as generalists
While many people celebrated March 17as St. Patrick’s Day, medical studentsfrom the Class of 2005 had another reason to celebrate. There were shouts,cheers and tears of joy at HarknessBallroom on Match Day, the half-century-old ritual that will likely determine the course of their careers. Nationwide,almost 94 percent of medical schoolseniors matched to residencies this year.
Students applied to programsaround the country, but a larger numberthan ever before—27 out of 94—arestaying in Connecticut, mostly at Yale-New Haven Hospital. “People worryabout New Haven—is it keeping goodstudents? Well, it’s keeping really goodstudents,” said Nancy R. Angoff, m.p.h.’81, m.d. ’90, hs ’93, associate dean forstudent affairs. Another trend at Yale isthat more students this year are goinginto internal medicine, primary careand pediatrics than in past years, whichsaw higher numbers of graduating seniors entering surgical subspecialties.
For the most part, students werecalm and poised as they approached the
tables stacked with the envelopes thatheld news of their futures for the nextfour years. But Michael Shapiro wasunable to contain himself as he sprinted ahead of the crowd, ripped open hisenvelope, let out a yell and then burstinto tears. He was accepted to theUniversity of Pittsburgh MedicalCenter’s plastic surgery program, hisgoal after volunteering for OperationSmile two years ago, when he went to Morocco to assist with reconstructivesurgery. “It sounds schmaltzy,” he said, “but it’s been my dream.”
Many students whipped out cellphones to share the good news withfamily and friends, but Brad Raphaelwas able to share it in person with hisfather, Irving G. Raphael, m.d. ’71, whowas on hand. “It’s excitement, nervous-ness and relief all combined into one,”the younger Raphael said before open-ing his envelope. Upon learning thegood news—that he was going to theHospital for Special Surgery at CornellUniversity Weill Medical College to pur-sue orthopaedic surgery—he huggedhis father, also an orthopaedist, andsaid, “It’s exactly where I want to be.I’m feeling euphoria right now.”
—Jill Max
2005 residency placements for Yale medical students
The Office of Student Affairs has pro-
vided the following list, which outlines
the results of the National Resident
Matching Program for Yale’s medical
graduates. Some names appear twice
because the graduate is entering a one-
year program before beginning a specialty
residency. The transitional designation
is a one-year program with three-month
rotations in different specialties.
CaliforniaHarbor–ucla Medical Center, TorranceLeo Kim, medicine-preliminary
Stanford University ProgramsJeffrey Chi, internal medicineDouglas Jacobson, medicine-
preliminaryInna Landres, obstetrics and
gynecologyChristoph Lee, diagnostic radiologyNir Modiano, internal medicine
ucla Medical Center, Los AngelesEdidiong Ikpe, emergency
medicine/internal medicine
University of California,San FranciscoNeelendu Dey, internal medicineJessica Yager, internal medicine
University of Southern California,Los AngelesLeo Kim, ophthalmology
ColoradoHealthone Presbyterian/St. Luke’sMedical Center, DenverMariah Ruth, transitional
University of Colorado School ofMedicine, DenverHeidi Cook, obstetrics and
gynecologyMariah Ruth, dermatology
ConnecticutHospital of Saint Raphael’s, NewHavenAnnika Dronge, transitionalDavid Ornan, transitional
Middlesex Hospital Program,MiddletownKohar Jones, family practice
Brad Raphael was joined by his father, IrvingRaphael, an orthopaedist who graduated fromthe medical school in 1971.
Douglas Jacobson, Michele Flagge, ChristopherKwong, David Ornan, Brendon Graeber, SuzanneBaron and Christoph Lee toasted their matches.

39
Yale-New Haven HospitalDavid Aversa, psychiatryAnamika Chaudhuri, internal
medicineStephanie Colegio-Eisenbarth,
laboratory medicineGina Constantine, internal
medicine/primaryVicente Diaz, ophthalmologyAnnika Dronge, ophthalmologyThomas Fernandez, psychiatry-
adult/childJohn Forrest, internal medicineAdam Gafni-Kane, obstetrics and
gynecologyBarton Kenney, pathology-anatomic
and clinicalBrett King, dermatologyEleanor Knopp, dermatologyChristopher Kwong, internal
medicine/primaryCatherine Loerke, surgery-preliminaryJavier Lopez, obstetrics and gynecologyCoeurlida Louis, internal
medicine/primaryErnest Mandel, internal medicineDeanne Nakamoto, medicine-
primary-preliminary, ophthalmologySarah Nikiforow, internal medicineDamani Piggott, medicine/pediatricsDavid Ross, psychiatryIsaac Sasson, obstetrics and gynecologyGrace Smith, medicine-preliminaryCurtis Weiss, internal medicineCarlos Wesley, emergency medicine
FloridaJackson Memorial Hospital, MiamiMatthew Whitley, otolaryngology
GeorgiaEmory University School of Medicine,AtlantaMichele Flagge, emergency medicineAndre Matthews, emergency
medicine
HawaiiUniversity of Hawaii Program,HonoluluChristoph Lee, transitional
IndianaIndiana University School ofMedicine, IndianapolisNicholas Countryman, dermatology
IowaUniversity of Iowa (Des Moines)ProgramAndrew Chen, medicine-preliminary
MarylandJohns Hopkins Hospital, BaltimoreYuri Agrawal, surgery-preliminary,
otolaryngologyAmy Duffield, pathologyNaudia Lauder, internal medicineMartine Solages, pediatrics
MassachusettsBeth Israel Deaconess MedicalCenter, BostonJillian Catalanotti, internal medicineDagan Coppock, internal medicineEric Golding, internal medicine Joshua Klein, medicine-preliminary
Boston University Medical CenterKatherine Gergen Barnett,
family practice
Brigham and Women’s Hospital,BostonCristina Baseggio, internal
medicine/primaryMichael Herce, internal medicineEleanor Knopp, medicine-preliminaryJanelle Luk, obstetrics and
gynecology
Harvard Combined Program, BostonSusan Rushing, pediatric neurology
Massachusetts General Hospital,BostonSuzanne Baron, internal medicineBrett King, medicine-preliminaryMandy Krauthamer, internal
medicine/primaryErin Mahony, pediatricsBrian Nahed, surgery-preliminary,
neurosurgery
Massachusetts General Hospital/ Brigham and Women’s Hospital,BostonJoshua Klein, neurology
Massachusetts General Hospital(Harvard Combined)Ariel Frey, medicine/pediatrics
MichiganUniversity of Michigan Hospitals,Ann ArborRaymond Lynch, general surgery
MississippiKeesler Medical Center Program,Keesler afbKwabena Blankson, pediatrics
New Hampshire Dartmouth-Hitchcock MedicalCenter, LebanonDaniel Gibson, surgery-preliminary,
neurosurgery
New YorkAlbert Einstein College/MontefioreMedical Center, BronxMargo Simon, family practice
Flushing Hospital Medical CenterDaniel Khaimov, transitional
Hospital for Special Surgery/CornellMedical CenterBradley Raphael, orthopaedic surgery
Mount Sinai HospitalJocelyn Soffer, psychiatry
New York-Presbyterian Hospital–ColumbiaRohit Chandwani, general surgeryDaniel Khaimov, anesthesiologyAimee Lee, internal medicine
New York-Presbyterian Hospital–CornellJennifer Davids, general surgeryMatthew Davids, internal medicineElena Gimenez-Hubbard, surgery-
preliminary, urologyEdison Machado, internal
medicine/primary
New York University School ofMedicineHelena Hansen, psychiatryDavid Ornan, diagnostic radiology
nyu Downtown HospitalVicente Diaz, medicine-preliminary
Sound Shore Medical Center ofWestchester, New RochelleNeil Lester, medicine-preliminary
Staten Island University HospitalNeil Lester, diagnostic radiology
University of Rochester/StrongMemorial HospitalLorky Libaridian, medicine/pediatrics
North CarolinaDuke University Medical Center,DurhamHardean Achneck, general surgeryRichard Chung, medicine/pediatricsSean Lee, general surgery
University of North CarolinaHospitals Program, Chapel HillJesse James, internal medicineTrevor Phillips, emergency medicine
PennsylvaniaChildren’s Hospital of PhiladelphiaFrances Balamuth, pediatricsChristina Lynch, pediatrics-
preliminary, pediatric neurology
Hospital of the University ofPennsylvania, PhiladelphiaNiya Jones, internal medicineJune Spector, internal medicine/
primary
University of Pittsburgh MedicalCenterMichael Shapiro, plastic surgery
WashingtonUniversity of Washington AffiliatedHospitals, SeattleChloe Atreya, internal medicineAndrew Chen, ophthalmologyJing Feng, dermatologySharon Gill, internal medicine/
primaryLianne Hirano, internal medicineDouglas Jacobson, ophthalmology
WisconsinMedical College of WisconsinProgram, MilwaukeeMatthew Streckert, emergency
medicine
St. Joseph Regional Medical Center,MilwaukeeJing Feng, transitional
Three students are pursuing careeropportunities other than residency.Julie Cantor will be an associate atMunger, Tolles & Olson, a law firm inLos Angeles. Eric Poolman has a pub-lic health postdoctoral fellowship atthe School of Medicine. Louis Morenohas a position as research managerat Gerson Lehrman Group, a firm inManhattan that specializes in cus-tomized research for business.
l e f t to r i g h t Edidiong Ikpeand Niya Jones were ecstatic withtheir matches. Ikpe is pursuingemergency medicine and internalmedicine at ucla and Jones isdoing an internal medicine resi-dency at the Hospital of the
University of Pennsylvania.Erin Mahony shared her news—a residency in pediatrics atMass General. News of his resi-dency brought Michael Shapiro to tears of joy.
jake
wym
an (
5)

yale
med
icin
esu
mm
er20
0540 students
Boffo reviews for GoldenProbe!! Raves for Alpern!!Überstein rocks Harkness!!
The excitement was palpable at theFirst Annual Golden Probe Awards, theClass of 2007’s entry in the ever-popular parade of shows put on annu-ally by second-year medical students at Yale. Fans gathered behind a ropeline at the entrance to Harkness Audi-torium to greet the nominees and wonder who among them would winthe statues of gilded hands with erectindex fingers honoring the best in thebusiness. Fans cheered and snappedphotos at the sight of celebrity docs onthe other side of the rope.
Inside, it was all about entertain-ment, not to mention the minutiae ofbeing a medical student. The nod forBest Situation Comedy went to SeinfelderXXY, a spoof melding the televisionshow Seinfeld with Klinefelter XXY syn-drome, a common chromosomal abnor-mality. Erotic Admissions took the awardfor Best Pornographic Film (heavens!),with a cast starring admissions deanThomas L. Lentz, m.d. ’64, and adult-film actress Jenna Jameson, portrayed byDanielle Guez, as an applicant willing to get into med school “at any cost.”(Line from script: “The mcat is so longand hard!”) There was even an award for Best Physiology Textbook, pittingCostanzo’s Physiology, a top-rated text formed students, against Medical Physiologyby local heroes Boron and Boulpaep. Itended in a tie.
Dean Robert J. Alpern, m.d., madehis Yale singing debut with the themesong from Dean Alpern’s Neighborhood,the winner of Best Children’s Show,which evoked the late Fred Rogers,
complete with nerdy sweater and bluetennis shoes. The rock band Übersteinraised the roof with their original com-position, “New Haven Blues,” and themusicians—Michael Martinez and EricHuebner on guitars, Brian Yablon onkeyboards, Dario Englot on bass andpublic health student Jared Novak ondrums—played the four nominationsfor Best Oldies Song. The titles? “ThisGlans is Made for You and Me,” byWoody Urethrie; “Doc Around theClock,” by Bill Frist and the Congress;“Here Comes the Shunt,” by theNeedles; and “Don’t Know Much” byCram Booke.
When it came to the cluelessnessthat defines at least a part of secondyear, the last entry said it all:
Don’t know much biochemistry
Don’t know much physiology
Don’t know much about a histo book
Don’t know much about those pills you took …
Of course that will all change in twoyears, when the singers and dancers of ’07 will have traded their status asresident comedians for the real dramaof residency. Stay tuned!
—Cathy Shufro
b e l o w Caryn St. Clair, Cicely Williams andDanielle Guez sang and danced the show finale,“Bust Your Ass,” based on the 1990s Young M.C. hit: “This here’s a jam for all the students,tryin’ to get by, but it’s such a nuisance, getshut down cuz of your impudence. Studying abit would show some more prudence.”
terr
y d
agra
di
(3)
m i d d l e Ryan Kelly sang “Hey, Yale,” a songabout the Yale System, to the tune of Outkast’s“Hey Ya.”
b ot to m Michael Martinez of Überstein, aband with four medical students and one publichealth student, brought down the house withone original song and covers of oldies adaptedto medical themes.

41
Balancing the bedside and the bench, and having funalong the way
As he delivered the 18th annual FarrLecture at Student Research Day inMay, Arthur L. Horwich, m.d., hs ’78,fw ’83, described his own path to acareer in research. He trained as apediatrician, but the lure of the labora-tory ultimately proved too strong to resist. Still, he found a balance, hesaid. “Research and the bedside,” hesaid, “are inextricably linked.” Horwich,a geneticist whose work has shownhow proteins fold, still consults onclinical cases.
“You cannot predict exactly whatyou will be doing in some balance ofresearch and clinical medicine,” saidHorwich, the Eugene Higgins Profes-sor of Genetics and professor of pedi-atrics, as he offered some advice.“Make sure it is a balance that reallycauses you to have fun.”
Among the 75 students who pre-sented this year was second-yearmedical student Mary Dombrowski,who examined whether transplants ofolfactory ensheathing cells can regen-erate myelin. She chose the topicbecause her father has multiple scle-rosis. In her experiments with ratsshe found that the cells did encouragemyelin growth. “It has stimulated myinterest in neurology as a careerchoice,” she said.
Fourth-year student Hardean E.Achneck found the bright side to a dev-astating disease. Ascending aorticaneurysms are associated with adecrease in systemic atherosclerosis,and there may be a genetic mechanisminvolved, he said. “If we find out what
the genes are, we may find the mecha-nism of this and, eventually, treat ath-erosclerosis,” he said.
Research topics ranged from a mixof basic science and clinical findings toat least one offbeat subject. David A.Ross, a student in the m.d./ph.d. pro-gram, studied the phenomenon ofabsolute pitch. “The vast majority ofgreat composers,” he said, “have hadperfect pitch.” Alison H. Norris, alsoan m.d./ph.d. student, studied the hivrisk for workers on a sugar plantationin Tanzania. Helena Hansen, whocompleted the m.d./ph.d. program inMay, studied faith-based substanceabuse treatment in a Pentecostal com-munity in Puerto Rico.
Five students were chosen to makeoral presentations: Margo D. Simon,Eric Poolman, Suzanne J. Baron,Raymond Lynch and Joshua Klein.
—John Curtis
b e l o w The five students chosen to make oral presentations—Eric Poolman, Raymond Lynch,Margo Simon, Suzanne Baron and Joshua Klein—joined John Forrest, director of studentresearch, keynote speaker Arthur Horwich and Dean Robert Alpern before their talks.
terr
y d
agra
di
(3)
m i d d l e David Ross studied the phenomenonof perfect pitch.
b ot to m Jenna Giltnane described her researchin protein expression to Linda Bi.

yale
med
icin
esu
mm
er20
0542 alumni faces
65 years out of Yaleand still practicingHistory taking and the physical examremain at the heart of pediatricianRichard Dormont’s practice.
In Minot, N.D. (population 36,567), thelocal tourism board had to make up aslogan to help outsiders remember theplace’s name. (Why not Minot? rhymeswhen pronounced correctly.) Yet thesmall north-central North Dakota town draws families from large cities in surrounding states and Canada whocome seeking medical help for children with hard-to-diagnose diseases. Theycome to consult pediatrician Richard E.Dormont, m.d. ’40. Still in practice atthe age of 89, Dormont enjoys a repu-tation as a brilliant diagnostician aswell as a dedicated doctor available topatients at all hours. For several years,he has had a reduced patient load andshorter office hours, which allows moretime for bird-watching and for visitinghis four daughters. But retirement isnot on his radar.
“I like keeping busy and using my skills,” Dormont said, 65 yearsafter earning his medical degree.
A voracious reader of journals and a regular at medical conferences,Dormont is scrupulous about keepingup with new science. But he believespassionately that the tools he relied on in the early days of his practice—history taking and physical examina-tion—remain the bedrock of medi-cine. Recently a couple raised in Minotbrought their 19-month-old child home to consult Dormont after severalphysicians were puzzled by the child’sbreathing problems. He made thepotentially lifesaving diagnosis of con-
genital heart disease with equipmentno more high-tech than a stethoscopeand his own ears. The other doctors,Dormont said, had focused on breath-ing problems and examined the lungsrather than the heart. In addition, hesaid, physicians nowadays too often failto perform a thorough physical exam.
Minot parents keep bringing himtheir newborns for routine care. “Everytime someone has a new addition, theysay, ‘Now you can’t retire until so-and-so’s 18!’,” said Leann Hayton, l.p.n.
Hayton met Dormont in 1968when she came to work in pediatrics at Trinity Hospital in Minot. At first,Dormont’s “encyclopedic” knowledgewas intimidating, but he quickly puther at ease. “Dr. Dormont is a wonder-ful and patient teacher,” she said. “Ilearned more listening to and workingwith him than I could have in anyamount of schooling.”
Ruth Ann Rexine, r.n., also cameto know Dormont through hospital
pediatrics. She remembers his routineof making rounds before 7 a.m. (afterbreakfasting over medical journals),spending the day in his office, thendoing rounds again at 5 p.m. If achild’s condition worsened, day ornight, Dormont would be at the hospi-tal in minutes. “Always in a suit andbow tie,” Rexine remembered.
She chose Dormont for her ownchildren because of his legendary thor-oughness, his custom of answeringparents’ questions by phone everymorning from 8:30 to 9 a.m. and forthe way he could put children at ease.
Dormont had initially planned topursue a career in internal medicine.But when he lost the residency hewanted, his pediatrics professor cameto the rescue with a job in the pediatricoutpatient department at JohnsHopkins Hospital. He saw diseasesthat have disappeared or are a rarity—polio, measles, mumps—and each ofthe 55 patients he saw every day got a
When he’s not caring for children,pediatrician Richard Dormont is often out birding near his home in Minot, North Dakota.
eric
ste
rud

43
physical examination. “It can be done,”Dormont said.
After Johns Hopkins, Dormonttaught at Louisiana State University fortwo years, but decided academic medi-cine was not for him. “You have to be a politician,” he said. “I’m the world’sworst politician.”
Dormont served in the SouthPacific during World War II and alsopracticed briefly in Texas. In 1953 hecame to Minot, drawn by the chance to work in a group clinic. “That wasalmost considered communist on theEast Coast,” he remembered.
But the practice suited him becauseit provided him with his own lab, was connected to a hospital and, mostimportantly, allowed him his ownmedical library.
Dormont has spent the later years ofhis career in solo practice. “That can bedangerous,” said James Moller, m.d., aUniversity of Minnesota pediatric cardi-ologist who regularly comes to Minot forconsultations. But, said Moller, Dormontis so intellectually rigorous that he chal-lenges himself the way a good partnerwould. “He is always questioning, look-ing up things, studying,” Moller said.
Known universally as “Dr. Dormont,”he has cared for most of his commu-nity at one time or another.
“Whenever I’m birding, someonewill stop and say hello. Usually it’s oneof my patients,” Dormont said.
He estimates that he’s seen severalhundred thousand patients during his career. As long as they keep seek-ing him out, he said, his practice will stay open.
—Colleen Shaddox
Last November David Graham told a Senate committee that the Food and DrugAdministration had mishandled the drug Vioxx, which he considered dangerous.
fda’s top safety critic keeps a watchful eye on the public good
Whenever David J. Graham, m.d., m.p.h.,hs ’81, wonders whether he made the right career move from Yale-NewHaven Hospital resident to residentcritic of the Food and Drug Adminis-tration (fda), he recalls with remorse a patient who died under his care.
At the time, 1979-1981, he wasdoing a residency in internal medicineat Yale after graduating from the JohnsHopkins School of Medicine and plan-ning to become an expert on viral infec-tions of the central nervous system. But the patient died of an unexpectedadverse drug reaction, and even thoughGraham was not at fault, “I was the person who had prescribed the drug,”Graham says. The incident “contributedto my interest in studying drug safety.”
He also discovered during his timeat Yale that he “didn’t enjoy the day-to-day grind of patient care,” so he settledon epidemiology. Since then, he hashad a 20-year career as an epidemiolo-gist at the fda, forgoing more lucrative
offers in the private sector. He is nowassociate director for science and medi-cine in the agency’s Office of DrugSafety. Despite (and because of) thattitle, he has also become the fda’smost vocal and listened-to critic.
For years, Graham, 51, has been thefda’s equivalent of an ingrown toenail,causing his employer pain as he wentpublic with allegations that the agencywas allowing prescription drugs itapproved to stay on the market despiteevidence from its own researchers thatthe medications were harming andkilling people by the thousands.
In Graham’s view, the drug safetyproblems began in 1992 with the pas-sage of a law aimed at getting lifesav-ing drugs onto the market faster. Tospeed up approvals, the law forcedpharmaceutical companies to footmost of the bill for the review process.That left the fda “captured by indus-try,” says Graham. “He who pays thepiper calls the tune.” In the meantime,the same officials who approved thedrugs were being asked to monitortheir safety after they’d hit the market.If there’s evidence of harm, “now
reu
ters
/kev
in l
amar
qu
e

yale
med
icin
esu
mm
er20
0544 alumni faces
they’ve got to do an about-face,” hesays. “At its heart, that is an inherentstructural conflict of interest.”
Graham said a former boss told himthat the drug industry was the fda’sclient, but Graham, an assistant scout-master and devout Catholic with sixchildren, didn’t buy it. If he sees that adrug may be harmful, he’ll investigate.If the evidence warrants it, he’ll chal-lenge the fda’s regulatory position inter-nally, even if it earns him the enmity of his superiors, which it often has. Thefda labeled one of his studies “junkscience,” and forbade him to publishit in a major medical journal. (Sixweeks later the fda changed its mindand the article was published, lastFebruary, in The Lancet.)
Graham has called for the with-drawal of a dozen prescription drugs,and almost all of them have since beenremoved from the market—often aftera fight with his superiors—in somecases by the drugmakers themselves.One case made Graham a star witnessbefore the United States Senate’sfinance committee in 2004, whenMerck & Co. suddenly removedVioxx, its popular painkiller, after thecompany’s studies showed a higher risk of heart attacks and strokes amongusers of the drug. Graham had beenwarning about Vioxx for years, but thefda refused to pull the drug on his recommendations. He testified that theagency also urged him to change theconclusions of another damning studyabout Vioxx just before Merck’s sur-prising announcement. The voluntarywithdrawal placed the agency in anunwelcome spotlight over its allegedfailures to protect Americans againstunsafe drugs. Meanwhile, Graham
sought whistleblower status, and tele-phone calls disparaging him to theGovernment Accountability Project, anonprofit that protects maverick insiders, were traced back to the fda.(fda officials say they allow employeesto speak their minds, and couldn’texplain the incident.)
“The fda has let the American peopledown and, sadly, betrayed a public trust,”Graham told the Senate committee.
“I think I’ve had a substantial impact,as much as fda officialdom wants tobad-mouth me,” he says. “I point to theevidence and I say, ‘Look, I’m almostalways right.’ I don’t recklessly recom-mend the withdrawal of drugs.”
He says he hopes to finish hiscareer at the agency, even if more diffi-culty lies ahead. He has two sugges-tions for improving drug safety. First,the government should create a drugsafety center parallel to the fda’s drug approval center. The new centerwould oversee postmarketing regula-tion and would be able to call on the fda commissioner to pull a drug it deems unsafe. Second, this centershould be provided with enoughmoney to do its job. (A bipartisanSenate bill co-sponsored by DemocratChristopher J. Dodd of Connecticutand Republican Charles E. Grassley ofIowa would do just that.)
“I feel fairly certain that I’ve prob-ably saved more lives taking the careerpath I have taken than I would havewith another career path,” Graham says.“That’s something that colleagues bothwithin government and in academiaremind me of periodically when I tellthem of my tales of woe at the fda—they remind me that I’m doing good.”
—John Dillon
With an interest in the past,admissions dean doubles as a chronicler of local lore
Two years after receiving his medicaldegree, Thomas L. Lentz, m.d. ’64,made the decision, along with his wife,Judith, to leave New Haven and moveto the country. They found a pre-Revolutionary War house in Killing-worth, Conn., about 40 minutes fromLentz’s job as an instructor in anatomyat the School of Medicine. (When themedical school offered him a positionhe decided not to pursue a residency.)
Soon everything started growing:the Lentz family, the size of their new home, the Ohio native’s involve-ment in his adopted community andhis role at the School of Medicine,where he is now associate dean foradmissions and financial aid and pro-fessor of cell biology.
On moving day the Killingworthhouse was “livable,” but needy. “Therewas a lot of work to do,” said Lentz. “Itnever ends.” He painstakingly restoredan antique barn that was reduced to itsstone foundation. He and his wifebought surrounding parcels as theybecame available. Today their place inthe country is an 80-acre spread thatrequires a great deal of landscapingwork, though the five sheep they raisefor wool keep the grass trimmed.
Restoring a 1759 house piquedLentz’s interest in Killingworth history.He was a founding member of the his-torical society and serves as historianof the Congregational Church inKillingworth. (He also is a member ofthe town’s land trust and an electedmember of the planning and zoningcommission.) In 1976 when the his-

45
Familiar FacesDo you have a colleague who is makinga difference in medicine or public health or has followed an unusual pathsince leaving Yale? We’d like to hearabout alumni of the School of Medicine,School of Public Health, PhysicianAssociate Program and the medicalschool’s doctoral, fellowship and residency programs. Drop us a line [email protected] or write to Faces,Yale Medicine, P.O. Box 7612, New Haven,CT 06519-0612.
porters of the Yale System,” said JamesD. Jamieson, m.d., ph.d., professorand past chair of cell biology. “It’s beena joy to work with him, because I’velearned so much from him.”
Jamieson is impressed with Lentz’slow-key style in the lab and classroom.With some students coming fromhumanities backgrounds, Lentz’s thor-ough, methodical teaching of histologyleaves each student excellently pre-pared, said Jamieson. Lentz fine-tuneslectures he has given literally hundredsof times, added Jamieson, to incorpo-rate new information and increase his effectiveness.
While Lentz’s students still spendtime bent over traditional microscopes,his lab also uses a “virtual micro-scope”—high-resolution scans of slidesthat students can view and manipulateon computer screens. The new tech-nology makes it easier for students towork together and with faculty, as everyone is viewing the same imagesimultaneously.
The soft-spoken professor is slow tospeak about his own accomplishmentsbut quick to talk about his department,which began as a section in 1973 underthe leadership of Rockefeller University scientist George E. Palade, m.d.,who would win a Nobel Prize twoyears later. In addition to pursuing hisown research on primitive nervous systems, structure-function relation-ships of the nicotinic acetylcholinereceptor and, more recently, the entryand transport of rabies virus in neu-rons, Lentz serves as the department’shistorian—he stores departmental photographs and papers and wrote ahistory of cell biology at Yale for thedepartment website.
The history of his department andof the School of Medicine itself is palpable in Lentz’s office. He rescuedfrom the garbage the chair he offers to visitors. It belonged to Thomas R.Forbes, ph.d., who came to Yale in1945. Forbes eventually became theEbenezer K. Hunt Professor ofAnatomy and chaired the admissionscommittee throughout the 1950s and1960s. Lentz had sat in that chair forhis own admissions interview. It giveshim a good deal of pleasure to offerthe chair to accomplished hopefulstoday. “They inspire me,” he said.
—Colleen Shaddox
In the almost 40 years that Thomas Lentz haslived in Killingworth, he has restored an 18th-century house, helped found the town historicalsociety and served on the land trust and planning and zoning commission. He recently published a softcover book with more than 200 historical photographs of the town.
torical society was raising funds torestore a 19th-century schoolhouse,Lentz assembled a pamphlet of oldphotographs from the town that soldfor $5. This year a copy sold on eBayfor $180. Clearly, there is a market forvintage Killingworth images. So inanother attempt to enrich the historicalsociety, Lentz wrote A PhotographicHistory of Killingworth, a much moreambitious project. The softcover bookfeatures more than 200 photographsalong with his narrative.
Lentz said that he wrote the book “in his spare time,” a curious choice ofwords for a man with teaching respon-sibilities, his own research interests anda passionate commitment to selectingapplicants who will be not only excep-tional physicians, but also leaders intheir profession. “It never gets old andstale, because there’s always somethingnew,” Lentz said of his interactions withstudents and applicants. “These kids aredoing such amazing things that it’sreally exciting to talk with them. I wish I could take them all.”
The typical applicant has changedsince Lentz began serving on the admissions committee in 1968. Todaymany arrive at the medical school with postcollege experience working inhealth care as well as authorship of one or more scientific articles. Lentzwondered whether the medical schoolwould accept him today.
“We went to college, we majoredin biology, maybe we belonged to thepremed club. We worked summers as an orderly in a hospital. We mighthave worked a semester in the lab,”Lentz said.
Lentz is particularly suited to admis-sions as “one of the staunchest sup-
isab
el c
hen
ow
eth

yale
med
icin
esu
mm
er20
0546 alumni notes
send alumni news toClaire M. Bessinger, Yale Medicine,
P.O. Box 7612, New Haven, CT 06519-0612, or via e-mail to [email protected]
visit us on the webyalemedicine.yale.edu
1930s
John P. Ferguson,m.d. ’39, droppedus a note recently, recalling thathe “won the Yale Golf Champion-ship in the year 1934-35. Now I’ve found out they don’t makethe balls as good as they used to. They don’t go as far!”
1960s
John J. Schrogie, m.d. ’60, vicepresident for periapproval andgeriatric research studies atOmnicare Clinical Research inKing of Prussia, Pa., has receivedthe 2005 Henry W. Elliott Distin-guished Service Award from theAmerican Society for ClinicalPharmacology and Therapeutics.
Donald G. Skinner, m.d. ’64,received the 2005 PresidentialMedallion in March from theUniversity of Southern California(usc), where he is professor andchair of the Catherine and JosephAresty Department of Urologyand holds the Hanson-WhiteChair in Medical Research at theKeck School of Medicine of usc.
1970s
C. Gene Cayten, m.d., m.p.h. ’72,professor of surgery, communityand preventive medicine atNew York Medical College, hasbeen appointed senior associ-ate dean of Our Lady of MercyMedical Center in the Bronx.At the college he has served asdirector and senior advisor ofthe Institute for Trauma andEmergency Care and was pro-gram director of the college’ssurgical residency programs at Our Lady of Mercy and Lincoln Hospital.
Howard K. Koh, m.d. ’77, has beennamed the first recipient of theHarvey V. Fineberg Professorshipof Public Health at the HarvardSchool of Public Health. Thechair honors a former dean ofthe school. Koh previouslyserved as Massachusetts’ com-missioner of public health.
Pamela H. Nagami, m.d. ’76, ofthe Kaiser Permanente Wood-land Hills Medical Center, wasone of 12 physicians to receivethe Southern California Perma-nente Medical Group 2004Physicians’ Exceptional Contri-bution Award. The award recog-nizes physicians who have madenoteworthy contributions totheir communities.
Andrew B. Newman, m.d. ’75, isthe chair and managing directorof the newly founded OceanMedicine Foundation in Califor-nia. He will maintain his pul-monary practice and adjunctclinical faculty position atStanford while working with the foundation to improve thehealth of people on islands byincreasing the quality of island-based health care and ocean science and by preventing theglobal spread of epidemics.
1980s
Patrick A. Charmel, m.p.h. ’83, hasbeen appointed to the NationalAdvisory Council for HealthcareResearch and Quality, whichadvises the U.S. Department ofHealth and Human Services and its Agency for HealthcareResearch and Quality. Charmel is president and ceo of GriffinHospital and its parent com-pany, Griffin Health ServicesCorp., in Derby, Conn.
Jonathon S. Lewin, m.d. ’85, hs’86, a neuroradiologist with aresearch interest in mri-guidedinterventional procedures, wasnamed the Martin W. DonnerProfessor and director of theDepartment of Radiology atJohns Hopkins. He and his wife,Linda O. Lewin, m.d. ’87, and theirchildren live in Baltimore, Md.
James S. Marks, m.d., m.p.h. ’80,has been named senior vicepresident and director of thehealth group of the RobertWood Johnson Foundation. He isthe former acting director of theCoordinating Center for HealthInformation and Service at theCenters for Disease Control andPrevention.
Edward S. Tyau, m.d. ’85, of theKaiser Permanente RiversideMedical Center, was one of 12 physicians to receive the South-ern California PermanenteMedical Group 2004 Physicians’Exceptional Contribution Award.The award recognizes physicianswho have made noteworthy con-tributions to their communities.
1990s
Senda Benaissa, m.p.h. ’95, wasmarried to Mario Hernandez inOctober. Benaissa is a researchscientist at Gallaudet ResearchInstitute and consultant at theWorld Bank in Washington, D.C.,focusing on health care andinternational disability.
Mark Coyle, pa ’96, and Stacey L.Frasca, pa, were married on Sep-tember 12. Both the bride andgroom work as physician assis-tants at St. Vincent Hospital atWorcester (Mass.) Medical Center.
Michelle P. Dequina, m.p.h. ’98,currently studying for her m.b.a.at Yale, and Neal K. Nakra, m.d., afellow in pediatric pulmonologyat Yale-New Haven Hospital,were married on January 14.
Manendiu A. Ndoping, m.p.h. ’98,a manager at the Health Strat-egies Consultancy in Washington,D.C., and Reginald P. Bazile, a con-sultant in Washington, weremarried on December 30.
Cynthia Carver Smith, m.p.h. ’90,writes to say that she and herhusband, Lt. Col. David B. Smith,usmc (Ret.), celebrated theirfourth wedding anniversary lastSeptember. David is an IT executive for the Securities andExchange Commission, andCynthia owns a telecommunica-tions company in the Washing-ton, D.C., area. In 1999 Cynthiaand David founded Cynthia’s Kids,a nonprofit devoted to the well-being of children, and theyrecently made a gift to YaleSchool of Medicine’s Departmentof Obstetrics, Gynecology andReproductive Services in memoryof their twins, Jack and JuliaSmith.
2000s
Aviv Halpert, pa ’01, a pediatricphysician assistant at MontefioreMedical Center in New York, wasmarried to Jessica Pitt, a pediatricoccupational therapist, onNovember 26, 2003.
Andrew Newman Patrick CharmelJohn Ferguson Michelle DequinaHoward Koh Edward TyauJonathon Lewin
47in memoriam
send obituary notices toClaire M. Bessinger, Yale Medicine,
P.O. Box 7612, New Haven, CT 06519-0612, or via e-mail to [email protected]
Elisha Atkins, m.d., professoremeritus of medicine, died onApril 22 at the age of 84 inBelmont, Mass. With Yale col-league Phyllis Bodel, m.d., Atkinsdemonstrated the close relation-ship between the induction of fever and the ability to resistinfection, and was author ofnumerous research articles onfever and infection. At the Schoolof Medicine, Atkins served on the admissions committee andfor a year was acting associatedean. He also served as master of Saybrook College, one of Yale’s undergraduate residen-tial colleges.
John E. Bowers, m.d. ’47, died onFebruary 10 at the age of 80.Bowers was a lieutenant in theU.S. Navy during the Korean Warand was the chief of staff atPlantation General Hospital inPlantation, Fla.
Sonja M. Buckley, m.d., a Yalevirologist who in 1969 helped toidentify the deadly Lassa virus,which originated in Africa, diedon February 2 in Baltimore atthe age of 86. Buckley receivedher medical degree from theUniversity of Zurich in 1944. Aftercoming to the United States,she worked first as a researchassistant at John Hopkins, thenat the Sloan-Kettering Institute,where she became head of thesolid tumor program in 1949.She began working on viruses at the Rockefeller Foundation in1957 and came to Yale in 1964.She retired in 1994.
Marshall Edelson, m.d., ph.d.,died at the age of 76 on January16 in Woodbridge, Conn. Edelsonwas a professor emeritus of psy-chiatry at the School of Medicine,where he taught for over 30years. He wrote nine books ontopics ranging from grouptherapy to psychoanalytic theoryand received many awards for his teaching and scholarship.
Nicholas M. Greene, m.d., founderof the Department of Anes-thesiology at Yale, died in NewHaven on December 28 atthe age of 82. Greene, one ofthe founding fathers of modernanesthesiology, served as direc-tor and chair of the departmentfor 18 years. He is credited withtransforming the service at Yalefrom a technical subspecialty of surgery into a medical andacademic discipline in its ownright. He published severalbooks and more than 200 arti-cles about education and thephysiological changes associ-ated with anesthesia. In 2001the School of Medicine honoredGreene with the establishmentof the Nicholas M. GreeneProfessorship in Anesthesiology,an endowed chair.
William E. Laupus, m.d. ’45, diedon February 14. Laupus taughtat New York Hospital beforegoing into private practice inDetroit. He returned to teachingat the Medical College ofGeorgia, Augusta, as assistantprofessor of pediatrics, and thenbecame chair of the departmentof pediatrics at the MedicalCollege of Virginia in Richmond.As founding dean, he trans-formed the School of Medicineat East Carolina University,Greenville, N.C., into an accreditedfour-year program.
James M. Malloy, m.p.h. ’67, diedon January 27. After his gradu-ation Malloy worked for YaleUniversity and then WaterburyHospital. He also served as theceo of three medical centersbefore moving to Jackson, Miss.,where he founded one of thestate’s first hmos. He subse-quently started a health careconsulting practice. Malloyraised money for health care ini-tiatives serving underinsuredcommunities in Mississippi,earning him the DistinguishedAlumni Service Award from theSchool of Public Health in 2004.
Yvedt L. Matory, m.d. ’81, died onApril 15 in Needham, Mass., ofcomplications from melanoma.She was 48. Matory was an asso-ciate surgeon in the Division ofSurgical Oncology and co-chairof the Women’s Cancer Programat Brigham and Women’sHospital in Boston. In 2000 shestarted HospitalCareOnline, acompany that uses computersand remote monitoring to carefor patients after their dischargefrom the hospital.
Eric W. Mood, m.p.h. ’43, died onDecember 31. Mood was a vet-eran of World War II, who servedin Italy and the South Pacific. Heretired from the Army Reserve asa colonel. He worked as directorof the Bureau of EnvironmentalSanitation for the New HavenHealth Department before join-ing the Yale public health facultyas a lecturer. In the mid-1960s hedeveloped the Division of Envi-ronmental Health and served asits director. His research focusedon food sanitation, waste watertreatment, swimming pool stan-dards, drinking water quality, airpollution and the health aspectsof housing.
Alvin Novick, m.d., professor ofecology and evolutionarybiology, died in New Haven ofprostate cancer on April 10 atthe age of 79. After serving inWorld War II, during which hewas a prisoner of war inGermany, Novick studied medi-cine at Harvard. He taughtbiology at Yale for 48 years andwas a world-renowned experton bat echolocation. Starting in1982, however, he turned hisattention to the aids crisis. Hewas chair of the Mayor’s TaskForce on aids in New Haven anda founder of aids Project NewHaven and Leeway, Connecticut’sonly nursing home for the treat-ment of people living with aids.
George A. Silver, m.d., died onJanuary 7 at the age of 91 inChevy Chase, Md. A professoremeritus of public health atYale, Silver served as deputyassistant secretary for healthand scientific affairs at the U.S.Department of Health, Educa-tion and Welfare from 1965 until1968. He served in the ArmyMedical Corps in Europe duringWorld War II, helping to liberateDachau and other concentrationcamps. After the war, he waschief of the social medicine divi-sion at Montefiore Hospital inNew York. He served on theWorld Health Organization’sexpert committee on medicalcare and was secretary of theFederation of AmericanScientists’ national council.

yale
med
icin
esu
mm
er20
0548 follow-up archives 50 and 25 years ago
winter /spring 1980Yale Medicine
Match Day 1980
“Match Day is the culmination ofseveral months of planning, coun-seling, and decision making on the part of senior medical stu-dents, deans and faculty, as well as hospitals participating in theNational Resident Matching Pro-gram (nrmp). The program wasdeveloped during the 1950s whenthere were more internship posi-tions available than there weremedical school graduates to fillthem. As a result, many hospitalswere exerting pressure on stu-dents to sign contracts for theirinternships early in their senioryear; some even pressed for deci-sions early in the sophomore orjunior years. In 1953, after severalattempts to establish an equitablesystem for internship appoint-ments, the basic rules of the exist-ing nrmp were set. …
“This year, March 12 was MatchDay. At Yale, of the 96 members of the Class of 1980, 42 studentsreceived appointments to the hos-pital of their first choice; 19 wereappointed to the hospital theylisted as second choice; and 10 totheir third choice.”
october 1955Alumni Bulletin
New Graduate Program inMedical Sociology
“Yale University will start a newgraduate program in medical soci-ology—the first of its kind in thenation to train students to applythe knowledge and techniques ofsociology to the fields of medicineand public health. The new pro-gram will attempt to bridge thegap between medicine and sociol-ogy—between the doctor and the society which he serves. It willprepare students for teaching,research and administrative posi-tions involving the social aspectsof health and medicine. …
“The first year will be spent incourses designed to meet specialinterests and training needs.The student will study the appli-cation of medical knowledge topublic health problems, as well asthe relationship of public healthto various sociological phenom-ena. Courses will be taken in boththe Department of Sociology and the School of Medicine. Thesecond year of the program willbe devoted to a thesis in the fieldof health or medical problemsand society.”
Antibiotic-resistant ribosomes unmasked
Five years ago, Yale scientists made a splash with the long-sought atomic structure of the large subunit of the ribosome,the protein-synthesizing factory of the cell and a target formany antibiotics (See “Yale Researchers Solve Structure of theRibosome,” Fall 2000/ Winter 2001). It was the largest asym-metric structure to be solved up to that time, and the work,coming from the laboratories of Thomas A. Steitz, ph.d.,Sterling Professor of Molecular Biophysics and Biochemistryand a Howard Hughes Medical Institute investigator, and PeterB. Moore, ph.d., Sterling Professor of Chemistry and professorof molecular biophysics and biochemistry, settled many long-standing questions about protein synthesis.
This spring the Yale group offered a new collection of structures that explain how some bacteria escape the killingeffects of some antibiotics. With antibiotic resistance threat-ening to undo years of progress against infectious disease, thework provides a road map to new antimicrobial drugs.
Many commonly used antibiotics bind to the samelarge pocket in the bacterial ribosome and block its ability tosynthesize proteins. In a study published in the April 22 issueof the journal Cell, Steitz and Moore investigated how azithro-mycin and four other antibiotics bind to the ribosome in drug-resistant and nonresistant bacteria. All are affected bythe same crucial change in just one of the 3,000-plus rnanucleotides that make up the large subunit.
“We found that mutations creating resistance result inthe insertion of one extra polar bump into the drug bindingsite that pushes a bound drug a little further away from itspreferred position than it would like to be,” said Moore. “Theshape and charge complementarity go from nice to not quiteso nice, and you go from sensitive to resistant because theamount of drug it now takes to inhibit these bacteria is morethan patients can tolerate.”
Knowing the problem suggests its solution—redesignantibiotics so they can fit around the bump. Now researcherscan exploit structure-based drug design, a technique that hasyielded successful treatments for aids and cancer. That effortwill continue close to home, at Rib-X Pharmaceuticals, theNew Haven startup that Steitz, Moore and several Yale col-leagues co-founded back in 2001, in the wake of solving theirfirst ribosome structure.
—Pat McCaffrey
daq
i tu
end note
A F T E R 1 8 Y E A R S , A FA R E W E L L TO YA L E
Visitors to the Office of Alumni Affairs will still be able to helpthemselves to a donut or some candy from the ever-presentdish by the door. But the cheery smile and boundless enthusiasmSharon R. McManus brought to her job as director of alumni affairs, a post she assumed in 2000, will be absent. (Not to mentionthe Irish soda bread she brought each year on St. Patrick’s Day.)
Alumni around the country got to know McManus duringher frequent trips organizing receptions and meetings, as well as at the annual reunion where she was, as office administratorPatricia DiNatale said, the “ambassador of smiles.” In addition toplanning and overseeing the annual reunion, McManus launcheda Web-based program to enlist alumni as mentors for currentstudents, especially during the residency application process.
After 18 years at Yale, including 16 at the School of Medi-cine, McManus left in May to join the staff of the Nightingale-Bamford School, a K-12 school for girls in New York City.
At a farewell party in early May, an ode to McManus writ-ten by a colleague recalled her “smiling face, that sweet Irishlaughter … For all who visit alumni affairs, you’re engulfed withthe feeling someone truly cares!”
joh
n c
urt
is
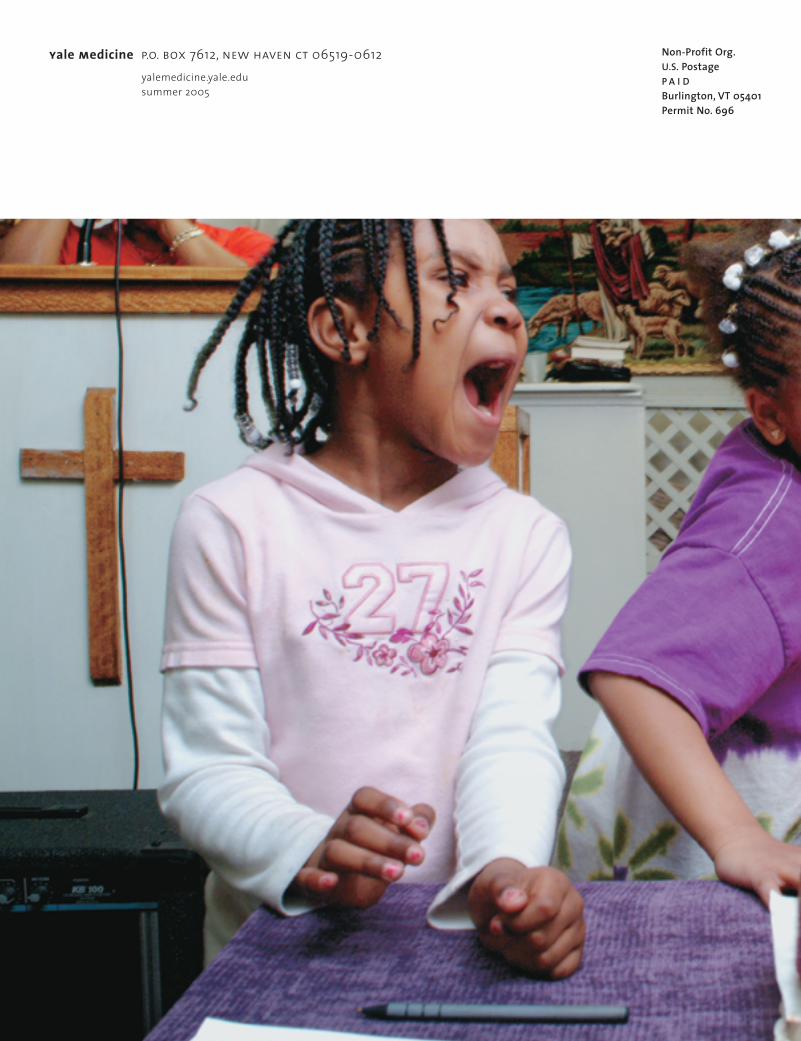
yale medicine p.o. box 7612, new haven ct 06519-0612 yalemedicine.yale.edusummer 2005
Non-Profit Org.U.S. PostageP A I DBurlington, VT 05401Permit No. 696




















