11-10612-shl Doc 427 Filed 03/16/12 Entered 03/16/12 16:44 ...
Upload
khangminh22Category
view
1download
0
A Learning Organisation
Annual report 2015/16
training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development
2
training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development
A Learning OrganisationContents
1 Foreword from the Chairman and Chief Executive 4
2 Our vision and objectives 6
3 The first full year of our new Trust 7
4 Quality and performance against key targets 11
5 Researching to innovate 16
6 Celebrating staff excellence 18
7 Our patients’ feedback 22
8 Our estate 24
9 Information governance 27
10 Our Trust Board 28
11 Annual governance statement 35
12 Financial report 48
13 Remuneration report 94
Annual report 2015/16

3
training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development
2015/16 saw teams participating in international, national and local research
activities, with over 70 consultants active in
projects and 3,500 plus patients involved in
research-led services.
Our staff which includes 1,300 doctors, 4,000
nurses as well as therapists, scientists and support staff,
serve a diverse population of approximately 850,000
Examples of excellence can be seen in our stroke service which is rated the best in the
country and at St. Mark’s Hospital, an
internationally renowned specialist centre for colorectal
diseases.
A ground-breaking research study using robot assisted
training to help stroke patients regain movement in their
affected arm was launched at Northwick Park Hospital.

4
Foreword from the Chairman and Chief Executive1
A learning organisationAs one of the largest integrated acute and community care trusts in the country, our focus is to ensure that we provide services of the highest quality to the people who live and work in North West London. Our aim is to be the Trust of choice for patients and staff.
In delivering this care we face some significant challenges but have started to see good progress against these during 2015/16. Our financial position remains difficult, partly as a legacy of the merger. However, thanks to the collective efforts of staff across the Trust and the support of our commissioners, we ended the financial year on plan. This was particularly impressive given the significant financial pressures experienced across the NHS last year. The aim now must be to maintain this good performance and ensure that we use our resources as effectively and efficiently as possible.
A&E performance is another important area where we are beginning to see improvement. In January 2016 a new ward block opened at Northwick Park Hospital providing 63 additional beds and an Assessment Unit and Short Stay Unit. These units are helping to improve patient flow through the hospital. In addition to the extra beds, we have introduced new procedures and forged close links with the London Ambulance Service and
Clinical Commissioning Groups (CCGs) to better manage demand and ensure patient safety at all times.
We continue to lead the way in a number of other areas. Examples of excellence can be seen in our stroke service which is rated the best in the country and at St. Mark’s Hospital, an internationally renowned specialist centre for colorectal diseases.
The nature of our work means that we must ensure that we make the best use of our resources across all of our community and hospital sites and services. The NHS Five Year Forward View (FYFV) set out a new shared vision for the future of the NHS based around the new models of care involving stakeholders working collaboratively across the local healthcare system. To help deliver the FYFV local sustainability and transformation plans (STPs) are being set up across the country. The Trust is part of the North West London STP, bringing together primary, acute, community, mental health
and social care organisations with local authorities to agree on a shared approach to improving health and healthcare. The work of the STP will be a driver for change during the coming years.
The STP for North West London has the advantage of building on some important relationships already forged through the Shaping a Healthier Future (SaHF) programme. In June 2015 the maternity unit at Ealing Hospital closed as part of the SaHF plans to reshape maternity services across the whole sector. A review into those changes found that they were made safely with patients seeing improvements to their care. The SaHF programme will see changes to children’s services at Ealing Hospital come into effect from summer 2016 and our paediatric team have worked to plan for these during the past year.
Major changes of this kind cannot be made without staff feeling well supported and well informed. During the year we have held weekly, Chief Executive-led, open staff forums across all of our sites. These
Jacqueline Docherty, DBE Chief Executive Officer
Peter Worthington Chairman

5
With your continued support we will be able to further develop and strengthen the Trust, enhance the experience of patients and realise our full potential.
Jacqueline Docherty, DBE Chief Executive Officer
Peter Worthington Chairman
meetings have focused on a different theme each month and work to encourage two-way conversations with the executive team.
The theme of this year’s annual report is a learning organisation, one that prides itself on innovation, transformation, training, research & development – and learning from our patients through feedback and involvement opportunities at the Trust. There are some fantastic examples inside the report of the work that our teams are doing across all of our sites. The report also shines the spotlight on our annual staff awards. Now in
their third year the ‘Pride in our Staff LNWH staff Excellence Awards’ celebrate outstanding achievement by individuals and teams.
Without our staff, dedicated volunteers and associated charities we would not be able to provide excellent care to the many thousands of patients who use our hospital and community services each year. It is also important to acknowledge the support we receive from our CCGs, Health and Wellbeing Boards, local councils, Local Healthwatch, clinical and business partners and of course our patients.
Members of the Trust’s Ambulatory Care Team at Northwick Park Hospital.

6
Our vision and objectives2Our 9,000 plus staff which include 1,300 doctors, 4,000 nurses as well as therapists, scientists and support staff, serve a diverse population of approximately 850,000 from:
• Central Middlesex Hospital
• Ealing Hospital
• Northwick Park Hospital
• St. Mark’s Hospital
• Community services including Clayponds Rehabilitation Hospital
• Meadow House Hospice, Denham Unit and Willesden Centre.
VisionTo evolve we must create an identity and culture that will support the ambitions we have for our hospital and community services. Five core objectives will drive this work helping the Trust to achieve its vision ‘to provide excellent clinical care in the right setting by being compassionate, responsive and innovative.’
ObjectivesImproving our focus on safety and quality
• We will work with our patients to ensure that the Trust complies with the recommendations made by the Francis Inquiry into the events at Mid-Staffordshire NHS Foundation Trust
• We will continue to ensure the safety and wellbeing of all patients in our care.
Improving patient experience, satisfaction and engagement
• We will work with all our stakeholders to develop a culture of openness, caring and compassion
• We will actively involve patients and carers in all aspects of care and service delivery and act on their feedback
• We will complete our programme to improve our estate, including the operating theatres, emergency department and infrastructure at the Northwick Park site.
Creating a sustainable workforce that is engaged in developing and improving services
• We aim to become the employer of choice for healthcare staff
• We will ensure our values are understood and embedded.
Ensure financial sustainability• We will deliver a financial strategy that supports the Trust but does
not undermine our focus on patient safety.
Planning for our future• We will support implementation of the Shaping a Healthier Future
programme to enable better standards of care for our patients.
London North West Healthcare NHS Trust is one of the largest integrated care trusts in the country, bringing together hospital and community services across the boroughs of Brent, Ealing and Harrow.
training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development

7
Crick Ward assessment unit and Darwin Ward short stay facility are helping to improve the flow of patients through the hospital. Patients are able to be admitted more quickly from A&E to the ward and then on to a safe discharge home.
Elgin Ward infectious diseases unit has 15 single rooms all with en-suite facilities and an infectious diseases assessment room for outpatient care.
Upper gastrointestinal and colorectal cancer development
The Trust receives, on average, over 120 referrals for patients with suspected
New wards help to reduce patient stay
The new Acute Medical Unit at Northwick Park Hospital provides a state-of-the-art working environment for staff and an enhanced experience for patients. Opened in January 2016 the Crick, Darwin and Elgin wards provide a total of 63 new beds.
We are proud of our teams meeting core standards, while innovating and developing services for patients at the same time. This section of the annual report includes some of the highlights from our first full year operating as London North West Healthcare NHS Trust.
The first full year of our new Trust3
The Trust has pledged to be a learning organisation, one that learns from its patients, staff, best practice, education, research and developments internationally.
training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development
Members of the health visiting team at Wembley Centre For Health and Care.

8
Pushing the boundaries in cardiac care
The Trust is taking part in the international ISCHEMIA trial that is researching the best outcomes for people with stable coronary heart disease such as angina. Northwick Park Hospital is the highest recruiting centre in the world for the trial, which looks at medication and lifestyle changes versus stenting and surgery, or a combination of the two, to ultimately recommend a best standard of care internationally.
Improvements for liver disease patients
Clinicians at Central Middlesex Hospital launched a new treatment approach that is speeding up the assessment and diagnosis of liver disease. The innovative technology called Acoustic Radiation Force Impulse (ARFI) delivers full liver assessments for patients in a single day. The approach allows patients to have a full liver assessment in one day, rather than across three hospital visits.
information exchange and further expansion of community services.
The rapid access clinic enables local GPs to refer children needing specialist review more quickly. The aim is to reduce the number of children coming to A&E by referring them from the GP surgery direct to the appropriate paediatric specialist in hospital.
The Paediatric Care Information Exchange offers parents access to a web-based child health record. The pilot project benefits those parents with children who have multiple and complex needs. These patients often receive care from a number of places so the online approach makes sharing and updating information much easier.
Community services in Southall were given a boost with the launch of Connected Care for Children (CC4C). CC4C focuses on providing more care and support from venues closer to home and, in the process, reduces the need for families to come to hospital.
upper gastrointestinal (GI) and colorectal cancer every week. During 2015/16 a new service was launched at St. Mark’s Hospital to improve the experience of patients by speeding up the referral to diagnosis and treatment.
Endoscopy, Radiology, Outpatient Services (EROS) was developed by consultants and specialist nurses to improve the whole patient pathway. Its focus on improving communications has reduced diagnosis times, provided a single point of contact for patients and GPs and improved the speed of appointments. Our clinicians are now reviewing patients’ results in record time, resulting in a quicker discharge from the pathway.
Better support for patients surviving GI cancer
A new approach to caring for cancer survivors is improving quality of life for those living with the disease. Most GI cancer survivors do not experience ongoing problems after treatment and surgery but, for those that do, the side-effects can be debilitating. The Trust has introduced a new service to support this group of patients. Managed by two gastroenterologists and a Macmillan nurse consultant, the service is multi-disciplinary and one of only two in London. GPs are able to refer patients through a single point of contact and referrals have increased week on week since it started.
Improving care for children
A number of developments in children’s services were introduced at Ealing Hospital including a new rapid access clinic, a paediatric care
The first full year of our new Trust
A new hi-tech theatre that is purpose built for integrating 2D and 3D imaging systems.

9
computer screen and places their arm onto the robotic device. The therapist then asks the patient to undertake some arm exercises such as moving between targets on the computer screen. If the person is unable to move their arm then the robot moves it to complete the task. If the patient initiates movement, the robot provides adjustable levels of assistance to facilitate the arm movement – all of which helps the brain and arm to learn to work together again.
One of the first patients to have therapy using the robotic arm was 50-year-old Bindiya Panya. She says: “I had a stroke in March 2015, lost movement down my right side and couldn’t walk. It’s very hard for people to understand how difficult that is to accept. I feel very lucky to have been asked to take part in this trial. The robotic arm has made such a difference to use of my right arm.”
involving support from a consultant-led multidisciplinary team including therapists, a dietician and rehab assistant. Patients are supported with getting to grips with day to day tasks such as dressing and cooking.
Robot research benefits for stroke patients
A ground-breaking research study using robot assisted training to help stroke patients regain movement in their affected arm was launched at Northwick Park Hospital.
During the training, the patient sits at a table facing a
High tech theatre is first to integrate 2D and 3D imaging
St. Mark’s Hospital is the first in the country to be purpose built for an innovative new approach to bowel surgery. The theatre fully integrates 2D and 3D imaging systems including sterile touch screens to control the equipment. The theatre combines keyhole surgery with simultaneous flexible endoscopy – a long, thin tube that has a light source and video camera at one end. The benefits to patients are that bowel operations will be smaller, safer and faster which means better and reduced recovery times.
Sharing pharmacy expertise
A new online training course was introduced by Ealing Hospital’s Pharmacy Department to support community services staff working alone with patients in their own homes. Lone workers have less opportunity than hospital-based colleagues to check medication queries with peers and multi-disciplinary teams. The online training enables them to stay up-to-date on how medicines should be administered, handled, stored and safely disposed of.
Stroke rehabilitation at home
A new approach to stroke rehabilitation is focused on providing patients with the right care in the right setting. Patients spend on average 17 days in hospital after a stroke with the majority of that time being spent in rehabilitation. Funded by Brent Clinical Commissioning Group, the pilot programme enables patients to receive the rehabilitation element of their care at home. The packages of care last up to six weeks,
Robot assisted training is helping stroke patients.
Staff in the upgraded decontamination unit at Central Middesex Hospital.
10
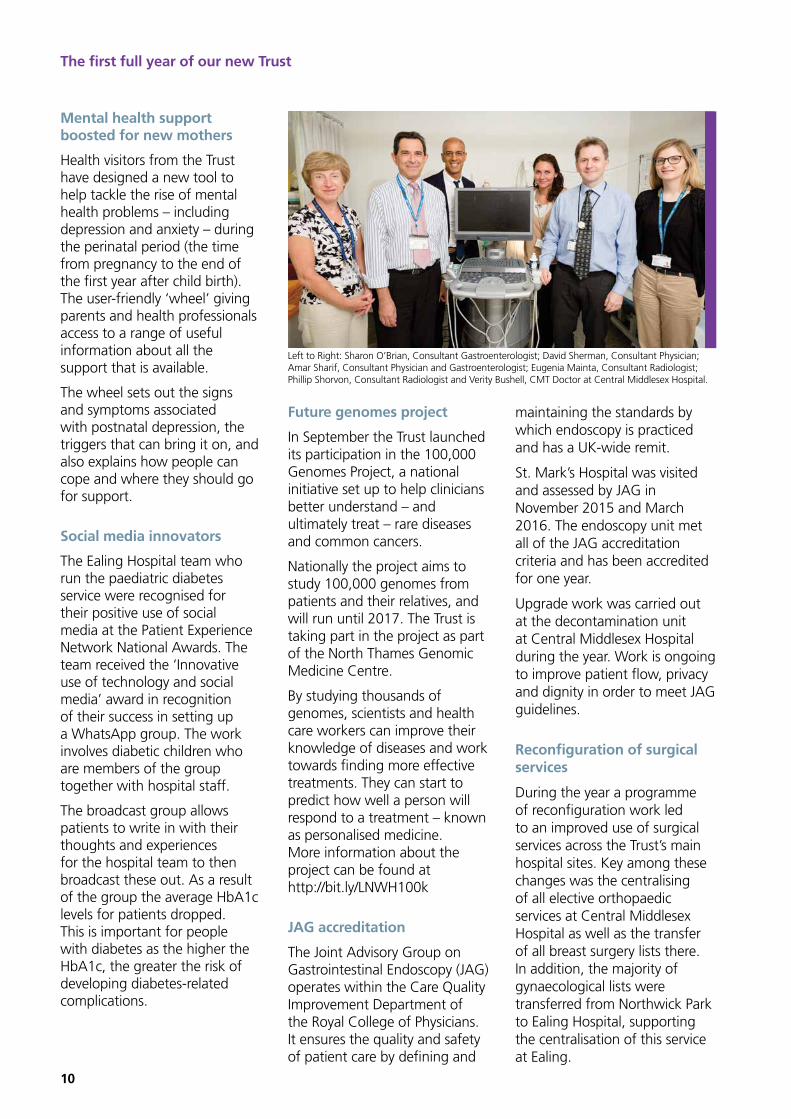
Future genomes project
In September the Trust launched its participation in the 100,000 Genomes Project, a national initiative set up to help clinicians better understand – and ultimately treat – rare diseases and common cancers.
Nationally the project aims to study 100,000 genomes from patients and their relatives, and will run until 2017. The Trust is taking part in the project as part of the North Thames Genomic Medicine Centre.
By studying thousands of genomes, scientists and health care workers can improve their knowledge of diseases and work towards finding more effective treatments. They can start to predict how well a person will respond to a treatment – known as personalised medicine. More information about the project can be found at http://bit.ly/LNWH100k
JAG accreditation
The Joint Advisory Group on Gastrointestinal Endoscopy (JAG) operates within the Care Quality Improvement Department of the Royal College of Physicians. It ensures the quality and safety of patient care by defining and
Mental health support boosted for new mothers
Health visitors from the Trust have designed a new tool to help tackle the rise of mental health problems – including depression and anxiety – during the perinatal period (the time from pregnancy to the end of the first year after child birth). The user-friendly ‘wheel’ giving parents and health professionals access to a range of useful information about all the support that is available.
The wheel sets out the signs and symptoms associated with postnatal depression, the triggers that can bring it on, and also explains how people can cope and where they should go for support.
Social media innovators
The Ealing Hospital team who run the paediatric diabetes service were recognised for their positive use of social media at the Patient Experience Network National Awards. The team received the ‘Innovative use of technology and social media’ award in recognition of their success in setting up a WhatsApp group. The work involves diabetic children who are members of the group together with hospital staff.
The broadcast group allows patients to write in with their thoughts and experiences for the hospital team to then broadcast these out. As a result of the group the average HbA1c levels for patients dropped. This is important for people with diabetes as the higher the HbA1c, the greater the risk of developing diabetes-related complications.
maintaining the standards by which endoscopy is practiced and has a UK-wide remit.
St. Mark’s Hospital was visited and assessed by JAG in November 2015 and March 2016. The endoscopy unit met all of the JAG accreditation criteria and has been accredited for one year.
Upgrade work was carried out at the decontamination unit at Central Middlesex Hospital during the year. Work is ongoing to improve patient flow, privacy and dignity in order to meet JAG guidelines.
Reconfiguration of surgical services
During the year a programme of reconfiguration work led to an improved use of surgical services across the Trust’s main hospital sites. Key among these changes was the centralising of all elective orthopaedic services at Central Middlesex Hospital as well as the transfer of all breast surgery lists there. In addition, the majority of gynaecological lists were transferred from Northwick Park to Ealing Hospital, supporting the centralisation of this service at Ealing.
The first full year of our new Trust
Left to Right: Sharon O’Brian, Consultant Gastroenterologist; David Sherman, Consultant Physician; Amar Sharif, Consultant Physician and Gastroenterologist; Eugenia Mainta, Consultant Radiologist; Phillip Shorvon, Consultant Radiologist and Verity Bushell, CMT Doctor at Central Middlesex Hospital.

11
Quality
1 Reducing patient harm
Our reducing patient harm programme focused on reducing grade three and four Trust-acquired pressure ulcers, reducing urinary tract infections in patients with catheters, reducing harm from falls and developing a supportive infrastructure to enable clinical supervision for frontline staff.
This is the largest element of the quality agenda and is focused on making sure that patients experience good outcomes from the care they receive. Our performance is on the table on page 15, with key highlights described below.
Quality and our performance against key targets4
Sign up to safety campaign
We became a member of the Sign up to Safety campaign, which aims to make the NHS the safest healthcare system in the world. The long-term objective is to halve avoidable harm and save 6,000 lives over the next three years.
Falls, VTE and the standard hospital
mortality indicator
Our staff made excellent progress in reducing harm from falls, to strengthen compliance with venous thromboembolism (VTE) standards and to maintain the standard hospital mortality indicator. For our falls prevention work, we are now below the 2010 National Patient Safety Association (NPSA) national average for acute trusts and we are working with our clinical commissioning groups to spread this good practice to nursing and residential homes.
Pressure ulcers and UTIs
Pressure ulcers are largely preventable and we strengthened monitoring and practice standards in this area. Our performance improved thanks to the improved governance, data usage and stronger ‘Ward to Board’ processes that now include senior daily reviews of all pressure ulcer patient cases. It was a similar case with
At the heart of everything we do is a strong focus on quality to make sure that our patients receive the best and safest care. We made progress against three main priorities which were reducing patient harm, improving the patient experience and improving the emergency care pathway. We also hosted an announced inspection in October from the Care Quality Commission (CQC). The visit has provided valuable insight into how our services benchmark nationally against peer organisations.

12
2 Improving patient experience
The annual patient surveys provide a rich source of feedback to help us make improvements that ensure patients have a good experience in our care. Satisfaction levels have an impact on the reputation of the Trust and we use the information patients give us to focus our work for the year.
While the survey results show a rise in patient satisfaction compared to the previous year, there is still much work to do for our performance to reach best practice standards. Key objectives for 2016/17 are to get more patients participating in the surveys, plus improving appointment booking and change processes.
Improving the quality of discharge processes
Good discharge processes are central to a positive patient experience. A delayed or poorly planned discharge can lead to a number of issues both for the patient and wider service.
lead at Brent, Harrow and Hillingdon Clinical Commissioning Group a total of 22 cases were reclassified as non – trajectory cases. Therefore our end of year position was 27 cases against the trajectory of 37.
We have a number of strategies to reduce the risk of Clostridium difficile infection and these include prudent prescribing and antibiotic stewardship. The Trust rate of Clostridium difficile per 100,000 bed days is 11.67, compared to the England rate of 15.23.
• MRSA bloodstream infection has a zero tolerance target in the acute hospital setting. The Trust unfortunately reported a total of six cases. This equates to a rate of 2.12 per 100,000 bed days, compared to 0.89 in England. Eliminating MRSA bloodstream infection is a key priority in the coming year.
reducing urinary tract infections (UTIs), where a more robust bladder care pathway has led to reducing numbers of patients with catheters developing UTIs.
Nasogastric tubes and cancer patient pathway
We were disappointed not to meet our targets for better management of patients with nasogastric tubes and improved cancer patient pathways. These areas will be priorities for 2016/17 and we will continue to improve governance processes and the use of data for closer monitoring and review.
Infection control
Our services remained committed to reducing all avoidable healthcare associated infections. Our performance in key areas is noted below:
• A ceiling of no more than 37 cases of Clostridium difficile was set for the Trust in 2015/16. A total of 49 cases were reported as part of the mandatory reporting system. However, following review with our commissioning
Quality and our performance against key targets
Staff mark the opening of the new modular ward block at Northwick Park Hospital.

13
Our performance was as follows:
Almost 95 out of every 100 patients (94.8 per
cent) who were referred to the Trust by an NHS cancer screening service received their first definitive treatment within 62 days, against a national standard of at least 90 per cent.
Almost 95 out of every 100 patients (94.2 per
cent) referred with suspected cancer to the Trust by their GP were seen by a clinician within two weeks. The national standard is 93 per cent.
99 out of every 100 patients (98.8 per cent)
were treated for cancer within 31 days of a decision to treat. This meets the national standard of at least 96 per cent.
More than eight out of every 10 patients (81.9 per
cent) received their treatment within 62 days following an urgent GP referral for suspected cancer. This was below the national standard of 85 per cent. These are often complex pathways, involving a number of healthcare providers and multiple diagnostics. We have been working with our local commissioners, external trust
Performance against key access targets Cancer
Throughout the year we carried out a range of improvement initiatives to support performance against national cancer standards, which included:
• Planning for an upgraded cancer information management system to support the tracking of patients throughout their assessment and treatment plan.
• Removing, where possible, unnecessary waits in the diagnostic phase of patient pathways.
• Strengthening multi-disciplinary team meetings across tumour sites to plan the next steps for an individual’s care.
• Improving communication with other NHS trusts when shared diagnostics and treatments are required.
The introduction of discharge coordinators at Northwick Park and Ealing hospitals has helped to improve our performance for patients alongside closer working with other health and social care partners to develop a single access point into services.
PLACE, end of life care and wellbeing
We were disappointed to miss our Patient-led Assessment of the Care Environment (PLACE) end of life care and wellbeing promotion targets. These areas will have close attention in the current year. In end of life care, we have set up a steering group which has reviewed our practice against best standards of care nationally and identified five priority areas.
3 Improving the emergency care pathway
Improving the emergency care pathway is aimed at supporting patients to access the right services, at the right time, to get the right standard of care. Our objectives in this area covered reducing waiting times for patients, work with the London Ambulance Service, discharge processes and the emergency pathway for frail elderly patients.
Care for frail elderly patients
We achieved our targets for frail elderly patients with the introduction of a dedicated Older People’s Assessment Liaison Service. The service has helped to reduce the re-attendance of elderly patients by five per cent. This has been supported by the introduction of a rotational programme that has improved elderly care consultant cover at all hospitals.
Staff in the new Diabetes and Endocrinology Centre.

14
for patients who have had, or are at risk of having, a stroke. Our Hyper Acute Stroke Service provides such specialist support, contributing to our strong performance in this area.
96 out of every 100 patients admitted with a stroke spent
at least 90 per cent of their stay on the stroke unit. This met the national standard of at least 90 per cent and is important because it shows that these patients were in the most appropriate place to receive specialist treatment.
The Trust treated 100 per cent of all patients
diagnosed with a transient ischaemic attack (TIA) within 24 hours. This met the national standard of at least 90 per cent.
Inpatient care
As one of the largest NHS trusts in the UK, we have a large inpatient bed base that we have to manage as efficiently as possible. During the year a number of schemes led to improvements for patients including quicker transfers between emergency departments to inpatient settings, increasing numbers of consultant-led ward rounds, improved treatment planning and discharge planning with community partners.
Almost 96 per cent (95.8 per cent) of patients
admitted to the Trust received an assessment for VTE, achieving the national standard (95 per cent).
Since 2013 all NHS trusts have been required to
eliminate mixed-sex accommodation, except where it is in the overall clinical interest of the patient. Across the year there were six unacceptable mixed sex accommodation breaches and this is an area of attention for 2016/17.
community services, social care and clinical commissioning groups to improve our performance against this standard.
Ambulance handovers
Following joint working with the London Ambulance Service (LAS) an improvement plan was developed, based on ensuring a timely handover of patients to the Trust. In total 52,680 ambulances took patients to the A&E departments in 2015/16, on average 49 a day to Ealing Hospital and 96 a day to Northwick Park Hospital. Handovers between ambulance and A&E must take place within 15 minutes where possible and the Trust has to report handover breaches taking longer than 30 minutes and 60 minutes.
The average time for ambulance handover to the
A&E Team improved by 17% to an average of 21 minutes. Improvements continue into 2016/17, with an average of 19 minutes reported across April and May.
Of the total LAS arrivals, 5,935 (11.3%) handovers to
A&E took longer than 30 minutes.
Of the total LAS arrival, 1,199 (2.3%) handovers to
A&E took longer than 60 minutes.
Good progress is being made with performance in April and May showing a 23.5% reduction in handovers taking longer than 60 minutes. This is within an overall 11.7% increase of LAS journeys to the Trust.
Stroke
Access to specialist care is essential for the best outcomes
colleagues and primary care to improve processes through a detailed improvement plan.
More than 95 out of every 100 women (95.4 per cent)
referred for a breast surgery appointment were seen within two weeks. This met the national standard of at least 93 per cent.
Accident and Emergency
A joint plan was developed with our local commissioners and social care partners that identified a range of improvements. This included improving processes within the Emergency Department; processes for managing impatient beds, reducing delays to investigations and improving inpatient short stay capacity. These improvements were developed in the latter part of the year with a robust winter plan. The emergency improvement plan also included redesigning the workforce, recruiting more permanent staff and re-aligning staffing rosters.
The redesign work included improvements in access to emergency short stay, ambulatory care, urgent care centres, short stay inpatient units and specialist inpatient beds. We have also improved our patient transport services to avoid the need for unnecessary overnight hospital stays so as to free up more beds for urgent situations.
Our performance was as follows:
Despite our efforts we missed the national target of
at least 95 per cent of patients attending an A&E or Urgent Care Centre to be admitted, discharged or transferred to an alternative service within four hours. Our performance was 89.4 per cent (almost nine out of 10 patients). We are working with all our partners in primary care,
Quality and our performance against key targets

15
The table below summarises our performance, the full picture of which is available in our annual Quality Account published on our website.
Priorities Target Status
Reduce Patient harm
Reduce the number of grade 3 and grade 4 Trust-acquired pressure ulcers
Reduce the number of patients with a urinary catheter developing urinary tract infections
Ensure effective management of a patients requiring a naso-gastric tube
Ensure sustained effective management of the cancer pathway
Reduce harm from falls
Strengthen compliance with VTE standards
Reduce the number of Trust attributed health care associated infections
Maintain the standard hospital mortality indicator below 90
Embed a culture of learning from complaints and incidents
Develop a supportive infrastructure to enable clinical supervision to front line staff
Improve recruitment and retention
Improvement data quality and information assurance
Improve patient experience
Sustain and improve performance of the suite of national patient satisfaction surveys
Improve compliance with PLACE audit standards
Improve the quality of the discharge process
Improve the end of life experience for patients and their relatives
Improve patients’ health and wellbeing by providing activities to support their holistic needs
Improve access and emergency care
Improve patient information to support timely access to services
Reduce LAS breaches
Reduce the time patients have to wait to be seen
Improve the pathway of care for frail elderly patients
Ensure appropriate seven day patient discharge for patients attending the hospital
Improve 4 hour performance in line with agreed trajectory

16
Researching to innovate5The creation of the new Trust has enhanced our research and development programme which is resulting in improvements for patient care.
2015/16 saw teams participating in international, national and local research activities, with over 70 consultants active in projects and 3,500 plus patients involved in research-led services.
training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development
Since the new Trust’s launch, 56 studies have received permission within 15 days, resulting in a 90 per cent score against the National Institute for Health Research (NIHR) national metric target of 80 per cent.
The number of staff both in the acute and community setting requesting support for research and quality improvement
projects continued to rise. The R&D Department also started collaborating with local clinical commissioning groups on some key performance indicators (KPIs), including projects to help prevent falls.
Key successes in quality improvement and enhanced patient outcomes follow.
Performance highlightsCollaboration for Leadership in Applied Health Research and Care (CLAHRC)
The Trust has an excellent working relationship with CLAHRC whose role is to embed research findings into patient care. As the ‘Outer London Hub’ for CLAHRC, we lead on some high profile projects, of which the heart failure programme is showing successful outcomes as it enters the completion phase.
The 100,000 Genomes Project
This is a national project set up to help clinicians better understand and treat rare inherited diseases and common cancers. The Trust, part of the North West Thames Regional Genetics Service, has exceeded its recruitment target for rare diseases in the first phase,
100,000 genomes project leads, Sunder Chita and Dr Joan Pitkin.

17
have reported over a 100 per cent increase in the number of patients entering into their research studies.
The Trust Cardiology department continues to be the leading global recruiter for the ISCHEMIA study and has now successfully taken on the lead coordinating centre role for the UK.
The LOLIPOP follow-up and Diabetic Genetic Variants sub-study team were the highest recruiting observational studies in 2015/16, recruiting over 1,981 patients.
Patient Research Forum The forum is gaining a strong reputation with other patient groups and is helping to raise the Trust’s profile across the North West London sector and beyond.
resulting in our position as the most successful recruiter in the UK.
Enhancing treatment techniques
A new technique for advanced rectal polypectomy, known as TASER, has been developed by researchers at St Mark’s Hospital, allowing polyps from the colon to be removed more effectively. St Mark’s has also had input into Ulcerative Colitis NICE guidelines for the management of the disease in both adults and children.
Focus on rehabilitation
Northwick Park houses an extensive programme of R&D in rehabilitation, run in partnership with the Cicely Saunders Institute at King’s College London. This applied programme of health services research has had substantial impact on patient care over the last few
years, especially for patients with profound and complex disabilities.
Trainee research collaborative
The Trust launched the Maxillofacial Trainee Research Collaborative (MTReC) in April 2015. The collaborative offers the specialty the opportunity to run large-scale, multi-centre audits and clinical trials, by bringing together trainees into one collaborative group.
Robotics stroke programme
The Trust is a member of The RATULS Trial (UKCRN ID 15309), making it one of only four centres in the UK to participate in this innovative robotics stroke study. Read about the project in more detail in chapter three.
Recruitment success
Cardiovascular, Gastroenterology, Genetics, Health Service Delivery & Surgery specialties
Research Officer Chris Kinsey with Grace Young, UK Country Coordinator for the ISCHEMIA trial, a major international study looking at how best to care for patients with stable coronary artery disease.

18
Celebrating staff excellence6The 2016 Pride in Our Staff Excellence Awards provided the opportunity to celebrate everything outstanding about our people. Over 200 nominations were received for individuals and teams.
The winners:
Caring excellence teamWinners: Rheumatology Department 1
Caring excellence individualWinner: Conrad Jaggwe, A&E Housekeeping 2
Patient safety teamWinners: Clinical Governance Datix implementation team 3
Patient safety individualWinner: Ann Deacon, Advanced Nurse Specialist Practitioner 4
Stronger together teamWinners: Acute Medical Unit team 5
Stronger together individualWinner: Shushila Faruqi, paediatric liaison health visitor 6
Unsung hero teamWinners: Complex discharge co-ordinators 7
Unsung hero individualWinner: Christine Buttle, ED receptionist 8
1 2
3 4
5 6
7 8
LNWH staff awardsPride in our Staff…recognising staff who go the extra mile

19
1211
189 10
13 14
15 16
1917
Patient experience teamWinners: The Speech and language ENT team 9
Patient experience IndividualWinner: Anne Kennedy, medical secretary, orthopaedics 10
Innovator of the year teamWinners: Brent Integrated Diabetes Service 11
Innovator of the year individualWinner: Mary FcFarlane, lead principal speech and language therapist 12
Volunteer of the yearWinner: Audrey Alpe 13
Winner: Beryl Carr 14
Student of the yearWinner: Joycelyn Temu, staff nurse 15
Winner: Siobhan Hickey, midwife 16
Winner: Claire Warriner, trainee health visitor 17
Chairman’s awardWinners: Medical records team across all sites 18
Winner: Dr Charles Cayley, medical director 19

20
Workforce in numbersIn 2015/16 the Trust’s headcount included 8,778 staff (8,116 full time equivalent staff (WTE)) and 1,891 part-time workers. Our part-time workforce continues to rise as we offer more flexible ways of working and family-friendly employment opportunities.
The year-end vacancy rate rose slightly to 13 per cent up from 11 per cent in 2014/15. This is close to the vacancy figure recorded when the Trust was first formed in October 2014. It reflects some movement in the workforce as the merger of services took shape and the difficult labour market faced by the public sector in London where the cost of living is very high. Our overall staff turnover rate was 16 per cent, compared to 13 per cent in the previous year. The reported sickness rate was 3.7 per cent, against a national figure of 4 per cent.
We focused our efforts to ensure mandatory training rates improved, which substantially increased the figure of staff compliant in this area. We now report 75 per cent of staff participating in mandatory training, along with a rise in the number of staff receiving appraisals. This latter figure almost doubled during the year, from 40 per cent in 2014/15 to 74.7 per cent in 2016.
Backlog Electrical £3.2m
Community Info Systems £2.1m
Developments £5.0m
Health & Safety £1.6m
IT & IT Infrastructure £4.5m
Medical Equipment £2.9m
Extra Item
Extra Item
Extra Item
38%
14%13%
9%
8%
6%
5%4% 3%
Additional professional scientific and technical 3.4%
Additional clinical services 17.8%
Administrative and clerical 19.2%
Allied health professionals 9.2%
Estates and ancillary 0.8%
Healthcare scientists 0.9%
Medical and dental 14.1%
Nursing and midwifery registered 34%
Students 0.6%
Backlog Electrical £3.2m
Community Info Systems £2.1m
Developments £5.0m
Health & Safety £1.6m
IT & IT Infrastructure £4.5m
Medical Equipment £2.9m
Extra Item
Extra Item
Extra Item
38%
14%13%
9%
8%
6%
5%4% 3%
Asian 30.2%
Black 16.8%
Chinese/other 7.8%
Mixed 2.4%
Not stated 5.8%
White 37%
Staff groups as a percentage of our workforce Staff ethnicity as a percentage of workforce
Celebrating staff excellence
Backlog Electrical £3.2m
Community Info Systems £2.1m
Developments £5.0m
Health & Safety £1.6m
IT & IT Infrastructure £4.5m
Medical Equipment £2.9m
Extra Item
Extra Item
Extra Item
38%
14%13%
9%
8%
6%
5%4% 3%
Additional professional scientific and technical 3.4%
Additional clinical services 17.8%
Administrative and clerical 19.2%
Allied health professionals 9.2%
Estates and ancillary 0.8%
Healthcare scientists 0.9%
Medical and dental 14.1%
Nursing and midwifery registered 34%
Students 0.6%
Backlog Electrical £3.2m
Community Info Systems £2.1m
Developments £5.0m
Health & Safety £1.6m
IT & IT Infrastructure £4.5m
Medical Equipment £2.9m
Extra Item
Extra Item
Extra Item
38%
14%13%
9%
8%
6%
5%4% 3%
Asian 30.2%
Black 16.8%
Chinese/other 7.8%
Mixed 2.4%
Not stated 5.8%
White 37%
Community staff In the Denham Unit.

21
How we work in partnership We work in partnership with our recognised trade unions. In line with our jointly agreed change management policy, we remain committed to consultation when staff are affected by changes to the way services are run.
Our Joint Negotiating and Consultative Committee (for all staff) and the Local Negotiating Committee (for medical staff) work together to agree policies and support staff consultations where formal changes to the organisation are required.
Communicating with staffWe are committed to creating and supporting an open and honest culture at the Trust. The executive team are very visible across the organisation and the Chief Executive takes the lead on weekly ‘Ask Jacqueline’ open forums.
In addition, there are established Trust communications channels including the Today staff e-bulletin, Chief Executive’s This Week message and monthly all-staff Team Talk core brief.
Committed to equality and diversityWe have a number of responsibilities under equality legislation and are committed to being an inclusive employer. We recently completed a consultation on new equality objectives, which are designed to help us meet and exceed our responsibilities and develop the Trust as a highly regarded inclusive service provider and employer.
Other progress that has been made this year includes:
• publishing data for the Workforce Race Equality Standard
• working with partners to introduce new technology to support more accessible and flexible service delivery
• continued development of our mediation service and training up new mediators throughout the Trust
• offering greater flexibility in order to make it easier for our staff and patients to access interpreters.
We are committed to employing disabled people and adopt the principles of the ‘positive about disabled people’ symbol as part of our job application process. This means that the Trust guarantees applicants with disabilities an interview if they meet the basic conditions for the job.
What our staff told usNHS trusts send an annual survey to staff to find out how they rate their working life. The 2015 NHS Staff Survey was sent out in the autumn and the results published in February 2016.
In summary, compared to their national benchmark group, our staff felt more motivated and more able to personally provide quality services. They also reported feeling happier with their appraisals and non-mandatory training opportunities. However, staff at the Trust are less likely to report problems such as errors, near misses, incidents and unsafe clinical practice, as well as bullying, harassment and abuse. They are also less confident about equal treatment in career progression and more likely to consider that they have experienced discrimination.
The top five areas in which we compared favourably with other acute and community trusts were:
• staff satisfaction with the quality of work and patient care they are able to deliver
• staff motivation at work
• quality of appraisals
• percentage of staff agreeing that their role makes a difference to patients / service users
• quality of non-mandatory training, learning and development.
Areas in which we compared less favourably with our peer trusts include:
• percentage of staff believing that the organisation provides equal opportunities for career progression or promotion
• percentage of staff / colleagues reporting most recent experience of harassment, bullying or abuse
• percentage of staff experiencing discrimination at work in the last 12 months
• staff confidence and security in reporting unsafe clinical practice
• percentage of staff reporting errors, near misses or incidents witnessed in the last month.
Action plans have been produced to tackle all the areas where we perform less well.

22
Our patients’ feedback7The Trust encourages feedback from anyone who uses or has contact with our services. Patients, their families, carers and visitors’ views provide a rich source of information from which we make improvements and innovate for the future.
• assisting complainants to help them understand the complaints procedure
• demonstrating that learning through complaints to improve services has been effective.
During the year we received 914 formal complaints across acute and community sites. Over 98 per cent of the complaints were acknowledged within three days of receipt – either by email, phone or in writing – with details of advocacy services should the complainant need further assistance in making their complaint.
Themes from complaints
Across the Trust the top four themes from complaints were:
• queries about clinical treatment
• issues with staff attitude
• issues with appointments including delays and cancellations
• issues around communications.
ComplimentsWe received 481 formal compliments across the organisation, praising the work of our staff and services. These were in addition to the many cards, letters and tokens of appreciation received directly by wards and departments.
ComplaintsWe place high importance on offering a systematic, accessible, impartial and positive process for dealing with all complaints. This means making sure that any issues are acknowledged, handled sensitively and resolved to the complainant’s satisfaction wherever possible. We are committed to:
• dealing with complaints fairly and proficiently
• properly investigating complaints, and providing adequate responses
• treating complainants with respect, courtesy and being open
Patient Advice & Liaison Service (PALS) PALS provides a one-stop service for anyone with queries, comments, complaints or compliments about our services. The service received 3,464 enquiries from patients and visitors in 2015/16. A large number of problems/concerns were resolved by the PALS team without the need for a formal complaint.
Themes from PALS
The top four themes emerging from PALS enquiries were:
• queries about clinical treatment
• queries about appointments
• issues with verbal communication and information for patients
• issues with staff attitude.
training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development

23
implemented in January 2016 for the merged organisation, and there is work ongoing to make sure that all data is registered, verified and used appropriately.
Another focus for the new PRT is to develop training to support staff to deal with, support and respond more effectively to complainants. Often complaints are dealt with by junior staff who benefit from extra support in order to facilitate the best outcomes in complaints cases.
Friends and Family TestWhether friends and family would recommend our services to each other has become an important quality indicator for the NHS. In 2015/16 25,358 people told us that they would recommend our services.
have started to make videos with patients happy to share their stories which is helping to create greater understanding from the ward to the Board of the issues they face. The stories are leading to service improvements and even greater compassion by encouraging more shared understanding between teams and their patients.
Patient Relations TeamDuring the year there were some resource issues within the Patient Relations Team (PRT) that facilitates the complaints process. This is currently being resolved in a reconfiguration of departments to ensure that an efficient service is offered at all times across the whole Trust.
A new Datix complaints management system was
These themes reflect national issues identified by the Health & Social Care Information Centre (HSCIC). The HSCIC monitors written hospital and community complaints and this information is published on an annual basis. The data is collected and reported on a quarterly basis, with quarters 1-3 validated by the HSCIC and quarter 4 pending validation.
The Trust handles all complaints in the strictest confidence and they are kept separately from patient medical records.
Principles for remedy
The Trust adheres to the Parliamentary and Health Service Ombudsman’s (PHSO) six principles for remedy in our handling of complaints. The principles for remedy outline best practice for organisations to encourage the fair, open and accountable treatment of complainants, alongside appropriate and proportionate remedies.
Complainants can ask the PHSO to review the way in which their complaints have been handled if they remain dissatisfied with the investigation and action taken by us in response to their complaint.
During 2015/16, 21 complaints were referred to the PHSO, of which one has been upheld. To date five have been partially upheld and three have not been upheld.
Improvements to how we learn from complaints and how they are handled
We actively encourage positive and negative feedback about our services and recognise how powerful it is for patients’ stories and emotions to be shared. We A new mum and baby with the homebirth team.

24
hospital to support the delivery of improved ambulatory care and haematology day care services.
New wards
A new modular building opened its doors in January providing three new wards, a state-of-the-art working environment for staff and an enhanced experience for patients. Read more about the unit in section three.
Non-emergency patient transport service
In February the Trust successfully migrated over to a new contractor that provides a single Trust-wide non-emergency patient transport service.
SustainabilityWe are committed to improving future sustainability and a range of initiatives took us forward in our efforts to become a greener organisation.
Our estate8The quality of environment provided by our Trust has a significant impact on our patients’ experience. That is why during the present year we will be investing more to ensure that our estate and facilities match up to the high standards of care and treatments provided by our staff.
A priority for 2016/17 will be to address some of the weaker areas highlighted in our Patient-led Assessment of the Care Environment (PLACE) 2015 scores.
Improvements completed Over £35m was spent on improvements to the physical environment and new equipment in 2015/16. Examples of this work include:
Ealing Hospital
Theatres
A £700,000 refurbishment of theatre 2 to meet modern day standards, including the capacity for new laser treatments and surgery.
Central Middlesex Hospital
Theatres
The conversion of one theatre to a Laminar facility, meaning that capacity has improved with surgeons now able to undertake more orthopaedic operations on the site.
Decontamination
The Endoscopy Decontamination
Unit underwent a £260,000 upgrade. The unit plays an important role in infection prevention with responsibility for the high quality decontamination of all endoscopes used at the hospital.
Northwick Park Hospital
Children’s services
Jack’s Place children’s unit underwent a major refurbishment to improve the ward and bring the quality of environment up to modern day standards. An important element of the project was improving the children’s play and recreational space. Contractors and staff managed the work in a number of phases over 15 weeks, with the unit remaining open at all times to ensure the least disruption to services.
Remodelling of space
Following changes to A&E services a £600,000 project has now completed involving the remodelling of space at the

25
An Environment Management Group and Environment Waste Management Group ensure that sustainability is considered in all areas of our business.
At Ealing the 1MWe Combined Heat and Power (CHP) unit which integrates the production of usable heat and power (electricity) – in one single, more efficient process – was repaired and is now fully operational. This is already reducing energy usage and electricity costs.
The EU emissions trading system (EU ETS) report for Northwick Park Hospital was successfully submitted. This is an emissions cap system on the total emissions that are allowed from the site. Northwick Park is our only hospital that qualifies for meeting the requirement.
The Carbon Reduction Commitment Energy Efficiency Scheme report for 2015/16 has been submitted showing the Trust as fully compliant. This is a UK government scheme designed to improve energy
efficiency and cut carbon dioxide (CO2) emissions in high-energy use private and public sector organisations.
Safety standardsFire
During 2015/16 we enhanced fire safety provision, recruiting two full-time fire safety advisors to support the Fire Safety Manager. The new advisors bring with them extensive experience as senior fire safety officers previously with the London Fire Brigade.
Significant investment has been made in upgrading physical fire precautions throughout the Trust, including a rolling programme of fire compartmentation works in Northwick Park Hospital’s main wards and the upgrading of the fire containment systems in the surgical theatres at Ealing Hospital. The new Acute Medical Unit at Northwick Park
also includes a state-of-the-art automatic fire suppression system, ensuring the highest levels of fire safety for patients and staff.
Asbestos
We have strengthened our position in relation to our duty to manage risks in relation to asbestos. This work includes an Asbestos Action Plan and Asbestos Safety Group which reports to the Trust-wide Health and Safety Group.
PLACEPatient-led assessments of the care environment (PLACE) were carried out across inpatient areas between January and June 2015. Our patient representatives make up at least 50 per cent of our assessment teams, providing the Trust with an effective and valuable appraisal of the key areas involved in the assessments.
The new Jack’s Place Children’s Unit.

26
an MPS database. This new system assists with any reported crime and ensures that retrieved items can be returned to owners in a timely way. The PPT also works closely with the Trust’s Counter Fraud Team.
Emergency preparednessOur Emergency Planning Team works to ensure that the Trust is adequately prepared for any emergencies. We have in place plans that are fully compliant with the requirements of the NHS England Emergency Preparedness Framework 2015 and associated guidance.
During 2015/16 we worked collaboratively with our partner agencies across all three London boroughs to plan for and ensure appropriate management of all
• A refurbishment programme has been completed for a number of patient bathroom and toilet areas.
Improving securityOur local security management specialists continue to support staff by communicating about security awareness and good practice, and by promoting a pro-security culture. This includes security awareness training and the involvement of the Metropolitan Police Service (MPS) in awareness days across the Trust.
In addition, and in conjunction with the Personal Property Team (PPT - part of the Safer Neighbourhood Team), staff and visitors have been offered an identification service for personal property, which is logged onto
Cleanliness FoodPrivacy, dignity and wellbeing
Condition appearance and
maintenance Dementia
2014 2015 2014
2015
2014 2015 2014 2015 2015Food
Organi-sational
foodWard food
Northwick Park And St. Mark’s
98.35% 91.68% 72.02% 76.56% 68.53% 78% 78.05% 63.63% 89.20% 79.30% 59.16%
Central Middlesex Hospital
97.03% 88.72% 69.58% 73.83% 70.42% 75.13% 72.64% 62.33% 92.14% 78.81% 63%
Ealing Hospital 97.05% 97.39% 87.17% 87.28% 79.43% 89.27% 74.12% 67.73% 86.98% 81.97% 60.20%
Willesden Centre For Health and Care
99.47% 99.42% 97.14% 95.71% 94.04% 96.58% 81.15% 65.20% 96.96% 89.68% 65.63%
Meadow House 100% 100% 90.32% 78.44% 86.57% 73.08% 100% 88.24% 88.96% 88.24% 65.03%
Denham Unit 94.66% 98.67% 92.63% 84.09% 81.23% 87.14% 84.78% 92.86% 85.85% 90% 100%
Clayponds Hospital
98.08% 95.87% 95.26% 89.91% 91.53% 88.42% 84.93% 84.23% 93.75% 90.36% 77.11%
Red = More than 5% fall in score Amber = Less than 5% fall in score Green = Score the same
Blue = Improved score Italics = Less than national average
Our PLACE scores for the five key areas were:
In some key areas the results were disappointing but the implementation of an action plan has already resulted in a number of positive impacts, notably:
• Investment in a new patient meal service at Northwick Park, St. Mark’s and Central Middlesex hospitals, including the introduction of an electronic patient meal ordering system. Patients are now able to order their meals as close to meal service time as possible.
• A cleaning standards training awareness programme has been implemented across the clinical divisions.
• A new Protected Mealtimes Policy is now in place throughout all areas.
Our estate

27
Information governance ensures that our staff use information ethically and legally. Through this work, we adhere to strict national guidelines to ensure the confidential and sensitive treatment of any data and information belonging to those who use or have contact with our services.
Incidents relating to information are actively managed and monitored through the Trust’s Information Governance Group, which reports to the Integrated Governance Board Sub-Committee of the Corporate Quality and Risk Committee. The Trust takes a risk-based approach to information governance and a risk register is in place for the key areas of information security, records management and data quality. Any risks that are rated highly using the national NHS 5x5 risk matrix are then entered onto our Corporate High Risk Register.
The Trust has a senior information risk owner who is the Director of Strategy. The Director has a deputy who has responsibility for information governance, corporate records and medical records. They work closely with the Trust’s Caldicott Guardian, one of our consultant gastroenterologists.
IncidentsAll incidents are rated according to severity using Health and Social Care Information Centre (HSIC) definitions, with 0 being the lowest rating and 2 the highest. Any level 2 rated incidents must be notified to the Information Commissioner’s Office who is the regulator for data protection in England. They are also placed on the Strategic Executive Information System, the national incident reporting system.
There were two level 2 incidents reported during 2015/16, although following the outcome of a detailed investigation, one of the incidents was reclassified as a level 1.
The following table illustrates reported level 2 incidents for the year.
Category Nature of incidentTotal of level 2 incident reports
1 Loss of inadequately protected electronic equipment devices or paper documents from secured NHS premises
None
2 Loss of inadequately protected electronic equipment devices or paper documents from outside secured NHS premises
None
3 Insecure disposal of inadequately protected electronic equipment, devices or paper documents
None
4 Unauthorised disclosure One
5 Other None
Information governance9types of significant and major
incidents. The Trust emergency planning team has been involved in several exercises throughout the year including a pan London heat-wave exercise, a hazardous material/contaminated patient exercise and two community rest centre exercises with colleagues from local authorities.
In July 2015 the major Incident response was tested by the Trust’s participation in an Emergo exercise. More than 60 staff from all areas and grades participated in the day-long exercise organised by Public Health England (PHE). The incident, a fictitious high-speed rail collision involving hazardous materials, allowed staff to test the response in real-time by coordinating people, equipment and services. PHE provided a detailed report on how we responded and the overall result was positive. Learning points were shared and appropriate action taken.
Throughout the year we responded to several local incidents that occurred on our premises. These internal incidents are not managed by implementing the Trust Major Incident Plan, but through business continuity planning and response. The incidents included power outages, localised flooding, and IT interface issues. Following each incident the Trust continues to take forward lessons learned and good practice to better prepare for the future.
Looking forward to 2016/17, we will continue to develop and consolidate our emergency planning work programme through exercises and local business continuity planning.
28
Our Trust board10
Non-Executive Directors
Dr Vineta Bhalla
Andrew Farrell
Janet Rubin
Professor David Taube
Andrew van Doorn
Ruwan Weerasekera
Martin West
Non-Executive Director
Non-Executive Director
Non-Executive Director
Designate Non-Executive Director
Non-Executive Director
Non-Executive Director
Non-Executive Director
Executive Directors
Lee Martin
Amanda Pye
Dr Charles Cayley
Simon Crawford
Jon Bell
Claire Gore
Nigel Myhill
Chief Operating Officer
Chief Nurse Medical Director
Director of Strategy
Chief Financial Officer
Director of Human Resources
Director of Estates and Facilities
Our current* members of the Trust Board are as follows. There were a number of changes in non-executive and executive directors during the year which are noted in the Annual Governance Statement.
Peter Worthington
Jacqueline Docherty
Chair Chief Executive Officer
*April 2016
Chair and Chief Executive Officer

29
Board Accountable Roles
Role Executive Lead Non-Executive Director Lead
Accountable Officer Jacqueline Docherty
Allegations against professional misconduct
Claire Gore
Caldicott Guardian Delegated by C Cayley to Simon Gabe
Controlled drugs Dr Charles Cayley
Counter fraud Jon Bell Andrew Farrell
CQC Amanda Pye
Doctors in difficulty Dr Charles Cayley Prof David Taube
Emergency planning Lee Martin
End of life care Dr Charles Cayley Prof David Taube
Equality and diversity Amanda Pye (Patients) Claire Gore (Staff)
Fire safety Nigel Myhill
Health and safety Nigel Myhill Martin West
Infection control Jacqueline Docherty / Fiona Coogan
Patient safety Dr Charles Cayley Prof David Taube
Responsible officer Dr Charles Cayley
Safeguarding adults Amanda Pye Peter Worthington
Safeguarding children Amanda Pye Peter Worthington
Security Nigel Myhill
Senior Information Responsible Officer
Kevin Connolly (Simon Crawford Board member)
Whistleblowing Amanda Pye (Clinical) Claire Gore (Non-clinical)
Ruwan Weerasekera

30
Our Trust Board
Name
Title Dire
ctor
ship
(inc
ludi
ng n
on-e
xecu
tive
dire
ctor
ship
s he
ld in
priv
ate
com
pani
es o
r PL
Cs)
or
com
pany
sec
reta
ry
Ow
ners
hip
or p
art-
owne
rshi
p of
priv
ate
com
pani
es, p
artn
ersh
ips,
bus
ines
s or
co
nsul
tanc
ies
doin
g bu
sine
ss w
ith t
he N
HS
Maj
ority
or
cont
rolli
ng s
hare
hold
ings
in
orga
nisa
tions
doi
ng b
usin
ess
or li
kely
or
poss
ibly
se
ekin
g to
do
busi
ness
with
the
NH
S
Posi
tion
of a
utho
rity
in a
cha
rity
or v
olun
tary
bo
dy in
the
fiel
d of
hea
lthca
re, s
ocia
l car
e or
ho
usin
g
Any
mat
eria
l con
nect
ion
with
a v
olun
tary
or
othe
r bo
dy c
ontr
actin
g fo
r se
rvic
es w
ith N
HS
orga
nisa
tions
Ass
ocia
ted
inte
rest
of
part
ners
or
clos
e fa
mily
m
embe
rs s
houl
d al
so b
e de
clar
ed
Oth
er r
elev
ant
inte
rest
/inco
me
Dat
e of
dec
lara
tion/
upda
te
Votin
g di
rect
or o
f LN
WH
T Bo
ard
Amanda Pye Chief Nurse (from 1 Sep 2015)
Nil Nil Nil Nil Nil Nil Nil 30 Dec 2015
Yes
Andrew Farrell Non-Executive Director
Director North Ten Limited. August 2015
Nil Nil Nil Nil Nil Nil 22 Apr 2016
Yes
Andrew Van Doorn Non-Executive Director
Nil Nil Nil Deputy CEO, HACT 49-51 East Road, London N1 6AH, Housing Innovation Charity (May 2003 to present)
Chair, Stonewell Housing, Leroy House, 436 Essex Road, London N1 3QP, support provider for LGBT people (Feb 2009 to present)
As above, current contracts with NHS organisations
Nil Nil 2 Mar 2016
Yes
Carole Flowers Chief Nurse Left 7 Jun 2015
Nil Nil Nil Nil Nil Nil Nil Nil Nil
Caroline Corby Non-Executive Director Left 13 Jun 2015
Director of the Probation Association (until Jul 2014)
Chair of the London Probation Trust (until Jul 2014)
Board member of JML since Jan 2014
Non-Executive Director Criminal Cases Review Commission (July 2014).
Non-Executive Director of Children and Family Court Advisory Service (CAFCASS) (Dec 2014).
Nil Nil Member; Management Committee of the Parole Board (January 2015).
Nil Nil Nil Nil Nil
Chris Pocklington COO (until 6 Sep 2015 then on secondment)
Director Imperial College Health Partners (end Sep 2015)
Nil Nil Nil Nil Nil Nil Nil Nil
Board Declaration of Interests

31
Name
Title Dire
ctor
ship
(inc
ludi
ng n
on-e
xecu
tive
dire
ctor
ship
s he
ld in
priv
ate
com
pani
es o
r PL
Cs)
or
com
pany
sec
reta
ry
Ow
ners
hip
or p
art-
owne
rshi
p of
priv
ate
com
pani
es, p
artn
ersh
ips,
bus
ines
s or
co
nsul
tanc
ies
doin
g bu
sine
ss w
ith t
he N
HS
Maj
ority
or
cont
rolli
ng s
hare
hold
ings
in
orga
nisa
tions
doi
ng b
usin
ess
or li
kely
or
poss
ibly
se
ekin
g to
do
busi
ness
with
the
NH
S
Posi
tion
of a
utho
rity
in a
cha
rity
or v
olun
tary
bo
dy in
the
fiel
d of
hea
lthca
re, s
ocia
l car
e or
ho
usin
g
Any
mat
eria
l con
nect
ion
with
a v
olun
tary
or
othe
r bo
dy c
ontr
actin
g fo
r se
rvic
es w
ith N
HS
orga
nisa
tions
Ass
ocia
ted
inte
rest
of
part
ners
or
clos
e fa
mily
m
embe
rs s
houl
d al
so b
e de
clar
ed
Oth
er r
elev
ant
inte
rest
/inco
me
Dat
e of
dec
lara
tion/
upda
te
Votin
g di
rect
or o
f LN
WH
T Bo
ard
Christopher Blake Commercial Director
Nil Nil Nil Nil Nil Nil Nil 15 Feb 2016
No longer a Board member
Claire Gore Director of HR & OD (from 1 Mar 2016)
Nil Nil Nil Nil Nil Nil Nil 6 Apr 2016
Yes
David Taube Non-Executive Director
Director Imperial College Academic Health Science Centre
Nil Nil Advisor National Kidney Federation
Trustee St Mary’s Kidney Patients Association
Nil Nil Nil 1 Oct 2014
Yes
Dr Charles Cayley Medical Director
Nil Nil Nil Patron of Sudbury neighbourhood centre
Nil Nil Nil 15 Feb 2016
Yes
Dr Vineta Bhalla Non-Executive Director
Health System Dynamics Ltd (2013 to present)
Nil Nil Nil Nil Nil Nil 2 Mar 2016
Yes
Gary Munn Interim Director of Estates and Facilities (25 May to 6 Sept 2015)
Nil Nil Nil Nil Nil Nil Nil Nil Nil
Jacqueline Docherty CEO
Director Imperial College Health Partners (April 2015 to present)
Director, The Cancer Vanguard, Royal Marsden Partners Accountable Clinical Network (Cancer) (September 2015 to present)
Nil Nil Nil Nil Nil Nil 16 Feb 2016
Yes
Janet Rubin Non-Executive Director
Director of Janet Rubin Human Resource Consultancy Ltd (1997 to present)
Nil Nil Ambassador, Kids Out Charity (2005-2016)
An Associate with Praesta Partners who undertake Executive Coaching in all sectors including the NHS (May 2014 to present)
Nil Nil 25 Feb 2016
Yes

32
Our Trust Board
Name
Title Dire
ctor
ship
(inc
ludi
ng n
on-e
xecu
tive
dire
ctor
ship
s he
ld in
priv
ate
com
pani
es o
r PL
Cs)
or
com
pany
sec
reta
ry
Ow
ners
hip
or p
art-
owne
rshi
p of
priv
ate
com
pani
es, p
artn
ersh
ips,
bus
ines
s or
co
nsul
tanc
ies
doin
g bu
sine
ss w
ith t
he N
HS
Maj
ority
or
cont
rolli
ng s
hare
hold
ings
in
orga
nisa
tions
doi
ng b
usin
ess
or li
kely
or
poss
ibly
see
king
to
do b
usin
ess
with
the
NH
S
Posi
tion
of a
utho
rity
in a
cha
rity
or v
olun
tary
bo
dy in
the
fiel
d of
hea
lthca
re, s
ocia
l car
e or
ho
usin
g
Any
mat
eria
l con
nect
ion
with
a v
olun
tary
or
othe
r bo
dy c
ontr
actin
g fo
r se
rvic
es w
ith N
HS
orga
nisa
tions
Ass
ocia
ted
inte
rest
of
part
ners
or
clos
e fa
mily
m
embe
rs s
houl
d al
so b
e de
clar
ed
Oth
er r
elev
ant
inte
rest
/inco
me
Dat
e of
dec
lara
tion/
upda
te
Votin
g di
rect
or o
f LN
WH
T Bo
ard
Jeanne Spinks Non-Executive Director Left 31 Aug 2015
Nil Nil Nil Member of the Advisory Panel to the Welsh Ministers about the Public Policy Institute for Wales
Nil Nil Nil Nil Nil
Jon Bell Interim CFO (from 5 Oct 2015)
Carbery Consulting Ltd Carbery Consulting Ltd
Nil Nil Nil Wife is self-employed currently engaged by Chelsea and Westminster NHS FT
Nil 16 Feb 2016
Yes
Kevin Connolly Director of ICT
Nil Nil Nil Nil Nil Nil Nil 4 Mar 2016
No longer a Board member
Lee Martin COO (from 2 Nov 2015)
Nil Nil Nil Nil Nil Nil Nil 1 Mar 2016
Yes
Mark Gammage, Interim HR Lead Adviser (from 1 Jun 2015)
Managing Partner Dearden LLP – a management consultancy organisation; Managing Partner Dearden HR – a specialist HR Consultancy; Managing Director Dearden Interim – an interim management organisation; Managing Director Mark Gammage Ltd – a management consultancy organisation; HR Lead – Shaping a Healthier Future – the programme overseeing the changes to healthcare provision across NW London
Nil Nil Nil Nil Nil Nil 7 Jan 2016
No
Martin West Non-Executive Director
Non-Executive Director of NHS Property Services Ltd (NHSPS)
Non-Executive Director of Kent Surrey and Sussex Academic Health Science Network
Nil Nil Nil Nil Nil Nil 1 Oct 2014
Yes
Board Declaration of Interests

33
Name
Title Dire
ctor
ship
(inc
ludi
ng n
on-e
xecu
tive
dire
ctor
ship
s he
ld in
priv
ate
com
pani
es o
r PL
Cs)
or
com
pany
sec
reta
ry
Ow
ners
hip
or p
art-
owne
rshi
p of
priv
ate
com
pani
es, p
artn
ersh
ips,
bus
ines
s or
co
nsul
tanc
ies
doin
g bu
sine
ss w
ith t
he N
HS
Maj
ority
or
cont
rolli
ng s
hare
hold
ings
in
orga
nisa
tions
doi
ng b
usin
ess
or li
kely
or
poss
ibly
see
king
to
do b
usin
ess
with
the
NH
S
Posi
tion
of a
utho
rity
in a
cha
rity
or v
olun
tary
bo
dy in
the
fiel
d of
hea
lthca
re, s
ocia
l car
e or
ho
usin
g
Any
mat
eria
l con
nect
ion
with
a v
olun
tary
or
othe
r bo
dy c
ontr
actin
g fo
r se
rvic
es w
ith N
HS
orga
nisa
tions
Ass
ocia
ted
inte
rest
of
part
ners
or
clos
e fa
mily
m
embe
rs s
houl
d al
so b
e de
clar
ed
Oth
er r
elev
ant
inte
rest
/inco
me
Dat
e of
dec
lara
tion/
upda
te
Votin
g di
rect
or o
f LN
WH
T Bo
ard
Nigel Myhill
Director of Estates & Facilities (from 7 Sep 2015)
Nil Nil Nil Nil Nil Nil Nil 15 Feb 2016
No
Patricia Williamson Deputy Chairman Left 30 Sep 2015
Director PMW HR Consulting Ltd
Nil Nil Nil HR Lead Hinchingbrooke Healthcare NHS Trust
Nil Nil 29 Apr 2015
Nil
Paul Kingsmore Director of Estates and Facilities (until 31 May 2015)
Director Institute of Healthcare Engineering and Estate Management Ltd
Nil Nil Patron of the Association of Healthcare Cleaning Professionals
Nil Nil Nil 1 Mar 2015
Nil
Paul Stanton Interim HR Director (until 29 May 2015)
Nil Nil Nil Nil Nil Nil Nil Nil No longer a Board member
Peter Worthington Chairman
LP Origination Limited
Chesilton Consultancy Limited
Charter House (Flat Owners) Limited
Charter House Flats Management (Drury Lane) Limited
MRIMC Management Company LLP
Midway Resources International (Exempt private limited liability)
Dates: For all of the above, since appointment as chairman and continuing
Nil Nil Nil Nil Nil 15 Feb 2016
Yes

34
Our Trust Board
Name
Title Dire
ctor
ship
(inc
ludi
ng n
on-e
xecu
tive
dire
ctor
ship
s he
ld in
priv
ate
com
pani
es o
r PL
Cs)
or
com
pany
sec
reta
ry
Ow
ners
hip
or p
art-
owne
rshi
p of
priv
ate
com
pani
es, p
artn
ersh
ips,
bus
ines
s or
co
nsul
tanc
ies
doin
g bu
sine
ss w
ith t
he N
HS
Maj
ority
or
cont
rolli
ng s
hare
hold
ings
in
orga
nisa
tions
doi
ng b
usin
ess
or li
kely
or
poss
ibly
see
king
to
do b
usin
ess
with
the
NH
S
Posi
tion
of a
utho
rity
in a
cha
rity
or v
olun
tary
bo
dy in
the
fiel
d of
hea
lthca
re, s
ocia
l car
e or
ho
usin
g
Any
mat
eria
l con
nect
ion
with
a v
olun
tary
or
othe
r bo
dy c
ontr
actin
g fo
r se
rvic
es w
ith N
HS
orga
nisa
tions
Ass
ocia
ted
inte
rest
of
part
ners
or
clos
e fa
mily
m
embe
rs s
houl
d al
so b
e de
clar
ed
Oth
er r
elev
ant
inte
rest
/inco
me
Dat
e of
dec
lara
tion/
upda
te
Votin
g di
rect
or o
f LN
WH
T Bo
ard
Ruwan Weeresekera Non-Executive Director
Weera Consulting Limited (09546470) Director Appointed on 16 April 2015
The Bridge Academy, Hackney (05195911) Director Appointed on 12 February 2015
Nil Nil London Works Agency Limited (08525614)
Director Appointed on 23 June 2015
Nil Partner on Harrow Safeguarding Board
Nil 30 Dec 2015
Yes
Simon Crawford Director of Strategy (from 12 Oct 2015, previously CFO and SRO)
Director Imperial College Health Partners
Director Imperial College Health Partners (October 2015 to present)
Nil Nil Nil Nil Nil 17 Mar 2016
Yes
Siobhan Jordan Interim Chief Nurse 27 May to 31 Aug 2015
Nil Nil Nil Nil Nil Nil Nil Nil Nil
Stella Dutton Non-Executive Director Left 31 Oct 2015
Nil Nil Nil Nil Nil Nil Nil Nil Nil
Tina Benson Director of Operations (Interim COO from 7 Sept to 1 Nov 2015)
Nil Nil Nil Nil Nil Nil Nil 22 Feb 2016
No longer a Board member
Yvonne Leese Director of Community Services
Nil Nil Nil Nil Nil Nil Nil Nil No longer a Board member
Each director states that, as far as they are aware, there is no relevant audit information of which the Trust’s auditors are unaware, and that they have taken all steps to ensure they and the auditors are aware of any relevant audit information.
Board Declaration of Interests

35
Scope of Responsibility: April 2015 to March 2016As Accountable Officer I have responsibility for maintaining a sound system of internal control that supports the achievement of the NHS Trust’s policies, aims and objectives, whilst safeguarding quality standards and the public funds and departmental assets for which I am responsible, in accordance with the responsibilities assigned to me. I am also responsible for ensuring that the NHS Trust is administered prudently and economically and that resources are applied efficiently and effectively. I also acknowledge my responsibilities as set out in the NHS Accountable Officer Memorandum.
I have used the Board Assurance Framework (BAF), risk register, internal audit, counter fraud and external audit to ensure proper arrangements are in place for discharge of statutory functions, as well as to detect and act upon any irregularities found and to ensure that the Trust is able to discharge its statutory functions in a legally compliant manner.
The Trust is compliant with all 12 of the Monitor licence requirements for NHS trusts as set out in the NHS TDA Accountability Framework. Work is continuing to improve the financial position of the Trust and address issues raised by the
Care Quality Commission (CQC) in regard to one of its legacy organisations, The North West London Hospitals NHS Trust and actions arising from the CQC inspection in October 2015.
The Governance Framework of the OrganisationThe Trust is governed by a Trust Board made up of eight Non-Executive Directors, (including the Chairman), and six Executive Directors, including the Chief Executive. The Director of Estates and Facilities and the Director for Human Resources and Organisational Development/Interim HR Lead Adviser attended the Trust Board in a non-voting capacity. Until June 2015 the Director of Community Services, Head of Communications, the Director of Operations, the Director of IM&T and the Director of Commercial Development attended the Trust Board in a non-voting capacity.
The Trust Board has overall responsibility for determining the future direction of the Trust and ensuring delivery of safe and effective services in accordance with legislation and the principles of the NHS. The Trust Board must also ensure the organisation complies with relevant regulatory standards. During the year, workshops have been held to assess the effectiveness of the Board covering topics such as strategic risk management, Board Assurance Framework, annual
plan, well-led Board and a review of the Trust’s Committee governance reporting structure.
Non-Executive Directors of NHS Trusts are appointed by the NHS Trust Development Authority*. They are not employees of the Trust but receive remuneration for the role which is agreed nationally. Executive Directors are employees of the Trust. Details of directors’ remuneration are set out in the Remuneration Report, which is part of the Annual Report. The Trust Board met 10 times in public and 11 times in private during the period April 2015 to March 2016. In addition six Board workshops were held during the year.
In September 2015 a new Board Assurance Accountability Structure was established to strengthen governance reporting and assurance from operational meetings through to the Board via Executive and Board Committees. These replaced some of the existing committees as described below and are operating effectively. Going forward an annual review of Board Committee effectiveness will be carried out. There are eight standing committees which carry out functions delegated to them by the Trust Board and seek assurance on behalf of the Board. These committees report directly to the Trust Board. These formal Board committees are:
• Audit Committee
• Strategy Committee
• Finance and Performance Committee
London North West Healthcare NHS Trust
Annual Governance Statement11
*The NHS TDA has since become NHS Improvement

36
• Integrated Governance Committee
• Charitable Fund Management Committee
• Remuneration Committee
• Patient and Staff Committee
• Clinical Excellence Committee.
Prior to September 2015, the following board committees were in place and then replaced by the committees above:
• Strategy, People and Communications Committee
• Audit, Governance and Risk Committee
• Finance, Investment, Estates and Facilities Committee
• Clinical, Performance and Patient Experience Committee
• Senior Appointments and Remuneration Committee.
Audit Committee, formerly Audit, Governance and Risk Committee
The Audit Committee reviews and provides assurance on internal controls, including financial controls. This Committee received regular reports on the work and findings of the internal and external auditors and counter fraud services. The Committee is chaired by a Non-Executive Director and the membership includes three other Non-Executive Directors, with at least one member having recent, relevant financial experience. The lead Executive Director is the Chief Financial Officer.
Annual governance statement
The Finance and Performance Committee, formerly Finance, Investment and Estates Committee
The primary purpose of the Finance and Performance Committee is to provide assurance to the Trust Board that the financial strategy, financial policies and efficiency plans effectively support the organisational strategy and to undertake, on behalf of the Trust Board, objective scrutiny of the Trust’s annual financial plans, long-term financial strategy, investment policy, estates strategy and major investment decisions, including those relating to the Trust’s estate and IT. The Committee is chaired by a Non-Executive Director with two additional Non-Executive Directors as members. The lead Executive Director is the Chief Financial Officer.
Remuneration Committee, formerly Senior Appointments and Remuneration Committee
The purpose of the Committee is to oversee the process of appointment, remuneration, suspension, termination and succession planning for all non-executive and executive directors and to ensure the Board has the appropriate level, balance and quality of resources. The Committee is chaired by the Chairman of the Trust with three other Non-Executive Directors as members. Membership of the Remuneration Committee is made up exclusively of Non-Executive Directors; Executive Directors have no involvement in determining their own remuneration.
Clinical Excellence Committee, formerly Clinical Performance and Patient Experience Committee
The primary purpose of the Committee is to support the Board in the objective scrutiny and challenge of all aspects of clinical safety, quality and effective performance and patient experience. The Committee is chaired by a Non-Executive Director supported by three other Non-Executives. The lead Executive Director is the Chief Nurse.
Strategy Committee, formerly Strategy, People and Communications Committee
The primary purpose of the committee is to provide strategic direction, scrutiny, challenge around strategy development and implementation, including clinical, financial, workforce, estate and IT strategy development; and facilitate organisational development. The Committee is chaired by a Non-Executive Director. The membership includes two additional Non-Executive Directors. The lead Executive Director is the Director of Strategy.
Charitable Fund Management Committee
The Trust Board acts as Trustee to the London North West Healthcare Charitable Funds for the organisation and has established a Charitable Fund Management Committee with delegated authority to manage the charitable funds on its behalf. The purpose of the Committee is to ensure that Trust Funds are managed and invested properly in accordance with the Charities Act and the NHS Trust’s Standing

37
Financial Instructions (SFIs). The Committee is chaired by a Non-Executive Director and comprises two other Non-Executive Directors and two Executive Directors, one of whom is the Chief Financial Officer.
Patient and Staff Committee
The Committee’s purpose is to ensure that there is a culture of continuous, positive improvement and engagement with patients/users. To ensure initiatives including positive engagement with staff and external stakeholders to make a difference to patients/users’ experience in receiving high quality care; ensure the Trust has a robust approach to recruitment and retention of staff; and ensure the Trust continues to fulfil requirements as determined by the CQC and other regulators. The Committee oversees activity relating to equality, diversity, complaints and workforce development. The Committee is chaired by a Non-Executive Director and includes two other Non-Executive Directors. The lead Executive Directors are the Chief Nurse and Director of Human Resources and Organisational Development.
Integrated Governance Committee
The purpose of the Committee is to ensure the implementation of integrated risk management Trust-wide and to consider the Trust Risk Register and Board Assurance Framework. This Committee works in collaboration with the Audit Committee to determine the audit requirements for the Trust. The Committee is chaired by a Non-Executive Director and includes two other Non-
Executive Directors. The lead Executive Directors are the Chief Financial Officer and the Chief Operating Officer.
Service Change to Directors
Patricia Williamson, Deputy Chair and Non-Executive Director. Last day of service 30th September 2015
Stella Dutton, Non-Executive Director. Last day of service 31st October 2015
Jeanne Spinks, Non-Executive Director. Last day of service 31st August 2015
Caroline Corby, Non-Executive Director. Last day of service 13th June 2015
Simon Crawford, Director of Finance until 11th October 2015
Jon Bell, Interim Chief Financial Officer from 12th October 2015
Mark Gammage, Interim Lead HR Adviser from 1st June 2015 to 29th February 2016
Paul Stanton, Director of HR until 29th May 2015
Tina Benson, Acting Chief Operating Officer from 7th September 2015 to 1st November 2015
Christopher Pocklington, Chief Operating Officer. On Secondment from LNWHT from 6th September 2015 to 6th March 2016.
Siobhan Jordan, Interim Chief Nurse from 27th May 2015 to 31st August 2015
Carole Flowers, Director of Nursing until 27th May 2015
Paul Kingsmore, Director of Estates and Facilities until 24th May 2015
Gary Munn, Acting Director of Estates and Facilities from 25th May 2015 to 6th September 2015
Tina Benson, Director of Operations until 6th September 2015
Andrew Farrell, Non-Executive Director from 1st August 2015
Ruwan Weerasekera, Non-Executive Director from 1st September 2015
Janet Rubin, Non-Executive Director from 15th February 2016
Dr Vineta Bhalla, Non-Executive Director from 21st February 2016
Andrew van Doorn, Non-Executive Director from 1st March 2016
Compliance with the Code of Governance
The London North West Healthcare NHS Trust operates as a unitary Board which means that all Board members work together as equals to act in the best interests of the organisation. The Trust Board met the criteria set out in the Code of Governance in relation to the independence of Non-Executive Directors.
Board Assurance Framework The Assurance Framework is reported regularly to the Board and two Board workshops were held in the reporting period specifically to discuss the Board Assurance Framework and progress in mitigating risks to delivery. The Framework is continually updated in order to ensure that it covers all areas on which the Board should be seeking assurance. This information is supplemented and enhanced by the other performance management

38
Annual governance statementN
ame
Role
Boa
rd P
ublic
Boar
d Pr
ivat
e
Aud
it, G
over
nanc
e &
Ris
k C
omm
ittee
Mar
to
Aug
201
5
Aud
it C
omm
ittee
Oct
201
5
to M
ar 2
016
LNW
H C
harit
able
Fun
d M
anag
emen
t C
omm
ittee
Clin
ical
Per
form
ance
& P
atie
nt
Expe
rienc
e M
ar t
o Se
pt 2
015
Clin
ical
Exc
elle
nce
Com
mitt
ee
Oct
201
5 to
Mar
201
6
Fina
nce,
Inve
stm
ent
& E
stat
es
Mar
to
Sept
201
5 [P
rivat
e]
Fina
nce
and
Perf
orm
ance
C
omm
ittee
Oct
201
5 to
Mar
201
6 [P
rivat
e]
Inte
grat
ed G
over
nanc
e ne
w f
rom
Se
pt 2
015
[Priv
ate]
Patie
nt a
nd S
taff
new
fro
m
Sept
201
5
Rem
uner
atio
n C
omm
ittee
(f
orm
erly
Sen
ior
App
oint
men
ts a
nd
Rem
uner
atio
n) -
Con
fiden
tial
Stra
tegy
, Peo
ple
& C
omm
unic
atio
n M
ar t
o Se
pt 2
015
[Priv
ate]
Stra
tegy
Com
mitt
ee O
ct 2
015
to
Mar
201
6
TOTAL NUMBER OF MEETINGS 2015-16 10 11 2 4 3 4 5 5 [2]
6 [6]
4 [1]
6 5 3 [2]
4
Peter Worthington Chairman 10 9 1 4 2 2 5 3 [1]
6 [6]
4 [1]
5 5 2 [1]
4
Patricia Williamson Deputy Chair and Non-Executive Director (left 30 Sept 2015)
4 5 1
Stella Dutton Non-Executive Director (left 31 Oct 2015)
3 4 2 2 3 [2]
1 1 [1]
1
Jeanne Spinks Non-Executive Director (left 31 Aug 2015)
4 5 2 2 3 [2]
Caroline Corby Non-Executive Director (left 13 Jun 2015)
1 1 1 3 2 2 [1]
Martin West Non-Executive Director 9 10 2 4 4 [2]
5 [5]
3 1 4
Prof. David Taube Non-Executive Director 9 9 4 4 2 1 [1]
1
Ruwan Weeraskera Non-Executive Director (from 1 Sept 2015)
5 5 2 4 6 [6]
3 [1]
5 2 3
Andrew Farrell Non-Executive Director (from 1 Aug 2015)
7 7 4 2 5 6 [5]
4 [1]
5 4 3
Janet Rubin Non-Executive Director (from 15 Feb 2016)
2 2 1 1 [1]
1 1 1 1
Dr Vineta Bhalla Non-Executive Director (from 21 Feb 2016)
1 1 1 1 1 1
Andrew van Doorn Non-Executive Director (from 1 Mar 2016)
1 1 1 1 [1]
1 1
Jacqueline Docherty Chief Executive 10 11 2 4 1 4 3 3 [2]
5 [5]
3 [1]
5 5 2 [1]
3
Simon Crawford Chief Financial Officer (until 11 Oct 2015)
5 6 2 2 1 4 [2]
1 [1]
1 1 [1]
Simon Crawford Director of Strategy (from 12 Oct 2015)
5 5 5 [5]
2 [1]
2
Jon Bell Interim Chief Financial Officer (from 7 Oct 2015)
4 4 2 5 [5]
2 4
Dr Charles Cayley Medical Director 9 11 2 4 5 4 [1]
5 3
Paul Stanton Director of HR (until 29 May 2015)
3 3 1 1 1
Mark Gammage Interim Lead HR Adviser (1 Jun 2015 to 29 Feb 2016)
4 5 [1] 5 4 1 [1]
1
Claire Gore Director of HR and OD (from Mar 2015)
1 1 1
Chris Pocklington Chief Operating Officer (until 6 Sept 2015)
3 4 2 1 3 [1]
3 [2]
Lee Martin Chief Operating Officer (from Nov 2015)
2 2 2 3 2 [3]
2 1
Tina Benson Acting Chief Operating Officer (7 Sept to Nov 2015)
1 1 1 1 [1]
1 1
Tina Benson Director of Operations (until 7 Sept 2015)
4 2 1 [1]
Carole Flowers Director of Nursing (until 27 May 2015)
2 2 2
Siobhan Jordan Interim Chief Nurse (27 May to 31 Aug 2015)
2 3 2 1 [1]
Amanda Pye Chief Nurse (from Sept 2015)
5 5 3 4 [1]
6
Paul Kingsmore Director of Estates & Facilities (left 31 May 2015)
1 1 2 2
Nigel Myhill Director of Estates and Facilities (from Sept 2015)
6 6 3 4 [4]
2 [1]
2 1
Gary Munn Acting Director of Estates and Facilities (25 May to 6 Sept 2015)
2 3 2 [2]
2 [1]
Yvonne Leese Director of Community Services 2 2 1 2 2
Kevin Connolly Director of IM&T 2 5 3 [2]
2 [1]
4
Christopher Blake Director of Commercial Development
2 2 3 [2]
2 [1]
2 [1]
3
Trust Board Attendance and Committee membership April 2015 to March 2016

39
in 2015/16 which included the creation of clinical governance and audit leads in each division. These roles have been fundamental in the divisions bringing together the relevant clinical performance data for review by the divisions and validation into the Trust governance processes. This has facilitated learning from clinical audits, complaints, Datix, SIs, patient feedback and operational performance.
The Trust has improved its responsiveness to complaints over the last 12 months with increased emphasis on the timeliness and quality of response and again this is a key aspect of review at the divisional performance review meetings as well as more assertive follow-up from the central complaints team.
Mortality
The Trust has recognised that it needs to strengthen its routine reporting and understanding of all mortality indicators. A reformed Mortality Review Group (MRG), chaired by the Medical Director was established during 2015/16; and a standard report format is being developed and will be in place by 2016/17.
The Trust Board routinely has oversight of the mortality data and the detail relating to deaths is discussed at the Clinical Excellence Board Committee. The aim is to continue to be transparent and clear on any individual service outliers even where the overall performance of the Trust is satisfactory. Divisional and local speciality mortality committees will continue. The Trust had no specific CQC alerts in 2015/16. Mortality data was also considered in the full CQC review during October 2015.
The finance section of the integrated performance report includes a full monthly review of financial performance, covering income and expenditure against budget, analysis of the pay, non-pay and income position, performance against the Cost Improvement Programme target and also reports the balance sheet, working capital and cash position of the Trust.
The Board takes collective responsibility for the operational performance of the organisation and has maintained a strong focus on patient safety, ensuring that clinical safety has not been compromised by the financial pressures facing the organisation and has applied a range of measures to access, clinical standards, the output of clinical quality and patient experience surveys, the causes of serious incidents, the reasons for complaints and the effectiveness of our services.
Clinical Governance FrameworkRevised Board assurance arrangements were put in place during 2015/16 under which oversight of quality takes place through the Integrated Governance Committee of the Board and the two reporting executive committees for Clinical Quality and Risk (chaired by the Chief Operating Officer), and Corporate Quality and Risk (Chaired by the Chief Financial Officer). The executive lead for Quality and Risk within the Trust is the Chief Nurse.
Divisions’ own governance frameworks were reviewed
tools presented, including the Integrated Performance Report. This report provided a comprehensive performance overview to the Board on adherence with regulatory targets, quality indicators, financial delivery and workforce metrics.
The five key Corporate objectives were agreed in April 2015 with detailed sub-objectives for delivery which are monitored through the monthly Integrated Performance Report and Board Assurance Framework. The Board strives to improve the effectiveness of the process for setting challenging but deliverable objectives and continually reviews the controls that are in place for monitoring and supporting the delivery of corporate objectives. The Trust Board has exercised its duty to monitor performance through the integrated performance reports that it receives at each monthly meeting which are scrutinised in detail in the Finance and Performance Committee. These reports are a product of the revised monthly Divisional performance meetings chaired by the Chief Operating Officer that review Divisional performance against all key National and local targets as well as performance in respect of incident reviews, complaints and expected services changes.
The operational performance section of the integrated performance report has continued to develop throughout 2015/16 and provides a summary report against all key national and Trust agreed performance targets as well as more detailed analysis against the key care domains of safety, caring, effective, responsive and well led.

40
National publications
In 2015/16 the Trust reviewed relevant national publications including the Lampard and Morecambe Bay reports. A dedicated Board workshop considered the Morecambe Bay findings with the women and children division highlighting key issues and how the Trust compared and what action was or needed to be taken to address any remaining deficiencies.
Care Quality Commission (CQC)
London North West Healthcare NHS Trust is registered with the Care Quality Commission (CQC) without conditions. In 2015/16 the Trust had its first formal CQC assessment as a merged Trust. The formal report is still awaited from the CQC although the Trust did receive a letter in December 2015 with specific areas of concern. The Trust has set out its response to the issues identified in a letter of reply on 7th January 2016. The Trust will develop an overall action plan to address any areas of concern identified in the final CQC report.
Quality Improvement Plan
The Trust in 2015/16 has reviewed its quality improvement plan and continues the monitoring of the key indicators, reporting these in the monthly integrated performance report to the Board. Priorities in the Trust’s quality improvement plan for 2016/17 have been developed and consulted on internally with key work stream operational and overarching leads, and at a strategic level with commissioners.
Annual governance statement
Quality improvement is supported through the application of nationally recognised methodologies, such as Lean, to maintain and sustain change. The organisation in 2015/16 signed up to the Sign up to Safety campaign and this will continue in 2016/17 and be embedded in the Trust’s overall emphasis on safety and learning.
Quality Account
The Quality Account will be produced in accordance with relevant national guidance. In accordance with best practice there have been external and internal workshops held to help shape this year’s Quality Account. It is produced by the Chief Nurse and will be reviewed both internally and externally as per the guidance and approved by the Trust Board.
Staff wellbeing
The Trust reviewed the feedback from staff surveys and has taken action to improve communication, develop its service strategy, provide feedback on issues raised, improve its appraisal processes and be clear about its staffing levels and processes for agreeing additional staffing. The Trust has also identified service areas where broader team development would be beneficial and has made arrangements to facilitate this. The Trust will also be undertaking a broader organisational development programme in 2016/17.
A key area of activity for the Trust during 2015/16 was to improve the compliance rates of staff with appraisals and mandatory training, with particular emphasis on those staff requiring safeguarding
children and adults training. Compliance rates have significantly improved as a result and ongoing monitoring and provision of courses will ensure this improvement is maintained.
Safer staffing
The Trust has reviewed its nursing and midwifery workforce in 2015/16 using the safer nursing tool which has informed the review of nursing establishments, roles, functions and budgets. Daily acuity reviews of patients’ needs are now in place which support the planning and rostering of staff to ensure patient safety is not compromised. Monthly safer staffing reports were developed in Autumn 2015 and provide detail on individual ward/service area staffing levels and how these relate to the acuity of patients being cared for.
Safeguarding
The Trust in 2015/16 reviewed its safeguarding controls for both adults and children. This has led to a number of improvements in the reporting and measuring of safeguarding referrals, including ensuring the Trust Board through the Integrated Performance report monthly updates. Further work is required in 2016/17 to ensure that the Trust continues to strengthen its safeguarding processes and systems with a particular focus on learning disability and children who do not attend.
Clinical Audit
London North West Healthcare NHS Trust has structures and processes in place to ensure that external and internal statutory / mandatory clinical audit requirements are met. Each year

41
the Trust agrees a priority audit programme for the forthcoming year, which includes relevant national, record keeping, NICE guidance and local policy audits. Results of these audits and their accompanying action plans allow the organisation to assure itself that it is following good practice, implementing new guidance effectively and monitoring outcomes.
The Clinical Standards and Effectiveness Group (CSEG) sets the strategic direction for clinical audit within the organisation and is responsible for monitoring the national priority audits. The CSEG reviews and agrees the Trust priority programme before it is submitted for approval at the Clinical Cabinet.
The divisions have established governance groups, which are responsible for ensuring standards are achieved within their services. The divisional governance groups receive monthly audit reports to enable them to review progress of their audits. Each division is required to exception report to the Clinical Quality and Risk Group regarding their audit completion rate and any areas of concern.
Annually the Trust’s Annual Clinical Audit & Effectiveness Report provides detail on all audits undertaken along with improvement actions taken as a result of audit. The Clinical Audit and Effectiveness Team provide details of the national audits the Trust is eligible to participate in, and the number of cases submitted: this information is included in the Trust‘s annual Quality Account.
Counter Fraud and Bribery
The Trust is committed to promoting and maintaining an absolute standard of honesty and integrity, and to eliminating fraud and illegal acts committed within the Trust. It undertakes rigorous investigation and disciplinary action where appropriate and seeks recovery of any losses where possible. The Trust has adopted best practice, as recommended by NHS Protect.
The Trust publicises widely the procedure for staff to report any concerns about potential fraud and corruption. Any concerns raised are investigated by our local counter-fraud specialists or NHS Protect as appropriate and all investigations are reported to the Audit Committee and the Integrated Governance Committee.
The Local Counter Fraud Specialist completed the Standards Review Tool Kit (SRT) for the Trust for 2015/16 but NHS Protect has yet to release the results.
Risk and Internal Control Framework Internal Control
The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can, therefore, only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an on-going process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of
London North West Healthcare NHS Trust, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically.
The overall responsibility for the management of risk lies with the Chief Executive as the Accountable Officer. The Board of Directors, collectively and individually, ensures that systems of internal control and management are in place. The Board sought assurance through scrutiny of the Board Assurance Framework and the receipt of reports to the Board from the eight board committees. The committees and, in particular, the Audit Committee, receive exception reports from a number of sub-committees that closely monitor areas of risk. The Trust aims to facilitate a proactive approach to risk management and learning from incidents and good practice through investigating incidents and learning from what went wrong, staff training and other awareness raising initiatives. Monthly news magazines are published on the Trust intranet and information sharing is encouraged through presentation of performance reports at specialist committees and other meetings.
The system of internal control is underpinned by compliance with the Trust’s terms of authorisation and the requirement of regulatory bodies relevant to NHS trusts. These requirements are reflected in the Trust’s risk management strategy and policy.
The Trust involves key stakeholders in its risk management processes as appropriate. These include

42
• monitoring the implementation and completion of actions.
Actions taken so far include:
• review of the organisation’s processes for the reporting, investigating and learning from SIs;
• implementation of weekly SI monitoring meetings with divisional governance leads; and
• development and sign-off of the new Trust process for the management of SIs.
Data security incidents
Incidents relating to information are actively managed and monitored through the Trust’s Information Governance Group, which meets quarterly and reports to the Integrated Governance Board Committee through the Corporate Quality and Risk Committee. The Trust takes a risk-based approach to Information Governance and a risk register is in place for each of the key areas covered by the Information Governance Toolkit including: information security, records management, and data quality. This approach allows clear and unambiguous day-to-day management with a framework for reporting upwards and escalation. Any risks that are scored 12 or greater using the NHS 5x5 risk matrix are submitted for entry onto the Corporate Risk Register.
The Senior Information Responsible Officer for the Trust is the Director of Strategy. There is also a Deputy Senior Information Responsible Officer with responsibility for information governance, corporate records and medical records who also works closely with the Trust’s Caldicott
Never Event incidents
There were eight Never Events within the Trust From April 2015 to March 2016.
Duty of Candour Theme Occurrences Met?
Wrong blood transfusion 2 Yes
Wrong ocular lens inserted 2 Yes
Wrong site surgery 1 Yes
Misplaced NG tube 1 Yes
Wrong route intravenous medication 1 Yes
Fall from window 1 Yes
Serious incidents
The Chief Nurse has reviewed the process of SI management at LNWH Trust. It is evident that there are gaps in timeliness of meeting the NHS target of 60 days (the Board is sighted on this) and the follow-up of actions and the robustness of action plan templates. There is now a meeting in place for executive review of completed SI reports which has increased the oversight and sign-off process. Further development in 2016/17 will include the following:
• ownership by the senior leadership of the SIs;
• human factors training;
• root cause analysis (RCA) training;
• review of action plan template to make it SMART; and
the clinical commissioning groups, Healthwatch, staff side representatives, voluntary or statutory organisations, patients and the public and others as required.
Incident reporting and lessons learned
During the last year the Trust has identified deficiencies in the process of reporting and learning from serious incidents (SIs) and Datix reports. In response the Trust has re-issued guidance to staff on the need to comply with the incident reporting policy, ensured that there is monthly discussion of incident reporting, investigation and timely closure of reviews at the divisional performance review meetings. It has also improved reporting of Datix incidents and the closure of investigations to the Board and its sub-committees.
The Trust commenced a roll-out programme on lessons learnt in 2015/16. This will continue into 2016/17 and will place a significant emphasis on learning from SIs and the substantial body of valuable information within Datix reports. Achievements and lessons learned from the 2015/16 Quality Improvement Programme will be provided in the final Annual Plan submission.
Annual governance statement

43
Summary of personal data related incidents in 2015/16 showing the number of Level 2 incidents by defined category for the London North West Healthcare NHS Trust from April 2015 to March 2016
Category Nature of incident Total
1Loss of inadequately protected electronic equipment devices or paper documents from secured NHS premises
NONE
2Loss of inadequately protected electronic equipment devices or paper documents from outside secured NHS premises
NONE
3Insecure disposal of inadequately protected electronic equipment, devices or paper documents
NONE
4 Unauthorised disclosure 1
5 Other NONE
Guardian (Dr Simon Gabe, Consultant Gastroenterologist).
Incidents are rated according to severity as defined by the Health & Social Care Information Centre (0 being the lowest, 2 being the highest). All information incidents rated at a level 2 are notified to the Information Commissioner’s Office (the regulator for data protection in England) via the Health & Social
Care Information Centre (HSCIC) Information Governance Incident Reporting Tool, and are also placed on STEIS, the national incident reporting system.
There were two Level 2 incidents reported during the period April 2015 to March 2016. Please note that following on from a detailed investigation, including discussions with the Information Commissioner’s Office, one of these incidents
was reduced to a Level 1 classification. The confirmed Level 2 incident related to a staff member’s health record being inappropriately accessed by colleagues, which was then subject to action under Trust disciplinary policy. The second incident, reduced to Level 1, related to inappropriate disposal of copy health records which had been held at an off-site outreach clinic.

44
Annual governance statement
supported by detailed divisional and local directorate risk registers which are reviewed, validated and monitored by the divisional governance groups and presented to the Clinical and Corporate Quality and Risk committees. The register is configured under six main headings. These are clinical quality of care, governance and capital resourcing, estates, workforce, strategic change and finance.
Risks were managed in line with the Trust’s Risk Management Strategy and Policy. These use pre-existing structures to oversee and manage risk in addition to quarterly performance reviews by the executive team.
Risks entered on the Corporate Risk Register have a score of 12 or above and have been reviewed and agreed for addition to the register by an Executive Director. The Corporate Risk Register is
Training on risk management, including incident reporting and risk assessment for staff is provided in a number of forums, these include: induction for all staff, mandatory update training for all staff, risk assessment training, e-learning for incident reporting and Datix use, online guidance for Datix use (reporting and managers), ad-hoc training delivered to teams and departments based on identified requirements.
Risk Assessment
The Trust has adopted the Health and Safety Executive and National Patient Safety Agency’s Five Steps to Risk Assessment as the basis for the procedure for undertaking risk assessment and documentation has been developed to support this approach. The diagram below describes the process by which local risk assessment is escalated through the organisation and describes Board and Executive overview mechanisms.
The Corporate Risk Register is maintained by the Chief Nurse.
High and significant risks and the maintenance of the Risk Register are the responsibility of the Executive Director Team.
Any issues material to corporate objectives are brought to the attention of the Trust Board immediately; otherwise the Trust Board reviews
the Risk Register quarterly.
Divisional management teams complete risk assessments and manage divisional risk registers.
Risks requiring resources feed into service development planning and/or capital and business case processes.
Risk assessments at ward and departmental level and local risk registers are completed.
Moderate and serious risks are reported to and incorporated into each divisional management team’s risk register.

45
resources) to meet the 4 hour Accident and Emergency target. Despite the pressures the Trust has performed reasonably well but this will continue to be an area that is closely monitored.
• Referral to treatment time – Following a challenging year, this is expected to be fully mitigated by August 2016. Within this cancer waiting times are a particular issue due to increasing numbers of referrals.
• Staff shortages - In the context of a national shortage of nurses, high levels of staff turnover and the SaHF impact, the Trust is experiencing difficulty in recruiting, and service expansion is compounding nurse shortages at ward level which may, if unmitigated, impact on the quality of care. There are a number of initiatives in place to mitigate this and quality of care is closely monitored.
• Patient Experience. There is a need to continue to improve the patient’s experience. (Primarily inpatient, maternity and cancer services).
• Low levels of compliance with Mandatory Training leading to concern for patient safety.
• Delivering the challenging cost improvement programme to meet the financial pressures faced by the Trust and at the same time maintain operational performance in the context of a material financial deficit and significant changes in the provision of services.
• Channelling staff engagement to deliver the significant service changes
Major risks to the Trust identified during 2015/16 included:
The Trust has described the principal strategic and operational risks that it faces in the Annual Report. The principal current strategic risks are identified as follows:
• Financial – The Trust has an underlying financial deficit that will not be fully resolved until the North West London sector agrees resolutions to structural deficits at Ealing and Central Middlesex hospitals. The financial pressures in the NHS affect our ability to meet our key financial targets and our financing strategy for future capital developments.
• Shaping a Healthier Future – Significant service change including structural change in the North West London sector as part of proposals under Shaping a Healthier Future (SaHF) will entail material changes for providers in the sector. It is expected that this will bring both challenges in the scale of change to services at Central Middlesex and Ealing hospital sites but also potential benefits in the form of additional activity to the Trust on the Northwick Park site. These plans are in the process of further development and will be reflected in the Sustainability and Transformation Plans (STPs) for North West London.
With regard to operational risks the principal current risks are identified as follows:
• Emergency Department flow - Risk of insufficient capacity (in terms of beds, theatres, outpatient and diagnostic
required to deliver both the Trust’s business plan and the wider NHS reform agenda.
• Maintaining the provision of high quality services in the context of the challenges of wider patient choice, qualitative performance measures and provider competition.
• Insufficient timely, accurate capture of activity data in both the community and acute settings within the Trust.
• Poor Estates infrastructure on the Northwick Park Hospital and St. Marks site.
• Low appraisal rates across the Trust. Failure of managers to complete appraisals to identify talent.
The mitigation and the current status for each of these risks are described in more detail in the Annual Report, the Board Assurance Framework and Risk Register. Although the risks above are current risks to the Trust, they are also expected to continue into the future. The risks associated with financial pressures in the NHS are expected to increase. As a consequence there is a risk that the Trust’s planned developments, including new hospital buildings and investment in a new electronic health records system will not go ahead to the timescale planned, thereby delaying the delivery of the expected benefits.
Significant issuesOperational performance
The Board informed the NHS TDA that the Trust has faced difficulties in maintaining A&E performance due to high levels

46
Annual governance statement
of emergency admissions and capacity constraints, particularly in terms of acute medical beds. The Trust did not achieve the 95% national four hour standard, with a year-end position of 89.4%.The Trust Board has focused specifically on this area and committed to ongoing investment with increased bed resource being made available in the period and further increases in capacity planned for 2015/16. The Trust is working across the health economy to establish the correct capacity in the right setting to care for our population.
During October 2014 to March 2015 the Trust did not meet the 18 week target for admitted patients and non-admitted patients with admitted figures of 83.34% and non-admitted figures of 94.24%. The Trust is making progress to address these issues and delivery of the capacity will be the key focus for 2015/16. To assure the Board over data quality in relation to the 18 week target there are weekly waiting times meetings that review patients on incomplete elective pathways and the development and deployment of waiting times information that flags pathways requiring additional capacity or validation. Performance reports have been developed that provide information for the Board and front line teams. RTT and waiting list management were a core part of the Trust’s Data Quality Audit completed in quarter 4 2015/16. This was completed by independent validation.
A team of external RTT subject matter experts reviewed the pathway for validation which was completed during February to March 2015. RTT data quality, utilisation of internal
validation systems and all audit findings are reviewed through the Data Quality Group, with appropriate issues escalated to the Information Assurance Board which reports up to Audit Committee and Integrated Governance Committee. Data quality issues in regard to community and acute activity are being addressed by data quality programmes, monitored through a dedicated group with weekly KPI reporting produced for managers. A merged Trust Data Quality Policy was approved in December 2014.
In quarter 3 the Trust breached the 62 day GP referral to treatment target, and whilst those patients affected are small in number, patient-initiated delays may have caused this breach. Work continues to ensure the target is recovered where patients are ready for treatment.
The Trust underachieved against the national standards for MRSA in 2015/16 and the C. Diff objective. There were a total of 6 MRSA blood stream infections, four of which following a Post Infection Review were deemed unavoidable. A total of 49 C. diff cases were reported as part of mandatory surveillance. A total of 22 cases have been reclassified by the commissioning lead as on-trajectory cases, equating to a total of 27 cases against an objective of no more than 37 cases. The Trust rate per 100,000 bed days is 11.67 compared to 15.23 across England. In 2015/16 The Trust signed up to the National Infection Prevention Control Collaborative 90 day Improvement Programme. An overall action plan is being developed for 2016/17 which will be monitored by the
Trust Board and Integrated Governance Committee.
The Trust in 2015/16 reviewed safeguarding controls in both adults and children. This has led to a number improvements in the reporting and measuring of safeguarding referrals, including ensuring that the Trust Board, through the Performance Report, has monthly updates. Further work is required in 2016/17 to ensure that the Trust continues to strengthen its safeguarding processes and systems with a particular focus on learning disability and children who do not attend.
Financial Performance
The Trust agreed a planned deficit control total of £88.3m for 2015/16 and has delivered an out-turn deficit of £88.2m. The plan for 2016/17 is a deficit control total of £61.5m after the receipt of £21.5m from the Sustainability and Transformation Fund. Within the 2016/17 plan is a savings target of £34.7m (4.5% of expenditure), excluding £15.8m from the full year effect of 2015/16 savings. The Trust is working with the sector to address the issue of long term financial sustainability which is contingent on further transformation change across the organisation and the reconfiguration of services as part of the Shaping a Healthier Future strategy.
Workforce capacity has been a challenge partly due to the recommendations for safer staffing levels and a shortage of qualified clinical staff. The Trust has commenced a recalibration of staff requirements across the Trust to ensure adequate and safe levels of staffing. There is a Board focus on recruitment

47
Specific actions and recommendations from reviews have been agreed with responsible officers and implementation dates are set to address the recommendations. The Audit Committee and the Integrated Governance Committee monitor progress and outcomes of these recommendations.
Chief Executive’s StatementThis Annual Governance Statement sets out the arrangements for the governance of London North West Healthcare NHS Trust which I consider to be reasonable and robust for the period 1st April 2015 to 31st March 2016.
Accountable Officer: Jacqueline Docherty DBE, Chief Executive
Organisation: London North West Healthcare NHS Trust
Signature:
Date: 25th May 2016
The Trust Quality Account describes key priorities the new Trust intends to meet during the year ahead and these are subject to consultation with key stakeholders. Both draft and final versions of the document are seen by the Board for comment and approval.
The Trust has a serious incident and incident reporting policy which outlines criteria for the reporting of incidents and uses the Datix risk management web based system across the organisation.
Serious incidents and Never Events are reported in line with national guidance and deadlines. These are overseen by both the Trust Board and the Integrated Governance Committee on behalf of the Board. This Integrated Governance Committee also monitors progress with action plans related to serious incident reports.
Head of Internal Audit OpinionThe Trust is in receipt of its Head of Internal Audit Opinion that based on the work undertaken in the financial year, reasonable assurance can be given that there are adequate and effective management and internal control processes to manage the achievement of the organisation’s objectives.
Over the 12 month period, nine audits were completed of which four ‘limited assurance’ opinion were issued and comprised of Management of DNAs, Private Patients, HR Workforce Planning and Temporary Staffing within Community Services and Health and Safety.
and retention and as part of the retention strategy there will be a need for appraisal compliance, so as to identify talent, support staff and maximise their opportunities to develop a career within the Trust. There is a need to enhance levels of mandatory training undertaken by staff which will be addressed by the use of real time reporting, agreed schedules of training and the frequency of updates allowing for alignment with the individual’s Personal Development Plan.
Review of the effectiveness of risk management and internal controlI have drawn on the content of the Quality Reports and this Annual Report and other performance information available to me. My review is also informed by comments made by the external auditors in their reports.
I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the Board, the Audit Committee, and a plan to address weaknesses and ensure continuous improvement of the system will be in place.
The Board ensures the effectiveness of the system of the internal control through clear accountability and reporting arrangements.
The Board monitors the Assurance Framework and objectives, ensuring actions to address gaps in control and gaps in assurance are progressed.
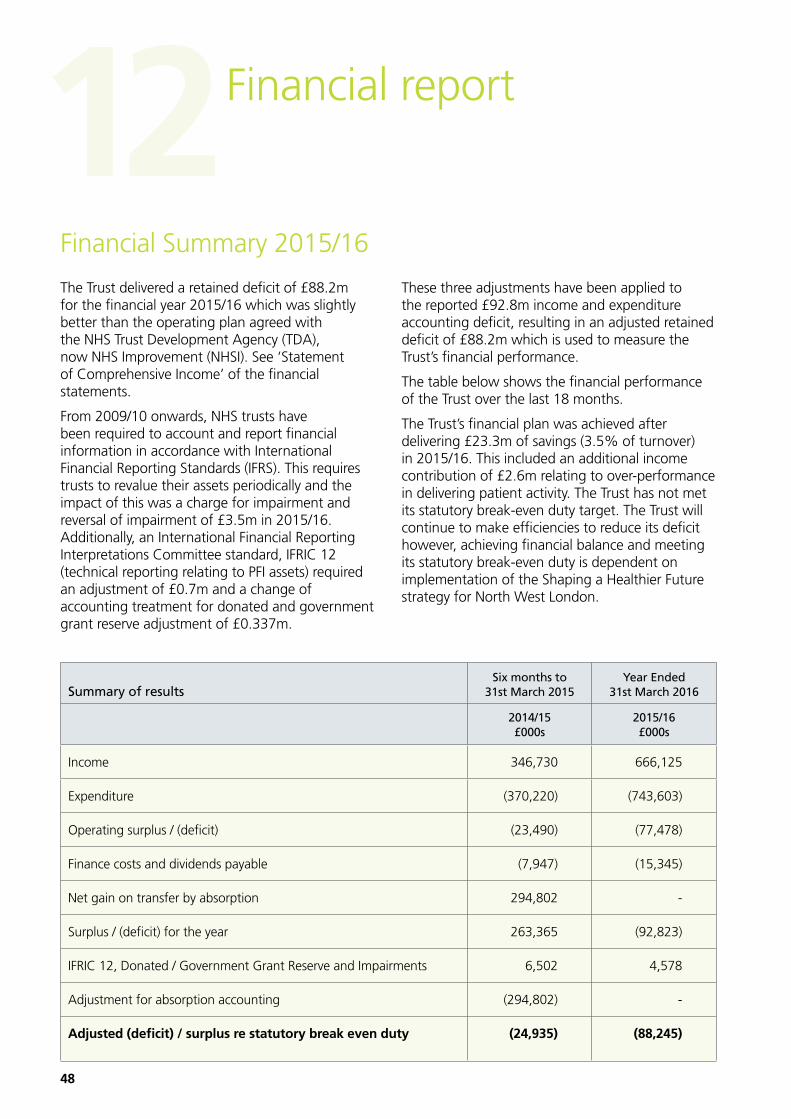
48
The Trust delivered a retained deficit of £88.2m for the financial year 2015/16 which was slightly better than the operating plan agreed with the NHS Trust Development Agency (TDA), now NHS Improvement (NHSI). See ‘Statement of Comprehensive Income’ of the financial statements.
From 2009/10 onwards, NHS trusts have been required to account and report financial information in accordance with International Financial Reporting Standards (IFRS). This requires trusts to revalue their assets periodically and the impact of this was a charge for impairment and reversal of impairment of £3.5m in 2015/16. Additionally, an International Financial Reporting Interpretations Committee standard, IFRIC 12 (technical reporting relating to PFI assets) required an adjustment of £0.7m and a change of accounting treatment for donated and government grant reserve adjustment of £0.337m.
These three adjustments have been applied to the reported £92.8m income and expenditure accounting deficit, resulting in an adjusted retained deficit of £88.2m which is used to measure the Trust’s financial performance.
The table below shows the financial performance of the Trust over the last 18 months.
The Trust’s financial plan was achieved after delivering £23.3m of savings (3.5% of turnover) in 2015/16. This included an additional income contribution of £2.6m relating to over-performance in delivering patient activity. The Trust has not met its statutory break-even duty target. The Trust will continue to make efficiencies to reduce its deficit however, achieving financial balance and meeting its statutory break-even duty is dependent on implementation of the Shaping a Healthier Future strategy for North West London.
Summary of resultsSix months to
31st March 2015Year Ended
31st March 2016
2014/15 £000s
2015/16 £000s
Income 346,730 666,125
Expenditure (370,220) (743,603)
Operating surplus / (deficit) (23,490) (77,478)
Finance costs and dividends payable (7,947) (15,345)
Net gain on transfer by absorption 294,802 -
Surplus / (deficit) for the year 263,365 (92,823)
IFRIC 12, Donated / Government Grant Reserve and Impairments 6,502 4,578
Adjustment for absorption accounting (294,802) -
Adjusted (deficit) / surplus re statutory break even duty (24,935) (88,245)
Financial Summary 2015/16
Financial report12

49
IncomeThe Trust income was £666m in 2015/16.
The graph below shows that 59% of the Trust’s income is derived from three main commissioners (clinical commissioning groups - CCGs) – Brent CCG (21%), Harrow CCG (17%) and Ealing CCG (21%). The Trust continues to provide services to Hillingdon and Barnet patients, with 5% of the Trust’s income coming from these two CCGs.
NHS England accounts for 15% of the Trust’s income and this is largely related to specialist patient healthcare. Research and education makes up another 5% of the Trust’s income.
The Trust continues to be principally a public sector NHS provider of services, with just 1% of income derived from private patient activity.
Where the money comes from
Expenditure The Trust’s total operating expenditure for the year was £743.6m
The Trust spent a total of £474.9m on pay in the year, with 70% of this spent directly on doctors and nursing staff.
How much we spend on staff - £millions
Nursing
Scientific, technicaland professional
50 100 150
£m
200 250
Medical
Admin and clerical
Professions allied tomedicine
Other staff
Other
20 40 60
£m
80 100 120 140 160
Non-clinical supplies
Establishmentand transport
Research,development education
and training
Nursing
Scientific, technicaland professional
50 100 150
£m
200 250
Medical
Admin and clerical
Professions allied tomedicine
Other staff
Other
20 40 60
£m
80 100 120 140 160
Non-clinical supplies
Establishmentand transport
Research,development education
and training
Non-pay expenditure The chart below illustrates our non-pay expenditure for the year. The largest category of non-pay spend was on clinical supplies which directly supports patient care on our wards and within our services.
Impairments in the year were £3.5m as a result of the revaluation of the Trust’s estate assets. This is excluded from the Trust’s reported deficit, against which we are performance managed.
Non-pay expenditure - £millions
Nursing
Scientific, technicaland professional
50 100 150
£m
200 250
Medical
Admin and clerical
Professions allied tomedicine
Other staff
20 40 60
£m
80 100 120 140 160
Clinical supplies
Other
Premises
Non-clinical supplies
Depreciation
Establishmentand transport
Impairments
Research,development education
and training
NHS Ealing CCG 21%
NHS Brent CCG 21%
NHS Harrow CCG 17%
NHS England 15%
Other 7%
Other CCG 6%
Education & Research 5%
NHS Hillingdon CCG 3%
Local Authorities 2%
NHS Barnet 2%

50
Cash and LiquidityThe Trust received in cash £19.1m of revenue Public Dividend Capital (PDC) and £11.6m for Capital PDC, £58.4m of Working Capital Loan (of which £45m has been paid back) and an Interim Revenue Loan of £76.9m in 2015/16 from the Department of Health to support the financing of the Trust’s planned deficit as a result of income not covering the in-year expenditure.
The Trust retained £3.3m cash in the bank at the period end. We have managed our cash within the External Financing Limit with a small undershoot of £0.4m.
Capital investmentThe Trust invested £34.8m in a capital programme in 2015/16. This significant investment has allowed us to continue with our substantial programme to improve facilities and equipment for patient care. The capital programme was financed by £13.8m of internally generated funds, £1.2m PFI allocation, £11.6m public dividend capital (PDC) and an £8.1m Interim Capital Investment Loan from the Department of Health (DH).
The Trust has maintained capital expenditure within its capital resource limit agreed with the NHS TDA.
The next chart shows how our capital was spent. Total spend on key projects amounted to £22.5m, or 64%, and comprised the following schemes:
• The modular project consists of a brand new facility at the Northwick Park site which has been set up as a three warded unit providing both flexibility and additional bed capacity Trust-wide.
• Improvement to the mortuary facility to accommodate current and expected future capacity.
• Backlog electrical works aimed at improving and upgrading the current electrical infrastructure on the Northwick Park & St. Mark’s site.
• Completion of a community information systems scheme resulting in the use of the same system across all our community services.
• New medical equipment including a brand new Catheterisation Laboratory, endoscopy equipment and operating tables.
The balance of capital spending, £12.3m, consisted of smaller schemes under the following categories – Infrastructure, IT, Equipment, Health and Safety and PFI (lifecycle replacement cost).
Capital Spend 2015/16 - £millions
Backlog Electrical £3.2m
Community Info Systems £2.1m
Developments £5m
Health & Safety £1.6m
IT & IT Infrastructure £4.5m
Medical Equipment £2.9m
Modular £13.4m
Mortuary £1m
PFI £1.2m
38%
14%13%
9%
8%
6%
5%4% 3%
Financial report

51
The Better Payment Practice Code (BPPC) requires the Trust to aim to pay 95% of undisputed invoices by the due date or within 30 days of the receipt of goods and services or a valid invoice, whichever is later. The Trust paid 51.7% by value of its Non-NHS suppliers within 30 days. We are addressing a number of process issues which, along with the cash constraints resulting from the deficit, contributed to the failure to meet this target in 2015/16.
Challenging financial environmentThe major financial concern for the Trust was to deliver a challenging savings programme and maintain financial stability, while also meeting the demands of increased activity and national operational performance targets.
The Trust has an Improvement Delivery Team in place, which monitors and manages the savings programme. We have managed to achieve the savings target of £23.3m in 2015/16 through cost reductions and efficiency savings as well as a £2.6m efficiency contribution from the additional income gained from extra activity. In spite of the significant progress made in reducing our costs this year it is expected that the coming year will continue to be very challenging in terms of our finances. The Trust has set a target of £34.6m of further cost improvements in 2016/17, in addition to the full year effect of savings commenced in 2015/16. The Trust will also be in receipt of £21.5m from the Sustainability and Transformation Fund, giving a planned deficit for 2016/17 of £61.5m. We are seeking agreement with the Department of Health for the necessary funding to mitigate the cash impact of the expected deficit position, to be provided through either PDC support or a working capital loan.
In spite of the ongoing challenges the Trust has clear plans to reduce the deficit through further transformational savings and synergies as well as an ongoing review of the cost base for delivering services. The Trust also had confirmation of NHS Improvement support for the level of cash needed in the next 12 months to maintain our trading position. The directors, therefore, have a reasonable expectation that the Trust has adequate resources to continue in operational existence for the foreseeable future. Consequently, we continue to adopt the ‘going concern’ basis in preparing the annual accounts.
Financial accountabilityGrant Thornton UK LLP is the appointed external auditor to the Trust. During 2015/16, the fees payable to Grant Thornton for its statutory external audit were £138k. There were no other fees paid to Grant Thornton in 2015/16.
Counter fraud and corruptionThe Trust is committed to promoting and maintaining an absolute standard of honesty and integrity, and to eliminating fraud and illegal acts committed within the Trust. We undertake rigorous investigation and disciplinary action where appropriate and seek recovery of any losses where possible. The Trust has adopted best practice, as recommended by NHS Protect, and is also involved in the National Fraud Initiative, which is led by the Cabinet Office.
We have widely publicised our procedure for staff to report any concerns about potential fraud and corruption. Any concerns raised are investigated by our local counter-fraud specialists or the NHS Protect as appropriate and all investigations are reported to the Audit Committee.
Jon Bell
Interim Director of Finance
Date: 27 May 2016

52
Independent auditor’s report to the directors of London North West Healthcare NHS TrustWe have audited the financial statements of London North West Healthcare NHS Trust (the “Trust”) for the year ended 31 March 2016 under the Local Audit and Accountability Act 2014 (the “Act”). The financial statements comprise the Statement of Comprehensive Income, the Statement of Financial Position, the Statement of Changes in Taxpayers’ Equity, the Statement of Cash Flows and the related notes. The financial reporting framework that has been applied in their preparation is applicable law and International Financial Reporting Standards (IFRSs) as adopted by the European Union, and as interpreted and adapted by the 2015/16 Government Financial Reporting Manual (the 2015/16 FReM) as contained in the Department of Health Group Manual for Accounts 2015/16 (the 2015/16 MfA) and the Accounts Direction issued by the Secretary of State with the approval of HM Treasury as relevant to the National Health Service in England (the Accounts Direction).
This report is made solely to the Directors of London North West Healthcare NHS Trust, as a body, in accordance with Part 5 of the Act and as set out in paragraph 43 of the Statement of Responsibilities of Auditors and Audited Bodies published by Public Sector Audit Appointments Limited. Our audit work has been undertaken so that we might state to the Directors of the Trust those matters we are required to state to them in an auditor’s report and for no other purpose. To the fullest extent permitted by law, we do not accept or assume responsibility to anyone other than the Trust and the Directors of the Trust, as a body, for our audit work, for this report, or for the opinions we have formed.
Respective responsibilities of Directors, the Accountable Officer and auditor
As explained more fully in the Statement of Directors’ Responsibilities, the Directors are responsible for the preparation of the financial statements and for being satisfied that they give a true and fair view. Our responsibility is to audit and
Financial report
express an opinion on the financial statements in accordance with applicable law and International Standards on Auditing (UK and Ireland). Those standards require us to comply with the Auditing Practices Board’s Ethical Standards for Auditors.
As explained in the statement of the Chief Executive’s responsibilities, as the Accountable Officer of the Trust, the Accountable Officer is responsible for the arrangements to secure economy, efficiency and effectiveness in the use of the Trust’s resources. We are required under Section 21(3)(c) and Schedule 13 paragraph 10(a) of the Act to be satisfied that the Trust has made proper arrangements for securing economy, efficiency and effectiveness in its use of resources and to report our opinion as required by Section 21(4)(b) of the Act.
We are not required to consider, nor have we considered, whether all aspects of the Trust’s arrangements for securing economy, efficiency and effectiveness in its use of resources are operating effectively.
Scope of the audit of the financial statements
An audit involves obtaining evidence about the amounts and disclosures in the financial statements sufficient to give reasonable assurance that the financial statements are free from material misstatement, whether caused by fraud or error. This includes an assessment of whether the accounting policies are appropriate to the Trust’s circumstances and have been consistently applied and adequately disclosed; the reasonableness of significant accounting estimates made by the Directors; and the overall presentation of the financial statements. In addition, we read all the financial and non-financial information in the Annual Report to identify material inconsistencies with the audited financial statements and to identify any information that is apparently materially incorrect based on, or materially inconsistent with, the knowledge acquired by us in the course of performing the audit. If we become aware of any apparent material misstatements or inconsistencies we consider the implications for our report.

53
Scope of the review of arrangements for securing economy, efficiency and effectiveness in the use of resources
We have undertaken our review in accordance with the Code of Audit Practice, having regard to the guidance on the specified criteria issued by the Comptroller and Auditor General in November 2015, as to whether the Trust had proper arrangements to ensure it took properly informed decisions and deployed resources to achieve planned and sustainable outcomes for taxpayers and local people. The Comptroller and Auditor General determined these criteria as those necessary for us to consider under the Code of Audit Practice in satisfying ourselves whether the Trust put in place proper arrangements for securing economy, efficiency and effectiveness in its use of resources for the year ended 31 March 2016, and to report by exception where we are not satisfied.
We planned our work in accordance with the Code of Audit Practice. Based on our risk assessment, we undertook such work as we considered necessary to form a view on whether, in all significant respects, the Trust had put in place proper arrangements to secure economy, efficiency and effectiveness in its use of resources.
Opinion on financial statements
In our opinion the financial statements:
• give a true and fair view of the financial position of London North West Healthcare NHS Trust as at 31 March 2016 and of its expenditure and income for the year then ended; and
• have been prepared properly in accordance with IFRSs as adopted by the European Union, as interpreted and adapted by the 2015/16 FReM as contained in the 2015/16 MfA and the Accounts Direction.
Opinion on other matters
In our opinion:
• the parts of the Remuneration and Staff Report to be audited have been properly prepared in accordance with IFRSs as adopted by the European Union, as interpreted and adapted by the 2015/16 FReM as contained in the 2015/16 MfA and the Accounts Direction; and
• the other information published together with the audited financial statements in the Annual Report is consistent with the audited financial statements.
Matters on which we are required to report by exception
We are required to report to you if we refer a matter to the Secretary of State under section 30 of the Act.
We have a duty under the Act to refer the matter to the Secretary of State if we have reason to believe that the Trust, or an officer of the Trust, is about to make, or has made, a decision which involves or would involve the body incurring unlawful expenditure, or is about to take, or has begun to take a course of action which, if followed to its conclusion, would be unlawful and likely to cause a loss or deficiency.
On 25 May 2016, we referred a matter to the Secretary of State under section 30 of the Act as in March 2016, the Trust Board agreed a draft deficit budget of £61.5 million for the year ending 31 March 2017. Given the planned deficit in 2016/17 and the significant deficit accumulated to 31 March 2016, the Trust’s expenditure is likely to exceed income for the three year periods ending 31 March 2017 and 31 March 2018. We have reason to believe that the Trust has taken a course of action that, if followed to its conclusion, will lead to a breach of the Trust’s break-even duty for the three year periods ending 31 March 2017 and 31 March 2018.
We are required to report to you if we are not satisfied that the Trust has put in place proper arrangements to secure economy, efficiency and effectiveness in its use of resources.
Basis for adverse value for money conclusion
Our review of the Trust’s arrangements identified the following matters:
• The Trust’s outturn position for 2015/16 records a £88.2 million deficit in line with budget after the delivery of a £23.3 million cost improvement plan. The deficit represents 12 per cent of the Trust’s gross annual expenditure.
• The Trust has set a further deficit plan for 2016/17 of £61.5 million in accordance with the control total set by the NHS Trust

54
Financial report
Development Authority, which is a lower deficit budget than 2015/16, but includes £21.5 million of non-recurrent funding.
• During the year the Trust has been developing its long term financial model which aims to bring the Trust into financial balance in 2023/24 subject to the implementation of the North West London Shaping a Healthier Future Strategy and the resolution of structural deficits in the Trust. Therefore, as at the date of this report, the Trust does not have a financial plan which brings the Trust back into financial balance in the medium term.
• During the year the Trust has reported to its Board that it has failed to meet the national priority targets in relation to A&E 4 hour waits, 18 week Referral to Treatment and 62 day cancer waits against a backdrop of increased activity. Annual performance against these targets has declined from 2014/15. Although action plans are in place these are yet to result in evidence of sustained improvements in performance.
These matters identify weaknesses in the Trust’s arrangements for:
• setting a sustainable budget with sufficient capacity to absorb emerging cost pressures due to the current configuration of services
• responding to service delivery issues and increases in activity effectively to support the sustainable delivery of strategic priorities.
These issues are evidence of weaknesses in proper arrangements for:
• planning finances effectively to support the sustainable delivery of strategic priorities and maintain statutory functions
• understanding and using appropriate cost and performance information to support informed decision making and performance management.
Adverse value for money conclusion
On the basis of our work, having regard to the guidance issued by the Comptroller & Auditor General in November 2015, because of the significance of the matters described in the Basis for adverse value for money conclusion paragraph we are not satisfied that, in all significant respects, London North West Healthcare NHS Trust put in place proper arrangements for securing economy, efficiency and effectiveness in its use of resources
for the year ended 31 March 2016.
We have nothing to report in respect of the following matters where we are required to report to you by exception if:
• in our opinion the governance statement does not comply with guidance issued by the NHS Trust Development Authority; or
• we issue a report in the public interest under section 24 of the Act; or
• we make a written recommendation to the Trust under section 24 of the Act.
Certificate
We certify that we have completed the audit of the accounts of London North West Healthcare NHS Trust in accordance with the requirements of the Act and the Code of Audit Practice.
Emily Hill
for and on behalf of Grant Thornton UK LLP, Appointed Auditor
Grant Thornton House Melton Street London NW1 2EP
Date: 2 June 2016

55
Statement of Comprehensive Income for year ended 31 March 2016
2015-16
Six month accounts period ended 31 March
2015
NOTE £000 £000
Gross employee benefits 9.1 (474,876) (241,463)
Other operating costs 7 (268,727) (128,757)
Revenue from patient care activities 4 595,323 309,522
Other operating revenue 5 70,802 37,208
Operating (deficit) (77,478) (23,490)
Investment revenue 11 70 33Other gains and (losses) 12 (4) (78)
Finance costs 13 (7,077) (3,277)
(Deficit) for the financial year (84,489) (26,812)
Public dividend capital dividends payable (8,334) (4,626)
Transfers by absorption - gains 0 473,443
Transfers by absorption - (losses) 0 (178,641)
Net Gain/(loss) on transfers by absorption 0 294,802
Retained (deficit)/surplus for the year (92,823) 263,364
Other Comprehensive IncomeNet gain on revaluation of property, plant & equipment 7,548 814
Total other comprehensive Income 7,548 814
Total comprehensive income for the year (85,275) 264,178
Financial performance for the yearRetained (deficit)/surplus for the year (92,823) 263,364
IFRIC 12 adjustment (including IFRIC 12 impairments) (1,364) 3,324
Impairments (excluding IFRIC 12 impairments) 5,605 2,992
Adjustments in respect of donated gov’t grant asset reserve elimination
337 187
Adjustment re absorption accounting 0 (294,802)
Adjusted retained (deficit) (88,245) (24,935)
The Trust’s reported NHS financial position is derived from its retained deficit/surplus, but adjusted for the following:
a) The revenue cost of bringing PFI assets onto the balance sheet (due to the introduction of International Financial Reporting Standards (IFRS) accounting in 2009/10) - NHS Trusts’ financial performance measurement needs to be aligned with the guidance issued by HM Treasury measuring Departmental expenditure. Therefore, the incremental revenue expenditure resulting from the application of IFRS to PFI, which has no cash impact and is not chargeable for overall budgeting purposes, should be reported as technical. This additional cost £0.723m is not considered part of the organisation’s operating position.
b) The Trust is required to revalue its Land and Building on a regular basis as a result of the IFRS implementation and this has resulted in a net impairment of its Building by £3.518m, of which zero was available to absorbed by the revaluation reserve. Therefore, an impairment of £3.518m has been recognised in the I&E account. The impairment for Trust owned buildings is £5.605m and an increase in valuation of £2.087m for PFI buildings. The increase in valuation on the PFI has been credited to the Income and Expenditure account in line with IAS 36, whereby a reversal of an impairment loss on the same asset to the extent that it reverses that was recognised previously in the Income and Expenditure account. Impairments are specifically excluded from measurement of the Trust’s financial performance.
c) Due to a change in accounting requirement, elimination of donated and government grant reserve has resulted in net income of £0.337m. Therefore, the reduction of income resulting from the application of change to donated and government grant account treatment, which has no cash impact and is not chargeable for overall budgeting purposes, should be reported as technical. This is not considered part of the organisation’s operating position.
The notes on pages 59 to 93 form part of this account.
Annual accounts for the year ended 31 March 2016

56
Annual accounts for the year ended 31 March 2016
Statement of Financial Position as at 31 March 2016
NOTE31 March 2016
£00031 March 2015
£000
Non-current assets:Property, plant and equipment 14 437,723 419,094
Intangible assets 15 8,731 2,179
Total non-current assets 446,454 421,273
Current assets:Inventories 19 9,851 8,034
Trade and other receivables 20.1 41,597 49,154
Cash and cash equivalents 21 3,315 1,043
Sub-total current assets 54,763 58,231
Total current assets 54,763 58,231
Total assets 501,217 479,504
Current liabilitiesTrade and other payables 22 (99,935) (110,608)
Provisions 26 (1,092) (3,528)
Borrowings 23 (1,815) (2,070)
DH capital loan 23 (136) (136)
Total current liabilities (102,978) (116,342)
Net current assets/(liabilities) (48,215) (58,111)
Total assets less current liabilities 398,239 363,162
Non-current liabilitiesProvisions 26 (4,102) (4,116)
Borrowings 23 (56,013) (57,520)
DH revenue support loan 23 (90,239) 0
DH capital loan 23 (2,137) (1,273)
Total non-current liabilities (152,491) (62,909)
Total assets employed: 245,748 300,253
Finance by:Public dividend capital 361,647 330,877
Retained earnings (124,261) (31,438)
Revaluation reserve 8,362 814
Total Taxpayers’ Equity: 245,748 300,253
London North West Healthcare was established 1st October 2014, therefore, prior period comparators are only meaningful for the Statement of Financial Performance and have been included where relevant. Prior period comparators for the Statement of Comprehensive Income and associated notes only reflect six months trading position for the period 1st October 2014 to 31st March 2015.
The notes on pages 59 to 93 form part of this account.
The financial statements on pages 55 to 58 were approved by the Audit Committee and adopted by the Board on 25th May 2016 and signed on its behalf by:
Jacqueline Docherty DBE Jon Bell Chief Executive: Interim Chief Financial Officer:
Date: 27th May 2016 Date: 27th May 2016

57
Statement of Changes in Taxpayers’ Equity for the year ending 31 March 2016
Public Dividend capital
Retained earnings
Revaluation reserve
Total reserves
£000 £000 £000 £000
Balance at 1 April 2015 330,877 (31,438) 814 300,253
Changes in taxpayers’ equity for the year ended 31 March 2016
Retained (deficit) for the year 0 (92,823) 0 (92,823)
Net gain on revaluation of property, plant, equipment 0 0 7,548 7,548
Reclassification adjustments
Permanent PDC received - cash 30,770 0 0 30,770
Net recognised revenue/(expense) for the year 30,770 (92,823) 7,548 (54,505)
Balance at 31 March 2016 361,647 (124,261) 8,362 245,748
Balance at 1 October 2014 0 0 0 0
Changes in taxpayers’ equity for the period ended 31 March 2015
Retained surplus/(deficit) for the year 0 263,364 0 263,364
Net gain on revaluation of property, plant, equipment 0 0 814 814
Reclassification adjustments
Transfers to/(from) other bodies within the resource account boundary
0 (294,802) 0 (294,802)
Originating capital for Trust established in year 294,802 0 0 294,802
New temporary and permanent PDC received - cash 36,075 0 0 36,075
Net recognised revenue/(expense) for the year 330,877 (31,438) 814 300,253
Balance at 31 March 2015 330,877 (31,438) 814 300,253

58
Annual accounts for the year ended 31 March 2016
Statement of Cash Flows for the Year ended 31 March 2016
2015-16 Six month accounts period ended
31 March 2015
NOTE £000 £000
Cash flows from operating activities
Operating (deficit) (77,478) (23,490)
Depreciation and amortisation 7 13,690 6,878
Impairments and reversals 16 3,518 6,027
Interest paid (7,017) (3,202)
Pdc dividend (paid) (8,704) (4,410)
(Increase) in inventories (1,817) (124)
(Increase)/decrease in trade and other receivables 7,920 (986)
(Decrease) in trade and other payables (10,449) (5,581)
Provisions utilised (576) (254)
Increase/(decrease) in movement in non cash provisions (1,931) 3,000
Net cash (outflow) from operating activities (82,844) (22,142)
Cash flows from investing activities
Interest received 70 33
(Payments) for property, plant and equipment (34,386) (17,471)
(Payments) for intangible assets (680) (526)
Rental revenue 0 3,159
Net cash (outflow) from investing activities (34,996) (14,805)
Net cash (outflow) before financing (117,840) (36,947)
Cash flows from financing activities
Gross temporary (2014/15 only) and permanent PDC received 30,770 36,075
Loans received from DH - new capital investment loans 1,000 0
Loans received from DH - new revenue support loans 135,300 0
Loans repaid to DH - capital investment loans repayment of principal
(136) (68)
Loans repaid to DH - working capital loans/revenue support loans
(45,061) 0
Cash transferred to NHS Foundation Trusts or on dissolution 0 2,877
Capital element of payments in respect of finance leases and On-SoFP PFI and LIFT
(1,761) (894)
Net cash inflow from financing activities 120,112 37,990
Net increase in cash and cash equivalents 2,272 1,043
Cash and cash equivalents (and bank overdraft) at beginning of the period
1,043 0
Cash and cash equivalents (and bank overdraft) at year end
21 3,315 1,043

59
Notes to the accounts
1. Accounting PoliciesThe Secretary of State for Health has directed that the financial statements of NHS Trusts shall meet the accounting requirements of the Department of Health Group Manual for Accounts, which shall be agreed with HM Treasury. Consequently, the following financial statements have been prepared in accordance with the DH Group Manual for Accounts 2015-16 issued by the Department of Health. The accounting policies contained in that manual follow International Financial Reporting Standards to the extent that they are meaningful and appropriate to the NHS, as determined by HM Treasury, which is advised by the Financial Reporting Advisory Board. Where the Manual for Accounts permits a choice of accounting policy, the accounting policy which is judged to be most appropriate to the particular circumstances of the Trust for the purpose of giving a true and fair view has been selected. The particular policies adopted by the Trust are described below. They have been applied consistently in dealing with items considered material in relation to the accounts.
1.1 Accounting conventionThese accounts have been prepared under the historical cost convention modified to account for the revaluation of property, plant and equipment, intangible assets, inventories and certain financial assets and financial liabilities.
Going ConcernThe Trust recorded an adjusted retained deficit of £88.245m for the year ended 31st March 2016, slightly better than the £88.339m agreed with the NHS Trust Development Authority, now known as NHS Improvement from 1st April 2016.
The financial statements have been prepared on a going concern basis. In accordance with IAS 1, management has made an assessment of the Trust’s ability to continue as a going concern. For the financial year commencing 1 April 2016, the Trust has forecast a deficit of £61.5m after a savings requirement of £34.7m. This plan is under discussion with NHS Improvement and requires additional cash support through PDC and/or loan funding. The Trust has received written confirmation from NHS Improvement that it is reasonable to expect that this cash financing will be made available such that the organisation is able to meet its liabilities in the next twelve months.
The merged Trust will intend, over the period of Shaping a Healthier Future (SaHF) implementation, to deliver substantial clinical innovation, efficiencies and
synergies to maintain financial stability. Additionally, the new organisation will be better placed to respond swiftly to the rapidly changing healthcare environment, in effect sustaining long term resilience. Shaping a Healthier Future is the programme to reshape hospital and out of hospital health and care services in North West London. North West London has a growing and ageing population, and at present, specialist care is too thinly spread over too many sites and some facilities are inadequate.
1.2 Charitable FundsUnder the provisions of IFRS 10 Consolidated and Separate Financial Statements, those Charitable Funds that fall under common control with NHS bodies are consolidated within the entity’s financial statements. In accordance with IAS 1 Presentation of Financial Statements, restated prior period accounts are presented where the adoption of the new policy has a material impact.
1.3 Critical accounting judgements and key sources of estimation uncertainty In the application of the NHS Trust’s accounting policies, management is required to make judgements, estimates and assumptions about the carrying amounts of assets and liabilities that are not readily apparent from other sources. The estimates and associated assumptions are based on historical experience and other factors that are considered to be relevant. Actual results may differ from those estimates and the estimates and underlying assumptions are continually reviewed. Revisions to accounting estimates are recognised in the period in which the estimate is revised if the revision affects only that period or in the period of the revision and future periods if the revision affects both current and future periods.
1.3.1 Critical judgements in applying accounting policiesThe following are the critical judgements, apart from those involving estimations (see below) that management has made in the process of applying the NHS Trust’s accounting policies and that have the most significant effect on the amounts recognised in the financial statements.
Following Treasury’s agreement to apply IFRS 10 to NHS Charities, London North West Healthcare has established that as the Trust is the corporate Trustee of the London North West Healthcare Charitable Fund, charity number 1083634, it effectively has the power to exercise control so as to obtain economic benefits.
Total income received by the charity during the period 1st April 2015 to 31st March 2016 was £1.39m which is only 0.2% of London North West Healthcare NHS

60
Annual accounts for the year ended 31 March 2016
Trust’s Exchequer Income. There were no substantive legacies or grant income received during this period.
IAS 1, Presentation of Financial Statements, says that specific disclosure requirements set out in individual standards or interpretations need to be satisfied if the information is not material and is reiterated in the NHS Manual for Accounts 2015-16.
Charitable funds are not consolidated into London North West Healthcare NHS Trust accounts on grounds of materiality.
1.3.2 Key sources of estimation uncertainty The following are the key assumptions concerning the future and other key sources of estimation uncertainty at the end of the reporting period, that have a significant risk of causing a material adjustment to the carrying amounts of assets and liabilities within the next financial year.
A model provided by the Department of Health has been used to calculate the effect of bringing the PFI scheme on to the Trust balance sheet. This is not expected to yield a result that is materially different from other means of calculation.
A desktop valuation and review of remaining lives of the Trust’s estate was conducted by professional Chartered Surveyors Cushman and Wakefield using data from BCIS (Building Cost Information Services) and RICS (Royal Institute of Chartered Surveyors).
The Trust has used this valuation in its 2015/16 accounts. The impact of the assessment of the Trust’s estate will be an overall increase in the valuation as at 31st March 2016 and will result in a depreciation profile that is a more accurate reflection of the useful economic life of the land and buildings.
The methodology adopted meets the requirements of International Accounting Standards (IAS) 16; Property, plant and equipment and does not deviate from the principles therein.
Provisions for credit notes have been made in order to ensure that any charges arising from subsequently cancelling disputed NHS invoices or refunding SLA contractual and over performance values are chargeable against the correct financial period and are included within the amounts disclosed for NHS payables and receivables.
Data for the pension provision is provided by NHS Pensions and uses data tables of expected lives for males and females provided by the National Statistics Office. The provision has been discounted at a rate of 1.37%
1.4 Revenue Revenue in respect of services provided is recognised when, and to the extent that, performance occurs,
and is measured at the fair value of the consideration receivable. The main source of revenue for the Trust is from commissioners for healthcare services. Revenue relating to patient care spells that are part-completed at the year end are apportioned across the financial years on the basis of costs incurred to date compared to total expected costs.
Where income is received for a specific activity that is to be delivered in the following year, that income is deferred.
The NHS Trust receives income under the NHS Injury Cost Recovery Scheme, designed to reclaim the cost of treating injured individuals to whom personal injury compensation has subsequently been paid e.g. by an insurer. The NHS Trust recognises the income when it receives notification from the Department of Work and Pension’s Compensation Recovery Unit that the individual has lodged a compensation claim. The income is measured at the agreed tariff for the treatments provided to the injured individual, less a provision for unsuccessful compensation claims and doubtful debts, currently at 21.99%, an increase from last year’s rate of 18.9%
1.5 Employee Benefits
Short-term employee benefitsSalaries, wages and employment-related payments are recognised in the period in which the service is received from employees. The cost of leave earned but not taken by employees at the end of the period is recognised in the financial statements to the extent that employees are permitted to carry forward leave into the following period.
Retirement benefit costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme. The scheme is an unfunded, defined benefit scheme that covers NHS employers, General Practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, the scheme is accounted for as if it were a defined contribution scheme: the cost to the NHS body of participating in the scheme is taken as equal to the contributions payable to the scheme for the accounting period.
For early retirements other than those due to ill health the additional pension liabilities are not funded by the scheme. The full amount of the liability for the additional costs is charged to expenditure at the time the Trust commits itself to the retirement, regardless of the method of payment.

61
1.6 Other expensesOther operating expenses are recognised when, and to the extent that, the goods or services have been received. They are measured at the fair value of the consideration payable.
1.7 Property, plant and equipment
RecognitionProperty, plant and equipment is capitalised if:
• it is held for use in delivering services or for administrative purposes;
• it is probable that future economic benefits will flow to, or service potential will be supplied to the Trust;
• it is expected to be used for more than one financial year;
• the cost of the item can be measured reliably; and
• the item has cost of at least £5,000; or
• collectively, a number of items have a cost of at least £5,000 and individually have a cost of more than £250, where the assets are functionally interdependent, they had broadly simultaneous purchase dates, are anticipated to have simultaneous disposal dates and are under single managerial control; or
• items form part of the initial equipping and setting-up cost of a new building, ward or unit, irrespective of their individual or collective cost.
Where a large asset, for example a building, includes a number of components with significantly different asset lives, the components are treated as separate assets and depreciated over their own useful economic lives.
ValuationAll property, plant and equipment are measured initially at cost, representing the cost directly attributable to acquiring or constructing the asset and bringing it to the location and condition necessary for it to be capable of operating in the manner intended by management. All assets are measured subsequently at fair value.
Land and buildings used for the Trust’s services or for administrative purposes are stated in the statement of financial position at their revalued amounts, being the fair value at the date of revaluation less any impairment.
Revaluations are performed with sufficient regularity to ensure that carrying amounts are not materially different from those that would be determined at the end of the reporting period. Fair values are determined as follows:
• land and non-specialised buildings – market value for existing use
• specialised buildings – depreciated replacement cost.
HM Treasury has adopted a standard approach to depreciated replacement cost valuations based on modern equivalent assets and, where it would meet the location requirements of the service being provided, an alternative site can be valued.
The Trust have engaged Cushman and Wakefield, an external independent body who are RICS qualified
practitioners, to carry out a desktop valuation of the Trust’s Land and Buildings including Dwellings. The calculated value was £387,895,000.
Properties in the course of construction for service or administration purposes are carried at cost, less any impairment loss. Cost includes professional fees but not borrowing costs, which are recognised as expenses immediately, as allowed by IAS 23 for assets held at fair value. Assets are revalued and depreciation commences when they are brought into use.
Fixtures and equipment are carried at depreciated historic cost as this is not considered to be materially different from fair value.
An increase arising on revaluation is taken to the revaluation reserve except when it reverses an impairment for the same asset previously recognised in expenditure, in which case it is credited to expenditure to the extent of the decrease previously charged there. A revaluation decrease that does not result from a loss of economic value or service potential is recognised as an impairment charged to the revaluation reserve to the extent that there is a balance on the reserve for the asset and, thereafter, to expenditure. Impairment losses that arise from a clear consumption of economic benefit should be taken to expenditure. Gains and losses recognised in the revaluation reserve are reported as other comprehensive income in the Statement of Comprehensive Income.
Subsequent expenditureWhere subsequent expenditure enhances an asset beyond its original specification, the directly attributable cost is capitalised. Where subsequent expenditure restores the asset to its original specification, the expenditure is capitalised and any existing carrying value of the item replaced is written-out and charged to operating expenses.
1.8 Intangible assets
RecognitionIntangible assets are non-monetary assets without physical substance, which are capable of sale separately from the rest of the trust’s business or which arise from contractual or other legal rights. They are recognised only when it is probable that future economic benefits will flow to, or service potential be provided to, the Trust; where the cost of the asset can be measured reliably, and where the cost is at least £5,000.
Intangible assets acquired separately are initially recognised at current value. Software that is integral to the operating of hardware, for example an operating system, is capitalised as part of the relevant item of property, plant and equipment. Software that is not integral to the operation of hardware, for example application software, is capitalised as an intangible asset. Expenditure on research is not capitalised: it is recognised as an operating expense in the period in which it is incurred. Internally-generated assets are

62
Annual accounts for the year ended 31 March 2016
recognised if, and only if, all of the following have been demonstrated:
• the technical feasibility of completing the intangible asset so that it will be available for use• the intention to complete the intangible asset and use it• the ability to sell or use the intangible asset• how the intangible asset will generate probable future economic benefits or service potential• the availability of adequate technical, financial and other resources to complete the intangible asset and sell or use it• the ability to measure reliably the expenditure attributable to the intangible asset during its development
MeasurementThe amount initially recognised for internally-generated intangible assets is the sum of the expenditure incurred from the date when the criteria above are initially met. Where no internally-generated intangible asset can be recognised, the expenditure is recognised in the period in which it is incurred.
Following initial recognition, intangible assets are carried at fair value by reference to an active market, or, where no active market exists, at amortised replacement cost (modern equivalent assets basis), indexed for relevant price increases, as a proxy for fair value. Internally-developed software is held at historic cost to reflect the opposing effects of increases in development costs and technological advances.
1.9 Depreciation, amortisation and impairmentsFreehold land, properties under construction, and assets held for sale are not depreciated.
Otherwise, depreciation and amortisation are charged to write off the costs or valuation of property, plant and equipment and intangible non-current assets, less any residual value, over their estimated useful lives, in a manner that reflects the consumption of economic benefits or service potential of the assets. The estimated useful life of an asset is the period over which the NHS Trust expects to obtain economic benefits or service potential from the asset. This is specific to the NHS Trust and may be shorter than the physical life of the asset itself. Estimated useful lives and residual values are reviewed each year end, with the effect of any changes recognised on a prospective basis. Assets held under finance leases are depreciated over their estimated useful lives.
At each reporting period end, the NHS Trust checks whether there is any indication that any of its tangible or intangible non-current assets have suffered an impairment loss. If there is indication of an impairment loss, the recoverable amount of the asset is estimated to determine whether there has been a loss and, if so, its amount. Intangible assets not yet available for use are tested for impairment annually.
A revaluation decrease that does not result from a loss of economic value or service potential is recognised as an impairment charged to the revaluation reserve to the extent that there is a balance on the reserve for the asset and, thereafter, to expenditure. Impairment losses that arise from a clear consumption of economic benefit should be taken to expenditure. Where an impairment loss subsequently reverses, the carrying amount of the asset is increased to the revised estimate of the recoverable amount but capped at the amount that would have been determined had there been no initial impairment loss. The reversal of the impairment loss is credited to expenditure to the extent of the decrease previously charged there and thereafter to the revaluation reserve.
1.10 Donated assetsDonated non-current assets are capitalised at their fair value on receipt, with a matching credit to income. They are valued, depreciated and impaired as described above for purchased assets. Gains and losses on revaluations, impairments and sales are as described above for purchased assets. Deferred income is recognised only where conditions attached to the donation preclude immediate recognition of the gain.
1.11 Government grants Government grant funded assets are capitalised at their fair value on receipt, with a matching credit to income. Deferred income is recognised only where conditions attached to the grant preclude immediate recognition of the gain.
1.12 Non-current assets held for saleNon-current assets are classified as held for sale if their carrying amount will be recovered principally through a sale transaction rather than through continuing use. This condition is regarded as met when the sale is highly probable, the asset is available for immediate sale in its present condition and management is committed to the sale, which is expected to qualify for recognition as a completed sale within one year from the date of classification. Non-current assets held for sale are measured at the lower of their previous carrying amount and fair value less costs to sell. Fair value is open market value including alternative uses.
The profit or loss arising on disposal of an asset is the difference between the sale proceeds and the carrying amount and is recognised in the Statement of Comprehensive Income. On disposal, the balance for the asset on the revaluation reserve is transferred to retained earnings.
Property, plant and equipment that is to be scrapped or demolished does not qualify for recognition as held for sale. Instead, it is retained as an operational asset and

63
its economic life is adjusted. The asset is de-recognised when it is scrapped or demolished.
1.13 LeasesLeases are classified as finance leases when substantially all the risks and rewards of ownership are transferred to the lessee. All other leases are classified as operating leases.
The Trust as lesseeProperty, plant and equipment held under finance leases are initially recognised, at the inception of the lease, at fair value or, if lower, at the present value of the minimum lease payments, with a matching liability for the lease obligation to the lessor. Lease payments are apportioned between finance charges and reduction of the lease obligation so as to achieve a constant rate on interest on the remaining balance of the liability. Finance charges are recognised in calculating the Trust’s surplus/deficit.
Operating lease payments are recognised as an expense on a straight-line basis over the lease term. Lease incentives are recognised initially as a liability and subsequently as a reduction of rentals on a straight-line basis over the lease term.
Contingent rentals are recognised as an expense in the period in which they are incurred.
Where a lease is for land and buildings, the land and building components are separated and individually assessed as to whether they are operating or finance leases.
The NHS Trust as lessorAmounts due from lessees under finance leases are recorded as receivables at the amount of the NHS Trust’s net investment in the leases. Finance lease income is allocated to accounting periods so as to reflect a constant periodic rate of return on the Trust’s net investment outstanding in respect of the leases.
Rental income from operating leases is recognised on a straight-line basis over the term of the lease. Initial direct costs incurred in negotiating and arranging an operating lease are added to the carrying amount of the leased asset and recognised on a straight-line basis over the lease term.
1.14 Private Finance Initiative (PFI) transactions
HM Treasury has determined that government bodies shall account for infrastructure PFI schemes where the government body controls the use of the infrastructure and the residual interest in the infrastructure at the end of the arrangement as service concession arrangements, following the principles of the requirements of IFRIC 12. The Trust therefore recognises the PFI asset as an item of
property, plant and equipment together with a liability to pay for it. The services received under the contract are recorded as operating expenses.
The annual unitary payment is separated into the following component parts, using appropriate estimation techniques where necessary:
a) Payment for the fair value of services received;
b) Payment for the PFI asset, including finance costs; and
c) Payment for the replacement of components of the asset during the contract ‘lifecycle replacement’.
Services receivedThe fair value of services received in the year is recorded under the relevant expenditure headings within ‘operating expenses’.
PFI assetThe PFI assets are recognised as property, plant and equipment, when they come into use. The assets are measured initially at fair value in accordance with the principles of IAS 17. Subsequently, the assets are measured at current value, which is kept up to date in accordance with the Trust’s approach for each relevant class of asset in accordance with the principles of IAS 16.
PFI liabilityA PFI liability is recognised at the same time as the PFI assets are recognised. It is measured initially at the same amount as the fair value of the PFI assets and is subsequently measured as a finance lease liability in accordance with IAS 17.
An annual finance cost is calculated by applying the implicit interest rate in the lease to the opening lease liability for the period, and is charged to ‘Finance Costs’ within the Statement of Comprehensive Income.
The element of the annual unitary payment that is allocated as a finance lease rental is applied to meet the annual finance cost and to repay the lease liability over the contract term.
An element of the annual unitary payment increase due to cumulative indexation is allocated to the finance lease. In accordance with IAS 17, this amount is not included in the minimum lease payments, but is instead treated as contingent rent and is expensed as incurred. In substance, this amount is a finance cost in respect of the liability and the expense is presented as a contingent finance cost in the Statement of Comprehensive Income.
Lifecycle replacementComponents of the asset replaced by the operator during the contract (‘lifecycle replacement’) are
64
Annual accounts for the year ended 31 March 2016
capitalised where they meet the Trust’s criteria for capital expenditure. They are capitalised at the time they are provided by the operator and are measured initially at their fair value.
The element of the annual unitary payment allocated to lifecycle replacement is pre-determined for each year of the contract from the operator’s planned programme of lifecycle replacement. Where the lifecycle component is provided earlier or later than expected, a short-term finance lease liability or prepayment is recognised respectively.
Where the fair value of the lifecycle component is less than the amount determined in the contract, the difference is recognised as an expense when the replacement is provided. If the fair value is greater than the amount determined in the contract, the difference is treated as a ‘free’ asset and a deferred income balance is recognised. The deferred income is released to the operating income over the shorter of the remaining contract period or the useful economic life of the replacement component.
Assets contributed by the NHS Trust to the operator for use in the schemeAssets contributed for use in the scheme continue to be recognised as items of property, plant and equipment in the NHS Trust’s Statement of Financial Position.
Other assets contributed by the NHS Trust to the operatorAssets contributed (e.g. cash payments, surplus property) by the NHS Trust to the operator before the asset is brought into use, which are intended to defray the operator’s capital costs, are recognised initially as prepayments during the construction phase of the contract. Subsequently, when the asset is made available to the NHS Trust, the prepayment is treated as an initial payment towards the finance lease liability and is set against the carrying value of the liability.
1.15 InventoriesInventories are valued at the lower of cost and net realisable value using the first-in first-out (FIFO) cost formula. This is considered to be a reasonable approximation to fair value due to the high turnover of stocks.
1.16 Cash and cash equivalentsCash is cash in hand and deposits with any financial institution repayable without penalty on notice of not more than 24 hours. Cash equivalents are investments that mature in 3 months or less from the date of acquisition and that are readily convertible to known amounts of cash with insignificant risk of change in value.
In the Statement of Cash Flows, cash and cash equivalents are shown net of bank overdrafts that are repayable on demand and that form an integral part of the NHS Trust’s cash management.
1.17 ProvisionsProvisions are recognised when the NHS Trust has a present legal or constructive obligation as a result of a past event, it is probable that the NHS Trust will be required to settle the obligation, and a reliable estimate can be made of the amount of the obligation. The amount recognised as a provision is the best estimate of the expenditure required to settle the obligation at the end of the reporting period, taking into account the risks and uncertainties. Where a provision is measured using the cash flows estimated to settle the obligation, its carrying amount is the present value of those cash flows using HM Treasury’s discount rate of 0.8% in real terms, 1.37% for employee early departure obligations.
When some or all of the economic benefits required to settle a provision are expected to be recovered from a third party, the receivable is recognised as an asset if it is virtually certain that reimbursements will be received and the amount of the receivable can be measured reliably.
A restructuring provision is recognised when the Trust has developed a detailed formal plan for the restructuring and has raised a valid expectation in those affected that it will carry out the restructuring by starting to implement the plan or announcing its main features to those affected by it.
The merger of the two legacy trusts, Ealing Hospital NHS Trust and North West London Hospitals NHS Trust, has resulted in structural changes which have been implemented, at the reporting date, not all of these plans have not been developed in sufficient detail to give rise to a restructuring provision. The measurement of a restructuring provision includes only the direct expenditures arising from the restructuring, which are those amounts that are both necessarily entailed by the restructuring and not associated with ongoing activities of the entity.
1.18 Clinical negligence costsThe NHS Litigation Authority (NHSLA) operates a risk pooling scheme under which the Trust pays an annual contribution to the NHSLA which in return settles all clinical negligence claims. The contribution is charged to expenditure. Although the NHSLA is administratively responsible for all clinical negligence cases the legal liability remains with the NHS Trust. The total value of clinical negligence provisions carried by the NHSLA on behalf of the Trust is disclosed at Note 26.

65
1.19 Non-clinical risk poolingThe NHS Trust participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling schemes under which the NHS Trust pays an annual contribution to the NHS Litigation Authority and, in return, receives assistance with the costs of claims arising. The annual membership contributions, and any excesses payable in respect of particular claims are charged to operating expenses as and when they become due.
1.20 Carbon Reduction Commitment Scheme (CRC)CRC and similar allowances are accounted for as government grant funded intangible assets if they are not expected to be realised within 12 months, and otherwise as other current assets. They are valued at open market value. As the NHS body makes emissions, a provision is recognised with an offsetting transfer from deferred income. The provision is settled on surrender of the allowances. The asset, provision and deferred income amounts are valued at fair value at the end of the reporting period.
1.21 ContingenciesA contingent liability is a possible obligation that arises from past events and whose existence will be confirmed only by the occurrence or non-occurrence of one or more uncertain future events not wholly within the control of the NHS Trust, or a present obligation that is not recognised because it is not probable that a payment will be required to settle the obligation or the amount of the obligation cannot be measured sufficiently reliably. A contingent liability is disclosed unless the possibility of a payment is remote.
A contingent asset is a possible asset that arises from past events and whose existence will be confirmed by the occurrence or non-occurrence of one or more uncertain future events not wholly within the control of the NHS Trust. A contingent asset is disclosed where an inflow of economic benefits is probable.
Where the time value of money is material, contingencies are disclosed at their present value.
1.22 Financial assets Financial assets are recognised when the NHS Trust becomes party to the financial instrument contract or, in the case of trade receivables, when the goods or services have been delivered. Financial assets are derecognised when the contractual rights have expired or the asset has been transferred.
Financial assets are classified into the following categories: financial assets at fair value through profit and loss; held to maturity investments; available for sale financial assets, and loans and receivables. The classification depends on the nature and purpose of the
financial assets and is determined at the time of initial recognition.
Financial assets at fair value through profit and lossEmbedded derivatives that have different risks and characteristics to their host contracts, and contracts with embedded derivatives whose separate value cannot be ascertained, are treated as financial assets at fair value through profit and loss. They are held at fair value, with any resultant gain or loss recognised in calculating the NHS Trust’s surplus or deficit for the year. The net gain or loss incorporates any interest earned on the financial asset.
Held to maturity investmentsHeld to maturity investments are non-derivative financial assets with fixed or determinable payments and fixed maturity, and there is a positive intention and ability to hold to maturity. After initial recognition, they are held at amortised cost using the effective interest method, less any impairment. Interest is recognised using the effective interest method.
Available for sale financial assetsAvailable for sale financial assets are non-derivative financial assets that are designated as available for sale or that do not fall within any of the other three financial asset classifications. They are measured at fair value with changes in value taken to the revaluation reserve, with the exception of impairment losses. Accumulated gains or losses are recycled to surplus/deficit on de-recognition.
Loans and receivablesLoans and receivables are non-derivative financial assets with fixed or determinable payments which are not quoted in an active market. After initial recognition, they are measured at amortised cost using the effective interest method, less any impairment. Interest is recognised using the effective interest method.
Fair value is determined by reference to quoted market prices where possible, otherwise by valuation techniques, such as recent market transactions.
The effective interest rate is the rate that exactly discounts estimated future cash receipts through the expected life of the financial asset, to the initial fair value of the financial asset.
At the end of the reporting period, the NHS Trust assesses whether any financial assets, other than those held at ‘fair value through profit and loss’ are impaired. Financial assets are impaired and impairment losses recognised if there is objective evidence of impairment as a result of one or more events which occurred after the initial recognition of the asset and which has an

66
Annual accounts for the year ended 31 March 2016
impact on the estimated future cash flows of the asset.
For financial assets carried at amortised cost, the amount of the impairment loss is measured as the difference between the asset’s carrying amount and the present value of the revised future cash flows discounted at the asset’s original effective interest rate. The loss is recognised in expenditure and the carrying amount of the asset is reduced directly.
If, in a subsequent period, the amount of the impairment loss decreases and the decrease can be related objectively to an event occurring after the impairment was recognised, the previously recognised impairment loss is reversed through expenditure to the extent that the carrying amount of the receivable at the date of the impairment is reversed does not exceed what the amortised cost would have been had the impairment not been recognised.
1.23 Financial liabilities Financial liabilities are recognised on the statement of financial position when the NHS Trust becomes party to the contractual provisions of the financial instrument or, in the case of trade payables, when the goods or services have been received. Financial liabilities are de-recognised when the liability has been discharged, that is, the liability has been paid or has expired.
Loans from the Department of Health are recognised at historical cost. Otherwise, financial liabilities are initially recognised at fair value.
Financial guarantee contract liabilitiesFinancial guarantee contract liabilities are subsequently measured at the higher of:
• The amount of the obligation under the contract, as determined in accordance with IAS 37 Provisions, Contingent Liabilities and Contingent Assets; and
• The premium received (or imputed) for entering into the guarantee less cumulative amortisation.
Financial liabilities at fair value through profit and lossEmbedded derivatives that have different risks and characteristics to their host contracts, and contracts with embedded derivatives whose separate value cannot be ascertained, are treated as financial liabilities at fair value through profit and loss. They are held at fair value, with any resultant gain or loss recognised in the NHS Trust’s surplus/deficit. The net gain or loss incorporates any interest payable on the financial liability.
Other financial liabilitiesAfter initial recognition, all other financial liabilities are measured at amortised cost using the effective interest method, except for loans from Department of Health, which are carried at historic cost. The effective interest
rate is the rate that exactly discounts estimated future cash payments through the life of the asset, to the net carrying amount of the financial liability. Interest is recognised using the effective interest method.
1.24 Value added taxMost of the activities of the Trust are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
1.25 Foreign currenciesThe Trust’s functional currency and presentational currency is sterling. Transactions denominated in a foreign currency are translated into sterling at the exchange rate ruling on the dates of the transactions. At the end of the reporting period, monetary items denominated in foreign currencies are retranslated at the spot exchange rate on 31 March. Resulting exchange gains and losses for either of these are recognised in the Trust’s surplus/deficit in the period in which they arise.
1.26 Third party assetsAssets belonging to third parties (such as money held on behalf of patients) are not recognised in the accounts since the Trust has no beneficial interest in them. Details of third party assets are given in Note 35 to the accounts.
1.27 Public dividend capital (PDC) and PDC dividendPublic dividend capital represents taxpayers’ equity in the NHS Trust. At any time the Secretary of State can issue new PDC to, and require repayments of PDC from, the Trust. PDC is recorded at the value received. As PDC is issued under legislation rather than under contract, it is not treated as an equity financial instrument.
An annual charge, reflecting the cost of capital utilised by the Trust, is payable to the Department of Health as public dividend capital dividend. The charge is calculated at the real rate set by HM Treasury (currently 3.5%) on the average carrying amount of all assets less liabilities (except for donated assets and cash balances with the Government Banking Service). The average carrying amount of assets is calculated as a simple average of opening and closing relevant net assets.
In accordance with the requirements laid down by the Department of Health (as the issuer of PDC), the dividend for the year is calculated on the actual average relevant net assets as set out in the “pre-audit” version of the annual accounts. The dividend thus calculated is

67
not revised should any adjustment to net assets occur as a result the audit of the annual accounts.
1.28 Losses and special paymentsLosses and special payments are items that Parliament would not have contemplated when it agreed funds for the health service or passed legislation. By their nature they are items that ideally should not arise. They are therefore subject to special control procedures compared with the generality of payments. They are divided into different categories, which govern the way that individual cases are handled.
Losses and special payments are charged to the relevant functional headings in expenditure on an accruals basis, including losses which would have been made good through insurance cover had the Trust not been bearing their own risks (with insurance premiums then being included as normal revenue expenditure).
1.29 Research and developmentResearch and development expenditure is charged against income in the year in which it is incurred, except insofar as development expenditure relates to a clearly defined project and the benefits of it can reasonably be regarded as assured. Expenditure so deferred is limited to the value of future benefits expected and is amortised through the SOCI on a systematic basis over the period expected to benefit from the project. It should be revalued on the basis of current cost. The amortisation is calculated on the same basis as depreciation, on a quarterly basis.
1.30 Accounting standards that have been issued but have not yet been adoptedThe HM Treasury Financial Reporting Manual (FReM) does not require the following Standards and Interpretations to be applied in 2015-16. These standards are still subject to HM Treasury FReM interpretation, with IFRS 9 and IFRS 15 being for implementation in 2018-19, and the government implementation date for IFRS 16 still subject to HM Treasury consideration.
• IFRS 9 Financial Instruments – Application required for accounting periods beginning on or after 1 January 2018, but not yet adopted by the FReM: early adoption is not therefore permitted.
• IFRS 15 Revenue for Contracts with Customers - Application required for accounting periods beginning on or after 1 January 2017, but not yet adopted by the FReM: early adoption is not therefore permitted.
• IFRS 16 Leases – Application required for accounting periods beginning on or after 1 January 2019, but not yet adopted by the FReM: early adoption is not therefore permitted.

68
Annual accounts for the year ended 31 March 2016
2. Operating segments
As per NHS guidance, the Trust is considered to have only one segment i.e. that of healthcare provision. However, the Board reviews financial performance by community and acute services.
Some categories of income are not uniformally credited to individual services, for example some cost per activity is credited to ‘central income’ and other cost per case activity is credited to individual services. The same is true for some expenditure categories, for example certain overheads are charged to ‘corporate’ whereas other overheads are charged to individual services.
Therefore the operating deficit includes a significant number of estimates and adjustments and should be treated as an indicator of costs only. However, on a Trust level, the total net deficit of £88.245m is the same as the Trust’s overall reported adjusted deficit.
Community services Acute services Total
2015-16
Six month accounts period
ended 31 March
2015 2015-16
Six month accounts period
ended 31 March
2015 2015-16
Six month accounts period
ended 31 March
2015
£000 £000 £000 £000 £000 £000
Income 114,404 66,253 551,721 287,012 666,125 353,265
Expenditure (119,130) (75,838) (635,240) (302,362) (754,370) (378,200)
Operating deficit (4,726) (9,585) (83,519) (15,350) (88,245) (24,935)
Net assets are not reported by segment.
3. Income generation activities
The Trust undertakes income generation activities with an aim of achieving profit, which is then used in patient care. The Trust received income of £15.354m from income generation activities. This includes £1.0m from a drug manufacturing scheme and pharmacy services provided and £1.25m from car parking income.
Summary table - Drug manufacturing scheme 2015-16
Six month accounts period ended
31 March 2015
£000 £000
Income 1,006 902
Full cost (824) (824)
Surplus 182 78

69
4. Revenue from patient care activities 2015-16 Six month accounts
period ended 31 March 2015
£000 £000
NHS trusts 534 432
NHS England 101,313 50,227
Clinical commissioning groups 464,618 246,009
Foundation trusts 258 226
NHS other (including Public Health England and Prop Co) 2,215 1,041
Non-NHS:
Local authorities 16,461 7,075
Private patients 4,475 2,368
Overseas patients (non-reciprocal) 2,199 550
Injury costs recovery 1,924 1,031
Other 1,326 563
Total revenue from patient care activities 595,323 309,522
5. Other operating revenue 2015-16 Six month accounts
period ended 31 March 2015
£000 £000
Education, training and research 31,842 16,923
Non-patient care services to other bodies 2,389 605
Income generation (other fees and charges) 15,354 11,170
Rental revenue from operating leases 7,241 3,160
Other revenue 13,976 5,350
Total other operating revenue 70,802 37,208
Total operating revenue 666,125 346,730
6. Overseas visitors disclosure 2015-16 Six month accounts
period ended 31 March 2015
£000 £000
Income recognised during 2015-16 (invoiced amounts and accruals) 2,199 550
Cash payments received in-year (re receivables at 31 March 2015) 638 625
Cash payments received in-year (iro invoices issued 2014-15) 625 368
Amounts added to provision for impairment of receivables (re receivables at 31 March 2014)
0 109
Amounts added to provision for impairment of receivables (iro invoices issued 2014-15)
394 169
Amounts written off in-year (irrespective of year of recognition) 379 103

70
Annual accounts for the year ended 31 March 2016
7. Operating expenses 2015-16
Six month accounts period ended
31 March 2015
£000 £000
Trust Chair and Non-executive Directors 53 33
Supplies and services - clinical 147,218 71,288
Supplies and services - general 27,562 11,059
Consultancy services 2,604 682
Establishment 7,546 3,587
Transport 4,683 2,175
Service charges - ON-SOFP PFIs and other service concession arrangements 2,176 1,065
Business rates paid to local authorities 3,261 0
Premises 22,919 11,245
Hospitality 138 76
Insurance 545 243
Legal fees 874 541
Impairments and reversals of receivables 3,455 798
Inventories write down 220 0
Depreciation 12,394 6,544
Amortisation 1,296 334
Impairments and reversals of property, plant and equipment 3,518 6,027
Internal audit fees 67 0
Audit fees 126 140
Other auditor’s remuneration 12 10
Clinical negligence 21,946 7,047
Research and development (excluding staff costs) 832 333
Education and training 1,956 1,006
Change in discount rate (3) (21)
Other 3,329 4,545
Total operating expenses (excluding employee benefits) 268,727 128,757
Employee benefits
Employee benefits excluding board members 473,721 240,744
Board members 1,155 719
Total employee benefits 474,876 241,463
Total operating expenses 743,603 370,220

71
8. Operating Leases
8.1 London North West Healthcare NHS Trust as lessee
London North West Healthcare holds operating leases under the following four categories - buildings, equipment, cars and printers.
2015-16
Six month accounts period ended 31
March 2015
Land Buildings Other Total Total
£000 £000 £000 £000 £000
Payments recognised as an expense
Minimum lease payments 1,878 793
Total 1,878 793
Payable:No later than one year 0 339 1,411 1,750 275
Between one and five years 0 1,355 1,297 2,652 128
After five years 0 1,355 0 1,355 0
Total 0 3,049 2,708 5,757 403
Total future sublease payments expected to be received: 0 0
8.2 London North West Healthcare NHS Trust as lessor 2015-16
Six month accounts period ended 31
March 2015
£000 £000
Recognised as revenue
Rental revenue 7,241 3,160
Total 7,241 3,160

72
Annual accounts for the year ended 31 March 2016
9. Employee benefits and staff numbers
9.1 Employee benefits 2015-16
TotalPermanently
employed Other£000 £000 £000
Employee benefits - Gross expenditure
Salaries and wages 411,393 321,823 89,570
Social security costs 30,485 27,944 2,541
Employer contributions to NHS BSA - pensions division 36,757 36,757 0
Termination benefits 972 972 0
Total employee benefits 479,607 387,496 92,111
Employee costs capitalised 4,731 400 4,331
Gross employee benefits excluding capitalised costs 474,876 387,096 87,780
Six month accounts ended 31 March 2015
Total £000
Permanently employed
£000Other £000
Employee benefits - Gross expenditure - Six month accounts ended 31 March 2015
Salaries and wages 207,232 158,520 48,712
Social security costs 16,063 14,607 1,456
Employer Contributions to NHS BSA - Pensions Division 18,851 18,014 837
Termination benefits 105 105 0
TOTAL - including capitalised costs 242,251 191,246 51,005
Employee costs capitalised 788 770 18
Gross employee benefits excluding capitalised costs 241,463 190,476 50,987
9.2 Staff numbers
2015-16 2014-15
Total
Number
Permanently employed
Number
Other
Number
Total
Number
Average staff numbers
Medical and dental 1,367 1,161 206 1,393
Administration and estates 1,940 1,629 311 2,061
Healthcare assistants and other support staff 1,377 1,123 254 1,292
Nursing, midwifery and health visiting staff 3,349 2,754 595 3,462
Scientific, therapeutic and technical staff 1,410 1,242 168 1,416
Total 9,443 7,909 1,534 9,624
Of the above - staff engaged on capital projects 39 15 24 27

73
9.3 Staff Sickness absence and ill health retirements
2015-16 2014-15
Number Number
Total days lost 61,620 63,526Total staff years 8,080 7,862
Average working days lost 7.63 8.08
2015-16 2014-15
Number Number
Number of persons retired early on ill health grounds 0 0
£000 £000Total additional pensions liabilities accrued in the year 0 0
9.4 Exit packages agreed in 2015-162015-16
Exit package cost band (including any special payment element)
*Number of compulsory
redundancies
Cost of compulsory
redundancies
Number of other departures
agreed
Cost of other departures
agreed
Total number of exit
packagesTotal cost of
exit packages
Number £ Number £ Number £
Less than £10,000 8 28,027 0 0 8 28,027
£10,000-£25,000 1 19,658 0 0 1 19,658
£25,001-£50,000 2 81,198 0 0 2 81,198
£50,001-£100,000 3 281,283 0 0 3 281,283
£100,001 - £150,000 0 0 0 0 0 0
£150,001 - £200,000 1 153,333 0 0 1 153,333
>£200,000 1 319,687 0 0 1 319,687
Total 16 883,186 0 0 16 883,186
Six month accounts period ended 31 March 2015
Exit package cost band (including any special payment element)
*Number of compulsory
redundancies
Cost of compulsory
redundancies
Number of other departures
agreed
Cost of other departures
agreed.Total number of
exit packagesTotal cost of exit
packages
Number £ Number £ Number £
Less than £10,000 0 0 0 0 0 0
£10,000-£25,000 1 12,463 0 0 1 12,463
£25,001-£50,000 0 0 0 0 0 0
£50,001-£100,000 1 92,198 0 0 1 92,198
£100,001 - £150,000 0 0 0 0 0 0
£150,001 - £200,000 0 0 0 0 0 0
>£200,000 0 0 0 0 0 0
Total 2 104,661 0 0 2 104,661
Redundancy and other departure costs have been paid in accordance with the provisions of the NHS pension scheme. Exit costs in this note are accounted for in full in the year of departure. Where London North West Healthcare (LNWH) has agreed early retirements, the additional costs are met by the LNWH and not by the NHS pensions scheme. Ill-health retirement costs are met by the NHS pensions scheme and are not included in the table.
This disclosure reports the number and value of exit packages agreed in the year. Note: The expense associated with these departures may have been recognised in part or in full in a previous period.

74
Annual accounts for the year ended 31 March 2016
9.5 Pension costs Past and present employees are covered by the provisions of the two NHS pension schemes. Details of the benefits payable and rules of the schemes can be found on the NHS Pensions website at www.nhsbsa.nhs.uk/pensions. Both are unfunded defined benefit schemes that cover NHS employers, GP practices and other bodies, allowed under the direction of the Secretary of State in England and Wales. They are not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, each scheme is accounted for as if it were a defined contribution scheme: the cost to the NHS body of participating in each scheme is taken as equal to the contributions payable to that scheme for the accounting period.
In order that the defined benefit obligations recognised in the financial statements do not differ materially from those that would be determined at the reporting date by a formal actuarial valuation, the FReM requires that “the period between formal valuations shall be four years, with approximate assessments in intervening years”. An outline of these follows:
a) Accounting valuation A valuation of scheme liability is carried out annually by the scheme actuary (currently the Government Actuary’s Department) as at the end of the reporting period. This utilises an actuarial assessment for the previous accounting period in conjunction with updated membership and financial data for the current reporting period, and are accepted as providing suitably robust figures for financial reporting purposes. The valuation of scheme liability as at 31 March 2016, is based on valuation data as 31 March 2015, updated to 31 March 2016 with summary global member and accounting data. In undertaking this actuarial assessment, the methodology prescribed in IAS 19, relevant FReM interpretations, and the discount rate prescribed by HM Treasury have also been used.
The latest assessment of the liabilities of the scheme is contained in the scheme actuary report, which forms part of the annual NHS Pension Scheme (England and Wales) Pension Accounts. These accounts can be viewed on the NHS Pensions website and are published annually. Copies can also be obtained from The Stationery Office.
b) Full actuarial (funding) valuation The purpose of this valuation is to assess the level of liability in respect of the benefits due under the schemes (taking into account their recent demographic experience), and to recommend contribution rates payable by employees and employers.
The last published actuarial valuation undertaken for the NHS Pension Scheme was completed for the year ending 31 March 2012.
The Scheme Regulations allow for the level of contribution rates to be changed by the Secretary of State for Health, with the consent of HM Treasury, and consideration of the advice of the Scheme Actuary and appropriate employee and employer representatives as deemed appropriate.

75
10. Better Payment Practice Code
10.1 Measure of compliance
2015-16 2015-16
Six month accounts period ended 31
March 2015
Six month accounts period ended 31
March 2015
Number £000 Number £000
Non-NHS Payables
Total non-NHS Trade invoices paid in the year 173,035 439,627 70,581 164,083
Total non-NHS Trade invoices paid within target 46,996 227,332 26,498 95,349
Percentage of NHS Trade invoices paid within target 27.16% 51.71% 37.54% 58.11%
NHS Payables
Total NHS Trade invoices paid in the year 2,598 23,866 2,081 11,201
Total NHS Trade invoices paid within target 328 2,544 489 1,436
Percentage of NHS Trade invoices paid within target 12.63% 10.66% 23.50% 12.82%
The Better Payment Practice Code requires the NHS body to aim to pay all valid invoices by the due date or within 30 days of receipt of a valid invoice, whichever is later.
11. Investment Revenue 2015-16
Six month accounts period ended
31 March 2015
Interest Revenue £000 £000
Bank interest 70 33Subtotal 70 33Total investment revenue 70 33
12. Other Gains and Losses 2015-16
Six month accounts period ended
31 March 2015
£000 £000
(Loss) on disposal of assets other than by sale (PPE) (4) (78)Total (4) (78)
13. Finance Costs 2015-16
Six month accounts period ended
31 March 2015
£000 £000
Interest Interest on loans and overdrafts 982 24 Interest on obligations under finance leases 136 77Interest on obligations under PFI contracts: - main finance cost 3,884 2,086 - contingent finance cost 2,015 1,015Total interest expense 7,017 3,202Provisions - unwinding of discount 60 75Total 7,077 3,277
The Trust received revenue support loans to the value of £90.239m to fund its planned deficit. The Trust also received capital investment loans of £1m to fund an IT project within its capital programme. This has resulted in an increase in interest charges for 2015-16.

76
Annual accounts for the year ended 31 March 2016
14. Property, plant and equipment
14.1 Property, plant and equipment
2015-16 Land
Buildings excluding dwellings Dwellings
Assets under construction &
payments on account
Plant & machinery
Information technology
Furniture and
fittings Total £000 £000 £000 £000 £000 £000 £000 £000
Cost or valuation: At 1 April 2015 63,586 374,509 6,245 23,790 92,937 46,762 4,453 612,282
Additions of assets under construction
0 0 0 12,777 0 0 0 12,777
Additions purchased 0 21,165 0 0 911 0 9 22,085Reclassifications 0 3,652 0 (15,794) 3,661 506 127 (7,848)Disposals other than for sale
0 0 0 (21) 0 0 0 (21)
Upward revaluation/positive indexation
1,105 7,049 (606) 0 0 0 0 7,548
Impairment/reversals charged to operating expenses
0 (3,518) 0 0 0 0 0 (3,518)
At 31 March 2016 64,691 402,857 5,639 20,752 97,509 47,268 4,589 643,305
DepreciationAt 1 April 2015 10,391 69,330 40 0 69,298 40,715 3,414 193,188Charged during the year 0 5,442 89 0 4,467 2,157 239 12,394At 31 March 2016 10,391 74,772 129 0 73,765 42,872 3,653 205,582Net Book Value at 31 March 2016
54,300 328,085 5,510 20,752 23,744 4,396 936 437,723
Asset financing:Owned - purchased 54,300 245,019 5,510 20,752 22,728 4,394 859 353,562Owned - donated 0 7,458 0 0 291 2 77 7,828Owned - government granted
0 3,324 0 0 30 0 0 3,354
Held on finance lease 0 0 0 0 695 0 0 695On-SOFP PFI contracts 0 72,284 0 0 0 0 0 72,284Total at 31 March 2016
54,300 328,085 5,510 20,752 23,744 4,396 936 437,723
Revaluation reserve balance for property, plant & equipment
Land Buildings Dwellings
Assets under construction &
payments on account
Plant & machinery
Information technology
Furniture and
fittings Total £000 £000 £000 £000 £000 £000 £000 £000
At 1 April 2015 505 (306) 615 0 0 0 0 814
Movements (revaluation)
1,105 7,049 (606) 0 0 0 0 7,548
At 31 March 2016 1,610 6,743 9 0 0 0 0 8,362
Additions to Assets Under Construction Balance in 2015-16£000
Buildings excl dwellings 11,834
Plant & machinery 943
Balance as at YTD 12,777

77
14.2 Property, plant and equipment prior-period
2014-15 Land
Buildings excluding dwellings Dwellings
Assets under construction & payments on account
Plant and
machineryInformation technology
Furniture and
fittings Total
£000 £000 £000 £000 £000 £000 £000 £000
Cost or valuation:
At 1 October 2014 0 0 0 0 0 0 0 0
Additions of assets under construction
0 0 0 13,958 0 0 0 13,958
Additions purchased 0 2,833 0 0 1,999 0 0 4,832
Reclassifications 0 20,244 0 (22,810) 2,089 56 403 (18)
Disposals other than for sale
0 0 0 0 (330) 0 0 (330)
Revaluation 505 (306) 615 0 0 0 0 814
Transfers (to)/from other public sector bodies under absorption accounting
63,081 351,738 5,630 32,642 89,179 46,706 4,050 593,026
At 31 March 2015 63,586 374,509 6,245 23,790 92,937 46,762 4,453 612,282
Depreciation
At 1 October 2014 0 0 0 0 0 0 0 0
Disposals other than for sale
0 0 0 0 (249) 0 0 (249)
Impairments/negative indexation charged to operating expenses
0 6,027 0 0 0 0 0 6,027
Charged during the year 0 2,671 40 0 2,205 1,508 120 6,544
Transfers (to)/from other public sector bodies under absorption accounting
10,391 60,632 0 0 67,342 39,207 3,294 180,866
At 31 March 2015 10,391 69,330 40 0 69,298 40,715 3,414 193,188
Net book value at 31 March 2015
53,195 305,179 6,205 23,790 23,639 6,047 1,039 419,094
Asset financing:
Owned - purchased 53,195 225,448 6,205 23,790 22,388 6,043 932 338,001
Owned - donated 0 7,046 0 0 419 4 0 7,469
Owned - government granted
0 3,191 0 0 38 0 0 3,229
Held on finance lease 0 0 0 0 794 0 107 901
On-SOFP PFI contracts 0 69,494 0 0 0 0 0 69,494
PFI residual: interests 0 0 0 0 0 0 0 0
Total at 31 March 2015 53,195 305,179 6,205 23,790 23,639 6,047 1,039 419,094

78
Annual accounts for the year ended 31 March 2016
14.3 Property, plant and equipment
Of the totals as at 31st March 2016, £54.3m related to land valued at open market and £5.510m related to dwellings valued at open market value.
The current value of buildings excluding dwellings is £328.085m
Land and buildings were revalued as at 31st March 2016 by Cushman and Wakefield, the Trust’s appointed valuers. The valuation was undertaken by surveyors who were suitably experienced and qualified members of the Royal Institute of Chartered Surveyors.
The valuation was carried out in accordance with the RICS Appraisal and Valuation Manual insofar as these terms are consistent with the agreed requirements of the Department of Health and HM Treasury.
Details of asset lives are:
Buildings and dwellings between 10 and 90 years.
Plant and machinery between 5 and 15 years.
Information technology between 5 and 10 years.
Furniture and fittings between 2 and 10 years.
Software licenses between 3 and 10 years.
15. Intangible non-current assets
15.1 Intangible non-current assets
2015-16Computer
licensesLicenses and trademarks Patents
Development expenditure -
internally generated Total
£000 £000 £000 £000 £000
At 1 April 2015 6,370 0 0 0 6,370
Reclassifications 7,848 0 0 0 7,848
At 31 March 2016 14,218 0 0 0 14,218
Amortisation
At 1 April 2015 4,191 0 0 0 4,191
Charged During the Year 1,296 0 0 0 1,296
At 31 March 2016 5,487 0 0 0 5,487
Net Book Value at 31 March 2016 8,731 0 0 0 8,731
Asset Financing: Net book value at 31 March 2016 comprises:
Purchased 8,731 0 0 0 8,731
Donated 0 0 0 0 0
Total at 31 March 2016 8,731 0 0 0 8,731

79
15.2 Intangible non-current assets prior period
2014-15Computer
licensesLicenses and trademarks Patents
Development expenditure -
internally generated Total
£000 £000 £000 £000 £000
Cost or valuation:At 1 October 2014 0 0 0 0 0Additions - purchased 167 0 0 0 167Reclassifications 18 0 0 0 18Transfer (to)/from Other Public Sector bodies under Absorption Accounting
6,185 0 0 0 6,185
At 31 March 2015 6,370 0 0 0 6,370
AmortisationAt 1 October 2014 0 0 0 0 0Charged during the year 334 0 0 0 334Transfer (to)/from Other Public Sector bodies under Absorption Accounting
3,857 0 0 0 3,857
At 31 March 2015 4,191 0 0 0 4,191
Net book value at 31 March 2015 2,179 0 0 0 2,179Net book value at 31 March 2015 comprises:Purchased 2,179 2,179Total at 31 March 2015 2,179 0 0 0 2,179
16. Analysis of impairments and reversals recognised in 2015-16
31 March 2016
Six month accounts period ended 31 March 2015
Total Total
£000 £000
Property, plant and equipment impairments and reversals taken to SoCIChanges in market price 3,518 6,027Total charged to Annually Managed Expenditure 3,518 6,027
Total Impairments of Property, plant and equipment changed to SoCI
3,518 6,027
Overall Total Impairments 3,518 6,027
17. Commitments
17.1 Capital CommitmentsContracted capital commitments at 31 March not otherwise included in these financial statements:
31 March 2016
Six month accounts period ended 31 March 2015
£000 £000
Property, plant and equipment 6,726 21,800
Total 6,726 21,800

80
Annual accounts for the year ended 31 March 2016
18. Intra-Government and other balances
Current receivables
Non-current receivables
Current payables
Non-current payables
£000 £000 £000 £000
Balances with other central government bodies 0 0 9,045 0
Balances with local authorities 0 0 19 0
Balances with NHS bodies inside the departmental group 25,356 0 13,841 92,376
Balances with bodies external to government 16,241 0 78,981 56,013
At 31 March 2016 41,597 0 101,886 148,389
Prior period:
Balances with other central government bodies 0 0 9,331 0
Balances with local authorities 1,136 0 69 0
Balances with NHS bodies outside the departmental group 0 0 101 0
Balances with NHS bodies inside the departmental group 32,452 0 11,124 1,273
Balances with bodies external to government 15,566 0 92,189 57,520
At 31 March 2015 49,154 0 112,814 58,793
19. Inventories
Drugs Consumables EnergyLoan
Equipment Other Total
£000 £000 £000 £000 £000 £000
Balance at 1 April 2015 4,403 3,506 125 0 0 8,034
Additions 66,276 922 0 0 0 67,198
Inventories recognised as an expense in the period
(65,158) 0 (3) 0 0 (65,161)
Write-down of inventories (including losses)
(220) 0 0 0 0 (220)
Balance at 31 March 2016 5,301 4,428 122 0 0 9,851

81
Current Non-current
20.1 Trade and other receivables31 March
201631 March
201531 March
201631 March
2015
£000 £000 £000 £000
NHS receivables - revenue 25,202 32,452 0 0
Non-NHS receivables - revenue 14,822 16,795 0 0
Non-NHS prepayments and accrued income 3,621 3,461 0 0
PDC Dividend prepaid to DH 154 0
Provision for the impairment of receivables (4,725) (6,187) 0 0
VAT 2,523 2,633 0 0
Total 41,597 49,154 0 0
Total payables (current and non-current) 41,597 49,154
Included in NHS receivables are prepaid pension contributions: 0
The great majority of trade is with clinical commissioning groups (CCGs). As CCGs are funded by Government to buy NHS patient care services, no credit scoring of them is considered necessary.
20.2 Receivables past their due date but not impaired31 March
2016
Six month accounts period ended
31 March 2015
£000 £000
By up to three months 667 283
By three to six months 4,338 4,684
Total 5,005 4,967
20.3 Provision for impairment of receivables
2015-16
Six month accounts period ended
31 March 2015
£000 £000
Balance at 1 April 2015 (6,187) 0
Amount written off during the year 4,917 0
(Increase)/decrease in receivables impaired (3,455) (798)
Transfers (to)/from other public sector bodies under absorption accounting
0 (5,389)
Balance at 31 March 2016 (4,725) (6,187)
20. Trade and other receivables

82
21. Cash and Cash Equivalents 31 March 2016 31 March 2015
£000 £000
Opening balance 1,043 2,877
Net change in year 2,272 1,834
Closing balance 3,315 1,043
Made up of
Cash with Government banking service 3,251 924
Commercial banks 41 96
Cash in hand 23 23
Cash and cash equivalents as in statement of financial position 3,315 1,043
Cash and cash equivalents as in statement of cash flows 3,315 1,043
Third party assets - bank balance (not included above) 3 4
22. Trade and other payables
Current Non-current
31 March 2016
31 March 2015
31 March 2016
31 March 2015
£000 £000 £000 £000
NHS payables - revenue 11,510 10,772 0 0
NHS accruals and deferred income 2,195 0 0 0
Non-NHS payables - revenue 37,878 39,524 0 0
Non-NHS payables - capital 6,280 6,504 0 0
Non-NHS accruals and deferred income 32,890 44,269 0 0
Social security costs 4,418 4,493 0 0
PDC dividend payable to DH 0 216 0 0
Accrued interest on DH loans 144 0 0
Tax 4,620 4,830 0 0
Total 99,935 110,608 0 0
Total payables (current and non-current) 99,935 110,608
Included above:
Outstanding pension contributions at the year end 5,311 5,381
Annual accounts for the year ended 31 March 2016
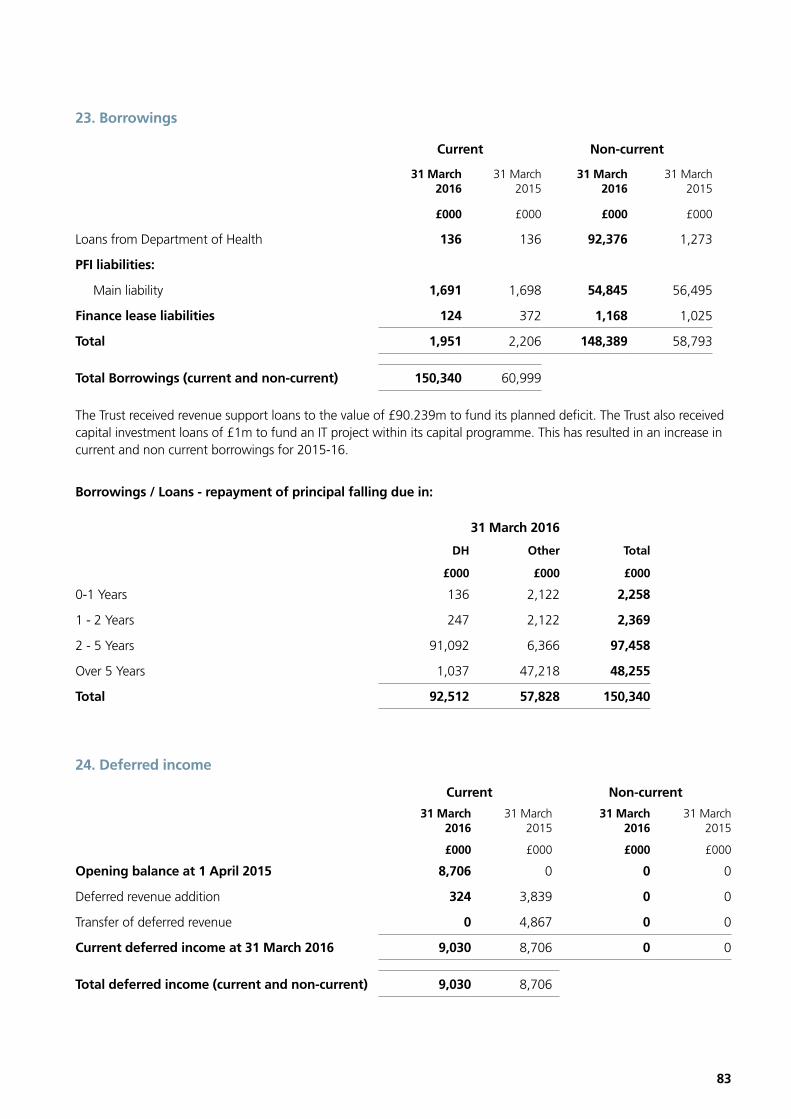
83
23. Borrowings
Current Non-current
31 March 2016
31 March 2015
31 March 2016
31 March 2015
£000 £000 £000 £000
Loans from Department of Health 136 136 92,376 1,273
PFI liabilities:
Main liability 1,691 1,698 54,845 56,495
Finance lease liabilities 124 372 1,168 1,025
Total 1,951 2,206 148,389 58,793
Total Borrowings (current and non-current) 150,340 60,999
The Trust received revenue support loans to the value of £90.239m to fund its planned deficit. The Trust also received capital investment loans of £1m to fund an IT project within its capital programme. This has resulted in an increase in current and non current borrowings for 2015-16.
Borrowings / Loans - repayment of principal falling due in:
31 March 2016
DH Other Total
£000 £000 £000
0-1 Years 136 2,122 2,258
1 - 2 Years 247 2,122 2,369
2 - 5 Years 91,092 6,366 97,458
Over 5 Years 1,037 47,218 48,255
Total 92,512 57,828 150,340
24. Deferred income
Current Non-current
31 March 2016
31 March 2015
31 March 2016
31 March 2015
£000 £000 £000 £000
Opening balance at 1 April 2015 8,706 0 0 0
Deferred revenue addition 324 3,839 0 0
Transfer of deferred revenue 0 4,867 0 0
Current deferred income at 31 March 2016 9,030 8,706 0 0
Total deferred income (current and non-current) 9,030 8,706

84
Annual accounts for the year ended 31 March 2016Annual accounts for the year ended 31 March 2016
25. Finance lease obligations as lessee
London North West Healthcare holds a finance lease for Beds. The lease was taken out in the Financial Year 2008/09 under a 15 year term.
The lease does not have a fixed rental per annum and is due to expire in 2022/23.
The present value of the minimum payments has been calculated using the Trust’s cost of capital, which is currently 3.5%
Amounts payable under finance leases (Other)Minimum lease
payments
Present value of minimum
lease payments
31 March 2016
31 March 2015
31 March 2016
31 March 2015
£000 £000 £000 £000
Within one year 235 704 124 372
Between one and five years 1,234 995 917 774
After five years 267 268 251 251
Less future finance charges (444) (570) 0 0
Minimum Lease Payments / Present value of minimum lease payments
1,292 1,397 1,292 1,397
Included in:
Current borrowings 124 372
Non-current borrowings 1,168 1,025
1,292 1,397

85
26. Provisions
Total
Early departure
costsLegal
claims Other Redundancy
£000 £000 £000 £000 £000
Balance at 1 April 2015 7,644 4,353 746 1,797 748
Arising during the year 896 242 334 0 320
Utilised during the year (576) (257) 0 0 (319)
Reversed unused (2,827) (33) (568) (1,797) (429)
Unwinding of discount 60 60 0 0 0
Change in discount rate (3) (3) 0 0 0
Balance at 31 March 2016 5,194 4,362 512 0 320
Expected Timing of Cash Flows:
No later than one year 1,092 260 512 0 320
Later than one year and not later than five years 1,040 1,040 0 0 0
Later than five years 3,062 3,062 0 0 0
Amount Included in the Provisions of the NHS Litigation Authority in respect of clinical negligence liabilities:
As at 31 March 2016 188,688
As at 31 March 2015 118,144
The early departure cost relating to staff refers to pension payments for staff retiring early through ill health. These figures are provided by NHS Pensions Authority. The discount rate for pensions relating to other staff has increased from 1.3% to 1.37% in line with HM Treasury and Department of Health guidelines. Settlements of these claims are determined using statistics provided by The Office of National Statistics (ONS).
Legal claims refer to public and employers liability claims and also provisions in relation to ongoing employment cases. Value of these claims will be subject to the relevant judgements or subsequent settlements made by the relevant employment tribunals.
The redundancy provision relates to potential senior management redundancies.
27. Contingencies
31 March 2016
31 March 2015
£000 £000
Contingent liabilities
NHS Litigation Authority legal claims (85) (128)
Employment Tribunal and other employee related litigation
(445) (527)
Net value of contingent liabilities (530) (655)

86
Annual accounts for the year ended 31 March 2016
28. PFI - additional information
The information below is required by the Department of Heath for inclusion in national statutory accounts
Under the PFI contract, which ends on 16th March 2036, the Trust’s PFI provider ByCentral Limited has constructed the Brent Emergency Care and Diagnostoic Center (BECaD) on the site of Central Middlesex Hospital and provides facilities management of existing and new premises for the duration of the contract. At the conclusion of the contract, ownership of the asset will revert to the Trust. Under IFRIC 12, the asset is treated as an asset of the Trust.
Charges to operating expenditure and future commitments in respect of ON and OFF SOFP PFI 2015-16
Six month accounts period ended
31 March 2015
£000 £000
Service element of on SOFP PFI charged to operating expenses in year 2,176 1,065
Total 2,176 1,065
Payments committed to in respect of off SOFP PFI and the service element of on SOFP PFI
No later than one year 1,625 1,586
Later than one year, no later than five years 6,918 6,749
Later than five years 32,867 34,662
Total 41,411 42,997
The current PFI contract assumed an inflation rate of 2.5% (£42,997k), however if the assumption that the inflation rate was 0%, then the total payments would have been £33,906k. Additionally, if inflation was 5%, the payment would have been £57,842k.
Imputed “finance lease” obligations for on SOFP PFI contracts due 2015-16
Six month accounts period ended
31 March 2015
£000 £000
No later than one year 5,626 5,711
Later than one year, no later than five years 21,244 21,883
Later than five years 79,189 84,176
Subtotal 106,059 111,770
Less: interest element (49,523) (53,577)
Total 56,536 58,193
Present Value Imputed “finance lease” obligations for on SOFP PFI contracts due 2015-16 2014-15
Analysed by when PFI payments are due £000 £000
No later than one year 1,691 1,657
Later than one year, no later than five years 6,648 6,812
Later than five years 48,197 49,724
Total 56,536 58,193
Number of on SOFP PFI Contracts
Total Number of on PFI contracts 1

87
29. Impact of IFRS treatment - current year
The information below is required by the Department of Heath for budget reconciliation purposes
2015-16
Six month accounts period ended 31 March
2015
Income Expenditure Income Expenditure
£000 £000 £000 £000
Revenue costs of IFRS: Arrangements reported on SoFP under IFRIC12 (e.g. PFI)
Depreciation charges 0 963 0 476
Interest Expense 0 5,896 0 3,010
Impairment charge - AME 0 (2,087) 0 3,035
Other Expenditure 0 2,176 0 1,065
Impact on PDC dividend payable 0 473 0 146
Total IFRS Expenditure (IFRIC12) 0 7,421 0 7,732
Revenue consequences of PFI / LIFT schemes under UK GAAP / ESA95 (net of any sublease revenue)
0 (8,785) 0 (4,408)
Net IFRS change (IFRIC12) 0 (1,364) 0 3,324
Capital Consequences of IFRS : LIFT/PFI and other items under IFRIC12
Capital expenditure 2015-16 1,237 505
UK GAAP capital expenditure 2015-16 (Reversionary Interest)
1,237 505
2015-16 2015-16
Income/ Expenditure IFRIC
12 YTD
Income/ Expenditure ESA
10 YTD
£000 £000
Revenue costs of IFRS12 compared with ESA10
Depreciation charges 963 0
Interest Expense 5,896 0
Impairment charge - AME (2,087) 0
Other Expenditure
Service charge 2,176 8,785
Impact on PDC Dividend Payable 473 0
Total Revenue Cost under IFRIC12 vs ESA10 7,421 8,785
Revenue Receivable from subleasing 0 0
Net Revenue Cost/(income) under IFRIC12 vs ESA10 7,421 8,785

88
Annual accounts for the year ended 31 March 2016
30. Financial Instruments
30.1 Financial risk management
Financial reporting standard IFRS 7 requires disclosure of the role that financial instruments have had during the period in creating or changing the risks a body faces in undertaking its activities. Because of the continuing service provider relationship that the NHS Trust has with clinical commissioning groups (CCGs) and the way those CCGs are financed, the NHS Trust is not exposed to the degree of financial risk faced by business entities. Also financial instruments play a much more limited role in creating or changing risk than would be typical of listed companies, to which the financial reporting standards mainly apply. The NHS Trust has limited powers to borrow or invest surplus funds and financial assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks facing the NHS Trust in undertaking its activities.
The Trust’s treasury management operations are carried out by the finance department, within parameters defined formally within the Trust’s standing financial instructions and policies agreed by the Board of Directors. The Trust’s treasury activity is subject to review by its internal auditors.
Currency risk
The Trust is principally a domestic organisation with the great majority of transactions, assets and liabilities being in the UK and sterling based. The Trust has no overseas operations. The Trust therefore has low exposure to currency rate fluctuations.
Interest rate risk
The Trust borrows from government for capital expenditure, subject to affordability as confirmed by NHS Improvement. The borrowings are for 1 – 25 years, in line with the life of the associated assets, and interest is charged at the National Loans Fund rate, fixed for the life of the loan. The Trust therefore has low exposure to interest rate fluctuations.
Credit risk
Because the majority of the Trust’s revenue comes from contracts with other public sector bodies, the Trust has low exposure to credit risk. The maximum exposures as at 31 March 2016 are in receivables from customers, as disclosed in the trade and other receivables note.
Liquidity risk
The Trust’s operating costs are incurred under contracts with CCGs, which are financed from resources voted annually by Parliament. The Trust funds its capital expenditure from funds obtained within its prudential borrowing limit. For the financial year commencing 1 April 2016, the Trust has forecast a deficit of £61.5m. This plan is under discussion with NHS Improvement and requires additional cash support through PDC and/or loan funding. The Trust has received written confirmation from NHS Improvement that it is reasonable to expect that this cash financing will be made available such that the organisation is able to meet its liabilities in the next 12 months.

89
30.2 Financial Assets
At ‘fair value through profit and loss’
Loans and receivables
Available for sale Total
£000 £000 £000 £000
Receivables - NHS 0 27,485 0 27,485
Receivables - non-NHS 0 13,478 0 13,478
Cash at bank and in hand 0 3,315 0 3,315
Total at 31 March 2016 0 44,278 0 44,278
Receivables - NHS 0 31,250 0 31,250
Receivables - non-NHS 0 12,550 0 12,550
Cash at bank and in hand 0 1,043 0 1,043
Total at 31 March 2015 0 44,843 0 44,843
30.3 Financial Liabilities At ‘fair value through
profit and loss’ Other Total
£000 £000 £000
Embedded derivatives 0 0 0
NHS payables 0 11,510 11,510
Non-NHS payables 0 64,674 64,674
Other borrowings 0 92,512 92,512
PFI & finance lease obligations 0 57,837 57,837
Other financial liabilities 0 0 0
Total at 31 March 2016 0 226,533 226,533
Embedded derivatives 0 0 0
NHS payables 0 13,621 13,621
Non-NHS payables 0 73,626 73,626
Other borrowings 0 1,409 1,409
PFI & finance lease obligations 0 59,590 59,590
Other financial liabilities 0 0 0
Total at 31 March 2015 0 148,246 148,246
31. Events after the end of the reporting period
There were no adjusting events after the reporting period.

90
32. Related party transactions
During the year none of the Department of Health Ministers, Trust Board members or members of the key management staff, or parties related to any of them, has undertaken any material transactions with London North West Healthcare NHS Trust.
The Department of Health is regarded as a related party. During the year, the Trust has had a significant number of material transactions with the Department, and with other entities for which the Department is regarded as the parent Department.
The most significant (over £100,000) cumulative transactions were as follows:
Organisation name Amounts owed to related party
Amounts due from related
party
£000 £000
Barnet CCG - 448
Brent CCG 137 2,788
Canterbury And Coastal CCG - 101
Central And North West London MH NHS Foundation Trust 124 354
Central London (Westminster) CCG - 921
Chelsea And Westminster Hospital NHS Foundation Trust 583 149
Community Health Partnerships 2,585 -
Ealing CCG - 2,951
Great Ormond Street Hospital for Children NHS Foundation Trust - 153
Guys And St Thomas NHS Foundation Trust 139 -
Hammersmith And Fulham CCG - 1,447
Harrow CCG - 6,701
Health Education England 1,610 789
Herts Valleys CCG - 303
Hillingdon CCG - 680
Hounslow and Richmond Community Healthcare NHS Trust 171 -
Hounslow CCG 270 -
Imperial College Healthcare NHS Trust 1,377 2,286
London Commissioning Hub - 4,507
London Region - 1,245
Moorfields Eye Hospital NHS Foundation Trust - 199
Nene CCG - 117
NHS England Core 351 -
NHS Property Services 3,323 -
Public Health England - 168
Royal Brompton And Harefield NHS Foundation Trust 150 148
Royal Free London NHS Foundation Trust 1,004 -
Royal National Orthopaedic Hospital NHS Trust - 329
South Central Local Office - 108
Slough CCG - 198
The Hillingdon Hospital NHS Foundation Trust 1,119 242
University College London NHS Foundation Trust 287 -
West London (K&C & Qpp) CCG 622 108
West London Mental Health NHS Trust 171 654
Annual accounts for the year ended 31 March 2016

91
The Trust has incurred transactions with NHS Property Services. Invoices to the value of £3.3m have been received. The Trust has on its Board, a Non-Executive Director who is also a Non-Executive Director of NHS Property Services.
The Trust has also received revenue and capital payments from a number of charitable funds, of which the trustees are also members of the Trust Board. The amounts due or to be paid at the end of the financial year are;
Amounts owed to related party
Amounts due from related party
£000 £000
London North West Healthcare Charitable Funds 332 75
33. Losses and special payments
The total number of losses cases in 2015-16 and their total value was as follows:
Total value of cases
Total number of cases
£
Losses 2,283,559 50
Special payments 3,259 13
Total losses and special payments 2,286,818 63
The total number of losses cases in 2014-15 and their total value was as follows:
Total value of cases
Total number of cases
£
Losses 278,284 210
Special payments 3,622 5
Total losses and special payments 281,906 215
Details of cases individually over £300,000
During the year, the Trust wrote off £2.2m debt associated with income relating to Road Traffic Accident Income.
This was as a result of aligning the Trust records for the legacy Ealing Hospital NHS Trust with those held by the Compensation Recovery Unit, responsible for making payments for Road Traffic Income.

92
Annual accounts for the year ended 31 March 2016
34. Financial performance targets
The figures given for periods prior to 2009-10 are on a UK GAAP basis as that is the basis on which the targets were set for those years.
34.1 Breakeven performance 2014-15 2015-16
£000 £000
Turnover 346,730 666,125
Retained surplus/(deficit) for the year 263,364 (92,823)
Adjustment for:
Timing/non-cash impacting distortions:
2007/08 PPA (relating to 1997/98 to 2006/07) 0 0
2008/09 PPA (relating to 1997/98 to 2007/08) 0 0
Adjustments for impairments 6,027 3,518
Adjustments for impact of policy change re donated/government grants assets 187 337
Consolidated Budgetary Guidance - adjustment for dual accounting under IFRIC12* 289 723
Absorption accounting adjustment (294,802) 0
Break-even in-year position (24,935) (88,245)
Break-even cumulative position (24,935) (113,180)
*Due to the introduction of International Financial Reporting Standards (IFRS) accounting in 2009-10, London North West Healthcare’s financial performance measurement needs to be aligned with the guidance issued by HM Treasury measuring Departmental expenditure. Therefore, the incremental revenue expenditure resulting from the application of IFRS to IFRIC 12 schemes (which would include PFI schemes), which has no cash impact and is not chargeable for overall budgeting purposes, is excluded when measuring Breakeven performance. Other adjustments are made in respect of accounting policy changes (impairments and the removal of the donated asset and government grant reserves) to maintain comparability year to year.
2014-15 2015-16
% %
Materiality test (I.e. is it equal to or less than 0.5%):
Break-even in-year position as a percentage of turnover (7.19) (13.25)
Break-even cumulative position as a percentage of turnover (7.19) (16.99)
The amounts in the above tables in respect of financial years 2005/06 to 2008/09 inclusive have not been restated to IFRS and remain on a UK GAAP basis.

93
34.2 Capital cost absorption rateThe dividend payable on public dividend capital is based on the actual (rather than forecast) average relevant net assets based on the pre audited accounts and therefore the actual capital cost absorption rate is automatically 3.5%.
34.3 External financing
The Trust is given an external financing limit which it is permitted to undershoot.
2015-16 2014-15
£000 £000
External financing limit (EFL) 118,260 37,089
Cash flow financing 117,840 36,947
Finance leases taken out in the year 0 0
External financing requirement 117,840 36,947
Under spend against EFL 420 142
34.4 Capital resource limit
The Trust is given a capital resource limit which it is not permitted to exceed.
2015-16 2014-15
£000 £000
Gross capital expenditure 34,862 18,957
Less: book value of assets disposed of (21) (81)
Charge against the capital resource limit 34,841 18,876
Capital resource limit 34,892 19,403
Underspend against the capital resource limit 51 527
35. Third party assets
The Trust held cash and cash equivalents which relate to monies held on behalf of patients or other parties. This has been excluded from the cash and cash equivalents figure reported in the accounts.
31 March 2016 31 March 2015
£000 £000
Third party assets held by the Trust 3 4

94
A B C D E F
Salary Expense Payments (taxable)*
Performance pay and bonuses
Long term performance
pay and bonuses
All pension - related benefits
Total
Executive Director
(bands of £5000)£000
(nearest £100)£000
(bands of £5000)£000
(bands of £5000)£000
(bands of £5000)£000
(bands of £5000)£000
Jacqueline Docherty Chief Executive 230 - 235 0 - - - 230 - 235
Lee Martin Chief Operating Officer (from 01/11/15) 55 - 60 0 - - 5 - 7.5 60 - 65
Don Fairley Director of Human Resources (to 10/11/15)
65 - 70 4 - - 15 - 17.5 80 - 85
Amanda Pye Chief Nurse (from 01/09/15)
80 - 85 0 - - 32.5 - 35 110 - 115
Paul Kingsmore Director of Estates and Facilities (to 31/05/15)
20 - 25 0 - - 5 - 7.5 25 - 30
Chris Pocklington Deputy Chief Executive Officer (to 06/03/16)
135 - 140 17 - - 7.5 - 10 145 - 150
Tina Benson Operational Director (to 31/03/16) 110 - 115 2 - - 32.5 - 35 145 - 150
Arthur Charles Cayley
Medical Director 210 - 215 8 - - - 210 - 215
Carole Flowers Chief Nurse (to 25/05/15) 30 - 35 0 - - 72.5 - 75 105 - 110
Nigel Myhill Director of Estates and Facilities (from 25/04/15)
65 - 70 0 - - 715 - 717.5 780 - 785
Claire Gore Director of Human Resources (from 01/03/16)
10 - 15 0 - - - 10 - 15
Simon Crawford Chief Financial Officer (to 04/10/15) Director of Strategy (from 05/10/15)
170 - 175 19 - - 52.5 - 55 225 - 230
Kevin Connolly Director of IT 95 - 100 0 - - 17.5 - 20 115 - 120
Paul Stanton Director of Human Resources 90 - 95 0 - - 97.5 - 100 190 - 195
Yvonne Lesse Operational Management 80 - 85 1 - - 40 - 42.5 125 - 130
Chris Blake Director of Transformation 100 - 105 19 - - 2.5 - 5 105 - 110
Gary Munn Acting Director of Estates and Facilities (from 25/05/15 - to 06/09/15)
90 - 95 0 - - 27.5 - 30 120 - 125
Jon Bell ** Interim Chief Financial Officer (from 5/10/15)
150 - 155 0 - - - 150 - 155
Peter Worthington Chairman 20 - 25 15 - - - 25 - 30
Patricia Williamson Non-Executive Director & Deputy Chair (to 30/09/2015)
0 - 5 0 - - - 0 - 5
Caroline Corby Non-Executive Director (to 12/06/15) 0 - 5 1 - - - 0 - 5
Stella Dutton Non-Executive Director (to 31/10/15) 0 - 5 15 - - - 5 - 10
David Taube Non-Executive Director 0 - 5 0 - - - 0 - 5
Jeanne Spinks Non-Executive Director (to 30/09/15) 0 - 5 36 - - - 5 - 10
Janet Rubin Non-Executive Director (from 15/02/16) 0 - 5 0 - - - 0 - 5
Andrew Farrell Non-Executive Director 0 - 5 0 - - - 0 - 5
Andrew Van Doorn Non-Executive Director (from 01/03/16) 0 - 5 0 - - - 0 - 5
Vinetta Bhalla Non-Executive Director (from 22/02/16) 0 - 5 0 - - - 0 - 5
Ruwan Weerasekera Non-Executive Director 0 - 5 0 - - - 0 - 5
Martin West Non-Executive Director 5 - 10 9 - - - 5 - 10
*Expense payments relate to expense allowances that are subject to UK tax
As non-executive members do not receive pensionable remuneration, there will be no entries in respect of pensions.
**The salary banding of the CFO includes irrecoverable VAT of £30,624.00, paid by the Trust.
Directors costs for the year ended 31 March 2016 (Subject to audit)
Remuneration report13
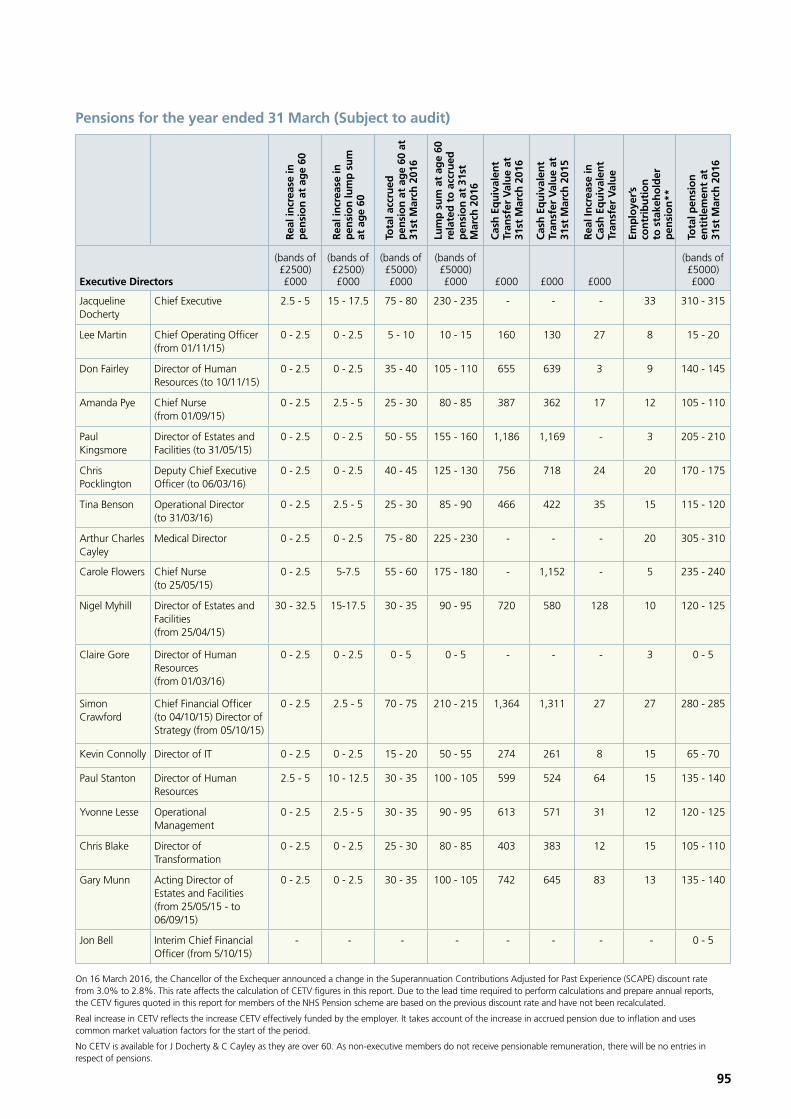
95
Pensions for the year ended 31 March (Subject to audit)
Rea
l in
crea
se in
p
ensi
on
at
age
60
Rea
l in
crea
se in
p
ensi
on
lum
p s
um
at
ag
e 60
Tota
l acc
rued
p
ensi
on
at
age
60 a
t 31
st M
arch
201
6
Lum
p s
um
at
age
60
rela
ted
to
acc
rued
p
ensi
on
at
31st
M
arch
201
6
Cas
h E
qu
ival
ent
Tran
sfer
Val
ue
at
31st
Mar
ch 2
016
Cas
h E
qu
ival
ent
Tran
sfer
Val
ue
at
31st
Mar
ch 2
015
Rea
l In
crea
se in
C
ash
Eq
uiv
alen
t Tr
ansf
er V
alu
e
Emp
loye
r’s
con
trib
uti
on
to
sta
keh
old
er
pen
sio
n**
Tota
l pen
sio
n
enti
tlem
ent
at
31st
Mar
ch 2
016
Executive Directors
(bands of £2500) £000
(bands of £2500) £000
(bands of £5000) £000
(bands of £5000) £000 £000 £000 £000
(bands of £5000) £000
Jacqueline Docherty
Chief Executive 2.5 - 5 15 - 17.5 75 - 80 230 - 235 - - - 33 310 - 315
Lee Martin Chief Operating Officer (from 01/11/15)
0 - 2.5 0 - 2.5 5 - 10 10 - 15 160 130 27 8 15 - 20
Don Fairley Director of Human Resources (to 10/11/15)
0 - 2.5 0 - 2.5 35 - 40 105 - 110 655 639 3 9 140 - 145
Amanda Pye Chief Nurse (from 01/09/15)
0 - 2.5 2.5 - 5 25 - 30 80 - 85 387 362 17 12 105 - 110
Paul Kingsmore
Director of Estates and Facilities (to 31/05/15)
0 - 2.5 0 - 2.5 50 - 55 155 - 160 1,186 1,169 - 3 205 - 210
Chris Pocklington
Deputy Chief Executive Officer (to 06/03/16)
0 - 2.5 0 - 2.5 40 - 45 125 - 130 756 718 24 20 170 - 175
Tina Benson Operational Director (to 31/03/16)
0 - 2.5 2.5 - 5 25 - 30 85 - 90 466 422 35 15 115 - 120
Arthur Charles Cayley
Medical Director 0 - 2.5 0 - 2.5 75 - 80 225 - 230 - - - 20 305 - 310
Carole Flowers Chief Nurse (to 25/05/15)
0 - 2.5 5-7.5 55 - 60 175 - 180 - 1,152 - 5 235 - 240
Nigel Myhill Director of Estates and Facilities (from 25/04/15)
30 - 32.5 15-17.5 30 - 35 90 - 95 720 580 128 10 120 - 125
Claire Gore Director of Human Resources (from 01/03/16)
0 - 2.5 0 - 2.5 0 - 5 0 - 5 - - - 3 0 - 5
Simon Crawford
Chief Financial Officer (to 04/10/15) Director of Strategy (from 05/10/15)
0 - 2.5 2.5 - 5 70 - 75 210 - 215 1,364 1,311 27 27 280 - 285
Kevin Connolly Director of IT 0 - 2.5 0 - 2.5 15 - 20 50 - 55 274 261 8 15 65 - 70
Paul Stanton Director of Human Resources
2.5 - 5 10 - 12.5 30 - 35 100 - 105 599 524 64 15 135 - 140
Yvonne Lesse Operational Management
0 - 2.5 2.5 - 5 30 - 35 90 - 95 613 571 31 12 120 - 125
Chris Blake Director of Transformation
0 - 2.5 0 - 2.5 25 - 30 80 - 85 403 383 12 15 105 - 110
Gary Munn Acting Director of Estates and Facilities (from 25/05/15 - to 06/09/15)
0 - 2.5 0 - 2.5 30 - 35 100 - 105 742 645 83 13 135 - 140
Jon Bell Interim Chief Financial Officer (from 5/10/15)
- - - - - - - - 0 - 5
On 16 March 2016, the Chancellor of the Exchequer announced a change in the Superannuation Contributions Adjusted for Past Experience (SCAPE) discount rate from 3.0% to 2.8%. This rate affects the calculation of CETV figures in this report. Due to the lead time required to perform calculations and prepare annual reports, the CETV figures quoted in this report for members of the NHS Pension scheme are based on the previous discount rate and have not been recalculated.
Real increase in CETV reflects the increase CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation and uses common market valuation factors for the start of the period.
No CETV is available for J Docherty & C Cayley as they are over 60. As non-executive members do not receive pensionable remuneration, there will be no entries in respect of pensions.

96
Remuneration report
Pay multiples 2015/16 (Subject to audit)
2015 - 16
Band of Highest Paid Director Remuneration (£000) 230-235
Median Total 30,530.53
Ratio 7.53
Reporting bodies are required to disclose the relationship between the salary of the most highly-paid individual in their organisation and the median earnings of the organisation’s workforce.
The banded remuneration of the highest paid director in London North West Healthcare in the financial year 2015-16 was 230-235 (270-275 2014/15). This was 7.53 (6.90 2014/15) times the median salary of the workforce, which was £30,530.53 (39,832.50 2014/15).
In 2015-16 1 employee received remuneration in excess of the highest paid director.
Total remuneration includes salary, non consolidated performance related pay, benefits in kind as well as severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pensions.
Staff exit packages 2015/16 (Subject to audit)
The disclosure reports the number and value of exit packages taken by staff leaving in the year.
2015/16 Six months accounts ended 31st March 2015
Exit package cost band (including any special payment element) *N
umbe
r of
co
mpu
lsor
y re
dund
anci
es
Cos
t of
com
puls
ory
redu
ndan
cies
Tota
l num
ber
of e
xit
pack
ages
Tota
l cos
t of
exi
t pa
ckag
es
Num
ber
of
com
puls
ory
redu
ndan
cies
Cos
t of
com
puls
ory
redu
ndan
cies
Tota
l num
ber
of e
xit
pack
ages
Tota
l cos
t of
exi
t pa
ckag
esNumber £ Number £ Number £ Number £
Less than £10,000 8 28,027 8 28,027 0 0 0 0
£10,000-£25,000 1 19,657 1 19,657 1 12,463 1 12,463
£25,001-£50,000 2 81,198 2 81,198 0 0 0 0
£50,001-£100,000 3 281,283 3 281,283 1 92,198 1 92,198
£100,001 - £150,000 0 0 0 0 0 0 0 0
£150,001 - £200,000 1 153,333 1 153,333 0 0 0 0
>£200,000 1 319,686 1 319,686 0 0 0 0
Total 16 883,184 16 883,184 2 104,661 2 104,661

97
Policy on the use of off-payroll engagement 2015/16
The Trust uses off-payroll engagements (contractors) for some tasks and roles. Sometimes interim cover is required for an established role or there is work to be undertaken for which specialist skills are required or which is of short duration. Such use of contractors is subject to approval by senior managers and regularly reviewed by the Trust’s senior management team.
Table 1: For all off-payroll engagements as of 31 March 2016, for more than £220 per day and that last longer than six months:
Number
Number of existing engagements as of 31 March 2016
Of which, the number that have existed:
for less than one year at the time of reporting 10
for between one and two years at the time of reporting 7
for between 2 and 3 years at the time of reporting 3
for between 3 and 4 years at the time of reporting 0
for 4 or more years at the time of reporting 0
Table 2: For all new off-payroll engagements between 1 April 2015 and 31 March 2016, for more than £220 per day and that last longer than six months:
Number
Number of new engagements, or those that reached six months in duration, between 1 April 2015 and 31 March 2016
7
Number of new engagements which include contractual clauses giving the London North West Healthcare the right to request assurance in relation to income tax and National Insurance obligations
7
Of which:
assurance has been received 4
assurance has not been received 3
engagements terminated as a result of assurance not being received 0
Table 3: For any off-payroll engagements of board members, and/or, senior officials with significant financial responsibility, between 1 April 2015 and 31 March 2016.
Number
Number of off-payroll engagements of board members, and/or senior officers with significant financial responsibility, during the financial year (1)
1
Total number of individuals on payroll and off-payroll that have been deemed “board members, and/or, senior officials with significant financial responsibility”, during the financial year. This figure should include both on payroll and off-payroll engagements. (2)
18
The recruitment of the Chief Financial Officer (CFO) post is expected to commence in mid-2016. The Trust has previously advertised the role on two occasions but has been unsuccessful in attracting the right calibre candidate. The Trust’s current CFO was employed through an off-payroll arrangement for six months until 31st March 2016. This arrangement was approved by NHS Improvement. From the 1st April, the CFO moved on to a fixed term contract on the payroll, with a contract end date of 31st March 2017.

98
Remuneration report
Staff numbers 2015/16 (Subject to audit)
Average Staff Numbers
2015-16 2014-15
TotalPermanently employed Other Total
Permanently employed Other
Number Number Number Number Number Number
Medical and dental 1,367 1,161 206 1,393 1,182 211
Ambulance staff 0 0 0 0 0 0
Administration and estates
1,940 1,629 311 2,061 1,727 334
Healthcare assistants and other support staff
1,377 1,123 254 1,292 983 309
Nursing, midwifery and health visiting staff
3,349 2,754 595 3,462 2,810 652
Nursing, midwifery and health visiting learners
0 0 0 0 0 0
Scientific, therapeutic and technical staff
1,410 1,242 168 1,416 1,247 169
Social Care Staff 0 0 0 0 0 0
Healthcare Science Staff
0 0 0 0 0 0
Other 0 0 0 0 0 0
Total 9,443 7,909 1,534 9,624 7,949 1,675

99
The information in this report is available in large print by calling 020 8869 3552.
If you would like a summary of this Annual Report in your own language please call 020 8869 3552 and state clearly in English the language you need and we will arrange an interpreter to speak to you.
If you would like a summary of the information contained in this annual report in your own language, please call 020 8869 2124 and state clearly, in English, the language you need and we will arrange for an interpreter to speak to you. Haddii aad jeclaan lahayd warka ku qoran warbixintaan gacan qabsiga loogu talogalay oo kooban oo luqaddaada ku qoran, fadlan soo wac 020 8869 3552 ka dibna si cad Ingiriis, ugu tilmaan, luqadda aad u baahan tahay waxaan markaas kuu diyaarin doonnaa turjumaan kula hadla. !-f<k!N{<mxqg<jgbqz<!-ml<ohx<Xt<t!uquvr<gtqe<!okiGh<H!dr<gt<!olipqbqz<!dr<gTg<Gk<!Okjuh<hMlieiz<?!kbUosb<K!020 8869 3552 we<x!w{<j{!okimIH!ogi{<M?!Nr<gqzk<kqz<?!oktquig!dr<gTg<Gk<!Okjuh<hMl<!olipqjb!Gxqh<hqm<miz<?!dr<gTme<!OhSukx<G!fir<gt<!yV!olipqohbIh<hitjv!Wx<hiM!osb<Ouil</!!+É ´ÉÉ̺ÉHí +¾àú´ÉɱɩÉÉÅ »É©ÉÉʴɺ`ò ©ÉÉʾúlÉÒ{ÉÉà »ÉÉ− ÷ÉÅ¶É Xà lÉ©É{Éà lÉ©ÉÉ− ÷Ò §ÉɺÉÉ©ÉÉÅ Xà<lÉÉà ¾úÉà«É lÉÉà, HÞí~ÉÉ Hí− ÷Ò{Éà 020 8869 3552 ~É− ÷ HíÉà±É Hí− ÷Éà +{Éà lÉ©ÉÉ− à÷ Wðà §ÉɺÉÉ{ÉÒ Wð°÷− ÷ ¾úÉà«É lÉà »~ɺ`ò °÷~Éà +ÅOÉàYð©ÉÉÅ WðiÉÉ´ÉÉà +{Éà lÉ©ÉÉ− ÷Ò Xàeàô ´ÉÉlÉ Hí−÷´ÉÉ +©Éà qÖö§ÉÉʺɫÉÉ{ÉÒ ´«É´É»oÉÉ Hí− ÷Ò +É~ÉÒ¶ÉÖÅ.
إذا آنت ترغب في الحصول على ملخص للمعلومات التي وردت في هذا التقرير السنوي بلغتك، واذآر بوضوح، باللغة اإلنجليزية، اللغة التي تحتاجها، 020 8869 3552اتصل على رقم
.سوف نقوم بتوفير مترجم ليتحدث إليكو
چنانچه تمايل داريد که خالصه اطالعات موجود در اين گزارش ساالنه را به زبان خود داشته تماس حاصل نمود و بطور واضح و با زبان 020 8869 3552باشيد، لطفا با شماره تلفن
بر اين اساس ما ترتيب حضور يک مترجم . انگليسی، زبان مورد نياز خود را اعالم فرمائيد .همزمان را بمنظور صحبت با شما خواهيم داد

training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation
transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation training research & development
learning from our patients feedback and involvement opportunities
innovation transformation research & development
training
learning from our patients feedback and involvement opportunities
innovation transformation research & development
Our Trust covers:
• Central Middlesex Hospital
• Ealing Hospital
• Northwick Park Hospital
• St. Mark’s Hospital
• Community services across Brent, Ealing and Harrow, including Clayponds Rehabilitation Hospital, Meadow House Hospice, Denham Unit and Willesden Centre.
Contact and follow us at:
Trust HQ London North West Healthcare NHS Trust Northwick Park Hospital Watford Road Harrow, HA1 3UJ
T. 020 8864 3232
E. [email protected] (general enquiries)
@LNWH_NHS
London North West Healthcare NHS Trust
www.lnwh.nhs.uk
Design: Jane Evans Design Limited Print: The Marstan Press Limited
Copyright © 2022 FDOKUMEN