Anaemia - RCP London
50
Anaemia Dr Dean Smith Haematology Consultant City Hospital, Nottingham
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Anaemia - RCP London

AnaemiaDr Dean Smith
Haematology ConsultantCity Hospital, Nottingham

Objectives
• 1. Be aware of different causes of anaemia• Dr Google tells us there are over 400 causes
• Will limit this to the more relevant, whilst identifying a framework for categorising the different causes
• 2. How to approach the investigation and management of an anaemic patient
• 3. When to transfuse
• 4. When to refer to haematology

Red Blood Cell (RBC) Lifecycle
• Erythropoiesis occurs in the bone marrow. Stimulated by erythropoietin (EPO) produced by the kidneys
• Just before and after leaving the bone marrow, the developing cells i.e. reticulocytes; theseconstitute about 1% of circulating red blood cells

Red Blood Cell (RBC) Lifecycle
• Average RBC lifespan is 120 days
• The ageing RBC undergoes changes in its plasma membrane, making itsusceptible to selective recognition by macrophages and subsequentphagocytosis in the mononuclear phagocyte system (spleen, liver and lymphnodes)his removes old and defective RBC
• This process normally occurs at the same rate of production by erythropoiesis,balancing the total circulating red blood cell count hence patients have a stableHb

Why do patients become anaemic?

Why do patients become anaemic?
• 1. Not making enough RBC• Reduced erythropoiesis (or
haematopoiesis)
• 2. Losing or breaking down RBC too quickly • Bleeding• Haemolysis

Causes of reduced erythropoiesis• 1. Haematinic deficiency
• Iron, folate, B12
• 2. Bone marrow disorders• Infiltration: Myeloma, leukaemia, lymphoma, myelofibrosis, metastatic cancer• Myelodysplasia• Aplastic anaemia
• 3. Myelosuppressive drugs • Chemotherapy, co-trimoxazole, multiple others
CAN CAUSE PANCYTOPENIA
Causes of reduced erythropoiesis• 4. CKD
• Reduced EPO
• 5. Chronic disease/inflammation• Infection, liver disease, autoimmune inflammatory disorders
• 6. Endocrine dysfunction• Hypothyroid, reduced testosterone

Case 1 – 28 yr old female
• Routine referral to haematology from GP with anaemia
• PC: Hb 92 g/l
• HPC: Menorrhagia. Not tolerating oral iron.
• Investigations: WCC 4.6, Platelets 250, MCV 72,
• Blood film – hypochromic, microcytic RBC, pencil cells. ferritin 12, transferrin saturation 10%
• IV iron (Ferrinject 1g) - 6 weeks later Hb 129, MCV 87

• Normal Blood Film • Iron Deficient
ferritin 12, transferrin saturation 10%
IV iron (Ferrinject 1g) - 6 weeks later Hb 129, MCV 87
Microcytic hypochromic
Pencil cell

Iron deficiency
• Iron absorbed in duodenum. Promoted by gastric Hcl.
• Ionized iron is toxic so nearly all on in the body is bound to protein• Eg. Hb, myoglobin, transferrin, ferritin, haemosiderin
• Iron is stored in 2 forms, ferritin and haemosiderin• Ferritin is soluble, haemosiderin insoluble
• Iron continuously circulates in plasma bound to transferrin

Causes of iron deficiency
• Inadequate intake
• Increased requirements, e.g. pregnancy
• Malabsorption, e.g. coeliac, gastrectomy
• Chronic haemorrhage

Diagnosing iron deficiency
• 1. MCV low
• 2. Blood film hypochromic, microcytic, pencil cells
• 3. A gold standard would be iron stain on bone marrow

Diagnosing iron deficiency• 4. Ferritin – roughly correlates with the amount of iron stored in tissues
• The exact ferritin level at which iron stores become deplete varies
• Hallberg et al 1993 studied 174 women. Correlated iron stores in bone marrow with ferritin.
• All women with Ferritin below 14 µg/l were iron deficient on marrow
• 25% of iron deficient women had iron levels above 14 µg/l
• Therefore don’t be guided completely by the lower limit of normal in the laboratory
• Ferritin levels increase in inflammatory conditions, e.g. acute or chronic infections, malignancy
• Therefore can be iron deficient with normal or high ferritin levels

Diagnosing iron deficiency• 5. Transferrin saturation
• Iron continually circulates in plasma bound to transferrin
• If iron levels are low, less transferrin has iron bound to it
• Hence transferrin saturation is a marker of iron state

Treating iron deficiency anaemia
• Oral iron • Suggest a trial of iron if ferritin <25 and/or TF saturation <20• Ferrous Sulphate 200mg = 65mg iron• Ferrous fumurate 210mg = 68mg iron• Ferrous gluconate 300mg = 35mg iron• Expect 10g/l Hb rise every 1-2 weeks if bleeding stopped• Continue at least 3 months to replenish stores• Suggest take od, then bd then tds for compliance
• IV iron if not absorbing or tolerating – QMC day case or renal outpatients
• Treat underlying cause

Case 2 - 47 year old man
• PC: Fatigue
• HPC: Went to GP and had FBC. Abnormal. Pancytopenia.• Urgent haem referral. ?leukaemia
• Hb 67, WBC 1.8, Neut 0.9, Platelets 84• MCV 114• Blood film – oval macrocytes, hypersegmented neutrophils (5+ lobes)

• Normal Blood Film • Iron Deficient
B12 98, Intrinsic Factor Antibody positive
IM B12 replacement (3 x per week for 2 weeks then 3 monthly)
Hypersegmented neutrophilOval macrocyte
Tear drop

3. B12 deficiency• B12 in food is mainly bound to protein
• Pepsin in the stomach releases B12 from protein
• B12 binds to intrinsic factor.
• Function of intrinsic factor is to transport B12 into the epithelia cells of the distal half of small intestine
• Intrinsic factor is produced by gastric parietal cells in the stomach
• Body generally has stores for 2+ years
• Patients with B12 deficiency may develop neurological symptoms, e.g. peripheral neuropathy, subacute combined degeneration of the cord
Causes of B12 deficiency
• Inadequate intake
• Inadequate secretion of intrinsic factor• Pernicious anaemia - Antibodies against intrinsic factor and/or gastric parietal cells
• Gastrectomy
• Malabsorption• Crohns, ileal resection
• NB B12 levels will measure s low if patient is taking OCP or HRT.

• Raised MCV• Blood film as per folate deficiency• Low B12• Test for intrinsic factor antibodies. GPC antibodies not recommended
by BSH – positive in 10% of normal cases

Management of B12 deficiency
• If true pernicious anaemia then would need hydroxocobalamin replacement life long
• BSH suggests is strong suspicion or IF antibody positive, e.g. low level or symptoms, IM replacement
• If incidental finding and moderate level and IF antibody negative could trial oral replacement. If levels don’t improve IM replacement could

Can be a complex decision! D/W haem if not clear cut.

Folate deficiency
• Folate absorbed in duodenum and jejunum
• Body generally has stores for c. 5-6 months

Causes of folate deficiency
• Inadequate intake
• Increased requirements• Pregnancy, haemolytic anaemia
• Malabsorption• Coeliac disease, jejunal resection

Diagnosing folate deficiency
• Raised MCV
• Blood film –macrocytes, hypersegmented neutrophils – same picture as B12 deficiency
• Reduced folate – can measure serum or red cell• Serum folate levels are readily affected by a short period of negative folate
balance• Red cell folate often a more reliable assessment of folate stores

Management of folate deficiency
• Folic acid 5mg daily – at least 3 months
• Can use 5mg tds if needed, e.g. in severe haemolysis
• Treat underlying cause
• In my experience, borderline/slightly low B12 and/or folate doesn't cause significant anaemia. Replace, but monitor and further investigations if no improvement.

Case 3 – 59 year old man
• PC: Presented to GP with fatigue
• HPC: 1/12 history of lower back ache, no red flags. Pain had actually resolved by time he saw GP.
• No blood loss.
• Hb 102, WBC 5.6, Plts 290, MCV 92• Paraprotein not detected.• Kappa light chains 1200, Lambda 19.• BM biopsy – 40% plasma cells• Diagnosis myeloma

Bone marrow disorders
• Consider this if pancytopenia or other causes excluded
• Formal diagnosis generally requires a bone marrow biopsy
• Tests to request prior to haem referral• Paraprotein• Serum free light chains• Blood film

Case 4 - 74 year old female
• PC: Fatigue and Anaemia
• HPC: GP noted Hb 87 on bloods for fatigue.• Other symptom – recurrent UTIs• Haematinics normal. No paraprotein, serum free light chains normal.• MCV 98
• ESR 84, Cre 72• BM biopsy normal trilineage haematopoiesis

• Diagnosis - ?anaemia of chronic disease, ?related to recurrent UTI
• Plan: Commence EPREX 20,000 units once weekly• Autoimmune profile• CT CAP to exclude other malignancy/cause for anaemia of chronic
disease
• Hb increased to 103 after 4 weeks EPREX• CT – renal stone right ureter, hydropnephrosis and collection• Urology – removed stone, drained pus• 6 weeks later Hb 129, EPREX stopped. Hb remained normal.

Anaemia of chronic disease• Why does chronic disease cause anaemia?
• Slightly shortened RBC survival
• Decreases in both erythropoietin (EPO) production and marrow responsiveness to EPO.
• Iron metabolism is altered

• A diagnosis of exclusion but some markers are suggestive:• MCV low or normal• Haematinics and film normal• Raised inflammatory markers• Raised ferritin, low TF saturation
• Management• Serum EPO• Iron may help to ensure adequate response to EPO• Treat the underlying cause
Iron Deficient ACD
MCV Low Low or Normal
Ferritin Low Normal or Raised
TF saturation Low Low

Causes of Haemolysis• Congenital
• Sickle cell anaemia• Thalassaemia• G6PD deficiency
Causes of Haemolysis• Acquired – Immune
• Warm-reactive antibodies “AIHA”• Idiopathic • Secondary to CLL, lymphoma, other autoimmune conditions e.g. SLE
• Cold Hemagglutinin Disease (CHAD)• Idiopathic• Secondary to Mycoplasma pneumonia, infectious mononucleosis, lymphomas
Causes of Haemolysis• Acquired Non-Immune
• Microangiopathic haemolytic anaemia (MAHA)• HUS, TTP, DIC• Malignant HTN
• Mechanical trauma• Heart valve disease/replacement
• March Haemoglobinuria

AIHA

CHAD

MAHA
• Blood film in TTP
• Note fragments and lack of platelets

Case 5 - 62 year old man
• PC: Fatigue ++
• HPC: Known CLL, last treated with chemo 3 years ago. • 1-2/52 history of extreme fatigue. No blood loss. No B symptoms • Last CLL clinic 6 weeks ago – CLL stable.
• Hb 73, WCC 17, Neut 3, Lymph 13, Plts 210• MCV 105• Ferritin/B12/Folate normal
• LDH 1126, reticulocytes 189, bilirubin 48, haptoglobin <0.3
• Direct Coombes test positive
• i.e. haemolysis screen positive
• Diagnosis AIHA
• Management:• Transfused• Pred 1mg/kg• Folic acid• Consider treating underlying CLL

Diagnose haemolysis
• Reticulocytes• LDH• Haptoglobin• Bilirubin
• Conjugated and unconjugated
• Direct coombs test• Blood film – will see reticulocytes, spherocytes, ?fragments

Management of haemolysis
• Depends on the type
• Always folic acid as stores will be depleted by the increased RBC turnover
• Immune haemolysis – immune suppression• Steroids 1st line• Rituximab• Steroid sparing agents
• If secondary, e.g. to CLL, treat the underlying cause of doesn't response to immune suppression.

How to approach an anaemic patient
• 2 key questions:• Isolated anaemia or pancytopenia
• Pancytopenia more suggestive of bone marrow disorder
• What is MCV?• Low, normal or raised
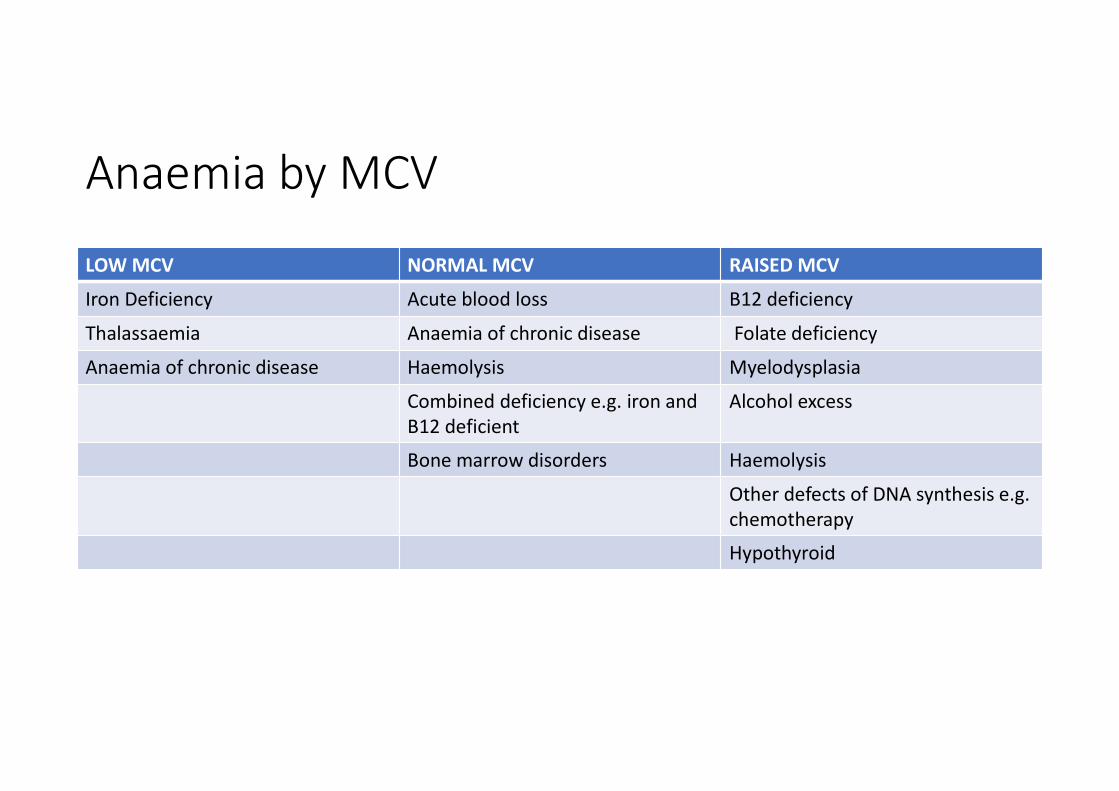
Anaemia by MCV
LOW MCV NORMAL MCV RAISED MCV
Iron Deficiency Acute blood loss B12 deficiency
Thalassaemia Anaemia of chronic disease Folate deficiency
Anaemia of chronic disease Haemolysis Myelodysplasia
Combined deficiency e.g. iron and B12 deficient
Alcohol excess
Bone marrow disorders Haemolysis
Other defects of DNA synthesis e.g. chemotherapy
Hypothyroid

Anaemia investigations
• B12, folate, ferritin, transferrin saturation• Blood film• Reticulocyte count• LDH, haptoglobin, bilirubin
• DAT • Immunoglobulins, serum free light chains• Review medication chart
BEFORE TRANSFUSION!

• No universal trigger
• Do not transfuse for chronic anaemias from haematinic deficiency unless haemodynamic instability
• <70 g/L• ICU, PICU, sepsis• Acute upper GI bleed• Massive haemorrhage (Hb 70-90)
• ?<80-90 g/L with acute coronary syndrome
• <90 if bleeding or haemolysing
Transfusion Threshold

When to refer
• If haematinics normal
• No drugs as obvious cause
• No acute bleed

Summary/Review of Objectives• 1. Be aware of different causes of anaemia
• Ineffective erythropoiesis
• Increased red cell breakdown
• Blood loss
• 2. How to approach the investigation and management of an anaemic patient
• Is patient anaemic or pancytopenic
• What is the MCV
• Request haematinics, haemolysis screen, blood film, myeloma screen.
• Review medications
• Consider anaemia of chronic disease.

Summary/Review of Objectives• 3. When to transfuse
• Hb <70
• Hb 80-90 if elderly/cardiac history
• Not if haematinic deficiency unless haemodynamically unstable
• Hb <90 if bleeding or haemolysing
• 4. When to refer to haematology• If haematinics normal
• No drugs as obvious cause
• No acute bleed