An open-label study of anakinra for the treatment of moderate to severe hidradenitis suppurativa
9
ORIGINAL ARTICLES An open-label study of anakinra for the treatment of moderate to severe hidradenitis suppurativa Kieron S. Leslie, DTM&H, FRCP, Shivani V. Tripathi, MD, Tien V. Nguyen, MD, Mariela Pauli, MS, and Michael D. Rosenblum, MD, PhD San Francisco, California Background: Hidradenitis suppurativa (HS) is a chronic inflammatory disorder characterized by sterile abscesses and fistulae predominantly affecting the axillae and groin. Various biologic agents have been attempted for HS, but there is still no definitive treatment. Objectives: We sought to evaluate the efficacy, safety, and tolerability of anakinra in the treatment of moderate to severe HS. Methods: Six patients with moderate to severe HS were enrolled in an open-label study with all patients receiving active treatment for 8 weeks with an additional 8 weeks of follow-up off therapy. Results: The 5 patients who completed the 8-week therapy showed a significant mean decrease in their modified Sartorius score of 34.8 points. The physician and patient global assessment of overall activity showed significant reductions between baseline and 8 weeks of therapy: 45.8 points and 35.6 points, respectively. The Dermatology Life Quality Index showed a significant reduction after 8 weeks of treatment with anakinra. Functional T-cell analysis revealed that patients had increased percentages of CD3 1 T cells in lesional skin compared with nonlesional skin before therapy. Limitations: The limited number of patients and lack of control group are limitations. Conclusions: Anakinra demonstrated decreased HS disease activity by both objective and subjective measures. ( J Am Acad Dermatol 2014;70:243-51.) Key words: anakinra; inflammation; interleukin-1; hidradenitis suppurativa; T cells; treatment. H idradenitis suppurativa (HS) is a chronic inflammatory disorder characterized by sterile abscesses and fistulae predominantly affecting the axillae and groin. It causes significant morbidity from pain and drainage and is associated with significantly compromised quality of life. 1 There are few epidemiologic data but prevalence rates have been reported from 0.05% in North America 2 to 4% in Denmark. 3 There is increasing evidence that the immune system plays a crucial role in the development and persistence of HS. Overproduction of cytokines associated with innate immunity (including interleu- kin [IL]-1b and tumor necrosis factor [TNF]-alfa) have From the Department of Dermatology, University of California, San Francisco. Swedish Orphan Biovitrum AB provided study drug but all other funding was from internal research funds. Disclosure: Dr Leslie has served as a consultant and is on the speaker’s bureau for Novartis Pharmaceuticals. Drs Tripathi, Nguyen, and Rosenblum, and Ms Pauli have no conflicts of interest to declare. Accepted for publication September 19, 2013. Reprint requests: Kieron S. Leslie, DTM&H, FRCP, Department of Dermatology, University of California, San Francisco, 1701 Divisadero St, San Francisco, CA 94115. E-mail: lesliek@derm. ucsf.edu. Published online December 5, 2013. 0190-9622/$36.00 Ó 2013 by the American Academy of Dermatology, Inc. http://dx.doi.org/10.1016/j.jaad.2013.09.044 Abbreviations used: CI: confidence interval DLQI: Dermatology Life Quality Index HS: hidradenitis suppurativa IL: interleukin Th: helper T cell TNF: tumor necrosis factor VAS: visual analog scale 243
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of An open-label study of anakinra for the treatment of moderate to severe hidradenitis suppurativa

ORIGINAL ARTICLES
An open-label study of anakinra for the treatmentof moderate to severe hidradenitis suppurativa
Kieron S. Leslie, DTM&H, FRCP, Shivani V. Tripathi, MD, Tien V. Nguyen, MD, Mariela Pauli, MS,and Michael D. Rosenblum, MD, PhD
San Francisco, California
From
Fr
Swed
fu
Discl
sp
N
in
Acce
Background: Hidradenitis suppurativa (HS) is a chronic inflammatory disorder characterized by sterileabscesses and fistulae predominantly affecting the axillae and groin. Various biologic agents have beenattempted for HS, but there is still no definitive treatment.
Objectives: We sought to evaluate the efficacy, safety, and tolerability of anakinra in the treatment ofmoderate to severe HS.
Methods: Six patients with moderate to severe HS were enrolled in an open-label study with all patientsreceiving active treatment for 8 weeks with an additional 8 weeks of follow-up off therapy.
Results: The 5 patients who completed the 8-week therapy showed a significant mean decrease in theirmodified Sartorius score of 34.8 points. The physician and patient global assessment of overall activityshowed significant reductions between baseline and 8 weeks of therapy: 45.8 points and 35.6 points,respectively. The Dermatology Life Quality Index showed a significant reduction after 8 weeks of treatmentwith anakinra. Functional T-cell analysis revealed that patients had increased percentages of CD31 T cellsin lesional skin compared with nonlesional skin before therapy.
Limitations: The limited number of patients and lack of control group are limitations.
Conclusions: Anakinra demonstrated decreased HS disease activity by both objective and subjectivemeasures. ( J Am Acad Dermatol 2014;70:243-51.)
Key words: anakinra; inflammation; interleukin-1; hidradenitis suppurativa; T cells; treatment.
Abbreviations used:
CI: confidence intervalDLQI: Dermatology Life Quality IndexHS: hidradenitis suppurativaIL: interleukinTh: helper T cellTNF: tumor necrosis factorVAS: visual analog scale
Hidradenitis suppurativa (HS) is a chronicinflammatory disorder characterized bysterile abscesses and fistulae predominantly
affecting the axillae and groin. It causes significantmorbidity from pain and drainage and is associatedwith significantly compromised quality of life.1 Thereare few epidemiologic data but prevalence rates havebeen reported from 0.05% in North America2 to 4% inDenmark.3
There is increasing evidence that the immunesystem plays a crucial role in the development andpersistence of HS. Overproduction of cytokines
the Department of Dermatology, University of California, San
ancisco.
ish Orphan Biovitrum AB provided study drug but all other
nding was from internal research funds.
osure: Dr Leslie has served as a consultant and is on the
eaker’s bureau for Novartis Pharmaceuticals. Drs Tripathi,
guyen, and Rosenblum, and Ms Pauli have no conflicts of
terest to declare.
pted for publication September 19, 2013.
associated with innate immunity (including interleu-kin [IL]-1b and tumor necrosis factor [TNF]-alfa) have
Reprint requests: Kieron S. Leslie, DTM&H, FRCP, Department of
Dermatology, University of California, San Francisco, 1701
Divisadero St, San Francisco, CA 94115. E-mail: lesliek@derm.
ucsf.edu.
Published online December 5, 2013.
0190-9622/$36.00
� 2013 by the American Academy of Dermatology, Inc.
http://dx.doi.org/10.1016/j.jaad.2013.09.044
243

J AM ACAD DERMATOL
FEBRUARY 2014244 Leslie et al
been observed from HS skin cultures.4 In addition,expression of cytokines that directly modulate theadaptive immune system (including IL-10, IL-12,IL-17, and IL-23) are observed in HS skin.4,5
Although these studies have implicated variouscytokines and inflammatory pathways in initiatingand maintaining inflammation in patients with
CAPSULE SUMMARY
d Effects of anakinra therapy onhidradenitis suppurativa were evaluatedin this open-label clinical trial.
d Anakinra resulted in significantreductions in the modified Sartoriusscore and improvement in quality of life.
d Anakinra has potential as a treatment forhidradenitis suppurativa.
HS, the dominant cytokine(s)that drive this disease haveyet to be determined.Understanding the dominantcytokines that CD41 helperT cells (Th) produce in theskin is critical in attemptsto better define the patho-genesis of HS. Th differenti-ation (ie, Th1, Th2, Th17)dictates the type of cutane-ous inflammation and pro-vides a rationale approachfor therapies that target
specific cytokines and immune pathways.Therapy with biologic agents that inhibit specificcytokines have been increasingly attempted forpatients with severe and refractory disease.TNF-alfa blockade with infliximab has been reportedin a randomized double-blind crossover study todecrease the severity score of HS in the majority ofpatients as compared with placebo.6 Initialreports suggested etanercept as an useful agent7,8
although subsequent trials showed little to noefficacy.9,10 More recently, a large multicenterstudy11 demonstrated that after 16 weeks of therapy,adalimumab achieves a clinical response in 17.6% ofpatients as compared with 9.6% in patients dosedevery over week and 3.9% in the placebo group.Clinical improvements in patients treated withthe p40 inhibitor, ustekinumab, have also beenreported.12-14 Despite these encouraging results,highly efficacious therapy for patients with HS andsevere disease has yet to be elucidated.
We recently reported a marked reduction indisease activity in a patient with HS and concom-itant pyoderma gangrenosum who was treatedwith anakinra, an IL-1 receptor antagonist,15 afterfailing multiple other therapies. Both HS andthe autoinflammatory syndromes are characterizedby recurrent noninfectious inflammatory episodeswithout autoantibodies or antigen-specific Tcells.16 Indeed, most autoinflammatory syndromeshave been shown to be remarkably responsiveto IL-1 blockade such as cryopyrin-associatedperiodic syndrome,17 TNF receptoreassociatedperiodic syndrome,18 and familial Mediterraneanfever.19
The objective of this study was to evaluate theefficacy, safety, and tolerability of anakinra in thetreatment of moderate to severe HS. The study’sdesign was open-label, with all patients receivingactive treatment for 8 weeks with an additional8 weeks of follow-up off therapy. In addition tomeasuring clinical disease, we functionally defined
skin-infiltrating T cells andT-cell cytokine productionin these patients to deter-mine the nature of theadaptive immune responsein HS and the influence ofIL-1 blockade.
METHODSStudy patients
This was an investigator-initiated clinical trial thatwas approved by the localinstitutional review board
and was registered with ClinicalTrials.gov(NCT01516749). Patients aged 18 years or olderwith moderate to severe HS were recruited from anacademic dermatology practice in San Francisco, CA.Informed consent was obtained before study entry.Patients were included if they had minimummodified Sartorius score20 of 25 or greater and activedisease in at least 2 anatomic regions. Patients wereallowed oral or topical antibiotic therapy for their HSas long as they were receiving a stable dose for atleast 4 weeks before baseline visit and were willingto remain on a stable dose for the full duration of thestudy. Exclusion criteria included concurrent activeinfections such as HIV, hepatitis B, hepatitis C, andtuberculosis; history of malignancy; and use of otherimmunosuppressive therapies within 12 weeks ofthe baseline visit.
Study designThis was an open-label pilot study, where all
patients received active therapy of anakinra(Kineret) for 8 weeks, followed by an additional8 weeks of follow-up off therapy.
Treatment and assessmentsAll study patients were treated with self-
administered daily anakinra (100 mg) via subcuta-neous injection. At each study visit, the samephysician examined patients, and the modifiedSartorius score was calculated. In addition, thephysician assessed disease activity on visualanalog scale (VAS) ranging from 0 mm (absent) to100 mm (worst imaginable) as a physicians globalassessment. Similarly, the patients reported overall

J AM ACAD DERMATOL
VOLUME 70, NUMBER 2Leslie et al 245
(global) disease activity of HS, in addition to focusedsubjective measures of pain, drainage, and odor withappropriate VAS. Patient were asked, ‘‘What is theoverall activity (pain, discharge, odor, and presenceof new lesions) of hidradenitis at this visit?’’ with ascale of 0 = no activity to maximal activity = 100. TheDermatology Life Quality Index (DLQI) wascompleted at every visit in addition to the ShortForm (36) Health Survey; these questionnaires wereboth self-administered. Clinical photographs weretaken of all affected body sites.
Skin digestion and flow cytometrySkin biopsies of lesional and unaffected skin were
performed at the baseline visit and after completing8 weeks of therapy. Skin was minced finely withdissection scissors and digested overnight in bufferconsisting of 0.8 mg/mL collagenase type 4(Worthington 4188, Biochemical Corp, Lakewood,NJ), 0.02 mg/mL deoxyribonuclease (Sigma DN25-1G, St Louis, MO), 10% fetal bovine serum, 1%hydroxyethyl piperazineethanesulfonic acid, and 1%penicillin/streptavidin in Roswell Park MemorialInstitute medium. For detection of intracellular cyto-kine production, punch biopsy specimens were stim-ulated with 1 �g/mL lipopolysaccharide (Sigma) for 6hours, 70 ng/mL of phorbol myristate acetate, and 700ng/mL of ionomycin in the presence of BrefeldinA (Sigma) for 4 to 5 hours. Data were acquired by anLSRFortessa (BD Biosciences, San Jose, CA) and ana-lyzed using FlowJo software (Tree Star, Ashland, OR).
SafetyVital signs and physical examination were
undertaken at every visit. The investigators assessedadverse events throughout the study by directpatient query, observation by study personnel, andspontaneous patient reporting. Blood chemistrywas assessed at baseline, week 4 (on therapy), andweek 12 (off therapy). No Formal adverse eventquestionnaire was used in this study.
Study end pointsThe primary end point measure was the
proportion of patients who had a significantreduction in modified Sartorius score at the end ofthe treatment period, week 8 compared with week 0.Secondary end points included VAS scores for thephysician’s global assessment and subjective patientratings of overall disease activity, pain discharge,and odor. Other measures included quality-of-lifeevaluation with DLQI and SF36. Acute phaseresponse, with C-reactive protein levels, was alsoevaluated throughout the trial.
Statistical analysisDescriptive statistics (SD, mean, minimum, and
maximum) by visit were computed for the outcomevariables. Parametric tests (paired t test) were usedto analyze efficacy of the treatment. Significancewas accepted at P less than .05. Analysis softwarewas Stata, Version 12.0 (StataCorp LP, CollegeStation, TX).
RESULTSEleven patients were screened for this study, and 6
fit the criteria and were enrolled. Baseline character-istics are depicted in Table I. Five patients completedthe treatment phase of the studywith anakinra; oneofthese patients was subsequently lost to follow-upbecause of difficult socioeconomic factors prevent-ing attendance at follow-up study visits. The sixthpatient received treatment for 2weekswith anakinra,at which point, he had shown improvement in allstudy outcomes (modified Sartorius score, physicianglobal assessment, and all patient subjective mea-sures). He did not report any treatment side effects.Subsequent to this visit he was lost to follow-up. Theonly side effect reported by patients globally was theinjection site reaction that subsided for all patients byweek 2 of treatment. No adverse events were seen inany of the study participants in either the treatmentphase or follow-up phase of the study.
The 5 patients who completed the 8-week therapyshowed a significant mean decrease in theirmodified Sartorius score of 34.8 points (P = .024,95% confidence interval [CI] 7.56-62.05). The meanvalue for the modified Sartorius scores showedprogressive improvement during the treatmentperiod, and rebound during the follow-up post-treatment period (Fig 1, A and Fig 2).
The physician global assessment and patientglobal assessment of overall activity using VAS(maximum score 100) showed significant reductionsin mean values between baseline and 8 weeks oftherapy: 45.8 points (P = .006, 95% CI 22.1-69.5) and35.6 points (P = .019, 95% CI 9.83-61.4), respectively(Fig 1, B). Rebound in these values was appreciatedin the follow-up phase of the study. Other subjectivepatient assessments that showed a significant changefrom baseline to end of treatment phase includedpain, which showed a mean reduction of 35.2(P = .033, 95% CI 4.66-65.74) and discharge severity(mean change 27.4, P = .019, 95% CI 0.07-54.11).Odor severity mean showed a 30.0-point reductionalthough was not significant for the 5 patients(P = .079, 95% CI e5.53 to 65.53) (Fig 1, C ).
The DLQI, measuring the extent to which diseaseaffects quality of life with higher score (maximum 30)reflecting a larger negative effect of disease onquality
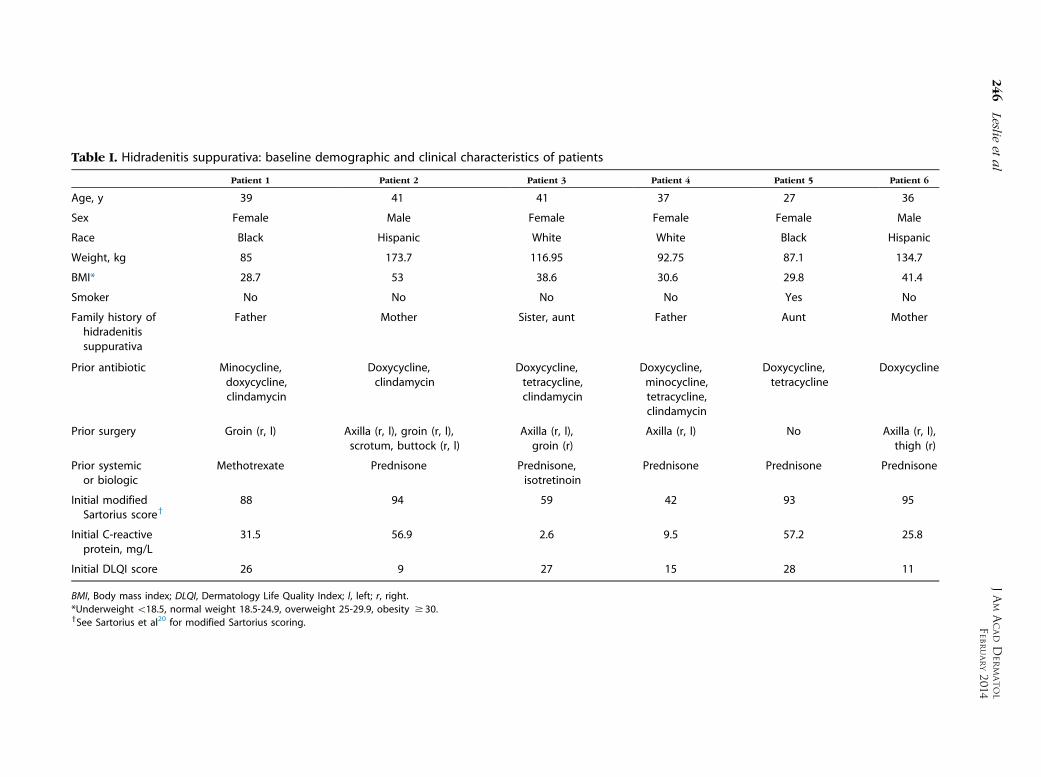
Table I. Hidradenitis suppurativa: baseline demographic and clinical characteristics of patients
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6
Age, y 39 41 41 37 27 36
Sex Female Male Female Female Female Male
Race Black Hispanic White White Black Hispanic
Weight, kg 85 173.7 116.95 92.75 87.1 134.7
BMI* 28.7 53 38.6 30.6 29.8 41.4
Smoker No No No No Yes No
Family history ofhidradenitissuppurativa
Father Mother Sister, aunt Father Aunt Mother
Prior antibiotic Minocycline,doxycycline,clindamycin
Doxycycline,clindamycin
Doxycycline,tetracycline,clindamycin
Doxycycline,minocycline,tetracycline,clindamycin
Doxycycline,tetracycline
Doxycycline
Prior surgery Groin (r, l) Axilla (r, l), groin (r, l),scrotum, buttock (r, l)
Axilla (r, l),groin (r)
Axilla (r, l) No Axilla (r, l),thigh (r)
Prior systemicor biologic
Methotrexate Prednisone Prednisone,isotretinoin
Prednisone Prednisone Prednisone
Initial modifiedSartorius scorey
88 94 59 42 93 95
Initial C-reactiveprotein, mg/L
31.5 56.9 2.6 9.5 57.2 25.8
Initial DLQI score 26 9 27 15 28 11
BMI, Body mass index; DLQI, Dermatology Life Quality Index; l, left; r, right.
*Underweight\18.5, normal weight 18.5-24.9, overweight 25-29.9, obesity $ 30.ySee Sartorius et al20 for modified Sartorius scoring.
JAM
ACADD
ERM
ATOL
FEBRUARY20
14246
Leslieet
al

Fig 2. Hidradenitis suppurativa, patient 1: left axilla atweeks 0 (baseline), 8 (on treatment), and 16 (off treatment).
Fig 1. Hidradenitis suppurativa.A, Modified Sartorius scorefor patients 1 to 6 at weeks 0 (premedication); 2, 4, and 8(treatment period); and 12 and 16 (follow-up). B, Meanphysician versus patient global assessments of diseaseactivity; visual analog scale (VAS ) (0-100). C, Mean patientVAS scores for pain, discharge, and odor. D, Mean Derma-tology Life Quality Index (DLQI ) for patients at each visit.
J AM ACAD DERMATOL
VOLUME 70, NUMBER 2Leslie et al 247
of life, showed a significant reduction in mean scoresafter 8 weeks of treatment with anakinra, a meandecreaseof 8.4 points (P= .046, 95%CI 0.23-16.57). Atfollow-up DLQI scores worsened and reflected thepretreatment scores (Fig 1, D).
Baseline C-reactive protein levels varied tremen-dously from 2.6 to 57.2 mg/L (normal \3.1 mg/L)

Fig 3. A, Immunoflow cytometry on nonlesional and lesional skin from patients withhidradenitis suppurativa (HS) before and after treatment (tx) with anakinra. Percentages ofCD3-, interleukin (IL)-17-, or interferon-g (IFNg)-secreting cells in nonlesional and lesional skinof patients with HS before tx with anakinra. B, Flow cytometry of patient 1 before and after txwith anakinra. Plots are pregated on viable CD31CD41 cells.
J AM ACAD DERMATOL
FEBRUARY 2014248 Leslie et al
with a mean of 30.6 (SD 23.03) (n = 6). C-reactiveprotein levels showed a mean reduction of16.7 points from baseline to end of treatment phase.This change was not significant (P = .076, 95% CIe2.784 to 36.14) although suggests a trend forreduction in acute phase response.
Functional T-cell analysis of the patients revealedthat all patients had increased percentages of CD31 Tcells in lesional skin compared with nonlesional skinbefore therapy (Fig 3, A). All patients had skewingaway from Th17 differentiation in lesional skin com-pared with nonlesional skin (ie, T cells from HS skinproduced less IL-17 comparedwith clinically normal-appearing skin harvested from the same patient) (Fig3, A, bottom left). Interestingly, the patient with the
best clinical response (patient 1) had a predominantTh1 skew in lesional skin comparedwith nonlesionalskin, with marked increased in interferon-g produc-tion from T cells infiltrating diseased skin in thispatient (Fig 3,A, bottom right). In addition, treatmentwith anakinra completely reversed the Th1 skewobserved in this patient (Fig 3, B).
DISCUSSIONTo our knowledge, this clinical trial is the first to
prospectively address the efficacy and safety ofanakinra, an IL-1 receptor antagonist for thetreatment of moderate to severe HS. Previous casereports have had conflicting results with both areduction in disease activity15 or no response to

J AM ACAD DERMATOL
VOLUME 70, NUMBER 2Leslie et al 249
IL-1 inhibition.21 In this open-label study, anakinraappeared to be well tolerated and demonstrated astatistically significant decrease in disease activity ofHS by both objective and subjective measures.The 8-week observation period enabled us toidentify potential rebound. Limitations of this studyinclude the lack of a control group and a smallnumber of participants.
The modified Sartorius score is a validatedinstrument that assesses disease activity in HS andhas been used in other therapeutic studies.11 In the 5patients who completed the treatment phase of thestudy, a significant and clinically meaningfulreduction of score by a mean of 34.8 points wasrecorded. This was evident at all time points from 2weeks onward but was maximal at 8 weeks. Ourresults compare favorably with a large blindedrandomized study comparing adalimumab, weeklyversus every other week dosing against placebo,11
which also used the modified Sartorius score as anend point. This study found a median 30-pointreduction in score at 16 weeks of treatment withadalimumab 40 mg weekly versus 16-pointreduction in the every other week group versus7.5-point reduction in the placebo group. Inaddition, we saw a significant rebound in the scoreduring the follow-up phase for the 4 patients whoremained in the study with a mean increase of 52.5points at 16 weeks compared with 8 weeks.
The quality of life in patients with HS is severelyimpacted with considerable pain,22 emotional dis-tress,23 and sexual health.24 The minimal clinicallymeaningful reduction in DLQI score is considered tobe between �6.96 and �4.05.25 Clinical trials usingTNF-alfa-blocking agents have reported reductionsin DLQI scores ranging from �6.911 to no significantchange26,27 with adalimumab, �106 to �9.128 withinfliximab, and variable results with etanercept from�11.6,7 �4,10 to no change.9 Our study showed amean reduction in DLQI score of �8.4 after 8 weeksof therapy (P = .047). This improvement in meanDLQI score is similar to that reported by Kimballet al11 of �6.3 in patients treated with weeklyadalimumab. Again rebound back to baseline scoreswere seen in the DLQI for the 4 remaining patients inour study during the follow-up (observation) phase.
Anakinra was well tolerated in this study with 5of the 6 enrolled patients completing treatment.There were no adverse events. Daily injections arerequired because of its short half-life of 6 hours,which may limit its acceptability as a treatment forpatients. All of our patients reported painfulinjection site reactions, which decreased inseverity after a few weeks of treatment. Injectionsite reactions with anakinra have been commonly
reported.29 Otherwise anakinra has a favorableside-effect profile when compared with otherbiologics. Increased risk of infection30 andneutropenia are the most commonly reported. Noassociation with an increased risk of malignancyhas been reported.31
Clinically, we show that IL-1 blockade isefficacious in treating HS. On a cellular andmolecular level, we show that HS is associated withskewing away from Th17 differentiation, and thepatient with the best response to anakinra haddisease that was dominated by Th1 cytokineproduction. IL-1a and IL-1b are pleiotropiccytokines with multiple effects on the immunesystem.32 IL-1a is produced by many cell types,including endothelial cells and keratinocytes, and isthought to act locally. In contrast, expression of IL-1bappears to be relatively restricted to monocytes andmacrophages and can act systemically. Thebiologicalactivities of IL-1a and IL-1b are mediated by bindingto IL-1 receptor type I, which is expressed on widevariety of cell types.33 The IL-1 pathway is one of themost potent proinflammatory pathways and IL-1-mediated inflammation has been shown to induceand enhance both Th17- and Th1-type T-cell re-sponses.34 It has been proposed that IL-1 signalingmay promote Th1 immunity through increasedsurvival and expansion of interferon-g-producingT cells, possibly through augmentation of thenuclear factor kappa B pathway.34-36 Here, weshow that HS is not associated with Th17-typeinflammation, suggesting that IL-1 does not contrib-ute to HS pathogenesis by augmenting Th17responses. Instead, we speculate that in the settingof diminished Th17 disease, the dominant role of IL-1is to increase the survival and expansion of Th1. Thisis supported by the observation that blocking IL-1signaling in a patient with HS and predominant Th1disease led to a complete reversal of Th1 cytokineproduction and near complete disease resolution.Thus, we speculate that biologic therapy that prefer-entially inhibits Th1 differentiation and/or Th1 cyto-kine production will most likely be more efficaciousin treating HS than those that target Th2 or Th17cytokines. Of course, a larger study with morepatients is needed to definitively test this.
In conclusion, our study demonstrated that dailyanakinra is an effective treatment in patients with HSwith significant reduction in subjective andobjective measurements of disease activity.However HS disease activity rebounded rapidlywhen off therapy. The current cost of anakinraas listed by Epocrates (https://online.epocrates.com/home) is $22,516 (annual cost) compared withweekly adalimumab, which costs $50,700 (annual

J AM ACAD DERMATOL
FEBRUARY 2014250 Leslie et al
cost). Future research should address whether theseresults are replicated in a larger randomizedblinded placebo-controlled study. Ultimately, aclinical trial comparing IL-1 inhibition with thecurrent gold standard of biological therapy of TNFblockers is warranted in moderate to severe HS.
The authors are very grateful to Charles McCulloch,PhD, Department of Epidemiology, University ofCalifornia, San Francisco, for his advice regarding statisticalanalysis, and to the patients for their participation in thisstudy.
REFERENCES
1. Onderdijk AJ, van der Zee HH, Esmann S, Lophaven S, Dufour
DN, Jemec GB, et al. Depression in patients with hidradenitis
suppurativa. J Eur Acad Dermatol Venereol 2013;27:473-8.
2. Cosmatos I, Matcho A, Weinstein R, Montgomery MO, Stang P.
Analysis of patient claims data to determine the prevalence of
hidradenitis suppurativa in the United States. J Am Acad
Dermatol 2013;68:412-9.
3. Jemec GB, Heidenheim M, Nielsen NH. The prevalence of
hidradenitis suppurativa and its potential precursor lesions.
J Am Acad Dermatol 1996;35:191-4.
4. van der Zee HH, de Ruiter L, van den Broecke DG, Dik WA,
Laman JD, Prens EP, et al. Elevated levels of tumor necrosis
factor (TNF)-a, interleukin (IL)-1b and IL-10 in hidradenitis
suppurativa skin: a rationale for targeting TNF-a and IL-1b.
Br J Dermatol 2011;164:1292-8.
5. Schlapbach C, H€anni T, Yawalkar N, Hunger RE, et al. Expres-
sion of the IL-23/Th17 pathway in lesions of hidradenitis
suppurativa. J Am Acad Dermatol 2011;65:790-8.
6. Grant A, Gonzalez T, Montgomery MO, Cardenas V, Kerdel FA.
Infliximab therapy for patients with moderate to severe
hidradenitis suppurativa: a randomized, double-blind,
placebo-controlled crossover trial. J Am Acad Dermatol
2010;62:205-17.
7. Cusack C, Buckley C. Etanercept: effective in the management
of hidradenitis suppurativa. Br J Dermatol 2006;154:726-9.
8. Giamarellos-Bourboulis EJ, Pelekanou E, Antonopoulou A,
Petropoulou H, Baziaka F, Karagianni V, et al. An open-label
phase II study of the safety and efficacy of etanercept for the
therapy of hidradenitis suppurativa. Br J Dermatol 2008;158:
567-72.
9. Adams DR, Yankura JA, Fogelberg AC, Anderson BE. Treatment
of hidradenitis suppurativa with etanercept injection.
Arch Dermatol 2010;146:501-4.
10. Lee RA, Dommasch E, Treat J, Sciacca-Kirby J, Chachkin J,
Williams S. A prospective clinical trial of open-label etanercept
for the treatment of hidradenitis suppurativa. J Am Acad
Dermatol 2009;60:565-73.
11. Kimball AB, Kerdel F, Adams D, Mrowietz U, Gelfand JM,
Gniadecki R, et al. Adalimumab for the treatment of moderate
to severe hidradenitis suppurativa: a parallel randomized trial.
Ann Intern Med 2012;157:846-55.
12. Gulliver WP, Jemec GBE, Baker KA. Experience with ustekinu-
mab for the treatment of moderate to severe hidradenitis
suppurativa. J Eur Acad Dermatol Venereol 2012;26:911-4.
13. Sharon VR, Garcia MS, Bagheri S, Goodarzi H, Yang C, Ono Y,
et al. Management of recalcitrant hidradenitis suppurativa
with ustekinumab. Acta Derm Venereol 2012;92:320-1.
14. Baerveldt EM, Kappen JH, Thio HB, van Laar JA, van Hagen PM,
Prens LP. Successful long-term triple disease control by
ustekinumab in a patient with Behcet’s disease, psoriasis
and hidradenitis suppurativa. Ann Rheum Dis 2013;72:626-7.
15. Hsiao JL, Antaya RJ, Berger T, Maurer T, Shinkai K, Leslie KS.
Hidradenitis suppurativa and concomitant pyoderma gangre-
nosum: a case series and literature review. Arch Dermatol
2010;146:1265-70.
16. Stojanov S, Kastner DL. Familial autoinflammatory diseases:
genetics, pathogenesis and treatment. Curr Opin Rheumatol
2005;17:586-99.
17. Leslie KS, Lachmann HJ, Bruning E, McGrath JA, Bybee A,
Gallimore JR, et al. Phenotype, genotype, and sustained
response to anakinra in 22 patients with autoinflammatory
disease associated with CIAS-1/NALP3 mutations. Arch Der-
matol 2006;142:1591-7.
18. Obici L, Meini A, Cattalini M, Chicca S, Galliani M, Donadei S,
et al. Favorable and sustained response to anakinra in tumor
necrosis factor receptor-associated periodic syndrome (TRAPS)
with or without AA amyloidosis. Ann Rheum Dis 2011;70:
1511-2.
19. Stankovic Stojanovic K, Delmas Y, Torres PU, Peltier J, Pelle G,
J�eru I, et al. Dramatic beneficial effect of interleukin-1 inhibitor
treatment in patients with familial Mediterranean fever com-
plicated with amyloidosis and renal failure. Nephrol Dial
Transplant 2012;27:1898-901.
20. Sartorius K, Emtestam L, Jemec GBE, Lapins J. Objective
scoring of hidradenitis suppurativa reflecting the role
of tobacco smoking and obesity. Br J Dermatol 2009;161:
831-9.
21. Van der Zee HH, Prens EP. Failure of anti-interleukin-1 therapy
in severe hidradenitis suppurativa: a case report. Dermatology
2013;226:97-100.
22. Smith HS, Chao JD, Teitelbaum J. Painful hidradenitis
suppurativa. Clin J Pain 2010;26:435-44.
23. Esmann S, Jemec GBE. Psychosocial impact of hidradenitis
suppurativa: a qualitative study. Acta Derm Venereol 2011;91:
328-32.
24. Kurek A, Peters EM, Chanwangpong A, Sabat R, Sterry W,
Schneider-Burrus S. Profound disturbances of sexual health in
patients with acne inversa. J Am Acad Dermatol 2012;67:
422-8.e1.
25. Shikiar R, Willian MK, Okun MM, Thompson CS, Revicki DA. The
validity and responsiveness of three quality of life measures in
the assessment of psoriasis patients: results of a phase II study.
Health Qual Life Outcomes 2006;4:71.
26. Miller I, Lynggaard CD, Lophaven S, Zachariae C, Dufour DN,
Jemec GB. A double-blind placebo-controlled randomized trial
of adalimumab in the treatment of hidradenitis suppurativa.
Br J Dermatol 2011;165:391-8.
27. Amano M, Grant A, Kerdel FA. A prospective open-label clinical
trial of adalimumab for the treatment of hidradenitis
suppurativa. Int J Dermatol 2010;49:950-5.
28. Mekkes JR, Bos JD. Long-term efficacy of a single course of
infliximab in hidradenitis suppurativa. Br J Dermatol 2008;158:
370-4.
29. Belani H, Gensler L, Bajpai U, Meinhardt E, Graf J, Pincus L,
et al. Neutrophilic urticaria with systemic inflammation: a case
series. JAMA Dermatol 2013;149:453-8.
30. Fleischmann RM, Schechtman J, Bennett R, Handel ML,
Burmester GR, Tesser J, et al. Anakinra, a recombinant
human interleukin-1 receptor antagonist (r-metHuIL-1ra), in
patients with rheumatoid arthritis: a large, international,
multicenter, placebo-controlled trial. Arthritis Rheum 2003;
48:927-34.
31. Lopez-Olivo MA, Tayar JH, Martinez-Lopez JA, Pollono EN,
Cueto JP, Gonzales-Crespo MR, et al. Risk of malignancies in

J AM ACAD DERMATOL
VOLUME 70, NUMBER 2Leslie et al 251
patients with rheumatoid arthritis treated with biologic ther-
apy: a meta-analysis. JAMA 2012;308:898-908.
32. Sims JE, Smith DE. The IL-1 family: regulators of immunity.
Nat Rev Immunol 2010;10:89-102.
33. Sims JE, March CJ, Cosman D, Widmer MB, MacDonald HR,
McMahan CJ, et al. cDNA expression cloning of the IL-1
receptor, a member of the immunoglobulin superfamily.
Science 1988;241:585-9.
34. Ben-Sasson SZ, Caucheteux S, Crank M, Hu-Li J, Paul WE. IL-1
acts on T cells to enhance the magnitude of in vivo immune
responses. Cytokine 2011;56:122-5.
35. Weber A, Wasiliew P, Kracht M. Interleukin-1 (IL-1) pathway.
Sci Signal 2010;3:cm1.
36. Vallabhapurapu S, Karin M. Regulation and function of
NF-kappaB transcription factors in the immune system.
Annu Rev Immunol 2009;27:693-733.