
An Elevated Level of Physical Activity Is Associated With Normal Lipoprotein(a) Levels in...
10
An Elevated Level of Physical Activity Is Associated With Normal Lipoprotein(a) Levels in Individuals From Maracaibo, Venezuela Valmore Bermu ´ dez, MD, MPH, PhD, 1 * Daniel Aparicio, BSc, 1 Edward Rojas, BSc, 1 Lianny Pen ˜ aranda, BSc, 1 Freddy Finol, BSc, 1 Luis Acosta, BSc, 1 Edgardo Mengual, MD, 1 Joselyn Rojas, MD, 1 Nailet Arra ´ iz, MSc, PhD, 1 Alexandra Toledo, BSc, 1 Carlos Colmenares, BSc, 1 Jesica Urribarı ´, BSc, 1 Wireynis Sanchez, BSc, 1 Carlos Pineda, BSc, 1 Dalia Rodriguez, BSc, 1 Judith Faria, BSc, 1 Roberto An ˜ ez, BSc, 1 Raquel Cano, MD, MgSc, 1 Clı ´maco Cano, PharmD, 1 Luis Sorell, PhD, 2 and Manuel Velasco, MD, FRCP Edin 3 Coronary artery disease is the main cause of death worldwide. Lipoprotein(a) [Lp(a)], is an independent risk factor for coronary artery disease in which concentrations are genetically regulated. Contradictory results have been published about physical activity influence on Lp(a) concentration. This research aimed to determine associations between different physical activity levels and Lp(a) concentration. A descriptive and cross-sectional study was made in 1340 randomly selected subjects (males = 598; females = 712) to whom a complete clinical history, the International Physical Activity Questionnaire, and Lp(a) level determination were made. Statistical analysis was carried out to assess qualitative variables relationship by x 2 and differences between means by one-way analysis of variance considering a P value ,0.05 as statistically significant. Results are shown as absolute frequencies, percentages, and mean 6 standard deviation according to case. Physical activity levels were ordinal classified as follows: low activity with 24.3% (n = 318), moderate activity with 35.0% (n = 458), and high physical activity with 40.8% (n = 534). Lp(a) concentration in the studied sample was 26.28 6 12.64 (IC: 25.59–26.96) mg/dL. Lp(a) con- centration according to low, moderate, and high physical activity levels were 29.22 6 13.74, 26.27 6 12.91, and 24.53 6 11.35 mg/dL, respectively, observing statistically significant differences between low and moderate level (P = 0.004) and low and high level (P , 0.001). A strong association (x 2 = 9.771; P = 0.002) was observed among a high physical activity level and a normal concentration of Lp(a) (less than 30 mg/dL). A lifestyle characterized by high physical activity is associated with normal Lp(a) levels. Keywords: physical activity, lipoprotein(a), lifestyle, cardiovascular risk INTRODUCTION Cardiovascular diseases constitute one of the main causes of death in the adult population worldwide, but it was not always like this. Less than three decades ago, prevention and control of conditions related to cardiovascular and cerebrovascular diseases were not the priority. In fact, they were considered industrialized countries diseases, often labeled the ‘‘Westernized lifestyle diseases’’ as a result of their distinct character- istics that were far from the usual traits seen in the developing countries. Today, they are a high-priority 1 Endocrine and Metabolic Diseases Research Center ‘‘Dr. Fe ´lix Go ´mez,’’ School of Medicine, University of Zulia, Maracaibo, Venezuela; 2 Angiology and Vascular Surgery Institute, Genetic Engineering and Biotechnology Center, La Habana, Cuba; and 3 Clinical Pharmacology Unit, Vargas Medical School, Central University of Venezuela, Caracas, Venezuela. This work was supported by research grant No. S1-2002000445 from the National Fund for Science, Technology and Innovation (FONACIT), Ministerio del Poder Popular para la Ciencia y la Tecnologı ´a, Repu ´blica Bolivariana de Venezuela. *Address for correspondence: The University of Zulia, Endocrine and Metabolic Diseases Research Center, 20th Avenue, Maracaibo, 4004, Venezuela. E-mail: [email protected]; [email protected] American Journal of Therapeutics 17, 341–350 (2010) 1075–2765 Ó 2010 Lippincott Williams & Wilkins www.americantherapeutics.com
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of An Elevated Level of Physical Activity Is Associated With Normal Lipoprotein(a) Levels in...
An Elevated Level of Physical Activity Is
Associated With Normal Lipoprotein(a) Levels in
Individuals From Maracaibo, Venezuela
Valmore Bermudez, MD, MPH, PhD,1* Daniel Aparicio, BSc,1 Edward Rojas, BSc,1
Lianny Penaranda, BSc,1 Freddy Finol, BSc,1 Luis Acosta, BSc,1
Edgardo Mengual, MD,1 Joselyn Rojas, MD,1 Nailet Arraiz, MSc, PhD,1
Alexandra Toledo, BSc,1 Carlos Colmenares, BSc,1 Jesica Urribarı, BSc,1
Wireynis Sanchez, BSc,1 Carlos Pineda, BSc,1 Dalia Rodriguez, BSc,1
Judith Faria, BSc,1 Roberto Anez, BSc,1 Raquel Cano, MD, MgSc,1
Clımaco Cano, PharmD,1 Luis Sorell, PhD,2 and Manuel Velasco, MD, FRCP Edin3
Coronary artery disease is the main cause of death worldwide. Lipoprotein(a) [Lp(a)], is an independentrisk factor for coronary artery disease in which concentrations are genetically regulated. Contradictoryresults have been published about physical activity influence on Lp(a) concentration. This research aimedto determine associations between different physical activity levels and Lp(a) concentration. A descriptiveand cross-sectional study was made in 1340 randomly selected subjects (males = 598; females = 712) towhom a complete clinical history, the International Physical Activity Questionnaire, and Lp(a) leveldetermination were made. Statistical analysis was carried out to assess qualitative variables relationshipby x2 and differences between means by one-way analysis of variance considering a P value ,0.05 asstatistically significant. Results are shown as absolute frequencies, percentages, and mean 6 standarddeviation according to case. Physical activity levels were ordinal classified as follows: low activity with24.3% (n = 318), moderate activity with 35.0% (n = 458), and high physical activity with 40.8% (n = 534).Lp(a) concentration in the studied sample was 26.28 6 12.64 (IC: 25.59–26.96) mg/dL. Lp(a) con-centration according to low, moderate, and high physical activity levels were 29.22 6 13.74, 26.27 6 12.91,and 24.53 6 11.35 mg/dL, respectively, observing statistically significant differences between low andmoderate level (P = 0.004) and low and high level (P , 0.001). A strong association (x2 = 9.771; P = 0.002)was observed among a high physical activity level and a normal concentration of Lp(a) (less than30 mg/dL). A lifestyle characterized by high physical activity is associated with normal Lp(a) levels.
Keywords: physical activity, lipoprotein(a), lifestyle, cardiovascular risk
INTRODUCTION
Cardiovascular diseases constitute one of the maincauses of death in the adult population worldwide, butit was not always like this. Less than three decades ago,prevention and control of conditions related tocardiovascular and cerebrovascular diseases were not
the priority. In fact, they were considered industrializedcountries diseases, often labeled the ‘‘Westernizedlifestyle diseases’’ as a result of their distinct character-
istics that were far from the usual traits seen in thedeveloping countries. Today, they are a high-priority
1Endocrine and Metabolic Diseases Research Center ‘‘Dr. FelixGomez,’’ School of Medicine, University of Zulia, Maracaibo,Venezuela; 2Angiology and Vascular Surgery Institute, GeneticEngineering and Biotechnology Center, La Habana, Cuba; and3Clinical Pharmacology Unit, Vargas Medical School, CentralUniversity of Venezuela, Caracas, Venezuela.This work was supported by research grant No. S1-2002000445from the National Fund for Science, Technology and Innovation(FONACIT), Ministerio del Poder Popular para la Ciencia y laTecnologıa, Republica Bolivariana de Venezuela.*Address for correspondence: The University of Zulia, Endocrine andMetabolic Diseases Research Center, 20th Avenue, Maracaibo, 4004,Venezuela. E-mail: [email protected]; [email protected]
American Journal of Therapeutics 17, 341–350 (2010)
1075–2765 � 2010 Lippincott Williams & Wilkins www.americantherapeutics.com
Valmore
Inserted Text
r

problem in the agenda of almost every country in theworld, including the developing countries. By 2001, thetotal death toll for nontransmissible diseases was up to32 millions, of which almost its half—16.7 million—were the result of cardiovascular diseases.1 Venezueladoes not escape this reality. According to the yearbookof mortality, by 2006, more than 28% of the diagnoseddeaths were the result of cardiovascular disease, withcardiac problems the first cause of death (20.63%) andcerebrovascular disease the fourth (7.76%).2
Traditionally, the main risk factors for coronaryartery disease are smoking habit, Westernized diet, andsedentary lifestyle, all of these expressed in a phenotypecharacterized by an unfavorable lipid profile, hyper-glycemia, elevated body mass index, and high bloodpressure. It has been argued that these factors explainat least 75% of the new cases of coronary disease.1,3
Today, new risk factors have emerged4 and havebeen identified and analyzed; such is the case of theunique lipoprotein(a) [Lp(a)]. Investigations show thathigh concentrations of this particle are associated withthree- or fourfold risk for myocardial infarction5,6 andischemic cerebrovascular disease,7–9 although somestudies have shown controversial results.10 Ability ofLp(a) to enhance cardiovascular risk is the result of itsatherogenic and pro-thrombotic properties,11 as a resultof its similarity to the low-density lipoprotein particleand structural homology to plasminogen, but lackingits fibrinolytic activity.
It is worth commenting that there is no consensusdefining the cutoff values of Lp(a), but commonlya value of 30 mg/dL or greater has been used. Yet,many authors believe that levels above 25 mg/dL areimportant predictors of cardiovascular risk; yet evensome consider accepting a 20-mg/dL level as a high-risk cutoff point.12
A sedentary lifestyle constitutes an independent andmodifiable risk factor for cardiovascular disease. Thereis not a clear definition on what a sedentary lifestyle isor what an active lifestyle is. Some authors definea sedentary person as one who invests a low amount ofminutes during the day for activities during their freetime,18 activity that would actually consume 4 metabolicequivalent tasks (METs), with minimal time activity forexecution, which has been established as 25 minutes forwomen and 30 minutes for men. Other authors define itas someone who invests less than 10% of their dailyenergy consumption doing physical activity that requires4 or more METs (any physical activity equivalent or supe-rior to walking fast). A MET is the energy consumption ofan individual at rest, which is approximately 1 kcal/kg/hour, meaning, 4.184 kJ/kg/hour.14 This concept hasbeen useful in the measurement of physical activity level,making it accepted and applied worldwide.
Meanwhile, the benefits of physical activity havebeen extensively documented.14 Various studies showthat regular physical activity lowers fasting andpostprandial glycemia and insulin resistance,15,16 bodymass index,17 and elevated blood pressure.18 Likewise,it positively influences parameters in the lipid profile,like elevating high-density lipoproteins, lowering low-density lipoprotein cholesterol, and triglycerides.19
Although the beneficial effects of exercise in thecardiovascular area have been widely documented, therelationship between physical activity and Lp(a)concentration has not been well studied. Thus, thepurpose of this study was to determine the associationbetween Lp(a) and physical patterns in individualsfrom an urban population from Venezuela.
MATERIALS AND METHODS
Study design
A cross-sectional and comparative study was made in1310 adult individuals, 712 females (54.4%) and 598males (45.6%), randomly selected from MaracaiboDistrict, Zulia State, Venezuela, during the periodAugust 2007 to March 2009 to whom previousinformed written consent, a complete medical historywas made, and the Long Form of the InternationalPhysical Activity Questionnaire (IPAQ) was applied.After 8 to 12 hours of fasting, all patients underwentvenous blood sampling to determine Lp(a) concentra-tion. This work is part of a large cross-sectional studyconducted by our center, ‘‘The Maracaibo CityMetabolic Syndrome Study.’’
According to the 2001 Venezuelan population census,the population of Maracaibo District was of 1,219,927habitants20 with a 2007 estimate of 1,428,043 people.Likewise, 59.7% of the population will be made ofindividuals older than 18 years of age. To take thesedata as accurate, the size needed for the requiredpopulation sample for a confidence level of 99% anda fixed error limit of 3.5% is 1399 individuals with ages18 years old or older.
Statistical analysis
Statistical analysis was done using Statistical Packagefor the Social Sciences for Windows, Version 15.0 (SPSSInc., Chicago, IL). Normal distribution of the quantita-tive variables was assessed by the Geary test. To establishthe association between physical activity as an ordinalvariable and the presence or not of high levels of Lp(a),Pearson’s x2 test was used. To find significant differencesbetween means of quantitative variables, grouped accord-ing to physical activity categories, one-way analysis of
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
342 Bermudez et al

variance was used (With Tukeys post hoc test),considering significant values of P , 0.05. The resultswere expressed as absolute and relative frequencies andmean 6 standard deviation according to the case.
Determination of lipoprotein (a)
After centrifugation for 10 minutes at 4000 rpm, serumwas obtained from the blood sample taken from eachpatient. Lp(a) concentration was determined using theturbidimetric latex test method (Human Gesellschaftfur Biochemica und Diagnostica mbH, Wiesbaden,Germany).21 In this method, the sample inducesagglutination of latex particles coated with anti-Lp(a)antibodies. The agglutination is proportional to thelevels of Lp(a) and can be measured by turbidimetry.
Classification of physical activity levels
Categorization of physical activity was made accord-ing to the IPAQ Research Committee,22 classifying itinto three levels: 1) low—no activity is reported orsome activity is reported but not enough to meetcategories 2 or 3; 2) moderate—either of the followingthree criteria: a) 3 or more days of vigorous-intensityactivity of at least 20 minutes per day or b) 5 or moredays of moderate-intensity activity and/or walking ofat least 30 minutes per day or c) 5 or more days of anycombination of walking, moderate-intensity or vigor-ous-intensity activities achieving a minimum of at least600 MET-minutes/week; 2) high—any one of thefollowing two criteria: a) vigorous-intensity activityon at least 3 days and accumulating at least 1500 MET-minutes/week or b) 7 or more days of any combinationof walking, moderate- or vigorous-intensity activitiesaccumulating at least 3000 MET-minutes/week.
RESULTS
Study sample composition
A total of 1310 individuals from both sexes, 712 females(54.4%) and 598 males (45.6%), met all criterionnecessary to be included in this study. Mean age was39.42 6 15.82 years and body mass index arithmeticmean was 28.24 6 6.55 kg/m2.
Maracaibo is a multiethnic population The samplewas mainly constituted by persons of Venezuelan–mixed race (n = 980 [74.8%]), Hispanic white people(n = 244 [18.6%]), African–Venezuelan (n = 41 [3.1%]),Venezuelan Indians (Wayuu ethnicity) (n = 33 [2.5%]),Asian population (n = 4 [0.3%]), among others.
The socioeconomic status distribution according toGraffar scale (modified by Mendez-Castellano) wasstructured as follows: upper class: n = 24 (1.8%), high-middle class: n = 277 (21.1%), middle class: n = 461
(35.2%), low class: n = 468 (35.7%), and lower class orextreme poverty: n = 48 (3.7%).
Lipoprotein (a) behavior according to physicalactivity intensity
Lp(a) distribution in our population was near tonormal according to histogram, Q-Q graphics, andthe normality Gaerys test. Lp(a) concentration for thetotal population examined was 26.28 6 12.64 mg/dL(IC: 25.59–26.96). There were no significant differencesin Lp(a) levels between both sexes; females with26.54 6 12.56 mg/dL (IC: 25.63–27.44) versus maleswith 25.97 6 24.80 mg/dL (IC: 24.92–27.02).
According to the IPAQ analysis, 24.3% of the samplehad low physical activity (n = 318), 35.0% had mod-erate physical activity (n = 458), and 40.8% exhibitedhigh physical activity (n = 534). When comparing METscalculated by IPAQ for low (448.72 6 860.38; IC:353.79–543.64), moderate (1541.39 6 933.45; IC: 1455.67–1627.10), and high (8640.52 6 6733.34; IC: 8068.13–9212.92) physical activity levels, significant differenceswere found among all groups: low vs moderate (P =0.002); low vs high (P , 0.001) and finally, moderate vshigh (P , 0.001).
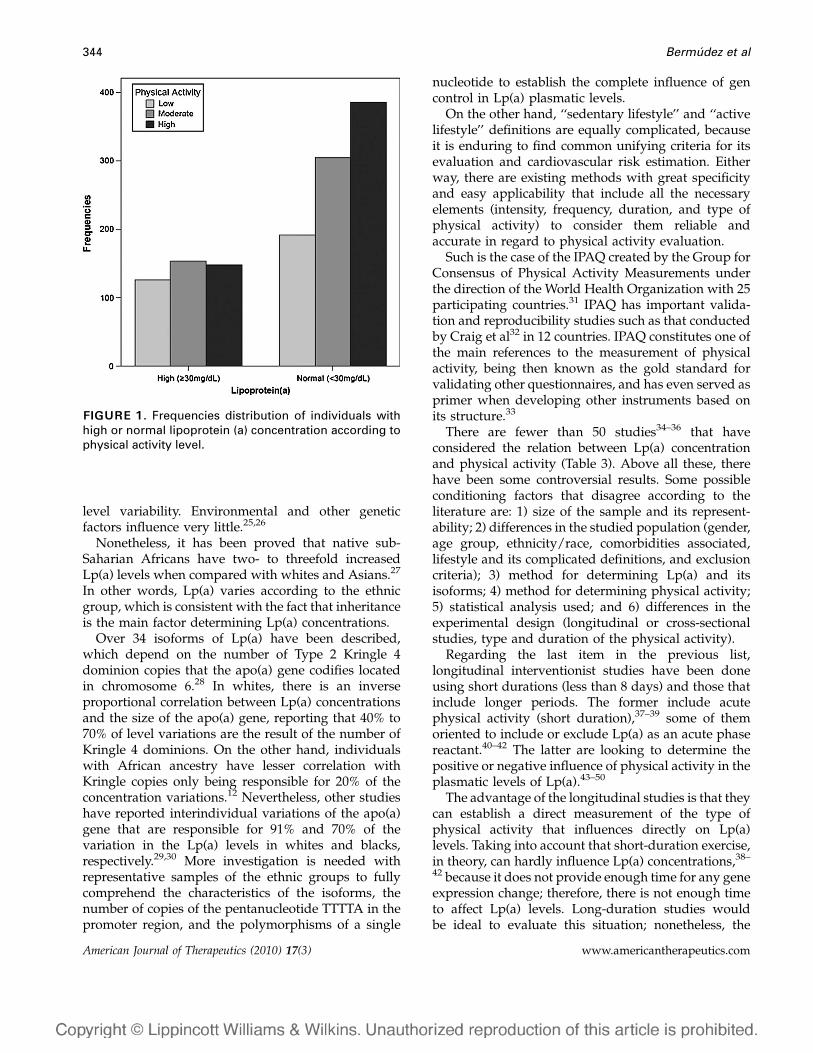
Individuals with high (30 mg/dL or greater) ornormal Lp(a) levels (less than 30 mg/dL) were groupedaccording to their physical activity intensity and thenclassified according to physical activity intensity(Fig. 1), showing a greater number of patients withnormal Lp(a) levels and high physical activity whencompared with Lp(a) levels in individuals with normaland low physical activity with a significant differenceas evidenced in Table 1. Moreover, the associationbetween the presence or not of high Lp(a) levelsaccording physical activity categories through Pear-son’s x
2 test was strong and statistically significant (x2
= 13.073, P = 0.001) indicating that those with a highlevel of physical activity do not show a high Lp(a) level.The mean Lp(a) plasma concentration for each physicalactivity level (low, moderate, and high) was 29.22 6
13.74, 26.27 6 12.91, and 24.53 6 11.35 mg/dL,respectively, evidencing significant differences whencomparing these values (P , 0.05; Fig. 2; Table 2).
DISCUSSION
It is widely accepted that Lp(a) concentration is geneti-cally regulated in 90%, at least in whites.23 Maybeapproximately 40% of this variability is the result ofquantitative polymorphisms in the internal sequence ofthe Apo (a) structural gene and other polymorphismsin the promoter site account for other 10% to 14%24
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Physical Activity and Lipoprotein(a) Levels 343
level variability. Environmental and other geneticfactors influence very little.25,26
Nonetheless, it has been proved that native sub-Saharian Africans have two- to threefold increasedLp(a) levels when compared with whites and Asians.27
In other words, Lp(a) varies according to the ethnicgroup, which is consistent with the fact that inheritanceis the main factor determining Lp(a) concentrations.
Over 34 isoforms of Lp(a) have been described,which depend on the number of Type 2 Kringle 4dominion copies that the apo(a) gene codifies locatedin chromosome 6.28 In whites, there is an inverseproportional correlation between Lp(a) concentrationsand the size of the apo(a) gene, reporting that 40% to70% of level variations are the result of the number ofKringle 4 dominions. On the other hand, individualswith African ancestry have lesser correlation withKringle copies only being responsible for 20% of theconcentration variations.12 Nevertheless, other studieshave reported interindividual variations of the apo(a)gene that are responsible for 91% and 70% of thevariation in the Lp(a) levels in whites and blacks,respectively.29,30 More investigation is needed withrepresentative samples of the ethnic groups to fullycomprehend the characteristics of the isoforms, thenumber of copies of the pentanucleotide TTTTA in thepromoter region, and the polymorphisms of a single
nucleotide to establish the complete influence of gencontrol in Lp(a) plasmatic levels.
On the other hand, ‘‘sedentary lifestyle’’ and ‘‘activelifestyle’’ definitions are equally complicated, becauseit is enduring to find common unifying criteria for itsevaluation and cardiovascular risk estimation. Eitherway, there are existing methods with great specificityand easy applicability that include all the necessaryelements (intensity, frequency, duration, and type ofphysical activity) to consider them reliable andaccurate in regard to physical activity evaluation.
Such is the case of the IPAQ created by the Group forConsensus of Physical Activity Measurements underthe direction of the World Health Organization with 25participating countries.31 IPAQ has important valida-tion and reproducibility studies such as that conductedby Craig et al32 in 12 countries. IPAQ constitutes one ofthe main references to the measurement of physicalactivity, being then known as the gold standard forvalidating other questionnaires, and has even served asprimer when developing other instruments based onits structure.33
There are fewer than 50 studies34–36 that haveconsidered the relation between Lp(a) concentrationand physical activity (Table 3). Above all these, therehave been some controversial results. Some possibleconditioning factors that disagree according to theliterature are: 1) size of the sample and its represent-ability; 2) differences in the studied population (gender,age group, ethnicity/race, comorbidities associated,lifestyle and its complicated definitions, and exclusioncriteria); 3) method for determining Lp(a) and itsisoforms; 4) method for determining physical activity;5) statistical analysis used; and 6) differences in theexperimental design (longitudinal or cross-sectionalstudies, type and duration of the physical activity).
Regarding the last item in the previous list,longitudinal interventionist studies have been doneusing short durations (less than 8 days) and those thatinclude longer periods. The former include acutephysical activity (short duration),37–39 some of themoriented to include or exclude Lp(a) as an acute phasereactant.40–42 The latter are looking to determine thepositive or negative influence of physical activity in theplasmatic levels of Lp(a).43–50
The advantage of the longitudinal studies is that theycan establish a direct measurement of the type ofphysical activity that influences directly on Lp(a)levels. Taking into account that short-duration exercise,in theory, can hardly influence Lp(a) concentrations,38–
42 because it does not provide enough time for any geneexpression change; therefore, there is not enough timeto affect Lp(a) levels. Long-duration studies wouldbe ideal to evaluate this situation; nonetheless, the
FIGURE 1. Frequencies distribution of individuals withhigh or normal lipoprotein (a) concentration according tophysical activity level.
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
344 Bermudez et al
Table
1.
Ass
oci
ati
on
be
twe
en
lip
op
rote
in(a
)[L
p(a
)]le
ve
lsa
nd
ph
ysi
cal
act
ivit
yp
att
ern
s.
Hig
hL
p(a
)(3
0m
g/d
Lo
rg
rea
ter)
Ph
ysi
cal
act
ivit
y
Lo
wM
od
era
te
Me
nW
om
en
To
tal
Me
nW
om
en
To
tal
n%
n%
n%
n%
n%
n%
Ye
s5
93
9.3
67
39
.91
26
39
.66
93
48
43
2,9
15
33
3,4
No
91
60
.71
01
60
.11
92
60
.41
34
66
17
16
7,1
30
56
6,6
To
tal
15
01
00
16
81
00
31
81
00
20
31
00
25
51
00
45
81
00
x2
(Pv
alu
e)
4.1
20
(0.0
42
)5
.32
9(0
.02
1)
9.4
39
(0.0
02
)0
.26
7(0
.60
5)
(0.0
23
)(0
.87
9)
(0.2
11
)(0
.64
6)
Od
ds
rati
o(C
l)1
.3(1
.01
–1.7
7)
1.3
72
(1.0
5–1
.79
)1
.3(1
.1–.
15
)1
.06
4(0
.84
2–1
.34
)1
.01
6(0
.82
–1.2
5)
1.0
1(0
.8–1
.25
)x
2(P
va
lue
)1
3.0
73
(0.0
01
)
Hig
hL
p(a
)(3
0m
g/d
Lo
rg
rea
ter)
Ph
ysi
cal
act
ivit
y
Hig
h
Me
nW
om
en
To
tal
n%
n%
n%
Ye
s6
72
7,3
81
28
14
82
7,7
No
17
87
2,7
20
87
23
86
72
,3T
ota
l2
45
10
02
89
10
05
34
10
0x
2(P
va
lue
)5
.22
9(0
.02
2)
4,5
98
(0,0
32
)9
,77
1(0
,00
2)
Od
ds
rati
o(C
l)0
.77
8(0
.62
–0.9
7)
0,8
06
(0,6
5–0
,98
)0
.7(0
,6–0
,9)
x2
(Pv
alu
e)
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Physical Activity and Lipoprotein(a) Levels 345

majority do not last over 3 months43,45,47 to evaluatea possible genetic regulation, and the very few that dolast over 3 months usually have a population samplethat is either too small or nonrepresentative.46,49,50
Cross-sectional studies can be divided into twogroups: one that compares the lifestyle of a certaingroup that has a vast physical activity (sportsmanship)versus sedentary individuals.51–54 Others take a ran-dom population, to which physical activity question-naires are applied to really get to know their lifestylesand categorize them into levels, evaluating Lp(a)concentrations.55–60
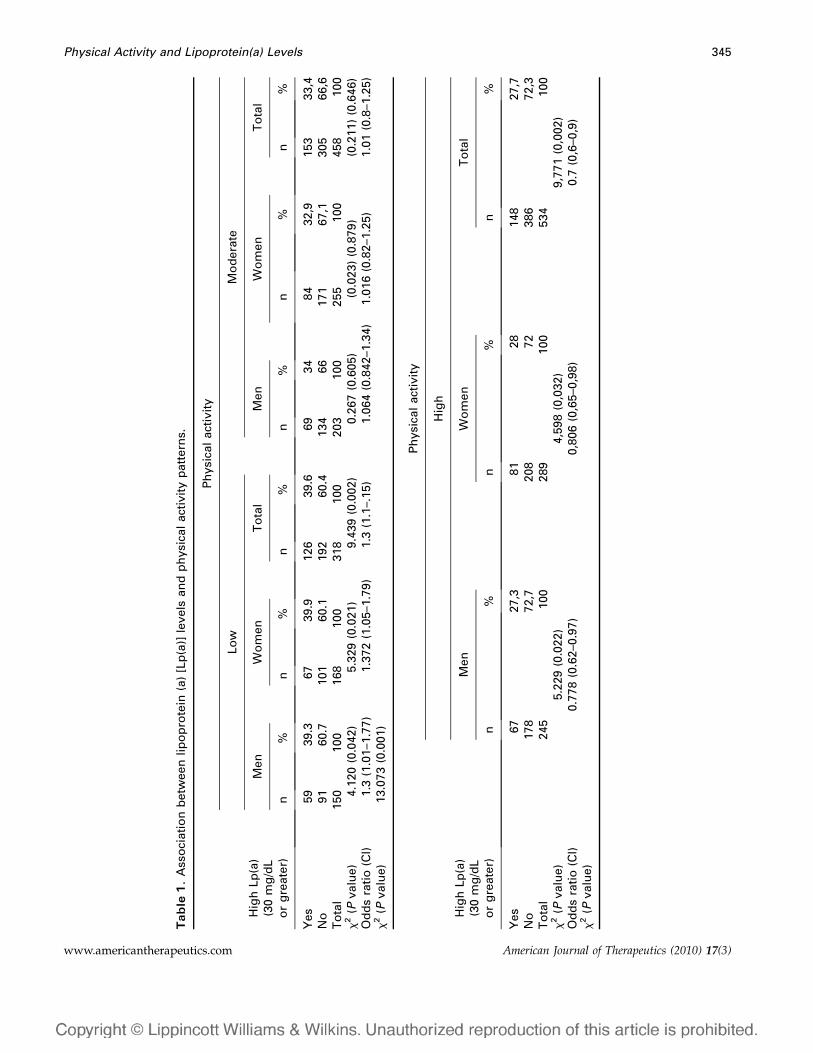
Our study shows an association between high Lp(a)concentrations (30 mg/dL or greater) and the threecategories for physical activity (x2 = 13.073; P = 0.001)with the main conclusion that people with high
physical activity do not show elevated concentrationsof Lp(a). When evaluating this finding, there was astrong association between high physical activity andLp(a) levels below 30 mg/dL (x2 = 9.771; P = 0.002), butthere is no association with moderate physical activity(x2 = 0.211; P = 0.646). In the same manner, those whodo not have a low physical activity level have Lp(a)levels below 30 mg/dL (x2 = 9.439; P = 0.002). Theserelations were maintained in the presence of high orlow Lp(a) concentrations at each physical activity levelaccording to gender (Table 1), which concurs withhaving found no difference between Lp(a) concen-trations in both genders.
Additionally, Figure 2 shows the significant differ-ences between Lp(a) levels from all the individuals forlow physical activity comparing it with those withmoderate (P = 0.004; IC: 0.80–5.09) and high (P , 0.001;IC: 2.60–6.76) physical activity, but not betweenmoderate and high (P = 0.076; IC: –0.13–3.60) physicalactivity.
As mentioned before, there are some discrepanciesconcerning the influence of physical activity on Lp(a)levels. One of the oldest studies reported a loweringeffect on Lp(a) with acute physical activity, meaning,8 days of daily cross- country skiing –12 to 25 km ina cold weather and dramatic dietary alterations.44
These conclusions contrast with other studies, whichhave found no evidence of this influence39–42; one inparticular was done by Durstine et al38 who argue thatin the cross country skiing study, plasmatic volumechange, cold exposure, and weight lost have to be takeninto account. It also shows the deficiency of plasmaticvolume determination in studies related to raisingLp(a) values after some exercises like that done byrunners, because the plasmatic volume can changeover 10% during the exercise and days after.
Table 2. Lipoprotein (a) [Lp(a)] concentration according to physical activity patterns and gender
Physical activity
Low Moderate
Men Women Both Men Women Both
Lp(a) 29.48 6 13.69 28.98 6 13.81 29.22 6 13.74 25.94 6 13.60 26.53 6 12.36 26.27 6 12.91Cl 27.27–31.69 26.88–31.09 27.70–30.73 24.05–27.82 25.01–28.06 25.08–27.45
Physical activity
High
Men Women Both
Lp(a) 23.84 6 11.77 25.12 6 10.98 24.53 6 11.35Cl 22.36–25.32 23.85–26.39 23.57–25.50
FIGURE 2. Lipoprotein (a) concentration according physicalactivity level.
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
346 Bermudez et al
Set on to evaluate the influence of physical activityon Lp(a) levels, Ponjee et al49,50 subjected 36 sedentaryindividuals to a training regimen of three to four timesa week for 9 months, in which after 24 weeks, subjectsran a 15-km race and after 36 weeks a 21-km marathon.Their conclusions were that an exercise program thatincludes running marathons to longer distancesincreases Lp(a) concentrations. Contributing to thisdebate, Cardoso et al59 suggested that the elevation ofLp(a) in high-exercise athletes can represent a normalmetabolic response to small repetitive lesions in tissuesproduced by massive muscle movement in prolongedand frequent periods.
On the other hand, Austin et al37 evaluated patientswith Type 1 diabetes and showed an inverse relation-ship between Lp(a) and lipid profile with the use of thestatic bicycle with a standard ergonometer, pointingout that physical activity is a beneficial tool incontrolling these patients. Another study furtherconfirms positive influence of physical activity inpatients with Type 1 and Type 2 diabetes.48
Cross-sectional studies also have published contro-versial results. Comparing 57 endurance runners and62 control subjects showed no significant differences,54
which concurs with previous studies that have failed torecognize any difference using cardiorespiratory
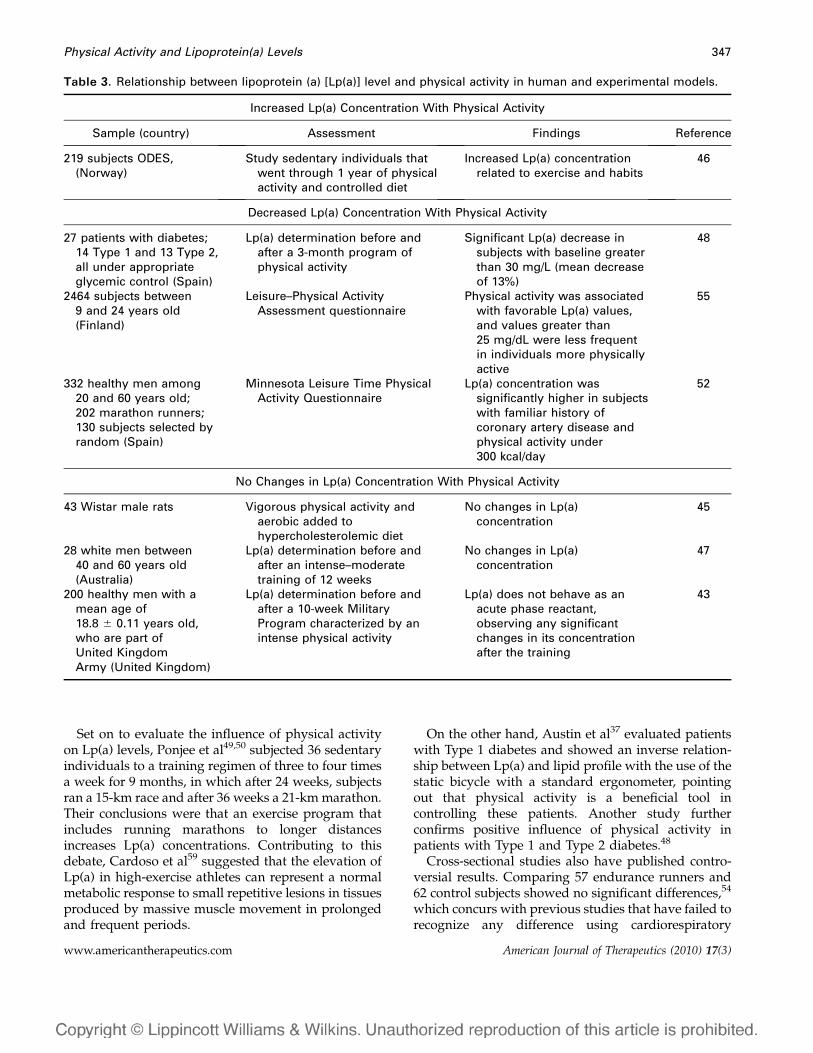
Table 3. Relationship between lipoprotein (a) [Lp(a)] level and physical activity in human and experimental models.
Increased Lp(a) Concentration With Physical Activity
Sample (country) Assessment Findings Reference
219 subjects ODES,(Norway)
Study sedentary individuals thatwent through 1 year of physicalactivity and controlled diet
Increased Lp(a) concentrationrelated to exercise and habits
46
Decreased Lp(a) Concentration With Physical Activity
27 patients with diabetes;14 Type 1 and 13 Type 2,all under appropriateglycemic control (Spain)
Lp(a) determination before andafter a 3-month program ofphysical activity
Significant Lp(a) decrease insubjects with baseline greaterthan 30 mg/L (mean decreaseof 13%)
48
2464 subjects between9 and 24 years old(Finland)
Leisure–Physical ActivityAssessment questionnaire
Physical activity was associatedwith favorable Lp(a) values,and values greater than25 mg/dL were less frequentin individuals more physicallyactive
55
332 healthy men among20 and 60 years old;202 marathon runners;130 subjects selected byrandom (Spain)
Minnesota Leisure Time PhysicalActivity Questionnaire
Lp(a) concentration wassignificantly higher in subjectswith familiar history ofcoronary artery disease andphysical activity under300 kcal/day
52
No Changes in Lp(a) Concentration With Physical Activity
43 Wistar male rats Vigorous physical activity andaerobic added tohypercholesterolemic diet
No changes in Lp(a)concentration
45
28 white men between40 and 60 years old(Australia)
Lp(a) determination before andafter an intense–moderatetraining of 12 weeks
No changes in Lp(a)concentration
47
200 healthy men with amean age of18.8 6 0.11 years old,who are part ofUnited KingdomArmy (United Kingdom)
Lp(a) determination before andafter a 10-week MilitaryProgram characterized by anintense physical activity
Lp(a) does not behave as anacute phase reactant,observing any significantchanges in its concentrationafter the training
43
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Physical Activity and Lipoprotein(a) Levels 347

fitness.57,60 A study using a sample of 1600 Irish peoplesuggested that the increment of physical activityproduced small changes in Lp(a) concentrations.56
It is proper to emphasize the lack of definition ofsedentary lifestyle that is used in some studies.Meanwhile, other studies have used questionnairesand/or classifications for physical activity that weremade by the investigating team and not approvedtools. There are existing limitations in these kinds ofquestionnaires; one of the frequent fouls found is notmeasuring the leisure time and daily work56 that couldeven place a person considered as sedentary in a highercategory of physical activity.
On the contrary, our results show a clear relationshipbetween physical activity level and Lp(a) concentra-tion. A previous study showed similar results, Taimelaet al55 did a multicentric study in 2464 children,adolescents, and young adults between 9 and 24 yearsof age evaluating the risk factors for cardiovasculardisease. They concluded that physically active indi-viduals seldom had Lp(a) levels above 25 mg/dLwithout any relation with age, gender, or othercardiovascular risk factor.
Our study overcomes the usual obstacles to extrap-olate results, because of its size and representativepopulation of Maracaibo. The results concur for bothgenders, application of measurement questionnaire ofphysical activity—internationally validated—and, us-ing appropriate statistical analysis, bearing significantresults.
Nevertheless, this research presents some interestinglimitations. The cross-sectional design of this workcannot corroborate if a determined exercise done ina specific way for a given amount of time is capable ofreducing Lp(a) concentrations. Either way, IPAQevaluated daily activities (exercise at work, trans-portation method, leisure time, domestic life, andgardening), which sheds some light to the type oflifestyle, beyond the programmed activities scheduledfor a brief period of time. It is also recognized thatisoforms of Lp(a) nor its different polymorphisms wereundetermined, being unable, hypothetically, to relatedto the level of physical activity with the diminishmentof certain specific isoforms and not others. Likewise,the lowering effect of physical activity on Lp(a) levelscan influence only the concentration of a specificpolymorphism.
CONCLUSIONS
Our study shows that a lifestyle characterized by highphysical activity is associated with Lp(a) concentra-tions below 30 mg/dL in an urban Venezuelan–mixed
population. This relationship is reinforced by thefinding that significantly lower Lp(a) concentrationsare found in individuals with moderate to highphysical activity compared with those with lowphysical activity.
REFERENCES
1. Beaglehole R, Irwin A, Prentice T. The World Health Report:2003: Shaping the Future. Geneva: World Health Organi-
zation; 2003.2. Ministry of Popular Power For Health. Mortality statis-
tics 2006. General Direction of Epidemiology. Caracas,
Venezuela: Information and Health Statistics Direction;
2007.3. Magnus P, Beaglehole R. The real contribution of the
major risk factors to the coronary epidemics: time to end
the �only–50%� myth. Arch Intern Med. 2001;161:2657–
2660.4. Harjai KJ. Potential new cardiovascular risk factors: left
ventricular hypertrophy, homocysteine, lipoprotein(a),
triglycerides, oxidative stress, and fibrinogen. Ann InternMed. 1999;131:376–386.
5. Kamstrup PR, Benn M, Tybjærg-Hansen A, et al. Extreme
lipoprotein(a) levels and risk of myocardial infarction in
the general population: the Copenhagen City Heart
Study. Circulation. 2008;117:176–184.6. Jones GT, van Rij AM, Cole J, et al. Plasma lipoprotein(a)
indicates risk for 4 distinct forms of vascular disease. ClinChem. 2007;53:679–685.
7. Jurgens G, Taddei-Peters WC, Koltringer P, et al. Lipopro-
tein(a) serum concentration and apolipoprotein(a) phe-
notype correlate with severity and presence of ischemic
cerebrovascular disease. Stroke. 1995;26:1841–1848.8. Ariyo AA, Thach Ch, Tracy R. Lp(a) lipoprotein, vascular
disease, and mortality in the elderly. N Engl J Med. 2003;
349:2108–2115.9. Smolders B, Lemmens R, Thijs V. Lipoprotein(a) and
stroke: a meta-analysis of observational studies. Stroke.
2007;38:1959–1966.10. Ridker PM, Stampfer MJ, Hennekens CH. Plasma
concentration of lipoprotein(a) and the risk of future
stroke. JAMA. 1995;273:1269–1273.11. Bermudez V, Arraiz N, Cano C, et al. Lipoprotein(a):
molecular and epidemiologic basis about its role in
cardiovascular diseases. Revista Latinoamericana de Hiper-tension. 2008;3:113–122.
12. Enas EA, Chacko V, Senthilkumar A, et al. Elevated
lipoprotein(a)—a genetic risk factor for premature vas-
cular disease in people with and without standard risk
factors: a review. Dis Mon. 2006;52:5–50.13. Cabrera de Leona A, Rodrıguez-Perez MC, Rodrıguez-
Benjumedab LM, et al. Sedentary Lifestyle: physical
activity duration versus percentage of energy expendi-
ture. Rev Esp Cardiol. 2007;60:244–250.
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
348 Bermudez et al

14. Lakka TA, Laaksonen DE. Physical activity in preventionand treatment of the metabolic syndrome. Appl PhysiolNutr Metab. 2007;32:76–88.
15. Healy GN, Shaw JE, Dunstan DW, et al. Objectivelymeasured light-intensity physical activity is indepen-dently associated with 2-h plasma glucose. Diabetes Care.2007;30:1384–1389.
16. LaMonte MJ, Blair SN, Church TS. Role of exercise inreducing the risk of diabetes and obesity: physical activityand diabetes prevention. J Appl Physiol. 2005;99:1205–1213.
17. Mora S, Lee IM, Buring JE, et al. Association of physicalactivity and body mass index with novel and traditionalcardiovascular biomarkers in women. JAMA 2006;295:1412–1419.
18. Chobanian AV, Bakris GL, Black HR, et al; National HighBlood Pressure Education Program Coordinating Com-mittee. Seventh Report of the Joint National Committeeon Prevention, Detection, Evaluation, and Treatment ofHigh Blood Pressure. Hypertension. 2003;42:1206–1252.
19. Skoumas J, Pitsavos C, Panagiotakos DB, et al. Physicalactivity, high density lipoprotein cholesterol and otherlipids levels, in men and women from the ATTICA study.Lipids in Health and Disease. 2003;2:1–7.
20. Health Statistic Report of Zulia State 2003. Table 9. Maincauses of death according to gender, rates and percentage.Zulia State: Maracaibo Municipality; 2003.
21. Human Gesellschaft fur Biochemica und DiagnosticambH, Alemania. Latex enhanced immunoturbidimetrictest. Available at: www.bganalizadores.com.ar/insertos_productos/inserto288.pdf. Accessed May 3, 2009.
22. IPAQ Research Committee. Guidelines for the dataprocessing and analysis of the International PhysicalActivity Questionnaire 2005. Available at: www.ipaq.ki.se. Accessed May 3, 2009.
23. Boerwinkle E, Leffert CC, Lin J, et al. Apolipoprotein(a)gene accounts for greater than 90% of the variationin plasma lipoprotein(a) concentrations. J Clin Invest.1992;90:52–60.
24. Lippi G, Guidi G. Lipoprotein(a): from ancestral benefit tomodern pathogen? Q J Med. 2000;93:75–84.
25. Sorell L, Bermudez F, Bermudez V, et al. Lipoprotein(A):From a novel antigen to a cardiovascular diseasepredictor. Revista Latinoamericana de Hipertension. 2007;2:165–178.
26. Sentı M, Pedro-Botet J, Rubies-Prat J, et al. Influenceof apolipoprotein(a) genetic polymorphism on serumlipoprotein(a) concentration in patients with ischemiccerebrovascular disease. Cerebrovasc Dis. 1994;4:298–303.
27. Bermudez V, Arraiz N, Rojas E, et al. Abnormally highlipoprotein(a) leves in African-American communitiesfrom Venezuela faced to other African-descendingpopulations: are ethnic origins related? Revista Latin-oamericana de Hipertension. 2008;3:66–72.
28. Kamstrup PR, Tybjærg-Hansen A, Steffensen R, et al.Apolipoprotein(a) pentanucleotide repeat polymor-phism, lipoprotein(a) levels and risk of ischemic heartdisease. J Clin Endocrinol Metab. 2008;93:3769–3776.
29. Chretien JP, Coresh J, Berthier-Schaad Y, et al. Threesingle-nucleotide polymorphisms in LPA account formost of the increase in lipoprotein(a) level elevation inAfrican Americans compared with European Americans.J Med Genet. 2006;43:917–923.
30. Mooser V, Scheer D, Marcovina SM, et al. The Apo(a)gene is the major determinant of variation in plasmaLp(a) levels in African Americans. Am J Hum Genet. 1997;61:402–417.
31. Dartagnan P, Correa C, Ribeiro J. Reproducibility andvalidity of the International Physical Activity Questionnairein adolescents. Rev Bras Med Esporte. 2005;11:147e–154e.
32. Craig C, Marshall A, Sjostrom M, et al. InternationalPhysical Activity Questionnaire: 12-country reliabilityand validity. Med Sci Sports Exerc. 2003;35:1381–1395.
33. Arvidsson D, Slinde F, Hulthen L. Physical activityquestionnaire for adolescents validated against doublylabelled water. Eur J Clin Nutr. 2005;59:376–383.
34. Mackinnon LT, Hubinger LM. Effects of exercise onlipoprotein(a). Sports Med. 1999;28:11–24.
35. Mackinnon LT, Hubinger LM, Frank L. Effects of physicalactivity and diet on lipoprotein(a). Med Sci Sports Exerc.1997;29:1429–1436.
36. Seixas-Prado E, Martin-Dantas EH. Effects of aerobicphysical exercises and force in lipoproteins HDL, LDLand Lipoprotein(A). Arq Bras Cardiol. 2002;79:429–433.
37. Austin A, Warty V, Janosky J, Arslanian S. The relation-ship of physical fitness to lipid and lipoprotein(a) levels inadolescents with IDDM. Diabetes Care. 1993;16:421–425.
38. Durstine JL, Ferguson MA, Szymanski LM, et al. Effect ofa single session of exercise on lipoprotein(a). Med SciSports Exerc. 1996;28:1277–1281.
39. Szymanski LM, Durstine JL, Davis PG, et al. Factorsaffecting fibrinolytic potential: cardiovascular fitness,body composition, and lipoprotein(a). Metabolism. 1996;45:1427–1433.
40. Durstine JL, Davis PG, Ferguson MA, et al. Effects ofshort-duration and long-duration exercise on lipoprotei-n(a). Med Sci Sports Exerc. 2001;33:1511–1516.
41. Hubinger L, Mackinnon LT, Lee B, et al. Acute effects oftreadmill running on lipoprotein(a) levels in males andfemales. Med Sci Sports Exerc. 1997;29:436–442.
42. Gruden G, Olivetti C, Taliano C, et al. Lipoprotein(a) afteracute exercise in healthy subjects. lnt J Clin Lab Res. 1996;26:140–141.
43. Byrne DJ, Jagroop IA, Montgomery HE, et al. Lipoprotein(a) does not participate in the early acute phase responseto training or extreme physical activity and is unlikely toenhance any associated immediate cardiovascular risk.J Clin Pathol. 2002;55:280–285.
44. Hellsten G, Boman K, Hallmans G, et al. Lipids andendurance physical activity. Atherosclerosis. 1989;75:93–94.
45. Dantas R, Seixas E, Almeida L, et al. Lipoprotein(A) andbody mass in mice which were submitted to hypercho-lesterolemia and strength and aerobic physical trainings.Fit Perf J. 2008;7:137–144.
46. Holmes I, Urdalb P, Anderssenc S, et al. Exercise-inducedincrease in lipoprotein(a). Atherosclerosis. 1996;122:97–104.
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Physical Activity and Lipoprotein(a) Levels 349

47. Hubinger L, Mackinnon LT. The effect of endurancetraining on lipoprotein(a) [Lp(a)] levels in middle-agedmales. Med Sci Sports Exerc. 1996;28:757–764.
48. Rigla M, Sanchez-Quesada JL, Ordonez-Llanos J, et al.Effect of physical exercise on lipoprotein(a) and low-density lipoprotein modifications in type 1 and type 2diabetic patients. Metabolism. 2000;49:640–647.
49. Ponjee GA, Janssen EM, van Wersch JW. Long-termphysical exercise and lipoprotein(a) levels in a previouslysedentary male and female population. Ann Clin Biochem.1995;32:181–185.
50. Ponjee GA, Janssen EM, Hermans J, et al. Regularphysical activity and changes in risk factors for coronaryheart disease: a nine months prospective study. Eur J ClinChem Clin Biochem. 1996;34:477–483.
51. Halle M, Berg A, Von-Stein T, et al. Lipoprotein(a) inendurance athletes, power athletes, and sedentary con-trols. Med Sci Sports Exerc. 1996;28:962–966.
52. Martin S, Elosua R, Covas MI, et al. Relationship of lipo-protein(a) levels to physical activity and family historyof coronary heart disease. Am J Public Health. 1999;83:383–385.
53. Thomas TR, Ziogas G, Harris WS. Influence of fitnessstatus on very-low-density lipoprotein subfractions andlipoprotein(a) in men and women. Metabolism Clinical andExperimental. 1997;46:1178–1183.
54. Hubinger L, Mackinnon LT, Lepre F. Lipoprotein(a)[Lp(a)] levels in middle-aged male runners and sedentarycontrols. Med Sci Sports Exerc. 1995;27:490–496.
55. Taimela S, Viikari JSA, Porkka KVK, et al. Lipoprotein (a)levels in children and young adults: the influence ofphysical activity. The Cardiovascular Risk in Young FinnsStudy. Acta Paediatr. 1994;83:1258–1263.
56. MacAuley D, McCrum EE, Stott G, et al. Physical activity,lipids, apolipoproteins, and Lp(a) in the Northern IrelandHealth and Activity Survey. Med Sci Sports Exerc. 1996;28:720–736.
57. Drowatzky KL, Durstine JL, Irwin ML, et al. Theassociation between physical activity, cardiorespiratoryfitness, and lipoprotein(a) concentrations in a tri-ethnicsample of women: The Cross-Cultural Activity Partici-pation Study. Vasc Med. 2001;6:15–21.
58. Craig SB, Bandini LG, Lichtenstein AH, et al. Theimpact of physical activity on lipids, lipoproteins, andblood pressure in preadolescent girls. Pediatrics. 1996;98:389–395.
59. Cardoso GC, Posadas C, Orvananos OO, et al. Long distancerunners and body-builders exhibit elevated plasma levels oflipoprotein(a). Chem Phys Lipids. 1994;67–68:207–221.
60. Israel RG, Sullivan MJ, Marks RH, et al. Relationshipbetween cardiorespiratory fitness and lipoprotein(a)in men and women. Med Sci Sports Exerc. 1994;26:425–431.
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
350 Bermudez et al




















