
Evaluating Obesity Prevention Efforts - Multiple Chronic ...
Upload
khangminh22Category
view
3download
0
1/8https://e-cmsj.org
ABSTRACT
Background and Objectives: Elevated blood pressure and obesity are important contributors to cardiovascular diseases. We aimed to elucidate the combined effect of elevated blood pressure and obesity on diastolic function.Methods: We included individuals without known cardiovascular disease or hypertension (n=779) based on health check-up data from a tertiary hospital in Korea. Study participants were categorized by their blood pressure (BP) and body mass index (BMI). BP was divided into 3 categories (optimal BP <120/80, normal BP 120–129/80–84, and high normal BP 130–139/85–89 mmHg) and defined obesity as BMI ≥25 kg/m2. Diastolic dysfunction was defined as an E/e′ ≥10. Multivariate logistic regression analysis was used to identify the independent risk of having diastolic dysfunction of each BP/BMI category.Results: Across BP and BMI categories, a gradual decrease in e′ velocity and increase in the E/e′ ratio were observed. High normal BP/obese group had the highest risk of diastolic dysfunction (odds ratio [OR], 7.4; 95% confidence interval [CI], 3.7–14.7), followed by normal BP/obese group (OR, 4.8; 95% CI, 2.5–9.2), optimal BP/obese group (OR, 3.0; 95% CI, 1.5–5.8), high normal BP/non-obese group (OR, 2.1; 95% CI, 1.1–4.2), and normal BP/non-obese group (OR, 1.4; 95% CI, 0.8–2.4) than the optimal BP/non-obese group after adjustment for covariates.Conclusions: High normal BP was associated with worse diastolic function than normal BP, not to mention optimal BP, in both BMI categories. Moreover, the adverse association was pronounced when combined with obesity.
Keywords: Obesity; Blood pressure; Prehypertension; Diastole; Exercise tolerance
INTRODUCTION
Elevated blood pressure (BP) and increased body mass index (BMI) are major risk factors of cardiovascular diseases, including heart failure with preserved ejection fraction.1-4 Recently, novel anti-diabetic drugs, such as sodium-glucose transport-2 inhibitors and glucagon-
Cardiometab Syndr J. 2022 Mar;2(1):e1https://doi.org/10.51789/cmsj.2022.2.e1pISSN 2734-1143·eISSN 2765-3749
Original Article
Received: Jul 28, 2021Revised: Sep 1, 2021Accepted: Sep 23, 2021
Correspondence toSang-Hyun Ihm, MD, PhDDivision of Cardiology, Department of Internal Medicine, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, 327, Sosa-ro, Bucheon 14647, Korea.E-mail: [email protected]
Copyright © 2022. Korean Society of CardioMetabolic SyndromeThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ORCID iDsMi-Hyang Jung https://orcid.org/0000-0003-0224-5178Sang-Hyun Ihm https://orcid.org/0000-0001-5017-5421Dae Young Cheon https://orcid.org/0000-0001-6713-4300
Conflict of InterestThe authors have no financial conflicts of interest.
Author ContributionsConceptualization: Jung MH, Ihm SH; Data curation: Jung MH; Formal analysis: Jung MH; Investigation: Jung MH, Ihm SH, Lee DH, Cheon DY, Park MS, Kim DY, Lee S, Choi JH, Han S, Youn HJ, Ryu KH; Software: Jung MH; Validation: Jung MH, Ihm SH, Lee DH, Cheon
Mi-Hyang Jung , MD1, Sang-Hyun Ihm , MD, PhD2, Dong-Hyeon Lee, MD3, Dae Young Cheon , MD1, Myung Soo Park, MD1, Do Young Kim, MD1, Sunki Lee, MD1, Jae Hyuk Choi, MD1, Seongwoo Han, MD1, Ho-Joong Youn, MD3, and Kyu-Hyung Ryu, MD1
1Cardiovascular Center, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea
2Division of Cardiology, Department of Internal Medicine, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
3Cardiovascular Center, College of Medicine, Seoul St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea
Combined Effect of Elevated Blood Pressure and Obesity on Left Ventricular Diastolic Function
Provisional
Provisional

DY, Park MS, Kim DY, Lee S, Choi JH, Han S, Youn HJ, Ryu KH; Writing - original draft: Jung MH, Ihm SH; Writing - review & editing: Jung MH, Ihm SH, Lee DH, Cheon DY, Park MS, Kim DY, Lee S, Choi JH, Han S, Youn HJ, Ryu KH.
like-peptide-1 receptor agonists, have drawn much attention owing to their cardiovascular benefits.5 Although the exact mechanism behind the cardiovascular benefit needs to be clarified, they shared two features of reducing BP and moderating body weight to some degree.5 This implies that the combined effect of elevated BP and BMI might be deleterious to cardiovascular health.
Globally, the prevalence of obesity and hypertension is increasing and Korean population is not an exception. According to a recent report by the Korean Society of Hypertension, 1 in 4 (25.9%) of the Korean population has BP in prehypertension range (120–139 mmHg) and the prevalence of this category is expected to increase further.6 From the standpoint of primary prevention, it would be clinically worthwhile to accurately stratify the risk related to the prehypertension and identify the vulnerable population who need intensive risk modification or close monitoring.
Through this study, we sought to identify the combined effect of elevated BP and increased BMI on left ventricular (LV) diastolic dysfunction. In particular, we focused on diastolic function because it reflects heart status in various cardiovascular diseases, including atherosclerotic heart disease and heart failure.7-9
METHODS
Study population and data collectionHealthy individuals of 20–79 years of age with available comprehensive health check-up data from a tertiary hospital in Korea were included in the current study. To identify the independent role of elevated BP and BMI on diastolic function, we excluded those individuals with the following conditions: those who had known cardiovascular disease, hypertension, diabetes, asymptomatic but significant structural heart disease detected by echocardiography, significant lung disease confirmed by chest radiography or pulmonary function test, anemia, early termination of an exercise test for other reasons, and non-Korean populations. Therefore, 779 individuals were included in the main analyses.
Based on BP (3 categories: optimal [BP <120/80 mmHg], normal [BP 120–129/80–84 mmHg], and high normal BP [BP 130–139/85–89 mmHg]) and BMI (2 categories: non-obese [BMI <25 kg/m2] and obese [BMI ≥25 kg/m2]), individuals were classified into 6 categories of optimal BP/non-obese (n=295), normal BP/non-obese (n=151), high normal BP/non-obese (n=77), optimal BP/obese (n=88), normal BP/obese (n=96), and high normal BP/obese (n=72). In accordance with the recent hypertension guidelines,10 we divided those with 120–139/80–89 mmHg (previously called prehypertension in Joint National Committee [JNC] 7 report11) further into 120–129/80–84 mmHg (normal BP) and 130–139/85–89 mmHg (high normal BP) to evaluate the risk associated with BP level.
All participants were interviewed for their demographic details, health-related behaviors, and medical history. A trained nurse measured their height and weight under the standardized protocol. Blood pressure was measured at least twice after resting for at least 10 minutes using an automated BP device (TM-2665P; A&D, Tokyo, Japan), and the average value was taken. Blood samples were drawn from the antecubital vein after overnight fasting. We acquired body composition data from a bioelectrical impedance analysis device (InBody 720; Biospace, Seoul, Korea). Exercise capacity was assessed using a cardiopulmonary
2/8https://doi.org/10.51789/cmsj.2022.2.e1
Combined Effect of BP and Obesity
https://e-cmsj.org
Provisional
Provisional
exercise test (Schiller, Baar, Switzerland) and recorded in 2 forms (peak VO2 [mL/kg/min] and percent-predicted peak VO2 [%]). The detailed methods are provided elsewhere.12,13 The local institutional review board approved this study and exempted the requirement for obtaining informed consent considering the retrospective study design.
Echocardiographic evaluationAccording to the guidelines, 2-dimensional, M-mode, and Doppler images were acquired by a trained sonographer using a GE Vivid 7 Ultrasound System (GE Healthcare Service, Milwaukee, WI, USA). LV mass was assessed in the parasternal long axis using M-mode and indexed to body surface area. LV systolic function (LV ejection fraction) was evaluated in the apical window through Simpson's method. LV diastolic function was assessed in the same window using pulse-wave Doppler method at the mitral leaflet tips (E and A velocity) and tissue Doppler recordings at the septal annulus (e′ and a′ velocity). Thereby, E/e′ ratio was calculated. Diastolic dysfunction was defined as an E/e′ ratio ≥10.
Statistical methodsCategorical variables were presented as number with frequency (%) and continuous variables as mean with standard deviation. The group characteristics by BP/BMI categories were evaluated using analysis of variance, χ2 test, or Fisher's exact test. Bonferroni post hoc analysis was performed to identify subgroup differences. To adjust the difference in baseline characteristics (age and sex), analysis of covariance was further applied. Multivariate logistic regression analysis (backward stepwise approach) was performed to identify the independent risk of having diastolic dysfunction of each BP/BMI category after controlling for confounders (age, sex, and triglyceride), which showed the differences across the groups in terms of baseline characteristics. Covariates were carefully chosen to avoid collinearity. A p-value <0.05 was considered statistically significant. The analyses were conducted using SPSS version 21.0 software (SPSS, Inc., Chicago, IL, USA).
RESULTS
Baseline characteristicsA total of 779 participants (42.5% women) were included in the present study. Mean age was 52.7±8.8 years. Half of the study population had optimal BP (n=383, 49.2%). Non-obese individuals comprised approximately two-third of the study population (n=523, 67.1%). Obese individuals comprised more men (47.6% vs. 77.7%) with higher BP (117.4±10.7 vs. 122.7±9.1 mmHg) and triglyceride levels (97.4±63.5 vs. 144.5±93.3 mg/dL), and lower exercise capacity (percent-predicted peak VO2, 97.1±27.6% vs. 81.2±22.0%) than non-obese individuals (all p<0.05). Detailed baseline characteristics according to BP/BMI categories are summarized in Table 1.
Cardiac structure and function by their combined BP/BMI categoriesAcross BP categories (from optimal BP to high normal BP), LV wall thickness increased in each BMI group. LV wall thickness of high normal BP/non-obese individuals was comparable to that of optimal BP/obese individuals. LV systolic function, assessed with LV ejection fraction, did not differ between the groups (Table 2).
Regarding diastolic function, gradual increase in A velocity and decrease in e′ velocity were demonstrated in both non-obese and obese individuals. E/e′ ratio, which reflects the LV filling
3/8https://doi.org/10.51789/cmsj.2022.2.e1
Combined Effect of BP and Obesity
https://e-cmsj.org
Provisional
Provisional
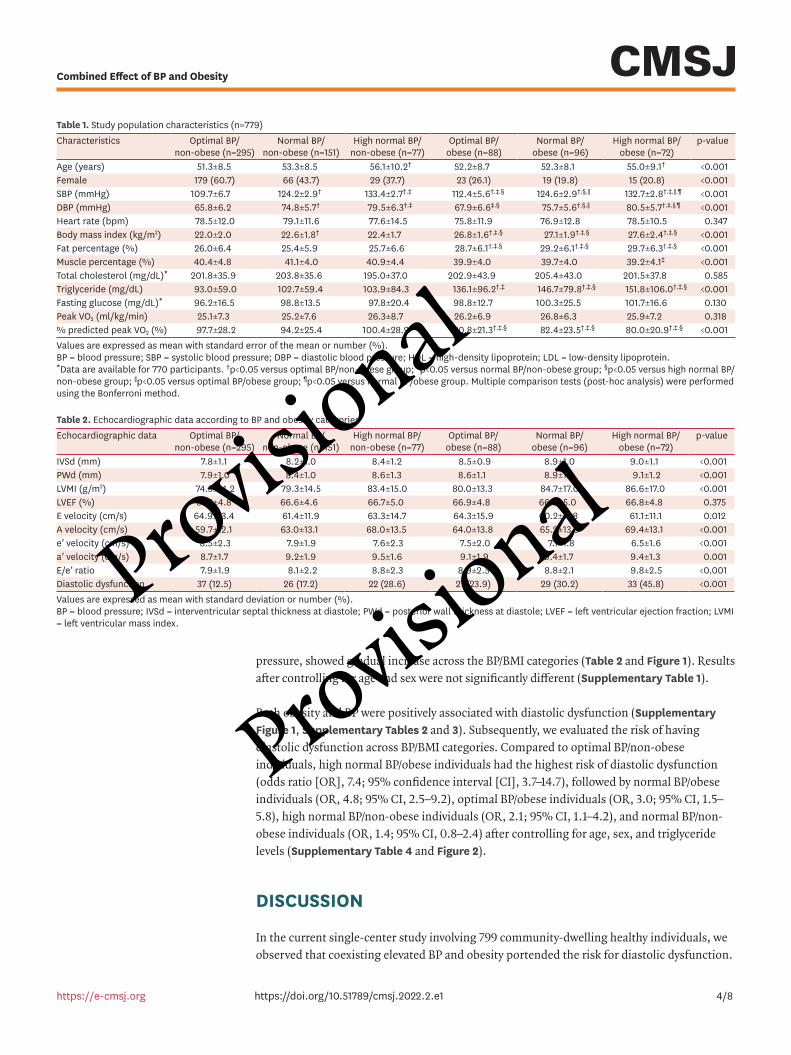
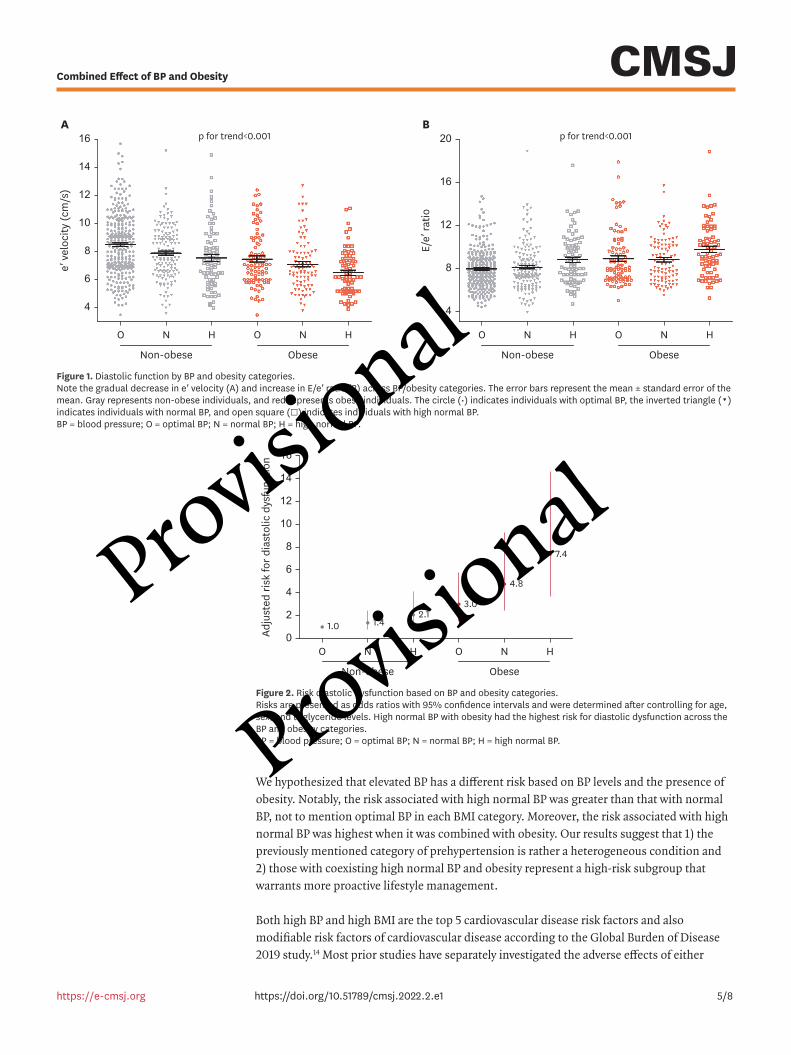
pressure, showed gradual increase across the BP/BMI categories (Table 2 and Figure 1). Results after controlling for age and sex were not significantly different (Supplementary Table 1).
Both obesity and BP were positively associated with diastolic dysfunction (Supplementary Figure 1, Supplementary Tables 2 and 3). Subsequently, we evaluated the risk of having diastolic dysfunction across BP/BMI categories. Compared to optimal BP/non-obese individuals, high normal BP/obese individuals had the highest risk of diastolic dysfunction (odds ratio [OR], 7.4; 95% confidence interval [CI], 3.7–14.7), followed by normal BP/obese individuals (OR, 4.8; 95% CI, 2.5–9.2), optimal BP/obese individuals (OR, 3.0; 95% CI, 1.5–5.8), high normal BP/non-obese individuals (OR, 2.1; 95% CI, 1.1–4.2), and normal BP/non-obese individuals (OR, 1.4; 95% CI, 0.8–2.4) after controlling for age, sex, and triglyceride levels (Supplementary Table 4 and Figure 2).
DISCUSSION
In the current single-center study involving 799 community-dwelling healthy individuals, we observed that coexisting elevated BP and obesity portended the risk for diastolic dysfunction.
4/8https://doi.org/10.51789/cmsj.2022.2.e1
Combined Effect of BP and Obesity
https://e-cmsj.org
Table 1. Study population characteristics (n=779)Characteristics Optimal BP/
non-obese (n=295)Normal BP/
non-obese (n=151)High normal BP/
non-obese (n=77)Optimal BP/
obese (n=88)Normal BP/
obese (n=96)High normal BP/
obese (n=72)p-value
Age (years) 51.3±8.5 53.3±8.5 56.1±10.2† 52.2±8.7 52.3±8.1 55.0±9.1† <0.001Female 179 (60.7) 66 (43.7) 29 (37.7) 23 (26.1) 19 (19.8) 15 (20.8) <0.001SBP (mmHg) 109.7±6.7 124.2±2.9† 133.4±2.7†,‡ 112.4±5.6†,‡,§ 124.6±2.9†,§,∥ 132.7±2.8†,‡,∥,¶ <0.001DBP (mmHg) 65.8±6.2 74.8±5.7† 79.5±6.3†,‡ 67.9±6.6‡,§ 75.7±5.6†,§,∥ 80.5±5.7†,‡,∥,¶ <0.001Heart rate (bpm) 78.5±12.0 79.1±11.6 77.6±14.5 75.8±11.9 76.9±12.8 78.5±10.5 0.347Body mass index (kg/m2) 22.0±2.0 22.6±1.8† 22.4±1.7 26.8±1.6†,‡,§ 27.1±1.9†,‡,§ 27.6±2.4†,‡,§ <0.001Fat percentage (%) 26.0±6.4 25.4±5.9 25.7±6.6 28.7±6.1†,‡,§ 29.2±6.1†,‡,§ 29.7±6.3†,‡,§ <0.001Muscle percentage (%) 40.4±4.8 41.1±4.0 40.9±4.4 39.9±4.0 39.7±4.0 39.2±4.1‡ <0.001Total cholesterol (mg/dL)* 201.8±35.9 203.8±35.6 195.0±37.0 202.9±43.9 205.4±43.0 201.5±37.8 0.585Triglyceride (mg/dL) 93.0±59.0 102.7±59.4 103.9±84.3 136.1±96.2†,‡ 146.7±79.8†,‡,§ 151.8±106.0†,‡,§ <0.001Fasting glucose (mg/dL)* 96.2±16.5 98.8±13.5 97.8±20.4 98.8±12.7 100.3±25.5 101.7±16.6 0.130Peak VO2 (ml/kg/min) 25.1±7.3 25.2±7.6 26.3±8.7 26.2±6.9 26.8±6.3 25.9±7.2 0.318% predicted peak VO2 (%) 97.7±28.2 94.2±25.4 100.4±28.9 80.8±21.3†,‡,§ 82.4±23.5†,‡,§ 80.0±20.9†,‡,§ <0.001Values are expressed as mean with standard error of the mean or number (%).BP = blood pressure; SBP = systolic blood pressure; DBP = diastolic blood pressure; HDL = high-density lipoprotein; LDL = low-density lipoprotein.*Data are available for 770 participants. †p<0.05 versus optimal BP/non-obese group; ‡p<0.05 versus normal BP/non-obese group; §p<0.05 versus high normal BP/non-obese group; ∥p<0.05 versus optimal BP/obese group; ¶p<0.05 versus normal BP/obese group. Multiple comparison tests (post-hoc analysis) were performed using the Bonferroni method.
Table 2. Echocardiographic data according to BP and obesity categoriesEchocardiographic data Optimal BP/
non-obese (n=295)Normal BP/
non-obese (n=151)High normal BP/
non-obese (n=77)Optimal BP/
obese (n=88)Normal BP/
obese (n=96)High normal BP/
obese (n=72)p-value
IVSd (mm) 7.8±1.1 8.2±1.0 8.4±1.2 8.5±0.9 8.9±1.0 9.0±1.1 <0.001PWd (mm) 7.9±1.0 8.4±1.0 8.6±1.3 8.6±1.1 8.9±1.1 9.1±1.2 <0.001LVMI (g/m2) 74.3±14.2 79.3±14.5 83.4±15.0 80.0±13.3 84.7±17.0 86.6±17.0 <0.001LVEF (%) 67.3±4.8 66.6±4.6 66.7±5.0 66.9±4.8 66.0±5.0 66.8±4.8 0.375E velocity (cm/s) 64.9±13.4 61.4±11.9 63.3±14.7 64.3±15.9 60.2±11.8 61.1±11.1 0.012A velocity (cm/s) 59.7±12.1 63.0±13.1 68.0±13.5 64.0±13.8 65.2±13.3 69.4±13.1 <0.001e′ velocity (cm/s) 8.5±2.3 7.9±1.9 7.6±2.3 7.5±2.0 7.1±1.8 6.5±1.6 <0.001a′ velocity (cm/s) 8.7±1.7 9.2±1.9 9.5±1.6 9.1±1.9 9.4±1.7 9.4±1.3 0.001E/e′ ratio 7.9±1.9 8.1±2.2 8.8±2.3 8.9±2.5 8.8±2.1 9.8±2.5 <0.001Diastolic dysfunction 37 (12.5) 26 (17.2) 22 (28.6) 21 (23.9) 29 (30.2) 33 (45.8) <0.001Values are expressed as mean with standard deviation or number (%).BP = blood pressure; IVSd = interventricular septal thickness at diastole; PWd = posterior wall thickness at diastole; LVEF = left ventricular ejection fraction; LVMI = left ventricular mass index.
Provisional
Provisional
We hypothesized that elevated BP has a different risk based on BP levels and the presence of obesity. Notably, the risk associated with high normal BP was greater than that with normal BP, not to mention optimal BP in each BMI category. Moreover, the risk associated with high normal BP was highest when it was combined with obesity. Our results suggest that 1) the previously mentioned category of prehypertension is rather a heterogeneous condition and 2) those with coexisting high normal BP and obesity represent a high-risk subgroup that warrants more proactive lifestyle management.
Both high BP and high BMI are the top 5 cardiovascular disease risk factors and also modifiable risk factors of cardiovascular disease according to the Global Burden of Disease 2019 study.14 Most prior studies have separately investigated the adverse effects of either
5/8https://doi.org/10.51789/cmsj.2022.2.e1
Combined Effect of BP and Obesity
https://e-cmsj.org
4
8
12
6
10
14
16
O N
Non-obese
A B
Obese
H O N H
e′ v
eloc
ity (c
m/s
)
p for trend<0.001
4
8
12
16
20
O N
Non-obese Obese
H O N H
E/e′
ratio
p for trend<0.001
Figure 1. Diastolic function by BP and obesity categories. Note the gradual decrease in e′ velocity (A) and increase in E/e′ ratio (B) across BP/obesity categories. The error bars represent the mean ± standard error of the mean. Gray represents non-obese individuals, and red represents obese individuals. The circle (•) indicates individuals with optimal BP, the inverted triangle (▾) indicates individuals with normal BP, and open square (□) indicates individuals with high normal BP. BP = blood pressure; O = optimal BP; N = normal BP; H = high normal BP.
0
4
8
12
16
2
6
10
14
O N
Non-obese Obese
H O N H
1.0 1.42.1
3.0
4.8
7.4
Adju
sted
risk
for d
iast
olic
dys
func
tion
Figure 2. Risk diastolic dysfunction based on BP and obesity categories. Risks are presented as odds ratios with 95% confidence intervals and were determined after controlling for age, sex, and triglyceride levels. High normal BP with obesity had the highest risk for diastolic dysfunction across the BP and obesity categories. BP = blood pressure; O = optimal BP; N = normal BP; H = high normal BP.
Provisional
Provisional
elevated BP or higher BMI on diastolic function, despite their simultaneous occurrence.12,15,16 If any, they have focused on overt hypertension, not the precursor state of it.17,18 From a primary prevention viewpoint, prehypertension might be a more potential target given that prehypertension is a more reversible state. In the current study, gradual risk elevation was demonstrated when BP category was elevated, even below 140/90 mmHg. Furthermore, we observed the highest risk of diastolic dysfunction when high normal BP coexisted with obesity. These findings highlight the importance of a multi-dimensional risk assessment in clinical practice. Physicians tend to evaluate a single dimension of cardiovascular risk factors (such as each of BP, BMI, or glucose), and to focus on a single risk factor that is of high significance. In the real world, however, the vulnerable point might be where high BP and elevated BMI intersect. Considering that many individuals have multiple risk factors in common, correction of two or more minor risk factors simultaneously (shown in studies of exercise and/or anti-diabetic drugs) might lead to greater health benefits.5,19
The possible explanation for this is that BP and BMI deleteriously affect each other. Julius et al.20 previously described the phenomenon as ‘a 2-way street.’ Enhanced sympathetic tone, over-activation of renin-angiotensin-aldosterone system, insulin resistance, and obstructive sleep apnea are intricately intertwined and lead to diastolic dysfunction and ultimately adverse cardiovascular outcomes.20,21 In the current study, the effect of obesity on BP-related diastolic dysfunction was additive, not multiplicative (interaction p>0.05, data are not shown). This might be due to the preclinical stages of BP intervals, which we examined. A previous study showed the multiplicative effect of combined BP and BMI, in a more advanced stage of highest BP (>135 mmHg) and BMI (>30 kg/m2).22
This study has several limitations. The current study is based on cross-sectional data; therefore, causal relationship cannot be drawn. The influence of residual confounding factors that were not assessed in this study needs to be also considered. Selection bias might have affected the results because the study population represents a high-income population who could afford comprehensive health check-ups (including cardiopulmonary exercise test and echocardiography) and are proactive about their health and wellness. Further, this study cannot be generalized to the populations of other ethnicities, because the current study population included only Koreans.
In a community-dwelling healthy population without overt hypertension or cardiovascular disease, gradual risk elevation was observed across BP/obesity categories. Our study indicates that previously categorized prehypertension comprised heterogeneous groups. Those coexisting with high normal BP and obesity were found to have the highest risk for subclinical heart problems. Therefore, clinical attention and proactive preventive management are needed for those with coexisting high normal BP and obesity to prevent irreversible changes.
SUPPLEMENTARY MATERIALS
Supplementary Table 1Age- and sex- adjusted mean E/e′ ratio by BP and obesity categories
Click here to view
6/8https://doi.org/10.51789/cmsj.2022.2.e1
Combined Effect of BP and Obesity
https://e-cmsj.org
Provisional
Provisional
Supplementary Table 2Risk of diastolic dysfunction based on obesity
Click here to view
Supplementary Table 3Risk of diastolic dysfunction based on BP
Click here to view
Supplementary Table 4Risk of diastolic dysfunction according to BP and obesity categories
Click here to view
Supplementary Figure 1Correlation between E/e′ and body mass index/blood pressure.
Click here to view
REFERENCES
1. Park J, Kim HL, Kim MA, et al. Traditional cardiovascular risk factors and obstructive coronary disease in patients with stable chest pain: gender-specific analysis. Cardiometab Syndr J 2021;1:101-10. CROSSREF
2. Pfeffer MA, Shah AM, Borlaug BA. Heart failure with preserved ejection fraction in perspective. Circ Res 2019;124:1598-617. PUBMED | CROSSREF
3. Jung MH, Yi SW, An SJ, Yi JJ. Age-specific associations between systolic blood pressure and cardiovascular mortality. Heart 2019;105:1070-7. PUBMED | CROSSREF
4. Jung MH, Yi SW, An SJ, Balkau B, Yi JJ, Kim H. Complex interaction of fasting glucose, body mass index, age and sex on all-cause mortality: a cohort study in 15 million Korean adults. Diabetologia 2020;63:1616-25. PUBMED | CROSSREF
5. Wilcox T, De Block C, Schwartzbard AZ, Newman JD. Diabetic agents, from metformin to SGLT2 inhibitors and GLP1 receptor agonists: JACC Focus Seminar. J Am Coll Cardiol 2020;75:1956-74. PUBMED | CROSSREF
6. Kim HC, Ihm SH, Kim GH, et al. 2018 Korean Society of Hypertension guidelines for the management of hypertension: part I-epidemiology of hypertension. Clin Hypertens 2019;25:16. PUBMED | CROSSREF
7. Ohara T, Little WC. Evolving focus on diastolic dysfunction in patients with coronary artery disease. Curr Opin Cardiol 2010;25:613-21. PUBMED | CROSSREF
8. Zile MR, Brutsaert DL. New concepts in diastolic dysfunction and diastolic heart failure: Part I: diagnosis, prognosis, and measurements of diastolic function. Circulation 2002;105:1387-93. PUBMED | CROSSREF
9. Obokata M, Reddy YN, Borlaug BA. Diastolic dysfunction and heart failure with preserved ejection fraction: understanding mechanisms by using noninvasive methods. JACC Cardiovasc Imaging 2020;13:245-57. PUBMED | CROSSREF
10. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial
7/8https://doi.org/10.51789/cmsj.2022.2.e1
Combined Effect of BP and Obesity
https://e-cmsj.org
Provisional
Provisional
hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens 2018;36:1953-2041. PUBMED | CROSSREF
11. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003;289:2560-72. PUBMED | CROSSREF
12. Jung MH, Ihm SH, Lee DH, et al. Sex-specific associations of obesity with exercise capacity and diastolic function in Koreans. Nutr Metab Cardiovasc Dis 2021;31:254-62. PUBMED | CROSSREF
13. Jung MH, Ihm SH, Park SM, et al. Effects of sarcopenia, body mass indices, and sarcopenic obesity on diastolic function and exercise capacity in Koreans. Metabolism 2019;97:18-24. PUBMED | CROSSREF
14. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol 2020;76:2982-3021. PUBMED | CROSSREF
15. Wei FF, Yang WY, Thijs L, et al. Conventional and ambulatory blood pressure as predictors of diastolic left ventricular function in a Flemish population. J Am Heart Assoc 2018;7:e007868. PUBMED | CROSSREF
16. Russo C, Jin Z, Homma S, et al. Effect of obesity and overweight on left ventricular diastolic function: a community-based study in an elderly cohort. J Am Coll Cardiol 2011;57:1368-74. PUBMED | CROSSREF
17. Kim J, Kim MG, Kang S, et al. Obesity and hypertension in association with diastolic dysfunction could reduce exercise capacity. Korean Circ J 2016;46:394-401. PUBMED | CROSSREF
18. Thomas F, Bean K, Pannier B, Oppert JM, Guize L, Benetos A. Cardiovascular mortality in overweight subjects: the key role of associated risk factors. Hypertension 2005;46:654-9. PUBMED | CROSSREF
19. Fiuza-Luces C, Garatachea N, Berger NA, Lucia A. Exercise is the real polypill. Physiology (Bethesda) 2013;28:330-58. PUBMED | CROSSREF
20. Julius S, Valentini M, Palatini P. Overweight and hypertension : a 2-way street? Hypertension 2000;35:807-13. PUBMED | CROSSREF
21. Narkiewicz K. Obesity and hypertension--the issue is more complex than we thought. Nephrol Dial Transplant 2006;21:264-7. PUBMED | CROSSREF
22. Silventoinen K, Magnusson PK, Neovius M, et al. Does obesity modify the effect of blood pressure on the risk of cardiovascular disease? A population-based cohort study of more than one million Swedish men. Circulation 2008;118:1637-42. PUBMED | CROSSREF
8/8https://doi.org/10.51789/cmsj.2022.2.e1
Combined Effect of BP and Obesity
https://e-cmsj.org
Provisional
Provisional
Copyright © 2022 FDOKUMEN




















