
Schizophrenic patients with type 2 diabetes - Semantic Scholar
Upload
independentCategory
view
0download
0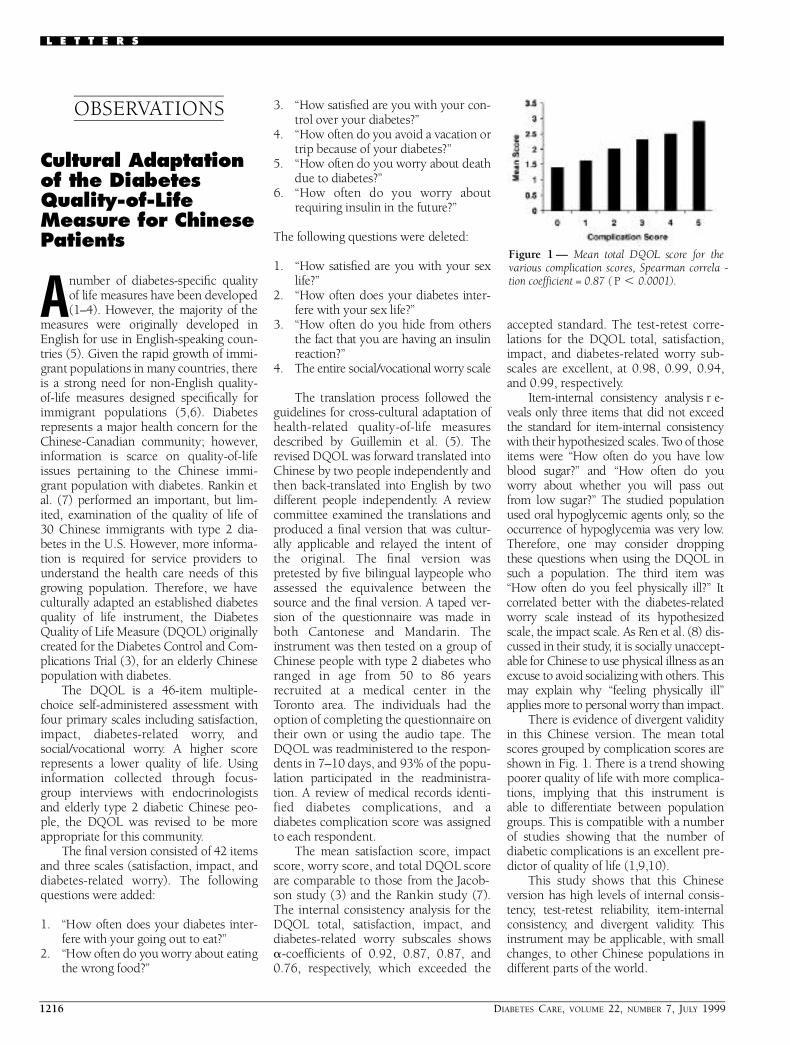
1216 DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999
O B S E RVAT I O N S
Cultural Adaptationof the DiabetesQ u a l i t y - o f - L i f eM e a s u re for ChineseP a t i e n t s
Anumber of diabetes-specific qualityof life measures have been developed(1–4). However, the majority of the
m e a s u res were originally developed inEnglish for use in English-speaking coun-tries (5). Given the rapid growth of immi-grant populations in many countries, thereis a strong need for non-English quality-of-life measures designed specifically forimmigrant populations (5,6). Diabetesre p resents a major health concern for theChinese-Canadian community; however,i n f o rmation is scarce on quality-of-lifeissues pertaining to the Chinese immi-grant population with diabetes. Rankin etal. (7) perf o rmed an important, but lim-ited, examination of the quality of life of30 Chinese immigrants with type 2 dia-betes in the U.S. However, more inform a-tion is re q u i red for service providers tounderstand the health care needs of thisg rowing population. There f o re, we haveculturally adapted an established diabetesquality of life instrument, the DiabetesQuality of Life Measure (DQOL) originallyc reated for the Diabetes Control and Com-plications Trial (3), for an elderly Chinesepopulation with diabetes.
The DQOL is a 46-item multiple-choice self-administered assessment withfour primary scales including satisfaction,impact, diabetes-related worry, andsocial/vocational worry. A higher scorere p resents a lower quality of life. Usingi n f o rmation collected through focus-g roup interviews with endocrinologistsand elderly type 2 diabetic Chinese peo-ple, the DQOL was revised to be morea p p ropriate for this community.
The final version consisted of 42 itemsand three scales (satisfaction, impact, andd i a b e t e s - related worry). The followingquestions were added:
1 . “How often does your diabetes inter-f e re with your going out to eat?”
2 . “How often do you worry about eatingthe wrong food?”
3 . “How satisfied are you with your con-t rol over your diabetes?”
4 . “How often do you avoid a vacation ortrip because of your diabetes?”
5 . “How often do you worry about deathdue to diabetes?”
6 . “How often do you worry aboutrequiring insulin in the future ? ”
The following questions were deleted:
1 . “How satisfied are you with your sexl i f e ? ”
2 . “How often does your diabetes inter-f e re with your sex life?”
3 . “How often do you hide from othersthe fact that you are having an insulinre a c t i o n ? ”
4 . The entire social/vocational worry scale
The translation process followed theguidelines for cross-cultural adaptation ofh e a l t h - related quality-of-life measure sdescribed by Guillemin et al. (5). Therevised DQOL was forw a rd translated intoChinese by two people independently andthen back-translated into English by twod i ff e rent people independently. A re v i e wcommittee examined the translations andp roduced a final version that was cultur-ally applicable and relayed the intent ofthe original. The final version wasp retested by five bilingual laypeople whoassessed the equivalence between thes o u rce and the final version. A taped ver-sion of the questionnaire was made inboth Cantonese and Mandarin. Thei n s t rument was then tested on a group ofChinese people with type 2 diabetes whoranged in age from 50 to 86 yearsre c ruited at a medical center in theTo ronto area. The individuals had theoption of completing the questionnaire ontheir own or using the audio tape. TheDQOL was re a d m i n i s t e red to the re s p o n-dents in 7–10 days, and 93% of the popu-lation participated in the re a d m i n i s t r a-tion. A review of medical re c o rds identi-fied diabetes complications, and adiabetes complication score was assignedto each re s p o n d e n t .
The mean satisfaction score, impacts c o re, worry score, and total DQOL scorea re comparable to those from the Jacob-son study (3) and the Rankin study (7).The internal consistency analysis for theDQOL total, satisfaction, impact, andd i a b e t e s - related worry subscales showsa- c o e fficients of 0.92, 0.87, 0.87, and0.76, re s p e c t i v e l y, which exceeded the
accepted standard. The test-retest corre-lations for the DQOL total, satisfaction,impact, and diabetes-related worry sub-scales are excellent, at 0.98, 0.99, 0.94,and 0.99, re s p e c t i v e l y.
I t e m - i n t e rnal consistency analysis re -v e a l s only three items that did not exceedthe standard for item-internal consistencywith their hypothesized scales. Two of thoseitems were “How often do you have lowblood sugar?” and “How often do youw o rry about whether you will pass outf rom low sugar?” The studied populationused oral hypoglycemic agents only, so theo c c u rrence of hypoglycemia was very low.T h e re f o re, one may consider dro p p i n gthese questions when using the DQOL insuch a population. The third item was“How often do you feel physically ill?” Itc o rrelated better with the diabetes-re l a t e dw o rry scale instead of its hypothesizedscale, the impact scale. As Ren et al. (8) dis-cussed in their study, it is socially unaccept-able for Chinese to use physical illness as anexcuse to avoid socializing with others. Thismay explain why “feeling physically ill”applies more to personal worry than impact.
T h e re is evidence of divergent validityin this Chinese version. The mean totals c o res grouped by complication scores areshown in Fig. 1. There is a trend showingp o o rer quality of life with more complica-tions, implying that this instrument is able to diff e rentiate between populationg roups. This is compatible with a numberof studies showing that the number of diabetic complications is an excellent pre-dictor of quality of life (1,9,10).
This study shows that this Chineseversion has high levels of internal consis-t e n c y, test-retest re l i a b i l i t y, item-intern a lc o n s i s t e n c y, and divergent validity. Thisi n s t rument may be applicable, with smallchanges, to other Chinese populations ind i ff e rent parts of the world.
L E T T E R S
F i g u re 1 — Mean total DQOL score for the various complication scores, Spearman correla -tion coefficient = 0.87 ( P , 0.0001).

DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999 1217
Letters
ALICE Y. CHENG, MD
ELAINE Y. TSUI, MD
ANTHONY J.G. HANLEY, MSC
BERNARD ZINMAN, MDCM
F rom the Departments of Medicine (A.Y.C.) andPublic Health Sciences (A.J.G.H.) and the Bantingand Best Diabetes Centre (B.Z.), University ofTo ronto; and the Samuel Lunenfeld Research Insti-tute (A.J.G.H., B.Z.), Mount Sinai Hospital (E.Y. T. ) ,To ronto, Ontario, Canada.
A d d ress correspondence to Dr. Bern a rd Zinman,Mount Sinai Hospital, 600 University Ave., Suite782, To ronto, Ontario M5G 1X5, Canada. E-mail:z i n m a n @ m s h r i . o n . c a .
R e f e re n c e s1 . Boyer JG, Earp JAL: The development of
an instrument for assessing the quality oflife of people with diabetes: Diabetes-39.Med Care 35:440–453, 1997
2 . Hammond GS, Aoki TT: Measurement ofhealth status in diabetic patients: diabetesimpact measurement scales. Diabetes Care15:469–477, 1992
3 . Jacobson A, Barofsky I, Cleary P, Rand L:Reliability and validity of a diabetes qual-ity-of-life measure for the Diabetes Contro land Complications Trial (DCCT). D i a b e t e sC a re 11:725–732, 1988
4 . Kotsanos JG, Vignati L, Huster W, Andre-jasich C, Boggs MB, Jacobson AM, Marre roD, Mathias SD, Patrick D, Zalani S, Ander-son J: Health-related quality-of-life re s u l t sf rom multinational clinical trials of insulinl i s p ro. Diabetes Care 20:948–958, 1997
5 . Guillemin F, Bombardier C, Beaton D:C ross-cultural adaptation of health-re l a t e dquality of life measures: literature re v i e wand proposed guidelines. J Clin Epidemiol46:1417–1432, 1993
6 . Wa re JE, Keller SD, Gandek B, Brazier JE,Sullivan M: Evaluating translations ofhealth status questionnaires: methodsf rom the IQOLA project. Int J Tech AssessHealth Care 11:525–550, 1995
7 . Rankin SH, Galbraith ME, Huang P: Qual-ity of life and social environment asre p o rted by Chinese immigrants with non-insulin-dependent diabetes mellitus. Diabetes Educ 23:171–177, 1997
8 . Ren XS, Amick B, Zhou L, Gandek B:Translation and psychometric evaluation ofa Chinese version of the SF-36 health sur-vey in the United States. J Clin Epidemiol51:1129–1138, 1998
9 . Jacobson AM, De Groot M, Samson JA:The evaluation of two measures of qualityof life in patients with type I and type IIdiabetes. Diabetes Care 17:267–274, 1994
1 0 . Glasgow RE, Ruggiero L, Eakin EG, Dry-foos J, Chobanian L: Quality of life andassociated characteristics in a larg enational sample of adults with diabetes.Diabetes Care 20:562–567, 1997
A m i n o t r a n s f e r a s eActivity and Acarbose Tre a t m e n tin Patients Wi t hType 2 Diabetes
Re c e n t l y, two cases of acute and severehepatotoxic reactions in diabetic sub-jects under acarbose treatment have
been re p o rted (1,2). For both cases, theauthors hypothesize cytonecrotic damagedue to an idiosyncratic reaction to acar-bose. Consequently, the monitoring ofs e rum aminotransferase activity (SAA) dur-ing acarbose treatment was warranted toa v e rt this unpredictable, but potentiallys e v e re, complication. However, ,1% ofthe therapeutic dose of acarbose isabsorbed by the gut in man (3), and re a c-tions of this kind seem to be extre m e l yr a re. In a previous work, we documentedthe safety and efficacy of 300 mg acarboseper day in 42 patients with type 2 diabetesand well-compensated posthepatitic liverc i rrhosis over a 28-week period (4). Stimu-lated by the above-mentioned re p o rts, wereevaluated our outpatients treated withacarbose alone for at least 12 months andselected 770 further patients with type 2diabetes (302 men and 468 women, meanage 57 ± 7 years, diabetes duration 9 ± 3years, HbA1 c 7.6 ± 1.1 by high-perf o r-mance liquid chromatography). Allpatients underwent questioning on riskfactors for hepatitis infection and alcoholor drug consumption, physical examina-tion, and assay of HBsAg (AUS-RIA II;Abbott, Milan, Italy) and HCV-Ab (HCV-ELISA III; Ortho Diagnostics, Milan, Italy).The patients with one alteration of one orm o re parameters underwent abdominalultrasonography and autoantibody assays(anti-mitochondrial antibody, anti–smallmuscle antibody, anti-nuclear antibody).All SAA values re p o rted in the clinicalre c o rds over a 12-month period before andafter the beginning of the acarbose tre a t-ment were analyzed. SAA alterations wereo b s e rved in 136 of 770 (17.7%) patients(values ,1.5 times the upper normal limitin 101 patients and between 1.5 and 2.5times in 35). SAA values before acarbosew e re altered in 95 of 136 (69.8%) patients,n o rmal in 16 (11.8%), and not available in25 (18.4%). Of the 16 patients with nor-mal SAA before treatment, one hadhepatomegaly with coarse ultrasono-graphic pattern, and the other 15 were
n o rmal with respect to all parameters con-sidered, including antibodies againstE p s t e i n - B a rr or cytomegaloviruses, ands e rum a-1-antitripsin, ceruloplasmin, iro n ,b i l i rubin, alkaline phosphatase, and cop-per levels. All patients with SAA alterationsu n d e rwent, by informed consent, liverbiopsy by Tru-cut needle, except the latter15 patients, who refused this investigation.In these 15 patients with indeterminate eti-o l o g y, acarbose was discontinued and SAAre t u rned to normal within 2–3 months.Thus, in our study, SAA alterations werea l ready present before the beginning of theacarbose treatment in 15.7% of patients. Inp a rt i c u l a r, 13.1% (101 patients) had asilent chronic liver disease (100 chro n i cactive hepatitis and 1 liver cirrhosis, with ap revalence comparable with that in thegeneral population of our country), and2.6% (20 patients) had fatty liver withouthepatitis. Acarbose treatment did not mod-ify the extent of SAA increase in 95 of 136patients, as previously observed (4). Onthe other hand, slight and reversible alter-ations of SAA were observed in only 15patients (1.9%) after the beginning of thet reatment with acarbose. Our observ a t i o n sa re in complete agreement with pre v i o u sre p o rts of limited alterations of SAA duringacarbose treatment in diabetic patientswith no prior history of liver disease (3).These alterations were interpreted as notbeing due to acute liver toxicity because oftheir prompt and complete re v e r s i b i l i t y(3). Such reactions are by no means com-parable to the severe hepatotoxic re a c t i o n sin the above-mentioned re p o rts (1,2); sim-ilar limited effects have been describedwith many drugs of current use.
On these grounds, we agree that thes e v e re hepatotoxic reactions re p o rted inpatients under acarbose treatment (1,2) canbe safely considered to be idiosyncraticand, as such, as possible and unpre d i c t a b l ewith any other drug. The simultaneousintake of glibenclamide, fluphenazine, andalcohol in one case might be considered afavorable condition (5). In addition, wewould not recommend a diff e rent schemefor the monitoring of SAA during acarboset reatment than the one currently used during therapy with other oral hypogly-cemic agents.
SANDRO GENTILE, MD
SALVATORE TURCO, MD
GIUSEPPINA GUARINO, MD
FERDINANDO C. SASSO, MD
ROBERTO TORELLA, MD

1218 DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999
Letters
F rom the Departments of Geriatrics and MetabolicDisease (S.G., G.G., F.C.S., R.T.) and Clinical andExperimental Medicine (S.T.), Federico the 2ndUniversity and 2nd University of Naples, Naples,I t a l y.
A d d ress correspondence to Prof. Sandro Gentile,D e p a rtment of Geriatrics and Metabolic Disease,2nd University of Naples, Via Nicolardi, Parco Arc a-dia 4, 80131 Naples, Italy.
R e f e re n c e s1 . C a rrascosa M, Pascual F, Aresti S: Acar-
bose-induced acute severe hepatotoxicity.Lancet 349:698–699, 1997
2 . Andrade RL, Lucena MI, Rodriguez-Men-dizabar M: Hepatic injury caused by acar-bose (Letter). Ann Int Med 125:931, 1996
3 . Acarbose for diabetes mellitus (Editorial).Med Lett 38:9–10, 1996
4 . Gentile S, Tu rco S, Rossi E, To rella R: Non-insulin-dependent diabetes mellitus andliver cirrhosis: effect of treatment withacarbose. In F ront Diabetes. Belfio re F,L o renzi M, Molinatti GM, Porta M, Eds.Basel, Karg e r, 1998, p. 167–171
5 . Lee WM: Drug-induced hepatotoxicity. N Engl J Med 333:1118–1127, 1995
High-Dose Vitamin CS u p p l e m e n t a t i o nI n c reases PlasmaG l u c o s e
High-dose ascorbic acid (vitamin C[ VitC]) supplementation may have ab e n e ficial effect in type 1 diabetes. It
may improve glycemic control, loweringboth fasting plasma glucose and HbA1 c
(1). Also, it has recently been suggestedthat antioxidant treatment using high-dose VitC may help to prevent renal injuryin type 1 diabetic rats (2). Although theseresults suggest that high-dose VitC supple-mentation in diabetes may be benefic i a l ,h e rein is re p o rted a potential detrimentale ffect of high-dose VitC supplementation,an increase in plasma glucose that con-founded a diagnosis of type 2 diabetes.
A 49-year-old slight-to-moderatelyobese, but otherwise healthy, male Cau-casian was found on routine examinationto have an elevated fasting plasma glucoseof 6.6 mmol/l. The patient demonstratedno increases in glycosylated hemoglobin,nor did he have detectable glucose in hisurine. The patient was subsequently diag-nosed as likely having type 2 diabetesbased on his age, obesity, and a repeat elevated fasting plasma glucose level
(6.8 mmol/l) and impaired glucose toler-ance (1 h, 12.2 mmol/l; 2 h, 8.5 mmol/l);h o w e v e r, it was noted that the plasma glu-cose results were not conclusive. Thepatient was, there f o re, re f e rred to a dia-betes clinic for further evaluation.
The patient himself suggested thatp e rhaps a high dosage of VitC that he wastaking had resulted in the elevation of thefasting and postprandial glucose re s u l t s .The patient had been taking 4,500 mg of asynthetic unsweetened VitC product eachday for the past 5 years.
Without change in his diet or activity,the patient was asked to discontinue hiss u p p l e m e n t a ry VitC, and his fastingplasma glucose level was retested. After 7 days without VitC, the patient’s fastingglucose was found to be within the norm a lrange, at 5.9 mmol/l, and continued tod rop to 5.5 mmol/l after 10 days withoutVitC. The patient re s t a rted 4,500 mg/dayof VitC and, when tested after 1 week,again had an elevation of his fastingplasma glucose, to 6.1 mmol/l. The Vi t Cwas again discontinued, and after 1 weekt h e re was no change in the glucose level;h o w e v e r, when tested after 3 weeks with-out VitC, his glucose was 4.4 mmol/l.
The observed increase in plasma glu-cose when the patient was taking high-dose VitC was not likely due to interf e r-ence of the VitC with the method of glu-cose measurement. Glucose hexokinaseenzyme assay was used to determine glu-cose levels. This method is similar to glucose oxidase methods (3), and is notsubject to direct interf e rence by ascorbatein routine plasma glucose measure m e n t s(4). Banhegyi and colleagues (5,6) havep reviously shown in vitro that VitC caninduce glucose production from a numberof diff e rent cells, sometimes resulting inhigh glucose production (7). The elevatedfasting plasma glucose level measured inthis patient was only demonstrable whenthe patient had been taking a very highdosage ($4,500 mg/day) of VitC for atleast 1 week prior to testing that persistedin elevation until at least 8–10 days afterdiscontinuance of the VitC. These re s u l t sshow for the first time, in humans, thats u p p l e m e n t a ry VitC can increase plasmaglucose levels. Elevated plasma glucosedue to very high-dose VitC could result ina questionable or misdiagnosis of diabetesand/or additional unnecessary testing, as inthis case. More o v e r, VitC-induced pro d u c-tion of glucose may interf e re in the glucosemonitoring of true diabetic patients.
The patient refused to eliminate sup-p l e m e n t a ry VitC, but reduced theamount taken to 1,500 mg/day. At thisdosage, multiple repeat testing of hisplasma glucose showed results within then o rmal range. In the very few studies thathave been done, VitC up to 2,000 mg/dayhas been shown not to result in ani n c rease in plasma glucose (1,8), andthese dosages are suggested to be benefi-cial (1). There f o re, a dosage of1,500–2,000 mg/day would provide theexpected beneficial effects of supplemen-t a ry VitC in diabetes (1,8,9), but may noti n t e rf e re with plasma glucose determ i n a-tions and confound a diagnosis or tre a t-ment of this disord e r.
This is the first re p o rt of supplemen-t a ry VitC in humans causing an unex-pected elevation of plasma glucose levelsconfounding a diagnosis of type 2 dia-betes. However, this may be more com-mon if further examined, particularly inb o rderline cases in which patients are tak-ing high-dose VitC supplements. To insureaccurate interpretation of the fasting orpostprandial plasma glucose measure-ments, it may be advisable for individualstaking megadoses of VitC to be asked torefrain from ingesting supplementary Vi t Cfor at least 1 week prior to testing.
DONALD R. BRANCH, PHD
F rom the University of To ronto, Department ofMedicine, The To ronto Hospital and CanadianBlood Services, To ronto, Ontario, Canada.
A d d ress correspondence to Dr. Donald R.Branch, The To ronto Hospital, 67 College St.,To ronto, Ontario, Canada M5G 2M1. E-mail:d o n . b r a n c h @ u t o ro n t o . c a .
R e f e re n c e s1. Eriksson J, Kohvakka A: Magnesium and
ascorbic acid supplementation in diabetesmellitus. Ann Nutr Metab 3 9 : 2 1 7 – 2 2 3 ,1 9 9 5
2. Craven PA, DeRubertis FR, Kagan VE,Melhem M, Studer RK: Effects of supple-mentation with vitamin C or E on albu-minuria, glomerular TGF-beta, andg l o m e rular size in diabetes. J Am SocN e p h ro l 8:1405–1414, 1997
3. Genter PM, Ipp E: Accuracy of plasma glu-cose measurements in the hypoglycemicrange. Diabetes Care 17:595–598, 1994
4. Fiorani M, De Sanctis R, Scarlatti F, StocchiV: Substrates of hexokinase, glucose-6-phosphate dehydrogenase, and glycer-adldehyde-3-phosphate dehydro g e n a s ep revent the inhibitory response induced
DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999 1219
Letters
by ascorbic acid/iron and dehydro a s c o r b i cacid in rabbit ery t h rocytes. A rch BiochemB i o p h y s 356:159–166, 1998
5. Braun L, Puskas F, Csala M, Gyorffy E,G a rzo T, Mandl J, Banhegyi G: Gluconeo-genesis from ascorbic acid: ascorbate re c y-cling in isolated murine hepatocytes. F E B SL e t t 390:183–186, 1996
6. Banhegyi G, Braun L, Csala M, Puskas F,Mandl J: Ascorbate metabolism and itsregulation in animals. F ree Radic Biol Med23:793–803, 1997
7. Braun L, Puskas F, Csala M, Meszaros G,Mandl J, Banhegyi G: Ascorbate as a sub-strate for glycolysis or gluconeogenesis:evidence for an intero rgan ascorbatecycle. F ree Radic Biol Med 2 3 : 8 0 4 – 8 0 8 ,1 9 9 7
8. Davie SJ, Gould BJ, Yudkin JS: Effect of vit-amin C on glycosylation of proteins. D i a -betes 41:167–173, 1992
9. Cunningham JJ: The glucose/insulin sys-tem and vitamin C: implications ininsulin-dependent diabetes mellitus. J AmColl Nutr 17:105–108, 1998
Revised Standard sfor the Treatment ofType 2 Diabetes inTe x a s
In 1996, the Texas Diabetes Council(TDC) and the Texas Department ofHealth endorsed a treatment algorithm
for people with type 2 diabetes (1) thatwas implemented as a standard of care bymanaged care organizations operatingwithin the state. Recently, a number ofdevelopments have altered the manage-ment of patients with type 2 diabetes,necessitating evolution of the TDC algo-rithm. The American Diabetes Associa-tion (ADA), for example, has revised itsdiagnostic criteria and the standards andgoals of treatment (2,3), and results fro mthe U.K. Prospective Diabetes Study have recently confirmed the dramaticb e n e fits of intensive glucose control inpatients with type 2 diabetes (4,5).F i n a l l y, new pharmacologic agents for thet reatment of type 2 diabetes have alsobecome available, greatly expandingt reatment options.
On the basis of these new data and therecommendations of consultants, the TDChas amended the algorithm for tre a t m e n tof patients with type 2 diabetes. The newguidelines re flect awareness that mores c rupulous management of fasting plasma
glucose (FPG) and glycated hemoglobin( H b A1 c) concentrations, coupled withg reater attention to normalizing bodyweight and lipid concentrations, are nowdeemed necessary to properly managepatients with type 2 diabetes and tod e c rease the incidence and severity of microvascular and macrovascular com-plications. Key revisions are summariz-ed below.
• Treatment goals for FPG and HbA1 c
concentrations (,126 mg/dl and,7.0%, respectively) now re flect 1998ADA recommendations. Thro u g h o u tthe entire treatment course, manage-ment of diabetes is deemed inadequate,and treatment pro g resses to the nextstage when FPG $126 mg/dl andH b A1 c #7 . 0 % .
• Routine home glucose monitoring hasbeen identified as an essential baselinei n t e rvention for all individuals withtype 2 diabetes.
• P h a rmacologic therapy should bei n t roduced within 1 month if glycemicgoals are not achieved with initial non-p h a rmacologic interventions. Whilestill stressing the importance of diet,e x e rcise, and other nondrug interv e n-tions, the new guidelines emphasizerapid and effective treatment of hyper-g l y c e m i a .
• A metform i n / s u l f o n y l u rea combina-tion is now designated as the pre f e rre dsecond-line therapy if first-line met-f o rmin or sulfonylurea monotherapy atoptimal doses does not provide ade-quate glycemic control. An altern a t ec a t e g o ry of “Other MonotherapyOptions” has also been added for usein patients whose health status or con-comitant medication profile con-traindicate use of the designated fir s t -line agents.
• Physicians may now add a third oralagent when combination therapy withm e t f o rmin and a sulfonylurea does notp rovide adequate glucose contro l .
G reater knowledge of up-to-datet reatment options is paramount in devel-oping patient programs and health sys-tem changes that will help control thetide of type 2 diabetes. Pre l i m i n a ry data,f rom a recent outcome study in 154patients newly diagnosed with type 2 dia-betes, have revealed that this algorithm,when implemented by a diabetes nursec a s e - m a n a g e r, reduced mean HbA1 c c o n-
centrations by 1.9% after 1 year( D e F ronzo RA, Anderson E, unpublishedo b s e rvations). We hope that this re v i s e dalgorithm will help clinicians thro u g h o u tthe U.S. to minimize the incidence andseverity of long-term complications intheir patients with type 2 diabetes.
Acknowledgments — Texas Diabetes Coun-cil members and advisory board membersinclude: Maria C. Alen, MD, Chair; Lawre n c eB. Harkless, DPM, Vice Chair; Gene Bell, RN,C F N P, CDE, Secre t a ry; Stuart Fitts; Vi c t o rHugo Gonzalez, MD; Judith L. Haley; Jan B.Hamilton, PhD, RD/LD; Richard S. Hayley;Thomas R. McCann; Cheryl Jenkins Port e r,RD, LD, CDE; Philip Ricks II; Rosa M. Va l e n-zuela, MSSW, LMSW; Linda G. Browne, Te x a sCommission for the Blind; Kay Priest, RN,Texas Department of Human Services; PhilipHuang, MD, MPH, Texas Department ofHealth; Leeda Womack, Texas RehabilitationCommission; Tommy Flemming, Texas Edu-cation Agency; Lee Forshay, MD, physician inprivate practice, Fort Wo rth, TX; Sure n d u r aVa rma, MD, Texas Tech School of Medicine;Charles Reasner, MD, University of Te x a sHealth Sciences Center; Ralph DeFronzo, MD,University of Texas Health Sciences Center;Alan J. Garber, MD, PhD, Baylor College ofMedicine; and Jaime Davidson, MD, physi-cian in private practice, Dallas, TX.
JAIME DAVIDSON, MD
F rom the Texas Department of Health, Austin, Te x a s .A d d ress correspondence to Jaime A. Davidson, MD,
Endocrine & Diabetes Association of Texas, 7777F o rest Lane, B-445, Dallas, TX 75230.
J.D. has received re s e a rch funding from Bayer,Bristol-Meyers Squibb, Eli Lilly, Parke-Davis, HoechstMarion Roussel, Mylan, Novartis, Novo Nordisk, andSchering Plough and consulting or speaking feesf rom Bayer, Bristol-Meyers Squibb, Eli Lilly, Merc k ,Bio Control Technologies, Parke-Davis, NovoN o rdisk, and Boehringer Mannheim.
R e f e re n c e s1. Davidson JA: The treatment of type II dia-
betes in Texas: current issues for managedc a re and employers. Diabetes Care 2 0 :446–451, 1997
2. American Diabetes Association: Standard sof medical care for patients with diabetesmellitus. Diabetes Care 21 (Suppl.1):S23–S31, 1998
3. American Diabetes Association. Scre e n i n gfor type 2 diabetes. Diabetes Care 2 1(Suppl. 1):S20–S22, 1998
4. UK Prospective Diabetes Study Gro u p :E ffect of intensive blood-glucose contro lwith metformin on complications in over-weight patients with type 2 diabetes(UKPDS 34). L a n c e t 352:854–865, 1998

1220 DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999
Letters
5. UK Prospective Diabetes Study Gro u p :Intensive blood-glucose control withs u l p h o n y l u reas or insulin compared withconventional treatment and risk of com-plications in patients with type 2 diabetes(UKPDS 33). L a n c e t 352:837–853, 1998
Glycemic Control and CAD Risk: aH e retical Thought
Now that the dust has settled after therelease of the U.K. Prospective Dia-betes Study results (1), it is time to
reassess the evidence relating the degree ofglycemia in diabetes and its control to car-diovascular risk. Clearly, the interv e n t i o ntrials to date (1–3) in type 2 diabetes thathave tried to assess the benefits ofi m p roved glycemic control have failed toshow a major benefit. Similarly, the follow-up of the Diabetes Control and Complica-tions Trial (DCCT) cohort (Epidemiologyof Diabetes Interventions and Complica-tions) shows no relationship betweenintensive therapy (or HbA1) during theDCCT and either carotid wall thickness(4) or ankle-brachial index (5) (two earlysubclinical markers of athero s c l e rosis) inthis young type 1 diabetic cohort, which isc u rrently too young to have suff e red suff i-cient coro n a ry art e ry disease events and,thus, to analyze fully.
While all of these studies (as indeeddo most studies) have major limitations,these results should not surprise usbecause the epidemiologic data have, fordecades, thrown doubt on a simple re l a-tionship (6,7). Explanations, to date, forthese contradictory findings have usuallyfocused on potential adverse effects of sul-f o n y l u reas, and/or hyperinsulinemia(which may result from sulfonylurea orinsulin therapy). Though these arg u m e n t smay have some merit, they do not fullyexplain the epidemiologic evidence. Is itpossible that, instead of the trial tre a t-ments being bad, hyperglycemia itself (atleast in diabetes) both predicts and pro-tects against coro n a ry athero s c l e rosis andclinical events? Such a hypothesis hasg reat appeal and could operate via thee ffects of advanced glycosylation endp roducts (AGEs) (8) and/or stimulation ofg rowth factors (9). It is proposed thath y p e rglycemia in diabetes, along withmany other facets of diabetes, enhancesa t h e ro s c l e rosis, but, at the same time,
because of AGE formation and pro t e i nc ross-linking (8) and/or stimulation ofg rowth factors (9), the stability of theresulting plaques is increased, re n d e r i n gthem somewhat less likely to ru p t u re andcause events. If this, or a similar model,w e re true, it might reconcile the epidemio-logic and clinical trial data because thep redicted result might be a weak positiverelationship between glycemia and epi-demiological events, while one might pre-dict, as seen in clinical trials, that loweringblood sugar may have a weak negativee ffect as a result of reducing the stabiliza-tion of an increased number of plaques.
P roving such a hypothesis would bed i fficult and would re q u i re either larg edetailed pathologic, or conceivably longi-tudinal angiographic, studies looking for alower number of vulnerable plaques (orru p t u res) as a pro p o rtion of total plaque(or stenotic) burden in diabetic versusnondiabetic subjects. Does anyone havesuch data?
TREVOR J. ORCHARD, MBBCH, MMEDSCI
F rom the Department of Epidemiology, GraduateSchool of Public Health, University of Pittsburg h ,P i t t s b u rgh, Pennsylvania.
A d d ress correspondence to Trevor J. Orc h a rd ,MD, University of Pittsburgh, Epidemiology, 34605th Ave., Rangos Bldg., Pittsburgh, PA 15213. E-mail: [email protected].
T.J.O. has received grant support from theAlteon Company.
R e f e re n c e s1 . UK Prospective Diabetes Study (UKPDS)
G roup: Intensive blood-glucose contro lwith sulphonylureas or insulin compare dwith conventional treatment and risk ofcomplications in patients with type 2 dia-betes (UKPDS 33). L a n c e t 3 5 2 : 8 3 7 – 8 5 2 ,1 9 9 8
2 . Seltzer HS: A summary of criticisms of thefindings and conclusions of the UniversityG roup Diabetes Program (UGDP). D i a -b e t e s 21:976–979, 1972
3 . Abraira C, Colwell JA, Nuttall FQ, SawinC T, Nagel NJ, Comstock JP: Ve t e r a n sa ffairs cooperative study on glycemic con-t rol and complications in type II diabetes( VA CSDM). Diabetes Care 1 8 : 1 1 1 3 – 1 1 2 3 ,1 9 9 5
4 . Zinman B, Cleary P, O’Leary D, Orc h a rd T:The effect of intensive diabetes tre a t m e n ton carotid art e ry wall thickness in the Epi-demiology of Diabetes Interventions andComplications (Abstract). D i a b e t e s 4 5(Suppl. 2):188A, 1996
5 . O rc h a rd T, Cleary P, Genuth S, Nathan D:
C o rrelates of lower extremity arterial dis-ease in type 1 diabetes (Abstract). D i a -b e t o l o g i a 41 (Suppl. 1):334A, 1998
6 . B a rrett-Connor E: Does hyperg l y c e m i areally cause coro n a ry heart disease? D i a -betes Care 20:1620–1623, 1997
7 . O rc h a rd TJ: Hyperglycemia and coro n a ryh e a rt disease. Diabetes Care 2 1 : 3 2 1 – 3 2 2 ,1 9 9 8
8 . Bucala R, Vlassara H: Advanced glycosyla-tion end products in diabetic renal andvascular disease. Am J Kidney Dis 2 6 :875–888, 1995
9 . Clemmons DR: Role of peptide gro w t hfactors in development of macro v a s c u l a rcomplications of diabetes. Diabetes Care14:153–156, 1991
L o w - D e n s i t yL i p o p rotein Part i c l eSize as an Independent P redictor of Glycated Low-DensityL i p o p rotein Level
The increased glycation of apolipopro-tein has been suggested to have ani m p o rtant role in the accelerated
development of athero s c l e rosis in patientswith diabetes (1,2). Small dense LDL par-ticles are a recognized risk factor for coro-n a ry heart disease (3,4). Thus, both theglycation of LDL and the predominance ofsmall dense LDL particles may contributeto the increased risk of athero s c l e rosis inpatients with diabetes. However, littlei n f o rmation is available re g a rding the re l a-tionship between the glycated LDL leveland LDL particle size. In the present study,our objective was to determine whetherthe glycated LDL level and LDL part i c l esize are re l a t e d .
A total of 175 subjects undergoing aroutine medical checkup were enrolled inthe present study. Informed consenta p p roved by the ethics committee ofNagoya University was obtained from allsubjects, and none of them had been diag-nosed as having diabetes. The peak size ofLDL particles was determined by use of2–16% nondenaturing polyacry l a m i d egradient gel electro p h o resis as describedp reviously (5). The competitive enzyme-linked immunosorbent assay with amonoclonal antibody that was capable ofrecognizing a specific epitope of glycated

DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999 1221
Letters
a p o l i p o p rotein B within the LDL complexwas used for the determination of glycatedLDL levels (6).
The mean age of the 175 subjects was49.7 ± 8.4 (mean ± SD) years. There were132 men, aged 27–73 years, and 43women, aged 30–65 years. The mean lev-els of fasting glucose, HbA1 c, and fastinginsulin were 5.39 ± 1.49 mmol/l, 5.74 ±1.23%, and 34.8 ± 27.7 pmol/l, re s p e c-t i v e l y, all of which were within norm a lrange. The mean LDL particle size was263 ± 8 Å. The glycated LDL level showeda significant inverse correlation with theLDL particle size (r = 20.440, P ,0.0001) and positive correlations with age(r = 0.200, P = 0.0080) and the plasmalevels of total cholesterol (r = 0.227, P =0.0026), LDL cholesterol (r = 0.161, P =0.0334), triglycerides (r= 0.225, P= 0.0027),fasting glucose (r = 0.322, P , 0 . 0 0 0 1 ) ,and HbA1 c (r = 0.309, P , 0.0001). Thef o rw a rd stepwise re g ression analysisshowed that the LDL particle size corre-lated best with the glycated LDL level (R2 =0.194). The next factor that contributeds i g n i ficantly to the correlation coeff i c i e n twas the plasma fasting glucose level. Thetotal variance explained by these twoparameters was 0.235.
We analyzed these relationships sepa-rately for the male and female subjectsbecause it has been re p o rted that LDL par-ticle size is influenced by sex and, inwomen, by menopausal status (7,8). Forthe men, glycated LDL level was s i g n i fi-cantly correlated with LDL particle size (r =20.411, P , 0.0001). The women alsoshowed a strong correlation between gly-cated LDL level and LDL particle size (r =20.461, P = 0.0019). No significant re l a-tionship was observed between glycatedLDL level and menopausal status (r =0.116, NS) of the women. Regre s s i o nanalysis for the men showed associationssimilar to those for all subjects (total R2 =0.215). LDL particle size was the onlyindependent factor that influenced the gly-cated LDL level in the women (R2 = 0.213).
In the present study, mean plasma lev-els of triglycerides, fasting glucose, HbA1 c,and fasting insulin were within norm a lrange, and the correlation between gly-cated LDL level and LDL particle size wass i g n i ficant. These results suggest that thec o rrelation between glycated LDL leveland LDL particle size may be seen even inthe absence of diabetes or abnormal lipidmetabolism. In addition, LDL particle sizewas found to be a determinant of the gly-
cated LDL level. The separate analyses ofmale and female subjects in the pre s e n tstudy also suggest that the corre l a t i o nbetween glycated LDL level and LDL part i-cle size exists independent of sex ormenopausal status. It has been re p o rt e dthat LDL particle size is determined notonly by metabolic status and therapeutici n t e rventions, but also by genetic factors(9,10). This implies that LDL may have alonger residence time in plasma in someindividuals than in others, allowing it tobecome more glycated and potentiallym o re atherogenic on this count. Individu-als with genetically small LDL part i c l e smay re q u i re more strict glycemic contro lthan those with normal-sized LDL.
In the present study, the fasting glu-cose level was also an independent factorthat influenced the glycated LDL level.H o w e v e r, it was a weaker determinant ofthe glycated LDL level than LDL part i c l esize. This may be because most subjects inthe present study had normal plasma glu-cose levels.
In summary, we observed a signific a n tnegative correlation between glycated LDLlevel and LDL particle size. LDL part i c l esize was shown to independently pre d i c tthe glycated LDL level. The separate analy-ses of male and female subjects had similarresults re g a rding the relationship betweenglycated LDL level and LDL particle size.Small LDL particles are likely to underg oglycation, even in the normal plasma glu-cose state. This change is accelerated byh y p e rglycemia, possibly influencing thep ro g ression of art e r i o s c l e rosis in patientswith diabetes.
HIDEO MATSUI, MD
KENJI OKUMURA, MD
YUKIO TOKI, MD
TETSUO HAYAKAWA, MD
F rom Internal Medicine II, Nagoya UniversitySchool of Medicine, Nagoya, Japan.
A d d ress correspondence to Hideo Matsui, MD,I n t e rnal Medicine II, Nagoya University School of Med-icine, 65 Ts u rumai-cho, Showa-ku, Nagoya 466-8550,Japan. E-mail: hideom@tsuru . m e d . n a g o y a - u . a c . j p .
R e f e re n c e s1 . Colaco CALS, Roser BJ: Athero s c l e ro s i s
and glycation. B i o e s s a y s 1 6 : 1 4 5 – 1 4 7 ,1 9 9 4
2 . Lyons TJ, Jenkins AJ: Lipoprotein glyca-tion and its metabolic consequences. C u rrOpin Lipidol 8:174–180, 1997
3 . Austin MA, Breslow JL, Hennekens CH,Buring JE, Willett WC, Krauss RM: Low-
density lipoprotein subclass patterns andrisk of myocardial infarction. J A M A260:1917–1921, 1988
4 . Campos H, Genest JJ Jr, Blijlevens E,McNamara JR, Jenner JL, Ordovas JM,Wilson PWF, Schaefer EJ: Low densityl i p o p rotein particle size and coro n a rya rt e ry disease. A rterioscler Thro m b12:187–195, 1992
5 . Nichols AV, Krauss RM, Musliner TA :Nondenaturing polyacrylamide gradientgel electro p h o resis. Methods Enzymol128:417–431, 1986
6 . Shea EA, Cohen MP: Immunologic detec-tion and measurement of glycateda p o l i p o p rotein B with site specific mono-clonal antibodies. J Immunol Methods162:85–95, 1993
7 . Campos H, McNamara JR, Wilson PWF,O rdovas JM, Schaefer EJ: Diff e rences inlow density lipoprotein subfractions anda p o l i p o p roteins in premenopausal andpostmenopausal women. J Clin EndocrinolM e t a b 67:30–35, 1988
8 . Wiliams PT, Vranizan KM, Krauss RM:C o rrelations of plasma lipoproteins withLDL subfractions by particle size in menand women. J Lipid Res 3 3 : 7 6 5 – 7 7 4 ,1 9 9 2
9 . Austin MA, Krauss RM: Genetic control ofl o w - d e n s i t y - l i p o p rotein subclasses. L a n c e t2:592–595, 1986
1 0 . Rotter JI, Bu X, Cantor RM, Wa rden CH,B rown J, Gray RJ, Blanche PJ, Krauss RM,Lusis AJ: Multilocus genetic determ i n a n t sof LDL particle size in coro n a ry art e ry dis-ease families. Am J Hum Genet 5 8 :585–594, 1996
Hypersensitivity toRegular and I n t e rmediate, butNot to Cry s t a l l i z e d ,Insulin as an Aggravation Factorfor UnderlyingBulimia Nervosa ina Patient With Type 1 Diabetes
The use of recombinant human insulinhas decreased the incidence of allerg i cresponses to insulin, but has not elim-
inated them. In most cases, such allerg i cresponses are induced by IgG antibodiesand target concomitant materials such asp rotamine or pre s e rvatives (1). There arer a re cases of immediate type hypersensitiv-

1222 DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999
Letters

DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999 1223
Letters
ity to regular and intermediate-type insulin,but not to long-acting insulin (2,3). Thecoexistence of eating disorders with type 1diabetes is common among young femalepatients and significantly complicates man-agement (4–6). We re p o rt a patient whodemonstrated an allergic response to all butultralente human insulin and had anunderlying eating disord e r.
A 22-year-old woman was diagnosedas having type 1 diabetes when she beganto experience thirst, muscle cramps,polydipsia, and a loss of body weight inDecember 1995. Body weight on the fir s thospital admission was 35 kg (BMI 15.1k g / m2). Fasting plasma glucose was 15.9mmol/l, HbA1 c was 14.1% (normal range4.2–5.7), and anti-GAD antibody waspositive in her serum, at 23 U/ml (norm a lrange ,5). Treatment was initiated withp remixed 70:30 insulin, with a subse-quent improvement in HbA1 c to 6.6%.The patient feared diabetic complicationsand became very preoccupied with herblood glucose level. For several monthsafter the first hospitalization, she wasv e ry compliant in her treatment pro g r a m .H o w e v e r, she gradually tended to con-sume more sweets, sugar, and fatty richfoods instead of the high-fiber diet thathad been prescribed. In September 1996,the patient noticed local itchy wheal-and-fla re reactions at the sites of injection andoccasionally felt nausea. The emerg e n c eof insulin allergy began to disturb herblood glucose levels, resulting in ani n c rease in insulin re q u i rement. Thei n c reased dose of insulin triggered con-c e rn about becoming obese, and shebegan self-induced vomiting for weightc o n t rol. Her menstrual periods ceased.She was hospitalized again in Marc h1997 and fulfilled the criteria for bulimian e rvosa in Diagnostic and Statistical Man -ual of Disorders, Fourth Edition ( D S M - I V )(7) because she had a history of binge-eating and purging episodes. The patientstopped self-induced vomiting, but thenused laxatives to reduce her body weightand occasionally reduced her dose orstopped injecting insulin. Physical exam-ination revealed that she was 152 cm talland weighed 36.2 kg. She had a smallsubcutaneous induration at the site of herinsulin injection. Her Achilles tendonre flex could not be elicited. Her skin wasd ry, and her palms were yellow. Ocularfundus photography revealed no sign ofre t i n o p a t h y. Laboratory tests wereremarkable for ery t h rocyte: 368 3 1 04
per µl; HbA1 c was 11%. Her serum bind-ing to 1 2 5I-labelled human insulin was84% of nonspecific binding (,10%), andIgE to human insulin was positive asshown by the titer of 4.54 U/ml (,0 . 3 5 ) .Her HLA was positive for DR6/9,DR52/53, and DQ1/3. She did not haveHLA-DR4, which has been re p o rted to beassociated with an immune response toinsulin (8). All types of available re c o m-binant human insulin showed positivereactions except recombinant ultralentehuman insulin (Novolin U/Ultratard ;Novo Nordisk A/S, Bagsvaerd, Denmark;not available in U.S.) (Table 1). Nonaller-gic recombinant ultralente insulin usesthe same buffer agents as Humalin N andNovolin N, and the same isotonic agentsand pre s e rvatives as Monotard humaninsulin. The skin test was perf o rmed bythe same batches of syringes and diluentusing 50 µl of 0.01 U/ml each insulin.The cutaneous responses were negativeafter challenge by diluents for Humulin R(containing concentrated glycerin and m-c resol), Humulin N (containing pro t a-mine sulfate, concentrated glycerin, m-c resol, and phenol), and Humulin L/U(containing ZnO and methyl parahy-d roxy benzoate) from Eli Lilly (Indi-anapolis, IN). There f o re, the allergy isattributed to the conformational changeof insulin itself. Takatsuki et al. (2) alsore p o rted a similar response in a patientwith type 2 diabetes, and they concludedthat antibodies recognized insulin itselfbecause originally nonallergic ultralentehuman insulin acquired antigenicity afterinsulin was decrystallized by acidifyingwith acetic acid. Treatment with a neu-tralizing and crystallizing maneuver mayinduce conformational change and re s u l tin less antigenicity. Treatment with cry s-tallized human insulin (Novolin U/Ultra-t a rd) and the least allergic regular insulin(Novolin R) was started, along with oraladministration of antihistamine (mex-tazine) to reduce the allergic response asmuch as possible. Blood glucose declinedto an acceptable range, and her glycosy-lated HbA1 c declined from 10.7 to 7.1%.She gradually accepted proper bodyweight control and recognized her dis-t o rted body image. Her menstru a t i o nresumed 6 months after the final men-s t ruation period.
The allergy to insulin undermined thisp a t i e n t ’s eff o rts to achieve glycemic contro l .The complication of immediate-typehypersensitivity to human insulin is rare ,
while eating disorders are common amonginsulin-treated women with diabetes.T h e re f o re, careful attention must be paid tothe care of young women with type 1 dia-betes, especially when presenting withunexplained poor glycemic contro l .
A c k n o w l e d g m e n t s — The authors gratefullyacknowledge the review of the manuscript byD r. B.L. Furman (Department of Physiologyand Pharm a c o l o g y, University of Strathclyde).The authors also thank N. Takekawa for secre-tarial assistance.
MITSUYASU ITOH, MD
KEIKO UCHIMURA, MD
MASAKI MAKINO, MD
TAKAKO KOBAYASHI, MD
HIROAKI KAKIZAWA, MD
MUTSUKO NAGATA, MD
KENTARO FUJIWARA, MD
SEIYA KATO, MD
YASUTOSHI ITOH, MD
AKIO NAGASAKA, MD
F rom the Division of Endocrinology and Metabo-lism, the Department of Internal Medicine, FujitaHealth University, School of Medicine, To y a k e ,Aichi, Japan.
A d d ress correspondence to Mitsuyasu Itoh, MD,Division of Endocrinology and Metabolism, Depart-ment of Internal Medicine, Fujita Health University,School of Medicine, 1-98 Dengakugakubo, Kut-sukake, Toyoake, Aichi 470-1192, Japan. E-mail:m i t u y a s u @ f u j i t a - h u . a c . j p .
R e f e re n c e s1 . K u rtz AB, Gray RS, Markanday S, Nabarro
JD: Circulating IgG antibody to pro t a m i n ein patients treated with pro t a m i n e - i n s u l i n s .D i a b e t o l o g i a 25:322–324, 1983
2 . Takatsuki H, Ishii H, Yamauchi T,Nakashima N, Nagase S, Hisatomi A,Umeda F, Nawata H: A case of insulina l l e rgy: the crystalline human insulin maymask its antigenicity. Diabetes Res ClinP r a c t 12:137–139, 1991
3 . Takagi M, Kamoi K, Kaneko K: A case ofinsulin allergy with reaction to short - a c t-ing and intermediate-acting insulins butnot to long-acting insulins. J Japan Diab Soc39:205–210, 1996
4. Hudson JI, Wentworth SM, Hudson MS,Pope HG Jr: Prevalence of anorexia nervosa and bulimia among young dia-betic women. J Clin Psychiatry 46:88–89, 1985
5 . Rydall AC, Rodin GM, Olmsted MP,Devenyi RG, Daneman D: Disord e red eat-ing behavior and microvascular compli-cations in young women with insulin-dependent diabetes mellitus. N Engl J Med336:1849–1854, 1997
6 . Rodin GM, Daneman D: Eating disord e r s

1224 DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999
Letters
and IDDM. Diabetes Care 1 5 : 1 4 0 2 – 1 4 1 2 ,1 9 9 2
7 . American Psychiatric Association: D i a g -nostic and Statistical Manual of Disord e r s ,F o u rth Edition. Washington, DC, AmericanPsychiatric Association, 1994
8 . S c h e rnthaner G: Immunogenicity anda l l e rgenic potential of animal and humaninsulins. Diabetes Care 16 (Suppl. 3):155–165, 1993
Endothelial Dysfunction Is NotReversed by Simvastatin Treatment in Type 2Diabetic Patients Wi t hH y p e rc h o l e s t e ro l e m i a
Patients with type 2 diabetes are asso-ciated with a marked increase in therisk of coro n a ry heart disease death.
R e c e n t l y, Celermajor et al. (1) developed anoninvasive method to measure vascularendothelial function by assessing the dila-tion of the brachial art e ry in response tothe increase in blood flo w, a response thatis mediated by the release of nitric oxidef rom endothelial cells. By administrationof nitrate, which causes smooth musclerelaxation, it can also be used to distin-guish endothelial-dependent and -inde-pendent vascular dysfunction. Although ithas been re p o rted that cholesterol lower-ing improves brachial vasoactivity inh y p e rc h o l e s t e rolemic subjects (2), it is notknown whether lowering serum choles-t e rol improves endothelial function inthose type 2 diabetic patients who are sus-ceptible to or who already have endothe-lial injury (3).
We re c ruited 21 type 2 diabetic sub-jects with hyperc h o l e s t e rolemia and 21age-, sex-, and BMI-matched nondiabeticc o n t rol subjects. After baseline evaluations,patients were assigned to take 10 mg sim-vastatin every night for a total of 24 weeks.
Brachial art e ry vasoactivity was evalu-ated as described previously (1). After deter-mination of baseline arterial diameter andblood flow velocity, a blood pre s s u re cuffwas inflated to a pre s s u re of 200 mmHg andmaintained for 5 min. The brachial art e rywas scanned before and immediately afterc u ff deflation and then for 20 min. After 20min, nitroglycerin (0.6 mg) was adminis-t e red sublingually for an additional 20 min.
The result showed that baselinebrachial art e ry diameter, either expre s s e das absolute values (4.71 ± 0.17 vs. 4.41 ±0.16 mm, P 5 NS) or divided by bodys u rface area (2.70 ± 0.08 vs. 2.60 ± 0.06m m / m2, P 5 NS), was relatively similarin type 2 diabetic patients and nondia-betic subjects. Baseline brachial art e ryflow did not differ between diabetic indi-viduals and control subjects (127 ± 11 vs.100 ± 5 ml/min, P 5 NS). Peak perc e n t-age change in diameter was signific a n t l ysmaller in the diabetic than in the nondi-abetic group (6.1 ± 0.8 vs. 9.5 ± 1.2, P ,0.05). Percent changes of nitro g l y c e r i n -induced vasodilatation were also signifi-cantly smaller in diabetic subjects than innondiabetic individuals (14.5 ± 1.0 vs.19.7 ± 2.1, P , 0 . 0 5 ) .
In response to simvastatin tre a t m e n t ,total cholesterol decreased from (mean ±SEM) 6.3 ± 0.1 mmol/l to 5.1 ± 0.2, 4.8 ±0.2, and 4.7 ± 0.2 at weeks 4, 12, and 24,respectively (P , 0.001). LDL cholestero lvalues fell from 4.2 ± 0.1 mmol/l to 3.1 ±0.2, 2.8 ± 0.2, and 2.7 ± 0.2 mmol/l (P ,0.001). Fasting plasma triglyceride levelsd e c reased from 2.1 ± 0.2 mmol/l to 1.9 ±0.2, 1.9 ± 0.2, and 1.6 ± 0.2 mmol/l (P ,0.05), while HDL cholesterol levels didnot change after simvastatin administra-tion. Baseline diameter and flow ofbrachial art e ry did not change after sim-vastatin administration for 24 weeks( Table 1).
P revious studies of lipid-loweringtherapy on endothelial function in hyper-c h o l e s t e rolemic subjects have pro d u c e dc o n t roversial findings. Treatment withsimvastatin for 12 weeks improved brachiala rt e ry vasoactivity in a group of m i d d l e -aged men (4). However, lipid-loweringt reatment for 6 months could not com-pletely re s t o re acetylcholine-inducedvasodilatation in the coro n a ry arteries ofh y p e rc h o l e s t e rolemic subjects (5). Ve ry
re c e n t l y, an Armed Forces Regre s s i o nStudy showed that pharmacological ther-apy for 30 months did not pro d u c echanges in flow-mediated brachial vasodi-lation (6). Despite a 26–35% reduction inLDL cholesterol levels, we failed to detectan improvement in flow-mediated orn i t roglycerin-induced vasodilation in type 2diabetic subjects with hyperc h o l e s-t e rolemia after simvastatin treatment for24 weeks. All of our diabetic subjects havehad a history of diabetes for .5 years andless than satisfactory glucose contro l ,which might lead to severe and irre-versible vascular change (3).
In summary, type 2 diabetic patientswith hyperc h o l e s t e rolemia had impaire dendothelium-dependent and -independentbrachial art e ry vasoactivities when com-p a red with nondiabetic individuals. Despiteits effect of lowering circulating cholestero lconcentrations, simvastatin therapy for 24weeks did not produce significant changesin endothelium-dependent or -indepen-dent brachial art e ry vasoactivity.
A c k n o w l e d g m e n t s —This study was sup-p o rted by grants from the National ScienceCouncil, Taiwan, ROC (NSC 88-2314-B075A-014) and from Veterans General Hospital,Taichung, Taiwan (TCVGH 883503C andVGHTH 87-025-3).
WAYNE HUEY-HERNG SHEU, MD, PHD
BEEN-LIN JUANG, MS
YING-TSUNG CHEN, MD
WEN-JANE LEE, PHD
F rom the Divisions of Endocrinology and Metabo-lism (W. H . - H . S . , W.-J.L.) and Cardiology (Y. - T. C . ) ,D e p a rtment of Internal Medicine, Taichung Ve t e r-ans General Hospital; the Department of ChemicalEngineering (B.-L.J.), Tunghai University; andChung-Shan Medical and Dental College, Ta i c h u n g ;and the National Yang-Ming University, Taipei, Ta i-wan, Republic of China.
A d d ress correspondence to Wayne Huey-Hern gSheu, MD, PhD, No. 160, Section 3, Chung-Kang
Table 1—Brachial artery vasoactivity in type 2 diabetic patients with hypercholesterolemiabefore and after administration of simvastatin
Week0 4 12 24
BaselineDiameter (mm) 4.71 ± 0.17 4.67 ± 0.17 4.87 ± 0.18 4.83 ± 0.17Flow (ml/min) 127 ± 11 130 ± 14 152 ± 13 149 ± 16
Peak diameter percent change (%)Flow-mediated 6.1 ± 0.8 7.2 ± 0.7 7.0 ± 0.8 7.7 ± 0.9Nitrate-induced 14.5 ± 1.0 ND 13.2 ± 1.2 13.3 ± 1.3
Data are means ± SEM. ND, not done.

DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999 1225
Letters
Road, Division of Endocrinology and Metabolism,Taichung Veterans General Hospital, Taichung, Taiwan 407. E-mail: [email protected]. t w.
R e f e re n c e s1 . C e l e rmajor D, Sorensen K, Gooch V,
Spegelhalter D, Miller O, Sullivan I, LloydJ, Deanfield J: Non-invasive detection ofendothelial dysfunction in children andadults at risk of athero s l c e rosis. L a n c e t340:1111–1115, 1992
2 . S t roes SG, Koomans HA, de Bruin TWA ,Rabelink TJ: Vascular function in the fore-a rm of hyperc h o l e s t e rolemic patients offand on lipid-lowering medications. L a n c e t346:467–471, 1995
3 . Stehouwer CDA, Lambert J, Donker AJM,van Hinsbergh VWM: Endothelial dys-function and pathogenesis of diabetica n g i o p a t h y. C a rdiovascular Res 3 4 : 5 5 – 6 8 ,1 9 9 7
4 . Vogel RA, Corretti MC, Plotnick GD:Changes in flow-mediated brachial art e ryvasoactivity with lowering of desirablec h o l e s t e rol levels in healthy middle-agedmen. Am J Card i o l 77:37–40, 1996
5 . Leung WH, Lau CP, Wong CK: Benefic i a le ffect of cholesterol-lowering therapy onc o ro n a ry endothelium-dependent re l a x-ation in hyperc h o l e s t e rolemic patients.L a n c e t 341:1496–1500, 1993
6 . A n d rews TC, Whitney EJ, Green G, Kalen-ian R, Personius BE: Effect of gemfib rozil ±niacin ± cholestyramine on endothelialfunction in patients with serum low den-sity lipoprotein cholesterol level ,1 6 0mg/dl and high density lipoprotein choles-t e rol level ,40 mg/dl. Am J Card i o l80:831–835, 1997
C O M M E N T S A N DR E S P O N S E S
Clinical Features ofElderly Patients Wi t hType 2 Diabetes
Few studies have surveyed the clinicalf e a t u res of elderly patients with type 2diabetes, even though their numbers
a re pro g ressively increasing (1–3). Aging isa major risk factor for glucose intolerance,and both impaired insulin secretion andinsulin resistance appear to contribute toa g e - related risk (4–6). We compare delderly patients with type 2 diabetes withmiddle-aged patients to identify diff e r-
ences and similarities and to help in deter-mining how best to treat elderly patientswith this disease.
A total of 337 consecutive patientswith type 2 diabetes were divided into twog roups: 174 patients aged $65 years(elderly patients; 85 men, 89 women), and163 patients aged ,65 years (middle-agedpatients; 99 men, 64 women). In addition,the 174 elderly patients were divided intos u b g roups by age at onset (before or after65 years) and duration of diabetes (moreor less than 10 years). Clinical features ofelderly patients with type 2 diabetes are asfollows: BMI was lower (21.8 ± 2.9 vs.22.9 ± 3.2 kg/m2, P , 0.001 by unpaire dS t u d e n t ’s t test) and the percentage of bodymass re p resented by fat was higher (27.2 ±6.3 vs. 24.7 ± 5.8%, P , 0.001) in elderlythan in middle-aged patients. HbA1 c l e v e l sand fasting serum C-peptide concentra-tions were similar between groups. As form i c ro a n g i o p a t h y, the relative frequency ofnondiabetic retinopathy was lower (67.8vs. 82.2%, P , 0.01 by x2 test), while fre-quencies of macroalbuminuria and severen e u ropathy were higher (12.6 vs. 3.7%, P , 0.01; 21.8 vs. 8.0%, P , 0 . 0 0 5 ,respectively), in elderly patients. Amongelderly patients, HbA1 c levels were lower(6.4 ± 1.0 vs. 7.0 ± 1.0%, P , 0.001) inpatients whose age at onset was at least 65 years (late-onset subgroup). Relativef requencies of nondiabetic re t i n o p a t h yand normoalbuminuria were higher (85.3 vs. 54.5%, P , 0.001; 65.3 vs.43.4%, P , 0.01, respectively) and thoseof pro g ressive diabetic retinopathy andinsulin use were lower (2.7 vs. 22.2%, P ,0.005; 17.3 vs. 38.4%, P , 0.01, re s p e c-tively) in the late-onset subgroup than inpatients whose age at onset was under 65 years (early-onset subgroup). Fastings e rum C-peptide concentrations werelower (0.53 ± 0.30 vs. 0.70 ± 0.40 nmol/l,P , 0.001) and HbA1 c levels were higher(7.1 ± 0.9 vs. 6.3 ± 1.1%, P , 0.001) inpatients with a duration of diabetes of atleast 10 years (long-duration subgro u p ) .Relative frequencies of nondiabeticre t i n o p a t h y, normoalbuminuria, and tre a t-ment with diet alone were lower (45.8 vs.87.9%, P , 0.001; 42.2 vs. 62.6%, P ,0.05; 4.8 vs. 29.7%, P , 0.001, re s p e c-tively) and those of pro g ressive diabeticretinopathy and insulin use were higher(26.5 vs. 2.2%, P , 0.001; 45.8 vs.11.0%, P , 0.001, respectively) in thelong-duration subgroup than in the short -duration patients.
In summary, elderly patients with type 2diabetes had a high ratio of body fat to l e a nbody mass and more advanced micro a n-giopathy than middle-aged patients, whilec o n t rol of diabetes, endogenous insulinrelease, and prevalences of tre a t m e n tmodalities were similar. Many patientsachieved good control without insulin useand diabetic microangiopathies were lesss e v e re in the late-onset than in the early-onset subgroup. Furt h e rm o re, endoge-nous insulin release was diminished in thelong-duration subgroup, where control ofdiabetes was poorer despite a high pre v a-lence of insulin use, and diabetic micro a n-giopathies were more advanced, than inthe short-duration subgroup. In conclu-sion, elderly patients with early onset andlong duration of type 2 diabetes re q u i respecial attention to glycemic control andassessment of and interventions againstm o re advanced micro a n g i o p a t h i e s .
MICHIAKI FUKUI, MD
NAOTO NAKAMURA, MD
TAKAAKI MIZUTANI, MD
MOTOHARU KONDO, MD
F rom the Department of Medicine and EndocrineUnit (M.F., T.M.), Ayabe Municipal Hospital; andthe First Department of Internal Medicine (M.F. ,N.N., M.K.), Kyoto Prefectural University of Medi-cine, Kyoto, Japan.
A d d ress correspondence to Michiaki Fukui, theD e p a rtment of Medicine and Endocrine Unit, Ay a b eMunicipal Hospital, 20-1 Otsuka Aono-cho, Ay a b eC i t y, Kyoto 623-0011, Japan.
R e f e re n c e s1 . H a rris MI, Hadden WC, Knowler WC,
Bennett PH: Prevalence of diabetes andi m p a i red glucose tolerance and plasmaglucose levels in U.S. population aged20–74 yr. Diabetes 36:523–534, 1987
2 . Meneilly GS, Elliott T, Tessier D, Hards L,Tildesley H: NIDDM in the elderly. D i a -betes Care 19:1320–1325, 1996
3 . Jackson RA, Blix PM, Matthews JA, Ham-ling JB, Din BM, Brown DC, Belin J,Rubenstein AH, Nabarro JD: Influence ofageing on glucose homeostasis. J ClinEndocrinol Metab 55:840–848, 1982
4 . Shimizu M, Kawazu S, Tomono S, Ohno T,Utsugi T, Kato N, Ishii C, Ito Y, Murata K:A g e - related alteration of pancreatic b- c e l lfunction. Diabetes Care 19:8–11, 1996
5 . Gumbiner B, Polonsky KS, Beltz WF, Wa l -lace P, Brechitel G, Fink RI: Effects of agingon insulin secretion. Diabetes 3 8 : 1 5 4 9 – 1 5 5 6 ,1 9 8 9
6 . Rowe JW, Minaker KL, Pallotta JA: Charac-terization of the insulin resistance of aging.J Clin Invest 71:1581–1587, 1983

1226 DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999
Letters
Response to Fukuiet al.
The letter by Fukui et al. (1) re p re-sents an interesting contribution tothe literature. As the authors cor-
rectly state, few studies have surveyed theclinical features of elderly patients withtype 2 diabetes, even though their num-bers are pro g ressively increasing. How-e v e r, several issues need to be addre s s e din re g a rd to their submission. First, theauthors suggest that insulin resistance is amajor contributing factor to the glucoseintolerance of aging. Recent studies sug-gest that insulin resistance may be lessi m p o rtant than previously thought (2).When interpreting the data, North Amer-ican and European readers should notethat the BMI (,22) and HbA1 c (,7 % )levels in the elderly patients are substan-tially lower than is generally seen in Cau-casian populations, limiting the general-izability of the results. The elderly sub-jects had a lower BMI but a higherp e rcentage of body fat than young sub-jects. Was there a diff e rence in fat distri-bution between groups, such as a diff e r-ence in waist-to-hip ratio? The methodfor determining body fat should bestated, since certain methods are inaccu-rate in the elderly. The authors state thatelderly patients had a lower frequency ofretinopathy but a higher frequency ofm a c roalbuminuria and neuropathy whenc o m p a red with young subjects. Howw e re these complications diagnosed?We re young and old subjects matched forduration of diabetes, which would obvi-ously affect the likelihood of complica-tions? Elderly patients who developedthe disease after age 65 years had a lowerf requency of retinopathy and nephro p a-t h y. Since the subjects who developeddiabetes after age 65 presumably had as h o rter duration of disease, the lower fre-quency of complications in this gro u pwas probably the result of shorter diseaseduration, and not an effect of the agingp rocess. Other risk factors such as hyper-tension, smoking, and hyperlipidemiap resumably alter the risk of complicationin elderly patients with diabetes. We rethese factors evenly distributed in the dif-f e rent patient groups? Finally, the authorsneglect to re f e rence several import a n tpapers that have found that bothglycemic control and duration of diabetesmodify the risk of macrovascular and
m i c rovascular complications in theelderly patient with diabetes (3–6).
In summary, this submission is a valu-able contribution to the literature, but thedata need to be carefully interpre t e d .
GRAYDON S. MENEILLY, MD
A d d ress correspondence to Graydon S. Meneilly, MD,S-169, 2211 We s b rook Mall, Va n c o u v e r, BC, V6T 2B5,C a n a d a .
R e f e re n c e s1 . Fukui M, Nakamura N, Mizutani T,
Kondo M: Clinical features of elderlypatients with type 2 diabetes (Letter). D i a -betes Care 22:1225, 1999
2 . F e rrannini E, Vichi S, Beck-Nielsen H,Laakso M, Paolisso G, Smith U, Euro p e a nG roup for the Study of Insulin Resistance(EGIR): Insulin action and age. D i a b e t e s45:947–953, 1996
3 . Kuusisto J, Mykkanen L, Pyorala K, LaaksoM: NIDDM and its metabolic control pre-dict coro n a ry heart disease in elderly sub-jects. D i a b e t e s 43:960–967, 1994
4 . Kuusisto J, Mykkanen L, Pyorala K,Laakso M: Non–insulin-dependent dia-betes and its metabolic control are impor-tant predictors of stroke in elderly sub-jects. S t roke 25:1157–1164, 1994
5 . Nathan DM, Singer DE, Godine JE, Har-rington DH, Perlmuter LC: Retinopathy inolder type 2 diabetics: association with glu-cose contro l . D i a b e t e s 35:797–801, 1986
6 . Morisaki N, Watanabe S, Kobayashi J,Kanzaki T, Takahashi K, Yokote K, Te z u k aM, Ta s h i ro J, Inadera H, Saito Y: Diabeticc o n t rol and pro g ression of retinopathy inelderly patients: five-year follow-up study.J Am Geriatr Soc 42:142–145, 1994
2 - Year Pro s p e c t i v eAudit of the Effect ofthe Introduction ofInsulin Lispro inPatients With S p e c i fic C l i n i c a lI n d i c a t i o n s
Clinical studies have shown thatinsulin lispro (Humalog; Eli Lilly,Indianapolis, IN) may lead to
i m p roved glycemic control with long-termtherapy in type 1 diabetes (1,2) and that itis associated with less weight gain andi m p roved patient satisfaction (3) whenc o m p a red with soluble insulin. An
i m p rovement in HbA1 c by 0.3–0.4% as aresult of using insulin lispro has also beendemonstrated in some of these studies(4,5). These results may be due to thenotable diff e rences in the pharm a c o k i n e t-ics of insulin lispro, specific a l l y, fasteronset and shorter duration of action and ahigher peak concentration.
After the introduction of insulin lisproin the U.K., we conducted a pro s p e c t i v eaudit of its use to study efficacy in selectedpatients attending our clinic. Insulin lisprowas off e red to patients who had one of thefollowing clinical indications: 1) inabilityto wait between injections and meals, 2) excessive postprandial hyperg l y c e m i a ,3) late postprandial hypoglycemia, or 4) nocturnal hypoglycemia. Soluble insulinin basal bolus therapy was replaced withinsulin lispro, with no change in theo v e rnight insulin type. Insulin lispro wass t a rted in 221 diabetic patients (type 1 n =198, type 2 n = 23), average age 41.3 ±11.6 years, mean duration of diabetes 18 ±1 years. Ethnic backgrounds consisted ofwhite Caucasian (209), South Asian (8),A f ro-Caribbean (3), and Chinese (1).
B e f o re commencement of insulinl i s p ro, mean HbA1 c was 9.11 ± 0.15%. At6 months, mean HbA1 c fell signific a n t l yto 8.56 ± 0.19% (n = 211, P , 0 . 0 0 5 )and mean insulin dose fell from 63.2 ± 5 to 56.4 ± 3.9 U/day (P , 0.01). After 1 year, mean HbA1 c was 8.78 ± 0.20% (n= 177, P , 0.005 compared with base-line values); 49 and 22 patients oninsulin lispro were followed up for 18months and 2 years, re s p e c t i v e l y. At 18months, mean HbA1 c was 8.66 ± 0.33 (P, 0.005), and at 2 years, mean HbA1 c
was 8.36 ± 0.37% (NS).The mean weight gain of the patients
on insulin lispro has been 1.5 ± 1.48k g / y e a r. The number of patients whore p o rted severe hypoglycemic episodesrequiring assistance from another personin the preceding 6 months was similar (12vs. 13) before and after insulin lispro tre a t-ment. In a further audit of 30 patientsf rom the group, however, the self-assessedhypoglycemia score fell signific a n t l y, fro m1.32 ± 0.1 to 0.25 ± 0.01 U (P , 0.01). Atotal of 14 episodes of diabetic ketoacido-sis occurred in 10 individuals over the 2-year period. Only nine patients re t u rn e dto using soluble insulin.
Our prospective audit of insulin lisproin patients with specific clinical indica-tions shows that the improvement inH b A1 c and reduction in hypoglycemic

DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999 1227
Letters
events are similar or better than thatre p o rted in clinical studies (4,5). In ourpractice, lispro insulin has been an addi-tional useful tool in assisting our patientsto achieve improved glycemic contro lwithout excessive weight gain, hypogly-cemia or diabetic ketoacidosis.
SUDESNA CHATTERJEE, MBBS
IAN W. GALLEN, MD, MRCP
LAURENCE SANDLER, MD, FRCP
F rom the Ciltern Diabetes Centre, Wycombe Hospi-tal, High Wycombe, Buckinghamshire, U.K.
A d d ress correspondence and reprint requests toIan W. Gallen, MD, Wycombe Hospital, QueenAlexandria Road, High Wycombe, Bucking-h a m s h i re HP11 2TT, U.K.
R e f e re n c e s1 . Zinman B, Ross S, Campos R, Strack T, the
Canadian Lispro Study Group: A doubleblind randomized controlled trial compar-ing NPH and Ultralente as basal insulinreplacement with LISPRO insulin (Abstract).Diabetes 46 (Suppl. 1):43A, 1997
2 . Feinglos MN, Thacker CH, English J, BethelMA, Lane J: Modification of postprandialh y p e rglycemia with insulin lispro impro v e sglucose control in patients with type 2 dia-betes. Diabetes Care 20:1539–1542, 1997
3 . Kotsanos JG, Vignati L, Huster W, Andre-jasich C, Boggs MB, Jacobson AM, Marre roD, Mathias SD, Patrick D, Zalani S, Ander-son J: Health-related quality-of-life re s u l t sf rom multinational clinical trials of insulinl i s p ro: assessing benefits of a new diabetest h e r a p y. Diabetes Care 20:948–958, 1997
4 . Zinman B, Tildesley H, Chiasson JL, Ts u iE, Strack T: Insulin lispro in SCII: re s u l t sof a double-blind cross-over study. D i a -betes 46:440–443, 1997
5 . Ebeling P, Jansson PA, Smith U, Lalli C,Bolli GB, Koivisto VA: Strategies towardi m p roved control during insulin lisprotherapy in IDDM: importance of basalinsulin. Diabetes Care 20:1287–1289, 1997
6 . Kovisto VA: The human insulin analogueinsulin lispro. Ann Med 30:260–266, 1998
E ffect of Fiber Intakeand Meal Pattern onG a s t ro i n t e s t i n a lSymptoms Wi t hA c a r b o s e
We were interested to read the art i-cle by Wolever et al. (1) in whichthey re p o rted that gastro i n t e s t i n a l
symptoms in diabetic subjects treated with
acarbose were not related to carbohydrateintake. Like the authors, we wondere dwhether a high carbohydrate and highfiber intake would be associated with theg reatest amount of colonic ferm e n t a t i o nand, hence, gastrointestinal side effects. Toassess this problem, we prospectively fol-lowed 80 type 2 diabetic patients (47 men,33 women, aged 47–66 years) who failedto be adequately controlled on diet aloneand who were subsequently treated withacarbose. On the basis of a dietary assess-ment, they were divided into two gro u p s :a high-fiber group, taking $50% of theire n e rgy from carbohydrate (58.5%), and al o w - fiber group, taking ,50% of theire n e rgy from carbohydrate (41.5%). Thepatients were also assigned to two otherg roups related to meal pattern. Those witha regular meal pattern were in one gro u p(71%), and those who ate irregularly werein another (29%).
The patients were followed for 1 year,and during this period, 37% of patientsceased treatment with acarbose as a result ofside effects. Overall, 42.5% of the patientscomplained of flatulence, 11% of diarrh e a ,7.5% of both, and 5% of abdominal disten-tion, giving a total side effect rate of 66%.
Of those patients in the high-fib e rg roup, 29% had side effects, and in thel o w - fiber group, 24% had side effects. Sidee ffects were noted in 39% of the re g u l a rmeal pattern group and in 20% of thei rregular meal pattern group. None of thesed i ff e rences were statistically signific a n t .
Our data are broadly in keeping withthose of Wolever et al., demonstrating ahigh side-effect rate with acarbose, butwith no relationship with fiber content ofdiet or meal pattern .
ANDREW D.B. HARROWER, FRCPE
ALISON HARROWER, BA
HELEN JACK, SRD
F rom the Diabetes Centre, Monklands Hospital,A i rdrie, Scotland.
A d d ress correspondence to Dr. A.D.B. Harro w e r,FRCPE, Diabetes Centre, Monklands Hospital, Air-drie, ML6 OJS, Scotland.
R e f e re n c e s1 . Wolever TMS, Chiasson J-L, Josse RG,
Hunt JA, Palmason C, Rodger NW, RossSA, Ryan EA, Tan MH: No re l a t i o n s h i pbetween carbohydrate intake and effect ofacarbose on HbA1 c or gastro i n t e s t i n a lsymptoms in type 2 diabetic subjects con-suming 30–60% of energy from carbohy-drate. Diabetes Care 21:1612–1618, 1998
a- To c o p h e rol InducesLeptin Expression inHealthy Individualsand In Vi t ro
Shimizu et al. (1) have recently shownthat troglitazone reduces the plasmaleptin concentration in poorly con-
t rolled type 2 diabetic patients. The mech-anism through which troglitazone aff e c t splasma leptin levels has not been deter-mined so far, but potentially involves thei m p rovement of insulin sensitivity or dire c tactivation of peroxisome pro l i f e r a t o r- a c t i-vated receptor (PPA R ) -g (2). Anotherpotential mechanism through which tro g l i-tazone influences leptin expressioninvolves its antioxidative pro p e rties: tro g l i-tazone has an a- t o c o p h e rol moiety, and afunctional binding side for the re d o x - s e n s i-tive transcription factor C/EBP exists in theleptin promoter (3). However, the effect ofoxidative stress on leptin expression hasnot been evaluated so far. There f o re, wedecided to determine the effect of a- t o c o-p h e rol on plasma leptin levels in healthyindividuals and on o b-mRNA pro d u c t i o nin diff e rentiated 3T3-L1 cells.
The study consisted of 24 healthy indi-viduals (BMI 20–30 kg/m2) who wereasked to omit any vitamin supplementationand to stay on a normal diet for 4 weeksb e f o re and 2 weeks during D-a- t o c o p h e ro lsupplementation (800 U/day). All bloodsamples were taken in the morning afterfasting. Plasma leptin levels were measure dusing a radioimmunoassay (Linco Researc h ,St. Charles, MO) according to the manufac-t u re r ’s guidelines.
C u l t u re and diff e rentiation of 3T3L 1 – p readipocytes (American Type Cul-t u re Collection, Rockville, MD) were per-f o rmed according to Krieger-Brauer andKather (4). D-a- t o c o p h e rol, dissolved in a10% ethanol solution, was added to dif-f e rentiated 3T3-L1 cells for a final a-t o c o p h e rol concentration of 20 µg/ml.The same amount of ethanol without a-t o c o p h e rol served as control. mRNA wasobtained using the Rneasy Mini Kit (Qia-gen, Hilden, Germany) according to them a n u f a c t u re r ’s instructions. cDNA ob-tained by reverse transcription (AMVreverse transcriptase; Promega, Heidel-b e rg, Germany) of 2 µg total RNA wasused for polymerase chain reaction (PCR)a c c o rding to Yoshida et al. (5), and s a m-ples were electro p h o resed on a 2% agaro s e

1228 DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999
Letters
gel. Signal intensity was evaluated densito-m e t r i c a l l y, calculating for each PCR pro d-uct the ratio of leptin to b- a c t i n .
Data are given as means ± SD and arec o m p a red using the paired Student’s ttest, with P , 0.05 being statisticallysignificant. Statistics were calculatedusing SAS software .
In 24 healthy individuals, oxidatives t ress as determined by the plasmaticparameters malonaldehyde MDA) and 4 - h y d roxy-3(E)-uonenal (4HNE) was onlym a rginally reduced (MDA from 9.64 to9.27, 4-HNE from 12.07 to 11.59). Plasmaleptin levels increased from 12.8 to 15.0ng/ml (P = 0.039). RNA was isolated fro md i ff e rentiated 3T3-L1 adipo-cytes grown inthe presence or absence of a- t o c o p h e ro l .Intensity of o b-mRNA signals, as deter-mined by reverse transcription– P C R ,i n c reased to 470% after 24 h and to 622%after 48 h of a- t o c o p h e rol exposure. Noinduction of o b-mRNA was seen after expo-s u re to ethanol only. Thus, the antioxidantD-a- t o c o p h e rol induces o b-mRNA expre s-sion in diff e rentated 3T3-L1 cells, consis-tent with the induction of plasma leptin lev-els observed in healthy volunteers.
These observations showing an induc-tion of plasma leptin concentration after a- t o c o p h e rol supplementation are in con-trast to the recently described reduction ofplasma leptin concentration seen in poorlyc o n t rolled type 2 diabetic patients aftert roglitazone treatment. A reduction ofplasma leptin levels after treatment witht roglitazone has so far only been shown intype 2 diabetic patients (1) and in animalmodels of type 2 diabetes (6), but no eff e c ton plasma leptin levels has been observed inpatients with polycystic ovarian syndro m e(PCOS) (7) or in obese nondiabetic people(8), despite a reduction of plasma insulinlevels. There f o re, it seems possible that thee ffect of troglitazone on plasma leptin istransmitted through diff e rent and potentiallyopposing effects of troglitazone on insulins e n s i t i v i t y, PPA R -g activation, and oxidatives t ress. The present data show for the fir s ttime that the antioxidant a- t o c o p h e rol influ-ences leptin expression in healthy individu-als and in vitro. To further clarify the role ofantioxidants and oxidative stress in the re g u-lation of leptin expression, future studiesevaluating plasma leptin concentrations inhealthy individuals and in diabetic patientsshould include markers of oxidative stre s s .
BEREND ISERMANN, MD
ANGELIKA BIERHAUS, PHD
HANS TRITSCHLER, MD
REINHARD ZIEGLER, MDPETER PAUL NAWROTH, MD
F rom the First Medical Clinic (B.I., A.B., R.Z.,P. P.N.), University of Heidelberg, Department ofEndocrinology and Metabolism, Heidelberg; andAsta Medica (H.T.), Frankfurt, Germ a n y.
A d d ress correspondence to Berend Isermann, MD,Blood Research Institute, PO Box 2178, Milwaukee,WI 53212-2178. E-mail: bhiserm a n n @ b c s e w. e d u .
R e f e re n c e s1 . Shimizu H, Tsuchiya T, Sato N, Shimo-
mura Y, Kobayashi I, Mori M: Tro g l i t a z o n ereduces plasma leptin concentration buti n c reases hunger in NIDDM patients. Diabetes Care 21:1470–1474, 1998
2 . De Vos P, Lefebvre AM, Miller SG, Guerre -Millo M, Wong K, Saladin R, Hamann LG,Staels B, Briggs MR, Auwerx J: Thiazo-lidinediones re p ress ob gene expression inrodents via activation of peroxisome pro-l i f e r a t o r-activated receptor g. J Clin Invest98:1004–1009, 1996
3 . DeLa Brousse FC, Shan B, Chen JL: Identi-fication of the promoter of mouse obesegene. P N A S 93:4096–4101, 1996
4 . K r i e g e r-Brauer HI, Kather H: Antagonistice ffects of diff e rent members of the fib ro b l a s tand platelet-derived growth factor familieson adipose conversion and NADPH-depen-dent H2O2 generation in 3T3 L1-cells.Biochem J 307:549–556, 1995
5 . Yoshida T, Monkawa T, Hayashi M, Saru t aT: Regulation of expression of leptinmRNA and secretion of leptin by thyro i dh o rmone in 3T3-L1 adipocytes. B i o c h e mBiophys Res Commun 232:822–826, 1997
6 . Okuno A, Tamemoto H, Tobe K, Ueki K,Mori Y, Iwamoto K, Umecono K,Akanuma Y, Fujiwara T, Horikoshi H,Yazaki Y, Kadowaki T: Tro g l i t a z o n ei n c reases the number of small adipocyteswithout the change of white tissue mass inobese Zucker rats. J Clin Invest 1 0 1 :1354–1361, 1998
7 . M a n t z o ros CS, Dunaif A, Flier JS: Leptinconcentrations in the polycystic ovary syn-d rome. J Clin Endocrinol Metab 8 2 : 1 6 8 7 –1691, 1997
8 . Nolan JJ, Olefsky JM, Nyce MR, ConsidineRV, Caro JF: Effect of troglitazone on leptinp roduction: studies in vitro and in humansubjects. D i a b e t e s 45:1276–1278, 1996
Response toI s e rmann et al.
We appreciate the important obser-vations of Dr. Isermann and associ-ates in healthy individuals and in
v i t ro (1). Thiazolidinediones have beenre p o rted to re p ress o b gene expression inthe rodent via peroxisome pro l i f e r a t o r- a c t i-vated receptor (PPA R ) -g. Their fin d i n g
indicated that the reduction of circ u l a t i n gleptin concentrations by troglitazone maynot be attributable to the modulation of afunctional binding site for the re d o x - s e n s i-tive transcription factor C/EBP in the leptinp ro m o t e r. To clarify the mechanism of ourfindings, their observation should bei m p o rtant. Their observation was found inhealthy individuals, while our data havebeen obtained from poorly controlled dia-betic patients. Since there may be diff e r-ences in the effects of troglitazone on circ u-lating leptin concentrations amongnonobese, diabetic, and nondiabetic obesesubjects, the effects of D-a- t o c o p h e rol sup-plement should be determined in nonobesepoorly controlled diabetic subjects to con-clude this issue.
In addition, our recent pre l i m i n a ryfindings have demonstrated that circ u l a t i n gleptin concentrations in poorly contro l l e dtype 2 diabetic patients were not re d u c e dby a 4-week administration of metform i n ,which improves hyperglycemia through thereduction of hepatic glucose pro d u c t i o nand the enhancement of glucose uptake inmuscle and adipose tissues. However, 4-week administration of troglitazone obvi-ously decreased circulating leptin concen-tration in poorly controlled type 2 diabeticpatients, as we have previously re p o rt e d .Both metformin and troglitazone re d u c einsulin resistance by diff e rent mechanisms,resulting in the improvement of glycemicc o n t rol in poorly controlled type 2 diabeticpatients, but the effect on circulating leptinconcentrations is quite diff e rent. It has beenre p o rted that the existence of diabetes doesnot affect circulating leptin concentrations.It is possible that an improvement ofinsulin resistance by troglitazone does notplay an important role in the reduction ofc i rculating leptin concentrations.
HIROYUKI SHIMIZU, MD, PHD
TAKAHUMI TSUCHIYA, MD
MASATOMO MORI, MD, PHD
F rom the First Department of Internal Medicine, GunmaUniversity School of Medicine, Maebashi, Gunma, Japan.
A d d ress correspondence to Hiroyuki Shimizu,MD, PhD, First Department of Internal Medicine,Gunma University School of Medicine,3-39-22 Showa-machi, Maebashi, Gunma 371-8511Japan. E-mail: [email protected].
R e f e re n c e s1 . I s e rmann B, Bierhaus A, Tritschler H,
Ziegler R, Nawroth PP: a- To c o p h e ro linduces leptin expression in healthy indi-viduals and in vitro (Letter). Diabetes Care22:1227–1228, 1999

DIABETES CARE, VOLUME 22, NUMBER 7, JULY 1999 1229
Erratum
Jovanovic L: Retinopathy risk: What is responsible? Hormones, hyperglycemia, or humalog? Diabetes Care 22:846–848, 1999
Two errors were introduced during typesetting in the above article.
The first sentence of the article should be as follows:
T h e re are three re p o rted situations in which rapid normalization of blood glucose levels increases the risk for deteriora-tion of diabetic retinopathy: puberty (1), pregnancy (2), and high concentrations of gro w t h - p romoting hormones (3).
The fourth sentence of the second paragraph is incorrect. It should be replaced by the following two sentences:
In addition, other placental growth hormone variants have been found to increase prolactin throughout pre g n a n c y,along with human somatomammotropin (9). Prolactin, a pituitary hormone that increases during pre g n a n c y, hasg ro w t h - p romoting characteristics.
Copyright © 2022 FDOKUMEN




















