AMERICAN FAMILYPHYSICIAN®
74
www.aafp.org/afp A MERICAN F AMILY P HYSICIAN ® AN EDITORIALLY INDEPENDENT, PEER EVIEWED JOURNAL OF THE AMERICAN ACADEMY OF FAMILY PHYSICIANS June 1, 2019 664 Letters to the Editor 670 Editorials: Cardiovascular Disease 676 Cochrane for Clinicians 708 Curbside Consultation 712 FPIN’s Help Desk Answers 713 Photo Quiz 716 POEMs 719 Practice Guidelines 673 CME Quiz is worth 6 credits. 682 Varicose Veins: Diagnosis and Treatment 689 Adolescent Substance Use and Misuse 699 Caregiver Care American Family Physician Vol. 99 No. 11 pp. 661-726 Varicose Veins Adolescent Substance Use and Misuse Caregiver Care June 1, 2019 afp20190601 cover.indd 1 5/15/19 11:21 AM
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of AMERICAN FAMILYPHYSICIAN®

www.aafp.org/afp
AMERICAN FAMILY PHYSICIAN®
AN EDITORIALLY INDEPENDENT, PEER EVIEWED JOURNAL OF THE AMERICAN ACADEMY OF FAMILY PHYSICIANS
June 1, 2019
664 Letters to the Editor
670 Editorials: Cardiovascular Disease
676 Cochrane for Clinicians
708 Curbside Consultation
712 FPIN’s Help Desk Answers
713 Photo Quiz
716 POEMs
719 Practice Guidelines
673 CME Quiz is worth 6 credits.
682 Varicose Veins: Diagnosis and Treatment
689 Adolescent Substance Use and Misuse
699 Caregiver Care
Am
erican F
amily P
hysician
Vol. 99
No. 11
pp. 661-726 V
aricose Veins
Adolescent Substance U
se and Misuse
Caregiver C
are June 1, 2019
afp20190601 cover.indd 1 5/15/19 11:21 AM

AAFP
GLOBAL
HEALTH
SUMM
IT
Impa
ctin
g G
loba
l Hea
lth
thro
ugh
Fam
ily M
edic
ine
Sept
embe
r 12-
15Ja
ckso
nvill
e, F
L
AAFP
GLOBAL
HEALTH
SUMM
IT
HOP19020251
Make a (sustainable) difference. Register now.
Save 15% when you attend both events. AAFP Global Health Summit WONCA World Rural Health ConferenceOctober 10–12 | aafp.org/ghs October 12–15 | wrhc19.org
Primary Health Care and Family Medicine: Health Equity for AllOctober 10–12 | Albuquerque, New Mexico(Health equity pre-conferences | October 9)
WRHC 2019Explore rural health in the land of enchantment
aafp.org/ghs
2019 AAFP GLOBAL HEALTH SUMMIT
19020251 GHS Full Page Ad.indd 1 5/6/19 2:21 PM

American Family Physician (ISSN 0002-838X) is published semimonthly by the Journal Media Division, American Academy of Family Physicians, 11400 Tomahawk Creek Parkway, Leawood, KS 66211-2680; phone: 800-274-2237. The journal is indexed in MEDLINE and CINAHL.
One-year print and digital subscription: AAFP student members, $40; AAFP inter national members, $110; physicians and other individuals, $290—U.S.A.; institutions, $730—U.S.A.; medical students, residents, allied health care professionals, and medical office manage ment staff, $185—U.S.A., when payment is accompanied by identification of profession. For complete rates outside the U.S.A., plus digital-only rates, go to https://www.aafp.org/afp/subscribe. Remit in U.S. dollars, drawn on a U.S. bank. All subscriptions include web access and the mobile app edition. To order by VISA, MasterCard, Discover, or American Express, call 800-274-2237, or go to https://www.aafp.org/afp/subscribe. Print copies of back issues are $20 a copy, plus shipping for addresses outside the U.S.A. (volume discounts available). Online access to restricted issues is $39.95 per issue. Periodicals postage paid at Shawnee Mission, Kan., and at additional mailing offices. Printed in the U.S.A. Copyright © 2019 by the American Academy of Family Physicians.
POSTMASTER: Send address changes to American Family Physician 11400 Tomahawk Creek Parkway, Leawood, KS 66211-2680
Cover illustration by Jonathan Dimes, Baltimore, Md.
AMERICAN FAMILY PHYSICIAN®
AN EDITORIALLY INDEPENDENT, PEER EVIEWED JOURNAL OF THE AMERICAN ACADEMY OF FAMILY PHYSICIANS
June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 661
682 Varicose Veins: Diagnosis and TreatmentJaqueline Raetz, Megan Wilson, and Kimberly Collins
The pathophysiology of varicose veins involves a genetic predisposition, incompetent valves, weakened vascular walls, and increased intravenous pres-sure. Established risk factors include family history of venous disease, female sex, older age, chronically increased intra-abdominal pressure, deep venous thrombosis, and arteriovenous shunt-ing. Over the past 10 years, there has been a significant change in treatment recommendations for symptomatic varicose veins, largely because of the lack of evidence supporting the use of compression stockings and the rise of minimally invasive endovascular tech-niques. Current guidelines recommend endovenous thermal ablation as first-line therapy for nonpregnant patients, followed by endovenous sclerotherapy and surgery. CME
689 Adolescent Substance Use and Misuse: Recog-nition and ManagementJessica A. Kulak and Kim S. Griswold
Adolescent use of illicit substances imposes burdens to all levels of society. The types of substances that adolescents use have changed over the past decade, with a decrease in alcohol and increase in marijuana and opioid use. Primary care physicians can help identify ado-lescents who use illicit substances; the American Academy of Pediatrics recommends several types of screening tools. A split-visit model encourages parents to participate in part of the clinical visit and allows adolescents to have confidential conversations with physicians. Evidence-based treatments range from school- and parent-based interventions to medication-assisted treatment. Motivational interviewing may be useful in addressing adolescent substance use. Prevention efforts can supplement cessation programs. CME
699 Caregiver CareKristine Swartz and Lauren G. Collins
Caregiving is associated with physical, psychological, and financial burdens, and the demand for caregivers is expected to rise during the next few decades. Family physicians can offer practical, individualized interventions such as caregiver assessments that direct the caregiver to local area agen-cies on aging, websites, and respite care. Additionally, the caregiver’s quality of life can be increased by psychoeduca-tion, skills training, and therapeutic counseling, all of which decrease the caregiver’s burden. CME
Patient information available online: Caregiver Care
Volume 99, Number 11 June 1, 2019
afp20190601 contents.indd 661 5/10/19 9:22 AM

AMERICAN FAMILY PHYSICIAN®
Follow AFPJournal at https://www.twitter.com/AFPJournal.
Follow AFP at https://www.facebook.com/AFPJournal.
662 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
664 Letters to the Editor• Medical Content Should Be Equitable and Inclusive
of Diverse Populations Shokoufeh Dianat
reply: Sumi Sexton, Kenny Lin• Preoperative Nutritional Optimization in Older
Patients Reduces Complications Daniel S. Orlovich
reply: Chandrika Kumar
670 Editorials• Rethinking Aspirin for the Primary Prevention
of Cardiovascular Disease Kenneth W. Lin, Jennifer Middleton
672 Close-ups• My Kidney Donation: Unexpected Twists
Caroline Wellbery
673 CME Quiz
675 AFP Clinical Answers• Measles Vaccine, Acute Appendicitis, Screening
for Heart Disease, Abdominal Pain, Hyperhidrosis
676 Cochrane for Clinicians CME
• Anticoagulation for the Long-term Treatment of VTE in Patients with Cancer
Michael J. Arnold, Noah Cooperstein, Christopher Jonas
• Alternative Interventions for Chronic Prostatitis/Chronic Pelvic Pain Syndrome in Men
Anne L. Mounsey, Elizabeth Parks
708 Curbside Consultation• An Unhappily Married Patient
Matthew Alexander, Shaista Qureshi
712 FPIN’s Help Desk Answers• Attention-Deficit/Hyperactivity Disorder: Screening
and Evaluation Payal Gaba, Matthew Giordanengo
713 Photo Quiz• A Bump on the Gum
Nguyet-Cam Lam, Tue T. Te
716 POEMs
719 Practice Guidelines CME
• Cancer Screening: ACS Releases Annual Summary of Recommendations
Lisa Croke
Available Online and in the Mobile App Edition
Patient Information• Caregiver Care
Medicine by the Numbers • Antibiotic Prophylaxis in Patients with COPD Robert Murrey Brown, Rory Spiegel
Reader Services
666 Corrections
723 Classified Information
726 CME Course Information
727 Advertiser Index
CME This article is included as part of this issue’s continuing medical education (CME) activity. See CME Quiz, p. 673. For a complete listing of CME courses, go to the AAFP CME Center at https://www.aafp.org/cme.
Available Online For online-only content, see the table of contents at https://www.aafp.org/afp/2019/0601.
Mobile App EditionAFP is available for Android, iOS, and Kindle Fire devices.
Full TextOnline archives for AFP are available at https://www.aafp.org/afp. AFP is also available on Clinical Key.
CommentingAAFP members and AFP sub-scribers may post comments to all content online. Others may e-mail [email protected].
AFP By TopicFor the Editors’ Choice of Best Available Content, go to https://www.aafp.org/afp/topics.
E-mail Table of ContentsAnyone may enroll to receive AFP ’s table of contents by e-mail at https://www.aafp.org/afp/etoc.
Information for AuthorsInformation for authors and author statement forms are available at https://www.aafp.org/afp/authors.
AFP PodcastAvailable on iTunes and Google Play Music or at https://www.aafp.org/afppodcast.
afp20190601 contents.indd 662 5/10/19 9:22 AM

EDITOR-IN-CHIEF
Sumi M. Sexton, MD, Georgetown University
DEPUTY EDITOR
Kenny Lin, MD, MPH, Georgetown University
DEPUTY EDITOR FOR EVIDENCE-BASED MEDICINE
Mark H. Ebell, MD, MS, University of Georgia
ASSOCIATE DEPUTY EDITOR
Caroline Wellbery, MD, Georgetown University
ASSOCIATE MEDICAL EDITORS
Barbara S. Apgar, MD, MS, University of Michigan
John E. Delzell, Jr., MD, MSPH, Northeast Georgia Health System
Anne D. Walling, MD, University of Kansas School of Medicine-Wichita
Barry D. Weiss, MD, University of Arizona
ASSISTANT MEDICAL EDITORS
Corey D. Fogleman, MD, Lancaster General Hospital Family Medicine Residency
Dean A. Seehusen, MD, MPH, Eisenhower Army Medical Center
Allen F. Shaughnessy, PharmD, MMedEd, Tufts University
CONTRIBUTING EDITORS
Jacob S. Anderson, DO, University of Arizona College of Medicine–Phoenix Family Medicine Residency; Assistant Editor, AFP Podcast
Steven R. Brown, MD, University of Arizona College of Medicine–Phoenix Family Medicine Residency; Editor, AFP Podcast
Christopher W. Bunt, MD, Medical University of South Carolina
Sarah Coles, MD, University of Arizona College of Medicine–Phoenix Family Medicine Residency; Assistant Editor, AFP Podcast
Jennifer L. Middleton, MD, MPH, OhioHealth Riverside Methodist Hospital
Aaron Saguil, MD, MPH, Uniformed Services University of the Health Sciences
Elizabeth Salisbury-Afshar, MD, MPH, American Institutes for Research, Chicago
MEDICAL EDITING FELLOW
Michael Arnold, MD
EDITOR EMERITUS
Jay Siwek, MD, Georgetown University
EXECUTIVE EDITOR
Joyce A. Merriman
SENIOR EDITOR and AFP ONLINE ADMINISTRATOR
Matthew Neff
SENIOR EDITORS
Monica Preboth, Genevieve W. Ressel
SENIOR ASSOCIATE EDITORS
Carrie Armstrong, Amber Randel
ASSOCIATE EDITOR AND AFP ONLINE COORDINATOR
Laurie Costlow
ASSOCIATE EDITOR
Lindsey Hoover
EDITORIAL COORDINATORS
Holly Messerschmidt, Jennifer Wilkes
EDITORIAL ASSISTANT
Elizabeth Jahns
ART COORDINATOR
David Klemm
DIRECTOR OF JOURNAL MEDIA
Stephanie Hanaway
DIRECTOR OF OPERATIONS
Darren Sextro
ADMINISTRATIVE COORDINATOR
Marilyn Harvey
DIRECTOR OF ADVERTISING
John Payne
DIRECTOR OF ADVERTISING SALES
John Molluso
NATIONAL ACCOUNT MANAGER
Mickey Cotter
ADVERTISING SERVICES SPECIALISTS
Frances Spitsnogle, Linda A. Porter
ADVERTISING SALES OFFICE MANAGER
Stefanie Valenzano
SUBSCRIPTION MANAGER
Susi Cordill
SUBSCRIPTION STRATEGISTS
Alan Fagen, Rebecca Harp
DATA MANAGEMENT AND MARKET INSIGHTS MANAGER
Tiffany M. Long
PRODUCTION DIRECTOR
Bret A. Taylor
PRODUCTION GRAPHICS MANAGER
Stacey Herrmann
SENIOR GRAPHIC ASSOCIATE
Bryan Colley
GRAPHIC ASSOCIATE
Randy Knittel
DIGITAL PRODUCTION SPECIALIST
Evan Palmer
EXECUTIVE VICE PRESIDENT
Douglas E. Henley, MD
SENIOR VICE PRESIDENT FOR EDUCATION
Clif Knight, MD
Editorial/Production Offices 11400 Tomahawk Creek Pkwy. Leawood, KS 66211-2680 913-906-6205
Advertising Sales Office 500 Route 17 South Hasbrouck Heights, NJ 07604-3121 201-288-4440
AMERICAN FAMILY PHYSICIAN®
AFP DirectoryArticle proposals—Contact Sumi M. Sexton, MD, editor-in-chief (e-mail: [email protected]).
Other editorial questions—Call 913-906-6205 or send a fax to 913-906-6086. Use the list below to find the person who can best help you:• Reader feedback—Contact Joyce A. Merriman, executive editor (e-mail:
[email protected]). For letters to the editor, follow the instructions on the first page of “Letters to the Editor” in each issue or in the Authors’ Guide at https://www.aafp.org/afp/authors.
• Delivery problems, back issues—Contact the content sales and distribu-tion department (800-274-2237; e-mail: [email protected]).
• Subscriptions, address changes—Refer to the ordering information on the first page of the table of contents, at the bottom of the page. For address changes: click on “Manage Subscriptions” at https://www.aafp.org/afp/subscribe.
Permission to reuse material from AFP:• Academic use, general photocopying, electronic use—See www.copy-
right.com and enter ISSN 0002-838X in the search box; or contact the Copyright Clearance Center ([email protected]; 978-750-8400; fax: 978-646-8700).
• Bulk reprints, e-prints—Contact Dan Woodall at AAFP ([email protected]).
• Other requests—Contact AAFP intellectual property coordinator ([email protected]).
Display advertising—Contact John Molluso, director of advertising sales (e-mail: [email protected]), or Mickey Cotter, national account manager (e-mail: mcotter @ aafp.org); telephone: 201-288-4440; fax: 201-288-4914.
Classified information—Contact Community Brands (e-mail: AAFP@community brands.com; 727-497-6568).
Other AAFP information—800-274-2237
Editorial PoliciesThe purpose of AFP is to serve the medical profession and provide continu-ing medical education (CME). The information and opinions presented in AFP reflect the views of the authors, not those of the journal or the American Academy of Family Physicians, unless so stated. Advertising is accepted only if judged to be in harmony with the purpose of the journal; however, AFP reserves the right to reject any advertising at its sole discretion. Acceptance does not constitute endorsement by AFP or the American Academy of Family Physicians of a particular policy, product, procedure, or advertorial.
It is the policy of the American Academy of Family Physicians that all individuals in a position to affect the content of a CME activity disclose relationships that they or their spouse/partner have with commercial enti-ties. Further, should any such relationship be determined to be in possible conflict of interest as it relates to the individual’s proposed role in the CME activity, the conflicts of interest must be resolved before confirmation of the individual’s participation. We inform readers of any pertinent relationships disclosed. A disclosure statement is published at the end of relevant articles. The medical and professional editors of AFP have disclosed all relation-ships with commercial interests. There are no relevant conflicts of interest to disclose.
AFP publishes trade names of drugs for the readers’ convenience only; pub-lished names are based on what is currently available. This does not imply endorsement of any product by AFP or the American Academy of Family Physicians.
CME Objectives 1. To provide updates on the diagnosis and treatment of clinical conditions man-
aged by family physicians. 2. To provide reference citations to support statements referring to clinical
studies, new information, controversial material, specific quantitative data, and any other information not generally found in reference textbooks on the subject.
3. To provide balanced discussions of the strengths and weaknesses of diagnostic and treatment strategies (controversial or speculative material is identified).
4. To provide evidence-based guidelines or consensus viewpoint in preference to personal opinion.
staff-V20.indd 663 5/10/19 9:22 AM

664 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
Letters to the EditorMedical Content Should Be Equitable and Inclusive of Diverse Populations
To the Editor: I am writing to bring your attention to the need for more racially inclusive language and equity-driven content in Ameri-can Family Physician (AFP). For example, I was struck by the noninclusivity of one sentence in the article on vitamin D screening and supple-mentation in the February 15, 2018, issue.1 In the context of describing recommended dietary allowances of vitamin D, the authors wrote, “Suf-ficient sun exposure to produce a light-pink skin hue (one minimal erythema dose) is equivalent to 20,000 IU of oral vitamin D.”1 By writing about light-pink skin hue without qualifying the sen-tence, the authors implied that light pink is the only skin hue relevant to the reader. I suggest that sentences that apply only to a portion of the pop-ulation be preceded by qualifiers, such as, “For those with light skin color, […].” The sentence should then be followed by a statement relating the effects of sun exposure on vitamin D levels of people with darker skin colors.2
The American Academy of Family Physicians has made efforts to reduce health disparities by launching the EveryONE project, which seeks to address the social determinants of health at the home and neighborhood levels (https://www.aafp.org/patient-care/social-determinants-of-health/cdhe/everyone-project.html). Eliminat-ing health disparities requires a multipronged and multilevel approach involving every insti-tution and sector of society. As one component, AFP is well positioned to help readers address inequities in our one-on-one patient encounters
through improving the quality of care that we provide to marginalized groups. I have three suggestions:
1. Provide Continuing Medical Education (CME) content that uses inclusive language to guide care for all of our diverse patients. Language used in the journal should be inclusive of all skin colors, genders, ranges of able-bodiedness, and socioeconomic backgrounds that our patients represent.
2. Highlight the gaps in literature when research studies underrepresent marginal-ized groups. Consider making it a criterion for authors of AFP to critically apply a health equity lens and to make it transparent when a content area is lacking in generalizability.3
3. Acknowledge and address the impact of implicit bias. One factor that contributes to health care disparities in the United States is implicit racial biases that affect physician-patient inter-actions and influence medical decision-making.4 One step toward reducing implicit biases is to make physicians aware of their susceptibility to biases so that engrained habits can be actively and intentionally dismantled.5 Wherever evi-dence for implicit biases negatively affecting care is available, AFP review articles can draw upon existing work and propose specific strategies to disrupt the perpetuation of biases from one gen-eration of physicians to the next.6
Shokoufeh Dianat, DOSan Francisco, Calif. E-mail: [email protected]
Author disclosure: No relevant financial affiliations.
References 1. LeFevre ML, LeFevre NM. Vitamin D screening and supple-
mentation in community-dwelling adults: common ques-tions and answers. Am Fam Physician. 2018;97(4):254-260.
2. Khalid AT, Moore CG, Hall C, et al. Utility of sun-reactive skin typing and melanin index for discerning vitamin D deficiency. Pediatr Res. 2017;82(3):444-451.
3. Geller SE, Koch A, Pellettieri B, Carnes M. Inclusion, analysis, and reporting of sex and race/ethnicity in clin-ical trials: have we made progress? J Womens Health. 2011;20(3):315-320.
4. Dovidio JF, Fiske ST. Under the radar: how unexamined biases in decision-making processes in clinical interac-tions can contribute to health care disparities. Am J Public Health. 2012;102(5):945-952.
5. Byrne A, Tanesini A. Instilling new habits: addressing implicit bias in healthcare professionals. Adv Health Sci Educ Theory Pract. 2015;20(5):1255-1262.
6. Brooks KC. A piece of my mind. A silent curriculum. JAMA. 2015;313(19):1909-1910.
Send letters to [email protected], or 11400 Tomahawk Creek Pkwy., Leawood, KS 66211-2680. Include your complete address, e-mail address, and telephone number. Letters should be fewer than 400 words and limited to six refer-ences, one table or figure, and three authors.
Letters submitted for publication in AFP must not be sub-mitted to any other publication. Possible conflicts of inter-est must be disclosed at time of submission. Submission of a letter will be construed as granting the AAFP permis-sion to publish the letter in any of its publications in any form. The editors may edit letters to meet style and space requirements.
This series is coordinated by Kenny Lin, MD, MPH, Deputy Editor.
june 1 letters.indd 664 5/10/19 9:22 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 665
LETTERS TO THE EDITOR
In Reply: Thank you for your insightful com-ments. We agree that it is essential that topics covered in AFP be inclusive of diverse popula-tions. Given the concise nature of our articles, the emphasis is often on practical evidence-based points that are supported in the existing litera-ture rather than highlighting knowledge gaps and making recommendations for further research. We can certainly be more mindful of noninclu-sive language, but here are the ways we’ve already been addressing diversity and health equity in the journal:
1. A recent editorial on social determinants of health highlighted the EveryONE Project resources (https://www.aafp.org/afp/2019/0415/p476.html).1
2. We’ve published articles on dermatologic conditions in skin of color (https://www.aafp.org/afp/2013/0615/p850.html and https://www.aafp.org/afp/2013/0615/p859.html)2,3 and also a recent article on transgender care (https://www.aafp.org/afp/2018/1201/p645.html)4 that has been acknowledged as an important resource in other articles (https://www.medscape.com/view-article/909885#vp_1 [login required]).5
3. We have an AFP By Topic collection of con-tent on Care of Special Populations, including historically marginalized groups (https://www.aafp.org/afp/populations).
4. We constantly reevaluate medical terminol-ogy to make sure that it’s inclusive and does not promote implicit bias (e.g., “patient with opioid use disorder” instead of “opioid-dependent” or “opioid addict”).
As always, we appreciate reader feedback and your interest in making AFP applicable to all of the patients family physicians care for.Sumi Sexton, MD, Editor-in-Chief
Kenny Lin, MD, MPH, Deputy Editor
References 1. Sherin K, Adebanjo T, Jani A. Social determinants of
health: family physicians’ leadership role. Am Fam Physi-cian. 2019;99(8):476-477.
2. Kundu RV, Patterson S. Dermatologic conditions in skin of color: part I. Special considerations for common skin dis-orders. Am Fam Physician. 2013;87(12):850-856.
3. Kundu RV, Patterson S. Dermatologic conditions in skin of color: part II. Disorders occurring predominantly in skin of color. Am Fam Physician. 2013;87(12):859-865.
4. Klein DA, Paradise SL, Goodwin ET. Caring for transgender-diverse persons: what clinicians should know. Am Fam Physician. 2018;98(11):645-653.
5. Citroner GW. Confronting transphobia in healthcare. Med-scape. March 8, 2019. https://www.medscape.com/view-article/909885 [login required]. Accessed April 24, 2019.
Preoperative Nutritional Optimization in Older Patients Reduces Complications
Original Article: Preoperative Assessment in Older Adults: A Comprehensive Approach
Issue Date: August 15, 2018
See additional reader comments at: https://www.aafp.org/afp/2018/0815/p214.html
To the Editor: This article is deserving of praise for its thoroughness and recognition of an important issue. I wish to reiterate the signifi-cance of nutrition and offer practical recommen-dations for nutritional optimization.
More than 50% of older surgical patients are thought to have malnutrition.1 Poor nutrition is associated with increased postoperative compli-cations, prolonged length of hospitalization, and increased health care costs.2 In terms of modifi-able preoperative risk factors, malnutrition is one of the few that is associated with poor surgical outcomes, including mortality.3,4 Although refer-ral to a dietitian may be ideal for certain patients, there can be multiple barriers to implementation. Only one out of five patients receives any nutri-tional intervention in the preoperative and post-operative periods.5
Herein lies an opportunity for the family phy-sician to make two recommendations. The first is supplementation with arginine and fish oil, and the second is high-protein supplements taken two to three times daily (minimum of 18 g of pro-tein per serving).5 Both may be obtained at local pharmacies or ordered online. Supplementation for a minimum of five days for low-risk patients and seven days for those at higher risk has been recommended.5 A patient at higher risk would have an albumin level of less than 3.0 g per dL (30 g per L) or would meet any of the following criteria: body mass index of less than 20 kg per m2 if older than 65 years, unplanned weight loss of more than 10% of total body weight in the past six months, or eating less than 50% of a person’s nor-mal diet in the past week. In addition, one could communicate that total protein content is more important than total caloric intake.5
Daniel S. Orlovich, MD, PharmDStanford, Calif. E-mail: [email protected]
Author disclosure: No relevant financial affiliations.
References 1. Damulevičienė G, Lesauskaitė V, Macijauskienė J. Nutri-
tional status of elderly surgical patients. Medicina (Kaunas). 2008; 44(8): 609-618.
june 1 letters.indd 665 5/10/19 9:22 AM

666 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
LETTERS TO THE EDITOR
2. Gregg JR, Cookson MS, Phillips S, et al. Effect of preopera-tive nutritional deficiency on mortality after radical cystec-tomy for bladder cancer. J Urol. 2011; 185(1): 90-96.
3. Malietzis G, Currie AC, Athanasiou T, et al. Influence of body composition profile on outcomes following colorec-tal cancer surgery. Br J Surg. 2016; 103(5): 572-580.
4. Vaid S, Bell T, Grim R, Ahuja V. Predicting risk of death in general surgery patients on the basis of preoperative vari-ables using American College of Surgeons National Sur-gical Quality Improvement Program data. Perm J. 2012; 16(4): 10-17.
5. Williams JD, Wischmeyer PE. Assessment of perioperative nutrition practices and attitudes—a national survey of col-orectal and GI surgical oncology programs. Am J Surg. 2017; 213(6): 1010-1018.
In Reply: Thank you for your comments on nutrition in older adults. Given the breadth of material we wanted to cover on the perioperative visit, we focused our nutritional assessment and intervention recommendations on areas with the strongest supporting data. The study by Williams and Wischmeyer quoted by Dr. Orlovich in his letter looked primarily at colorectal and gastro-intestinal surgical oncology programs; although they comprise a large number of surgeries that older adults undergo, they are not inclusive of all the types of surgeries in older adults.
Malnutrition increases length of hospital stay and related costs and is associated with an increased risk of adverse postoperative events. Assessment should include history of unintentional weight loss and documentation of baseline weight, height, and albumin level. If available, and if time permits, patients identified to have poor nutrition may ben-efit from referral to a dietitian for a comprehensive plan to optimize nutritional status. Nutrition rec-ommendations may include modifications to diet, food consistency changes, and nutritional supple-ments. Compared with no intervention, dietary advice and/or nutritional supplements improve body weight, muscle bulk, and strength, although there is inconclusive evidence of improved survival. Patients with dentures should be reminded to bring them to the hospital to facilitate appropriate caloric intake postoperatively.1
Current studies are too heterogeneous and lack conclusive evidence that preoperative oral nutri-tional support with dietary supplements improves outcomes for patients undergoing surgery.2
Other barriers include adding supplements in patients who may already take a number of medications and our limited understanding of how these natural supplements may or may not interact with a patient’s current medications, especially given concerns around the lack of U.S.
Food and Drug Administration monitoring for nutritional supplements. Cost is also a major fac-tor for older adults.
We agree that a focus on nutritional support and supplementation is an important area of further research, although it remains unclear whether it improves surgical outcomes or mor-tality for older adults when started before surgery.Chandrika Kumar, MD, FACPWest Haven, Va. E-mail: [email protected]
Author disclosure: No relevant financial affiliations.
References 1. Chun A. Medical and preoperative evaluation of the older
adult. Otolaryngol Clin North Am. 2018; 51(4): 835-846.
2. Bruns ER, Argillander TE, Van Den Heuvel B, et al. Oral nutrition as a form of pre-operative enhancement in patients undergoing surgery for colorectal cancer: a sys-tematic review. Surg Infect (Larchmt). 2018; 19(1): 1-10.
CorrectionsStrength of evidence. The article, “The Preg-nant Patient: Managing Common Acute Medical Problems” (November 1, 2018, p. 595), contained an error in the third sentence of the second para-graph of the “Common Symptoms During Preg-nancy” section in the second column on page 597. This sentence stated that there was modest evidence that P6 acupressure can be a first-line therapy for nausea in patients who are pregnant, rather than stating the level of evidence was weak and that P6 acupressure can be a treatment option in this population. This sentence should have read, “There is weak evidence that P6 acu-pressure can also be a treatment option.” The online version of the article has been corrected.
Incorrect disease risk. The article, “The Preg-nant Patient: Managing Common Acute Medical Problems” (November 1, 2018, p. 595), contained an error in the third sentence of the second para-graph of the “Dysuria” section in the first column on page 601 regarding the use of trimethoprim/sulfamethoxazole in pregnant patients and the associated risks to the newborn. This sentence should have read, “Trimethoprim/sulfamethox-azole is generally not recommended for use in pregnancy because of risks of neural tube defects in early pregnancy, as well as kernicterus in the newborn and permanent neonatal neurologic damage.” The online version of the article has been corrected. ■
june 1 letters.indd 666 5/10/19 9:22 AM

The BioFire® FilmArray® Respiratory Panel (RP) EZ uses a molecular syndromic approach to accurately detect and identify a wide range of pathogens—not just Flu A and B. As a healthcare provider, this means your patients can receive the right treatment the �rst time, potentially leading to higher patient satisfaction and lower costs. And as the name implies, it’s easy and can be performed right in your of�ce or clinic.1 1 test. 14 respiratory pathogens. All in about an hour.
biofiredx.com
BioFire RP EZ Pathogens
VirusesAdenovirusCoronavirusHuman MetapneumovirusHuman Rhinovirus/EnterovirusIn�uenza A
In�uenza A/H1In�uenza A/H1-2009In�uenza A/H3In�uenza BParain�uenza VirusRespiratory Syncytial Virus
BacteriaBordetella pertussisChlamydophila pneumoniaeMycoplasma pneumoniae
Nail it with one swab.Syndromic respiratory infection testing now CLIA-waived
CLIA WAIVED
1 CLIA Certi�cate of Waiver required to perform testing.
For more information contact+1 801-736-6354 ext. 1947
BFDX-MKT-0234

from the AAFPNews
Policy and Health Issues From AAFP News
For more news, visit AAFP News at www.aafp.org/news.
Academy Takes Aim at Maternal Mortality Crisis
Even as they are dropping worldwide, ma-ternal mortality rates are rising in the United States.
Family physicians can play a key role in reversing the trend and the AAFP is working with partners on several fronts.
AAFP President John Cullen, M.D., of Val-dez, Alaska, was scheduled to be a featured speaker May 11 during the March for Moms rally on the National Mall in Washington, D.C. The AAFP was a partner in the event, which aimed to raise awareness.
The rally was planned to occur in the wake of an advocacy day May 10 on Capitol Hill to address legislation on issues such as family leave and health disparities.
In addition, the AAFP aims to build a coalition of partners to address maternal mortality. Academy representatives met March 26 in Washington with representatives from the American College of Obstetricians and Gynecologists and the National Rural Health Association.
Both organizations are participating in the AAFP’s maternal mortality task force, which had its first meeting in April and is scheduled to meet again June 29. It is expected to report back to the COD when it meets Sept. 23-25 in Philadelphia.
Cullen also was scheduled to speak during a May 5 maternal safety meeting hosted by the CDC’s Division of Reproductive Health and ACOG during ACOG’s annual meeting in Nashville, Tenn., and to participate in a CMS forum on rural maternal health June 12 in Washington.
For more, go to https://www.aafp.org/news/health-of-the-public/ 20190501maternalmortality.html.
New CMS Initiative Draws on AAFP Payment Model
HHS has announced new payment models influenced, in part, by the AAFP’s Ad-vanced Primary Care Alternative Payment Model and other physician input, with the intention of initiating valued-based trans-formation in primary care settings around the country.
AAFP Vice Speaker Russell Kohl, M.D., of Stilwell, Kan., joined HHS Secretary Alex Azar, CMS Administrator Seema Verma, M.P.H., and Adam Boehler, director of CMS’ Center for Medicare & Medicaid Innovation, on stage in Washington, D.C., for the April 22 unveiling of the models in the CMS Primary Cares Initiative.
Kohl said the initiative represents import-ant movement toward acknowledging the vital role of primary care “by placing greater emphasis on the investments we make in family medicine and other primary care practices.”
CMMI designed the models with consider-able stakeholder input, including ideas put forth in the AAFP’s APC-APM, which the Physician-Focused Payment Model Tech-nical Advisory Committee had previously recommended that HHS begin testing.
The AAFP is analyzing the details of the CMS Primary Cares Initiative and will pre-pare an executive summary to help guide family physicians moving forward.
For more, go to https://www.aafp.org/news/government-medicine/ 20190424cmsprimarycares.html.
AAFP Advocates for State Primary Care Spending Bills
The AAFP and state chapters have thrown their support behind several efforts to
increase spending on primary care.
In Oregon, where lawmakers in 2017 unanimously passed legislation requiring that 12% of all health spending go toward primary care, the Academy expressed support for a bill introduced this session that would maintain the 12% mandate while updating the law to solidify family medicine’s gains there the past few years. The Oregon AFP, meanwhile, submitted separate testimony supporting the updated law.
In Vermont, the AAFP and the state chap-ter endorsed legislation that would, the Academy said in a letter, “increase health care spending investment and transparen-cy in primary care.”
And in Missouri, the AAFP and the state chapter have written to both chambers of the General Assembly to advocate for passage of twin bills that would require all health insurance carriers to report their annual health care medical expenditures and their total primary care medical expen-ditures to the state each year, for review by legislators.
Primary care spending legislation has been introduced in five other states, as well — Colorado, Hawaii, Maine, Washing-ton and West Virginia — in some cases, gaining traction with chapter support.
For more, go to https://www.aafp.org/news/government-medi-cine/20190424statespending.html.
— AAFP News Staff
20190601_yellow_sheet.indd 1 5/6/2019 4:23:20 PM

Learn, Apply, Improve with AAFP CMEaafp.org/summerlive • (800) 274-2237
AAFP Live CME events are offered in a variety of great locations throughout the year. Join us for these can’t-miss, collaborative courses to: • Attend up-to-date, evidence-based sessions created by family physicians for family physicians. • Earn CME while you network with colleagues. • Participate in hands-on courses to enhance your procedural skills and patient outcomes.*
REGISTER EARLY TO SAVE!
Learn the latest, earn credit, and enjoy a summer getaway —AAFP Live CME
Learn the latest, earn credit,
*Additional fees apply for optional workshops.
18111694 2019 Summer LIVE_Journal Ad FP.indd 1 2/14/19 9:12 AM

670 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
EditorialsRethinking Aspirin for the Primary Prevention of Cardiovascular DiseaseKenneth W. Lin, MD, MPH, Georgetown University Medical
Center, Washington, District of Columbia
Jennifer Middleton, MD, MPH, OhioHealth Riverside Meth-
odist Hospital, Columbus, Ohio
Administering aspirin during a heart attack or stroke can be lifesaving. The benefits of daily low-dose (81 mg) aspirin therapy to prevent recurrent cardiovascular disease (CVD) events are also well established.1 Aspirin’s routine use for primary prevention, however, has been the subject of con-troversy because of questionable benefits and increased bleeding risk.2,3 Aspirin therapy may reduce the relative risk of a first heart attack or stroke, but this benefit could be out-weighed by the risk of gastrointestinal bleeding.4 According to a 2011-2012 national survey, one-third of Americans 40 years or older take a daily aspirin, including 28% of adults without known CVD5; therefore, delineating these risks and benefits has significant implications.
The U.S. Preventive Services Task Force (USPSTF) cur-rently recommends that adults 50 to 59 years of age start taking a daily low-dose aspirin if they have a 10% or greater 10-year CVD risk, do not have bleeding risk factors, and are willing to take a daily aspirin for at least 10 years. Adults 60 to 69 years of age with similar CVD risk may consider starting low-dose aspirin therapy but are at higher risk of bleeding and less likely to benefit overall, according to the USPSTF. The USPSTF found insufficient evidence to assess the balance of benefits and harms of starting low-dose aspi-rin therapy for primary prevention in adults younger than 50 or older than 69 years.6
Supporting evidence for the 2016 USPSTF recommen-dations included a systematic review of 11 randomized, controlled trials of aspirin therapy with myocardial infarc-tion and stroke outcomes published between 1988 and 20147 with a review of major gastrointestinal bleeding and hem-orrhagic strokes in trial participants.8 According to one member of the USPSTF at the time of the 2016 recom-mendation, the goal was to select adults at high enough cardiovascular risk that their expected benefit from aspi-rin therapy (including a possible reduction in the risk of developing colorectal cancer)6 would outweigh the harms of bleeding.9 However, in the decade or more since most of the trials analyzed by the USPSTF took place, fewer U.S. adults are smoking, and more have become eligible for statins and antihypertensives, which could have reduced aspirin’s incremental benefit. Also, the USPSTF review sug-gested that the presence of diabetes mellitus did not alter the effectiveness of aspirin therapy in reducing CVD events, but only three trials specifically recruited these patients.7
In 2014, the U.S. Food and Drug Administration, citing concerns about insufficient evidence, advised the general public against using low-dose aspirin therapy for primary prevention of heart attack or stroke.10 Indeed, three recent studies’ findings are more supportive of the U.S. Food and Drug Administration recommendation than the USPSTF recommendation. In the Aspirin to Reduce Risk of Initial Vascular Events (ARRIVE) trial, more than 12,000 Euro-pean and U.S. adults 55 years or older without diabetes were randomized to take 100 mg of enteric-coated aspirin or placebo daily for a median follow-up of five years. The researchers for the ARRIVE trial enrolled participants determined to be at a moderate risk of CVD (participants’ mean atherosclerotic CVD risk score was 17.3% to 17.4%). With the caveat that less than 5% of participants had a car-diovascular event during the study, no difference occurred between the groups in a composite outcome of cardiovas-cular death, myocardial infarction, unstable angina, stroke, or transient ischemic attack. However, 1% of the aspirin group experienced gastrointestinal bleeding compared with only 0.5% of the placebo group (hazard ratio = 2.11; 95% confidence interval, 1.36 to 3.28).11
The aspirin-placebo comparison in the ARRIVE trial was mirrored by another trial, A Study of Cardiovascular Events in Diabetes, but this trial enrolled 15,000 adults 40 years or older with diabetes in U.K. primary care practices. After a mean follow-up of 7.4 years, a lower percentage of the aspi-rin group had experienced serious vascular events than the placebo group, but this benefit was offset by an increased percentage of major bleeding events. The researchers calcu-lated a number needed to treat of 91 to prevent a vascular event and number needed to harm of 112 to cause a major bleeding event, from which they concluded that aspirin pro-vided no net benefit.12
Finally, the Aspirin in Reducing Events in the Elderly trial examined the effect of five years of daily low-dose aspirin therapy on community-dwelling adults 70 years or older in the United States and Australia. There were no differ-ences in the primary endpoint of disability-free survival (a composite of death, dementia, and persistent physical dis-ability) or the prespecified secondary endpoint of CVD deaths, events, and hospitalizations.13,14 However, the aspi-rin group had a significantly higher rate of major hemor-rhage and higher all-cause mortality.15
A meta-analysis that pooled data from older primary prevention trials with these three new studies calculated a number needed to treat of 265 to prevent a composite car-diovascular outcome (cardiovascular mortality, nonfatal myocardial infarction, and nonfatal stroke) and number needed to harm of 210 to prevent a major bleeding event, suggesting that aspirin provided no net benefit.16 Studies
edit lin.indd 670 5/10/19 9:22 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 671
EDITORIALS
with an estimated population 10-year CVD risk of greater than 10% experienced a similar balance of benefits and harms (number needed to treat = 196; number needed to harm = 152).
Though not designed to determine whether long-term use of daily aspirin reduces colorectal cancer incidence or mor-tality, as other evidence has suggested,17 the new evidence should prompt the USPSTF to reevaluate their 2016 aspi-rin guideline. The new data do not exclude the possibility that aspirin may still benefit adults at very high CVD risk (e.g., 20% or more over 10 years) or those at lower risk who are unable to tolerate statins, but the data otherwise suggest that the risks of low-dose aspirin therapy for primary pre-vention outweigh any potential benefits. For most patients, we should be deprescribing aspirin for primary preven-tion of CVD. To prevent heart attacks and strokes, family physicians should focus instead on smoking cessation and lifestyle changes, controlling high blood pressure, and pre-scribing statins when indicated.
Editor’s Note: Portions of this editorial are adapted, with permission, from a previous Medscape commentary by Dr. Lin (https:// www.medscape.com/viewarticle/902186; login required). Dr. Lin and Dr. Middleton are Deputy Editor and Contributing Editor, respectively, for AFP.
Address correspondence to Kenneth W. Lin, MD, MPH, at kenneth.lin@ georgetown.edu. Reprints are not available from the authors.
Author disclosure: No relevant financial affiliations.
References 1. Baigent C, Blackwell L, Collins R, et al.; Antithrombotic Trialists’ (ATT)
Collaboration. Aspirin in the primary and secondary prevention of vas-cular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009; 373(9678): 1849-1860.
2. Bailey AL, Smyth SS, Campbell CL. The case against routine aspirin use for primary prevention in low-risk adults. Am Fam Physician. 2011; 83(12): 1387-1390.
3. Miser WF. Appropriate aspirin use for primary prevention of cardiovas-cular disease. Am Fam Physician. 2011; 83(12): 1380-1386.
4. Sutcliffe P, Connock M, Gurung T, et al. Aspirin in primary prevention of cardiovascular disease and cancer: a systematic review of the balance
of evidence from reviews of randomized trials. PLoS One. 2013; 8(12): e81970.
5. Gu Q, Dillon CF, Eberhardt MS, Wright JD, Burt VL. Preventive aspirin and other antiplatelet medication use among U.S. adults aged ≥ 40 years: data from the National Health and Nutrition Examination Survey, 2011-2012. Public Health Rep. 2015; 130(6): 643-654.
6. Bibbins-Domingo K; U.S. Preventive Services Task Force. Aspirin use for the primary prevention of cardiovascular disease and colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2016; 164(12): 836-845.
7. Guirguis-Blake JM, Evans CV, Senger CA, O’Connor EA, Whitlock EP. Aspirin for the primary prevention of cardiovascular events: a system-atic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2016; 164(12): 804-813.
8. Whitlock EP, Burda BU, Williams SB, Guirguis-Blake JM, Evans CV. Bleed-ing risks with aspirin use for primary prevention in adults: a systematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2016; 164(12): 826-835.
9. Owens DK. Aspirin for the prevention of cardiovascular disease and colorectal cancer: new recommendations from the USPSTF. Am Fam Physician. 2017; 95(4): 222-223.
10. U.S. Food and Drug Administration. Use of aspirin for primary pre-vention of heart attack and stroke. May 2, 2014. Updated December 30, 2016. http:// www.fda.gov/Drugs/ResourcesForYou/Consumers/ucm390574.htm. Accessed September 26, 2018.
11. Gaziano JM, Brotons C, Coppolecchia R, et al.; ARRIVE Executive Committee. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a ran-domised, double-blind, placebo-controlled trial. Lancet. 2018; 392(10152): 1036-1046.
12. Bowman L, Mafham M, Wallendszus K, et al.; ASCEND Study Collabo-rative Group. Effects of aspirin for primary prevention in persons with diabetes mellitus. N Engl J Med. 2018; 379(16): 1529-1539.
13. McNeil JJ, Woods RL, Nelson MR, et al.; ASPREE Investigator Group. Effect of aspirin on disability-free survival in the healthy elderly. N Engl J Med. 2018; 379(16): 1499-1508.
14. McNeil JJ, Wolfe R, Woods RL, et al.; ASPREE Investigator Group. Effect of aspirin on cardiovascular events and bleeding in the healthy elderly. N Engl J Med. 2018; 379(16): 1509-1518.
15. McNeil JJ, Nelson MR, Woods RL, et al.; ASPREE Investigator Group. Effect of aspirin on all-cause mortality in the healthy elderly. N Engl J Med. 2018; 379(16): 1519-1528.
16. Zheng SL, Roddick AJ. Association of aspirin use for primary prevention with cardiovascular events and bleeding events: a systematic review and meta-analysis. JAMA. 2019;321(3):277-287.
17. Chubak J, Kamineni A, Buist DS, Anderson ML, Whitlock EP. Aspirin use for the prevention of colorectal cancer: an updated systematic evidence review for the U.S. Preventive Services Task Force. AHRQ publication no. 15-05228-ER-1. Rockville, Md.: Agency for Healthcare Research and Quality; September 2015. ■
edit lin.indd 671 5/10/19 9:22 AM

672 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
Close-upsA Patient’s Perspective
My Kidney Donation: Unexpected Twists
Some years ago, a close family friend told me his chronic kidney disease had progressed and he would need a new kidney to avoid dialysis. I volunteered to donate my kidney, and as it turned out, I was a near perfect match. But, our celebration did not last long. While I was being worked up for surgery, the transplant team found some ureteral abnormalities that made me ineligible for the donation.
A few years later, I began experienc-ing flank pain, which was bad enough to send me to the emergency room. I was told my right kidney was no lon-ger functional and would have to be removed. The surgery went smoothly. It was hard to believe that a nephrec-tomy could seem like minor surgery (although admittedly, recovery was slow).
Still, this was not the outcome I had hoped for: instead of losing my kidney to give life, my surgery brought me face-to-face with my own mortality. Fortunately, I am now in good health. I am working again and have rejoined my running group. To our great joy, my friend finally reached the top of the transplant list and is doing beautifully with his new kidney.—M.K.
CommentaryM.K.’s story brings to mind Johanna Shapiro’s definition of empathy: an engaged act in which “the physician must draw closer to the patient, putting the interests of others above those of self, even at some sacrifice to oneself.” M.K, a phy-sician herself, is one of those people for whom altruism is a natural way of life. She inspires us to reenvision the reach of relationship-centered care, while reminding us that even when things do not turn out as we intend, we are all connected in unexpected ways. Caroline Wellbery, MD
ResourcesNational Kidney Foundation: https:// www.kidney.org/transplantation/beadonor
Reese PP, Allen MB, Carney C, et al. Outcomes for individuals turned down for living kidney donation. Clin Transplant. 2018; 32(12): e13408.
Tong A, Chapman JR, Wong G, Kanellis J, McCarthy G, Craig JC. The motivations and experiences of living kidney donors: a thematic synthesis. Am J Kidney Dis. 2012; 60(1): 15-26. ■
The editors of AFP welcome submissions for Close-ups. Guidelines for contributing to this feature can be found in the Authors’ Guide at https:// www.aafp.org/afp/authors.
This series is coordinated by Caroline Wellbery, MD, Associate Deputy Editor, with assistance from Amy Crawford-Faucher, MD; Jo Marie Reilly, MD; and Sanaz Majd, MD.
A collection of Close-ups published in AFP is available at https:// www.aafp.org/afp/closeups.
jun 1 closeups.indd 672 5/10/19 9:22 AM

BONUS DIGITAL CONTENTAAFP Members and AFP Subscribers: Click here to take the quiz now
June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 673
CME Quiz
ArticlesVaricose Veins: Diagnosis and Treatment (p. 682)
Q1. Which one of the following findings in the evalua-tion of varicose veins is an early sign of advanced venous disease? (check one)
l A. Throbbing.
l B. Hemodynamically significant external hemorrhage.
l C. Corona phlebectatica.
l D. Relief with leg elevation.
Q2. Which one of the following imaging modalities is the best way to evaluate varicose veins in preparation for an interventional procedure? (check one)
l A. Venography.
l B. Venous duplex ultrasonography.
l C. Plethysmography.
l D. Magnetic resonance imaging.
Q3. Which one of the following statements about the treatment of varicose veins is correct? (check one)
l A. Endovenous thermal ablation should be consid-ered only after a trial of conservative treatment.
l B. Surgery is considered the best interventional treatment option.
l C. Sclerotherapy is better at maintaining saphenous vein occlusion at six months than endovenous laser ablation or surgery.
l D. Endovenous thermal ablation is considered first-line therapy for nonpregnant patients.
Adolescent Substance Use and Misuse: Recognition and Management (p. 689)
Q4. Which one of the following statements about adoles-cent substance use is correct? (check one)
l A. Traditional cigarette use is rising.
l B. Marijuana is the most commonly used substance.
l C. Hospitalization from prescription opioid poison-ing is rising.
l D. Adolescent males have higher rates of nonmed-ical use of amphetamines and tranquilizers than adolescent females.
Q5. What is the U.S. Preventive Services Task Force and the American Academy of Family Physicians recommen-dation for primary care–based behavioral interventions to prevent or reduce illicit substance use or nonmedical pharmaceutical use in children or adolescents? (check one)
l A. Routinely recommended.
l B. Selectively recommended.
l C. Recommended against.
l D. Insufficient evidence to determine harms and benefits.
Q6. Which one of the following statements about the split-visit model is correct? (check one)
l A. Parents participate in the clinical visit for a limited time and then leave the room.
l B. Parents do not participate in the clinical visit.
l C. Parents stay in the room with the adolescent the whole time during the clinical visit.
l D. The American Academy of Family Physicians dis-courages adolescent-physician confidential visits.
AAFP members and other physicians and health care professionals who receive the print version of AFP in their own name can submit responses for CME credit at https:// www.aafp.org/afpquiz. Quiz questions are featured below for your convenience. This issue is approved for up to 6 Prescribed and AMA PRA Category 1 credits. The total credit for this issue is based on one credit for each article included in the Quiz. Credits may be claimed for one year from the date of this issue. Questions? Call 800-274-2237.
jun 1 quiz.indd 673 5/10/19 9:23 AM

674 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
CME QUIZ
Caregiver Care (p. 699)
Q7. Which one of the following statements about assess-ing caregiver needs and burdens is correct? (check one)
l A. A caregiver is defined as someone who spends more than 24 hours per week with the care recipient.
l B. Care recipients are less likely to provide reliable information when interviewed alone.
l C. Anyone who identifies as a caregiver should be offered an assessment.
l D. There are no validated tools available for assess-ing caregiver burden.
Q8. Which one of the following aspects of care is one of the most burdensome challenges for caregivers caring for people with heart failure? (check one)
l A. Managing pain.
l B. Enforcing dietary restrictions.
l C. Lifting.
l D. Behavior disturbances.
Q9. Which one of the following statements about caring for a person at the end of life is most accurate? (check one)
l A. The care recipient’s transfer to a long-term care facility has a positive effect on the caregiver’s burden.
l B. Caregivers are most likely to need intensified support for depression after the care recipient’s death.
l C. Early palliative care interventions for patients with serious illness improves quality of life.
l D. Life-prolonging interventions in the late stages of heart failure have been shown to relieve caregiver burden.
Cochrane for CliniciansAnticoagulation for the Long-term Treatment of VTE in Patients with Cancer (p. 676)
Q10. Which one of the following statements about the prevention of recurrent venous thromboembolism (VTE) in patients with cancer is correct? (check one)
l A. Use of low-molecular-weight heparin (LMWH) reduces the risk of recurrent VTE to a greater extent than vitamin K antagonists.
l B. Use of LMWH reduces the risk of recurrent VTE to a greater extent than direct oral anticoagulants.
l C. Use of LMWH increases bleeding risk compared with direct oral anticoagulants.
l D. Use of LMWH increases bleeding risk compared with vitamin K antagonists.
Alternative Interventions for Chronic Prostatitis/Chronic Pelvic Pain Syndrome in Men (p. 677)
Q11. Which one of the following statements about nonpharmacologic therapies for men with long-standing pelvic pain and urinary symptoms is correct? (check one)
l A. Transrectal thermotherapy and physical therapy are likely to be clinically beneficial.
l B. Extracorporeal shock wave therapy and acupunc-ture are likely to be clinically beneficial.
l C. Prostatic massage improves prostatitis symptoms.
l D. There is high-quality evidence for the effec-tiveness of lifestyle modifications for urinary symptoms.
Practice GuidelinesCancer Screening: ACS Releases Annual Summary of Recommendations (p. 719)
Q12. Which one of the following statements about the 2018 cancer screening recommendations from the Amer-ican Cancer Society (ACS) is correct? (check one)
l A. Colorectal cancer screening should be offered at age 40 in average-risk patients.
l B. Lung cancer screening in high-risk patients should occur biannually after shared decision-making.
l C. Prostate cancer screening can be done at age 50 in average-risk patients who opt for testing after a physician-initiated discussion.
l D. Cervical cancer screening should occur before age 21 in those with early onset sexual activity.
Answers to this issue’s quiz are on the inside back cover.
jun 1 quiz.indd 674 5/10/19 9:23 AM

BONUS DIGITAL CONTENT
June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 674A
Medicine by the NumbersA Collaboration of TheNNT.com and AFP
➤ Antibiotic Prophylaxis in Patients with COPDRobert Murrey Brown, MD, and Rory Spiegel, MD
Details for This ReviewStudy Population: Patients older than 40 years with spirometry-proven diagnosis of moderate to severe chronic obstructive pulmonary disease (COPD)
Efficacy End Points: COPD exacerbations, fre-quency of exacerbations, time to first exacerba-tion, and health-related quality of life as measured by the St. George’s Respiratory Questionnaire or the Chronic Respiratory Diseases Questionnaire
Harm End Points: Drug resistance as measured by micro-bial sensitivity, adverse drug effects, hospitalization, and all-cause mortality
Narrative: COPD is defined as persistent respiratory symp-toms and airflow obstruction caused by alveolar and airway dysfunction resulting from exposure to noxious parti-cles and gases.1 It is common throughout the world and is the third leading cause of death in the United States.2 Morbidity from COPD is costly, reducing the capacity for work3 and increasing the number of emergency department visits and hospitalizations.4 It can profoundly reduce qual-ity of life, causing social isolation and depression.5,6 Viral infections account for most exacerbations, but bacterial colonization increases with the severity of COPD, and bac-terial infections are more common in acute exacerbations.7
In theory, antibiotics provide their benefit by decreas-ing bacterial growth, potentially limiting the inflamma-tory effects of the bacteria.8,9 Prophylactic antibiotics were routinely administered for cases of chronic bronchitis 30 years ago, but this practice declined amid concern for antibiotic resistance without evidence of efficacy.
The Cochrane group identified 14 randomized controlled trials of antibiotics compared with placebo, with end points of prevention of COPD exacerbations or improved quality of life. The studies were pub-lished or presented between 2001 and 2017 and included a total of 3,932 participants. Nine trials stud-ied continuous macrolide antibiotic treatment (1,925 participants); two
examined antibiotics administered three times weekly (176 participants); two studied pulsed antibiotics given three days per month or five days every eight weeks (1,732 partici-pants), and one trial compared three arms: continuous dox-ycycline vs. azithromycin (Zithromax) administered three times weekly vs. moxifloxacin (Avelox) for five days every month (99 participants). The heterogeneity of the studies was moderate.
The number needed to treat to prevent one exacerbation of COPD was 8. The effect was evident only when patients received antibiotics at least three times weekly. There was no significant impact on the frequency of hospitalization, all-cause mortality, or quality of life.
Data reporting for adverse drug events and microbial resistance was inadequate for a formal meta-analysis. A sin-gle study demonstrated a number needed to harm of 25 to cause one case of diarrhea and 18 to cause a single case of hearing loss. Single-study analyses of microbial resistance demonstrated a risk of rapid resistance to moxifloxacin in patients colonized with Pseudomonas. All but two studies, both of shorter duration (six months or less), demonstrated an increase in the minimum inhibitory concentration of bacteria cultured from sputum of patients exposed to pro-
phylactic antibiotics.
Caveats: Optimization of preven-tive regimens, including long-acting muscarinic antagonists, long-acting beta agonists, inhaled corticoste-roids, phosphodiesterase-4 inhib-itors, and mucolytics, was not reported and potentially limited the validity of these results. In an attempt to control for this source of
ANTIBIOTIC PROPHYLAXIS IN PATIENTS WITH COPD
Benefits Harms
1 in 8 had an exacerbation of chronic obstructive pulmonary disease prevented
No hospitalizations were prevented
No deaths were prevented
1 in 25 developed diarrhea
1 in 18 developed hearing loss
The NNT Group Rating System
Green Benefits greater than harms
Yellow Unclear benefits
Red No benefits
Black Harms greater than benefits
jun 1 nnt.indd 1 5/10/19 9:23 AM

674B American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
MEDICINE BY THE NUMBERS
bias, the authors examined studies published from 2005 to 2009, 2010 to 2014, and 2015 onward. Despite improvements in medical management of COPD over this period, the authors found no change in the effectiveness of antibiotic prophylaxis when examining earlier vs. later studies.
In addition, three studies were not double-blinded, eight did not clearly blind the outcome assessment, four were subject to attrition bias, one had selective reporting, and another was at unclear risk because no prospective trial reg-istration or protocol could be evaluated. When the authors performed a sensitivity analysis, removing all trials at high risk of bias, the results were similar to the primary analysis.
This research fails to determine whether the modest poten-tial benefits of prophylaxis outweigh the risk of resistance. Antibiotic prophylaxis is proposed to work by decreasing bacterial colonization, but slow-multiplying bacteria, such as those found in biofilms, are profoundly tolerant to anti-biotics.10 Lengthy, multidrug regimens are required to kill these bacteria. Single-agent coverage may temporarily tar-get rapidly multiplying bacteria and halt exacerbations, but lengthy courses with single agents may lead to resistance. Longer-term studies might uncover an increased cost and mortality for treating pneumonia in patients with COPD in which resistance has been worsened by ineffective chronic suppressive therapy. Copyright © 2019 MD Aware, LLC (theNNT.com). Used with permission.
This series is coordinated by Dean A. Seehusen, MD, MPH, AFP Assistant Medical Editor, and Daniel Runde, MD, from the NNT Group.
A collection of Medicine by the Numbers published in AFP is available at https:// www.aafp.org/afp/mbtn.
Author disclosure: No relevant financial affiliations.
References 1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy
for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2018 report). https:// goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-revised-20-Nov_WMS.pdf. Accessed January 25, 2019.
2. National Center for Health Statistics. Health, United States 2015: with Special Feature on Racial and Ethnic Health Disparities. Hyattsville, Md.: U.S. Department of Health and Human Services; 2016.
3. Wheaton AG, Cunningham TJ, Ford ES, Croft JB; Centers for Disease Control and Prevention (CDC). Employment and activity limitations among adults with chronic obstructive pulmonary disease—United States, 2013. MMWR Morb Mortal Wkly Rep. 2015; 64(11): 289-295.
4. Wheaton AG, Ford ES, Cunningham TJ, Croft JB. Chronic obstructive pulmonary disease, hospital visits, and comorbidities: National Survey of Residential Care Facilities, 2010. J Aging Health. 2015; 27: 480-499.
5. Liu Y, Croft JB, Anderson LA, Wheaton AG, Presley-Cantrell LR, Ford ES. The association of chronic obstructive pulmonary disease, disabil-ity, engagement in social activities, and mortality among US adults aged 70 years or older, 1994-2006. Int J Chron Obstruct Pulmon Dis. 2014; 9: 75-83.
6. Cunningham TJ, Ford ES, Rolle IV, Wheaton AG, Croft JB. Association of self-reported cigarette smoking with chronic obstructive pulmonary disease and co-morbid chronic conditions in the United States. COPD. 2015; 12(3): 276-286.
7. Woodhead M, Blasi F, Ewig S, et al.; Joint Taskforce of the European Respiratory Society and European Society for Clinical Microbiology and Infectious Diseases. Guidelines for the management of adult lower respiratory tract infections—full version. Clin Microbiol Infect. 2011; 17(suppl 6): E1-E59.
8. Matkovic Z, Miravitlles M. Chronic bronchial infection in COPD. Is there an infective phenotype? Respir Med. 2013; 107(1): 10-22.
9. Martinez FJ, Curtis JL, Albert R. Role of macrolide therapy in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2008; 3(3): 331-350.
10. Hu Y, Coates A. Nonmultiplying bacteria are profoundly tolerant to anti-biotics. In: Coates AR, ed. Antibiotic Resistance. Handbook of Experi-mental Pharmacology. Vol. 211. New York, NY: Springer; 2012: 99-120. ■
jun 1 nnt.indd 2 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 675
AFP Clinical Answers
Measles Vaccine, Acute Appendicitis, Screening for Heart Disease, Abdominal Pain, Hyperhidrosis
What are the risks associated with delaying the first dose of MMR vaccine after 12 to 15 months of age?Febrile seizures that occur seven to 10 days after the first dose of the measles, mumps, and rubella (MMR) vaccine are rare (0.04% of chil-dren between 12 and 15 months), but the risk is increased when the first dose is delayed after the recommended age. In a retrospective cohort study of 840,348 U.S. children who received measles vaccination between 2001 and 2011, those who received a measles vaccination at 16 to 23 months of age had a greater increase in seizure risk (relative risk = 6.5; 95% confidence interval, 5.3 to 8.1) than those who received a vaccination at 12 to 15 months of age (relative risk = 3.4; 95% confidence interval, 3.0 to 3.9), conferring an attributable risk of 5.5 additional cases per 10,000 vaccines given.
https://www.aafp.org/afp/2017/0615/p786.html
https://www.aafp.org/afp/2014/0515/p786.html
How does intravenous antibiotic therapy for acute appendicitis in adults compare to initial appendectomy?Antibiotic treatment for adults with appendicitis results in decreased complications, less sick leave or disability, and less need for pain medication compared with initial appendectomy. However, 40% of patients who receive antibiotic therapy will require appendectomy within one year.
https://www.aafp.org/afp/2018/0701/p25.html
Should asymptomatic patients be screened for heart disease with ECG?Screening asymptomatic patients with electro-cardiography (ECG) has an extremely low yield in detecting significant pathology and leads to many false-positive findings. The U.S. Preventive Services Task Force recommends against screen-ing with ECG to predict coronary artery disease
in low-risk patients and found insufficient evi-dence to assess the benefits and harms of screen-ing in individuals at intermediate or high risk.
https://www.aafp.org/afp/2018/1115/p561.html
In children with recurrent abdominal pain, what characteristics can distinguish organic from nonorganic disease?Organic disease is suggested by the presence of fever, vomiting, blood in the stool, more than three alarm symptoms, or history of urinary tract infections.
https://www.aafp.org/afp/2018/0615/p785.html
What is the first-line treatment for most persons with primary focal hyperhidrosis?Topical 20% aluminum chloride (Drysol) should be used as first-line treatment in most cases of primary hyperhidrosis, regardless of severity and location. Iontophoresis may be effective as first- or second-line treatment for primary hyperhi-drosis of the palms or soles.
https://www.aafp.org/afp/2018/0601/p729.html
Tip for Using AFP at the Point of CareLooking for more information about vaccines? You can find more in AFP ’s Immunizations col-lection at https://www.aafp.org/afp/immuniza-tions. Check out more than 60 other collections in AFP By Topic at https://www.aafp.org/afp/topics. When you find your favorite topics click “Add to Favorites” to add them to your personal Favorites list. Find a summary of the 2019 immu-nization schedules at https://www.aafp.org/afp/2019/0215/p264.html.
A collection of AFP Clinical Answers published in AFP is available at https://www.aafp.org/afp/answers. All AFP departments are available at https://www.aafp.org/afp/collections.
june 1 ca.indd 675 5/10/19 9:23 AM

676 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
Cochrane for CliniciansPutting Evidence into Practice
Anticoagulation for the Long-term Treatment of VTE in Patients with Cancer
Michael J. Arnold, MD, Uniformed Services University of the Health Sciences, Bethesda, Maryland
Noah Cooperstein, MD, Saint Louis University South-west Illinois Family Medicine Residency Program, O’Fallon, Illinois
Christopher Jonas, DO, Uniformed Services Univer-sity of the Health Sciences, Bethesda, Maryland
Author disclosure: No relevant financial affiliations.
Clinical QuestionWhat is the preferred anticoagulant for long-term prevention of recurring venous thrombo-embolism (VTE) in patients with cancer?
Evidence-Based AnswerLow-molecular-weight heparin (LMWH), vita-min K antagonists, and direct oral anticoagu-lants, when used to prevent recurrent VTE, have a similar impact on all-cause mortality. Compared with vitamin K antagonists, LMWH reduces recurrent VTE in patients with cancer (num-ber needed to treat = 19), with similar adverse event profiles.1 (Strength of Recommendation: A, consistent, good-quality patient-oriented evi-dence.) Direct oral anticoagulants reduce VTE risk to the same extent as LMWH but at an increased risk of major bleeding (number needed to harm = 34).1 (Strength of Recommendation: B, based on inconsistent or limited-quality patient-oriented evidence.)
Practice PointersPatients with cancer have an annual VTE risk of 1.3%, which is six times higher than patients
without cancer.2 The risk of VTE recurrence in patients with cancer can reach 29% at one year, leading to recommendations for long-term anticoagulation.3 Cancer also conveys a high risk of major bleeding—up to 20% at one year for patients with both cancer and VTE.4 This Cochrane review evaluated the safety and effec-tiveness of long-term anticoagulation to prevent VTE recurrence in patients with cancer.1
Sixteen randomized controlled trials involv-ing 5,167 patients with cancer and diagnostically confirmed initial VTE were identified. Patients of all ages with solid or hematologic cancers at any stage were studied. The primary outcome was all-cause mortality; secondary outcomes included recurrent symptomatic VTE and major bleeding. The review evaluated large, multicenter trials and local studies with as few as 35 patients. Most multicenter trials were multinational, whereas the single-center trials were conducted in North America or Europe. Studies varied greatly in the medications used within each class. The larger studies were funded by the sponsoring pharma-ceutical company.
Five studies that included 1,781 patients com-pared LMWH and vitamin K antagonists. There was no difference in mortality between groups. LMWH reduced recurrent symptomatic VTE compared with vitamin K antagonists (number needed to treat = 19; 95% CI, 14 to 34) in patients with cancer, with no difference in major bleeding between the two groups. One study reported no difference in thrombocytopenia between patients receiving LMWH and those receiving vitamin K antagonists.
Four studies with a total of 1,031 patients com-pared direct oral anticoagulants and vitamin K antagonists and found similar mortality rates, recurrent symptomatic VTE rates, and bleeding events between the groups. Data were low qual-ity because of imprecise reporting and inclusion criteria.
Two studies compared LMWH and direct oral anticoagulants, but only one study, which included 1,016 patients, contained data sufficient for analysis. Mortality risk was similar between the groups, and there was no significant differ-ence in recurrent symptomatic VTE between the direct oral anticoagulant and LMWH treatment
These are summaries of reviews from the Cochrane Library.
This series is coordinated by Corey D. Fogle-man, MD, Assistant Medical Editor.
A collection of Cochrane for Clinicians pub-lished in AFP is available at https://www.aafp.org/afp/cochrane.
CME This clinical content conforms to AAFP criteria for continuing medical education (CME). See CME Quiz on page 673.
jun 1 cochrane.indd 676 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 677
COCHRANE FOR CLINICIANS
arms (relative risk = 0.69; 95% CI, 0.47 to 1.01). Patients using direct oral anticoagulants had an increased risk of major bleeding events compared with patients using LMWH (number needed to harm = 34; 95% CI, 13 to 2,439).
A recent systematic review concluded that direct oral anticoagulants do not significantly reduce VTE recurrence compared with LMWH, but they do increase major bleed-ing.5 Guidelines from the American Society of Clinical Oncology, the American College of Chest Physicians, the European Society for Medical Oncology, and the National Institute for Health and Care Excellence recommend LMWH as first-line treatment for recurrent VTE in patients with cancer, which is consistent with the results of this Cochrane review.1,6-8
The practice recommendations in this activity are available at http:// www.cochrane.org/CD006650.
Editor’s Note: The numbers needed to treat and to harm, and the corresponding confidence intervals, were calculated by the authors based on raw data provided in the original Cochrane review.
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of the Air Force, Uni-formed Services University of the Health Sciences, Department of Defense, or the U.S. government.
References
1. Kahale LA, Hakoum MB, Tsolakian IG, et al. Anticoagulation for the long-term treatment of venous thromboembolism in people with can-cer. Cochrane Database Syst Rev. 2018; (6): CD006650.
2. Horsted F, West J, Grainge MJ. Risk of venous thromboembolism in patients with cancer: a systematic review and meta-analysis. PLoS Med. 2012; 9(7): e1001275.
3. Chee CE, Ashrani AA, Marks RS, et al. Predictors of venous throm-boembolism recurrence and bleeding among active cancer patients: a population-based cohort study. Blood. 2014; 123(25): 3972-3978.
4. Kamphuisen PW, Beyer-Westendorf J. Bleeding complications during anticoagulant treatment in patients with cancer. Thromb Res. 2014;133 (suppl 2): S49-S55.
5. Li A, Garcia DA, Lyman GH, Carrier M. Direct oral anticoagulant (DOAC) versus low-molecular-weight heparin (LMWH) for treatment of cancer associated thrombosis (CAT): a systematic review and meta-analysis. Thromb Res. 2018; 173: 158-163.
6. Lyman GH, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2013; 31(17): 2189-2204.
7. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE dis-ease: CHEST guideline and expert panel report [published correction appears in Chest. 2016; 150(4): 988]. Chest. 2016; 149(2): 315-352.
8. National Institute for Health and Care Excellence (NICE). Venous thromboembolic diseases: diagnosis, management and thrombophilia testing. Clinical guideline [CG144]. Updated November 2015. https:// www.nice.org.uk/Guidance/cg144. Accessed September 17, 2018.
Alternative Interventions for Chronic Prostatitis/Chronic Pelvic Pain Syndrome in Men
Anne L. Mounsey, MD, and Elizabeth Parks, MD, University of North Carolina, Chapel Hill, North Carolina
Author disclosure: No relevant financial affiliations.
Clinical QuestionAre nonpharmacologic therapies safe and effective for men with long-standing pelvic pain and lower urinary tract symptoms, also known as chronic prostatitis/chronic pelvic pain syndrome?
Evidence-Based AnswerIn men with chronic pelvic pain and urinary dysfunction who have not responded to standard medical management, extracorporeal shock wave therapy reduces symptoms and increases quality of life. Acupuncture may also provide benefit to some patients.1 (Strength of Recommendation: B, based on limited-quality patient-oriented evidence.)
Circumcision, transrectal thermotherapy, and physi-cal activity demonstrated a statistically but not clinically
SUMMARY TABLE: COMPARISON OF ANTICOAGULANTS TO PREVENT RECURRENT VTE AND MAJOR BLEEDING IN PATIENTS WITH CANCER
Intervention Control Outcomes NNT/NNHNumber of participants (number of studies)
Quality of evidence
LMWH Vitamin K antagonists
Recurrent VTE NNT = 19 (95% CI, 14 to 34) Favored LMWH
1,781 (5 RCTs) Moderate
Major bleeding No difference
Direct oral anticoagulants
Vitamin K antagonists
Recurrent VTE No difference 1,031 (4 RCTs) Low
Major bleeding No difference
Direct oral anticoagulants
LMWH Recurrent VTE No difference 1,016 (1 RCT) Low
Major bleeding NNH = 34 (95% CI, 13 to 2,439)
LMWH = low-molecular-weight heparin; NNH = number needed to harm; NNT = number needed to treat; RCT = randomized controlled trial; VTE = venous thromboembolism.
jun 1 cochrane.indd 677 5/10/19 9:23 AM

678 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
COCHRANE FOR CLINICIANS
significant reduction in symptoms. It is unclear whether lifestyle modifications or prostatic massage provides any benefit. Most nonpharmacologic interventions are not asso-ciated with an increased risk of adverse events.1 (Strength of Recommendation: B, based on limited-quality patient-oriented evidence.)
Practice PointersProstatitis is a common disorder affecting 10% to 14% of men in the United States, and it accounts for 1% of primary care visits each year.2,3 Chronic prostatitis/chronic pelvic pain syndrome, defined as pelvic pain and lower urinary tract symptoms lasting more than three months, is a diag-nosis of exclusion and comprises most cases. Men typi-cally present with pain in the lower abdomen, perineum, testicles, or penis, as well as urinary symptoms and sexual dysfunction, including ejaculatory pain. The variety of pre-sentations likely reflects the unclear etiology of this disease. As such, there is no standard first-line pharmacologic inter-vention. Antibiotics, nonsteroidal anti-inflammatory drugs, pregabalin (Lyrica), alpha blockers, and 5-alpha reductase inhibitors are most commonly used, and response to medi-cal management is often limited.
This Cochrane review of 38 randomized controlled tri-als involving 3,290 men evaluated the effectiveness of several nonpharmacologic interventions for chronic pros-tatitis/chronic pelvic pain syndrome.1 Participants were younger than 50 years. In 11 of 12 studies included in this meta-analysis, previous pharmacologic therapy had been unsuccessful. The primary outcome was the previously val-idated 13-question, 43-point National Institutes of Health–Chronic Prostatitis Symptom Index (NIH-CPSI) scale, which assessed pain, urinary symptoms, and quality of life. On this scale, the minimal clinically important difference is considered a six-point reduction from baseline.
Extracorporeal shock wave therapy applied at the perineum demonstrated significant improvement in NIH-CPSI score vs. sham procedure at six weeks in three studies (mean difference [MD] = –6.18; 95% CI, –7.46 to –4.89), but this effect was no longer present at 12 and 24 weeks. Mod-erate evidence in one study supported improvement in sex-ual dysfunction with extracorporeal shock wave therapy vs. control.
Three high-quality studies (N = 204) found that acupunc-ture vs. a sham procedure likely improved symptoms at six to eight weeks (NIH-CPSI score MD = –5.79; 95% CI, –7.32 to –4.26). One study demonstrated persistent benefit at 24 weeks. However, there was no improvement in sexual dysfunction. In two lower-quality studies with inadequate blinding (N = 78), acupuncture provided statistical benefit
(MD = –4.09; 95% CI, –6.87 to –1.30) compared with phar-macotherapy (i.e., levofloxacin [Levaquin], ibuprofen, or pollen extract).
Of the other interventions evaluated, few provided meaningful benefit. In one study of 700 men, circumci-sion provided statistical benefit on the NIH-CPSI score (MD = –3.00; 95% CI, –3.82 to –2.18) without a signifi-cant increase in adverse events at 12 weeks of follow-up. In one study of transrectal thermotherapy alone vs. medical therapy and another study of transrectal thermotherapy plus medical therapy vs. medical therapy alone, transrec-tal thermotherapy provided statistical, but not clinical, improvement (MD = –2.5; 95% CI, –3.8 to –1.2 and MD = –4.34; 95% CI, –5.65 to –3.04, respectively). Interest-ingly, in one low-quality study, physical activity reduced pain and increased quality of life, but worsened urinary symptoms. Prostatic massage, ultrasound, myofascial trig-ger point release, transurethral thermotherapy, transure-thral needle ablation, and sono-electromagnetic therapy did not improve prostatitis symptoms. Evidence for the effectiveness of biofeedback, lifestyle modifications, laser therapy, tibial nerve stimulation, and transcutaneous elec-trical nerve stimulation was very low-quality because of the potentially high risk of bias.
Consensus guidelines suggest using individualized, symptom-based treatment for chronic prostatitis/chronic pelvic pain syndrome. Multimodal therapy is recom-mended because of the complex nature of this syndrome similar to other chronic pain disorders.4 Evidence for non-pharmacologic interventions is generally limited, and many of the interventions are expensive and not widely avail-able. Yet, given the desperate situation of many patients in whom standard medical management has failed, even small improvements in symptoms may be beneficial. Therefore, family physicians should consider extracorporeal shock wave therapy and acupuncture for the management of chronic prostatitis/chronic pelvic pain syndrome.The practice recommendations in this activity are available at http:// www.cochrane.org/CD012551.
References 1. Franco JV, Turk T, Jung JH, et al. Non-pharmacological interventions
for treating chronic prostatitis/chronic pelvic pain syndrome. Cochrane Database Syst Rev. 2018; (5): CD012551.
2. Bajpayee P, Kumar K, Sharma S, et al. Prostatitis: prevalence, health impact and quality improvement strategies. Acta Poloniae Pharmaceu-tica. 2012; 69(4): 571-579.
3. Collins MM, Stafford RS, O’Leary MP, et al. How common is prostatitis? A national survey of physician visits. J Urol. 1998; 159(4): 1224-1228.
4. Magistro G, Waenlaher FM, Grabe M, et al. Contemporary management of chronic prostatitis/chronic pelvic pain syndrome. European Urol. 2016; 69(2): 286-297. ■
jun 1 cochrane.indd 678 5/10/19 9:23 AM

The EveryONE ProjectAdvancing health equity in every community
In its first major development for The EveryONE Project, the AAFP compiled an in-depth toolkit to help physicians recognize and respond to social factors that impact the health of patients.
The EveryONE Project toolkit is validated, intuitive, action oriented, and free. Utilize it to:
• Raise awareness about the effects of social determinants of health.
• Discover specific health risks in patients of all backgrounds.
• Understand and manage potential biases that may exist.
• Connect patients with essential resources in their area. Reveal and address the unseen health hurdles your patients face every day. Start using The EveryONE Project toolkit now.
aafp.org/EveryONE/tools
• Build community engagement and partnerships for support.• Engage legislators at the local, state, and federal levels.
Achieve healthier outcomes—for everyone.
17101839 Everyone Full Page.indd 1 12/11/17 11:20 AM

682 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
Varicose veins are subcutaneous veins dilated to at least 3 mm in diameter when measured with the patient in an upright position. They are part of a continuum of chronic venous disorders ranging from fine telangiectasias, also called spi-der veins, (less than 1 mm; Figure 1) and reticu-lar veins (1 to 3 mm; Figure 1) to chronic venous insufficiency, which may include edema, hyper-pigmentation, and venous ulcers. Chronic venous disease is most commonly described using the CEAP (clinical, etiologic, anatomic, pathophysi-ologic) classification system (Table 1).1
Varicose Veins: Diagnosis and TreatmentJaqueline Raetz, MD; Megan Wilson, MD; and Kimberly Collins, MD
University of Washington Family Medicine Residency, Seattle, Washington
CME This clinical content conforms to AAFP criteria for continuing medical education (CME). See CME Quiz on page 673.
Author disclosure: No relevant financial affiliations.
Patient information: A handout on this topic is available at https:// family doctor.org/condition/varicose-veins.
Varicose veins are twisted, dilated veins most commonly located on the lower extremities. The exact pathophysiology is debated, but it involves a genetic predisposition, incompetent valves, weakened vascular walls, and increased intravenous pressure. Risk factors include family history of venous disease; female sex; older age; chronically increased intra-abdominal pressure due to obesity, preg-nancy, chronic constipation, or a tumor; and prolonged standing. Symptoms of varicose veins include a heavy, achy feeling and an itching or burning sensation; these symptoms worsen with prolonged standing. Potential complications include infection, leg ulcers, stasis changes, and thrombosis. Con-servative treatment options include external compression; lifestyle modifications, such as avoidance of prolonged standing and straining, exercise, wearing nonrestrictive clothing, modification of car-diovascular risk factors, and interventions to reduce peripheral edema; elevation of the affected leg; weight loss; and medical therapy. There is not enough evidence to determine if compression stock-ings are effective in the treatment of varicose veins in the absence of active or healed venous ulcers. Interventional treatments include external laser thermal ablation, endovenous thermal ablation, endo-venous sclerotherapy, and surgery. Although surgery was once the standard of care, it largely has been replaced by endovenous thermal ablation, which can be performed under local anesthesia and may have better outcomes and fewer complications than other treatments. Existing evidence and clinical guidelines suggest that a trial of compression therapy is not warranted before referral for endove-nous thermal ablation, although it may be necessary for insurance coverage. (Am Fam Physician. 2019; 99(11): 682-688. Copyright © 2019 American Academy of Family Physicians.)
FIGURE 1
Telangiectasia, or spider veins, (black arrow) are small dilated superficial veins less than 1 mm in diameter. They are present in 43% of men and 55% of women.3 Reticular veins (white arrow) are 1 to 3 mm in diameter.
raetz.indd 682 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 683
VARICOSE VEINS
Varicose veins are common on the lower extrem-ities, with widely varying estimates of prevalence.2 A recent study found that telangiectasias occur in 43% of men and 55% of women, and varicose veins occur in 16% of men and 29% of women.3 In a pop-ulation with a mean age of 60 years, the prevalence of CEAP classification C0 to C6 is 29%, 29%, 23%, 10%, 9%, 1.5%, and 0.5%, respectively.4
EtiologyVenous disease resulting in valvular reflux appears to be the underlying cause of varicose veins.5 The exact pathophysiology is debated, but it involves a genetic predisposition, incompetent valves, weakened vascular walls, and increased intravenous pressure. In most cases, the valvular dysfunction is presumed to be caused by a loss of elasticity in the vein wall, with failure of the valve leaflets to fit together. Rather than blood flowing from distal to proximal and superficial to deep, failed or incompetent valves allow blood to flow in the reverse direction. With increased pressure on the affected venous system, the larger veins may become elongated and tortuous. Shear stress on venous endothelial cells due to reversed or turbulent blood flow and inflammation are also important etiologic factors for venous disease.6
Varicose veins in the legs may involve the main axial superficial veins (the great saphe-nous vein and the small saphenous vein or their superficial tributaries).7 Established risk fac-tors for varicose veins include family history of
venous disease; female sex; older age; chronically increased intra-abdominal pressure due to obe-sity, pregnancy, chronic constipation, or a tumor; prolonged standing; deep venous thrombosis causing damage to valves and secondary revas-cularization; and arteriovenous shunting.8,9
DiagnosisCLINICAL PRESENTATION
The clinical presentation of varicose veins varies, and some patients may be asymptomatic.10 Local-ized symptoms may be unilateral or bilateral and include pain, burning, itching, and tingling at the site of the varicose veins. Generalized symptoms consist of aching, heaviness, cramping, throb-bing, restlessness, and swelling in the legs.7,11 Symptoms are often worse at the end of the day, especially after prolonged standing, and usually resolve when patients sit and elevate their legs. Women are significantly more likely than men to report lower limb symptoms.12 Patients are more likely to have symptoms and increasing severity of symptoms with increasing CEAP clinical class (C0 to C6).6
Although varicose veins may cause varying degrees of discomfort or cosmetic concern, they are rarely associated with significant complica-tions. Signs of a more serious underlying vascular insufficiency may include changes in skin pigmen-tation, eczema, infection, superficial thrombo-phlebitis, venous ulceration, loss of subcutaneous tissue, and lipodermatosclerosis (a decrease in
SORT: KEY RECOMMENDATIONS FOR PRACTICE
Clinical recommendationEvidence rating References Comments
There is not enough evidence to determine if compression stockings are effective in the treatment of varicose veins in the absence of active or healed venous ulcers.
B 7, 15, 19-21 Based on a Cochrane review and clinical guidelines based on systematic reviews; consensus guidelines and expert opinion
Horse chestnut seed extract (Aesculus hippocastanum) and other phlebotonics may ease the symptoms of varicose veins, but long-term studies of the safety and effectiveness of phlebotonics are lacking.
B 23-25 Based on systematic reviews/Cochrane review of lower-quality RCTs
Referral for interventional treatment of symptomatic vari-cose veins in nonpregnant patients should not be delayed for a trial of external compression. Interventional treat-ment should be offered if valvular reflux is documented.
C 7, 15 Clinical guidelines based on systematic reviews; consensus guidelines and expert opinion
Endovascular laser ablation may be better tolerated than sclerotherapy and surgery, with fewer adverse effects and equal effectiveness.
B 30, 31 Based on a Cochrane review of lower- quality RCTs and an RCT on quality-of-life outcomes
RCT = randomized controlled trial.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease- oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https:// www.aafp.org/afpsort.
raetz.indd 683 5/10/19 9:23 AM

684 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
lower leg circumference due to chronic inflam-mation, fibrosis, and contraction of the skin and subcutaneous tissues). Although rare, hemo-dynamically significant external hemorrhage resulting from the perforation of a varicose vein has been reported.13
Evaluation of patient risk factors, symptoms, and typical physical examination findings helps determine a diagnosis. Through inspection and palpation, the examiner should note the size and distribution of varicose veins, the presence and type of edema, and the presence of skin discol-oration, excoriation, or ulceration. Fan-shaped varicose veins in the ankle (corona phlebectatica; Figure 2) are considered an early sign of advanced venous disease. Decreased ankle mobility, atro-phie blanche (a circular whitish area of scar tissue surrounded by dilated capillaries), and lipoder-matosclerosis are also signs of advanced venous disease.1 Noting locations of other varicosities is important. Perineal, vulvar, or groin varicosi-ties may be a sign of pelvic vein incompetence or obstruction, which may include abdominal, pel-vic, or renal masses.7 Bedside clinical tests used to detect the site of reflux, such as palpation for a retrograde transmitted impulse from the saphe-nofemoral junction through the long saphenous vein (tap test) or for transmission of a thrill or impulse with coughing at the saphenofemoral junction (cough test), are of limited value because of their poor sensitivity or specificity.14
IMAGING STUDIES
When venous disease is severe or interventional therapy is being considered, venous duplex ultra-sonography is the modality of choice.7,15 Duplex ultrasonography is a simple, noninvasive,
TABLE 1
The Basic CEAP Classification System for Chronic Venous Disease
Classification Description
Clinical*
C0 No visible or palpable signs of venous disease
C1 Telangiectasias or reticular veins
C2 Varicose veins
C3 Edema
C4a Pigmentation or eczema
C4b Lipodermatosclerosis or atrophie blanche
C5 Healed venous ulcer
C6 Active venous ulcer
Etiologic
Ec Congenital
Ep Primary
Es Secondary (postthrombotic)
En No venous cause identified
Anatomic
As Superficial veins
Ap Perforating veins
Ad Deep veins
An No venous location identified
Pathophysiologic
Pr Reflux
Po Obstruction
Pr,o Reflux and obstruction
Pn No venous pathophysiology identifiable
Note: The CEAP classification system provides a framework to characterize venous disease, including varicose veins. The first por-tion of the CEAP classification system can be used alone in practice. For example, a patient presenting to the office with varicose veins with mild edema and aching but no hemosiderin staining of the lower extremities could be documented as having C3S venous dis-ease. Venous studies would be needed to further classify the patient using the remainder of the CEAP system.
*—The presence or absence of symptoms is noted with a subscript “S” or “A,” for example C1A (asymptomatic telangiectasias) or C5S (symptomatic healed venous ulcer). Symptoms include aching, pain, tightness, skin irritation, heaviness, muscle cramps, and other symptoms attributable to venous dysfunction.
Adapted with permission from Eklöf B, Rutherford RB, Bergan JJ, et al.; American Venous Forum International Ad Hoc Committee for Revision of the CEAP Classification. Revision of the CEAP classifi-cation for chronic venous disorders: consensus statement. J Vasc Surg. 2004; 40(6): 1251-1252.
FIGURE 2
Corona phlebectatica with edema. Corona phlebec-tatica can include blue veins, blue telangiectasia, red telangiectasia, and darker stasis spots. It is consid-ered an early sign of advanced venous disease. Using the CEAP classification system (Table 1), this patient would be classified as having C3 vascular disease.
raetz.indd 684 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 685
VARICOSE VEINS
painless, and readily available modality that can assess the anatomy and physiology of the lower extremity venous system. It can help determine which saphenous junctions are incompetent, the diameter of the junctions, the extent of reflux, and the location and size of other incompetent perforating veins. It can also assess for acute and occult deep venous thrombosis and superficial thrombophlebitis. Reflux is defined as a retrograde flow duration of more than 350 milliseconds in the perforating veins, more than 500 milliseconds in the superficial and deep calf veins, and more than 1,000 milliseconds in the femoropopliteal veins.16,17 Other imaging modalities, such as computed tomography, magnetic resonance imaging, venography, and plethysmography, are used only if venous ultrasonography is inconclusive or for more complex surgical situations.7
TreatmentUse of the CEAP classification system is important for diagnosis but does not provide guidance
for treatment decisions. Treatment options for varicose veins include conservative management and interventional therapies such as thermal ablation, endovenous sclerotherapy, and surgery (Table 2).7,15,18 The decision to proceed with treatment and the choice of treatment are based on symptoms and patient preferences. Other considerations include cost, potential for complications, availability of resources, insurance reimbursement, and physician training. The presence or absence of deep venous insufficiency and the characteristics of the affected veins can also help guide treatment.17
Over the past 10 years, there has been a significant change in the recommendations for treatment of symptomatic varicose veins. This is in large part because of the lack of evidence supporting the use of compression stockings and the rise of minimally invasive endovascular techniques.
CONSERVATIVE MANAGEMENT
Conservative treatment options include external compression; lifestyle modifications, such as
TABLE 2
Treatment Options for Varicose Veins
Treatment Comments
Conservative measures
Compression (e.g., bandages, support stockings, intermittent pneumatic compression devices)
Compression stockings can provide relief from discomfort, although evidence is lacking; external compression is first-line treatment only in pregnant women
Elevation of the affected leg May improve symptoms in some patients
Lifestyle modifications Examples include avoidance of prolonged standing and straining, exer-cise, wearing nonrestrictive clothing, modification of cardiovascular risk factors, and interventions to reduce peripheral edema
Weight loss Weight loss may improve symptoms in patients who are obese
Phlebotonics Most are available as dietary supplements (often with multiple agents in one supplement) and are sold over the counter in the United States; horse chestnut seed extract (Aesculus hippocastanum) may provide symptom-atic relief, but long-term studies are lacking
Interventional
Thermal ablation
External laser thermal ablation Works best for telangiectasias
Endovenous thermal ablation (using a laser or radio waves)
Used for larger vessels, including the greater saphenous vein
Endovenous sclerotherapy A variety of agents may be used, including hypertonic saline, sodium tetradecyl (Sotradecol), and polidocanol (Varithena)
Surgery (ligation and stripping or phlebectomy with multiple small incisions)
Although surgery has historically been the most widely recommended treatment option, a growing body of literature does not consistently sup-port surgery as the best interventional treatment option; updated surgical techniques use small incisions to reduce scarring, blood loss, and com-plications and limit removal of the superficial axial veins from the groin to knee, and may be performed under local or regional anesthesia
Adapted with permission from Jones RH, Carek PJ. Management of varicose veins. Am Fam Physician. 2008; 78(11): 1292, with additional information from references 7 and 15.
raetz.indd 685 5/10/19 9:23 AM

686 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
VARICOSE VEINS
avoidance of prolonged standing and straining, exercise, wearing nonrestrictive clothing, modi-fication of cardiovascular risk factors, and inter-ventions to reduce peripheral edema; elevation of the affected leg; weight loss; and phlebotonics. These measures are recommended for patients who are not candidates for endovenous or surgi-cal management, do not desire intervention, or are pregnant.7,15
Compression has long been recommended as initial therapy for varicose veins. However, there is not enough evidence to determine if compression stockings are effective in the treat-ment of varicose veins in the absence of active or healed venous ulcers.7,19-21 The 2013 National Institute for Health and Care Excellence clinical guidelines recommend offering external com-pression only if interventional treatment is inef-fective and as first-line therapy only in pregnant women.15
In some cases, a trial of external compression may be required by insurance companies before approval of interventional treatments. Although the optimal length and pressure for effective treatment has not been determined, typical rec-ommendations include wearing 20 to 30 mm Hg elastic compression stockings with a gradient of decreasing pressure from the distal to proximal extremity.22
Phlebotonics are oral and topical therapies that may increase venous tone, improve capillary hyperpermeability, and decrease blood viscosity with the goal of decreasing symptoms of chronic venous insufficiency.23 They include flavonoids or other compounds often extracted from plants, such as rutin (also called rutoside), diosmin, hidrosmin, disodium flavodate, French mari-time pine bark extract (Pycnogenol), grape seed extract, and horse chestnut seed extract (Aesculus hippocastanum). Diosmiplex (Vasculera) is the only prescription formulation available in the United States.23 Diosmiplex is derived from orange rinds and is categorized as a medical food, not a drug. The usual dosage is 630 mg daily.
Horse chestnut seed extract appears to be safe and effective in reducing pain, edema, and pru-ritus from chronic venous insufficiency when used for two to 16 weeks. The common dosage is 300 mg twice daily or 50 mg of escin, the active compound.24 There is moderate-quality evidence that other phlebotonics may improve edema and
possibly decrease symptoms such as cramps, rest-less legs, and paresthesia.25
Most phlebotonics are available as dietary sup-plements in the United States, and many formu-lations contain multiple phlebotonics in a single supplement. Long-term studies of the safety and effectiveness of phlebotonics for the treatment of varicose veins are lacking.25
INTERVENTIONAL TREATMENTS
Thermal Ablation. Thermal ablation destroys damaged veins using an external laser or via endovenous catheter using a laser (endovenous laser ablation) or radio waves (radiofrequency ablation). External laser thermal ablation works best for telangiectasias. In this therapy, hemoglo-bin absorbs the laser light leading to thermoco-agulation.26 Endovenous thermal ablation can be used for larger vessels, including the great saphe-nous vein. Under ultrasound guidance, a laser optical fiber or radiofrequency catheter electrode is inserted into the vein in a distal to proximal direction. Heat from the laser or radio waves coagulates the blood in the vein, resulting in clo-sure of the vein and redirection of blood flow to functional veins.26,27
Endovenous thermal ablation is performed after a local anesthetic is injected around the vein. Patients can walk after the procedure and may be discharged home the same day. Patients may return quickly to work and other activities. There is a risk (approximately 7%) of surround-ing nerve damage attributed to thermal injury; however, most nerve damage is temporary.27 Endovenous thermal ablation is recommended as first-line treatment for nonpregnant patients with symptomatic varicose veins and documented val-vular reflux, and need not be delayed for a trial of external compression.7,15
Endovenous Sclerotherapy. Endovenous sclero-therapy involves using ultrasound guidance to inject superficial veins with an agent that causes inflammation of the endothelium, resulting in fibrosis and occlusion in the vein.27 Sclerother-apy is typically used for small (1 to 3 mm) and medium (3 to 5 mm) veins or to treat recurrent varicose veins after surgery; however, there is not a precise diameter used to make treatment decisions.28
A needle is inserted into the vein lumen and the sclerosing agent is injected, often with air to
raetz.indd 686 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 687
VARICOSE VEINS
create a foam. The foam displaces the blood and reacts with the vascular endothelium, sealing and scarring the vein. A variety of agents may be used, including hypertonic saline, sodium tetra-decyl (Sotradecol), and polidocanol (Varithena). There is no evidence that any of these agents is superior to the others in terms of effectiveness or patient satisfaction.29
Surgery. Historically, surgery with ligation and stripping of the great or small saphenous vein has been the standard of care for the treatment of varicose veins after the failure of conservative therapy. However, a growing body of literature does not consistently support surgery as the best interventional treatment option, and the 2013 National Institute for Health and Care Excellence clinical guidelines recommend surgery as third-line therapy after endovenous thermal ablation and sclerotherapy.15,30,31
Updated surgical techniques use small inci-sions to reduce scarring, blood loss, and compli-cations and limit removal of the superficial axial veins from the groin to knee. Some of these pro-cedures can be performed under regional or local anesthesia.7 Ligation and stripping of the great and small saphenous vein are probably the best-known procedures. Typically, the vein is divided proximally, a vein stripper is passed distally to an incision made near the knee to access the tip of the stripper. The proximal end of the stripper is secured to the vein and the vein is then removed as the stripper is pulled distally. Nonsaphenous and smaller veins can be removed via phlebec-tomy, during which a scalpel or large-gauge nee-dle is used to create punctures every 2 to 3 cm along a varicose vein. Segments of the damaged vein are removed using forceps or small hooks.
OUTCOME DATA
A 2014 Cochrane review concluded that endo-venous laser ablation, radiofrequency ablation, and foam sclerotherapy are as effective as sur-gery for great saphenous vein varices.30 Prior literature suggested that traditional surgical treatment of varicose veins with great saphenous vein ligation at the saphenofemoral junction and stripping has a five-year recurrence rate of 20% to 28%.30 Clinical recurrence of varicose veins at five years was measured in only one study in the Cochrane review and suggested no difference between endovenous laser ablation and surgery.30
Maintaining saphenous vein occlusion at six months is less likely with sclerotherapy than with endovenous laser ablation or surgery (43% vs. 80%).31 Endothermal ablation resulted in less recurrence of reflux at one year compared with surgery when treating varicose veins of the small saphenous vein resulting from incompetence of the saphenous-popliteal junction.27
Nonsurgical therapies may have faster return-to-work and recovery times than surgery. Endo-venous laser ablation may be better tolerated than sclerotherapy and surgery, with fewer adverse effects and equal effectiveness.30,31 For all three therapies, rates of minor and major complica-tions, including numbness, persistent bruising or tenderness, skin ulceration, skin staining, and lumpiness, are relatively low (1% to 7%).31 Hema-tomas occur more often with surgical treatment than with foam sclerotherapy or radiofrequency ablation. Endovenous laser ablation appears to be superior to surgery in terms of technical failure and neovascularization. Although all interven-tional treatment leads to symptomatic improve-ment, the improvement at six months may be more significant with endovenous laser ablation and surgery than with foam sclerotherapy.31
This article updates a previous article on this topic by Jones and Carek.18
Data Sources: A search was performed in Essen-tial Evidence Plus. Additionally, PubMed and the Cochrane database were searched using the key term varicose veins. The PubMed search was limited to English language, humans, 10 years, and system-atic reviews. Search dates: March 15, 2018; June 6, 2018; and February 21, 2019.
The Authors
JAQUELINE RAETZ, MD, is an associate professor in the University of Washington Family Medicine Residency program, Seattle.
MEGAN WILSON, MD, is an assistant professor in the University of Washington Family Medicine Residency program.
KIMBERLY COLLINS, MD, is an assistant professor in the University of Washington Family Medicine Residency program.
Address correspondence to Jaqueline Raetz, MD, 331 NE Thornton Place, Seattle, WA 98125 (e-mail: jraetz@ uw.edu). Reprints are not available from the authors.
raetz.indd 687 5/10/19 9:23 AM

688 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
VARICOSE VEINS
References 1. Eklöf B, Rutherford RB, Bergan JJ, et al.; American Venous
Forum International Ad Hoc Committee for Revision of the CEAP Classification. Revision of the CEAP classifica-tion for chronic venous disorders: consensus statement. J Vasc Surg. 2004; 40(6): 1248-1252.
2. Eberhardt RT, Raffetto JD. Chronic venous insufficiency. Circulation. 2014; 130(4): 333-346.
3. Kaplan RM, Criqui MH, Denenberg JO, Bergan J, Fronek A. Quality of life in patients with chronic venous disease: San Diego population study. J Vasc Surg. 2003; 37(5): 1047-1053.
4. McLafferty RB, Passman MA, Caprini JA, et al. Increasing awareness about venous disease: The American Venous Forum expands the National Venous Screening Program. J Vasc Surg. 2008; 48(2): 394-399.
5. Clarke GH, Vasdekis SN, Hobbs JT, Nicolaides AN. Venous wall function in the pathogenesis of varicose veins. Surgery. 1992; 111(4): 402-408.
6. Bergan JJ, Schmid-Schönbein GW, Smith PD, Nicolaides AN, Boisseau MR, Eklof B. Chronic venous disease. N Engl J Med. 2006; 355(5): 488-498.
7. Gloviczki P, Comerota AJ, Dalsing MC, et al. The care of patients with varicose veins and associated chronic venous diseases: clinical practice guidelines of the Soci-ety for Vascular Surgery and the American Venous Forum. J Vasc Surg. 2011; 53(5 suppl): 2S-48S.
8. Beebe-Dimmer JL, Pfeifer JR, Engle JS, Schottenfeld D. The epidemiology of chronic venous insufficiency and varicose veins. Ann Epidemiol. 2005; 15(3): 175-184.
9. Sadick NS. Advances in the treatment of varicose veins: ambulatory phlebectomy, foam sclerotherapy, endovas-cular laser, and radiofrequency closure. Dermatol Clin. 2005; 23(3): 443-455, vi.
10. Teruya TH, Ballard JL. New approaches for the treatment of varicose veins. Surg Clin North Am. 2004; 84(5): 1397-1417, viii-ix.
11. Langer RD, Ho E, Denenberg JO, Fronek A, Allison M, Criqui MH. Relationships between symptoms and venous disease: the San Diego population study. Arch Intern Med. 2005; 165(12): 1420-1424.
12. Bradbury A, Evans C, Allan P, Lee A, Ruckley CV, Fowkes FG. What are the symptoms of varicose veins? Edinburgh vein study cross sectional population survey. BMJ. 1999; 318(7180): 353-356.
13. Racette S, Sauvageau A. Unusual sudden death: two case reports of hemorrhage by rupture of varicose veins. Am J Forensic Med Pathol. 2005; 26(3): 294-296.
14. Kim J, Richards S, Kent PJ. Clinical examination of varicose veins—a validation study. Ann R Coll Surg Engl. 2000; 82(3): 171-175.
15. National Institute for Health and Care Excellence. Vari-cose veins: diagnosis and management. Clinical guideline 168. July 2013. https:// www.nice.org.uk/guidance/cg168. Accessed May 21, 2018.
16. Labropoulos N, Tiongson J, Pryor L, et al. Definition of venous reflux in lower-extremity veins. J Vasc Surg. 2003; 38(4): 793-798.
17. Coleridge-Smith P, Labropoulos N, Partsch H, Myers K, Nicolaides A, Cavezzi A. Duplex ultrasound investigation of the veins in chronic venous disease of the lower limbs—UIP consensus document. Part I. Basic principles. Eur J Vasc Endovasc Surg. 2006; 31(1): 83-92.
18. Jones RH, Carek PJ. Management of varicose veins. Am Fam Physician. 2008; 78(11): 1289-1294.
19. Shingler S, Robertson L, Boghossian S, Stewart M. Com-pression stockings for the initial treatment of varicose veins in patients without venous ulceration. Cochrane Database Syst Rev. 2013;(12): CD008819.
20. O’Meara S, Cullum N, Nelson EA, Dumville JC. Compres-sion for venous leg ulcers. Cochrane Database Syst Rev. 2012;(11): CD000265.
21. Nelson EA, Bell-Syer SE. Compression for preventing recurrence of venous ulcers. Cochrane Database Syst Rev. 2014;(9): CD002303.
22. Lam Ey, Giswold ME, Moneta GL. Venous and lymphatic disease. In: Dries DJ, ed. Schwartz’s Principles of Surgery. 8th ed. New York, NY: McGraw-Hill; 2005: 823-825.
23. Bush R, Comerota A, Meissner M, Raffetto JD, Hahn SR, Freeman K. Recommendations for the medical manage-ment of chronic venous disease: the role of micronized purified flavonoid fraction (MPFF) [published correction appears in Phlebology. 2017; 32(10): NP36]. Phlebology. 2017; 32(1 suppl): 3-19.
24. Pittler MH, Ernst E. Horse chestnut seed extract for chronic venous insufficiency. Cochrane Database Syst Rev. 2012;(11): CD003230.
25. Martinez-Zapata MJ, Vernooij RW, Uriona Tuma SM, et al. Phlebotonics for venous insufficiency. Cochrane Data-base Syst Rev. 2016; (4): CD003229.
26. Reichert D. Evaluation of the long-pulse dye laser for the treatment of leg telangiectasias. Dermatol Surg. 1998; 24(7): 737-740.
27. Paravastu SC, Horne M, Dodd PD. Endovenous ablation therapy (laser or radiofrequency) or foam sclerotherapy versus conventional surgical repair for short saphenous varicose veins. Cochrane Database Syst Rev. 2016; (11): CD010878.
28. Tisi PV, Beverley C, Rees A. Injection sclerotherapy for varicose veins. Cochrane Database Syst Rev. 2006; (4): CD001732.
29. Schwartz L, Maxwell H. Sclerotherapy for lower limb telangiectasias. Cochrane Database Syst Rev. 2011; (12): CD008826.
30. Nesbitt C, Bedenis R, Bhattacharya V, Stansby G. Endove-nous ablation (radiofrequency and laser) and foam sclero-therapy versus open surgery for great saphenous vein varices. Cochrane Database Syst Rev. 2014; (7): CD005624.
31. Brittenden J, Cotton SC, Elders A, et al. A randomized trial comparing treatments for varicose veins. N Engl J Med. 2014; 371(13): 1218-1227.
raetz.indd 688 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 689
Adolescent use of illicit substances imposes an enor-mous burden on individuals, families, and communities. Substance use has correlations with violence, including adolescent homicides1 and relationship victimization.2 Adolescence (typically encompassing youth 10 to 19 years of age)3 is a time of development, including ongoing matur-ing of the brain; therefore, it is essential to consider the pathophysiology of substance use.4,5 Adolescent brains are more vulnerable to the temptation to use substances and to the effects of these substances because reward pathways develop before prefrontal cognition.5 Sustained substance use can affect neuropsychological functioning, resulting in attention deficits, memory problems, and decreased cognitive flexibility.5
Scope and Prevalence Adolescents who participated in the Youth Risk Behav-ior Survey (a survey of students in grades 9 to 12) in 2015 indicated that 32.8% of them have used alcohol and that 10.8% of them have smoked cigarettes in the past 30 days.6
Nearly 10% of high school students have used two or more tobacco products in the past 30 days,7 and dual users (i.e., users of two or more tobacco products) are at greater risk of engaging in other risky behaviors (e.g., other substance use) compared with nontobacco users and single-product users.8
One in five U.S. adolescents had used marijuana in 2015,6 and Monitoring the Future (a survey of 8th, 10th, and 12th graders) results indicated a significant increase in adoles-cent marijuana use in 2017 because of adolescents’ lowered risk perceptions.9 Alcohol is the substance most consumed by adolescents; however, the Youth Risk Behavior and
Adolescent Substance Use and Misuse: Recognition and Management
Jessica A. Kulak, PhD, MPH, and Kim S. Griswold, MD, MPH, State University of New York at Buffalo, Buffalo, New York
CME This clinical content conforms to AAFP criteria for continuing medical education (CME). See CME Quiz on page 673.
Author disclosure: No relevant financial affiliations.
Adolescent use of illicit substances imposes an enormous burden on individuals, families, and communities. The types of illicit substances adolescents are using have changed drastically over the past decade with decreases in alcohol use (includ-ing binge alcohol use) offset by increases in electronic cigarette, marijuana, and opioid use. Primary care physicians have the opportunity to identify adolescents who use illicit substances. The U.S. Preventive Services Task Force and the American Academy of Family Physicians found insufficient evidence to assess the balance of benefits and harms of primary care–based behavioral interventions to prevent or reduce illicit substance use or nonmedical pharmaceutical use in children or adoles-cents. The American Academy of Pediatrics recommends that clinicians become familiar with Screening, Brief Intervention, and Referral to Treatment initiatives. Validated screening tools that may be used in primary care include the CRAFFT, POSIT, AUDIT, and NIAAA Screening Guide. During the clinical visit, a split-visit model encourages parents to participate in the visit for a limited time but also allows adolescents to have confidential conversations with physicians. Evidence-based treatment modalities range from school- and parent-based interventions to medication-assisted treatment. Brief interventions using components of motivational interviewing may be suitable for addressing substance use, even among adolescents not seeking treatment. Prevention efforts can supplement cessation programs to maximize program effectiveness. (Am Fam Physician. 2019;99(11): 689-696. Copyright © 2019 American Academy of Family Physicians.)
WHAT IS NEW ON THIS TOPIC
Adolescent Substance Use and Misuse
In 2017, e-cigarettes were the most commonly used nicotine- delivery product among high school students.
Approximately 27% of adolescents 13 to 18 years of age who drink alcohol mix it with energy drinks. These adolescents are at increased risk for using tobacco and marijuana and for nonmedical use of prescription stimulants.
Seventeen percent of adolescents have taken prescription drugs without a doctor’s prescription.
kulak.indd 689 5/10/19 9:23 AM

690 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
ADOLESCENT SUBSTANCE USE AND MISUSE
Monitoring the Future surveys show decreases in 30-day, annual, and lifetime use in 2015, including significant declines in current and binge drinking.10 Approximately 27% of alcohol-using adolescents 13 to 18 years of age mix alcohol with energy drinks, which is a risk factor for tobacco, marijuana, and nonmedical use of prescription stimulants.11
In 2015, adolescent use of illicit substances was reported to be 2.1% for heroin, 5.2% for cocaine, 6.4% for hallu-cinogens, and 9.2% for synthetic marijuana.6 National estimates indicate that approximately 5% of adoles- cents had used ecstasy/methylenedioxymethamphetamine (MDMA).6 Other research, however, indicates that the estimate could be as high as 8% because many adolescents do not realize that the substance they know as Molly is a form of ecstasy.12 Approximately 16.8% of adolescents have taken prescription drugs without a physician’s prescrip-tion (nonmedical use of prescription drugs).6 In some high school seniors, the nonmedical use of prescription stim-ulants is associated with substance use disorders (SUDs) in adulthood,13 and lifetime nonmedical use of prescrip-tion opioids is a risk factor for lifetime heroin use among adolescents.14
The opioid epidemic does not spare the younger popula-tion. From 1997 to 2012, hospitalizations for prescription opioid poisoning in children and adolescents increased 165% (1.40 to 3.71 per 100,000); for adolescents older than 15 years, hospitalizations for heroin and methadone poison-ing increased 161% (0.96 to 2.51 per 100,000) and 950% (0.10
to 1.05 per 100,000), respec-tively.15 Nonmedical con-sumption of codeine cough syrup is sometimes an intro-duction to opioid misuse among youth.16 The cough syrup is typically mixed with soda or occasionally alcohol and is colloquially known as lean, sizzurp, or purple drank.17 Previous research showed that misuse of codeine cough syrup was primarily by black youth. Other research, however, indicates that the use of lean is also high among His-panic and Native American youth; males; homosexual, bisexual, and transgender individuals; and youth from urban areas.17
The types of products and the ways in which they are used have changed drastically over the past decade. Tra-ditional cigarette use is low and declining, but high school students’ use of any tobacco product within 30 days (19.6%) has not changed significantly from 2011 to 2017,18 primarily because of the increase in hookah and electronic cigarette (e-cigarette) use. The use of cigarillos (smaller, unfiltered cigars) is also prevalent. Cigarillo users often empty the tobacco and replace the contents with mari-juana, creating a blunt.19
In 2017, e-cigarettes were the most commonly used nicotine-delivering product among high school students.18 E-cigarette usage, or vaping, has also become a method for administering marijuana; in national and community sam-ples of high school students, rates of vaporizing marijuana by using e-cigarettes were high (10%9 to 29.2%20). In 2018, 21% of U.S. 12th graders reported vaping nicotine in the past 30 days.21 A JUUL is a popular vaping tool that delivers high concentrations of nicotine and has a sleek appearance similar to a computer flash drive.22 JUUL products are promoted on social media platforms whose primary audiences are youth or young adults. JUUL Labs, Inc., and retailers selling the JUUL product have received warning letters from the U.S. Food and Drug Administration22 and have been subjected to fines for illegally selling these products to minors.23
Physicians are valued as a trustworthy source of infor-mation, so they may be asked to provide information about vaping and e-cigarettes to patients and their families.24 The role of e-cigarettes as a form of nicotine delivery continues to
SORT: KEY RECOMMENDATIONS FOR PRACTICE
Clinical recommendationEvidence rating References
The American Academy of Pediatrics recommends that physicians become knowledgeable about the Screening, Brief Intervention, and Referral to Treatment (SBIRT) guidelines.
C 35
The U.S. Preventive Services Task Force and the American Academy of Family Physicians conclude that the current evidence is insufficient to assess the balance of benefits and harms of primary care–based behavioral interventions to prevent or reduce illicit substance or non-medical pharmaceutical use in children and adolescents.
C 48, 49
Primary care treatment for adolescent substance use should be coor-dinated with treatment from other mental health experts.
C 50
Brief interventions using components of motivational interviewing may reduce illicit substance use among adolescents.
C 41, 53
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https:// www.aafp.org/afpsort.
kulak.indd 690 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 691
ADOLESCENT SUBSTANCE USE AND MISUSE
be debated, but physicians can provide accurate information on meaningful differences in product risks.25
Sociodemographic Differences Between 2002 and 2014, male and female adolescents 12 to 17 years of age had similar 12-month preva-lence rates of SUDs and decreasing trends in use of illicit substances. Male adolescents are typically more likely to use most illicit substances; female adolescents are more likely to use nonmedical amphetamines and tranquilizers.10 Risk factors for illicit substance use include dropping out of high school and ease of access to sub-stances.26 Rural adolescents reported easier access to tobacco products and steroids; urban adolescents reported greater access to alcohol, mari-juana, cocaine, methamphetamines, inhalants, ecstasy, hallucinogens, and prescription drugs.27 Neighborhood economic disadvantage, social dis-order, and high unemployment rates may play a larger role than individual- level factors in the variance of alcohol and illicit substance use among black adolescents compared with white adolescents.28
Screening and Diagnosis Mild, moderate, or severe SUD is iden-tified in persons who meet criteria in the Diagnostic and Statistical Manual of Mental Disorders, 5th ed., indicating significant clinical and/or functional impairment (Table 1).29 Because 81% of patients seeking SUD treatment had been seen by a primary care physician during the previous year, primary care physicians have the opportunity to iden-tify adolescents who use substances.30 However, few primary care physicians screen adolescents according to guide-lines,30 likely because of low reported levels of preparedness,31 knowledge,30 and low perceived confidence32 to iden-tify and treat substance use.
TABLE 1
Diagnostic Criteria for Substance Use Disorder
A. A problematic pattern of use of an intoxicating substance not able to be classified within the alcohol; caffeine; cannabis; hallucinogen (phencyclidine and others); inhalant; opioid; sedative, hypnotic, or anxiolytic; stimulant; or tobacco categories and leading to clinically significant impairment or distress, as manifested by at least two of the following, occurring within a 12-month period:
1. The substance is often taken in larger amounts or over a longer period than was intended.
2. There is a persistent desire or unsuccessful efforts to cut down or control use of the substance.
3. A great deal of time is spent in activities necessary to obtain the substance, use the substance, or recover from its effects.
4. Craving, or a strong desire or urge to use the substance.
5. Recurrent use of the substance resulting in a failure to fulfill major role obligations at work, school, or home.
6. Continued use of the substance despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of its use.
7. Important social, occupational, or recreational activities are given up or reduced because of use of the substance.
8. Recurrent use of the substance in situations in which it is physically hazardous.
9. Use of the substance is continued despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance.
10. Tolerance, as defined by either of the following:
a. A need for markedly increased amounts of the substance to achieve intoxi-cation or desired effect.
b. A markedly diminished effect with continued use of same amount of the substance.
11. Withdrawal, as manifested by either of the following:
a. The characteristic withdrawal syndrome for other (or unknown) substance (refer to Criteria A and B of the criteria sets for other [or unknown] substance withdrawal).
b. The substance (or a closely related substance) is taken to relieve or avoid withdrawal symptoms.
Specify if:
In early remission: After full criteria for other (or unknown) substance use disor-der were previously met, none of the criteria for other (or unknown) substance use disorder have been met for at least 3 months but for less than 12 months (with the exception that Criterion A4, “Craving, or a strong desire or urge to use the substance,” may be met).
In sustained remission: After full criteria for other (or unknown) substance use dis-order were previously met, none of the criteria for other (or unknown) substance use disorder have been met at any time during a period of 12 months or longer (with the exception that Criterion A4, “Craving, or a strong desire or urge to use the substance,” may be met).
Specify if:
In a controlled environment: This additional specifier is used if the individual is in an environment where access to the substance is restricted.
Reprinted with permission from American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013: 577-578.
kulak.indd 691 5/10/19 9:23 AM

692 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
ADOLESCENT SUBSTANCE USE AND MISUSE
To assist physicians in managing substance use in ado-lescents, the Substance Abuse and Mental Health Services Administration (SAMHSA) launched the Screening, Brief Intervention, and Referral to Treatment (SBIRT) initiative.33 Screening flowcharts based on the SBIRT model are available (http:// pediatrics.aappublications.org/content/128/5/e1330 and http:// pediatrics.aappublications.org/content/138/1/ e20161211). The American Academy of Pediatrics (AAP) recommends that physicians become familiar with adoles-cent SBIRT practices.34,35
SCREENING TOOLS
Several validated screening tools that may be used in primary care,29,36 including the CRAFFT questionnaire, Problem Ori-ented Screening Instrument for Teenagers (POSIT), Alcohol
Use Disorders Identification Test (AUDIT), and the National Institute on Alcohol Abuse and Alcoholism Screening Guide, are reviewed in Table 236-38; the CAGE questionnaire is not recommended for use with adolescents because of its low sensitivity. Self-administered computer screening may be a valid and time-efficient alternative to in-person screening.39 Physicians who choose to screen adolescents for substance use may want to provide examples of specific drugs (e.g., if querying ecstasy use, indicate that the substance known as Molly is a form of ecstasy; if querying e-cigarette use, indicate this includes the use of vapes or JUULs).
CONFIDENTIALITY
Confidentiality in adolescent health care visits is a signifi-cant predictor of the number and subject matter of health
TABLE 2
Key Characteristics of Substance Use Screening Tools
Screening tool Patients Time to administer
Optimal cut-point associated with problem use
Sensitivity (95% CI)
Specificity (95% CI)
Alcohol Use Disorders Iden-tification Test (AUDIT)37
13 to 19 years of age; college stu-dents; emergency department patients
2 minutes 2 0.88 (0.83 to 0.93) 0.81 (0.77 to 0.85)
CAGE Questionnaire*37 Adults (not recom-mended for use with adolescents)
Not appli-cable (not recommended for use with adolescents)
1 0.37 (0.29 to 0.44) 0.96 (0.94 to 0.98)
CRAFFT Questionnaire†37 14 to 18 years of age
74 seconds via paper; 49 seconds via computer
1 0.92 (0.88 to 0.96) 0.64 (0.59 to 0.69)
National Institute on Alco-hol Abuse and Alcoholism (NIAAA) Screening Guide38
Offers age-specific screening questions (9 to 11, 11 to 14, and 14 to 18 years of age)
Not documented; only two ques-tions in length
Varies by age 0.87 (0.76 to 0.94) 0.84 (0.82 to 0.86)
Problem Oriented Screening Instrument for Teenagers (POSIT)37
12 to 19 years of age
20 to 30 minutes 1 0.84 (0.79 to 0.90) 0.89 (0.86 to 0.92)
Note: Links to the screening tools are available at https:// www.drugabuse.gov/nidamed-medical-health-professionals/tool-resources-your- practice/screening-assessment-drug-testing-resources/chart-evidence-based-screening-tools-adults.36
*—CAGE = Have you ever felt you should Cut down on your drinking? Have people Annoyed you by criticizing your drinking? Have you ever felt bad or Guilty about your drinking? Have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover (Eye opener)?†—CRAFFT = Have you ever ridden in a Car driven by someone (including yourself) who was high or had been using alcohol or drugs? Do you ever use alcohol or drugs to Relax, feel better about yourself, or fit in? Do you ever use alcohol or drugs while you are by yourself, Alone? Do you ever Forget things you did while using alcohol or drugs? Do your family or Friends ever tell you that you should cut down on your drinking or drug use? Have you ever gotten into Trouble while you were using alcohol or drugs?
Information from references 36 through 38.
kulak.indd 692 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 693
ADOLESCENT SUBSTANCE USE AND MISUSE
topics discussed.40 Adolescents particularly fear that alcohol, tobacco, or illicit substance use may be disclosed to their par-ents and/or legal authorities.41 Physicians should be aware of federal and state laws that apply to adolescent minor confiden-tiality because these may differ among states42 (https:// www.guttmacher.org/state-policy/explore/overview-minors- consent-law). Parental support for adolescent confidentiality can be mixed, so research suggests a split-visit model. This model encourages parents to participate in the clinical visit for a limited time but then requests that parents leave the examination room to allow for an adolescent-physician con-fidential conversation.40 The American Academy of Family Physicians supports offering adolescents examinations and counseling separate from parents.42 It is essential for phy-sicians and other health care professionals to explain the benefits of this model and to clarify adolescent and parent expectations and boundaries.40,43,44
LABORATORY TESTING
Laboratory (urine or serum) testing has limited use for diagnostic purposes and documenting history of substance use.45 Guidelines on the use of drug testing in children and adolescents are not clear, although the AAP supports fur-ther study of its safety and effectiveness.46 The AAP further recommends against implementing school- and home-based testing and supports informing concerned parents about the limitations of such testing.47
Prevention and TreatmentThe U.S. Preventive Services Task Force and American Academy of Family Physicians have found insufficient evi-dence to assess the balance of benefits and harms of primary care–based behavioral interventions to prevent or reduce illicit substance use or nonmedical pharmaceutical use in children or adolescents.48,49
Although early identification is ideal, screening and interventions can be useful at any stage of illicit substance use.50 Prevention and treatment strategies often go together; prevention efforts can supplement cessation programs to maximize program effectiveness.51 Prevention program-ming aims to decrease risk and to promote protective factors while considering specific population character-istics, cultural influences, and determinants of health.29 Among Monitoring the Future survey participants, 40% of past year users of narcotics stated that they were originally prescribed their narcotics.52 To deter nonmedical use of pre-scription drugs by adolescent patients, prescribing physi-cians should consider reducing the number of prescriptions or amount in the prescription. As in treatment planning and delivery, prevention strategies focus on families, schools, and communities (Table 3). Treatment should address the
needs of the whole person.50 Coexisting mental health prob-lems should be identified and treated in conjunction with SUD,50 and primary care physicians should refer, as appro-priate, to child/adolescent psychiatrists. Evidence-based treatment modalities range from school- and parent-based interventions that seek to involve the family in treatment to medication-assisted treatment (such as buprenorphine and naltrexone [Revia] in the treatment of opioid use disorder; Table 4).50
TABLE 3
Adolescent Substance Use Resources
General information
The Community Guide: Adolescent Health
https:// www.thecommunityguide.org/topic/adolescent-health?field_recommendation_tid=All&items_per_page=5
National Institute on Drug Abuse: Children & Teens
https:// www.drugabuse.gov/children-and-teens
SAMHSA
https:// www.samhsa.gov/
Support and treatment
American Academy of Addiction Psychiatry: Find a Specialist
http:// www.aaap.org/?page_id=658?sid=658
American Academy of Child and Adolescent Psychiatry: Child and Adolescent Psychiatrist Finder
http:// www.aacap.org/AACAP/Families_and_Youth/Resources/CAP_Finder.aspx
American Society of Addiction Medicine: Search Membership Directory
https:// asam.ps.membersuite.com/directory/SearchDirectory_Criteria.aspx
National Institute on Alcohol Abuse and Alcoholism Screening Guide
https:// pubs.niaaa.nih.gov/publications/Practitioner/YouthGuide/YouthGuidePocket.pdf
SAMHSA: Behavioral Health Treatment Services Locator
800-662-4357 (800-662-HELP) https://www.findtreatment.samhsa.gov
SAMHSA – TIP 31: Screening and Assessing Adolescents for Substance Use Disorders
https:// store.samhsa.gov/product/TIP-31-Screening-and-Assessing-Adolescents- for-Substance-Use-Disorders/SMA12-4079
Cultural awareness
SAMHSA – TIP 59: Improving Cultural Competence
https:// store.samhsa.gov/system/files/sma14-4849.pdf
SAMHSA = Substance Abuse and Mental Health Services Adminis-tration; TIP = treatment improvement protocol.
kulak.indd 693 5/10/19 9:23 AM
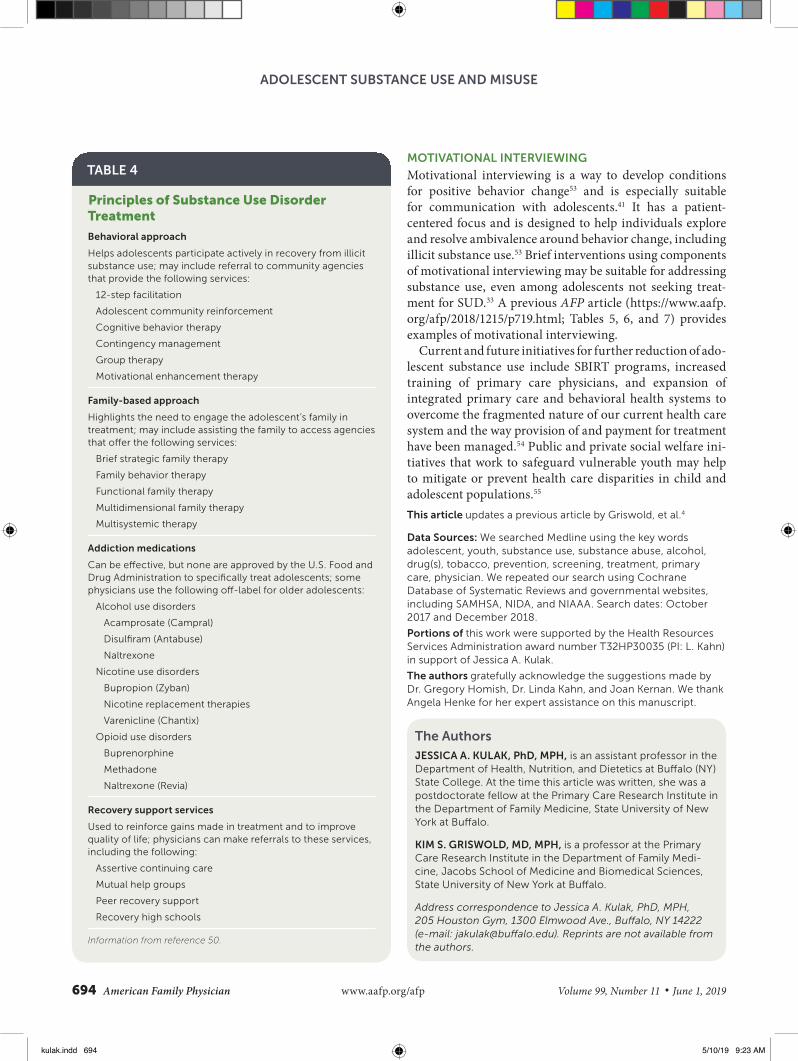
694 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
ADOLESCENT SUBSTANCE USE AND MISUSE
MOTIVATIONAL INTERVIEWING
Motivational interviewing is a way to develop conditions for positive behavior change53 and is especially suitable for communication with adolescents.41 It has a patient- centered focus and is designed to help individuals explore and resolve ambivalence around behavior change, including illicit substance use.53 Brief interventions using components of motivational interviewing may be suitable for addressing substance use, even among adolescents not seeking treat-ment for SUD.33 A previous AFP article (https:// www.aafp.org/afp/2018/1215/p719.html; Tables 5, 6, and 7) provides examples of motivational interviewing.
Current and future initiatives for further reduction of ado-lescent substance use include SBIRT programs, increased training of primary care physicians, and expansion of integrated primary care and behavioral health systems to overcome the fragmented nature of our current health care system and the way provision of and payment for treatment have been managed.54 Public and private social welfare ini-tiatives that work to safeguard vulnerable youth may help to mitigate or prevent health care disparities in child and adolescent populations.55
This article updates a previous article by Griswold, et al.4
Data Sources: We searched Medline using the key words adolescent, youth, substance use, substance abuse, alcohol, drug(s), tobacco, prevention, screening, treatment, primary care, physician. We repeated our search using Cochrane Database of Systematic Reviews and governmental websites, including SAMHSA, NIDA, and NIAAA. Search dates: October 2017 and December 2018.
Portions of this work were supported by the Health Resources Services Administration award number T32HP30035 (PI: L. Kahn) in support of Jessica A. Kulak.
The authors gratefully acknowledge the suggestions made by Dr. Gregory Homish, Dr. Linda Kahn, and Joan Kernan. We thank Angela Henke for her expert assistance on this manuscript.
The Authors
JESSICA A. KULAK, PhD, MPH, is an assistant professor in the Department of Health, Nutrition, and Dietetics at Buffalo (NY)State College. At the time this article was written, she was a postdoctorate fellow at the Primary Care Research Institute in the Department of Family Medicine, State University of New York at Buffalo.
KIM S. GRISWOLD, MD, MPH, is a professor at the Primary Care Research Institute in the Department of Family Medi-cine, Jacobs School of Medicine and Biomedical Sciences, State University of New York at Buffalo.
Address correspondence to Jessica A. Kulak, PhD, MPH, 205 Houston Gym, 1300 Elmwood Ave., Buffalo, NY 14222 (e-mail: jakulak@ buffalo.edu). Reprints are not available from the authors.
TABLE 4
Principles of Substance Use Disorder Treatment
Behavioral approach
Helps adolescents participate actively in recovery from illicit substance use; may include referral to community agencies that provide the following services:
12-step facilitation
Adolescent community reinforcement
Cognitive behavior therapy
Contingency management
Group therapy
Motivational enhancement therapy
Family-based approach
Highlights the need to engage the adolescent’s family in treatment; may include assisting the family to access agencies that offer the following services:
Brief strategic family therapy
Family behavior therapy
Functional family therapy
Multidimensional family therapy
Multisystemic therapy
Addiction medications
Can be effective, but none are approved by the U.S. Food and Drug Administration to specifically treat adolescents; some physicians use the following off-label for older adolescents:
Alcohol use disorders
Acamprosate (Campral)
Disulfiram (Antabuse)
Naltrexone
Nicotine use disorders
Bupropion (Zyban)
Nicotine replacement therapies
Varenicline (Chantix)
Opioid use disorders
Buprenorphine
Methadone
Naltrexone (Revia)
Recovery support services
Used to reinforce gains made in treatment and to improve quality of life; physicians can make referrals to these services, including the following:
Assertive continuing care
Mutual help groups
Peer recovery support
Recovery high schools
Information from reference 50.
kulak.indd 694 5/10/19 9:23 AM
June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 695
ADOLESCENT SUBSTANCE USE AND MISUSE
References 1. Hohl BC, Wiley S, Wiebe DJ, Culyba AJ, Drake R, Branas CC. Asso-
ciation of drug and alcohol use with adolescent firearm homicide at individual, family, and neighborhood levels. JAMA Intern Med. 2017; 177(3): 317-324.
2. Walsh K, Moreland AM, Hanson RF, Resnick HS, Saunders BE, Kilpatrick DG. Relationship violence victimization and binge drinking trajectories among a nationally representative sample of adolescents. J Adolesc. 2017; 58: 49-55.
3. World Health Organization, 2014. Recognizing adolescence. http://apps.who.int/adolescent/second-decade/section2/page1/recognizing-adolescence.html. Accessed July 6, 2018.
4. Griswold KS, Aronoff H, Kernan JB, Kahn LS. Adolescent substance use and abuse: recognition and management. Am Fam Physician. 2008; 77(3): 331-336.
5. Squeglia LM, Gray KM. Alcohol and drug use and the developing brain. Curr Psychiatry Rep. 2016; 18(5): 46.
6. Kann L, McManus T, Harris WA, et al. Youth risk behavior surveillance—United States, 2015. MMWR Surveill Summ. 2016; 65(6): 1-174.
7. Jamal A, Gentzke A, Hu SS, et al. Tobacco use among middle and high school students—United States, 2011-2016. MMWR Morb Mortal Wkly Rep. 2017; 66(23): 597-603.
8. Creamer MR, Portillo GV, Clendennen SL, Perry CL. Is adolescent poly-tobacco use associated with alcohol and other drug use? Am J Health Behav. 2016; 40(1): 117-122.
9. Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the future: national survey results on drug use 1975-2017: 2017 overview. Key findings on adolescent drug use. http:// monitoringthefuture.org/pubs/monographs/mtf-overview2017.pdf. Accessed October 16, 2018.
10. Peiper NC, Ridenour TA, Hochwalt B, Coyne-Beasley T. Overview on prevalence and recent trends in adolescent substance use and abuse. Child Adolesc Psychiatr Clin N Am. 2016; 25(3): 349-365.
11. Khan SR, Cottler LB, Striley CW. Correlates of use of alcohol mixed with energy drinks among youth across 10 US metropolitan areas. Drug Alcohol Depend. 2016; 163: 236-241.
12. Palamar JJ, Keyes K, Cleland CM. Underreporting of ecstasy use among high school seniors in the US. Drug Alcohol Depend. 2016; 165: 279-282.
13. McCabe SE, Veliz P, Wilens TE, Schulenberg JE. Adolescents’ prescrip-tion stimulant use and adult functional outcomes: a national prospec-tive study. J Am Acad Child Adolesc Psychiatry. 2017; 56(3): 226-233.e4.
14. Palamar JJ, Shearston JA, Dawson EW, Mateu-Gelabert P, Ompad DC. Nonmedical opioid use and heroin use in a nationally representative sample of US high school seniors. Drug Alcohol Depend. 2016; 158: 132-138.
15. Gaither JR, Leventhal JM, Ryan SA, Camenga DR. National trends in hospitalizations for opioid poisonings among children and adolescents, 1997 to 2012. JAMA Pediatr. 2016; 170(12): 1195-1201.
16. Peters RJ Jr., Kelder SH, Markham CM, Yacoubian GS Jr., Peters LA, Ellis A. Beliefs and social norms about codeine and promethazine hydro-chloride cough syrup (CPHCS) onset and perceived addiction among urban Houstonian adolescents: an addiction trend in the city of lean. J Drug Educ. 2003; 33(4): 415-425.
17. Agnich LE, Stogner JM, Miller BL, Marcum CD. Purple drank preva-lence and characteristics of misusers of codeine cough syrup mixtures. Addict Behav. 2013; 38(9): 2445-2449.
18. Wang TW, Gentzke A, Sharapova S, Cullen KA, Ambrose BK, Jamal A. Tobacco product use among middle and high school students—United States, 2011-2017. MMWR Morb Mortal Wkly Rep. 2018;67(22): 629-633.
19. Giovenco DP, Miller Lo EJ, Lewis MJ, Delnevo CD. “They’re pretty much made for blunts”: product features that facilitate marijuana use among young adult cigarillo users in the United States. Nicotine Tob Res. 2017; 19(11): 1359-1364.
20. Morean ME, Kong G, Camenga DR, Cavallo DA, Krishnan-Sarin S. High school students’ use of electronic cigarettes to vaporize cannabis. Pedi-atrics. 2015; 136(4): 611-616.
21. Miech R, Johnston L, O’Malley PM, Bachman JG, Patrick ME. Adoles-cent vaping and nicotine use in 2017-2018—U.S. national estimates. N Engl J Med. 2019;380(2):192-193.
22. Huang J, Duan Z, Kwok J, et al. Vaping versus JUULing: how the extraordinary growth and marketing of JUUL transformed the US retail e-cigarette market. Tob Control. 2019;28:146-151.
23. U.S. Food and Drug Administration. Warning letters and civil money penalties issued to retailers for selling JUUL and other e-cigarettes to minors. Updated September 12, 2018. https:// www.fda.gov/tobaccoproducts/newsevents/ucm605278.htm. Accessed January 2, 2019.
24. Singh B, Hrywna M, Wackowski OA, Delnevo CD, Jane Lewis M, Stein-berg MB. Knowledge, recommendation, and beliefs of e-cigarettes among physicians involved in tobacco cessation: a qualitative study. Prev Med Rep. 2017; 8: 25-29.
25. Kozlowski LT, Sweanor DT. Young or adult users of multiple tobacco/nicotine products urgently need to be informed of meaningful differ-ences in product risks. Addict Behav. 2018; 76: 376-381.
26. Tice P, Lipari RN, Van Horn SL. Substance use among 12th grade aged youths, by dropout status. The CBHSQ Report: August 15, 2017. Rock-ville, Md.: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration; 2013: 1-7.
27. Warren JC, Smalley KB, Barefoot KN. Perceived ease of access to alco-hol, tobacco and other substances in rural and urban US students. Rural Remote Health. 2015; 15(4): 3397.
28. Cooper HL, West B, Linton S, et al. Contextual predictors of injection drug use among black adolescents and adults in US metropolitan areas, 1993-2007. Am J Public Health. 2016; 106(3): 517-526.
29. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Asso-ciation; 2013: 577-578.
30. Sterling S, Kline-Simon AH, Wibbelsman C, Wong A, Weisner C. Screening for adolescent alcohol and drug use in pediatric health-care settings: predictors and implications for practice and policy. Addict Sci Clin Pract. 2012; 7: 13.
31. Shapiro B, Coffa D, McCance-Katz EF. A primary care approach to sub-stance misuse. Am Fam Physician. 2013; 88(2): 113-121.
32. Midboe AM, Cucciare MA, Trafton JA, Ketroser N, Chardos JF. Imple-menting motivational interviewing in primary care: the role of provider characteristics. Transl Behav Med. 2011; 1(4): 588-594.
33. Borus J, Parhami I, Levy S. Screening, brief intervention, and referral to treatment. Child Adolesc Psychiatr Clin N Am. 2016; 25(4): 579-601.
34. Levy SJ, Williams JF; Committee on Substance Use and Prevention. Substance use screening, brief intervention, and referral to treatment. Pediatrics. 2016; 138(1): e20161211.
35. Committee on Substance Abuse; Levy SJ, Kokotailo PK. Substance use screening, brief intervention, and referral to treatment for pediatricians. Pediatrics. 2011; 128(5): e1330-e1340.
36. National Institute on Drug Abuse. Chart of evidence-based screening tools and assessments for adults and adolescents; June 2018. https://bit.ly/2t5N5Sk. Accessed October 16, 2018.
37. Knight JR, Sherritt L, Harris SK, Gates EC, Chang G. Validity of brief alco-hol screening tests among adolescents: a comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcohol Clin Exp Res. 2003; 27(1): 67-73.
38. D’Amico EJ, Parast L, Meredith LS, Ewing BA, Shadel WG, Stein BD. Screening in primary care: what is the best way to identify at-risk youth for substance use? Pediatrics. 2016; 138(6): e20161717.
39. Harris SK, Knight JR Jr., Van Hook S, et al. Adolescent substance use screening in primary care: validity of computer self-administered versus clinician-administered screening. Subst Abus. 2016; 37(1): 197-203.
kulak.indd 695 5/10/19 9:23 AM

696 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
ADOLESCENT SUBSTANCE USE AND MISUSE
40. Gilbert AL, Rickert VI, Aalsma MC. Clinical conversations about health: the impact of confidentiality in preventive adolescent care. J Adolesc Health. 2014; 55(5): 672-677.
41. National Institute on Alcohol Abuse and Alcoholism. Alcohol screening and brief intervention for youth: a practitioner’s guide; 2015. https:// pubs.niaaa.nih.gov/publications/Practitioner/YouthGuide/YouthGuide.pdf. Accessed October 16, 2018.
42. American Academy of Family Physicians. Adolescent health care, confidentiality. July 2018. https:// www.aafp.org/about/policies/all/adolescent-confidentiality.html. Accessed October 16, 2018.
43. Ham P, Allen C. Adolescent health screening and counseling. Am Fam Physician. 2012; 86(12): 1109-1116.
44. Klein DA, Hutchinson JW. Providing confidential care for adolescents. Am Fam Physician. 2012; 85(6): 556-560.
45. Winters KC, Kaminer Y. Screening and assessing adolescent substance use disorders in clinical populations. J Am Acad Child Adolesc Psychia-try. 2008; 47(7): 740-744.
46. Levy S, Siqueira LM, Ammerman SD, et al.; Committee on Substance Abuse. Testing for drugs of abuse in children and adolescents. Pediat-rics. 2014; 133(6): e1798-e1807.
47. American Society of Addiction Medicine. Appropriate use of drug test-ing in clinical addiction medicine; April 5, 2017. https://bit.ly/2DRS1Am. Accessed October 16, 2018.
48. Moyer VA. Primary care behavioral interventions to reduce illicit drug and nonmedical pharmaceutical use in children and adolescents: U.S.
Preventive Services Task Force recommendation statement. Ann Intern Med. 2014; 160(9): 634-639.
49. American Academy of Family Physicians. Clinical Preventive Ser-vice Recommendation: illicit drug use; 2018. https:// www.aafp.org/ patient-care/clinical-recommendations/all/ill icit-drug-use.html. Accessed June 18, 2018.
50. National Institute on Drug Abuse. Principles of adolescent substance use disorder treatment: a research-based guide; January 2014. https://bit.ly/1VVAVW0. Accessed October 16, 2018.
51. Sussman S, Skara S, Ames SL. Substance abuse among adolescents. Subst Use Misuse. 2008; 43(12-13): 1802-1828.
52. Miech RA, Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the future: national survey results on drug use 1975-2017: 2017 volume 1. Secondary school students. http:// www.monitoringthefuture.org//pubs/monographs/mtf-vol1_2017.pdf. Accessed January 2, 2019.
53. Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. New York, NY: Guilford; 2013.
54. Sterling S, Weisner C, Hinman A, Parthasarathy S. Access to treatment for adolescents with substance use and co-occurring disorders: chal-lenges and opportunities. J Am Acad Child Adolesc Psychiatry. 2010; 49(7): 637-646.
55. Cluver LD, Orkin FM, Meinck F, Boyes ME, Yakubovich AR, Sherr L. Can social protection improve sustainable development goals for adoles-cent health? PLoS One. 2016; 11(10): e0164808.
kulak.indd 696 5/10/19 9:23 AM

The future of health begins with youThe more researchers know about what makes each of us unique, the more tailored our health care can become.
Join a research effort with one million or more people nationwide to create a healthier future for all of us.
JoinAllofUs.org/togetherPrecision Medicine Initiative, PMI, All of Us, the All of Us logo, and “The Future of Health Begins with You” are service marks of the U.S. Department of Health and Human Services.
18060884 STP All of Us Journal Insert.indd 1 6/15/18 11:10 AM

We’re calling on one million people to lead the way toward better health.
Precision Medicine Initiative, PMI, All of Us, the All of Us logo, and “The Future of Health Begins with You” are service marks of the U.S. Department of Health and Human Services.
What is precision medicine?
Precision medicine is health care that is based on you as an individual. It takes into account factors like where you live, what you do, and your family health history. The goal is to be able to tell people the best ways to stay healthy. If someone does get sick, precision medicine may help health care teams fi nd the treatment that will work best.
What is the All of Us Research Program?
The All of Us Research Program is a large research program. The goal is to help researchers understand more about why people get sick or stay healthy. People who join will give us information about their health, habits, and what it’s like where they live. By looking for patterns, researchers may learn more about what affects people’s health.
How do I join the All of Us Research Program?
There are three ways to join:
• Visit the All of Us website JoinAllofUs.org.• Download the All of Us app.• If you get health care at one of our affi liated health
care provider organizations, you can join there.
Because the All of Us Research Program is research, you will be asked to complete an informed consent process. This process tells more about what is involved, and the risks and benefi ts of joining.
What will you ask me to do?
If you decide to join All of Us, we will ask you to share different kinds of information. We will ask you basic information like your name and where you live, questions about your health, family, home, and work. If you have an electronic health record, we may ask for access. We might also ask you to give samples, like blood or urine.
How long will the All of Us Research Program last?
All of Us may last for at least 10 years. We hope you will stay involved over time. If you join, you can withdraw at any time for any reason without penalty.
Why should I join the All of Us Research Program?
You will be contributing to research that may improve health for everyone. Here are some examples of what researchers might be able to discover:
• Better tests to see if people are sick or are atrisk of getting sick.
• Better mobile apps to encourage healthy habits.• Better medicine or information about how much
of a medicine is right for each person.
What will you do to protect my privacy?
We will take great care to protect your information. Here are a few of the steps we will take:
• Information we have about you will be stored onprotected computers. We will limit and keep trackof who sees the information.
• We will remove your name and other directidentifi ers (like your date of birth) from yourinformation and replace them with a code.
• Researchers must promise not to try to fi ndout who you are.
• We will tell you if there is a data breach.• The All of Us Research Program has Certifi cates
of Confi dentiality from the U.S. government. Thiswill help us fi ght legal demands (such as a courtorder) to give out information that could identify you.
[email protected](844) 842-2855 JoinAllofUs.org/together
18060884 STP All of Us Journal Insert.indd 2 6/15/18 11:10 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 699
A family caregiver is broadly defined as a friend or rel-ative who provides unpaid assistance for a person with a chronic or disabling condition.1 Eighty percent of adults requiring long-term care currently live at home in the com-munity, and unpaid family caregivers provide 90% of their care.2 These caregivers fill an important role for the fam-ily and provide a substantial cost savings of an estimated $470 billion nationwide in 2013.3 Family caregivers serve as a critical extension of the U.S. health care system, and sup-porting this “invisible and isolated army” has emerged as a national public health priority.3,4
In the next few decades, the demand for family care-givers is expected to increase.5 This growing demand is attributed to shorter hospital stays, limited hospital dis-charge planning, and an aging U.S. population. By 2030, one in five adults will be 65 years or older, and a signifi-cant number of these older adults will require assistance with instrumental activities of daily living or activities of
daily living.5 Table 1 lists common characteristics of care recipients.6
Caregiver BurdenCaring for loved ones is associated with several benefits, including personal satisfaction in relieving another’s dis-comfort, feeling useful and needed, and finding more meaning in life. Caregiving is also associated with signifi-cant physical, psychological, and financial burden for care providers (Table 2).1,3,6-12 Stressors associated with care-giving situations are often persistent, uncontrollable, and unpredictable, and one-third of all caregivers describe a high burden of care. Caregivers reporting the highest
Caregiver CareKristine Swartz, MD, and Lauren G. Collins, MD, Thomas Jefferson University, Philadelphia, Pennsylvania
CME This clinical content conforms to AAFP criteria for continuing medical education (CME). See CME Quiz on page 673.
Author disclosure: No relevant financial affiliations.
Patient information: A handout on this topic, written by the authors of this article, is available at https:// www.aafp.org/afp/2019/0601/p699-s1.html.
Eighty percent of adults requiring long-term care currently live at home in the community, and unpaid family caregivers provide 90% of their care. Family caregivers serve as a critical extension of the U.S. health care system, and the demand for family caregivers is expected to increase during the next few decades. Caring for loved ones is associated with several benefits, including personal fulfillment; however, caregiving is also associated with physical, psychological, and financial burdens. Family physicians can aid in the identification, support, and treatment of caregivers by offering caregiver assess-ments—interviews directed at identifying high levels of burden—as soon as caregivers are identified. Repeat assessments may be considered when there is a change in the status of the caregiver or the care recipient. Caregivers should be directed to appropriate resources for support, including national caregiving organizations, local elder care agencies, websites, and respite care. Psychoeducation, skills training, and therapeutic counseling interventions for caregivers have shown small to moderate success by decreasing caregiver burden and increasing caregiver quality of life. Additional research is needed to further identify strategies to offset caregiver stress, depression, and poor health outcomes. Support and anticipatory guid-ance for the caregiver is especially helpful during care transitions and at the care recipient’s end of life. (Am Fam Physician. 2019; 99(11): 699-706. Copyright © 2019 American Academy of Family Physicians.)
TABLE 1
Characteristics of Care Recipients
Average age: 69 years
Behavioral problems (7%)
Female (65%)
Hospitalized in past 12 months (53%)
Memory problems (26%)
Need assistance with activities of daily living (59%)
Need assistance with instrumental activities of daily living (99%)
Information from reference 6.
swartz.indd 699 5/10/19 9:23 AM

700 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
CAREGIVER CARE
burden are more likely to be less educated, to live with the care recipient, to provide more than 21 hours of caregiving per week, to care for someone with cognitive impairment or difficult to manage behaviors, and to perceive they had no choice in assuming the caregiver role (Table 3).6 It is less common to have multigenerational family homes in the United States, which may place a more direct burden on one family member. Spousal caregivers are at high risk of care-giver burden, often providing a high number of care hours and assisting with medical tasks, and they are less likely to have additional help.6 Most caregivers report having less time for family and friends, having increased emotional stress, and neglecting self-care, such as healthy sleep, exer-cise, and dietary habits.5,13
Caregiver AssessmentCaregiver assessment refers to a systematic, family-centered process of gathering information about a caregiver situation to identify needs and resources. Assessment can be performed by the family physician or other health care team member.1 Ideally, caregivers and care recipients should be interviewed together and separately to allow assessment of confidential information such as elder abuse or caregiver stress.14
Initial assessment may be performed as soon as a per-son self-identifies as a caregiver. This may include the pri-mary caregiver as well as other family members, friends, or neighbors who consider themselves caregivers. Repeat assessments can be offered as the care recipient’s or caregiv-er’s condition changes. These changes may be triggered by the diagnosis of a medical condition associated with high burden (i.e., care requiring more than 21 hours per week), change in functional status of a caregiver or care recipi-ent, or care transitions, and should involve development of a care plan for additional support and resources.12 The National Consensus Development Conference for Care-giver Assessment developed practice guidelines that have been incorporated in the Guided Care model15 and pro-moted by numerous national organizations.1,12,16,17 See a caregiver assessment table at https:// www.caregiver.org/ caregivers-count-too-section-3-caregiver-assessment- table for practical in-office questions,16 and the Modified
TABLE 2
Elements of Caregiver BurdenFinancial effects6
Increased absenteeism or reduced work hours
Increased self-reported financial strain
Loss of promotional and training opportunities
Loss of salary and benefits
Reduction in retirement savings and Social Security benefits
Health effects
Higher inflammatory burden and other biomarkers of poor health in caregivers for people with dementia7
Higher rates of insomnia and depression8
Higher risk of serious illness9
Increased mortality for spousal caregivers10
Less likely to engage in preventive care10
Subjective sense of worsening health11
Inadequate preparation, knowledge, and skills
Lack of information on how to care for recipient: safety, activities of daily living1,3,12
Lack of information on self-care: coping with stress, find-ing time for self 1,3,12
Lack of information on support services1,3,12
Information from 1, 3, 6 through 12.
TABLE 3
Characteristics of Caregivers
Average age: 49 years
Average hours of care provided per week: 24.4
Feel they had no choice in role (50%)
Female (60%)
Help with medical and nursing tasks (57%)
Provide care more than five years (24%)
Provide care more than 21 hours per week (26%)
Information from reference 6.
WHAT IS NEW ON THIS TOPIC
Caregiver Care
Online interactive programs significantly reduce patient physical symptoms and decrease caregiver burden and depressive symptoms.
In caregivers of people with dementia, a meta-analysis showed that multicomponent interventions (e.g., edu-cation, resiliency training, problem solving) can reduce depressive symptoms, improve quality of life, and reduce caregiver burden.
The National Family Caregiver Support Program is the first federally funded program to formally recognize caregiv-ers. However, in 2016, the program received only $150 million in federal funding, approximately one-twentieth of one percent of the estimated value of caregiver contribu-tions to the health system.
swartz.indd 700 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 701
CAREGIVER CARE
Caregiver Strain Index at https:// consultgeri.org/try-this/general-assessment/issue-14.pdf.18 The adapted Zarit Burden Interview is another validated tool that can be used to assess caregiver burden; see appendix at https:// bit.ly/2Hso3qt.19
Caregiver SupportDespite many published research trials showing effective interventions, such as multidimensional and psychoedu-cational interventions,20-22 there has been a delay in trans-lating the research into resources that are readily accessible to caregivers. This requires development of best practices, assessment of clinical relevance, and restructuring of reim-bursements to allow for sustainability. Until this happens, family physicians can focus on practical, individualized interventions aimed at assisting caregivers.23
Caregivers should be encouraged to take a break, join a support group, and pursue their own interests. They should be encouraged to take care of their own health, including preventive health care, and to seek respite care when needed.5
Family physicians should provide accurate, disease- specific education and resources for obtaining more infor-mation1,6,13,16 (Table 4). Online toolkits, such as the AARP’s Prepare to Care: A Planning Guide for Families, can be eas-ily accessed and provided during an office visit.24 Caregiv-ers should be offered training in medical tasks and specific care needs with the help of therapists and nurses. Referrals should be made to appropriate resources such as local elder care agencies, home health care services, adult day pro-grams, and meal delivery services.
Family physicians should encourage caregivers to partic-ipate in the health care of the recipient. Evidence suggests that when care recipients and caregivers are treated as a dyad, outcomes for both are improved.25 Caregivers often know the most about the needs of the care recipient and can be vital allies in the care management plan. Evidence shows that caregiver involvement and agreement with the care plan increases adherence to recommendations.26
There is strong evidence that early palliative care inter-ventions for patients with serious illness improve quality of life and family satisfaction, and can reduce caregiver bur-den.27 Family physicians are uniquely positioned to provide primary palliative care, such as facilitating goals of care discussions and advance care planning. Addressing the care recipient’s symptoms of chronic illness can improve the caregiver’s quality of life and help relieve the caregiver’s dis-tress over the recipient’s discomfort.28
Caregiver care often necessitates offering innovations in self-management through technology. Family caregiv-ers can now access educational materials as well as con-nect with other caregivers online.13 Websites and apps are available to schedule tasks and help families coordinate
caregivers, meal delivery, and appointments. Wearable technology and remote monitoring systems are expand-ing and hold promise for improving the lives of caregiv-ers.29 Online interactive programs have shown reductions in patient physical symptoms and in caregiver burden and depressive symptoms.30,31 Advancements in smart home environments allow caregivers to monitor care recipients from remote locations, detecting changes and preventing adverse events in the care recipient.32 Telehealth options are expanding and offer real-time access to health care teams. Table 5 lists apps and services recommended by reputable online resources such as AARP and the National Alliance on Caregiving. Despite potential benefits of new technol-ogies, these innovations may be limited by the ability of caregivers to access and learn how to operate new devices, overcome cost barriers, and avoid the perception of deper-sonalized care.32
Specialized CaregivingCANCER
Changes in health care and insurance reimbursement have led to much of cancer care being provided at home, with the family assuming more responsibilities.33 A 2017 meta- analysis found that psychoeducational interventions were the most common intervention researched; however, they often require significant time, making them hard to trans-late to clinical practice.34 Pain management skills and symptoms assessment are the largest caregiver needs.34 A 2015 study found that interdisciplinary palliative care interventions such as educational sessions and self-care plans improved caregivers’ social well-being scores, low-ered psychological distress scores, and significantly reduced caregiver burden.35 Continued research with a focus on pal-liative care interventions, the effect on caregivers, and ways to increase the availability of these services is needed.
DEMENTIA
Caregiving for a person with dementia is associated with high levels of strain caused by associated behavior distur-bances, intense physical tasks, and the need for constant vigilance. High caregiver strain has been identified as a predictor of long-term care placement in these patients; therefore, family physicians should identify caregivers early and provide support.36 Fact sheets available from Family Caregiver Alliance are free, easy to download, and provide practical guidance on topics such as understanding and managing dementia behaviors, controlling frustration, self-care, and end-of-life decision making.1
Evidence to support caregiver interventions in this subgroup is fairly robust.37-39 Structured education pro-vided in home and telephone-based sessions to improve
swartz.indd 701 5/10/19 9:23 AM

702 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
CAREGIVER CARE
caregiver coping skills and management of behaviors have decreased caregiver burden and improved quality of life for the caregiver and care recipient.37 A meta-analysis showed that multicomponent interventions (e.g., education, resil-iency training, problem solving) can reduce depressive symptoms, improve quality of life, and reduce caregiver burden.38 Interventions are cost saving or cost neutral by
helping to keep care recipients in the community longer.39 Additional resources are needed to translate these inter-ventions into opportunities accessible to all caregivers.
HEART FAILURE
Caregivers of patients with heart failure report similar issues as those caring for patients with other chronic illnesses.40
TABLE 4
Caregiver Resources
Organization Website Resources
National organizations
AARP https:// www.aarp.org/caregiving/ Prepare to Care guide, legal and financial infor-mation, local resources
American Academy of Family Physicians
https:// family doctor.org/caregiver-stress/ General information on caregiver self-care
Caregiver Action Network https:// caregiveraction.org/ Scenario-specific tips and toolbox, caregiver connections
Family Caregiver Alliance, National Center on Caregiving
https:// www.caregiver.org/ Disease- and issue-specific fact and tip sheets, caregiver connections, policy and advocacy information
Mather Lifeways Institute on Aging https:// www.matherlifewaysinstituteonaging.com/category/caregiving/
Caregiver-specific articles, senior housing initiatives
National Institute on Aging https:// www.nia.nih.gov/health/caregiving Caregiving tips with focus on dementia and older adults
Rosalynn Carter Institute for Caregiving
http:// rci.gsw.edu Caregiver workshops and resources, research
Caregiver education and respite care
Alzheimer’s Association and AARP https:// www.communityresourcefinder.org Programs, resources for housing, caregivers
American Elder Care Research Organization
https:// www.payingforseniorcare.com Resources for paying for care, managing insur-ance, reducing costs
ARCH National Respite Network and Resource Center
https:// archrespite.org/ Respite locator and funding by state
AssistGuide Information Services http:// www.agis.com Explanation of government resources, Medi-care/Medicaid, assistive devices
Caring Today http:// caringtoday.com/blog/ Caregiver blog
Family Caregiver Alliance Camp for Caring
https:// www.caregiver.org/camp-caring Respite camp for caregivers and recipients
Hospice Foundation of America https:// www.hospicefoundation.org Information about hospice care
United Hospital Fund Next Step in Care
https:// www.nextstepincare.org Focus on helping caregivers with transitions in care, communication with health care teams
U.S. Administration on Aging https:// www.eldercare.gov Local community resources
U.S. Administration on Aging https:// www.longtermcare.gov Resources for long-term care placement
Specific caregiving scenarios
Caregiving.com https:// www.caring.com/support-groups/caring-for-a-spouse
Caregiver blog for spouses, topics including finances, intimacy, and managing symptoms
Centers for Disease Control and Prevention
https:// www.cdc.gov/ncbddd/disability andhealth/family.html
Tips for caregivers of people with disabilities
National Organization for Rare Disorders
https:// rarediseases.org/for-patients-and- families/connect-others/find-patient- organization/
Disease-specific resource for support groups
Parent to Parent http:// www.p2pusa.org/ Resources with local options for families of children who have special needs
U.S. Department of Veterans Affairs https:// www.caregiver.va.gov/ Resource for caregivers, mentoring program, hotlines, access to support coordinator
Well Spouse Association https:// wellspouse.org Support group locator, national conference, social community
swartz.indd 702 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 703
CAREGIVER CARE
The most burdensome aspects of care are enforcing dietary restrictions and monitoring for signs and symptoms of heart failure.40,41 Care recipients with heart failure may have fre-quent exacerbations requiring hospitalization and a more uncertain clinical trajectory that can increase caregiver strain. During the past decade, there have been signifi-cant advances in the availability of advanced heart failure
therapies (e.g., left ventricular assist devices, inotropic med-ications) that can lower hospitalization and mortality rates. Availability of these therapies may increase life expectancy, but often leave care recipients with a higher degree of func-tional disability, thereby increasing the burden of care-giving.42 Overall, few interventions have been thoroughly studied to effectively support caregivers of patients with
TABLE 5
Technology and Apps for Caregivers
Organization Website Resources
General information
AARP https:// www.aarp.org/caregiving/home-care/info-2017/technology-apps-ag.html
Tips for choosing caregiving apps
Family coordination
AARP Caregiving App https:// states.aarp.org/aarp-caregiving-app Calendar, caregiver coordination
CareZone https:// carezone.com/home Caregiver coordination health care record keeping, scheduling
Caring Bridge https:// www.caringbridge.org Calendar, scheduling, forum for updates, fundraising
Caring Village https:// www.caringvillage.com Calendar, communication, document storage, to-do lists
Evernote https:// evernote.com Organization, to-do lists
Google Calendar, Google Docs https:// www.google.com Calendar and shared documents
Lotsa Helping Hands https:// lotsahelpinghands.com Calendar, forum for updates
Transportation
AARP Transportation Services https:// www.aarp.org/caregiving/ home-care/transportation-services/ ?intcmp=CAR-LRS-R3-C2
General information
Arrive
GoGoGrandparent
https:// arriverides.com
https:// gogograndparent.com
Links to Uber and Lyft without need for smartphone
Remote monitoring
Blipcare (blood pressure monitoring) http:// www.blipcare.com Various monitoring tools using wearable deviceseCare 21 https:// ecare21.com
GPS SmartSole (trackable shoes) http:// gpssmartsole.com/gpssmartsole
Luna Lights (automated lighting) https:// lunalights.org
SafeinHome (alerts) http:// www.safeinhome.com
Consumer Reports: Medical Alert Systems
https:// www.consumerreports.org/ medical-alert-systems/how-to-choose- a-medical-alert-system
How to choose medical alert system
Medication management
Medisafe
MyMeds
MyMedSchedule
https:// medisafe.com
https:// www.my-meds.com
https:// secure.medactionplan.com/mymedschedule
Medication management, reminders
Telehealth services
AARP Telehealth Services https:// www.aarp.org/caregiving/health/telehealth-services/?intcmp=CAR-LRS-R3-C1
General information
swartz.indd 703 5/10/19 9:23 AM

704 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
CAREGIVER CARE
heart failure.43 Given the high level of symptom monitor-ing, caregiver burden, and uncertainty in disease trajectory, many experts are calling for earlier and concurrent involve-ment of palliative care with the goal of improving caregiver education and confidence, assistance with management of symptoms, and skilled advanced care planning.43
STROKE
Stroke is the leading cause of serious long-term disabil-ity, and most stroke survivors return home.44 These care recipients often require significant assistance with activi-ties of daily living and instrumental activities of daily liv-ing.44 A review of caregiver interventions shows that those with a focus on dyad interventions may help survivor out-comes; however, interventions targeted specifically toward caregivers are needed to improve caregiver outcomes.45 Skill-building interventions (e.g., problem solving, tips for communicating with health care professionals, strate-gies for lifting) were more effective at improving caregiver outcomes than providing information about the diagnosis alone.45 Appropriate referrals to home health care, skilled therapy, and respite care should be offered by the family physician in addition to options for home modifications.
TRANSITIONS IN CARE
Many caregivers experience a decrease in depressive symp-toms after the death of a care recipient, which may mark the end of the care recipient’s discomfort. The placement of a care recipient into a long-term care facility is not associated with
positive effects on the caregiver and may be accompanied by an increase in caregiver anxiety.46 This implies that the relief of the daily caregiving burden does not account for the reduc-tion in depressive symptoms in bereaved caregivers. To ease these care transitions, family physicians should provide antic-ipatory guidance, assistance with advance care planning, and appropriate resources for respite, long-term, and end-of-life care.36,37,43 It may be more useful to intensify resources and support in the time preceding death rather than afterwards.47
Public PolicyProviding optimal care for the patient and caregiver man-dates an understanding of financial reimbursement strat-egies. The Family and Medical Leave Act allows qualified employees to take up to 12 weeks of continuous or intermit-tent unpaid leave to provide care. The United States is one of the few developed economies that does not offer mandatory paid leave, a topic that has emerged as a new public policy interest. The National Family Caregiver Support Program was the first federally funded program to formally recog-nize caregivers. However, in 2016, the program received only $150 million in federal funding, approximately one-twentieth of one percent of the value of caregiver con-tributions.47 Consumer-, participant-, and self-directed care programs are now available in nearly every state, allowing informal caregivers, such as a spouse or other family mem-ber, to be paid for the services they provide. Most programs are based on Medicaid home- and community-based ser-vice waiver programs that provide in-home assistance for
SORT: KEY RECOMMENDATIONS FOR PRACTICE
Clinical recommendationEvidence rating References
All caregivers should be offered assessment to identify high levels of caregiver burden. C 1, 12, 16
Encouraging caregivers to take a break, take care of their own health, seek preventive health care, join a support group, and seek respite care when needed are key ways that a family physician can provide direct caregiver support.
C 5
Caregivers identified as having unmet educational or informational needs should be directed to appropri-ate resources for support.
C 1, 6, 13, 16
Psychoeducational, skills training, and therapeutic counseling interventions for caregivers of patients with chronic conditions (e.g., dementia, cancer, stroke, heart failure) have small to moderate success in decreasing caregiver burden and increasing caregiver quality of life.
B 34, 35, 37-39
Anticipatory guidance, assistance with advance care planning, and information about appropriate resources should be provided to the care recipient and caregiver during care transitions and at the end of life.
C 36, 37, 43
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease- oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https:// www.aafp.org/afpsort.
swartz.indd 704 5/10/19 9:23 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 705
CAREGIVER CARE
nursing home–eligible care recipients who qualify for Med-icaid services. However, options have expanded to include non-Medicaid programs, veterans’ programs, life insur-ance, and long-term care insurance to allow family mem-bers to be paid caregivers.48
This article updates previous articles on this topic by Parks and Novielli,49 and by the authors.50
Data Sources: A PubMed search was completed using Clinical Queries and the key terms caregiver, burden, and stress. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. Also searched were the Agency for Healthcare Research and Quality evidence reports, Clinical Evidence, the Cochrane database, and the Institute for Clinical Systems Improvement. Search dates: February 15, 2018, and January 2, 2019.
The Authors
KRISTINE SWARTZ, MD, is an assistant professor in the Department of Family and Community Medicine at Thomas Jefferson University, Philadelphia, Pa.
LAUREN G. COLLINS, MD, is a Josiah Macy Jr. Foundation Faculty Scholar and an associate professor in the Department of Family and Community Medicine at Thomas Jefferson University.
Address correspondence to Kristine Swartz, MD, Thomas Jefferson University, 1015 Walnut St., Ste. 401, Philadelphia, PA 19107 (e-mail: kristine.swartz@ jefferson.edu). Reprints are not available from the authors.
References 1. Family Caregiver Alliance. Caregiver assessment: principles, guidelines
and strategies for change. Report from a national consensus develop-ment conference. Volume 1. April 2006. https:// www.caregiver.org/caregiver/jsp/content/pdfs/v1_consensus.pdf. Accessed February 11, 2018.
2. U.S. Institute of Medicine; Committee on the Future Health Care Work-force for Older Americans. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC.: National Academies Press; 2008.
3. Reinhard SC, Feinberg LF, Choula R, Houser A. Valuing the invaluable: 2015 update. AARP Public Policy Institute. July 2015. https:// www.aarp.org/content/dam/aarp/ppi/2015/valuing-the-invaluable-2015-update-new.pdf. Accessed February 15, 2018.
4. U.S. Department of Health and Human Services. Healthy People 2010: general data issues. https:// www.cdc.gov/nchs/data/hpdata2010/hp2010_general_data_issues.pdf. Accessed February 15, 2018.
5. National Association of Chronic Disease Directors; Centers for Dis-ease Control and Prevention; Health Benefits ABCs. CDC seeks to protect health of family caregivers. January 15, 2009. https:// c.ymcdn.com/sites/www.chronicdisease.org/resource/resmgr/healthy_aging_critical_issues_brief/ha_cib_healthoffamilycaregiv.pdf. Accessed Feb-ruary 15, 2018.
6. AARP Public Policy Institute; National Alliance for Caregiving. Execu-tive summary: caregiving in the U.S. June 2105. https:// www.aarp.org/content/dam/aarp/ppi/2015/caregiving-in-the-united-states-2015-executive-summary-revised.pdf. Accessed February 15, 2018.
7. von Känel R, Dimsdale JE, Mills PJ, et al. Effect of Alzheimer caregiving stress and age on frailty markers interleukin-6, C-reactive protein, and D-dimer. J Gerontol A Biol Sci Med Sci. 2006; 61(9): 963-969.
8. Kelly K, Reinhard SC, Brooks-Danso A. Professional partners supporting family caregivers. Am J Nurs. 2008; 108(9 suppl): 6-12.
9. Haley WE, Roth DL, Howard G, Safford MM. Caregiving strain and esti-mated risk for stroke and coronary heart disease among spouse care-givers: differential effects by race and sex. Stroke. 2010; 41(2): 331-336.
10. Schulz R, Beach SR. Caregiving as a risk factor for mortality: the Care-giver Health Effects Study. JAMA. 1999; 282(23): 2215-2219.
11. Roth DL, Fredman L, Haley WE. Informal caregiving and its impact on health: a reappraisal from population-based studies. Gerontologist. 2015; 55(2): 309-319.
12. Family Caregiver Alliance. Family caregiving: state of the art, future trends. March 6, 2007. https:// www.caregiver.org/sites/fca.huang.radicaldesigns.org/files/pdfs/2007_asa_preconference_proceedings.pdf. Accessed February 15, 2018.
13. Canadian Institute for Health Information. Supporting informal caregivers— the heart of home care: executive summary. August 2010. https:// secure.cihi.ca/free_products/Caregiver_Distress_AIB_2010_EN.pdf. Accessed August 28, 2018.
14. Greene MG, Majerovitz SD, Adelman RD, Rizzo C. The effects of the presence of a third person on the physician-older patient medical inter-view. J Am Geriatr Soc. 1994; 42(4): 413-419.
15. Johns Hopkins University. Guided care: comprehensive primary care for complex patients. http:// www.guidedcare.org/. Accessed February 15, 2018.
16. Family Caregiver Alliance. Caregivers count too! A toolkit to help practitioners assess the needs of family caregivers. June 2006. https:// www.caregiver.org/sites/caregiver.org/files/pdfs/Assessment_Toolkit_20060802.pdf. Accessed February 15, 2018.
17. American Medical Association. Caring for the caregiver: a guide for physician. https:// www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/public-health/caregiver-burnout-guide.pdf. Accessed February 15, 2018.
18. Thornton M, Travis SS. Analysis of the reliability of the modified care-giver strain index. J Gerontol B Psychol Sci Soc Sci. 2003; 58(2): S129.
19. Bédard M, Molloy DW, Squire L, Dubois S, Lever JA, O’Donnell M. The Zarit Burden Interview: a new short version and screening version. Ger-ontologist. 2001; 41(5): 652-657.
20. Van’t Leven N, Prick AE, Groenewoud JG, Roelofs PD, de Lange J, Pot AM. Dyadic interventions for community-dwelling people with demen-tia and their family caregivers: a systematic review. Int Psychogeriatr. 2013; 25(10): 1581-1603.
21. Gitlin LN, Belle SH, Burgio LD, et al. Effect of multicomponent interven-tions on caregiver burden and depression: the REACH multisite initiative at 6-month follow-up. Psychol Aging. 2003; 18(3): 361-374.
22. Adelman RD, Tmanova LL, Delgado D, Dion S, Lachs MS. Caregiver bur-den: a clinical review. JAMA. 2014; 311(10): 1052-1060.
23. Gitlin LN, Marx K, Stanley IH, Hodgson N. Translating evidence-based dementia caregiving interventions into practice: state-of-the-science and next steps. Gerontologist. 2015; 55(2): 210-226.
24. AARP. Prepare to care: a planning guide for families. April 2010. https:// www.aarp.org/caregiving/prepare-to-care-planning-guide/. Accessed November 30, 2018.
25. Schulz R, O’Brien A, Czaja S, et al. Dementia caregiver intervention research: in search of clinical significance. Gerontologist. 2002; 42(5): 589-602.
26. Bogardus ST Jr, Bradley EH, Williams CS, Maciejewski PK, Gallo WT, Inouye SK. Achieving goals in geriatric assessment: role of caregiver agreement and adherence to recommendations. J Am Geriatr Soc. 2004; 52(1): 99-105.
27. Ornstein KA, Schulz R, Meier DE. Families caring for an aging America need palliative care. J Am Geriatr Soc. 2017; 65(4): 877-878.
swartz.indd 705 5/10/19 9:23 AM

706 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
CAREGIVER CARE
28. Quill TE, Abernethy AP. Generalist plus specialist palliative care—creat-ing a more sustainable model. N Engl J Med. 2013; 368(13): 1173-1175.
29. Adler R, Mehta R. Catalyzing technology to support family caregiving. National Alliance for Caregiving. July 2014. http:// ajuntament.barcelona.cat/familia/sites/default/files/arxius-noticies/Catalyzing-Technology-to-Support-Family-Caregiving_FINAL.pdf. Accessed March 27, 2018.
30. Gustafson DH, DuBenske LL, Namkoong K, et al. An eHealth system supporting palliative care for patients with non-small cell lung cancer: a randomized trial. Cancer. 2013; 119(9): 1744-1751.
31. DuBenske LL, Gustafson DH, Namkoong K, et al. CHESS improves can-cer caregivers’ burden and mood: results of an eHealth RCT. Health Psychol. 2014; 33(10): 1261-1272.
32. Chi NC, Demiris G. The roles of telehealth tools in supporting family caregivers: current evidence, opportunities, and limitations. J Gerontol Nurs. 2017; 43(2): 3-5.
33. van Ryn M, Sanders S, Kahn K, et al. Objective burden, resources, and other stressors among informal cancer caregivers: a hidden quality issue? Psychooncology. 2011; 20(1): 44-52.
34. Ferrell B, Wittenberg E. A review of family caregiving intervention trials in oncology. CA Cancer J Clin. 2017; 67(4): 318-325.
35. Sun V, Grant M, Koczywas M, et al. Effectiveness of an interdisciplinary palliative care intervention for family caregivers in lung cancer. Cancer. 2015; 121(20): 3737-3745.
36. Yaffe K, Fox P, Newcomer R, et al. Patient and caregiver characteristics and nursing home placement in patients with dementia. JAMA. 2002; 287(16): 2090-2097.
37. Nichols LO, Martindale-Adams J, Burns R, Graney MJ, Zuber J. Transla-tion of a dementia caregiver support program in a health care system—REACH VA. Arch Intern Med. 2011; 171(4): 353-359.
38. Laver K, Milte R, Dyer S, Crotty M. A systematic review and meta-analysis comparing carer focused and dyadic multicomponent interventions for carers of people with dementia. J Aging Health. 2017; 29(8): 1308-1349.
39. Foldes SS, Moriarty JP, Farseth PH, Mittelman MS, Long KH. Medicaid savings from the New York University caregiver intervention for families with dementia. Gerontologist. 2018; 58(2): e97-e106.
40. Pressler SJ, Gradus-Pizlo I, Chubinski SD, et al. Family caregiver out-comes in heart failure. Am J Crit Care. 2009; 18(2): 149-159.
41. Annema C, Luttik ML, Jaarsma T. Reasons for readmission in heart fail-ure: perspectives of patients, caregivers, cardiologists, and heart failure nurses. Heart Lung. 2009; 38(5): 427-434.
42. Joo H, Fang J, Losby JL, Wang G. Cost of informal caregiving for patients with heart failure. Am Heart J. 2015; 169(1): 142-148.
43. Nicholas Dionne-Odom J, Hooker SA, Bekelman D, et al.; IMPACT-HF National Workgroup. Family caregiving for persons with heart failure at the intersection of heart failure and palliative care: a state-of-the- science review. Heart Fail Rev. 2017; 22(5): 543-557.
44. Oliva-Moreno J, Peña-Longobardo LM, Mar J, et al. Determinants of informal care, burden, and risk of burnout in caregivers of stroke: the CONOCES study. Stroke. 2018; 49(1): 140-146.
45. Bakas T, McCarthy M, Miller ET. Update on the state of the evidence for stroke family caregiver and dyad interventions. Stroke. 2017; 48(5): e122-e125.
46. Burton LC, Zdaniuk B, Schulz R, Jackson S, Hirsch C. Transitions in spousal caregiving. Gerontologist. 2003; 43(2): 230-241.
47. Administration for Community Living. National family caregiver support program. 2017. https:// www.acl.gov/programs/support-caregivers/ national-family-caregiver-support-program. Accessed February 15, 2018.
48. Paying for Senior Care. Receive payment as a caregiver: cash and coun-seling and other options. April 2018. https:// www.payingforseniorcare.com/longtermcare/resources/cash-and-counseling-program.html. Accessed February 15, 2018.
49. Parks SM, Novielli KD. A practical guide to caring for caregivers. Am Fam Physician. 2000; 62(12): 2613-2622.
50. Collins LG, Swartz K. Caregiver care. Am Fam Physician. 2011; 83(11): 1309-1317.
swartz.indd 706 5/10/19 9:23 AM
Spring is here and with better weather come more outdoor activities, making anyone
a potential bullseye for a tick bite. When your patient thinks that they've been affected,
they’ll want answers — fast. It doesn’t help that current testing options may take hours or
days for results. Not anymore! Sofia 2 Lyme FIA uses a finger-stick whole blood sample to
provide accurate, objective and automated results in as few as 3 minutes, getting doctor
and patient on a path to treatment much sooner.
Sofia 2 Lyme FIA is the only rapid, near-patient testing solution that provides IgM and IgG
differentiated results in a single test. It has demonstrated accuracy comparable to
laboratory testing — all with less than 1 minute hands-on-time. And with the power of
Virena, you will have near real time prevalence data and incidence mapping for your
area providing greater information and allowing for better healthcare decisions.
AD20
3196
00EN
00 (0
4/19
)
Where families go out to play, ticks lie in wait to prey.
For more information contact Quidel Inside Sales at 858.431.5814 Or go to our website at Sofia2Lyme.com
CLIAWAIVED 3ART ≥
minsAdvance Result Technology
Sofia 2 Lyme FIA: CLIA-waived Results in minutes, not days.
Quidel_Sofia2_PicnicLyme_AAFP.qxp_Layout 1 4/18/19 12:08 PM Page 1

This handout is provided to you by your family doctor and the American Academy of Family Physicians. Other health-related information is available from the AAFP online at https://familydoctor.org.
This information provides a general overview and may not apply to everyone. Talk to your family doctor to find out if this information applies to you and to get more information on this subject. Copyright © 2019 American Academy of Family Physicians. Individuals may photocopy this material for their own personal reference, and physicians may photocopy for use with their own patients. Written permission is required for all other uses, including electronic uses.
INFORMATION from Your Family Doctor
Who is a caregiver?A caregiver is a friend or relative who provides unpaid care for someone with a chronic or disabling condition.
What are the benefits and challenges of caregiving?Caregiving is associated with personal satisfaction in helping a loved one. However, most caregivers feel unprepared to provide care. Caregivers report having less time to spend with other family members and friends. They may have trouble with money because of their caregiving expenses. They also are less likely to make time for regular health care for themselves. Caregivers with high stress levels are at risk of serious medical problems.
What can my doctor do to help?When taking the person you are caring for to the doctor, it is important to tell the doctor that you are the caregiver. The doctor may ask how you feel about caregiving, how much help your loved one needs, and how you provide this care. The doctor may refer you to other resources for help.
What can I do to help myself?Make sure to take time for yourself. Find ways to help relieve your stress, such as talking to friends or
family, exercising, meditating, or praying. It may help to find other support services in your area. Make sure to visit your doctor on a regular basis to help protect your own health.
Where can I find more information?
Your doctor
AAFP’s Patient Information Resource https://familydoctor.org/familydoctor/en/seniors/caregiving/caregiver-health-and-wellness.html
https://familydoctor.org/familydoctor/en/seniors/caregiving/caregiver-stress.html
AARP https://www.aarp.org/families/caregiving
Family Caregiver Alliance https://www.caregiver.org
Caregiver Action Network https://caregiveraction.org/
U.S. Administration on Aging Eldercare Locator https://www.eldercare.gov
June 2019
Page 1 of 1
Caregiver Care
BONUS DIGITAL CONTENT
swartz pated.indd 1 5/10/19 9:23 AM

REGISTER SOON TO SECURE YOUR SPOT AT THE LOWEST PRICE.
• Learn and Earn: Up to 28 Live credits through 300 educational sessions covering 125 topics
• Explore the Expo: 50 product categories of technologies and patient care solutions
• Connect with Peers: Thousands of family docs networking at social events and activities
• Be Inspired: Thought-provoking speakers during three main stage sessions throughout the week
• Tour America’s City: A world-renowned art scene, fabulous food, outdoor adventures, and American history
THE AAFP’S LARGEST ANNUAL FAMILY MEDICINE EVENT
Full_Page_Bleed.indd 1 3/4/19 4:31 PM

708 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
Curbside Consultation
An Unhappily Married PatientCommentary by Matthew Alexander, PhD, and Shaista Qureshi, MD
Department of Family Medicine, The University of North Carolina, Atrium Health, Charlotte, North Carolina
Case Scenario A 45-year-old woman presented to my office with initial symptoms of headaches and insomnia. My initial screening showed mild depression; her physical examination was normal. I asked her how things were at home, and she told me that she and her husband fight all the time. She added that her husband complains that they never have sex and that she is afraid he may be interested in a coworker. She stated that her attempts to talk with her husband about their situation have been met with anger and defensiveness. She is begin-ning to shut down her feelings in the relationship.
During my training, I was encouraged to explore relationship issues between committed partners; however, doing this in a busy office set-ting is challenging. What practical recommen-dations can be offered? What indicators should prompt a more thorough evaluation and/or refer-ral for additional care?
Commentary Overall, marriage enhances health.1 Men gain greater health benefits from marriage than their wives. Conversely, wives are more negatively affected by a bad marriage than their husbands.2,3 In general, the health benefit of marriage is max-imized in a good marriage but negated in a bad marriage.4,5
Physicians receive little training in couple dynamics, however. Only a few articles in the medical literature address the treatment of inter-personal stress in committed couples. This is par-ticularly alarming because family physicians have traditionally been trusted to address family issues, and patients want family physicians to be knowl-edgeable about and helpful with these issues.6
ManagementWomen are more likely to share concerns in the physician’s office7; however, men may be willing to share if properly encouraged with open-ended questions. Relationship issues present in same-sex marriages are similar to those in heterosex-ual marriages. The goal is to address the patient’s concerns with appropriate sensitivity while remaining on schedule during a busy clinical day.
INTERVIEWING
First, gather information about the marital situ-ation in a timely manner. Be aware of the risk of triangulation; physicians should remember that they are hearing only one side of the story and should be careful before recommending specific actions without obtaining a complete picture. Physicians should also make every effort to be sensitive to cultural differences about marriage and to be self-aware of unconscious bias.
Physicians can achieve a relatively complete picture in a short amount of time by asking these questions:• How did you and your spouse meet? • How long have you been in your partnership? • Is this your first marriage? • Do you have any children or grandchildren?• What types of external stressors (e.g., money,
career, in-laws, medical issues) currently affect your relationship?
• Have you tried anything to fix this problem?• What would your spouse say about this situa-
tion if your spouse were in the office now? • What bothers you the most about this situation?• What are you willing to do to help this
situation?• Would it be okay if I offer some suggestions?
Case scenarios are written to express typical situations that family physicians may encounter; authors remain anonymous. Send scenarios to afpjournal@ aafp.org. Materials are edited to retain confidentiality.
This series is coordinated by Caroline Wellbery, MD, Associate Deputy Editor.
A collection of Curbside Consultation published in AFP is available at https:// www.aafp.org/afp/curbside.
Author disclosure: No relevant financial affiliations.
may 15 curbside.indd 708 5/10/19 9:24 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 709
CURBSIDE CONSULTATION
• Would you be willing to attend couple ther-apy with your spouse? (It is helpful if you ask patients whether they have past experience see-ing therapists or whether any barriers to seeing a therapist [e.g., cost, pride, fear] would keep them from following through.)
RECOMMENDATIONS FOR SOLUTIONS
Several real-world recommendations are effective for unhappily married patients when address-ing typical problems, including fighting, sexual libido incongruities, and trust and communica-tion issues. Table 1 lists examples of simple sug-gestions to help spouses connect.8
Constant Fighting• Take a 10-minute break if fighting gets intense;
discuss again only after both parties have calmed down.
• Express more appreciation to your spouse; a five-to-one ratio of positive to negative inter-actions is associated with marital satisfaction.9
• Try to empathize and understand what might be bothering your spouse.
• Practice emotional regulation techniques such as diaphragmatic breathing and time-out to prevent fights from escalating; meditation has also been found to improve emotional regulation.10,11
• Ask your spouse to come to the office to discuss relationship issues. A possible script: “I saw our doctor today and was asked about relationship problems. Based on what I shared, our doctor recommended that you come in with me next time so that both sides of the story can be heard and recommendations could be made to help us. Would you consider going with me?” Alter-natively, ask your spouse to consider couple therapy.
Sexual Libido Incongruities• Accept that differences in libido exist, includ-
ing that a man’s libido is sometimes less than a woman’s libido.
• Schedule sex on the same night every week.
Lack of Trust and Communication• Set aside time to talk without distractions (e.g.,
talking while walking, putting cell phones away during dinner).
• Ask your spouse to express what is really both-ersome by using I statements (e.g., I feel angry when you…).
• Watch a relationship-oriented movie together; research shows that couples who watch and discuss relationship movies on a regular basis are less likely to divorce12 (e.g., The Story of Us [1999], Hope Springs [2012]).
• Increase your involvement in activities that promote connection, including novel activi-ties that have benefit in facilitating connection (e.g., riding motorized scooters to have dinner in a previously unvisited restaurant).13
• Read books about marriage; bibliotherapy is an effective intervention for a variety of psy-chological problems14,15 (e.g., Hold Me Tight by Susan Johnson, The Seven Principles for Mak-ing Marriage Work by John Gottman and Nan Silver, The Sex-Starved Marriage by Michele Weiner Davis).
• See a licensed marriage therapist; therapists who practice Emotionally Focused Couple Therapy typically provide the best outcome.16,17
RED FLAG REFERRALS
Substance abuse, infidelity, high levels of con-tempt, or intimate partner violence indicate the need for specific referrals (i.e., addiction treat-ment center, couple therapy, anger management therapy, women’s shelter, respectively). Physi-cians should follow safety protocols if exposure to volatile patients is an issue.
Case ResolutionThe physician in the case scenario should recom-mend that the patient have a conversation with her husband and suggest to him that they have a scheduled date night once a week. The patient could be encouraged to read a book on marital health or sexuality and to engage in more fun activities with her husband on a regular basis. She should be encouraged to come back in a month
TABLE 1
Cultivating Connection
Be nice and appreciative
Engage in fun and novel activities
Have one date night per week
Meet emotional as well as sexual needs
Say I love you
Share housework
Talk for 10 minutes a day
Information from reference 8.
may 15 curbside.indd 709 5/10/19 9:24 AM

710 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
CURBSIDE CONSULTATION
to report whether the situation has improved. If it has not improved, the physician should offer a referral to a qualified couple therapist. The authors thank Dave Slawson, MD, for his expert assistance in developing this article.
Address correspondence to Matthew Alexander, PhD, at Matthew.Alexander@ atriumhealth.org. Reprints are not available from the authors.
References 1. Robles TF, Slatcher RB, Trombello JM, McGinn MM. Marital
quality and health: a meta-analytic review. Psychol Bull. 2014; 140(1): 140-187.
2. Kiecolt-Glaser JK, Glaser R, Cacioppo JT, et al. Marital conflict in older adults: endocrinological and immunolog-ical correlates. Psychosom Med. 1997; 59(4): 339-349.
3. Kiecolt-Glaser JK, Newton TL. Marriage and health: his and hers. Psychol Bull. 2001; 127(4): 472-503.
4. Ross CE, Mirowsky J, Goldsteen K. The impact of the fam-ily on health: the decade in review. J Marriage Fam. 1990; 52(4): 1059-1078.
5. Holt-Lunstad J, Birminghan W, Jones BQ. Is there some-thing unique about marriage? The relative impact of mari-tal status, relationship quality, and network social support on ambulatory blood pressure and mental health. Ann Behav Med. 2008; 35(2): 239-244.
6. Hansen JP, Bobula J, Meyer D, Kushner K, Pridham K. Treat or refer: patients’ interest in family physician involvement in their psychosocial problems. J Fam Pract. 1987; 24(5): 499-503.
7. Mental Health Foundation. Survey of people with lived experience of mental health probems reveals men less likely to seek medical support; November 6, 2016. https://www.mentalhealth.org.uk/news/survey-people-lived-experience-mental-health-problems-reveals-men-less-likely-seek-medical. Accessed April 1, 2019.
8. Nelson T. Date nights: they make your marriage work. Huff-ington Post. Updated April 9, 2012. https:// www.huffpost.com/entry/date-nights-they-make-you_n_1264207. Accessed March 1, 2019.
9. Gottman J, Silver N. The Seven Principles for Making Mar-riage Work. London, United Kingdom: Cassell Illustrated; 2018.
10. Carson JW, Carson KM, Gil KM, Baucom DH. Self-expansion as a mediator of relationship improvements in a mindfulness intervention. J Marital Fam Ther. 2007; 33(4): 517-528.
11. Kimmes JG, May RW, Siebert GS, Jaurequi ME, Fincham FD. The association between trait mindfulness and car-diovascular reactivity during marital conflict. Mindfulness. 2018; 9(4): 1160-1169.
12. Rogge RD, Cobb RJ, Lawrence E, Johnson MD, Bradbury TN. Is skills training necessary for the primary prevention of marital distress and dissolution? A 3-year experimental study of three interventions. J Consult Clin Psychol. 2013; 81(6): 949-961.
13. Aron A, Norman CC, Aron EN, McKenna C, Heyman RE. Couples’ shared participation in novel and arousing activ-ities and experienced relationship quality. J Pers Soc Psy-chol. 2000; 78(2): 273-284.
14. Wilson DM, Cash TF. Who reads self-help books? Devel-opment and validation of the self-help reading attitudes survey. Personality and Individual Differences. 2000; 29(1): 119-129.
15. Cuijpers P. Bibliotherapy in unipolar depression: a meta-analysis. J Behav Ther Exp Psychiatry. 1997; 28(2): 139-147.
16. Johnson SM, Hunsley J, Greenberg L, Schindler D. Emo-tionally focused couples therapy: status and challenges. J Clinical Psychology: Science and Practice. 1999; 6(1): 67-79.
17. Makinen JA, Johnson SM. Resolving attachment injuries in couples using emotionally focused therapy: steps toward forgiveness and reconciliation. J Consult Clin Psychol. 2006; 74(6): 1055-1064. ■
may 15 curbside.indd 710 5/10/19 9:24 AM

Because you want practice and patient care advice designed for family doctors, from family doctors
Why FPM ?
Get FPM in print
JRM
1703
0612
For a better practice, healthier patients, and a rewarding career.
Don’t wait.Subscribe today.
aafp.org/fpm/forfamilydocs
Better practice.
Healthier patients.
Rewarding career.
Family Practice Management | A peer-reviewed journal | May/June 2018
Screening for Social Determinants of Health 7
Developing Standing Orders to Help Your Team 13
Five Mobile Apps for Mindfulness 21
The Role of Humility in Leadership 25
How to Be Happy in Practice for 30-Plus Years 40
Opinion: Making Deprescribing Doable 5
Coding Q&A: Diabetic Shoe Certification 33
Practice Pearls: Managing Online Ratings 34
CME Quiz: Earn 5 Credits 35
AAFP SUPPLEMENT
MAKING SENSE
OF MACRA 17
A FOUR-PART PROCESS
Deprescribing
Unnecessary
Medications 28
www.aafp.org/fpm* AAFP member rate only $50/year. Non-member physician rate $125.

712 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
FPIN’s Help Desk Answers
Attention-Deficit/Hyperactivity Disorder: Screening and Evaluation
Payal Gaba, MD, Kadlec Family Medicine Residency, Richland, Washington
Matthew Giordanengo, DO, Montana Family Medicine Residency, Billings, Montana
Clinical QuestionWhat are the best screening tools for the evaluation and diag-nosis of attention-deficit/hyperactivity disorder (ADHD)?
Evidence-Based AnswerThe Conners Abbreviated Symptom Questionnaire has the best combination of positive and negative likelihood ratios (eTable A). (Strength of Recommendation [SOR]: B, based on a meta-analysis of observational studies.) The Vanderbilt ADHD Diagnostic Teacher and Parent Rating Scales also have moderate sensitivity and specificity in ele-mentary school–aged children. (SOR: B, based on a single cohort study.)
Evidence SummaryA 2016 meta-analysis of 25 cross-sectional, cohort, and case-control studies evaluated the accuracy of the Child Behavior Checklist–Attention Problem Scale (CBCL-AP) and three versions of the Conners Rating Scales–Revised (CRS-R) for diagnosing ADHD in children and adoles-cents three to 18 years of age.1 Patients had all three types of ADHD: predominantly hyperactive/impulsive, pre-dominantly inattentive, and combined. In addition to the CBCL-AP (14 studies) and the three versions of the CRS-R, the Conners Parent Rating Scale–Revised short form (four studies), the Conners Teacher Rating Scale–Revised short form (five studies), and the Conners Abbreviated Symptom Questionnaire (five studies) were evaluated. The reference standard was a clinical examination performed by a qual-ified professional using diagnostic criteria from the Diag-nostic and Statistical Manual of Mental Disorders (DSM),
3rd or 4th ed., and corresponding diagnosis codes from the International Classification of Diseases, 9th or 10th revision. All scales had moderate sensitivity, specificity, and positive and negative likelihood ratios for diagnosing ADHD. The Conners Abbreviated Symptom Questionnaire may be the most effective diagnostic tool for ADHD because of its brev-ity and high diagnostic accuracy, and the CBCL-AP could be used for more comprehensive assessments.
A 2013 cohort study compared the Vanderbilt ADHD Diagnostic Parent/Teacher Rating Scales with a structured diagnostic psychiatric interview using DSM-IV criteria.2,3 Participants were selected from a random sample of ele-mentary school students in urban, suburban, and rural school districts in Oklahoma. The Vanderbilt parent and teacher scales were moderately sensitive and specific for diagnosing ADHD.Copyright © Family Physicians Inquiries Network. Used with permission.
Address correspondence to Payal Gaba, MD, at [email protected]. Reprints are not available from the authors.
References 1. Chang LY, Wang MY, Tsai PS. Diagnostic accuracy of rating scales for
attention-deficit/hyperactivity disorder: a meta-analysis. Pediatrics. 2016; 137(3): e20152749.
2. Bard DE, Wolraich ML, Neas B, Doffing M, Beck L. The psychometric properties of the Vanderbilt attention-deficit hyperactivity disorder diagnostic parent rating scale in a community population. J Dev Behav Pediatr. 2013; 34(2): 72-82.
3. Wolraich ML, Bard DE, Neas B, Doffing M, Beck L. The psychometric properties of the Vanderbilt attention-deficit hyperactivity disorder diagnostic teacher rating scale in a community population. J Dev Behav Pediatr. 2013; 34(2): 83-93. ■
Additional content at https://www.aafp.org/afp/2019/0601/p712.html.
Help Desk Answers provides answers to questions submitted by practicing family physicians to the Family Physicians Inquiries Network (FPIN). Members of the network select questions based on their relevance to family medicine. Answers are drawn from an approved set of evidence-based resources and undergo peer review. The strength of recommendations and the level of evidence for individual studies are rated using criteria developed by the Evidence-Based Medicine Working Group (http:// www.cebm.net).
The complete database of evidence-based questions and answers is copyrighted by FPIN. If interested in submitting questions or writing answers for this series, go to http:// www.fpin.org or e-mail: questions@ fpin.org.
This series is coordinated by John E. Delzell Jr., MD, MSPH, Associate Medical Editor.
A collection of FPIN’s Help Desk Answers published in AFP is available at https:// www.aafp.org/afp/hda.
Author disclosure: No relevant financial affiliations.
jun 1 fpin hda.indd 712 5/10/19 9:24 AM

BONUS DIGITAL CONTENT
June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 712A
HELP DESK ANSWERS
eTABLE A
Diagnostic Accuracy of Tests for Attention-Deficit/Hyperactivity Disorder
Test Studies Participants Sensitivity (95% CI) Specificity (95% CI) Positive LR Negative LR
Child Behavior Checklist–Attention Problems Scale
14 3,296 77% (69% to 84%) 73% (64% to 81%) 2.9 0.3
Conners Parent Rating Scale–Revised short form
4 596 75% (64% to 84%) 75% (64% to 84%) 3.0 0.3
Conners Teacher Rating Scale–Revised short form
5 733 72% (63% to 79%) 84% (69% to 93%) 4.6 0.3
Conners Abbreviated Symptom Questionnaire
5 972 83% (59% to 95%) 84% (68% to 93%) 5.3 0.2
Vanderbilt ADHD Diagnostic Parent Rating Scale
1 560 80% (71% to 87%) 75% (66% to 83%) 3.2 0.3
Vanderbilt ADHD Diagnostic Teacher Rating Scale
1 370 69% (43% to 87%) 84% (78% to 89%) 4.3 0.4
ADHD = attention-deficit/hyperactivity disorder; LR = likelihood ratio.
Information from:
Bard DE, Wolraich ML, Neas B, Doffing M, Beck L. The psychometric properties of the Vanderbilt attention-deficit hyperactivity disorder diagnostic parent rating scale in a community population. J Dev Behav Pediatr. 2013; 34(2): 72-82.
Chang LY, Wang MY, Tsai PS. Diagnostic accuracy of rating scales for attention-deficit/hyperactivity disorder: a meta-analysis. Pediatrics. 2016; 137(3): e20152749.
Wolraich ML, Bard DE, Neas B, Doffing M, Beck L. The psychometric properties of the Vanderbilt attention-deficit hyperactivity disorder diagnostic teacher rating scale in a community population. J Dev Behav Pediatr. 2013; 34(2): 83-93.
jun 1 fpin hda.indd 1 5/10/19 9:24 AM
advanced care planning | symptom management last hours | grief and bereavement
Relieve Suffering, Offer Compassion
Self-Study
NEW! Hospice and Palliative Care Self-Study Package
aafp.org/hospicepalliative
GET IT NOW 11.5 AAFP Prescribed credits

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 713
Photo Quiz
A Bump on the GumNguyet-Cam Lam, MD, FAAFP, and Tue T. Te, MD
St. Luke’s Family Medicine Residency Program, Bethlehem, Pennsylvania
A 10-year-old girl was brought to the family medicine clinic by her mother with a painful lesion on the left upper gum. The lesion was first noted about two months before the visit, when it was approximately 3 mm in diameter. The lesion had gradually increased in size. There was no dis-charge, but the patient had noticed a change in sensation in her gum. She had no constitutional symptoms or history of injury to the permanent tooth. However, the mother recalled that one of her baby teeth was pulled in preparation for braces two years earlier.
Physical examination revealed a lesion on the left upper anterior gingiva above the canine tooth (Figure 1). The round, erythematous lesion measured 8 mm in diameter. It was firm, non-pulsatile, and tender to palpation, and it did not bleed.
Question
Based on the patient’s history and physical examination findings, which one of the follow-ing is the most likely diagnosis?
l A. Dental abscess.
l B. Langerhans cell histiocytosis.
l C. Mucocele.
l D. Pyogenic granuloma.
See the following page for discussion.
The editors of AFP welcome submissions for Photo Quiz. Guidelines for preparing and submitting a Photo Quiz manuscript can be found in the Authors’ Guide at https:// www.aafp.org/afp/photoquizinfo. To be considered for publication, submissions must meet these guidelines. E-mail submissions to afpphoto@ aafp.org.
This series is coordinated by John E. Delzell Jr., MD, MSPH, Associate Medical Editor.
A collection of Photo Quiz published in AFP is available at https:// www.aafp.org/afp/photoquiz.
Previously published Photo Quizzes are now featured in a mobile app. Get more information at https:// www.aafp.org/afp/apps.
Author disclosure: No relevant financial affiliations.
FIGURE 1
jun 1 photo.indd 713 5/10/19 9:24 AM

714 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
PHOTO QUIZ
DiscussionThe answer is A: dental abscess. Den-tal abscess is a subtype of odonto-genic infection, which is one of the most common diseases of the oral and maxillofacial region.1 Classifications of dental abscess include periapical, periodontal, gingival, pericoronal, and combined periodontal-endodontic. Pain is one of the most common symptoms of dental abscess for which patients seek medical attention. The pain is usually moderate to severe and can be intermittent or persistent and sharp, throbbing, or shooting. Pain is absent in some acute cases. Swelling is almost always present, whether it is the acute or subacute phase. Patients sometimes describe a toothache with sensitivity to hot and cold and may have a history of a recent dental procedure.
Odontogenic infection is diagnosed with physical exam-ination and imaging findings. The choice of imaging study varies with clinical setting. Computed tomography is par-ticularly sensitive for osseous structures and is the modality of choice for most odontogenic infections.2 Fluid collection and tissue biopsies should be examined for evidence of acute or chronic inflammation and infection.
A spreading infection is more serious than localized swelling of gingival tissue, because the infection could spread outward from the root of the tooth throughout the bone and periosteum.3 Failure to recognize a systemic infection can lead to chronic infections or life-threatening complications, such as airway obstruction, mediastinitis, necrotizing fasciitis, cavernous sinus thrombosis, cerebral abscess, orbital abscess, and sepsis.4 Severe complications require intravenous antibiotics, incision and drainage, and probable removal of the source of infection.3 A localized infection is usually not urgent and can be managed in the outpatient setting.
Langerhans cell histiocytosis is a rare histiocytic disorder that most commonly affects children one to three years of age, although it can occur at any age. In young children, it is an acute disseminated multisystem disease.5 Bone and skin are most commonly affected. There is oral involvement in about 13% of cases,6 usually manifesting as an intraoral mass, gingivitis, mucosal ulcers, and loose teeth. Lesions of the bones or soft tissue are painful.7
Mucocele is an area of mucin drainage in soft tissue resulting from rupture of a salivary duct. Mucocele is most common in children and young adults who usually have multiple episodes of swelling lesions with periodic rupture.
Long-standing lesions may develop fibrosis, which is non-tender on palpation.8 Mucocele is most commonly located on the inside of the lower lip.9
Pyogenic granuloma is a rapidly growing lesion that devel-ops in response to local irritations, such as poor hygiene, overhanging dental fillings, and trauma. The lesion can be from millimeters to centimeters in diameter. Pyogenic granulomas are erythematous, nonpainful, and smooth, and bleed easily when touched.8 Address correspondence to Nguyet-Cam Lam, MD, FAAFP, at Nguyet-Cam.Lam@ sluhn.org. Reprints are not available from the authors.
References 1. Zamiri B, Hashemi SB, Hashemi SH, Rafiee Z, Ehsani S. Prevalence of
odontogenic deep head and neck spaces infection and its correlation with length of hospital stay. J Dent (Shiraz). 2012; 13(1): 29-35.
2. Hurley MC, Heran MK. Imaging studies for head and neck infections. Infect Dis Clin North Am. 2007; 21(2): 305-353.
3. Hay W Jr., Levin M, Deterding R, Abzug M, Sondheimer J. In: Oral med-icine and dentistry. Current Diagnosis and Treatment: Pediatrics. 22nd ed. New York, NY: McGraw-Hill; 2014.
4. Bali RK, Sharma P, Gaba S, Kaur A, Ghanghas P. A review of complications of odontogenic infections. Natl J Maxillofac Surg. 2015; 6(2): 136-143.
5. Baumgartner I, von Hochstetter A, Baumert B, Luetolf U, Follath F. Langerhans’-cell histiocytosis in adults. Med Pediatr Oncol. 1997; 28(1): 9-14.
6. Grois N, Pötschger U, Prosch H, et al.; DALHX- and LCH I and II Study Committee. Risk factors for diabetes insipidus in Langerhans cell histio-cytosis. Pediatr Blood Cancer. 2006; 46(2): 228-233.
7. Huang W, Yang X, Cao D, et al. Eosinophilic granuloma of spine in adults: a report of 30 cases and outcome. Acta Neurochir (Wien). 2010; 152(7): 1129-1137.
8. Gonsalves WC, Chi AC, Neville BW. Common oral lesions: part II. Masses and neoplasia. Am Fam Physician. 2007; 75(4): 509-512.
9. Bodner L, Manor E, Joshua Z, Shaco-Levy R. Oral mucoceles in children—analysis of 56 new cases. Pediatr Dermatol. 2015; 32(5): 647-650. ■
SUMMARY TABLE
Condition Characteristics
Dental abscess Moderate to severe pain, swelling, sensitivity to hot and cold; may have history of a recent dental procedure
Langerhans cell histiocytosis
Bone and skin are most commonly affected; oral involve-ment is possible, most often manifesting as an intraoral mass, gingivitis, mucosal ulcers, and loose teeth; most common in children one to three years of age
Mucocele Multiple episodes of swelling with periodic rupture, non-tender, often appears inside the lower lip, most common in young children
Pyogenic granuloma
Rapidly growing, erythematous, nonpainful, smooth lesions that bleed easily
jun 1 photo.indd 714 5/10/19 9:24 AM

AAFP NEWS Your Primary Source for Family Medicine UpdatesAAFP News provides accurate and frequent news
updates and blog posts to AAFP members, plus
developments on family medicine advocacy issues.
• Updated throughout the week at www.aafp.org/news • Available on the AAFP mobile app
• Delivered directly to your inbox
aafp.org/news
Share your voice! AAFP members can comment on individual AAFP News stories.

716 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
POEMsPatient-Oriented Evidence That Matters
Overview of New ACC/AHA Lipid Guidelines
Clinical QuestionWhat do cardiologists recommend for the management of hyperlipidemia?
Bottom LineThese updated guidelines, made without any input from primary care physicians who manage most patients with hyperlipidemia, are more complex than the 2013 guide-lines and will likely lead to even more recommendations for statins, ezetimibe (Zetia), and PSK9 inhibitors. Rather than a “fire and forget” strategy involving a risk-based prescrip-tion of a moderate- or high-intensity statin, we are supposed to go back to monitoring low-density lipoprotein (LDL) levels and targeting a percentage reduction in LDL choles-terol—and in very high-risk patients targeting an LDL level of less than 70 mg per dL (1.81 mmol per L). (Level of Evi-dence = 1a–)
SynopsisThis is an update to the 2013 American College of Cardiol-ogy/American Heart Association (ACC/AHA) guidelines, which were the first to base treatment decisions primarily on the 10-year risk of an atherosclerotic cardiovascular dis-ease (ASCVD) event rather than on specific LDL targets. This guideline reemphasizes regularly measuring lipids and a return to an LDL target for assessing effectiveness and deciding when to prescribe one of the new and pricey PSK9 inhibitors ($14,000 to $15,000 per year at http://www.goodrx.com, December 1, 2018). Statins are divided into high intensity (atorvastatin [Lipitor], 40 to 80 mg; rosuvasta-tin [Crestor], 20 to 40 mg), moderate-intensity (atorvastatin,
10 to 20 mg; simvastatin [Zocor], 20 to 40 mg; rosuvastatin, 5 to 10 mg), and low-intensity (simvastatin, 10 mg) groups. For primary prevention in people 20 to 39 years of age, the guidelines recommend an assessment of the lifetime risk of ASCVD as a way to frighten patients into compliance with lifestyle changes. For people 20 to 39 years of age with LDL levels greater than 160 mg per dL (4.14 mmol per L) or a fam-ily history of premature ASCVD, a statin is recommended. For patients 40 years and older, a high-intensity statin is recommended for an LDL level greater than 190 mg per dL (4.92 mmol per L) and a moderate- or high-intensity statin (depending on other risk factors) for those with diabetes mellitus.
For all other patients, the Pooled Cohort Equations are used to place patients into one of four risk groups; the old guideline had only three. If the 10-year risk of an ASCVD event is less than 5%, no statin is recommended. If the 10-year risk is 5% to 7.5%, consider a moderate-intensity statin if there is also a “risk enhancer,” such as LDL level greater than 160 mg per dL, family history of premature ASCVD, chronic kidney disease, metabolic syndrome, South Asian ancestry, preeclampsia, HIV, rheumatoid arthritis, or psoriasis. For persons with a 7.5% to 20% risk, they recommend a moderate-intensity statin for most patients to target a 30% to 49% reduction in LDL choles-terol. Finally, if the risk is greater than 20%, a statin to target a 50% or more reduction in LDL cholesterol is rec-ommended. For prevention in persons with known vascu-lar disease, a new category of very high risk is described. It is defined as two or more of the following major events: acute coronary syndrome in the past 12 months, previous myocardial infarction, previous ischemic stroke, or symp-tomatic peripheral artery disease. A patient is also very high risk if he or she has one of those major ASCVD events and multiple high-risk conditions, such as familial hyper-cholesterolemia, age of at least 65 years, hypertension, dia-betes, chronic kidney disease, tobacco use, heart failure, or LDL level greater than 100 mg per dL (2.59 mmol per L) despite maximal statin plus ezetimibe therapy. Patients in this category should be taking a high-intensity statin, add-ing ezetimibe if necessary, to target an LDL level of 70 mg per dL. If that is not achieved, a PSK9 inhibitor should be considered.
Regarding PSK9 inhibitors, it is notable that the guide-line cautions that “the long-term safety (more than 3 years) is uncertain and cost effectiveness is low at mid-2018 list prices.” Although the previous guideline was silent on the question of monitoring lipid levels, this one recom-mends regular monitoring (at least once per year) to verify
POEMs (patient-oriented evidence that matters) are pro-vided by Essential Evidence Plus, a point-of-care clinical decision support system published by Wiley-Blackwell. For more information, see http:// www.essentialevidenceplus.com. Copyright Wiley-Blackwell. Used with permission.
For definitions of levels of evidence used in POEMs, see http:// www.essentialevidenceplus.com/product/ebm_loe.cfm?show=oxford.
To subscribe to a free podcast of these and other POEMs that appear in AFP, search in iTunes for “POEM of the Week” or go to http:// goo.gl/3niWXb.
This series is coordinated by Sumi Sexton, MD, Editor-in-Chief.
A collection of POEMs published in AFP is available at https:// www.aafp.org/afp/poems.
june 1 poems.indd 716 5/10/19 9:24 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 717
POEMS
adherence to the medication and to estimate the percentage reduction in LDL level. It is also worth noting which organi-zations were not among the 12 that endorsed this guideline: the American Academy of Family Physicians (AAFP) and the American College of Physicians (ACP). This is reminis-cent of the recent, aggressive hypertension guidelines from the ACC/AHA that the AAFP and ACP also did not partic-ipate in or endorse. Study design: Practice guideline
Funding source: Government
Setting: Various (guideline)
Reference: Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;S0735-1097(18)39034-X.
Mark H. Ebell, MD, MSProfessor University of Georgia, Athens, Ga.
Aspirin, Eicosapentaenoic Acid, and Placebo Equally Effective in Preventing Colorectal Adenomas in High-Risk Patients
Clinical QuestionIs aspirin or eicosapentaenoic acid (EPA) effective in pre-venting colorectal adenomas in patients with previous high-risk colorectal neoplasia?
Bottom LineAfter 12 months, neither aspirin nor EPA, alone or in com-bination, are any better than placebo at preventing colorec-tal adenomas in patients with high-risk neoplasia. (Level of Evidence = 1b)
SynopsisThe Systematic Evaluation of Aspirin and Fish Oil (seA-FOod) Polyp Prevention Trial was a factorial trial that randomized patients with high-risk colorectal neoplasms detected on screening colonoscopy. The included patients had three or more adenomas, one of which had to be 1 cm in diameter, or they had five or more smaller adenomas. The researchers randomized patients to receive EPA (1,000 mg twice daily; n = 179) plus placebo, aspirin (300 mg daily; n = 177) plus placebo, EPA plus aspirin (n = 177); or pla-cebo plus placebo (n = 176). The researchers performed a follow-up colonoscopy 12 months after enrollment. Sixty-six patients (9%) did not have a follow-up colonoscopy and were excluded from the analysis. The rate of subsequent adenomas at follow-up was high (61% to 63%) and not sta-tistically significantly different for each group. The rate of adverse events was low in all groups.
Study design: Randomized controlled trial (double-blinded)
Funding source: Government
Allocation: Concealed
Setting: Outpatient (any)
Reference: Hull MA, Sprange K, Hepburn T, et al.; seAFOod Collaborative Group. Eicosapentaenoic acid and aspirin, alone and in combination, for the prevention of colorectal adenomas (seAFOod Polyp Prevention trial): a multicentre, randomised, double-blind, placebo-controlled, 2 x 2 factorial trial. Lancet. 2018;392(10164):2583-2594.
Henry C. Barry, MD, MSProfessor Michigan State University, East Lansing, Mich.
Probiotic Ineffective for Treatment of Acute Gastroenteritis in Young Children
Clinical QuestionIs the probiotic Lactobacillus rhamnosus GG safe and effec-tive for the treatment of acute gastroenteritis in young children?
Bottom LineTreatment with the probiotic L. rhamnosus GG does not result in faster symptomatic improvement or less moder-ate or severe diarrhea in young children with acute gastro-enteritis. (Level of Evidence = 1b)
SynopsisAlthough some studies have shown a benefit to probiot-ics for the treatment of acute gastroenteritis in children, they have generally been small, funded by industry, or had methodologic flaws. This study was a large, well-designed randomized trial that attempted to more definitively answer this question. Children three months to four years of age with at least three watery stools per day for less than seven days were identified in 10 university pediatric emer-gency departments. Children were excluded if they or their caregivers were potentially immunocompromised, or if the children were taking long-term corticosteroids, had been premature, or had chronic gastrointestinal disease. Chil-dren were also excluded if they had any biliary tract dis-ease, hematochezia, or allergies to the study medication or to any antibiotics used to treat invasive L. rhamnosus infec-tion. They were then randomized to receive the probiotic or placebo once daily for five days, stratified by presenta-tion within or later than 48 hours of the onset of illness, and with the first dose given in the emergency department. Of the 971 patients randomized, 943 completed the study, with a similar rate of loss to follow-up in both groups. The median age of participants was 1.4 years, 53% were male, and the median duration of diarrhea was 53 hours; groups were balanced at the start of the study. After 14 days, the
june 1 poems.indd 717 5/10/19 9:24 AM

718 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
POEMS
likelihood of moderate to severe symptoms based on the modified Vesikari scale score was similar between groups (11.8% in the probiotic group and 12.6% in the placebo group). There were also no differences between groups regarding secondary symptom outcomes such as the dura-tion or frequency of diarrhea. There was more wheezing in the probiotic group (5 vs. 0; P = .03). Study design: Randomized controlled trial (double-blinded)
Funding source: Government
Allocation: Concealed
Setting: Emergency department
Reference: Schnadower D, Tarr PI, Casper TC, et al. Lactoba-cillus rhamnosus GG versus placebo for acute gastroenteritis in children. N Engl J Med. 2018;379(21):2002-2014.
Mark H. Ebell, MD, MSProfessor University of Georgia, Athens, Ga.
Benefits and Harms for Low-Dose Aspirin in Patients with Diabetes Mellitus
Clinical QuestionWhat are the benefits and harms of low-dose aspirin in adults with diabetes mellitus?
Bottom LineThe 7,740 patients who took low-dose aspirin experienced 51 fewer vascular deaths, nonfatal myocardial infarctions (MIs), or nonfatal ischemic strokes; 29 fewer transient isch-emic attacks (TIAs); and 44 fewer revascularizations than patients who took placebo over a mean of 7.4 years. This is balanced by an additional 69 major bleeding episodes during that period, with no effect on vascular or all-cause deaths, and no difference in the incidence of cancer. (Level of Evidence = 1b)
SynopsisThis British study recruited adults 40 years and older with diabetes, no known cardiovascular disease, no contrain-dications to aspirin, and no major comorbidity that would keep them from participating in the study for at least five years. After a placebo run-in period to assure adherence, 15,480 participants were randomized to receive aspirin 100 mg once daily or matching placebo. They were also randomized to receive an omega-3 fatty acid capsule or placebo; those results are reported separately. The groups were balanced at the start of the study: the patients had a mean age of 63 years, 63% were men, and 96% were white. Almost all (94%) had type 2 diabetes. A validated risk score determined that approximately 40% of participants were at low risk of vascular events (less than 5% at five years), 40% had a five-year risk of 5% to 10%, and the remainder were at
high risk. Because the trial was ongoing, the authors added TIA to the original primary composite efficacy outcome of vascular death, nonfatal MI, or nonfatal stroke (excluding intracranial hemorrhage). The primary safety outcome was a composite of intracranial hemorrhage, intraocular hem-orrhage that threatens sight, gastrointestinal bleeding, or any other serious bleeding event. After a mean follow-up of 7.4 years, 99% of patients had complete follow-up data, with outcomes adjudicated for more than 90% by a committee masked to treatment assignment. The authors also looked at the effect of adding revascularization to the composite efficacy outcome. There was no difference between groups in the original efficacy outcome of vascular death, nonfa-tal MI, and nonfatal ischemic stroke (7.0% with aspirin vs. 7.6% with placebo; hazard ratio [HR] = 0.92; 95% CI, 0.82 to 1.03). When you add TIA to the composite outcome, the difference between groups is statistically significant (8.5% vs. 9.6%; HR = 0.88; CI, 0.79 to 97; number needed to treat [NNT] = 90 for 7.4 years). Adding revascularization to the original efficacy outcome had a similar result (10.8% vs. 12.1%; HR = 0.88; CI, 0.80 to 0.97; NNT = 77 for 7 years). When examining results stratified by vascular risk, those at moderate and higher vascular risk also experienced more major bleeding events (8.9 to 9.6 vs. 2.8 per 5,000 person-years in the low-risk group). The number of serious vascular events avoided per 5,000 person years was 5.7 in the low-risk group, 11.2 in the moderate-risk group, and only 4.9 in the high-risk group. For the composite harm outcome, there was a significantly increased risk of major bleeding, primar-ily due to more serious gastrointestinal and other bleeds (4.1% vs. 3.2%; HR = 1.29; CI, 1.09 to 1.52; number needed to treat to harm = 111 over 7 years). There was no difference in fatal bleeding events or hemorrhagic strokes. There was no difference in the incidence of cancer (11.6% for aspirin vs. 11.5% for placebo), including for gastrointestinal can-cers (2.0% vs. 2.0%). There were no significant differences between groups in all-cause mortality or in vascular deaths. Study design: Randomized controlled trial (double-blinded)
Funding source: Industry and foundation
Allocation: Concealed
Setting: Outpatient (any)
Reference: Bowman L, Mafham M, Wallendszus K, et al.; ASCEND Study Collaborative Group. Effects of aspirin for pri-mary prevention in persons with diabetes mellitus. N Engl J Med. 2018; 379(16): 1529-1539.
Mark H. Ebell, MD, MSProfessor University of Georgia, Athens, Ga.
Editor’s Note: Dr. Ebell is Deputy Editor for Evidence- Based Medicine for AFP and cofounder and Editor-in-Chief of Essential Evidence Plus. ■
june 1 poems.indd 718 5/10/19 9:24 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 719
Practice Guidelines
Cancer Screening: ACS Releases Annual Summary
of Recommendations
The American Cancer Society (ACS) pro-vides a summary of recommendations for can-cer screening (Table 1) each year, including any updates and recent data, and advice for when recommendations cannot be made. In addition to this summary, the 2018 report outlines issues that affect screening for breast, cervical, colorec-tal, and prostate cancer; further explains the 2013 recommendations for lung cancer screening via low-dose computed tomography; compares the ACS recommendations with those of other pro-fessional health care organizations; and provides information from the National Health Interview Survey.
Breast CancerBreast cancer is the most common cancer in women living in the United States, with an esti-mated 266,120 patients diagnosed with invasive
breast cancer in 2018 and an associated 40,920 deaths. The ACS screening rec-ommendations in women at average risk were updated in 2015 and have not changed. This guideline underscores the importance of yearly screening in women 45 to 54 years of age and those 40 to 44 years who choose ear-lier screening, because evidence has shown that such screening in pre-menopausal women is associated with a significantly decreased risk of iden-tifying advanced breast cancer com-pared with screening performed every other year. Postmenopausal women do
not have similar benefits associated with yearly screening, unless they are currently receiving hormone treatment for menopause; therefore, women 55 years or older can receive screening every other year or yearly, depending on patient preference. An age to stop screening is not iden-tified, but continued screening may be beneficial in certain women 75 years or older, taking into account mortality, age, comorbidities, and func-tion. These recommendations were made after a review of the burden of disease and of the benefits and harms of screening. An update to the 2007 screening recommendations in women at greater than average risk is currently being completed.
Cervical CancerAn estimated 13,240 persons will be diagnosed with invasive cervical cancer in 2018, with an associated 4,170 deaths. The ACS, American
Coverage of guidelines from other organizations does not imply endorsement by AFP or the AAFP.
This series is coordinated by Sumi Sexton, MD, Editor-in-Chief.
A collection of Practice Guidelines published in AFP is available at https:// www.aafp.org/afp/practguide.
CME This clinical content conforms to AAFP criteria for continuing medical education (CME). See CME Quiz on page 673.
Author disclosure: No relevant financial affiliations.
Key Points for Practice
• The ACS recommends yearly screening for breast can-cer in women 45 to 54 years of age and those 40 to 44 years of age who choose earlier screening.
• Women with atypical squamous cells of undeter-mined significance on cervical cancer screening that were found to be negative for HPV should have repeat screening in three years.
• Physicians should initiate discussions on prostate cancer with those at average risk starting at 50 years of age, at 45 years with higher risk, and at 40 years in those at even higher risk.
From the AFP Editors
jun 1 pg cancer.indd 719 5/10/19 9:24 AM
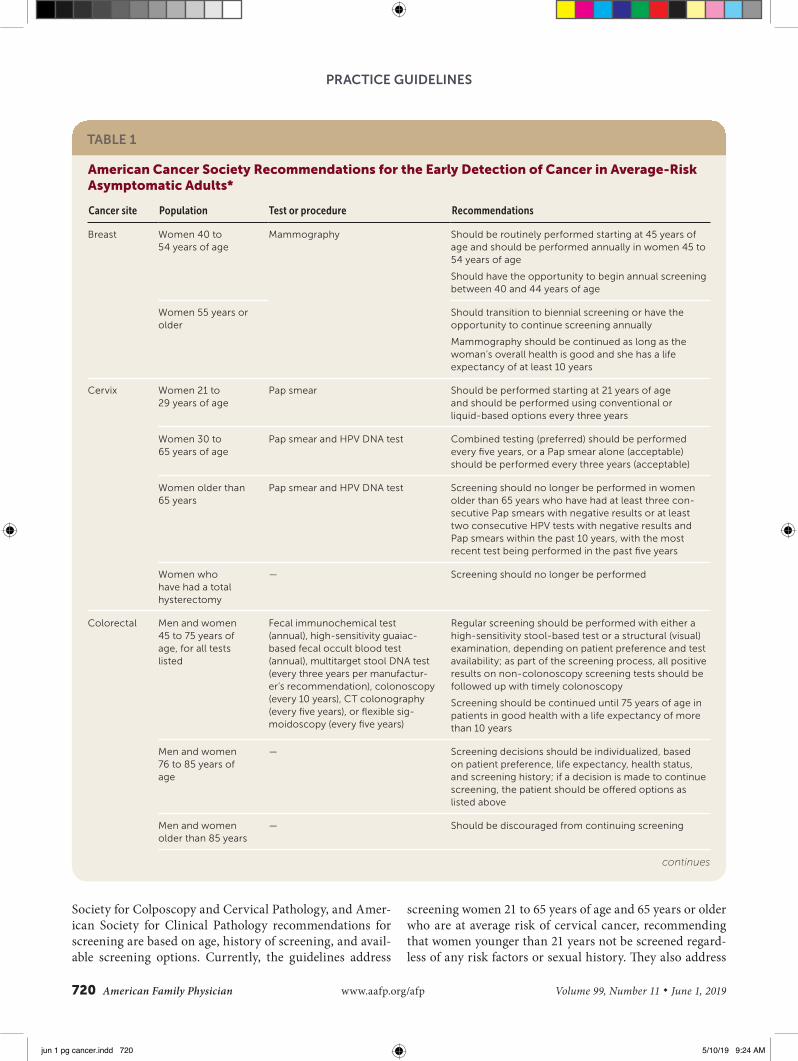
720 American Family Physician www.aafp.org/afp Volume 99, Number 11 ◆ June 1, 2019
PRACTICE GUIDELINES
Society for Colposcopy and Cervical Pathology, and Amer-ican Society for Clinical Pathology recommendations for screening are based on age, history of screening, and avail-able screening options. Currently, the guidelines address
screening women 21 to 65 years of age and 65 years or older who are at average risk of cervical cancer, recommending that women younger than 21 years not be screened regard-less of any risk factors or sexual history. They also address
TABLE 1
American Cancer Society Recommendations for the Early Detection of Cancer in Average-Risk Asymptomatic Adults*
Cancer site Population Test or procedure Recommendations
Breast Women 40 to 54 years of age
Mammography Should be routinely performed starting at 45 years of age and should be performed annually in women 45 to 54 years of age
Should have the opportunity to begin annual screening between 40 and 44 years of age
Women 55 years or older
Should transition to biennial screening or have the opportunity to continue screening annually
Mammography should be continued as long as the woman’s overall health is good and she has a life expectancy of at least 10 years
Cervix Women 21 to 29 years of age
Pap smear Should be performed starting at 21 years of age and should be performed using conventional or liquid-based options every three years
Women 30 to 65 years of age
Pap smear and HPV DNA test Combined testing (preferred) should be performed every five years, or a Pap smear alone (acceptable) should be performed every three years (acceptable)
Women older than 65 years
Pap smear and HPV DNA test Screening should no longer be performed in women older than 65 years who have had at least three con-secutive Pap smears with negative results or at least two consecutive HPV tests with negative results and Pap smears within the past 10 years, with the most recent test being performed in the past five years
Women who have had a total hysterectomy
— Screening should no longer be performed
Colorectal Men and women 45 to 75 years of age, for all tests listed
Fecal immunochemical test (annual), high-sensitivity guaiac-based fecal occult blood test (annual), multitarget stool DNA test (every three years per manufactur-er’s recommendation), colonoscopy (every 10 years), CT colonography (every five years), or flexible sig-moidoscopy (every five years)
Regular screening should be performed with either a high-sensitivity stool-based test or a structural (visual) examination, depending on patient preference and test availability; as part of the screening process, all positive results on non-colonoscopy screening tests should be followed up with timely colonoscopy
Screening should be continued until 75 years of age in patients in good health with a life expectancy of more than 10 years
Men and women 76 to 85 years of age
— Screening decisions should be individualized, based on patient preference, life expectancy, health status, and screening history; if a decision is made to continue screening, the patient should be offered options as listed above
Men and women older than 85 years
— Should be discouraged from continuing screening
continues
jun 1 pg cancer.indd 720 5/10/19 9:24 AM

June 1, 2019 ◆ Volume 99, Number 11 www.aafp.org/afp American Family Physician 721
PRACTICE GUIDELINES
the human papillomavirus (HPV) vaccine and other spe-cial considerations. The current guidelines recommend that women with atypical squamous cells of undetermined significance that were found to be negative for HPV should have repeat screening in three years. The recommenda-tions on atypical squamous cells of undetermined signifi-cance and HPV vaccines have been added since the 2012 guideline, and a full update of the cervical cancer screening guidelines is currently being completed.
Colorectal CancerAn estimated 140,250 persons will be diagnosed with col-orectal cancer in 2018, with an associated 50,630 deaths. Despite this, the incidence and mortality rates have been decreasing in persons 50 years or older, based mainly on the use of screening for prevention and early identification. In 2018, the ACS updated its recommendations for screening in persons at average risk, with the most notable change being to start screening at 45 years of age; emphasizing screening in general via a variety of options, with appro-priate guidance about their benefits and harms, rather than a preference for certain screening options; and describing follow-up protocols in patients with concerning results on
stool testing. The guidance specific to persons at increased and high risk was last updated in 2001.
Prostate CancerProstate cancer is the second most common cancer in U.S. men, with an estimated 164,690 diagnoses in 2018 and an associated 29,430 deaths. Recommendations for early iden-tification of prostate cancer were last published in 2010, with a full update anticipated for 2019. Decisions about screening should be made using an informed decision-making process, with physicians initiating discussions with those at average risk starting at 50 years of age, with those at high risk (e.g., black, family history of a diagnosis at younger than 65 years) at age 45, and those at even higher risk (e.g., family history of multiple diagnoses at younger than 65 years) at age 40.
Lung CancerIn its 2013 guidance, the ACS recommended that physi-cians discuss current smoking, as well as smoking history, with persons 55 to 74 years of age. Subsequently, physicians who have contacts with high-quality treatment facilities also should discuss screening methods and their associated
TABLE 1 (continued)
American Cancer Society Recommendations for the Early Detection of Cancer in Average-Risk Asymptomatic Adults*
Cancer site Population Test or procedure Recommendations
Endometrial Women, at menopause
— Should be informed about risks and symptoms of endometrial cancer and strongly encouraged to report any unexpected bleeding or spotting to their physicians
Lung Current or former smokers 55 to 74 years of age in good health with at least a 30-pack-year his-tory of smoking
Low-dose helical CT Should be performed annually in adults who currently smoke or have quit within the past 15 years, and who have at least a 30-pack-year smoking history; receive evidence-based smoking cessation counseling (if they are current smokers); have undergone a process of informed or shared decision-making that included information about the potential benefits, limitations, and harms of screening with low-dose CT; and have access to a high-volume, high-quality lung cancer screening and treatment center
Prostate Men 50 years or older
Prostate-specific antigen test with or without digital rectal examination
Men who have a life expectancy of at least 10 years should have an opportunity to make an informed deci-sion with their health care professional about whether to be screened after receiving information about the potential benefits, risks, and uncertainties associated with screening; should not occur without an informed decision-making process
CT = computed tomography; HPV = human papillomavirus; Pap = Papanicolaou.
*—All persons should become familiar with the potential benefits, limitations, and harms associated with cancer screening.
Adapted with permission from Smith RA, Andrews KS, Brooks D, et al. Cancer screening in the United States, 2018: a review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin. 2018; 68(4): 299.
jun 1 pg cancer.indd 721 5/10/19 9:24 AM

PRACTICE GUIDELINES
benefits and harms with those patients in good health who have at least a 30-pack-year history of smoking, who smoke currently, or who only quit smoking in the past 15 years. This recommendation, however, has been misconstrued by some physicians to mean that decisions to screen should involve shared decision-making, instead of a firm recom-mendation to screen combined with appropriate discus-sions with the patient.
To clarify this recommendation and appropriately place the emphasis, as ACS intended, on a firm recommendation for screening, in 2017, the ACS modified the wording to say that yearly screening should be performed with low-dose computed tomography in this patient population, combined with counseling on smoking cessation in current smokers and provision of information about benefits and harms of such screening. In addition, smoking cessation counseling was emphasized as an important component of identifying adults who should receive screening, which is not a replace-ment for smoking cessation.
Editor’s Note: The AAFP’s screening recommendations differ in some important respects from those of the ACS. The AAFP recommends starting routine mammography and colorectal cancer screening at age 50 in average-risk adults, and supports providing prostate specific antigen–based screening only to men 55 to 69 years of age who express a clear preference for the test after shared decision-making. In contrast to the ACS’s “firm recommendation to screen” for lung cancer in persons 55 to 74 years of age with at least a 30-pack-year history of smoking, the AAFP concluded that the evidence was insufficient to recommend for or against annual low-dose computed tomography in this population. In its recommendation, the AAFP cited concerns about high false-positive rates, unknown long-term harms of radiation exposure from follow-up full-dose computed tomography, and the lack of replication of the National Lung Screening Trial results in community settings (https:// www.aafp.org/patient-care/clinical-recommendations/all/lung-cancer.html).—Kenny Lin, MD, MPH, Deputy Editor
Guideline source: American Cancer Society
Evidence rating system used? Yes
Systematic literature search described? No
Guideline developed by participants without relevant financial ties to industry? No
Recommendations based on patient-oriented outcomes? Yes
Published source: CA Cancer J Clin. July/August, 2018; 68(4): 297-316
Available at: https:// onlinelibrary.wiley.com/doi/full/10.3322/caac.21446
Lisa CrokeAFP Senior Associate Editor ■
Advanced Life Support in Obstetrics (ALSO®)
Effectively manage and respond to obstetrical emergencies with comprehensive training that saves lives.
• Standardized, multi-disciplinary approach
• Prepare for real-life, emergency situations
• Hands-on simulation training
• Helpful testing tools and mnemonics
Schedule an essential ALSO trainingfor you and your team today.
(800) 274-2237, ext. 8722 aafp.org/ALSO
®
Advanced Life Support in Obstetrics
18060984 ALSO Journal Ads Half Vert.indd 1 8/27/18 9:43 AM
jun 1 pg cancer.indd 722 5/10/19 9:24 AM

• Open 8 to 8 every day• Flexible schedules, no call• Guaranteed $240,000 averaging 4
shifts a week• Additional bonus pay based on
productivity• Malpractice coverage• Medical and dental for physician and
dependents at no cost• Long term disability insurance• Retirement plan with matching funds
PHYSICIAN OPPORTUNITIES
Contact Merl O’Brien, MD, at:(916) 791-1300, ext.11111; or email CV to:[email protected].
Physicians WantedCALIFORNIAARIZONA
To advertise in AAFP CareerLink Classifi eds contact our Media Sales Team at: (727) 497-6568; E-mail: [email protected]
CAREERLINK CLASSIFIEDS
PHYSICIAN – FAMILY MEDICINELocated in Vista, California, Vista Community Clinic is a private, nonprofit outpatient community clinic located in North San Diego County serving people who experience social, cultural or economic barriers to health care in a comprehensive, high quality setting.
• Position: Full-time, Part-time and Per Diem Family Medicine Physicians.
• Responsibilities: Provides outpatient care to clinic patients and ensures quality assurance. Malpractice coverage is provided by Clinic.
• Requirements: California license, DEA license, CPR certification and board certified in family medicine. Bilingual English/Spanish preferred.
• Contact Us: Visit our website at www.vistacommunityclinic.org Forward resume to [email protected] or fax resume to 760 414 3702.
EEO/AA/M/F/Vet/ Disabled
JOIN OURPRIMARY CARE TEAM!
Tsehootsooi Medical Center, Fort Defiance, AZ seeks BE/BC Family Practice Physicians and Internal
Medicine Physicians. Innovation is the unique difference in a truly diverse multi-cultural medical
community in northeastern Arizona.
• Integrated healthcare systemincludes (1) satellite clinic,ancillary services, WellnessCenter, on-site clinicalpharmacists, behavioralhealth, case managers andsocial services.
• Flexible Work Schedules• Paid Benefits include: Health
Benefits, Federal TortMalpractice Coverage, PaidVacation, Paid CME attendance
• Salary is Negotiable, Sign-OnBonus, Relocation Incentive
• Incentive Pay based on AnnualPerformance
• 1-4 Bedroom Homes• Loan Forgiveness Options:NHSC,
I.H.S. and Arizona State LRPFor more information, please contact:
Ra’el AugareMedical Recruiting Mngr.928.729.8309Ophelia AnthonyMed. Recruiting Coord.928.688.5653 / (520) 391-0679
www.fdihb.org
American Family Physician isn’t just read, it’s studied.
Advertise your FPopportunities and services in AFP.
(727) 497-6568 [email protected]
June 1, 2019 Volume 99, Number 11 www.aafp.org/afp American Family Physician 723
AFP_06012019.indd 1 5/4/19 3:45 AM

FLORIDA
• Open 8 to 8 every day• Flexible schedules, no call• Guaranteed $240,000 averaging 4
shifts a week• Additional bonus pay based on
productivity• Malpractice coverage• Medical and dental for physician and
dependents at no cost• Long term disability insurance• Retirement plan with matching funds
PHYSICIAN OPPORTUNITIES
Contact Merl O’Brien, MD, at:(916) 791-1300, ext.11111; or email CV to:[email protected].
Physicians WantedCALIFORNIA FLORIDA
PHYSICIAN – FAMILY MEDICINELocated in Vista, California, Vista Community Clinic is a private, nonprofit outpatient community clinic located in North San Diego County serving people who experience social, cultural or economic barriers to health care in a comprehensive, high quality setting.
• Position: Full-time, Part-time and Per Diem Family Medicine Physicians.
• Responsibilities: Provides outpatient care to clinic patients and ensures quality assurance. Malpractice coverage is provided by Clinic.
• Requirements: California license, DEA license, CPR certification and board certified in family medicine. Bilingual English/Spanish preferred.
• Contact Us: Visit our website at www.vistacommunityclinic.org Forward resume to [email protected] or fax resume to 760 414 3702.
EEO/AA/M/F/Vet/ Disabled
COME ENJOY BEAUTIFUL WEATHER YEAR ROUND!
We are expanding & looking for full-time BC/BE Family Medicine physicians to staff the lower acuity areas of our emergency departments.
Multiple facilities all along the North Florida & South Georgia coast - you can choose to work near the following beaches/islands:
• Golden Isles of Georgia• Fernandina Beach, FL• Jacksonville Beach, FL• St. Augustine Beach, FL
• No office overhead (work in hospital)• Flexible shift schedule (9-10 hr shifts)• Cool procedures (foreign bodies,
abscesses, lacerations)• Gratifying treatment results (emergent)• Base pay + RVU salary (very
competitive)• Malpractice Insurance provided• Alternating holiday block schedules• Great camaraderie w/ low attrition (our
docs are happy)
We don’t use recruiters. We want to talk to you directly. Please send your CV or inquiries to Dr. Christina Caro at [email protected].
ADVERTISE WITH THE#1 BRAND
IN PRIMARY CARE.
(727) [email protected]
Northern CA hospital-owned network of practices is adding three physicians and expanding several of its clinics. The clinics are about an hour from and in between Sacramento and San Francisco. This position offers a great work-life balance: it’s outpatient only with no call of any kind and flexible schedule options. The great location, strong salary, and complete benefits will appeal to you.
For more information, please contact Roberta Margolis directly at
203.663.9335 or email your CV and references to [email protected].
Quick Facts• Monday - Friday, 8 am to 5 pm • Option to work four 10-hour days • 17 - 22 patients daily • Possible academic affiliation • Health with dental and vision for doctor
and family • Loan repayment available • Paid malpractice with no tail • Very generous PTO plus CME time • Relocation reimbursement and sign-on bonus
Opportunity available for family physicians and internists.
Search jobs, upload anonymous CVs and set up email alerts to
be notified when great jobs are posted.
AAFPCareerLink.org
464 American Family Physician www.aafp.org/afp Volume 98, Number 7 October 1, 2018
To advertise in AAFP CareerLink Classifieds contact our Media Sales Team at: (727) 497-6568; E-mail: [email protected]
CAREERLINK CLASSIFIEDS
With an outstanding staff, Patient First supports you in providing excellent care.We are looking for full and part-time physicians. With over 70 locations throughout greater Washington, D.C., Maryland,Virginia, Pennsylvania, and New Jersey, Patient First physicians have been providing urgent and primary care for over 35years. In addition to flexible schedules and career advancement opportunities, we offer a comprehensive compensationpackage that includes:• Excellent salary • Loan assistance• Relocation package • Outstanding malpractice insurance• Licensure and certification assistance and reimbursement• Health, dental, vision, life, and disability insurance, plus more.
To learn more, contact RecruitmentCoordinator Eleanor Hertzler at 804-822-4478or [email protected], or visitwww.patientfirst.com/PatientFirstCareers
Physician Founded Patient Focused 6.5 x 4.375_Layout 1 12/5/17 2:24 PM Page 1MULTI-STATE
724 American Family Physician www.aafp.org/afp Volume 99, Number 11 June 1, 2019
Readers turn to AFPfor information on upcoming courses and programs
Advertise your CME opportunity in AFP.
(727) 497-6568
AFP_06012019.indd 2 5/4/19 3:45 AM

June 1, 2019 Volume 99, Number 11 www.aafp.org/afp American Family Physician 725
OREGON
Oregon Health & Science University
OHSU’s Family Medicine Department is ranked in the top 5 for primary care, residency, rural medicine and research.
We are hiring providers to care for pati ents and support our academic mission.
Locati ons range from Portland area to rural Klamath Falls and The Dalles, Oregon. All clinics are certi ied Pati ent-Centered Primary Care Medical Homes.
Interested in shaping the future of primary care?
Visit www.ohsu.edu/fmcareers.
TENNESSEE
The University of Tennessee, Department of Family Medicine, is seeking a full time Addiction Medicine physician to join the faculty of their Center for Addiction Science in Memphis, Tennessee. Qualifi ed applicants should possess a DATA 2000 waiver for the prescribing of buprenorphine.
Responsibilities will include:• Participation in a broad spectrum of treatment
services for individuals with substance use disorders, including inpatient and outpatient care and consultative services
• Training and supervision of fellows, residents and students in Addiction Medicine
• Clinical research involvement• Community outreach
Interested applicants should submita cover letter and CV to:Muneeza Khan, MD, FAAFPUniversity of Tennessee Health Science CenterDepartment of Family Medicine1301 Primacy Pkwy, Memphis, TN 38119
Academic rank and salary dependent upon experience. American Board of Addiction Medicine certifi cation by the American Board of Preventive Medicine is highly desirable. The University of Tennessee is an EE)/AA/Title VI/Title IX/Section 504/ADA/ADEA institution in the provision of its education and employment programs and services.
ADVERTISE WITH THE#1 BRAND
IN PRIMARY CARE.
(727) [email protected]
Put your opportunity in front of physicians, whenever, however they want — in print, online and on their mobile devices.
Advertise with the #1 brand in primary care.
To advertise in American Family Physician, FPM, and on AAFPCareerLink.org call us at (727) 497-6568, or [email protected].
AFP_06012019.indd 3 5/4/19 3:46 AM

Medical Equipment
• Bionet CardioCare 2000 $1,255.00• Schiller AT-2 Plus* $2,275.00 *add Spirometry $1,000.00• Burdick ELI 250c $3,188.00 $3,188.00 • Welch Allyn CP150 with Interp $3,258.00
AFP is the most well-read journal
among primary care physicians
(727) [email protected]
AAFPCareerLink.org
CME Course Information
The American Academy of Stem Cell Physicians invites you to discover everything you need to know about Stem Cells.
AASCP’s “Master Workshop” is the most comprehensive stem cell therapy workshop. Never before has a workshop brought in BM, SVF, UCB, Peptides, Cytokines and Exosomes under the same roof. Get real hands on experience on patients as well as cadavers. See one, do one, and teach one.
Earn your CME and become board certi� ed by the American Academy of Stem Cell Physicians.
August 2-4, 2019
aaoscp.com or call305-891-4696
Search jobs, upload anonymous CVs and set up email alerts to
be notifi ed when great jobs are posted.
AAFPCareerLink.org
Comprehensive MRO Training Including Hair, Sweat, Oral Fluid, Interpretation of
Opiates, Alcohol Testing, and AAMRO Certification Exam (Friday–Sunday)
Nashville, TN August 9–11, 2019 Las Vegas, NV December 6–8, 2019
Approved for 21.75 AAFP Prescribed credits
NEW! Advanced Comprehensive MRO Training and Certification Exam
(Saturday–Sunday) (1.5 Day Program—Certified MROs only)
Nashville, TN August 10–11, 2019 Approved for 13.25 AAFP Prescribed credits
Special CME Programs
Medical Review Officer Training
(800) 489-1839 www.aamro.com
726 American Family Physician www.aafp.org/afp Volume 99, Number 11 June 1, 2019
AFP_06012019.indd 4 5/4/19 3:46 AM

Advertiser Index
AAFP . . . . . . . . . . . . . . . . . . . . . 667*, 679*, 680*, 707*, 711*, 715*
All of Us Research Program/AAFP/SANOFI PASTEUR . . . . . . .697
ALSO/AAFP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .722
Aleve/BAYER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .669
ASTRAZENECA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2nd Cover
Cologuard/PFIZER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 711*
Eucrisa/PFIZER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 672A*
FilmArray RP EZ/BIOFIRE DIAGNOSTICS . . . . . . . . . . . . . . . . . . . .667*
GILEAD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4th Cover
Jornay/IRONSHORE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .679
Longitudinal Assessment Self-Study Package/AAFP . . . . . . . . . . . . . . . . . . . . . . 3rd Cover
PFIZER & LILLY CORPORATE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .715*
QUIDEL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .707*
*DOES NOT APPEAR IN ALL COPIES .
Answers to This Issue’s CME Quiz Q1. C Q2. B Q3. D
Q4. C Q5. D Q6. A
Q7. C Q8. B Q9. C
Q10. A Q11. B Q12. C
New!
Feel confident about the Family Medicine Certification Longitudinal Assessment (FMCLA) with an invaluable new study tool from the AAFP. Study anytime, anywhere and address specific knowledge gaps with the combined learning power of the Board Review Self-Study Package and FP Comprehensive™.
Make the Longitudinal Assessment Self-Study Package your all-in-one FMCLA companion and earn up to 52 AAFP Prescribed credits.
New test. New AAFP study tool.
aafp.org/lassp • (800) 274-2237
19020314_BR FMCLA_Concept_Print Ad HP.indd 1 3/21/19 12:29 PMafp20190601 ad index.indd 3 5/10/19 9:24 AM

Discover how membership can power you.
THE AAFP POWERS ME TO FIGHT FOR OUR SPECIALTY.Andrew Lutzkanin III, MDAAFP MemberHershey, PA
aafp.org/powering-you